
The odyssey of medical education in Indonesia
Published online: 2 January, TAPS 2019, 4(1), 4-8
DOI: https://doi.org/10.29060/TAPS.2019-4-1/GP1077
Rita Mustika1,2, Hiroshi Nishigori3, Sjamsuhidajat Ronokusumo1 & Albert Scherpbier4
1Medical Education Department, Faculty of Medicine, Universitas Indonesia, Indonesia; 2The Indonesian Medical Education and Research Institute (IMERI), Faculty of Medicine, Universitas Indonesia, Indonesia; 3Center of Medical Education, Graduate School of Medicine, Kyoto University, Japan; 4Faculty of Health, Medicine, and Life Sciences, Maastricht University, Netherland
Abstract
Medical education in Indonesia has undergone a long journey. It began with the establishment of medical training for native youth in a military hospital in Jakarta during the Dutch colonial period in 1849. Since then, the number of medical schools has increased according to socio-political needs. Currently, there are 83 medical schools, public and private, which generate approximately 8000 graduates per year. The explosion in the number of medical schools challenged quality of medical education. Indeed, several curriculum changes and improvements applied to elevate the quality. Undergraduate program was initially implementing Dutch curriculum, but was then changed into American curriculum. The improvement continued by implementing the first and the second national curriculum. Since 2005 a national level competency-based curriculum (CBC) was carried out for undergraduate programs, while for postgraduate clinical training the CBC began later on. Moreover, Medical Internship Program and the National Competency-based Examination were introduced following the CBC. Nevertheless, some problems with advancement of medical schools were identified, including lack of staff and facilities, existing learning cultures and limitation of experts. Accordingly, many efforts have been made, including enactment of law on medical education and national accreditation. In the future, support from international organizations in terms of financial, consultation, faculty development and accreditation should be optimized. In addition, collaboration with medical education community elsewhere would be beneficial to overcome the challenges and promote the quality of medical education.
Keywords: Medical Schools, Curriculum Changes, Medical Education, Indonesia
Practice Highlights
- Medical education in Indonesia has travelled a long journey since the first medical training program was established in 1849. Currently, there are 83 medical schools and 8,000 annual graduates.
- The implementation of the CBC and the dramatic growth of medical schools have raised concerns about the quality of medical education nationwide.
- Enactment of laws on medical education, accreditation of medical programs, faculty development, and the national competency-based examination have been instituted to improve the quality of medical education.
- Partnerships and collaborations with other medical education communities in and outside the country should be encouraged to continuously improve educational conditions.
I. INTRODUCTION
Indonesia is the largest archipelago, located between Asian and Australian continent, and Indian and Pacific oceans. There are 17.504 islands forming 1.904.569 km2 land area with 257.600.000 inhabitants, making it the fourth most populated country. Most of the population lives in Java. Diverse ethnicities exist, mostly Javanese (40.1%), followed by Sundanese, Malay, Batak, Madurese, Betawi, Minangkabau, Buginese, Bantenese, Banjarese, Balinese, Acehnese, Dayak, Sasak, Chinese and others. Furthermore, 700 languages are spoken and various religions exist, Islam is the religion observed by most of the population (80%), followed by Christianity, Buddhism, Hinduism, and others (Central Bureau Statistics of Indonesia, 2016). Indonesia had been a Dutch colony for 3.5 centuries and declared its independence on August 17th, 1945 after being occupied by Japan for 3.5 years. Long history of colonialism influenced education and health systems in Indonesia.
During the last decade, Indonesia has emerged as a relatively stable country, economically and politically. Moreover, life expectancy reached 71 years (Central Bureau Statistics of Indonesia, 2016). The health system is provided and funded by private and public sectors. In 2014, the government launched a National Health Insurance Program and a plan for universal health coverage in 2019 (Marzuki, 2016). The education system is organized into 3 levels: basic and secondary education in 12 years, followed by higher education. Compulsory age for education is 7-15 years. Higher-education is managed by the Ministry of Research, Technology, and Higher Education. While the basic secondary education is managed by the Ministry of Education and Culture (Marzuki, 2016).
II. MEDICAL EDUCATION DURING THE COLONIAL PERIOD
Medical education in Indonesia began in the Dutch colonial period around 17th century. Since the first medical training initiated in 1849, was established as School of Java Doctor in 1851 to train native youngster to treat smallpox. Dr. W. Bosch, chief of the military-health services was appointed as Head of the school. Students were selected based on ability to write and speak Malay, and the graduate worked as smallpox-caretaker. In 1902, the school transformed into ‘School tot Opleiding van Inlandsche Artsen (School of Medicine for Indigenous Doctors)’ or STOVIA and the Dutch became an academic language. STOVIA only accepted natives and granted title ‘Inlandsch Arts’, meaning doctor from original area. The Nederland Indische Artsen (NIAS) was a second school established in 1913 in Surabaya and accepted students’ from various background. To ensure the ability to speak Dutch, students required to learn Dutch in the first 3 years before they learn medicine for 7 years (Hesselink, 2011).
The medical school as a higher education institute was established in August 16th, 1927 named Geneeskundige Hoogeschool (Higher School of Medicine) to replace STOVIA. The study period was 6 years and the school granted a certificate similar to that of the medical school in the Netherlands ‘Artsen’.
In August 17th, 1945, Indonesia declared its independence. Due to political instability, Geneeskundige Hoogeschool was moved to central Java and NIAS was closed. A year later, Geneeskundige Hoogeschool returned to Jakarta, while in Yogyakarta, a new medical school was established. In the same year, the Government stated that academic activities should be delivered in Bahasa Indonesia (Hesselink, 2011).
