
Faculty’s perception of their role as a tutor during Problem-Based Learning activity in undergraduate medical education
Submitted: 17 August 2023
Accepted: 21 December 2023
Published online: 2 April, TAPS 2024, 9(2), 87-91
https://doi.org/10.29060/TAPS.2024-9-2/SC3114
Isharyah Sunarno1,2, Budu Mannyu2,3, Suryani As’ad2,4, Sri Asriyani2,5, Irawan Yusuf 2,6, Rina Masadah2,7 & Agussalim Bukhari2,4
1Department of Obstetrics and Gynecology, Faculty of Medicine, Hasanuddin University, Indonesia; 2Department of Medical Education, Faculty of Medicine, Hasanuddin University, Indonesia; 3Department of Ophthalmology, Faculty of Medicine, Hasanuddin University, Indonesia; 4Department of Clinical Nutrition, Faculty of Medicine, Hasanuddin University, Indonesia; 5Department of Radiology, Faculty of Medicine, Hasanuddin University, Indonesia; 6Department of Physiology, Faculty of Medicine, Hasanuddin University, Indonesia; 7Department of Pathological Anatomy, Faculty of Medicine, Hasanuddin University, Indonesia
Abstract
Introduction: The study aimed to ascertain how the faculty at the Faculty of Medicine, Hasanuddin University perceived their role as a tutor during a problem-based learning activity during the academic phase of medical education, based on the length of time they acted as a tutor.
Methods: This was prospective observational research with an explanatory sequential mixed-method design, which was performed at the Undergraduate Medical Study Program, Faculty of Medicine, Hasanuddin University, from January 2023 until May 2023. Research subjects were divided into two groups: a) the Novice group and b) the Expert group. Quantitative data were collected by giving a questionnaire containing six categories with 35 questions and distributed by Google form. An independent t-test was used to compare the faculty’s perception, with a p-value <.05 significant. Followed by Focus Group Discussion (FGD) for qualitative data, which then were analysed by thematic analysis. The last stage is integrating quantitative and qualitative data.
Results: There were statistically significant differences in seven issues between the two groups. Most of the tutors in both groups had favorable opinions, except for the expert group’s disagreement with the passive role of the tutor in the tutorial group. Eight positive and twelve negative perceptions were found in the FGD.
Conclusion: Most tutors positively perceived their role in PBL, with the expert group having more dependable opinions and well-reasoned suggestions.
Keywords: Problem-Based Learning, Undergraduate Medical Education, Focus Group Discussion
I. INTRODUCTION
The transition from teacher-centered to student-centered learning occurs with the introduction of active learning based on the needs of the students. The majority of effective active learning activities in the classroom were created in small groups using the Problem-Based Learning (PBL) approach. PBL has no worse outcomes in terms of academic performance and is more effective than conventional methods at enhancing social and communication skills, problem-solving abilities, and self-learning abilities, and allows the students to collaborate while integrating science, theory, and practice (Trullàs et al., 2022; Wiggins et al., 2017). A tutor or a facilitator is a pertinent element for the success of tutorial activities in PBL, thus evaluating periodically their perception and understanding about PBL activities, will help determine the need for resource development at the faculty level. Based on the aforementioned background, the author is intrigued to understand how the faculty at the Undergraduate Faculty of Medicine at Hasanuddin University perceived their role as a tutor during a PBL activity based on the duration they acted as a tutor.
II. METHODS
Short-case PBL tutorial is the model being implemented in our institution. An explanatory sequential mixed-methods observational prospective design study was carried out from January 2023 to May 2023. Informed consent was obtained from all the participants (ethics approval recommendation number: 99/UN4.6.4.5.31/PP36/2022). The study was conducted in three stages (Figure 1):
A. Stage 1
Gathering quantitative data via a survey disseminated using Google form, after which the information was analysed using SPSS version 25. The Likert scale, which ranged from 1 (extremely disagree) to 5 (extremely agree), was used to evaluate the 35 items in the questionnaire that served as the study’s primary data collection tool (Table 1 which is openly available on Figshare). The validity and reliability test for the study’s questionnaire was carried out as the first step and the Pearson Correlation was used to examine the outcome; all questions were valid with Cronbach’s α .951. The next step was to collect data through convenience sampling. Inclusion criteria were lecturers who: have attended training to become PBL tutors, are actively involved in PBL activities, and are willing to participate in the research projects to completion. Exclusion criteria were lecturers who were not familiar with the Google form application. Subjects with other commitments that prevented them from finishing the research activities and with a conflict of interest in continuing the study were considered dropouts. The research participants were split into two groups: the novice group (participants who served as tutors for less than five years) and the expert group (participants who served as tutors for five years or more). The Slovin formula was used to determine the minimum sample size, and the result was 32 people for each group. Characteristics of the study subjects were presented descriptively. An independent t-test was used to compare the faculty’s perception of their role as a tutor during a problem-based learning activity, with a p-value <.05 significant.
B. Stage 2
Focus Group Discussions (FGD) were held to collect qualitative data. The participants in the FGD were divided into two groups using the identical criteria utilised for the quantitative group categorisation, and each group consisted of six subjects. Each participant received a set of open-ended questions to be discussed during the FGD. All events and discussions were recorded, and then all conversations were transcribed using the VERBATIM app. MAXQDA 2020 was then used to tag and categorise the data. Thematic analysis was used to assess qualitative data. We used an audit trail and triangulation during data collection and conducted a peer review during data analysis to ensure the validity of the qualitative data.
C. Stage 3
Integrating quantitative and qualitative data was performed by linking data, followed by integration at the interpretation and reporting level which was conducted by integration through a narrative with a weaving approach.
III. RESULTS
A. Characteristics of the Subjects
The subjects in the novice groups were all under 45 years old, but the expert group was predominately made up of older faculty members. Both groups were predominately female. At the time of the research, medical doctors dominated the novice group, but the expert group included people with a range of educational backgrounds. Characteristics of the study subjects are openly available in Table 2 on Figshare.
B. Quantitative Data
Seven question items from four categories significantly differed between the novice and expert groups as shown in Table 3 which is openly available on Figshare.
C. Qualitative Data
Thematic analysis from the FGD revealed that the expert group only has negative perceptions, whereas the novice group has both negative and positive perceptions. The data are openly available in Table 4 on Figshare.
D. Integration of Quantitative and Qualitative Data
Faculty staff has the same perception about almost all concepts about the role of a PBL tutor, except for seven concepts that were statistically significantly different (Figure 1):
1) PBL as Pedagogical Method: Q5 (group tutorials help students share experiences) and Q9 (PBL is a great tool for student learning) were significantly different, with the majority of the novice group agreeing with it while the majority of the expert group were extremely agreeable. Nevertheless, while the novice had a positive perspective shown in the discussion, the expert expressly stated that “(PBL) increased the (student’s) ability to discuss but not the depth of knowledge.”
2) Supervising Problem Processing in Tutorial Groups: Q12 (I function as a resource person in the group) and Q13 (I participate in creating a positive work environment for the group) were significantly different, with most of the novice group agreeing to the concept while the majority of the expert group were extremely agreeable. The novice group stated in the FGD that “PBL is very effective for building students’ analytical skills because the students can interact with each other to express their opinions and find key problem-solving strategies.” Both groups had the same perception that some tutors attended the PBL activities “just as a formality.” Q17 (I am sensitive to the wishes of the students regarding their need for support) was also significantly different, with most participants in both groups agreeing that tutors are sensitive to the student’s need for support, but 5.71% of the novices extremely disagreed. In contrast, none of the experts in the expert group disagreed with the concept. From the FGD results, the expert group suggested that the “tutor should give feedback and guidance to the students”.
3) Potential Barriers to Student Learning in PBL: the majority of both groups agreed that the group size is just right from a tutorial point of view (Q24), but the novice group had a wide range of responses (from extremely disagree to extremely agree), while 77.14% of the expert group agreed. “Six to eight students in one PBL group” is an elaborate suggestion made by the expert group as a result of the FGD.
4) There was a statistically significant difference between the two groups regarding the role of the tutor, which is usually passive in the tutorial group (Q29), with the expert group’s consensus on the matter being unfavorable, whereas the novice group’s responses were evenly split between neutral and disagree. The FGD’s results revealed that the novice merely stated, “If the students had a misleading concept, the tutor could not be kept silent,” whereas the expert suggested, “The tutor should be the chairman of the group discussion,” and “Questions and keywords must be made by the tutor.”
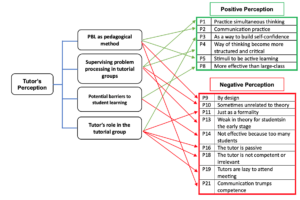
Figure 1. Integration of Quantitative and Qualitative Data
IV. DISCUSSION
PBL can be regarded as a multidisciplinary method that allows the learners to resolve real-life problems and situations in every aspect, learn how to construct new information meaningfully, put away the understanding of ready-to-use knowledge, and acquire critical thinking skills. Problem processing or facilitation is a challenging task (Aydogmus & Mutlu, 2019). Since PBL can be used in specific topics and can break up the monotony of traditional didactic teaching, it has become a popular alternative teaching strategy for undergraduate medical students. It can also be used as a method of integrated teaching. Overall, it is a great tool for students learning (Gadicherla et al., 2022).
The group size is one of the possible obstacles to students’ learning in PBL. All students will not be able to participate in a team that is too big. A team that is too small could not have enough members to address the learning objectives or enough diverse opinions to guarantee a robust discussion. The tutor should be aware of how the participants play their roles, noting those who do not contribute to debates or who are silent. Therefore, they must pay close attention to what is happening in the group process to intervene and provide feedback, promoting the participants’ individual and group progress. The tutor can assist the student in identifying their requirements through motivated evaluations and simple feedback, fostering the growth of self-confidence, autonomy, and, ultimately, integration into group dynamics. PBL teams ideally consist of 6–10 students (Dent et al., 2017).
V. CONCLUSION
Aside from seven concepts, both groups mostly had positive perceptions about their role as tutors, with the expert group having more dependable opinions and well-reasoned suggestions.
Notes on Contributors
Isharyah Sunarno made the following contributions to the study: conceptualised, created the initial draft and study design, investigated and collected data, conducted formal analysis, looked for research references, performed critical revision of the article, reviewed and edited the article, and approved the study’s final published version.
The following are the contributions Budu Mannyu made to the study: provided insights into the methodology, suggested research references, served as a peer reviewer of the study’s findings, performed critical revision of the article, and gave his approval of the final draft to be published.
Suryani As’ad contributed the following to the study: she offered insights into the methodology, proposed research references, served as a peer reviewer of the study’s findings, revised the article critically, and approved the final draft of the manuscript to be published.
The study benefited from Sri Asriyani’s efforts, which included: suggestion for research references, peer review of the study’s findings, and performed critical revision of the article.
The following contributions were made to the study by Irawan Yusuf: peer reviewing of the result, supervising the research activities, and critical editing of the publication.
The following are the contributions Rina Masadah contributed to the study: provided ideas into the original draft, supervised the research activities, and edited the publication critically.
Agussalim Bukhari made the following contributions to the study: offered insights into the methodology, oversaw the research activities, critically revised the final version of the article.
Ethical Approval
The study was approved by the Research Ethical Committee Faculty of Medicine Hasanuddin University with recommendation number: 99/UN4.6.4.5.31/PP36/ 2022.
Data Availability
The authors confirm that the data supporting the findings of this study are available within the article and its Supplementary material for research instrument in https://doi.org/10.6084/m9.figshare.23646918
Acknowledgement
Authors would like to express our sincere gratitude to all the tutors who participated in this study. A special appreciation is given to Ichlas Nanang Affandi and A. Tenri Rustam from the Psychology Study Program, Faculty of Medicine, Hasanuddin University for their valuable support throughout the research process, including their role as the facilitator of the FGD. We also would like to thank Andriany Qanitha and the CRP team from Faculty of Medicine, Hasanuddin University for their support in developing the manuscript. We are also grateful to the Department of Medical Education, Faculty of Medicine, Hasanuddin University for providing us with the resources and support we needed to complete this study.
Funding
This research received no external funding.
Declaration of Interest
The authors declare no conflict of interest.
References
Aydogmus, M., & Mutlu, A. (2019). Problem-based learning studies: A content analysis. Turkish Studies-Educational Sciences, 14(4), 1615–1630. https://doi.org/10.29228/turkishstudies.23012
Dent, J. A., Harden, R. M., & Hunt, D. (2017). A practical guide for medical teachers (5th ed.). Elsevier.
Gadicherla, S., Kulkarni, A., Rao, C., & Rao, M. Y. (2022). Perception and acceptance of problem-based learning as a teaching-learning method among undergraduate medical students and faculty. Azerbaijan Medical Journal, 62(03), 975–982.
Trullàs, J. C., Blay, C., Sarri, E., & Pujol, R. (2022). Effectiveness of problem-based learning methodology in undergraduate medical education: A scoping review. BMC Medical Education, 22(1), 1–12. https://doi.org/10.1186/s12909-022-03154-8
Wiggins, B. L., Eddy, S. L., Wener-Fligner, L., Freisem, K., Grunspan, D. Z., Theobald, E. J., Timbrook, J., & Crowe, A. J. (2017). ASPECT: A survey to assess student perspective of engagement in an active-learning classroom. CBE Life Sciences Education, 16(2), 1–13. https://doi.org/10.1187/cbe.16-08-0244
*Isharyah Sunarno
Jl. Perintis Kemerdekaan Km. 11,
Faculty of Medicine, Hasanuddin University
+62411-585859
Email: isharyahsunarno@gmail.com
Submitted: 12 June 2023
Accepted: 24 October 2023
Published online: 2 April, TAPS 2024, 9(2), 81-86
https://doi.org/10.29060/TAPS.2024-9-2/SC3066
Lean Heong Foo1, Nurul Haziqah Binte Suhaimi2, Saudha Binte Sadimin2, Marianne Meng Ann Ong1
1Department of Restorative Dentistry, National Dental Centre, Singapore; 2Dental Assisting, National Dental Centre, Singapore
Abstract
Introduction: An online survey was conducted on 16 National Institute of Technical Education Certificate (NITEC) Dental Surgery Assistant (DSA) trainees in National Dental Centre Singapore to find out their perceptions and understanding of mental well-being.
Methods: The 43-item survey included (i) Psychological General Well-being Index (PGWB) with 22 items based on 6 domains (anxiety, depression, positive well-being, self-control, general health, and vitality); (ii) 5 items on mental health knowledge; (iii) 4 items on lifestyle; and (iv) 12 items on perceptions of mental well-being and working in the dental clinic. Responses were collated for descriptive analysis and Cronbach’s alpha analysis was done for internal consistency for Likert scale items.
Results: The average PGWB score was 61.5 (range 18-89). Fourteen trainees (75%) indicated they were feeling depressed and 31.2% of trainees felt under stress in the past month. The majority (81.3%) of trainees recognised the role of exercise in maintaining mental health and 75% of trainees were able to differentiate between sadness and depression. However, 56.3% and 87.5% of the trainees incorrectly answered that mental and psychological disorders are not preventable conditions and mental disorders are caused by a wrong way of thinking respectively. The Cronbach’s alpha on PGWB (a = 0.87) and trainees’ perception of working in the clinic (a = 0.76) revealed good internal consistency.
Conclusion: The PGWB scores and survey analysis indicate there is a knowledge gap about mental health and the need to improve mental well-being in this cohort of NITEC DSA trainees.
Keywords: Mental Well-being, Dental Surgery Assistant Trainee, Psychological General Well-being Index
I. INTRODUCTION
In National Dental Centre Singapore (NDCS), Dental Surgery Assistant (DSA) trainees are required to complete a 1-year National Institute of Technical Education Certificate (NITEC) DSA programme to be qualified as a DSA. Similar to the training of dental students, DSA trainees undergo a significant transition from learning in a classroom setting (4 weeks pre-clinical didactic and observation) to a high-stress dental clinic work environment (clinical) when they start on-the-job training 1 month after commencing their programme. During this transition period, they need to multi-task and adapt to new clinical responsibilities related to infection control, patient management, and assisting clinicians. It has been reported that 80% of 299 Israeli DSAs suffered from a high level of burnout where the most stressful work-related factors were low income, high workload, and work hazards (Uziel et al., 2019). A survey was thus conducted to gain insights into the perceptions of mental well-being and working in the dental clinic among NDCS’s NITEC DSA trainees. This was a needs analysis survey done in June 2022 for a mental wellness module that aimed to provide support to DSA trainees enrolled in the 1-year NITEC DSA programme.
