
Gamification through collaborative learning in medical education
Submitted: 30 Nov 2022
Accepted: 30 Jan 2023
Published online: 4 July, TAPS 2023, 8(3), 45-49
https://doi.org/10.29060/TAPS.2023-8-3/SC2921
Sasikala Devi Amirthalingam1, Shamala Ramasamy2 & Sharifah Sulaiha Hj Syed Aznal3
1Department of Family Medicine, International Medical University, Kuala Lumpur, Malaysia; 2Department for Psychology, International Medical University, Kuala Lumpur, Malaysia; 3Department of Obstetrics and Gynaecology, International Medical University, Kuala Lumpur, Malaysia
Abstract
Introduction: Introduction to Health Profession (IHP) was designed to teach first-year medical students the importance of self-directed learning, accountability, and teamwork in healthcare. Due to the COVID 19 pandemic, the course was delivered virtually, incorporating elements of gamification.
Methods: Gamification features included collaborative teamwork to simulate and record the roleplay for assignments based on crisis management scenarios. The syllabus involves knowledge checks to promote self-directed learning and personal accountability as well as online questionnaires to identify personality traits followed by discussion. Games like Chinese whispers and charades were introduced to identify listening skills. Additional gamification features include progress mechanics for collecting badges upon successful completion of knowledge checks / assessments and completing collaborative teamwork activities.
Results: Results from the descriptive study on the educational usefulness of the IHP module was found to be satisfactory. The feedback was encouraging as >95% of students gave positive feedback that the IHP activities enabled them to understand the value of teamwork, effective communication, professional behavior and enabled them to be resilient and adaptable. 92% agreed that the IHP activities helped to make connections and network with their peers during the pandemic
Conclusion: Gamification of IHP course was successful in terms of practicality and usefulness in promoting communication, collaborative work, experiential learning, and teamwork. Students were empowered to take charge of their own learning of both content and development of interpersonal skills and teamwork through gamification. The isolation caused by the pandemic was alleviated by the networking that occurred during collaborative group activities.
Keywords: Gamification, Self-directed Learning, Collaborative Learning
I. INTRODUCTION
Introduction to Health Profession (IHP) course was initiated during Covid-19 pandemic and conducted at the beginning of our medical program enrolment to introduce freshmen to the real world and value systems of health professional. The learning activities were designed to provide real life experiences, exposing to communication skills within the community and peers, professionalism including teamwork and ethics, and the value of self-reflecting practice. The isolation caused by the pandemic was alleviated by networking that occurred during collaborative group activities and online interactive discussion with invited speakers of health professionals. The group activities were gamified to make learning fun, memorable, engaging and motivating. It is designed to promote a sense of accomplishment while learning through discovery and during the social interaction.
Gamification in education has existed since time immemorial but with the advent of wireless technology, it has given rise to unique ways to improve student engagement (Dodson, 2021) in learning. Gamification is defined as “the craft of deriving all the fun and addicting elements found in games and applying them to real-world or productive activities” (Chou, 2012). There is growing evidence for gamification in a wider pedagogical context and the concept is gaining traction within the medical education community. These “fun and addicting elements” include progress mechanics such as badges, narrative structure and immediate feedback. The gamification features introduced in the IHP module are badges, immediate feedback, challenges in the form of knowledge checks and roleplay in virtual reality in crisis management scenarios.
II. METHODS
Collaborative group activities were conducted by dividing 171 first year students into 16 small groups. Activities were carried out using synchronous and asynchronous virtual platforms to accommodate about 40 % of international students who were still in their home countries. Lessons in IHP consisted of recognising personality traits, application of communication skills, ethics and professionalism and recognising teamwork as intrinsic requirements for delivery of effective healthcare.
Asynchronous sessions required students to individually go through the prepared learning materials followed by knowledge checks. Test repetition without penalty is allowed within an allotted time frame until learners reach a satisfactory result. Following successful completion of knowledge check, students would earn their badge of completion.
Activities like ‘discovering personality traits’ are conducted as online synchronous workshops and facilitated by a group of psychologists. Self-administered questionnaire was administered to determine personality traits, followed by a psychologist-led group discussion to share feedback and reflection. Having the session on a virtual platform provided the students with a degree of anonymity, which enabled them to share profound reflections and feedback. Through the questionnaire responses, the psychologists were able to identify red flags and reach out to the students.
During the online ‘communication skills’ workshop, games such as Chinese whispers and charades were used to cultivate active listening skills and understand nonverbal communication. Students were assigned to group works comprising of preparing oral presentations on scenarios involving ethics and professionalism. In addition, they were tasked to solve issues in selected crisis management scenarios using role-plays and virtual reality. Creativity is highly encouraged and weighted with high percentage. This encourages social interaction and influences learning by creating a subjective sense of presence to facilitate virtual experiential learning.
Upon completion of the IHP activities, students are required to complete a self-administered questionnaire to feedback on the efficacy of the module, hence implied consent is given. The questionnaire measured whether the gamification of IHP achieved the learning outcomes of enabling the understanding of the value of teamwork, effective communication, professional behaviour and to be adaptable and resilient. In addition, the questionnaire inquired if participation in IHP activities helped them create contacts and network with their peers. Open comments are sought after for thematic analysis.
III. RESULTS
51.4% of the cohort responded to the self-administered online questionnaire. Feedback was encouraging as >95% of students gave positive feedback. They felt IHP activities enabled them to understand the value of teamwork, effective communication, professional behaviour and being resilient and adaptable. Most agreed IHP activities helped to make connections and network with peers during the pandemic. Many agreed they developed some insight about themselves during IHP activities. Several themes were drawn from the collected feedback. The primary theme is teamwork where students demonstrate co-operation in working together in teams to attain mutual goals and learn leadership qualities. Majority felt they developed skills in active listening, organisation, patience, self-confidence, and showing empathy. Other characteristics learnt were resilience building, controlling emotions, adaptation, overcoming challenges, professionalism and ethical behaviour.
Common comments on areas to improve are their lack of confidence and discomfort in expressing one’s thoughts. Both being too rigid and overly flexible were commented. Other comments were not feeling at ease with working in a team, becoming overwhelmed, paying excessive attention to detail, and becoming frustrated. Being shy and quiet as well as not being assertive were among the constructive feedback (See Table 1). A copy of the survey questions and the additional tables of survey results are openly available at https://doi.org/10.6084/m9.figshare.21656864.
|
Student Feedback for the Introduction to Health Profession (IHP) module Total number of respondents: 88 |
|||
|
NO. |
THEMES |
OPEN FEEDBACK FROM STUDENTS |
|
|
Majority of the positive responses are as follows: |
Common comments on areas to improve self: |
||
|
1 |
Teamwork |
|
|
|
2 |
Effective Communication |
|
|
|
3 |
Professional Behavior |
|
|
|
4 |
Adaptability and resilience |
|
|
|
5 |
Making connections and networking with peers |
|
|
|
6 |
Insight to self |
|
|
|
Table 1. Student Feedback from IHP Cohort ME121 |
|||
IV. DISCUSSION
IHP is a new course with the objectives of introducing students to the real world and value systems of the health professional, focusing on communication skills, medical ethics, teamwork, and the importance of self-reflective practice. The learning is mainly facilitated by group work and formative assessment through immediate provision of feedback and self-reflection. Due to pandemic-related restrictions, the initial plans for real life experience and exposure in IHP course had to be converted to the online platform. An instructional method such as gamification was selected to help retain student engagement and encourage participation (Chou, 2012). Applying the design elements and principles found in games to education was useful in sparking student interest and motivation (Chou, 2012).
Knowledge checks challenged the minds, improved cognition and knowledge retention (Singhal et al., 2019). Progress mechanics in the form of earning ‘a badge on completion’ of assigned activities, going through the provided learning material and completing the knowledge check to an acceptable level, promoted self-directed learning, created a sense of achievement and retained student engagement. This reward system fosters student participation, as it is a tangible reward (Dodson, 2021).
The seclusion from real life interaction is feared to mentally and psychologically affect students. A study in Switzerland has shown a significant impact on the mental health of learners due to the lockdown in 2020 (Elmer et al., 2020). In another study, social interaction is recognised as an important factor for enhancing learning especially in areas of critical thinking and problem solving (Hurst et al., 2013). The group works in the IHP course, though set virtually, have assisted students in networking and socialising during the pandemic. This was agreed by majority of the students who participated in IHP activities.
Effective leadership is essential in delivering high standards of clinical practice. The students learnt leadership skills through organising group work, delegating roles and responsibilities among team members. Among the examples of group work are problem- solving scenarios like managing a fire in CCU or multiple vehicle accident on the highway. The instructional content was related to the teamwork and roles and responsibilities of the different health professionals involved in managing the crisis and it was gamified by adding elements of game fiction such as the different themes, settings and characters. As students had to self- produce scripts after some brief research of relevant contents, they had some autonomy over the depth and breadth of their learning. Working in teams towards common goals lead to improved productivity and self-esteem and created supportive relationships during the collaborative learning (Singhal et al., 2019). Narrative synthesis and role playing in scenarios managing crisis situations stimulated reflective practice whilst integration of cause and effect enabled experiential learning.
Overall feedback was encouraging as almost all students enjoyed the activities and found them both educational and engaging. They discovered characteristics in themselves that helped them to improve team spirit and communication. The groupwork on the various projects developed learning communities and promoted interpersonal skills, integrating diverse learner types with a wide range of knowledge, skills, past experiences and personal attributes. This was effectively utilized in the groupwork and collaborative learning.
Some setbacks occurred when both the faculty and students were unfamiliar with online gamification. The synchronous sessions with international students in different time zones, made group discussions challenging. Support from the Information Technology team is valuable but poses an exorbitant cost. Students having expectations of medical school learning to be more didactive, instead had to adapt to being adult learners, for more extensive self- directed learning and reflective practice.
V. CONCLUSION
In conclusion, gamification of IHP module encouraged student engagement, teamwork and collaborative learning. IHP course was accessible virtually, which was a boon for our international students who could interact virtually with peers and access and take part in the lessons. The gamification features used were reproducible. Gamification is useful in medical education and can be pursued as a method to deliver lessons and engage students. It is a tool to allow learning in depth and for experiential learning on the virtual platform.
Notes on Contributors
Dr Sasikala Devi Amirthalingam is the first author, contributing to the abstract, introduction, discussion and literature review. She agrees to be accountable for all aspects of the work.
Dr Shamala Ramasamy is the second author, contributing to methodology, results and literature review. She agrees to be accountable for all aspects of the work.
Prof Sharifah Sulaiha Hj Syed Aznal is the third author, contributing to abstract, introduction, discussion and revising it critically for important intellectual content. She agrees to be accountable for all aspects of the work.
Ethical Approval
The dean of School of Medicine, International Medical University has given a letter to say that there is no objection to sharing of findings for educational purpose.
Data Availability
The data that support the finding are openly available in the Figshare repository. https://doi.org/10.6084/m9.figshare.21656864
Acknowledgement
We would like to acknowledge Fareeza Marican Bt Abu Backer and Norhasliza Binti Hashim from E Learning Department from International Medical University for the technical assistance in the gamification features to the module.
Funding
There is no financial support or any financial relationships that may pose a conflict of interest.
Declaration of Interest
There is no conflicting interest to any parties concerned.
References
Chou, Y. K. (2012). What is gamification. Yukai Chou: Gamification and Behavioral Design. https://yukaichou.com/gamification-examples/what-is-gamification/
Dodson, K. R. (2021). Can gamification drive increased student engagement? Educause Review. https://er.educause.edu/articles/sponsored/2021/10/can-gamification-drive-increased-student-engagement
Elmer, T., Mepham, K., & Stadtfeld, C. (2020). Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE, 15(7), Article e0236337. https://doi.org/10.1371/journal.pone.0236337
Hurst, B., Wallace, R., & Nixon, S. B. (2013). The impact of social interaction on student learning. Reading Horizons: A Journal of Literacy and Language Arts, 52(4), Article 5. https://scholarworks.wmich.edu/reading_horizons/vol52/iss4/5
Singhal, S., Hough, J., & Cripps, D. (2019). Twelve tips for incorporating gamification into medical education. MedEdPublish, 8(3), Article 216.
*Sasikala Devi Amirthalingam
International Medical University,
Kuala Lumpur, Malaysia
+60133513435
Email: SasikalaDevi@imu.edu.my
Submitted: 5 August 2022
Accepted: 2 November 2022
Published online: 4 April, TAPS 2023, 8(2), 76-79
https://doi.org/10.29060/TAPS.2023-8-2/SC2861
Poh-Sun Goh1 & Elisabeth Frieda Maria Schlegel2
1Department of Diagnostic Radiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Department of Science Education, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hofstra University, United States
Abstract
Introduction: The aim of this short communication is to examine the journey of scholarship in health professions education (HPE).
Methods: We will focus on tangible small steps to start, sustain, and succeed along this journey. Through a proposed innovation in scholarship – micro-scholarship – we will describe how this is similar to and an extension of bite-size or micro-learning, and workplace micro-practice related to just-in-time (JiT) learning settings.
Results: We will demonstrate how the small steps for generating and engaging with micro-content can be similarly applied to micro-scholarship. Then, progressive and iterative refinement of output and practice of micro-scholarship can be combined and result in macro-scholarship after cycles of public engagement for final digital or print publication. This stepwise approach creates an accessible, sustainable strategy to achieve success as a scholar in HPE. We will elaborate on micro, macro, and meta matters and celebrate how these small steps encourage and allow broad participation in the creation, critique, and progressive refinement of scholarship.
Conclusion: Small, sustainable, steps leads to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Keywords: Micro-Scholarship, Micro-Learning, Just-In-Time (JiT) Learning, Community of Practice (CoP), Technology, Network Effects, Post-Publication Peer Review (PPPR)
I. INTRODUCTION
Modern changes in the pace and way we conduct and experience teaching and learning have resulted in production and consumption of smaller chunks of content. Succinct, bite-size content is easier to remember and consumes less cognitive bandwidth with reduced cognitive load. In addition, it is also significantly easier to share and engage with within a professional community of practice (CoP). Compact modular, bite-size content is also ideal for just-in-time (JiT) micro-learning and workplace micro-practice (Yilmaz et al., 2022), or on-demand learning and practice, with which we are all familiar. In this paper, we will extend this idea of micro-learning and micro-practice to scholarship, by examining the “new” idea of micro-scholarship – defined as “the process of making visible the smallest accessible and assessable steps that document a scholarly journey, which can then be assembled and presented as an outcome of academic scholarship” (Goh et al., 2021). Mobile technology tools and platforms support open display, access to, and iterative engagement with this content by a community of practice (CoP), both in learning and scholarship (Goh et al., 2021; Goh & Sandars, 2020; Schlegel, 2021).
II. MICRO-MATTERS
Just as a musical composition is made up of individual notes, a construction from its individual parts, and a meal of its individual ingredients, commonly accepted and acknowledged finished works of scholarship in HPE are composed of its individual parts. A conference presentation or journal paper, peer reviewed, read by and engaged with by a CoP, contains core components – e.g., the title (which includes key ideas); key words (which are defined and illustrated in the presentation or paper); and cited published work by earlier authors (from a review of the field, including takeaways from the author(s) that are relevant and that the authors intend to discuss, elaborate, and build upon). However, a close examination and reflection of these core parts of finished works of scholarship show that they not only form the ingredients of the final work, but that they also fall within the categories of scholarship proposed by Boyer, with evaluation criteria described by Hutchings and Shulman; (Goh et al., 2021; Goh & Sandars, 2020). Boyer’s model for scholarship includes (1) integration, (2) application, (3) teaching and learning, and (4) discovery.
