
Teleconferencing as a teaching modality for clinical year medical students: Lessons from COVID-19
Submitted: 18 October 2020
Accepted: 1 March 2021
Published online: 5 October, TAPS 2021, 6(4), 17-25
https://doi.org/10.29060/TAPS.2021-6-4/OA2418
Xin Rong Goh1, Chee Wai Ku2,4, Rajeswari Kathirvel1,2,4,5 & Kok Hian Tan1,3,4
1Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore; 2Department of Obstetrics and Gynaecology, KK Women’s & Children’s Hospital, Singapore; 3Department of Maternal Fetal Medicine, KK Women’s & Children’s Hospital, Singapore; 4Duke-NUS Medical School, Singapore; 5Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: Disease outbreaks (DO) result in unprecedented changes to the healthcare industry with far-reaching implications for medical education. The need to adapt to the fluidity during DO requires the delivery of the clinical medical curriculum to be flexible and effective. There is a lack of well-established guidelines on how medical education should be delivered during DO. This study aimed to explore the efficacy of teleconferencing-based platforms (TBP) as a teaching modality to overcome the challenges of clinical year medical education amidst a global pandemic and possibility of its use when there are no disease outbreaks (NDO).
Methods: A cross-sectional survey amongst 144 undergraduate clinical year students from a medical school in Singapore was conducted from May to June 2020, to explore their perspectives on TBP compared to physical venue-based platforms (PVBP). The survey consisted 5-point Likert scale and open-ended questions. Statistical and thematic analyses were performed.
Results: TBP provides greater convenience in travelling, note-taking and ability to overcome administrative challenges. Students strongly recommended its use in DO and NDO. However, students faced increased distractibility, decreased engagement and ease of raising questions, with a lower efficacy in content delivery. The above is dependent on the type of lessons delivered – clinical skills-based or didactic sessions.
Conclusion: TBP is a promising teaching modality for DO with promising possibility of extending its use to NDO. We propose a tri-faceted approach to target improvement in content delivery on TBP, mainly with measures to target propensity for decreased engagement and increased distractibility and to address the technology-related concerns.
Keywords: Medical Education, Teleconferencing, Teaching Modalities, Medical Students, COVID-19, Disease Outbreaks, Pandemics
Practice Highlights
- TBP was strongly recommended as substitute teaching modality during disease outbreaks.
- Students recommended TBP as a supplement for teaching even when there are no disease outbreaks.
- TBP enabled more convenience in travelling, note-taking and overcoming administrative challenges.
- Decreased engagement and increased distractibility noted when sessions are conducted on TBP.
- TBP can be improved via use of teaching aids and contextualising it to the lesson type.
I. INTRODUCTION
Singapore has experienced the escalation of its Disease Outbreak Response System Condition (DORSCON) status to ‘Orange’ due to COVID-19 outbreak on 7th February 2020. This has had significant implications in multiple sectors of the healthcare industry, including that of medical education (Samarasekera, Goh & Lau, 2020). It called for the rapid remodelling of the delivery of the medical education curriculum during a time when social containment and avoidance of large groups gatherings were enforced (Samarasekera & Gwee, 2021). In particular, to contain and prevent the spread of COVID-19, clinical rotations in healthcare institutions were temporarily suspended during the DORSCON Orange period (Chandratre, 2020; Samarasekera, Goh, Yeo et al., 2020).
Many institutions had since employed teleconferencing-based platforms (TBP) to deliver curriculum (Kanneganti et al., 2020; Srinivasan, 2020). TBP is defined as an avenue of e-learning that is ‘internet and local-networking based’ (Al-Shorbaji et al., 2015), enabling the provision of ‘synchronous’ (Dhir et al., 2017) real time audio-visual online interactions across different locations (Lamba, 2011). The literature exploring the use of TBP during DO is limited. Most studies on TBP focused on its use when there are no disease outbreaks (NDO). They described its facilitation of direct teacher-student engagement with quieter students (Fox, 2004) and raised its comparable effectiveness in fulfilling learning outcomes to traditional face-to-face lectures (Bertsch et al., 2007). TBP nonetheless faces deterrents to its implementation, including those of financial implications (Lim et al., 2009) and technical difficulties (Boatin et al., 2015; Lamba, 2011). During DO, it had helped to overcome concerns of social distancing and allowed the continuation of medical training (Kanneganti et al., 2020; Lim et al., 2009).
In spite of the above, it should be recognised that the temporary suspension of clinical rotations represent the absence of a cornerstone in delivery of the medical curriculum (Govindarajan et al., 2018; Jacobs & Samarasekera, 2012; Lim et al., 2009; Rawekar et al., 2016). This study thus chose to specifically focus on the clinical year students owing to the potential application of these findings to post-graduate clinical trainings. Furthermore, the different content and focus during the pre-clinical years (e.g. lack of clinical rotations, presence of anatomy and science practical) would likely raise concerns that are unique and non-generalisable to students in the clinical years. Pre-clinical students were therefor excluded from the current study.
While the use of TBP is largely commended (Fatani, 2020), it is pertinent to compare its efficacy to traditional physical venues-based platforms (PVBP) as a potential replacement or supplement for the delivery of the clinical curriculum during DO. This study aims to understand the ground-up perspective of clinical year students on TBP as an education tool during DO, as compared to PVBP. It also explored TBP’s suitability and effectiveness for the delivery of the undergraduate medical education when there are no disease outbreaks (NDO).
II. METHODS
A. Ethics Review
The following study was approved by NTU Institutional Review Board (IRB Reference number: 2020-05-003) with an exempt status.
B. Survey Design and Study Population
All undergraduate clinical year medical students from the Lee Kong Chian School of Medicine who had used teleconferencing as a part of their curriculum were invited to participate in an online survey via email and social-messaging platform that included an explanation of the study’s details. Informed consent was implied when the participant accessed the online survey administered via SurveyMonkeyÓ platform. Personal identifiers were not collected.
The cross-sectional survey consisted of a mix of 5-point Likert scale questions and open-ended questions. It was anticipated to be completed in 10 minutes. The questions were designed to evaluate their familiarity with teleconferencing and their opinions on teleconferencing as an educational tool as compared to physical venue-based sessions, e.g. traditional lectures, bedside and small group tutorials, and team-based learning. Their willingness to extend teleconferencing as a supplementary delivery tool for medical education in both DO and NDO situations were also explored.
The survey questions were developed de-novo with reference to the existing literature. The themes of platform accessibility and ease of raising questions were adapted from Al-Neklawy (2017) while that of engagement and distractibility were adapted from the Danielson’s Framework for Teaching – The classroom environment (Alvarez & Anderson-Ketchmark, 2011). The survey was then piloted amongst a group of medical students and faculty to assess content and face validity.
C. Statistical Analysis
Self-reported estimates on the number of prior use of teleconferencing were divided by 52 to determine weekly usage. Numerical values were awarded for the 5-point Likert scale as follows: Strongly agree (5), agree (4), neutral (3), disagree (2) and strongly disagree (1).
Paired 2 tailed T test was performed to determine the significance of difference in subjective efficacy of PVBP and TBP. To compare effect of gender on subjective efficacy for the two platforms and recommendations for TBP, independent T test and Fisher’s exact test were performed respectively. Pearson Correlation testing was performed to look for correlations between the variables. Kruskal-Wallis H test was used to study the effect of year of study on the responses. A p value of < 0.05 indicated statistical significance. Data analysis was performed using SPSSTM software (V.24.0).
D. Qualitative Analysis
Thematic analysis was performed for the elaborations and justifications provided by survey respondents. Concepts that were similar were used to guide the development of themes.
III. RESULTS
A. Sociodemographic Characteristics
A total of 144 out of 315 clinical year medical students completed the survey over a 3-week period from May to June 2020 (Year 3: n = 51; Year 4: n = 64; Year 5: n = 29). The survey response rate was 45.7%. Majority of students who responded were female (58.3%) and Year 4 (44.4%).
B. Teleconferencing Usage Patterns
Majority (73.6%) of students had used a teleconferencing platform, for educational and non-education purposes, in the past year prior to declaration of DORSCON Orange. The top three teleconferencing platforms by corrected mean weekly usage prior to DORSCON orange were Skype© (0.2), FaceTime© (0.2) and ZOOM© (0.1). During DOSRCON orange, the top three platforms for educational purposes by corrected mean weekly usage were ZOOM© (4.0), Skype© (0.3), Facetime© (0.1). (Table 1)
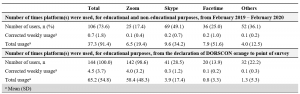
Table 1. Use of teleconferencing-based platforms by medical students
Corrected weekly usage was calculated as follows: (A) Total usage divided by 52, (B) Total usage divided by number of weeks from declaration of DOSRSCON orange to point of survey (For example: 1 week + 1 day would be considered as 2 weeks)
Others included: Whatsapp©, Microsoft Teams©, Google Hangouts©, WebEx©, Discord©, Houseparty©
C. Physical-Venue Based (PVBP) vs Teleconferencing-Based (TBP) Platforms
Students felt PVBP had significant engagement (mean = 4.0) and less distractibility (mean = 2.7). TBP had notable convenience (mean = 4.6), with negligible concerns on its safety (mean = 2.3) on a 5-point Likert scale. (Table 2)
When comparing TBP to PVBP, there was a significant increase in convenience (mean = 4.6 vs 3.8; p <0.001) with TBP. However, this was faced with increased distractibility (mean = 3.7 vs 2.7; p <0.001), decreased engagement (mean = 3.5 vs 4.0; p <0.001), ease of raising questions (mean: 3.4 vs 3.7; p =0.008) and efficacy in the delivery of content (mean: 4.0 vs 3.8; p =0.001). (Table 2)
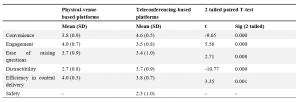
Table 2: Comparison of subjective efficacy of physical venue-based vs teleconferencing based platforms by clinical year medical students surveyed from May to June 2020 on a 5-point Likert Scale
Numerical values were assigned as follows: Strongly disagree (1), Disagree (2), Neutral (3), Agree (4), Strongly agree (5)
D. Correlations Between Responses
Based on Pearson’s correlation, students who were engaged on PVBP, tend to be more comfortable in raising questions (r = 0.301, p <0.001) and less distracted (r = -0.337, p <0.001) with PVBP. Similarly, students who felt engaged on TBP tend to feel comfortable in raising questions on TBP (r = 0.301, p <0.001), less distracted (r = – 0.353, p <0.001) and agree on its efficacy in content delivery (r = 0.570, p <0.001). Students who felt more distracted on PVBP tend to also be more distracted on TBP (r = 0.176, p <0.05). No significant correlations were found between prior teleconferencing experience on self-reported rating of PVBP and TBP.
Kruskal-Wallis H test showed a statistically significant difference in rating of convenience for TBP between different years of study (χ2 (2) = 18.1, p <0.001, mean (Year 3) 87.1, (Year 4) 69.8, (Year 5) 53.0). There were no statistically significant effects of gender on the responses.
E. Recommendations of Teleconferencing Platform
An overwhelming majority of students recommended use of TBP in DO (n = 143, 99.3%), 54.9% (n = 79) recommended it as a substitute, and 44.4% (n = 64) as a supplement for learning, whereas one student did not recommend it at all. A significant proportion continued to favour its use even during NDO (n = 121, 84.0%), although there was a slight shift in preference for it to be used as a supplement (Supplement: n = 108, 75%; Substitute: n = 13, 9.0%). (Table 3A)
There were no statistically significant effects of gender or year of study on the responses.
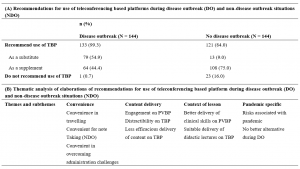
Table 3. Recommendations and suggested improvements for use of teleconferencing platforms during disease and non-disease outbreak situations by clinical year medical students surveyed from May to June 2020
N refers to the total number of elaborations provided for each type of recommendations, of which percentage (%) calculated reflects the percentage of respondents who raised a particular theme in their elaborations. n refers to the number of times the theme appeared per respondent.
Representative elaborations were quoted and tagged by the respondent’s demographic (Recommendation, Year of Study, Gender)
F. Qualitative Analysis
Thematic analyses revealed 10 main areas of discussion. These were categorised into three main themes that were common for both DO and NDO: convenience, content delivery and context of lesson (Table 3B). For the analysis for DO recommendations, a new theme materialised: Pandemic-specific considerations. Suggestions for improvements of TBP mainly fell into 3 categories – enhanced use of TBP teaching aids, ZOOM© fatigue and connectivity and technological concerns.
1) Convenience: Students indicated that TBP reduced their need to travel to teaching destinations, thereby saving on expenditure and time. This was especially useful when they were scheduled with a full day of lectures that did not require any clinical setting training, and during the exam period. For example, one student reported, “I value the time saved on travelling… more than the increased concentration and engagement of a face-to-face tutorial, given that exams are looming.” (Year 4, Female)
The ability to stream these sessions from home was advantageous as students could take additional measures to help sustain their attention, including the ease of taking refreshment breaks. Students valued the ease of taking notes as elaborated by one student as “easier to take screenshots of the slides so we don’t waste time copying the points.” (Year 5, Female)
Students noted TBP to be more convenient in arranging lectures across institutions. Specific to NDO, TBP was suggested as a potential mean to allow “teaching very large groups of people… combined stream classes” (Year 3, Male) and across medical schools. TBP also offered flexible scheduling arrangements. Examples included situations where participants are “feeling unwell but are worried about missing class” (Year 3, Female), “tutors with very busy or unpredictable schedules… which would require students to meet at odd or inconvenient timings” (Year 4, Male), hence minimising need for students to “stay back” (Year 5, Female) in the late evening.
2) Content delivery: Students discussed how triadic interactions between tutors and students, and amongst themselves were better afforded on PVBP. Nuances of social cues like facial expressions were cited as potentially beneficial for tutors to gauge students’ engagements. One student shared that “the tutor can gauge whether or not the content is appropriate based on the body language/facial expressions of the students which may be hard to do so on an online platform.” (Year 5, Female) Students also noted how TBP changed the nature of social interactions, making participants “less likely to speak up or participate… [with] the tutor [feeling] more distant.” (Year 4, Female)
The interactions between students as a reinforcement for learning surfaced as a crucial component. As one student shared, PVBP gave the “chance for the team to meet and learn from each other… quizzing each other, clarifying doubts, or sharing fun facts and important information [that]… cannot be done over teleconferencing.” (Year 3, Female)
Students reported that it was harder to stay focused during TBP sessions as one was in a “more comfortable location with no one monitoring your movements and actions” (Year 3, Male), unable to see the tutor in person and may have concomitant activities surrounding them. The implications of such distractibility were noted that TBP made it easier “to hide away and therefore not be present.” (Year 4, Female)
3) Context of lesson: Students felt their subjective assessment of TBP versus PVBP should factor in the type of lessons being delivered. It was unanimous that clinical-based teachings required use of PVBP to develop soft skills and appreciate clinical signs. To illustrate, one student shared, “medicine is an apprenticeship – there are many skills that cannot be learnt theoretically but must be observed in a clinical setting… Physical sessions are still very important to teach such skills, and should proceed with adequate safety measures in place. Otherwise, we will become doctors with good theoretical knowledge but poor practical/people skills” (Year 5, Female). However, many agreed that didactic lectures which involved pure unidirectional delivery of content could be suitably delivered over TBP as “lecturer… can still speak and present slides as usual.” (Year 3, Male)
4) Pandemic specific considerations: Students acknowledged the risk-benefit ratio of disease transmission and accommodation for the schedule of clinical tutors. One student summarised, “Additional benefits gained through physical venue-based outweighed by risks of disease transmission due to physical interaction.” (Year 3, Male) TBP was hence considered to be a safe and only suitable alternative to ensure continuity of curriculum delivery during DO.
5) Identified areas of improvement: Students raised suggestions to overcome the drawbacks of TBP in 3 main domains. Firstly, they recommended the enhanced used of teaching aids to increase engagement peer-peer interactions. Secondly, they raised the phenomenon of “ZOOM© fatigue” and the need to manage scheduling of tutorials. For example, one student shared, “People seem to think that online lectures are less mentally taxing since you’re at home, and proceed to pack the entire day full of lectures for couple weeks on end… there is no time to consolidate knowledge especially in the absence of opportunity to apply in a clinical setting.” (Year 4, Male) Hence, students suggested tutors to avoid “bombarding students with back-to-back tutorials, leading to information overload” (Year 4, Female) and decrease the maximum time per day to less than 4-5 hours. The inclusion of breaks between sessions as a mental break since tutors who are “swapping in… would not know if students are still engaged or fatigued.” (Year 4, Male)
Lastly, presence of poor connectivity contributed to streaming lags, with negative implications on students “concentration and ability to follow the lecture.” (Year 4, Female) The possibility of increasing tutors’ familiarity with the platform was cited to have facilitated a smoother conduct of lessons.
IV. DISCUSSION
A. Summary of Results
An overwhelming majority of students recommended the continued use of TBP during both DO and NDO. This is most likely due to the increased convenience in travelling, taking down notes, overcoming administrative challenges, and its suitable replacement for didactic lectures. The student’s perception of convenience of TBP correlated to the year of study, with the earlier clinical year students finding it more convenient than the final year students. Nevertheless, this should be evaluated against the background that end users range from enthusiastic ‘technophiles’ to ‘technophobes’, which influences the receptiveness towards e-learning platforms (Bruce, 1997; Fox, 2004).
Specifically during DO, it was viewed to be the best available alternative when considering the disease transmission risk and the busy schedules of the clinical tutors as they may have new responsibilities as front-liners in pandemics (Branch et al., 1997; Cook, 2006; Goh, 2020; Harden & Crosby, 2000; Ramani & Leinster, 2008).
The shift in preference of use of TBP as a substitute to supplement during NDO was noticeable. This can be due to many factors. There is a decreased engagement due to the reduced ability of tutors to assess nuances of social cues (Fox, 2004), greater distractibility and decreased ease of raising questions on TBP. Notably, peer-peer interaction is lost over TBP. Each student’s interaction is multidirectional: student with resource materials, with educator, and between students (Dhir et al., 2017). The value of such interactions and study groups in medical education should be duly taken into consideration (Burgess et al., 2014). Poorer engagement were further compounded by challenges with technology-related concerns and risks of “ZOOM© fatigue”.
Distractibility on TBP could be due to learning in a non-classroom environment (Fox, 2004) with a device that could also be used for non-educational purposes (Walsh, 2015). “ZOOM© fatigue” was likely due to lack of pre-fixed maximal time duration and the tendency for tutors to over-deliver and pile extra study materials (Fox, 2004) causing student’s to “feel tired and restless” (Srinivasan, 2020).
Interestingly, students’ innate personality and learning attitudes potentially influenced their perceptions of PVBP and TBP. Students who were more engaged on a platform, also felt more comfortable raising questions, were less distracted and believed that the platform was efficacious in delivering content. This demonstrates the difference between the “active and engaged learners” and the majority who are “silent lurkers (Fox, 2004). Similarly, students who felt more distracted on PVBP appeared to also be more distracted on TBP.
B. Recommendations
TBP as a teaching modality has an indisputable role during both DO and NDO. It is well-established that medical students experience significant psychological impact during DO (AlAteeq et al., 2020; Ullah & Amin, 2020), possibly related concerns on the impact of their studies (Lyons et al., 2020). Hence with the increased use of TBP, it is imperative that medical educators develop a deeper understanding on the potential short-comings of the platform and how best to maximise its utility as a teaching modality.
Nonetheless, it is vital to recognise that the efficacy of any new education tool depends on both educators and students. It would be better facilitated if the end user is familiar with the platform. It should be considered in light of its application and configuration (Cook, 2006) and ideally be managed and monitored by trained staff (Dhir et al., 2017; Harden, 2018). Moving forward, we recommend a tri-faceted approach to improve the content delivery of TBP during both DO and NDO (Figure 1).

Figure 1. Correlation of domains assessed for efficacy of teleconferencing-based platforms (TBP) with themes identified and suggestions to improve content delivery on TBP
1) Domain 1: Contextual use of TBP: Disease outbreak situations:
- Where physical appreciation of clinical skills through bedside tutorial or real-life clinical interactions might not be feasible, consider use of media and standardised patients to simulate clinical exposure.
- The supplemental use of standardised patients (Peters & Thrien, 2020) hones student’s clinical competence while facilitating the training of relevant skills needed for future practice (Khoo et al., 2020), a notable example in these evolving recent times also includes that of telemedicine (Williams & Song, 2016).
No disease outbreak situations
- TBP should mainly be used for didactic or team-based learning sessions, large group teaching sessions and for students who are unable to physically attend the lecture.
2) Domain 2: Targeting decreased engagement and increased distractibility:
- Use of multi-modal teaching aids, e.g. virtual quizzes, breakout rooms for small group engagement, drawing functions to better visually illustrate explanations.
- Monitoring of students’ current fatigue level in session via live polls at regular hourly intervals.
- Engagement of a central coordinator to regulate the maximum hours of online sessions per day, with considerations of suitable breaks between sessions.
- Prior assessment of student’s learning attitudes and class dynamics to enable tailored use of teaching aids.
3) Domain 3: Smoothening transition to TBP:
- Engagement of central coordinator to brief tutors on the functionality of TBP of choice to minimise technology unfamiliarity and maximise its utility in conducting sessions.
- Educational institutions to consider providing infrastructural support to students and educators, including dedicated spaces, electronic devices with internet connections, and easy access to technical support. These would help minimise network connectivity challenges and providing a conducive study environment for those who might face difficulties accessing TBP off-campus.
- Selective use of TBP as a supplement during NDO to increase both students and educator’s familiarity with the platform and as a learning tool, thereby enabling a smoother transition during DO.
C. Limitations
Our study has few limitations. We surveyed clinical year students from a single medical school and therefore, our study may not reflect the views of students from other medical schools with different teaching pedagogies and those of pre-clinical year students. Future studies should consider exploring the opinions of clinical tutors on PVBP and TBP and their perspective as educators in delivering such curriculum. In addition, given our limited sample size, some statistically significant sub-group patterns may not have been evident.
V. CONCLUSION
TBP is an important teaching modality during DO and NDO, especially with its increased convenience. However, it has certain issues including context-specific use, decreased engagement, increased distractibility and technological challenges. Our proposed potential interventions may help to maximise its utility and facilitate transition of its use in subsequent DO.
Notes on Contributors
Xin Rong Goh designed the study, recruited the participants, administered the survey, analysed the data and wrote the first and subsequent drafts of the manuscript. Rajeswari Kathirvel and Chee Wai Ku contributed to analysis of the data and writing of the manuscript. Kok Hian Tan contributed to the study design and reviewed the manuscript. All authors have read and approved the final manuscript.
Ethical Approval
The following study was approved by NTU Institutional Review Board (IRB Reference number: 2020-05-003) with an exempt status.
Data Availability
The ethical approval by NTU Institutional Review Board was based on the conditions that while the data is deidentified data, only study team members will have access to the raw data that will be stored on a password protected PC. The data could thus not be uploaded on a public data sharing platform.
Acknowledgement
The authors acknowledge Dr Joel Shi Quan Tan, Yong Loo Lin School of Medicine, National University of Singapore, for his contribution to the statistical analysis of the paper.
Funding
No funding sources was used for this research study.
Declaration of Interest
The authors have no conflicts of interest to declare.
References
AlAteeq, D. A., Aljhani, S., & AlEesa, D. (2020). Perceived stress among students in virtual classrooms during the COVID-19 outbreak in KSA. Journal of Taibah University Medical Sciences, 15(5), 398–403. https://doi.org/10.1016/j.jtumed.2020.07.004
Al-Neklawy, A. F. (2017). Online embryology teaching using learning management systems appears to be a successful additional learning tool among Egyptian medical students. Annals of Anatomy, 214, 9–14. https://doi.org/10.1016/j.aanat.2017.07.001
Al-Shorbaji, N., Atun, R., Car, J., Majeed, A., & Wheeler, E. (2015). eLearning health professional for undergraduate education. World Health Organistion. https://www.who.int/hrh/documents/14126-eLearningReport.pdf
Alvarez, M. E., & Anderson-Ketchmark, C. (2011). Danielson’s framework for teaching. Children and Schools, 33(1), 61–63. https://doi.org/10.1093/cs/33.1.61
Bertsch, T. F., Callas, P. W., Rubin, A., Caputo, M. P., & Ricci, M. A. (2007). Applied research: Effectiveness of lectures attended via interactive video conferencing versus in-person in preparing third-year internal medicine clerkship students for clinical practice examinations (CPX). Teaching and Learning in Medicine, 19(1), 4–8. https://doi.org/10.1080/10401330709336616
Boatin, A., Ngonzi, J., Bradford, L., Wylie, B., & Goodman, A. (2015). Teaching by teleconference: A model for distance medical education across two continents HHS public access. Open Journal of Obstetrics and Gynecology, 5(13), 754–761. https://doi.org/10.4236/ojog.2015.513106
Branch, W. T., Kroenke, K., & Levinson, W. (1997). The clinician-educator – Present and future roles. Journal of General Internal Medicine, 12(Suppl. 2), 1–4. https://doi.org/10.1046/j.1525-1497.12.s2.16.x
Bruce, B. C. (1997). Literacy technologies: What stance should we take? Journal of Literacy Research, 29(2), 289–309.
Burgess, A., McGregor, D., & Mellis, C. (2014). Medical students as peer tutors: A systematic review. BMC Medical Education, 14,115. https://doi.org/10.1186/1472-6920-14-115
Chandratre, S. (2020). Medical students and COVID-19: Challenges and supportive strategies. Journal of Medical Education and Curricular Development, 7. https://doi.org/10.1177/2382120520935059
Cook, D. A. (2006). Where are we with web-based learning in medical education? Medical Teacher, 28(7), 594–598. https://doi.org/10.1080/01421590601028854
Dhir, S. K., Verma, D., Batta, M., & Mishra, D. (2017). E-learning in medical education in India. Indian Pediatrics, 54(10), 871–877. https://doi.org/10.1007/s13312-017-1152-9
Fatani, T. H. (2020). Student satisfaction with videoconferencing teaching quality during the COVID-19 pandemic. BMC Medical Education, 20(1), 396. https://doi.org/10.1186/s12909-020-02310-2
Fox, R. (2004, December). SARS epidemic: Teachers’ experiences using ICTs. In R. Atkinson., C. McBeath., D. Jonas-Dwyer. & R. Phillips (Eds.), Beyond the comfort zone: Proceedings of the 21st Annual Conference of the Australasian Society for Computers in Learning in Tertiary Education (ASCILITE) (pp. 319-327). Australasian Society for Computers in Learning in Tertiary Education. http://www.ascilite.org.au/conferences/perth04/procs/fox.html
Goh, C. T. (2020, May 3). COVID-19: Guarding against burnout, compassion fatigue and trauma in frontline healthcare workers. Channel News Asia. https://www.channelnewsasia.com/news/singapore/covid-19-guarding-against-burnout-trauma-ttsh-ncid-frontline-12669280
Govindarajan, S., Vasanth, G., Kumar, P. A., Priyadarshini, C., Radhakrishnan, S. S., Kanagaraj, V., Balasubramanian, N., Kumar, P. N., Divya, T. J., & Aishwarya, C. N. (2018). Impact of a comprehensive early clinical exposure program for preclinical year medical students. Health Professions Education, 4(2), 133–138. https://doi.org/10.1016/j.hpe.2017.06.002
Harden, R. M. (2018). Medical teacher E-learning-caged bird or soaring eagle? Medical Teacher, 30(1), 1–4. https://doi.org/10.1080/01421590801938878
Harden, R. M., & Crosby, J. (2000). AMEE guide no 20: The good teacher is more than a lecturer – The twelve roles of the teacher. Medical Teacher, 22(4), 334–347. https://doi.org/10.1080/014215900409429
Jacobs, J. L., & Samarasekera, D. D. (2012). How we put into practice the principles of embedding medical students into healthcare teams. Medical Teacher, 34(12), 1008–1011. https://doi.org/10.3109/0142159X.2012.731097
Kanneganti, A., Sia, C.-H., Ashokka, B., & Ooi, S. B. S. (2020). Continuing medical education during a pandemic: An academic institution’s experience. Postgraduate Medical Journal, 96, 384- 386. https://doi.org/10.1136/postgradmedj-2020-137840
Khoo, S. A., Aswin, W., Shen, G. Q. Y., Haq, H. M., Junaidah, B., Yiew, J. L., Abiramy, M., & Sashikumar, G. (2020). Improving provider-patient communication skills among doctors and nurses in the children’s emergency department. The Asia Pacific Scholar, 5(3), 28–41. https://doi.org/10.29060/TAPS.2020-5-3/OA2160
Lim, E. C. H., Oh, V. M. S., Koh, D. R., & Seet, R. C. S. (2009). The challenges of “continuing medical education” in a pandemic era. Annals of the Academy of Medicine Singapore, 38(8), 724–726.
Lyons, Z., Wilcox, H., Leung, L., & Dearsley, O. (2020). COVID-19 and the mental well-being of Australian medical students: Impact, concerns and coping strategies used. Australasian Psychiatry, 28(6), 649–652. https://doi.org/10.1177/1039856220947945
Lamba, P. (2011). Teleconferencing in medical education: A useful tool. Australasian Medical Journal, 4(8), 442–447. https://doi.org/10.4066/AMJ.2011.823
Peters, T., & Thrien, C. (2020). The digital use of simulated patients in times of the corona pandemic – Considerations and proposals. GMS Journal for Medical Education, 37(7), Doc 93. https://doi.org/10.3205/zma001386
Ramani, S., & Leinster, S. (2008). AMEE guide no. 34: Teaching in the clinical environment. Medical Teacher, 30(4), 347–364. https://doi.org/10.1080/01421590802061613
Rawekar, A., Jagzape, A., Srivastava, T., & Gotarkar, S. (2016). Skill learning through early clinical exposure: An experience of Indian medical school. Journal of Clinical and Diagnostic Research, 10(1), JC01–JC04. https://doi.org/10.7860/JCDR/2016/17101.7022
Samarasekera, D. D., Goh, D. L. M., & Lau, T. C. (2020). Medical school approach to manage the current COVID-19 crisis. Academic Medicine, 95(8), 1126–1127. https://doi.org/10.1097/ACM.0000000000003425
Samarasekera, D. D., Goh, D. L. M., Yeo, S. P., Ngiam, N. S. P., Aw, M. M., Lim, M. M., Pillai, S., Lee, S. S., Mahadevan, M., Kow, A., Chong, Y. S., & Lau, T. C. (2020). Response and lessons learnt managing the covid-19 crisis by school of medicine, National University of Singapore. MedEdPublish, 9(1), 92, https://doi.org/10.15694/mep.2020.000092.1
Samarasekera, D. D., & Gwee, M. C. E. (2021). Adapting to change during challenging times. The Asia Pacific Scholar, 6(1), 1-2. https://doi.org/10.29060/TAPS.2021-6-1/EV6N1
Srinivasan, D. K. (2020). Medical students’ perceptions and an anatomy teacher’s personal crisis experience using an e-learning platform for tutorials during the Covid-19 crisis. Anatomical Sciences Education, 13(3), 318-319. https://doi.org/10.1002/ase.1970
Ullah, R., & Amin, S. (2020). The psychological impact of COVID-19 on medical students [Letter]. Psychiatry Research, 288, 113020. https://doi.org/10.1016/j.psychres.2020.113020
Walsh, K. (2015). Mobile learning in medical education: Review. Ethiopian Journal of Health Sciences, 25(4), 363–366. https://doi.org/10.4314/ejhs.v25i4.10
Williams, B., & Song, J. J. Y. (2016). Are simulated patients effective in facilitating development of clinical competence for healthcare students? A scoping review. Advances in Simulation (London, England), 1, 6. https://doi.org/10.1186/s41077-016-0006-1
*Goh Xin Rong
11 Mandalay Road,
Singapore 308232
Email: xinronggoh@yahoo.com.sg
Submitted: 26 September 2020
Accepted: 1 March 2021
Published online: 5 October, TAPS 2021, 6(4), 7-16
https://doi.org/10.29060/TAPS.2021-6-4/OA2415
Rasika Manori Jayasinghe1, Indika Priyanthi Thilakumara1, Bandara Dhanushka Leuke2, Gishan Edirisinghe3, Manil Christopher Nishan Fonseka3, Manjula Attygalla4 & Ruwan Duminda Jayasinghe2
1Department of Prosthetic Dentistry, Faculty of Dental Sciences, University of Peradeniya, Sri Lanka; 2Department of Oral Medicine and Periodontology, Faculty of Dental Sciences, University of Peradeniya, Sri Lanka; 3Department of Restorative Dentistry, Faculty of Dental Sciences, University of Peradeniya, Sri Lanka; 4Department of Oral Surgery, Faculty of Dental Sciences, University of Peradeniya, Sri Lanka
Abstract
Introduction: E-learning resulted in a revolution in dental education with continuous educational experiences. General objective of this study was to assess the perspective of undergraduate dental students on effectiveness of e-learning in the Bachelor of Dental Surgery (BDS) programme. Specific objectives were to identify students’ opinion on the factors that promote e-learning, awareness on the effectiveness of using different platforms and social media, barriers imposed and suggestions for the improvement of e-learning in the BDS programme.
Methods: This was a cross sectional descriptive study among undergraduate dental students of the Faculty of Dental Sciences, University of Peradeniya, Sri Lanka using a self-administered pre-tested questionnaire administered via a web-based survey form. Frequencies and percentages were obtained for categorical data and Chi-square test was used to determine the association between variables.
Results: The majority received the e-learning experience well. Fifty-four percent of the participants felt it was better compared to traditional face-to-face learning and the difference between the semesters (p=0.000) and genders was statistically significant (p=0.000). Difference in overall satisfaction on e-learning material across the different semesters was statistically significant. Students felt that e-learning should be used as a supplementary tool mainly by means of procedural videos during delivery of the skill component. Fifty percent participants felt that conducting assessments online is fair for all the students.
Conclusion: A positive learning experience was achieved through the e-learning modalities in comparison to traditional face-to-face learning though in terms of skills training, e-learning modalities should only be considered as a supplementary tool.
Keywords: E-Learning, Perspective, Dental Undergraduates, Dental Education
Practice Highlights
- Majority felt e-learning was better compared to traditional face-to-face learning.
- Majority were satisfied with interactions with teachers and teacher responses to clarifications.
- Students felt that e-learning used as a supplementary tool during delivery of the skill component.
I. INTRODUCTION
E-learning has resulted in a revolutionising dental education to an extent that more interactive and intuitive e-learning options have evolved which provide students with an enjoyable and meaningful continuum to their educational experience. During the current COVID-19 pandemic electronic learning tools have been invaluable in the delivery of knowledge in many higher education institutions (Li & Lalani, 2020). One of the great advantages of e-learning is the possibility of transferring knowledge and skills to a large number of recipients irrespective of the time of delivery of knowledge (Asiry, 2017). In addition, students can repeatedly peruse the material and follow it in their own pace at a relatively low cost. This is considered an excellent method of overcoming certain difficulties faced with the traditional system of teaching such as the lack of space especially within the lecture halls and a shortage of human resources (Asiry, 2017). However, socio-economic factors play an important role in deciding the type of teaching. Students in the developed countries prefer e-learning modalities while students in the developing countries prefer it as a supplementary method (Schlenz et al., 2020). A study by Asiry (2017) identified e-learning as a helpful supplementary learning method among Saudi Arabian dental students rather than a replacement for traditional teaching methods. According to authors’ experience, though there was much resistance in adopting to e-learning at its infancy, it has now been universally accepted as a learning modality not only by teachers but also by the students. Many are of the view that assimilation of knowledge could be best achieved purely through e-learning modalities where as it should be supplementary in nature in skills acquisition. The popularity of books and hard copies of journals have seen a steady decline due to the availability of e-learning resources and even publishers have realised this trend and supply both hard and electronic versions of their publications which in future may progressively be replaced by electronic educational materials.
The success of e-learning is dependent on a multitude of factors. Computer literacy, availability of appropriate technology, accessibility and having a good high bandwidth internet connection are some of the key factors (Asiry, 2017; Linjawi & Alfadda, 2018). According to a study by Gunawardane and Wijekoon (2017), it was revealed that dental students in the Faculty of Dental Sciences, University of Peradeniya, Sri Lanka had adequate computer literacy and facilities. Although Linjawi and Alfadda (2018) identified that the perceived impact of e-learning and readiness for e-learning though popular and satisfactory among Saudi Arabian dental students, declined as they proceeded to higher semesters. Imparting the skills component has been identified as a major challenge in using e-learning and students were in need of more support in the skills domain (Linjawi & Alfadda, 2018). Students have been shown to have better skills and motivation for use of online tools for personal or non-educational purposes than for learning purposes. Thus, this should be carefully considered when developing a successful strategy to motivate them for e-learning (Linjawi & Alfadda, 2018). Apart from the above mentioned factors, student characteristics, cognitive factors (performance expectations) and the social environment (learning climate) are considered as some predictors of the perceived satisfaction among students (Venkatesh et al., 2019). Most of the students prefer a combined approach comprising traditional and e-learning methods than relying on e-learning methods alone. Some of the preferred methods of delivery of e-learning resources for pre-clinical dental undergraduates were online flash lectures and procedural videos (Asiry, 2017). Video demonstrations enabled students to reflect on their predominant learning approaches, which emphasise self-directed learning and avoid surface learning techniques (Chonkar et al., 2019). Some dental schools in the developed countries have introduced tools such as Technology Enhanced Learning (TEL) in both pre-clinical and clinical courses with the development of innovative learning platforms and they further assess and monitor student performance in relation to the new approach (Wong et al., 2020). Further, Faculty of Dentistry, National University of Singapore has implemented a multi-stage framework for the academic staff to grasp technology in various aspects such as reflecting teaching practice, designing new technology options and identifying learner impact with changes on teaching methods.
However, not everyone is in agreement with the benefits of e-learning. University administrators and experts in information technology working in universities have varying opinion (ranging from majority of teaching on traditional classroom mode to predominant e-learning mode) regarding the need of administrational change created by e-learning, generation of resources, impact on enrolment, responsibility for course design and content and the impact on the mission of the university. However, there is a general agreement on challenges such as the requirement of resources and cost of maintenance, need for motivating the teachers to keep abreast with the latest technology and the necessity for cooperation to improve e-learning (Hillenburg et al., 2006).
