
Issue 51
Aug 2024
PEOPLE OF NUS MEDICINE

NUS alumnus and Cambridge-trained Roger Foo is NUS Medicine’s Vice-Dean for Research. The mild-mannered heart specialist is the inaugural chair of the Zayed bin Sultan Al Nahyan Professorship of Medicine at the National University of Singapore (NUS), Director of the NUHS Cardiovascular Metabolic Disease Translational Research Programme, Senior Consultant at the National University Heart Centre Singapore (NUHCS) where he is Clinical Lead for the Cardiac Genetics Service, Director at the Cardiovascular Research Institute (CVRI), and also Research Director at the A*STAR Institute of Molecular and Cell Biology (IMCB). He is also Chair of the Ministry of Health Clinician Scientist Residency Research Panel.
After his undergraduate medical education here at the Yong Loo Lin School of Medicine, National University of Singapore (NUS Medicine), Roger underwent graduate clinical training at King’s College Hospital in London and also at Addenbrooke’s Hospital, Cambridge. His research training was spent in the labs of the late Professor David de Bono (British Heart Foundation Chair of Cardiology, Leicester), Professor Morris Brown (past president British Hypertension Society, and Professor of Clinical Pharmacology, Cambridge), Professor Martin Bennett (BHF Chair of Cardiovascular Sciences, Cambridge) and Professor Rick Kitsis (The Dr. Gerald and Myra Dorros Chair in Cardiovascular Disease, Albert Einstein College of Medicine, New York), where he was continuously funded by both The Wellcome Trust and the British Heart Foundation with fellowships and project grants.
Altogether, Roger trained and worked in Cambridge, UK, for over 20 years at the Division of Cardiovascular Medicine (University of Cambridge) and also at the Addenbrooke’s Hospital NHS Trust before moving his lab to Singapore in 2013. At the National University Heart Centre, Singapore, he established Singapore’s first Cardiac Genetics clinical service, and has since been leading the Cardiovascular Epigenomics and Molecular Epigenetics Themes for many of the largest Cardiovascular grant awards in the country.
Research in his lab makes use of genomic technology to study cardiac epigenome and hunt for novel Heart Failure mechanisms. Roger, 55, enjoys reading scientific, historical and current affairs literature, as well as travel with his wife. He keeps as much as possible to a daily swimming regime and uses WhatsApp and Instagram to keep in touch with his 2 adult children who live abroad.
Q: Describe your time in medical school. Did you have this irrepressible urge to excel and what did you excel at in medical school anyway?
A: I was never excellent in medical school! I topped my primary school for all 6 years, and there ended the peak of my school academic career. I did well enough in secondary school and junior college to scrape through into med school, and passed each year in med school to make it out with a medical degree. No distinctions, no dean’s list, no prizes. Just an average student who probably spent too much time watching movies and hanging out with friends, doing aimlessly nothing, and scrambling madly the few months before each year-end exam. None of my med school classmates will remember me in association with the word excel.
Q: What is a clinician-scientist? A medical hybrid?
A: They’re people who are trained clinicians, practise in a clinical capacity, and yet also work on the science, i.e. run experiments or clinical trials that lead to discoveries and set standards or drugs for treatment or management of patients. Clinician-scientists are on the cutting edge of medical science: they are the ones who discover the molecules and the drugs that can be used to treat patients tomorrow.
Q: How did you end up here? Did you take a wrong turn, or choose the straight and narrow path that leads through valleys of dark shadows?
A: It wasn’t a “wrong” turn because I love what I do today, so it’s turned out absolutely right for me. But I don’t deny that it was an unexpected turn. I knew I wanted to be a cardiologist as early as when I was a third year medical student. In fact, he who inspired me on the path of cardiology was Professor Chia Boon Lock. He conducted the first cardiology tutorial I attended in the small teaching room outside Ward 44 of Singapore General Hospital. I was completely mesmerised by his tutorial on angiotensin-converting enzyme (ACE) inhibitors (a new drug at that time!) and was subsequently introduced to his wonderful world of electrocardiogram (ECG). His ECG textbook, including a recently revised edition, is matchless. Prof Chia set me on the path—in love with the heart and all things cardiology. I stuck copies of patients’ abnormal ECGs all over my wall when I was a trainee, and felt quite special by being able to read the waves and squiggles, as if they were hieroglyphics. So when it came to picking a speciality for myself, there was no question which one it was going to be. What was the surprise was how much I came to love research and working in a wet lab when I had the chance to do that while working in the UK. I love that I am in research and in science because it means that I can always claim to know only a little, since research is all about learning more.
