
Virtual Integrated Patient: An AI supplementary tool for second-year medical students
Submitted: 31 August 2020
Accepted: 9 December 2020
Published online: 13 July, TAPS 2021, 6(3), 87-90
https://doi.org/10.29060/TAPS.2021-6-3/SC2394
Juanita S. M. Kong1*, Boon See Teo2*, Yueh Jia Lee1, Anu Bharath Pabba1, Edmund J.D. Lee1 & Judy C. G. Sng1
1Department of Pharmacology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Department of Family Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
*Equal contribution; first co-authors are in alphabetical order
Abstract
Introduction: With the COVID-19 pandemic, Singapore underwent a national lockdown in which most organisations, including schools were closed. Halting face-to-face tutorials resulting in decreased clinical contact for medical students. Prior to the pandemic, we had developed the Virtual Integrated Patient (VIP). Equipped with conversational technology, it provides students online practice in various clinical skills such as history-taking, physical examination and investigations. The aim of this paper is to describe the supplementary use of VIP in the second-year class, in which a pilot study was conducted.
Methods: The VIP platform was introduced to the cohort and used to supplement the teaching of history-taking in the “Communication with Patients” (CWP) module for second-year students. Traditionally, CWP tutorials involve face-to-face history-taking from standardised patients (SPs). Students, who consented to participating in the trial, had an additional 3 weeks’ access to VIP to practice their history-taking skills. They completed a survey on their user experience and satisfaction at the end of the 3 weeks.
Results: Out of the 106 participants, 87% strongly agreed or agreed that using VIP helped in remembering the content while 69% of them felt that VIP increased their confidence and competence in history-taking.
Conclusion: VIP was well-received by students and showed promise as a tool to supplement history-taking tutorials, prior to students’ encounter with SPs and real patients. Hence, this trend showed its potential as an alternative when clinical rotations were delayed or cancelled. Further research can be done to evaluate its effectiveness in this context.
Keywords: Medical Education Tool, Virtual Patients, Communication, Skill Acquisition, Chatbot, Conversational
I. INTRODUCTION
Clinical skills that are commonly practised face-to-face were a challenge for students to practise during the onset of the Novel Coronavirus (COVID-19) in Singapore. Singapore underwent a 2-month lockdown during which time most non-essential organisations, including medical schools were closed nationwide. In our institution, lectures and tutorials were moved online and face-to-face clinical teaching on campus and in hospitals were cancelled. This move necessitated the use of virtual tools, such as remote meeting through Zoom and the use of virtual patient simulators that do not require the students to be physically on campus.
Virtual patient simulators have been used in a wide range of medical education settings, ranging from the teaching of clinical reasoning, procedural skills, communication skills, and integrated performance to critical thinking (Kononowicz et al., 2019). In recent years, there has been increasing use of virtual patients in the healthcare sector and technology improvements will continue to grow. The Virtual Integrated Patient (VIP) is a virtual patient simulator that was created by our team prior to the pandemic. It leverages on artificial intelligence (AI) technology advancements in the area of naturalistic conversational technology. Prior to VIP, existing technology platforms were focused on the linear, semi-linear and menu-driven (with drop-down option boxes) simulators and there were very few developed in free-text conversations (Kononowicz et al., 2015). The VIP has a natural language processor that is flexible to adapt and adjust to conduct a realistic conversation that can enhance specific skill acquisition (Cendan & Lok, 2012; Kononowicz et al., 2019).
The next unique feature of the VIP is the random patient generator (Figure 1a and b). Every time a student logs in, a new patient is generated. They can revisit the past patients if they have not completed the case and restart where they have left off. The random patient generator provides a realistic situation for users that no two doctors will see the same patient at the same time increasing in variability of patients and potentially, diagnoses. Users can also probe into their virtual patients’ history in their unique ways. Integration of natural language processing using conversational technology has allowed users to chat with the virtual patient as though they are chatting with a real person (Figure 1c). The virtual patient is trained with data sets and is AI-learning enabled. Wi-fi connectivity allows VIP to be accessed anywhere and at any time. It is a safe environment where students are able to make mistakes without any penalty and learn from it. VIP has interfaces for history-taking through a chatbot, physical examination, and laboratory investigations as seen in Figure 1c to d.
The aim of this short communication is to describe how VIP has been employed in a history-taking module for second-year medical students. VIP may play a role in providing a platform for users to consistently practise their skills during a global pandemic where face-to-face tutorials are limited.

Figure 1. a to d. Screenshots of the Virtual Integrated Patient (VIP) interface; b. An example of a random patient generator with no same patient; c. In the history-taking screen, the user can chat with a randomly generated virtual patient, who generates answers using the pre-loaded content and the natural language processor; d. Left: The physical examination screen. d. Right: The laboratory investigations screen which provides realistic case information given explicit buttons throughout interface for easy navigation. Bottom Panel: e to f: Skill Retention Confidence survey results.
II. METHODS
This study’s information sheet, study plan, instruction slides, and survey forms were submitted to the National University of Singapore’s (NUS) institutional review board (IRB) for assessment. It was approved with the study approval code of S-19-263.
VIP was introduced to Phase II “Communications with Patients” (CWP) module in Academic Year (AY) 2019/2020. In this module, students usually clerk a total of three to six standardised patients (SPs) for three sessions over a course of 3 weeks. VIP was introduced to supplement the CWP curriculum. On top of clerking three to six SPs in 3 weeks, participants were given access to VIP during the same 3 weeks. VIP was loaded with cases that complemented and reinforced the contents taught during tutorials, with the aim to deepen students’ understanding of the tutorial content and train them to use the history-taking framework taught during the module.
The VIP team introduced the VIP computer programme and how to use it during the first lecture of the CWP module. Recruitment was done and informed consent was taken from the willing participants for the study. All Phase II students enrolled in the course (n=296) were divided into two groups: the first group received access at the first tutorial (intervention group) and the other group with no access (control group). Eventually, all students from both groups (intervention and control) had received access to the VIP by the end of first week and they could practise over the remaining 2 weeks of the study. Participants were asked to complete a survey at the end of 3 weeks. This is to provide an insight on their confidence levels in executing the history taking exercise and key takeaways with VIP usage at the end of the study.
Students who declined to participate in the study would still have received access to the VIP, but only after the study period of 3 weeks. This ensured fairness for all second-year medical students to have 6 months to practice on the VIP system before their OSCE (Objective Structured Clinical Examination) at the end of the semester.
Following the 3 weeks of tutorials, students were encouraged to continue practising using the VIP prior to the OSCE which was scheduled to be at the end of the academic year. The original study protocol included collection of participants’ history-taking scores at the OSCE, but this was not possible as the OSCE was cancelled due to the COVID-19 situation in Singapore.
III. RESULTS
We obtained quantitative survey responses (n=106 respondents out of 298; 35% response rate). They indicated positively to VIP with 87% of students feeling that using VIP helped in remembering the content. And 69% of the students strongly agreeing or agreed that VIP increased their confidence in taking history (Figure 1f and g).
Students also provided qualitative responses of the key takeaways with the supplementary usage of VIP with their curriculum. First, they indicated that they were able to execute the history-taking procedures more efficiently with additional practice on the VIP. Second, students indicated that they could better remember the methodological content taught in class after repeated usage, thus reinforcing the procedural history-taking skills. Last but not least, survey respondents also reported enhanced understanding of the multiple facets of presenting cases. Where they learnt more about each diagnosis from the summary page after each case completion.
IV. DISCUSSION
VIP was well-received by students in CWP. Users’ survey responses reiterated that more practice aided their skill acquisition, helping them to score in their examinations. By keeping the simulation realistic, they could transfer the skills back into their clinical attachments in future. Also, adding VIP supplementary to the planned curriculum, students were provided additional practice that past years students have requested for in course feedback.
Traditionally, CWP students could only clerk three to six SPs during the whole course of module over a span of 3 weeks. Thereafter, they would not have any chance to practice their history-taking skills through the clerking of SPs until their OSCE which would happen half a year later. Over the years, students provided feedback that they did not receive adequate practice prior to the OSCE and practising on their friends was not feasible due to the hectic nature of their curricular commitments. However, this barrier could not be overcome due to the constraints of the packed timetable of the Phase II students. Therefore, current phase II students who reported that VIP enhances their efficiency and has provided them with adequate practice suggest that VIP is a promising supplement for the course.
One key objective of the VIP is to focus on the processes of getting to a diagnosis rather than just the right diagnosis itself. Medical students’ focus usually stems from the diagnoses to symptom as they are taught in that framework. The enhanced understanding of case definition through the case summaries were welcomed due to the realistic nature of their experiences and how it can be related in the actual clinics. This therefore enhances the students’ enthusiasm toward the usage of the platform. Furthermore, the intention of this was to ease the performance anxiety faced by the students by preparing them in a low-stakes environment, helping them to boost their confidence, in facing SPs or real patients. The study results resonated with this purpose as the students reported greater confidence and efficiency in taking family history after using VIP.
Moreover, the availability of VIP appealed to the students. Due to their curricular commitments, students are more often than not, on the go. While travelling or waiting for a class, where there is available Wi-Fi connectivity, they can log on and practise clerking patients on the simulator. Some students who were not able to attend tutorials were slightly disadvantaged as they would lose one or two SP clerking from the 3 weeks.
V. CONCLUSION
With greater confidence and better utilisation of CWP framework among the students who utilised VIP, VIP is promising as a tool to supplement face-to-face history-taking tutorials. It may have potential use in a pandemic situation where medical students have reduced access to in-person clinical teaching. However, further research is needed to establish its effectiveness as an alternative to in-person clinical teaching.
Notes on Contributors
Author 1, Juanita Kong, was involved in the data collection, analysis, writing, reading, and the final submission of this manuscript. Author 2, Teo Boon See was involved in the planning and execution of this study, writing, reading, and the submission of this manuscript. Both Authors 1 and 2 have equal contribution to the manuscript. Author 3, Lee Yueh Jia, was involved in the data collection, analysis and the reading of this manuscript. Author 4, Anu Bharath Pabba, was involved in the data collection and programming of the tool. Author 5, Edmund Lee was involved in the conceptualisation of the study, data collection, analysis, reading and the final approval of this manuscript. Judy Sng, was involved in the conceptualisation of the study, data collection, analysis, reading and the final approval of this manuscript.
Acknowledgements
We would like to thank the students who participated and provided us with additional feedback when we requested for it. Additionally, we would like to thank all the people who has helped us along the way. Last but not the least, we are grateful for the people who believed in this project.
Funding
The development of the VIP was initially funded by the MOE Tertiary Research Funding (2018 to 2020). It is currently supported by the Yong Loo Lin School of Medicine, under the Innovation Project.
Declaration of Interest
There are no conflicts of interests in this study.
References
Cendan, J., & Lok, B. (2012). The use of virtual patients in medical school curricula. Advances in Physiology Education, 36(1), 48–53. https://doi.org/10.1152/advan.00054.2011
Kononowicz, A. A., Zary, N., Edelbring, S., Corral, J., & Hege, I. (2015). Virtual patients – What are we talking about? A framework to classify the meanings of the term in healthcare education. BMC Medical Education, 15(1), 1–7. https://doi.org/10.1186/s12909-015-0296-3
Kononowicz, A. A., Woodham, L. A., Edelbring, S., Stathakarou, N., Davies, D., Saxena, N., Tudor Car, L., Carlstedt-Duke, J., Car, J., & Zary, N. (2019). Virtual patient simulations in health professions education: Systematic review and meta-analysis by the digital health education collaboration. Journal of Medical Internet Research, 21(7), e14676. https://doi.org/10.2196/14676
*Judy C. G. Sng
Department of Pharmacology,
Yong Loo Lin School of Medicine,
National University of Singapore
MD3, 16 Medical Drive #04-01
Singapore 117600
Tel: +65-65163676
Email: phcsngj@nus.edu.sg
Submitted: 30 August 2020
Accepted: 12 November 2020
Published online: 13 July, TAPS 2021, 6(3), 83-86
https://doi.org/10.29060/TAPS.2021-6-3/SC2390
Rahman Habeebul
Department of Psychiatry, Tan Tock Seng Hospital, Singapore
Abstract
Introduction: Archetypes in psychology are complete models of behaviours, thoughts and feelings, representative of universal experiences. From Plato’s description of Forms to Jung’s analytical introduction to archetypes in psychology, to common use of Moore’s masculine archetypes in popular culture, we use such “complete representations” to enable change.
Methods: In examining psychologically driven responses to the recent and ongoing pandemic crisis, the use of a graphic representation of interacting archetypes is proposed—the ‘archetypogram’.
Results: Drawing on concepts from psychodynamic therapy practise, including Transactional Analysis and Jungian theory, four main archetypes are proposed for their interdependence—the prisoner, the soldier, the sage and the jester/trickster, and a model describing their interactions is presented with the intention of enabling helpful behaviours in response to crisis. The model further proposes positive and negative positions within each archetype, labelled as ‘creating’ and ‘consuming’ behaviours respectively. The ‘archetypogram’ thus is a visual representation of three main components – the four archetypes, creating vs consuming behaviours, and movement between the various positions. Use of the ‘archetypogram’ is aimed at enabling individuals in crisis to move from consuming to creating behaviours.
Conclusion: The ‘archetypogram’ is a model of change which may be applied to persons distressed in crisis, and is able to move behaviours towards positive and creating self-states.
Keywords: Archetypes, Psychology, Crisis, Distress
I. INTRODUCTION
This was a crisis borne on the wings of travellers, leaving in its wake the term ‘a new norm’. In reflecting on observed and experienced emotional responses to the crisis, a structure emerged that identified three main themes—1) feelings of helplessness 2) seemingly never-ending activity and 3) a wish to be able to rise above billowing waves of information and misinformation. Hence the archetypes of a prisoner, a soldier and a sage seemed appropriate.
It was expected that psychological reactions of anxiety, worry, grief and helplessness would run their course in this new crisis, but behavioural responses were unpredictable, from hoarding of toilet roll to disregard of rules and breaking of lockdown laws, to apathy. Why was there a difference between a leader of a nation (Luce, 2020) and a 9-year-old girl (Harris, 2020); one denying the problem at its outset, and the other, deciding to sew personal protective equipment (PPE) gowns to help her local doctors? What enables one person to do what needs to be done in crisis, and yet paralyses another into inaction? Many concepts have been put forth, with names such as grit, resilience, and growth mindset, but are there quick descriptors we can apply, that can help us move out of unhelpful states into more effective, useful ways of being?
II. OBSERVATIONAL PERSPECTIVE
We gravitate towards archetypes—“whole” descriptions of images that we identify with externally, and which we identify within ourselves internally. Jung’s description of archetypes has enabled a scaffold on which we can build our understanding of basic human reactions and behaviours in a Gestalt manner. In archetypes we unite both unconscious and conscious domains of being, and place intention second to observation.
The first evident experiences observed in the thick of the outbreak were feelings of being stuck, or being held hostage by the situation with feelings of helplessness that imprison the person. The prisoner was both angry and sad, and endured a mind filled with comparisons e.g. “Were there other prisoners being better treated? Was the suffering equal? Would someone else gain whilst we were denied of something possibly essential to our well-being, such as PPE?” Locus of control was felt externally (Rotter, 1954).
Amongst those who would put action to thought, a different set of behaviours was noted. There was a sense of constant effort, of having to negotiate endless tasks for a small ‘win’. Life was a blur of activity with anticipation of further problems, and resentment (signalling a slip back into prisoner state), but most times the effort of doing kept away negative emotions. This seemed to be the role of a tireless soldier, who would get wounded through unpreparedness.
There was yet a third group, who seemed untouched by the outbreak. They would go about their usual activities, or turn to alternatives effortlessly. This group I called the sage, and hypothesised that few of us would achieve the transcendental nature they exuded, in keeping with Maslow’s topmost hierarchy of being values (Maslow, 1998).
However, referencing Transactional Analysis (Berne, 1961) where the ego-states of Parent, Adult and Child were further divided into negative and positive functional states depending on how stable they were, a further split within the three archetypes could be seen, with negative positions and positive positions. Hence, for the prisoner archetype, whilst inactivity was observed as a behaviour, the prisoner in a positive position was able to plan, or conserve parts of themselves for further action, to either rise as a soldier or guide as a sage.
