
“Booster Shots” of Humanism at Bedside Teaching
Published online: 5 May, TAPS 2020, 5(2), 45-47
https://doi.org/10.29060/TAPS.2020-5-2/PV1085
Chi-Wan Lai
Koo Foundation Sun Yat-Sen Cancer Center, Taipei, Taiwan
I. INTRODUCTION
Most medical education programmes in Taiwan accept students upon high school graduation. Medical education used to consist of seven years with the last year being an internship. Since 2013, medical students have graduated at the end of six years, and the internship has been moved to a postgraduate year. In both formats, students have been offered medical humanities courses in the “pre-med” phase, i.e. the first two years of medical school. From the third year onward, however, students rarely have exposure to subjects related to humanism, other than courses on medical ethics and some problem-based learning case discussions. Moreover, medical students have had very little exposure to humanities in high school. Such limited exposure to humanities during medical school can have detrimental effects on cultivating humanistic physicians in Taiwan.
It is known that the majority of medical schools in the U.S. are post-baccalaureate system, i.e. most of the medical students have already had exposure to humanities courses during undergraduate years. Yet research shows that medical students in the U.S. have problems with empathy decline as they advance through medical school (Neumann et al., 2011). The Arnold P. Gold Foundation has been advocating for infusing the human connection into healthcare, and Plant, Barone, Serwint, & Butani (2015) articulated very well the need to take humanism back to the bedside. Lacking these efforts, the empathy decline among medical students in Taiwan could conceivably be even more serious than in the U.S.
This paper advocates for the importance of instilling humanism at the bedside during clinical rotations to serve as “booster shots” to enhance the medical humanities learned by students in the pre-med phase.
II. MY PERSONAL EXPERIENCES IN LEARNING AND TEACHING AT THE BEDSIDE
Following my graduation from medical school at National Taiwan University School of Medicine in 1969, I completed a four-year residency in the Neurology & Psychiatry Department at Taiwan Medical University Hospital (1970-1974) and did an attending year before I went to the University of Minnesota to start another residency program in Neurology (1975-1978). In Minnesota, I was deeply impressed by the bedside teaching of my respected mentor, Dr. A. B. Baker, the chairman of the Neurology Department. I vividly remember one unforgettable incident – before he did a “straight leg raising test” (Swartz, 2014) on a female patient suffering from sciatica, he first asked for a towel to cover the area between the patient’s legs before raising her leg to test the possibility of sciatic nerve entrapment. He clearly demonstrated sensitivity to the patient’s potential feeling of embarrassment caused by performing such a test while surrounded by students and residents. Through several of these “enlightening moments” at the bedside, he demonstrated his famous quote: “Students learn from observing how you do, rather than from what you say.”
Since then, I have continued my interest in bedside teaching while teaching at the University of Kansas Medical Center (1979-1998) and upon my return to Taiwan in 1998.
It is my personal conviction that bedside teaching should include not only medical knowledge and skills but also bedside manner, sympathetic listening and empathetic communication. Such teaching can serve as “booster shots” during clinical years to enhance the humanism that medical students learn in earlier years. For more than a decade, I have been conducting regular bedside teaching in three teaching hospitals for 5th or 6th year medical students at National Yang Ming Medical University, National Taiwan University, and National Cheng-Kung University during their clerkship rotating through neurology.
I would like to present the following two cases to illustrate how to enhance students’ sensitivity to the suffering of others (patients and their families), while also teaching neurological examination techniques, differential diagnoses, and management.
III. CASE 1: A PATIENT WITH MYASTHENIA GRAVIS WHO SUFFERS FROM DIPLOPIA
The diagnosis was delayed by his presenting chief complaints as “dizziness,” for which he visited several ENT doctors, until finally he was referred to neurologists. Students were puzzled by how the patient could “confuse” diplopia (“double vision”) with dizziness. I then demonstrated to students how to self-induce diplopia by stretching out their left arm, with index finger pointed to the sky, and then continue to stare at this finger while trying to apply pressure to their right eyeball with their right hand. This would artificially create different positions of the eyeballs (dysconjugation), resulting in problems with the fusion of two images projected from the retinae to the brain. This caused “double vision” and a dizzy feeling, which was exactly what happened to this patient. Students then appreciated what the patient was suffering and understood why the patient could perceive “double vision” as “dizziness.”
IV. CASE 2: A PATIENT AT THE END-STAGE OF AMYOTROPHIC LATERAL SCLEROSIS, A DEVASTATING MOTOR NEURON DISEASE THAT HAS NO EFFECTIVE TREATMENT
After the student presented the history of the patient, I reminded students to find out how we could help such a seemingly “medically helpless” patient. After observing severe bulbar symptoms and demonstrating the coexistence of upper and lower motor neuron signs at bedside, I thought it might be a good case to lead the patient into a discussion of serious issues related to end-of-life.
So I posed a question – “What do you worry about the most?” – trying to lead the patient into a discussion of whether he would consider accepting emergent intubation followed by long term ventilation when he developed difficulty with breathing. Unexpectedly, the patient responded, “What I worry about the most is my daughters’ education.” He then went on to share with us his story of how his lack of formal education due to poverty led him to the life-long misery of humiliation at work. Consequently, he has tried to save as much money as possible for his two daughters’ college education. Unfortunately, his financial status had been seriously compromised by his loss of job and increasing medical expenses since he became ill, at a time when his two daughters would soon graduate from high school.
After we left the patient and started discussing the patient’s neurological findings, one student reminded us that we had not discussed how to help this patient. She went on to share with us her thoughts: she would like to see the patient’s daughters, discuss with them whether they themselves were interested in going to college, and if so, she would urge them to speak to their father about their desire to work in the daytime and to attend college through evening school.
We were all impressed by this student’s thoughtful proposal, and I went on to praise her, saying that she had beautifully illustrated the truth of the following statement: “Although there is nothing more that can be done for the body, this does not mean that there is nothing more that can be done for the sick person” (Cassell, 2004).
V. GENERAL DISCUSSION OF HOW I CONDUCT BEDSIDE TEACHING
At the end of my bedside teaching, I usually ask students to share what they have learned. Students tend to recall cognitive learning, i.e. medical knowledge of diagnosis and treatment as well as clinical skills in neurological exam. Then under prompting, they begin to share their observations of behavioral/affective aspects and express their empathy towards the suffering of patients and their families. Some of them voice their appreciation for bedside manner and communication skills demonstrated by the medical team. At the end, I have consistently tried to raise their sensitivity and draw attention to the patient’s suffering. Lately, I like to share with students the joy of reading Dr. Charon’s succinct article, “To See the Suffering,” in which she writes, “To see the suffering might be what the humanities in medicine are for, and that those who become capable of seeing the suffering around them in medical practice both experience the cost of countenancing the full burden of illness and death and, simultaneously, comprehend with clarity the worth of this thing, this life.” (Charon, 2017)
VI. MY PERSONAL PLEA FOR THE INTEGRATION OF CLINICAL MEDICINE AND HUMANITIES IN MEDICAL EDUCATION PROGRAM
Attention to humanistic issues at the bedside demonstrates to students the relevance and application of humanities in individual cases and leads to a deeper appreciation of what they have learned about medical humanities during their pre-med years. Consequently, such bedside teaching can serve as “booster shots” to rekindle students’ interest in the humanistic aspects of patient care. However, it is difficult to expect lasting effects on the attitudes and behaviors of medical trainees unless such teaching can be frequently and widely practiced throughout clinical rotations.
Therefore, I would like to recommend that more attending physicians in teaching hospitals should be encouraged to teach humanism at the bedside. Medical schools should set a high priority for the clinical faculty to help students enhance their sensitivity “to see the suffering” and develop empathy towards patients. If possible, such efforts should be incorporated into faculty development programs for clinical teachers from all clinical departments in teaching hospitals.
Note on Contributor
Chi-Wan Lai, M.D. is the chair professor of medical education, attending physician in the Division of Neurology, Koo Foundation Sun Yat-Sen Cancer Center, Taipei, Taiwan.
Funding
The author declares no funding is involved for this paper.
Declaration of Interest
The author declares no conflicts of interest.
References
Cassell, E. J. (2004). The nature of suffering and the goals of medicine (2nd ed., p. 118). United Kingdom: Oxford University Press.
Charon, R. (2017). To see the suffering. Academic Medicine, 92(12), 1668-1670. https://doi.org/10.1097/ACM.0000000000001989
Neumann, M., Edelhäuser, F., Tauschel, D., Fischer, M. R., Wirtz, M., Woopen, C., … Scheffer C. (2011). Empathy decline and its reasons: A systematic review of studies with medical students and residents. Academic Medicine, 86(8), 996-1009. https://doi.org/10.1097/ACM.0b013e318221e615
Plant, J., Barone, M. A., Serwint, J. R., & Butani, L. (2015). Taking humanism back to the bedside. Pediatrics, 136(5), 828-830. https://doi.org/10.1542/peds.2015-3042
Swartz, M. H. (2014). Textbook of physical diagnosis: History and Examination (7th ed., p. 564). Philadelphia, PA: Elsevier.
*Lai Chi-Wan
125 Lih-Der Road,
Pei-Tou District, Taipei, Taiwan
Telephone: +886 2 2897-0011
Email address: chiwanlai@gmail.com
Published online: 5 May, TAPS 2020, 5(2), 57-58
https://doi.org/10.29060/TAPS.2020-5-2/LE2221
Muhammad Raihan Jumat
Office of Education, Duke-NUS Medical School
I read with great interest Samarasekera and Gwee’s article in TAPS (January, 2020) entitled: “Grit in healthcare education practice”. The authors cited Duckworth’s seminal studies on grit and its strong correlation with success. The authors suggested that grit be used to select for medical students and for healthcare systems to adopt organisational grit. I applaud the authors’ call for implementing organisational grit in healthcare. This is a step forward in working out the multiple issues plaguing healthcare. Interestingly, the call to implement organisational grit might not make it necessary to select for grit upon medical school admission.
Duckworth had posited that the mere assembly of gritty individuals might not necessarily create a gritty organisation (Duckworth, 2016). Students who test as gritty upon admission might be gritty in a different context than that of a medical school. Medical school has its own specific set of challenges which are not shared in many other pre-medical school experience. Hence, students who type as gritty on a medical school entry exam might not remain gritty in medical school.
Grit needs to be developed as a team within an organisation with a shared goal (Duckworth, 2016; Lee & Duckworth, 2018). This development starts with assembling a group of individuals with similar interests. These individuals are then encouraged to work together with chances to carry out deliberate practice and constant reminders of their shared purpose. This group should be even encouraged to fail and learn from those failures. This group will then develop grit as a unit (Duckworth, 2016).
Creating an environment which is demanding yet nurturing is key in promoting grit (Lee & Duckworth, 2018). Team-based or problem-based learning provides a conducive setting for such an environment to thrive in medical school. Students are grouped in teams and are faced with demanding challenges which would force them to work together over an extended period of time. These students are allowed to fail and learn from their mistakes. Over time, the team develops grit.
The formation of a culture which promotes and breeds grit within an organisation would be a stronger force to withstand the demanding challenges of healthcare than just a selection of gritty individuals. Structural changes in healthcare to allow for organisational grit to take root should be undertaken. Increased reports of physician burnout necessitate that healthcare workers be given support. Organisational grit would give healthcare workers the support they require.
Note on Contributor
Muhammad Raihan Jumat, PhD, is an Education Fellow in the Office of Educaiton at Duke-NUS Medical School. The author conceived the idea and wrote this letter.
Acknowledgements
The author would like to thank Professors Scott Compton and Sandy Cook for their advice and encouragement in writing this letter.
Funding
No funding was involved in this letter.
Declaration of Interest
The author does not have any competing interests.
References
Duckworth, A. (2016). Grit: The power of passion and perseverance (First Scribner hardcover ed.). New York, NY: Scribner.
Lee, T. H. & Duckworth, A. L. (2018). Organizational grit. Retrieved from Harvard Business Review, https://hbr.org/2018/09/organizationalgrit
*Muhammad Raihan Jumat
Office of Education,
Duke-NUS Medical School,
8 College Road,
Singapore 169857
Tel: +6 56516 4771
E-mail: raihan.jumat@duke-nus.edu.sg
Published online: 5 May, TAPS 2020, 5(2), 41-44
https://doi.org/10.29060/TAPS.2020-5-2/SC2134
Sok Mui May Lim1,2, Zi An Galvyn Goh2 & Bhing Leet Tan1
1Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore; 2Centre for Learning Environment and Assessment Development (CoLEAD), Singapore Institute of Technology, Singapore
Abstract
The use of standardised patients has become integral in the contemporary healthcare and medical education sector, with ongoing discussion on exploring ways to improve existing standardised patient programs. One potentially untapped group in society that may contribute to such programs are persons with disabilities. Persons with disabilities have journeyed through the healthcare system, from injury to post-rehabilitation, and can provide inputs based on their experiences beyond their conditions. This paper draws on our experiences gained from a two-phase experiential learning research project that involved occupational therapy students learning from persons with disabilities. This paper aims to provide eight highly feasible, systematic tips to involve persons with disabilities as standardised patients for assessments and practical lessons. We highlight the importance of considering persons with disabilities when they are in their role of standardised patients as paid co-workers rather than volunteers or patients. This partnership between persons with disabilities and educators should be viewed as a reciprocally beneficial one whereby the university and the disability community learn from one another.
Keywords: Standardised Patients, Objective Structured Clinical Examination (OSCE), Persons with Disabilities, Inclusion, Role-play, Script, Practical Lessons
I. INTRODUCTION
The use of standardised patients (SPs) has become integral to the contemporary healthcare and medical education sector. While an SP is commonly defined as a person trained to portray a scenario, an SP can also be an actual patient using his or her own history and physical exam findings (Kowitlawakul, Chow, Salam, & Ignacio, 2015). Presently, persons with disability (PWDs) have participated in SP programs, albeit less frequently and on a smaller scale (Long-Bellil et al., 2011; Minihan et al., 2004; Wells, Byron, McMullen, & Birchall, 2002). SPs with disabilities have also been used in Singapore hospitals, but mainly as patients to be examined for their own medical conditions. PWDs have a lot to offer in clinical education beyond sharing about their conditions.
A. Why Incorporate Persons with Disabilities into SP Programs?
There are many benefits in involving PWDs in SP programs. PWDs may be able to impart knowledge that ‘goes beyond the textbook’, due to their experiences of receiving services from various healthcare professionals – from the time the disability occurred to the post-rehabilitation phase of living independently in society. The input given based on their individual experiences would, therefore, be authentic (Wells et al., 2002). Students can get practice working with real PWDs in a safe setting where they can make mistakes and receive feedback before going for their clinical placements and meeting with real patients (Minihan et al., 2004). This can nurture a new generation of healthcare professionals who may be more proficient in treating PWDs, thereby raising the service delivery standard for the entire sector.
B. Perspectives Gained From Previous Experiential Learning Project
This paper is based on our experiences gained from a previous experiential learning research project. PWDs participated in a two-phase experiential learning research project that spanned two years (Lim, Tan, Lim, & Goh, 2018). In phase one, the PWDs acted as community teachers to occupational therapy student groups, interacting with them in the community while performing their daily activities. This paper draws from our experiences in Phase Two of the study, in which a group of PWDs were trained to and worked as SPs in practical classes and Objective Structured Clinical Examinations (OSCEs). Upon the conclusion of the research project, PWDs continue to be part of the degree programme contributing as community teachers and SPs. The paper aims to provide practical helpful tips in bringing PWDs onboard as SPs.
II. DISCUSSION
A. Tip 1 – Interviewing and Selecting PWDs Who Are Suitable for Acting
PWDs were selected based on six criteria determined by faculty members in the health profession who have prior experience working with SPs. First, the PWD has an interest in healthcare education and wants to work with students for the purpose of educating them as future healthcare professionals. Second, the PWD should have come to terms and accepted their disability. It is very difficult for them to talk about their disability or role-play as a patient when they are still struggling emotionally with their own conditions. Third, the PWD does not have cognitive impairment and is able to understand and remember the script for role-playing. Fourth, he/she must be able to communicate clearly and coherently. Fifth, the PWD should be willing to learn the basics of acting or role-playing. Sixth, he/she must understand the objectives of the training or assessment, such as being impartial to all students and being honest in giving feedback when required.
B. Tip 2 – Training Should Be Conducted in Gradual Phases
Training PWDs as SPs can be carried out in a gradual phase as outlined in details in Figure 1. In the first phase, novice PWD SPs are taught the basics of role-play by faculty and experienced SPs. In the second phase, the entire group goes through a common script. Novice PWD SPs observe the faculty and experienced SPs enact the script. Then, the novice PWD SPs practice amongst themselves and receive feedback.
After the training, faculty should speak to the PWDs individually to determine if they are comfortable with role-playing and address any queries that they may have. It is only after they attempt the role of an SP that they can personally assess their comfort level and confidence. This can ensure that the PWDs who participate are comfortable with their roles and feel engaged and respected by the institution.
In the third phase, PWD SPs can progress to non-graded practical lessons with students, which are less stressful for both students and PWD SPs. In subsequent phases, the faculty can then decide to select PWD SPs whom they deem are ready for summative assessments such as the OSCE.
C. Tip 3 – Start Novice PWD SPs with Simple and Suitable Scripts
Initial scripts should be simple and should not require complex acting skills. It takes time to gain confidence in memorising required lines, maintaining their roles as well as acting in scenarios which require more expression of emotions. Scripts that involve more sophisticated acting skills (e.g., maintenance of strong emotions) should be reserved for SPs who are experienced and confident with acting. The PWD SPs should be matched to suitable scripts that do not conflict with their disability. For example, a PWD SP who uses a wheelchair cannot be paired with a script that involves walking. The combination of progressing gradually and usage of suitable scripts allows for PWD SPs to refine their skills and ensure that their acting skills do not compromise the students’ learning experience.
D. Tip 4 – Prepare Students Not to Be Surprised By Real Disability
Prior to the interaction session, students should be pre-empted by the faculty that they would be working with PWDs who may have a range of disabilities. This is to prevent unnecessary surprise. In addition, students should be reminded that the disability may or may not be the focus of the scenario, depending on the instruction given to the student. For example, in an OSCE scenario, students may be tasked to explain a medical error or demonstrate a procedural skill instead of addressing the disability of the SP. This pre-empting can be complemented with teaching communication skills geared towards interacting with PWDs.
E. Tip 5 – Checking Accessibility – Within and Outside of the Venue
Ensuring accessibility prior to the session is important. This includes the route from the nearest public transport node (e.g., train station) to the venue. Things to take note of are the availability of ramps and lifts for wheelchair users and the presence of accessible parking lots. In addition, the venue where the lesson or assessment is going to take place needs to be inspected to ensure that the entrances and exits are wide enough for wheelchairs access.
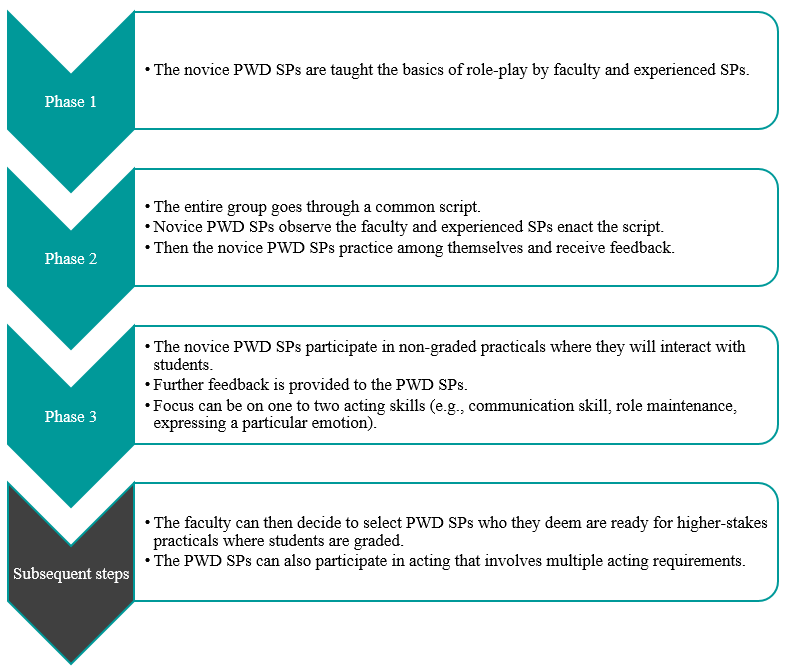
Figure 1. Diagram to outline general recommended steps for training PWD SPs
F. Tip 6 – Pay PWDs at Market Rates and Accord Them Identical Contractual Rights
PWD SPs should be remunerated at market rates that are equal to SPs without disability. They also sign the same SP contract and fulfil the same legal obligations. In performing the role of the SP, they are treated as co-workers of the university, not volunteers or patients. This reflects the principles of equality and diversity, as well as the seriousness of their roles as active members of the healthcare and medical education system. If there are certain risks involved in their interaction with students, such risks should be made clear to the PWD SPs, so they can make an informed decision on accepting the job.