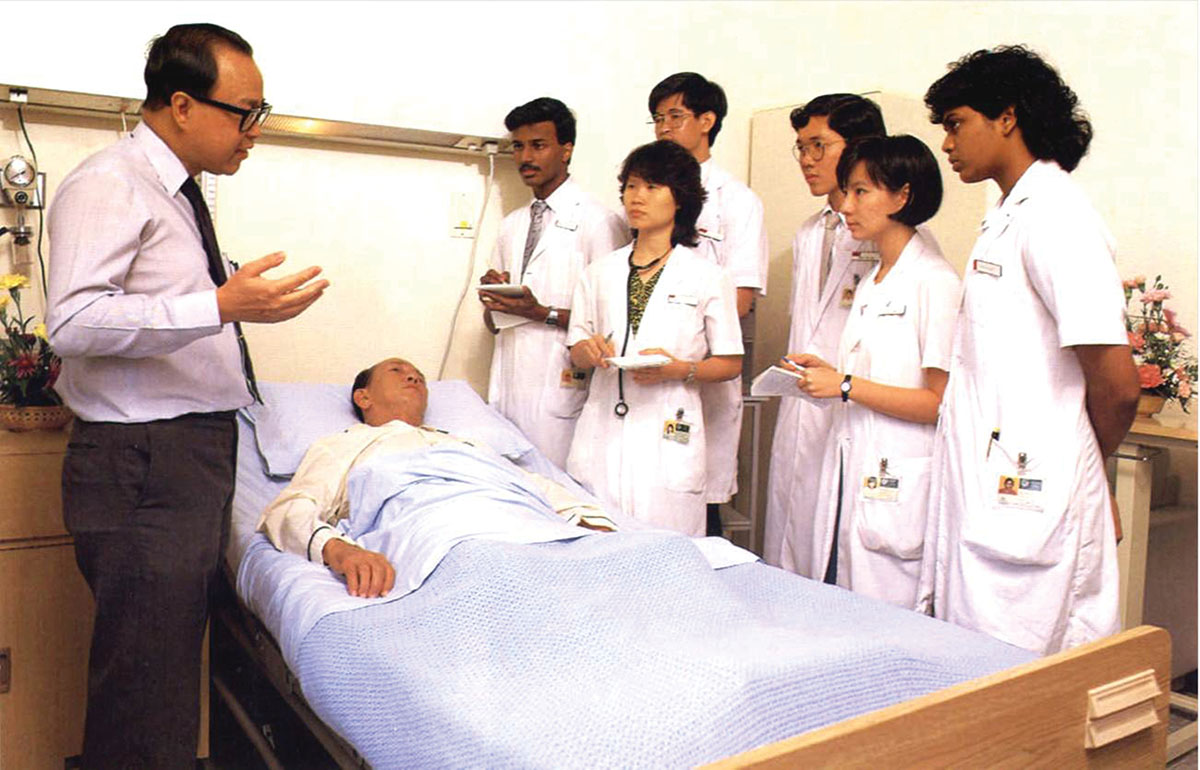

The late Prof Chia Boon Lock at his mesmerising best.
Q: What is the difference between a dry lab and a wet lab? What swimmers do you wear when you enter your wet lab? Is the water cool?
A: Haha. My son attended Eton College and at his school, every boy is either a “wet bob” or a “dry bob”. Wet lab refers to the lab where biochemical, molecular and cellular experiments are carried out. For example, proteins are run in a Western blot, DNA is amplified by polymerase chain reaction (PCR) and cells are cultured in vitro. Most of these processes involve fluids of some form. Dry lab refers to the lab where scientists work at desks on computers, analysing data, processing data through software pipelines, devising algorithms for data and numbers, and generating graphs and plots. A dry lab consists of computers and servers, not usually anything that is liquid or fluid.
Q: You wear 7 hats at work, including the newest one of Vice-Dean for Research here at NUS Medicine. How do you see the scientific work here contributing to Singaporeans’ health and well-being? What new areas need investigation and interrogation?