II. METHODS
An online anonymous survey with written consent was disseminated via Form.SG to the 2022 cohort of DSA trainees to complete three months after starting their 1-year programme. The 43-item survey included (i) Psychological General Well-being Index (PGWB) with 22 items based on 6 domains (anxiety, depressed mood, positive well-being, self-control, general health and vitality) (Dupuy, 1984); (ii) 5 items on knowledge about mental health; (iii) 4 items on lifestyle; and (iv) 2 items on perception of mental well-being (adapted from Puspitasari et al., 2020) and 10 items on working in a dental clinic (crafted based on NDCS context). DSA trainees rated their level of agreement based on a 6-point Likert scale for PGWB (5 -most favourable response to 0 – unfavourable response) and a 5-point Likert scale for the perception of mental health and working in a dental clinic (5 – strongly agree to 1 – strongly disagree). The PGWB score ranges from 0 to 110, effectively representing an individual’s comprehensive subjective well-being. Additionally, the six dimensions of the PGWB index provide valuable insights into the subjective well-being associated with each specific dimension. The survey responses were collated for descriptive analysis and Cronbach’s alpha analysis was done for internal consistency for Likert scale items.
III. RESULTS
The entire cohort of sixteen DSA trainees {all female; age 17-50, mean 28.19 (23.39-32.99)} completed the online survey (100% response rate). The data of this study are openly available in the Figshare repository at http://doi.org/10.6084/m9.figshare.23501136.
Only 25% of trainees (4/16) had more than 1 year of prior working experience in a dental clinic. Their collated responses based on their second-month experience of the 1-year programme are as follows:
A. Psychological General Well-being Index (PGWB)
The average PGWB score for this cohort was 61.5 (range 18-89, 95% CI 52.80 – 70.20), indicating lower than average general well-being in this cohort {normal range 68-83 (Dupuy, 1984)}. No significant correlation was found between age and dental clinic experience on PGWB (r=-0.03; -0.06). The Cronbach’s alpha in PGWB (a = 0.93) indicated good internal reliability with a good individual domain analysis of 0.85 for all the domains (Appendix A: Table 1, Figures 2 and 3).
1) General health: The trainees achieved a mean score of 8.94 (Range 0-15) in general health. The majority (68.75%, 11/16) of trainees agreed they felt healthy enough to function.
2) Positive well-being: The trainees experienced a lower than moderate level of positive emotion and life satisfaction with a mean score of 9.94 (Range 0-20). Only 5 out of 16 trainees (31.25%) were happy with their personal life most of the time.
3) Self-control: The trainees possessed a moderate to higher level of self-control in regulating their behavior and emotions (mean 56, Range 0-15). However, about half of the cohort (56.25%, 9/16) admitted they felt a lack of control over their action in the past month.
4) Vitality: The trainees exhibited a moderate level of energy and vitality (mean 10.31, Range 0-20). However, 7 trainees (43.75%) admitted they felt worn out and exhausted most of the time in the past month.
5) Depressed mood: The trainees, on average, experienced a relatively moderate level of depressive symptoms in the past month (mean:88, Range 0-15). Fourteen trainees (75%) admitted they were feeling depressed and 31.2% of trainees (5/16) had felt under stress in the past month.
6) Anxiety: The trainees exhibited a moderate level of anxiety (mean 12.88, Range 0-25). Majority (81.25%, 13/16) of trainees admitted they felt high-strung quite a good bit of time in the past month.
B. Knowledge about Mental Health
Majority of DSA trainees (81.3%, 13/16) recognised the role of exercise in maintaining mental health and 75% (12/16) of trainees were able to differentiate between sadness and depression. However, 56.3% (9/16) of the trainees incorrectly answered that mental and psychological disorders are not preventable conditions, and a majority (87.5%, 14/16) incorrectly answered that mental disorders are caused by a wrong way of thinking (Appendix B).
C. Lifestyle
Half of the cohort exercised at least once a week. Only 50% of the cohort had self-care activities for themselves. Majority of the trainees (15/16) did not meditate and 50% of the trainees sought help from their friends and family when necessary (Appendix B).
D. Perception of Mental Well-being and Working in a Dental Clinic
Majority of the trainees also gave a neutral response (75%, 12/16) to the statement related to stress from working in the dental clinic. Majority agreed that mental health is important for their general health (87.5%, 14/16). Only half of the cohort indicated they were comfortable to work in the dental clinic (56.3%, 9/16) (Figure 1). About ¾ of the cohort believed they could complete the training programme and were confident to perform the on-the-job training (75%, 12/16). Majority (81.3%, 13/16) were willing to seek help if they encountered problems working in the dental clinic (Figure 1). The Cronbach’s alpha of trainees’ perceptions of working in the clinic (a = 0.76) revealed good internal consistency.

Figure 1. Perceptions of DSA trainees of mental well-being and working in the dental clinic in the second month of their 1-year programme
IV. DISCUSSION
Mental well-being is associated with one’s ability to cope with normal stresses of life and work productivity. This is particularly important in health professionals, including DSAs, to ensure the quality of patient care and professional satisfaction. To our knowledge, this is the first local survey to investigate DSA trainees’ perceptions of mental well-being and working in the dental clinic. The PGWB analysis revealed this cohort of DSA trainees had a lower-than-normal score that was even lower than a group of 320 Japanese dental students (61.5 versus 68.63) (Sugiura et al., 2005). Additionally, the trainees also demonstrated moderate levels of depression and anxiety, with a detailed analysis indicating a significant number experiencing stress. This observation highlighted the transition from pre-clinical to clinical training phase can be challenging and stressful with increased workload and responsibility, as evident among DSAs who demonstrated a moderate level of professional burnout (Uziel et al., 2019). A similar trend was observed in this transition phase for dental students, where stress was associated with increased responsibility and demands associated with caring for real patients (de Souza Ferreira et al., 2023). Despite the difference in curriculum and a larger student cohort, the Japanese dental students (Sugiura et al., 2005) appeared to cope with their training better as their PGWB revealed they were more relaxed (Anxiety 16.43 versus 12.88) and cheerful (Depression 11.24 versus 9.88) compared with our DSA trainees. This finding reflects the need for providing mental well-being support for our DSA trainees in their programme.
The misconceptions about mental health and infrequent self-care practices among trainees suggest a lack of awareness of mental wellness. Implementing a mental wellness module focusing on positive psychology, coping techniques like breathing exercises and meditation, and resource awareness can help address these issues. The Trainees’ willingness to seek help and recognise exercise’s role in mental health shows openness to support and intervention. Our pilot data is constrained by a small sample size and the absence of a control group for comparison, making it insufficient for general population inferences. The limitation of PGWBI includes only 6 dimensions and the potential of bias due to self-reported data. Future recommendations involve re-evaluating the impact of the mental wellness module at the end of the 1-year program, inclusion of qualitative data, and establishing a supportive work environment with accessible mental health resources and mentorship to enhance the well-being and job satisfaction of DSAs.
V. CONCLUSION
In conclusion, the survey findings from this small cohort of DSA trainees underscore the importance of addressing mental health and well-being in this group of learners. The high prevalence of depressive symptoms and reported stress among the trainees highlights the need for targeted interventions and support systems to promote mental well-being. Hence, a mental wellness module will be introduced to this cohort of DSA trainees and this survey will be repeated 3 months after the module completion to assess any changes in this cohort’s perception of mental well-being and working in the dental clinic.
Notes on Contributors
FLH reviewed the literature, contributed to the study conception, data acquisition, and data analysis, drafted, and critically revised the manuscript.
NHS contributed to the data acquisition, data analysis, and critically revised the manuscript.
SS contributed to the data acquisition, data analysis, and critically revised the manuscript.
MO contributed to the study conception, data acquisition and critically revised the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Ethical Approval
This study was exempted from the formal Centralised Institutional Review Broad review by SingHealth Institutional Review Board (CIRB Ref: 2022/2122).
Data Availability
The data that support the findings of this study are openly available in the Figshare repository http://doi.org/10.6084/m9.figshare.23501136.
Acknowledgement
We would like to thank Ms Liu Yanting for her help in data preparation and collection.
Funding
There was no funding involved in the preparation of the manuscript.
Declaration of Interest
The authors declare no conflict of interest.
References
de Souza Ferreira, F., Barros, I., da Costa Neves, T., Pazos, J. M., & Garcia, P. P. N. S. (2023). Stress amongst dental students in the transition from preclinical training to clinical training: A qualitative study. European Journal of Dental Education. 27(3), 568-574.
Dupuy, H. J. (1984). The Psychological General Well-Being (PGWB) index. In: Wenger NK, Mattson ME, Furberg CF, & Elinson J (Eds). Assessment of quality of life in clinical trials of cardiovascular therapies. 170-183. Le Jacq.
Puspitasari, I. M., Garnisa, I. T., Sinuraya, R. K., & Witriani, W. (2020). Perceptions, knowledge, and attitude toward mental health disorders and their treatment among students in an Indonesian university. Psychology Research and Behaviour Management, 27(13), 845-854.
Sugiura, G., Shinada, K., & Kawaguchi, Y. (2005). Psychological well-being and perceptions of stress amongst Japanese dental students. European Journal of Dental Education. 9(1),17-25.
Uziel, N., Meyerson, J., Birenzweig, Y., & Eli, I. (2019). Professional burnout and work stress among Israeli dental assistants. Psychology, Health & Medicine, 24(1), 59-67.
*Foo Lean Heong
National Dental Centre Singapore
5, Second Hospital Avenue
168938 Singapore
Email: foo.lean.heong@singhealth.com.sg
Submitted: 20 April 2023
Accepted: 23 August 2023
Published online: 2 January, TAPS 2024, 9(1), 54-57
https://doi.org/10.29060/TAPS.2024-9-1/SC3048
Atul Kumar1, Amol Gawande1, Meghana Bhilare2, Vishal Wadajkar2, Indrajit Ghoshal3 & Shirish Raibagkar4
1Dr.D.Y. Patil B-School, Pune, India; 2Dr.D.Y. Patil Institute of Management and Research, Pune, India; 3Faculty of Computer Science and Engineering, Poornima University, Jaipur, India; 4Savitribai Phule Pune University, Pune, India
Abstract
Introduction: The purpose of this study is to carry out a comparative analysis of the job satisfaction of nurses working in India based on the different types of the hospital they are working with. The study tests the null hypothesis that the job satisfaction of nurses from India across different types of hospitals is the same.
Methods: Four hundred nurses divided into 100 each for four popular types of hospitals – (1) Educational; (2) Government; (3) Charitable Trust; and (4) Private, from all over India were surveyed. Two ANOVA tests were performed. The first one was performed, taking overall job satisfaction as the dependent variable. The second ANOVA was performed by taking the monetary and compensation factors, work environment and management support, and job-related factors as the dependent variables.
Results: The overall mean of job satisfaction was -0.73 (SD 0.60). Overall, 65 percent of the variability of the dependent variable, job satisfaction, is explained by the type of hospital and is statistically significant (p<0.0001).
Conclusion: Monetary and compensation factors, work environment and management support, and job-related factors impact nurses’ job satisfaction. These factors vary with the type of hospital, and hence it can be concluded that due to variation in these factors depending on the type of hospital, the job satisfaction of nurses varies. Implications of our study are for the educational, government, and charitable trust hospitals to improve their work culture, management, and work environment so that nurses will have higher job satisfaction.
Keywords: Nurses, Job Satisfaction, India, Hospitals, Government, Private, Charitable Trust, Educational
I. INTRODUCTION
India’s ratio of nurses per 1000 population is only 1.96 as against the WHO norm of 3 per 1000 population. Another 4.3 million more nurses are required by India by the year 2024 to meet the World Health Organization (WHO) standard of 3 nurses per 1000 population (Business Standard, 2021). Job satisfaction of nurses assumes significance given the huge gap between its current ratio of nurses per 1000 and the WHO norm. But studies investigating linkages between types of hospitals (legal structure of the hospital) and their impact on the job satisfaction of nurses are relatively low. Different types of hospitals can be found in India – Educational, Government, Charitable Trust, Private, Military, Missionary, Railway, and a few more. A sizable amount of literature is available which suggests that factors like organisational culture matters in the job satisfaction of nurses (Rahnavard et al., 2018). But there are few studies correlating these factors with the type of hospital. The association between the factors and the type of hospital remains unexplored. This research attempts to provide empirical evidence supporting the association of the factors influencing job satisfaction and the type of hospitals. The study expects to generate valuable insights for nurses and their employers of different types. It is based on a survey of 100 nurses each from the four most popular types of hospitals – (1) Educational; (2) Government; (3) Charitable Trust; and (4) Private owned.
II. METHODS
The size of the Indian population of nurses is more than 3 million. At a 95 percent confidence interval, the sample size for this population works out to 384, which we rounded off to 400, giving an equal representation of 100 nurses each from the four types of hospitals – educational, government, charitable trust, and private owned. The task of collecting 100 responses for each type of hospital was distributed among the authors. Convenience and purposive sampling method were used. However, to make the study group more inclusive, the sample included nurses from all regions and parts of India – urban, semi-urban, and rural. The questionnaire was administered through Google Forms. The survey was conducted in March 2023. Express written consent for participation was obtained from each respondent.
The study got ethics committee approval number DYP202301, from the Dr.D Y Patil (Deemed to be) University, Pune, India, and Dr.Ajeenkya D Y Patil University, Pune, India.
A scale developed by Chang et al. (2017) to measure the job satisfaction of healthcare workers was largely referred to while designing our scale, which was duly tested for validity and reliability (Cronbach Alpha 0.96). We spoke to a few senior nurses who advised us to consider monetary and compensation factors while assessing the job satisfaction of nurses. Monetary benefits are important for any working human in any part of the world. Studies on job satisfaction (conducted in developed, developing, and underdeveloped countries) include monetary benefits as a parameter. Based on our discussion with the senior nurses and the existing literature, we identified three main factors as determinants of job satisfaction for Indian nurses – monetary and compensation factors, work environment and management support, and job-related factors. monetary and compensation Factors included items like “The salary pay-scales are satisfactory”, “Benefits like provident fund, and gratuity are duly given”, and others. work environment and management support included items like “The management of this organization is supportive of me”, “The management makes changes based on my suggestions and feedback”, and others. job-related factors included items like “I receive the right amount of support and guidance from my direct supervisor”, “I am provided with all trainings necessary for me to perform my job”, and others.
III. RESULTS
Some of the distinctive features of the profile information include a relatively high concentration of respondents in the work experience groups of 10-15 years (158 respondents representing 40 percent of the sample), very low representation of postgraduate educational qualification (10 respondents representing 3 percent of the sample); very low representation of hospitals with a standing of <10 years (11 respondents representing 3 percent of the sample). All these 11 hospitals with a standing of <10 years were private hospitals. The data that support the findings of this study are openly available at https://www.openicpsr.org/ openicpsr/project/190042/version/V1/view (Bhilare, 2023).
A. Descriptive Statistics
Table 1 shows descriptive statistics of the sample.
|
Type |
Total |
Monetary |
Work Env. |
Job related |
||||
|
Mean |
SD |
Mean |
SD |
Mean |
SD |
Mean |
SD |
|
|
Educational |
-0.22 |
0.86 |
-0.21 |
0.87 |
-0.27 |
0.89 |
-0.19 |
0.90 |
|
Govt. |
-1.55 |
0.40 |
-1.53 |
0.39 |
-1.60 |
0.47 |
-1.54 |
0.44 |
|
Trust |
-1.57 |
0.46 |
-1.51 |
0.47 |
-1.65 |
0.50 |
-1.53 |
0.50 |
|
Private |
0.42 |
0.68 |
0.39 |
0.74 |
0.39 |
0.68 |
0.48 |
0.71 |
|
Total |
-0.73 |
0.60 |
-0.71 |
1.05 |
-0.78 |
1.09 |
-0.70 |
1.09 |
Table 1. Descriptive statistics of the sample
The overall job satisfaction mean scores of the hospitals were -0.22 (0.86) for educational hospitals, -1.55 (0.40) for Government hospitals, -1.57 (0.46) for Trust hospitals, and 0.42 (0.68) for private hospitals. For all the 400 respondents taken together, the mean job satisfaction score was -0.73 (SD 0.60).
In the case of educational hospitals, all three factors of job satisfaction were negative – monetary and compensation factors (M= -0.21, SD 0.87), work environment and management support (M= -0.27, SD 0.89), and Job-related factors (M= -0.19, SD 0.90). The same was the case with government hospitals which reported negative job satisfaction for all three factors – monetary and compensation factors (M= -1.53, SD 0.39), work environment and management support (M= -1.60, SD 0.47), and Job-related factors (M= -1.54, SD 0.44).
Further, charitable trust hospitals too reported negative job satisfaction for all three factors – monetary and compensation factors (M= -1.51, SD 0.47), work environment and management support (M= -1.65, SD 0.50), and job-related factors (M= -1.53, SD 0.50). However, private hospitals were the only type of hospitals that reported positive job satisfaction for all three factors – monetary and compensation factors (M= 0.39, SD 0.74), Work environment and management support (M= 0.39, SD 0.68), and job-related factors (M= 0.48, SD 0.71).