The positive position of soldier archetype was decisive, enabling energy to effect change without burning themselves out, and able to make difficult decisions. Behaviour was internally motivated and pragmatically guided by agency.
For the sage archetype, the positive position enabled them to nurture those around, lending stability to the system while being transcendental- as encompassed in the description by Maslow who placed this at the apex of the hierarchy of needs. Such a person is ‘care-ing’, not just caring of those around him or her, but also actively engaged in ‘care’ which is a constant state of being present.
III. INTERVENTIONAL PERSPECTIVE
Pathological emotions, thoughts and behaviours were proposed to arise from a primary prisoner state. Subsequently, as responses to helplessness and anger, three main behaviours were noted. 1) Continued inactivity (staying in the helpless prisoner state). 2) Busyness in ‘doing’, but where excessive activity was used to deflect uncomfortable feelings of helplessness (escape into soldiering) or 3) Non-responsiveness, where the uncomfortable feelings are avoided altogether (escape into sageing). These corresponded to efforts to defeat the source of conflict, but being ineffective, resulted in inaction (self-defeat), ineffective activity (other-defeat) or avoidance (reality-defeat).
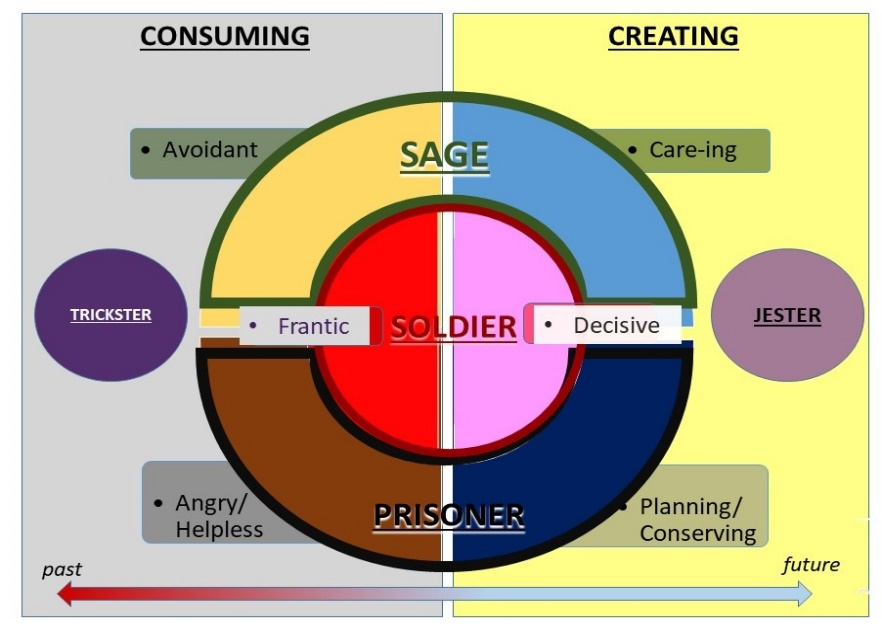
Figure 1. The Crisis Archetypogram
If we were to look to the negative positions, we see the behaviours as ‘consuming’, where either time, effort or emotional energy are consumed with poor outcomes, or no change in adapting to crisis.
If we were to look to the positive positions, we see the behaviours as ‘creating’ – ideas are born, work is done to engage parts of the system, there is nurturing of others and effort is concise, allowing adaptation and solving of problems.
In looking at ‘creating’ from the positive position, a further archetype emerges—that of the jester. This was the archetype who was flexible and not imprisoned, not always embattled nor always aloof and calm. This archetype would defuse tense situations with humour as a mature defence mechanism. The utility of the jester lies in the ability to bind people (and oneself) to a common cause; in the absence of hugs, laughter does a fair job of oxytocin production, and of fostering attachment. Pulled into negativity however, the jester’s negative position manifests as a trickster who would undermine with cunning the work done by the planning prisoner, the decisive soldier and the nurturing sage. The trickster at work was observed in the form of self-sabotage, or by disrupting efforts of the group with jokes belittling the efforts of others.
A. Completing the Circle – The ‘Archetypogram’
The ‘Archetypogram’ in Figure 1 seeks to visually represent the interconnectedness of the various archetypes, in positive (creating) and negative (consuming) positions. How may we use such a crisis archetypogram to help ourselves and those around us?
The first step would be to identify where we are in the archetypogram—remembering that the position we are holding is temporary and a state (a current and temporary manner of being or interacting in domains of thoughts, feelings and behaviour), not a trait (longer term more durable repeated patterns of interactions).
The second regular step is to move to creating rather than consuming, and meeting the needs of the future instead of being mired in the past. In times of crisis, resources are limited. By moving to a creating state (which is often creative), we make better use of resources available, or contribute more if we agree to change. In a consuming state, time is a price to pay for opportunity lost when not moving forward, even if no other resources are used (anxiety paralysis).
B. Limitations in Change
Having applied the archetypogram in change management, limitations in effectiveness have been observed in situations where either there was a clinical disorder giving rise to anxiety and depression, or if there was resistance to the idea of change being possible within the archetypogram (similar to being in the pre-contemplative state of change). It is hoped that with development of the archetypogram, limited therapy sessions may be used to address clinical disorders.
IV. CONCLUSION
Whilst it is ideal that we move in the general direction of actualization we need to be mindful of limitations in resources; flexibility in approach is paramount, as is being kind to ourselves no matter the approach we adopt.
In a crisis, the ‘work to do’ therefore is to:
1. Identify the state we are in – Prisoner/ Soldier/ Sage/ Jester-Trickster.
2. Identify the outcome of our behaviours – creating or consuming.
3. Identify how we can move ourselves from a consuming to a creating position, first by moving within our archetype (e.g. from angry/ helpless prisoner, to a conserving/ planning prisoner), then up archetypes (eg on to a decisive soldier, and eventually to a nurturing and care-ing sage). The movement can be internal via self-awareness (a practiced skill incorporating conservation of energy by mindfulness/ relaxation exercises and problem solving) or external via a coach, counsellor or therapist.
4. Be aware of the tendency to move upwards within the consuming rank states where avoidance and burnout from the sage and soldier states respectively can reinforce a primary angry / helpless prisoner’s distressed negative position.
5. Be mindful that the distressed position is often at the base of what one feels and thinks as ‘problems’. Emotional responses of grief, anxiety and anger arise from helplessness or loss, and these responses can be true of individuals as well as groups, but still amenable to working through with the aid of the archetypogram.
In conclusion, while the use of archetypes in verbal tradition is established, the visual archetypogram proposes an exciting model to move behaviours in crisis towards positive and creating self-states, in fields ranging from coaching, to counselling, to psychotherapy.
Note on Contributor
Dr Habeebul Rahman is solely responsible for all observations and ideas contained within this manuscript.
Ethical Approval
Ethics review (including informed consent) was not sought for this manuscript owing to the hypothetico-deductive nature of the paper.
Acknowledgement
The writer wishes to acknowledge TTSH Department of Psychiatry, Organisational Development and Operations for their contribution to the development of this work.
Funding
No funding was sought or obtained for this paper.
Declaration of Interest
No conflicts of interest.
References
Berne, E. (1961). Transactional analysis in psychotherapy: A systematic individual and social psychiatry. Grove Press.
Harris, E. (2020, May 11). For Malaysian schoolgirl, homework is sewing PPE gowns to help beat coronavirus. Reuters https://www.reuters.com/article/us-health-coronavirus-malaysia-protectiv-idUSKBN22N037
Luce, E. (2020, May 17). Inside Trump’s coronavirus meltdown. The Straits Times. https://www.straitstimes.com/world/united-states/inside-trumps-coronavirus-meltdown
Maslow, A. H. (1998). Toward a psychology of being. Wiley.
Rotter, J. B. (1954). Social learning and clinical psychology. Prentice-Hall.
*Rahman Habeebul
Tan Tock Seng Hospital,
11 Jalan Tan Tock Seng,
Singapore 308433
Email: habeebul_rahman@ttsh.com.sg
Submitted: 16 July 2020
Accepted: 16 September 2020
Published online: 13 July, TAPS 2021, 6(3), 95-98
https://doi.org/10.29060/TAPS.2021-6-3/SC2342
Shin Ying Thng, Bao Yu Geraldine Leong, Guat Keng Yvonne Goh, Ching Ching Elaine Tan, Jimmy Kock Keng Goh & Kaibin Kelvin Kuan
Emergency Department, Changi General Hospital, Singapore
Abstract
Introduction: Singapore was one of the earliest countries affected by the COVID-19 outbreak, requiring our emergency department to respond urgently to this surge. A designated Fever Area (FA) with a resuscitation room was rapidly set up to manage patients at risk of COVID-19. Our paper describes measures put into this new area to optimise safety outcomes of these patients.
Methods: Plan-Do-Study-Act (PDSA) cycles incorporating in-situ simulation in the FA resuscitation room were conducted. Using varied resuscitation scenarios and facilitated debriefing, we identified safety gaps and took immediate steps to rectify them in a collaborative manner involving various respective stakeholders.
Results: Following reflective debriefing and studying of work processes, latent safety threats were identified resulting in successful improvements and modifications to protocols, equipment, staffing and processes in the FA resuscitation area.
Conclusion: PDSA cycles involving in-situ simulation helped to identify safety threats and refine work processes in a newly set up FA facility. As a result, our healthcare team was more prepared to manage the complexities of COVID-19 patients in a high-risk environment.
Keywords: Simulation, COVID-19, Medical Education
I. INTRODUCTION
Singapore was one of the first countries to be affected by the COVID-19 pandemic and has the highest number of Covid-19 cases in South East Asia to date. When the COVID-19 outbreak first reached Singapore, healthcare facilities had to prepare for a surge of patients with suspected or confirmed COVID-19. Our Emergency Department (ED) serves a 1006 bed hospital and sees an average of 400 patients daily pre-COVID-19. We were required to quickly reconfigure our space, equipment and staff. There was a need to segregate high risk or suspect COVID cases to be seen in a separate area in order to minimise cross-infection risks to our vulnerable patients. There was also a need to limit exposure of high-risk patients to a designated team of doctors and healthcare professionals in order to ensure continuity of services.
An area comprising the original admission transit area (with three isolation negative pressure rooms) and unused outpatient clinics next to the main ED underwent reconfiguration to become the new designated Fever Area (FA). This was to allow easy access to shared ED resources. The new FA had a combined capacity of 58 patients. Two FA resuscitation rooms were set up to cater for rapidly deteriorating patients that will require endotracheal intubation and resuscitation, both for COVID related complications as well as non-infectious related medical emergencies, such as an acute myocardial infarction or an acute surgical abdomen. Adequate resuscitation and stabilisation facilities in the FA were needed to minimise unnecessary movements of these infectious critically ill patients to the resuscitation area in the main ED, thus, decreasing the risk of cross-infection in other personnel.
The first few patient resuscitations conducted in the FA were challenging. There were many issues raised by the healthcare team concerning resuscitating and performing high-risk procedures in an unfamiliar environment. The FA team recognised an urgent need to improve system workflow competence in the FA resuscitation area. The healthcare team had to be shown that the improved FA resuscitation rooms were as well equipped as the main ED resuscitation area to handle critically ill patients and that such patients can be stabilized effectively there.
II. METHODS
In-situ simulation was the chosen modality as many of the difficulties encountered were systemic issues related to acute care in the unfamiliar FA resuscitation rooms and appropriate usage of Personal Protective Equipment (PPE) in such a scenario. In-situ simulation occurs where the case scenario is simulated in the actual clinical care area with real inter-professional teams instead of in an artificial setting in the simulation centre. By carrying out in-situ simulation, the team hoped to be able to recognise and remedy potential active failures and latent threats (Couto et al., 2018) present in the FA resuscitation rooms before any real-life adverse outcomes (Raemer et al., 2018) can occur.
Four emergency physicians and two nurse clinicians experienced in simulation design and debriefing conducted four in-situ simulation sessions with a high-fidelity mannequin in the FA (Dieckmann et al., 2020). Safety of all faculty, staff and patients were a priority and careful measures were taken to ensure participants and patients were not put at risk by simulating in-situ (Knight et al., 2018). Simulation sessions were conducted at the time of lowest patient load and all participants were outfitted in full PPE. They were also educated prior on potential safety hazards of in-situ simulation. Participant numbers for each simulation session were kept small at five to six with two facilitators.
The simulation scenarios, comprising of COVID-19 patients deteriorating from acute myocardial infarction, respiratory failure and cardiac arrest, were designed to challenge the complexities of adapting clinical management, manpower and equipment requirement and existing workflows to an infectious setting.
A multidisciplinary team comprising of eight nurses, six doctors and two radiographers involved in patient care at the FA participated in four simulation sessions held over two months. Verbal informed consent was taken from participants prior to simulation and confidentiality of participants was ensured. Centralised Institution Review Board (CIRB) review was submitted and waiver of consent was obtained. After each simulation scenario, formalised debriefing was carried out immediately, focusing on work process issues, communication failures and latent threats identified within the FA. Questions were crafted to guide participants to attain dialogical reflection and to move past a description of errors. They were encouraged to consider the implications of observations and come up with solutions for change using Fleck’s framework of reflection levels (Kihlgren et al., 2015).
The list of ideas generated was gathered and studied for common themes. A separate session was held where clinical, operational and administrative representatives brainstormed to find feasible and practical solutions to each problem identified. Immediate steps were taken to implement improvements and modifications to clinical protocols, equipment, staffing and workflows. Plan-Do-Study-Act (PDSA) quality improvement cycles were used to evaluate the improvements instituted after each simulation. This was carried out by a multidisciplinary team, comprising of medical, nursing and allied health staff.
III. RESULTS
The latent safety threats that surfaced were broadly categorised into five descriptive categories: Equipment, Organization, Staffing, Communication and Protocol (Refer to Table 1).
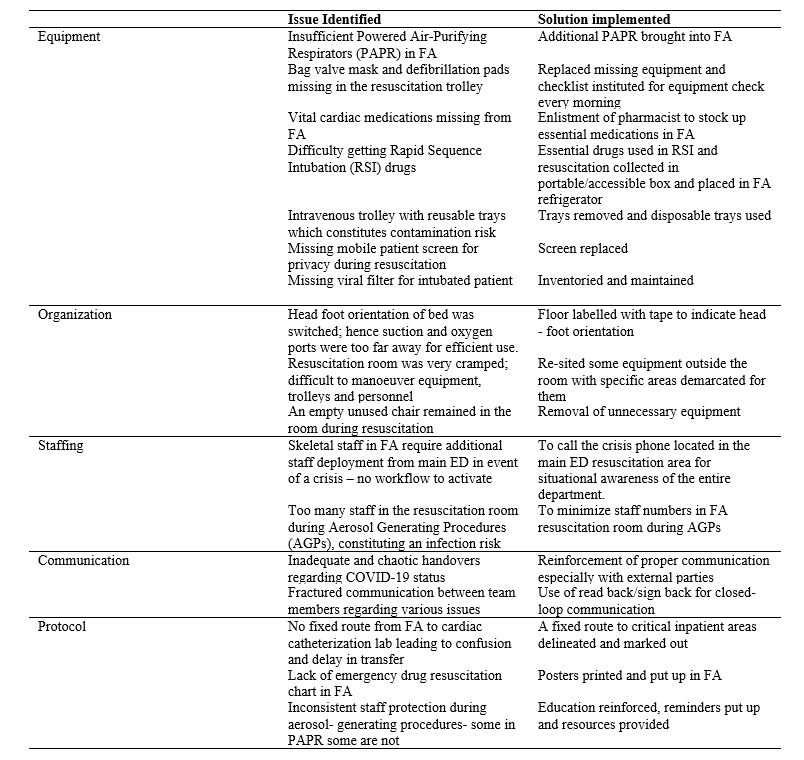
Table 1: Results
In-situ simulation uncovered the problems of insufficient Powered-Air Purifying Respirators (PAPR) and viral filters, as well as, missing defibrillator pads and bag valve masks from resuscitation trolleys. A checklist of essential equipment and medications was created with mandatory checks and re-stocking carried out by the FA nurses every morning. Medications vital for resuscitation were also found to be inadequate. A pharmacist was recruited to draw up and stock an essential list of drugs in the FA. Medications, which required refrigeration, were packed in a portable box so they could be easily brought to the FA resuscitation room from the fridge when required. Drug and resuscitation charts were put up as reminders and easy reference to improve patient safety.