G. Tip 7 – Provide Opportunity for PWDs to Give Feedback
PWDs can be a valuable resource in providing feedback to faculty, scenario developers and other SPs. Similarly, they may be able to give insightful feedback to students. It is important to train the PWD SPs on the methods of providing feedback to students. Given their lived experience, they can provide insight into how real patients would respond and react while suggesting ways for trainee healthcare professionals to respond in a more patient-centred manner.
H. Tip 8 – Reflect and Improve
Carrying out an evaluation with the respective stakeholders, whether they are PWD SPs, faculty, or students, is key to the success of an inclusive SP program. This can also ensure quality assurance of the program. The following are several broad questions which can be considered in the evaluation. Firstly, whether the stakeholder faced any challenges during the session. Secondly, whether the scenarios or scripts worked well for PWD SPs to interact with students. Thirdly, whether there are any other ways that the learning experience can be improved. This can provide rich data for the SP program developers to reflect and improve upon the pedagogy. We have received positive feedback from both students and PWDs in this project.
III. CONCLUSION
It is important to empower PWDs and create a dynamic relationship between them and healthcare professionals/
educators. For an inclusive SP program to be effective, educators must change their own mindset about PWDs. We have to switch the lens from viewing them as patients to co-workers. This partnership should be viewed as a reciprocally beneficial one whereby the university and the disability community learn from one another. Through the process of engagement, both educators and students learn from PWD SPs about knowledge that goes beyond the textbook, and the factors that enhance or diminish the quality of healthcare/medical service delivery from individuals who have experienced going through the healthcare/medical system. With time and with more training institutions engaging PWDs as SPs, this can be a potentially viable employment option for PWDs.
Notes on Contributors
Associate Professor May Lim is the Director of the Centre for Learning Environment and Assessment Development (CoLEAD) at the Singapore Institute of Technology, and a faculty in the Health and Social Sciences Cluster teaching occupational therapy.
At the time when this work was done, Mr Goh Zi An Galvyn was a research assistant in the Centre for Learning Environment and Assessment Development (CoLEAD) at the Singapore Institute of Technology.
Associate Professor Tan Bhing Leet is the Deputy Cluster Director (Applied Learning) of the Health and Social Sciences Cluster, and Programme Director of the Bachelor of Science in Occupational Therapy degree programme at the Singapore Institute of Technology.
Ethical Approval
Ethics approval was granted by the Singapore Institute of Technology Institutional Review Board for this project (IRB number: 20150002).
Acknowledgements
The authors thank all faculty, students, PWD and non-PWD standardised patients who were involved in the Singapore Institute of Technology Bachelor of Science in Occupational Therapy degree programme. In addition, we would like to extend our deepest gratitude to Associate Professor Tham Kum Ying, Education Director of Tan Tock Seng Hospital Pre-Professional Education Office and senior lecturers Miss Heidi Tan and Mr Lim Hua Beng from the Singapore Institute of Technology.
Funding
Funding was provided from the Singapore Ministry of Education (MOE Tertiary Education Research Fund grant: R-MOE-A203-A002).
Declaration of Interest
The authors declare no conflict of interest concerning any aspect of this research.
References
Kowitlawakul, Y., Chow, Y., Salam, Z., & Ignacio, J. (2015). Exploring the use of standardized patients for simulation-based learning in preparing advanced practice nurses. Nurse Education Today, 35(7), 894-899. https://doi.org/10.1016/j.nedt.2015.03.004
Lim, S. M., Tan, B. L., Lim, H. B., & Goh, Z. A. G. (2018). Engaging persons with disabilities as community teachers for experiential learning in occupational therapy education. Hong Kong Journal of Occupational Therapy, 31(1), 36-45. https://doi.org/10.1177/1569186118783877
Long-Bellil, L. M., Robey, K. L., Graham, C. L., Minihan, P. M., Smeltzer, S. C., Kahn, P., & Alliance for Disability in Health Care Education. (2011). Teaching medical students about disability: The use of standardized patients. Academic Medicine, 86(9), 1163-1170. https://doi.org/10.1097/ACM.0b013e318226b5dc
Minihan, P. M., Bradshaw, Y. S., Long, L. M., Altman, W., Perduta-Fulginiti, S., Ector, J., … Sneirson, R. (2004). Teaching about disability: Involving patients with disabilities as medical educators. Disability Studies Quarterly, 24(4). https://doi.org/10.18061/dsq.v24i4.883
Wells, T. P. E., Byron, M. A., McMullen, S. H. P., & Birchall, M. A. (2002). Disability teaching for medical students: Disabled people contribute to curriculum development. Medical Education, 36(8), 788-790. https://onlinelibrary.wiley.com/doi/abs/10.1046/j.1365-2923.2002.01264_1.x
*Lim Sok Mui
Singapore Institute of Technology,
SIT@Dover, 10 Dover Drive,
Singapore 138683
Email: may.lim@singaporetech.edu.sg
Published online: 5 May, TAPS 2020, 5(2), 32-40
https://doi.org/10.29060/TAPS.2020-5-2/OA2194
Suriyakumar Mahendra Arnold1, Sepali Wickrematilake2, Dinusha Fernando3, Roshan Sampath1, Palitha Karunapema4 & Pasyodun Koralage Buddhika Mahesh5
1Quarantine Unit, Ministry of Health Sri Lanka; 2Regional Director of Health Services Office, Matale, Sri Lanka; 3Regional Director of Health Services Office, Puttalam, Sri Lanka; 4Health Promotion Bureau, Ministry of Health, Sri Lanka; 5Ministry of Health, Sri Lanka
Abstract
Background: The duties of Public Health Inspectors (PHI) includes those related to food legislation. Effective methods are being explored in providing refresher training for them amidst the constraints of resources.
Objective: To assess the knowledge, attitudes and skills of the PHI on food legislation and to evaluate the effectiveness of a Distance Education (DE) programme in improving these.
Methodology: The study included quasi-experimental educational intervention with a pre- and post- assessments. 105and 109 PHI were recruited for the intervention and control groups. Pre and post interventional assessments on the knowledge, attitudes, self-assessed competencies and performance were done with a self-administered questionnaire and observational checklist. Intervention group was exposed to an educational intervention through a distance education programme. Post-assessments were done following four months of the intervention.
Results: The pre interventional knowledge and performance was poor. PHI had unfavorable views. Post intervention mean knowledge and performance scores revealed that a statistically significant improvement (P<0.001) has occurred in the intervention group. Change in the opinions on usefulness of in-service training on food safety to develop knowledge and skills, was statistically significant (P<0.01) in the intervention group.
Conclusion: The DE method used in the present study was feasible to implement and was effective in significantly improving the knowledge and performance of the PHI.
Keywords: Distance Education, Continuing Education, Public Health Inspector, Food Legislation
Practice Highlights
- Continues Education is important for development of knowledge and skills of healthcare staff.
- Distance Education can be successfully used for Continues Education for staff geographically scattered.
I. INTRODUCTION
Learning is an active, continuous, sequential process. Learning takes place more rapidly when the learner has the opportunity to practice and experience what is being learned in a variety of situations. It is facilitated when it takes place in or near the real situation in which the learner expects to work (Schunk, 2012). There is an increasing recognition of the need for health workers to continue their education throughout their career (Price & Reichert, 2017). The changes that take place in health needs and health care policies necessitate continued learning.
Continuing education (CE) should be an integral part of an employment. Adequate provision should therefore be made for it in terms of manpower, study level and financial reimbursement. Whenever possible, CE must be provided at the place of work and must be relevant to the immediate needs of the health care workers and the community he/she serves (Billett et al, 2015; Cedefop, 2015; Kenny, Ralph & Brown, 2006; Sherman & Chappell, 2018).
Professional and technical education with traditional methods of training are often inflexible, time- and place- constrained and too expensive to meet the demand for training (Asian Development Bank, 2014; Scott, 2010). Efforts like technological advancements and distance education techniques have created an immense impact in molding the education methods (Chay, 2019). Distance education (DE) seems to offer a way of providing flexible, effective job-related training.
To be successful, DE programme must be systematically designed, interactively motivational and suited to the needs of the audience (Balaban-Sali, 2008). Distance education has the potential of delivering more educational opportunities to more people than ever before, at lower average cost and most importantly, at a higher quality than most people can get in other ways (Marcinkiewicz, Cybart & Chrominska-Szosland, 2002).
The problem of updating the knowledge and skills of health personnel already on the job still remains as a challenge (Murray & Christison, 2018). It is almost impossible to have them re-trained at the institutions they occupy with face-to-face contact with the physical presence of trainers. Hence it is important to develop novel programmes in updating and refreshing of the health personnel amidst the feasibility constraints.
Food borne diseases account for a major toll on health. According to the World Health Organization (WHO), up to one-third of the populations of developed countries are affected by foodborne illnesses and the problem is likely to be far widespread in developing countries (World Health Organisation, 2002). The administration and implementation of food laws requires a qualified, trained, and efficient food inspection service (Food and Agriculture Organization of UN & WHO, 2003; Sri Lanka Accreditation Board for Conformity Assessment, 2013). Hence, proper training of food inspectors (PHI) is a prerequisite for an efficient food control system.
The need of providing training to PHI to improve their performance has been identified in the National Health Development Plan (NHDP) of Sri Lanka (Ministry of Health Sri Lanka, 2016). Public Health Inspector is one of the main authorised officers to implement public health laws in Sri Lanka. Of their many duties, PHI play a major role in maintaining food safety in the community. In addition, the food legislation is one area where major responsibility in implementation lies with the health sector. Therefore, educational interventions to improve the implementation could be carried out successfully as a part and parcel of the NHDP of Sri Lanka.
This study was done to assess the knowledge, attitudes and skills of the PHI on food legislation and to evaluate the effectiveness of a DE programme in improving these.
II. METHODS
A. Study Design
The study consisted of 3 components; Pre-interventional assessment, a quasi-experimentation and a post-interventional assessment. In the pre- and post-tests assessment of knowledge, attitudes, self-assessment of competencies (SAC) and observation of performance of PHI on implementation of legislation on food safety was carried out.
B. Study Setting
The study was conducted in Gampaha and Kurunegala districts. Range PHI (PHI serving in an allocated PHI range in a MOH area) serving in these districts were selected as the study population. PHI performing duties of specialized campaigns were excluded as they do not carry out activities on food safety. In allocating PHI to the intervention and control groups, all PHI in a single district were allocated to either the intervention or the control group. Random allocation within a district was not possible in this educational intervention as cross-contamination would have occurred if PHI serving in the same area or adjacent areas were included in both the intervention and control groups. Assessment of knowledge, self-assessment of competencies and attitudes were carried out in all the PHI in both groups. However, the performance was assessed in a sub-sample of 25% of PHI in each group due to feasibility-related practical constraints.
C. Study Instruments
Self-administered questionnaires were used for the assessment of knowledge, attitudes and SAC. Performances were assessed by direct observation in the filed and the office settings using check lists. The questionnaires and checklist were developed using Delphi Technique with the participation of Public Health Specialists, Medical Officers of Health, Food & Drugs Inspectors and Public Health Tutors. Knowledge questionnaire had 15 short answer question with a maximum score of 50 marks. Attitude questionnaire had 15 5-point Likert Scale statements and SAC questionnaire had 15 statements with a 4-point rating scale ranging from very competent to cannot perform. Three checklists were for assessment of food handling establishments, food sampling and record keeping in the PHI office. Checklists were administered by the principal investigator. Following the pre-interventional assessment the intervention group was exposed to a distance education programme using distance education modules. The control group was not exposed to this educational programme.
D. Training Needs Assessment
A Training Needs Assessment followed by selection of study topics, development of the curriculum and development of course materials were carried out in preparation of the three distance education modules. Through the training needs-assessment the specific training needs in the poorly performed areas of the pre-test were identified. Topics that were to be incorporated in the distance education modules were selected using the Nominal Group Technique. The topics selected for the three modules were; “1.Legislation on food safety”, “2.Food sampling, Inspection and rating of food establishments and maintenance of records in food safety” and “3.Legal procedures in food safety”.
E. Distance Education Programme
The DE programme was conducted using the printed media. Three DE modules were distributed at monthly interval for three months. Each module contained a tutorial and the participants were requested to answer after studying the entire module. The questions were based on subject matter covered by all the lessons in the module.
Post intervention assessment was conducted after a lapse of four months of administering the final module. The tools used for this assessment i.e. questionnaires and checklists, were identical to those used in the pre intervention assessment.
III. RESULTS
There were 105 PHI in the intervention group and 109 in the control group.
|
Component |
Intervention Group | Control Group | ||||
| Pre | Post |
Signifi cance |
Pre | Post |
Significance |
|
| Mean | Mean | Mean | Mean | |||
|
Enactments on food safety
|
29.4 | 61.3 | P < 0.001 |
30.6
|
32.1 | NS |
|
Food labelling
|
52.4 | 68.1 | P < 0.001 | 54.2 | 56.4 | NS |
|
Food sampling
|
24.0 | 63.4 | P < 0.001 | 24.9 | 26.8 | NS |
|
Meat and fish inspection
|
54.4 | 67.6 | P < 0.001 | 53.6 | 55.6 | NS |
| Legal procedures | 40.3 | 67.8 | P < 0.001 | 41.4 | 43.5 | NS |
Table 1. Comparison of PHI in the intervention and control groups by mean scores of theknowledge assessment before and after the intervention
| Intervention Group | Control Group | ||
| Component | Difference between post and pre mean scores | Difference between post and pre mean scores | Significance |
| Enactments on food safety | +31.9 | +1.5 | P< 0.001 |
| Food labelling | +15.7 | +2.2 | P< 0.001 |
| Food sampling | +39.4 | +1.9 | P< 0.001 |
| Meat and fish inspection | +13.2 | +2.0 | P< 0.001 |
| Legal procedures | +27.5 | +2.1 | P< 0.001 |
Table 2. Comparison of the changes in the mean scores of the knowledge assessment between the intervention and control groups
A. Knowledge
In comparison of the pre and post intervention knowledge scores, PHI in the intervention group has shown statistically significant (P<0.001) improvements in all components. Control group failed to achieve a significant improvement (Table 1).
In the intervention group highest change was seen in the knowledge on ‘food sampling’ (+39.4 marks) and was closely followed by ‘enactments in food safety’ (+31.9 marks). The difference of scores between the two groups achieved a statistical significance at P < 0.001 (Table 2).
B. Attitudes
Except for the change in the attitudes on usefulness of in-service training to develop knowledge and skills where there was a 25.4% increase in the number of PHI of the intervention group who agreed with this statement and showed a statistically significant difference (P<0.01), there was no other significant changes of the attitudes of PHI in both groups (refer Appendix A, Supplementary Table 1).
C. Self assessed competencies
At both pre and post tests a high proportion of the PHI in both groups rated themselves either ‘very competent’ or ‘competent’ in performing activities. Only a minority indicated that they cannot perform the listed activities. The only deviation of this pattern was seen in the intervention group in two activities, “correctly identifying the legislation in which different violations of food safety be prosecuted” and “performing court procedures in court cases in food safety” where an increase of 16.6% and 25.4% respectively was seen from the pre intervention value, which were statistically significant (refer Appendix B, Supplementary Table 2).
D. Performance
In comparison of the mean performance scores obtained in the pre and post intervention assessments the intervention group showed a significant increase (P < 0.001) at the post-intervention assessment in all 3 activities: inspection and categorization of food establishments, food sampling and documentation and maintenance of records. In the control group there was a marginal increase in the mean scores at the post intervention assessment and was not statistically significant (Table 3).
| Intervention Group | Control Group | |||||
| Component |
Pre n=30 |
Post n=30 |
Signifi cance |
Pre n=30 |
Post n=30 |
Significance |
| Mean | Mean | Mean | Mean | |||
| Inspection and categorization of food establishments | 40.1 | 69.3 | P < 0.001 | 42.2 | 44.1 | NS |
| Food sampling | 50.7 | 70.9 | P < 0.001 | 53.5 | 55.1 | NS |
| Planning, documentation and maintenance of records | 29.8 | 47.3 | P < 0.001 | 31.2 | 32.9 | NS |
Table 3. Comparison of mean performance scores before and after intervention
The difference of the pre and post mean performance scores of the intervention and control group showed that the changes in the mean performance scores were marginal in the control group in comparison to the changes of the intervention group (Table 4). The difference of scores between the two groups achieved a statistical significance (P< 0.001).
| Intervention Group | Control Group | ||
| Component | Difference between post and pre means | Difference between post and pre means | Significance |
| Inspection and categorization of food establishments | +29.2 | +1.9 | P< 0.001 |
| Food sampling | +20.2 | +1.6 | P< 0.001 |
| Planning, documentation and maintenance of records | +17.5 | +1.7 | P< 0.001 |
Table 4. Comparison of the changes in mean performance scores between the intervention and control groups
IV. DISCUSSION
This is the first documented local study testing a DE method for improving the knowledge, attitude and skills of PHI on food legislation. CE is a process, including the experiences after initial training that helps the personnel to attain competencies relevant to their work (Gaspard & Yang, 2016). Of the methods available, distance education method has been used successfully in many countries to provide CE for health care workers. With the advances in the healthcare system, it is essential that Sri Lanka evaluate the effectiveness of different strategies in updating the primary healthcare workers. Hence this study is an eye-opener for the policy-planners in relation to the in-service training of the health staff.
Pre-intervention assessment results showed that the overall knowledge was poor in both groups. Similarly there was no significant difference in attitudes, self-assessed competencies and performance between the two groups, thus the intervention and control groups were comparable before the intervention. Therefore, these results also discount the selection bias in the present study.
The findings of the pre-intervention assessment pointed to the need of CE as the total knowledge scores obtained was unsatisfactory. Only 17.1% of the study group and 23.9% of the control group have undergone any training on food safety during the past three years. Thus a majority of the PHI have had no opportunity for CE to improve and update their knowledge. The findings also revealed that the knowledge and performance in enactments in food safety, food sampling and legal procedures were poor. These findings were taken into consideration in selecting study topics for the distance education modules. Gap analysis is important in planning CE (Moore, Green, & Gallis, 2009) and identifying of needs has an impact on performance outcome in CE (Cervero & Gaines, 2015).
In training a large number of health care workers at different geographical locations, it is important to maintain uniformity of such training. In addition, the quality of educational materials provided will have an effect on the outcome of the intervention. The present study considered these factors and the services of experts were obtained in developing DE modules which were technically sound and of high quality. Uniformity was maintained by administering the modules in a similar manner at all centres where the training programme was conducted.
Since a time lag between the intervention and the post intervention assessment is needed to ascertain the sustainability of the effectiveness of the intervention, the post-intervention assessment was carried out four months after administering the final module.
In general there was no change in the attitudes towards implementation of food legislation in both intervention and control groups except for the views expressed on usefulness of in-service training. One of the reasons for no change in views in both groups may be due to the fact that there was no significant change in their working environment, resources and support services. However, these factors were outside the control of the present intervention.
CE activities can lead to improved competencies and performance (Moore et al., 2009). This study revealed that DE strategy used here was effective in improving the knowledge and performance significantly in the intervention group.
The intervention used in the present study was carried out with minimal interference to the routine duties of the trainees. Unlike institutional-based training programmes or workshops, trainees did not have to be away from the work place resulting in incurring a minimal cost. In the present educational intervention, printing cost incurred for the three distance education modules was minimal. Thus as a developing country with health care workers scattered throughout the island, due consideration should be given to shift from traditional institutional-based training at the central level to providing continuing education at the local setting using feasible, cost-effective methods such as DE where appropriate.
The study was limited to two districts in two provinces. This study was conducted in two districts as a quasi-experimental study. Since then the probability of a selection bias cannot be totally excluded. Overall picture could have been obtained if this study was conducted as an island-wide study. These were taken into account in the interpretation of findings. Sustainability of the improved performance as a result of the DE programme would have been better monitored if post interventional assessments were carried out at one-year and two-year period.
V. CONCLUSION
The present intervention was effective in improving the knowledge and performance of the PHI in implementing legislation on food safety indicating the effectiveness of providing continues education to PHI using distance education method. As this method proved to be feasible, of low cost and has the ability to provide training without mobilizing the staff, it can be incorporated into the existing training system for health care workers.
Notes on Contributors
Mahendra Arnold, Sepali Wickramatilake, Dinusha Fernando, Roshan Sampath and Palitha Karunapema are Public Health Specialists attached to the Ministry of Health. Pasyodun Koralage Buddhika Mahesh is a Senior Registrar in Community Medicine of the Ministry of Health.
Ethical Approval
Ethical approval was obtained from Ethics Committee, Faculty of Medicine, University of Colombo.
Acknowledgements
The authors would like to acknowledge the Public Health Inspectors who participated in this study.
Funding
This study did not receive any external funding.
Declaration of Interest
The authors do not have any conflict of interest to declare.
References
Asian Development Bank (2014). Innovative Strategies in Technical and Vocational Education and Training for Accelerated Human Resource Development in South Asia. Mandaluyong City, Philippines: Asian Development Bank.
Billett, S., Choy, S., Dymock, D., Smith, R., Henderson, A., Tyler, M., & Kelly, A.(2015). Towards more effective continuing education and training for Australian workers, NCVER, Adelaide.
Balaban-Sali, J. (2008). Designing motivational learning systems in distance education. Turkish Online Journal of Distance Education-TOJDE, 9(3), 149-159.