B. Testing of the Hypotheses
Two ANOVA tests were performed. The first one was performed, taking overall job satisfaction as the dependent variable (R2 0.65, p<0.0001). The second ANOVA was performed by taking the monetary and compensation factors (R2 0.62, p<0.0001), work environment and management support (R2 0.64, p<0.0001), and job-related factors (R2 0.64, p<0.0001) as the dependent variables.
IV. DISCUSSION
The overall job satisfaction score of the entire sample size of 400 respondents is -0.73 (SD 0.60), which is close to -1, indicating somewhat dissatisfied. Thus, on an overall basis, Indian nurses have reported job dissatisfaction. An important reason for this is the mismatch between the guidelines of the Nursing Council about the working conditions and the actual working conditions at the various hospitals. The analysis shows that for all the three factors, namely, the Monetary and compensation factors, the work environment and management support factors, and job-related factors the scores are range-bound. This indicates a close relationship between these three factors.
However, when we look at the analysis by the type of hospitals, major variations are seen. Three out of the four types: educational hospitals, government hospitals, and charitable trust hospitals, show negative job satisfaction, whereas only one type, the private owned hospitals, show positive job satisfaction. This is because private hospitals offer a much better and more professional work culture leading to higher job satisfaction among the nurses (Srimulyani & Hermanto, 2022). Interestingly, there is not much difference between the job satisfaction scores of government hospitals and charitable trust hospitals. The standard deviations associated with these two high negative scores are also similar. Scores of government hospitals and charitable trust hospitals can be taken as lying between somewhat dissatisfied and strongly dissatisfied ratings, pointing out a big gap between the prescribed norms of working conditions and the actual working conditions. The score of -0.22 indicates relatively much lesser job dissatisfaction in the case of educational hospitals (as compared to government and charitable trusts). It indicates that the control over educational hospitals is better as compared to the other two types of hospitals. The positive score of 0.42 in the case of private hospitals lies between neutral and somewhat satisfactory pointing a positive and professional work culture.
An important observation that emerges from the analysis is that for each of the four types of hospitals, there is little variation in the three factors of job satisfaction or dissatisfaction. This is because the three factors are closely related to each other.
V. CONCLUSION
Indian nurses, on an overall basis, are somewhat dissatisfied with their jobs. However, when we look into different types of hospitals, it is concluded that nurses working in private hospitals are moderately satisfied, those working in educational hospitals are moderately dissatisfied, and those working in government and charitable trust hospitals are highly dissatisfied. monetary and compensation factors, work environment and management support, and job-related factors impact nurses’ job satisfaction. These factors vary with the type of hospital, and hence it can be concluded that due to variation in these factors depending on the type of hospital, the job satisfaction of nurses varies. This impact is strong on an overall basis, as well as for the three factors (monetary and compensation Factors, work environment and management support, and job-related factors) separately. Interestingly there is a strong correlation among the three factors that we have used for measuring the job satisfaction of nurses. We conclude that positive and relatively higher job satisfaction among nurses working in private hospitals (Srimulyani & Hermanto, 2022) can be attributed to professional working culture, better monetary and compensation factors, better co-worker relationships, and other factors.
Notes on Contributors
Dr. Atul Kumar contributed to the conceptualization of the entire study. Dr. Amol Gawande contributed in designing methods for the study. Dr. Meghana Bhilare contributed to data collection. Dr. Vishal Wadajkar contributed to data analysis. Dr. lndrajit Ghoshal contributed in deducing findings and writing the discussion. Dr. S S Raibagkar contributed in writing the full paper including the conclusion. All the authors have read and approved the final manuscript.
Ethical Approval
The study got ethics committee approval number DYP202301, from the Institutional Review Boards of Dr.D Y Patil (Deemed to be) University, Pune, India, and Dr.Ajeenkya D Y Patil University, Pune, India.
Data Availability
All 400 responses were collated in a data set that has been deposited in a repository and can be accessed at https://www.openicpsr.org/openicpsr/project/190042/version/V1/view
Funding
No external funding was used for the study.
Declaration of Interest
We declare that there is no conflict of interest or competing interest of any sort with any individual or organization.
References
Bhilare, M. (2023). Data set Nurses Job Satisfaction (ICPSR 190042; Version V1) [Data set]. ICPSR. https://www.openicpsr.org/openicpsr/project/190042/version/V1/view
Business Standard. (2021, September 2). India in need of 4.3 mn more nurses by 2024 to meet who norms: Nurse org. Retrieved March 29, 2023, from https://www.business-standard.com/article/ current-affairs/india-in-need-of-4-3-mn-more-nurses-by-2024-to-meet-who-norms-nurse-org-121090201448_1.html
Chang, E., Cohen, J., Koethe, B., Smith, K., & Bir, A. (2017). Measuring job satisfaction among healthcare staff in the United States: a confirmatory factor analysis of the Satisfaction of Employees in Health Care (SEHC) survey. International Journal for Quality in Health Care, 29(2), 262-268. https://doi.org/10.1093/intqhc/mzx012
Rahnavard, F., Sadati, A. K., Hemmati, S., Ebrahimzade, N., Sarikhani, Y., Heydari, S. T., & Lankarani, K. B. (2018). The impact of environmental and demographic factors on nursing job satisfaction. Electronic Physician, 10(4), 6712. https://doi.org/10.19082%2F6712
Srimulyani, V. A., & Hermanto, Y. B. (2022). Organizational culture as a mediator of credible leadership influence on work engagement: empirical studies in private hospitals in East Java, Indonesia. Humanities and Social Sciences Communications, 9(1), Article 274. https://doi.org/10.1057/s41599-022-01289-z
*Shirish S Raibagkar
Savitribai Phule Pune University,
Ganeshkhind, Pune, India
Email: ssrssr696@gmail.com
Submitted: 5 March 2023
Accepted: 2 August 2023
Published online: 2 January, TAPS 2024, 9(1), 49-53
https://doi.org/10.29060/TAPS.2024-9-1/SC3016
Thamudi D Sundarapperuma1, Eranthi Weeratunga1, Prabhavi Wijesiriwardhana2, Eranga Silva2, Shanika Karunanayaka3, & Kithmini Yasarathne3
1Department of Nursing, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka; 2Department of Medical Laboratory Science, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka; 3Department of Pharmacy, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka
Abstract
Introduction: Several nations around the world had to close schools, colleges, universities, and other educational institutions as they were badly affected by the spread of COVID-19. The purpose of this study was to measure the effectiveness of online vs physical teaching during the COVID-19 pandemic, at the Faculty of Allied Health Sciences (FAHS), University of Ruhuna (UoR) Sri Lanka.
Method: A cross-sectional study was conducted among 200 undergraduates. The data were collected through displayed/approved results sheets of the students of selected batches in the Department of Nursing, Department of Pharmacy, and Medical Laboratory Science (MLS). Paired sample T-test was used to compare the results of undergraduates.
Results: The examination results of 47-54 undergraduates in nursing, 28 in pharmacy, and 22 in MLS were analysed. Significant differences in Psychiatry in Nursing and Nursing Clinical Attachment were identified in the Department of Nursing (p=0.001). In the Department of Pharmacy, only Pharmaceutical Chemistry I (p=0.012) reported a significant difference. The undergraduates of MLS who underwent online theory sessions had scored more in Microbiology and Immunology (p=0.022) and Basic Genetics and Molecular Biology (p=0.000) whereas in Research Methodology and Epidemiology, the undergraduates who participated in physical lectures had scored more marks (p=0.001).
Conclusion: Practical/interactive session-based course units and clinical appointments had a higher impact on the mode of teaching than many theoretical course units. The results might serve as a primer for the creation of an action plan to support the academics and clinical/practical components of undergraduates.
Keywords: Undergraduates, Online Teaching, Physical Teaching, Examination Results, COVID-19
I. INTRODUCTION
The provisional closure of educational institutions during the coronavirus disease-19 (COVID-19) pandemic has unexpectedly transformed the Sri Lankan education landscape in favour of distance learning or online learning. As a result of this, drastic changes in digital platforms and applications i.e., digital learning management systems became common among universities (Ariyananda et al., 2022). These universities used existing modular object-oriented dynamic learning environment-based learning management systems (Moodle) and the Lanka Education and Research Network (LEARN) was connected to university web servers and used for online education to mitigate the effects of disrupted learning (Hayashi et al., 2020).
Online teaching was a novel experience for university lecturers and undergraduates, and it was a huge challenge for both parties. In the beginning, both parties had to face several issues due to the unfamiliarity of these novel methods, the unavailability of basic facilities, and insufficient network coverage in Sri Lanka. Though it would be an effective alternative to conduct Zoom lectures again as physical lectures once the university reopened, we were unable to conduct lectures due to limited time during the semester. Therefore, the need emerged to identify a more effective mode to deliver lectures to undergraduates. This study aims to address the effectiveness of online vs. physical teaching during the COVID-19 pandemic, by analysing the examination results at the Faculty of Allied Health Sciences (FAHS), University of Ruhuna (UoR).
II. METHODS
A cross-sectional study was conducted to measure the effectiveness of online teaching vs. traditional/physical teaching and its impact on the performance of undergraduates. The data were collected through displayed/approved results sheets of the students of selected batches in the Department of Nursing, Pharmacy, MLS, FAHS, UoR. Nursing, though considered as a separate discipline from other para-medical disciplines in other countries, is considered under the Faculties of Allied Health Science in Sri Lanka. The examination results of two batches of undergraduates in a similar semester but who had learned in a different mode (in this group one batch has completely learned online while another batch has learned physically) were purposefully selected from each department. All lectures done via Zoom were recorded and distributed among students. Both groups underwent the same types of examination, mainly multiple-choice questions (MCQs) and short structured questions (SEQ) for theoretical knowledge. Practical and clinical skills were assessed using practical-based examination and patient-based clinical examination respectively. These examinations had been conducted in 2021 and 2022 and results were released in 2022. The analysis of results was conducted in January and February 2023.
Data from approximately 208 proper undergraduates (who sat for the first time) were analysed. The population was composed of nursing (n=108), pharmacy (n=56), and MLS (n=44) students. However, the results of repeat undergraduates were excluded. Six subjects were considered under the Department of Nursing. The number of candidates for the subjects was not equal. To analyse the effectiveness, a comparative analysis of the results of the end-semester examinations was performed by three departments separately. Mainly, in the Department of Nursing and Pharmacy the end semester examination results (two examinations/academic year) were evaluated while in the Department of MLS, the final term results were evaluated (three examinations /academic year).
Statistical Package for Social Science (SPSS) 26 software was used to analyse data. The mean and standard deviation (SD) values of the results sheets were analysed using descriptive statistics. After considering the distribution of the data set, paired sample T-test was used to compare the means of two batches. All results were regarded as statically significant at p < 0.05.
Ethical approval was obtained to analyse the published data from the Ethics Review Committee, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka (Ref. no. 200.01.2023). Consent was obtained from all relevant authorities before taking results from the notice board.
III. RESULTS
Two batches were selected in the nursing department and each batch consisted of 54 undergraduates. An equal number of candidates had not participated in every subject and therefore results were analysed based on students’ attendance for the different subjects. Under the nursing department, there were six subjects for students. Four subjects out of these six subjects consisted only of theory components. One subject had both theory and clinical components and the other subject had only clinical-based examination.
All the subjects had only a theory component in the selected semester in the pharmacy department. Under the department of MLS, all subjects consisted of theory and practical components.
|
Course units |
Component (Theory/ practical/clinical) |
Physical mode |
Virtual mode |
p-value |
||||
|
|
|
n |
Mean value |
+SD |
n |
Mean value |
+SD |
|
|
Nursing (2nd year 1st semester results) |
2016/2017 batch |
2017/2018 batch |
||||||
|
Pharmacology in Nursing |
T |
50 |
55.9 |
15.9 |
50 |
60.16 |
19.14 |
0.24 |
|
Medical Nursing 1 |
T |
50 |
54.9 |
7.8 |
50 |
68.09 |
15.6 |
0.053 |
|
Surgical Nursing 1 |
T |
47 |
57.83 |
8.47 |
47 |
57.61 |
10.08 |
0.914 |
|
Psychiatry in Nursing |
T+C |
51 |
59.53 |
7.38 |
51 |
66.03 |
10.69 |
0.001* |
|
Psychology in Nursing |
T |
54 |
67.41 |
12.88 |
54 |
62.51 |
14.5 |
0.071 |
|
Nursing Clinical Attachment III |
C |
47 |
71.85 |
9.79 |
47 |
66.03 |
10.69 |
0.001* |
|
Pharmacy (1st year 1st semester results) |
2017/2018 batch |
|
The 2019/2020 batch |
|||||
|
Pharmaceutical Chemistry I |
T |
28 |
66.14 |
10.49 |
28 |
69.62 |
12.11 |
0.012* |
|
Pharmaceutics IA |
T |
28 |
76.96 |
9.43 |
28 |
76.56 |
14.50 |
0.412 |
|
Mathematics |
T |
28 |
66.25 |
19.09 |
28 |
62.10 |
16.10 |
0.230 |
|
MLS (2nd year-end examination results) |
2016/2017 batch |
2017/2018 batch |
||||||
|
Microbiology and Immunology |
T+P |
22 |
68.11 |
4.86 |
22 |
72.69 |
7.94 |
0.022* |
|
Statistics, Research Methodology & Epidemiology |
T+P |
22 |
62.01 |
5.28 |
22 |
57.09 |
5.14 |
0.001* |
|
Haematology |
T+P |
22 |
57.22 |
3.58 |
22 |
60.42 |
4.98 |
0.058 |
|
Medical Parasitology |
T+P |
22 |
68.26 |
6.14 |
22 |
70.53 |
5.41 |
0.185 |
|
Basic Genetics, Molecular Genetics & Molecular Biology |
T+P |
22 |
61.32 |
5.98 |
22 |
70.31 |
5.68 |
0.000* |
|
Transfusion Medicine |
T+P |
22 |
66.68 |
6.84 |
22 |
69.87 |
6.20 |
0.163 |
Table 1. Comparison of results among undergraduates
*Paired sample T-test p < 0.05; T-theory, P-practical, C-clinical
IV. DISCUSSION
Online teaching was a big challenge to Sri Lankan undergraduates and teachers due to inadequate internet and infrastructural facilities for online teaching at the beginning of the COVID-19 pandemic. There was no other substitution except to conduct lectures online to provide continuous education during the lockdown. Therefore, this study was carried out to analyse the effectiveness of online teaching and student performances in selected batches of the FAHS, University of Ruhuna, Sri Lanka.
The mean value of the students’ marks for the several theoretical subjects was comparable in both groups. These findings show that the undergraduates in all three courses have appropriately adhered to the online method, and it may probably show the adherence of the lecturers to the technology. Indeed, free access to the LEARN platform may provide a huge impact on the results and the high information literacy of the undergraduates and lecturers may be the reason for it (Sample survey division, 2021). Though poor internet facilities disturbed and demotivated the undergraduates, the opportunity to listen to video recordings repeatedly may have mitigated the effect of this barrier. The reasons for the higher marks scored by the students who learned via Zoom than physical mode might be the favourable environment that prevailed by listening to lectures at their homes; fewer travel costs and time; the opportunity to have a better conversation with lecturers; having more time for self-learning/studying; and minimum disturbances from colleagues.
However, the mean value for the practical and clinical subjects was significantly low among the online group compared to the physical group. The clinical component is an essential part of the nursing undergraduate since it is vital to have adequate clinical exposure to gain competence to work in a real patient situation. Mainly, students learn how to handle patients with various disease conditions during their clinical practices. Furthermore, undergraduates can apply their theoretical knowledge in a real patient environment (e.g. evidenced-based practice); understand real patient matters; get technical and caring skills through interaction with patients and healthcare workers; and develop empathetic attitudes. Undergraduates did not get an opportunity to continue their clinical attachments as done previously due to the COVID-19 outbreak in Sri Lanka. During their clinical placements, they had to face several internal (fear, anxiety, etc.) and external (maintaining distance, lockdowns, close contacts, PPEs, etc.) constraints. It may be the reason for the lower performance.
However, another study conducted with final-year medical students found that some part of clinical exposure can be gained by providing online interactive learning materials (Ariyananda et al., 2022). Simulations are the recommended method for students to develop their clinical skills (Koukourikos et al., 2021) but these methods are not very popular in Sri Lanka due to the high cost of such kind of manikin. Likewise, practical subjects are essential to have a factual environment to get adequate training and robust hands-on skills. Nursing procedures/practical was not conducted due to the closure of the university and the limitations of close contact. This may also reduce the practical skills of nursing undergraduates. Under the pharmacy department, a significant difference was observed for the subject of Pharmaceutical Chemistry 1, which contains a lot of physical interactive parts. In the Zoom platform, it was difficult to conduct that much of interactive sessions with limited resources. That might be the reason for the difference. However, MLS and pharmacy departments have provided recorded practical sessions which may be the reason for the different results among departments.
