
Fixing the leaky pipeline: Tips to promote gender equity in Academic Medicine
Submitted: 18 December 2020
Accepted: 12 April 2021
Published online: 5 October, TAPS 2021, 6(4), 1-6
https://doi.org/10.29060/TAPS.2021-6-4/GP2451
Dora J. Stadler1,2, Halah Ibrahim3,4, Joseph Cofrancesco Jr4 & Sophia Archuleta5,6
1Department of Medicine, Weill Cornell Medical College, Doha, Qatar; 2Walter Reed National Military Medical Center in Bethesda, United States of America; 3Department of Medicine, Sheikh Khalifa Medical City, Abu Dhabi, United Arab Emirates; 4Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, United States of America; 5Division of Infectious Diseases, Department of Medicine, National University Hospital, Singapore; 6Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, National University Health System, Singapore
Abstract
Introduction: Gender equity in academic medicine is a global concern. Women physicians lag behind men in salary, research productivity, and reaching top academic rank and leadership positions.
Methods: In this Global Perspective, we provide suggestions for overcoming gender bias, drawn from a multidisciplinary literature and personal experiences working as clinician educators in the international academic arena. These suggestions are not exhaustive but inform a tool kit for institutions and individuals to support the advancement of women in academic medicine.
Results: Barriers include limited access to same gender role models and mentors, fewer networking opportunities, fewer nominations for awards and speakership opportunities, as well as implicit gender bias. Institutional interventions can address disparities along the career continuum focusing on scholarship, promotion and leadership opportunities. Women faculty can also seek out professional development programmes and mentorship to support their own advancement. Informal and formal networking opportunities, using a variety of platforms, including social media, can help build relationships to enhance career development and success, and provide social, emotional and professional support to women at all stages of their career. The National University Health System’s Women in Science and Healthcare project is an example of a successful group formed to empower women and foster personal and professional development.
Conclusion: Successful incentives and policies need to consider local institutional and cultural contexts, as well as approaches to mitigate implicit bias. Achieving gender parity in academic medicine will promote a personally and professionally fulfilled global healthcare workforce to improve patient care and clinical outcomes worldwide.
Practice Highlights
- The gender gap in academic medicine persists worldwide, especially at higher academic rank & leadership positions.
- Institutions should develop strategies to address gender equity in faculty recruitment, retention & advancement.
- Female faculty can help to advance themselves and each other through seeking self-development, mentorship and networking opportunities, utilising local as well as global resources available through a variety of channels, including social media.
- Women faculty groups can facilitate networking opportunities and create a critical mass of individuals, who can provide effective personal and professional support.
I. THE STATE OF GENDER EQUITY IN INTERNATIONAL ACADEMIC MEDICINE
Gender inequity in academic medicine has been a global concern for several decades. Although the enrolment of women in medical schools has reached or exceeded parity in many parts of the world, disparities remain in academic rank, career advancement, and leadership positions internationally (Stadler et al., 2017). Women faculty lag behind their male colleagues in several domains, including salaries, research productivity, and resource allocation. Various terminologies have been used to describe this phenomenon, including the leaky pipeline, sticky floor, broken rungs, and glass ceiling. Regardless of the phrasing, the outcome remains the same – the gender gap persists, particularly at the highest academic ranks and in medical leadership positions. As recent studies have linked physician female gender to improved patient clinical outcomes, hospitals and academic institutions now have additional incentives to train and retain a diverse workforce.
Though much of the literature on gender disparity in academic medicine is Western-based, global studies also document ongoing inequity. For example, a comparative study in Scandinavian countries found significantly fewer women in higher income specialties and in leadership positions, despite policies and cultural attitudes that support and promote work-life balance. Even in countries, such as Russia, where the majority of the physician workforce is comprised of women, the authors found significantly fewer women in prestigious specialties, tertiary care and academic medicine. In a multinational study of newly accredited postgraduate training programs in Singapore, Qatar and the United Arab Emirates, women comprised 25% of the clinician educator workforce and only 18% of hospital CEO/ CMOs, and were significantly less likely to hold an academic appointment (Stadler et al., 2017).
There are multiple barriers to female physician advancement, including limited access to same gender role models and mentors, fewer networking opportunities, lower salaries, less funding and resources (administrative staff, laboratory space), and fewer nominations for awards and conference speakership opportunities (Ibrahim et al., 2019a). These disadvantages start early in a female physician’s career and continue throughout her education, training and employment and, ultimately, impact her career trajectory. The cause is multifactorial, but there is a large body of literature that suggests that implicit gender biases play a significant negative role in the recruitment, retention and promotion of female physicians. Gender stereotype threat, which goes beyond how women are perceived and evaluated, and affects how they actually perform, could further augment disparity. There is currently a dearth of literature on successful initiatives to improve gender equity in the international arena and further research is needed to identify effective interventions in local contexts. Given the complexity of the underlying causes of gender inequity, initiatives to advance women in academic medicine should be comprehensive and multi-pronged, and include both institutional and individual interventions.
II. INSTITUTIONAL INITIATIVES
International academic institutions can vary considerably in faculty gender composition, resources available, and institutional culture. International medical education is evolving, and now is the time for healthcare institutions to assess the diversity of their faculty and review policies and protocols for any evidence of systemic bias, as well as formally assess organisational climate. The leaky pipeline model offers a framework to address these issues along the continuum of a female physician’s career. First, explicit policies to recruit, hire and retain more female academic faculty are necessary. Institutions need to analyse their current status and set goals for improvement (Ibrahim et al., 2019b), and need to ensure equity in advancement, with a focus on success in scholarship, promotion and leadership. Contributors to the leaky pipeline and a summary of possible approaches to resolve issues are described in Figures 1 and 2, respectively.
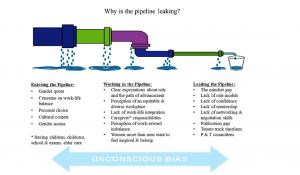
Figure 1. Barriers to recruitment, retention, and advancement
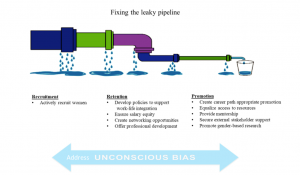
Figure 2. Institutional strategies to support female faculty recruitment, retention and promotion
Implicit or unconscious bias affects all aspect of this process; therefore, continued training to recognise and mitigate its effects is vital to success. Effective institutional policies for recruitment of a diverse faculty have included bias training for members of search and promotion committees, ensuring committee diversity (representative of gender, minorities and clinical tracks), as well as accountability through tracking of female faculty applicants and hires. Successful initiatives for retention of faculty have focused on development of policies that facilitate work-life balance and integration, such as part-time work, job sharing, and on-site childcare. The facilitation of an institutional culture that makes these options accessible without fear of stigma or penalty is crucial for these programs to succeed. Transparency in policies and salaries, systematic review and adjustment of pay structure, as well as offering negotiation workshops for female faculty, have all been shown to be successful in equalising the salary gap. Formal institutional support in terms of funding, space, time allotment, and interdepartmental activities to foster collaboration can boost research productivity and decrease isolation reported by female academic faculty. Structured professional development for faculty at all career levels, with a family friendly schedule, can be a positive factor in women physicians’ career satisfaction and retention.
Institutional review and focus on parity in advancement can help to identify and fix the ‘broken rungs’ on the ladder to promotion and leadership positions for women. Adjusted promotion and tenure guidelines to account for childcare and part-time work are also integral to advancement. While many of these recommendations are based on literature from Western academic institutions, the overall framework and guiding principles can be adapted globally. Further, gender-based research in international academic institutions is needed to better address inequity and barriers in local contexts.
III. INDIVIDUAL INITIATIVES
Institutional change is a long-term process and transforming institutional culture can take time. Despite the systemic gender bias, women physicians can take proactive steps to advancement. Women physicians face a set of internal challenges such as their own implicit bias, susceptibility to gender stereotype threat that can affect performance, and higher rates of imposter syndrome. Individual faculty members can seek out and request to participate in faculty development programs that support addressing these topics, as well those that support career advancement. Women can seek mentors and sponsors at their own or other institutions through local, regional and national networks. In addition to structured faculty development and formal mentorship processes, networking, a less formal relationship, can be utilised to support female faculty. Networking, a process used to build, maintain and use relationships to enhance career development and success, can provide social, emotional and professional support to women at all stages of their career. It can also combat professional and personal isolation often experienced by female faculty. In today’s globally dispersed and pandemic affected medical communities, the power of social media cannot be undervalued. Social media platforms can be used to form communities to share knowledge, address isolation, facilitate networking, and provide mentoring (Ibrahim et al., 2020). These platforms also serve as effective venues to broadcast and celebrate accomplishments. Networking can occur through individual channels and through grassroots efforts to build a community of women with shared goals and interests. A useful guide to building an international women’s group to facilitate and support female physician networking is illustrated in Figure 3 and exemplified through the following project.
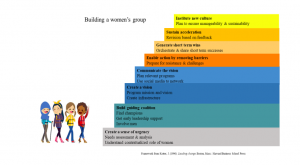
Figure 3. Framework for building a women’s group
IV. AN EXAMPLE OF SUCCESS IN THE LOCAL ARENA: THE WISH PROJECT
Solutions to achieve meaningful change require multidimensional and comprehensive strategies. However, there is limited information in the medical literature about developing or running an academic women’s group, especially in the international arena where policies and support systems for gender parity may be lacking. Often, a “bottom-up” approach, by women for women, is needed. Therefore, in 2017, to help the advancement of women at our institution, we formed the National University Health System Women in Science and Healthcare (NUHS WISH), dedicated to empowering and supporting women in healthcare and science fields in the NUHS ecosystem (Yoong et al., 2019). We viewed this group as more than a social opportunity, but rather as a vehicle for women’s empowerment. Borrowing from a multidisciplinary literature on group formation and change management, we structured our initiative according to John Kotter’s 8-step process of transformational change, as seen in Figure 3. First, we assembled a small team of passionate and dedicated women who served as transformation leaders. With the simple mission of supporting the personal and professional advancement of women in healthcare, the team communicated their vision through word of mouth and social media. Next, the transformation leaders worked with institution leadership to highlight and address barriers to female advancement in healthcare. We shared short-term wins, and planned for the future. Viewing the women’s group as an opportunity for culture change, rather than a single initiative, encourages sustainability and innovation. We deliberately alternated informal social gatherings and formal structured events. Workshops were planned for women at all career stages, with specific focus on the development of skills essential for success in healthcare, including leadership and mentorship. Given the varied professions and career stages of the members, we provided early career professionals the opportunity to network with experienced women, who offered career-related and other advice. Senior members benefitted from interacting with individuals in key leadership positions. WISH is now in partnership with senior leadership, and has grown to be a strong group of empowered female health professionals. We believe this network of developmental relationships is critical for the retention and success of women in academic medicine.
In conclusion, ensuring gender equity should be an important goal for academic medicine institutions worldwide. Our recommendations are based on personal experiences, as well as a review of best practices. The suggestions are not exhaustive and we are cognisant that no single model fits all institutions; culture and context must always be considered. Nonetheless, we believe that multilevel, institution-wide approaches to support the advancement of female faculty will benefit the institution as a whole, and help to foster inclusivity and equality in the international medical workforce. Women can also create structures to help support their advancement. By supporting all healthcare professionals to reach their full potential, we can strive for a personally and professionally fulfilled global healthcare workforce to improve patient care and clinical outcomes worldwide.
Notes on Contributors
Dora J. Stadler conceived the manuscript design, reviewed the literature and drafted the manuscript. Halah Ibrahim reviewed the literature and drafted the manuscript, Joseph Cofrancesco Jr. advised the manuscript design and gave critical feedback to the manuscript. Sophia Archuleta conceived the manuscript design, reviewed the literature and gave critical feedback to the manuscript. All authors have read and approved the final manuscript.
Acknowledgement
The authors wish to thank Siok Ching Chia, BS, National University Hospital for her assistance in preparing the manuscript for submission.
Funding Statement
There were no funding sources for this study.
Declaration of Interest
The authors declare no conflicts of interest.
References
Ibrahim, H., Abdel-Razig, S., Stadler, D. J., Cofrancesco, J., Jr., & Archuleta, S. (2019a). Assessment of gender equity among invited speakers and award recipients at US annual medical education conferences. JAMA Network Open, 2(11), e1916222. https://doi.org/10.1001/jamanetworkopen.2019.16222
Ibrahim, H., Stadler, D. J., Archuleta, S., Anglade, P., & Cofrancesco, J., Jr. (2019b). Twelve tips for developing and running a successful women’s group in international academic medicine. Medical Teacher, 41(11), 1239-1244. https://doi.org/10.1080/0142159X.2018.1521954
Ibrahim, H., Anglade, P., & Abdel-Razig, S. (2020). The use of social media by female physicians in an international setting: A mixed methods study of a group WhatsApp chat. Women’s Health Reports, 1(1), 60-64. https://doi.org/10.1089/whr.2019.0015
Stadler, D. J., Archuleta, S., Ibrahim, H., Shah, N. G., Al-Mohammed, A. A., & Cofrancesco J., Jr. (2017). Gender and international clinician educators. Postgraduate Medical Journal, 93(1106), 719-724. http://doi.org/10.1136/postgradmedj-2016-134599
Yoong, J., Alonso, S., Chan, C. W., Clement, M.-V., Lim, L. H. K., & Archuleta, S. (2019). Investing in gender equity in health and biomedical research: A Singapore perspective. The Lancet, 393(10171), e21-e22. https://doi.org/10.1016/S0140-6736(18)32096-8
*Sophia Archuleta
1E Kent Ridge Road
NUHS Tower Block, Level 10
Singapore 119228
Tel: +65 6772 6188
Email: sophia@nus.edu.sg
Submitted: 24 December 2020
Accepted: 10 March 2021
Published online: 13 July, TAPS 2021, 6(3), 10-13
https://doi.org/10.29060/TAPS.2021-6-3/GP2455
Young-Mee Lee1 & Hyunmi Park1,2
1Department of Medical Education, Korea University College of Medicine, Seoul, South Korea; 2Department of Brain Convergence Research Center, Korea University College of Medicine, Seoul, South Korea
Abstract
Introduction: We describe the circumstances and adaptations in the South Korean medical education during the COVID-19 pandemic and discuss areas in need of improvement in preparation of a worsening situation or for similar future public health crises.
Methods: Literature reviews, focusing on research papers about medical educational changes in South Korea during the COVID-19 pandemic were performed. Selective data collected from a nationwide online survey by the Korean Association of Medical Colleges on the status of curricular changes in medical schools during the COVID-19 was presented.
Results: All lectures have moved online, but clinical students continued their hospital placements during the pandemic, except for the first 3-5 weeks during the first surge in 2020. Initial technical naivety of the faculty and lack of technical resources were short-lived and the medical students settled well showing a much higher than expected student satisfaction level over online education. Practical skills sessions which benefit most from onsite hands-on experiences such as anatomy dissection, were delivered through a blended approach in some medical school. Student evaluation is the area of least change, mainly due to the students’ lack of trust in online assessments.
Conclusion: South Korea’ underwent major changes in medical education brought upon COVID-19 and the readiness of the technology adoption has been much increased. Student evaluation is the area of least transformation. Adoption of a programmatic assessment system should be considered to enhance not only learning but also improve trust among stakeholders of medical schools.
Practice Highlights
- Medical education in South Korea has evolved rapidly due to COVID-19.
- Korea’s medical schools moved all its lectures online with positive student responses.
- Clinical placements continued under strict personal protection equipment.
- The readiness of technology adoption in education bore fruit during the current pandemic.
- Assessment is the area of least change, but to prepare for the future, adaptations are necessary.
I. INTRODUCTION
However, from the beginning of December 2020, the daily positive COVID-19 patients have steadily increased reaching the new 1,000 mark by mid-December. The government having raised its social distancing level up to 2.5 in the Seoul metropolitan area, is contemplating raising it to the maximum, which will become akin to the European lockdown with most non-essential businesses and institutions shutting down. At the time of writing this paper in the middle of December the whole country is trying hard to avoid lockdown.
In this paper, the authors described the circumstances and adaptations in the South Korean medical education during the COVID-19 pandemic with some specific examples and discuss areas in need of improvement in preparation of a worsening situation or for similar future public health crises.
II. OVERALL ADAPTATIONS IN MEDICAL SCHOOL WITH SPECIFIC EXAMPLES
On the 30th of January 2020, the Korean government, via the Central Disease Control Headquarters, raised the infectious disease alert level to three out of the four-tier system, and the Korean Association of Medical Colleges (KAMC) produced its first recommendation for its 40 medical schools. This recommendation included advice to medical schools to enhance its infection control measures, augment communication with the students and hospitals, and provide adequate personal protective equipment (PPE) to all students in the clinical hospital rotation. On the 23rd of February 2020, the Korean government raised its infectious disease alert to the highest level. On the 24th of February 2020, KAMC released its second guidance to all medical schools, relaying the advice from the ministry of education on delaying the school opening date for 2 weeks and suspending all clinical rotations.
To explore the overall adaptations in medical schools by the mid-May 2020, KAMC conducted a nationwide online survey which 37 deans out of the 40 medical schools in South Korea participated in. This survey showed that all 37 medical schools had changed to online education for their preclinical courses. Laboratory skills in basic science subjects moved online, but anatomy dissection laboratory varied: online e-Anatomy replaced them in 11 schools, and 14 schools delayed it to the end of semester, and 10 schools proceeded with on-campus cadaveric dissection under strict infection control measures when the government social distancing level decreased to level 2 (the daily new positive COVID-19 patient fell under 100). The early glitches derived from the technical naivety of the faculty and lack of technical resources did not last long, and all students, faculty and institutions adapted rapidly, which resulted in a much higher than expected student satisfaction level on online education. The area of least change was in the student assessment. The student assessment was mostly delayed, and held later in face-to-face format at the end of the semester.
