
Are residents learners or workers? A historical perspective in Japan
Submitted: 12 July 2020
Accepted: 18 August 2020
Published online: 5 January, TAPS 2021, 6(1), 122-124
https://doi.org/10.29060/TAPS.2021-6-1/PV2339
Hirohisa Fujikawa1, Daisuke Son1,2 & Masato Eto1
1Department of Medical Education Studies, International Research Center for Medical Education, Graduate School of Medicine, The University of Tokyo, Japan; 2Department of Community-based Family Medicine, School of Medicine, Tottori University Faculty of Medicine, Japan
I. INTRODUCTION
Many countries enforce limits on the number of hours that medical residents work. For example, in the United States, regulations about duty hours were instituted by the Accreditation Council of Graduate Medical Education as early as in 2003, reinforcing those limits in 2011 and again in 2017 (Accreditation Council for Graduate Medical Education, 2017). These reforms triggered discussion in medical education literature about their wide-ranging effects on resident education, resident wellness, and patient care (Bolster & Rourke, 2015).
In Japan, restrictions on working hours will be implemented for physicians in April 2024 (Shibuya & Unno, 2019). Because of its rapidly shifting demographics to being a super-aged society with a low birth rate, Japan is now facing issues with residents’ learning and working that other countries will need to confront in the near future as their populations shift as well (as of late 2020). Here we report on the history and current situation of postgraduate medical education in Japan, which are highly relevant to re-evaluating postgraduate training in other countries.
II. INTRODUCTION OF WESTERN-STYLE MEDICAL EDUCATION TO JAPAN
Up to and throughout the Edo period (1603–1868), there were no qualifications required for someone to become a physician; they learned in apprenticeship or learned by reading medical books on their own (Izumi & Isozumi, 2001).
At the beginning of the Meiji era (1868–1912), the Japanese government introduced German medicine to the medical education system in Japan. In 1871, the government invited German medical teachers to the precursor of the University of Tokyo (Daigaku To-ko) (Izumi & Isozumi, 2001). In the years that followed, many graduates from that school were in charge of medical education at medical schools nationwide. The German-style medical education system, therefore, spread throughout Japan and the German impact on the Japanese system of medical education is still evident. For example, Japan’s current six-year undergraduate medical educational system has Germanic origin. Thus, although Japan introduced Western-style medical education, there was no systematic system of postgraduate medical education in this era.
III. EARLY INTERNSHIP PROGRAMME AND DEVELOPMENT OF NEW POSTGRADUATE MEDICAL TRAINING SYSTEM
From the end of World War II until the 1980s, the Japanese medical education system was reconstructed as a result of Japan coming under American influence. In 1946, the present national licensing system for physicians and first medical internship system were implemented. The educational content of this early internship programme, however, was lacking, as were the financial arrangements for the interns. Trainees had no guarantee of their status, and the first-year residents were required to work as volunteers before taking the national medical license examination (Shukan Igakukai Shimbun, 2004).
In the late 1960s, protests by medical students at the University of Tokyo for the improvement of interns’ working conditions progressively intensified and spread to other universities as well. Students across the country boycotted the medical license test and those in Tokyo occupied the Yasuda Auditorium (a symbol of the University of Tokyo) in protest. There was recognition that the internship programme as it was, with its overworked trainees, could lead to patient safety issues related to possible errors by the fatigued interns. This problem of patient safety is still a topic of discussion worldwide, and led to the limit of 80 hours of work per week for residents in U.S. training programmes mentioned in the introduction.
As a result of the protest, the internship system was discontinued in 1968, and a postgraduate medical training system was introduced to replace it. In this system, students took the medical license examination following graduation, and then received specific training for at least two more years. This strengthened the quality of the education compared to the previous system, but the status and pay of the trainees remained unstable (Shukan Igakukai Shimbun, 2004). Graduate students were forced to work part-time jobs during their training. They also raised issues related to the content of their education, inadequate guidance system, and insufficient evaluation of the training received.
In 2004, a new two-year mandatory postgraduate medical training system was implemented in all training programmes (Shukan Igakukai Shimbun, 2004). In this system, all medical school graduates spend two years rotating through the seven specialties (internal medicine, surgery, emergency medicine or anaesthesiology, paediatrics, psychiatry, community-based medicine, and obstetrics and gynaecology). Then only after the two-year training, can young physicians enter specialty-based residencies. Owing to this reform, the average resident salary has increased, and residents are paid sufficiently to concentrate on their training. Moreover, with respect to learning, this system has enabled residents to obtain more experience and become more confident about their clinical skills and the efficiency of their general knowledge (Nomura et al., 2008).
IV. WORK STYLE REFORM
The Japanese economy grew dramatically after World War II. At that time, ideal workers were considered to be those who spent all their time working. The epitome of this attitude is captured in the phrase “Can you work for 24 hours?” which became popular after originating from a Japanese TV advertisement for an energy drink. Japan was notorious for its long working hours, and because it also became an aging society, where a relatively small number of working-age people must support a large senior population, there was a need to raise productivity. Death by overworking was so frequently occurring in Japan that it even had its own name, Karoshi, which literally means “death by overwork.” As a result, work-life balance started to get a lot of attention as the solution to avoid this social problem.
Medical care in Japan has long been supported by the self-sacrificing work of physicians, especially young doctors in their twenties and thirties (Shibuya & Unno, 2019). According to an investigation performed by the Ministry of Health, Labour and Welfare (MHLW), 40% of physicians exceed the norm for hours worked by workers in other sectors. More than 10% of physicians work more than 1860 hours of overtime per year (Ministry of Health, Labour and Welfare, 2019). Because of this, the MHLW drew up a contentious plan to restrict physicians’ working hours through a regulation that will take effect in 2024. In particular, physicians’ overtime hours will be restricted to 960 hours per year, to keep hours below what is called the “Karoshi Line” (the number of hours beyond which a death is presumed to be related to overwork). There will still be allowances in the regulation for some physicians to work up to 1,860 hours yearly overtime, far above the Karoshi Line, if necessary to maintain community health care or to work intensively for the purpose of learning and becoming specialists.
V. RESIDENT AS LEARNER OR WORKER?
In Japan, the view of residents has vacillated over time between the perspective of “resident as learner” and that of “resident as worker.” Until the repeal of the early internship system in 1968, the viewpoint of “resident as learner” was dominant, and trainees were obliged to work unpaid. In the course of abolition of the early internship system, the standpoint of “resident as worker” was enhanced. The perspective of “resident as learner” was revisited through the process of the new two-year postgraduate training system implementation in 2004.
Nowadays, the viewpoint of “resident as worker” draws attention because physicians and residents are still forced to work for prolonged hours. Because of this, burnout among medical residents has become a critical problem, and several studies have been conducted on the mental health of residents in Japan. This suggests that the pendulum has swung too far and the perspective of “resident as learner” is now lacking. We must develop and implement resident education that emphasises their roles as both learners and workers, for the sake of the patients they care for and for society’s sake.
The implication of this is that we will need to educate residents effectively and efficiently within a limited number of work hours. The duty hour restrictions will raise the number of trainees caring for a particular patient on any given day, and will push up the demand for meaningful and efficient transfer of information. We will have to teach “new professionalism.” New professionalism derives from sharing responsibility for patient care, as contrasted with nostalgic professionalism, which is defined as continuously giving priority to a patient’s needs over one’s own personal needs (Arora, Farnan, & Humphrey, 2012). Trainees have to be taught a new view of their responsibilities and new skills for directing team-based care. More specifically, they should be taught the skills of quickly summarising and communicating pertinent sign-out information at the end of shifts to support patient care. The model of continuity-enhanced handovers may be useful (Arora, Reed, & Fletcher, 2014).
It is our responsibility as educators and leaders to seek breakthrough solutions to promote an educational system that emphasises both the perspective of “resident as learner” and that of “resident as worker.” It is time for change.
Notes on Contributors
Hirohisa Fujikawa contributed to the acquisition, analysis and interpretation of the data and the drafting of the manuscript. He approved the final manuscript, and agreed to be accountable for all aspects of the work in ensuring that questions related to any part of the work are appropriately investigated and resolved.
Daisuke Son contributed to the conception and design of the study, and the revision of the manuscript. He approved the final manuscript, and agreed to be accountable for all aspects of the work in ensuring that questions related to any part of the work are appropriately investigated and resolved.
Masato Eto contributed to the conception and design of the study, and the revision of the manuscript. He approved the final manuscript, and agreed to be accountable for all aspects of the work in ensuring that questions related to any part of the work are appropriately investigated and resolved.
Acknowledgement
The authors wish to express sincere appreciation to Ms. Kayo Kondo, School of Politics, Philosophy, Language and Communication Studies, University of East Anglia, who assisted us in translating the manuscript.
Funding
The authors have no funding to report.
Declaration of Interest
The authors declare no conflicts of interest associated with this manuscript.
References
Accreditation Council for Graduate Medical Education. (2017). Common Program Requirements Section VI with Background and Intent [PDF file]. Retrieved from https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRs_Section%20VI_with-Background-and-Intent_2017-01.pdf.
Arora, V. M., Farnan, J. M., & Humphrey, H. J. (2012). Professionalism in the era of duty hours: Time for a shift change? JAMA, 308(21), 2195–2196. https://doi.org/10.1001/jama.2012.14584
Arora, V. M., Reed, D. A., & Fletcher, K. E. (2014). Building continuity in handovers with shorter residency duty hours. BMC Medical Education, 14(Suppl 1), S16. https://doi.org/10.1186/1472-6920-14-S1-S16
Bolster, L., & Rourke, L. (2015). The effect of restricting residents’ duty hours on patient safety, resident well-being, and resident education: An updated systematic review. Journal of Graduate Medical Education, 7(3), 349–363. https://doi.org/10.4300/JGME-D-14-00612.1
Izumi, Y., & Isozumi, K. (2001). Modern Japanese medical history and the European influence. The Keio Journal of Medicine, 50(2), 91–99. https://doi.org/10.2302/kjm.50.91
Ministry of Health, Labour and Welfare. (2019). On the upper limit for overtime among doctors (in Japanese). Document 2 presented at the 19th Committee on the Work Style Reform of Doctors [PDF file]. Retrieved from https://www.mhlw.go.jp/content/10800000/000481338.pdf
Nomura, K., Yano, E., Aoki, M., Kawaminami, K., Endo, H., & Fukui, T. (2008). Improvement of residents’ clinical competency after the introduction of new postgraduate medical education program in Japan. Medical Teacher, 30(6), e161–e169. https://doi.org/10.1080/01421590802047307
Shibuya, K., & Unno, N. (2019). Unpaid doctors in Japanese university hospitals. The Lancet, 393(10176), 1096–1097. https://doi.org/10.1016/S0140-6736(19)30472-6
Shukan Igakukai, Shimbun. (2004). The History of clinical training in Japan (in Japanese) [PDF file]. Retrieved from http://www.igaku-shoin.co.jp/nwsppr/n2004dir/n2566dir/n2566_02.pdf
*Hirohisa Fujikawa
The University of Tokyo,
7-3-1 Hongo, Bunkyo-ku,
Tokyo 113-0033, Japan
Tel: +81-3-5841-3480
Email: hirohisa.fujikawa@gmail.com
Submitted: 1 April 2020
Accepted: 26 May 2020
Published online: 5 January, TAPS 2021, 6(1), 128-131
https://doi.org/10.29060/TAPS.2021-6-1/PV2240
Sonia Kumar, Rachel Browne, Jeffrey Wu & Simon Tso
Department of Dermatology, South Warwickshire NHS Foundation Trust, Warwick, United Kingdom
I. FACTORS INFLUENCING MOTIVATION TO PURSUE GRADUATE-ENTRY MEDICINE
The decision to pursue medicine is a significant step for individuals, particularly those for whom this involves a career change. While medicine in the UK has traditionally been an undergraduate course, graduate-entry medicine (GEM) programmes were introduced in 2000 and offer an accelerated course for suitably qualified candidates with a Bachelor’s degree. Students have a variety of motivations for undertaking a GEM programme (Carter & Peile, 2007), and we herein explore the factors that influence this range of motivations.
Literature suggests that students of GEM programmes can broadly be categorised into two groups: individuals who do not consider medicine when choosing their first degree, or individuals who selected a degree subject that would keep medicine open as a career (Sulong et al., 2014). Key motivating factors to pursue GEM include prior health service experience (as a patient or as a health professional), professional autonomy, and influence from others. The most frequently cited factor influencing the decision was a desire to help people (Sulong et al., 2014). Other literature suggests a lack of job satisfaction and limited career development opportunities are key factors drawing individuals away from their original career paths and into medicine.
The other group includes individuals who had previously failed to gain entry to medical school at the undergraduate level, studying alternative subjects but maintaining a goal of studying medicine. These individuals have demonstrated motivation by completing a degree that was not their first choice, and this can continue throughout their medical studies. A comparison of Leicester Medical School GEM and undergraduate-entry medicine (UEM) students found higher general pass rates for GEM students with a biomedical science background when compared to their UEM peers (Carter & Peile, 2007).
II. STUDENT EXPERIENCES
A semi-structured interview-based study exploring the experiences of twenty-one students from the University of Warwick GEM programme was conducted by the author Simon Tso as part of his doctoral research thesis (Tso, 2017). Students were asked to describe their motivations to pursue GEM. Three broad groups of student journeys into GEM were identified: ‘medicine as an end goal’, ‘career indecision’ and ‘career switchers’. The ‘medicine as an end goal’ group represented students within the study and students in this group recalled a longstanding ambition to pursue medicine. The ‘career indecision’ group consisted of students who had previously considered medicine as a potential career but instead chose an alternative path. The ‘career switchers’ comprised of students who left their previous career to pursue GEM.
A. Why Pursue Medicine as a Career?
Motivations to pursue GEM were attributed to a combination of ‘pull’ and ‘push’ factors. ‘Pull’ factors included those that the students regarded as positive experiences or perceived incentives of choosing medicine as a career. A few, however, experienced negative ‘pull’ factors, recalling pressure and expectation from family to pursue medicine simply because they were good at science. Often, the reassurance of a guaranteed job following the degree influenced this pressure.
A key theme for motivations reported by this group was their general interest in human health, a desire to improve people’s lives and to do “meaningful work”. In most instances, many had received positive encouragements from other individuals who supported and positively influenced their career choice. One student, however, recalled a negative experience in secondary school when he expressed an interest in applying for UEM to a teacher. This teacher subsequently discouraged application expressing that they did not believe the student would meet the expected entry requirements. The student felt that extra support from their teachers rather than discouragement could have guided them to have studied UEM rather than having to apply for a GEM programme later in life.
‘Push’ factors were reasons why some students chose to cease continuing on their original career path and consider alternative careers instead. Reasons given highlighted the disillusionment they felt with certain aspects of their original career path and therefore felt pushed to consider an alternative career. These included lack of career progression opportunities, lack of job satisfaction and lack of autonomy in their roles. The students perceived that medicine could offer the opportunities they desired from a career.
III. OUR REFLECTIONS
A. What Factors Influence Motivation to Study GEM?
The Self Determination Theory devised by Ryan and Deci (2000) can be applied to the understanding of why people choose to study GEM. The Self Determination Theory suggests that three factors are required for psychological growth: autonomy, competence and connection. Although thought to be innate, these factors are affected by environmental interactions and can influence our proactivity or passivity. The degree of self-determination is also influenced by whether the factors that motivate us are:
- Intrinsic–where an activity is done for the pleasure or enjoyment of the activity itself.
- Extrinsic–where a task is performed for a possible reward or fear of punishment.
- In some instances, factors that make us demotivated–the lack of desire to act or, act without intent.
Typical intrinsic factors recalled as motivations for pursuing GEM were the desire to do something fulfilling or to help others. For others it was the desire to commit to lifelong learning or a career where their interest in biological sciences could be applied to human physiology.
Extrinsic factors such as family pressures or socioeconomic background also have been known to impact career choice and journey. In some cultures, professions such as medicine, engineering or pharmacy are held in high esteem and children from these backgrounds can be encouraged to pursue these subjects at university. These careers are often associated with job and financial stability, factors that may be of high importance to individuals from a disadvantaged or low socioeconomic background. In these instances, a career in medicine can be perceived as a mode of upwards social mobility.
B. What Factors Contribute to Career Indecision?
Gati, Krausz and Osipow (1996) describe a theoretically driven taxonomy of career decision that can be applied to the career indecisions reported by the medical students in their study. The taxonomy was categorised into three broad clusters; lack of readiness, lack of information, and inconsistent information, all of which can explain why individuals may be hesitant or indecisive when considering a career in medicine.
Typically, students in the United Kingdom consider a career in medicine aged 16-18, applying to medical school in the second year of the A-Level programme. The decision to pursue medicine is difficult, and some may be lacking the required information to adequately prepare them, both to apply and to succeed in the application process. This is particularly relevant to students from disadvantaged backgrounds or resource-poor schools that may find it challenging to support the aspirations of their students and prepare them for medical school interviews.
Widening participation (WP) is an umbrella term referring to coordinated efforts that encourage and support individuals from underrepresented or disadvantaged backgrounds to consider pursuing academic careers such as engineering, medicine and law. The idea behind the programmes is to ensure that all students have access to equal opportunities, regardless of their background. These schemes often provide interview support, work experience schemes and checking of personal statements. They can provide further insight into the career, and also provide workshops on the special entrance tests required for medical school admission.
A medical student in our study was supported by a WP scheme to gain admission into her first degree which served as a stepping-stone into a GEM programme. An increase in provision and access to WP schemes would seek to level the playing field in the application process to medical school at both UEM and GEM level. The provision of extra support and information would enable these students to make informed career choices and make the medical school application process fairer.
IV. CONCLUSION
GEM programmes provide individuals the opportunity to pursue medicine as a career at a later stage, and their additional life and work experience can engender a more diverse and experienced cohort of graduates (Carter & Peile, 2007). WP schemes at the university level could further contribute to this diversity, and it would be interesting for future studies to explore whether students who were unsuccessful or did not attempt to gain entry at the UEM level could have benefited from secondary school WP programmes.
It is clear that there are multiple reasons individuals decide to pursue GEM, whether as a long-term ambition from school age or as a career change. These multifactorial motivations consist of both intrinsic and extrinsic factors and more work is needed to understand their influence on students’ motivations. Identifying common themes allows for more effective recruitment and teaching of these non-traditional students who will eventually contribute to a more diverse medical workforce.
Notes on Contributors
Dr Sonia Kumar is a graduate of the University of Warwick graduate-entry medicine degree programme and is a newly qualified Foundation Year 1 doctor at the South Warwickshire NHS Foundation Trust. Dr Kumar made substantial contributions to the conception, design, editing of this piece and approval of the final manuscript.
Dr Rachel Browne completed a Masters in Medical Education at the University of Warwick. She is a Speciality Registrar in Dermatology and former Clinical Education Fellow at the South Warwickshire NHS Foundation Trust. Dr Browne contributed to the design and editing of this piece including approving this final manuscript.
Dr Jeffrey Wu is a graduate of the University of Warwick graduate-entry medicine programme and former undergraduate Teaching Assistant at the University of California, San Diego. He is training in Internal Medicine at South Warwickshire NHS Foundation Trust. Dr Wu contributed to the design, edit and approval of this manuscript.
Dr Simon Tso completed a doctoral (MD) degree at the University of Warwick. He is a Fellow of the Higher Education Academy and Consultant Dermatologist at the South Warwickshire NHS Foundation Trust. Dr Tso made substantial contribution to the conception, data analysis/interpretation editing and authorising the final manuscript.
Ethical Approval
This study was part of a larger study investigating the experience of graduate-entry medicine degree programme students, which has received ethical approval from the University of Warwick Biomedical Research Ethics Sub-Committee (Reference: 169-01-2012).
Acknowledgements
The authors would like to thank Asim Yousuf, Nina Owen, Mike Smith and Dr Jane Kidd for their assistance with the design and development of the study.
Funding
This study was part of a larger study investigating the experience of graduate-entry medicine degree programme students, which was funded by the Institute for Advanced Teaching and Learning, University of Warwick, United Kingdom.
Declaration of Interest
The authors have no conflict of interest, including no financial, consultant, institutional and other relationships that might lead to bias.
References
Carter, Y. H., & Peile, E. (2007). Graduate entry medicine: High aspirations at birth. Clinical Medicine, 7(2), 143–147. https://doi.org/10.7861/clinmedicine.7-2-143
Gati, I., Krausz, M., & Osipow, S. H. (1996). A taxonomy of difficulties in career decision making. Journal of Counselling Psychology, 43(4), 510–526. https://doi.org/10.1037/0022-0167.43.4.510
Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist, 55(1), 68–78. https://doi.org/10.1037/0003-066X.55.1.68
Sulong, S., McGrath, D., Finucane, P., Horgan, M., O’Flynn, S., & O’Tuathaigh, C. (2014). Studying medicine – A cross-sectional questionnaire-based analysis of the motivational factors which influence graduate and undergraduate entrants in Ireland. JRSM Open, 5(4), 204253331351015. https://doi.org/10.1177/2042533313510157
Tso, S. H. Y. (2017). The graduate-entry medical student: Challenges to transition through medical school (Doctoral dissertation, University of Warwick, Coventry, United Kingdom). Retrieved from http://wrap.warwick.ac.uk/99890/
*Sonia Kumar
Lakin Road, CV34 5BW
South Warwickshire NHS Foundation Trust,
Warwick, United Kingdom
Email: Sonia.kumar@doctors.org.uk
Submitted: 21 February 2020
Accepted: 3 June 2020
Published online: 5 January, TAPS 2021, 6(1), 125-127
https://doi.org/10.29060/TAPS.2021-6-1/PV2228
Chooi Peng Ong, Cindy Shiqi Zhu, Desmond SL Ong & Ying Pin Toh
Family Medicine Residency, National University Health System, Singapore
I. INTRODUCTION
Family medicine training encompasses the need to develop a diverse skillset and the ability to practice in different settings. During three years of training, family medicine residents from National University Health System (NUHS) rapidly transit through many hospital rotations with varying specialty-specific competency requirements. Throughout this period, each resident is rostered to run a half-day primary care clinic on the same day each week and is assigned a dedicated faculty member to supervise him during the session. Each faculty member is assigned up to four to six residents for the half-day sessions every week. There is a need to contextualise what is learnt in hospital to primary care, and to effectively integrate knowledge across disciplines. We describe here a tool that the NUHS family medicine residency has used to bring together faculty and residents of varying seniorities and locations for discussion, reflection, and growth.
II. METHODS
A. What We Did
Over the past few years, learners’ groups have been created by residency faculty and residents on a voluntary basis, using an internet-based group messaging platform. As described here, the group is defined by a common supervising faculty member and is formed for the duration of the academic year. The supervisor is also the group administrator and main facilitator.
The platform described here is the WhatsApp messaging platform. It was chosen because of the ubiquity of its use by the faculty and resident bodies as well as the closed nature of the groups, in that membership is by invitation, and messages are encrypted (WhatsApp Inc., n.d.). An additional benefit was that, unlike some dedicated healthcare messaging applications, the messages and shared resources are not automatically deleted (Geron, 2011) after a period of time.
The WhatsApp group chat functions as a virtual community board for clinical learning, questions, answers, and clarification. Topics discussed usually arise from residents’ clinic encounters, and the emphasis of discussion is on contextualising knowledge from books and hospital learning to real-life primary care practice. For example, a patient is seen for chronic disease management and is noted to smoke cigarettes. The post-consultation debrief may include a suggestion to read up on nicotine replacement strategies (NRT), following which the resident may upload an update on NRT to the chat group. Case-based discussion proceeds asynchronously and is facilitated by the supervisor and contributed to by all group members. Notably, case discussions involving patients are anonymised, and the use of unique personal identifiers is prohibited. Additionally, the group platform allows discussion and opinion to evolve on current issues relating to professionalism and ethics. Over time, the group chat messages become a useful depository of contextualised, opportunistic, experiential learning for the group.
III. DISCUSSION
A. Potential Pitfalls
The commonest pitfall is the tendency for resources shared to be comprehensive textbook-like knowledge updates, whereas the more useful type of update is a distilled, pragmatic one that can be directly applied to practice. It is often noted that group participation tends to wane as the year progresses, possibly due to an increase in coursework and examination preparation. Some group members tend to participate more freely than others. Unlike a face-to-face group, the quiet members may be virtually forgotten by others over the course of the year unless effort is made to engage them.
The openness of the discussion can be affected by traditional medical hierarchies and the facilitator may need to intentionally address this. It is important to recognise that the richness of discourse is largely dependent on the quality of moderation and on participant engagement. Finally, as topics for discussion are identified opportunistically, the same topics may be repeatedly identified.
