
Increasing the value of Community-Based Education through Interprofessional Education
Submitted: 11 February 2022
Accepted: 21 July 2022
Published online: 4 April, TAPS 2023, 8(2), 4-13
https://doi.org/10.29060/TAPS.2023-8-2/OA2755
Tri Nur Kristina1, Fatikhu Yatuni Asmara2, Sudaryanto Sudaryanto1, Nuryanto Nuryanto3 & Saekhol Bakri1
1Department of Medicine, Faculty of Medicine, Universitas Diponegoro, Indonesia; 2Department of Nursing, Faculty of Medicine, Universitas Diponegoro, Indonesia; 3Department of Nutrition, Faculty of Medicine, Universitas Diponegoro, Indonesia
Abstract
Introduction: This study aimed to examine the usefulness of Community Based-Education (CBE) and Interprofessional Education (IPE) to community health outcomes.
Methods: The design was a mixed-method study. Each small group worked together to identify family health problems, implement interventions, and evaluate the results. The Readiness for Interprofessional Learning Scale (RIPLS) questionnaire was applied to compare students’ perceptions before and after the implementation. In addition, qualitative data were acquired from students’ comments on the questionnaire, interviews with community representatives, and FGDs with instructors at the end of the program.
Results: Three hundred and sixty-seven out of 465 students returned the completed paired questionnaire (78.9 % response rate). Paired t-test showed that student perception of responsibility slightly increased, whereas teamwork and collaboration, negative and positive professional identity decreased somewhat. However, most pre-post students’ responses already trended to the positive side (scales 4 and 5). Moreover, the Chi-square test showed that pre-post students’ confidence levels significantly increased. Most small groups of students successfully empowered the community to solve health problems. Students, instructors, and representatives of community members appreciated the program. However, several students felt their instructors were not motivated to mentor their tasks, and sometimes they had difficulty conducting home visits together.
Conclusion: This study showed that the combination of CBE-IPE contributes to more favourable community health outcomes. However, it was challenging in several aspects of preparation, including highly motivated instructors. Nevertheless, pre and post-implementation students’ attitudes are still positive.
Keywords: Interprofessional Education (IPE), Community Based Education (CBE), Health Profession Students, Readiness
I. INTRODUCTION
Community-based education (CBE) programs for medical and other health professionals expose students to community health problems, in which they will work in the future as health professionals. However, the CBE program is usually implemented within a single discipline, whereas community health problems must be solved collaboratively among a health care team (Housley et al., 2018).
Interprofessional Education (IPE) has been identified as a valuable method of learning experiences to increase the collaboration and communication of health professionals in healthcare settings. Several studies have reported positive student perceptions of IPE, including improved patient and community outcomes (Dynes et al., 2013). For example, the Leicester Model of IPE demonstrated that students and healthcare professionals gain valuable insights into the balance task of patient-related issues and offer clarity about the effectiveness of collaborative opportunities in addressing patients’ needs (Lennox & Anderson, 2012). Carr (2015) also reported that after the IPE experience, students perceived strong confidence in communication with other professions, increased knowledge of the importance of teamwork and collaboration, learning professional roles, respecting other professional points of view, and improved communication skills.
The goal of undergraduate education for students in the health professions is mainly to produce graduates who can solve community health problems and increase community health, particularly in primary health care. Moreover, community health problems should be solved collaboratively. Thus, Community Based Education (CBE) combined with IPE is needed to be implemented in health professions schools. Several studies have implemented IPE in the community and positively affected students. For example, a study in the Philippines showed the usefulness of the IPE in the community, such as: learning about collaboration, appreciation of roles, holistic care, service to the community, and unique learning experience (Opina-Tan, 2013). A qualitative study in Australia also concluded that students who were voluntarily involved in an IPE program appreciate the opportunity to have direct practice experience in a community context and see this as a valuable way of engaging in interprofessional learning (Stewart et al., 2015). Furthermore, Wagner et al. (2011) stated that IPE in the community improved teamwork.
However, the IPE implementation in community-setting in Indonesia is not yet promising. Lestari et al. (2020) reported that communication and mutual support were problems faced by students. Furthermore, Randita et al. (2019) also stated that collaborative patient-centred competence has a moderate effect when IPE is implemented in the community setting. Therefore, IPE in Indonesia needs further exploration, especially when it is implemented in the community setting with a large number of students who are not volunteers but are obliged to be involved in such programs. In addition, it is anticipated that a learning model combining CBE and IPE will have additional benefits in supporting community health. Thus, the research question of this study was, is the combination of CBE-IPE valuable on community health outcomes, and what are the students’ attitudes and perceptions towards the new program?
II. METHODS
A. The Combination CBE-IPE Model
Before implementation, we matched the curricula of three health professions study programs (Medicine, Nursing, and Nutrition) at the Faculty of Medicine Universitas Diponegoro (a government medical school in Semarang, Indonesia). Based on the acquired competencies and timing possibility, we agreed that the new CBE-IPE program should be implemented for students in the 6th semester. In the 6th semester, all 465 health professions students (212 medical students, 127 nursing students, and 126 nutrition students) participated in this program during one semester.
Before implementation, we discussed with the head of the district health office and the director of the community health centre (CHC) to receive suggestions related to this program, especially in conjunction with the population health situation. As a result, we agreed that students should be assigned to families with pregnant women to support the local government health program in reducing maternal mortality. Thirty-six cadres (voluntary community members) were requested to participate in the project by the director of the CHC and agreed to help them in the program implementation. All cadres had been trained to conduct simple health promotion by the CHC.
A total of 465 health professions students were divided into 126 small groups consisting of 1-2 medical and nursing students and one nutrition student. One small group was attached to one family with a pregnant woman. To have experiences with a continuum of care, small groups of students added one other family if the first family had no children or elderly. Students had to work together to measure the health status of all family members, identify health problems, and propose a solution for identified health problems in discussions with their instructors. Based on those discussions, the students worked collaboratively with the cadres to implement collaborative interventions and eventually evaluated the result of their interventions. During this implementation, groups of students presented their work three times in seminars attended by all instructors and coordinators from three departments. The head of CHC received final reports for follow-up.
B. Study Design and Subjects
The design of this study was a mixed-method study to combine quantitative and qualitative data, in which the qualitative data was used to enrich the quantitative ones. Quantitative data was acquired by asking all students (465 health professions students) to fill out questionnaires before and after implementing the CBE-IPE program. We used the Readiness for Interprofessional Learning Scale (RIPLS) to evaluate students’ perceptions. This questionnaire has been widely used to collect students’ attitudes and perceptions to measure the readiness of healthcare professional students to undertake shared learning activities (Hertweck et al., 2012; Parsell & Bligh, 1999). Negative professional identity items represented negative statements regarding the value of working with other healthcare students. Therefore, this study reversed scored items so that high scores indicated IPE readiness (McFadyen et al., 2006). We used RIPLS in the Indonesian language version, which was developed by Tyastuti et al. (2014). It used exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). The EFA accounted for 59.9% of the total variance, while the alpha coefficient of CFA was > 0.7. Furthermore, construct validity was acceptable goodness of fit. Thus, the RIPLS in the Indonesian language version is a valid tool to assess students’ attitudes toward IPE.
The qualitative data were gained by collecting student comments in the questionnaire by asking: “Please write your words regarding this new program.” Moreover, TNK conducted interviews one by one with representatives of community members: two housewives and three cadres. At the end of the program, we conducted a workshop, including two times FGD conducted by TNK, FYA, and SB with 16 instructor’s representatives. Verbatim of all qualitative data was completed by TNK. The result of students’ intervention for patients and families was identified from students’ reports.
C. Data Analyses
We described the student’s characteristics and the result of student intervention on community outcomes. Paired-sample t-tests were used to compare the pre-post students’ responses to RIPLS. In addition, students’ perceptions related to self-confidence before and after the implementation were compared using chi-square. SPSS v22 was used to analyse the quantitative data. The students’ comments and interviews with community member representatives and instructors were analysed using content analysis according to Braun and Clarke (2006). First, keywords were identified as codes, and we used a matrix consisted three columns, namely keywords, categories, and themes. TNK and FYA conducted qualitative data analysis. Different coding was discussed to reach a consensus.
D. Ethical Consideration
We verbally explained this study to all participants before collecting the data. Especially for students, we guaranteed that their perceptions would not affect their scores. Then, we asked for participants’ agreement to join this study by signing the informed consent. The author would confidentially keep their identity.
III. RESULTS
Three hundred and sixty-seven out of 465 students returned the completed paired questionnaire (78.9 % response rate). Table 1 shows the subject’s characteristics of this study.
|
No |
Subject’s characteristics |
Categories |
Quantity |
Percentage |
|
1. |
Students (n= 367) |
|||
|
The study program |
Medicine |
167 |
45.4 |
|
|
Nursing |
100 |
27.3 |
||
|
Nutrition |
100 |
27.3 |
||
|
Gender |
Male |
73 |
20 |
|
|
Female |
294 |
80 |
||
|
2. |
Instructors (n: 16) |
|||
|
The study program |
Medicine |
6 |
38 |
|
|
Nursing |
5 |
31 |
||
|
Nutrition |
5 |
31 |
||
|
Gender |
Male |
4 |
25 |
|
|
Female |
12 |
75 |
||
|
Age |
31-40 |
6 |
37 |
|
|
41-50 |
10 |
63 |
||
|
3 |
Representative of community members |
|||
|
Age |
30-40 |
3 |
60 |
|
|
41-50 |
2 |
40 |
||
|
Gender |
Male |
0 |
0 |
|
|
Female |
5 |
100 |
||
Table 1. Characteristics of study subjects
A. The Result of Students’ Intervention in the Community Outcomes
Various health problems were identified and successfully managed by the students in collaboration with cadres (Table 2 and 3). Students also recognised that most families with low social-economic status and little education did not have health insurance. The head of the CHC agreed to follow up on some parts of the identified health problems, such as visiting pregnant women with high risk to ensure that they will deliver in the hospital, giving intervention for malnutrition toddlers, and vitalizing the post-health for the elderly.
|
No |
Problems identified |
Students’ interventions |
Results
|
|
1 |
One pregnant woman with an abortion |
Students and cadre provided education and accompanied the mother to the hospital. |
a. The mother should be curettage by the doctor in the hospital. b. The mother healthy and agrees to postpone the next pregnancy. |
|
2 |
Only 20% of pregnant women without risk factors who follow gymnastic program in CHC |
Motivation to follow gymnastic for pregnant women |
Moderate-high compliance
|
|
3 |
About 40% of pregnant women have low knowledge about monitoring of pregnancy and low compliance with routine ANC |
Direct education and gave motivation |
Increasing knowledge and compliance for ANC |
|
4 |
25.4% of pregnant women with risk factors according to the standard of WHO and 0.04% with high risk |
Motivation to routinely ANC and monitoring |
High compliance |
|
5 |
42.1% of pregnant women do not have health insurance |
Education to apply government health insurance |
25% have insured key person agrees to follow up |
|
6 |
Social and cultural problem (do not want to eat fish) |
Direct education |
Moderate-high compliance |
|
7 |
83.3% of pregnant women not enough nutrition in their daily diet (2 days recall) |
Gave leaflet and an example of healthy food |
Moderate-high compliance |
|
8 |
20% of pregnant women with anemia)
|
Gave Fe from CHC or midwives. |
Low compliance (reason: not good taste and felt nausea) |
Table 2. Students’ work-related pregnant women in the community
|
No |
Problems identified |
Students’ interventions |
Results
|
|
Baby and Toddlers |
|||
|
1 |
10% with malnutrition |
Education to mother and giving an example of healthy food |
Head of CHC followed up based on student’s report |
|
2 |
Acute Respiratory Infection |
Education and Suggested to CHC |
Cured |
|
3 |
Diarrhoea |
Education and Suggested to CHC |
Cured |
|
4 |
Motoric low development |
Education and Suggested to CHC |
Still to be followed up |
|
5 |
Difficult to eat, low knowledge of mother about healthy food |
Education to mother and give an example of healthy food |
Increasing knowledge |
|
6 |
One child with hydrocephalus |
Motivation to go to the hospital and finding the agency of hydrocephalus |
Has been tackled by the agency of hydrocephalus |
|
Puberty |
|||
|
1 |
Low knowledge about reproductive health |
Direct education |
Increasing knowledge and Head of CHC agree to follow up |
|
2 |
Smoking habit & Narcotic consumption |
Direct education |
|
|
3 |
Anemia among girl |
Direct education |
|
|
Adult |
|||
|
1 |
Low knowledge of occupational accident |
Direct education |
Increasing knowledge |
|
2 |
Low knowledge about family planning |
Direct education |
Increasing knowledge |
|
Elderly |
|||
|
1 |
Hypertension, Knee osteoarthritis, DM type II, Low Back Pain, Stroke, Low quality of life due to osteoarthritis and LBP |
Education and Suggestion to routinely to CHC |
Have been followed up by CHC
|
|
2 |
Only 15% routinely come to the integrative post health for elderly |
Education and Motivation |
Low compliance
|
Table 3. Students’ work with other family members
B. Pre-post Comparison of Students’ Perceptions
Students’ perceptions using RIPLS (5-point Likert scale) from all study programs showed a slight decrease in team collaboration, professional identity, and the cumulative sub-scale. Only student perception of responsibility slightly increased (Table 4). However, most pre-post students’ responses to the RIPLS questionnaire already trended to the positive side (scales 4 and 5). Comparison of pre-post students’ self-assessment of their confidence level significantly increased (Table 5).
|
No |
Subscale |
Pre Mean ± SD |
Post Mean ± SD |
P |
|
1 |
Teamwork & Collaboration |
38.96 ± 3.2 |
36.93 ± 4.0 |
< 0.001* |
|
2 |
Negative professional identity |
6.01 ± 2.4 |
5.29 ± 1.9 |
< 0.001* |
|
3 |
Positive Professional identity |
20.91 ± 1.9 |
20.23 ± 2.5 |
< 0.001* |
|
4 |
Role of responsibility |
5.38 ± 1.3 |
5.56 ± 1.5 |
0.07 |
|
5 |
Total subscale |
70.57 ± 5.0 |
68.74 ± 5.9 |
< 0.001* |
Table 4. Comparison of all students’ perception using RIPLS pre and post implementation (n: 367)
*Significance (p < 0.05) with paired t test
|
No |
Level of Confidence |
Pre |
Post |
Sig |
|
1 |
Not so confident |
69 (18.8%) |
3 (0.8%) |
< 0.00* |
|
2 |
Confident |
272 (74.1%) |
281 (76.6%) |
|
|
3 |
Very confident |
26 (7.1%) |
83 (22.6%) |
Table 5. Level of students’ Confidence (N: 367)
*Significance (p < 0.05) with chi-square test
C. Students’ Comments
Only 141/367 (38%) students wrote their comments in the questionnaire. However, most students (94% of 141 students) appreciated this program and suggested it be continued.
“The program is good; it can help community member to solve their health problem”
F23Nurs
“I agree if the program will be continued”
F50Nurs
Positive aspects raised by the students were:
- Opportunity to have direct communication with the community member (68%),
“I have the opportunity to communicate directly with patients and family, which is difficult to do when I’m only studying in the class”
M13Med
- Understanding each other when exploring and sharing knowledge to solve the identified health problems (32%),
“I feel amazed that each of us has our roles in solving health problems”
F67Med
- Learning about health team collaboration in the actual situation (40%),
“I learn a lot about how to collaborate with other health students in the real situation”
F90Nut
- Feeling proud that they had the opportunity to contribute to managing community health problems (69%).
“This program gives me an opportunity to collaborate with other professions to solve community health problems”
F44Nurs
The student’s complaints were as follows:
- Their task of working with a continuum of care was too heavy and exhausting.
“Focus on one family problem for one small team would be more useful.”
F57Med
- Several students (13%) also felt that their instructors were not motivated to mentor their tasks.
“It is difficult to make an appointment with the instructors, so we don’t have enough time to get feedback from him”
F21Med
- They had difficulty conducting home visits together (73%).
“Our biggest problem is matching the schedule to do a home visit.”
M98Nut
D. Interviews with Representatives of Community Members (two housewives, three cadres)
Both housewives and cadres appreciated the students’ work. They believed the students already had enough competencies to help their health problems. Cadres were still committed to participating in the following program and working with the students to implement, monitor, and evaluate the intervention.
“We are so happy that students help us a lot to identify and to solve our health problems”
F01HW
“Yes, of course, we will help students to communicate with the family as well as report the result of students’ intervention to Community Health Centre”
F03C
Community members thought they were not receiving enough information about the students’ purpose for visiting their house. They suggested that the cadre should have explained to them this program. However, they welcomed the students and told them to make an appointment before the home visit.
“There was no information from cadres of CHC that students will come to our house, but we still welcoming the students because it gives many benefits for us”
FHW02
E. FGD with Instructors at the End of the Program
Most instructors (94,5%) appreciated the value of this program. However, they needed more detailed information about the program, especially assessing students. They also thought it was too hard for students to add one family after already concentrating on one family’s health problem. They agreed that a tiny group should only be attached to one family with a pregnant woman. To strengthen collaboration competencies, all groups of students should implement a “collaborative intervention” that involves all disciplines.
“Sometimes students implemented their intervention within a single discipline that they thought more appropriate to solve the specified health problem.”
F05Inst
The instructors suggested that the assessment include peer assessment to increase students’ attitudes toward valuing each other. It was finally agreed that in the next implementation, various types of assessment would be implemented, namely students’ activities, presentation and discussion, peer assessment, and students’ assessment by the family members.
“Various assessment methods are preferable to capture students’ performance from the different side”
M09Inst
IV. DISCUSSION
This study aimed to examine the impact of implementing the CBE-IPE model on the outcomes of student intervention in the community and students’ attitudes and perceptions towards the new program. Within the CBE-IPE program, the health professions students successfully worked together to empower the community to solve most community health problems. The CBE-IPE program aims to give health profession students direct experiences in working as a health team in dealing with community health problems that might correlate with the social and economic backgrounds of community members. In this study, students identified several health problems in the family with low financial status, low education, and did not have any health insurance. Hence, the health profession students within this program also had an opportunity to learn several principles, including the level of education and economic aspects when implementing their interventions. It is in line with the study by Ngo et al. (2021), who reported that hypertension and cardiovascular risk could be identified by conducting CBE-IPE in homeless adults.
We implemented the CBE-IPE program without any serious obstacles due to the support from the local health government and the director of CHC. Cadres and representatives of community members also commented that the students’ presence and work were beneficial. They stated that they would be involved in the program and work with students to implement, monitor, and evaluate the result. It is important to involve cadres in this program because they will handle the follow-up under the supervision of CHC. Some studies also involved non-health workers in IPE implementation, such as Akter et al. (2016), who involved lay health workers, and Dynes et al. (2013), that involved health extension workers and community health promoters in improving maternal and neonatal health outcomes.
A. Students’ Attitudes and Perceptions Toward the CBE-IPE Program
This study showed that students’ attitudes and perceptions toward this program have improved, especially regarding the role of responsibility and confidence level. In this study, students have tasks to implement health intervention after discussing health problems identified with their instructor, which might increase their commitment and confidence. Tan et al. (2021) also demonstrated the importance of feedback and discussion, in which IPE participants noted that the debriefing process improves their compliance and teamwork.
Students’ perceptions as assessed by the RIPLS in aspects of team collaboration and interprofessional identity were slightly lower, although statistically significant. These statistically significant differences might result from the large sample size of this study. Several studies have shown that one-time IPE implementation is unlikely to change attitudes, whereas multiple or longitudinal IPE experiences elicit attitudinal change with a more positive response (Hammick et al., 2007; Pollard et al., 2006). Hind et al. (2003) reported little to no change in the health professions students’ perception of the RIPLS between pre-and post-implementation. Schreiber et al. (2014) also reported a slight increase and no statistically significant differences in the pre-post response to the RIPLS because the students already had positive attitudes toward IPE. Torsvik et al. (2021) reported that RIPLS tends to have a ceiling effect. Therefore, RIPLS no longer seems suitable for measuring and evaluating the impact of interprofessional learning. In this study, “most pre-post students’ responses to the RIPLS questionnaire already trended to the positive side.” Thus, the RIPLS also possibly has a ceiling effect in this study.
B. Wrapped up CBE-IPE Program Evaluation
Evaluation of this initial program demonstrates that students felt favourable toward the CBE-IPE program and felt more confident when dealing with community health problems. In line with Wong et al. (2018) study, the final students of six health programs have a positive attitude towards working together in an interprofessional health care team.
Nevertheless, students also complained that their tasks in working within a continuum of care were too heavy. As a result, they felt exhausted and less motivated to identify other health problems in another family. This complaint was in line with the instructors’ opinion. It concurred that students could learn from each other when they presented and discussed their work in the seminar. The recommendations included an adjustment in the tasks, scheduling, and improvements in the communication and quality of supervision. Therefore, the students’ tasks must be adjusted to accommodate these suggestions in the following implementation. Sunguya et al. (2014) reported that curriculum is an essential challenge in implementing IPE, which is in line with the study conducted by Thistlethwaite (2012) and Herath et al. (2017), which states that teaching methods and learning activities can be problems faced when implementing IPE. Furthermore, scheduling is one of the problems faced by faculty who implement the IPE program (Ngabonzima et al., 2020)
The instructors mentioned that the students’ interventions were not always “collaborative disciplines” since sometimes only a single discipline intervention for some health problems, and very little content was contributed by the other students in the specified group. Therefore, these circumstances might influence the lower perception of negative professional identity after the program implementation (Hind et al., 2003). Milot et al. (2015) also reported that it could sometimes be challenging to combine heterogeneous student teams during the learning together phase, where every discipline should be represented.
Understanding the attitudes of health professional students and the factors that influence their perceptions, including the situation they face during implementation, may help implement the program in several stages. There are four levels for the students to join the interprofessional collaborative practice. These include level 1: intra-professional education: the foundation of group skills, level 2: introduction to interprofessional education and collaboration: exposure to the healthcare team, level 3: interprofessional collaboration, and level 4: becoming an influential member of the healthcare team (Salfi et al., 2012).
C. Limitations
This study’s limitation lies in the type of data collection that only uses a closed-ended questionnaire and asks the students to write their comments on the program. Although the students raised several positive attributes, this study did not obtain sufficient information about what happened during the implementation and what was behind the students’ rated aspects. Therefore, FGDs with students are still needed to understand program implementation in-depth. Further, direct participation in program implementation might identify obstacles regarding when students should collaborate in their intervention program. Additionally, limitations in this study are acknowledged as data were collected from less than 80% of students participating in the program. Finally, no formal feedback was collected from the community members, although verbal input in the interview was positive. A collection of more detailed data would have provided a deeper understanding of the program’s impact on community perceptions.
We realize that implementing the CBE-IPE program in the community, which involves many students, was challenging and needed more careful preparation. Moreover, the lecturers’ motivation might be increased by encouraging and facilitating them to include field epidemiology research in the same area, with research funding from the faculty. Several changes should be made based on this evaluation, including more detailed guidance for the students and instructors.
V. CONCLUSION
This study revealed that the combination of CBE-IPE for 6th-semester health profession students had been perceived as a valuable learning experience to build community health. Nevertheless, it was challenging for many students in several aspects of the preparation. Moreover, highly motivated lecturers are required, which might be increased by encouraging and facilitating field epidemiology research in the same area. Finally, further research is needed to explore students’ experiences during implementation, primarily how they work as a team and their belief in professional identity. It is also important to identify the result of a combination of CBE-IPE implementation in terms of the satisfaction of students, instructors, and family members.
Notes on Contributors
Tri Nur Kristina conceptualised and designed the research, participated in the analysis and intepretation of data, drafted and revised the manuscript, and giving final approval of the version to be published.
Fatikhu Yatuni Asmara conceptualised of the program implementation, participated in the data collection, and revised the manuscript.
Sudaryanto conceptualised of the program implementation.
Nuryanto conceptualised of the program implementation and participated in the data collection.
Saekhol Bakri conception of the program implementation and participated in the data collection.
Ethical Approval
The Medical and Health Research Ethics Committee (MHREC), Faculty of Medicine Diponegoro University-Dr. Kariadi General Hospital had approved this study (No. 519/EC/FK/2020).
Data Availability
Author could not share the data of this study widely because of its privacy. It also contains qualitative data.
Acknowledgement
The authors would like to thank the Faculty of Medicine Universitas Diponegoro for providing the funding for this study.
Funding
This work supported by Faculty of Medicine Universitas Diponegoro (Grant number: 233-71/UN7.6.1/PP/2020).
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
References
Akter, T., Sibbritt, D., & Dawson, A. (2016). Workforce interventions to deliver postnatal care to improve neonatal outcomes in low- and lower-middle-income countries: A narrative synthesis. Asia-Pacific Journal of Public Health, 28(8), 659–681. https://doi.org/10.1177/1010539516656435
Braun, V., & Clarke, V. (2006). Qualitative research in psychology using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101.
Carr, S. (2015). Examining health professional students’ attitudes on interprofessional education. (Publication no. 309) [Doctoral Dissertations, University of Rhode Island]. DigitalCommons@URI. http://digitalcommons.uri.edu/oa_diss/309
Dynes, M., Buffington, S. T., Carpenter, M., Handley, A., Kelley, M., Tadesse, L., Beyene, H. T., & Sibley, L. (2013). Strengthening maternal and newborn health in rural Ethiopia: Early results from frontline health worker community maternal and newborn health training. Midwifery, 29(3), 251–259. https://doi.org/10.1016/j.midw.2012.01.006
Hammick, M., Freeth, D., Koppel, I., Reeves, S., & Barr, H. A. (2007). A best evidence systematic review of interprofessional education. BEME guide no.9. Medical Teacher, 29(8), 735-751. https://doi.org/10.1080/01421590701682576
Herath, C., Zhou, Y., Gan, Y., Nakandawire, N., Gong, Y., & Lu, Z. (2017). A comparative study of interprofessional education in global health care: A systematic review. Medicine, 96(38), 1-7. https://doi.org/10.1097/MD.0000000000007336
Hertweck, M., Hawkins, S., Bednarek, M., Goreczny, A., Schreiber, J., & Sterrett, S. (2012). Attitudes towards interprofessional education: Comparing physician assistant and other health care professions students. The Journal of Physician Assistant Education, 23(2), 8-15.
Hind, M., Norman, I., Cooper, S., Gill, E., Hilton, R., Judd, P., & Jones, S. (2003). Interprofessional perceptions of health care students. Journal of Interprofessional Care, 17(1), 21-34. https://doi.org/10.1080/1356182021000044120
Housley, C. L., Neill, K. K., White, L. S., Tedder, A. T., & Castleberry, A. N. (2018). An evaluation of an interprofessional practice-based learning environment using student reflections. Journal of Interprofessional Care, 32(1), 108–110. http://doi.org/10.1080/13561820.2017.1356808
Lennox, A., & Anderson, E. S. (2012). Delivering quality improvements in patient care: the application of the Leicester Model of interprofessional education. Quality in Primary Care, 20(3), 219–226.
Lestari, E., Scherpbier, A., & Stalmeijer, R. (2020). Stimulating students’ interprofessional teamwork skills through community-based education: A mixed methods evaluation. Journal of Multidisciplinary Healthcare, 13, 1143–1155. http://doi.org/10.2147/JMDH.S267732
McFadyen, A. K., Webster, V. S., & Maclaren, W. M. (2006). The test-retest reliability of a revised version of the Readiness for Interprofessional Learning Scale (RIPLS). Journal of Interprofessional Care, 20(6), 633-639. https://doi.org/10.1080/13561820600991181
Milot, E., Dumont, S., Aubin, M., Bourdeau, G., Azizah, G. M., Picard, L., & St‑Germain, D. (2015). Building an interfaculty interprofessional education curriculum: What can we learn from the Université Laval Experience? Education for Health, 28(1), 58-63. https://doi.org/10.4103/1357-6283.161896
Ngabonzima, A., Kenyon, C., Hategeka, C., Utuza, A. J., Banguti, P. R., Luginaah, I., & F Cechetto, D. (2020). Developing and implementing a novel mentorship model (4+1) for maternal, newborn and child health in Rwanda. BMC Health Services Research, 20(1), Article 924. https://doi.org/10.1186/s12913-020-05789-z
Ngo, A. N., Islam, M. A., Aoyagi, J., Sandor, Z., & Sandor, S. (2021). Prevalence of hypertension in homeless adults: An interprofessional education community-based health fairs cross-sectional study in urban long beach, California. High Blood Pressure and Cardiovascular Prevention, 28(1), 63-68. https://doi.org/ doi: 10.1007/s40292-020-00424-8
Opina-Tan, L. A. (2013). A pilot implementation of interprofessional education in a community‑academy partnership in the Philippines. Education for Health, 26(3), 164-171. https://doi.org/10.4103/1357-6283.125992
Parsell, G., & Bligh, J. (1999). The development of a questionnaire to assess the readiness of healthcare students for interprofessional learning (RIPLS). Medical Education, 33(2), 95-100. https://doi.org/10.1046/j.1365-2923.1999.00298.x
Pollard, K. C., Miers, M. E., Gilchrist, M., & Sayers, A. (2006). A comparison of interprofessional perception and working relationship among health and social care students: The results of a 3-year intervention. Health and Social Care in the Community, 14(6), 541-552. https://doi.org/10.1111/j.1365-2524.2006.00642.x
Randita, A. B. T., Widyandana, W., & Claramita, M. (2019). IPE-COM: A pilot study on interprofessional learning design for medical and midwifery students. Journal of Multidiscipline Health Care, 12, 767–775. http://doi.org/10.2147/JMDH.S202522
Salfi, J., Solomon, P., Allen, D., Mohaupt, J., & Patterson, C. (2012). Overcoming all obstacles: A framework for embedding interprofessional education into a large, multisite bachelor of science nursing program. Journal of Nursing Education, 51(2), 106-110. https://doi.org/10.3928/01484834-20111230-05
Schreiber, J., Goreczny, A., Bednarek, M. L., Hawkins, S. R., Hertweck, M. L., & Sterret, S. E. (2014). The effects of single event interprofessional education (IPE) experience on occupational therapy students’ attitude toward IPE. The Internet Journal of Allied Health Sciences and Practice, 12(1), 1-8. https://doi.org/10.46743/1540-580X/2014.1467
Stewart, V., Betts, H., Chee, P., & Ingamells, A. (2015). Interprofessional learning: Health and allied health students in a community context. Advance in Social Work & Welfare Education, 17(2), 70-85.
Sunguya, B. F., Hinthong, W., Jimba, M., & Yasuoka, J. (2014). Interprofessional education for whom? – Challenges and lessons learned from its implementation in developed countries and their application to developing countries: A systematic review. PLoS ONE, 9(5), e96724. https://doi.org/10.1371/journal.pone.0096724
Tan, K. W., Ong, H. K., & Mok, U. S. (2021). Using simulation and inter-professional education to teach infection prevention during resuscitation. The Asia Pacific Scholar, 6(1), 93-108. https://doi.org/10.29060/TAPS.2021-6-1/OA2229
Thistlethwaite, J. (2012). Interprofessional education: a review of context, learning and the research agenda. Medical Education, 46(1), 58–70. https://doi.org/10.1111/j.1365-2923.2011.04143.x
Torsvik, M., Johnsen, H. C., Lillebo, B., Reinaas, L. O., & Vaag, J. R. (2021). Has “the ceiling” rendered the readiness for interprofessional learning scale (RIPLS) outdated? Journal of Multidisciplinary Healthcare, 14, 523–531. https://doi.org/10.2147/JMDH.S296418
Tyastuti, D., Onishi, H., Ekayanti, F., & Kitamura, K. (2014). Psychometric item analysis and validation of the Indonesian version of the Readiness for Interprofessional Learning Scale (RIPLS). Journal of Interprofessional Care, 28(5), 426-432. https://doi.org/10.3109/13561820.2014.907778
Wagner, J., Liston, B., & Miller, J. (2011). Developing interprofessional communication skills. Teaching and Learning in Nursing, 6(3), 97-101. https://doi.org/10.1016/j.teln.2010.12.003
Wong, P. S., Hasan, S. S., Ooi, J., Lim, L. S. H., & Nadarajah, V. D. (2018). Assessment of attitude for interprofessional team working and knowledge of health professions competencies for final year health professional students. The Asia Pacific Scholar, 3(1), 27-37. https://doi.org/10.29060/TAPS.2018-3-1/OA1064
*Fatikhu Yatuni Asmara
Department of Nursing, Faculty Medicine,
Universitas Diponegoro
Jl. Prof Soedarto, SH, Tembalang,
Semarang, Indonesia
+6281229495962
Email: f.y.asmara@fk.undip.ac.id
Submitted: 28 July 2022
Accepted: 12 October 2022
Published online: 3 January, TAPS 2023, 8(1), 25-32
https://doi.org/10.29060/TAPS.2023-8-1/OA2850
Choon Peng Jeremy Wee1, Mingwei Ng1 & Pim W. Teunissen2
1Department of Emergency Medicine, Singapore General Hospital, Singapore; 2School of Health Professions Education (SHE), Faculty of Health Medicine and Life Sciences, Maastricht University, Maastricht, The Netherlands
Abstract
Introduction: This study was performed to understand how fixed clinical teams affected informal learning in Emergency Medicine Residents. Better understanding the effects of team dynamics on informal learning may help to optimise learning and improve performance.
Methods: From 8th February 2020 till 27th September 2020, the Singapore General Hospital Emergency Department adopted a fixed team system. Zoom interviews were carried out amongst Emergency Medicine Residents who worked in the fixed team system using a semi-structured iterative interview guide. A qualitative content analysis was used for this exploratory study. The interviews were transcribed verbatim, anonymised and coding via template analysis performed. Data collection and analysis were performed until data sufficiency.
Results: The themes identified centred around relationship dynamics, team composition and motivation for learning. The first was how improved relationships led to improved trust, communications and camaraderie among team members. This improved peer learning and clinical supervision and provided a more personalised learning experience. A balanced team composition allowed learners to be exposed to experts in various subspecialties. Finally, there was an initial increase in motivation, followed by a decrease with time.
Conclusion: In postgraduate medical education, working in a fixed team system with balanced members had positive effects on informal learning by strengthening relationships and communications.
Keywords: Informal Learning, Workplace Learning, Fixed Teams, Medical Education, Postgraduate
Practice Highlights
- Fixed teams can strengthen relationships between members through better trust, familiarity and communication.
- A balanced fixed team with members having different areas of expertise allows a variety of perspectives.
- Rotation of team members may achieve a balance between the stronger relationship and familiarity of the members of fixed teams and the greater variance in perspectives from a non-fixed team system.
I. INTRODUCTION
Fixed teams (FT) and non-fixed teams (NFT) exist in medicine because of differing service requirements and manpower resources. Examples of FTs can exist in ward round teams and operating surgical teams (Eddy et al., 2016; Stepaniak et al., 2012) where personnel stay within the same work team for long periods. In other areas of healthcare like the Emergency Departments (ED), a NFT system is usually employed where teams are formed according to the personnel rostered to work on that shift and team members change every shift. This allows a more flexible system for the team members as they can request off days and leave according to their personal schedule and yet allows for 24-hour coverage in the ED.
High levels of performance are required of medical teams, both fixed and non-fixed, to achieve good patient outcomes. Therefore, team members should learn how to work effectively together to deliver the best patient care. There are studies, both within healthcare and other industries, which showed mixed results when FT were compared with NFT with regards to team performance. A systematic review on minimal invasive surgical teams found that the FTs had better teamwork and had reduced rates of technical mistakes compared to NFTs (Gjeraa et al., 2016). However, an aviation study showed that FTs made more minor errors compared to NFTs due to FT members being too familiar with each other and overlooking errors (Barker et al., 1996). Although it is unclear how transferable specific research findings from non-healthcare domains are, what is clear is that FTs and NFTs are different in the way teams were formed and the amount of time team members spend working together. There is a lack of understanding if and how these differences affect the way learning takes place in FT and NFTs; which could translate to the performance of the team and its members.
Workplace learning occurs through informal learning by experiencing work challenges and via interpersonal relationships. Informal learning can be supported through learner engagement by encouraging active participation in work activities and aligning learners’ interests with that of the organisation’s objectives towards improving the individuals’ and organisation’s capabilities (Billett, 2007). Informal learning is now widely accepted as a form of workplace learning that occurs out of a formal planned teaching program. It usually occurs during work activities which are not primarily aimed towards education, with learning objectives not planned beforehand (Callanan et al., 2011; Rogoff et al., 2016; Watkins et al., 2018). Although informal learning had been studied, there are very few studies looking at how being in FTs affects informal learning. A review on the involvement of employees in workplace learning (Kyndt & Baert, 2013) revealed that there was a paucity of literature on whether any team system improves the involvement of employees in informal learning. Thus, it remains to be studied what effects working in a FT system has on informal learning especially of the more junior team members.
An integrative literature review on informal learning found that some of the important components of informal learning within members of a team and between teams included interpersonal relationships, feedback, networking and leadership (Jeong et al., 2018). Therefore, there may be differences in interpersonal relationships and feedback between the different team systems. It is known that good interpersonal relationships include good supervisor and peer support and both affect whether what is learnt is applied at the workplace (Burke & Hutchins, 2016), there was little published data on whether supervisor and peer support or even the supervisory relationship were affected by the amount of time spent together. Within some healthcare systems both FTs and NFTs consists of members with varying levels of experience, differing expertise and roles. In a FT, the learners are only supervised by supervisors within that team; therefore, each learner’s supervised time is divided within a small group of supervisors as compared to a NFT system where each learner’s supervised time is spread amongst a larger number of supervisors. Thus, despite this increased time spent together in a FT, it is not clear if working in a FT impacts supervisory or interpersonal relationship.
Having a good trusted learner-supervisor relationship can result in the establishment of an “Educational Alliance” (Telio et al., 2015). This is because feedback from a credible trusted source was more readily accepted and feedback is another important component of effective informal learning within a team (Jeong et al., 2018).
Furthermore, a study among social work students and their supervisors in a rotational placement model, found that the longer the amount of time they spent with each other the greater the trust between them (Vassos et al., 2017). On the other hand, being in a FT could restrict networking and socialisation to a smaller group of people as contact with other teams’ members could be reduced however it is not known how this could affect informal learning.
Understanding how informal learning takes place within FT and NFT may allow optimisation of learning within each and perhaps even configure teams to enhance learning and thus ultimately improve performance. Our study aimed to fill this gap in the literature by exploring how fixed clinical teams affected the experience of informal learning for Emergency Medicine (EM) Residents. By doing so we hope to understand how informal learning can be supported via the appropriate implementation of team systems especially where high performance is expected from the teams.
II. METHODS
To study how being in fixed clinical teams affected the experience of informal learning for EM Residents we conducted an exploratory qualitative study based on a constructivism research paradigm using content analysis of individual interviews. This is because informal learning could not be quantified with specific learning outcomes.
A. Setting
EDs teams manage a large number of critically ill patients who may need time sensitive interventions. These teams would comprise of experienced Emergency Physicians (EPs) and more junior Medical Officers (MOs) and Residents. The Residents are postgraduate doctors who are training to graduate as EPs; therefore, informal workplace learning is a crucial part of their training. Hence the residents would be good study subjects to investigate the effect of team systems on informal learning.
The Singapore General Hospital (SGH) ED functioned via NFTs where the composition and number of members in the team differed with each 8 hour shifts accordingly to the anticipated patient load. The COVID-19 pandemic provided a naturalistic setting where the effect of a FT system can be compared to a NFT system which had existed before hand. After COVID-19 was declared a pandemic by the World Health Organisation (WHO) on the 11th March 2020 (World Health Organisation, 2020). There was an emphasis on infection control to contain the pandemic. Many countries had instituted social distancing measures which included curfew-like measures and travel restrictions (Lake, 2020). Similarly, the Singapore government had instituted legislative measures to limit face-to-face interactions. In the ED of SGH, measures were put in place to limit the spread of COVID-19.
Thus, from 8th February till 27th September 2020, as part of infection control measures, doctors were organised into 5 FTs, each having between 5-7 Consultants, 3-5 EM Senior Residents, 2-3 EM Junior Residents and 7-9 non-EM Medical Officers (MO) (Liu et al., 2020; Quah et al., 2020). The Senior Emergency Physicians (SEPs) consisted of certified specialists in EM (Associate Consultants, Consultants and Senior Consultants); they played supervisory and educational roles to the junior doctors (JD) which included MOs, Junior Residents and Senior Residents. Each FT worked 12-hour shifts. Interactions between teams were kept to a minimum and members from different teams were not allowed to mingle. Thus, the residents were only supervised by their team’s SEPs. Informal learning would now occur within these FTs.
Formal learning was converted to a remote online platform because of infection control measures. Lectures and tutorials were held and recorded using software which enabled online asynchronous access e.g. Zoom (Zoom, 2016) as not all residents could be given protected learning time together. Sessions which could not be transferred onto an online platform (e.g. hands on simulation and procedure skills training) were cancelled. Formal summative examinations were also cancelled.
B. Interviews
Interviews were conducted and recorded via Zoom (Zoom, 2016) to maintain social distancing. The primary investigator performed 11 interviews and a coinvestigator performed the remaining 4 out of a total of 15 interviews. A semi-structured iterative interview guide was developed based on Eraut’s typology on informal learning which included team activities, tasks and enabling/disabling factors (Eraut, 2010) was used, and the interviews were audio-recorded and transcribed verbatim and anonymised. The interviews allowed positive and negative aspects to be explored and being semi structured the questions asked varied according to the interviewees’ responses. This helped to focus the interviewees to what informal learning was with examples when it could occur within team activities. The guide was iteratively amended with each interview to enhance clarity which helped to obtain more in-depth data in later interviews.
C. Participants
Twenty-four ED residents were working in the FT system in the ED of SGH during COVID-19. Fifteen were Junior Residents and 9 were Senior Residents. Purposive sampling was carried out with at least two Residents from each team being sampled. This is to ensure that there was good representation for all of the fixed clinical teams. All 24 residents were invited to participate via email and WhatsApp messaging platform with written consent being obtained. Fifteen individual interviews were conducted before data sufficiency was achieved where no new data would change the outcome of the study, thus no further interviews were conducted beyond data sufficiency (Varpio et al., 2017). Eleven interviewees were Junior Residents (4 females and 7 males) and 4 were Senior Residents (3 females and 1 male).
D. Data Analysis
Data analysis was performed via template analysis by the primary and coinvestigator independently (Brooks et al., 2015). Eraut’s typology developed from his research on informal learning was used as a priori themes in the initial coding template (Eraut, 2010). Coding template modifications were made as the analysis of the transcripts continued. Themes were categorised into hierarchical clusters and relationships between them were studied and defined. After final modifications, the coding template was applied to the entire data set. Coding themes were compared and discussed between the primary investigator and the coinvestigator until consensus was reached.
E. Ethics
Waiver for approval was granted by the Singhealth Institutional Ethics Board. The primary investigator was a core faculty within the Singhealth Emergency Medicine Residency Program and although the interview was conducted among EM residents the primary investigator did not conduct the interviews when the interviewees were from the same team as the primary investigator. These were conducted by the coinvestigator. The coinvestigator was an EM Senior Resident who was not involved in the FT system. A reflexivity diary was kept, and peer debrief was done.
III. RESULTS
Three main themes emerged on how working in FTs affected informal learning amongst our participants (Figure 1). These included changes in relationship dynamics between members, effect of FT composition on informal learning of the participants and influence on motivation.
