The remote past
When the Straits and Federated Malay States Government Medical School opened its doors on 3 July 1905 in what was to be the historical beginning of medical education in the region, 16 young persons presented themselves for the full five-year course that would lead, on successful completion, to their qualification as medical practitioners1 and in the words of one of the recommendations of the Kynnersley Commission of 1902 on the system of English Education in Singapore, “supply the demand for Assistant Surgeons and General Practitioners among the native population and the poorer inhabitants”.2
As remembered 60 years later by one of the seven successful candidates who passed the final examination in Medicine, Surgery and Midwifery in the shortest prescribed time in 1910, the late Dr Chen Su Lan, “The Medical School was born without a flourish of trumpets”.3 Indeed, as measured by the subsequent evolution of the medical school and the achievements of its graduates, the original educational and professional objectives must seem to contemporary eyes relatively modest and circumscribed.
For some who yearn nostalgically for those simpler times, one fact is worth pointing out. The Government, in its reply to the signatories of the memorandum of 1904 that petitioned for the establishment of a medical school stated that the candidates for admission should “have passed the seventh standard in one or other of the secondary schools of the Colony or the Federated Malay States”.4 Standard 7 was the highest achievable attainment in English schools at that time. Primary school comprised two primary classes and Standard I, elementary school comprising Standards II to V, and secondary school comprised standards VI to VII.2 This meant that the 16 students in 1905 had an average age of 14 years (assuming that schooling began at age 6) and that of the seven successful licentiates in 1910, the average age was no more than 19 years. Viewed in our contemporary context, young men of the latter age would still be serving their National Service unless this had been deferred.
The early years
Dr RD Keith, the second principal of the School from 1909 to 1917, had written that the medical course was based largely on the programme prevailing in England, especially London and it consisted of an initial two years in the basic sciences followed by clinical clerkships in Medicine, Surgery and Midwifery during the next three years.5 The main subjects in the first year were Chemistry, Botany and Physics. The study of elementary Anatomy and Physiology begun in this year extended into the second year.
Majestic facade of the old Faculty of Medicine Building, a wonderful work of architecture to behold even today.
Dr Chen Su Lan,3 in his reminiscences, recalled that a month after the opening of the medical school, practical Anatomy began under the supervision of the first principal, Dr GD Freer. Two cadavers were available for study, a muscular young man and a young woman. How were the bodies preserved? Formalin was used as a fixative in the 1890s. In the US during the same period, various agents were used either alone or in different combinations in departments of Anatomy.6 Among these agents were carbolic acid, glycerine, arsenic, chloral hydrate, zinc chloride, mercuric bi-chloride, alcohol, potassium carbonate, sodium bicarbonate, sodium chloride, methyl spirit, formalin, potassium nitrate and boric acid. The agents were injected directly into the subjects. In some instances, the subjects were preserved by cold storage. In this connection, one of the recommendations of the committee on Medical Education in 1869 of the General Medical Council of Great Britain was that Anatomy and dissections be conducted in the first and second winter sessions of the medical course because even at that time, bodies could only be preserved in winter.7 Undoubtedly, Dr Freer and his part-time lecturers recruited from the Government Medical Service settled on a workable formula for preserving human subjects in Singapore’s perennially warm and humid conditions. Appropriately, the large building used for dissections was situated far behind the main college buildings in the refurbished former lunatic asylum.3 What were the physical conditions like? No extant description seems available. Was the building electrically lighted or were kerosene lamps still in use? Perhaps in sunny Singapore, natural light would have served. What about ventilation? Were electrically driven high ceiling fans a feature or did open windows suffice? There was nothing like the centrally air-conditioned comforts that are currently enjoyed.
Of the curriculum itself, what precisely was subsumed under “Anatomy”? Dr Chen Su Lan3 remembered that there were lectures in Osteology and that textbooks were lent to students. What were these textbooks? Of dissection guides, Professor DJ Cunningham’s Manual of Practical Anatomy had been published in 1893. Did students also have access to Henry Gray’s famous “Anatomy”? Was Histology taught under the aegis of Anatomy or was it part of the province of Physiology, as was the practice then in many medical schools in Britain? The fact that, according to Dr Chen Su Lan,3 the microscopes which arrived in 1906 were housed in the Physiology building suggested that the second possibility was probably the case. Were Neuroanatomy and descriptive Embryology also taught then? We shall have to be content with these and other questions of those early years remaining unanswered.
The recent past
As one approaches the recent past, one is on firmer ground, especially since the medical school’s observance of its 50th, 60th and 75th anniversaries. A department as such was non-existent until the first Chair of Anatomy was established in 1922.4 With this event and the provision of staff, the curriculum would have expanded to bring it in line with that of other medical schools in the British colonies, particularly those in London. By the time of the Faculty of Medicine’s diamond jubilee, the Department of Anatomy had assumed responsibility for courses for second year medical, dental, science, and third year medical as well as postgraduate (surgically aspiring) students. Besides traditional gross Anatomy, lectures and practical classes were also conducted in Neuroanatomy, Histology and descriptive Embryology.
