
Text analysis of personal statements written in English by Japanese medical students
Submitted: 11 November 2021
Accepted: 27 January 2022
Published online: 5 April, TAPS 2022, 7(2), 51-55
https://doi.org/10.29060/TAPS.2022-7-2/SC2710
Rintaro Imafuku, Kaho Hayakawa & Takuya Saiki
Medical Education Development Center, Gifu University, Japan
Abstract
Introduction: Personal statements are important documents in the admission and programme application processes, including international elective programmes, in medical education. However, writing these is challenging for international applicants not only because of their unfamiliarity with this genre but also their English academic writing skills. This study aims to explore the organisation and elaboration of text in personal statements written by Japanese medical students for international elective programme application.
Methods: Drawing on genre analysis, the first draft of personal statements written by eight fifth-year medical students at a Japanese university were analysed. The text data were deductively classified into moves and steps, using Chiu’s framework of the personal statement genre.
Results: In the introduction, Japanese medical students commonly described the context and issues of healthcare in Japan and the future goals for physicians. In the move of the relevant background, it was notable that six out of eight personal statements showed personality. Although a range of moves was covered when writing about the reasons for applying, only two students described their understanding of programmes and institutional attributes. In the move of conclusion, they focused more on writing their goals of future success and contribution to the course. Furthermore, no applicant expressed self-promotion and praise for academics, programmes, and institutions.
Conclusion: The findings of this study can provide a springboard for the development of support for Japanese students’ academic writing in English in medical education across cultures.
Keywords: Medical Education, International Electives, Personal Statement, Genre Analysis, Discourse, Rhetorical Patterns, Written Communication
I. INTRODUCTION
The personal statement, as a promotional academic genre, is an important document in the admission process for higher education. However, numerous applicants face difficulties while preparing application materials because of their unfamiliarity with the genre of discourse and audience expectations (Ding, 2007). In medical education, particularly institutions in Western countries, several instances require the submission of personal statements for application to, for instance, medical schools, international electives, residency programmes, and research programmes.
Globalisation in medical education has promoted worldwide student mobility. Currently, many Asian medical students, including Japanese students, participate in international electives in Western countries. International electives provide several benefits to medical students, including cultural competence, communication skills, and clinical reasoning (Imafuku et al., 2021). However, because some institutions require the submission of personal statements for application to the international elective programme, it can be challenging for international applicants not only because of their unfamiliarity with the genre of discourse but also their English academic writing skills.
As the preparation of application materials, including personal statements, can be challenging for Asian medical students, educators must facilitate a more comprehensive pre-departure course, along with providing support for composing such documents. Specifically, a better understanding of the linguistic features of their personal statements is fundamental for developing academic writing support for their application documents. Therefore, this study used the genre analysis framework (Swales, 1990) to explore the organisation and elaboration of text in personal statements written by Japanese medical students for the international elective programme application. Specifically, the following research question was developed: What are the rhetorical characteristics of Japanese medical students’ personal statements written in English?
II. METHODS
A. Setting
International electives, which allow the students at the Gifu University School of Medicine to study overseas, are optional modules of either four or eight weeks in the final year of the clinical clerkship programme with the goals of observation, understanding and experiencing clinical practices in different cultural contexts. Through this programme, every year, 10–15 medical students study clinical medicine in a foreign country and gain cross-cultural experience in a clinical setting. As some highly competitive overseas institutions require the submission of personal statements, letters of recommendation, and curriculum vitae during the application, faculty members of the medical education division provide some support for their preparation, if required by the students. Although the guidebook for international electives briefly explains the definition and role of personal statements, the students are not officially given any sample or format of English personal statements.
B. Data Collection and Analysis
This study collected personal statements written in English by fifth-year medical students (n=8; Student A-H) at a Japanese university, from 2013 to 2017, as part of the application documents for international electives in institutions in the United Kingdom (UK) or the United States (US). Their TOEFL (Test of English as a Foreign Language) (iBT) score ranges from 90 to 101. Written informed consent to participate was obtained from them. Their first drafts were analysed through the lens of move analysis as an element of genre analysis (Swales, 1990) to reveal rhetorical patterns from a cultural perspective. The first draft, which has not been revised using feedback from others, directly reflects their cultural and linguistical influences regarding the rhetorical patterns. Text data were analysed by the first author, who has a background in applied linguistics and medical education. Subsequently, the preliminary findings of the text analysis were discussed by all the research team members to establish the credibility and dependability of the data analysis.
Genre analysis aims to describe the organisational patterns of text in a specific context, and genres are viewed as staged goal-oriented social processes of the written or spoken practice. For example, in written communication, reader expectations, document structure, and rhetoric development vary depending on the genre, such as research articles, invitation letters, and reminder emails. A move is an analytical unit defined as a rhetorical component shifting from one part of a text to another that performs a specific communicative function (Swales, 1990, p.140). Each move is subcategorised into one or more functional units called steps.
Specifically, this study applied Chiu’s (2016) framework of moves and steps in the context of personal statements for graduate school application to medical education. Drawing on this analytical framework that comprises five moves: introduction, relevant background, reasons for applying, extra-curricular information, and conclusion, the text data were deductively classified into moves and steps.
Ethical approval was obtained from the Gifu University Ethics Committee (No. 25–367). Students were assured of the confidentiality of the contents.
III. RESULTS
The average length of the personal statements was 535.5 words (range: 314–873 words). The deidentified data of personal statements by some participants who gave their consent to share the whole text that support the findings of this study are available in Figshare at http://doi.org/10.6084/m9.figshare.17030705. All the data set can be available from the corresponding author on reasonable request. Table 1 indicates the total number of personal statements that consists of any step of each move and shows the representative text in each move.
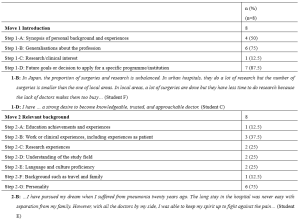

Table 1. Moves and steps of the personal statements for international electives written in English by Japanese medical students
As can be seen from Table 1, in the introduction, Japanese medical students commonly described the context and issues of healthcare in Japan (1-B) and future goals for physicians (1-D). Expressions of their research and clinical interests (1-C) were made the least in the introduction move. In the relevant background move, it is notable that six out of eight personal statements in this study showed personality (2-G), which is much higher than the rest of the other steps. In the reasons for applying move, six Japanese medical students made the rhetorical step of personal development and ambition, whereas only two students described their understanding of programmes and institutional attributes (3-C) and disciplinary and research reasons (3-E). Extra-curricular information (Move 4) was not provided by the applicants in this study. In the move of conclusion, Japanese medical students focused only on their future success goals (5-A) and contribution to the course (5-E). Furthermore, no applicant expressed self-promotion (5-B) and praise for academics, programmes, and institutions (5-D) in this study.
IV. DISCUSSION
Drawing on genre analysis (Swales, 1990), this study revealed the rhetorical patterns of personal statements written by Japanese medical students. Although the participants had high or adequate English proficiency, they seemed to struggle with personal statement writing due to the unfamiliar genre of discourse. Imafuku et al. (2021) found that the participants faced several difficulties related to linguistic, sociolinguistic, and sociocultural aspects during the international electives, whereas this study showed that the applicants had already experienced difficulties of cross-cultural communication at the pre-departure stage.
Genre analysis offers a useful theoretical framework and an analytical perspective of people’s communicative practices in a cultural context, especially allowing educators or researchers to examine how language is used in specific contexts for particular purposes, thus contributing to the knowledge of specific writing instructions (Ding, 2007). Writing a personal statement is a common issue not only in medical education but also in higher education. Personal statements are a type of promotional academic genre in admissions to higher education institutions or programmes that expects textual self-aggrandisement by applicants. Chiu (2016), who examined personal statements in the areas of educational policy, language and literacy, and higher education, demonstrated that self-promotion or evaluation is an important step in the conclusion move for graduate school applications in the UK and the US. As a response to Chiu’s (2016) study, the finding of this study that self-promotion or evaluation is not indicated in the move of conclusion by Japanese medical students suggests their need to learn not only the rhetorical structure and reader expectations but also ways of logically and effectively expressing their own strengths. The results of this study can be a useful learning resource to understand what rhetorically characterises a personal statement.
Reflecting on the rhetorical patterns of the students in a given genre is pivotal to communicative achievement in intercultural settings. In this sense, contrastive rhetoric studies have provided useful implications for a better understanding of writing patterns from a cross-cultural viewpoint. For example, contrastive rhetoric studies of Japanese and English to date have shown different discourse organisations of and approaches to writing in a variety of genres, such as newspaper columns, doctoral dissertations, and narrative essays (Connor, 1996). In the previous studies reviewed by Connor (1996), Japanese writing was characterised by a reader-responsible language and a deductive rhetorical pattern. Furthermore, the Japanese are oriented to share values of indirectness, and the reader is expected to interpret what the writer intended to convey. This study suggests that understanding the rhetorical features in the writer’s own cultural context is essential to writing in the target genre of discourse in different cultural contexts.
Although this study illuminates written communication across cultures through the text analysis of personal statements, investigation should be undertaken continuously for further data collection, as the sample size of text data from eight students is limited to a particular institution. Furthermore, follow-up interviews are worthwhile to explore students’ writer identity and cognitive process during writing.
V. CONCLUSION
There are increased opportunities for cross-cultural communication, including both spoken and written formats, in globalised contexts, such as medicine. For written communication, in the genre of personal statements in medical education, this study found that Japanese students shared limited information about the relevant background (Move 2) and did not express adequate self-promotion (Move 5). The findings can act as a springboard for the development of support for Japanese students’ academic writing in English in medical education across cultures.
Notes on Contributors
Rintaro Imafuku reviewed the literature, designed the study, conducted text analysis, and wrote the manuscript.
Kaho Hayakawa was involved in data collection and analysis of the text.
Takuya Saiki was involved in data collection and analysis of the text.
All the authors have read and approved the final manuscript.
Ethical Approval
This study was approved by the Gifu University Ethics Committees (No. 25–367). Consent was obtained from all participants for the research study. Confidentiality was assured for the contents of students’ writing. All participants have given written consent for their data to be used in the research and for publication.
Data Availability
Deidentified data of personal statements by the participants who gave their consent to share the whole text are openly available at http://doi.org/10.6084 /m9.figshare.17030705. The data are available from the corresponding author on reasonable request.
Funding
This work was supported by the JSPS KAKENHI [Grant number 20K10374].
Declaration of Interest
The authors report no conflicts of interest.
References
Chiu, Y.-L. T. (2016). ‘Singing your tune’: Genre structure and writer identity in personal statements for doctoral applications. Journal of English for Academic Purposes, 21, 48-59. https://doi.org/10.1016/j.jeap.2015.11.001
Connor, U. (1996). Contrastive rhetoric: Cross-cultural aspects of second language writing. Cambridge University Press.
Ding, H. (2007). Genre analysis of personal statements: Analysis of moves in application essays to medical and dental schools. English for Specific Purposes, 26(3), 368-392. https://doi.org/10.1016/j.esp.2006.09.004
Imafuku, R., Saiki, T., Hayakawa, K., Sakashita, K., & Suzuki, Y. (2021). Rewarding journeys: Exploring medical students’ learning experiences in international electives. Medical Education Online, 26(1), 1913784. https://doi.org/10.1080/10872981.2021.1913784
Swales, J. (1990). Genre analysis: English in academic and research settings. Cambridge University Press.
*Rintaro Imafuku
1-1 Yanagido, Gifu, Gifu, 501-1194
Email: rimafuku@gifu-u.ac.jp
Submitted: 30 July 2021
Accepted: 17 January 2022
Published online: 5 April, TAPS 2022, 7(2), 46-50
https://doi.org/10.29060/TAPS.2022-7-2/SC2662
Kheng Tian Lim1 & Bao Yun Koh2
1Department of General Surgery, Khoo Teck Puat Hospital, Singapore; 2Education Development Office, Khoo Teck Puat Hospital, Singapore
Abstract
Introduction: Medical students (MS) may lack the knowledge and experience in performing basic surgical skills (BSS) when they first commence their postgraduate surgical training. We conducted a pilot BSS workshop with specific learning outcomes for MS.
Methods: Our BSS workshop program consisted of reading the pre-workshop online modules, watching the instructional videos of skills demonstration, and completing the pre-workshop multiple-choice questions (MCQ). MS attended the onsite workshop a week later, which consisted of a basic surgical theory lecture, live demonstration of the skills by the teaching faculty and, supervised skills training coupled with feedback. Surgical skills taught were knot tying, suturing techniques, laparoscopic peg transfer, precision cutting, application of endoloop ties. A standardised surgical skills rubric was used to assess the competency and safety of BSS. A post-workshop MCQ was administered to assess the knowledge learned. The criteria for successful completion of BSS were a satisfactory grade in the surgical skills assessment and a pass score in the MCQ.
Results: All the participating MS achieved a satisfactory grade in the surgical skills assessment and passed the MCQ. Several pedagogical methods were used to enhance knowledge learning and practical skills competency including a flipped classroom in blended learning, technology-enhanced learning, kinesthetic learning, and providing effective feedback.
Conclusion: MS taught in BSS workshop can achieve competency in knowledge, skills, safe attitude and prepare them for future postgraduate surgical training. In the current COVID-19 pandemic, our challenge is to develop similar BSS in a safe environment using technology-enhanced tools such as online instructional videos and online feedback.
Keywords: Assessment, Basic Surgical Skills, Competency, Feedback, Medical Students, Outcome-based Education
I. INTRODUCTION
Medical students (MS) may lack the knowledge and experience in performing certain basic surgical skills (BSS) when they first commence their postgraduate surgical training in hospitals. Traditionally, BSS are usually not taught formally in the undergraduate medical curriculum until much later in the postgraduate level. The opportunity for teachers to teach BSS and for MS to learn is much dependent on the situation in operating rooms during assigned core surgical postings or student selective postings.
In Singapore, Yong Loo Lin School of Medicine, National University of Singapore (NUS) provides basic and advanced clinical procedural simulation training to undergraduate MS. Skills taught include gowning, scrubbing techniques, suturing, and knot-tying. Lee Kong Chian School of Medicine, Nanyang Technological University (NTU) teaches suturing and knot-tying skills in dry laboratory to undergraduate MS. All these stimulated practical skills and experience acquired by MS are transferrable to real patients’ environments. In addition, SingHealth Academy, an educational arm of SingHealth, provides BSS workshop training at the postgraduate level for interested learners. In the United Kingdom and Ireland, the BSS course is a curriculum-mandated course for postgraduate Core Surgical Training programmes.
Healthcare institution partners such as Khoo Teck Puat Hospital (KTPH), provide clinical training for MS of NUS and NTU. Our Department of General Surgery (GS) identifies the need in the learning outcomes for the graduating MS, to equip them with the competent foundation of BSS for postgraduate surgical training, although not a graduating competency requirement set by Singapore Medical Council. We conducted a small pilot workshop at our institution, aiming at educational quality improvement for our MS in three learning domains, namely surgical knowledge, practical surgical skills, and attitudes in safety that are common to all forms of surgery.
II. METHODS
A. Workshop organization, MS and Teaching Faculty, Teaching Materials
The Department of GS and Education Development Office (EDO), KTPH organised a 1-day BSS workshop for MS with the request from MS and was scheduled on 20th December 2019. Planning over three months was required to prepare the learning objectives and outcomes, workshop programme schedule, venue, teaching materials, surgical scrubs, sustenance, and coordination by the workshop director and EDO. Both the local and overseas MS were invited and recruited for training. Experienced local teaching faculty members were invited and briefed on the teaching methodology, feedback provision, and assessment criteria.
MS who agreed to participate were given instructions to read the pre-workshop fundamentals of the BSS document, watch the instructional video clips of the BSS demonstration and, complete pre-workshop multiple-choice questions (MCQ), all of which were provided online 1 week before the workshop. These pre-workshop activities may help to motivate the MS and provide an opportunity for self-assessment of their understanding of the BSS topics. MS were allowed to post questions to the workshop director for guidance. The course content and MCQ were prepared by the course director to be appropriate to the MS level.
The workshop was divided into morning and afternoon sessions to cater to a larger group of interested MS coming from overseas. The onsite workshop consisted of a short basic theory lecture, a live demonstration of the practical BSS, MS performing the practical BSS with direct supervision and corrective feedback. BSS taught were knot tying using one-hand, two-hand, and instrumental techniques. Suturing techniques taught included simple, mattress, interrupted, continuous suture. More advanced laparoscopic skills such as laparoscopic peg transfer, precision cutting, and application of endoloop ties were taught. A post-workshop MCQ was administered.