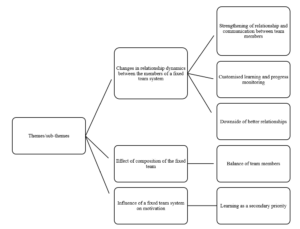
Figure 1. Themes and sub-themes
Theme 1: Changes in Relationship Dynamics between FT Members
From the interviews, the participants felt that the FT system resulted in more familiarity, trust, teamwork and improved communications between team members including SEPs, Residents and MOs. Interviewees felt that this strengthened the relationship dynamics between FT members as compared to a NFT. This meant that FT members were able to coordinate and exchange information better. It led to an increase in familiarity in knowing each member’s style of practice and way of thinking. The team members could understand each other better and how they reasoned.
The strengthened relationship between residents and SEPs changed with dynamics. Having a “closer rapport” and “deeper bond” allowed the residents to “tag along” with SEPs “more often” and gave the residents more insight as to why the SEPs behaved in a certain way as to “how they had practiced medicine” and the rationale behind each step was “more easily communicated to the residents who were tagging along” (Resident A), resulting in residents having a deeper understanding of why things were done in addition to how things were done. This strengthened relationship was also present between the residents and their peers. Therefore, peer learning improved within the FTs as junior residents reported feeling less reservation in asking each other questions.
Resident D felt that peer learning was better within FTs because of the improved relationship, there were less reservations which had prevented him from asking his peers questions in a NFT setting.
He elaborated:
“Fixed team [was] definitely better for peer learning. For the same reasons, because you know each other better, you’re more familiar. We don’t only talk to each other about work… after a while, when you go for meals together… or rather like resting together and no cases around you sit and talk. So there’s a lot more familiarity with the person you’re working with, and… you’re just more comfortable with asking questions… you don’t feel like this is somebody who’s going to judge you if [you] asked a stupid question”
This was not just amongst the residents but also with SEPs. Resident G felt that it was easier for the residents to speak to the SEPs because of familiarity and resulted in less workplace stress:
“Over the time as we knew each other better … the workplace stress was much lower… so I could… work with less stress at workplace… Because if you didn’t really know the consultant you tend to be afraid to talk to them; then of course your stress levels will be higher. But if you know that consultant and you know what kind of person, he or she is then you could be more comfortable to talk to them…”
“…It is more comfortable to… approach the senior because you know every day… we have a fixed team so naturally we feel that our relationship is closer…”
“… so, I won’t be too afraid to speak out or to talk to them to discuss with them.”
Contributing to additional ways of informal learning, communication within FTs even during work took on a more “friendly [and] social” form with greater congeniality and via more “communication platforms” (WhatsApp and Tiger Text) which continued even “outside of work” (Resident H). These platforms were also used as learning tools to facilitate case discussions, share learning points and experiences. This was not previously present in the NFTs. The residents felt that learning was more customised because of the change in relationship dynamics. In FTs, there was closer supervision of residents by SEPs. The residents “spent more time” with the same group of supervisors, thus the supervisors were able to better “assess both strengths, weaknesses and address any particular loopholes” of the residents (Resident A).
However, there were some adverse effects of this change in relationship dynamics. Some residents felt that with a closer relationship between team members, supervisors sometimes were more tolerant of the learners’ shortcomings and be less likely to point it out because of not wanting to affect the relationship. This closer relationship could result in residents taking “shortcuts” and “flying under the radar” because they knew the SEPs could tolerate or would not scrutinise the learners closely once “trust” was established (Resident L). Resident H gave an example of how familiarity could lead to less critical thinking by the learner:
“If… the senior always does like… [Rapid Sequence Intubation] … even though I question the first time I saw him do that… subsequently … every time I work with him I will do [it] this way. I won’t really think does the patient really need this way [of management] or will the patient benefit in a different way… if you are working with different bosses then every case you need to restart your thinking…”
Theme 2: Effect of Composition of the FT
All interviewees felt that the composition of the FT had affected informal learning, and that having a balanced team in terms of a wide range of years of practice amongst both the SEPs as well as the JDs would help improve informal learning. Having a team where the JDs were of differing seniorities of practice could help with peer learning because the senior ones could help the junior ones more. This also applied to the SEPs as that provided a wider perspective to clinical issues due to having different clinical experience and expertise in different subspecialties. Furthermore, if the JDs in a FT were of a similar level of practice, Resident C expressed that they could be “competing with each other for cases and procedures” which adversely affected informal learning with fewer opportunities to perform procedures. In a NFT the members would be constantly changing and it would be unlikely its JD would be always of the same level of practice.
The interviewees expressed concern that within a FT system that, although residents had close contact with a fixed group of supervisors, they lacked contact with the other teams’ SEPs. Many residents felt that this had adversely impacted informal learning because the SEPs were experts in different subspecialties (e.g., Trauma, Toxicology, Ultrasound, etc). By not interacting with many SEPs, residents were unable to learn from them. Furthermore, different supervisors had different perspectives and approaches to patients which the residents may not be exposed to if they were not in the same team as these seniors. However, this was mitigated by having a team with a balanced variation in the areas of specialty of the seniors. Resident F summarised this:
“…a team with… people from different seniorities are essential… (even) juniors can teach seniors… the way that my team was composed… it was a good mix… there are people from different… specialties… from different seniorities even within the juniors … like first posting to… [senior post graduate years]… offers different perspectives, learning of different things… people from different [subspecialties] can offer insight into the systems-based learning or component from other parts of the institution…”
Theme 3: Influence of a FT System on Motivation
Many residents felt that having FTs increased their motivation to learn. This resulted from their supervisors being able to inspire them and follow up with their learning progress more closely. Resident M was motivated to learn because his “friends (FT members) were very motivating” and “enthusiastic”; this encouraged him to learn more. Furthermore, resident C felt more motivated to learn in a FT because he “always sees the same senior” and this more frequent contact results in him being “more likely to take their feedback and opinion more seriously and work harder”
However, “after some time everyone is comfortable with each other” and some participants feared that their motivation “might go down” (Resident N). This was because there was a feeling of complacency as time went on within a FT, hence the motivation to learn started to dwindle after an initial increase.
Other reasons for this decline were related to COVID-19, the focus was more on facing the threat rather than learning and the priority to learn was secondary. The motivation to learn “was a bit less” as “the mood was more to survive than to learn”; Resident L was “less driven to learn” because there was a “general bleakness in the whole situation of [COVID-19] which made his “inner desire to learn… wane a bit”
IV. DISCUSSION
This study explored how working in fixed clinical teams affected informal learning for EM Residents. There are many pros and cons to fixed team rostering however the focus of this study is on informal learning. The findings highlighted the importance of having a balanced team composition where team members were able to establish trust and a strong bidirectional relationship because of the longer time spent working together. Motivation to learn increased initially; however after some time, some felt a decrease. This was consistent with prior work which highlighted team dynamics and commitment and that feedback which was given often and in a socially interactive environment were factors which helped to enable effective work-based learning (Attenborough et al., 2019; Jeong et al., 2018; Kyndt et al., 2016). Unlike in Attenborough’s work where team leadership was one of the factors identified; our respondents did not mention the effect of team leadership on informal learning. Their focus was more on the relationships between the different team members. From this study the predominant factors which positively affected informal learning included teamwork, collaborative task performance, where good communication was needed between different people, and personal development especially in building interpersonal relationships and group decision making.
Limited studies were done on how FTs affect informal learning. Our study found that FTs resulted in more (informal) communication channels (e.g. WhatsApp) being formed which was not present in NFTs, resulting in more learning activities including sharing ideas, resources and experiences. These sharing activities were some of the major forms of informal learning activities identified in the literature (Lohman, 2006). FTs resulted in open communication and quality feedback which was well received, and were found to be beneficial towards informal learning (Jeong et al., 2018). Our study showed that working in a FTs led to more customised learning. Findings of improved communications and strengthened relationships in a bidirectional manner involving teacher and learner alike, supports a shift from a predominantly teacher to learner type of dynamics to a team learning dynamics where all team members can learn with and from one another. This is important because informal learning takes place effectively when learning from past mistakes and feedback exchange occurs, involving both cognitive and social interactions (Jeong et al., 2018).
FTs had negative effects on informal learning as well. Familiarity resulted in supervisors being more tolerant of shortcomings and FTs limited learners’ contact with other teams’ supervisors and adversely affected informal learning. This was because informal learning also takes place when there is sharing of ideas, expertise and experience (Lohman, 2006) and limiting the number of supervisors limits the variance of shared viewpoints.
Our study has limitations. Firstly, interviewee recall bias was possible because 6 months had passed after the FT system was stopped before the interviews. Therefore, some details may not have been accurately recalled given this period which could affect the trustworthiness of results. Secondly, the participants were likely to be comparing their experiences in the FT system during COVID-19 to a NFT system without a pandemic. Thus, some of the experienced changes may be because of the pandemic rather than purely due to the FT system. Thirdly, there are many pros and cons to FTs however the focus of this study is on informal learning thus other factors not investigated with this study may affect the feasibility of FT. Lastly there could be power differential effects between the interviewers and the interviewees because the interviewers performed supervisory and roles to the residents. However, to mitigate this, a reflexivity diary was kept, and peer debrief between the two interviewers was performed. Furthermore, the interviewers did not interview members who had been in the same team as them.
V. CONCLUSION
In conclusion, FTs impact informal learning by building strong relationships with improved team communications and adding a social dimension for learning. A balance of team members as well as rotating the residents across different FTs may be beneficial for improving informal learning for EM Residents.
Notes on Contributors
Dr Wee Choon Peng Jeremy submitted the CIRB application, (with the help of the last author) conceptualised the study and its design. He performed the literature review, recruited and interviewed the participants, collected and transcribed the data, performed the thematic analysis of the data and wrote the manuscript.
Dr Ng Mingwei helped to recruit and interview some of the participants, transcribed and collected the data. Dr Ng helped perform the thematic analysis of the data and helped edit the manuscript.
Prof. Dr. Pim Teunissen was central to the conceptualisation of the study, advised on the design of the study and gave critical feedback to the writing of the manuscript and edited the manuscript extensively
All the authors have read and approved the final manuscript.
Ethical Approval
We have included the letter for waiver of CIRB via email. Ethics approval for waiver of written informed consent was obtained from the Singhealth Institutional Review Board (CIRB Ref: 2020/3114).
Data Availability
As the data set is qualitative in nature, we are not able to upload that in any public repository.
Funding
There is no funding for this paper/study.
Declaration of Interest
The authors report there are no competing interests to declare.
References
Attenborough, J., Abbott, S., Brook, J., & Knight, R. A. (2019). Everywhere and nowhere: Work-based learning in healthcare education. Nurse Education in Practice, 36, 132-138. https://doi.org/10.1016/j.nepr.2019.03.004
Barker, J. M., Clothier, C. C., Woody, J. R., McKinney, E. H., Jr., & Brown, J. L. (1996). Crew resource management: A simulator study comparing fixed versus formed aircrews. Aviation, Space, and Environmental Medicine, 67(1), 3-7.
Billett, S. (2007). Constituting the workplace curriculum. Journal of Curriculum Studies, 38(1), 31-48. https://doi.org/10.1080/00220270500153781
Brooks, J., McCluskey, S., Turley, E., & King, N. (2015). The utility of template analysis in qualitative psychology research. Qualitative Research in Psychology, 12(2), 202-222. https://doi.org/10.1080/14780887.2014.955224
Burke, L. A., & Hutchins, H. M. (2016). Training transfer: An integrative literature review. Human Resource Development Review, 6(3), 263-296. https://doi.org/10.1177/1534484307303035
Callanan, M., Cervantes, C., & Loomis, M. (2011). Informal learning. Wiley Interdisciplinary Reviews Cognitive Science, 2(6), 646-655. https://doi.org/10.1002/wcs.143
Eddy, K., Jordan, Z., & Stephenson, M. (2016). Health professionals’ experience of teamwork education in acute hospital settings: a systematic review of qualitative literature. JBI Database of Systematic Reviews Implementation Reports, 14(4), 96-137. https://doi.org/10.11124/JBISRIR-2016-1843
Eraut, M. (2010). Informal learning in the workplace. Studies in continuing education, 26(2), 247-273. https://doi.org/10.1080/158037042000225245
Gjeraa, K., Spanager, L., Konge, L., Petersen, R. H., & Ostergaard, D. (2016). Non-technical skills in minimally invasive surgery teams: A systematic review, Surgical Endoscopy, 30(12), 5185-5199. https://doi.org/10.1007/s00464-016-4890-1
Jeong, S., Han, S. J., Lee, J., Sunalai, S., & Yoon, S. W. (2018). Integrative literature review on informal learning: Antecedents, conceptualizations, and future directions. Human Resource Development Review, 17(2), 128-152. https://doi.org/10.1177/1534484318772242
Kyndt, E., & Baert, H. (2013). Antecedents of employees’ involvement in work-related learning. Review of Educational Research, 83(2), 273-313. https://doi.org/10.3102/0034654313478021
Kyndt, E., Vermeire, E., & Cabus, S. (2016). Informal workplace learning among nurses. Journal of Workplace Learning, 28(7), 435-450. https://doi.org/10.1108/JWL-06-2015-0052
Lake, M. A. (2020). What we know so far: COVID-19 current clinical knowledge and research. Clinical Medicine, 20(2), 124-127. https://doi.org/10.7861/clinmed.2019-coron
Liu, Z., Teo, T. L., Lim, M. J., Nadarajan, G. D., Segaram, S. S. C., Thangarajoo, S., Wee, L. E., Wee, J. C. P., & Tan, K. B. K. (2020). Dynamic emergency department response to the evolving COVID-19 pandemic: The experience of a tertiary hospital in Singapore. Journal of the American College of Emergency Physicians Open, 1(6),1395-1403. https://doi.org/10.1002/emp2.12264
Lohman, M. C. (2006). Factors influencing teachers’ engagement in informal learning activities. Journal of Workplace Learning, 18(3), 141-156. https://doi.org/10.1108/13665620610654577
Quah, L. J. J., Tan, B. K. K., Fua, T. P., Wee, C. P. J., Lim, C. S., Nadarajan, G., Zakaria, N. D., Chan, S. J., Wan, P. W., Teo, L. T., Chua, Y. Y., Wong, E., & Venkataraman, A. (2020). Reorganising the emergency department to manage the COVID-19 outbreak. International Journal of Emergency Medicine, 13(1), Article 32. https://doi.org/10.1186/s12245-020-00294-w
Rogoff, B., Callanan, M., Gutiérrez, K. D., & Erickson, F. (2016). The organization of informal learning. Review of Research in Education, 40(1), 356-401. https://doi.org/10.3102/0091732×16680994
Stepaniak, P. S., Heij, C., Buise, M. P., Mannaerts, G. H., Smulders, J. F., & Nienhuijs, S. W. (2012). Bariatric surgery with operating room teams that stayed fixed during the day: A multicenter study analyzing the effects on patient outcomes, teamwork and safety climate, and procedure duration. Anesthesia and Analgesia, 115(6), 1384-1392. https://doi.org/10.1213/ANE.0b013e31826c7fa6
Telio, S., Ajjawi, R., & Regehr, G. (2015). The “Educational Alliance” as a framework for reconceptualizing feedback in medical education. Academic Medicine, 90(5), 609-614. https://doi.org/10.1097/ACM.0000000000000560
Varpio, L., Ajjawi, R., Monrouxe, L. V., O’Brien, B. C., & Rees, C. E. (2017). Shedding the cobra effect: Problematising thematic emergence, triangulation, saturation and member checking. Medical Education, 51(1), 40-50. https://doi.org/10.1111/medu.13124
Vassos, S., Harms, L., & Rose, D. (2017). Supervision and social work students: Relationships in a team-based rotation placement model. Social Work Education, 37(3), 328-341. https://doi.org/10.1080/02615479.2017.1406466
Watkins, K. E., Marsick, V. J., Wofford, M. G., & Ellinger, A. D. (2018). The evolving Marsick and Watkins (1990) theory of informal and incidental learning. New Directions for Adult and Continuing Education, 2018(159), 21-36. https://doi.org/10.1002/ace.20285
World Health Organisation. (2020). World Health Organisation emergencies press conference on coronavirus disease outbreak – 11 March 2020. https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020
Zoom. (2016). Security guide. Zoom Video Communications Inc.
*Wee Choon Peng Jeremy
Outram Road,
Singapore 169608
Email: jeremy.wee.c.p@singhealth.com.sg
Submitted: 26 November 2021
Accepted: 21 July 2022
Published online: 3 January, TAPS 2023, 8(1), 33-42
https://doi.org/10.29060/TAPS.2023-8-1/OA2712
Jaime Maria Tan1, Junaidah Binte Badron1 & Sashikumar Ganapathy1,2
1Department of Emergency Medicine, KK Women’s & Children’s Hospital, Singapore; 2Duke-NUS Medical School, Singapore
Abstract
Introduction: Perceptions towards the working and learning environment as well as coping mechanisms have been studied across different healthcare sectors. They have shown to reduce stress and burnout. However, perceptions of the work environment in the Emergency Department (ED) setting have not been studied in depth. The literature surrounding coping mechanisms also mostly focuses on their impacts rather than the mechanisms utilised. In addition, these were often investigated using surveys. This study aimed to use a phenomenological approach to explore the perceptions and coping strategies of junior doctors working in a paediatric ED.
Methods: Sixteen junior doctors working in the Paediatric ED were recruited. Semi-structured interviews were conducted after conducting literature reviews. Data was collected until saturation point. All interviews were recorded and transcribed verbatim manually and subsequently analysed.
Results: The greatest fears of junior doctors starting their paediatric emergency posting were lack of knowledge due to inexperience in the subspecialty; fear of the work environment due to unfamiliarity as well as workload and the intrinsic high-stress environment. The main coping strategies were ensuring clinical safety, obtaining psychosocial support from loved ones and colleagues, and placing focus on spirituality and wellbeing.
Conclusion: In this study, the perceptions and coping strategies of the junior doctors in the Paediatric ED were explored. The findings from this study will help to structure and improve the support given to future junior doctors who rotate to the department as well as better orientate them to allay their pre-conceived notions.
Keywords: Coping Behaviours, Perceptions, Paediatric Emergency Department, Stressors, Interviews
Practice Highlights
- Participants worried about knowledge, workload and responsibilities prior to starting their posting.
- Perceptions were mostly of an anticipatory nature, influenced by seniors’ past experiences.
- In work, support from senior staff was helpful in allaying their fears and increasing patient safety.
- Participants felt psychosocial support, spirituality and wellness were useful coping strategies.
- Maladpative coping strategies did not come up as a main theme in our study.
I. INTRODUCTION
Perceptions toward the work and learning environment can strongly impact experiences and even lead to large amounts of stress (Chan et al., 2016). A poorer perception of the learning environment is also associated with greater levels of burnout (Chew et al., 2019; Sum et al., 2019). Conversely, a positive perception of the work environment helps to alleviate stress (Abraham et al., 2018). Workers’ perception of their work environment contributes significantly to their overall experiences.
Main factors contributing to stress in the ED include heavy workload and critically ill patients. Workplace violence, trauma, abuse and morbidity also add to the stress and burnout experienced (Burbeck et al., 2002; Copeland & Henry, 2018; Healy & Tyrrell, 2011; Xu et al., 2019). In the paediatric setting, added stressors include dealing with sexual abuse and non-accidental injury as well as death and the inability to provide optimal care for children (Alomari et al., 2021; Basu et al., 2016; Durand et al., 2019; Greenslade et al., 2019; Shanafelt et al., 2012; Watson et al., 2019).
Given these significant stressors, individuals utilise different coping mechanisms to mediate these experiences (Howlett et al., 2015).
Some coping strategies discussed in previous studies include socialising with friends and family (Gribben et al., 2019). Focusing on physical wellbeing, clinical variety, reflectivity, and organizational activities were also helpful in alleviating burnout in other areas of healthcare (Barham et al., 2019; Koh et al., 2015).
Several studies also found that the use of maladaptive coping mechanisms, such as alcohol use and self-blame increased with the frequency of burnout (Jackson et al., 2016; Oreskovich et al., 2015; Ryali et al., 2018; Talih et al., 2018).
While many studies studied stressors and the effectiveness of the coping mechanisms used, the actual components of coping mechanisms were not well studied. In studies that did look at coping mechanisms and their effectiveness, these studies were also often done via the survey method and were only evaluated on the surface.
Most studies looked at healthcare workers in general. Few studies looked solely at the doctor population. This makes conclusively evaluating the doctor component of coping mechanisms and their effects difficult.
While other studies looked at an adult emergency perspective, there were also few studies looking at the paediatric ED. It has been reported that dealing with paediatric emergencies causes more stress compared to their adult equivalents. Some of the contributing factors are related to the nature of working with children. These, in itself, are unmodifiable (Guise et al., 2017). Therefore, it is important to study how the paediatric context can affect the experiences of the doctors who care for them.
In our study, we studied the perceptions of junior doctors at the beginning of their posting. We subsequently explored their coping mechanisms in the Singaporean context.
The element of stress in the ED among junior doctors is significant as the ED is often part of many specialist training pathways (Mason et al., 2015). During the time of training, the doctors are still learning and developing. Hence, many doctors experience sharp learning curves during their postings. This brings about more stress (McPherson et al., 2003). In some cases, the stress can even lead to doctors thinking about leaving clinical practice altogether (Degen et al., 2014).
In the Singaporean context, paediatric emergency postings are part and parcel of speciality training for junior doctors (especially for those in emergency medicine and family medicine training). Because of this, junior doctors spend the majority of their paediatric postings in the paediatric emergency. As such, a Singapore-specific context would give light on the challenges of this sizable group.
The nature of the healthcare system in Singapore is unique. Up to 60% of the consultations in the paediatric ED were for nonurgent conditions due to the overall perception of the severity of symptoms and parental preference towards paediatric specialist facilities (Ganapathy et al., 2015). This would lead to an increased workload for the paediatric ED. The distribution in workload may also differ compared to a global perspective, with the load of severe paediatric trauma in Singapore being low (Pek et al., 2019).
These subtleties in the paediatric ED in Singapore can influence the experiences of junior doctors differently. With these key differences in mind, we aimed to investigate the perceptions of junior doctors towards their paediatric ED posting in Singapore and how they subsequently coped with the challenges faced.
II. METHODS
A. Design
In this study, we examined the experiences of doctors in their paediatric ED rotation and how their thoughts and actions influenced their stress during their rotation. We deemed the phenomenological approach to be the most appropriate for this study. Phenomenology is defined as the study of how individuals see and experience a phenomenon and what this means to the individuals in their own experience (Neubauer et al., 2019; Smith, 2021).
The approach we chose was that of an interpretive phenomenological analysis in which we aimed to investigate the experience through the participants’ own experiences and perceptions. With the help of the various participants’ accounts, themes and ideas bound by their experiences were explored (Tuffour, 2017).
B. Methods
The members of the study performed a preliminary literature review on the topic and explored plausible methods of data collection. The study team decided on semi-structured interviews as it promotes sharing and would allow for sufficient privacy.
The team members included a senior consultant, a staff physician and a medical officer. Together, after discussions about concepts that the team was keen to explore, an interview guide was drawn up.
Subsequently, a proposal was submitted to the Hospital Centralised Institutional Review Board for approval.
One-on-one interviews were conducted with the participants by investigator A, a medical officer who was rotating within the department at the time of the study. This was done to reduce the power differential. Interviews were conducted at a location and time convenient to the participant.
Prior to the interviews, consent was sought and all interviews were recorded and subsequently transcribed verbatim. The interviews were conducted over a 1-month period in December 2019.
Questions were open-ended and allowed participants to share ideas that they were keen to raise with no restrictions to the topics brought up. Interview questions were tweaked alongside subsequent interviews so that they were easier to understand and would encourage sharing. Additional questioning in subsequent interviews was adopted to improve clarity. For example, one of the questions that featured early in the interviews was ‘What are some of the coping mechanisms you use?’ During subsequent interviews we noticed some participants utilised coping mechanisms before work to prepare themselves, some used other strategies during work to cope with the stress, while others dealt with their stressors after getting off work. We tweaked the question to include ‘during the shift or outside of the shift’ to help participants widen their perspective about certain coping methods they may have used but were not immediately conscious of when answering the questions. No new questions referring to particular themes were inserted although interviewers were aware of the themes that had been highlighted in previous interviews. This was done in addition to the initial interview guide and ensured the broad nature of questioning was not compromised and the breadth of interviews was maintained.
Themes were identified from the interviews until data saturation was reached. Data saturation was noted at the 12th interview. The team continued to learn from subsequent interviews, with interviews contributing additional depth to the issues explored. Further interviews were conducted to confirm that no new theme was being identified.
The interviews were then transcribed and de-identified. They were subsequently reviewed by 2 reviewers (Investigator A and Investigator B). Data was analysed using a step-by-step thematic analysis method (Braun & Clarke, 2006). Investigators A and B independently analysed the transcripts, identified themes and later reported the common themes. These themes were discussed for concurrence. When any differences in opinion arose, these would be reviewed by investigator C to resolve any disagreement.
C. Setting
The research was conducted within the Paediatric ED in KK Women’s and Children’s Hospital, a tertiary paediatric hospital.
The Children’s Emergency of KK Women’s and Children’s Hospital is the largest paediatric emergency unit in Singapore. During the time of the interviews, the department treated over 400 patients daily. The Children’s Emergency sees all children under the age of 18 years for all medical complaints.
The department is staffed by over 60 junior doctors at a single time. These junior doctors come from various backgrounds and pass through the department for varying amounts of time. Thus, their experience can be very heterogeneous.
The job scope and responsibilities of all the junior doctors are primarily the same despite the different levels of experience. They are expected to treat the patients that present to the ED. These doctors can seek advice from the senior doctors who are on the ground. However, for the majority of the time, they would be tasked to treat patients on their own.
D. Participants
Participants were recruited through an email that was circulated to all junior doctors in the department. Participation in the study was voluntary and participants were not remunerated.
A total of 16 junior doctors were recruited and interviewed over a 1-month period. Due to the busyness of the ED and the limited time frame in which the interviews were conducted, only 16 interviews were conducted. Convenience sampling was chosen for the sampling method. The first 16 volunteers who had volunteered were interviewed. However, it was noted that saturation point was reached prior to the conclusion of the interview process.
The variety within the ED was well represented. The details of participant breakdown are elaborated on in Table 1.
|
Experience & Training Information |
|
|
|
|
|
Mean post-graduate year, 3.6 (2-6)* |
|
|
|
|
|
|
Emergency Medicine |
Family Medicine |
Paediatric Medicine |
Not in a training program at time of study |
|
Training Program (n=16) |
5 |
2 |
1 |
8 |
|
Epidemiological Data |
|
|
|
|
|
|
Chinese |
|
Indian |
|
|
Race (n=16) |
13 |
|
3 |
|
|
|
Male |
|
Female |
|
|
Gender (n=16) |
6 |
|
10 |
|
Table 1: Characteristics of Participants
*Mean (Range)
E. Analysis
All transcripts were reviewed by JT and SG. Coding was done manually using Microsoft Word. During the process, themes were identified and substantiating quotes were recorded. Iterative data analysis was done so that interviewers were aware of themes that were previously mentioned. However, the themes were not specifically explored unless brought up by the subsequent interviews.
III. RESULTS
Through the interviews, we collected information about the experiences within the ED. Interview transcripts collected as a part of this study are openly available on Figshare at http://doi.org./10.6084/m9.figshare.19204761 (Tan et al., 2022). From the interviews conducted, the experience was divided into the initial perceptions and coping mechanisms.
A. Perceptions
The perceptions of the paediatric emergency rotation in the ED were largely contributed by the experiences of the individuals who had previously worked in the department. This was achieved through consultation with friends or colleagues prior to starting the posting to find out more about the rotation.
“Before I started doing the posting, I asked some people who have done or were currently doing the posting…to find out what I was getting myself into”
(P7)
The broad themes elicited about the perceptions and inherent worries of the incoming medical officers were that of being unprepared due to ‘inadequate knowledge’ or ‘unfamiliarity’, as well as the impending ‘work load’ and ‘work factors’.
1) Fear of subject matter: Participants who were not familiar with the paediatric content were worried about their competency and adequacy in treating children. Oftentimes, participants cited that exposure to the paediatric subject matter may have been inadequate or dated and as a result, resulted in fears of being unprepared or being unsafe.
“I’ve not done any paediatric postings before as a doctor so that was a bit worrying.”
(P4)
“I’ve never dealt with paediatrics before so it was quite scary to come onto the posting”
(P14)
In participants who did however have some background in paediatrics, additional fears of specialised emergency knowledge also emerged with participants feeling nervous about the posting.
“Some of the things included technical skills such as doing back slabs, manipulation and reduction, and I guess managing trauma and more complicated acute conditions such as diabetic ketoacidosis and haemophilia and oncological and metabolic related conditions.”
(P11)
“When I started I learnt about resuscitation cases which I felt was a bit nerve-wracking to start with”
(P12)
2) Unfamiliarity: Even though participants may have been at different time points in their careers during the posting, they were all expected to perform mostly the same duties and responsibilities. As a result, a section of the participants cited worries about adjusting to the roles and environment that they may have been new to. These included concerns about being new to the system used. These added to the worries that participants often had about starting a new posting and made participants even more fearful.
“Coming from the UK, this was my first job in Singapore as a MO and thus had close to 0 experience of working in Singapore”
(P8)
“I was also not very familiar with the system. It added to the fear and unpreparedness before starting the posting.”
(P9)
3) Work factors: As a place with high turnover and workload, the picture painted to many of the participants was that it may be difficult to cope with the high workload. This would result in participants being overloaded and overwhelmed. A level of uncertainty was also described. Many participants were left feeling fearful, apprehensive and unsure of what to expect during the upcoming posting. Some were also worried about the expectations they may have to live up to and the nature of the environment being extremely stressful.
“I just heard that it can be quite busy with many patients and at the beginning, it can feel a bit of a throw into the deep end as we often don’t know what to expect and the learning curve can be quite steep”
(P12)
“I was also a bit apprehensive as I heard how busy the posting could get”
(P10)
“It’s quite a stressful working environment because the seniors have a certain working expectation and if you can’t live up to the expectations.”
(P16)
Practically, participants were also worried about the potential to get sufficient rest. Many participants heard that manpower may be tight and would result in having fewer or insufficient off days and would run the risk of feeling tired and burnt out.
“I heard that it was also difficult to get leave that you want and that you would also be really tired during the posting”
(P13)
B. Coping Mechanisms
We then explored the different ways the participants utilised to cope with their experiences in the ED. Participants used a variety of means that we broadly classified into broad themes of ensuring clinical safety, psychosocial support and spirituality.
1) Clinical safety: Participants were inevitably worried about competency and had inherent fears of patient safety in their practice. Coping strategies in this realm could be divided into preparation, senior supervision and collegial opinion.
Preparation was often seen in speaking to doctors who had previously rotated through the posting to allow junior doctors to prepare themselves mentally.
“I asked around and tried to mentally prepare myself for what people told me to expect”
(P3)
In addition, the perceived knowledge gaps and lack of experience were dealt with by many participants through studying and reading up to cover these gaps as well as to prevent them from feeling out of depth.
“I had actually read the guidelines prior especially for the things that I was not familiar with.”
(P10)
On the ground, participants found the availability and approachability of help and support from senior colleagues helpful in easing the worry and anxiety experienced in the emergency department. This also helped participants feel more safe and secure in their practices in the emergency department.
“I appreciate the nice seniors. Most of the seniors are approachable and they treat us like fellow colleagues. They respect our opinions and try to keep it in mind”
(P10)
“I feel very safe at work and very well supported by the seniors. In general, it is easy to ask for help from most of the seniors.”
(P8)
In addition, many participants also felt that their fellow medical officer colleagues were also important in ensuring safety in their practice. With different levels of experience, they could bounce ideas off each other and get a second opinion from their peers. Furthermore, their colleagues also helped to pick up the workload when they felt overwhelmed.
“Everyone is willing to help out when you get stuck. Help is useful and it is easy to come by”
(P1)
“I feel like I have a good relationship with them (peers) and that helps me and I can also get second opinions from them if I’m unsure.”
(P9)
2) Psychosocial support: In the high-strung environment of the emergency department, there is a lot of stress and emotions that come with the job. We found that many participants shared about the social component involved in unpacking these emotions and relieving their stress. The components of the collegial environment and support from loved ones appeared to be crucial coping mechanisms that helped participants.
The work climate was cited to be collegial and relationships between co-colleagues were described as friendly. Many participants felt comfortable with their co-colleagues such that they could ventilate their emotions and experiences with one another. These helped participants process and debrief their experiences.
“We generally laugh about the situation together and it gets better. Sometimes they give advice based on what they have seen and how to avoid such circumstances and we try and help each other.”
(P7)
“It’s useful amongst colleagues because we go through the same things and we get to exchange ideas and I feel we get to debrief this way as well. That helps because we don’t feel like we go through it alone because we have similar experiences.”
(P8)
Apart from the work environment, supportive loved ones and close friends also helped participants cope with difficult days. Participants cited that out of work encounters helped them to get through tough days and relieve their stress.
“Sometimes I also talk about it with someone. Usually that helps and my stress doesn’t usually last beyond the same day.”
(P6)
“I guess these 3 things, my family, friends and colleagues help me with tough days.”
(P7)
3) Spirituality and wellness: Spirituality and wellbeing were also important in dealing with the experiences and stressors the participants faced. Apart from dealing with the clinical stressors and unpacking the experiences with others, participants also spoke about coming to terms with their experiences and emotions on their own. This involved components of religion and reflexivity. Participants also spoke about the role of maintaining their wellbeing with leisure and self-care activities.
Participants spoke about reflecting and reviewing the good as well as the bad moments at work. These helped the participants make sense of their experiences and as a result, helped them improve and learn.
“I usually pray and reflect on my day and think about what are the good points I can get out of the day.”
(P9)
Religion also featured as a means of coping with emotions in the sometimes chaotic environment seen in the ED. These helped participants work better and feel more focused at work.
“I feel like I’m stable when I pray … and I think more thoughts are more ordered. That helps me.”
(P15)
Focusing on physical wellbeing also helped to reduce the stress experienced. Participants cited different activities – food, sleep, exercise, self-care and hobbies that helped them take their minds off work and help them get rejuvenated before the next working day.
“Eating and relaxing help me after a tough day”
(P4)
“I find exercising is helpful, and it helps me feel fresher and less sleepy”
(P3)
“Listening to music and watching videos and just going about non-work related normal daily life.”
(P11)
“I ensure that I have a good work-life balance… I go for a massage, go for a buffet, watch a movie and enjoy myself.”
(P13)
“I draw, I paint. I learn languages. Sometimes I travel. These things help me relax and cope with stress.”
(P16)
IV. DISCUSSION
We sought to understand the perceptions of junior doctors starting out in the emergency department as well as the subsequent coping strategies they undertook for challenges that they faced. During the process, we interviewed sixteen junior doctors who spoke in detail about their experiences.
The perceptions that the junior doctors in our study described consisted mainly of their worries and concerns prior to the start of the posting. Most of the perceptions and worries were centred on knowledge, workload and responsibilities that came with the posting.
A large proportion of participants expressed worry regarding competency and personal comfort levels in managing children. As the ED is a broad one and knowledge is inexhaustible, the concerns in lack of competency are seen in the other elements of emergency care and not strictly paediatric emergency (Jelinek et al., 2013; Kennelly et al., 2012; Yong & Ng, 2016).
Many of the worries described by the participants were of an anticipatory nature, from hearing their predecessors’ experiences. Anticipation of negative experiences can lead to anxiety and stress in individuals (Carlson et al., 2010; Grupe & Nitschke, 2013). Participants had anxiety about the workload and certain work factors prior to the start of the posting. While predecessors’ recounts are helpful in preparing doctors for their upcoming experience, the anxiety that comes with this preparation may not be. Positive effects can also be seen when a positive picture is painted of the upcoming experience (Gangwal et al., 2014; Luo et al., 2018). As it is difficult to balance the negative anxiety and the positive effects of preparation, it may be helpful for junior doctors to receive a formal handover from existing doctors who themselves have had a positive experience so as to prevent excessive anxiety.
We next explored the coping strategies involved to help the participants through the difficult parts of their experiences.
In areas of safety, participants commented on how the support from the senior staff helped allay their fears and increase patient safety at work. Other studies showed similar themes with HCWs expressing the desire for support, professional help and preventive action in the ED (Mikkola et al., 2019; Povedano-Jimenez et al., 2020; Ruotsalainen et al., 2015). In situations where support was provided, these corresponded to higher levels of satisfaction at work (Hunsaker et al., 2015). This is especially so in HCWs who were exposed to traumatic situations (Zhao et al., 2015).
Social support is an important factor in dealing with stressful situations (Gribben et al., 2019). In our cohort, our participants also engaged in social interactions with family, friends and colleagues in an attempt to deal with stressors in the ED. The collegial environment was also beneficial in dealing with stress and helping participants better process their experiences (Povedano-Jimenez et al., 2020).
Apart from expressing emotions and stressors, participants also sought to ensure mental and physical wellness of oneself. This was done by focusing on their spirituality as well as physical wellness and self-care. These strategies utilised were similar to those seen in other studies (Gribben et al., 2019; Hoonpongsimanont et al., 2013; McPherson et al., 2003; Palmer Kelly et al., 2020; Xu et al., 2019).
Maladaptive coping strategies did not come up as a main theme in our interviews.
A. Limitations
The study was conducted in a single ED at a single time point. Efforts were taken to diversify the population interviewed with participants experiencing different durations within the department. However, interviews of participants who had experienced the ED at different time points could have brought about different views and themes.
The primary investigator was also working within the same department during the time of the study. As the investigator was also a junior doctor during the study, a power dynamic effect was minimised.
The setting was limited to a single centre in the Singapore setting and thus, was extremely specific. Singapore is a city-state with easy access to healthcare. In addition, due to strict legislation, violence is minimal compared to other areas. As such, the patient load and patient type may differ from other ED and may raise the question of applicability in a different setting.
In addition, this study was conducted prior to the COVID-19 pandemic and the findings were representative of the climate at that time. The pandemic has led to multiple changes in workflow and work culture in the paediatric ED, and these may affect the applicability of our findings.
B. Future Research and Practical Implications
The study is the first qualitative in-depth study looking at perceptions and coping strategies in a paediatric emergency setting among junior doctors in a single centre. It is the first study to explore the individual perceptions and coping mechanisms of doctors, with a focus on the subset of junior doctors. The group was relatively small and conducted at a single time point. As such, the study can be expanded to include a larger group of participants across different time points and centres to illustrate a bigger picture.
Many of the participants also talked about the challenges they experienced in the paediatric emergency. They also raised possible improvements that could be made to help with stressors and challenges in the ED. This could be studied further and future research could focus on how we could target these factors and how effective these adjustments can be.
The findings of this research echoed the findings of prior studies. This study also sheds light and gives us more depth in terms of the early perceptions prior to the start of the postings and the coping strategies that were used.
These findings can also help future doctors rotating through the ED picture the experience. This would give doctors an opportunity to decide how best to prepare themselves. It could also help the doctors feel united with their current colleagues and predecessors in their challenges. And that they are not alone in their experiences.
V. CONCLUSION
In this study, the perceptions of junior doctors and coping strategies of junior doctors in an Asian Paediatric ED were studied. We looked at the perceptions and coping strategies utilised. Many factors were established in contributing to the experience. Improvements and suggestions to improve the experience were also brought up. Other HCWs can also understand how to best work with the junior doctors to facilitate an effective and pleasant working environment.
Notes on Contributors
Jaime Tan undertook literature reviews, conducted and analysed interviews and drafted the manuscript. Junaidah Badron reviewed the interviews and drafted and reviewed the manuscript. Sashikumar Ganapathy conceived the idea of the study, reviewed and analysed interview transcripts and advised the manuscript design. All authors have read and approved the final manuscript.
Ethical Approval
This project was submitted to the Centralised Institutional Review Board for approval (CIRB Ref 2019.2772). All participants consented to the research study.
Data Availability
All data collected in this study are openly available on Figshare repository, http://doi.org/10.6084/m9.figshare.19204761
Acknowledgement
We would like to thank all participants for volunteering their time and agreeing to participate in this study.
Funding
No funding was involved in this study.
Declaration of Interest
The authors declare that they have no conflicts of interest.
References
Abraham, L. J., Thom, O., Greenslade, J. H., Wallis, M., Johnston, A. N., Carlström, E., Mills, D., & Crilly, J. (2018). Morale, stress and coping strategies of staff working in the emergency department: A comparison of two different-sized departments. Emergency Medicine Australasia, 30(3), 375-381. https://doi.org/10.1111/1742-6723.12895
Alomari, A. H., Collison, J., Hunt, L., & Wilson, N. J. (2021). Stressors for emergency department nurses: Insights from a cross‐sectional survey. Journal of Clinical Nursing, 30(7-8), 975-985. https://doi.org10.1111/jocn.15641
Barham, D., De Beer, W., & Clark, H. (2019). The role of professional supervision for palliative care doctors in New Zealand: A quantitative survey of attitudes and experiences. The New Zealand Medical Journal, 132(1501), 10–20.