III. CURRICULUM CHANGES
By 1950, 3 medical schools existed in Indonesia: Faculty of Medicine Universitas Indonesia (UI) in Jakarta, University of Gadjah Mada (UGM) in Yogyakarta, and faculteit der geneeskunde branch of UI in Surabaya (Hesselink, 2011). During this period, many Dutch physicians who also were lecturers returned to the Netherlands because of inflation, difficulty to teach in Bahasa Indonesia, and hostility toward them. Moreover, the existing schools generated few physicians yearly. The Dutch curriculum was identified as one of the reasons for few graduates. The curriculum emphasized on research-individual study, and the students decided individually when to sit for the examination, resulting only 5-10 students graduated annually. To solve the problem, government opened 3 new schools.
Furthermore, international support was sought to transform the curriculum into American curriculum; the support came from University of California and World Health Organization (WHO). The American curriculum fostered problem solving-critical thinking, study methods were a balance between lectures, laboratory, community, and clerkship. Assessment was in cohort groups. Around 1956, the American curriculum was implemented. Notwithstanding the curriculum succeeding to increase the number of graduates 2-3 times, the shortage of physicians in certain areas persisted, because the graduates still prefer to work in urban areas. Furthermore, the curriculum evaluation revealed that most schools lacked faculty and facilities to continuously implement it. Consequently, in 1970 medical schools returned to the Dutch curriculum (Hesselink, 2011). Other effort was the policy of requiring graduates to serve as rural physicians for 3-5 years before accepting permanent post. With support from WHO, the curriculum was changed into community-oriented curriculum to prepare the graduates to the rural (Indonesian Consortium of Health Sciences, 2013).
In 1984, finally Indonesia developed its own national curriculum, named KIPDI I. It was a community-oriented curriculum and was implemented nationwide. This was followed by KIPDI II, a content- and discipline-based curriculum in 1995. In 2005, influenced by a changing paradigm in medical education globally, from a structure- and process-based to a competency-based curriculum, Indonesia introduced a competency-based curriculum (CBC). At the same time, the Indonesia Medical Council was established with tasks to manage the registration of medical doctors and dentists, authorize medical education standards, and maintain quality of medical practice (Indonesian Consortium of Health Sciences, 2013).
IV. THE GROWTH OF MEDICAL SCHOOLS IN INDONESIA
Medical schools were mushrooming since 1960. Five public and 1 private medical schools in 1960, became 9 public and 10 private medical schools in 1970. The number continuously rose, and in 2005, there were 24 public and 27 private schools. Moreover, in 2010, there was a policy that every island should establish at least one medical school, resulting in 6 public and 14 private new medical schools (Indonesian Consortium of Health Sciences, 2013). Currently, 71 medical schools have already been accredited by the National Accreditation Body for Higher Education (BAN-PT).
In 2016, there were 12 newly established, but not yet accredited, medical schools. In total, presently there are 83 medical schools in Indonesia. Figure 1 shows the growth of medical schools in Indonesia (Indonesian Medical Council, 2017).
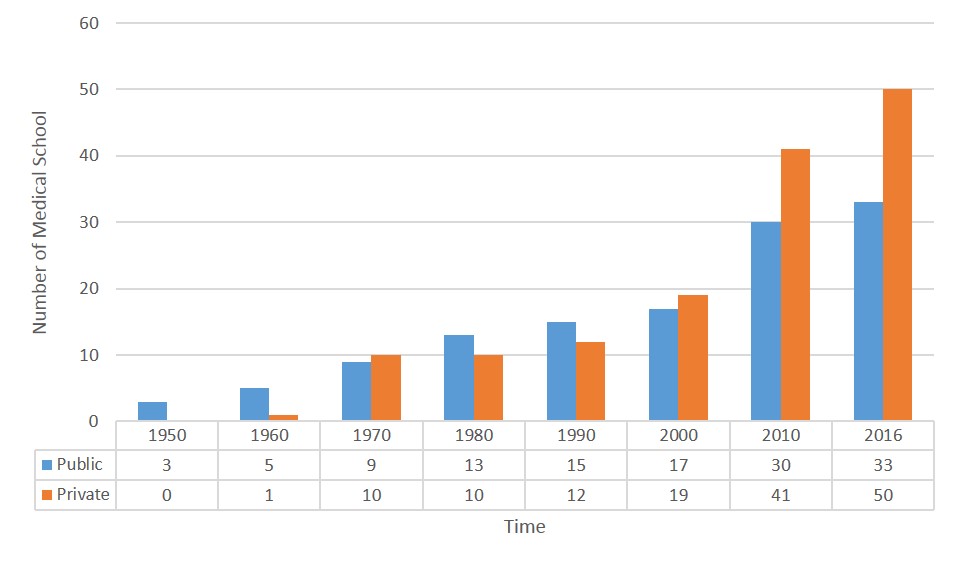
Figure 1. The growth of medical school over time
V. CURRENT SITUATION
A. Undergraduate Medical Education
Medical schools in Indonesia are part of a university, public or private. Besides organizing a regular program, some schools collaborate with schools abroad and offer an International Class Program. The selection process of public medical schools is based on the high school performance or a written test (national and independent written test). Some medical schools add Multiple Mini Interview (MMI) or psychometric test for selection. The private schools organize their own selection. Only high school graduates from science track could apply for selection. Study period of the undergraduate program is at least 3,5 years of pre-clinical studies, followed by a 2-year clinical phase. Strategy for implementing the CBC mandated the medical school to implement at least 50% vertical and horizontal integration in the curriculum. Most medical schools implemented their curriculum based on organ systems in modules. Specific skills such as procedural skills, research, and professional development are integrated within curriculum. Early clinical exposure is achieved by using clinical scenarios for triggering discussion. Mostly community-oriented education is implemented from the beginning of the program (Indonesian Medical Council, 2017).
B. Medical Internship Program
After passing the national examination, since 2010, graduates are required to attend a 1-year medical internship program before they could work independently (Indonesian Medical Council, 2017). The Indonesian Medical Internship program is managed by a committee established in 2009, comprising all stake holders, under the Ministry of Health of the Republic of Indonesia. The graduates were appointed to a healthcare institute close to their medical schools’ location. During internship, an intern works in a primary health care centre and a local hospital, under the supervision of a trained senior physician. Most of the internship is located in the rural areas, but since 2015, Jakarta – the capital – also welcomed interns (Indonesian Medical Council, 2017). The law on medical education mandated a 2-year, primary care physician program for a post-intern to become a primary care physician. Currently, this program is still in preparation.