B. Assessment in Knowledge, Skills, and Attitudes
The surgical knowledge was assessed using the pre-and post-workshop MCQ, based on the course content prepared for MS.
The surgical skills assessment was carried out by direct observation of procedural skills (DOPS) using a standardised surgical skills rubric. Open surgery skills assessment included instrument selection and handling, knotting techniques, tissue handling, and suturing techniques. Laparoscopic surgery skills assessment included instrument selection and handling, peg transfer, precision cutting, and ligating loop. The overall summative assessment of global grading in the surgical skills domain by the teaching faculty was either satisfactory or unsatisfactory.
MS were assigned to work in pairs with the ratio of MS: teaching faculty as 2:1. Assessment in the attitude and behavior domain was based on direct observation in the safe handling of sharps and needles, general assisting, and laparoscopic camera assisting skills.
C. Feedback and Competency
The teaching faculty used DOPS to provide feedback on the practical BSS performed by the MS which allowed the MS to improve and progress from a novice to a competent learner level in the skills and attitude domains. The specific, timely, and purposeful feedback served as a channel for MS to improve and reflect on their learning outcomes in these domains.
The competency criteria for successful completion of the BSS workshop were set as a pass mark of 60% in the summative MCQ test and a satisfactory grade in the summative skills assessment by the teaching faculty. A Certificate of Attendance would be awarded to MS who have acquired the competency criteria.
III. RESULTS
Assessment and evaluation data gathered for this workshop and pre-workshop MCQ questions were uploaded to an online repository for archiving and validation purposes. It may be assessed through the following Digital Object Identifier (DOI): https://doi.org/10.6084/m9.figshare.16884877.v2 (Lim & Koh, 2021).
A total of 38 MS signed up for the BSS workshop with 1 dropout. Thirty-seven MS attended the workshop of which 25 were from overseas medical schools. Thirty-six MS attempted the pre-workshop MCQ (10 questions). Thirty-seven MS passed the post-workshop MCQ (15 questions). All MS achieved satisfactory grades in practical skills. There was no needle stick injury reported.
The BSS workshop program evaluation form was administered and completed anonymously for the quality improvement process after verbal consent was taken from the participants. (Table 1).
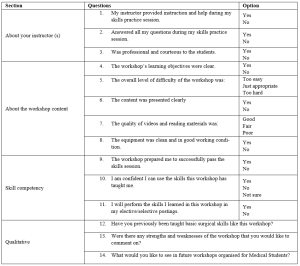
Table 1. BSS Workshop for MS Program Evaluation
IV. DISCUSSION
Bloom’s Taxonomy comprises three learning domains known as cognitive (knowledge), affective (attitude), and psychomotor (skills). Each domain has a hierarchy that corresponds to distinct levels of learning which is important for students to develop holistically. The learning objectives of the BSS workshop for MS are thus designed to fulfil these three domains, specifically to: 1) acquire the fundamental knowledge of BSS (knowledge), 2) demonstrate a variety of surgical knots and suturing skills effectively (skills) and, 3) handle and use of surgical instruments and tissue safely (attitude).
Harden et al. (1999) described an outcome-based education framework that comprises six levels of training to achieve the outcomes. These six levels of training are: 1) awareness of the procedure, 2) full theoretical understanding of the procedure, 3) observation of the procedure, 4) carrying out part of the procedure, 5) undertaking the procedure under the supervision and, 6) undertaking the procedure unsupervised. Similarly, the programme activities of the BSS workshop for MS were developed to cover these six levels of training. The learning outcomes of this workshop are to equip the MS with the competency of BSS for postgraduate surgical training. The teaching faculty members share their knowledge, demonstrate their expertise, advise MS, and provide feedback to improve technical skills and promote learning.
Effective feedback is necessary to enhance learning. Pendleton et al. (2003) described a four-step process for carrying out a feedback session. Ramani and Krackov (2012) described twelve tips for clinical teachers to provide effective feedback to undergraduate and graduate medical trainees. Our teaching faculty members were able to provide effective feedback to MS using these frameworks to establish a respectful learning environment, feedback on direct observation, make feedback timely, reinforce and correct observed behaviors, use specific language to focus on performance, confirm the learner’s understanding and conclude with an action plan.
The assessment for learning in the BSS workshop for MS was designed to align with the three learning domains using: 1) pre-and post-workshop MCQ to test surgical knowledge, 2) DOPS by the teaching faculty to test surgical skills and, 3) DOPS in the safe handling of sharps and needles, general assisting and laparoscopic camera assisting skills to test the attitude and behavior. A standardised surgical skills rubric was used for DOPS.
Technology-enhanced learning (TEL) intervention and enhancement can be characterised by 1) replicating existing teaching practices, 2) supplementing existing teaching or, 3) transforming teaching, learning processes, and outcomes (Kirkwood & Price, 2014). Several pedagogical methods were used in this BSS workshop to enhance knowledge learning and skills acquisition such as flipped classroom in blended learning, a mixture of the three characteristics of TEL, kinesthetic learning, and providing effective feedback. In the current COVID-19 pandemic, there are challenges to conducting such a practical workshop. TEL tools that combine online educational materials, instructional videos, feedback, and face-to-face online interaction such as Zoom, and Microsoft Teams are the new norm.
The limitation of this workshop includes the lack of MCQ standardisation process and the quality of the video clips which we intend to improve in the next workshop.
V. CONCLUSION
Conducting a BSS workshop for MS with specific learning outcomes is feasible where the MS can achieve competency in knowledge, skills, safe attitude and prepare them for postgraduate surgical training. In the current COVID-19 pandemic, our challenge is to develop similar BSS in a safe environment using TEL tools.
Notes on Contributors
Dr. Lim Kheng Tian designed the work, reviewed the literature, drafted the work, revised the content critically, and wrote the manuscript. Ms. Koh Bao Yun contributed to the design and administration of the work, gave critical feedback to the content, and revised the manuscript. All authors have read and approved the final manuscript.
Ethical Approval
This 1-day workshop program was conducted for educational quality improvement (QI) with approval from the Department of GS and EDO, KTPH. This article was submitted with Institutional Review Board/Ethical approval for exemption from full review. We have attached the local IRB waiver document NHG DSRB Ref: 2021/00888.
Data Availability
Inline to make research available to the scientific community for data replication and scientific progress, the dataset of this workshop may be found for free through the Figshare website: https://doi.org/10.6084/m9. figshare.16884877.v2
Acknowledgement
The authors want to thank all the MS and teaching faculty who participated in the workshop. We would like to acknowledge Dr. Lee Yao Zong, Associate Consultant of the Department of GS, KTPH for providing help in the laparoscopic educational content. We would like to acknowledge the technical help of Mr. Mohamad Sean Abdullah, former Experimental Surgical Services Development Executive of the Department of GS, KTPH. We would like to acknowledge equipment support from KARL STORZ Endoscopy Singapore Sales Pte Ltd for providing the reusable laparoscopic trainer and laparoscopic instruments. We also like to acknowledge NHG Education for linking up EDO, KTPH with the Singapore Medical Society of Australia and New Zealand (SMSANZ).
Funding
There is no funding for this paper. The suturing materials used in the workshop were funded by the Pre-Employment Clinical Training (PECT) Funds received by KTPH for local MS whilst overseas MS were self-funded. The funder was not involved in the design, delivery of the workshop, or submission of the paper.
Declaration of Interest
All authors declare no conflicts of interest, including financial, consultant, institutional, and other relationships that might lead to bias or a conflict of interest.
References
Harden, R. M., Crosby, J. R., Davis, M. H., & Friedman, M. (1999). AMEE Guide No. 14: Outcome-based education: Part 5-From competency to meta-competency: A model for the specification of learning outcomes. Medical Teacher, 21(6), 546–552. https://doi.org/10.1080/01421599978951
Kirkwood, A., & Price, L. (2014). Technology-enhanced learning and teaching in higher education: What is ‘enhanced’ and how do we know? A critical literature review. Learning, Media and Technology, 39(1), 6–36. https://doi.org/10.1080/17439884.2013.770404
Lim, K. T., & Koh, B. Y. (2021). Start small and aim big in conducting a basic surgical skills workshop for medical students—Repository data (p. 11710 Bytes) [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.16884877.v2
Pendleton, D., Schofield, T., Tate, P., & Havelock, P. (2003). The New Consultation. Oxford University Press.
Ramani, S., & Krackov, S. K. (2012). Twelve tips for giving feedback effectively in the clinical environment. Medical Teacher, 34(10), 787–791. https://doi.org/10.3109/0142159X.2012.684916
*Lim Kheng Tian
Department of General Surgery,
Khoo Teck Puat Hospital,
90 Yishun Central,
Singapore 768828.
Tel: +65 65558000
Email: lim.kheng.tian@ktph.com.sg
Submitted: 22 August 2021
Accepted: 28 December 2021
Published online: 5 April, TAPS 2022, 7(2), 42-45
https://doi.org/10.29060/TAPS.2022-7-2/SC2682
Lee Man Xin1*, Zhang Yuan Helen2* & Fatimah Lateef2,3
1Changi General Hospital Emergency Department, Singapore; 2Singapore General Hospital Emergency Department, Singapore; 3Singhealth Duke-NUS Institute of Medical Simulation (SIMS) Education Office, Singapore
*Joint first authors
Abstract
Introduction: Advanced Cardiac Life Support (ACLS) course is one of the mandatory certifications for the majority of medical as well as some nursing professionals. There are, however, multiple variations in its instruction model worldwide. We aim to evaluate the efficacy of traditional ACLS course versus a hybrid ACLS course utilised during the COVID-19 pandemic.
Methods: This retrospective study was carried out at SingHealth Duke-NUS Institute of Medical Simulation using course results of participants in the centre’s ACLS course between May to October 2019 for the traditional course were compared with participants attending the hybrid course from February to June 2021.
Results: A total of 925 participants were recruited during the study period. Of these, 626 participants were from the traditional group and 299 participants were from the hybrid learning group. There is no statistically significant difference between the two group (χ2=1.02 p = 0.313) in terms of first pass attempts; first pass attempt at MCQ (p=0.805) and first pass attempt at practical stations (p=0.408). However, there was statistically significant difference between the mean difference in results of traditional vs hybrid MCQ score, -0.29 (95% CI: -0.57 to -0.01, p=0.0409). Finally, senior doctors were also found to perform better than junior doctors in both traditional (p=0.0235) and hybrid courses (p=0.0309) at the first pass attempt of ACLS certification.
Conclusion: Participants in the hybrid ACLS course demonstrated at least equal overall proficiency in certification of ACLS as compared to the traditional instruction.
Keywords: Advanced Cardiac Life Support, Teaching Model, COVID-19, Hybrid Learning
I. INTRODUCTION
Cardiopulmonary resuscitation (CPR) represents an emergency lifesaving procedure for cardiac arrest patients. It is a core skillset for every licensed physician, graduating medical students and paramedics. It provides evidence-based algorithms to be executed to optimise the likelihood of survival in cardiac arrest patients. Cardiac arrest poses a major public health challenge. Worldwide, sudden and unexpected cardiac death is one of the most common causes of death. Given such a substantial disease burden, structured and continued training of physicians and first responders on advanced cardiac life support (ACLS) is extremely crucial. In Singapore, about 3000 people have a sudden cardiac arrest every year (Ong, 2020).
The first Advanced Cardiac Life Support (ACLS) course in Singapore, was started in late 1985 and traditionally it has been conducted over two days. It comprises of pre-reading from a manual outlining the procedure algorithms, a combination of face-to-face didactics and hands-on skills stations conducted by licensed providers and instructors, followed by multiple-choice theory and practical certification tests. It mainly focuses on technical knowledge and skills which needs to be recertified every two years (Anantharaman, 2017). Since the implementation of social distancing measures under DORSCON Orange in Singapore in response to the COVID-19 disease outbreak on 7th February 2020, ACLS teaching model has since been modified to multimedia lectures followed by small-group (maximum 5 people) practical lessons, which was further adjusted to include an online self-administered pre-lecture quiz from 18th February 2021 onwards. Limited evidence has shown that written evaluation is not a predictor for skills performance in an ACLS course and there is now, a growing body of advocates for high-fidelity mannequin-based simulation supplementing ACLS curricula. Multiple research studies have focused on the efficacy of various educational and instructional methods for ACLS teaching in terms of improvement to the resuscitation knowledge and clinical skills (Thorne et al., 2017).
We aim to retrospectively evaluate the efficacy of our new hybrid ACLS teaching model based on participants passing rate of both theory and practical tests as compared to the traditional ACLS instruction model. The primary goal is to provide enhanced insights into the way ACLS training should be conducted and further refine our courses as we evolve in the new norm of living with the COVID-19 pandemic. Institutional Review Board waiver has been obtained through Singapore Health Service (CIRB: 2021/2499).
II. METHODS
A. Study design and participants
This retrospective study was carried out at SingHealth Duke-NUS Institute of Medical Simulation (SIMS) using the course results of participants in the centre’s Advanced Cardiac Life Support (ACLS) course. A waiver of consent was approved by the institute’s CRIB committee as the results were anonymised.
The ACLS course traditionally comprises face-to-face didactic lecture components and practical skills stations culminating in MCQ and practical assessment. Successful completion of both MCQ and practical assessment results in certification or recertification for the participants.
In the hybrid ACLS learning model, the didactic lecture component has been replaced with an interactive online learning platform while maintaining the same practical skills stations with reduced instructor to student ratio because of safe distancing measures. To facilitate learning, a pre- and post-lesson quiz, with 25 MCQ questions, was administered on the online learning platform.
Course results of participants attending the traditional course from May to October 2019 were compared with participants attending the hybrid course from February to June 2021. No participants were found to have attended both the traditional and hybrid ACLS courses, to date. We did not differentiate between recertification and certification courses since there are no differences in assessments.
B. Outcome measures
Our primary outcome measure was the proportion of participants with successful first pass attempt at course certification between traditional and hybrid ACLS courses.
For secondary outcomes, we analysed the mean difference in MCQ scores and first pass attempts at practical stations between traditional and hybrid ACLS instructions. We also compared differences between pre- and post-lesson quiz scores administered during the hybrid learning to assess retention of theoretical knowledge. Lastly, we conducted a sub-group analysis comparing the proportion of senior doctors and junior doctors who pass the course at the first attempt, in both the traditional and hybrid learning groups. Here, senior doctors refer to individuals with specialist registration while junior doctors refer to all other registered medical practitioners.
C. Statistical analysis
A priori sample size estimation was carried out with the assumption that 90% of participants will pass with the first attempt in both traditional and hybrid ACLS teaching models. We used a non-inferiority margin of 10%. Taking α = 0.05 and a statistical power of 80%, we determined that would require at least 155 participants per group.
Statistical analysis was performed using Microsoft Excel 2019. T-test was used when comparing means, Chi-square test was used when comparing categorical variables.
III. RESULTS
A total of 925 participants were recruited during the study period. Of these, 626 participants were from the traditional group and 299 participants, from the hybrid learning group. No participants were excluded from the study. Table 1 shows the characteristics of both groups. The data supporting this study are openly available at https://doi.org/10.6084/m9.figshare.15131664.v1 (Lee et al., 2021).
For the traditional group, 87.7% (549 of 626) passed at the first attempt, whilst for the hybrid group, 90.0% (269 of 299) passed at first attempt (See Table 1). There was no statistically significant difference between the two groups (p = 0.313).
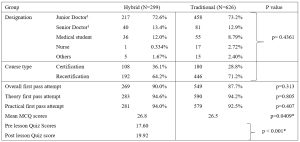
Table 1. Baseline Demographics of Participants for the ACLS Courses and comparison of primary and secondary outcome measures between the Hybrid and Traditional ACLS courses participants
1 Senior doctors are registered specialists under Singapore Medical Council. Junior doctors are all other registered medical practitioners under Singapore Medical Council.
There were no statistically significant differences between the two groups in terms of proportion of first pass attempt at MCQ (p=0.805) and first pass attempt at practical stations (p=0.408). There was however, a statistically significant difference, but with a very small effect size, between the mean difference in results of traditional vs hybrid MCQ score, -0.29 (95% CI: -0.57 to -0.01, p=0.0409).
We also compared the pre- and post-lesson quiz scores in the hybrid learning group. 21 participants were excluded from the analysis due to incomplete pre- or post- test results. We found a mean score difference of 2.32 (95% CI: 1.84 to 2.80, p < 0.001), out of a maximum score of 25, which was higher in post-test group.