Basu, S., Yap, C., & Mason, S. (2016). Examining the sources of occupational stress in an emergency department. Occupational Medicine, 66(9), 737–742. https://doi.org/10.1093/occmed/kqw155
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101. https://doi.org/10.1191/1478088706qp063oa
Burbeck, R., Coomber, S., Robinson, S. M., & Todd, C. (2002). Occupational stress in consultants in accident and emergency medicine: A national survey of levels of stress at work. Emergency Medicine Journal, 19(3), 234–238. https://doi.org/10.1136/emj.19.3.234
Carlson, J. M., Greenberg, T., Rubin, D., & Mujica-Parodi, L. R. (2010). Feeling anxious: Anticipatory amygdalo-insular response predicts the feeling of anxious anticipation. Social Cognitive and Affective Neuroscience, 6(1), 74–81. https://doi.org/10.1093/scan/nsq017
Chan, C. Y. W., Sum, M. Y., Lim, W. S., Chew, N. W. M., Samarasekera, D. D., & Sim, K. (2016). Adoption and correlates of Postgraduate Hospital Educational Environment Measure (PHEEM) in the evaluation of learning environments – A systematic review. Medical Teacher, 38(12), 1248–1255. https://doi.org/10.1080/0142159x.2016.1210108
Chew, Q. H., Ang, L. P., Tan, L. L., Chan, H. N., Ong, S. H., Cheng, A., Lai, Y. M., Tan, M. Y., Tor, P. C., Gwee, K. P., & Sim, K. (2019). A cross-sectional study of burnout and its associations with learning environment and learner factors among psychiatry residents within a National Psychiatry Residency Programme. BMJ Open, 9(8), e030619. https://doi.org/10.1136/bmjopen-2019-030619
Copeland, D., & Henry, M. (2018). The relationship between workplace violence, perceptions of safety, and professional quality of life among emergency department staff members in a Level 1 Trauma Centre. International Emergency Nursing, 39, 26–32. https://doi.org/10.1016/j.ienj.2018.01.006
Degen, C., Weigl, M., Glaser, J., Li, J., & Angerer, P. (2014). The impact of training and working conditions on junior doctors’ intention to leave clinical practice. BMC Medical Education, 14(1). https://doi.org/10.1186/1472-6920-14-119
Durand, A. C., Bompard, C., Sportiello, J., Michelet, P., & Gentile, S. (2019). Stress and burnout among professionals working in the emergency department in a French university hospital: Prevalence and associated factors. Work, 63(1), 57–67. https://doi.org/10.3233/wor-192908
Ganapathy, S., Lim, S. Y., Kua, J. P., & Ng, K. C. (2015). Non-urgent paediatric emergency department visits: Why are they so common? A Singapore perspective. Annals of the Academy of Medicine, Singapore, 44(7), 269–271. https://doi.org/10.47102/annals-acadmedsg.v44n7p269
Gangwal, R. R., Rameshchandra Badjatia, S., & Harish Dave, B. (2014). Effect of exposure to positive images of dentistry on dental anxiety among 7 to 12 years old children. International Journal of Clinical Pediatric Dentistry, 7(3), 176–179. https://doi.org/10.5005/jp-journals-10005-1260
Greenslade, J. H., Wallis, M., Johnston, A. N. B., Carlström, E., Wilhelms, D. B., & Crilly, J. (2019). Key occupational stressors in the ED: an international comparison. Emergency Medicine Journal, 37(2), 106–111. https://doi.org/10.1136/emermed-2018-208390
Gribben, J. L., Kase, S. M., Waldman, E. D., & Weintraub, A. S. (2019). A cross-sectional analysis of compassion fatigue, burnout, and compassion satisfaction in paediatric critical care physicians in the United States*. Paediatric Critical Care Medicine, 20(3), 213–222. https://doi.org/10.1097/pcc.0000000000001803
Grupe, D. W., & Nitschke, J. B. (2013). Uncertainty and anticipation in anxiety: An integrated neurobiological and psychological perspective. Nature Reviews Neuroscience, 14(7), 488–501. https://doi.org/10.1038/nrn3524
Guise, J. M., Hansen, M., O’Brien, K., Dickinson, C., Meckler, G., Engle, P., Lambert, W., & Jui, J. (2017). Emergency medical services responders’ perceptions of the effect of stress and anxiety on patient safety in the out-of-hospital emergency care of children: A qualitative study. BMJ Open, 7(2), e014057. https://doi.org/10.1136/bmjopen-2016-014057
Healy, S., & Tyrrell, M. (2011). Stress in emergency departments: Experiences of nurses and doctors. Emergency Nurse, 19(4), 31–37. https://doi.org/10.7748/en2011.07.19.4.31.c8611
Hoonpongsimanont, W., Murphy, M., Kim, C. H., Nasir, D., & Compton, S. (2013). Emergency medicine resident well-being: Stress and satisfaction. Occupational Medicine, 64(1), 45–48. https://doi.org/10.1093/occmed/kqt139
Howlett, M., Doody, K., Murray, J., LeBlanc-Duchin, D., Fraser, J., & Atkinson, P. (2015). Burnout in emergency department healthcare professionals is associated with coping style: A cross-sectional survey. Emergency Medicine Journal, 32(9), 722–727. https://doi.org/10.1136/emermed-2014-203750
Hunsaker, S., Chen, H. C., Maughan, D., & Heaston, S. (2015). Factors that influence the development of compassion fatigue, burnout, and compassion satisfaction in emergency department nurses. Journal of Nursing Scholarship, 47(2), 186–194. https://doi.org/10.1111/jnu.12122
Jackson, E. R., Shanafelt, T. D., Hasan, O., Satele, D. V., & Dyrbye, L. N. (2016). Burnout and alcohol abuse/dependence among U.S. medical students. Academic Medicine, 91(9), 1251–1256. https://doi.org/10.1097/acm.0000000000001138
Jelinek, G. A., Weiland, T. J., Mackinlay, C., Gerdtz, M., & Hill, N. (2013). Knowledge and confidence of Australian emergency department clinicians in managing patients with mental health-related presentations: Findings from a national qualitative study. International Journal of Emergency Medicine, 6, Article 2. https://doi.org/10.1186/1865-1380-6-2
Kennelly, S. P., Morley, D., Coughlan, T., Collins, R., Rochford, M., & O’Neill, D. (2012). Knowledge, skills and attitudes of doctors towards assessing cognition in older patients in the emergency department. Postgraduate Medical Journal, 89(1049), 137–141. https://doi.org/10.1136/postgradmedj-2012-131226
Koh, M. Y. H., Chong, P. H., Neo, P. S. H., Ong, Y. J., Yong, W. C., Ong, W. Y., Shen, M. L. J., & Hum, A. Y. M. (2015). Burnout, psychological morbidity and use of coping mechanisms among palliative care practitioners: A multi-centre cross-sectional study. Palliative Medicine, 29(7), 633–642. https://doi.org/10.1177/0269216315575850
Luo, Y., Chen, X., Qi, S., You, X., & Huang, X. (2018). Well-being and anticipation for future positive events: Evidences from an fMRI Study. Frontiers in Psychology, 8. https://doi.org/10.3389/fpsyg.2017.02199
Mason, S., O’Keeffe, C., Carter, A., & Stride, C. (2015). A longitudinal study of well-being, confidence and competence in junior doctors and the impact of emergency medicine placements. Emergency Medicine Journal, 33(2), 91–98. https://doi.org/10.1136/emermed-2014-204514
McPherson, S., Hale, R., Richardson, P., & Obholzer, A. (2003). Stress and coping in accident and emergency senior house officers. Emergency Medicine Journal, 20(3), 230–231. https://doi.org/10.1136/emj.20.3.230
Mikkola, R., Huhtala, H., & Paavilainen, E. (2019). Development of a coping model for work‐related fear among staff working in emergency department in Finland – Study for nursing and medical staff. Scandinavian Journal of Caring Sciences, 33(3), 651–660. https://doi.org/10.1111/scs.12658
Neubauer, B. E., Witkop, C. T., & Varpio, L. (2019). How phenomenology can help us learn from the experiences of others. Perspectives on Medical Education, 8(2), 90–97. https://doi.org/10.1007/s40037-019-0509-2
Oreskovich, M. R., Shanafelt, T., Dyrbye, L. N., Tan, L., Sotile, W., Satele, D., West, C. P., Sloan, J., & Boone, S. (2015). The prevalence of substance use disorders in American physicians. The American Journal on Addictions, 24(1), 30–38. https://doi.org/10.1111/ajad.12173
Palmer Kelly, E., Hyer, M., Payne, N., & Pawlik, T. M. (2020). A mixed-methods approach to understanding the role of religion and spirituality in healthcare provider well-being. Psychology of Religion and Spirituality, 12(4), 487–493. https://doi.org/10.1037/rel0000297
Pek, J. H., Ong, Y. K. G., Quek, E. C. S., Feng, X. Y. J., Allen, J. C., Jr., & Chong, S. L. (2019). Evaluation of the criteria for trauma activation in the paediatric emergency department. Emergency Medicine Journal, 36(9), 529–534. https://doi.org/10.1136/emermed-2018-207857
Povedano-Jimenez, M., Granados-Gamez, G., & Garcia-Caro, M. P. (2020). Work environment factors in coping with patient death among Spanish nurses: A cross-sectional survey. Revista Latino-Americana de Enfermagem, 28. https://doi.org/10.1590/1518-8345.3279.3234
Ruotsalainen, J., Verbeek, J., Mariné, A., & Serra, C. (2015). Preventing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews, 2015(4), CD002892. https://doi.org/10.1002/14651858.cd002892.pub5
Ryali, V. S. R., Sreelatha, P., & Premlal, L. (2018). Burnout and coping strategies among residents of a private medical college in South India: A cross-sectional study. Industrial Psychiatry Journal, 27(2), 213-218. https://doi.org/10.4103/ipj.ipj_53_18
Shanafelt, T. D., Boone, S., Tan, L., Dyrbye, L. N., Sotile, W., Satele, D., West, C. P., Sloan, J., & Oreskovich, M. R. (2012). Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Archives of Internal Medicine, 172(18), 1377-1385. https://doi.org/10.1001/archinternmed.2012.3199
Smith, D. W. (2021). Stanford Encyclopaedia of Philosophy. https://plato.stanford.edu.
Sum, M. Y., Chew, Q. H., & Sim, K. (2019). Perceptions of the learning environment on the relationship between stress and burnout for residents in an ACGME-I accredited national psychiatry residency program. Journal of Graduate Medical Education, 11(4s), 85–90. https://doi.org/10.4300/jgme-d-18-00795
Talih, F., Daher, M., Daou, D., & Ajaltouni, J. (2018). Examining burnout, depression, and attitudes regarding drug use among Lebanese medical students during the 4 years of medical school. Academic Psychiatry, 42(2), 288–296. https://doi.org/10.1007/s40596-017-0879-x
Tan, M. Y., Ng, N. B. H., Aw, M. M., & Lin, J. B. (2022). Perceived stress & sentiments of housemen starting work during the COVID-19 Pandemic in Singapore. The Asia Pacific Scholar, 7(2), 56–60. https://doi.org/10.29060/taps.2022-7-2/sc2686
Tuffour, I. (2017). A critical overview of interpretative phenomenological analysis: A contemporary qualitative research approach. Journal of Healthcare Communications, 2(4). https://doi.org/10.4172/2472-1654.10009
Watson, A. G., Saggar, V., MacDowell, C., & McCoy, J. V. (2019). Self-reported modifying effects of resilience factors on perceptions of workload, patient outcomes, and burnout in physician-attendees of an international emergency medicine conference. Psychology, Health & Medicine, 24(10), 1220–1234. https://doi.org/10.1080/13548506.2019.1619785
Xu, H. G., Johnston, A. N., Greenslade, J. H., Wallis, M., Elder, E., Abraham, L., Thom, O., Carlström, E., & Crilly, J. (2019). Stressors and coping strategies of emergency department nurses and doctors: A cross-sectional study. Australasian Emergency Care, 22(3), 180–186. https://doi.org/10.1016/j.auec.2018.10.005
Yong, A. M. Y., & Ng, J. (2016). Assessing the level of knowledge of emergency department physicians in recognition of common skin lesions. Annals of Clinical and Laboratory Research, 4(1). https://doi.org/10.21767/2386-5180.100073
Zhao, S., Liu, H., Ma, H., Jiao, M., Li, Y., Hao, Y., Sun, Y., Gao, L., Hong, S., Kang, Z., Wu, Q., & Qiao, H. (2015). Coping with Workplace Violence in Healthcare Settings: Social Support and Strategies. International Journal of Environmental Research and Public Health, 12(11), 14429–14444. https://doi.org/10.3390/ijerph121114429
*Jaime Maria Tan
KK Women’s and Children’s Hospital,
100 Bukit Timah Road,
Singapore 229899
+6590303124
Email: jaime.tan@mohh.com.sg
Submitted: 19 May 2022
Accepted: 21 September 2022
Published online: 3 January, TAPS 2023, 8(1), 3-12
https://doi.org/10.29060/TAPS.2023-8-1/OA2817
Junji Haruta1,2, Ayumi Takayashiki2, Ryohei Goto2, Takami Maeno2, Sachiko Ozone2 & Tetsuhiro Maeno2
1Medical Education Center, School of Medicine, Keio University, Japan; 2Department of Primary Care and Medical Education, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan
Abstract
Introduction: The pandemic caused by the novel coronavirus (COVID-19) has produced dramatic changes in the learning environment for clinical practice in medical education, and the impact on medical students has been significant. However, few program evaluation studies involving professional identity, now emphasised in medical education, have compared current with pre-COVID-19 programs. Here, we compared the professional identity recognised by medical students in the years before and during COVID-19.
Methods: Medical students who participated in clinical practice were evaluated using the Japanese version of the Professional Self-Identity Questionnaire (PSIQ), a 9-item inventory rated using 7-point Likert scales. They answered on the first day of a 4-week clinical practice module within a community-based medical education (CBME) program and at graduation in 2018-2019 (pre-COVID-19 pandemic) and in 2019-2020 (during-COVID-19 pandemic). We compared the mean difference in total PSIQ score of the 2019-2020 students to those of the 2018-2019 students as a historical cohort using an unpaired t-test.
Results: Participants were 104 medical students in the 2018-2019 academic year and 92 in the 2019-2020 academic year. PSIQ was increased at graduation. Mean difference in total PSIQ score was statistically higher for the 2019-2020 students (13.5 ± 9.4) than for the 2018-2019 students (10.3 ± 8.1) (t =2.6, df =195, p = 0.01).
Conclusion: Although clinical practice was restricted by COVID-19, this had some positive impact on the strengthening of professional identity recognised by medical students. This finding may have been influenced by the imprinting of professional norms and changes in society.
Keywords: Novel Coronavirus Infection, Professional Identity, Clinical Practice, Questionnaire Survey, Program Evaluation
Practice Highlights
- Professional identity recognised by medical students in Japan was assessed by questionnaire.
- Changes during clinical practice were compared between two grades using a historical cohort.
- Medical students’ recognised professional identity scores improved after one year in both cohorts.
- Medical students experienced the COVID-19 pandemic showed some positive impact on professional identity.
- Medical students internalised their role as healthcare professionals owing to COVID-19 pandemic.
I. INTRODUCTION
The pandemic caused by the novel coronavirus (COVID-19) has caused unprecedented disruption to medical education systems around the world (Kaul et al., 2021; Khasawneh et al., 2020; Lucey & Johnston, 2020; Papapanou et al., 2021). In particular, the pandemic has made it difficult to continue medical educational programs, including regular lectures, and face-to-face lectures, experiments, and clinical practice involving patients (Al Samaraee, 2020; Emanuel, 2020; Shankar & Wilson, 2020). The Association of American Medical Colleges took the unprecedented decision to suspend clinical practice and issued guidance instructing medical students to avoid clinical practice involving direct patient contact (Association of American Medical Colleges, 2020). The many university hospitals in the U.S. have made it a priority to utilise students in controlling the spread of COVID-19 infection. Other countries followed this precedent. Medical students accordingly lost the opportunity to learn through patients in clinical practice. In Japan also, clinical practice was suspended at many universities.
Commonly implemented alternative teaching methods were online interactive discussions and video lectures (Chiodini, 2020; Mian & Khan, 2020). To prevent the spread of COVID-19 from medical students in clinical practice (Alsoghair et al., 2021), students were required to socially distance not only from patients but also from healthcare providers and faculty members. However, implementing the requisite changes to curricula, such as interrupting or drastically postponing clinical practice, was difficult, forcing faculties to develop curricula that provided students with opportunities to supplement their ongoing clinical practice as early as possible, while making use of online devices (Ross, 2020). These changes in the learning environment affected medical students’ learning. For example, a survey of 2nd-6th grade students at the University of Geneva found that 2/3 of the medical students experienced decreased motivation and concentration in distracting learning environments such as home, whereas some medical students who were exposed to clinical practice during the COVID-19 pandemic showed an increased sense of belonging to the profession (Wurth et al., 2022). A change in perception with remote learning in response to the COVID-19 pandemic among Canadian undergraduate students also revealed a significant decrease in students’ achievement goals, engagement, and perceptions of success, and an increase in perceptions of cheating (Daniels et al., 2021). Perceptions of learning due to changes in the curriculum due to COVID-19 have been investigated and controversially reported, but few reports have investigated professional identity as a foundation for becoming a physician.
To be effective clinicians, it is important that medical students acquire not only knowledge and skills but also professional identity formation (Cruess et al., 2014; Hafferty & Franks, 1994). Professional identity is defined as “attitudes, values, knowledge, beliefs, and skills shared with others in a professional group” (Crossley & Vivekananda-Schmidt, 2009). Professional identity formation is noted as an ongoing process influenced by several factors, including practice experience and professional socialisation (Adams et al., 2006). In this study, we adopted a theoretical framework which is based on a concept that illustrates the interplay of professional identity formation and socialisation through a complex conscious and unconscious process centered on role models, mentors, and the accumulation of individual experiences (Cruess et al., 2015). Because clinical practice is a period in which medical students meet role models and mentors and gain their first experiences as a healthcare provider, clinical practice is major contributor to the development of professional identity in medical students (Haruta et al., 2020).
Although studies have reported that medical education programs altered by the COVID-19 pandemic have affected medical students’ perceptions of the role of the physician and their learning strategies (Findyartini et al., 2020; Wurth et al., 2022), little is known about the influence of curricula changes on medical students with regard to their professional identity formation as physicians affected by role models, mentors, and individual experience (Stetson et al., 2020).
Here, we aimed to compare professional identity as a physician as perceived by medical students in clinical practice before and during COVID-19 using the Professional Self Identity Questionnaire (PSIQ).
II. METHODS
A. Setting
Japan first faced the challenge of the COVID-19 pandemic in January 2020, and a state of emergency was declared for all regions of Japan on April 16, 2020 (Prime Minister’s Office of Japan, 2020). During that time, some medical universities suspended clinical training and implemented online education instead. The COVID-19 Outline of Measures for COVID-19 formulated by the Japanese Ministry of Education, Culture, Sports, Science and Technology was sent to all higher education institutions, including medical schools, on June 5, 2020 (Hayashi et al., 2022), with the main advice that universities should operate in a resilient manner for experiential educational practices such as clinical practice. Under these circumstances, leaders of Japanese medical schools were asked to consult various stakeholders and make decisions on whether or not to continue clinical practice, often leaving detailed instructions to local operations managers in each field (Hayashi et al., 2022). In contrast, primary care physicians were forced to adapt to local conditions (Haruta et al., 2021).
Students enter medical school in Japan after graduating from high school, and the curriculum is six years long. Clinical training usually takes place in the fourth to sixth years. This schedule is also implemented at the University of Tsukuba in Japan: clinical training is divided into a first half from October of the fourth year to September of the fifth year and a second half from October of the fifth year to June of the sixth year, for a total of 78 weeks. After clinical training, medical students spend time studying for graduation and national exams, in addition to attending lectures.
The first phase of this clinical practice consists of a four-week rotation in basic departments such as internal medicine, surgery, obstetrics and gynecology, pediatrics, and emergency medicine, mainly at affiliated hospitals. The second phase incorporates some elective subjects and includes 4 weeks’ mandatory clinical practice in a CBME curriculum and a further 4 weeks’ clinical practice in a department of interest. Typically, 15 to 17 students rotate every 4 weeks through clinical practice in the CBME curriculum. This clinical training was conducted before the pandemic, but was discontinued in response to it at the end of March 2020. In March, medical students continued clinical training while all elementary and junior high schools were closed. All clinical training was then cancelled in April 2020 and replaced with report assignments only. These were replaced in May and June with online training and on-demand assignments. Sixth-year students in the class of 2020, and subsequently also in 2021 and 2022, were required to adhere to health observation recording and infection prevention behaviors in accordance with the University of Tsukuba Hospital staff behavior guidelines, which had not been previously followed. Similarly, they were also restricted from participating in training hospital tours and extracurricular activities, which were usually a part of their training.
B. Study Design
Training in clinical practice at the University of Tsukuba consists of a first phase for 4th and 5th year students and a second phase for 5th and 6th year students. CBME is included in the latter phase. Data from 5th-year medical students who participated in clinical practice in a 4-week community-based medical education (CBME) program from October 2019 to March 2020 and who graduated in March 2021 were compared to those of the previous year’s students (2018-2019) as a historical cohort. This cohort included 6th-year medical students who graduated in March 2020 and who had participated in a similar clinical practice program the previous year, from October 2018 to May 2019. As in the 2018-2019 academic year, a questionnaire was administered using the PSIQ in the 2019-2020 academic year. The PSIQ, conducted as part of program evaluation of the CBME program, was administered on the first day of the 4-week clinical practice of the program and at graduation. Study participants included 118 fifth- and sixth-year medical students who participated in clinical practice in the CBME program from October 2018 to May 2019 (pre-COVID-19 pandemic) and 100 fifth- and sixth-year medical students who participated from October 2019 to March 2020 (during-COVID-19 pandemic). The 35 participants from April-May 2020, when the 4-week clinical practice in the CBME program was switched to online practice due to COVID-19, were excluded because they could not be pre-evaluated.
C. Instrument: Japanese Version of the Professional Self Identity Questionnaire (PSIQ)
The Professional Self-Identity Questionnaire (PSIQ) is a 9-item inventory which is rated using 7-point Likert scales (Crossley & Vivekananda-Schmidt, 2009). This instrument measures the sense of students in identifying their current position on a continuum between ‘first-day student’ and ‘qualified doctor’ when engaged in each of nine domains of professional activity. These nine domains include “Teamwork,” “Communication,” “Conducting assessment,” “Cultural awareness,” “Ethical awareness,” “Using records,” “Dealing with emergencies,” “Reflection,” and “Teaching”. Each item is rated on a 7-point Likert scale. For this research, we set 1 point as “equivalent to the first day of clinical practice” and 7 points as “equivalent to the first day of initial residency”. The PSIQ is an assessment sheet form originally designed in English. The original study was validated in a sample of 496 medical students across multiple phases of education, and the overall internal reliability (Cronbach’s alpha) was reported to be 0.93 (Crossley & Vivekananda-Schmidt, 2009). Previously, we developed a Japanese version of the PSIQ and operationally defined PSIQ scores as professional identity as a physician as perceived by medical students. Cronbach’s alpha of the Japanese PSIQ was reported to be 0.93 (Haruta et al., 2021), which allows students to measure changes in their own professional identity by tracking each of the nine professional activities over time. We set the total score on this scale as the main outcome of this study. The study showed that this was a reliable and valid tool for program evaluation during clinical practice (Haruta et al., 2021).
D. Participants and Data Collection
In 2018-2019 (pre-COVID-19 pandemic) and 2019-2020 (during-COVID-19 pandemic), we assessed the professional identity of medical students from October of their fifth year to May of the sixth year using PSIQ. The survey was administered on the first day of clinical practice in the CBME program as PSIQ 1 (September 2018 to May 2019 and September 2019 to March 2020) and at graduation as PSIQ 2 (2020 January, and January 2021) (Figure 1).
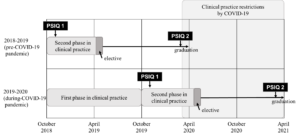
Figure 1. Timing in clinical practice and the PSIQ in 2018-2019 and 2019-2020
On the first day of clinical practice in the CBME program, the authors (JH, TaM, AT) explained the purpose of the study to the students. The authors informed the students that the study would be undertaken as a program evaluation and research, and that their grades would not be influenced in case they did not agree to participate. Those students who agreed to participate signed a consent form giving permission to use their data. Subsequently, the authors asked medical students to fill out the PSIQ as a paper-based, self-administered questionnaire, and to include their student ID number. At graduation, all medical students completed the PSIQ on the internet or on paper as a self-administered questionnaire, again with their student ID number. The study was approved by the Ethics Committee of the University of Tsukuba (No. 1329).
E. Data Analysis
To evaluate the differences in total PSIQ and scores for each item between the first day of clinical practice in the CBME program and the time of graduation, effect sizes (Cohen’s d) were determined for the total PSIQ and scores for each item. In addition, the Shapiro-Wilk test was performed to determine data distribution. For comparison of means for the difference in total PSIQ between 2018-2019 and 2019-2020, an unpaired t-test was applied. The Shapiro-Wilk test confirmed that data distribution for both PSIQ 1 and 2 were not normal. However, since the distribution of PSIQ 2-1 was consistent with normality, a t-test was employed. Missing values were excluded. Data analysis was conducted using SPSS ver. 26 with significance set at the p<0.05 level for total scores as the primary outcome of the PSIQ. Additionally, to deal with the possibility of multiplicity in the simultaneous assessment of each item score, significance levels were Bonferroni corrected, with p< 0.005 (Lee & Lee, 2018).
III. RESULTS
As shown in Table 1, participants analysed in the 2018-2019 academic year (pre-COVID-19 pandemic) included 104 medical students (response rate: 88.1%) who responded at both time points (first day of clinical practice in the CBME program and at graduation), 33 of whom were female. In the 2019-2020 academic year (during-COVID-19 pandemic), 92 medical students (response rate: 92.0%) who responded at both time points were included, 33 of whom were female. One student who did not give consent to have their data used in this study was excluded.
|
2018-2019 (pre-COVID-19 pandemic) |
2019-2020 (during-COVID-19 pandemic) (n=92) |
|
|
Age, mean ± standard deviation |
20.6±1.5 |
21.2±3.4 |
|
Gender, number of persons (%) |
||
|
Male |
66 (63.5) |
51 (55.4) |
|
Female |
33 (31.7) |
33 (35.9) |
|
Unknown |
5 (4.8) |
8 (8.7) |
Table 1. Characteristics of medical students included in the analysis
Table 2 shows that the means of total PSIQ scores and each PSIQ item for 2018-2019 and 2019-2020 were increased at graduation. A comparison of the mean for the difference using the unpaired t-test in total PSIQ score for 2018-2019 and 2019-2020 revealed that it was statistically higher for the 2019-2020 students (13.5 ± 9.4) than for the 2018-2019 students (10.3 ± 8.1) (t =2.6, df =195, p = 0.01). However, there were no statistically significant differences using the unpaired t-test with Bonferronni correction at a 0.005 level of significance in mean scores for 9 items of the PSIQ, namely “Teamwork” (t=0.96 df=195, p=0.341), “Communication” (t=1.84, df=195, p=0.068), “Conducting assessment” (t=2.31, df=195, p=0.24) “Cultural awareness” (t=1.41, df=195, p=0.022), “Ethical awareness” (t=2.25, df=195, p=0.161), “Using records” (t=2.67, df=195, p=0.026), “Dealing with emergencies” (t=2.33, df=195, p=0.008), “Reflection” (t=2.32, df=195, p=0.021) and “Teaching” (t=2.19, df=195, p=0.030). The effect size (Cohen’s d) for total PSIQ scores from the first day of clinical practice in the CBME program to graduation was Δ1.3 in 2018-2019 and Δ1.4 in 2019-2020. The effect size (Cohen’s d) for each item of the PSIQ was Δ1.4 in 2018-2019. Range for items was Δ0.8-1.1 in 2018-2019 and Δ0.9-1.2 in 2019-2020.
|
|
Fiscal year (usually April 1 to March 31) |
First day of the CBME program (1) |
At graduation (2) |
Mean difference in PSIQ (2)-(1) |
t score |
Df |
p-value |
Cohen’s d |
|
Total score (Main outcome) |
2018-2019 (pre-COVID-19 pandemic) |
28.5±7.6 |
38.8±8.5 |
10.3±8.1 |
2.60 |
195 |
0.01 |
1.3 |
|
2019-2020 (during-COVID-19 pandemic) |
28.0±6.6 |
41.6±9.2 |
13.5±9.4 |
1.4 |
||||
|
Sub-analysis |
|
|
||||||
|
Teamwork |
2018-2019 |
3.0±1.2 |
4.4±1.0 |
1.4±1.2 |
0.96 |
195 |
0.341 |
1.1 |
|
2019-2020 |
3.0±1.1 |
4.6±1.1 |
1.6±1.3 |
1.2 |
||||
|
Communication |
2018-2019 |
3.7±1.1 |
4.7±1.1 |
1.0±1.2 |
1.84 |
195 |
0.068 |
0.8 |
|
2019-2020 |
3.5±1.1 |
4.9±1.1 |
1.4±1.3 |
1 |
||||
|
Conducting assessment |
2018-2019 |
3.2±1.0 |
4.4±1.1 |
1.2±1.2 |
2.27 |
195 |
0.024 |
1 |
|
2019-2020 |
3.1±1.0 |
4.7±1.1 |
1.6±1.3 |
1.2 |
||||
|
Cultural awareness |
2018-2019 |
2.9±1.1 |
4.2±1.3 |
1.3±1.3 |
2.31 |
195 |
0.022 |
1 |
|
2019-2020 |
2.8±1.1 |
4.5±1.3 |
1.8±1.5 |
1.2 |
||||
|
Ethics awareness |
2018-2019 |
3.4±1.2 |
4.5±1.1 |
1.1±1.3 |
1.41 |
195 |
0.161 |
0.9 |
|
2019-2020 |
3.5±1.2 |
4.9±1.1 |
1.4±1.4 |
1 |
||||
|
Using record entries |
2018-2019 |
3.4±1.0 |
4.5±1.1 |
1.0±1.1 |
2.25 |
195 |
0.026 |
0.9 |
|
2019-2020 |
3.4±0.9 |
4.8±1.1 |
1.4±1.3 |
1.1 |
||||
|
Dealing with emergencies |
2018-2019 |
2.5±1.1 |
3.8±1.3 |
1.3±1.2 |
2.67 |
195 |
0.008 |
1.1 |
|
2019-2020 |
2.3±1.2 |
4.1±1.4 |
1.9±1.7 |
1.1 |
||||
|
Reflection |
2018-2019 |
3.3±1.1 |
4.3±1.1 |
1.0±1.3 |
2.32 |
195 |
0.021 |
0.8 |
|
2019-2020 |
3.2±0.9 |
4.6±1.3 |
1.4±1.5 |
1 |
||||
|
Teaching |
2018-2019 |
3.1±0.9 |
4.1±1.1 |
0.9±1.1 |
2.19 |
195 |
0. 030 |
0.8 |
|
2019-2020 |
3.2±1.0 |
4.5±1.2 |
1.3±1.4 |
1 |
Table 2. Unpaired t-test analysis and effect sizes for the Professional Identity Self-Assessment Form
IV. DISCUSSION
We found that the means of total and each PSIQ score of medical students who graduated during the COVID-19 pandemic were statistically increased compared to those of students graduating before the pre-COVID-19 pandemic. These findings indicate that, compared with students in the preceding year, the COVID-19 pandemic had a certain positive impact on professional identity formation in medical students with regard to clinical practice.
Considering the framework we used, in which the interaction and reflection of role models, mentors, and individual experiences are key, we believe that all participants were influenced by COVID-19. In addition, professional identity formation is reported to be strongly influenced by environment, context, and other personal variables. (Jarvis-Selinger et al., 2012) The increase in total PSIQ score from the previous year’s medical students may have been due not only to changes in clinical practice, but also to changes in what is expected of medical students by the university hospital and society. In light of these factors, medical students had fewer opportunities to acquire the knowledge and skills required of physicians in the clinical setting directly from role models and mentors, but may nevertheless have been affected by compliance with COVID-19 control measures conducted by the university hospital, and thereby followed the norms of medical professionals communicated through intentional and unintentional messaging. In addition, with the all-engrossing impact of the COVID-19 pandemic throughout society, we speculate that at least some of the students in the COVID-19 group were consulted by family and social contacts as experts and authorities on a daily or more frequent basis, and that such constant reinforcement might also have encouraged PIF. That is, medical students under the COVID-19 pandemic may have internalised the values and norms of the medical professional (Kinnear et al., 2021). Since professional identity formation involves social and relational factors, it is possible that the students’ life and social changes due to COVID-19 reinforced their recognised professional identity (Goldie, 2012).
The more uncertain and ambiguous the period, the more important reflection becomes in PIF. To cope with such uncertainties as the transition from the classroom curriculum to online platforms, rapid changes in the clinical practice environment, and the isolation caused by social distancing, medical students need a well-formed professional identity and socialisation practices (Costello, 2005). Poor PIF is reported to manifest in burnout (Abedini et al., 2018), and depression and anxiety disorders have increased in COVID-19 (Daniels et al., 2021). Since a core component of PIF is the acceptance of uncertainty and ambiguity, medical educators may have provided reflection opportunities for medical students to consciously consider the social factors manifested in COVID-19, such as individual and professional duties, resource priorities, and health disparities, all of which have a positive impact on PIF and socialisation (Stetson et al., 2020). Alternatively, emotion-focused coping strategies (e.g., arts engagement) and problem-solving strategies (e.g., volunteering) to reduce medical students’ anxiety, fear, and stress may be effective (Moula et al., 2022). Students require time and space to reflect on their emergent identity as professionals in these crisis situations (Moula et al., 2022). The extended time for independent learning may have allowed the students to subconsciously reflect on their professional identity, taking seriously the changes in society caused by COVID-19. PIF scores may have accordingly increased in this study.
In general, medical teachers should have made efforts to promote medical students’ professional identity formation even during the COVID-19 pandemic (Goldhamer et al., 2020). Professional identity formation is not a process that should be left to chance; it should be explicitly supported through systematic support and curriculum initiatives (Cruess et al., 2015; Schumacher et al., 2012). In reality, it is necessary to require rapid changes in clinical practice to prevent infection caused by COVID-19, and it has been difficult to promote systematic support for professional identity formation for medical students. However, COVID-19 might not have negatively affected the professional identity recognised by medical students who were in clinical practice immediately after the pandemic. The efforts of Japanese medical educators to implement online and other types of learning to replace clinical practice, and the well-considered efforts of faculty to make clinical practice as feasible as possible may have served as role models or mentors, and influenced medical students’ professional identity formation.
This study has three limitations. First, because there was a difference of 8-17 months between the first day of clinical practice in the CBME program and graduation, given that more clinical practice experience may strengthen the professional identity recognised by medical students, it is possible that differences in clinical practice experience may have affected PSIQ scores. Second, extrapolation from this study should be done with care, since it is a comparison of a one-year questionnaire survey at a single university. Third, a degree of response bias may be present due to the self-reporting design, with inclusion of student ID number. Fourth, evaluation at three or more points may allow a more precise comparison of changes, given that professional identity formation is a dynamic process. Even allowing for these limitations, our findings provide meaningful feedback to medical students and faculty, particularly given the paucity of studies evaluating and comparing changes in professional identity formation – which consists of multiple factors – before and during the COVID-19 pandemic. For the future of medical education, it is imperative to track the professional identity recognised by physicians whose student experience in clinical practice was restricted under the COVID-19 pandemic, and was accordingly significantly changed compared with other years.
V. CONCLUSION
Comparison of the professional identity recognised by medical students whose experience of clinical practice was affected by the COVID-19 pandemic to that of students in the previous year showed some positive impact on professional identity. This lack of negative difference in recognised professional identity even under restricted clinical practice may have been influenced by the imprinting of professional norms and changes in society.
Notes on Contributors
JH, AT, SO, TaM and TeM were involved in the conception and design of this study. JH, AT, and TaM collected the data. JH and RG conducted data analysis. JH mainly wrote the paper. AT, SO, TaM and TeM gave critical feedback on the manuscript. All authors have read and approved the final manuscript.
Ethical Approval
This study was approved by the Ethics Committee of the University of Tsukuba’s Faculty of Medicine and Medical Sciences (No. 1329). All participants have given written consent for their data to be used in the research and for publication.
Data Availability
It is not possible to share data since we did not obtain consent from participants to share all data collected.
Acknowledgement
We thank the faculty staff members Shoji Yokoya, Hisashi Yoshimoto, Shogen Suzuki, Naoto Sakamoto, Yu Yamamoto, Yoshihiro Kataoka, Shoichi Masumoto, Haruka Kuno, Takashi Inaba, Shuhei Hamada, Shogo Kawada, and Sayaka Nin of the Department of Primary Care and Medical Education, Faculty of Medicine, University of Tsukuba. Additionally, we thank the healthcare staff who taught the medical students at the CBME program sites in clinical practice.
Funding
This study was funded by the education/research fund of Department of Primary Care and Medical Education, Faculty of Medicine, University of Tsukuba.
Declaration of Interest
There are no companies or other entities with which the authors have conflict of interest relationships that should be disclosed in relation to the content of the paper.
References
Abedini, N. C., Stack, S. W., Goodman, J. L., & Steinberg, K. P. (2018). “It’s not just time off”: A framework for understanding factors promoting recovery from burnout among internal medicine residents. Journal of Graduate Medical Education, 10(1), 26–32. https://doi.org/10.4300/JGME-D-17-00440.1
Adams, K., Hean, S., Sturgis, P., & Clark, J. M. (2006). Investigating the factors influencing professional identity of first-year health and social care students. Learning in Health and Social Care, 5(2), 55–68. https://doi.org/10.1111/j.1473-6861.2006.00119.x
Al Samaraee, A. (2020). The impact of the COVID-19 pandemic on medical education. British Journal of Hospital Medicine, 81(7), 1-4. https://doi.org/10.12968/HMED.2020.0191
Alsoghair, M., Almazyad, M., Alburaykan, T., Alsultan, A., Alnughaymishi, A., Almazyad, S., Alharbi, M., Alkassas, W., Almadud, A., & Alsuhaibani, M. (2021). Medical Students and COVID-19: Knowledge, preventive behaviors, and risk perception. International Journal of Environmental Research and Public Health, 18(2), 842. https://doi.org/10.3390/ijerph18020842
Association of American Medical Colleges. (2020). Guidance on medical students’ participation in direct in-person patient contact activities. https://www.aamc.org/system/files/2020-08/meded-August-14-Guidance-on-Medical-Students-on-Clinical-Rotations.pdf
Chiodini, J. (2020). Online learning in the time of COVID-19. Travel Medicine and Infectious Disease, 34, Article 101669. https://doi.org/10.1016/j.tmaid.2020.101669
Costello, C. Y. (2005). Professional identity crisis: Race, class, gender, and success at professional schools. Vanderbilt University Press.
Crossley, J., & Vivekananda-Schmidt, P. (2009). The development and evaluation of a professional self identity questionnaire to measure evolving professional self-identity in health and social care students. Medical Teacher, 3(12), e603–e607. https://doi.org/10.3109/01421590903193547
Cruess, R. L., Cruess, S. R., Boudreau, J. D., Snell, L., & Steinert, Y. (2014). Reframing medical education to support professional identity formation. Academic Medicine, 89(11), 1446–1451. https://doi.org/10.1097/ACM.0000000000000427
Cruess, R. L., Cruess, S. R., Boudreau, J. D., Snell, L., & Steinert, Y. (2015). A schematic representation of the professional identity formation and socialization of medical students and residents: A guide for medical educators. Academic Medicine, 90(6), 718–725. https://doi.org/10.1097/ACM.0000000000000700
Emanuel, E. J. (2020). The inevitable reimagining of medical education. JAMA, 323(12), 1127–1128. https://doi.org/10.1001/jama.2020.1227
Findyartini, A., Anggraeni, D., Mikhael Husin, J., & Greviana, N. (2020). Exploring medical students’ professional identity formation through written reflections during the COVID-19 pandemic. Journal of Public Health Research, 9(s1), 1918. https://doi.org/10.4081/jphr.2020.1918
Goldhamer, M. E. J., Pusic, M. V., Co, J. P. T., & Weinstein, D. F. (2020). Can covid catalyze an educational transformation? Competency-based advancement in a crisis. New England Journal of Medicine, 383(11), 1003–1005. https://doi.org/10.1056/NEJMP2018570
Goldie, J. (2012). The formation of professional identity in medical students: Considerations for educators. Medical Teacher, 34(9), e641–e648. https://doi.org/10.3109/0142159X.2012.687476
Hafferty, F. W., & Franks, R. (1994). The hidden curriculum, ethics teaching, and the structure of medical education. Academic Medicine, 69(11), 861–871. https://doi.org/10.1097/00001888-199411000-00001
Haruta, J., Maeno, T., Takayashiki, A., Goto, R., Ozone, S., & Maeno, T. (2021). Validation of the professional self-identity questionnaire for medical students during clinical practice in Japan. International Journal of Medical Education, 12, 160–165. https://doi.org/10.5116/ijme.610d.104b
Haruta, J., Ozone, S., & Hamano, J. (2020). Doctors’ professional identity and socialisation from medical students to staff doctors in Japan: Narrative analysis in qualitative research from a family physician perspective. BMJ Open, 10(7), e035300. https://doi.org/10.1136/bmjopen-2019-035300
Hayashi, M., Saiki, T., Kanter, S. L., & Ho, M. J. (2022). Leaders’ perspectives and actions to manage challenges in medical education presented by the COVID-19 pandemic: A nationwide survey of Japanese medical colleges. BMC Medical Education, 22(1), 144. https://doi.org/10.1186/s12909-022-03193-1
Jarvis-Selinger, S., Pratt, D. D., & Regehr, G. (2012). Competency is not enough: Integrating identity formation into the medical education discourse. Academic Medicine, 87(9), 1185–1190. https://doi.org/10.1097/ACM.0b013e3182604968
Kaul, V., Gallo de Moraes, A., Khateeb, D., Greenstein, Y., Winter, G., Chae, J. M., Stewart, N. H., Qadir, N., & Dangayach, N. S. (2021). Medical education during the COVID-19 pandemic. CHEST, 159(5), 1949–1960. https://doi.org/10.1016/j.chest.2020.12.026
Khasawneh, A. I., Humeidan, A. A., Alsulaiman, J. W., Bloukh, S., Ramadan, M., Al-Shatanawi, T. N., Awad, H. H., Hijazi, W. Y., Al-Kammash, K. R., Obeidat, N., Saleh, T., & Kheirallah, K. A. (2020). Medical students and COVID-19: Knowledge, attitudes, and precautionary measures. A descriptive study from Jordan. Frontiers in Public Health, 8, 253. https://doi.org/10.3389/fpubh.2020.00253
Kinnear, B., Zhou, C., Kinnear, B., Carraccio, C., & Schumacher, D. J. (2021). Professional identity formation during the COVID-19 pandemic. Journal of Hospital Medicine, 16(1), 44–46. https://doi.org/10.12788/jhm.3540
Lee, S., & Lee, D. K. (2018). What is the proper way to apply the multiple comparison test? Korean Journal of Anesthesiology, 71(5), 353-360. https://doi.org/10.4097/KJA.D.18.00242
Lucey, C. R., & Johnston, S. C. (2020). The transformational effects of COVID-19 on medical education. JAMA, 324(11), 1033–1034. https://doi.org/10.1001/jama.2020.14136
Mian, A., & Khan, S. (2020). Medical education during pandemics: A UK perspective. BMC Medicine, 18(1), 100. https://doi.org/10.1186/s12916-020-01577-y
Moula, Z., Horsburgh, J., Scott, K., Rozier-Hope, T., & Kumar, S. (2022). The impact of COVID-19 on professional identity formation: An international qualitative study of medical students’ reflective entries in a global creative competition. BMC Medical Education, 22(1), 545. https://doi.org/10.1186/s12909-022-03595-1
Papapanou, M., Routsi, E., Tsamakis, K., Fotis, L., Marinos, G., Lidoriki, I., Karamanou, M., Papaioannou, T. G., Tsiptsios, D., Smyrnis, N., Rizos, E., & Schizas, D. (2021). Medical education challenges and innovations during COVID-19 pandemic. Postgraduate Medical Journal, 98, 321-327. https://doi.org/10.1136/postgradmedj-2021-140032
Prime Minister’s Office of Japan. (2020). [COVID-19] Declaration of a state of emergency in response to the Novel Coronavirus Disease. https://japan.kantei.go.jp/ongoingtopics/_00020.html
Ross, D. A., & the members of National Neuroscience Curriculum Initiative “Quarantine Curriculum” Committee (2020). Creating a “Quarantine Curriculum” to enhance teaching and learning during the COVID-19 pandemic. Academic Medicine, 95(8), 1125–1126. https://doi.org/10.1097/ACM.0000000000003424
Schumacher, D. J., Slovin, S. R., Riebschleger, M. P., Englander, R., Hicks, P. J., & Carraccio, C. (2012). Perspective: Beyond counting hours: The importance of supervision, professionalism, transitions of care, and workload in residency training. Academic Medicine, 87(7), 883–888. https://doi.org/10.1097/ACM.0b013e318257d57d
Shankar, P. R., & Wilson, I. G. (2020). The COVID-19 pandemic and undergraduate medical student teaching-learning and assessment. Canadian Medical Education Journal, 12(1), e190–e191. https://doi.org/10.36834/cmej.70800
Stetson, G. V., Kryzhanovskaya, I. V., Lomen-Hoerth, C., & Hauer, K. E. (2020). Professional identity formation in disorienting times. Medical Education, 54(8), 765–766. http://doi.org/10.1111/medu.14202
Wurth, S., Sader, J., Cerutti, B., Broers, B., Nadia Bajwa, M., Carballo, S., Escher, M., Galetto-Lacour, A., Grosgurin, O., Lavallard, V., Savoldelli, G., Serratrice, J., Nendaz, M., & Audétat-Voiro, M. C. (2022). Correction to: Medical students’ perceptions and coping strategies during the first wave of the COVID-19 pandemic: Studies, clinical implication, and professional identity. BMC Medical Education, 22(1), Article 232. https://doi.org/10.1186/s12909-022-03307-9
*Junji Haruta
35 Shinanomachi Shinjukuku Tokyo
160-8582, Japan
Email: junharujp@keio.jp
Submitted: 12 May 2022
Accepted: 3 August 2022
Published online: 3 January, TAPS 2023, 8(1), 13-24
https://doi.org/10.29060/TAPS.2023-8-1/OA2810
Audrey Lim1, Vicki Xafis2 & Clare Delany3
1Health and Social Sciences Cluster, Singapore Institute of Technology (SIT), Singapore; 2Graduate School of Humanities and Social Sciences, University of Melbourne, Melbourne, Australia; 3Department of Medical Education, School of Medicine, University of Melbourne, Melbourne, Australia
Abstract
Introduction: Workplace contexts, including political and sociocultural systems influence health professions’ perception and experience of ethical issues. Although established health ethics principles are relevant guiding values, they may be experienced and interpreted differently within different health contexts. How should ethics education account for this? This paper presents ethical dilemmas and concerns encountered by physiotherapists practicing in Singapore and discusses the implications for ethics education.