A: The analogy is that of conducting a large orchestra with its full suite of instruments encompassing strings, woodwind, brass, percussion and more. Each section is doing its best towards Singaporeans’ health and well-being as you rightly indicated, and the conductor is responsible for getting all the sections to play synchronously, in tune and harmoniously, sharing resources, expertise and complementarity. The conductor isn’t only me because there are many of us playing different roles in the coordination and organisation. It is wonderful to be surrounded by so many talented clinicians and basic scientists here at NUS Medicine. We are a very lucky ecosystem, to have the talent, and also the resource to bring a large number of projects together. Many around the world already envy the healthcare that we have in Singapore, so before us is the challenge to make things even better because we are acutely aware of what needs fixing and where pressing medical needs are at the frontier of medical science.

It is wonderful to be surrounded by so many talented clinicians and basic scientists here at NUS Medicine. We are a very lucky ecosystem, to have the talent, and also the resource to bring a large number of projects together. Many around the world already envy the healthcare that we have in Singapore, so before us is the challenge to make things even better because we are acutely aware of what needs fixing and where pressing medical needs are at the frontier of medical science.”
Q: The English philosopher George Bernard Shaw reportedly said “Science is always wrong; it is the very artifice of men. Science can never solve one problem without raising 10 more problems.” Does science answer questions or raise new ones in a never-ending dialectic? To what end?
A: The preceding part of that quote is “We call one side of humanity religion, and the other science. Religion is always right, and science is always wrong; it is the very artifice of men….” Even in his best form, George Bernard Shaw has been pronounced a polemicist, with expressed views that are often contentious, and at one time he even promoted eugenics. On this quote though, it touches a raw nerve of mine at the interface between religion and science. There are those (including Richard Dawkins) who believe the 2 to be opposite poles. Science is ready to be proven wrong, and the very basis of science is to work towards proving whether the hypothesis is correct or wrong. That is also why science textbooks have to be revised, to keep up with the newest and latest evidence. These notions are quite the opposite from religion which is unfalsifiable, and is always right. Religion is not for asking the question why, but instead by believing through faith, and based upon age-old teachings from ancient scripture. I have to leave it here for those with faith to resolve the 2 ends of this.
Q: What’s the secret sauce for success in research work, and how do you define success?
A: There must be many versions of success, and each version to me, is equally worth celebrating. Winning a grant, getting a piece of work peer-reviewed and published. Being recognised by my community to have contributed to a piece of knowledge, or better still a change in practice. Having a trainee or student win a prize, or successfully defend his/her thesis. I am always excited with every form of success that I see among our colleagues and teams around here. Each one is always very well-deserved. How does one get to success? Nothing takes the place of tenacious hard work, paying attention to mentor advice, yet not simply or blindly following trends, but following the science, and respecting what your experimental results are saying to you. Working well in teams seems also to make for a very helpful ingredient towards bigger success today. There must be many roads to success, but the one that is most obviously wrong is quitting.
Q: Which comes first—the doctor or the scientist?
A: Doctor for sure. That is the role in which we make the difference to every patient we see, and to his/her family. Science is what satisfies our scientific selves because we may be doing something that can make a big impact on many more patients in the future. But today, that one patient in front of us is what matters.
Q: Which is more challenging—attending to a medically complex patient, or tackling a scientifically impossible piece of work in your lab?
A: I no longer attend to medically complex patients in the ward or clinic, but refer these to my colleagues who spend much more time than me seeing patients. It isn’t fair to patients to have me see the most complex cases, given that I spend more time in research at the bench, rather than in the clinic. These days, in clinic, I am really only focussed on patients with genetic heart disease, so to me, those are not usually complex, and I manage them comfortably. For genetic cases that are complex, I am very glad that there is now a very friendly and collaborative network and community of cardiac geneticists around the world, and we share knowledge and experience for complex cases readily.
Q: Please share about your years at Cambridge University. Is the place really as good as it’s cracked up to be?
A: Cambridge was utterly inspiring! It is hard to know where to begin on this one, and even harder to know where to end. Cambridge opened my eyes to what science really is. How medical discoveries are made, and how one can really do what one loves and feel so rewarded for it. When I was at Cambridge, the lab next door to mine was THE lab that mapped out the first 11 genes explaining obesity. The first monoclonal antibody that was first used to cure cancer was presented there in the grand round.
