
A peer observation program for the professional development of laboratory tutors
Published online: 3 January, TAPS 2017, 2(1), 21-24
DOI: https://doi.org/10.29060/TAPS.2017-2-1/SC1017
Helen Naug1, Natalie Colson1, Andrew Pearson1, Eugene DuToit1, Grace Qi2
1School of Medical Science, Griffith University, Australia; 2School of Languages Humanities and Social Sciences, Griffith University, Australia
Abstract
As undergraduate allied health programs continue to expand, there is increasing reliance on laboratory tutors, to engage, mentor and teach students. The bioscience laboratory is a specialised, tightly regulated learning environment and a potentially rich learning platform for students, but when the laboratory tutors are inadequately trained, the flow-on effects to the students can produce unfavourable learning outcomes. Traditionally, new tutors attend a generic sessional training workshop offered by the university. Due to the added health & safety considerations and the type of learning (kinaesthetic) that occurs in the laboratory, we identified a need for a specific professional development program for laboratory tutors. Our aim was to develop a program that allowed tutors to work within a framework tailored for laboratory teaching and, in a supportive environment, build teaching skills that promote student learning. Based on Lave’s theory of situated learning (Lave, 1991) and the recognised approach of supported reflective practice (Bell, 2001) we placed opportunities for peer observation at the centre of the program. The framework presented here (3P’s) was developed specifically for laboratory tutors and served as behavioural guidelines for peer observation sessions. Ten participants volunteered for the pilot program which concluded in 2015. Peer observation records and focus group data were gathered to evaluate the pilot program. Tutor feedback has initiated improvements in the program, and due to its overall success, it has been embedded into the recruitment/induction process for laboratory tutors in our department.
Keywords: Peer Observation, Laboratory Teaching, Bioscience Education, Professional Development
I. INTRODUCTION
In the laboratory teaching environment, creating a safe learning space for inexperienced undergraduate students is a significant responsibility for the laboratory tutor/instructor. While the university provides a generic teaching and learning workshop centrally, we identified the need for a specifically tailored framework for training the laboratory tutors. In response to this need we developed
1) A framework listing the professional qualities of a laboratory tutor (3P’s matrix) and
2) An efficient on-the-job training program (peer observation)
A. Laboratory learning environment
The need for discipline-specific academic training programs is gaining recognition, particularly for laboratory-based learning (Good et al, 2015). Due to the potential hazards encountered in the laboratory environment there is a certain behavioural code of conduct for laboratories that tutors need to teach and model without coming across as ‘authoritarian’. Tutors need to be able to coach students as they learn skills kinaesthetically, and guide them to make connections between the laboratory and lecture content.
Situated learning and reflective practice served as the theoretical underpinnings of our peer observation design. In her theory of situated learning, Lave describes learning as a ‘social phenomenon constituted in the experienced, lived-in world, through legitimate peripheral participation in ongoing social practice’ (Lave, 1991, p64). In addition to situated learning, our approach emphasises reflective practice where activities involving observation ‘… encourage shared critical reflection on real-life teaching experiences-and can lead to transformation of both perspective and practice.’ (Bell, 2001).
This report details the framework and methodology for implementing this program which was piloted in 2014/2015 and, due to its success, is now embedded in our department as a prescribed training program for novice laboratory tutors.
II. METHODS
Formal ethical clearance was obtained before the commencement of the pilot program. Sessional laboratory tutors/instructors were invited to be part of the professional development program at the commencement of the teaching semester in 2014/2015. Ten tutors (4 experienced and 6 novice tutors) volunteered for the program.
A. Induction workshop
As part of the program, a specifically designed two-hour induction workshop was delivered to the participants which highlighted effective teaching practices in the laboratory; it also included an explanation of the peer observation process. Two of the project team members (NC and HN) designed a matrix to create some structure for the tutoring role, termed the 3P’s framework. 3P’s is an acronym for preparation, participation and professionalism, key terms which categorise observable qualities of good laboratory teaching (see Table 1). All the resources (including the 3P’s matrix) were made available to the program participants.
| Laboratory Tutor Professional Development Matrix | |||
| Competency | Evidence
Level C Poor |
Evidence
Level B Average |
Evidence
Level A Excellent |
| Professionalism |
Insufficient evidence E.g.,
|
Moderate evidence E.g.,
|
Significant evidence E.g.,
|
| Preparation |
Insufficient evidence E.g.,
|
Moderate evidence E.g.,
|
Significant evidence
E.g.,
|
| Participation |
Insufficient evidence E.g.,
|
Moderate evidence E.g.,
|
Significant evidence
E.g.,
|
Table 1. 3P’s Matrix
B. Formation of the triad
An excel spreadsheet was electronically shared with the participants who filled in times indicating their availability to be observed, and to observe another tutor or peer. Course convenors also made themselves available to observe the participants as an “expert”. Once a triad was formed (observer, observee and expert) the observation session would proceed.
C. Peer observation process
The peer observation process was modelled on the university’s peer review of teaching program (Martin & Double, 1998) which most of the academic team in this program had experienced first-hand. The modified process we developed for sessional laboratory tutors included 3 episodes:
1) Observee prepares a summary of the teaching session
2) Peer observer and “expert” observer attend the session and observe the tutor and complete the feedback peer observation sheet which includes alignment with the 3P’s matrix and any other comments
3) The triad decide on a time to meet and give feedback (30 minutes) which is then followed by a second observation usually 3-5 weeks later
D. Evaluation
1) Focus group discussion: Five of the participant tutors ( 3 novice and 2 experienced) volunteered to discuss their experience of the program in a 10 minute focus group session which took place the final week of semester after completion of the program. The focus group discussion was recorded, transcribed and analysed for relevant themes. The analytical procedures were based on the Conventional Content Analysis suggested by Hsieh and Shannon (2005).
2) Peer observation sheets: The peer observation sheets were analysed for tutor’s observed alignment to the 3P’s matrix.
III. RESULTS
A. Focus group discussion
1) Theme 1- Receiving feedback:
Participants recognized the need to receive feedback on their performance as tutors and agreed that it was a good initiative:
“In previous years there was never any critical feedback on our performance as tutors… and I always wondered how we know whether our performance is good or bad or how to improve…”
“It’s a two-way process…you get feedback when you are observed, but when I was observing someone I realised that I could learn so much… you don’t just pick up on their mistakes but you can learn new ways of doing things to improve your own teaching”
2) Theme 2- Expectations:
Participants were not sure what to expect from the program.
“I was hesitant about starting the program because I felt that the labs I was going to be observed in I would be very anxious…doubtful in my knowledge and confidence…and I didn’t think I would be able to perform well…but as it turned out I was really calm”
3) Theme 3- Preparation and professionalism:
Participants feel the program helps formalise their teaching and give it meaning.
“ One experience I had in one of the first lab sessions was quite negative in that I couldn’t troubleshoot the software problems the students were having…I spent most of the session trying to understand the software because I hadn’t properly prepared myself on how to use it…through that lab so many students were having problems and I felt helpless as a tutor and disappointed in myself…and I don’t think I would have reflected on that experience so greatly if I hadn’t been part of the program…I would have just taken it as a bad run..”
“I received some critical feedback on health & safety issues that I had disregarded…I simply forgot to take notice…usually I am so strict with health & safety… but I had become complacent…”
“I liked the way we had the matrix as something concrete to focus on…”
B. Peer Observation sheets
Based on the peer observation reports, participants were able to demonstrate moderate or significant evidence of the key attributes that we identified as important for the role of laboratory tutor, as defined in the 3P’s matrix. Only in 8 of the 60 observed teaching sessions did the observed tutor demonstrate insufficient evidence of a key attribute. We can infer from these peer observations that on the whole, the tutors had made an effort to model the attributes, and initiate improvements in their approach to teaching.
IV. DISCUSSION
This report details a professional development program for laboratory tutors which incorporates strategies based on peer observation (situated learning) and feedback sessions (reflective practice). Results show that tutors in the program relied on the 3P’s matrix in preparation for the observed sessions (over 90% of the teaching sessions observed showed alignment with the 3P’s matrix).This indicates that with the 3P’s framework tutors can learn “on the job” and form new practices to improve their teaching; a demonstrable outcome of situated learning. In addition, tutors agree that they “learn something” by observing their peers, another key component of situated learning (Lave, 1991).
Focus group discussions indicate that tutors appreciated the critical feedback regarding their teaching performance which generally resulted in improved performance in the subsequent observations. The feedback sessions encouraged reflective practice, leading to changes in “perspective and practice” (Bell, 2001). Not only did tutors acknowledge errors in their practice but developed confidence in practice initiatives. Such changes in attitude and practice are desirable outcomes in any professional development program..
V. CONCLUSION
This program is innovative as it focuses specifically on the professional development of laboratory tutors. It has fulfilled its primary purpose to create a framework to assist tutors to develop skills for teaching in bioscience laboratories. As we continue to encourage the development of expertise among tutors, experienced academics involved in the program also improve their skills by contributing to what essentially is a community of practice. Future evaluations of the program will incorporate a measurable comparison between the two observation episodes for novice tutors, based on the 3P’s matrix. This will more clearly demonstrate, and help quantify, improvements in performance. The overriding aim of this program is improved learning in undergraduate laboratories, and our future course evaluations will target measurable student feedback on laboratory learning.
Notes on Contributors
Helen Naug PhD is a senior lecturer and academic lead for the common foundation year program for the Health faculty. Natalie Colson PhD is senior lecturer in Genetics and program director for the Bachelor of Biomedical Science program. Andrew Pearson PhD is senior lecturer and first year co-ordinator for the School of Medical Science. Grace Qi is a PhD candidate for the school of languages, humanities and social sciences. Eugene DuToit is associate professor and program director for the Bachelor of Biomedical Science with Honours program.
Declaration of Interest
The authors declare that they have no competing interests.
References
Bell, M. (2001). Supported reflective practice: a programme of peer observation and feedback for academic teaching development. International Journal for Academic Development, 6(1), 29-39.
Good, J., Colthorpe, K., Zimbardi, K., & Kafer, G. (2015). The Roles of Mentoring and Motivation in Student Teaching Assistant Interactions and in Improving Experience in First-Year Biology Laboratory Classes. Journal of College Science Teaching, 44(4), 88-98.
Hsieh, H. & Shannon, S. E. (2005). Three approaches to Qualitative Content Analysis. Qualitative Health Research, 15(9), 1277-1288. doi: 10.1177/1049732305276687
Lave, J. (1991). Situating learning in communities of practice in Resnick, Lauren B. (Ed); Levine, John M. (Ed); Teasley, Stephanie D. (Ed), Perspectives on socially shared cognition. (pp. 63-82). Washington, DC, US: American Psychological Association, xiii, 429 pp. http://dx.doi.org/10.1037/10096-003
Martin, G.A. & Double, J.M. (1998). Developing Higher Education Teaching Skills through Peer Observation and Collaborative Reflection. Innovations in Education and Training International, 35(2) 161-170.
Published online: 3 January, TAPS 2017, 2(1), 16-20
DOI: https://doi.org/10.29060/TAPS.2017-2-1/SC1010
Giat Yeng Khee, Jia Yuan Tay, Sei Keng Koh, Melissa Mee Yin Chow, Wan Chee Ong and Paik Shia Lim
Department of Pharmacy, Singapore General Hospital, Singapore
Abstract
Aim: To assess trainee’s knowledge and practice behavior changes with the revised basic MMS training program.
Methods: Kirkpatrick’s four-level evaluation model was adopted in this study. A questionnaire was used to seek trainees’ feedback on the training program. For learning progression, trainees’ self- perception of their competency pre- and post-training, and results from a multiple-choice questions (MCQ) test were assessed.
Thirty-eight behavioral changes in the patient care delivery and problem solving competency cluster of the General Level Competency Framework (GLF) were compared pre- and 6 months post-training. Evaluation of level-4 results is pending as advanced training is in progress.
Results: Fourteen out of fifteen trainees who had completed the basic MMS training responded to the online questionnaire. Eleven trainees (78.6%) rated basic MMS training program as good or excellent. Positive response was highest in tutorials (84.3%), followed by continuous education sessions (70.6%) and clinic attachments (67.6%). Suggestions for improvement include increasing the frequency and opportunities of hands-on patient interview at clinic attachments.
Sixty-four percent of trainees perceived improvement (p<0.013) in delivering patient care post-training (median=3; IQR: 3-4) than pre-training (median=3; IQR: 2.75-3). All but one trainee passed the MCQ test (median score: 80; IQR: 76-86). A greater proportion of patient care delivery and problem solving behaviors (69.2% and 35.9% respectively) in GLF was graded highest performance at post-training compared to pre-training (35.3% and 14.3% respectively).
Conclusions: The revised training program is well-received by trainees and feedback from trainees provides insights into future improvements in the content and delivery of the program.
Keywords: Medication Management, Pharmacist, Training, Kirkpatrick
I. INTRODUCTION
Pharmacist-provided Medication Management Service (MMS) aims to improve patients’ outcomes by promoting effective and safe medication use. Essential knowledge and skills in chronic disease management are required in providing good quality pharmaceutical care. An in-house 6-month MMS training program was first developed in January 2013 to impart essential skills of a competent MMS pharmacist. It focused primarily on self-directed learning, using reading materials provided by a sole trainer, amidst the heavy daily workload of trainees. Successful completion of the original training program therefore relied greatly on the trainees’ motivation and commitment. Consequently, completion rate within 6 months as a trained MMS pharmacist was unsatisfactory. Furthermore, the growth of other clinical pharmacy services was affected as the completion of MMS training was a pre-requisite before embarking on other specialized services.
As detailed in Diagram 1, a revised training program which adopted outcome-based education approach was implemented in April 2014. It was divided into basic and advanced phase, which each lasts for 6 months. The basic MMS training program aimed to facilitate learning and enhance competency of pharmacists in medication review and dispensing, while the advanced program aimed to ensure broad- based competency and clinical skills of pharmacists before embarking on pharmacist-provided ambulatory care services. In the revised program, there were significantly more engagement between the trainers and trainees in facilitating trainees’ learning. Prior to this study, a systematic evaluation of the MMS training program has not been conducted. As a first step in evaluating the effectiveness of the revised MMS training program, in this study, we aimed to assess trainees’ knowledge and practice behavior changes following completion of basic MMS training and to identify areas for improvement.
| Original MMS Training Program (6 months) | Revised MMS Training Program (12 months) |
| Reading material provided
Self-directed learning by trainees for 6 months Multiple-choice questions (MCQ) test Completion of MMS training
|
Four monthly tutorials* + Three MMS clinic attachments
MCQ test
(Basic MMS training – 6 months)
Completion of basic MMS training Conducting 15 MMS reviews under supervision
(Advanced MMS training** – 6 months)
MCQ test Completion of advanced MMS training |
*Topics discussed during tutorials include cardiology, endocrinology, geriatric & nephrology
**Basic MMS training is compulsory for all outpatient pharmacists in SGH whereas the advanced MMS training is optional.
Diagram 1. Original and revised MMS training program in Singapore General Hospital
II. METHODS
In this study, the Kirkpatrick’s four-level evaluation model, developed for measuring training effectiveness, was utilized (Kirkpatrick, 1998). This systematic approach offers multiple levels of evaluation using different data sources and it allows evaluation of both qualitative and quantitative data. All pharmacists who had received basic MMS training in year 2014 were recruited to participate in the study. No ethic approval required based on Singapore Health Services centralized institutional review board. All four- level outcomes were measured as follows:
A. Kirkpatrick level I: Reaction
An online questionnaire, developed by a group of MMS trainers and trainees who were not recruited in the study, was administered to trainee post-basic MMS training. Trainees rated the effectiveness of the basic MMS training program including the various training modalities (tutorials, continuous education sessions and clinic attachments) on a 5-point Likert-scale and provided suggestions for improvement.