In the study conducted in one faculty of the University of Ruhuna, a low number of participants were limitations of the study. A mixed-method study approach with a larger sample was recommended and further recommendations were made to assess the experience of undergraduates and lecturers.
V. CONCLUSION
Mode of teaching had not impacted the theoretical course units of undergraduates whereas practical/interactive session-based course units and clinical appointments had a greater impact on the mode of teaching. The findings can act as a primer for the development of an action plan to support university undergraduates’ academic and clinical works during pandemics. Further, the findings of this study would be helpful in robust the quality of online teaching methods in future pandemics.
Note on Contributors
TDS and EW contributed to the data analysis, manuscript drafting, and final editing of the revised manuscript. PW and SK contributed to the data analysis and manuscript drafting. ES and KY contributed to the data analysis. All authors read and approved the final revised manuscript.
Ethical Approval
Ethical approval was obtained from the Ethics Review Committee, Faculty of Allied Health Sciences, University of Ruhuna, Galle, Sri Lanka (Ref. no. 200.01.2023). Permission was obtained from the Dean/Faculty of Allied Health Sciences, University of Ruhuna, Assistant registrar/Faculty of Allied Health Sciences, University of Ruhuna, and Heads of the Department of Nursing, Department of Medical Laboratory Science, and Department of Pharmacy/Faculty of Allied Health Sciences, University of Ruhuna.
Data Availability
Data sets analysed during the current study would be available from the corresponding author upon reasonable request.
Acknowledgement
The authors are grateful to the Dean, Assistant Registrar, and the three Heads of the departments mentioned above for granting permission. Further, Ms. Chithra Ranasinghe, a Former WHO consultant is acknowledged for her contribution to language editing.
Funding
The authors received no funding for this study.
Declaration of Interest
The authors declare that they have no competing interests.
References
Ariyananda, P. L., Chin, J. H., Raman, R. K., Athif, A. L., Tan, Y. Y., & Hafiz, M. (2022). Online learning during the COVID pandemic lockdown: A cross sectional study among medical students. The Asia Pacific Scholar, 7(3), 46-50. https://doi.org/10.29060/taps.2022-7-3/sc2715
Hayashi, R., Garcia, M., Maddawin, A., & Hewagamage, K. P. (2020). Online Learning in Sri Lanka’s Higher Education Institutions during the COVID-19 Pandemic. Asian Development Bank. https://doi.org/10.22617/brf200260-2
Koukourikos, K., Tsaloglidou, A., Kourkouta, L., Papathanasiou, I. V., Iliadis, C., Fratzana, A., & Panagiotou, A. (2021). Simulation in clinical nursing education. Acta Informatica Medica, 29(1), 15-20. https://doi.org/10.5455/aim.2021.29.15-20
Sample Survey Division. (2021). Computer Literacy Statistics 2021 Annual Bulletin. Department of Census and Statistics. http://www.statistics.gov.lk/Resource/en/ComputerLiteracy/Bulletins/AnnualBuletinComputerLiteracy-2021.pdf
*Thamudi Sundarapperuma
Department of Nursing,
Faculty of Allied Health Sciences,
University of Ruhuna,
Galle, 80 000, Sri Lanka
+94 71 31 86 524
Email: chamudi2006@yahoo.com,
thamudids@ahs.ruh.ac.lk
Submitted: 24 January 2023
Accepted: 2 August 2023
Published online: 2 January, TAPS 2024, 9(1), 42-48
https://doi.org/10.29060/TAPS.2024-9-1/SC2997
Rahizan Zainuldin1 & Heidi Siew Khoon Tan1,2
1Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore; 2Pre-Professional Education Office, Tan Tock Seng Hospital, Singapore
Abstract
Introduction: Singapore Institute of Technology’s undergraduate (UG) occupational therapy (OT) and physiotherapy (PT) programs are one of the first implementors of Entrustable Professional Activities (EPAs) in the respective allied health professions training. The aim of the paper is to report the outcomes of the first year of EPAs implementation in clinical practice education (CPE) and share next steps refining implementation.
Methods: A quality improvement (QI) study using the Plan-Do-Check-Act (PDCA) cycle was conducted. UG OT Year 2 and Year 3 students, UG PT Year 3 students and their clinical educators (CEs) who experienced the use of EPAs for the first time were surveyed at the end of the clinical block.
Results: There was generally high agreement (>70% agreed or strongly agreed) among all groups in using EPAs to better understand the learning objectives of CPE and practice expectations as future entry-level practitioners at conditional-registration. More than 70% of OT respondents but less than 50% PT respondents found the EPA assessment forms easy to use. Less than 60% of both program CEs did not include colleagues for EPA assessments. 55% of both OT and PT CEs found the EPA training and resources adequate. Overall, PT respondents showed lower agreement than OT respondents in five survey items.
Conclusion: The first implementation cycle of EPA in the undergraduate OT and PT CPE had mixed acceptability to the EPA assessment tools. Three strategic changes were made for the second implementation cycle., i.e., redesign of EPA-based assessment forms, training focus and ‘just-in-time’ training with streamlined resources.
Keywords: Clinical Training, Entrustable Professional Activities, Occupational Therapy, Physiotherapy, Undergraduate, Workplace-based Assessment
I. INTRODUCTION
In 2021, the occupational therapy (OT) and physiotherapy (PT) undergraduate programs at Singapore Institute of Technology (SIT) added a novel assessment, Entrustable Professional Activities (EPAs), to the extant competency-based assessment tools in clinical practice education (CPE). EPAs are units of professional activities entrusted to a learner determined by five levels of supervision, once the learner has demonstrated the required competence (ten Cate & Taylor, 2020). OT EPAs and PT EPAs (Zainuldin & Tan, 2021) were developed and introduced to SIT CPE as part of the Ministry of Health’s review of healthcare professions’ training standards. EPA-based assessments are relevant in CPE where students perform professional activities at workplace, supervised by onsite clinical educators (CEs). Previous CPEs assessed only OT and PT student competencies using the validated Student Practice Evaluation Form-Revised Edition (SPEF-R) (Turpin et al., 2011) and the Clinical Competency and Reasoning Assessment (CCRA), respectively. Conceptually, the pairing of EPAs with SPEF-R or CCRA potentially offer CEs an opportunity to empower students through graduated levels of entrustment supported by appropriate proficiency levels. Operationally, EPA assessment does not add new activities. OT and PT CEs can utilise routine observations of students’ tasks, case discussions and case-notes documentation as sources to inform entrustment levels in EPAs.
No EPA implementation in any OT and PT curricula has been documented. At SIT, EPA implementation in CPE needs evaluation. Recognising that implementing process changes requires an iterative approach, SIT embarked on a quality improvement study using the Plan-Do-Check-Act (PDCA) cycle. This paper reports the results of operationalising EPAs for the first time in OT and PT CPE, including the use of EPA-based assessment forms. The Methods section describes the Plan and Do, followed by the Results section reporting outcomes of the Check and the Discussion section highlighting the Act to improve implementation.
II. METHODS
A. CPE Structure
OT CPE consists of four blocks of seven weeks each and interspersed between academic modules in Years 2, 3 and 4. PT CPE consists of five consequent blocks (four core and one elective) of six weeks each, begins only after all academic modules are completed in Year 3 and continues to Year 4. OT and PT students complete different clinical settings for each CPE block.
B. Participants and Study Design
OT Year 2 and Year 3 students, PT Year 3 students and their CEs who experienced EPA use for the first time were surveyed at the end of a clinical block. An online EPA survey is incorporated with routine post placement feedback for both students and CEs, therefore no consent was required. The QI study was exempt from ethics review (SIT Institutional Review Board, No. 2022122). Survey results were extracted from February to December 2021.
C. PDCA Cycle: Plan-Do
OT and PT have five core EPAs each. EPA-based assessment activities are short practice observations, entrustment-based discussions and case-notes evaluations. These activities serve as sources of information (SOIs), or workplace-based assessments (WBAs) in OT CPE, to inform entrustment decision-making. OT CE assesses EPAs by documenting in a single patient case form with all three WBAs per EPA. PT CE assesses EPAs for every patient case anchored by three different SOI forms with written justifications. OT and PT CEs and students were trained on nuts and bolts of EPAs and on using WBA/SOI forms in CE training workshops and student pre-CPE briefing, respectively.
Each OT EPA requires a total of six patient cases entrusted to students at Level 3 entrustment (indirect supervision) across four CPE blocks. Each PT EPA requires six cases at Level 3 entrustment at each core clinical block, which totals 24 cases by end of the program. Appendix 1 and 2 provides visualisation of EPA implementation across multiple CPE blocks.
The EPA survey has ten items. The first eight items are scored on a 4-point Likert-scale (strongly disagree-strongly agree). The final two questions seek qualitative feedback on benefits and challenges and suggestions for improvements. Unless indicated, items are phrased in the same manner in both student and CE surveys.
D. Data Collection and Analysis
Data were counted as proportions of respondents who agreed (pooled response from ‘agree’ and ‘strongly agree’) and proportions disagreed (pooled from ‘disagree’ and ‘strongly disagree’). The authors grouped the qualitative narrative into benefits and challenges.
III. RESULTS
A. PDCA Cycle: Check
There were 99.0% response rate from OT Year 2 students (105/106), 97.7% from Year 3 OT students (85/87), 93.2% from PT Year 3 students (137/147), 98.5% from OT CEs (199/202) and 92.5% from PT CEs (247/267). Proportion of respondents who agreed with each item statement is shown in Table 1. Data on item scores for each student and CE are available at online repository, http://doi.org/10.6084/m9.figshare.21941288
|
Survey Items |
OT Year 3 students |
OT Year 2 students |
PT Year 3 students |
OT CEs
|
PT CEs
|
|
(n = 85) |
(n = 105) |
(n = 137) |
(n = 199) |
(n = 247) |
|
|
Q1 – Using EPAs in CPE helps me better understand and meet future conditional-registration requirements.
|
90.6 |
98.1 |
75.2 |
89.4 |
71.7 |
|
Q2 – The EPA documents help me to better understand the learning objectives in CPE.
|
84.7 |
98.1 |
72.3 |
75.9 |
71.7 |
|
Q3 – The WBA/SOI forms are easy to use.
|
76.5 |
85.7 |
38.7 |
73.4 |
47.8 |
|
Q4 – CE: The WBA/SOI forms are adequate for me to determine students’ competence and entrustment level. / Student: The WBAs/SOIs help me to better gauge my progress and level of competence.
|
91.8 |
97.1 |
70.1 |
72.9 |
64.6 |
|
Q5 – I understand the connection between OT EPAs and SPEF-R2 competencies or PT EPAs and CCRA.
|
84.7 |
97.1 |
72.3 |
69.8 |
83.0 |
|
Q6 – CE: I use the EPA documents explicitly with students during clinical teaching and assessment. / Student: I use the EPA documents to guide my learning goals during CPE.
|
62.4 |
92.4 |
51.1 |
87.9 |
59.1 |
|
Q7 – CE: I involve other colleagues in doing WBAs/SOIs to calibrate students’ entrustment level. / Student: Besides my CE, I also received feedback from other OTs or other PTs who were involved in my WBAs/SOIs.
|
44.7 |
66.7 |
54.0 |
58.8 |
45.3 |
|
Q8 – I feel the current briefing/training/resources are adequate for me to incorporate the use of EPAs in CPE. |
70.6 |
89.5 |
56.2 |
55.3 |
55.9 |
Table 1. Proportion of OT and PT students and CEs who agree with the EPA survey items
PT CEs and students were almost unanimous that SOI forms were difficult to use (Q3). Common to OT and PT CEs, many did not involve colleagues in EPAs (Q7) and felt that training to understand EPAs was inadequate (Q8).
Qualitatively, both disciplines benefitted from the use of WBA/SOI forms to scaffold learning through structured feedback and action plans when addressing identified competency gaps. Feedback from OT and PT students below closely exemplified the appreciation:
“EPAs allow me to track my progress over the weeks and transfer my reflections into action when given the opportunity to receive objective and qualitative feedback from the EPA form.”
OT Student#45
“The discussions with the CE on what to do if the situation was different made me realise the importance of planning even for the worst-case scenario…enabled me to identify the gaps in knowledge and skills that had to be worked on.”
PT Student#67
However, PT groups cited complicated forms design and copious paperwork from numerous SOIs time-consuming and stressful. Ambivalence on its practicality was best summed by PT CE#31, “As a first-time user of the SOIs, I found it quite difficult to navigate the forms, took me some tries to understand how I can determine the students’ competence and entrustment level. As there were many forms, it was quite confusing, and hence stressful and time-consuming. Otherwise, they are useful tools.”
The most common challenge among OT CEs was assessing certain EPAs, such as planning care transition, in some settings. “Some EPAs are harder to do in some settings, for example, in the hands therapy setting; it is harder to do the handover/discharge EPA as there are less of these patients.” (OT CE#32). Calling for more support, one CE suggested “SIT go through a round of training on the different EPAs and give relevant case examples to help us better understand them.” (OT CE#4).
IV. DISCUSSION
Response rates were excellent. The convergence of high agreement rates with narrative feedback on using EPAs and WBA/SOIs for teaching/learning, understanding the CPE learning objectives and meeting practice expectations as future entry-level practitioners suggest early indication that EPAs may facilitate SIT OT and PT students transit to new practitioners. The positive experience in this regard resonated with other EPA survey on final-year dietetics students and their clinical supervisors in Australia (Bramley et al., 2021). Practical challenges with the SOI forms, resulting in onerous and time-consuming evidence collection; low levels in involving colleagues in EPA assessments; and inadequate EPA training/resources for CEs were identified as key areas for change in both disciplines.
A. PDCA Cycle: Act
First, to reduce assessment burden, WBA and SOI forms were redesigned and harmonised in preparation towards a standardised EPA online assessment system currently developed in-house. Multiple WBA/SOI forms were combined into a single-page checklist form with a small open-ended section. A checklist was similarly suggested for nursing EPAs assessment, citing convenience as a reason (Lau et al., 2020). On the single-page form, CEs tick entrustment levels for each WBA/SOI associated to each EPA with all EPAs on the same page. The only narrative section is where CEs describe key justifications supporting their entrustment decisions, followed by students’ reflections. Second, to bridge assessment expectations among clinicians and increase propensity to share EPA assessments with colleagues, EPA training was refined to emphasise balance of supervision control with autonomy and clearer definitions between entrustment levels 2 (direct supervision) and 3 (indirect supervision) through case examples. Third, ‘just-in-time’ refresher training was added to activate volition in assessing EPAs. Toolkits containing briefing videos and streamlined resources in short bites, such as 3-minute videos, powtoons, form samplers and frequently-asked-questions, were released for OT and PT CEs closer to placement block. PT CEs also received a refresher at early weeks of every placement block.
V. CONCLUSION
The PDCA cycle is used to inform and make iterative adaptations to each cycle of EPA implementation. The Plan-Do stage completed the first implementation cycle of EPA in the undergraduate OT and PT CPE in 2021. The Check stage revealed mixed experiences to EPA use. The lowest agreement was the ease of using SOI forms among PT students and CEs. While EPAs were accepted as teaching and learning tools, CEs did not involve colleagues in EPA assessments. Training on EPA assessment for CEs was inadequate. Consequently, the Act stage yielded changes in form design, training focus and streamlined resources for the next implementation cycle.
Notes on Contributors
Rahizan Zainuldin (RZ) led the design of the quality improvement and implementation of EPAs, submitted the study to SIT IRB, analysed and interpreted both quantitative and qualitative data for the PT CPE, prepared the manuscript, wrote the initial draft and finalised for submission.
Heidi Siew Khoon Tan (HSKT) led the design of the EPA survey, analysed and interpreted both quantitative and qualitative data for the OT CPE, provided a critical review of the manuscript, and concurred on the final version.
Ethical Approval
The QI study was exempt from ethics review (SIT Institutional Review Board, No. 2022122).
Data Availability
Data on item scores for each student and CE are available at online repository, publicly accessed at http://doi.org/ 10.6084/m9.figshare.21941288. While the data is available for readers’ perusal and no permission from the authors is needed, please write an email of intention to use the data for any purposes to the corresponding author.
Acknowledgement
We would like to acknowledge the OT and PT CPE committee members who have contributed in the planning and implementation of the EPA. We would also like to thank Ms Annie Wang Haiyan, Manager, Academic Programmes Administration, SIT, for uploading the survey on and extracting the survey results from the online assessment portal of our Clinical Practice Education portal.