B. Tips for Managing the Group
The tone and culture of the group will greatly affect the efficacy of group interactions. It is important to set ground rules of courtesy, freedom to question, and expectations of participation early in the group’s life cycle. Also, while the facilitator needs to encourage active participation with provocative questioning, the senior residents need to help set the tone of egalitarian discussion, in order for younger participants to feel sufficiently comfortable to contribute willingly. Having a co-facilitator who is another faculty member or a resident who was a member of a past-year group has helped in establishing the group’s openness and activeness, with varying degrees of success.
It is important for the facilitator to have an idea of what broad topics ought to be discussed over the lifespan of the group, which is often the duration of the academic year. This ensures that discussions are guided beyond the strictly opportunistic. The length of contributions should not exceed the attention span of those reading. As a suggestion, the length of an uploaded update should not exceed the size of a smartphone screen, the emphasis being on curated pearls.
It is important to emphasise an academic focus, to ensure the group does not devolve into a social support group. This is not because social support is secondary, but because these WhatsApp groups, as described here, were set up to further academic objectives. Social greetings are therefore largely relegated to alternative message boards and private messages. Nevertheless, it is recognised that a functional group will have social elements, and that social greetings may be an indicator of group cohesion and viability (Salas, Grossman, Hughes, & Coultas, 2015).
As with any group that interacts over time, an informal curriculum (Rogoff, Callanan, Gutiérrez, & Erickson, 2016) will run in parallel with the explicit curriculum and will eventually impact on learner attitudes and even values. It is important for the facilitator to reflect on the elements of his informal/implicit curriculum and to intentionally drive it. Examples of these elements may include personal integrity, collegiality, or independent questioning.
IV. CONCLUSION
The WhatsApp chat groups described here have allowed us to extend study group discussions beyond the clinic. This is particularly useful in family medicine training where the contextualization of a broad knowledge base needs to be constant and relentless, and opportunities for face-to-face meetings are limited by logistics. The extended virtual discussion is also a useful platform by which to teach affective domain skills, such as attitudes and values. Because of the iterative nature of clinic sessions intercalated with online discussions, learning can be reflected on and applied and may be postulated to occur at up to Kirkpatrick level 3 (Kirkpatrick & Kirkpatrick, 2006). Finally, by bringing together learners of varying seniorities, role modelling, mentoring, camaraderie, and certain emotional support are happy by-products.
Notes on Contributors
Ong Chooi Peng is a faculty member of the NUHS family medicine residency program. She runs several virtual groups, reviewed the literature, and wrote the manuscript.
Desmond Ong is a faculty member of the NUHS family medicine residency program. He also runs virtual groups and helped edit the manuscript.
Cindy Zhu Shi Qi and Toh Ying Pin are residents within the NUHS family medicine residency program. They belong to virtual groups and helped edit the manuscript.
Acknowledgements
The authors acknowledge the generations of NUHS family medicine residents who have contributed to the development and evolution of the virtual groups, to the current form of WhatsApp groups described here.
Funding
The authors received no funding for this work.
Declaration of Interest
The authors declare no conflict of interest.
References
Geron, T. (2011, June 15). TigerText secures (and erases) your text messages. Retrieved January 20, 2020, from https://tigerconnect.com/newsroom/tigertext-secures-and-erases-your-text-messages/
Kirkpatrick, D. L., & Kirkpatrick, J. D. (2006). Evaluating Training Programs. New York, NY: Macmillan Publishers.
Rogoff, B., Callanan, M., Gutiérrez, K., & Erickson, F. (2016). The organization of informal learning. Review of Research in Education, 40(1), 356-401. https://doi.org/10.3102/0091732×16680994
Salas, E., Grossman, R., Hughes, A., & Coultas, C. (2015). Measuring team cohesion. Human Factors: The Journal of the Human Factors and Ergonomics Society, 57(3), 365-374. https://doi.org/10.1177/0018720815578267
WhatsApp Inc. (2020, January 20). WhatsApp Security: Privacy and Security is in our DNA. Retrieved from http://www.whatsapp.com/security/
*Cindy Shiqi Zhu
1E Kent Ridge Road,
Singapore 119228
National University Health System (NUHS)
Email: Shi_Qi_ZHU@nuhs.edu.sg
Submitted: 20 April 2020
Accepted: 29 April 2020
Published online: 1 September, TAPS 2020, 5(3), 88
https://doi.org/10.29060/TAPS.2020-5-3/LE2252
Wenqi Chiew
Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Dear Editor,
I read with great interest your editorial “Grit in healthcare education and practice” published on The Asia Pacific Scholar (Dujeepa & Gwee, 2020). I agree that grit is an important trait to develop in healthcare, especially for patient care. In addition to focusing on grit at the institutional level, we could look at it on an individual level. The question henceforth is that–How do we develop or strengthen the grit in ourselves? Angela Duckworth proposed 5 ways to develop grit–pursue what interests you; practice; find purpose; have hope; and join a gritty group (Barker, 2016). Personally, I feel that finding purpose plays a large role in developing passion and perseverance.
I would like to share this poem that I wrote after my first attempt on blood taking on a patient. Amidst hectic schedules and difficult tasks in medical school, this promise that I made years ago helped kept my passion and perseverance alive.
With shaking hands and a sweaty palm
I slide the needle in and try to calm
And I heave a sigh of great relief
As I watch the backflow fill beneath
Just minutes before, my mentor had asked
“Do you mind if my student try this task?”
With trusting eyes and a reassuring grin,
The patient said, “go ahead, do your thing.”
The trust that you have given to me
Even though I may now be unworthy
Inspires me and greatly spurs me on
To be a better doctor hereupon.
Notes on Contributors
Wenqi Chiew is listed as the first author and she wrote this paper.
Funding
There is no funding provided.
Declaration of Interest
There is no conflict of interest, including financial, consultant, institutional or otherwise for the author.
References
Barker, E. (2016). This is how to increase grit, according to research. Retrieved from TIME, https://time.com/4323260/how-to-increase-grit-perseverance/
Dujeepa, D. S., & Gwee, M. C. E. (2020). Grit in healthcare education and practice. The Asia Pacific Scholar, 5(1), 1-2. https://doi.org/10.29060/TAPS.2020-5-1/EV5N1
*Wenqi Chiew
Yong Loo Lin School of Medicine,
1E Kent Ridge Road,
National University of Singapore,
Singapore 119228
Email: wenqi@u.nus.edu
Submitted: 17 March 2020
Accepted: 3 April 2020
Published online: 1 September, TAPS 2020, 5(3), 83-87
https://doi.org/10.29060/TAPS.2020-5-3/SC2238
Cristelle Chow1, Cynthia Lim2 & Koh Cheng Thoon3
1General Paediatrics Service, Department of Paediatrics, KK Women’s and Children’s Hospital, Singapore; 2Nursing Clinical Services, KK Women’s and Children’s Hospital, Singapore; 3Infectious Disease Service, Department of Paediatrics, KK Women’s and Children’s Hospital, Singapore
Abstract
Background: Effective communication between doctors and patients leads to better compliance, health outcomes and higher doctor and patient satisfaction. Although in-person communication skills training programs are effective, they require high resource utilisation and may provide variable learner experiences due to challenges in standardisation.
Objective: This study aimed to develop and implement an evidence-based, self-directed and interactive online communication skills training course to determine if the course would improve learner application of communication skills in real clinical encounters.
Methods: The course design utilised the Kalamazoo Consensus framework and included videos based on common paediatric clinical scenarios. Final year medical students in academic year 2017/2018 undergoing a two-week paediatric clerkship were divided into two groups. Both groups received standard clerkship educational experiences, but only the intervention group (88 out of 146 total students) was enrolled into the course. Caregiver/patient feedback based on students’ clinical communication was obtained, together with pre- and post-video scenario self-reported confidence levels and course feedback.
Results: There were minimal differences in patient feedback between intervention and control groups, but the control group was more likely to confirm caregivers’/patients’ agreement with management plans and provide a summary. However, caregivers/patients tended to feel more comfortable with the intervention compared to the control group. Median confidence levels increased post-video scenarios and learners reported gains in knowledge, attitudes and skills in paediatric-specific communication.
Conclusion: Although online video-based communication courses are useful standardisation teaching tools, complementation with on-the-job training is essential for learners to demonstrate effective communication.
Keywords: Online Learning, Undergraduate Medicine, Professionalism, Communication Skills, Patient Feedback
I. INTRODUCTION
Effective doctor-patient communication leads to better compliance, health outcomes and higher doctor and patient satisfaction. Online video-based communication skills courses can be feasible, with learners reporting increased confidence in key communication skills (Kemper, Foy, Wissow, & Shore, 2008). However, these evaluation methods have been limited to the Kirkpatrick levels of “reaction” and “learning”, instead of “behaviour” and “results”, which are more reflective of applied learning.
While in-person communication skills training programs simulate clinical environments, they can have inconsistent delivery because facilitators and standardised patients provide variable training experiences. In order to replace traditional role-play sessions, this study aimed to develop and implement a pilot online communication skills course to provide standardised, video-based scenarios in a self-directed interactive learning format using an evidence-based framework.
Our research questions are as follows:
- Would an online communication course improve the application of communication skills in real clinical encounters?
- What is the impact of an online communication course on learner-rated confidence levels in paediatric-specific clinical communication encounters?
- What are the self-reported aspects of learning that participants of an online communication course experience?
II. METHODS
This course design utilised the Kalamazoo Consensus framework (Makoul, 2001) which included the essential elements of clinical communication: Open the discussion, gather information, understand patient’s perspective, share information, reach agreement and provide closure.
Through Bandura’s social learning theory, people learn through observing others’ behaviour. The attitudes and outcomes of those behaviours then guide subsequent actions. This course therefore utilised videos featuring positive doctor-caregiver interactions, to encourage modelling through observation. The 3-5-minute video scenarios acted by practicing healthcare professionals were based on commonly encountered general paediatric clinical situations.
The course was designed using Articulate© software. “Pop-up” prompts highlighting important clinical or communication points, a pre- and post-test and in-video multiple-choice questions were included to increase learner engagement. To evaluate the impact of the course on learner-rated confidence levels, students were shown a clinical vignette, and asked to rate their self-confidence on a 4-point Likert scale before and after each video. Each video concluded with a summary, emphasising the utilisation of the Kalamazoo Consensus Framework.
|
Q1: Did the student introduce his/ her name? |
Q2: Did the student allow you to express your concerns? |
|
⃝ Yes ⃝ No ⃝ Not sure |
⃝ Yes, ALL my concerns ⃝ Not really, only SOME of my concerns ⃝ No, NONE of my concerns |
|
Q3: How much was the student interested in your point of view (e.g. expectations, ideas, beliefs, values) when he/she was asking you questions? |
Q4: How much was the student interested in your point of view (e.g. expectations, ideas, beliefs, values) when he/she was planning and explaining things? |
|
⃝ Very interested ⃝ Somewhat interested ⃝ Somewhat uninterested ⃝ Not interested at all |
⃝ Very interested ⃝ Somewhat interested ⃝ Somewhat uninterested ⃝ Not interested at all |
Q5: Did you feel that the student listened to you? |
Q6: How well do you feel the student explained things to you? |
|
⃝ Listened all the time ⃝ Listened sometimes ⃝ Did not listen at all |
⃝ Very well – I understood all the explanation ⃝ Fairly well – I understood some of the explanation ⃝ Not well at all – I did not understand all of the explanation |
|
Q7: Did the student check if you were agreeable with the management plan? |
Q8: Did the student provide a summary of the problem/ plans at the end of the conversation? |
|
⃝ Yes ⃝ No ⃝ Not sure |
⃝ Yes ⃝ No ⃝ Not sure
|
|
Q9: Overall, how comfortable were you interacting with the student? |
Q10: What do you think this student could improve in? E.g. Be more courteous/ respectful, speak or explain more clearly, listen more, check my understanding, answer my queries etc. |
|
⃝ Very comfortable – I would like to have him/ her be my/ my child’s doctor ⃝ Somewhat comfortable ⃝ Somewhat uncomfortable ⃝ Not comfortable at all – I do not want him/ her to be my/ my child’s doctor |
|
Table 1. Caregiver/Patient Feedback Form
To evaluate the self-reported learning points from the course, students were asked upon course completion to provide course feedback, including free-text completion of the phrase: “Things I have learnt include…” To evaluate whether the course improved the application of communication skills in real clinical encounters, caregiver/patient feedback was obtained towards the end of the paediatric clerkship for all students, regardless of course participation (Table 1). This form was modified based on course content from a family feedback instrument utilised in a paediatric setting (Zimmer, Solomon, Siberry, & Serwint, 2008). Implied informed consent was obtained from all participants.
Final year medical students from a five-year Singapore undergraduate medical program were enrolled over one academic year (2017/2018). Alternate batches (2nd, 4th, 6th, 8th) were enrolled into the course. Each student was provided a unique username and password for course access on any internet-enabled device throughout his/her 2-week paediatric clerkship and course participation was strongly recommended. Students from other batches (1st, 3rd, 5th, 7th) were analysed as controls. All students integrated into paediatric clinical teams, participated in ward rounds and communicated plans to patients/caregivers.
Statistical analysis was performed using SPSS© Statistics version 25.0 and chi-square analysis was used for patient feedback analysis.
This study was exempted from formal Centralized Institutional Review Board review and implied informed consent was granted by the SingHealth Centralized Institutional Review Board.
III. RESULTS
A total of 146 students were posted to the study institution in academic year 2017/2018 and 88 students were enrolled into the course. There were 80 (90.9%) attempts at the course, of which 76 (95%) students provided course feedback. The median time needed for course completion was 59 minutes. Patient feedback was successfully collected for 94 students, of which 44 (46.8%) attempted the course. Main reasons for unsuccessful collection were fast patient turnovers and patients/caregivers rejecting the request to provide feedback, usually due to perceived insufficient student contact time.
A. Application of Communication Skills – Evaluated via Patient Feedback
Although there were generally no differences in patient feedback between intervention and control groups, the control group was more likely to check with caregivers/patients whether they were agreeable with the management plan (76.0% vs. 56.8%, p<0.05) and provided a summary to the caregiver/patient (74.0% vs. 47.7%, p<0.05). Approaching statistical significance was the finding that caregivers/patients were more likely to feel very comfortable with the intervention compared to the control group (65.9% vs. 48.0%, p=0.062).
B. Course Impact on Self-Reported Confidence Levels
For scenario 1, the median confidence level increased from 3 (“somewhat confident”) to 4 (“very confident”). For the subsequent scenarios, this increased from 2 (“a little confident”) to 3 (“somewhat confident”).
C. Self-Reported Learning Points –Evaluated via Course Feedback
1) Knowledge: The majority of students mentioned learning about the clinical management and discharge advice for gastroenteritis and urinary tract infection, and the need for procedural sedation in uncooperative young children. Students reported that they had learnt general frameworks and principles for communication, and concepts of consent-taking. Students also frequently mentioned “practical”, in terms of “practical knowledge” and “practical tips” for communication.
2) Attitude: Students mentioned that they learnt about the importance of empathy. They also reported important aspects of patient-centred care, such as understanding the parent’s or patient’s perspective to formulate a treatment plan together and ensuring mutual understanding via “checking back to ensure the parent truly understands” and “to have a closed loop at the end of each communication”.
3) Skills: On a broader perspective, students described that they had learnt “how to properly structure communication with a patient’s parents” and “how to better communicate with parents using the various strategies”. Almost all students reflected that they had learnt specific communication skills, particularly with regards to dealing with challenging situations such as “how to approach parents who may not be cooperative/willing to listen to you” and “how to address angry parents” as well as “how to address their concerns and manage their expectations”. Two students also mentioned that they may not have been exposed to similar scenarios in their daily work: “… handle scenarios which are often not taught within lectures.”
IV. DISCUSSION
Computer-based communication courses have shown to improve students’ self-efficacy in performing communication tasks and assessments of students’ perceptions and practice of communication skills (Kemper et al., 2008), which was also demonstrated in this study’s improvement in self-reported confidence levels. It is however, expected that most students would experience increased confidence immediately after receiving new information about an unfamiliar topic.
This study provides an example of how a course that is traditionally delivered face-to-face can be designed to be delivered online, utilising less time and manpower resources while providing standardised teaching instruction in an evidence-based manner.
The qualitative findings in this study have not been replicated elsewhere, and provide an interesting perspective to student course perception. Students gained practical knowledge which is not readily available in clinical clerkships due to patient case variability and gained insight into an applicable framework for future clinical communication encounters. It is possible that the interactive nature of the course increased student presence and participation, resulting in improved learning outcomes in this aspect (Ammenwerth et al., 2019). Empathy, an important professional skill not easily taught but reflected as a learning point, was likely acquired through non-verbal communication demonstrated in the videos. Although it is not guaranteed that self-reported knowledge, skills and attitudes will translate into practice, future e-learning communication courses can be designed as pre-course material for traditional role-play facilitators to enhance learning experiences.
This study’s use of patient feedback provides unique insight into applied learning. Interestingly, the control group fared better in the actions of checking with caregivers/patients about management plan agreement and providing caregivers/patients with a summary. As clerkships also provide opportunities to observe healthcare professionals conducting clinical communication, it is likely that the control group learnt these behaviours from real-life encounters. Caregivers/patients tended to feel more comfortable with the intervention group, which could be explained through unmeasurable, subtle behaviours that the group may have learnt from the course, such as empathy, attentiveness and appropriate body language. Although the use of standardised patients for comparing both groups might have shown different results, it is known that how learners behave in the classroom and with real patients when unobserved is often less reflective of true workplace behaviours (Malhotra et al., 2009).
This study is limited by small participant and patient feedback numbers. Culturally, many patients forget their healthcare providers and experiences. An ideal situation would be direct clinical encounter observation, but due to the Hawthorne effect, a less truthful version of student behaviour may be observed instead.
V. CONCLUSION
Although online video-based communication courses can be used as a standardised teaching tool to improve student self-reported confidence levels and self-perceived knowledge, skills and attitudes, it remains to be proven if they can result in a change in student behaviour. It is likely that on-the-job experiences also contribute to their ability to demonstrate effective communication, which supports the supplementation, rather than the replacement of such practical experiences with online video-based course material.
Notes on Contributors
CC, CL and TKC contributed to the conception and design of the work. CC, CL and TKC also analysed data and drafted the work . CC, CL and TKC approved the final published version and are agreeable to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. CC, CL and TKC collectively contributed equally to this paper.
Ethical Approval
This study was exempted from formal Centralized Institutional Review Board review by the SingHealth Centralized Institutional Review Board (CIRB Ref: 2017/2178).
Acknowledgements
The authors would like to acknowledge the SingHealth Paediatrics Academic Clinical Programme in providing the grant funding for this project.
Funding
The study was funded by the SingHealth Paediatrics Academic Clinical Programme Tan Cheng Lim Fund Grant which was awarded in 2017 (Grant Reference: PAEDACP-TCL/2017/EDU/001).
Declaration of Interest
All authors disclose that there are no potential conflicts of interest, including financial, consultant, institutional and other relationships that could have direct or potential influence or impart bias on the work.
References
Ammenwerth. E., Hackl, W. O., Dornauer, V., Felderer, M., Hoerbst, A., Nantschev, R., & Netzer, M. (2019). Impact of students’ presence and course participation on learning outcome in co-operative online-based courses. Studies in Health Technology and Informatics, 262, 87-90.
Kemper, K. J., Foy, J. M., Wissow, L., & Shore, S. (2008). Enhancing communication skills for paediatric visits through on-line training using video demonstrations. BMC Medical Education, 8, 8.
Makoul, G. (2001). Essential elements of communication in medical encounters: the Kalamazoo consensus statement. Academic Medicine, 76(4), 390-393.
Malhotra, A., Gregory, I., Darvill, E., Goble, E., Pryce-Roberts, A., Lundberg, K., & Hafstad, H. (2009). Mind the gap: Learners’ perspectives on what they learn in communication compared to how they and others behave in the real world. Patient Education and Counseling, 76(3), 385-90.
Zimmer, K. P., Solomon, B. S., Siberry, G. K., & Serwint, J. R. (2008). Continuity-structured clinical observations: assessing the multiple-observer evaluation in a pae1diatric resident continuity clinic. Pediatrics, 121(6), e1633-1645.
*Cristelle Chow
Department of Paediatrics,
KK Women’s and Children’s Hospital
100 Bukit Timah Road,
Singapore 229899
Email: cristelle.chow.ct@singhealth.com.sg
Submitted: 8 February 2020
Accepted: 9 April 2020
Published online: 1 September, TAPS 2020, 5(3), 71-82
https://doi.org/10.29060/TAPS.2020-5-3/OA2226
May Eng Loo1, Brenda Wong2, Yee Mun Lee3
1Health Outcomes and Medical Education Research (HOMER), National Healthcare Group, Singapore; 2Group Education, National Healthcare Group, Singapore; 3Department of Urology, Tan Tock Seng Hospital, Singapore
Abstract
In order to understand what constitutes unprofessional online behaviour from the perspectives of stakeholders, there have been studies that examine the perceptions of doctors and the public on hypothetical online postings. However, the considerations and reasoning of the participants when they evaluate online posts have not been explored in-depth. This project aimed to examine the main considerations and possible conflicting considerations of faculty and residents when they evaluate the appropriateness of Facebook posts, and how they might negotiate any conflicts. Faculty and residents from the National Healthcare Group – Alexandra Health Pte Ltd Residency in Singapore were randomly presented Facebooks posts as part of an online questionnaire, rated their appropriateness, and provided explanations for their ratings. Responses were coded for main considerations and responses with 2 or more conflicting considerations were further analysed to describe the conflict and the way they were negotiated. 182 faculty and residents rated the appropriateness of three out of six Facebook posts and explained their evaluation. Except for one post which was evaluated as ‘Neither appropriate nor inappropriate’ by the majority (37%) of the respondents, all other posts were rated as either ‘Very inappropriate’ or ‘Inappropriate’ by the majority of respondents (34%-69%). Despite similar evaluation of inappropriateness, faculty and residents take into account a wide range of considerations. These considerations tend to conflict with one another when the respondents considered freedom of expression of the poster and the educational purpose of a post. Understanding physicians’ negotiation of conflicting considerations provides insight into their outworking of professionalism in social media context.
Keywords: Professionalism, Social Media, Postgraduate Education
Practice Highlights
- Doctors within the same Residency do not necessarily have a uniform set of professional priorities regarding social media.
- They may also have to manage conflicting professional and personal values in different contexts.
- Educators of professional values could recognise the complexity of such conflicts and be sensitive to this in their teaching.
- We recommend creating platforms for doctors to have conversations on social media use.
I. INTRODUCTION
In June 2017, Mark Zuckerberg announced that the Facebook community was officially two billion people. While seeking to understand how social media can be maximised for good, Chief Product Officer Chris Cox was conscious of Facebook’s responsibility to ‘curtail any way that it can be misused or turned into something sad’ (Constine, 2017). In healthcare education and practice, social media has both the potential to be maximised for good (e.g. facilitating communication and improving knowledge) as well as the potential to be misused, compromising patient confidentiality and eroding public confidence in the medical profession (Greysen, Kind, & Chretien, 2010; Hamm et al., 2013). In their commentary, Chretien and Kind (2014) propose that in order to reap the benefits of social media use for healthcare, physicians need to be first aware of the risks of using social media and address concerns of unprofessional online behaviour.
In order to understand what constitutes unprofessional online behaviour from the perspectives of stakeholders, there have been studies that examine the perceptions of doctors and the public on hypothetical online postings (Chretien, Farnan, Greysen, & Kind, 2011; Dawkins, King, Boateng, Nichols, & Desselle, 2017; Greysen et al., 2013; Jain et al., 2014; Kesselheim, Batra, Belmonte, Boland, & McGregor, 2014; Kind, Greysen, & Chretien, 2012; Rocha & de Castro, 2014). These studies found that online behaviour that participants judged as unprofessional include patient privacy violations, patient content in general and negative comments about faculty and staff. However, the considerations and reasoning of the participants when they evaluate online posts have not been explored in-depth, and especially for posts that may be inappropriate but may not appear obviously unprofessional. Such ‘grey posts’ may include patient storytelling posts where, for example, a patient’s identity is not revealed but details are shared to encourage reflection or request support through social media (Wells, Lehavot, & Isaac, 2015). Professional or personal values may sometimes come into conflict when they seem equally important in such situations. However, not much is known about what these conflicting considerations are when doctors evaluate such online posts and how these conflicting considerations are resolved or negotiated.