B. Kirkpatrick level II: Learning
The same online questionnaire was used to examine the trainees’ perception on the impact of the MMS training program, either positively or negatively affecting their competency in delivering patient care. Results of the multiple-choice questions (MCQ) test administered 6-month post training were examined. The MCQ test that consisted of 50 recall and case-based questions was developed by two MMS trainers, who were the content experts, so as to assess trainees’ clinical knowledge and reasoning. Questions were scrutinised to ensure that they represented an accurate measure of the learning outcomes.
C. Kirkpatrick level III: Behaviour
Changes in observed practice behaviours were assessed using the United Kingdom-adapted General Level Competency Framework (GLF). This is an assessment and developmental tool consisting of 63 behavioural statements distributed into 3 competency clusters: delivery of patient care, problem solving, and professionalism (Rutter et al., 2012). Thirty-eight behavior statements, representing the areas where basic MMS training could have a major influence on, were measured pre- and post-basic MMS training. The performance-level rating for each behaviour (1=rarely; 2=sometimes; 3=usually; 4=consistently) was based on the consistency in demonstration in practice, which was rated according to the assessor’s observation.
D. Kirkpatrick level IV: Results
Currently, the advanced MMS training is still in progress. In advanced MMS training, 15 case reviews by the trainees will be assessed. Trainee with satisfactory achievements in both the final MCQ test and 15 case reviews will be deemed eligible as trained MMS pharmacist.
E. Data Analysis
Descriptive statistics were used to summarize the trainees’ characteristics, reactions to basic MMS training programme and learning outcomes. Behavioural changes pre- and post-basic MMS training were assessed and compared using Wilcoxon signed rank test. SPSS, version 21 (SPSS Inc., an IBM Company Chicago, USA) was used for statistical analysis and a p-value of <0.05 was defined to be statistically significant.
III. RESULTS
Fourteen out of fifteen trainees who had completed the basic MMS training participated in this study. Half of the trainees completed their pharmacy undergraduate program in Singapore while the rest completed their studies overseas.
A. Kirkpatrick level I: Reaction
Fourteen trainees responded to the online questionnaire. Eleven trainees (78.6%) rated basic MMS training program as good or excellent. Positive response was highest in tutorials (84.3%), followed by continuous education (CE) sessions (70.6%) and clinic attachments (67.6%). Suggestions for improvement include increasing the frequency and opportunities of hands-on patient interview at clinical attachments.
B. Kirkpatrick level II: Learning
Nine trainees (64.0%) perceived significant improvement in delivering patient care post-training (median=3; IQR: 3-4) as compared to pre-training (median=3; IQR: 2.75-3) (p<0.013). As for the MCQ test conducted post-training, all but one trainee passed the MCQ test, achieving a median score of 80 (IQR: 76-86).
C. Kirkpatrick level III: Behaviour
Thirteen trainees had completed pre- and post-training GLF assessment for observed practice behaviours. Overall, 23 out of the 38 behaviors (60.5%) were found to have significant improvement at repeated observation post-training. Greater proportion of behaviors in delivering patient care cluster was graded to perform consistently at highest performance level post-training compared to pre-training (69.2% vs 35.3%). Similar improvement was observed in the problem solving cluster where 14.3% and 35.9% of the behaviors were graded consistent performance at pre- and post-training respectively. There was no significant improvement observed in 3 behaviors as the trainees were practicing at the highest level during the pre-training evaluation. Performance level for other behaviors was maintained over the 6- month training.
IV. DISCUSSION
Assessment of the training program provides valuable information to trainers and its institution in seeking ways to improve the training program. The revised basic MMS training program has likely achieved its aim to provide broad-based training that enhances trainee’s competency in patient care as positive results were observed in trainee’s attitude, knowledge and performance (level 2 and 3). Feedback (level 1) from the trainees was encouraging and indicated that the revised training program with the inclusion of tutorials, CE sessions and clinic attachments, was well-received and trainees had perceived improvement in their competency at providing patient care. Engagement between trainers and trainees in our revised program has been increased, as compared to the original program. This increased engagement between the trainers and trainees may have enhanced the trainees’ learning experiences through regular feedback from the trainers and reflection of their learning process, thus resulting in better performance post-training. From the high rate of positive response from trainees, it demonstrated that such interaction with trainers was in favor to support learning.
Clinic attachment was ranked lowest amongst all training activities as trainees commented that the opportunities for clinic attachments were sparse, with 3 clinic attachments distributed over 6 months. However, increasing the frequency of clinic attachments is not feasible in view of the large pool of trainees and limited training resources. Proposed plans for enhancement of the program include restructuring tutorial or CE sessions to problem-based learning. Simulation cases could be used to facilitate the application of knowledge and prepare trainees better for hands-on experiences during clinic attachments.
There were limitations to our study. First, positive changes observed in attitude, knowledge and performance may not be solely contributed by the MMS training program due to the lack of a control group. Improvement in behaviors observed in GLF assessment could be contributed by other sources of training such as the 5-weekly outpatient clinical group discussion, feedback or suggestions from their GLF assessor, self-directed learning and lecture series from other continuing professional education provided by external parties. Second, pre-training MCQ test was not performed. Therefore, the extent of improvement in trainees’ knowledge level was not established.
V. CONCLUSION
Our assessment shows that the revised basic MMS training program is well-received by trainees and feedback from trainees provides insights into future improvements in the content and delivery of the program. The results of the advanced MMS training are pending, therefore, the effectiveness of the revised MMS program is yet to be evaluated.
Notes on Contributors
Khee Giat Yeng is a board certified pharmacotherapy specialist at Singapore General Hospital where she is involved in the provision of ambulatory care services in the medication management service, rheumatology monitoring clinic and anticoagulation clinic. She is also actively involved in teaching medical students, pre-registration pharmacists, pharmacists and post-graduate students.
Tay Jia Yuan is a pharmacist in Singapore General Hospital and is currently participating in the advanced training program for the medication management service in SGH.
Koh Sei Keng is involved in the provision of anticoagulation services at the ambulatory care clinic in the Singapore General Hospital.
Melissa Mee Yin Chow a senior pharmacist at Singapore General Hospital with a board certification in pharmacotherapy. She is involved with training of pre-registration pharmacists and registered pharmacists. She also provides ambulatory care services in medication management, anti-coagulation and haemodialysis disease management clinics.
Ong Wan Chee is a senior clinical pharmacist at Singapore General Hospital. She is actively involved in the provision of ambulatory care services including medication management service, patient outreach program, inflammatory bowel disease, and rheumatology monitoring clinic. She also teaches the medical students, pharmacists, pre-registration pharmacists and postgraduate students.
Lim Paik Shia is a principal clinical pharmacist, practicing in ambulatory care clinics at Singapore General Hospital. She is actively driving the pharmacist-provided clinics, in particularly medication management service to outpatients and hemodialysis patients. She is also a clinical educator for pharmacists, residents, postgraduate students and pre-registration pharmacists.
Acknowledgements
The authors would like to thank all MMS trainers for their contributions in this study. We would like to acknowledge the guidance provided by Mr Chang Wei Terk who had pioneered the original MMS training program and his instrumental role in the revision of the program.
Declaration of Interest
The authors declare no conflict of interest or any sources of funding for this study.
References
Kirkpatrick, D. L. (1998). Evaluating training programs: The four levels (2nd ed.). San Francisco, CA: Berrett-Koehler.
Rutter, V., Wong, C., Coombes, I., Cardiff, L., Duggan, C., Yee, M. L., Lim, K. W., & Bates, I. (2012). Use of a general level framework to facilitate performance improvement in hospital pharmacists in Singapore. American Journal of Pharmaceutical Education, 76(6), 107.
Published online: 2 May, TAPS 2017, 2(2), 30-33
DOI: https://doi.org/10.29060/TAPS.2017-2-2/SC1013
Akalanka P. Hettihewa, Indika M. Karunathilake & M. N. S. K. Perera
Medical Education Development and Research Centre (MEDARC), Faculty of Medicine, University of Colombo, Sri Lanka
Abstract
Introduction & Objectives: Faculty of Medicine, University of Colombo, Sri Lanka conducts MBBS and BSc physiotherapy degree programs following SPICES model where educators have to play diverse roles in order to fulfil their responsibilities. Looking at them from a student’s perspective will help understand what students perceive as important roles of educators and help the students understand the educators’ different capacities. An effective medical educator possesses a range of qualities. Looking at them from students’ point of view indicates what they expect from teachers as professionals.
Methods: Harden and Crosby (2000) paper on 12 roles of a medical teacher was the conceptual framework for this study. Based on previous literature a questionnaire was developed with 20 different roles and 15 qualities of an educator. Study followed an analytical cross-sectional design with participation of 188 physiotherapy and medical undergraduates.
Results: Study findings indicated that the students’ perception on importance of different roles of teachers had a close overlap with Harden’s 12 roles. Information provider as a lecturer in class room in clinical settings, in practical settings, developing learning materials for lectures, clinical educators etc. Importance of being an examiner and curriculum planner was rated relatively low by students. Students perceived good communication skills, professional skills, knowledge and respect for patients as most important qualities in an educator.
Conclusion: Findings will help educators understand what learners expect from them and help students understand the different capacities of educators.
Keywords: 12 Roles of a Medical Teacher; Ideal Medical Teacher; Student Perception; Survey
I. INTRODUCTION
The purpose of teaching is to facilitate personal growth and development that impact the professional, social and political aspects of learners (Galbraith, 2004). Since global trend of medical education is moving towards a more humanistic approach to patient care, medical teachers need to become educators, interacting with individual students (McLean, 2001).
Faculty of Medicine, Colombo, Sri Lanka conducts a 5 year MBBS degree programme and a 4 year BSc. Physiotherapy degree programme. Both programmes follow innovative student-centred curricula and incorporate features of SPICES model in their teaching. This context involves diverse learners, various teaching methods and a range of teaching settings. This student-centred learning environment expects the teachers to guide the learners with diverse abilities, knowledge and different levels of comprehension towards self-directed study. In order to fulfil their responsibilities in this context teachers have to play a variety of roles.
Harden and Crosby (2000) have identified that with rapid changes in medical education the role of the medical teacher is changing. They have identified 12 roles of the medical teacher falling into six categories.
According to Cross (1995) discrepant perceptions of roles and behaviours in clinical education may have an adverse effect on student learning. So it is important that
students should have an understanding of different roles of the teacher and the faculty should understand the students’ perception on the different roles of a medical educator and how the students perceive the importance of different roles to them as undergraduates.
Successful completion of these demanding and complex roles requires teachers to possess a range of professional and personal qualities. Different studies have identified a variety of characteristics as the best qualities in a medical educator. Looking at them from a student’s point of view will help understand what students perceive as being important and what they expect from their teachers as educators and medical professionals.
The findings of this study will help students understand the different capacities of educators and how to get the maximum aid from their educators in these different capacities. Findings will also help the educators understand what leaners expect from them as teachers and medical professionals.
II. METHODOLOGY
Objectives of this study were to:
- Identify the medical and physiotherapy undergraduates’ perception on importance of different roles of a medical teacher.
- Identify the medical and physiotherapy undergraduates’ perception on important qualities in a medical teacher.
- Compare the differences of students’ perception regarding the importance of different roles in a medical teacher based on their academic year.
- Compare the differences of students’ perception regarding the importance of different roles in a medical teacher based on students’ programme of study.
This study followed an analytical cross sectional study design; it was carried out in faculty of Medicine, Colombo, Sri Lanka. At a confidence interval of 95% and a 5 % margin of error the target sample was 300 undergraduates representing three academic years of the faculty.
A self-administered questionnaire with 20 roles and 15 qualities of a medical teacher was developed to collect the data. Harden’s (2000) paper on 12 roles of a medical teacher was used as a conceptual frame to identifying the different roles of a medical teacher. Based on these 12 roles, 14 different roles of teachers were identified. To better suit the study setting and participants the learning facilitator role was re-categorized as facilitator of small group discussions (SGD) and facilitator of problem based learning (PBL) sessions, role of clinical or practical teacher was divided as information provider in clinical settings and information provider in practical settings. Other 10 original roles of Harden’s (2000) study were also included. Based on previous literature 6 more roles were added, as tutors, personal advisors, clinical educators, researchers, administrators and community health developers. Based on previous study findings, 15 important personal and professional qualities of a medical teacher were added to the questionnaire.
Students’ perception was obtained through a likert scale, 5 being very important, 4, considerably important to 1 being not important. Participants marked the importance of roles and qualities according to their perception. Data was analysed using the 16th version of SPSS. First and second objectives were analysed using descriptive analyses and third and fourth objectives were analysed using chi square.
III. RESULTS
Total of 188 students participated in the study at a response rate of 62.67% representing three academic years of the faculty. Out of which 139 were MBBS undergraduates and 159 were females.
According to the responses, the students perceived following roles of medical teachers to be very important. Majority perceived the most important role of a teacher was being an information provider in clinical settings. Following roles are listed according to majority’s perception of their importance.
- Information provider in practical settings
- Information provider as a lecturer in class room
- Clinical Educator
- Developing learning materials for lectures (Presentations/ handouts)
- On-the-job role model (Clinic/ward)
- Role model in teaching setting
- Learning facilitator in SGDs
- Learning facilitator in PBLs
- Examiner of formal examinations
- Curriculum Planner
- Curriculum Evaluator
The roles teachers’ play as researchers, course organizers and resource developers were rated low by the students. Undergraduates’ perceived that the least important role of a medical teacher is of an administrator. Being a mentor and a personal advisor were also rated as less important by the participants.
There was no statistically significant difference found in students’ perception on different roles of a medical teacher based on the participants’ academic year. No statistically significant difference was found in students’ perception for majority of educators’ roles; however physiotherapy undergraduates had a more positive perception towards educators’ role as researchers and course organizers than MBBS undergraduates. Difference in perception was statistically significant (P > 0.05).
Students perceived that the most important qualities of a medical teacher were having, good communication skills, knowledge, professional skills and humanistic approach to patient care. Having good knowledge in technology was rated as the quality with lowest importance and having honesty and integrity were also rated low by the participants.