Funding
No funding source is provided.
Declaration of Interest
Rahizan Zainuldin and Heidi Siew Khoon Tan disclose there is no conflict of interest of any form.
References
Bramley, A. L., Thomas, C. J., McKenna, L., & Itsiopoulos, C. (2021). E-portfolios and entrustable professional activities to support competency-based education in dietetics. Nursing and Health Sciences, 23(1), 148-156. https://doi.org/10.1111/nhs.12774
Lau, S. T., Ang, E., Samarasekera, D. D., & Shorey, S. (2020). Evaluation of an undergraduate nursing entrustable professional activities framework: An exploratory qualitative research. Nurse Education Today, 87, Article 104343. https://doi.org/10.1016/j.nedt.2020.104343
ten Cate, O., & Taylor, D. R. (2020). The recommended description of an entrustable professional activity: AMEE Guide No. 140. Medical Teacher 43(10), 1106-1114. https://doi.org/10.1080/0142159X.2020.1838465
Turpin, M., Fitzgerald, C., & Rodger, S. (2011). Development of the Student Practice Evaluation Form Revised Edition Package. Australian Occupational Therapy Journal, 58(2), 67-73. https://doi.org/10.1111/j.1440-1630.2010.00890.x
Zainuldin, R., & Tan, H. Y. (2021). Development of entrustable professional activities for a physiotherapy undergraduate programme in Singapore. Physiotherapy, 112, 64-71. https://doi.org/10.1016/j.physio.2021.03.017
*Rahizan Zainuldin
10 Dover Road,
Singapore 138683
+6596522418
Email: Rahizan.Zainuldin@singaporetech.edu.sg
Submitted: 18 February 2023
Accepted: 28 March 2023
Published online: 3 October, TAPS 2023, 8(4), 40-45
https://doi.org/10.29060/TAPS.2023-8-4/SC3010
Kit Mun Tan1, Chan Choong Foong2, Donnie Adams3, Wei Han Hong2, Yew Kong Lee4 & Vinod Pallath2
1Department of Medicine, Faculty of Medicine, Universiti Malaya, Malaysia; 2Medical Education and Research Development Unit (MERDU), Faculty of Medicine, Universiti Malaya, Malaysia; 3Department of Educational Management, Planning and Policy, Faculty of Education, Universiti Malaya, Malaysia; 4Department of Primary Care, Faculty of Medicine, Universiti Malaya, Malaysia
Abstract
Introduction: The global COVID-19 pandemic had greatly affected the delivery of medical education, where institutions had to convert to remote learning almost immediately. This study aimed to measure undergraduate medical students’ readiness and factors associated with readiness for remote learning.
Methods: A cross-sectional quantitative study was conducted amongst undergraduate medical students using the Blended Learning Readiness Engagement Questionnaire, during the pandemic where lessons had to be delivered fully online in 2020.
Results: 329 students participated in the study. Mean scores for remote learning readiness were 3.61/4.00 (technology availability), 3.60 (technology skills), 3.50 (technology usage), 3.35 (computer and internet efficacy), and 3.03 (self-directed learning). Male students appeared more ready for remote learning than females, in the dimensions of self-directed learning and computer and internet efficacy. Students in the pre-clinical years showed a lower level of readiness in the technology availability domain compared to clinical students. The lowest score however was in the self-directed learning dimension regardless of the students’ year of studies.
Conclusion: The pandemic had created a paradigm shift in the delivery of the medical program which is likely to remain despite resumption of daily activities post-pandemic. Support for student readiness in transition from instructor-driven learning models to self-directed learning models is crucial and requires attention by institutions of higher learning. Exploring methods to improve self-directed learning and increase availability of technology and conducting sessions to improve computer and internet efficacy can be considered in the early stages of pre-clinical years to ensure equitable access for all students.
Keywords: Remote Learning, Student’s Readiness, Medical Education
I. INTRODUCTION
The COVID-19 pandemic and global emergency from the end of January 2020 had greatly affected the education sector, with many institutions including undergraduate medical schools converting to remote learning within a short timeframe.
Previous studies have shown that e-learning methods were effective and acceptable among medical undergraduate students (Chen et al., 2020). Studies have also suggested that students may struggle in adapting to a self-directed learning process (Vaughan, 2007), prefer traditional face-to-face lectures and possibly lacking the technological skills and infrastructure for a satisfactory remote learning experience.
It is important to determine the remote learning readiness of undergraduate medical students to facilitate the adaptation of these practices to maximise student competencies. Therefore, the primary objective of this study was to determine the readiness for remote learning in undergraduate medical students in a South-East Asian university and the secondary objective was to identify factors associated with their remote learning readiness.
II. METHODS
This was a cross-sectional quantitative study to measure medical students’ readiness towards remote learning using the BLREQ questionnaire. This study was approved by the Research Ethics Committee (Reference UM.TNC2/UMREC-889) of the university.
In the Covid-19 enforced scenario at that time, the physical face-to-face teaching in our institution was moved to online almost immediately, requiring the students to adapt their learning approaches rapidly to suit the needs of a virtual learning environment.
The duration of the study was one month, from the 19th of June to the 19th of July 2020. Our country implemented a national lockdown (and emergency remote learning) due to COVID-19 on the 18th of March 2020. Thus, data collection occurred in the first few months of the remote learning situation and represented students’ experiences and readiness during the early phase of the change.
The students were from all five years of study in the medical undergraduate program. They were contacted via their online educational platform and WhatsApp group chats with details of the study, participant’s consent form, link to the online self-administered questionnaire and weekly reminders to encourage participation. Participation was voluntary and consent was obtained from the students. Data were anonymised and not traceable to a particular individual.
This study utilised Section A and B of the BLREQ questionnaire which is a validated questionnaire on the readiness and engagement of students in blended learning (Adams et al., 2018). Although ‘Blended Learning’ is defined as a combination of e-learning (online) and traditional education (face-to-face) approaches, the BLREQ is appropriate for this study as it primarily measures students’ readiness for remote learning. Section A contained basic demographic questions (i.e., age, gender, year of study). Section B had 37 items in five dimensions which addressed various aspects of students’ readiness for remote learning. A 4-point Likert-type scale ranging from strongly disagree (1) to strongly agree (4) was provided with only one response allowed per item.
The data was analysed using IBM SPSS version 25. The data was non-normally distributed; hence the Mann-Whitney U test was used to test for significant difference in scores between gender and stages of study.
III. RESULTS
There were 329 complete responses out of 734 invited participants (44.8% response rate). Most respondents were aged between 20 to 24 years old (Mean=21.9; SD=1.8). Approximately 59% were female and 59% were clinical students.
The total dimension and individual item mean scores are reported in Table I with the highest and lowest scores of each dimension annotated. The dimensions of remote learning readiness arranged in descending order of total mean score are Technology Availability (3.61+50), Technology Skills (3.60+.43), Technology Usage (3.50+.44), Computer and Internet Efficacy (3.35+.49), and Self-directed Learning (3.03+.51) (Table 1). Research data of this study are available at https://doi.org/10.6084/m9.figshare.21443100
Analysed by gender, the mean scores of male students were significantly higher than female students in the dimensions of Self-directed Learning; 3.13 vs 2.96 (U=10354.5, z=-3.18, p=.001), and Computer and Internet Efficacy; 3.39 vs 3.32 (U=11332.5, z=-2.02, p=.044). Individual items in which male students scored significantly higher in each dimension were [SDL1], [SDL4], [CIE2] and [CIE3].
When comparing between stages of study, the mean score of clinical students was significantly higher than pre-clinical students only in the Technology Availability dimension; 3.65 vs 3.55 (U=11376.0, z=-2.13, p=.034) An individual item which clinical students scored significantly higher in Technology Availability dimension was [TA3].
|
Dimensions and items |
Mean |
SD |
|
[TS] Technology Skills dimension |
3.60 |
.43 |
|
[TS1] I know the basic functions of a computer/laptop and its peripherals like the printer, speaker, keyboard, mouse etc.** |
3.76 |
.45 |
|
[TS2] I know how to save and open documents from a hard disk or other removable storage device. |
3.67 |
.52 |
|
[TS3] I know how to open and send email with file attachments. |
3.72 |
.48 |
|
[TS4] I know how to log on to Wi-Fi |
3.74 |
.46 |
|
[TS5] I know how to navigate web pages (go to next or previous page). |
3.68 |
.50 |
|
[TS6] I know how to download files using browsers (e.g., Google Chrome, Internet Explorer, Firefox) and view them. |
3.67 |
.51 |
|
[TS7] I know how to access an online library or database.* |
3.19 |
.78 |
|
[TS8] I know how to use Word processing software (e.g., Microsoft (MS) Word). |
3.62 |
.53 |
|
[TS9] I know how to use Presentation software (e.g., MS PowerPoint). |
3.60 |
.53 |
|
[TS10] I know how to use Spreadsheet software (e.g., MS Excel). |
3.30 |
.75 |
|
[TS11] I know how to open several applications at the same time and move easily between them. |
3.60 |
.60 |
|
[TU] Technology Usage [TU] dimension |
3.50 |
.44 |
|
[TU1] I often use the internet to find information.** |
3.86 |
.37 |
|
[TU2] I often use e-mail to communicate.* |
2.93 |
.93 |
|
[TU3] I often use office software (e.g., MS Word, PowerPoint, Excel). |
3.62 |
.56 |
|
[TU4] I often use social networking sites to share information (e.g., Facebook, Twitter, Instagram, Snapchat). |
3.39 |
.83 |
|
[TU5] I often use instant messaging (e.g., WhatsApp, Viber, WeChat, Line, Telegram). |
3.72 |
.54 |
|
[TU6] I often use cloud-based file hosting services to store or share documents (e.g., Google Drive, Dropbox, One drive). |
3.44 |
.69 |
|
[TU7] I often use learning management systems (e.g., Blackboard, Moodle). |
3.28 |
.69 |
|
[TU8] I often use mobile technologies (e.g., Smartphone, Tablet) to communicate. |
3.72 |
.51 |
|
[TA] Technology Availability dimension |
3.61 |
.50 |
|
[TA1] I have a computer/laptop with an internet connection.** |
3.74 |
.53 |
|
[TA2] I have a computer/laptop with adequate software for learning (e.g., Microsoft (MS) Office). |
3.63 |
.57 |
|
[TA3] I have speakers for courses with video presentations.* |
3.50 |
.72 |
|
[TA4] I have a computer/laptop and its peripherals like the printer, speaker, keyboard, mouse etc. |
3.57 |
.66 |
|
[SDL] Self-directed Learning dimension |
3.03 |
.51 |
|
[SDL1] I am a highly independent learner. |
3.12 |
.69 |
|
[SDL2] I am able to learn new technologies.** |
3.60 |
.55 |
|
[SDL3] I do not need direct lectures to understand materials.* |
2.36 |
.92 |
|
[SDL4] I would describe myself as a self-starter in learning using technology. |
3.18 |
.79 |
|
[SDL5] I am not distracted by other online activities when learning online (e.g., Facebook, Gaming, Internet surfing). |
2.42 |
1.04 |
|
[SDL6] I can read the online instructional materials on the basis of my needs. |
3.49 |
.58 |
|
[CIE] Computer and Internet Efficacy dimension |
3.35 |
.49 |
|
[CIE1] I feel confident in using online tools (e.g., email, internet chat, instant messenger) to communicate effectively with others. |
3.48 |
.65 |
|
[CIE2] I feel confident in expressing myself (e.g., emotions and humour) in my university’s learning management systems (e.g., Blackboard, Moodle) |
2.89 |
.83 |
|
[CIE3] I feel confident in posting questions in online discussions.* |
2.87 |
.82 |
|
[CIE4] I feel confident in performing the basic functions of Word processing software (e.g., MS Word). |
3.59 |
.55 |
|
[CIE5] I feel confident in performing the basic functions of Presentation software (e.g., MS PowerPoint). |
3.48 |
.62 |
|
[CIE6] I feel confident in performing the basic functions of Spread sheet (e.g., MS Excel). |
3.26 |
.78 |
|
[CIE7] I feel confident in using web browsers (e.g., Google Chrome, Mozilla Firefox) to find or gather information for online learning.** |
3.67 |
.53 |
|
[CIE8] I feel confident in using computer or tablet or mobile phone for online learning. |
3.56 |
.63 |
Table 1. Dimension and individual item mean scores of student readiness to engage in remote learning
** highest score in the dimension
*lowest score in the dimension
IV. DISCUSSION
This study aimed to identify medical students’ readiness for remote learning across five dimensions and to identify factors associated with their readiness during the early months of the COVID-19 online learning transition period. Although there is significant resumption of usual activities post-COVID-19 pandemic, many of the online and self-directed components of learning are likely to remain as the way forward in the medical curriculum. Therefore, we feel that this study still has relevance currently.
All mean scores of the subscales Technology Availability (TA), Technology Skills (TS), Technology Usage (TU), Computer and Internet Efficacy (CIE) and Self-directed Learning (SDL), were above 3 on a scale of 1 to 4. The mean scores in our study were much higher and have less deviation than Adams et al’s study conducted in a similar setting before the COVID-19 pandemic, in which the five dimensions scored lower than 3.00, with SDL scoring the lowest mean in the other study at 1.25+1.55 (Adams et al., 2018). Adams et al’s study also did not show much difference when comparing between medicine, social science, science and engineering students (Adams et al., 2018), indicating that readiness for online learning was much lower overall pre-COVID-19.
Despite the increase compared to Adams et al’s study, SDL still scored the lowest in our study out of the five dimensions. An implication of this is that universities need to help learners transition from facilitator/ instructor-driven learning models to self-directed learning models. This can be done by making training in ‘learning to learn’ (L2L) an essential component of student support. In our setting, this training should address items which scored lowest in SDL as these indicate areas of struggle for students; [SDL3] and [SDL5]. It is also possible that some facilitators are not aware of what SDL is, therefore facilitators can also benefit from training for SDL methods.
Our study demonstrated significantly higher readiness for remote learning among male students in comparison to female students in the domains of SDL and CIE. While some studies indicate no gender differences in e-Learning readiness, other studies also report gender differences such as males having more positive attitudes toward online learning; males being more ready for online learning (Adams et al., 2018) and males using more learning strategies and having better technical skills than females (Alghamdi et al., 2020). In the CIE domain, males scored higher in the items [CIE2] and [CIE3] which are both related to communication through a virtual platform. This resulted in males scoring higher in the CIE domain in general. The gender disparity in remote learning readiness needs to be addressed as female students are increasingly the majority (and therefore primary stakeholders) in medical schools worldwide.
The mean score of clinical students was significantly higher than pre-clinical students only in the Technology Availability domain with clinical students reporting better hardware and infrastructure access compared to pre-clinical students. It is likely that as the learners progress through a course, they become more aware of the technological requirements of the course and invest in better devices and internet access. It is also possible that the students’ socioeconomic status at the beginning of their course may not have been good, for example if they were awaiting scholarships to be processed, which subsequently became available later in their course of study. This may have then enabled the students to purchase better hardware and infrastructure further on in their course, during the clinical years. However, this financial aspect was not included our study. It is still worth considering future programs early in the course, where there could be subsidies for students to purchase necessary technological equipment for their studies.
A. Limitations and Recommendations
One limitation of this study was that it looked at remote learning in general and did not look at clinical elements such as using online simulated patients for history taking classes, or procedural skills videos. The study also only looked at student perspectives, and not faculty perspectives to get a complete picture of the online learning experiences. Future studies should explore student readiness for clinical online learning as this would be a struggle for students even if the transition was under normal circumstances (Vaughan, 2007). The perspectives of faculty members on readiness to move towards online learning also need to be explored. The strength of this study was that it used a previously validated questionnaire which allowed some comparison on students’ remote learning readiness with pre-COVID-19 studies.
V. CONCLUSION
In conclusion, the study explored medical undergraduates’ remote learning readiness in a public medical school in Malaysia during the COVID-19 pandemic. In general, students were found to be ready for remote learning. However, the lowest scores were for the domain of self-directed learning and computer and internet efficacy. Based on our findings, we feel that support for student readiness in transition from instructor-driven learning models to self-directed learning models is crucial and requires attention by institutions of higher learning. Exploring methods to improve self-directed learning and increase availability of technology and conducting sessions to improve computer and internet efficacy can be considered in the early stages of pre-clinical years to ensure equitable access for all students. There should also be efforts to train the educators to develop online learning activities which incorporate the socio-relational aspects of learning into the remote learning experience.
Notes on Contributors
Kit Mun, Tan is the first author and person who initiated the study, contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Chan Choong, Foong contributed to the design of study, data collection and analysis, writing and approval of the final version of the manuscript.
