
Resilience workshop: Building resilience for academic success – From stumble to soar
Submitted: 18 May 2024
Accepted: 25 November 2024
Published online: 1 April, TAPS 2025, 10(2), 4-7
https://doi.org/10.29060/TAPS.2025-10-2/GP3347
Juliet Mathew1, Hazlina Binti Abu Bakar2 & Shilpa Murthy2
1Clinical Skills & Simulation Centre and School of Medicine, IMU University, Malaysia; 2Department of Clinical Skills and School of Medicine, IMU University, Malaysia
Abstract
Introduction: Medical students are known to have a higher prevalence of psychological distress although they begin medical school with better mental health than their peers. Depression and burnout rates are high among them and many of these students do not seek help due to the associated stigma linked with mental health concerns. At present, there are several known resilience-enhancing modules incorporated within the curriculum to improve students coping skills, however, there are no known modules yet that introduce this concept within the early medical curriculum, especially within the pre-clinical years.
Methods: IMU University introduces a Resilience Workshop within early pre-clinical years to appropriately engage students to recognise and address common challenges. This can be tackled by understanding the various coping mechanisms that can be adopted. This workshop describes four main areas: introduction to resilience, interactive activities, discussions, and reflection platforms. This initiative aligns with the university’s curriculum focus on person-centred care, emphasising personalised care as a priority.
Results: Preliminary results suggest that the Resilience Workshop can aid in developing suggested and self-regulated interventions to manage adversities faced by medical students. Attention to individual students’ coping reservoirs can help promote well-being and minimise burnout. Formal and informal offerings within medical schools can help fill the reservoir.
Conclusion: This article provides a perspective on fostering resilience building within the early medical curriculum to cultivate core strengths among medical students for managing adversities.
Practice Highlights
- Psychological distress is prevalent among medical students.
- Challenges occur in medical students seeking help.
- Resilience strength is vital to medical students to recognise and address common challenges.
- A gap exists in the curriculum to improve medical students’ coping skills in the early years.
- Fostering resilience in early medical curricula can cultivate core strengths among medical students for managing adversities.
I. INTRODUCTION
IMU University’s Resilience Workshop was designed and implemented within the medical curriculum in pre-clinical years to develop students’ core inner strengths to their possible highest growth. This is so that they are fully equipped and ready to meet the challenges of competent care delivery to patients. In line with IMU University’s revised medical curriculum’s direction which focuses on the philosophy of person-centred care with humanistic values, this workshop emphasises self-care as a priority before embarking on to selfless care of patients.
In this revised curriculum, much emphasis is placed on the development of skills, behaviours, and attitudes within the delivery of care to patients, encompassing the basic concepts of human interaction, patient safety, quality improvement, and systems thinking; while enhancing the skills of teamwork, effective communication, leadership, negotiation, and cooperation.
The aim has been to best prepare our graduates to practice within the needs of the health profession in the 21st century. This includes equipping them in communication, clinical, cultural, interpersonal, research, and system thinking competencies. These prepare our students to be ready for any advanced clinical training within local or international institutions.
The curriculum’s goal is also to produce graduates who are person-centred and with humanistic values, with professional attributes of being empathetic, compassionate, responsive, and adaptive besides being a transformative leader, lifelong learner, and professionally competent.
Thus, the new curriculum emphasises graduates’ wellness, person-focus services, effective communication, personalised care, multi-disciplinary collaboration & approach, coordinated, continuous & seamless care delivery manner; & application of system thinking and value-based care.
In aligning with this direction and ensuring that our graduates are fit to practice as global doctors with opportunities to practice internationally, the Resilience Workshop engages and guides students in building their own core coping mechanisms while reviewing the principles of determinants of resilience. It is designed to inspire and empower students to be resilient. The postulation is that the students would have retained a substantial knowledge base which constitutes an increasing resource for coping with the diverse challenges they will be exposed to in their medical journey, and for building core resilience strength.
II. METHODS
A. Structured Workshop Flow
The lesson outcomes from this workshop aim at achieving student’s understanding of the importance of adapting well in the face of adversity, threats, or even significant sources of stress, as well as engaging in resilience throughout medical school. With inspiring themes such as “Bend, But Do Not Break” in semester two and “Be Managing Adversities Delightfully (Be MAD)” in semester four, pre-clinical medical students are exposed to challenging scenarios that they may encounter. These scenarios extend beyond their roles as students, to include their relationships with friends, roommates, peers, and more.
The workshop is designed to engage students in four main areas:
Session 1: Introduction to Resilience
Session 2: Activity on Resilience
Session 3: Discussions on Resilience
Session 4: Reflection on Resilience
At the beginning of the workshop, students are provided with The Brief Resilience Scale adapted from Ohio University. It consists of simple and focused scoring scales. It is concise and has good psychometric properties including strong validity and reliability, capturing resilience effectively. Students can score and gauge their resilience levels with easy-to-follow instructions. This allows them to understand their coping strengths, identify their ability to recover from adversities, focus on areas for improvement, and guide them toward improved performances within medical training.
Subsequently, students are introduced to the concept of resilience. They are then led into small group discussions to engage, brainstorm scenarios presented, and grasp levels of coping and managing difficult scenarios that are commonly encountered. They are also given opportunities to share their experiences and discuss possible solutions to the scenarios and their insights. Debriefing includes discussions based on structured questions that could engage students in their thought processes and emotional experiences. It also focuses on their possible courses of action, ideas, or solutions in managing difficult situations within the scenario presented.
B. Reflection Analysis
Students are encouraged to reflect on their experiences and take-home messages from the workshop. They are required to submit a 500-word essay via e-mail, documenting the challenges and strengths that surfaced for them during the session. This must be submitted within a stipulated time frame after the workshop, via e-mail to facilitators for assessment. These reflection essays are reviewed and students with potential mental health concerns are identified. They are then followed personally or referred to their mentors for appropriate support.
III. RESULTS
The scenarios used exposed students to common issues encountered during their early medical training. It encompassed adjustments to the new environment on campus and hostels, adjustments to a new culture of peers, understanding new subjects, meeting professionalism requirements, and addressing unique and individualised adversities.
These scenarios stimulated discussions in the breakout sessions, where standard questions were posed to ignite the development of possible solutions to the simulated adversities faced: (A) How would you handle this situation? (B) What would you do? (C) How would you feel? (D) Explain.
Students were encouraged to narrate their experiences and explore their thoughts and emotions. This helped students realise that there are common issues that are endured by many. Most students reported that the workshop helped them to understand the various coping mechanisms that can be adopted to solve issues that may arise within their journey and progress in medical school. Verbal responses received include:
“I didn’t realise how important managing stress was until I was hit by a personal issue. It affected my studies. This workshop showed me how I can handle stress better…”
“I didn’t want to attend this workshop at first. But the scenarios discussed were mostly what I had endured. I wish I knew these coping strategies earlier…”
IV. DISCUSSION
Students can establish strong foundations in coping strategies, emotional intelligence, and stress management by introducing resilience throughout the preclinical years. The hurdles are mostly theoretical and academic, making it a less demanding environment to begin honing these talents. Students can study the fundamentals of resilience, through such workshops. The basic ideas from the preclinical years could be modified and built upon to deal with the interpersonal, ethical, and emotional difficulties that may arise in their academic obligations and their clinical practice.
The challenges encountered can be described within the following phases:
A. Pre-workshop Challenges
The lack of facilitators with adequate skills in resilience science and mental health advocacy was the main challenge. As mental health issues require more in-depth management, the deliverance of such workshops had to be done by facilitators who are skilled in strong communication skills, empathy, patience, and compassion. The initial perspective was that all faculty would be well-equipped with these skills, however, it became clear post-workshop, that this was not the case. The selection of such facilitators to deliver the context of this workshop in a non-lecturing but inspiring way posed a challenge. The solution is to include training for faculty before the workshop.
B. Workshop Challenges
During the Malaysian Movement Control Order (M.C.O.) when this workshop was first introduced to help students cope, it was delivered online. Hence, the active involvement of students was limited as being on camera had its challenges. Further, many students considered such a workshop to be non-mainstream and non-exam oriented, thus, needing much encouragement to participate fully. The solution is to introduce face-to-face workshops to better engage students.
C. Post-workshop Challenges
Most students who attended the workshop completed and e-mailed the reflection exercises. However, a certain percentage of them failed to do so. This presents a challenge in identifying any student who may have a serious underlying issue with managing adversities resiliently. The solution is to track attendance when delivering assignments.
A possible way to capture all reflections would be to make attendance marked only upon receiving the assignment. As these are medical students in their early years, this approach may not be effective and can lead to non-genuine or robotic responses. While addressing and reinforcing professionalism may be another goal for obtaining reflective essays, it may seem forced. More self-regulating and motivating strategies should hence be developed and applied.
This two-hour workshop is a brief intervention within the time-limited curriculum within semesters two and four. Moving forward, a half-day workshop with more time for interaction with peers and educators could better engage students. A survey could be conducted post-workshop to assess students’ feedback. Providing progression reports of students’ resilience levels could be a more accurate measure of the workshop’s impact. Also, the BRS could be re-used in semester four, to review recovery or the ability to regain equilibrium after adversity.
The students’ submissions of their reflective essays constitute a dataset that can be analysed for further studies in this field, to address and create various aspects of positive interventions within mental health access and stress-relief resources. The aim is, to create better impacts on students’ learning and experience in medical school.
V. CONCLUSION
Above all, we need to understand that resilience is a lifelong ability that cannot be acquired in a single workshop. It needs to be constantly supported through different educational stages, within challenging and stressful circumstances.
Attention to individual students’ coping reservoirs can help promote well-being and minimise burnout. Formal and informal offerings within medical schools can contribute to this effort. Helping students cultivate the skills to sustain their well-being throughout their careers has important payoffs for the overall medical education enterprise.
IMU University’s Resilience Workshop can aid in the development of suggested as well as self-regulated interventions to manage adversities faced by medical students. A formal study is ongoing to substantiate this. Further to this, the development of a student-led multifaceted approach that promotes not only care-taking behaviours but also focuses on institutional and cultural change to empower students to participate in these resiliency strategies can be considered.
This and other models of coping should be empirically validated, for students to not stumble through medical school, but soar.
Notes on Contributors
Dr Juliet Mathew is the first author who designed and wrote this article. Director of the Clinical Skills & Simulation Centre at IMU University, she teaches simulation concepts to pre-clinical students. She confirms sole responsibility for this article’s conception, design, analysis, interpretation of results of context, and manuscript preparation.
Dr Hazlina Binti Abu Bakar supervised the conception of this project and contributed to the critical review of the manuscript. She is a lecturer teaching clinical skills and simulation concepts at the School of Medicine University, IMU University. She also holds a master’s degree in healthcare and medical simulation.
Dr Shilpa Murthy contributed to the continuous review of the important intellectual content and final version of the manuscript. She also contributed to the conception of this project. She is a senior lecturer teaching clinical skills and simulation concepts to pre-clinical medical students at the School of Medicine, IMU University.
Acknowledgements
The authors would like to express our sincere appreciation to Dr Cheah Xian-Yang for his invaluable assistance in proofreading this article. We also extend our gratitude to Associate Professor Dr Sow Chew Fei for her guidance.
Funding
There is no funding for this paper.
Declaration of Interest
The authors of this paper have no conflicts of interest to declare.
References
Bird, A., Tomescu, O., Oyola, S., Houpy, J., Anderson, I., & Pincavage, A. (2020). A curriculum to teach resilience skills to medical students during clinical training. MedEdPORTAL, 16, Article 10975. https://doi.org/10.15766/mep_2374-8265.10975
Cook, M. C., & Stewart, R. (2023). Resilience and sub-optimal social determinants of health: Fostering organizational resilience in the medical profession. Primary Care: Clinics in Office Practice, 50(4), 689-698. https://doi.org/10.1016/j.pop.2023.04.013
Omari, O. A., Yahyaei, A. A., Wynaden, D., Damra, J., Aljezawi, M., Qaderi, M. A., Ruqaishi, H. A., Shahrour, L. A., & AlBashtawy, M. (2023). Correlates of resilience among university students in Oman: A cross-sectional study. BMC Psychology, 11, Article 2. https://doi.org/10.1186/s40359-022-01035-9
Rotenstein, L. S., Ramos, M. A., Hom, J., & Gardner, A. (2016). Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: A systematic review and meta-analysis. JAMA, 316(21), 2214-2236.https://doi.org/10.1001/jama.2016.17324
Thompson, G., McBride, R. B., Hosford, C. C., & Halaas, G. (2016). Resilience among medical students: The role of coping style and social support. Teaching and Learning in Medicine, 28(2), 174-182. https://doi.org/10.1080/10401334.2016.1146611
*Dr Juliet Mathew
IMU University, 126, Jalan Jalil Perkasa 19,
Bukit Jalil, 57000 Kuala Lumpur
Federal Territory of Kuala Lumpur
+6012 – 574 1723
Email: julietmathew@imu.edu.my
Submitted: 15 June 2024
Accepted: 12 September 2024
Published online: 1 April, TAPS 2025, 10(2), 8-12
https://doi.org/10.29060/TAPS.2025-10-2/GP3440
Galvin Sim Siang Lin1, Tong Wah Lim2 & Mariana Minatel Braga3
1Department of Restorative Dentistry, Kulliyyah of Dentistry, International Islamic University Malaysia, Malaysia; 2Division of Restorative Dental Sciences, Faculty of Dentistry, The University of Hong Kong, Hong Kong S.A.R.; 3Department of Orthodontics and Pediatric Dentistry, School of Dentistry, University of São Paulo, Brazil
Abstract
Introduction: Dental education is undergoing a major transformation due to evolving healthcare needs, technological advancements, and the demand for dental practitioners to meet the diverse needs of a global patient community. Competency-based education (CBE) is at the forefront of this change, focusing on what students are competent in upon graduation. Unlike traditional models, CBE emphasises practical skills, critical thinking, and problem-solving.
Methods: This article explo res the shift towards CBE in dental education, examining frameworks that support CBE like Miller’s Pyramid and guidelines from organisations such as the Accreditation Council for Graduate Medical Education (ACGME) and the American Dental Education Association (ADEA). It also involves a detailed analysis of these frameworks and their application in designing competency-based curricula.
Results: The findings reveal that CBE facilitates a student-centric approach, enhancing critical thinking, problem-solving, and autonomous self-assessment. These frameworks guide the design of curricula including identifying core competencies, defining competency levels, mapping competencies to learning outcomes, selecting effective teaching methods and utilising various assessment strategies. However, implementing CBE faces challenges, including measuring soft skills and resistance from educators and students.
Conclusion: CBE represents a paradigm shift in dental education, ensuring graduates are not only knowledgeable but proficient in practical skills. Future recommendations include incorporating technology-enhanced learning, global health competencies, and sustainability practices into the curriculum. Continuous professional development for educators and robust feedback mechanisms are needed to maintain the curriculum’s relevance and effectiveness, ensuring dental graduates are well-equipped to meet the demands of modern dental practice.
Practice Highlights
- Dental education is evolving to meet global healthcare needs and technological advancements.
- CBE focuses on practical skills, critical thinking, and problem-solving
- CBE ensures dental graduates are competent and ready for modern practice challenges.
- Several frameworks can be used to guide CBE in developing clinical
- Designing CBE curricula involves defining core competencies and using diverse assessment methods.
I. INTRODUCTION
Dental education is at a pivotal moment, facing a profound transformation influenced by the dynamic intersection of changing healthcare needs, technological advancements, and the urgent call for dental practitioners to cater to the diverse requirements of a globalised patient community. Amid this swiftly evolving landscape, traditional approaches to dental education are undergoing a fundamental reimagination. The aim is to nurture a generation of dental professionals not only well-versed in theoretical knowledge but, crucially, equipped with the competencies vital for thriving in modern dental practice. Competency-based education (CBE) emerges as a key player in this educational revolution. This approach to curriculum design and teaching revolves around a central question: What should students be able to do or achieve at the culmination of their course or program? In the realm of dental education, CBE moves beyond the traditional focus on accumulating knowledge and places a spotlight on the practical skills students need to excel in their future roles. It is not just about what students know; it is about what they can proficiently do. Why adopt competency-based education in dentistry? The answer lies in its power to enhance student learning by emphasising hands-on skills, critical thinking, and problem-solving abilities. CBE ensures that graduates are not merely well-informed in dental theory but are also competent practitioners capable of meeting the ever-changing demands of contemporary dental care.
II. THE SHIFT TOWARDS COMPETENCY-BASED DENTAL EDUCATION
In recent years, the field of dental education has undergone a transformative shift, pivoting away from the traditional education models to embrace the principles of competency-based dental education. This evolution is rooted in a fundamental recognition that the mastery of dental skills and knowledge is a dynamic process, necessitating an educational paradigm that transcends mere adherence to a predetermined timeframe (Chuenjitwongsa et al., 2018). While various definitions of competency-based education exist, there is a consensus that it revolves around outcome-based learning, ensuring the production of graduates with the requisite knowledge, skills, and attitudes to serve society effectively, meeting the standards of national qualifications frameworks, stakeholders, and the labour market.
Traditional-based dental education has faced criticisms for its potential to produce graduates who may lack practical proficiency or struggle to adapt to emerging trends in dentistry. It emphasises time spent in the classroom, irrespective of individual mastery. Furthermore, traditional models may sometimes struggle to keep pace with the rapid advancements in dental technology and shifting paradigms in patient care, underscoring the need for a more adaptive and outcomes-focused approach. On the other hand, CBE signifies a departure from traditional education, characterised by its teacher-centred, examination-focused, time-constrained, and discipline-oriented approach. It transitions towards a student-centric educational model using an outcome-based approach that enhances students’ capabilities in critical thinking, problem-solving, and autonomous self-assessment.
Moreover, in CBE, the focus shifts from completing a predefined course of study to ensuring that learners attain proficiency in specific competencies, enabling them to navigate the complexities of dental practice effectively. In a competency-based framework, success is measured by demonstrating specific skills, ensuring that graduates are not merely knowledgeable but possess the practical expertise required for clinical practice. Besides, future professionals tend to be able to make decisions even when ideal/learned circumstances are changed. This paradigm shift promotes a deeper understanding of concepts and fosters a culture of continuous improvement. In CBE, novice dental students commence their training in simulation laboratories, preparing them to progressively attain beginner and competent levels in clinical settings.