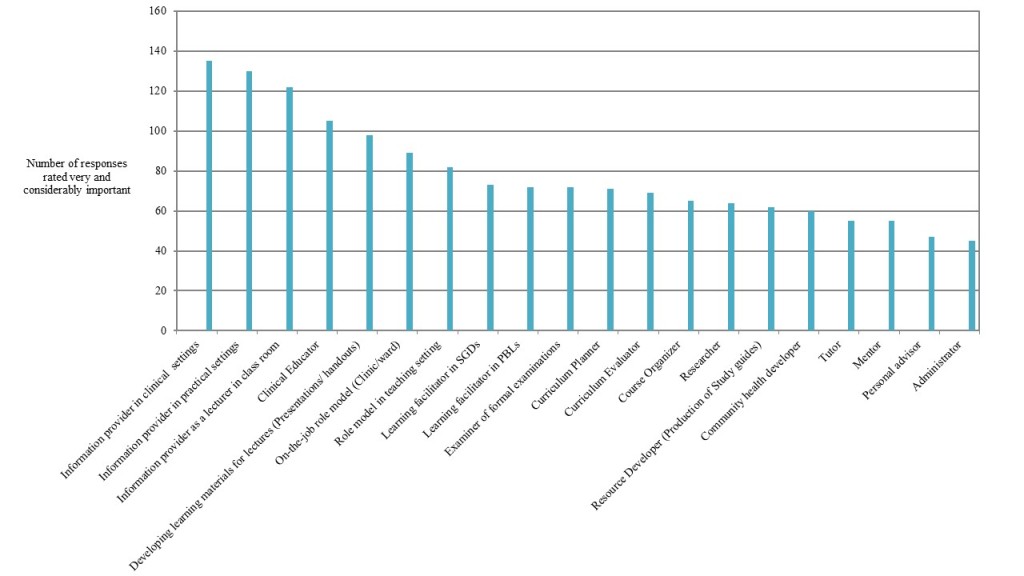
Figure 1: Undergraduates’ Perceived Importance of Different Roles of a Medical Teacher
IV. DISCUSSION
Students’ perception on importance of different roles of teachers had a close overlap with the 12 roles identified by Professor Harden (2000). However, students didn’t perceive the roles of being a mentor, course organizer, and resource material developer (study guides) as being important as Harden (2000) found. This might be due to the fact that students don’t get an opportunity to observe educators in these roles at the faculty and the responsibilities they have in these roles. Even though these roles have a strong impact on the curriculum and curriculum development educators don’t directly contact with students through these roles so the students might not perceive their importance as much as the faculty does.
Educators can play an important role as a mentor and a personal advisor to the students in their personal and professional lives. However students had rated both these roles as not being “very important” roles of a medical teacher. Can this be due to the fact that the students have not observed their educators in these roles frequently and closely? It may also be due to the fact that with the cultural and social factors involved in the Sri Lankan educational and clinical settings students are not familiar with seeking advice from their educators on personal issues.
Students had identified many of the qualities in the questionnaire as being “very important” for a medical teacher to have. However following medical ethics, honesty and integrity were ranked relatively low by the students. It is an interesting observation and the reasons for this should be identified.
Physiotherapy undergraduates had a more positive perception towards educators’ role as researchers and course organizers than MBBS undergraduates. This could be due to better student to staff ratio in the Physiotherapy training program. The Physiotherapy program has only 30 students per intake every year whereas MBBS program has 200 students in each intake. Therefore the physiotherapy students have more opportunity to work closely with their educators getting more exposure to their teachers involved in variety of different teaching roles as course organizers and researchers than the MBBS students.
V. CONCLUSION
Findings indicate that the participants understand that teachers play a range of important roles other than being just a teacher. They had also identified that to fulfil these roles educators need to possess a range of personal and professional qualities.
Findings from this study will help students understand the different capacities of educators and will also help educators understand what learners expect from them as medical professionals. This will lead to better student-teacher interactions.
Notes on Contributors
Ms. Akalanka Hettihewa is a physiotherapist from Faculty of Medicine, University of Colombo, Sri Lanka, currently employed at the Medical Education Development and Research Centre (MEDARC) Faculty of Medicine Colombo, Sri Lanka.
Dr. Indika Karunathilake is the director of the Medical Education Development and Research Centre (MEDARC) Faculty of Medicine Colombo Sri Lanka.
Dr. M.N.S.K Perera is a MBBS graduate from Faculty of Medicine, Colombo, currently working at the National Hospital Sri Lanka (NHSL) Colombo.
Ethical Approval
The approval for this study was obtained from the Ethics Review Committee, Faculty of Medicine, Colombo, Sri Lanka.
Declaration of Interest
The authors declare that they have no competing interests.
References
Cross, V. (1995). Perceptions of the Ideal Clinical Educator in Physiotherapy Education, Physiotherapy, 81(9), 506-513.
Galbraith, M.W. (2004). Adult learning methods: A guide for effective instruction (3rd ed.). Florida, Krieger publishing Company.
Harden, R.M., & Crosby, J. (2000). AMEE Guide No 20: The good teacher is more than a lecturer, the twelve roles of the teacher, Medical Teacher, 22(4), 334-347.
McLean, M. (2001). Qualities attributed to an ideal educator by medical students: should faculty take cognizance? Medical Teacher, 23(4), 367-370.
*Akalanka P. Hettihewa
110, Sri Dharmarama Rd, Fort, Matara
Tel: +94783641866
Email: akalankahettihewa26@gmail.com
Published online: 5 September, TAPS 2017, 2(3), 24-25
DOI: https://doi.org/10.29060/TAPS.2017-2-3/SC1042
Shahla Siddiqui
Department of Anaesthesia, Khoo Teck Puat Hospital, Singapore
Abstract
There is a gap between the teaching and practice of clinical ethics. Many students learn bioethics at an undergraduate level in lectures and through tutorials. They may also learn case based ethical reflection; however, discussing ethical issues of real ICU patients and families is a novel form of experiential teaching which engages undergraduate students and helps them see practical and quick consideration in very sick patients. Often ICU patients present complex and difficult ethical dilemmas which can demonstrate real life scenarios that students can relate to when learning in a classroom.
Keywords: Ethics Teaching, Interprofessionalism, Experiential Learning
I. INTRODUCTION
The The Intensive Care Unit is an environment where myriad complex clinical situations present and these are often closely intertwined with ethical dilemmas (Svantesson, Anderzén-Carlsson, Thorsén, Kallenberg & Ahlström, 2008). ‘Ethical dilemmas’ constitute many complex situations which can surround a patient’s clinical care that often involve an apparent mental conflict between moral imperatives, in which to obey one would be opposing the other (Braunack Mayer, 2001). Situations range from triage, surrogate decision making, organ donation, family communication and patient autonomy. An example of this may be a family insisting on non-beneficial life sustaining therapy in an elderly patient. Many times such situations are not explicitly presented to medical students and they rarely get a chance to witness how doctors deal with real complex clinical ethics issues in a situation where time is essence (Oberle & Hughes, 2001). Coping with these problems is crucial to the development of medical students and an exposure to how a multi-disciplinary team of doctors, social workers, nurses and palliative care physicians may help solve hard cases is very useful. The interaction and cooperation between different professions also helps to consolidate the roles of each allied health team and highlights to the medical student an integrated professional attitude (Udén, Norberg & Lindseth, 1992).
The aim of this educational qualitative study was to evaluate the narrative feedback of medical students after being exposed to Ethics rounds in a 14 bedded surgical ICU of a teaching hospital by a multi-disciplinary ICU team.
II. METHODS
After IRB approval, medical students posted to our hospital for an Anaesthesia rotation were invited to participate in the study. A verbal consent was obtained with specific instructions to maintain patient confidentiality. The author who is an intensivist led the rounds of all ICU patients. This included a multi -disciplinary round comprising of nurses, social workers and allied health staff such as a pharmacist, a physiotherapist and a dietician. All staff had been conducting daily ICU rounds on the patients and were familiar with their ethical issues. The students were briefed about ethics issues that may have arisen in each patient’s case and how they were resolved by the team. There was input from the other team members especially the social workers and the nurses. Students were encouraged to reflect and ask questions about each case and offer their own input. Some cases were straightforward and did not have many ethical questions, however some others had complex problems that needed more time. Some issues were resolved already whilst others were ongoing and the students were encouraged to offer solutions based on their past learning. All students belonged to the fourth year of medical school and had received a longitudinal ethics teaching. At the end students were asked to write down an anonymous narrative feedback for the author.
III. RESULTS
Overall the six medical students were very happy to be part of the 1 hour ICU ethics round. They appreciated the real life practical application of the issues facing a team of professionals daily and the aspects of care we need to consider when resolving such issues.
“ I felt that the session was very informative and helped clarify many perceptions we had towards the ICU.”
It reinforced their view of an inter-professional approach to ICU care:
“The involvement of other healthcare workers of the ICU team helped us better appreciate the multi- disciplinary nature of ICU care and the role each person plays.”
“Having the allied healthcare team there to offer their thoughts also brought a new perspective to patient care for me. I feel that these lessons are more valuable than what we may take away from a didactic lecture alone.”
They were able to appreciate the ethical challenges faced by the team:
“I really enjoyed it and it gave me an insight not only on the logistical side of the ICU but also the ‘heart’ behind it and the ethical dilemmas that the healthcare professionals go through every day.”
A patient perspective and human aspect was also highlighted by the input from nurses, physician and social workers which is different from the often cold clinical picture on rounds:
“It was interesting to learn about the various patients in the ICU and the challenges they themselves face in getting better.”
“This enabled us to tie in the things that we had heard of during lectures and tutorials, and the many issues that we may have not been exposed first hand to.”
The practical aspects of clinical care was exposed:
“It was also a good way to see the practical aspects of ICU care ….being able to see different ICU patients and hear their stories we got a real feel of the ICU”.
“We also felt easy asking pertinent questions about their management to you.”
IV. DISCUSSION
Experiential learning and case based clinical bioethics teaching is a practical and effective way of imparting explicit knowledge, skills and role modeling attitudes for medical students (Widdershoven, Abma & Molewijk, 2009). This should not be solely dedicated to ICU or for ethics. Many ethical issues faced in ICUs are commonplace in ward settings as well (Rathert & Fleming, 2008). Effective communication, empathy, cultural nuances and professionalism are all learning that medical students can pick up from such ethics rounds in the ICU.
Notes on Contributors
Shahla Siddiqui is a Senior Consultant and Intensivist as well as a graduate student in medical ethics.
Declaration of Interest
The author declares no conflict of interest.
References
Svantesson, M., Anderzén-Carlsson, A., Thorsén, H., Kallenberg, K., & Ahlström, G. (2008). Interprofessional ethics rounds concerning dialysis patients: Staff’s ethical reflections before and after rounds, Journal of Medical Ethics, 34(5), 407-13.
Braunack Mayer, A. J. (2001). What makes a problem an ethical problem? An empirical perspective on the nature of ethical problems in general practice. Journal of Medical Ethics, 27 (2), 98-103.
Oberle, K., & Hughes D. (2001) Doctors’ and nurses’ perceptions of ethical problems in end-of-life decisions, Journal of Advanced Nursing, 33(6), 707-15.
Udén, G., Norberg, A., & Lindseth, A. (1992). Ethical reasoning in nurses’ and physicians’ stories about care episodes. Journal of Advanced Nursing, 17(9), 1028-34.
Widdershoven, G., Abma, T. & Molewijk, B. (2009) Empirical ethics as dialogical practice. Bioethics, 23(4), 236-48.
Rathert, C., & Fleming, D. A. (2008). Hospital ethical climate and teamwork in acute care: The moderating role of leaders. Health Care Manage Review, 33(4), 323-31.
*Shahla Siddiqui
Tel: 0065 66022137
Email: shahlasi@yahoo.com
Published online: 2 January, TAPS 2018, 3(1), 42-49
DOI: https://doi.org/10.29060/TAPS.2018-3-1/SC1059
Bikramjit Pal, M. V. Kumar, Htoo Htoo Kyaw Soe, Sudipta Pal
Melaka Manipal Medical College, Manipal University, Malaysia
Abstract
Introduction: Simulation is the imitation of the operation of a real-world process or system over time. Innovative simulation training solutions are now being used to train medical professionals in an attempt to reduce the number of safety concerns that have adverse effects on the patients.
Objectives: (a) To determine its usefulness as a teaching or learning tool for management of surgical emergencies, both in the short term and medium term by students’ perception. (b) To plan future teaching methodology regarding hi-fidelity simulation based on the study outcomes and re-assessment of the current training modules.
Methods: Quasi-experimental time series design with pretest-posttest interventional study. Quantitative data was analysed in terms of Mean, Standard Deviation and standard error of Mean. Statistical tests of significance like Repeated Measure of Analysis of Variance (ANOVA) were used for comparisons. P value < 0.001 was considered to be statistically significant.
Results: The students opined that the simulated sessions on high fidelity simulators had encouraged their active participation which was appropriate to their current level of learning. It helped them to think fast and the training sessions resembled a real life situation. The study showed that learning had progressively improved with each session of simulation with corresponding decrease in stress.
Conclusion: Implementation of high fidelity simulation based learning in our Institute had been perceived favourably by a large number of students in enhancing their knowledge over time in management of trauma and surgical emergencies.
Keywords: High fidelity simulation, Simulation in medical education, Stress in simulation
I. INTRODUCTION
High fidelity simulation is an innovative and effective strategy to address increasing student enrolment, faculty shortages, and limited clinical sites (Schoenig, Sittner, & Todd, 2006). The value of simulation in undergraduate medical education is now well established; it basically animates the curriculum. Medical training in the current era is multi-modular and simulation based learning may play a pivotal role in improving training standards in medical schools (Joseph et al., 2015). High Fidelity Patient Simulators replicate patient care scenarios in a realistic environment and have advantage of repetition of the same scenario in a controlled environment which allows practice without risk to patient thereby minimizing chances of medical error and thus, make them a useful tool for student assessment. It is also recognized that putting the learners into a simulated critical care environment subjects them to stresses which have not been well studied. There were many studies on the use of simulation (mainly low and medium fidelity) in medical education but few studies were done on the effectiveness of high fidelity simulation based teaching in under-graduate medical students. The importance of simulation in training medical students are being recognized by academic institutions around the world. In spite of proven benefits, it has so far not been formally introduced as a part of curriculum in medical colleges in our settings. With this background, this study was conducted to explore the perception of medical students on the usefulness of high fidelity patient simulation.
II. METHODS
This was an ongoing research study about the impact of high fidelity patient simulation in undergraduate medical education. METIman Pre-Hospital High Fidelity Patient Simulator (Serial number: MMP-0418/2013; CAE Healthcare, USA) was used in this study. The final year MBBS students of MMMC were the subjects of this study. The students of these batches who volunteered were recruited during their surgical posting after obtaining their informed consent. The proportion of students who volunteered was 92.73% (204 students out of total number of 220 students).