C. Postgraduate clinical training programme and Continuing Medical Education/ Continuing Professional Development (CME/CPD)
Postgraduate clinical training program started after the independence. Students were recruited based on their undergraduate performance. In 1979, the government established a Consortium of Health Sciences (CHS) to structure the program and produce a general guidelines. Since 2013, the programs are managed by medical schools in coordination with specialist association. Currently, there are 36 specialist associations within 17 medical schools. Quality is assured with an accreditation process by neutral organizations at the national level. In general, the requirement to join the programs is completing internship, but some specialties required additional 1-2 years of clinical experience. The selection included a written test, an English proficiency test, an interview (multiple mini interview [MMI] or regular interview), and a psychometric test. Most programs are implementing a CBC-modular approach (Indonesian Consortium of Health Sciences, 2013).
Lifelong learning and the re-certification process required physicians to join CME/CPD programs. The providers of CME/CPD are The Indonesian Medical Association, the Specialist Association, the medical schools, and the Ministry of Health. Activities vary from academic conferences, seminars, workshops, to e-learning, journal or magazine. Most specialist organizations organize an annual academic conference at the regional, national, and international level. Quality is monitored by the Indonesian Medical Doctor Association (Indonesian Medical Council, 2017).
VI. MAJOR CHALLENGES AND FUTURE PERSPECTIVE
The Implementation of CBC requires many adjustments. A WHO consultant guided the initiation, and some international institutions were supporting financially to develop the system. Despite the support, diverse locations and infrastructure make medical schools vary in implementing CBC. Moreover, students and teachers are struggling to adapt to the new teaching-learning culture. This is aggravated by the lack of medical teachers in the schools.
To support the CBC implementation, the Government paired new schools with the more established ones. The support was in terms of curriculum, faculty development, and resources. Alternative active learning methods were introduced to suit the limited resources. However, the implementation at the national level needs continuous monitoring.
The increasing number of schools not only increases the number of graduates, but also raises concerns about quality. The admission process could be less competitive and problematic, and the availability of teaching hospitals could also be a problem. The Government has set a quota for admission based on the level of accreditation to address this. The other effort is the Government imposing standards and national accreditation guidelines, benchmarked to the Global Standards of Medical Education from World Federation of Medical Education (WFME) (Indonesian Medical Council, 2012). All programs have to undergo a national accreditation processes every 5 years. Medical schools are expected to identify their weaknesses and seek continuous improvement through the accreditation process. Meanwhile, only 20 out of 71 (28%) accredited undergraduate programs were granted ‘A’, the highest level of accreditation grade (Indonesian Medical Council, 2017).
Currently, more medical schools participate in medical education associations and research collaborations. For example, The South East Asia Regional Association for Medical Education (SEARAME) and The Association for Medical Education in Europe (AMEE). Some medical schools organized national medical education meetings annually and invite international speakers. UI organized Jakarta Meeting on Medical Education (JAKMED) conference annually since 2008.
Medical education in Indonesia has come through a long impressive journey. Progressing tremendously over time. The importance of high quality of medical education has been acknowledged by the enactment of the new Law on Medical Education and the support from all stakeholders. Hence, the medical education community should focus on improving quality of education. The Government needs to continuously support in terms of developing regulations for medical education, career paths for medical-clinical teachers, and allocate standard facilities. Furthermore, partnership and collaboration within and outside the country has been proven to be worthwhile, facilitating learning from each other and effectively solving problems. Indonesia medical education community needs to enhance participation in promoting high quality medical education globally.
Note on Contributors
Rita Mustika is a senior lecturer at Department of Medical Education, Faculty of Medicine, Universitas Indonesia and Coordinator of Collaboration in Medical Education at The Indonesian Medical Education and Research Institute (IMERI).
Hiroshi Nishigori is an Associate Professor at the Centre for Medical Education, Graduate School of Medicine, Kyoto University, Japan.
Sjamsuhidajat Ronokusumo is a former Chair of Indonesian Consortium of Health Sciences and Professor emeritus at Department of Medical Education, Faculty of Medicine, Universitas Indonesia.
Albert Scherpbier is a Professor of Quality Promotion in Medical Education and Dean of the Faculty of Health, Medicine, and Life Sciences of Maastricht University, Netherlands.
Acknowledgements
The authors wish to express sincere appreciation to Professor Agus Purwadianto for a fruitful discussion during the finalization of this manuscript.
Funding
This manuscript was initiated during fellowship program at the centre for medical education, Kyoto University, funded by the Medical Education and Research Institute (IMERI).
Declaration of Interest
All authors confirm that they do not have conflict of interest in connection with this manuscript including financial, consultant, institutional and other relationships that might lead to bias or conflict of interest.
References
Central Bureau Statistics of Indonesia. (2016). Statistik Indonesian 2016 [Statistical yearbook of Indonesia], 113–133. Indonesia: BPS-Statistics Indonesia.
Hesselink, L. (2011). Healers on the colonial market; Native doctors and midwives in the Dutch East Indies. Leiden – Boston: Brill. Retrieved from http://www.oapen.org/record/400271.
Indonesian Consortium of Health Sciences. (2013). Perkembangan pendidikan kedokteran di Indonesia. Sistem Pendidikan Kedokteran di Indonesia menuju 2045 [Development of medical education in Indonesia. Medical Education System in Indonesia Toward 2045]. Indonesia: Indonesian Consortium of Health Sciences.
Indonesian Medical Council. (2017). Profil Konsil Kedokteran Indonesia [Profile of Indonesia Medical Council]. Retrieved October 21, 2017, from http://www.kki.go.id/index.php/subMenu/983.
