
From conflict zones to classrooms: Humanitarian deployments as catalysts for medical education
Submitted: 17 December 2025
Accepted: 6 April 2026
Published online: 7 July, TAPS 2026, 11(3), 1-7
https://doi.org/10.29060/TAPS.2026-11-3/GP3968
Mohamad Hamim Mohamad Hanifah1 & Jubaida Paraja2
1Department of Emergency Medicine and 2Department of Pathology and Microbiology, Faculty of Medicine and Health Sciences, Universiti Malaysia Sabah, Kota Kinabalu, Sabah, Malaysia
Abstract
Introduction: Medical education increasingly values experiential learning, yet the profound pedagogical potential of humanitarian deployments remains underexplored. This narrative review, based on a clinician-educator’s first-hand field experiences, argues that humanitarian fieldwork in conflict and resource-limited settings serves as a powerful catalyst for innovation in medical education, offering unique lessons that can transform teaching and learning.
Methods: Drawing on the author’s humanitarian missions in Bangladesh, Myanmar, Afghanistan, and Lebanon, this paper employs a reflective, practice-based analysis from a clinician-educator’s perspective. Key experiences are examined and systematically aligned with established educational theories, including transformative and experiential learning, to extract transferable educational principles and pedagogical strategies.
Results: The analysis identifies four critical themes from humanitarian fieldwork: ethics-in-action, cultural humility, resilience, and clinical improvisation. These themes were translated into concrete educational strategies–low-resource simulation, narrative medicine, case-based ethics, and train-the-trainer models–when integrated into formal curricula, significantly enrich student learning. They foster not only clinical competence but also empathy, ethical reasoning, and a sense of global citizenship.
Conclusion: Humanitarian medicine represents a powerful form of transformative professional development, where discomfort becomes a catalyst for growth. Integrating these field-derived lessons enhances teaching effectiveness, deepens reflective practice, and strengthens institutional capacity for global health education. These insights highlight the educational value of humanitarian experiences in cultivating resilient, ethical, and compassionate educators–qualities essential for preparing future-ready healthcare professionals.
Practice Highlights
- Humanitarian fieldwork generates critical educational themes.
- Low-resource simulation is a powerful, transferable pedagogical tool.
- Integrating authentic field narratives and ethical dilemmas into curricula.
- The “Train-the-Trainer” model empowers learners and builds sustainable capacity.
- Humanitarian deployments should be recognised as valuable faculty development.
I. INTRODUCTION
Modern medical education prioritises experiential learning to shape competent and compassionate healthcare professionals (Taylor & Hamdy, 2013). Among the most potent yet underutilised sources of this learning are humanitarian deployments. These missions place clinicians in conflict zones, disaster areas, and resource-limited settings, demanding not only clinical skill but also ethical sensitivity, cultural awareness, and logistical adaptability. For educators, they offer a transformative lens through which to re-examine teaching and curriculum design.
This narrative review is grounded in my first-hand experiences with humanitarian organisations in Bangladesh, Myanmar, Afghanistan, and Lebanon. Each mission, set against a backdrop of crisis, provided unique insights into healthcare delivery under extreme duress. More importantly, they revealed the essential competencies for humane and effective practice–skills increasingly vital in today’s unpredictable global health landscape.
I argue that humanitarian fieldwork, when critically reflected upon, is a powerful engine for educational innovation. By aligning field-based lessons with established educational frameworks, I demonstrate how these experiences can enrich mainstream medical education. My aim is to advocate their structured integration to foster a new standard of clinical excellence, empathy, resilience, and global citizenship.
II. FIELD-BASED LEARNING: THE WORLD AS A CLASSROOM
Humanitarian deployments are immersive, high stakes learning environments where conventional medical training is both tested and transcended. Far from the structured confines of academia, these missions unfold in unpredictable and resource-constrained contexts. They demand real-time clinical decision-making, deep cultural sensitivity, and the ability to improvise–skills often peripheral in standard curricula. My experiences across four distinct settings illustrate how such environments become unparalleled classrooms.
A. Bangladesh-Myanmar Food Flotilla (2017): Learning through Adaptability
During a maritime aid mission, bureaucratic delays in port clearance were inevitable. Instead of idling, we transformed this time into a training opportunity. Onboard the vessel, we conducted capacity-building sessions for volunteers, using realistic simulation drills for man-overboard and mass casualty scenarios. This was not abstract theory; it was essential preparation for potential emergencies at sea. The core educational insight was clear: when original plans fail, meaningful learning can still thrive if we reimagine our objectives with flexibility and purpose.
B. Afghanistan (2024): Education Amidst Extreme Scarcity
A mission to a high-volume maternity hospital in Kabul presented a starkly different challenge: profound resource scarcity. With only two CTG monitors for hundreds of high-risk patients, the constraint was omnipresent. Yet, the commitment of local staff was extraordinary.
Despite exhausting clinical shifts, they engaged deeply in hands-on workshops on basic life support (BLS), advanced life support (ALS), neonatal resuscitation, obstetric emergencies, and point-of-care ultrasound (POCUS). Navigating Dari and Pashto language barriers through interpreters and translated materials embedded inclusivity into our teaching. The most powerful validation came hours into the training, when a resident successfully revived a newborn using the techniques just practiced–a direct testament to the life-saving impact of contextually relevant education.
C. Lebanon (2025): Building Community Capacity
In Beirut’s Shatila refugee camp, the focus shifted to sustainable, community-based learning. Within the camp’s dense and fragile infrastructure, we delivered interactive simulation workshops on BLS, ALS, trauma care, and pain management to Palestinian healthcare providers. Physical space was limited, necessitating creative scheduling and use of communal areas. A pivotal moment occurred when a volunteer physiotherapist excelled in an ALS simulation. Recognising her potential, we empowered her to become a trainer herself. This outcome embodies a core educational principle: sustainable capacity is built by identifying and empowering talent within the community.
Collectively, these missions reveal field-based learning as a multidimensional crucible. It forges not only clinical competence but also emotional intelligence, cultural humility, and emergent leadership. This process aligns perfectly with Kolb’s (1984) experiential learning cycle, where concrete experience sparks reflection, conceptualisation, and active experimentation. In each setting, the field itself–with all its challenges–became the most authentic and relevant curriculum. A summary of these missions, their challenges, and derived educational themes is provided in Table 1.
|
Mission Location |
Context |
Key Challenges |
Educational Themes |
Pedagogical Translation |
|
Bangladesh (2017) |
Maritime humanitarian aid |
Restricted clinical access |
Flexibility, resilience |
Emergency drills, BLS training |
|
Afghanistan (2024) |
Maternity hospital |
Resource scarcity, language barriers |
Ethics-in-action, cultural humility |
Low-resource simulation, translated materials |
|
Lebanon (2025) |
Refugee camp |
Infrastructure limitations |
Empowerment, improvisation |
Train-the-Trainer model, peer teaching |
Table 1. Summary of Humanitarian Missions and Educational Insights
III. CORE EDUCATIONAL THEMES FROM THE FIELD
Beyond technical skills, humanitarian deployments expose broader, transformative themes that are difficult to replicate in a traditional classroom. From my missions, four essential themes emerge as critical for holistic physician development.
A. Ethics in Action
Medical ethics are often taught as abstract principles. In Kabul’s maternity hospital, they became urgent, daily dilemmas. With only two CTG monitors, deciding which high-risk patient received monitoring was a matter of distributive justice in real time. Allocating the last ICU bed or final dose of a critical drug required instant ethical reasoning rooted in clinical urgency and compassion. These experiences underscore that ethics must be taught as a dynamic, context-sensitive process, not a detached philosophical debate.
B. Cultural Humility and Linguistic Sensitivity
Effective cross-cultural practice requires cultural humility–an ongoing openness to self-reflection and acknowledgment of one’s limitations. In Kabul, this meant adapting all materials and using interpreters for Dari and Pashto speakers. In Shatila, it involved localising content into Arabic and framing it within the Palestinian refugee experience. These efforts shift the paradigm from one-way knowledge transfer to building collaborative learning partnerships that respect and integrate linguistic and cultural realities.
C. Resilience and Emotional Intelligence
The emotional weight of humanitarian work is profound. In Bangladesh, our team faced moral distress when logistical barriers prevented direct clinical care. Pivoting our role from healers to educators required significant emotional resilience and a reframing of purpose. Witnessing local providers in Lebanon continue to offer dignified care amidst overwhelming adversity highlighted the indispensable role of emotional intelligence–self-awareness, empathy, and peer support–as a core clinical competency.
D. Improvisation and Clinical Agility
Each mission demanded creative problem-solving. On a ship’s rolling deck in Myanmar, we adapted emergency drills to the moving environment. In Afghanistan, we taught ALS using minimal equipment, relying on inventive substitutions. In Lebanon’s cramped spaces, we redesigned schedules and used community resources innovatively. These experiences cement the value of “thinking on one’s feet”–maintaining safety and efficacy despite severe constraints, a skill of increasing relevance in all healthcare settings.