Donnie, Adams is the creator of the original Blended Learning Readiness Questionnaire (BLREQ) and contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Wei Han, Hong contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Yew Kong, Lee contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Vinod, Pallath is the corresponding author and contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Ethical Approval
This study received ethical approval from the Universiti Malaya Ethics Review Committee with the approval number of UM.TNC2/UMREC-889.
Data Availability
Research data of this study are available at https://doi.org/10.6084/m9.figshare.21443100.
Readers may access the anonymised data freely with the above URL. Kindly contact the authors for permission if you wish to use the data for a subsequent study or collaboration.
Acknowledgement
We would like to acknowledge and express gratitude to the undergraduate medical students who took the time to participate in this study.
Funding
There was no external funding for this study.
Declaration of Interest
All the authors do not have a conflict of interest to declare.
References
Adams, D., Sumintono, B., Mohamed, A., & Mohamad Noor, N. S. (2018). E-learning readiness among students of diverse backgrounds in a leading Malaysian higher education institution. Malaysian Journal of Learning and Instruction, 15(2), 227-256. https://doi.org/10.32890/mjli2018.15.2.9
Alghamdi, A., Karpinski, A. C., Lepp, A., & Barkley, J. (2020). Online and face-to-face classroom multitasking and academic performance: Moderated mediation with self-efficacy for self-regulated learning and gender. Computers in Human Behavior, 102, 214-222. https://doi.org/10.1016/j.chb.2019.08.018
Chen, J., Zhou, J., Wang, Y., Qi, G., Xia, C., Mo, G., & Zhang, Z. (2020). Blended learning in basic medical laboratory courses improves medical students’ abilities in self-learning, understanding, and problem solving. Advances in Physiology Education, 44(1), 9-14.
Vaughan, N. (2007). Perspectives on blended learning in higher education. International Journal on E-Learning, 6(1), 81-94. https://www.learntechlib.org/primary/p/6310/
*Associate Professor Dr Vinod Pallath
Medical Education Research and Development Unit,
Faculty of Medicine, Universiti Malaya,
50603 Kuala Lumpur
Email: vinodpallath@um.edu.my
Submitted: 9 February 2023
Accepted: 22 March 2023
Published online: 3 October, TAPS 2023, 8(4), 36-39
https://doi.org/10.29060/TAPS.2023-8-4/SC3000
Komson Wannasai1, Wisanu Rottuntikarn1, Atiporn Sae-ung2, Kwankamol Limsopatham2, Wiyada Dankai1
1Department of Pathology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 2Department of Parasitology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
Abstract
Introduction: Global medical and healthcare education systems are increasingly adopting team-based learning (TBL). TBL is an interactive teaching programme for improving the performance, clinical knowledge, and communication skills of students. The aim of this study is to report the learning experience and satisfaction of participants with the TBL programme in the preclinical years of the Faculty of Medicine, Chiang Mai University.
Methods: Following the implementation of TBL in the academic year 2022, we asked 387 preclinical medical students, consisting of 222 Year 2 and 165 Year 3 medical students who attended the TBL class to voluntarily complete a self-assessment survey.
Results: Overall, 95.35% of the students were satisfied with the structure of the TBL course and agreed to attend the next TBL class. The overall satisfaction score was also high (4.44 ± 0.627). In addition, the students strongly agreed that the TBL programme improved their communication skills (4.50 ± 0.796), learning improvement (4.41 ± 0.781), and enthusiasm for learning (4.46 ± 0.795).
Conclusion: The survey findings indicated that students valued TBL-based learning since it enabled them to collaborate and embrace learning while perhaps enhancing their study abilities. However, since this is a pilot study, further investigations are warranted.
Keywords: Team-based Learning, Small Group Interaction, Medical Education, Implementation
I. INTRODUCTION
Team-based learning (TBL) is a form of small-group teaching which can improve student performance, clinical knowledge, and communication skills. It has been employed in medical and healthcare education in the US, Australia, Austria, Japan, South Korea, and Singapore (Burgess et al., 2014; Michaelsen & Sweet, 2008). Since 2000s, this model has been used in medical education to foster deep learning across a variety of subjects and educational contexts, benefiting teachers and helping academically weak and strong students achieve the same or better results than with conventional methods (Parmelee et al., 2012). In addition, it is more effective for engaging students than lecturing in a large class with few teachers (Burgess et al., 2020b).
The key elements of TBL include pre-class preparation to encourage self-study, teamwork, and instant feedback. These key elements promote active learning and critical thinking (Burgess et al., 2020a; Parmelee et al., 2012). The steps in TBL include pre-class preparation, individual readiness assurance test (iRAT), team readiness assurance test (tRAT), feedback, and team application (Burgess et al., 2014). In the tRAT and team application phase, students work in small groups to demonstrate the use of teamwork for problem-solving. Clinical problem-solving exercises by students lead to class discussions and instructor comments (Burgess et al., 2020a; Michaelsen & Sweet, 2008). The teacher’s feedback can help clarify students’ responses by discussing their answers. In the academic year 2022, TBL was implemented on second- and third-year medical students in the Faculty of Medicine, Chiang Mai University, and self-assessment questionnaires were used to assess students’ satisfaction with the TBL model. This research aims to examine the impact of team-based learning on whether or not students were able to build their own learning processes, as well as to measure student satisfaction with teaching and learning in the TBL paradigm in order to improve further TBL classrooms in the faculty.
II. METHODS
A. Sampling and Participants
In 2022, 387 pre-clinic medical students from Chiang Mai University’s Faculty of Medicine were studied (222 from Year 2 and 165 from Year 3). Year 2 medical students studied human skin and the connective tissue system, while Year 3 medical students studied human haematology. Each TBL class consisted of 50 teams of mixed-gender and grades. Each team contained five members.
B. Structure and Components of TBL
The TBL programme was first implemented in the 2022 academic year, covering preclinical academic Years 2 and 3 at the Faculty of Medicine, Chiang Mai University. The TBL structure comprised two major phases: pre-class and in-class. The TBL topics included automated haematology and venomous snakes for Year 3 medical students. The skin infection topic was selected for Year 2 medical students.
After TBL, the non-researcher academic team informed medical students about the study and sought volunteers to avoid a conflict of interest between the instructors and the medical students. The non-researchers urged students interested in the experiment to complete a Google Forms questionnaire outlining the study’s relevance, including an explanation of the topic, data gathering, and the pros and cons of participation. If participants agreed to answer the questionnaire, they could complete the Google Form to consent and submit the questionnaire, with their personal information remaining anonymous.
For validity, a questionnaire to explore students’ views on TBL was prepared via a literature study, student review (two students), peer review (faculty members from two departments), and expert opinion (a TBL expert). It also examined students’ perceptions of teams and their beliefs and values in collaboration. The outcomes of the different years of student were then compared.
C. Data Collection and Analysis
Upon completing the TBL class, participant students were invited to voluntarily take the self-assessment survey to explore their thoughts on the assertions made in the TBL literature. The questionnaire was in Thai and we used a five-point Likert scale (1 = strongly dissatisfied, 2 = unsatisfied, 3 = neither satisfied nor dissatisfied, 4 = satisfied, 5 = strongly satisfied). Students were asked about the preparation for the TBL class, including student material, classroom, teaching content, self-preparation, orientation programme, class material, and the overall programme. The self-assessment survey also asked about promoting self-understanding, including communication skills, learning improvement, and enthusiasm in learning using a five-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = strongly agree).
The TBL self-assessment survey data were analysed according to mean and standard deviation (SD) using STATA version 16 (STATA Corp., Texas, USA). The Pearson’s Chi-square test was used to analyze the difference between second- and third-year medical students’ percentages of satisfaction or agreement in each aspect. Statistical significance was accepted at p < 0.05. The reliability of the questionnaire was calculated using Cronbach’s alpha.
III. RESULTS
In years 2 and 3, Cronbach’s alpha of the medical students’ questionnaire was 0.869. In total, 369/387 (95.35%) participants appreciated the course structure and agreed to attend the next TBL session. Students rated the TBL class 4.44 ± 0.627 on a five-point Likert scale, with 1 being severely dissatisfied and 5 very pleased. Students also liked the classroom (4.48 ± 0.738), TBL structure (4.41 ± 0.771), and self-preparation (4.28 ± 0.780). The orientation programme, instructional material, pre-recorded video, and handouts were also well-received. Most students (69.25%, 268/387) spent 1–2 days self-preparing before the TBL class, followed by 3–4 days (24.55%, 95/387) and 5–7 days (5.43%, 21/387), while 0.78% (3/387) did not self-prepare.
On a five-point Likert scale from 1 to 5, students assessed their self-understanding progress, stating that TBL increased their communication, learning, and enthusiasm (4.50 ± 0.796, 4.41 ± 0.781, 4.46 ± 0.795).
The student t-tests revealed no significant differences between students in years 2 and 3. Except time for preparation (Pearson’s Chi-square test; p < 0.005), medical students in years 2 and 3 had similar self-assessment survey scores. In addition, Year 3 medical students also scored better in enthusiasm for studying than Year 2 medical students in increasing self-understanding (Student t-test; p = 0.023) (Table 1).
|
|
Year 2 |
Year 3 |
p-value |
|
Student satisfaction towards the TBL class |
|||
|
Agree to attend the next TBL class: % (n) |
95.95% (213/222) |
94.55% (156/165) |
0.519 |
|
Classroom: mean (SD) |
4.49 (0.671) |
4.47 (0.823) |
0.903 |
|
TBL structure: mean (SD) |
4.38 (0.73) |
4.45 (0.822) |
0.377 |
|
Orientation programme: mean (SD) |
4.46 (0.628) |
4.40 (0.810) |
0.417 |
|
Teaching material: mean (SD) |
4.67 (0.568) |
4.56 (0.578) |
0.064 |
|
Student preparation time: mean (SD) |
4.20 (0.788) |
4.40 (0.755) |
0.012 |
|
Time for preparation: % (n) 1–2 days 3–4 days 5–7 days No preparation |
80.18% (178/222) 14.41% (32/222) 4.50% (10/222) 0.90% (2/222) |
54.55% (90/165) 38.18% (63/165) 6.67% (11/165) 0.61% (1/165) |
< 0.005 |
|
Promotion of learning skills |
|||
|
Communication skills: mean (SD) |
4.46 (0.734) |
4.56 (0.674) |
0.154 |
|
Understanding of the topics: mean (SD) |
4.36 (0.729) |
4.47 (0.845) |
0.180 |
|
Enthusiasm for learning: mean (SD) |
4.38 (0.797) |
4.56 (0.783) |
0.023 |
|
Cronbach’s alpha |
0.869 |
0.869 |
|
Table 1. Comparison between the satisfaction of medical students in years 2 and 3 towards the TBL class and agreement to the promotion of self-understanding
IV. DISCUSSION
TBL changes how students learn by encouraging them to become more accountable by preparing for the team assurance test and application exercise (Burgess et al., 2020a). Teacher-directed pre-class preparation for advanced tasks may involve reading textbooks, reference articles, or instructor-created material while the readiness assurance test enhances students’ enthusiasm for TBL (Parmelee et al., 2012). However, students may resist TBL or active learning because it varies from passive lecture-based learning. Teachers must be aware of this and advocate TBL-style learning to improve ability and encourage students to be more prepared. This research examines the attitudes of medical students towards the two courses post-TBL and provides valuable input on TBL strategies, regardless of the course schedule.
Student feedback can improve teaching and student satisfaction. Students agreed that TBL can improve communication, learning, and passion. Second-year medical students were less motivated than third-year (p = 0.023), implying they need to focus on the core content of the preclinical module rather than TBL preparation, while third years have more time management experience for pre-class self-study. Students liked the teaching material because, in addition to textbooks, the instructors prepared PowerPoint presentations, recorded VDOs, and documentation, allowing those with different learning styles to make the appropriate choice.
Interestingly, both classes found the TBL structure and location less satisfying, possibly because first-time students could not comprehend group activities. Students can further grasp the TBL framework and enjoy the structured process with a revamped instructional layout and additional classes. As for the classroom, the seat layout may prevent suitable group conversations, with a small-group or smart classroom being more appropriate for TBL.
The preparation time satisfaction results are significantly difference, with Year 2 students being considerably less satisfied than Year 3 (p = 0.012). Most second-year medical students spent one to two days planning, and third years one to four (p = 0.005), primarily because the third-year course was longer. Second-year medical students attended a two-week course on human skin and the connective tissue system with a TBL class in the second week, whereas third years took a five-week haematological system course with a TBL class in the fourth week. Both classes received course material on Mondays, while the TBL was on Fridays in the same week. Second-year medical students may need to study the basic science aspects and be unable to independently assess the pre-class material, whereas third-year students had more time. Accordingly, a TBL course should last at least three to four weeks to allow medical students to understand the basic TBL instructional material and independently assess it.
This study has limitations. The questionnaire was expert-evaluated without instructor facilitation. In addition, our study focused on students’ satisfaction with TBL, hence we didn’t include academic outcomes to prove the value of TBL.
V. CONCLUSION
The survey showed that students appreciated TBL-based learning since it helped them to work together and embrace learning, while potentially improving their study skills. A diversity of pre-class material allows students to choose learning tactics depending on their individual abilities. Students found the activity venue inadequate and classroom improvements would boost their satisfaction level.
Notes on Contributors
KW reviewed the literature, designed the study, analysed data, co-wrote the manuscript, critically reviewed and edited the manuscript, and then read it through prior to final approval.
WD reviewed the literature, analysed the data, co-wrote the manuscript, and critically reviewed and edited the manuscript.
WR gave critical feedback on the writing of the manuscript.
AS and KL provided scientific insight and advice, and critically reviewed and edited the manuscript.
Ethical Approval
This research was approved by the institutional ethics committee of the Faculty of Medicine at Chiang Mai University (Study code: PAT-2565-09243).
Data Availability
On reasonable request, the corresponding author will provide data to support the conclusions of this study. Due to privacy and ethical considerations, the data cannot be made public.
Acknowledgement
The authors wish to express their sincere appreciation to Ms. Naorn Sriwangdang for assisting with the preparation of the research proposal.
Funding
This study was supported by the Faculty of Medicine, Chiang Mai University, grant no. 062-2566.
Declaration of Interest
The authors confirm they have no potential conflicts of interest.
References
Burgess, A., Bleasel, J., Hickson, J., Guler, C., Kalman, E., & Haq, I. (2020a). Team-based learning replaces problem-based learning at a large medical school. BMC Medical Education, 20, Article 492. https://doi.org/10.1186/s12909-020-02362-4
Burgess, A., van Diggele, C., Roberts, C., & Mellis, C. (2020b). Team-based learning: Design, facilitation and participation. BMC Medical Education, 20(Suppl 2), Article 461. https://doi.org/10.1186/s12909-020-02287-y
Burgess, A. W., McGregor, D. M., & Mellis, C. M. (2014). Applying established guidelines to team-based learning programs in medical schools: A systematic review. Academic Medicine, 89(4), 678–688. https://doi.org/10.1097/ACM.0000000000000162
Michaelsen, L. K., & Sweet, M. (2008). The essential elements of team-based learning. New Directions for Teaching and Learning, 2008(116), 7–27. https://doi.org/10.1002/tl.330
Parmelee, D., Michaelsen, L. K., Cook, S., & Hudes, P. D. (2012). Team-based learning: A practical guide: AMEE Guide No. 65. Medical Teacher, 34(5), e275–e287. https://doi.org/10.3109/0142159X.2012.651179
*Komson Wannasai
Department of Pathology,
Faculty of Medicine,
Chiang Mai University,
110 Inthavaroros road, Sriphume
Meaung, Chiang Mai, 50200
+6653935442
Email: komson.wanna@gmail.com
Submitted: 11 September 2021
Accepted: 22 March 2023
Published online: 4 July, TAPS 2023, 8(3), 58-61
https://doi.org/10.29060/TAPS.2023-8-3/SC2694
Maria Isabel Atienza & Noel Atienza
San Beda University College of Medicine, Philippines
Abstract
Introduction: An evaluation of the online medical course was conducted to assess student readiness, engagement, and satisfaction at the San Beda University College of Medicine in Manila during the COVID-19 pandemic.
Methodology: A convergent mixed methods approach was done with a quantitative online survey and a qualitative thematic analysis of focus group discussions (FGD) with medical students. A total of 440 students participated in the survey while 20 students participated in the FGDs.
Results: The medical students were sufficiently equipped with computers and internet connections that allowed them to access the online medical course from their homes. The 5 themes identified during the study that were relevant to education were: Student readiness for online learning, Learning Management System (LMS) and internet connectivity, teaching and learning activities, the value of engagements, and teaching effectiveness of the faculty. The combined quantitative and qualitative analysis revealed vital issues that affect student learning. This included the need for students to interact with fellow students and to be engaged with their faculty. The issues that affect teaching included the need for continuing faculty training and management skills in delivering the full online course.