In response to concerns about unprofessional behaviour on social media, guidelines have been published by medical associations in various countries like the USA, UK, Canada, Australia, New Zealand as well as Singapore (American College of Physicians Ethics, Professionalism, and Human Rights Committee, 2012; Australian Medical Association, 2010; Canadian Medical Association, 2011; General Medical Council, 2013; Singapore Medical Council, 2016). These existing guidelines are generally comprehensive, providing principles for social media use and examples of unprofessional behaviour to avoid. Regarding posting online, concerns about patient confidentiality, professionalism, collegiality and preserving patients’ and the public trust in the medical profession are key issues raised by the guidelines. In particular, the Singapore Medical Council gives a list of inappropriate posts, examples include ‘speaking and writing in an indiscreet, bigoted, rude, and obscene or profane manner’ and ‘posting personal or derogatory comments about patients or colleagues’ (Singapore Medical Council, 2016).
Our study seeks to explore the considerations and possible competing or conflicting considerations of faculty and residents in the National Healthcare Group – Alexandra Health Pte Ltd (NHG-AHPL) Residency program when they evaluate online postings, especially grey posts. This study also aims to examine how the participants resolve or negotiate these conflicting considerations. Identifying the considerations of faculty and residents when they evaluate the posts sheds light on what constitutes unprofessional online posts and provides a platform for further discussion on existing social media use guidelines. Furthermore, understanding how doctors negotiate at times conflicting norms and obligations also provides insight into how they perceive the outworking of professionalism in the social media context.
II. METHODS
Six Facebook posts deemed inappropriate were identified from an online search. One author (L.M.E.) searched Google News on 30th June 2016 using a Boolean search: (social media OR Facebook OR twitter OR blog OR online OR internet OR web) AND (doctor OR physician OR medical student OR hospital OR clinic OR ward) AND (inappropriate OR unprofessional OR wrong OR unethical). The search was restricted to the first 20 pages of results (10 hits/page) and four posts (Posts 1, 2, 4 and 5) that appeared inappropriate but were not clearly unprofessional were selected. The remaining two posts (Post 3 and 6) were re-used from a pilot phase of the study. The characteristics of the posts are described in Table 1 and the screenshots of the six posts can be found in Appendix A.
|
|
Content domain |
Poster’s seniority |
Possible issues |
|
Post 1 |
Work: patient-related |
Not stated |
Breach of confidentiality, privacy |
|
Post 2 |
Personal: interpersonal conflict |
Medical student
|
Harsh language bordering on criminal threat |
|
Post 3 |
Work: patient-related |
Doctor |
Negativity towards patient, breach of confidentiality |
|
Post 4 |
Personal: opinion |
Medical student |
Harsh language on a controversial topic |
|
Post 5 |
Work: patient-related |
Junior doctor |
Breach of confidentiality, insensitive language |
|
Post 6 |
Work: colleague-related |
Intern |
Negativity towards colleague |
Table 1. Characteristics of posts
As part of an online questionnaire administered between 8th September and 30th October 2016 on social media use, faculty and residents from the NHG-AHPL Residency program in Singapore were asked to rate the appropriateness of three of these posts and to explain their evaluation. All respondents provided informed consent at the start of the questionnaire. Considerations were identified using structural coding which is a question-based code that acts as a labelling and indexing device (Saldana, 2012). For example, the following response was coded ‘Purpose’, ‘Language’ and ‘Respect’ based on the question “What do respondents consider when they evaluate posts?”
Someone has just died. Instead of showing empathy to the family of the deceased who had just lost a loved one, she uses swear words in a callous, insensitive way. Even though her intentions might have been good to ask people to wear a crash helmet, the way she said it was offensive and highly inappropriate given the circumstances. (F5.3)
In the first round of coding, two authors (L.M.E, B.W.) coded each response independently and resolved coding discrepancies through discussions. Using a codebook developed from the first round of coding as a guide, each response was revisited and coded. Coding discrepancies were resolved through more extensive discussions. The second round of coding added new codes to the codebook. Responses with two or more conflicting considerations were further analysed to describe the conflict and the way they were negotiated. Conflicting considerations were identified based on the plain reading of the response, prompted by the use of conjunctions such as ‘but’, ‘even though’ and ‘while’. Appendix B gives a full description of the codes used. Ethics approval was obtained from the institution’s Domain Specific Review Board.
III. RESULTS
A total of 182 respondents (36.8%)–64 faculty and 118 residents–rated the appropriateness of three out of six Facebook posts. 463 responses–169 responses from faculty and 294 responses from residents–were analysed. Table 2 provides a summary of the results for each post.
|
|
Evaluation of appropriateness |
Considerations |
Conflicting considerations |
|
Post 1 |
n=86 ‘Very inappropriate’ (34%)
‘Inappropriate’ (34%)
‘Neither appropriate nor inappropriate’ (30%).
‘Appropriate’ (1%)
‘Very appropriate’ (1%)
|
n=74 1. ‘Consent’ (n=41) 2. ‘Confidentiality’ (n=20) 3. ‘Context’ (n=11) 4. ‘Respect’ (n=10) 5.’Professionalism'(n=6) 6 ‘Purpose'(n=6) 7. ‘Consequences'(n=3) 8. ‘Language'(n=3) 9. ‘Safety'(n=3) 10. ‘Audience'(n=1) 11. ‘Behaviour'(n=1) 12. ‘Platform’(n=1) |
n=3 Positive tone of the post versus patient confidentiality, whether consent was taken, consequences and sensitivity towards the baby’s parents
|
|
Post 2 |
n=93 ‘Very inappropriate’ (39%)
‘Inappropriate’ (39%)
‘Neither appropriate nor inappropriate’ (18%)
‘Appropriate’ (3%)
|
n=77 1. ‘Platform’ (n=24) 2. ‘Behaviour’ (n=16) 3. ‘Freedom'(n=16) 4. ‘Professionalism’ (n=16) 5. ‘Lawfulness'(n=13) 6. ‘Method of resolution'(n=13). 7. ‘Language'(n=8) 8. ‘Reflection'(n=8) 9. ‘Audience'(n=3) 10. ‘Consequences'(n=2) 11. ‘Trends and norms'(n=2) 12. ‘Context'(n=1) 13. ‘Purpose'(n=1) 14. ‘Seniority'(n=1).
|
n=6 Personal nature of the post and the poster’s freedom to express his anger and how his anger is justifiable versus considerations of professionalism, the method used for resolution, consequences and lawfulness
Norms on the internet versus how the post reflects negatively upon the poster’s personality
|
|
Post 3 |
n=95 ‘Very inappropriate’ (36%)
‘Inappropriate’ (44%)
‘Neither appropriate nor inappropriate’ (20%)
‘Appropriate’ (0%)
‘Very appropriate’ (1%)*
|
n=81 1.‘Professionalism’ (n=48) 2. ‘Confidentiality’ (n=24) 3. ‘Platform’ (n=14) 4. ‘Consequences'(n=5) 5. ‘Language'(n=5) 6. ‘Reflection’(n=5) 7. ‘Boundary’(n=4) 8. ‘Freedom’(n=4) 9. ‘Purpose'(n=4) 10. ‘Behaviour'(n=2) 11. ‘Method of resolution'(n=2) 12. ‘Audience'(n=1)
|
n=4 Poster’s right to state a fact or express his feelings and poster posting in jest versus considerations of professionalism
|
|
Post 4 |
n=96
‘Very inappropriate’ (27%)
‘Inappropriate’ (28%)
‘Neither appropriate nor inappropriate’ (37%)
‘Appropriate’ (4%)
‘Very appropriate’ (1%)*
No response (1%)
|
n=79 1. ‘Freedom’ (n=33) 2. ‘Behaviour’ (n=14) 3. ‘Context’ (n=13) 4. ‘Platform’ (n=11) 5. ‘Language’ (n=8) 6. ‘Professionalism’ (n=7) 7.‘Boundary’ (n=6) 8. ‘Trends and norms’ (n=5) 9. ‘Consequences’ (n=3) 10. ‘Method of resolution’ (n=3) 11. ‘Anonymity’ (n=2) 12. ‘Respect’ (n=2) 13. ‘Audience’ (n=1) 14. ‘Confidentiality’ (n=1).
|
n=13 Poster’s freedom to express his personal opinion versus considerations, of professionalism, language, audience, behaviour, context, platform and consequences.
Norms on social media versus harsh language |
|
Post 5 |
n=91 ‘Very inappropriate’ (24%)
‘Inappropriate’(42%)
‘Neither appropriate nor inappropriate’ (24%)
‘Appropriate’(1%)
‘Very appropriate’ (9%)
|
n=79 1. ‘Confidentiality’ (n=38) 2. ‘Language’ (n=24) 3. ‘Purpose’ (n=23) 4. ‘Respect’ (n=17) 5. ‘Professionalism’ (n=10) 6. ‘Behaviour'(n=8) 7. ‘Platform'(n=7) 8. ‘Audience’(n=6) 9. ‘Consequences’(n=4) 10. ‘Freedom’(n=4) 11. ‘Boundary'(n=1) 12. ‘Context'(n=1) 13. ‘Reflection'(n=1) 14. ‘Trends and norms'(n=1)
|
n=15 Educational message versus considerations of language and tone, respect, platform, audience and consequences
Freedom of the poster to post what she wants without patient identifiers versus consideration of the language used |
|
Post 6 |
n=89 ‘Very inappropriate’(69%)
‘Inappropriate’ (20%)
‘Neither appropriate nor inappropriate’ (4%)
‘Appropriate’ (0%)
‘Very appropriate’ (2%)
No response (2%)
|
n=91 1.‘Platform’ (n=22) 2. ‘Collegiality’ (n=21) 3.’Method of resolution’ (n=20) 4. ‘Professionalism’ (n=18) 5. ‘Consequences’ (n=13) 6. ‘Language'(n=11) 7. ‘Lawfulness’(n=6) 8. ‘Confidentiality’(n=4) 9. ‘Behaviour’(n=3) 10. ‘Context'(n=3) 11.’Anonymity'(n=2) 12. ‘Freedom’ (n=1) 13. ‘Purpose’ (n=1) 14. ‘Respect'(n=1)
|
n=1 Consideration that the poster might be trying to resolve an issue versus considerations of the inappropriateness of the post in terms of collegiality |
Table 2. Summary of results for Posts 1-6
A. Evaluation and Considerations
Except for Post 4 which was evaluated as ‘Neither appropriate nor inappropriate’ by the majority (37%) of the respondents, all other posts were rated as either ‘Very inappropriate’ or ‘Inappropriate’ by the majority of respondents (34%-69%). In particular, Post 5 has a relatively high proportion of respondents (10%) rating it as either ‘Appropriate’ or ‘Very appropriate’. Respondents have a broad range of considerations with ‘Professionalism’, ‘Language’, ‘Behaviour’ and ‘Platform’ repeated across all six posts.
‘Platform’ was the main consideration for Post 2 and Post 6. Respondents considered the inappropriateness of posting on a public platform what should only be said or done in private, “FB is a public forum. People should settle personal grievances NOT online but privately” (R2.57; Post 2); “Publicly criticizing a colleague is inappropriate. Feedback should always be given in a private setting” (R6.33; Post 6).
For the other posts, the main considerations were ‘Consent’ (Post 1), ‘Professionalism’ (Post 3), ‘Freedom’ (Post 4) and ‘Confidentiality’ (Post 5). More than half of the respondents (55%) for Post 1 considered whether consent or permission was obtained before posting. For Post 3, more than half of the respondents (59%) considered professionalism generally or more specifically in terms of attitude. For Post 4, 42% of the respondents considered the freedom of speech of the poster including the freedom of the poster to post personal matters in a personal capacity, with personal accountability. Confidentiality and privacy of patients was considered by 24% of respondents on Post 5.
B. Negotiation of Conflicting Considerations
Among the six posts, Post 5 had the most number of respondents with conflicting considerations (n=15), followed by Post 4 (n=13).
For Post 5, fourteen respondents considered that the poster has an educational purpose versus other considerations and one respondent considered freedom of expression versus language. To negotiate the conflicting considerations for Post 5, six respondents reasoned that the educational message of the post and the poster’s good intentions need to be subjected to (or at least seen in the light of) considerations of confidentiality, language, professionalism and respect. For example, two faculty members, F5.3 and F5.5, thought that although the poster had good intentions and the message was educational, her language and tone were inappropriate.
Someone has just died. Instead of showing empathy to the family of the deceased who had just lost a loved one, she uses swear words in a callous, insensitive way. Even though her intentions might have been good to ask people to wear a crash helmet, the way she said it was offensive and highly inappropriate given the circumstances (F5.3).
F5.5 also considered the possible identification of the victim, “although message was ‘correct’ strong language including expletives used which is inappropriate timing and location of post may allow identification of victim” (F5.5).
However, there were nine respondents for Post 5 who considered educational purpose and freedom of expression at the same level of importance as other considerations. Rating Post 5 as ‘Neither inappropriate nor appropriate’, F5.6 reasoned that the possible breach in Professionalism/Confidentiality may be justified by educational purpose, “I don’t think it’s appropriate to talk about patient experiences on Facebook but I believe she has done so with the intention of encouraging others to wear helmets” while R5.39 reasoned that the inappropriate language use may also be justified by the freedom of the poster to say what she wants as long as there were no patient identifiers, “While her choice of words may not be the best, there were no patient identifiers. Again, she can say what she wants”.
For Post 4 which had 13 respondents with conflicting considerations, 12 respondents considered that the poster should have the freedom to express his personal opinion versus a variety of other considerations, including that of ‘Professionalism’,’ Language’, ‘Audience’,’ Behaviour’, ‘Context’, ‘Platform’ and ‘Consequences’. One respondent considered norms on social media versus the harsh language used.
To negotiate the conflicting considerations for Post 4, six respondents prioritised professionalism and other considerations like audience and consequences over freedom of expression. For example, a resident reasoned that while medical professionals can have their own political views, the poster should consider the possible consequences of such a post being seen by a wider audience and being used against him, “Everyone is entitled to his own view, medical professionals can have their own political views, but caution needs to be exercised if this information is used against him. might need to restrict to close friends only” (R4.43).
Seven respondents, however, considered freedom of expression and norms on social media at the same level of importance as other considerations. For example, respondents R4.51 and R4.60 rated Post 4 as ‘Neither inappropriate nor appropriate’. They reasoned that the harsh language used or the negative consequences of the post may be justified by the poster’s entitlement to freedom of expression, “He is entitled to his beliefs and freedom of speech about political and religious issues. Even though these comments are harsh and mean, we can’t possibly control how everyone speaks” (R 4.51); “Everyone is entitled to free speech and he has every right to say what he wants. But again this does not look good on his reputation” (R 4.60).
The number of respondents with conflicting considerations for the other posts ranged from 1 to 6. In general, respondents negotiated the conflicting considerations mainly by prioritising professionalism over and above the other considerations.
IV. DISCUSSION
A total of 182 faculty and residents (36.8%) from the NHG-AHPL Residency program in Singapore rated the appropriateness of Facebook posts and 463 evaluation responses were analysed. One of three postgraduate medical education programs in Singapore, the NHG-AHPL Residency comprises 27 residency programs within a few institutions including hospitals and nine polyclinics. Faculty and residents who explained their evaluation took into account a wide range of considerations and these considerations tended to conflict with one another when the respondents considered freedom of expression of the poster and the educational purpose of a post. These findings suggest that doctors within the same Residency do not necessarily have a uniform set of professional priorities and may have to manage conflicting professional and personal values in different contexts. The teaching and evaluation of professionalism should thus increasingly take conflict and context into consideration (Ginsburg et al., 2000). Educators of professional values could recognise the complexity of such conflicts and be sensitive to this in their teaching, whether formally or informally.
Freedom of speech or expression appears to be a recurrent consideration for posts not just in the personal domain (Posts 2 and 4) but also those in the work-related domain as well (Posts 3 and 5). Given that freedom of expression is not commonly encouraged or emphasised in Asian cultures (Kim & Sherman, 2007), it may be somewhat surprising that this was a recurrent consideration for doctors in Singapore. This consideration thus deserves more attention from developers of social media use guidelines and online professionalism course facilitators who can seek to start addressing these considerations by first recognising and acknowledging them. While existing social media guidelines could and should be tempered by recognising doctors’ right to free speech, doctors and medical students would also need to exercise critical judgment to consider whether their freedom of expression is appropriate in view of the guidelines (Farnan et al., 2009).
This study found that the post that elicited the most number of conflicting considerations was Post 5. This post by a junior doctor contained insensitive language and patient-related content but had an educational purpose. It is unclear whether if the post had been written more sensitively, it would elicit even more conflicting considerations. This may be a valid cause for concern given the potential negative consequences of such posts (Wells et al., 2015). Although the victim was not named, it is still possible that enough details are given for him to be identified. Such a post may also violate family members’ expectations of privacy. Public trust could also possibly be undermined because of the insensitivity and lack of empathy displayed by a doctor. It may be helpful for faculty to engage residents or students with such issues informally or formally during relevant courses and to explore alternative avenues for patient storytelling.
Based on the findings of our study, we recommend creating platforms for conversations on social media use to take place among faculty and residents. Using existing social media use guidelines and relevant findings from studies as material for discussion, faculty and residents could consider various perspectives, discuss how guidelines may moderate some considerations and explore further considerations arising from the conversation. Discussions like these require doctors to exercise critical judgments on ethical dilemmas and arrive at possible ways to negotiate conflicting considerations in various circumstances within the social media context. In her commentary on social media and medical professionalism, Fenwick (2014) discusses how doctors in contemporary practice must deal with conflicting priorities and urges a more pluralistic approach to understanding the notion of professionalism while thinking critically about social media’s current and future implications for practice. Such conversations can provide opportunities for the doctors to do so and perhaps more crucially, to consider how social media can be used creatively for better patient and health outcomes.
In a recent systematic review on the use of social media in graduate medical education, the authors found ten studies pertaining to resident professionalism (Sterling, Leung, Wright, & Bishop, 2017). However, most were exploratory, surveying residents about their social network behaviour and exploring how program directors use social media to monitor unprofessional behaviour of residents. Although our study was limited to the faculty and residents in one Residency in Singapore, to our knowledge, this is the first study to shed light on how residents as well as faculty negotiate conflicting considerations when evaluating online posts. Instead of hypothetical Facebook posts (whereby it would be possible to address potential biases by varying factors like the age or gender of the poster), we used authentic posts (except Post 6) which respondents might find more relevant and might be more motivated to evaluate and discuss them. Another limitation of the study was that we did not consider how factors like the respondents’ age, type of residency program or their actual usage of social media may influence their evaluation of the posts. However, we followed a systematic, transparent process for coding the written responses and we achieved a high interrater reliability through extensive discussions.
Future work should focus on understanding the complexities of how doctors negotiate conflicting professional values. In this study, respondents were asked to explain their evaluation after rating the appropriateness of the posts and the length of responses varied from one word to several sentences. Due to the limitation of such a study design, the reasoning process of some respondents could not be examined. Conducting interviews or focus groups could enable more in-depth analysis of how participants negotiate conflicting values. Research in moral psychology has shed light on how a person makes moral judgments. According to cognitive developmentalists a person may spontaneously have a new intuition that contradicts the initial intuitive judgment during the course of thinking about a situation (Kohlberg, 1969; Piaget, 1965). He/she comes to see a dilemma from more than one perspective and experiences competing intuitions. In particular, focus-group discussions could shed light on how the moral judgments of participants in the group might influence one another (Haidt, 2001). Studies designed to focus on examining how doctors resolve conflicting professional values can deepen our understanding of medical professionalism and what it constitutes, within the social media context and beyond.
V. CONCLUSION
This study aimed to explore the considerations and possible competing or conflicting considerations of faculty and residents in the NHG-AHPL Residency program when they evaluate online postings, especially grey posts. Faculty and residents who explained their evaluation took into account a wide range of considerations and these considerations tended to conflict with one another when the respondents considered freedom of expression of the poster and the educational purpose of a post. These findings suggest that doctors within the same Residency do not necessarily have a uniform set of professional priorities and may have to manage conflicting professional and personal values in different contexts. Educators of professional values could recognise the complexity of such conflicts and be sensitive to this in their teaching, whether formally or informally. We recommend creating platforms for conversations on social media use to take place among faculty and residents.
Notes on Contributors
Ms Loo May Eng is Research Analyst at Health Outcomes and Medical Education Research (HOMER), National Healthcare Group. She is the primary author of this manuscript and was involved in the study design, data collection and analysis of this project.
Dr Lee Yee Mun is Senior Consultant at the Department of Urology, Tan Tock Seng Hospital. He was involved in the conceptualisation of this project.
Ms Brenda Wong is Program Coordinator at Group Education, National Healthcare Group. She was involved in data collection and analysis.
Ethical Approval
Ethics approval was obtained from the institution’s Domain Specific Review Board (NHG DSRB Ref: 2015/00584).
Acknowledgements
The authors would like to thank all residents and faculty who participated in the questionnaire.
Funding
The research did not receive any specific grant from funding agencies.
Declaration of Interest
There is no conflict of interest to declare.
References
American College of Physicians Ethics, Professionalism, and Human Rights Committee. (2012). American College of Physicians Ethics Manual: Sixth edition. Annals of Internal Medicine, 156(1 Pt 2), 73–104. https://doi.org/10.7326/0003-4819-156-1-201201031-00001
Australian Medical Association. (2010). Social media and the medical profession. Retrieved from https://ama.com.au/article/social-media-and-medical-profession
Canadian Medical Association. (2011). Social media and Canadian physicians: Issues and rules of engagement. Retrieved from https://www.cma.ca/En/Pages/social-media-use.aspx
Chretien, K. C., Farnan, J. M., Greysen, S. R., & Kind, T. (2011). To friend or not to friend? Social networking and faculty perceptions of online professionalism. Academic Medicine, 86(12), 1545-1550. https://doi.org/10.1097/ACM.0b013e3182356128
Chretien, K. C., & Kind, T. (2014). Climbing social media in medicine’s hierarchy of needs. Academic Medicine, 89(10), 1318–1320. https://doi.org/10.1097/ACM.0000000000000430
Constine, J. (2017, June 27). Facebook now has 2 billion monthly users… and responsibility. Retrieved October 20, 2017, from TechCrunch website http://social.techcrunch.com/2017/06/27/facebook-2-billion-users/
Dawkins, R., King, W. D., Boateng, B., Nichols, M., & Desselle, B. C. (2017). Pediatric residents’ perceptions of potential professionalism violations on social media: A US national survey. JMIR Medical Education, 3(1). https://doi.org/10.2196/mededu.5993
Farnan, J. M., Paro, J. A. M., Higa, J. T., Reddy, S. T., Humphrey, H. J., & Arora, V. M. (2009). Commentary: The relationship status of digital media and professionalism: it’s complicated. Academic Medicine, 84(11), 1479–1481. https://doi.org/10.1097/ACM.0b013e3181bb17af
Fenwick, T. (2014). Social media and medical professionalism: Rethinking the debate and the way forward. Academic Medicine, 89 (10), 1331–1334. https://doi.org/10.1097/ACM.0000000000000436
General Medical Council. (2013). Doctors’ use of social media. Retrieved from http://www.gmc-uk.org/guidance/ethical_guidance/21186.asp
Ginsburg, S., Regehr, G., Hatala, R., McNaughton, N., Frohna, A., Hodges, B., … Stern, D. (2000). Context, conflict, and resolution: A new conceptual framework for evaluating professionalism. Academic Medicine, 75(Supplement), S6–S11.
Greysen, S. R., Johnson, D., Kind, T., Chretien, K. C., Gross, C. P., Young, A., & Chaudhry, H. J. (2013). Online professionalism investigations by state medical boards: First, do no harm. Annals of Internal Medicine, 158(2), 124–130. https://doi.org/10.7326/0003-4819-158-2-201301150-00008
Greysen, S. R., Kind, T., & Chretien, K. C. (2010). Online Professionalism and the Mirror of Social Media. Journal of General Internal Medicine, 25(11), 1227–1229. https://doi.org/10.1007/s11606-010-1447-1
Haidt, J. (2001). The emotional dog and its rational tail: A social intuitionist approach to moral judgment. Psychological Review, 108 (4), 814–834.