The suspension of clinical rotations varied widely between schools, from the first week of March to the last week of May 2020, with a median of 21 days. 14 schools provided online teaching and one school provided alternative simulation lessons but without patient contact during the closure or delay of clinical rotations. Before making the decision on restarting clinical rotations, there were high tensions between medical schools and students and even parents who were concerned and nervous on the potential infection risk to students that the hospital rotations potentially posed. To reduce this anxiety, medical schools held a series of meetings with student representatives and after putting in place safeguards against the risk of COVID-19 infection including PPE, the clerkships restarted. KAMC’s great efforts in the procurement of masks for medical students was critical for restarting clinical rotations, and medical schools were able to provide five masks per student per week even during the period of extreme masks shortage (Park et al., 2020).
A. Blended Anatomy Learning: Does Students’ Satisfaction Equal Achievement of Intended Learning Outcomes?
In the authors’ medical school, the COVID-19 pandemic forced the anatomy course to change from the traditional large group lectures and cadaveric dissection to blended anatomy courses. The theory lectures were delivered entirely online and the anatomy dissection course, resulted in an inadvertent flipped learning effect. The e-Anatomyâ videos (Panmun Education, Seoul, Republic of Korea), and Complete Anatomyâ (Elsevier, Amsterdam, Netherlands) online platform were provided to students as home assignment while on-campus dissection sessions were suspended. At the end of April, face-to-face cadaver dissections recommenced following the infection prevention measures guidelines with the use of proper PPE.
Although the students’ responses to the online anatomy teaching were remarkably positive, the anatomy department faculty at the authors’ school were concerned about the effectiveness of the altered teaching methods in achieving the intended learning outcomes. Therefore, Yoo et al. (2021) examined the educational outcomes of the online and blended learning approach in anatomy, and the results showed the anatomy achievement scores of the blended learning group (the 2020 class) being higher than those of traditional lectures (2019 class). The authors of this study interpreted that in-advance self-study at home using online learning videos before the actual on-campus dissection labs induced a flipped learning effect, and online education let the students to achieve more self-study time and individual tailored learning.
B. Adaptations in Paediatric Clerkship Education
As described earlier, most university-based hospital rotations restarted around March 16th with limited patient contact in respiratory and primary community clinics. Although the reduced patient volume which students could come into contact was inevitable, this situation was most serious in paediatric clinical clerkships. Paediatric patients visiting primary clinics and even tertiary university hospitals drastically decreased down in South Korea during the COVID-19 pandemic. In addition, the paediatric parents’ refusal or complaints on being seen by medical students worsened and the number of medical students allowed into hospital rotations were restricted in some hospitals.
To overcome the shortcomings of paediatric clerkship education, the authors of the study (Lee, K. D. Park et al., 2020) created an actual patient encounter-based role play. One student within the student group (usually 3-4 students in one group) performed a history taking and physical examination of a hospitalised child with a guardian, who later played the role of the parent, with another student in the same group taking the doctor’s role, interacting with each other in front of faculty physicians, residents, and the rest of the peer students. This role play session facilitated the provision of feedback and discussion. The students’ responses to the alternative educational approaches were positive, but the students required more discussion, and detailed feedback from the faculty physicians on their performance.
C. Online Medical Education Seminar for Faculty
Although the advantages of webinars in higher education and professional training have already been proven, they have not been widely used in South Korea before the COVID-19 pandemic. However, currently webinars and online academic conferences have almost totally replaced onsite gatherings. The COVID-19 pandemic has forced the Faculty Academy of Medical Education (FAME) seminars at Korea University College of Medicine (KUCM) to go online (Lee, H. Park et al., 2020). The authors of this study reported that FAME was established to enhance the teacher’s educational competency and promote a positive educational culture, but the participation of faculty members in this seminar has not been very active. When FAME had to be abruptly changed to online, the authors moved the seminar format online with pessimistic expectations of further decrease in the number of participants. However, such expectations were thoroughly shattered on April 8th by the login attendance of 210 faculty members on the first webinar which was the highest attendance since its inception in 2012. Although the webinar for faculty development was launched successfully and received positive reviews, further studies should follow to examine its educational effectiveness.
D. Medical Licensing Examination
The Korean Medical licensing exam consists of two parts; the written test takes place annually in January and the clinical skills test is held the previous year usually between September and October. During the span of 35 days 3,100 participants are examined in one examination centre. This year, the clinical exam was planned to be held between September 1st and October 27th, at its usual centre under strict infection control measures. However, another unprecedented crisis was added on the present COVID-19 pandemic in South Korea. In August 2020 Korean doctors held a series of national strikes as the government tried to push new policies amidst a pandemic where healthcare workers have been working tirelessly over the previous half a year to maintain the COVID-19 cases at bay and protecting the public. The doctors’ national protest was triggered by a sudden governmental announcement on critical policy changes without any previous discussion or consultation to medical associations or medical education authorities. The policies included the foundation of a ‘public medical school’ funded by taxpayers’ money with a non-transparent admission criterion and an exemption from the standard accreditation process to accelerate its building. This policy only focused on increasing the total number of doctors with the hope to fill the currently essential specialties which residents undersupply without dealing with the core underlying problem.
The national doctors strike resulted in 86% of medical students forfeiting their application for the national licensing exams (Kim & Choi, 2020) with only around 400 students undertaking the clinical exam on site wearing masks. All the stations were carried out as before with only the oral cavity examination being replaced for a verbal explanation.
III. DISCUSSION
Korea has managed the COVID-19 situation relatively well and only the lectures were moved online, whilst exams were carried face-to-face, and almost near-normal clinical practice training ensued in medical education. This double edge sword situation might not have prepared us as a nation in the event of a worse pandemic in the future. Fortunately, we can learn from the published experiences of other countries such as virtual rounds, virtual patient encounters, clinical skills simulations through the use of information technology (IT), and from virtual or augmented reality experiences used in resident skills training.
Remarkable advances in the Korean medical education in recent decades, especially, the readiness of technology adoption in education bore fruit during the current pandemic. More importantly, the experiences gained by educators during COVID-19 have consolidated student-centred education which was previously a concept rather than an actioned need. Nevertheless, student evaluation is the area of least transformation. The main reason for the resistance by the students towards online assessments is the lack of trust in the security and fairness of such method. The students’ negative perceptions over online assessments are mainly due to their belief that no technical method can 100% prevent cheating. Some medical educators pointed out that having to consider using various devices to prevent cheating during online exams is born out of the schools’ mistrust towards students, a non-educational behaviour in need of reconsideration. However, in Korea, the distrust among student peers is a bigger issue than the mistrust between the schools and students. To reduce the distrust surrounding examination, we should reconsider the current competitive summative assessment system. We could aspire for a better model, which can promote student learning instead of focusing on achieving good grades only. It is time to discuss a transition to a programmatic assessment and investigate ways on its adaptation and incorporation in medical education.
The authors of this article described major changes in medical education brought upon COVID-19 and the lessons what we’ve learned in South Korea. Since each country has faced differing levels of the COVID-19 crisis, our experience in South Korea may not be directly transferrable to other countries or contexts. However, sharing eclectic experiences from differing countries the mounting literature that can be tapped into by countries who find themselves in similar situations as ours in the future. Medical educators should actively share their novel ideas, experiences and hardships encountered on medical education through the current health crisis, as such cooperation will prepare us all against the uncertain medical future.
Notes on Contributors
Young-Mee Lee is a professor at the Department of Medical Education, Korea University College of Medicine, Seoul, South Korea, reviewed the literature, developed the methodological framework for the study, performed data analysis and developed the manuscript, gave critical feedback to the writing of the manuscript.
Hyunmi Park, MBChB, FRCS, PhD, is a research professor at the Department of Brain Convergence Research Center, Korea University, Seoul, South Korea, reviewed the literature, analysed the data and was involved in the writing of the draft, review and editing of the manuscript.
Both authors have read and approved the final manuscript.
Acknowledgments
We, authors of this study, are very grateful to KAMC for sharing the national survey data so we could perform the analysis and interpretation of such data. We wish to show our deepest gratitude to every single one of the Korean medical school deans, who not only have taken their time to participate in our study, but have tirelessly worked during the worst pandemic in living memory to ensure the safety of students and staff whilst maintaining the highest of standards in medical education.
Funding
There are no funding sources to declare.
Declaration of Interest
No conflicts of interest to declare.
References
Kim, M., & Choi, H. (2020). S. Korean government to not let over 2,700 medical students another shot at medical licensing exam. Hankyoreh. http://english.hani.co.kr/arti/english_edition/e_national/961515.html
Lee, Y. -M., Park, H., Pyun, S. B., & Yoon, Y. W. (2020). Enforced format change to medical education webinar during the coronavirus disease 2019 pandemic. Korean Journal of Medical Education, 32(2), 101–102. https://doi.org/10.3946/KJME.2020.158
Lee, Y. – M., Park, K. D., & Seo, J. H. (2020). New paradigm of pediatric clinical clerkship during the epidemic of COVID-19. Journal of Korean Medical Science, 35(38), 1–5. https://doi.org/10.3346/JKMS.2020.35.E344
Park, J., Park, H., Lim, J. E., Rhim, H. C., & Lee, Y. -M. (2020). Medical students’ perspectives on recommencing clinical rotations during coronavirus disease 2019 at one institution in South Korea. Korean Journal of Medical Education, 32(2), 223–229. https://doi.org/10.3946/KJME.2020.170
Yoo, H., Kim, D., Lee, Y. -M., & Rhyu, I. J. (2021). Adaptations in anatomy education during COVID-19. Journal of Korean Medical Science, 36(1), e13. https://doi.org/10.3346/jkms.2021.36.e13
*Young-Mee Lee
Department of Medical Education,
Korea University College of Medicine,
73 Goryodae-ro, Seongbuk-gu,
Seoul, 02841, Republic of Korea
Email: ymleehj@korea.ac.kr
Submitted: 15 October 2020
Accepted: 17 February 2021
Published online: 13 July, TAPS 2021, 6(3), 5-9
https://doi.org/10.29060/TAPS.2021-6-3/GP2430
Wei-Han Hong1a, Vinod Pallath1b, Chan Choong Foong1, Christina Phoay Lay Tan2, Mary Joseph Marret3, Yang Faridah Abdul Aziz4 & Jamuna Vadivelu1
1Medical Education Research and Education Unit, Faculty of Medicine, Universiti Malaya, Malaysia; 2Department of Primary Care Medicine, Faculty of Medicine, Universiti Malaya, Malaysia; 3Department of Paediatrics, Faculty of Medicine, Universiti Malaya, Malaysia; 4Department of Biomedical Imaging, Faculty of Medicine, Universiti Malaya, Malaysia
a,bJoint first author
Abstract
Introduction: The article is a succinct summary of events and process for emergency digitisation and transition to remote teaching during the COVID- 19 pandemic. The challenges of such transition included the need for enhanced infrastructure facilities, compliance to directives from regulatory bodies, providing an equivalent learning experience in the virtual learning environment (VLE) and ensuring the end user capacity to utilise the VLE created.
Methods: To accomplish this task a suitable instructional design and transition model was utilised to create an integrated Moodle and Microsoft Teams platform as the VLE. The curriculum was recreated in the VLE through review of existing infrastructure and resources, deconstructing the demands of the curriculum, reconstructing the learning experiences of curriculum in VLE and innovating to improve. The end user training was also provided using the same VLE created, which ensured capacity building. Virtual Clinical Assessments (VCA) were created to ensure the completion of assessment tasks.
Results: The utilisation of the ACTIONS transition model resulted in the evolution of instructional delivery from a Web Enhanced approach to a customised Web Centric approach and implementation of Virtual Clinical Assessments. Students expressed their satisfaction in the learning experience through VLE, but were anxious about their clinical training and connectivity issues.
Conclusion: This transition demonstrated the need of future directions in terms of learner readiness to be more self-directed and self-determined, design thinking for transformation to a Web Centric curriculum, faculty readiness to change and develop the competency of Technological Pedagogical Content Knowledge (TPACK).
Practice Highlights
- ACTIONS model is an appropriate design and transition model.
- Exigent transition is an opportunity to augment the capabilities of VLE and innovate.
- Ensure the recreation of an equivalent virtual learning experience to the onsite learning experience
- TPACK has emerged as an essential trainer competency.
I. INTRODUCTION
The COVID-19 pandemic has been a catalyst for extraordinary transformation in medical education. Malaysia underwent a form of lockdown under the Movement Control Order (MCO). The MCO was initiated on 18th March 2020 for two weeks and extended several times until 9th June 2020, with changing levels of restrictions in phases. With the designation of their usual clinical learning environment as a COVID Hospital, it was inevitable that medical students at the Universiti Malaya experienced major disruptions in clinical teaching.
The exodus of all students to their hometowns at the start of the MCO necessitated overnight conversion of teaching and learning processes into online delivery. With the emergence of the initial four weeks of the MCO as a fluid, unpredictable and undefined landscape, the medical faculty formulated a range of teaching and learning modalities adaptable to different conditions.
These adaptations were made while maintaining compliance with requirements of various regulatory bodies and policy makers, including the Ministry of Higher Education, Malaysian Medical Council, the Malaysian Qualifying Agency and university governance. This process of assimilation within a rapidly evolving milieu was a formidable challenge. This article aims to provide a succinct summary of events and processes for emergency digitisation and transition to remote teaching during the COVID-19 pandemic. This summary will function as a model for transformation on the run to manage the implementation and delivery of higher education programme during a major crisis or disaster.
II. METHODS
As events preceding the implementation of the MCO unfolded, sequential meetings were held to brainstorm on the safety, mode of delivery in emergency transition, preparation for training of students and staff, and evaluation of the changes. The faculty of medicine seized the opportunity to plan and implement a comprehensive online learning experience during the MCO period. Designated teams explored the various technologies available to support learning and shared best practices in an explosion of webinars. It became evident that dedicated teamwork to deal with sudden and enforced changes was crucial for this transition to be effective.
A. Theoretical Framework to Support the Digital Transition
An exigent digital transition like this required an instructional design model to affect a transition that was sustainable and future-ready. There was also a need to ensure that learning objectives envisaged for a physical face-to-face curriculum delivery model could be achieved with digital transition. The most practical model for such a transition was the ACTIONS model by Tony Bates (as cited in Boettcher & Conrad, 1999). ACTIONS is an acronym for Access, Costs, Teaching and learning, Interaction and user friendliness, Organisational issues, Operational and implementation expenses, Novelty and Speed.
B. The Development Approach – Review, Deconstruct, Reconstruct and Innovate
Recreating the entire learning experience in the VLE required the following steps
1) Review of existing e-resources and mapping them to curriculum: The existing e-resources available at Faculty of Medicine and Library were reviewed to analyse the need for additional resources. Contents of the e- resources were also mapped to the curriculum to understand the alignment of available resources with topics covered in different stages.
2) Deconstruct the existing curriculum and detailing its demands: The Universiti Malaya Medical Programme (UMMP) comprises five stages. Stages 1 and 2 (years 1 and 2) provide the preclinical and Stages 3. 1, 3.2 and 3.3 (years 3 to 5) provide the clinical learning experiences to students. The unique instructional demands of each stage were carefully analysed to clarify the possibilities and limitations of the VLE created. This step enabled categorisation of learning experiences which were suitable for delivery in the VLE and learning experiences which were not suited to a VLE with regard to the achievement of learning outcomes.
3) Reconstruct the learning experiences of curriculum in VLE: While contents of the curriculum were already available on a university learning management system (LMS) called Student Powered e- Collaborative Transforming UM (SPeCTRUM), the Moodle-based segment of the VLE, learning spaces had to be created within the Microsoft Teams segment to enable synchronous collaboration. The design principle adopted was to replicate physical facilities of Faculty of Medicine as closely as possible by providing virtual large and small group learning spaces (virtual classrooms) within Microsoft Teams. Each stage was denoted as a team. Designated channels were then created within each team for system-based blocks in preclinical stages and specialty-based postings in clinical stages. Small group teaching activity spaces including PBL rooms were created as separate channels within respective teams.
4) Innovate and improve: Although it was an exigent digital transition, the opportunity to innovate and improve could not be missed. Through deep linking of Moodle-based SPeCTRUM and Microsoft Teams, a seamless login and navigation experience was created. The learning spaces created in Microsoft Teams were provided with direct access to e-resources in the forms of ‘tabs’, simulating the existence of resource libraries within the learning spaces. OneNote was made available in these tabs as potential ‘white boards’. A complete transition to ‘flipped classes’ was also adopted by the faculty, replacing the traditional lectures.
C. Ensuring the Effective Utilisation of the VLE and Digital Instructional Delivery – The End User Training
Effective digital transition was enabled through utilisation of the VLE itself as the learning space for training of end-users. Detailed user guides were prepared. A series of synchronous hands-on sessions were also provided. All training sessions were recorded and accessible in the VLE for future reference. Continuous one-to-one support was provided on request for end-users. This dynamic transition support became an opportunity for upskilling faculty members and administrators.
D. Evaluation of Learning Experiences of the Students
A 13-item questionnaire was developed to examine learning experiences of students. The development considered existing institutional expectations of teaching, standards for problem-based learning and online learning, and generic criteria for learning environments. In addition, two open-ended questions were created for students to express what they liked and what did not work well. One week after commencement of the VLE, students were invited to relate their learning experiences via this questionnaire. This early feedback from the perspective of end-users was vital to identify aspects of the newly-constructed VLE which required adjustments.