Methods: Qualitative methods informed by interpretivism and phenomenology were employed. In-depth interviews with 42 physiotherapists from different workplace settings in Singapore were conducted. Participants described everyday ethical challenges they encountered. Inductive content analysis was used to analyse the interview transcript data.
Results: Ethical issues occurred within and across three spheres of ethics: micro, meso and macro. Ethical issues at the micro sphere centered around physiotherapist-patient relationships, interactions with colleagues, and therapists’ feelings of moral distress. In the meso sphere, ethical challenges related to influences arising from the organizational resources or systems. In the macro sphere, ethical challenges developed or were influenced by sociocultural, religious, economic, and political factors.
Conclusion: The findings reflect current literature indicating that context can influence ethical situations, as experienced and perceived by physiotherapists in their unique settings. Such empirical data might inform the development of ethics curricula to ensure that universal ethical principles are situated within the realities of clinical practice. Locally relevant and realistic ethical case studies will better enable students to recognise and address these situations.
Keywords: Ethics, Physiotherapy, Health Professions Education, Ethics Education, Asian Context, Singapore, Healthcare Principles, Health Ethics Principles
Practice Highlights
- Context can influence the ethical situations experienced and interpreted by healthcare professionals.
- Contextualised cases studies need to be developed to make ethics real and relevant to students.
- Ethics education should incorporate local context and not focus only on ethics epistemic knowledge.
- Ethics education should incorporate the dynamic influence of macro, meso and micro factors.
I. INTRODUCTION
The established health ethics principles articulated by Beauchamp and Childress (2001): autonomy, beneficence, non-maleficence, and justice guide healthcare practice, including physiotherapy (Carpenter & Richardson, 2008; Edwards, Delany, et al., 2011). Although these principles were originally proposed as universally relevant and foundational to health ethics, health professionals interpret them differently, depending on their professional and personal background, their values, and the culture of the community and settings in which they work (Fuscaldo et al., 2013). In physiotherapy ethics scholarship, there is growing recognition that the universal nature of principlism as a supporting ethical decision-making framework, may not be a sufficient guide for physiotherapists in their ethical decision-making, because of the plurality of values and diverse contexts of healthcare practice (Carpenter, 2010; Carpenter & Richardson, 2008; Edwards, Wickford, et al., 2011; Fryer et al., 2021; Greenfield, 2006; Hudon et al., 2019; Oyeyemi, 2011; Souri et al., 2020; Sturm et al., 2022). Consequently, there is increasing pedagogical interest in using case studies drawn from everyday practice to bring authenticity and contextual relevance to ethics education (Aguilar-Rodríguez et al., 2019; Fuscaldo et al., 2013).
In physiotherapy, empirical studies have shown that different work contexts, political and sociocultural systems have a direct influence on physiotherapists’ perception and experience of ethical issues (Delany et al., 2018; Fryer et al., 2021; Sturm et al., 2022). A recent example is the study of ethical issues physiotherapists experienced by Sturm et al. (2022). The authors reported physiotherapists working in specific countries described having to compromise their professional integrity due to overt threats and intimidation by suppressive professional organisations or leaders. They were directed to follow the societal or organisational hierarchies or risk jeopardizing their careers. Studies of ethical experiences of physiotherapists practicing in the African nations (Aderibigbe & Chima, 2019; Chigbo et al., 2015; Nyante et al., 2020; Oppong, 2019; Oyeyemi, 2011) and the Greater Middle East region (Edwards, Wickford, et al., 2011; Qamar et al., 2014; Souri et al., 2020) similarly discussed how cultural influences, such as religion or spirituality can directly affect ethical practice and decision-making. Despite increasing empirical evidence globally, the influence of cultural and societal contexts on ethical decision-making and therapists’ interpretation of health values has not been examined in the East and Southeast Asian regions. There has also been little exploration of how societal and cultural context in which physiotherapy is practiced might be used to inform and shape curricula for ethics education.
In this paper, we present data about the ethical situations physiotherapists in Singapore encounter in their everyday clinical practice. Singapore is multi-racial, multi-religious and multi-cultural. The values of Singaporean people are very much rooted in their Asian heritage, with Confucianism as the prevailing social model (Ong, 2020; Tan, 1989; Yang et al., 2006). This research aims to contribute to knowledge about the influence of context on clinical ethical issues and decision-making, as interpreted by physiotherapists in Singapore. The empirical data will then be used to inform subsequent ethics curricula. Identifying and analysing the factors influencing ethical issues, as they are experienced and interpreted by physiotherapists in the Singaporean context, is an important pedagogical strategy to inform the development of health ethics curricula.
II. METHODS
We used a qualitative methodology drawing on the research paradigm of phenomenology and conducted in-depth interviews. We recruited physiotherapy clinicians using purposive (Palys, 2008) and snowball sampling (Holloway & Galvin, 2016). Written and verbal consent was obtained. Semi-structured interviews were conducted by AL and ranged from 44 to 123 minutes. Audio recordings were professionally transcribed verbatim and were reviewed by AL. Content analysis was used to analyse the transcribed data, with interviewer’s written field notes as supporting reference. Data was systematically coded and categorised with the aim of identifying themes, their frequency, and relationships, through both description and interpretation (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005; Lindgren et al., 2020; Vaismoradi et al., 2013). Assisted by QSR NVivo 12 Software, the data analysis was organised into five steps (Figure 1). Although illustrated as a linear, chronological sequence, analysis occurred in a non-linear, iterative manner till there was clarity and meaning in the themes that were identified.
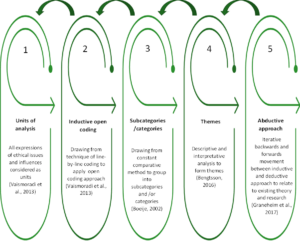
Figure 1. Sequence of data analysis
III. RESULTS
A total of 42 physiotherapists from four settings: acute, community, specialised institutions, and private practice participated (Table 1). All participants have been practicing physiotherapists in Singapore for the past three years, with 33.3 % in geriatrics and neuro rehabilitation, 45.3% in musculoskeletal and sports, and 21.4% in cardiopulmonary and other niche specialties. Thirty-six participants are Singaporeans and six are from Malaysia, Philippines, Hong Kong, New Zealand, and the UK. Ages ranged from 27 to 54 years old.
|
WORK SETTINGS |
ACUTE
Restructured public hospitals & subsidiaries |
COMMUNITY
Government supported intermediate & long- term care facilities |
SPECIALISED INSTITUTIONS
Government supported facilities for medical specialties/ niche populations
|
PRIVATE
Independent private physio clinics |
TOTAL (n) |
|
Number of Participants (n) |
16 |
13 |
6 |
7 |
42 |
|
Percentage (%) |
38.1 |
31.0 |
14.3 |
16.6 |
100 |
|
Gender (n) |
|
||||
|
Female |
9 |
12 |
5 |
2 |
28 |
|
Male |
7 |
1 |
1 |
5 |
14 |
|
Age Group in Years (n) |
|
||||
|
26-35 |
10 |
5 |
2 |
2 |
19 |
|
36-45 |
4 |
5 |
3 |
3 |
15 |
|
46-55 |
2 |
3 |
1 |
2 |
8 |
|
Professional Qualifications (n) |
|
||||
|
Diploma/Degree |
7 |
9 |
2 |
1 |
19 |
|
Postgraduate |
9 |
4 |
4 |
6 |
23 |
|
Number of Years in Healthcare (n) |
|
||||
|
< 10 |
9 |
6 |
1 |
2 |
18 |
|
10-20 |
5 |
5 |
4 |
3 |
17 |
|
> 20 |
2 |
2 |
1 |
2 |
7 |
n = number of participants
Table 1. Participants demographics
Six key themes were identified from the ethical situations described by the participants in their everyday physiotherapy practice: 1) managing healthcare resource constraints – encompassing ethical situations regarding the financial cost of healthcare, resource limitations and healthcare system inadequacies, 2) conforming to healthcare norms in Singapore – covering particular ethical challenges related to Singapore’s sociocultural context, including healthcare norms, 3) negotiating the complexity of the work environment – comprising challenges participants encountered in fulfilling their multiple obligations, especially in a negative work environment, 4) adapting to the intricacies of different healthcare settings – representing the unique ethical issues specific to the four different settings in Singapore, 5) balancing professional obligations and personal wellbeing – emerging from the participants’ struggle with their duty as moral agents, entrusted with the care of their patients while safeguarding their personal wellbeing and 6) advocating for patients: the predicament of relationships – exploring the relational aspects of a physiotherapist’s role, including defining professional boundaries, advocating for patients while managing their responsibilities to patients’ family and their colleagues. Complete quotes (QN1- QN18) illustrating the six themes are presented in Table 2.
|
Themes |
Quotations (QN) |
|
Managing healthcare resource constraints |
QN1: “I feel that these boundaries are set…because… at the end of the day it’s [healthcare] a business … we have to meet our finances. We have to balance our cheque books”. (P25) QN2: “If it’s something beyond our control, like the health system in Singapore itself, it can also be a potential barrier to our ethical practice. Because it’s not that we don’t want to do it. But … our hands are tied and it’s because of all these external factors that is affecting us.” (P38) |
|
Conforming to healthcare norms in Singapore |
QN3: “The subsidized cases actually are more complex than the private patients because private patients once they have a problem, they will get medical attention immediately… Whereas the subsidized patients…they usually drag…if they are being managed by a fresh grad that has no idea what is going on, then I think is unfair for them. And so, the cases that they [juniors] see, a lot of time is much more complex than the cases that the seniors see.” (P15) QN4: “I think insisting on certain types of equipment that we don’t feel or don’t agree with, that the patient really needs, but we do have to give because the doctor will keep on insisting on it, no matter how much we tell them that it may not be beneficial to the patient and all that. I think that’s one of the ethical things that I feel that I encounter.” (P33) QN5: “Breaking bad news seems to be also a bit of a two-way thing, where you have to go around to the family member first, before telling the patient even now. I mean, 20 years ago when I first started work it was like that, and I thought it would have moved on right? No. So I think is the education and is the perception of our Asian values, of the very paternalistic values that I think our families, or our patient’s families have.” (P09) |
|
Negotiating the complexity of the work environment |
QN6: “Because all you [i.e. the organisation] care about is earning money, all you [i.e. the organisation] care about is how many patients I can see a day and not caring whether I see it well, I’m seeing it correctly, whether I have provided value to the client.” (P13) QN7: “I see a patient, I read the history and I do the minimum, I do no harm. Patient may not get very well or recover as fast as they should…In terms of assessment, we need to be a bit more holistic, we need to assess thoroughly, but we don’t have the time…to me is clinically not ethical, but that’s how we’ve been working in a clinical setting because of time constraint, resources constraint.” (P22) QN8: “When I see something, I will just say it out to my superior, hoping that something can be done. And I can say it a few times, but once I see this is not going to work, because simply nobody responds to you, then just have to let it be, or if you really cannot take it, then you leave the organization.” (P15) |
|
Adapting to the intricacies of different healthcare settings |
QN9: “So, the proper procedure is that we refer them back to the doctor and get a new referral for the new problem. I find it quite silly to do that, the patient is right in front of me, and I know what’s the problem. I can instantly give a solution to the problem, why do I need to go and get a referral, and then delay for another three months before the patient can come back and see me for another problem?” (P26 – in acute setting) QN10: “If I make this person too mobile, family member cannot cope, he’s falling down, so this is my moral dilemma. I want him to be better, physically better. But he’s moving all over the place and he’s prone to fall and he’s much bigger size than the carer, (who) is only 40kg. I’m in a moral dilemma, how much should I give? How much should I train, or should I just give a little bit more just to maintain him? Must see from carer’s perspective. I don’t live with the person. I can come in once in a while, that one hour or just 45 minutes. But this person stays 24 hours, that’s where I’m stuck.” (P02 – in community setting) QN11: “However, then comes to work organisation that you need to understand the needs of the organisation and even the greater picture, therefore, you may not give the patient the best anymore.” (P03 – in specialised institution setting) QN12: “It’s very correlation or causation, or whatever. Often the treatment plan will miraculously be the same length as the [number] of sessions given by insurance, which you know is coincidence right? That it always happens to be the same length. You’ve got 10 sessions via insurance. That’s how long it’s going to take you to get better.” (P29 explained in a satirical manner – in private practice clinic) |
|
Balancing professional obligations and personal wellbeing
|
QN13: “Yes, so every day, we’ll carry him out on a chair for two hours… we’ll carry him back to bed and it’s two to three times max assist…this actually gave my senior some backache…because every day, is every day…because for such heavy patient, there’s no real technique already… So, this is a dilemma.” (P36) QN14: “Because I thought it was like part of my job. Probably he accidentally touched…when we do transfer, it tends to like, hands go flare anywhere. So, I thought never mind because I need to do my job. I need to transfer him. Of course, I don’t want him to fall down. So, I have to do all this contact.” (P34) QN15: “If it is a young female patient, then you try to have the female TA (therapy assistant) to be in as your chaperon. If it’s Ah Ma (older lady), then just keep the door open. It’s okay. I don’t know how is that right or wrong. But so far, it doesn’t give me any problem with that kind of practice. Usually, the Ah Ma doesn’t complain.” (P11) |
|
Advocating for patients: the predicament of relationships |
QN16: “Of course, the patient did give verbal consent. So, by right, by legal standpoint, it means that it’s fine. Then you start thinking a little bit deeper, sometimes when you’re in a clinic, patient will actually feel that they have to do that. If they don’t agree to your examination, then they are here for no purpose…Does it make the patient feel that we are coercing them? And they don’t really have a choice to really say, I don’t want it in that sense.” (P41) QN17: “I’m trying to fight for my client’s welfare. But a lot of times, if the family do not seek that welfare for the client, there is nothing I can do…. Do I train the caregiver who’s not willing to learn? Do I charge this family when the family has already expressed interest in no longer paying for equipment, or even therapy? Do I force it down their throat?” (P04)
QN18: “I guess maybe to me it really depends on the extent of that incident, how bad of that it is to the profession as a whole. If it is something that is minor and understandable, then probably I will not. But if it is something that is…pretty bad, maybe I would. I don’t know, it’s still a struggle, I can’t because it’s my fellow friends and colleagues. So, it’s a bit tough to be honest.” (P27) |
Table 2. Quotes to illustrate the six themes
A. Managing Healthcare Resource Constraints
Participants were aware of their ethical responsibility to act in the patient’s best interest in the provision of care but felt the pressure of finite resources and financial constraints (QN1). They described how they struggled to fulfill their professional obligations whilst at the same time managing patients’ expectations about availability of resources. Some therapists found loopholes to bypass government funding requirements. One participant (P26) summarised it as being a “discrepancy between the ideal care for the nation as a whole versus what is ideal for the patient’s health right before my eyes”. Some participants spoke about how key performance indicators (KPIs) intended to manage healthcare costs can drive change in organisational and clinician behaviour to practice defensively rather than using evidence-based practice to meet patients’ needs. Participant 09 described it as “funding drives behaviour” and gave the example of how a KPI that tracks fall rates may sway clinicians to be overly conservative to prevent falls, rather than challenging patients’ balance to maximise recovery. A lack of clear workflows and integration between different clinical settings was another ethical challenge preventing best available care for patient. Community and private practice physiotherapists indicated that they lack access to medical records and diagnostic results to seek clarity on a patient’s condition. This resulted in therapists feeling frustrated, as they had to delay treatment or proceed without a clear understanding of the patient’s medical status (QN2).
B. Conforming to Healthcare Norms in Singapore
For some participants, the allocation of only senior clinicians to private patients and junior clinicians to subsidised patients was viewed as unjust practice, where allocation of clinicians’ expertise is not based on the needs of patients. Participant 15 shared that the subsidised patients tended to be more complex cases as they may not have the resources to seek medical attention early (QN3). Most participants acknowledged this as an accepted practice in Singapore’s healthcare system and not just specific to physiotherapy, with participant 39 highlighting that “no one addresses it”. Adding to the social class differentiation, nearly all participants commented on the acceptance of hierarchical differentiation in healthcare with doctors at the top. Many participants spoke about paternalism being widely practiced and accepted by patients, and shared incidents where doctors dictated treatment plans, and even overrode patients’ wishes. Participants felt obliged to comply regardless of their own professional judgement (QN4).
Familialism may also compromise patients’ autonomy. Participants shared stories where family members dominated decision-making or demanded withholding information from patients. There were also geriatric patients who chose to relinquish their autonomy to their children. Many participants viewed this as an accepted part of Asian norms (QN5). A few participants stressed that many Singaporeans still hold conservative views and highlighted the importance of remaining sensitive to racial, religious, and cultural differences. For example, participant 22 disclosed that it is not accepted practice for male physiotherapists to place electrocardiogram (ECG) leads on a female patient even with the patient’s consent and a chaperon present.
C. Negotiating the Complexity of the Work Environment
Organisations have to manage the financial cost of patient care and ensure business sustainability. With resource limitations, clinicians face the challenge of conflicting obligations to their organisation and their patients. Participant 13 expressed her frustration and resentment that physiotherapy outcomes are determined by organisational financial values (QN6). Another participant (P31) shared how she had to discharge patients “prematurely” to meet organisational expectations. Other participants coped by settling for minimum treatment and doing no harm to patients (QN7).
Adding to this complexity was a negative work culture, expressed by participants as the pressure to conform to the organisation’s expectations, norms, and practices. Examples given included unreasonable workloads, biasness towards preferred staff, belittling remarks, fault-finding, and masked threats of poor appraisals. Staff were expected to conform and follow the rules, leading to a culture of fear, where safety incidents went unreported for fear of repercussions. This was further perpetuated by the lack of supervisors’ moral courage, who ignored such ethical infringements, thus normalizing ethical silence as accepted behaviour. Participant 13 disclosed her moral distress when her concerns regarding fraudulent behaviour by a colleague who falsely documented and charged for services, were disregarded by her seniors. Some participants dispiritedly added that often no action was taken and they either learnt to accept the status quo and found their own solutions or left the organisation (QN8).
D. Adapting to the Intricacies of Different Healthcare Settings
1) Acute settings: The different organisational structure and systems in each setting gave rise to specific ethical concerns. Many ethical issues in the acute settings related to the structured systems, established practices and workflows. One such practice was physiotherapists not being allowed as first contact practitioners in public institutions. Patients can only be seen with a referral from doctors and only be treated for the problem for which they were referred. This was ethically challenging for physiotherapists wanting to manage patients holistically (QN9). Several participants also raised concerns regarding minimal charging per session. In some acute settings, the on-call duty was rostered for all physiotherapists, regardless of their inpatient competency or speciality. Concerns were raised about whether this was ethically good clinical practice and in patients’ best interests.
2) Community settings: Some participants commented that community settings have varied and diverse services, making it difficult to implement guidelines that are applicable and fair to all services. This can encourage clinicians to circumvent the rules to benefit their patients. In integrating a patient back to their community, the patient’s psychological, social, and family issues can become the major consideration. Participant 02 shared her dilemma in having to factor in the caregiver’s coping ability when progressing a patient with mental health issues, who had little comprehension of fall risks, to independent mobility (QN10). A few participants commented that community physiotherapists generally have greater independence and flexibility in their work schedule, but this can engender accountability issues in terms of documentation and the standard of services provided. Some participants felt that the lack of awareness of community services available and an unsubstantiated perception that community physiotherapists are not as skilled, may deter some patients from continuing their care in the community and could have contributed to a shortage of community allied health professionals.
3) Specialised institutions: For some specialised institutions where healthcare is not the core business, physiotherapists reported being constrained by the organisational goals when caring for their patients. The needs of the organisation and the deliverables expected factored greatly in both the patient’s and clinician’s decision-making. Consequently, the best interest of the patient may not take precedence (QN11). Participants commented that the hierarchical order in such institutions tended to be more overt, with instructions directed by leaders in charge rather than team discussions.
4) Private practice clinics: Participant 27 described the business aspect of private practice as having to wear two hats: one as a clinician and one as a businessman. This can lead to maximising profits through overcharging, overservicing and maximising insurance claims. Participant 27 further disclosed that most people kept it hushed, “it’s one of those things that everyone knows is happening, but no one wants to rock the boat”. Participant 29 shared how he had to see post-op cases twice weekly, regardless of whether it was necessary, “because that’s just the way things are done” and how the cost of treatment or number of sessions needed for recovery consistently matched the insurance claim limits (QN12). Other participants raised issues which bordered on being illegal. One common example shared was fee-splitting, whereby commission was given for the referral of patients. Private clinicians commented that private practice is loosely regulated, with no standardisation or best practice guidelines and that there is little collaboration or accountability to the profession. They further elaborated that private practice is very competitive, with some clinicians making exaggerated claims about their skills or effectiveness of their treatment.
E. Balancing Professional Obligations and Personal Wellbeing
Participants described conflicts between their work responsibilities and their personal wellbeing. They shared their insecurities about whether they had positively fulfilled their professional obligations. Demanding expectations or long working hours imposed by organisations forced some participants to sacrifice their personal life, compromise their mental health and even sustain work-related injuries. Participants detailed episodes of transferring or ambulating patients without equipment or sufficient manpower (QN13). The nature of physiotherapy often requires close physical contact with patients. Participant 34 disclosed her distressing encounter with a patient with mental health issues, who repeatedly touched her inappropriately but denied it. On why she continued treatment, she replied that she needed to do her job and convinced herself that it was probably accidental (QN14). Participant 11 shared his dilemma with regard to treating female patients when there was a lack of chaperones. To protect staff from allegations of misconduct, it is accepted practice to leave the consultation room door open, leading to a possible violation of patients’ privacy (QN15). Participants also disclosed unethical and even illegal incidents which reflected the therapists’ conflict between protecting themselves and their professional responsibilities. These included false documentation of clinical notes, dishonesty about treatment errors, or not reporting safety violations.
Having self-doubt about one’s competency, whether it is due to inexperience, being out of practice or due to a lack of access to resources led some participants to question whether they had done patients a disservice or whether they were practicing beyond their capability. At times, clinicians also found it challenging to bill patients for physiotherapy services, especially if patients had financial difficulties.
F. Advocating for Patients: The Predicament of Relationships
Several participants highlighted the crossing of professional boundaries as an ethical concern. This included patients constantly calling or messaging, asking for free advice or personal favours. The nebulous zone where a professional relationship crossed over into friendship or even a dependency worried many participants. Numerous participants shared their turmoil when dealing with special populations such as patients with mental health conditions. The dilemma of overriding a patient’s autonomy became harder to resolve when the patient’s safety was at risk or where there was a possibility of detrimental consequences. Participant 41 pondered about the unspoken power differential between the patient and the healthcare professional, which can lead to patients feeling pressured to consent to treatment (QN16).
Another common dilemma expressed by participants was gaining caregivers’ and families’ support. Family members felt justified in their demands as the payer and viewed themselves as the spokesperson. Some participants expressed their helplessness with family members unwilling to pay for needed services or equipment (QN17).
Participants shared views about maintaining collegiality and not disrespecting colleagues’ viewpoints, specifically when there were conflicting patient management strategies. Some participants resented the loss of their professional autonomy but yielded to maintain harmony, and to avoid confusion for the patient. A number of participants reinforced this strong sense of fraternity, including unwillingness to expose wrongdoing even if colleagues had crossed ethical and legal boundaries (QN18). Some participants spoke about the move towards transdisciplinary practice in Singapore and the blurring of professional boundaries. One participant (P04) elaborated on resource limitations in home-based therapy, prompting her to take on other healthcare roles to prescribe home equipment and even change patients’ wound dressings. She expressed her dilemma in having to consider the patient’s perspective, her organisation’s views, and her own competency as well as the professional and legal implications of providing the wrong advice.
Further analysis revealed that the ethical challenges encountered mapped to the three overall spheres of ethics previously identified by Glaser (2005) and Sippel et al. (2015), namely the micro, meso and macro spheres. Ethical issues at the micro sphere centered around physiotherapist-patient relationships, physiotherapist’s interactions with colleagues and their own needs. The meso sphere consists of four quarters that represented the four settings, and issues included structural problems and challenges related to organizational resources or systems. The macro sphere comprises ethical issues rooted in the influence of cultural, sociological, religious, economic, and political contexts (Sippel et al., 2015). The modified illustration of spheres of ethics with the meso sphere encircling the micro sphere and the macro sphere encircling the meso sphere, show the connection and interdependence of all three spheres (Figure 2).

Figure 2. Spheres of ethics (six themes)
IV. DISCUSSION
This study is the first to report on the clinical ethics issues faced by physiotherapists practicing in Singapore. It also provides some insights into the influence of context in ethical decision-making. The six themes identified were further organised into micro, meso and macro spheres or contexts of ethics. The micro sphere themes included ethical issues that have previously been identified in other physiotherapy study findings (Delany et al., 2018; Fryer et al., 2021; Praestegaard & Gard, 2013; Sturm et al., 2022). The notable points of difference specific to Singapore were themes residing in the meso and macro spheres. These themes offered potential insights into the particular context of physiotherapy practice in Singapore. One example in the meso sphere is the influence of different healthcare settings (acute, community, specialised institutions, and private practice) on ethical dimensions of physiotherapy practice within Singapore’s healthcare system. There were differences in the predominance or perceived importance of certain ethical issues due to each setting’s unique organisational structure and systems. These findings appear to reflect current literature which reported on differences in physiotherapists’ ethical experiences due to the influence of healthcare settings (Cantu, 2018, 2019; Hudon et al., 2015).
At the macro sphere, participants reported that fulfilling government set KPIs or outcome measures which determined healthcare funding exerted indirect pressure on them. They grappled with patients’ expectations of advocacy on their behalf and societal expectations of cost containment (Dronberger, 2003). In meeting the requirements, participants had to balance their view about what was a good enough treatment constrained by the system, versus the best treatment available. The findings suggest that having to meet quantitative statistical numbers such as discharge rates was interpreted by some therapists as neglecting the quality of care and negatively affecting the therapist-patient relationship. This finding is consistent with that of Hudon et al. (2015), who highlighted institutional and economic influence on the quality of physiotherapy service and public trust. Another theme in the macro sphere concerned the negative effects of hierarchies and power differentials, which therapists believed led to paternalistic practice. Factors contributing to paternalism can include time limitations on treatment, patient’s literacy levels, societal values of respecting seniority and the accepted practice of patients handing over decision-making to authority or their family. Familialism is prevalent in Singaporean culture, where a family centric approach or interest will outweigh individual’s autonomy (Krishna, 2012). It is viewed as an accepted part of Asian values and needs to be acknowledged in order to provide the best possible care for the patient. Ethical issues related to familialism have also been reported by studies in the African context (Chigbo et al., 2015; Nyante et al., 2020; Sippel et al., 2015).
A. Relevance to Ethics Education
There is agreement that ethics cannot be taught independent of context, with a focus only on the epistemic knowledge, but that it needs to incorporate the dynamic influence of macro, meso and micro factors (Barradell, 2017; Cantu, 2018; Greenfield et al., 2015; Ladeira & Koifman, 2017). The themes in this study can directly inform the ethics curriculum, highlighting to students the influence of resource constraints, local healthcare norms, organisational culture, challenges of different settings, as well as balancing multiple obligations. Beyond awareness, students must be equipped with the abilities and skillsets to address and navigate these ethical situations. Elaboration on each theme’s implications for the local ethics curriculum is outlined in Table 3.
|
Spheres of ethics |
Themes |
How understanding of spheres of ethics can inform physiotherapy ethics curricula |
|
MACRO: Conflict of ethical principles versus societal expectations, culture, and practices |
Managing healthcare resource constraints |
· Incorporate understanding of financial aspects of healthcare and its influence on physiotherapy practice (Finch et al., 2005). · Learn to anticipate and navigate the potential conflicts between equitable use of resources (justice) and best care for each patient (beneficence). |
|
Conforming to healthcare norms in Singapore |
· Be consciously aware of local cultural and practices. Acknowledging and respecting both universal health ethics principles and culturally based differences in values by taking into account relevant contextual considerations in application of ethical principles (Fuscaldo et al., 2013). · Learn to reason and negotiate for common moral ground without compromising one’s moral integrity (Fuscaldo et al., 2013). |
|
|
MESO: Contention between ethical principles and organisational values and norms |
Negotiating the complexity of the work environment |
· Recognise the complexities of the work environment, including managing obligations to employers versus professional duty to their patients. · Develop strategies and skillsets to overcome negative work culture (e.g. by building an advisory support system and network within the organisation or the national professional body). |
|
Adapting to the intricacies of different healthcare settings |
· Understand the strengths and limitations of different workplace settings in Singapore and potential ethical challenges. |
|
|
MICRO: Conflict of ethical principles or the struggle between self-interest versus altruism |
Balancing professional obligations & personal wellbeing |
· Reinforce importance of personal integrity and learn coping strategies for self -care to prevent professional burn out or moral distress. |
|
Advocating for patients: the predicament of relationships |
· Appreciate that relational aspects of physiotherapy practice go beyond patient-therapist interactions to include colleagues and caregivers. · Emphasise physiotherapists’ role as a moral agent and advocate for patients. |
Table 3. Implications for ethics curricula
The study findings can be used to inform the development of realistic and contextualised case studies that have the potential to resonate with students’ clinical experience and improve the relevance of ethics education (Barnitt & Roberts, 2000; Fuscaldo et al., 2013; Triezenberg & Davis, 2000). The data in this study highlighted therapists’ emotions of frustration, anger, and concern. Disregarding contextual differences may create indifference, cynicism, or even moral distress when students begin practice and experience the realities of clinical practice (Greenfield & Jensen, 2010; Mohr & Mahon, 1996; Nalette, 2010). Students may dismiss ethics as irrelevant or feel disrespected that their culture and practices have not been considered in the materials taught (Fuscaldo et al., 2013).
Developing realistic case studies for ethics curricula has four possible effects: 1) it assists in dispelling the notion that ethics is based on abstract and idealist considerations (Seedhouse, 1995), 2) it can stimulate practical reflection and be action guiding to help students reason and navigate ethical challenges (Geddes et al., 2009; Swisher et al., 2012), 3) it can address the dissonance between what they learn in the classroom and what they experience in clinical practice (Dutton & Sellheim, 2017), 4) it can assist to increase ethics literacy and ethical courage. Case studies based on local experiences can provide the physiotherapy community with the ethical language to express their thoughts (Barnitt & Partridge, 1997). This shared language may enable students and clinicians to share experiences and learn how to speak up or seek help. Only when ethical issues that are pertinent to the local physiotherapy community are voiced, articulated, and discussed, can there be engagement of the community to confront identified ethical concerns, commit to creating change, and to strive towards ethical clinical practice.
B. Limitations
Participant recruitment and interviews were completed under the permeating influence of the global COVID crisis amidst shortage of healthcare staff. Due to the sensitivity of the topic, participants may have been guarded and not freely shared their views.
V. CONCLUSION
This study explored the ethical issues experienced and interpreted by physiotherapists across a range of practice settings in Singapore and examined how these experiences could inform ethics education. Our results have further substantiated current literature that context plays a critical influencing role on ethical situations, as they are experienced and perceived by physiotherapists in their unique geographical and clinical settings. The ability to act ethically has to be understood within the context and complexity of the sociocultural and political framework, along with the explicit and implicit influences, obligations, and commitments as part of a community, in order to directly address the everyday frustrations and concerns that clinicians face in trying to provide the best care for patients. With this knowledge, ethics educators and clinical supervisors will be better equipped to prepare students for clinical practice in Singapore.
Notes on Contributors
AL reviewed the literature, conceptualised and designed the study, conducted the interviews, analysed and interpreted the data, drafted the manuscript and wrote the final version submitted. This study is part of her PhD thesis.
CD is the first author’s primary PhD supervisor, who is involved in finalising the study and manuscript conceptualisation, and supervised the study from the beginning to the final version of the manuscript.
VX is the first author’s local PhD supervisor for data collection and supervised the study from the beginning to the final version of the manuscript.
Both CD and VX gave critical feedback on the direction and writing of the manuscript.
Ethical Approval
Ethics approval for this study was obtained from the University of Melbourne, Medicine and Dentistry Human Sub-Committee on 25 October 2019 (ID 1955123), and from the Singapore Institute of Technology, Institutional Review Board on 25 November 2019 (Project 2019146).
Data Availability
As the topic is of a sensitive nature and part of a larger PhD study, transcripts from the interviews are confidential and the authors do not have consent to upload onto a repository.
Acknowledgement
The authors would like to thank the 42 participants who have consented and graciously gave their time to participate in this study.
Funding
This study was completed with support from Singapore Institute of Technology (SIT) SEED grant (R-MOE-E103-C019).
Declaration of Interest
The authors declare that they have no competing interests.
References
Aderibigbe, K. S., & Chima, S. C. (2019). Knowledge and practice of informed consent by physiotherapists and therapy assistants in Kwazulu-Natal Province, South Africa. South African Journal of Physiotherapy, 75(1), a1330. https://doi.org/10.4102/sajp.v75i1.1330
Aguilar-Rodríguez, M., Marques-Sule, E., Serra-Añó, P., Espí-López, G. V., Dueñas-Moscardó, L., & Pérez-Alenda, S. (2019). A blended-learning programme regarding professional ethics in physiotherapy students. Nursing Ethics, 26(5), 1410–1423. https://doi.org/10.1177/0969733017748479
Barnitt, R., & Partridge, C. (1997). Ethical reasoning in physical therapy and occupational therapy. Physiotherapy Research International, 2(3), 178–194. https://doi.org/10.1002/pri.v2:3
Barnitt, R. E., & Roberts, L. C. (2000). Facilitating ethical reasoning in student physical therapists. Journal of Physical Therapy Education, 14(3), 35–41. https://doi.org/10.1097/00001416-200010000-00007
Barradell, S. (2017). Moving forth: Imagining physiotherapy education differently. Physiotherapy Theory & Practice, 33(6), 439–447. https://doi.org/10.1080/09593985.2017.1323361
Beauchamp, T. L., & Childress, J. F. (2001). Principles of biomedical ethics. Oxford University Press.
Bengtsson, M. (2016). How to plan and perform a qualitative study using content analysis. NursingPlus Open, 2, 8–14. https://doi.org/10.1016/j.npls.2016.01.001
Boeije, H. (2002). A purposeful approach to the constant comparative method in the analysis of qualitative interviews. Quality and Quantity, 36, 391–409. https://doi.org/10.1023/a:1020909529486
Cantu, R. (2018). Physical therapists’ perception of workplace ethics in an evolving health-care delivery environment: A cross-sectional survey. Physiotherapy Theory and Practice, 35(8), 724–737. https://doi.org/10.1080/09593985.2018.1457744
Cantu, R. (2019). Physical therapists’ ethical dilemmas in treatment, coding, and billing for rehabilitation services in skilled nursing facilities: A mixed-method pilot study. Journal of the American Medical Directors Association, 20(11), 1458–1461. https://doi.org/10.1016/j.jamda.2019.06.013
Carpenter, C. (2010). Moral distress in physical therapy practice. Physiotherapy Theory & Practice, 26(2), 69–78. https://doi.org/10.3109/09593980903387878
Carpenter, C., & Richardson, B. (2008). Ethics knowledge in physical therapy: A narrative review of the literature since 2000. Physical Therapy Reviews, 13(5), 366–374. https://doi.org/10.1179/174328808×356393
Chigbo, N. N., Ezeome, E. R., Onyeka, T. C., & Amah, C. C. (2015). Ethics of physiotherapy practice in terminally ill patients in a developing country, Nigeria. Nigerian Journal of Clinical Practice, 18(7), S40–S45. https://doi.org/10.4103/1119-3077.170826
Delany, C., Edwards, I., & Fryer, C. (2018). How physiotherapists perceive, interpret, and respond to the ethical dimensions of practice: A qualitative study. Physiotherapy Theory and Practice, 35(7), 663–676. https://doi.org/10.1080/09593985.2018.1456583
Dronberger, J. (2003). Fraud and negligence in physical therapy practice: A case example. Physiotherapy Theory and Practice, 19(3), 151–159. https://doi.org/10.1080/09593980307961
Dutton, L. L., & Sellheim, D. O. (2017). Academic and clinical dissonance in physical therapist education: How do students cope? Journal of Physical Therapy Education, 31(1), 61–72. https://doi.org/10.1097/00001416-201731010-00009
Edwards, I., Delany, C. M., Townsend, A. F., & Swisher, L. L. (2011). New perspectives on the theory of justice: Implications for physical therapy ethics and clinical practice. Physical Therapy, 91(11), 1642–1652. https://doi.org/10.2522/ptj.20100351.10
Edwards, I., Wickford, J., Adel, A. A., & Thoren, J. (2011). Living a moral professional life amidst uncertainty: Ethics for an Afghan physical therapy curriculum. Advances in Physiotherapy, 13(1), 26–33. https://doi.org/10.3109/14038196.2010.483015
Elo, S., & Kyngäs, H. (2008). The qualitative content analysis process. Journal of Advanced Nursing, 62(1), 107–115. https://doi.org/10.1111/j.1365-2648.2007.04569.x
Finch, E., Geddes, E. L., & Larin, H. (2005). Ethically-based clinical decision-making in physical therapy: Process and issues. Physiotherapy Theory and Practice, 21(3), 147–162. https://doi.org/10.1080/09593980590922271
Fryer, C., Sturm, A., Roth, R., & Edwards, I. (2021). Scarcity of resources and inequity in access are frequently reported ethical issues for physiotherapists internationally: An observational study. BMC Medical Ethics, 22, Article 97. https://doi.org/10.1186/s12910-021-00663-x
Fuscaldo, G., Russell, S., Gillam, L., Delany, C., & Parker, M. (2013). Addressing cultural diversity in health ethics education: Final Report 2013. http://www.research-matters.com.au/publications/FinalReport.pdf
Geddes, E. L., Salvatori, P., & Eva, K. W. (2009). Does moral judgement improve in occupational therapy and physiotherapy students over the course of their pre-licensure training? Learning in Health and Social Care, 8(2), 92–102. https://doi.org/10.1111/j.1473-6861.2008.00205.x
Glaser, J. W. (2005). Three realms of ethics:An integrating map of ethics for the future. In R. B. Purtilo, G. M. Jensen, & C. B. Royeen (Eds.), Educating for moral action: A sourcebook in health and rehabilitation ethics (pp. 169-184). F.A. Davies.
Graneheim, U. H., Lindgren, B. M., & Lundman, B. (2017). Methodological challenges in qualitative content analysis: A discussion paper. Nurse Education Today, 56, 29–34. https://doi.org/10.1016/j.nedt.2017.06.002
Greenfield, B., & Jensen, G. M. (2010). Beyond a code of ethics: Phenomenological ethics for everyday practice. Physiotherapy Research International, 15(2), 88–95. https://doi.org/10.1002/pri.481
Greenfield, B. H. (2006). The meaning of caring in five experienced physical therapists. Physiotherapy Theory and Practice, 22(4), 175–187. https://doi.org/10.1080/09593980600822859
Greenfield, B. H., Jensen, G. M., Delany, C. M., Mostrom, E., Knab, M., & Jampel, A. (2015). Power and promise of narrative for advancing physical therapist education and practice. Physical Therapy, 95(6), 924-933. https://doi.org/10.2522/ptj.20140085
Holloway, I., & Galvin, K. (2016). Data analysis: Procedures, practices and use of computers. In Qualitative research in nursing and healthcare(4th ed., 287–302).Wiley-Blackwell.
Hsieh, H. F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research, 15(9), 1277–1288. https://doi.org/10.1177/1049732305276687
Hudon, A., Drolet, M. J., & Jones, B. W. (2015). Ethical issues raised by private practice physiotherapy are more diverse than first meets the eye: Recommendations from a literature review. Physiotherapy Canada, 67(2), 124–132. https://doi.org/10.3138/ptc.2014-10
Hudon, A., Ehrmann Feldman, D., & Hunt, M. (2019). Tensions living out professional values for physical therapists treating injured workers. Qualitative Health Research, 29(6), 876–888. https://doi.org/10.1177/1049732318803589
Krishna, L. R. (2012). Best interests determination within the Singapore context. Nursing Ethics, 19(6), 787–799. https://doi.org/10.1177/0969733011433316
Ladeira, T. L., & Koifman, L. (2017). Interface entre fisioterapia, bioética e educação: revisão integrativa [Interface between physical therapy, bioethics and education: Integrative review]. Revista Bioética, 25(3), 618–629. https:/doi.org/10.1590/1983-80422017253219
Lindgren, B. M., Lundman, B., & Graneheim, U. H. (2020). Abstraction and interpretation during the qualitative content analysis process. International Journal of Nursing Studies, 108. https://doi.org/10.1016/j.ijnurstu.2020.103632
Mohr, W. K., & Mahon, M. M. (1996). Dirty hands: The underside of marketplace health care. Advances in Nursing Science, 19(1), 28–37. https://doi.org/10.1097/00012272-199609000-00005
Nalette, E. (2010). Constrained physical therapist practice: An ethical case analysis of recommending discharge placement from the acute care setting. Physical Therapy, 90(6), 939–952. https://doi.org/10.2522/ptj.20050399
Nyante, G. G., Andoh, C. K., & Bello, A. I. (2020). Patterns of ethical issues and decision-making challenges in clinical practice among Ghanaian physiotherapists. Ghana Medical Journal, 54(3), 179–185. https://doi.org/10.4314/gmj.v54i3.9
Ong, E. K. (2020). The impact of sociocultural influences on the COVID-19 measures—reflections from Singapore. Journal of Pain and Symptom Management, 60(2), e90–e92. https://doi.org/10.1016/j.jpainsymman.2020.04.022
Oppong, S. (2019). When the ethical is unethical and the unethical is ethical: Cultural relativism in ethical decision-making. Polish Psychological Bulletin, 50(1), 18–28. https://doi.org/10.24425/ppb.2019.126014
Oyeyemi, A. (2011). Ethics and contextual framework for professional behaviour and code of practice for physiotherapists in Nigeria. Journal of the Nigeria Society of Physiotherapy, 19(1–2), 49–53. https://academicjournals.org/journal/JNSP/article-full-text -pdf/0AA592B65221
Palys, T. (2008). Purposive sampling. In L. M. Given (Ed.), The sage encyclopedia of qualittaive research methods (Vol. 2, pp. 697–698). Los Angeles: Sage.