Hamm, M. P., Chisholm, A., Shulhan, J., Milne, A., Scott, S. D., Klassen, T. P., & Hartling, L. (2013). Social media use by health care professionals and trainees: A scoping review. Academic Medicine, 88(9), 1376–1383. https://doi.org/10.1097/ACM.0b013e31829eb91c
Jain, A., Petty, E. M., Jaber, R. M., Tackett, S., Purkiss, J., Fitzgerald, J., & White, C. (2014). What is appropriate to post on social media? Ratings from students, faculty members and the public. Medical Education, 48(2), 157–169. https://doi.org/10.1111/medu.12282
Kesselheim, J. C., Batra, M., Belmonte, F., Boland, K. A., & McGregor, R. S. (2014). New professionalism challenges in medical training: An exploration of social networking. Journal of Graduate Medical Education, 6(1), 100–105. https://doi.org/10.4300/JGME-D-13-00132.1
Kim, H. S., & Sherman, D. K. (2007). “Express yourself”: Culture and the effect of self-expression on choice. Journal of Personality and Social Psychology, 92(1), 1-11. https://doi.org/10.1037/0022-3514.92.1.1
Kind, T., Greysen, S. R., & Chretien, K. C. (2012). Pediatric clerkship directors’ social networking use and perceptions of online professionalism. Academic Pediatrics, 12(2), 142–148. https://doi.org/10.1016/j.acap.2011.12.003
Kohlberg, L. (1969). Stage and sequence: The cognitive development approach to socialization. In D. Goslin (Ed.), Handbook of socialization theory (pp. 347–480). Chicago: Rand McNally.
Piaget, J. (1965). The moral judgment of the child. Retrieved from http://archive.org/details/moraljudgmentoft005613mbp
Rocha, P. N., & de Castro, N. A. A. (2014). Opinions of students from a Brazilian medical school regarding online professionalism. Journal of General Internal Medicine, 29(5), 758–764. https://doi.org/10.1007/s11606-013-2748-y
Saldana, J. (2012). The Coding Manual for Qualitative Researchers. London: SAGE.
Singapore Medical Council. (2016). smc handbook on medical ethics. Retrieved from http://www.healthprofessionals.gov.sg/content/hprof/smc/en/topnav/guidelines/ethical_code_and_ethical_guidelines.html
Sterling, M., Leung, P., Wright, D., & Bishop, T. F. (2017). The Use of Social Media in Graduate Medical Education: A Systematic Review. Academic Medicine, 92(7), 1043–1056. https://doi.org/10.1097/ACM.0000000000001617
Wells, D. M., Lehavot, K., & Isaac, M. L. (2015). Sounding Off on Social Media: The Ethics of Patient Storytelling in the Modern Era. Academic Medicine, 90(8), 1015–1019. https://doi.org/10.1097/ACM.0000000000000668
*Loo May Eng
Health Outcomes and Medical Education Research,
National Healthcare Group
Tel: (65) 6359 6362
Email: may_eng_loo@nhg.com.sg
Submitted: 16 October 2019
Accepted: 11 February 2020
Published online: 1 September, TAPS 2020, 5(3), 62-70
https://doi.org/10.29060/TAPS.2020-5-3/OA2204
Benny Kai Guo Loo1, Koh Cheng Thoon2, Jessica Hui Yin Tan1, Karen Donceras Nadua2 & Cristelle Chu-Tian Chow1
1General Paediatric Service, KK Women’s and Children’s Hospital, Singapore; 2Infectious Diseases Service, KK Women’s and Children’s Hospital, Singapore
Abstract
Introduction: Residents-as-teachers (RAT) programmes benefit both medical students and residents. However, common barriers encountered include busy clinical duties, congested lesson schedules and duty-hour regulations.
Methods: The study aimed to determine if providing a structured teaching platform and logistic support, through the Paediatric Residents As Teaching Advocates (PRATA) programme, would enhance residents’ teaching competencies and reduce learning barriers faced by medical students. The programme was held over 23 months and participated by 502 medical students. Residents were assigned as intervention group tutors and conducted bedside teachings. The evaluation was performed by medical students using paper surveys with 5-point Likert scales at the start and end of the programme.
Results: We found that students in the intervention groups perceived residents to be more competent teachers. The teaching competencies with the most significant difference were residents’ enthusiasm (intervention vs control: 4.34 vs 3.92), giving constructive feedback (4.23 vs 3.83) and overall teaching effectiveness (4.27 vs 3.89). Higher scores indicated better teaching competency. Similarly, the intervention groups perceived fewer barriers. More improvement was noted in the intervention groups with regards to busy ward work as a teaching barrier as the scores improved by 0.49, compared to 0.3 in the control groups.
Conclusion: This study demonstrated that providing a structured teaching platform could enhance residents’ teaching competencies and logistic support could help overcome common barriers in RAT programmes. This combination could enhance future RAT programmes’ effectiveness.
Keywords: Paediatric, Resident-As-Teacher, Teaching Competency, Barrier, Clinical Duty, Lesson Schedule, Duty-Hour Regulation
Practice Highlights
- RAT programme with structured, dedicated teaching platforms can improve residents’ teaching competencies.
- Assigning tutor responsibilities to residents can increase their level of enthusiasm and perception of self-importance as a tutor.
- Busy work commitment, congested lesson schedules and duty-hour regulations are barriers in RAT programmes.
- Logistic support is effective in overcoming common barriers in RAT programmes.
I. INTRODUCTION
Residents play a vital role in the education of medical students. They spend up to 25% of their time teaching and research has shown that they can improve medical students’ knowledge and examination scores (McKean, & Palmer, 2015). With the shift of postgraduate medical training in Singapore to the residency system under Accreditation Council on Graduate Medical Education-International (ACGME-I) in 2011, teaching is recognised as an important competency for residents (Accreditation Council for Graduate Medical Education, 2017).
Studies have demonstrated the benefits of residents-as-teachers (RAT) programmes for both residents and medical students (Hill, Yu, Barrow, & Hattie, 2009). A controlled trial of RAT programme involving 24 obstetrics and gynaecology residents showed that their teaching skills have improved via objective structured teaching examination (Gaba, Blatt, Macri, & Greenberg, 2007). Subjectively, residents feel that teaching improves their clinical knowledge (Post, Quattlebaum, & Benich III, 2009). A successful RAT programme also enhances the students’ perception of the resident as a physician (Wamsley, Julian, & Wipf, 2004), as well as higher overall satisfaction with the clinical posting (Huynh, Savitski, Kirven, Godwin, & Gil, 2011). Furthermore, effective resident teachers can influence the students’ future career choices (Musunuru, Lewis, Rikkers, & Chen, 2007).
Although residents acknowledge that teaching is part of their duty and have the desire to teach, there are also many barriers encountered. A common problem is the heavy burden of clinical duties and lack of uninterrupted time (Wamsley et al., 2004). The limitation of time was further worsened by the introduction of duty-hour regulations (Brasher, Chowdhry, Hauge, & Prinz, 2005). The residents understandably prioritise clinical work and are exhausted after completion of clinical duties, leaving little time or energy to focus on education. Other challenges include a lack of confidence and insufficient training as an educator (Yedidia, Schwartz, Hirschkorn, & Lipkin, 1995). A survey of paediatric residents indicated that prior training in teaching can benefit the residents in teaching students (Busari, Scherpbier, Van Der Vleuten, & Essed, 2000).
A. Conceptual Framework
As learning involves knowledge organisation through the continuous addition and modification of concepts and relations over time, it is understandable that experts would have a more complex knowledge structure compared to novices (Meller, M. Chen, R. Chen, & Haeseler, 2013). The difference in knowledge structure between the experts and novices would be significant. Intermediate learners, such as paediatric residents, in this case paediatric residents, with a knowledge structure more similar to novices, would, therefore, be able to better appreciate and address the cognitive problems encountered by the medical students. Paediatric residents would be in an optimal position to minimise the distance between what the novice already knows and what needs to be learned, also referred to as the “zone of proximal development” (Ten Cate, Snell, Mann, & Vermunt, 2004).
Engaging residents as teachers utilise the principles of near-peer teaching. Social and cognitive congruence, demonstrated by Schmidt and Moust (1995), as well as Lockspeiser, O’Sullivan, Teherani, and Muller (2008), supports the near-peer teaching relationship. Social congruence enables residents to communicate with students in an informal, empathic way which in turn encourages student engagement and drives learning (Schmidt & Moust, 1995). Cognitive congruence, whereby residents have a better appreciation of students’ deficits in knowledge, enables residents to clarify problems at a level appropriate and relevant to students (Lockspeiser et al., 2008).
Utilising these principles, we have developed the RAT programme, Paediatric Residents As Teaching Advocates (PRATA), for our residents to engage in formal, structured teaching duties. The authors believe that residents can teach more effectively with a structured teaching platform, and medical students will experience fewer barriers with logistic support from RAT programme.
II. METHODS
A controlled, prospective, pre-post study was carried out at KK Women’s and Children’s Hospital (KKH), Department of Paediatric Medicine, from June 2014 to April 2016. As this study was categorised as an education quality improvement, Singhealth Centralised Institutional Review Board (CIRB) indicated that formal IRB review was not required. Implied informed consent was obtained from participants during a briefing prior to the data collection.
A. Study Setting and Participants
KKH is the largest academic paediatric medical centre in Singapore, with a capacity of more than 800 inpatient beds. The paediatric residency programme also trains more than half of the paediatric residents nationwide.
Third-year medical students from the NUS Yong Loo Lin School of Medicine are attached to KKH for 1-month clinical posting as part of their paediatric training. Every batch of students consists of 6 tutorial groups and each group has 5 to 6 students. Each tutorial group is assigned to a ward team for the entire posting. The students are also required to evaluate and provide feedback on their tutors at the end of the posting.
Four to five paediatric consultants are assigned to each tutorial group as their dedicated tutors. These consultants are paediatric specialists who have completed a recognised training programme and are accredited by the Specialist Accreditation board. Every consultant has more than 3 years’ experience of teaching medical students.
All paediatric residents in their first 3 years of training (n=49) had attended workshops on “Effective Bedside Teaching using the Five-Minute Preceptor” (half-day programme with lectures and practice sessions on microteaching skills for effective clinical teaching) and “Giving Effective Feedback” (half-day programme with lectures and role-play sessions on a 4-step model for constructive feedback). These residents were invited to take part in the PRATA programme through email and participation was voluntary. Thirty-three paediatric residents (67%) participated in the PRATA programme.
B. Study Implementation
The study coordinators randomly assigned 3 medical student tutorial groups to be intervention groups and the remaining 3 groups as controls at the beginning of each posting. A total of 51 intervention and 51 control groups were assigned over 17 batches of students. The intervention included assigning 1 resident to the tutor group with a structured teaching schedule to assist with logistics coordination (Figure 1). The resident was to conduct 2 bedside teaching sessions, focusing on history taking and physical examination techniques. Two administrators from the education office were involved in the scheduling of the teaching roster according to the residents’ ward roster and work commitments, and in line with ACGME-I duty-hour restrictions. This ensured that the arrangements were specifically catered for the respective residents as they were often in different areas of work and thus have varying work commitments.
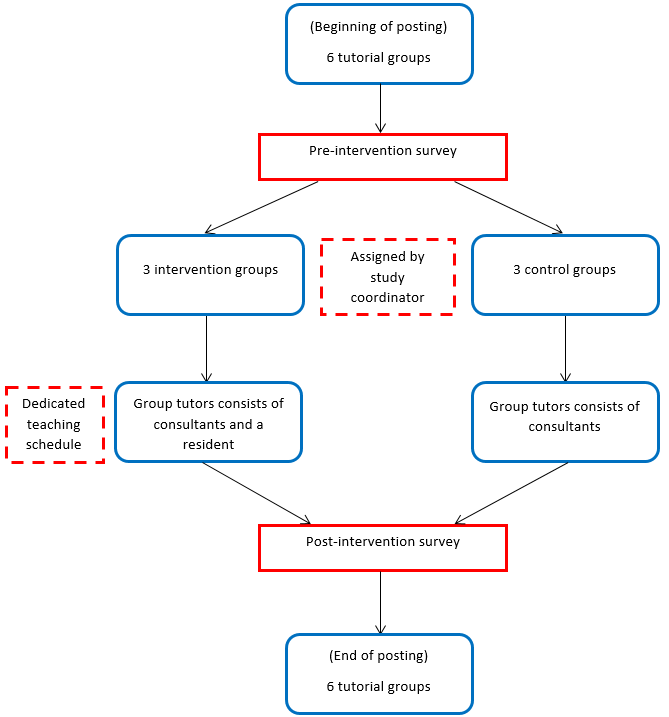
Note: A total of 17 batches of students with 51 intervention and 51 control groups participated in the programme.
Figure 1. PRATA programme protocol diagram (per batch)
For comparison, the existing teaching interactions between residents and medical students in the wards were evaluated in the control groups. As the students were attached to the same ward team for the posting, the residents in the ward team could teach the medical students. Often, these teaching sessions were unplanned, brief and limited by the burden of clinical work.
Apart from the additional resident tutor in the intervention groups, both groups of students received the same standard of medical education, comprising of the same series of planned lectures, the number of bedside tutorials by the consultants, and the duration of ward and clinic attachments.
C. Survey Forms
Paper surveys were given to all students at the beginning (9-question survey) and the end of the posting (18-question survey). These surveys were anonymised and collected by the study coordinators. The survey design was based on 2 studies by Copeland and Hewson (2000), and Hill et al. (2012). These rating instruments were chosen as they were widely used in assessing RAT programmes, applicable in a variety of clinical setting and frequently cited to date. To suit the local context, relevant questions were extracted by the study coordinators based on residents’ feedback and modified accordingly. A 5-point Likert scale was used for the questions, ranging from strongly disagree to strongly agree. A free-text box was included for any comments on both surveys.
|
Effectiveness of Resident Teaching |
Strongly Disagree |
Disagree |
Neutral |
Agree |
Strongly Agree |
|
My medical knowledge and/or clinical skills have improved significantly during the clerkship after being taught by residents |
|
|
|
|
|
|
We received adequate teaching from residents during the clerkship |
|
|
|
|
|
|
The resident established a good learning environment |
|
|
|
|
|
|
The resident stimulated me to learn independently |
|
|
|
|
|
|
The resident offered regular and constructive feedback (both positive and negative) in a timely manner and in an appropriate setting |
|
|
|
|
|
|
The resident clearly specified what we were expected to know and do for the tutorial |
|
|
|
|
|
|
The resident was able to adjust the teaching according to my needs (experience, competence, interest) |
|
|
|
|
|
|
The resident asked questions that promoted learning (e.g. clarification, reflective questions) |
|
|
|
|
|
|
The resident gave clear explanations or reasons for his/her opinions, advice and actions etc. |
|
|
|
|
|
|
The resident was able to effectively coach me on my clinical skills |
|
|
|
|
|
|
The resident taught or demonstrated effective patient and/or family communication skills |
|
|
|
|
|
|
The residents are enthusiastic about teaching |
|
|
|
|
|
|
The resident made teaching relevant to patient care |
|
|
|
|
|
|
Overall, the resident was an effective teacher |
|
|
|
|
|
|
Barriers to Resident Teaching |
Strongly Disagree |
Disagree |
Neutral |
Agree |
Strongly Agree |
|
Ward work was too busy and residents had no time for teaching |
|
|
|
|
|
|
There were too many lectures and tutorials outside of the ward to allow for resident teaching |
|
|
|
|
|
|
Personal Impact of Resident Teaching |
Strongly Disagree |
Disagree |
Neutral |
Agree |
Strongly Agree |
|
The resident tutor was a positive role model for me |
|
|
|
|
|
|
After being taught and interacting with my resident teacher, it would make me more likely consider/select Paediatrics as my choice for future residency training |
|
|
|
|
|
|
Any other comments:
|
The pre-programme survey (Appendix) asked the students about their expectations of residents as teachers, as well as the perceived barriers to receiving resident teachings. The post-programme survey (Table 1) focused on the students’ evaluation of residents’ teaching competencies, the impact of resident teachings and the barriers encountered. For the post-programme survey, the intervention groups evaluated the resident from their tutor group, whereas the control groups evaluated the resident from the ward team.
D. Statistical Analysis
Data were expressed as mean scores with standard deviations. For questions about residents’ teaching competencies, post-programme differences were evaluated between groups using the Mann-Whitney U test. For questions on barriers to receiving resident teachings, pre and post-programme differences were evaluated within and between groups using the Wilcoxon signed-rank test and the Mann-Whitney U test respectively. A p-value of less than 0.05 was taken to be significant for all tests. Analyses were conducted using SPSS version 19.
III. RESULTS
A. Participant Demographics
A total of 502 medical students from 17 batches participated in the PRATA programme over 23 months. Overall, there was 100% pre-programme and 81% (410 students) post-programme participation. The post-programme participation was 74% in the control group and 88% in the intervention group. The baseline demographics were comparable between the groups.
B. Resident Teaching Competencies
A higher score indicated better teaching competency. The intervention group students gave significantly better scores across all aspects for the residents’ teaching competencies as compared to the control groups (Table 2). The biggest difference was noted in the question of the enthusiasm shown by the residents. The intervention groups scored 4.34 and the control groups scored 3.92. The next greatest difference was from the question of residents giving regular and constructive feedback. The scores for the intervention and control groups were 4.23 and 3.83 respectively. The overall assessment of residents as effective teachers showed a similar trend as the intervention groups scored 4.27 and the control groups scored lower at 3.89. The differences in these competencies were all statistically significant.
|
Post-programme survey questions on resident teaching competencies |
Control (n = 188) |
Intervention (n = 222) |
P# |
|
Mean* (SD) |
Mean* (SD) |
||
|
My medical knowledge and/or clinical skills have improved significantly during the clerkship after being taught by residents |
3.92 (0.53) |
4.05 (0.65) |
0.01 |
|
We received adequate teaching from residents during the clerkship |
3.62 (0.79) |
3.94 (0.75) |
<0.01 |
|
The resident established a good learning environment |
3.94 (0.59) |
4.27 (0.57) |
<0.01 |
|
The resident stimulated me to learn independently |
3.88 (0.61) |
4.10 (0.62) |
<0.01 |
|
The resident offered regular and constructive feedback (both positive and negative) in a timely manner and in an appropriate setting |
3.83 (0.66) |
4.23 (0.61) |
<0.01 |
|
The resident clearly specified what we were expected to know and do for the tutorial |
3.72 (0.68) |
4.09 (0.68) |
<0.01 |
|
The resident was able to adjust the teaching according to my needs (experience, competence, interest) |
3.91 (0.64) |
4.22 (0.66) |
<0.01 |
|
The resident asked questions that promoted learning (e.g. clarifications, probes, reflective questions) |
3.94 (0.62) |
4.24 (0.61) |
<0.01 |
|
The resident gave clear explanations or reasons for his/her opinions, advice and actions etc. |
3.95 (0.58) |
4.28 (0.58) |
<0.01 |
|
The resident was able to effectively coach me on my clinical skills |
3.84 (0.68) |
4.17 (0.65) |
<0.01 |
|
The resident taught or demonstrated effective patient and/or family communication skills |
3.89 (0.69) |
4.20 (0.62) |
<0.01 |
|
The residents are enthusiastic about teaching |
3.92 (0.65) |
4.34 (0.67) |
<0.01 |
|
The resident made teaching relevant to patient care |
3.90 (0.61) |
4.26 (0.59) |
<0.01 |
|
Overall, the resident was an effective teacher |
3.89 (0.63) |
4.27 (0.67) |
<0.01 |
Note: *Higher mean score indicates better competency.
#Mann-Whitney U test used for between-group comparisons.
Table 2. Results of survey questions relating to resident teaching competencies
C. Barriers to Resident Teachings
A lower mean score indicated less significant barrier to receiving resident teachings. Generally, the mean scores on barriers reported by the intervention groups decreased more than the control groups after the programme. For the question on busy ward work as a barrier for residents to teach, both groups started with the same mean score of 3.52. At the end of the posting, more improvement was noted in the intervention groups as the mean score decreased to 3.03, as compared to 3.22 in the control groups. Although the difference was statistically significant within the groups, it was not significant when comparing the post-programme difference between the groups (Table 3). For the question about too many lectures and tutorials as a barrier for students to attend resident teachings, the score decreased from 2.90 to 2.59 in the intervention groups. In contrast, the scored increased from 2.90 to 3.07 in the control groups, which meant that the barrier remained significant throughout their posting. The difference in the intervention groups and the post-programme difference between the groups were both statistically significant (Table 3).
|
Survey questions on barriers to resident teaching |
Control group (n = 188) |
Intervention group (n = 222) |
Control vs Intervention |
||||
|
Pre-programme Mean* (SD) |
Post-programme Mean* (SD) |
Pre-Post Difference P# |
Pre-programme Mean* (SD) |
Post-programme Mean* (SD) |
Pre-Post Difference P# |
Post Difference P^ |
|
|
Ward work was too busy and residents had no time for teaching |
3.52 (0.81) |
3.22 (0.89) |
<0.01 |
3.52 (0.79) |
3.03 (1.01) |
<0.01 |
0.42 |
|
There were too many lectures and tutorials outside of the ward to allow for resident teaching |
2.90 (0.76) |
3.07 (0.87) |
0.31 |
2.90 (0.82) |
2.59 (0.95) |
<0.01 |
<0.01 |
Note: *Lower mean score indicates less severe barrier.
#Wilcoxon signed-rank test used for within-group comparisons.
^Mann-Whitney U test used for between-group comparisons.
Table 3. Results of survey questions relating to barriers to receiving resident teachings
IV. DISCUSSION
RAT programmes have demonstrated improvement in residents’ teaching competencies and contribute significantly to the education of medical students (Hill et al., 2009). Although barriers to resident teachings such as excessive workload and duty hour regulations have been identified (Wamsley et al., 2004), there is limited literature on overcoming these obstacles in RAT programmes.
The main aims of the PRATA programme are to provide paediatric residents with a structured teaching platform to improve their teaching competencies and logistic support to overcome common barriers in RAT programmes. The residents in the PRATA programme had the added elements of a dedicated environment for teaching and assuming the role and responsibility as a teaching faculty. The education office also provided these residents with logistic support to reduce scheduling conflicts and duty-hour violations.
This study revealed that the PRATA programme improved the students’ perceptions of the residents’ teaching competencies. This is consistent that RAT programmes enhance resident teaching skills (Zackoff, Jerardi, Unaka, Sucharew, & Klein, 2015). The residents in the intervention groups achieved higher scores in all teaching competency domains, and this included innate characteristics (displaying enthusiasm), techniques (giving constructive feedback) and bedside skills (demonstrating effective communication). A higher score indicated better proficiency in that domain. Although both groups of residents were equipped with the same set of teaching skills, those in the PRATA programme were provided with a structured teaching platform as compared to the unpredictable and potentially chaotic ward setting in the control groups. Furthermore, assigning the residents responsibility as the group tutors possibly increased their level of enthusiasm and perception of self-importance as a tutor. Our study demonstrated that residents in RAT programmes that provide structure to apply their teaching skills can be perceived as better educators.
The results also showed that students from both student groups were very worried about the barriers to receiving resident teachings before the programme. They were more concerned about the residents’ busy work commitments as compared to their congested lesson schedules. Our programme was able to reduce the impact of these barriers as both scores improved significantly in the intervention groups. In contrast, the control groups continued to perceive after the posting that their lesson schedules did not permit residents to teach. Overall, the students from the intervention groups seemed to have a more positive learning experience as there were 20% more students who considered working in Paediatric Medicine in the future. The PRATA programme highlighted that logistic support was an important factor to decrease the students’ concerns of these barriers, which could impede them seeking learning opportunities from the residents.
We have identified some limitations of our study. Firstly, the residents participated in the programme voluntarily, therefore we could have recruited residents who were more passionate or more experienced in teaching. Therefore, we aim to recruit all residents and stratify them by their level of training for the subsequent studies. Secondly, there was no standardisation of the teaching topics. The residents in the intervention groups could have taught in the areas they were more confident in, whereas the residents in the control group could only teach about the patients in the ward. For future studies, we can assign the same teaching topics when evaluating the residents’ teaching competencies. Lastly, the improvement of scores in the intervention groups, although statistically significant, can be complex to interpret in the practical setting. A qualitative study on these aspects can give more insight, such as the specific traits or techniques that residents in the programme displayed, or the practical burden of the barrier on the students’ learning.
V. CONCLUSION
This study demonstrated that providing a structured teaching platform could enhance residents’ teaching competencies. This was an important factor as existing resident teachings commonly occur while performing clinical work and in the chaotic ward setting. The study also showed that logistic support could help overcome common barriers in RAT programmes, such as busy work commitments. We believe this combination is important to include in future RAT programmes.
Notes on Contributors
Dr Benny Kai Guo Loo is an Associate Consultant in General Paediatric Service at KK Women’s and Children’s hospital. He has a keen interest in medical education and is currently a Co-ordinator for Yong Loo Lin School of Medicine, NUS and Physician Faculty for Singhealth Paediatric Residency Programme.
A/Prof Koh Cheng Thoon is the Head and Senior Consultant of Infectious Diseases Service at KK Women’s and Children’s hospital. He is also the Academic Vice-Chair for Education in Singhealth Duke-NUS Paediatric Academic Clinical Programme and he was awarded the Wong Hock Boon Society-SMA Charity Fund Outstanding Mentor Award in 2016.