The COVID-19 pandemic has made it necessary to impart changers in the modalities of education all over the world. Since schools and universities have been closed to prevent the spread of infection, conducting e-learning sessions has become the prime mode of teaching. The situation in Sri Lanka was without exception. Most programmes including the Bachelor of Dental Surgery had to comply with this requirement in order to provide the students a continuous educational experience during the pandemic situation. E-learning has been used in a very primitive level in the Faculty of Dental Sciences, University of Peradeniya for a long time but had not been utilised to its full potential. As dentistry is mostly a skill based professional degree programme, delivering course content online was a challenge. In addition, resistance to change was evident among the staff due to the fact that they were comfortable with the traditional time tested methods. However, with the new norms, e-learning platforms such as Zoom, Google Meet and WhatsApp discussions were used at the Faculty of Dental Sciences for the learning along with narrated PowerPoint presentations, video demonstrations and online quizzes uploaded onto the existing e-learning platform Dent Moodle. Due to this novel experience, it was considered important to analyse the students’ opinion on e-learning, the difficulties faced by them and expectations to improve e-learning in the field of dentistry. Further, it would be beneficial to identify barriers of e-learning when designing and revising the dental undergraduate curriculum in the future.
II. OBJECTIVES
General objective of the study was to assess the undergraduate dental students’ perception on the effectiveness of e-learning utilised in the Bachelor of Dental Surgery (BDS) programme. The specific objectives were to identify students’ opinion on the factors that promote e-learning, awareness on the effectiveness of using different platforms and social media, barriers imposed and suggestions for the improvement of e-learning in the BDS study programme.
III. MATERIALS AND METHODS
A cross sectional descriptive study was carried out on a sample comprising of undergraduate dental students of the Faculty of Dental Sciences, University of Peradeniya who had enrolled and followed all online lectures and assignments based on the content taught via e-learning in the first, third, fifth and seventh semesters. A self-administered and pre-tested (25 students representing all batches for the pilot and their responses were excluded from the study sample) questionnaire was administered via a web-based survey form. A covering letter, information sheet and consent form were also annexed to this form. Those respondents who gave the informed consent were able to fill the questionnaire. The survey link was disseminated among the dental students via the email by the faculty administration unit. The questionnaire used in this study comprised of 23 close-ended questions which consisted of demographic data and specific questions on awareness, attitude and practice of e-learning. Examples of e-learning platform stated in the questionnaire were live Zoom presentations, Google Meet, Power Point presentations with voice narrations and supplementary material such as web links, video demonstrations and YouTube and other video links.
Confidentiality and anonymity of the data provided were assured by keeping the questionnaire anonymous. No identification details were included in the questionnaire. Data management and statistical analysis was performed using the statistical software SPSS version 21.0. Frequencies and percentages were obtained for categorical data and Chi-square test was used to determine the association between variables. Ethical clearance was obtained from the Ethics Review Committee of the Faculty of Dental Sciences, University of Peradeniya (ERC/ FDS/UOP/I/2020/21).
IV. RESULTS
The response rate was 82% (250 participants out of 305 of all undergraduates). The sample comprised 19% from the first semester, nearly 25% from the third semester, 26% from the fifth semester and nearly 30% from the seventh semesters of the Bachelor of Dental Surgery (BDS) programme. Seventy-two percent (72%) were females. Approximately 41% claimed that they have either very good or excellent literacy on information technology (IT). Fifty-four percent of the respondents claimed that their English language literacy is very good or excellent. A majority of the population accessed e-learning content using their mobile devices. Half of the sample had experienced some kind of interruptions during e-learning.
A. Satisfaction on E-learning
Seventy-one percent (71%) responded that they were either satisfied or highly satisfied about e-learning materials they received. More than one third of the respondents (39%) felt encouraged to collaborate and interact with their teachers during e-learning time compared to the in-class teaching sessions. A similar percentage of respondents felt that they were more encouraged to work on course materials compared to the traditional learning sessions received at the university. Around 74% of the students felt that the teachers were friendly during e-learning sessions. Moreover, 62% of them were either satisfied or highly satisfied with the provision to ask questions during e-learning sessions. Sixty percent (60%) of respondents was satisfied or highly satisfied with the answers received for the clarifications they requested. Seventy percent (70%) of the students claimed that the interactions between the lecturers and students during question and answer sessions, case scenarios and case discussions were essential for the success of e-learning experience. Fifty-five percent (55%) of them were satisfied with the interactions they experienced during e-learning sessions in their study period. Interestingly, more than one third of the respondents were of the opinion that online lectures were more effective than traditional live lectures. Moreover, 54% of the sample felt that the overall e-learning experiences was better than the traditional learning opportunities they received in the university and the possibility of following the coursework at their own pace (14.8%) was chosen as the main reason for this response.
Females had better overall e-learning experiences than the learning opportunities they received at the university compared to male students and this difference was statistically significant (p=0.000) (Table 1).
Surprisingly, only 1% of the respondents had identified social media as a positive influence on e-learning.
Table 1 describes participants’ response to the questionnaire according to their gender.
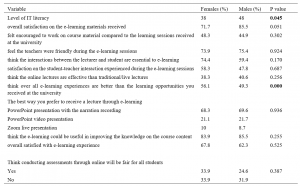
Table 1. Comparison of participants’ response according to their gender (in percentages)
B. Preference on Methods of E-learning
Sixty-four percent (64%) of the participants were familiar with Zoom as an e-learning platform. Majority of the students preferred PowerPoint presentations with narrations (68%) to receive lectures. In addition, 69% felt that e-learning materials had helped them to improve their knowledge on the course content specified in the Intended Learning Outcomes (ILOs). Around 34% had identified video demonstrations as an important tool in imparting skills training to achieve the course ILOs. Over 70% rated it as highly useful when students’ opinion is taken in consideration in improving knowledge on the course content.
Sixty-four percent (64%) felt that that e-learning material should be used as supplementary materials for in-class learning within the skills domain. The e-learning materials considered appropriate were video demonstrations, procedural steps described in text documents, YouTube links and case discussions. Majority of the courses in the first semester (Anatomy, Dental Anatomy and Physiology related), third semester (Tooth morphology and occlusion, Human Diseases, Dental Biomaterials), fifth semester (Operative Dentistry, Population Oral Health, Clinical and Diagnostic Oral Sciences [CDOS1] and Child and Adolescent Oral Health [CAOH1]) and seventh semester (Adult Oral Health, CDOS2 and CAOH2) were rated as suitable for e-learning activities.
C. Opinion on Assessment via E-Learning Platforms
The Multiple Choice Questions (MCQ) and Short Answer Questions (SAQ) were the more common forms of assessments provided to the participants. However, some students (9%) had experience with essays too. These assessments were formative in nature whereby the questions were posted after each learning session in order to assess the effectiveness of the learning process. These questions were marked by the teachers or self-marked by the students. Sixty-nine percent (69%) felt that conducting assessments online is fair.
D. Opinion on Barriers Identified in E-Learning
Though the majority of first semester students had identified inadequate opportunities to work with other batch mates as a stumbling block, the majority of the seventh semester had identified technical difficulties in accessing the e-learning resources as the major barrier in e-learning. However, there was no significant difference in the responses between the genders and the semester of study of the student.
E. Suggestions to Improve E-Learning
When the students were requested to suggest ways to use the e-learning to improve the required skills, approximately half (52%) of the respondents preferred video demonstrations on clinical and lab procedures. Furthermore, multiple choice questions, use of charts to explain presentations, discussion forums, quizzes, assignments, web links and supplementary reading material were other ways of improving the learning experience as suggested by the participants. However, 3% of the students had clearly mentioned that e-learning could not be used to improve the required skills in dentistry.
There were multiple suggestions by the majority to improve the overall effectiveness of their e-learning experience. Some of the suggestions were uploading of lectures coupled with assignments, video demonstrations especially for practical scenarios, lectures followed by discussions and lectures on Zoom followed by case discussions. However, the statistical significance could not be assessed between genders or semesters as the number of responses for each option was small.
F. Analysis of Results According to the Respondents’ Current Semester
When the results were assessed according to the current semester, a majority of the first, third and seventh semesters students preferred video demonstrations for e-learning sessions. However, a majority of the fifth semester students preferred a combination of video demonstrations and a text document describing procedural steps or video demonstrations combined with YouTube links and discussion forums. Respondents from first semester had the highest overall satisfaction on e-learning materials they received and the difference between the semesters was statistically significant. (p=0.002). Over two-thirds of the seventh semester students (being the students who were exposed to conventional classroom learning experience for more than three years) confirmed that their overall e-learning experiences were better than the traditional classroom learning opportunities they received at the university and the difference was statistically significant (p=0.000) (Table 2). Further, students’ rating of e-learning materials received from teachers (p=0.002) (Figure 1) and encouragement to work on course material compared to the learning sessions received at the university (p=0.015) (Figure 2) were statistically significant when the semester of study were considered.
Table 2 describes participants’ response to the questionnaire according to their semester of study.
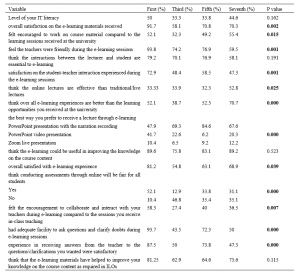
Table 2. Variations of participants’ response according to their semester of study (in percentages)
Figure 1 shows students’ rating of e-learning materials received from teachers according to their semester of study.
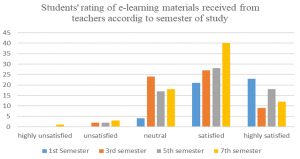
Figure 1. Students’ rating of e-learning materials received from teachers according to their semester of study
Figure 2 shows students’ feeling of encouragement to work on course material compared to conventional learning sessions received at the university.
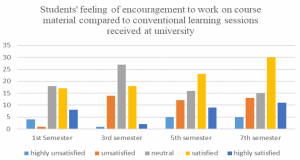
Figure 2. Students’ feeling of encouragement to work on course material compared to conventional learning sessions received at the university according to their semester of study
When the results were analysed according to theory based courses (Anatomy, Oral Biology, Human Diseases, Tooth morphology and Occlusion, Dental Biomaterials) against practical, lab based and clinical training courses (Adult Oral Health, Population Oral Health, Clinical and Diagnostic Oral Sciences, Child and Adolescent Oral Health), the participants’ overall e-learning experience in theory based courses was significantly higher than practical and clinical courses (p= 0.03).
All data are available at https://figshare.com/s/c6c7b8f1d5cfd0076808.
V. DISCUSSION
E-learning is a broad term which encompasses the use of software applications to support learning, whether online or offline (Piccoli et al., 2001). The efficacy of an e-learning experience is dependent on many factors such as availability of devices, access to internet, knowledge on IT and uninterrupted internet connectivity (Asiry, 2017; Linjawi & Alfadda, 2018).
In the present study, half of the sample experienced some interruption during the e-learning sessions. It has been demonstrated in previous studies that students generally have a positive outlook to e-learning in spite of technical problems and related stresses (Brumini et al., 2014). Other studies have also highlighted positive experiences in isolated dental specialties (Bains et al., 2011; Gonzalez & Gadbury-Amyot, 2016; Qi et al., 2013; Reissmann et al., 2015). Our results revealed that students had a better learning experience with e-learning in comparison to traditional methods which was compatible with the findings of similar studies (Turkyilmaz et al., 2019). A study in Germany involving undergraduate dental students stated that participation in online learning was higher compared to “face-to-face” courses which was similar to the findings of the present study (Schlenz et al., 2020). Reasons for popularity of e-learning material over face-to-face learning are that it not only provides flexibility in the learning process (p=0.003) but also saves time (p = 0.012) (Anwar et al., 2021).
When the students’ perception on e-learning resources were analysed, males showed better IT literacy in comparison to female students. Even though the female students were not as confident as male students, a majority of them expressed that the overall e-learning experience was better than the conventional learning. These findings endorse the observations of Linjawi and Alfadda (2018) where the students claimed that they had better skills and motivation for e-learning than conventional learning activities. The identification of social media platforms for e-learning opportunities by a very few students in our study corroborate the fact that formal modalities of delivering e-learning resources should be implemented rather than relying on generic platforms.
Participants’ overall e-learning experience in theory based courses were significantly higher than practical and clinical courses due to the need of hands on experience, simulator training and working with patients for the practical and clinical courses than listening, reading and writing practice. This fact should be carefully considered when developing and planning the modes of content delivery as the knowledge and skills domains should be separately considered. More theory could be delivered through e-learning modalities and this time saved could be utilised for the face to face delivery of practical and clinical procedural teaching in predominantly skills based courses such as the Bachelor of Dental Surgery. However, the findings contradict the previous belief of the faculty that e-learning should only be used as a supplementary tool. There is a possibility to incorporate classroom and e-learning as a blended learning experience when imparting theory components in the future to save time, improve efficient use of limited infrastructure and to focus more on much needed skill development in dentistry. Incorporation of e-learning facilities to the maximum possible level should also be considered in future planning of the state universities in the delivery of undergraduate education in countries such as in Sri Lanka to enhance the quality of learning using the minimal physical and human resources available. Reports from experience in other countries highlight that e-learning processes are also cost effective, due to the availability of low cost or free online tools and platforms which can be used by teachers with a sound background of pedagogical knowledge (Goh, 2018).
First semester had the highest overall satisfaction on e-learning. This group consisted of students who hardly had any noteworthy face-to-face learning experience in the Faculty of Dental Sciences due to the abrupt closure during pandemic situation. Therefore, it seems that they could not effectively compare the two learning methods. Though less than first semester, more than 50% of the seventh semester students had a positive attitude towards e-learning experience. Our finding is in agreement with the findings of a previous study where it was shown that the perceived impact of e-learning and readiness for e-learning became less acceptable as students became mature (Linjawi & Alfadda, 2018).
Positive feedback regarding e-learning experience showed statistically significant differences between students of different semesters in relation to overall satisfaction on the e-learning materials received; encouragement to work on course materials; feeling that the teachers were friendly during the e-learning sessions; satisfaction on the student-teacher interaction during e-learning sessions. These findings should be considered when modes of learning for different components are planned by the Faculty of Dental Sciences during future revisions to the curriculum. Similarly, a recent report on undergraduate dental education during the COVID-19 pandemic has described that e-learning has been appreciated not only by students and teachers, but also in relation to the teacher-student interaction (Bennardo et al., 2020).
A majority of the students felt that the best way to receive the theory component was through PowerPoint presentation with voice narrations. This was statistically significant when compared among different semesters. This is in contrast with the preferred e-learning method among the Saudi Arabian dental students whereby online flash lectures were the most preferred method (Asiry, 2017).
Similar to our findings, a study on health care students belonging to 11 countries among the developed and developing nations also identified that 60% agreed that clinical and practical skills are best learned in clinics and laboratories (Abbasi et al., 2020). Another study involving over 3000 medical students of all years from over 13 schools in Libya has revealed only 21% agreed that e-learning could be used for clinical aspects, as compared with 55% who disagreed with this statement and 24% who were neutral (Alsoufi et al., 2020). The students ‘most preferred mode to learn skills as prescribed in the ILOs was through the use of procedural videos. A previous study carried out in the same institute to investigate the efficacy of procedural video versus live demonstrations revealed that that there was no appreciable difference in the development of skills in dental laboratory technology procedures (Thilakumara et al., 2018). This outcome could be applied to our findings that e-learning sessions, if followed by discussion forums with the teachers, as suggested by the participants would dramatically improve the e-learning experience.
E-learning with its virtual learning environment also requires different skills and a positive attitude from instructors. The positive attitude of the instructors towards technology, the interactive teaching style, and control over the technology were found to have an important influence on students’ reactions to the learning environment (Piccoli et al., 2001). This highlights the importance of professional development in two main aspects; technical and e-pedagogical areas (Conole & Oliver, 2002). The significance of institutional support should be highlighted. Therefore, the need of training for the teachers in the use of efficient methods for e-learning is emphasised. Furthermore, the faculty needs to have a long-term plan to encourage learning facilities through the use of different platforms, use of web links and production of supplementary video for demonstrations in order to encourage students towards a lifelong learning experience. Investment in more user-friendly and versatile software and resources to improve e-learning activities should be prioritised in order to make this endeavour more effective, interactive and receptive to the end users.
A. Limitations of the Study
Our study was performed in a single country and in a single institution as the country has only one dental school. Therefore, the results may not be generalised to other countries and to the region. The results must be validated through further multi-centre studies in order to obtain an overall opinion. Multi-national studies would provide a better understanding on how e-learning could replace the bulk of conventional dental undergraduate clinical learning and provide cost effective solutions for the developing countries with limited physical and human resources to avoid disruption of clinical training during difficult times such as the present COVID-19 pandemic. Another limitation is the cross-sectional nature of the study design, which limited our ability to identify causal associations.
VI. CONCLUSION
A positive learning experience was achieved through the e-learning modalities by the undergraduate dental students in comparison to traditional face-to-face learning. In terms of skills training, e-learning should only be considered as a supplementary tool. These findings will be useful when designing the study courses as a major part of theory component via e-learning mode and skill component with combined e-learning and conventional modes in the future.
We recommend adapting interactive e-learning platforms by using highly sophisticated technologies along with virtual clinical experience with combined clinical scenarios and assessments based on discussions of patient cases. Cost-effective solutions are needed to reduce disruption of undergraduate dental education especially in developing countries in the region like Sri Lanka and there should be new collective effort by the countries in the South Asian region in planning and sharing less expensive e-learning solutions in order to overcome financial issues. Such measures may vary from learning theory and virtual clinical and lab-based experience, followed by limited hands-on experience on live patients in a safe environment during difficult times of this nature.
Notes on Contributors
Principal and corresponding author (Rasika Jayasinghe) conceptualised the research and edited the initial draft and wrote the results after analysis. She also did the final approval of the version to be published and agreed to be accountable for all aspects of the work.
Manjula Attygalla edited the initial draft of the manuscript and supported in modification of the questionnaire. He also did the final approval of the version to be published and agreed to be accountable for all aspects of the work.
Manil Fonseka supported planning of the study, edited the research proposal and manuscript. He also did final editing and approval of the version to be published and agreed to be accountable for all aspects of the work.
Dhanushka Leuke Bandara supported planning of the study, designed the Google form, carried out the survey and entered the data in addition to editing of the manuscript. She also did final approval of the version to be published and agreed to be accountable for all aspects of the work.
Gishan Edirisinghe carried out the literature survey and did the final approval of the version to be published and agreed to be accountable for all aspects of the work.
Ruwan Jayasinghe supported planning of the study, prepared the initial draft of the research proposal and edited the final draft of the manuscript. He did the final approval of the version to be published and agreed to be accountable for all aspects of the work.
Indika Thilakumara supported planning of the study, edited the first draft and wrote the discussion. She did the final approval of the version to be published and agreed to be accountable for all aspects of the work.
Ethical Approval
Ethical clearance has been granted by Ethics Review Committee, Faculty of Dental Sciences, University of Peradeniya. (ERC/FDS/UOP/I/2020/21).
Data Availability
All data are available at https://figshare.com/s/c6c7b8f1d5cfd0076808 and can be accessed on request and approval from the corresponding author.
Funding
No funding sources are associated with this study.
Declaration of Interest
Authors declare that they do not have possible conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
Abbasi, M. S., Ahmed, N., Sajjad, B., Alshahrani, A., Saeed, S., Sarfaraz, S., Alhamdan, R. S., Vohra, F., & Abduljabbar, T. E. (2020). E-Learning perception and satisfaction among health sciences students amid the COVID-19 pandemic. Work, 67(3), 549-556. https://doi.org/10.3233/WOR-203308
Alsoufi, A., Alsuyihili, A., Msherghi, A., Elhadi, A., Atiyah, H., Ashini, A., Ashwieb, A., Ghula, M., Hasan, H. B., Abudabuos, S., Alameen, H., Abokhdhir, T., Anaiba, M., Nagib, T., Shuwayyah, A., Benothman, R., Arrefae, G., Alkhwayildi, A., Alhadi, A., … Elhadi, M. (2020). Impact of the COVID-19 pandemic on medical education: Medical students’ knowledge, attitudes, and practices regarding electronic learning. PLOS ONE, 15(11), e0242905. https://doi.org/10.1371/journal.pone.0242905
Anwar, A., Mansoor, H., Faisal, D., & Khan, H. S. (2021). E-learning amid the COVID-19 lockdown: Standpoint of medical and dental undergraduates. Pakistani Journal of Medical Sciences, 37 (1), 217-222. https://doi.org/10.12669/pjms.37.1.3124
Asiry, M. A. (2017). Dental students’ perceptions of an online learning. The Saudi Dental Journal, 29(4), 167–170. https://doi.org/10.1016/j.sdentj.2017.03.005
Bains, M., Reynolds, P. A., McDonald, F., & Sherriff, M. (2011). Effectiveness and acceptability of face-to-face, blended and e-learning: A randomised trial of orthodontic undergraduates. European Journal of Dental Education, 15(2), 110–117. https://doi.org/10.1111/j.1600-0579.2010.00651.x
Bennardo, F., Buffone, C., Fortunato, L., & Giudice, A. (2020). COVID-19 is a challenge for dental education—A commentary. European Journal of Dental Education, 24(4), 822-824. https://doi.org/10.1111/eje.12555
Brumini, G., Špalj, S., Mavrinac, M., Biočina-Lukenda, D., Strujić, M., & Brumini, M. (2014). Attitudes towards e-learning amongst dental students at the universities in Croatia. European Journal of Dental Education, 18(1), 15-23. https://doi.org/10.1111/eje.12068
Chonkar, S. P., Qi, H. L. C., Ha, T. C., Lim, M., Ng, M. J., & Tan, K. H. (2019). Can digital media affect the learning approach of medical students? The Asia Pacific Scholar, 4(1), 13- 23. https://doi.org/10.29060/TAPS.2019-4-1/OA1058
Conole, G. C., & Oliver, M. (2002). Embedding theory into learning technology practice with toolkits. Journal of Interactive Media in Education (8), 2- 3. https://doi.org/10.5334/2002-8
Goh, P. S. (2018). eLearning in medical education – Costs and value add. The Asia Pacific Scholar, 3(2), 58- 60. https://doi.org/10.29060/TAPS.2018-3-2/PV1073
Gonzalez, S. M., & Gadbury-Amyot, C. C. (2016). Using Twitter for teaching and learning in an oral and maxillofacial radiology course. Journal Dental Education, 80(2), 149–155. https://doi.org/10.1002/j.0022-0337.2016.80.2.tb06070.x
Gunawardane, S., & Wijekoon, P. (2017). Changes in perceived computer use and knowledge in Sri Lankan dental students in the last ten years. Scholars Journal of Dental Sciences, 4(5), 216-219.
Hillenburg, K. L., Cederberg, R. A., Gray, S. A., Hurst, C. L., Johnson, G. K., & Potter, B. J. (2006). E-learning and the future of dental education: Opinions of administrators and information technology specialists. European Journal of Dental Education, 10, 169–177. https://doi.org/10.1111/j.1600-0579.2006.00413.x
Li, C., & Lalani, F. (2020). The COVID-19 pandemic has changed education forever. This is how. World Economic Forum. https://www.weforum.org/agenda/2020/04/coronavirus-education-global-covid19-online-digital-learning
Linjawi, A. I., & Alfadda, L. S. (2018). Students’ perception, attitudes, and readiness toward online learning in dental education in Saudi Arabia: A cohort study. Advances in Medical Education and Practice, 9, 855–863. https://doi.org/10.2147/AMEP.S175395
Piccoli, G., Ahmed, R., & Ives, B. (2001). Web-based virtual learning environments: A research framework and a preliminary assessment of effectiveness in basic IT skills training. MIS Quarterly, 25(4), 401-426. https://doi.org/10.2307/3250989
Qi, S., Yan, Y., Li, R., & Hu, J. (2013). The impact of active versus passive use of 3D technology: A study of dental students at Wuhan University, China. Journal of Dental Education, 77(11), 1536–1542.
Reissmann, D. R., Sierwald, I., Berger, F., & Heydecke, G. (2015). A model of blended learning in a preclinical course in prosthetic dentistry. Journal of Dental Education, 79(2), 157–165. https://doi.org/10.1002/j.0022-0337.2015.79.2.tb05870.x
Schlenz, M. A., Michel, K., Wegner, K., Schmidt, A., Rehmann, P., & Wöstmann, B. (2020). Undergraduate dental students’ perspective on the implementation of digital dentistry in the preclinical curriculum: A questionnaire survey. BMC Oral Health, 20, 78. https://doi.org/10.1186/s12903-020-01071-0
Thilakumara, I. P., Jayasinghe, R. M., Rasnayaka, S. K., Jayasinghe, V. P., & Abeysundara, S. (2018). Effectiveness of procedural video verses live demonstrations in teaching laboratory techniques to dental students. Journal of Dental Education; 82(8), 898-904. https://doi.org/ 10.21815/JDE.018.086
Turkyilmaz, I., Hariri, N. H., & Jahangiri, L. (2019). Student’s perception of the impact of e-learning on dental education. Journal of Contemporary Dental Practice, 20(5), 616-621.
Venkatesh, S., Rao, Y. K., Nagaraja, H., Woolley, T., Alele, F. O., Bunmi, S., & Malau-Aduli, B. S. (2019). Factors influencing medical students’ experiences and satisfaction with blended integrated e-learning. Medical Principles and Practice, 29, 296-402. https://doi.org/10.1159/000505210
Wong, M. L., Lee, T. W. O., Allen, P. F., & Foong, K. W. C. (2020). Dental education in Singapore: A journey of 90 years and beyond. The Asia Pacific Scholar, 5(1), 3- 7. https://doi.org/10.29060/TAPS.2020-5-1/GP1086
*RM Jayasinghe
Department of Prosthetic Dentistry,
Faculty of Dental Sciences,
University of Peradeniya
Tel: +94777806314
Email: manorija@pdn.ac.lk/ manoripathiraja@yahoo.com
Submitted: 19 July 2020
Accepted: 7 October 2020
Published online: 13 July, TAPS 2021, 6(3), 67-74
https://doi.org/10.29060/TAPS.2021-6-3/OA2347
Tess Lin Teo, Jia Hao Lim, Choon Peng Jeremy Wee & Evelyn Wong
Department of Emergency Medicine, Singapore General Hospital, Singapore
Abstract
Introduction: Singapore experienced the COVID-19 outbreak from January 2020 and Emergency Departments (ED) were at the forefront of healthcare activity during this time. Medical students who were attached to the EDs had their clinical training affected.
Methods: We surveyed teaching faculty in a tertiary teaching hospital in Singapore to assess if they would consider delivering clinical teaching to medical students during the outbreak and conducted a thematic analysis of their responses.
Results: 53.6% felt that medical students should not undergo clinical teaching in the ED and 60.7% did not wish to teach medical students during the outbreak. Three themes arose during the analysis of the data – Cognitive Overload of Clinical Teachers, Prioritisation of Clinical Staff Welfare versus Medical Students, and Risk of Viral Exposure versus Clinical Education.
Conclusion: During a pandemic, a balance needs to be sought between clinical service and education, and faculty attitudes towards teaching in high-risk environments can shift their priorities in favour of providing the former over the latter.
Keywords: Disease Outbreak, Pandemic, Faculty, Medical Students, Attitudes, Clinical Teaching, Emergency Medicine
Practice Highlights
- In a pandemic, a balance needs to be sought between clinical education and risking learner exposure to the virus.
- A crisis situation can affect educators’ priorities and attitudes towards the provision of clinical education, in favour of providing crucial clinical services.
I. INTRODUCTION
Since the first reported cases of COVID-19 infections in Wuhan, in December 2019, the month of January 2020 saw Singapore’s Ministry of Health (MOH) issue guidelines and implement a series of calibrated defensive measures to reduce the risk of imported cases and community transmission (Lin et al., 2020; WHO, 2020). Singapore has a Disease Outbreak Response System Condition (DORSCON) framework, which guides the nation’s response to various emerging infectious diseases outbreaks. The four-level colour-coded system of Green, Yellow, Orange and Red, describes the increasing severity of the outbreak in the community (Quah et al., 2020).
The Department of Emergency Medicine (DEM) of Singapore General Hospital saw 130 000 visits in 2019 (SGH, 2019). It hosted 158 medical students (MS) through the year. Aside from some elective students, the majority were in their second year of clinical postings. Formal clerkships consisted of four weeks of clinical exposure in which they were expected to clerk and present cases to teaching faculty and perform minor procedures such as intravenous cannulation and insertion of bladder catheters etc., with about nine hours of classroom tutorials.
In early January 2020, DORSCON yellow was declared, indicating either a severe outbreak outside Singapore or that the disease was contained locally with no significant community spread (Quah et al., 2020). All DEM staff were required to wear personal protective equipment (PPE). Hospital elective surgeries were postponed. Other outbreak measures included setting up new isolation areas for patients. DEM staff had their leave embargoed to ensure that there was adequate manpower to staff these areas in anticipation of a gradually worsening outbreak (Chua et al., 2020).
On 7 February 2020, the outbreak alert rose to DORSCON Orange (DO) as there were cases of community transmissions (Quah et al., 2020). Based on previous experience managing the Severe Acute Respiratory Syndrome (SARS) outbreak 17 years prior, the DEM transitioned to an Outbreak Response Roster, where physicians and nurses of the DEM were split into teams that worked 12 hour shifts, with no overlapping shifts, hence limiting staff contact to only those within their teams (Chua et al., 2020). With DO in effect, the department needed to come to a rapid decision about whether or not to accept MS in the ED. A group of 12 MS that the DEM was supposed to host this April already had their clerkship cancelled due to concerns of breaching infection control and safe distancing measures. There have been no studies to date on faculty attitudes towards clinical teaching of MS during a pandemic, although papers have been published about students’ attitudes towards clinical training during disease outbreaks. The Clerkship Director conducted a short and focused survey amongst the faculty between the 27th-29th of March, amidst rising public concerns that the country might soon be locked down, to explore their attitudes on having MS clerkships during the COVID-19 pandemic. The results of this survey allowed the Director to quickly understand the sentiments of the faculty and thus decided that an entirely remote, online teaching program would be created instead. 9 days after the survey, on the 7th of April, the Singapore government officially announced the implementation of a lockdown, known locally as a ‘circuit breaker’ (Quah et al., 2020).
II. METHODS
Clinical teachers of the DEM were issued an anonymous survey over a period of three days via an online survey tool, SurveyMonkey (www.surveymonkey.com). Participants were informed prior to completing the survey that it was anonymous, and by proceeding with the survey they consented to the results being used for research purposes. The data collected included their professional appointments in the department and two yes/no questions: “Do you think medical students should be performing their EM clerkship during DO?” and “Are you keen on teaching MS clinically during DO?”. Participants answering “No” to the latter were asked to elaborate. All participants were asked to write about any concerns they had about having MS in the emergency department (ED) during DO. No other personal identifying information was sought. The survey was deliberately kept short and easy to answer to promote staff participation within the short timeframe the DEM had to make the decision about accepting students. Informed consent was waived as per the Institutional Review Board (IRB).
A simple descriptive quantitative analysis of responses to the 1st two yes-no questions identified the overarching sentiment of the department towards hosting MS during DO and was followed by a thematic analysis of the free-text answers to the last two open-ended questions (Braun & Clarke, 2006).
As many participants used the last question (‘any other comments?’) to emphasise or elaborate on the preceding question (‘why aren’t you keen to teach?’), the majority of the qualitative data gathered pertains to the issues of having MS in the department during DO. There was a paucity of data detailing why participants were in favour of teaching MS, as the survey did not specifically ask this. Hence, the authors chose to focus on analysing the responses of participants who were not keen to teach during this time. This analysis yielded three different themes. However, a small number of respondents supportive of MS felt strongly about teaching and volunteered their reasons in response to the last question. While this data is insufficient to support a robust thematic analysis, a small section is included at the end in order to present as complete a discussion as possible.
III. RESULTS
A. Participant Background
Participants consisted of Emergency Medicine (EM) specialists, permanent registrars or middle grade staff and EM senior residents. These groups were chosen because they each hold significant roles, such as being named supervisors or clinical instructors of MS, and have considerably more contact time with MS in the DEM as opposed to nursing staff or junior doctors.
B. Quantitative Results
A total of 28 out of 45 (62.3%) responses were recorded. Except for two individuals, all other respondents in favour of hosting MS in the ED during DO (46.4%) were also keen to teach them. About two-thirds of the participants (60.7%) were not keen to teach MS during DO. However, of this latter group, 23.5% of respondents offered (without prompting) a compromise – where they proposed teaching only during the relatively less busy night shifts, in their response to ‘Any other comments?’ Table 1 shows the breakdown of responses.

Table 1: Responses broken down by question.
[1]Number of participants who offered the compromise of teaching during the relatively less busy night shifts despite indicating they were not keen to teach MS.
C. Qualitative Results – Reasons Against
Each of the three themes presented here begins with a short paragraph that describes the situational context in which this survey took place, followed by a series of selected statements, and ends with a general summary and discussion of the responses within the respective theme. In order to maintain the authenticity of the data, each response is reproduced verbatim, sometimes in Singlish, the local colloquial variety of Standard Singaporean English (Bokhorst-Heng, 2005). Any edits to the text for clarification purposes have been clearly identified.
1) First theme: Cognitive overload of clinical teachers– There is only so much one can handle: Emergency physicians are no strangers to high stress environments, and are aware that as frontline workers they will be at the forefront in dealing with any emerging infectious disease. The move into DO represented the shifting of the local virus epidemiology from predominantly imported cases that could be easily identified and isolated, into the community-at-large. With this shift came changes to existing workflows and the re-arrangement of department space to form isolation areas for treating potential infectious cases. The implementation of a strict team-based roster described earlier meant that almost half the entire department would not physically meet the other half, and a surge in manpower requirements saw many junior doctors from other departments being rotated into the ED to help tackle the increased clinical load. Being new to the DEM, these new doctors required more supervision and assistance in adapting to the unfamiliar work environment. Responses that supported this theme include:
“High clinical load, long hours. Already cognitively overloaded. Not conducive for teaching. New [junior doctors] need to be taught also.”
Participant #6, Specialist
“Focus on daily evolving challenge first.” and in response to the last question “Please no.”
Participant #2, Senior Resident
“During DORSCON ORANGE we are in stress, if clinical teaching sessions start then other [doctors’] stress and workload level will increase.”
Participant #25, Staff registrar
“May be more a hassle if we have to look after the new [junior doctors] rotating and students [as well].”
Participant #4, Specialist
“We are also in a 12-hour outbreak roster which is physically, emotionally and mentally draining. Teaching students in this environment is far from ideal” and in response to the last question “Am fairly strongly against this idea”.
Participant #8, Specialist
“Day shifts no bandwidth to teach […] also can’t pay attention to [medical students] during day shifts, too tiring and too busy […] but I feel I can’t do [medical students] justice because I can’t debrief after a shift either, too tired.”
Participant #17, Specialist
Many of these responses conveyed a sense of exhaustion, reflecting the toll that constant workflow changes, longer work hours and relative social isolation was taking on the faculty. Teaching and supervising MS appeared to be viewed as a “hassle” or “extra work”, an additional drain to a clinical faculty’s energy during a busy and stressful shift.
This brought the department to a discussion on the provision of clinical services versus clinical education – whether teaching the next generation of future doctors was as important as treating the patient in front of us. One school of thought held that as clinician educators, physicians should – as the name implies – be clinicians first before educators. However, the interplay between these two roles is likely dependent on the faculty’s attitudes towards learners, as will be described later. Being cognitively overloaded naturally results in a shuffling of One’s priorities, which is seen next.
2) Second theme: Prioritisation of staff welfare – whose welfare is more important, staff or students? : It is well known that mental health can be adversely affected in crisis situations, and as the COVID-19 situation unfolded, boosting morale and maintaining the welfare of all staff became an important consideration (Matsuishi et al., 2012; McAlonan et al., 2007). At the forefront of this effort was the need to provide the staff with a supply of good quality personal protective equipment (PPE) so the staff would feel safe and confident in existing infection control measures. Although Singapore had yet to experience a shortage of PPE, there was still a concerted effort made by all hospitals to conserve these resources. Staff wellness was a theme seen in several responses:
“[I] can’t do the [junior doctors] justice because having a [medical student] attached to them is another stressor in an already stressful shift.”
Participant #17, Specialist
“Having to keep our doctors and nurses safe takes up a lot of energy. Students are young and naïve and will require even more time and resources to ensure they are safe.”
Participant #22, Specialist
“Furthermore, they will need to use PPE and again this should be conserved during the period of the outbreak.”
Participant #27, Specialist
“Medical students are important for future but I feel staff currently working in the department should be look after well.”
Participant #25, Staff registrar
“Waste PPE.”
Participant #20, Specialist
The importance of conserving PPE during a pandemic is undisputed and the concern that MS would use them up is valid. It was interesting to note in these responses hints of an “us-versus-them” mentality, where MS were seen as competition for the limited resources of PPE, time, and energy. Students were not viewed as part of the DEM team and perceived more as “stressors”, who required attention because they were “young and naïve”, and their use of PPE was viewed as a “waste”. This identification of an “in-group” of staff and an “out-group” of students led to a prioritisation or favouring of the former over the latter. This behaviour can be explained by the Social Identity Theory (SIT), which states that part of an individual’s self-image or self-concept is derived from the social groups to which they perceive themselves to belong to (Hogg & Reid, 2006; Tajfel & Turner, 1979). Thus, in order to maintain a positive self-image, there is a tendency for people to favour the in-group and discriminate against the out-group. This phenomenon was famously demonstrated by Tajfel et al in their Minimal Group Paradigm studies, which essentially showed that the mere perception of belonging to one of two distinct groups was enough to trigger social discrimination between the groups (Tajfel et al., 1971). Behaviour like this is indicative that a significant number of the department hold the belief that there is a distinct divide between students and staff, rather than seeing MS as belonging to the wider group of the medical fraternity. Creating such a divide between staff and student is problematic because it hinders effective teaching, especially because MS will eventually transition from the “out-group” of students to the “in-group” of staff upon graduation, and clinician educators are responsible for providing a safe environment for them to learn in. However, beyond this discussion of intergroup competition, there were concerns amongst the faculty with regards to the appropriateness of siting clinical learning in the high-risk, front-line location of the ED in a pandemic, as discussed in the next theme.