III. RESULTS
A. The Challenge Made into an Opportunity – The Digital Transition
The school faced a huge hurdle as these sudden changes required augmented capabilities, stretching the existing connectivity infrastructure to its limits. As Information Technology (IT) professionals addressed the obvious task of ensuring good connectivity for all faculty members, administrators and students, others worked to transform mindsets of the eager and less-willing to adapt to the new norm of providing emergency online teaching to the students.
Universiti Malaya had an existing web-enhanced blended learning approach which utilised SPeCTRUM to support e-learning. The pandemic compelled transition from a Web-Enhanced approach with a physical classroom as the primary site of instruction to a web-centric approach with a virtual online platform as the primary site of instruction. To effect this change, capabilities of the existing LMS were enhanced to provide experiences of asynchronous and synchronous communication together with collaboration possibilities in a robust Virtual Learning Environment (VLE).
The ACTIONS model facilitated the evaluation of issues including uniform access to the selected web-based tools, adaptability of existing teaching learning methods to the VLE, organisational constraints and support needed for implementation, reliability and future-readiness of the VLE platform as well as the speed or ease with which the curriculum could be fully transitioned to a Web-Centric mode. Such planning resulted in the decision of deep linking and combining the capabilities of Moodle-based SPeCTRUM and Microsoft Teams as a VLE solution for the instantaneous digital transition.
B. Transition in Assessments
Assessment activities also had to be aligned with teaching and learning, taking into account guidelines of various regulatory bodies. During the MCO, existing written assessment components, which were in the form of single best answer (SBA) and extended matching type questions, were administered using online software in the SBA format.
Clinical end-of-rotations examinations posed a greater challenge. During the MCO, it was not possible to conduct examinations in the clinical environment with actual patients or a simulated clinical environment where both examiners and students could have face-to-face interaction with standardised patients. We therefore created Virtual Clinical Assessments (VCAs), writing clinical scenarios which could be used in a format similar to a structured oral examination online. Each VCA lasted 30 minutes with components of history-taking, physical examination, differential diagnoses, investigations and management along the lines of an “observed long case” clinical examination. Examiners or standardised patients were trained to role play for history-taking. De-identified clinical photographs were used for the physical examination component. Investigations such as biomedical images and laboratory results provided data for interpretation. An existing final-year examiner clinical assessment mark sheet with reference rubric was adapted for use, with components of history-taking, examination, clinical reasoning, management, knowledge, communication skills and professionalism. Specific trigger questions to assess these components were incorporated into each scenario. This assessment format could be utilised on a totally virtual platform or in a partially virtual assessment, combining face-to-face interaction with simulated patients/caregivers and clinical photographs or videos, complying with prevailing restrictions at different phases of the MCO.
C. Students’ Experiences of the Virtual Learning Environment
Students recognised and appreciated the Faculty’s efforts in establishing the online learning system for them to continue their studies. Students reported several aspects that worked well. These included pre-recorded teaching materials which allowed students to learn at their own pace. Students were also able to obtain adequate information and understood the information delivered during the virtual problem-based learning sessions. They were also less inhibited to ask questions from behind the screen during synchronous sessions.
However, there were also some areas of concern. Some students encountered internet stability issues. They needed time to adapt to the online learning platform, such as learning how to avoid speaking at the same time during the problem-based learning sessions. While acknowledging the usefulness of videos for some clinical exposure, they yearned to return to hands-on practice of clinical skills and receive feedback on their performance.
D. Prioritising Safety
With the relaxation of MCO restrictions in June to a “recovery MCO” when final year medical students were allowed back, guidelines and protocols were established to ensure safety of students, staff as well as patients. Students returned in batches and were provided with instructions to self-assess their risks before travelling. Subsequent orientation was given to perform risk assessments whenever they checked into their hostel, other buildings within the university campus, and into the hospital. The Occupational Safety, Health and Environment (OSHE) and hospital infection control teams developed a software application for the purpose of tracking the entry of patients, students and staff into the hospital premises. Students were placed on a staggered schedule within their clinical rotation to avoid overcrowding of wards and clinics. Students and staff were constantly reminded to adhere to social distancing and safety guidelines from the Ministry of Health.
IV. CONCLUSION- FUTURE DIRECTIONS
The COVID-19 pandemic has enhanced the use of technology-enhanced learning and instructional delivery as a medium for education. To adapt to this paradigm shift and ensure future readiness, the following areas require immediate attention:
A. Student Readiness
Ensuring readiness of learners to become self-directed and self-determined as they move from higher secondary/ high school to University education. Students should also be supported to develop effective online learning approaches.
B. Academic Faculty Readiness and TPACK as a competency
Academic faculty readiness to facilitate learning among the generation Z learners needs to be ensured. This essentially means that faculty members need to develop Technological Pedagogical Content Knowledge (TPACK, Figure 1) (Koehler & Mishra, 2009), as an essential competency to be effective in technology integration to facilitate learning. TPACK essentially represents the fundamental understanding of faculty members on effectively facilitating the learning process using technology, using appropriate pedagogical approaches to meet the instructional demands of each discipline/ specialty. The importance of up-skilling and re-skilling academic faculty members to equip them with latest tools available for teaching and learning is getting emphasised here.
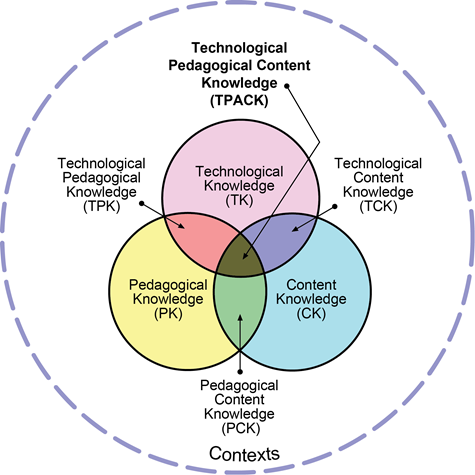
Figure 1: Technological Pedagogical Content Knowledge (TPACK). Reproduced by permission of the publisher (Koehler, 2011)
C. Infrastructure Development
Infrastructure planning, development and resource allocation to meet the future needs of technology-enhanced learning becomes a necessity to ensure the implementation of curriculum.
Notes on Contributors
Dr. Wei Han Hong involved in development of the concept, contributed to the creation of VLE through the inputs of curriculum requirements and ensured implementation, participated in the trials and troubleshooting of VLE, coordinated and contributed to the manuscript writing and approved the final version.
Associate Professor Dr. Vinod Pallath involved in conceptualising and development of the VLE, coordinated the development of VLE and lead the training of the faculty members through the VLE, contributed to manuscript writing and performed critical revisions to make the final version and approved the final version.
Dr. Chan Choong Foong involved in development of the concept, ensured the integration of quality requirements in the VLE, participated in the trials and troubleshooting of VLE, contributed to the manuscript and approved the final version.
Professor Dr. Christina Tan Phoay Lay involved in development of the concept, coordinated and contributed to development of assessments in the VLE, participated in the training, contributed to the manuscript and approved the final version.
Professor Dr. Mary Joseph Marret involved in development of the concept, coordinated and contributed to development of assessments in the VLE, participated in the training, contributed to the manuscript and approved the final version.
Professor Dr. Yang Faridah binti Abdul Aziz involved in development of the concept, supported the development of VLE in the capacity of Deputy Dean (undergraduate), ensured the demands of the curriculum are met through the VLE, contributed and critically reviewed the manuscript and approved the final version.
Professor Dr. Jamuna Vadivelu involved in development of the concept, supported the development of VLE in the capacity of Head of Unit, ensured the demands of the curriculum are met through the VLE, contributed and critically reviewed the manuscript and approved the final version.
Acknowledgement
Authors acknowledge the technical contributions and administrative support received from Medical Education and Research Development Unit and Dean’s Office, Faculty of Medicine, Universiti Malaya.
Funding Statement
There was no funding for the process described in the manuscript.
Declaration of Interest
The authors declare that there is no conflict of interest related to this manuscript.
References
Boettcher, J. V., & Conrad, R. M. (1999). Faculty guide for moving teaching and learning to the web. League for Innovation in the Community College.
Koehler, M. (2011, May 11). Using the TPACK image. TPACK.ORG. http://matt-koehler.com/tpack2/using-the-tpack-image/
Koehler, M., & Mishra, P. (2009). What is technological pedagogical content knowledge (TPACK)? Contemporary Issues in Technology and Teacher Education, 9(1), 60-70. https://doi.org/10.1177/002205741319300303
*Jamuna Vadivelu
Medical Education and Research Development Unit,
Faculty of Medicine,
University of Malaya,
50603 Kuala Lumpur, Malaysia.
Email: jamuna@ummc.edu.my
Submitted: 31 July 2019
Accepted: 6 October 2019
Published online: 1 September, TAPS 2020, 5(3), 5-9
https://doi.org/10.29060/TAPS.2020-5-3/GP2178
Rachmadya Nur Hidayah1, Richard Fuller2 & Trudie E. Roberts3
1Department of Medical Education and Bioethics, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Indonesia; 2School of Medicine, Faculty of Health and Life Sciences, University of Liverpool, United Kingdom; 3Leeds Institute of Medical Education, Faculty of Medicine and Health, University of Leeds, United Kingdom
Abstract
Southeast Asian region has been experiencing significant challenges to their health care systems, driving some countries establishing policies to ensure the quality of the medical workforce through the introduction of national licensing examinations. This paper examines the experiences of Southeast Asian countries in implementing licensing examinations, highlighting the changes and development of the education policy and its impact on medical education. The lesson learnt from the high-stakes assessment policy offers a new perspective on how medical licensing examinations could represent a potential regional approach for a better health care.
Practice Highlights
- ASEAN countries have been implementing national licensing examinations to ensure the quality of health care education and practice, while at the same time, anticipate the increasing migration of health care professionals in the region.
- The consequences of medical licensing examinations on education varied between countries and regions implementing the policy. The development of National Licensing Examinations in Southeast Asia region has been driving changes in education as its consequences. Looking at the impact, there is a possibility that this policy will lead to greater impact on health care, which may be different than the consequences of similar policy in the Northern America and European context.
- The experience of ASEAN countries such as Indonesia, Thailand, and Lao, offers an insight on how the licensing examination policy drives improvement in medical education through collaboration between stakeholders. This effort should work alongside the strengthening of accreditation system for medical education. The improvement is necessary to support health care policy and produce better quality of medical and health care professionals.
I. BACKGROUND
Healthcare in Southeast Asia faces a major challenge–that of delivering high quality, safe care to one of the most populated areas in the world, alongside rapid regional development. The trend in disease burden is shifting to non-communicable diseases, along with the challenge of globalisation which contributes to the migration of patients and health care professionals. It is known that the migration from low- and middle- income countries, or from developing to developed countries, is more common than the opposite (Tangcharoensathien et al., 2018). The migration of health care workforce has been followed by the international movement in medical education (e.g. offshore medical schools), which have created global-local tensions in medical education. In the interest of ensuring the quality of care and patient safety, the WHO through its Global Code of Practice on the International Recruitment of Health Personnel, recommended the implementation of mandatory national licensing examinations (NLEs) by regulatory bodies have been viewed as supporting this high-stakes education policy, which was in line with the increasing practice of licensing examinations in Southeast Asia countries (Tangcharoensathien et al., 2018).
II. NATIONAL LICENSING EXAMINATIONS: LESSONS FROM NORTH AMERICA AND EUROPE
The policy of using licensing examinations for quality assurance of graduates (and arguably supporting better health care outcomes) has been used in other parts of the world. The United States Medical Licensing Examination (USMLE) and the Medical Council of Canada Qualifying Examination (MCCQE) are the most notable examples. Although firstly established as an effort to reduce variation among practitioners, the USMLE has been developed to an assessment system for international medical graduates as well as home graduates who wish to be licensed in the US or Canada. Both the USMLE and MCCQE went through changes in the administration; from essay and oral examination into a more systematic MCQ and clinical skills assessment in the last two decades. Licensure’s focus shifted into educational outcomes, projecting of continuing medical education and revalidation, the use of technology and psychometrics. NLEs in the Northern America are viewed as effort on ensuring the quality of both home medical graduates and migrating health care professionals.
The impact of NLEs in both countries have been a topic for research in this area. Changes in medical schools’ curricula, especially after the implementation of clinical skills assessment, were reported. Better performance in NLEs have been associated with better preventive and management in primary care; fewer patient complaints; better patient care for international graduates and better performance in postgraduate assessment. However, there were no evidence showing direct impact of NLEs to patients, which raises debate on whether the NLEs ensure patient safety. Despite the debate, the NLEs in both countries have become cornerstones of educational quality assurance system, which also relies on the accreditation system of medical schools and continuing professional development.
European countries have different approaches to the issue of health care professionals’ migration and quality assurance. As European Union (EU) member countries recognise the qualification of health care professionals graduating from other EU countries, there are equal opportunities for them to work within the EU, particularly for medical doctors. Although there are examinations for foreign graduates, the focus is more on language competency rather than medical knowledge and skills. Whilst there are concerns about the diversity of curricula among EU countries, many experts believed that the accreditation systems were sufficient to assure the quality of their graduates (Archer et. al, 2017). Despite this, countries such as Switzerland, Poland, and Germany, have established medical licensing examinations for their home graduates and non-European Economic Area (EEA) countries’ graduates. In 2015, the General Medical Council in the United Kingdom followed this step and plans to start their medical licensing assessment (MLA) (Archer et al., 2017) which the GMC will put into action in 2023. The MLA is designed to be embedded in medical schools’ assessment, which means that there will be consequences in education that could be anticipated in the future.
The two regions might have different approach in quality assuring the graduates and medical practice depending on how the education and healthcare system work in the regions. However, it is worth to notice that the policy, along with accreditation systems, could change the practice of education and possibly the health care system.
III. NATIONAL EXAMINATIONS IN ASEAN: THE POSSIBILITY OF REGIONAL APPROACH FOR BETTER CARE?
Although the approaches taken by the EU countries and ASEAN countries are similar, it is worth noting that the context of patient management policies in both settings are different, as well as their education systems. As they work towards the ASEAN Vision 2020 on Partnership in Dynamic Development, ASEAN countries agreed a number of frameworks to enable the free flow of services for professionals in health care. The mutual recognition arrangements (MRA) for nurses, medical and dental practitioners in ASEAN countries were created in 2006-2009 in response to the partnership. This arrangement required countries to establish regulations for migration of health care professionals. The regulations came in the form of a licensing examination, which have subsequently shaped health care professions education policies in a number of member states.
For these countries, introducing national licensing examinations was not solely about the need to regulate foreign health care professionals, but also to improve the quality of graduates. Most of ASEAN member states are developing countries sharing similar challenges: inadequate numbers of physicians, uneven distribution of health care professionals, and a developing education and health care system (Kittrakulrat, Jongjatuporn, Jurjai, Jarupanich, & Pongpirul, 2014; Sonoda et al., 2017; Tangcharoensathien et al., 2018). The challenges are often followed by the increasing number of medical schools to produce more doctors –as in Indonesia’s case, without a rigid quality assurance system, raising concern of lower quality of graduates. As these countries lacked regulation of health care professionals through existing licensing and re-licensing policies, they started to introduce the NLE as a way of using education and assessment to achieve better health care globally.
Four out of ten ASEAN member countries have implemented NLEs to date: Thailand, Philippines, Indonesia, and Malaysia. Each country has different reasons for introducing the policy. Thailand and Indonesia introduced the NLE for home and international graduates in 2006-2007, to ensure the quality of competent doctors and to improve the quality of their medical schools. In Indonesia, there has been an increasing number of medical schools in the last decade, leading to concerns of differential quality of education delivered which impact on the Government’s policy to improve the quality of health professions education. Philippines and Malaysia, both had NLEs for international graduates only, whose number has been increasing in the recent years. Even though the other countries in the South East Asia region currently do not have NLEs, the topic is being discussed amongst policy makers (Kittrakulrat et al., 2014; Sonoda et al., 2017). Vietnam and Lao are in the process of developing NLEs, and India is considering the NLE as part of their policy in ensuring international graduates are prepared to work in its healthcare system. The increasing trend of health care professions’ migration (Tangcharoensathien et al., 2018) means that the NLE is a relevant issue aligned with the idea of ASEAN Economic Community (AEC), where medical professions can be qualified to practice medicine in another country in this region (Kittrakulrat et al., 2014). For a comparison, other countries in Asia such as Taiwan and South Korea have been establishing medical/ health care professionals licensing examinations, which showed impact on medical education.
Although ASEAN countries have been implementing NLEs to address the influx of international graduates, the fact that the examinations are mostly delivered in local languange makes it complicated for a regional approach of licensing examinations in the era of AEC. Similarly, the difference in culture, economy, education and health care system, also poses another challenge for the free-flow of health care professionals in AEC. Variation of methods and types of licensing examinations exist in countries implementing NLEs; although the knowledge and clinical skills are the most common outcome to be assessed (Price et al., 2018). Even so, the current practice of NLEs might open opportunities for finding common and equal standard for patient care and medical education in ASEAN.
IV. LESSON LEARNT FROM MEDICAL LICENSING EXAMINATIONS IN ASEAN: INVESTING IN HEALTH CARE PROFESSIONALS’ EDUCATION
The development of the NLE in developing countries such as ASEAN members offers a pathway for improving medical and to further extent, health care professionals’ education systems. For these countries, even though the number of overseas qualified doctors may not be significant compared to domestic graduates, the policy was considered an important step towards producing competent health care professionals. It is about how a country moves forward by changing policies, improving education system, and aiming to produce better health care providers.