III. FRAMEWORK FOR COMPETENCY-BASED DENTAL EDUCATION
A. Miller’s Pyramid
The Miller Pyramid of Competence, introduced by psychologist George Miller in 1990 (Miller, 1990), stands as a foundational framework for evaluating clinical proficiency in healthcare education. This pyramid encapsulates a four-tiered hierarchy, delineating the progressive stages of competence acquisition. At its base, the pyramid begins with “knowledge”, representing the foundational cognitive understanding of concepts typically assessed in classroom-based environments. Moving upwards, the tiers evolve into “competence” and subsequently “performance”, encompassing knowledge translation into practical skills through simulated clinical settings. The higher echelons of the pyramid, namely “action”, signify the culmination of clinical competence in real-world scenarios. Here, learners demonstrate their ability to apply theoretical knowledge and practical skills in authentic clinical environments. The Miller Pyramid’s distinction between cognitive and behavioural components is particularly noteworthy. The lower tiers, focusing on knowledge and competence, mention the importance of classroom-based assessments in gauging cognitive understanding. In contrast, the apex tiers of performance and action underline the significance of evaluating behavioural aspects within simulated and real clinical settings. This hierarchical structure provides a great understanding of competency development, guiding educators in designing competency-based curricula.
B. Accreditation Council for Graduate Medical Education (ACGME)
The ACGME plays a role in shaping the educational standards for healthcare professionals. ACGME has delineated six core competencies, transcending traditional disciplinary boundaries and applicable to various healthcare practitioners (Batalden et al., 2002). These competencies form a holistic approach to evaluating the proficiency of healthcare professionals and are integral to fostering well-rounded practitioners capable of meeting the complex demands of modern healthcare. The six core competencies identified by ACGME are Patient Care, Medical Knowledge, Professionalism, Interpersonal and Communication Skills, Practice-Based Learning and Improvement, and Systems-Based Practice. Patient Care centres on delivering compassionate, effective, evidence-based care to individuals and populations, while medical knowledge encompasses the understanding needed for sound clinical decision-making. Professionalism emphasises ethical behaviour, accountability, and a commitment to the well-being of patients. Interpersonal and Communication Skills are crucial for effective collaboration and patient interaction, whereas practice-Based Learning and Improvement involves the ability to critically assess and improve one’s own clinical practice continuously. Systems-Based Practice involves comprehending healthcare delivery systems and endorsing high-quality and cost-effective patient care within the broader healthcare system context. Customising these competencies for the dental context allows dental educators to align educational objectives, ensuring their curriculum imparts technical skills while cultivating the ethical, communication, and systemic perspectives essential for a well-rounded dental practitioner.
C. American Dental Education Association (ADEA) Competencies for the New General Dentist
The ADEA has crafted the Competencies for the New General Dentist, a set of guidelines tailored specifically for dental education (American Dental Education Association, 2017). Ratified by the ADEA House of Delegates on 2nd April 2008, this framework is a decisive step in defining the essential competencies for individuals entering the dental profession as general dentists., This document reflects a departure from the 1997 competencies, aligned with patient care responsibilities, public oral health needs, and contemporary trends in dental practice and draws inspiration from the 2002 Institute of Medicine’s core competencies with a heightened emphasis on quality patient care and safety. Structured into six domains—Critical Thinking, Professionalism, Communication and Interpersonal Skills, Health Promotion, Practice Management and Informatics, and Patient Care—the competencies are thoughtfully organised, allowing for more flexible and adaptable integration into dental education curricula. This framework serves as a central resource for the ADEA at the national level and individual dental schools at the local level, fostering an environment conducive to innovation in predoctoral dental school curricula. Overall, the ADEA competencies serve as a benchmark, enabling dental educators to design curricula that not only meet but exceed the contemporary expectations and requirements of the dental profession.
D. The Graduating European Dentist Curriculum
The Graduating European Dentist Curriculum, under the auspices of the Association for Dental Education in Europe (ADEE), presents a contemporary framework embodying the optimal academic practices for undergraduate dental education in Europe (Field et al., 2017). This curriculum is structured across five integral domains, each contributing to a comprehensive educational experience: (1) Professionalism, (2) Safe and Effective Clinical Practice, (3) Patient-Centred Care, (4) Dentistry and Society, and (5) Research. Crafted through a collaborative process involving consultation, consensus-building, and collegial learning, this curriculum highlights the importance of patient safety, teamwork, and teaching excellence. Aligned with European Quality in Higher Education benchmarks, “The Graduating European Dentist” introduces an innovative approach reflecting the pinnacle of academic standards in European dental education. The revised framework features a more explicit linkage between “Learning Outcomes” and the defined curriculum, accompanied by detailed guidance specific to each competence domain, encompassing “Methods of Teaching and Learning” and “Methods of Assessment”. It is anticipated that this framework would facilitate an enriched educational experience for dental students across Europe.
IV. DESIGNING A COMPETENCY-BASED DENTAL CURRICULUM
To effectively design and develop a competency-based dental curriculum, educators need a comprehensive framework that aligns with the unique challenges and requirements of dental practice. The following components are some of the basic summarised steps that serve as foundational guides for the implementation of a competency-based curriculum:
A. Identifying Core Competencies
Begin by identifying the core competencies that future dental practitioners must possess. This involves collaboration with practitioners, educators, and stakeholders to ensure that the curriculum reflects the evolving needs of the dental profession. Core competencies might encompass knowledge acquisition, clinical skills, patient communication, ethical practice, and the ability to integrate new research findings into practice.
B. Defining Competency Levels
Once core competencies have been identified, it is crucial to define distinct competency levels for each skill or knowledge area. These levels serve as benchmarks for assessing student progress and proficiency. They facilitate a granular approach to education, where learning and assessment can be tailored to students’ individual needs, recognising that learners progress at different rates and may require differentiated levels of support to achieve competency.
C. Mapping Competencies to Learning Outcomes
Each identified competency should be mapped to specific learning outcomes within the curriculum. This mapping process ensures that the curriculum is logically structured, with a clear progression from foundational knowledge to applying skills in complex clinical scenarios. It allows educators to design courses and modules that systematically build upon each other, guiding students on a clear path towards achieving the essential competencies required for successful dental practice.
D. Selecting Effective Teaching Methods
Adopt diverse and innovative teaching methods that cater to different learning styles and encourage active engagement. Techniques such as problem-based learning (PBL), case-based learning (CBL), team-based learning (TBL), simulation exercises, and hands-on clinical practice are effective in helping students develop critical thinking and practical skills. Incorporating technology, such as virtual reality (VR) and digital simulations, can also enhance learning experiences and prepare students for real-world challenges.
E. Utilising Assessment Strategies
Implement a variety of assessment methods to evaluate students’ competency levels. This may include practical exams, case-based assessments, and objective structured clinical examinations (OSCEs). These should be complemented by regular, formative assessments and feedback, which are instrumental in identifying areas where students may struggle and providing them with the support needed to overcome these challenges. The ultimate goal of assessment within a competency-based curriculum is not merely to test knowledge but to facilitate the development of skilled, reflective, and adaptable dental practitioners.
V. LIMITATIONS AND CHALLENGES IN IMPLEMENTING A COMPETENCY-BASED CURRICULUM
Authenticity and the ability to accurately measure skills have been identified as the primary challenges in CBE for dentistry. In this field, knowledge and skills are often assessed as separate entities, leading to a potential loss of authenticity throughout the learning process. While CBE incorporates a variety of subjective and objective evaluations, measuring certain soft skills, such as clinician-patient communication, ethics, and values, remains a challenge due to their complex and intangible nature. Moreover, implementing CBE in dental education may face additional obstacles, including the limited availability of established theoretical frameworks to guide the teaching-learning process, insufficient training for educators in adapting to this curriculum style, and resistance from both teaching staff and students. Addressing these challenges is essential for ensuring the successful adoption and integration of competency-based education within dental programs.
VI. CONCLUSION
The transition towards competency-based dental education marks a significant paradigm shift aimed at equipping future dental professionals with the practical skills, ethical understanding, and critical thinking abilities necessary for success in the contemporary dental landscape. Future recommendations include the further integration of technology-enhanced learning tools, the development of global health competencies, and the emphasis on sustainability and ethical practices within the curriculum. Additionally, establishing robust feedback mechanisms and promoting continuous professional development among educators will be crucial in maintaining the curriculum’s relevance and effectiveness.
Notes on Contributors
GSSL and TWL were involved in the conception and design of the study. GSSL, TWL and MMB reviewed the literature, collected the data, and wrote the original draft. TWL edited the original draft. All authors have read and approved the final manuscript.
Funding
No funding is required for this paper.
Declaration of Interest
All authors have no conflicts of interest.
References
American Dental Education Association. (2017). ADEA competencies for the new general dentist. Journal of Dental Education, 81(7), 844-847. https://doi.org/10.1002/j.0022-0337.2017.81.7.tb06299.x
Batalden, P., Leach, D., Swing, S., Dreyfus, H., & Dreyfus, S. (2002). General competencies and accreditation in graduate medical education. Health Affairs (Millwood), 21(5), 103-111. https://doi.org/10.1377/hlthaff.21.5.103
Chuenjitwongsa, S., Oliver, R., & Bullock, A. D. (2018). Competence, competency‐based education, and undergraduate dental education: A discussion paper. European Journal of Dental Education, 22(1), 1-8. https://doi.org/10.1111/eje.12213
Field, J. C., Cowpe, J. G., & Walmsley, A. D. (2017). The graduating European dentist: A new undergraduate curriculum framework. European Journal of Dental Education, 21 Suppl 1, 2-10. https://doi.org/10.1111/eje.12307
Miller, G. E. (1990). The assessment of clinical skills /competence/performance. Academic Medicine, 65(9), S63-67. https://doi.org/10.1097/00001888-199009000-00045
*Galvin Sim Siang Lin
Department of Restorative Dentistry,
Kulliyyah of Dentistry,
International Islamic University Malaysia,
Kuantan Campus, Pahang, Malaysia
Email: galvin@iium.edu.my
Submitted: 5 July 2024
Accepted: 25 November 2024
Published online: 1 April, TAPS 2025, 10(2), 13-16
https://doi.org/10.29060/TAPS.2025-10-2/GP3456
Eng Koon Ong1-4,7 & Wen Shan Sim4-6
1Division of Supportive and Palliative Care, National Cancer Centre Singapore, Singapore; 2Office of Medical Humanities, SingHealth Medicine Academic Clinical Programme, Singapore; 3Division of Cancer Education, National Cancer Centre Singapore, Singapore; 4Duke-NUS Graduate Medical School, Singapore; 5Maternal Fetal Medicine, KK Women’s and Children’s Hospital, Singapore; 6PGY1 Programme, SingHealth, Singapore; 7Assisi Hospice, Singapore
Abstract
Introduction: The medical humanities (MH) have the potential to support medical education (ME) by developing observational skills, promote reflective practice and transformative growth. However, contextual content and methods relevant to our local and regional learners and teachers are lacking.
Methods: We describe three MH-based ME programmes within SingHealth to illustrate our considerations in the choice of conceptual frameworks and content selection in programme development and evaluation.
Results: Highlighting pertinent challenges in developing the field due to poor awareness, lack of resources and research capability, we emphasise the importance of interdisciplinarity, engaging leadership, and generating research output. Broad strategies to achieve these goals are then presented.
Conclusion: Highlighting challenges due to the lack of awareness, administrative and funding support, and research capability, we propose strategies to overcome such barriers and hope that readers will be inspired to contribute to this developing landscape where science and art intersect.
Practice Highlights
- Established frameworks and methods should be employed in programme development and evaluation.
- Art, literature, and theatre may be employed in medical humanities-programmes.
- Interdisciplinarity, leadership engagement and development of research capability are essential.
- Alignment with organisational needs and vision will ensure relevance and sustained support.
- The impact of the humanities on fostering wellbeing should not be neglected.
I. INTRODUCTION
The medical humanities (MH) is an interdisciplinary field characterised by critical enquiry and engagement of humanities disciplines. In medical education (ME), content or pedagogy derived from the arts and humanities may be employed to develop observational skills, promote reflective practice and transformative growth, and support humanistic clinical practice and communications (Dennhardt et al., 2016). However, while the integration of the MH in ME in Western countries has been widely supported and reported, a similar movement within Asian countries appears to be lacking and challenging. Educators in Arab-Muslim environments have lamented the lack of culturally-relevant content and concepts that remain predominantly Western-centric (Daher-Nashif & Kane, 2022), while additional challenges cited in China, Hong Kong, and Taiwan include limited awareness exacerbated by conflicting priorities of academic institutions (Tan et al., 2021; Wu & Chen, 2018). These factors result in a lack of impetus for higher education reform and slow research advancement of the field. To address these gaps, we first describe three educational programmes to highlight how local content and methods of co-facilitation may be employed. Next, we list the respective conceptual frameworks, learning objectives and programme evaluation methods selected. Finally, we discuss strategies to increase awareness, maintain leadership and participant interest, secure sustained funding, and promote scholarly efforts. We hope that this article will support and inspire like-minded clinician educators with structurally relevant guidance that is currently lacking in the literature.
II. PROGRAMME DESCRIPTION
One of the first programmes we implemented was the HAPPE (Humanistic Aspirations as a Propellor for Palliative care Education) workshop, a 1.5-hour small group discussion session for junior doctors in a palliative care rotation at the Division of Supportive and Palliative Care, National Cancer Centre Singapore, facilitated by an accredited clinical psychologist and art therapist. Schon’s theory of Reflective Practice defined by reflection-in-action and reflection-on-action guided the discussions that focused on the participants’ experience with challenging clinical encounters that they expressed through readings of literary work and art-based craftwork. Parts of Gagne’s model of lesson planning such as the importance of gaining the learner’s attention, stimulating recall, presenting stimulus, and providing learning guidance were aptly supported by our choice of materials and facilitation. The themes of empathy and wellbeing were discussed and highlighted the importance of reflective practice on past challenging encounters. As a pilot educational intervention started since 2018, we chose to investigate the feasibility and acceptability of the MH-based workshop using self-reported quantitative scales such as the Consultation and Relational Empathy (CARE) Measure and Jefferson Physician Empathy Scale (JPES) pre- and post-workshop. Both scores improved after attendance of the workshop, supporting continual efforts for future runs of the workshop.
One year later, the half-day ADEPT (Arts and Drama to Enable Perspective Taking) workshop was implemented. In contrast to HAPPE, ADEPT was conducted for final year medical students from the Duke-NUS medical school within their core rotation to palliative care. Addressing the lack of adequate clinical exposure and role-modelling due to the brevity of the week-long rotation, a full recording of a local play A Good Death which portrayed theatrical presentations of severe pain, end-of-life conversations, and physician burnout was shown to the students. They then participated in small group discussions about perceptions of palliative care, professional identity formation, clinical communications, and physician wellbeing. These discussions were co-facilitated by a palliative care specialist, trained counsellor, and the director of the play and served to dispel myths about palliative care, promote self-awareness, and introduce coping strategies. The workshop was guided by Knowles’ theory of adult-learning and we ensured that a sense of agency and empowerment was promoted, with the students participating in self-directed reflection and learning. Building on the quantitative results of the HAPPE workshop, ADEPT was evaluated through a qualitative lens where students were invited to participate in individual semi-structured interviews by an independent interviewer to share their experiences of the workshop.
Finally, the full-day HEARTEN (Harnessing Educational approaches with the Arts to encourage End of life Conversations) workshop was started in 2022 and employed theatre-based techniques to address healthcare professionals’ discomfort in initiating advanced care planning (ACP) conversations with patients. The workshop marked our first formal collaboration with a local professional theatre group (ArtsWok) external to the SingHealth Duke-NUS Academic Medicine Centre and was attended by physicians, nurses, and various allied health professionals. This collaboration further cemented our approach of engaging local content and co-facilitators. Together, the team of physicians, social workers, art therapists, humanities researchers, and a theatre director employed Mezirow’s framework of transformational change to design experiential theatre- and acting-based exercises to trigger discussions about deep-seated perceptions and misgivings about initiating ACP discussions. We evaluated participants’ change in confidence levels in ACP discussions pre- and post-workshop through the Self-Competence in Death Work Scale (SC-DWS) survey quantitatively. An open-ended question was also embedded within the post-workshop survey to allow triangulation of the quantitative data collected. Preliminary data analysis showed an improvement in the SC-DWS surveys, with participants reflecting that their pre-existing concerns about triggering unhappiness and anxiety in patients might have been unfounded.
III. CHALLENGES
The HAPPE, ADEPT, and HEARTEN workshops illustrate a spectrum of MH-based ME programmes in terms of scale (5 to 20 participants per workshop; workshop durations of 1.5 to 8 hours), learning objectives, involvement of co-facilitators, choice of materials, and evaluation methods. In addition, all three workshops were supported by local institutional academic research funding, the amount of which increased over the years (SGD$5,000 – $42,000). By clearly enunciating our choice of educational conceptual frameworks and validated scales for programme evaluation, and consistently incorporating local content and engaging local stakeholders, we posit that some of the challenges such as the lack of contextually relevant content and frameworks and rigor in programme development and evaluation may be addressed.
However, several pertinent challenges exist. Firstly, awareness about the MH remains poor, with its integration into ME at a nascent stage compared to Western countries. Competing with other educational programmes that are better established, the small group size and similar pools of participants who enrolled in our programmes risk the case of “preaching to the choir.” This in turn may lead to challenges in garnering leadership support to encourage staff participation. In addition, securing sustained programme funding is challenging as education grants are limited to smaller, project-based programmes. Relative to clinical research, institutional management and administrative teams have less experience and expertise in supporting medical education research. Often, the project team members find themselves overwhelmed with administrative tasks including financial processes and manpower recruitment. These barriers towards research capacity building may deter interested but busy clinician educators from contributing to scholarly work that is crucial to support the growth of the field.
IV. PROPOSED STRATEGIES
We propose three areas of consideration that we have found helpful in navigating challenges in the landscape. While our experience stems from a single local healthcare centre, similar cultural, societal, and systemic factors in other parts of the Asia-Pacific region will allow applicability and relevance to other clinician educators.