Cervero, R. M., & Gaines, J. K. (2015). The impact of CME on physician performance and patient health outcomes: An updated synthesis of systematic reviews. Journal of Continuing Education in the Health Professions, 35(2), 131–138.
Chay, O. M. (2019). Transformation of medical education over the years – A personal view. The Asia Pacific Scolar, 4(1), 59-61
Food and Agriculture Organization of the United Nations [UN], & World Health Organization [WHO] (2003). Assuring Food Safety and Quality: Guidelines for Strengthening National Food Control Systems,_FAO Food and Nutrition Paper 76. A Joint FAO/WHO publication. http://www.fao.org/3/a-y8705e.pdf
Gaspard, J., & Yang, C. (2016). Training needs assessment of health care professionals in a developing country: The example of Saint Lucia. BMC Medical Education, 16, 1-6. https://bmcmededuc.biomedcentral.com/articles/10.1186/s12909-016-0638-9
Kenny, M., Ralph, S., & Brown, M. (2006) Lifelong learning, professional development and community work. Research in Post-Compulsory Education, 5(1), 51-62.
Marcinkiewicz, A., Cybart, A., & Chrominska-Szosland, D. (2002). Distance learning in postgraduate training of professionals: Example of occupational medicine specialization. Wiad Lek, 55(1), 330-334.
Ministry of Health Sri Lanka. (2016). National health strategic master plan 2016 -2025. Colombo, Sri Lanka: Ministry of Health
Moore, D. E., Green, J. S., & Gallis, H. A. (2009). Achieving Desired Results and Improved Outcomes: Integrating Planning and Assessment Throughout Learning Activities. Journal of Continuing Education in The Health Professions, 29(1), 1–15.
Murray, D. E., & Christison, M. (2018). Online Language Teacher Education: A Review of the Literature. Aqueduto, Norwich.
Price, S., & Reichert, C. (2017). The importance of continuing professional development to career satisfaction and patient care: Meeting the needs of novice to mid- to late-career nurses throughout their career span, Administrative Sciences, 7(2), 17. https://www.mdpi.com/2076-3387/7/2/17.
Schunk, D. H. (2012). Learning Theories, An Educational Perspective (6th Ed.). Boston, MA: Pearson Education, Inc.
Scott, S. G. (2010) Factors Impacting the Selection of Training-Delivery Systems and Training Methodology of Virginia Training Professionals (doctoral dissertation). Blacksburg, VA: Faculty of the Virginia Polytechnic Institute and State University.
Sherman, L. T., & Chappell, K. B. (2018). Global perspective on continuing professional development. The Asia Pacific Scolar, 3(2), 1-5.
Sri Lanka Accreditation Board for Conformity Assessment. (2013). Specific Criteria for Food Inspection, (Doc No. IB-GL(P)-03). Retrieved from http://www.slab.lk/Support/Publications/Inspection%20Bodies/IB-Specific-Criteria-for-Food-Inspection.pdf
World Health Organization. (2002). WHO Global Strategy for Food Safety: Safer food for better health. Retrieved from https://apps.who.int/iris/handle/10665/42559
*Mahendra Arnold
52/18, Pulinathalarama Road,
Magammana, Ragama, Sri Lanka
Tel: +94714199953
Email: mahendra_arnold@yahoo.com
Published online: 5 May, TAPS 2020, 5(2), 22-31
https://doi.org/10.29060/TAPS.2020-5-2/OA2173
Andrea Thompson1, Tanisha Jowsey1, Helen Butler1, Augusta Connor2, Emma Griffiths2, Hadley Brown2 & Marcus Henning1
1University of Auckland, New Zealand; 2Mercy Hospice, Auckland, New Zealand
Abstract
Objective: The aim of this study was to identify the impact of a series of palliative care educational packages on pharmacists’ practice for improved service delivery. We asked, what are the educator and learner experiences of a short course comprised of workshops and a series of palliative care learning packages, and how have learners changed their practice as a result of the course?
Method: Semi-structured interviews were conducted and transcribed verbatim. Interpretive thematic analysis was undertaken.
Results: Eight people participated in this study; five pharmacists who had completed learning packages in palliative care and three educators who facilitated teaching sessions for the learning packages. The teaching and assessment approaches were applied and transferable to the clinical setting. The teaching strategies stimulated engagement, enabling participants to share their ideas and personal experiences. Participants’ understanding of palliative care was improved and they developed confidence to engage in deeper conversations with patients and/or their families and carers. Although the completion of assessment for the learning packages enabled credit for continuing professional development, their impact on the long-term practice of pharmacists was not established.
Conclusions: The findings of this study suggest that interactive teaching methods assisted the interviewed pharmacists to further develop their understanding of palliative care, and communication skills for palliative care patients and/or their families/carers. Pharmacists were better equipped and felt more comfortable about having these potentially difficult conversations. We recommend educators to place more emphasis on reflective activities within learning packages to encourage learners to develop more meaning from their experiences.
Keywords: Palliative Care Education, Pharmacist, Hospice, Interactive Learning, Communication, Learning Packages
Practice Highlights
- The course studied informs pharmacists’ practice for improved service delivery.
- The course led to more meaningful palliative care conversations.
- Interactive teaching methods supports learner engagement.
- Educators sharing personal experiences supports learning.
I. INTRODUCTION
There have been recommendations in the literature for over 30 years that pharmacists should receive more education around end-of-life issues and care (Dickinson, 2013). While inadequate training and knowledge in palliative care leads to poor palliative care provision (Furstenberg et al., 1998; Vernon, Brien, & Dooley, & Spruyt, 1999), effective palliative education can positively transform care provision (Institute of Medicine, 2015).
Research shows that effective palliative care education for pharmacists can deepen their understanding of their role in symptom and therapy management and psychosocial care during end-of-life stages, including reducing death anxiety among patients (Atayee, Best, & Daniels, 2008; Dickinson, 2013; Needham, Wong & Campion, 2002). Learning about palliative care encourages collaboration and continuity in service provision, and appropriate, timely and individualised care (Dickinson, 2013). Additionally, with extra training, community pharmacists can become more actively involved in their palliative patients’ care, including providing patient education, prescribing advice to physicians and facilitating continuity between healthcare settings (O’Connor, Pugh, Jiwa, Hughes, & Fisher, 2011). Australian community pharmacists report that completing a flexible online palliative care education programme positively impacts their practice (Hussainy, Marriott, Beattie, Nation, & Dooley, 2010). Hussainy et al. (2010) recommend future educational courses to include face-to-face weekly workshops in order to increase participation. In New Zealand, undergraduate pharmacy students receive palliative care training and upon graduation they manage various palliative care needs. To booster pharmacist palliative care knowledge and communication skills, and in response to the call from Hussainy et al. (2010), in 2016, educators at a metropolitan hospice in New Zealand ran a short course for pharmacists. The authors, including the educator participants in this study, were not involved in the course design. Here we explore participant experiences of the course including application of new knowledge/skills to practice.
The seminal pedagogical approaches of Schön (1983), Kolb (1984) and Knowles (1984) are relevant. Learning occurs when professionals reflect on their tacit knowledge and make sense of their experiences; therefore reflective practice is a central pedagogical approach (Schön, 1983). With this in mind, opportunities for reflective practice ought to be integrated into the design of educational initiatives. Kolb’s (1984) experiential learning model suggests learners have a concrete experience and then reflect on it, enabling them to formulate abstract concepts and generalisations. Learners can then try out their new understanding through the process of active experimentation. The need to be self-directed, the role of the learner’s experiences, motivation, and readiness to learn are examples of assumptions embedded in Knowles’ adult learning theory (Knowles, Holton, & Swanson, 2015).
In this paper, we explore the course in terms of teaching delivery and learning. We undertook a small interpretive thematic study to explore the participants’ experiences of the course. It is important for educators to be involved in researching and reflecting on their own teaching (Henning, Hu, Webster, Brown & Murphy, 2015; Steinert, Cruess, Cruess, & Snell, 2005) and we therefore included the teaching staff as participants alongside learner participants in this study.
A. Research Questions
We asked, what are the educator and learner experiences of a short course comprised of workshops and a series of palliative care learning packages, and how have learners changed their practice as a result of the course?
II. METHODS
A. Participants and Description of Educational Intervention
Learner participants were pharmacists who were enrolled in the course. The course learning packages were part of Hospice New Zealand’s Fundamentals of Palliative Care education programme (Appendix A). Figure 1 outlines the mode of delivery and educational frameworks for the learning packages. A two-hour workshop was offered for each learning package and the participants were given access to online resources such as a workbook, pre-reading and reflection activities. Learners were required to complete the pre-reading and reflection activities prior to each workshop. Learners engaged in classroom-based teaching activities, which largely included group discussions. The total number of learning packages that each learner participant completed is shown in Appendix A.
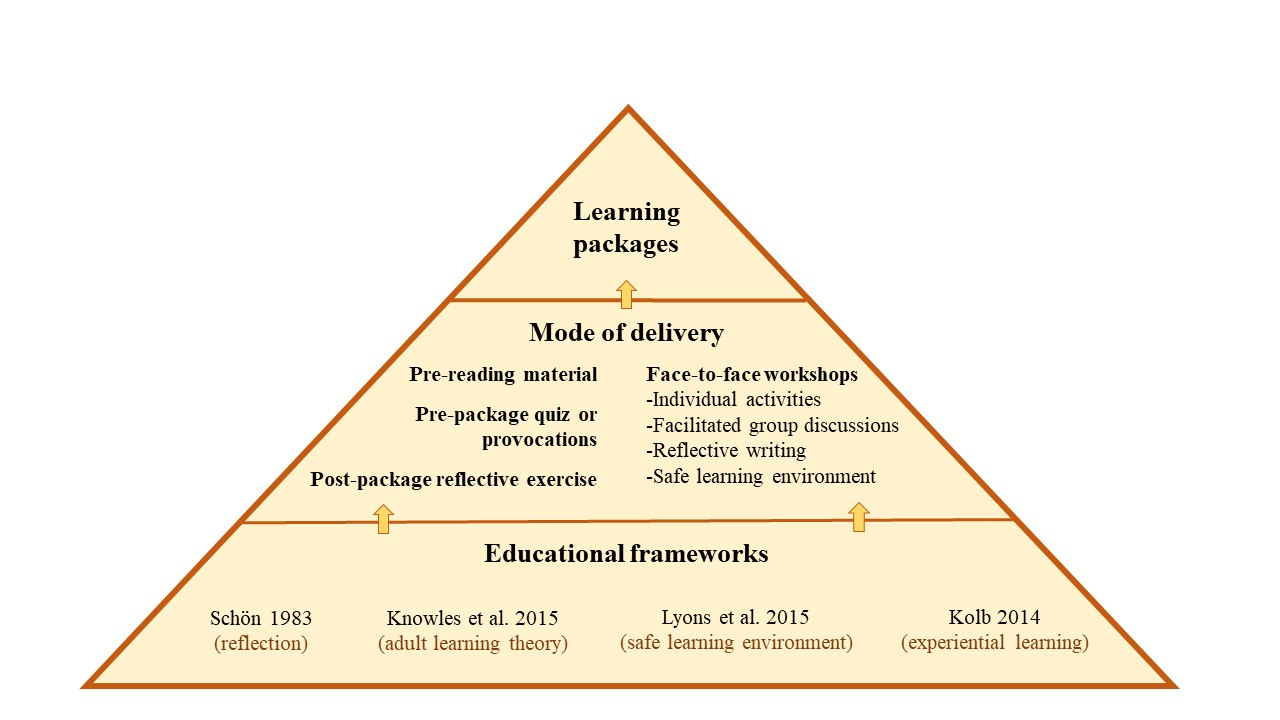
Figure 1. Mode of delivery and educational frameworks
Educator participants were three experienced facilitators (with pharmacy and nursing backgrounds) who were employed by the hospice. Each had an interest in education and had undertaken formal training sessions in palliative care delivery prior to facilitating the course.
B. Data Collection
Course educators and learners were invited via email to partake in a one-off face-to-face or phone interview to discuss their experiences of the course. One member of the research team (author 4) conducted all interviews following a semi-structured interview guide (Appendix B). Interviews were audio-recorded and transcribed verbatim. Data were collected between December 2016 and March 2017.
C. Data Analysis
Following Morse and Field (1995) and Saldaña(2016), we used general purpose interpretive thematic analysis. Transcripts were de-identified then uploaded into a qualitative data management system, QSR NVivo 11 software. Three members of the research team (authors 1, 2 and 7) read the transcripts and iteratively created a coding scheme. This involved looking for recurrent words, phrases and concepts within the data, which were termed codes. An initial coding scheme was developed iteratively containing primary codes, subsidiary codes and their definitions. There was a defined protocol for when to code the concepts. Two members of the research team (authors 1 and 2) independently coded each transcript and this coding was then checked by author 7 to ensure consistency and rigour. Two of our authors (3 and 5) were educator participants in this study. They were interviewed by a member of the research team, using the same questions posed to the third educator participant. To minimise bias, these authors were not involved in any aspect of the data analysis.
As the analysis progressed, some of the codes and sub-codes and their definitions were modified to ensure they conveyed the meaning participants had expressed during interviews. Assumptions about the relationships within and between concepts were proposed and explored. The codes were iteratively formed into themes and subthemes (Table 1). These themes were manually cross-checked for consistency. The QSR NVivo 11 software query functions were used to confirm relationships between themes and subthemes. These themes were discussed and refined between the three members of the analysis team.
|
Theme |
Subthemes |
|
A. Application to Practice |
1) Developing an understanding of palliative care 2) Developing empathy, listening and communication skills |
|
B. Learner Engagement |
1) Methods of teaching 2) Engagement – interactive style of teaching works 3) Drawing on personal experience 4) Feeling safe to share and learn |
|
C. Assessment and Evaluation |
1) The role of assessment and evaluation |
Table 1. Themes and subthemes of participant experiences
III. RESULTS
Eight females participated in this study, including five learners (course participants) and three educators. Their reflections on the course that they had attended as either an educator or learner rotated around three core themes: (1) application to practice, (2) learner engagement, and (3) assessment and evaluation (Table 1).
A. Application to Practice
Learner participants reported that the packages had increased their sense of preparedness for having real-life discussions with patients and family members/carers about death and dying/palliative care options, and ethical issues. Learners reported that this sense of preparedness had encouraged them to engage more deeply in conversations concerning palliative care.
1) Developing an understanding of palliative care: Educator and learner participants said the course enhanced their skills and understanding of communication with patients, their families/carers and other health professionals. Learners particularly valued information concerning the following subjects: the impact of a cancer diagnosis on significant others; medication; pharmacology; symptom and pain management; caring for palliative patients; ethical dilemmas; and dementia. A greater understanding of palliative care meant that learners reported they found they were able to make decisions about pharmaceuticals (without needing to check with another health professional), which they saw as likely to save time while maintaining quality of care. Further, learners’ understanding was influenced by the educators’ passion for teaching in the area of palliative care.
You might be thinking why on earth are they using Dexamethasone to increase this patient’s appetite – that doesn’t sound right. I need to ring the doctor. Whereas now they understand this is normal, this is the dose range, so they’re better equipped to supply the medication because they understand why. They’re not having to constantly ring the GP [general practitioner].
(Educator 1)
They [educators] know their topic inside out and they do their best to pass on … every ounce of knowledge that they have, which is great to see in colleagues. I just found it incredibly, inspiring to have that sort of passion for a topic.
(Learner 2)
2) Developing empathy, listening and communication skills: The learning modules enabled learner participants to develop awareness, empathy, and communication skills–particularly listening skills. They gave specific examples of empathic behaviour when dealing with patients and their families, for example, recognising and attempting to understand the multiple losses and life changes one might experience with a cancer diagnosis. Further, the content and delivery of the learning packages gave learners opportunities to be more prepared to engage in difficult conversations around death and dying.
It’s just being able to have more empathy for the people because you appreciate what they’re going through and what’s happening … just being a bit more available I suppose and realise in the end you spend time listening to what they have to say and trying to do the best for them.
(Learner 1)
And I guess when I’m talking to people, [recognising] that they’re going through a lot of losses and because of their cancer for example, they may have lost their job, I mean, if they can’t work anymore, their role in the family, they may have physical changes and loss around that.
(Learner 3)
The importance of ‘giving special time’ for conversation was an additional skill participants learned through completion of the modules. They recognised the importance of moving beyond the patient’s prescription and taking time to listen and engage in conversation with the patients and/or their families/carers.
Well actually at the time we had a customer–a man whose wife was dying of cancer, and I think instead of taking the prescription and things like that, you went out and took a special time and talked to them and spent a bit of time without actually asking too many specific questions.
(Learner 5)
In addition to communicating with patients and their families/carers, learner participants reported that the delivery of the learning modules helped equip and gave learners confidence to communicate more effectively with other health professionals.
“I deal a lot with rest homes and private hospitals so being able to assist the RNs [registered nurses] and to be able to relate to them.”
(Learner 2)
“And so, I sort of feel a lot more comfortable about that and comfortable talking to the doctors, you know, when something’s happening. So, I’ve learnt that.”
(Learner 4)
B. Learner Engagement
1) Methods of teaching: All participants discussed methods of teaching as having direct impact on their learning. Educator participants discussed teaching methods in more depth and greater frequency than pharmacist learner participants. They identified that when interactive strategies were utilised (videos, small group activities, case scenarios, demonstrations, and brainstorms), the learners absorbed/embedded more information and valued the teaching material more than when the information was presented didactically.
If I have to use a PowerPoint [slide presentation] I will learn it so that it’s behind me and I’m speaking to the audience and using eye contact, engaging from them their interest and whether they’re understanding. And I like to encourage questions to be asked as I’m talking because that then helps to add another layer of explanation. I also like case scenarios and preparing a case scenario or an ethical situation for groups to break off and discuss in their small groups and then to feedback so that each group can learn from everybody else.
(Educator 1)
The exception to this pattern was Educator 3’s observation that didactic teaching was an effective teaching strategy to begin the learning session, as it is a teaching format familiar to learners. Once the class was underway a more engaging method was needed.
“[Learners] were quite happy to be led initially, [using] didactic teaching. But I don’t think the sessions would have been as effective if we had continued that route.”
(Educator 3)
The relevance of content was also important to both the educator and learner participants. They valued material that was relevant and applicable to the pharmacists’ ‘specific care populations and practices of care.’
I was satisfied that I was able to provide consultant specialist advice and make it real for the pharmacists…. I put in a number of extra slides that were specific to pharmacists and some of the pharmacology of the drugs etcetera.
(Educator 1)
“It was kind of practical stuff [content] that you could easily translate when dealing with people when they came into the pharmacy.”
(Learner 1)
2) Engagement–Interactive style of teaching works: The teaching methods that learner participants had most to say about were interactive ones. This included facilitated whole-group conversation that was supported by small group activities.
There were a lot of different points of view and a lot of different people who were at different levels of experience in different areas and I think having the whole group there that were all pharmacists was really helpful. We all learned from each other.
(Learner 3)
In contrast, when educators discussed interactive teaching, they talked about it in terms of group dynamics and managing the discussions so that all learners had opportunity to voice their opinions.
There’s nothing worse than having somebody that just has to answer every question, has to share everything because they just need to be heard. So, you have to manage that and … manage the person that just sits there and doesn’t say anything.
(Educator 2)
3) Drawing on personal experience: Three educators and two learners reported that some educators drew on their personal experience–such as from the hospice pharmacist setting–to illustrate the relevance of material. When learners discussed their relevant personal experiences, it was equally valued.
“We all learned from each other.”
(Learner 3)
“We even had one pharmacist kind of stand up and say ‘This happened to me and I want you guys to learn from this’, so there was a lot of them talking about their experiences and sharing stuff.”
(Educator 3)
A learner reflected that the course material had value for her in her personal life.
I’d also gone through it [living and caring for a palliative care patient] with a flatmate early on and I felt that I hadn’t actually coped with it particularly well. So, it [the course] was a little bit for my own good as well.
(Learner 5)
Likewise, an educator made the observation that the course material was applicable to learners in their personal as well as their professional lives.
There was a strong feeling from pharmacists that they were also doing this to learn for their own personal lives because everybody will be touched by palliative care at some point in their lives, whether it be family or friends and it’s helped them to be better equipped with that.
(Educator 1)
The telling of personal experience can be linked with our first theme of Developing empathy, listening and communication skills. It is both telling and listening that comprises effective communication, which is core to pharmacist practices of care.
4) Feeling safe to share and learn: Feeling safe is important to supporting people’s learning. This was explicitly discussed by participants, and implicitly presented in other participants’ accounts.
She [Educator 2] talked to us, she encouraged you to give your opinion or your thoughts as well and you were never made to feel like what you said wasn’t right or was not significant. I thought she was great. It was very much an open forum, so you could relate, add bits in or ask questions and you felt comfortable doing that.
(Learner 4)
Educators were strategic in providing effective learning safe learning environments:
One of the skills of palliative care education is talking about topics that can be really quite difficult for some people if they’ve had a recent loss or they’ve had a situation in their personal life and it’ll trigger, so ground rules are really important to try and keep–to make sure people feel safe. So, you ensure when you start a session that people know that they can share stuff of a personal nature, but that information stays in the room and that it’s not to go outside. And you want people to be respectful.