The policy to improve the quality of health professionals is in line with WHO strategy to invest in transforming the education and training of human resources in health. The transformational strategy emphasised by WHO relies on collaborative work between higher education and the health sectors through establishing national policies to secure the education standard and funding. Therefore, for ASEAN countries implementing the NLE, it represents an investment for health education improvement, and a means to support their health care systems in the future.
Lao’s experience in developing the NLE showed how the country changed its policy and strengthened their education system (Sonoda et al., 2017). In the process of establishing the NLE, Lao needed to strengthen their education system through policies and working with their stakeholders. In Lao’s case, these efforts were considered as significant moves toward better healthcare. The government took note that to produce competent health care professionals, they needed to improve the education system which made them revise educational curricula and assessment practices. The example from Lao’s experience showed that the introduction of NLE drives improvement in health care professions education which is necessary to produce competent professionals (Sonoda et al., 2017). In Thailand, the licensing examination drove changes in undergraduate education (e.g. recognising at-risk students) and postgraduate education. While in Singapore, the national examinations have been introduced in postgraduate studies for ensuring quality assurance (Ruth et al., 2018).
The extent of the NLEs’ roles in bringing health care improvement in ASEAN countries is potentially greater still. In Indonesia, which has the largest population in ASEAN, the NLE for medical graduates was part of government strategies to empower human resources for health and improve the quality of health care professionals. As reported by the Joint Committee on Medical Doctor Competence examination in 2013, the examination was designed to lever the quality of medical education, including medical schools, in the long run. Emergent work from Indonesia (Hidayah, 2018) highlights that the NLEs led to a number of positive consequences for medical education: improvement in educational practices, improvement of learning resources and facilities, and collaboration between education institutions and health care providers. Since its implementation in 2007, other health care professionals such as dentistry, nursing, and midwifery have been developing, along with the strengthening of accreditation system. The collaboration between stake holders and the culture of Indonesia led to the collective work in scaling up the education. Hidayah’s work (2018) revealed that medical schools have been upgrading their education quality to produce competent graduates. The effort came in the form of increasing collaboration for curriculum and assessment development, expanding clinical placements, and collaboration for faculty development. For example, there have been regional collaboration for assessment practice between medical schools as reported by the National Committee in Indonesia. Especially for new and private schools, this collaboration helps them in leveraging their educational practice. Research highlights that in the context of developing medical education such as Indonesia, the NLE acts as a catalyst to drive improvement, linking the vital role of the regulator (i.e. the government) and major stakeholders (e.g. association of medical schools) (Hidayah, 2018). In the long term, this improvement in the quality of education is expected to bring improvement in health care by ensuring the quality of medical education and medical graduates.
In the broader field of health professions education, national licensing examinations remain a hotly debated policy (Archer et al., 2017). However, the experience of ASEAN countries in implementing NLEs reveals opportunities for a bigger role for this high-stakes assessment in the quality assurance system of health care professionals in order to enhance the quality of health care. In the future, lessons learnt from how an education policy can support developing countries in improving their health care quality, has the potential to enhance the approach to health care problems globally.
Notes on Contributors
Rachmadya Nur Hidayah conducted the research as her PhD project, and its results were used in this article. She conducted literature search, designed the concept of this review and write the manuscript.
Richard Fuller supervised the research project, contributed to the concept design of the manuscript and revised the draft of the manuscript.
Trudie E. Roberts supervised the research project, contributed to the concept design of the manuscript and revised the draft of the manuscript.
Ethical Approval
The authors sincerely thank Rebecca O’Rourke for her helpful feedback for the manuscript.
Acknowledgements
The authors sincerely thank Rebecca O’Rourke for her helpful feedback for the manuscript.
Funding
The work by Hidayah cited in this study was a doctoral study, fully funded by the Indonesia Endowment Fund for Education (LPDP – Lembaga Pengelola Dana Pendidikan), the Ministry of Finance, Republic of Indonesia.
Declaration of Interest
Although the study referred in this manuscript was a doctoral project funded by the government of Indonesia, the authors declare that there is no conflict interest related to the discussion presented in the manuscript.
References
Archer, J., Lynn, N., Coombes, L., Roberts, M., Gale, T., & Regan de Bere, S. (2017). The medical licensing examination debate. Regulation & Governance, 11(3), 315-322. https://doi.org/10.1111/rego.12118
Hidayah, R. N. (2018). Impact of the national medical licensing examination in Indonesia: Perspectives from students, teachers, and medical schools (Doctoral dissertation, University of Leeds). Retrieved from http://etheses.whiterose.ac.uk/20215/
Kittrakulrat, J., Jongjatuporn, W., Jurjai, R., Jarupanich, N., & Pongpirul, K. (2014). The ASEAN economic community and medical qualification. Global Health Action, 7, 24535. https://doi.org/10.3402/gha.v7.24535
Price, T., Lynn, N., Coombes, L., Roberts, M., Gale, T., de Bere, S. R., & Archer, J. (2018). The international landscape of medical licensing examinations: A typology derived from a systematic review. International journal of health policy and management, 7(9), 782. https://doi.org/10.15171/ijhpm.2018.32
Lim, M. C. R., Tsou, Y. K. K., Ong, C. P., Wong, K. W. S., Tan, C. S. G., Soon, S. W. W., … & Cruz, M. S. P. (2018). Family medicine post-graduate examination reforms in Singapore: A value-driven practical and contextual approach. The Asia Pacific Scholar, 3(3), 39-42. https://doi.org/10.29060/TAPS.2018-3-3/SC1057
Sonoda, M., Syhavong, B., Vongsamphanh, C., Phoutsavath, P., Inthapanith, P., Rotem, A., & Fujita, N. (2017). The evolution of the national licensing system of health care professionals: a qualitative descriptive case study in Lao People’s Democratic Republic. Human Resources for Health, 15(51), 1-13. https://doi.org/10.1186/s12960-017-0215-2
Tangcharoensathien, V., Travis, P., Tancarino, A. S., Sawaengdee, K., Chhoedon, Y., Hassan, S., & Pudpong, N. (2018). Managing in-and out-migration of health workforce in selected countries in South East Asia region. International journal of health policy and management, 7(2), 137. https://doi.org/10.15171/ijhpm.2017.49
*Rachmadya Nur Hidayah
Jl.Farmako Sekip Utara,Yogyakarta 55281
Faculty of Medicine, Public Health, and Nursing
Universitas Gadjah Mada, Indonesia
Email: r.nurhidayah@ugm.ac.id
Submitted: 30 May 2019
Accepted: 20 June 2019
Published online: 1 September, TAPS 2020, 5(3), 1-4
https://doi.org/10.29060/TAPS.2020-5-3/PV2164
Bonny L. Dickinson1, Zhi Xiong Chen2 & Aviad Haramati3
1Department of Biomedical Sciences, Western Michigan University Homer Stryker M.D. School of Medicine, Kalamazoo, Michigan, USA; 2Department of Physiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 3Centre for Innovation and Leadership in Education, Georgetown University School of Medicine, Washington, DC, USA
Abstract
Medical science educators are faculty members primarily responsible for teaching the medical sciences to healthcare profession students. These educators also have roles in other academic areas such as curriculum development, learner assessment, advising and mentoring, clinical duties, research, institutional service, leadership and administration. Academic institutions worldwide are increasingly focused on excelling in cutting-edge research, a major criterion for university rankings, which has led to significant resources and attention invested in those endeavours. At the same time, the primary goal of academic institutions is to educate and train healthcare professionals. As a result, medical science educators are often caught in the middle of these competing interests, leading to the ambiguity between personal career development and institutional priorities. It is in this context that we consider how medical science educators might navigate these issues and how academic institutions can support and strengthen this important cohort of faculty. First, with an attempt at humour, we begin by considering three stereotypical identities of medical science educators. We then discuss how the growing number of medical education associations and programs designed to support medical science educators are making a difference. Our goal is to provide a clear direction for the current career trajectory of medical science educators.
Keywords: Recognition, Promotion, Innovation and Leadership in Education, Teaching Academy
Practice Highlights
- Medical science educators are critical to the mission of academic institutions.
- Institutions need to adopt guidelines to recognise, reward and promote medical science educators.
- The formation of a vibrant educator community to drive innovation and scholarship is important.
- Establishing a center for innovation and leadership can support and develop faculty in education.
I. THE MULTIPLE IDENTITIES OF THE MEDICAL SCIENCE EDUCATOR
Medical science educators have many roles, the most important of which is to educate students in the health professions. The many roles, responsibilities and expectations placed on these educators can shape distinct personalities or identities. Here, in a tongue-in-cheek fashion, we describe three stereotypical educator identities. The first is the ‘homemaker’. These educators engage in multiple routine tasks that few faculty enjoy (e.g., writing examination questions, directing courses, learner assessment, etc.). The ‘homemaker’ educators are usually in managerial roles, overworked, under-appreciated and often frustrated with the lack of time available to pursue scholarship or other rewarding endeavours. ‘Homemaker’ educators perceive them-selves as lacking the liberty or empowerment to actually embody their career aspirations.
The second stereotypical personality is the ‘punch clock employee’. These educators also often perform routine tasks, do what they are told, and rarely desire to excel beyond what they are expected to do. They perceive themselves as trapped in a cycle driven by their routines and, as a result, lack the motivation and aspiration to grow and develop as scholars.
The third identity is the ‘talk show host’ medical science educator. This identity is difficult to distinguish from those educators who are well versed in pedagogy and genuinely student-centric. The ‘talk show host’ educators enjoy teaching and may even be well-liked by students. This can, however, be borne out of a narcissistic need to be popular, in lieu of adopting a sincere concern for students’ learning. Their teaching approaches may also come across as self-absorbed and gimmicky, bordering on showboating. The ‘talk show host’ educator believes that what is important is what the teacher does, not what the students do (Biggs, 1999). Perhaps not surprising, ‘talk show host’ educators tend to accumulate teaching awards and steadily advance in their careers but lack a serious scholarship to accompany their teaching accolades. This makes it difficult to distinguish them from educators with a genuine interest in students’ learning who insist on using evidence-based teaching techniques that may be unpopular with students, yet proven to support and optimise learning effectively.
What then is the ideal identity for medical science educators? We propose the ‘servant’ educator identity to describe educators who are genuinely interested in what the student does and how the student learns (Biggs, 1999). How can this ‘servant’ educator identity be supported? We propose that two ‘I’s must play a role: individual and institution. At the individual level, the one question that all medical science educators should ask themselves is, “What is the reason that you have chosen to be an educator?” If the answer is to inspire and educate the next generation of health professionals, then the educator is on the right track. To support this goal, institutions must foster an environment that supports educator development to help them to discover, grow and achieve their career aspirations. This requires the institution to identify, encourage, recognise, reward, and promote educators who possess such attitudes (Bligh & Brice, 2009). Finally, institutions should aim to focus on the long-term vision instead of short-term gains, ‘heartware’ instead of hardware, and to support medical science educators and their work. Below, we discuss two ways that institutions can help nurture the ‘servant’ medical science educator.
II. SUPPORTING THE PROMOTION OF MEDICAL SCIENCE EDUCATORS
Medical schools have a long history of using well-established guidelines for granting promotion and tenure to faculty based largely on the number and quality of peer-reviewed publications and a track record of grant support for biomedical research. The recognition that these standards do not translate to the evaluation of faculty with predominant roles in teaching (both in the classroom and the clinic) and medical education scholarship has launched a now decades-long conversation about how to evaluate medical science educators for the purposes of appointment, promotion and tenure. In response to this challenge, the 2006 Consensus Conference on Educational Scholarship developed a portfolio-based format for documenting scholarly activity, using evidence of quantity, quality, and engagement with the education community (Simpson et al., 2007). In 2010, the Association of American Medical Colleges Task Force on Educator Evaluation created consensus guidelines to supplement the 2006 report for use by those responsible for evaluating the educational contributions of faculty. In that work, the task force also clearly articulated the need for institutional adoption of the criteria to recognise educators through academic promotion.
Today, faculty entering the field of medical education have access to a literature replete with guidelines for evaluating medical school faculty and recommendations for defining and strengthening scholarship in medical education. Faculty also have access to a rapidly expanding number of training programs to develop faculty as educational scholars. In addition, a growing number of medical education organisations, such as the International Association of Medical Science Educators (IAMSE) and the Association for Medical Education in Europe, and educational programs for health profession educators, have come into existence over the past 25 years. Whether this growth has translated into the formal adoption of clear guidelines for the recognition, reward, and promotion of medical science educators was recently examined by the Committee for the Advancement of Medical Science Educators (CAMSE), a subcommittee of the IAMSE Professional Development Committee. Following a comprehensive review of existing criteria for recognising excellence and professional advancement in medical education, CAMSE surveyed the IAMSE membership to assess whether the work of Boyer, Glassick, and others have influenced institutional adoption of guidelines for recognising, rewarding, and promoting medical science educators, and to evaluate biomedical science faculty awareness of these guidelines and their own institutional policies (Dickinson et al., 2018). The results of the survey identified several needs: 1) more time for faculty to pursue scholarship and innovation in medical education; 2) greater institutional recognition of medical science educators and their scholarly contributions; and 3) increased institutional support and resources for educator activities. An additional finding was that some medical science educators do feel recognised and rewarded for their work, as over half of respondents (57%) indicated that medical science educators can be promoted at their institutions based on their work as educators.
To further facilitate the reward, recognition, and promotion of medical science educators, CAMSE is creating toolkits for educators and those charged with evaluating educators. The toolkits will be applicable to a breadth of health science institutions with an international scope, and are framed using the quantity, quality, and engagement model advocated by Simpson, et al (Simpson et al., 2007). The educator toolkit provides a structured approach to developing a strong educator portfolio by helping faculty clearly translate their educational work and scholarship into a readily understood format for department chairs, promotion committee members, and other institutional leaders. Worksheets and detailed instructions provided with the toolkit are tailored to document quantity, quality, and engagement model in teaching, learner assessment, advising and mentoring, curriculum development, and leadership and administration. The evaluator toolkit is designed as a companion to this toolkit and is intended for institutional leaders tasked with evaluating educators. The focus of the toolkits on medical science educators addresses the gap in the recognition of their scholarly teaching and educational scholarship. Further, these toolkits may be readily adapted for use by clinician-educators. We anticipate that these user-friendly, open-access, IAMSE-recommended toolkits will be widely used by educators and adopted by institutions to enhance recognition, reward, and promotion of biomedical science educators.
III. SUPPORT FOR INNOVATION AND LEADERSHIP IN EDUCATION: BUILDING A COMMUNITY OF EDUCATORS
Medical education is undergoing rapid changes in many fundamental ways. Curricula are becoming more integrated, both horizontally across science disciplines and vertically with the incorporation of earlier clinical experiences. Teaching sessions are being shifted to more active learning formats, and assessment is now a strategy for learning, as much as it has been a measurement of learning. At the same time, the role of the teacher is moving dramatically from deliverer of information to facilitator of learning. These changes require core teaching faculty to possess specific skills gained through additional training. As institutions grapple with the challenges of helping content experts become educators, profound changes are happening to faculty members themselves. There are real shifts in terms of faculty members’ identity and how they view their role at the institution. As mentioned earlier, there are key challenges for academic institutions as to how to nurture, develop and reward these educators and ensure that they have a career path for promotion and advancement.
At Georgetown University Medical Center (GUMC), the leadership of the institution encouraged and supported the creation of a Center for Innovation and Leadership in Education (CENTILE). Specifically, this was a school-wide investment in faculty development in education, which enabled the formation of an inter-professional community of educators that drive innovation and scholarship. The goals of CENTILE are to promote excellence in teaching, to foster programmatic innovation in education, to facilitate scholarship in health professions education, and to develop future educational leaders. CENTILE aims to help faculty gain the necessary skills through a variety of programs such as Education Grand Rounds and workshops from visiting leaders around the globe, and by convening an annual Colloquium for GUMC Educators in the Health Professions, wherein faculty share their creative innovations in education, and learn valuable insights and skills from one another.
Another important development has been the establishment of the GUMC Teaching Academy in the Health Sciences, which provides opportunities for faculty to receive peer-recognition of accomplishments in education. There are several levels of membership that aim to create a growth trajectory for faculty, beginning with the Protégé level, for residents and post-doctoral fellows with an interest in education; and the Associate Member, for new members of the faculty eager to explore their interest in education. The level of Principal Member, is one in which a faculty member is judged to have achieved excellence in one of five domains: Direct Teaching, Mentoring and Advising, Instructional Design/Curricular Development, Educational Scholarship or Educational Leadership. Each of those domains has specific criteria and requires submission of examples of quality, quantity, innovation and dissemination of accomplishments in that area (as described by Simpson et al., 2007). The highest level of recognition is the Distinguished Member, in which a faculty member is deemed to have achieved excellence in three of the five domains listed above. Those applications are reviewed by both an internal group and two external reviewers. At present (May 2019), there are 110 members of the Teaching Academy at GUMC, of which 29 are at the Principal level and only 3 have attained the Distinguished Educator status. One of the important outcomes that has occurred in the 4 years since the establishment of the GUMC Teaching Academy is that the promotion and tenure committee has adopted the GUMC Teaching Academy criteria when reviewing applications for faculty appointment and promotion.
CENTILE was established to fill a need at GUMC and has a clear mandate to advance the educational mission of the academic medical centre by Educating the Educators (Haramati, 2015). Those members of the faculty who are determined to devote their careers in education now have a clear trajectory to obtain the necessary skills as well as to be evaluated and rewarded for their educational achievements. We believe that every academic health centre should identify resources, develop programs and standards, and ultimately, enable medical and health professions educators to pursue education in practice and in scholarship, and to be recognised appropriately for those accomplishments.