Innovative JiT micro-content on mobile platforms is easily accessible for members of a CoP to engage with, evaluate, critique, and build upon. All online content, including, e.g., on Twitter, blogs, or modular courses, is subject to creative reader collectives, which post comments, repost, reshare, and create new meaning and value from individual posts of content, contributing to group engagement, which has many of the characteristics of scholarship (Schlegel & Primacio, 2021). We propose that these artefacts and activities illustrate examples of Boyer’s Scholarship categories, including demonstrating the Scholarship of Teaching and Learning SoTL. Digital and online content and platforms support and scale our efforts as learners and scholars, no different yet more facile as compared to in-person activities, with increased importance placed on being a public professional, and respecting intellectual property, shown by proper citation of digital content, and use of this content with permission where applicable, followed by data-driven dissemination (Arrington & Cohen, 2015; Kern et al., 2015). This public reaction and appraisal of content compares to wide audience post-publication peer review (PPPR) with the added value of a feedback-loop through responses on comments. Just as developing bite-size, short format, JiT digital, online content, has transformed and continues to transform our educational and professional practices, a similar process can now facilitate and support granular, open digital display and engagement of both our initial and subsequent steps when engaging in scholarship in HPE, similar to and an extension of micro-learning. Practicing micro-scholarship involves encountering a “new idea”; researching its meaning; adding relevance to specific discussion themes and takeaways; discovering key published and presented work; and then both taking note of and making notes on these findings during reflection and discussions within a local CoP. This micro-scholarship is subsequently made open and visible to a global readership or a CoP, through private, semi-private, and public engagement platforms. Micro-scholarship content gets progressively refined through iterative engagement with members of a CoP, through discussion, feedback, critique, and personal reflection. The relevance and usefulness of this content, as well as confidence in the authors of this micro- scholarship content, is progressively enhanced. We also learn how and where this content is best disseminated and presented, and best ways this might be combined and stacked. The iterative in- person and scalable digital conversations amplifying the spread and engagement with this material to create meaning, in step-by-step fashion, form the core practices of both micro-scholarship (Goh et al., 2021) and bite-size engagement with material (Schlegel, 2021). After refinement, these pieces can be combined into larger pieces of finished work of macro-scholarship. Thus, activities undertaken as part of micro-learning or micro-scholarship are accessible, independent, and sustainable small, step-wise efforts that can and do add-up. Progression along the developmental path of a scholar will include a variety of conversations within a CoP, such as the supportive networks of peers, senior practitioners, mentors and coaches, including collaborative (team)work and initially supervised instruction as part of a successful scholar’s journey. Conversations and engagement within a CoP do range from positive and helpful to (those that are or perceived to be) occasionally provocative and challenging. However, professional and good-natured discussion generally guide scholarly development similar to trial and error, and progressive improvement and iterative steps enable learning and growth.
III. MACRO-MATTERS
Simply put, a finished larger work is made up small pieces that have been selected and refined, through an iterative process of reflection and feedback, by engaging with a CoP or specialised collective of readers. Open (digital) practice from an early stage, the platforms (places and readers) we engage in, and our active participation in professional CoP of global specialised readers provide both “informed” and “critical” feedback – and review of these “early” and “small” or “micro” pieces of work – from a (much wider) audience. The key distinction is who engages with this work, from as wide a spectrum of professional practice, experience, and expertise as possible, and from a diversity of points of view. Digital tools and practices facilitate and scale this process. This is similar to the work of artists, who engage in open sketching, including showcasing early drafts and ideas, prototyping, drawing, and artistic creation in open studios. When members of a CoP engage through digital platforms the impact from their individual and collective input can scale exponentially through network effects (Azhar, 2021).
IV. META-MATTERS
The process of scholarship mirrors the stepwise, sequential, cumulative process of learning, and training for proficiency and mastery in any area of practice. Our roles as practitioners, educators and scholars are all informed by learning science. Digital devices, tools, platforms, and practices exponentially scale up the impact of our efforts through applied network theory and interactions. Ultimately, we live and practice professionally within our CoP, which provides both the audience and peer reviewers of our public work, thus driving a fruitful evolution of our profession. Our ultimate aim is to engage a CoP in conversations, including broader participation in the production, refinement, and consumption of products of scholarship, in form and format, and through processes accessible for all. Micro-scholarship is a starting point that allows wider participation and engagement in the process of scholarship. The components of micro-scholarship, when refined and confidently presented, are contained within published finished macro-scholarship outputs. Then, micro-scholarship and macro-scholarship add collaboration and value within a larger scholarship ecosystem and professional CoP, a meta-level practice or meta-system, within which micro- and macro- level activities occur. An explicit example of the outputs and process of moving from micro, through macro, to meta practice illustrated https://www.slideshare.net/dnrgohps/illustrated-stacked-microscholarship-steps-along-academic-path-of-educational-scholar.
Another example of enhancing scholarship of teaching and learning SoTL across different levels might include, e.g. a remote consultation with members of scholarly project teams, prompting to publish a themed blog post, which, in return, becomes now a generalizable, transferrable offering to the global CoP, moving from the meta-system to the macro-level, as evidenced by comments from different institutions and subsequent implementation of ideas (Arrington & Cohen, 2015).
V. CONCLUSION
In this paper, we have examined, showcased, and celebrated the small sustainable steps to success as a scholar in HPE, describing micro, macro, and meta matters and illustrating how combining small components of scholarship is an effective strategy for dissemination, access, engagement, conversation and collaboration within a CoP in HPE.
Notes on Contributors
Poh-Sun Goh pitched initial idea, was involved in active discussion and brainstormed with co-author iterative refinement of core message(s), wrote first draft, and actively revised series of subsequent drafts, and submitted final draft. This manuscript built on previous collaborative work, cited in article on Micro-Scholarship and Digital Scholarship.
Elisabeth Schlegel was involved in active discussion and brainstormed with co-author iterative refinement of core message(s), and actively revised series of subsequent drafts, and including and approving final draft. This manuscript built on previous work, cited in article including on bite-sized learning.
Ethical Approval
As this manuscript is a description of an innovative approach to scholarship, ethical approval and IRB application was not required.
Data Availability
There is no additional data separate from available in cited references.
Acknowledgement
No technical help and/or financial and material support or contributions was received in preparation of this manuscript.
Funding
Both authors have no funding source to declare.
Declaration of Interest
Both authors declare that there are no possible conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
Arrington, N. M., & Cohen, A. L. (2015). Enhancing scholarship of teaching and learning through micro-level collaboration across two disciplines. International Journal of Teaching and Learning in Higher Education, 27(2), 194.
Azhar, A. (2021). The exponential age: How accelerating technology is transforming business, politics and society. Diversion Books.
Goh, P. S., Roberts-Lieb, S., & Sandars, J. (2021). Definition of Micro-Scholarship. https://microscholarship.blogspot.com/
Goh, P. S., & Sandars, J. (2020). Rethinking scholarship in medical education during the era of the COVID-19 pandemic. MedEdPublish, 9(97). https://doi.org/10.15694/mep.2020.000097.1
Kern, B., Mettetal, G., Dixson, M., & Morgan, R. K. (2015). The role of SoTL in the academy: Upon the 25th anniversary of Boyer’s scholarship reconsidered. Journal of the Scholarship of Teaching and Learning, 15(3), 1-14. https://doi.org/10.14434/josotl.v15i3.13623
Schlegel, E. (2021). (Not only) for medical students: Get involved in medical education research & scholarship. https://elisabeth-fm-schlegel.weebly.com/elearning-bites/not-only-for-medical-students-get-involved-in-medical-education-research-scholarship
Schlegel, E., & Primacio, J. (2021). Blogging for the continuum of medical education: Engaging diverse communities of learners. MedEdPublish, 10, Article 136. https://doi.org/10.15694/mep.2021.000136.1
Yilmaz, Y., Papanagnou, D., Fornari, A., & Chan, T. M. (2022). The learning loop: Conceptualizing Just-in-Time faculty development. AEM Education and Training, 6(1), e10722. https://doi.org/10.1002/aet2.10722
*Poh-Sun Goh
Department of Diagnostic Radiology
National University Hospital,
Main Building, Lobby F, Level 4
#04-398, DDI Library
5 Lower Kent Ridge Road, Singapore 119074
+6567724211
Email: dnrgohps@nus.edu.sg
Submitted: 28 April 2022
Accepted: 19 August 2022
Published online: 4 April, TAPS 2023, 8(2), 70-75
https://doi.org/10.29060/TAPS.2023-8-2/SC2802
Sok Mui Lim, Ramesh Shahdadpuri & Ching Yee Pua
Centre for Learning Environment and Assessment Development (CoLEAD), Singapore Institute of Technology, Singapore
Abstract
Introduction: Coaching has gained acceptance in the education field as a way to enable learners to achieve their fullest potential. In the endeavor to set up a coaching ecosystem in our university, we started by equipping our educators with fundamental coaching skills and techniques. Our training workshop, Coaching As An SIT Educator, covers the key coaching competencies and is highly practice focused. Participants get hands-on skills practice using contextualised scenarios that are based on realistic academic, workplace and clinical placement settings.
Methods: To address concerns on time-effectiveness, we adopt a solution-focused approach to coaching. We want to create a mindset shift for educators, from subject experts providing advice and solutions, to coaches asking powerful coaching questions that help students make discoveries and work towards their goals. We encourage our educators to engage students holistically by finding coachable moments in their daily student interactions.
Results: Competency-based assessments are conducted to determine achievement of the learning outcomes, articulated by the knowledge, attitude, and demonstration of coaching skills with students. Assessments consist of a reflection, multiple-choice question (MCQ) quiz, and scenario-based coaching role plays. Participants achieved the learning outcomes as demonstrated from the assessments.
Conclusion: The coach training workshop is the major pillar of our coaching initiative. Beyond the workshop, ongoing coaching development is supported through other activities and resources, including community of practice, coaching circle and knowledge repository. Opportunities for continuous learning and conversation platforms for sharing coaching experiences are part of the growing coaching ecosystem at SIT.
Keywords: Assessments, Coaching Competencies, Coaching Conversations, Coaching Ecosystem, Coachable Moments, Faculty Development, Feedback, Holistic Development, Solution-Focused
I. INTRODUCTION
Coaching has gained greater awareness and wider acceptance in the education field in the past decade, led by the efforts of innovative educators and more evidence-based research. Coaching has been described as a very powerful approach that facilitates personal and professional change through deep level listening, questioning, setting the right challenges and providing support along the process (Griffiths, 2005). More specifically, academic coaching is defined as individualised practice of asking students reflective, motivation-based questions, providing opportunities for formal self-assessment, sharing effective strategies, and co-creating a tangible plan that promotes accountability (Deiorio et al., 2017).
In traditional educational settings, communication tends to be mostly directive, where the educator is the subject expert who gives instructions, solutions or advice to students. From this “telling” or “pushing” stance where the focus is on problem solving and advice giving, shifting to coaching conversations requires an “asking” or “pulling” communication approach. Engaging in coaching conversations involves the educator coaching students through powerful questioning, active listening and guiding them to explore possibilities so as to discover new ideas and find solutions for themselves.
In 2020, Singapore Institute of Technology (SIT) introduced internal coach training for all academic staff with the aim to build educators’ capability to work with students at a deeper level. This highly contextualised academic coaching training was made mandatory for all educators. This was essential for the creation of a strong coaching ecosystem in the university and adopting coaching practices across a variety of learning contexts, such as providing assignment feedback, consultations on projects and supervising students at the workplace. In working with students towards their preferred futures, SIT educators can help the students develop confidence and self-efficacy, enabling them to achieve their fullest potential.
II. METHODS
This section highlights the critical elements of the faculty development programme.
A. Solution-focused Approach
One of the top concerns of many educators is time. There are underlying concerns on whether coaching students will take up too much time, and what happens if they uncover student issues that they cannot deal with. A solution-focused coaching approach alleviates some of these concerns. The basic principle of the solution-focused approach is to help coachees reflect and design their solutions, rather than go down the path of root cause analysis. Its forward-oriented solution approach contrasts with other traditional psychological techniques, which tend to look back at the past or are problem-focused (Grant & Gerrard, 2020).
The solution-focused approach is known for its simplicity, attention to language and time effectiveness. The conversation is steered to a preferred future of the issue at hand without dwelling on the troubled past. The coach encourages the coachee to focus on their strengths and positive resources, to think about their resourceful past, and to draw on positive lessons from when they have been at their best. After identifying their desired outcomes and considering their options in the context of present realities, the coach guides the coachee to think about the next steps to progress towards their preferred future.
B. Mindset Shift
In higher education, many coachable opportunities outside the formal contact hours can be easily missed. For example, instead of merely deducting marks for repeated late submissions of assignments, the educator could coach the student on improving time management. In clinical fieldwork, when a student complains about limited interaction with the busy clinical educator, the university supervisor can coach the student on how best to schedule time for feedback. Our daily encounters and interactions with students present many coachable moments that offer just-in-time and authentic learning opportunities to support students in their development to become work-ready graduates.
Students may initially find coaching sessions difficult as it is easier to just ask for solutions than to discover solutions for oneself. However, with time, students will realise the value of coaching as they witness their progress. In an Asian context, where many students are respectful and value advice from authoritative figures, such as professors, coaching can require a mindset shift for both students and faculty (Lim, 2021).
C. Tailoring the Coaching Training to Education Context
The Coaching As An SIT Educator workshop is an in-house designed 2-day program. It is highly contextualised for the needs of SIT academic staff, to equip them to be versatile and agile educators, performing the role of Teacher-Coach-Mentor. The workshop covers the key coaching fundamentals and is highly practice-oriented. The programme design was intended for participants to develop hands-on coaching skills with contextualised role play scenarios (see Appendix A for an example), so that they can apply what they have learnt with their students immediately after the workshop.
While we do not intend to train credentialed professional coaches, the key International Coaching Federation (ICF) coaching competencies were referenced to guide the design of the SIT workshop. The GROW model (Whitmore, 2019) was introduced as a framework for the participants to organise and manage the flow of the coaching conversation. Drawing on inputs from academic staff, realistic student-centric scenarios were created for class discussions and role plays. The coaching practice sessions are conducted in dyad, triad, and hot seat formats. The workshop design and facilitation ensure that there is psychological safety, providing a trusting space for constructive debriefing, feedback sharing and open questions and answers to take place.
To manage the workshop time and resources effectively, e-learning content was developed in-house, specifically to complement the interactive classroom session. A week before the start of the workshop, the participants can access materials in the form of an asynchronous pre-recorded webinar. The webinar consists of five micromodules, covering topics such as Mindset, Motivation, Emotional Intelligence, and Feedback Skills (refer to Appendix B for more details). As many participants may already be familiar with these topics, this self-learning component serves as a good refresher to prepare participants for the coaching workshop.
Please refer to Table 1 for details of the Coaching as An SIT Educator workshop.
|
Workshop: Coaching As An SIT Educator |
|
|
Learning Outcomes By the end of this course, participants will be able to:
|
|
|
Topics Covered |
|
|
Pre-Workshop: eLearning
|
Workshop Day 1:
Workshop Day 2:
|
|
Assessments (Day 2) |
|
|
Role Plays: Standardised Students & Assessors Scenarios (each – 20 minutes):
|
Quiz: Multiple Choice Questions (MCQs)
|
Table 1. Coaching As An SIT Educator Workshop
III. EVALUATION OF COACHING COMPETENCY
To assess the attainment of the learning outcomes and development of the participants’ coaching competence (knowledge, skills, attitude), assessments and reflection exercises are incorporated into the workshop. As this is not a certification program, assessments are formative in nature, with focus on providing the educators quality feedback. Coaching knowledge is assessed through a multiple-choice question (MCQ) quiz. Attitude and mindset shift is evaluated through pre- and post- workshop surveys, and reflection questions.