(Educator 2)
C. Assessment and Evaluation
1) The role of assessment and evaluation: Educator participants highlighted the importance of assessment to enhance learning. Two assessment methods; reflective activities undertaken during the learning packages and quizzes completed at the end of the packages were formatively assessed methods. Educator participants pointed out there is a mechanism for assessment to be recognised by the Pharmaceutical Society of New Zealand. In this case, successful completion of assessment therefore becomes a summative assessment.
“[The] Pharmaceutical Society approves questions and if participants gain more than 80% then … the Society awards them learning points that contribute to their compulsory continuing education.”
(Educator 1)
Along with the assessment methods described, the Hospice NZ programme gives learners the opportunity to complete an evaluation which includes questions about learning value for each learning package. The inclusion of assessment and evaluation methods fosters learners to think about how process (teaching delivery) and content have contributed to their learning.
Although educators promoted the merits of assessment comprising part of the learning modules, they acknowledged that assessment gauges learning only in the short term. It is not possible to determine the long-term impact on practice from the assessment and evaluation methods currently utilised. Further, participants identified some confusion around the reflective activities.
“We struggle with assessing their learning long-term – what have they taken away a year later? What are they using in their practice? That’s what we haven’t been able to establish.”
(Educator 1)
“Participants appeared confused about the requirements for the pre and post session reflective activities which they were required to complete in the learning packages.”
(Learner 1)
IV. DISCUSSION
Effective palliative education for pharmacists enables participants to understand their role in end of life care, reduces death anxiety, prepares them to relate to people who are dying and facilitates psychological and emotional competence (Dickinson, 2013). It offers people knowledge and confidence to engage in the types of conversations that enrich peoples’ lives by making them feel heard and cared for. Dau Voire said, “be brave enough to start a conversation that matters” (Bravery Sayings & Bravery Quotes, n.d.). Is it bravery for pharmacists to engage patients in conversations about life and death? It absolutely is because the conversation may necessitate reflecting on your own life, mortality, and wishes.
We have shown that pharmacists valued this palliative care course because it developed key skills–and increased their bravery–to engage in deeper, more meaningful palliative care conversations in their professional and personal lives. We discuss the findings in turn.
A. Learning Engagement
Teaching delivery, which is primarily focused on interactive teaching methods such as small group activities, case scenarios, demonstrations, discussions and brainstorms markedly supported learner engagement. They valued opportunities to learn through discussing learner and educator experiences. These findings are consistent with Knowles’ adult learning theory, which suggests that the learners’ experiences ought to be tapped into (Knowles, et al., 2015). Teachers can help learners by using experiential techniques to acknowledge and utilise learners’ experiences through group discussions, activities to foster reflection, simulation exercises, and problem-solving activities (Knowles et al., 2015; Kolb, 1984; Schön 1983). In our view, one of the strengths of the learning packages is that they align with key educational frameworks (Figure 1).
Learners and educators in this study promoted a safe learning environment to optimise participation and learning (Lyons et al., 2015). This is echoed by existing education literature (Brown, 1988; Douglas, 1976). A safe climate, atmosphere or environment enables participants to feel comfortable about discussing personal experiences, including those which are difficult or challenging.
B. Assessment and Evaluation
When reflection is not encouraged in the clinical setting learning opportunities may be lost (Branch & Paranjape, 2002; Schön, 1983). In this course, learning was promoted through reflection and this was valued by learners, although they reported confusion about requirements for reflection activities. The opportunity for completion of modules to contribute to pharmacists’ continuing professional development (CPD) requirements was a key driver for participants completing the summative assessment. It is unlikely that meeting CPD requirements is the sole requirement for engaging in CPD. Further motivators for CPD may be to enhance professional knowledge and competence (Ryan, 2003).
C. Application to Practice
Several elements of the course were reportedly taken forward by participants to change their practices of care which had the flow-on effect of reducing their need to contact another health professional (for example, the patient’s general practitioner) to assist in decision-making processes. This improved the patient’s continuity of care. The value of palliative education is supported by the evaluation of an online programme in palliative care for pharmacists which demonstrated that the programme positively influenced the knowledge, confidence and practice of community pharmacists (Hussainy et al., 2010).
Delivery of the learning packages enabled pharmacists to develop a greater understanding of the impact of life-limiting illnesses and fostered both their development of empathy and ability to communicate with patients and their families and/or carers. The need for developing communication skills was strongly emphasised in a study which examined the community pharmacist’s role in palliative care (O’Connor et al., 2011). Emotional issues were seen as a major source of stress for general practitioners in an earlier study that identified the importance of the need for training and education to support general practitioners in managing emotional responses for palliative care patients and their families (O’Connor, Fisher, & Guilfoyle, 2006).
D. Limitations
Only females consented to participate in this study. We cannot speak to male pharmacist experiences of the course. The number of course participants was small and we had difficulty recruiting people to our study, partly because the interviews were held several months after the conclusion of the course. Our sample size was therefore small and our findings may not be generalisable. To increase study participation, future research of palliative care pharmacy courses could seek to recruit participants on workshop days or within a week of the course conclusion. Two of the authors on this paper were participants in the study. They were not involved in any aspect of the data analysis but they did contribute to the introduction and discussion sections of this article. The study did not establish the longer-term impact of the educational initiative on pharmacists’ practice. This is an opportunity for future research.
V. CONCLUSION
It is clear that effective palliative care education such as the learning packages discussed here is valued by pharmacists and relevant to their practice. Pharmacists in this study found the learning packages enhanced their understanding of palliative care, sharpened their communication skills and bolstered their confidence to engage in deeper conversations with patients and their families/carers and other health professionals. The interactive teaching methods promoted participant engagement and gave them opportunities to share their ideas and personal experiences and to listen to the experiences of others. Improving communication was a key feature for participants in this study. We therefore recommend that community pharmacists continue to be offered effective palliative care education, and that promotion of communication skills remain central to course method and content. An increased focus on critical reflection activities within such courses needs to be encouraged so that pharmacists can make meaning of their experiences and learning opportunities are not lost.
Notes on Contributors
Andrea Thompson is a Professional Teaching Fellow at the Centre for Medical and Health Sciences Education, University of Auckland.
Tanisha Jowsey is a medical anthropologist and a Senior Lecturer at the Centre for Medical and Health Sciences Education, University of Auckland.
Helen Butler was formerly employed at a Hospice in New Zealand and is now a Professional Teaching Fellow in the School of Nursing at the University of Auckland.
Augusta Connor, was formerly a research assistant at a Hospice in New Zealand and now works in health economics in the United Kingdom.
Emma Griffiths works at a Hospice in New Zealand as a specialist palliative care pharmacist.
Hadley Brown was formerly employed at a Hospice in New Zealand and is now self-employed. He has been involved in management within in the New Zealand hospice sector.
Marcus Henning is an Associate Professor at the Centre for Medical and Health Sciences Education, University of Auckland.
Ethical Approval
This study was approved by the University of Auckland Human Participants Ethics Committee (Reference Number: 016800).
Acknowledgements
We would like to acknowledge the participants who shared their experiences of teaching and learning.
Funding
A research assistant who conducted and transcribed the interviews was funded by Mercy Hospice, Auckland, New Zealand.
Declaration of Interest
Two authors were participants in the study. Although they were involved in the design of the study and contributed to writing the paper they were not involved in analysis of the data.
References
Atayee, R., Best, B., & Daniels, C. (2008). Development of an ambulatory palliative care pharmacist practice. Journal of Palliative Medicine, 11(8), 1077-1082. https://doi.org/10.1089/jpm.2008.0023
Branch, T., & Paranjape, T. (2002). Feedback and reflection: Teaching methods for clinical settings. Academic Medicine, 77(12), 1185-1188. https://doi.org/10.1097/00001888-200212000-00005
Bravery Sayings & Bravery Quotes (n.d.). Bravery sayings and quotes. Retrieved from http://www.wiseoldsayings.com/bravery-quotes/
Brown, G. (1988). Effective teaching in higher education. London: Methuen.
Dickinson, G. (2013). End-of-life and palliative care education in US pharmacy schools. American Journal of Hospice and Palliative Medicine, 30(6), 532-535. https://doi.org/10.1177/1049909112457011
Douglas, T. (1976). Groupwork practice. London: Tavistock Publications.
Furstenberg, C., Ahles, T., Whedon, M., Pierce, K., Dolan, M., Roberts, L., & Silberfarb, P. (1998). Knowledge and attitudes of health-care providers toward cancer pain management: A comparison of physicians, nurses, and pharmacists in the state of New Hampshire. Journal of Pain and Symptom Management, 15(6), 335-349. https://doi.org/10.1016/S0885-3924(98)00023-2
Henning, M., Hu, J., Webster, C., Brown, H., & Murphy, J. (2015). An evaluation of Hospice New Zealand’s interprofessional fundamentals of palliative care program at a single site. Palliative & Supportive Care, 13(3), 725-732.
Hussainy, S., Marriott, J., Beattie, J., Nation, R., & Dooley, M. (2010). A palliative cancer care flexible education program for Australian community pharmacists. American Journal of Pharmaceutical Education, 74(2), 1-9. https://doi.org/10.5688/aj740224
Institute of Medicine (2015). Committee on Approaching Death: Addressing, Key End-of-Life Issues. Dying in America: Improving quality and honoring individual preferences near the end of life. Washington, D.C.: National Academies Press.
Knowles, M. (1984). The adult learner: A neglected species (3rd Ed.). Houston: Gulf Pub. Co.
Knowles, M., Holton, E., & Swanson, R. (2015). The adult learner. (8th Ed.). New York: Routledge.
Kolb, D. (1984). Experiential learning: Experience as the source of learning and development. Englewood Cliffs, N.J.: Prentice-Hall c1984.
Lyons, R., Lazzara, E. H., Benishek, L. E., Zajac, S., Gregory, M., Sonesh, S. C., & Salas, E. (2015). Enhancing the effectiveness of team debriefings in medical simulation: More best practices. The Joint Commission Journal on Quality and Patient Safety, 41(3), 115. https://doi.org/10.1016/S1553-7250(15)41016-5
Morse, J. & Field, J. (1995). Qualitative research methods for health professionals (2nd Ed.). Thousand Oaks: Sage Publications.
Needham, D. S., Wong, I. C. K., & Campion, P. D. (2002). Evaluation of the effectiveness of UK community pharmacists’ interventions in community palliative care. Palliative Medicine, 16(3), 219-225. https://doi.org/10.1191/0269216302pm533oa
O’Connor, M., Fisher, C., & Guilfoyle, A. (2006). Interdisciplinary teams in palliative care: A critical reflection. International Journal of Palliative Nursing, 12(3), 132-137. https://doi.org/10.12968/ijpn.2006.12.3.20698
O’Connor, M., Pugh, J., Jiwa, M., Hughes, J., & Fisher, C. (2011). The palliative care interdisciplinary team: Where is the community pharmacist? Journal of Palliative Medicine, 14(1), 7-11. https://doi.org/10.1089/jpm.2010.0369
Ryan, J. (2003). Continuous professional development along the continuum of lifelong learning. Nurse Education Today, 23(7), 498-508. https://doi.org/10.1016/S0260-6917(03)00074-1
Saldaña, J. (2016). The coding manual for qualitative researchers (3rd Ed.). London: Sage.
Schön, D. (1983). The reflective practitioner. New York, NY: Basic Books.
Steinert, Y., Cruess, S., Cruess, R., & Snell, L. (2005). Faculty development for teaching and evaluating professionalism: From programme design to curriculum change. Medical Education, 39(2), 127-136.
Vernon, J., Brien, J., Dooley, M., & Spruyt, O. (1999). Multidisciplinary treatment paths and medication management of palliative care patients. Proceedings of the Australian Society of Clinical and Experimental Pharmacologists and Toxicologists, 7, 74.
*Andrea Thompson
University of Auckland,
Building 599, Level 12,
Auckland City Hospital
Private Bag 92019,
Auckland 1142
Tel: +6499231906
Email: andrea.thompson@auckland.ac.nz
Published online: 7 January, TAPS 2020, 5(1), 79-81
DOI: https://doi.org/10.29060/TAPS.2020-5-1/CS2092
Rajeev Ramachandran1, 2, Clarice Chong3 & Lee Gan Goh3
1Khoo Teck Puat – National University Children’s Medical Institute, National University Health System, Singapore; 2Department of Paediatrics, Yong Loo Lin School of Medicine, National University of Singapore; 3Department of Family Medicine, National University Health System, Singapore & Yong Loo Lin School of Medicine, National University of Singapore
I. INTRODUCTION
Family Medicine (FM) is an applied and integrative discipline. In 2011, the Ministry of Health introduced FM Residency Program in Singapore to train aspiring Family Physicians (FP). There are three sponsoring institutions, namely, Sing-Health Polyclinics, National Healthcare Group Polyclinics, and National University Health System (NUHS).
The Singapore FM Residency programs have rotations involving 13 disciplines, one of which is Paediatrics. As part of training in Paediatrics, the NUHS program has set up an outpatient Paediatric Longitudinal Clinic (PLC) staffed by FM Residents. This PLC is a service cum training clinic. It is supervised jointly by a Paediatrician core-faculty and a FM core-faculty. The FM Residency program aims at training a FP to provide primary, personal, and preventive care; and comprehensive, continuing and coordinated care to the patient and their family (Goh & Ong, 2014).
We report a case study of using a patient with a genetic syndrome to illustrate the Family Medicine approach in the training of the FP in a FM Residency Program. This Approach consists of the 3 Ps (personal, primary, and preventive care) to define care needs; and 3Cs (comprehensive, continuing and coordinated care) in managing the patient and family.
II. OBJECTIVE AND METHODS
The objective of this paper is to illustrate the potential of using FM approach in managing a patient with a rare multi-system genetic disorder. This teaching event took place at the PLC. The patient was clerked by the FM resident on duty. The one-year-old patient who looked dysmorphic to us (having microcephaly, broad thumbs and great toes, poor growth, and mental slowness), presented with constipation. The resident discovered that he was regularly seeing a neonatologist, neurologist, dietitian and gastroenterologist for the multiple problems he was having.
Using the FM approach, we defined the patient’s primary, personal, and preventive care needs and formulated a comprehensive, continuing, and coordinated care approach in managing the patient and family. Through this approach we hoped to reduce fragmentation of care, duplication of services, and forestall complications through preventive care.
III. LEARNING POTENTIAL FOR THE FM RESIDENT
All three subspecialists managing this patient have worked independently of one another. The neonatologist with the help of a dietitian was following up the patient for failure to thrive. The height and weight centiles were < 3% and this did not improve with nutritional intervention. The neurologist was following up for microcephaly and gastroenterologist was treating the patient for constipation. In this particular instance, it was the constipation that brought the patient to Children’s Emergency and she was followed up by us in the PLC a week later.
During the case discussion with the FM Resident, the General Paediatrician recognized that microcephaly, broad thumbs and great toes are prominent features of Rubinstein-Taybi syndrome which is a genetic syndrome. The FM faculty encouraged the resident to read about this condition and find out if the presentation of the patient matches with what is described in text books as well as explore the strategies to reduce fragmentation of care and work with various members of the health care team to increase the integration of care (Newbronner, Borthwick, Finn, Scales, & Pearson, 2017; Starfield, Shi, & Macinko, 2005). In the follow-up discussion, the patient’s care needs of the 3Ps (primary care, personal care, and preventive care needs) were defined. With a better understanding of the genetic syndrome, the FM Resident was able to formulate the 3Cs of management care needs (comprehensive, continuing, and co-ordinated care) of the patient and family. Table 1 shows the scope of the 3Ps and 3Cs in this case study (Gandhi, 2016).
|
| Source: Gandhi, 2016 |
Table 1. Components of the family medicine approach in the clinical case of a patient with genetic syndrome
IV. DISCUSSION
The FM approach in the integration of care in Paediatrics is illustrated in this case study of a genetic syndrome. The potential of using such a clinical case is rich. What is also important is the paradigm shift from the focus of studying biomedical features of syndromic rarities to integrate care of the patient.
The Rubinstein-Taybi syndrome (Gandhi, 2016) encountered in this patient is one example of a genetic syndrome that can be used to teach the scope and breadth of the FM approach. There are other genetic syndromes that can be used, e.g., the patient with Trisomy 21; Duchenne progressive muscular atrophy, or Spinal muscular atrophy (SMA).
Some of the day-to-day medical problems found in such genetic syndromes can be dealt with by the Family Physician alone, e.g., constipation. Other problems may need shared care of two or more clinical disciplines, as for example, the care for mental retardation, skeletal abnormalities, organ abnormalities, and slow physical growth. These are common features encountered in genetic syndromes.
The 3Ps: Defining the primary, personal, and preventive care needs of the patient.
Primary care is first level care. Constipation is an outpatient problem that the FP can help.
Personal care is important in connection with monitoring growth and development and providing acute care for common problems. The FP needs to help the patient and family define the tasks and provide recommendations where these are needed.
Preventive care has its role too. The preventive treatment of constipation, orthopaedic problems, mental stimulation, can be jointly coordinated by the FP and the Paediatric subspecialists (neonatologist, neurologist, and gastroenterologist in this case study).
The 3Cs: Managing the comprehensive care, continuing care, and coordinated care needs of the patient and family.
Comprehensive care spans the physical domain of the patient’s clinical features, social domain of the patient (parents, helpers) which will include the caregivers who need to know the medical condition that the child is having, as well as symptoms and treatment that will be needed e.g. constipation, schooling, and other life-course preparation for the child. The treatment of this condition is based on symptoms.
Continuing care is needed. In view of the multisystem involvement, anticipatory care may be needed e.g., dental care, intellectual and social development needs of the child.
Co-ordination of care is also needed. The child is under the care of the neonatologist, neurologist, and gastroenterologist. The FP could certainly co-ordinate the care between the specialists and in this way reduce duplication of care.
V. MOVING FORWARD
The Family Medicine Approach in teaching the management of the patient with a genetic syndrome shifts the focus from learning just biomedical rarities to teaching a system of defining the care needs that can be remembered as 3Ps; and the management of these needs as the 3Cs.
Through the co-ordination of care, reduction in fragmentation and duplication of care can be achieved and the inter-professional collaborative practice helps to deliver high quality, safe patient-centred services to achieve best possible long term health outcomes. Through prevention, some of the complications of multi-system diseases can be reduced.
Notes on Contributors
Rajeev Ramachandran, MD, FAAP, is an American Board certified General Paediatrician and Senior Consultant in the Department of Paediatrics, National University Hospital, Singapore and a Core Faculty for the Family Medicine Residency Program, National University Health Systems, and Singapore. He conceived this construct and intervention, wrote the manuscript, and agreed to its publication in its final form.
Clarice Chong, MBBS, MMED (Family Medicine), was a Family Medicine resident at the Family Medicine Residency Program, National University Health Systems, Singapore. She has since passed her MMed. (Family Medicine) specialty examination. She conceived this construct and intervention and agreed to its publication in its final form.
Goh Lee Gan, MMED (Internal Medicine), FCFP(Singapore), FRCGP, FRACGP, is a Senior Consultant and Professorial Fellow in the Department of Family Medicine, National University Hospital, Singapore and Associate Program Director for the Family Medicine Residency Program, National University Health Systems, Singapore. He conceived this construct and intervention, wrote the manuscript, and agreed to its publication in its final form.
Acknowledgements
We thank Dr Dimple Rajgor for her assistance in formatting, reviewing, and in submitting the manuscript for publication.
Funding
No funding is involved in this paper.
Declaration of Interest
There is no conflict of interest, including financial, consultant, institutional or otherwise for any of the authors involved in this manuscript.
References
Gandhi, A. (2016). Rubinstein-Taybi Syndrome. Retrieved from https://patient.info/doctor/rubinstein-taybi-syndrome-pro
Goh, L. G., & Ong, C. P. (2014). Education and training in family medicine: Progress and a proposed national vision for 2030. Singapore Medical Journal, 55(3), 117-23. https://doi.org/10.11622/smedj.2014031
Newbronner, E., Borthwick, R., Finn, G., Scales, M., & Pearson, D. (2017). Creating better doctors: Exploring the value of learning medicine in primary care. Education for Primary Care, 28(4), 201-209. https://doi.org/10.1080/14739879.2016.1277789
Starfield, B., Shi, L., & Macinko, J. (2005). Contribution of primary care to health systems and health. The Milbank Quarterly, 83(3), 457-502. https://doi.org/10.1111/j.1468-0009.2005.00409.x
*Rajeev Ramachandran
NUHS Tower Block Level 12,
1E Kent Ridge Road,
Singapore 119228
Tel: + 65 6772 3615
Fax: +65 67797486
Email: rajeev_ramachandran@nuhs.edu.sg
Published online: 7 January, TAPS 2020, 5(1), 76-78
DOI: https://doi.org/10.29060/TAPS.2020-5-1/PV1083
C. Rajasoorya
Department of General Medicine, Sengkang General Hospital, SingHealth, Singapore
I. INTRODUCTION
Reflections represent exploration and explanation of events and may reveal anxieties, errors and weaknesses; they do however have positive influences highlighting strengths and successes for better future outcomes. The author reflects on his practice as a clinician-educator close to four decades and shares a perspective of his retrospectively pleasant but arduous journey into medical education.