A. Promoting Interdisciplinary Teaching and Learning
The MH is defined by an interdisciplinary approach and we adopt a collaborative approach in engaging various stakeholders such as local and regional humanities scholars, creative arts therapists, professional artistes, and community arts organisations. This allows us access to content from diverse subjects including anthropology, literature, history, philosophy, and other social sciences and to methods such as narrative inquiry, close reading, narrative therapy, and conversational analysis which were previously unfamiliar to us. Learners have described our programmes as refreshing and eye-opening. However, we are also mindful that some may not take to the arts and humanities naturally. Thus, co-facilitators take extra care to emphasise that learners need not be experts in the arts to engage in reflective practice, and co-facilitators from the humanities are always paired with a clinician educator to ensure the discussions are balanced and relevant.
B. Alignment with Individual Needs and Organisational Goals
An awareness about existing needs and organisational vision is crucial to ensure relevance of the MH programmes. In the SingHealth Duke-NUS Academic Medicine Centre (AMC), our programmes support pillars of the medical education (ME) masterplan such as interprofessional education, educational excellence, and fostering wellbeing. By including other health professions besides doctors, approaching programme development and evaluation through established educational frameworks and methods, and promoting wellbeing by engaging in the arts, the ADEPT workshops have now been adopted by the SingHealth College of Allied Health and Singapore Institute of Technology for allied health professionals and trainees respectively. Notably, the impact of the arts in fostering wellbeing by providing an avenue for expression of difficult emotions, building a sense of community, and processing grief for healthcare professionals provides further impetus for leadership support of our programmes. While MH programmes are not psychotherapy-based per se, participants have shared that the experience was therapeutic and with an increased awareness about struggles, some have been prompted to seek support from professional mental health professionals after programme attendance. Seeing the value of the MH, various offices of the medical humanities have been set up within the AMC since 2019. In 2023, the SingHealth Duke-NUS Medical Humanities Institute was established to further provide centre-wide administrative and funding support for MH programmes within ME. Supported by social media platforms, these offices have organised webinars, colloquiums, and Medical Humanities conferences that increase the visibility of our endeavours and continue to engage leadership, increase interest, and sustain awareness of MH-based programmes.
C. Developing Research Capability
Despite its rich history and diverse cultural perspectives, research in the medical humanities (MH) in medical education (ME) within Asian countries remains at a nascent stage compared to our Western counterparts. To develop research capability, we adopt a two-pronged approach. Firstly, all of our programmes follow a best practice approach towards development and evaluation guided by established educational theoretical frameworks and methods respectively. Secondly, all of our programmes include a scholarly component, as illustrated above. We are currently analysing qualitative data collected from the ADEPT and HEARTEN workshops and preliminary findings suggest that more data is needed to guide the choice of content, teaching methods, learning objectives, and matching of these aspects to different learner populations. Future funding from the MH offices coupled with national and regional funding on a larger scale made possible by our cross-institutional and interdisciplinary collaborations will allow us to embark on further research to address these gaps.
V. CONCLUSION
The medical humanities (MH) have the potential to impact medical education (ME) learning and teaching outcomes but contextual content and methods relevant to our local and regional learners are lacking. We have described three MH-based ME programmes to illustrate considerations in programme development and evaluation. Highlighting considerations in awareness, administrative and funding support, and research capability, we propose strategies to overcome such challenges and hope that readers will be inspired to contribute to this developing landscape where science and art intersect.
As Carlo Rubbia, Nobel prize winner in physics says,
“Science for me is very close to art. Scientific discovery is an irrational act. It’s an intuition which turns out to be reality at the end of it – and I see no difference between a scientist developing a marvellous discovery and an artist making a painting.”
Notes on Contributors
Both OEK and SWS contributed to the conceptualisation of the paper through their experience and work in both undergraduate and postgraduate training. With repeated discussions, the approach towards explaining the value of the paper and learning points for readers were finalised. Both authors worked on the initial draft of the manuscript, before refining the contents though an iterative process of literature review and discussions with other educators and participants of the various programs. The final draft of the paper was reviewed by both authors who reached the consensus that the paper was ready for submission for publication. Both authors agree to be accountable for all aspects of the paper.
Acknowledgements
We would like to thank Ms Chiam Min and Ms April Thant Aung for proofreading the article.
Funding
No funding was received.
Declaration of Interest
Both OEK and SWS state no conflicts of interest.
References
Daher-Nashif, S., & Kane, T. (2022). A culturally competent approach to teach humanities in international medical school: Potential frameworks and lessons learned. MedEdPublish, 12(6). https://doi.org/10.12688/mep.18938.1
Dennhardt, S., Apramian, T., Lingard, L., Torabi, N., & Amtfield, S. (2016). Rethinking research in the medical humanities: A scoping review and narrative synthesis of quantitative outcome studies. Medical Education, 50(3), 285-299. https://doi.org/10.1111/medu.12812
Ong, E. K., & Anantham, D. (2019). The medical humanities: Reconnecting with the soul of medicine. Annals of the Academy of Medicine Singapore, 48(7), 233-237.
Tan, M. K. B., Tan, C. M., Tan, S. G., Yoong, J., & Gibbons, B. (2021). Connecting the dots: The state of arts and health in Singapore. Arts & Health, 15(2), 119-134. https://doi.org/10.1080/17533015.2021.2005643
Wu, H. Y. J., & Chen, J. Y. (2018). Conundrum between internationalisation and interdisciplinarity: Reflection on the development of medical humanities in Hong Kong, Taiwan and China. MedEdPublish, 7(184). https://doi.org/10.15694/mep.2018.0000184.1
*Ong Eng Koon
National Cancer Centre Singapore
30 Hospital Blvd, Singapore 168583
Email: ong.eng.koon@assisihospice.org.sg
Submitted: 24 December 2023
Accepted: 31 July 2024
Published online: 7 January, TAPS 2025, 10(1), 4-9
https://doi.org/10.29060/TAPS.2025-10-1/GP3201
Muhamad Saiful Bahri Yusoff1,2
1Department of Medical Education, School of Medical Sciences, Universiti Sains Malaysia, Malaysia; 2Centre for the Development of Academic Excellence, Universiti Sains Malaysia, Malaysia
Abstract
Introduction: This article explores the dynamic relationship between the Scholarship of Teaching and Learning (SoTL) and the well-being of students and educators within the context of medical education.
Methods: The author critically reviewed the salient views and knowledge at the intersection of SoTL, well-being, and resilience. By critically examining literature, insights from various studies were synthesised, offering a detailed overview of the current state of knowledge in this field. This review guided the identification of key practices and recommendations.
Results: SoTL emerges as a transformative force, enhancing well-being for both students and educator through evidence-based practices and innovative teaching methods. The article explores the crucial role of SoTL in fostering resilience, not only among students but also among educators. Despite promising evidence, challenges in implementing SoTL for well-being persist, requiring strategic approaches to overcome traditional paradigms. The discussion extends to the global implications of SoTL, emphasising the need for collaborative efforts to foster better educational practices and establish inclusive learning environments.
Conclusion: As we assess the evidence for transformative change, a call-to-action echoes, urging global collaboration, research endeavors, and institutional support to realise the full potential of SoTL, ultimately creating environments where both learners and educators thrive.
Practice Highlights
- Employ evidence-based teaching methods derived from SoTL practices.
- Prioritise individuals’ mental, emotional, and social growth through SoTL practices.
- Cultivate adaptive learning approaches to enhance student resilience through SoTL practices.
- Acknowledge and bolster the well-being of educators through SoTL practices.
- Embrace cross-cultural collaboration within the realm of SOTL practices.
I. INTRODUCTION
The Scholarship of Teaching and Learning (SoTL) involves a systematic examination of teaching practices and their impact on student outcomes, aiming to achieve optimal educational results and contribute to societal enhancement (Luan et al., 2019). Rooted in research, evidence, and critical reflection, SoTL enhances practices within specific disciplines and professions (Coleman et al., 2023). Typically led by discipline-specific teachers, SoTL-based projects focus on improving both teaching methods and students’ learning experiences (Coleman et al., 2023). In the evolving educational landscape, including advancements in technology and shifts in learning methods, SoTL is essential for improving instructional techniques and evaluating their impact on both academic success and the well-being of students and educators. Wellbeing signifies the state of positive emotions, effective functioning, the realisation of one’s potential, a sense of control, purpose, and positive relationships (Ruggeri et al., 2020). Within traditional teaching methods, a pivotal research question arises: Do we have enough evidence to advocate for a significant change acknowledging the diverse experiences of educators and learners? This prompts a close examination of the current educational landscape, evolving roles of educators and learners, and the urgent need for a comprehensive understanding of well-being and resilience in the context of SoTL.
II. METHODS
The author critically reviewed the salient views and knowledge at the intersection of SoTL, well-being, and resilience. By critically examining selected literature from diverse studies, insights were synthesised to present a detailed overview of the current state of knowledge in this field. The approach allowed for an in-depth exploration of how SoTL principles are implemented and their impact on the well-being of students and educator. The synthesis of study findings resulted in a comprehensive understanding and practical recommendations for transformative educational practices.
III. RESULTS
A. Current Landscape of Teaching and Learning
The current way we teach relies heavily on traditional methods, often involving direct instruction and focusing on course content. While these methods have traditionally aimed at spreading knowledge, we are now questioning their impact on the well-being of students and educator (Coleman et al., 2023; Khairul Anhar Holder et al., 2023). Conventional teaching, with its emphasis on standardised assessments and delivering content, might unintentionally lead to increased stress and reduced resilience among learners. It’s clear that education is changing, and there is a growing call for a more comprehensive approach to teaching and learning. This means exploring methods that not only promote academic success but also prioritising the well-being and resilience of everyone involved in education.
B. Current Concept of Scholar of Teaching and Learning (SoTL)
SoTL is a dynamic approach to education, dedicated to improving teaching methods and enhancing student learning experiences (Coleman et al., 2023; Luan et al., 2019). It employs transformative teaching methods that connect academic content with real-world contexts, fostering critical thinking skills. SoTL involves reflective practice, where educators systematically assess and improve teaching using evidence-based research and educational theory. SoTL promotes knowledge sharing among educators, encouraging collaboration and professional development. Through educational inquiry, SoTL engages educators in thorough investigations, contributing to knowledge creation that enhances teaching practices. Ultimately, SoTL serves as a catalyst for transforming education by advocating for experiential learning, innovative teaching methods, and inclusive strategies, preparing students for success in a changing global landscape. SoTL encompasses transformative pedagogy, reflective practice, teacher dissemination, educational inquiry, and educational transformation (see Figure 1).
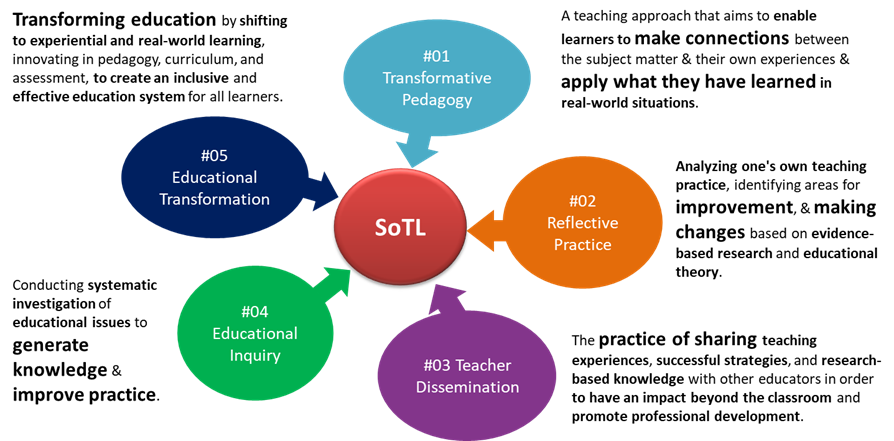
Figure 1. The key characteristics of SoTL
C. Defining Well-being and Resilience in Medical Education
In medical education, well-being goes beyond simply being stress-free (Roslan et al., 2022; Ruggeri et al., 2020). Alongside well-being, resilience becomes essential for overcoming challenges since it is the ability to recover from setbacks, adapt to changing circumstances, and thrive in adversity (Khairul Anhar Holder et al., 2023; Roslan et al., 2022). Figure 2 illustrates the interconnected components and outcomes of well-being in medical education. The left side highlights factors contributing to well-being such as resilience, while the right side shows the outcomes of enhanced well-being, such as better patient care, and reduced burnout.
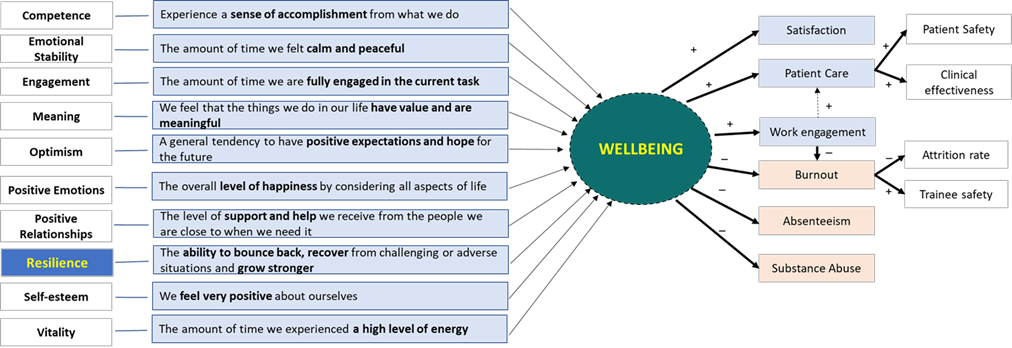
Figure 2. The interconnectedness of wellbeing and resilience in medical education
D. Roles of SoTL in Enhancing Well-being and Resilience
SoTL proves to influence student well-being enhancement within educational environments (Coleman et al., 2023; Luan et al., 2019). As educators embrace evidence-based practices, the imperative of prioritising well-being in pedagogical discourse becomes evident. SoTL, employing rigorous research and reflective teaching, seeks strategies that not only elevate academic success but also positively contributes to the student experience. Research findings highlight the substantial impact of teaching practices guided by SoTL principles on student engagement, motivation, and satisfaction (Coleman et al., 2023; Khairul Anhar Holder et al., 2023). This intertwining of SoTL with well-being underscores its pivotal role in shaping a more comprehensive and enriching educational experience (Coleman et al., 2023).
E. Educator Well-being
Teaching, with its inherent demands and complexities, can significantly influence educators’ well-being. SoTL recognises the critical role of supporting educator well-being as essential for sustainable and effective teaching practices. Educator well-being extends beyond workload management to encompass the emotional and intellectual dimensions of teaching. Institutions embracing SoTL principles prioritise initiatives such as professional development, mentorship programs, and fostering a conducive work environment (Coleman et al., 2023; Luan et al., 2019). These endeavors not only elevate teaching quality but also contribute to the personal and professional growth of educators, leading to their well-being.
F. Student Well-being
The core of SoTL lies in its significant impact on students’ well-being, surpassing traditional measures of academic success by recognising the intricate connection between a student’s educational success and their overall well-being (Khairul Anhar Holder et al., 2023). The implementation of evidence-based teaching practices, guided by SoTL principles, establishes an environment conducive to positive mental, emotional, and social development among students. Research indicates that students exposed to such approaches report higher levels of satisfaction, motivation, and a sense of belonging within the academic setting (Coleman et al., 2023). Through innovative teaching methods, SoTL fosters holistic student development, addressing diverse needs and serve as a catalyst for student well-being, cultivating a rewarding and supportive educational experience (Coleman et al., 2023; Luan et al., 2019).
G. Challenges in Implementing SoTL for Well-being
Despite the potential of SoTL to improve student and educator well-being, its implementation faces challenges, notably overcoming traditional teaching paradigms. Resistance to change within academic institutions, often rooted in institutional cultures and ingrained beliefs, can hinder the integration of SoTL-informed practices. Cultural and institutional barriers may also manifest in the allocation of resources and recognition. SoTL demands time, collaboration, and institutional support for meaningful implementation, posing challenges for institutions in prioritising these aspects over more traditional academic pursuits (Luan et al., 2019). The complex challenges associated with integrating SoTL for well-being underscore the necessity for strategic approaches to overcome these obstacles and pave the way for transformative changes in educational practices (Coleman et al., 2023).
H. The Need for Resilience in Learning Environments
In the ever-evolving field of education, resilience stands out as a crucial quality for navigating the complexities of learning environments (Khairul Anhar Holder et al., 2023; Roslan et al., 2022; Ruggeri et al., 2020). Students who develop resilience not only excel academically but also build a mindset that prepares them for uncertainties in the future. SoTL plays a vital role in fostering resilience by promoting pedagogical strategies that encourage adaptive learning. Through experiential approaches, collaborative projects, and real-world applications of knowledge, SoTL contributes to the development of resilient learners (Coleman et al., 2023). SoTL emphasises the transformative potential of educational practices that not only convey knowledge but also equip learners with the resilience needed to thrive in an ever-changing world (Coleman et al., 2023; Luan et al., 2019).
I. Evaluating the Evidence for Transformational Change
Do we have enough evidence to support a transformative change in educational practices? Recent studies indicate a strong connection between SoTL-informed teaching practices and positive outcomes, both academically and well-being (Coleman et al., 2023). However, challenges exist due to variability in methodologies, research scope, and the need for longitudinal studies to assess sustained effects. The evidence is promising, showing improved student engagement, increased educator satisfaction, and positive learning environments (Coleman et al., 2023). Further research is needed to establish causal relationships and identify specific SoTL elements contributing significantly to well-being. A global perspective is crucial, requiring collaborative, cross-cultural research efforts to enrich the evidence base and ensure global applicability of transformative changes.
J. Implications for Global Medical Education
Exploring SoTL’s impact on student and educator well-being has profound implications for global medical education. Applied globally, SoTL principles can transcend cultural and institutional boundaries, fostering a more inclusive and responsive educational landscape (Roslan et al., 2022; Ruggeri et al., 2020). Successful SoTL implementations globally offer insights for transformative changes in education (Coleman et al., 2023; Luan et al., 2019). However, addressing cultural nuances, regional differences, and institutional variations requires a careful global approach to applying SoTL principles. Global medical education benefits from collective efforts, fostering cross-cultural exchanges of SoTL best practices (Coleman et al., 2023). The wide-reaching implications of SoTL, underscored by a system-learner-oriented framework for well-being (Figure 3), highlight the need for collaborative endeavors to shape a more equitable global educational experience. SoTL should be reimagined as an emerging practice for researchers to impact teaching, learning, and assessment, promoting well-being (Coleman et al., 2023).