3) Third Theme: Risk of viral exposure vs clinical education – What is the price to pay and who pays it?: During the initial period of DO, medical schools pulled MS out of the clinical environment and moved to online learning, with the aim of protecting them from unnecessary exposure to the virus and for safe distancing. However, when they proposed that students be allowed back into the hospitals after undergoing PPE training, this risk of exposure had not changed, as the number of positive cases was rising daily still. Responses that reflected this theme included:
“Don’t think it’s appropriate to have students around in a high-risk environment.”
Participant #4, Specialist
“Having medical students around not only will expose them to infection it will also compromise the rest of the staff in the event of a breach in infection [protocols]. Also, them just hanging around & not allowed to have hands-on [participation] in the procedures, clerking, [patient] contact etc will not be of any benefit [to them] at this time.”
Participant #7, Senior Resident
“Student safety issue. No minder to ensure students’ adherence to strict PPE as Doctors and Nurses will be busy with clinical service.”
Participant #11, Specialist
“I think medical students are not providing clinical care to patients and having them in the ED increases risk to patients (without the attendant benefits) and increases risk to themselves (without the moral obligation to do so as doctors) and their family.”
Participant #27, Specialist
“Can students be [held] responsible for their own health? Or the school or the department? As doctors, we know it as our duty and occupational hazard. But as students – their duty is to learn (best done in a safe environment), not put their health at risk.”
Participant #6, Specialist
Responses that addressed the risk of virus exposure in the ED could be divided into two groups –those that were predominantly concerned about the students themselves catching the virus, and those that were more concerned about the consequences of such an event. The risk of catching the virus was seen as too high a cost – one that was borne not only by the individual student but by the patients and the staff as well. The benefits of clinical bedside instruction were called into question, as students’ movements would be restricted to low or medium-risk areas only. More than one participant raised the potential issue of students breaching infection control protocol or needing supervision in donning their PPE, despite reassurances given that schools would send MS for PPE training. This reflected a lack of trust in MS – themselves adult learners – who could be reasonably expected to understand the importance of infection control protocols. It begs the question of how big a role the educator plays in the personal safety of a MS and that of the patients and staff they interact with.
D. Qualitative Results – Reasons For
The survey design did not specifically ask responders about their reasons for supporting teaching MS during this pandemic. However, some participants felt strongly enough about this to advocate for clinical postings. Their reasons are shared below.
1) Theme: For the sake of tomorrow – In defence of teaching amidst a crisis:
“I feel we can still provide a meaningful learning experience for these students. We just need to lay out clear instructions and precautions for them to follow. It is a good opportunity to show to students how emergency medicine is adaptive, versatile, and for them to appreciate how quickly workflows can change, or how triage works in a disaster setting.”
Participant # 15, Specialist
“The way it is done has to be different […] the traditional method of teaching, where the students look to the seniors and may expect some form of spoon feeding […] Only when this mind-set is removed, will the tutors […] look at them as part of the team and incorporate them […], and will students see […] themselves as Drs to be [sic], practice safe habits from the very start and protect themselves as the patient’s doctor. This sense of ownership, accountability, professionalism can be started from that stage as a medical student. This is the perfect opportunity to state that this is what is expected and groom them likewise.”
Participant #19, Specialist
“I feel that the teaching should as much as possible be a simulation of working life and that working in high-risk areas such as these gives a semblance of pressure which cultivates good habits such as mindfulness of hand hygiene, donning of PPE etc.”
Participant #26, Senior Resident
The responses share a commonality of seeing the pandemic as an opportunity for modelling positive attitudes that would benefit the student in the future. This point of view advocates for the acknowledgement of the realities of being a doctor and assumes that students are already part of the “in-group” of the medical team rather than the “out-group” as seen in the earlier discussion.
IV. DISCUSSION
A. Limitations
This study has its limitations, chiefly being the lack of qualitative data representing the opinions of those who were keen to teach MS as the initial survey was conducted with the purpose of gauging whether or not the department would be open to receiving MS during DO. This lack of data meant that this study is at best a one-sided representation of the department’s opinion.
Additionally, all four of the authors have a keen interest in the education of MS and two of the authors are actively involved in faculty development. They were all both participants in the study as well as its evaluators. Prior to evaluation of results, the authors themselves suspected that majority of the faculty would be too overwhelmed with the changes the pandemic wrought to want to teach students, which may have contributed to confirmation bias in the analysis of the data. However, throughout the analysis, every attempt was made to ensure that the themes uncovered remained true to the data, and much of the original data was reproduced here faithfully to maintain transparency, such that the reader may draw their own conclusions.
Another limitation of the study was that the survey was unable to measure shifts in the attitudes of faculty as the pandemic evolved, which would have allowed us to understand the amplitude of the effect of the pandemic itself more clearly.
B. New Insights
It was worth noting that nearly two-thirds of the department did not want to teach MS during DO, despite each participant having taught MS routinely prior to this pandemic. Initial analysis of the reasons given for this refusal revealed three distinct themes of Cognitive Overload of Teachers, the need to Prioritise Staff Welfare and the Risk of Viral Exposure to Students – themes that are transferrable to many departments involved in pandemic response, regardless of locality.
Expounding further on this topic, it can be seen in some of the responses detailed under the themes of Cognitive Overload and Prioritising Staff Welfare, that there was a perceived increase in the need to supervise the new junior doctors rotating into the department on short notice (as opposed to the junior doctors who were already in the middle of their rotation and thus more familiar with the department’s protocols). This supervision is an important component of the continuing clinical education of junior doctors, which in itself is part of a larger debate surrounding the competing aims of clinical service versus clinical education that has been ongoing for many years (Woods, 1980). It is often the case in EM that when overwhelmed with patients, clinical education is sacrificed for clinical service without much short-term complications. Indeed, even amongst EM residents, more research is needed to define the optimal balance between service and education (Quinn & Brunett, 2009). However, a pandemic presents a rather unique situation in that most junior doctors will not have worked in a pandemic before. Thus, the need to educate junior doctors on both pandemic response and the importance of personal safety – with its direct impact on patient safety – now cannot be sacrificed without directly affecting the provision of clinical service.
It is beyond the scope of this paper to comment on whether educating MS on pandemics through clinical immersion programs during a pandemic better prepares them for future outbreaks, or in the broader sense, whether the clinical education of today’s MS by immersive learning can bolster the clinical service of tomorrow’s junior doctors. In fact, it seems almost premature to consider this question given the paternalistic attitude many of our faculty appeared to have towards students, perceiving them as learners to be looked after – to the extent that they could not even be trusted with their own safety and that of the patients and staff they interact with. Interestingly, this view seems to be shared by MS themselves – an electronic survey conducted at one of Singapore’s medical schools showed that a third of currently enrolled MS were concerned that they might introduce possible risks to the patient should they return to the clinical setting (Compton et al., 2020). These findings are indicative of a more deeply rooted mindset in which the social hierarchy draws a clear line between Teacher and Student. This becomes clearer when one considers that in Confucian Heritage Cultures such as Singapore (Biggs, 1998), the teacher holds great authority and students brought up in such cultures tend to defer to such authority as a matter of course (Ho, 2020). Given the multiple factors that contribute to this debate, it is unlikely that we will be able to arrive at a clear answer without further research, but what is certain is that medical students are not essential workers and, in a pandemic, medical schools need to balance their educational needs and ethical obligations to keep students safe (Menon et al., 2020).
Within our paper, it is heartening that many participants who were not keen to teach still tried to offer a compromise of teaching during the relatively less busy night shifts instead, and that 46% of our department were willing to accept MS during this period. COVID-19 allowed us to uncover some of the underlying attitudes towards MS and to consider them in the context of Singapore’s cultural heritage. These attitudes are important for us to address if we are to improve the delivery of medical education in the ED and we would like to invite the reader to consider whether the same uncovering has occurred in their respective departments.
V. CONCLUSION
The balance between clinical service and clinical education is a precarious one that appears to shift quickly in favour of the former in the high-risk environment of an evolving pandemic, which presents significant challenges even for experienced educators to overcome. As seen in our paper, cognitive overload of educators and the need to prioritise the welfare of junior staff inexperienced in pandemic response takes clear precedence over the education of MS. The paternalistic view that majority of our faculty hold leads to doubts about the ability of MS to keep themselves and their patients safe from virus exposure, doubts that are surprisingly shared by MS as well, and is indicative of the social hierarchy deeply ingrained in Confucian Heritage Cultures such as Singapore and surrounding countries in the region, where students tend to defer to authority as a matter of course. In order to improve as medical educators, we must place further effort into uncovering the underlying attitudes of both faculty and MS and address them in ways specific to our cultural heritage.
Notes on Contributors
Author Teo TL analysed the transcripts, conducted the primary thematic analysis and wrote the manuscript. Author Lim JH co-wrote the manuscript. Author Wee JCP conducted the literature review and developed the manuscript. Author Wong E designed and conducted the study, performed the data collection and developed the manuscript. All the authors have read and approved the final manuscript.
Ethical Approval
IRB approval for this study was obtained (SingHealth CRIB reference number 2020/2134).
Acknowledgement
The authors would like to acknowledge all participants of the survey.
Funding
No funding sources are associated with this study.
Declaration of Interest
All authors work in SGH DEM and answered the survey as participants.
References
Biggs, J. (1998). Learning from the confucian heritage: So size doesn’t matter? International Journal of Educational Research, 29(8), 723–738. https://doi.org/10.1016/S0883-0355(98)00060-3
Bokhorst-Heng, W. D. (2005). Debating singlish. Multilingua, 24(3), 185–209. https://doi.org/10.1515/mult.2005.24.3.185
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Chua, W. L. T., Quah, L. J. J., Shen, Y., Zakaria, D., Wan, P. W., Tan, K., & Wong, E. (2020). Emergency department ‘outbreak rostering’ to meet challenges of COVID-19. Emergency Medicine Journal, 37(7), 407–410. https://doi.org/10.1136/emermed-2020-209614
Compton, S., Sarraf-Yazdi, S., Rustandy, F., & Radha Krishna, L. K. (2020). Medical students’ preference for returning to the clinical setting during the COVID-19 pandemic. Medical Education, 54(10), 943–950. https://doi.org/10.1111/medu.14268
Ho, S. (2020). Culture and learning: Confucian heritage learners, social-oriented achievement, and innovative pedagogies. In C. Sanger & N. Gleason (Eds.), Diversity and inclusion in global higher education (pp. 117–159). Palgrave Macmillan. https://doi.org/10.1007/978-981-15-1628-3
Hogg, M. A., & Reid, S. A. (2006). Social identity, self-categorization, and the communication of group norms. Communication Theory, 16(1), 7–30. https://doi.org/10.1111/j.1468-2885.2006.00003.x
Lin, R. J., Lee, T. H., & Lye, D. C. B. (2020). From SARS to COVID-19: The Singapore journey. The Medical Journal of Australia, 212(11), 497-502.e1. https://doi.org/10.5694/mja2.50623
Matsuishi, K., Kawazoe, A., Imai, H., Ito, A., Mouri, K., Kitamura, N., Miyake, K., Mino, K., Isobe, M., Takamiya, S., Hitokoto, H., & Mita, T. (2012). Psychological impact of the pandemic (H1N1) 2009 on general hospital workers in Kobe. Psychiatry and Clinical Neurosciences, 66(4), 353–360. https://doi.org/10.1111/j.1440-1819.2012.02336.x
McAlonan, G. M., Lee, A. M., Cheung, V., Cheung, C., Tsang, K. W. T., Sham, P. C., Chua, S. E., & Wong, J. G. W. S. (2007). Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Canadian Journal of Psychiatry, 52(4), 241–247. https://doi.org/10.1177/070674370705200406
Menon, A., Klein, E. J., Kollars, K., & Kleinhenz, A. L. W. (2020). Medical students are not essential workers: Examining institutional responsibility during the COVID-19 pandemic. Academic Medicine, 95(8), 1149–1151. https://doi.org/10.1097/ACM.0000000000003478
Quah, L. J. J., Tan, B. K. K., Fua, T. P., Wee, C. P. J., Lim, C. S., Nadarajan, G., Zakaria, N. D., Chan, S. J., Wan, P. W., Teo, L. T., Chua, Y. Y., Wong, E., & Venkataraman, A. (2020). Reorganising the emergency department to manage the COVID-19 outbreak. International Journal of Emergency Medicine, 13(1), 32. https://doi.org/10.1186/s12245-020-00294-w
Quinn, A., & Brunett, P. (2009). Service versus education: Finding the right balance: A consensus statement from the council of emergency medicine residency directors 2009 academic assembly “Question 19” working group. Academic Emergency Medicine, 16(SUPPL. 2), 15–18. https://doi.org/10.1111/j.1553-2712.2009.00599.x
SGH. (2019). Hospital Overview – Singapore General Hospital. Retrieved August 17, 2020, from https://www.sgh.com.sg/about-us/corporate-profile/Pages/hospital-overview.aspx
COVID-19 (Temporary Measures) Act 2020. (2020). https://sso.agc.gov.sg/Act/COVID19TMA2020
Tajfel, H., Billig, M. G., Bundy, R. P., & Flament, C. (1971). Social categorization and intergroup behaviour. European Journal of Social Psychology, 1(2), 149–178. https://doi.org/10.1002/ejsp.2420010202
Tajfel, H., & Turner, J. C. (1979). An integrative theory of intergroup conflict. In W. G. Austin & S. Worchel (Eds.), The social psychology of intergroup relations (pp. 33–47). Brooks/Cole.
WHO. (2020). IHR emergency committee for pneumonia due to the novel coronavirus 2019-nCoV transcript of a pressing briefing. Retrived January 30, 2020, from https://www.who.int/docs/default-source/coronaviruse/transcripts/ihr-emergency-committee-for-pneumonia-due-to-the-novel-coronavirus-2019-ncov-press-briefing-transcript-30012020.pdf?sfvrsn=c9463ac1_2
Woods, D. (1980). Service and education in residency programs. A question of balance. Canadian Medical Association Journal, 123(1), 44.
*Evelyn Wong
Department of Emergency Medicine,
Singapore General Hospital
Outram Road
Singapore 169608
Email: evelyn.wong@singhealth.com.sg
Submitted: 30 August 2020
Accepted: 9 December 2020
Published online: 13 July, TAPS 2021, 6(3), 56-66
https://doi.org/10.29060/TAPS.2021-6-3/OA2440
Gayathri Devi Nadarajan1, Kirsty J Freeman2, Paul Weng Wan1, Jia Hao Lim1, Abegail Resus Fernandez2 & Evelyn Wong1
1Department of Emergency Medicine, Singapore General Hospital, Singapore; 2Office of Education, Duke-NUS Medical School, Singapore
Abstract
Introduction: COVID-19 challenged a graduate medical student Emergency Medicine Clinical Clerkship to transform a 160-hour face-to-face clinical syllabus to a remotely delivered e-learning programme comprising of live streamed lectures, case-based discussions, and telesimulation experiences. This paper outlines the evaluation of the telesimulation component of a programme that was designed as a solution to COVID-19 restriction.
Methods: A mixed methods approach was used to evaluate the telesimulation educational activities. Via a post-course online survey student were asked to rate the pre-simulation preparation, level of engagement, confidence in recognising and responding to the four clinical presentations and to evaluate telesimulation as a tool to prepare for working in the clinical environment. Students responded to open-ended questions describing their experience in greater depth.
Results: Forty-two (72.4%) out of 58 students responded. 97.62% agreed that participating in the simulation was interesting and useful and 90.48% felt that this will provide a good grounding prior to clinical work. Four key themes were identified: Fidelity, Realism, Engagement and Knowledge, Skills and Attitudes Outcomes. Limitations of telesimulation included the inability to examine patients, perform procedures and experience non-verbal cues of team members and patients; but this emphasised importance of non-verbal cues and close looped communication. Additionally, designing the telesimulation according to defined objectives and scheduling it after the theory teaching contributed to successful execution.
Conclusion: Telesimulation is an effective alternative when in-person teaching is not possible and if used correctly, can sharpen non-tactile aspects of clinical care such as history taking, executing treatment algorithms and team communication.
Keywords: Telesimulation, COVID-19, Emergency Medicine, Programme Evaluation
Practice Highlights
- Telesimulation doesn’t replace but can be an effective alternative when in-person teaching is not possible.
- When implemented correctly, it can sharpen non-tactile aspects of clinical care.
- It is possible to achieve a level of fidelity and realism in a telesimulation environment.
- Simulation faculty needs to be skilled in debriefing techniques that enable the learner to reflect.
- Limitations of telesimulation can be reframed as learning opportunities.
I. INTRODUCTION
COVID-19 brought about unexpected challenges to medical education, especially to student clinical clerkships where medical students would spend time within a clinical discipline, interacting with clinicians and learning from patients. Healthcare institutions restricted student movement within clinical environments and barred students from entering the high-risk frontline areas to reduce exposure risk.
Prior to COVID-19, students undertaking an Emergency Medicine (EM) Clinical Clerkship, would have the opportunity to manage and deliver care to high acuity patients, with bedside teaching, small group tutorials, problem-based learning and simulation modalities. With COVID-19, students were not permitted into the Emergency Department (ED) and face-to-face teaching activities were halted. Hence this clerkship had to be conducted remotely. The EM clerkship was transformed from a 160-hour clinical programme to a remotely administered programme comprising 40 hours of e-learning, 40 hours of interactive live online session and 15 hours of telesimulation. As part of this programme, we decided to utilise telesimulation to help students achieve some of the objectives of a clinical clerkship.
Telesimulation is defined as the “Process by which telecommunication and simulation resources are utilised to provide education, training and/or assessment to learners at an off-site location” (McCoy et al., 2017). By allowing simulation to be conducted through devices such as the computer and phone, it mitigates the problem of physical proximity. Though telesimulation has existed for about a decade, its utilisation appears limited to the rural settings and studies mainly describe its usage for learning skills (Mikrogianakis et al., 2011; Naik et al., 2020; Okrainec et al., 2010) rather than for emergency management of patients. With the need to adapt teaching to remote experiences, telesimulation is gaining popularity (Sa-Couto & Nicolau, 2020).
A. Programme Overview
This remote learning programme was developed in a tertiary ED in Singapore which receives both undergraduate and postgraduate medical students for their EM clerkship. There were 58 postgraduate medical students undertaking their 4-week EM clerkship in June 2020. The EM core clinical training curriculum was taught by EM faculty via online modules and interactive classroom sessions delivered via the video conferencing platform, Zoom. The learners spent the mornings in interactive online sessions with faculty, and afternoons in self-study as part of a flipped classroom learning, using provided learning materials. The telesimulation session was scheduled in the last week, over five days. The students were split into ten groups each comprising of five to six students, where two groups participated in one telesimulation session each day.
Our objectives for this telesimulation programme was to ensure that the students could take a focused clinical history from the simulated patients, communicate with them, construct a list of differentials and manage them accordingly in the emergency setting. The secondary objectives were to train them to prioritise the investigations and management of critically ill patients and to communicate and work effectively within a team. Using Kern’s six step approach, the team of simulation and clinical educators’ planned and implemented the telesimulation activity to achieve these outcomes (Harden et al., 1999; Smith & Dollase, 1999) during their EM clerkship.
As medical students, the learners are at a novice stage according to The Dreyfus Model of Skill Acquisition (Benner, 2004; Dreyfuss & Dreyfus, 1980). Hence, the deliberate attempt not to assess skills such as intubation or defibrillation through telesimulation as it may create unnecessary anxiety and feelings of incompetence (Papanagnou, 2017). Furthermore, it was deemed challenging to conduct procedural skill teaching through this modality. Instead, the focus was on clinical reasoning and patient management. The clinical students fall under the category of “show how” within the Miller’s pyramid, with regards to history taking, clinical reasoning and management. As adult learners, a problem centred (Knowles, 1990), experiential learning approach (Kolb, 1984) would be more valuable. Hence telesimulation was an appropriate modality.
Each telesimulation session was conducted by two simulation and one physician faculty. There was a total of four scenarios for each session, where one group, consisting of five to six students, will participate in the scenario, while the other group observes, before switching. This allowed each group of students to participate in two clinical scenarios. The topics chosen for telesimulation were Anaphylaxis, Cardiac Arrest, Meningitis, and Syncope where the theory was covered in the core topics in the preceding weeks. Each of these scenarios began with the students taking a history from the simulated patient, before the patient progressively deteriorated and required resuscitation. Figure 1 shows a summary of the scenarios. The scenarios were selected as they did not require much procedure-based interventions (e.g. chest tube insertion in a poly trauma victim) which would be difficult to assess via Zoom.
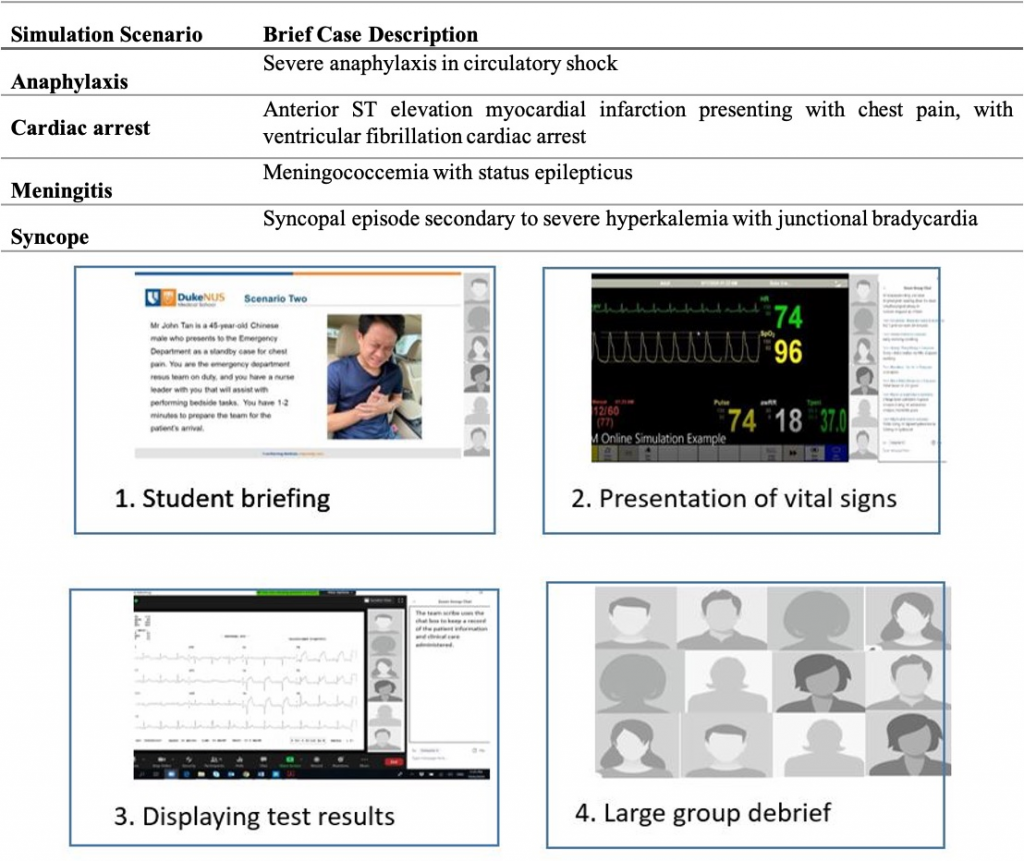
Figure 1. Brief case description of simulation scenarios and visual presentation of the flow of the telesimulation experience
The sessions commenced with a briefing where the students were orientated to the online environment, including the use of video and microphones. As depicted in Figure 1, using the share screen feature, the simulation technician switched between different views. The briefing included a photo of the patient as a visual cue, along with the text of the presenting case. One of the simulation faculty played the circulating nurse, providing prompts to aid students’ engagement and asking participants to clarify their statements or orders as the scenario progressed. Using existing mannequin software and ensuring sharing of screen sounds, real-time patient monitoring was provided to the learners when requested. Upon request, additional visual cues of investigation results would be displayed, reverting back to either a picture of the patient or the patient monitoring. With their video off, the clinical faculty voiced the patient. At the conclusion of the scenario, all participants and faculty turned their video and microphones back on to participate in the large group debrief before proceeding on to the next scenario.
The objective of this paper is to describe the students’ experience of telesimulation as part of an online clerkship programme and how such techniques can be used to meet learning outcomes (Harden et al., 1999) in various settings. At the time of writing, there is no literature describing evaluation of the use of a telesimulation programme within the ED for medical student education, with this paper aiming to address this gap.
II. METHODS
A mixed methods approach was used to evaluate the introduction of telesimulation to the EM online clerkship, and to gain students’ perspective on learning through telesimulation. Programme evaluation research aligns with a mixed methods approach as the collection of both quantitative and qualitative data provide a deeper understanding of the student experience (Cohen et al., 2011).
A. Participants, Data Collection and Analysis
58 final year medical students who participated in the EM Online Clerkship programme were invited to participate in a post-telesimulation activity evaluation survey. Using a 5-point Likert scale, students were asked to indicate their agreement on 11 items addressing pre-simulation preparation, their level of engagement, confidence in recognising and responding to the four clinical presentations and telesimulation as a tool to prepare for working in the clinical environment. Seven open-ended questions were asked to enable the students to describe their experience in greater depth. 24hrs after completing the telesimulation session, students received an email with a link to the survey. Qualtrics online survey software was used to build, distribute and collect the survey responses. Voluntary consent was assumed by participation in the anonymised online evaluation. A statement outlining the purpose of the survey was included at the start of the survey and require an agreement before the survey could be commenced. Completion of the survey therefore implied consent. The survey took between three and five minutes to complete, all responses were anonymous, with no identifiable data collected.
Descriptive statistics was used to analyse the responses to the Likert scale questions, with thematic analysis of the open-ended survey questions. Author one (GN) and author two (KF) reviewed the transcripts separately, making note of key phrases, outline possible categories or themes. Both authors then jointly rearranged and renamed the codes, developing higher order themes. NVivo 12™ was used to store, code and manage the qualitative data.
III. RESULTS
Of the 58 students who were invited to participate in the survey, 42 complete responses were received, a response rate of 72.4%. As seen in table 2, the results demonstrated that 97.62% of respondents agreed/strongly agreed that participating in the telesimulation session was interesting and useful to their learning. In relation to the use of visual and auditory cues, 93% of respondents felt that these helped them engage in the simulation. In relation to their level of preparedness to participate in the telesimulation experience, nearly 17% of respondents reported that the pre-session handout did not adequately preparing them for what to expect in the session.
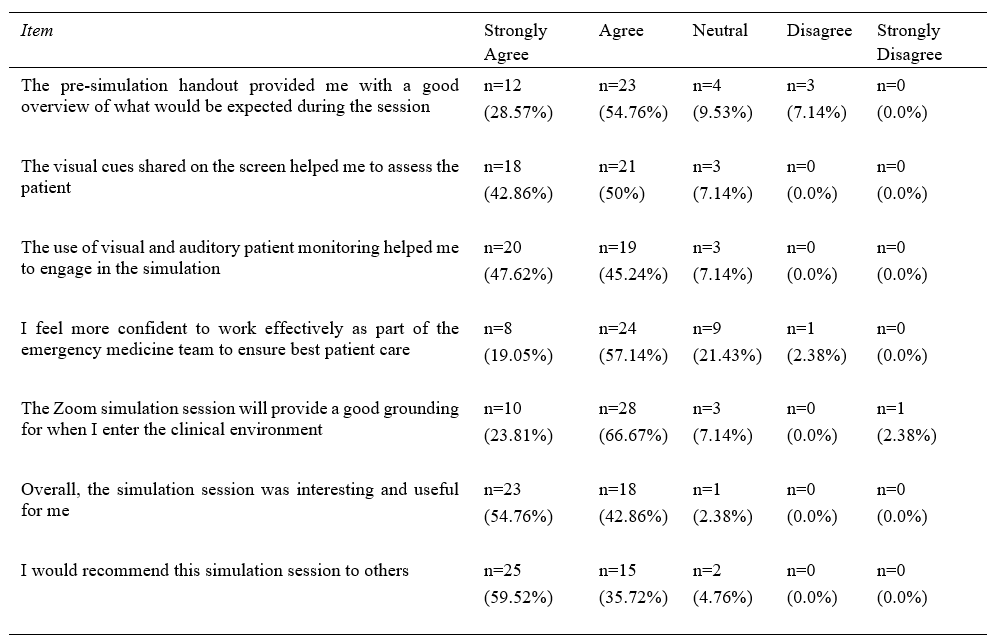
Table 1. Results of the student responses to the Likert scale items
When asked to rate if they felt more confident recognising and responding to the four clinical presentations (anaphylaxis, cardiac arrest, meningitis, and syncope), between 90% and 93% agreed/strongly agreed that participating in the telesimulation sessions resulted in them feeling more confident in recognising and responding to the specific clinical presentations (Figure 2).
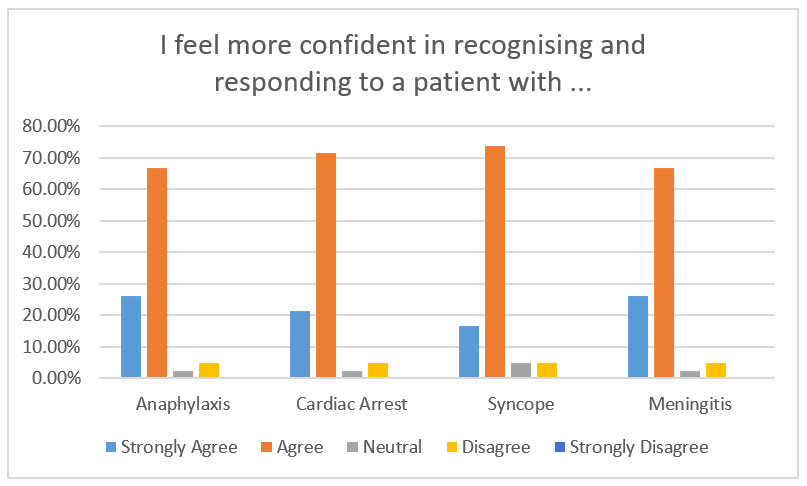
Figure 2. Student rating to the question “I feel more confident in recognising and responding to a patient with …”
Four key themes were identified following the data analysis of the open-ended survey questions, describing around the telesimulation experience of the respondents: 1) Fidelity; 2) Realism; 3) Engagement; and 4) Outcomes. As demonstrated in Figure 3, the themes do not exist in isolation, but intersect as they describe the telesimulation experience that the students had. The students feedback reflected the benefits and limitations which fall under these main themes.
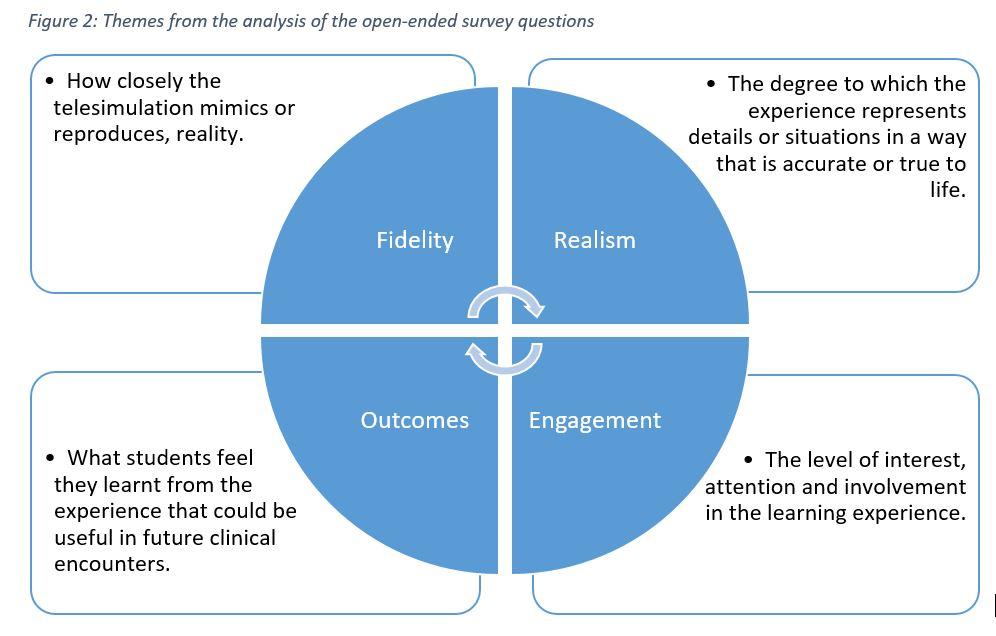
Figure 3. Themes reflecting the students experience with telesimulation
A. Fidelity – Physical, Psychological and Conceptual
The theme Fidelity reflects how closely the telesimulation mimics or reproduces, reality. Subthemes of conceptual, physical and psychological fidelity were also reflected. The students’ feedback reflected limitations in physical fidelity while conceptual and psychological fidelity was present mostly.
They reported that the auditory and visual stimulus from the dynamic display of investigations and real-time vital signs monitoring, provided a high level of physical fidelity.
“Auditory and visual information on patients’ vitals and results were really helpful in generating the differential list.”
Student 37
“The noise and sights is a good proxy for real life cases in a virtual environment.”
Student 4
“Seeing the vitals of the patient in real-time allows us to experience the importance of time in managing critically ill patients”
Student 20
However, aspects of physical fidelity, particularly related to the patient assessment, were reported as challenging via telesimulation. With the patient represented as a static picture, voiced by the clinical faculty, students shared how the lack of non-verbal and visual cues from the patient impacted their ability to perform a physical assessment of their patient.
“….we don’t get to observe the body language of the patient as much as we would like”
Student 12
“More difficult than in real life. Seeing and hearing a real patient gives much information”
Student 15
“I think what is lacking is being able to visually evaluate the patient”
Student 21
In terms of the level of psychological fidelity, the auditory cues from the ‘patient’ and the real-time vital signs monitoring simulated the ED resuscitation room, which appears to have instilled a similar sense the stress and the need to think under pressure, as reflected by the students’ feedback.
“Have to work around the distractions of beeping monitors, seizing patient, teammates asking questions/suggestions.”
Student 33
“It’s dynamic and gives us the opportunity to think under pressure.”
Student 13
“Stressful but probably close to reality?”
Student 35
The students’ statements reflected the subtheme of conceptual fidelity, where they felt the context and sequence was similar to what they would encounter in the ED, where they are required to deliver timely and lifesaving treatment. This was possibly because the faculty made deliberate attempts to ensure that events during the simulation would unfold as it usually would in the ED room, based on the learners’ actions.
“It simulates a clinical environment with real time updates of vitals and test results in addition to the history and communications.”
Student 5
What the students did report struggling with however, was the limitations of the platform in terms of multiple actions occurring simultaneously. Unlike in real life, multiple tasks could not be performed at the same time over the online platform, and this impeded the conceptual fidelity.
“In reality, multiple interventions would be carried out in tandem.”
Student 35
“More challenging to perform tasks concurrently over Zoom.”
Student 36
“…many things cannot occur concurrently.”
Student 2
B. Realism
The theme Realism captures the degree to which the experience represented details or situations in a way that is accurate or true to life. Students reported that aspects of the telesimulation experience represented what they thought an actual ED encounter would be like.
“I think the process is similar to the actual clinical environment, it is difficult, especially when the patient is deteriorating in front of you, and your team are waiting for you to make the decisions.”
Student 41
“The pictures/videos and the beeping of the monitor, they make it more real”.
Student 42
“It was realistic as getting the differentials was time sensitive”.
Student 13
The students also acknowledged the limitations in achieving realism presented by telesimulation as the various team members could not perform tasks simultaneously and take in cues from the patient to assess the outcome of their actions.
“Harder to communicate with my teammates compared to real life because only one person could speak at a time while in real life, multiple conversations could be occurring”
Student 3
“More difficult than taking a history in real life – more technical issues (can’t hear properly), Can’t see the patient”
Student 8
C. Engagement
The theme Engagement relates to the level of interest, attention and involvement in the learning experience. The level of fidelity and realism impacts the level of engagement of the learners. Most students were able to immerse themselves and fully engage in the scenarios, possibly because aspects of fidelity and realism were deliberately given close attention during the preparation phase.
“I actually forgot that the patient was being voiced by the clinical tutor”
Student 41
“My heart was racing doing the simulation – what will I be like when I am there for real?”
Student 41
However, on the downside, without being together in the same place, some felt that the scenario was too “messy” and “chaotic” and found it difficult to follow.
“It was a little hectic with the many other ongoing tasks in the background”
Student 6
“Easier to detach oneself from the patient (less affected by patient’s appearance, tone of voice, blood, gore, suffering etc.)”
Student 28
At the same time, some students faced technical difficulties, such as small or flickering screen, poor internet connection or poor audio, which were barriers to their engagement.
“…there were some issues hearing the faculty clearly which may affect the quality of learning.”
Student 6
By addressing the concepts of realism and fidelity, the students reported increased levels of engagement, although it appears that technical barriers unique to telesimulation provide challenges for some students achieving a greater level of engagement.
D. Outcomes- Knowledge, Skills and Attitudes
The theme Outcomes encompasses what students feel they learnt from the experience that could be useful in future clinical encounters. Under outcomes, there were sub-themes of knowledge, skills and attitudes. From a knowledge perspective, students reported that the telesimulation reinforced their clinical reasoning to arrive at a differential list.
“It was very useful and helped with our clinical reasoning. It was also useful in learning how to generate differential diagnoses as a team and going down the path of a working differential diagnosis while keeping others in mind.”
Student 32
Whilst the lack of hands-on practice was acknowledged, the telesimulation environment required them to practice the skills of prioritisation, leadership, teamwork and effective, close loop communication to manage the patient and this accounted for their skills gained.