Notes on Contributors
Bonny L. Dickinson, PhD, MS-HPEd is a Professor and Vice-Chair of Biomedical Sciences at the Western Michigan University Homer Stryker M.D. School of Medicine, Kalamazoo, Michigan, USA.
Chen Zhi Xiong, BSc, MHPE, PhD is a senior lecturer and Integration Lead Educator (Medicine) at the Yong Loo Lin School of Medicine, and Assistant Dean of Students at the National University of Singapore.
Aviad Haramati, PhD is a Professor, Division of Integrative Physiology in the Department of Biochemistry, Molecular and Cellular Biology and Director of the Center for Innovation and Leadership in Education (CENTILE), Georgetown University School of Medicine, Washington, DC, USA.
Acknowledgement
The authors wish to thank the organisers of the Asia Pacific Medical Education Conference for selecting this work for presentation at the 2019 conference.
Funding
Funding for the manuscript was supported by each of the institutions involved.
Declaration of Interest
There is no conflict of interest from any of the authors with regards to this paper.
References
Biggs, J. (1999). What the student does: Teaching for enhanced learning. Higher Education Research & Development, 18(1), 57-75. https://doi.org/10.1080/0729436990180105
Bligh, J., & Brice, J. (2009). Further insights into the roles of the medical educator: The importance of scholarly management. Academic Medicine, 84(8), 1161-1165. https://doi.org/10.1097/ACM.0b013e3181ace633
Dickinson, B, L., Deming, N., Coplit, L., Huggett, K. N., Quesnelle, K., Sheakley, M., … Wragg, S. (2018). IAMSE member perspectives on the recognition, reward, and promotion of medical science educators: An IAMSE sponsored survey. Medical Science Educator, 28(2), 335-343. https://doi.org/10.1007/s40670-018-0548-z
Haramati, A. (2015). Educating the educators: A key to curricular integration. Academic Medicine, 90(2), 133-135. https://doi.org/10.1097/ACM.0000000000000444
Simpson, D., Fincher, R. E., Hafler, J. P., Irby, D. M., Richards, B. F., Rosenfeld, G. C., & Viggiano, T. R. (2007). Advancing educators and education by defining the components and evidence associated with educational scholarship. Medical Education, 41(10), 1002-1009. https://doi.org/10.1111/j.1365-2923.2007.02844.x
*Aviad Haramati
Center for Innovation and Leadership in Education,
Georgetown University School of Medicine,
Washington, DC 20057
Tel: 202-687-1021
Email: haramati@georgetown.edu
Published online: 5 May, TAPS 2020, 5(2), 1-4
https://doi.org/10.29060/TAPS.2020-5-2/GP1084
Colm Bergin1 & Mary Horgan2,3
1School of Medicine Trinity College Dublin, Ireland; 2Royal College of Physicians of Ireland, Ireland; 3School of Medicine, University College Cork, Ireland
Abstract
Medical education and training has evolved over the centuries. Ireland has a long history of leading on aspects of training that remain relevant today, focussing on the apprenticeship model coupled with a robust modern medical education framework. The practice of medicine is changing rapidly driven by expanding knowledge, advances in technology and use of artificial intelligence, demographic shifts and the expectations of patients and society. Medical training and education need to adapt to ensure that our current knowledge and future medical workforce is prepared for modern-day patient-centric practice. Ireland has emerged as a world leader in medical device technology, pharmaceutical research and development and social media technology support which offer the opportunity for the future of medical training. Knowledge, emotional intelligence, critical thinking, compassion, resilience and leadership are key attributes to which we as a profession aspire. There is an opportunity to leverage Ireland’s global position in technology and finance to train our modern-day medical workforce whilst retaining the attributes of the compassionate practice of the art of medicine. This paper explores the past, present and future of medical education and training in Ireland.
Practice Highlights
- Ireland has a history of leading in medical education.
- Training focusses on the blended apprenticeship model.
- Ireland is now a world leader in medical device technology, pharmaceutical research and social media technology.
- Agility, diversity and flexibility are embedded in the modern day medical training model.
- Compassion and communication remain pivotal to the practice of medicine.
I. INTRODUCTION
Ireland is a small island on the westerly fringe of Europe separated from Great Britain by the Irish Sea and with a population size similar to Singapore. Although Ireland is a small nation, its global impact is large due to the high value we, as a nation, put in educating our population. Ireland now ranks fourth in the world in the UN’s Human Development Index, a widely accepted measure of living conditions or quality of life across the globe. Ireland is ranked second to Singapore in reading performance in Organisation for Economic Co-operation and Development (OECD, 2019) rankings. The enrolment of 17-year-olds in Ireland’s secondary education system is 99.3%, with well over the OECD average continuing on to tertiary level education. Ireland is a hub for many major pharmaceutical, medical devices and technology companies which has allowed growth in research. Partnerships between industry and Irish universities facilitate innovation and research in the medical and life sciences sectors. There are six medical schools in the Republic of Ireland, one of which dates from the 17th century and four from the 19th century. Ireland is justly proud of the history and quality of its medical education. This article outlines the past, present and future of undergraduate and postgraduate education in Ireland.
II. THE PAST
Ireland has a long history of being at the forefront of medical education. Many of the Presidents of the Royal College of Physicians of Ireland (RCPI), which was founded in 1654, have played eminent roles in innovation in medical education since the 17th century (Coakley, 1992). Medical education started in Ireland with the appointment of John Stearne as the first professor of medicine at Trinity College in the 1650s. The School of Anatomy in Trinity College did not open until 1711; however, following its opening, the medical school flourished.
Worldwide, doctors and medical students associate the name of Robert Graves with the disease of the thyroid gland however few are aware of the key role he played in the development of bedside teaching. During the early 19th century, Graves introduced two elements of radical change in medical education: the distribution of the care of patients to senior medical students and the changing of teaching from the lecture room to the bedside of the patient. These fundamental changes in medical education developed the skill of observation and ensured that errors in clinical judgement were corrected on the spot (Coakley, 1992). Grave’s method of teaching was adopted in the English-speaking world and continues to this day. Graves constantly exhorted students to spend time on the wards gaining practical experience. Graves appreciated the importance of what is now called continuing professional development by stating that “if a teacher is to maintain the credibility of his students he must keep up with modern advances” (Coakley, 1992, p. 91).
While Graves and his colleague Dr Stokes (the condition Cheyne Stokes respiration bears his name) “were not the first to make use of beside teaching, they did so consistently and so successfully that it was adopted by clinical teachers elsewhere” (p. 94) according to Professor Daniel Reisman writing in the Medical History of the College of Physicians of Philadelphia in 1921 (Coakley, 1992).
In the late 19th century, the first generation of women doctors found the Irish medical hierarchy to be unusually open-minded with regard to the question of women’s admission in contrast to the policy in Great Britain. The Royal College of Physicians of Ireland (previously known as King and Queen’s College of Physicians in Ireland) was the first institution in the British Isles to admit women who had taken their studies abroad to their licentiate examinations in 1877 thereby allowing the first registration of female doctors in Great Britain and Ireland. Sophia Jex Blake, a leading campaigner for women’s admission to the medical profession from the 1860s, remarked that this decision was “the turning point” in the societal shift to gender equality in medicine as a profession.
III. THE PRESENT
A. Undergraduate Medical Education
Medical education in Ireland is provided by six medical schools. In 2006, the Irish government commissioned a report “Medical Education in Ireland: A New Direction”, the Fottrell report (Working Group on Undergraduate Medical Education and Training, 2006), which addressed core issues such as funding, selection criteria for medical school entry and intake numbers, curriculum reform, clinical training and oversight of undergraduate education. The implementation of the report resulted in, 1) expanded and new access routes to medical school with the addition of Graduate Entry Medical programmes in four of the schools, 2) curricular reform with outcomes linked to objectives, content, delivery methodologies, and assessment thereby expanding the methods by which education is delivered in line with international standards, 3) increased funding for faculty and infrastructure, 4) expansion of teaching to primary care facilities and, 5) accreditation of all clinical sites in partnership with Ireland’s national health service, the Health Service Executive (HSE).
Admission to medical school for Irish students is highly competitive, with ten applicants for each place. For school leavers, places are awarded on the basis of a combination of marks achieved in their high school exit examination and the recently introduced Health Professions’ Aptitude Test Ireland. Graduate entry students must achieve at a minimum upper second class honours primary degree and are then admitted on the basis of performance in the Graduate Medical School Admissions Test. Places at Irish medical schools are highly sought after by international students because of the international reputation for high-quality medical education in Ireland, and the safe, welcoming nature of the country. Students apply through international agents and are offered places based on academic performance, interviews and personal statements.
The Medical Council of Ireland regulates undergraduate medical education in accordance with the World Federation for Medical Education Standards. Irish medical schools have long been recognised for their strengths in providing an excellent grounding in foundational sciences, coupled with high-quality clinical teaching, experiential training and an emphasis on professionalism. Recent decades have seen innovation in the areas of inter-professional learning and team-based practice, research and innovation skills, the humanities in medical education, simulation and other forms of technology-enhanced learning. The universities have established academic units specifically dedicated to medical education and offer masters level qualifications in medical education.
Undergraduate medical education in Ireland shares many challenges with other jurisdictions including the continued provision of high-quality clinical learning environments for placements, supporting students’ health and wellbeing, and ensuring that graduates are well prepared for modern-day practice. Irish medical schools have retained the formal observed examination of bedside practice and communication as a significant component of the final year medical examinations.
International partnerships to support medical student exchange programmes are underpinned by memoranda of understanding. These facilitate high-quality research and clinical electives to enhance the student experience and prepare them for future practice in differing healthcare settings.
B. Postgraduate Medical Education
The governance of postgraduate education and training is under the remit of the Royal Colleges which are funded by the HSE to provide training on clinical sites. There are 13 postgraduate training bodies across all domains of practice. The RCPI is the largest training body with 1500 trainees in the specialities of medicine: paediatrics, obstetrics and pathology. Following a year’s internship, trainees enter two years of general professional training (residency) followed by a five-year fellowship of speciality training during which many trainees undertake formal research training to the level of MD/PhD. Partnership between the universities and the postgraduate training bodies has led to the establishment of structured training programmes to train academic clinicians such as the Irish Clinical Academic Training Programme.
The tradition of Irish doctors doing part of their training overseas is a well-established practice. Since the 1950s, the well-educated Irish diaspora have emigrated to develop professionally and return to Ireland to contribute their new knowledge and skills to society. Specifically, the Irish healthcare system has benefitted greatly from these medical graduates returning to Ireland bringing not only the expertise of their particular medical speciality but also the benefits gained from the experiences of working in different health systems.
In recent years, the Irish government published two reports on postgraduate medical education and training: “Preparing Ireland’s Doctors to Meet the Health Needs of the 21st Century”, Buttimer report (Postgraduate Medical Education and Training Group, 2006) and “Strategic Review of Medical Training and Career Structures”, McCraith report (Department of Health, 2014). These reports address the global challenges of doctor recruitment and retention, emerging healthcare needs of the population and the need for medical training and practice to incorporate use of modern-day technologies and fiscal responsibility and stewardship.
IV. THE FUTURE
There are three key elements to consider in the future planning of medical education and training: the modern-day workforce, the patient and the workplace environment. The increased financial challenge from rising healthcare costs is a central consideration for the future of medical education and training. Medical training needs to provide diversity in who we train and what we train doctors for, flexibility in training and work practice, and agility in how we respond to new challenges. We need models of collaboration with the sharing of learning material across borders, avoiding “reinventing the wheel” in a resource-scarce world.
The modern-day workforce is the most educated of all generations. They embrace technology and look for opportunities to innovate. They want a work-life balance that ensures job satisfaction and avoids burnout. The “one size fits all” model of a doctor needs to be “retired” to allow smart young medical professionals to adapt to the needs of the modern-day work patient and work environment. The future will require doctors to leave their comfort zones and work with other professionals outside healthcare. To achieve this, medical training will need to embrace innovation and entrepreneurship, providing doctors with experiential learning in the disciplines of business, science, engineering and law. Ireland is well-positioned to leverage on experiential learning and internships with global pharmaceutical, medical technology and medical device companies, as most of the world’s major companies are based in the country. Programmes, such as Bioinnovate Ireland, establish teams of doctors, other healthcare professionals, engineers and business school graduates who partner to identify innovative solutions to healthcare delivery. Health Innovation Hub Ireland brings innovation in and out of the health service and is a partnership between the medical schools and teaching hospitals and is funded by the Irish government through Enterprise Ireland. Initiatives such as this offer a new funding structure through which these companies sponsor applicants. The output from such partnerships will ensure that doctors become skilled innovators who can provide leadership in tackling global health issues such as disparity and inequality in healthcare access and healthcare provision, embedded in a sustainable financial model.
The new generation of doctors wants the option to practice differently. Modern-day society and individuals have increasing expectations of the healthcare system and their doctors. Doctors need to be effective in managing these expectations through knowledge exchange and communication. The modern-day practice is impacted by external influences, some predictable such as demographic shifts and workforce and resource scarcity; others unpredictable, such as new technological and therapeutic breakthroughs and shifts in global economic power. What is certain is a finite healthcare budget, so cost-consciousness must be built into our training programmes. What is uncertain is how we can deal with the unpredicted nature of quality healthcare provision.
Notes on Contributors
Professor Colm Bergin is a consultant physician in Infectious Diseases at St James’ Hospital and a clinical professor of medicine at Trinity College Dublin, Ireland. He is Director of Training Site accreditation RCPI and Censor in RCPI. He is the former director of Wellcome HRB Clinical Research Facility, Trinity College Dublin
Professor Mary Horgan is the president of the Royal College of Physicians of Ireland and former Dean of the School of Medicine, University College Cork. She is a consultant physician in Infectious Diseases at Cork and has served on numerous government-appointed boards and Governor of University Board.
Acknowledgements
Professor Tim O’Brien National University of Ireland Galway (NUIG), Dr Carmel Malone NUIG, Professor Michael Keane University College Dublin (UCD), Professor Paula O’Leary University College Cork (UCC), Dr Deirdre Bennett UCC and Dr Roisin Craven Royal College of Physicians of Ireland (RCPI).
Funding
There is no funding involved for this paper.
Declaration of Interest
The authors declare no conflict of interest.
References
Coakley, D. (1992). Irish masters of medicine. Dublin, Ireland: Town House.
Department of Health. (2014). Strategic review of medical training and career structure: Report on medical career structures and pathways following completion of specialist training. Retrieved from https://www.lenus.ie/handle/10147/317460
Organisation for Economic Co-operation and Development. (2019). Population [Indicator]. https://doi.org/10.1787/d434f82b-en
Postgraduate Medical Education and Training Group. (2006). Preparing Ireland’s doctors to meet the health needs of the 21st century. Retrieved from https://www.lenus.ie/handle/10147/42920
Working Group on Undergraduate Medical Education and Training. (2006). Medical education in Ireland: A new direction. Retrieved from https://www.lenus.ie/handle/10147/43350
*Mary Horgan
Royal College of Physicians of Ireland,
19 South Frederick Street, Dublin 2, Ireland
Tel: +35 32149 01596
Email: m.horgan@ucc.ie
Published online: 2 January, TAPS 2018, 3(1), 1-5
DOI: https://doi.org/10.29060/TAPS.2018-3-1/GP1071
Ronald M. Harden
University of Dundee, United Kingdom
I. SUMMARY
The ASPIRE-to-Excellence Initiative was established in 2013 to provide a mechanism where Excellence in teaching in a medical school received international recognition. Excellence was recognised in one or more of the following areas – Student Assessment, Student Engagement with the curriculum, Social Accountability of the medical school, Faculty Development and Simulation. Dental and Veterinary schools were included in the programme in 2015. To date, 23 schools from 12 countries around the world have received an ASPIRE award in one or more of the areas.
Experience gained with the ASPIRE-to-Excellence programme has established that it is possible to develop criteria on which excellence can be assessed and that schools benefit from participating in the programme and from the feedback received. The ASPIRE-to-Excellence initiative has created de facto standards for best practice in each of the areas assessed.
II. THE IMPORTANCE OF TEACHING
The importance attached by universities and medical schools to their teaching responsibilities has come under scrutiny. Does the school make explicit the appropriate learning outcomes expected of the student? Does it offer a suitable range of learning opportunities and experiences to facilitate the students’ achievement of the learning outcomes? Does it have a valid, reliable and fair system of student assessment? Are staff trained with regard to their teaching responsibilities and are students engaged in the curriculum planning and development? These questions are key in relation to the responsibilities a medical school has in training doctors who will be competent to meet the needs of the community they will serve following qualification.
III. THE BIRTH OF ASPIRE
When excellence in teaching is considered and when the issue of evaluating excellence in teaching is raised, the question frequently asked is whether it is possible to evaluate excellence in teaching in the same way as excellence in research. The evidence used to assess research excellence includes the number of research papers published and their citations and the research grant income received. What criteria can be used to determine excellence in teaching? Indeed, is this possible? David Wilkinson, then Dean of the University of Queensland, Australia suggested that excellence could be measured. He highlighted at a meeting during the Asia-Pacific Medical Education Conference in Singapore in 2010, the need for a form of quality assurance that recognised excellence which rightly falls outside the formal accreditation process as the remit of professional education bodies. He argued that a programme should be established that goes beyond the traditional accreditation process and that recognised that the education programme in a school can be subjected to peer review against an agreed set of standards or benchmarks that identified world-class excellence in education. AMEE, a leading international medical education organisation, he proposed, should respond to this challenge by establishing a mechanism where excellence in education in a medical school was recognised. The ASPIRE-to-Excellence initiative was born.