Conclusion: The success of online education rests heavily on the interactions of the students, the teachers, and the knowledge. Student interactions, managerial and skills training for the faculty, and providing students with a mix of synchronous and asynchronous activities are the most effective means to ensure the effective delivery of online medical courses.
Keywords: Medical Curricular Revision, Formative Evaluation, Student Engagement, Synchronous and Asynchronous Online Learning, Cognitive Overload
I. INTRODUCTION
The COVID-19 pandemic necessitated a shift to online teaching and a revision of the medical curriculum with synchronous and asynchronous online activities. Medical schools worldwide adapted teaching strategies utilising Video Conferencing and Learning Management Systems.
This program evaluation of the online medical course aimed to evaluate the effectiveness of instruction using the various components of online learning. The study centered on the perspectives of students using a mixed methods design (Fitzpatrick et al., 2011). The study focused on the interplay of digital capabilities, students’ perceptions and satisfaction with the interactions and engagements during the online course.
II. METHODS
The mixed methods research protocol was approved by the Institutional Ethics Board of San Beda University. The study utilised a convergent mixed method design with a quantitative online survey that was conducted on 440 respondent students representing each of the four-year levels of the medical school. Six focus group discussion (FGD) sessions were conducted on 20 students. All student participants provided a signed informed consent form to participate in the survey and in the FGDs. The 25-item online survey questionnaire included a 5-point Likert scale for items on readiness for the online course, overall satisfaction, and engagement. The online FGD sessions were conducted using an open-ended questionnaire guide on student capabilities for the online course, student satisfaction, and student engagement.
The FGD recordings were transcribed and subjected to thematic analysis to identify major themes. Quantitative and qualitative data were analysed simultaneously through a joint display of the two sets of results. A joint display using pillar integration was done to demonstrate the themes where the data corroborated or validated each other. The conceptual framework, data collection tools, the data results, and the pillar integration table are posted in a data repository file for this study can be accessed through a repository at: https://doi.org/10.6084/m9.figshare.16682569.v2 (Atienza & Atienza, 2021).
III. RESULTS
The survey revealed that students were adequately equipped with the necessary computers and smartphones needed to access the online course. Only 50% of the students were taking the online course from their homes within the same city as the medical school. While 72% encountered internet connectivity problems, 88% of students were successful in the use of the LMS and the videoconferencing platform to access the course and take online examinations.
Seventy-eight percent of students found online student-to-student and faculty-to-class interactions to be beneficial to student learning. Among the synchronous activities, 63% of students preferred live online lectures. Among the asynchronous activities, 52% of students preferred uploaded video lectures. Overall, around 52% of students experienced being overloaded with study requirements while 48% of students felt there was sufficient time for independent study.
The results of the survey and the thematic analysis of the FGDs were organised into themes and subthemes. These themes were generated from the integration of the quantitative and qualitative data. The schematic diagram (Figure 1) demonstrates how the themes are related to the effectiveness of learning based on the perspective of the students.
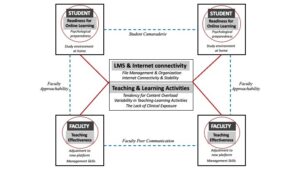
Figure 1. Schematic diagram of themes and subthemes identified in a mixed methods analysis of a fully online medical course at SBU-COM during the COVID pandemic
A. Student Readiness
The first theme that surfaced from the results was Student Readiness to engage in online learning. Students found their readiness to be dependent on two subthemes:
1) Study environment at home: Students expressed that the sudden shift to studying from home required that they designate sufficient time and space for studying. Students recognised that responsibilities at home and to the family could be distractions if not managed properly.
2) Psychological preparedness: The students also expressed the value of psychological preparedness as essential in dealing with stress and fatigue resulting from the unexpected shift to the online learning mode.
B. LMS and Internet Connectivity
The second theme highlights the importance of having computers and a stable internet connection as major determinants of student satisfaction with the online course. The introduction of an LMS for the medical course required immediate training for both the students and the faculty. While 81% of the students had the necessary gadgets and a good internet signal, 17% experienced major connection problems that disrupted up to 50% of live lectures and offline recorded videos. Student satisfaction with online learning was dependent on how timely and how organised the learning materials were uploaded into the LMS.
C. Teaching and Learning Activities
The third theme refers to the blend of online and offline activities for the different courses. The major subthemes included cognitive overload, variability of teaching and learning activities across courses, and the lack of clinical exposure.
1) Cognitive overload: Students had a perception of being overloaded by the volume of information delivered through the online course. The introduction of new forms of assessments such as video assignments, group reports, and research outputs contributed to the perceived cognitive overload.
2) Variability of teaching and learning activities: The variability in the blend of online and offline activities across the different courses required varying degrees of adjustments from the students. The students expressed their preference for live or recorded lectures over small group discussions and live laboratory demonstrations.
3) Lack of clinical exposure: Students in the 3rd and 4th year levels were apprehensive about the lack of clinical exposure in the actual medical environment due to the restrictions brought about by the pandemic. They recognise that they may not have the necessary skills training needed for internship.
D. The Value of Engagements
Unexpectedly, the fourth theme that students found important in the shift to online learning was the value of engagements.
1) Student-to-student online interactions: Up to 78% of students found support through interactions with other students. These interactions were useful not only for sharing the academic workload but also for mental and emotional support highlighting the value of student camaraderie despite being limited to virtual interactions.
2) Faculty-to-class interactions: Up to 80% of students expressed appreciation for the efforts of the faculty to get student feedback, answer clarificatory questions, and provide explanations when necessary. The students also expressed greater satisfaction with courses delivered online. Both faculty interactions with the class and with individual students were recognised as faculty approachability.
E. Teaching Effectiveness of The Faculty
The fifth theme Teaching pertains to the ability of the faculty to manage the online platform for teaching.
1) Faculty management skills: Teaching effectiveness is facilitated by the ease by which the faculty manages virtual teaching.
2) Faculty peer communication: Students recommend that the faculty within and across different courses coordinate their activities so that students can more easily manage their time and learning.
IV. DISCUSSION
The experience of delivering the medical course online has been very limited in the past. The teaching and learning strategies for medical courses to be delivered fully online require extensive preparation of the three main points in the transaction of learning: the learners, the teachers, and the course content. Learner readiness entails a clear delineation of the study environment in terms of time and space for study. Proper orientation to the online learning environment and psychological support should be made available to the students before the course begins. An inventory of the students’ computers and internet connectivity should also be done to ensure readiness for the course.
Delivering the course online necessitates faculty training on teaching and learning strategies for synchronous and asynchronous delivery as well as the proper navigation of the LMS and its available features. The faculty must maximise the benefits of technology as well as pedagogy in the online learning environment.
This study showed that in the shift of medical education to an online mode during the pandemic, student learning relies heavily on interactions between the learners, the teachers, and the course content. In an online course that relies so much on technology as a means of course delivery and integration, teaching and learning success depends on how well the interactions are established among these three points (Ifinedo & Rikala, 2019).
The design of courses must facilitate student-to-student interactions while faculty-to-class interactions using both synchronous and asynchronous activities would provide a good learning experience for students (Rhim & Han, 2020; Seymour-Walsh et al., 2020).
V. CONCLUSION
To succeed in the delivery of the online medical course, sufficient time must be given for faculty-to-student interactions during synchronous sessions and after the online classes. The faculty must demonstrate approachability by being open to continuing interactions with students outside the synchronous sessions. The coordination of faculty members within and across different courses must be enhanced to reflect efficiency in delivering their respective courses.
This study was performed during the early phase after the shift to full online delivery of the medical course. While the study is based on the perceptions of the students, the results of this study may be valuable in planning for continuing the online delivery of the medical course. The results of this study may be more robust with the inclusion of faculty perceptions and indicators of student academic performance.
Notes on Contributors
Dr. Maria Isabel Atienza conceptualised, designed, and implemented this study. She conducted the focus group discussions, prepared the thematic analysis, and wrote the manuscript for this study.
Dr. Noel Atienza helped in the design and conduct of the online survey and was involved in the data processing and data analysis of the survey. He was also involved in the preparation and editing of the final manuscript.
Ethical Approval
The research protocol SBU-REB # 2020-028 for this study was reviewed and approved by the San Beda University Research Ethics Board on November 28, 2020.
Data Availability
Data collection tools and research data are available and can be accessed by any interested reader through a repository at: https://doi.org/10.6084/m9.figshare.16682569.v2. The data in the repository may not be copied or cited without written permission from the authors.
Acknowledgment
The authors would like to acknowledge the support provided by the Alumni of San Beda and their commitment to promoting faculty research activities.
Funding
This study was funded by the Jesus P. Francisco Distinguished Professorial Chair Research Grant from the San Beda College Alumni Foundation, Inc.
Declaration of Interest
There are no conflicts of interest in this study.
References
Atienza, M., & Atienza, N. (2021). An online medical course during the COVID-19 pandemic: A mixed methods analysis. [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.16682569.v2
Fitzpatrick, J., Sanders, J., & Worthen, B. (2011). Program evaluation: Alternative approaches and practical guidelines 4th Edition. Pearson Education, Inc.
Ifinedo, E., & Rikala, J. (2019). TPACK and educational interactions: Pillars of successful technology integration. World Conference on E-Learning. Association for the Advancement of Computing in Education, 295-305. https://www.learntechlib.org/primary/p/211094/
Rhim, H., & Han, H. (2020). Teaching online: Foundational concepts of online learning and practical guidelines. Korean Journal of Medical Education, 32(3), 175-183. https://doi.org/10.3946/kjme.2020.171
Seymour-Walsh, A., Bell, A., Weber, A., & Smith, T. (2020). Adapting to a new reality: COVID-19 coronavirus and online education in the health professions. Rural and Remote Health, 20, 6000. https://doi.org/10.22605/RRH6000
*Maria Isabel Maniego Atienza
San Beda University, Mendiola Street,
Barangay San Miguel,
City of Manila, Philippines
+639178668751
Email: mimatienza@yahoo.com
Submitted: 15 August 2022
Accepted: 20 December 2022
Published online: 4 July, TAPS 2023, 8(3), 54-57
https://doi.org/10.29060/TAPS.2023-8-3/SC2867
Seow Chong Lee & Foong May Yeong
Department of Biochemistry, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: In the first weeks of medical school, students learn fundamental cell biology in a series of lectures taught by five lecturers, followed by a mass tutorial session. In this exploratory study, we examined students’ perceptions of the mass tutorial session over two academic years to find out if they viewed the tutorials differently after minor tweaks were introduced.
Methods: Reflective questions were posted to the undergraduate Year 1 Medical students at the end of each mass tutorial session in 2019 and 2020. Content analysis was conducted on students’ anonymous responses, using each response as the unit of analysis. The responses were categorised under the learning objectives, with responses coded under multiple categories where appropriate. The distribution of the counts from responses in 2019 and 2020 was compared, and the tutorial slides used over the two years were reviewed in conjunction with students’ perceptions to identify changes.
Results: In 2019, we collected 122 responses which coded into 127 unique counts, while in 2020, 119 responses coded into 143 unique counts. Compared to 2019, we noted increases in the percentage of counts under “Link concepts” and “Apply knowledge”, with concomitant decreases in percentage of counts in “Recall contents”. We also found that the 2020 tutorial contained additional slides, including a summary slide and lecture slides in their explanations of answers to the tutorial questions.
Conclusion: Minor tweaks in the tutorial presentation could improve students’ perceptions of our mass tutorials.
Keywords: Mass Tutorials, Students’ Reflections, Apply Knowledge, Link Concepts, Minor Tweaks
I. INTRODUCTION
In the first few weeks of medical school, students learn about cell biology which is fundamental to what they need to know about tissues, organs, and the whole body in a series of lectures co-taught by five lecturers. In the lectures, efforts are made to highlight basic cellular processes, and illustrate how these are inter-connected in a cell. Where appropriate, how knowledge in the biomedical sciences underpins applications in clinical settings is also illustrated by the lecturers. At the end of the series of lectures, the lecturers will co-facilitate a mass tutorial session aimed at summing up the topics.
The mass tutorial session has several learning objectives. These include basic levels of learning such as recalling concepts, preparing for assessments, and building knowledge on topics, to higher levels of learning such as applying concepts to solve real life problems, and linking concepts between topics. Being the only teaching and learning activity that all lecturers co-teach, the mass tutorial provides the best opportunity to demonstrate links and apply the consolidated knowledge learnt during the different lectures.
Once the teaching and learning activities are completed, the coordinator of the lectures Foong May Yeong (YFM) reviews the curriculum to ensure that the teaching and learning activities delivered the intended learning objectives. Such reviews include students’ experiences of the curriculum (Erickson et al., 2008), which the coordinator (YFM) routinely collect through posting reflective questions at the end of the tutorial. In this exploratory study, we analysed students’ reflections from 2019 and 2020, and categorised them under different learning objectives of the tutorial. We noted an increase in percentage counts under “Apply knowledge” and “Link concepts” in 2020 compared to 2019. A review of the tutorial slides revealed the addition of summary and lecture slides in 2020. Our results suggest that minor tweaks to the tutorial presentation are sufficient to help students see the intended usefulness and relevance of tutorials.
II. METHODS
A. Format of Mass Tutorials
The mass tutorial was conducted after completion of the cell lectures. For 2019, this was a face-to-face session. For 2020, due to the COVID-19 pandemic, the tutorial was conducted online via Microsoft Teams. The class size was 281 for 2019, and 280 for 2020. Four out of five lecturers taught the same topics for both years. For both years, during the mass tutorial, each lecturer used Poll Everywhere to pose a mix of five to six recall and application questions linked to their topic. Identical questions were used in 2019 and 2020. Students discussed among themselves before answering these questions. The class responses were then revealed, after which the lecturer explained the solutions to their questions. The cycle was repeated until all the lecturers completed their parts.
B. Collection of Student Reflections
After each tutorial, the coordinator (YFM) posted two reflection questions on Poll Everywhere. The two questions were: 1. “What were the key points you learned in this session?”, 2. “Any questions?”. Answering these reflection questions were voluntary and anonymous. A waiver of informed consent was approved by Yong Loo Lin School of Medicine Medical Sciences Departmental Ethics Review Committee. The responses to question 1 obtained from students in 2019 and 2020 were analysed in this study.
C. Content Analysis
The responses to question 1 were coded and categorized into the different learning objectives of the mass tutorial, using each response as a unit of analysis. Each response could be coded into multiple categories when appropriate. The counts under each category were represented as a percentage of all counts coded from the responses. The tutorial slides used in 2019 and 2020 were also reviewed to understand students’ perceptions.
III. RESULTS
In 2019, we collected 122 responses which were coded into 127 unique counts. In 2020, we collected 119 responses which were coded into 143 unique counts. The number of responses and unique counts coded were largely similar between the two years. The unique counts were categorised into the five learning objectives and their percentage counts were presented in Figure 1. Supplemental data containing an overview of the categories and samples of students’ responses, as well as the counts under each category, are openly available in Tables 1 and 2 shared at Figshare at http://doi.org/10.6084/m9.figshare.20484498 (Lee & Yeong, 2022). The distribution of the counts differed between the two years. In 2019, majority of the counts were categorized to “Recall contents” (37.0%), with low numbers categorized as “Apply knowledge” and “Link concepts” (15.0% and 3.1% respectively). In comparison, in 2020, we observed a decrease in percentage of counts in “Recall contents” (to 21.0%), with an increased percentage in counts in “Apply knowledge” and “Link concepts” (to 22.4% and 15.4% respectively). Overall, there is a shift in distribution of counts, from a skewed distribution in 2019, to an even distribution in 2020.
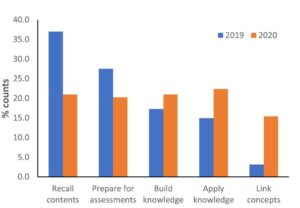
Figure 1. Categorisation of students’ responses into the learning objectives
Given that tutorial questions used in the two years were largely identical, we reviewed the tutorial slides used in these two years to look for possible differences. In 2020, firstly, a summary slide detailing the different aspects of the cell was added to the start of the tutorial slides. Secondly, lecture slides were included in the tutorial slides to explain the answers to the tutorial questions. The lecture slides could come from the lecturer teaching the topic of interest, or from other lecturers if connections across topics were important. These additions could have altered students’ perceptions of the mass tutorial session in 2020.
IV. DISCUSSION
In this study, we examined students’ reflections collected across two academic years to understand their perceptions of the mass tutorial sessions that capped the teaching of cell biology. One of the intentions of the lecturers when designing the tutorial questions was to demonstrate links across topics, and illustrate how questions can be solved using connections across topics. The decrease in percentage of counts under “Recall contents” in 2020 suggested an increase in students’ awareness of the usefulness and relevance of the tutorial sessions when minor changes were made in the presentation of the overview of the cell biology topic and the answers to the tutorial questions.