Marzuki, P. (2016). Case study 24.5: Establishing a quality assurance system of medical education in Indonesia. In K. Abdurahman, S. Mennin, R. Harden, & C. Kennedy (1st Ed.), Routledge International Handbook of Medical Education (pp. 340–342). London: Routledge.
*Rita Mustika, MD, M. Epid
Medical Education Department,
Faculty of Jl. Salemba Raya no 6
Jakarta Pusat, Indonesia
Telephone/fax: +62218901814
Email Address: ritakobe@gmail.com
Published online: 2 January, TAPS 2019, 4(1), 1-3
DOI: https://doi.org/10.29060/TAPS.2019-4-1/GP1072
Julie Drendall & John J. Norcini
Foundation for Advancement of International Medical Education and Research, United States
I. INTRODUCTION
The Foundation for Advancement of International Medical Education and Research (FAIMER®) is a non-profit foundation committed to improving the health of communities by enhancing the quality of health professions education. This article highlights several of FAIMER’s international efforts, with particular emphasis on the fellowship programs developed in partnership with institutions in the Asia-Pacific region.
II. PERSONAL VIEW
FAIMER’s work has historically been concentrated in lower-income regions of Asia, Africa, and Latin America, and has focused on three specific strategies: faculty development, targeted research that informs health workforce policy and practice, and development of data that advances educational quality improvement decisions. FAIMER’s fellowship programs, in particular, enable us to build partnerships with local experts aimed at creating meaningful and sustained improvements in the systems that produce health care providers. These programs provide health professions educators with opportunities to learn new methodologies in teaching and assessment, develop leadership and management skills, exchange educational expertise, and pursue advanced degrees in health professions education (Burdick, 2014). Participants apply this knowledge to improve teaching and learning at their home institutions, with the ultimate goal of improving health outcomes.
The FAIMER Institute is a two-year, part-time fellowship program for international health professions faculty who have demonstrated the potential to play key roles in improving education at their institutions and in their regions. Fellows receive training, tools, and support that enables them to become agents of change — creators of meaningful and sustainable advances in health professions education. The curriculum is organized around four overlapping themes: education methods, project management and evaluation, leadership and management, and education research. Practical application of the knowledge and skills acquired in these four areas is demonstrated through individual, locally relevant education projects, which are proposed during the application process, endorsed by the Fellows’ home institutions, and developed and implemented over the course of the two-year fellowship.
The FAIMER Institute is designed to foster professional support and collaboration with other educators as each Fellow becomes a member of a global health professions education community of practice (Burdick et al., 2010). The program consists of two brief residential sessions in the United States, each followed by a one-year distance learning session. The residential sessions are scheduled so that incoming Fellows overlap with returning Fellows, which means that over the course of the two-year fellowship, each Fellow has the opportunity to work closely with nearly 50 other health professions educators. During the distance learning sessions, Fellows participate in a series of web-based discussions with other Fellows and Institute faculty while implementing their projects at their home institutions. Fellows also interact regularly with each other via a listserv and receive individual coaching and mentoring throughout the program from international experts.
FAIMER’s Regional Institute fellowship programs are modelled after the FAIMER Institute, adapting the curriculum and content to meet the needs of specific regions. To date, FAIMER has established 11 Regional Institutes, located in India, Brazil, Sub-Saharan Africa, China, Chile, Egypt, and Indonesia. Generally hosted by local medical schools, these regional programs draw their participants from the area. This regional concentration facilitates the development of a strong local professional community for collaboration and peer support (Burdick, 2014). Like the FAIMER Institute, the Regional Institute programs include both residential and distance learning sessions, and participants are required to propose and implement education innovation projects that are supported by their home institutions.
To date, we have more than 1,500 FAIMER Fellows, representing more than 50 countries. Slightly more than half of them are from the Asia-Pacific region. The largest concentrations of FAIMER Fellows in the Asia-Pacific region are in India and China, where six of FAIMER’s existing Regional Institutes are located: four in India, developed in partnership with Seth G.S. Medical College (Mumbai), Christian Medical College (Ludhiana), PSG Institute of Medical Sciences and Research (Coimbatore), and Manipal University (Manipal); and two in China, developed in partnership with China Medical University (Shenyang) and Southern Medical University (Guangzhou). The FAIMER Regional Institute of Indonesia for Educational Development and Leadership will welcome its first class of Fellows in Yogyakarta in February 2019, and current Asia-Pacific FAIMER Fellows also hail from Malaysia, Indonesia, Nepal, Pakistan, Sri Lanka, the Philippines, Vietnam, Mongolia, and Fiji.
This international, project-centered approach and emphasis on bringing together a mix of health professions educators from different disciplines make FAIMER’s fellowship programs relatively unique. One of our newer Regional Institutes, the Manipal University-FAIMER International Institute for Leadership in Interprofessional Education, has gone even a step further by inviting participation not just from health professions educators, but from all of the professions (e.g., engineers, urban designers) that contribute to the health of communities. Participants in this program design interprofessional projects, which foster interaction and collaboration among faculty of diverse professional backgrounds.
Central to FAIMER’s fellowship model, the Fellows’ education innovation projects serve as excellent learning experiences, but are also intended to address specific educational needs at participants’ home institutions. Projects with the potential to improve the health of the applicant’s community, country, or region, and which have full institutional support, are given higher priority in the fellowship selection process. For example, a project designed by FAIMER Institute Fellow Rukhsana Ayub Aslam utilized high school and medical students to supplement the care provided by public health workers through service learning projects in four different communities of Pakistan. Its primary focus was to raise awareness about the causes, effects, and prevention of iron deficiency anaemia, a common condition among women of reproductive age in Pakistan. The initial project was supported by local institutions and NGOs but within a few years, it had attracted international partners including Flinders University in Australia and Global Health through Education, Training and Service (GHETS), a U.S.-based NGO, which enabled it to add point-of-care testing and treatment components that have yielded measurable positive health outcomes (Aslam, 2015).