II. BAPTISM INTO CLINICAL TEACHING
I embarked on teaching medical students because I did not want them to encounter the same struggles I had with learning voluminous medical facts and lists. Moving into clinical years and with more experience, I understood the importance and applicability of basic sciences with greater clarity. As a way of guiding juniors and preparing for my own higher examinations, I got interested in teaching clinical medicine. Repeatedly ringing in me is what a clinical-skills foundation teacher profoundly reminded us that teaching is a way to expose our knowledge gaps and help us remember better. Being fortunate to have been taught by some of the doyens of medicine as well as having a high clinical load, it surprises me on how much I learnt from both my students and patients.
III. REJUVENATION AND EVOLUTION
Once, I had wrongly succumbed to the idea “the new generation is different and is less interested in learning”. Disillusioned, I almost contemplated giving up teaching. Fortunately, I closely worked with a few brilliant, enthusiastic and hardworking interns who rekindled my interest in teaching and awakened in me the need to customise teaching to the generation we are dealing with (not vice versa). A teacher must accept that his experience in the early years will not mirror those of his students, rather than reminisce the past. The new generation is learning and practising in a different era where patient expectations are different, knowledge has been democratised and voluminous knowledge can be easily accessed via the internet and smartphones. Clinical teachers may take benefit to emphasise on clinical application and reasoning rather than factual content.
When I had a family of my own, the similarities between teacher-student and parent-child stirred in me the importance of ownership, responsibility, and avoidance of the remark “no time to teach”. It also dawned on me the extent of pressure we inflict on our students and how it contributes to vanishment of the joy of learning. I learnt that learning can be intuitive, varied and supplanted by metaphors of daily activities of life and knowledge application.
For a long time in my career, I used to go on an ordered line of questioning whenever I dealt with clinical groups. There was predictability who was going to be asked next. I learnt subsequently such an order of questioning stops the thinking process in all except the one in the “hot seat”; the rest passively “switched-off”. I have now adopted a routine (albeit, struggled) to get to know my students by name and ask questions in a random order which allows everyone to think; besides making them feel appreciated being called by their name.
I have found it useful to open difficult questions to the entire group – letting the student know it is a difficult question and providing a challenge to the brilliant to attempt it. At times I have openly admitted that I did not know the answer to that question at their age (or even later!). This resonates very well with students who feel teachers understand their difficulties. The dictum that no question is ever a stupid question cannot be overemphasised.
An experienced teacher can sense which student is struggling and distract attention quickly to another party so that the embarrassment to the individual struggling student is removed. It is important to recognise a student with the knowledge but hesitant to answer; cajoling the answer out of him is an art that comes with experience. Where a wrong answer is provided, it would be useful to ask for the reasoning rather than brush it aside with an emphatic “no”. A couple of years ago, I asked one of my rather always quiet students why she volunteered to be in the “hot seat” for a short clinical case – her answer of not being intimidated by me and having confidence that I would not embarrass her was a powerful lesson on how fear kills enthusiasm. I was fascinated to hear in later times that she had expressed a desire to be a clinical teacher!
Experienced teachers will be bold enough to admit they do not know. Admittedly, this was never easy for me during the growing years, until recent times. An occasional bright spark student may know the answer and he or she should be given credit for educating the teacher. Mutual respect promotes learning for all involved. Time and again, I had experienced and learnt from my colleagues (particularly from my overseas stints) of how protecting ego and hiding ignorance serves only to retard the process of learning. Eating humble pie may seem daunting and embarrassing, but I now accept it as fulfilling and enriching. Teaching and learning are intertwined and run in both directions – one must break the cultural barrier that the teacher has all the knowledge and the student some or none. It took a young medical officer to unravel a misconception I had for more than 20 years that chronic malaria and tropical splenomegaly syndrome were different entities.
We often do clinical teaching on cases we already know accompanied by its inherent biases. Teaching on cases we are blinded to is a mind-boggling experience. In the last few years, I have experimented and adventured with teaching on cases where I am blinded to the findings or diagnosis. Both the student and the teacher can learn a lot and we get better as we express our thoughts and disrobe our thinking processes openly. This to me is akin to practising clinical reasoning live.
Most of my initial clinical teachings concentrated on artificial situations where we selected “good cases” — this, unfortunately creates an artificial divide of what we see as clinicians and how patients present to us. I am even more convinced, over the years, that every case is a good case to teach; choosing the slant and emphasis in every situation is critical.
We tend to cram information to students, as much as I did in the past. Now, I ask myself before a tutorial or lecture on what is the primary target of my teaching. Teaching must be customised to the audience. I used to joke with my students in the early years whenever an examiner asks you for causes of a certain abnormality – a second-year student gives two, third-year student three and final year student gives five, as a rough rule. This joke highlights the need to avoid unintentionally submerging our students in a factual journey and overloading them, forgetting how we acquired skills in a graduated manner.
Leonardo da Vinci is attributed to suggesting that simplicity is the ultimate sophistication. Great teachers have a way of simplifying complex concepts. Nobel laureates Michael Brown and Joseph Goldstein likened lipoprotein traffic to navigating the maze in the London underground system while explaining lipoprotein metabolism. Prober and Heath (2012) remind us of the importance of making lessons “stickier” by making it comprehensible and memorable. Efforts to make things “simple is often harder than complex”, as profoundly highlighted by Steven Jobs (as cited in Reinhardt, 1998).
IV. PRINCIPLES AND PHILOSOPHIES
Over the decades, I have gradually moulded myself into believing in some philosophical concepts on clinical teaching shared below:
- Clinical teaching can be likened to planting a seed in a soil (student in the health care environment). We need to ensure the presence of sunshine, rain (stimulus) and fertile soil (conducive environment); as in nurturing, the wind (pressure and currents) cannot be too strong. A clinical teacher must look after the student welfare in preventing burnout, disillusionment or wilting away.
- For busy clinicians, giving committed time and effort to teaching can be challenging. It is worthwhile reminding us that to be a “doctor” means “to teach”. With ownership, we never generally say we lack time or rewards to teach and guide. Sharing our experiences and difficulties make students feel they are in good company.
- Teachers must learn to squeeze the best out of their students rather than looking negatively at their lack of knowledge. Beneath every “F-student” is an “A student” waiting in line and time to pop-out! A teacher must take part-responsibility and embarrassment for students’ failures, as much as we take pride and pleasure in their successes.
- Teachers should take extra effort to simplify concepts and to remind themselves that if they face difficulty in understanding certain concepts, it is unreasonable to expect their students to grasp these same concepts easily.
- Teaching should not concentrate on voluminous facts that are so easily accessible. It must be customised to deal with diversity in the audience as well as cater to the level of expertise of the student. Clinical teaching should focus on clinical reasoning.
- We must be bold enough to try teaching methods to reflect the plasticity we have within ourselves to adapt, grow and regenerate our knowledge and its transmission.
V. CONCLUSION
Medical education has changed over the few decades that I have practised in. The fundamentals have remained – to train our doctors as future physicians and specialists. The core values must be preserved while stimulating progress incorporating new ways of practice. Experience and reflections are excellent tools in our armamentarium of methodologies. I have never regretted my adventure into clinical teaching.
Notes on Contributors
Professor Rajasoorya is a senior consultant, endocrinologist, Campus Education Director at Sengkang General Hospital; clinical professor at NUS School of Medicine; and adjunct professor of Duke-NUS Medical School. He has undertaken various leadership, administrative/advisory positions in medical education, curriculum development and is the recipient of numerous education and teaching awards.
Acknowledgements
I gratefully acknowledge the inspiration, experience, and knowledge of my students, my patients and my teachers that has moulded my philosophy in teaching.
Funding
No funding was obtained in the preparation and production of the paper.
Declaration of Interest
The author declares no conflict of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
Reinhardt, A. (1998, May 25). Steve Jobs: ‘There’s sanity returning’. Bloomberg Businessweek. Retrieved from https://www.bloomberg.com/businessweek
Prober, C. G., & Heath, C. (2012). Lecture halls without lectures – A proposal for medical education. The New England Journal of Medicine, 366(18), 1657-1659.
*C. Rajasoorya
Department of General Medicine,
Sengkang General Hospital,
110 Sengkang East Way,
Singapore 544886
Tel: +65 6930 2221
Email: c.rajasoorya@singhealth.com.sg
Published online: 7 January, TAPS 2020, 5(1), 70-75
DOI: https://doi.org/10.29060/TAPS.2020-5-1/SC2065
Carmel Tepper, Jo Bishop & Kirsty Forrest
Faculty of Health Sciences and Medicine, Bond University, Australia
Abstract
Bond University Medical Program recognises the importance of workplace based assessment as an integrated, authentic form of assessment. In partnership with a software company, the Bond Medical Program has designed and implemented an online Student Clinical ePortfolio, utilising a mobile-enabled, secure, digital platform available on multiple devices from any location allowing a range of clinically relevant assessments “at the patient bedside”. The innovative dashboard allows meaningful aggregation of student assessment to provide an accurate picture of student competency. Students are also able to upload evidence of compliance documentation and record attendance and training hours using their mobile phone.
Assessment within hospitals encourages learning within hospitals, and the Student Clinical ePortfolio provides evidence of multiple student-patient interactions and procedural skill competency. Students also have enhanced interprofessional learning opportunities where nurses and allied health staff, in conjunction with supervising clinicians, can assess and provide feedback on competencies essential to becoming a ‘work-ready’ doctor.
Keywords: Authentic Assessment, Interprofessional Learning, Technology-Enhanced Learning, Feedback, Workplace-Based Assessment
I. INTRODUCTION
The medical education community is rapidly embracing workplace based assessment (WBA) as a more authentic form of assessment of medical students’ clinical competence. These clinical interactions are complex, with integrated competencies observed in real-life settings. For the safety of patients, however, it is essential that medical schools have evidence that their graduates have attained sufficient standards in core skills and activities as indicated by their relevant accrediting institutions’ graduating doctor competency frameworks. This includes evidence not only of sufficient maintenance of compliance documentation, attendance in clinical settings and teaching sessions, but also the ability of the student to interact competently with a variety of patients.
Student clinical placements within medical schools are often undertaken in multiple locations with a variety of clinical supervisors. At Bond University, Australia this process involves over 150 locations with up to 800 clinical supervisors observing, assessing and providing feedback on student performance. Previous manual, paper-based processes were inefficient, time-consuming, prone to error, and limited the opportunity for real-time feedback to students. Difficulty aggregating information resulted in difficulty making pass-fail decisions on student performance on rotation and delayed intervention for students requiring remediation for either compliance, attendance or clinical performance.
Whilst clear and validated documentation of proficiency required of a “work-ready” graduate is often challenging to obtain, this aggregation of multiple data points to build a more complete picture of student competence is central to the concept of programmatic assessment (van der Vleuten, 2016). A portfolio of evidence with timely feedback on performance is seen as essential for demonstrating the growing development of student clinical skills.
An electronic, or ePortfolio, represents the technological evolution from paper-based to electronic clinical assessments (Garrett, McPhee, & Jackson, 2013). There are multiple ePortfolios and learning management systems available which can be used in the workplace and electronically collect in-progress assessments and accomplishments (Kinash, Wood, & McLean, 2012). Some ePortfolios also allow students to manage continuing professional development. Bond Medical Program, however, sought to develop an ePortfolio specifically designed for undergraduate medical students that could aggregate not only attendance and compliance but also competency assessment data in a meaningful way to build an accurate picture of student competency in the hospital setting.
The aim of this short communication is to describe why and how a new version of a bespoke electronic portfolio was designed and implemented.
II. METHODS
Bond University partnered with a software company, which had healthcare experience, in the development of a digital student Clinical ePortfolio. The business requirement specification was for a fully mobile-enabled, secure, digital platform available on any device from any location that would allow a range of clinically relevant WBAs to be captured by clinicians “at the bedside” with the ability to provide immediate feedback to students. In addition, the software was to contain a process for students to provide evidence of compliance documentation and attendance at compulsory teaching sessions and on rostered placement shifts. The initial plan was to replicate all paper-based processes onto an electronic platform. The development of the software was iterative to the needs of the university using a road cycle improvement process. An app-based product was developed to house the clinical portfolio.
| Feature | Benefit | Replacing |
| Tablet and mobile phone-enabled clinical assessment | Readily available, user-friendly, allows for opportunistic assessment
Guest assessors (allied health and nursing) can participate in medical student education |
Paper assessment which had to be collected and collated |
| Compliance | Simple to scan and upload by students
Dashboard shows aggregate of compliance completion to ensure all required documentation has been provided |
Time-consuming, laborious paper trail of compliance documentation |
| Attendance with GPS tracking | Students take responsibility for being on rotation when rostered
Specific number of absences can trigger early student support processes Accurate record of which students attended compulsory classes |
Paper sign-on forms |
| Dashboard – Summary data | Student and clinical staff can view aggregated summary data showing attendance, compliance, student patient logs and WBAs | Multiple individual paper WBAs that could not be aggregated |
| Personal student learning | Students can log personal patient interactions as a record of their learning on rotation | Paper patient logs |
| Learning Modules with associated procedural skills assessment | Students watch a ‘best-practice’ learning module, demonstrate their understanding by answering a short quiz and then generate an assessment for a clinical supervisor. The clinical assessor guides and observes the skill performance and then provides a ‘trust level’ competency rating. Students can repeat the assessment until competency achieved | Skills performed in hospital setting not formally captured |
| Feedback to student | Voice recorded or typed, feedback is provided to student as soon as submitted by the assessor – timely and relevant to the performance | Verbal feedback or occasional comment on a form |
| CPD | Students can log personal continuing professional development to capture more fully their learning journey |
Table 1. Bond eportfolio features
In August 2017, the compliance portion of the portfolio was piloted with a single clinical year cohort of medical students and supervisors. In 2018, attendance and WBAs were conducted at the bedside of patients across all clinical years.
Delivering the project across many sites required the support of all supervisors, along with timely stakeholder engagement, and change management considerations. The needs of busy clinicians were surveyed, and a low-key launch by way of an online training video was preferred by the majority, with face-to-face on-site training available upon request. There are several barriers to timely feedback in the busy clinical environment with ‘opportunistic assessment’, multiple demands on clinician time and multiple students and/or trainees under supervision at any one time (Algiraigri, 2014). Feedback using the ePortfolio can be provided in the moment, recorded as either typing or voice recording and reviewed by students within their own time. Feedback from clinicians described it as “easy to complete on the go” and “easy to assess then and there (at the bedside)”. Table 1 describes the features and benefits of the Bond ePortfolio.
An example of the compliance dashboard, and the assessment portfolio front page is shown in the Appendix.
III. RESULTS
The new platform successfully delivered the required features through the Bond Student Clinical Portfolio. The Portfolio is accessible to both student and supervising clinicians using mobile phones or office desktop computers. Students indicate their attendance using a GPS geolocating attendance application. Compliance documents, clerked cases, reflections and other assessment components including the final in-training assessment are uploaded for supervisor assessment, whilst Mini-Clinical Evaluation Exercises are now completed by supervisors using a mobile phone at the patient bedside. All assessments are housed in one cloud-based portal, accessible to the decision-making committees.
An added advantage of this system is improving student digital literacy and self-directed learning, assisting them to become familiar with the process of self-documenting evidence of competence and skills obtained a valuable and highly sought-after skill for a graduated doctor.
A. Workplace Based Assessment
Evaluation of the 2018 pilot demonstrated significant efficiencies in documentation collection of WBA. Previously, professional staff would have collated 2,350 components of high-stakes assessment per year to be reviewed and presented to the Board of Examiners (BoE). Faculty can now track student progress during clinical rotation, with a process in place to identify students who require additional support to succeed. Faculty receive automatic notifications for review of submitted assessment items. During meetings of decision-making committees such as the BoE, student assessment items can be viewed by the committee to verify students who are borderline or those who receive commendations.
B. Attendance
Key members of the medical programme have a ‘dashboard’ on their homepage with ‘live’ attendance data. The Professional Staff Team can run reports when required but the platform will monitor students who meet the nominated ‘concern’ percentage of missed sessions which notifies the team that a support email may be required. In our experience, concerns around student well-being often present with non-attendance patterns. Supervisors in the clinical setting can now electronically track the progress of students allocated to their teams during rotations. In addition, they can identify students who require additional support in a timelier manner, helping to provide the best education experience possible.
C. Feedback
The clinicians’ ability to utilise their preferred method of feedback delivery allows flexibility and improved engagement in the process. For instance, the ability to voice record was introduced, enabling students to immediately access assessor feedback. This has resulted in increased communication between students and their assessors and a very positive response from the student body.
Feedback on students’ experience of this platform has been sought through ongoing discussion with the initial pilot group, and regular updates on their learning management system, and representative year specific feedback through staff-student liaison committees. The attendance monitoring has had mixed reviews from students who “appreciate not having to sign in on paper” but have been impacted by technical issues around non-syncing with certain mobile devices.
IV. DISCUSSION
Our belief is that assessment within hospitals will encourage learning within hospitals. Our intention is to remove Objective Structured Clinical Examinations (OSCEs) from the final year assessment to be replaced with authentic WBAs that are reliable and valid. OSCEs will continue to be used in the earlier years of the medical programme. There may be limitations as the very nature of the hospital environment is opportunistic. Students will have multiple patient (data) interactions to support their developing portfolio with evidence of competencies achieved. Students can personalise their studies and identify areas of focus for skill development during placement, to ultimately build confidence in their work readiness as a day one doctor. Ultimately, assessment information “should tell a story about the learner” (van der Vleuten, 2016, p. 888).
This platform offers many advantages over other platforms. The selection of the software partner was a competitive process. A full needs analysis and tender process was performed which for brevity has not been presented here. The advantages over other platforms identified at procurement were the opportunity to customise and the ability to have all the processes (compliance, attendance, placement and assessment) on one platform. Subsequent advantages made clear after implementation, and not delivered by other platforms included; the ability for students to take the portfolio into the workforce, a dashboard for attendance, and working with a partner based in health care who understood all stakeholder requirements, with an emphasis on safe patient care.
The next step will be to utilise the platform for training, progression and maintenance of competency of procedural skills before graduation. Specific procedural skills, required by accrediting bodies and relevant to the year of learning, will be assigned to the student for completion during a rotation. The student, in addition to the routine clinical practice of for example intravenous cannulation, will observe an interactive learning module about that skill, complete a short assessment to test their understanding of the module, and the system will then generate an assessment assigned to a clinical supervisor. The student will then perform the skill on the patient and the supervisor will submit the completed assessment on a ‘trust level’ scale of competency (ten Cate, 2013). If the student is not yet able to perform the skill sufficiently independently, there are opportunities to practice and repeat the assessment until competency is obtained.
V. CONCLUSION
Digitising the processes for monitoring attendance, conducting and collating compliance documentation, clinical assessment and delivering feedback at sites of clinical exposure has created significant efficiencies in the delivery of our programme. Preliminary feedback indicates that this leads to a vastly improved student experience with real-time, enhanced feedback on assessment performance and timely student remediation to assist students in becoming safe and competent ‘work-ready’ doctors. Live updates that notify of absenteeism allow for more timely support and personalised care. The aggregation of data into one personalised student clinical ePortfolio will allow decision-making bodies to make intelligent and safe pass-fail decisions based on evidence of student clinical performance.
Notes on Contributors
Carmel Tepper is the Academic Assessment Lead at Bond University. She has a special interest in exam blueprinting, item analysis and assessment technologies.
Jo Bishop is the Academic Curriculum Lead and Associate Dean, Student Affairs and Service Quality at Bond University. Jo is an expert on curriculum planning and development and has a passion for enhancing the student experience.
Kirsty Forrest is the Dean of Medicine at Bond University. She has been involved in medical educational research for 15 years and is co-author and editor of several best-selling medical textbooks including ‘Medical Education at a Glance’ and ‘Understanding Medical Education: Evidence Theory and Practice’.
Ethical Approval
Ethical approval was not required.
Acknowledgements
An e-poster presentation on some of this work was presented at 15th anniversary APMEC and awarded a merit.
Funding
There is no funding involved for this paper.
Declaration of Interest
Other institutional uptake of the new designed Student Clinical Portfolio may financially benefit Bond University.