Praestegaard, J., & Gard, G. (2013). Ethical issues in physiotherapy – Reflected from the perspective of physiotherapists in private practice. Physiotherapy Theory & Practice, 29(2), 96–112. https://doi.org/10.3109/09593985.2012.700388
Qamar, M. M., Basharat, A., Rasul, A., Basharat, S., & Ijaz, M. J. (2014). Perception of physical therapy students and professionals about the importance of professional ethics. International Journal of Medicine and Applied Health., 2(2), 57–61. https://www.academia.edu/11604067/perception_of_physical_therapy_students_and_professionals_about_the_importance_of_professional_ethics
Seedhouse, D. (1995). There’s Logic, and then there’s what we do around here. Health Care Analysis, 3(2), 87–90. https://doi.org/10.1007/BF02198208
Sippel, D., Marckmann, G., Atangana, E. N., & Strech, D. (2015). Clinical ethics in Gabon: The spectrum of clinical ethical issues based on findings from in-depth interviews at three public hospitals. PLoS ONE, 10(7), e0132374. https://doi.org/10.1371/journal.pone.0132374
Souri, N., Moghadam, A. N., & Shahbolaghi, M. (2020). Iranian physiotherapists’ perceptions of the ethical issues in everyday practice. Iranian Rehabilitation Journal, 18(2), 125–136. https://doi.org/10.32598/irj.18.2.221.5
Sturm, A., Edwards, I., Elizabeth Fryer, C., & Roth, R. (2022). (Almost) 50 shades of an ethical situation-international physiotherapists’ experiences of everyday ethics: A qualitative analysis. Physiotherapy Theory and Practice. https://doi.org/10.1080/09593985.2021.2015812
Swisher, L. L., Kessel, G. V., Jones, M., Beckstead, J., & Edwards, I. (2012). Evaluating moral reasoning outcomes in physical therapy ethics education: stage, schema, phase, and type. Physical Therapy Reviews, 17(3), 167–175. https://doi.org/10.1179/1743288X12Y.0000000011
Tan, C. H. (1989). Confucianism and nation building in Singapore. International Journal of Social Economics, 16(8), 5–16. https://doi.org/10.1108/03068298910133106
Triezenberg, H. L., & Davis, C. M. (2000). Beyond the code of ethics: Educating physical therapists for their role as moral agents. Journal of Physical Therapy Education, 14(3), 48–58. https://doi.org/10.1097/00001416-200010000-00009
Vaismoradi, M., Turunen, H., & Bondas, T. (2013). Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nursing and Health Sciences, 15(3), 398–405. https://doi.org/10.1111/nhs.12048
Yang, S., Shek, M. P., Tsunaka, M., & Lim, H. B. (2006). Cultural influences on occupational therapy practice in Singapore: a pilot study. Occupational Therapy International, 13(3), 176–192. https://doi.org/10.1002/oti.217
*Audrey Lim
Health and Social Sciences Cluster
Singapore Institute of Technology (SIT)
10 Dover Road
Singapore 138683
+65 6592 3390
Email: Audrey.Lim@SingaporeTech.edu.sg
Submitted: 22 January 2022
Accepted: 4 May 2022
Published online: 4 October, TAPS 2022, 7(4), 50-58
https://doi.org/10.29060/TAPS.2022-7-4/OA2748
Nguyen Tran Minh Duc, Khuu Hoang Viet & Vuong Thi Ngoc Lan
University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam
Abstract
Introduction: The Scholarly Project provides medical students with an opportunity to conduct research on a health and health care topic of interest with faculty mentors. Despite the proven benefits of the Scholarly Project there has only been a gradual change to undergraduate medical education in Vietnam. In the academic year of 2020-2021, the University of Medicine and Pharmacy (UMP) at Ho Chi Minh City launched the Scholarly Project as part of an innovative educational program. This study investigated the impact of the Scholarly Project on the research skills perception of participating undergraduate medical students.
Methods: A questionnaire evaluating the perception of fourteen research skills was given to participants in the first week, at midterm, and after finishing the Scholarly Project; students assessed their level on each skill using a 5-point Likert scale from 1 (lowest score) to 5 (highest score).
Results: There were statistically significant increases in scores for 11 skills after participation in the Scholarly Project. Of the remaining three skills, ‘Understanding the importance of “controls”’ and ‘Interpreting data’ skills showed a trend towards improvement while the ‘Statistically analyse data’ skill showed a downward trend.
Conclusion: The Scholarly Project had a positive impact on each student’s perception of most research skills and should be integrated into the revamped undergraduate medical education program at UMP, with detailed instruction on targeted skills for choosing the optimal study design and follow-up assessment.
Keywords: Study Skills, Scholarly Project, Undergraduate, Medical Education, Self-Assessment
Practice Highlights
- The Scholarly Project is an essential component of the undergraduate medical education curriculum.
- Targeted researching skills is a valuable method to optimise competency-based criteria.
- The initial choice of study design is important to the overall research skill self-perceptive improvement.
I. INTRODUCTION
Scholarly Project has emerged as an essential component of the modern undergraduate medical curriculum. This entails mentored study in a single topic area and may include classical hypothesis-driven research, literature reviews, or the creation of a medically-related product (Boninger et al., 2010). By researching a topic, designing and implementing experiments and analysing the results, students not only gain knowledge and experience but also essential skills including critical thinking, time management, collaboration, information technology and confidence, all of which benefit their academic endeavours and result in higher undergraduate graduation rates (Bickford et al., 2020; Carson, 2007). Furthermore, the Scholarly Project program, which allows students to learn about research, was rated positively by most undergraduates. In addition, it provides faculty members with assistance in their research projects and the chance to influence future generations (Dagher et al., 2016). It has also been noted that the process of exposing undergraduate students to research benefits the researchers who take part as instructors by refining and shaping their scientific minds (Zydney et al., 2002).
The number of research studies with Vietnamese authorship published in ISI-indexed journals increased considerably between 2001 and 2015, with an annual growth rate of 17%. However, the majority of this growth (77%) was accounted for by international collaboration research rather than domestic-only projects, especially in the clinical medicine area. Thus, scientific research in Vietnam had not changed considerably or achieved independence in this field (Nguyen et al., 2016).
In the academic year of 2020-2021, the University of Medicine and Pharmacy at Ho Chi Minh City (UMP), Vietnam, pioneered the launch of a one-year Scholarly Project for all fifth-year medical students. This medical student population is the first generation to learn under the refreshed Undergraduate Medical Curriculum of the UMP and the first class to experience the Scholarly Project. Undergraduate research experiences are characterised by four features: mentorship, originality, acceptability, and dissemination (Kardash, 2000). Assessment of undergraduate research experience, which determines whether students gained any research skills (such as identifying the research question, collecting data, thinking independently and creatively) is best performed after completing the research program (Blockus et al., 1997; Manduca, 1997). The quasi-experimental work presented here provides one of the first investigations into how the Scholarly Project at the UMP, Vietnam, impacted on the participating students’ perception of how their medical research skills improved in the academic year of 2020-2021.
II. METHODS
A. Description of the Scholarly Project
The Scholarly Project is a compulsory academic module that aims to enable fifth-year medical students to conduct medical research early in their careers. It provides these students with an active experience in conducting a research project with faculty members starting at the beginning of the fifth academic year. The data reported here were collected from medical students and mentors who participated during the 2020-2021 academic year.
For most medical students, the Scholarly Project provides the first exposure to the field of research. There are 48 groups of nine medical students, including one team leader, one secretary, and team members, with one faculty mentor. Medical students are expected to contribute actively to the best of their ability in committed teamwork and an ethical manner.
Members of the faculties of Medicine and Public Medicine who have active ongoing research projects are eligible to participate in the Scholarly Project. Faculty members act as mentors to the students and facilitate the students’ learning process by providing supervision, guidance, and support. In addition, members should allocate suitable tasks for each student based on their skills, expertise, interests, and background.
B. Scholarly Project Steps
1) Student orientation: Student orientation occurred in the first week, informing students of the program’s procedure, and their roles and responsibilities (Figure 1). Also, in the first week, the medical student curriculum included a medical research course, describing the formation of research ideas, study design and statistics, literature searching and referencing, and research ethics. Students were also provided with important dates and deadlines for the Scholarly Project stage.
2) Matching: Matching is the process of pairing students with project mentors. From the first weeks of the Scholarly Project, each student team is required to create a team profile on the university website, including the scientific interest, skill, and research fields of interest for each team member. Each medical student team then chose a mentor from a provided list, taking into account medical research fields and their research curriculum vitae. Each team picked up to 2 mentors, in order of preference. After the deadline, mentors chose which team they would like to work with based on the students’ choice; this process continued until all teams were paired.
3) Work initiation: Students were expected to initiate contact with the faculty member after being notified via the university website that they have been matched to a project. During the second week of the Scholarly Project, faculty members and students discussed the research project, and the roles and responsibilities. Upon finalising the agreement between the two parties, students completed a meeting report form, which was signed by both the mentor(s) and the team leader. During online learning periods due to COVID-19, online meetings were encouraged, along with completion of the meeting report form. This meeting report form included information about topics discussed during the meeting, future work, each student’s role in the research project, and confirmed the next appointment date. Student teams and faculty members scheduled meetings based on the design of their study. In follow-up meetings, faculty mentors continued to discuss and evaluate the medical students’ work, and further plans were discussed. There was no upper limit for the number of meetings. However, there was a second required meeting at the third week of the Scholarly Project, which was nearly the end of the modules, for the research team to update the collected data, trouble-shooting solutions, or feedback.
4) Presentation: In the final week of the fifth-year curriculum, a Scholarly Project Symposium provided the opportunity for research teams to present their project findings. This allowed the scientific committee to evaluate both the performance of each student and the research project in general. Another aim of the symposium was for medical students to learn and share their findings with other teams, and the presentation also provides a valuable reference for the subsequent classes.

Figure 1. Integration of the Scholarly Project into the new reformed undergraduate and postgraduate medical curriculum in Vietnam.
C. Study Setting and Participants
This one-group pretest-posttest study had a quasi-experimental design. Research skills assessed were chosen based on fourteen individual research skills (Kardash, 2000). The questionnaire has been used previously, with a Cronbach’s alpha calculated at 0.9 and item-total correlation varied between 0.49 to 0.76 (Kardash, 2000). The questionnaire was translated into Vietnamese, then the local language version was pre-tested and the final text was amended as necessary. The translation process was undertaken in accordance with Guidelines for the Cross-Cultural Adaptation Process (Beaton et al., 2000). Translations were evaluated and compared with the original questionnaire by the Education and Research Council of the UMP to ensure accuracy of the Vietnamese version prior to study initiation. Medical student surveys were administered during the first week of the Scholarly Project and students were asked to indicate their current level of performance for each skill and the extent to which they hoped that the project would develop each skill on a 5-point Likert scale from 1–5 (where higher scores indicate greater skill level). Surveys were repeated at midterm and during the last week of the Scholarly Project module; at these times the students used the same scale to rate the extent to which they felt capable of performing each skill and how they believed the internship had developed their skills in general. Medical students had to provide informed consent on the first page of the electronic form before accessing the rest of the questionnaire.
D. Statistical Analysis
Raw data were extracted from the online survey link for each participating medical student and saved in Excel sheets. R (R Core Team, Vienna, Austria) was applied to analyse data. First, scores for each skill at baseline were compared with those obtained after project completion using a paired t-test (Student’s t-test). The same method was used to compare expected skill level evaluated at baseline and the actual skill level rating at the end of the Scholarly Project. A p-value of <0.05 was considered to be statistically significant.
III. RESULTS
A. Response Rate and Participant Data
Of 384 students participating in the Scholarly Project, 194 (50.5%) completed the survey. The majority of participants were male (60%) and had the role of project team member (75.3%) (See Table 1). The most common Scholarly Project design was a cross-sectional study (47.9%), followed by study protocol development (21.1%), case/case series report (11.9%), and literature review (10.3%) (Table 1). Twenty-one different departments with a wide range of specialties provided scientific mentors for the Scholarly Projects undertaken by 48 research groups (See Table 1).
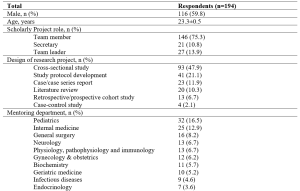
Table 1. Demographic and project characteristics for survey respondents.
Values are mean ± standard deviation, or number of respondents (%).
B. Research Skills at Baseline, Midterm and Project Completion
At baseline, self-rated competency was highest for ‘Understand the importance of “controls”’, ‘Understand contemporary concepts’, ‘Identify a specific question’, and ‘Observe and collect data’ (Figure 2). All skills had self-evaluating levels above “moderate” (score of >3), except for ‘Write research for publication’ (mean score 2.696). Students expected that all skills would increase after participating in the Scholarly Project (p<0.001).
In the midterm survey, five skill groups showed significant improvement from baseline (Figure 2). These were ‘Make use of scientific literature’, ‘Identify a specific question’, ‘Observe and collect data’, ‘Relate results to the “bigger picture”’, and ‘Orally communicate research project skills’. Conversely, there was a significant decrease in self-rated skill for ‘Statistically analyse data’ and ‘Interpret data skills’, while other skill ratings were stable (Figure 2).
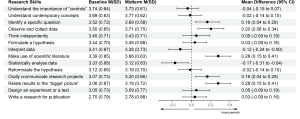
Figure 2. Change in self-rated medical research skills of 194 participants from baseline to the midterm of the Scholarly Project
M: mean; SD: standard deviation; CI: confidence interval
At the completion of the Scholarly Project, the five skills that showed improvement at the midterm assessment showed continued improvement, and another six skills had also improved significantly compared with baseline (Figure 3). However, scores for ‘Understand the importance of “controls”’, ‘Interpret data’ and ‘Statistically analyse data” did not change significantly from baseline, and the mean score for the latter parameter was actually slightly below baseline (Figure 3).
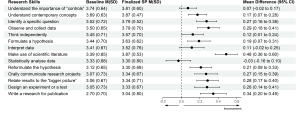
Figure 3. Change in self-rated medical research skills of 194 participants from baseline to completion of the Scholarly Project (SP)
M: mean; SD: standard deviation; CI: confidence interval.
Looking more closely at analytical skills relating to six types of study design showed that self-rated skill for the ability to interpret data for a literature review decreased significantly, as did self-rated skill scores for statistically analyse data in relation to study protocol development and literature review (Table 2). In contrast, there was a significant improvement in self-rated skill for data interpretation for cross-sectional studies and for statistical analysis of data in cohort studies (Table 2).

Table 2. Self-evaluated skill level scores for ‘Interpret data’ and ‘Statistically analyse data’ from baseline to completion of the Scholarly Project
Values are mean ± standard deviation. *p<0.05 vs baseline.
IV. DISCUSSION
A. Impact of Scholarly Project on Students’ Perception of Research Skills
Our results show that ratings for most skills increased during and after the Scholarly Project. Increases in ratings for ‘Identifying a specific question’, ‘Orally communicate research projects’, and ‘Relate results to the “bigger picture”’ in our study were consistent with data from Schor et al. (2005), who reported that the Scholarly Project could be beneficial by fostering analytical thinking skills, improving oral communication skills, and enhancing skills for evaluating and applying new knowledge to their profession (Schor et al., 2005). A significant increase in ‘Make use of scientific literature’ in our study reflects the idea-forming process at the study design stage of the Scholarly Project, during which students could practice the ability to read and critically evaluate medical literature. These are essential components of undergraduate medical education, irrespective of whether students intend to pursue a career in academic medicine or in public or private clinical practice (Holloway et al., 2004).
B. Data-related Skills and the Concept of a Control Group
The two skills of ‘Statistically analyse data’ and ‘Interpret data’ are introduced mainly in the Advanced Statistics Module with a training period of 2 weeks before starting the Scholarly Project, and briefly presented in the ‘Basic statistics informatics’ module during the first year of training and in the ‘Basic epidemiology’ module during the third year of the undergraduate curriculum. Therefore, baseline assessments in our study took place after the Advanced Statistics Module, which could have influenced ratings on the above skills. Given that our midterm assessment was performed at a time when most students had not had the opportunity to practice these skills, there may have been a negative impact on self-evaluation. The change in scores for ‘Statistically analyse data’ and ‘Interpret data’ at the midterm assessment was therefore influenced by an external factor (the Advanced Statistics Module) and an internal factor (the Scholarly Project). Therefore, future assessments of the impact of the Scholarly Project on learning should not have the quasi-experimental design used here, but instead, use an interrupted time-series design. This will mean that several surveys would be conducted before starting the Advanced Statistics Module, with the aim of eliminating confounding factors.
The final assessment showed significant improvements in scores for ‘Statistically analyse data’ and ‘Interpret data skills’ compared with the midterm survey. When applied in students’ projects, the improvement of these two skills indirectly supported the aforementioned context. This highlights the value of active learning compared with passive learning. It has conclusively been shown that cramming statistical knowledge means that students do not understand basic concepts to apply appropriately (Leppink, 2017). As noted by Leppink, statistics should be integrated into medical subjects; familiarity with these subjects and the repeated use of these skills provides opportunities to develop statistical skills. The Scholar Project is a typical example of this trend. However, only the ‘Statistically analyse data skill’ showed a downward pattern, while the ‘Interpret data skill’ increased slightly, suggesting that the Scholarly Project should focus more on these skills. Additional studies that take these variables into account are needed.
The control group concept is taught in Basic Epidemiology during the third year of Basic Science and the first sessions of the Scholarly Project. The control group has a pivotal role in study design should have elements that match the experimental group’s characteristics, except for the intervention/variable applied to the latter (Kinser & Robins, 2013). This scientific control group enables the experimental study of one variable at a time, and it is an essential part of the scientific method. Two identical experiments are carried out in a controlled experiment: in one of them, the treatment or tested factor is applied (experimental group), whereas in the other group (control), the tested factor is not applied (Pithon, 2013). However, due to the limitation that only four respondents had a project with a case-control study design, the ‘Understand the importance of “controls”’ skill only showed a modest improvement, despite having been taught previously, which is similar to a previous undergraduate research study (Kardash, 2000). Compared with cross-sectional study design, which was the most popular design for studies in this Scholarly Project, case-control studies often required a greater amount of human and facility resources. We suggest that a case-control study with a small sample size of 10–20 could be a suitable study design for medical students to understand how best to conduct research with a control group.
Of the 194 respondents in our study, 56.7% of the cohort should have been able to fully experience all fourteen of the skills assessed. In contrast, those who participated in study protocol development, literature review, and case/case series report projects had limited opportunities to practice analytical skills. Similar to our findings, a previous study demonstrated that only 13% of 475 projects conducted by medical students contained four main research skill areas, including research methods, information gathering, critical analysis and review, and data processing (Murdoch-Eaton et al., 2010). Furthermore, the COVID-19 outbreak during the academic year 2020-2021 significantly impacted the originally planned Scholarly Project data collection process. As a result, some research teams switched to more feasible design studies such as study development or literature review, which potentially influenced the two skills of statistical analysis and data interpretation skills. Therefore, it could be hypothesised that these conditions are less likely to occur if participants recognise the skills required for research before designing the study protocol. Thus, there is room for further progress in determining the optimal project descriptions provided to medical students participating in the Scholarly Project to allow them to benefit from the research opportunities and fully develop essential skills.
C. The Role of Scholarly Project in Medical Education in Vietnam
This Scholarly Project is an essential step in curriculum reform for Vietnam’s medical education system. In the last two decades, medical educators in Vietnam have collaborated to promote the social trend for undergraduate medical education, and identify the goals and outcomes of learning from medical graduates in expected knowledge, attitudes, and skills (Hoat et al., 2009). Furthermore, Vietnamese policymakers created an environment that enabled academic innovation by implementing the necessary changes to national university autonomy policies (Duong et al., 2021). These policies enable public universities to be financially independent, manage their operation and human resources, prioritise technology, and develop new curricula. The Scholarly Project helps to train physicians who are better prepared to meet patient requirements and health needs (Fan et al., 2012). Based on competency in medical education, the Scholarly Project focuses on outcomes, emphasises the application of knowledge and practice, and promotes greater learner-centeredness (Carraccio et al., 2002; Frank et al., 2010; Iobst et al., 2010). In addition, the Scholarly Project helps to reduce the time spent in passive lectures, which can negative affect medical students (Deslauriers et al., 2019; Schwartzstein et al., 2020; Schwartzstein & Roberts, 2017). Instead, students are encouraged to explore research topics based on their interests, human and institutional resources, and university mentors’ guidance and follow-up. Compared with the large class sizes from Vietnam’s traditional teaching method, the Scholarly Project (with an average of eight students and one mentor) provides low faculty-to-students ratios, creating desired small group learning. Starting for the first time in the 2020-2021 school year, Scholarly Project had to adapt to the impact of the COVID-19 pandemic, with two periods of online learning required in September 2020 and May 2021 due to local COVID-19 outbreaks. To help manage this, the university applied for technical assistance from Microsoft Office 365 with a full-access subscription to maintain the scheduled small group meetings between students and their mentors while optimising social distancing (Duong et al., 2021).
We recommend introducing the 14-skill questionnaire as a tool for medical students to self-monitor their improvement during participation in the Scholarly Project. From the mentors’ perspective, the questionnaire provides a reliable and convenient reference for providing feedback to students and suggestions about areas that need further improvement. These approaches could also be utilised in other institutions, either locally or internationally, who include a Scholarly Project for a number of reasons: (1) the Scholarly Project is a lengthy module that could be impacted by unexpected events (e.g. COVID-19); (2) the need for routine self-check and mentor feedback to facilitate the required research skills improvement; and (3) because the questionnaire is a validated, convenient and accessible method for both medical students and mentors.
D. Study Limitations
Although the survey was sent to all medical students participating in the Scholarly Project, only just over half of students responded. Therefore, the impact of the Scholarly Project on non-responding medical students may not reflect the trends reported here, limiting the generalizability of our findings. Nonresponse bias is another potential limitation, although this is not necessarily associated with a lower response rate (Davern, 2013; Halbesleben and Whitman, 2012). Participants might perceive that self-evaluation about how much their research skills had improved could indirectly reflect their level of participation in Scholarly Project, the contribution of their mentor, and the level of their academic performance, leading to social desirability bias in their responses. We attempted to reduce nonresponse and social desirability bias, and any perception that responses could impact on academic assessments, by making survey responses anonymous and keeping the study survey completely separate from any academic assessments (e.g. grade-point average). Another limitation is the lack of a control group of medical students, but this is difficult because participation in the Scholarly Project is mandatory for all students. Using a control group would have strengthened the study from a methodological perspective and allowed investigation of the impact of specific aspects of the Scholarly Project.
Respond shift bias is inevitable while conducting this research. To reduce this, instead of completing self-evaluation for all fourteen skills initially and then after the completion of the whole project, students should assess their skill level immediately after the completion of each Module. However, response shift bias happened because respondents perceived the purpose of the survey as assessing the program’s effectiveness. In the context of our research, even if assessments were completed after each Module, students would realise the aim of the survey meaning that respond-shift bias would not decrease considerably.
V. CONCLUSION
Scholarly Project is an excellent learning opportunity for medical students in the refreshed undergraduate medical curriculum. Participating in a Scholarly Project provides students with research experience, including the knowledge, structure, and support needed to engage in scholarly work. By providing the foundations for scholarly work, medical students can enter the health care workforce with solid clinical expertise and the basic skills required to conduct high-quality projects that improve the safety and quality of care delivered to patients. We suggest integrating the Scholarly Project curriculum throughout the undergraduate medical education curriculum in Vietnam. This is important in terms of early experience of medical research and fostering a good understanding of medical scientific research for all future doctors, regardless of their ultimate career destination.
Notes on Contributors
N.T.M.D. and K.H.V. drafted and revised the manuscript. V.T.N.L. helped in reviewing the manuscript. All authors (N.T.M.D., K.H.V., V.T.N.L.) have made substantial contributions to the conception and design of the work and the acquisition, analysis, and interpretation of data. All authors read and approved the final manuscript.
Ethical Approval
The authors declare that this study did not require human ethics approval and did not include experiments on animal or human subjects. This study was submitted to the Institutional Review Board (IRB) at University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam. This project was determined to be exempt from IRB review. All methods were carried out in accordance with relevant guidelines and regulations. Respondents were informed that their participation in the survey was completely voluntary and there were no risks associated with their participation.
Data Availability
The datasets generated and/or analysed during the current study are not publicly available for reasons of data protection but are available from the corresponding author on reasonable request.
Acknowledgement
The authors would very much like to acknowledge Ms. Le Minh Chau, Mr. Ung Nguyen Vu Hoang, Ms. Duong Kim Ngan, Mr. Nguyen Hai Dang, Ms. Tran Thi Hong Ngoc, Mr. Giang Luu Thanh Hoang, and Mr. Nguyen Hoang Nhan (University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam) for their support of this study.
Funding
No funding has been received for the study.
Declaration of Interest
The authors declare that they have no competing interests.
References
Beaton, D. E., Bombardier, C., Guillemin, F., & Ferraz, M. B. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures. Spine, 25(24), 3186-3191. https://doi.org/10.1097/00007632-200012150-00014
Bickford, N., Peterson, E., Jensen, P., & Thomas, D. (2020). Undergraduates interested in STEM research are better students than their peers. Education Sciences, 10(6), 150. https://doi.org/10.3390/educsci10060150
Blockus, L., Kardash, C. M., Blair, M., & Wallace, M. (1997). Undergraduate internship program evaluation: A comprehensive approach at a research university. Council on Undergraduate Research, 18, 60–63.
Boninger, M., Troen, P., Green, E., Borkan, J., Lance-Jones, C., Humphrey, A., Gruppuso, P., Kant, P., McGee, J., Willochell, M., Schor, N., Kanter, S. L., & Levine, A. S. (2010). Implementation of a longitudinal mentored scholarly project: An approach at two medical schools. Academic Medicine, 85(3), 429–437. https://doi.org/10.1097/acm.0b013e3181ccc96f
Carraccio, C., Wolfsthal, S. D., Englander, R., Ferentz, K., & Martin, C. (2002). Shifting Paradigms. Academic Medicine, 77(5), 361–367. https://doi.org/10.1097/00001888-200205000-00003
Carson, S. (2007). A new paradigm for mentored undergraduate research in molecular microbiology. CBE—Life Sciences Education, 6(4), 343–349. https://doi.org/10.1187/cbe.07-05-0027
Dagher, M. M., Atieh, J. A., Soubra, M. K., Khoury, S. J., Tamim, H., & Kaafarani, B. R. (2016). Medical Research Volunteer Program (MRVP): Innovative program promoting undergraduate research in the medical field. BMC Medical Education, 16(1), Article 160. https://doi.org/10.1186/s12909-016-0670-9
Davern, M. (2013). Nonresponse rates are a problematic indicator of nonresponse bias in survey research. Health Services Research, 48(3), 905–912. https://doi.org/10.1111/1475-6773.12070
Deslauriers, L., McCarty, L. S., Miller, K., Callaghan, K., & Kestin, G. (2019). Measuring actual learning versus feeling of learning in response to being actively engaged in the classroom. Proceedings of the National Academy of Sciences, 116(39), 19251–19257. https://doi.org/10.1073/pnas.1821936116
Duong, D. B., Phan, T., Trung, N. Q., Le, B. N., Do, H. M., Nguyen, H. M., Tang, S. H., Pham, V. A., Le, B. K., Le, L. C., Siddiqui, Z., Cosimi, L. A., & Pollack, T. (2021). Innovations in medical education in Vietnam. BMJ Innovations, 7(Suppl 1), s23–s29. https://doi.org/10.1136/bmjinnov-2021-000708
Fan, A. P., Tran, D. T., Kosik, R. O., Mandell, G. A., Hsu, H. S., & Chen, Y. S. (2012). Medical education in Vietnam. Medical Teacher, 34(2), 103–107. https://doi.org/10.3109/0142159x.2011.613499
Frank, J. R., Snell, L. S., Cate, O. T., Holmboe, E. S., Carraccio, C., Swing, S. R., Harris, P., Glasgow, N. J., Campbell, C., Dath, D., Harden, R. M., Iobst, W., Long, D. M., Mungroo, R., Richardson, D. L., Sherbino, J., Silver, I., Taber, S., Talbot, M., & Harris, K. A. (2010). Competency-based medical education: Theory to practice. Medical Teacher, 32(8), 638–645. https://doi.org/10.3109/0142159x.2010.501190
Halbesleben, J. R. B., & Whitman, M. V. (2012). Evaluating survey quality in health services research: A decision framework for assessing nonresponse bias. Health Services Research, 48(3), 913–930. https://doi.org/10.1111/1475-6773.12002
Hoat, L. N., Lan Viet, N., van der Wilt, G., Broerse, J., Ruitenberg, E., & Wright, E. (2009). Motivation of university and non-university stakeholders to change medical education in Vietnam. BMC Medical Education, 9(1), Article 49. https://doi.org/10.1186/1472-6920-9-49
Holloway, R., Nesbit, K., Bordley, D., & Noyes, K. (2004). Teaching and evaluating first and second year medical students’ practice of evidence-based medicine. Medical Education, 38(8), 868–878. https://doi.org/10.1111/j.1365-2929.2004.01817.x
Iobst, W. F., Sherbino, J., Cate, O. T., Richardson, D. L., Dath, D., Swing, S. R., Harris, P., Mungroo, R., Holmboe, E. S., & Frank, J. R. (2010). Competency-based medical education in postgraduate medical education. Medical Teacher, 32(8), 651–656. https://doi.org/10.3109/0142159x.2010.500709
Kardash, C. M. (2000). Evaluation of undergraduate research experience: Perceptions of undergraduate interns and their faculty mentors. Journal of Educational Psychology, 92(1), 191–201. https://doi.org/10.1037/0022-0663.92.1.191
Kinser, P. A., & Robins, J. L. (2013). Control group design: enhancing rigor in research of mind-body therapies for depression. Evidence-Based Complementary and Alternative Medicine, 2013. https://doi.org/10.1155/2013/140467
Leppink, J. (2017). Helping medical students in their study of statistics: A flexible approach. Journal of Taibah University Medical Sciences, 12(1), 1–7. https://doi.org/10.1016/j.jtumed.2016.08.007
Manduca, C. (1997). Broadly defined goals for undergraduate research projects: A basis for program evaluation. Council on Undergraduate Research, 18(2), 64–69.
Murdoch-Eaton, D., Drewery, S., Elton, S., Emmerson, C., Marshall, M., Smith, J. A., Stark, P., & Whittle, S. (2010). What do medical students understand by research and research skills? Identifying research opportunities within undergraduate projects. Medical Teacher, 32(3), e152–e160. https://doi.org/10.3109/01421591003657493
Nguyen, T. V., Ho-Le, T. P., & Le, U. V. (2016). International collaboration in scientific research in Vietnam: An analysis of patterns and impact. Scientometrics, 110(2), 1035–1051. https://doi.org/10.1007/s11192-016-2201-1
Pithon, M. M. (2013). Importance of the control group in scientific research. Dental Press Journal of Orthodontics, 18(6), 13–14. https://doi.org/10.1590/s2176-94512013000600003
Schor, N. F., Troen, P., Kanter, S. L., & Levine, A. S. (2005). The scholarly project initiative: Introducing scholarship in medicine through a longitudinal, mentored curricular program. Academic Medicine, 80(9), 824–831. https://doi.org/10.1097/00001888-200509000-00009
Schwartzstein, R. M., Dienstag, J. L., King, R. W., Chang, B. S., Flanagan, J. G., Besche, H. C., Hoenig, M. P., Miloslavsky, E. M., Atkins, K. M., Puig, A., Cockrill, B. A., Wittels, K. A., Dalrymple, J. L., Gooding, H., Hirsh, D. A., Alexander, E. K., Fazio, S. B., & Hundert, E. M. (2020). The Harvard Medical School pathways curriculum: Reimagining developmentally appropriate medical education for contemporary learners. Academic Medicine, 95(11), 1687–1695. https://doi.org/10.1097/acm.0000000000003270
Schwartzstein, R. M., & Roberts, D. H. (2017). Saying goodbye to lectures in medical school — Paradigm shift or passing fad? New England Journal of Medicine, 377(7), 605–607. https://doi.org/10.1056/nejmp1706474
Zydney, A. L., Bennett, J. S., Shahid, A., & Bauer, K. W. (2002). Impact of undergraduate research experience in engineering. Journal of Engineering Education, 91(2), 151–157. https://doi.org/10.1002/j.2168-9830.2002.tb00687.x
*Nguyen Tran Minh Duc
217 Hong Bang Street, Ward 11,
District 5, Ho Chi Minh City, Vietnam
+84 988 127 948
Email: ntmduc160046@ump.edu.vn
Submitted: 13 January 2022
Accepted: 9 May 2022
Published online: 4 October, TAPS 2022, 7(4), 35-49
https://doi.org/10.29060/TAPS.2022-7-4/OA2699
Yuan Kit Christopher Chua1*, Kay Wei Ping Ng1*, Eng Soo Yap2,3, Pei Shi Priscillia Lye4, Joy Vijayan1, & Yee Cheun Chan1
1Department of Medicine, Division of Neurology, National University Hospital Singapore, Singapore; 2Department of Haematology-oncology, National University Cancer Institute Singapore, Singapore; 3Department of Laboratory Medicine, National University Hospital Singapore, Singapore; 4Department of Medicine, Division of Infectious Diseases, National University Hospital Singapore, Singapore
*Co-first authors
Abstract
Introduction: In-class engagement enhances learning and can be measured using observational tools. As the COVID-19 pandemic shifted teaching online, we modified a tool to measure the engagement of instructors and students, comparing in-person with online teaching and different class types.
Methods: Video recordings of in-person and online teachings of six identical topics each were evaluated using our ‘In-class Engagement Measure’ (IEM). There were three topics each of case-based learning (CBL) and lecture-based instruction (LLC). Student IEM scores were: (1) no response, (2) answers when directly questioned, (3) answers spontaneously, (4) questions spontaneously, (5) initiates group discussions. Instructor IEM scores were: (1) addressing passive listeners, (2) asking ≥1 students, (3) initiates discussions, (4) monitors small group discussion, (5) monitoring whole class discussions.
Results: Twelve video recorded sessions were analysed. For instructors, there were no significant differences in percentage time of no engagement or IEM scores when comparing in-person with online teaching. For students, there was a significantly higher percentage time of no engagement for the online teaching of two topics. For class type, there was overall less percentage time of no engagement and higher IEM scores for CBL than LLC.
Conclusion: Our modified IEM tool demonstrated that instructors’ engagement remained similar, but students’ engagement reduced with online teaching. Additionally, more in-class engagement was observed in CBL. “Presenteeism”, where learners were online but disengaged was common. More effort is needed to engage students during online teaching.
Keywords: Engagement, Observational Tool, Online Learning, E-learning, COVID-19, Medical Education, Research
Practice Highlights
- Lectures to large class (LLC) and case-based learning (CBL) are associated with lower levels of student engagement when conducted on a virtual platform.
- Instructors’ engagement during online teachings remained similar to that of in-person teachings.
- LLC is associated with reduced student engagement than CBL.
I. INTRODUCTION
Educational theories suggest that learning should be an active process. According to social constructivist theory, learning can be better achieved by social interactions in the learning environment (Kaufman, 2003). Active learning strategies fostering the students to interact with each other and the instructor such as discussions, talks, questions, may yield desirable learning outcomes in terms of knowledge, skills, or attitudes (Rao & DiCarlo, 2001). Therefore, using in-class learner engagement as an important keystone of active learning strategies is known to stimulate and enhance the learner’s assimilation of content and concepts (Armstrong & Fukami, 2009; Watson et al., 1991).
There is good evidence for the importance of engagement in online learning and use of an engagement metric has been advocated to better understand student online interactions to improve the online learning environment (Berman & Artino, 2018). While medical literature suggests that virtual education games foster engagement (McCoy et al., 2016), the level of engagement and learning fostered by online methods for group discussion and teaching is unknown. Teleconferencing is among some of the methods suggested for maintaining education during the COVID-19 pandemic (Chick et al., 2020).
Possible methods of quantifying student engagement include direct observation and student self-report. O’Malley et al. (2003) has published a validated observation instrument called STROBE to assess in-class learner engagement in health professions without interfering with learner activities. This observation instrument is used to document observed dichotomized types of instructor and student behaviors in 5-minute cycles and quantify the number of questions asked by the instructor and students in different class subtypes. This instrument as well as revised forms of this instrument has since been used as “in-class engagement measures” to compare instructor and student behaviors in different class types (Alimoglu et al., 2014; Kelly et al., 2005).
In our institution, a hybrid curriculum of case-based learning as well as lecture-style courses is used to teach the post graduate year one (PGY-1) interns. We had video recordings of these courses performed in-person prior to the COVID-19 pandemic. With the advent of the pandemic, these courses were shifted onto Zoom teleconferencing platform, but delivered by the same instructors, in the same class format.
We therefore aimed to determine and compare in-class learning engagement levels via observing instructor and student behaviours in different platforms of learning (either observed online or in-person retrospectively via video recording) delivered by the same instructor before and during the COVID-19 pandemic. We also aimed to compare instructor and student behaviours in different class types (either case-based learning or lecture style instruction). To do this, we planned to modify a known in-person observational tool for student engagement – “STROBE” (O’Malley et al., 2003) for use in analysing and recording the behaviours of students in both online and in-person teaching.
II. METHODS
A. Observed Class Types
In this study, we observed two different class types, case-based learning (CBL), as well as lecture-based instruction to teach basic medical/surgical topics to a large classroom (LLC) of PGY-1 interns. Video recordings of these in-person teachings were made in 2017. Both these class types were replicated in the same format on an online Zoom teleconferencing platform and were delivered by nearly all of the same tutors using the same content and Powerpoint slides during the COVID-19 pandemic in 2020. We aimed to view the 2017 video-recordings of the in-person teachings and compare them with the 2020 online teaching of PGY-1 interns. Written consent was obtained from the tutors and implied consent from the students. Students were informed beforehand via email that the sessions were going to be observed and they were again reminded at the start of each session where they had the chance to opt out. Subsequently, all student feedback and observation scores were amalgamated and de-identified. This study was approved by the institution’s ethics board.
Three topics each of case-based learning as well as lecture-style instruction were selected in chronological order as scheduled for students. Each topic of instruction was allotted up to a maximum of 90 minutes of time, but the instructor could choose to end the class earlier if the session was completed. Description of both class types are below.
1) Description of case-based learning in large classroom
The content of the learning was designed by the instructor, and consisted of clinical cases involving patient scenarios, where the main pedagogy was problem-solving and answering case-based questions relating to the patient scenario (e.g., diagnosis, reading clinical images or electrocardiograms, creating an investigation or treatment plan). Each case would typically take about 15 to 20 minutes to complete, and there would typically be five to six cases. Students were expected to answer the questions, and the instructor gave feedback on the answers and provided additional information, sometimes via additional Powerpoint slides. Class discussions were encouraged where students were encouraged to debate and discuss with each other over their classmates’ answers. The titles of the case-based learning were “ECG – tachydysrhythmias”, “Approach to a confused patient” and “Approach to chest pain”.
2) Description of lecture in large classroom
This is a typical lecture-style instruction performed with participation of around 86 PGY1-interns and one instructor. The instructor delivers information via a Powerpoint slide presentation and rarely adds clinical case-based questions into the slides to invite student discussion. The titles of the lectures were “Cardiovascular health – hypertensive urgencies”, “Trauma – chest, abdomen and pelvis” and “Stroke”.
B. Instructor and Student Characteristics
The instructors all had at least ten years of teaching experience in medical education, and all had been teaching the same topics to the PGY-1 interns for at least the last five years. Student feedback scores on their teaching activities have been satisfactorily high (mean 4.63 for 2019, the year prior to the shift to online learning for the pandemic). All the tutors (except for one instructor who taught “Stroke”) had taught the same topics using the same content and Powerpoint slides in 2017 via in-person teaching which was caught on camera.
The students were all PGY-1 interns, who have been asked by the institution to attend at least 70% of a mandatory one-year long teaching program where they are given weekly instruction on various medical or surgical topics. The teaching program commences from May of each year. There were 86 PGY-1 interns commencing their rotations in our institution and attending the teaching program from May 2020. There were 75 PGY-1 interns attending the teaching program in the video recordings caught in 2017.
C. Observation Tool
A revised form of STROBE (O’Malley et al., 2003) was used to analyze and record the behaviors of the instructor and students in classes, to provide a more objective third-person measure of student engagement. The original STROBE tool was an instrument that was developed to objectively measure student engagement across a variety medical education classroom settings. The STROBE instrument consists of 5-minute observational cycles repeated continuously throughout the learning session with relevant observations recorded on a data collection form. Within each cycle, observers record selected aspects of behavior from a list of specified categories that occur in each interval recorded. Observations include macrolevel elements such as structure of class, major activity during time, and a global judgment of the proportion of class members who appear on task, as well as microlevel elements such as instructor’s behavior and the behaviors of four randomly selected students. Observers also record who the behaviours of instructors and students were directed at. After which, observers tally the number of questions asked by the students and instructor in the remainder of the 5 minutes. The revision of this tool was made by the 3 Clinician-educators from the research team (CYC, YES, KN), having discussed what kind of instructor and student behaviors were considered as “active student engagement”, keeping the main statements and principles of the original STROBE tool. The scale was modified to make it suitable for use in an online learning setting, where the observers may not be able to observe the student’s body language cues when the student does not turn on his/her video function. We called this modified scale our ‘In-class engagement measure’. The modified scales were as follows:
A 5-item list of instructor and student behaviors was therefore created and rated from 1 to 5 each, with different scales for instructor and student. For the student behavior scale, each item was to show progressively increasing levels of interaction, and perceived engagement, both with the instructor and with each other. For the instructor behavior list, each item was also about progressively interactive behaviors by the instructor to get the students to engage. We called these scales our “In-class Engagement Measure (IEM)”. The scales were as follows:
Student:
- No response even when asked
- Answers only when directly questioned
- Answers questions spontaneously
- Speaks to instructor spontaneouslyg.,Poses questions, discusses concepts
- Speaks to instructor and 1 or more other student during a discussion
Instructor:
- Talking to entire class while all the students are passive receivers
- Telling/asking to one or a group of students, or teaching/showing an application on a student
- Starting or conducting a discussion open to whole class, or assigning some students for some learning tasks
- Listening/monitoring actively discussing one or a group of students
- Listening/monitoring actively discussing entire class
For the student behaviour list, we also sub-categorized the student behaviour item “1”, where “1*” was defined as no response when a question was posed to a specific student and not just the whole class, where the student-in-question would have his/her name called by the tutor.