The simulation sessions were conducted with one sub-group of 12 to 15 students which were further divided into 3 teams of 4 to 5 students. The participants were briefed about the simulation sessions and expected learning outcomes. The duration of each simulation session was 50 minutes: Briefing (10 minutes), Simulation (25 minutes) and Debriefing (15 minutes). A theoretical briefing was given by the investigator on ATLS protocol for trauma management and management of surgical emergencies like hypovolemic shock, tension pneumothorax and head injury. This briefing was done as an interactive lecture to the whole subgroup. Each team then participated in a trauma simulation session and the scenario was chosen randomly from among the conditions mentioned above. The three teams in a subgroup were assigned three different scenarios. The teams were then debriefed in order to achieve the learning outcomes. The same team had participated second time in the simulation of the same scenario after 1 week and third time after 3 – 4 weeks to test their short to medium term retention of knowledge and practical skills, followed by final debriefing. Thus, at the end of the course, each student was expected to perform satisfactorily any of the roles during the management of the standard scenarios.
Each student was assessed individually in terms of their progress in knowledge, confidence and stress reduction. We developed a standardized five point (very poor to excellent) Likert scale questionnaire (Appendix I), to collect initial background knowledge of the students on the first day of the training course in terms of ATLS protocol for management of acute trauma, management of hypovolemic shock, management of tension pneumothorax and management of head injury. The same questionnaire was repeated after every session for post-session knowledge assessment.
Another set of five point Likert scale questionnaire was designed to obtain participant feedback after each session on the relevance and usefulness of the simulation experience, effectiveness of briefing and debriefing and stressor assessment. It was an ordinal scale used by respondents to rate the degree to which they agree or disagree to a statement (Appendix II). The stressor questionnaire contained thirteen items (Appendix III). They resembled pre and post tests for comparison to note progress in confidence and stress reduction. Finally, a third set of questionnaire was administered to the students at the completion of training for their feedback assessment of training course (Appendix IV).
We used Microsoft Excel for data entry and SPSS software (SPSS Inc. Released 2009. PASW Statistics for Windows, Version 18.0. Chicago: SPSS Inc.) for data analysis. We calculated descriptive statistics such as frequency and percentage for categorical data; mean and standard deviation for total score of knowledge, simulation assessment and stressor assessment. We used one-way repeated measure ANOVA to determine the statistically significant difference in simulation assessment (total score) and stressor assessment (total score). We also used Friedman test to determine the statistically significant difference in individual item of knowledge assessment, simulation assessment and stressor assessment. P value <0.001 was taken to be statistically significant in our study.
III. RESULTS
The cohort of 204 participants in this study were selected from four batches of final year MBBS students (October 2015 to April 2016).
Friedman test of simulation assessment for individual items showed significant difference of simulation assessment over time. One-way repeated measure ANOVA of stressor assessment (total score) revealed statistically significant difference (p < 0.001) of total score of stressor assessment over time. Total score of stressor assessment was decreased from 27.09 (Mean) / 7.41(SD) at pre-simulation to 25.63 (Mean) / 8.06(SD) at post-simulation I, to 23.92 (Mean) / 8.92(SD) at post-simulation II and to 23.75 (Mean) / 9.77(SD) at post-simulation III.
For assessment of stress during simulation sessions, we used Likert scale of 1 to 5 (low stress to maximum stress). There was significant difference (p < 0.001) of stressor assessment during simulation over time (Friedman test) for following individual items where majority of the students had the opinion of “moderate stress” regarding “Competition with team members”, “Limited time during simulation sessions”, “Participation in debriefing” and “high stress” regarding “Death of simulated patient”.
|
Item
|
Pre | Post I | Post II | Post III | P value |
| Median (Q1, Q3) | |||||
| 1 – strongly disagree, 2- tend to disagree, 3 – neither agree or disagree, 4 – tend to agree, 5 – strongly agree | |||||
| The session level was appropriate to my present level of knowledge and experience | 4.0 (3.0, 4.0) | 4.0 (4.0, 4.0) | 4.0 (4.0, 4.0) | 4.0 (4.0, 4.0) | <0.001* |
| It encouraged my active participation | 4.0 (4.0, 4.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | <0.001* |
| Clinical management more easily learned | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 4.0) | 4.0 (4.0, 4.0) | 0.996 |
| The training session resembled a real life situation | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 0.011* |
| It helps me to think quickly | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 0.003* |
| Repetition of the scenario during training is essential | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 0.001* |
| Time for the scenario was adequate | – | 4.0 (3.0, 4.0) | 4.0 (4.0, 4.0) | 4.0 (4.0, 4.0) | 0.149 |
| Briefing and Debriefing: | |||||
| Time for initial briefing was adequate | 4.0 (4.0, 5.0) | 4.0 (4.0, 4.0) | 4.0 (4.0, 4.0) | 4.0 (4.0, 4.0) | <0.001* |
| Time for debriefing was adequate | – | 4.0 (3.0, 4.0) | 4.0 (4.0, 4.0) | 4.0 (4.0, 4.0) | 0.184 |
| Debriefing helped me to learn better | – | 4.0 (4.0, 4.0) | 4.0 (4.0, 4.0) | 4.0 (4.0, 4.0) | 0.273 |
| Affective: | |||||
| I want to have further sessions on the simulator | – | 5.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | <0.001* |
| I feel that simulation is essential to train in trauma management | 4.0 (3.0, 5.0) | 5.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | <0.001* |
| Learning Outcomes: | |||||
| I am confident of managing a trauma scenario in real life | – | 3.0 (3.0, 4.0) | 4.0 (3.0, 4.0) | 4.0 (3.0, 4.0) | <0.001* |
Table 1. Simulation assessment at pre-simulation, post-simulation I, post-simulation II and post-simulation III (individual item)
IV. DISCUSSION
High fidelity simulators have revolutionised training as almost any emergency situation can be replicated. Simulation sessions have provided opportunity for clinical students to collaborate and apply both cognitive and psychomotor skills. Our main objective was to determine usefulness of high fidelity simulation as a teaching or learning tool for management of surgical emergencies. The study showed that high fidelity simulators had made a difference in enhancing the knowledge over time in management of trauma and surgical emergencies as perceived by our students. It also showed that learning had significantly improved with each session of simulation and learners’ attitudes were supportive of simulation. Wayne, Barsuk, O’Leary, Fudala, & McGaghie (2008) showed that internal medicine residents had increased knowledge and skills using simulation technology and deliberate practice. Participants in one study (Okuda et al., 2009) felt simulation based teaching was a reliable tool for assessing learners by providing good feedback on performance which was similar to our observation. In a study by Founds, Zewe, & Scheuer (2011), participants felt that high fidelity simulators can present simulations that were closer to real life situations which was similar to opinion of most of our students. The study revealed that simulation sessions with high fidelity simulators encouraged active participation of students who need further sessions on simulation for better understanding of clinical problems and knowledge acquisition. The finding in one of the main area of study: “Clinical management more easily learned” was not satisfactorily documented (p < 0.996). It showed that simulation did not always help in better understanding of management of clinical problems. The drop in stress was significant at week II and III but flattened out in week IV which might be due to participants’ increasing adaptability to simulated atmosphere. The time for briefing was adequate but participants felt that time for debriefing was inadequate and debriefing did not help them to learn better. This was an area of utmost concern to us as we concluded that there was a definite lacuna in our debriefing process. We planned to rectify our shortcomings and deficiencies in this matter. For long term assessment we planned to get these students back during their internship period and do a re-test to validate the improved outcome. Most of the students had a favourable perception about high fidelity patient simulation indicating that it has bright prospect for its inclusion in under-graduate curriculum in near future.
V. CONCLUSION
Few studies have been done with regards to students’ perception on the effectiveness of high fidelity simulators in training under-graduate medical students. This innovative training method may help to improve the quality of medical care and safety of the patient. The limitation of this study: This was a single centre study and participants who volunteered were only recruited. Hence findings may not be applicable to other settings. Even though training with high fidelity simulators was perceived positively by the students, it remained unclear whether the learning skills acquired with this teaching methodology would translate into improved patient care.
Notes on Contributors
Bikramjit Pal MBBS, DA (Anesthesiology), MS (Surgery); Associate Professor, Department of Surgery and Chairman of Clinical Skills Learning Committee, Member of the International Forum of Teachers of the UNESCO Chair in Bioethics, Melaka-Manipal Medical College, Manipal University, Malaysia
MV Kumar BSc, MBBS, FRCS Ed; Professor and Ex-HOD, Department of Surgery and member of Clinical Skills Learning Committee, Melaka-Manipal Medical College, Manipal University, Malaysia
Htoo Htoo Kyaw Soe MBBS, MPH, PhD; Associate Professor, Department of Community Medicine and member of Statistics Committee, Melaka-Manipal Medical College, Manipal University, Malaysia
Sudipta Pal MBBS, PGDMCH; Lecturer, Department of Community Medicine, Melaka-Manipal Medical College, Manipal University, Malaysia
Ethical Approval
Duly taken from the IRB & IEC, Melaka-Manipal Medical College.
Acknowledgements
The final year MBBS students of Melaka-Manipal Medical College who had participated in this research project, the faculty of the Department of Surgery, the lab assistants and technicians of Clinical Skills Lab, the Management of Melaka-Manipal Medical College and last but not the least, Prof. Dinker Pai (Ex-Head of Department of Surgery, MMMC), for his inspiration, initiation and conceptualization of this research project.
Declaration of Interest
The authors have not received any funding or benefits from industry or elsewhere to conduct this study and have no conflicts of interest.
References
Founds, S. A., Zewe, G., & Scheuer, L. A. (2011). Development of high fidelity simulated clinical experiences for baccalaureate nursing students. Journal of Professional Nursing, 27(1), 5–9.
Joseph, N., Nelliyanil, M., Jindal, S., Utkarsha., Abraham, A.E., Alok, Y., … Lankeshwar, S. (2015). Perception of Simulation based Learning among Medical Students in South India. Annals of Medical and Health Sciences Research, 5(4), 247–252. doi: 10.4103/21419248.
Okuda, Y., Bryson, E. O., De Maria, S. Jr., Jacobson, L., Quinones, J., Shen, B., & Levine, A. l. (2009). The utility of simulation in medical education: What is the evidence? Mount Sinai Journal of Medicine, 76(4), 330–43. doi: 10.1002/msj.20127.
Schoenig, A. M., Sittner, B. J., & Todd, M. J. (2006). Simulated clinical experience: nursing students’ perceptions and the educators’ role. Nurse Education, 31 (6), 253-8.
Wayne, D. B., Barsuk, J. H., O’Leary, K. J., Fudala, M. J., & McGaghie, W. C. (2008). Mastery Learning of Thoracentesis Skills by Internal Medicine Residents Using Simulation Technology and Deliberate Practice. Society of Hospital Medicine, 3(1), 48-54. doi: 10.1002/jhm.268.
*Bikramjit Pal
Associate Professor (Surgery),
Melaka-Manipal Medical College
Jalan Batu Hampar, Bukit Baru,
75150, Melaka, Malaysia.
Mobile: +60-1118728085.
Landline (Office): +60-6-2896662-1116; +60-6-2925849/50/51.
FAX: +60-6-2817977.
E-mail: bikramjit.pal@manipal.edu.my
Alternative email: drbikramjitpal@gmail.com
Published online: 2 January, TAPS 2018, 3(1), 38-41
DOI: https://doi.org/10.29060/TAPS.2018-3-1/SC1040
Sean Wu1, Julia Farquhar1, 2, Scott Compton1
1Duke-NUS Medical School, Singapore; 2School of Medicine, Duke University, USA
Abstract
Aim: Evidence suggests that Team Based Learning (TBL) is an effective teaching method for promoting student learning. Many people have also suggested that TBL supports other complex curriculum objectives, such as teamwork and communication skills. However, there is limited rigorous, substantive data to support these claims. Therefore, the purpose of this study was to assess medical educators’ perceptions of the outcomes affected by TBL, thereby highlighting the specific areas of TBL in need of research.
Methods: We reviewed the published research on TBL in medical education, and identified 21 unique claims from authors regarding the outcomes of TBL. The claims centred on 4 domains: learning, behaviours, skills, and wellbeing. We created a questionnaire that asked medical educators to rate their support for each claim. The survey was distributed to the medical educators with experience teaching via TBL and who were active users of the Team Based Learning Collaborative listserv.
Results: Fifty responses were received. Respondents strongly supported claims that TBL positively impacts behaviours and skills over traditional, lecture based teaching methods, including the promotion of self-directed learning, active learning, peer-to-peer learning, and teaching. In addition, respondents strongly supported claims that TBL promotes teamwork, collaboration, communication and problem solving. Most participants reported that TBL is more effective in promoting interpersonal, accountability, leadership and teaching skills.
Conclusion: Medical educators that use TBL have favourable perceptions of the practice across a variety of domains. Future research should examine the actual effects of TBL on these domains.
Keywords: Team Based Learning; Medical Education; Teaching
I. INTRODUCTION
Team-based learning (TBL), originally developed for use in business schools, is now a growing teaching modality in medical education. The process of TBL is comprised of three components: advance preparation, individual and team readiness assurance tests (RATs), and in-class application of content through team exercises (Parmelee, Michaelsen, Cook, & Hudes, 2012). In a TBL course, students are typically assigned into teams of 5 to 7, and receive preparatory materials before class. At the beginning of the TBL process, each individual completes a readiness assurance test (I-RAT). Students next re-take the same readiness assurance test during class as a team (T-RAT), reaching consensus to select a single best answer, and receive immediate feedback. Students typically then have the option to write evidence-based appeals for their wrong answers, and finally an instructor clarifies lingering questions. Following the readiness assurance phase, the teams then work on solving applied problems, followed by whole class discussions. Evidence suggests that TBL is a popular teaching modality, with approximately one-third of US schools and colleges of pharmacy implementing it into the curriculum (Allen et al., 2013).
A number of studies have shown TBL to be as academically effective or more effective than traditional lecture-based courses by promoting mastery over several core medical subjects (Fatmi, Hartling, Hiller, Campbell, & Oswald, 2013; Koles, Stolfi, Borges, Nelson, & Parmelee, 2010; Nieder, Parmelee, Stolfie, & Hudes, 2005). These studies have focused specifically on the academic outcomes of TBL, yet TBL as a teaching modality is often assumed to support complex curriculum objectives such as teamwork and communication skills. Despite these assumptions, little substantive data exists to support these claims. For the current body of research to progress and to improve our understanding of the true effects of TBL, these assumed outcomes need to be explicitly described and articulated. Following which, individual outcomes can be studied and interventions can be proposed to further develop TBL as a medical teaching modality. Therefore, the purpose of this study was to assess TBL medical educators’ perceptions of the outcomes affected by TBL, thereby providing a framework for future research.