Lastly, we compared the proportion of first pass test attempts between senior and junior doctors in both traditional and hybrid learning groups. Senior doctors consistently performed better than junior doctors in both traditional (96.3% vs 87.8% p=0.0235) and hybrid settings (100% vs 89.4% p=0.0309).
IV. DISCUSSION
ACLS is one of the most basic yet crucial skills of medical practitioners worldwide receiving special attention in the framework of various international and national resuscitation councils and societies (Thorne et al., 2017). Clinical educators must explore modalities and evolving technologies that can overcome the barriers of cost, access, and frequency of exposure, while balancing flexibility and applicability that follow deliverable sequelae. Thus far, participants of blended e-learning ACLS courses are known to demonstrate similar scores on the knowledge test, skills test and their final passing rate. The e-learning ACLS course also demonstrates equivalence to traditional face-to-face learning in equipping participants with ACLS skills when compared to the traditional course. This was demonstrated in our results as well. This is a value-added benefit, especially when considering factors such as increased autonomy, cost-effectiveness, decreased instructor burden and improved standardisation of course material (Thorne et al., 2017).
As we shift more towards andragogy among adult professionals, the principles for ACLS instruction should also focus more on self-directed, self-motivated and experiential instruction. Evidence does support that the form and content of these highly structured/model courses are important to transfer the clinical competence that is needed, especially in unstructured, emergencies (Rasmussen et al., 2013). Hence, exploring a sustainable model of ACLS knowledge translation is another important point since further research is needed to develop the optimal evaluation system for the ACLS training program which includes evaluation of the participants, the instructors, and the overall program. The goal should be to assess the degree to which the ACLS program is meeting its objective: to educate medical practitioners, first responders and rescuers.
The COVID-19 pandemic has affected simulation centres where ACLS courses are routinely held. Alternative education modalities have been employed, which include computer-based simulation where technology is used to enhance, augment or even at times, replace real-life simulation. It not only offers the professionals convenience but, complies with safe-distancing or ‘work-from-home’ restrictions put forth by regulatory bodies in many countries. Online modules of virtual reality have also been explored as these can be accessed anywhere electronically and can reduce the amount of face-to-face time that routine training normally requires.
V. CONCLUSION
Hybrid instruction of ACLS training for certification should be recommended as one of the main formats of course delivery as it is as effective compared to the traditional face-to-face training program. From our results it has performed well enough to allow for the safe transition and application of ACLS training in this new era.
Notes on Contributors
Lee Man Xin is involved in conceptualising the study, analysing and interpreting the data, drafting the above manuscript and approving the version to be published. He agrees to be accountable for all aspects of the work.
Zhang Yuan Helen is involved in conceptualising the study, interpreting the data, drafting the above manuscript and approving the version to be published. She agrees to be accountable for all aspects of the work.
Lateef Fatimah is involved in finalising the study conceptualisation and determining key elements for analysis. She is involved in the revision and final approval of the version to be published. She agrees to be accountable for all aspects of the work.
Ethical Approval
Institutional Review Board waiver has been obtained through Singapore Health Service (CIRB: 2021/2499).
Data Availability
The data supporting this study are openly available at figshare repository: https://doi.org/10.6084/m9.figshare.15131664.v1
Acknowledgement
The authors would like to thank Mr Billy Tee, Ms Suppiah Madhavi and Ms Angeline Ng from Singhealth Duke-NUS Institute of Medical Simulation (SIMS) Singapore for providing the data sets.
Funding
This paper receives no funding from outside sources.
Declaration of Interest
Authors have nothing to declare, nor any conflict of interests.
References
Anantharaman, V. (2017). The National Resuscitation Council, Singapore, and 34 years of resuscitation training: 1983 to 2017. Singapore Medical Journal, 58(7), 418–423. https://doi.org/10.11622/smedj.2017069
Lee, M. X., Lateef, F., & Zhang, H. Y. (2021). Hybrid ACLS model (version 1). [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.15131664.v1
Ong, M. E. (2020, October 2). Improving outcomes for Out-of-Hospital cardiac arrest victims. The Straits Times. https://www.singhealth.com.sg/rhs/news/research/improving-outcomes-for-out-of-hospital-cardiac-arrest-victims
Rasmussen, M. B., Dieckmann, P., Barry Issenberg, S., Østergaard, D., Søreide, E., & Ringsted, C. V. (2013). Long-term intended and unintended experiences after Advanced Life Support training. Resuscitation, 84(3), 373–377. https://doi.org/10.1016/j.resuscitation.2012.07.030
Thorne, C. J., Lockey, A. S., Kimani, P. K., Bullock, I., Hampshire, S., Begum-Ali, S., & Perkins, G. D. (2017). e-Learning in Advanced Life Support-What factors influence assessment outcome? Resuscitation, 114, 83–91. https://doi.org/10.1016/j.resuscitation.2017.02.014
*Lee Man Xin
Changi General Hospital Emergency Department
2 Simei Street 3, Singapore 529889
Email: Lee.Man.Xin@singhealth.com.sg
Submitted: 10 August 2021
Accepted: 28 October 2022
Published online: 5 April, TAPS 2022, 7(2), 37-41
https://doi.org/10.29060/TAPS.2022-7-2/SC2670
Qianhui Cheng1, Joanna Pearly Ti1,2, Wai Yung Yu1,2, Hui Ping Oh1, Yih Yian Sitoh1,2
1Department of Neuroradiology, National Neuroscience Institute, Singapore; 2Duke NUS Graduate Medical School, Singapore
Abstract
Introduction: Magnetic Resonance (MR) safety is critically important in any Radiology Department, and MR-related accidents are preventable. Serious games provide opportunities for learners to build MR safety awareness through play in an immersive learning environment by using simulated scenarios such as screening virtual patients and managing an MR-related accident.
Methods: We developed a serious game, in partnership with a game developer, introducing MR safety concepts to learners as they navigate through a virtual 3D Radiology department. Drag-and-drop minigames are incorporated to aid the learner to identify hazards in and around the MR environment. Virtual patients are placed in waiting areas to provide realism, and learners are tasked to screen them as part of MR Safety Screening checks. A simulation of an MR-related accident prompts learners to make decisions or take actions to ensure safety and mitigate further risks during the accident. The learner also role-plays as a Risk Officer to identify the multiple key incidents that led to the accident. These formative assessments, with instantaneous feedback, assesses the learners’ knowledge of MR safety.
Results: Pilot feedback of this serious game revealed that it is realistic, engaging and relatable. The instructions within the game were clear and aided learning. The game has also been scaled up and customised for the radiology departments of 3 other healthcare institutions.
Conclusion: Serious games provide a training solution to raise MR safety awareness by simulating real-life scenarios in an immersive learning environment. It supplements face-to-face training and is scalable to other healthcare institutions.
Keywords: Medical Education, Technology-Enhanced Learning, Gamification, MR Safety, Workplace Safety, Simulation
I. INTRODUCTION
Magnetic Resonance (MR) safety plays a critical role in any Radiology Department to ensure the safety of patients and healthcare workers. MR is an imaging tool that uses a magnetic field to acquire detailed images of the body for the investigation of diseases.
MR-related incidents are prevalent; for instance, the US Food and Drug Administration (US FDA) received 1568 adverse events reports for MR-related incidents over 10 years between 2008 and 2017 (Delfino et al., 2019). These reported adverse events included mechanical events (eg. crushed injuries) and projectiles that are caused by objects pulled in by the magnetic field.
Hence, caution must be taken as the MR scanner’s magnetic field is always on and poses safety risks when MR safety protocols are not adhered to. Ferromagnetic objects can become projectiles within or near the magnetic field and pose a danger to patients and staff members present within it. MR-related accidents are preventable and are caused by MR safety lapses, occasionally resulting in deadly outcomes. Hence, building MR safety awareness for all levels of healthcare staff, from ward staff to those who work in the radiology department, is crucial.
Today’s generation of learners, coined as ‘digital natives’ are accustomed and receptive to the digital world and game-based learning (Girard et al., 2013). Serious games refer to digital games with the specific purpose of training learners to meet an educational objective (Girard et al., 2013). It has been used as an educational tool to realistically simulate incidents for disaster risk management (DRM) and to raise awareness (Solinska-Nowak et al., 2018). Similarly, it has also been used as training tools in health professional education for patient safety (Ricciardi & De Paolis, 2014).
Serious games can virtually replicate the MR environment and simulate MR incidents that are too dangerous to re-enact in the real world, thus preparing the healthcare professionals for such scenarios. The serious game is an ideal training solution to complement face-to-face training of healthcare professionals on MR safety and can be incorporated into the standardised curriculum design. The intended learning outcomes can be achieved through the constructive alignment of learning activities (within the game and on-the-job) and coupled with assessment and in-game feedback.
Using a learner-centric approach, serious games provide learners with risk-free decision-making opportunities, enhancing MR safety competency through play within an immersive, yet safe, virtual learning environment. These allow learners to exercise the safety behaviours and actions required at the workplace to handle situations that they may encounter.
This short communication aims to describe how this serious game was developed and how the game was evaluated at the pilot stage.
II. METHODS
The team was awarded the Learning Technology Adoption Grant in January 2020 offered by SkillsFuture Singapore (SSG). It is a grant to fund medical education serious games in SingHealth. SingHealth Academy partnered the team with game developers, including instructional designers who helped with the game development.
MR safety lapses can be deadly, and the learning outcomes of the game are to gain knowledge of MR safety and accident risk management, and to be able to demonstrate understanding of these concepts by application of knowledge in the application scenarios within the game and at the workplace.
The target audience for this game includes radiology staff, healthcare staff or ancillary staff, such as housekeeping personnel, who may enter the MR environment and thus, are required to ensure MR safety in their line of work.
The game sets out in a virtual radiology department, modelled after the Neuroradiology department at the National Neuroscience Institute. The virtual world includes virtual patients, staff as player and non-player characters in institutional uniforms, and medical devices that mirror real-life equipment in the radiology department.
Two games were created in the MR safety series. In the first game, learners navigate as an avatar to interact with objects in the MR environment, such as medical devices and virtual patients. The learning outcome of the first game is to understand the key MR safety concepts which follow the American College of Radiology (ACR) guidelines (American College of Radiology, 2020).
The second game was modelled on an MR-related accident. Learners assess the accident scenario (Fig 1a) and consider strategies for risk management, evaluating their options within the game. Critical wrong decisions or actions made during the gameplay may trigger an abrupt end to the game. This emphasises the urgency of actions required in an MR-related accident when a life is in danger and the immediate steps required to be taken to reduce the risk for further injuries. Beyond the virtual accident, the learner role-plays as a Risk Officer to assess and identify several key incidents that led to the accident as part of a root cause analysis investigation.

Figure 1a (left): MR accident scenario within the serious game
Figure 1b (right): Application of MR safety labelling near the MR scanner
Minigames are used as formative assessments, and learners receive instantaneous in-game feedback from their attempts. By screening virtual patients and placement of medical devices in their appropriate location, as part of the MR safety screening checks, the game assesses learners’ ability to identify hazards in and around the MR environment (Fig 1b), with correct placement demonstrating their learning.
For the purpose of game development, beta testers from the Neuroradiology department were included to gather preliminary feedback about the game through implied consent. A survey was administered, and responses ranged on a Likert scale (1=Strongly disagree to 5= Strongly agree).
III. RESULTS
In the initial phase of game development, beta testing of the game was conducted on 11 staff, including radiographers, radiologists, radiography assistants, radiology nurses and administrative staff with differing years of MR work experience. Beta-testers were also selected for their experiences in playing games, ranging from none to some experience. Data reported below as ‘agreed’ is aggregated to reflect ‘agreed’ and ‘strongly agree’ responses (Cheng et al., 2021).
In terms of the learning instructions, all respondents (100%) were aware of the learning outcomes. 81.82% found the instructions clear, and they knew what to do at every stage.
In terms of the virtual game environment, respondents generally felt the game has realistic engagement regarding the design. All respondents (100%) agreed that the game environment was realistic; the avatars (player characters) and objects in the game resembled those at the workplace (100%), and the background sound aided the engagement with the game (81.82%). 90.91% of respondents could also relate to the main player character within the game.
On the contrary, some respondents had trouble operationalising the game mechanics; 27.27% had trouble using the controls, and 36.36% found it difficult navigating within the game.
Overall, 90.91% found the game was fun, and engaging (100%). 81.82% agreed that their past experience helped them to overcome some of the obstacles in the game. Furthermore, 81.82% agreed that the results are a fair reflection of their skill and competency in MR safety.
Arising from the positive preliminary feedback of this serious game, the game has been shared and further adopted by radiology departments from three other healthcare institutions [Singapore General Hospital (SGH), KK Women’s and Children’s Hospital (KKH) and Sengkang General Hospital (SKH)]. The respective teams are working with the game developers to customise and adapt the environment to the local site, including medical devices and safety labels in their local settings for MR safety education.
IV. DISCUSSION
The MR safety game is an educational tool to assess and align MR safety competency for healthcare staff. Furthermore, the game can be incorporated into the orientation curriculum of radiographers as part of a competency checklist onboarding package, supplementing face-to-face training.
Being accustomed to the digital games, ‘digital natives’ as the target generation of learners would find this mode of delivery more relatable, engaging and realistic (Girard et al., 2013). At the same time, it also incorporates a structured learning design, constructively aligned with clear learning outcomes, learning activities and assessment coupled with instantaneous in-game feedback.
However, we acknowledge that some learners may experience difficulties with navigation in a virtual world. Hence, clear instructions by the facilitator on gaming instructions need to be incorporated in the pre-briefing to learners for more effective engagement and outcomes.
As learners navigate the virtual environment, they pick up MR safety knowledge and apply them to game scenarios as part of active learning. Role-playing as a Risk Officer also makes them more aware of the possible safety lapses that may occur and lead to an MR-related accident. Post-game play feedback should also be incorporated for learners to align the behaviours expected of learners at the workplace.
Beyond the institution, it is scalable to staff from other radiology departments and hospital ward staff, such as nurses and doctors who have no prior knowledge of MR safety but would have adhoc opportunity to be in the MR environment, for example, accompanying a patient to the radiology department for an MR scan.
Finally, through experiential learning, the game emphasises that everyone plays a critical role in MR safety and that safety lapses can lead to accidents.
V. CONCLUSION
Purpose-built simulation serious games that mimic a virtual radiology department provide an ideal training solution for MR safety education. Serious games provide an immersive learning environment where simulated scenarios such as safety screening of virtual patients and MR-related accidents is made possible. Simulation of dangerous scenarios that are impossible to recreate in the real world provides opportunities to raise MR safety awareness and is also scalable to the wider healthcare community.
Notes on Contributors
Cheng Qianhui contributed to the conceptualisation and design of this serious game, drafting the manuscript and approved the final version to be published.
Joanna Pearly Ti contributed to the conceptualisation and design of this serious game, revised the manuscript for intellectual content and approved the final version to be published.
Yu Wai-Yung is a mentor to the team, revised the manuscript for intellectual content and approved the final version to be published.
Oh Hui Ping contributed to the conceptualisation and design of this serious game, revised the manuscript for intellectual content and approved the final version to be published.
Sitoh Yih Yian is a mentor to the team, revised the manuscript for intellectual content and approved the final version to be published.
Ethical Approval
Review not required as stipulated by CIRB (CIRB Reference No.: 2021/2397).
Data Availability
The beta testing evaluation data presented in this manuscript is available in the Figshare data repository: https://doi.org/10.6084/m9.figshare.14473074.v1
Acknowledgement
We would like to thank SingHealth Academy and Playware Studios for their tremendous contribution for the creation of this serious game. We are also thankful to NNI neuroradiology staff for their help with the pre-testing of the game, contributing to the game development through honest feedback. We are thankful to Serious Games Asia and Singapore University of Technology and Design (SUTD) for co-developing the survey evaluation. We sincerely thank our scale-up teams, the radiology departments from Singapore General Hospital (SGH), Sengkang General Hospital (SKH) and KK Women’s and Children’s Hospital (KKH) so that more staff across SingHealth can benefit from MR safety training through this serious game.
This project has been presented as Free Communication at the Asia Pacific Medical Education Conference 2021, and the author was awarded the Young Scholar Award Runner-up.
Funding
The game development and scale-up is funded by Learning Technology Adoption Grant (LTAG) offered under SkillsFuture Singapore (SSG), which SingHealth Academy has applied to jumpstart medical education serious games in SingHealth institutions. SingHealth Academy is the education arm in SingHealth to coordinate the application with SSG.
Declaration of Interest
The authors declare no conflict of interest.