D. Observation Process
Drawing from the described process for the STROBE observation tool (O’Malley et al., 2003), as well as other described modifications of the STROBE tool (Alimoglu et al., 2014), we used the same observation units and cycles. Modifications to the original described process for the STROBE observation tool was made to make it suitable for not being in-person when observing a large group of students and their instructor. Three observers from the research team (CYC, YES, KN) observed and recorded the instructor and student behaviors for the three case-based learning and three lecture-style learning conducted live online in 2020, and as a video recording of in-person teaching in 2017. A total of 12 lectures were therefore analyzed. One observation unit was a 5-minute cycle. The 5-minute cycle would proceed as such: The observer would write the starting time of the cycle and information about the class (number of students, title of session). The observer would select a student from the class and observe that student for 20 seconds and mark the type of engagement observed according to the IEM scale created. As the observers were not in-person for the teaching at either the 2017 video recording, and for the 2020 online learning, students who responded to the instructor or posed questions were marked at the same time by all the three observers. The 5-minute cycle would consist of four 20-second observations of individual learners, so marking of student engagement would be performed four times within that cycle with different students in succession. The observer would also observe the instructor for that 5-minute cycle and similarly mark the instructor’s behavior once for that 5-minute cycle. For the remainder of the modified STROBE cycle, the observer would tally the number of questions asked by all the students and the instructor.
Observers independently and separately observed and marked the students’ and instructors’ behaviors. Due to the lack of in-person observation, students who responded or posed questions during the session were uniformly chosen for marking by the three observers. If a student had already been marked once during that cycle, the same student was not used for remaining three observations within the same cycle. At the end of the marking, two observers (KN and YES) compared their scores for both students and instructor. The marks given by the third observer (CYC) was used to validate the final score awarded and used as the tiebreaker when there was a discrepancy in the marks given by the first two observers.
E. Collation of Post Teaching Survey Feedback
Apart from the data derived from our modified observational tool, we also reviewed data from surveys conducted by the educational committee after each of these teaching sessions (see Table 1). These were general surveys used to solicit student feedback on the teaching sessions. They were distributed in-person in 2017, with the same forms distributed to the students online in 2020. Responses from the students were in response to five statements, with scoring 0 to 5 (1 for Strongly disagree, 2 for disagree, 3 for neither agree nor disagree, 4 for agree, and 5 for Strongly agree). These feedback forms had an overall feedback score marked by the student, as well as a score marked by the student in response to a question assessing for self-reported engagement – “The session was interactive and engaging”. The other questions were “The session has encouraged self-directed learning and critical thinking”, “The session was relevant to my stage of training”, “The session helped me advance my clinical decision-making skills”, and “The session has increased my confidence in day-to-day patient management”. Means of the feedback scores were taken as a qualitative guide, and we analyzed the overall feedback scores (“Overall feedback score” in Table 1), and the scores in response to the question assessing for self-reported engagement (“Self-reported engagement feedback score” in Table 1).
F. Statistical Analyses
Descriptive statistics were used to determine frequencies and median number of questions asked, as well as mean student feedback scores and absolute duration of each teaching session. Fisher exact test was also performed to analyze the differences in scores between different lectures and case-based learning, and the scores in the 2017 in-person learning versus that of the 2020 online learning. For analysis of the scores, we dichotomized our scores using the cut-off of “1”, or our first item on the behavior list for both students and instructors, as we felt that the first item reflected an extreme non-participation for both student and instructor, which if left to continue, can result in negative learning and teaching behaviors.
III. RESULTS
A. Class Types, Characteristics, Feedback Scores
A total of 12 sessions were observed, consisting of in-person and online teaching sessions of six topics (Table 1). There were 3 topics of CBL and LLC each. Duration of the class sessions range from 30-55 minutes for the in-person sessions and 40-90 minutes for the online sessions. Total number of PGY-1 students eligible to attend the in-person teaching sessions in 2017 was 82, and 86 for the online teaching sessions in 2020. Student attendance for the in-person sessions ranged from 11 (13.4%) to 31 (37.8%) and that for the online session ranged from 28 (32.6%) to 77 (89.5%). Median (range) of feedback scores for in-person sessions were 4.57 (4.25 to 4.72) vs 4.32 (4.04 to 4.61) for online sessions. Median (range) of self-reported engagement scores for in-person sessions were 4.55 (4.25 to 4.79) vs 4.34 (4.00 to 4.67) for online sessions (Table 1).
Table 1. Class types and characteristics (*Different tutors, but using same content)
B. Instructors’Engagement Behaviour
1) Comparing in-person vs online teaching: Percentage time during which there is no engagement/interaction (or scoring “1” on the IEM score). This ranges from 0-80% for in-person teaching vs 0-100% for online teaching (Table 2A). For each topic, there is no significant difference between percentage time of no engagement.
Most frequent IEM scores. Most frequent IEM scores for each 5-minute segment were 3 for in-person teaching (48.9%) and online teaching (52.9%) (Table 2B).
2) Comparing CBL vs LLC: Percentage time during which there is no engagement/interaction. This ranges from 0-23.1% for CBL vs 50-100% for LLC (Table 2A).
Most frequent IEM scores. Most frequent IEM score was 3 for CBL (77.3%) and 1 for LLC (71.4%). (Table 2B).
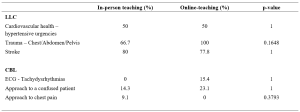
Table 2A. Comparison of instructors’ behaviour showing percentage time with no engagement (scoring “1” on the IEM score)
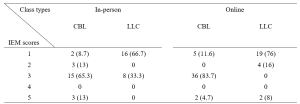
Table 2B. Numbers (percentages) of a particular IEM score received for a 5-minutes segment of teaching – for instructors
C. Students’ Engagement Behaviour
1) Comparing in-person vs online teaching: Percentage time during which there is no engagement/interaction. This ranges from 0-95% for in-person teaching vs 78.8-100% for online teaching (Table 3A). There is significant difference in percentage time of no engagement in two topics (ECG, chest pain), where there is higher percentage of no engagement time with online teaching.
Most frequent IEM scores. Most frequent IEM scores were 1 for both in-person teaching (63.8%) and online teaching (85.1%) (Table 3B).
2) Comparing CBL vs LLC: Percentage time during which there is no engagement/interaction. This ranges from 0-81.9% for CBL vs 84.4-100% for LLC (Table 3A).
Most frequent IEM scores.
Most frequent IEM scores were 1 for both CBL (65.3%) and LLC (91.8%) (Table 3B).
Presence of 1* scores, where “1*” was defined as no response when a question was posed to a specific student called by name. There was no 1* IEM score for in-person teaching for either CBL or LLC, and 8.4% (12/143) of the “1” responses were 1* for online-teaching for CBL and 6.5% (6/92) of the “1” responses were 1* for LLC.
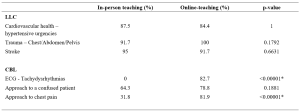
Table 3A. Comparison of students’ behaviour showing percentage time with no engagement (scoring “1” on the IEM score)
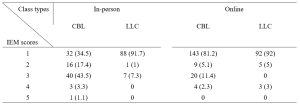
Table 3B. Numbers (percentages) of a particular IEM score received for a 5-minutes segment of teaching – for students
D. Number of Questions Asked Per 5-minute Cycle
Median number of questions asked by instructors ranged from 0-2 for in-person teaching and 1-3 for online teaching (See Appendix 1). These range from 1-3 for CBL vs 0-1 for LLC.
Median number of questions asked by students in all sessions were 0.
The results for this study can be derived from the dataset uploaded onto the online repository accessed via https://doi.org/10.6084/m9.figshare.18133379.v1 (Chua et al., 2022).
IV. DISCUSSION
We modified the known STROBE instrument (O’Malley et al., 2003) to create an observational tool “IEM” which could be used to quantify instructor and student engagement despite the observer not being present in-person. Our IEM scores were derived by taking scores that were in agreement when independently scored by two main observers (YES and KN). The third observer (CYC) was used as the validator of the scores by the two main observers. When there was a discrepancy in the scores awarded by the two observers, the score which was in agreement with the score awarded by CYC was used. To give an indication of the IEM tool’s effectiveness where the observer is not present in-person, we postulated that our modified IEM score should still demonstrate the well-documented difference in engagement between lecture-style learning and case-based learning sessions (Kelly et al., 2005). Our modified IEM score did indeed show more frequent higher scores as expected for case-based learning sessions (Tables 2B and 3B). We also compared our IEM scores with the students’ self-reported engagement scores (Table 1) that had been collected as part of student feedback. The general correlation in the trend of observed IEM scores with that of the students’ self-reported engagement scores also suggest the usefulness of our modified STROBE tool in situations where the observer is not present in-person, although this needs to be further validated in prospective studies.
Our initial study hypothesis was that students may find themselves more engaged in online teaching sessions and open to posing questions to the instructor and their peers, due to the presence of the “chat”, “likes” and “poll” functions available on the Zoom tele-conferencing platform, which may be more familiar to a younger generation accustomed to using social media. We had postulated that live online lectures would encourage further engagement from students who would not otherwise participate in-person, due to the less intimidating online environment where they can ask and answer questions more anonymously (Kay & Pasarica, 2019; Ni, 2013). In an Asian-pacific context, video conferencing had been found to be able to improve access for participation for more reticent participants who prefer written expression, through alternative communication channels like the ‘chat box’, although there was a potential trend to reduced engagement. (Ong et al., 2021).
Our data, shows, that Zoom teleconferencing during the COVID-19 pandemic can be associated with reduced student engagement. The percentage time where there was no engagement was significantly higher with online sessions (Table 3A) and the most frequent IEM score was lower (1 for online vs 3 for in-person), for CBL sessions (Table 3B). This phenomenon in medical education during the COVID-19 pandemic has previously been described. Using student and instructor feedback, students were more likely to have reduced engagement during virtual learning (Longhurst et al., 2020; Dost et al., 2020), and would have increased difficulties maintain focus, concentration and motivation during online learning (Wilcha, 2020).
Our data also suggests that for the instructor to even try to achieve close to the same levels of engagement as before, a longer duration of time was spent by each instructor per topic when executing CBL (Table 1). This may include time where the instructor needs multiple attempts at questioning and discussion before there is a student response. It is also possible that for in-person learning, the instructor relies greatly also on non-verbal cues (e.g., body language, nods of the head, collective feel of the room) to determine if a question has been satisfactorily answered, and therefore can move on quicker than when on a Zoom platform where one cannot see most, or even every student.
The higher number of attendees for online learning compared to in-person attendance (see Table 1) highlights one of the strengths of online learning, which is where online learning is more easily accessible for students who would save on time getting to a designated lecture room and provides flexibility for students to enter and exit (Dost et al., 2020). Unfortunately, this also likely encourages the phenomenon of “presenteeism”, where students are not focused on the learning session, but instead engage in other tasks simultaneously, e.g., reading or composing emails, or completing work tasks instead of having dedicated protected teaching time. Resident learners have been described to participate in nearly twice as many non-teaching session related activities per hour during an online session than when in-person (Weber & Ahn, 2020). This has likely contributed to the number of 1* scores we had, where the student has logged into the Zoom platform, but is not available to even respond in the negative when called upon to answer a question. This presenteeism, however, is not just a problem for online learning, but even for in-person learning, where pretending to engage has been found to be a significant unrecognized issue (Fuller et al., 2018).
The main implication that our study highlights that to improve student engagement when using online learning, a face-to-face platform cannot simply be transposed into a virtual platform. It had been suggested that engagement during live virtual learning could be enhanced with the use of interactive quizzes with audience polling functions (Morawo et al., 2020) and possibly other methods such as “gamification” (Nieto-Escamez & Roldan-Tapia, 2021). Our instructors for the CBL sessions had used both poll functions and live questioning for their sessions, but without increased success in engagement. Smaller groups are likely required to enhance student engagement, but this would lead to the need for increased time and teaching manpower. Increasing the opportunity for interaction via a virtual platform would also require the need to create additional online resources, which would take up more faculty time where creating new resources can take at least three times as much work compared to a traditional format (Gewin, 2020). Online resources would need to be modified in such a way that increases student autonomy to increase student engagement in medical education (Kay & Pasarica, 2019). Our study also shows that as a first step, in time and resource-limited settings, a case-based approach to teaching would be more ideal to enhance student engagement than lecture style teaching.
A culture of accountability also needs to be fostered within the online teaching sessions, where students need to be educated on how Zoom meetings can be more enriching when cameras are on (Sharp et al., 2021). PGY-1 interns, as recent graduates, also need to be educated on the aspect of professionalism when entering the medical work force, where they can be called upon to answer questions during meetings or conferences. When initial questions are not voluntarily answered, our tutors often practice “cold-calling”, which can help keep learners alert and ready (Lemov, 2015). Unfortunately, these evidence-based teaching methods that work well when the student is in-person, ultimately will fail if online students are not educated on their need to be accountable to the instructor or their peers.
This study has several limitations. Firstly, the level of student engagement may also be affected by external factors, such as a different physical learning environment, class size and avenues of communication. The stresses of the on-going pandemic may also have affected student engagement, as a decrease in quality of life and stress would negatively impact student motivation (Lyndon et al., 2017). Secondly, the topics for lecture to large class and case-based learning were not identical as these topics were picked in chronological order and there were no topics in the curriculum that had material for both the lecture and case-based learning class types. This difference in topics may have potentially contributed to confounding when we try to make direct comparisons between the two class types, although, we have attempted to mitigate this by including a variety of topics in each class type. Thirdly, the improved student engagement and feedback scores for in-person learning may also have had some bias given the smaller student size for in-person learning. It is also possible that only the more motivated, and hence more likely to be engaged students, would turn up for in-person learning. Fourthly, due to the online nature as well as the retrospective viewing of the video recordings, the observers were not present in-person to observe the non-verbal cues of the students or instructors. The tool, however, was modified to take into account only the verbal output that could be observed online or via video recording. Lastly, our IEM tool will benefit from more studies and research to further confirm its validity in observing students when the observer is not present in-person.
V. CONCLUSION
Lectures are associated with reduced student engagement than case-based learning, while both class types are associated with lower levels of student engagement when conducted on a virtual platform. Instructor levels of engagement, however, remain about the same. This highlights that a face-to-face platform cannot simply be transposed into a virtual platform, and it is important to address this gap in engagement as this can lower faculty satisfaction with teaching and ultimately result in burnout. Blended teaching or smaller group teaching as the world turns the corner in the COVID-19 pandemic may be one way to circumvent the situation but is also constrained by faculty time and manpower. Our study also shows that as a first step, in time and resource-limited settings, a case-based approach to teaching would be more ideal to enhance student engagement than lecture style teaching.
Notes on Contributors
Dr Ng Wei Ping Kay and Dr Chua Yuan Kit Christopher are co-first authors and contributed to conceptual development, acquisition, analysis, and interpretation of data for the work. They contributed to drafting and revising the work and approved the final version to be published. They agree to be accountable for all aspects of the work.
Dr Lye Pei Shi Priscillia contributed to conceptual development, acquisition, analysis, and interpretation of data for the work. She contributed to drafting and revising the work and approved the final version to be published. She agrees to be accountable for all aspects of the work.
Dr Joy Vijayan contributed to conceptual development, acquisition, analysis, and interpretation of data for the work. He contributed to drafting and revising the work and approved the final version to be published. He agrees to be accountable for all aspects of the work.
Dr Yap Eng Soo contributed to conceptual development, acquisition, analysis, and interpretation of data for the work. He contributed to drafting and revising the work and approved the final version to be published. He agrees to be accountable for all aspects of the work.
Dr Chan Yee Cheun contributed to conceptual development, acquisition, analysis, and interpretation of data for the work. He contributed to drafting and revising the work and approved the final version to be published. He agrees to be accountable for all aspects of the work.
Ethical Approval
I confirm that the study has been approved by Domain Specific Review Board (DSRB), National Healthcare Group, Singapore, an institutional ethics committee. DSRB reference number: 2020/00415.
Data Availability
The data that support the findings of this study are openly available in Figshare at https://doi.org/10.6084/m9.fig share.18133379.v1.
Acknowledgement
We would like to acknowledge Ms. Jacqueline Lam for her administrative support in observing the recordings and online-teaching.
Funding
There was no funding for this research study.
Declaration of Interest
The authors report no conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
Alimoglu, M. K., Sarac, D. B., Alparslan, D., Karakas, A. A., & Altintas. (2014). An observation tool for instructor and student behaviors to measure in-class learner engagement: A validation study. Medical Education Online, 19(1), 24037. https://doi.org/10.3402/meo.v19.24037
Armstrong, S. J., & Fukami, C. V. (2009). The SAGE Handbook of Management Learning, Education and Development. SAGE Publications Ltd. https://www.doi.org/10.4135/9780857021038
Berman, N. B., & Artino, A. R. J., (2018). Development and initial validation of an online engagement metric using virtual patients. BMC Medical Education, 18(1), 213. https://doi.org/10.1186/s12909-018-1322-z
Chick, R. C., Clifton, G. T., Peace, K. M., Propper, B. W., Hale, D. F., Alseidi, A. A., & Vreeland, T. J. (2020). Using technology to maintain the education of residents during the COVID-19 Pandemic. Journal of Surgical Education, 77(4), 729–732. https://doi.org/10.1016/j.jsurg.2020.03.018
Chua, Y. K. C., Ng, K. W. P., Yap, E. S., Lye, P. S. P., Vijayan, J., & Chan, Y. C. (2022). Evaluating online learning engagement (Version 1) [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.18133379.v1
Dost, S., Hossain, A., Shehab, M., Abdelwahed, A., & Al-Nusair, L. (2020). Perceptions of medical students towards online teaching during the COVID-19 pandemic: A national cross-sectional survey of 2721 UK medical students. BMJ Open, 10(11), e42378. https://doi.org/10.1136/bmjopen-2020-042378
Fuller, K. A., Karunaratne, N. S., Naidu, S., Exintaris, B., Short, J. L., Wolcott, M. D., Singleton, S., & White, P. J. (2018). Development of a self-report instrument for measuring in-class student engagement reveals that pretending to engage is a significant unrecognized problem. PLOS ONE, 13(10), e0205828. https://doi.org/10.1371/journal.pone.0205828
Gewin, V. (2020). Five tips for moving teaching online as COVID-19 takes hold. Nature, 580(7802), 295–296. https://doi.org/10.1038/d41586-020-00896-7
Kaufman, D. M. (2003). Applying educational theory in practice. BMJ, 326(7382), 213–216. https://doi.org/10.1136/bmj.326.7382.213
Kay, D., & Pasarica, M. (2019). Using technology to increase student (and faculty satisfaction with) engagement in medical education. Advances in Physiology Education, 43(3), 408–413. https://doi.org/10.1152/advan.00033.2019
Kelly, P. A., Haidet, P., Schneider, V., Searle, N., Seidel, C. L., & Richards, B. F. (2005). A comparison of in-class learner engagement across lecture, problem-based learning, and team learning using the STROBE classroom observation tool. Teaching and Learning in Medicine, 17(2), 112–118. https://doi.org/10.1207/s15328015tlm1702_4
Lemov, D. (2015). Teach like a champion 2.0: 62 techniques that put students on the path to college. (2nd ed.). Jossey-Bass.
Longhurst, G. J., Stone, D. M., Dulohery, K., Scully, D., Campbell, T., & Smith, C. F. (2020). Strength, weakness, opportunity, threat (SWOT) analysis of the adaptations to anatomical education in the United Kingdom and Republic of Ireland in response to the Covid-19 pandemic. Anatomical Sciences Education, 13(3), 301–311. https://doi.org/10.1002/ase.1967
Lyndon, M. P., Henning, M. A., Alyami, H., Krishna, S., Zeng, I., Yu, T.-C., & Hill, A. G. (2017). Burnout, quality of life, motivation, and academic achievement among medical students: A person-oriented approach. Perspectives on Medical Education, 6(2), 108–114. https://doi.org/10.1007/s40037-017-0340-6
McCoy, L., Pettit, R. K., Lewis, J. H., Allgood, J. A., Bay, C., & Schwartz, F. N. (2016). Evaluating medical student engagement during virtual patient simulations: A sequential, mixed methods study. BMC Medical Education, 16, 20. https://doi.org/10.1186/s12909-016-0530-7
Morawo, A., Sun, C., & Lowden, M. (2020). Enhancing engagement during live virtual learning using interactive quizzes. Medical Education, 54(12), 1188. https://doi.org/10.1111/medu.14253
Ni, A. Y. (2013). Comparing the effectiveness of classroom and online learning: Teaching research methods. Journal of Public Affairs Education, 19(2), 199-215. https://doi.org/10.1080/15236803.2013.12001730
Nieto-Escamez, F. A., & Roldan-Tapia, M. D. (2021). Gamifica- tion as online teaching strategy during COVID-19: A mini-review. Frontiers in Psychology, 12, 648522. https://doi.org/10.3389/fpsyg.2021.648552
O’Malley, K. J., Moran, B. J., Haidet, P., Seidel, C. L., Schneider, V., Morgan, R. O., Kelly, P. A., & Richards, B. (2003). Validation of an observation instrument for measuring student engagement in health professions settings. Evaluation & the Health Professions, 26(1), 86–103. https://doi.org/10.1177/0163278702250093
Ong, C. C. P., Choo, C. S. C., Tan, N. C. K., & Ong, L. Y. (2021). Unanticipated learning effects in videoconference continuous professional development. The Asia Pacific Scholar, 6(4), 135-141. https://doi.org/10.29060/TAPS.2021-6-4/SC2484
Rao, S. P., & DiCarlo, S. E. (2001). Active learning of respiratory physiology improves performance on respiratory physiology examinations. Advances in Physiology Education, 25(2), 55–61. https://doi.org/10.1152/advances.2001.25.2.55
Sharp, E. A., Norman, M. K., Spagnoletti, C. L., & Miller, B. G. (2021). Optimizing synchronous online teaching sessions: A guide to the “new normal” in medical education. Academic Pediatrics, 21(1), 11–15. https://doi.org/10.1016/j.acap.2020.11.009
Watson, W. E., Michaelsen, L. K., & Sharp, W. (1991). Member competence, group interaction, and group decision making: A longitudinal study. Journal of Applied Psychology, 76(6), 803–809. https://doi.org/10.1037/0021-9010.76.6.803
Weber, W., & Ahn, J. (2020). COVID-19 conferences: Resident perceptions of online synchronous learning environments. Western Journal of Emergency Medicine, 22(1), 115–118. https://doi.org/10.5811/westjem.2020.11.49125
Wilcha, R. J. (2020). Effectiveness of virtual medical teaching during the COVID-19 crisis: Systematic review. JMIR Medical Education, 6(2), e20963. https://doi.org/10.2196/20963
*Chua Yuan Kit Christopher
5 Lower Kent Ridge Road,
National University Hospital,
Singapore 119074
+65 7795555
Email: christopher_chua@nuhs.edu.sg
Submitted: 6 January 2022
Accepted: 4 May 2022
Published online: 4 October, TAPS 2022, 7(4), 22-34
https://doi.org/10.29060/TAPS.2022-7-4/OA2735
Amelah Abdul Qader1,2, Hui Meng Er3 & Chew Fei Sow3
1School of Postgraduate Studies, International Medical University, Kuala Lumpur, Malaysia; 2University of Cyberjaya, Faculty of Medicine, Cyberjaya, Malaysia; 3IMU Centre for Education, International Medical University, Kuala Lumpur, Malaysia
Abstract
Introduction: The direct ophthalmoscope is a standard tool for fundus examination but is underutilised in practice due to technical difficulties. Although the smartphone ophthalmoscope has been demonstrated to improve fundus abnormality detection, there are limited studies assessing its utility as a teaching tool for fundus examination in Southeast Asian medical schools. This study explored the perception of medical students’ toward using a smartphone ophthalmoscope for fundus examination and compared their abilities to diagnose common fundal abnormalities using smartphone ophthalmoscope against direct ophthalmoscope.
Methods: Sixty-nine Year-4 undergraduate medical students participated in the study. Their competencies in using direct ophthalmoscope and smartphone ophthalmoscope for fundus examination on manikins with ocular abnormalities were formatively assessed. The scores were analysed using the SPSS statistical software. Their perceptions on the use of smartphone ophthalmoscopes for fundus examination were obtained using a questionnaire.
Results: The students’ competency assessment scores using the smartphone ophthalmoscope were significantly higher than those using the direct ophthalmoscope. A significantly higher percentage of them correctly diagnosed fundus abnormalities using the smartphone ophthalmoscope. They were confident in detecting fundus abnormalities using the smartphone ophthalmoscope and appreciated the comfortable working distance, ease of use and collaborative learning. More than 90% of them were of the view that smartphone ophthalmoscopes should be included in the undergraduate medical curriculum.
Conclusion: Undergraduate medical students performed better in fundus examination on manikins with ocular abnormalities using smartphone ophthalmoscope compared to direct ophthalmoscope. Their positive perceptions toward smartphone ophthalmoscope support its use as a supplementary teaching tool in undergraduate medical curriculum.
Keywords: Medical Students, Smartphone, Ophthalmoscope, Teaching Tool
Practice Highlights
- The smartphone ophthalmoscope is a useful supplementary teaching tool for fundus examination in undergraduate medical education.
- Fundus examination is performed at a safe working distance from the patient using a smartphone ophthalmoscope.
- Students are able to detect fundus abnormalities with greater ease and accuracy using a smartphone ophthalmoscope compared to a direct ophthalmoscope.
- Students appreciate the collaborative learning through peer discussion of the fundus findings using the smartphone ophthalmoscope.
I. INTRODUCTION
Fundus examination is one of the essential procedures which provides information about ocular conditions that may compromise the quality of vision and lead to blindness (Leonardo, 2018). The direct ophthalmoscope (DO) is one of the robust ocular clinical examination tools to be grasped during clinical skill training in medical schools as well as clinical practice. However, students have difficulty mastering the technique of using it (Kim & Chao, 2019), particularly when they have to coordinate their hand movements at a very near distance to the patient and close one eye when examining the patient’s fundus through the pupil (MacKay et al., 2015). They also have to adjust the power of the direct ophthalmoscope lenses to get a clearer picture if there is a refractive error with the patient’s eye or their own eyes. Instead of concentrating on detecting fundus findings, the students are preoccupied with adjusting the direct ophthalmoscope.
Technical constraints may be the main reason for the underuse of direct ophthalmoscopes. Experienced physicians who use the direct ophthalmoscope may lack confidence and frequently miss significant abnormalities (Purbrick & Chong, 2015), causing delayed diagnosis of preventable eye disorders and permanent vision impairment (Myung et al., 2014). This has led to the exploration of alternative tools to overcome some of these challenges (Giardini et al., 2014; Kim & Chao, 2019). Smartphone ophthalmoscope, for example, is a breakthrough digital portable retinal imaging system that allows medical practitioners to view the fundus with high-definition images or video of a routine ophthalmoscope examination.
The D-EYE smartphone ophthalmoscope was developed by Doctor Andrea Russo in 2015 (Russo et al., 2015). It is a small, portable, and inexpensive retinal imaging system that can capture retinal images using an attachment to a smartphone that uses a cross-polarisation technique to reduce corneal reflections. It is integrated with the smartphone’s autofocus feature to accommodate the patient’s refractive error.
A. Problem and Rationale
Fundus examination requires extensive practice to develop adequate interpretation skills (Leonardo, 2018). Medical students are taught to use the direct ophthalmoscope in order to recognise retinal signs of life-threatening disorders (Benbassat et al., 2012). The International Council of Ophthalmology recognises direct ophthalmoscope examination as one of the seven core ocular medical education competencies. All graduating medical students are expected to recognise common abnormalities of the ocular fundus using a direct ophthalmoscope (Dunn et al., 2021). However, there is a lack of competencies among the medical graduates using this tool (MacKay et al., 2015). This needs to be addressed as at least 2.2 billion people globally have visual impairment or blindness, of which at least 1 billion have deterioration in vision that could have been prevented if they were screened or detected earlier, World Health Organization (2019). Tan et al. (2020) reported several favourable studies carried out in Italy, UK, and India on the advantages of smartphone ophthalmoscopes for fundus examination and visualisation of the retinal image. In a randomised cross-over study done by Curtis et al. (2021) on the ease of use of D-EYE smartphone ophthalmoscope versus direct ophthalmoscope, 44 Year-one medical students in Canada examined the patients’ fundus for optic disc assessment and compared their findings with the respective photographs provided. The ease of use and confidence was more significant with the D-EYE smartphone ophthalmoscope.
Although the smartphone ophthalmoscope is available in Southeast Asian countries such as Malaysia, it is not commonly used in public hospitals and general practitioner clinics. This is probably due to resource constraint issues in developing countries. Moreover, there are limited studies assessing its use, in particular, there is no literature report on such studies among undergraduate medical students in Southeast Asia. However, based on the positive findings from the literature, it has been proposed that smartphone ophthalmoscope be included in clinical skill training for fundus examination among undergraduate medical students at the university where this study was conducted. Therefore, this study was carried out to explore the students’ perceptions of using smartphone ophthalmoscopes for fundus examination and determine whether their competencies in fundus examination improved using this tool compared to using the direct ophthalmoscope. In this study, the D-EYE smartphone ophthalmoscope was chosen over the other types of smartphone ophthalmoscope due to reasons including the ease of data management using the available app facility, cost feasibility and convenience. The two research questions of the study were:
1) What were the perceptions of medical students on the use of smartphone ophthalmoscope for fundus examination?
2) Was there a difference between students’ competencies in fundus examination when using the smartphone ophthalmoscope compared to the direct ophthalmoscope?
The cognitive theory of multimedia learning can be applied in the context of fundus examination using a smartphone ophthalmoscope. Using a smartphone ophthalmoscope, the student can visualise the fundus on the smartphone screen. According to the cognitive theory of multimedia learning (Figure 1), the students engage in active cognitive processing in order to create a cohesive mental representation of their experiences based on their recall knowledge of fundus structures and ocular abnormalities. This will allow them to integrate the findings with other relevant information. They can then describe their findings and organise the selected images into a “mental model” of the items they are learning. Finally, their prior knowledge of ocular disorders is incorporated and reconciled with these verbal explanations and graphical representations.
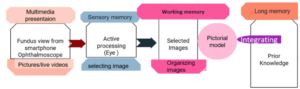
Figure 1. Cognitive theory of multimedia learning
According to the social constructivism theory, learning is social, active and constructed through social interaction (Lötter & Jacobs, 2020). Technologies have been shown to enhance students’ problem solving by breaking down complex concepts into sub-problems (Kim & Hannafin, 2011). A smartphone ophthalmoscope is an appropriate tool for encouraging active interaction between the students and lecturer to work on real-world problems in the teaching and learning environment. When the students perform fundus examination using the smartphone ophthalmoscope, they can see the findings on the screen together with their peers and the lecturer. This will allow them to gain more knowledge and understanding as they can discuss and link the new ideas in the context of their prior knowledge.
II. METHODS
The study was approved by the International Medical University Joint-Committee on Research and Ethics (IMU-JC). Informed consent was obtained from all respondents. The nature and purpose of the study were explained to them. The respondents were assured of anonymity and confidentiality of the collected information.
A. Study Setting
The data were collected from Year-4 undergraduate medical students who undertook ophthalmology rotation for the academic year 2020/2021, at the University of Cyberjaya, Malaysia.
In the fourth year of the medical curriculum, the students undertake four major postings (Orthopedic, Family Medicine, Psychiatry and a speciality posting) over two semesters (Semesters 7 and 8). These are conducted in four rotations per year (rotations 1 & 2 in Semester 7, rotations 3 & 4 in Semester 8). The speciality posting includes Ophthalmology, Anaesthesia, ENT and Radiology. The duration of each of these speciality posting is two weeks. In the ophthalmology posting the students are taught the principles of history taking and ocular examination in the Clinical Skill Training Department and in the hospital, where they clerk patients with eye conditions. Additionally, they learn about basic common eye conditions during interactive sessions and case-based discussion sessions in small groups. However, during the COVID-19 pandemic, the posting was affected by lockdown measures. Therefore, the case-based discussion sessions were conducted online, and ocular examination was demonstrated through online interactive video sessions. Nevertheless, there was a window of opportunity where the students could return to the campus physically for a one-week revision. During this period, the students practice ophthalmoscopy examination on manikins in the Clinical Skill Training Department.
B. Study Design
The direct ophthalmoscope examination technique was introduced to the students virtually through video demonstrations and during online interactive discussion sessions. During the revision week, the students were trained for two hours to perform fundus examination using the direct ophthalmoscope. For the smartphone ophthalmoscope, they were briefed and trained on its use for 20-30 minutes. The training was conducted by a member of the teaching staff (who is the researcher in this study, AMAQ). Following that, the students were required to examine various slides of fundus images provided in the manikins (M1 and M2).
The selected slides on the manikins represented the common pathological fundus findings, i.e. optic disc swelling, branch retinal vein occlusion, optic atrophy/glaucoma and diabetic retinopathy/ maculopathy. Each student performed the fundus examination on M1 and M2 using the direct and smartphone ophthalmoscopes separately (approximately 2-3 minutes on each manikin) on the same day. The students were required to fill in their findings based on their observation (without discussing with their peers) on the formative assessment forms (shown in Appendix 1) and indicate the tools they utilised (direct or smartphone ophthalmoscopes). The formative assessment form was adapted from Mamtora et al. (2018) and had been validated by two ophthalmologists in the department.
To avoid bias, all the completed formative assessment forms were collected and submitted to another researcher (SCF) who was not involved in marking (to remove information on the tool used by the student on each form). These were then returned to the researcher in this study, (AMAQ) for marking.
After completing the formative assessment, the students were requested to fill in an online questionnaire regarding their perception on the use of smartphone ophthalmoscope for fundus examination. This questionnaire (Appendix 2) was adapted from Nagra & Huntjens (2020). In addition, the students were requested to provide the reasons for their suggestions to include smartphone ophthalmoscopes or replace direct ophthalmoscopes with smartphone ophthalmoscopes in the medical curriculum.
C. Data Analysis
All data were statistically analysed using SPSS version 23. The paired t-test was used to compare the performance of the students in the formative assessments using direct ophthalmoscopes and smartphone ophthalmoscopes. The number of students getting the correct diagnosis using both tools was statistically analysed using the McNemar (Chi Square) test (Liao & Lin, 2008). The statistical significance was determined based on the p-values (the difference is significant if p ≤ 0.05). The responses of the students in the perceptions questionnaire related to the ease of use, confidence, and preference were analysed.
III. RESULTS
Sixty-nine Year-4 medical students participated in this study. The demographic data are shown in Table 1.
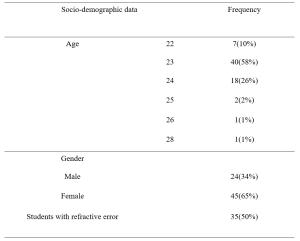
Table 1: Demographic data
A. Comparison of Formative Assessment Scores Using Smartphone Ophthalmoscope and Direct Ophthalmoscope
The mean scores of the students were higher using the smartphone ophthalmoscope (59%) than the direct ophthalmoscope (39%). The same trend was observed for the students with and without refractive error. The results are shown in Table 2. A higher number of students were able to make the correct diagnosis for all fundus abnormalities using the smartphone ophthalmoscope compared to the direct ophthalmoscope. The difference is statistically significant (p-value < 0.05). The results are presented in Table 3. The data that support the findings are openly available in Figshare at https://figshare.com/s/d45da87ea42c596e714b
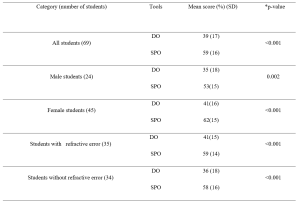
Table 2: Comparison of formative assessment scores using direct ophthalmoscope (DO) and smartphone ophthalmoscope (SPO).
*p-value (paired t-test)
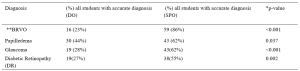
Table 3: Comparison of correct diagnosis using direct ophthalmoscope and smartphone ophthalmoscope.
*McNemar (Chi square) test (Liao & Lin, 2008),
**(Branch retinal vein occlusion)
A. Students’ Perceptions on the Use of Smartphone Ophthalmoscope for Fundus Examination
A total of 69 students participated in the online questionnaire. All the students appreciated that their peers could share the findings with them on the smartphone screen. Most of the students (87%) preferred using smartphone ophthalmoscopes over direct ophthalmoscopes, and 86% felt confident when using the smartphone ophthalmoscope. In addition, the comfortable working distance was appreciated by 87% of the students. The responses of the participants are shown in Table 4.
|
Online student evaluation Form
|
Likert scale 1= Strongly disagree 2= disagree, 3 = Neutral, 4 =agree, 5= Strongly agree |
||||
|
Section 1 Perception on smartphone ophthalmoscope use |
1 |
2 |
3 |
4 |
5 |
|
I feel confident while using it |
1.4% |
2.9% |
8.7% |
56.5% |
30.4% |
|
I feel easy to view the fundus |
0.0% |
5.8% |
11.6% |
44.9% |
37.7% |
|
I feel comfortable when my peer can observe with me the findings |
0.0% |
0.0% |
0.0% |
30.4% |
69.6% |
|
My hand is steady while I am performing examination |
0.0% |
4.3% |
20.3% |
40.6% |
34.8% |
|
I can pick the finding faster |
0.0% |
4.3% |
21.7% |
42.0% |
31.9% |
|
Smartphone ophthalmoscope user-friendly |
0.0% |
1.4% |
7.2% |
39.1% |
52.2% |
|
I prefer to use it
|
0.0% |
4.3% |
8.7% |
40.6% |
46.4% |
|
Online student evaluation Form |
Likert scale 1= Strongly disagree 2= disagree, 3 = Neutral, 4 =agree, 5= Strongly agree
|
||||
|
Section 2 Efficiency of smartphone ophthalmoscope |
1 |
2 |
3 |
4 |
5 |
|
It takes shorter duration to detect finding |
0.0% |
4.3% |
27.5% |
33.3% |
34.8% |
|
It has comfortable working distance |
0.0% |
0.0% |
13.0% |
40.6% |
46.4% |
|
I found difficulty in handling it |
10.1% |
44.9% |
21.7% |
20.3% |
2.9% |
|
I think Smartphone ophthalmoscope must be added to the medical curriculum |
0.0% |
0.0% |
4.3% |
47.8% |
47.8% |
|
I think direct ophthalmoscope should be replaced by smartphone ophthalmoscope |
1.4% |
10.1% |
26.1% |
33.3% |
29.0% |
Table 4: Responses of participants in the questionnaire to evaluate their perception and efficiency on the use of smartphone ophthalmoscope for fundus examination
B. Students’ Preference for Types of Ophthalmoscopes
Most of the students (94%) suggested that the smartphone ophthalmoscope be included in the medical curriculum, and 62% suggested to replace the direct ophthalmoscope with the smartphone ophthalmoscope. Their preference was mainly attributed to the efficiency, ease of use (for those with refractive error and amblyopia (lazy eye)), autofocus function using the smartphone, and the possibility of using both eyes to see the images on the smartphone screen. In addition, the comfortable working distance, ease of cleaning after use and peer discussion were cited. Meanwhile, 11% of the students suggested keeping direct ophthalmoscope alongside the smartphone ophthalmoscope in the curriculum. They opined that smartphone ophthalmoscope should be included as an additional teaching and learning tool for fundus examination but disagreed that it should replace direct ophthalmoscope totally as the smartphone ophthalmoscope might not be readily available in all healthcare settings. One of the participants commented that “eye examination using direct ophthalmoscope was thought to be a basic procedural skill that doctors must-have. Smartphone ophthalmoscope was a newer technology that might not be available in hospitals, unlike direct ophthalmoscope, which was more common“.
IV. DISCUSSION
The students scored significantly higher in the formative assessment for fundus abnormalities using the smartphone ophthalmoscope compared to the direct ophthalmoscope. The findings from this study were consistent with those of Kim and Chao (2019) and Dunn et al. (2021). In addition, the study also showed that the difference was statistically significant regardless of the presence of refractive error.
The students with refractive error and amblyopia have commented that they found the smartphone ophthalmoscope more convenient and efficient than the direct ophthalmoscope. They stated that they had difficulty using their amblyopic eye when performing the examination using the direct ophthalmoscope as they had to follow the ‘Three R rule’ in which students should use their right eye and their right hand when examining the right eye of the patient at the side of the patient at about 45 degrees to avoid kissing position with the patient. The students with refractive errors highlighted another issue that they needed to adjust the direct ophthalmoscope very frequently to get a proper and clear view. However, when they used the smartphone ophthalmoscope, they were able to perform the examination using both eyes, as they could view the fundus on the smartphone screen without having to close one eye. Fifty percent of the students in this study reported they had refractive errors. In the study by Al-Rashidi et al. (2018), it was found that 89 out of 162 medical students (54 %) had refractive errors. In this study, a significantly higher number of students obtained the correct diagnosis of branch retinal vein occlusion (86%) and glaucoma (62%) using the smartphone ophthalmoscope compared to the direct ophthalmoscope (p-value < 0. 001).
In a study conducted by Mrad et al. (2021) on the accurate method for glaucoma screening, they found that the D-EYE smartphone ophthalmoscope was more accurate for capturing fundus images and assessing the optic disc in detecting glaucoma compared to the direct ophthalmoscope. In addition, Mamtora et al. (2018) reported that it was more convenient and easier to detect optic disc and blood vessels using the D-EYE smartphone ophthalmoscope. Providing alternative tools in medical education could help students learn and perform more efficiently during their teaching and learning activities.
In our study, 86% of the students felt confident using the smartphone ophthalmoscope, and 83% of them found it easy to view the fundus. The majority of the students (91%) found the smartphone ophthalmoscope user friendly, and 73% indicated that they were able to identify the findings quickly while using the smartphone ophthalmoscope. It has been reported previously that medical students preferred smartphone ophthalmoscopes to direct ophthalmoscopes and were more likely to make correct and faster diagnoses (Nagra & Huntjens, 2020). Though mastering the technique of using the direct ophthalmoscope is important, it is equally paramount to be able to identify the fundus findings accurately. The cognitive load theory states that the human working memory can only hold a certain number of interrelated objects (Chu, 2014). Motivational components can enhance student learning by boosting generative processing as long as the learner is not constantly overburdened with needless processing or diverted from critical processing (Mayer, 2014). The technical challenges faced while using the direct ophthalmoscope could hamper the students’ ability to recognise the features associated with fundus abnormalities. The smartphone ophthalmoscope offers an advantage in this context.
In this study, 87 % of the students found that the working distance of a smartphone ophthalmoscope was more comfortable compared to the typical 1–3 cm working distance of a direct ophthalmoscope. This finding was similar to the study conducted by Huntjens & Nagra (2020), where they found that 92% of the students preferred the longer working distance of 20–60 cm of the D-EYE smartphone ophthalmoscope.
The use of smartphone ophthalmoscope as a teaching tool increases student engagement and enhances their learning experience. All students appreciated that their peers could observe the findings together with them on the smartphone screen. They were able to discuss among themselves, as well as with the lecturer. Learning must be an engaging and meaningful experience for the learners to be productive (Mellis et al., 2013). Learners will utilise strategies developed earlier in their training to optimise their knowledge and skills through reflection. When the students record the fundus images, they can discuss their interpretation of findings with the lecturers and peers. Feedback from this process will improve their learning efforts (Kaufman, 2019). The feedback and reflection facilitate the construction of new knowledge, as well as strategies for improving the performance as all of them could see the same findings on the smartphone screen and discuss accordingly.