Workspace organization issues that surfaced from in-situ simulation included the need to maintain patient privacy with mobile screens during resuscitation. Confusion over the head-foot orientation of the trolley bed resulted in suction and oxygen ports being too far for efficient use when it was placed in the wrong configuration. To correct this, the FA resuscitation room floor was labelled with tape indicating the proper orientation. The small FA resuscitation room area made manoeuvring equipment, trolleys and personnel difficult. Efforts were taken to re-site equipment to specific demarcated areas outside the FA resuscitation room, with the added benefit of reducing equipment contamination. A crisis phone was set up so that existing staff in FA could quickly call for additional staff deployment in event of a surge, thus improving communication and increasing situational awareness of the entire department to emergent needs at the FA.
Protocols were also adapted to the needs of the FA. During a resuscitation scenario, too many healthcare workers crowded into the room, raising a safety concern. It was protocolised that staff numbers should be minimized in the FA resuscitation room, especially during Aerosol Generating Procedures (AGP). PPE use was a barrier to communications, with “handovers” and “read back” being disrupted or unclear. The importance of adhering to these communication tools was reinforced. There was no fixed route identified for the transport of infectious patients to critical inpatient areas, thus, these were delineated so as to minimize confusion and decrease the infectious footprint, and risk of cross-infection to others. Staff protection during AGP was found to be inconsistent; hence PPE education was reinforced and educational resources provided to staff.
IV. CONCLUSION
Many issues were surfaced and lessons learnt via in-situ simulation, which allowed immediate risk mitigation to be carried out. Simple, immediate changes were made in FA with the available resources, resulting in improved patient and staff safety—which is especially important during surges due to the COVID-19 pandemic. We have successfully used in situ simulation with PDSA cycles to test and develop new facilities and protocols whilst managing the demands of a pandemic. Similar outcomes had also been demonstrated in other in-situ simulation studies. Using this modality to test pre-existing protocols and equipment in the FA resuscitation rooms offered an opportunity for the identification of potential threats and service gaps that would otherwise not have been detected as efficiently via conventional reporting systems (Knight et al., 2018). This method of PDSA testing is useful in the rapidly evolving COVID-19 situation, and may be replicated in other hospitals and regions safely when required. It ensures the safety of healthcare workers and actively improves patient safety despite the limitations of the pandemic.
A follow-up study to look at the usage of the FA resuscitation area, number of critically ill patients in the FA being transferred into the main ED resuscitation room, and patient morbidity and mortality data would be necessary to further determine the success of our intervention at a higher Kirkpatrick level of behavioural change to improve patient outcomes in the FA.
Notes on Contributors
Dr Elaine Tan carried out the literature search and instituted the changes. Dr Geraldine Leong ran the simulation, wrote the manuscript and instituted the changes. Dr Jimmy Goh set up the fever area, advised regarding the manuscript and instituted the changes. Dr Kelvin Kuan ran the simulation, wrote the manuscript and instituted the changes. Dr Thng Shin Ying designed the simulation, ran the simulation, and wrote the manuscript. Dr Yvonne Goh designed the simulation, ran the simulation and wrote the manuscript.
Ethical Approval
This study was exempted from CIRB review- 2020/2640.
Acknowledgements
The authors would like to acknowledge the staff of Changi Simulation Institute for their technical help and assistance with this project. We would also like to thank Dr Syahid Hassan for providing his expertise in the methodology of this project.
Funding
No funding was required.
Declaration of Interest
The authors state no conflict of interest.
References
Couto, T. B., Barreto, J. K. S., Marcon, F. C., Mafra, A. C. C. N., & Accorsi, T. A. D. (2018). Detecting latent safety threats in an interprofessional training that combines in situ simulation with task training in an emergency department. Advances in Simulation, 3(1), 23. https://doi.org/10.1186/s41077-018-0083-4
Dieckmann, P., Torgeirsen, K., Qvindesland, S. A., Thomas, L., Bushell, V., & Langli Ersdal, H. (2020). The use of simulation to prepare and improve responses to infectious disease outbreaks like COVID-19: Practical tips and resources from Norway, Denmark, and the UK. Advances in Simulation, 5, 3. https://doi.org/10.1186/s41077-020-00121-5
Kihlgren, P., Spanager, L., & Dieckmann, P. (2015). Investigating novice doctors’ reflections in debriefings after simulation scenarios. Medical Teacher, 37(5), 437-443. https://doi.org/10.3109/0142159X.2014.956054
Knight, P., MacGloin, H., Lane, M., Lofton, L., Desai, A., Haxby, E., Macrae, D., Korb, C., Mortimer, P., & Burmester, M. (2018). Mitigating latent threats identified through an embedded in situ simulation program and their comparison to patient safety incidents: A retrospective review. Frontiers in Pediatrics, 5, 281. https://doi.org/10.3389/fped.2017.00281
Raemer, D., Hannenberg, A., & Mullen, A. (2018). Simulation safety first: An imperative. Simulation in Healthcare, 13, 373-375. https://doi.org/10.1097/SIH.0000000000000341
*Thng Shin Ying
Changi General Hospital
2 Simei Street 3
Singapore, 529889
Email: thng.shin.ying@singhealth.com.sg
Submitted: 2 April 2020
Accepted: 3 June 2020
Published online: 5 January, TAPS 2021, 6(1), 109-113
https://doi.org/10.29060/TAPS.2021-6-1/SC2243
Wen Hao Chen1, Shairah Radzi1, Li Qi Chiu2, Wai Yee Yeong3, Sreenivasulu Reddy Mogali1
1Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore; 2Department of Emergency Medicine, Tan Tock Seng Hospital, Singapore; 3Singapore Centre for 3D Printing, School of Mechanical and Aerospace Engineering, Nanyang Technological University, Singapore
Abstract
Introduction: Simulation-based training has become a popular tool for chest tube training, but existing training modalities face inherent limitations. Cadaveric and animal models are limited by access and cost, while commercial models are often too costly for widespread use. Hence, medical educators seek a new modality for simulation-based instruction. 3D printing has seen growing applications in medicine, owing to its advantages in recreating anatomical detail using readily available medical images.
Methods: Anonymised computer tomography data of a patient’s thorax was processed using modelling software to create a printable model. Compared to a previous study, 3D printing was applied extensively to this task trainer. A mixture of fused deposition modelling and material jetting technology allowed us to introduce superior haptics while keeping costs low. Given material limitations, the chest wall thickness was reduced to preserve the ease of incision and dissection.
Results: The complete thoracostomy task trainer costs approximately SGD$130 (or USD$97), which is significantly cheaper compared to the average commercial task trainer. It requires approximately 118 hours of print time. The complete task trainer simulates the consistencies of ribs, intercostal muscles and skin.
Conclusion: By utilising multiple 3D printing technologies, this paper aims to outline an improved methodology to produce a 3D printed chest tube simulator. An accurate evaluation can only be carried out after we improve on the anatomical fidelity of this prototype. A 3D printed task trainer has great potential to provide sustainable simulation-based education in the future.
Keywords: Medical Education, Chest Tube, Thoracostomy, Simulation, 3D Printing
I. INTRODUCTION
Training opportunities in procedures such as chest tube insertions are increasingly limited amidst a growing population of trainees. Yet, the deliberate practice remains essential to improving proficiency and preventing possible complications such as lung parenchymal damage (Hernandez, El Khatib, Prokop, Zielinski, & Aho, 2018). Hence, many institutions have adopted simulation-based training to provide realistic training opportunities while mitigating harm to patients.
Cadaveric and animal models are limited by access and cost, and raise religious and ethical concerns (Kovacs, Levitan, & Sandeski, 2018). In addition, commercial models tend to be very costly (e.g. Trauma-Man® at USD~$25,000). As such, new modalities are desired.
Three-dimensional (3D) printing can accurately recreate anatomical details from imaging data through precision modelling and a wide range of compatible printing materials (Mogali et al., 2018). Together with its decreasing cost, it has become an attractive technology for creating inexpensive and anatomically accurate simulation modalities.
A previous study from the Federal University of Parana, Brazil (Bettega et al., 2019) outlined the development and evaluation of a low-cost chest tube simulator. The bony structures were 3D printed, while the remainder of the model was manually assembled using silicone sheets, foam pads, and balloons.
They compared 2 groups of participants using a porcine rib model, and their 3D printed simulator respectively. They found subjective improvements in confidence and safety amongst both groups and showed no difference between the objective grades. Hence, they concluded that their 3D printed simulator was equivalent to the animal model concerning the simulation of a chest tube placement.
However, there exist many other 3D printing technologies and materials, which can potentially be applied to create superior haptics and anatomical detail. Hence, this paper aims to outline a methodology of integrating multiple 3D printing modalities to create a cost-efficient 3D printed chest tube simulator.
II. METHODS
An anonymised computerized tomography (CT) file of a healthy human thorax (2.5 mm slices thickness) in Digital Communication in Medicine (DICOM) format was downloaded from the databank provided by 3D Slicer (https://www.slicer.org/, Version 4.10.2). The CT data was available freely for research and educational use at the time of this study.
3D Slicer was employed to segment the thoracic bony structures using a radiodensity based threshold algorithm, which traces the bone based on the Hounsfield units. Due to a lack of contrast possibly from the poor resolution of the CT images, we were not able to segment the respective soft tissue layers using thresholding. Hence, the intercostal muscles were manually drawn with the paintbrush function. Intrathoracic organs were all removed to create a central cavity. From initial experimentation, we found that incision and dissection were too difficult to perform if the task trainer was printed at the true thoracic thickness. Hence, a decision was made to thin out the chest wall. At the 4th and 5th intercostal space midaxillary line, the mean chest wall thickness is 39mm (Laan et al., 2016), but our model measured at 18mm at this corresponding anatomical landmark.
Further processing was done to smoothen the contours of the model (see Appendix, A). Subsequently, the anatomical structures were saved as stereolithography (STL) file and exported into Materialise Magics (Version 20 by Materialise, Belgium).
On Magics, cut and Boolean techniques were used to create the replaceable component. This space was demarcated by the 5th to 6th intercostal space, between anterior axillary to the mid axillary line. To create a secure fit for the replaceable piece, a groove was created and reinforced using the cut and punch function which generates teething to maximise friction. The main frame measured 23cm (length) x 19.5cm (width) x 23.5cm (height), while the replaceable part measured 9cm (length x 8.1cm (width) x 0.8cm (height). The Fix Wizard and Shrink Wrap Part functions were used to repair the surface mesh and eliminate holes and loose shells. The models were then exported using IdeaMaker® (Raise3D, USA) and uploaded to the printer.
The model was printed in two parts: the main frame was printed using fusion deposition modelling (FDM). This technology extrudes a continuous filament of melted thermoplastic, repeated by layer based on the design coordinates. Bones were printed with polylactic acid (PLA) which is a rigid material while the intercostal muscles were printed with thermoplastic urethane (TPU) which is a flexible material. Support was printed using PLA. We utilised a dual nozzle extrusion printer (Raise3D Pro 2, Raise3D, USA) to allow us to print the bony and soft tissue simultaneously, thereby increasing convenience. The following settings were used: printing speeds were reduced to 25mm/s, retraction of the TPU extrusion head was disabled, nozzle temperatures were set at 200°C, and build plate temperature was at 65°C. Post-print processing was done to remove the support, with subsequent filing and sanding.
The replaceable part was printed using Objet500 Connex 3 (Stratasys Ltd, Eden Prairie, MN), a multi-material printer utilising material jetting technology. This technology drops liquid photopolymers onto the build tray and simultaneously cures the material using UV light. As such, we can mix plastic and rubber to create hybrid consistencies (Mogali et al., 2018) of varying shore hardness. Two materials were selected to achieve the desired haptics: VeroWhite (FullCure, RGD835) was the stiff plastic photopolymer used for bones, while Tango Plus (FullCure, 930) was the rubber photopolymer used for simulating soft tissue. Support resin (FullCure, 706) was also used for printing. Post-printing processing was required to remove the support resin.
Skin coloured silicone sheets of 5 mm thickness were wrapped around the model using generic superglue. The task trainer was cable tied to stainless steel supports and screwed onto a laminated wood baseplate. Cut sponges were wrapped in duct tape to simulate the lung parenchyma and placed into the central cavity created.
III. RESULTS
The completed task trainer is shown in Figure 1. Both the main frame and replaceable piece provided simulation for the ribs, intercostal muscles, and skin.
The 3D thoracostomy task trainer costs approximately SGD$130 (or USD$97) (excluding manpower and printer cost)–see Appendix, B). The baseplate and mount were repurposed and did not add to costs.
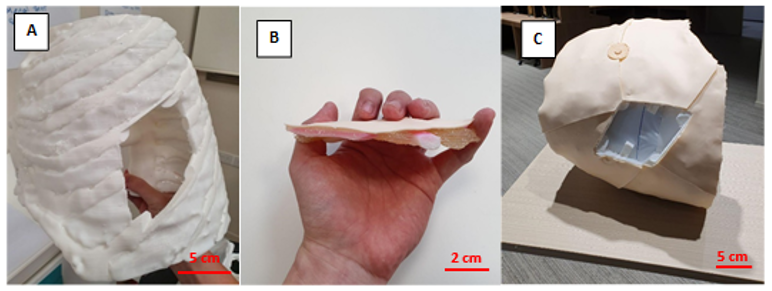
Note. A = completed hemithorax main frame using FDM printing; B= replaceable piece; C = task trainer without the replaceable piece. Figure 1. Photos of the completed task trainer
The main frame required 676g of polylactic acid and 114g of thermoplastic urethane. The replaceable piece required 30g of VeroWhite, 22g of Tango Plus, and 66g of Support706. It took a total of approximately 118 hours to print the entire task trainer.
IV. DISCUSSION
Our methodology addressed several issues with the model as outlined by the Brazilian team (Bettega et al., 2019). The proposed methodology here required less manual assembly of components, thereby saving time and improving fabrication. By utilising dual extrusion printing, construction was simplified while integrating an additional material for varying consistencies. The creation of a replaceable piece also meant long term savings in the cost of utilising this model. These logistical advantages would make it easier to adopt our proposed task trainer.
Secondly, simple materials such as foam pads and silicone sheets were inferior in simulating human tissue. Our utilisation of material jetting technology with the Objet500 Connex 3 (Stratasys Ltd, Eden Prairie, MN) printer allowed us to blend plastic and rubber materials to better recreate the consistency of human tissue. This technology and blend of materials have been extensively validated in other simulation models (Mogali et al., 2018).
Cost remains an important impedance to the widespread use of simulation in procedural education. We performed a surface comparison of our product against an existing commercial model in use by a local hospital in Singapore (LF03770U by Lifeform, NASCO, USA). The task trainer outlined here (~USD$97) is significantly cheaper than the commercial trainer (~USD$1,800). Also, our material blend provides superior haptics and bony structures in the replaceable component, as compared to a plain silicone insert in the Lifeform model. These should provide improvements in the quality and quantity of simulation opportunities for training physicians.
Unfortunately, we were not able to recreate the anatomical thickness of the thorax given our material limitations at the time of writing. This inaccurate depth of dissection creates a confounding variable when evaluating our task trainer against existing cadaveric or commercial simulators. Hence, an evaluation of this task trainer was withheld to address this limitation in our future prototype. Moving forward, we plan to invite physicians to validate the efficacy of our improved task trainer.
V. CONCLUSION
We have outlined the methodology for creating a 3D printed tube thoracostomy task trainer using a combination of printing technologies. The outlined task trainer could potentially provide superior haptics at a lower cost while improving fabrication. However, an equitable validation against an existing modality of simulation can only be done after we achieve a comparable anatomical fidelity.