Coaching skills are assessed via role plays (with standardised students). The role play format involves two 20-minute coaching sessions with the participant (playing the role of an educator) having a coaching conversation with standardised students (who act as coachees) and are conducted virtually in real time over the Zoom platform, using breakout rooms. The role plays that are based on common scenarios in university and workplace supervision settings. An invaluable part of the learning in this assessment comes from the feedback conversation between the participant (coach) and assessor, who observes the coaching conversation. Many participants regard the skills assessment and individualised feedback on their coaching skills as the highlight of the training programme.
IV. DISCUSSION
Many readily available coaching materials or vendor-run workshops are geared towards executive or corporate scenarios. While the skills of coaching may be transferable, it is difficult for educators to draw relevance to student engagement. Therefore, Coaching As An SIT Educator workshop focuses on case studies of university scenarios, and supervision for work-integrated learning (e.g., internship, clinical placement). Participants get to work with fellow learners in group work and discussions, to engage in personal reflection, and takeaway practical knowledge and skills on their learnings in a safe space.
For a sustained effort to practice coaching and build an on-going coaching culture, a mandatory workshop is inadequate. Other coaching resources are available to support coaching practice and promote continuous learning in SIT:
- Community of Practice: Coaching Conversations @SIT (offered to any interested academic staff)
- Coaching Circle (offered to all alumni of the coaching workshop)
- Coach Academy (knowledge repository with academic and coaching industry resources).
V. CONCLUSION
In coaching, there lies great potential for students to be developed holistically if we tap on coachable moments in higher education. A contextualised, well-developed coaching development programme is an enabler for this potential to be fulfilled. Drawing on evidence-based research from academia and professional practice, a practice-oriented programme which focuses on developing hands-on coaching skills will be impactful, as educators can put these skills into action in their interaction with students.
Notes on Contributors
Associate Professor Lim Sok Mui (May) led the Center for Learning Environment and Assessment Development (CoLEAD) and spearheaded the coaching initiative in the university, contributed to the conception, drafted and critically revised the manuscript.
Ramesh Shahdadpuri is the senior educational developer in CoLEAD and plays the role of the coaching trainer for the faculty training program. reviewed the literature, contributed to the conception and assisted in revising the manuscript.
Pua Ching Yee is the learning analyst in CoLEAD and plays the role of coordinating the coaching training and assessment of the participants. She assisted in critically reviewing, revising and formatting the manuscript.
All authors gave their final approval and agree to be accountable for all aspects of the work.
Ethical Approval
This is a narrative review related to coaching training program with no data presented and no ethical approval is required.
Data Availability
This paper is a narrative review with no data analysis.
Acknowledgement
The authors would like to thank Miss Cherine Foo for her significant contribution of the coaching program.
Funding
There is no funding involved in the preparation of the manuscript.
Declaration of Interest
The authors declare no conflict of interest.
References
Deiorio, N. M., Skye, E., & Sheu, L. (2017). Introduction and definition of academic coaching. In N. M. Deiorio & M. M. Hammoud (Eds.), Coaching in medical education: A faculty handbook (pp. 1-5). American Medical Association.
Grant, A. M., & Gerrard, B. (2020). Comparing problem-focused, solution-focused and combined problem-focused/solution-focused coaching approach: solution-focused coaching questions mitigate the negative impact of dysfunctional attitudes. Coaching: An International Journal of Theory, Research and Practice, 13(1), 61-77. https://doi.org/10.1080/17521882.2019.1599030
Griffiths, K. (2005). Personal coaching: A model for effective learning. Journal of Learning Design, 1(2), 55–65. http://dx.doi.org/10.5204/jld.v1i2.17
Lim, S. M. (2021, May 27). The answer is not always the solution: using coaching in higher education. Times Higher Education. https://www.timeshighereducation.com/campus/answer-not-always-solution-using-coaching-higher-education
Whitmore, J. (2019). Coaching for performance: The principles and practice of coaching and leadership (5th ed.). Nicholas Brealey Publishing.
*Lim Sok Mui
Singapore Institute of Technology,
10 Dover Drive, Singapore 138683
+65 65921171
Email: may.lim@singaporetech.edu.sg
Submitted: 4 October 2022
Accepted: 5 December 2022
Published online: 4 April, TAPS 2023, 8(2), 66-69
https://doi.org/10.29060/TAPS.2023-8-2/SC2894
Simon Field1, Pat Croskerry2, Susan Love3, & Peggy Alexiadis Brown4
1Undergraduate Medical Education and Emergency Medicine, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 2Critical Thinking Program, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 3Faculty Development, Continuing Professional Development, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 4Dalhousie Medicine New Brunswick, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada
Abstract
Introduction: For all clinical providers in healthcare, decision-making is a critical feature of everything they do. Every day physicians engage in clinical decision-making where knowledge, evidence, experience, and interpretation of clinical data are used to produce decisions, yet, it is fair to say that most do not have an explicit insight or understanding of this complex process. In particular, few will have training in teaching and assessing the cognitive and affective factors that underlie clinical decision-making.
Methods: To foster an increased awareness and understanding of these factors, the Dalhousie Critical Thinking Program was established with the mandate to develop and deliver curriculum for critical thinking in the 4-year undergraduate program. To assist teaching faculty with the goal and objectives of the program, the Teaching and Assessing Critical Thinking Program (TACT) was introduced.
Results: Using the dual process model as a platform for decision-making, this program introduces general principles of critical thinking and provides tools to teach learners how to strengthen their critical thinking skills. To offer flexible learning, an online approach was chosen for delivery of the program.
Conclusion: To date, we have offered eleven iterations of Part 1 to a total of 261 participants and six iterations of Part 2 to a total of 89 participants. Evaluations show the online approach to content delivery was well received and the content to be of practical use.
Keywords: Critical Thinking, Clinical Decision-Making, Faculty Development, Asynchronous Learning
I. INTRODUCTION
This paper provides a review of a two-part Teaching and Assessing Critical Thinking (TACT) program which was developed to help faculty understand vulnerability to bias and the role of metacognitive processes in clinical decision-making. The objective of the TACT program is to better prepare faculty to teach learners these important skills. In this paper, we describe how it was implemented, how participants perceived the program, and what changes were needed to address this important hidden ‘soft’ skill within the clinical setting.
II. METHODS
Physicians are constantly required to interpret information when they interact with patients, communicate with colleagues, review medical histories and laboratory reports, conduct physical exams, review the medical literature, and attend rounds. All of these clinical activities demand a sustained level of accuracy, clarity, and especially rationality. Critical thinking (CT) does not guarantee rationality but is one of its more important features and is essential for the role of physician.
Reliable and accurate diagnosis is the barometer of good clinical decision-making and will have a direct impact on treatment outcomes and patient safety. One in 20 (or roughly 12 million) American adult outpatients are affected by diagnostic errors every year. The overall number of fatalities associated with diagnostic failure is not known, but it is estimated that 40,000 – 80,000 deaths occur annually in hospitalised patients in the USA due to diagnostic failure.
A number of studies have shown that training in the development of CT skills in undergraduate students is effective. (Abrami et al., 2015) However, given that most faculty in medical schools today will not have had explicit CT training, specific initiatives in teaching it seem appropriate, not only for the faculty themselves but, importantly, for the students they teach.
To better prepare learners, Dalhousie’s Faculty of Medicine established the Critical Thinking Program in 2012. The program incorporated principles from the Foundation for Critical Thinking into a general model of clinical reasoning (Croskerry, 2018). The Dalhousie critical thinking curriculum reflects a consensus in the current medical literature that the dual process model (System 1 and System 2) is the most appropriate platform for reviewing the clinical decision-making process (See Figure 1).
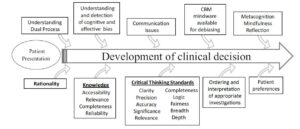
Figure 1. The Dalhousie University model for clinical decision making. (Reproduced with Permission)
A key component in the delivery of this curriculum is helping faculty develop the skills they will need to teach and mentor critical thinking in the clinical environment. Most educators have limited understanding of the advances in medical decision-making and how to best teach critical thinking and clinical reasoning.
The TACT Program comprises two distinct courses: TACT 1 and TACT 2. The program is structured to develop a sound knowledge of critical thinking principles in TACT 1, followed by a focus on teaching and learning in TACT 2. TACT 1 centres on three main themes: How Physicians Make Decisions, Cognitive and Affective Biases, and Cognitive Debiasing Strategies. TACT 2 centres on two main themes: Fundamentals of Medical Education and Strategies for Teaching and Assessing CT. In TACT 2, participants choose one of four elective options: Evidence Based Medicine, Competency Based Medical Education, Medical Humanities, or Curriculum Development.
The TACT Program uses an asynchronous online approach to reach Dalhousie faculty who are distributed across the Canadian Maritime Provinces. This approach mediates potential barriers for participation such as distance and time constraints and allows for individualised learning experiences while building an interactive online community of practice experience (Cook & Steinert, 2013). We use a combination of curricular tools including online didactic lectures, independent study activities, webinars, and discussion boards.
To date (Winter 2022), we have held 11 iterations of TACT 1 and 6 iterations of TACT 2, with 163 of 261 participants completing TACT 1 and 78 of 89 registrants completing TACT 2.
Of those who completed TACT 1, 55 % went on to enrol in TACT 2.
We initially developed the TACT Program for Dalhousie faculty (primarily physicians); however, due to growing interest in the topic, we have opened enrolment to include participants from around the world, including the United States, Mexico, United Kingdom, Australia, New Zealand, Turkey and Brazil. We also opened enrolment to participants from a variety of health professions and other fields of study. By opening the program to participants with diverse backgrounds in practice and location we have increased the diversity of perspectives and the richness of reflections posted to the discussion boards.
Prior to starting the TACT Program, we asked participants to complete a survey measuring their current knowledge of teaching and assessing CT, and motivation for taking the course.
Participants reported little satisfaction with previous knowledge in CT (Mean: 2.67 ± 0.84 on a Likert Scale of 1 (not at all satisfied) to 5 (very satisfied)). The following themes were identified as motivators for taking the TACT Program — a desire to: learn, improve clinical reasoning by increasing knowledge, understand the impact of critical thinking, provide better clinical care, decrease diagnostic error, and become a better educator.
We administered a summative evaluation following both TACT 1 and TACT 2. For TACT 1, 75% (121/162) completed the final evaluation and for TACT 2, 90% (63/70). In the summative evaluation, we asked participants to rate their course in a number of areas from course delivery to the effectiveness of increasing their knowledge and comfort in teaching critical thinking. Consent to data collection was implied as part of the administration of the evaluation. We found that participants were very satisfied with delivery methods.
III. RESULTS
A. What Did We Learn about the Participants?
All participants taking the TACT Program shared a similar motivation: the intent to improve their critical thinking skills and to teaching others. Steinert et al. (2002) found that faculty are more likely to enrol in an online program if they believe it would meet a perceived need. Our participants identified a desire to improve their own practice, confidence and awareness, to make the unconscious conscious, and to develop the language to name, identify and act on cognitive biases and those circumstances that create biases. This enabled them to better teach and mentor CT.
Participants also identified the value of communicating with others who offered a different perspective on clinical work and life experiences.
Physicians may not readily share/disclose mistakes they make in the clinical setting. In medical training environments, overconfidence and reluctance to admit mistakes are often the norm, which may work against fostering a culture of reflection (Brezis et al., 2016). Due to the confidentiality of the discussion boards, our participants could freely reflect on what factors contribute to errors they have made/seen and share those lessons with peers without fear of loss of reputation and embarrassment.
B. What Did We Learn about the Delivery?
We found that the online delivery was successful in reaching a broad base of participants. Some participants appreciated the mode of delivery as well.
A benefit of online courses is the ease with which faculty can control their pace of instruction. When asked, we found that 97.4% of respondents identified they would do more faculty development programs online.
When we reviewed the online tracking statistics, we found that our participants were accessing materials at all hours. Participants, each with their own learning style, appreciated the mix of interactivity and self-study the online format offered.
IV. DISCUSSION
Ideally, we would like to know how effectively participants in the TACT program incorporated the teaching principles into their own practices in the real clinical world. However, it is very challenging methodologically to do this, and it appears the best we can do is to ask about participant impressions and insight into their experience.
It appeared that the TACT program provided a rich opportunity for participants to interact and share their quest to understand and refine the metacognitive aspects associated with their clinical decision-making and critical thinking processes. It also provided our participants with the language to describe and teach these processes to trainees.
V. CONCLUSION
In summary, the TACT program shows promise in engaging distributed faculty to further their curiosity and interest in how to improve, teach and foster critical thinking skills within medical education and in their own practice. We recognise that although this online asynchronous mode of delivery may not be appropriate to meet the diverse learning styles of all potential participants, the favourable reviews we have received from our program graduates highlighted that the flexible interactivity with the content contributed to the success of the TACT program.
Notes on Contributor
Simon Field assisted in the initial development of the TACT program and contributed to the data analysis and writing of the article.
Pat Croskerry was a founding member of the Critical Thinking Advisory Group, and contributed to the development of the TACT program and to the writing of the article.
Susan Love has been an active contributor to the running of the TACT program, designed the survey tools, collected and analyzed qualitative and quantitative data from the program evaluation, and contributed to the writing of the article.
Peggy Alexiadis Brown collected and analyzed qualitative and quantitative data from the program evaluation survey tools, and contributed to the writing of the article.
All authors have reviewed and approved the final manuscript.
Ethical Approval
The data gathered for this article was collected anonymously as part of Program Evaluation, and a written waiver has been obtained stating that it is exempt from full institutional Research Ethics approval.
Acknowledgement
We acknowledge the valuable support and contribution of Deirdre Harvey and other members of the Critical Thinking Advisory Group. For further information on how to implement a similar program in your region, please feel free to contact us.
Funding
There is no funding associated with this project.
Declaration of Interest
None of the authors have any conflicts of interest to declare, and they do not receive any financial assistance or funding for their participation in the TACT program.
References
Abrami, P. C., Bernard, R. M., Borokhovski, E., Waddington, D. I., Wade, C. A., & Persson, T. (2015). Strategies for teaching students to think critically: A meta-analysis. Review of Educational Research, 85(2), 275-314. https://doi.org/10.3102%2F0034654314551063
Brezis, M., Orkin-Bedolach, Y., Fink, D., & Kiderman, A. (2016). Does physician’s training induce overconfidence that hampers disclosing errors? Journal of Patient Safety, 15(4) 296-298. https://doi.org/10.1097/pts.0000000000000255
Cook, D. A., & Steinert, Y. (2013). Online learning for faculty development: a review of the literature. Medical Teacher, 35(11), 930-937. https://doi.org/10.3109/0142159X.2013.827328
Croskerry, P. (2018). A model for clinical decision-making in medicine. Medical Science Educator, 27(Suppl 1), S9-S13. https://doi.org/10.1007/s40670-017-0499-9
Steinert, Y. L., McLeod, P. J., Conochie, L., & Nasmith, L. (2002). An online discussion for medical faculty: An experiment that failed. Academic Medicine., 77(9), 939-940. https://doi.org/10.1097/00001888-200209000-00046
*Simon Field
Dept of Emergency Medicine,
Dalhousie University, Halifax,
Nova Scotia, Canada
Email: simonfield@dal.ca
Submitted: 22 February 2022
Accepted: 3 August 2022
Published online: 3 January, TAPS 2023, 8(1), 47-50
https://doi.org/10.29060/TAPS.2023-8-1/SC2764
Kye Mon Min Swe1 & Amit Bhardwaj2
1Department of Population Medicine, University Tunku Abdul Rahman, Malaysia; 2Department of Orthopaedics, Sengkang General Hospital, Singapore
Abstract
Introduction: During the era of COVID-19 pandemic, online learning has become more prevalent as it was the most available option for higher education training which has been a challenging experience for the students and the lecturers especially in the medical and health sciences training. The study was conducted to determine the perceptions of clinical year medical students on online learning environments during the COVID-19 pandemic.