IV. PEDAGOGICAL TRANSLATION: FROM FIELD TO CURRICULUM
Transforming the raw lessons of humanitarian fieldwork into structured medical education requires more than storytelling–it demands intentional pedagogical design (Milota et al., 2019). My experiences have been translated into educational strategies, simulations, and reflective exercises that enrich clinical teaching and professional identity formation. These core strategies, their origins, and their educational benefits are outlined in Table 2.
|
Strategy |
Origin |
Educational Benefit |
Classroom Application |
|
Low resource simulation |
Afghanistan, Myanmar |
Adaptability, teamwork |
Emergency medicine modules |
|
Narrative medicine |
Lebanon, Bangladesh |
Empathy, identity formation |
Reflective writing assignments |
|
Train-the-Trainer |
Lebanon |
Leadership, sustainability |
Peer-led BLS/ALS sessions |
|
Case-based ethics |
Kabul |
Ethical reasoning |
Tutorials on distributive justice |
Table 2. Pedagogical Strategies Derived from Humanitarian Deployments
A. Simulation-Based Learning in Low-Resource Contexts
Simulation was a cornerstone of all field missions, proving that high-fidelity learning doesn’t require advanced technology. Inspired by maritime drills in Myanmar and low-equipment ALS simulations in Afghanistan, I developed low-resource simulation modules for students. These exercises challenge learners to manage emergencies with limited personnel and tools, emphasising adaptability, teamwork, and clinical reasoning over technical dependence.
B. Ethics and Cultural Humility through Case-Based Discussion
The ethical dilemmas of Kabul and the cultural adaptations of Shatila have been transformed into compelling case studies. Students now grapple with scenarios like triaging the last ICU bed, sparking deep discussions on justice in resource-poor settings. Cases involving language barriers prompt reflection on informed consent and cross-cultural trust-building, grounding abstract ethical principles in tangible complexity.
C. Narrative Medicine and Reflective Writing
Authentic field stories are powerful catalysts for discussion. The journey of the Shatila physiotherapist who became a trainer sparks conversations about identity, potential, and medicine’s social mission. Reflections on the pivot from clinical care to training in Bangladesh form the basis of writing assignments that help students process concepts of frustration, failure, and purpose, humanising their own educational journey.
D. Train-the-Trainer and Peer Teaching Models
The success of empowering local providers in Lebanon inspired the adoption of peer-teaching models in my home institution. Senior medical students now co-facilitate BLS and trauma sessions for their juniors. This reinforces their knowledge while developing essential skills in leadership, communication, and mentorship, creating a self-sustaining educational culture.
These translations are rooted in Mezirow’s (1991) transformative learning theory. The “disorienting dilemmas” faced in the field–ethical, cultural, logistical–act as powerful triggers for critical reflection. When imported into the classroom via simulation and narrative, they disrupt students’ assumptions about healthcare and their role within it, fostering the perspective shift essential for transformative growth. The complete model for translating humanitarian fieldwork into curricular innovation is illustrated in Figure 1.
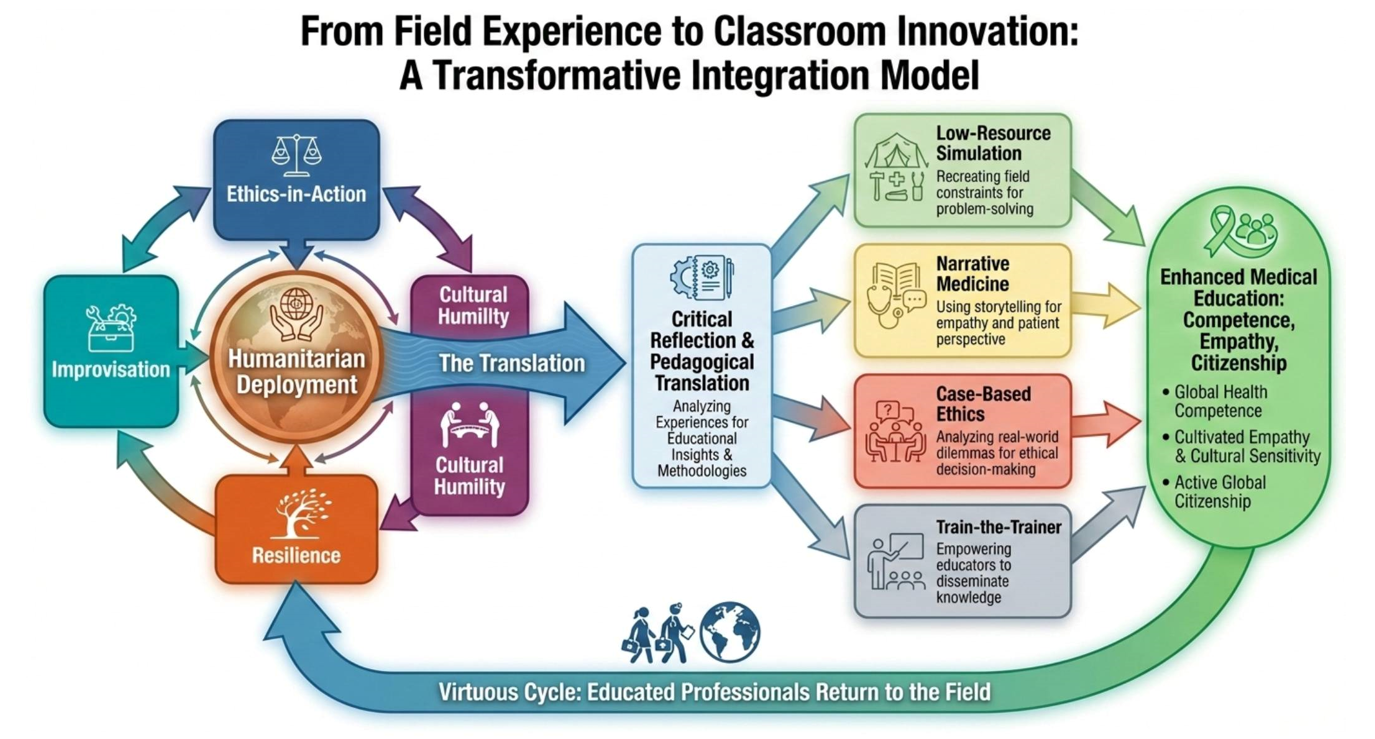
Figure 1: From Humanitarian Fieldwork to Curricular Innovation: A Model for Transformative Integration in Medical Education
(Note: This diagram illustrates the authors’ original conceptual framework and was visually rendered using OpenAI’s DALL-E 3 image generation tool on 17 December 2025.)
V. DISCUSSION: THEORETICAL ALIGNMENT AND INSTITUTIONAL IMPLICATIONS
The case for integrating humanitarian field experiences into medical education is strengthened by its firm grounding in foundational learning theories. This alignment provides a robust rationale for formal inclusion in faculty development and curriculum design.
A. Transformative Learning in Practice
Mezirow’s (1991) theory finds vivid expression in these missions. The discomfort and dissonance encountered are not impediments but the essential catalysts for deep learning. When educators model the vulnerability of grappling with ethical ambiguity or logistical failure, they give students permission to engage in the critical self-reflection necessary for their own transformative professional development.
B. Enacting the Experiential Cycle
These deployments perfectly illustrate Kolb’s (1984) experiential learning cycle. The concrete experience of teaching neonatal resuscitation in Kabul leads to reflective observation (debriefing), then to abstract conceptualisation (understanding the power of low-resource simulation), and finally to active experimentation (designing and implementing a new curriculum module). This cycle ensures field learning is an active, iterative process of knowledge creation, not a passive event.
C. Building Communities of Practice
The Train-the-Trainer model’s success in Lebanon is a direct embodiment of Lave and Wenger’s (1991) situated learning theory. By progressing from peripheral participant to central trainer, local volunteers fully entered their community of practice. Similarly, when students engage with these global health narratives, they begin to envision themselves as part of an international community of healthcare providers, fostering a sense of shared responsibility and belonging.
To harness this potential, institutions must act. Humanitarian work should be formally recognised as valuable Continuing Professional Development (CPD) for educators. Faculty development programs should incorporate modules on “contextual pedagogy,” teaching in low-resource settings, and using narrative and simulation drawn from global health. Creating structured platforms–such as dedicated grand rounds or digital story repositories–for faculty to share field-based insights can enrich an institution’s entire educational ecosystem.
Ultimately, humanitarian medicine teaches us to reframe discomfort. The field’s unpredictability, emotional intensity, and ethical complexity create a fertile ground for the deepest form of learning. By embracing these experiences as central to our educational mission, we can prepare a generation of physicians who are not only clinically expert but also emotionally intelligent, culturally humble, and equipped to lead in an uncertain future.