References
American College of Radiology. (2020). ACR manual on MR safety. https://www.acr.org/-/media/ACR/Files/RadiologySafety/MRSafety/Manual-on-MR-Safety.pdf
Cheng, Q., Ti, J. P., Yu, W.-Y., Oh, H. P., & Sitoh, Y. Y. (2021). MR safety beta testing data [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.14473074.v1
Delfino, J. G., Krainak, D. M., Flesher, S. A., & Miller, D. L. (2019). MRI‐related FDA adverse event reports: A 10‐yr review. Medical Physics, 46(12), 5562–5571. https://doi.org/10.1002/mp.13768
Girard, C., Ecalle, J., & Magnan, A. (2013). Serious games as new educational tools: How effective are they? A meta-analysis of recent studies. Journal of Computer Assisted Learning, 29(3), 207–219. https://doi.org/10.1111/j.1365-2729.2012.00489.x
Ricciardi, F., & De Paolis, L. T. (2014). A comprehensive review of serious games in health professions. International Journal of Computer Games Technology, 2014, Article 787968. https://doi.org/10.1155/2014/787968
Solinska-Nowak, A., Magnuszewski, P., Curl, M., French, A., Keating, A., Mochizuki, J., Liu, W., Mechler, R., Kulakowska, M., & Jarzabek, L. (2018). An overview of serious games for disaster risk management – Prospects and limitations for informing actions to arrest increasing risk. International Journal of Disaster Risk Reduction, 31, 1013–1029. https://doi.org/10.1016/j.ijdrr.2018.09.001
*Cheng Qianhui
National Neuroscience Institution
11 Jalan Tan Tock Seng,
Singapore 308433
Singapore 117593
Email: qianhui_cheng@nni.com.sg
Submitted: 14 April 2021
Accepted: 24 June 2021
Published online: 4 January, TAPS 2022, 7(1), 98-101
https://doi.org/10.29060/TAPS.2022-7-1/SC2517
Lean Heong Foo & Marianne Meng Ann Ong
Department of Restorative Dentistry, National Dental Centre Singapore, Singapore
Abstract
Introduction: Team-based learning (TBL) pedagogy is a structured, flipped classroom approach to promote active learning. In April 2019, we designed a TBL workshop to introduce the New Classification of Periodontal Diseases 2017 to a group of general dental practitioners (GDPs). We aimed to investigate GDPs feedback on learning this new classification using TBL pedagogy.
Methods: Two articles related to the 2017 classification were sent to 22 GDPs 2 weeks prior to a 3-hour workshop. During the face-to-face session, they were randomly assigned to five groups. They participated in individual and group readiness assurance tests. Subsequently, the GDPs had inter- and intragroup facilitated discussions on three simulated clinical cases. They then provided feedback using a pen-to-paper survey. Based on a 5-point Likert scale (1-strongly disagree to 5-strongly agree), they indicated their level of agreement on items related to the workshop and their learning experience.
Results: Majority (94.7%, 18 out of 19 GDPs) agreed the session improved their understanding of the new classification and they preferred this TBL pedagogy compared to a conventional lecture. All learners agreed they can apply the knowledge to their work and there was a high degree of participation and involvement during the session. They found the group discussion and the simulated clinical cases useful.
Conclusion: A TBL workshop is suitable for clinical teaching of the New Classification of Periodontal Diseases 2017 for GDPs. Its structure promotes interaction among learners with the opportunity to provide feedback and reflection during the group discussions. This model might be a good pedagogy for continuing dental education.
Keywords: Team-based Learning, General Dental Practitioners, New Classification of Periodontal Diseases
I. INTRODUCTION
Team-based learning (TBL) is a flipped classroom, structured learning pedagogy that was introduced by Larry Michaelsen and has gained popularity among healthcare educators recently. TBL is learner-centric and dialectic based, and practices logical discussion used for determining the truth of a theory or opinion (Michaelsen et al., 2008). It provides the opportunity for peer-teaching by group members and can assist weaker students in understanding course materials.
Several dental educators have utilised TBL in undergraduate dentistry programmes and observed higher engagement among learners, less student contact time and faculty time, and higher course grades (Haj-Ali & Al Quran, 2013). General dental practitioners (GDPs), unlike undergraduate dental students, juggle between busy dental practice and family life. Hence, GDPs might seek active learning with direct knowledge application to manage their continuing dental education needs efficiently. The World Workshop of Periodontology recently revamped the diagnosis of periodontal diseases and proposed a new classification of staging (Stage I-IV; based on severity of disease) and grading (Grade A-C; based on disease progression) for periodontitis (Tonetti et al., 2018). We aimed to investigate GDP feedback on learning this new classification using TBL pedagogy.
II. METHODS
This is a descriptive study on GDPs’ feedback on learning the New Classification of Periodontal Diseases 2017 using a TBL approach. 22 GDPs attended the TBL workshop in April 2019.
Two articles related to the new classification were sent to the GDPs 2 weeks prior to the 3-hour workshop. Five multiple-choice questions were crafted from the two articles (Individual Readiness Assurance Test, IRAT) to assess learners’ basic understanding of the new classification. Learners were divided into five groups to discuss IRAT and provide answers using the immediate feedback assessment technique card (Group Readiness Assurance Test, GRAT). Faculty then highlighted key elements of the new classification. Three clinical periodontal cases crafted based on the 4S framework principles i.e. same problem, significant problem, specific choice, and simultaneous reporting, were used in the application process (Michaelsen et al., 2008). The key question was to diagnose the periodontal condition based on the staging and grading criteria. Lastly, learners provided implied consent by answering an anonymous pen-to-paper survey voluntarily. They answered based on their level of agreement on a 5-point Likert scale (5 indicating strongly agree, 1 indicating strongly disagree). The survey comprising 13 education-related statements: two statements related to programme content, two to presentation, six to learning experience, and three about the workshop. Three qualitative questions in the survey were: “What do you like most about the workshop?”, “What aspects of the session could be improved?” and “Other comments and feedback”.
III. RESULTS
Nineteen out of the 22 GDPs who attended the TBL workshop responded to the survey (response rate 86.4%). Results are summarised in Figure 1. We conducted a reliability analysis on the perceived task values scale comprising two subscales (learning experience and workshop) with at least three items.
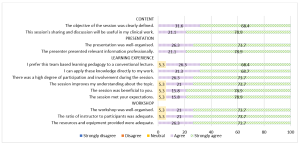
Figure 1. Learners’ feedback about the workshop
A. Content (Two items)
During the workshop, we highlighted the staging and grading criteria for the new classification. Learners provided a mean score of 4.74 (standard deviation, SD, 0.446; median 5) in two statements related to content. In general, 68.4% of them strongly agreed and 31.6% agreed the objective of the workshop was clearly defined. There were 78.9% and 21.1% of learners who strongly agreed and agreed respectively that the sharing and discussion during the workshop was useful to their clinical work.
B. Presentation (Two items)
Learners gave a mean score of 4.76 for presentation (SD 0.431; median 5). There were 73.7% learners who strongly agreed and 26.3% who agreed that the presentation was well-organised. In addition, 78.9% and 21.1% of the learners strongly agreed and agreed respectively that the presenter presented relevant information professionally.
C. Learning Experience (Six items)
Cronbach’s alpha for the learning experience subscale reached acceptable reliability at α = 0.81. The mean score for learning experience was 4.70 (SD 0.531; median 5). There were 68.4% learners who strongly agreed and 26.3% who agreed that they prefer TBL pedagogy to a conventional lecture. Also, 68.7% of the learners strongly agreed and 31.3% agreed they could apply the knowledge directly to their work. All learners agreed that there was a high degree of participation and involvement during the session. 18 learners (94.7%) agreed that the session met their expectations and improved their understanding about the topic.
D. Workshop (Three items)
The mean score for learners’ feedback on the workshop was 4.71 (SD 0.533; median 5). 18 learners (94.7%) agreed that the workshop was well organised with an adequate ratio of instructor to participants (2:22). There were 73.7% learners who strongly agreed and 26.3% who agreed that resources and equipment provided were adequate. Cronbach’s alpha for the workshop subscale reached acceptable reliability at α = 0.75.
E. Qualitative Feedback
The learners cited the following themes as their favourite component of the workshop: “group interaction and discussion” (4), “clinical case discussion” (3), “useful and relevant clinical cases” (1), “interesting readiness assurance test” (1), and “pre-reading material” (1). They also cited “active learning” (1), “correct wrong understanding” (1), “discussion improves my understanding” (1), and “great information and lecturer” (1) as positive learning experiences. Three different learners provided feedback of “best workshop ever attended”, “well done”, and “very good” respectively. One learner commented that the air-conditioning in the room was cold. One learner commented on small font size in dental charting and another learner suggested “less tests at the start”.
IV. DISCUSSION
The flipped classroom concept in TBL was suitable for GDPs to study the pre-reading articles at their own pace. The structured workshop enabled them to correct any misconception immediately and deepen their understanding about the new classification. This observation concurs with the finding that all GDPs agreed they could apply the knowledge to their work and preferred this pedagogy over a traditional lecture. This active learning process differs from a conventional didactic lecture, which is faculty-centric with less feedback and interaction. Hence, this pedagogy can be applied for some continuing dental education programmes by improving the delivery and application of new concepts. The 4S framework in the application cases are key elements to promote productive and logical discussion similar to a debate facilitated by faculty. The problem-solving aspect of TBL, along with the scaffolding and guidance by faculty, can enhance the metacognition process among learners (Hrynchak & Batty, 2012). Almost all learners agreed there was an adequate ratio of faculty to participants, emphasising the benefit of using TBL workshops to teach a large group of learners with less faculty. However, faculty needs to work more in planning and preparing the teaching materials, executing, and facilitating the session following the TBL structure and process. In addition, hurdles in conducting TBL include acceptance from faculty and learners, difficulty in supervising a large group, the customisation of the course content, and adequate training and expertise to conduct TBL effectively.
The learners also cited “group interaction and discussion” as their favourite component of the workshop. The learning theory underpinning TBL is the constructivist learning theory where the faculty exposes knowledge inconsistency during group discussion, subsequently allowing a new mental framework to be built upon the new understanding (Hrynchak & Batty, 2012). TBL is useful in healthcare education since it can promote good critical thinking and teamwork. In addition, the intra- and intergroup formal discussion provides the opportunity to reflect, give feedback, and enable peer-teaching. Self-reflection enables learners to make a judgement when modifying their existing knowledge. Peer-to-peer teaching in TBL enhances learning and aids weaker learners to understand the course material (Park et al., 2014).
Some limitations of our study were that the sample size was small, reporting participants’ self-perception on how they felt after attending the workshop and the lack of longitudinal follow-up on retention of knowledge. In addition, we did not have a separate didactic lecture on the new classification as a control group to truly compare the two different modes of teaching. Future recommendation includes having two groups of GDPs to collate their perceptions as well as include a pre and post assessment to investigate the difference in improvement and in knowledge retention comparing TBL workshop and traditional didactic lecture, and include peer evaluation in TBL to increase accountability among learners. Besides, ethnographic research method can be explored to provide insight to researchers to understand the essence of how dental professionals learn during TBL. It would be meaningful to follow up this group of GDPs to assess the accuracy of their periodontal diagnoses based on the new classification to investigate the effectiveness of the TBL workshop. Of note, TBL workshops can be adapted into an online format; this is particularly useful during the current COVID-19 pandemic to engage learners and promote active learning in an online setting.
V. CONCLUSION
In conclusion, TBL pedagogy may be another mode of teaching for GDPs in continuing dental education where participants are actively engaged, and direct application of knowledge gained can be made. During this pandemic, where face-to-face sessions are minimised, educators can consider adopting TBL pedagogy on an online platform to improve learning experience and engagement of their learners.
Notes on Contributors
Dr Lean Heong Foo is a Consultant Periodontist in Department of Restorative Dentistry and Head to the Dental Surgery Assistant Certification Programme in National Dental Centre Singapore. FLH reviewed the literature, contributed to study conception, data acquisition, data analysis, drafted and critically revised the manuscript.
Dr Marianne M. A. Ong is a Senior Consultant Periodontist & Director of Education in National Dental Centre Singapore. MO contributed to study conception, data acquisition and critically revised the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Ethical Approval
This study was exempted from formal Centralised Institutional Review Broad review by SingHealth Institutional Review Board (CIRB Ref: 2021/2133).
Data Availability
Data is deposited at Figshare. https://doi.org/10.6084/m9.figshare.14411858
Acknowledgement
The authors would like to thank Ms Safiyya Mohamed Ali for providing editorial support.
Funding
There was no funding involved in the preparation of the manuscript.
Declaration of Interest
The authors declare no conflict of interest.
References
Haj-Ali, R., & Al Quran, F. (2013). Team-based learning in a preclinical removable denture prosthesis module in a United Arab Emirates dental school. Journal of Dental Education, 77(3), 351–357.
Hrynchak, P., & Batty, H. (2012). The educational theory basis of team-based learning. Medical Teacher, 34(10), 796–801.https://doi.org/10.3109/0142159X.2012.687120
Michaelsen, L. K., Parmelee, D. X., McMahon, K. K., & Levine, R. E. (2008). Team-based learning for health professions education: A guide to using small groups to improving learning. Stylus.
Park, S. E., Kim, J., & Anderson, N. K. (2014). Evaluating a team-based learning method for detecting dental caries in dental students. Journal of Curriculum and Teaching, 3(2), 100-105. https://doi.org/10.5430/jct.v3n2p100
Tonetti, M. S., Greenwell, H., & Kornman, K. S. (2018). Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. Journal of Periodontology, 89(Suppl 1), S159–S172. https://doi.org/10.1002/JPER.18-0006
*Foo Lean Heong
National Dental Centre Singapore,
5, Second Hospital Avenue,
168938 Singapore
Email: foo.lean.heong@singhealth.com
Submitted: 29 March 2021
Accepted: 28 September 2021
Published online: 4 January, TAPS 2022, 7(1), 102-105
https://doi.org/10.29060/TAPS.2022-7-1/SC2508
Mairi Scott & Susie Schofield
Centre for Medical Education (CME), School of Medicine, University of Dundee, Scotland, United Kingdom
Abstract
Introduction: The switch to online off-campus teaching for universities worldwide due to COVID-19 will transform into more sustainable and predictable delivery models where virtual and local student contact will continue to be combined. Institutions must do more to replace the full student experience and benefits of learners and educators being together.
Methods: Our centre has been delivering distance blended and online learning for more than 40 years and has over 4000 alumni across five continents. Our students and alumni come from varied healthcare disciplines and are at different stages of their career as educators and practitioners. Whilst studying on the programme students work together flexibly in randomly arranged peer groups designed to allow the establishment of Communities of Practice (CoP) through the use of online Discussion Boards.
Results: We found Discussion Boards encouraged reflection on learning, sharing of ideas with peers and tutors, reduce anxiety, support progression, and enable benchmarking. This led to a highly effective student sense of belonging to each other, our educators, and the wider University, with many highlighting an excellent student experience and maintaining a thriving CoP within the alumni body.
Conclusion: Despite being based on one large postgraduate programme in medical education, our CoP approach is relevant to any undergraduate programme, particularly those that lead to professional qualification. With our mix of nationalities, we can ‘model the way’ for enabling strong CoP’s to share ideas about best practice with a strong student and alumni network which can be shared across the international healthcare community.
Keywords: Communities of Practice, Sense of Belonging, Student Experience
I. INTRODUCTION
The sudden switch to online, dual delivery and on-campus/off-campus teaching for Universities worldwide will not be reversed at the end of the current COVID-19 crisis but will transform into a more sustainable and predictable delivery model where virtual and local student contact will continue to be combined. The switch, known as Emergency Remote Teaching (ERT) (Hodges et al., 2020) achieved much in a short timeframe but institutions need to do more to truly replace the full student experience and benefits of learners and educators being together on-site. The need for this new approach is acute in professional-based courses such as medicine where students need to learn complex skills within the context of healthcare delivery. These skills are acquired through multiple interactions with clinical colleagues in the workplace which, although often brief, are focused in real-time.
Given that the learning environment is dependent on the institutional ‘personality, spirit, and culture’ (Holt & Roff, 2004, pp. 553), human interaction is necessary to create that culture. We must develop new approaches to delivering medical education by merging established educational technologies with virtual approaches to establish on-line interaction with peers and senior colleagues such as can be achieved in Communities of Practice (CoPs) (Lave & Wenger, 1991). CoPs are social structures where people can share ideas, stories, and experiences relevant to the community’s activities. They help participants make sense of new knowledge and enable novices to benefit from working with experts, thus reducing anxiety, supporting progression, and enabling benchmarking. These components lead to the creation of a rich environment for information-sharing which has become increasingly important within healthcare delivery organisations during the COVID-19 pandemic.