“I will be able to apply the concept of teamwork, thinking on my feet, thinking broad, and constant reassessment of the unstable patient in my clinical training over the next few months”
Student 6
“Stay calm, go back to first principles, have the approach at your fingertips, make an effort to remember drug doses and administration route”
Student 2
IV. DISCUSSION
In relation to Kirkpatrick’s model for evaluating educational outcomes, the results of this study (table 1) demonstrate achievement of both level one (reactions) and level two (learning) outcomes (Kirkpatrick & Kirkpatrick, 2009). Whilst these findings may not determine the effectiveness of telesimulation, it does however provide insight into the learners’ experience that have highlighted the strengths and limitations of telesimulation, which the authors of this paper believe provides a foundation upon which others can build.
It is well documented in the simulation literature that fidelity and realism are important concepts that need to be considered when planning simulation-based education (Oliver, 2002). And this was an initial concern by the educators. The lack of a physical ‘patient’ on which to carry out procedures and physical examination could limit the effectiveness of the telesimulation experience. To address this limitation, faculty briefed the learners about the limitations and the strategies, such as the use of a ‘nurse confederate’ to provide clinical information, as well as having visual cues such as pictures and videos to trigger their actions. Interestingly, the feedback suggests that the lack of a physical ‘patient’ to examine, resulted in more emphasis being placed on the audio and visual cues during the session. This allowed the learners to proactively compensate for the lack of tactile cues with audio and visual ones, reinforcing the importance of clinical alerts and alarms. The inability to perform a physical examination provided an opportunity for the debriefer to emphasise the importance of the skill in clinical care.
There was a deliberate attempt to create scenarios that were commonly seen in the ED in as much details as possible to achieve realism in the virtual space. This limited the scenarios that could be used as we had to use ensure procedures were not required for the patient management to progress (for example, trauma was deemed inappropriate). The faculty feel that the typical, non-complex ED scenarios compounded with the sequence of events as it would occur in real life possibly contributed to the student’s perception of realism during the telesimulation.
Instructional scaffolding was key to student engagement. The faculty configured the telesimulation session to be held after three weeks of interactive and didactic sessions on Zoom. This allows the learners to acquire essential knowledge which they can then apply during the telesimulation session. With the background baseline knowledge, the telesimulation setup and audio and visual prompts of a real ED environment, the faculty felt that they were able to immerse the students within the scenario rather than conducting it as an online Problem-Based-Learning session. This may have contributed to their engagement.
Communication skills were a common thread reported by the students, both positively and negatively in many of their statements. They described the shortcomings of communication over Zoom and felt that the session highlighted how non-verbal cues and the physical presence influences the way one communicates. At the same time, the absence of visual and tactile stimuli forced them to practice good communication to get their points across when managing the patients.
Interestingly, though many students scored high on the Likert scale about feeling confident in managing emergencies, with the open-ended questions, they reflected feelings of nervousness, fear and a lack of confidence to working in the ED, showing that perhaps this cannot replace patient contact.
Cognisant of the limitations of telesimulation, most of the learners enjoyed the session. This may have been due to the novelty of it and ED room mimics such as the beeping of the monitors and the realistic scenarios. Faculty also realise that the limitations of telesimulation and used them as discussion points to highlight elements that one may take for granted during their patient encounters, such as the non-verbal cues and the tactile stimuli.
Key to this successful telesimulation session was establishing realistic and focused objectives (Harden et al., 1999). Failing to recognise that telesimulation differs from conventional simulation and therefore emphasising on tactile skills such as procedures and physical examination will minimise the effectiveness of the session. Knowing the inherent limitations helped faculty to prepare holistically for the session. Learning objectives focused on non-tactile aspects, such as history taking and executing treatment algorithms. In addition, as tactile cues are limited in the telesimulation setting, all other cues such as visual and audio were optimised.
Debriefing during the telesimulation sessions has an even more vital role in student learning compared to conventional simulation sessions (Fanning & Gaba, 2007). The debriefer not only has to highlight salient clinical points regarding the case, but also probe learners to think about limitations of the telesimulation modality. Therein, understanding the importance of highlighting tactile and visual feedback. For example, one learner recognised that he was “unable to visually observe and direct the teammate”; another came to the conclusion that “being able to see the patient and physical expression of fellow doctors/nurses is crucial”. This allows the educator to discuss the importance of situational awareness and non-verbal cues in enhancing team dynamics. However, if the debriefer fails to address this limitation, the learners may leave the session feeling dissatisfied or inadequate with their performance at the session. The uniqueness of telesimulation adds another facet to debriefing where the debriefer needs to be able to address the limitations of telesimulation and relate it back to clinical relevance. Therefore, there might be a need to provide additional training for educators in debriefing telesimulation sessions.
Simulation-based training is an effective modality to teach procedural skills, put into practice treatment algorithms and hone soft-skill relevant to team dynamics. (Lateef, 2010; Sirimanna & Aggarwal, 2014). As demonstrated through this innovative programme, it has an important role to play in medical education during such a pandemic where it might be used to mitigate the negative educational impact of no patient contact, team-based training and protocol development and testing (Chaplin et al., 2020; Dieckmann et al., 2020). All this is done within a psychologically and physically safe environment.
Based on the feedback collected, a conceptual framework below (Figure 4) was drawn, showing the relationship between the concepts of fidelity and realism in the telesimulation experience to the level of engagement and therefore outcomes perceived by the learners. This is supported by the objectives, experiential learning and a safe learning environment.
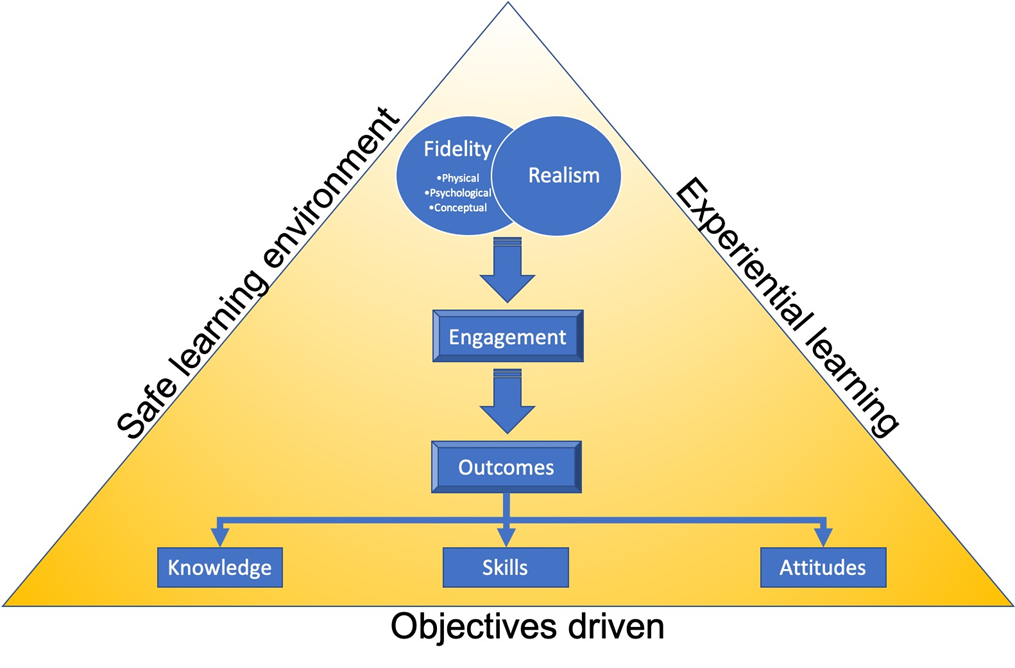
Figure 4. Conceptual framework
V. CONCLUSION
The role of face-to-face interactions with patients and immersing oneself in the acute care environment in bridging the theory to practice gap experienced by all healthcare students is essential to their clinical training. The restrictions encountered due to COVID-19 have required clinical educators to be agile and innovative in their approach the clinical clerkships. The EM clerkship telesimulation programme set out to provide an avenue for medical students to hone their clinical skills (history taking) and clinical reasoning (deriving differential diagnosis) in a safe environment. The evaluation of this programme has highlighted key areas of telesimulation which educators need to consider when planning to use it. The feedback from the students is promising and it highlights certain teaching points which may not be reflected upon during in-person simulation. Educators who wish to implement a telesimulation programme should pay particular attention to the learning objectives and debriefing methods. Whilst this paper has outlined how telesimulation can be implemented during a pandemic, it is envisaged that educators from other healthcare disciplines could use these findings to support the adoption of telesimulation in a variety of educational contexts. Telesimulation is a good alternative in settings such as this pandemic or during distance training programmes and may be a convenient way to hone history taking, clinical reasoning and communication skills without the use of an expensive simulation laboratory. The modality needs to meet the learning objectives and the debriefing should be adopted for telesimulation. However, the authors/faculty feel it cannot replace the full benefits of in-person simulation or learning from direct patient contact.
Notes on Contributors
Gayathri Devi Nadarajan and Kirsty J Freeman conceptualised the article, undertook the thematic analysis, contributed to article sections, and reviewed and revised manuscript based on suggestions from the other authors.
Lim Jia Hao, Wan Paul Weng and WONG Evelyn contributed to the conceptualisation of the paper, contributed to the article sections, reviewed and revised drafts.
Abegail Resus Fernandez undertook the quantitative analysis, and reviewed drafts.
All authors were involved in the development and delivery of the EM Clerkship Telesimulation Programme. All the authors have read and approved the final manuscript.
Ethical Approval
The SingHealth Centralised Institutional Review Board (CIRB) granted an exemption, CIRB Ref. No.: 2020/2719, as this study was assessed as a quality improvement project.
Data Availability
All relevant data are within the manuscript.
Acknowledgement
We would like to thanks the students who participated in this unit and their willingness to adapt to the online platform with grace and enthusiasm.
Funding
This work has not received any external funding.
Declaration of Interest
All authors declare that there are no conflicts of interest.
References
Benner, P. (2004). Using the dreyfus model of skill acquisition to describe and interpret skill acquisition and clinical judgment in nursing practice and education. Bulletin of Science, Technology and Society, 24(3), 188–199. https://doi.org/10.1177/0270467604265061
Chaplin, T., McColl, T., Petrosoniak, A., & Hall, A. K. (2020). Building the plane as you fly: Simulation during the COVID-19 pandemic. Canadian Journal of Emergency Medicine, 22(5), 576–578. https://doi.org/10.1017/cem.2020.398
Cohen, L., Manion, L., & Morrison, K. (2011). Research methods in education. Routledge. https://doi.org/10.4324/9780203720967
Dieckmann, P., Torgeirsen, K., Qvindesland, S. A., Thomas, L., Bushell, V., & Langli Ersdal, H. (2020). The use of simulation to prepare and improve responses to infectious disease outbreaks like COVID-19: Practical tips and resources from Norway, Denmark, and the UK. Advances in Simulation, 5(1), 1–10. https://doi.org/10.1186/s41077-020-00121-5
Dreyfuss, S. E., & Dreyfus, H. L. (1980). A five-stage model of the mental activities involved in directed skill acquisition. Berkeley. https://apps.dtic.mil/dtic/tr/fulltext/u2/a084551.pdf
Fanning, R. M., & Gaba, D. M. (2007). The role of debriefing in simulation-based learning. Simulation in Healthcare, 2(2), 115–125. https://doi.org/10.1097/SIH.0b013e3180315539
Harden, R. M., Crosby, J. R., & Davis, M. H. (1999). AMEE Guide No. 14: Outcome-based education: Part 1 – An introduction to outcome-based education. Medical Teacher, 21(1), 7–14. https://doi.org/10.1080/01421599979969
Kirkpatrick, D. L., & Kirkpatrick, J. D. (2009). Evaluating: Part of a ten-step process. In evaluating training programs. Berrett-Koehler Publishers.
Knowles, M. S. (1990). The adult learner: A neglected species. Gulf Publishing Co.
Kolb, D. A. (1984). The process of experiential learning. Experiential learning: Experience as the source of learning and development (pp. 20-38). Prentice Hall.
Lateef, F. (2010). Simulation-based learning: Just like the real thing. Journal of Emergencies, Trauma, and Shock, 3(4), 348. https://doi.org/10.4103/0974-2700.70743
McCoy, C. E., Sayegh, J., Alrabah, R., & Yarris, L. M. (2017). Telesimulation: An innovative tool for health professions education. Academic Emergency Medicine Education and Training, 1(2), 132–136. https://doi.org/10.1002/aet2.10015
Mikrogianakis, A., Kam, A., Silver, S., Bakanisi, B., Henao, O., Okrainec, A., & Azzie, G. (2011). Telesimulation: An innovative and effective tool for teaching novel intraosseous insertion techniques in developing countries. Academic Emergency Medicine, 18(4), 420–427. https://doi.org/10.1111/j.1553-2712.2011.01038.x
Naik, N., Finkelstein, R. A., Howell, J., Rajwani, K., & Ching, K. (2020). Telesimulation for COVID-19 Ventilator management training with social-distancing restrictions during the coronavirus pandemic. Simulation and Gaming, 51(4), 571–577. https://doi.org/10.1177/1046878120926561
Okrainec, A., Henao, O., & Azzie, G. (2010). Telesimulation: An effective method for teaching the fundamentals of laparoscopic surgery in resource-restricted countries. Surgical Endoscopy, 24(2), 417–422. https://doi.org/10.1007/s00464-009-0572-6
Oliver, R. G. (2002). Simulation-based medical education. In R. M. Harden & J. A. Dent (Eds.), A practical guide for medical teachers (4th ed., Vol. 29, Issue 2, pp. 226–233). Churchill Livingstone.
Papanagnou, D. (2017). Telesimulation: A paradigm shift for simulation education. Academic Emergency Medicine Education and Training, 1(2), 137–139. https://doi.org/10.1002/aet2.10032
Sa-Couto, C., & Nicolau, A. (2020). How to use telesimulation to reduce COVID-19 training challenges: A recipe with free online tools and a bit of imagination. MedEdPublish, 9(1), 1–7. https://doi.org/10.15694/mep.2020.000129.1
Sirimanna, P. V., & Aggarwal, R. (2014). Patient safety. In Levine, A., DeMaria, S., Jr., Schwartz, A. D., & Sim. A. J. (Eds.). The comprehensive textbook of healthcare simulation. Springer.
Smith, S. R., & Dollase, R. (1999). AMEE guide No. 14: Outcome-based education: Part 2 – Planning, implementing and evaluating a competency-based curriculum. Medical Teacher, 21(1), 15–22. https://doi.org/10.1080/01421599979978
*Gayathri Devi Nadarajan
Department of Emergency Medicine
Singapore General Hospital
1 Outram Road, Singapore 169608
Tel: +65 96804724
Email: gayathri.devi.nadarajan@singhealth.com.sg
Submitted: 14 August 2020
Accepted: 6 November 2020
Published online: 13 July, TAPS 2021, 6(3), 45-55
https://doi.org/10.29060/TAPS.2021-6-3/OA2377
Nathalie Khoueiry Zgheib1, Ahmed Ali2 & Ramzi Sabra1
1Department of Pharmacology and Toxicology, American University of Beirut Faculty of Medicine, Beirut, Lebanon; 2Medical Education Unit, American University of Beirut Faculty of Medicine, Beirut, Lebanon
Abstract
Introduction: The forced transition to online learning due to the COVID-19 pandemic has impacted medical education significantly.
Methods: In this paper, the authors compare the performance of Year 1 and 2 classes of medical students who took the same courses either online (2019-2020) or face-to-face (2018-2019), and compare their evaluation of these courses. The authors also present results of three survey questions delivered to current Year 1 medical students on the perceived advantages and disadvantages of online learning and suggestions for improvement.
Results: Performance and evaluation scores of Year 1 and 2 classes was similar irrespective of the mode of delivery of the course in question. 30 current (2019-2020) Year 1 students responded to the survey questions with a response rate of 25.4%. Some of the cited disadvantages had to do with technical, infrastructural and faculty know-how and support. But the more challenging limitations had to do with the process of learning and what facilitates it, the students’ ability to self-regulate and to motivate themselves, the negative impact of isolation, loss of socialisation and interaction with peers and faculty, and the almost total lack of hands-on experiences.
Conclusion: Rapid transition to online learning did not affect student knowledge acquisition negatively. As such, the sudden shift to online education might not be a totally negative development and can be harnessed to drive a more progressive medical education agenda. These results are particularly important considering the several disadvantages that the students cited in relation to the online delivery of the courses.
Keywords: Online Learning, COVID-19 Pandemic, Medical Students
Practice Highlights
- The authors report on the forced transition to online learning due to the COVID-19 pandemic.
- The performance and evaluation scores were similar in online delivery vs face-to face.
- The sudden shift to online education might not be a totally negative development despite the several disadvantages that students cited.
I. INTRODUCTION
The COVID-19 pandemic has impacted medical education significantly. Students were sent home and many schools were forced to shift their teaching, almost overnight, from face-to-face encounters to virtual, online delivery, in many cases without having had substantial previous experience with this mode of delivery. This disruption spanned the clinical and preclinical years. In previous events, researchers prioritised the synthesis of available evidence in terms of training medical students to respond and mitigate the effects of different types of disasters (Ashcroft et al., 2020). While there was more attention to find solutions for medical education in difficult settings (McKimm et al., 2019), including few examples that came to light after the outbreaks of H1N1 and H5N1 influenza, the severe acute respiratory syndrome (SARS) (Patil et al., 2003), and most recently, Ebola (Woodward & McLernon-Billows, 2018), there is paucity of literature that could inform adaptations of medical education methods during or post disasters, conflicts, or outbreaks. Recent articles have reflected on these changes and challenges and have suggested means of responding to the new reality, and offered advice on adopting new tools to ensure the best possible delivery of the curriculum (Daniel, 2020; Fawn et al., 2020; Liang et al., 2020; Ross, 2020; Sandars et al., 2020).
A recent meta-analysis that compared offline and online undergraduate medical education (under normal circumstances) revealed either no difference in outcomes on knowledge tests or a slightly higher performance for those who received online learning (Pei & Wu, 2019). In addition, a review of the literature showed that the adoption of E-Learning, in comparison with mostly traditional and other means of learning, expands access to education and increases the pool of faculty, in low resource settings (Frehywot et al., 2013). These data suggest that for preclinical education, there might not be a major negative impact of moving to online learning. It should be noted, however, that the situation brought about by the COVID-19 pandemic, which necessitated an abrupt transition to online education, may not be identical to that in which online delivery was a, planned and well-designed method to deliver at least part of the curriculum of the medical school; thus, the outcomes in knowledge acquisition during the recent COVID-19- forced transition to online teaching cannot be confidently predicted (Lim et al., 2009).
The American University of Beirut Faculty of Medicine (AUBFM), which follows the American model of medical education, suspended all in-person physical classes and assessments for years 1 and 2 on March 12, 2020. Thus, faculty, students and staff had to shift to online learning practically immediately. In this paper, we report our experience with this forced transition to online learning, specifically addressing Year 1 and 2 students’ perceptions of and response to it, and examining whether this transition affected their knowledge acquisition as reflected by their performance on written examinations.
II. METHODS
This is not a research study, as confirmed by our Institutional Review Board (IRB), since our purpose was to describe our experience with the delivery of the medical school curriculum after the sudden shift to online education, and whether that affected the students’ performance on their examinations and their evaluation of the courses. This was neither a planned intervention nor a systematic approach to test a specific hypothesis.
A. Setting
We analysed data from Year 1 and 2 classes of medical students who took the same courses either online (2019-2020) or face-to-face (2018-2019). We examined student performance in two courses, one for first year medical students (115 Class of 2022 students as face-to-face in 2018-2019 versus 118 Class of 2023 students as online in 2019-2020) entitled The Blood, and the other for second year medical students (114 Class of 2021 students as face-to-face in 2018-2019 versus 115 Class of 2022 students as online in 2019-2020) entitled Human Development and Psychopathology. Both courses are integrated modules that cover the histology, pathology, physiology, biochemistry, pathophysiology, pharmacology of the blood and lymphatic system and of neuropsychiatry, as well as the clinical, social, ethical, and behavioural aspects of related disorders.
Both courses extend over four weeks and end with a final summative examination. The main teaching activities consist of lectures and team-based learning (TBL) sessions, along with other small or large group discussions sessions dealing with epidemiology, evidence-based medicine, medical ethics, and social determinants of health relevant to the medical topics being covered.
The transition to online learning with the current medical students (2019-2020) was as follows: The didactic lectures were delivered either as asynchronous Voice-Over-PowerPoint (VOP) recordings or synchronous live lectures using Webex, which were recorded live. These recordings were made available to students on Moodle, the learning management system used at AUBFM. Faculty chose which of the two modes best suited them. As for the TBLs and group discussion sessions, they were run live using either Webex or Zoom applications. The latter was particularly appropriate for TBL sessions as it allowed virtual breakout rooms for team discussions.
The Respondus lockdown browser, with camera recordings serving as a virtual proctor, was adopted for written assessments, which included the individual Readiness Assurance Tests (i-RAT) of the TBLs as well as the final examinations. All these assessments utilise single-best answer multiple choice questions. Previous to the transition to online learning in 2018-2019, all i-RATs and group-RATs (g-RATs) were paper-based with physical proctoring, while the final course examinations, which used single best answer multiple choice questions, were computer-based, and were run on American University of Beirut (AUB) secure computers, also with physical proctoring.
Prior to COVID-19, final examinations were a hybrid of locally generated questions and National Board of Medical Examiners (NBME) customised examinations. During the COVID-19 pandemic, NBME examinations were not available and final examinations were totally locally generated. With regard to TBL’s, during the online transition, no g-RATs were performed due to our inability to ensure their security; thus, automatic feedback, which was an integral part of the TBL process, was not possible, and was replaced by a brief review of the questions by the TBL preceptor.
In addition, and in order to reduce the potential for cheating and communication among students, we reduced the time allotted for final examinations from 1.2 minutes per question to 1 minute per question. Reducing the on-line time during examinations was also done in order to minimise connectivity problems that arise due to the poor internet infrastructure in Lebanon and due to the frequent cuts in electricity.
B. Students’ Attitudes
At AUBFM, at the end of every course, students are expected to anonymously fill an online course evaluation form. This form includes twelve statements on various aspects of the course with which the students express a level of agreement (Sup. Table 1). Scores are assigned to their responses as follows: 1: Strongly disagree, 2: Disagree, 3: Neither agree nor disagree, 4: Agree, 5: Strongly agree. One of the items on that form (# 4) addresses the effectiveness of the teaching methods. An overall course rating is calculated as the average score for all 12 items. We compared the scores on both item #4 and the overall rating for the course given online (2019-2020) for both Year 1 and 2 medical students with the scores for the same course when delivered face-to-face (2018-2019).
Due to the lack of survey items that are specifically tailored to online teaching in the regular course evaluation forms, we asked the students to respond to 3 additional open-ended questions. This part was administered only to the current (2019-2010) first year medical students who had completed the Blood course and were the following:
1) In your opinion, what are the advantages of online teaching and learning over face-to-face teaching and learning?
2) In your opinion, what are the disadvantages of online teaching and learning over face-to-face teaching and learning?
3) Please provide suggestions for improvement of the online teaching and learning process.
C. Performance on the Final Examinations
Overall performance in the same courses was compared between the current classes (online) and the previous year’s classes (face-to-face). Thus, for the current Year 1 class (Class of 2023) the comparator class was the current Year 2 class (Class of 2022), and for the latter the comparator class was the current Year 3 class (Class of 2021). We restricted the comparisons of final examination grades to performance of the various classes on the locally generated questions.
In order to ensure that any two classes being compared did not differ in terms of academic or cognitive abilities, we also compared the performance of the current and the previous year’s classes according to: 1) their scores on the Medical College Admissions Test (MCAT) taken prior to admission to medical school; and 2) their overall grades in other courses that were given face-to-face during the current year (i.e. in the earlier part of the 2019-2020 academic year); these courses included one entitled Cellular and Molecular Basis of Medicine (CMM) given during year 1, and another entitled The Kidney and Urinary System given during year 2; these were the first courses to be delivered during the current year.
In comparing grades and scores on courses and examinations, we took into account the passing standards set for each. At AUBFM, we use criterion based absolute passing grades for every assessment. For written assessments such as final examinations using multiple choice questions, the Angoff method is utilised to set the passing grade. Similarly, the passing grade for a course is calculated based on the weighting of the individual assessment tools in that course. Thus, for any two courses or examinations that we compared, we first did the analysis using the raw grades, and then, when needed, we also compared the adjusted grades after equalising the passing grades.
D. Data Analysis
For the three survey questions, answers were downloaded on excel for systematic and iterative thematic analysis. Answers were manually coded by one of the authors. The compiled codes were then discussed, compared and consolidated into themes by two of the authors over 3 meetings. The focus was on main themes, commonalities and conflicting views of participants, and relationships between themes. Findings were tabulated with relevant quotes. For the evaluation scores and performance on exam, data were available on excel and statistical comparisons were conducted using the Student’s unpaired t-test.
III. RESULTS
A. Students’ Attitudes
Twenty-six of the 118 current medicine one student filled the survey, and four more sent an email to the course coordinator, the response rate is hence 24.5%. Several themes emanated for each of the three questions especially concerning disadvantages of online learning; these are tabulated in Table 1 with representative quotes. The main advantages of online learning were the time flexibility with asynchronous learning coupled with better overall well-being as a result of staying at home. VOPs were valued because they allowed students to control their learning pace.
As for disadvantages, there were several. These included: the loss of motivation, the potential for procrastination, the problems arising from a bad internet connection leading to greater internet costs, inadequacy of the home environment for learning, less interaction with teachers and students, paucity of immediate feedback, loss of hands on experiences, and struggles because of the faculty’s deficiencies in the area of information technology in general, and in online teaching, in particular.
The students made several suggestions to improve the process, and these included proposals for faculty development, and provision of better technical support and knowhow. In addition, they proposed to decrease or cancel synchronous lectures and provide all didactic lectures as VOPs, to be followed by synchronous online sessions for questions and feedback. They also proposed to imbed questions within the VOPs to stimulate students to think (akin to audience response polls used in live lectures), as well as forum discussions to increase interactions with peers and faculty. Students also insisted that they receive more detailed feedback on their performance on examinations and i-RAT questions.
Despite the many disadvantages cited and the clear room for improvement for online teaching and learning, the overall course ratings as well as the evaluation of teaching for the online courses were not different from their face-to-face counterparts (Tables 2 and 3).
|
Survey question |
Theme |
Quote |
|
Advantages of online teaching and learning in comparison to face to face teaching and learning |
Time flexibility with asynchronous learning |
“Better scheduling that allows us to sleep and rest at night in order to wake up better prepared to ace those PowerPoints” (S9) “Easier to manage our time” (S18) |
|
Control of learning pace with VOP |
“Being able to speed through slides/concepts we already understood and pausing and replaying concepts that we have trouble with makes the whole learning process a lot more efficient and focused” (S27) |
|
|
More wellbeing |
“Less time to commute which allows more time to rest and take care of oneself” (S9) “Having a very healthy diet with my family in the village” (S12) “The [exam] performance is better and stress in minimal” (S23) |
|
|
Disadvantages of online teaching and learning in comparison to face to face teaching and learning |
Potential for procrastination and loss of motivation |
“Less motivation, harder to follow the schedule, requires strong time management skills” (S5) “Face to face teaching helps me organize my day better” (S4) “Being at university with other students around studying during the day motivated me” (S26) |
|
Bad internet connection |
“Internet connection in our country is not stable to hold a class or an exam, so we are resorting to 3g/4g. This leads to a lot of extra expense” (S3) “Time consuming” (S2) and “Sessions would run for more than their original allocated time” (S3) “Longer exams might coincide with the times of the electricity shut offs. This would automatically freeze Respondus and the student will have to restart their computer and so on. Although we are given extra time this adds a lot of stress to an already stressful situation” (S19) “Asking questions are much more difficult and needs much more time” (S7) “WebEx needed a stronger Wi-Fi in some sessions which leads to a harder way to grasp the information” (S18) “The internet connection everywhere in Lebanon is not the best, sometimes we have trouble listening. Sometimes it also gets really crowded when everyone wants to talk at the at the same” (S21) |
|
|
Home environment less conducive to learning |
“Not everybody has the privilege of adjusting their environments to their liking, whether that be because of their dog barking or their family members not respecting their study time” (S28) “This experience helped my appreciate how much I concentrate better in the library” (S9)
|
|
|
Loss of interaction with teachers |
“No direct interaction, harder to communicate directly with professors” (S2) “Face to face interaction was lost: no clues to non-verbal clues, no gestures seen” (S17) “It is true that we can always email the doctors for any additional questions but that does not compare to in person interactions” (S19)
|
|
|
Loss of interaction with students |
“not being able to interact with my friends” (S12) “Students lose their social skills as they interact less with each other-more into introversion” (S17) “You feel there is a barrier between you and the students” (S17) |
|
|
Lack of immediate feedback |
“One problem is during exams not being able to see my mistakes” (S15) “Not correcting our exam and not seeing our mistakes was a huge disadvantage for the online learning” (S18) “Restricting questions to only emails” (S11) and “some professors don’t respond to emails” (S16) and “the response may be delayed” (S29) |
|
|
Loss of hands on experiences |
“No hands-on experience for courses like clinical skills” (S3) “Mainly missing out on clinical skills” (S22) |
|
|
Faculty’s lack of IT knowhow or experience |
“Professors have different abilities and effectiveness in knowing how to do a VOP/online lecture” (S11) “Most Drs. don’t know how to use zoom or WebEx” (S6) “Many instructors are not technically inclined or are outright aversive to it” (S13) “So much time is wasted on technical issues” (S19) “Professors sometimes don’t see the raised hands and sometimes it doesn’t even work. In some lectures we had to wait for the professor to give us access, so we spent time waiting while they didn’t see that some people are trying to access the lecture” (S21) “One of the disadvantages is using the live WebEx sessions. Some professors are losing their recordings, others have a poor connection” (S23) |
|
|
Effect on faculty’s teaching skills |
“Some professors …just read instead of teaching” (S7) “Many professors are not exactly cooperative in terms of explaining mainly because they read their PowerPoints” (S23) “Can’t explain a topic and be passionate about it if talking to a screen or microphone” (S23) |
|
|
Suggestions to improve the current online teaching |
Technical support and knowhow |
“Train the staff on the proper way of utilising the platforms” (S2) “Make IT staff more readily available to help instructors” (S16) “Agree on one way to give the lecture via WebEx as some professors used WebEx team, where we had to ask permission for access, and it was kind of chaotic. It would also be better if the professor agreed on one way to have the questions asked to avoid interruptions and multiple people talking at the same time” (S21) |
|
More VOPs and less WebEx for lectures |
“I think VOP is a much safer option and a less tiring one” (S23) “Revert from live WebEx sessions to VOP” (S3) |
|
|
More interaction and immediate feedback |
“Open forums for discussion” (S3) “Adding analytical questions in PowerPoints” (S9) “See exams and mistakes” (S15) “If the professors want to use WebEx … then they should allow questions at all times and not only at the end of the session” (S11) “Include small assessment questions (clicker like questions) at the end of each major concept so that the students can assess their understanding” (S19) “Recording voice over PowerPoint for lectures, with every group of lectures followed by a WebEx session where the professor answers questions” (S24) “Review/Q&A session once a week” (S25) |
Table 1. Themes Generated from the Three Survey Questions with Selected Representative Quotes
VOP: Voice Over PowerPoint
|
Medicine class of |
2022 |
2023 |
P-value |
|
Academic Year 1 |
2018-2019 |
2019-2020 |
|
|
Number of students |
115 |
118 |
|
|
|
Baseline performance |
||
|
MCAT scores |
509±6 |
510±6 |
0.119 |
|
Class average on the final exam of the CMM course |
82.6±6.1 |
84.3±7.4 |
0.011 |
|
Passing grade for the final exam of the CMM course |
64.1 |
64.7 |
|
|
Adjusted grade for the final exam of the CMM coursea |
83.2±6.1 |
84.3±7.4 |
0.065 |
|
|
Performance in The Blood course |
||
|
Course delivery |
Face to Face |
Online |
|
|
Number of questions on the final exam |
50 |
77 |
|
|
Class average on the final exam |
83±9 |
81±9 |
0.043 |
|
Passing grade for the final exam |
65 |
61 |
|
|
Adjusted grade for the final exama |
83±9 |
85±9 |
0.091 |
|
|
Student Evaluation of The Blood Course |
||
|
Rating of teaching methods |
4.0±0.8 |
4.0±1.0 |
0.920 |
|
Overall course rating |
4.0±0.7 |
4.1±0.8 |
0.754 |
Table 2. Comparison of Performance of Year 1 Students in Various Courses and Examinations and Their Evaluation of the Blood Course
Data are presented as Mean ± Standard Deviation
P-values were generated by Student’s unpaired t-test
MCAT: Medical College Admissions Test; CMM: Cellular and Molecular Basis of Medicine
aadjusted after equalizing the passing grades on the examinations in the 2 different years
|
Medicine class of |
2021 |
2022 |
P-value |
|
Academic Year 2 |
2018-2019 |
2019-2020 |
|
|
Number of students |
114 |
115 |
|
|
|
Baseline performance |
||
|
MCAT scores |
509±5 |
509±6 |
0.842 |
|
Class average on the final exam of the CMM course |
83.8±6.4 |
82.6±6.1 |
0.156 |
|
Passing grade for the final exam of the CMM course |
65.3 |
64.1 |
|
|
Adjusted grade for the final exam of the CMM coursea |
82.6±6.4 |
82.6±6.1 |
0.455 |
|
Performance on the final exam of The Kidney course |
78.1±7.9 |
78.7±7.2 |
0.558 |
|
Passing grade for the final exam of The Kidney course |
62.2 |
62.3 |
|
|
|
Performance in the Human Development and Psychopathology course |
||
|
Course delivery |
Face to Face |
Online |
|
|
Number of questions on the final exam |
45 |
75 |
|
|
Class average on the final exam |
83.7±7.4 |
83.5±6.8 |
0.892 |
|
Passing grade for the final exam |
68.0 |
64.8 |
|
|
Adjusted grade for the final exama |
83.7±7.4 |
86.7±6.8 |
0.002 |
|
|
Student evaluation of the Human Development and Psychopathology course |
||
|
Rating of teaching methods |
4.2±0.9 |
4.1±0.9 |
0.426 |
|
Overall course rating |
4.3±0.7 |
4.1±0.8 |
0.251 |
Table 3. Comparison of Performance of Year 2 Students in Various Courses and Examinations and Their Evaluation of the Human Development and Psychopathology Course
Data are presented as Mean ± Standard Deviation
P-values were generated by Student’s unpaired t-test
MCAT: Medical College Admissions Test; CMM: Cellular and Molecular Basis of Medicine
aadjusted after equalizing the passing grades on the examinations in the 2 different years
B. Performance of Students in the Courses and Examinations
As shown in Tables 2 and 3, there were no statistically significant differences in the MCAT scores between any two classes that were compared. The performance of the Year 1 students on the CMM course during the current academic year (online) was higher than that of students during the previous year (face-to-face); however, the passing grade for the two courses was slightly different. When the passing grades were equalised, there was no longer a difference between the two classes. Similarly, there was no difference in the performance of the Year 2 students on either the CMM course they took in Year 1, or on The Kidney and Urinary System course between the current class and the previous year’s class (all face-to-face).
With regard to The Blood course, the grade on the final examination was significantly lower for current students (online) relative to their predecessors (face-to-face); however, the passing grades on these examinations were different, with the current year’s examination having a lower passing grade than last year’s. When the passing grades were equalised, there was no longer a difference in the performance on the final examination.
The performance of the students in the Human Development and Psychopathology course’s final examination was almost identical in the online group compared with their predecessors (all face-to-face). Interestingly, the passing grade on this year’s examination was lower than that on last year’s examination, such that when the passing scores were equalized, the current class had better performance on the final examination than last year’s class.
IV. DISCUSSION
Medical education scholars have been increasingly disseminating opinions about sudden transitioning to online education to COVID-19 and the adaptations that are being implemented. Few studies have documented the actual institutional experiences, the perspectives of students, and the lessons learned in different medical courses or curricula such as TBL (Gaber et al., 2020), anatomy (Srinivasan, 2020) and continuing medical education in obstetrics and gynaecology (Kanneganti et al., 2020). Only one report from Wuhan, China, evaluated nursing interns’ outcomes on emergency medicine theoretical and practical examination scores (Zhou et al., 2020). The current paper is the first to examine the impact of this abrupt transition to online learning, which occurred in numerous countries worldwide, on the performance of our medical students in knowledge-based examinations. It reveals that the sudden shift to full online learning that our medical school had to adopt did not have a negative influence on the students’ knowledge acquisition as judged by their performance on final examinations. It also did not affect their overall reception and evaluation of the courses. These results are particularly interesting and important considering the many disadvantages that the students cited in relation to the online delivery of the courses.
Many of the limitations and disadvantages of online education cited by students had to do with technical and infrastructural matters and with faculty know-how and IT support. These are problems that can, theoretically, be easily remedied. The more challenging, however, limitations had to do with the process of learning, what facilitates or hampers it, the students’ ability to self-regulate and to motivate themselves, the negative impact of isolation, loss of socialisation and interaction with peers and faculty, and the almost total lack of hands-on experiences.
These limitations did not affect the students’ ability to achieve learning, at least in the domain of knowledge acquisition and application. It is clear that students in the three classes that were examined had, at baseline, a similar level of achievement meaning that any differences in student performance in the courses that were given online this year cannot be ascribed to differences in the academic performance or ability of the students. Therefore, the lack of difference in performance between classes taking the course online versus those taking it face-to-face suggests a consistency in performance that was not affected adversely by the sudden transition to online learning.
One reason for this lack of difference in performance between online and face-to-face delivery of the courses may be that the outcomes that were being sought and assessed were essentially knowledge acquisition and knowledge application. This agrees with the overall results of multiple studies that compared online vs offline learning in medical school, and which, in fact, tended to favour online learning (Pei & Wu, 2019). Indeed, even before our sudden shift to total online education, many of our students had adopted their own approaches to achieve the knowledge learning outcomes. Even though lectures were not available online, attendance at face-to-face lectures (which was not mandatory) was never complete, and for the majority of students, the rate of attendance ranged between 25% and 75% (unpublished data). In fact, the students indicated that they depended instead on notes and voice recordings made during the lecture that were shared by their classmates or predecessors, and that they used several Web-based resources. In contrast, attendance at TBL exercises and other interactive and small group sessions is mandatory at our school, and students uniformly participated in them, as they did in the online Zoom-based sessions. Thus, our students were probably well prepared for this sudden shift. In line with this view, Ferrel and Ryan (2020), in a recent editorial on the impact of COVID-19 on medical education, predicted that many medical students in their didactic years may perceive little change in their study schedule, since many of them already use outside resources and watch school lectures after they have been presented.