Both lecture and summary slides likely promoted links in different ways. The lecture slides represent theoretical knowledge for each topic, and also add visuals to the explanations of tutorial questions. Inclusion of lecture slides allow students to use both visual and audio channels to process the explanations, instead of using only the audio channel to listen to explanations when they were delivered verbally without visuals (Mayer, 2014). Using both channels could lower the cognitive load for students to learn and construct meaningful frameworks to solve problems. Summary slides juxtaposed different topics within a slide, allowing students to visualize connections between topics in the proper functioning of a cell (Bae & Watson, 2014). Adding these slides require little effort from the lecturers as the slides are readily available. Such small changes in improving the instructional approach could result in improvements in student learning (Lang, 2016).
There are several limitations to our study. Firstly, we only reviewed the tutorial slides, which covers part of the enacted curriculum. Secondly, the tutorial in 2019 was conducted face-to-face while the one in 2020 was conducted online. Online learning normally is not something students view positively, hence the improvements in student perceptions was surprising. Students prefer the social aspects of learning, which is abundant in face-to-face learning but greatly diminished in online learning (Siah et al., 2022). However, the diminished opportunities for peer-learning in online environment might contribute to increased attention diverted to lecturers for explanations.
V. CONCLUSION
Surveying and analysing students’ reflections at the end of mass tutorial proved to be informative in evaluating and improving our tutorials. In our preliminary analysis, a change in students’ perceptions of the tutorial from recalling of concepts to application of knowledge and linking concepts corresponded to minor tweaks in our tutorial presentation slides. Such minor tweaks, requiring little time, but yet are effective in helping students see the usefulness and relevance of tutorials, is an approach that even busy academics can do.
Notes on Contributors
Seow Chong Lee contributed to the analysis and interpretation of data, drafting and revising of the manuscript.
Foong May Yeong contributed to the conception and design of the study, interpretation of data, drafting and revising of the manuscript.
Ethical Approval
Ethics approval was obtained from Yong Loo Lin School of Medicine Medical Sciences Departmental Ethics Review Committee (Reference code: MSDERC-2022-006).
Data Availability
An overview of the categorization of responses into categories and samples of students’ responses, as well as the counts under each category are openly available in Figshare at https://doi.org/10.6084/m9.figshare.20484498.
Funding
This paper receives no funding from outside sources.
Declaration of Interest
The authors have no conflict of interest to declare.
References
Bae, J., & Watson, B. (2014). Toward a better understanding and application of the principles of visual communication. In W. Huang (Ed.), Handbook of Human Centric Visualization (pp. 179-201). Springer. https://doi.org/10.1007/978-1-4614-7485-2_7
Erickson, F., Bagrodia, R., Gook-Sather, A., Espinoza, M., Jurow, S., Shultz, J. J., & Spencer, J. (2008). Students’ experience of school curriculum: the everyday circumstances of granting and withholding assent to learn. In F. M. Connelly, M. F. He, & J. Phillion. (Eds.), The SAGE Handbook of Curriculum and Instruction (pp. 198-218). https://doi.org/10.4135/9781412976572.n10
Lang, J. M. (2016). Small Teaching: Everyday Lessons from the Science of Learning (1st ed.). Jossey-Bass.
Lee, S. C., & Yeong, F. M. (2022). Minor tweaks to tutorial presentation improved students’ perceptions of our mass tutorial. https://doi.org/10.6084/m9.figshare.20484498
Mayer, R. E. (2014). Multimedia instruction. In M. Spector, D. Merrill, J. Elen, & M. J. Bishop (Eds.), Handbook of Research on Educational Communications and Technology (pp. 385-399). https://doi.org/10.1007/978-1-4614-3185-5_31
Siah, C. R., Huang, C. M., Poon, Y. S. R., & Koh, S. S. (2022). Nursing students’ perceptions of online learning and its impact on knowledge level. Nurse Education Today, 112, Article 105327. https://doi.org/10.1016/j.nedt.2022.105327
*Foong May Yeong
MD4, 5 Science Drive 2,
S117545
+65 6516 8866
Email: bchyfm@nus.edu.sg
Submitted: 28 April 2022
Accepted: 9 February 2023
Published online: 4 July, TAPS 2023, 8(3), 50-53
https://doi.org/10.29060/TAPS.2023-8-3/SC2798
Olivia MY Ngan1,2, Jasmine YN Hui3 & Sihan Sun4
1Medical Ethics and Humanities Unit, School of Clinical Medicine, LKS Faculty of Medicine, The University of Hong Kong, HKSAR; 2Centre for Medical Ethics and Law, Faculty of Law and LKS School of Medicine, The University of Hong Kong; 3Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR; 4CUHK Centre for Bioethics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR
Abstract
Introduction: Didactic pedagogy and passive learning in bioethics and medical humanities teaching are ineffective in engaging students and gauging learning interests. As a result, medical students are unaware of why and how bioethics and medical humanities relate to their learning and thus prioritising acquiring clinical knowledge in their medical education.
Methods: This project involves a teacher-student collaboration to develop a teaching approach, which bridges historical events and contemporary issues, acknowledging how ethics and humanities are interwoven in clinical and everyday life. The objectives are to (1) highlight landmark historical events in bioethics and medical humanities and (2) recognise the evolving nature of values and social norms that inform current practice.
Results: The three activities include the use of historical narratives, annual newsletter publications, and social media to augment didactic classroom teaching and learning. Video narratives of landmark events in bioethics were developed to strengthen historical knowledge and encourage self-reflection. The newsletter invited students to write about any topic in bioethics and medical humanities and enabled them to experience a peer-review process. It allowed students to critically appraise everyday issues. Social media engagement via Instagram offered a flexible and informal medium to diversify the traditional bioethics content taught in the classroom. The advantages and obstacles of each element are discussed.
Conclusion: A holistic approach using historical narratives, newsletters, and social media engages students’ learning and allows students to become conscious of how past events shape the present.
Keywords: Bioethics, Medical Ethics, Medical Humanities, Education, History, Curriculum Development, Social Media, Student as Partner, Newsletter
I. INTRODUCTION
With modern bioethics taking shape in the late 1960s, the introduction of formal bioethics teaching in medical schools developed slowly in Europe and Northern America over the subsequent decades. It was recognised that professional ability not only encompassed scientific knowledge and clinical skills, but also embodied a high standard of professional ethics, values, and moral conduct. A paradigm shift in how medical education shaped students’ moral compasses and holistic decision-making abilities was needed. In 1987, the Liaison Committee on Medical Education stated that medical schools must incorporate bioethics and medical humanities teaching into their curricula (Carrese et al., 2015). In 1993, the British General Medical Council published a white paper, Tomorrow’s Doctors, which outlined a blueprint for reforming the curriculum and affirmed that teaching ethics and law was an integral part of medical education (Mattick & Bligh, 2006).
Bioethics teaching started relatively late in Asia-Pacific and is strategically less developed in its teaching content, methodology, and assessment (Qian et al., 2018; Sim et al., 2019). There is little discussion on how to best deliver bioethics education through a multidisciplinary lens, as the disciplines of humanities (e.g., philosophy, history, and law), social sciences (e.g., anthropology and sociology), and arts (e.g., literature) are extensive. Our team recognised that passive learning using conventional pedagogy (e.g., didactic lectures and tutorials) had significant drawbacks. Earlier studies showed that teachers adopting these methods struggled to engage and stimulate students’ reception to ethics learning (Ganguly et al., 2022; Ngan & Sim, 2021). They were unaware of why and how bioethics and medical humanities were related to their science background, called them “soft” subject, and thus prioritised acquiring clinical knowledge (Leo & Eagen, 2008).
This paper describes a new teaching approach that draws reference from the philosophy of history teaching, using the past to understand and predict present and future actions. We describe three activities, including using historical narratives, annual newsletter publications, and social media to augment classroom teaching and learning in hopes of promoting ethical sensitivity to students’ clinical and everyday life experiences. Our learners are medical students undertaking a six-year undergraduate medical degree programme. These activities were implemented to support pre-clinical year teaching, though also applicable to clinical year students.
II. DESCRIPTIONS OF THREE TEACHING ACTIVITIES
A. Historical Narratives
The adoption of historical narratives in bioethics teaching draws reference from the philosophy of history teaching, using the past to appreciate the present and the future. But its history is often neglected in the curriculum due to time constraints. Students perceived a disconnection between themselves and unethical events, struggling to understand the significance and effects specific past events may have had on present society (Ngan & Sim, 2021). Gerald L. Gutek (1995), History Educator, advocated that “[teaching] should illuminate the past in order to provide the perspective in time and place that we need to make reflective decisions on the [medical] education choices that face us today. Understanding the importance of bioethics history reminds ourselves about the wrongdoings in science, either due to procedural insensitivity or limited guidelines, and may also improve individual behaviour and organisational culture, re-enforcing a high standard of professional conduct. The video narratives reinforce historical knowledge and the ability to discern and scrutinize the similarities and differences between the past and present.
In this pilot project supported by the faculty’s teaching development grant, landmark historical events were developed as short video narratives that complemented the teaching curriculum topic. Table 1 is a non-exhaustive list of examples describing key events in ethics and how they relate to contemporary issues. In our experience, the video productions were well-received by students’ feedback evaluation. The high cost, however, would be a concern. Should the video improve students’ sensitivity towards bioethics, a comprehensive development of bioethics history video should be invested as an educational media to support teaching.
|
Historical Events |
Related Ethical Concerns |
Contemporary Issues |
|
Eugenics measures in the United States (1896- 1940), Germany (1933-45), and Japan (1948-1996) |
Eugenics |
Emerging technologies (e.g., gene-editing technologies, preimplantation diagnosis, and prenatal diagnosis) |
|
The “God” Committee: Rationing dialysis machines (1961) |
Equity, fair allocation approach, transplantation ethics |
Allocation of scarce resources (e.g., vaccine, ICU bed, funds) |
|
Tuskegee Syphilis Study, (1972) |
Research ethics (e.g., informed consent, exploitation of vulnerable populations) |
Research involving vulnerable populations (e.g., homeless, inmates) |
|
Stanford Prison Experiment (1971)
Milgram’s “destructive obedience” Study (1974) |
Unethical research conduct was uncovered (e.g., psychological harms, deception) |
Social and behaviour research illuminates the need for participant protection beyond the scope of biomedical studies. |
|
Table 1. Implications of Landmark Events on Present-day |
||
B. Bioethics Newsletter
In this pilot project, our team incepted a student-led bioethics newsletter aiming to draw ethical sensitivity in everyday life. Medical students were invited to contribute and write a commentary based on a topical issue of their interest; stimuli may have ranged from the news, movies, dramas, documentaries, plays, clinical ward experiences, and overseas observations. The opportunity provided students with a platform to voice and elucidate their opinions. It also allowed students to be more receptive to opposing ideas, developing a greater awareness of ethical dilemmas.
We published three annual newsletters and reflected on our experience. In the first issue, there was no peer-review process. We felt that the absence of a communication medium between the student writers and student editors hindered the quality of submissions. A peer-review process was implemented starting from the second issue, which was perceived to be beneficial as students were able to receive feedback and enhance intellectual rigour. More importantly, students were also exposed to the peer-reviewing process, which is useful for their future professional career development in academia.
Several obstacles relating to the submission process and the future sustainability of the newsletter were also met. In the first issue, interest was generated primarily through word-of-mouth and promotion on social media. In the second issue, prize incentives were given to best-written submissions. Participation gained momentum in the second and third issues, where we saw an average of 15-20 submissions. Sustainability was also a concern in terms of reader engagement and recruiting altruistic junior students to take over the project. To encourage multidisciplinary engagement, we aim to call for submissions in both written Chinese and English and accept entries from all students within the medicine faculty. We have a long-term goal of fostering a multidisciplinary collaboration across the Faculties.
C. Social Media
Given the generational influx of physicians and medical educators, the use of social media in medical education has seen rising popularity in recent years. Platforms like Twitter, Instagram, YouTube, and LinkedIn are easily accessible, user-friendly and encourage users’ interaction in a local and international setting. The flexibility of social media may also promote active learning pedagogies and personalised education, allowing students to build upon the knowledge they perceive to be interesting.
We started an Instagram page (IG: cubioethics) in June 2020 and curated content on a monthly basis. Content covered a broad range of bioethical topics, including several themed series: a news roundup named “Ethics in the News” and a series based on biotechnology seen in the sci-fi television series, Black Mirror. Each post consisted of a short synopsis on the topic and multiple discussion points were raised to incite critical thinking and reflection.
The flexibility and informal nature of Instagram allowed us to diversify the traditional bioethics content taught in the classroom. For example, it offered an experimental opportunity to teach through television and film. Moreover, the Instagram page allowed us to connect with students and professionals from local and international institutes. Engagement was reflected in post shares, likes, comments, and page follows. As the bioethics community on Instagram remains relatively small, it was easy to establish rapport. This community was able to help expand our audience via mutual post sharing and furthered the ethical debate raised in our posts.
Maintaining an Instagram page was not easy – content creation, the design process, and engaging with readers required careful planning and time. Also, from a cultural standpoint, it seemed as if there was a stronger tendency for international users to publicly participate in the conversation by commenting rather than local students. This may be due to worries about online criticism or the pervasive nature of social media and how it may no longer be viewed as a “safe space” for controversial discourse.
III. CONCLUSION
We reflected on our experience refining traditional didactic pedagogy by adopting three activities: historical narratives, newsletters, and social media. Each component presents unique educational benefits (e.g., recounting the evolution of today’s achievements, exposing students to peer-review publishing experience, cultivating sensitivities to everyday life) and operational barriers (e.g., budget constraints, altruistic students’ recruitment, time- and labour-intensive). Our teaching pedagogy may also be adopted in bioethics teaching in other disciplines, including biomedical and life sciences.
Notes on Contributors
OMYN conceived the study, developed the narration scripts, facilitated the newsletter peer-review as a teacher editor, reviewed the literature, and drafted the intellectual content of the manuscript.
JYNH led the newsletter peer-review as a student editor, managed the social media platform, and drafted the intellectual content of the manuscript.
SS reviewed newsletter entries and critically revised the manuscript for intellectual content. All authors are accountable for all aspects of the work and approve the final manuscript.
Ethical Approval
This study involves a theoretical discussion only and does not require ethical approval.
Data Availability
The data that support the findings of this study are openly available in the Figshare repository. http://doi.org/10.6084/m9.figshare.19768264
Funding
The study is supported by the Teaching Development and Language Enhancement Grant (TDLEG) for the 2019-22 Triennium. The funders had no role in the content review of the manuscript.
Declaration of Interest
The authors declare no conflict of interest.
References
Carrese, J. A., Malek, J., Watson, K., Lehmann, L. S., Green, M. J., McCullough, L. B., Geller, G., Braddock III, C. H., & Doukas, D. J. (2015). The essential role of medical ethics education in achieving professionalism: The Romanell Report. Academic Medicine, 90(6), 744–752. http://doi.org/10.1097/ACM.0000000000000715
Ganguly, B., D’Souza, R., & Nunes, R. (2022). Challenges in the teaching–learning process of the newly implemented module on bioethics in the undergraduate medical curriculum in India. Asian Bioethics Review. https://doi.org/10.1007/s41649-022-00225-2
Gutek, G. L. (1995). A history of the western educational experience (2nd ed.). Waveland Press, Inc.
Leo, T., & Eagen, K. (2008). Professionalism education: The medical student response. Perspectives in Biology and Medicine, 51(4), 508–516. https://doi.org/10.1353/pbm.0.0058
Mattick, K., & Bligh, J. (2006). Teaching and assessing medical ethics: Where are we now? Journal of Medical Ethics, 32(3), 181–185. http://doi.org/10.1136/jme.2005.014597
Ngan, O. M. Y., & Sim, J. H. (2021). Evolution of bioethics education in the medical programme: A tale of two medical schools. International Journal of Ethics Education, 6, 37–50. https://doi.org/10.1007/s40889-020-00112-0
Qian, Y., Han, Q., Yuan, W., & Fan, C. (2018). Insights into medical humanities education in China and the West. Journal of International Medical Research, 46(9), 3507–3517.
Sim, J. H., Ngan, O. M. Y., & Ng, H. K. (2019). Bioethics education in the medical programme among Malaysian medical schools: Where are we now? Journal of Medical Education and Curricular Development, 6.
*Olivia M.Y Ngan
Medical Ethics and Humanities Unit,
School of Clinical Medicine,
Li Ka Shing Faculty of Medicine,
The University of Hong Kong, Pokfulam,
Hong Kong Island, Hong Kong SAR
Email: olivian1@hku.hk
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