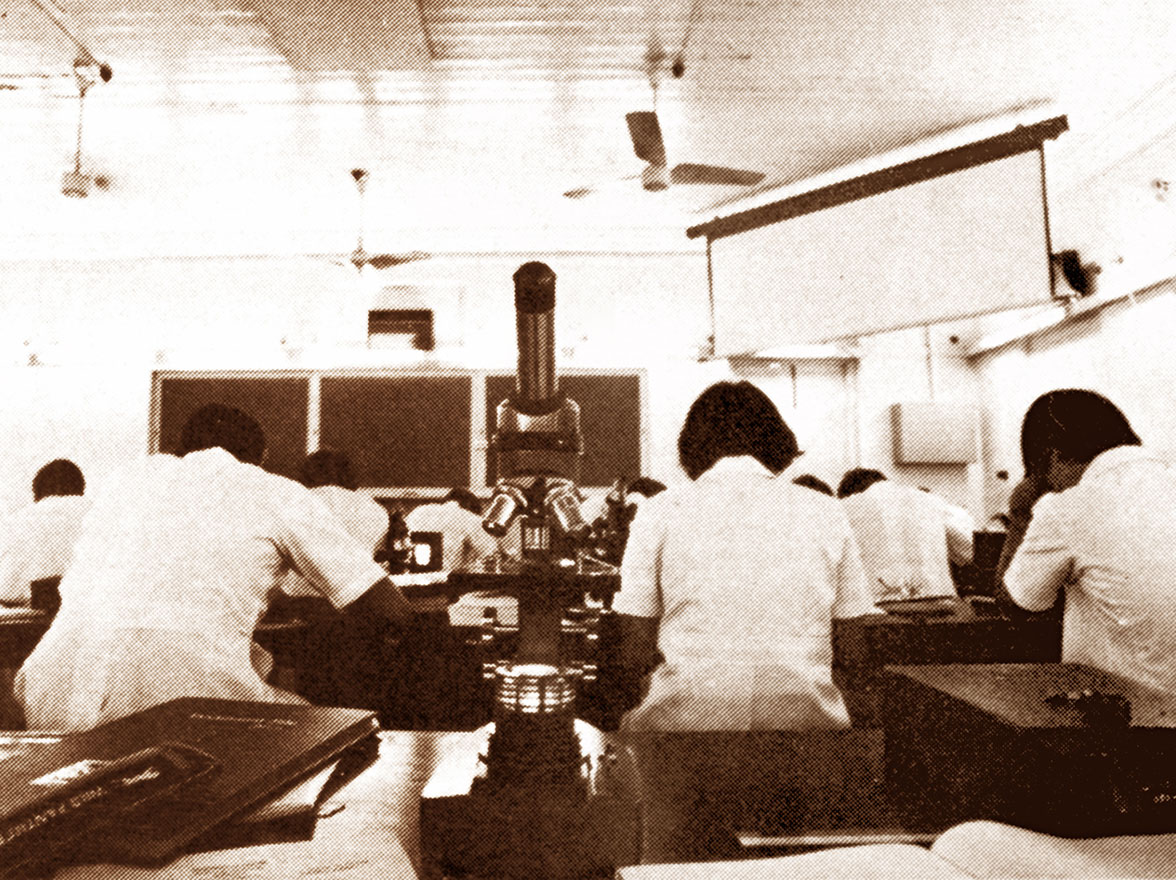
Old Histology Laboratory in the Tan Teck Guan Building.
From the mid-1960s to the mid-1990s, the course of Anatomy for medical students spanned three semesters (in 1½ academic sessions) and was conducted in such a way that gross Anatomy, Embryology, Neuroanatomy and Histology were delivered in a coordinated fashion. Emphasis was given to the clinical application where appropriate, constantly drawing the students’ attention to the professional relevance of the course. A regular feature of the course was the series of applied Anatomy lectures given by clinicians from both the public and private sectors. By the early 1980s, the gross Anatomy course was structured in such a way that at the commencement of each week, a pre-dissection lecture was given in which the week’s dissection was reviewed and the important structures that would be encountered were indicated. When the students had completed their practical study, they were divided into small groups, where individual tutors reviewed the tutorial objectives that had been made available earlier. Besides its responsibility to medical students, the Anatomy department also took part in the teaching of dental, science, pharmacy and postgraduate students.
The late 20th and early 21st centuries
In the late 1990s and early 2000s, the NUS medical curriculum was further substantially revised to meet the challenges of the time in anticipation that medical practice would be characterised by the following:
|
a)
|
The rapid expansion of biomedical knowledge.
|
|
b)
|
Advances in medical technology based on a better understanding of molecular and cellular processes in the human body.
|
|
c)
|
The rapid expansion of the Internet and related electronic media/resources.
|
|
d)
|
Better-educated and well-informed patients.
|
|
e)
|
Complex ethical issues that evolve in parallel with advances in medicine.8,9
|
In view of the above, a current medical student will need to have a thorough knowledge of basic medical sciences to support and strengthen future medical practice. A strong and factual foundation in Human Biology is essential for understanding human diseases. Various educational objectives were introduced recently, viz:
|
1)
|
Basic science foundation for clinical practice.
|
|
2)
|
Clinical competence.
|
|
3)
|
Communication.
|
|
4)
|
Appropriate attitudes.
|
|
5)
|
Professional development.
|
In line with the above educational objectives, the core M1 curriculum was organised into three tracks, namely:
|
1)
|
Structural and Cell Biology,
|
|
2)
|
Human Structure and Development, and
|
|
3)
|
Systems Biology.
|
Staff members at the Sepoy Lines Campus (1980).
In this track system, Human Anatomy classically fell into the Human Structure and Development Track. The original 1½-year Anatomy programme of the mid-1990s was tailored into a one-year programme with a drastic reduction in teaching/ contact hours. The teaching of core anatomical knowledge has been further streamlined to synchronise with the teaching in Cell Biology and Systems Biology. In this way, knowledge learnt by a medical student can be integrated, with a better understanding of the structure and functions of the human body.