II. METHODOLOGY
A. Development of Questionnaire
We identified 21 claims of the positive effects of TBL in various published papers and textbooks. We categorized these claims into 4 domains: learning, behaviours, skills, and well-being. Examples of references to each claim are available from the corresponding offer. We subsequently compiled those claims and used them as the basis for a questionnaire in order to assess the support for each claim among TBL users.
The final questionnaire consisted of 6 demographic questions, followed by the claims within each domain: learning (4 questions), behaviours (4 questions), skills (8 questions) and wellbeing (5 questions). In addition, we asked 3 questions related to the extent that TBL skills learned in classroom settings translates to clinical settings.
Cognitive interviews were conducted with ten TBL educators to determine if the questions were clear and interpreted as intended. Relevant edits were made and the questionnaire was revised. We then assessed reliability using the test-retest method. Eight TBL educators responded to the questionnaire twice within two weeks. The test-retest reliability of the instrument was 0.927 (df = 8, p<0.001) based on Spearman’s correlation coefficient, thus demonstrating its suitability for research use.
B. Dissemination
The final survey was uploaded onto surveymonkey.com and submitted to the Team-Based Learning Collaborative (TBLC) listserv with a request for medical educators to respond. The TBLC listserve is comprised of people interested in TBL, and is open to all educators. The introductory email made explicit that medical educators were the target of the survey.
III. RESULTS
A total of 50 medical educators replied. The participants were a seasoned group of medical educators, having an average of 14 years’ experience in the field. Most respondents were senior faculty members (25% professor, 36% associate professors), while 19% were assistant professors and 20% had other academic appointments. Overall the respondents had substantial experience in using TBL: 96% had created TBL materials, 98% had facilitated TBL discussions, and 78% had designed course curriculum with TBL as the primary educational modality.
As shown in Figure 1, respondents tended to strongly support the various claims that suggest TBL positively impacts learning, behaviour, and skills. In fact, most participants reported that TBL promotes “Deep Learning” and “Application of knowledge” much more, 83% and 98% respectively, than conventional lecture based modalities. Nearly all (96%) reported that TBL is more effective in promoting retention of knowledge than lecture and most (64.5%) replied that TBL is more effective in promoting breadth of knowledge. A minority (25%) of respondents indicated that there is no difference between the two teaching modalities in student learning.
In terms of student behaviour, respondents reported that TBL promotes self-directed learning, active learning, peer-to-peer learning and teaching much more than lecture based teaching modalities. Most (98%) answered that TBL is more effective in teaching self-directed learning, peer-to-peer learning, and peer-to-peer teaching than lecture. All answered that TBL promotes active learning more than traditional lecture based teaching. Only one replied that TBL and lecture-based teaching are equally effective in promoting the aforementioned student behaviours.
Most respondents replied that TBL is more effective than lecture-based teaching in promoting a multitude of student skills. All answered that TBL is better at promoting teamwork, collaboration, communication and problem solving. Most of participants reported that TBL is more effective in promoting interpersonal, accountability, leadership and teaching skills.
Figure 1 also demonstrates that there is less support for the claims surrounding TBL promotion of wellbeing. Nearly half (44%) of the respondents answered that TBL resulted in more competition than lecture-based teaching whereas a quarter replied the opposite. Half reported that TBL leads to more anxiety whereas a quarter replied otherwise. More than half reported that TBL promoted empathy more so than lecture, whereas 35% of respondents were unsure or thought the two teaching modalities equal. Most respondents answered that lecture-based teaching was easier than TBL, yet also answered that TBL was more enjoyable. Interestingly, respondents also reported that TBL-learned skills translated well to the clinical setting. Most, 89.5%, 83.3%, and 66.7% respectively, answered that teamwork, communication, and leadership skills learned in a TBL classroom were applicable to the clinical rotations.
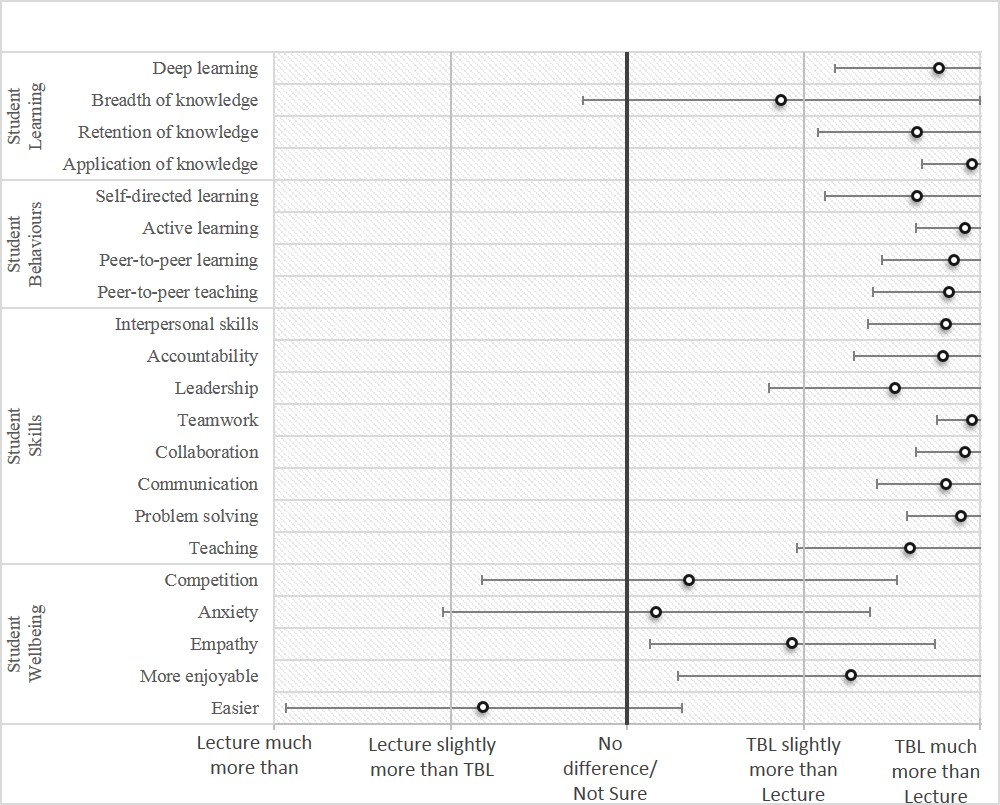
Figure 1. Medical educators’ ratings: lecture-based teaching versus team based learning in promoting different skills
IV. DISCUSSION
The results of the study indicate that TBL medical educators believe TBL to be better than traditional lecture-based teaching in achieving a vast variety of outcomes. According to the survey results, educators believe that TBL promotes students’ mastery of subject content by encouraging deep and active learning as well as the retention and application of knowledge. They also believe that TBL develops behaviours such as peer-to-peer learning and teaching. An important point is that most TBL educators believe TBL fosters development of key skillsets such as accountability, teamwork, collaboration, and communication that play vital roles in the successful transition of students from classroom learning to clinical clerkships. Yet respondents to this survey may be wary that TBL may negatively affect student wellbeing by increasing competition and difficulty. Interestingly, many of the TBL educators appeared confident that TBL aids in the development of medical students that are independent learners, teamwork-oriented and effective leaders. However, to date, there is little substantive data to suggest that any of these claims are true. Likewise, there was strong support for the notion that skills learnt in classroom TBL sessions translate to the clinical setting. Again, little evidence currently exists to support this claim.
This study is limited by the small convenience sample drawn from the TBL collaborative listserv. The participants may not be representative of TBL educators as a whole. However, the participant profiles reveal that these respondents have extensive experience in medical education and using TBL in the classroom.
V. CONCLUSION
This study should serve as a call to action to educational researchers to investigate the claims of the effects of TBL, particularly those associated with non-academic factors, such as teamwork, leadership, and communication. In fact, the results of this study could serve as the foundation for future research. Ensuing studies can provide evidence towards determining the validity of these assumptions, thereby providing direction for the development of TBL as a teaching modality in medical education.
Notes on Contributors
Sean Wu, MD, is a graduate of the Duke-NUS Medical School and currently an Internal Medicine resident at NUHS. Julia Farquhar is a medical student at the Duke School of Medicine, Durham, NC, USA.
Scott Compton, PhD, is the Associate Dean and Associate Professor of Medical Education, Research, and Evaluation at Duke-NUS Medical School.
Ethical Approval
The approval for this study was obtained from the Institutional Review Board, National University of Singapore.
Declaration of Interest
The authors declare that they have no competing interests.
References
Allen, R. E., Copeland. J., Franks, A. S., Karimi, R., McCollum, M., & Riese, D. J. (2013). Team-based learning in US colleges and schools of pharmacy. The American Journal of Pharmaceutical Education, 77(6). DOI: 10.5688/ajpe776115
Fatmi, M., Hartling, L., Hillier, T., Campbell, S., & Oswald, A.E. (2013). The effectiveness of team-based learning on learning outcomes in health professions education: BEME Guide No. 30. Medical Teacher, 35(12), 1608-24. DOI: 10.31.09/0142159X.2013.849802
Koles, P. G., Stolfi, A., Borges, N. J., Nelson, S., & Parmelee, D.X. (2010). The impact of team-based learning on medical students’ academic performance. Academic Medicine, 85(11), 1739-1745. DOI: 10.1097/ACM.0b013e3181f52bed
Nieder, G. L., Parmelee, D. X., Stolfi, A., & Hudes, P. D. (2005). Team‐based learning in a medical gross anatomy and embryology course. Clinical Anatomy, 18(1), 56-63. DOI: 10.1002/ca.20040
Parmelee, D., Michaelsen, L.K., Cook, S., & Hudes, P.D. (2012). Team-based learning: A practical guide: AMEE Guide No. 65. Medical Teacher, 34(5), e275-e287. DOI: 10.3109/0142159X.2012.651179
* Scott Compton, PhD
Medical Education, Research and Evaluation Department
Duke-NUS Medical School
8 College Road, Singapore 169857.
Tel: +65 6601 1565.
Email: scott.compton@duke-nus.edu.sg
Published online: 4 September, TAPS 2018, 3(3), 39-42
DOI: https://doi.org/10.29060/TAPS.2018-3-3/SC1057
Lim Mien Choo Ruth, Keith Tsou Yu Kei, Chooi Peng Ong, Sabrina Wong Kay Wye, Gilbert Tan Choon Seng, Winnie Soon Shok Wen, Joanne Quah Hui Min & Marie Stella P. Cruz
Division of Graduate Medical Studies, Yong Loo Lin School of Medicine, National University of Singapore
Abstract
This paper describes the revision of a national post-graduate medical examination to incorporate formal quality assurance and psychometrics. We discuss the considerations and rationale leading to the new format, challenges faced and lessons learned in making the change. The processes described were successfully implemented in the 2015 examination administration. We continue to reflect on and analyse these processes to improve the examination.
Keywords: Post-graduate, Examination Reform, Quality Assurance, Psychometrics, Family Medicine, Standardised Patient
I. CONTEXT
In Singapore, population growth and a swiftly inverting population pyramid have diametrically changed the job scope of the family physician, impacting training and certification.
Postgraduate Family Medicine certification in Singapore formally began with the Membership of the College of General Practitioners (MCGP) in 1972, and was replaced in 1993 by the Master of Medicine in Family Medicine (MMed FM) examination. This examination comprised a theory portion, a viva voce and a clinical examination (Table 1).
In 2011, Singapore adopted the American Accreditation Council for Graduate Medical Education-International (ACGME-I) Residency system. Family Medicine Residency culminates in a summative multiple-choice question (MCQ) examination administered by the American Board of Medical Specialties (ABMS) with no clinical component.
With these training and contextual changes, the time was appropriate for a review and revision of the MMed FM examination. We describe the considerations and processes leading to the new MMed FM examination in 2015.
II. FROM THE OLD TO THE NEW
A. Family Medicine Examination Committee
In 2012, the Family Medicine Examination Committee (FMEC) was set up to administer and review the examination, reporting to the Division of Graduate Medical Studies (DGMS), with education consultative support from the Centre for Medical Education, National University of Singapore. Senior family physicians from different training institutions form the FMEC.
B. Reviewing the Old Examination
| Old MMed FM Examination | 2015 MMed FM Examination | Rationale for change | |
| Format | Theory
Essays, Short Answers, MCQ, Slides, Viva voce |
Theory
250 MCQ Paper |
Increased sampling points to increase reliability |
| Clinical Examination
2 Long Cases, 4 Short Cases |
Clinical Examination
Slides, Viva voce, 3 Long Consultations, 5 Short Consultations, 3 Physical Examinations |
Increased sampling points to increase reliability
|
|
| Duration of Clinical Examination | 150 minutes | 218 minutes | Increased testing time |
| Domains Tested | Knowledge – Theory papers, Long Cases
Synthesis, Psychomotor skills – Short Cases Professional Communication – Long Cases, Viva voce
|
Knowledge, Interpretation, Application – Context-rich MCQs
Synthesis, Application, Patient Communication – Consultations Psychomotor skills – Physical Examinations Professional Communication – Viva voce |
Increased number of domains tested
Higher level of cognitive domains tested |
| Blueprinting | Theory
No formal blueprinting |
Theory
Formal blueprinting |
Defined composition of testing points |
| Clinical Examination
Long Cases were “eyeballed” to cover adult and paediatric problems Short Cases blueprinted by broad body systems and “eyeballed” such that a candidate did not have similar Long and Short cases |
Clinical Examination
Formal blueprinting across Consultations and Physical Examination stations |
Defined composition of testing points
|
|
| Clinical Material used | Real Patients (RP) | Real Patients
Standardised Patients (SP) |
Increased number of sampling points
Increased type of testing points Richness of clinical material with use of RP Standardisation of clinical material with use of SP |
| Quality Assurance | Blueprinting | Blueprinting | Increased content validity with new blueprint |
| Examiner training by observation | Formal Examiner Training & Feedback | Systematisation of examiner training | |
| Pre-set Pass Mark | Standard setting methods and psychometrics in Pass/Fail decisions | Better defensibility of Pass/Fail decisions | |
| External Examiner | External Examiner | Independent audit of examination process |
Table 1. Summary of main components of the old and 2015 examinations
The previous long case involved assessing the patient and discussing management with the examiner. The short case was a physical examination station. Two long cases provided insufficient insight into the candidate’s mastery of the breadth of the Family Medicine curriculum (Swanson, Norman, & Linn, 1995). With real patients, standardisation of testing points across a cohort was not possible. Management was discussed with the examiner only, so communication with the patient about management was not assessed.
The old pass mark was pre-defined at 50%, regardless of difficulty of cases.
C. Developing the New Examination
We developed the new examination following review of literature (Swanson, Norman, & Linn, 1995; Van der Vleuten & Schuwirth, 2005; Mookherjee, Chang, Boscardin, & Hauer, 2013) and discussion to determine best practice. Our priorities were to improve the representativeness and reliability of testing within a practicable framework.
The new examination includes theory and clinical components, and psychometrics to analyse candidate performance. The theory component is now the ABMS MCQ examination. Candidates who are successful may sit the clinical examination.