Methods: A cross sectional study was conducted to clinical year medical students at University Tunku Abdul Rahman. The validated Online Learning Environment Survey (OLES) was used as a tool to conduct the study.
Results: Total 84 clinical year students participated in the study. Among four domains of OLES questionnaire, the domain; “Support of online learning” had the highest mean perception scores, 4.15 (0.55), followed by “Usability of online learning tools” 3.89 (0.82), and “Quality of Learning; 3.80 (0.68) and the domain “Enjoyment” was the lowest mean perception scores 3.48 (1.08). Most of the students (52.4%) rated the overall satisfaction of online teaching experiences “Very good” while (13.1) % rated “Excellent”.
Conclusion: In conclusion, the perceptions of clinical year medical students on online learning environments during the COVID-19 pandemic were satisfactory although there were challenging online learning experiences during the pandemic. It was recommended to include qualitative method in future studies to provide more useful in-depth information regarding online learning environment.
Keywords: Online Learning Environment, Perceptions, Medical Students, Malaysia, COVID-19
I. INTRODUCTION
Online learning is defined as learning via web-based technology and students interact with their peers and educators through web-based communication tools (Bonk & Reynolds, 1997). The usability of the web-based learning system is important as are its applications such as interactive video, forums, chat rooms, email, and document sharing systems (Klein et al., 2006).
Online learning is regarded nowadays as a new way of interaction in the educational process and online learning facilities offer various opportunities to get new knowledge and develop students’ skills through engagement and interaction in new learning environments. (Samoylenko et al., 2022)
Due to the novel coronavirus pandemic, all the higher education training has converted to online teaching and assessments including medical programs. To fulfil the student physical learning time requirement, the academic year of MBBS clinical year programmes (Year 3 to Year 5) has been divided into Phase 1; purely online teaching as medical students were not allowed to be posted to hospitals followed by Phase 2; face to face physical clinical training at the hospital. Phase 1 teaching for clinical years include, online task-based learning, online lectures and online case-based discussion, online clinical skill, and procedures. This research study was conducted to evaluate the online learning environment of clinical year students and to find out differences in students’ perceptions between the academic years.
II. METHODS
A cross sectional study was conducted to (total=135) Year 3 to Year 5 clinical year medical students. 43 students were in Year 3, 49 students were in Year 4 and 43 students were in Year 5 at University Tunku Abdul Rahman (UTAR), Selangor, Malaysia. All the clinical year students were invited to participate in the study by sending electronic invitations emails, informed consent was taken. Data was collected via google form and the information was anonymised.
A validated Online Learning Environment Survey (OLES) (Pearson & Trinidad, 2005) was used to evaluate the online learning environment of medical students of UTAR during Phase 1 of purely online teaching. The questionnaire consists of two sessions. Section (I) general demographic information, Section (II) contains 50 items of OLES questionnaires developed by Pearson and Trinidad (2005). The validity of the tool was recorded as Cronbach’s Alpha Coefficient value of 0.79 to 0.90. The OLES consists of nine scales: Computer Usage (CU); Teacher Support (TS); Student Interaction & Collaboration (SIC); Personal Relevance (PR); Authentic Learning (AL); Student Autonomy (SA); Equity (EQ); Enjoyment (EN); and A-synchronicity (AS) which can further classified into four domains: (1) Support for learning; (2) Quality of learning; (3) Usability of online learning tools; and (4) Enjoyment. Responses were recorded against a five-point scale with the following representations: 1- Never; 2- Seldom; 3- Sometimes; 4- Often; and 5- Almost Always. (Pearson & Trinidad, 2005)
Data were analysed by using SPSS (Statistical Package for Social Science) for Windows, version 26.0. The categorical variables were described by frequency and percentage. Student t-test and Analysis of variance (Anova) test was used to compare means between the groups of different academic years. Ethical approval was acquired from the Scientific Ethical Review Committee of the UTAR.
III. RESULTS
A total of 84 clinical year medical students participated from Year 3 to Year 5. There were 27 out of 43 Year 3 students (62.79%), 26 out of 49 Year 4 students (53.06%), 31 out of 43 Year 5 students (72.09%) who completed the questionnaire. Approximately 82 (97.6%) students were aged between 21 to 25 years and (63.1%) were female students.
The online learning environment survey (OLES) tool consists of four domains to evaluate student online learning environments such as “Support of Online learning”, “Usability of online learning tools”, “Quality of Learning” and “Enjoyment”. Among four domains of OLES tool, the domain; “Support of online learning” had the highest mean perception scores 4.15 (0.55), followed by “Usability of online learning tools” 3.89 (0.82), and “Quality of Learning; 3.80 (0.68) and the domain “Enjoyment” was the lowest mean perception scores 3.48 (1.08).
|
Domains of perceptions of online learning environment |
Subscales of perceptions of online learning environment |
Mean (SD) |
Mean (SD) |
|
Support for learning |
Computer Usage |
4.24 (0.64) |
4.15 (0.55) |
|
Teacher Support |
4.09 (0.78) |
||
|
Student Interaction and Collaboration |
4.02 (0.78) |
||
|
Equity |
4.25 (0.82) |
||
|
Quality of learning |
Personal Relevance |
3.60 (0.87) |
3.80 (0.68) |
|
Authentic Learning |
3.66 (0.82) |
||
|
Student Autonomy |
4.16 (0.76) |
||
|
Usability of online learning tools |
A-synchronicity |
3.89 (0.81) |
3.89 (0.82) |
|
Enjoyment |
Enjoyment |
3.48 (1.08) |
3.48 (1.08) |
Table 1: The mean perception scores of domains and subscales of online learning environment
Regarding the relation between academic year and student perception on different domains of the online environment, Year 5 students 3.89 (1.01) enjoyed the online learning as compared to Year 3 3.25(0.95) and Year 4 students 3.22 (1.18) respectively and the difference was statistically significant (P<0.027). Year 4 students perceived more positive on domains support of learning (P=0.658) and quality of learning (P=.396) and Year 5 students perceived online learning tools were useful (P=0.681).
The students were asked to rate their online learning experience via 5 points scale, poor to excellent and (52.4%) of the students found online learning experiences very good followed by (29.4%) good and (13.4%) rated excellent. The data for this research can be accessed at http://doi.org/10.6084/m9.figshare.19322297
IV. DISCUSSION
During COVID-19 pandemic era, medical clinical teaching via online was a challenging experience for both clinical lecturers and clinical year students and this study was to determine the perceptions of clinical year medical students on online learning environments during the COVID-19 pandemic.
A. Evaluating Online Learning Environment
In the literature, there were quite several tools which have been developed to specifically evaluate online learning environments such as Constructivist On-Line Learning Environment Survey (COLLES), Web-Based Learning Environment Inventory (WEBLEI), Technology-Rich Outcomes-Focused Learning Environment Inventory (TROFLEI), and Online Learning Environment Survey (OLES). The OLES instruments have been used to evaluate the university’s online learning environment and found to be a useful tool to evaluate online learning environments as the questionnaires were applicable to our local setting of online teaching. The OLES tool consists of four domains to evaluate student online learning environments such as Support of Online learning, Usability of online learning tools, Quality of Learning and Enjoyment. (Chew, 2015) The scores on scales which received specific attention for online educators to monitor the online learning environment provided for students.
1) Support of online learning: This domain includes four sub scales and it is the most important part for the students to be able to cope with the online learning environment. Regarding support for computer usage, the findings indicate the students received good support from the university regarding online learning such as the providing internet package for students, laptops, online learning tools and platforms such as Microsoft team. The support from lecturers and peers were also important in regarding clinical case discussion and group works. But in some cases, the students need to go and use internet at their relative’s house. On the “Lecturer Support Scale” and “Equity scale”, that the students got support and equivalent chances to contribute in class discussion. (Chew, 2015)
2) Usability of online learning tools: This domain includes asynchronicity subscale. Asynchronicity allows students to learn on their own schedule, within a certain timeframe. In this study, there were high mean scores for the “Asynchronicity” scale which indicates that the students found it easier to communicate online. But the result was contrary to a study by Chew (2015), found out that the students found it challenging to communicate online depends on the availability of internet and usage of social media.
3) Quality of learning: This domain includes three subscales: Personal Relevance, Student Autonomy, and Authenticity learning. The findings indicate that the students were able to manage and play significant roles in their learning in the online learning climates.
4) Enjoyment: The Enjoyment scale was used to evaluate the extent of enjoyment of learning in an online learning environment. Among all four domains, the enjoyment was the least mean perception score which indicated that although the students received support from university and lecturers, they enjoyed less with the online classes as the classes were entirely online. The result was similar to a study by Chew (2015), stated that the students had limited enjoyment in online learning environments due to lack of motivation and technical problems.
B. Limitations of the study
The study was conducted in a private medical university and quantitative approach. A mixed methods approach with larger sample was recommended for future investigations. Validation of the survey recommends carrying out for local setting.
C. Implication of the study
The present study evaluates the online learning environment experienced by clinical year medical students which found to be useful by giving them different learning opportunities and this can be used to implicate future clinical teaching as hybrid mode to create an effective and safe learning environment. The information from this study about the students’ perceptions on online learning, provided significant implications in the field such as implementation of hybrid learning, telemedicine in medical curriculum.
V. CONCLUSION
In conclusion, the perceptions of clinical year medical students on online learning environments during the COVID-19 pandemic were satisfactory although there were challenging online learning experience during the pandemic. It was recommended to include qualitative method in future studies to provide more useful in-depth information regarding online learning environment.
Notes on Contributors
Dr Kye is the corresponding author for this paper. She designed the study, analysed the data, prepared the manuscript working together with the co-author.
Dr Amit Bhardwaj made substantial contributions to the design, editing and preparation of the final manuscript.
Ethical Approval
The research study was approved by Universiti Tunku Abdul Rahman Scientific and Ethical Review committee on 20th July 2020 (Approval number: U/SERC/92/2020).
Data Availability
The data that support the findings of the study are openly available at http://doi.org/10.6084/m9.figshare.19322297
Acknowledgement
We would like to acknowledge the clinical medical students of UTAR (Academic Year 2020/2021) for voluntary participation in this study.
Funding
There was no funding for this research study.
Declaration of Interest
The authors declare that there are no conflicts of interest, including financial, consultant, institutional and other relationships.
References
Bonk, C. J., & Reynolds, T. H. (1997). Learner-centred web instruction for higher order thinking, teamwork, and apprenticeship. In B. H. Khan (Ed.), Web-based instruction (pp.167-178). Englewood Cliffs.
Chew, R. (2015). Perceptions of online learning in an Australian University: Malaysian students’ perspective – Support for Learning. International Journal of Information and Education Technology, 5(8), 587-592. https://doi.org/10.7763/ijiet.2015.v5.573
Klein, H. J., Noe, R. A., & Wang, C. W. (2006). Motivation to learn and course outcomes: The impact of delivery mode, learning goal orientation, and perceived barriers and enablers. Personnel Psychology, 59(3), 665–702. http://doi.org/10.1111/j.1744-6570.2006.00050.x
Samoylenko, N., Zharko, L., & Glotova, A. (2022). Designing online learning environment: ICT tools and teaching strategies. Athens Journal of Education, 9(1), 49-62. https://www.athensjournals.gr/education/2022-9-1-4-Samoylenko.pdf
Pearson, J., & Trinidad, S. (2005). OLES: An instrument for refining the design of e-learning environments. Journal of Computer Assisted Learning, 21(6), 396- 404. https://doi.org/10.1111/j.1365-2729.2005.00146.x
*Kye Mon Min Swe
Jalan Sungai Long, Bandar Sungai Long,
43000 Kajang, Selangor
+601115133799
Email: drkyemonfms@gmail.com
Submitted: 29 May 2022
Accepted: 16 August 2022
Published online: 3 January, TAPS 2023, 8(1), 43-46
https://doi.org/10.29060/TAPS.2023-8-1/SC2807
Kirsty Foster
Academy for Medical Education, Medical School, University of Queensland, Brisbane, Australia
Abstract
Introduction: A series of workshops was held early in our MD curriculum redesign with two aims: gaining stakeholder input to curriculum direction and design; engaging colleagues in the curriculum development process.
Methods: Workshops format included rationale for change and small-group discussions on three questions: (1) Future challenges in healthcare? (2) our current strengths? (3) Future graduate attributes? Small-group discussions were audio-recorded, transcribed and fieldnotes kept and thematically analysed. We conducted a literature review looking at best practice and exemplar medical programs globally.
Results: Forty-seven workshops were held across 17 sites with more than 1000 people participating and 100 written submissions received. Analysis showed alignment between data from workshops, written submissions and the literature review.
The commitment of our medical community to the education of future doctors and to healthcare was universally evident.
Six roles of a well-rounded doctor emerged from the data: (1) Safe and effective clinicians – clinically capable, person-centered with sound clinical judgement; (2) Critical thinkers, scientists and scholars with a thorough understanding of the social and scientific basis of medicine, to support clinical decision making; (3) Kind and compassionate professionals – sensitive, responsive, communicate clearly and act with integrity; (4) Partners and team players who collaborate effectively and show leadership in clinical care, education and research; (5) Dynamic learners and educators – adaptable and committed to lifelong learning; and (6) Advocates for health improvement – able to positively and responsibly impact the health of individuals, communities and populations
Conclusion: Deliberate stakeholder engagement implemented from the start of a major medical curriculum renewal is helpful in facilitating change management.
Keywords: Medical Education, Medical Curriculum, Stakeholder Engagement, Collaboration
I. INTRODUCTION
The quality of the medical education we provide to future doctors is directly related to the quality of care they will provide to their future patients (Torralba & Katz, 2020). It is the responsibility of those involved and of medical schools to promote the highest standards of medical education and medical student learning. At the University of Queensland, a major reimagining of the MD Program is underway to ensure that our already strong medical program remains informed by best practice in both medicine and in education. This is crucial to enabling our medical graduates to be optimally equipped for their internship, pre-vocational and specialist training. It is our responsibility to enable our graduates to be ready for the future medical needs of the people and communities they serve.
Medical programs are complex and involve many people. As well as University academic and professional staff, medical students are taught, supervised and supported by a wide variety of doctors and other health professionals during the four years of our postgraduate degree. At our university we have approximately 4,500 affiliates who may have a role in teaching, supervising or otherwise influencing one or more medical students at some point during their four-year MD program. Many of these are clinical teachers or supervisors who work for the health services with which UQ has a student placement agreement in place. Cognisant that major curricular review is challenging we implemented a deliberate strategy of engagement with as many of our stakeholders as possible from the start of the MD Design project in 2019. In the first stage we planned a series of engagement workshops with key stakeholders and this is the basis of the study.
The purpose of our study was twofold:
Firstly, to gain input from a wide range of stakeholders early in the process to futureproof our curriculum – that is, to inform the vision on what our graduates need to be able to know, do, and be, to succeed in internship and beyond.
Secondly, to involve our key stakeholders in the curriculum design process as a component of change management.