VI. CONCLUSION
Humanitarian medicine is more than service; it is a transformative educational journey. Stepping beyond institutional comfort zones fosters profound growth. These missions demanded a synthesis of clinical expertise, emotional resilience, cultural humility, and ethical clarity–the very qualities that define a compassionate, globally minded physician.
Challenges like language barriers, scarcity, and human suffering were not obstacles but essential catalysts for learning. These “disorienting dilemmas” prompted deep reflection, reshaped my professional identity, and inspired innovative approaches to teaching.
By integrating humanitarian narratives, low-resource simulations, and real-world ethical dilemmas into curricula, we bridge the gap between theoretical knowledge and practical wisdom. We invite learners to explore not just how to treat disease, but what it means to serve, lead, and care in adversity. These lessons cultivate empathy, global citizenship, and a service-oriented mindset–qualities indispensable in our interconnected world.
For educators, humanitarian deployments are unparalleled faculty development. They refine pedagogy, deepen reflective practice, and foster knowledge co-creation with diverse communities. Academic institutions must recognise and support these experiences not as extracurricular, but as essential to health professions education.
The most powerful education occurs in the messiness of real life–in refugee camps, on ships, in under-equipped hospitals, in moments of shared humanity. Here, textbook knowledge meets compassion, theory is tested by reality, and both learners and educators grow. Humanitarian medicine must be embraced not only as service but as a transformative force that teaches with both knowledge and heart.
Notes on Contributors
Mohamad Hamim Mohamad Hanifah conceived the work based on firsthand field experiences; acquired and interpreted the narrative data and drafted the initial manuscript and its critical intellectual content.
Jubaida Paraja contributed to the conceptual design of the pedagogical translation framework and critically revised the manuscript for important intellectual content.
All Authors provided final approval of the version to be published and agree to be accountable for all aspects of the work.
Acknowledgement
We are deeply grateful to the humanitarian partners and the dedicated local health teams in each field location for their partnership, resilience, and shared commitment to care under extreme conditions. Their work is the foundation of this reflection. We also thank our peers for their insightful comments during the development of this article.
Funding
No specific grant was received from any funding agency for the writing of this manuscript. The humanitarian deployments described were conducted in a voluntary capacity with various non-governmental organisations.
Declaration of Interest
The authors declare no conflicts of interest related to the research, authorship, or publication of this article.
Declaration of AI and AI-assisted Technologies in the Writing Process
All structural mapping, pedagogical pathways, and textual content were defined solely by the authors. Figure 1 illustrates the authors’ original conceptual framework and was visually rendered using OpenAI’s DALL-E 3 image generation tool on 17 December 2025.
References
Kolb, D. A. (1984). Experiential learning: Experience as the source of learning and development. Prentice-Hall.
Lave, J., & Wenger, E. (1991). Situated learning: Legitimate peripheral participation. Cambridge University Press. https://doi.org/10.1017/CBO9780511815355
Mezirow, J. (1991). Transformative dimensions of adult learning. Jossey-Bass.
Milota, M. M., van Thiel, G. J. M. W., & van Delden, J. J. M. (2019). Narrative medicine as a medical education tool: A systematic review. Medical Teacher, 41(7), 802–810. https://doi.org/10.1080/0142159X.2019.1584274
Taylor, D. C. M., & Hamdy, H. (2013). Adult learning theories: Implications for learning and teaching in medical education: AMEE Guide No. 83. Medical Teacher, 35(11), e1561–e1572. https://doi.org/10.3109/0142159X.2013.828153
*Assoc. Prof. Dr. Jubaida Paraja
Faculty of Medicine and Health Sciences,
Universiti Malaysia Sabah,
88400 Kota Kinabalu,
Sabah, Malaysia
Email: jubaida@ums.edu.my
Submitted: 8 August 2025
Accepted: 18 November 2025
Published online: 7 April, TAPS 2026, 11(2), 4-8
https://doi.org/10.29060/TAPS.2026-11-2/GP3842
Dujeepa D. Samarasekera1, Chung-Hsien Chaou2, Ardi Findyartini3, Jamuna Vadivelu4, Malcolm Mahadevan5, Yang Faridah Abdul Aziz6, Faith Chia7, Yeo Su Ping1 & Lee Shuh Shing1
1Centre for Medical Education (CenMED), Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Department of Emergency Medicine & Medical Education Research Center, Chang Gung Memorial Hospital, Linkou Branch, Taiwan; 3Department of Medical Education, Faculty of Medicine, University of Indonesia, Indonesia; 4Medical Education and Research Development Unit (MERDU), Faculty of Medicine, University of Malaya, Malaysia; 5Department of Emergency Medicine, National University Hospital, National University Health System (NUHS), Singapore; 6Department of Biomedical Imaging & Medical Education and Research Unit, Faculty of Medicine, University of Malaya, Malaysia; 7Department of Rheumatology, Allergy and Immunology, Tan Tock Seng Hospital, Singapore
Abstract
Introduction: The COVID-19 pandemic significantly impacted postgraduate medical education (PGME). This led to rapid adaptations to ensure training continuity and to develop competent healthcare professionals.
Methods: This descriptive study focusses on the sustainable innovations made in Indonesia, Malaysia, Singapore, Taiwan and the USA PGME residency training. Draft country sections were written by co-authors with direct, current knowledge of postgraduate training in those settings.
Results: Key lessons emerged from curricular adjustments, digital transformation, operational agility, assessments, and faculty development. Curriculum changes included integrating pandemic-specific content, such as COVID-19 management and public health priorities, into training programs. Singapore’s rapid revision efforts and Indonesia’s compulsory topic introduction are typical examples. Despite movement restrictions and constraints on clinical training, innovative solutions like simulations and telemedicine preserved skill development. Digital transformation played a crucial role, with countries adopting virtual platforms and hybrid simulation models. Technology-driven innovations like augmented reality and teleconsultation expanded training scopes. However, challenges like engagement, transitioning faculty to remote learning systems and unstable internet connectivity remained challenges. Operational agility was demonstrated through cross-institutional collaborations. Assessment formats evolved, with hybrid models and virtual logbooks introduced to maintain educational standards. Accreditation processes were adapted, with flexibility granted in assessment delivery while ensuring quality. Faculty development was accelerated with Singapore leveraging international trends to ensure resilience in local training programs.
Conclusion: The pandemic instigated a paradigm shift from reactive adaptation to proactive transformation in PGME, positioning systems as global exemplars of how medical education can evolve amidst complexity and incorporate necessary changes envisioning long-term strengthening of the systems.
Practice Highlights
PGME adaptation during COVID-19 pandemic and transformation post pandemic is supported by:
- Implementation of operational agility by placing residents in diverse environments and fostering national collaborations to sustain training.
- Integration of simulations and telemedicine to maintain skill development amid constraints during crisis situations.
- Development of teleconsultation and hybrid learning models to enhance inclusivity, accessibility, and resilience in medical education.
- Adoption of flexible models to accredit and sustain quality of training and accreditation of programmes.
- Evolvement of assessment and accreditation with hybrid models and virtual tools to preserve educational standards and flexibility.
I. INTRODUCTION
The COVID-19 pandemic has profoundly impacted postgraduate medical education (PGME) worldwide. The challenges and opportunities have led to significant transformations in how medical training is delivered (Sklar, 2020). This manuscript examines the experiences and adaptations to PGME in Singapore, Indonesia, Malaysia, Taiwan, and the USA. Draft country sections were written by co-authors with direct, contemporary knowledge of postgraduate training in each setting (authors are listed under Notes on Contributors). We used a shared template (curriculum changes; clinical exposure; digital transformation; assessments; faculty development; operational agility) to ensure comparability. Country drafts were iteratively edited centrally to harmonise scope and remove duplication. This manuscript is a descriptive synthesis of these country reports and the peer-reviewed literature cited.
A. Curricular Adjustments and Clinical Exposure
The onset of COVID-19 served as a catalyst for revising PGME curricula across the globe. In Singapore, the curriculum was quickly adjusted to include COVID-19 management and public health priorities. The curriculum in internal medicine and infectious diseases was updated to cover outbreak containment, infection prevention, and control. Emergency medicine and surgical specialties underwent targeted curricular revisions to embed pandemic-specific protocols and essential skills (Oon et al, 2023).
In Indonesia, while the curriculum remained largely unchanged, COVID-19 management became a compulsory knowledge area, with online courses and skills training introduced to equip residents for frontline duties. Residents gained competencies in global health problem management, highlighting the need for an integrated curriculum approach.
Malaysia adopted remote learning platforms for curricular delivery, introducing virtual ward rounds and telemedicine consultations. Training e-portfolios were developed to record and review trainee progress systematically. This shift presented new training opportunities, allowing engagement in telehealth and familiarisation with hospital delivery systems.