In our continued search for sustainable simulation models, 3D printing shows great potential in reproducing anatomical detail with superior cost efficiency. The growing availability of 3D printing infrastructure makes the large-scale adoption of such task trainers ever more realistic. It makes it therefore worthwhile to invest in the creation of the perfect 3D printed task trainer.
Notes on Contributors
Mr. Wen Hao Chen is an undergraduate medical student with the Lee Kong Chian School of Medicine, Singapore. He was involved in the development of the task trainer, along with co-authoring the submitted manuscript.
Dr. Shairah Radzi is a research fellow with the Lee Kong Chian School of Medicine, Singapore. She was involved in the development of the task trainer, along with co-authoring the submitted manuscript.
Dr. Li Qi Chiu is a consultant physician in the Department of Emergency Medicine in Tan Tock Seng Hospital, Singapore. She was involved in the development of the task trainer, along with co-authoring the submitted manuscript.
Assoc. Prof Wai Yee Yeong is the Associate Chair (Students) of the School of Mechanical and Aerospace Engineering, Nanyang Technological University, Singapore. She was involved in the development of the task trainer, providing her technical expertise on the 3D printing process, along with co-authoring the submitted manuscript.
Asst. Prof Sreenivasulu Reddy Mogali is the Head of Anatomy and Principal Investigator in Clinical Anatomy and Medical Education at Lee Kong Chian School of Medicine, Singapore. He was involved in the development of the task trainer, along with co-authoring the submitted manuscript. He serves as the principal investigator.
Ethical Approval
Approved by Nanyang Technological University’s Institutional Review Board (2019-07-017). The CT scans used were anonymised and provided free for education and research use by 3D Slicer (https://www.slicer.org/, Version 4.10.2).
Acknowledgement
The authors thank the staff and faculty of the Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore for supporting this research; Singapore Centre for 3D Printing, Nanyang Technological University for their technical support.
Funding
This project was funded by the Ministry of Education Research Start-Up Grant, Lee Kong Chian School of Medicine, Nanyang Technological University Singapore.
Declaration of Interest
All authors declare no conflict of interest. The authors alone are responsible for the content and writing of the article.
References
Bettega, A. L., Brunello, L. F. S., Nazar, G. A., De-Luca, G. Y. E., Sarquis, L. M., Wiederkehr, H. de A., … Pimentel, S. K. (2019). Chest tube simulator: Development of low-cost model for training of physicians and medical students. Revista Do Colégio Brasileiro de Cirurgiões, 46(1). https://doi.org/10.1590/0100-6991e-20192011
Hernandez, M. C., El Khatib, M., Prokop, L., Zielinski, M. D., & Aho, J. M. (2018). Complications in Tube Thoracostomy: Systematic review and Meta-analysis. The Journal of Trauma and Acute Care Surgery, 85(2), 410–416. https://doi.org/10.1097/TA.0000000000001840
Kovacs, G., Levitan, R., & Sandeski, R. (2018). Clinical Cadavers as a Simulation Resource for Procedural Learning. AEM Education and Training, 2(3), 239–247. https://doi.org/10.1002/aet2.10103
Laan, D. V., Vu, T. D. N., Thiels, C. A., Pandian, T. K., Schiller, H. J., Murad, M. H., & Aho, J. M. (2016). Chest Wall Thickness and Decompression Failure: A Systematic Review and Meta-analysis Comparing Anatomic Locations in Needle Thoracostomy. Injury, 47(4), 797–804. https://doi.org/10.1016/j.injury.2015.11.045
Mogali, S. R., Yeong, W. Y., Tan, H. K. J., Tan, G. J. S., Abrahams, P. H., Zary, N., … Ferenczi, M. A. (2018). Evaluation by medical students of the educational value of multi-material and multi-colored three-dimensional printed models of the upper limb for anatomical education. Anatomical Sciences Education, 11(1), 54–64. https://doi.org/10.1002/ase.1703
*Sreenivasulu Reddy Mogali
11 Mandalay Road, Singapore 308232
Lee Kong Chian School of Medicine,
Nanyang Technological University
Email: sreenivasulu.reddy@ntu.edu.sg
Submitted: 17 April 2020
Accepted: 05 August 2020
Published online: 5 January, TAPS 2021, 6(1), 114-118
https://doi.org/10.29060/TAPS.2021-6-1/SC2358
Warren Fong1,3,4, Yu Heng Kwan2, Sungwon Yoon2, Jie Kie Phang1, Julian Thumboo1,2,4 & Swee Cheng Ng1
1Department of Rheumatology and Immunology, Singapore General Hospital, Singapore; 2Programme in Health Services and Systems Research, Duke-NUS Medical School, Singapore; 3Duke-NUS Medical School, Singapore; 4Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: This study aimed to examine the perception of faculty on the relevance, feasibility and comprehensiveness of the Professionalism Mini Evaluation Exercise (P-MEX) in the assessment of medical professionalism in residency programmes in an Asian postgraduate training centre.
Methods: Cross-sectional survey data was collected from faculty in 33 residency programmes. Items were deemed to be relevant to assessment of medical professionalism when at least 80% of the faculty gave a rating of ≥8 on a 0-10 numerical rating scale (0 representing not relevant, 10 representing very relevant). Feedback regarding the feasibility and comprehensiveness of the P-MEX assessment was also collected from the faculty through open-ended questions.
Results: In total, 555 faculty from 33 residency programmes participated in the survey. Of the 21 items in the P-MEX, 17 items were deemed to be relevant. For the remaining four items ‘maintained appropriate appearance’, ‘extended his/herself to meet patient needs’, ‘solicited feedback’, and ‘advocated on behalf of a patient’, the percentage of faculty who gave a rating of ≥8 was 78%, 75%, 74%, and 69% respectively. Of the 333 respondents to the open-ended question on feasibility, 34% (n=113) felt that there were too many questions in the P-MEX. Faculty also reported that assessments about ‘collegiality’ and ‘communication with empathy’ were missing in the current P-MEX.
Conclusion: The P-MEX is relevant and feasible for assessment of medical professionalism. There may be a need for greater emphasis on the assessment of collegiality and empathetic communication in the P-MEX.
Keywords: Professionalism, Singapore, Survey, Assessment
I. INTRODUCTION
Medical professionalism is one of the core Accreditation Council for Graduate Medical Education competencies and forms the basis of medicine’s contract with society. Unprofessional behaviour during training of junior doctors has been shown to result in future unprofessional behaviour. Assessment of professionalism not only allows for timely feedback to residents to help them improve, but also allows for development of better curriculum to prevent lapses in medical professionalism. The Professionalism Mini-Evaluation Exercise (P-MEX) had previously been identified as a potential observer-based assessment tool (Kwan et al., 2018), but it has not been validated in a multi-ethnic and multi-cultural Asian context such as Singapore. According to International Ottawa Conference Working Group on the Assessment of Professionalism, professionalism varies across cultural contexts, and therefore cross-cultural validation of the assessment tool for medical professionalism is imperative (Hodges et al., 2011). The current assessment tools adopted in local institutions may not cover the entire continuum of medical professionalism. For example, in the Ministry of Health Holdings (MOHH) C1 form which is currently being used for the assessment of residents on a 6-monthly basis, the assessment of professionalism is summative and consists of only three items (1) Accepts responsibility and follows through on tasks, (2) Responds to patient’s unique characteristics and needs equitably, (3) Demonstrates integrity and ethical behaviour.
We aimed to (1) examine faculty perception of the relevance of the P-MEX for assessment of medical professionalism in the local context, and (2) determine the feasibility and comprehensiveness of the P-MEX as an assessment tool for medical professionalism in Singapore.
II. METHODS
A. Design and Participants
We invited faculty in the SingHealth residency programmes to participate in the study by completing an online anonymous questionnaire in July 2018 to August 2018. Participants were given one week to complete the survey, with three reminder emails sent at one-week, two-weeks and one-month after the deadline for submission. SingHealth Centralised Institutional Review Board approved the conduct of this study (Reference Number: 2016/3009). Implied informed consent was provided by participants before completing the online anonymous questionnaire.
B. Survey Questionnaire
The P-MEX consists of four domains (Doctor-patient relationship skills, Reflective skills, Time management and Inter-professional relationship skills) and 21 sub-domains. Faculty were asked to rate the relevance of each item in P-MEX using a 0-10 numerical rating scale (0 representing not relevant, 10 representing very relevant). The faculty were also asked the following open-ended questions to determine the feasibility and comprehensiveness of the P-MEX- (1) “In your opinion, is a P-MEX form with 21 items too long, making it not feasible for routine use? If so, which items should be removed?” and (2) “In your opinion, are there any missing items (observable actions of a medical professional) that should be included in this form? If so, what new items should be added?” The questionnaire also included additional questions related to demographic characteristics (age, gender, specialty and number of years since becoming a specialist).
C. Analysis
Items were deemed to be relevant to the assessment of medical professionalism when at least 80% of the faculty gave a rating of ≥8. This was determined by expert judgement and prior literature (Avouac et al., 2011). For the open-ended questions on feasibility and comprehensiveness, responses were categorised and the number of the respondents who deemed the 21-item P-MEX to be not feasible (too long) or not comprehensive (there were missing items that should be included) are presented.
III. RESULTS
In total, 555 faculty from 33 residency programmes participated in the survey (response rate 44%). The respondents were 59% male, median age 43 years old, age ranged from 30 to 78 years old. Specialists from medical and surgical disciplines made up 39% and 27% of the respondents respectively, with the remaining respondents coming from diagnostic radiology/nuclear medicine, anaesthesiology, paediatrics and emergency medicine (12%, 11%, 6% and 5% of the respondents respectively).
A. Relevance
Of the 21 items in P-MEX, 17 items were deemed to be relevant (at least 80% of the faculty gave a rating of ≥8). For the remaining four items ‘maintained appropriate appearance’, ‘extended his/herself to meet patient needs’, ‘solicited feedback’, and ‘advocated on behalf of a patient’, the percentage of faculty who gave a rating of ≥8 was 78%, 75%, 74%, and 69% respectively (Figure 1).
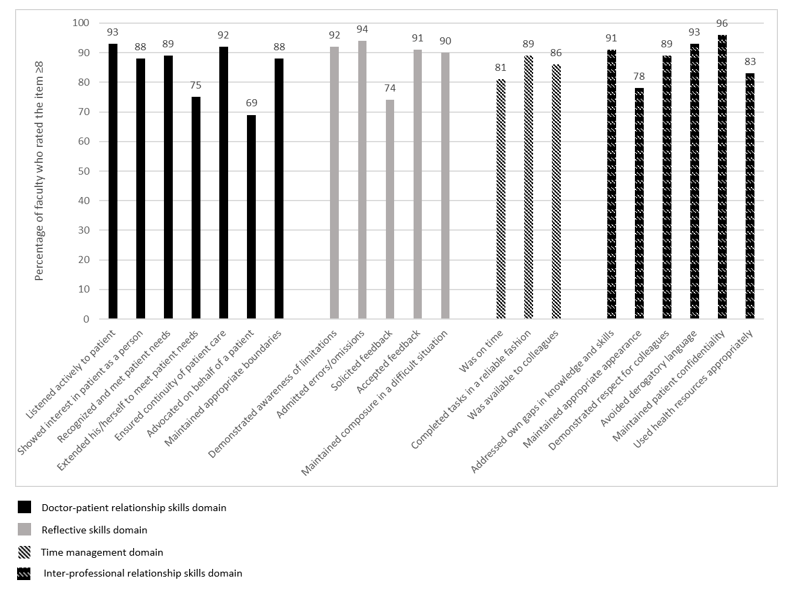
Figure 1: Percentage of faculty (n=555) who rated the item ≥8 on the relevance of the item in assessment of medical professionalism using a 0-10 numerical rating scale (0 representing not relevant, 10 representing very relevant).
B. Feasibility
There were 333 respondents for the question “In your opinion, is a P-MEX form with 21 items too long, making it not feasible for routine use? If so, which items should be removed?”, of which 34% (n=113) felt that there were too many questions in the P-MEX assessment form. The top four items chosen to be removed were “solicited feedback” (n=36), “extended his/herself to meet patient needs” (n=27), “advocated on behalf of a patient” (n=25), and “maintained appropriate appearance” (n=23). 208 (62%) respondents felt that the number of questions in the P-MEX assessment form was appropriate.
C. Comprehensiveness
There were 307 respondents to the question “In your opinion, are there any missing items (observable actions of a medical professional) that should be included in this form? If so, what new items should be added?”, of which 28% (n=85) faculty felt that there were missing items. The most frequently mentioned missing items were regarding assessment of ‘collegiality’ (n=54) and assessment of ‘communication with empathy’ (n=12).
Examples of ‘collegiality’ provided by faculty— “Collaboration with other healthcare professionals in the patients’ best interest”, “Demonstration of collaborative behaviour”
Examples of ‘communication with empathy ‘provided by faculty— “Communicate with empathy and effectively to patient and family, taking into account their level of understanding, education and socioeconomic background”, “Communication skills…should embrace empathy, listening skills, discretion, sensitivity and intelligence… sufficient information, counselling, planning and advice regarding medical condition and options.”
207 respondents (67%) felt that the P-MEX was comprehensive for the assessment of medical professionalism.
IV. DISCUSSION
This study provides preliminary evidence on the relevance, feasibility and comprehensiveness of the P-MEX in the assessment of medical professionalism in an Asian city state. The current study is part of a larger project to culturally adapt and validate the P-MEX. Based on our knowledge, this is the first study to explore the faculty perception on relevance, feasibility and comprehensiveness of the P-MEX in the assessment of medical professionalism in a multi-cultural and multi-ethnic context.
There were four items that were deemed to be less relevant (extended his/herself to meet patient needs, advocated on behalf of a patient, solicited feedback, maintained appropriate appearance). These findings were also similar in a validation study performed in Canada, where the items ‘extended his/herself to meet patient needs’ and ‘advocated on behalf of a patient’ were also frequently marked as ‘not applicable’, suggesting that the two items may be less relevant (Cruess, McIlroy, Cruess, Ginsburg, & Steinert, 2006). Qualitative methods can be used to explore the reasons why these items were deemed to be less relevant. About one-third of faculty felt that P-MEX was too long. Further study is warranted to evaluate the possibilities for shortening the P-MEX to reduce response burden and enhance routine use of the P-MEX.
In addition, our study revealed a need for greater emphasis on the assessment of collegiality. Some faculty felt that ‘collegiality’ was missing in the P-MEX despite the presence of items such as ‘demonstrated respect for colleagues’ and ‘avoided derogatory language’. This suggests that collegiality may encompass actions other than demonstrating respect and avoiding derogatory language in the local context, and further reinforces the emphasis of interprofessional collaborative practice.
Faculty also felt that there was also a lack of assessment of ‘communication with empathy’ in the P-MEX. The importance of empathetic communication is also supported by a study in Indonesia, a country in the same region, which found that patients considered communication as the most important attribute of medical professionalism (Sari, Prabandari, & Claramita, 2016).
This study has some limitations. The non-response rate raises concern about possible selection bias. Non-responders may have been less enthusiastic about the assessment of medical professionalism. Medical professionalism is affected by socio-cultural factors, therefore the findings from this study may not be entirely generalizable to another socio-cultural context. In addition, we were unable to elucidate the reasons for disagreement with the relevance of some of the items in the P-MEX as many faculty did not provide feedback and comments. Nevertheless, the findings of this study can serve as basis for future research, especially in countries with similar multicultural backgrounds.
V. CONCLUSION
Faculty agreed that most of the items in the P-MEX were relevant in the assessment of medical professionalism. Majority of the faculty also felt that the P-MEX was feasible to be used routinely in the assessment in medical professionalism. There may be a need for greater emphasis on the assessment of collegiality and communication with empathy in the modified P-MEX.
Notes on Contributors
Warren Fong reviewed the literature, designed the study, collected data, analysed data, and wrote manuscript. Yu Heng Kwan reviewed the literature, designed the study, collected data, analysed data, and wrote manuscript. Sungwon Yoon advised the design of study, analysed data, and gave critical feedback to the writing of manuscript. Jie Kie Phang collected data, analysed data, and wrote manuscript. Julian Thumboo advised the design of study, and gave critical feedback to the writing of manuscript. Swee Cheng Ng advised the design of study, collected data, analysed data, and gave critical feedback to the writing of manuscript. All authors have read and approved the final manuscript.