References
Algiraigri, A. H. (2014). Ten tips for receiving feedback effectively in clinical practice. Medical Education Online, 19(1), 25141. https://doi.org/10.3402/meo.v19.25141
Garrett, B. M., MacPhee, M., & Jackson, C. (2013). Evaluation of an eportfolio for the assessment of clinical competence in a baccalaureate nursing program. Nurse Education Today, 33(10), 1207-1213. https://doi.org/10.1016/j.nedt.2012.06.015
Kinash, S., Wood, K., & McLean, M. (2013, April 22). The whys and why nots of ePortfolios [Education technology publication]. Retrieved from https://educationtechnologysolutions.com/2013-/04/the-whys-and-why-nots-of-eportfolios/
ten Cate, O. (2013). Nuts and bolts of entrustable professional activities. Journal of Graduate Medical Education, 5(1), 157-158. https://doi.org/10.4300/JGME-D-12-00380.1
van der Vleuten, C. P. M. (2016). Revisiting ‘Assessing professional competence: From methods to programmes’. Medical Education, 50(9), 885-888. https://doi.org/10.1111/medu.12632
*Carmel Tepper
Faculty of Health Sciences,
Bond University,
14 University Drive, Robina QLD,
4226 Australia
E-mail: ctepper@bond.edu.au
Published online: 7 January, TAPS 2020, 5(1), 61-69
DOI: https://doi.org/10.29060/TAPS.2020-5-1/OA2152
Yoshitaka Maeda1, Yoshikazu Asada2, Yoshihiko Suzuki1 & Hiroshi Kawahira1
1Medical Simulation Centre, Jichi Medical University, Japan; 2Center for Information, Jichi Medical University, Japan
Abstract
Students in the early years of medical school should learn the skills of clinical site risk assessment. However, the effect of this training on clinically inexperienced students is not clear, and it is difficult for them to predict risks from a wide range of perspectives. Therefore, in this study, based on Kiken-Yochi Training (KYT) for risk prediction using what-if analysis, we examined how to expand risk prediction among clinically inexperienced medical students. We divided 120 students in the first year of medical school into small groups of seven to eight students. First, each group predicted risks in the standard KYT (S-KY) method, stating what risks exist in the illustrations. Next, they conducted a What-If KYT (W-KY) analysis, brainstorming situations that differed from the illustrations, and again conducted risk prediction. Three kinds of illustrations depicting medical scenes were used. Last, each student proposed solutions to prevent risks. In this study, we clarify differences in risk assessment tendencies for students between W-KY and S-KY. We found that students could predict a wide variety of risks about illustrations using W-KY, particularly risks about patient and medical personnel. However, for risks regarding management, clinical rules, and stakeholders, prediction in both S-KY and W-KY was difficult due students’ lack of knowledge, but solutions proposed by students covered these elements. Improving the format of discussion in W-KY might allow students to predict risk from a wider range of perspectives.
Keywords: Patient Safety Education, Undergraduate Education, Risk Assessment Skill, Kiken-Yochi Training, KYT, Risk Prediction, Clinically Inexperienced Medical Students
Practice Highlights
- This method helps inexperienced students brainstorm various scenarios needed for risk prediction.
- It was possible for students to practice risk assessment using What-If Kiken-Yochi Training (W-KY).
- Students could predict a wide variety of risks regarding patients and medical personnel using W-KY.
- It was difficult to predict management, clinical rules, and stakeholders’ risks even with W-KY.
I. INTRODUCTION
A. Issues on Patient Safety Education for Medical Students in Japan
In Japan, students enrol at medical schools immediately after graduating from high school. Safety education is often provided only at higher levels (4th or 5th year) in over 60% of medical schools in Japan, when clinical practice begins (Ishikawa, Hirao, & Maezawa, 2008). The following are the reasons: (1) educational practical methods for clinically inexperienced students are not specifically referred to in any guidelines or papers for students in the early years; (2) the educational effect on such students is unclear; (3) higher grade students have sufficient medical knowledge and can immediately apply their patient safety knowledge in clinical practice; and (4) there are few teachers specialising in medical safety, thus making it easier to determine the theme of education for higher grade students. On the contrary, 70% of medical schools only teach the minimum medical safety knowledge through lectures to students who have not yet practiced safety in clinical practice. The main contents of the lectures are analysis tools to prevent the recurrence of incidents, such as Root Cause Analysis and Failure Mode and Effects Analysis, legal responsibility knowledge, ethics, and infection (Mayer, Klamen, Gunderson, & Barach, 2009). However, as there are certain things that can be included immediately in clinical practice, it is difficult to keep students motivated.
The Telluride Interdisciplinary Roundtable (Mayer et al., 2009) and Lucian Leape Institute (2010) indicated that patient safety education should be conducted through a longitudinal curricular approach (including patient safety education in the curriculum of all grades), and it is important to educate lower grade students who have no clinical experience. This would enable students to learn the necessity and importance of patient safety knowledge, and to consider patient safety as implementation science while continuously practicing patient safety skills (Nakajima, 2012). Ishikawa et al. (2008) also emphasised the importance of continuous patient safety education, starting with beginner students so they can acquire good safety habits.
The Telluride Interdisciplinary Roundtable (Mayer et al., 2009) and Lucian Leape Institute (2010) outlined the patient safety competencies that students should acquire. In particular, students lack education on “non-technical skills” (Nakajima, 2012). Some of the necessary non-technical skills students need when they start working after graduation are risk assessment (situational awareness) skills to prevent accidents. This involves advance awareness of safety weaknesses and threats (risks) in the workplace or operations and the ability to avoid these risks (Doi, Kawamoto, & Yamaguchi, 2012; Takahashi, 2010). The World Health Organization’s (WHO’s) Patient Safety Curriculum Guide shows in Topic 6 (Understanding & Managing Clinical Risk) that students have to take correct action when they see an unsafe situation or environment (Walton et al., 2010). For example, when they see wet steps, they should predict the possibility of patients falling. WHO’s guide outlines the four-step process to manage clinical risks: (1) identify the risk, (2) assess the frequency and severity of the risk, (3) reduce or eliminate the risk, and (4) assess the costs saved by reducing the risk versus the costs of not managing the risk. However, this guide does not explain the teaching methods to enable students to identify or predict risks.
B. Educational Method Issues for Risk Assessment in Japan
Kiken-Yochi Training (KYT), a type of risk prediction training, was created by Sumitomo Metal Industries Co., LTD in 1974 (Chen & Mao, 2011), and helps workers understand risks in many kinds of industries, including the medical field (Doi et al., 2012; Hirokane, Shiraki, & Ohdo, 2010). KYT originated in Japan (Ito, Taguchi, & Fujinami, 2014) and has become a common safety management method (Ji, 2014). It increases workers’ awareness of risks and motivation to practice in a team and improves their problem-solving skills (Chen & Jin, 2012). KYT also enables workers to easily conduct on-site risk assessment. In a metal auto parts factory, the accident rate fell by six percent one year after the implementation of KYT (Poosanthanasarn, Sriboorapa, Fungladda, & Lohachit, 2005). In recent years, KYT use has also begun to spread in the medical field in countries other than Japan (Noor, Irniza, Emilia, Anita, & Suriani, 2016). In standard KYT (S-KY), the facilitator presents the learner with illustrations or photographs depicting the work site and guides them through four steps: (1) extracting items and risks considered to be dangerous in the illustration, (2) rating each item’s risk, (3) planning solutions, and (4) selecting urgent solutions (Japan Industrial Safety & Health Association, 2008). In particular, an important skill for medical staff at clinical sites is the ability to predict a myriad of risks from a broad perspective using the illustration in Step 1. More effective KYT has recently been designed, such as KYT using video instead of illustrations and KYT applications for tablets that enable students to easily take risk assessment training alone, such as during breaks, and KYT combining medical simulations of real clinic situations (Kadoyanagi, 2016; Nagamatsu, Miyazaki, & Harada, 2011; Takahashi et al., 2017; Yoneda et al., 2017).
However, in S-KY, the ability of experts to predict risks is higher than that of novices because novices do not have enough knowledge of important areas in the illustrations (Murata, Hayami, & Moriwaka, 2009). Hirokane et al. (2010) pointed out that experts are able to predict risks specifically in order to consider effective solutions to prevent accidents. Therefore, KYT is usually conducted for clinically experienced students, and is rarely implemented for inexperienced students. The reasons are as follows: (1) in S-KY, risk prediction in the illustrations is limited to “specific circumstances”; (2) if medical students practice risk prediction using only these illustrations, they cannot accurately identify risks at clinical sites when they encounter a situation different from the “specific circumstances” in the illustration in the future; and (3) if teachers use illustrations of scenes from non-medical sites to avoid the inability to predict risks in clinically inexperienced students who do not have enough medical knowledge, it is difficult for students to link the risk prediction content with actual clinical sites, to become motivated to learn, and to obtain educational effects from the training.
C. Hypothesis: What-If KYT (W-KY) Applicability
What-If analysis is used as a brainstorming method. It is widely used in the field of service design and brainstorms what kind of things will occur if a particular situation changes (Stickdorn & Schneider, 2012). Based on this method, Mochizuki and Komatsubara (2016) propose a step 0 prior to the existing risk assessment in KYT that is aimed at traffic safety, letting the participants identify various alternate situations: “If the situation of the illustration were different”. Next, the participants perform a risk assessment for each situation developed in Step 0. For example, the facilitator shows participants illustrations depicting sunny daytime “driving scenes on a straight road”. Participants conduct what-if brainstorming and consider various situations, such as “if the weather is different from the illustration”, “if it was night-time”, or “if it is a mountain pass”. They then conduct a risk assessment for each situation. This modification is called the W-KY. The subsequent steps are the same as the S-KY (Steps 1 to 4). By adding Step 0, participants are then better able to predict various risks from the illustrations, and their risk sensitivity increases.
Based on these articles related to S-KY and W-KY, S-KY might be more feasible for clinically experienced students than inexperienced students. Therefore, W-KY might be feasible for clinically inexperienced students, because the What-If analysis (Step 0) might help students’ brainstorming. It also might increase motivation to practice and improve students’ problem-solving capabilities. The central question of this paper is whether the W-KY is effective and feasible for clinically inexperienced students. Existing studies have not adopted the W-KY to medical treatment, and the effect on clinically inexperienced students is unclear.
D. Purpose of This Study
In this study, based on the W-KY, we propose and implement a training method to help clinically inexperienced students predict risks. We also clarify differences in the risk assessment tendencies of students in W-KY versus the S-KY.
II. METHODS
A. Methods in W-KY
We conducted the S-KY and W-KY for 120 medical students half a year after admission in 70-minute compulsory classes. The purpose of these classes was to teach diversity of thinking and thinking of others through discussions in small groups of seven to eight people. The S-KY and W-KY were conducted over two classes (140 minutes). Specifically, the students conducted group work in the following order using three kinds of illustrations (Figure 1) depicting clinical sites. In our class, after individual students brainstormed ideas, they shared ideas with others and learned about the diversity of ideas.
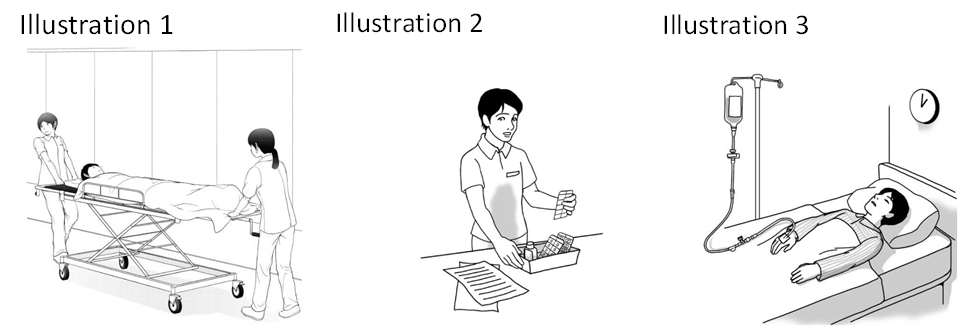
Figure 1. Illustrations used in S-KY and W-KY (Courtesy of Japan Industrial Safety & Health Association [n.d.])
Step 1 (S-KY Step): Individual students predicted what risks exist in the three illustrations, then they used posters to share their prediction results with the group.
Step 2 (W-KY Step): Individual students brainstormed “situations that differed from the illustration” for each of the three illustrations. For example, in Illustration 1, one student thought of “a situation in which only one person was guiding the gurney”.
Step 3 (W-KY Step): Individual students predicted what risks exist in the situations they brainstormed in Step 2, then shared the results in their groups using posters.
Step 4 (S-KY and W-KY Steps): Each student considered solutions to mitigate the risks that they had predicted and submitted a report on them at the end of the class. Specifically, each student selected one risk considered to be the biggest risk in each illustration, and considered three solutions to prevent the risk.
B. Clarification of Differences in Risk Assessment Tendency of Students Between W-KY and S-KY
We compared the prediction results of S-KY in Step 1 and W-KY in Step 3 using the P-mSHELL model (Kawano, 2002). This model shows that factors of medical incidents are patient, management, software, hardware, environment, and liveware (individuals/ teams). P-mSHELL represents the initials of these factors. To evaluate the effectiveness of safety education, it is necessary to ensure that risks related to Human Factors can be predicted from a broad viewpoint. There are several models that explain the cause of Human Factors issues: Lewin’s equation model (human behaviour is determined by factors related to the person and their environment; Lewin, 1936), the 4M model (factors related to Man, Machine, Media, and Management), and Reason’s categories (factors related to patient and provider; task, technology, and tool; and team, environment, and organisation; Reason, 1997). All models consider both human and environmental factors as the background of Human Factors issues. Among these models, P-mSHELL is a highly detailed model that explains human and environmental factors in medicine, thus making it easy to evaluate the effectiveness of safety education. The P-mSHELL model is based on the SHEL model that has been used in analysis of Human Factors issues in aviation. Molloy and O’Boyle (2005) pointed out this model is useful in examining errors in clinical site, and may have some potential in training medical staff about Human Factors. Therefore, the P-mSHELL model is frequently referenced to understand human error in medical care. It is expected that the target students of this research will be able to predict the safety weaknesses (risks) in the clinical site from the point of view of P-mSHELL and to take preventative solutions. For this reason, this study verifies the educational effect by comparing the danger predicted by S-KY and W-KY using this model. We also summarise student brainstorming results in Step 2 “regarding situations that differ from the illustration” and examine its effect on student risk assessment. Then, we classify the solutions described in the report by students from the point of view of P-mSHELL.
C. Ethical Considerations in This Research
Regarding the ethical use of the results of S-KY and W-KY conducted in the class for research, we emphasised and explained to students that cooperation in this study was voluntary and that declining to cooperate would have no influence on their grades. We explained that students’ grades are scored based on the rubric described in the syllabus and that consent to cooperate in the research could be withdrawn at any time. It was explained that the results of this study may be published after processing, but the student’s personal information would not be revealed in the publication. The students entered their consent to use the results of S-KY and W-KY for this research in the e-learning system, Moodle, and 120 out of 123 students agreed to participate. In this research, we analysed data from students who agreed to participate. This study was considered exempt by the Jichi Medical University Review Board (protocol number 18-014).
III. RESULTS
A. Results of Predicted Risk by S-KY and W-KY
Figure 2 (left) shows the total number of risks predicted by students for each illustration. In addition, Figure 2 (right) shows the average number of predicted risks for each student group. We clarified the difference between S-KY and W-KY using the students’ t-test.
First, students were able to predict a variety of risks regardless of whether S-KY or W-KY was used. With the exception of liveware (team) in Illustration 3, the risks for all elements of P-mSHELL were predicted. In addition, the risks varied widely in the ease of prediction by the illustration (Figure 2, left). In Illustration 1, patient, environment, and liveware (individual) risks were predicted in S-KY and W-KY. In Illustration 2 predicted risks were liveware (person), and in Illustration 3, patient. Risks related to management, software, and liveware (team) were very few in both S-KY and W-KY, and for some illustrations, student groups predicted no risks in some categories.
Despite W-KY being implemented after S-KY, patient and environment risks had approximately the same number in S-KY and the W-KY. The number of liveware (individual) and hardware risks predicted in W-KY was less than in S-KY—liveware (individual): t(16) = 3.47, p < .05; Hardware: t(16) = 3.44, p < .05. In W-KY, many were predicted in Illustrations 1 and 2.
For example, in scenario 1, risks such as, “staff transferred patient to the wrong room” and “the patient would be injured if the stretcher breaks” were predicted in S-KY. In W-KY, risks such as, “If the corridor is dark, staff are not able to notice changes in the patient’s condition”, “If the corridor gets wet, the stretcher may slip and fall”, “If the patient is elderly, the patient will fracture a bone due to impact”, “If the patient has dementia, he forgets about treatment when he wakes up and removes the infusion tube himself”, and “If the staff is busy, he forgets to change the drip, emptying the drip and harming the patient” were predicted.
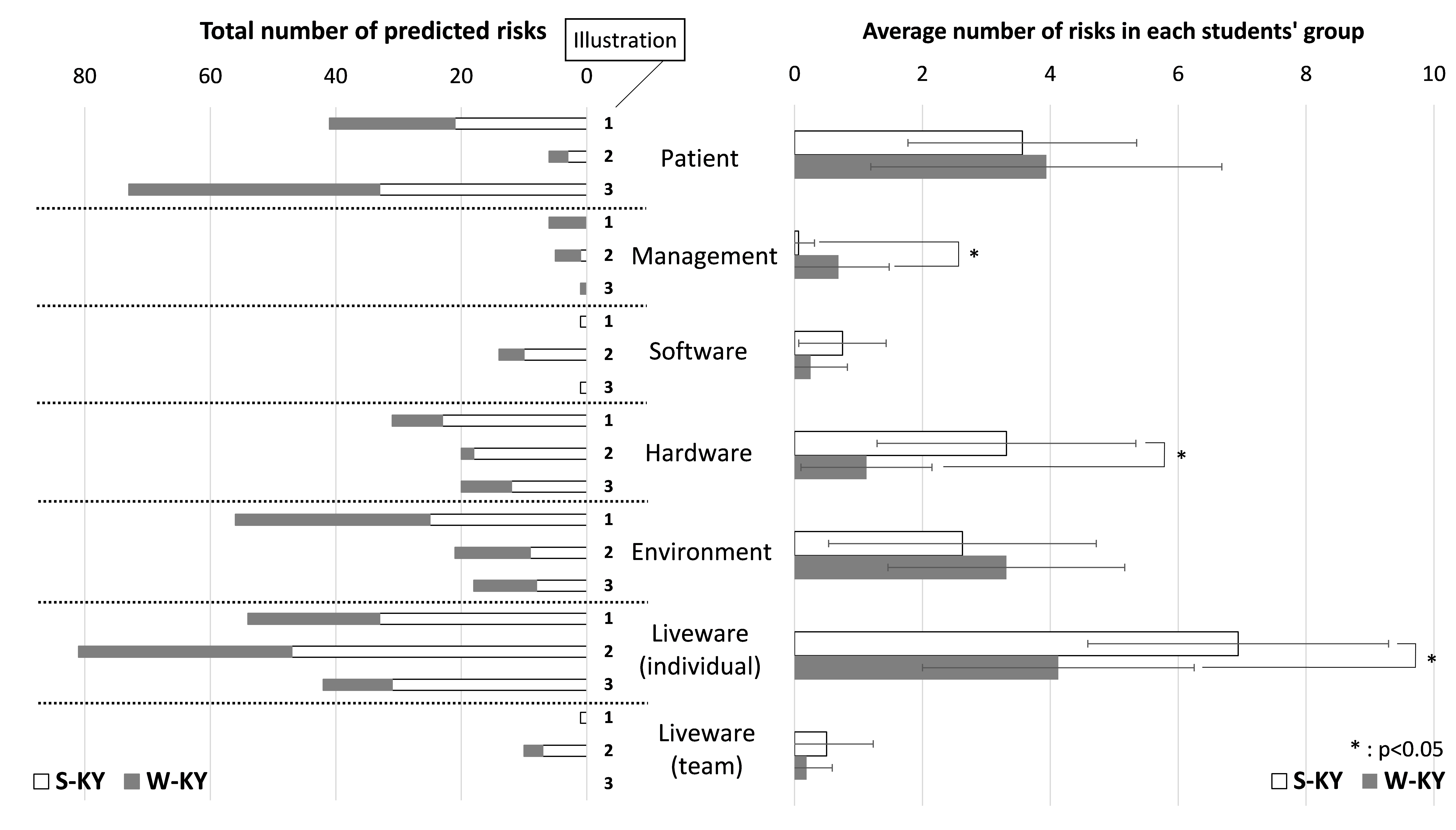 Figure 2. Result of predicted risk by S-KY and W-KY (Based on the classification of P-mSHELL)
Figure 2. Result of predicted risk by S-KY and W-KY (Based on the classification of P-mSHELL)
B. Results of Brainstorming Situations That Differed from the Illustration in Step 2
Table 1 shows how the students brainstormed situations that differed from each illustration in Step 2 as mentioned in the Methods section (refer to A. Methods in W-KY). In Table 1, the situations brainstormed by the students are organised based on each element of P-mSHELL.
First, the situations brainstormed by the students were remarkably diverse regarding patient, liveware (individual), hardware, and environmental factors. Although the number of liveware (individual) and hardware risks predicted in W-KY were less than in S-KY, the liveware (individual) risks predicted in W-KY were diverse.