We have built on over 40 years’ experience of delivering distance, blended and online Masters-level accredited medical education learning across five continents to ‘model the way’ to providing a strong student experience for online learners. Our students and alumni come from various interdisciplinary healthcare disciplines, at different stages of their career as educators and practitioners.
II. METHODS
Several Discussion Boards (DBs), usually one per study week plus one for assignment questions are created in each 12-week Moodle-based module. Students are randomly assigned to groups to work together flexibly within these peer groups. Each discussion has a ‘prompt’ linked to that week’s work, designed to create CoPs and a highly effective student sense of belonging (SoB) to each other and programme educators. In the first module students are actively encouraged to participate, with emphasis being on the ‘safe space’ created that allows them to learn effectively from and with each other. DB comments are used as part of programme enhancement and quality assurance. Students give informed consent to their evaluation comments within DBs being extracted for overall programme review.
III. RESULTS
As students move from legitimate peripheral participant to experienced member, they often express increased confidence that their posts will allow them to share their view and help colleagues. The forum posts have been analysed as part of a much larger study; the following diagram (Figure 1) highlights some of the benefits.
Figure 1. Sample of comments in DBs posts
Our experience over the last four years is that student levels of interaction increase the further into the programme they go, suggesting that they value and enjoy it. Overall, when asked specifically if that assumption is correct, feedback from students is exceptionally positive and they comment on their achievement of a SoB through engagement with the DBs. Many highlight the excellent student experience. Another indirect indication of success is that student module success rate averages 93% across the modules, which is high for an online learning programme.
The benefits of using DBs are threefold:
- They allow for reflection on learning in real-time due to regular module-specific weekly activities requiring students to reflect on that week’s educational materials and post their thoughts on the DBs.
- They allow sharing with peers and tutors, establishing CoPs: The DB posts create peer-to-peer dialogue, encouraging students to practise the language of the discipline in a safe, supported environment. Learning activities are based on the principle of linking previous experience with the interpretation of new knowledge, thus enabling an escalation of the complexity of questions to enhance deeper connection and dialogue. Although essentially (and importantly) it is the students as peers who are encouraged to respond to each other’s questions and comments, the tutors do monitor posts, providing input when necessary and desirable. In some modules, students are required to give peer feedback on draft assignments using a 1:4 ratio to encourage a range of views and expertise, increasing the depth and extent of their critical thinking and analysis. This also gives them practice in giving and receiving feedback, an essential skill for future medical educators.
- CoPs build trust in colleagues and a SoB within the learning environment, leading to an excellent learning experience. Students state that they value the tutor contribution as this increases the confidence they have in their own online comments, sometimes shifting the discussion to a more profitable area for new learning in a way that was not pre-planned or even at times expected.
IV. DISCUSSION
Our approach to the creation of CoPs is based on the principle that in order to establish student trust and a SoB DBs are an essential tool. Management research describes trust within organisations as being multifaceted, with the main components being capability, well-meaning intent, and integrity (Ridings et al., 2002). It is accepted that within our programmes both tutor and student capabilities have been established. Integrity is established by clearly explaining the expected mode of student behaviour at the outset and demonstrated as students work through the programme. Well-meaning intent is demonstrated by acts of positive reciprocation built up over time by asking students to give peer feedback frequently and around increasingly complex activities. Both integrity and well-meaning intent therefore need to have a continued focus during module design and delivery and throughout the assessment process.
Now that medical education has been forced to re-evaluate the place of online learning as a consequence of the COVID-19 crisis, it seems inevitable that many of the discovered benefits will lead to significant changes in the way we teach and learn. Davis (2018) explored a future medical school being one ‘without walls’ by which he meant that the artificial separation of the ‘classroom and the clinic’ would inevitably diminish as we embraced flipped classrooms and online collaborative learning.
If we adopt this approach for student learning it may also change the way we think about faculty development, as we could create extensive networks of faculty development special interest grouped CoPs beyond the ‘walls’ of our own schools. A recent study by Chan et al. (2018) in McMaster describes the creation of a Faculty Incubator – a virtual CoP which uses a longitudinal, asynchronous, online platform to deliver a one-year curriculum to support early-to mid-career educators from 30 different locations with their professional development. This widespread (geographically) collaborative approach was found to be well received, with lively interactions which broke down some of the boundaries that normally prevent early career academics from approaching unknown colleagues in different locations, colleagues they would normally never have met in person.
An additional challenge created by the COVID-19 pandemic was the necessity for healthcare professionals to make clinical decisions in an ‘evidence-poor’ disease by gathering emerging data (often by word-of-mouth) and treating patients without the certainty of a knowledge base built up over decades of robust randomised controlled trial (RCT) evidence. This is described by Rosenquist (2021, pp. 8) as a kind of “Bayesian fatigue”: a stress-induced dysphoria experienced when the corpus of knowledge that is the foundation of one’s work acquired over decades, becomes less important than information being gathered from disparate sources in real time.’ The ‘disparate sources’ referred to here are groups of widely dispersed practitioners (within current and new CoPs) who are sharing individual and collective rapid learning by experience that has become necessary when treating patients with COVID-19. These CoPs are based on the collective trust healthcare professionals express in valuing the views of colleagues struggling with similar challenges. This helps reduce that ‘Bayesian’ impact when it comes to making difficult clinical decisions in real time with limited evidence. However, trust within a CoP also comes from previous positive experience of being within other CoPs, and so it is important that we as medical educators enable our students to have experience of the value of sustainable CoPs in their own learning. Despite the limitations of the range of the study comments, we believe that given the extent of the sudden switch to ERT our findings of use of DBs to establish much appreciated CoPs justifies early dissemination through this short communication.
V. CONCLUSION
As medical educators we must have the skills necessary to establish strong and sustainable CoPs to educate current and future healthcare professionals in this effective way of learning from each other. This can be done as effectively with online learning as with on-campus interaction, allowing the possibility of the widespread creation of truly effective international CoPs sustainable for years to come.
Notes on Contributors
Professor Mairi Scott reviewed the literature, selected the data, wrote the manuscript, created the presentation and presented the materials virtually to the Conference. Dr Susie Schofield reviewed the literature, advised on the selection of the data and gave critical feedback on the manuscript. Both authors have read and approved the final manuscript.
Ethical Approval
Ethics approved was granted by School of Medicine & School of Life Sciences Research Ethics Committee, University of Dundee, Dundee, DD1 4HN on 03/05/19. Application Number: 19/41.
Data Availability
Ethical approval specified that raw data would not be made available for others out with the Centre ‘beyond the anonymised published or reported versions within the dissemination strategy’.
Acknowledgement
The authors would like to thank Dr Thillainathan Sathaananthan (PhD student) and Dr Linda Jones (PhD supervisor, Senior Lecturer) CME, University of Dundee, who produced some of the outcomes as part of research into student experiences with online learning and the use of Discussion Boards.
Funding
No grant or external funding was received for this work.
Declaration of Interest
Both authors have no conflict of interest to declare.
References
Chan, T. M., Gottlieb, M., Sherbino, J., Cooney, R., Boysen-Osborn, M., Swaminathan, A., Ankel, F., & Yarris, L. M. (2018). The ALiEM faculty incubator: A novel online approach to faculty development in education scholarship. Academic Medicine, 93(10), 1497–1502. https://doi.org/10.1097/ACM.0000000000002309
Davis, D. (2018). The medical school without walls: Reflections on the future of medical education. Medical Teacher, 40(10), 1004–1009. https://doi.org/10.1080/0142159X.2018.1507263
Hodges, C., Moore, S., Lockee, B., Trust, T., & Bond, A. (2020). The difference between emergency remote teaching and online learning. EDUCAUSE Review. https://er.educause.edu/%20articles/2020/3/the-difference-between-emergency-remote-teaching-and-online-learning
Holt, M. C., & Roff, S. (2004). Development and validation of the Anaesthetic Theatre Educational Environment Measure (ATEEM). Medical Teacher, 26(6), 553-558. https://doi.org/10.1080/01421590410001711599
Lave, J., & Wenger, E. (1991). Situated learning: Legitimate peripheral participation. Cambridge University Press.
Ridings, C. M., Gefen, D., & Arinze, B. (2002). Some antecedents and effects of trust in virtual communities: The Journal of Strategic Information Systems, 11(3-4), 271–295. https://doi.org/10.1016/S0963-8687(02)00021-5
Rosenquist, J. N. (2021). The stress of Bayesian medicine—Uncomfortable uncertainty in the face of COVID-19. New England Journal of Medicine, 384(1), 7-9. https://doi.org/10.1056/NEJMp2018857
*Mairi Scott
Centre for Medical Education,
University of Dundee
Email: m.z.scott@dundee.ac.uk
Submitted: 15 January 2021
Accepted: 12 April 2021
Published online: 5 October, TAPS 2021, 6(4), 142-145
https://doi.org/10.29060/TAPS.2021-6-4/SC2489
Anne Thushara Matthias1, Gam Aacharige Navoda Dharani1, Gayasha Kavindi Somathilake2 & Saman B Gunatilake1
1Faculty of Medical Sciences, University of Sri Jayewardenepura, Gangodawila, Sri Lanka; 2 National Centre for Primary Care and Allergy Research, University of Sri Jayewardenepura, Sri Lanka
Abstract
Introduction: Multiple factors influence doctor-patient communication. A good consultation starts with an introduction of him or herself by the doctor to the patient. The next step is to address patients in a manner they prefer. There is a paucity of data about how best to address patients in an Asian country. This study investigates how patients prefer to be addressed by doctors.
Methods: This is a cross-sectional study conducted from July 1st to August 31st, 2020 at a single Centre: Colombo South Teaching Hospital in Sri Lanka.
Results: Of 1200 patients, 63.25% reported that doctors never introduced themselves and 97.91% of patients reported, doctors never inquired how to address them. 49.9% preferred to be addressed informally (as mother, father, sister) than by the name (first name, last name, title). The older female patients, married patients, patients of lower education, and lower monthly income preferred to be addressed informally.
Conclusion: Most doctors did not introduce themselves to patients during medical consultations and did not inquire how patients wish to be addressed.
Keywords: Doctor-Patient Relationship, Medical Consultation, Professionalism, Introduction, Doctor’s Name Badge, South Asian, Sri Lanka
I. INTRODUCTION
Professionalism plays an important role in the practice of medicine. The Charter on Medical Professionalism has a set of 10 commitments. Commitment to professional responsibilities is one of them. It includes the way doctors dress and conduct themselves during a consultation (Blank et al., 2003). Abiding by these principles, doctors can improve their interaction with patients resulting in a better outcome (Gillen et al., 2018) A good introduction will facilitate a positive attitude from the patient towards the doctor. “#hellomynameis” campaign in the UK was initiated to create awareness about the importance of an introduction (Egener et al., 2017).
Professionalism is impacted by social, cultural, and economic factors. It is believed that the translation of professionalism concepts across the world should consider national cultural difference. Studies from western populations have shown that most patients prefer being addressed by their first name and for the doctor to be introduced by their full name and title (Egener et al., 2017). There is a paucity of data on how Asian patients wish to be addressed.
The Sri Lankan society is hierarchical based on age, caste, wealth, educational qualifications, and profession. Respect for doctors comes naturally in this system. Doctors are treated with great respect in rural communities. It is quite common to find doctors not introducing themselves to the patient and expecting them to know who you are. In Sri Lanka, doctors tend to address the patients mostly informally addressing the patient as a family member- ‘father, mother, uncle, sister, etc.’, in the local language assuming it would connect with the patient better. This study explores the way doctors address patients in an Asian cultural setting and the patient’s expectations.
II. METHODS
A cross-sectional study was conducted from 1st July to 31st August 2020 at the Colombo South Teaching Hospital. A total of 1200 patients were selected from the wards in a sequential, systematic manner with a skip interval of one. Informed verbal consent was obtained from the participants. The first part of the questionnaire contained demographics. Some questions asked the participants about how they wish to be addressed and how doctors addressed them and how they would like their doctor to introduce themselves. Informal methods of address were mother, father, sister, etc. Formal methods were the use of the first name, last name, or titles.
Statistical analysis including the statistical significance tests was performed using SPSS IBM SPSS Statistics Version 20 IBM Corp. (2017), IBM SPSS Statistics for Windows. Armonk, NY: IBM Corp. Pearson Chi-Square Association Test was used to identify the statistically significant associations between the categorical variables at a confidence level of 95%.
III. RESULTS
A. Demographics
(See Table 1)
Of the 1200 participants, 868 (72.33%) were female. Of the sample, 1022 (85.16%) were from urban areas.
|
Characteristics |
Number of participants (%) |
||||
|
Informal method
|
First name
|
Last name
|
No preference
|
||
|
Total |
|
599 |
427 |
77 |
79 |
|
Age |
Below 40 (< 40) (664) |
253 (38.10%) |
312 (46.99%) |
33 (4.97%) |
49 (7.38%) |
|
Above 40 (> = 40) (536) |
346 (64.55%) |
115 (21.46%) |
44 (8.21%) |
30 (5.60%) |
|
|
Education Level |
Post Graduate & Graduate (147) |
54 (36.73%) |
56 (38.1%) |
10 (6.8%) |
9 (6.12%) |
|
|
Grade 6-A/L (986) |
501 (50.81%) |
359 (36.41%) |
60 (6.09%) |
66 (6.69%) |
|
|
Grade 1-5 & Not educated (67) |
44 (65.67%) |
12 (17.91%) |
7 (10.44%) |
4 (5.97%) |
|
Income |
>100,000 (61) |
15 (24.6%) |
23 (37.7%) |
4 (6.56%) |
6 (9.84%) |
|
|
20,000-100,000 (982) |
490 (49.9%) |
357 (36.35%) |
66 (6.72%) |
64 (6.52%) |
|
|
<20000 (157) |
94 (59.87%) |
47 (29.93%) |
7 (4.45%) |
9 (0.75%) |
|
Occupation |
Skilled Occupations (581) |
251 (43.2%) |
230 (39.59%) |
40 (6.88%) |
84 (14.46%) |
|
|
Unskilled occupations (591) |
339 (57.36%) |
178 (30.11%) |
37 (6.26%) |
37 (6.36%) |
|
|
A/L & Uni students (28) |
9 (32.14%) |
19 (67.86%) |
– |
– |
Table 1. Difference between how patients wish to be addressed and vice versa
B. How Doctors Addressed Patients
Of the 1200 patients, 1175 (97.91%) reported that doctors never inquired how to address them at the beginning of the consultation (Matthias, 2021). A large proportion, 1124 (93.66%) reported that doctors have addressed them informally and 599 (49.9%) preferred being addressed informally, 427 (35.58%) preferred to be addressed by their first name, and 77 (6.41%) by their last name. Only 18, preferred to be addressed by their title (Dr/Rev).
More females preferred to be addressed informally when compared to the males (451/868 (51.96%) vs 148/332 (44.58%) (Pearson Chi-Square = 4.345, p = 0.037). Married patients preferred to be addressed informally when compared to the unmarried/divorced/separated (578/1089 (53.1%) vs 21/111 (18.9%), Pearson Chi-Square = 54.339, p < 0.001). The ethnicity of the patients and the area they are from (Urban/Rural) had no significant impact on how they desired to be addressed.
Over 65% of the patients (44/67) with a lower level of education preferred being addressed in an informal way whereas only 36.7% (54/147) of the graduates/post graduates preferred the informal way (Pearson Chi-Square = 23.264, p < 0.001). Monthly family income was a statistically significant variable and patients with a higher family income (Over LKR 100,000) preferred to be addressed more formally when compared to patients with an income below LKR 20,000 (40/61 = 65.57% Vs 54/157 = 34.39%, Pearson Chi-Square = 23.928, p < 0.001). The occupations of the patients are also a significant factor which affected their preference in the way being addressed with 57.4% of the patients with unskilled occupations (UN) and 43.2% of the ones with skilled occupations preferring the informal way (339/591 = 57.36% vs 251/581 = 43.20%, Pearson Chi-Square = 34.771, p < 0.001). Older patients (40 and above) preferred to be addressed informally when compared to others. (346/536 = 64.6% Vs 253/664 = 38.1%, p < 0.001).
Of 1059 patients, 495 (46.7%) preferred being addressed the informal way as they felt it made the doctor-patient relationship more personal and 627 (59.2%) patients felt the doctor treated them as their relative. Of the Doctors, 759 (63.25%) did not introduce themselves to the patients and 865 patients (72.08%) prefer doctors to wear a name badge. 718(59.8%) wanted doctors to introduce themselves with the title, doctor’s designation and specialty. 246(20.5%) wanted doctors to tell their title and first name. Only 4(0.3%) didn’t want doctors to introduce themselves.