Individual project topics vary widely, but some of the most common areas of focus are teaching methods, curriculum change, program evaluation, alignment with health system/context, and student assessment (FAIMER Brief Reports, n.d.). In the Asia-Pacific region, specifically, the most common areas of concentration have been teaching methods, curriculum change, assessment, clinical skills, and faculty development; other popular areas of focus include problem-based learning, computer-based learning, student affairs, and community-based education.
We routinely evaluate our work and have found that through their projects, Fellows have successfully introduced new educational approaches, faculty development initiatives, curriculum reform, and the creation and/or strengthening of medical education units and departments at their home institutions. Fellows report improvements in the quality of teaching and collaboration at their schools, as well as an increased interest in research and scholarship pertaining to health professions education (FAIMER Brief Reports, n.d.). Many of the projects that have been incorporated successfully at an institutional level are then expanded and replicated at other institutions in Fellows’ countries and regions—creating a ripple or multiplier effect. A significant number of these projects are also having a direct effect on health, through faculty and student-led patient education initiatives, health surveillance projects, and community-based interventions aimed at increasing access to care (Burdick, Amaral, Campos, & Norcini, 2011).
Aside from the projects, we have evidence of the personal and professional growth of our Fellows over the course of their fellowships and beyond. Our data suggest that the leadership training Fellows receive improves their confidence, which contributes to professional advancement and enables them to have increased impact and influence on health education practice and policy, institutionally, regionally, and internationally (FAIMER Brief Reports, n.d.). Many are appointed to key leadership roles at their institutions, and some go on to become members of specialized groups and committees, serve on regulatory bodies, and are appointed to national commissions and councils.
A number of our Fellows expressed the need for additional training with academic recognition, as have other educators around the world. Consequently, we created the FAIMER Distance Learning program in partnership with Keele University and the Centre for Medical Education in Context (CenMEDIC). It aims to empower health professions educators with the knowledge and skills to take educational standards and practice to a higher level— to develop their own practice, improve health professions education at their institutions and in their communities, and ultimately help bring about real and lasting advances in local health care. Participants are able to earn a Certificate, Diploma, or Master’s Degree in Health Professions Education with a focus on accreditation and assessment. The Certificate and Diploma programs are conducted entirely online, and the Master’s Degree is a blended learning program that includes a brief residential session and a dissertation. Our inaugural Masters class graduated in 2016, and it included six educators from the Asia-Pacific region.
The improvement of health professions education may not be the most obvious or immediate means of improving global health outcomes, but evidence from FAIMER’s 18 years indicates that it has a definite impact. We are privileged to be able to do this work, and we are extremely proud of the accomplishments of our Fellows.
Note on Contributors
Julie Drendall, MSS, MLSP, is the Administrative Manager for Communications of the Foundation for Advancement of International Medical Education and Research (FAIMER).
John J. Norcini, PhD, is the President and CEO of the Foundation for Advancement of International Medical Education and Research (FAIMER).
Funding
No funding is involved in this paper.
Declaration of Interest
Both authors report no competing interests.
References
Aslam, R. A. (2015, September). Service learning to develop students’ social responsibility and improve women’s health. Project presented at the Annual Conference of The Network: Towards Unity for Health, Gauteng Province, South Africa.
Burdick, W. P. (2014). Global faculty development: Lessons learned from the Foundation for Advancement of International Medical Education and Research (FAIMER) initiatives. Academic Medicine, 89(8), 1097-1099.
Burdick, W. P., Amaral, E., Campos, H., Norcini, J. (2011). A model for linkage between health professions education and health: FAIMER international faculty development initiatives. Medical Teacher, 33(8), 632-637.
Burdick, W. P., Diserens, D., Friedman, S. R., Morahan, P. S., Kalishman, S., Eklund, M. A., … Norcini, J. J. (2010). Measuring the effects of an international health professions faculty development fellowship: The FAIMER Institute. Medical Teacher, 32(5), 414-421.
FAIMER Brief Reports. Retrieved from http://www.faimer.org/education/program-evaluation.html.
*John Norcini
Email: jnorcini@faimer.org
Mailing address: 3624 Market Street,
3rd Floor, Philadelphia,
PA 19104-2685 USA
Published online: 7 January, TAPS 2020, 5(1), 3-7
DOI: https://doi.org/10.29060/TAPS.2020-5-1/GP1086
Mun Loke Wong1, Teresa Woon Oi Lee2, Patrick Finbarr Allen3, Kelvin Weng Chiong Foong4
Disciplines of 1Primary Dental Care & Population Oral Health; 2Oral Sciences; 3Endodontics, Operative Dentistry & Prosthodontics; 4Orthodontics & Paediatric Dentistry, Faculty of Dentistry, National University of Singapore, Singapore
Abstract
In 2019, the Faculty of Dentistry celebrated its 90th anniversary. Since its beginning, the Faculty has grown from strength to strength and its efforts at nurturing generations of oral healthcare professionals have evolved. Such growth and evolution ensure that the Faculty’s mission of education remains contemporaneous, effective and relevant to future-proof its graduates to play an instrumental role in helping the population achieve good oral health. This article documents the Faculty’s early years; highlights its journey and educational endeavours which have transformed teaching and learning in dentistry. It also sheds light on key drivers of change which will shape the way the Faculty seeks to transform dental education for the future.
Practice Highlights
- Dental education plays a pivotal role in training future generations of oral healthcare professionals.
- Dental education will evolve and transform with time as new pedagogical approaches emerge and shape its delivery.
- The planning and delivery of dental education will also be influenced by a myriad of other factors including demographic shifts such as the increasingly ageing population.
- Critical thinking and problem solving skills are essential skillsets to be cultivated through dental education.
- Technology can be a useful and powerful lever to advance and transform teaching and learning in dentistry.