The lack of significant differences in scores and attitudes may also attest to our – and indeed all – medical students’ resilience and adaptability to difficult situations, for they are high-achieving and resourceful students who have been selected from among an exceedingly competitive group of applicants, and likely have the cognitive powers and non-cognitive qualities to meet such challenges. Ferrel and Ryan (2020) also emphasised the need for medical students to adapt and be innovative during the pandemic, and to devise ways by which they can exhibit their skills, work ethics and teamwork. In fact, one of the advantages of the online shift that our students cited was the flexibility this approach afforded them in managing their time, setting their schedules, controlling their pace of learning and achieving better self-care. Nevertheless, some of them found it challenging to do so, and to regulate their environment and motivate themselves; rather, they seemed to require external cues or assistance to get into a learning mode, and found difficulty in establishing boundaries between work and home, as suggested recently by Rose (2020). In this context, it is noteworthy that our students preferred asynchronous to synchronous learning, and this is consistent with Daniel’s recommendation to use this approach because it gives teachers “flexibility in preparing learning materials and enables students to juggle the demands of home and study” (Daniel, 2020).
Our findings also raise questions about certain assumptions regarding student learning and the optimal teaching approaches for knowledge-based objectives, such as the value and benefits of face-to-face interactions among students and with faculty in a didactic context. Our results suggest that students can achieve these knowledge objectives without the personal interaction and contact with faculty. This, of course, does not address the non-cognitive learning outcomes that might be negatively affected by pure online learning. As summarised by Fawn et al. (2020), while content may be covered well in such abrupt transitions to online learning, we cannot be sure that the valuable non-cognitive learning that happens as a result of the “social activity, the relationship-building, the problem-solving, the dialogue and generation of ideas and the students’ own discovery of other content that has not been pre-defined by the teacher” has been achieved.
We cannot make definite, long-term conclusions from this single account that is restricted to 2 courses in the preclinical years, a brief period of time, and one institution, and a low response rate for the survey questions, but the results are encouraging, and may have implications for educational practice. The lack of decline in cognitive performance may suggest that the sudden shift to online education might not be a totally negative development. If our findings are reproduced or generalised, one can use them to validate what progressive medical educators have been advocating for years, that: online educational technology must change the way we educate our students; didactic lecturing should give way to flipped classrooms; and valuable teacher time must be expended to help students apply knowledge rather than to simply transfer information in scheduled lectures. Quoting Ezekiel Emanuel (2020), who in a recent article stated that the reconfiguration of medical education, fuelled by online educational technology, seemed inevitable, Wolanskyj-Spinner (2020) suggested that the coronavirus epidemic appears to be an inflection point that is forcing a disruption in how we teach medicine. At AUBFM, we have long pressed the faculty who teach medical students to record their lectures and use the scheduled class time thus saved to implement flipped classrooms, employing small-group-based, problem-solving and interactive sessions. While many responded, many also hesitated, objected, and even resisted. The following two additional comments provided by two students illustrate their frustration with the resistance of faculty and their hopes to move in that direction:
“I really hope we can make online learning standard coming out of this phase … There was an attempt a few years ago but many instructors refused to be recorded or to fiddle with computers; we must seize the opportunity now.”
“Please never stop recording lectures, regardless of the status of live classes!”
Ahmed et al. (2020) recently reported that during the 2003 SARS epidemic in China, novel online problem-based learning techniques had to be implemented in one medical school that proved to be so popular that they were applied as part of the regular curriculum in later years. We believe that medical educators can harness the current disruption in how we teach medical students, and make use of to implement novel and sound educational practices and adopt a wide variety of valid approaches and tools that, otherwise, might have been resisted by unwilling individuals with entrenched ideas.
V. CONCLUSION
In conclusion, rapid transition to online learning did not affect student knowledge acquisition negatively. As such, the sudden shift to online education might not be a totally negative development and can be harnessed to drive a more progressive medical education agenda. These results are particularly important considering the several disadvantages that the students cited in relation to the online delivery of the courses.
Notes on Contributors
Nathalie Zgheib developed the concept, collected and analysed data, and wrote the first draft of the manuscript. Ahmed Ali also developed the concept, performed the literature review, and revised the manuscript write-up. Ramzi Sabra also developed the concept, collected and analysed data, and revised the manuscript write-up. The three authors read and approved the final version of the manuscript.
Data Availability
The data that support the findings of this manuscript are available from the corresponding author upon reasonable request.
Ethical Approval
This is a report of experience with educational practices. It was confirmed by our Institutional Review Board (IRB) that the activities described in this article do not constitute human subject research.
Acknowledgments
The authors wish to thank AUBFM faculty and medical students for their support, diligence and flexibility during the COVID-19 pandemic.
Funding
This study did not receive any funding.
Declaration of interest
The authors do not have any conflict of interest to declare.
References
Ahmed, H., Allaf, M., & Elghazaly, H. (2020). COVID-19 and medical education. The Lancet Infectious Diseases, 20(7), 777-778. https://doi.org/10.1016/S1473-3099(20)30226-7
Ashcroft, J., Byrne, M. H. V., Brennan, P. A., & Davies, R. J. (2020). Preparing medical students for a pandemic: A systematic review of student disaster training programmes. Postgraduate Medical Journal, Advance online publication. https://doi.org/10.1136/postgradmedj-2020-137906
Daniel, S. J. (2020). Education and the COVID-19 pandemic. Prospects, 49, 91-96. https://doi.org/10.1007/s11125-020-09464-3
Emanuel, E. J. (2020). The inevitable reimagining of medical education. Journal of the American Medical Association, 323(12), 1127-1128. https://doi.org/10.1001/jama.2020.1227
Fawn, T., Jones, D., & Aitken, G. (2020). Challenging assumptions about “moving online” in response to COVID-19, and some practical advice. MedEdPublish, 9(1), 83. https://doi.org/10.15694/mep.2020.000083.1
Ferrel, M. N., & Ryan, J. J. (2020). The impact of COVID-19 on medical education. Cureus, 12(3), e7492. https://doi.org/10.7759/cureus.7492
Frehywot, S., Vovides, Y., Talib, Z., Mikhail, N., Ross, H., Wohltjen, H., Koumare, A. K., & Scott, J. (2013). E-learning in medical education in resource constrained low- and middle-income countries. Human Resources for Health, 4(11), 4. https://doi.org/10.1186/1478-4491-11-4
Gaber, D. A., Shehata, M. H., & Amin, H. A. A. (2020). Online team-based learning sessions as interactive methodologies during the pandemic. Medical Education, 54(7), 666-667. https://doi.org/10.1111/medu.14198
Kanneganti, A., Lim, K. M. X., Chan, G. M. F., Choo, S. N., Choolani, M., Ismail-Pratt, I., & Logan, S. J. S. (2020). Pedagogy in a pandemic – COVID-19 and virtual continuing medical education (vCME) in obstetrics and gynecology. Acta Obstetetricia et Gynecologica Scandinavica, 99(6), 692-695. https://doi.org/10.1111/aogs.13885
Liang, Z. C., Ooi, S. B. S., & Wang, W. (2020). Pandemics and their impact on medical training: Lessons from Singapore. Academic Medicine, 95(9), 1359-1361. https://doi.org/10.1097/ACM.0000000000003441
Lim, E. C., Oh, V. M., Koh, D. R., & Seet, R. C. (2009). The challenges of “continuing medical education” in a pandemic era. Annals of Academic Medicine Singapore, 38(8), 724-726.
McKimm, J., Mclean, M., Gibbs, T., & Pawlowicz, E. (2019). Sharing stories about medical education in difficult circumstances: Conceptualizing issues, strategies, and solutions. Medical Teacher, 41(1), 83-90. https://doi.org/10.1080/0142159X.2018.1442566
Patil, N. G., Chan, Y., & Yan, H. (2003). SARS and its effect on medical education in Hong Kong. Medical Education, 37(12), 1127-1128. https://doi.org/10.1046/j.1365-2923.2003.01723.x
Pei, L., & Wu, H. (2019). Does online learning work better than offline learning in undergraduate medical education? A systematic review and meta-analysis. Medical Education Online, 24(1), 1666538. https://doi.org/10.1080/10872981.2019.1666538
Rose, S. (2020). Medical student education in the time of COVID-19. Journal of the American Medical Association, 323(21), 2131-2132. https://doi.org/10.1001/jama.2020.5227
Ross, D. (2020). Creating a “quarantine curriculum” to enhance teaching and learning during the COVID-19 pandemic. Academic Medicine, 95(8), 1125-1126.
Sandars, J., Correia, R., Dankbaar, M., de Jong, P., Sun Goh, P., Hege, I., Oh, S., Patel, R., Premkumar, K., Webb, A., & Pusic, M. (2020). Twelve tips for rapidly migrating to online learning during the COVID-19 pandemic. MedEdPublish, 9(1), 82. https://doi.org/10.15694/mep.2020.000082.1
Srinivasan, D. K. (2020). Medical students’ perceptions and an Anatomy teacher’s personal experience using an e-learning platform for tutorials during the Covid-19 crisis. Anatomical Sciences Education, 13(3), 318-319. https://doi.org/10.1002/ase.1970
Wolanskyj-Spinner, A. (2020). COVID-19: The global disrupter of medical education. ASH Clinical News, https://www.ashclinicalnews.org/viewpoints/editors-corner/covid-19-global-disrupter-medical-education/
Woodward, A., & McLernon-Billows, D. (2018). Undergraduate medical education in Sierra Leone: A qualitative study of the student experience. BMC Medical Education, 18(1), 298. https://doi.org/10.1186/s12909-018-1397-6
Zhou, T., Huang, S., Cheng, J., & Xiao, Y. (2020). The distance teaching practice of combined mode of massive open online course micro-video for interns in emergency department during the COVID-19 epidemic period. Telemedicine Journal and E-Health, 26(5), 584-588. https://doi.org/10.1089/tmj.2020.0079
*Ramzi Sabra
Department of Pharmacology and Toxicology,
Faculty of Medicine,
American University of Beirut,
PO. Box 11-0236, Riad El Solh,
Beirut, Lebanon
Tel: +961-1-350000 Ext: 4848
Email: rsabra@aub.edu.lb
Submitted: 28 August 2020
Accepted: 3 March 2021
Published online: 13 July, TAPS 2021, 6(3), 32-44
https://doi.org/10.29060/TAPS.2021-6-3/OA2385
Judy McKimm1, Subha Ramani2 & Vishna Devi Nadarajah3
1Swansea University Medical School, United Kingdom; 2Harvard Medical School, United States of America; 3International Medical University, Malaysia
Abstract
Introduction: The COVID-19 pandemic has caused huge change and uncertainty for universities, faculty, and students around the world. For many health professions’ education (HPE) leaders, the pandemic has caused unforeseen crises, such as closure of campuses, uncertainty over student numbers and finances and an almost overnight shift to online learning and assessment.
Methods: In this article, we explore a range of leadership approaches, some of which are more applicable to times of crisis, and others which will be required to take forward a vision for an uncertain future. We focus on leadership and change, crisis and uncertainty, conceptualising ‘leadership’ as comprising the three interrelated elements of leadership, management and followership. These elements operate at various levels – intrapersonal, interpersonal, organisational and global systems levels.
Results: Effective leaders are often seen as being able to thrive in times of crisis – the traditional ‘hero leader’ – however, leadership in rapidly changing, complex and uncertain situations needs to be much more nuanced, adaptive and flexible.
Conclusion: From the many leadership theories and approaches available, we suggest some specific approaches that leaders might choose in order to work with their teams and organisations through these rapidly changing and challenging times.
Keywords: Leadership, Followership, Management, Health Professions Education, Change, Crisis, Uncertainty, Emotional Intelligence, COVID-19 Pandemic, Universities
Practice Highlights
- In rapid change and uncertainty, different leadership approaches are needed.
- Primal leadership and emotional intelligence are essential.
- Followers need to feel safe, physically and psychologically.
- Authentic and inclusive leadership draws from diverse views.
- Adaptive and regenerative leadership acknowledges interrelated systems.
I. INTRODUCTION
The COVID-19 pandemic has caused huge change and uncertainty for universities and their stakeholders around the world. For many health professions education (HPE) leaders, the pandemic has caused an unforeseen crisis, the ripples from which will probably be felt for years to come. Effective leaders are often seen as being able to thrive in times of crisis – the traditional ‘hero leader’ – however, leadership in rapidly changing, complex and uncertain situations need to be much more nuanced and flexible. In this article we explore leadership approaches, some of which are more applicable to times of crisis, and others which will be required to take forward a vision for the ‘new normal’ to ensure that we learn from our experiences during the pandemic.
In this article we focus on leadership and change. We start with an overview of the leadership triad, a discussion of the educational challenges imposed by the COVID-19 pandemic, followed by detailed discussion of effective leadership styles and competencies during challenging situations, approaching these through three lenses: Intrapersonal, referring to characteristics that successful leaders possess; interpersonal, referring to leadership styles and approaches leaders can adopt when they interact with others; and system level, which refers to leadership attributes to effectively lead organisations during a crisis. We conceptualise ‘leadership’ as comprising three interrelated elements: leadership, management, and followership (see Figure 1), which we call the ‘leadership triad’ (McKimm & O’Sullivan, 2016).

Figure 1: The Leadership Triad
Note: From “When I say … leadership,” by J. McKimm, and H. O’Sullivan, 2016, Medical Education, 50(9), 896–897. https://doi.org/10.1111/medu.13119
Leadership is about change and movement, putting the power and energy into a system or initiative, whereas management provides the means of enacting the leadership vision and making change happen. Leadership is always about ‘people’ (motivating them towards goals or activities) whereas management is about systems, processes and policies and we structure the article around this approach (Scouller, 2011). Followership provides the leadership with the ‘people power’ to enact the change; without followers, leadership cannot happen as leaders cannot do everything themselves. Even the most senior leaders do not ‘lead’ all the time, in ‘real life’ we move around these three elements as we lead, manage, and follow in various situations.
As leaders in HPE ourselves (Refer to Appendix A), we reflect and ask, what can a leader do during this period to ensure the best interest of all stakeholders? What lessons can we offer from our own experiences and the experiences of other leaders to those who need guidance to weather and even thrive after the crisis? The approach we have taken is to first examine the major challenges facing health professions’ leaders during this crisis, we then offer specific leadership approaches that can effectively address these challenges, concluding with change management approaches required to prepare and sustain the new normal.
II. CRISIS AND CHALLENGES FOR HEALTH PROFESSIONS EDUCATION
2020 has been a hugely challenging year for all higher education leaders across the world. From managing the rapid switch to online learning, answering student calls for some form of refund or reduction in fees, to expanded support for students and staff including emotional support, the COVID-19 pandemic has forced educational leaders to manage a different type of crisis altogether.
HPE leadership has been hugely tested during the pandemic ‘crisis’ which is very different from leading in ‘normal’ times. How do we define a crisis? A crisis is any event that could lead to an unstable, difficult and/or dangerous situation affecting an individual, group, community, or whole society. It means that difficult or important decisions must be made amidst great uncertainty and lack of information about what the future might hold. In the middle of a crisis everything can feel like it is failing or impossible. The pandemic accelerated and exacerbated many of the challenges already being experienced in HPE, including the rising costs of operating universities, increase in tuition fees and accessibility to higher education, and competition from commercial and online learning providers. Leaders in HPE face additional and different sets of challenges, as they service and are dependent on both the education and health care sectors for student education and postgraduate training. The crisis is not only experienced at organisational or team level, but the pandemic has also impacted individuals (students, academic faculty, clinical teachers, and healthcare staff) whose normal coping mechanisms may be insufficient.
However, this is not all negative and leaders need to tap into a growth mind-set, which has been defined as one that views failure and challenges as learning opportunities (Dweck, 2016). For example, Kanter (2020) suggests that it is possible to come out of a crisis stronger than before if leaders operate with a ‘people first culture’ and pay ‘attention to three things: establish clear accountability in the leadership ranks; develop a nuts-and-bolts, collaborative plan for getting through the crisis; and appoint a separate group in charge of defining the “new normal,” when the worst is over’.
It is also important to recognise that the pandemic (set alongside climate change and causes related to systemic social injustices) has foregrounded and increased awareness on inequalities across the globe in many areas, including HPE. Leadership in these times needs to pay close attention to this and seize the moment to facilitate and mobilise real change within their institutions or communities. Perhaps more so when such institutions train future health professionals and develop future leaders, who need to believe that a positive change is possible and that their own cultural context can be celebrated.
III. WHAT SORT OF LEADERSHIP IS NEEDED TO ADDRESS THESE CHALLENGES?
Inevitably changes are to be expected as the impact of the pandemic is unprecedented and is a matter of national security and public health. In most countries, governance and decision making during this crisis will be by National security councils with advisories or guidelines offered by ministries of health higher education, home affairs, or other relevant bodies. This means that universities and educational leaders who usually have autonomy in decision making are subject to stricter controls and frequent changes from authorities who are understandably making decisions at national and international levels. For people in leadership positions, this is unchartered territory and given the ‘traditional’ power and authority hierarchies and processes in higher education and health professions education, it is unsurprising that leaders may feel helpless during a crisis such as this. In Figure 2, we list four levels along which leadership needs to be enacted, and some suggested approaches to help leaders move out of this feeling of helplessness so that they can lead the people for whom they are responsible.
Figure 2: Four levels of leadership for addressing challenges during a crisis
Note: Drawing from “ABC of clinical leadership,” by T. Swanwick and J. McKimm, 2017, John Wiley & Sons.
A. The Intrapersonal Level: Working with Emotional and Social Intelligence
Challenging circumstances which force change, such as the COVID-19 pandemic, result in a range of emotional responses among leaders and all those for whom they are responsible.
In 1998, Daniel Goleman proposed that leadership skills such as toughness, vision, determination, and intelligence alone are insufficient. He stated that the most successful leaders also possess a high degree of emotional intelligence (EI) which includes the traits of self-awareness, self-regulation, motivation, empathy, and social skills (Goleman, 1998). Boyatzis and Goleman went to analyse the core attributes that were present in those identified by a variety of companies as their most successful leaders. As a result, twelve competencies of emotional and social intelligence were described under four domains and depicted in Figure 3. The four domains include: Self-awareness, self-management, social awareness, and relationship management; these are critical attributes for leaders to operate effectively through own and others’ emotions during challenging circumstances such as the COVID-19 pandemic. These competencies and behaviours help to simplify a complex construct such as EI and can facilitate leadership development in this area.
Figure 3: Intrapersonal leadership attributes: Emotional and social intelligence competencies essential to lead and manage change during challenging circumstances.
Note: Adapted from “Competencies as a behavioral approach to emotional intelligence,” by R. E. Boyatzis, 2009, Journal of Management Development, 28(9), 749–770. https://doi.org/10.1108/02621710910987647
While the construct of EI and competencies can serve as a useful guide to leaders in leading and managing change, the actual behaviours that are most effective depend on the organisational culture and the societal culture within which an organisation is situated. Moreover, at institutions which feature diversity in the composition of its leaders, staff and learners, leaders should recognise that individuals on a team might have different emotional reactions even when working towards a common goal. All four domains of EI competencies are essential for leaders to manage the groups of people they lead (See Table 1).
|
1. Self-awareness allows leaders to recognise their assumptions and biases, and how they affect their worldview. 2. Self-management promotes thought before action and ability to manage own emotions and reactions, important in reigning in negative emotion. 3. Social awareness allows leaders to understand the individuals who make up their team and recognise differences in viewpoints and personalities. 4. Relationship management is essential to welcome a variety of perspectives, nurture talent, and maximise the potential and productivity of individuals, teams, and the organisation. Mentoring and coaching skills fall under this domain.
|
Table 1: The impact of the four EI domains
A. The Interpersonal Level: Influencing Others and Drawing on Their Individual and Collective Strengths
In rapid change and uncertainty, what people want from their leaders is an authentic voice and to feel that leaders are listening, taking their concerns seriously and that they have the expertise and authority to lead and manage change. Leaders are created and maintained by how their followers see, relate to, and trust them (Uhl-Bien & Carsten, 2018). Simon Sinek talks about how followers will follow their leaders into highly unsafe situations (such as war) if they feel their leaders can keep them safe and that they are ‘in it’ together (Sinek, 2014). Whilst internally, leaders may feel as lost and at sea as those for whom they are responsible, they must draw on their own resilience and ‘grit’ (Duckworth & Duckworth, 2016) to step up and provide effective leadership. This involves displaying courage, putting personal interests aside to achieve what needs to be done and acting on convictions and principles even when it requires personal risk-taking. In crisis or uncertainty, followers need leaders who can communicate clearly, transparently, and regularly, who can make decisions (even if these are unpopular or later change) and who look out for and care for them (Paixão et al., 2020).
Primal leadership, described by EI experts, emphasises that leaders’ emotional affect and mood is a major driver of the mood and behaviours of others around them (Goleman et al., 2001). Thus, during a crisis, leaders need to be optimistic, yet, authentic and realistic. Positive emotion or resonance is critical to motivate people, allow them to be productive amidst chaos and preserve their wellbeing. As the pandemic spread around the world, some academic leaders demonstrated a highly person-centred approach in relation to staff and students, recognising their fears and anxieties, encouraging virtual education and work whenever possible, thus demonstrating primal leadership as well as cultural intelligence (Liao & Thomas, 2020; Velarde et al., 2020). If we want people to work interprofessional, pay attention to well-being and motivation, and work together to meet organisational goals, then flattening hierarchies is essential to generate ideas and functional collaboration (Barrow et al., 2011; Barrow et al., 2014) (Refer to Appendix B).
Whilst leaders may need to take a ‘command and control’ type of leadership in times of great crisis because important decisions must be taken and communicated quickly, after the immediate crisis other approaches will be helpful. For example, authentic, altruistic, person-centred, and inclusive leadership (Avolio & Gardner, 2005; Cardiff et al., 2018; Hollander, 2012; Sosik et al., 2009) approaches are very much focussed on the leader drawing from their own strengths and, through awareness and acknowledgement of their own weaknesses and biases, proactively seeking a range of perspectives on issues and demonstrating that they value and listen to those around them. When leaders are trying to make impactful decisions in times of uncertainty, having a range of views and ideas is essential. Leaders may also need to show intellectual humility – admitting mistakes, learning from criticism and different points of view, and acknowledging and seeking contributions of others to overcome limitations. As tasks are defined, leaders need to empower and demonstrate their confidence in people by delegating and holding them responsible for activities they can control.
B. The Complex Organisation or System Level: Adaptive Leadership
While conventional approaches to leadership and management have their place, as the pandemic elapsed around the world leaders needed to be highly adaptive and flexible, adjusting their outcomes and approaches based on rapidly changing information. Because we live in a VUCA (Volatile, Uncertain, Complex, Ambiguous)
(Worley & Jules, 2020) and RUPT (Rapid, Uncertain, Paradoxical, Tangled) (Till, Dutta, McKimm, 2016) world, leadership is needed that is flexible and agile enough to adapt to circumstances which most HPEs have not experienced before.
Adaptive leadership (Heifetz et al., 2009; Randall & Coakley, 2007) is specifically focussed on leadership in complex systems or situations and is helpful when thinking about how to respond to change, uncertainty, and crisis. Adaptive leaders do not simply work in a technical way (by just applying familiar management processes and ways of working) but involve people throughout the organisation to help solve ‘wicked’ problems, which may not have a clear solution and may require new ways of working. Adaptive leaders create the organisational conditions that enable dynamic networks and environments to achieve agreed goals in uncertain environments. Adaptive leadership focuses on four dimensions: Navigating organisational/system environments; leading with empathy; learning through self-correction and reflection and creating win-win solutions. These dimensions have many parallels with EI competencies. One of the most useful concepts in adaptive leadership which helps leaders to make decisions, is the ability to diagnose the ‘precious’ from the ‘expendable’ (Heifetz et al., 2009). What do we mean by this? The ‘precious’ is what is vitally important to the organisation; in education this is the learners themselves, the faculty, and the quality of educational provision – you do not want to lose the focus on these as you respond to crisis and change. What is ‘expendable’? Because of campus closures due to the pandemic, suddenly the large lecture theatres, shiny new buildings, and campuses that many universities see as artefacts of success and prestige, were expendable. Once the ‘new normal’ emerges, we will no doubt see a return to campuses and utilisation of buildings again, but adaptive leaders recognise what is precious and make sure that this is looked after and nurtured. We must remember this once the immediate crises are past (Refer to Appendix C).
C. The Global Eco-System Level: A Focus on Healing and Regeneration
The pandemic has highlighted starkly that the world, its countries, people, and structures are highly interconnected. In such times what affects one country, and actions (or inactions) cause ripples across the globe. We have already alluded to the need for leaders to work collaboratively and share practices, and during the pandemic we have seen multiple examples of international collaboration and the sharing of practice by HPEs everywhere. When we are all in the same boat, we need to sail in the same direction.
As well as being willing and proactive in collaborating on finding solutions to common challenges, leaders in HPE also need to consider the wider implications of the impact of climate change and human activities on health and health care. McKimm and McLean (2020) make the case for an ‘eco-ethical’ leadership approach which focuses leaders’ minds on the need for sustainable health professions’ education and practices. Another approach that is very relevant to HPE and its response to the pandemic is that of ‘regenerative’ leadership (Hutchins & Storm, 2019). In stimulating the recovery of health professions’ education and the organisations that provide it, leaders will need to pay attention to ensuring the conditions for healing, regeneration and thriving are present, so that people (faculty and students) feel safe to return to campuses and a more ‘normal’ way of working.
IV. PREPARING FOR A ‘NEW NORMAL’
A. Planning and Implementing Change
As countries, organisations and individuals start to look forward and prepare for mass returns to campus, leaders will need to support students and faculty for a ‘new normal’. This requires managing expectations as well as physical and psychological safety as discussed above. Management is all about maintaining stability and order (as Drucker (2007) says: ‘doing the thing right’) therefore, in addition to choosing appropriate leadership approaches, leaders will need to utilise a range of management tools to help plan how universities and their research, education programmes and other activities will function.
B. Risk Assessment
In an ideal world, all changes would be able to be planned for and there would be no surprises. However, successful organisations (and individuals) also plan for unforeseen circumstances to stay resilient and help mitigate risk. There are a few ways of assessing risks, with one of the most widely used being a ‘risk matrix’ (Ni et al., 2010). This is used during risk assessment to define the level of risk by considering the category of probability or likelihood against the category of consequence severity. This simple tool helps to increase the visibility of risks and assist management decision making. At university level as well as departmental and programme levels, a risk analysis should be carried out and updated regularly. In stable times, risk analysis helps the organisation keep aware of external and internal risk factors and put plans in place, but during the pandemic it is essential.
C. Managing Change
A widely used tool to lead, accelerate and manage change is Kotter’s (2007) eight-stage process (Refer to Appendix D).
The pandemic itself provided a sense of urgency as universities and teachers scrambled to respond, and leaders needed a good understanding of organisational resources, the external environment, and educational responses worldwide to develop meaningful and realistic strategies (Schwartzstein et al., 2008). The fluidity and volatility of the pandemic situation early on made any progress along Kotter’s steps difficult to see at either individual or institutional level. Whilst it can feel very unsettling to have to return to an earlier Step, after moving a few steps forward, it is often necessary to do so and Kotter’s model acknowledges that change is iterative, not linear. Kotter’s and similar models are very useful both for planning the changes needed as well as offering a framework for analysis of where change efforts are faltering or failing. A formal communications strategy is essential which provides consistent messages, opportunities for questions to be answered for all key stakeholders and celebrates ‘quick visible wins’, such as learners returning to their studies or a successfully run online assessment or graduation ceremony.
D. Focus on Outcomes
Across the world, universities (many of which had never provided online learning or assessment) suddenly had to decide how (or whether) they would (or could) provide educational opportunities for their students. Cameron and Green (2019) suggest that leaders responding to or stimulating change need to balance their efforts across three dimensions of any change: outcomes, interests, and emotions. In terms of ‘outcomes’, they stress that clear outcomes (deliverables) must be developed and implemented. Outcomes (goals, targets or objectives) need to be SMART (specific, measurable, achievable, realistic and time bound). In times of immediate crisis, some goals will need to be very short-term (e.g. ‘ensure all faculty are able and prepared to work from home by the end of next week’), whereas strategically, senior leaders have the responsibility to keep the longer terms outcomes in mind, e.g. ‘ensure that the university remains financially viable’. In terms of ‘emotions’, Cameron and Green (2019) suggest that the role of the leader is to enable people and the culture to adapt to the change and leaders also need to pay attention to (what may be competing) interests, here they need to mobilize their influence, authority and power to enact the change.
E. Planning and Implementation
McKimm and Jones (2018) suggest using project management techniques for operational planning and implementation. During the pandemic, plans will need to be devised and aligned in a range of areas (learning and teaching, student and faculty wellbeing, research, estates, finance etc.) and at many levels: whole university, department, and programme.
A project management approach sees activities as temporary, non-routine, acknowledging uncertainty and with a defined end point. Techniques taking a ‘linear’ view of change such as Lewin’s ‘freeze/unfreeze’ model (Cummings et al., 2016; Lewin, 1951) can be useful in framing the response into simple terms rather than getting bogged down in complexity. These look at the change process as comprising three steps: current state (how the university, schools and programmes ran pre-pandemic) – transitional state (how the university runs during the pandemic) – desired state (how might everything run after the pandemic, in the ‘new normal’). Once the broad elements and strategy have been agreed, then the detailed planning and implementation stages begin.
F. Sustaining Change
1) Recognising the dynamism of change: While crisis can bring about opportunities for real change, realistically there will be challenges sustaining the change. Buchanan et al. (2005) suggests organisational sustainability is contextual and dependent of various factors, including changes in market demands, financial viability, or political decisions. The drivers of sustainability will also differ based on organisational levels for example whether at the individual, managerial or leadership role. Given the uncertainties that leaders will face, an important step in sustaining change with positive outcomes would be an awareness that change, and sustainability is not static but is instead dynamic, requiring an improvement trajectory over time. This concept can also be described as dynamic stability: a process of continual, small, and possibly innovative changes that involve the modification or enhancement existing practices and business models (Hodges & Gill, 2014). When translated into practice, sustaining change requires as much attention from leaders as when developing and implementing change.
2) Supporting individuals at multiple levels: As sustainability of change is also dependent at the individual level, leaders should strongly promote and support initiatives that promote both individual professional and personal development. In the context of HPE, staff support is often interpreted as faculty development activities and more often is the form of workshops or, more recently, webinars. It is important for institutions to broaden the support activities to include non-faculty staff, provide activities other than workshops and implement initiatives for wellness and mental health wellbeing at the workplace. Another example of staff supports activities that has gained traction during this crisis are global community of practices. Given the similar challenges faced, global community of practices offer an opportunity to share strategies of mutual interest and benefit and build networks of educators across socio-cultural contexts (Thampy et al., 2020). As health professions’ leaders and educational organisations brace for the financial impact of the crisis, the case to reduce funding for staff support and investment in people maybe put forward. Leaders need to reflect and balance the impact reducing operating costs with enhancing the skills of staff to embrace, work with and sustain change.
3) Exchanging and co-creating global solutions: Sustaining change requires a vision for a new way of leadership and ways of working (McKimm & McLean, 2020). The recent COVID-19 crisis has highlighted that solutions to manage and sustain positive outcomes may not come from familiar local sources or authorities. The crisis also challenged the previously held assumptions of standards and readiness of healthcare systems and governance of it in some countries, suggesting much can be learned from successful approaches taken across the globe. Leaders in HPE should work collaboratively to acknowledge that solutions can come from across boundaries and draw from it lessons and guidelines for a global approach in the training of health professionals.
V. CONCLUSION
Although this paper provides a roadmap and suggested approaches for HPE leaders and followers alike to reflect on as they work through various waves of the pandemic, it is critical for leaders to be flexible and adaptive and adopt an emotionally intelligent and person-centred approach. Psychological safety is integral for professionals at all levels to successfully accomplish individual and institutional goals during challenging circumstances, along with leaders who provide stability and vision. What has become abundantly clear during the pandemic is that health professions’ educators from around the world have common as well as unique challenges and are increasingly seeking a diverse, multicultural global community of practice, sharing best practices and seeking to understand other cultural, regional and national educational context. These insights emphasise that health professions educators, regardless of their geographical location, cannot succeed in their leadership roles without a culturally sensitive, competent and grounded approach. No longer can experts from one group of countries impose their best practices on another region of the world without opening themselves to learning from other cultures and contexts.
Notes on Contributors
Judy McKimm conceptualised the idea for the article, wrote specific sections, and reviewed and edited the full article prior to submission.
Subha Ramani helped design the structure for this perspective, wrote content sections, edited, read and approved the final manuscript.
Vishna Devi Nadarajah helped design the structure for this perspective, wrote content sections, edited, read and approved the final manuscript.
Ethical Approval
No ethics approval was required as this is an opinion piece supported by a literature review and does not relate to primary research.
Funding
No funding sources are associated with this paper.
Declaration of Interest
I confirm that the manuscript is original work of authors which has not been previously published or under review with another journal.
I confirm that all research meets the legal and ethical guidelines.
I confirm that I have stated all possible conflicts of interest in my manuscript and explicitly stated even if there is no conflict of interest.
I am not using third-party material that requires formal permission.
References
Ashokka, B., Ong, S. Y., Tay, K. H., Loh, N. H. W., Gee, C. F., & Samarasekera, D. D. (2020). Coordinated responses of academic medical centres to pandemics: Sustaining medical education during COVID-19. Medical Teacher, 42(7), 762–771. https://doi.org/10.1080/0142159x.2020.1757634
Avolio, B. J., & Gardner, W. L. (2005). Authentic leadership development: Getting to the root of positive forms of leadership. The Leadership Quarterly, 16(3), 315–338. https://doi.org/10.1016/j.leaqua.2005.03.001
Barrow, M., McKimm, J., & Gasquoine, S. (2011). The policy and the practice: early-career doctors and nurses as leaders and followers in the delivery of health care. Advances in Health Sciences Education, 16(1), 17–29. https://doi.org/10.1007/s10459-010-9239-2
Barrow, M., McKimm, J., Gasquoine, S., & Rowe, D. (2014). Collaborating in healthcare delivery: Exploring conceptual differences at the “bedside.” Journal of Interprofessional Care, 29(2), 119–124. https://doi.org/10.3109/13561820.2014.955911
Boyatzis, R. E. (2009). Competencies as a behavioral approach to emotional intelligence. Journal of Management Development, 28(9), 749–770. https://doi.org/10.1108/02621710910987647
Buchanan, D., Ketley, D., Gollop, R., Jones, J. L., Lamont, S. S., Neath, A., & Whitby, E. (2005). No going back: A review of the literature on sustaining strategic change. International Journal of Management Review, 7 (3). https://doi.org/10.1111/j.1468-2370.2005.00111.x
Cameron, E., & Green, M. (2019). Making sense of change management: A complete guide to the models, tools, and techniques of organizational change. Kogan Page Publishers.
Cardiff, S., McCormack, B., & McCance, T. (2018). Person-centred leadership: A relational approach to leadership derived through action research. Journal of Clinical Nursing, 27(15–16), 3056–3069. https://doi.org/10.1111/jocn.14492
Cummings, S., Bridgman, T., & Brown, K. G. (2016). Unfreezing change as three steps: Rethinking Kurt Lewin’s legacy for change management. Human Relations, 69(1), 33-60.
Duckworth, A. (2016). Grit: The power of passion and perseverance (Vol. 234), Scribner. https://doi.org/10.1111/peps.12198
Dweck, C. (2016). What having a “growth mindset” actually means. Harvard Business Review, 13, 213-226.
Goleman, D. (1998). The emotionally competent leader. The Healthcare Forum Journal, 41(2), 36-38.
Goleman, D., Boyatzis, R., & McKee, A. (2001). Primal leadership: The hidden driver of great performance. Harvard Business Review, 79(11), 42-53.
Heifetz, R. A., Heifetz, R., Grashow, A., & Linsky, M. (2009). The practice of adaptive leadership: Tools and tactics for changing your organization and the world. Harvard Business Press.
Hodges, J., & Gill, R. (2014). Sustaining change in organizations (1st ed.). SAGE Publications.
Hollander, E. P. (2012). Inclusive leadership: The essential leader-follower relationship (Applied Psychology Series) (1st ed.). Routledge.
Hutchins, G., & Storm, L. (2019). Regenerative Leadership: The DNA of life-affirming 21st century organizations. Wordzworth Publishing.
Kanter, R. M. (2020). Leading your team past the peak of a crisis. Harvard Business Review
Kotter, J. (2007). Leading change: Why transformation efforts fail. Harvard Business Review, 86, 97-103.
Lazarus, G., Mangkuliguna, G., & Findyartini, A. (2020). Medical students in Indonesia: An invaluable living gemstone during coronavirus disease 2019 pandemic. Korean Journal of Medical Education, 32(3), 237–241. https://doi.org/10.3946/kjme.2020.165
Lewin, K. (1951). Field theory in social science: Selected theoretical papers (D. Cartwright, Ed.). Harpers.
Liao, Y., & Thomas, D. C. (2020). Conceptualizing Cultural Intelligence. In Cultural Intelligence in the World of Work (pp. 17-30). Springer.
McKimm, J., & Jones, P. K. (2018). Twelve tips for applying change models to curriculum design, development and delivery. Medical Teacher, 40(5), 520-526.
McKimm, J., & McLean, M. (2020). Rethinking health professions’ education leadership: Developing ‘eco-ethical’leaders for a more sustainable world and future. Medical Teacher, 42(8), 855-860.