Figure 3. A System-Learner-Oriented SoTL for Wellbeing Framework
IV. DISCUSSION
The current education landscape is undergoing a significant shift away from traditional teaching practices due to their potential unwanted impact on student and educator well-being (Coleman et al., 2023; Khairul Anhar Holder et al., 2023). This recognition has led to a growing urgency for transformative changes aligned with global academic needs. SoTL, encompassing transformative pedagogy, reflective practice, teacher dissemination, educational inquiry, and transformation, emerges as a guiding light in this educational shift, committing to enhancing teaching methodologies and student learning experiences despite facing challenges (Coleman et al., 2023; Luan et al., 2019).
Implementing SoTL for well-being faces many challenges, including resistance to change, institutional cultures, and fixed beliefs (Coleman et al., 2023; Luan et al., 2019). The need for resources, time, collaboration, and institutional support becomes apparent for meaningful implementation. This highlight potential lack of awareness amongst educator regarding SoTL practices, emphasising the importance of strategic approaches. Additionally, resilience in learning environments is vital for maintaining well-being and achieving academic success (Roslan et al., 2022; Ruggeri et al., 2020). In medical education, building resilience among students and educator is essential for coping with challenges (Khairul Anhar Holder et al., 2023) and recovering from setbacks effectively (Roslan et al., 2022).
Evaluating the current evidence on SoTL and its impact on well-being reveals promising connections but shows up the need for further research (Coleman et al., 2023). Recognising the variability in methodologies, research scope, and the necessity for longitudinal studies is crucial. Comprehensive evaluations and robust evidence are needed to validate the effectiveness of SoTL practices and their long-term impact on both student and educator well-being. This includes an in-depth examination of SoTL’s potential benefits and challenges to ensure that its implementation leads to meaningful and sustainable improvements in educational practices.
Advocating for a global perspective highlight diverse educational contexts worldwide. Collaborative, cross-cultural research efforts are vital to enrich the evidence base and ensure the global applicability of transformative changes. The extension of educational experiences and innovations through sharing practices and policies will be crucial. By integrating SoTL principles, fostering a culture of continuous improvement, and prioritising well-being, global medical education can create supportive, resilient, and effective learning environments that cater to the holistic development of students and educator.
V. CONCLUSION
Integrating SoTL with student and educator well-being signifies a transformative shift in global education. The evidence reveals that adoption of SoTL principles as a pathway to comprehensive educational experiences, emphasising the connection between teaching methods and well-being. A resounding call to action emphasises the essential need for global collaboration, dedicated research, and institutional support to unlock SoTL’s full potential. Only through these collective efforts can educational environments foster the flourishing of student and educator, marking a paradigm shift worldwide.
Notes on Contributors
MSBY contributes to the conception of the work, the acquisition of data for the work, drafts the work or revising it critically for important intellectual content, approves the final version to be published, and agrees to be accountable for all aspects of the work.
Acknowledgement
The content of this article is mainly based on a presentation titled “SOTL in Student and Faculty Well-being and Resilience – Do We Have Enough Evidence for a Transformational Change?” given by the author at the 20th Asia Pacific Medical Education Conference in Singapore. This article has undergone language editing by ChatGPT 3.5 to enhance its syntax and improve overall clarity.
Funding
This paper has not received any fundings.
Declaration of Interest
The author declared no conflict of interests.
References
Coleman, K., Uzhegova, D., Blaher, B., & Arkoudis, S. (2023). The educational turn: Rethinking the scholarship of teaching and learning in higher education. Springer Nature, Singapore. https://doi.org/10.1007/978-981-19-8951-3
Luan, W. S., Khambari, M. N. M., Razali, A. B. M., Rashid, S. A. & Ching, F. T. H. (2019). Scholarship of teaching and learning @UPM. Centre for Academic Development (CADe), Universiti Putra Malaysia, Malaysia. https://cade.upm.edu.my/upload/doku men/20220624103811eBook_-_SoTL@UPM_(Complete).pdf
Ruggeri, K., Garcia-Garzon, E., Maguire, Á., Matz, S., & Huppert, F. A. (2020). Well-being is more than happiness and life satisfaction: A multidimensional analysis of 21 countries. Health and Quality of Life Outcomes, 18(1), 1-16. https://doi.org/10.1186/ s12955-020-01423-y
Roslan, N. S., Yusoff, M. S. B., Morgan, K., Razak, A. A., & Shauki, N. I. A. (2022). Evolution of resilience construct, its distinction with hardiness, mental toughness, work engagement and grit, and implications to future healthcare research. Education in Medicine Journal, 14(1), 99-114. https://doi.org/10.21315/eimj 2022.14.1.9
Khairul Anhar Holder, N. A., Pallath, V., Vadivelu, J., & Foong C. C. (2023). Using document phenomenology to investigate academic failure among year 1 undergraduate Malaysian medical students. BMC Medical Education, 23(310), 1-19. https://doi.org/10.1186/s12909-023-04285-2
*Assoc. Prof. Dr Muhamad Saiful Bahri Bin Yusoff
Department of Medical Education,
School of Medical Sciences,
Universiti Sains Malaysia,
Kelantan, Malaysia
+60169629640
Email: msaiful_bahri@usm.my
Submitted: 3 January 2023
Accepted: 29 May 2024
Published online: 1 October, TAPS 2024, 9(4), 1-5
https://doi.org/10.29060/TAPS.2024-9-4/GP2940
Sengkhoun Lim1, Steve Vilhem2, Sambath Cheab1, Laura Goldman3, Aklinn Nhem1, Ponndara Ith1 & Youttiroung Bounchan1
1University of Health Sciences, Cambodia; 2Institute of Humanities in Medicine CHUV, Switzerland; 3Boston University, United States of America
Abstract
Introduction: There is a global call for transforming medical education to meet evolving healthcare needs. However, navigating the challenges of educational change in resource-limited contexts requires key stakeholders, from leaders to educators and students, to adopt innovative approaches. This paper presents practical examples of such innovations from the University of Health Sciences (UHS) in Cambodia’s experiences, followed by discussions on enabled and hindered factors of their initiation, implementation, and sustainability. This paper also aims to inspire future medical education innovations.
Methods: This paper relied on internal document reviews, including strategic plans, project proposals & planning, course syllabi, and evaluation reports, and the collective working experiences of co-authors in initiating, implementing, and leading these innovations.
Results: Three innovative projects at UHS illustrated how creative ideas are put into practice, including (1) The elective International Programme (IP) with a dual objective of training local trainers while preparing students for international mobility, (2) The Master of Health Professions Education (MHPE), a cost-effective faculty development programme delivered in-person at UHS campus by faculty of a university partner, and (3) Peer-assisted Learning (PAL), a student-led initiative to promote learning skills.
Conclusion: Medical education innovations are needed in resource-limited contexts. The success of these initiatives resulted from multi-factors, notably long-term strategic planning, supportive leadership, active partnerships, policy commitment, local champions, resourcefulness, and student engagement. The late adoption of technology-enhanced learning, the necessity for robust faculty development programmes, and early investment in student leaders, coupled with post-graduate retention planning, represent challenges that present strategic opportunities.
Practice Highlights
- Medical education innovations are needed in a resource-limited country like Cambodia.
- Piloting before widespread implementation allows for tailoring to a specific local context.
- Long-term partnerships between external experts and internal faculty foster contextualisation, local capacity-building, and stakeholder buy-in.
- Continuous and supportive leadership with strategic planning is essential for driving and sustaining educational innovations.
- Identifying and nurturing local champions to carry out innovations is key to sustainability.
I. INTRODUCTION
The 1910 Flexner report inspired the transformation of medical education to a science and knowledge-based curriculum. A century later, an influential Lancet report called for transforming health professions education to meet changing population healthcare needs (Frenk et al., 2010). However, in resource-limited contexts, doctor training has not kept pace with public health challenges like an increase of chronic diseases. Moving away from the Flexnerian model presents significant challenges to the status quo because it involves leadership, technical, financial, and administrative commitments, specifically in Cambodia (Lim et al., 2024). To address these issues, key stakeholders, from leaders to educators and students, must adopt innovative approaches to medical education that are culturally and contextually appropriate.
This paper showcases three innovations that exemplify how creative ideas are put into practice at the university level: the elective programme, faculty development, and student-led initiative. Innovation, by definition, refers to the ability to introduce novel and useful ideas within a specific context. These examples are considered new and beneficial for stakeholders in the Cambodian context. The first two are practices adapted from other countries, while the last is an initiative of, by, and for students from within the university. The “Triple I” model of three phases of initiation, implementation, and institutionalisation, is used to discuss these innovations, especially the challenges to sustainability (Fullan, 2015). This paper also aims to inspire future innovations in medical education.
II. THREE INNOVATIONS IN MEDICAL EDUCATION
University of Health Sciences (UHS) is the oldest and largest state-owned university of health sciences in Cambodia. In late 2001, UHS became a public administrative institution entrusted by the Ministry of Health to be a leading university in medical education reforms. Below are three medical education innovations at UHS.
A. Elective Programme
Launched in 2013 by UHS-Faculty of Medicine (FoM) with financial and technical assistance from development partners, especially France, the International Programme (IP) is a tool for educational innovation and strengthening international relationships. This 3-year elective programme annually selects 60 outstanding students during their clinical phase (years 4-6). The IP has a dual objective: training of trainers (ToT) and student preparation for international mobility. To achieve these goals, UHS brings foreign professors from partner universities to role model a new generation of Cambodian trainers in modern teaching. Students actively engage in four main activities: academic training, language courses, research methodology, and socio-cultural activities. Visiting professors teach IP undergraduate students in the mornings and post-graduate residents in the afternoons to maximise their in-country time. Local trainers co-train with these professors in their respective disciplines to learn new teaching methods. French, English, and Khmer languages are mediums of instruction.
The IP has functioned as a pilot initiative, introducing student-centered learning, simulation-based education, and standardized assessment to the medical curriculum. These approaches have been well-received by faculty and students. In 2017, case-based learning (CBL) and simulation were scaled up to all students at FoM. The IP is considered an achievement because of its contribution to UHS’s strategic goals: educational innovation, ToT, and strengthening international relations. Presently, UHS has a pool of at least 60 trainers in CBL and simulation at FoM. Furthermore, the IP model was replicated within UHS’s nursing and pharmacy programmes in 2015 and 2018, respectively.
B. Faculty Development Programme
Faculty development (FD) is key to supporting educators in their multifaceted roles. UHS has invested in FD programmes to equip faculty with knowledge and skills, specifically responding to reforms in health professions education (HPE). A key initiative was a 2-year Master of Health Professions Education (MHPE) programme, offered in partnership with University of the Philippines (UP)-Manila from 2011 to 2016. Funded by the WHO and French Cooperation, the programme catered to two cohorts of 28 health professionals, including doctors, dentists, pharmacists, nurses, and medical laboratory technicians.
The programme’s hybrid delivery model was a historical first at UHS. It combined intensive 5-day on-site sessions led by visiting UP-Manila faculty, followed by distance learning modules. The MHPE programme is not only for individual professional development but also institutional development. While the programme faced challenges with language barriers, inter-professional learning, and technology limitations, it yielded positive outcomes in local human resource development in HPE. Eight students graduated with master’s degrees, while 12 received diplomas. Many graduates now contribute significantly to UHS, staffing the pedagogy unit and different faculties.
Building on local expertise, those MHPE graduates embarked on own FD programme development at UHS, beginning with a mandatory 4-day basic pedagogy course for all educators in 2015. The pedagogy unit has trained over 518 teachers in basic pedagogy. Currently, UHS’s FD programmes include short courses and workshops; strategically tailored to address national, institutional, and teacher needs. These programmes focus on competency-based course development, lesson planning, writing MCQs, and practical teaching skills (e.g., interactive lectures, small group, and simulation-based facilitation). For sustainability, UHS prioritises FD initiatives that are competency-based, cost-effective, and fit to the Cambodian context. Most FD programmes are now designed and delivered in Khmer by local trainers. UHS still collaborates with international partners to develop different FD programmes, especially for new HPE topics like interprofessional education (IPE).
C. Student-led Initiative
The value of students as active partners in education is well-established. Recognizing this notion, UHS actively promotes student engagement, particularly student roles in teaching. Through the Global Health through Education Training and Service (GHETS) grant (2016-2022), six cohorts of 56 students participated in the Essential Skills in Medical Education (ESME) online course. A group of student champions from the first cohort (including two authors: SL and SC) partnered with UHS-Medical Student Association (MSA) to launch the Peer-assisted Learning (PAL) club. PAL initially began as a 3-month extra-curricular course designed to integrate learning skills with basic science subjects. It has currently evolved into a hub for student-led initiatives, offering the Annual Medical Education Conference (AMEC), training courses, workshops, and socio-cultural events. Most activities were postponed during the pandemic, and some were restarted by UHS-MSA in 2023.
III. DISCUSSION
The “Triple I” model describes three phases of educational change over time (Fullan, 2015). The first phase is initiation, an attempt to embrace innovations. The second phase is implementation, the process of putting ideas into action. The third phase is institutionalisation when innovations become routine. The goal of change is institutionalisation; however, it does not occur without innovative adoptions being successfully initiated and implemented. This model is a conceptual framework used to discuss enabled and hindered factors in medical education innovations at UHS, Cambodia.
Active collaboration with development partners drives educational change at national and institutional levels in Cambodia (Lim et al., 2024). The IP and FD are examples of technical cooperation, directly contributing to the university’s long-term goals of educational innovation, human resource capacity-building, and international relations strengthening. Aligning innovations with organisational goals, shared beliefs, and core values is crucial for acceptability and implementation effectiveness (Century et al., 2012). Such partnerships hold particular significance in resource-limited contexts. Through external expertise and funding, medical schools can overcome barriers such as stakeholder buy-in, technical and resource constraints.
Innovations utilizing existing or external resources are more likely to gain approval from university leaders. Student engagement can positively enhance the university’s reputation on the international and national stage. UHS continues supporting PAL student-led activities, which were initially cost-free and run by highly motivated student volunteers, despite not aligning directly with strategic priorities and may not be perceived as needed by stakeholders.
Innovation characteristics influence the process of putting ideas into action. Relevant stakeholders may struggle to perceive the necessity for change because needs are often unclear at the beginning of innovation. Educational change is inherently complex, demanding shifts in educational philosophy, teaching strategies, and even skillsets. While this complexity poses implementation challenges, it also results in greater change because more is being attempted (Fullan, 2015). The IP was initially co-led with international experts, and local stakeholders ensured contextual and cultural relevance through co-creation and co-teaching. The IP marked a radical departure from the status quo, transitioning from teacher-centered to student-centered instruction. This shift presented significant challenges to many UHS teachers whose teaching practices rely on didactic lectures. Considerable efforts are needed to increase faculty buy-in, commitment, and capacity-building. Placing teachers as co-trainers alongside visiting professors is one way to overcome these challenges and contribute to the success.
Piloting is another enabling factor in which innovations are tested before committing to their full adoption. The IP, FD, and PAL all started as small-scale, elective experimentations before scaling up to benefit all.
Sustainability remains a persistent challenge in resource-limited contexts. Innovative projects will likely cease after a few years of implementation due to a lack of financial, technical, or stakeholder commitment. At UHS, the IP, FD, and PAL are examples of sustainable innovations. Several factors contribute to sustainability. Changing university policies is key to ensuring medical schools engage in long-term transformation (Bland et al., 2000). These three initiatives were built into organisational and programme structures through policy change, budgeting, or academic calendar. For instance, UHS incorporated PAL student-led activities into its 5-year strategic plan (2019-2023) and allocated a small stipend for student peer-teaching. Additionally, students receive recognition through certificates and further opportunities. PAL is sustained through MSA, an established organisational structure at UHS.
Strong leadership is paramount for driving and sustaining innovations (Bland et al., 2000). Beyond mere initiation, innovation implementation requires ongoing evaluation, revision, and expansion plans to sustain success. UHS strategic plans (2014-2018 and 2019-2023) made public commitment by setting clear indicators for innovative activities such as the IP and FD. These programmes had local leaders do hard work overtime. Empowering local champions to carry out innovations is key to sustainability. UHS exemplifies this through proactive approaches such as identifying and training faculty and student leaders, providing them opportunities to engage in impactful work. Notably, most FD programmes at UHS are now developed and conducted in Khmer by local trainers, underscoring institutional commitment to local capacity-building and sustainability.
Many challenges still exist. The university’s late adoption of technology-enhanced learning hindered its response to the COVID-19 pandemic, causing disruptions when moving to distance learning. Limited resources add another layer of complexity. To ensure effectiveness and sustainability, UHS must invest in technology-enhanced and robust FD programmes, especially in the context of transitioning toward competency-based medical education. Securing funding can be achieved through collaborative partnerships and increased budgets from UHS itself. Investing in student leaders early holds promise; however, results may not be immediately apparent. It takes a bird’s view to allocate resources to develop future leaders, and a transition plan is needed to retain these student champions at UHS after their graduation.
IV. CONCLUSION
Medical education innovations are needed in a resource-limited country like Cambodia. UHS strategically launched three small-scale programmes to meet institutional goals in medical education reforms. The sustainability of these programmes is due to several factors. Leveraging both internal and external resources, including development partners, local faculty and students, enabled knowledge transfer, and maximised resources. Long-term partnerships between international experts and local faculty resulted in contextualisation, capacity-building, and stakeholder buy-in at the home institution. Identifying and nurturing leaders and champions among faculty and students was a key feature alongside piloting innovations, allowing for local adaptations before scaling up. The challenges facing the university can be strategically turned into further opportunities.
Notes on Contributors
Sengkhoun Lim conceptualized and designed the study, collected and analyzed data, and wrote the manuscript.
Steve Vilhem analyzed data and drafted the International Programme part.
Sambath Cheab provided input on the initial study design and participated in data collection and analysis.
Laura N. Goldman provided guidance on manuscript writing, contributed to the discussion section, and edited the whole manuscript into plain English.
Aklinn Nhem provided source documents, validated information, gave feedback, and proofread.
Ponndara Ith validated information, gave feedback, proofread, and edited the text.