On the other hand, the situation about management, software and liveware (team) were small in number (Table 1). This is also reflected in the low number of risks predicted for these factors (Figure 2).
| Description in the illustration | Situations brainstormed by students (in W-KY) | |
| Patient | One adult patient | Infants, elderly patients, infections, dementia, allergies, acute diseases, tall, obese patient, angry, sleeping, turning over many times, excited, removing the tube, patient with the same name exists, the patient’s family (child) is present, the operation is refused for religious reasons |
| Management | N/A | Staff shortage |
| Software | Directions | Mistaken, hard to read handwriting |
| Hardware
|
Gurney | Broken, screw loose, unstable |
| Bed | Narrow, nurse call button is broken | |
| Drip stand, tube | Fall, break, clogged tube, multiple drops exist | |
| Environment | Corridor | Crowded, wet in the rain, slippery, narrow, blackout |
| Room | Dark, bumpy, flickering, large number of patients | |
| Workspace | Messy | |
| Liveware (individual) |
One nurse | Fatigue, poor health, infection, lack of sleep, after working late, rushing, novice, lack of technology, lack of knowledge, presbyopia |
| Liveware (team) |
Nurse | Does not exist, bad relationship, noisy |
Table 1. Results of brainstorming in Step 2 about “situation different from illustration”
C. Solutions Proposed by Students to Mitigate the Risks
In Figure 3, the solutions proposed by the students to mitigate the risks were classified by P-mSHELL. In addition, Table 2 shows a concrete example of solutions for each element. In this paper, it has not been possible to analyse what kind of solutions were considered for each risk in S-KY and W-KY because students considered solutions in a post-class report.
In both S-KY and W-KY, students were able to consider a wide variety of solutions for almost all P-mSHELL factors. Although predicted risks related to management, software, and liveware (team) were very few, students were able to propose a lot of solutions related to them. There were many solutions, especially for software and hardware. For example, for software, double-checking, pointing and calling (occupational safety method), and creating a checklist were suggestion; in hardware, changing the shapes and names of the medicine in order to make it difficult to make mistakes was proposed.
| Patient | Patient participation Patient education Counseling, informed consent |
| Management | Work-life balance Rest management Staffing |
| Software | Creation of procedures (patient transport, patient fixation, dispensing, medication, patient assistance, etc.)
Examination of check method (pointing and calling, etc.) Efficiency of preparation work |
| Hardware
|
Improvement of hospital facilities
Improvement and computerisation of medical records and prescriptions Change of medicine shape and name Automation |
| Environment | Sorting Setting-in-order Shining Standardising Sustaining the discipline |
| Liveware (individual) |
Education and training Counseling Studying medical knowledge Attention/concentration Multitasking prevention Qualifications |
| Liveware (team) |
Good communication Thorough double check Establish a contact system |
Table 2. Examples of solutions considered by students
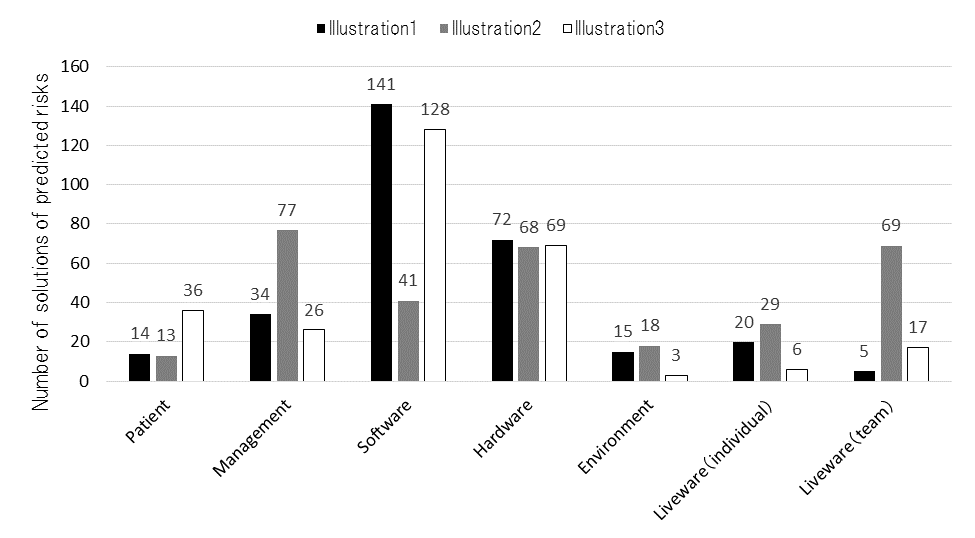 Figure 3. Result of solutions of predicted risks (based on the classification of P-mSHELL)
Figure 3. Result of solutions of predicted risks (based on the classification of P-mSHELL)
IV. DISCUSSION
A. Similarity and Difference Between S-KY and W-KY
Students should be able to predict risks in all elements of P-mSHELL as they can minimally experience the risks of each element in a clinical site. The results show that the elements of risk in P-mSHELL in both S-KY and W-KY are similar. Students could predict many patient and environment risks. These elements were drawn in advance in each illustration as shown in Figure 1. In other words, it was possible for students to brainstorm risks regarding stakeholders and medical devices drawn in illustrations in S-KY and W-KY. One of the possible reasons students could predict several patient and environment risks is that even a clinically inexperienced medical student has experience as a patient or has experienced the same situation (e.g., fatigue, immorality, lack of knowledge, etc.) as liveware (individual). Kazaoka, and Otsuka (2003) indicate that nursing students tend to recognise risks that they can imagine as their own and consider important, such as liveware (individual). On the other hand, management, software, and liveware (team) risks were very few in both S-KY and W-KY. The number of patient, environment, management, software, and liveware (team) risks had approximately the same number in S-KY and W-KY. The number of liveware (individual) and hardware risks in W-KY was less than in S-KY. In other words, it is considered that W-KY may cover the risks that can be predicted with S-KY.
Next, we discuss the strengths of W-KY. The risk description by students in W-KY included the risks and information related to various situations. Particularly in W-KY, students were able to brainstorm a wide variety of situations regarding patient, liveware (individual), hardware, and environmental risks (Table 1). This tendency is the same as the risk prediction tendency of S-KY and W-KY, and the reason for this tendency is considered to be the same. In W-KY, for example, regarding the transporting of stretchers, inexperienced students could consider various dynamic situations that can cause accidents, such as wet corridors, crowded corridors, violent or acutely ill patients, and lack of human resources. These situations that students brainstormed, listed in Table 1, are paraphrased as medical accident risks. In other words, in S-KY, students predict only medical accidents related to illustrations (results of accidents), whereas in W-KY, students were able to predict many high-risk situations that can cause medical accidents, and medical accidents (possible cause and results of accidents).
Through W-KY, students may have learned what a high-risk situation is and that clinical tasks can change into various dynamic situations that differ from illustrations. As a result, they may have learned the necessity of risk prediction in clinical practice and the significance of learning patient safety. These points will be explored in future research. In addition, Hirokane et al. (2010) pointed out that it is very important to predict risks specifically to prevent accidents. Therefore, it is possible that even inexperienced students can do this by using W-KY.
B. Limitations of W-KY
Only few students could predict risks management, software, and liveware (team) in S-KY and W-KY. However, students were able to consider solutions for almost all P-mSHELL factors (Figure 3). Contrary to the results of predicting risks in W-KY and S-KY, students were able to propose many solutions related to the aforementioned elements. This means that students can brainstorm these elements. In particular, regarding the software, students can mention the establishment and thoroughness of rules and manuals when planning solutions, and can think sufficiently from that viewpoint. Therefore, improving the format of discussion in W-KY may allow students to predict risks from a wider range of perspectives.
V. CONCLUSION
In this research, we proposed and implemented a training method to help clinically inexperienced students predict various risks. W-KY (brainstorming situations in illustrations and predicting risks based on them), as implemented in this research, allowed clinically inexperienced students to predict risks. We found that the elements of risk in P-mSHELL in both S-KY and W-KY are similar. Students could predict many patient and environment risks. However, with regard to management, software, and liveware (team) factors, S-KY and W-KY appeared to be difficult.
In addition, W-KY enables the prediction of high-risk situations that can cause medical accidents. This is important for predicting risks—including possible causes of accidents—specifically to prevent accidents.
In summary, W-KY can cover the risks that can be predicted by S-KY, and also allows students to consider various dynamic high-risk situations that can cause accidents. This suggests that W-KY can be used instead of S-KY.
In this study, it was not possible to analyse what kind of solutions to prevent risks were considered for each risk in S-KY and W-KY, as students considered solutions in a post-class report. Because this study was conducted as part of the class, we could not obtain data of student perspectives on learning outcomes or transferring learning to practice. The first-year medical school students in this research have the opportunity to receive medical safety education again when they are in the fourth year. At that time, we have plans to provide opportunities for practicing skills by applying W-KY in clinical practice, which will be explored in a future research. In addition, comparisons between students with clinical experience and inexperienced students and between W-KY/S-KY and other educational programs on accident prevention are also future topics of this research.
Notes on Contributors
Yoshitaka Maeda, PhD, is a research associate at the Medical Simulation Center at Jichi Medical University, Japan. He conducted the research supervision, class implementation, and data analysis.
Yoshikazu Asada, PhD, is an assistant professor at the Center for Information at Jichi Medical University, Japan. He contributed to the data compilation regarding the effect of this education.
Yoshihiko Suzuki, MD, is an assistant professor at the Medical Simulation Center at Jichi Medical University, Japan. He contributed to the design and planning of this class.
Hiroshi Kawahira, MD, is a professor at the Medical Simulation Center at Jichi Medical University, Japan. He gave advice on writing this paper and on data aggregation.
Ethical Approval
This study was approved by the Jichi Medical University Institutional Review Board (Protocol number 18-014).
Funding
There is no funding involved for this paper.
Declaration of Interest
The authors report no conflict of interest. The authors alone are responsible for the content and writing of this article.
References
Chen, Q., & Jin, R. (2012). Safety4Site commitment to enhance jobsite safety management and performance. Journal of Construction Engineering and Management, 138(4), 509-519. http://doi.org/10.1061/(ASCE)CO.1943-7862.0000453
Chen, N., & Mao, Y. (2011). Specific statistics and control method study on unsafe behavior in Chinese coal mines. Procedia Engineering, 26, 2222-2229. https://doi.org/10.1016/j.proeng.2011.11.2428
Doi, T., Kawamoto, K., & Yamaguchi, K. (2012). Difference in the level of patient treatment safety analysed by the years of experience of the radiological technologies. Nihon Hoshasen Gijutsu Gakkai zasshi [Japanese Journal of Radiological Technology], 68(5), 608-616. http://doi.org/10.6009/jjrt.2012_jsrt_68.5.608
Hirokane, M., Shiraki, W., & Ohdo, K. (2010). Hazard prediction activities for safety education. Doboku Gakkai Ronbunshuu F/JSCE Journal of Construction Engineering and Management, 66(1), 55-69. https://doi.org/10.2208/jscejf.66.55
Ishikawa, M., Hirao, T., & Maezawa, M. (2008). Study of patient safety education for undergraduates. Igaku Kyoiku / Medical Education (Japan), 39(2), 115-119. https://doi.org/10.11307/mededjapan1970.39.115
Ito, K., Taguchi, H., & Fujinami, K. (2014). Posing questions during experimental operations for safety training in university chemistry experiments. International Journal of Multimedia and Ubiquitous Engineering, 9(3), 51-62. http://dx.doi.org/10.14257/ijmue.2014.9.3.06
Japan Industrial Safety and Health Association. (2008). Sugu ni jissen shirīzu Anzen wo Sakidori Kiken Yochi [Practice series: Ahead of safety, risk prediction]. Tokyo, Japan: JISHA.
Japan Industrial Safety and Health Association. (n.d.). Iryō kango | kiken yobō kunren (KYT) muryō irasutoshīto-shū [Medical/Nursing | Risk prediction training (KYT) free illustration sheet collection]. Retrieved from https://www.aemk.or.jp/kyt/iryo/page/5
Ji, H. J. (2014). A study on safety culture construction for coal mine. Applied Mechanics and Materials, 644-650, 5949-5952. https://doi.org/10.4028/www.scientific.net/AMM.644-650.5949
Kadoyanagi, T. (2016). Shūdan sanka taiken-gata kōshū-yō kizai (dōga KYT)-tō no un’yō jōkyō ni tsuite (tokushū jukō-sha no tokusei ni ōjita kōtsū anzen kyōiku) (Operation of group training equipment [Video KYT]. [Traffic safety education according to the characteristics of the students]). Gekkan Kōtsū, 47(7), 44-55.
Kawano, R. (2002). Iryō risuku manējimento seminā tekisuto [Medical risk management seminar text]. Tokyo, Japan: Tepco Systems.
Kazaoka, T., & Otsuka, K. (2003). Study of nursing students’ recognition of the risks of medical treatment accidents: Using the scenario of role playing drug misadministrations. Journal of Japan Society of Nursing Research, 26(5), 133-143. https://doi.org/10.15065/jjsnr.20030912009
Lewin, K. (1936). Principles of topological psychology. New York, NY: McGraw-Hill. http://dx.doi.org/10.1037/10019-000
Lucian Leape Institute. (2010). Unmet needs: Teaching physicians to provide safe patient care. Boston, MA: National Patient Safety Foundation.
Mayer, D., Klamen, D. L., Gunderson, A., & Barach, P. (2009). Designing a patient safety undergraduate medical curriculum: The telluride interdisciplinary roundtable experience. Teaching and Learning in Medicine, 21(1), 52-58. https://doi.org/10.1080/10401330802574090
Mochizuki, R., & Komatsubara, A. (2016). Proposal of traffic KYT with using What-if analysis. The Human Factors in Japan, 20(2), 79-82.
https://doi.org/10.11443/jphf.20.2_79
Molloy, G. J., & O’Boyle, C. A. (2005). The SHEL model: A useful tool for analyzing and teaching the contribution of Human Factors to medical error. Academic Medicine, 80(2), 152-155.
Murata, A., Hayami, T., & Moriwaka, M. (2009). Visual information processing characteristics of drivers in prediction of dangerous situation-comparison among novice, expert and non-licensed person. In Proceedings: Fifth international workshop on computational intelligence & applications, 2009(1), 254-257. Hiroshima, Japan: IEEE SMC Hiroshima Chapter.
Nagamatsu, I., Miyazaki, I., & Harada, C. (2011). Kango kiso kyōiku ni okeru kiken yochi torēningu (KYT) wo toriireta iryō anzen kyōiku ni kansuru kōsatsu: Dōga jirei o mochiita puroguramu no kōka [A study on medical safety education incorporating risk prediction training (KYT) in nursing education: Effects of programs using movie]. Nihon kango gakkai ronbun-shū. Kango kyōiku, 42, 158-161. Retrieved from
https://iss.ndl.go.jp/books/R000000004-I023685394-00?ar=4e1f&locale=e
Nakajima, K. (2012). 4. Patient safety and quality improvement education for undergraduate medical students. Nihon Naika Gakkai Zasshi [Journal of the Japan Society of Internal Medicine], 101(12), 3477-3483. https://doi.org/10.2169/naika.101.3477
Noor, A. Y., Irniza, R., Emilia, Z. A., Anita, A. R., & Suriani, I. (2016). Kiken yochi training (KYT) in reducing accidents at workplaces: A systematic review. International Journal of Public Health and Clinical Sciences, 3(4), 123-132.
Poosanthanasarn, N., Sriboorapa, S, Fungladda, W., & Lohachit, C. (2005). Reduction of low back muscular discomfort through an applied ergonomics intervention program. The Southeast Asian Journal of Tropical Medicine and Public Health, 36(Suppl. 4), 262-270.
Reason, J. T. (1997). Managing the risks of organizational accidents. Aldershot, England: Ashgate Publishing Limited.
Stickdorn, M., & Schneider, J. (2012). This is service design thinking: Basics-tools-cases. Amsterdam, The Netherlands: BIS Publishers.
Takahashi, A., Mishina, M., Takagi, M., Shimazaki, K., Ishida, T., & Umezaki, S. (2017). Taburetto tanmatsu wo mochiita anzen kyōzai no kunren kōka to anzen kanri e no ōyō: Teisō jūtaku kenchiku genba wo taishō to shite [Effect of safety teaching materials using tablet and its application to safety management: For low-rise residential building]. Specific research reports of National Institute of Occupational Safety and Health, 47, 39-44.
Takahashi, R. (2010). Nontekunikkusukiru torēningu e no chosen [Challenge to non-technical skills training]. In K. Nakajima, & Y. Kodama (Eds.), Iryō anzen koto hajime [Beginning of medical safety] (pp. 36-51). Tokyo, Japan: Igaku Syoin.
Walton, M., Woodward, H., Van Staalduinen, S., Lemer, C., Greaves, F., Noble, D., … Barraclough, B. (2010). The WHO patient safety curriculum guide for medical schools. BMJ Quality & Safety, 19(6), 542-546. http://dx.doi.org/10.1136/qshc.2009.036970
Yoneda, T., Itami, K., Seki, K., Kawabata, A., Kubota, Y., Yasuhara, O., & Maesako, T. (2017). Changes in nursing students’ risk awareness and understanding of medical incidents after exposure to a simulated incident. Japan Journal of Educational Technology, 41(Suppl.), 17-20.
https://doi.org/10.15077/jjet.S41011
*Yoshitaka Maeda
Medical Simulation Center,
Jichi Medical University,
3311-1, Yakushiji,
Shimotsuke-shi, Tochigi, Japan
Tel: +81 285 58 7455
Email: y-maeda@jichi.ac.jp
Published online: 7 January, TAPS 2020, 5(1), 54-60
DOI: https://doi.org/10.29060/TAPS.2020-5-1/OA2095
Min Jia Chua1, Gen Lin Foo2 & Ernest Beng Kee Kwek2
1National Healthcare Group, Ministry of Health Holdings, Singapore; 2Department of Orthopaedic Surgery, Woodlands Health Campus, Singapore
Abstract
Introduction: Mentoring is a vital component of a well-rounded medical teaching environment, as evidenced by its implementation in many residency programmes. This study aims to evaluate the perceived value of mentoring by faculty and near-peer mentoring to the orthopaedic surgery resident.
Methods: An online survey comprising multiple choice questions and scaled-response questions with a few open-ended questions was created and distributed to all residents, from residency years 2 to 5, within an orthopaedic residency programme in Singapore to gather their views on a tiered mentorship programme.
Results: 100% of surveyed residents responded. 68.4% of junior residents had a senior resident mentor while 84.8% of all residents had a faculty mentor. Junior residents generally viewed senior resident mentors as being crucial and beneficial for training, with scores comparable to those for faculty mentors. Residents who had mentors, in particular those who had chosen their own mentors, tended to be more satisfied than their counterparts. The most desired characteristics of mentors among the residents included approachability, willingness to share, being able to give feedback and experience. 66.7% of residents felt that near-peer mentorship should be required in the residency programme but only 30.3% of them felt that it should be formalised. 78.8% of residents surveyed felt that mentorship by faculty was required.
Conclusion: Residents viewed mentoring by faculty and near-peer mentoring as being beneficial and crucial to their orthopaedic residency training. We propose that an ideal mentoring programme should be tiered, allow choice of mentors and include near-peer mentoring as a requirement but not necessarily monitored.
Keywords: Orthopaedic Surgery, Resident Education, Mentoring, Medical Teaching, Tiered Mentorship
Practice Highlights
- Study to evaluate value of mentoring by faculty and near-peer mentoring to orthopaedic surgery resident.
- Residents viewed mentoring by faculty and near-peer mentoring programmes as being beneficial and crucial.
- Ideal mentoring programme should be tiered and allow choice of mentors.
- Near-peer mentoring should be a requirement but not necessarily monitored.
I. INTRODUCTION
Mentoring has long been a crucial element of effective resident medical education (Sambunjak, Straus, & Marusic, 2006), with many programmes adopting mentoring by faculty as an integral component of their residency programme. Various models of mentoring and types of mentoring activities have been described including didactic sessions, regular mentor-mentee meetings and group projects (Kashiwagi, Varkey, & Cook, 2013). The benefits of mentoring have also been shown in various studies, by aiding personal and professional development during residency, helping with
career preparation (Ramanan, Taylor, Davis, & Phillips, 2006), improving professional and social skills (increased self-confidence, improved communication skills; Buddeberg-Fischer, & Herta, 2006).
There is however, little data looking at how Orthopaedic residents view mentorship programmes (Flint, Jahangir, Browner, & Mehta, 2009). Furthermore, most studies look at mentoring by faculty with little emphasis on near-peer mentoring. In fact, a literature review has shown that no studies have looked at and compared the two entities in orthopaedic residency programmes.
In our residency programme, a tiered mentorship framework, where both mentoring by faculty and near-peer mentoring are practised, has been in place since 2014. In the former, a mentor of associate consultant grade and above who is in post-fellowship training will mentor a resident while in the latter, a senior resident mentor will mentor a junior resident two residency years below him or her.
The objective of having a near-peer mentorship framework in our programme was to bridge some of the gaps in traditional mentorship. In mentorship by faculty models, there will inevitably be hierarchical distance between mentors and mentees and residents may not feel as at ease approaching their mentors for certain issues. Furthermore, there may be a shortage of faculty members who are also strapped for time and may not be able to devote enough time for holistic mentorship of residents. These mentors are also further away from their residency training years and may not be able to understand some of the issues their mentees face in the current residency climate. It was envisaged that senior residents who are near-peers on the ground will be able to address some of the abovementioned shortcomings in the traditional mentorship model.
Currently, mentorship by faculty is formally monitored by the programme and mandates at least bi-annual meetings with a mentoring form to be filled in while near-peer mentorship is a self-directed initiative by the residents which is more informal with no stipulated frequency of meetings and no compulsory documentation under the residency programme requirements.