I. INTRODUCTION
A. The Early Years of Dental Education
In 1922, the Council of King Edward VII College of Medicine mooted the idea of establishing a dental school. The first dental course was introduced in 1926 (Ho, Keng & Tay, 1989). A year later, a Department of Dental Surgery in King Edward VII College of Medicine was formed. The early Dental School, the only one in the British Crown Colonies in the East at that time (Lee, 2006), operated from five small rooms in a disused ward (Norris Block) in the General Hospital, Sepoy Lines. Between 1926 and 1927, seven students enrolled in a four-year Licentiate in Dental Surgery (LDS) course but all dropped out of the course after the first year.
Mr E. K. Tratman from Bristol was appointed Professor of Dental Surgery and Head of the Dental School in 1929. Under his leadership, the LDS was lengthened to five years to align with similar courses offered by British schools and with the eventual intention for it to be recognised by the United Kingdom (UK) General Medical Council. The dental course re-started in April 1929 with three of the pioneer LDS students. A new “Dental School and Clinic” building opened in 1938 in Sepoy Lines to cater for an increased student intake (Ho, Keng & Tay 1989; Lee, 2006).
During the war from 1939 to 1945, the Dental School was closed as the premises were occupied by the Japanese Military. At the end of World War II, the UK General Medical Council recognised the LDS in 1946. In 1949, the University of Malaya was formed and the Dental School became the Dental Department within the Faculty of Medicine. In 1950, Professor Tratman retired. Professor R J S Tickle took over as Professor of Dental Surgery, University of Malaya. That year, the dentistry course was revised to conform with the UK General Dental Council requirements and the degree of Bachelor of Dental surgery (BDS) replaced the LDS (Ho, Keng, & Tay, 1989).
B. Becoming a Dental Faculty
An extension to the Dental School building in Sepoy Lines was completed in 1955. Facilities and equipment were upgraded. The School, comprising three main clinical units – Conservative Dentistry, Oral Surgery and Prosthetic Dentistry, doubled its enrolment to 124 students (Ho, Keng, & Tay, 1989; Tan & Keng, 2005).
In 1962, the Dental Department became part of the University of Singapore, a separate entity from the University of Malaya (Singapore). The Dental School became a Faculty independent of the Faculty of Medicine in 1966. Professor Edmund Tay Mai Hiong, a graduate from the local Dental School, became the first Dean of the new Faculty of Dentistry. The Faculty continued to develop with newer facilities added to it and was later re-structured into three Departments – Operative Dentistry, Oral Surgery and Prosthetic Dentistry. A new School of Postgraduate Dental Studies was also established (Ho, Keng, & Tay, 1989).
In 1986, the Faculty of Dentistry moved to the Kent Ridge campus (Ho, Keng, & Tay, 1989), occupying three floors in the National University Hospital (NUH) Main Building. In 2010, the Faculty moved to a new location on Kent Ridge where the undergraduate teaching clinics, classrooms, pre-clinical simulation and dental laboratories, the graduate clinic for residency training in Orthodontics and Prosthodontics, the Dean’s office and academic staff offices were housed. Clinical services for the public and residency training for Endodontics, Periodontology as well as Oral and Maxillofacial Surgery remained at the Dental Centre in the NUH Main Building. Research laboratories were housed separately in a neighbouring building.
C. A New Home – the National University Centre for Oral Health, Singapore
On 5 July 2019, the National University Centre for Oral Health, Singapore (NUCOHS) was officially opened. Education, research and administrative functions of the NUS Faculty of Dentistry and the clinical services of the NUH University Dental Cluster came under one roof.
| Year | Dean |
| 1986 – 1994 | Professor Loh Hong Sai |
| 1995 – 2000 | Professor Chew Chong Lin |
| 2001 – 2009 | Associate Professor Keson Tan |
| 2010 – 2016 | Associate Professor Grace Ong |
| 2016 – Present | Professor Patrick Finbarr Allen |
Table 1. Deans of the Faculty of Dentistry at Kent Ridge Campus
II. CELEBRATING THE EVOLUTION OF DENTAL EDUCATION
The fundamental goal of nurturing, educating and training competent oral healthcare professionals to deliver high quality and safe care remains a cornerstone of the Faculty’s mission. While this has not changed, significant changes have emerged in the delivery of dental education.
Such changes stemmed from two factors. The first was a shift from the traditional teacher-centred approach to a more student-centred one. The view that teachers are experts solely responsible for delivering content and student learning is no longer sacrosanct. Instead, students play a significant role in directing their learning while teachers facilitate it. Secondly, the Faculty moved towards a competency-based curriculum driven by clearly defined competencies expected of a newly qualified dentist. This was in line with global best practices in dental education. These changes led to the introduction of various new initiatives between 1990 and 2000.
A. Competency-Based Curriculum
The traditional approach of a requirement-based curriculum where students were deemed competent on completing a fixed number of dental procedures was replaced by a competency-based curriculum. This gave students more flexibility in learning procedures by attaining expected performance standards. It also reduced the attendant stress students faced from the former approach.
B. High-Fidelity Simulation Technology
The first high fidelity pre-clinical simulation training system was introduced in the Operative Dentistry curriculum using real-time augmented reality feedback to inform students and academic staff of the quality of the students’ performance.
C. Problem-Based Learning
Problem-based Learning (PBL) was introduced to help students become more self-directed in their learning. Under the guidance of PBL facilitators, students took the lead to ask questions and find answers related to pertinent oral health conditions presented through case-based discussions.
D. Undergraduate Research Opportunities Programme (UROP)
Introduced in 1996, UROP comprises a compulsory mini-research project which students undertake over 16 to 18 months. Academic and clinical staff guide students to either develop hypothesis-driven projects or conduct literature reviews of key topics. Through UROP, the students’ intellectual curiosity is piqued and they are guided to discover answers systematically. The students share their findings at an annual Faculty Research Day with the best teams representing the Faculty at regional and international scientific competitions.