Taiwan leveraged its experience from previous outbreaks to make pandemic-related curricular adjustments, including telemedicine. Their curriculum stability stemmed from existing frameworks that allowed swift incorporation of new competencies such as video-assisted intubations.
In the USA, tele-supervision and tele-health were integrated into curricula, accommodating training disruptions with an emphasis on tele-consultation skills. The ACGME’s flexibility enabled programs to maintain educational continuity despite the challenges.
Clinical exposure faced challenges due to movement restrictions and infection control measures. In Singapore, inter-hospital rotations were halted. This limited the breadth of exposure but ensured procedural training through simulations and telemedicine. Indonesia encountered similar constraints. In addition to this, residents were developed as frontline healthcare workers combating the pandemic in the healthcare system. These circumstances led to urgent and creative adaptations in teaching and supervision formats to support skill acquisition. Cognitive components were taught online, while skill development was conducted in person in various possible and safe forms. These online learning methods have been further developed and integrated into current residency training programmes (Balakrishnan et al., 2020).
B. Digital Transformation in Teaching
The pandemic catalysed a rapid digital transformation in PGME, redefining teaching methodologies across countries. Singapore quickly transitioned to virtual platforms for didactic sessions, ensuring continuity and increasing accessibility. Simulation-based learning adapted to hybrid models, preserving educational value while meeting safety requirements. Emerging technologies like augmented reality have redefined surgical training, providing scalable educational models (Balakrishnan et al., 2020) (Renaud et al., 2021).
Indonesia embraced online learning, integrating video learning and flipped classrooms for cognitive acquisitions. However, engagement challenges persisted due to unstable internet connections and multitasking of both the consultants and residents during online sessions. Practical skill development continued in clinical settings with enhanced simulations and adapted supervision system.
Malaysia’s teaching innovations partially replaced face-to-face interactions with a hybrid approach, enhancing attendance monitoring and assessment efficiency. However, the “hidden curriculum” often delivered through personal interactions was less effectively communicated online (Yusoff et al., 2020).
Taiwan’s use of virtual simulations and online OSCEs (Objective Structured Clinical Examinations) allowed for skill development in an online environment. Challenges included financial limitations and resistance to change. Although most faculty members and students have become accustomed to online courses and virtual meetings in the post-pandemic era, face-to-face interaction still offers irreplaceable benefits, particularly in communication, engagement, and collaborative learning.
During the COVID-19 pandemic, postgraduate programmes across the USA reported a rapid expansion of both remote didactic sessions and tele-health patient encounters, though adoption varied widely across specialties. Psychiatry, internal medicine and paediatrics shifted substantial portions of clinical care and teaching online, whereas procedure-intensive fields such as surgery and obstetrics transitioned more selectively. Programme evaluations highlight that learning outcomes were most positive when virtual teaching incorporated interactive case discussions, small-group sessions, and real-time feedback rather than passive online lectures. Concurrently, the ACGME issued time-limited flexibilities on supervision and clinical learning environments, endorsing tele-supervision in appropriate contexts while safeguarding procedural competency standards. These experiences have accelerated national discussions on how tele-education and tele-supervision can be safely integrated into residency training. The ACGME’s ongoing review of its Common Program Requirements aims to include evidence-informed guidance on remote education, supervision, and competency assessment. Going forward, US training programmes are encouraged to document the impact of these modalities on trainee performance, patient outcomes, and wellbeing to inform sustainable, equitable models of postgraduate medical education.
C. Operational Agility and Workforce Planning
The pandemic presented unprecedented challenges for PGME operational management, requiring adaptive strategies to sustain training and healthcare delivery. Singapore implemented a “fostering” approach, integrating residents into alternative hospital environments to maintain clinical exposure. This model enriched training and spurred national coordination of residency programs, fostering cross-institutional collaborations. This is now ongoing and residents from different sponsoring Institutions (SI) have the opportunity to train and use learning resources from another Sis (Renaud et al., 2021).
Indonesia and Malaysia adapted their operational frameworks for remote learning, employing proctoring systems and modifying assessment methods. While these adaptations ensured quality, challenges remained in creating learning resources and encouraging faculty transition to online formats.
Taiwan maintained operational stability by leveraging past outbreak management experiences, while the USA’s ACGME allowed temporary emergency statuses for flexibility in training requirements.
D. Assessment and Accreditation
Assessment and accreditation processes were restructured to accommodate pandemic constraints while maintaining educational integrity. In Singapore, summative assessments shifted to hybrid formats, preserving fairness and rigour. Virtual logbooks and electronic portfolios were introduced, enriching formative assessment ecosystems.
Indonesia’s accreditation processes were simplified, conducting online exams with real-time monitoring. Malaysia faced accreditation delays due to SOP adjustments for virtual formats but integrated online assessments into credentialing processes.
Taiwan’s credentialing remained stable, with minor shifts toward competency-based medical education. Relevant assessment tools, such as milestones and Entrustable Professional Activities (EPAs), have been widely adopted across various specialty training programs nationwide. The USA maintained accreditation standards, adapting supervision practices and reporting on pandemic impacts in PGME activities.
E. Educational Innovations
The pandemic drove enduring innovations in PGME, including teleconsultation and hybrid learning models. The observed differences map to four system-level features. First, health system structure focusing on centralised systems (e.g., Singapore’s national clusters) were able to coordinate cross-institutional resources faster than highly fragmented systems. Second, resource availability determined technological sophistication (high in Singapore/US, constrained in parts of Indonesia/Malaysia). Third, accreditation flexibility and governance (e.g., ACGME guidance vs local regulator timelines) influenced how quickly assessments could be adapted. Finally, learning culture and prior outbreak experience (Taiwan’s SARS legacy) shaped faculty and trainee readiness to adopt remote modalities. Recognising these drivers helps tailor recommendations: resource-intensive tech works where funding and digital literacy permit, whereas low-cost simulation and task-sharing strategies are more applicable in lower-resource settings.
F. Faculty Development and Pedagogical Shifts
The global transformation in faculty development was accelerated by the pandemic, compelling educators to rethink teaching, assessment, and mentorship delivery. Singapore harnessed international innovations to enhance local faculty development, adopting flipped classroom models and microlearning inspired by global trends.
Participation in international faculty development programs enriched local practices, building faculty champions who guided reforms and shared Singapore’s innovations on global platforms. The USA encouraged programs to document faculty adaptation, recognising resilience as crucial to PGME sustainability.
By observing and adapting international best practices, local institutions weathered the pandemic’s educational storm and emerged with a more agile, inclusive, and scholarly approach to faculty development.
G. Postgraduate Medical Education in the Post-Covid Era
The COVID-19 pandemic disrupted traditional models of postgraduate medical education, prompting rapid shifts towards digital learning. Initially driven by necessity, these changes have since evolved into permanent components of contemporary curricula, reflecting the adaptability of residents, faculty, and institutions.
During the pandemic, clinical exposure was significantly curtailed, and the informal curriculum typically acquired through in-person interactions and experiential learning was diluted. In response, digital simulations, telemedicine, and virtual case-based discussions were introduced to bridge the gap. While these tools could not fully replicate the complexity of real patient care, they laid the groundwork for blended learning models that are now being refined and embedded into routine training.
Faculty development became a priority, with short, focused programmes in digital pedagogy helping educators gain confidence and competence in online teaching. Peer support networks and institutional incentives have further encouraged sustained engagement. These efforts have led to more inclusive and flexible teaching approaches, better suited to diverse learner needs.
Assessment practices also underwent transformation. Hybrid models combining online and in-person evaluations were trialled and are now being formalised, offering greater adaptability while maintaining rigour. Cross-institutional collaborations, initially formed to share resources during the crisis, have matured into structured partnerships that enhance access and quality across programmes.
Today, interactive digital platforms, gamification, and real-time feedback mechanisms are routinely used to foster engagement and recreate aspects of the informal curriculum. Augmented reality and high-fidelity simulations are increasingly integrated into clinical skills training, complementing supervised patient encounters. These innovations are not temporary fixes but strategic enhancements to educational delivery.
Equity remains a central concern. Institutions are investing in infrastructure and inclusive teaching strategies to ensure all trainees regardless of background can participate fully and benefit equally. The pandemic revealed gaps, but it also accelerated progress towards more resilient, responsive, and equitable systems.
Postgraduate medical education has not simply recovered it has reoriented. The adaptations made under pressure have become embedded practices, shaping a future that is more flexible, collaborative, and inclusive.
II. CONCLUSION
The COVID-19 pandemic influenced and accelerated innovations both necessary and lasting transformations in postgraduate medical education. Our cross-country comparison shows that the nature and scale of innovations were shaped by health-system structure, resource/digital readiness, accreditation flexibility and learning culture. Future resilience will depend on tailoring strategies to these systemic features investing in scalable, equity-minded digital solutions where resources permit, and prioritising low-cost, high-impact simulation and regional collaborations in lower-resourced settings.