In our study, 93% of the students’ suggested that smartphone ophthalmoscopes should be included in the medical curriculum. It was easier for them to see the findings without spending a longer time trying to focus by squinting and shutting one eye to look for the findings, as the image is automatically adjusted in a smartphone ophthalmoscope. This has been highlighted as one of the advantages of using the smartphone ophthalmoscope in medical training and screening in primary care centres (Nagra & Huntjens, 2020). Smartphone-based fundus image could even replace the direct ophthalmoscope in clinical medicine (Wintergerst et al., 2020). In our study, out of the 69 students, only eight students (11%) opined that the direct ophthalmoscope should not be totally replaced with a smartphone ophthalmoscope. From their point of view, the direct ophthalmoscope is a must-know clinical skill that contributes to their professional identity. In particular, the smartphone ophthalmoscope may not be easily available in developing countries due to resource constraints. The direct ophthalmoscope is one of the fundamental skills that all clinicians should be able to perform. It is included in the assessment of the final year undergraduate curriculum as well as the postgraduate membership assessment. (Purbrick & Chong, 2015).
With a specific instructional scaffolding strategy, smartphone ophthalmoscopes can be used as a prologue to the direct ophthalmoscope. Students will be able to share the fundus pictures with their peers through the screen simultaneously for the same patient during clinical practice sessions in packed clinics, without having to struggle with the technical challenges of the direct ophthalmoscope. As a result, patients will be less burdened in terms of examination time, and students will be able to evaluate more patients with fundus abnormalities in a shorter amount of time. The concept of just-in-time learning can be a useful pedagogical tool for medical academicians to improve their teaching and learning approach in the age of technology. The just-in-time learning idea uses technology to deliver teaching and learning activities, allowing learning communities to understand better and practise (Naseem et al, 2019). According to Riel (2000), academics continue to play an essential role in encouraging learners to apply their knowledge effectively. As new technologies emerge, educators must prepare students to be lifelong learners who are digitally literate and resourceful in their application of technology.
A. Limitations of the Study
As the study was conducted during the COVID-19 pandemic, the duration for recruitment and training of the students was limited. As a result, the students had a shorter period of face-to-face clinical training. This limited the student’s exposure to performing fundus examinations on real patients in the hospital and using the various ophthalmoscopic tools. In addition, the lack of practice could have affected the students’ performance in the formative assessment on fundus examination using the smartphone and direct ophthalmoscopes. Therefore, we recommend repeating this study when the COVID-19 situation is resolved.
Another limitation of the study was that the students performed the fundus examination on the same manikins using the direct ophthalmoscope followed by the smartphone ophthalmoscope (or vice versa) on the same day. This could result in bias in their judgement in identifying the fundus abnormalities. Nevertheless, the students were reminded to be objective and record their findings accurately based on their observations using either tool.
V. CONCLUSION
Smartphone ophthalmoscope is an effective teaching tool for improving the skills in detecting common clinical ocular diseases. It provides a comfortable working distance and promotes collaborative learning by enabling peer discussion. It is also convenient for students with refractive errors. Therefore, the smartphone ophthalmoscope is a valuable supplementary teaching tool for fundus examination and is highly recommended to be included in the undergraduate medical curriculum.
Notes on Contributors
AMAQ designed and conducted the study, reviewed the literature, analysed the data and wrote the manuscript EHM designed the study, analysed the data, gave critical feedback and edited the manuscript before submission. SCF designed the study, gave critical feedback and edited the manuscript before submission.
Ethical Approval
The study was approved by the International Medical University Joint-Committee on Research and Ethics (IMU-JC), Project ID No.: MHPE I/2021(01). Informed consent was obtained from all respondents, and the nature and purpose of the study were explained to them. The respondents were assured of anonymity and confidentiality of the collected information.
Data Availability
All data are available at https://figshare.com/s/d45da87ea42c596e714b and can be accessed on request and approval from the corresponding author.
Acknowledgement
The authors would like to thank the medical students at the University of Cyberjaya who showed their enthusiasm for learning. And special thanks to the statisticians, Dr Norhafizah Ab Manan, University of Cyberjaya and Dr Shamala Ramasamy, International Medical university, for their advice on statistical tests. The authors would also like to thank Professor Ian Wilson for proofreading the manuscript.
Funding
This study was funded by the International Medical University, Malaysia. MHPE I/2021(01)
Declaration of Interest
Authors declare that they do not have possible conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
Al-Rashidi, S. H., Albahouth, A. A., Althwini, W. A., Alsohibani, A. A., Alnughaymishi, A. A., Alsaeed, A. A., Al-Rashidi, F. H., & Almatrafi, S. (2018). Prevalence refractive errors among medical students of Qassim University, Saudi Arabia: Cross-sectional descriptive study. Open Access Macedonian Journal of Medical Sciences, 6(5), 940–943. https://doi.org/10.3889/oamjms.2018.197
Benbassat, J., Polak, B. C. P., & Javitt, J. C. (2012). Objectives of teaching direct ophthalmoscopy to medical students. Acta Ophthalmologica, 90(6), 503–507. https://doi.org/10.1111/j.1755-3768.2011.02221.x
Chu, H.-C. (2014). Potential Negative Effects of Mobile Learning on Students’ Learning Achievement and Cognitive Load—A Format Assessment Perspective. Educational Technology & Society, 17 (1), 332–344
Curtis, R., Xu, M., Liu, D., Kwok, J., Hopman, W., Irrcher, I., & Baxter, S. (2021). Smartphone Compatible versus Conventional Ophthalmoscope: A Randomized Crossover Educational Trial. Journal of Academic Ophthalmology, 13(02), e270–e276. https://doi.org/10.1055/s-0041-1736438
Dunn, H. P., Kang, C. J., Marks, S., Witherow, J. L., Dunn, S. M., Healey, P. R., & White, A. J. (2021). Perceived usefulness and ease of use of fundoscopy by medical students: A randomised cross-over trial of six technologies (eFOCUS 1). BMC Medical Education, 21(1), 41. https://doi.org/10.1186/s12909-020-02469-8
Giardini, M. E., Livingstone, I. A. T., Jordan, S., Bolster, N. M., Peto, T., Burton, M., & Bastawrous, A. (2014). A smartphone based ophthalmoscope. [paper presentation]. 36th Annual International Conference of the Engineering in Medicine and Biology Society, EMBC, Chicago, United States. https://doi.org/10.1109/EMBC.2014.6944049
Kaufman, D. M. (2019). Teaching and Learning in Medical Education. How Theory can Inform Practice. Tim Swanwick, Kirsty Forrest, Bridget C. O’Brien (Eds), Understanding medical education evidence, theory, and practice (pp. 37-69). The Association for the Study of Medical Education.
Kim, M. C., & Hannafin, M. J. (2011). Scaffolding problem solving in technology-enhanced learning environments (TELEs): Bridging research and theory with practice. Computers & Education, 56(2), 403-417. Elsevier Ltd. https://www.learntechlib.org/p/67172/.
Kim, Y., & Chao, D. L. (2019). Comparison of smartphone ophthalmoscopy vs conventional direct ophthalmoscopy as a teaching tool for medical students: The COSMOS study. Clinical Ophthalmology, 13, 391–401. https://doi.org/10.2147/OPTH.S190922
Leonardo, D. (2018). Development of a virtual reality ophthalmoscope prototype: Mechatronic Engineering Program Faculty of Engineering, Universidad Militar Nueva Granada, Bogotá D.C., Colombia. http://hdl.handle.net/10654/17843
Liao, Y. Y., & Lin, Y. M. (2008). McNemar test is preferred for comparison of diagnostic techniques. American Journal of Roentgenology, 191(4), 2008. https://doi.org/10.2214/AJR.08.1090
Lötter, M. J., & Jacobs, L. (2020). Using smartphones as a social constructivist pedagogical tool for inquiry-supported problem-solving: An exploratory study. Journal of Teaching in Travel & Tourism, 20(4), 347–363. https://doi.org/10.1080/15313220.2020.1715323
MacKay, D. D., Garza, P. S., Bruce, B. B., Newman, N. J., & Biousse, V. (2015). The demise of direct ophthalmoscopy: A modern clinical challenge. Neurology: Clinical PraFalctice, 5(2), 150–157. https://doi.org/10.1212/CPJ.0000000000000115
Mamtora, S., Sandinha, M. T., Ajith, A., Song, A., & Steel, D. H. W. (2018). Smart phone ophthalmoscopy: A potential replacement for the direct ophthalmoscope. Eye (Basingstoke), 32(11), 1766–1771. https://doi.org/10.1038/s41433-018-0177-1
Mayer, R. E. (2014). Cognitive theory of multimedia learning. The Cambridge Handbook of Multimedia Learning, Second Edition, 43–71. https://doi.org/10.1017/CBO9781139547369.005
Mellis, S., Carvalho, L., & Thompson, K. (2013, December 1-5). Applying 21st century constructivist learning theory to stage 4 design projects. [Conference presentation]. Joint Australian Association for Research in Education Annual Conference, Adelaide. https://files.eric.ed.gov/fulltext/ED603249.pdf
Mrad, Y., Elloumi, Y., Akil, M., & Bedoui, M. H. (2021). A Fast and Accurate Method for Glaucoma Screening from Smartphone-Captured Fundus Images. Irbm, 1, 1–11. https://doi.org/10.1016/j.irbm.2021.06.004
Myung, D., Jais, A., He, L., Blumenkranz, M. S., & Chang, R. T. (2014). 3D Printed Smartphone Indirect Lens Adapter for Rapid, High Quality Retinal Imaging. Journal of Mobile Technology in Medicine, 3(1), 9–15. https://doi.org/10.7309/jmtm.3.1.3
Nagra, M., & Huntjens, B. (2020). Smartphone ophthalmoscopy: Patient and student practitioner perceptions. Journal of Medical Systems, 44(1), Article 10. https://doi.org/10.1007/s10916-019-1477-0
Naseem, A., Ghias, K., Bawani, S., Shahab, M. A., Nizamuddin, S., Kashif, W., Khan, K. S., Ahmad, T., & Khan, M. (2019). Designing EthAKUL: A mobile just-in-time learning environment for bioethics in Pakistan. Scholarship of Teaching and Learning in the South, 3(1), 36–56. https://doi.org/10.36615/sotls.v3i1.70
Purbrick, R. M. J., & Chong, N. V. (2015). Direct ophthalmoscopy should be taught to undergraduate medical students—No. Eye, 29(8), 990-991. https://doi.org/10.1038/eye.2015.91
Riel, M. (2000). Education in the 21st century: Just-in-Time learning or learning communities, Technology and Learning, 137-160.
Russo, A., Morescalchi, F., Costagliola, C., Delcassi, L., & Semeraro, F. (2015). Comparison of smartphone ophthalmoscopy with slit-lamp biomicroscopy for grading diabetic retinopathy. American Journal of Ophthalmology, 159(2), 360-364. https://doi.org/10.1016/j.ajo.2014.11.008
Tan, C. H., Kyaw, B. M., Smith, H., Tan, C. S., & Car, L. T. (2020). Use of smartphones to detect diabetic retinopathy: Scoping review and meta-analysis of diagnostic test accuracy studies. Journal of Medical Internet Research, 22(5), e16658.
Wintergerst, M. W. M., Jansen, L. G., Holz, F. G., & Finger, R. P. (2020). Smartphone-Based Fundus Imaging-Where Are We Now? Asia-Pacific Journal of Ophthalmology, 9(4), 308–314. https://doi.org/10.1097/APO.0000000000000303
World Health Organization. (2019). Report of the 4th global scientific meeting on trachoma: Geneva, 27–29 November 2018. World Health Organization.
*Amelah Mohammed Abdul Qader
University of Cyberjaya Campus
Persiaran Bestari, Cyber 11, 63000 Cyberjaya,
Selangor Darul Ehsan, Malaysia
Email: amelah@cyberjaya.edu.my/ dramelahariqi@gmail.com
Submitted: 22 September 2021
Accepted: 27 April 2022
Published online: 4 October, TAPS 2022, 7(4), 1-21
https://doi.org/10.29060/TAPS.2022-7-4/OA2785
Yao Chi Gloria Leung1*, Kennedy Yao Yi Ng2*, Ka Shing Yow3*, Nerice Heng Wen Ngiam4, Dillon Guo Dong Yeo4, Angeline Jie-Yin Tey5, Melanie Si Rui Lim6, Aaron Kai Wen Tang7, Bi Hui Chew8, Celine Tham9, Jia Qi Yeo10, Tang Ching Lau11,12, Sweet Fun Wong13,14, Gerald Choon-Huat Koh15,16** & Chek Hooi Wong14,17**
1Department of Anaesthesiology, Singapore General Hospital, Singapore; 2Department of Medical Oncology, National Cancer Centre Singapore, Singapore; 3Department of General Medicine, National University Hospital, Singapore; 4Department of General Medicine, Singapore General Hospital, Singapore; 5Department of General Medicine, Tan Tock Seng Hospital, Singapore; 6Department of General Paediatrics, Kandang Kerbau Hospital, Singapore, 7Department of Psychiatry, Singapore General Hospital, Singapore; 8Tan Tock Seng Hospital, Singapore; 9Ng Teng Fong General Hospital, Singapore, 10National Healthcare Group Pharmacy, Singapore, 11Department of Medicine, NUS Yong Loo Lin School of Medicine, Singapore; 12Division of Rheumatology, University Medicine Cluster, National University Hospital, Singapore; 13Medical Board and Population Health & Community Transformation, Khoo Teck Puat Hospital, Singapore; 14Department of Geriatrics, Khoo Teck Puat Hospital, Singapore; 15Saw Swee Hock School of Public Health, National University of Singapore, Singapore; 16Future Primary Care, Ministry of Health Office of Healthcare Transformation, Singapore; 17Health Services and Systems Research, Duke-National University of Singapore Medical School, Singapore
*Co-first authors
**Co-last authors
Abstract
Introduction: Tri-Generational HomeCare (TriGen) is a student-initiated home visit programme for patients with a key focus on undergraduate interprofessional education (IPE). We sought to validate the Readiness for Interprofessional Learning Scale (RIPLS) and evaluate TriGen’s efficacy by investigating healthcare undergraduates’ attitude towards IPE.
Methods: Teams of healthcare undergraduates performed home visits for patients fortnightly over six months, trained by professionals from a regional hospital and a social service organisation. The RIPLS was validated using exploratory factor analysis. Evaluation of TriGen’s efficacy was performed via the administration of the RIPLS pre- and post-intervention, analysis of qualitative survey results and thematic analysis of written feedback.
Results: 79.6% of 226 undergraduate participants from 2015-2018 were enrolled. Exploratory factor analysis revealed four factors accounting for 64.9% of total variance. One item loaded poorly and was removed. There was no difference in pre- and post-intervention RIPLS total and subscale scores. 91.6% of respondents agreed they better appreciated the importance of interprofessional collaboration (IPC) in patient care, and 72.8% said MDMs were important for their learning. Thematic analysis revealed takeaways including learning from and teaching one another, understanding one’s own and other healthcare professionals’ role, teamwork, and meeting undergraduates from different faculties.
Conclusion: We validated the RIPLS in Singapore and demonstrated the feasibility of an interprofessional, student-initiated home visit programme. While there was no change in RIPLS scores, the qualitative feedback suggests that there are participant-perceived benefits for IPE after undergoing this programme, even with the perceived barriers to IPE. Future programmes can work on addressing these barriers to IPE.
Keywords: Interprofessional Education, Student-Initiated Home Visit Programme, RIPLS, Validation
Practice Highlights
- We validated the Readiness for Interprofessional Learning Scale (RIPLS) in Singapore, a multi-ethnic Asian country.
- A student-initiated, interprofessional, longitudinal home visit program is feasible.
- While there was no significant change in RIPLS scores, participants reported qualitative benefits of the programme in their attitudes towards IPE.
- Qualitative feedback highlighted four main barriers to IPE: Time constraints, unmotivated teammates, administrative burden, and unsuitable patients.
I. INTRODUCTION
Interprofessional education (IPE) aims to prepare healthcare professionals for effective collaboration, and while becoming increasingly common, is challenging to initiate, implement, evaluate and sustain (Fahs et al., 2017). Key challenges include designing a curriculum that integrates IPE with traditional academic frameworks, active engagement of facilitators and students, and accommodating various professions (Sunguya et al., 2014). IPE is context-specific, evolving, and involves continuous interaction and interdependence, and many traditional top-down approaches such as forums and lectures do not effectively teach it (Briggs & McElhaney, 2015).
Experiential IPE programmes employ a ground-up approach and potentially tackle some of the aforementioned challenges. Students involved in on-the-ground interprofessional healthcare visits to older adults showed that such experiences improved student collaboration and students’ self-perception of interprofessional team care-related skills (Blythe & Spiring, 2020; Conti et al., 2016; McManus et al., 2017; Toth-Pal et al., 2020; Vaughn et al., 2014). Therefore, a group of undergraduates from the National University of Singapore (NUS) Yong Loo Lin School of Medicine initiated an experiential student-led IPE programme which is aimed at improving health outcomes in older people with frequent hospital readmissions. This longitudinal service-learning programme was anchored by several educational aims including enhancing students’ IPE outcomes and improving attitudes towards IPE.
Formal evaluation of such programmes and investigating student IPE attitudes after being involved in a longitudinal home visit programmes are lacking in the current IPE literature (Grice et al., 2018). This study aims to evaluate TriGen’s effectiveness by investigating student IPE attitudes through the use of the Readiness for Interprofessional Learning Scale (RIPLS). Since the RIPLS has not been validated in the Singapore context, this study also aims to validate this scale.
II. METHODS
A. Programme Design
TriGen is a collaboration between NUS Yong Loo Lin School of Medicine, Khoo Teck Puat Hospital, a Northern regional hospital in Singapore, and North West Community Development Council, a grassroots organisation (Ng et al., 2020a, 2020b). A non-profit ground-up social initiative by healthcare undergraduates, it has the dual aim of i) serving the medical and social needs of older patients by providing longitudinal home visits by interprofessional student teams; ii) educating and empowering undergraduate students through a service-learning approach, with a key focus on improving attitudes towards IPE. The programme was designed under the mentorship of university faculty members, and was earmarked as a co-curricular activity aimed at improving students’ attitudes towards IPE and IPC. Older patients with frequent hospital readmissions (three or more times over six months) were followed up by healthcare undergraduates enrolled in Medicine, Nursing, Pharmacy, Social Work, Physiotherapy or Occupational Therapy courses in Singapore.
The programme begins with healthcare undergraduates undergoing didactic, skill-based training and team-based simulation training covering possible scenarios encountered during home visits (Annex 1). Each team comprising 2-3 interdisciplinary undergraduates conduct fortnightly visits to 1-2 patients over 6 months. At the midpoint and endpoint of the programme, healthcare undergraduates assessed the patients’ needs and presented at multi-disciplinary meetings (MDMs) chaired by healthcare professionals and grassroots staff, who guided the undergraduates to execute a management plan.
This IPE programme was designed based on educational principles for adult learners outlined by Knowles (1984). First, it provided healthcare undergraduates with opportunities for experiential learning anchored in the service-learning approach. Second, it was largely problem-based group learning with most training sessions being team-based and scenario-based. MDMs were also problem-based and encouraged undergraduates to brainstorm ideas to address their patients’ issues. Third, the service they provided in this programme modelled the work they may engage in after graduation. What they learned in this programme was of immediate relevance to their current study and future practice. Lastly, the programme provided autonomy to healthcare undergraduates to direct their own learning. This programme was voluntary and allowed participants’ flexibility for further self-study of topics of interest. Key student outcomes include readiness for IPE (including teamwork and collaboration, professional identity, roles and responsibility), and a better appreciation for IPC.
B. Evaluation Approach
This study used the framework by Kirkpatrick (1959) expanded by Barr et al. (2005) to evaluate the effectiveness of TriGen in improving healthcare undergraduates’ attitudes towards IPE, particularly in evaluation levels 1, 2a and 2b, which centre on learner’s reactions, attitude perceptions, and acquisition of knowledge or skills (Table 1). The use of quantitative and qualitative data collection in a survey was thought to be most appropriate in capturing the data and making the evaluation richer, and was hence the approach utilised for this research (Figure 1).
|
Evaluation Level |
Methods and Measures |
Timeframe |
|
Level 1: Learners’ reactions Participants’ views of their learning experience and opinions about the program |
Participants’ self-reported feedback of IPE learning |
Post-intervention |
|
Qualitative feedback |
Post-intervention |
|
|
Level 2a: Modification of attitudes perceptions |
Participants’ self-reported feedback of IPE learning |
Post-intervention |
|
Qualitative feedback |
Post-intervention |
|
|
|
Readiness for Interprofessional Learning Scale |
Pre- and post-intervention |
|
Level 2b: Acquisition of knowledge/skills Concepts, procedures, principles, and skills |
Qualitative feedback |
Post-intervention |
Table 1: Components of Kirkpatrick/Barr et al. evaluation framework as applied to TriGen
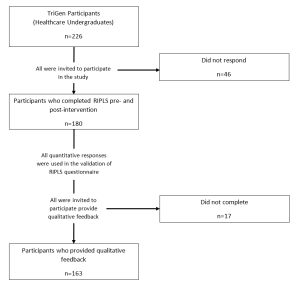
Figure 1: Flowchart of study components
C. Quantitative Measures
The RIPLS (Parsell & Bligh, 1999) was among the first scales developed for measurement of attitudes towards interprofessional learning. It assesses student readiness for IPE and IPC with other health care professionals and has been reported to be sensitive to differences in the students’ attitude towards IPE (Berger-Estilita et al., 2020). While there are a few studies validating it in Asian countries (China, Indonesia, Japan), none have been performed in Singapore (a multi-ethnic Asian country with English language as a predominant language of instruction (Ganotice & Chan, 2018; Lestari et al., 2016; Li et al., 2018; Tamura et al., 2012).
The RIPLS, a 19-item questionnaire comprising 4 subscales (“Teamwork and Collaboration”; “Positive Professional Identity”; “Negative Professional Identity” and “Roles and Responsibilities”), was administered pre- and post-intervention (McFadyen et al., 2005). Higher RIPLS scores imply greater readiness for interprofessional learning. This study validates the RIPLS in the Singapore context for the first time, then employs it for quantitative evaluation of TriGen. Additionally, separate from the RIPLS, three questions were added as a direct measure of participants’ reaction (Level 1), “I better appreciate the importance of IPC in the care of patients through the programme”, “The multidisciplinary meetings organised were important for my learning”, and “I would recommend the programme to my friends.”
1) Statistical Analysis: The Shapiro-Wilk test was used to assess if the data followed a normal distribution (Shapiro & Wilk, 1965). Factor analysis was conducted to explore the construct validity of the RIPLS, and Cronbach’s alpha was computed to determine internal consistency. The suitability of the correlation matrix was determined by the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity. The numbers of factors retained for the initial solutions and entered into the rotation were determined with the application of Kaiser’s criterion (eigenvalues >1). The initial factor extraction was performed using principal component analysis. Exploratory factor analysis was then conducted based on the RIPLS four-subscale structure. A paired t-test comparing baseline and post-intervention responses was computed for each survey item to determine significant differences (p ≤ 0.05). One-way ANOVA was performed to assess for demographic factors that correlated with pre-intervention and magnitude of change in RIPLS scores; if it demonstrated an overall difference between groups, post-hoc Tukey’s HSD was performed. For all statistical analyses, the Statistical Package for Social Sciences (SPSS, Version 23.0, Chicago, Illinois) was used.
D. Qualitative Measures
Post-intervention qualitative feedback regarding participants’ learning experiences was collected through online surveys. Questions include: What did you learn about interprofessional collaboration? What are your learning points after completing the project? Would you recommend this project to your peers, and what are your reasons? These questions were chosen to better understand participants’ reaction to the programme, their attitudes toward IPE and IPC, and other key learning points they may have.
1) Thematic Analysis: All survey participants were encouraged to participate in the qualitative research, with a total of 163 recruited to give written qualitative feedback on the programme. Given the relatively large sample of data, thematic analysis was chosen to explore and interpret the dataset, distilling it into recurring ideas (Braun & Clarke, 2006; Kiger & Varpio, 2020). Analysis was performed on participants’ qualitative descriptions of their learning experiences, with constant comparison analysis used to identify patterns in participants’ responses and develop a coding schema. Two coders independently identified major themes from the text within all transcripts, with reference to the research questions. They discussed and resolved any disagreements. No member checking was performed. A common coding schema was generated and applied to all the transcripts.
E. Ethical Approval
Ethical approval was obtained from the NUS institutional review board (B-15-272). Study participation was entirely voluntary and anonymous. Informed consent was taken from participants before data collection commenced, and they were allowed to withdraw from the research at any point in time. No incentives were provided to study participants.
III. RESULTS
226 healthcare undergraduates participated in TriGen from 2015-2018. Response rate for the RIPLS was 79.6%.
A. Demographics
Median age was 21 (range 18-41). 62.2% of participants were female, 37.8% were male. 31.7% were medical students, 12.8% nursing students, 42.2% pharmacy students, 10.0% social work students, and 3.3% therapy students. First- and second-year students comprised 62.2% of participants, while third- to fifth-years comprised 37.8%. 65.0% participated in previous IPE activities.
B. Construct Validity
The KMO index was 0.902, indicating sampling adequacy. The chi-square index for Barlett’s test of sphericity was 1919.445 (df171, p<0.001), indicating suitability for factor analysis.
Principal component analysis yielded four components largely consistent with the four-subscale model of the RIPLS (Barr et al., 2005) (Annex 2). However, one item, “I am not sure what my professional role will be”, had a low loading value of 0.285 under the original subscale of “Roles and Responsibility” and a borderline low loading value of 0.459 under the subscale of “Negative Professional Identity”. It was removed from subsequent analyses in view of its poor fit into the theoretical construct (Table 2).
|
No |
Statements |
Teamwork and Collaboration |
Negative Professional Identity |
Positive Professional Identity |
Roles and Responsibilities |
|
1 |
Shared learning will help me to think positively about other healthcare professionals. |
0.794 |
|
|
|
|
2 |
Learning with other health and social care students before qualification would improve relationships after qualification. |
0.781 |
|
|
|
|
3 |
Team-working skills are essential for all health and social care students to learn. |
0.773 |
|
|
|
|
4 |
Shared learning will help me to understand my own limitations. |
0.767 |
|
|
|
|
5 |
Communication skills should be learnt with other health and social care students. |
0.746 |
|
|
|
|
6 |
Learning with other students/professionals will make me become a more effective member of a health and social care team. |
0.742 |
|
|
|
|
7 |
For small group learning to work, students need to trust and respect each other. |
0.739 |
|
|
|
|
8 |
Shared learning with other healthcare students will increase my ability to understand clinical problems. |
0.723 |
|
|
|
|
9 |
Patients would ultimately benefit if health and social care students/professionals worked together to solve patient problems. |
0.650 |
|
|
|
|
10 |
It is not necessary for undergraduate health and social care students to learn together. |
|
0.882 |
|
|
|
11 |
I don’t want to waste time learning with other health and social care students. |
|
0.854 |
|
|
|
12 |
Clinical problem-solving skills can only be learnt with students from my own department. |
|
0.799 |
|
|
|
13 |
Shared learning will help to clarify the nature of patient problems. |
|
|
0.658 |
|
|
14 |
Shared learning before qualification will help me become a better team worker. |
|
|
0.642 |
|
|
15 |
I would welcome the opportunity to work on small group projects with other health and social care students. |
|
|
0.614 |
|
|
16 |
Shared learning with other health and social care professionals will help me to communicate better with patients and other healthcare professionals. |
|
|
0.567 |
|
|
17 |
The function of nurses and therapists is mainly to provide support for doctors. |
|
|
|
0.836 |
|
18 |
I am not sure what my professional role will be. |
|
0.459* |
|
0.285 |
|
19 |
I have to acquire much more knowledge and skills than other health or social care students. |
|
|
|
0.517 |
Table 2: Exploratory Factor Analysis of the RIPLS – Contribution of Items to Each Component
*The highest loading value of each item under the four subscales are shown (except for item 18). A loading value of >0.5 was taken to be satisfactory. Item 18, “I am not sure what my professional role will be.”, was deemed borderline satisfactory at a loading value of 0.459 in the subscale Negative Professional Identity. Its loading value was lower at 0.285 in its original subscale Roles and Responsibility.
C. Internal Consistency
Cronbach’s alpha is 0.848 for RIPLS total score, suggesting good internal consistency.
D. Baseline RIPLS Score
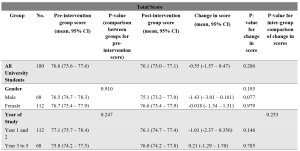
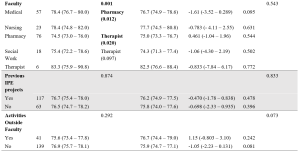
Table 3: Total RIPLS scores.
Subscale scores can be found in Annexes 3 to 6.
The mean baseline total RIPLS score was 76.6 (95% CI 75.6 – 77.6). There was a baseline difference between faculties (p=0.001), with medical and therapy undergraduates having higher scores as compared to pharmacy students (mean difference 3.85, 0.59–7.11, p=0.012 and mean difference 8.83, 0.94–16.7, p=0.020, respectively) (Table 3). As for subscales, there was a difference in “Teamwork and Collaboration” baseline scores between years of study, with Year 1–2 undergraduates had a higher baseline score of 40.8 (40.0–41.5) versus Year 3–5 undergraduates with a score of 39.5 (38.6–40.4) (p=0.038) (Annex 3). Medical undergraduates had higher baseline scores for the “Teamwork and Collaboration” 41.2 (40.2–42.2)) and “Positive Professional Identity” 17.9 (17.4–18.5) subscales compared to pharmacy undergraduates 39.3 (38.4–40.1) (p=0.034), and 17.0 (16.6–17.4) (p=0.036) respectively (Annexes 3-4). Social work undergraduates have the lowest baseline “Roles and Responsibility” score, averaging 4.94 (4.34–5.55) compared to all other faculties (Annex 6).
E. Change in RIPLS Score Post-Intervention
There was no significant difference between the pre- and post-intervention RIPLS total score and the subscale score under the “Teamwork and Collaboration” subscale (Table 3, Annex 3). Under the “Positive Professional Identity” subscale, there was a decrease in post-intervention scores of Year 1-2 students (mean difference -0.500 (-0.931– -0.069), p=0.023) and students with no participation in activities outside of the faculty (mean difference -0.403 (-0.768 – -0.037), p=0.031) (Annex 4). Under the “Negative Professional Identity” subscale, there was a decrease in post-intervention score in medical students (mean difference -0.667 (-1.31– – 0.020), p=0.44) and social work students (-0.889 (-1.70– -0.073), p=0.035) (Annex 5). There was an increase in the post-intervention score amongst female students under the “Roles and Responsibility” subscale (mean difference 0.384 (0.065–0.703), p=0.019) (Annex 6).
F. Individual Item Analysis
Negatively coded statements like “the function of nurses and therapists is mainly to provide support for doctors” (Item 17) and “I am not sure what my professional role will be” (Item 18) showed significant increases in scores post-intervention (0.23, p=0.005 and 0.17, p=0.016 respectively). Other significant findings include a decrease in scores for the statements “Shared learning with other health and social care professionals will help me to communicate better with patients and other healthcare professionals” (Item 13) (-0.14, p=0.013), and “Shared learning will help to clarify the nature of patient problems (Item 15) (-0.10, p=0.034) (Table 4).
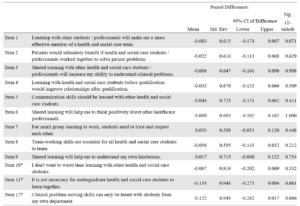

Table 4: RIPLS (Individual items analysis)
G. Self-Reported Feedback on Interprofessional Learning
91.6% participants agreed they could “better appreciate the importance of interprofessional collaboration in the care of patients”. 72.8% said MDMs were important for their learning and 91.9% of respondents would recommend the programme to their friends.
H. Qualitative Feedback
163 of 180 survey respondents participated in the qualitative research (response rate 90.6%). (Fig 1) 34.4% of respondents were male and 65.6% female. 33.1% of respondents were studying Medicine, 12.3% Nursing, 40.5% Pharmacy, 11.0% Social Work and 3.1% Therapy. 54.6% of respondents were in early years of study (Year 1–2). 74.8% had previous exposure to IPE. Thematic analysis yielded the following themes:
1) Learning and teaching one another: Healthcare undergraduates found value in learning from one another. They shared knowledge and skills gained from their respective curriculum with one another.
“I feel more equipped and prepared to teach and learn from other healthcare professionals”
21-year-old female third-year medical student
“I learnt a lot from my social work team leader and how to consider the social aspects of issues the elderly face”
20-year-old male first-year medical student
2) Understanding the role of other healthcare professionals: Healthcare undergraduates learned the role of other healthcare professionals and gained new insights into how different healthcare professionals contributed to the care of the patient.
[I have] learn[ed] … how we can tap on each other[’s] strengths to come up with a care plan for the patients
21-year-old female third-year pharmacy student
Understanding what medicine, nursing [and] pharmacy does make quite a lot of difference to how we perceive and thus, work with them.
23-year-old female second-year social work student
3) Understanding one’s own role: Healthcare undergraduates reported developing a greater understanding of the roles and responsibilities they played as a part of a multi-disciplinary team.
I am now more aware of the role and responsibility I have as a healthcare professional.
21-year-old female first-year pharmacy student
Working in a multi-disciplinary team gave me a feel of how it may be like caring for a patient as a team in my future career.
20-year-old female first-year social work student
4) Teamwork: Healthcare undergraduates appreciated the need for collaboration and teamwork within a multi-disciplinary team. They learned about the importance of compromise.
Working with different people, in terms of personality, faculty, etcetera – I learnt to give and take and be more understanding towards the others.
21-year-old second-year social work student
It has allowed me to better understand … how the different professions can come together to better serve the needs of patients.
20-year-old female second-year pharmacy student
5) Opportunity to meet people from other faculties: Healthcare undergraduates valued meeting people from other faculties and developing collaborative relationships they would otherwise not have had the opportunity to.
I got to know seniors in medicine and peers from pharmacy.
20-year-old female first-year nursing student
It is a very unique experience, having the chance to interact with … other university students from different healthcare faculties.
20-year-old female second-year pharmacy student
6) Factors limiting learning: Factors limiting learning included time constraints, unmotivated teammates, administrative burden and lack of suitable patients. For the latter, some undergraduates felt that their care was restricted to companionship for patients who were already able to manage their own chronic conditions well and did not require further help from the healthcare undergraduates.
IV. DISCUSSION
A. Validation of the RIPLS in Singapore
This study validated the RIPLS in the Singapore context. The final model is the same as proposed by McFadyen et al. (2005). without item 18 “I am not sure what my professional role will be”, from “Roles and Responsibility” subscale. The poor fit of this item into this study’s theoretical construct could be because participants are mostly in their pre-clinical years and may not understand professional roles and responsibilities due to their limited on-job experience, a reason also proposed by McFadyen et al. (2005) and Tyastuti et al. (2014). Tyastuti et al. (2014) found this item, along with “I have to acquire much more knowledge and skills than other healthcare students” (item 19) from the same subscale had loading factors of <0.5 and removed the entire “Roles and Responsibility” subscale from the Indonesian version of the RIPLS. Other studies validating the RIPLS also experienced issues with this subscale (Lauffs et al., 2008; Lestari et al., 2016; McFadyen et al., 2005).
B. Baseline RIPLS score
The mean baseline RIPLS score is comparable with that by Chua et al. (2015), another study conducted in Singapore which measured change in the RIPLS after a one-day IPE conference. They also found higher baseline RIPLS scores for medical undergraduates versus other faculties, a finding also noted in this study and another done in a culturally similar country (Lestari et al., 2016). However, this finding seems inconsistent as other studies (Aziz et al., 2011; de Oliveira et al., 2018) have found the contrary.
Chua et al. (2015) also found that prior IPE experience resulted in higher baseline RIPLS scores, a finding not replicated in this study. We hypothesise that while 65.0% of this study’s participants had previous IPE exposure (versus 10.6% in Chua et al. (2015)), the heterogenous nature of IPE programmes they previously participated in may have had differing efficacy in improving IPE attitudes.
This study found undergraduates in their later years had a lower baseline “Teamwork and Collaboration” subscale score, versus those in their early years. We postulate that undergraduates with more clinical experience better understand the challenges of IPE in practice, a finding echoed by Judge et al. (2015).
That pharmacy students, but not medical students, were mandated by their curriculum to fulfil volunteering hours which could explain the former’s lower baseline scores for total RIPLS and subscales “Teamwork and Collaboration” and “Positive Professional Identity” since they are likely less motivated by IPE when choosing to participate.
Social work undergraduates’ low baseline “Roles and Responsibility” score likely reflects their minimal exposure to medical social work unless they elected for healthcare modules in their senior years of study.
C. Change in Pre- and Post-intervention RIPLS Scores
Our study did not show a significant difference between the pre- and post-intervention RIPLS total score and the “Teamwork and Collaboration” subscale. Additionally, there was a decrease seen in post-intervention scores under the “Positive Professional Identity” subscale for Year 1-2 students and the “Negative Professional Identity” subscale in medical students and social work students. This is in contrast with the literature, where previous studies involving conferences (Chua et al., 2015) or solitary learning modules (Wakely et al., 2013; Zaudke et al., 2016) demonstrated a significant difference in the total RIPLS score pre- and post- intervention. Possible reasons for this are further discussed in section E.
There was a significant increase in the post-intervention score amongst female students under the “Roles and Responsibility” subscale. Previous studies have suggested that there are gender specific differences in perception towards IPE with female students having a more positive attitude towards IPE (Hansson et al., 2010; Wilhelmsson et al., 2011). In addition, the individual item analysis showed that negatively coded statements relating to the subscale of “Roles and Responsibility” such as “the function of nurses and therapists is mainly to provide support for doctors” (Item 17) and “I am not sure what my professional role will be” (Item 18) had significant increases in scores post-intervention. This is encouraging and demonstrates the success of the programme in helping students understand the respective roles and responsibility of each profession which is a crucial part of IPE and eventually IPC.
Other significant findings in the individual item analysis include a decrease in scores for the statements “Shared learning with other health and social care professionals will help me to communicate better with patients and other healthcare professionals” (Item 13), and “Shared learning will help to clarify the nature of patient problems” (Item 15). These findings suggest that the programme can be improved by incorporating more modules on communication between healthcare professionals and shared problem-solving.
D. Qualitative Feedback
While the lack of a significant difference between the pre- and post-intervention RIPLS scores suggest no changes in attitudes, the qualitative data revealed that the majority of undergraduates better appreciated the importance of IPC for patient care and many felt that that MDMs were useful for their learning.
Qualitative analysis revealed five major themes in the undergraduates’ learning pertaining to IPE. Participants learned from and taught each other. Being able to freely learn from and teach one another requires mutual trust and respect which are key elements of collaborative practices (de Oliveira et al., 2018). Participants reported better understanding of their own and other healthcare professionals’ roles; these are recognised as crucial components of collaborative practice (Canadian Interprofessional Health Collaborative, 2010). Undergraduates also shared that they learned about teamwork, specifically, conflict resolution and compromise. Finally, undergraduates appreciated the opportunities to meet fellow undergraduates from different faculties. It has been observed in many successful IPE programmes that informal social interactions are potentially as important as the actual IPE activities (Lie et al., 2016). We observed that the relationships built between participants of the programme often persisted beyond the completion of the programme; these relationships could benefit the institution and healthcare system (Hoffman et al., 2008).
E. Possible Reasons Underlying Lack of Improvement in RIPLS Scores
First, as mentioned earlier, the RIPLS has been described to have psychometrics issues, with multiple researchers modifying the subscales (Mahler et al., 2015). Second, Schmitz and Brandt (2015) suggested that RIPLS is insensitive to course improvements and to pre- versus post-intervention change in attitudes. We chose the RIPLS at the start of 2014 as it had been widely used and validated and simple to administer, and we also sought to validate it in Singapore for the first time. Unfortunately, few studies on its potential issues had been published at the time to inform the design of this study. Third, the longitudinal nature of the programme may have permitted undergraduates greater insight to the challenges of IPE and realities of collaborating within interprofessional teams, tampering their idealism.
Lestari et al. (2016) described how nursing and midwifery undergraduates had lower RIPLS scores as compared to medical and dentistry undergraduates as they had prior clinical experience and likely observed less than exemplary interactions amongst members of healthcare teams. Similarly, Makino et al. (2013) found that graduates of an IPE programme had a lower mean score on the Modified Attitudes Toward Health Care Teams Scale (ATHCTS) as compared to current students. The authors suggested that the alumni’s negative attitude may be due to their real-world experience. Several structural issues in clinical practice have been identified that contribute to this trend, for example competition between professionals (Tremblay et al., 2010) and power struggles (Paradis & Whitehead, 2015).
F. Barriers to IPE
Undergraduates reported four main barriers: time constraints, unmotivated teammates, administrative burden, unsuitable patients. Other studies including Alexandraki et al. (2017) and West et al. (2016) have also faced time constraints. As this programme is voluntary, undergraduates had to take time off their already packed curriculum to participate, and the selection of volunteers was not a stringent process. Additionally, as participants were contributing to clinical care, documentation of visits is required. Multiple studies showed that physicians deemed documentation and administrative work burdensome and excessive time spent on these may be associated with physicians’ burnout (Patel et al., 2018; Wright & Katz, 2018).
In addressing these barriers, incorporating academic credits for participation, a more stringent selection of participants, streamlining administrative work and prudent choice of patients may be considered. These measures are already being implemented by the programme organisers to improve the programme.
G. Strengths and Limitations
The strength of this study lies in the use of both quantitative and qualitative data grounded on an established framework by Kirkpatrick (1959) for the evaluation of a novel experiential IPE programme. The limitations of our study include it being single-institution and that the participants are volunteers which thus form a self-selected group. Hence, the results may not be generalisable. There was also no control arm for the intervention. In addition, there was a large variation in baseline RIPLS score seen in the programme, which can be potentially improved with a more robust study design that controls for baseline differences. Lastly, the use of only a survey for data collection may limit the depth of qualitative data obtained. Further studies could include qualitative interviews.
V. CONCLUSION
We validated the RIPLS in Singapore and demonstrated the feasibility of an interprofessional student-initiated home visit programme. While there was no significant change in RIPLS scores, the qualitative feedback suggests that there are participant-perceived benefits for IPE after undergoing this programme, even with the perceived barriers to IPE. Future programmes can work on addressing these barriers to IPE.