The re-designed clinical examination comprises thirteen stations, with the slides and viva voce stations being holdovers from the old format. The remaining eleven comprise five short consultations, three long consultations, and three physical examination stations, an increase over the previous six stations (Swanson et al, 1995). This increases the number of sampling points and testing time and hence reliability (Van der Vleuten & Schuwirth, 2005).
For the consultations, the candidate evaluates, and then discusses management with the patient. He is judged on his handling of the consultation, not on his interaction with examiners. A long consultation tests multiple and more complex issues than a short consultation. Consultations are set in a primary care context, representing Family Medicine practice in Singapore.
The standardised patient (SP) was introduced, and consultations involve real and standardised patients. The three physical examination stations continue to use real patients.
The viva voce was retained to allow testing of professional communication and discussion of clinical reasoning.
Instead of a pre-defined standard, we introduced the use of psychometrics to determine the pass marks, and collaborated with a medical educationist who has been trained in assessment psychometrics. At the same time, we implemented examiner training (Van der Vleuten, Luyk, Ballegooijen, & Swanson, 1989), calibration, and standard setting. The passing standard is defined as that of a proficient family physician on the Dreyfus model of skill acquisition (Goh & Ong, 2014).
A new mark sheet, assessing clinical skills and global assessment of the candidate’s performance, was introduced.
D. Evaluating the New Examination
The FMEC committed to incorporating quality assurance measures into the design and implementation of the new clinical examination.
For the first time, an examination blueprint was formally developed. Testing points were chosen across the curriculum to reflect competencies required in Family Medicine practice (Mookherjee et al, 2013).
The blueprint guided recruitment of real patients and SP case development. FMEC members tested the SP cases for authenticity and reasonableness. Before each clinical examination bloc, all examiners participated in calibration sessions during which clinical history and signs were confirmed and salient points agreed upon.
Borderline regression and modified Angoff methods were used to set pass marks. Performance and reliability of individual stations and the entire examination were studied. Examiner performance was analysed and feedback given.
The examination, conducted under the auspices of the DGMS, conformed to standard operating procedures, access and security measures used in other DGMS examinations.
An external examiner (EE) observed the examination (Associate Professor Neil Spike). This EE had observed previous MMed FM examinations.
III. CHALLENGES AND LESSONS
The old examination format had been in place for forty-three years (1972 – 2014). The new format introduced standard setting, examination validity as an evidence-based concept, the use of SPs, and the use of statistics to analyse results.
Stakeholder engagement was, and remains, paramount. There was a need for consistent, sustained communication to trainers, residents and examiners.
With the consultation as test encounter, we are assessing for relevant history and hypothesis-driven physical examination. This differs from traditional assessment that rewards comprehensiveness. Examiners debated the boundaries of relevance and hypothesis-driven practice, to help form their expert judgement of what is required of proficiency.
With the many changes introduced, we set a requirement for examiners to have attended examiner training sessions before appointment. This is common in many examinations but new to us.
The format, as presented here, will remain for 2016 and 2017, after which time we will review the programme of assessment. At this time, we are in the process of gathering feedback and reviewing the outcomes for the examination administrations of 2015 and 2016.
Notes on Contributors
Dr Ruth Lim is the Chairperson of the Family Medicine Examination committee, Chief Examiner for the Master of Medicine (Family Medicine) Examination and Director of Education for SingHealth Polyclinics.
Dr Keith Tsou is the Deputy Chairperson of the Family Medicine Examination committee, Deputy Chief Examiner for the Master of Medicine (Family Medicine) Examination and Director of Clinical Services for National University Polyclinics.
Dr Ong Chooi Peng is member of the Family Medicine Examination committee, Senior Consultant of the Department of Family Medicine, National University Health System.
Dr Sabrina Wong is member of the Family Medicine Examination committee, Assistant Director of Clinical Services for National Healthcare Group Polyclinics.
Dr Gilbert Tan is member of the Family Medicine Examination committee, Assistant Director of Clinical Services for SingHealth Polyclinics.
Dr Winnie Soon is member of the Family Medicine Examination committee, Consultant Family Physician for National Healthcare Group Polyclinics.
Dr Joanne Quah is member of the Family Medicine Examination committee, Director for Outram Polyclinics under SingHealth Polyclinics.
Dr Marie Stella P. Cruz is member of the Family Medicine Examination committee, Family Physician and Adjunct Lecturer for Department of Medicine and Division of Graduate Medical Studies, National University of Singapore.
Ethical Approval
No IRB approval is involved.
Declaration of Interest
Authors declare no conflict of interest.
References
Swanson, D. B., Norman, G. R., & Linn, R. L. (1995). Performance-based assessment: Lessons from the health professions. Educational Research, 24(5), 5-11. https://doi.org/10.3102/0013189X024005005.
Van der Vleuten, C. P. M., & Schuwirth, L. W. T. (2005). Assessing professional competence: from methods to programmes. Medical Education, 39, 309-17. Retrieved from https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1365-2929.2005.02094.x.
Vleuten, C. V., Luyk, S. V., Ballegooijen, A. V. & Swanson, D. B. (1989). Training and experience of examiners. Medical Education, 23(3), 290-6.
Goh, L. G. & Ong, C. P. (2014). Education and training in family medicine: progress and a proposed national vision for 2030. Singapore Medical Journal, 55(3), 117-23. http://dx.doi.org/10.11622/smedj.2014031.
Mookherjee, S., Chang, A., Boscardin, C. K. & Hauer, K. E. (2013). How to develop a competency-based examination blueprint for longitudinal standardized patient clinical skills assessments. Medical Teacher, 35(11), 883-90. https://doi.org/10.3109/0142159X.2013.809408.
*Ruth Lim
Division of Graduate Medical Studies,
Yong Loo Lin School of Medicine,
National University of Singapore
Blk MD3, Level 2, 16 Medical Drive,
Singapore 117600
Email: ruth.lim@singhealth.com.sg
Contact: +65-63777018
Published online: 4 September, TAPS 2018, 3(3), 35-38
DOI: https://doi.org/10.29060/TAPS.2018-3-3/SC1062
Li-Phing Clarice Wee
Ng Teng Fong General Hospital, Singapore
Abstract
Objectives: Do Not Attempt Resuscitation (DNAR) orders have been used in hospitals worldwide for the past 30 years, but are still considered to be a challenging and difficult area of practice. Nurses being the frontline healthcare professionals should be involved during the decision-making process and are required to have good understanding of the DNAR order, in order to provide effective and efficient care. Our aim was to investigate: nurses’ involvement during decision-making process, level of understanding of issues surrounding DNAR orders; and how they perceive care for patients with DNAR orders.
Methods: A descriptive crossed sectional study design using electronic questionnaires was adopted for the study. The study was conducted among 400 nurses at a tertiary hospital in Singapore.
Results: This study showed that 44.5% of nurses reported physicians did not involve them in decisions for DNAR orders; only 8% felt that they should be involved in the decision-making process. Even if they did not agree with the order, 63.2% would still comply whilst 21% of them were willing to discuss this further with the treatment teams. Most agreed that antibiotics, intravenous fluids, oxygen therapy and artificial feeding were appropriate for patients with DNAR orders. Majority (57.1%) expressed uneasiness in discussing end of life issues with patients even in specialty areas.
Conclusion: Nurses should be encouraged to advocate for their patient and take part in the decision-making process. Communication between the medical team and nurses can be improved and there is an obvious need for further improvement in education and collaboration in this area.
Keywords: Do Not Attempt resuscitation, End-of-Life, Withdrawal, Palliative Care
I. INTRODUCTION
Do-Not-Attempt Resuscitation (DNAR) orders have been used in hospitals worldwide for over the past 30 years with the intention of preventing non-beneficial treatments for hospitalized patients. These orders provide direction for the medical team and often take place after discussion with the patient, their family members and the multidisciplinary team as this decision is often complex with possible legal, ethical and moral implications. Although these decisions are typically initiated by physicians, nurses play a key role in DNAR discussions as well (Gendt et al., 2006).
Nurses are often the first point of contact for a patient and have the responsibility to act as patient advocates (Fitz, Fuld, Haydock & Palmer, 2010). They are in the best position to fulfil a liaison role between physicians and patients; conveying patient preferences to the physicians and influencing acceptance by the patient or surrogate decision-maker of the medical recommendations of DNAR (Gendt et. al, 2006). Many studies have shown that healthcare workers tend to provide less medical care to DNAR patients and inconsistencies around what continuing care should be given to patients exist. Similarly, DNAR orders can also influence the delivery of nursing care. Fitz et. al (2010)’s study showed that a significant number of nurses believed a DNAR order altered nursing observation frequency, pain relief and fluids administered.
Though end-of-life care and patients with DNAR orders can co-exist, there might be a fine line in terms of treatment goals and outcomes. A study done by Stewart and Baldry (2010) found that a DNAR decision is perceived by some as equivalent to withdrawal of active treatment. The aim of the study was to identify nurses’ involvement during the decision-making process, level of understanding of issues surrounding DNAR orders; and how they perceive care for patients with DNAR orders.
II. METHODS
A. Design and Setting
A descriptive crossed sectional study design using electronic questionnaires was adopted for the study. It was conducted at 700-bedded hospital in Singapore where approximately 2500 nurses work full-time.
B. Sample
Convenience sampling method was adopted for the recruitment of nurses in the study and 400 nurses participated in the study.
C. Instruments Used
The questionnaire was adapted from a previous study with the author’s permission (O’Hanlon, O’Connor, S., Peters & O’Connor, M., 2013) and piloted on 50 nurses working in the ICU and High Dependency Unit (HDU). Thereafter, the questionnaire was further modified and consisted of 24 questions to improve the clarity of some questions and to better address the aims of the study.
D. Data Collection and Analysis
Ethical approval was obtained from the Institutional Review Board prior to data collection. Data was collected over a period of 5 months (June – October 2016). Consent was assumed if the survey was completed. Responses were collected anonymously through an electronic platform with a secured login. Responses were confidential and descriptive statistics analysis was used to analyse the data.
III. RESULTS
Majority of respondents were 21-30 years old females, with an average work experience of less than 5 years. Most of the participants were Chinese and an equal number of participants had a degree or Masters as their highest qualification. Majority of the participants were staff nurses who work in a medical ward, whilst other responses were collected from nurses working in the ICU, emergency department (ED) and surgical wards.
A. Involvement in the Decision-Making Process
Nurses thought that the patient (75.5%), family members (83.5%) and physicians (79%) should be involved in DNAR decision-making process as shown in Figure 1. However, only 8% thought that nurses should be involved in this process. A proportion of nurses (13.8%) reported that they had previously disagreed with a DNAR decision, but 63.2% said that they would still comply with the orders even if they did not agree. Majority (57.1%) of the nurses reported that they were not comfortable discussing end-of-life issues with patients and their family members and a sub-group analysis revealed that this was also true for nurses working in specialty areas like the Intensive Care Unit, High Dependency Unit and Emergency Department.
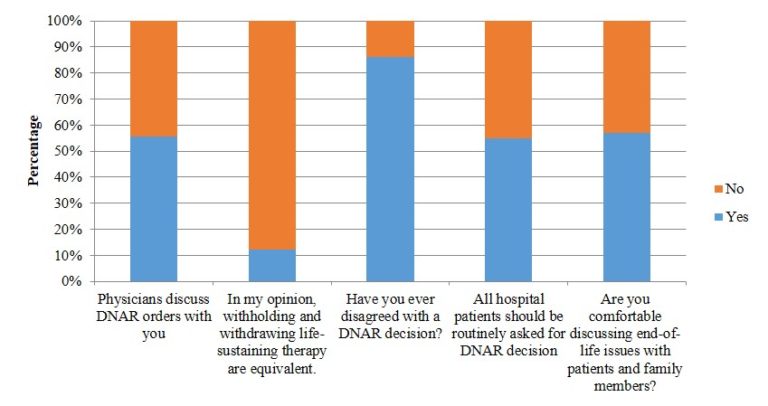
Figure 1. Involvement in the decision-making process (N=400)
B. Perceptions and Understanding
The results in Figure 1 showed that majority (63%) felt that withholding and withdrawing life-sustaining therapy were equivalent. There was no consensus with regards to the survival rate for out-of-hospital cardiac arrest and in-hospital cardiac arrest rates and these were generally overestimated. If a patient had a DNAR order in place, therapies like antibiotics, intravenous fluids, oxygen therapy and nasogastric feeds were deemed to be appropriate. Other therapies like intubation, cardiac compression, defibrillation, surgery, transfer to HD or ICU, dialysis and antiarrhythmic for life threatening cardiac rhythm were thought to be less appropriate. There were no differences observed between junior and senior nurses.
IV. DISCUSSION
To our knowledge, this study is the first to investigate nurses’ involvement during the decision-making process; and how they perceive care for patients with DNAR orders in a Singapore.
The study provided insight to gaps in communication that exist amongst the medical and nursing team; and the central importance of communication between these two teams. From the study, an alarming number of nurses revealed that they were not comfortable discussing end-of-life issues with patients or family members, even if they worked in critical areas.
Unlike Western countries, Singapore does not have a national policy on DNAR or an established framework to guide end-of-life care. Various studies have reported that the distinction between withholding and withdrawing treatment is not always recognised, and an assumption is often made that DNAR equates to withdrawal of active treatment (Stewart & Baldry, 2010). This is also observed in this study as majority of the respondents felt that withholding and withdrawing life-sustaining measures were equivalent. There is often an overlap between the two areas but more importantly, these decisions should be individualised to patients.
Results of the study showed that respondents of this study generally overestimated the survival rate of out-of-hospital cardiac arrest rates, in-hospital survival rates, recovery with good neurological function and survival to discharge. This study also revealed that nurses regarded therapies like IV fluids, antibiotics, oxygen therapy and nasogastric tube feeding as appropriate for patients with a DNAR order. The findings differed from O’Hanlon et. al (2013)’s study that surfaced some confusion over palliation and DNAR orders and only 36% of nurses felt that nasogastric tube feeding was appropriate for patients with DNAR orders. A recent study exploring physician attitudes towards withholding and withdrawal of life-sustaining treatments in end-of-life care saw that most were more ready to withhold and withdraw haemodialysis than enteral feeds (Phua et. al, 2015). This difference could perhaps reflect cultural differences as the Asian culture consider food and nutrition as basic rather than medical care, representing love and hope for health and an expression of filial piety (Phua et. al, 2015).
Being a single-centred questionnaire-based study, there are limitations to be considered. Half of the respondents only had 5 years or less of working experience. Religious beliefs of the participants were also not included in this study and this could potentially contribute to the nurses’ views on end-of-life care. As such, findings should not be generalised to the nursing population in Singapore or Asia and a larger study is recommended to replicate the study findings.