Notes on Contributors
Yang Faridah Abdul Aziz, Chung-Hsien Chaou, Faith Chia, Ardi Findyartini, Malcolm Mahadevan Jamuna Vadivelu drafted the respective portion for their countries and subsequently, the manuscript was combined and edited by Dujeepa Samarasekera, Lee Shuh Shing and Yeo Su Ping. All the authors read the final version and provided their suggestions and/or approvals.
Acknowledgement
We would like to thank Prof Timothy Brigham and Prof Lynne Kirk for their perspectives on the initiatives rolled out in the United States of America during the pandemic.
Funding
There is no funding for this study.
Declaration of Interest
The authors declare no conflict of interest.
References
Ashokka, B., Ong, S. Y., Tay, K. H., Loh, N. H. W., Gee, C. F., & Samarasekera, D. D. (2020). Coordinated responses of academic medical centres to pandemics: Sustaining medical education during COVID-19. Medical Teacher, 42(7), 762-771. https://doi.org/10.1080/0142159X.2020.1757634
Oon, J. E. L., Mok, S. F., Samarasekera, D. D., & Teunissen, P. (2023). Training infectious diseases senior residents during COVID-19: The impact and the lessons learnt. Medical Teacher, 45(9), 1005-1011. https://doi.org/10.1080/0142159X.2023.2168182
Renaud, C. J., Chen, Z. X., Yuen, H. W., Tan, L. L., Te Pan, T. L., & Samarasekera, D. D. (2021). Impact of COVID-19 on health profession education in Singapore: Adoption of innovative strategies and contingencies across the educational continuum. The Asia Pacific Scholar, 6(3), 14-23. https://doi.org/10.29060/TAPS.2021-6-3/RA2346
Sklar, D. P. (2020). COVID-19: Lessons from the disaster that can improve health professions education. Academic Medicine, 95(11), 1631-1633. https://doi.org/10.1097/ACM.0000000000003547
Yusoff, M. S. B., Hadie, S. N. H., Mohamad, I., Draman, N., Al-Aarifin, I. M., Rahman, W. F. W. A., … & Yaacob, N. A. (2020). Sustainable medical teaching and learning during the COVID-19 pandemic: Surviving the new normal. The Malaysian Journal of Medical Sciences: MJMS, 27(3), 137-142. https://doi.org/10.21315/mjms2020.27.3.14
*Dujeepa D. Samarasekera
Yong Loo Lin School of Medicine,
National University of Singapore, Singapore
10 Medical Drive, Singapore 117597
Email: dujeepa@nus.edu.sg
Submitted: 21 December 2024
Accepted: 14 May 2025
Published online: 6 January, TAPS 2026, 11(1), 4-8
https://doi.org/10.29060/TAPS.2026-11-1/GP3610
Ganesh Ramachandran1, Aung Ko Ko Min2 & Vivian Fernandez1
1School of Medicine, Faculty of Health & Medical Sciences, Taylor’s University, Malaysia; 2Faculty of Medicine, MAHSA University, Malaysia
Abstract
Introduction: The provision of higher education has been for the longest time the responsibility of the state. With increasing demands for places in institutions of higher learning, there has been increasing involvement of the non-public (private) sector in this area. The extent of this involvement is wide and encompasses both nonprofessional and professional qualifications. This involvement has brought the issue of ensuring that graduates from the non-public sector institutions are on par with their public sector counterparts.
Methods: This paper looks at strategies that are in place or that may be employed to ensure that the non-public sector plays its part in developing holistic and fit for purpose healthcare practitioners with a primary focus on the Malaysian doctor. It is largely based on the local landscape, referring to global standards, expectations and recommendations.
Results: Developing a holistic healthcare practitioner begins with appropriate selection and delivering accredited standardised training and assessment.
Conclusion: It is expected that these strategies are similar for all healthcare professionals, and that adhering to the required measures will meet the expectations of the primary stakeholder, the patient.
Practice Highlights
- A holistic healthcare professional is knowledgeable, skilled and will have the required affective attributes to provide safe, high quality and empathetic healthcare with an emphasis on prevention of disease and staying healthy.
- This requires the selection of appropriate candidates, standardised training and assessment to produce a fit for needs practitioner.
- Defined standards will ensure that we are able to meet this aim more effectively.
I. INTRODUCTION
The Good Medical Practice Guide of the Malaysian Medical Council (2019) states that “the doctor is traditionally held in esteem by society as a highly qualified professional who is expected to serve his fellow human beings in a dedicated and selfless manner. His opinion on matters, not just medical, is often sought and received with respect.
As such while theoretical knowledge, practical and clinical skills are a given requirement for a doctor or any healthcare professional, these must be complemented by a good standard of soft skills that are necessary to meet the demands of the end users, primarily the patient, family and the employing authority (AlThukair & Rattray, 2023).
II. DEVELOPING A HOLISTIC HEALTHCARE PRACTITIONER
Traditionally, tertiary education as a whole and tertiary education leading to a professional qualification in particular has always been within the realm of the public sector or the state.
This has changed because of increasing demands and “democratisation” of all areas of education including higher education. Regulations have been modified to attract international students and develop “educational hubs” in some countries. Economic considerations have resulted in decreased funding of public sector institutions making them unable to meet demands and appear inefficient in delivery, paving the way for the non-public or private sector.
The non-public sector contribution to higher education may be in the form of government aided institutions, not-for-profit institutions and for-profit institutions.
In developed economies such as the United Kingdom and the United States of America, private higher education providers comprise about 3% and 23% respectively of total enrolment. This is in contrast to Asia where as much as 80% depend on the private sector for higher education. In India, more than 50% of students are enrolled in private institutions. Korea reports figures as high as 85%, and in Malaysia up to 52% are enrolled in private institutions. Almost all of these are for profit institutions.
A study by the United Kingdom’s Centre for Global Higher Education looked at for-profit providers in six countries (USA, Germany, Australia, Poland, Japan, and Chile) and reported that the standards in these institutions tend to be inferior to that of a public institution. This finding gives rise to the possibility that standards in these institutions may be more malleable and that is worrisome for countries where the numbers seeking private higher education is high. This situation, if not addressed, will be detrimental to the healthcare provisions in the country in the middle and long term.
Inevitably, the perception of private institutions is usually negative. They are perceived to be for profit and not particularly interested in quality, without any positive impact for the stakeholders and community. However, this is not entirely accurate. In many countries including Malaysia, these providers are regulated and must meet the standards of the accreditation agency in the country. In the case of Malaysia, it is the Malaysian Qualifications Agency and for medicine the standards are determined by the Malaysian Medical Council and contained in a document called the Standards for Undergraduate Medical Education (2nd edition 2022). All medical schools are regularly monitored, and accreditation is a requirement for recognition and registration with the council prior to employment as interns.
Having more medical schools will address the need for more locally qualified doctors and meet the needs of an increasing population. Prospective students will have increased choices in terms of institutions they choose to attend.
In the long run it will reduce dependence on an expatriate workforce by providing local doctors for a local populace. Job opportunities for qualified specialist staff will also increase with healthy competition between the public and private sectors.
Private institutions are also able to operate without too much dependence on policies driven by politics of the land and may be able to introduce more cutting-edge teaching and learning technologies because of financial viability and less red tape.
On the other hand, private institutions must always guard against being overwhelmed by the for-profit motive and must ensure that standards are not diluted. The institution must ensure employment of adequate numbers of trained academics to prevent any compromise in teaching, while investing in physical infrastructure, laboratory equipment, simulators, cadavers and prosected specimens among others. These schools may not be able to address the needs of the whole community because they are likely to be situated in urban and affluent environments and may contribute to a lack of racial diversity among the student population.
Additionally, unplanned expansion may also result in excessive numbers which may lead to a reflex moratorium on new schools, this in turn may impact numbers down the line leading to a shortage of doctors as seen in Malaysia currently.
A robust accrediting body and medical council which sets standards and guards against the above is always required to ensure compliance. In the Malaysian landscape this is largely in place to ensure standards of all local graduates from the public and private educational sector. Evidence from the Ministry of Health Malaysia seems to indicate that most attrition is due to mental health and coping issues as well as disciplinary matters such as non-completion of logbooks and tardiness in fulfilment of required duties. This means that checks and balances regarding theoretical and practical competence are largely in place, with the problems being related to attitudes, resilience and expected standards of conduct. This is a real challenge and must be addressed to ensure holistic medical practice.
A holistic healthcare practitioner is one who takes consideration of all the patient’s needs as far as possible when delivering care. This implies a practitioner who is theoretically and practically sound with the necessary soft skills to provide care for the patient under their charge. The practitioner must also be resilient, mindful and be aware of the expectations of the community they serve in.
While many of us assume that our stakeholders want healthcare providers that are competent and fit for purpose in terms of expertise, it appears that there are unmet needs in many encounters.