Dr Jessica Hui Yin Tan is a Senior Resident in General Paediatrics Service at KK Women’s and Children’s hospital. She is also a clinical lecturer at the Yong Loo Lin School of Medicine, NUS.
Dr Karen Donceras Nadua is an Associate Consultant in Infectious Diseases Service at KK Women’s and Children’s hospital. She is also a clinical teacher at the Lee Kong Chian School of Medicine.
Dr Cristelle Chu-Tian Chow is a Consultant in General Paediatrics Service at KK Women’s and Children’s hospital. She obtained her Master of Health Professions Education from Maastricht University and is currently the Associate Programme Director for Singhealth Paediatric Residency Programme.
Ethical Approval
The study was categorised as an education quality improvement hence formal Singhealth Centralised Institutional Board review is not required.
Acknowledgements
The authors would like to thank Paediatric Graduate Medical Education and Academic Clinical Programme secretariat, faculty and residents who have helped to make PRATA programme a success. We would also like to thank Prof Sandy Cook, Senior Associate Dean in Duke-NUS, for her guidance in the writing of this manuscript.
Funding
The authors report no funding source for this study.
Declaration of Interest
The authors declare no conflict of interest.
References
Accreditation Council for Graduate Medical Education (2017). Common program requirements. Retrieved from https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRs_2017-07-01.pdf.
Brasher, A. E., Chowdhry, S., Hauge, L. S., & Prinz, R. A. (2005). Medical students’ perceptions of resident teaching: Have duty hours regulations had an impact? Annals of Surgery, 242(4), 548.
Busari, J. O., Scherpbier, A. J. J. A., Van Der Vleuten, C. P. M., & Essed, G. E. (2000). Residents’ perception of their role in teaching undergraduate students in the clinical setting. Medical Teacher, 22(4), 348-353.
Copeland, H. L., & Hewson, M. G. (2000). Developing and testing an instrument to measure the effectiveness of clinical teaching in an academic medical center. Academic Medicine, 75(2), 161-166.
Gaba, N. D., Blatt, B., Macri, C. J., & Greenberg, L. (2007). Improving teaching skills in obstetrics and gynecology residents: Evaluation of a residents-as-teachers program. American Journal of Obstetrics and Gynecology, 196(1), 87-e1.
Hill, A. G., Srinivasa, S., Hawken, S. J., Barrow, M., Farrell, S. E., Hattie, J., & Yu, T. C. (2012). Impact of a resident-as-teacher workshop on teaching behavior of interns and learning outcomes of medical students. Journal of Graduate Medical Education, 4(1), 34-41.
Hill, A. G., Yu, T. C., Barrow, M., & Hattie, J. (2009). A systematic review of resident‐as‐teacher programmes. Medical Education, 43(12), 1129-1140.
Huynh, A., Savitski, J., Kirven, M., Godwin, J., & Gil, K. M. (2011). Effect of medical students’ experiences with residents as teachers on clerkship assessment. Journal of Graduate Medical Education, 3(3), 345-349.
Lockspeiser, T. M., O’Sullivan, P., Teherani, A., & Muller, J. (2008). Understanding the experience of being taught by peers: The value of social and cognitive congruence. Advances in Health Sciences Education, 13(3), 361-372.
McKean, A. J. S., & Palmer, B. A. (2015). Psychiatry resident-led tutorials increase medical student knowledge and improve national board of medical examiners shelf exam scores. Academic Psychiatry, 39(3), 309-311.
Meller, S. M., Chen, M., Chen, R., & Haeseler, F. D. (2013). Near-peer teaching in a required third-year clerkship. The Yale Journal of Biology and Medicine, 86(4), 583.
Musunuru, S., Lewis, B., Rikkers, L. F., & Chen, H. (2007). Effective surgical residents strongly influence medical students to pursue surgical careers. Journal of the American College of Surgeons, 204(1), 164-167.
Post, R. E., Quattlebaum, R. G., & Benich III, J. J. (2009). Residents-as-teachers curricula: A critical review. Academic Medicine, 84(3), 374-380.
Schmidt, H. G., & Moust, J. H. (1995). What Makes a Tutor Effective? A Structural Equations Modelling Approach to Learning in Problem-Based Curricula. Academic Medicine, 70(8), 708-714
Ten Cate, O., Snell, L., Mann, K., & Vermunt, J. (2004). Orienting teaching toward the learning process. Academic Medicine, 79(3), 219-228.
Wamsley, M. A., Julian, K. A., & Wipf, J. E. (2004). A literature review of “resident-as-teacher” curricula. Journal of General Internal Medicine, 19(5), 574-581.
Yedidia, M. J., Schwartz, M. D., Hirschkorn, C., & Lipkin, M. (1995). Learners as teachers. Journal of General Internal Medicine, 10(11), 615-623.
Zackoff, M., Jerardi, K., Unaka, N., Sucharew, H., & Klein, M. (2015). An observed structured teaching evaluation demonstrates the impact of a resident-as-teacher curriculum on teaching competency. Hospital Paediatrics, 5(6), 342-347.
*Benny K. G. Loo
Division of Paediatric Medicine
KK Women’s and Children’s Hospital
100 Bukit Timah Road, Singapore 229899
Tel: +65 62255554
Email: benny.loo.k.g@singhealth.com.sg
Submitted: 7 July 2019
Accepted: 30 January 2020
Published online: 1 September, TAPS 2020, 5(3), 54-61
https://doi.org/10.29060/TAPS.2020-5-3/OA2170
Kieng Wee Loh1, Jerome Ingmar Rotgans2, Kevin Tan3, Nigel Choon Kiat Tan3
1National Healthcare Group, Ministry of Health Holdings, Singapore; 2Office of Medical Education, Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore; 3Office of Neurological Education, Department of Neurology, National Neuroscience Institute, Singapore
Abstract
Introduction: Clinical reasoning is the cognitive process of weighing clinical information together with past experience to evaluate diagnostic and management dilemmas. There is a paucity of literature regarding predictors of clinical reasoning at the postgraduate level. We performed a retrospective study on internal medicine residents to determine the sociodemographic and experiential correlates of clinical reasoning in neurological localisation, measured using validated tests.
Methods: We recruited 162 internal medicine residents undergoing a three-month attachment in neurology at the National Neuroscience Institute, Singapore, over a 2.5 year period. Clinical reasoning was assessed on the second month of their attachment via two validated tests of neurological localisation–Extended Matching Questions (EMQ) and Script Concordance Test (SCT). Data on gender, undergraduate medical education (local vs overseas graduates), graduate medical education, and amount of clinical experience were collected, and their association with EMQ and SCT scores evaluated via multivariate analysis.
Results: Multivariate analysis indicated that local graduates scored higher than overseas graduates in the SCT (adjusted R2 = 0.101, f2 = 0.112). Being a local graduate and having more local experience positively predicted EMQ scores (adjusted R2 = 0.049, f2 = 0.112).
Conclusion: Clinical reasoning in neurological localisation can be predicted via a two-factor model–undergraduate medical education and the amount of local experience. Context specificity likely underpins the process.
Keywords: Clinical Reasoning, Context Specificity, Extended Matching Questions, Neurological Localization, Script Concordance Test
Practice Highlights
- Clinical reasoning is a combination of two concurrent processes–pattern recognition in familiar circumstances (illness scripts); and deliberate analysis in unfamiliar scenarios (hypothetico-deductive approach).
- Validated tools exist to assess aspects of clinical reasoning–Script Concordance Tests (SCTs) for illness scripts; and Extended Matching Questions (EMQs) for hypothetico-deductive reasoning.
- Doctors who (a) were educated locally; and (b) worked locally for a longer period, tend to reason more similarly to local expert clinicians in the area of neurological localization.
- Development of clinical reasoning in neurology appears to be specific to a given clinical context
- To optimize the development of clinical reasoning in neurology, internal medicine residency programmes could consider maximizing trainees’ exposure to the local medical context before rotating them to a neurology posting.
I. INTRODUCTION
Clinical reasoning is the cognitive process of integrating and weighing clinical information together with past experiences to evaluate diagnostic and management dilemmas (Monteiro & Norman, 2013). Together with an appropriate knowledge base, this is central to clinical competence (Elstein, Shulman, & Sprafka, 1990; Groen & Patel, 1985), Clinical reasoning is especially important for the skill of neurological localisation (Gelb, Gunderson, Henry, Kirshner, & Jozefowicz, 2002; Nicholl & Appleton, 2015), which involves interpreting clinical signs and symptoms to identify the site of neuroanatomical abnormalities–a crucial first step in making a neurologic diagnosis. Accurate clinical reasoning is an important core competency (Connor, Durning & Rencic, 2019), and is essential in minimising diagnostic errors (Durning, Trowbridge, & Schuwirth, 2019).
The ‘dual process’ paradigm of clinical reasoning proposes that a combination of rapid intuition and deliberate analysis is employed in clinical decision making (Elstein, 2009; Eva, 2005; Monteiro & Norman, 2013). In familiar circumstances, relevant clinical information is compared with past experiences to arrive at a diagnosis (Elstein, 2009), akin to pattern recognition. This content-specific knowledge is organised into mental networks (‘illness scripts’) for easy retrieval (Boushehri, Arabshahi, & Monajemi, 2015; Norman, Young, & Brooks, 2007). In unfamiliar situations, however, a ‘hypothetico-deductive’ approach is utilised instead, where hypotheses are formulated through conscious deliberations and later tested (Boushehri et al., 2015; Elstein, 2009; Monteiro & Norman, 2013). These reasoning processes work in parallel, but experts are more adept at switching between both approaches whilst maintaining a higher performance level in each (Boushehri et al., 2015; Eva, 2005; Monteiro & Norman, 2013).
Several studies have examined predictors of academic performance in medical undergraduates (Ferguson, James, & Madeley, 2002; Hamdy et al., 2006; Kanna, Gu, Akhuetie, & Dimitrov, 2009). Previous studies have examined sociodemographic characteristics and educational background as potential predictors, as these have practical relevance in reviewing admission criteria and teaching methods for undergraduate programmes. Female gender (Adams et al., 2008; Ferguson et al., 2002; Guerrasio, Garrity, & Aagaard, 2014; Stegers-Jager, Themmen, Cohen-Schotanus, & Steyerberg, 2015; Woolf, Haq, McManus, Higham, & Dacre, 2008), ethnic majority status (Stegers-Jager et al., 2015; Vaughan, Sanders, Crossley, O’Neill, & Wass, 2015; Woolf, Cave, Greenhalgh, & Dacre, 2008; Woolf & Haq et al., 2008; Woolf, Potts, & McManus, 2011) and older age (Kusurkar, Kruitwagen, Ten Cate, & Croiset, 2010) were found to be significant predictors; educational background (Kusurkar et al., 2010) and past academic performance (Ferguson et al., 2002; Hamdy et al., 2006; Kanna et al., 2009; Stegers-Jager et al., 2015; Woloschuk, McLaughlin, & Wright, 2010) also showed positive associations. However, academic performance does not solely reflect reasoning skill, especially in postgraduates (Woloschuk et al., 2010; Woloschuk, McLaughlin, & Wright, 2013).
The ‘dual process’ theory also identifies clinical experience as important for clinical reasoning, especially in the formation of illness scripts (Elstein, 2009; Eva, 2005; Monteiro & Norman, 2013). Yet this is seldom explored, with few studies on postgraduates, a group where clinical experience might be more relevant.
The current Singapore postgraduate training system is based on the United States’ residency system (Huggan et al., 2012). Medical graduates, whether local or overseas-trained, must first register with the Singapore Medical Council (SMC) to start practising medicine locally. They can then apply for graduate medical education programmes (‘residency’) in various sponsoring institutions to train in a speciality; residency entry can occur immediately after or several years after graduation.
In Singapore, internal medicine residents rotate between subspecialty departments (such as cardiology or neurology) in no fixed order, hence two residents rotated to neurology may differ in the amount of working experience as a resident, as a clinician practising locally, and as a doctor in general. Moreover, experiences may differ between the various sponsoring institutions, and also between disparate undergraduate medical programmes. These differences might influence clinical reasoning.
Additionally, most Singaporean male graduates defer their medical careers to complete a two-year stint with the Singapore Armed Forces (SAF), as part of their compulsory National Service. Within the SAF, medicine is rarely practised in conventional clinical settings, and the quality of clinical experience may be affected. Clinical experience may hence differ between genders.
Several instruments have been designed to assess clinical reasoning (Amini et al., 2011; Boushehri et al., 2015), but these were infrequently used in studies (Groves, O’rourke, & Alexander, 2003; Postma & White, 2015). Some studies utilised unvalidated questionnaires (Groves et al., 2003); others did not specifically assess clinical reasoning (Postma & White, 2015). Moreover, the focus of each instrument varies–Extended Matching Questions (EMQ; Beullens, Struyf, & Van Damme, 2005) on ‘hypothetico-deductive’ reasoning; Script Concordance Test (SCT; Lubarsky, Charlin, Cook, Chalk, & van der Vleuten, 2011) on illness scripts (Amini et al., 2011; Boushehri et al., 2015). As both approaches are complementary, it may thus be prudent to employ multiple instruments to better evaluate clinical reasoning as an outcome measure, especially for the important skill of neurological localisation (Gelb et al., 2002; Nicholl & Appleton, 2015).
Given the gaps in the extant literature, we thus aimed to determine predictors of postgraduate performance in clinical reasoning tests, within the context of neurological localisation.
II. METHODS
A. Subjects
Subjects comprised 162 internal medicine residents from two sponsoring institutions (National Healthcare Group and Singapore Health Services). Each resident completed a three-month neurology rotation at the National Neuroscience Institute (NNI), Singapore, from January 2014 to June 2016. Waiver of further ethical deliberation was granted by the SingHealth Centralised Institutional Review Board (CIRB) for this education program improvement project; subjects were anonymised and implied informed consent was obtained from all participants. We excluded 17 subjects who failed to complete the required assessments, leaving 145 (90%) subjects for eventual analysis.
B. Predictor Variables
We investigated three sociodemographic characteristics–gender, undergraduate medical education (UME) and graduate medical education (GME). UME denotes the location of undergraduate training institution, and was classified into local (Singapore) and overseas. GME refers to the residency programmes of the two sponsoring institutions, anonymised as ‘A’ and ‘B’.
Clinical experience was judged by three metrics–overall experience (OE), local experience (LE) and residency experience (RE; Figure 1). OE and LE were calculated as the number of months from graduation and SMC registration respectively, to the month of test attempt. RE, defined as the residency training year, was categorised as ‘Year 1’, ‘Year 2’ and ‘Year 3’.
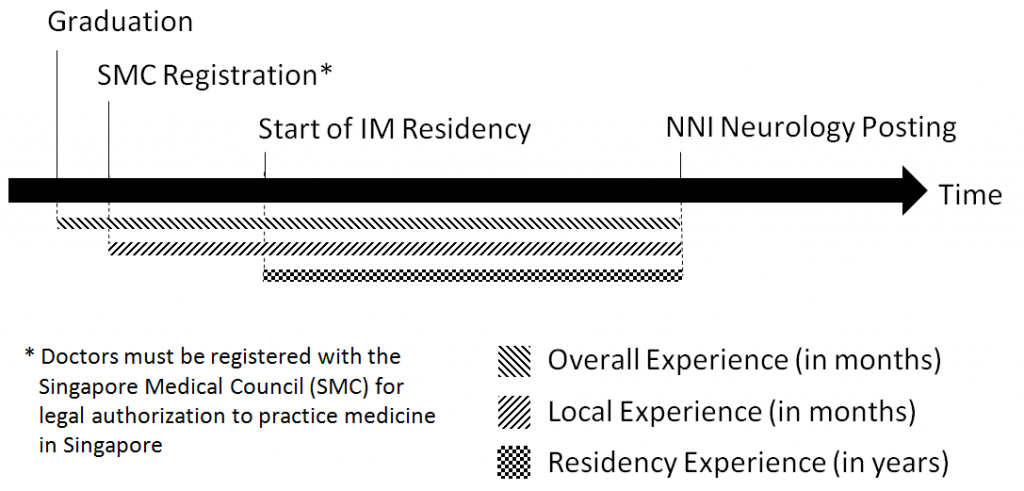
Figure 1. Measures of clinical experience
We obtained data on gender, GME and RE from our institution records; UME and month of SMC registration were obtained from the SMC Registry of Doctors. Graduation month was derived from our institution records for local graduates and estimated for overseas graduates from the dates of their alma mater’s most recent graduation ceremony, available online.
C. Outcome Measures
We used two validated methods of assessment, Script Concordance Test (SCT; Lubarsky et al., 2011) and Extended Matching Questions (EMQ; Beullens et al., 2005), to evaluate clinical reasoning in neurological localisation. We specifically selected the SCT and EMQ tests that had previously demonstrated construct validity and reliability in our Singapore context (Tan, Tan, Kandiah, Samarasekera, & Ponnamperuma, 2014; Tan et al., 2017).
An SCT contains case scenarios with 3-5 part questions (Fournier, Demeester, & Charlin, 2008; Figure 2)–a relevant diagnostic or management option; a new clinical finding; and a five-point Likert Scale indicating the new finding’s effect on the initial option. A scoring key is derived from scores by an expert panel; subsequent test-takers are then scored for degree of concordance to the experts (Fournier et al., 2008; Wan, 2015).
Our locally-validated SCT (Tan et al., 2014) contained 14 scenarios, each with 3–5 question items, totalling 53 items; reliability and generalisability were acceptable (Cronbach α 0.75, G-coefficient 0.74). Questions and scoring keys were derived from local experts. We analysed only the neurological localisation component (7 scenarios).
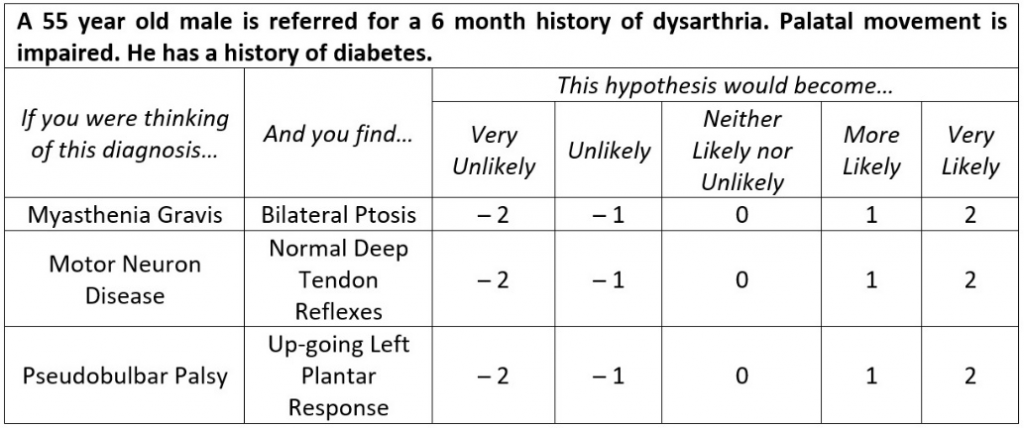
Figure 2. Script Concordance Test (SCT)–Sample questions (Tan et al., 2017)
EMQs are multiple-choice questions consisting of case scenarios, each with a single answer drawn from a shared list of at least 7 options (Case & Swanson, 1993; Fenderson, Damjanov, Robeson, Veloski, & Rubin, 1997). Our locally-validated EMQ (Tan et al., 2017) contained 45 scenarios with a shared answer list of 25 options (Figure 3); reliability and generalisability were excellent (Cronbach α 0.85, G-coefficient 0.85).
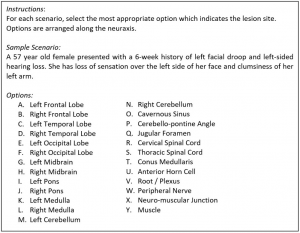
Figure 3. Extended Matching Questions (EMQ)–Sample questions (Tan et al., 2014)
Subjects completed both timed closed-book tests via an online portal during the second month of their three-month neurology rotation, done as a formative assessment. Scores were expressed in percentages. Subjects had no prior exposure to the SCT or EMQ during their neurology rotation or as practising doctors, and were introduced to the test format on the day of assessment. One worked example of the SCT and EMQ was provided to the subjects before the test.
D. Statistical Analysis
Descriptive statistics were calculated to test assumptions of normality before proceeding with multivariate analysis. We used SPSS Statistics version 20, and considered p-values <0.05 as statistically significant; all tests were two-tailed.
Multivariate stepwise linear regression models were used to assess the relationship between predictor variables (gender, UME, GME, OE, LE and RE) and outcome measures (SCT and EMQ scores). Tolerance values were computed to assess multicollinearity, with values below 0.60 considered problematic (Chan, 2004). Overall model performance was assessed using Nagelkerke’s R2, and effect sizes measured with Cohen’s f2. Effect sizes of 0.02, 0.15 and 0.35 were considered low, medium and large respectively (Cohen, 1988).
III. RESULTS
The majority of the 145 subjects were female, local graduates and belonged to residency ‘B’ (Table 1).Mean and standard deviation of SCT and EMQ scores were 68.03 ± 8.24% and 81.84 ± 12.17% respectively. Population statistics did not reveal a need for non-parametric tests.
|
|
|
n |
% |
|
Sociodemographic Characteristics |
|||
|
Gender |
Male |
61 |
42.07 |
|
Female |
84 |
57.93 |
|
|
Undergraduate Medical Education (UME) |
Local |
87 |
60.00 |
|
Overseas |
58 |
40.00 |
|
|
Graduate Medical Education (GME) |
Residency ‘A’ |
46 |
31.72 |
|
Residency ‘B’ |
99 |
68.28 |
|
|
Clinical Experience (months)* |
|||
|
Overall Experience (OE) |
38.34 ± 21.32 |
||
|
Local Experience (LE) |
33.43 ± 16.50 |
||
|
Residency Experience (RE) |
Year 1 |
55 |
37.93 |
|
Year 2 |
55 |
37.93 |
|
|
Year 3 |
35 |
24.14 |
|
|
Test Scores (%)* |
|||
|
Script Concordance Test (SCT) |
68.03 ± 8.24 |
||
|
Extended Matching Question (EMQ) |
81.84 ± 12.17 |
||
|
* Values expressed in Mean ± Standard Deviation |
|||
Table 1. Characteristics of subject population (n = 145)
Since both EMQ and SCT assess clinical reasoning, albeit different aspects, their inclusion in Multivariate analysis (Table 2, Model A) were potentially contentious. Additional models excluding these were therefore created (Model B).
|
Model |
Outcome |
Co-Variable |
B |
95% CI‡ |
SE |
Sig. |
Adjusted R2 |
f2 |
|
1A |
SCT Score |
UME* |
4.5 |
2.0 – 7.0 |
1.3 |
0.001 |
0.204 |
0.256 |
|
EMQ Score |
0.2 |
0.1 – 0.3 |
0.1 |
< 0.001 |
||||
|
1B |
SCT Score |
UME |
5.5 |
2.9 – 8.1 |
1.3 |
< 0.001 |
0.101 |
0.112 |
|
2A |
EMQ Score |
LE† |
0.1 |
0.0 – 0.2 |
0.1 |
0.025 |
0.164 |
0.196 |
|
SCT Score |
0.5 |
0.3 – 0.8 |
0.1 |
< 0.001 |
||||
|
2B |
EMQ Score |
UME |
4.7 |
0.7 – 8.7 |
2.0 |
0.021 |
0.049 |
0.052 |
|
LE |
0.1 |
0.0 – 0.2 |
0.1 |
0.041 |
||||
|
* Undergraduate Medical Education, Overseas (reference) vs Local (comparator) † Local Experience ‡ All Tolerance values >0.89 |
||||||||
Table 2. Multivariate correlation of outcome measures with predictor variables
Local graduates and better EMQ performers tended to have higher SCT scores (adjusted R2 = 0.204, f2 = 0.256; Model 1A). Residents with more local experience and higher SCT scores also had higher EMQ scores (adjusted R2 = 0.164, f2 = 0.196; Model 2A).
In the additional models, UME remained as the sole association for SCT scores (adjusted R2 = 0.101, f2 = 0.112; Model 1B). However, UME became significant for EMQ scores (adjusted R2 = 0.049, f2 = 0.052), with local graduates scoring higher (Model 2B).
IV. DISCUSSION
As there is a paucity of literature about postgraduate performance in clinical reasoning, this study provides a unique opportunity to evaluate its predictors, especially clinical experience. We used validated instruments to measure clinical reasoning skills in neurological localisation, and elucidated multivariate associations between clinical reasoning, clinical experience, and sociodemographic characteristics of our subjects.