Youttiroung Bounchan provided source documents, validated information, gave feedback, proofread, and edited the manuscript. All authors have read and approved the final manuscript.
Acknowledgement
The authors thank Professor Vonthanak Saphonn, Rector of the University of Health Sciences, for his continuous and supportive leadership in these medical education innovations and Professor Mam Bunsocheat for his contributions to the International Programme at the University of Health Sciences, Cambodia.
Funding
There is no funding involved for this paper.
Declaration of Interest
The authors report no conflict of interest.
References
Bland, C. J., Starnaman, S., Wersal, L., Moorehead-Rosenberg, L., Zonia, S., & Henry, R. (2000). Curricular change in medical schools: How to succeed. Academic medicine, 75(6), 575–594. https://doi.org/10.1097/00001888-200006000-00006
Century, J., Cassata, A., Rudnick, M., & Freeman, C. (2012). Measuring enactment of innovations and the factors that affect implementation and sustainability: Moving toward common language and shared conceptual understanding. The Journal of Behavioral Health Services & Research, 39(4), 343–361. https://doi.org/10.1007/s11414-012-9287-x
Frenk, J., Chen, L., Bhutta, Z. A., Cohen, J., Crisp, N., Evans, T., Fineberg, H., Garcia, P., Ke, Y., Kelley, P., Kistnasamy, B., Meleis, A., Naylor, D., Pablos-Mendez, A., Reddy, S., Scrimshaw, S., Sepulveda, J., Serwadda, D., & Zurayk, H. (2010). Health professionals for a new century: Transforming education to strengthen health systems in an interdependent world. The Lancet, 376(9756), 1923–1958. https://doi.org/10.1016/S0140-6736 (10) 61854-5
Fullan, M. (2015). The new meaning of educational change (5th ed.). Teachers College Press.
Lim, S., Cheab, S., Goldman, L. N., Ith, P., & Bounchan, Y. (2024). The past, present and future of medical education in Cambodia. Medical Teacher, 46(6), 842-848. https://doi.org/10.1080/014 2159X.2024.2327490
*Sengkhoun Lim
73 Preah Monivong Blvd (93),
Phnom Penh, Cambodia
+855 92 222 622
Email: sengkhounlim@ymail.com
Submitted: 8 July 2023
Accepted: 21 September 2023
Published online: 2 April, TAPS 2024, 9(2), 1-4
https://doi.org/10.29060/TAPS.2024-9-2/GP3089
Lamiaa Mohsen1, Marwa Shabrawy1, Waleed Hassan1, Zakia Arfeen2 & Mohammed Ahmed Rashid2
1School of Medicine, Newgiza University, Cairo, Egypt; 2UCL Medical School, Faculty of Medical Sciences, University College London, London, United Kingdom
Abstract
Introduction: In 2016, a new university opened in Egypt that sought to ‘challenge the ordinary’ in a country with a long and rich heritage of knowledge production. Newgiza University (NGU), located adjacent to the ancient pyramids of Giza outside Cairo, launched with a foundational focus on health sciences, through undergraduate courses in medicine, dentistry, and pharmacy. Each programme was co-developed through an academic collaboration with University College London (UCL), a high-ranking, research-intensive, UK university.
Methods: As the collaboration passes a key juncture of graduating the first cohorts of doctors, dentists, and pharmacists from these courses who embark on their professional careers, we examine and reflect on the journey to date. In particular, this article reviews the growing academic literature about international partnerships in medical education, describes how curricula, assessments, and management structures in the three NGU healthcare courses were adapted and finessed to fit the Egyptian context, and shares the lessons learnt by the academic leadership teams responsible for this challenging but stimulating collaboration project.
Results: The collaboration between NGU and UCL is an example of an international education partnership approach that seems to be growing in popularity globally. The overriding importance of building trust and respect between partners was clear in this collaboration, as was the need for clear communication channels to guide the necessarily complex decision-making that underpinned it.
Conclusion: Given inevitable power imbalances in such collaborations, critical examinations of their impacts on organisations, staff, and students are an important research priority in the future.
Practice Highlights
- International education partnerships are growing in popularity and there is a growing academic literature exploring different collaboration models.
- Co-development of healthcare professions education curricula across national borders requires attention to relational factors including trust and respect.
- Power differentials make it crucial to evaluate such partnerships using a critical lens.
I. INTRODUCTION
Egypt has a long and rich intellectual and cultural heritage dating back millennia. In the last century, Egyptian higher education sector has been shaped both by globalisation and a series of governmental policies (Reid, 2002). Against this backdrop, a new university was conceptualised that would ‘challenge the ordinary’ by creating a diverse community of staff and students to spearhead academic and scientific advancement in Egypt and beyond. Endorsed by Presidential Decree as a non-profit, private university in April 2010, Newgiza University (NGU) officially opened in 2016 with an initial focus on healthcare sciences, launching schools in Medicine, Dentistry, and Pharmacy.
As part of its mission to create an exciting learning environment that is filled with energy, talent, and cultural diversity to redefine the future of Egypt, NGU had a strategic objective to partner with a leading overseas university with a strong track-record in health professions education (HPE) to co-develop these new programmes. After briefly considering the literature on international education partnerships, this article will describe the experiences of an academic collaboration between NGU and University College London (UCL) to co-develop new undergraduate programmes in Medicine, Dentistry, and Pharmacy, that graduated their first cohorts in early 2023.
An emerging phenomenon in recent decades has been the delivery of curricula outside of the country in which they were developed. A variety of terms have been used to describe such arrangements, including ‘offshore education’, ‘transnational education’, and ‘crossborder curriculum partnerships’. The purpose of these partnerships is to provide comparable educational experiences in both institutions and can be attractive for students who are seeking a foreign qualification but do not wish to move overseas.
A literature review on international curriculum partnerships noted that almost all identified articles were about early-stage developments, reflecting that this is a growing and evolving topic (Waterval et al., 2015). It found that the most common reason for partnerships to deteriorate is mistrust and ‘disturbed relationships’, going on to conclude that there are no quick fixes to resolve cultural differences and that personal collaborations at all levels should be prioritised. As was noted in a subsequent systematic review, the academic literature is currently dominated by single case studies and there are many possible directions for future research (Kosmützky et al., 2016). Within HPE, Hodges et al. (2009) observed the growing trend of international education partnerships within a rapidly evolving globalisation discourse within the field more broadly. A later study that focussed on challenges and solutions in the context of international education partnerships in medicine suggested that there are both financial and academic advantages to both institutions (Waterval et al., 2016).
II. METHODS
From its inception, the stated vision of NGU has been to establish healthcare programmes that inspire and educate a new generation of clinicians by moving away from structures and practices of traditional universities in the region that limit effective learning. The NGU leadership team sought to reduce class sizes, focus on innovation and leadership, and move away from didactic and theoretical teaching, and towards a more patient-centred and practice-focused model of education. University College London (UCL) is based in the heart of London in the UK and is consistently ranked as one of the world’s best universities. It has schools of medicine, dentistry, and pharmacy, which each focuses on providing integrated and patient-focused education.
The underlying ethos of this collaboration has been of respectful co-development, with each team mindful of what they bring ‘to the table’ by way of expertise and experience. As such, a paradoxical success of this collaboration has been that it has shrunk and scaled back since the outset, as NGU academic, managerial, and administrative teams have taken on increasing levels of independent responsibility and their counterpart UCL teams have evolved to play roles of advisor and mentor accordingly. Although UCL curricula, assessments, and policies have been the basis for the corresponding NGU programmes in each of the three disciplines, these have gradually been adapted and contextualised to fit with the vision and operating environment of NGU.
The collaboration was structured around a three-phase approach. Phase one involved an exercise to clarify the vision and high-level structure for the three programmes and agree the legal and academic basis for the collaboration project. Phase two involved the detailed co-design and implementation of curricula and assessments across the three programmes to support their launch and delivery. Phase three, which is currently in progress, involves the ongoing operationalisation and continuous improvement of the programmes and the further development of the schools in other domains, including postgraduate education and research. These three phases are underpinned by a service contract between the two universities that takes the shape of work packages, which set the parameters and arrangements for each aspect of the collaboration.
III. RESULTS
Although geopolitical unrest was identified as a risk by both parties at the outset, this has not affected the project thus far. Instead, it has been a pandemic, COVID-19, that has proved to be the greatest disruption. Restrictions to air travel and international movement meant that for almost two years, the UCL-NGU collaboration shifted to an entirely virtual format.
This period of physical distance between the respective teams illuminated the importance of in-person visits. Seeing each other’s campuses and witnessing the contexts in which the two universities function was undoubtedly an important part of strengthening the relationship. That the project had been established for four years at the time of the onset of the pandemic meant that this was fortunately already well developed. As well as the important contextual understanding that these visits provided, it also allowed teams to socialise together and rich conversations over coffee breaks and meals often blurred the boundaries between professional and personal relationships. Indeed, close relationships between NGU and UCL counterparts was central to the success of the collaboration.
A particularly intellectually engaging aspect of this collaboration has been the adaptation of curricula content for a context that differs in social, political, cultural, epidemiological, and clinical domains. Whilst many scientific and technical aspects of HPE curricula seemingly transfer across countries readily, collaborators on both sides were surprised by the extent to which they required modification. For example, the many epidemiological and health system differences between the UK and Egypt meant there were important differences in disease patterns, drug availability, and technical equipment that need to be reflected in curricula to prepare students adequately for clinical practice. Likewise, significant areas of each curricula focus on topics linked to professional practice, including communication, healthcare ethics and law, and patient safety and clinical governance. These topic areas required significant adaptation to align with Egyptian legal and social practices, often prompting stimulating discussions and several iterative stages of development to contextualise individual teaching resources.
As well as drawing on UCL curricula structure and teaching resources to establish the new courses across the three healthcare schools, NGU also utilised UCL assessment policies and items to develop NGU assessments in each of the schools. There were, though, important adaptations. For example, the regulatory context in Egyptian higher education meant that a greater proportion of assessment weighting had to be given to ‘in semester’ assessment, necessitating a shift in emphasis from the UCL approach. Rather than using UCL assessment items directly in summative exams, the approach from the NGU schools was instead to use these to help their own faculty recognise the characteristics of high-quality items as they developed their own items. This was supplemented by many assessment writing workshops, which were often cross-disciplinary in the early phases of the collaboration as each faculty grew in size. Assessment tools used at UCL, including objective structured clinical examinations and workplace-based assessments, are not widely used in undergraduate education in Egypt and took time to embed.
One of the benefits of designing three undergraduate healthcare programmes together, launching simultaneously on a purpose-built modern campus, was the opportunity to maximise interprofessional education opportunities. This was realised through an ambitious introductory module for students from all three programmes. Not only did this provide an opportunity for students from all three NGU healthcare courses to learn together and from each other, it also embedded an inter-disciplinary approach across the three NGU schools, with faculty members from different schools often co-leading particular sessions or components of the module. On top of these benefits, it also enabled the three UCL schools to work much more closely and ensure alignment across all of their approaches. This interprofessional collaboration helped to foster closer working between schools at both NGU and UCL in other domains, which was an unexpected but pleasing consequence of this collaboration.
IV. DISCUSSION
A striking finding for teams from both universities was the central importance of human and relational factors to the collaboration. The formation of a new university creates distinct requirements in terms of leadership and culture, which can be challenging for any education leader or team. The additional layer of complexity of managing an international partner heightens this challenge, and meant the NGU leadership teams had to manage many more stakeholders than one might ordinarily have to contend with. This was especially so given the history and prestige associated with UCL, being from a high-income country with a reputation for academic excellence. The history of the UK as a former colonising country and Egypt as a former colonised country can also not be ignored. Together, these power imbalances and perceived knowledge hierarchies inevitably created a context that can easily slip to being unequal and exploitative.
By recognising the tensions faced by the NGU leadership and the potentially problematic power structures inherent to this collaboration, the teams in this collaboration acutely recognised the need for flexibility and understanding. The principle of respect and friendship was of overriding importance as it framed this collaboration not as one underpinned by ‘neutrality’, as such a thing does not exist, but rather through an outlook of deeply caring about the experiences and success of your partner team. Throughout the operational and academic aspects of the collaboration, this overriding focus on co-development and respect allowed both partners to ensure they were holding themselves and one another to account for the sake of the project mission.
Another crucial area of learning for both teams has been a sense of regret at the lack of formal scholarship and research that has been embedded in this collaboration. From the outset, the unwavering focus has been to help NGU achieve high-quality education programmes and to ensure that NGU students have an excellent student experience. This relentless focus on educational delivery, assessment, and quality management of the programmes left little time to focus on scholarship, despite a clear desire from both sides to do so. In particular, both teams recognise the many avenues of research that could have been explored through the collaboration thus far, including psychometric analyses comparing assessment performance between NGU and UCL cohorts all the way through to in-depth work using theories that help understand the complex relational factors through lenses of power and globalisation, and much between. Fortunately, this has become a priority as the collaboration moves to its next stage.
V. CONCLUSION
As the first student cohorts from its three healthcare courses graduate, NGU will enter a new stage of its development, and plans are underway to extend and deepen the collaboration with UCL across these schools. This article has summarised the dearth of academic literature on international partnerships in HPE and juxtaposed this with a complex and rich story that highlights the many different insights that can emerge from a single multi-professional collaboration. In our increasingly globalised world, the cross-cultural and relational issues raised through these partnerships have the potential to have wide-ranging and beneficial findings that extend beyond those communities working specifically on international partnerships. The importance of embedding scholarship into international HPE collaborations is clear to the academic teams on both sides of the UCL-NGU collaboration. As we plan for this in the next stages of our work together, we encourage others involved in international education partnerships to do the same and contribute to a scholarly area of growing importance in the field.
Notes on Contributors
LM led the collaboration on behalf of the NGU school of medicine, conceptualised the study, analysed the literature, and co-wrote the manuscript.
MS co-ordinated the collaboration on behalf of NGU, conceptualised the study, and developed the manuscript.
WH managed the collaboration on behalf of the NGU school of medicine, conceptualised the study, and developed the manuscript.
ZA co-ordinated the collaboration on behalf of UCL medical school, conceptualised the study, and developed the manuscript.
MAR led the collaboration on behalf of UCL medical school, reviewed the literature, conceptualised the study, and co-wrote the manuscript.
Funding
No funding was received.
Declaration of Interest
All authors were engaged in the academic collaboration described in this article.
References
Hodges, B. D., Maniate, J. M., Martimianakis, M. A., Alsuwaidan, M., & Segouin, C. (2009). Cracks and crevices: Globalization discourse and medical education. Medical teacher, 31(10), 910-917.
Kosmützky, A., & Putty, R. (2016). Transcending borders and traversing boundaries: A systematic review of the literature on transnational, offshore, cross-border, and borderless higher education. Journal of Studies in International Education, 20(1), 8-33.
Reid, D. M. (2002). Cairo University and the making of modern Egypt (Vol. 23). Cambridge University Press.
Waterval, D. G., Frambach, J. M., Driessen, E. W., & Scherpbier, A. J. (2015). Copy but not paste: A literature review of crossborder curriculum partnerships. Journal of Studies in International Education, 19(1), 65-85.
Waterval, D. G., Frambach, J. M., Oudkerk Pool, A., Driessen, E. W., & Scherpbier, A. J. (2016). An exploration of crossborder medical curriculum partnerships: Balancing curriculum equiva- lence and local adaptation. Medical teacher, 38(3), 255-262.
*Mohammed Ahmed Rashid
University College London,
Gower Street, London,
WC1E 6AE, United Kingdom
Email: ahmed.rashid@ucl.ac.uk
Submitted: 6 September 2022
Accepted: 1 March 2023
Published online: 3 October, TAPS 2023, 8(4), 1-4
https://doi.org/10.29060/TAPS.2023-8-4/GP2878
Saroj Jayasinghe1, Santhushya Fernando2
1Department of Clinical Medicine, Faculty of Medicine, University of Colombo, Sri Lanka; 2Department of Medical Humanities, Faculty of Medicine, University of Colombo, Sri Lanka
Abstract
Introduction: Medical Humanities is the interface of health sciences and humanities and an emerging field of interest. Several papers have outlined the status of this field in the Asian region where a diversity of teaching and learning approaches have been used. We share developments initiated in a Sri Lankan medical school and discuss its relevance to the southern Asian region, especially in using arts in medical humanities.
Methods: Historical records, narratives, grey literature, and published resources were collated to describe the initiative in the Faculty of Medicine, University of Colombo. The data was collected, synthesized and described especially in the context of the region.
Results: We observe a structured development of medical humanities in the curriculum. The novelty of the curriculum is that it evolving to include wider experiences from the visual and performance arts, in order to achieve the goal of promoting humaneness. The contents were locally developed, based on needs with an indigenous cultural bias giving rise to a unique southern Asian perspective of medical humanities.
Conclusion: There are diverse experiences and initiatives in medical humanities in Asian, and some are not captured in published literature. It is challenging to follow these diverse trends in different locations, share experiences and learn from each other, and place medical humanities in the regional and global maps of health professional education.
Practice Highlights
- Asia has seen several developments in the field of medical humanities.
- Sri Lanka has made significant progress and introduced it to medical education.
- One key innovation is the integration of arts to its teaching-learning.
- Southern Asia has rich and diverse religious, cultural and artistic traditions.
- The region could give a unique perspective to medical humanities.
I. INTRODUCTION
A recent scoping review traced the history of developments in the teaching / learning of humane care and recognition of its importance in medical training (Zhu et al., 2021). This paper also outlined the need to develop culturally relevant, effective, and integrative curricula that would promote humanistic attitudes and behaviours among medical students and physicians in Asia. There were developments of this field in Nepal that were shared in a subsequent correspondence (Shankar, 2022). These papers and several other publications have highlighted the developments in the field with a diversity of experiences.
We share a few developments from Sri Lanka that demonstrate a widening interest in the field in southern Asia and opportunities to use its unique heritage to move forward.
II. SCOPE AND BACKGROUND INFORMATION
The Faculty of Medicine, University of Colombo is one of the oldest continuously functioning medical schools in Asia (from 1870). It has the distinction of pioneering an integrated curriculum in the country in 1995 and establishing the first Department of Medical Humanities in 2016.