Patients want to be treated as a person not a number. They want community-based care that addresses social issues and family involvement in decision making. Patients also expect affordable care, destigmatisation of certain types of diseases, and avoiding stereotyping (Natafgi et al., 2022).
This then is the expectation, and the challenge is how we meet these. The Institute of Medicine (National Academies of Science, Engineering, and Medicine, Washington USA) in 2019 has outlined the six aims to improve health care delivery. It emphasises safety, effectiveness, equity, efficiency, timeliness, and a patient centred focus (Torralba & Katz, 2020) which broadly resonates with patient expectations outlined previously.
The BMJ in 2002 posed two questions to its readers, “what makes a good doctor?” and “how can we make one?” Answers varied but some important takeaways regarding a good doctor were that
- A good doctor had to be a good human being.
- A good doctor had to be one that genuinely liked people and wanted to help them.
- A good doctor had to be special in some way, extra dedicated, extra humane or extra selfless.
- A good doctor had to take care of themselves first.
- A good doctor had to find medicine fun, fascinating, and stimulating (Rizo, 2002).
Producing a good doctor appears to be more challenging. It is a given that providing quality healthcare requires quality medical education. Correspondingly, providing quality medical education depends on
- good student selection mechanisms.
- attracting and maintaining highly qualified academic and practice staff.
- designing a curriculum that is current and reviewed regularly to ensure active learning, problem solving, and critical thinking with appropriate use of technology grounded in real life examples.
- basing curriculum design and renewal on multiple stakeholder feedback and on real time performance of graduates in the workplace.
- a high standard of cognitive and psychomotor learning coupled with affective attributes of safe, ethical, and empathetic practice.
- designing valid assessments that ensure achievement of learning outcomes in the area of cognitive, psychomotor and affective skills.
- adequate investment in infrastructure in terms of classrooms, laboratories, libraries and clinical teaching sites that are all equipped to provide quality teaching and learning.
- developing links with other institutions of learning and practice to benchmark standards and provide opportunities for internships and elective placements in preparation for their future careers.
- incorporating quality assurance in all aspects of teaching, learning and assessment.
All of these are generally the norm and are contained in accreditation standards which are based on the recommendations of the World Federation of Medical Education.
In effect, all medical schools, public or private need to commit to producing a competent practitioner who is knowledgeable, skilled, and has the necessary positive affective attributes to deliver holistic care. We have got it right to a large extent in the areas of cognitive and psychomotor competence which are tangible and measurable. The affective competencies in terms of soft skills, resilience, coping mechanisms, and mental health are something that we all continue to work on. It is less tangible and is ever changing because of the changing expectations of all stakeholders. To ensure a competent professional we also have to take into consideration the environmental and animal health issues that have an increasing impact on our health. There is a need to refine our curriculums to move from one that emphasises treatment to one that emphasises prevention and staying healthy. Additionally, incorporation of digital skills and the utilisation of artificial intelligence is another space that needs to be explored and incorporated into the curriculum aiming to create a holistic and complete healthcare professional.
This will require the implementation of a minimum acceptable standard for entry that is based on a set of acceptable qualifications, or a standardised entrance test. Selection of a student should also take into account affective attributes, needs background, and aptitude. This entails the use of interviews, multiple mini-interviews and aptitude tests in the selection process. Complying to a required curriculum standard with a common exit examination for all medical schools will help achieve the above targets (Aftab et al., 2021).
We will also need to explore and incorporate elements of the one health curriculum, preventive medical care and digital competencies into an already packed curriculum in a meaningful and practical manner.
Different countries and institutions are on different stages of this path but what is evident is that there is an acknowledgement of the need to set a common minimum standard of entry, competency and outcome.

Figure 1. Attributes and the regulatory mechanisms to achieve this aim. Solid arrows are the processes in place and dotted arrows are the processes in progress.
III. CONCLUSION
In conclusion, the Shushruta Samhita an ancient Indian text of surgery, harking back to 400 BC perhaps put it well by saying “A physician well versed in the principles of the science of medicine but incompetent in the art because of want of practice, as well as the physician, experienced in his art but short on the knowledge of Ayurveda, is like a one-winged bird that is incapable of soaring high in the sky”.
This statement encompasses the requirements expected of a holistic practitioner and is time tested across the ages. This is the holy grail we all aspire to whether in the public or private sector of medical education. By and large, we have the regulations and mechanisms required in place. Continuous quality enhancement and working together will enhance standards in our aspiration to produce holistic, balanced graduates who are global and flexible in their outlook and employability.
Notes on Contributors
All authors were involved in the literature review, writing, editing and proof reading of this article. The concept is attributed to GR the first author. All authors have approved the final version of this article.
Acknowledgement
The authors thank the faulty leadership for permission to write and submit this article.
Funding
There was no funding support involved.
Declaration of Interest
All authors are from private universities that provide an accredited undergraduate medical programme in Malaysia.
References
Aftab, W., Khan, M., Rego, S., Chavan, N., Rahman-Shepherd, A., Sharma, I., Wu, S., Zeinali, Z., Hasan, R., & Siddiqi, S. (2021). Variations in regulations to control standards for training and licensing of physicians: A multi-country comparison. Human Resources for Health, 19, Article 91. https://doi.org/10.1186/s12960-021-00629-5
AlThukair, D., & Rattray, J. (2023). What makes a high-quality medical education and graduate? The Saudi Arabia labor market’s perspective. In Innovations in higher education teaching and learning (pp. 67-83). https://doi.org/10.1108/s2055-364120230000054004
Natafgi, N., Ladeji, O., Blackwell, S., Hong, Y. D., Graham, G., Cort, M., & Mullins, C. D. (2022). Similar values, different expectations: How do patients and providers view ‘health’ and perceive the healthcare experience? Health Expectations, 25(4), 1517-1528. https://doi.org/10.1111/hex.13493
Rizo, C. A. (2002). What’s a good doctor and how do you make one? BMJ, 325(7366), 711. https://doi.org/10.1136/bmj.325.7366.711
Torralba, K. M. D., & Katz, J. D. (2020). Quality of medical care begins with quality of medical education. Clinical Rheumatology, 39(3), 617-618. https://doi.org/10.1007/s10067-019-04902-w
*Ganesh Ramachandran
School of Medicine,
Faculty of Health and Medical Sciences,
Taylor’s University, Malaysia
+6 012 373 2201
Email: Ganesh.Ramachandran@taylors.edu.my
Submitted: 29 January 2025
Accepted: 16 April 2025
Published online: 6 January, TAPS 2026, 11(1), 9-13
https://doi.org/10.29060/TAPS.2026-11-1/GP3651
Michael Krasner
Department of Medicine, University of Rochester School of Medicine and Dentistry, United States of America
Abstract
Introduction: The growing prevalence of burnout among healthcare professionals has emerged as a global crisis, adversely affecting individual well-being, patient care, and healthcare systems while imposing significant economic burdens. Addressing this systemic problem requires innovative, scalable interventions that target the root causes of burnout. Mindful Practice in Medicine (MPIM), developed at the University of Rochester School of Medicine and Dentistry, represents a promising approach. MPIM fosters self-awareness, emotional intelligence, teamwork, and compassion. With over 20 years of evidence-based implementation, MPIM has demonstrated substantial improvements in clinician well-being, burnout, empathy, teamwork, and patient-centered care.
Methods: This global perspective highlights the program’s global impact through case studies of MPIM-trained facilitators who have embeded these programs into undergraduate, graduate, and postgraduate medical education as well as into institutional healthcare systems.
Results: Examples from Switzerland, the United States, the United Kingdom, Australia, and Canada illustrate MPIM’s adaptability and effectiveness for fostering systemic cultural changes, restoring joy in medicine, and promoting organisational resilience.
Conclusion: These efforts underscore the potential of MPIM to catalyse a global paradigm shift in healthcare, improving outcomes for both professionals and patients. Further research and strategic scaling are necessary to maximise MPIM’s reach and sustainability and to address the intertwined crises of professional burnout and healthcare quality.
Practice Highlights
- MPIM programs integrates contemplative practices, narrative medicine, and appreciative inquiry.
- MPIM demonstrates sustainable improvement in burnout, wellness, teamwork, and patient centered care.
- MPIM facilitators have implemented global programs across the medical training and care continuum.
- MPIM interventions can be scaled to address individual and systemic health professional challenges.
- MPIM may help provide solutions for improving healthcare quality and health professional wellbeing.
Everybody complains about the weather, but nobody does anything about it.