E. Developing 21st Century Skills
Critical thinking and problem solving skills are especially important in a constantly and rapidly evolving clinical dentistry landscape. Towards this end, the BDS curriculum was reviewed in 2015 to reduce content fragmentation and redundancy to allow more opportunity to develop critical thinking and problem solving skills in the students. For instance, the three complementary subjects of Oral Pathology, Oral Medicine and Oral Radiology were integrated to form a new module spanning Years 2 – 4 of the BDS curriculum. This synergised the learning in these areas to help the students better appreciate the diagnostic and clinical aspects of Oral Pathologies and critically apply the knowledge to address real life clinical issues which often involve Oral Medicine and Oral Radiology too.
F. Harnessing Technology
With the proliferation of technology-enhanced learning (TEL), the Faculty has harnessed the potential of emerging technology to enrich the educational journeys of its students. In light of this, the Faculty has intentionally embraced technology on various fronts.
1) Technology-Infused pre-clinical simulation: Simulation training in the Faculty has advanced further with virtual reality simulators that incorporate haptic force-feedback to complement the conventional simulation training used to teach tooth restorations. Students now have a more authentic experience of these clinical procedures prior to managing their patients. Simulation, which brings together 3D printing and augmented reality technology, has also come to the forefront in teaching students to deliver Inferior Dento-Alveolar Nerve blocks effectively and safely. An iBook has also been developed to help students electronically navigate the theory behind such anaesthetic techniques. Extraction of mandibular first molars of complex root forms and minor surgical removal of wisdom teeth of varying impactions have also leveraged similar 3D-printed simulations in undergraduate teaching.
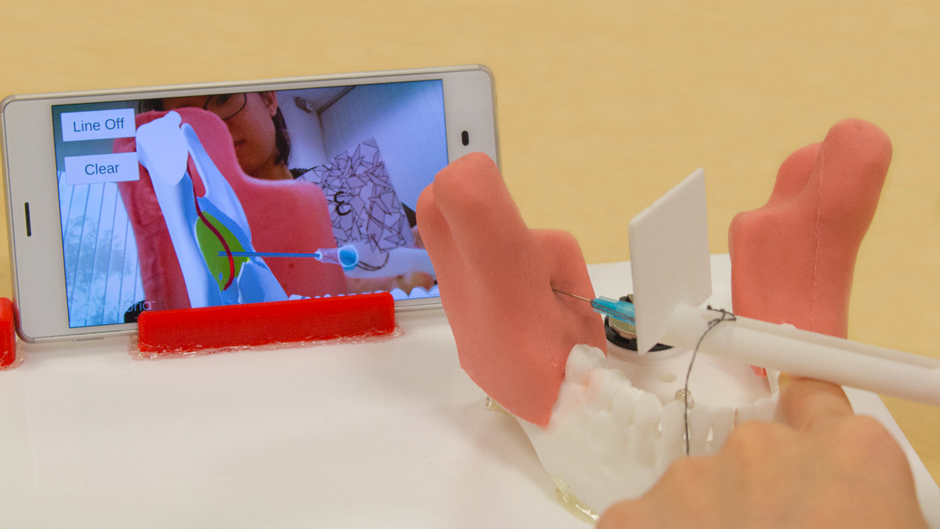
Figure 1. A simulator with augmented reality technology provides real-time visual feedback to students on the placement of the injection needle for Inferior Alveolar Nerve Local Anaesthesia
2) Eye tracking of X-ray reading: A more recent TEL development supported by the MOE Tertiary Education Research Fund employed eye tracking technology to understand eye gaze patterns of students when they read X-rays. In so doing, academic staff are able to tailor their teaching to their students’ needs and guide them more effectively in interpreting radiographs.
G. Technology in Clinical Education
Beyond pre-clinical training, the Faculty has also used technology in these areas of clinical education:
1) Visualisation of anatomy with Cone-Beam Computed Tomography (CBCT): Diagnostic 3D CBCT technology was introduced in 2009. Dental students, residents and clinical staff use this modality to visualise complex anatomy for diagnosis and to plan treatment of impacted teeth, dental edentulism, and jaw deformity.
2) Digital impressions and analysis of virtual dental models: Digital models from digital impressions are generated in PDF file for 360-degree viewing. This facilitates analysis of the dental models by Orthodontics residents.
Given the potential of technology in dental education, the Faculty has introduced a six-stage framework to guide the development, use, and evaluation of technology in teaching and learning. These six stages encourage academic staff to embrace technology in teaching through a systematic approach to:
- Reflect on teaching practice;
- Identify learning gap;
- Design, Develop, and Implement technology solution;
- Assess learner satisfaction (usability);
- Assess learner gain (outcomes); and
- Assess learner impact (behaviours).
With this framework, academic staff can tap on a Faculty-level Technology in Dental Education (TIDE) Fund to champion their technology-enhanced learning (TEL) efforts. In so doing, they will also be able to gather useful data on how their TEL interventions contribute to student learning. Through this fund, academic staff have since developed innovative teaching platforms such as iRadiate and iRadiate 3D which use a multi-media platform and augmented reality technology, respectively, to train dental students to accurately position the intra-oral X-ray tube.
In line with a more student-centric approach of learning, the Faculty has leveraged new technology-driven capabilities to longitudinally track students’ first piece of work to graduation with the Longitudinal Learning and Coaching Management (LLCM) system. With its full roll-out, students’ performance in clinics, laboratories and classrooms can be triangulated to yield patterns of performance for analysis. Through this, students’ poor performance can be more expeditiously identified by academic staff for timely remedial interventions.
H. Responding to Continuing Professional Development
The Faculty has also been proactive in responding to the professional development needs of practising dentists. This is supported by the Division of Graduate Dental Studies (DGDS) and Centre for Advanced Dental Education (CADE) which oversee speciality training and continuing professional development programmes. In 2014, a new three-year full time Master of Dental Surgery Paediatric Dentistry programme was introduced to address a national need to train more specialists in the management of oral diseases in children. CADE introduced a two-year part-time Graduate Diploma in Dental Implantology around 2006 to address the need to train general dentists in dental implantology. A more recent programme in Geriatric Dentistry was introduced to equip dentists with additional skills to manage the oral health needs of the older adults.