Ethical Approval
Ethical approval for this was granted by the SingHealth Institutional Review Board (Reference Number: 2016/3009).
Acknowledgement
The authors wish to thank all the study participants for contributing to this work.
Funding
This research was supported by SingHealth Duke-NUS Medicine Academic Clinical Programme Education Support Programme Grant (Reference Number: 03/FY2017/P2/03-A47). Funder was not involved in the design, delivery or submission of the research.
Declaration of Interest
The authors declare that they have no competing interests.
References
Avouac, J., Fransen, J., Walker, U., Riccieri, V., Smith, V., Muller, C., … Matucci-Cerinic, M. (2011). Preliminary criteria for the very early diagnosis of systemic sclerosis: Results of a Delphi Consensus Study from EULAR Scleroderma Trials and Research Group. Annals of the Rheumatic Diseases, 70(3), 476-481. doi:10.1136/ard.2010.136929
Cruess, R., McIlroy, J. H., Cruess, S., Ginsburg, S., & Steinert, Y. (2006). The professionalism mini-evaluation exercise: A preliminary investigation. Academic Medicine, 81(10), S74-S78.
Hodges, B. D., Ginsburg, S., Cruess, R., Cruess, S., Delport, R., Hafferty, F., . . . Ohbu, S. (2011). Assessment of professionalism: Recommendations from the Ottawa 2010 Conference. Medical Teacher, 33(5), 354-363.
Kwan, Y. H., Png, K., Phang, J. K., Leung, Y. Y., Goh, H., Seah, Y., . . . Lie, D. (2018). A systematic review of the quality and utility of observer-based instruments for assessing medical professionalism. Journal of Graduate Medical Education, 10(6), 629-638.
Sari, M. I., Prabandari, Y. S., & Claramita, M. (2016). Physicians’ professionalism at primary care facilities from patients’ perspective: The importance of doctors’ communication skills. Journal of Family Medicine and Primary Care, 5(1), 56-60. https://doi.org/10.4103/2249-4863.184624
*Warren Fong
SingHealth Rheumatology,
Senior Residency Programme,
20 College Road,
Singapore 169856
Tel: +6563214028
Email: warren.fong.w.s@singhealth.com.sg
Submitted: 17 March 2020
Accepted: 3 April 2020
Published online: 1 September, TAPS 2020, 5(3), 83-87
https://doi.org/10.29060/TAPS.2020-5-3/SC2238
Cristelle Chow1, Cynthia Lim2 & Koh Cheng Thoon3
1General Paediatrics Service, Department of Paediatrics, KK Women’s and Children’s Hospital, Singapore; 2Nursing Clinical Services, KK Women’s and Children’s Hospital, Singapore; 3Infectious Disease Service, Department of Paediatrics, KK Women’s and Children’s Hospital, Singapore
Abstract
Background: Effective communication between doctors and patients leads to better compliance, health outcomes and higher doctor and patient satisfaction. Although in-person communication skills training programs are effective, they require high resource utilisation and may provide variable learner experiences due to challenges in standardisation.
Objective: This study aimed to develop and implement an evidence-based, self-directed and interactive online communication skills training course to determine if the course would improve learner application of communication skills in real clinical encounters.
Methods: The course design utilised the Kalamazoo Consensus framework and included videos based on common paediatric clinical scenarios. Final year medical students in academic year 2017/2018 undergoing a two-week paediatric clerkship were divided into two groups. Both groups received standard clerkship educational experiences, but only the intervention group (88 out of 146 total students) was enrolled into the course. Caregiver/patient feedback based on students’ clinical communication was obtained, together with pre- and post-video scenario self-reported confidence levels and course feedback.
Results: There were minimal differences in patient feedback between intervention and control groups, but the control group was more likely to confirm caregivers’/patients’ agreement with management plans and provide a summary. However, caregivers/patients tended to feel more comfortable with the intervention compared to the control group. Median confidence levels increased post-video scenarios and learners reported gains in knowledge, attitudes and skills in paediatric-specific communication.
Conclusion: Although online video-based communication courses are useful standardisation teaching tools, complementation with on-the-job training is essential for learners to demonstrate effective communication.
Keywords: Online Learning, Undergraduate Medicine, Professionalism, Communication Skills, Patient Feedback
I. INTRODUCTION
Effective doctor-patient communication leads to better compliance, health outcomes and higher doctor and patient satisfaction. Online video-based communication skills courses can be feasible, with learners reporting increased confidence in key communication skills (Kemper, Foy, Wissow, & Shore, 2008). However, these evaluation methods have been limited to the Kirkpatrick levels of “reaction” and “learning”, instead of “behaviour” and “results”, which are more reflective of applied learning.
While in-person communication skills training programs simulate clinical environments, they can have inconsistent delivery because facilitators and standardised patients provide variable training experiences. In order to replace traditional role-play sessions, this study aimed to develop and implement a pilot online communication skills course to provide standardised, video-based scenarios in a self-directed interactive learning format using an evidence-based framework.
Our research questions are as follows:
- Would an online communication course improve the application of communication skills in real clinical encounters?
- What is the impact of an online communication course on learner-rated confidence levels in paediatric-specific clinical communication encounters?
- What are the self-reported aspects of learning that participants of an online communication course experience?
II. METHODS
This course design utilised the Kalamazoo Consensus framework (Makoul, 2001) which included the essential elements of clinical communication: Open the discussion, gather information, understand patient’s perspective, share information, reach agreement and provide closure.
Through Bandura’s social learning theory, people learn through observing others’ behaviour. The attitudes and outcomes of those behaviours then guide subsequent actions. This course therefore utilised videos featuring positive doctor-caregiver interactions, to encourage modelling through observation. The 3-5-minute video scenarios acted by practicing healthcare professionals were based on commonly encountered general paediatric clinical situations.
The course was designed using Articulate© software. “Pop-up” prompts highlighting important clinical or communication points, a pre- and post-test and in-video multiple-choice questions were included to increase learner engagement. To evaluate the impact of the course on learner-rated confidence levels, students were shown a clinical vignette, and asked to rate their self-confidence on a 4-point Likert scale before and after each video. Each video concluded with a summary, emphasising the utilisation of the Kalamazoo Consensus Framework.
|
Q1: Did the student introduce his/ her name? |
Q2: Did the student allow you to express your concerns? |
|
⃝ Yes ⃝ No ⃝ Not sure |
⃝ Yes, ALL my concerns ⃝ Not really, only SOME of my concerns ⃝ No, NONE of my concerns |
|
Q3: How much was the student interested in your point of view (e.g. expectations, ideas, beliefs, values) when he/she was asking you questions? |
Q4: How much was the student interested in your point of view (e.g. expectations, ideas, beliefs, values) when he/she was planning and explaining things? |
|
⃝ Very interested ⃝ Somewhat interested ⃝ Somewhat uninterested ⃝ Not interested at all |
⃝ Very interested ⃝ Somewhat interested ⃝ Somewhat uninterested ⃝ Not interested at all |
Q5: Did you feel that the student listened to you? |
Q6: How well do you feel the student explained things to you? |
|
⃝ Listened all the time ⃝ Listened sometimes ⃝ Did not listen at all |
⃝ Very well – I understood all the explanation ⃝ Fairly well – I understood some of the explanation ⃝ Not well at all – I did not understand all of the explanation |
|
Q7: Did the student check if you were agreeable with the management plan? |
Q8: Did the student provide a summary of the problem/ plans at the end of the conversation? |
|
⃝ Yes ⃝ No ⃝ Not sure |
⃝ Yes ⃝ No ⃝ Not sure
|
|
Q9: Overall, how comfortable were you interacting with the student? |
Q10: What do you think this student could improve in? E.g. Be more courteous/ respectful, speak or explain more clearly, listen more, check my understanding, answer my queries etc. |
|
⃝ Very comfortable – I would like to have him/ her be my/ my child’s doctor ⃝ Somewhat comfortable ⃝ Somewhat uncomfortable ⃝ Not comfortable at all – I do not want him/ her to be my/ my child’s doctor |
|
Table 1. Caregiver/Patient Feedback Form
To evaluate the self-reported learning points from the course, students were asked upon course completion to provide course feedback, including free-text completion of the phrase: “Things I have learnt include…” To evaluate whether the course improved the application of communication skills in real clinical encounters, caregiver/patient feedback was obtained towards the end of the paediatric clerkship for all students, regardless of course participation (Table 1). This form was modified based on course content from a family feedback instrument utilised in a paediatric setting (Zimmer, Solomon, Siberry, & Serwint, 2008). Implied informed consent was obtained from all participants.
Final year medical students from a five-year Singapore undergraduate medical program were enrolled over one academic year (2017/2018). Alternate batches (2nd, 4th, 6th, 8th) were enrolled into the course. Each student was provided a unique username and password for course access on any internet-enabled device throughout his/her 2-week paediatric clerkship and course participation was strongly recommended. Students from other batches (1st, 3rd, 5th, 7th) were analysed as controls. All students integrated into paediatric clinical teams, participated in ward rounds and communicated plans to patients/caregivers.
Statistical analysis was performed using SPSS© Statistics version 25.0 and chi-square analysis was used for patient feedback analysis.
This study was exempted from formal Centralized Institutional Review Board review and implied informed consent was granted by the SingHealth Centralized Institutional Review Board.
III. RESULTS
A total of 146 students were posted to the study institution in academic year 2017/2018 and 88 students were enrolled into the course. There were 80 (90.9%) attempts at the course, of which 76 (95%) students provided course feedback. The median time needed for course completion was 59 minutes. Patient feedback was successfully collected for 94 students, of which 44 (46.8%) attempted the course. Main reasons for unsuccessful collection were fast patient turnovers and patients/caregivers rejecting the request to provide feedback, usually due to perceived insufficient student contact time.
A. Application of Communication Skills – Evaluated via Patient Feedback
Although there were generally no differences in patient feedback between intervention and control groups, the control group was more likely to check with caregivers/patients whether they were agreeable with the management plan (76.0% vs. 56.8%, p<0.05) and provided a summary to the caregiver/patient (74.0% vs. 47.7%, p<0.05). Approaching statistical significance was the finding that caregivers/patients were more likely to feel very comfortable with the intervention compared to the control group (65.9% vs. 48.0%, p=0.062).
B. Course Impact on Self-Reported Confidence Levels
For scenario 1, the median confidence level increased from 3 (“somewhat confident”) to 4 (“very confident”). For the subsequent scenarios, this increased from 2 (“a little confident”) to 3 (“somewhat confident”).
C. Self-Reported Learning Points –Evaluated via Course Feedback
1) Knowledge: The majority of students mentioned learning about the clinical management and discharge advice for gastroenteritis and urinary tract infection, and the need for procedural sedation in uncooperative young children. Students reported that they had learnt general frameworks and principles for communication, and concepts of consent-taking. Students also frequently mentioned “practical”, in terms of “practical knowledge” and “practical tips” for communication.
2) Attitude: Students mentioned that they learnt about the importance of empathy. They also reported important aspects of patient-centred care, such as understanding the parent’s or patient’s perspective to formulate a treatment plan together and ensuring mutual understanding via “checking back to ensure the parent truly understands” and “to have a closed loop at the end of each communication”.
3) Skills: On a broader perspective, students described that they had learnt “how to properly structure communication with a patient’s parents” and “how to better communicate with parents using the various strategies”. Almost all students reflected that they had learnt specific communication skills, particularly with regards to dealing with challenging situations such as “how to approach parents who may not be cooperative/willing to listen to you” and “how to address angry parents” as well as “how to address their concerns and manage their expectations”. Two students also mentioned that they may not have been exposed to similar scenarios in their daily work: “… handle scenarios which are often not taught within lectures.”
IV. DISCUSSION
Computer-based communication courses have shown to improve students’ self-efficacy in performing communication tasks and assessments of students’ perceptions and practice of communication skills (Kemper et al., 2008), which was also demonstrated in this study’s improvement in self-reported confidence levels. It is however, expected that most students would experience increased confidence immediately after receiving new information about an unfamiliar topic.
This study provides an example of how a course that is traditionally delivered face-to-face can be designed to be delivered online, utilising less time and manpower resources while providing standardised teaching instruction in an evidence-based manner.
The qualitative findings in this study have not been replicated elsewhere, and provide an interesting perspective to student course perception. Students gained practical knowledge which is not readily available in clinical clerkships due to patient case variability and gained insight into an applicable framework for future clinical communication encounters. It is possible that the interactive nature of the course increased student presence and participation, resulting in improved learning outcomes in this aspect (Ammenwerth et al., 2019). Empathy, an important professional skill not easily taught but reflected as a learning point, was likely acquired through non-verbal communication demonstrated in the videos. Although it is not guaranteed that self-reported knowledge, skills and attitudes will translate into practice, future e-learning communication courses can be designed as pre-course material for traditional role-play facilitators to enhance learning experiences.
This study’s use of patient feedback provides unique insight into applied learning. Interestingly, the control group fared better in the actions of checking with caregivers/patients about management plan agreement and providing caregivers/patients with a summary. As clerkships also provide opportunities to observe healthcare professionals conducting clinical communication, it is likely that the control group learnt these behaviours from real-life encounters. Caregivers/patients tended to feel more comfortable with the intervention group, which could be explained through unmeasurable, subtle behaviours that the group may have learnt from the course, such as empathy, attentiveness and appropriate body language. Although the use of standardised patients for comparing both groups might have shown different results, it is known that how learners behave in the classroom and with real patients when unobserved is often less reflective of true workplace behaviours (Malhotra et al., 2009).
This study is limited by small participant and patient feedback numbers. Culturally, many patients forget their healthcare providers and experiences. An ideal situation would be direct clinical encounter observation, but due to the Hawthorne effect, a less truthful version of student behaviour may be observed instead.
V. CONCLUSION
Although online video-based communication courses can be used as a standardised teaching tool to improve student self-reported confidence levels and self-perceived knowledge, skills and attitudes, it remains to be proven if they can result in a change in student behaviour. It is likely that on-the-job experiences also contribute to their ability to demonstrate effective communication, which supports the supplementation, rather than the replacement of such practical experiences with online video-based course material.
Notes on Contributors
CC, CL and TKC contributed to the conception and design of the work. CC, CL and TKC also analysed data and drafted the work . CC, CL and TKC approved the final published version and are agreeable to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. CC, CL and TKC collectively contributed equally to this paper.
Ethical Approval
This study was exempted from formal Centralized Institutional Review Board review by the SingHealth Centralized Institutional Review Board (CIRB Ref: 2017/2178).
Acknowledgements
The authors would like to acknowledge the SingHealth Paediatrics Academic Clinical Programme in providing the grant funding for this project.
Funding
The study was funded by the SingHealth Paediatrics Academic Clinical Programme Tan Cheng Lim Fund Grant which was awarded in 2017 (Grant Reference: PAEDACP-TCL/2017/EDU/001).
Declaration of Interest
All authors disclose that there are no potential conflicts of interest, including financial, consultant, institutional and other relationships that could have direct or potential influence or impart bias on the work.
References
Ammenwerth. E., Hackl, W. O., Dornauer, V., Felderer, M., Hoerbst, A., Nantschev, R., & Netzer, M. (2019). Impact of students’ presence and course participation on learning outcome in co-operative online-based courses. Studies in Health Technology and Informatics, 262, 87-90.
Kemper, K. J., Foy, J. M., Wissow, L., & Shore, S. (2008). Enhancing communication skills for paediatric visits through on-line training using video demonstrations. BMC Medical Education, 8, 8.
Makoul, G. (2001). Essential elements of communication in medical encounters: the Kalamazoo consensus statement. Academic Medicine, 76(4), 390-393.
Malhotra, A., Gregory, I., Darvill, E., Goble, E., Pryce-Roberts, A., Lundberg, K., & Hafstad, H. (2009). Mind the gap: Learners’ perspectives on what they learn in communication compared to how they and others behave in the real world. Patient Education and Counseling, 76(3), 385-90.