II. METHODS
A series of stakeholder workshops was held. The format of each workshop was to start with a brief outline of the drivers and rationale for curricular change, followed by small-group interactive discussions focusing on three questions:
- What are the major future challenges in relation to healthcare?
- What are our current strengths as a Medical Program, as a university and as a health community?
- What are the important attributes for our future graduates to achieve to best prepare them for their careers?
Ethics approval for the study was granted by the University of Queensland Human Research Ethics Committee (Approval number 2019001725). At the start of each workshop attendees were provided with information about the study and given the opportunity to withdraw. Their participation in the workshop was regarded as consent. All small-group discussions were overseen by KF, audio-recorded and transcribed. KF and the administrative team kept field notes capturing any elements additional to the spoken word such as the general atmosphere of the workshop. KF and JH analysed the transcripts thematically identifying key elements in each focus area. In parallel a literature review was conducted looking at best practice medical education and exemplar medical programs across the globe were explored.
III. RESULTS
Over a period 15 months between July 2019 and January 2021 47 workshops were held across 17 sites with more than 1100 people participating. More than 100 written submissions were received and 5814 people and organisations contacted. Analysis demonstrated general agreement that major change was needed and there was good alignment between feedback received from stakeholder workshops, written submissions and the key findings from the current state analysis as outlined above. There were some stakeholders who felt that they needed to see more substantial evidence that the current curriculum needed refreshing. This group felt reluctant to embark on further change in view of modifications already made in recent years. They were also concerned that ‘change fatigue’ may be a challenge especially among our health service colleagues who contribute to the program.
A key finding was that the passion and commitment of our medical community to the education of future medical doctors and to make a positive contribution to healthcare was universally evident.
The resulting vision for our new MD program is:
To nurture and educate future medical graduates who are clinically capable, team players, kind and compassionate, serve responsibly and are dedicated to the continual improvement of the health of people and communities in Queensland, Australia and across the globe.
To enhance the capability of our graduates to meet the needs of their future patients a set of six roles of the all-round high-quality doctor was developed from the data. These roles map to the four domains that the Australian Medical Council require for primary medical degrees (Australian Medical Council (AMC), 2012), and have been adopted as the vertical themes of the new MD program. They are:
- Critical thinkers, scientists and scholars who have a thorough knowledge and understanding of the social and scientific basis of medicine, and able to apply evidence and research to inform and support clinical decision making.
- Dynamic learners and educators who continue to adapt, are curious, agile, motivated, self-directed, with the ability to honestly and humbly appraise their own learning needs, and have a commitment to lifelong learning.
- Advocates for health improvement who stand with people and are able to positively and responsibly impact the health of individuals, communities and populations. Are able to apply an understanding of health inequalities to strive for health equity, and incorporates prevention and advocacy into clinical practice in all settings.
- Partners and team players who collaborate effectively and show leadership when appropriate in the provision of clinical care and health-related education and research.
- Kind and compassionate professionals who are sensitive, responsive, communicate clearly and act with integrity. Compassion and professionalism are linked not only to improved patient outcomes but to better practitioner outcomes including job satisfaction and to better institutional outcomes.
- Safe and effective clinicians who are clinically capable, person-centred and demonstrate sound clinical judgement – and who can see that they cannot be safe and effective unless they are also capable in all other roles.
The new MD program is structured as five fully integrated courses, three year-long and two semester long courses in final year, with assessment focused on growth and development of knowledge skills and attitudes through active engagement in learning. Assessment for learning as well as of learning is fundamental in enabling all students to reach their full potential. The project has progressed through development of staged learning outcomes for each year of the program and now into detailed and appropriately sequenced learning activities.

Figure 1. The six roles of a well-rounded doctor
IV. DISCUSSION
Communication throughout a period of major change is challenging especially where there are many diverse stakeholders across a large and complex organisation like a medical school (Velthuis et al., 2018). Our strategy was a deliberate one to retain connection and involvement during a lengthy process. Our initial engagement work reported here gave us a good start by actively involving as many people as possible from the beginning of the project. As the project has progressed stakeholders have remained engaged and have been particularly keen on seeking the detail needed to assist in implementation of the new curriculum. This has, on occasion, been challenging when tension between some specialist discipline areas protecting their ‘patch’ and the needs of medical students at primary medical degree level emerge. We also found that education is not regarded as a specialist field by some of our experienced clinical teachers. A lack of understanding about the iterative process of outcomes-based curriculum development contributed to colleagues seeking answers about what is to be taught being frustrated at what they saw as a laborious process of careful scaffolding and integration. This contesting of curriculum is recognised within institutions where it can inhibit development of more effective curricula which promote learning and are more than simply identification of content to be taught (Prideaux, 2003). By engaging with stakeholders from the earliest stage of the curriculum development process we feel that we have minimised this effect.
V. CONCLUSION
Our experience demonstrates that a deliberate stakeholder engagement strategy implemented from the start of a major curriculum renewal is helpful in maintaining key stakeholder involvement. We found that facilitating a collective discussion about the direction and underpinning values of an innovative medical curriculum was a helpful strategy although some stakeholders felt that, since their wishes had not been adopted, they had not been involved. Despite this, we found that, in most cases, stakeholder involvement from the start led to ongoing collaboration in the change management of implementing a new medical program.
We must ensure that our graduates are optimally prepared to begin their careers as medical practitioners over the next 30 to 40 years, and are ready to meet the needs of the people of Queensland, Australia and globally. We are confident that our early engagement on MD Design will help to achieve that goal.
Notes on Contributors
KF conceptualised, led the workshops where data were collected, contributed to data analysis and wrote the manuscript.
Ethical Approval
Ethics Approval for the study was obtained from the University of Queensland Human Research Ethics Committee, Application number 2019001725 granted June 2019. Potential participants were provided with study information prior to the workshops and their active participation in the ensuing workshop was taken to indicate consent.
Data Availability
Data is not currently stored in the UQ Data repository because of its nature, as transcripts of meeting discussions where the partipants may be identified would breach the conditions of ethics approval.
Acknowledgement
The curriculum design project described in this study is an endeavour involving a large number of people. The author would especially like to thank Professor Stuart Carney, Dean of the Medical School for his support in many of the engagement sessions, Dr Jane Hallos for her assistance with data collection, analysis and literature review, Ms Alexandra Longworth for assistance in data collection and all workshop participants for their input.
Funding
The study was funded as part of the MD Design project led by the Faculty of Medicine at the University of Queensland. There was no specific grant funding but the Mayne Bequest supported medical education research expenses.
Declaration of Interest
The author has no conflict of interest to declare.
References
Australian Medical Council (AMC). (2012). Standards for assessment and accreditation of primary medical programs by the Australian Medical Council 2012. Australian Medical Council Ltd.
Prideaux, D. (2003). ABC of teaching and learning in medicine: Curriculum design. BMJ, 326(7381), 268-270. https://doi.org/10.1136/bmj.326.7383.268
Torralba, K. M. D., & Katz, J. D. (2020). Quality of medical care begins with quality of medical education. Clinical Rheumatology, 39, 617-618. https://doi.org/10.1007/s10067-019-04902-w
Velthuis, F., Varpio, L., Helmich, E., Dekker, H., & Jaarsma, A. D. C. (2018). Navigating the complexities of undergraduate medical curriculum change: change leaders’ perspectives. Academic Medicine, 93(10), 1503-1510. https://doi.org/10.1097/ACM.0000000000002165
*Kirsty Foster OAM
Academy for Medical Education, Medical School,
Level 6, Oral Health Centre,
288 Herston Road
Herston QLD 4006 Australia
+61 7 3346 4676
Email: Kirsty.foster@uq.edu.au
Submitted: 8 January 2022
Accepted: 26 April 2022
Published online: 5 July, TAPS 2022, 7(3), 51-56
https://doi.org/10.29060/TAPS.2022-7-3/SC2738
Yiwen Koh1, Chengjie Lee2, Mui Teng Chua1,3, Beatrice Soke Mun Phoon4, Nicole Mun Teng Cheung1 & Gene Wai Han Chan1,3
1Emergency Medicine Department, National University Hospital, National University Health System, Singapore; 2Department of Emergency Medicine, Sengkang General Hospital, Singapore; 3Department of Surgery, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 4Department of Nursing, National University Hospital, National University Health System, Singapore
Abstract
Introduction: During the first wave of the COVID-19 pandemic in Singapore, clinical attachments for medical and nursing students were temporarily suspended and replaced with online learning. It is unclear how the lack of clinical exposure and the switch to online learning has affected them. This study aims to explore their perceptions of online learning and their preparedness to COVID-19 as clinical postings resumed.
Methods: A cross-sectional study was conducted among undergraduate and graduate medical and nursing students from three local universities, using an online self-administered survey evaluating the following: (1) demographics; (2) attitudes towards online learning; (3) anxieties; (4) coping strategies; (5) perceived pandemic preparedness; and (6) knowledge about COVID-19.
Results: A total of 316 responses were analysed. 81% agreed with the transition to online learning, most citing the need to finish academic requirements and the perceived safety of studying at home. More nursing students than medical students (75.2% vs 67.5% p=0.019) perceived they had received sufficient infection control training. Both groups had good knowledge and coping mechanisms towards COVID-19.
Conclusions: This study demonstrated that medical and nursing students were generally receptive to this unprecedented shift to online learning. They appear pandemic ready and can be trained to play an active part in future outbreaks.
Keywords: Medical Students, Nursing Students, COVID-19, Pandemic, Online Learning, Survey
I. INTRODUCTION
During the first wave of the COVID-19 pandemic in Singapore, the government implemented safe distancing and movement restriction orders in a bid to flatten the epidemiological curve. These measures from 7th April to 1st June 2020 were coined the “circuit breaker” period. Clinical attachments for medical and nursing students were suspended to lower the risk of COVID-19 transmission and to focus the hospitals’ efforts towards dealing with the outbreak.
Before the pandemic, students were embedded within clinical teams where they received bedside teachings, practised communications with patients and acquired practical skills. Students perceive online learning during the pandemic to be less effective for acquiring clinical skills due to the absence of patient interaction and real-world practice (Wilcha, 2020). As the pandemic situation stabilised in Singapore, healthcare students gradually returned to the hospitals from May 2020. In one study, students were concerned about returning to the clinical settings as they perceived themselves as untrained and worried about the risks they might introduce to patients (Hernández-Martínez et al., 2021). This may arise from a lack of pandemic preparedness, which is not commonly incorporated into the medical and nursing school curriculum.
To date, there are no studies evaluating the perceptions of both local medical and nursing students towards the disruption of their studies by the pandemic, and whether these perceptions would be similar to those cited in the aforementioned study. Specifically, we aim to describe the perceptions of online learning and pandemic preparedness of medical and nursing students in Singapore during the “circuit breaker” period. Understanding this will help us create more effective learning strategies and reinforce their preparation for future pandemics.
II. METHODS
A. Study Design and Setting
This was a cross-sectional survey involving medical and nursing students from Yong Loo Lin School of Medicine (YLLSOM) and Alice Lee Centre for Nursing Studies (ALCNS), National University of Singapore (NUS); Duke-NUS Medical School (Duke-NUS); and Lee Kong Chian School of Medicine (LKCSOM), Nanyang Technological University (NTU). Students doing clinical attachments in healthcare institutions during the “circuit breaker” period were sent a link to a self-administered, anonymous online questionnaire. Participation was voluntary. Ethics approval for waiver of written informed consent was obtained from NUS Institutional Review Board (Reference number: NUS-IRB-2020-129).
B. Study Instrument
The questionnaire comprised six parts with a total of 74 questions: (1) socio-demographic characteristics; (2) attitudes towards halting clinical attachments and shift to online learning; (3) anxieties towards the pandemic; (4) coping strategies; (5) perceived pandemic preparedness; and (6) specific knowledge about COVID-19. Responses were collected on Likert scales and the questionnaire was adapted from previous studies with permission. Minor modifications were made to standardise the terms used to refer to COVID-19 and online learning and to ensure understandability in Singapore’s context, while preserving the original intent of the source studies. Content validity of the questionnaire was examined by three board-certified emergency physicians involved in undergraduate and postgraduate medical education.
C. Survey Dissemination
The survey was disseminated to eligible students via email by each school’s administrative staff, who were not part of the study team. Four reminder emails were sent from September to October 2020.
D. Statistical Analysis
Results were analysed using Stata 14 (StataCorp LP, College Station, TX). Categorical variables were reported as proportions in percentages and analysed using χ2 test or Fisher’s exact test, as indicated. A p-value of < 0.05 was considered statistically significant.
III. RESULTS
A total of 316 students were recruited between September and December 2020. 64.2% (203/316) were medical students, most of whom were from YLLSOM (147/203, 72.4%). The majority were between 21 and 29 years of age (250/316, 79.1%).
Table 1 details the respondents’ attitudes towards clinical attachment and their perceived pandemic preparedness. Overall, 57% (180/316) of respondents agreed or strongly agreed with stopping clinical attachments. 81% (256/316) agreed with the shift to online learning. The two main reasons for preferring online learning were the need to finish academic requirements and the perceived safety of studying at home. Of those who disagreed, most preferred learning in the clinical areas and felt there was a lack of personal interaction with tutors and classmates via online learning.
With regards to pandemic preparedness, more nursing students agreed or strongly agreed they had received sufficient infection control training in school or the hospitals they were posted to (75.2% vs 67.5% p=0.019) and had someone to turn to for advice on the use of personal protective equipment if uncertain (p<0.001), compared to the medical students. They were also more likely to have received influenza vaccination (p<0.001) or were recommended to do so (p=0.020).
More than 70% of students used healthy coping strategies such as participating in relaxation activities and interacting with family and friends for support. More than 90% were aware of the basic facts about COVID-19, such as its origin, symptoms, transmission, and prevention methods. Supplementary tables of the complete survey results have been made openly available online at https://doi.org/10.6084/m9.figshare.19646340 .
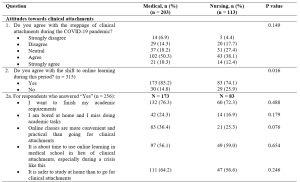
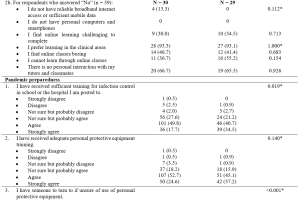
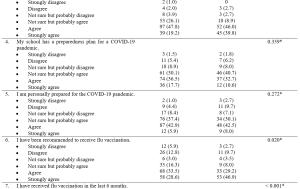
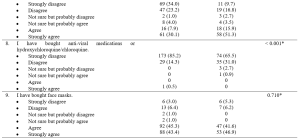
Table 1. Attitudes towards clinical attachments during Singapore’s circuit breaker period (7 April to 1 June 2020) and their perceived pandemic preparedness
*Fisher’s exact test
Cronbach’s alpha for 9 items of pandemic preparedness = .60
IV. DISCUSSION
A. Paradigm Shift to Online Learning
Our study found that the majority were agreeable with transitioning to online learning during the pandemic. Unsurprisingly, given Singapore’s digital connectivity, students in this study did not lack a reliable internet connection or access to technological devices – reasons why students in other countries found virtual teaching challenging (Wilcha, 2020). Among those who disagreed with the transition to online learning, more than 90% indicated they preferred learning in the clinical areas. They were also concerned about the lack of personal interaction with tutors and classmates. These were similar concerns reflected by medical and nursing students in other studies, who felt that online teaching could not adequately replace clinical teachings and learning of practical clinical skills, in the absence of direct patient contact. Lack of physical interaction with tutors and classmates can also result in reduced student engagement levels which may lead to less effective learning (Wilcha, 2020).