Charles Dudley Warner
I. THE PROBLEM OF HEALTH PROFESSIONAL BURNOUT AND WELLBEING
Awareness of physician and health professional burnout and efforts to promote their well-being have gained significant attention in recent years, especially as the COVID-19 pandemic underscored the critical role of physician wellbeing in achieving healthcare’s mission of providing quality patient care. Burnout, a work-related syndrome characterised by emotional exhaustion, depersonalisation, and a reduced sense of personal accomplishment, has become a global public health crisis. More than 50% of physicians, both in training and in practice, exhibit burnout symptoms, leading to negative impacts on patient care, healthcare systems, and health professionals’ mental health, compromising professionalism and care quality, and imposing substantial economic costs. The worldwide economic impact is difficult to assess but estimates six years ago from within the United States healthcare system amounted to $4.6 billion, or approximately $7,600 per employed physician annually (Han et al., 2019).
The drivers of health professional burnout are not rooted in the health professional’s individual shortfalls, a lack of resilience, or insufficient experience managing complex personal, interpersonal, and medical dynamics within the complicated maze found in healthcare systems. Rather, it is derived primarily from systemic issues including excessive workloads, inefficient processes, administrative burdens, work-life conflicts, and a lack of organisational support and control over workplace decisions (West et al., 2018). Demographic factors also contribute, with burnout rates higher among female and younger physicians. Addressing this crisis thus requires organisational level strategies like redesigning work processes and increasing clinical support as well as fostering a culture of supportive leadership and collaboration.
Yet, many interventions developed in response to this crisis fall short of addressing these systemic and medical cultural challenges. Among such interventions that show promise are mindfulness-based stress reduction programs, small-group community building programs, and initiatives to promote meaning and connection in the workplace. These interventions, primarily individually oriented, have demonstrated tangible benefits when aligned with the specific drivers of burnout and hold the potential to mitigate its widespread effects and enhance both physician well-being and healthcare system performance. However, in many ways they are not designed nor intended to specifically address systemic issues, and thus far have failed to improve causal structural and cultural factors (Shanafelt, 2021).
II. MINDFUL PRACTICE IN MEDICINE/FLOURISHING IN MEDICINE
This Global Perspective discusses an intervention called Mindful Practice in Medicine (MPIM). In addition to empirically published evidence on its salutary effects on physician burnout and wellbeing and its demonstrated flexibility, the work of a growing number of trained MPIM facilitators worldwide has begun to address the systemic, organisational, and medical culture changes needed to begin to have an impact on this epidemic and move healthcare systems toward healthier, stabler, and higher quality. This report presents an overview of MPIM programs and training, and a sampling of how its trained facilitators impact systems of medicine across the continuum of undergraduate, graduate, and post-graduate medical education, as well as within academic healthcare educational and delivery culture.
MPIM/Flourishing in Medicine, developed at the University of Rochester School of Medicine and Dentistry 20 years ago, provides educational skills training designed to empower health professionals and organisations to thrive by restoring joy in medicine, fostering community, and promoting excellence in healthcare. Through interactive in-person and online workshops, seminars, and presentations, these programs serve physicians, medical educators, trainees, other health professionals, and leaders within the healthcare ecosystem at individual, organisational, and institutional levels. The approach emphasises self-awareness, emotional intelligence, deep listening, interpersonal dynamics, teamwork, and compassion, while actively engaging participants with a focus on relationship-centered care.
Rooted in a biopsychosocial framework, MPIM integrates contemplative and awareness-building practices, narrative medicine, and appreciative inquiry to enhance clinician well-being, relational dynamics, individual and group resilience, and quality of patient care. Research conducted at the University of Rochester and replicated globally demonstrates significant improvements in well-being, burnout, empathy, teamwork, work satisfaction, and a stronger psychosocial orientation in patient care delivery. Participants consistently highlight the program’s emphasis on its ability to foster collegial community, the contemplative practices, narrative medicine skills, the application of appreciative inquiry, and a focus on self-care as keys to its effectiveness in transforming both individual and organisational healthcare experiences. (Epstein et al., 2022; Krasner et al., 2009). Several thousand health professionals worldwide have participated in this training with nearly two hundred completing facilitator or advanced teacher training. The following examples highlight a few interventions and programs that MPIM teacher trainees have implemented in their medical communities across the globe. These demonstrate real-world responses to the crisis in healthcare systems and medical culture across a continuum of medical education.
MPIM is being implemented globally with adaptations that align with diverse cultural and educational contexts, ensuring its relevance and effectiveness in various healthcare environments. Unlike conventional mindfulness programs, MPIM is specifically designed for the medical professional, integrating self-awareness, emotional intelligence, and relationship-centered care into clinical practice. Its flexibility allows trained facilitators to tailor interventions to local healthcare systems, addressing both individual well-being and systemic cultural challenges. By embedding mindfulness-based principles within medical education and institutional frameworks, MPIM goes beyond individual stress reduction, acting as a catalyst for systemic change in healthcare, ultimately improving physician well-being, team dynamics, and patient care quality on a global scale. Figure 1 shows the global presence of mindful practice in medicine programmes.

Figure 1. Global presence of mindful practice in medicine programs (locations of intensive workshops or advanced teacher trainees)
III. GLOBAL APPLICATIONS ACROSS LEVELS OF MEDICAL EDUCATION
A. Undergraduate Medical Training, University of Fribourg, Switzerland
Dr. Raphael Bonvin, an MPIM Advanced Teacher Training graduate, came to the University of Fribourg Faculty of Science and Medicine to improve academic performance by addressing the intrinsic motivations of undergraduate medical students. Directing the second half of the six-year undergraduate medical education curriculum, he has embedded pedagogy and programs influenced by MPIM. The new curriculum highlights contemplative practices, self-awareness and self-care, mind-body medicine, and a humanistic approach to assessments that focus on formative assessment as a primary motivator of the development of individual learning plans with the goal of improved preparation for graduate medical training and the practice of medicine. Outcomes to date of this curricular redesign, now in its fifth year, demonstrate this program as leading Swiss medical schools’ federal licensing exam scores that reflect clinical skills and knowledge. The undergraduate medical education at Fribourg also demonstrates significantly improved sense of autonomy and efficacy among graduates who have now moved on to graduate medical training programs.
B. School of Medicine, The University of Missouri Kansas City, USA
Dr. Jodi Jackson, an MPIM Advanced Teacher Training graduate, created the Mindfulness in Medicine Scholars Program, now in its second full year. It is a yearlong training program for a combined group of undergraduate medical students and medical school faculty with a goal of enhancing self-awareness, professional relationships, quality of medical care, and personal wellness, leading to a designation for the students of Distinction in Mindfulness in Medicine upon graduation. The program is based directly on the MPIM formal curriculum and taught over a ten-month period. Outcomes to date (not yet published) have demonstrated significant improvements in self-efficacy, mindfulness, and burnout for students, and improvements in mindfulness and burnout for faculty.
C. University of Warwick Medical School, West Midlands, UK
Dr. Majid Khan, an MPIM Advanced Teacher Training graduate, and Dr. Manuel Villareal, an MPIM Facilitator Training graduate, along with their colleague Dr. Petra Hanson, have developed an MPIM program for graduate medical education general practitioner trainees in the United Kingdom. They have demonstrated not only feasibility for this program but also significant improvements in burnout, wellbeing, engagement, stress, and mindfulness. Based on these findings they are implementing a more widespread integration of this MPIM program into other graduate medical training programs at their institution.
D. Barwon Health, Geelong, Victoria, Australia
Based on his experience as an MPIM Advanced Teacher Training graduate, and to introduce MPIM to clinician members of his hospital staff, Dr. Ross Carne has created an MPIM-informed program called Belonging in Medicine which is delivered as a post-graduate educational experience within a community hospital setting. Feedback from the first few cohorts of this program include a request for more MPIM-informed programming for medical staff, a strong recommendation of the program to physicians more junior in training to support their professional development and health, and a greater sense of connection of participants with their colleagues, their work, and themselves.
E. University of Calgary Cumming School of Medicine, Calgary, Alberta, Canada
Dr. Todd Hill and Dr. Ward Flemon, both MPIM Facilitator Training graduates, have engaged senior leadership at their institution to support the training of a critical number of MPIM facilitators within their institution with the goal of embedding MPIM-informed programs vertically and longitudinally into the healthcare institution at every level (undergraduate, graduate, and post-graduate medical education as well as more broadly across other health professional teams such as behavioral health, nursing, public health, and community health). Over the past several years over one-hundred thirty faculty physicians and medical trainees have undergone MPIM Core Training, and sixteen faculty have recently completed the MPIM Facilitator Training and are now developing and implementing MPIM-informed interventions that are supported by senior administration leadership within their academic medical center to improve the institutional culture, the work experience of health professionals, and the quality of care delivered to patients.
IV. CONCLUSION
The increasing prevalence of burnout among healthcare professionals jeopardises the well-being of the practitioners, adversely affects patient care, and imposes significant economic burdens on healthcare systems. Addressing this issue necessitates creative and comprehensive organisational strategies that impact underlying systemic and cultural factors. The healthcare system globally finds itself in the initial stages of developing feasible, effective, and scalable interventions to address this problem, and requires more efforts to succeed.