Zimmer, K. P., Solomon, B. S., Siberry, G. K., & Serwint, J. R. (2008). Continuity-structured clinical observations: assessing the multiple-observer evaluation in a pae1diatric resident continuity clinic. Pediatrics, 121(6), e1633-1645.
*Cristelle Chow
Department of Paediatrics,
KK Women’s and Children’s Hospital
100 Bukit Timah Road,
Singapore 229899
Email: cristelle.chow.ct@singhealth.com.sg
Published online: 5 May, TAPS 2020, 5(2), 41-44
https://doi.org/10.29060/TAPS.2020-5-2/SC2134
Sok Mui May Lim1,2, Zi An Galvyn Goh2 & Bhing Leet Tan1
1Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore; 2Centre for Learning Environment and Assessment Development (CoLEAD), Singapore Institute of Technology, Singapore
Abstract
The use of standardised patients has become integral in the contemporary healthcare and medical education sector, with ongoing discussion on exploring ways to improve existing standardised patient programs. One potentially untapped group in society that may contribute to such programs are persons with disabilities. Persons with disabilities have journeyed through the healthcare system, from injury to post-rehabilitation, and can provide inputs based on their experiences beyond their conditions. This paper draws on our experiences gained from a two-phase experiential learning research project that involved occupational therapy students learning from persons with disabilities. This paper aims to provide eight highly feasible, systematic tips to involve persons with disabilities as standardised patients for assessments and practical lessons. We highlight the importance of considering persons with disabilities when they are in their role of standardised patients as paid co-workers rather than volunteers or patients. This partnership between persons with disabilities and educators should be viewed as a reciprocally beneficial one whereby the university and the disability community learn from one another.
Keywords: Standardised Patients, Objective Structured Clinical Examination (OSCE), Persons with Disabilities, Inclusion, Role-play, Script, Practical Lessons
I. INTRODUCTION
The use of standardised patients (SPs) has become integral to the contemporary healthcare and medical education sector. While an SP is commonly defined as a person trained to portray a scenario, an SP can also be an actual patient using his or her own history and physical exam findings (Kowitlawakul, Chow, Salam, & Ignacio, 2015). Presently, persons with disability (PWDs) have participated in SP programs, albeit less frequently and on a smaller scale (Long-Bellil et al., 2011; Minihan et al., 2004; Wells, Byron, McMullen, & Birchall, 2002). SPs with disabilities have also been used in Singapore hospitals, but mainly as patients to be examined for their own medical conditions. PWDs have a lot to offer in clinical education beyond sharing about their conditions.
A. Why Incorporate Persons with Disabilities into SP Programs?
There are many benefits in involving PWDs in SP programs. PWDs may be able to impart knowledge that ‘goes beyond the textbook’, due to their experiences of receiving services from various healthcare professionals – from the time the disability occurred to the post-rehabilitation phase of living independently in society. The input given based on their individual experiences would, therefore, be authentic (Wells et al., 2002). Students can get practice working with real PWDs in a safe setting where they can make mistakes and receive feedback before going for their clinical placements and meeting with real patients (Minihan et al., 2004). This can nurture a new generation of healthcare professionals who may be more proficient in treating PWDs, thereby raising the service delivery standard for the entire sector.
B. Perspectives Gained From Previous Experiential Learning Project
This paper is based on our experiences gained from a previous experiential learning research project. PWDs participated in a two-phase experiential learning research project that spanned two years (Lim, Tan, Lim, & Goh, 2018). In phase one, the PWDs acted as community teachers to occupational therapy student groups, interacting with them in the community while performing their daily activities. This paper draws from our experiences in Phase Two of the study, in which a group of PWDs were trained to and worked as SPs in practical classes and Objective Structured Clinical Examinations (OSCEs). Upon the conclusion of the research project, PWDs continue to be part of the degree programme contributing as community teachers and SPs. The paper aims to provide practical helpful tips in bringing PWDs onboard as SPs.
II. DISCUSSION
A. Tip 1 – Interviewing and Selecting PWDs Who Are Suitable for Acting
PWDs were selected based on six criteria determined by faculty members in the health profession who have prior experience working with SPs. First, the PWD has an interest in healthcare education and wants to work with students for the purpose of educating them as future healthcare professionals. Second, the PWD should have come to terms and accepted their disability. It is very difficult for them to talk about their disability or role-play as a patient when they are still struggling emotionally with their own conditions. Third, the PWD does not have cognitive impairment and is able to understand and remember the script for role-playing. Fourth, he/she must be able to communicate clearly and coherently. Fifth, the PWD should be willing to learn the basics of acting or role-playing. Sixth, he/she must understand the objectives of the training or assessment, such as being impartial to all students and being honest in giving feedback when required.
B. Tip 2 – Training Should Be Conducted in Gradual Phases
Training PWDs as SPs can be carried out in a gradual phase as outlined in details in Figure 1. In the first phase, novice PWD SPs are taught the basics of role-play by faculty and experienced SPs. In the second phase, the entire group goes through a common script. Novice PWD SPs observe the faculty and experienced SPs enact the script. Then, the novice PWD SPs practice amongst themselves and receive feedback.
After the training, faculty should speak to the PWDs individually to determine if they are comfortable with role-playing and address any queries that they may have. It is only after they attempt the role of an SP that they can personally assess their comfort level and confidence. This can ensure that the PWDs who participate are comfortable with their roles and feel engaged and respected by the institution.
In the third phase, PWD SPs can progress to non-graded practical lessons with students, which are less stressful for both students and PWD SPs. In subsequent phases, the faculty can then decide to select PWD SPs whom they deem are ready for summative assessments such as the OSCE.
C. Tip 3 – Start Novice PWD SPs with Simple and Suitable Scripts
Initial scripts should be simple and should not require complex acting skills. It takes time to gain confidence in memorising required lines, maintaining their roles as well as acting in scenarios which require more expression of emotions. Scripts that involve more sophisticated acting skills (e.g., maintenance of strong emotions) should be reserved for SPs who are experienced and confident with acting. The PWD SPs should be matched to suitable scripts that do not conflict with their disability. For example, a PWD SP who uses a wheelchair cannot be paired with a script that involves walking. The combination of progressing gradually and usage of suitable scripts allows for PWD SPs to refine their skills and ensure that their acting skills do not compromise the students’ learning experience.
D. Tip 4 – Prepare Students Not to Be Surprised By Real Disability
Prior to the interaction session, students should be pre-empted by the faculty that they would be working with PWDs who may have a range of disabilities. This is to prevent unnecessary surprise. In addition, students should be reminded that the disability may or may not be the focus of the scenario, depending on the instruction given to the student. For example, in an OSCE scenario, students may be tasked to explain a medical error or demonstrate a procedural skill instead of addressing the disability of the SP. This pre-empting can be complemented with teaching communication skills geared towards interacting with PWDs.
E. Tip 5 – Checking Accessibility – Within and Outside of the Venue
Ensuring accessibility prior to the session is important. This includes the route from the nearest public transport node (e.g., train station) to the venue. Things to take note of are the availability of ramps and lifts for wheelchair users and the presence of accessible parking lots. In addition, the venue where the lesson or assessment is going to take place needs to be inspected to ensure that the entrances and exits are wide enough for wheelchairs access.
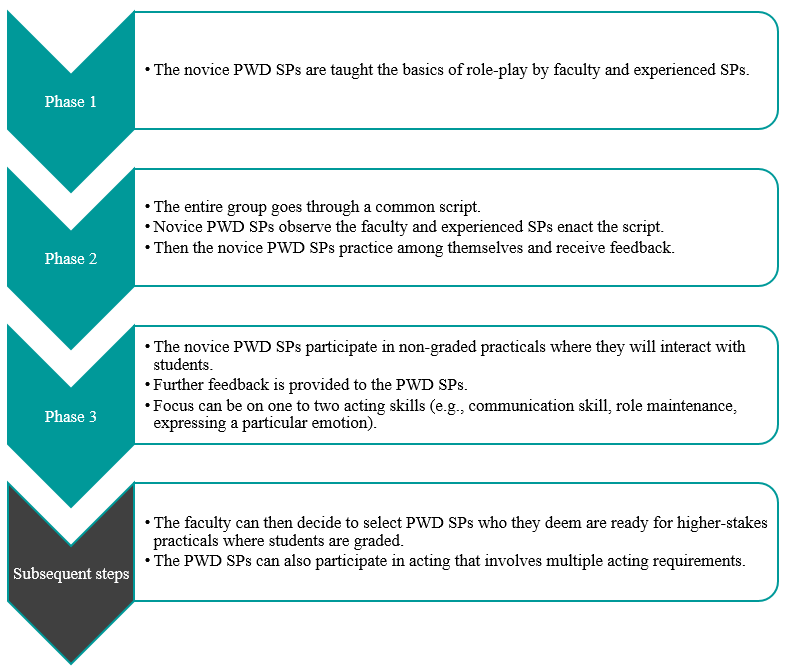
Figure 1. Diagram to outline general recommended steps for training PWD SPs
F. Tip 6 – Pay PWDs at Market Rates and Accord Them Identical Contractual Rights
PWD SPs should be remunerated at market rates that are equal to SPs without disability. They also sign the same SP contract and fulfil the same legal obligations. In performing the role of the SP, they are treated as co-workers of the university, not volunteers or patients. This reflects the principles of equality and diversity, as well as the seriousness of their roles as active members of the healthcare and medical education system. If there are certain risks involved in their interaction with students, such risks should be made clear to the PWD SPs, so they can make an informed decision on accepting the job.
G. Tip 7 – Provide Opportunity for PWDs to Give Feedback
PWDs can be a valuable resource in providing feedback to faculty, scenario developers and other SPs. Similarly, they may be able to give insightful feedback to students. It is important to train the PWD SPs on the methods of providing feedback to students. Given their lived experience, they can provide insight into how real patients would respond and react while suggesting ways for trainee healthcare professionals to respond in a more patient-centred manner.
H. Tip 8 – Reflect and Improve
Carrying out an evaluation with the respective stakeholders, whether they are PWD SPs, faculty, or students, is key to the success of an inclusive SP program. This can also ensure quality assurance of the program. The following are several broad questions which can be considered in the evaluation. Firstly, whether the stakeholder faced any challenges during the session. Secondly, whether the scenarios or scripts worked well for PWD SPs to interact with students. Thirdly, whether there are any other ways that the learning experience can be improved. This can provide rich data for the SP program developers to reflect and improve upon the pedagogy. We have received positive feedback from both students and PWDs in this project.
III. CONCLUSION
It is important to empower PWDs and create a dynamic relationship between them and healthcare professionals/
educators. For an inclusive SP program to be effective, educators must change their own mindset about PWDs. We have to switch the lens from viewing them as patients to co-workers. This partnership should be viewed as a reciprocally beneficial one whereby the university and the disability community learn from one another. Through the process of engagement, both educators and students learn from PWD SPs about knowledge that goes beyond the textbook, and the factors that enhance or diminish the quality of healthcare/medical service delivery from individuals who have experienced going through the healthcare/medical system. With time and with more training institutions engaging PWDs as SPs, this can be a potentially viable employment option for PWDs.
Notes on Contributors
Associate Professor May Lim is the Director of the Centre for Learning Environment and Assessment Development (CoLEAD) at the Singapore Institute of Technology, and a faculty in the Health and Social Sciences Cluster teaching occupational therapy.
At the time when this work was done, Mr Goh Zi An Galvyn was a research assistant in the Centre for Learning Environment and Assessment Development (CoLEAD) at the Singapore Institute of Technology.
Associate Professor Tan Bhing Leet is the Deputy Cluster Director (Applied Learning) of the Health and Social Sciences Cluster, and Programme Director of the Bachelor of Science in Occupational Therapy degree programme at the Singapore Institute of Technology.
Ethical Approval
Ethics approval was granted by the Singapore Institute of Technology Institutional Review Board for this project (IRB number: 20150002).
Acknowledgements
The authors thank all faculty, students, PWD and non-PWD standardised patients who were involved in the Singapore Institute of Technology Bachelor of Science in Occupational Therapy degree programme. In addition, we would like to extend our deepest gratitude to Associate Professor Tham Kum Ying, Education Director of Tan Tock Seng Hospital Pre-Professional Education Office and senior lecturers Miss Heidi Tan and Mr Lim Hua Beng from the Singapore Institute of Technology.
Funding
Funding was provided from the Singapore Ministry of Education (MOE Tertiary Education Research Fund grant: R-MOE-A203-A002).
Declaration of Interest
The authors declare no conflict of interest concerning any aspect of this research.
References
Kowitlawakul, Y., Chow, Y., Salam, Z., & Ignacio, J. (2015). Exploring the use of standardized patients for simulation-based learning in preparing advanced practice nurses. Nurse Education Today, 35(7), 894-899. https://doi.org/10.1016/j.nedt.2015.03.004
Lim, S. M., Tan, B. L., Lim, H. B., & Goh, Z. A. G. (2018). Engaging persons with disabilities as community teachers for experiential learning in occupational therapy education. Hong Kong Journal of Occupational Therapy, 31(1), 36-45. https://doi.org/10.1177/1569186118783877
Long-Bellil, L. M., Robey, K. L., Graham, C. L., Minihan, P. M., Smeltzer, S. C., Kahn, P., & Alliance for Disability in Health Care Education. (2011). Teaching medical students about disability: The use of standardized patients. Academic Medicine, 86(9), 1163-1170. https://doi.org/10.1097/ACM.0b013e318226b5dc
Minihan, P. M., Bradshaw, Y. S., Long, L. M., Altman, W., Perduta-Fulginiti, S., Ector, J., … Sneirson, R. (2004). Teaching about disability: Involving patients with disabilities as medical educators. Disability Studies Quarterly, 24(4). https://doi.org/10.18061/dsq.v24i4.883
Wells, T. P. E., Byron, M. A., McMullen, S. H. P., & Birchall, M. A. (2002). Disability teaching for medical students: Disabled people contribute to curriculum development. Medical Education, 36(8), 788-790. https://onlinelibrary.wiley.com/doi/abs/10.1046/j.1365-2923.2002.01264_1.x
*Lim Sok Mui
Singapore Institute of Technology,
SIT@Dover, 10 Dover Drive,
Singapore 138683
Email: may.lim@singaporetech.edu.sg
Published online: 1 June, TAPS 2016, 1(1), 23-25
DOI: https://doi.org/10.29060/TAPS.2016-1-1/SC1009
Richard Hays
University of Tasmania, Australia
Abstract
A curriculum is an important component of a medical program because it is the source of information that learners, teachers and external stakeholders use to understand what learners will experience on their journey to recognition as a medical graduate. While many focus on and debate the content of a medical curriculum, with some suggestions that there should be national curricula for each jurisdiction or even a global curriculum for all medical programs, the curriculum content is only one factor to consider when designing, revising or accrediting a curriculum. Just as important are the alignment with the program’s mission and health workforce needs, the presence of agreed graduate outcomes, the theoretical bases of the curriculum, the prior learning of commencing students, the curriculum implementation models, the assessment of student progress and program evaluation processes. This paper presents a framework for this more holistic approach to reviewing a curriculum, proposing triangulation of information from several sources – documents, websites, learners, teachers and employers – and considering several accreditation standards that impact on curriculum design and delivery.
Keywords: Curriculum design; curriculum review; accreditation; social accountability; program evaluation
I. BACKGROUND
In medical education the curriculum defines medical programs, guides the teaching by faculty and informs the learning by students of what is required to become a doctor. For basic medical education, the outcome is recognition as a novice practitioner, and for subsequent levels there are more specific outcomes related to particular specialties. The term ‘curriculum’ is defined in the Oxford Dictionary as ‘the subjects comprising a course of study in a school or college’, which suggests an emphasis on the content, whereas learning may depend significantly on how the content is delivered, learned and assessed.