McKimm, J., & O’Sullivan, H. (2016). When I say … leadership. Medical Education, 50(9), 896–897. https://doi.org/10.1111/medu.13119
Nadarajah, V. D., Er, H. M., & Lilley, P. (2020). Turning around a medical education conference: Ottawa 2020 in the time of COVID‐19. Medical Education, 54(8), 760–761. https://doi.org/10.1111/medu.14197
Ni, H., Chen, A., & Chen, N. (2010). Some extensions on risk matrix approach. Safety Science, 48(10), 1269–1278. https://doi.org/10.1016/j.ssci.2010.04.005
Paixão, G., Mills, C., McKimm, J., Hassanien, M. A., & Al-Hayani, A. A. (2020). Leadership in a crisis: Doing things differently, doing different things. British Journal of Hospital Medicine, 81(11), 1–9. https://doi.org/10.12968/hmed.2020.0611
Randall, L. M., & Coakley, L. A. (2007). Applying adaptive leadership to successful change initiatives in academia. Leadership & Organization Development Journal, 28(4), 325–335. https://doi.org/10.1108/01437730710752201
Schwartzstein, R. M., Huang, G. C., & Coughlin, C. M. (2008). Development and implementation of a comprehensive strategic plan for medical education at an academic medical center. Academic Medicine, 83(6), 550–559. https://doi.org/10.1097/acm.0b013e3181722c7c
Scouller, J. (2011). The three levels of leadership: How to develop your leadership presence, knowhow, and skill. Management Books 2000.
Sinek, S. (2014). Leaders eat last: Why some teams pull together and others don’t. Penguin.
Sosik, J. J., Jung, D., & Dinger, S. L. (2009). Values in authentic action. Group & Organization Management, 34(4), 395–431. https://doi.org/10.1177/1059601108329212
Swanwick, T., & McKimm, J. (2017). ABC of clinical leadership. John Wiley & Sons.
Thampy, H. K., Ramani, S., McKimm, J., & Nadarajah, V. D. (2020). Virtual speed mentoring in challenging times. The Clinical Teacher, 17(4), 430–432. https://doi.org/10.1111/tct.13216
Till, A., Dutta, N., & McKimm, J. (2016). Vertical leadership in highly complex and unpredictable health systems. British Journal of Hospital Medicine, 77(8), 471–475. https://doi.org/10.12968/hmed.2016.77.8.471
Uhl-Bien, M., & Carsten, M. (2018). Reversing the lens in leadership: Positioning followership in the leadership construct. In Leadership now: Reflections on the legacy of Boas Shamir. Emerald Publishing Limited.
Velarde, J. M., Ghani, M. F., Adams, D., & Cheah, J.-H. (2020). Towards a healthy school climate: The mediating effect of transformational leadership on cultural intelligence and organisational health. Educational Management Administration & Leadership. https://doi.org/10.1177/1741143220937311
Worley, C. G., & Jules, C. (2020). COVID-19’s uncomfortable revelations about agile and sustainable organizations in a VUCA world. The Journal of Applied Behavioral Science, 56(3), 279–283. https://doi.org/10.1177/0021886320936263
*Judy McKimm
Swansea University Medical School,
Swansea University
Swansea, UK, SA1 8PP
Email: j.mckimm@swansea.ac.uk
Submitted: 28 July 2020
Accepted: 3 December 2020
Published online: 13 July, TAPS 2021, 6(3), 75-82
https://doi.org/10.29060/TAPS.2021-6-3/OA2366
Kirsty J Freeman1 & Brid Phillips2
1Office of Education, Duke-NUS Medical School, Singapore; 2Health Professions Education Unit, The University of Western Australia, Australia
Abstract
Introduction: Healthcare requires its practitioners, policymakers, stakeholders, and critics to have empathetic awareness and skills in critical thinking. Often these skills are neglected or lost in current educational programs aimed at those interested in the field of health. Health humanities and, in particular narrative medicine, aim to redress this omission.
Methods: We used a mixed methods approach to explore the experience of health humanities students in creative writing and staged readings to foster empathic awareness and critical thinking. Data was collected from 20 second-year students enrolled in an undergraduate health humanities unit via a post-assessment survey, and thematic analysis of a reflective paper.
Results: 92.9% of the students felt that writing a creative piece helped them to understand the health topic from a different perspective, with 85.7% reporting that the use of creative writing helped to create emotional connections. From the reflective paper, six themes were elicited through the thematic data analysis: (1) The value of language; (2) Insights into the patient experience; (3) Giving voice to the patient; (4) Creating empathic exchanges; (5) Illness and emotion; and (6) Reflective practice.
Conclusion: By offering a mode of experiential learning involving both creative writing and staged readings, students develop empathic ways of thinking and being while deepening their critical engagement with a range of health topics. Students were able to understand the need to make humanistic sense of the health and well-being narrative, providing them with a range of transferable skills which will be an asset in any workplace.
Keywords: Narrative Medicine, Empathy, Critical Thinking, Staged Reading, Health Humanities
Practice Highlights
- Creative writing and staged readings are effective in fostering empathetic awareness and critical thinking.
- Narrative medicine techniques result in greater understanding about the perspectives of others.
- Developing creative language leads to enhanced communication skills and nuanced ways of thinking.
- Staged readings delivered online provide effective teaching and learning opportunities.
I. INTRODUCTION
Health humanities, and the attendant field of medical humanities, refer to the application of the creative or fine arts (visual arts, performing arts etc.) and humanities disciplines (literary studies, law, history, philosophy, etc.) to discussions and explorations on the nature of human health and well-being (Crawford et al., 2010). Within this broad umbrella lies the discipline of narrative medicine. The application of humanities to health has had a long pedigree, but the distinct disciplines of both narrative medicine and health humanities only began to emerge over the first decade of the 21st Century. In part, they emerged from a growing concern about an increasing lack of empathy in health professionals (Dean & McAllister, 2018; Lai, 2020). Narrative medicine with its interest in creativity and ambiguity strives to address this concern. Through narrative medicine, skills in thinking reflectively, listening actively, observing more closely and writing creatively can be developed. It has been shown that there is a positive impact on empathy and communication following narrative medicine education (Barber & Moreno-Leguizamon, 2017). This is important as the empathy conveying physician is more successful in promoting better clinical outcomes for patients. However, ‘[d]espite the centrality of stories to many of the tasks that clinicians perform it remains that explicit and formal teaching of knowledge and methods in narrative is relatively novel’ (Boudreau et al., 2012, p. 152).
One of the educational techniques embraced in narrative medicine is staged readings. A staged reading is an event which may have some rehearsal time, but the readers use scripts on stage. There is minimal staging, costuming, and props. This is pertinent as the use of theatre in academic teaching represents a new model of education that reminds students of the humanity of people (Baker et al., 2019). This form of engagement involves an emotional transaction through the spectacle of theatre which, as the Greeks understood it, was an occasion that provided recognition, catharsis, and release for both the individual and the wider community (Shapiro & Hunt, 2003). Health topics are also more easily understood through the medium of performance (Ünalan et al., 2009). Ünalan et al. (2009) also surmised that theatrical performance could increase empathy levels. There are similar benefits to be had from staged medical readings which foster introspection and reflection (Matharu et al., 2011). The purpose of this study was to determine whether the use of creative writing and staged readings could develop empathy and critical thinking in second year university students enrolled in an undergraduate health humanities unit of study. Student enrolment information confirms majority of students are on a pathway to studying medicine, pharmacy, dentistry, ophthalmology, or global health.
A. Context
In semester one of 2020, 20 second-year students were enrolled in a narrative medicine unit, as part of their undergraduate bachelor’s degree. By delivering an undergraduate unit in narrative medicine, the goal is to give students the opportunity:
- To dip their toes into the world of literary fiction.
- To present their own creative pieces relating to health topics.
- To gain an understanding of health issues from the perspective of others as this increases empathetic awareness.
Through a series of scaffolded assessments, students have a unique opportunity to develop empathetic awareness and critical thinking skills through creative presentations mimicking staged readings.
Two of the three assessments related to the staged reading, the second assessment was a creative piece and the third was a reflection on process of creating the piece and the health topic to which it related. The purpose of these assessments was to demonstrate different modes of narrative writing. This was achieved through the construction of a creative piece that explored a health topic using narrative medicine techniques including but not limited to short story writing, poetry, and play writing.
The unit involved supporting students to devise a short creative writing piece. Within the piece, themes of empathy, communication, cultural difference, and societal biases and assumptions around the students’ chosen health topics were explored. The piece was then to be presented as a staged reading by the students for an invited audience. The audience would include the wider university community of undergraduate and postgraduate students, staff, and invited guests such as health professionals to the reading. Immediately following their reading, the students, supported by academic staff, were to hold a guided discussion on the significance of health topics in the piece. This discussion would bring biases and assumptions into focus and heighten the individual’s awareness of emotional dynamics at work in the healthcare context while also offering insights into the perspective of others. Similar programs have been used to educate bioethical students, help them to develop discussion questions, and enhance their critical self-reflection (Kerr et al., 2020; Robeson & King, 2017).
Students were required to read a literary fiction novel, Extinctions (Wilson, 2020). The act of reading itself has demonstrated benefits of improving processing of experiences and developing empathy. Reading literature also improves our social awareness and our ability to see the perspectives of others (Fennelly, 2020; Kaptein et al., 2018). In the novel Extinctions, there are many discernible health topics such as traumatic brain injury, drug use, ageing, mobility issues, death and dying, and loss of independence. There is also a range of characters involved in these issues from a young girl with a drug problem to the protagonist, Fred, a man in his declining years. It was important to foster student engagement with the project by offering a fully scaffolded experience to allay performance anxieties. Scaffolding has been shown to support students as they negotiate a challenging environment and allow them to make meaning for themselves rather than have it imposed on them from an autocratic perspective (Wilson, 2016). Each week from the first week of semester, the seminar included both a close reading exercise and a creative writing exercise. The scaffolding also included several resource folders addressing the main genres the students were encouraged to explore – short story, poetry, drama. The folders contained videos, book chapters, blog posts, and journal articles that introduced the students to ways of writing creatively. There was also a dedicated workshop which explored these techniques and answered any questions the students had on creative writing.
Due to COVID-19 restrictions on social gatherings and the cancellation of face-to-face interactions, the presentation aspect had to be cancelled at short notice and instead, presentations took place online without the wider audience participation. The creative pieces were read in an online forum limited to students and the unit coordinator. The students had the opportunity to read their work to other participating students and to lead a short discussion on their health topic. This sharing is important as ‘representation is always a dialogue, in which, the receiver of the work contributes a necessary response to the creator of the work’ (Charon et al., 2016, p. 347). As the students based their pieces on fully rounded characters from the novel, this process shares similarities with verbatim theatre. Verbatim theatre has been shown to allow positive exploration of emotional behaviours (Scott et al., 2017). After this process, students were encouraged to incorporate feedback from the presentations into their pieces before submission of the creative piece.
The third assessment component of the unit required the students to submit a reflective essay on the experience where they discuss the creative process and their representation of the health topic which they had chosen. They had to discuss the significance of the health topic and examine their personal responses to the topic and how it was influenced by their research, the creative process, and the discussions which took place following the presentation of the piece. To support the reflective process, we developed a reflective writing toolkit which illustrates both the process and its importance.
II. METHODS
A cross-sectional mixed methods design was used to evaluate the experience of health humanities students in creative writing and staged readings to foster empathic awareness and critical thinking. 20 second-year students who were enrolled in a narrative medicine unit between January and June 2020 were invited to participate.
A. Data Collection and Analysis
Data was collected at two points over the semester, an online survey in week 10, and a reflective paper at the end of semester in week 13.
1) Creative writing and staged reading assessment student experience survey: All 20 undergraduate students enrolled in the unit in semester one, 2020, were invited to participate in an online survey examining the student experience of participating in the creative writing and staged reading assessment. The survey tool curated by author one (KF) was designed to collect basic demographic data about the student, along with information about their current enrolment. The survey was designed to evaluate the first two level of Kirkpatrick’s model of program evaluation, level one being reaction and level two learning (Frye & Hemmer, 2012). Given that this is the first time the program had been offered, the authors felt that the data collected would provide a baseline upon which further detailed evaluations can build upon. Students were asked to rate their experience with the staged reading project using a five-point Likert scale, as well as responding to open-ended questions designed to further expand on the students’ experience. A statement of voluntary consent was included at the start of the survey and the participant had to agree to the consent before the survey could commence. Thus participation in the anonymized online evaluation indicates consent. Descriptive statistics were calculated for the demographic data. Categorical data are presented as number and percentage. The analyses were performed using IBM SPSS Statistics Version 25.0. Thematic analysis of the open-ended questions was then undertaken. Researcher bias was minimised by having author one (KF), who was not involved in delivering the course, undertake the analysis of the survey data.
2) Staged reading reflective essay: The second data collection point was a reflective essay (n=20). Thematic analysis of the text was undertaken by both authors. Each author reviewed the transcripts separately, making note of key phrases, outline possible categories or themes. Discussion of our interpretations took place over teleconference, as we then jointly rearranged and renamed the codes, developing higher order themes. NVivo 12™ was used to manage the qualitative data (QSR International., 2018). This mixed methods design combines quantitative and qualitative data to provide a richer source of information about the experience of staged readings.
III. RESULTS
A. Creative Writing and Staged Reading Assessment Student Experience Survey
Of the 20 students enrolled in the unit, 14 completed the student experience survey, a response rate of 70%. Table 1 summarises the demographic characteristics of the respondents. As can be seen in Table 1, the students were enrolled in one of three bachelor degrees. The degree enrolled by majority of students in is science based, with only 1 respondent studying an Arts based degree. 92.8% of respondents had not previously completed an undergraduate degree. Three respondents spoke languages other than English at home.
When asked to rate their experience in the staged reading project 92.9% of the respondents felt that writing a creative piece helped them to understand the health topic from a different perspective; with 85.7% reporting that the use of creative writing helped to create emotional connections (Table 2).
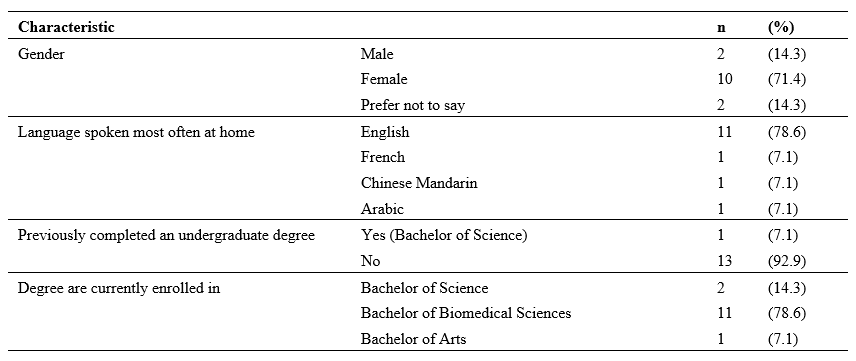
Table 1. Summary of demographic characteristics of respondents
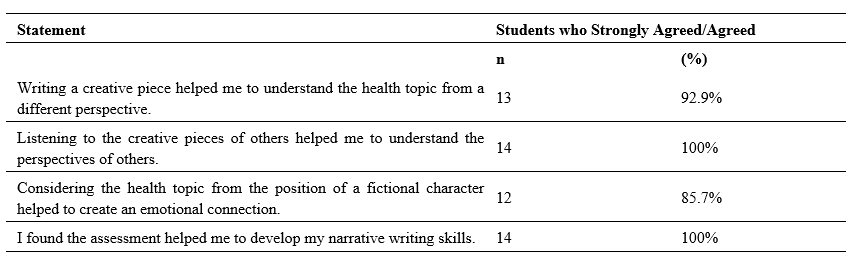
Table 2. Student rating of creative writing and staged reading assessment
When asked to describe their experience of the staged reading assessment in the free text survey questions students reported feeling daunted, nervous and apprehensive about the prospect of writing a creative piece, as many of them shared that they had little or no experience with creative writing. With several students describing to task as challenging, on reflection they expressed feeling fulfilled, enriched, sharing that they found the task rewarding.
A. Staged Reading Reflective Essay
The qualitative data analysis resulted in six themes being identified: (1) The value of language; (2) Insights into the patient experience; (3) Giving voice to the patient; (4) Creating empathic exchanges; (5) Illness and emotion; and (6) Reflective practice (Figure 2). These themes are described in this section, illustrated with representative quotes.
Figure 1. Overview of the staged reading themes
1) The value of language: as they worked through their creative piece, students discovered the value and power of language as a tool for expression and communication. Students commented on their appreciation of language:
Since I wanted to create a powerful and emotional piece, I experimented using literacy techniques to achieve a desperate and anxious tone.
Student 2
I learnt that the use of language is also vital in writing a creative piece, emphasising the importance of communication between the author and readers.
Student 14
2) Insights into the patient experience: Students developed an awareness of the value of research when trying to understand the issues surrounding health topics. Better equipped with quality knowledge and research, they were able to give more nuanced accounts of health experiences. Students learned the value of looking beyond the symptom to see the whole person and, thus the value and importance of person-centred care:
Acknowledging that my research and reflections had resulted in greater understandings of both the health topic and the importance of seeing a patient beyond their physical disease.
Student 2
It is very important to take into consideration all aspects of what a person is experiencing in order to make the best assessment and to come up with the best route of action to help the patient overcome whatever it is they are suffering from.
Student 1
3) Giving voice to the patient: Students gained an insight into the need to give a voice to patients in order to gain better understanding of the perspectives of others. They reflected on the powerlessness and silence that often surrounds certain conditions and situations:
I felt that I was able to give Katie an authentic voice, through which readers were then able to empathise with, and better understand, her struggles.
Student 4
Furthermore, the narratives of victims can empower them by giving them a voice in times when they are often silenced.
Student 7
4) Creating empathetic exchanges: Students gained an understanding of empathetic exchanges and in some instances understood the need to create opportunities for the development of empathy. The students did not always articulate the word empathy but instead alluded to the concept by talking about experiencing and understanding the emotions and perspectives of others:
I felt increased levels of empathy towards individuals dealing with the disorder as I now understand the many other challenges and hurdles that accompany eating disorders that I didn’t know prior to this assignment.
Student 8
When using these descriptions, I felt that I was able to build an emotional connection with Katie’s character, thus encouraging readers to also empathise with her situation.
Student 4
5) Illness and emotion: Students discovered that emotional transactions and states are intertwined with health and illness. They understood, through their work, the interconnectiveness of emotional responses and illness. Some of their observations included:
I have become more sensitive to the idea that human beings are inherently emotional and can be affectively moved when provided with an impetus.
Student 3
The purpose of the piece was unearthing the complex thoughts and emotions individuals with eating disorders and substance abuse go through.
Student 8
6) Reflective Practice: On topics where students previously had felt knowledgeable, deeper reflection and considerations revealed their own misconceptions and lack of knowledge. Within this paradigm, they also showed a maturation of habits and behaviours. Their comments were insightful:
I entered a phase of reflection where I realised that I would have previously contributed to these harmful views.
Student 2
I learnt and later researched further the differences in the perception of STEM women in both Western and Asian populations. This is something I would attempt to change. It was really interesting for me to discover that I had this unconscious bias forcing me to further expand my learning and knowledge in the area.
Student 18
IV. DISCUSSION
While the use of creative writing and staged readings is a developing area in health humanities, the findings of this study suggest that they are effective in fostering emotional awareness and critical thinking. McDonald et al. (2015) found that ‘[a]nalysis of the student’s writing showed that they demonstrated the ability to “stand in another’s shoes” and, interestingly, the students’ comments on their own writing showed that their ability to relate to characters they initially felt little affinity for deepened’ (McDonald et al., 2015, p. 9).
By taking part in the creative writing project and the accompanying reflection piece, students were exposed to an innovative and experiential form of learning that provided a unique pedagogical experience. Whilst the students reported being daunted at the thought of constructing a creative piece, the self-reflective processes and actively engaging with the perspectives of others, ensured students were able to enhance their critical thinking skills. In the creative writing and staged reading assessment student experience survey, 100% of students agreed, “Listening to the creative pieces of others helped me to understand the perspectives of others”. This accords with the work of Deloney and Graham who note “[e]xperiential learning activities increase student engagement and are a helpful tool to connect abstract ideas with concrete knowledge” (Deloney & Graham, 2003, p. 249).
The findings of this study highlight the value of language as a tool for expression and communication. Educators need to be mindful of their student population when contemplating incorporating creative writing and staged readings into their programs. For students to be accepted for enrolment at The University of Western Australia they must demonstrate a minimum level of English language proficiency necessary for academic studies. Whilst there has been several studies examining what Hyland calls “linguistics disadvantage in terms of a Native/non-Native divide” (Hyland, 2016, p. 61) in academic writing (Badenhorst et al., 2015; Bocanegra-Valle, 2014; Zhao, 2017), the impact of this linguistic divide in creative writing and staged readings has not been fully explored.
The students gained insights into holistic care relating to both themselves and others. As these are undergraduate students, many on a pathway to a career in health, insights into holistic care and self-care are valuable life lessons. There was also an indication that the process contributed to the social and cultural well-being of themselves and others. Nagji et al. (2013) note that theatre based programs/novel humanities based curriculum items contribute to student well-being, an increasingly important area for universities to address particularly during a pandemic. Although the student population participating in this unit are studying science-based degrees where creative writing is not commonplace, the learning strategies were structured in a way that enabled development of narrative writing skills.
By integrating the narrative medicine techniques of creative writing and staged readings the students were able to give more nuanced accounts of health experiences. Students learned the value of looking beyond the symptom to see the whole person and, thus the value and importance of person-centred care. This gave them valuable insights into the patient experience. During this process, students gained an insight into the need to give a voice to patients in order to gain better understanding of the perspectives of others. They learnt about the powerlessness and silence that often surrounds certain conditions and situations. In their responses, the students did not always articulate the word empathy but instead alluded to the concept by talking about experiencing and understanding the emotions and perspectives of others. Students gained an understanding of the power of empathetic exchanges and in some instances understood the importance of creating empathetic exchanges opportunities. Another important theme which was uncovered, was a growing awareness amongst students that emotional transactions and states are intertwined with health and illness. They understood, through their work, the interconnectiveness of illness and emotion. On topics where students previously had felt knowledgeable, deeper reflection and considerations revealed their own misconceptions and lack of knowledge. Within this paradigm, they also showed a maturation of habits and behaviours leading to improved reflective practices.
There were limitations with the project as we had to move from face-to-face to online teaching due to constraints placed upon teaching during the COVID-19 pandemic. However, the online format did have some unexpected benefits, with a number of students feeling less intimidated when presenting online compared to a face-to-face workshop. Despite the move to online teaching, the cohort remained present and engaged in the project. Many expressed regrets at losing physical contact and the incidental discussions that happen before and after classes but overall with support they adapted well.
V. CONCLUSION
This study has described the experience of students engaging in creative writing and staged readings as part of a narrative medicine unit. Students completing the unit and its attendant assessments developed useful life skills including critical thinking, understanding the perspectives of others, and the positive use of narrative in appreciating the experiences of others. The work engaged them in new and innovative ways evidenced by some statements which noted that their experience in this unit was unique in their university journey. Having autonomy over the health topic they chose, the character they explored, and the creative medium they used to express their thinking, enhanced the learning experience and allowed them to meet the learning outcomes of the unit.
Notes on Contributors
Kirsty J Freeman crafted the paper with her co-author, performed the data collection and analysis of the survey, and undertook thematic analysis of the reflective essays. Dr Brid Phillips crafted the paper with her co-author, conducted the literature search, and undertook thematic analysis of the reflective essays. All the authors have read and approved the final manuscript.
Ethical Approval
Ethics approval was granted by The University of Western Australia Human Research Ethics Committee: HREC RA/4/20/5254.
Data Availability
All relevant quantitative data are within the manuscript. The qualitative data collected for this manuscript originates from assessment items submitted as part of the participants’ academic studies. The authors do not have consent to upload this data into a data repository.
Acknowledgement
We would like to thanks the students who participated in this unit and their willingness to adapt to the online platform with grace and enthusiasm.
Funding
This work has not received any external funding.
Declaration of Interest
All authors declare that there are no conflicts of interest.
References
Badenhorst, C., Moloney, C., Rosales, J., Dyer, J., & Ru, L. (2015). Beyond deficit: Graduate student research-writing pedagogies. Teaching in Higher Education, 20(1), 1-11. https://doi.org/10.1080/13562517.2014.945160
Baker, H. F., Moreland, P. J., Thompson, L. M., Clark-Youngblood, E. M., Solell-Knepler, P. R., Palmietto, N. L., & Gossett, N. A. (2019). Building empathy and professional skills in global health nursing through theatre monologues. The Journal of Nursing Education, 58(11), 653-656. https://doi.org/10.3928/01484834-20191021-07
Barber, S., & Moreno-Leguizamon, C. J. (2017). Can narrative medicine education contribute to the delivery of compassionate care? A review of the literature. Medical Humanities, 43(3), 199-203. https://doi.org/10.1136/medhum-2017-011242
Bocanegra-Valle, A. (2014). ‘English is my default academic language’: Voices from LSP scholars publishing in a multilingual journal. Journal of English for Academic Purposes, 13(1), 65-77. https://doi.org/10.1016/j.jeap.2013.10.010
Boudreau, J. D., Liben, S., & Fuks, A. (2012). A faculty development workshop in narrative-based reflective writing. Perspectives on Medical Education, 1(3), 143-154. https://doi.org/10.1007/s40037-012-0021-4
Charon, R., Hermann, N., & Devlin, M. J. (2016). Close reading and creative writing in clinical education: Teaching attention, representation, and affiliation. Academic Medicine, 91(3), 345-350. https://doi.org/10.1097/ACM.0000000000000827
Crawford, P., Brown, B., Tischler, V., & Baker, C. (2010). Health humanities: The future of medical humanities? Mental Health Review Journal, 15(3), 4-10. https://doi.org/10.5042/mhrj.2010.0654
Dean, S., & McAllister, M. (2018). How education must reawaken empathy. Journal of Advanced Nursing, 74(2), 233-234. https://doi.org/10.1111/jan.13239
Deloney, L. A., & Graham, C. J. (2003). Wit: Using drama to teach first-year medical students about empathy and compassion. Teaching and Learning in Medicine, 15(4), 247-251. https://doi.org/10.1207/S15328015TLM1504_06
Fennelly, B. A. (2020, May 15). What’s the use of reading? Literature and empathy [Video] . https://youtu.be/9nJv8sxpUKU
Frye, A. W., & Hemmer, P. A. (2012). Program evaluation models and related theories: AMEE guide no. 67. Medical Teacher, 34(5), e288-299. https://doi.org/10.3109/0142159x.2012.668637
Hyland, K. (2016). Academic publishing and the myth of linguistic injustice. Journal of Second Language Writing, 31, 58-69. https://doi.org/10.1016/j.jslw.2016.01.005
Kaptein, A., Hughes, B., Murray, M., & Smyth, J. (2018). Start making sense: Art informing health psychology. Health Psychology Open, 5(1), 205510291876004. https://doi.org/10.1177/2055102918760042
Kerr, A., Biechler, M., Kachmar, U., Palocko, B., & Shaub, T. (2020). Confessions of a reluctant caregiver palliative educational program: Using readers’ theater to teach end-of-life communication in undergraduate medical education. Health Communication, 35(2), 192-200. https://doi.org/10.1080/10410236.2018.1550471
Lai, C.-W. (2020). “Booster shots” of humanism at bedside teaching. The Asia Pacific Scholar, 5(2), 45-47. https://doi.org/10.29060/TAPS.2020-5-2/PV1085
Matharu, K. S., Howell, J., & Fitzgerald, F. (2011). Drama and empathy in medical education: Drama and empathy. Literature Compass, 8(7), 443-454. https://doi.org/10.1111/j.1741-4113.2011.00778.x
McDonald, P., Ashton, K., Barratt, R., Doyle, S., Imeson, D., Meir, A., & Risser, G. (2015). Clinical realism: A new literary genre and a potential tool for encouraging empathy in medical students. BMC Medical Education, 15(1), 112-112. https://doi.org/10.1186/s12909-015-0372-8
Nagji, A., Brett-MacLean, P., & Breault, L. (2013). Exploring the benefits of an optional theatre module on medical student well-being. Teaching and Learning in Medicine, 25(3), 201-206. https://doi.org/10.1080/10401334.2013.801774
QSR International. (2018). NVivo 12 [Software]. In https://qsrinternational.com/nvivo/nvivo-products/
Robeson, R., & King, N. (2017). Performable case studies in ethics education. Healthcare, 5(3), 57. https://doi.org/10.3390/healthcare5030057
Scott, K. M., Berlec, Š., Nash, L., Hooker, L., Dwyer, P., Macneill, P., River, J., & Ivory, K. (2017). Grace under pressure: A drama-based approach to tackling mistreatment of medical students. Medical Humanities, 43(1), 68. https://doi.org/10.1136/medhum-2016-011031
Shapiro, J., & Hunt, L. (2003). All the world’s a stage: The use of theatrical performance in medical education. Medical Education, 37(10), 922-927. https://doi.org/10.1046/j.1365-2923.2003.01634.x
Ünalan, P. C., Uzuner, A., Ifçili, S., Akman, M., Hancolu, S., & Thulesius, H. O. (2009). Using theatre in education in a traditional lecture oriented medical curriculum. BMC Medical Education, 9(1), 73-73. https://doi.org/10.1186/1472-6920-9-73
Wilson, J. (2020). Extinctions. UWA Publishing.
Wilson, K. (2016). Critical reading, critical thinking: Delicate scaffolding in english for academic purposes (EAP). Thinking Skills and Creativity, 22, 256-265. https://doi.org/10.1016/j.tsc.2016.10.002
Zhao, J. (2017). Native speaker advantage in academic writing? Conjunctive realizations in EAP writing by four groups of writers. Ampersand, 4, 47-57. https://doi.org/10.1016/j.amper.2017.07.001
*Kirsty J Freeman
Duke-NUS Medical School
8 College Road, Singapore 169857
Tel:+65 89219676
Email: kirsty.freeman@duke-nus.edu.sg
Submitted: 1 October 2020
Accepted: 3 December 2020
Published online: 4 May, TAPS 2021, 6(2), 78-87
https://doi.org/10.29060/TAPS.2021-6-2/OA2406
Yoshitaka Maeda1, Yoshikazu Asada2, Yoshihiko Suzuki1, Akihiro Watanabe3, Satoshi Suzuki3 & Hiroshi Kawahira1
1Medical Simulation Center, Jichi Medical University, Japan; 2Center for Information, Jichi Medical University, Japan; 3Faculty of Health and Medical Sciences, Kanagawa Institute of Technology, Japan
Abstract
Introduction: Students in the early years of medical school should learn clinical site risk assessment skills. However, the effect of this training on clinically inexperienced students is not clear, and it is difficult for students to predict risks from a wide range of perspectives. This study aims to develop and implement three patterns of safety walk rounds (SWR) in a class of students with no clinical experience.
Methods: Three types of SWR were conducted: (A) 37 students observed a familiar classroom and predicted safety risks; (B) 39 students created a profile of a fictitious student in advance and then used Type A parameters; (C) 100 students participated. First, Type A was conducted as a practice. Next, students observed a hospital and predicted risks. All participants in Types A to C had no clinical experience. We classified all risks into perception, comprehension, and action.
Results: For each safety walk-round, there were two types of risk prediction. In Type A, risks such as perception and comprehension were more than 80%. In Types B and C, action risks were 60%. Students had little experience in observing facilities and none at finding safety risks.
Conclusion: Each method had a different risk prediction tendency. Combining the methods could enable students to acquire comprehensive skills in assessing hidden environmental patient safety risks.
Keywords: Patient Safety Education, Undergraduate Education, Risk Assessment Skill, Safety Walk-Rounds
Practice Highlights
- Proposes a patient safety education method incorporating safety walk rounds (SWR).
- Clarifies the risk prediction tendency of clinically inexperienced students in each SWR pattern.
- Students conducting SWR in familiar classrooms tend to predict certain risks.
- Creating fictitious user profiles before SWR enables prediction of action risks.
- Combining different SWR types could enable comprehensive risk assessment skills.
I. INTRODUCTION
In Japan, first-year medical students are recent high school graduates. 60% of universities that train medical professionals provide patient safety education to fourth year medical students at the start of clinical training (Ishikawa et al., 2008). Further, lower grade educational methods do not include specific guidelines for patient safety education, and students in lower grades do not have sufficient medical knowledge to immediately apply their patient safety knowledge in clinical practice. This problem has been pointed out not only in Japan but also in the US and Canada (Alper et al., 2009). Conversely, the Telluride Interdisciplinary Roundtable (Mayer et al., 2009) and Lucian Leape Institute (2010) showed that patient safety education should be included in the curriculum of all grades. This would enable students to learn the necessity and importance of patient safety knowledge and consider patient safety as an implementation science while continuously practising patient safety skills (Nakajima, 2012).
However, many medical schools teach basic patient safety knowledge through lectures on accident analysis tools, legal responsibility knowledge, ethics, and infection (Mayer et al., 2009); however, students lack education on non-technical skills (Mayer et al., 2009; Nakajima, 2012; Walton et al., 2010). Students should be trained in awareness of safety weaknesses, threats (risks) in the workplace or operations, and how to avoid these risks (Doi et al., 2012). Topic 6 of the World Health Organization’s (WHO’s) Patient Safety Curriculum Guide indicates that students need to take appropriate corrective action when they see an unsafe situation or environment (Walton et al., 2010). However, the WHO guidelines do not explain how these risk assessment skills can be taught to students. Literature that examines the effectiveness of risk assessment skills training for early-year medical students is deficient.
To address these issues, we focused on Safety walk rounds (SWR), in which a safety manager goes to a workplace, listens to staff opinions on safety, and observes the workplace to identify safety issues before an accident (Hafey, 2017; Womack, 2013). Singer and Tucker (2014) pointed out that SWR enhances safety culture. The effects of SWR in the radiology department have reduced the number of unsafe events by half (Donnelly et al., 2008). Additionally, other studies reported that safety managers grow more sensitive to safety issues using SWR and that motivation regarding safety is increased (Frankel et al., 2003; Singer & Tucker, 2014). However, its educational effect and applicability to educating clinically inexperienced students are not clear since SWR has not been used for education.
This study aims to develop and implement three patterns of SWR in a class of students with no clinical experience. We clarify the risk prediction tendency of students in each SWR pattern and discuss the effects.
II. METHODS
A. Development Process of Three Types of SWR
We developed three patterns of SWRs to help clinically inexperienced students predict risk and considered what motivates students to learn. We used the ARCS model proposed by J. M. Keller in 1983, which is a framework using four elements: Attention (stimulating the learner’s interest, intellectual curiosity, and inquisitiveness); Relevance (making the content familiar and meaningful); Confidence (encouraging learners to learn); and Satisfaction (giving the learner a sense of satisfaction and motivation to learn more) (Keller, 1987). ARCS is an acronym for these elements.
· SWR in daily situations (SWR-D): Experts are better at predicting risks than novices as the latter has limited knowledge of important aspects of each situation (Murata et al., 2009). Hence, clinically inexperienced students might find it difficult to predict risks in clinical situations. Using the ARCS model, students need to be given Attention, Confidence and Satisfaction. Therefore, we developed SWR in daily situations (SWR-D). Students observe daily situations in classrooms and school buildings for instances of safety risk and take pictures. We use daily situations as classrooms and school buildings are familiar environments for students, and there are many safety risks for educating students.
· SWR in daily situations using the Persona method (SWR-DP): It may be difficult for students who have never performed SWR to observe safety risks in daily situations, and students’ Confidence should be high. Therefore, we combined the persona method with SWR to create a virtual profile of a virtual user, including name, gender, age, and information about the system (e.g., technological literacy). The Persona method has been used to examine the safety of driving support systems (Lindgren et al., 2007). We hypothesize that the Persona method would help students to predict risk from the perspective of a specific user. The student considers the problems the virtual user will face and their behaviour (Cooper, 2004; Mulder & Yaar, 2006). Students created fictitious student profiles (personas) and conducted SWR assuming that the persona students would spend one day in school buildings and classrooms.
· SWR in clinical situations (SWR-C): It may be difficult for students to associate SWR with patient safety in clinical practice, as SWR in daily situations were not related to clinical practice conducted. Further, students might not be motivated to learn—using the ARCS model, students need to see Relevance and Satisfaction. Therefore, we developed the SWR in clinical situations (SWR-C). First, to practice SWR, students performed SWR-D. After SWR-D, they observed clinical situations in hospitals to predict risks (SWR-C).
B. Description of Participants and SWR Implementation Process
This study involved first-year medical students and third-year students in the medical engineer training courses who had no clinical experience. After participating in each SWR pattern, students were asked for their opinions.
1) SWR-D: The participants included 37 students in the third-year medical engineer training course and 100 students who had been in medical school for one month. SWR-D was administered to the third-year (2018) medical engineer training students in one session. SWR-D was implemented as one of the required general education courses for first-year medical students in 2019. An exercise using SWR-D was given to all participants who worked in groups of four to five. Students photographed incidences of safety risk (30 minutes) and collaborated to identify the risks in each photo (20 minutes).
2) SWR-DP: The participants included 39 students (different from SWR-D) in the third-year medical engineer training course. SWR-DP was administered to the third-year (2019) medical engineering students in one session and conducted in groups of four to five. Each group considered one persona (virtual student profile) for the first 20 minutes, and SWR-D was conducted as before.
3) SWR-C: The participants included 100 students (same as SWR-D) who had been in medical school for one month. Each student was assigned one clinical department in advance. Two weeks after the SWR-D, early exposure training was conducted. During training, students found safety risks in clinical situations and outlined the identified risks in reports as photography was not allowed for confidentiality.
C. Statistical Analysis
The risks predicted by students in each SWR pattern were counted and classified into the following: perception—difficulty perceiving something that exists in the outside world (e.g., signs that are difficult to read); comprehension—difficulty understanding the meaning of something that exists in the outside world and in planning what action to take (e.g., signs that are difficult to understand); and action—difficulty performing the intended action (e.g., places where it is difficult to walk).
These classifications are based on Norman’s seven stages of action (Norman & Draper, 1986) where human actions are classified into seven stages: forming the goal, forming the intention, specifying an action, executing the action, perceiving the state of the world, interpreting the perception, and evaluating the outcome (Norman, 1988). This is a representative model widely used for the design evaluation of man-machine systems such as computers (Fleming & Koman, 1998) to understand human cognitive behaviour that leads to human error in medical treatment (Zhang et al., 2002; Zhang et al., 2004).