To address the perceived weaknesses of online learning, educators worldwide have increasingly adopted novel teaching methods. These include virtual simulations and ward rounds where students can interact with real patients, and simulated set-ups at home for clinical skills practice. In several studies, positive feedback was cited in terms of an increase in medical knowledge, clinical reasoning, and communication skills with these teaching methods (Wilcha, 2020). Our study focused on their perceptions of online learning in the initial phase of the pandemic. As the pandemic persists and with more experience in these innovative ways of online engagement, it is unclear whether the students may view online learning differently now.
It is also uncertain whether online learning is less effective in acquiring knowledge compared to clinical placements. Weston and Zauche (2021) found no difference in standardised assessment scores between nursing students who completed an in-person paediatric clinical practice versus those who used high-fidelity virtual simulation software with pre-briefing and debriefing components. More research is needed to evaluate the effectiveness of technology-assisted education in imparting clinical competency compared with traditional bedside teaching.
B. Pandemic Preparedness
In this study, we found most of the medical and nursing students felt they were prepared for the pandemic. However, a greater proportion of nursing students perceived they had received sufficient infection control training or had someone to seek advice on the use of personal protective equipment. More had also received the influenza vaccination or were recommended to do so. A previous study found that nursing students were superior to medical students in hand hygiene performance (Cambil-Martin et al., 2020). This was attributed to curriculum differences and less practical training in the healthcare setting for medical students. Our results may reflect similar curriculum disparities, suggesting a need to narrow this gap in pandemic preparation education.
A systematic review by Martin et al. (2020) found that medical students were keen to assist in responses to pandemics and other global health emergencies, in both clinical and non-clinical roles, citing social responsibility and an obligation to help. Having adequate training and knowledge were some factors encouraging their participation. In this study, we did not directly examine if students were willing to serve in the pandemic should the need arise. They however did demonstrate satisfactory basic knowledge about COVID-19 and had healthy coping strategies. This suggests they may be pandemic-ready and may be recruited to play a more active part in future outbreaks.
C. Limitations
Our study has its limitations. First, the voluntary survey results are subjected to non-response bias. However, the demographics of responders were similar to the entire student body and should be representative of the cohort. Second, a cross-sectional survey does not allow the tracking of changes in responses over time. Third, the results may not be generalisable to other countries at varying stages of socio-economic development. Lastly, the results cannot capture responses outside the pre-set questionnaire. For this, qualitative studies would be required to further explore the impact of COVID-19 on the students’ perceptions towards online learning and pandemic preparedness.
V. CONCLUSION
The COVID-19 pandemic has disrupted the education of medical and nursing students in Singapore, causing an unprecedented shift from classroom teaching and bedside clinical attachments to online learning. Although this study demonstrated that medical and nursing students were generally receptive towards this paradigm shift, there is a need to continue implementing and refining online learning methods, especially in teaching clinical skills that are traditionally acquired at the bedside. Additionally, our study found that local medical and nursing students may be pandemic ready and can be trained to take an active part in future outbreaks.
Notes on Contributors
Yiwen Koh reviewed the literature, designed the study, analysed the data and wrote the manuscript. Chengjie Lee performed data collection, analysed the data and critically revised the manuscript. Mui Teng Chua advised on statistical analysis methods, analysed the data and critically revised the manuscript. Beatrice Soke Mun Phoon performed data collection and critically revised the manuscript. Nicole Mun Teng Cheung designed the study instrument and critically revised the manuscript. Gene Wai Han Chan reviewed the literature, conceptualised the overall design of the study and critically revised the manuscript. All authors have read and approved the final manuscript.
Ethical Approval
Ethics approval for waiver of written informed consent was obtained from the NUS Institutional Review Board (Reference number: NUS-IRB-2020-129).
Data Availability
The ethical approval by NUS Institutional Review Board was based on the conditions that only study team members will have access to the raw data that will be stored in a password-protected file. A copy of the survey questions and the additional tables of survey results are openly available at https://doi.org/10.6084/m9.figshare.19646340
Acknowledgement
The authors would like to thank the administrative staff of the Yong Loo Lin School of Medicine, Duke-NUS Medical School, Lee Kong Chian School of Medicine and Alice Lee Centre for Nursing Studies for their kind assistance with this study.
Funding
No funding sources were used for this research study.
Declaration of Interest
The authors have no conflicts of interest to declare.
References
Cambil-Martin, J., Fernandez-Prada, M., Gonzalez-Cabrera, J., Rodriguez-Lopez, C., Almaraz-Gomez, A., Lana-Perez, A., & Bueno-Cavanillas, A. (2020). Comparison of knowledge, attitudes and hand hygiene behavioral intention in medical and nursing students. Journal of Preventive Medicine and Hygiene, 61(1), E9–E14. https://doi.org/10.15167/2421-4248/jpmh2020.61.1.741
Hernández-Martínez, A., Rodríguez-Almagro, J., Martínez-Arce, A., Romero-Blanco, C., García-Iglesias, J. J., & Gómez-Salgado, J. (2021). Nursing students’ experience and training in healthcare aid during the COVID-19 pandemic in Spain. Journal of Clinical Nursing. https://doi.org/10.1111/jocn.15706
Martin, A., Blom, I. M., Whyatt, G., Shaunak, R., Viva, M., & Banerjee, L. (2020). A rapid systematic review exploring the involvement of medical students in pandemics and other global health emergencies. Disaster Medicine and Public Health Preparedness, 1–13. https://doi.org/10.1017/dmp.2020.315
Weston, J., & Zauche, L. H. (2021). Comparison of virtual simulation to clinical practice for prelicensure nursing students in pediatrics. Nurse Educator, 46(5), E95–E98. https://doi.org/10.1097/NNE.0000000000000946
Wilcha, R. J. (2020). Effectiveness of virtual medical teaching during the COVID-19 crisis: systematic review. JMIR Medical Education, 6(2), e20963. https://doi.org/10.2196/20963
*Chengjie Lee
110 Sengkang East Way,
Singapore 544886
Email: lee.chengjie@singhealth.com.sg
Submitted: 7 June 2021
Accepted: 20 January 2022
Published online: 5 July, TAPS 2022, 7(3), 46-50
https://doi.org/10.29060/TAPS.2022-7-3/SC2715
Pilane Liyanage Ariyananda, Chin Jia Hui, Reyhan Karthikeyan Raman, Aishath Lyn Athif, Tan Yuan Yong, Muhammad Hafiz
International Medical University, Malaysia
Abstract
Introduction: We aimed to find out how medical students coped with online learning at home during the COVID 19 pandemic ‘lockdown’.
Methods: A cross-sectional study was carried out from July to December 2020, using an online SurveyMonkey Questionnaire®, with four sections: biodata; learning environment; study habits; open comments; sent to 1359 students of the International Medical University, Malaysia. Responses of strongly disagree, somewhat disagree, neither agree nor disagree, somewhat agree and strongly agree for the closed-ended questions on the learning environment and study habits, were scored on a 5-point Likert scale. Percentages of responses were obtained for the closed ended questions.
Results: There were 323 (23.8%) responses. This included 207 (64%) students from the preclinical semesters 1 – 5 and 116 (36%) students from clinical semesters 6 – 10. Of the respondents, more than 90% had the necessary equipment, 75% had their own personal rooms to study, and 60% had satisfactory internet connections. Several demotivating factors (especially, monotony in studying) and factors that disturbed their studies (especially, tendency to watch television) were also reported.
Conclusion: Although more than 90% of those who responded had the necessary equipment for online learning, about 40% had inadequate facilities for online learning at home and only 75% had personal rooms to study. In addition, there were factors that disturbed and demotivated their online studies.
Keywords: Online Learning, Self-directed Learning, Self-regulated Learning, Learning Environment, Malaysian Medical Students
I. INTRODUCTION
In response to the COVID 19 pandemic, the government of Malaysia imposed a movement control order which is referred to as a lockdown, on 18, March 2020. The International Medical University (IMU), which is a private medical university in Malaysia has been relatively resourceful with respect to e-learning even before the occurrence of the lockdown as it had Moodle®, an online Learning Management System (LMS) platform, in its e-learning portal. Like most educational institutions, the IMU, within a short period of time, had to shift the teaching and learning process from a face-to-face mode to an online mode using Microsoft Teams® most of the time during the lockdown.
The objectives or our study were: to describe the learning environment and the study habits of undergraduate medical students while attending online learning sessions during the lockdown; to determine whether undergraduate medical students used the online resources to practice clinical skills (such as communication skills, physical examination skills) and to develop clinical reasoning.
II. METHODS
A literature search was done in PubMed and Google Scholar using search words: online learning, self-directed learning, self-regulated learning, and learning environment. Study setting and sample selection: Our study population was undergraduate medical students of the IMU. Sample size was calculated to be 293, using the formula provided by Fluid Surveys (2020), for a population size of 1359, with a confidence level of 95% and a margin of error of 5%. A cross-sectional study was carried out using an online SurveyMonkey Questionnaire®, from July to December 2020. As online surveys are well known to have high non-response rates, the questionnaire was sent to all the undergraduate medical students in the IMU, during the lockdown. Data collection and analysis: Informed written consent was obtained from all participants. The questionnaire had four sections: biodata; learning environment; study habits and open comments. There was a total of 12 questions with questions 4, 10 and 11 being closed-ended and having 4, 5 and 14 subsidiary questions, respectively within them. Responses to the closed-ended questions were scored on a 5-point Likert scale: strongly disagree; somewhat disagree; neither agree nor disagree; somewhat agree; strongly agree. Percentages of responses were calculated for the closed-ended questions. Data were analysed using software SPSS version 26.0 (IBM Corporation), and summarised, and descriptive statistics are presented.
III. RESULTS
Data that support the study are openly available in Figshare at http://doi.org/10.6084/m9.figshare. 16909384 (Ariyananda et al., 2021). 323 students (23.7%) responded. This included 207 (64%) students from the preclinical semesters 1 – 5 and 116 (36%) students from clinical semesters 6 – 10. 75% were in their homes and the remainder were in rented accommodation close to the university. Data mentioned below are summarised in Table 1. More than 98% had either a laptop or a tablet and a smart phone. 93% had Internet and WiFi connections, but the internet connection was stable only for 59.4% and only 64.7% had uninterrupted power supply. The locations of their study areas were as follows: personal room 75%; common ‘living room’15.8%; twin shared room 6.5%; varying locations 2.7%. The following demotivating factors were reported: monotony in studying (70.6%); lack of access to real patients (56.3%); lack of support from peers and mentors (50.5%); inadequacy of e-learning resources (25.7%). In addition, 85.7% reported a variety of other causes as demotivating factors. Factors that distracted were watching television (83.6%); sleeping (55.4%); distractions from other members of the family (40.2%) and house chores (40.2%). For demotivating factors and distractions students were invited to offer one or more responses. Ability to obtain feedback, learn clinical skills, learn clinical reasoning and to prepare for assessments were rated as insufficient (scored as strongly disagree, somewhat disagree or neither agree or disagree) as 55.1, 80.5, 57.2 and 56.6 percent, respectively. Those who strongly agreed or somewhat agreed or neither agreed or disagreed that following issues impair their study performances were: inability to access educational resources physically (62.8%) and deterioration of self-discipline (74.3%).
To determine which online resources were statistically significant with respect to their perception of adequacy to learn and practice clinical skills, an independent sample t test was used to compare the mean score on perception of adequacy of different online resources for 63 (19.5%) students who answered ‘yes’ (strongly agree & somewhat agree) against 260 (80.5%) who answered ‘no’ (strongly disagree, somewhat disagree & neither agree nor disagree). A similar statistical comparison was done regarding learning clinical reasoning during online learning to 138 (42.7%) students who answered ‘yes’, with 185 (57.3%) who answered ‘no’ with respect to perception regarding adequacy of resources. Both comparisons yielded highly significant p values.
|
Statement |
Strongly Disagree n (%) |
Somewhat Disagree n (%) |
Neither Agree nor Disagree n (%) |
Somewhat Agree n (%) |
Strongly Agree n (%) |
|
There was adequate lighting for me to study |
5 (1.5) |
15 (4.6) |
9 (2.8) |
81 (25.1) |
213 (65.9) |
|
I had adequate workspace study |
8 (2.5) |
22 (6.8) |
10 (3.1) |
86 (26.6) |
197 (61) |
|
There were no external distractions around my study |
48 (14.9) |
95 (29.4) |
53 (16.4) |
66 (20.4) |
61 (18.9) |
|
Comfort factor (prepared meals and clean laundry) helped to make a more productive studying environment |
22 (6.8) |
19 (5.9) |
37 (11.5) |
77 (23.8) |
168 (52) |
|
The inability to access resources (textbooks, quiet study environment etc.) from a physical library affected the quality of my studies. |
59 (18.3) |
61 (18.9) |
70 (21.7) |
88 (27.2) |
45 (13.9) |
|
I required supervision from lecturers to effectively study. |
84 (26) |
86 (26.6) |
77 (23.8) |
49 (15.2) |
27 (8.4% |
|
I struggled with self-discipline to concentrate fully on my studies while at home. |
33 (10.2) |
50 (15.5) |
39 (12.1) |
97 (30) |
104 (32.2) |
|
I prefer studying in groups rather than in isolation. |
68 (21.1) |
81 (25.1) |
75 (23.2) |
49 (15.2) |
50 (15.5) |
|
I was able to manage my time better during the lockdown for my studies. |
54 (16.7) |
64 (19.8) |
75 (23.2) |
93 (28.8) |
37 (11.5) |
|
I am confident to use online resources for my studies. |
0 (0.0%) |
19 (5.9%) |
51 (15.8%) |
133 (40.9%) |
120 (37.2%) |
|
IMU e-learning resources were adequate to facilitate my studies. |
17 (5.3) |
37 (11.5) |
88 (27.2) |
131 (40.6) |
50 (15.5) |
|
I was able to navigate my way through IMU e-learning to get the materials required for my studies. |
6 (1.9) |
29 (9) |
60 (18.6) |
143 (44.3) |
85 (26.3) |
|
I found online teaching sessions helpful to me to achieve the learning outcomes. |
20 (6.2) |
44 (13.7) |
89 (27.6) |
109 (33.7) |
61 (18.6) |
|
Scheduled online sessions helped me organize my time for my studies. |
27 (8.4) |
43 (13.3) |
67 (20.7) |
108 (33.7) |
78 (23.8) |
|
Scheduled online sessions helped me motivate myself to do my own self-study. |
32 (9.9) |
48 (14.9) |
75 (23.2) |
99 (30.7) |
69 (21.4) |
|
I was able to participate in online discussions with ease. |
19 (5.9) |
43 (13.3) |
76 (23.5) |
123 (38.1) |
62 (19.2) |
|
I was able to receive relevant feedback from my mentors on my performance through online sessions. |
25 (7.7) |
63 (19.5) |
90 (27.9) |
84 (26) |
61 (18.9) |
|
I was able to learn clinical skills (previously through CSSC sessions / Clinical Postings) through online sessions. |
122 (37.8) |
93 (28.8) |
45 (13.9) |
48 (14.9) |
15 (4.6) |
|
I was able to apply clinical reasoning in cases discussed through online sessions. |
32 (9.9) |
58 (17.6) |
94 (29.7) |
110 (34.1) |
29 (8.7) |
|
I was able to prepare well for assessments through online sessions. |
31 (9.6) |
66 (20.4) |
86 (26.6) |
101 (31.3) |
39 (12.1) |
|
I had stable Internet connection for online sessions. |
30 (9.3) |
44 (13.6) |
57 (17.6) |
108 (33.4) |
84 (26) |
|
I did not experience any power outages which interrupted online sessions. |
19 (5.9) |
61 (18.9) |
34 (10.5) |
81 (25.1) |
128 (39.6) |
Table 1. Information about the online resources and learning environments.