Notes on Contributors
Gloria Yao Chi Leung contributed to the conception and design of the work, the acquisition, analysis, and interpretation of data for the work, drafting and revising the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Kennedy Yao Yi Ng contributed to the conception and design of the work, analysis and interpretation of data for the work, drafting and revising the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Yow Ka Shing contributed to the conception and design of the work, the acquisition and interpretation of data for the work, drafting and revising the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Nerice Heng Wen Ngiam contributed to the conception and design of the work, the acquisition of data for the work, drafting the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Dillon Guo Dong Yeo contributed to the conception and design of the work, drafting the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Angeline Jie-Yin Tey contributed to the conception and design of the work, drafting the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Melanie Si Rui Lim contributed to the conception and design of the work, drafting the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Aaron Kai Wen Tang contributed to the conception and design of the work, drafting the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Chew Bi Hui contributed to the conception and design of the work, drafting the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Celine Yi Xin Tham contributed to the conception and design of the work, drafting the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Yeo Jia Qi contributed to the conception and design of the work, drafting the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Lau Tang Ching contributed to the conception and design of the work, critical revision of the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Wong Sweet Fun contributed to the conception and design of the work, critical revision of the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Gerald Choon Huat Koh contributed to the conception and design of the work, interpretation of the data for the work, critical revision of the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Wong Chek Hooi contributed to the conception and design of the work, interpretation of the data for the work, critical revision of the manuscript, approves of the publishing of the manuscript, and agrees to be accountable for the accuracy of the work.
Ethical Approval
Ethical approval was obtained from the NUS institutional review board (B-15-272). Study participation was entirely voluntary and anonymous. Informed consent was taken from participants before data collection commenced, and they were allowed to withdraw from the research at any point in time. No incentives were provided to study participants.
Data Availability
According to institutional policy, research dataset is available on reasonable request to the corresponding author.
Acknowledgement
The authors would like to thank the Tri-Generational HomeCare Organising Committee from 2014 to 2018 for supporting the study. They would like to extend their thanks to the National University of Singapore, Yong Loo Lin School of Medicine, Dean’s Office; the North West Community Development Council; Khoo Teck Puat Hospital, Singapore; Geriatric Education and Research Institute, Singapore. Finally, they would like to thank the volunteers for their generosity and the patients for their hospitality.
Funding
National University of Singapore, Yong Loo Lin School of Medicine, Dean’s Office; the North West Community Development Council; Khoo Teck Puat Hospital, Singapore provided funding support for the purchase of medical consumables, refreshments and logistics for the program.
Declaration of Interest
There are no conflicts of interest.
References
Alexandraki, I., Hernandez, C. A., Torre, D. M., & Chretien, K. C. (2017). Interprofessional education in the internal medicine clerkship post-LCME standard issuance: Results of a national survey. Journal of General Internal Medicine, 32(8), 871–876.https://doi.org/10.1007/s11606-017-4004-3
Aziz, Z., Teck, L. C., & Yen, P. Y. (2011). The attitudes of medical, nursing and pharmacy students to inter-professional learning. Procedia – Social and Behavioural Sciences, 29, 639–645. https://doi.org/10.1016/j.sbspro.2011.11.287
Barr, H., Koppel, I., Reeves, S., Hammick, M., & Freeth, D. (2005). Effective interprofessional education: argument, assumption, and evidence (1st edition). Wiley-Blackwell.
Berger-Estilita, J., Fuchs, A., Hahn, M., Chiang, H., & Greif, R. (2020). Attitudes towards interprofessional education in the medical curriculum: A systematic review of the literature. BMC Medical Education, 20(1), Article 254. https://doi.org/10.1186/s12909-020-02176-4
Blythe, J., & Spiring, R. (2020). The virtual home visit. Education for Primary Care, 31(4), 244–246. https://doi.org/10.1080/14739879.2020.1772119
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Briggs, M. C. E., & McElhaney, J. E. (2015). Frailty and interprofessional collaboration. Interdisciplinary Topics in Gerontology and Geriatrics, 41, 121–136. https://doi.org/10.1159/000381204
Canadian Interprofessional Health Collaborative. (2010). A national interprofessional competency framework. https://phabc.org/wp-content/uploads/2015/07/CIHC-National-Interprofessional-Competency-Framework.pdf
Chua, A. Z., Lo, D. Y., Ho, W. H., Koh, Y. Q., Lim, D. S., Tam, J. K., Liaw, S. Y., & Koh, G. C. (2015). The effectiveness of a shared conference experience in improving undergraduate medical and nursing students’ attitudes towards inter-professional education in an Asian country: A before and after study. BMC Medical Education, 15, Article 233. https://doi.org/10.1186/s12909-015-0509-9
Conti, G., Bowers, C., O’Connell, M. B., Bruer, S., Bugdalski-Stutrud, C., Smith, G., Bickes, J., & Mendez, J. (2016). Examining the effects of an experiential interprofessional education activity with older adults. Journal of Interprofessional Care, 30(2), 184–190. https://doi.org/10.3109/13561820.2015.1092428
de Oliveira, V. F., Bittencourt, M. F., Navarro Pinto, Í. F., Lucchetti, A. L. G., da Silva Ezequiel, O., & Lucchetti, G. (2018). Comparison of the readiness for interprofessional learning and the rate of contact among students from nine different healthcare courses. Nurse Education Today, 63, 64–68. https://doi.org/10.1016/j.nedt.2018.01.013
Fahs, D. B., Honan, L., Gonzalez-Colaso, R., & Colson, E. R. (2017). Interprofessional education development: Not for the faint of heart. Advances in Medical Education and Practice, 8, 329–336. https://doi.org/10.2147/AMEP.S133426
Ganotice, F. A., & Chan, L. K. (2018). Construct validation of the English version of Readiness for Interprofessional Learning Scale (RIPLS): Are Chinese undergraduate students ready for ‘shared learning’? Journal of Interprofessional Care, 32(1), 69–74. https://doi.org/10.1080/13561820.2017.1359508
Grice, G. R., Thomason, A. R., Meny, L. M., Pinelli, N. R., Martello, J. L., & Zorek, J. A. (2018). Intentional interprofessional experiential education. American Journal of Pharmaceutical Education, 82(3), Article 6502. https://doi.org/10.5688/ajpe6502
Hansson, A., Foldevi, M., & Mattsson, B. (2010). Medical students’ attitudes toward collaboration between doctors and nurses – A comparison between two Swedish universities. Journal of Interprofessional Care, 24(3), 242–250. https://doi.org/10.3109/13561820903163439
Hoffman, S. J., Rosenfield, D., Gilbert, J. H. V., & Oandasan, I. F. (2008). Student leadership in interprofessional education: Benefits, challenges and implications for educators, researchers and policymakers. Medical Education, 42(7), 654–661. https://doi.org/10.1111/j.1365-2923.2008.03042.x
Judge, M. P., Polifroni, E. C., & Zhu, S. (2015). Influence of student attributes on readiness for interprofessional learning across multiple healthcare disciplines: Identifying factors to inform educational development. International Journal of Nursing Sciences, 2(3), 248–252. https://doi.org/10.1016/j.ijnss.2015.07.007
Kiger, M. E., & Varpio, L. (2020). Thematic analysis of qualitative data: AMEE Guide No. 131. Medical Teacher, 42(8), 846–854. https://doi.org/10.1080/0142159X.2020.1755030
Kirkpatrick, D. L. (1959). Techniques for Evaluation Training Programs. Journal of the American Society of Training Directors, 13, 21–26.
Knowles, M. S. (1984). Andragogy in Action: Applying Modern Principles of Adult Learning (1st edition). Jossey-Bass.
Lauffs, M., Ponzer, S., Saboonchi, F., Lonka, K., Hylin, U., & Mattiasson, A.-C. (2008). Cross-cultural adaptation of the Swedish version of Readiness for Interprofessional Learning Scale (RIPLS). Medical Education, 42(4), 405–411. https://doi.org/10.1111/j.1365-2923.2008.03017.x
Lestari, E., Stalmeijer, R. E., Widyandana, D., & Scherpbier, A. (2016). Understanding students’ readiness for interprofessional learning in an Asian context: A mixed-methods study. BMC Medical Education, 16, Article 179. https://doi.org/10.1186/s12909-016-0704-3
Li, Z., Sun, Y., & Zhang, Y. (2018). Adaptation and reliability of the Readiness for Inter Professional Learning Scale (RIPLS) in the Chinese health care students setting. BMC Medical Education, 18(1), Article 309. https://doi.org/10.1186/s12909-018-1423-8
Lie, D. A., Forest, C. P., Walsh, A., Banzali, Y., & Lohenry, K. (2016). What and how do students learn in an interprofessional student-run clinic? An educational framework for team-based care. Medical Education Online, 21(1), Article 31900. https://doi.org/10.3402/meo.v21.31900
Mahler, C., Berger, S., & Reeves, S. (2015). The Readiness for Interprofessional Learning Scale (RIPLS): A problematic evaluative scale for the interprofessional field. Journal of Interprofessional Care, 29(4), 289–291. https://doi.org/10.3109/13561820.2015.1059652
Makino, T., Shinozaki, H., Hayashi, K., Lee, B., Matsui, H., Kururi, N., Kazama, H., Ogawara, H., Tozato, F., Iwasaki, K., Asakawa, Y., Abe, Y., Uchida, Y., Kanaizumi, S., Sakou, K., & Watanabe, H. (2013). Attitudes toward interprofessional healthcare teams: A comparison between undergraduate students and alumni. Journal of Interprofessional Care, 27(3), 261–268. https://doi.org/10.3109/13561820.2012.751901
McFadyen, A. K., Webster, V., Strachan, K., Figgins, E., Brown, H., & McKechnie, J. (2005). The Readiness for Interprofessional Learning Scale: A possible more stable sub-scale model for the original version of RIPLS. Journal of Interprofessional Care, 19(6), 595–603. https://doi.org/10.1080/13561820500430157
McManus, K., Shannon, K., Rhodes, D. L., Edgar, J. D., & Cox, C. (2017). An interprofessional education program’s impact on attitudes toward and desire to work with older adults. Education for Health, 30(2), 172–175. https://doi.org/10.4103/efh.EfH_2_15
Ng, K. Y. Y., Leung, G. Y. C., Tey, A. J.-Y., Chaung, J. Q., Lee, S. M., Soundararajan, A., Yow, K. S., Ngiam, N. H. W., Lau, T. C., Wong, S. F., Wong, C. H., & Koh, G. C.-H. (2020a). Bridging the intergenerational gap: The outcomes of a student-initiated, longitudinal, inter-professional, inter-generational home visit program. BMC Medical Education, 20(1), Article 148. https://doi.org/10.1186/s12909-020-02064-x
Ng, K. Y. Y., Leung, G. Y. C., Yow, K. S., Ngiam, N. H. W., Yeo, D. G. D., Tey, A. J.-Y., Lim, M. S. R., Tang, A. K. W., Chew, B. H., Tham, C. Y. X., Yeo, J. Q., Lau, T. C., Wong, S. F., Wong, C. H., & Koh, G. C.-H. (2020b). Impact of an interprofessional, longitudinal, undergraduate student-initiated home visit program towards interprofessional education. Research Square. https://doi.org/10.21203/rs.3.rs-23744/v1
Paradis, E., & Whitehead, C. R. (2015). Louder than words: Power and conflict in interprofessional education articles, 1954-2013. Medical Education, 49(4), 399–407. https://doi.org/10.1111/medu.12668
Parsell, G., & Bligh, J. (1999). The development of a questionnaire to assess the readiness of health care students for interprofessional learning (RIPLS). Medical Education, 33(2), 95-100. https://doi.org/10.1046/j.1365-2923.1999.00298.x
Patel, R. S., Bachu, R., Adikey, A., Malik, M., & Shah, M. (2018). Factors related to physician burnout and its consequences: A review. Behavioural Sciences, 8(11), Article 98. https://doi.org/10.3390/bs8110098
Schmitz, C. C., & Brandt, B. F. (2015). The Readiness for Interprofessional Learning Scale: To RIPLS or not to RIPLS? That is only part of the question. Journal of Interprofessional Care, 29(6), 525–526. https://doi.org/10.3109/13561820.2015.1108719
Shapiro, S. S., & Wilk, M. B. (1965). an analysis of variance test for normality (complete samples). Biometrika, 52(3/4), 591–611. https://doi.org/10.2307/2333709
Sunguya, B. F., Hinthong, W., Jimba, M., & Yasuoka, J. (2014). Interprofessional education for whom? – Challenges and lessons learned from its implementation in developed countries and their application to developing countries: A systematic review. PloS One, 9(5), Article e96724. https://doi.org/10.1371/journal.pone.0096724
Tamura, Y., Seki, K., Usami, M., Taku, S., Bontje, P., Ando, H., Taru, C., & Ishikawa, Y. (2012). Cultural adaptation and validating a Japanese version of the readiness for interprofessional learning scale (RIPLS). Journal of Interprofessional Care, 26(1), 56–63. https://doi.org/10.3109/13561820.2011.595848
Toth-Pal, E., Fridén, C., Asenjo, S. T., & Olsson, C. B. (2020). Home visits as an interprofessional learning activity for students in primary healthcare. Primary Health Care Research & Development, 21, Article e59. https://doi.org/10.1017/S1463423620000572
Tremblay, D., Drouin, D., Lang, A., Roberge, D., Ritchie, J., & Plante, A. (2010). Interprofessional collaborative practice within cancer teams: Translating evidence into action. A mixed methods study protocol. Implementation Science, 5, Article 53. https://doi.org/10.1186/1748-5908-5-53
Tyastuti, D., Onishi, H., Ekayanti, F., & Kitamura, K. (2014). Psychometric item analysis and validation of the Indonesian version of the Readiness for Interprofessional Learning Scale (RIPLS). Journal of Interprofessional Care, 28(5), 426–432. https://doi.org/10.3109/13561820.2014.907778
Vaughn, L. M., Cross, B., Bossaer, L., Flores, E. K., Moore, J., & Click, I. (2014). Analysis of an interprofessional home visit assignment: Student perceptions of team-based care, home visits, and medication-related problems. Family Medicine, 46(7), 522–526
Wakely, L., Brown, L., & Burrows, J. (2013). Evaluating interprofessional learning modules: Health students’ attitudes to interprofessional practice. Journal of Interprofessional Care, 27(5), 424–425. https://doi.org/10.3109/13561820.2013.784730
West, C., Graham, L., Palmer, R. T., Miller, M. F., Thayer, E. K., Stuber, M. L., Awdishu, L., Umoren, R. A., Wamsley, M. A., Nelson, E. A., Joo, P. A., Tysinger, J. W., George, P., & Carney, P. A. (2016). Implementation of interprofessional education (IPE) in 16 U.S. medical schools: Common practices, barriers and facilitators. Journal of Interprofessional Education & Practice, 4, 41–49. https://doi.org/10.1016/j.xjep.2016.05.002
Wilhelmsson, M., Ponzer, S., Dahlgren, L. O., Timpka, T., & Faresjö, T. (2011). Are female students in general and nursing students more ready for teamwork and interprofessional collaboration in healthcare? BMC Medical Education, 11, Article 15. https://doi.org/10.1186/1472-6920-11-15
Wright, A. A., & Katz, I. T. (2018). Beyond burnout — Redesigning care to restore meaning and sanity for physicians. The New England Journal of Medicine, 378(4), 309–311. https://doi.org/10.1056/NEJMp1716845
Zaudke, J. K., Paolo, A., Kleoppel, J., Phillips, C., & Shrader, S. (2016). The impact of an interprofessional practice experience on readiness for interprofessional learning. Family Medicine, 48(5), 371–376.
*Chek Hooi WONG
90 Yishun Central,
Khoo Teck Puat Hospital,
Singapore 768828
9 Lower Kent Ridge Rd, Level 10,
+65 6807 8001
Email: wong.chek.hooi@ktph.com.sg
Submitted: 5 January 2022
Accepted: 24 February 2022
Published online: 5 July, TAPS 2022, 7(3), 33-41
https://doi.org/10.29060/TAPS.2022-7-3/OA2739
Javier Zheng Huan Thng1, Fion Yun Yee Tan1, Marion Margaret Hui Yong Aw1,2 & Shijia Hu3
1Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Department of Paediatrics, Khoo Teck Puat-National University Children’s Medical Institute, National University Health System, Singapore; 3Faculty of Dentistry, National University of Singapore, Singapore
Abstract
Introduction: In paediatric practice, healthcare professionals are required to connect with the child and interact at his/her level. However, it can be very difficult for medical students to put themselves in the shoes of the young child, to empathize and understand how a child actually feels while being treated. The Teddy Bear Hospital (TBH) can serve as a platform for medical students to learn how to communicate and empathise with children. Additionally, virtual reality (VR) can be used to portray a child’s viewpoint. This study aims to assess how TBH and VR can improve learning outcomes for medical students.
Methods: A cohort study was conducted on 20 first-year medical students taking part in TBH sessions. The medical students did a Pre-, Post- and 1-year Post-intervention Jefferson Scale of Empathy to assess their empathy levels. They also completed a 1-year Post-intervention quantitative and qualitative survey on their experience.
Results: There was a significant increase in Jefferson score compared to Pre-intervention (116.95 ± 8.19) for both Post-intervention (121.65 ± 11.03) and 1-year Post-intervention (123.31 ± 8.86). More than 80% believed that participating in TBH improved their confidence and ability to interact with children, while 50% felt that VR scenarios helped prepare them for the TBH. Thematic analysis of qualitative responses described (1) Personal development, (2) Insights into interacting with children, and (3) Structure and curriculum.
Conclusion: TBH improved empathy and communication with children among pre-clinical medical students and the use of VR can be used to augment sessions.
Keywords: Education, Medical Student, Simulation Training, Teddy Bear Hospital, Virtual Reality
- The Teddy Bear Hospital sessions, consisting of physical simulation of medical scenarios with children, increased empathy of medical students.
- The use of virtual reality scenarios to portray the viewpoint of a child can augment the teaching of the Teddy Bear Hospital.
- The Teddy Bear Hospital and virtual reality sessions improved the comfort, increased confidence, and self-perceived ability of interacting with children in medical students.
I. INTRODUCTION
In paediatric practice, healthcare professionals are required to connect with the child and interact at his/her level. This is especially important, when the child is encountering new and unfamiliar situations or when they are unwell and face potentially challenging and painful procedures (Mead & Bower, 2002). However, it can be very difficult for new practitioners to put themselves in the shoes of the young child, to empathise and understand how a child actually feels while being treated (Dwamena et al., 2012). This is particularly true for medical students, who not only have to grapple with the unfamiliar medical aspects of pediatric disease, but may also need to manage a frightened and uncooperative child at the same time (MacDonald-Wicks & Levett-Jones, 2012). Furthermore, having limited interaction with children means that most medical students have a difficult time empathising with them.
Empathy is an important element in a physician-patient relationship, as it has shown to improve communication and therapeutic goals (Mercer & Reynolds, 2002). However, several studies have shown significant decrease in empathy over the course of medical school (Neumann et al., 2011). Although there have been numerous methods and approaches developed to enhance empathy in medical students (Batt-Rawden et al., 2013), including interventions based around the patient narrative (e.g. creative writing, blogging, drama, poetry, fiction, and film), problem-based learning, interpersonal skills training, patient interviews, and experiential learning (simulation of patient experience). Among these interventions, experiential (immersive) learning experiences have shown promising results (Halton & Cartwright, 2018). These scenarios can be conducted either physically or virtually. It can involve the learner completing a simulated task or experience a scenario from the point of view of someone else so as to put themselves in someone else’s shoes.
The advent and advancement of virtual reality (VR) media provide the opportunity for the portrayal of different viewpoints (Lok et al., 2006). A recent study found that empathy in medical students was improved with VR portraying the viewpoint of an older patient with conditions such as macular degeneration and hearing loss (Dyer et al., 2018). However, there has not been any research done on the use of VR to simulate the point of view of a child in a medical setting. The power of immersive media can be harnessed to simulate interactions between a child and healthcare professionals, exhibiting both positive and negative examples. More importantly, it can be used to introduce an inexperienced practitioner to the viewpoint of a child patient. This will help foster empathy and drive home the effectiveness of behaviour management skills (Stewart et al., 2013).
The Teddy Bear Hospital (TBH) is an international initiative, carried out by students from Medical Faculties, aimed at reducing children’s anxiety around medical environments, procedures and professionals (Bloch & Toker, 2008; Santen & Feldman, 1994; Siegel et al., 2018). TBH simulates the different medical environments and clinical situations which children may encounter in a friendly manner using they own toys (such as teddy bears). This simulation takes the form of multi-station role-plays, which could include a check-up by the doctor, watching a doctor applying a cast for a limb fracture or performing a procedure (e.g., taking a blood sample), or receiving an injection (all performed on teddy bears, who are the patients). In addition to reducing anxiety in young children, the TBH has also been used to teach medical students communication with children in a medical setting (Nheu et al., 2018; Ong et al., 2018). Although the qualitative feedback from medical students have been generally positive (Nheu et al., 2018; Ong et al., 2018), there have not been objective measures of the effect of the TBH on the empathy of medical students.
Both VR and TBH are immersive interventions that can potentially increase the empathy of medical student, they can also improve the learning experience by allowing students to experience effective techniques to interact with children and practice those techniques. However, each intervention has inherent disadvantages. VR usually follows a scripted scenario that does not allow students to practice and interact in real-time. While TBH is time and resource intensive, and cannot be conducted is situations such as a pandemic. Therefore, evaluating the effects of a combination of the 2 techniques can inform on the individual effectiveness as well as in combination.
This study aims to determine the effect of virtual and physical simulation on the empathy and learning experience of medical students. This will be done through a combination of VR instruction and practical simulation in a TBH experience, in which medical students are exposed to and educated on the positive interactions with a child patient in various medical scenarios.
II. METHODS
This is a cohort study of first year medical students who took part in TBH sessions in January 2020 and were followed up in January 2021. Subjects were recruited from volunteers who signed up to participate in TBH sessions. Subjects were reassured that their responses are strictly confidential and will have no impact on their grades or teaching received. Medical students who have participated in previous TBH sessions were excluded. Written informed consent was taken prior to participation. This study was approved by the Institutional Review Board (NUS-IRB Reference Number: S-19-151) and the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
As this was a pilot study, no sample size calculation was conducted prior to study initiation.
A. Survey Content and Timing
The Jefferson Scale of Empathy (Sidney Kimmel Medical College, Thomas Jefferson University, PA, USA) was used to assess the level of empathy (Hojat et al., 2018). It is a 20-item scale that was developed specifically to measure empathy in health professions education, including medical students. The S-version of the survey, for medical students, was administered in this study. The survey forms were purchased from Thomas Jefferson University, Center for Research in Medical Education and Health Care. The Jefferson scores were calculated out of a maximum of 140. The survey was conducted in its original English version as the language medium for education in Singapore is English and all participants are proficient.
1) Pre-intervention: Prior to the TBH session, the subjects completed the Jefferson Scale of Empathy to assess baseline empathy scores. The subjects then underwent a small group teaching session of one hour including viewing of two VR scenarios, conducted by the same instructors (JT & FT). The small group teaching sessions covered topics pertaining to doctor-patient relationship, and the developmental and psycho-affective challenges of interacting with children. The two VR scenarios depicted a child’s point of view in the setting of getting an injection (mooc vid, Scenario 1, 2019) and visiting the dentist (mooc vid, Scenario 2, 2019). The scenarios are interactive and the point of view can be manipulated by the viewer. After watching the VR scenarios, discussions where subjects can critique the healthcare providers’ actions and share their learning points were carried out. During this session, the subjects were also briefed about the different scenarios in the TBH session, including the content to be covered.
2) TBH session: The TBH session consisted of 5 scenarios namely: (1) Orthopedic Specialist: Meet Mr. Bones, (2) Respiratory Therapist: Help Teddy Breathe, (3) Family Medicine: Help Teddy Stay Healthy, (4) Personal Hygiene: Help Teddy Stay Clean, (5) Operating Theatre: Teddy has a Painful Tummy. The injection process and dental procedures were incorporated into scenarios 3 and 4 respectively. The medical students were divided into teams of 2 to 3, each interacting with a group of 5 to 8 children of the same age. Each team rotated through the different scenarios for 10 minutes. At each scenario, the medical students explained the task to the children and conducted hands-on simulation.
3) Post-intervention: After their first TBH session, the subjects completed a second Jefferson Scale of Empathy.
4) 1-year Post-intervention: One year after the TBH session, students completed a third Jefferson Scale of Empathy, along with a self-administered survey regarding the long-term impact of TBH sessions and the effectiveness of the VR scenarios.
To assess the long-term impact of TBH sessions and the effectiveness of the VR scenarios, a 1-year Post-intervention survey was administered in December 2020. The survey was adapted from a previous study (Ong et al., 2018) and piloted for understanding and readability.
The 1-year Post-intervention impact of TBH sessions was assessed using five questions on a 5-point Likert scale (strongly disagree, disagree, neutral, agree, strongly agree) regarding the effect of TBH sessions on improving the medical student’s ability, confidence and comfort level in communicating with children, and ability to empathize with children’s fear in the healthcare environment. Similarly, the effectiveness of the VR scenarios was assessed using three questions on a 5-point Likert scale, regarding the effect of the VR scenarios on preparation for TBH session, as well as improving the comfort level and confidence in engaging children. The remaining two questions obtained qualitative feedback regarding any difficulties faced as well as takeaways obtained during the TBH session.
B. Data Collection
The subjects completed the TBH sessions in small groups of up to eight volunteers, with up to 30 children, aged between 4 to 8 years old, in each session. It was explained to the children that they were participating in an activity to teach them about what happens during visits to a doctor. These sessions were conducted at the participating pre-schools with medical instruments and teddy bears as simulated patients.
Due to the COVID-19 pandemic situation and restrictions, the survey was collected via an online survey, instead of a planned Focused Group Discussion.
C. Data Analysis
Normality of data was checked using the Shapiro-Wilk test, data analysis of the Jefferson Scale of Empathy score was done via Paired samples correlation, Cohen’s d score and Paired Samples T test using Statistical Package for Social Sciences (SPSS) software (IBM SPSS Statistics 26, Armonk, NY, USA). Descriptive statistics were presented for the survey on learner experience.
Qualitative analysis was done on the medical students’ open-ended responses regarding the long-term impact of TBH sessions and the effectiveness of the VR scenarios. Using thematic content analysis and a qualitative descriptive framework (Creswell & Poth, 2019), emerging themes and illustrative quotes for each theme were extracted. The codes and themes were first done independently by two of the authors (JT & FT), any discrepancies were discussed and reconciled. After which, 2 other authors (SH & MA) reviewed and verified the finalised codes and themes, which were mapped for interpretation. Descriptive summaries and illustrative quotes were used to describe each theme.
III. RESULTS
A. Study Demographics
In total, 20 first time participants were recruited and consent was taken. All 20 were first year medical students; 9 males and 11 females. All participants (n=20) completed the Pre-intervention and Post-intervention survey while 16 completed the 1-year Post-intervention survey, with 4 participants declining to participate in the follow-up. The data that support the findings of this study are openly available in Figshare at https://doi.org/10.6084/m9.figshare.17973662 (Hu, 2022).
B. Jefferson Scale of Empathy
There was a significant (p=0.026) increase in the Jefferson score between the Pre-intervention (116.95 ± 8.19) and Post-intervention (121.65 ± 11.03). Similarly, there was a significant (p=0.002) increase from the Pre-intervention to 1-year Post-intervention (123.31 ± 8.86). (Figure 1) However, there was no difference between the Post-intervention and 1-year Post-intervention scores.
Cohen’s d score was used to determine the effect size of the intervention on the mean difference between the Pre- and Post-intervention score (0.48), and the Pre- and 1-year Post-intervention score (0.72). This corresponds to a medium effect of the intervention on the mean differences.
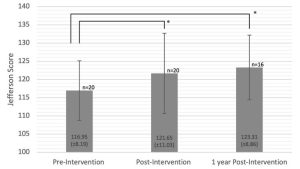
Figure 1. Jefferson Scale of Empathy Score before, immediately after and 1 year after TBH. Error bars represent the standard deviation. Asterisk (*) indicate significant differences between the groups, p<0.05.
C. Quantitative Survey
Quantitative responses from the survey on learner experience were categorised into positive responses (agree, strongly agree) and negative/neutral responses (neutral, disagree, strongly disagree). The total number of responses collected was 16 at 1-year Post-intervention (Table 1).
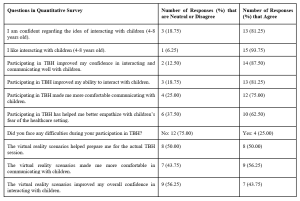
Table 1. Subject’s perception towards their TBH experience
The subjects were generally confident (75%) and enjoyed interacting with young children (94%). More than 80% believed that participating in TBH improved their confidence and ability to interact with children, and 75% felt that participating in TBH made them more comfortable communicating with children. 63% felt that TBH helped improve their ability to empathize with children’s fears of the healthcare setting. Overall, 75% of subjects did not face difficulties during the TBH sessions. In terms of the VR scenarios, around 50% felt that it was effective in preparing for the actual TBH session, with 56% feeling more comfortable and 44% feeling more confident interacting with children.
D. Qualitative Survey
Three major themes were generated from the analysis of the open-ended responses from 16 of the 20 subjects: (1) Personal development, (2) Insights into interacting with children and (3) Structure and curriculum of TBH. These themes were further categorised into sub-themes as shown in Table 2.
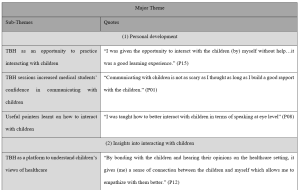
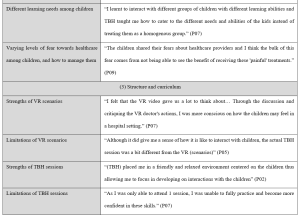
Table 2. Major themes, sub-themes and transcript highlights of qualitative survey
1) Personal development
TBH provided an opportunity for medical students in this study to interact with children in a safe and stress-free environment. These students would otherwise have limited experience communicating with children in that age-group, until actual clinical interactions with sick children.
“I was given the opportunity to interact with the children (by) myself without help…it was a good learning experience.” (P15)
The experience gave these medical students more confidence and reduced their anxiety about interacting with children, as they realized that it was not as difficult as they thought to communicate with children.
“Communicating with children is not as scary as I thought as long as I build a good rapport with the children.” (P01)
Medical students also learnt useful pointers on how to interact and communicate with children, which alleviated their worries and improved their confidence. These pointers include using simpler words, hand actions, speaking at eye level and being more expressive.
“(TBH) allowed me to practice how I interact with children (by) using easier words (and) hand actions” (P01)
“I was taught how to better interact with children in terms of speaking at eye level” (P08)
2) Insights into interacting with children
TBH was a unique platform to understand children’s learning needs and empathize with their views towards healthcare. This was achieved via interactions with the children.
“By bonding with the children and hearing their opinions on the healthcare setting, it gives (me) a sense of connection between the children and myself which allows me to empathize with them better.” (P12)
These interactions allowed medical students to learn how to adapt their teaching styles to suit the different needs of each individual child.
“I learnt to interact with different groups of children with different learning abilities and TBH taught me how to cater to the different needs and abilities of the kids instead of treating them as a homogenous group.” (P07)
These interactions also taught medical students that the children have different levels of fear towards healthcare. While some children were apprehensive, others were unafraid of the TBH sessions.
“The children shared their fears about healthcare providers and I think the bulk of this fear comes from not being able to see the benefit of receiving these ‘painful’ treatments.” (P09)
“The children seemed to be really excited during the TBH sessions, I don’t recall that the children expressed any fear about their experiences” (P16)
In addition to understanding the children’s fears towards healthcare, medical students learnt how to manage these fears by acknowledging them and putting themselves in the children’s shoes.
“We should never downscale a child’s fear towards healthcare. There is a need to try to understand where they are coming from, (and) to comfort and encourage them to the best of our ability.” (P13)
3) Structure and curriculum
To understand the impact of the newly added VR scenarios, feedback regarding its strengths and limitations were collated. One strength is that the students experienced various case studies through the VR scenarios. This allowed them to be better prepared for the TBH sessions and become more aware of the children’s emotions during their interaction.
“I felt that the VR video gave us a lot to think about… Through the discussion and critiquing the VR doctor’s actions, I was more conscious on how the children may feel in a hospital setting.” (P07)
Another strength is that during the training, medical students were also asked how they would respond to the hypothetical scenarios. By putting them in the hot seat, they were able to exchange ideas and learn from one another.
“The volunteer trainers asked us questions during the volunteer training, when I answered correctly it gave me more confidence and when I listen to other people’s answers, I feel more equipped to handle different situations too” (P15)
The VR scenarios were limited in terms of application to the actual TBH sessions. The scenarios only showed how to engage an individual child, which was different from actual TBH sessions, in which medical students had to teach a group of children.
“Although it did give me a sense of how it is like to interact with children, the actual TBH session was a bit different from the VR (scenarios)” (P05)
Feedback was also collated regarding the strengths and limitations of the TBH sessions.
One strength was the established curriculum so participants did not have to worry about the content but can instead focus on honing their communication skills. The fact that this was a student-run program, and that medical students had their peers as fellow participants, put them at ease and made it a more conducive environment.
“(TBH) placed me in a friendly and relaxed environment centred on the children thus allowing me to focus in developing on interactions with the children” (P02)
A limitation of the TBH sessions was that it was challenging for participants to balance teaching the children and empathising with them.
“I think it’s … difficult to see from the children’s perspective during the session… We are usually more focused on imparting rather than listening because of the inability to elicit responses from all of them.” (P13)
Another limitation of the TBH sessions was that participants are usually able to attend only one session. This may have held them back from being fully adept in their interactions with children.
“As I was only able to attend 1 session, I was unable to fully practice and become more confident in these skills.” (P07)
Finally, there were disagreements about whether the ratio of medical students to children was suitable. While some felt that it was appropriate, others had trouble managing the children.
“The ratio (of) facilitators to children were just nice (and) not overwhelming for either parties” (P15)
“It was just too chaotic and hard to manage so many of them especially since they’re so bubbly and curious” (P16)
IV. DISCUSSION
This was the first study to examine objectively and subjectively, the effect of TBH and VR training on the empathy levels of medical students. There was a statistically significant improvement in the medical student’s level of empathy immediately after the TBH session, which persisted 1 year after the TBH session. The outcomes of this study revealed that the medical students who participated in TBH augmented by VR training assisted them to better empathize with the children they worked with.
Compared with the previous work by Ong et al in the same institution, involving only traditional lecture preparation for TBH (Ong et al., 2018), it appears that the addition of VR training showed an increase in medical students’ perceived improvement in both interacting and teaching children. In that study conducted without the use of VR scenarios, 53% reported improvement in interacting with children and 39% reported improvement in teaching children, compared to the present study of 88% and 75% respectively. Moreover, VR training alone achieved improvements of 44% and 50% which is similar to TBH session alone. A recent study found that VR simulation alone improved the empathy of dental students when managing children (Hu & Lai, 2022), this is encouraging since the VR intervention was not as time and resource intensive as the TBH. Although the cohorts of medical students were different, each cohort is from the same year of training (i.e., first year medical students) and the TBH teaching was done with a standardised protocol and thus relatively similar across the cohorts. It appears that a combination of the 2 methods of training provided a greater magnitude to the student’s perceived improvement in interacting and teaching children. This suggests that although the VR training cannot replace the real TBH interaction with children, it can be used to augment the learning experience of students in communicating with children. Moreover, it can be deployed on a much larger scale to the entire cohort, instead of smaller groups like the labour intensive TBH teaching.
According to the qualitative analysis, the TBH is a good platform for medical students to practice and develop their communication skills with children. Through TBH, they pick up techniques on how to better communicate with children both from the trainers and their peers. Similar to previous studies, TBH has also been described to be a useful avenue to gain insights into children’s perspectives of the healthcare setting and therefore trains them to be better attuned to the needs and feelings of children (Nheu et al., 2018; Ong et al., 2018). Nonetheless, the medical students suggested some areas of improvements. For example, it was pointed out that the VR scenarios did not depict the actual TBH session, as such, it did not help in teaching children during TBH. However, the goal of the TBH session is to increase medical student’s empathy through teaching rather than training them to be educators. Therefore, the VR scenarios can still bring the desired benefits in terms of the medical student’s ability to empathize and communicate with children. Additionally, some felt that they are unable to fulfil both a teaching and learning role simultaneously and were overwhelmed. This may hinder them from achieving the desired outcome of increasing their empathy. A potential solution would be to expand the existing course material to further help those who struggle with engaging the children or having fewer children paired to each medical student teacher.
There were some limitations to this study. As there was no control group to compare against, it was difficult to determine if the improvements seen from Pre-intervention to Post-intervention were due to the VR training and participation in the TBH session alone. Future studies could consider including a control group in addition to the intervention group. The observed maintenance of the level of empathy from Post-intervention to 1-year Post-intervention could have been confounded by factors such as varying levels of clinical exposure. Additionally, the quantitative survey on learner experience was done 1 year after the TBH session and may be at risk for recall bias, future studies should consider collecting data at multiple time points to evaluate any difference between immediate and long-term effects of the interventions. However, all respondents provided feedback that were very detailed and informative, suggesting that they were able to recall the experience well. Moreover, due to the COVID-19 pandemic situation and restrictions, the survey was collected via an online survey, instead of the planned Focused Group Discussion, resulting in the inability to ask follow-up or clarifying questions. Lastly, the study was conducted on a small group of volunteers who may have biases due to interest in the discipline. However, a significant improvement was still noted in this small pilot study. Expansion of the program into the general curriculum to include a more diverse group of students will be needed to ascertain the effect of TBH on medical students in general.
V. CONCLUSION
In conclusion, the TBH experience for medical students was effective in increasing their levels of empathy and confidence in interacting and teaching children as it provides an opportunity for medical students to interact with children and understand their views of healthcare. The use of VR can augment the TBH experience or be used in situations where the student is unable to attend TBH sessions in person.
Notes on Contributors
JT and FT are considered co-first authors. JT participated in data collection, conducted the data analysis and interpretation, led the writing, and revised the manuscript for important intellectual content. FT participated in data collection, conducted the data analysis and interpretation, led the writing, and revised the manuscript for important intellectual content. MA conceived the idea and revised the manuscript for important intellectual content. SH conceived the idea, conducted the data analysis and interpretation, led the writing, and revised the manuscript for important intellectual content.
Ethical Approval
This study was approved by the Institutional Review Board (NUS-IRB Reference Number: S-19-151) and the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Data Availability
The data that support the findings of this study are openly available in Figshare repository, https://doi.org/10.6084/m9.figshare.17973662.
Acknowledgement
The authors would like to thank Dr Lee Shuh Shing and Ms Lim Yih Lin for their help with the statistical analysis and Manzalab for the help in creating the virtual reality scenarios.
Funding
This work was supported by the USPC-NUS Joint Innovative Projects in Higher Education grant (USPC-NUS 2018 SoM).
Declaration of Interest
The authors declare that they have no competing interests.
References
Batt-Rawden, S. A., Chisolm, M. S., Anton, B., & Flickinger, T. E. (2013). Teaching empathy to medical students: An updated, systematic review. Academic Medicine, 88(8), 1171-1177. https://doi.org/10.1097/ACM.0b013e318299f3e3
Bloch, Y. H., & Toker, A. (2008). Doctor, is my teddy bear okay? The “Teddy Bear Hospital” as a method to reduce children’s fear of hospitalization. Israel Medical Association Journal, 10(8-9), 597-599.
Creswell, J. W., & Poth, C. N. (2019). Qualitative inquiry & research design: Choosing among five approaches. SAGE.
Dwamena, F., Holmes‐Rovner, M., Gaulden, C. M., Jorgenson, S., Sadigh, G., Sikorskii, A., Lewin, S., Smith, R. C., Coffey, J., & Olomu, A. (2012). Interventions for providers to promote a patient‐centred approach in clinical consultations. Cochrane Database of Systematic Reviews, (12).
Dyer, E., Swartzlander, B. J., & Gugliucci, M. R. (2018). Using virtual reality in medical education to teach empathy. Journal of the Medical Library Association, 106(4), 498-500. https://doi.org/10.5195/jmla.2018.518
Halton, C., & Cartwright, T. (2018). Walking in a patient’s shoes: An evaluation study of immersive learning using a digital training intervention. Frontiers in Psychology, 9, 2124. https://doi.org/10.3389/fpsyg.2018.02124
Hojat, M., DeSantis, J., Shannon, S. C., Mortensen, L. H., Speicher, M. R., Bragan, L., LaNoue, M., & Calabrese, L. H. (2018). The Jefferson Scale of Empathy: a nationwide study of measurement properties, underlying components, latent variable structure, and national norms in medical students. Advances in Health Sciences Education, 23(5), 899-920.
Hu, S. (2022). Raw Jefferson Scores. [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.17973662
Hu, S., & Lai, B. W. P. (2022). Increasing empathy for children in dental students using virtual reality. International Journal of Paediatric Dentistry. https://doi.org/10.1111/ipd.12957
Lok, B., Ferdig, R. E., Raij, A., Johnsen, K., Dickerson, R., Coutts, J., Stevens, A., & Lind, D. S. (2006). Applying virtual reality in medical communication education: Current findings and potential teaching and learning benefits of immersive virtual patients. Virtual Reality, 10(3-4), 185-195.
MacDonald-Wicks, L., & Levett-Jones, T. (2012). Effective teaching of communication to health professional undergraduate and postgraduate students: A systematic review. JBI Evidence Synthesis, 10(28), 1-12. https://doi.org/10.11124/jbisrir-2012-327
Mead, N., & Bower, P. (2002). Patient-centred consultations and outcomes in primary care: A review of the literature. Patient education and counseling, 48(1), 51-61.
Mercer, S. W., & Reynolds, W. J. (2002). Empathy and quality of care. British Journal of General Practice, 52(Suppl), S9-S12.
mooc vid. (2019, September 13). Scenario 1 [Video]. YouTube. https://www.youtube.com/watch?v=4f6bZ_Kc2xw
mooc vid. (2019, September 13). Scenario 2 [Video]. YouTube. https://www.youtube.com/watch?v=oz4dm45Imkw
Neumann, M., Edelhäuser, F., Tauschel, D., Fischer, M. R., Wirtz, M., Woopen, C., Haramati, A., & Scheffer, C. (2011). Empathy decline and its reasons: A systematic review of studies with medical students and residents. Academic Medicine, 86(8), 996-1009. https://doi.org/10.1097/ACM.0b013e318221e615
Nheu, L., Uahwatanasakul, W., & Gray, A. (2018). Medical students’ experience of a Teddy Bear Hospital as part of a paediatric curriculum. Focus on Health Professional Education: A Multi-disciplinary Journal, 19(3), 40.
Ong, L., Chua, K. H., Soh, J. Y., & Aw, M. M. H. Y. (2018). Healthcare encounters in young children: Impact of Teddy bear Hospital, Singapore. The Asia Pacific Scholar, 3(3), 24-30. https://doi.org/10.29060/TAPS.2018-3-3/OA1055
Santen, L., & Feldman, T. (1994). Teddy bear clinics: a huge community project. MCN: The American Journal of Maternal/Child Nursing, 19(2), 102-106.
Siegel, B., Lewis, H., Bryan, L., & Batisky, D. (2018). The Teddy Bear Hospital as an outreach tool for reducing medical anxiety: A randomized trial. (2018). Pediatrics, 142(1_MeetingAbstract), 783. https://doi.org/10.1542/peds.142.1MA8.783
Stewart, M., Brown, J. B., Weston, W., McWhinney, I. R., McWilliam, C. L., & Freeman, T. (2013). Patient-centered medicine: Transforming the clinical method. CRC press.
*Shijia Hu
Faculty of Dentistry,
National University of Singapore
9 Lower Kent Ridge Road #10-01
National University Centre for Oral Health,
Singapore 119085
Email: denhus@nus.edu.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