D. Ethical Considerations in This Research
The ethical requirements in this study are in accord with the Declaration of Helsinki. We emphasized and explained to students that participation was voluntary and that declining to cooperate would have no influence on their grades. We also explained that consent to participate could be withdrawn at any time, that the results of this study may be published after processing, and that the students’ personal information would not be revealed. The students entered their consent in the e-learning system Moodle. This study was considered exempt by the Jichi Medical University Review Board (Number 18-014).
III. RESULTS
The total number of perception, comprehension, and action risks in each SWR is shown in Figure 1. Table 1 shows typical predicted risks and some of the images taken by students. The data that support the findings of this study are openly available in Figshare at <http://doi.org/10.6084/m9.figshare.13012664 (Maeda et al., 2021)>.
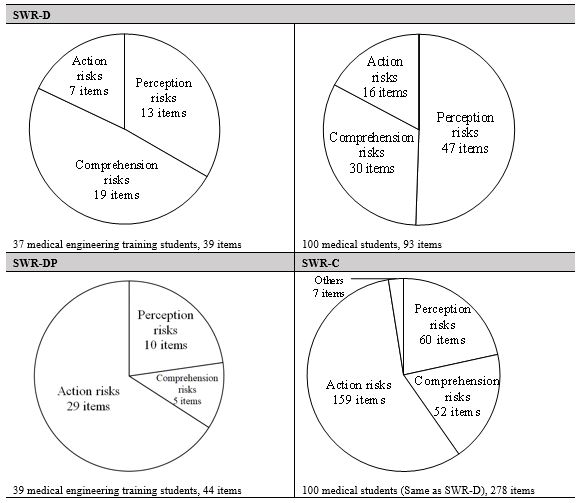
Figure 1. Classification results of risks predicted by students in each SWR pattern
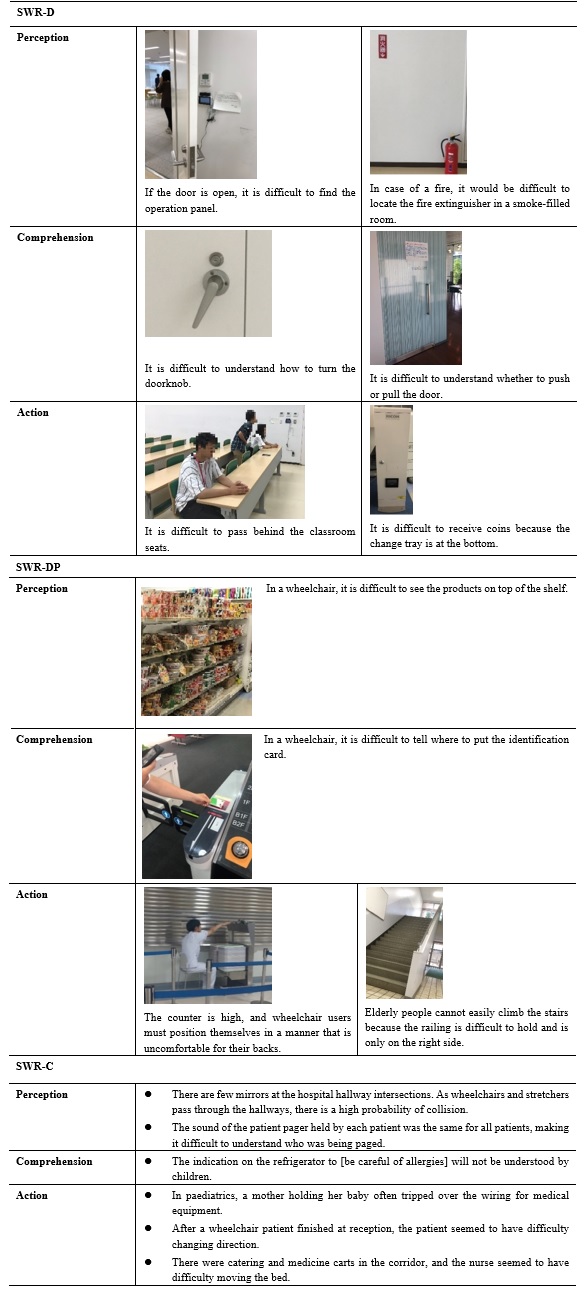
Table 1. Typical risks and captured images for each SWR pattern
In SWR-D, the number of action risks was lower than that of perception and comprehension risks. Risks related to guidance signs for school buildings and classrooms, signs, maps, doors, and operation panels for electric lights were predicted. Also, for example, a group of students who pointed out that it was difficult to find a fire extinguisher did not simply point out the problem of perception, but pointed out that “in the case of a fire, it would have been difficult to find the fire extinguisher in a room filled with smoke”. In other words, they imagined a fire situation that differed from the current conditions of the site they observed.
In SWR-DP, students created the persona shown in Table 2. Many students created fictitious profiles of students who had disabilities or who were elderly. Despite observing the same school building as SWR-D, the number of action risks is almost 70% of the total number (Figure 1). Table 1 shows that many students made extensive predictions from the same perspective as the persona—the risks associated with persons with some kind of disability. For example, from the height of the eyes of a person in a wheelchair, students predicted problems with the visibility of products in a shop, the height of a counter in a cafeteria, and with the routes, the persona would be likely to take within a building. Most identified problems pertained to a lack of easy access to the environment. In one image (Table 1), a student is seen simulating being in a wheelchair at the cafeteria counter.
|
Male, 70 years old, 160 cm, 55 kg, using a cane, hearing loss, narrow vision. He entered college to re-learn after retirement. He goes to school by bus. He is worried about being able to see the whiteboard. He is worried that he will be late for class because he moves more slowly. |
|
Male, 18 years old, 141 cm, 85 kg. He uses a wheelchair because he lost his left leg in a traffic accident. He is apprehensive about moving between classrooms. |
Table 2. Example of a persona (fictitious student profile) created by SWR-DP students
In SWR-C, action risks were the most frequent (Figure 1). Of the total 251 risks, approximately 90% were risks to patients and approximately 10% to healthcare professionals. From Table 1, regarding action, we can see that students observed the behaviour and embarrassment of patients at hospitals and predicted risks based on them (e.g., “The mother holding her baby was almost stumbling”; “Patients in wheelchairs were difficult to move”). In perception and comprehension, students brainstormed risks from the patients’ perspective (e.g., “The indication on the refrigerator to [be careful of allergies] will not be understood by children”). The students identified risks from the child’s perspective.
Table 3 shows the students’ opinions of each SWR. In all SWRs, students had little experience in observing the facilities they usually used, and finding safety risks was new to them. In SWR-DP, students said that although they were able-bodied, they could notice accessibility problems by observing the environments from the persona’s perspectives. For SWR-C, students noticed that there were many problems in the design and environment of the hospital facilities and that various safety measures had already been implemented.
|
SWR-D
SWR-DP
SWR-C
|
Table 3. Student opinion on SWR
IV. DISCUSSION
A. Student Risk Predicting Tendency in Each SWR Pattern
The importance of institutional design in patient safety has been pointed out in many publications. For example, environmental design is being considered to avoid various risks, such as falls and patient suicides, mixing up patients, and improper handling of tubes and connectors (Joseph & Rashid, 2007; Michalska & Szewieczek, 2007; Reiling, 2006; Reiling et al., 2003; Reiling et al., 2008). In particular, it has been pointed out that the indoor environment (e.g., noise and lighting) and interior design (e.g., furniture and materials) are important (Joseph & Rashid, 2007). When considering the design, it is necessary to predict both the direct impact risks and the indirect impact risks of accidents as points of view when predicting onsite risks. Direct impact risks are the aspects of hospital design that can directly impact safety outcomes, such as patient falls and medical errors (Joseph & Rashid, 2007). This is considered to correspond to “action” in this study. For example, a tall counter design is directly linked to the undesirable consequence of a wheelchair user being unable to receive a meal. Indirect impact risks are the aspects of hospital design that can cause users to make incorrect decisions that lead to accidents and errors (Joseph & Rashid, 2007). This is considered to correspond to “perception” and “comprehension” in this study. For example, a paediatric refrigerator’s “be careful of allergies” poster does not directly lead to an unsafe outcome; however, if a child is unable to understand, then an incorrect decision to eat food to which the child is allergic may lead to an unsafe outcome.
In SWR-D, many indirect impact risks (perception and comprehension) were predicted. Conversely, few action risks (direct impact risks) were predicted. SWR-DP and SWR-C results were the opposite to SWR-D; many direct impact risks and few indirect impact risks were identified.
In SWR, it is necessary to identify risks through brainstorming and simulation using the operators’ experience and reasoning (Okubo et al., 2014). However, different techniques identify different risk types. Indirect impact risks such as perception and comprehension are related to human internal thinking, such as incorrect decisions. To identify these risks, students need to observe from the perspective of the person concerned and brainstorm the risks. Conversely, the action is observable—a risk that students can predict by observing the actions of the concerned person or simulating behaviour as the concerned person. Subsequently, what caused each SWR to favour predicting one type of risk over another?
In SWR-D, most students observed a familiar daily situation from their (able-bodied) perspective. In SWR-DP, students observed a familiar daily situation from a persona’s point of view that differed from that of an able-bodied person. In SWR-C, they observed unfamiliar clinical situations from the patients’ perspective (it is unknown whether this perspective was different from their own). This suggests that when students observe a familiar environment from their own perspective, they concentrate on brainstorming about risks but do not conduct much action simulation (acting on a simulated basis and identifying risks). Consequently, the risks related to action were few.
Conversely, if students observe risk from others’ perspective, they may not be able to brainstorm well, and they may tend to predict risks by performing action simulations. In SWR-DP, many images of simulations, such as trying to use a cafeteria as a persona (for example, a wheelchair user), were recorded. Notably, novice nurses tend to observe bedsides without being able to imagine the patient’s condition or behaviour (Daikoku & Saito, 2017); it seems difficult to predict risks associated with unfamiliar subjects (people/environment) only by brainstorming.
However, during SWR-C, we asked students to predict risks only by observation to avoid interference with patient care, and students were unable to perform action simulations. Nevertheless, the risks associated with actions were the most predicted. According to the risks predicted by the students (Table 1), students likely found patients who were confused and observed their behaviour. In the clinical situation, there were several observable patients that students could predict many risks based on observable actions.
In summary, for clinically inexperienced students to predict many indirect impact risks (perception, comprehension), it is better for them to make observations from their own perspectives in a daily situation where brainstorming can be easily conducted. It is better to ask students to observe an unfamiliar person and environment to identify more direct impact risks (actions). It would be better to create a fictitious user profile (persona) and conduct SWR (SWR-DP) or conduct SWR in a clinical situation unfamiliar to students (SWR-C). In any case, if each SWR is implemented independently, the predicted risks are biased. Therefore, by combining each SWR, it may be possible to develop skills that enable students to find direct impact and indirect impact risks in a well-balanced manner.
B. Limitations
This study evaluates the educational benefits of three SWR patterns and discusses their effectiveness. We could not compare the three patterns of SWR for the following aspects. First, we could not examine the relationship between participants’ background and SWR. This study targeted first-year medical students (SWR-C) and third-year students in the medical engineer training course (SWR-D, SWR-DP). Each student’s age and expertise were different. Therefore, the background of each participant could have affected the participant’s risk prediction tendency. However, all students shared the common background of having no clinical experience and had basic education on patient safety and conducted SWR with a basic knowledge of human factors, such as medical accident analysis methods. Second, we could not conduct a comparative study of each SWR by statistical analysis as there were differences in the way each SWR was conducted. SWR-D and SWR-DP were administered as a group, while SWR-C was administered individually because of restrictions in clinical practice. We could not calculate the average number of hazard predictions per student.
Further, each SWR was conducted in a compulsory class; therefore, there were a large number of students per faculty member. Consequently, we could not observe all students. Therefore, we have little record of how students predicted risks, especially in SWR-C. This is because the simulation actions in clinical situations and photography were restricted.
Additionally, when examining the safety of facility design, it is important to predict risks to healthcare professionals as well as patients (Reiling et al., 2003). However, in SWR-C, 90% of the risks were related to patients. Future studies should examine training methods that enable clinically inexperienced students to predict risks to healthcare professionals.
V. CONCLUSION
In this study, we proposed a patient safety education method incorporating SWR. We conducted SWR-D, SWR-DP, and SWR-C sessions and clarified the risk assessment tendency of students in each SWR pattern. For students to predict many indirect impact risks (perception comprehension), it is better to have students observe a daily situation in which it is easy to identify risks from their own points of view (SWR-D). To find many direct impact risks (action), it is better for students to create a persona and observe a daily situation (SWR-DP) or clinical situation (SWR-C). This suggests that a combination of these SWRs would provide students with the skills to comprehensively predict the patient safety risks in facilities and the environment. By continuously conducting all SWR session types starting at lower grade levels, it is expected that skills related to risk assessment will be effectively acquired. It is expected that SWR education from pre-graduates will increase the number of medical professionals who can conduct an appropriate risk assessment in the field, resulting in improved quality and safety of healthcare.
Notes on Contributors
Yoshitaka Maeda, PhD, a Research Associate at the Medical Simulation Center at Jichi Medical University, Japan, contributed to the conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing (original draft, review, and editing), and visualization.
Yoshikazu Asada, PhD, an Assistant Professor at the Center for Information at Jichi Medical University, Japan, contributed to the methodology, validation, formal analysis, and visualization.
Yoshihiko Suzuki, MD, an Assistant Professor at the Medical Simulation Center at Jichi Medical University, Japan, contributed to the conceptualization and methodology.
Akihiro Watanabe, MS, a Research Associate at the Faculty of Health and Medical Sciences at Kanagawa Institute of Technology, Japan, contributed to the validation and investigation.
Satoshi Suzuki, PhD, a Professor at the Faculty of Health and Medical Sciences at Kanagawa Institute of Technology, Japan, contributed to the data curation, writing (review and editing), and visualization.
Hiroshi Kawahira, MD, PhD, FACS, a Professor at the Medical Simulation Center at Jichi Medical University, Japan, contributed to the writing (review and editing), supervision, and project administration.
All the authors have read and approved the final manuscript.
Ethical Approval
This study was approved by the Jichi Medical University Institutional Review Board (protocol number 18-014).
Data Availability
The data that support the findings of this study are openly available in Figshare repository, http://doi.org/10.6084/m9.figshare.13012664
Funding
There is no funder for this study.
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
Alper, E., Rosenberg, E. I., O’Brien, K. E., Fischer, M., & Durning, S. J. (2009). Patient safety education at US and Canadian medical schools: Results from the 2006 clerkship directors in internal medicine survey. Academic Medicine, 84(12), 1672-1676. https://doi.org/10.1097/acm.0b013e3181bf98a4
Cooper, A. (2004). The inmates are running the asylum: Why high-tech products drive us crazy and how to restore the sanity (Vol. 2). Sams Publishing.
Daikoku, R., & Saito, Y. (2017). Characteristics of gaze in expert nurses during observation at the bedside. Japanese Journal of Nursing Art and Science, 15(3), 218-226. https://doi.org/10.18892/jsnas.15.3_218
Doi, T., Kawamoto, K., & Yamaguchi, K. (2012). Difference by level of awareness and the years of experience to patient treatment safety. Japanese Journal of Radiological Technology, 68(5), 608-616. https://doi.org/10.6009/jjrt.2012_JSRT_68.5.608
Donnelly, L. F., Dickerson, J. M., Lehkamp, T. W., Gessner, K. E., Moskovitz, J., & Hutchinson, S. (2008). IRQN award paper: Operational rounds: A practical administrative process to improve safety and clinical services in radiology. Journal of the American College of Radiology, 5(11), 1142-1149. https://doi.org/10.1016/j.jacr.2008.05.017
Fleming, J., & Koman, R. (1998). Web navigation: Designing the user experience. O’Reilly Media.
Frankel, A., Gandhi, T. K., & Bates, D. W. (2003). Improving patient safety across a large integrated health care delivery system. International Journal for Quality in Health Care, 15(suppl_1), i31-i40. https://doi.org/10.1093/intqhc/mzg075
Hafey, R. B. (2017). Lean safety gemba walks: A methodology for workforce engagement and culture change. Productivity Press.
Ishikawa, M., Hirao, T., & Maezawa, M. (2008). Study of patient safety education for undergraduates. Medical Education, 39(2), 115-119. https://doi.org/10.11307/mededjapan1970.39.115
Joseph, A., & Rashid, M. (2007). The architecture of safety: Hospital design. Current Opinion in Critical Care, 13(6), 714-719. https://doi.org/10.1097/mcc.0b013e3282f1be6e
Keller, J. M. (1987). Development and use of the ARCS model of instructional design. Journal of Instructional Development, 10(3), 2-10. https://doi.org/10.1007/BF02905780
Lindgren, A., Chen, F., Amdahl, P., & Chaikiat, P. (2007). Using personas and scenarios as an interface design tool for advanced driver assistance systems. In: Stephanidis C. (eds) Universal Access in Human-Computer Interaction. Ambient Interaction. UAHCI 2007. Lecture Notes in Computer Science, vol 4555. Springer. https://doi.org/10.1007/978-3-540-73281-5_49
Lucian Leape Institute. (Eds.). (2010). Unmet needs: Teaching physicians to provide safe patient care. National Patient Safety Foundation.
Maeda, Y., Asada, Y., Suzuki, Y., Watanabe, A., Suzuki, S., & Kawahira, H. (2021). Proposal for safety walk-round education to develop risk prediction skills of novice health professional students [Data set]. Figshare. http://doi.org/10.6084/m9.figshare.13012664
Mayer, D., Klamen, D. L., Gunderson, A., & Barach, P. (2009). Designing a patient safety undergraduate medical curriculum: The Telluride interdisciplinary roundtable experience. Teaching and Learning in Medicine, 21(1), 52-58. https://doi.org/10.1080/10401330802574090
Michalska, J., & Szewieczek, D. (2007). The 5S methodology as a tool for improving the organization. Journal of Achievements in Materials and Manufacturing Engineering, 24(2), 211-214.
Mulder, S., & Yaar, Z. (2006). The user is always right: A practical guide to creating and using personas for the web. New Riders.
Murata, A., Hayami, T., & Moriwaka, M. (2009). Visual information processing characteristics of drivers in prediction of dangerous situation-Comparison among novice, expert and non-licensed person. In IEEE SMC Hiroshima Chapter (Eds.), Proceedings of Fifth International Workshop on Computational Intelligence & Applications, (pp. 254-257). IEEE SMC Hiroshima Chapter.
Nakajima, K. (2012). Patient safety and quality of medical care. Topics: III. Management of patient safety and quality of medical care: Theory and practice; 4. Patient safety and quality improvement education for undergraduate medical students. Nihon Naika Gakkai zasshi. The Journal of the Japanese Society of Internal Medicine, 101(12), 3477. https://doi.org/10.2169/naika.101.3477
Norman, D. A. (1988). The psychology of everyday things. Basic Books.
Norman, D. A., & Draper, S. W. (1986). User centered system design: New perspectives on human-computer interaction. L. Erlbaum Associates.
Okubo, Y., Kuroda, R., & Yamamoto, K. (2014). Health and safety patrol in universities. Journal of Environment and Safety, 5(3), 169-175. https://doi.org/10.11162/daikankyo.14C0702
Reiling, J. (2006). Safe design of healthcare facilities. BMJ Quality & Safety, 15(suppl 1), i34-i40. https://dx.doi.org/10.1136%2Fqshc.2006.019422
Reiling, J., Breckbill, C., Murphy, M., McCullough, S., & Chernos, S. (2003). Facility designing around patient safety and its effect on nursing. Nursing Economics, 21(3), 143.
Reiling, J., Hughes, R. G., & Murphy, M. R. (2008). The impact of facility design on patient safety. In Hughes, R. G (Ed.), Patient safety and quality: An evidence-based handbook for nurses. Agency for Healthcare Research and Quality.
Singer, S. J., & Tucker, A. L. (2014). The evolving literature on Safety walkrounds: Emerging themes and practical messages. BMJ Quality & Safety, 23(10), 789–800. http://dx.doi.org/10.1136/bmjqs-2014-003416
Walton, M., Woodward, H., Van Staalduinen, S., Lemer, C., Greaves, F., Noble, D., Ellis, B., Donaldson, L., & Barraclough, B. (2010). The WHO patient safety curriculum guide for medical schools. BMJ Quality & Safety, 19(6), 542-546. http://dx.doi.org/10.1136/qshc.2009.036970
Womack, J. (2013). Gemba walks: Expanded 2nd edition. Lean Enterprise Institute.
Zhang, J., Patel, V. L., & Johnson, T. R. (2002). Medical error: Is the solution medical or cognitive? Journal of American Medical Informatics Association, 9(6 Suppl 1), s75-77. https://dx.doi.org/10.1197%2Fjamia.M1232
Zhang, J., Patel, V. L., Johnson, T. R., & Shortliffe, E. H. (2004). A cognitive taxonomy of medical errors. Journal of Biomedical Informatics, 37(3), 193-204. https://doi.org/10.1016/j.jbi.2004.04.004
*Yoshitaka Maeda, PhD
3311-1, Yakushiji, Shimotsuke-shi,
(Kinen-tou 7th floor),
Tochigi,Japan, 329-0498
Tel: +81-285-58-7455
Email: y-maeda@jichi.ac.jp
Submitted: 30 April 2020
Accepted: 8 September 2020
Published online: 4 May, TAPS 2021, 6(2), 66-77
https://doi.org/10.29060/TAPS.2021-6-2/OA2391
Pauline Luk & Julie Chen
The University of Hong Kong, Hong Kong
Abstract
Introduction: A novel initiative allowed third year medical students to pursue experiential learning during a year-long Enrichment Year programme as part of the core curriculum. ‘connect*ed’, an online virtual community of learning was developed to provide learning and social support to students and to help them link their diverse experiences with the common goal of being a doctor. This study examined the nature, pattern, and content of online interactions among medical students within this community of learning to identify features that support learning and personal growth.
Methods: This was a quantitative-qualitative study using platform data analytics, social network analysis, thematic content analysis to analyse the nature and pattern of online interactions. Focus group interviews with the faculty mentors and medical students were used to triangulate the results.
Results: Students favoured online interactions focused on sharing and learning from each other rather than structured tasks. Multimedia content, especially images, attracted more attention and stimulated more constructive discussion. We identified five patterns of interaction. The degree centrality and reciprocity did not affect the team interactivity but mutual encouragement by team members and mentors can promote a positive team dynamic.
Conclusion: Online interactions that are less structured, relate to personal interests, and use of multimedia appear to generate the most meaningful content and teams do not necessarily need to have a leader to be effective. A structured online network that adopts these features can better support learners who are geographically separated and engaged in different learning experiences.
Keywords: Online Learning, Undergraduate, Interaction, Experiential Learning
Practice Highlights
- Image-based messages and less structured online activities focused on experience-sharing engage students and stimulate a more constructive discussion.
- The proactivity of students and mentors can foster a positive team dynamic and learning experience.
- A team or group leader is not always necessary to promote group interaction.
I. INTRODUCTION
Increasingly, medical schools are recognising the potential of a holistic, experiential curriculum to nurture the professional development of their students (Kallail et al., 2020). A growing body of evidence supports the benefits of experiential learning. Experiential learning has been associated with increasing interest in learning (Kallail et al., 2020) a better understanding of career choice (Lyons, 2017), and higher-order critical thinking skills (Alamodi et al., 2018).
Beginning in 2018-19, the Li Ka Shing Faculty of Medicine of The University of Hong Kong (HKUMed) introduced a mandatory, credit-bearing Enrichment Year for all third-year medical students. This initiative provided opportunities for substantive engagement in a personal area of interest related to research, service or humanitarian work, pursuit of a higher degree, or university exchange anywhere in the world in order to further the professional and personal development of students.
Recognising the difficulties students may encounter when they are off-campus and the need to support student experiential learning, we developed an online virtual community of learning called ‘connect*ed’ to provide learning and social support to students and to help them link their diverse experiences with their common goal of becoming a doctor. The idea of an online virtual learning space is well situated within the social constructivist theoretical framework (Vygotsky, 1978) which views social interaction as the basis for learning. Individuals develop and construct knowledge better when interacting with others rather than unilaterally receiving information, thereby conceptualising learning as a collaborative process. Building on this idea, Lave and Wenger discussed ‘communities of practice’ in which socially supported learning takes place (Lave & Wenger, 1991). In this related theory, social learning takes place within communities of practice defined as groups who have a common interest or domain, who engage and interact in shared activities thus developing a relationship. This dialogic interaction among the learner, peers and tutor evolves over time and can take place and be captured in the virtual learning space to support the evolution of work (Greenberg, 2006). In the higher education setting, online discussion forums, or web 2.0 technologies such as blogs and wikis draw on the benefits of social learning and communities of practice giving students time to think, contribute and give and receive feedback to help their learning.
This aim of this study is to examine the nature, pattern, and content of online interactions among medical students within the virtual community of learning, connect*ed, to identify features that support learning and personal growth. Findings will offer insight on how to further optimize collaborative online learning.
II. METHODS
A. Context
During the Enrichment Year, students were allocated to teams with a designated faculty mentor. Team composition was designed to maximise diversity of learning experiences, hence each team would have at least one student who was doing research, one doing service or humanitarian work, and one pursuing an exchange opportunity abroad. This allowed students to benefit from the experiences of their teammates. Prior to departure, a Launch Day was convened in June 2018 to facilitate team cohesion among members and their mentor, to familiarise with the connect*ed objectives, the e-learning platform, mentor and student teammates.
We chose to use the commercially developed e-platform, Workplace by Facebook to house connect*ed after extensive consultation and testing with stakeholders. The interface of Workplace is very similar to Facebook but operates in a closed community only accessible to registered connect*ed users. This helped to address legitimate privacy and confidentiality concerns while providing a user-friendly and familiar platform that students and teachers were willing to use.
Teams were encouraged to share their learning experience with each other and with their mentor on Workplace. Structured learning modules called “Inquiry Pods” (IP) were released online on a regular basis to help facilitate the sharing and discussion. The themes for the inquiry pods were communicator, ethical decision-maker, and global citizen, based on the six educational aims and learning outcomes of the university and the Bachelor of Medicine and Bachelor of Surgery (MBBS) programme (HKU, 2017). Students completed each IP by posting, commenting, and reacting to trigger material provided in the IP or based on their own/others Enrichment Year experience. Most of the posts were photos, video, text, or sharing of online information, via hyperlinks.
connect*ed is a graded component of the Enrichment Year and students must earn a pass (60%) in order to proceed to the next year of study. Team mentors graded each inquiry pod as a formative assessment, and at the end of the year, provided a summative assessment based the overall performance in the IP, online participation and team impact presentation. All the assessments were rubric-based (Appendix 1: Grading rubrics).
B. Study Design
This was a mixed methods quantitative-qualitative study that combined analyses of platform analytic data and qualitative information drawn from student work and focus group discussions (FGD) used to provide a richer understanding of online learning interactions among students (Ma, 2012).
C. Subjects
In the academic year 2018-19, 206 students participated in the Enrichment Year. They participated in 302 activities in Hong Kong and in 23 different cities around the world (Appendix 2: Activities undertaken by students in 2018-2019). These students were selectively divided into 33 teams of five to eight students, according to gender, destination and nature of activities, to ensure the most diversified combination of members.
D. Data Sources, Collection and Analysis
1) Level of activity: At the end of the first academic year, we evaluated the students’ online activity by analysing the usage data collected through the Application Programming Interface (API) of Workplace from June 2018 to May 2019. These showed the frequency of activity in terms of students, mentors and teams who posted, commented, replied, and reacted on the platform.
2) Social network interaction: Social network analysis is a method for studying the structure of relationships and the effect this social structure has on the attitudes, behaviour, and performance of the individual members of a group (Saqr et al., 2018). We extracted the Workplace data using Workplace Graph API, which allowed us to create objects by nodes and joined along edges, and developed a web tool (PHP +Vue.js+JQuery) to export data from Workplace. We focused our analysis on team members’ position and role in teams. The extracted data were imported to the open source software, Gephi that generated a graph for social network analysis. The software used nodes and edges to represent the connections between each member of the team and presented the interactions within the social network in terms of the size, gradient, and direction of the communication (Bastian et al., 2009).
3) Content of posts: The content of posts by each team was analysed for common themes based on the type of messages posted on the platform. Initial codes were generated based on the purpose of the posts and then categorised to find the essence of each theme. This allowed us to identify how students were using the platform and thereby understand the basic functions of the virtual community of learning.
4) Feedback and focus group discussion: We conducted FGD with students and mentors from March – June 2019. There were 13 FGD with 30 mentors and three with 9 students. Participation in FGD was voluntary and no monetary incentive was given to students or mentors. For mentors, the FGD was part of the evaluation, feedback and engagement effort to encourage mentors to continue their involvement in their project which is why all mentors were invited and most participated. Therefore, the participation rate was high. For the students’ sessions, there was a purposive selection of subjects based on student volunteers who were keen to share their experience and deliberate invitation to those who were comparatively inactive in the project. Each interview session lasted for 60 to 90 minutes. A semi-structured interview guide with pre-determined questions was used to focus the conversation on desired themes. The questions for both mentors and students were similar and covered participants’ experiences with connect*ed, using the Workplace platform, challenges and suggestions for improvement. All FGD were recorded by contemporaneous notes that were organised immediately following each session.
III. RESULTS
A. Level of Activity
There was a total of 815 posts, 8198 comments, and 6250 emoticon reactions: like (5843), love (169), haha (152), wow (71), sad (14), and angry (1) by 206 students and 33 mentors as summarised in Table 1.
|
Post (average) |
Comment (average) |
Reaction (average) |
|
Mentor N=33 |
539 (16.3) |
1484 (44.9) |
3017 (91.4) |
|
Students N=206 |
276 (1.3) |
6714 (32.6) |
3233 (15.7) |
|
Total |
815 |
8198 |
6250 |
Table 1. Summary of online interactions in 2018-19
B. Social Network Interaction
The pattern of interactions was visually represented in a social network analysis by Gephi. In the diagram, the red node represents the mentor, the green node represents the students. The edge between the nodes represents the interactions. The thicker and darker colour of the edge represents more interaction. The arrow represents the direction of the communication.
We categorised the patterns according to the number of responses of mentor and students. By comparing the frequency of responses (posts, comments, and reactions), we found that there were five common patterns of interaction that were reflected in all teams, regardless of their level of activity as summarised in Table 2.
Pattern |
Frequency of Posts |
Frequency of Comments |
Frequency of Reactions |
Team identifier |
|
1 |
High (from mentor) |
High (from mentor) |
High (from mentor) |
1, 9, 10, 11, 17, 21, 25, 26, 33, |
|
2 |
High from mentor |
High from mentor |
Average/Low from mentor |
2, 19, 31 |
|
3 |
High from mentor |
Low from mentor |
Average/Low from mentor |
3, 7, 14, 18, 28 |
|
4 |
High from mentor |
Low from mentor |
High from mentor |
4, 6, 12, 13, 15, 20, 23, 27, 29 |
|
5 |
High from mentor |
Average from mentor and students |
Any frequency |
5, 8, 16, 22, 24, 30, 32 |
Remark: H=high participation compare to team average; A=average participation that mentors are having similar amount of participation as students; L= low participation compare to team average
Table 2. Patterns of interactions among teams
In general, all mentors were more active than students as teachers initiated new posts and were often keen to share information with students (Appendix 3). Even when students were encouraged to create new posts, they tended to focus on completing the tasks in the Inquiry Pods.
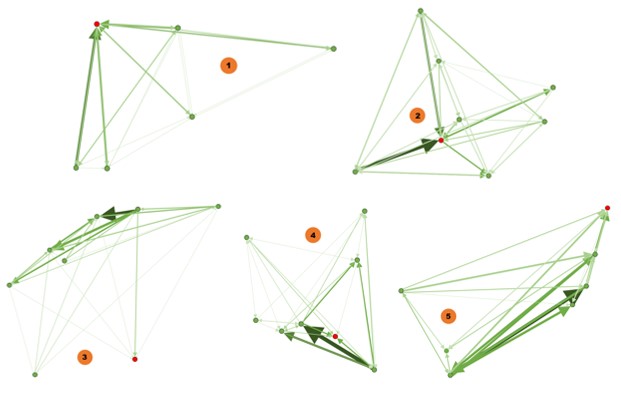
Diagram 1: Patterns of online interactions by teams
1) Pattern 1: Mentor degree centrality: We found that the number of responses from mentors were much higher than the students. For example, in Team 1, the mentor made 113 posts, 236 comments, and 227 reactions, while the five students made between 1-5 posts, 38-54 comments, and 14-43 reactions. Mentors were the centre point and driving force of the interaction. Students interact with others in response to mentor facilitation making the degree centrality towards to the mentor. The thickness of the edges is evenly distributed indicating a consistent level of interaction among all team members.
2) Pattern 2: Mentor degree centrality: Similar to Pattern 1, mentors were also active in posting and commenting, but gave much fewer reactions than students. The centre point is towards the mentor, and also the most active students in the team as shown by the two thick edges in the diagram. For instance, in team 2, the mentor posted 43 posts, 127 comments, and 19 reactions, while the seven students posted 1 to 12 post, 28 to 65 comments, and 8 to 66 reactions respectively. In this pattern, mentor was also the centre point, however, some nodes of students shared thicker edges.
3) Pattern 3: Student degree centrality: Team 3 is such an example, showing that the thick arrows are pointing towards students, meaning that the interaction is initiated by students. The mentor took a less important role in the conversations. The degree centrality is towards students and the mentor was outside of the interaction centre. For instance, in team 3, the mentor posted 12 posts, 19 comments, and 20 reactions, while the seven students posted 1 to 12 post, 17 to 68 comments, and 0 to 64 reactions respectively. In this pattern, mentor was situated outside the conversation circle. The degree of centrality shifted to students.
4) Pattern 4: Student degree centrality: The dynamics of interaction leaned towards active students, which were represented by the thick edges towards certain students. In this pattern, there were usually multiple centre points that did not include the mentor. For instance, in team 4, the mentor posted 11 posts, 27 comments, and 90 reactions, while the seven students posted 0 to 3 post, 28 to 78 comments, and 0 to 39 reactions respectively. The degree of centrality shifted to multiple students.
5) Pattern 5: Diversified degree centrality: Mentors were active in posting, having similar frequency of comments as the students and the number of comments among all members are the same, and having low reactions. In this pattern, there are multiple conversation nodes and most are interactions between students. Those interactions are more student-driven and indicate multi-centred conversation. For instance, in team 5, the mentor posted 18 posts, 36 comments, and 3 reactions, while the six students posted 0 to 3 post, 31 to 62 comments, and 4 to 29 reactions respectively. The degree of centrality shifted to more than one student. In this pattern, there is more interaction between students as shown by the bi-directional arrows. The degree centrality is low with diversified centres.
These patterns show that teams could have single-centred interaction (Pattern 1 & 2) or multi-centred interaction (Pattern 3, 4, & 5) with each representing different team interactions. Team activity, and not the centeredness of the interaction, was associated with the effectiveness of collaboration and the completion of tasks. In addition, most teams demonstrated one-way communication when interacting. That means the reciprocity of a network is low. In Teams 1 and 2, the interaction dynamics favoured the mentors, while in Teams 3, 4, and 5, the dynamics leaned towards active students. In contrast, team 5 demonstrated strong reciprocity.
However, after comparing the patterns of all 33 teams, there is no indication that a certain pattern was better than the others. There was no significant difference in the on-time completion rate for the IP assignments for the five most active teams (86.9%) compared with all 33 teams (85.5%).
C. Content of Posts
In connect*ed, students shared their Enrichment Year experience using text, photo, video, or related links of other websites. The nature of interactions was predominantly text-based, as it is easier to post and interact using the text. However, image-based messages attracted more attention and stimulated a more constructive discussion.
There were three particular areas that generated greater levels of interactivity. Firstly, students were very willing to share and reflect on their personal experiences. Taking the ‘Communicator’ Inquiry Pod as an example, students shared their observations on communication in their respective settings by posting on the team wall:
“There is a huge contrast here, where students actively ask questions even if the setting involves 80+ students. I suppose the background behind the two nationalities have a huge role in it, as Asians tend to be a bit more shy compared to the extrovertiveness commonly shared by Westerners. While we should embrace who we were and are, I think it is also beneficial to observe others and learn from such observations.”
Student A (studied abroad)
This text-based conversation thread compared and contrasted effective classroom communication in different countries. It enabled students to reflect and to draw on their own experiences to benefit all team members.
The second area of interest for students was social support. One of the most popular activities was the posting of photos and videos about their Enrichment Year activities including when they are performing social service missions, cooking a gourmet meal or joining group gatherings during festive occasions. Those posts generated numerous responses and reactions indicating a keen interest in reaching out and maintaining social connectedness.
Thirdly, students were more active online when there was information being shared related to the medical practice and they are more willing to discuss their views as shown in this sequence from Team 3:
“Being a MBBS student, people around may ask us for medical advice. They think we are knowledgeable to make a diagnosis based on their description and believe we are able to help. However, as we are not yet qualified, it is inappropriate for us to give any professional opinion. Sometimes, I would like to share what I have learnt and suggest some possible solutions. Nevertheless, at the same time, I am afraid my opinion would affect their health seeking behaviour, for instance, they might just follow what I share instead of seeing a doctor.”
Student B
“It’s true that we are not knowledgeable enough to give medical advice and it will be misleading to our relatives and friends if they take our opinions as professional advice and decide not to seek proper medical opinions. Thus, we should always remind ourselves of the role as medical students and think about the impacts of our words.”
Student C
“I understand your feeling as my relatives and friends also ask me for medical advice. It will be safer to advise them to seek help from medical professionals for diagnosis or other serious health issues. However, as a medical student, I think it is possible for us to give them some lifestyle advice without causing harmful consequences, for instance, smoking cessation, diet with lower cholesterol content and moderate exercise. Although we are not qualified to make a diagnosis at the moment, we can still use our medical knowledge as a way to promote public health and arise their health conscious.”
Student D
Students more actively express their opinions when the topics under discussion are related to the profession they are aiming to join.
D. Feedback and Focus Group Interviews
Although there were only 9 student interviewees, we found repeated themes and content suggesting data saturation. This may be because connect*ed comprised only 10% of the overall Enrichment Year and students did not pay particular attention to this component resulting in little variation in responses during the FGD.