Our results suggest that local graduates tend to score better in both clinical reasoning tests. Consistent with the existing literature (Postma & White, 2015), this indicates that educational background plays an important role in the development of clinical reasoning skills. Since SCT performance reflects the degree of concordance with verdicts made by local experts (Tan et al., 2014; Tan et al., 2017), this suggests that being educated locally may promote a similar outcome of reasoning. It is also possible that local undergraduate programmes provide better training in neurological localisation, as local graduates performed better in the EMQ, an instrument where scoring is independent of local experts’ views.
Interestingly, we found no significant associations between clinical experience and SCT performance. The accumulation of context-specific experiential knowledge is crucial for developing effective illness scripts (Elstein, 2009), hence SCT scores were expected to rise with increasing clinical experience (Boushehri et al., 2015; Kazour, Richa, Zoghbi, El-Hage, & Haddad, 2017; Lubarsky, Chalk, Kazitani, Gagnon, & Charlin, 2009; Norman et al., 2007). However, heuristics also play an important role (Boushehri et al., 2015; Elstein, 2009; Norman et al., 2007), suggesting that efficiency of knowledge organisation may be independent of clinical exposure. Alternatively, the study period may be insufficient for subjects to fully develop their illness scripts.
In contrast, more experienced doctors performed better at the EMQ, validating the premise that expertise is at least partially linked to experience and acquiring a strong knowledge base (Elstein et al., 1990; Monteiro & Norman, 2013; Neufeld, Norman, Feightner, & Barrows, 1981). Interestingly, only local experience was a significant predictor, but not overall experience. This suggests that overseas experience may not significantly improve clinical reasoning skills in neurological localisation and that the acquisition of such skills is a context-specific process (Durning, Artino, Pangaro, van der Vleuten, & Schuwirth, 2011; Durning et al., 2012; McBee et al., 2015).
Our findings have two potential implications for graduate medical education in Singapore. Firstly, the design of internal medicine residency programmes. To optimise the development of clinical reasoning in neurology, programmes could maximise local experience by assigning residents with less local experience to neurology only in the final year of the three-year residency. However, as local experience may also influence clinical reasoning in other subspecialties, further research is necessary to ascertain the optimal posting configuration that maximises clinical reasoning development across all disciplines.
Secondly, context appears to influence clinical reasoning in neurological localisation. Our results suggest that training location plays a role at both undergraduate and postgraduate levels. This might be due to context specificity, which attributes performance variations to situational factors (Durning et al., 2011; Durning et al., 2012; McBee et al., 2015). Since local exposure appears to be beneficial, it implies that overseas graduates and clinicians may require more time to acclimatise or familiarise themselves with the Singapore clinical context.
Our study has several strengths. We used validated, reliable tests to specifically assess clinical reasoning skills for neurological localisation. Homogeneity of the subject cohort, along with the consistent time-frame of test attempts, also allowed us to minimise confounders such as intrinsic motivation (Ferguson et al., 2002; Kusurkar et al., 2010; Vaughan et al., 2015), instructional design (Postma & White, 2015), and duration of neurology exposure.
There were also limitations. This is a single-centre, single subspecialty study with moderate sample size, and our results may not be applicable to other aspects of neurology besides neurological localisation. Further studies are needed to validate whether the results are generalisable beyond the neurology SCT and EMQ, and to other postgraduate populations. The study design was also limited due to the nature of secondary data analysis, thus information on other potentially important variables such as ethnicity (Adams et al., 2008; Guerrasio et al., 2014; Stegers-Jager et al., 2015; Woolf & Cave et al., 2008; Woolf & Haq et al., 2008), age (Woolf et al., 2011) and previous academic performance (Ferguson et al., 2002; Hamdy et al., 2006; Kanna et al., 2009; Stegers-Jager et al., 2015; Woloschuk et al., 2010) could not be fully obtained for evaluation. There is thus a possibility that other confounding variables may influence the findings in this study. Test questions may also intrinsically favour local graduates as they were formulated by local experts, but this is less likely as globally relevant clinical scenarios were tested.
V. CONCLUSION
In conclusion, our study suggests that local clinical experience and site of undergraduate education predict postgraduate clinical reasoning skill in validated tests of neurological localization. We believe context specificity likely underpins a significant part of clinical reasoning. Our findings have practical implications on residency programme design and highlight the need to provide overseas graduates and clinicians time to adapt to the local clinical context.
Notes on Contributors
Dr Loh Kieng Wee is a Medical Officer under the Ministry of Health Holdings, Singapore.
Jerome Ingmar Rotgans is an Assistant Professor at the Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore.
Dr Kevin Tan is Education Director, Vice-Chair (Education) and a Senior Consultant at the Department of Neurology, National Neuroscience Institute, Singapore.
Dr Nigel Choon Kiat Tan is Deputy Group Director Education (Undergraduate), Singapore Health Services, and a Senior Consultant at the Department of Neurology, National Neuroscience Institute, Singapore.
Ethical Approval
Ethical exemption has been granted from the SingHealth Centralised Institutional Review Board A, CIRB Ref: 2020/2228.
Acknowledgements
The authors would like to acknowledge the technical assistance & support provided by the Office of Neurological Education, National Neuroscience Institute, Singapore.
Funding
The research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Interest
Authors have no conflict of interest, including financial, institutional and other relationships that might lead to bias.
References
Adams, A., Buckingham, C. D., Lindenmeyer, A., McKinlay, J. B., Link, C., Marceau, L., & Arber, S. (2008). The influence of patient and doctor gender on diagnosing coronary heart disease. Sociology of Health and Illness, 30(1), 1–18.
Amini, M., Moghadami, M., Kojuri, J., Abbasi, H., Abadi, A. A., Molaee, N., & Charlin, B. (2011). An innovative method to assess clinical reasoning skills: Clinical reasoning tests in the second national medical science Olympiad in Iran. BMC Research Notes, 4(1), 418.
Beullens, J., Struyf, E., & Van Damme, B. (2005). Do extended matching multiple-choice questions measure clinical reasoning? Medical Education, 39(4), 410–417.
Boushehri, E., Arabshahi, K. S., & Monajemi, A. (2015). Clinical reasoning assessment through medical expertise theories: Past, present and future directions. Medical Journal of The Islamic Republic of Iran, 29(1), 222.
Case, S. M., & Swanson, D. B. (1993). Extended‐matching items: A practical alternative to free‐response questions. Teaching and Learning in Medicine, 5(2), 107–115.
Chan, Y. H. (2004). Biostatistics 201: Linear regression analysis. Singapore Medical Journal, 45(2), 55–61.
Cohen, J. (1988). Statistical Power Analysis for the Behavioural Sciences. Hillsdale, NJ: Lawrence Earlbaum Associates.
Connor, D. M., Durning, S. J., & Rencic, J. J. (2019). Clinical reasoning as a core competency. Academic Medicine. http://dx.doi.org/10.1097/ACM.0000000000003027
Durning, S., Artino, A. R., Pangaro, L., van der Vleuten, C. P., & Schuwirth, L. (2011). Context and clinical reasoning: Understanding the perspective of the expert’s voice. Medical Education, 45(9), 927–938.
Durning, S. J., Artino, A. R., Boulet, J. R., Dorrance, K., van der Vleuten, C., & Schuwirth, L. (2012). The impact of selected contextual factors on experts’ clinical reasoning performance (Does context impact clinical reasoning performance in experts?). Advances in Health Sciences Education, 17(1), 65–79.
Durning, S. J., Trowbridge, R. L., & Schuwirth, L. (2019). Clinical reasoning and diagnostic error: A call to merge two worlds to improve patient care. Academic Medicine. http://dx.doi.org/10.1097/ACM.0000000000003041
Elstein, A. S. (2009). Thinking about diagnostic thinking: A 30-year perspective. Advances in Health Science Education, 14(sup1), 7–18.
Elstein, A., Shulman, L., & Sprafka, S. (1990). Medical problem solving: A ten-year retrospective. Evaluation and the Health Professions, 13, 5–36.
Eva, K. W. (2005). What every teacher needs to know about clinical reasoning. Medical Education, 39(1), 98–106.
Fenderson, B. A., Damjanov, I., Robeson, M. R., Veloski, J. J., & Rubin, E. (1997). The virtues of extended matching and uncued tests as alternatives to multiple choice questions. Human Pathology, 28(5), 526–532.
Ferguson, E., James, D., & Madeley, L. (2002). Factors associated with success in medical school: Systematic review of the literature. British Medical Journal, 324(7343), 952–957.
Fournier, J. P., Demeester, A., & Charlin, B. (2008). Script concordance tests: Guidelines for construction. BMC Medical Informatics and Decision Making, 8, 18.
Gelb, D. J., Gunderson, C. H., Henry, K. A., Kirshner, H. S., & Jozefowicz, R. F. (2002). The neurology clerkship core curriculum. Neurology, 58(6), 849–852.
Groen, G. J., & Patel, V. L. (1985). Medical problem solving: some questionable assumptions. Medical Education, 19(2), 95–100.
Groves, M., O’rourke, P., & Alexander, H. (2003). The association between student characteristics and the development of clinical reasoning in a graduate-entry, PBL medical programme. Medical Teacher, 25(6), 626–631.
Guerrasio, J., Garrity, M. J., & Aagaard, E. M. (2014). Learner deficits and academic outcomes of medical students, residents, fellows, and attending physicians referred to a remediation program, 2006-2012. Academic Medicine, 89(2), 352–358.
Hamdy, H., Prasad, K., Anderson, M. B., Scherpbier, A., Williams, R., Zwierstra, R., & Cuddihy, H. (2006). BEME systematic review: Predictive values of measurements obtained in medical schools and future performance in medical practice. Medical Teacher. 28(2), 103–116.
Huggan, P. J., Samarasekara, D. D., Archuleta, S., Khoo, S. M., Sim, J. H., Sin, C. S., & Ooi, S. B. (2012). The successful, rapid transition to a new model of graduate medical education in Singapore. Academic Medicine, 87(9), 1268–1273.
Kanna, B., Gu, Y., Akhuetie, J., & Dimitrov, V. (2009). Predicting performance using background characteristics of international medical graduates in an inner-city university-affiliated Internal Medicine residency training program. BMC Medical Education, 9, 42.
Kazour, F., Richa, S., Zoghbi, M., El-Hage, W., & Haddad, F. G. (2017). Using the script concordance test to evaluate clinical reasoning skills in psychiatry. Academic Psychiatry, 41(1), 86-90.
Kusurkar, R., Kruitwagen, C., Ten Cate, O., & Croiset, G. (2010). Effects of age, gender and educational background on strength of motivation for medical school. Advances in Health Science Education, 15(3), 303–313.
Lubarsky, S., Chalk, C., Kazitani, D., Gagnon, R., & Charlin, B. (2009). The script concordance test: A new tool assessing clinical judgement in neurology. Canadian Journal of Neurological Sciences, 36, 326-331.
Lubarsky, S., Charlin, B., Cook, D. A., Chalk, C., & van der Vleuten, C. P. M. (2011). Script concordance testing: A review of published validity evidence. Medical Education, 45(4), 329–338.
McBee, E., Ratcliffe, T., Picho, K., Artino, A. R., Schuwirth, L., Kelly, W., … Durning, S. J. (2015). Consequences of contextual factors on clinical reasoning in resident physicians. Advances in Health Sciences Education, 20(5), 1225–1236.
Monteiro, S. M., & Norman, G. (2013), Diagnostic reasoning: Where we’ve been, where we’re going. Teaching and Learning in Medicine, 25(sup1), S26–S32.
Neufeld, V. R., Norman, G. R., Feightner, J. W., & Barrows, H. S. (1981). Clinical problem-solving by medical students: A cross-sectional and longitudinal analysis. Medical Education, 15, 315–322.
Nicholl, D. J., & Appleton, J. P. (2015). Clinical neurology: Why this still matters in the 21st century. Journal of Neurology, Neurosurgery and Psychiatry, 86(2), 229–233.
Norman, G., Young, M., & Brooks, L. (2007). Non-analytical models of clinical reasoning: The role of experience. Medical Education, 41(12), 1140–1145.
Postma, T. C., & White, J. G. (2015). Socio-demographic and academic correlates of clinical reasoning in a dental school in South Africa. European Journal of Dental Education, 10, 1–8.
Stegers-Jager, K. M., Themmen, A. P. N., Cohen-Schotanus, J., & Steyerberg, E. W. (2015). Predicting performance: Relative importance of students’ background and past performance. Medical Education, 49(9), 933–945.
Tan, K., Chin, H. X., Yau, C. W. L., Lim, E. C. H., Samarasekera, D., Ponnamperuma, G., & Tan, N. C. K. (2017). Evaluating a bedside tool for neuroanatomical localization with extended-matching questions. Anatomical Sciences Education, 11(3), 262-269.
Tan, K., Tan, N. C. K., Kandiah, N., Samarasekera, D., & Ponnamperuma, G. (2014). Validating a script concordance test for assessing neurological localization and emergencies. European Journal of Neurology, 21(11), 1419–1422.
Vaughan, S., Sanders, T., Crossley, N., O’Neill, P., & Wass, V. (2015). Bridging the gap: The roles of social capital and ethnicity in medical student achievement. Medical Education, 49(1), 114–123.
Wan, S. H. (2015). Using the script concordance test to assess clinical reasoning skills in undergraduate and postgraduate medicine. Hong Kong Medical Journal, 21(5), 455–461.
Woloschuk, W., McLaughlin, K., & Wright, B. (2010). Is undergraduate performance predictive of postgraduate performance? Teaching and Learning in Medicine, 22(3), 202–204.
Woloschuk, W., McLaughlin, K., & Wright, B. (2013). Predicting performance on the Medical Council of Canada Qualifying Exam Part II. Teaching and Learning in Medicine, 25(3), 237–241.
Woolf, K., Cave, J., Greenhalgh, T., & Dacre, J. (2008). Ethnic stereotypes and the underachievement of UK medical students from ethnic minorities: Qualitative study. British Medical Journal [Internet], 377, a1220. https://doi.org/10.1136/bmj.a1220
Woolf, K., Haq, I., McManus, I. C., Higham, J., & Dacre, J. (2008). Exploring the underperformance of male and minority ethnic medical students in first year clinical examinations. Advances in Health Science Education, 13(5), 607–616.
Woolf, K., Potts, H. W. W., & McManus, I. C. (2011). Ethnicity and academic performance in UK trained doctors and medical students: Systematic review and meta-analysis. British Medical Journal [Internet], 342, d901. https://doi.org/10.1136/bmj.d901
*Nigel Choon Kiat Tan
Office of Neurological Education,
Department of Neurology,
National Neuroscience Institute
11 Jalan Tan Tock Seng,
Singapore 308433
Email: nigel.tan@alumni.nus.edu.sg
Submitted: 1 July 2019
Accepted: 17 December 2019
Published online: 1 September, TAPS 2020, 5(3), 42-53
https://doi.org/10.29060/TAPS.2020-5-3/OA2166
Eng Lai Tan1, Sook Yee Gan1, Wei Meng Lim1, Peter C. K. Pook1 & Vishna D. Nadarajah2
1Institute for Research, Development & Innnovation, School of Pharmacy, International Medical University, Kuala Lumpur, Malaysia; 2IMU Centre for Education, School of Medicine, International Medical University, Kuala Lumpur, Malaysia
Abstract
This study measures the impact of the implementation of a dedicated research semester on various perceived competencies related to research. In 2016, surveys were conducted on final undergraduate Pharmacy students in regard to appraisal and critical thinking skills. Students’ perceptions of the impact of research in enhancing their employment potential were investigated. Our evaluation included students’ self-assessment of their writing, presentation, critical thinking and research skills. To assess qualitative parameters, the data obtained were analysed using the Wilcoxon signed-rank test. A total of 113 responses was received. A majority of students indicated that the research semester prepared them in undertaking their research projects. They acknowledged that research helped in building confidence and to acquire the ability to work independently. Most students perceived that the experience gained in research would enhance their employment potential. Overall, students developed critical thinking skills through their respective research project.
Keywords: Undergraduate Research, Pharmacy Programme, Critical Thinking, Research Ethics, Scientific Communication
Practice Highlights
- Competencies from research projects need to be transparent to both students and supervisors.
- Diversity of research projects should reflect the different career pathways of pharmacists.
- Ethical and professional dilemmas from research projects is opportunity for reflective learning.
I. INTRODUCTION
The Pharmacy profession has undergone tremendous changes over the years, and its scope has expanded. The roles of Pharmacists have extended beyond the traditional boundaries of drug preparation and distribution to ensuring that optimal therapeutic outcomes are achieved through patient-centred cognitive services (Bond, 2006; van Mil & Fernandez-Llimos, 2013). Pharmacists play increasing roles in patient education and counselling, health promotion and disease prevention, disease state management as well as being engaged in inter-professional consultation with other healthcare professionals in specialised patient settings (Holland & Nimmo, 1999; Tsuyuki & Schindel, 2008). The new roles for pharmacists evolve in parallel with evidence-based medicine (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Therefore, research skills are essential for both the practice and advancement of the pharmacy profession. In pharmacy, as in all undergraduate science programmes, research is a critical and essential component of the curriculum, although for pharmacy, being a professional degree, competency for practice takes precedence in the priority of the curriculum (Nykamp, Murphy, Marshall, & Bell, 2010). Nevertheless, there is a need to build a strong research program and culture within a pharmacy degree curriculum through sustainable educational initiatives that complement rather than compromise competencies needed for practice. Research being a critical part of scholarship is necessary for inculcating the attributes related to professional competency such as creative and critical thinking as well as problem-solving. Moreover, research also improves student learning skills and encourages the pursuit of research-related careers (Banks, Haynes, & Sprague, 2009; Nykamp et al., 2010).
The implementation of research in pharmacy curricula varies between institutions. Many colleges and universities require students to undertake coursework in research methodology, biostatistics, drug information, and literature evaluation, but only a small fraction of them chose to complete an extensive project with data collection, analysis, and reporting research findings (Murphy, Peralta, & Kirking, 1999). However, increasing emphasis and proportion of time allocated for actual data collection and analyses over the years attest to the recognition of research experience in pharmacy training (Murphy, Slack, Boesen, & Kirking, 2007). Undergraduate or first-degree research training requires a supportive environment and intellectual partnership amongst students and their faculty mentors. Through research, these students are able to apply knowledge gained in the classroom as they define new problems and formulate new research questions (Ash Merkel, 2003). Incorporating research into the curriculum is important as a means of inculcating scholarship in the community of learning, to motivate undergraduates to become independent thinkers and to prepare students for graduate programs (Adamsen, Larsen, Bjerregaard, & Madsen, 2003). A study by Tan revealed that undergraduate students who were guided by suitable research mentors experienced improved thinking, communication, and interpersonal skills. They also manifested heightened levels of self-confidence, resourcefulness, goal-consciousness, creativity and responsibility towards others. These were in contrast to the general feeling of insecurity and uncertainty at the beginning of the research endeavour (Tan, 2007).
Investing in research is often regarded as a costly endeavour which involves dedicated time from faculty members (Nykamp et al., 2010). Furthermore, providing research opportunities for undergraduate students inevitably involves internal funding as well as the involvement of considerable time and proportion of the faculty member. Several major barriers to implementing undergraduate research have been reported. Among these include a lack of faculty members with appropriate expertise and sufficient time for research supervision; other major impediments include the lack of dedicated time for data collection, opportunities, funding, training and support (Nykamp et al., 2010; Paalman, 2002). The logistics of managing research projects for a large number of students have been reported in some studies to be difficult or impossible. Universities have the option of eliminating laboratory experience from their undergraduate research project because of costs associated with maintaining laboratory personnel and the acquisition of expendable laboratory supplies and major equipment (Brandenberger, 1990).
Literature and contextual delivery of pharmacy programs across the world suggest the need to determine the impact of incorporating a research program for an undergraduate pharmacy curriculum (Awaisu & Alsalimy, 2015; Bunnett, 1984; Chopin, 2002; Doerschuk, 2004; Osborn & Karukstis, 2009; Warner, 1998). Will a semester dedicated to entirely research help students achieve the graduate competencies for the pharmacy profession through experiential learning? Hence, this study was conducted to evaluate the impact of a dedicated semester-long research program in an undergraduate pharmacy curriculum.
Before the commencement of the research semester, students select their research projects from a range of areas relevant to Pharmacy that include pharmacy practice, pharmaceutical technology, pharmacy chemistry and life sciences. These projects could be further categorised as laboratory-based, community-based or education research. Through the student mobility program and unique research partnership with other local and overseas institutions, students have opportunitiesto conduct their research projects in these external institutions. Students then defend their project proposals in the Research and Ethics Management Committee which ensures the quality, suitability and ethical aspects of a research project. In the Research Methodology module, students are given theoretical instructions in conducting a literature review, scientific writing and research ethics as well as training in statistics. The research semester spans a period of 16 weeks and should, therefore, be designed to provide an immersive experience in the rigours of research. This study measures the impact of the implementation of dedicated research semester on students’ perceived competencies related to research writing, presentation and critical thinking skills, ethical knowledge and preparedness to undertake research.
II. METHODS
This study is part of the regular programme audit conducted by the School of Pharmacy, the findings of which had been reported to the school’s curriculum and examination committee for quality assurance purpose. Student feedback was sought from final year undergraduate pharmacy students at the International Medical University in Kuala Lumpur, Malaysia in the second half of 2016. Students’ participation was on a voluntary basis after informed consent was obtained and was also a part of the periodic curriculum assessment conducted by the School of Pharmacy. Feedback was obtained from students using an online questionnaire before and after the research project. The questions were developed to measure a student acquiescence of specific perceived competencies relevant to pharmacists as informed by the literature. The face and content validity of the questionnaire were conducted with a small cohort of undergraduate pharmacy students prior to the survey. The pre-research online questionnaire consisted of questions related to the nature, types and placement sites of the projects as well as factors affecting students’ project preference. Ranking questions were also included for students’ self-assessment of their writing, presentation, critical thinking and research skills. In addition, there were also open questions that solicit information pertaining to students’ perceptions about their preparedness to undertake a research project, their knowledge about ethics in research and their anticipated career options. Where Likert-scale was used, the scores from each respondent were added up to achieve the final total. Wilcoxon sign-ranked test was used to compare all ranked data pertaining to students’ perception of their competencies. The post-research survey consisted of similar questions found in the pre-research questionnaire but with an additional section on evaluating the impact of research projects that the students have undertaken. It contained questions to solicit students’ perceptions on the enhancement of their knowledge in specific subject matter, the achievement of research objectives, the challenges they faced during the implementation of research project, skills developed and gained through the research project as well as the aspects of research ethics which are applicable to their future profession as pharmacists and the impact of research experience on their employment potential. All statistical tests were performed using SPSS Statistics and Microsoft Excel.
III. RESULTS
A. Study Population
Out of 180 students, a total of 113 responses was received in surveys conducted prior to and after the commencement of their research projects in the year 2016. These students were supervised by academic staff from all the four departments of the School of Pharmacy, namely life sciences (31%), pharmaceutical chemistry (21%), pharmaceutical technology (10%), pharmacy practice (22%) as well as the School of Dentistry (2%) and the School of Medicine (14%). Eighteen students were involved in community-based or education research while 95 students conducted lab-based research including those who were attached to other local institutions (eight students) or international partner universities (seven students) through collaborative research.
Most students of the cohort were successfully allocated to the project which was their first (61%), second (20%) or third choice (6%) although some (13%) were not allocated to the project of their choice. Interestingly, the main factor affecting the pharmacy students’ preference was research interest (61%). Some students selected the project based on their choice of supervisors (19%), their peer’s choice (10%) while other did not have a specific preference (10%).
B. Students’ Ratings on Preparedness, Ethics Understanding, Writing and Presentation Skills
In quantitative measures, we evaluate the percentage distribution of student ratings before and after the implementation of research projects pertaining to preparedness to undertake a research project, understanding of research ethics, writing skill and presentation skill. For preparedness to undertake a research project, students are more prepared to undertake a research project in the future, the percentage rating for good had increased from 30.1% to 40.7% (Appendix). However, the frequency distribution of the outcome measures of students’ preparedness after the project implementation was quite similar without any significant difference to before project implementation (p=0.472) (Figure 1A).
Before the research project, approximately 32.8% of students rated themselves for having good and excellence understanding in research ethics. However, after the research project, the percentage has increased to 45.1%. Statistical analysis showed significant improvement for the understanding of research ethics (p=0.002; Figure 1B).
There was 23.9% and 35.4% of students rated themselves for having good and excellent writing skill and presentation skill respectively. After the research project, the improvement is promising as the percentages had increased to 35.4% (p=0.001; Figure 1C) and 51.3% (p=0.001; Figure 1D) respectively.