IV. DISCUSSION
Although more than 90% of those who responded had the necessary equipment, about 40 % had inadequate facilities for online learning at home and only 75% had personal rooms to study. This is a substantial minority of students who are not equipped to carry out online learning effectively and it is a matter of concern. Areas that need urgent attention to improve online learning which would cater to 40% that lack facilities are: providing reliable power supply and fortification of web-based infrastructure and services (expansion of internet bandwidth and expansion of WiFi facilities, subsidized access to internet) and subsidizing hardware. It is known that use of the internet by medical students has not translated into improved online learning behaviour (Venkatesh et al., 2017). Previous studies suggest that self-study can be both efficient and inefficient depending on how the learners behave (Evans et al., 2020).
Majority of students strongly agreed and somewhat agreed with regards to adequacy of environmental factors/comforts such as illumination (91%), workspace (96.6%); and prepared meals and clean laundry (75.8%). Studies have shown that temperature, lighting, and noise have significant direct effects on university students’ academic performance (Realyvásquez-Vargas et al., 2020).
Furthermore, there were factors that disturbed and demotivated their online studies such as monotony in studying; lack of access to real patients; lack of support from peers and mentors and inadequacy of e-learning resources. Monotony when studying alone may be overcome by getting students to interact through peer online discussion groups and by providing gamified/interactive learning material online. Gaps due to lack of access to real patients may be reduced by use of photos (especially in dermatology and ophthalmology), images (such as radiographs, CT and MRI scans), video clips (in neurology to demonstrate involuntary movements and seizures), audio clips (to listen to abnormal heart sounds and murmurs) and by studying case scenarios. Examining parents and siblings at home may help to practice clinical examination techniques of different body systems. Role play by teachers and peers on predetermined scripts will help to develop clinical reasoning and communication skills. As non-verbal cues contribute to a great extent in data gathering during history taking, there is a high chance of students missing this aspect, as online learning is two-dimensional compared to three-dimensional experience they would get in real life. Our observations with regards to perceptions on learning clinical reasoning online is better than for learning clinical skills, as many as 42.7% perceive those resources at their disposal as adequate to learn clinical reasoning. This finding may be supported by the understanding that clinical reasoning can be learned without actual physical contact with patients.
However, these methods will not be able to substitute the kinaesthetic experiences of palpating abdominal lumps and uterus (at different stages of foetal development) as well as vaginal examination in normal and diseased states as done in clinical settings. As for learning clinical procedures, although theoretical aspects can be learned remotely, procedural skills cannot be properly acquired without performing in clinical settings. Simulations closely matching clinical settings using artificial intelligence, AR and VR technologies are available and would be further developed in the future.
Limitations: The main limitation of this study is the low response rate of 23.7% despite an email reminder and persuasion by the leader of each cohort. Although the sample exceeded the minimum sample size of 293, the findings may not be generalizable to the rest of the students at the IMU. The study does not address findings specific to different cohorts as subgroup analysis has not been done as sample sizes of cohorts were too small to arrive at valid conclusions. Since majority (64%) of students who responded are from the pre-clinical phase (whose clinical training is much less compared to clinical phase), pooled data regarding ability to learn clinical skills and clinical reasoning online would not be generalizable across all semesters.
V. CONCLUSION
It is concerning to find that 40% did not have stable internet and one-fourth did not have personal study rooms despite 90% possessing hardware. Furthermore, there were factors that disturbed and demotivated online studies. These should be remedied by providing reliable power supply and fortification of web-based infrastructure and services and by providing subsidised hardware.
Although acquisition of clinical reasoning and clinical skills were perceived to be possible, through online teaching/learning sessions, by one in five and two in five students respectively; every possible effort should be made to remedy shortcomings of the remaining students.
As the pandemic is likely to prevail for some time, we recommend further studies, especially to obtain perceptions of medical students studying in other medical schools in Malaysia and in poorly resourced countries and in the subset of clinical students.
Notes on Contributors
Pilane Liyanage Ariyananda contributed to the conception, design of the study, interpretation of data, and preparation of the paper. Chin Jia Hui, Reyhan Karthikeyan Raman, Aishath Lyn Athif, Tan Yuan Yong, Muhammad Hafiz contributed to conception, acquisition and analysis of data.
Ethical Approval
Permission was obtained from the Institutional Review Board (Project ID No.: IMU: CSc/Sem6 (34) 2020) of the IMU to collect and analyse the data.
Data Availability
A copy of the informed consent form, survey questionnaire and anonymized database are available at https://doi.org/10.6084/m9.figshare.16909384%20 under CC0 license.
Acknowledgement
We are grateful to IMU of Malaysia for permitting us to acquire and analyse data and to Professor IMR Goonewardene for his insightful comments on the manuscript. We thank students who participated in the study.
Funding
This work was supported by the International Medical University of Malaysia (Project ID No.: IMU: CSc/Sem6 (34) 2020).
Declaration of Interest
The authors have no competing interests.
References
Ariyananda, P. L., Hui, C. J., Raman, R. K., Athif, A. L., Yong, T. Y., & Hafiz, M. (2021). Online learning during the COVID pandemic lockdown: A cross sectional study among medical students [Data set]. Figshare. https://doi.org/10.6084/m9.figshare. 16909384
Evans, D. J. R., Bay, B. H., Wilson, T. D., Smith, C. F., Lachman, N., & Pawlina, W. (2020). Going virtual to support anatomy education: A STOPGAP in the midst of the COVID-19 pandemic. Anatomical Sciences Education. 13,279-283. http://doi:10.1002/ASE.1963
Fluid Surveys. (2020). http://fluidsurveys.com/university/survey-sample-size-calculator
Realyvásquez-Vargas, A., Maldonado-Macías, A. A., Arredondo-Soto, K. C., Baez-Lopez, Y., Carrillo-Gutiérrez, T., & Hernández-Escobedo, G. (2020). The impact of environmental factors on academic performance of university students taking online classes during the COVID-19 pandemic in Mexico. Sustainability, 12(21), 9194. https://doi.org/10.3390/su12219194
Venkatesh, S., Chandrasekaran, V., Dhandapany, G., Palanisamy, S., & Sadagopan, S. (2017). A survey on internet usage and online learning behaviour among medical undergraduates. Postgraduate Medical Journal, 93, 275–279. https://doi.org/10.1136/postgradmedj-2016-134164
*Pilane Liyanage Ariyananda
Clinical Campus,
International Medical University,
Jalan Rasah, Seremban 70300
Negeri Sembilan, Malaysia
Email: ariyananda@imu.edu.my
Submitted: 26 February 2022
Accepted: 22 April 2022
Published online: 5 July, TAPS 2022, 7(3), 42-45
https://doi.org/10.29060/TAPS.2022-7-3/SC2766
Gabriel Lee Keng Yan, Lee Yun Hui, Wong Mun Loke, & Charlene Goh Enhui
Faculty of Dentistry, National University of Singapore, Singapore
Abstract
Introduction: Nurturing preventive-minded dental students has been a fundamental goal of dental education. However, students still struggle to regularly implement preventive concepts such as caries risk assessment into their clinical practice. The objective of this study was to identify areas in the cariology curriculum that could be revised to help address this.
Methods: A total of 10 individuals participated and were divided into two focus group discussions. Thematic analysis was conducted, and key themes were identified based on their frequency of being cited before the final report was produced.
Results: Three major themes emerged: (1) Greater need for integration between the pre-clinical and clinical components of cariology; (2) Limited time and low priority that the clinical phase allows for practising caries prevention; and (3) Differing personal beliefs about the value and effectiveness of caries risk assessment and prevention. Participants cited that while didactics were helpful in providing a foundation, they found it difficult to link the concepts taught to their clinical practice. Furthermore, participants felt that they lacked support from their clinical supervisors, and patients were not always interested in taking action to prevent caries. There was also heterogeneity amongst students with regards to their overall opinion of the effectiveness of preventive concepts.
Conclusion: Nurturing preventive-mindedness amongst dental students may be limited by the current curriculum schedule, the prioritisation of procedural competencies, the lack of buy-in from clinical supervisors, and a perceived lack of relevance of the caries risk assessment protocol and should be addressed through curriculum reviews.
Keywords: Dental Education, Caries Risk Assessment, Cariology, Preventive Dentistry, Qualitative Study, Clinical Teaching, Cariogram
I. INTRODUCTION
According to the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019, dental caries in permanent teeth affects an estimated 2 billion people globally yet it is largely preventable. Thus, nurturing preventive-minded dental students has been a fundamental goal of dental education, and a recurring topic of discussion among dental educators (Pitts et al., 2018). Apart from the operative management of dental caries with fillings, dental students are taught to conduct caries risk assessments for their patients. This enables students to construct a tailored caries prevention plan leveraging the use of fluoride varnishes or dietary advice to prevent the onset or progression of carious lesions. However, studies have reported that while students are taught to assess patients’ risk for dental caries and customising preventive plans as part of the Cariology curriculum, they struggle to regularly incorporate prevention into their clinical practice (Calderon et al., 2007; Le Clerc et al., 2021).
The objective of this study was to identify areas in the Cariology curriculum that could be enhanced to help dental students become more prevention orientated in their clinical practice.
II. METHODS
A. Cariology Curriculum at NUS
The Faculty of Dentistry, National University of Singapore offers a four-year Bachelor of Dental Surgery (BDS) programme, mainly divided into pre-clinical and clinical phases. The Cariology curriculum begins in Year 1, where pre-clinical students are equipped with an understanding of the aetiology and pathogenesis of dental caries, along with its preventive and operative management. In Year 2, behavioural science and oral health education and promotion strategies are introduced. Commencing the clinical phase, Year 3 students are taught to utilise the Cariogram electronic assessment tool (D Bratthall, Computer software, Malmö, Sweden), to systematically assess a patient’s caries risk by using self-reported information on plaque control, dietary habits, fluoride exposure, and other caries-related risk factors. From the Cariogram results, a patient’s caries risk profile is generated to guide the development of a targeted caries prevention plan for the patient and aid in the delivery of patient education. A summative assessment is held during the final term of Year 4 where students are required to submit three patient case logs with caries risk assessments and prevention plans documented for one-to-one discussion with faculty members involved in the Cariology curriculum.
B. Study Design
An e-mail invitation was sent to the cohort of 2020 (N=55) within a month after the final examination results were released. Ten individuals responded, willing to participate and giving consent. Participants were divided into two groups where focus group discussions (FGDs) were conducted, held on a teleconferencing platform (Zoom Video Communications), facilitated by one study team member using a discussion guide. Audio recordings of the FGDs were transcribed by the facilitator and two other study team members. All the study team members conducted the thematic analysis. Key themes were identified based on their frequency of being cited.
III. RESULTS
Three major themes emerged from the FGDs.
A. Greater Need for Integration between the Pre-clinical and Clinical Components of Cariology
Participants felt that the pre-clinical lectures provided a foundational understanding of dental caries that they could draw from during their clinical phase of training. However, they suggested that the clinical application of Cariology, such as the use of the caries risk assessment (CRA), can be further emphasised at the beginning of the clinical phase of the BDS programme to reinforce its relevance and significance in the context of overall patient care.
“…not really on our mind when we enter clinics. Maybe the staff can run through the CRA assessment forms before entering clinics.”
[P6]
Participants also highlighted that the three cases due in Year 4 could be submitted and discussed with faculty staff earlier in the clinical phase of the course to concretise concepts and allow an opportunity to implement suggested modifications to their patients’ preventive plans.
“But CRA presentation could have been done earlier like in Year 3. Only after the discussion did it really stick in.”
[P10]
“By the time it made sense, clinic was over.”
[P6]
B. Limited Time and Low Priority to Practice Dental Caries Prevention in the Clinical Phase of Training
Participants shared that the main emphasis of a dental student’s limited clinical time was on operative procedures, as it would mean fulfilling clinical competency requirements essential for graduation.
“As students, we’re slow, so we want to maximise time for treatment rather than talking about prevention.”
[P2]
“…there are other more important requirements.”
[P9]
The low priority dental students accorded to dental caries prevention was also influenced by their clinical supervisors. Some participants noted that their clinical supervisors did not appear keen to discuss caries risk assessment findings during the clinical sessions and did not provide guidance on developing caries prevention plans.
“It is just a two-way thing between patients and students, and not with assessors”.
[P3]
“In the clinics no one really checks our caries risk assessments.”
[P1]
Participants also perceived a lack of interest among patients regarding prevention which discouraged them from providing advice.
“Out of the 30 (patients) I saw, only one was interested in oral hygiene instructions and good oral practices.”
[P2]
C. Differing Personal Beliefs about the Value and Effectiveness of Caries Risk Assessment and Prevention
There was a diverse spread of beliefs among participants about the value and effectiveness of caries risk assessment and caries risk management in clinical practice. Several participants saw the value of caries risk assessments and preventive management as necessary tools to help patients prevent the onset and progression of dental caries.
“Caries risk and prevention is what dentistry is about. It would shape preventive strategies and conversations.”
[P10]
“Knowing how to assess risk for the individual is meaningful as it helps employ more time-effective approaches to managing the patient.”
[P5]
Contrastingly, some participants felt that performing caries risk assessments had little added benefit in guiding their preventive advice as,
“…in the end the advice given is the same regardless…”
[P1]
“I didn’t really have to go through the caries risk assessment to tell them what good habits to have.”
[P7]
IV. DISCUSSION
The findings present several perceived barriers that students face from having a more prevention oriented clinical practice. As dental schools focus heavily on procedural competencies, students will place a larger emphasis on fulfilling these requirements and less on assisting their patients with preventive regimes. Furthermore, the duration of the clinical phase of dental training is insufficient to see the results of the preventive advice given, such as a reduction in incidence of new carious lesions, resulting in students finding its impact less meaningful or tangible as compared to placing a filling or extracting a tooth. One solution is to implement formative grading systems in place of the current summative assessments where students would actively identify patients at risk of caries and conduct one-to-one case discussions with their supervisors throughout the clinical phase and be graded accordingly. This system allows for opportunities to reinforce caries prevention concepts and patient management skills throughout the duration of the clinical training instead of only at the end. To address the scepticism some of the students may have with regard to caries risk assessment, steps to address misconceptions may need to be established (Maupome & Isyutina, 2013). A clearer delivery of concepts at the lecture sessions and opportunities during one-to-one case discussions could be implemented in the revised curriculum.
A frequent theme that emerged was the lack of buy-in from the clinical supervisors about carrying out caries risk assessments and preventive management in the student clinics. This may not be surprising as similar sentiments were reported in a recent qualitative study among practising dentists (Leggett et al., 2021). Majority of clinical supervisors are not involved in teaching Cariology and hence it may be necessary to align them with the teaching of caries management paradigms and their roles in informing preventive treatment plans. This can enable them to reinforce such concepts when they supervise the students in the clinics.
The lack of interest in preventive advice among the participants’ patients is similarly observed in other countries – patients know about prevention but are not interested to change (Leggett et al., 2021). Clinical supervisors can encourage dental students to consider different methods of patient engagement through techniques such as Motivational Interviewing, or even take the opportunity to exploit behavioural change models to effect a more pro-prevention lifestyle. In so doing, patients may appreciate better the importance of prevention from various perspectives including the associated cost savings with a reduction in the operative management of dental caries.
The issues highlighted through the FGDs are summarised in Table 1 together with possible modifications.