For decades, the curriculum was based on Flexner’s structures and was a conventional discipline-based curriculum with little inputs from the humanities. The reforms in 1995 led to a more integrated modular system with a longitudinal input from Behavioural Sciences (BS). The BS program had modules that focused on teaching / learning in topics related to personal development, communication skills, medical ethics, health management and professionalism (Jayasinghe, 2017). It was organized by appointing a group of academics to a Behavioural Science Stream (BSS) to coordinate the teaching / learning programs through the 5-year MBBS course.
However, inputs from the arts were minimal though it flourished outside the formal curriculum in the form of concerts, art festivals, photography exhibitions and musical events organized by the student body. These activities were heavily influenced by the urbanized Western culture and activities such as ball-room dancing, predominantly British literature, and Western models of theatre played a predominant role.
A qualitative change in the range of activities was observed around 1974 with the establishment of an Arts Circle in the Faculty of Medicine that promoted infusion of local culture. Interestingly, this coincided with changes in the admission criteria to universities that resulted in student intakes from diverse of social groups and a significant increase in entry from a wider range of districts and more rural schools.
In 2011, the BSS began to organize internal workshops to review its curriculum and propose future developments. During these discussions, participants expressed the need to promote more humaneness, empathy and compassion among students (Jayasinghe, 2017). This led to discussions on the potential role of the arts to meet these needs. The first lecture on “Illness from the perspective of humanities” was introduced in 2012. Soon a consensus view emerged to establish a Department of Medical Humanities in order to deliver a heavier educational input from humanities and thereby promote humane values in students. In August 2016, the Faculty of Medicine, University of Colombo, formally established the first Department of Medical Humanities in the country. In 2020 the BSS was renamed Humanities, Society and Professionalism Stream (HSPS) to reflect the introduction of new content to the curriculum.
III. EDUCATIONAL STRATEGIES
In order to identify contents for its new curriculum, the Department organized a series of invited lectures and discussions targeting the academic staff. It was titled “Exploring the Role of Humanities in Health”. The resource persons were experts on medical humanities and a diverse range of topics included “Role of Arts in Medicine”; “Approaches to teaching humanities to medical students”; “Medical narratives”; “Using poetry to inculcate attitudes”; and “Humanities in medicine: The Ruhuna Experiment”. Other opportunities, such as invitations to deliver guest lectures in conferences, were used by the authors to stimulate discussions on the potential role of the arts in health professional education (Jayasinghe, 2018).
The series of lectures culminated in the First International Conference on Medical Humanities held in 2018, on the theme “Learning to be more humane: The role of Medical Humanities” (Colombo Medical Humanities News, 2019). It included a half-day workshop on “Arts in Health Professional Education”. There was wide participation by experts in the field and the conference and workshop were used to refine the curriculum on medical humanities, especially on how to effectively introduce the arts to health professional education. This issue was further debated and discussed during seminars on Medical Humanities at the Colombo Medical Congress (in 2020) and orations dedicated to Medical Humanities (from 2021).
The knowledge gained from the above activities, were used to design an innovative curriculum that included a wider infusion from the arts and narrative-based learning. The main goals of the latter were to promote humaneness, encourage learners to develop a person-centred approach to clinical practice, and appreciate patient perspectives of illness. A range of educational strategies were used: assignment on appreciation of the arts and its relevance to empathy in care; student seminar to reflect on personal experiences of kind and unkind health professional behaviours, obtaining narratives from patients to highlight the humane and person-centered issues of illness; large-group lectures on topics such as “The Arts in Health and Illness” and “Empathy and Compassion”. The latter focused on research evidence from neurophysiology to demonstrate links between art appreciation and traits such as compassion and empathy.
In 2021, during the COVID pandemic, the HSPS and the Department of Medical Humanities introduced an innovative programme aimed at the students. A series of interactive multi-disciplinary webinars termed Humanitas were organied to explore contemporary issues connected to health and have continued as part of the teaching-learning programme. They have been held approximately at bi-monthly intervals and addressed a wide range of issues: life-experiences amidst environmental disasters, linguicism and decolonizing tertiary education, the world of animal welfare, lives of workers in the apparel industry, social and psychological issues faced by those with different sexual identities and orientations, and the emotional journey of a parent who lost her child to cancer.
Interviews from affected groups of people, artists, academics and intellectuals were creatively juxtaposed with short films, extracts from movies, selected musical scores. Examples of the latter included songs of peace sung during non-violent protests organised by Mahatma Gandhi and Martin Luther King Sr., and extracts of poetry and literature that drew attention to contemporary issues such as the plight of garment factory workers. Contributions were predominantly from Sri Lankan commentators reflecting our own historical and cultural context and local experiences.
Since the pandemic ended, Humanitas will be conducted in-person. The first for 2023 was titled ‘Dance and Life’, featuring live Indian and traditional Sri Lankan dance recitals by professional dancers. These performances were accompanied by commentaries by dancers on the emotions they felt while dancing, and the mechanisms of evoking feelings in the audience described by medical experts. These emotions and feelings were in turn linked to the ability of certain dances to generate compassion and empathy. The session ended with an expert dancer performing and describing how certain traditional dances of the Sinhalese (e.g. ‘Thovil’) were used as therapy for a diversity of illnesses.
The second recent innovation relates to activities on medical humanities organized for the 3rd Colombo Medical Congress in November 2022, an annual event in the University calendar and open to students. We organised a symposium exploring the neurophysiological correlates of music, poetry, and dance and complemented the academic program with a series of activities throughout the conference: free exhibitions of art, sculptures and photography, open-air musical events by students, and live sculpture and portrait sessions by professional artists. The latter live sessions enabled students and attendees to experience and interact with the process of artistic creations.
IV. DISCUSSION
Medical Humanities is an emerging field of interest in the interface of health sciences and humanities. The diversity of experiences in the Asian region has led to several initiatives. The initiative in Colombo used contemporary topics with contributions mainly from Sri Lankan commentators reflecting on our own historical and cultural contexts. We believe this enriched a field that is dominated by an allopathic or modern medical system that are predominantly Eurocentric and based on ‘Western’ values and culture.
We hope our experiences would diffuse in the Asian region. Southern Asia has a rich, historical and cultural heritage based predominantly from the Indian religions and include Hinduism, Sikhism, Jainism, Buddhism, and Islam that came from the Middle East and spread to the Indian sub-continent. The philosophical, cultural and religious foundations of this region give us a unique opportunity to give a novel perspective to the field. This will require a process of decolonizing our values and beliefs, and reconnecting to our own cultures and heritages. We also need to follow these trends in different locations, share experiences and learn from each other, often a difficult task because these initiatives may fail to reach mainstream journals or remain unpublished.
V. CONCLUSION
The paper highlights the need to have more collaborations within the southern Asian region and share knowledge that would be mutually beneficial. Southern Asia has a rich historical and cultural heritage. These roots could help develop a unique southern Asian version of Medical Humanities and place our version of medical humanities in the global maps of health professional education.
Notes on Contributors
Saroj Jayasinghe conceptualised and wrote the initial draft.
It was revised and expanded by Santhushya Fernando.
Both authors read and approved the manuscript.
Funding
The study was funded by personal funds.
Declaration of Interest
The authors have no conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias.
References
Our beginnings. (2019). Colombo Medical Humanities News, 1(1). https://med.cmb.ac.lk/medical-humanities/
Jayasinghe, S. (2017). Of course! We must look at the Arts… in its widest sense! Journal of the Ruhunu Clinical Society, 22(1), 4-5. http://doi.org/10.4038/jrcs.v22i1.26
Jayasinghe, S. (2018). Can the arts promote more humane health professionals? Exploring evidence from the neurosciences. Ceylon Journal of Medical Science, 55(1), 1-2. http://doi.org/10.4038/cjms.v55i1.4938
Shankar, P. R. (2022). Learning humanistic values in Nepal. The Asia Pacific Scholar, 7(3), 63-64. https://doi.org/10.29060/TAPS.2022-7-3/LE2777
Zhu, C. S., Yap, R. K. F., Lim, S. Y. S., Toh, Y. P., & Loh, V. W. K. (2021). Humanism in Asian medical education – A scoping review. The Asia Pacific Scholar, 7(1), 9-20. https://doi.org/10.29060/TAPS.2022-7-1/RA2460
*Saroj Jayasinghe
Faculty of Medicine,
University of Colombo,
No 25, Kinsey Road,
Colombo 8, Sri Lanka
+94718619331
Email: saroj@clinmed.cmb.ac.lk
Submitted: 15 October 2022
Accepted: 3 January 2023
Published online: 4 July, TAPS 2023, 8(3), 1-4
https://doi.org/10.29060/TAPS.2023-8-3/GP2903
Galvin Sim Siang Lin1, Yook Shiang Ng2 & Chan Choong Foong3
1Department of Dental Materials, Faculty of Dentistry, Asian Institute of Medicine, Science and Technology (AIMST) University, Malaysia; 2Conservative Dentistry Unit, School of Dental Sciences, Universiti Sains Malaysia, Health Campus, Malaysia; 3Medical Education and Research Development Unit (MERDU), Faculty of Medicine, Universiti Malaya, Malaysia
Abstract
Introduction: Dental materials science is one of the core courses for Malaysian undergraduate dental programmes, which has been primarily taught through a series of didactic lectures during the preclinical phase. In accordance with the newly revised national competency statement, Malaysian dental education is moving toward competency-based education, hence a reformation of the dental materials science curriculum is warranted.
Methods: Curriculum design including common teaching, learning and assessments methods for the Malaysian dental materials science were described and analysed. The common practices were reviewed and compared with latest national guidelines and literature.
Results: There is yet an initiative to establish a national curriculum for dental materials science. The use of traditional teaching strategies for this course also needs to be revamped from a teacher-centred to a student-centred approach. Furthermore, faculty members are facing significant challenges because the revamp requires them to explore cutting-edge pedagogical methods and develop appropriate learning opportunities, environments, resources, and assessments. Several recommendations are proposed, such as mapping the existing dental materials science curriculum to identify gaps, incorporating more hands-on sessions, implementing an integrated curriculum, introducing various formative and summative assessments, as well as recruiting faculty members with different areas of educational expertise.
Conclusion: It is hoped that this article offers a clearer pathway for Malaysian dental educators to pioneer new insight and transform the existing dental materials science curriculum.
I. INTRODUCTION
Malaysian dental curriculum is historically underpinned by the primary goal in nurturing clinically competent dentists to provide safe and high-quality oral healthcare treatment to the public. Although the curriculum has witnessed an array of revisions over the years, little has been done for dental materials science courses. In the present article, the authors outline an overview of the dental curriculum in Malaysia and describe how dental materials science courses are currently delivered. Subsequently, challenges and compelling needs are highlighted to envision the future curriculum.
II. OVERVIEW OF DENTAL CURRICULUM IN MALAYSIA
In May 1972, the Universiti Malaya established the country’s first dental school to offer a Bachelor of Dental Surgery (BDS) programme. Nowadays, dentistry has become one of the popular university programmes for high school leavers in Malaysia and the number of applicants has increased significantly over the past decades. Thirteen dental schools have been established of which six are public institutions and the remaining seven are private institutions. All dental schools in Malaysia operate independently as siloed institutions; there is no national standardised curriculum or licensing examination. Currently, each of these dental schools offers a five-year undergraduate dental programme leading to the conferment of BDS or Doctor of Dental Surgery (DDS), and all programmes are required to be accredited by the Malaysian Dental Council (MDC).
In general, undergraduate dental programmes in Malaysia are divided into two phases: preclinical and clinical phases. The preclinical phase encompasses the first two years of the undergraduate programmes. Undergraduate dental students are taught fundamental dental and medical concepts along with operative practical and laboratory skills through simulation exercises on mannequins or dummy heads. In the subsequent three years of the clinical phase, students are given the opportunities to manage and provide treatments to patients. At the end of the five-year programmes, dental students are expected to be clinically competent and practise evidence-based dentistry with ethics and professionalism.
III. DENTAL MATERIALS SCIENCE CURRICULUM IN MALAYSIA
A. Curriculum Content
Undergraduate dental programmes in Malaysia offer dental materials science courses as one of the core disciplines in the second year of preclinical phase. Dental materials science is a course that integrates underlying principles of chemical engineering and materials science into the practice of contemporary dentistry (Qazi et al., 2019). Typically, dental materials science is introduced as a stand-alone course distributed across several modules over the preclinical dental phase. The course usually starts with an introduction to dental materials and the properties of commonly used dental materials. In some dental schools, the course is divided into discipline-based such as dental materials used in conservative dentistry, prosthodontics, paediatric dentistry, orthodontics, or periodontics; whereas some schools divide the course into clinical-based and laboratory-based dental materials. Among the course content covered in clinical-based dental materials include amalgam, dental composite resin, glass ionomer cement and impression materials. On the other hand, denture-based polymers, dental ceramics, metal alloys, gypsum products as well as casting and investment materials are covered under laboratory-based dental materials. Additionally, most dental schools in Malaysia design and develop their dental materials science courses based on Bloom’s and Simpson’s taxonomies, with the bulk of the curriculum content lying within cognitive C1 (Remember) to C3 (Apply) and psychomotor P2 (Set) to P4 (Mechanism) levels.
B. Teaching, Learning and Assessment Methods
Dental materials science courses are usually delivered through a series of didactic lectures. Students are also exposed to practical hands-on sessions to examine the properties of commonly used dental materials and manipulate various dental materials. For instance, some dental schools in Malaysia introduce hands-on practical to evaluate the mechanical and viscoelastic properties of various dental materials as well as to mix clinical and laboratory-based dental materials, such as dental gypsum products, dental polymers, dental cement, and dental impression materials.
Nevertheless, since each dental school utilises a distinct set of course learning outcomes, it is infeasible to make a direct comparison between them. Moreover, students are required to meet the desired course learning outcomes upon completion of the courses. Most dental schools use either formative, summative, or a combination of both assessments to evaluate their students, though solely evaluating students based on formative assessment is rare. Students also might be evaluated through quizzes, presentation seminars, assignments, written assessments, and practical assessments such as objective-structured practical examinations (OSPE). Examples of written assessments include multiple-choice questions (MCQ) and short-answer questions (SAQ).
IV. CHALLENGES AND THE TURNING POINT
In June 2021, the Malaysian Dental Dean Council organised a workshop and proposed a revised national competency statement for future graduates in Malaysia, which was later endorsed by the Malaysian Dental Council in July 2021 (Malaysian Dental Council [MDC], 2021). The national competency statement was revised to align with the Malaysian Qualifications Framework version 2.0 competency-based education. Specifically, for dental materials science, the cognitive and psychomotor-related clusters have stated that future dental graduates should be able to justify the selection of dental materials based on the science and applications and related environmental issues (Cognitive: C4 Analyse) and to manipulate commonly used dental materials (Psychomotor: P5 Complex or overt response). Subsequently, Malaysian dental schools are prompted to revise their existing dental materials science curriculum to attain the intended learning outcomes. It is necessary to reform the dental materials science curriculum that is going to lead the attainment of cognitive and psychomotor competencies. Yet, there is no standardised national curriculum for dental materials science courses in Malaysia, despite there were a few attempts by faculty members from several dental schools.
Furthermore, pedagogical methods require improvement as dental materials science courses are often delivered via didactic lectures, whereby students claimed as a ‘dry’ subject (Soni et al., 2021). Implementation of traditional pedagogical methods does not only result in a lack of applications of pertinent knowledge, but these methods also reduce students’ interest and learning efficacies for the courses. Hence, the traditional pedagogical methods used to deliver dental materials science must be revamped to shift from teacher-centred approach to student-centred approach. There is a need to adopt diverse pedagogical methods in encouraging active students’ engagement during learning activities. This shift has posed a significant challenge to faculty members because not only do they need to explore innovative pedagogical methods that promote active learning, but they need to devise appropriate learning opportunities, learning locations, learning resources, and alternative assessments for students.
Different educational backgrounds of faculty members who teach dental materials courses are also a topic of discussion. Some Malaysian dental schools recruit experts with postgraduate degrees either in dental materials, conservative dentistry, prosthodontics, or restorative dentistry, while some schools might employ experts with a background in chemistry or material sciences. Students may miss the fundamental knowledge (if taught by BDS qualified) or fail to relate the clinical applications (if taught by scientists). At the present, teaching qualifications are encouraged but not mandatory for faculty members.
V. RECOMMENDATIONS FOR TOMORROW’S DENTAL MATERIALS SCIENCE CURRICULUM
The revised national competencies statement represents national advocacy for transformation in the dental curriculum. Hence, curriculum mapping is an initial step in transforming tomorrow’s dental materials science curriculum. Following curriculum mapping, dental educators can identify the gaps in the existing curriculum, suggest components to be maintained, revised, or removed with the purpose to achieve the desired cognitive and psychomotor competencies as listed in the national statement. Consequently, it also symbolises the significance to spur the call for the establishment of a designated dental education department in designing and developing comprehensive dental programmes in Malaysia. In hindsight, one may say that this notion served as the impetus for Malaysia to accomplish competency-based dental education in the 21st century.
Didactic lectures place a focus on the transmission of knowledge passively from lecturers to students. Students may find it difficult to understand the basic premises and practical applications of materials science and engineering due to its interdisciplinary nature in the field of dentistry. As students are required to comprehend and justify the selection of various dental materials, hands-on experience in their pre-clinical education is of utmost importance. For instance, practical sessions on manipulating different materials may be arranged following theoretical lectures. Thus, the ability to actively apply the theories of materials science to clinical content is what constitutes mastery in dental materials science courses, which goes beyond how well a student can recall and repeat factual information. In addition, to incorporate more hands-on sessions, the dental materials science curriculum should consider diverse pedagogical methods including but not limited to concept mapping, flipped classroom, micro-teaching, jigsaw, small-group discussions, and team-based learning. Although these methods are experimented in the literature, there is limited published evidence in Malaysia (Bhat et al., 2021).
The current discipline-based curriculum in Malaysian dental education consists of a stack of separate courses with their compartmentalised scopes and syllabus. Students may find it difficult to correlate theoretical knowledge and clinical application due to the lack of integration between preclinical and clinical courses. An integrated competency-based curriculum could overcome this dilemma by incorporating dental materials science into the list of courses that demand vertical and horizontal integration. Integrated curriculum as a visionary change could be regarded as one of the first instances in Malaysian dental education, where dental materials science is no longer viewed as a stand-alone course or under the aegis of a particular dental speciality. In fact, it will be divided into several subtopics that are integrated into several dental specialities across the preclinical and clinical phases. For instance, topics like amalgam and dental composite resin can be incorporated in conservative dentistry courses, whilst removable prosthodontics courses can cover dental materials like resin polymer and gypsum. As students are transitioning into clinical years, dental ceramics can be integrated into fixed prosthodontics courses.