A review of current practice at that time showed that no similar initiative existed. Over the past decade the move to recognise excellence in universities had been reflected in increasing attention being paid to university league tables with the results of university rankings placing universities in a global pecking order (Harden & Wilkinson, 2011). Such rankings paid no or little attention to teaching. The Shanghai ranking was based exclusively on research performance and quality of teaching, as most people would define it, had only a limited impact in the Times Higher rankings (Table 1). While there was growing pressure to treat teaching seriously as a professional activity with equal status to research (Skelton, 2005), there was no mechanism available at a global level for professional peer-review of excellence in teaching. National accrediting bodies and the World Federation for Medical Education were concerned, and correctly so, with basic standards and not with the assessment of excellence. The ASPIRE-to-Excellence initiative as proposed met the need for a mechanism where excellence in education could be assessed. The aim of the initiative was to recognise and promote outstanding performance and excellence in teaching and learning in medicine.
An ASPIRE-to-Excellence Foundation Board made up of international leaders in medical education was established and met for the first time in Glasgow in 2010. Membership of the current Board is given in table 2.
IV. THREE QUESTIONS
Three initial questions were addressed. Should an ASPIRE award recognise excellence across all aspects of the medical school performance or should excellence be recognised relating to specific aspects of the teaching? Should a single standard for excellence be established or should a school be rated at different levels and receive a gold, silver or bronze award? Finally, what criteria should be used to assess that excellence had been achieved?
With regard to the first question there was agreement that while eventually there might be a holistic assessment of excellence of a medical school’s teaching programme, at least in the first instance the assessment should focus on specific aspects of the programme. Three very different areas and elements of the teaching programme were agreed. These were the assessment of students, the engagement of students in the education programme and the social accountability of the medical school. The areas were chosen by the ASPIRE Board as they were considered important and reflected both traditional values for schools (such as ensuring that they graduated competent doctors), as well as newer concepts (students being partners in their own education and the importance of societal contributions that medical schools should make to their local health care provision). In 2015 a fourth area, faculty development, was added and in 2016 a fifth area, simulation. Curriculum is planned as a new area for 2017.
In relation to the second question there was agreement that the aim was not to identify “the best school” in each field but to recognise with an ASPIRE award all schools who had achieved the required standard of excellence. To date this has been seen as an absolute standard with schools either achieving it or not achieving it. Schools who demonstrated elements of excellence but not overall excellence in an area were commended on the aspects where they did demonstrate excellence. There is ongoing discussion, however, as to whether the ASPIRE-to-Excellence initiative should recognise excellence at different levels with gold, silver and bronze awards.
The final question related to the basis on which excellence would be assessed in a school in the different areas where a school chose to be assessed. An international panel of medical education experts under the guidance of a chair was established for each of the three initial areas and later the other areas. These panels worked independently and developed and refined the criteria for excellence in their area under the overall auspices of the ASPIRE Board. The criteria that resulted from the deliberations are described for each of the themes on the ASPIRE website (https://www.aspire-to-excellence.org/Areas+of+Excellence/).
Although the review process for each Theme Panel is slightly different, all applications are reviewed by teams of three Panel members who independently grade submissions against the individual criteria of the theme. Discrepancies in scoring between assessors are discussed and if agreement cannot be achieved more reviews are sought. Once consensus is reached, the Panel Chair then makes recommendations to the ASPIRE Board. Awards are then announced and presented at the annual AMEE meeting. Applications are confidential and unsuccessful schools are provided with detailed feedback to support their development and encourage further progress and successful reapplication.
Pilot studies were undertaken in each of the areas to test the criteria developed and the working of the review process.
V. PROGRESS TO DATE
The number of submissions and the number of awards made since the ASPIRE-to-Excellence programme was launched in 2013 are summarised in Table 3. Faculty development was launched as a theme in 2016. To date 23 schools from 12 countries around the world have received an ASPIRE-to-Excellence award. The schools together with the area where excellence in education is recognised are given in Table 4.
Since 2016, ASPIRE recognition has been extended to include veterinary and dental schools. In 2016 submissions were invited on a fifth area – Simulation. Seven submissions were received for this category by the closing date of 28th February 2017.
Each year, successful schools receive a trophy and are presented with their awards during a plenary session at the annual AMEE Conference.
| % Weighting | |
| Reputational survey (teaching) | 15% |
| PhD awards per academic | 6% |
| Undergraduates admitted per academic | 4.5% |
| Income per academic | 2.25% |
| PhDs/Undergraduate degrees awarded | 2.25% |
Table 1. THES world university ranking criteria and weighting for teaching
| Member | Country |
| Dan Hunt | USA (Chair) |
| Khalid Bin Abdulrahman | Saudi Arabia |
| Ducksun Ahn | Korea |
| Robbert Duvivier | Australia |
| Matthew Gwee | Singapore |
| Ronald Harden | UK |
| Martin Hart | UK |
| David Irby | USA |
| Barry Issenberg | USA |
| Hassan Khan | Pakistan |
| Tadahiko Kozu | Japan |
| Pat Lilley | UK |
| Stefan Lindgren | Denmark |
| Cristina Manzanares | Spain |
| Nivritti Patil | Hong Kong |
| Madalena Patricio | Portugal |
| Pablo Pulido | Venezuela |
| Trudie Roberts | UK |
| James Rourke | Canada |
| John Tegzes | USA |
| Cees van der Vleuten | Netherlands |
| Theanne Walters | Australia |
Table 2. Membership of ASPIRE-to-Excellence Board as of March 2017
| Assessment | Student Engagement | Social Accountability | Faculty Development | Total Submissions | Total Awards | |||||
| Year | Sub | Awards | Sub | Awards | Sub | Awards | Sub | Awards | ||
| 2013 | 7 | 2 | 12 | 6 | 10 | 3 | 29 | 11 | ||
| 2014 | 3 | 1 | 6 | 1 | 5 | 2 | 14 | 4 | ||
| 2015 | 2 | 0 | 7 | 6 | 7 | 0 | 16 | 6 | ||
| 2016 | 1 | 0 | 2 | 1 | 4 | 4 | 5 | 2 | 12 | 7 |
| Totals | 13 | 3 | 27 | 14 | 26 | 9 | 5 | 2 | 71 | 28 |
Table 3. Submissions and ASPIRE awards in the themes assessment, student engagement, social accountability and faculty development
| School | Country | Award |
| 2013 | ||
| Southern llinonis University School of Medicine | USA | Assess, St. Eng, Soc Acc |
| Aga Khan University | Paskistan | Assess, St. Eng |
| University of Maribor | Slovenia | St. Eng |
| International Medical University | Malaysia | St. Eng |
| University of Western Australia, Faculty of Medicine, Dentistry and Health Sciences | Australia | St. Eng |
| University of Minho | Portugal | St. Eng |
| Northern Ontario School of Medicine | Canada | Soc Acc |
| Hull York Medical School | UK | Soc Acc |
| 2014 | ||
| University of Leeds, School of Medicine | UK | Assess |
| University of Southampton | UK | St. Eng |
| Memorial University of Newfoundland | Canada | Soc Acc |
| University of New Mexico, School of Medicine | USA | Soc Acc |
| 2015 | ||
| The Charité – Universitätsmedizin, Berlin | Germany | St. Eng |
| University of Leeds, School of Medicine | UK | St. Eng |
| Utrecht University, Faculty of Medicine | The Netherlands | St. Eng |
| Uppsala University, School of Medicine | Sweden | St. Eng |
| Schulich School of Medicine and Dentistry | Canada | St. Eng |
| Chulalongkorn University, Faculty of Medicine | Thailand | St. Eng |
| 2016 | ||
| The School of Verterinary Medicine and Science, University of Nottingham | UK | St. Eng |
| Florida International University, Herbert Wertheim College of Medicine | USA | Soc Acc |
| Brody School of Medicine, East Carolina University | USA | Soc Acc |
| University of Leeds, School of Medicine | UK | Soc Acc |
| Leaders in Indigenous Medical Education (LIME) Network | Australia | Soc Acc |
| University of California, San Francisco | USA | Fac Dev |
| Royal Verterinary College, University of London | UK | Fac Dev |
| Assess= Student Assessment, St. Eng= Student Engagament with the curriculum, Soc Acc= Social Accountability of the school. Fac Dev= Faculty Development | ||
Table 4. Schools recognised with an ASPIRE-to-Excellence Award
VI. CONCLUSIONS
The ASPIRE-to-Excellence programme now in its fifth year has attracted favourable publicity and generally considered to be successful (Ahn & Ahn, 2014; Hunt & Harden, 2016; Patricio, 2016; Roberts, 2016). Experience gained in the ASPIRE programme has clearly established that it is possible to recognise excellence in teaching. Development of the criteria for excellence was a major activity which required a year’s work by each panel and pilot testing in schools. With the experience gained the application of the criteria has evolved over time and the evidence required to assess whether a school has met the criteria as set out has been refined. A separate submission from students in the school is seen as an important part of this process. Some criteria such as, in the case of the student engagement theme, full participation in a curriculum committee are seen as non-negotiable, while others such as responsible for the production of learning resource material are desirable but not essential.
It has become obvious that some schools, but not all schools, value the opportunity to assess and promote their excellence in teaching. The number of schools submitting for an application in one or more of the categories is still relatively small. Obviously ASPIRE Awards are relatively new and so schools may not be aware of the scheme but maybe some schools are wary of being judged and found not to be excellent. When the University Teaching Excellence framework was introduced in the UK some elite universities threatened to boycott the scheme and indicated that they did not wish to take part in an exercise where their teaching was assessed. It became apparent however that this was an unacceptable position to take.
Many elite medical schools while on the surface supporting the principles underpinning the ASPIRE-to-Excellence programme, have themselves not subjected themselves to an ASPIRE review. One reason may be that they fear they have more to lose than to gain from engaging with the assessment and that a possible rejection could damage their standing. It may be that as the importance of teaching as a function of a medical school is increasingly recognised and valued opting out of an exercise that assesses excellence in the area will be less attractive.
The benefits of submitting an ASPIRE-to-Excellence application have been documented. More than 90% of schools surveyed reported that the ASPIRE submission process and the feedback received as a result had a significant impact on their school, that it encouraged staff to reflect on their practice and often resulted in improvements. The ASPIRE award winners have now established an ASPIRE Academy which serves as a network of schools where excellence in education has been recognised.
In practice the ASPIRE-to-Excellence initiative has created de facto standards for best practice in the areas assessed. Schools who have not applied for an award have used these standards to evaluate their own education programme and used them as a basis for the further development. An awareness of what is recognised as excellence in a university is a component of striving towards excellence.
Notes on Contributors
Professor Ronald M Harden OBE MD FRCP(Glas) FRCS(Ed) FRCPC is the General Secretary of AMEE and Professor of Medical Education, University of Dundee, UK.
Declaration of Interest
The author declares no competing interests.
References
Ahn, E. & Ahn, D. (2014). Beyond accreditation: excellence in medical education. Medical Teacher, 36. 84-85.
Harden, R.M. & Wilkinson, D. (2011). Excellence in teaching and learning in medical schools. Medical Teacher 33(2). 95-96.
Hunt, D. & Harden, R.M. (2016). ASPIRE to excellence: a novel approach toward benchmarking excellence in medical schools. Educación Médica,. 17(3), 97-100.
Patricio, M. (2016). The ASPIRE initiative: excellence in student engagement in the school. Educación Médica, 17(3), 109-114.
Roberts, T.E. (2016). The ASPIRE initiative: excellence in assessment. Educación Médica, 17(3), 106-108.
Skelton, A. (2005). Towards a critical approach. Understanding teaching excellence in higher education. London and New York: Routledge Taylor and Francis Group.
*Prof Ronald M Harden
AMEE, 12 Airlie Place, Dundee, Scotland, DD1 4HJ
Tel: +44 1382 381953
Email: r.m.harden@dundee.ac.uk
Published online: 2 May, TAPS 2018, 3(2), 1-5
DOI: https://doi.org/10.29060/TAPS.2018-3-2/GP1074
Lawrence T. Sherman1 & Kathy B. Chappell2
1Academy for Global Interprofessional Learning and Education, Switzerland; 2American Nurses Credentialing Centre, United States of America
Abstract
Healthcare professionals worldwide participate in continuing professional development (CPD) to remain competent in practice, and to ensure they provide high-quality care to patients. Globally, CPD systems have evolved at different rates resulting in significant variation in structure, requirements, and oversight. In some countries, CPD has moved from single profession educational designs and formal didactic methods of delivery to educational models that are innovative, dynamic, and learner-centric. In other countries, CPD is a neglected part of the healthcare education continuum. This article provides a global perspective on the evolution of CPD over the past 20 years, and identifies opportunities for the future.
Practice Highlights
- CPD is a vital part of the medical education continuum.
- CPD systems vary worldwide.
- It is essential that healthcare professionals participate in CPD.
- CPD is moving from single profession education to interprofessional continuing education models.
- High-quality CPD is innovative, dynamic, and learner-driven.
I. INTRODUCTION
In the United States, the role of continuing professional development (CPD) as a strategy to ensure healthcare professionals are engaged in lifelong learning and maintaining clinical competence has evolved significantly over the past 20 years. Historically, CPD consisted primarily of didactic lectures delivered away from the work place setting, classroom style, and teacher-focused with little learner engagement. CPD was experts telling you how to practice. CPD was delivered in silos and in single profession models (as compared to interprofessional), with physicians lecturing to physicians, nurses to nurses, and similar.
A body of evidence linking CPD to improving clinical practice and patient outcomes has changed the field significantly, and for the better (Cervero & Gaines, 2014). CPD is now dynamic, flexible, and outcome-focused. Today’s CPD blends multiple educational methodologies to meet the needs of learners including but not limited to live (face-to-face) meetings, digital delivery, flipped classrooms, and simulation. CPD is embedded in the work place where experiential learning takes place, guided by expert faculty who provide opportunity for activities such as small group, problem-based learning built around real world problems. CPD is also embedding more opportunity for interprofessional continuing education (IPCE), as health care is delivered by teams of professionals in collaboration with patients and care givers, and research has demonstrated the positive impact of IPCE on team performance and patient outcomes (Reeves et al., 2016; Joint Accreditation, 2016).
II. CURRENT STATE OF GLOBAL CPD
Throughout the world, healthcare professional education starts with the undergraduate curriculum and continues through postgraduate training and specialization. CPD is the longest part of the continuum, often encompassing 40 or more years of a healthcare professional’s career, yet in many countries it is the least structured or regulated component of the continuum. Because new evidence in medicine and health care is published at an increasingly rapid rate, CPD is a vital component to ensuring healthcare professionals remain competent in practice and are able to deliver high-quality, evidence-based care. Unfortunately, there are still systems worldwide in which CPD is not considered a contiguous part of the healthcare education continuum, which poses a significant threat to maintaining healthcare providers’ competence and improving the quality of patient care. Globally, challenges in CPD include significant variability in how it is defined and structured, and the differing requirements and levels of oversight by country or region.
A. Definition of CPD
The definition of CPD varies greatly around the world. Most often, CPD is a catch-all term referring to the combination of formal continuing medical education (CME) and other types of activities designed to help healthcare professionals acquire knowledge and skills necessary for professional growth. Alternatively, others use the terms CPD and CME interchangeably, referring to only the educational components of learners’ ongoing development.
In the absence of a formal definition of CPD worldwide, the approaches to healthcare professional education for practicing clinicians vary widely. Countries that have more formal CPD systems are often those where participation in CPD is required for re-licensure, revalidation, or for financial/salary benefits. In countries where there is little or no need for documented, relevant CPD, there are fewer opportunities for physicians and other healthcare professionals to participate in high-quality CPD activities that have been designed to improve practice and outcomes.
B. Structured System for CPD
Another area of inconsistency globally is the structure of CPD systems. In North America, Australia and Europe, there are structured systems of CPD in which organizations that have met pre-established standards set forth by accrediting bodies (“accredited providers”) or organizations that develop certified educational activities using accreditation standards award continuing education (CE) credit to learners. While accredited providers vary in type, structure, and affiliation, they follow common practices when developing education. In systems that use accreditation standards, accredited provider types include but are not limited to academic medical centres, hospitals or healthcare systems, associations, specialty societies, government agencies, and medical education companies. In areas of the world that have not implemented accreditation standards, organizations that include commercial interests are able to develop education for healthcare professionals.
C. Activity Design, Evaluation and Credit
Healthcare professionals seek out and participate in CPD with the intent of improving their own knowledge and practice, and with a desire to provide the best care possible to the patients they serve. The design of educational activities including how they are evaluated, and the type of CE credit awarded (if any) reflect regional differences.
In countries using accreditation standards, accredited providers or organizations submitting activities for approval design educational activities to address professional practice gaps, or identified practice-based needs. Assessment of gaps, content development, implementation, and evaluation are the responsibility of the provider or organization. In some countries, however, CPD topics are selected by stakeholders such as governmental health authorities, and not determined by those who are responsible for designing and developing the education. This poses significant constraints for providers/organizations to conduct their own needs assessments and identify appropriate topics for CPD activities for their learners. In some areas of the world, commercial interest organizations are permitted to develop or participate in developing CPD that awards CE credit, while in others areas there is strict separation of commercial interest organizations from the educational activity design process.