A. Implications for Clinical Practice and Further Research
This study has multiple important implications. Firstly, there is clearly a need for more training and increased confidence to improve nurses’ involvement in the DNAR process. Nursing education has traditionally been focused on nursing diagnoses and the practical aspects of care. However, good communication skills surrounding end-of-life conversations are also required in order to advocate and better care for their patients. Perhaps nursing schools and hospitals should consider developing a structured programme to help improve communication skills surrounding difficult topics like end-of-life care and DNAR orders. Nurses should also be encouraged to be more involved in the DNAR process, encouraging open communication especially when expectations are not aligned with patients or family members and the treatment team.
Further research is recommended with a bigger population of nurses from various hospitals throughout Singapore and even Asia to provide more insight into this topic. Future research should also focus on testing the validity of the tool used in this study since it has not been tested after modification of the questionnaire.
As DNAR policies and issues surrounding withdrawal and withholding of care for these patients can vary from hospital to hospital, a national policy guiding physicians and nurses the matter could be developed to better equip healthcare workers with the necessary information needed to care for patients.
V. CONCLUSION
This study gives first insight into the perceptions and understanding of nurses surrounding DNAR orders and the care rendered for these patients. Being at the forefront, nurses should be encouraged to communicate openly with the medical team and advocate for their patients. In order to do so, structured programs and national policies should be considered so as to guide and support nurses through this process.
Notes on Contributors
Wee Li-Phing Clarice is an Advanced Practice Nurse at Ng Teng Fong General Hospital, Singapore.
Institutional Review Board (IRB)
Standard institutional review board (IRB) procedures were followed and approval was obtained by the author. IRB number 2016/00413.
Acknowledgements
The author would like to thank Dr. Ross Freebarin and Dr. Faheem Khan for their valuable suggestions towards the study design and questions; and Dr. Yanika Kowitlawakul for her help in reviewing the article. In addition, the author would also like to thank Ms Syairah Binte Mohd Reduan and Mr. Johnny Wong for their assistance during the pilot study that contributed towards the final questionnaire used in this study.
Declaration of Interest
The author does not have any declaration of conflict of interest, including financial, consultant, institutional and other relationships that might lead to bias.
References
Fitz, Z., Fuld, J., Haydock, S. & Palmer, C. (2010). Interpretation and intent: A study of the (mis)understanding of DNAR orders in a teaching hospital. Resuscitation, 81(9), 1138-1141. https://doi.org/10.1016/j.resuscitation.2010.05.014.
Gendt, C. D., Bilsen, J., Stichele, R. V., Noortgate, N. V. D., Lambert, M. & Deliens, L. (2007). Nurses’ involvement in ‘do not resuscitate’ decisions on acute elder care wards. Journal of Advanced Nursing, 57(4), 404-409.
O’Hanlon, S., O’Connor, S., Peters, C. & O’Connor, M. (2013). Nurses’ attitudes towards Do Not Attempt Resuscitation orders. Clinical Nursing Studies, 1(1), 43-50.
Phua, J., Joynt, G. M., Nishimura, M., Deng, Y., Myatra, S. N., Chan, Y. H. … Koh, Y. (2015). Withholding and withdrawal of life-sustaining treatments in intensive care units in Asia. JAMA Internal Medicine, 175(3), 363-371. https://doi.org/10.1001/jamainternmed.2014.7386.
Stewart, M. & Baldry, C. (2010). The over-interpretation of DNAR. Clinical Governance: An International Journal, 16(2), 119-128. https://doi.org/10.1108/14777271111124473.
*Wee Li-Phing Clarice
Email: clarice_wee@nuhs.edu.sg
Published online: 4 September, TAPS 2018, 3(3), 31-34
DOI: https://doi.org/10.29060/TAPS.2018-3-3/SC1056
Christie Anna1 & Lian Dee Ler2
1National Healthcare Group Polyclinics (NHGP), Singapore; 2Health Outcomes and Medical Education Research (HOMER), National Healthcare Group, Singapore
Abstract
Aims: The evidence on how reflection associates with clinical teaching is lacking. This study explored the reflection pattern of nursing clinical instructor trainees on their clinical teaching and its association with their teaching performance.
Methods: Reflection entries on two teaching sessions and respective teaching assessment data of a cohort of Registered Nurses participating in the National Healthcare Group College Clinical Instructor program (n=28) were retrieved for this study. Reflection entries were subjected to thematic analysis. Each reflection statement was coded and scored according to topics in relevance to three clinical teaching phases – preparation, performance and evaluation. Teaching assessment scores were then used to group the participants into different performance group. Reflection patterns derived from the coding scores were compared across these groups.
Results: Participants’ reflections focused on the performance phase (57% of reflected items), followed by preparation (30%) and evaluation (13%) phases. To assess the reflection pattern of trainees with differing teaching performance, participants whose teaching assessment scores were already high from first teaching session were classified into Consistently High group (score>22). Remaining participants were further categorized based on their improvement in teaching assessment scores into Higher Change (score difference>1) and Lower Change (score difference≤1). Compared to Lower Change group, participants in the Consistently High and Higher Change groups had higher trend of reflection focus on performance (57% and 59% vs 48%) and evaluation phases (14% and 14% vs 8%), but lower on preparation phase (29% and 27% vs 44%).
Conclusions: The finding suggests a possible role of reflection in teaching performance of nurse clinical instructors, warranting further investigation.
Keywords: Registered Nurses, Clinical Instructor, Reflective Thinking, Clinical Teaching, Reflective Journal
I. INTRODUCTION
The concept of reflection was first articulated by Dewey (Dewey, 1933) and it can be defined as ‘careful consideration and examination of issues of concern related to an experience’ (Kuiper & Pesut, 2004). Since its introduction, reflection has gained a lot of attraction in multiple disciplines and professions, including medicine and nursing. David Kolb, who developed the idea of ‘reflective learning’, is one of the most influential authors who proposed the incorporation of reflection as an educational approach (Kolb, 2015). Kolb suggested that learning should be a dialectic and cyclical process, and in his experiential learning model, suggested that experience is the basis of learning, which cannot take place without reflection. Meanwhile, reflection must be connected to action. In line to this conception, Donald Schön emphasized the importance of the ‘reflective practitioner’, describing reflective practice as the practice by which professionals can become aware of their implicit knowledge base and learn from their action or experience (Schön, 1983).
In the clinical setting, the focus of clinical teaching and learning has shifted from doing, to knowing and understanding (Won & Wong, 1987). In order to understand, one must process information or knowledge in a structured manner and reflect or link new experiences and knowledge with past experiences. This allows the learner to be a ‘reflective practitioner’ and learning to be meaningful. In addition, developing learners’ reflective skills enhances coherence between theoretical and practical components of education programmes (Hatlevik, 2012). Using reflection as a means to bridge the gap between theory and practice, and develop and articulate tacit knowledge is a widely used method in nursing literature (Johns & Joiner, 2002). As reflection is increasingly recognized as a crucial component in nursing education and practice (Nguyen, Fernandez, Karsenti, & Charlin, 2014), it was a timely initiative of the National Healthcare Group College (NHGC) to conduct a Clinical Instructor (CI) programme which factored reflection as an important aspect of the curriculum while assessing the association of reflection to nurses’ teaching performance.
The NHGC conducted a CI programme for the training and development of nursing clinical instructors. The development of reflective skills was incorporated as a methodology in the curriculum. The CI programme consisted of a total of sixteen days, of which six days were spent in the classroom, followed by ten days in the clinical setting as clinical practicum. In addition to the ten days clinical practicum period, participants were granted a one-month period, beginning from the last day of the programme to complete all assessment requirements of the programme. Participants of the programme were Registered Nurses (RNs) with a minimum of three years working experience in the clinical setting and a keen interest in the clinical teaching role. The aim of this study was to explore the reflective thinking of these nurse clinical instructors and its association with their clinical teaching performance during placement of the clinical practicum.
II. METHODOLOGY
Twenty-eight RNs were enrolled in the CI program and participated in this study which used quantitative thematic analysis to establish the relationship of reflective thinking and clinical teaching. During the one-month clinical practicum period of the programme, the CI trainees were required to carry out two clinical teaching sessions and log these cases into their Clinical Practicum Logbooks (CPL).
Clinical practicums took place in the same clinical setting where the RNs worked in. Following each clinical teaching session, they were to reflect upon their teaching and document their reflections in the Reflective Journal (RJ). The RJ contained a set of prompt questions to facilitate reflections: 1) what they had learnt from their clinical teaching; 2) what new learnings from classroom sessions they applied to the clinical setting; and 3) any concerns or doubts arose from their clinical teaching experiences. The CPL and RJ were in partial assessment requirements to successfully complete the CI programme.
At the end of the one-month clinical attachment period, both these documents were retrieved from the database for this study. The RJ was first subjected to thematic coding and analysis. The themes were coded deductively according to three clinical teaching phases – preparation, performance and evaluation. Two researchers who were initially blinded to participants’ teaching performances analysed the reflective journal. Each one independently read and coded each statement of the reflection from the first teaching log according to topics in relevance to the three clinical teaching phases. The two researchers’ respective coding results were then compared to ensure inter-coder reliability. Differences in interpretation were resolved through discussion until consensus was reached. To quantify the reflection themes, each reflective statement was coded as one reflected item. The frequency of reflected item for each clinical teaching phase was thus derived. For example, if a participant reflected on the preparation teaching phase, this reflected item was counted towards the reflection frequency for the preparation phase theme.
We also extracted the teaching assessment scores for both teaching sessions from participants’ CPL. Performance scores were then used to group participants according to their teaching performances; how groups were categorised is explained in detail in the results section. In order to analyse patterns of reflective thinking across these groups, the frequency of reflected item for each clinical teaching phase was converted to percentage over the total reflected items.
III. RESULTS
As suggested by Kolb, reflection is critical to connect experience to learning (Kolb, 2015). We thus analysed participants’ RJ on their first clinical teaching experience and explored their learning for clinical teaching through the change in their clinical teaching assessment scores between the first and second teaching sessions. Generally, participants’ reflections focused more on the performance (mean no. of reflected items = 3.8, 57%) as compared to preparation and evaluation (mean no. of reflected items are 2.0 and 0.9, or 30% and 13%, respectively) phases of clinical teaching (Figure 1). The teaching assessment scores of all participants either remained the same or improved across the two clinical teaching. The participants were classified into two groups according to their teaching assessment score in the first teaching. Fourteen participants whose teaching assessment scores were already high from the first teaching log were in the Consistently High group (score > 22). The remaining participants (score ≤ 22) were further classified based on the difference of teaching assessment scores between first and second teaching into Higher Change (difference > 1) and Lower Change (difference ≤ 1) for those with higher or lower improvements in clinical teaching, respectively. Participants in the Consistently High and Higher Change groups had higher trend of reflection focus on performance (57% and 59% vs 48%) and evaluation phases (14% and 14% vs 8%), but lower trend of reflection focus on preparation phase (29% and 27% vs 44%) when comparing to the Lower Change group.
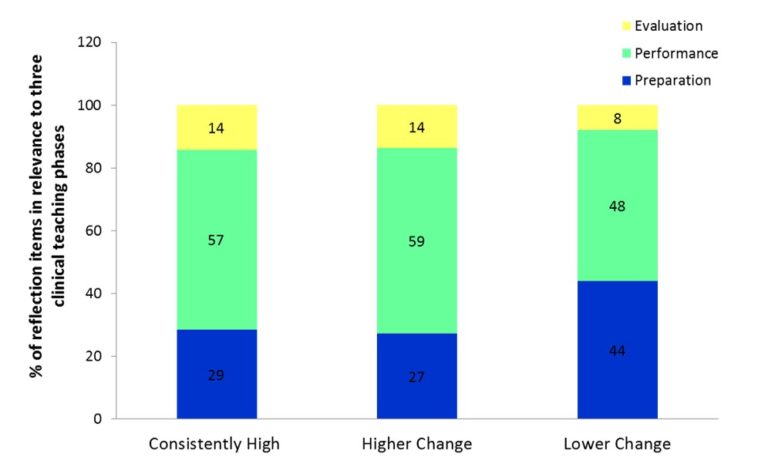
Figure 1. Percentage breakdown of participants’ reflections focus according to their group category
IV. DISCUSSION
The use of clinical logs and reflective journals in the programme was to allow learners to define their experiences in their own words through reflective writing following a practical experience, and thus to validate their own unique experiences. Kobert (1995) illustrated that clinical logs and reflection allowed the learner to see his/her world within a larger context. In addition, learning shifts from a passive to an active process (Callister, 1993). Reflecting on their practice, the clinical logs and reflective journals provided the learners with tools for developing and improving their metacognitive awareness. The ability to develop and subsequently improve reflective thinking skills begins with the awareness of one’s own thinking patterns (i.e. their metacognition) (Fonteyn & Cahill, 1998).
This pilot study set out to describe patterns of reflective thinking among RNs following experiencing clinical teaching sessions. Results from this study provide preliminary support of the relationship between the reflection on different clinical teaching phases and clinical teaching performance of CI trainees. While all participants’ reflection focused mostly on performance phase, those who attained consistent and improved teaching performance showed a higher trend of reflection focus in the performance and evaluation phases but a lower trend of reflection focus in the preparation phase when compared with other participants. In line with this research effort devoted to identify effective reflective practice education (Asselin & Fain, 2013), the understanding of how reflection associates with clinical teaching can inform curriculum design on how nurse educators can teach or scaffold reflection to enhance clinical instructors’ clinical teaching skills.
The assessment structure of the CPL could be a contributing factor in participants’ reflection focus of the teaching phases. The overall weightage of the CPL teaching assessment was 30% of the CI programme. Other assessment requirements for CI programme included developing a lesson plan based on a microteaching conducting session, class participation and presentations during classroom sessions, and doing an online quiz before commencement of the programme. The RJ entries carried a total weightage of 20%, which meant each reflective entry carried a hefty 10%. The CPL teaching performance of the trainees was assessed by their total performance scores in each of the three teaching phases, with the performance phase carrying the highest scores. The preparation and evaluation phases each carried 5 marks, while the performance phase carried 15 marks. The weightage distribution given to each clinical teaching phase could also have been a factor which contributed to participants’ reflection focus – where they tended to focus on the performance phase as it carried the highest weightage of scores among the three teaching phases.
It should be noted, that study limitations included the use of a small sample, all recruited from a single cohort of the CI programme. All participants of this cohort of the CI program were included in this study, with no exclusion criteria or eliminating factors. The RNs were of varying nationalities, with differing years of working experience, holding various educational qualifications, and even differing in age and gender. These factors were not considered in this study on their impact or influence towards their clinical teaching ability, depth of reflection potential or the capacity to translate reflective thoughts into writing. Future research, taking these factors into account, will be critical to further establish the relationship of reflective thinking and clinical teaching.
V. CONCLUSION
Different patterns of reflection were associated with clinical teaching in nurse clinical instructors. Those with consistently good teaching performance, when comparing to those with low or no improvement in teaching, have higher trend of reflection focus in the performance and evaluation phases but lower in preparation phase of their teaching. Similar reflection pattern was also observed in those showing high improvement in teaching. The finding thus suggested a possible role of reflection in clinical teaching performance of nurse clinical instructors which warrants further investigation.