IV. DISCUSSION
One important finding from our study was that doctors did not introduce themselves to patients. In most state sector hospitals in Sri Lanka, doctors do not wear a white coat or a name badge at present. A study done in the UK showed that 59.1% of patients and in our study 72% felt that doctors should wear name badges as a form of identification (Van Der Merwe et al., 2016). In our study, 98% of patients reported that doctors never inquired how to address them at the beginning of the consultation. To improve this aspect, these areas should be included in the objectives of the medical curriculum and continuous medical education programs of young doctors. The “Personal and professional development stream” which is taught in the medical faculty at Sri Jayewardenepura in Sri Lanka is an avenue that can be used for this purpose.
Social, cultural, ethnic, and other demographic factors can influence preferred modes of address. In our study, 50% prefer to be addressed in the informal way. There are several possible reasons for this. Sri Lankan people have long-standing cultural and religious beliefs. Sri Lankan traditions revolve around two dominant religions Buddhism & Hinduism. Filial piety, respect for one’s parents and elders, is a concept that is present in Asian countries. Addressing a person as a mother, father, son, etc. is considered as showing respect. The patients feel the doctors treat them as their own family or relative when they are addressed this way.
In studies done in most western countries, patients wish to be addressed by their first name. The higher the income and higher the education level of the patient, the lower is their preference for being addressed the informal way as they might perceive it as less professional. To solve the dilemma of whether to call the patient formally or informally and to make sure the patient is addressed according to their preference, the best approach would be to question the patient about their preferred name during their initial consultation and to record that in the patient’s records.
A. Strengths and Limitations
The large number of participants and recruiting from different wards; medical, surgical, paediatric, gynecology, and obstetrics to cover patients who were in the hospital for different illnesses are strengths. Not only did the study examine the patients’ preferred method of address, it examined the reasons behind the preference.
V. CONCLUSION
Our findings support a patient preference for informal greetings from their doctors in half the study population. It is not safe to assume that the patient can be addressed anyway the doctor deems right and it is good practice to ask patients how they prefer to be called at the beginning of the consultation. Doctors should introduce themselves clearly to patients and the current rates of introduction are inadequate. Majority of the patients prefer doctors to wear a name badge. In order to address patients in a culturally appropriate and patient preferred method it is always useful to ask the patient how they wish to be addressed.
Notes on Contributors
Anne Thushara Matthias was involved in conceptualisation, Methodology, Validation, Writing – Review & Editing, Supervision, Gam Aacharige Navoda Dharani was involved in investigation and data Curation, Gayasha Kavindi Somathilake was involved in formal analysis and Saman B Gunatilake was involved in writing final draft and review.
Ethical Approval
Ethical approval was from the Ethics Review Committee of the Colombo South Teaching Hospital(ERC 873/2020). There were no ethical issues. Informed consent was taken from the participants.
Data Availability
The datasets used during the current study are available from the corresponding author on reasonable request https://figshare.com/s/e6db9a7246f9ef08474a10.6084/m9.figshare.13633949 (Matthias, 2021).
Funding
No funding sources are associated with this paper.
Declaration of Interest
The authors declare that they have no competing interests.
References
Blank, L., Kimball, H., McDonald, W., & Merino, J. (2003). Medical professionalism in the new millennium: A physician charter 15 months later. Annals of Internal Medicine, 138(10), 839–841. https://doi.org/10.7326/0003-4819-138-10-200305200-00012
Egener, B. E., Mason, D. J., McDonald, W. J., Okun, S., Gaines, M. E., Fleming, D. A., Rosof, B. M., Gullen, D., & Andresen, M. L. (2017). The charter on professionalism for health care organizations. Academic Medicine, 92(8), 1091–1099. https://doi.org/10.1097/ACM.0000000000001561
Gillen, P., Sharifuddin, S. F., O’Sullivan, M., Gordon, A., & Doherty, E. M. (2018). How good are doctors at introducing themselves? #hellomynameis. Postgraduate Medical Journal, 94(1110), 204–206. https://doi.org/10.1136/postgradmedj-2017-135402
Matthias, T. (2021). Patient preferences of how they wish to be addressed in a medical consultation – Study from Sri Lanka. https://figshare.com/s/e6db9a7246f9ef08474a
Van Der Merwe, J. W., Rugunanan, M., Ras, J., Röscher, E. M., Henderson, B. D., & Joubert, G. (2016). Patient preferences regarding the dress code, conduct and resources used by doctors during consultations in the public healthcare sector in Bloemfontein, free state. South African Family Practice, 58(3), 94–99. https://doi.org/10.1080/20786190.2016.1187865
*Anne Thushara Matthias
Faculty of Medical Sciences,
University of Sri Jayewardenepura
Email: thushara.matthias@sjp.ac.lk
Submitted: 21 January 2021
Accepted: 16 April 2021
Published online: 5 October, TAPS 2021, 6(4), 135-141
https://doi.org/10.29060/TAPS.2021-6-4/SC2484
Caroline Choo Phaik Ong1,2, Candy Suet Cheng Choo1, Nigel Choon Kiat Tan2,3 & Lin Yin Ong1,2
1Department of Paediatric Surgery, KK Women’s and Children’s Hospital, SingHealth, Singapore; 2SingHealth Duke-NUS Academic Medical Centre, Singapore; 3Department of Neurology, National Neuroscience Institute, SingHealth, Singapore
Abstract
Introduction: The COVID-19 pandemic accelerated use of technology like videoconferencing (VC) in healthcare settings to maintain clinical teaching and continuous professional development (CPD) activities. Sociomaterial theory highlights the relationship of humans with sociomaterial forces, including technology. We used sociomaterial framing to review effect on CPD learning outcomes of morbidity and mortality meetings (M&M) when changed from face-to-face (FTF) to VC.
Methods: All surgical department staff were invited to participate in a survey about their experience of VC M&M compared to FTF M&M. Survey questions focused on technological impact of the learning environment and CPD outcomes. Respondents used 5-point Likert scale and free text for qualitative responses. De-identified data was analysed using Chi-squared comparative analysis with p<0.05 significance, and qualitative responses categorised.
Results: Of 42 invited, 30 (71.4%) responded. There was no significant difference in self-reported perception of CPD learning outcomes between FTF and VC M&M. Participants reported that VC offered more convenient meeting access, improved ease of presentation and viewing but reduced engagement. VC technology allowed alternative communication channels that improved understanding and increased junior participation. Participants requested more technological support, better connectivity and guidance on VC etiquette.
Conclusion: VC technology had predictable effects of improved access, learning curve problems and reduced interpersonal connection. Sociomaterial perspective revealed additional unexpected VC behaviours of chat box use that augmented CPD learning. Recognising the sociocultural and emotional impact of technology improves planning and learner support when converting FTF to VC M&M.
Keywords: Teleconferencing, Morbidity and Mortality Meeting, Continuous Professional Development, Sociomaterial Theory
I. INTRODUCTION
The COVID-19 pandemic instigated worldwide social distancing and rapid uptake of technology to replace face to face (FTF) communication. Healthcare professionals at clinical workplaces adopted educational technological tools to maintain teaching for students, trainees and continuous professional development (CPD) activities (Cleland et al., 2020). Likewise, our hospital-based department pivoted from FTF to interactive web-based videoconferencing (VC) (Zoom) to continue patient-care quality audits and CPD learning.
Before the pandemic, there was limited interest in teleconferencing for health professions education apart from remote learning and formal CPD webinars (Chipps et al., 2012). VC for informal CPD like the Morbidity and Mortality meeting (M&M) was mentioned only to boost attendance of faculty based at distant campuses. The M&M is a regular audit practice of surgical departments that constitutes an important type of informal CPD for individual and organisational learning (de Feijter et al., 2013). Many guidelines exist for FTF M&M but there are none for VC M&M.
Sociomaterial theory examines the mutual relationship of humans with sociomaterial forces and the resultant changes i.e., humans acting on and influenced by objects, nature, culture and/or technology. It provides a useful perspective to evaluate the effect of VC CPD learning and practice by highlighting the importance of materiality – in this case, technology – that is overlooked by other human-centric sociocultural educational theories (Fenwick, 2014). Using sociomaterial framing, we aimed to review the impact of changing from FTF to VC M&M in terms of CPD learning outcomes and user experience.
II. METHODS
A. Description of Context
On 7 Feb 2020, Singapore declared Orange Alert (severity level 3 out of 4) on the national Disease Outbreak Response System in response to the COVID-19 pandemic. Nationwide infection control measures required staff social distancing in public hospitals. Our department (Appendix A: department context and demographics) organises weekly Journal club and M&M as regular CPD; these were converted from FTF to VC meetings from 25 March 2020 till present. Singapore has widespread digital literacy and familiarity with computer usage; our hospital has used electronic health records since 2018. These factors facilitated our rapid pivot to VC meetings.
B. Description of Study
With institutional research board ethics waiver (CIRB Ref: 2020/2697), we sent an email inviting all department staff to participate in a survey about their experience of VC M&M compared to FTF M&M. The sampling frame comprised 18 permanent staff and 24 temporary staff on rotation in the department, from 1 April to 30 June 2020.
The primary outcomes of the survey were self-reported perceptions comparing FTF and VC M&M, addressing categories of CPD learning relevant to M&M: knowledge, practice change, attitude, user outcomes and intention to change (Table 1: Q1-Q3). We asked additional questions (Q4-14) about the FTF/ VC learning environments to elicit possible technological effects on primary outcomes. Face validity of the questionnaire was assessed by authors CCPOng, NCKTan and LYOng who are physicians familiar with M&M.
Recruitment, data collection, data entry and de-identification was performed by author CSChoo (clinical research coordinator) who is outside the department clinical hierarchy. Survey non-responders were given two reminders by CSChoo before the final 3-week deadline. Consent was implied if participants returned the completed survey. Authors CCPOng and CSChoo analysed the de-identified data. Participants responded whether they agreed with the statement, using a 5-point Likert scale. We carried out Chi-squared comparative analysis on 3 grouped categories: (strongly agree+ agree); (neutral) and (disagree+ strongly disagree).
III. RESULTS
A. Descriptive Demographics
We received responses from 30 people out of 42 invited (71.4%) with similar response rates for permanent staff 13/18 (72.2%) and temporary staff 17/24 (70.8%). Appendix A provides details on age, gender, job grade of respondents and prior familiarity with VC.
B. Survey Findings
The participants had attended on average 18.7 (SD 13.4) FTF M&M and 15.1(SD 8.3) VC M&M in the preceding 12 months. Apart from VC M&M, all had attended some other VC event such as administrative meetings, tutorials, webinars and non-work-related workshops or dinners.
|
Q |
Perception |
Analysis* group |
FTF M&M |
VC M&M |
p-value |
|||||||||
|
Strongly disagree & Disagree |
Neutral |
Strongly Agree & Agree |
Strongly disagree & Disagree |
Neutral |
Strongly Agree & Agree |
|||||||||
|
Q1 |
I learnt new medical knowledge |
whole |
0 |
5(16.7) |
25 (83.3) |
1 (3.3) |
0 |
29 (96.7) |
0.043 |
|||||
|
sub |
0 |
1 (4.2) |
23 (95.8) |
1 (4.2) |
0 |
23 (95.8) |
0.368 |
|||||||
|
Q2 |
I learnt new skills (e.g. clinical, teaching, communication, research, team, practical) |
whole |
0 |
7 (23.3) |
23 (76.7) |
1 (3.3) |
5 (16.7) |
24 (80.0) |
0.508 |
|||||
|
sub |
0 |
3 (12.5) |
21 (87.5) |
1 (4.2) |
3 (12.5) |
20 (83.3) |
0.599 |
|||||||
|
Q3 |
I would change my practice based on what I learnt |
whole** |
0 |
7 (24.1) |
22 (75.9) |
1 (3.3) |
3 (10.0) |
26 (86.7) |
0.233 |
|||||
|
sub** |
0 |
3 (13) |
20 (87.0) |
1 (4.2) |
2 (8.3) |
21(87.5) |
0.548 |
|||||||
|
Q4 |
Junior staff are comfortable presenting |
whole |
2 (6.7) |
8 (26.7) |
20 (66.7) |
1 (3.3) |
3 (10.0) |
26 (86.7) |
0.184 |
|||||
|
sub |
2 (8.3) |
3 (12.5) |
19 (79.2) |
1 (4.2) |
2 (8.3) |
21 (87.5) |
0.729 |
|||||||
|
Q5 |
Participants are comfortable to ask questions to clarify |
whole |
4 (13.3) |
9 (30.0) |
17 (56.7) |
3 (10.0) |
7 (23.3) |
20 (66.7) |
0.728 |
|||||
|
sub |
4 (17.7) |
5 (20.8) |
15 (62.5) |
3 (12.5) |
6 (25) |
15 (62.5) |
0.890 |
|||||||
|
Q6 |
Participants are comfortable to raise concerns or disagree with management |
whole |
3 (10.0) |
10 (33.3) |
17 (56.7) |
4 (13.3) |
5(16.7) |
21 (70.0) |
0.328 |
|||||
|
sub |
3 (12.5) |
6 (25.0) |
15 (62.5) |
4 (16.7) |
4 (16.7) |
16 (66.7) |
0.750 |
|||||||
|
Q7 |
Tone of discussion is respectful |
whole |
4 (13.3) |
10 (33.3) |
16 (53.3) |
1 (3.3) |
6 (20.0) |
23 (76.7) |
0.132 |
|||||
|
sub |
3 (12.5) |
6 (25.0) |
15 (62.5) |
1 (4.2) |
5 (20.8) |
18 (75.0) |
0.506 |
|||||||
|
Q8 |
Participants are engaged during the meeting |
whole |
2 (6.7) |
9 (30.0) |
19 (63.3) |
6 (20.0) |
8 (26.7) |
16 (53.3) |
0.314 |
|||||
|
sub |
2 (8.3) |
4 (16.7) |
18 (75.0) |
6 (25.0) |
7 (29.2) |
11(45.8) |
0.105 |
|||||||
|
Q9 |
I can see the slides clearly |
whole |
0 |
9 (30.0) |
21 (70.0) |
2 (6.7) |
1 (3.3) |
27 (90.0) |
0.01 |
|||||
|
sub |
0 |
4 (16.7) |
20 (83.3) |
2 (8.3) |
1 (4.2) |
21 (87.5) |
0.148 |
|||||||
|
Q10 |
I can follow the discussion well |
whole |
0 |
5 (16.7) |
25 (83.3) |
3 (10.0) |
3 (10.0 |
24(80.0) |
0.172 |
|||||
|
sub |
0 |
1 (4.2) |
23 (95.8) |
3 (12.5) |
3 (12.5) |
18 (75.0) |
0.100 |
|||||||
|
Q11 |
It is easy to provide comments during the meeting |
whole |
3 (10.0) |
8 (26.7) |
19 (63.3) |
6 (20.0) |
6 (20.0) |
18 (60.0) |
0.519 |
|||||
|
sub |
3 (12.5) |
3 (12.5) |
18 (75.0) |
6 (25.0) |
6 (25.0) |
12 (50.0) |
0.202 |
|||||||
|
Questions about VC M&M only |
||||||||||||||
|
Q12 |
I find it easy to navigate the buttons/ commands |
Strongly disagree & Disagree |
Neutral |
Strongly Agree & Agree |
||||||||||
|
3 (10%) |
3 (10%) |
24 (80%) |
||||||||||||
|
Q13 |
I prefer to ask questions / comment by |
Typing |
No preference |
Audio |
||||||||||
|
15 (50%) |
12 (40%) |
3 (10%) |
||||||||||||
|
Q14 |
I prefer to have the video on/ off for |
Myself |
Host |
Presenter |
Participant |
|||||||||
|
On |
4 (13.3%) |
12 (40%) |
21 (70%) |
2 (6.7%) |
||||||||||
|
Off |
22 (73.3%) |
3 (10%) |
1 (3.3%) |
8 (26.7%) |
||||||||||
|
No preference |
4 (13.3%) |
15 (50%) |
8 (26.7%) |
20 (66.7%) |
||||||||||
Table 1. Results of the survey
Table 1 shows the collated responses to survey questions comparing experience of FTF and VC M&M (Q1-11) and questions specific to VC technology (Q12-14). There were six participants who either had zero experience of FTF M&M or had experienced FTF M&M only in other departments, not ours. We carried out subgroup analysis excluding these 6 persons to remove possible influence of other M&M styles, since the study focus was on impact of VC technology.