A well-designed dental materials science curriculum must take assessments into consideration since it reflects how the documented curriculum is related to the outcomes (e.g., the student’s learning experiences, course learning outcomes and learning opportunities). If the dental materials science curriculum is to be revised to accommodate horizontal and vertical integrations, then a myriad of assessments should be utilised. Interdisciplinary care and evidence-based treatments with sound analytical and communication skills, are necessary for the successful and efficient delivery of tomorrow’s dental education. This justifies the need for assessment systems to be thorough and concrete enough to evaluate every stage of students’ progression. Although dental schools in Malaysia have been utilising written assessments (e.g., multiple choices questions, short answer questions) as the main assessment tool in dental materials science courses, alternative assessments such as modified Direct Observation of Procedural Skills (DOPS), peer- and self-assessments could be introduced in accordance with an integrated curriculum (Ferris & O’Flynn, 2015). These alternative assessments are valid and reliable in determining competencies and offering exceptional chances to combine summative and formative assessments. It is expected that students would be capable of recognising knowledge and skills, and they would value opportunities for improvement in their learning (i.e., self-reflection).
Moreover, Malaysian dental schools should consider recruiting faculty members with different areas of educational expertise in teaching dental materials science courses. Diversity of teaching staff will enhance and enrich the learning experiences of students. Experts with backgrounds in chemistry and materials science could involve in the teaching of fundamental principles of dental materials, while those with dental degrees may involve in translating the knowledge into practical applications. It is also worth noting that no single faculty member is recommended to cover the whole teaching and learning syllabus. Last, teaching qualifications are highly recommended for faculty members to apply and keep abreast with the latest instructional design. Nevertheless, the movement toward competency-based education (and moving away from traditional discipline-based or requirement-based education) would require more education research and academic discussions in Malaysia to rationalise and select appropriate teaching, learning and assessment methods as well as intellectual vibrancy, academic support, research, scholarship, and educational management in dental materials science courses.
VI. CONCLUSION
Malaysia is on the verge of advancing towards competency-based dental education along with the introduction of a diversity of teaching, learning and assessment methods. The path to change is not without obstacles and ambiguity. Thus, comprehensive education research and academic discussions among dental educators in Malaysia involved in the teaching of dental materials science are warranted to pioneer new insight to transform the existing dental materials science curriculum.
Notes on Contributors
GSSL and CCF was involved in conception and design of the study. GSSL and YSN reviewed the literature, collected the data, and wrote the original draft. CCF edited the original draft. All authors have read and approved the final manuscript.
Funding
No funding is required for this paper.
Declaration of Interest
All authors have no conflicts of interest.
References
Bhat, S., Madiyal, A., & Babu, G. S. (2021). Innovative teaching methods in dental education. Gülhane Medical Journal, 63, 8-13. https://doi.org/10.4274/gulhane.galenos.2020.1181
Ferris, H., & O’Flynn, D. (2015). Assessment in medical education; What are we trying to achieve? International Journal of Higher Education, 4(2), 139-144. https://doi.org/10.5430/ijhe.v4n2p139
Malaysian Dental Council. (2021). Competencies of new dental graduates, Malaysia-V2-2021. Retrieved September 23, 2022, from https://mdc.moh.gov.my/uploads/competencies_of_new_dental_grad_20222.pdf
Qazi, H. S., Ashar, A., & Ahmad, S. A. (2019). Impact of an innovative approach of teaching science of dental materials on the learning experiences of undergraduate students. Pakistan Armed Forces Medical Journal, 69, 582-588.
Soni, V., Kotsane, D. F., Moeno, S., & Molepo, J. (2021). Perceptions of students on a stand-alone dental materials course in a revised dental curriculum. European Journal of Dental Education, 25, 117-123.
*Galvin Sim Siang Lin
Department of Dental Materials,
Faculty of Dentistry,
Asian Institute of Medicine,
Science and Technology (AIMST) University,
08100, Bedong, Kedah, Malaysia
Email: galvin@aimst.edu.my
Submitted: 30 July 2021
Accepted: 4 October 2021
Published online: 5 April, TAPS 2022, 7(2), 1-5
https://doi.org/10.29060/TAPS.2022-7-2/GP2663
Mary Anne Reid1 & Kirsty Forrest2
1Senior Policy Officer, Medical Deans Australia and New Zealand, Australia; 2Dean of Medicine, Faculty of Health Sciences and Medicine, Bond University, Australia
Abstract
Introduction: This article summarises a report published in July 2021 by Medical Deans Australia and New Zealand (Medical Deans), the peak body representing the 23 medical programs in Australia and New Zealand. It explores how medical schools responded to the early impacts of COVID-19 in 2020, and how they might build on some of the changes to achieve fundamental improvements in medical education in Australia and New Zealand.
Methods: The Medical Deans report was based on: Responses to a survey midway through 2020 of its member schools about their experiences during the initial lockdowns; the contributions of presenters at the Medical Deans 2020 Annual Conference; subsequent discussions among communities of practice.
Results: Innovations introduced in response to the pandemic, included greater equity of learning opportunities across geographical locations; health services taking more responsibility for clinical placements; greater emphasis on competencies and less on clinical rotations in specific disciplines; strong collaboration between medical schools, and with providers in the medical training and research pipeline. Challenges include balancing the benefits of online learning with the need for human connection and a chronic lack of clinical training opportunities in community-based care.
Conclusion: While the impact of the pandemic on medical education and training was costly for all involved – both financially and personally – the scale of disruption provided a unique opportunity for step change. To fully realise this potential moving forward, medical schools will need to work in partnership with all those involved: students, health services, prevocational training, specialist colleges, regulators and governments.
Practice Highlights
- Equity of learning opportunities across rural, regional and urban locations using digital technology.
- Enhanced learning outcomes through a blend of remote and face-to-face teaching and assessment.
- Shared responsibility for medical students’ clinical placements as an essential part of the health system.
- More emphasis on student competencies and less on clinical rotations in specific disciplines.
- Strong collaboration between medical schools and across the training pipeline.
I. INTRODUCTION
Medical schools in Australia and New Zealand graduated close to the anticipated number of new doctors (3,800) at the end of 2020 – a significant feat given the size and number of shockwaves sent through the sector by the pandemic. Despite the immense stress COVID-19 placed on the sector, it was also the catalyst for significant innovation.
This article summarises the findings of a report published in July 2021 by the peak body representing the 23 medical schools in the two countries, Medical Deans Australia and New Zealand (Medical Deans). The report, Changing for good: What we learned in 2020 (Medical Deans Australia and New Zealand, 2021a), explored those innovations which occurred during the pandemic that medical schools want to retain and build on in the future. It also identified some critical gaps and problems highlighted by the pandemic that must be addressed moving forward.
II. METHODS
The report was authored on the basis of: responses to a survey run by Medical Deans Australia and New Zealand (MDANZ) midway through 2020; the contributions of presenters at the Medical Deans’ 2020 Annual Conference; subsequent discussions among Medical Deans’ communities of practice.
Where quotes are attributed to a particular person, they are drawn largely from the Annual Conference. Where quotes are attributed to a medical school rather than a person, they are drawn from the Medical Deans survey.
III. RESULTS
A. Innovation through Online Learning
As campuses closed early in 2020, schools employed a combination of pre-recorded sessions and interactive online lessons to deliver much of the non-clinical, and a small part of the clinical, medical curriculum to students. This created a sense of unity amongst students in different geographical locations as they all accessed the same lessons online – reducing disparities sometimes faced by those in regional and rural areas.
- University of Auckland: We have done much more synchronous learning across sites – we have eight sites in each clinical year across the north island – and we’re going to keep that.
- University of Newcastle: We’ve found that the expert facilitating a learning session can now be based anywhere and it works well.
- University of New South Wales: We have students at five metro hospitals and at least five rural ones, plus those in GP placements, who can now join each other in learning activities online. Prior to this, the rural students often felt left out of tutorials and activities that the metro students could get to.
The move out of the lecture theatre also allowed more flexibility for students in accessing lessons and interactivity, through online chat functions, and encouraged the use of advanced digital learning platforms. Small group tutorials used online tools to imitate some aspects of face-to-face clinical teaching and assessment, for example, Zoom rooms for interactions with actors or Objective Structured Clinical Examinations (OSCES).
- Sydney: The live Zoom component of the flipped classroom, with two experts (one monitoring chat), has proven very interactive and popular compared to a large lecture theatre. It also allows for more polling, which the students enjoy. With a cohort of 270, we saw increases from an average of 60-80 participants [25%] in lecture theatre mode to up to 210 participants on Zoom [75%].
However, there were also significant problems associated with delivering so much of the curriculum remotely. Online fatigue and the loss by students of a human connection with their peers and teachers was extremely stressful for many, particularly for international students, some of whom were far away from home for the first time. Another cohort at a particular disadvantage were the first-year students who did not get the chance to attend their university campus or make friends in this new phase of their life before the COVID lockdown.
Another issue for students was that access to adequate technology and learning space offsite was not always adequate, despite schools’ best efforts.
“The presumption in delivering medical training online is that all students have equal access to the technology, and that presumption is not correct,” said Professor John Fraser, University of Auckland’s Executive Dean of Medicine and Health Sciences. “Technology comes at a cost and not all students have enough resources to meet their technological needs. Also, the idea that each student has a space of their own to do their online learning is not always the case.”
Finally, medicine uses a very hands-on, apprentice-based educational approach, and there was only so much that could be done remotely.
Professor Fraser “There is so much subtlety in the way you learn in a clinical environment that it cannot be properly replicated online.”
The future of medical education lies in developing and refining the optimal blend of face-to-face and remote learning and assessment. Getting the balance right will be an ongoing priority for medical schools. By comparing approaches, medical schools have the best chance to determine the optimum mix of remote learning for their individual medical programs. This will be a continuing focus for medical schools, through the Medical Deans’ Medical Education Collaborative Committee (MECC). The University of Notre Dame Australia’s Dean of Medicine, Gervase Chaney, told the 2020 MDANZ Annual Conference that there was an opportunity to implement long-lasting change: “I think we’ve learned that if we are going to get value, we’re not going to be bringing our students on to campus four or five days every week. We’ll be looking at a more flexible learning approach and they can still be doing some clinical skills training – like the history-taking over Zoom or other online platforms. It’s a case of how we normalise this so that when students step into the clinical space, it’s a natural step for them.”
B. New Approaches to Clinical Learning
After an initial halt during the onset of the pandemic, clinical placements for later-year medical students were largely re-instated in 2020.
In Australia, one of the defining features of these new-style placements was the emphasis on shared responsibility between medical schools and health services. Medical schools collaborated as never before with each other and with health services on a range of clinical placement models and paid positions for medical students as part of the surge workforce. While remunerated roles already existed for final year students and pre-interns in other countries, including New Zealand, they were a first for Australia.
These new approaches to clinical placements and paid positions had the following features in common:
- the learning needs of the student were explicit and central
- the role of the student, and their scope of practice within the healthcare team, was more clearly defined and articulated
- medical schools and health services shared core responsibilities for students and the success of their placements
There was strong and widespread support from Australian medical schools for the benefits brought by this shared responsibility for medical students on placement or working within healthcare environments.
Another key shift in clinical training came about due to the need to minimise patient exposure to multiple healthcare workers: in many cases, students were placed for longer periods of time in general wards caring for patients with a range of medical conditions, and their rotations in some medical specialties were cancelled (e.g. obstetrics and gynaecology, intensive care). Students reported feeling more connected to the other health professionals they worked alongside during these longer placements and more able to make a valuable work contribution to patient care.
The Deputy Vice Chancellor, Tropical Health and Medicine at James Cook University, Richard Murray, believes this provided greater exposure for students to whole-of-patient care: “The clinical phase of medical education has traditionally been carved into different rotational experiences across medical disciplines and cemented in place through departments, budgets and staffing. COVID-19 has driven more learning around the integrated experience of patients. Rather than curriculum by a set of rotations, you have curriculum according to people of all ages and with all sorts of problems, which are often complex and interrelated. Learning is more integrated now.”
This discussion is furthered in the Medical Deans advocacy document Training tomorrow’s doctors – All pulling in the right direction (Medical Deans Australia and New Zealand, 2021b), with a number of recommendations for change. One of these is for regulators, medical schools and jurisdictional health service providers to build on the insights from the evaluation of the Assistants in Medicine role piloted in response to the pandemic in NSW in 2020 (New South Wales Health, 2021) and the New Zealand Trainee Intern model, to develop a shared and explicit understanding of what is needed to be prepared for practice; and to strengthen arrangements for students’ transition from medical school to employment.
C. Collaboration on Core Competencies
Also supporting this more generalist approach was the co-development by schools of an agreed set of core competencies needed for final-year medical students to progress to graduation.
This unprecedented collaboration between universities saw medical schools co-develop the common core competencies needed to graduate as a means of quality assuring the rapid and extensive changes made to their programs and placements due to the pandemic. Developed through the Medical Deans’ MECC, these core competencies were based on the schools’ own course outcomes and aligned with those required by the Australian Medical Council.
- Deakin University: We now have clear competencies mapped for internship – extended to the penultimate year. It is now less about the rotation and more about the competencies.
- University of Auckland: Based on our local graduate learning outcomes, we are emphasising core competencies over disciplinary learning outcomes. We are emphasising generic skills and capabilities.
The collaboration between medical schools during 2020 – culminating in the collaboration on core competencies – was amongst the most ranked highly ranked innovations of period which resulted in the Guidance statement: Clinical practice core competencies for graduating medical students (Medical Deans of Australia and New Zealand, 2020).
“The challenges of COVID made us create these dynamic and interactive education teams consisting of students, academics, professional support, design and IT staff all working together on re-developing format, content and assessments,” said University of NSW’s Associate Professor Torda. “At university level we did this across faculties; nationally, we worked more closely together, through Medical Deans in particular, to share and solve problems.” (Medical Deans Australia and New Zealand, 2021a)
D. Lack of Opportunities in Community-Based Care
A pre-existing lack of clinical training opportunities for medical students in community settings – in aged care in particular and, in some places, in general practice – only worsened during the COVID-19 pandemic.
National and international studies show that health systems which provide strong primary care are more cost-effective and associated with a more equitable distribution of healthcare across the population (Australian Department of Health, 2019). Yet GPs are not resourced in the same way as hospitals to provide clinical training for medical students, which fuels an over-emphasis on clinical training in hospitals. COVID-19 highlighted this problem, with GP placements becoming variable in 2020, as practices scrambled to secure the Personal Protective Equipment needed to provide patient services and tended to view medical students as an additional burden rather than as part of the health workforce response.
In the case of aged care, the limited training opportunities for clinical training that existed prior to the pandemic were lost completely in 2020, as facilities moved to shield their vulnerable elderly residents from COVID-19.
We know that the aging populations of Australia and New Zealand will increasingly require non-hospital-based care to manage the chronic and comorbidity conditions that typically occur in older populations (Australian Department of Health, 2019). Medical schools and health services must work together and with governments to ensure that more quality clinical training opportunities are available for students in both community-based aged care and general practice. In addition, to develop and implement solutions effectively there has to be continued and stronger collaboration right along the medical training and research pipeline, from medical schools to specialist training.
No single strategy will address this problem; it will require a coordinated effort. Medical Deans is advocating for Australian and New Zealand governments to establish a taskforce comprising the key stakeholders responsible for designing and delivering medical education and training across all stages of the continuum to:
- co-develop future training models that target the priority areas of workforce need; and
- explore the possibility of a “flipped” model for community-based PGY1 and PGY2 doctors where the majority of their experience occurs in a community-based setting, rotating into hospitals for training as required.
IV. CONCLUSION
While the impact of the pandemic on medical education and training in 2020 was costly – both financially and personally – the scale of disruption provided a unique opportunity for step change. In many cases, the sudden and massive changes created strong potential for lasting improvement. In other areas, the pandemic highlighted cracks that already existed within the health sector (e.g. lack of clinical placements in community healthcare settings), which will require coordinated effort beyond the medical education sector to fix.
Medical Deans has incorporated and built on these key learnings with the development of a number of advocacy positions and documents. In addition to those reports already mentioned, the learning has informed the student support document Creating a culture of support – For medical students transitioning to practice (Medical Deans Australia and New Zealand, 2021c), as well as the Medical Deans’ submission to the consultation for the Australian Medical Council’s Review of the Accreditation Standards for Primary Medical Programs.
Medical schools are looking to capitalise on the resourcefulness and innovation of 2020 in all the ways highlighted in this article and the full report by Medical Deans. To fully realise this potential, they will need to work in partnership with all those involved: students, health services, prevocational training, specialist colleges, regulators, and governments.
Notes on Contributors
Mary Anne Reid developed the Medical Deans survey of members schools and collated its findings. She integrated these with elements of the presentations made at the 2020 Annual Conference, and other member discussions, to develop the structure and write the text.
Kirsty Forrest provided key editorial and supervisory input as the member of the Medical Deans Executive supporting the report.
Acknowledgement
The authors acknowledge the support of Helen Craig, Chief Executive Officer of Medical Deans, who came up with the idea for the report and provided guidance throughout.
Funding
There are no funding sources to declare.
Declaration of Interest
The authors declare that there is no conflict of interest related to this manuscript.
References
Australian Department of Health. (2019). National Medical Workforce Strategy Scoping Framework.
Medical Deans Australia and New Zealand. (2020). Guidance statement: Clinical practice core competencies for graduating medical students. Unpublished. Please contact Medical Deans to request a copy at admin@medicaldeans.org.au
Medical Deans Australia and New Zealand. (2021a, July). Changing for good: What we learned in 2020. https://medicaldeans.org.au/md/2021/07/Changing-for-Good-What-We-Learned-in-2020-Medical-Deans-report-July-2021.pdf
Medical Deans Australia and New Zealand. (2021b, September). Training tomorrow’s doctors – All pulling in the right direction. https://medicaldeans.org.au/resource/training-tomorrows-doctors-all-pulling-in-the-right-direction/
Medical Deans Australia and New Zealand. (2021c, October). Creating a culture of support – For medical students transitioning to practice.