The main theme that arose from the FGD with students and mentors was about the most rewarding aspect of the online interaction in connect*ed. Both groups indicated that this was the social connectivity attained through student sharing of day-to-day life during the Enrichment Year.
“The photo and video did not need much effort to share with others, but they are more interesting and can let me know more about how others were doing during their Enrichment Year.”
Student E
“I am very interested in knowing the life of others in other universities. I hope they can share more and we could see others’ videos.”
Student F
“Sharing things we learned with the team could help us to be more socialized.”
Student G
Mentors also enjoyed knowing more about students’ Enrichment Year life and believed that students should enjoy themselves while learning.
“The connect*ed is a good example helping students to bridge their knowledge and core value. The sharing of experience (related to the Enrichment Year) is important, it engages students in the discussion”
Mentor X
“The platform support each other very well. This is a platform for socializing and communicating. I know what students are doing if they posted on the team wall.”
Mentor Y
The value of social connectivity for support was further emphasized by students suggesting that the platform was more useful for social networking than learning.
“connect*ed provided a platform for us sharing the struggles and support each other when I was having my Enrichment Year.”
Student I
This view was echoed by mentors who believed that connect*ed provided necessary support for students especially those who were overseas. Mentors used the chat function on Workplace to have personalized communication with their members and to offer advice.
“I used the chat function on the Workplace, which is more personal and can support each other very well…. I can have immediate interaction with students.”
Mentor Z
Students found mentors were motivating and encouraged them to interact in teams which led to some mentor-centric team interactions.
“Our mentor is very motivating and encourages all members to participate in the discussion. She guided us through to complete the inquiry pods.”
Student J
“In my team, there are some inactive members who have demotivated me to interact. If there is an active member, I think it would help.”
Student K
The findings also indicated that proactivity by student members, participation by the mentor, responsiveness, and social/non-academic discussions fostered a positive team dynamic and a positive online learning experience, regardless of whether the team interaction was primarily single-centred or multi-centred.
IV. DISCUSSION
This study examined the nature, pattern, and content of online interactions among medical students within a virtual community of learning among the inaugural cohort of the Enrichment Year to identify features that support learning and personal growth.
Our results found that students favoured online interactions that were less structured, image-rich and focused on sharing of experience to learn from each other and to support one another. Multimedia content, especially images, attracted more attention and stimulated discussion that was more constructive. This is consistent with findings in the literature that show that images have a positive influence on learning and engagement (Chan & Unsworth, 2011; Stuijfzand et al., 2016). Sharing of personal experience helped students to reflect on their own experience and explore how others experienced their Enrichment Year. The results support previous studies that suggest self-reflection and community building enhances experiential learning (Arnold & Paulus, 2010; Pai, 2016). This builds a virtual community that allows students to share their struggles which students found to be a crucial aspect of giving and receiving social support. The use of the different modes of communication available on Workplace, including the text messaging and voice calls as well as social media posting provided flexible avenues of support to students. The finding is very similar to the outcomes of a project involving a mobile application for experiential learning activities (Schnepp & Rogers, 2017). We also observed that the number of positive reactions (like, love, haha or wow) far exceeded the number of negative reactions (sad and angry). This is a visual form of encouragement from mentors and peers that reflected their interest in engaging with each other.
From the patterns derived from our social network analysis, we found that the interaction could be uni-directional or bi-directional, but there was no correlation of the interaction with team effectiveness in completing tasks on time. As seen in the social network patterns identified, active mentors can drive team interaction. However, in contrast with other findings in the literature, the degree centrality and reciprocity do not affect the team interactional dynamic (Jan & Vlachopoulos, 2019). Regardless of the directionality of the predominant interaction, if there are active members in the team or the mentors are motivating, these individuals are the key to generating more interaction and enhancing online learning experience of students.
Ideally, both mentors and all students should be active, but having at least one or two more active students, can raise the team dynamic. Once some students are willing to share their experience and give timely responses, it can stimulate others to join. Continued encouragement of active members and mentors can promote a positive team dynamic. In terms of degree centrality, the observation that no pattern of interaction was superior to the others suggests that a single leader is not always necessary to for the team to be effective.
This study suggests that interactions will occur most naturally when students are doing what they feel is useful such as maintaining social support with each other and their mentor. In order to be accepted, learning initiatives such as linking learning with experiential activities will need to be less formal and integrate more smoothly with students’ demonstrated desire for social support and interest to share experience. In addition, attention to team formation and ensuring opportunity develop team cohesion would be essential as students in the FGD, commented that when there were members they do not know well, it will be a hindrance for interaction. As the connect*ed is one of the graded components of the Enrichment Year, we observed that the assessment could serve as an external motivator encouraging students to contribute to the work and support their team. However, it could also have a negative impact as it is perceived as an additional burden and may pressure some students to participate for the sake of participating and doing so in an inauthentic way.
V. CONCLUSION
The online virtual community, connect*ed, to support experiential learning for medical students is still at an early stage. Features of connect*ed that facilitated learning and personal growth included a focus on student support and sharing especially with multimedia, less structured interactions, and teams with active members and/or mentor. It is important to note that interaction does not equate to learning (Jan & Vlachopoulos, 2019), and so the use of an online network that adopts these features may better support learners but the effectiveness of achieving formal learning outcome should be further studied. We will continue to modify and evaluate the functionality of the connect*ed community to ensure it is fit-for-purpose to support students’ needs and learning.
Notes on Contributors
Pauline Luk and Julie Chen contributed to the design and implementation of the research, analysis of the results and writing of the manuscript. PL drafted the manuscript, and JL edited and contributed to the intellectual content of the manuscript and provided overall supervision of the project. Both authors and approved the final manuscript.
Ethical Approval
This research received approval from the HKU Institutional Review Board (UW18-121). Consent was obtained from participants for the research study.
Acknowledgements
The authors sincerely appreciate the support from the mentors and students who participated in this study, the collaboration with the Education University of Hong Kong, and the administrative and technical support rendered by Mr. Francis Tsoi and Miss Joyce Tsang throughout the project.
Funding
This project was funded by the Hong Kong University Grants Committee (UGC) Funding Scheme for Teaching and Learning Related Proposals (2016-19 Triennium).
Declaration of Interest
The authors report no conflicts of interest.
References
Alamodi, A. A., Abu-Zaid, A., Eshaq, A. M., & Al-Kattan, K. (2018). The summer enrichment program: A multidimensional experiential enriching experience for junior medical students. The American Journal of the Medical Sciences, 356(2), 185-186. https://doi.org/10.1016/j.amjms.2018.05.005
Arnold, N., & Paulus, T. (2010). Using a social networking site for experiential learning: Appropriating, lurking, modeling and community building. The Internet and Higher Education, 13(4), 188-196. https://doi.org/10.1016/j.iheduc.2010.04.002
Bastian, M., Heymann, S., & Jacomy, M. (2009). Gephi: an open source software for exploring and manipulating networks. In the International AAAI Conference on Weblogs and Social Media. 361-362. Retrieved April 1, 2020, from https://vbn.aau.dk/ws/files/328840013/154_3225_1_PB.pdf
Chan, E., & Unsworth, L. (2011). Image–language interaction in online reading environments: Challenges for students’ reading comprehension. Australian Educational Researcher, 38(2), 181-202. https://doi.org/10.1007/s13384-011-0023-y
Greenberg, G. (2006). Can we talk? Electronic portfolios as collaborative learning spaces. In A. Jafari & C. Kaufman (Eds.), Handbook of Research on ePortfolios. Idea Group Inc.
HKU. (2017). Educational aims and institutional learning outcomes. Retrieved April 1, 2020, from http://www.handbook.hku.hk/ug/full-time-2017-18/important-policies/educational-aims-and-institutional-learning-outcomes
Jan, S., & Vlachopoulos, P. (2019). Social network analysis: A framework for identifying communities in higher education online learning. Technology, Knowledge and Learning, 24(4), 621-639. https://doi.org/10.1007/s10758-018-9375-y
Kallail, K. J., Shaw, P., Hughes, T., & Berardo, B. (2020). Enriching medical student learning experiences. Journal of Medical Education and Curricular Development, 7, 4. https://doi.org/10.1177/2382120520902160
Lave, J., & Wenger, E. (1991). Situated learning: legitimate peripheral participation. Cambridge University Press
Lyons, Z. (2017). Establishment and implementation of a psychiatry enrichment programme for medical students. Australasian Psychiatry, 25(1), 69-72. https://doi.org/10.1177/1039856216671663
Ma, L. (2012). Some philosophical considerations in using mixed methods in library and information science research. Journal of the American Society for Information Science and Technology, 63(9), 1859-1867. https://doi.org/10.1002/asi.22711
Pai, H. C. (2016). An integrated model for the effects of self-reflection and clinical experiential learning on clinical nursing performance in nursing students: A longitudinal study. Nurse Education Today, 45, 156. https://doi.org/10.1016/j.nedt.2016.07.011
Saqr, M., Fors, U., Tedre, M., & Nouri, J. (2018). How social network analysis can be used to monitor online collaborative learning and guide an informed intervention. PLoS One, 13(3). http://dx.doi.org/10.1371/journal.pone.0194777
Schnepp, J., & Rogers, C. (2017). Evaluating the acceptability and usability of EASEL: A mobile application that supports guided reflection for experiential learning activities. Journal of Information Technology Education: Innovations in Practice, 16, 195.
Stuijfzand, B. G., van Der Schaaf, M. F., Kirschner, F. C., Ravesloot, C. J., van Der Gijp, A., & Vincken, K. L. (2016). Medical students’ cognitive load in volumetric image interpretation: Insights from human-computer interaction and eye movements. Computers in Human Behavior, 62, 394-5632.
Vygotsky, L. S. (1978). Mind in Society. Harvard University Press. https://doi.org/10.2307/j.ctvjf9vz4
*Pauline Luk
5/F William MW Mong Block
21 Sassoon Road,
Pokfulam, Hong Kong
Email: pluk@hku.hk
Submitted: 21 August 2020
Accepted: 12 November 2020
Published online: 4 May, TAPS 2021, 6(2), 57-65
https://doi.org/10.29060/TAPS.2021-6-2/OA2378
Nicholas Beng Hui Ng1,2, Mae Yue Tan1,2, Shuh Shing Lee3, Nasyitah binti Abdul Aziz3, Marion M Aw1,2 & Jeremy Bingyuan Lin1,2
1Khoo Teck Puat-National University Children’s Medical Institute, National University Health System Singapore; 2Department of Paediatrics, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 3Centre for Medical Education (CenMED), Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: The coronavirus disease 2019 (COVID-19) pandemic has brought about additional challenges beyond the usual transitional stresses faced by a newly qualified doctor. We aimed to evaluate the impact of COVID-19 on interns’ stress, burnout, emotions, and implications on their training, while exploring their coping mechanisms and resilience levels.
Methods: Newly graduated doctors interning in a Paediatric department in Singapore, who experienced escalation of the pandemic from January to April 2020, were invited to participate. Participants completed the Perceived Stress Scale (PSS), Maslach’s Burnout Inventory (MBI), and Connor Davidson Resilience Scale 25-item (CD-RISC 25) pre-pandemic and 4 months into COVID-19. Group interviews were conducted to supplement the quantitative responses to achieve study aims.
Results: Response rate was 100% (n=10) for post-exposure questionnaires and group interviews. Despite working through the pandemic, interns’ stress levels were not increased, burnout remained low, while resilience remained high. Four themes emerged from the group interviews – the impacts of the pandemic on their psychology, duties, training, as well as protective mechanisms. Their responses, particularly the institutional mechanisms and individual coping strategies, enabled us to understand their unexpected low burnout and high resilience despite the pandemic.
Conclusion: This study demonstrated that it is possible to mitigate stress, burnout and preserve resilience of vulnerable healthcare workers such as interns amidst a pandemic. The study also validated a multifaceted approach that targets institutional, faculty as well as individual levels, can ensure the continued wellbeing of healthcare workers even in challenging times.
Keywords: COVID-19, Stress, Burnout, Resilience, Junior Doctor, Intern
Practice Highlights
- Intern doctors face additional and unique challenges in a pandemic, besides the usual stresses of their school-to-work transition.
- Our study shows that a multi-faceted approach that target institution, faculty and individual can lead to reduced burnout and preserved resilience in these doctors.
I. INTRODUCTION
With the coronavirus disease 2019 (COVID-19) pandemic, there are new stressors contributing to burnout in healthcare workers. We were particularly interested in evaluating the impact of COVID-19 on newly qualified doctors doing their internship, also known as House Officers or post-graduate year 1 doctors in Singapore. This is a particularly vulnerable group of healthcare workers as the school-to-work transitional year is traditionally a challenging period with high reports of burnout (Low et al., 2019; Sturman et al., 2017).
In Singapore, our first case of COVID-19 was on 23 January 2020. By February 2020, Singapore had one of the highest numbers of cases out of China (Chia & Moynihan, 2020). A global pandemic was declared on 12 March 2020. In early April 2020, the government tightened local measures with a ‘Circuit Breaker’, akin to the lockdowns in many countries (Ministry of Health Singapore, 2020).
Newly graduated doctors in Singapore complete a 12-month training period (4-month rotations in 3 different disciplines) prior to full medical registration. The period of January to April 2020 was during their third block and coincided with the full evolution of the pandemic, which came with multiple unexpected changes in work within the hospital. These included new protocols for personal protection, team segregation and mechanisms to cope with the increase in COVID-19 cases. In our department, interns and residents were divided into active and passive teams rotating fortnightly, where the active team had to shoulder the responsibility of caring for at risk or COVID-19 paediatric patients, with an intense overnight call duty schedule, different from the weekly frequency in the non-pandemic setting. In addition to work changes, there were also cancellation of overseas leave as well as cessation of scheduled teaching sessions.
With these changes, we aimed to evaluate the impact of the COVID-19 pandemic on interns in our department, focusing on their psychological well-being in terms of stress and burnout, and impact on clinical training. Our secondary aim was to explore the interns’ resilience, coping mechanisms and identify systemic measures they perceived as helpful during this pandemic.
II. METHODS
A. Study Design and Sample
This was a mixed-methods quantitative and qualitative study involving interns who worked from January to April 2020, in a paediatric department at a tertiary academic hospital that actively admitted COVID-19 patients. Informed consent was obtained from all participants for both the quantitative and qualitative components of the study.
B. Quantitative Data Methodology
Pre-pandemic data on perceived stress, burnout and resilience levels were collected a priori in early January 2020, when the interns first joined the department. This was part of a baseline evaluation of a separate study. We employed validated scales: the Perceived Stress Scale (PSS) (Cohen et al., 1983), the Maslach Burnout Inventory (MBI) for Health Services Survey (Maslach & Leiter, 2016), and the Connor-Davidson Resilience Scale 25-item (CD-RSIC 25) (Connor & Davidson, 2003) to measure stress, burnout and resilience respectively. The PSS measures the perception of stress, and is designed to tap how unpredictable, uncontrollable, and overloaded respondents find their lives. Scores ranging from 0-13, 14-26, and 27-40 are mild, moderate, and high perceived stress, respectively. The MBI is a 22-item inventory with scores in 3 domains of burnout: emotional exhaustion (EE), depersonalization (DP), and low personal accomplishment (PA) based on multiple questions for each of these subscales. We used a strict definition of burnout as having fulfilled criteria in all 3 domains of the MBI (i.e. high EE ≧ 27, high DP ≧ 10, and low PA ≦ 33). A liberal definition (i.e. high EE ≧ 27 and high DP ≧ 10 with or without a low PA) was also measured as both definitions are widely adopted in literature (Rotenstein et al., 2018). The CD-RISC 25-item (English version) is a validated scale to measure resilience. It gives a score ranging from 0 to 100, with higher scores reflecting greater resilience. On completion of the posting in end April 2020, the interns repeated the same set of questionnaires.
C. Qualitative Data Methodology: Group Discussions
We conducted group interviews to further evaluate the responses obtained from the questionnaires and to better understand the impact on the interns. Invitation emails were sent to all interns; participation was voluntary. The questions were developed to explore the challenges, emotions, psychological states and reflections of their coping mechanisms and supportive measures of the interns while working in the pandemic. The questions were developed and refined by the authors after discussion and consensus (Appendix 1). Two group interviews were conducted on separate days by the same interviewer, to maintain team segregation and physical distancing. Each group had 5 participants. The sessions were recorded and subsequently transcribed by an independent party.
D. Data Analysis
Quantitative data on the validated scales were scored according to the corresponding manuals. Descriptive and comparative analysis was done with SPSS, Version 23. For the interviews, thematic analysis was conducted. Two of the authors (SS & NAA) read the transcripts to understand fully the data, generated the initial codes independently. Next, codes with consistently similar content were grouped into sub-categories, and similar sub-categories were then combined into categories to form themes. In the event there were differing views on the coding or theme, they re-examined the primary data and further discussed to achieve consensus.
III. RESULTS
A. Quantitative Results
We had a 90% response rate (n=9) for the pre-exposure and 100% (n=10) for the post-exposure questionnaires. There was no change in PSS scores among the interns despite the pandemic, with both median scores in the moderate stress category at 17.5 post-exposure and 17 pre-exposure. There was no high perceived stress in all interns post-exposure. Using the strictest definition of burnout, burnout remained low at 20% post-exposure, compared to 11.1% pre-exposure (Table 1). When a more liberal definition of burnout is used as discussed in the methodology section, only 20% of participants were burnout post-exposure, compared to 66.7% of participants pre-exposure. High resilience levels were maintained, with median score of 74 pre-exposure and 72.5 post-exposure.
|
Measures |
Pre-exposure, (n=9) |
Post-exposure, (n=10) |
p value |
|
Perceived Stress Scale (PSS) |
|||
|
Median (SD) |
17 (6.75) |
17.50 (5.70)
|
N.A |
|
Low stress, n (%) |
4 (44.4%) |
3 (30%)
|
0.65 |
|
Moderate stress, n (%) |
4 (44.4%) |
7 (70%)
|
0.37 |
|
High stress, n (%) |
1 (11.1%) |
0 (0%)
|
0.474 |
|
Maslach Burnout Inventory (MBI) |
|||
|
No burnout, n (%) |
3 (33.3%) |
4 (40.0%) |
0.999 |
|
Strict definition of burnout, n (%) |
1 (11.1%) |
2 (20.0%)
|
0.999 |
|
Liberal definition of burnout, n (%) |
6 (66.7%) |
2 (20%) |
0.09 |
Table 1: Quantitative results showing scores on the Perceived Stress Scale and Maslach Burnout Inventory of the interns pre-pandemic, compared with scores post-exposure. (SD= Standard Deviation).
B. Qualitative Results
We had 100% participation in the group interviews (n=10). Four themes emerged from the qualitative analysis – psychological impact (feelings), impact on duties, impact on teaching and learning as well as preventive measures and support system. These are summarised in Table 2.
|
Key Theme 1: Psychological Impact (Feelings) |
|
|
Sub-themes |
Sample of quotations |
|
a) Loss of control coping with many changes
b) Emotional exhaustion (fear, burnout, uncertainty, loneliness)
c) Positive feelings |
“…throughout the pandemic, there were a lot of unexpected changes and uncertainty among the junior doctors especially the PGY1s (referring to interns)…”
“…COVID gives people much stress due to the uncertainty in a lot of things…” “the thought of COVID patients is scary” “…if I really contract this (COVID-19) I wouldn’t have too much concern (but) I was more scared I would pass it on to my family “…stress stemming from fear” “… cannot help but experienced feelings of isolation and loneliness… I avoided my mother, who is immunocompromised as I worry about passing the infection to her even when I am off active COVID-care duty…” “feeling of being protected alleviated stress and concerns related to contracting the virus” “…months during pandemic (in the posting) were enriching and enjoyable…” “working during pandemic is deemed as “a badge of honour” “felt the months during pandemic situation was a ‘good learning experience’”
|
|
Key Theme 2: Impact on Duties |
|
|
Sub-themes |
Sample of quotations |
|
a) Changes in clinical duties
b) Dealing with rapidly changing protocols
|
“felt that manpower shortage coupled with more frequent on-call duties within two weeks causes early burnout”
“…I think on the ground level the protocol is always bleak, for example who to swab and when…” “delayed updating of protocol online led to a bit of confusion” “not getting updated instantaneously and lack of accessible to the information” |
|
Key Theme 3: Impact on Teaching and Learning |
|
|
Sub-themes |
Sample of quotations |
|
a) Clinical exposure
b) Changes in teaching approaches |
“…in terms of the variety of cases in posting, it is significantly affected due to pandemic that changed demographic of attendees”
“…there wasn’t much teaching on-going until recently when we got the online platforms which I do feel is more helpful…” “due to having lesser patients, feels consultants have more time to teach” “while there is no group teaching, there is more teaching of cases on wards” |
|
Theme 4: Protective Measures and Support System |
|
|
Sub-themes |
Sample of quotations |
|
a) Rotation system which ensured sufficient manpower and rest
b) Institutional measures for personal protection against COVID-19 infection
c) Seniors, Peers and Staff support
d) Self-adaptability and resilience
|
“…we have enough manpower to actually toggle between the rotations for COVID-care and non-COVID services…”
“…PGY1s (Interns) are protected as we don’t swab the patients and we don’t have to expose ourselves to the possible aerolisation of the secretions, so I think that really protected us and relieved our stress…”
“… regular meetings (with) seniors that sat down to uncover our worries… seniors were open to taking feedback about rostering and manpower…” “…I really think it’s the support that has been given by the department and the institution, and the seniors especially have been very supportive…”
“…think of the hardships faced by other health professionals, one’s situation will not compare to theirs” “…stay strong, persevere, and that everyone will get through it together by supporting each other” “…remember that it was a choice and that it is also a privilege to be in medicine…” |
Table 2: Summary of key themes and sub-themes as well as verbatim quotations from our interns, from the group interviews.
1) Theme 1 – Psychological Impact (Feelings): Most interns perceived that the pandemic had caused drastic changes in their personal and work lives, with various psychological impacts. They expressed increased emotional exhaustion such as stress and burnout, that is mainly related to changes in their clinical duties (Theme 2). The interns also shared about risks of COVID-19 infection to self and especially to family and loved ones, increasing their worries and stress. Interns followed physical distancing measures and team segregation at work, but several interns avoided their loved ones at home, especially the elderly and immunocompromised. For these interns, they further shared feelings of isolation and loneliness. Positive emotions such as feeling secure, valued and protected existed simultaneously and were mainly associated with the protective measures and support systems (Theme 4) in the workplace. Some also reported that the posting was still enjoyable and felt proud to be working in the pandemic.
2) Theme 2 – Impact on Duties: The interns highlighted there were many changes in institutional work processes and their duties due to the pandemic. Due to manpower changes, there were pervasive reports of physical fatigue. There were however those who felt the workload was still manageable. Interns also raised the issue of non-timely information and unclear protocols which often led to confusion and uncertainty in their work.
3) Theme 3 – Impact on Teaching and Learning: There were mixed comments on this. As a result of strict physical distancing and team segregation, initial planned teaching sessions on general paediatrics were cancelled and the interns felt they “missed out” on their clinical training. Sessions were subsequently conducted using web-based platforms, which many found helpful. All interns felt that learning was restricted in the pandemic. Although it was beneficial to learn about pandemic response and management of suspected or affected COVID-19 patients, they felt their exposure to general paediatrics was reduced due to the limited variety of ward cases. However, there were some who felt there was better quality of teaching on the ward rounds as consultants had more time to teach with fewer elective and non-urgent cases in the rotations of non-COVID care.
4) Theme 4 – Preventive Measures and Support Systems: Despite the impacts on the interns’ psychology, duties and learning, they also shared on the various protective measures and support systems they perceived helped them cope. This was also the main reason for reported positive feelings of protection and support. Departmental and institutional work processes were implemented to take care of the interns’ physical and psychological welfare such as a rotational system of team segregation, which they reported provided a strict work-rest cycle as well as respite from COVID-care. In addition, seniors and faculty also ensured interns were competent and comfortable dealing with COVID-19 patients prior to taking on high risk duties such as swabbing patients. Support from multiple levels (seniors, department, institution) helped them through. In particular, the seniors and faculty provided support to the interns through regular “check-in” meetings where they could share concerns and provide feedback. The interns also shared that as a result of the strong support received, they were able to develop adaptability, perseverance and resilience, and they were even grateful to be in healthcare at this time.
IV. DISCUSSION
According to the demand-control-support model (Thomas, 2004), occupational stress causes burnout when job demands are high, individual autonomy is low and when job stress interferes with home life (Campbell et al., 2001; Linzer et al., 2001). On that note, we hypothesised that with the COVID-19 pandemic, interns would have increased stress and burnout, in addition to their routine difficulties in the transition from student to doctor. The pandemic-related concerns our interns had were similar to many healthcare workers globally – including the fear of contracting COVID-19 and more so transmitting it to vulnerable loved ones (Chen et al., 2020). Physical fatigue was also seen in our interns given the more intensive work schedule (Sasangohar et al., 2020). Although the total amount of admissions during the period was reduced to 40% of the usual load, the need for team segregation had led to a smaller pool of interns covering each clinical area. In addition, each intern had to do more in-house night calls while on active service. Segregation also meant that there would be less cross-coverage of duties where interns would receive less support from peers who would otherwise have been able to help with the workload on the ground. Another important aspect that had led to reported stress among many was the frequent changes in clinical workflows coupled with the lack of timely and reliable information (Wu et al., 2020). Many interns also highlighted concerns with regards to compromise and interference with their paediatric internship training (Liang et al., 2020). Despite all these, objectively the interns’ perceived stress was maintained without increase in burnout.
Burnout is known to be inversely related to resilience – this pattern is also reflected in our results. Resilience is the process of adapting well in the face of adversity, trauma, tragedy, threats or even significant sources of stress (Southwick et al., 2014). Our interns had high resilience scores, above what has previously been published among physicians (McKinley et al., 2020). One reason for this may be the development of resilience through a time of crisis, a phenomenon well encapsulated by the Crisis Theory: during a crisis or disequilibrium such as the current pandemic, people make attempts to adapt and seek solutions to restore stability. (Brooks et al., 2017; Caplan, 1964). The development of resilience is increasingly emphasised as an integral strategy to combat burnout. Potentially, the mitigating factors, coping mechanisms and support shared by our interns in the interviews, could explain their low burnout and high resilience.
Our interns perceived many systemic measures helped them cope with the pandemic – giving testament to the importance of institutional leadership in implementing safeguards for psychological health (Dewey et al., 2020; Wu et al., 2020). Protocols relating to staff protection, availability of personal protective equipment (Rasmussen et al., 2020) were some of the measures common to institutions worldwide. Furthermore, interns being the most junior member of the team, were spared from doing aerosolising procedures such as intubation, nebulisation administration and airway suctioning that were deferred to clinicians with prior experience and training. This allowed interns time to learn and improve in their competency and confidence prior to assuming these responsibilities. The interns were also thankful for the protected work-rest cycles (Wu et al., 2020), and that they were allowed to take paid leave – which is essential, more so in the pandemic to reduce fatigue and allowed time for rejuvenation.
Other than institutional support, direct support from seniors and faculty were significant in our interns’ responses in helping them, supporting the importance of mentorship (Ramanan et al., 2006). Despite feeling that they might not have reliable and timely access to important updates, they felt supported under the direct guidance of seniors who took the lead on the ground. Regular fortnightly ‘check-in’ sessions were conducted to elicit concerns, obtain feedback, and ensure continual wellbeing. This channel of communication was well received by interns: they appreciated the faculty’s concerns, had the autonomy of being able to input and contribute to the care of patients, the opportunity to air grievances confidentially and importantly, had closure on concerns they have raised regarding their rotations and training (Fischer et al., 2019). The enhanced collegiality between interns, support from seniors and improved cooperation among healthcare workers during this time of crisis naturally also contributed to reduced burnout levels, a finding well established in literature.(Li et al., 2013)
In terms of the impact of training, teaching sessions were initially discontinued to maintain physical distancing. Moreover, the interns had a higher proportion of time spent in the provision of COVID-19 care, which meant traditional general paediatric exposure was compromised. However, within 4 weeks of the pandemic, departmental teaching activities were restored via web-based sessions which interns found useful. The role of faculty in persisting with academic continuity, is again important in mitigating the impact of the pandemic on learning – some interns felt they had more teaching on the wards as consultants had more time to teach for each patient.
We believe that the perceived continual institutional and senior support for our interns allowed them to maintain high personal resilience, that could have mitigated their stress and burnout. In this pandemic, interns demonstrated adaptability and perseverance to the many changes, ability to persevere as well as finding gratitude amidst the challenges and focusing on their goal to help patients and fight the pandemic, which are all known features of resilience (Bird & Pincavage, 2016; Zwack & Schweitzer, 2013).
To our knowledge, this is the first research study in the pandemic that objectively evaluated the impact of the COVID-19 on interns’ psychological state, resilience and training. However, we recognise our study limitations. The small population would mean that it would be difficult to derive statistical comparisons in the pre- and post-exposure results. However, we believe the temporal exposure of the pandemic for this group of interns during their posting, made the pre- and post-pandemic results valid. The results were further supported by qualitative findings from a good group interview participation (100%) and in-depth discussion, that provided substantial explanations to the trend of results. We recognise that 2-4 months might be a short duration for negative psychological effects such as stress, and burnout to set in. Nonetheless, the amount of unprecedented changes and intensity of work for the interns involved within this period, were undoubtedly high. Another study limitation is the inclusion of Paediatric interns only and the possible lower exposure to COVID-19 as compared to their adult counterparts due to decreased disease morbidity and mortality in children. Although this factor could potentially result in less impact on the psychological factors studied, we believe other interns are likely to face similar concerns and challenges in the pandemic, due to their similar backgrounds and job scopes across most departments and disciplines.
This study elucidated the impact of the pandemic on interns in terms of their stress, burnout, as well as clinical duties and training. Despite increasing concerns on the psychological well-being of healthcare workers in the pandemic, our study has demonstrated that it is possible to mitigate their stress, burnout and preserve resilience, even in vulnerable new medical graduates. Our findings objectively validated the importance and effectiveness of the multi-faceted approach that target institution, faculty as well as the individual level, to build resilience and combat burnout in healthcare providers in this pandemic and beyond.
Notes on Contributors
Nicholas BH Ng contributed to conception and design of study, interpretation of data, drafting and critical revising of the article. Mae Yue Tan contributed to analysis and interpretation of data, drafting and critical revising of the article. Shuh Shing Lee contributed to analysis and interpretation of data, drafting and critical revising of the article. Nasyitah bte Abdul Aziz contributed to analysis and interpretation of data, drafting of the article. Marion M Aw contributed to interpretation of data, drafting and critical revising of the article. Jeremy BY Lin contributed to conception and design, interpretation of data, drafting and critical revising of the article. All authors gave final approval of the version to be published.
Data Availability
The data for this study can be found at https://doi.org/10.6084/m9.figshare.12924029.v1. The access to these datasets are available for use subject to approval of the authors of this article.
Ethical Approval
Ethics approval was obtained from the NHG Domain Specific Review Board (DSRB), with NHG DSRB reference number of 2020/00392.
Acknowledgement
The authors would like to thank the interns who participated in this study.
Funding
Funding for this study was obtained from NUHS Fund Limited – Medical Affairs (Education) Fund.
Declaration of Interest
All authors have no conflicts of interest to declare.
References
Bird, A., & Pincavage, A. (2016). A curriculum to foster resident resilience. MedEdPORTAL, 12, 10439. https://doi.org/10.15766/mep_2374-8265.10439
Brooks, S. K., Dunn, R., Amlôt, R., Rubin, G. J., & Greenberg, N. (2017). Social and occupational factors associated with psychological wellbeing among occupational groups affected by disaster: A systematic review. Journal of Mental Health, 26(4), 373-384. https://doi.org/10.1080/09638237.2017.1294732
Campbell, D. A., Jr., Sonnad, S. S., Eckhauser, F. E., Campbell, K. K., & Greenfield, L. J. (2001). Burnout among American surgeons. Surgery, 130(4), 696-702; discussion 702-695. https://doi.org/10.1067/msy.2001.116676
Caplan, G. (1964). Principles of preventive psychiatry. Basic Books.
Chen, Q., Liang, M., Li, Y., Guo, J., Fei, D., Wang, L., He, L., Sheng, C., Cai, Y., Li, X., Wang, J., & Zhang, Z. (2020). Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry, 7(4), e15-e16. https://doi.org/10.1016/s2215-0366(20)30078-x
Chia, R., & Moynihan, Q. (2020, February 20). This alarming map shows where the coronavirus has spread in Singapore, one of the worst-hit areas outside of China Business Insider Singapore. Business Insider. https://www.businessinsider.com/coronavirus-singapore-map-shows-spread-worst-hit-outside-china-2020-2?IR=T.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behaviour, 24(4), 385-396.
Connor, K. M., & Davidson, J. R. (2003). Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depression and Anxiety, 18(2), 76-82. https://doi.org/10.1002/da.10113
Dewey, C., Hingle, S., Goelz, E., & Linzer, M. (2020). Supporting clinicians during the COVID-19 pandemic. Annals of Internal Medicine, 172(11), 752-753. https://doi.org/10.7326/M20-1033
Fischer, J., Alpert, A., & Rao, P. (2019). Promoting intern resilience: Individual chief wellness check-ins. MedEdPORTAL, 15, 10848. https://doi.org/10.15766/mep_2374-8265.10848
Li, B., Bruyneel, L., Sermeus, W., Van den Heede, K., Matawie, K., Aiken, L., & Lesaffre, E. (2013). Group-level impact of work environment dimensions on burnout experiences among nurses: A multivariate multilevel probit model. International Journal of Nursing Studies, 50(2), 281–291. https://doi.org/10.1016/j.ijnurstu.2012.07.001
Liang, Z. C., Ooi, S. B. S., & Wang, W. (2020). Pandemics and their impact on medical training: Lessons From Singapore. Academic Medicine. https://doi.org/10.1097/acm.0000000000003441
Linzer, M., Visser, M. R., Oort, F. J., Smets, E. M., McMurray, J. E., & de Haes, H. C. (2001). Predicting and preventing physician burnout: results from the United States and the Netherlands. The American Journal of Medicine, 111(2), 170-175. https://doi.org/10.1016/s0002-9343(01)00814-2
Low, Z. X., Yeo, K. A., Sharma, V. K., Leung, G. K., McIntyre, R. S., Guerrero, A., Lu, B., Lam, C. C. S. F., Tran, B. X., Nguyen, L. H., Ho, C. S., Tam, W. W., & Ho, R. C. (2019). Prevalence of burnout in medical and surgical residents: A meta-analysis. International Journal of Environmental Research and Public Health, 16(9). https://doi.org/10.3390/ijerph16091479
Maslach, C. J. S., & Leiter, M. P. (2016). Maslach burnout inventory manual. Mind Garden Inc.
McKinley, N., McCain, R. S., Convie, L., Clarke, M., Dempster, M., Campbell, W. J., & Kirk, S. J. (2020). Resilience, burnout and coping mechanisms in UK doctors: A cross-sectional study. British Medical Journal Open, 10(1), e031765. https://doi.org/10.1136/bmjopen-2019-031765
Ministry of Health (MOH), Singapore. (2020). Circuit breaker to minimise further spread of COVID-19. https://www.moh.gov.sg/news-highlights/details/circuit-breaker-to-minimise-further-spread-of-covid-19. (Retrieved April 3, 2020)
Ng, N. B. H (2020). The COVID-19 Pandemic: Impact on Paediatric Postgraduate Year One Doctors [Data set]. Figshare. https://figshare.com/s/74c81ca193638a553ea2
Ramanan, R. A., Taylor, W. C., Davis, R. B., & Phillips, R. S. (2006). Mentoring matters. Mentoring and career preparation in internal medicine residency training. Journal of General Internal Medicine, 21(4), 340-345. https://doi.org/10.1111/j.1525-1497.2006.00346.x
Rasmussen, S., Sperling, P., Poulsen, M. S., Emmersen, J., & Andersen, S. (2020). Medical students for health-care staff shortages during the COVID-19 pandemic. The Lancet, 395(10234), e79-e80. https://doi.org/10.1016/s0140-6736(20)30923-5
Rotenstein, L. S., Torre, M., Ramos, M. A., Rosales, R. C., Guille, C., Sen, S., & Mata, D. A. (2018). Prevalence of burnout among physicians: A systematic review. The Journal of the American Medical Association, 320(11), 1131-1150. https://doi.org/10.1001/jama.2018.12777
Sasangohar, F., Jones, S. L., Masud, F. N., Vahidy, F. S., & Kash, B. A. (2020). Provider burnout and fatigue during the COVID-19 pandemic: Lessons learned from a high-volume intensive care unit. Anesthesia and Analgesia, 131(1), 106–111. https://doi.org/10.1213/ane.0000000000004866
Southwick, S. M., Bonanno, G. A., Masten, A. S., Panter-Brick, C., & Yehuda, R. (2014). Resilience definitions, theory, and challenges: Interdisciplinary perspectives. European Journal of Psychotraumatology, 5,(1), 25338. https://doi.org/10.3402/ejpt.v5.25338
Sturman, N., Tan, Z., & Turner, J. (2017). “A steep learning curve”: Junior doctor perspectives on the transition from medical student to the health-care workplace. BMC Medical Education, 17(1), 92. https://doi.org/10.1186/s12909-017-0931-2
Thomas, N. K. (2004). Resident burnout. The Journal of the American Medical Association, 292(23), 2880-2889. https://doi.org/10.1001/jama.292.23.2880
Wu, P. E., Styra, R., & Gold, W. L. (2020). Mitigating the psychological effects of COVID-19 on health care workers. Canadian Medical Association Journal, 192(17), E459-e460. https://doi.org/10.1503/cmaj.200519
Zwack, J., & Schweitzer, J. (2013). If every fifth physician is affected by burnout, what about the other four? Resilience strategies of experienced physicians. Academic Medicine, 88(3), 382-389. https://doi.org/10.1097/ACM.0b013e318281696b
*Jeremy Bingyuan Lin
1E Kent Ridge Road,
NUHS Tower Block Level 12,
Singapore 119228
Tel: (65) 6772 4847
Email: jeremy_lin@nuhs.edu.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