In general, self-reported perceptions of CPD outcomes were similar for both FTF and VC M&M. Participants appreciated that VC allowed us to continue M&M practice during the pandemic while acknowledging both positive and negative technological influences on process. Two questions (Q1 and Q9) had minor differences that were significant on whole group analysis but not significant on subgroup analysis. There was a trend towards decreased engagement for VC M&M compared to FTF M&M (Q8) that was not statistically significant.
When using VC (Table 1: Q12-14; Appendix B qualitative responses), more participants preferred to ask questions or comment by typing in the chat box than speaking on microphone. The most common reason given was to avoid interrupting meeting flow; some highlighted that the chat box facilitated junior staff participation. A few felt that keeping ‘video-on’ for all participants improved engagement but the rest preferred to have own ‘video-off’ with presenter ‘video-on’ to reduce distraction. Participants felt that while technology offered easier meeting access and simplified scheduling, it sometimes reduced engagement and interfered with community-building. Participants preferred more technological support, clearer guidance on expected VC behaviours, better infrastructure and connectivity.
A copy of the informed consent, survey questions and anonymised database are available at https://doi.org/10.6084/m9.figshare.13611611.v1.
IV. DISCUSSION
Sociomaterial perspectives offer new ways to conceptualise health professions education beyond individual cognitive and sociocultural educational lenses (Fenwick, 2014). Underpinned by diverse theories like cultural-historical activity theory, actor-network theory, and complexity theory, it recognises that “objects and humans act upon one another in ways that mutually transform their characteristics and activity” (Fenwick, 2014). Therefore, sociomaterial perspectives illuminate how technology (VC) and related infrastructure (devices and internet connectivity) interact with humans to modify the VC CPD learning environment.
In our context, widespread device penetration and free hospital Wi-Fi access aided rapid adoption of technology. Institution policy mandates internet separation from patient electronic health records, so staff use personal devices instead of hospital computers for meeting access, but it was otherwise straightforward to convert to VC M&M. Nevertheless, some unanticipated issues and VC behaviours manifested.
Introducing new technology is commonly associated with distress with learning how to use it. We chose Zoom as the most user-friendly VC platform because majority had no prior experience with VC. Unfortunately, early issues like ‘Zoom-bombing’ induced the company to make frequent user-interface changes that confused some users. A few participants (both younger and older) felt inadequately supported during their learning curve. We had provided a simple guidance document with link to online Zoom technical support but most preferred trial and error and asking for help during meetings.
Technical support alone is insufficient to address discomfort caused by social aspects of changed processes. We anticipated that uncertainty about protocols or inappropriate participant behaviours could lead to disengagement with poor CPD outcomes. We preempted these risks by following the same CPD framework as FTF M&M (e.g. moderator controls discussion, presentation template, focus on peer review learning without blame) and instituted additional VC safeguards for patient confidentiality by limiting patient identifiers, preventing recording and confirmation of attendee identity for meeting admission. We naturally evolved VC etiquette of queueing using the ‘raise-hand’ button while the moderator invites discussants by name and manages their order.
An ethnographic study of distributed VC in undergraduate medical education found that unintended ‘technologies of exposure’ – visual, curricular and auditory, discomforted the faculty and students (MacLeod et al., 2019). Similarly, many in our study disliked having their ‘video-on’. Although ‘video-on’ could improve interpersonal trust, visual exposure discomfort may interfere with aims of improved engagement and relationship-building. Originally, our department encouraged but did not mandate universal ‘video-on’. Gradually, it became the norm for all to have ‘video-off’ except the host and presenter. Despite ‘video-off’, we can maintain honest conversations necessary for M&M because of trust built through years of training and working together. Prolonged loss of FTF contact may erode trust, hence we created a departmental WhatsApp chat group to enhance social connection.
VC technology afforded unexpected learning contributions. The chat box promotes participation of reticent staff, both senior and junior, especially those preferring written expression; it augments understanding of audio discussion and allows sharing of links to supporting literature. The ease of participation empowers juniors and shifts focus from the vocal few who dominated FTF M&M. While the VC constraint of turn-taking for speakers slows down discussions, it improves interprofessional respect and meeting discipline when host can ‘mute’ the recalcitrant interrupter.
V. CONCLUSION
Sociomaterial perspectives highlight how VC technology changes the CPD learning environment of the M&M. VC provides improved access for participation and alternative communication channels but potentially reduces engagement. Recognising constraints and trade-offs of technology-driven enhancements allows better planning and learner support in VC CPD.
Note on Contributor
Caroline Choo Phaik Ong reviewed the literature, designed the study, analysed de-identified data and wrote the manuscript. Candy Suet Chong Choo performed data collection and de-identification, analysed the data and gave critical feedback to the writing of the manuscript. Nigel Choon Kiat Tan reviewed the literature, advised the design of the study and gave critical feedback to the writing of the manuscript. Lin Yin Ong advised design of the study and gave critical feedback to the writing of the manuscript. All the authors have read and approve the final manuscript.
Ethical Approval
This study received institutional research board ethics waiver (CIRB Ref: 2020/2697).
Acknowledgement
The authors would like to acknowledge the participants of the survey for sharing their responses freely.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Interest
All the authors have no declarations of conflicts of interest.
Data availability
A copy of the informed consent, survey questions and anonymised database are available at http://doi.org/10.6084/m9.figshare.13611611.v1 under CC0 licence.
References
Chipps, J., Brysiewicz, P., & Mars, M. (2012). A systematic review of the effectiveness of videoconference-based tele-education for medical and nursing education. Worldviews on Evidence-Based Nursing, 9(2), 78-87. https://doi.org/10.1111/j.1741-6787.2012.00241.x
Cleland, J., Tan, E. C. P., Tham, K. Y., & Low-Beer, N. (2020). How COVID-19 opened up questions of sociomateriality in healthcare education. Advances in Health Sciences Education, 25(2), 479-482. https://doi.org/10.1007/s10459-020-09968-9
de Feijter, J. M., de Grave, W. S., Koopmans, R. P., & Scherpbier, A. J. J. A. (2013). Informal learning from error in hospitals: what do we learn, how do we learn and how can informal learning be enhanced? A narrative review. Advances in Health Sciences Education, 18(4), 787-805. https://doi.org/10.1007/s10459-012-9400-1
Fenwick, T. (2014). Sociomateriality in medical practice and learning: Attuning to what matters. Medical Education, 48(1), 44-52. https://doi.org/10.1111/medu.12295
MacLeod, A., Cameron, P., Kits, O., & Tummons, J. (2019). Technologies of exposure: Videoconferenced distributed medical education as a sociomaterial practice. Academic Medicine, 94(3), 412-418. https://doi.org/10.1097/ACM.0000000000002536
*Caroline CP Ong
KK Women’s and Children’s Hospital,
100 Bukit Timah Road,
Singapore 229899
Tel: +65 63941113
Fax: +65 62910161
Email: Caroline.ong.c.p@singhealth.com.sg
Submitted: 27 January 2021
Accepted: 1 April 2021
Published online: 5 October, TAPS 2021, 6(4), 131-134
https://doi.org/10.29060/TAPS.2021-6-4/SC2478
Lean Heong Foo & Marianne Meng Ann Ong
Department of Restorative Dentistry, National Dental Centre Singapore, Singapore
Abstract
Introduction: The novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused the COVID-19 pandemic which started in 2020. This resulted in a disruption to educational activities across the globe. Dental education, in particular, was affected because of its vocational nature where learners come into close contact with patients when performing dental procedures.
Methods: This is a narrative review with no research data analysis involved.
Results: Social distancing measures introduced to curb the spread of the infection revolutionised the advancement of online education as the virtual environment is a safer place to conduct teaching compared to face-to-face teaching. In this article, we share our experience at the National Dental Centre Singapore (NDCS) in ensuring the safety of our faculty and learners when conducting didactic and clinical education during the pandemic. Didactic lectures were conducted in the virtual environment via synchronous and non-synchronous teaching. Essential clinical education was conducted in small groups with safe management measures in place. In addition, we provide guidelines to highlight the importance of meticulous planning, thorough preparation, and seamless delivery in conducting effective synchronous teaching.
Conclusion: Safe management measures put in place to ensure the well-being of our faculty and learners can ensure dental education continuity during the pandemic.
Keywords: Dental Education, Education Continuity, COVID-19
I. INTRODUCTION
The COVID-19 pandemic is severely affecting dental professionals since the Department of Labor Occupational and Health Administration United States of America (USA) published guidelines associating aerosol-generating procedures (AGP) in dentistry with SARS-CoV-2 virus spread. Many dental schools in the USA and Asia Pacific have desisted clinical practice and simulation sessions, causing severe disruption in dental training (Chang et al., 2021). Innovative guidelines were developed to conduct dental education during the pandemic (Hong et al., 2021). Singapore has undergone five phases during the pandemic: Pre-pandemic, Circuit Breaker (CB), Phase 1, Phase 2, and Phase 3 (current). We share our experience in continuing dental education for oral healthcare team learners (residents, dental technicians trainees, dental assistant trainees) in NDCS during the pandemic.
II. CLINICAL ADJUSTMENTS
After the Ministry of Health Singapore (MOH) raised the Diseases Outbreak Response System Condition (DORSCON) level from yellow to orange on 7th February 2020 (Pre-pandemic), NDCS senior management immediately adopted team segregation by establishing three self-contained teams comprising clinicians, dental surgery assistants, lab technicians, patient service associate executives, and health attendants (Tay et al., 2020). Learners at NDCS were also assigned to teams. All staff and learners were briefed on safe management measures to observe during clinical sessions. They were required to wear a surgical mask at all times except during meals, perform hand hygiene with an alcohol-based hand sanitiser, and report their temperature twice daily online. Triage and risk assessment of patients were carried out (Hong et al., 2021; Tay et al., 2020) and dental procedures were limited to emergency procedures to relieve pain, ongoing dental treatment, and dental clearance before medical procedures during CB. Use of personal protective equipment (PPE) comprising an eye shield, N95 mask or respirator, surgical gown, and gloves were indicated for all AGP while the use of an eye shield, surgical mask, and surgical gown was indicated for non-AGP following a risk-based assessment (Tay et al., 2020). Patients with suspected COVID-19 or who had close contact with a confirmed case were treated in a negative pressure room with proper PPE. All patients were required to rinse with cetylpyridinium chloride mouth rinse before their procedure. A 15-minute window in between patients was implemented to disinfect the operatory until Phase 3.
III. EDUCATION PROGRAMME ADJUSTMENTS
We conduct three structured education programmes in NDCS–National Institute of Technical Education (NITEC) Dental Assisting (DA), NITEC Dental Technology (DT), and National University of Singapore Master of Dental Surgery Residency Training Programme (RTP) for six dental specialties. In addition, Singapore Institute of Technology (SIT) Diagnostic Radiography (DR) students have observation attachments at NDCS. During CB, Phase 1, and Phase 2, we postponed the new intake of learners for DA due to logistic issues with our collaborators. The posting of DR learners to our centre was also halted. All existing DA and DT learners were allocated to the same clinical team and completed their programme during the pandemic. Residents in the RTP were divided into two groups; one group was based in NDCS and the other in National University Centre for Oral Health Singapore during the 7-week CB. From Phase 1 onwards, the two groups of residents started weekly alternating rotations for their clinical sessions between the two institutions.
NDCS education activities are classified into didactics and clinical sessions. We conducted didactics using synchronous and non-synchronous formats while clinical sessions gradually resumed from Phase 1 to 3 following prevailing MOH and institutional policies. Synchronous teaching and seminars were carried out using Zoom and WebEx online platforms. Voice annotated presentations and e-learning modules were launched in the SingHealth e-learning platform, Wizlearn, for non-synchronous teaching. Clinical sessions were conducted with a small clinical supervisor-learner ratio (1:5), triage of patients, use of complete PPE with an N95 mask, hand hygiene, and high suction evacuator for AGP (Tay et al., 2020). Face-to-face sessions for essential hands-on clinical skills building were organised in Phase 2 and 3 with safe management measures in place such as small instructor-learner ratio, safe distances between learners and instructors, segregation of learners and instructors in groups, donning of surgical masks, meticulous hand hygiene, and proper disinfection after equipment use (Tay et al., 2020).
IV. GUIDELINES FOR ONLINE SYNCHRONOUS TEACHING
Mayer’s theory of multimedia learning (Mayer, 2002) describes the learning process in online education by highlighting the dual channels (auditory and visual) and three stages of memory (sensory, working, and long-term) for processing information. The learner’s eyes and ears capture diagrams and text in the multimedia presentation with sensory memory input. These are converted into a pictorial and verbal mode respectively in the working memory and integrated with prior knowledge from the long-term memory. Educators should prevent cognitive overload in content planning, as learners have limited capacity to hold the pictorial and verbal mode in working memory. A three-phase guide highlighting salient information for conducting effective online synchronous teaching is provided.
A. Meticulous Planning
To understand learners, faculty can adopt a 5W and 1 H concept [(who (the learners), where (location of teaching), why (learning objectives), what (lesson content), when (duration), and how (online platform in this context)] when planning a teaching module. Besides, faculty can construct the learning objectives and teaching activities using Bloom’s taxonomy based on learning outcomes. Bloom’s taxonomy covers six cognitive domains in the following order: knowledge, comprehension, application, analysis, synthesis, and evaluation, where a higher-order is more complicated for the learners to master and demonstrate.
B. Thorough Preparation
Apart from teaching material, a faculty guide is recommended. It should contain the schedule and details of the teaching session, teaching activities, and probing questions and answers for reference; to ensure all the teaching tasks are completed within the planned schedule. Handouts are used to reduce cognitive overload and as a backup when the connection is down. Generally, a good camera, laptop or smartphone, internet connection, a simple background with light, and a quiet room are sufficient for online teaching.
C. Seamless Delivery
Good online synchronous teaching platforms include Zoom, WebEx, Microsoft Teams, Google Meet, Mikogo, and Slack with breakout rooms and annotation board features that are included in the premium subscription of these platforms. A dry run is recommended to familiarise oneself with the functions on the various platforms. Setting the learning climate during the session by preparing learners to respond at appropriate times is crucial. The faculty should look at the camera frequently to keep eye contact with learners. Backup plans that include standby internet access and soft copy handouts are useful when connection is down. Increased feedback and communication between faculty and learners is crucial in online teaching and can be achieved by:
i) Using a learning management system such as GoSoapBox to allow learners to input text individually, particularly useful for clinical case discussion.
ii) Using Slido or Poll Everywhere to conduct needs analysis or summative or formative assessment between teaching.
iii) Utilising the question and answer segment to assess learners’ responses and check progress.
iv) Using the chatbox to allow learners to post questions and comments.
Teleconferencing has limited non-verbal cues coupled with milliseconds delay in observation by other participants that can subconsciously force our brain to restore the synchrony present in face-to-face contact. This overworking can lead to tiredness and discomfort from virtual teleconferencing tools, termed as ‘Zoom fatigue’. Recommendations to reduce Zoom fatigue include taking a rest in between brief lessons and turning off the camera when muted to reduce stimulus and mental fatigue. Netiquette, a blend of ‘internet etiquette’, refers to a code of good behaviour for both educators and learners (Table 1) that should be practised in an online environment (Lateef, 2020) to promote courteous communication between learners and educators for a pleasant learning experience. Evaluation of online education can be conducted during the session by performing formative and summative assessment; assessing quality and completion rate of learners’ assignment; analysing learners feedback from the post-session questionnaire as well as learners’ grade during module assessment and performance in the clinic.
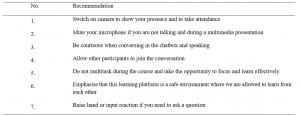
Table 1. Netiquette for online education
Note: Adapted from “Computer-based simulation and online teaching netiquette in the time of COVID 19,” by F. Lateef, 2020, EC Emergency Medicine and Critical Care, 4(8), 84-91.
V. MOVING FORWARD
It may take years to return to pre-COVID-19 normalcy, where physical interaction and large gatherings were social norms. Moving forward, we can consider a hybrid or blended learning module alongside limited face-to-face sessions confined to essential skill-based training. However, the effectiveness of online learning compared to traditional modes of clinical teaching has not been elucidated. Dentistry is a practical vocation that requires developing surgical and psychomotor skills to perform specific tasks. Online learning addresses the delivery of didactics but translating theory into practice which involves hands-on skills, teamwork and communication are challenging in the virtual setting. Virtual and augmented reality programmes such as Spatial, coupled with simulation video demonstration, may be suitable for skill-based training in dental education in the virtual environment. Psychological support for faculty and learners and forming a digital technology community of practice among educators can help to improve resilience and coping mechanisms during this challenging period. With safe management measures in place to ensure the well-being of our faculty and learners, we can adapt and continue education activities while looking for innovative ways to deliver clinical teaching effectively in dentistry amidst this pandemic.