I remember when that research was presented at grand round, every single person in the audience was amazed to learn how cancer was cured in the patients of that trial. Today, 2 out of 4 cancer patients can expect a cure of his/her cancer. It is research that saves the lives of thousands of people around the world today. My own mentor in Cambridge mapped out how somatic mutations in the adrenal gland explain why some patients have a curable form of hypertension, making it possible to cure hypertension in some. What remains for the latter is to work out the best diagnostic test to find the patients who have this form of hypertension who can be cured. Life in the medical campus at Cambridge was heaven. And when the choir sang in the college chapel at dusk at evensong, it took me even closer to heaven!

Q: Why do you think research is meaningful when the fact is that everyone dies eventually—and here in Singapore, the average lifespan is between 80 and 85 years?
A: It is not the lifespan but the health span that our research wants to tackle. Extending lifespan, but living the last years in ill health or worse, bed-bound, will not be meaningful. It is true that the one surest certainty in life is death, but I believe in the ultimate purpose of our research—which aims to help life to come to its conclusion as healthily, naturally and meaningfully as possible, and without causing burden to ourselves and our families.
Q: What makes you happy and what gets you down and what do you do to get back on your feet again?
A: What makes me happy is reading about amazing scientific breakthroughs or learning about new science. To me, nothing can be more real than science. The rest of life is so often about man-made or imagined realities. Science is the “real” reality. For example, just the other day a research fellow in the lab showed me an experimental result that suggests biochemical modifications on the tRNA from our heart cells seem to become drastically altered in the process of maturation. RNA does not only exist in the base form as it is often famously represented. Some of the bases are actually biochemically modified. The research fellow’s experimental result appears to suggest a significant wave of modification tracks with the maturation of the heart cell. If validated, this will be the first time that anyone has characterised this change, and if true, it could open up a new avenue for us to understand how the heart ages and fails, or even how to rejuvenate the heart or turn the clock back.
Every clinician-scientist will leave a mark somewhere by the research finding(s) that they contribute. I am very self-conscious of my own fallibility and inadequacies. Hubris is a big thing for me. I love that I am in research and in science because it means that I can always claim to know only a little, since research is all about learning more.”
Q: When are you at your productive, creative best?
A: In the evenings when the day is winding down. I make sure I spend time “going to the mountains”, which to me is metaphorically meditating and taking time to think deeply about what I am doing and review all my projects in my head. I chill by watching YouTube lectures and listening to audio books. I have a reading list that may be boring to some: I am currently working my way through all of Richard Dawkins books, and find myself deeply fascinated by his account of evolution. I love how much I am learning about the history of humanity and have gone down the rabbit hole with people like Robin May and Nick Lane, all great speakers on the subject. But I shouldn’t forget to mention that I am also spending a lot of time learning and familiarising myself with this new beast called artificial intelligence (AI). And I love winter in Cambridge for the log-fire. Sitting in front of a crackling fire after a long country walk in the misty cold, in my boots and jacket. Walking out into the cold winter mist fills me up immediately with inspiring thoughts of science and humanity.
Q: How does your family view the work that you do?
A: They are 100% supportive and I am ever grateful. My wife is a patient listener, and I think I am sufficiently good at storytelling to still be able to fascinate my grown-up children and their friends with our research results and ambitions.
Q: Complete this sentence: “Old clinician-scientists never fade away, they simply …………”
A: Old clinician-scientists never fade away, they simply start again inside the heart and mind of another young clinician-scientist who continues to push towards a new horizon. The true clinician-scientist leaves his mark by the science that he contributes to the world. Some clinician-scientists lead a clinical trial that confirms the use of a new medicine. Another finds the gene that is the target for new medicines today: for example, Semaglutide, the drug that came into global prominence recently as the first medicine that can be used successfully to treat obesity. How amazing to be the clinician-scientist looking after patients who benefit today. Every clinician-scientist will leave a mark somewhere by the research finding(s) that they contribute. I am very self-conscious of my own fallibility and inadequacies. Hubris is a big thing for me.
Q: And a life well-lived is?
A: To be remembered for the science I contribute, but probably even more so, for the fellow scientists and clinicians who I have worked with and helped supported in one way or another.
More from this issue

STUDENT MATTERS
Public Health Service
ETHICALLY SPEAKING
What Prompts People to Deliberately Expose Themselves to an Infection?

AFFAIRS OF THE HEART
Advancing Wellness: The Power of Human-Digital Collaboration in Chronic Illness Care