Residents were either assigned mentors or chose mentors at the start of the second year of their residency but due to various factors including efflux of faculty mentors or other administrative reasons, some residents do not have either senior resident or faculty mentors or both.
The objectives of this study were to 1) evaluate the orthopaedic surgery residents’ perception of mentoring by faculty and near-peer mentoring and 2) establish factors perceived as being important in mentors and a successful mentoring environment.
II. METHODS
An anonymised online survey with voluntary participation was administered to all orthopaedic surgery residents, from residency years 2 to 5 (R2 to R5), in our orthopaedic surgery residency programme. No identifiers were collected to ensure protection of the privacy of survey respondents. The choice of survey as the tool was to maximise response rates without compromising on data collection through comprehensive survey questions. There were two sets of questions evaluating the residents’ perception of mentoring by faculty and near-peer mentoring. The near-peer mentoring questions differed depending on whether the resident was a senior or junior resident and whether the resident possessed a mentee or mentor respectively. The mentoring by faculty questions varied depending on the presence of a mentor. The survey questions presented to the respondent were modified real-time based on their initial answers to the previous questions, hence eliminating questions which were not relevant.
These survey questions were adapted from a census survey conducted by the American Academy of Orthopaedic Surgeons (Flint et al., 2009) on residents with regard to their experience in, and opinion of mentorship programmes and the prevalence of such programmes.
The questions administered were largely multiple-choice questions and scaled-response questions with a few open-ended questions. The multiple-choice and scaled-response questions covered the characteristics and perception of the mentoring environment (including how beneficial and crucial they found the mentoring programme, their satisfaction with the programme, their ideal mentorship framework, etc.), the perception of the value of mentoring (for instance to what extent they felt it supported their educational experience, aided with networking and making career decisions) and the characteristics of an ideal mentor. For the scaled response questions, respondents were asked to rate the importance of and their satisfaction with the different facets of their mentoring experience or environment on a scale ranging from 1 to 5.
The open-ended section of the survey allowed residents to air what they had achieved or hoped to achieve through the mentorship programme as well as general comments about the programme and suggestions for improvement.
Standard institutional review board procedures were followed and ethics board approval was obtained. Data analysis was performed using SPSS.
III. RESULTS
The survey was administered to a total of 33 residents across the residency batches from R2 to R5 in the residency year, with a response rate of 100%. Of the respondents, 19 were junior residents (8 R2 and 11 R3) and 14 were senior residents (6 R4 and 8 R5).
Of the junior residents, 68.4% (13/19) of them had senior residents while 78.6% (11/14) of the surveyed senior residents had junior resident mentees, with two of the senior residents having two junior resident mentees. 84.8% (28/33) of surveyed residents had faculty mentors (further details in Table 1).
| Residency year | Number with faculty mentors | Number without faculty mentors | Number with SR mentors (R2 and R3) or mentees (R4 and R5) | Number without SR mentors (R2 and R3) or mentees (R4 and R5) |
| R2 | 6/8 (75%) | 2/8 (25%) | 7/8 (87.5%) | 1/8 (12.5%) |
| R3 | 11/11 (100%) | 0/11 (0%) | 6/11 (54.5%) | 5/11 (45.5%) |
| R4 | 3/6 (50%) | 3/6 (50%) | 4/6 (66.7%) | 2/6 (33.3%) |
| R5 | 8/8 (100%) | 0/8 (0%) | 7/8 (87.5%) | 1/8 (12.5%) |
Table 1. Breakdown of residents with faculty and senior resident (SR) mentors/mentees
Of the junior residents with a senior resident mentor, 53.8% (7/13) of them chose their own mentors while the rest had their mentors assigned. Of the residents with a faculty mentor, 60.7% (17/28) of them chose their own mentors. 69.2% (9/13) of junior residents met up with their senior resident mentors at least twice a year while 82.1% (23/28) of residents met up with their faculty mentors at least half-yearly or more frequently.
It was found that junior residents viewed senior resident mentors as being moderately beneficial and crucial to their training, with average scores of 3.92 on a scale of 1 to 5 (Figure 1). Of note, it was found that residents with senior resident mentors viewed near-peer mentorship as being more crucial and beneficial compared to their counterparts without senior resident mentors. Similar results were also echoed by the residents regarding their faculty mentors, with average scores of 3.89 and 4.14 for how crucial and beneficial faculty mentors were to residents with mentors and average scores of 3.6 and 4.0 for residents without mentors.
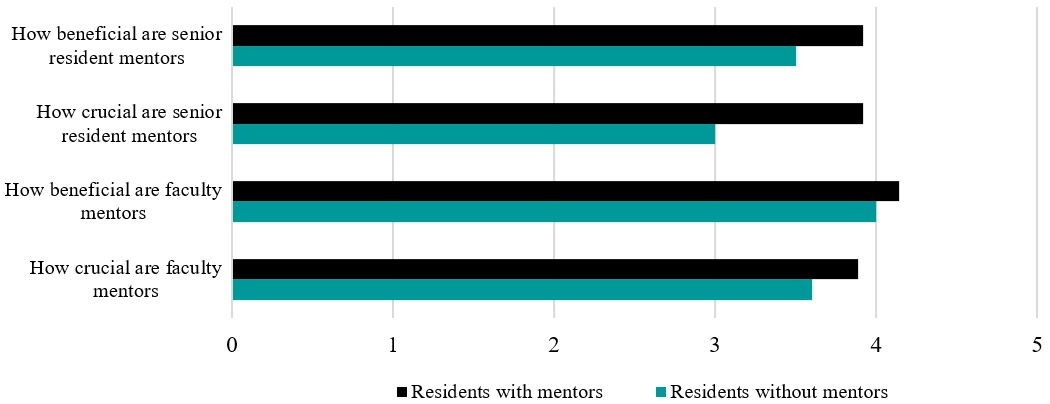
Figure 1. Chart showing how crucial and beneficial residents viewed senior resident and faculty mentors
In terms of satisfaction levels with the mentoring programme, residents with mentors (senior resident and faculty mentors) were also more satisfied with the mentoring programme than their peers without mentors, with average scores of 4.31 and 4.33 for residents with senior and faculty mentors respectively compared to average scores of 3.75 and 4.00 for residents without senior and faculty mentors.
A further subgroup analysis yielded that respondents with a self-selected mentor from both the senior resident and faculty mentor groups had higher scores for satisfaction levels (4.28 and 4.41 respectively) compared to those who had assigned mentors (4.16 and 4.20). Those with self-selected mentors in the faculty mentor group also felt that their mentor aided them more in supporting their educational experience and in making career decisions.
84.6% (11/13) of junior residents who had a senior resident mentor felt that their senior resident mentor was able to provide them with advice about career, employment, or difficult cases in the future while 89.3% (25/28) of residents with faculty mentors felt the same about their faculty mentors.
In terms of desired characteristics in a senior resident mentor, approachability, willingness to share and experience were the top three most desired characteristics (Figure 2A). Similar results were echoed in the results for faculty mentors, with ability to give feedback also highly valued (Figure 2B).
66.7% (22/33) of all residents felt that near-peer senior resident mentoring should be required in the resident programme but only 30.3% (10/33) thought that it should be formalised. Some of those who felt that near-peer mentoring should not be required expressed that they would like it to be up to the individual resident and that residents who are in need would approach senior residents directly of their own accord. 78.7% (26/33) of residents surveyed were of the opinion that faculty mentorship by faculty was required. Those who felt that faculty mentorship should not be required offered reasons including the hectic schedule of consultants and the unpredictable flow of faculty members into the private practice which would make it difficult for residents to maintain the same mentor throughout residency training.
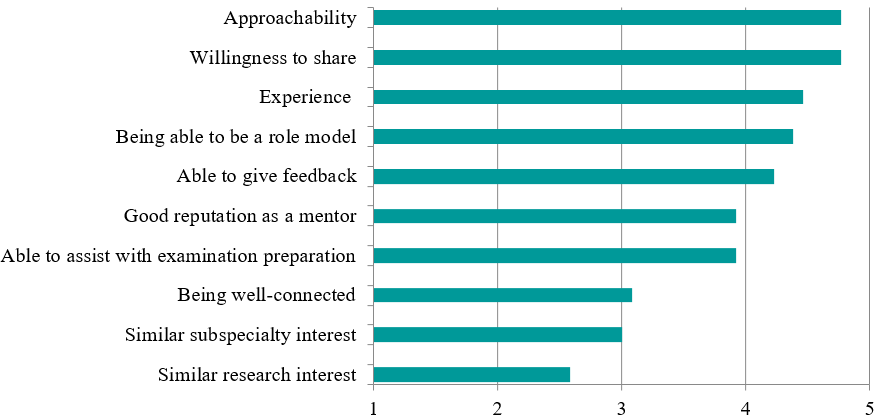
Figure 2A. Chart depicting the desired characteristics scores in senior resident faculty mentors, ranked from most to least desired
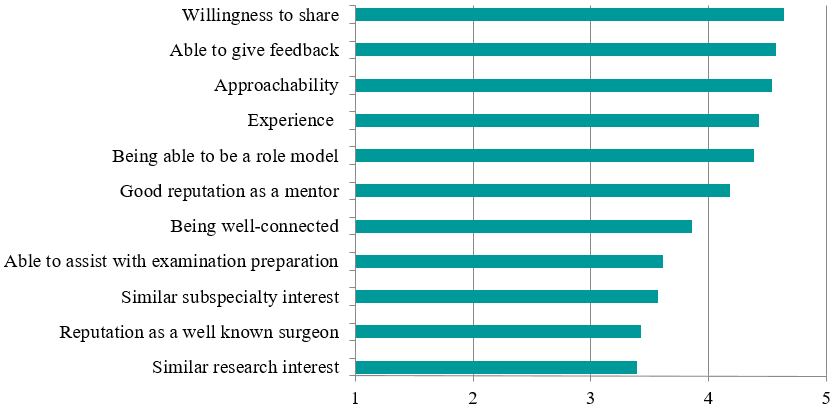
Figure 2B. Chart depicting the desired characteristics scores in faculty mentors, ranked from most to least desired
IV. DISCUSSION
Traditionally, the art of medicine and especially surgery has been passed down through an apprenticeship model (Gofton & Regehr, 2006). Multiple studies have shown that various aspects such as career paths, research output as well as personal development can be influenced greatly by mentorship (Calligaro, Dougherty, Sidawy, & Cronenwett, 2004; Gedde, Budenz, Haft, Lee, & Quigley, 2007). In fact, close to 80% of paediatric residents polled in a survey gave feedback that having a mentor was either very useful or crucial to survival during their residency years (Curtis, Adam, & Shelov, 1995). Over 20 years later, it appears that little has changed, with similar results being echoed in our study, with high scores reported for how crucial and beneficial faculty and senior resident mentorship was viewed as being by residents.
There are myriad challenges which one will face when mentoring orthopaedic residents. In comparison to teaching medical students, teaching an orthopaedic resident is often longer, more intense and calls for greater responsibility for teaching while compared to fellowship training (post-residency for subspecialty training); the mentor is teaching a much less knowledgeable and skilled protégé (Levine, Braman, Gelberman, & Black, 2013). There is hence an enhanced requirement for timely provision of feedback and assessment, and for nurturing the resident through his or her years of training. As Hill and Boone (2002) mentioned in their paper, mentoring aims “to provide a young aspiring professional with a tangible and immediate role model”. (p. 73)
For successful mentoring to occur, it requires reciprocity and has to be a “collaborative learning relationship” (Bland, Taylor, Shollen, Weber-Main, & Mulcahy, 2009). Levine et al. (2013) proposed certain obligations for a mentee to fulfil to maintain the mentor-mentee relationship and enhance the likelihood of success, including demanding and accepting feedback, seeking opportunities for self-improvement, following through, being prepared, requiring accountability, and more.
For the mentors, some traits which have been viewed as being important by surgical trainees include enthusiasm for the practice of surgery, commitment to excellence, good surgical technique, good leadership qualities, integrity and professionalism (Healy, Glynn, Malone, Cantillon, & Kerin, 2012). Certain more desirable traits of mentors which we have noted in our study include approachability, willingness to share and impart knowledge, experience as well as ability to give feedback. A mentor who has these traits will be better equipped to pass on his knowledge and skills to his mentee and hence provide a more well-rounded learning environment for the resident.
Nevertheless, we understand that mentoring is no mean feat and hence, it is recommended that both faculty members and senior residents take it upon themselves to train specific skill sets and develop desirable traits for mentoring which will enable them to successfully take on this mantle of responsibility. Mentoring workshops have been shown to improve mentoring competency and thereby improve outcomes for optimally mentored mentees (Lau et al., 2016; Gandhi & Johnson, 2016).
Our study also found that residents with self-selected mentors had higher satisfaction with the mentoring programme and felt that these mentors were able to support them more in their educational experience and making career decisions, a finding echoed in other studies (Yamada, Slanetz, & Boiselle, 2014). We postulate that this is because residents who selected their own mentors would be able to choose mentors who had desirable traits and whom they saw as ideal role models or were like-minded in their approach. Mentees have been shown to select role models—partners with whom they enjoy working and often report a mutual attraction or chemistry that sparks the development of the relationship (Kram, 1983).
As previously alluded to, mentoring by faculty is practised in many institutions and residency programmes but near-peer mentoring is often overlooked. The original intent of having a tiered mentorship framework in our programme was to ensure a holistic approach to mentoring of residents. It was envisioned that the senior resident mentor would be able to help ease the junior resident into the training programme and deal with immediate junior-level issues as well as assist in intermediate examination preparation while the senior faculty mentors would be able to provide a more overarching view as well as guidance and career advice. In the literature, it was found that mentees were generally less intimidated by near-peer mentors, felt they could relate better to them, and the near-peers understood them better as they had recently gone through situations they (the mentees) were now facing (Akinla, Hagan, & Atiomo, 2018). It was also shown that near-peer mentoring was a way of promoting professional and personal development, aid transition and maintain well-being of mentees (Akinla et al., 2018).
Residents in our programme were generally of the opinion that tiered mentorship was necessary but that near-peer mentoring should be informal, without any stipulated frequency of meetings, documentation of meetings and forms to fill up unlike mentoring by faculty. This is likely because senior residents are usually just a few years senior to the junior resident and both the mentors and mentees prefer a more informal environment and style of mentoring. This also enables junior residents to be more at ease to freely discuss any issues with the senior resident mentor. Furthermore, both the senior and junior residents have far more opportunities for interaction compared to the faculty mentor and the resident.
In the survey administered, aside from the previously mentioned results, we have also found that near-peer mentoring has positive effects on both the mentor as well as the mentee, with mentees commenting that senior resident mentors could provide pertinent directions as they started junior residency. Similarly, senior resident mentors felt that senior resident mentorship gave them an avenue to provide guidance and encouragement to their juniors, to allow them to benefit from past mistakes and to learn more efficiently. Furthermore, a tiered mentoring system contributes to a positive learning environment, creating a culture of camaraderie amongst seniors and juniors, resulting in a more closely-knit professional community.
Our residency programme encompasses both senior resident and faculty mentoring with the details on its implementation in our programme covered above. Moreover, it is the first to look at tiered mentoring and its impact on residents in orthopaedic surgery, with a 100% response rate among residents in our programme.
However, we acknowledge that this study does have some limitations. The first is that of the small sample size, which contributed to many of the variables being studied not having a statistically significant difference. Though we are limited by the small sample size due to the number of residents in the programme, we were able to achieve a high response rate as well as sub-divide the residents based on other variables including presence of a mentor and method of selection of mentor to allow for comparison between different groups. Other limitations include the fact that this study was only carried out in one institution which practised said model of mentorship. In addition, the mentorship programme had only been in place for two years when the survey was administered and its effects may not have been that far-reaching and apparent given the relatively short period of implementation, though this could form the basis for a longitudinal study in the future at further time points.
Future studies should be undertaken in the future to explore this field further. Studies involving various institutions which practice this model could be considered. Another area of study could be to look at objective measures like the Orthopaedic In-Training Examination and clinical rotation scores, exit examination success percentages and more. This would allow us to find out the tangible measurable effects that mentoring has on residents.
V. CONCLUSION
In conclusion, our study has found that mentoring by faculty and near-peer mentoring programmes are generally viewed as being beneficial and crucial to residency training and we believe that programmes should consider instituting tiered mentorship to reap the benefits.
We propose that an ideal mentoring environment should be 1) one that is tiered (encompassing both mentoring by faculty and near-peer mentoring), 2) a system that allows residents to choose their mentors, and 3) have near-peer mentoring as a required part of residency but on a more informal basis.
Notes on Contributors
Dr Chua Min Jia is a senior resident in orthopaedic surgery at the National Healthcare Group. He was involved in devising of the survey questionnaire, data collection and analysis and was the primary author of this manuscript.
Dr Foo Gen Lin is an associate consultant in the Department of Orthopaedic Surgery at the Woodlands Health Campus in Singapore. He was involved in devising of the survey questionnaire and editing of the manuscript.
Dr Ernest Kwek Beng Kee is a senior consultant and Chief of the Department of Orthopaedic Surgery at the Woodlands Health Campus in Singapore. He was involved in devising of the survey questionnaire, editing and approval of the final manuscript as well as overall supervision of the project.
Ethical Approval
This study was exempted by the National Healthcare Group Domain Specific Review Boards (DSRB).
Acknowledgement
The authors wish to thank all the orthopaedic surgery residents in our programme who participated in this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Interest
There is no conflict of interest to declare.
References
Akinla, O., Hagan, P., & Atiomo, W. (2018). A systematic review of the literature describing the outcomes of near-peer mentoring programs for first year medical students. BMC Medical Education, 18(1), 98.
Bland, C. J., Taylor, A. L., Shollen, S. L., Weber-Main, A. M., & Mulcahy, P. A. (2009). Faculty success through mentoring: A guide for mentors, mentees, and leaders. New York, NY: Rowman & Littlefield Education.
Buddeberg-Fischer, B., & Herta, K. D. (2006). Formal mentoring programmes for medical students and doctors – A review of the Medline literature. Medical Teacher, 28(3), 248-257.
Calligaro, K. D., Dougherty, M. J., Sidawy, A. N., & Cronenwett, J. L. (2004). Choice of vascular surgery as a specialty: Survey of vascular surgery residents, general surgery chief residents, and medical students at hospitals with vascular surgery training programs. Journal of Vascular Surgery, 40(5), 978-984.
Curtis, J. A., Adam, H., & Shelov, S. P. (1995). A formal mentoring program in a pediatric residency. Academic Medicine, 70(5), 453-454.
Flint, J. H., Jahangir, A. A., Browner, B. D., & Mehta, S. (2009). The value of mentorship in orthopaedic surgery resident education: The residents’ perspective. Journal of Bone and Joint Surgery America, 91(4), 1017-1022.
Gandhi, M., & Johnson, M. (2016). Creating more effective mentors: Mentoring the mentor. AIDS and Behavior, 20(Suppl 2), 294-303.
Gedde, S. J., Budenz, D. L., Haft, P., Lee, Y., & Quigley, H. A. (2007). Factors affecting the decision to pursue glaucoma fellowship training. Journal of Glaucoma, 16(1), 81-87.
Gofton, W., & Regehr, G. (2006). Factors in optimizing the learning environment for surgical training. Clinical Orthopaedics and Related Research, 449, 100-107.
Healy, N. A., Glynn, R. W., Malone, C., Cantillon, P., & Kerin, M. J. (2012). Surgical mentors and role models: Prevalence, importance and associated traits. Journal of Surgical Education, 69(5), 633-637.
Hill, J. A., & Boone, S. (2002). Personal perception on mentoring. Clinical Orthopaedics and Related Research, 396, 73-75.
Kashiwagi, D. T., Varkey, P., & Cook, D. A. (2013). Mentoring programs for physicians in academic medicine: A systematic review. Academic Medicine, 88(7), 1029-1037.
Kram, K. E. (1983). Phases of the mentor relationship. Academy of Management Journal, 26(4), 608-625.
Lau, C., Ford, J., Van Lieshout, R. J., Saperson, K., McConnell, M., & McCabe, R. (2016). Developing mentoring competency: Does a one session training workshop have impact? Academic Psychiatry, 40(3), 429-433.
Levine, W. N., Braman, J. P., Gelberman, R. H., & Black, K. P. (2013). Mentorship in orthopaedic surgery-road map to success for the mentor and the mentee: AOA critical issues. Journal of Bone and Joint Surgery America, 95(9), e59.
Ramanan, R. A., Taylor, W. C., Davis, R. B., & Phillips, R. S. (2006). Mentoring matters. Mentoring and career preparation in internal medicine residency training. Journal of General Internal Medicine, 21(4), 340-345.
Sambunjak, D., Straus, S. E., & Marusic, A. (2006). Mentoring in academic medicine: A systematic review. Journal of the American Medical Association, 296(9), 1103-1115.
Yamada, K., Slanetz, P. J., & Boiselle, P. M. (2014). Perceived benefits of a radiology resident mentoring program: Comparison of residents with self-selected vs assigned mentors. Canadian Association of Radiologists Journal, 65(2), 186-191.
*Chua Min Jia
Ministry of Health Holdings,
1 Maritime Square, Singapore 099253
Tel: +65 6357 7713
E-mail: minjia.chua@mohh.com.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