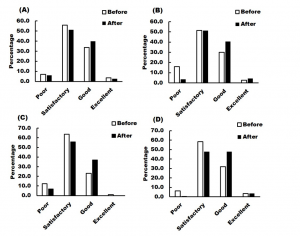
Note: The ratings before and after project implementation were compared and statistically analysed using the Wilcoxon signed-rank test.
Figure 1. Percentage distribution of student ratings before and after the implementation of research projects pertaining to their
(A) Preparedness to undertake research project (Mean value before=2.34, after=2.39, p=0.472);
(B) Understanding of research ethics (Mean value before=2.19, after=2.46, p=0.002);
(C) Writing skill (Mean value before=2.12, after=2.30, p=0.001); and
(D) Presentation skill (Mean value before=2.33, after=2.54, p=0.001).
C. Students’ Preparedness to Undertake a Research Project
Before the implementation of the research project, most students considered themselves well-prepared as they have improved their knowledge on the subject matter through personal reading and consultation with the respective supervisor (Table 1; Appendix A). They were well-informed about the research approach and techniques. However, these attributes were found lacking in those who have identified themselves as poor in preparation because they had less confidence and did not know what to expect. Students stated that they were now prepared to undertake research in the future because they have gained knowledge and exposure in research as well as trained with various laboratory and research skills (Table 1).
D. Students’ Self-Assessment of Their Writing and Presentation Skills
The surveys also considered students’ self-assessment on their writing and presentation skills. Overall, there was a significant improvement in both skills after the implementation of the research projects. They have contributed their improvement to the reading of journal articles, writing and presenting the research proposal and dissertation. Moreover, students perceived that writing a scientific report was different from writing other reports (Table 1). They found that it was challenging to discuss gathered information or results critically in a constructive manner as well as to ensure a good flow of content and clarity of the paper. As for presentation, some stated that stage fright affected their performance while others found that the question and answer section was quite challenging (Table 1).
E. Students’ Perceptions of Research Ethics
Students’ perceptions of their understanding of research ethics are shown in Table 1. They have related unethical practices as manipulation of data, dishonesty in data reporting as well as lack of objectivity and confidentiality (Table 1). They described good ethical practices as fairness, accountability, peer respect, minimising harm as well as respect for human dignity and rights. Students were able to learn about ethics through their research projects (Table 1). However, some of them indicated that they might have sound ethical knowledge but found themselves inadequate to make decisions and were unsure about how to apply it. Students were, however, able to identify several aspects of research ethics which are applicable to their future profession as pharmacists. These professional values include honesty, informed consent, evidence-based practice, patient safety, confidentiality, punctuality, integrity, responsibility and respect for others.
|
|
Students’ Comments |
|
|
Before Undertaking Research Project |
After Undertaking Research Project |
|
|
Preparedness to undertake research |
|
|
|
Research ethics |
|
|
|
Writing skill |
|
|
|
Presentation skill |
|
|
Table 1. Students’ perceptions of their preparedness to undertake research
F. Impact of Research on Future Career Options
Approximately 73.5% have indicated their interest in research while only 0.9% were highly interested and might have selected research or academia as their future career direction (Figure 2A). 25.6% indicated that they were not at all interested in research. Students were asked to rate their career preference before and after the research project; the result showed that research experience has no significant impact on career selection (Figure 2B). Majority of the students preferred to work in hospital and community setting, followed by business and industry setting, while academia and research are the least popular option.
G. Students’ Perceptions About the Impact of Research Experience on Their Employment Potential
As shown in Table 2 and in the Appendix B, the students’ perceptions were basically supported by skills that enhance their work-readiness. Other factors included largely personal development and project management skills. Some students stated that exposure to certain industry-related equipment and successful publication of research outputs would enhance their employment potential. On the other hand, students who were not agreeable to this perception stated that their research experience would not enhance their employment potential because their areas of research were not related to either community, industry or hospital pharmacy which they would be involved in the future and they were not keen to venture into research or academia. There were also students who thought that similar curriculum and research experience were available for most pharmacy graduates, hence there will be no difference among the graduates.
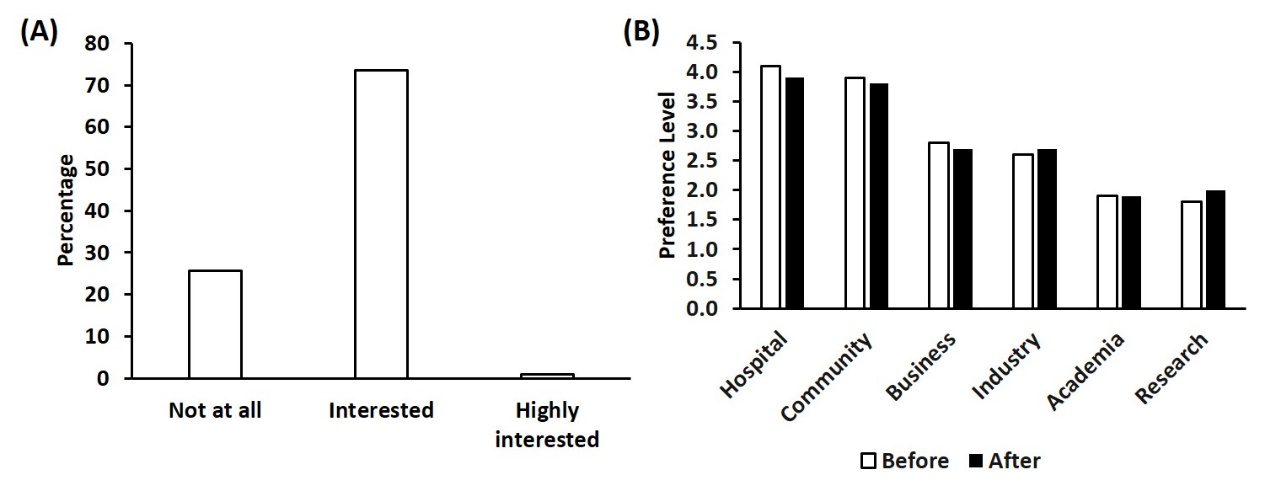
Note: Students were asked to rate their preferences in Likert scale ranging from level 1 (least preferred) to level 6 (most preferred).
Figure 2. (A) Students’ level of interest in research; (B) Students’ career preferences before and after the research project
|
Students’ Perception of Whether Research Experience Could Enhance Their Employment Potential |
Students’ Comments |
|
Yes |
|
|
No |
|
Table 2. Students’ perceptions about the impact of research experience on their employment potential
H. Students’ Perceptions of Their Research Achievements and Challenges
From the students’ perspective, the overall impact of the research projects that they appreciated was the acquisition of new practical knowledge in the rigours of research which could not be gained from lectures (Table 3). On the other hand, there were several issues and challenges faced by students during the project implementation. Students struggled on issues arising from interpersonal relations which include peers, supervisors and laboratory support staff as well as time constraint. Other challenges include limited study subjects and specialised equipment, poor time planning, poor knowledge in statistics and research techniques, unpredictable data and experimental failures, limited research fund and facilities. They also had difficulties with supervisors who were not helpful and who were too busy with other duties as well as delay in the arrival of research consumables.
|
Aspects |
Students’ Comments |
|
Achievement of research objectives |
|
|
Enhancement of knowledge in subject matter |
|
|
Skills gained |
|
|
Challenges faced |
|
Table 3. Students’ perceptions of the different aspects related to their research achievements and challenges
IV. DISCUSSION
This study confirmed that preparation for the research semester enhanced knowledge in topics of interest, research and collaborative skills for students. Through the research program, they are able to appreciate, explain, apply and relate the knowledge gained from research to lessons learnt in lectures. This exposure has enhanced their confidence in pursuing the research topics of interest after graduation. It would also improve their capability to work independently. This agrees with studies that confirmed that hands-on research experiences have been recognised to provide the best learning tools that enhance students’ learning, especially when done in collaboration with peers (Ash Merkel, 2003). The research program experience also had a positive impact on ethics and professionalism. Different instructional methods have been shown to be important for the comprehension of ethical knowledge, particularly those that involve intensive students’ participation and role-play (Guérin & Bussières, 2017). The research program described in this study provides the opportunity for application and comprehension as it requires full student participation for one semester and with preparation in the prior semester. The importance of engaging students in ethics and professionalism issues has been shown in a few studies related to pharmacy. In a study that compared the understanding of pharmaceutical ethical statements between pharmacy students and hospital pharmacists, a significant difference in understanding was reported in areas that were assessed, particularly in clinical research, advertising and marketing, dispensing medication, pharmaceutical care and code of ethics. The probable reason for this is knowledge in professional ethics obtained during undergraduate training might not be readily translated to actual professional practice (Guérin & Bussières, 2017). The importance of the right training in instilling ethical knowledge was again emphasised in another study in which the effectiveness of an early professional development series in a pharmaceutical care laboratory (PCL) course for first-year pharmacy students that highlighted the application of the Oath of a Pharmacist and the Pharmacists’ Code of Ethics. The results showed that while students entered their training with a strong appreciation for professionalism, they felt more confident in applying the Oath of a Pharmacist and the Pharmacists Code of Ethics to dilemmas in practice following each new learning activity that required active participation and application (Smith & Dinkins, 2015).
It was also noted that the research program could enhance skills related to scientific communication. Good writing and presenting skills are not naturally acquired skills but must be developed through multiple practice experience. Prior to the research program, these students have undergone several tasks that provided training to improve writing or presentation skills, namely assignments, practical reports, case reports, seminars and examinations in form of essays which were associated with the respective course. In addition, self-confidence was reported to be correlated with the writing ability or performance (Pajares & Johnson, 1994; Ranelli & Nelson, 1998). Another contributing factor to scientific communication is proficiency in the language of communication. Writing might pose a challenge to students who have poor language proficiency especially when it is a second language to students (Chokwe, 2013). In the context of this study, it is English language proficiency as the undergraduate pharmacy program is delivered in English while all students in this program are not native English speakers, but use English as a second language.
Participation in oral presentations was shown to enhance students’ critical-thinking and problem-solving skills especially when followed with a question and answer session. In addition to enhancing student learning experience and reflection, it provides an opportunity for students to evaluate their own as well as their fellow classmates’ presentations and develop their skills in providing constructive feedback (Hunter, Laursen, & Seymour, 2007). Moreover, the need for troubleshooting, critical analysis of the results and problem-solving during the course of the project contributed to the development of these skills. The benefits of faculty-mentored research projects have been well-recognised and shown to facilitate active learning, cultivate self-confidence as well as enhance students’ critical-thinking and communication skills (Bauer & Bennett, 2003; Lopatto & Tobias, 2010). Translating classroom teaching and reading into hands-on learning activities has been reported to promote personal skills development and enhance the learning experience (Chopin, 2002). The research programme has provided students with an insight into research and development, hence opening a new career option. It was noted that students with research experience were more prepared to pursue careers in science (Lopatto, 2007). Importantly, our findings suggest the skills and competencies gained from the research projects are aligned to the expanding roles of pharmacists that require evidence-based practices as reviewed by Bond (2006) and van Mil and Fernandez-Llimos (2013).
Several important practical points pertaining to the implementation of undergraduate pharmacy research projects are worthy of considerations. Perhaps the most important being the importance of a 16-week immersive experience in the rigours of research. In the current study, the number of laboratory projects exceeded the projects related to pharmacy practice and pharmacy education. A possible solution to this would be to encourage staff who are practising pharmacists to develop research ideas with their counterparts from other areas of expertise such that there are diversity and relevance of these research projects for future practice. Moreover, only perceived students’ competencies are addressed in this study and follow-up studies with objective measurement of competencies will be carried out.
V. CONCLUSION
Overall, the Pharmacy students surveyed in this study indicated that the impact of a research program has offered them an immersive experience to develop various skills and increased their perceived competencies, knowledge as well as confidence in carrying out research work in diverse disciplines. For academics implementing research programs for undergraduate pharmacists, this study also shows some of the challenges students faced.
Notes on Contributors
Eng Lai Tan (E.L.T.), PhD., is an Associate Professor in the Department of Life Sciences, School of Pharmacy, International Medical University (IMU). He is also the associated Dean of School of Postgraduate Studies, IMU.
Sook Yee Gan (S.Y.G), PhD., is an Associate Professor in the Department of Life Sciences, School of Pharmacy, IMU.
Wei Meng Lim (W.M.L.), PhD., is a lecturer in the Department of Pharmaceutical Technology, School of Pharmacy, IMU.
Vishna D. Nadarajah (V.D.N.), PhD., is the Pro-vice Chancellor of Education.
Peter C.K. Pook (P.C.K.P.), PhD., is the Deputy Vice Chancellor of IMU.
E.L.T., S.Y.G., V.D.N. and P.C.K.P. were involved in the design of the work. E.L.T. and S.Y.G. have administered data collection through surveys. E.L.T, S.Y.G. and W.M.L. conducted data analysis and interpretation. E.L.T and S.Y.G. drafted the article. V.D.N. and P.C.K.P. initiated the study and revised it critically. All authors approved the final version for publication in TAPS.
Ethical Approval
This study was exempted by Institutional Review Board (IRB). This study is part of the regular programme audit conducted by the School of Pharmacy, the findings of which had been reported to the school’s curriculum and examination committee for quality assurance purpose.
Acknowledgements
The authors wish to thank Semester 7 Pharmacy students who had participated in the surveys.
Funding
No funding source was required.
Declaration of Interest
The authors report no declaration of interest.
References
Adamsen, L., Larsen, K., Bjerregaard, L., & Madsen, J. K. (2003). Moving forward in a role as a researcher: the effect of a research method course on nurses’ research activity. Journal of Clinical Nursing, 12(3). https://doi.org/10.1046/j.1365-2702.2003.00708.x
Ash Merkel, C. (2003). Undergraduate Research at the Research Universities. New Directions for Teaching and Learning, 2003(93), 39-54. https://doi.org/10.1002/tl.87
Awaisu, A., & Alsalimy, N. (2015). Pharmacists’ involvement in and attitudes toward pharmacy practice research: A systematic review of the literature. Research in Social and Administrative Pharmacy, 11(6), 725-748. https://doi.org/10.1016/j.sapharm.2014.12.008
Banks, M. L., Haynes, K., & Sprague, J. E. (2009). A model for motivating PharmD students to pursue a PhD degree. Currents in Pharmacy Teaching and Learning, 1(2), 93-97. https://doi.org/10.1016/j.cptl.2009.10.008
Bauer, K. W., & Bennett, J. S. (2003). Alumni perceptions used to assess undergraduate research experience. The Journal of Higher Education, 74(2), 210-230. https://doi.org/10.1080/00221546.2003.11777197
Bond, C. (2006). The need for pharmacy practice research. International Journal of Pharmacy Practice, 14(1), 1-2. https://doi.org/10.1211/ijpp.14.1.0001
Bunnett, J. F. (1984). The education of butchers and bakers and public policy makers. Journal of Chemical Education, 61(6), 509. https://doi.org/10.1021/ed061p509
Chmielewski, J. G., & Stapleton, M. G. (2009). The biologists’ forum: The undergraduate research experience: it’s really not for everyone, students and faculty alike. BIOS, 80(2), 53-58. https://doi.org/10.1893/011.080.0201
Chokwe, J. M. (2013). Factors impacting academic writing skills of english second language students. Mediterranean Journal of Social Sciences, 4(14), 377. http://doi.org/10.5901/mjss.2013.v4n14p377
Chopin, S. F. (2002). Undergraduate research experiences: the translation of science education from reading to doing. The Anatomical Record, 269(1), 3-10. https://doi.org/10.1002/ar.10058
Doerschuk, P. (2004). A research and mentoring program for undergraduate women in computer science. Paper presented at the Frontiers in Education Conference, 34th Annual FIE 2004, S2H-7. http://doi.org/10.1109/FIE.2004.1408747
Guérin, A., & Bussières, J. (2017). Étude pilote du niveau d’accord à des énoncés sur l’éthique pharmaceutique d’étudiants en pharmacie et pharmaciens hospitaliers Québécois [A pilot study of the professional ethical thinking of Quebec hospital pharmacists and pharmacy students]. Annales Pharmaceutiques Francaises, 75(1), 67-76. https://doi.org/10.1016/j.pharma.2016.07.004
Holland, R., & Nimmo, C. (1999). Transitions, part 1: Beyond pharmaceutical care. The American Journal of Health-System Pharmacy, 56(17), 1758-1764. https://doi.org/10.1093/ajhp/56.17.1758
Hunter, A. B., Laursen, S. L., & Seymour, E. (2007). Becoming a scientist: The role of undergraduate research in students’ cognitive, personal, and professional development. Science Education, 91(1), 36-74. https://doi.org/10.1002/sce.20173
Lopatto, D. (2007). Undergraduate research experiences support science career decisions and active learning. CBE-Life Sciences Education, 6(4), 297-306. https://doi.org/10.1187/cbe.07-06-0039
Lopatto, D., & Tobias, S. (2010). Science in solution: The impact of undergraduate research on student learning. Washington, D.C.: The Council on Undergraduate Research. Retrieved from https://www.worldcat.org/title/science-in-solution-the-impact-of-undergraduate-research-on-student-learning/oclc/680773869
Murphy, J. E., Peralta, L. S., & Kirking, D. M. (1999). Research experiences and research-related coursework in the education of doctors of pharmacy. Pharmacotherapy, 19(2), 213-220. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2690916/
Murphy, J. E., Slack, M. K., Boesen, K. P., & Kirking, D. M. (2007). Research-related Coursework and Research Experiences in Doctor of Pharmacy Programs. The American Journal of Pharmaceutical Education, 71(6), 113. https://doi.org/10.1592/phco.19.3.213.30931
Nykamp, D. , Murphy, J. E. , Marshall, L. L., & Bell, A. (2010). Pharmacy students’ participation in a research experience culminating in journal publication. The American Journal of Pharmaceutical Education, 74(3), 47. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2865413
Osborn, J. M., & Karukstis, K. K. (2009). The benefits of undergraduate research, scholarship, and creative activity. Broadening participation in undergraduate research: Fostering excellence and enhancing the impact, 41-53. Retrieved from https://osborn.pages.tcnj.edu/files/2013/12/2-Osborn-and-Karukstis-2009.pdf
Paalman, M. H. (2002). Undergraduate research, education and the future of science. The Anatomical Record, 269(1), 1-2. https://doi.org/10.1002/ar.10059
Pajares, F., & Johnson, M. J. (1994). Confidence and competence in writing: The role of self-efficacy, outcome expectancy, and apprehension. Research in the Teaching of English, 313-331. Retrieved from https://www.jstor.org/stable/40171341
Ranelli, P. L., & Nelson, J. V. (1998). Assessing writing perceptions and practices of pharmacy students. The American Journal of Pharmaceutical Education, 62(4), 426. Retrieved from https://experts.umn.edu/en/publications/assessing-writing-perceptions-and-practices-of-pharmacy-students
Sackett, D. L., Rosenberg, W. M. C., Gray, J. A. M., Haynes, R. B., & Richardson, W. S. (1996). Evidence based medicine: what it is and what it isn’t. The British Medical Journal, 312(7023), 71-72. https://doi.org/10.1136/bmj.312.7023.71
Smith, M. G., & Dinkins, M. M. (2015). Early introduction to professional and ethical dilemmas in a pharmaceutical care laboratory course. The American Journal of Pharmaceutical Education, 79(10), 156. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4749904
Tan, E. B. (2007). Research Experiences of Undergraduate Students at a Comprehensive University. International Journal of Teaching and Learning in Higher Education, 19(3), 205-215. http://www.isetl.org/ijtlhe/past2.cfm?v=19&i=3
Tsuyuki, R. T., & Schindel, T. J. (2008). Changing Pharmacy Practice: The Leadership Challenge. Revue des Pharmaciens du Canada [Canadian Pharmacists Journal], 141(3), 174-180. https://journals.sagepub.com/doi/10.3821/1913701X2008141174CPPTLC20CO2
van Mil, J. W., & Fernandez-Llimos, F. (2013). What is ‘pharmaceutical care’ in 2013? Pharmacy Practice, 11(1), 1-2. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3780505/
Warner, J. W. (1998). A program for facilitating undergraduate research in biology. Journal of the Kentucky Academy of Sciences, 59, 2-5. Retrieved from https://www.biodiversitylibrary.org/item/104104#page/12/mode/1up
*Eng Lai Tan
School of Pharmacy,
International Medical University
126, Jalan Jalil Perkasa 19,
Bukit Jalil, 57000
Kuala Lumpur, Malaysia
Tel: +603-2731 7466
Email: englai_tan@imu.edu.my
Submitted: 15 May 2019
Accepted: 27 November 2019
Published online: 1 September, TAPS 2020, 5(3), 20-27
https://doi.org/10.29060/TAPS.2020-5-3/OA2157
Kosala N. Marambe1, Deepthi H. Edussuriya2 & Dharshana Jayawickrama1
1Medical Education Unit, Faculty of Medicine, University of Peradeniya, Sri Lanka; Department of Forensic Medicine, Faculty of Medicine, University of Peradeniya, Sri Lanka
Abstract
Introduction: Feedback reinforces good practice, identifies deficiencies and directs the learner to narrow the gap between actual and desired performance thus, playing a crucial role in the development of competence in medical training. However, feedback if not carefully handled can result in de-motivation and deterioration in performance.
It is believed that culture plays an important role in the way behaviours are valued and tolerated in educational settings.
Aim: To explore perceptions of Sri Lankan medical graduands on feedback received from teachers during clinical training.
Method: The study was conducted on a single intake of medical graduates after release of final MBBS results, ensured maximum variation sampling by including students from high, average and low performance categories. Participation was voluntary. Interviews were conducted using a short interview guide, transcribed and themes identified.
Results: 21 interviews were conducted. There were eight, six and seven volunteers from the high performing, average and poorly performing groups respectively. 63% were male.
Positive experiences encompassed; trainer taking a balanced approach to feedback by acknowledging good practices while indicating negative aspects, providing an emotionally supportive environment, clear articulation, offering focused learner support and motivating the learners through encouraging words and support to realize their potential. Negative experiences encompassed fault finding, biased nature and indiscreet behaviour of the trainers.
Conclusion: Sri Lankan medical graduands have experienced desirable and undesirable teacher behaviours during feedback episodes. Accurate conceptualization of ‘feedback process’ among clinical teachers and proactive measures to enhance the skills of teachers on giving feedback is needed.
Keywords: Undergraduate Clinical Training, Student Perceptions, Feedback
Practice Highlights
- Students call for a balanced approach in providing feedback.
- Sense of respect for the learner is solicited.
- Offering learner support is highly valued.
- Negative comments better be non-judgmental and descriptive.
- Accurate conceptualization of feedback process among trainers is a dire need.
I. INTRODUCTION
Feedback to a learner is an important aspect of teaching and learning and is essential in the acquisition of skills as well as development of competencies. In this era of outcome-based education, teacher feedback to learners plays a crucial role in the development of competence in medical training (Ende, 1983; Harden & Laidlaw, 2017). It becomes especially important in medical education in a hospital environment where teaching/learning occurs in an opportunistic manner in the presence of numerous other onlookers.
It is reiterated that in clinical practice, feedback reinforces good practice, identify deficiencies and directs the learner to narrow the gap between actual and desired performance (Bing-You, Paterson, & Levine, 1997; Bing-You & Trowbridge, 2009; Cantillon & Sargeant, 2008). Furthermore, Ponnamperuma (2015) argues desired performance should not be static but dynamic depending on the progress of the learner, emphasising the role of properly directed feedback in assisting enthusiastic learners to realise their potential. Similarly, Hesketh and Laidlaw (2002) argued feedback is essential element of the educational process that can help students reach their maximum potential. However, one should be mindful that feedback if not carefully handled can result in de-motivation and deterioration in performance (Cantillon & Sargeant, 2008).
Much highlighted educational alliance approach is based on a mutual understanding of purpose and of responsibility for learning. This alliance is complex with equal responsibility by the learner to learn and the teacher to teach (van de Ridder, Peters, Stokking, de Ru, & ten Cate, 2015). Barriers to effective feedback include, the purpose of feedback being unclear to the teacher (provider), and learner (recipient), unavailability of appropriate place or inadequate time to complete feedback and minimal or no training provided to the trainer in providing feedback (Hesketh & Laidlaw, 2002; Ponnamperuma, 2015).
van de Ridderet al. (2015) indicates that the effect of feedback may be small, if not given appropriately. However, it is well-known that for feedback to be of maximum benefit, learners’ too need to use and engage with the feedback processes appropriately. This concept which is known as “proactive recipience” includes, characteristics and behaviours of the receiver, sender; the message and context (Interpersonal communication variables); as well as recipient’s processes such as self-appraisal, assessment literacy, goal-setting, self-regulation, engagement and motivation (Winstone, Nash, Parker, & Rowntree, 2017).