Commercial interest organizations are defined by the Accreditation Council for Continuing Medical Education (ACCME) and other accrediting bodies as: produces, markets, sells or distributes health care goods or services consumed by or used on patients; is owned or operated, in whole or in part, by an organization that produces, markets, sells or distributes health care goods or services consumed by or used on patients; or advocates for use of the products or services of commercial interest organizations (Accreditation Council for Continuing Medical Education, 2004).
The vast majority of CPD developed globally is focused on single-profession education. While this “educational isolation” is common, it is not representative of the environment in which healthcare providers practice. The evolution of interprofessional continuing education (IPCE), in addition to single-specialty multidisciplinary education, has begun to emerge within North America, Europe, Australia, the Middle East, and Asia.
When evaluating CPD activities, the seven-level approach of Moore and colleagues (Figure 1) has been adopted in many areas worldwide (Moore, Green, & Gallis, 2009). Outside the US where accredited providers are required to measure at the level of competence or higher, the lower level outcome measures, participation and satisfaction, are assessed most frequently. Changes in knowledge are also measured, but the higher levels of measurement including changes in competence, performance, and patient or population health are measured far less often.

Finally, awarding of CE credit is inconsistent globally. In some countries, participation in CPD with associated CE credit is required for healthcare professionals to maintain a license to practice or for maintaining board certification. Some countries impose mandatory participation in CPD as a requirement for remuneration. In other areas, credit is not meaningful or relevant. This poses significant challenges for the global healthcare education community. There are no global standards for CPD, although accrediting bodies in some areas of the world have collaborated to use congruent standards and develop systems of mutual recognition, such as ACCME’s substantial equivalency evaluation process. In other areas of the world, standards have not been adopted. This is one of the major challenges to harmonize credit systems around the world.
III. THE EVOLUTION OF CPD IN THE UNITED STATES
A. Early 2000s
In the early 2000s, the CPD system in the United States was largely based on the concept of “formal” education delivered in live, face-to-face meetings. Commercial support, or funding from commercial interest organizations, was a significant driver of revenue for many continuing medical education (CME) companies. Educational activities were developed in a single profession model, with little opportunity for interaction or engagement between members of different health care professions. There was a lack of formal faculty training opportunities, and evaluation of educational activities was often based solely on satisfaction rather than higher level outcomes that reflected learning, practice change, and impact. The US accreditation system was strong, having implemented standards for commercial support and independence that required CME providers to prohibit commercial interest organizations from influencing the process of planning and presenting educational activities. The US accreditation system was also beginning to use its evidence-based criteria as a lever for change.
In 2006, the Accreditation Council for Continuing Medical Education (ACCME) began to require its providers design educational activities to change competence (ability to apply), performance, or patient outcomes. ACCME also required its providers to assess whether change in competence, performance, or patient outcomes occurred. Concurrently, the ACCME was also collaborating with the major accreditors in nursing and pharmacy to develop a joint accreditation system that recognized and promoted team-based learning. The foundation of the US accreditation system was based on provider accreditation rather than individual activity approval. A provider-based accreditation system allows for the review and approval a greater number of activities than an activity-based system, and facilitates an environment of self-regulation and educational innovation.
B. Present Day
CPD has evolved to encompass a wide range of educational experiences that reflect the needs of today’s healthcare professionals working within multiple and diverse health care settings. CPD includes activities such as conferences and formal meetings, but also incorporates less structured, informal learning that occurs in the workplace. CPD may include Grand Rounds, Tumor Boards, and organizational or unit-based quality improvement initiatives. CPD is incorporated within journals, and within poster presentations. CPD is flexible and adaptable, with better alignment across the education continuum – from undergraduate, to postgraduate, to the practice setting.
CPD is learner-focused and faculty-supported, in contrast to faculty-driven. Education is designed to meet the professional practice gaps of individual health care practitioners and of health care teams. CPD providers incorporate adult learning principles, active learning strategies, and longitudinal design interventions. CPD providers evaluate the impact of education using higher level outcomes that reflect competence (or intent to change practice), performance, and/or patient outcomes.
In the US, CPD is also moving from single profession to team-based models that incorporate multiple healthcare professionals into planning and designing educational activities. Accreditors across the major health care professions of medicine, nursing, and pharmacy have aligned expectations for continuing education providers, improving congruence and expectations. Three accreditors have also collaborated to create a joint accreditation program to promote IPCE in CPD. Providers that are jointly accredited have opportunity to award IPCE credit for team-based education, as well as retain the ability to award credit for single profession CE as appropriate (Joint Accreditation, 2016).
Although commercial support remains a source of funding for CME, there has been an overall reduction in the amount of support provided by commercial interest organizations. Data from the 2006 ACCME annual report indicated that 50% of the $2.4 billion spent on continuing medical education came from commercial support; this dropped to 28% of the $2.5 billion spent on CME as reported in the ACCME annual report in 2015, and only 11% of all CME activities in 2015 received commercial support (Accreditation Council for Continuing Medical Education, 2015).
Finally, CPD is being engaged as a strategy to address major public health issues in the US. Providers, accreditors, and the Food and Drug Administration (FDA) have combined forces to address opioid-related deaths through the Extended Release/Long Acting (ER/LA) Opioid Risk Evaluation and Mitigation Strategies (REMS) program. Funded by pharmaceutical manufacturers of ER/LA opioids, providers independently develop education designed for prescribers of these medications, while oversight of compliance is managed by the accreditors.
IV. CONCLUSION
CPD continues to evolve worldwide as it is increasingly recognized as an important part of the healthcare education continuum. Alignment is occurring among the healthcare accreditors in academia, post-graduate training, and practice. Changes and progress made in North America, Australia, and Europe are influencing and affecting change in countries throughout the rest of the world. This has led to the emergence of CPD professionals who have built the necessary skill set required to develop CPD activities worldwide. These changes are leading to the recognition of CPD as a critical element of the health care system, addressing health care gaps for individual practitioners, teams, patients, and the system.
Notes on Contributors
Lawrence Sherman, FACEHP, CHCP, is SVP at AGILE, a Swiss-based medical and interprofessional education provider, and has been involved in CME for24 years. He is an instructor at Northwell Health in New York, and Stony Brook University SOM. He co-chairs the CPD Committee for AMEE. He was host and creator of Lifelong Learning on ReachMD.
Dr. Chappell is SVP of Accreditation, Certification, Measurement, and Research at ANCC. She holds a BSN with distinction from the University of Virginia; an MSN and PhD from George Mason University. She is a Fellow in the American Academy of Nursing and Distinguished Scholar & Fellow in the National Academies of Practice.
Declaration of Interest
The authors of this paper have no conflicts of interest to declare.
References
Accreditation Council for Continuing Medical Education ACCME) (2004). Standards for Commercial Support: Standards to Ensure Independence in CME activities. Retrieved from http://www.accme.org/requirements/accreditation-requirements-cme-providers/standards-for-commercial-support.
Accreditation Council for Continuing Medical Education (2006). ACCME Annual Report Data – 2006. Retrieved from http://www.accme.org/news-publications/publications/annual-report-data/accme-annual-report-data-2006.
Accreditation Council for Continuing Medical Education (2015). ACCME Annual Report Data – 2015. Retrieved from http://www.accme.org/news-publications/publications/annual-report-data/accme-2015-annual-report.
Cervero, R., & Gaines, J. (2014). Effectiveness of continuing medical education: Updated synthesis of systematic reviews. Chicago: Accreditation Council for Continuing Medical Education.
Joint Accreditation (2016). By the Team for the Team: Evolving Interprofessional Continuing Education for Optimal Patient Care. Report from the 2016 Joint Accreditation Leadership Summit. Retrieved from http://www.jointaccreditation.org/sites/default/files/2016_Joint_Accreditation_Leadership_Summit_Report_0.pdf
Moore, D. E., Green, J. S., & Gallis, H. A. (2009). Achieving Desired Results and Improved Outcomes: Integrating Planning and Assessment Throughout Learning Activities. Journal of Continuing Education in the Health Professions, 29(1), 1 – 15.
Reeves, S., Fletcher, S., Barr, H., Birch, I., Boet, S., Davies, N., … Kitto, S.C. (2016). A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Medical Teacher, 38(7), 656 – 668.
*Lawrence Sherman
Email: meducate@gmail.com
Tel: +1.215.285.6034
Published online: 4 September, TAPS 2018, 3(3), 1-4
DOI: https://doi.org/10.29060/TAPS.2018-3-3/GP1070
Michelle A. Kelly1, Ashokka Balakrishnan2, & Krishnasamy Naren3
1School of Nursing, Midwifery and Paramedicine, Faculty of Health Sciences, Curtin University, Australia; 2Department of Anaesthesia, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 3Human Patient Simulation Centre, School of Medicine, Taylor’s University, Malaysia
I. INTRODUCTION
The ultimate goals of health professions education are to enhance practice readiness, improve delivery of safe patient care and ideally, improve patient outcomes. Simulation based education (SBE) is now well established as an educational approach, in undergraduate programs and for continuing professional education, that complements existing models in development of core clinical knowledge and skill acquisition for health professions students and clinicians. It is known that the various domains of learning, such as knowledge, the psychomotor, affective and behavioural elements of practice, can be incorporated into holistic patient care simulation scenarios (Kelly, Hopwood, Rooney & Boud, 2016). Ways of determining the impact of SBE are topics emerging in the literature. Increasingly, those who design and deliver SBE are becoming more attuned to the spectra of cultural considerations important for learning and practice (Bahreman & Swoboda, 2016).
Culture can be defined as ‘the social domain of practices and material expressions’ and ‘a way of life, customs and beliefs’ (Horvat, Horey, Romios, & Kis-Rigo, 2014). Further, culture is a consideration within the contexts of: organisational, ethnic, socio-economics, geographical, political, personal values and beliefs and societal standpoints (Horvat et al., 2014). For ease of discussion, we will focus on culture from the ethnic and geographical perspectives which influence approaches to learning and outcomes in educational settings. Specifically, we address the challenges – and opportunities – in addressing the cultural diversity in the student population. There is much in the literature about developing cultural competency in relation to patient care, but little acknowledging the diversity amongst health professions students and ways to maximise learning, specifically within SBE.
The cultural considerations of learners, as noted above, should be considered in all stages in SBE including the: formation of participant or observer groups; scenario topic and content presentation; preparation and participation of students and faculty; approaches to debriefing; post simulation reflection and benefits beyond the educational exercise. As SBE matures, educators are more cognisant of the importance of local contexts and nuanced practices as foundational features in designing and delivering simulations. Attention to students’ expectations of learning, embedded within their cultural norms, is critical for meaningful development of professional practice, as portrayed through SBE. These are important factors given the diversity in student cohorts, patients and the health workforce.
II. LEARNING EXPECTATIONS OF DIVERSE STUDENT COHORTS
Globalisation of the health workforce has an impact on universities, particularly in the Asia-Pacific region, in that there are significant numbers of ‘international’ students within health professions programs. These large, diverse student cohorts are distinctly heterogeneous in their cultural origins, language, educational backgrounds and clinical practice cultures (San Miguel & Rogan, 2015). Their expectations about learning often contrast with contemporary Western approaches. Rather than being the ‘font of all knowledge’ the contemporary role of teachers is to facilitate student learning. Group work, peer learning and Socratic dialogue are paradigms which significantly contrast with pre-university experiences, and often challenge the leaning expectations of students from Asian cultures (Kelly et al., 2016). For example, Asian students’ experiences from traditional college education are of assessments that personify rote learning so when students are suddenly exposed to approaches such as self-directed or problem based learning to promote deeper analytical processes, significant adjustment is required (personal experiences of all 3 authors). Some may say this is the case for students in many other countries. In any case, academics need to acknowledge the differences in these expectations and support students in the transition to higher education.
Culturally sensitive beliefs influence not only student learning but also clinical practice, and the expectations of clinical facilitators of ‘ideal’ student behaviours. The nuances of effective communication is a prime example here and one which can be addressed in SBE prior to students’ clinical placements. San Miguel and Rogan (2015) provide examples of facilitators’ comments about nursing students’ ‘ineffective’ communication abilities such as: avoiding eye contact, not engaging in ‘small talk’ and perceived lack of ‘seeking clarification’ in relation to clinical procedures. Many of these cultural considerations can be addressed using SBE to model ‘ideal’ professional behaviours to students as well as academics, and through peer teaching, offering those who facilitate SBE appreciation of student-centric approaches to learning.
III. KEEPING LEARNERS WITHIN THE SAME CULTURAL GROUPS?
We acknowledge there are benefits in combining learners from varied cultural backgrounds into ‘mixed groups’ for any educational approach, where diversity of contexts and values enrich awareness. However, when commencing a program of simulation, there may be benefit in configuring groups with similar cultural understandings, supported by a faculty member with an equivalent background. This approach may address the commonly reported levels of anxiety when participants are asked to ‘perform’ in simulation scenarios while others observe. Participants may then feel more able to interact using specific phrases, range of responses and practices inherent to their culture. Once the learners have reached a particular level of comfort with what is expected, a deliberate move to more heterogeneous groups may expand awareness of equally relevant responses from others’ cultural viewpoints. There is also value in academics’ modelling professional behaviours for students or clinicians, with respect to the context of the practice environment. These approaches may ease the transition to more demanding simulations that require greater learner engagement, more peer feedback and active participation in debriefing.
IV. PREPARATION TO FACILITATE LEARNING
SBE is a learner-centred approach, where participants and observers should feel comfortable in responding authentically to a given patient ‘situation’ and draw on tacit knowledge to personify holistic practices. Within SBE, learning and insight is facilitated through fluid interplay between participants (the socio-cultural) and with artefacts in the environment (the socio-material) (Kelly et al., 2016). Facilitating SBE requires multiple skills which may conflict with established, or comfortable, educational practices. Being mindful of what learners bring to the situation such as previous work and life experiences will also help facilitators support participants’ varied approaches to learning.
There is a dearth of literature on the influence culturally diverse faculty have on learners in SBE, another important point to discuss and explore. Planning how to facilitate simulations commences with agreement (if there are multiple faculty) on how to select active participants, the pace and complexity of the unfolding scenario, the level and type of support offered to participants, when to intervene if practice is unsafe, and when to stop the scenario.
Even the interactions between the simulation faculty and technical support team and how they choose to progress or deteriorate the ‘patient’ can vary based on the quality of interaction between them. These subtle differences can indeed influence the overall intended learning outcomes. Such factors can be minimised by having dry-runs of the scenario with all members of the simulation team, especially when they too are of diverse cultures. Pre-planning offers synchrony of intended simulation states with expected interventions and helps to shape the debriefing content.
V. ENGAGING OBSERVERS IN NOTICING
Attention is turning to those who observe simulations and ways to improve engagement in noticing what unfolds, to discuss during debriefing but to also trigger self-reflection of practice and beliefs. Several research groups are developing rubrics with varying levels of supportive prompts or sample answers to help students focus on the simulation action. Students can enter comments into the rubric about what they discern as professionally (and/or personally) important for a given patient care situation which provides opportunity to contribute opinions into the debriefing session. This may lead to more thoughtful and constructive comments rather than punitive tendencies or focusing on ‘what is right’. Students could also pair up to complete the rubrics which might highlight different opinions based on cultural values.
VI. DEBRIEFING DIVERSE STUDENT COHORTS
In the contexts of this paper, the cultural expectations of post-simulation debriefing are generally based on the principles of ‘seeking the absolute truth’ and ‘not settling for second best’. This conflicts with Western based models of debriefing where the facilitator probes students’ opinions in a ‘reflective mode’ approach. It is acknowledged that achieving stepwise deconstruction of the simulation exercise is important, namely – what went well, what does not fit in the expected plan, what went wrong, how could it be improved. A particular characteristic of culturally diverse learners is that they might choose not assert to embarrass their team mates when they knew of a superior alternative. However, it also important to note the students of Asian origin seem to be particularly keen to quickly reach the ‘essence of the matter’, being told what was not done to expected standards and which are the expected best practices that should be adopted. Hence the debriefing might have to dwell more on identifying the core misses and have a structured way of stating the expected.
Over time, techniques such as encouraging learners to lead discussions, learning how to phrase questions during debriefings, as well as allowing for periods of silence, might be viewed as a more useful and informative approach to reflection on and about practice. Simple trigger questions such as: what did you notice when …? what do others think? tell me more, and have you seen this before? might be useful in changing the format to debriefing conversations. Viewing other faculty as they model debriefing practices will help in implementing new approaches, as would peer-review of facilitation techniques.
VII. MAXIMISING STUDENT ENGAGEMENT AND REFLECTION
Simulation exercises are time, centre and faculty limited and have to progress within a frame of pre-planned events and activities. This is especially true when large student cohorts more than 200 have to rotate within a couple of days. Such schedules can limit the capacity to help learners who are shy performers when ‘being watched’, those with inability to be assertive in group sessions, and those who are ‘frozen’ when the session demands ‘action’ as a team. While culture can have influence on how students learn, inherently some students choose to lead the sessions, while some prefer to take instruction while the rest ruminate or stand inactive. The role of faculty in these situations is to maximise participation of all learners and guide them to achieve learning by being in teams.
VIII. SUPPORTING ONGOING LEARNING TO ENHANCE PRACTICE
Learning from the simulations needs to start before the actual sessions. Appropriate pre-reading to bring knowledge to the fore, pre-assessments immediately before or during simulation sessions to gauge knowledge retention and reflection, flagging current guidelines and core clinical information during the debriefing help to layer the learning experience. Following learners up after the simulations helps to determine if the minimum expectations as set by curricular goals has been achieved. With diverse student cohorts, there must be provision for extra sessions / open lab time for those who need more ‘deliberate practice’ following the simulations. Ongoing support can be offered through blended learning platforms. Options might include discussion forums or academic blogs that allow more ‘reserved’ students to clarify core principles with faculty and peers at a pace that suits their processing capacity and reflects their cultural belief systems.