The pace of medical curriculum review has increased globally due to several factors. Several new medical programs have been established, based on growing populations and rising health care standards, particularly in developing nations. Whether purchased from existing institutions or developed locally, new curricula have to be designed and most new programs face either mandatory or voluntary accreditation processes. Demographics are changing, particularly in developed nations, where the population is ageing and living with increasingly complex and chronic health care needs, requiring a larger and differently trained medical workforce (Duckett, 2005). Many universities are seeking efficiencies in program delivery, because the small group, clinician-led models preferred in medical education are expensive; leaders ask, perhaps not unreasonably, why medical education cannot be provided as effectively by less expensive methods, such as large group lectures supported by on-line resources and more junior faculty. We find ourselves in what might be termed a ‘post-PBL’ environment, where PBL programs have been criticised for gaps or lack of depth in anatomy, pathology and other foundation sciences, even though PBL models were developed in part to address the rapid increase in the knowledge base for medical practice, promoting peer-supported and self-directed learning (Dolmans et al, 2005). Can coping with this knowledge explosion be done differently?
Employers find that some medical graduates are not yet ‘work ready’, able to take responsibility for their actions or contribute to safe patient care without (ex-pensive) supervision and further training. Finally, regulators are becoming more vocal about challenges to the commonly used self-regulation model for the medical profession, amidst increasing complaints and concerns about competence and errors. Although most of these concerns relate to communication skills and professional behaviours of a small minority, regulators are increasing requirements for standards to be met by medical graduates outside of the traditional scientific knowledge domains. As a result, there are increasing requirements for accreditation or formal recognition of medical programs by regulatory authorities to ensure that programs produce the graduates needed to provide medical care. Arguably, the strongest accreditation systems are conducted by the General Medical Council for the UK, the Australian Medical Council for Australia and New Zealand, and the Liaison Committee for Medical Education (USA and Canada), but many other jurisdictions have, or are developing, strong accreditation processes. There are also global standards developed and promoted by the World Federation of Medical Education (WFME), which map reasonably well to most standards. While the World Federation of Medical Education is not an accrediting body, there are moves to mandate that accreditation standards and processes must comply with the WFME global standards for graduates to be eligible for recognition across jurisdictional borders (Karle, 2006).
There are therefore two broad categories of curriculum review. The first is that conducted by medical schools, new and old, to develop, maintain or refresh curricula that are current and fit for purpose. This should be a continuous process, with changes based on some kind of evidence, ideally evaluation data. The second category is that conducted by regulatory bodies during accreditation processes, in which the curriculum is always a major focus. For both categories, a broader, more holistic view of a curriculum, rather than just content, should be adopted. This means that a curriculum review should seek information or data from much more than just descriptions of the subject content. This paper presents a framework for achieving this more holistic approach.
II. METHOD
This paper is based on an analysis of the structure of standards and accreditation protocols of the General Medical Council, the Australian Medical Council, the Liaison Committee for Medical Education and the World Federation for Medical Education. In each case medical programs are measured against several standards, where only one standard might specifically address curriculum content, but other standards address delivery, assessment and evaluation. Sources of evidence for a curriculum review may therefore be found when considering almost all standards.
A. A framework for reviewing a medical curriculum
Although a curriculum should be well described in writing, such documents are a single source of information about what is intended. Judgements about curriculum content and process are best made through triangulation of information and data from a combination of potential sources that reflect a wide range of issues, as summarised in Table 1. Most of these sources should be readily accessible, although requires both electronic access (through a guest log in account) and a physical visit to inspect the facilities. Further information, particularly about implementation, can be obtained through observation of aspects of program delivery, such as teaching sessions and clinical examinations.
Constructive alignment of a curriculum, from the vision and mission through curriculum delivery and assessment, is important because it demonstrates that the curriculum is a more holistic, ‘connected’ entity. It shows that curriculum content, process and intended outcomes are planned and designed with an explicit intention to produce a particular kind of graduate. Ideally, the outcomes are the same as those of the accreditation body, although many schools will add some of their own. For example, while all schools in a particular jurisdiction may plan to produce ‘work ready’ graduates safe to enter postgraduate training, some may have additional outcomes relating to elite research performance or to meeting the needs of underserved populations, following the growing international trend towards social accountability (Boelen and Woollard, 2009).
There should be evidence of purposeful, theory-based educational design (Prideaux, 2003). There is a spectrum of pedagogical models, from separate subjects delivered to large groups by lectures, through to highly integrated (vertically and horizontally) programs delivered through interactive, small groups, following a case-based or problem-based learning model. While educators may have a preference for a particular model, all can work, so long as the content, delivery and assessment methods are done well. It is important to design the curriculum content and process to match the learners’ characteristics at entry. For example, school leaver programs tend to be longer and to have adjustment to university life and introductory foundation sciences early, followed by more integrated, clinically-immersed learning, whereas graduate entry programs commence with an assumption that students are ready to commence with the more integrated, clinically-oriented approach.
An additional consideration is cohort size, because interactive, small group models are difficult to deliver unless group size is appropriate (8-10 maximum?). This has implications for the physical facilities and intranet-based Learning Management System (LMS), because small group, interactive learning required larger numbers of tutorial rooms that are appropriately furnished and equipped, and accessible, flexible and interactive repositories of electronic learning resources.
Ideally, all learning outcomes are measurable – this may be a matter of wording – and then form the basis of assessment practices, such as method selection, blueprinting, item bank development and standard setting. It is important that an integrated curriculum has integrated assessment, otherwise students may focus on non-integrated sources (a ‘hidden curriculum’) rather than the curriculum. Finally, there should be evidence of evaluation processes that monitor the curriculum content and delivery. A medical curriculum should be a continuously evolving entity, with decisions for change based on the best available evidence. Such evidence may come from both the routine, annual or semester-based program-wide data on participation, and the more reflexive and exploration of specific questions or concerns that arise during academic years. There should be evidence of evaluation feedback being formally considered, with decisions to make changes and then evidence that the change has taken place and participants advised of the results of the evaluation.
|
Curriculum feature |
Information | sources | ||||||
|
Website /LMS |
Program outline | Unit/subject outlines | Assessment reports* | Faculty | Students* | Stakeholders |
Facilities Tour |
|
| Aligned with Vision & Mission | √ | √ | √ | √ | ||||
| Measurable graduate outcomes | √ | √ | √ | √ | √ | |||
| Purposeful design | √ | √ | √ | √ | ||||
| Appropriate for admission point | √ | √ | √ | |||||
| Suitability of facilities and LMS | √ | √ | √ | |||||
| Aligned with assessment | √ | √ | √ | √ | √ | √ | ||
| Evaluation explicit and built-in | √ | √ | √ | √ | √ |
Table 1. Framework for reviewing a medical curriculum
Table 1 includes the potential sources of information that should be sought when a curriculum is reviewed. This demonstrates the potential weakness of reviews based on only documents, because the documents describe what is intended to take place, not necessarily what does take place. Hence speaking with faculty (including part-time clinical teachers), students, employers and regulators can provide different information that describes the curriculum-in-action. Also important is the direct observation of teaching sessions of various types and of clinical assessment, both in the workplace and in OSCEs. It is not unusual for application to vary widely due to local ‘modifications’, despite apparently similar, ‘standard’ descriptions.
III. CONCLUSION
Reviewing a curriculum should be a continuous activity to maintain currency and fitness for purpose. The review should adopt a more holistic approach that includes curriculum content, delivery and assessment practices, as well as resourcing. This paper presents a framework to guide curriculum reviewers the issues to consider and the potential sources of information on which to base judgements.
Notes on Contributors
Richard Hays is an experienced medical educator with qualifications in both medicine and education. He has contributed to or led the design of several medical education programs and has also conducted formal medical program reviews at approximately 20 institutions in the United Kingdom, Europe and the Asia-Pacific region.
Ethical Approval
Ethical approval is not sought because there is no data presented and no possibility of identification of individual patients or students.
Declaration of Interest
There is no conflict of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
Boelen, C. & Woollard, R. (2009). Social accountability and accreditation: a new frontier for educational institutions. Medical Education, 43, 887-894.
Dolmans, D., De Grave, W., Wolfhagen I. & Van Der Vleuten, C. P. M. (2005). Problem-based learning: future challenges for educational practice and research. Medical Education, 39, 732-741.
Duckett, S. (2005). Health workforce design for the 21st century. Australian Health Review Quarterly, 29, 201-210.
Karle, H. (2006). Global standards and Accreditation in medical education: a view from the WFME. Academic Medicine, 81, S43-S48.
Prideaux, D. (2003). ABC of learning and teaching in medicine: Curriculum design. British Medical Journal, 326, 268-270.
Published online: 1 June, TAPS 2016, 1(1), 20-22
DOI: https://doi.org/10.29060/TAPS.2016-1-1/SC1011
Fong Jie Ming Nigel1*, Gan Ming Jin Eugene1*, Lim Yan Zheng Daniel1*, Ngiam Jing Hao Nicholas1*, Yeung Lok Kin Wesley1* & Tay Sook Muay2
1Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Department of Anaesthesia, Singapore General Hospital, Singapore
* Joint first authors
Abstract
The surgical physical examination is a fundamental part of medical training. We describe our experience with a near-peer teaching program for surgical physical examination skills, which involved senior medical students tutoring junior students starting their clinical rotations. We assessed scores on an Objective Structured Clinical Examination of the abdominal, vascular, and lumps examination before and after teaching. There was improvement in scores for all examinations and overall positive feedback from all students. This suggests that near-peer teaching may be a useful adjunct to faculty-led teaching of clinical skills.
Keywords: Near Peer Teaching; Physical Examination; Surgery
I. INTRODUCTION
Bedside clinical examination is fundamental to the practice of medicine. All 2nd year medical students at the National University of Singapore (NUS) undergo a 1 month Clinical Skills Foundation Course at the end of the academic year. This course is their maiden clinical posting and aims to introduce fundamentals of history taking and physical examination before they transit to their clinical years (3rd to 5th year). Unfortunately, it is challenging for faculty to effectively impart these skills due to increasing student numbers, busy clinical workloads and time constraints, leading to inadequate opportunities for learners’ active participation (versus passive observation), providing feedback, reflection and discussion (Spencer, 2003).
Near-peer teaching (NPT), using senior students to teach juniors, may supplement faculty-led teaching and ameliorate these difficulties. It has shown success in both case-based learning and teaching physical clinical examination (Blank et al, 2013). Beyond circumventing faculty constraints, NPT may promote a greater degree of active learning, knowledge application, and opportunities to correct misconceptions. Near-peer tutors may better understand learner challenges and share personal experience in overcoming these challenges (cognitive congruence), and promote a conducive, collaborative learning environment (social congruence) (Lockspeiser et al, 2008). Tutors who become role models may also benefit from deeper learning of content (Ten Cate et al, 2007) coupled with the development of higher cognitive skills whilst tutoring – to teach is to learn twice!
We describe a NPT initiative to teach surgical physical examination skills to students who are encountering clinical patients for the first time, in the ward via (i) a practical examination skills workshop and, (ii) the use of a novel course-book developed by the near-peer tutors as a teaching aid.
II. METHODS
Forty second-year students undergoing their maiden clinical posting at the Singapore General Hospital, Singapore, participated in a one-day workshop with IRB approval and written consent (Singhealth Centralised IRB Exemption 2015/2248, 27 March 2015). Students were divided into three groups and participated in three 2-hour long physical examination stations in a round-robin format. The stations were – (1) Abdominal examination, (2) Peripheral vascular examination, and (3) Lumps (skin, neck, breast, and groin). Five final-year students planned the workshop and served as near-peer tutors. A course book that served as a learning aid was written by near-peer tutors and vetted by faculty members. It was designed with the goal of encouraging the student to move beyond knowledge acquisition to application and synthesis of knowledge. Each section of the book introduced the sequence and rationale behind the steps of each surgical physical examination via a series of questions. These questions aimed to facilitate: (1) Understanding of the clinical significance and relationship between examination findings, (2) Clinico-pathological correlation and (3) Reasoning from first principles.
Instruction was modelled on Peyton’s four-step approach. Near-peer tutors explained the background to each examination, demonstrated the examination steps once, and discussed the technique, rationale, and possible findings in each step. Students then practiced on each other under supervision. To consolidate learning, near-peer tutors conducted post-tests based on objective structured clinical examination (OSCE) templates provided by the National University of Singapore, and provided qualitative feedback. Students also undertook identical OSCE pre-tests for comparison, and voluntarily completed anonymous feedback forms that made use of a 5-point Likert scale (Strongly Disagree to Strongly Agree) to evaluate various aspects of the workshop.
Statistical analysis was performed in R. Test scores were percentages of maximum possible score. Paired differences between individual pre-test and post-test scores were analyzed using Bayesian Estimation on weakly informative normal priors. Posterior probability distributions were approximated using Markov Chain Monte Carlo with 100,000 resamples.
III. RESULTS
| Exam | Mean pre-test score, out of 100 | Mean post-test score, out of 100 | Mean Paired Difference, absolute (95% credible interval) |
| Abdomen (n=40) | 73.3 | 91.4 | + 17.3 (10.0 – 24.6) |
| Arterial (n=40) | 41.6 | 91.3 | + 49.7 (41.7 – 57.8) |
| Lumps (n=38)* | 55.7 | 90.3 | + 34.7 (27.6 – 41.5) |
Table 1. Summary of pre-test and post-test results, and paired difference indicating the improvement from pre- to post-test
*Two students had to leave early
OSCE scores improved after teaching (Table 1), most markedly in the arterial examination (+49.7, credible interval 41.7-57.8), and also in the lumps (+34.7, credible interval 27.6-41.5) and abdominal examination (+17.3, credible interval 10.0-24.6). The abdominal examination started with the highest mean pre-test scores (73.3%), compared to the arterial (41.6%) and lumps examinations (55.7%). This may reflect greater exposure to the abdominal examination during prior faculty-led tutorials.
Out of the thirty-four students who provided feedback. 33 (97%) students agreed that the workshop helped them to pick up basic physical examination skills, and 32 (94%) were now more confident in performing these examinations on a real patient. Notably, all 34 students (100%) described better understanding of the rationale behind each clinical examination step, as opposed to performing the examinations mechanically; all (100%) found the small-group format conducive for learning. While all (100%) would encourage their juniors to attend this workshop next year, only 12 (35%) expressed interest to be a mentor themselves.
IV. DISCUSSION
We describe a student-initiated NPT initiative that supplements a faculty-led two-week surgical clinical rotation and physical examination teaching for students commencing their maiden clinical posting. This initiative has benefits to both students and near-peer tutors.
With regards to students, this initiative improved OSCE scores and was well received. The marked improvement in OSCE scores in areas less well-covered during faculty-led tutorials suggests that NPT sessions focusing on these gaps may complement and augment faculty-led tutorials particularly well. Physical examination stations with poorer OSCE scores may also highlight and objectively reflect areas in curriculum where faculty should focus on and refine. While it is encouraging that a number of students were keen to be mentors in the future, we are unsure as to why this aspiration was not a unanimous one amongst the entire student group. Possible reasons may include a lack of familiarity with the expectations of clinical teaching and lack of confidence given that this is their maiden clinical exposure.
Although the benefits to near-peer tutors were not formally evaluated, we propose that preparation of the course book and execution of the workshop required them to revisit their pre-clinical knowledge, understand its application to their current clinical knowledge, and synthesize and crystalize all the information to present it effectively, thus reinforcing their own learning.
With regards to the use of teaching aids, near-peer tutor developed examination revision notes for final year students accompanying NPT has been described (Rashid et al, 2011). Our course book, however, is a unique intervention that is primarily aimed at facilitating the building of links between pre-clinical knowledge and first clinical exposure. Future evaluation is necessary to determine the objective benefits of such a teaching aid.
Study limitations include a small sample size, potential observer bias because workshop tutors were OSCE assessors, and the lack of a comparison arm (e.g. Faculty teaching). These limitations can be addressed in the future by: Increasing our sample size by gradually extending subsequent editions of the workshop to all local teaching hospitals, recruiting more near-peers to serve as independent assessors to eliminate observe bias, and designing a study to compare faculty teaching alone against NPT in addition to faculty teaching.
We hope to highlight this valuable, yet under-utilized teaching modality which may be uniquely valuable in addressing the challenges faced in teaching clinical skills. We are optimistic that future studies may detail its academic, non-academic, and logistical benefits to students, near-peer tutors and faculty members alike.