A study conducted by Bose and Gijselaers (2013) supported the assumption that supervisors who promote residents to seek feedback with motives of self-improvement should also ensure that their students’ concerns of ego-protection and impression-defence are addressed during the process. van de Ridder et al. (2015) further states that the manner in which the message is framed, whether it is positive or negative affects students’ satisfaction and self-efficacy directly after the intervention even though it is known to fade-out over time.
Further it is believed that national culture plays an important role in the way behaviours are valued and tolerated in educational settings; Hofstede (2001), reported relatively higher power distance indices for South Asia. Sri Lanka being a South Asian country, the hierarchical nature of organisational arrangement is observed. Thus with the existence of high level of power distance between undergraduate students and academic staff, it is not customary for the students to argue with teachers or challenge teachers, even if the teachers deviate from accepted practices. In Asian cultures, the child-parent role pair is replaced by the teacher-student role pair (Hofstede, 2001) leading to observed paternalistic culture in Universities. Hence feedback tends be more of fault-finding with use of punitive measures as a means to change behaviour and it is likely that the trainees accept some of the negative behaviours of teachers (which are unlikely to be accepted by those in the West), considering it to have been done in good faith.
Bowen, Marshall and Murdoch-Eaton (2017) have identified three learner feedback behaviours; recognising, using, and seeking feedback. He proposes that core themes such as learner beliefs, attitudes, and perceptions; relationships; teacher attributes; mode of feedback; and learning culture influence these behaviours. Further, Perera, Lee, Win, Perera and Wijesuriya (2008) have reported perceived mismatch between the expectations of the provider and the receiver in an Asian context.
A survey on students’ perceptions of teacher feedback conducted in the Sri Lankan faculty by Mudiyanse, Pallegama and Marambe (2015) highlighted the existence of several deficiencies. Paucity of recent literature on perceptions of Sri Lankan undergraduate medical students on the feedback practices, prompted us to explore the issue of teacher feedback and its effect on students. As educationists, we believe an exploration of the actual situation would help understand the factors, which facilitate learning among Sri Lankan trainees, thus paving the way for informed decision-making. Hence the objective of the proposed study was to explore perceptions of Sri Lankan medical graduands to feedback received from teachers during clinical training.
II. METHODS
A qualitative inquiry informed by semi-structured interview was performed. The study sample was selected based on the final year results of a single intake of students in one medical Faculty within 3 months of release of results (this group of passed-out medical students awaiting award of degrees at the convocation is defined as graduands). Maximum variation within the sample was ensured through stratified random sampling technique. Fifteen students (8 males) were selected randomly by the research team from each achievement group namely, high achievers (those who secured classes–Group A), average students (those who secured ordinary passes–Group B) and poor performers (those who referred in any one final year subject–Group C).
Prospective participants were provided relevant information about the study via email and invited to be present for a short interview. They were informed that the interviews will be tape-recorded and transcribed for better comprehension and that confidentiality would be ensured. Those willing to participate in the study were instructed to contact the principal investigator by email. The volunteers were given appointments for the interview.
The nature of the study was explained to the volunteer and consent was obtained for audio recording by the Research Assistant (RA) prior to the scheduled interview. All interviews were conducted by the same interviewer in a sound-proof room, in the faculty-based on an interview schedule, which consisted of two open-ended questions. The probes used to obtain genuine responses were to recall a situation based on personal experience, during clinical training, where they were given, 1) constructive feedback and its impact on learning and 2) de-motivating feedback; and its impact on learning. Measures were taken to ensure anonymity.
Subsequently, the interviews were transcribed and read independently by three researchers with experience in qualitative research. Quotes were selected by the three researchers independently and grouped to identify broad themes. The broad themes identified were compared and consensus was achieved on common recurring themes, representative of the perceptions of undergraduate medical trainees on positive and negative experiences in receiving feedback.
III. RESULTS
Eight volunteers from the high achiever group (A), six from average group (B) and seven from referred group (C) amounting to a total of 21 students (63% males) were interviewed. Majority of the experiences with feedback (teacher to trainee) during clinical training in the third to fifth undergraduate year were rated as good. It was revealed feedback has been practiced more often, informally and systematically in the final year. According to interviewees, the majority of clinical teachers had listened to case histories presented by undergraduates and given feedback on the relevant and useful points for diagnosis and planning of management to the student concerned and others in the group during regular ward teaching sessions. Some of the assigned trainers have observed the physical examination techniques of students, clinical procedures and provided feedback to the student concerned, while others in the group also benefited from it.
Analysis of trainee perceptions of positive and negative feedback episodes during undergraduate medical training resulted in the identification of the four themes given below as those which motivated and enhance learning. Selected excerpts representative of all achievement groups, are included as evidence under each theme.
The positive experiences are centred on four themes presented below.
A. Balanced Approach to Feedback
Most of the interviewees valued when the feedback provider set the scene by acknowledging or appreciating the good aspects demonstrated by the trainee, while focusing on deficiencies whether it be history taking or examination.
“The teacher praised us for the good things we did in ward teaching sessions. Good practices were acknowledged during ward rounds … mistakes pointed out. Since the consultant capitalised on good things I did, I did not feel ‘belittled’.”
(A16)
“Teachers observed us, gave immediate feedback. First appreciated the thing done correctly, then advice was given to correct mistakes”
(B16)
“When good practices are highlighted we feel good. What we have missed were also pointed out … confidence increased”
(C7)
B. Demonstrating Respect for Learner
Respect for trainee and engaging in a dialogue, providing a non-threatening learning environment was mentioned as a factor which enhanced learning. These approaches include unbiased and unprejudiced behaviour, less hierarchical context, focus on specific performance and feedback phrased in descriptive, non-evaluative language. The other approaches include, use of neutral language, non-threatening tone of voice during feedback episodes, being sensitive to learners’ emotional status, taking measures to maintain privacy. The trainers’ behaviours underlying the episodes perceived as positive experiences by many interviewees consisted of features described above. Trainees sensed a lot of educational value in the caring, approachable, unbiased, respectful conduct of the trainers.
“The one-to-one feedback in clinical training is a good feature. We felt we could ask questions from the consultant and get some of the doubts clarified.”
(A15)
“We were treated like doctors. We could ask questions without fear, no big distance between student and teachers.”
(A5)
“So, I was encouraged to clarify my doubts in this manner. Never shout at us, so we were free to ask questions and behave in the ward. Adorable teacher, we could ask questions without fear.”
(A13)
“In a clinic setting, I was not thinking of privacy. Teacher called me to a room, … blamed for what was done. Got me to think if she was my mother … So, taught me about consent, privacy.”
(B15)
“The nature of the consultant, non-judgmental when I made mistakes, but tried to correct me by making a point clear. Not exceeding limits.”
(C11)
C. Clear Articulation and Offering Learner Support
Interviewees valued instances where the trainer provided focused advice, explained the mistakes made by trainees and offered adequate direction for improvement to the trainee. Providing clear descriptions of observed behaviour was felt to be more palatable and useful from the point of correcting one’s mistakes.
“I was okay with facts, I was observed during the process by a senior registrar and …, told me that I take more time–I was too slow. I was instructed to examine more abdomens of patients while in the ward, I did it and it became very useful.”
(A4)
“I was advised on how to organise histories, how to rearrange my history to suit final year requirements.”
(A8)
“We were supported, shown how to examine the patient correctly when we made mistakes. Directed us to read around …. Also, checked whether we have improved later”
(B1)
“What we have missed were also pointed out … We were shown correct techniques.”
(C7)
“end appointment viva, OSCE were held, one–to-one feedback. Wrong things we did were pointed out in a nice way. Focused, so we knew how to go about to improve knowledge.”
(C4)
D. Boosting Moral and Self- Esteem of Trainees
The interactions with trainees had been such that the trainer having identified the potential of students made them aware of it and motivated trainees to realise their full potential.
“I was identified as a good student by the clinician …, I was made aware of my potential, this I found encouraging and I tried to work better from then on in fact, it resulted me getting classes in later years.”
(A6)
“I was asked a simple question about ECG, when I did it right, I was praised… ‘you will become a consultant’, and later I came across an unusual heart sound and I told the consultant about it, he examined and also got the Registrars to listen to that so, I was encouraged to clarify my doubts.”
(A13)
“Third year teachers motivated me. They supervised us and corrected. All of us got a chance to do hands-on skills training.…supported learning”
(C3)
The negative experiences are centred on four themes presented below.
A. Fault-Finding and Judgmental Nature
Some of the expressions on negative experiences highlighted instances where feedback lacked acknowledgement of what was done right and encouragement, and being more of fault-finding exercise.
“When there are gaps in knowledge, the way teachers reacted at the start was not encouraging. We worked really hard, spent 3 whole nights in the ward. We get punished because 2-3 students in the group made mistakes. We are not rewarded for work we do.”
(B1)
“One clinician wanted to discuss a particular problem. … My patient had this problem found through a scan. …Unfortunately when the teacher examined, positive signs present because of full bladder. I was told that I will definitely repeat. I cried. I avoided the teacher. Still it haunts in me. Comments such as ‘you do not have a passing face’ was made, I was worried. Sad, when first impressions get carried through the appointment.”
(B15)
“I volunteered to present a case, I could not make a correct diagnosis and I was told I have cheated.”
(C11)
B. Biased Nature
Above refers to teacher referring to previous performance of a student in giving feedback to a new situation. Students feel if a mistake is made once that student gets noted and will be targeted and treated differently for the same mistake.
“Some students are treated differently. Even if we give correct answers, told not up to the mark.”
(B16)
“Some students were selected and they got scolded in front of everybody, I felt some of them worked very hard, when they make even a slight mistake, without giving credit to what was done right they got scolded.”
(A16)
“I felt expressions made following observations of performance were highly biased. Sometimes tend to generalise and make comments about students which are not true.”
(C3)
C. Indiscreet Behaviour of Trainers
Trainees perceived some environments as hostile, disrespectful, revealing things that should be private as illustrated by following phrases that were used to describe negative experiences.
“Embarrassing when … shouts at us, I think people have reasons for making mistakes. During ward rounds, scolding in front of patients in Sinhala, discourage students. Thereafter, students avoid these patients and lose chances of learning. I felt we were treated as school children.”
(B16)
“Certain appointments too scared of the consultant did not expect good feedback. Very harsh comments.”
(A18)
“Told you will fail, I did not see a fair reason to do so. Specially at a time when one is about to complete training before final exam. Last opportunity to learn in the course is lost. All your expectations are lost. There are better methods to motivate. What was done was unpleasant. Comments made are: you are bad- cannot do, I do not think you can pass.”
(B17)
D. Punishments in Addition to Feedback
Graduates also mentioned about instances where punishments were made in addition to negative feedback.
“Comparing students and scolding these students in front of others made them depressed. I have heard of students being punished when a wrong answer is given.”
(B14)
“Maybe one wrong answer, repeat for one month.”
(C5)
“Sometimes members of a group have to undergo punishment due to the fault of others in the group, like not presenting histories, being absent.”
(C14)
IV. DISCUSSION
It can be concluded that in most feedback episodes, interviewees have benefitted from trainer feedback, which has been balanced and supportive. Acceptance of more frequent, informal, timely, balanced and focused feedback was obvious in the expressions of trainees of all groups. However, the existence of variations among clinicians in the style of giving feedback was also evident. The Sri Lankan graduands valued acknowledgement, appreciation, praise of demonstrated good practices or desirable behaviours, by trainers during feedback sessions. In the Sri Lankan culture praise or words such as ‘excellent’, ‘very good’ and ‘good’ are used by teachers to acknowledge achievement of expected standard by students. Thus, interviewees endorsed the potential of simple measures in reinforcing good behaviour reported by Thorndike (1931) and Krackov (2009). Interestingly, Sri Lankan graduands, a group of South Asians, highlighted most of the characteristics of effective feedback found in literature under positive experiences, though hardly mentioned practices such as providing feedback as desired by the recipient and checking for understanding of the plan of action/ remedial measures (Matua, Seshan, Akintola, & Thanka, 2014; Ramani & Krackov, 2012; Rose, Best, & Higgs, 2005). Also, emphasis on reinforcing desirable behaviour during feedback episodes was not prominent in the expressions. In this regard, Ponnamperuma (2015) was of the view that ‘reinforcing desirable behaviour is rather conservative in South East Asian region’ compared to the West.
Similar to the findings of Hewson and Little (1998), most of the Sri Lankan interviewees endorsed feedback episodes where clinicians created a respectful environment were effective in enhancing learning and self-esteem. In such environments interviewees reported they are not in fear and hence tend to ask questions for clarification, and request support from different levels of clinical teachers, work with an inquiring mind and thereby enhance their knowledge and skills.
The trainees have perceived many advantages of balanced feedback that is trainer initiating the feedback dialogue by acknowledging and praising (which is more than acknowledgement) the observed good practices, later commenting on observed gaps in competencies, discussing remedial measures and finally incorporating monitoring strategies to ensure the attainment of competencies. Boud and Molloy (2013), have argued these as desirable aspects, which enhance learner engagement in a feedback model. Sri Lankans also endorsed the effect of such feedback on boosting confidence (Bing-You et al., 1997; Cantillon & Sargeant, 2008; Krackov, 2009, 2011). Ready acceptance of such balanced or even- handed feedback reported by Hewson and Little (1998) and Ramani and Krackov (2012) was apparent among Sri Lankan trainees.
Ponnamperuma (2015) indicated one of the expected roles of feedback is to challenge learners to realize their potential which demands extending the desirable level of competency for learners progressing well. It was encouraging to note that some of the interview excerpts referred to fulfilment of this role by the local trainers.
However, analysis of narratives on negative feedback episodes revealed desirable practices are not entirely prevalent in the Sri Lankan context. In describing features of negative feedback episodes, words such as ‘hostile’ and ‘tensed’ were frequently mentioned and majority doubted its effect on motivation and promoting learning. According to interviewees this situation has led to the emergence of ‘feedback phobia’, resulting in the avoidance of such teachers. Reflecting on the negative experiences of many interviewees, it is clear that the trainees request feedback to be made on direct observations of trainee performance in all encounters, using neutral language and a respectful tone which are the prescribed good practices in literature (Ramani & Krackov, 2012; van de Ridder et al., 2015). As reiterated in literature, it is important for trainers to maintain privacy and confidentiality particularly, when providing negative feedback (Ponnamperuma, 2015).
Further, being conscious of the tone and language used in feedback encounters is an absolute necessity to avoid de-motivation (Hewson & Little, 1998; van de Ridder et al., 2015). In this regard Ponnamperuma (2015) states negative feedback, if handled in a wrong way, can damage self -esteem, create a ‘feedback phobia’ leading to avoidance of such trainers and training opportunities.
Evidence suggests feedback phobia is not uncommon in the Sri Lankan context. Hence it is essential to frequently remind the trainers to be objective, unbiased and unprejudiced during informal feedback encounters and thereby ensure a favourable emotional climate, being sensitive to recipient’s emotions. A creative trainer would thus initiate a dialogue with the trainee, provide a space for the recipient/trainee to clarify the feedback and later offer guidance and support to enable accomplishment of competencies (Harden & Laidlaw, 2017). However, it is known that creativity requires time and effort on the part of a busy clinical trainer. In order to change the situation for the better, it is recommended regular faculty development programs include theory and practice of constructive feedback models (Boud & Molloy, 2013).
Quoting some of the observed undesirable practices in the South East Asian region, Ponnamperuma (2015) expressed doubt on accurate conceptualisation of feedback by both the provider and the recipient. Analysis of the negative experiences described by the graduands, raises concerns on the level of conceptualisation of feedback among some of the trainers in the Sri Lankan context. For example, interviewees revealed, though identifying undesirable behaviour was commonly practiced by the trainers, in most instances, they were not backed up with options and support for improvement. Hierarchical and paternalistic culture seems prominent in the Sri Lankan context leading to arrogant behaviours of some teachers during feedback episodes (Hofstede, 2001). Furthermore, as exemplified by interviewee quotes, the reaction of some of the clinical trainers had not been proportionate to the mistake made by the trainee concerned and trainees had been left with a sense of helplessness leading to negative repercussions such as emotional distress. Imposing punishments like non-signing off of clinical appointments, in addition to providing negative feedback has resulted in developing feedback phobia and avoidance of training opportunities (Ponnamperuma, 2015).
The graduands have experienced at least a few feedback encounters which were not effective, de-motivating and stressful; this need to be addressed constructively. Ende (1983) was optimistic that after some practice and planning, provision of feedback in clinical medicine is not as difficult as one might think. In this background, there is a need for the administrators to initiate a dialogue on institutional-level student feedback policy. Developing a contextualised feedback framework through active engagement of clinical teachers encompassing Pendleton’s rules (Pendleton, Schofield, Tate, & Havelock, 2003) or Agenda-Led Outcome Based Assessment (Chowdhury & Kalu, 2004), which are learner mediated, will be a step in the right direction.
Recently, Findyartini, Bilszta, Lysk and Soemantri (2019) had reported the effectiveness of employing strategies ensuring active engagement of participants during Faculty development initiatives, leading to cross-cultural adaptation of best practices in clinical teaching. Hence organising workshops for clinical teachers where they are made to reflect on student narratives of positive and negative feedback episodes in the light of good practices could be a useful strategy to promote adoption of desirable behaviours.
V. CONCLUSION
Positive and negative feedback experiences were revealed by Sri Lankan graduands. Features of effective and ineffective feedback episodes in the minds of Sri Lankan trainees are mostly the same as those reported in literature based on Western studies. However, graduands have perceived the existence of conservative behaviours among some of the teachers such as being more interested in fault-finding with less emphasis on discussing corrective measures. Hence it is speculated some of the trainers could be having a ‘culturally coloured’ concept of ‘feedback’, which needs urgent attention in order to realise the educational benefits of feedback. Since Feedback is a powerful learning tool in medical education, all efforts should be made to enhance the skills of trainers on giving feedback to learners.
Notes on Contributors
Kosala N. Marambe, MBBS, PhD (Maastricht), is Head of Medical Education Unit and professor in Medical Education. Has more than a decade of experience in organising staff development programs for Health professions educators, conducting and publishing qualitative research.
Deepthi H. Edussuriya, MBBS, MPhil, PhD (Sri Lanka), is a senior lecturer in the Department of Forensic Medicine and has experience in conducting and publishing qualitative research.
Dharshana Jayawickrama, MBBS, was formerly a temporary lecturer in the Medical Education Unit and served as a Research Assistant.
Ethical Approval
Ethics approval for the study proposal was obtained from the institutional ethics review committee of the University, Sri Lanka (Ethics approval number 2017/EC/69).
Acknowledgements
Authors wish to thank graduands who volunteered to share their experiences and Dr. T.M.S.H. Dharmaratne of the Medical Education Unit (MEU) for his assistance during identifying/selecting codes and identifying themes.
Funding
The research received no specific grant from any funding agency.
Declaration of Interest
The authors have no conflict of interest.
References
Bing-You, R. G., Paterson, J., & Levine, M. A. (1997). Feedback falling on deaf ears: Residents’ receptivity to feedback tempered by sender credibility. Medical Teacher, 19(1), 40–44. https://doi.org/10.3109/01421599709019346
Bing-You, R. G., & Trowbridge, R. L. (2009). Why medical educators may be failing at feedback. Journal of the American Medical Association, 302(12), 1330–1331. https://doi.org/10.1001/jama.2009.1393
Bose, M. M., & Gijselaers, W. H. (2013). Why supervisors should promote feedback-seeking behaviour in medical residency. Medical Teacher, 35(11), e1573-1583. https://doi.org/10.3109/0142159X.2013.803059
Boud, D., & Molloy, E. (2013). Rethinking models of feedback for learning: the challenge of design. Assessment & Evaluation in Higher Education, 38(6), 698-712. https://doi.org/10.1080/02602938.2012.691462
Bowen, L., Marshall, M., & Murdoch-Eaton, D. (2017). Medical student perceptions of feedback and feedback behaviors within the context of the “educational alliance”. Academic Medicine, 92(9), 1303–1312. https://doi.org/10.1097/ACM.0000000000001632
Cantillon, P., & Sargeant, J. (2008). Giving feedback in clinical settings. British Medical Journal, 337, 1292-1294. https://doi.org/10.1136/bmj.a1961
Chowdhury, R. R., & Kalu, G. (2004). Learning to give feedback in medical education. The Obstetrician & Gynaecologist, 6(4), 243-247. https://doi.org/10.1576/toag.6.4.243.27023
Ende, J. (1983). Feedback in clinical medical education. Journal of the American Medical Association, 250(6), 777-781. https://doi.org/10.1001/jama.1983.03340060055026
Findyartini, A., Bilszta, J., Lysk, J., & Soemantri, D. (2019). Transnational clinical teacher training: Lessons learned and cross cultural implications. The Asia Pacific Scholar, 4(3), 79-90. https://doi.org/10.29060/TAPS.2019-4-3/OA2088
Harden, R. M., & Laidlaw, J. M. (Ed.). (2017). Essential skills for a medical teacher-An introduction to teaching and learning in medicine (2nd Ed.). London, England: Elsevier.
Hesketh, E. A., & Laidlaw, J. M. (2002). Developing the teaching instinct: Feedback. Medical Teacher, 24(3), 245–248. https://doi.org/10.1080/014215902201409911
Hewson, M. G., & Little, M. L. (1998). Giving feedback in medical education: Verification of recommended techniques. Journal of General Internal Medicine, 13(2), 111–116. https://doi.org/10.1046/j.1525-1497.1998.00027.x
Hofstede, G. H. (2001). Culture’s consequences: Comparing values, behaviours, institutions, and organizations across nations (2nd Ed., pp.1-100). California, CF: Sage publications.
Krackov, S. K. (2009). Giving feedback. In J. A. Dent & R. M. Harden (Eds.), A practical guide for medical teachers (3rd Ed.). London, England: Elsevier.
Krackov, S. K. (2011). Expanding the horizon for feedback. Medical Teacher, 33(11), 873–874. https://doi.org/ 10.3109/0142159X.2011.617797
Matua, G. A., Seshan, V., Akintola, A. A., & Thanka, A. N. (2014). Strategies for providing effective feedback during preceptorship: Perspectives from an Omani hospital. Journal of Nursing education and practice, 4(10), 24-31. https://doi.org/10.5430/jnep.v4n10p24
Mudiyanse, R. M., Pallegama, R., & Marambe, K. (2015). Students’ perceptions of teacher feedback and the educational environment as measured by DREEM in a medical faculty in Sri Lanka. Journal of Medical science and clinical research, 3(6), 6101-6106.
Pendleton, D., Schofield, T., Tate, P., & Havelock, P. (2003). The consultation: An approach to learning and teaching. Oxford, England: Oxford University Press. https://doi.org/10.1093/med/9780192632883.001.0001
Perera, J., Lee, N., Win, K., Perera, J., & Wijesuriya, L. (2008). Formative feedback to students: The mismatch between faculty perceptions and student expectations. Medical Teacher, 30(4), 395–399. https://doi.org/10.1080/01421590801949966
Ponnamperuma, G. (2015). Feedback as conceptualized and practiced in South East Asia. In Chenicheri Sid Nair and Patricie Mertova (Eds.), Enhancing learning and teaching through student feedback in medical and health sciences (1st Ed., pp.43-59). Oxford, England: Chandos Elsevier. https://doi.org/10.1533/9781780634333.43
Ramani, S., & Krackov, S. K. (2012). Twelve tips for giving feedback effectively in the clinical environment. Medical Teacher, 34(10), 787-791. https://doi.org/10.3109/0142159X.2012.684916
Rose, M., Best, D., & Higgs, J. (2005). Transforming practice through clinical education, professional supervision and mentoring (1st Ed., pp. 143-159). Edinburgh, United Kingdom: Elsevier. https://doi.org/10.1016/B978-0-443-07454-7.50024-1
Thorndike, E. L. (1931). Human Learning (pp. 162-181). New York, NY: The Century Co. https://doi.org/10.1037/11243-000
van de Ridder, J. M. M., Peters, C. M. M., Stokking, K. M., de Ru, J. A., & ten Cate, O. T. J. (2015). Framing of feedback impacts student’s satisfaction, self-efficacy and performance. Advances in Health Sciences Education, 20(3), 803–816. https://doi.org/10.1007/s10459-014-9567-8
Winstone, N. E., Nash, R. A., Parker, M., & Rowntree, J. (2017). Supporting learners’ agentic engagement with feedback: A systematic review and a taxonomy of recipience processes. Educational Psychologist, 52(1), 17-37. https://doi.org/10.1080/00461520.2016.1207538
*Kosala N. Marambe
Faculty of Medicine,
University of Peradeniya,
Sri Lanka
Email: kosalnm@yahoo.com
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