In summary, culturally and linguistically diverse large cohorts are a challenge for many health professions educators. Understanding the different perspectives and expectations of these learners will assist faculty in creating and delivering culturally appropriate SBE experiences. Benefits would likely extend to all learners and offer insights about ways to enhance communication, teamwork and considerations when working in diverse teams or caring for diverse patient populations.
Notes on Contributors
Associate Professor Michelle Kelly PhD MN BSc brings varied clinical, educational and academic experience to her current role as Director: Community of Practice at Curtin University. Her practice and research in health professions education focuses on the varied ways simulation can be used to enhance and enable holistic clinical practice.
Dr Ashokka Balakrishnan is a consultant anaesthesiologist (NUH) and medical educationalist (CenMED, NUS) with 10 years’ experience in the use of high fidelity simulation. He has a Fellowship of the Australia New Zealand College of Anaesthesiologists (FANZCA) and a Masters in Health professions educations (MHPE) from Maastricht, Netherlands. His special interests are in interprofessional education through acute care simulation and multidisciplinary team training.
Dr Narendiren Krishnasamy MBBS, PG Dip in Diabetology, MBA (Hospital Management) runs the medical simulation learning programs at Taylor’s University, Malaysia. He strongly believes in “Raising the standards of medical education by promoting good healthcare and patient safety through simulation”.
Declaration of Interest
There are no specific conflicts of interest from any of the authors with regards to this paper. Views put forward are based on personal experiences, their own and others’ research.
References
Bahreman, N. T., & Swoboda, S. M. (2016). Honoring diversity: Developing culturally competent communication skills through simulation. Journal of Nursing Education, 55(2), 105-108. https://doi.org/10.3928/01484834-20160114-09
Horvat, L., Horey, D., Romios, P., & Kis-Rigo, J. (2014). Cultural competence education for health professionals. The Cochrane Database of Systematic Reviews (Online), 5(5), CD009405. https://doi.org/10.1002/14651858.CD009405.pub2.
Kelly, M. A., Hopwood, N., Rooney, D., & Boud, D. (2016). Enhancing students’ learning through simulation: Dealing with diverse, large cohorts. Clinical Simulation in Nursing, 12(5), 171-176. https://doi.org/10.1016/j.ecns.2016.01.010.
San Miguel, C., & Rogan, F. (2015). Assessing students’ English language proficiency during clinical placement: A qualitative evaluation of a language framework. Nurse Education Today, 35(6), 771-776. https://doi.org/10.1016/j.nedt.2015.02.014.
*Michelle A. Kelly
Email: Michelle.Kelly@curtin.edu.au
Published online: 2 January, TAPS 2019, 4(1), 9-12
DOI: https://doi.org/10.29060/TAPS.2019-4-1/GP2000
Klara E. Fransson1, Ingrid E. J. Lundahl1, Heidi K. Pasma1, Mohamed R. M. Rishard2 & Maduka de Lanerolle-Dias2
1Faculty of Medicine, Lund University, Sweden; 2Faculty of Medicine, University of Colombo, Sri Lanka
Abstract
Annually, a number of final year medical students from Lund University in Sweden travel to various healthcare facilities globally. We chose to go to the island of Sri Lanka, spending our elective at the department of Obstetrics and Gynaecology in Colombo. The dissimilarity between healthcare in Sweden and in Sri Lanka was evident throughout our stay. The design of healthcare facilities in Sri Lanka focused less on patient privacy and more on efficiency. The workload for doctors in Colombo was heavier than their Swedish counterparts. In general, outcome for Swedish patients is favourable when compared to Sri Lankan. We believe the difference in outcome is due to the unequal financial situations of the countries. Teaching approach in Sri Lanka diverted from Swedish practice by being more authoritarian but also exceedingly efficient. The large number of patients in wards and outpatient clinics allowed for us to experience a wide range of patient cases, offering important insights in medicine. It has been questioned whether the tradition of international electives is ethically justifiable. We therefore believe it important to stress that throughout our stay we were participating as observing students, not practicing doctors. We regard our elective a valuable experience, providing us with knowledge we will use in our future profession. Time spent observing Sri Lankan healthcare will also serve as a reminder to remain humble towards different cultures. We are now aware of the privileges we have, practicing medicine in a socioeconomically strong country.
Practice Highlights
- It is likely advantageous to include an international elective in medical training.
- Teaching methods and approach to teaching varies greatly between countries.
- It is important to respect and acknowledge cultural as well as financial differences between regions.
I. INTRODUCTION
Annually, a number of final year medical students from Lund University in Sweden travel to various healthcare facilities globally. We selected the Faculty of Medicine, University of Colombo, Sri Lanka for our elective. Sri Lanka has lately become a popular destination for outgoing elective students from Lund University. The overseas electives unit at the Faculty of Medicine at the University of Colombo was officially established in 2012, but the first students started coming in 1994. The unit now caters to over 100 students per year (125 students in 2016).
The main reason for our choice of Sri Lanka as our elective destination was the good reputation of the elective program, with the welcoming and friendly ambience known to be accompanied by an ambitious and demanding learning environment. The country remains an attractive elective destination for many doctors-to-be. The appeal of this island state seems to lie on the unique combination of advanced healthcare in a resource-limited setting spiced up with rare medical conditions and the aspects of tropical medicine. In addition, the island has much to offer in terms of the rich cultural heritage.
Obstetrics and Gynaecology was a natural choice of specialty for us since we all developed a growing interest in the field during our clinical rotation in Sweden. Also, we saw the elective as a precious opportunity to deepen our knowledge of Obstetrics and Gynaecology further, since our medical training in Sweden, including the 21-month post-graduate internship, only incorporates five weeks in the Obstetrics and Gynaecology department.
II. GLOBAL PERSPECTIVE
A. Healthcare Settings in Sri Lanka and Sweden
Although a fairly small island, Sri Lanka has a population of 21.2 million people as compared to 9.9 million people in our homeland Sweden. Sri Lanka has a gross domestic product (GDP) of around 81 billion USD and spends 3.0 % of this on healthcare. By comparison, Sweden has a GDP of 498 billion USD and a health expenditure of 11.0 % of GDP (The World Bank, 2015a, 2015b).
Within the field of Obstetrics and Gynaecology, Sri Lanka displays relatively low numbers of maternal and neonatal mortality. In 2015, the maternal mortality ratio in Sri Lanka was 30 in 100 000 live births, which was amongst the lowest in the region according to the World Health Organization (World Health Organization, 2015). The corresponding number in Sweden is 4 in 100 000 live births. The neonatal mortality rate was 6.3 in 1000 live births in Sri Lanka in 2015, as compared to 1.6 in 1000 live births in Sweden (The World Bank, 2015c).
Even though there are still obvious differences in mortality related to pregnancy and infancy when you compare Sweden and Sri Lanka, a lot of changes have been made in the latter country over the last decade. The focus on improving healthcare has resulted in a decrease in the risk of fatal outcomes in both mothers and children. For example, in 2007, 98.6 % of all deliveries are now supervised by a qualified attendant (The World Bank, 2015c). Also, considering the fact that the number of doctors in Sri Lanka was 0.7 physicians per 1000 people in 2010 while the corresponding number was 3.9 physicians per 1000 people in Sweden, the performance of Sri Lankan health care is evidently impressive (The World Bank, 2010).
We spent our four weeks’ elective programme at the De Soysa Women’s hospital in Colombo. The hospital, initially called the De Soysa Lying-In-Home, was founded in 1879 by a businessman named Sir Charles Henry de Soysa and is the second oldest maternal care centre in Asia. It was established with the purpose to provide maternal care for women with poor socioeconomic status, who by the time of foundation did not have access to proper maternal health care. Furthermore, the first Caesarean section in Sri Lanka was performed in the De Soysa Lying-in-Home in 1905. Since then, the hospital has played an important part in the development of improved maternal health care and in the education of obstetricians, gynaecologists, nurses, midwives and medical students (Seneviratne, 2004).
Colombo and its hospitals have been exposed to violence and disasters, as it suffered from the civil war that lasted between 1983 and 2009, as well as the tsunami in 2004 that destroyed parts of the city and killed thousands of people. When considering the preconditions and circumstances, it is impressive to notice that the quality of Sri Lanka’s healthcare still matches those of the wealthier countries (BBC, 2018).
B. Field Observations
Coming from a country where a delivery room holds one mother and her partner at a time, the number of patients held per square meter in the wards and in the labour rooms was sufficient to amaze us. For example, a ward held about 30 beds in the same room and there could be up to six women in the labour room simultaneously. Another surprise was delivered when we entered the outpatient clinics of De Soysa Hospital for Women. The doctors in those clinics could see 15 to 20 patients in two hours, which would roughly be equivalent to a day’s work in a Swedish outpatient clinic.
That there were several doctors working separately with different patients around the same table was also dissimilar to Swedish practice. In Sweden, integrity is highly valued and the strict confidentiality of each patient is legally established. Therefore, it was surprising to see how relaxed and natural the Sri Lankan women were among each other. The tranquil approach of the patients regarding gynaecological and obstetrical topics seemed to facilitate practice for the heavy burdened Sri Lankan doctors and was something that we were highly impressed by during our elective.
As proclaimed by our previous elective colleagues, the Sri Lankan doctors proved to have great depth of knowledge regarding physiology and clinical assessment. Luckily, throughout our stay at the De Soysa Hospital, doctors in general were very generous in sharing their knowledge with us, and teaching was regarded importantly by all staff members. The teaching approach in Sri Lanka is different from the one that is practiced in our country of residence. In Sweden students are encouraged to discuss, theorise and not to act too confident, whereas in Sri Lanka we were rebuked for using the word “maybe” when answering a question.
C. Learning Environment in the De Soysa Women’s Hospital
The learning environment in the outpatient clinic was quite different compared to what we are used to in Sweden. In Sri Lanka, the number of patients seen per doctor was substantially higher than in Sweden. This created a somewhat hectic learning environment but also provided an opportunity to discuss a large number of interesting cases in an efficient manner. We strongly feel that it was advantageous for us to partake in the outpatient clinics and it has been shown to be beneficial for students as it provides insight in various clinical topics and increased case exposure (Almoallim et al., 2015).
A common teaching method in Sweden is the discussion of prewritten patient cases in a classroom setting, whereas in Sri Lanka every patient is available for bedside case discussion. Applying theoretical knowledge on real patient cases seems to facilitate and rationalise learning as this allows for a holistic approach to learning (Salam, Siraj, Mohamad, Das & Rabeya, 2011). Unfortunately, because of a different perspective on patient integrity and high demands on patient-doctor communication, this kind of teaching is not applicable in Sweden.
We experienced a more pronounced hierarchy in Sri Lanka than in Sweden. This also affected the method of teaching, resulting in a more authoritarian approach. Not only were we unused to calling elder colleagues Sir and Madam, but also to the way hierarchy allowed for more experienced doctors to dictate the terms of the department. Questions were posed in a manner expecting straight and correct answers, not leaving any room for hesitation or speculation. Even though we were unfamiliar with this authoritarian climate, we still felt included and expected to partake in everyday work in a more natural manner than in Sweden.
D. Ethical Dilemmas Encountered as an Elective
Despite providing valuable experiences and practical training for students, it has been questioned whether the tradition of international electives is ethically justifiable (Gilbert, Miller, Corrick & Watson, 2013). Prior to departure, the importance of maintaining ethical standards during the elective was emphasised by our university. Hearing from students having gone to developing countries, this is not always an easy task, them being required to take responsibility beyond their level of training from the receiving institution. Luckily, we never faced such dilemmas in Sri Lanka. Throughout our stay, it was evident that we were participating as foreign students, not practicing doctors.
Something that did bother us throughout our elective was the fact that we could not properly communicate with the patients. The women were all very generous in letting us examine them, reading their medical charts, and observing them during a wide range of interventions and assessments. However, not being able to introduce ourselves and explain the purpose of our presence did feel wrong. The fact that Sri Lankan doctors often spoke English with us and when discussing patients amongst themselves facilitated our stay, but at the same time it disabled the patients to partake in discussions regarding their own health. While the Sri Lankan women might find this plausible, it could also be intimidating for patients to know they are the topic of discussion while being unable to comprehend what is being said.
Participating in an elective program in the Obstetrical and Gynaecological departments of Colombo was a rewarding experience for us. We were however curious how the hospital staff viewed such endeavours from foreign universities. Both doctors and nurses seemed to operate under a lot of pressure and our presence might have disturbed the hospital staff when performing their tasks. As elective students, we might unintentionally have gotten in the way, or delayed a nurse in performing her tasks. A doctor working fast to cope with workload might also have wasted precious time explaining a patient case to us. Regardless, it is important to note that we were very well received by everyone during our elective in Sri Lanka.
E. Potential Improvements
In the running of international electives, it is clear that the teaching habits, as well as the learning environment of sending and receiving institutes differ from one another. An exchange is beneficial not only for the foreign student, but also for the receiving institution, as it provides an opportunity to gain novel insights.
Coming from a culture where adhering to appointed times and locations is expected, we believe that an appointed supervisor and a more structured approach overall would be favourable. Also, giving students assignments such as case presentations during the course could support learning and improve contact with local doctors. As stated by Onishi in the Kaohsiung Journal of Medical Sciences, case presentation is an acknowledged learning method and can facilitate students’ clinical development (Onishi, 2008). Not surprisingly, it was in fact an integrated part of the training of junior doctors at the hospital.
Lastly, it would have been interesting to talk to Sri Lankan medical students to learn how their education is structured and what is expected of them. Unfortunately, this was not possible as they were on strike during our stay.
III. CONCLUSIONS
We regard our elective a valuable experience, providing us with important insights. Time spent observing Sri Lankan healthcare will in the future serve as a reminder to remain humble towards different cultures. Sweden being a country that has not waged war for centuries is at a financially advantageous point relative to Sri Lanka. We should remain mindful of how privileged we are, working as doctors in a socioeconomically strong country. Nevertheless, it is clear that there is much for us to learn and be inspired by from our colleagues in Sri Lanka.
Note on Contributors
K. E. Fransson, I. E. J. Lundahl and H. K. Pasma are all final year medical students at Lund University in Sweden.
Dr. M. R. M. Rishard is a practicing consultant in Obstetrics and Gynaecology at De Soysa’s Womens Hospital and National Hospital in Colombo, Sri Lanka.
Dr. M. de Lanerolle-Dias is a senior lecturer at the department of Biochemistry and Molecular Biology at the Faculty of Medicine, Sri Lanka, and is the chairperson of the International Unit, which coordinates electives for overseas students.
Acknowledgements
We would like to thank Dr Mohamed Rishard (University of Colombo) for encouragement and support while writing this paper as well as the de Soysa Women’s Hospital staff for contributing to our positive elective experience.
Also, we would like to thank Dr Lars Hagander (Lund University, Sweden), Dr Maduka de Lanerolle-Dias (University of Colombo, Sri Lanka) and Professor Athula Kaluarachchi for supervising our elective.
Funding
The authors received no specific funding for this work.
Declaration of Interest
The authors declare no conflicts of interest.
References
Almoallim, H., Minguet, J., Albazli, K., Alotaibi, M., Alwafi, S. & Feteih, M. (2015). Advantages and perspectives of teaching in outpatient clinics: A systematic review. Creative Education, 6, 1782-1789. http://dx.doi.org/10.4236/ce.2015.616181.
BBC News. (2018, February 26). Sri Lanka country profile. Retrieved from https://www.bbc.com/news/world-south-asia-11999611.
Gilbert, B. J., Miller, C., Corrick, F. & Watson, R. A. (2013). Should trainee doctors use the developing world to gain clinical experience? The annual Varsity Medical Debate – London, Friday 20th January, 2012. Philosophy, Ethics, and Humanities in Medicine, 8, 1. http://doi.org/10.1186/1747-5341-8-1.
Onishi, H. (2008). The Role of Case Presentation for Teaching and Learning Activities. The Kaohsiung Journal of Medical Sciences, 24(7), 356-360. https://doi.org/10.1016/S1607-551X(08)70132-3.
Salam, A., Siraj, H. H., Mohamad, N., Das, S., & Rabeya, Y. (2011). Bedside teaching in undergraduate medical education: Issues, strategies, and new models for better preparation of new generation doctors. Iranian Journal of Medical Sciences, 36(1), 1–6.
Seneviratne, H. R. (2004). De soysa hospital for women: 125 years service to the nation. Daily News. Retrieved from http://archives.dailynews.lk/2004/12/13/fea02.html.
The World Bank. (2010). Physicians (per 1000 people) [Data file]. Retrieved from https://data.worldbank.org/indicator/SH.MED.PHYS.ZS?locations=LK-SE.
The World Bank. (2015a). Current health expenditure (% of GDP) [Data file]. Retrieved from https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS?locations=LK-SE.
The World Bank. (2015b). Data for Sri Lanka, Sweden [Data file]. Retrieved from https://data.worldbank.org/?locations=LK-SE.
The World Bank. (2015c). Health [Data file]. Retrieved from https://data.worldbank.org/topic/health?locations=LK-SE.
World Health Organization (WHO). (2015). Health situation and trend assessment: Maternal mortality. Retrieved from
http://www.searo.who.int/entity/health_situation_trends/data/mnch_maternal-mortality-ratio/en/.
*Ingrid E. J. Lundahl
Email: lak12ilu@student.lu.se
Faculty of Medicine, Lund University
Box 117
SE-221 00 Lund
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