III. ADVANCING DENTAL EDUCATION INTO THE FUTURE
As the Faculty sets its sights on its centennial celebrations, it has put in place plans to advance dental education further. One area is continuing professional development of its academic staff. In line with this, the Dental Educators Empowerment Programme (DEEP) has been set up to support, engage, develop the capabilities of its academic staff and empower them to become effective dental educators.
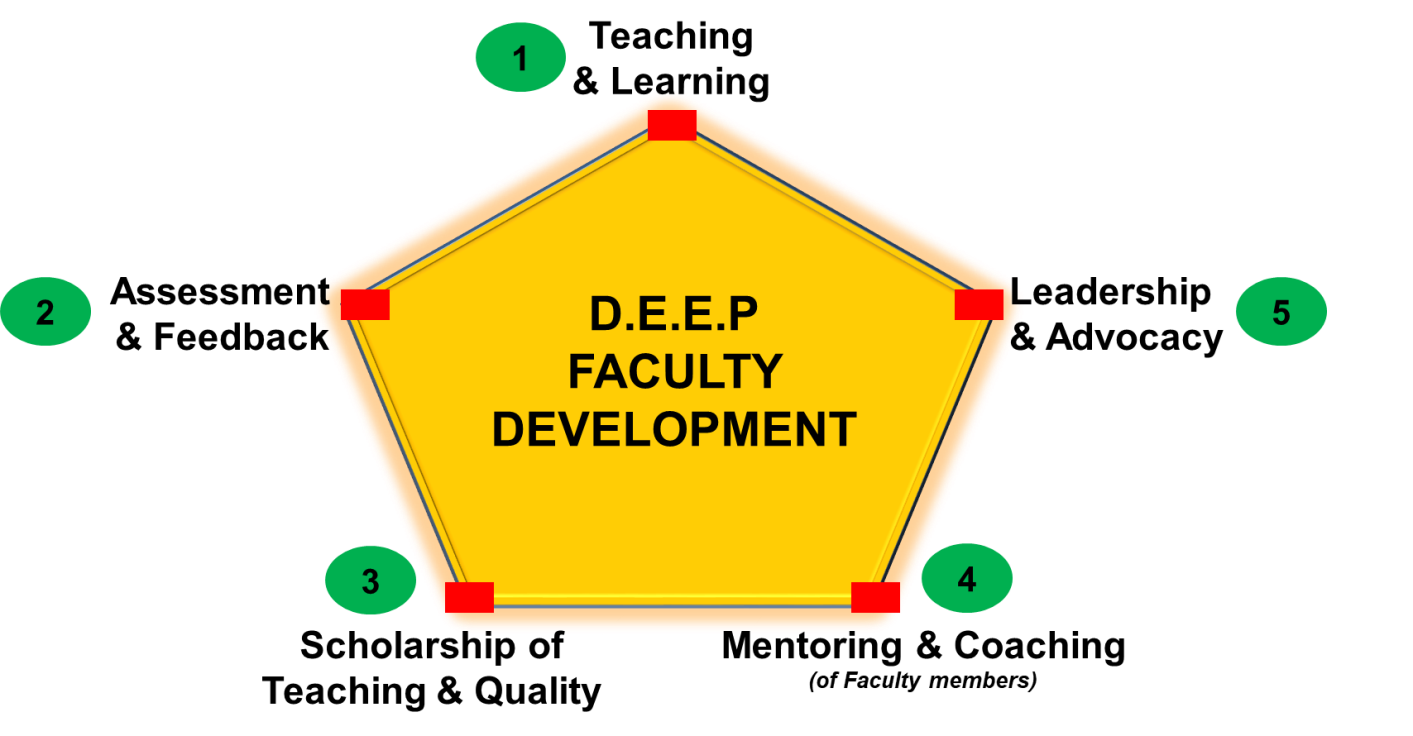
Figure 2. The DEEP framework and the domains of professional development for dental educators to empower themselves to advance dental education into the future
The demographic shifts resulting from an increasingly ageing population will also shape dental education of the future. The curriculum will need to be further enhanced to provide its undergraduates with added exposure in this area to meet the oral health needs of the elderly when they graduate. Increased exposure to the elderly in the community right from the first year of dental school is a possible trajectory for pre-clinical dental education.
Collaborative healthcare practice will also become a critical skillset for our future graduates as oral-systemic relationships become better established. Oral health care should be appreciated in the broader context of healthcare which requires multi-disciplinary and inter-professional engagements. This signals the need for increased opportunities in inter-professional education across the healthcare professions.
IV. CONCLUSION
Dental education is poised for change as it faces a myriad of factors ranging from new evidence-informed educational pedagogies, the advancement of educational technology as well as population changes. The Faculty of Dentistry will continue to embrace change to ensure that its graduates are ready to meet the evolving oral health needs of the population.
Notes on Contributors
Professor Patrick Finbarr Allen is Dean of Faculty of Dentistry.
Associate Professor Teresa Loh is from the Discipline of Oral Sciences.
Associate Professor Kelvin Foong is the Director of the Discipline of Orthodontics and Paediatric Dentistry.
Associate Professor Wong Mun Loke is the Vice Dean (Academic Affairs) of Faculty of Dentistry.
Funding
There is no funding involved for this paper.
Declaration of Interest
The authors declare no conflict of interest for this paper.
References
Ho, K. H., Keng, S. B., & Tay, D. K. L. (1989). 60 years of dental education (1929-1989). Faculty of Dentistry: National University of Singapore.
Tan, K. B. C., & Keng, S. B. (2005). Dental Education in Singapore – From the past to the future. Annals Academy of Medicine Singapore, 34(6), 196C-201C.
Lee, Y. K. (2006). Jottings on the history of dentistry in Singapore. Singapore Medical Journal, 47(4), 346-55.
*Kelvin Foong / Wong Mun Loke
9 Lower Kent Ridge Road,
National University Centre for Oral Health Singapore,
Singapore 119085
Email: denfwc@nus.edu.sg / denwml@nus.edu.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