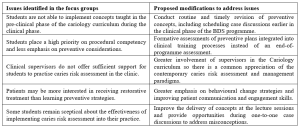
Table1. Issues identified in the FGDs and possible mitigating modifications to the current cariology curriculum
V. CONCLUSION
Nurturing preventive-mindedness among dental students may be limited by the current curriculum content and delivery, the prioritisation of procedural competencies, the lack of buy-in from clinical supervisors, and a perceived lack of relevance of the caries risk assessment protocol. Nevertheless, prevention remains the best cure for dental caries and the issues raised through the FGDs can be addressed through curricular modifications discussed earlier. This will, in turn, enhance the preventive-mindedness of the dental students.
Notes on Contributors
GLKY conceptualised the study, participated in data collection, analysis, and interpretation, drafted the manuscript, and approved the final version to be published.
LYH conceptualised the study, participated in data collection, analysis, and interpretation, critically revised the manuscript, and approved the final version to be published.
WML conceptualised the study, critically revised and approved the final version of the manuscript
CGE designed the methodology, participated in data collection, analysis, and interpretation, and critically revised and approved the final version of the manuscript.
Ethical Approval
This study was approved by the NUS Institutional Review Board (IRB No: S-20-141E).
Data Availability
The transcripts/data of this qualitative study are not publicly available due to confidentiality agreements with the participants.
Acknowledgement
The authors would like to thank the participants for their invaluable input and feedback.
Funding
There was no funding for this study.
Declaration of Interest
The authors have no conflicts of interest to declare.
References
Calderon, S. H., Gilbert, P., Zeff, R. N., Gansky, S. A., Featherstone, J. D., Weintraub, J. A., & Gerbert, B. (2007). Dental students’ knowledge, attitudes, and intended behaviors regarding caries risk assessment: impact of years of education and patient age. Journal of Dental Education, 71(11), 1420-1427. https://doi.org/10.1002/j.0022-0337.2007.71.11.tb04412.x
Le Clerc, J., Gasqui, M.-A., Laforest, L., Beaurain, M., Ceinos, R., Chemla, F., Chevalier, V., Colon, P., Fioretti, F., Gevrey, A., Kérourédan, O., Maret, D., Mocquot, C., Özcan, C., Pelissier, B., Pérez, F., Terrer, E., Turpin, Y.-L., Arbab-Chirani, R., . . . Doméjean, S. (2021). Knowledge and opinions of French dental students related to caries risk assessment and dental sealants (preventive and therapeutic). Odontology, 109(1), 41-52. https://doi.org/10.1007/s10266-020-00527-7
Leggett, H., Csikar, J., Vinall-Collier, K., & Douglas, G. (2021). Whose responsibility is it anyway? Exploring barriers to prevention of oral diseases across Europe. JDR Clinical & Translational Research, 6(1), 96-108. https://doi.org/10.1177/2380084420926972
Maupome, G., & Isyutina, O. (2013). Dental students’ and faculty members’ concepts and emotions associated with a caries risk assessment program. Journal of Dental Education, 77(11), 1477-1487. https://doi.org/10.1002/j.0022-0337.2013.77.11.tb05624.x
Pitts, N. B., Mazevet, M. E., Mayne, C., & Shaping the Future of Dental Education Cariology Group (2018). Shaping the future of dental education: Caries as a case-study. European Journal of Dental Education, 22 Suppl 1, 30–37. https://doi.org/10.1111/eje.12345
*Gabriel Lee Keng Yan
9 Lower Kent Ridge Rd, Level 10,
Singapore 119085
Email: dengabriellee@nus.edu.sg
Submitted: 23 August 2021
Accepted: 28 October 2021
Published online: 5 April, TAPS 2022, 7(2), 56-60
https://doi.org/10.29060/TAPS.2022-7-2/SC2686
Mae Yue Tan, Nicholas Beng Hui Ng, Marion Margaret Aw & Jeremy Bingyuan Lin
Khoo Teck Puat -National University Children’s Medical Institute, National University Health System, Singapore
Abstract
Introduction: The transition from medical student to houseman is well recognised as a stressful period for newly qualified doctors. This stress is likely to be heightened when the transition occurs during a pandemic. We aimed to evaluate the perceived stress levels of housemen as they begin housemanship and explore their sentiments and preparedness in starting work amidst the coronavirus disease 2019 (COVID-19) pandemic.
Methods: Housemen starting work at a tertiary institution in Singapore in May 2020 completed the following: (1) Perceived Stress Scale, (2) open-ended questions on perceived challenges and concerns and (3) questionnaire on preparedness and confidence in starting work. Descriptive statistics were used to analyse quantitative data and modified thematic analysis performed for qualitative data.
Results: Sixty-one housemen participated. Thirty-five (57.4%) reported high perceived stress. The themes for perceived challenges in this transition included coping with constant change, lack of reliable information from authorities, dealing with disappointment, physical fatigue, and loss of autonomy. The themes for concerns in beginning housemanship elicited relate to clinical competence, transitioning into new responsibilities, risk of infection with COVID-19, senior expectations, physical fatigue and training-related concerns. Despite these challenges and concerns, housemen were prepared to begin work during this pandemic.
Conclusion: Housemen transitioning during this pandemic experienced additional stressors and unique challenges pertaining to working in a pandemic. Encouragingly, they remain prepared to start work. Institutions and departments should be mindful of the specific concerns and challenges so that appropriate support can be put in place to support these junior doctors.
Keywords: COVID-19, Junior Doctor, Intern, Pandemic, Challenges, Preparedness
I. INTRODUCTION
Newly graduated doctors are a particularly vulnerable group of healthcare workers as they start work as housemen amidst the COVID-19 pandemic. The transition from student to doctor is already notorious for steep learning curves and increased stress (Sturman et al., 2017). Moreover, housemen in Singapore experienced drastic changes during their final year of medical school, a time which coincided with the surge of the pandemic in Singapore. Not only was clinical training was disrupted, this batch also experienced a modified form of final examinations, an earlier start to housemanship, and changes to posting selections, as manpower allocation was done centrally based on manpower demands. With that, we aimed to evaluate the perceived stress among housemen and explore their perceived challenges, concerns and preparedness just before they started work.
II. METHODS
We performed a cross-sectional anonymous survey on housemen at our institution on their first day of housemanship, in May 2020. The survey was administered before the hospital orientation by an independent institutional representative not part of the investigating team. Consent was implied through voluntary participation.
The Perceived Stress Scale (PSS) (Cohen et al., 1983) was used as a measure of stress. This tool is designed to assess how unpredictable, uncontrollable, and overloaded respondents find their lives. We also administered structured open-ended questions to elicit perceived challenges and major concerns while transitioning from medical school to starting work as a houseman. Participants also completed 7-point Likert rating scale modelled after an existing military instrument (Zagelbaum et al., 2014) to evaluate perceived preparedness and confidence in starting work.
Quantitative data was analysed using IBM SPSS (Version 23.0), with descriptive analysis. The qualitative data was analysed using modified thematic analysis, with NVivo software. All transcripts were coded independently by three authors. The coding method involved an inductive (ground up) method, looking at generating the unit of meanings, categorising the data and developing themes until data saturation was achieved. The kappa coefficient score for the qualitative data analysis was 0.87, indicating good agreement.
III. RESULTS
Sixty-one housemen participated (response rate 100%). A significant proportion (57.4%) rated high stress on the PSS.
Key themes of perceived challenges reported by the housemen transitioning from medical school to the workforce during the COVID-19 pandemic included: (1) coping with constant change, (2) lack of timely reliable information, (3) dealing with disappointment, (4) physical fatigue, (5) loss of autonomy (Fig 1). Examples of last-minute changes to examinations, work commencement and posting-related information were quoted as a major cause for significant uncertainties. Additionally, some had quoted the lack of timely nor reliable dissemination of the information, coming from third-party sources rather than relevant authorities. The shortened break between end of examinations and housemanship meant that typical traditions of personal and post-graduation plans, had to be cancelled, resulting in disappointment and reduced rest. Many also felt that the central distribution of manpower with increased rotations to pandemic heavy departments meant a loss of autonomy in selecting a posting or institution of choice.
The themes for perceived concerns about starting work during the pandemic included (1) clinical competence as a junior doctor, (2) transitioning into new responsibilities, (3) risk of infection, (4) failing to meet expectations of seniors, (5) physical fatigue and (6) training-related concerns. The lack of competence in patient management, “call” duties, and managing emergencies were a huge concern. This extended from concerns of manpower constraints and reduced supervision during pandemic times. Navigating the new job as a doctor with new responsibilities were also raised, with concerns on the long hours and overnight “calls” leading to burnout. There were also examples given on failing to meet the expectations of senior colleagues. Pandemic-specific concerns included the risk of contracting and transmitting COVID-19 to loved ones. Many had also expressed apprehension about the possible impact that the pandemic may have on their clinical training and career progression.
In terms of preparedness to start work amidst a pandemic, 82.0% (n = 50) housemen shared that they were mentally prepared to start work. Majority (86.8%) felt that their medical school had prepared them adequately to be a junior doctor. Three-quarters (75.4%) agreed that their medical school has prepared them adequately to deal with the pandemic and its related clinical demands. Majority (83.6%) felt confident in their clinical competency to effectively work as a junior doctor, and 77.0% felt confident in their clinical competency in dealing with the pandemic as a junior doctor. Interestingly, when asked about their confidence in managing stress, 80.3% reported being confident of dealing with stressors faced by a junior doctor while 77.0% felt confident in managing pandemic-related stress.

Figure 1. Perceived challenges in the transition period, and perceived concerns of new housemen just before starting their housemanship. The size of the boxes corresponds to the frequencies of the themes with examples of verbatim responses transcribed.
IV. DISCUSSION
Our results show that a significant proportion of housemen starting work in the current pandemic have high perceived stress; this appeared to be higher than what is reported in literature for medical students and house officers in non-pandemic settings (Drachev et al., 2020), and higher than healthcare workers during this pandemic (Chen et al., 2020). As such, we believe that this is a significant finding warranting attention.
The challenges of transitioning from medical school to housemanship is well established: not only do housemen have to cope with the responsibility of being a full-fledged doctor, there is also increased physical fatigue and professional expectations that need to be met. Some of these challenges specific to transitioning have also been raised by our housemen.
The sentiments of housemen transitioning during a pandemic are not unique to this group alone: dealing with frequent and constant change and the lack of reliable and timely information are challenges that have also been reported among other healthcare workers. However, there were specific points unique to this group of junior doctors we had studied, particularly the perceived insecurity over their qualifications due to disrupted student clinical training and modified final examinations. This we feel is an important point that medical schools should be aware of; in the event of disruptions or sudden changes to the process of assessment or accreditation, it is important that these be conveyed clearly to the student body, with appropriate engagement, opportunities for clarification and reassurance on any insecurities which they may result from these changes.
Significant pandemic-specific concerns included fears of contracting the COVID-19 infection and transmitting this to others. This fear is not uncommon among healthcare workers and has been reported in recent literature. There was also the additional concern of postgraduate training disruption, which was not unexpected given the disruptions to teaching, deployment to pandemic areas and the lack of choices in the selection of their postings.
We were encouraged to find that despite the higher perceived stress, reported challenges and concerns shared, the majority had felt that their medical schools had prepared them adequately to be a junior doctor, and to deal with pandemic related demands. Additionally, despite the concerns about starting work earlier, majority still reported being ready to start work and felt confident to work effectively – their response to readiness meant that they were not shying away from the call of duty during this pandemic.
Our study is not without limitations. Open-ended questions instead of interviews that were done in line with social distancing restrictions limited the depth of the qualitative data. That said, the 100% response rate provided us which rich data that could be analysed. Additionally, the use the modified questionnaire on preparedness not only lacked external validation; we are also aware that self-reported preparedness may not correlate with actual readiness.
We believe that the key sentiments we have reported on housemen starting work in a pandemic are likely to be universal and not unique to our institution alone. These data would be informative for institutions to provide targeted support for new housemen amidst the pandemic. These include:
- Providing clear and effective information transfer particularly on rapidly changing protocols.
- Emphasis on training on personal protection and infection prevention throughout their postings.
- If manpower resources permit, institutions may consider first deploying housemen to non-pandemic services with initial job-shadowing before sending them to pandemic areas.
- Close clinical supervision from immediate seniors.
- Specific teaching program catering to the learning needs of housemen during the pandemic.
- Enforcing strict work-rest cycles to ensure adequate rest.
- Dedicated mentors for housemen to share concerns and grievances. These mentors have the responsibility of identifying housemen who are struggling such that early support can be rendered.
- Appropriate resources for housemen who require additional support.
V. CONCLUSION
Newly qualified doctors beginning their housemanship during the COVID-19 pandemic have high perceived stress with specific pandemic-related concerns and challenges on top of the usual stressors in transitioning. That said, there is encouraging data on housemen preparedness in starting work during this time. Institutions should ensure that support systems are in place to support junior doctors in these likely protracted extraordinary times. A successful transition from medical school to workplace is the cornerstone that allows these junior doctors to integrate effectively to contribute to the workforce in the pandemic, and the long journey beyond.
Notes on Contributors
Mae Yue Tan contributed to analysis and interpretation of data, drafting and critical revising of the article.
Nicholas BH Ng contributed to analysis and interpretation of data, drafting and critical revising of the article.
Marion M Aw contributed to interpretation of data, drafting and critical revising of the article.
Jeremy BY Lin contributed to conception and design, interpretation of data, drafting and critical revising of the article.
All authors gave final approval of the version to be published.
Ethical Approval
Ethics approval was obtained from from the NHG Domain Specific Review Board (DSRB), with NHG DSRB reference number of 2020/00392.
Data Availability
The data for this study can be found at https://doi.org/10.6084/m9.figshare.16399107 and https://doi.org/10.6084/m9.figshare.16399419. The access to these datasets are available for use subject to approval of the authors of this article.
Acknowledgement
The authors would like to thank the housemen who participated in this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Interest
All authors have no conflict of interest to declare.
References
Chen, B., Li, Q. X., Zhang, H., Zhu, J. Y., Yang, X., Wu, Y. H., Xiong, J., Li, F., Wang, H., & Chen, Z. T. (2020). The psychological impact of COVID-19 outbreak on medical staff and the general public. Current Psychology, 1–9. https://doi.org/10.1007/s12144-020-01109-0
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behaviour, 24(4), 385-396.
Drachev, S. N., Stangvaltaite-Mouhat, L., Bolstad, N. L., Johnsen, J. K., Yushmanova, T. N., & Trovik, T. A. (2020). Perceived stress and associated factors in Russian medical and dental students: A cross-sectional study in North-West Russia. International Journal of Environmental Research and Public Health, 17(15), 5390. https://doi.org/10.3390/ijerph17155390
Sturman, N., Tan, Z., & Turner, J. (2017). “A steep learning curve”: Junior doctor perspectives on the transition from medical student to the health-care workplace. BMC Medical Education, 17(1), Article 92. https://doi.org/10.1186/s12909-017-0931-2
Zagelbaum, N. K., Heslin, K. C., Stein, J. A., Ruzek, J., Smith, R. E., Nyugen, T., & Dobalian, A. (2014). Factors influencing readiness to deploy in disaster response: Findings from a cross-sectional survey of the department of veterans affairs disaster emergency medical personnel system. BMC Emergency Medicine, 14, Article 16. https://doi.org/10.1186/1471-227X-14-16
*Tan Mae Yue
1E Kent Ridge Road,
NUHS Tower Block Level 12,
Singapore 119228
Tel: +65 6772 5555
Email: mae_yue_tan@nuhs.edu.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