Notes on Contributors
Christie Anna is a nurse educator at the National Healthcare Group Polyclinics, Singapore. She is involved in the development of nursing education.
Lian Dee Ler is a research analyst at NHG-HOMER, the research unit within Education Office of National Healthcare Group, Singapore. She is involved in health profession education research.
Ethical Approval
This study does not require ethics approval as determined by the NHG Domain Specific Review Board (DSRB), Reference 2017/00156.
Declaration of Interest
C. A. is an employee of National Healthcare Group Polyclinics and L.D.L. an employee of National Healthcare Group Singapore. The authors have no financial, consultant and other relationships that might lead to competing interests.
Acknowledgements
This pilot research project was supported by the following colleagues who provided their expertise that greatly assisted the research:
Lim Yong Hao, Research Analyst, NHG-HOMER, Group Education & Research;
Eileen So, Executive, NHG College;
Dong Lijuan, Assistant Director of Nursing, Nursing Services, NHG Polyclinics; and
Poh Chee Lien, Assistant Director of Nursing, NHG HQ, Group Education & Research.
Funding
The authors have no financial relationships.
References
Asselin, M. E., & Fain, J. A. (2013). Effect of reflective practice education on self-reflection, insight, and reflective thinking among experienced nurses: a pilot study. Journal for Nurses in Professional Development, 29(3), 111–119.
https://doi.org/10.1097/NND.0b013e318291c0cc.
Callister, L. C. (1993). The use of student journals in nursing education: Making meaning out of clinical experience. Journal of Nursing Education, 32(4), 185–186.
Dewey, J. (1933). How we think: a restatement of the relation of reflective thinking to the educative process. Lexington (Massachusetts): D. C. Heath.
Fonteyn, M. E., & Cahill, M. (1998). The use of clinical logs to improve nursing students’ metacognition: A pilot study. Journal of Advanced Nursing, 28(1), 149–154.
Hatlevik, I. K. R. (2012). The theory‐practice relationship: reflective skills and theoretical knowledge as key factors in bridging the gap between theory and practice in initial nursing education. Journal of Advanced Nursing, 68(4), 868–877.
Johns, C., & Joiner, A. (2002). Guided reflection: Advancing practice. Osney Mead, Oxford: Blackwell Science.
Kobert, L. J. (1995). In our own voice: Journaling as a teaching/learning technique for nurses. Journal of Nursing Education, 34(3), 140–142.
Kolb, D. A. (2015). Experiential Learning: Experience as the Source of Learning and Development. Upper Saddle River, New Jersey: Pearson Education.
Kuiper, R. A., & Pesut, D. J. (2004). Promoting cognitive and metacognitive reflective reasoning skills in nursing practice: Self-regulated learning theory. Journal of Advanced Nursing, 45(4), 381–391.
Nguyen, Q. D., Fernandez, N., Karsenti, T., & Charlin, B. (2014). What is reflection? A conceptual analysis of major definitions and a proposal of a five-component model. Medical Education, 48(12), 1176–1189.
https://doi.org/10.1111/medu.12583.
Schön, D. A. (1983). The reflective practitioner: How professionals think in action. New York: Basic books.
Won, J., & Wong, S. (1987). Towards effective clinical teaching in nursing. Journal of Advanced Nursing, 12(4), 505–513. https://doi.org/10.1111/j.1365-2648.1987.tb01360.x.
*Christie Ann
Email: christie_anna@nhgp.com.sg
*Lian Dee Ler
Email: lian_dee_ler@nhg.com.sg
Published online: 2 January, TAPS 2019, 4(1), 55-58
DOI: https://doi.org/10.29060/TAPS.2019-4-1/SC2000
Ikuo Shimizu, Junichiro Mori & Tsuyoshi Tada
Centre for Medical Education and Clinical Training, Shinshu University, Japan
Abstract
Consensus formation among faculties is essential to curriculum reform, especially for the clinical curriculum. However, there is limited evidence on the model of workshop that is necessary for curriculum reform. In the current project, we aimed at developing a beneficial workshop method for building consensus and reaching educational goals in curriculum reform. We compared the two types of workshop models. First, we conducted workshops using standard group work model with fixed group members. Then we used a revised workshop model. In the revised model, all but one group member moved their seats after the first round of discussion. In addition, we reserved time for plenary presentations and discussions after each round. We called the model “Modified World Café” workshop named after World Café, a collaborative dialogue method. With this design, not only we were able to achieve significant improvement of appropriate products and better consensus, but also attained several educative goals. Since the model combines characteristics of the standard group work and World Café concept, it might be useful in facilitating the sharing of new knowledge and creating consensus.
Keywords: Curriculum Reform, Workshop, Consensus Building, World Café
I. INTRODUCTION
When medical education managers conduct the curriculum reform in medical schools, they must plan for an effective implementation of the new outcomes of the curriculum, especially in the curriculum reform of clinical years when more diverse community clinician-educators at various educational environments are involved (Takamura, Misaki, & Takemura, 2017). Therefore, it is desirable that the curriculum is reformed by taking into accounts of the opinions from stakeholders at multiple specialties and reaching a consensus among them. In medical education, workshops have been performed for such a reform (Steinert, 2014). The standard workshop consists of small group discussions with fixed members throughout the schedule (Figure 1A), however, the effectiveness of this workshop design has not been well explored.
The World Café (Brown & Isaacs, 2005), a series of short group dialogues with table rotations (Figure 1B), is useful for building consensus since it relies on a participatory and collaborative network of conversations (Health Profession Opportunity Grants, 2015). However, one concern to apply World Café for establishing outcomes is that it may not be suitable to establish a new curriculum since it is just a dialogue process rather than a workshop to construct valid products and short discussion time may make discussions superficial and unfruitful.
Therefore, we designed a hybrid program of the standard workshop described above and World Café: the “Modified World Café” (Figure 1C). In this design, participants started the first round by providing a goal within a group to work on. After the first round, they share the discussion in the interim plenary presentation, then all members except one in each group (a “host”) move to a new table and start a new round of discussion. Finally, they return to their original table to summarise their discussions and finalise the product with a final presentation. While “Modified World Café” is similar to World Café in terms of process whereby all members except for one in each group move seats, there are two major differences: (1) each round is longer to discuss more deeply, and (2) participants have to collect opinions twice for interim and final presentations. These revisions are intended to finalise the products. We aimed at (1) evaluating the effectiveness of the “Modified World Café” to mix the various opinions and reach better consensus on the expected outcomes among participants, and (2) exploring the participants’ perceptions.
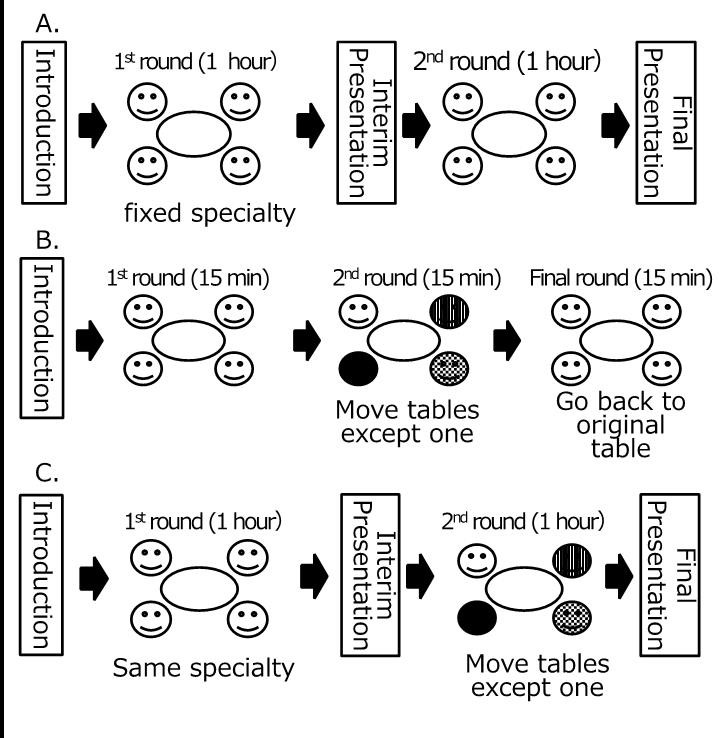
Note: 1A. The standard workshop (i.e., the model without moving tables),
1B. World Café dialogues (Brown, 2005), and
1C. “Modified World Café” workshop.
Figure 1. Three types of workshop models discussed in this article
II. METHODS
A. Setting
Shinshu University School of Medicine in Japan extended its clinical clerkship program from 15 to 21 months in 2015, by adding a 6-month elective clerkship program. In the new program, students are expected to rotate among the community teaching hospitals to acquire clinical competencies. Because of this reform, we conducted workshops to establish the learning outcomes of the new clinical clerkship program and share the outcomes from the 2014 to 2015 academic year. The workshop participants are clinician-educators of community teaching hospitals who teach medical students in the clinical clerkship program. Every teaching hospital was asked that at least one clinician-educator per hospital participated in one of the series of workshops.
B. Design of workshop
In the workshops, we used the following two workshop models for comparison. Firstly, we conducted two workshops with the standard group work model (Figure 1A), in which the participants engaged in two rounds of small group discussions. The groups consisted of five to seven participants each and were formed according to their clinical specialty, and members were fixed. Each group was asked to establish outcomes of its specialty for the reformed curriculum during the couple of rounds. Faculties of Shinshu University Hospital participated and facilitated the discussions. There were two presentation opportunities: interim and final sharing on what they have discussed.
We, then, conducted three workshops using the “Modified World Café”. The expected product, number of participants, the number and length of rounds, and the presence of facilitators were the same as the standard group work model. As described in the Introduction part (Figure 1C), all members except one in each group (a “host”) move to a new table in the second round. Two presentations (interim and final) were performed. The participants were briefed on process at the beginning of each workshop.
C. Evaluation
To evaluate these workshop models, the participants were asked to complete two anonymous questionnaires. The first one was an open-response evaluation sheet designed for participants to write their own perceptions (e.g. benefits, demerits, suggestions) on the group work in the workshop. The comments were analysed using thematic analysis, which involved iteratively exploring the data and comparing and refining the identified categories. Two team members read the data iteratively and analysed them thematically using the affinity diagram method (KJ method) (Scupin, 1997), identifying, analysing, and reporting themes within the data and developing an interpretive synthesis of the topic.
The second survey used a questionnaire comprising the following items: (1) the degree of perceived usefulness of the products, and (2) the degree of perceived consent of the products, and (3) the degree of active participation in the workshop. The responses were collected with a 5-point Likert scale ranged from 1 for “strongly disagree” to 5 for “strongly agree,” which we analysed statistically with the t-test.
III. RESULTS
A total of 120 educators from 37 hospitals participated in the five workshops (71 at the initial model and 49 at the revised model). Among them, 77.5% had been involved in postgraduate (residency) clinical teaching. The response rate of the questionnaire was 89.4%.
Analysing the open-response sheet in the initial model enabled the identification of four themes: preference for outcomes, usefulness of collaboration, attitude for participation, and need of inter-specialty discussions. From the comments after the Modified World Café, two more themes were emerged in addition to the four themes in the initial model: (1) suggestive opinions about educational views (“How should we address the diverse characteristics of students?” “Near-peer learning with residents can be useful”) and (2) an educational impact (“teaching strategies at the workplace,” “the importance of outcome-based education,” “an overview of legitimate peripheral participation”), all of which are theoretical bases of clinical clerkships.
The rating of the items in the questionnaire on the 5-point scale revealed that the mean degree of the usefulness of the products significantly improved from 3.77 to 4.00 (p = 0.017). The mean degree of perceived consent of the products also significantly improved from 3.61 to 4.05 (p = 0.001). The degree of active participation in the workshop did not change (4.05 and 3.95; p = 0.256).
IV. CONCLUSION
Our “Modified World Café” workshop shows not only improved the perceived usefulness and built better consensus but also yielded educational achievement from the analysis of open-response sheet. It is probably because of a benefit of World Café, which can visualize and share collective intelligence (Brown & Isaacs, 2005). By hybridizing the characteristics of the standard group work and World Café, our “Modified World Café” workshop can be a more suitable design. The degree of active participation did not change probably because the participants did not join in the workshop voluntarily. Better achievements with the same degree of active participation will still indicate a merit of “Modified World Café”.
On the other hand, there are some limitations. Firstly, since the participants attended only one workshop, our results might not be from any experimental design. Also, only three items were used in the questionnaire, although we observed significant improvement in some perceptions.
Since workshop tends to be dependent on its context (Steinert, 2014), the educational innovation in its design has been hindered. With this regard, our “Modified World Café” workshop may be applicable in other contexts which require highly collective processes for consensus creation, such as patient safety and interprofessional management.
Notes on Contributors
Ikuo Shimizu MD, MHPE, is an assistant professor at the Centre for Medical Education and Clinical Training in Shinshu University. He is also involved in the safety management office at Shinshu University Hospital.
Junichiro Mori, MD, PhD, is a lecturer at the Centre for Medical Education and Clinical Training in Shinshu University.
Tsuyoshi Tada, MD, PhD, is a professor at the Centre for Medical Education and Clinical Training in Shinshu University.
Ethical Approval
This work was approved by the Institutional Research Board at Shinshu University and carried out in accordance with the Declaration of Helsinki; in particular, anonymity was guaranteed and consented for analysis was obtained.
Acknowledgements
We thank all the other faculty members at the Centre for Medical Education and Clinical Training and the Shinshu University Hospital who contributed to the series of this workshop.
Funding
No funding is involved for this paper.
Declaration of Interest
The authors report no declarations of interest.
References
Brown, J., & Isaacs, D. (2005). The World Café: Shaping our futures through conversations that matter. San Francisco, CA: Berrett-Koehler Publishers.
Health Profession Opportunity Grants (2015). Using the World Café to Improve Instructor Engagement: A Guide for Health Profession Opportunity Grants Programs. Retrieved 1 March 2018, from https://www.acf.hhs.gov/ofa/resource/using-the-world-cafe-to-improve-instructor-engagement-a-guide-for-health-profession-opportunity-grants-programs.
Scupin, R. (1997). The KJ method: A technique for analysing data derived from Japanese ethnology. Human organisation, 56(2), 233-237.
Steinert, Y. (2014). Faculty development: Future directions. In Faculty Development in the Health Professions. Springer Netherlands.
Takamura, A., Misaki, H., & Takemura, Y. (2017). Community and interns’ perspectives on community – Participatory medical education: From passive to active participation. Family Medicine, 49(7), 507–513.
*Ikuo Shimizu, MD, MHPE
Safety Management Office
Shinshu University Hospital
3-1-1 Asahi, Matsumoto 3908621, Japan
Tel: +81 263 37 3359
Email: ishimizu@shinshu-u.ac.jp
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