Notes on Contributors
Fong Jie Ming Nigel, Gan Ming Jin Eugene, Lim Yan Zheng Daniel, Ngiam Jing Hao Nicholas and Yeung Lok Kin Wesley are final year medical students at the NUS Yong Loo Lin School of Medicine. They have an interest in medical education and have been involved in coordinating and implementing various near-peer teaching efforts in medical school. They conceived this initiative and were responsible for its implementation and preparation for publication.
Associate Professor Tay Sook Muay is a senior consultant anesthesiologist at the Singapore General Hospital (SGH), and the current Associate Dean for NUS Yong Loo Lin School of Medicine, SGH Campus. She is highly active in local and international teaching programs, education meetings and pedagogical committees. She is the faculty mentor for this near-peer teaching initiative.
Acknowledgements
We wish to acknowledge Cheng Kam Fei, Melissa Tang, and Krissie Chin from the Singapore General Hospital Associate Dean’s Office, for logistical support for the program.
Declaration of Interest
This is an unfunded study. All authors have no potential conflicts of interest.
References
Blank, W. A., Blankenfeld, H., Vogelmann, R., Linde, K., & Schneider, A. (2013). Can near-peer medical students effectively teach a new curriculum in physical examination? BMC Med Educ, 13, 165.
Lockspeiser, T. M., O’Sullivan, P., Teherani, A. & Muller, J. (2008). Understanding the experience of being taught by peers: the value of social and cognitive congruence. Adv Health Sci Educ Theory Pract, 13(3), 361-72.
Rashid, M. S., Sobowale, O., & Gore, D. (2011). A near-peer teaching program designed, developed and delivered exclusively by recent medical graduates for final year medical students sitting the final objective structured clinical examination (OSCE). BMC Med Educ, 11, 11.
Spencer, J. (2003). Learning and teaching in the clinical environment. BMJ, 326(7389), 591-4.
Ten Cate, O., & Durning, S. (2007). Peer teaching in medical education: twelve reasons to move from theory to practice. Med Teach, 29(6), 591-9.
Yong Loo Lin School of Medicine, National University of Singapore
1E Kent Ridge Road,
NUHS Tower Block, Level 11, Singapore 119228
Tel: 67723737
Email: nigelfong@gmail.com
Published online: 3 January, TAPS 2017, 2(1), 25-28
DOI: https://doi.org/10.29060/TAPS.2017-2-1/SC1001
Dipanshi Patel1, Namrata Baxi2, Abhishek Agarwal2, Kenyetta Givans1, Krystal Hunter2, Vijay Rajput3 & Anuradha Mookerjee2
1Cooper Medical School of Rowan University, Camden, New Jersey, United States of America; 2Cooper University Hospital, Camden, New Jersey, United States of America; 3Ross University School of Medicine, Miramar, Florida, United States of America
Abstract
Introduction: In graduate medical education, trainees have different academic and professional growth needs throughout their career, but these needs have not been well studied (Gusic, Zenni, Ludwig & First, 2010). Traditional mentoring programs in many disciplines including medicine, science, law, business and education report individuals with mentors having higher earnings, higher job satisfaction and higher rates of promotion, compared to individuals without mentors (Bussey-Jones et al.,2006; Sambunak, Straus & Marusic, 2010).
Methods: We developed a structured mentoring program in the Department of Medicine in Cooper University Hospital which encourages both academic and professional growth through a major emphasis on academic scholarship. We created a 21 questions survey to evaluate mentee satisfaction towards their assigned mentors. The questions fit into four categories consisting of the mentor’s personal attributes and action characteristics and mentee’s short term and long term career goals. Sixty junior trainees (Post Graduate Year 1-3) and 39 senior trainees (Post Graduate Year 4-7) completed the survey.
Results and Conclusions: Senior trainees were more satisfied with their mentors’ intrinsic qualities (96%) compared to junior trainees (93%), c2 (1, N=980) = 5.72, p=0.017. Additionally, senior trainees were more satisfied with their mentors’ action characteristics (95%) compared to junior trainees (91%), c2(1, N=677) = 4.03, p=0.045. Junior trainees had a lower satisfaction rating, compared to their senior colleagues, which might imply that their needs and desires were not properly addressed by their mentors. Both junior and senior trainees identified the lowest satisfaction rates in their mentors’ communication skills and ability to challenge them. This was an area of weakness within the mentorship program which requires further research and attention.
Keywords: Mentoring; Graduate Medical Education; Assessment
Practice Highlights
- Traditional mentoring programs in many disciplines including medicine, science, law, business, and education report mentees having higher earnings, higher job satisfaction and higher rates of promotion, compared to individuals without mentors (Bussey-Jones et al., 2006; Sambunak et al., 2010).
- There have been many variations to the mentorship framework, but there is a lack in scientific evidence to conclude which aspects of such a program holds the most beneficial characteristics (Bussey-Jones et al., 2006; Gusic et al., 2010).
- The professional and personal development needs for trainees change as they progress in their medical training.
- There is need for faculty development to enhance communication skills between mentor and mentee.
I. INTRODUCTION
Mentoring is an integral part of academic medicine and professional development during graduate medical education (Sambunak et al., 2010). Traditional mentoring programs in many disciplines including medicine, science, law, business, and education report individuals with mentors having higher earnings, higher job satisfaction and higher rates of promotion, compared to individuals without mentors (Bussey-Jones et al., 2006; Sambunak et al., 2010). Unfortunately, mentoring in academic medicine is often undervalued and not well studied (Sambunjak et al., 2006). Additionally, while many trainees and faculty form mentoring relationships independently, there is a lack of formal mentoring of postgraduate trainees in medicine (Sambunjak et al., 2006).
In recent years, many different forms of mentoring programs have been established in medical training. Omary et al. (2008) described multi-leveled mentorship as a way of “mentoring the mentors” which allowed for more well-rounded and thorough relationships. Conversely, Bussey-Jones et al. (2006) describes other organizations that established peer-to-peer mentoring programs which replace the claimed hierarchy and exploitation of traditional mentorship with mutual gain and friendship. However, these programs struggled with conflicts of competition to secure funding, publications, and networking opportunities. Gusic et al. (2010) explored the idea of an informal mentorship that allowed flexibility and fluidity in the mentorship, but later found that formal mentorship with structure and expectations was more beneficial than an informal one (Gusic et al., 2010). There have been many variations to the mentorship framework, but there is a lack of scientific evidence to conclude which aspects of such a program holds the most beneficial characteristics. Our mentoring program is designed to foster relationships between faculty and trainees regarding personal, clinical, and career goals. Academic growth is a major emphasis of this program for those trainee physicians who wish to follow an academic career pathway. With this research, we hope to better understand the dynamic between faculty and trainees in graduate medical education. We hypothesize that there will be no difference in satisfaction rates between junior and senior trainees in regards to their respective mentors.
II. METHODS
A. Participants
Participants consisted of 60 junior trainees (PGY 1-3) and 49 senior trainees (PGY 4-7) who were assigned to clinical facility mentors through a formal mentoring program in the Department of Medicine at Cooper University Hospital, Camden, NJ, for the 2013-2014 academic year.
B. Procedure
We have a formal mentoring program to foster relationships between faculty and trainees in Department of Medicine since 2011. PGY1 trainees were assigned a mentor within the first three months of their internship. Senior trainees were required to seek and identify a professional or academic mentor, preferably across the division and department boundaries. Program Directors and the Division Head of Medical Education helped to identify the mentors and mentees and establish the partnership. A list of mentor/mentee was developed and distributed to all the house staff. Mentor and mentee were required to sign a contract and meet in person for a one hour session at least two times a year at a local restaurant using provided meal vouchers. All meetings between mentor and mentee were recorded in narratives and brief encounter forms. They could continue their relationship outside this program as per their needs.
C. Instrumentation
We conducted IRB approved research by developing an anonymous, structured questionnaire modified based on a validated survey (Archer, Swanwick, Smith, O’Keeffe & Cater, 2013). The survey addressed the quality and satisfaction ratings of the existing mentoring program by identifying 21 areas of mentor qualities and attributes, using a four point agreement scale. The survey questions were grouped into categories that reflected traits which the mentors exhibited or goals which the mentors encouraged. The categories consisted of two competing groups: “personal attributes” versus “action characteristics” and “short-term goals” versus “long-term goals”(Archer et al., 2013) Table 1 lists the questions from the survey and the qualities and traits which correlated with them. Question 6, 11 and 17 from the survey were excluded from data analysis due to low response rates.
| Short Term | Long Term | Intrinsic | Action | |
| Q1- Remained up-to-date on your career | X | X | ||
| Q2- Showed genuine interest in your portfolio | X | X | ||
| Q3- Showed enthusiasm | X | |||
| Q4- Approachability | X | |||
| Q5- Ability to inspire you | X | |||
| Q6- Ability to seek help from other sources | ||||
| Q7- Ability to challenge you | X | |||
| Q8- Willingness to act to resolve problems in timely manner | X | X | ||
| Q9- Gave constructive feedback | X | |||
| Q10- Communication skills | X | X | ||
| Q11- Showed ability to communicate with your clinical supervisors | ||||
| Q12- Encouragement towards achieving excellence | X | X | ||
| Q13- Ability to take your supervision beyond a tick box exercise | X | |||
| Q14- Honesty and integrity | X | |||
| Q15- Ability to assure privacy and confidentiality | X | |||
| Q16- Ability to make time for you | X | X | ||
| Q17- Commitment to rearrange meetings | ||||
| Q18 – Interest in you as an individual | X | X | ||
| Q19 – Ability to be your advocate | X | |||
| Q20 – Ability to offer practical tailored advice for your long-term career planning | X | X | ||
| Q21 – Overall how do you rate your mentor |
Note: Modified from Archer et al., 2013
Table 1. Evaluation of principal mentor attributes
D. Data Analysis
We used Chi Square tests for statistical analyses. We also used reliability testing with Cronbach’s alpha to be sure that the question for each category was internally consistent. We compared the perception of junior trainees and senior trainees regarding their mentors’ personality traits and their mentors’ ability to address their long term and short term goals. We also analyzed the difference in satisfaction between trainees with known research interest versus no research interest.
III. RESULTS
When comparing satisfaction rates, senior trainees (PGY 4-7) were more satisfied (96%) compared to junior trainees (PGY1-3) (93%) regarding their mentors’ inherent qualities, c2 (1, N=980) = 5.72, p=0.017. Additionally, senior trainees were more satisfied (95%) compared to junior trainees (91%) regarding their mentors’ actions characteristics, c2 (1, N=677) = 4.03, p= 0.045. There were no statistical differences in mentor satisfaction rates irrespective of prior established research interest among trainees. When comparing PGY 1 to PGY 2-7 to identify if there were special needs for the first year junior trainees, there were no differences in satisfaction rates regarding how the mentees perceived their mentors and their career goals. The lowest satisfaction rates among all mentees (PGY 1-7) were regarding their mentors’ communication skills and ability to challenge them for their professional growth and career. Of all mentees, 13% did not believe their mentor showed ability to communicate with clinical supervisors and 14% did not believe their mentors adequately coached them on communication skills. Of all mentees, 11. % did not believe their mentor had the ability to take their supervision beyond a tick box exercise and 13. % did not believe their mentor was able to adequately challenge them.
There was strong reliability for each category of questions. The Crobach’s Alpha =.914 for the 9 items measuring “Inherent characteristic”. The Crobach’s Alpha =.915 for the 7 items measuring “Action characteristics”. The Crobach’s Alpha =.872 for the 4 items measuring “Short-Term”. The Crobach’s Alpha =.892 for the 4 items measuring “Long Term”.
IV. DISCUSSION and CONCLUSION
With this mentorship program, we hoped to foster the scholarly development of apprentices in graduate programs (Bussey-Jones et al., 2006). From the results of our survey, we see that senior trainees (95%) are more satisfied with their mentors learned skills compared to junior trainees (91%). While a mentor’s personal attributes are intrinsic within themselves and their nature, a mentor’s action characteristics (learned skills) can be improved through various training sessions and workshops (Archer et al., 2013). By identifying these areas of weakness and matching them with a plan of action, we can strengthen the mentorship program and provide services to accommodate mentees’ needs. Senior trainees (96%) also found more satisfaction in their mentors’ intrinsic characteristics than junior trainees (93%). It is possible that senior trainees are closer in maturity and life stage to their mentors or have more in common with their mentors compared to junior trainees. This highlights a potential area of improvement since it shows trainees have various needs and goals and we need to better address them. This finding warrants additional investigation to further the scope of the current research.
Junior and senior trainees (PGY 1-7) had lowest satisfaction rates regarding mentors’ coaching abilities in communication skills (13.5%) and mentors’ ability to communicate with clinical superiors (12.5%). Additionally, both junior and senior trainees (PGY 1-7) had the low satisfaction rates regarding mentors’ ability to challenge them (13.1%) and their ability to supervise them beyond a checkbox exercise (11.2%). Both of these components, communication and ability to challenge, are relatively teachable qualities, thus mentors might benefit from having educational workshops, which focus on those components of the mentoring experience.
Limitations which we encountered in our study included obtaining data from only one institution and having a small sample size. Additionally, the method with which the junior and senior trainees were matched with their mentors differed, which might impact the satisfaction rates. This was done because junior trainees are not familiar with the program’s faculty members and are less certain about which subspecialty they are interested in pursuing, compared to senior trainees.
Mentorship is a dynamic dyad interaction with immediate and long term impact. Establishing a mentor program fosters the scholarly development of apprentices in graduate programs (Sambunjak et al., 2006). Our program consisted of junior and senior trainees who might desire different skills and attributes from faculty mentors depending on their career goals and stage in training. Our aim was to identify areas of our mentor program which needed attention and restructuring to ensure a stronger program for the future. This research will help in developing future faculty development and mentoring programs across graduate medical education.
Notes on Contributors
Dipanshi Patel is a third year medical student at Cooper Medical School at Rowan University. She conducted literature review, assisted with data collection and data analysis, and contributed to the construction of short communications manuscript.
Dr. Namrata Baxi, MD is currently doing her specialty training in Nephrology at Robert Wood Johnson University in New Jersey. She collected and analyzed the data for this research while she was a senior post graduate trainee at Cooper University hospital.
Dr. Abhishek Agarwal, MD is currently a Chief resident at Cooper University hospital in the department of Internal Medicine. He assisted in collecting the data and analyzing it.
Kenyetta Givans is a third year medical student at Cooper Medical School at Rowan University, who contributed to the collection of the data.
Ms. Krystal Hunter, MBA is a statistician at Cooper Research Institute, and has contributed to the statistical analysis of this project. She has a valued interest in medical education research.
Dr. Vijay Rajput is Professor and Chair of Medicine at Ross University School of Medicine. He served as senior mentor for this research study. He has an extensive experience in medical education and has a passion for the holistic development of student and faculty.
Dr. Anuradha Mookerjee is Associate Professor of Medicine at Cooper University Hospital, in the Department of Internal Medicine. She helped in the design and implementation of this study. She has a marked interest in medical education and faculty development.
Acknowledgements
We have no additional acknowledgements.
Declaration of Interest
There is no conflict of interest, including financial, consultant, institutional or otherwise for any of the authors involved in this manuscript.
References
Archer, J., Swanwick, T., Smith, D., O’Keeffe, C., & Cater, N. (2013). Developing a Multisource Feedback Tool for Postgraduate Medical Educational Supervisors. Medical Teacher, 35, 245-154.
Bussey-Jones, J., Bernstein, L., Higgins, S., Malebranche, D., Paranjape, A., Genao, I., Lee, B., & Branch, W. (2006). Repaving the Road to Academic Success: The IMeRGE Approach to Peer Mentoring. Academic Medicine, 81, 674-679.
Gusic, M. E., Zenni, E. A., Ludwig, S. & First, L. R. (2010). Strategies to Design an Effective Mentoring Program. The Journal of Pediatrics, 156, 174-176.
Omary, M. B. (2008). Mentoring the Mentor: Another Tool to Enhance Mentorship. Gastroenterology, 315, 13-16.
Sambunak, D., Straus, S. E., & Marusic, A. (2010). A Systemic Review of Qualitative Research on the Meaning and Characteristics of Mentoring. Journal of General Intern Medicine, 25, 72-78.
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