New South Wales Health. (2021). Assistant in Medicine Evaluation Report.
https://www.health.nsw.gov.au/workforce/medical/Publications/aim-evaluation-report.pdf
*Mary Anne Reid
Medical Deans Australia and New Zealand,
19 Kent Street, Sydney, NSW 2000
Email: mreid@medicaldeans.org.au
Submitted: 14 June 2021
Accepted: 22 July 2021
Published online: 4 January, TAPS 2022, 7(1), 3-8
https://doi.org/10.29060/TAPS.2022-7-1/GP2655
Nagisa Shinagawa1, Tomoaki Inada2, Harumi Gomi3, Haruko Akatsu3, Motofumi Yoshida3 & Yutaka Kawakami3
1Graduate School of Medicine, International University of Health and Welfare, Japan; 2International Center, Jumonji University, Japan; 3School of Medicine, International University of Health and Welfare, Japan
Abstract
Introduction: The International University of Health and Welfare (IUHW) School of Medicine was founded in 2017 with the intention of providing medical content in English a historical first in Japan. Twenty international medical students have been accepted annually, with the majority possessing less than beginner level Japanese language proficiency at the time of enrolment. However, proficiency in Japanese, especially in the context of medicine is required for academic success and program completion. To address this, the IUHW School of Medicine has developed a course in medical Japanese with the objective of facilitating international students’ acquisition of medical Japanese and reinforcing such acquisition through various listening, speaking, reading, and writing activities. This study aims to describe the Japanese language education program for international students at the IUHW School of Medicine, with particular focus on the development of the curriculum and course content.
Methods: The course is designed based on the following educational strategies and their applications: (a) Synchronisation of both medical and Japanese contents; (b) Collaborative learning; (c) Japanese output of medical content learned in English; (d) Practical output through making/giving a presentation and discussion with medical experts; (e) Detailed language feedback from language experts; (f) Reinforcing the vocabulary knowledge by writing; and (g) Building up vocabulary and expressions with relevant contents.
Results: Our observations suggest that our international students have been able to continue their medical education in Japanese smoothly.
Conclusion: The content-based instructional design that includes second language acquisition strategies may also be applicable to other Asian languages such as Korean and Chinese.
Practice Highlights
- We have developed a medical Japanese language course to facilitate international students’ acquisition of Japanese medical language and to reinforce such acquisition through various listening, speaking, reading, and writing activities.
- According to the course design, Japanese language teachers introduce medical vocabulary and expressions into their lessons, and medical teachers determine their application by checking for errors in their Japanese-language presentation of medically-related content.
- This is the first effort in Japan to systematically teach medical Japanese to international students at the elementary level at a medical school.
- This approach has had a positive effect on international students’ acquisition of medical Japanese.
I. INTRODUCTION
International medical students’ need for linguistic educational support has been well reported by researchers in various countries. Many international students in Europe and the United States who have passed the language proficiency tests of their host institutions and are judged to have high language proficiency reportedly continue to have language-related problems in their academic and clinical work at medical schools (Michalski et al., 2017). To address this issue, educational courses for international students studying medicine in a second or third language are being implemented (Huhn et al., 2018). Although reports of such efforts in Chinese medical schools have surfaced in recent years (Zhang et al., 2019), no reports on systematic Japanese language education for international medical students have been published, in part due to the small number of international students in Japanese medical schools.
At the International University of Health and Welfare (IUHW) School of Medicine in Japan, 20 international medical students have been accepted annually since its foundation in 2017. However, the majority of admitted international students have possessed less than beginner level Japanese language proficiency at the time of enrolment. Notably, although international students have been accepted at university medical schools in Japan in the past, most of them have had high levels of Japanese language proficiency at the time of admission.
IUHW School of Medicine’s admission policy is as follows:
“Students must have achieved outstanding grades, outstanding English capability, a future-oriented and global outlook, and be strongly resolved to contribute to the development of the fields of health, medicine, and welfare in both their home country and the global community, in response to medical needs in Japan and overseas.”
This policy of accepting international students with limited Japanese proficiency is to facilitate the acceptance of outstanding students from Asia regardless of their Japanese ability and thus train them to become international medical doctors.
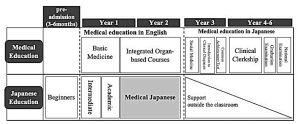
Figure 1. Medical Education Curriculum (top row) and Japanese Education Curriculum (bottom row) at International University of Health and Welfare School of Medicine, Japan
Figure 1 presents a simplified version of the curriculum of IUHW School of Medicine as well as the Japanese language education curriculum. At IUHW, medical education is carried out in English during the first two years of the six-year curriculum. International students come to Japan three to six months prior to entering medical school and attend several intensive pre-admission Japanese language courses. It is a condition of admission that students must acquire a beginner’s level of general Japanese before entering medical school. After enrolment, international students learn medicine together with Japanese students in English, while simultaneously continuing to learn Japanese. From the third year onwards, they learn medicine in Japanese and take the Common Achievement Tests (CAT) in Japanese; these comprise computer-based testing (CBT) for medical knowledge and an objective structured clinical examination (OSCE) on clinical skills. Both components are national tests that determine progression to the following year of study. All medical students in Japan must pass the CAT to proceed to a clinical clerkship. Essentially, passing the CAT is the prerequisite for passing the National Medical Licensure Examination, required to practice medicine as a physician in Japan.
To date, medical Japanese has rarely been research on the efficiency and methods of teaching medical Japanese to foreign students is rare due to the relatively small number of international medical students and foreign doctors in Japan. However, in recent years, research has revealed that medical Japanese is a distinct language that includes grammar and expressions that differ from general Japanese, with 80% of the vocabulary not covered in general Japanese language education curricula (Yamamoto et al., 2018).
Considering the precedents of other countries mentioned above, the Japanese language is not an exception for international medical students in Japan. However, if only general Japanese language classes are conducted, students will not only fail to acquire the knowledge and operational skills of medical Japanese but will be furthermore unable to acquire and retain the vast quantities of medical terminology they will encounter. As such, the IUHW School of Medicine has developed its own course in medical Japanese.
This study aims to describe the Japanese language education program for international students at the IUHW School of Medicine, with particular focus on the development of the “medical Japanese” course and its content. It is hoped that this paper will contribute to the development of educational curriculums for international medical students especially those from Asian countries who plan to study medicine in a second or third language.
II. SCOPE AND BACKGROUND INFORMATION
IUHW School of Medicine’s international students are currently, from Vietnam, Myanmar, Cambodia, Indonesia, Laos, Malaysia, Mongolia, Korea, China, and the United States (As of 2020). Most are from Southeast Asian countries, and, as noted, they arrive in Japan three to six months before beginning formal medical study with little or no Japanese language skills. At the IUHW School of Medicine, they begin learning Japanese from the “Hiragana”, a sort of Japanese language alphabet similar to the ABCs of English. After completing the beginner level course, they begin the formal study of medicine, and they will continue studying Japanese along with medicine in all years of study. The first and second semesters of the first year are dedicated to intermediate level study and the third term of the first year to the third term of the second year, they learn medical Japanese.
The objectives of the medical Japanese course are facilitating students’ acquisition of medical language through various listening, speaking, reading, and writing activities, reinforcing such acquisition, and developing their ability to deliver presentations in Japanese based on medical knowledge acquired in English. It was designed to provide content-based instruction (Grabe & Stoller, 1997) and was developed using various approaches to second language acquisition, such as collaborative learning and output-based activities.
Adult learning theory is the theoretical background for the development of this course. “A need to know” is an important element of adult learning theory. As students aim to become physicians in Japan, they often feel a strong need to acquire Japanese language skills and academic proficiency in Japanese. Particularly, since they know they will be studying medicine in Japanese from their third year on, they feel they must acquire medical Japanese before that time. As such, using medical content for Japanese language learning can satisfy this need and assist them in maintaining their internal motivation to learn. This leads us to “motivation to learn,” another important element of adult learning theory.
Adult learning theory focuses on self-directed learning involving the teaching of adults to be in control of their learning. Since students study medicine in English daily during their first two years of medical education, synchronising medical content with Japanese medical language learning facilitates their learning of medical terms, expressions, and phrases in Japanese using their existing knowledge. As they transit to studying medicine in Japanese from the third year onwards, international students become more autonomous inside and outside the classroom. Moreover, they work together with their Japanese classmates to utilise their content knowledge from the first two years to promote efficient acquisition of Japanese medical terms. From their third year of medical education onwards, since no additional formal Japanese language instruction is offered, international students are expected to primarily act as autonomous learners.
At the IUHW School of Medicine, from the third term in the first year to the end of the second year, the following 13 Integrated Organ-based Courses are provided: the Cardiovascular System, the Respiratory System, the Digestive System, the Endocrine System, the Renal System including Urology, the Gynecological System including the Mammary Gland, the Motor and Dermatological System including Connective Tissue, the Neurological System including Psychiatry, the Sensory Organ System, the Hematological System, Development and Abnormalities from Foetus to Child, Infectious Diseases, and Oncology including Radiotherapy and Palliative Care.
In the medical Japanese course, the units are aligned with the abovementioned specialties (see Figure 2). Group presentations are delivered on specific themes within those specialties. The composition of one unit is presented in Table 1. The teacher (hereafter “medical teacher”) of each organ-system subject selects four themes for each unit. For each theme, the key points to be learned in the second year are stipulated. For example, the Cardiovascular System medical teacher presents the key points, including pathology, epidemiology, diagnosis, treatment, and prognoses for various diseases (themes) such as hypertension, acute myocardial infarction, atrial fibrillation, and aortic stenosis.
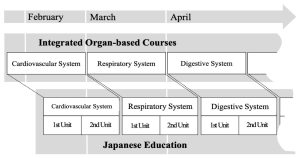
Figure 2. Linkage with Specialties
|
Time period |
Contents |
Details of Activities |
|
1 |
Vocabulary and contents learning |
Learning the vocabulary and contents of the theme using textbook. |
|
2 |
Presentation preparation |
Making the slides and the script |
|
3 |
Presentation rehearsal |
Check the slides and the script |
|
4 |
Presentation 1 |
・Presentation of the two groups ・Q&A session ・Plenary formative feedback session |
|
5 |
Presentation 2 |
・Presentation of the two groups ・Q&A session ・Plenary formative feedback session |
|
6 |
Presentation feedback |
・Individual feedback ・Overall general feedback ・Mini-reports |
|
7 |
Reading comprehension |
Reading the computer-based testing (CBT) workbook |
Table 1. Composition of One Unit
III. EDUCATIONAL STRATEGIES AND THEIR APPLICATIONS
We constructed the course based on educational strategies such as, synchronised medical contents and Japanese terms, small group discussion, and extensive reading, as detailed below.
A. Synchronisation of Both Medical and Japanese Contents
We intentionally synchronise the medical content and Japanese medical vocabulary to promote contextual learning for our students. The first hour of the session is preparatory time where the vocabulary and contents related to the particular theme. During this time, the vocabulary and expressions that are essential to the presentation are self-learned, after which class activities are carried out to reinforce understanding and apply content knowledge. As for the class activities, we conduct a variety of quizzes using interactive applications, such as Kahoot™ and Quizlet™. The Japanese language has three different sets of characters used in writing, and thus some medical terms are not easy for students to read. We use these interactive quiz applications to check for ability to read and comprehend each medical term.
B. Collaborative Learning
To promote deeper learning, group work for collaborative learning has been implemented.
In the second hour, students are divided into four groups, and presentation preparation is conducted. When the group leader initiates a review of the first session, the content of the theme is reconfirmed, along with the flow of the presentation and how the presentation frames should be distributed among the teammates.
Subsequently, students prepare the slides and presentation scripts individually, and then check with each other.
C. Japanese Output of Medical Content Learned in English
In the third hour, a rehearsal of the presentation is conducted, and two Japanese teachers listen to two group presentations (each 30 minutes per group). They write down any noteworthy points on a whiteboard and provide their feedback. They also check the slides for mistaken “Kanji” (Chinese characters in Japanese written format), for missing source references and pronunciation errors.
D. Practical Output through Making/Giving a Presentation, and Discussion with Medical Experts
In the fourth and fifth hours, presentations are made. In each hour, two groups deliver 15-minute presentations, each of which is followed by a 10-minute question and answer (Q&A) session and a 5-minute plenary formative feedback session. The medical teachers who teach the covered content in English listen to the presentations, answer questions, provide supplementary explanations, and correct students’ presentation as needed. The medical teachers use various categories to assess the presentations, such as the overall structure and appropriate application of medical knowledge. Simultaneously, the Japanese teachers assess the presentations for grammar and pronunciation.
E. Detailed Language Feedback by Language Experts
In the sixth hour, students will be given two types of feedback for the presentation: “individual feedback” and “feedback to everybody“. For the “individual feedback”, the students individually review their video-recorded presentations, based on a “presentation feedback sheet” created by the Japanese teachers. More specifically, this sheet includes comments about any pronunciation/expression errors made by the students. During “feedback to everybody”, the Japanese teacher explain and describe the Japanese expressions used by the students in the presentations and used by the medical teachers in the plenary formative feedback session, and the students further reflect on their Japanese.
F. Reinforcing the Vocabulary Knowledge by Writing
After receiving this feedback, the students write a mini-report. They are asked to summarise the contents of their presentations in a report, which is then reviewed by a Japanese teacher who corrects it and gives individual feedback later. It is generally desirable to learn specialised terms in the context of specialised subjects. It is also important to be exposed to the same words multiple times to acquire and retain vocabulary. By writing the summary related to the presentation contents, the students are given the opportunity to come into contact with medical terms multiple times.
G. Building Up Vocabulary and Expression with Relevant Content
In the seventh hour, extensive reading is conducted. Materials include the questions and commentaries for the 8–10 questions related to the presentation themes; these are selected by the medical teachers for each organ-system subject from a commercially available computer-based testing (CBT) workbook (Question Bank CBT, MEDIC MEDIA Co., Ltd.). It is important to note that the objective is not to answer comprehension questions but rather to understand the characteristic medical expressions, reinforce that understanding, and build vocabulary. Furthermore, the purpose is to familiarise the students with the question format in anticipation of the CBT examination they will undertake in their third year.
IV. DISCUSSION
This paper described the development of a medical Japanese course at the IUHW School of Medicine aiming to foster international students’ mastery of medical Japanese through various listening, speaking, reading, and writing activities.
Our observations suggest that IUHW School of Medicine’s international students have been able to continue their medical education in Japanese smoothly. The course assessment is based on the following two points: a vocabulary test for each Integrated Organ-based Course, and a rubric assessment by medical teachers and Japanese teachers at the time of presentation. In addition, we conducted questionnaires and interviews every end-of-semester with students. From the questionnaires, we could see that the students feel that this course will surely be useful for the medical school classes given in Japanese after the third year. The following compilation of comments from the interviews are illustrative: “I was able to reconstruct the fragmented knowledge in my mind by presenting in Japanese in this class what I learned in other medical courses in English.” “Since this class was synchronised with the medical courses, I was not only interested in giving my own presentation, but also in listening to other groups’ presentations.” “There were things that I did not understand in the medical courses that I was able to understand after listening to the presentations in this class.”
These results indicate that the Japanese medical course promotes students simultaneous learning of language forms (vocabulary, grammar, etc.) and medical content.
V. CONCLUSION
The content-based instructional design of our Japanese medical language course applies second language acquisition strategies simultaneously with adult learning theories such as contextual learning and collaborative learning. It is a teaching format for learning medical knowledge through the medium of English, and simultaneously learning another language other than English. In this case, the method was applied to Japanese language acquisition, specifically Japanese medical language acquisition. The method also offers scaffolding for international students to prepare them to continue their medical learning in Japanese on their own after the course. Having observed the Japanese language course over the three years since its implementation, we speculate that this method is applicable not only to the study of Japanese but also to the study in other Asian languages such as Korean and Chinese.
Notes on Contributors
NS reviewed the literature, designed the study and wrote the manuscript. TI advised the design of the study, gave critical feedback to the writing of the manuscript. HG gave scientific insight and advice, critically reviewed and edited the manuscript. HA, MY and YK have read and approved the final manuscript.
Acknowledgement
The authors wish to express sincere appreciation to Ahmed E. Hegab, Yuko Shiima, and Florescu M. Cosmin, International University of Health and Welfare, Medical School, for their constructive discussions and feedback during the preparation of this manuscript.
Funding
There is no funding for this paper.
Declaration of Interest
None of the authors have any competing interests.
References
Grabe, W., & Stoller, F. L. (1997). Content-Based Instruction: Research Foundations. https://carla.umn.edu/cobaltt/modules/principles/grabe_stoller1997/foundation.pdf (Accessed 7 April 2021).
Huhn, D., Al Halabi, K., Alhalabi, O., Armstrong, C., Castell Morley, A., Herzong, W., & Nikendei, C. (2018). Interactive peer-guided examination preparation course for second-year international full-time medical students: Quantitative and qualitative evaluation. GMS Journal for Medical Education, 35(5). https://doi.org/10.3205%2Fzma001203
Michalski, K., Farhan, N., Motschall, E., Vach, W., & Boeker, M. (2017). Dealing with foreign cultural paradigms: A systematic review on intercultural challenges of international medical graduates. PLOS ONE, 12(7), e0181330. https://doi.org/10.1371/journal.pone.0181330
Yamamoto, K., Inada, T., & Shinagawa, N. (2018). Ishikokkashikenno meishigoino taisuuyuudohini motozuku bunsekito kyoozaikaihatuno kanousei [Log-likelihood Analysis of Nouns in the National Examination for Medical Practitioners and the Development of Teaching Materials for International Medical Students]. Nihongo / Nihongo kyouiku. [Japanese/Japanese Education], (9), 245-260.
Zhang, J., Cheng, M., Guo, N., Xing, A., & Xu, L. (2019). ‘Standardized patients’ in teaching the communication skill of history-taking to four-year foreign medical undergraduates in the department of obstetrics and gynaecology. BMC Medical Education, 19(108). https://doi.org/10.1186/s12909-019-1541-y
*Nagisa Shinagawa
International University of Health and Welfare,
4-3 Kouzunomori, Narita,
Chiba 286-8686 Japan
Tel: +81-476-20-7701
Email: sinagawa@iuhw.ac.jp
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