Notes on Contributors
Dr Lean Heong Foo is a Consultant Periodontist in the Department of Restorative Dentistry and Head to the Dental Surgery Assistant Certification Programme. FLH reviewed the literature, contributed to the conception, data acquisition, drafted and critically revised the manuscript.
Dr Marianne Meng Ann Ong is a Senior Consultant Periodontist & Director of Education in National Dental Centre Singapore. MO contributed to the conception, data acquisition and critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of the work.
Ethical Approval
This is a narrative review related to dental education continuity during the COVID-19 pandemic and no ethical approval is required.
Data availability
This paper is a narrative review with no data analysis.
Acknowledgement
The authors would like to thank Ms Safiyya Mohamed Ali for providing editorial support.
Funding
There is no funding involved in the preparation of the manuscript.
Declaration of Interest
The authors declare no conflict of interest.
References
Chang, T., Hong, G., Paganelli, C., Phantumvanit, P., Chang, W., Shieh, Y., & Hsu, M. (2021). Innovation of dental education during COVID-19 pandemic. Journal of Dental Sciences, 16(1), 15-20. https://doi.org/10.1016/j.jds.2020.07.011
Hong, G., Chang, T., Terry, A., Chuenjitwongsa, S., Park, Y., Tsoi, J. K., Kusdhany, M. F. L. S., Egusa, H., Yamada, S., Kwon, J., Seow, L., Garcia, M. C. A. G., Wong, M. L., Ayuchai, P., & Hsu, M. (2021). Guidelines for innovation in dental education during the coronavirus disease 2019 pandemic. Journal of Oral Science, 63(1), 107-110. https://doi.org/10.2334/josnusd.20-0399
Lateef, F. (2020). Computer-based simulation and online teaching netiquette in the time of COVID 19. EC Emergency Medicine and Critical Care, 4(8), 84-91.
Mayer, R. E. (2002). Multimedia learning. Psychology of Learning and Motivation, 41, 85-139.
Tay, J. R. H., Ng, E., Ong, M. M. A., Sim, C., Tan, K., & Seneviratne, C. J. (2020). A risk-based approach to the COVID-19 pandemic: The experience in National Dental Centre Singapore. Frontiers in Medicine, 7. https://doi.org/10.3389/fmed.2020.562728
*Foo Lean Heong
National Dental Centre Singapore
5, Second Hospital Avenue,
168938 Singapore
Email: foo.lean.heong@singhealth.com.sg
Submitted: 31 August 2020
Accepted: 17 February 2021
Published online: 13 July, TAPS 2021, 6(3), 91-94
https://doi.org/10.29060/TAPS.2021-6-3/SC2353
Melissa Su Yi Yong, Xing Tong Yong, Olga Hillary Li Chew & Kuan Chen Zenne T’ng
Speech Therapy Department, Tan Tock Seng Hospital, Singapore
Abstract
Introduction: During the COVID-19 epidemic in Singapore, there was an urgent demand to train more nurses within a short timeframe to perform the Water Swallow Test (WST). The previous training model involved training with actual patients and was time-consuming. Hence, the model was revamped and standardised patients (SPs) were engaged for nurses’ training. This study further investigated nurses’ feedback about the new training model and compared the efficiency and learner-reported outcomes of the previous and new models.
Methods: Nurses who completed WST training from January 2018 to July 2020 were enrolled. Training records were accessed to determine the number of nurses trained under the previous and new models. Nurses were invited to complete post-training evaluation forms and their responses were analysed. Descriptive statistics and the Mann-Whitney U test were used for data analysis.
Results: Under the previous model, 52 nurses were trained over 2 years, whereas under the new model, 112 nurses were trained over two months. From the evaluation form responses, the majority of nurses trained under the new model agreed that they achieved the learning objectives and were confident in performing the WST. There was also no significant difference (p>0.05) found between learner-reported outcomes for both training models.
Conclusion: Our findings demonstrated that the new model that engaged SPs was more efficient in training more nurses. Nurses were also satisfied with the new training model, which achieved similar learner-reported outcomes as the previous model.
Keywords: Water Swallow Test, Standardised Patients, Train-the-Trainer, Dysphagia Screening
I. INTRODUCTION
The Water Swallow Test (WST) is a screening tool used to determine if a patient i) is at risk of aspiration, ii) requires swallowing assessment by a Speech Therapist (ST), and iii) can commence oral feeding (Suiter & Leder, 2008). In hospitals, doctors and nurses perform the WST on patients. Given the importance and potential medical sequelae of the WST, nurses require training before performing the test with patients.
At our institution, WST training is conducted using principles of train-the-trainer (Pearce et al., 2012) and flipped classroom model (Betihavas et al., 2016) to certify nurses as providers and trainers. A provider can conduct the WST on patients, and a trainer can train new providers and conduct the WST.
Previously, training was targeted at nurses in Stroke and Intensive Care Unit (ICU) wards. Trainers and providers had to complete an online module and quiz. Practical training was then conducted on actual patients either by a ST or certified trainer. Each practical was three hours and conducted with suitable patients.
When COVID-19 cases surged in Singapore, there was a pressing requirement to train more providers in ICU wards and at the National Centre for Infectious Diseases (NCID). However, there were challenges in continuing with the existing training model. Training with actual patients was too lengthy to meet the demand for more providers and could not be conducted during the outbreak to minimise patient contact. Therefore, the WST training model was revamped and standardised patients (SPs) were engaged (Kowitlawakul et al., 2015) to overcome the above challenges.
Under the new model, training was targeted at nurses in ICU, outbreak and general wards. Nurses had to complete an online module and quiz before attending training sessions in performing the WST with SPs. Eight providers were scheduled per session, which lasted three hours. The SPs were either a ST, nurse, or therapy assistant due to restrictions in the hospital’s visiting policy to engage professional SPs during the outbreak. The SP followed a standardised script demonstrating different signs of dysphagia. Figure 1 shows details on the previous and new training models.
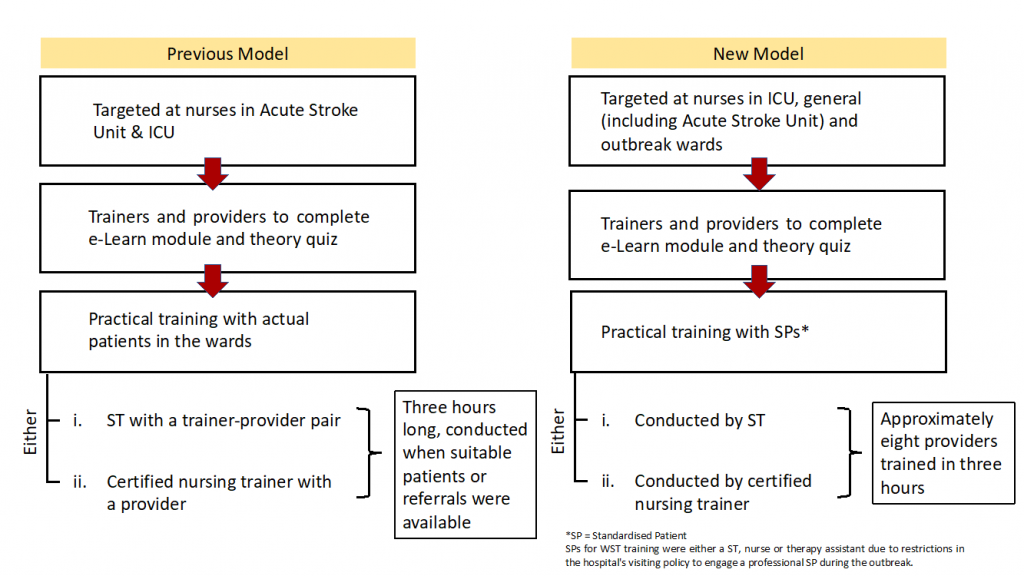
Figure 1: Previous and New Training Models
With the new training model implemented, the following research questions were posed:
1) Is the new training model more efficient in training providers to perform the WST compared to the previous model?
2) Are providers trained under the new model confident that they have achieved the learning objectives of the training and in performing the WST?
3) Is the new training model able to achieve similar learner-reported outcomes for providers as compared to the previous model?
It was hypothesised that:
1) The new training model is more efficient in training providers than the previous model.
2) Majority of providers trained under the new model will feel confident that they achieved the training learning objectives and in performing the WST.
3) The new training model will achieve similar learner-reported outcomes for providers when compared to the previous model.
II. METHODS
Nurses who completed WST training as providers from January 2018 – July 2020 were enrolled. Nurses were trained using the previous training model from January 2018 – April 2020. The new training model was implemented from May 2020.
In order to evaluate the efficiency in training providers under both models, nursing training records were accessed retrospectively to obtain the numbers and dates of providers who completed their training from January 2018 – July 2020. Total training hours under the previous model were computed based on the number of providers who completed training (three hours per provider). Under the new model, total training hours were calculated based on the number of training sessions (three hours per session) conducted from May – July 2020.
In order to evaluate the providers’ confidence in achieving the training’s learning objectives and in performing the WST, providers trained under both models were invited to complete an anonymous course evaluation form generated by the authors and select their responses on a 5-point Likert scale (i.e., strongly agree, agree, neutral, disagree, strongly disagree). The evaluation form was updated along with the new training model, however, these three statements remain unchanged in both versions and were used to analyse learner-reported outcomes:
1. I have a clear understanding of the contraindications of performing the WST.
2. I am confident of accurately identifying all the signs of dysphagia during the WST.
3. I am confident of performing the WST independently.
For data analysis, ‘strongly agree’ and ‘agree’ responses were collapsed into a single category and assigned a score of 1, ‘neutral’ response was assigned a score of 2, and ‘disagree’ and ‘strongly disagree’ responses were collapsed into a single category and assigned a score of 3. Statistical analysis was performed using SPSS statistics version 27.0. Descriptive statistics and the Mann-Whitney U test were used to analyse the evaluation form responses.
Implied consent was obtained from providers who voluntarily completed the form. This study was exempted from a formal NHG Domain Specific Review Board review.
III. RESULTS
A. Number of Providers Trained and Duration Required
Under the previous training model, 52 providers were trained over 24 months (January 2018 – December 2019). The total number of training hours was 156 hours (i.e., 52 providers x three hours). Under the new model, 112 providers were trained in 15 training sessions over two months (end May – mid-July 2020). The total training hours were 45 hours (i.e., 15 sessions x three hours).
Hence, one provider was trained every three-hourly training session and an average of 2.17 providers were trained per month under the previous model. Contrastingly, an average of 7.57 providers were trained every three-hourly training session and an average of 56 providers were trained per month under the new model.
B. Evaluation Form Responses
13 evaluation form responses (Nprevious = 13) were received under the previous model, and 111 responses (Nnew = 111) were received under the new model. The mean scores obtained for the three selected statements were:
1. I have a clear understanding of the contraindications of performing the WST (Previous model: M = 1.08, SD = 0.277; New model: M = 1.22, SD = 0.624).
2. I am confident of accurately identifying all the signs of dysphagia during the WST (Previous model: M = 1.08, SD = 0.277; New model: M = 1.23, SD = 0.567).
3. I am confident of performing the WST independently (Previous model: M = 1.15, SD = 0.555; New model: M = 1.22, SD = 0.563).
C. Comparison of Learner-Reported Outcomes
Scores from the new evaluation form (mean ranks = 62.76, 63.03, 62.90) were higher than scores from the previous form (mean ranks = 60.31, 57.96, 59.08) for all three statements. A Mann-Whitney U test indicated that the differences in scores between the previous and new model for all three statements were not statistically different, UStatement1 (Nnew = 111, Nprevious = 13) = 693.00, z = -0.438, p = 0.661; UStatement2 (Nnew = 111, Nprevious =13) = 662.50, z = -0.786, p = 0.432; UStatement3 (Nnew = 111, Nprevious = 13) = 677.00, z = -0.608, p = 0.543.
The above data set and analysis is available online (Yong et al., 2020).
IV. DISCUSSION
A. Efficiency of New Training Model
The new training model was more efficient than the previous model. Comparing the average number of providers trained per month, the new model was 25 times more efficient. Engagement of SPs allowed more staff to be trained in a single session by seven-fold, versus training with actual patients. Several factors made the new model more efficient: i) greater control over scheduling, ii) saving time from identifying suitable patients for training, and iii) reduced motion waste from accessing actual patients. Hence, more nurses could be trained to meet the needs of outbreak wards.
B. Feedback on Training
The mean rating scores for the three statements in the new evaluation form indicated that providers were satisfied with their training, as they mostly agreed or strongly agreed to achieving the training learning objectives and were confident in performing the WST.
C. Comparison of Learner-reported Outcomes under Both Models
No significant differences were found between responses in the previous and new evaluation forms. Thus, regardless of whether providers trained with actual patients or SPs, most perceived they fulfilled their learning objectives and felt confident to perform the WST independently. These findings indicated that providers did not perceive their training quality to be compromised with the use of SPs and shorter training duration.
D. Limitations
A limitation was that only 25% of providers completed the optional evaluation form under the previous model. The staff who responded likely had a positive training experience and this could lead to potential selection bias. We also acknowledge that the three statements from the evaluation form require further validity and reliability testing to analyse providers’ confidence levels and can be explored in future studies.
V. CONCLUSION
Our study demonstrated that having standardised patients as part of the training method translated to a significant increase in the efficiency of WST training. Potential scale-up of this WST training method can ensure that there is a steady pool of providers and trainers in the workforce to cope during peacetime and crises. Adopting the WST as part of routine dysphagia screening ultimately ensures safer feeding management and early access to Speech Therapy intervention. Further directions include investigating the effectiveness and validity of the new WST training model in various healthcare settings, such as acute and community hospitals and nursing homes, to improve training standards for dysphagia screening in the region, especially in light of the ongoing COVID-19 pandemic.
Notes on Contributors
Yong Su Yi Melissa and Yong Xing Tong evaluated the training model, conducted the training and wrote the manuscript. Olga Hillary Chew Li conducted the training and performed data collection. Zenne T’ng Kuan Chen initiated the design of the training model and gave critical feedback to the writing of the manuscript. All authors read and approved the final manuscript.
Ethical Approval
This study has been reviewed by NHG Domain Specific Review Board (DSRB) for determination of ethics requirement and does not require formal review (NHG DSRB Ref: 2020/00953).
Acknowledgements
We would like to acknowledge:
Senior Nurse Educator Kylie Tang and Nurse Educator Zhao Yue for their feedback in the design of the training model, accessing training records for data collection and collaboration in facilitating WST training for the Nursing Services department.
Senior Speech Therapist Ei Leen Fong for vetting the final manuscript
Principal Speech Therapist Kwong Seh Ling for her guidance in the data analysis and feedback on the manuscript.
Funding
There is no funding involved for this study.
Data Availability
All available data can be accessed publicly via https://doi.org/10.6084/m9.figshare.13110617.
Declaration of Interest
The authors declare there are no conflicts of interest.
References
Betihavas, V., Bridgman, H., Kornhaber, R., & Cross, M. (2016). The evidence for ‘flipping out’: A systematic review of the flipped classroom in nursing education. Nurse Education Today, 38, 15-21. https://doi.org/10.1016/j.nedt.2015.12.010
Kowitlawakul, Y., Chow, Y. L., Salam, Z. H., & Ignacio, J. (2015). Exploring the use of standardized patients for simulation-based learning in preparing advanced practice nurses. Nurse Education Today, 35(7), 894–899. https://doi.org/10.1016/j.nedt.2015.03.004
Pearce, J., Mann, M. K., Jones, C., van Buschbach, S., Olff, M., & Bisson, J. I. (2012). The most effective way of delivering a train-the-trainers program: A systematic review. The Journal of Continuing Education in the Health Professions, 32(3), 215–226. https://doi.org/10.1002/chp.21148
Suiter, D. M., & Leder, S. B. (2008). Clinical utility of the 3-ounce water swallow test. Dysphagia, 23(3), 244–250. https://doi.org/10.1007/s00455-007-9127-y
Yong, M., Yong, X. T., Chew, O., & Tng, Z. K. C. (2020). Training nurses to perform water swallow test with use of standardised patients (raw data & analysis) [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.13435310.v2
*Yong Su Yi Melissa
Tan Tock Seng Hospital,
11 Jalan Tan Tock Seng,
Singapore 308433
Tel: +65 8522 8013
Email: melissa_sy_yong@ttsh.com.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