The MPIM program, with its flexibility, broad applications as demonstrated in this Global Perspective across educational domains within medical training and healthcare delivery, and its global presence, represents one such intervention. MPIM programs integrate individual and group skills training that are relevant to the multiple layers of stakeholders within Medicine and focuses not solely on individual factors. As a result of MPIM’s impact on the experience of learners from levels of students to seasoned clinicians, it also function as a systemic change dynamic, creating ripples of effects horizontally (to other learners at the participant’s level), as well as vertically (to teams and staff as well as leadership and management), and thereby effects positive changes within the nested relationships in healthcare systems (the patients, the colleagues, the staff, the leaders, the management, and the larger community).
The challenges of scaling this program to impact larger numbers of healthcare systems and communities are significant, but not unsolvable. More research is required to consolidate MPIM’s feasibility and scalability as well as its impact on end points such as quality measures of patient care, sustainability of health professional wellbeing improvements, diminished job turnover, and demonstrable healthcare cost benefits. However daunting these challenges seem, the examples featured in this perspective provide a foundation for solutions. Equipping committed and trained health professionals with the facilitation and orgainsational skills and experience to design MPIM interventions tailored to their specific community’s needs provide the key. These efforts have the potential for more widespread acceptance, impact, and improvements in the experience of care and the experience of caring for both the patients we serve, and the professionals we are.
Notes on Contributors
Michael Krasner contributed to the conception of the work, the acquisition of data for the work, drafts the work or revising it critically for important intellectual content, approves the final version to be published, and agrees to be accountable for all aspects of the work.
Acknowledgement
The author acknowledges the commitment and creativity of the colleagues mentioned, listed in alphabetical order: Raphael Bonvin, M.D., Ross Carne, M.B.B.S., M.D., Ward Flemons, M.D., Todd Hill, Ph.D., Jodi Jackson, M.D., Majid Khan, M.D., & Manuel Villareal, M.D.
Funding
There is no funding involved.
Declaration of Interest
The author declares that there are no conflicts of interest.
References
Epstein, R. M., Marshall, F., Sanders, M., & Krasner, M. S. (2022). Effect of an intensive mindful practice workshop on patient-centered compassionate care, clinician well-being, work engagement, and teamwork. Journal of Continuing Education in the Health Professions, 42(1), 19-27. https://doi.org/10.1097/CEH.0000000000000379
Han, S., Shanafelt, T. D., Sinsky, C. A., Awad, K. M., Dyrbye, L. N., Fiscus, L. C., Trockel, M., & Goh, J. (2019). Estimating the attributable cost of physician burnout in the United States. Annals of Internal Medicine, 170(11), 784-790. https://doi.org/10.7326/M18-1422
Krasner, M. S., Epstein, R. M., Beckman, H., Suchman, A. L., Chapman, B., Mooney, C. J., & Quill, T. E. (2009). Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA, 302(12), 1284-1293. https://doi.org/10.1001/jama.2009.1384
Shanafelt, T. D. (2021). Physician well-being 2.0: Where are we and where are we going? Mayo Clinic Proceedings, 96(10), 2682-2693. https://doi.org/10.1016/j.mayocp.2021.06.005
West, C. P., Dyrbye, L. N., & Shanafelt, T. D. (2018). Physician burnout: Contributors, consequences and solutions. Journal of Internal Medicine, 283(6), 516-529. https://doi.org/10.1111/joim.12752
*Michael Krasner
601 Elmwood Ave,
Rochester, NY 14642,
United States
Email: m.krasner@medmal.com
Submitted: 28 March 2025
Accepted: 16 April 2025
Published online: 6 January, TAPS 2026, 11(1), 14-17
https://doi.org/10.29060/TAPS.2026-11-1/GP3708
Tang Ching Lau
Dean’s Office, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: The healthcare landscape is evolving rapidly, driven by technological advancements, an aging population, and the increasing complexity of patient care. The National University of Singapore (NUS)’s Common Curriculum for Healthcare Professional Education (CCHPE) is a comprehensive framework designed to foster collaboration, communication, and shared decision-making among future healthcare leaders. This article explores how NUS Medicine’s curriculum prepares students for the challenges of modern healthcare through a multi-disciplinary approach, with a focus on Singapore’s unique healthcare context.
Methods: NUS Medicine employs several strategies including: (1) Curriculum design with the CCHPE structured around five pillars that integrate multi-disciplinary perspectives; (2) Educational Strategies through the implementation of Interprofessional Education (IPE) initiatives, Longitudinal Patient Experience (LPE) programs, use of technology and digital tools, as well as the assessment and feedback mechanisms to foster collaboration among students of different healthcare disciplines; and (3) Stakeholder Management though relationship building and ensuring leadership support.
Results: The CCHPE enhances teamwork, communication, and patient outcomes, preparing graduates to thrive in team-based healthcare environments. NUS Medicine graduates are known for their ability to effectively work in multi-disciplinary teams, contributing to high standards of care in Singapore.
Conclusion: NUS Medicine’s CCHPE emphasises the importance of collaboration in modern healthcare, preparing students to meet complex healthcare challenges, and is essential for ensuring that our graduates are able to meet the demand for high-quality, team-based care in Singapore.
Practice Highlights
- Interprofessional Education (IPE) Initiatives involve joint training sessions and collaborative projects among students from different healthcare disciplines.
- Longitudinal Patient Experience (LPE) provides interdisciplinary experiential learning through home visits over one year.
- Utilising digital platforms and tools for collaborative learning, including virtual case discussions and online modules.
- Assessment with regular feedback to students on teamwork and communication skills, as well as conducting reflective practices to enhance learning.
- Agile Curriculum is designed with regular reviews and updates to adapt to evolving healthcare needs and technologies.
I. INTRODUCTION
The healthcare landscape is evolving rapidly, driven by technological advancements, an aging population, and the increasing complexity of patient care. In Singapore, the National University of Singapore (NUS) Yong Loo Lin School of Medicine has been a pioneer in medical education, adopting innovative approaches to train healthcare professionals who can work effectively in multi-disciplinary teams. Central to this effort is the school’s Common Curriculum for Healthcare Professional Education (CCHPE), a comprehensive framework designed to foster collaboration, communication, and shared decision-making among future healthcare leaders. This article explores how NUS Medicine’s curriculum prepares students for the challenges of modern healthcare through a multi-disciplinary approach, with a focus on Singapore’s unique healthcare context.
Healthcare delivery today requires the coordinated efforts of diverse professionals, including doctors, nurses, pharmacists, and allied health workers. Research consistently shows that effective teamwork in healthcare leads to better patient outcomes, reduced medical errors, and improved patient satisfaction (Brandt et al., 2019; Reeves et al., 2017). In Singapore, where the healthcare system is renowned for its efficiency and quality, the demand for collaborative practice is further amplified by an aging population, rising chronic disease burden, and the need for cost-effective solutions.
Recognising these challenges, NUS Medicine has embraced Interprofessional Education (IPE), where students from different healthcare disciplines learn together to develop the skills necessary for collaborative practice. The school’s Common Curriculum for Healthcare Professional Education (CCHPE) serves as a model for integrating multi-disciplinary learning into medical education, ensuring that graduates are equipped to thrive in team-based healthcare environments.
II. CURRICULUM STRUCTURE
The CCHPE is a cornerstone of NUS Medicine’s educational strategy. It is designed to provide students with a strong foundation in medical knowledge while emphasising the importance of collaboration, communication, and systems thinking. The curriculum is structured around five pillars, each addressing specific learning objectives with a focus on integrating multi-disciplinary perspectives.
A. Pillar 1 – Socio-Ecological Determinants of Health
This pillar introduces students to the social, ecological, and behavioral determinants of health, emphasising their influence on health and illness. Students learn to develop empathy for individuals embedded in various settings and systems that impact their health. This pillar aligns with Singapore’s Healthier SG initiative, which promotes population health through a life-course approach and targeted health measures for specific segments of society. By understanding these determinants, students are better equipped to address the root causes of health issues and work collaboratively to improve community health outcomes.
B. Pillar 2 – Professional Practice 1: The Foundations of Health Professionalism
In this pillar, students explore the professional attributes that underpin the identity of healthcare professionals, including compassion, honesty, integrity, empathy, responsibility, and respect. They learn to apply ethical principles to practical healthcare scenarios and understand the legal and regulatory frameworks that govern the health professions. This pillar also emphasises the importance of therapeutic communication and adopting a person-centered approach in professional practice, which is critical for building trust and rapport with patients and their families.
C. Pillar 3 – Professional Practice 2: Basic Skills in Health Professionalism
Building on the foundations of professionalism, this pillar focuses on developing interpersonal skills, cultural competence, and teamwork. Students learn to collaborate effectively in healthcare delivery, apply ethical reasoning, and navigate the ethical and regulatory considerations that arise in the context of vulnerable populations and health systems. They also learn to apply principles of conflict resolution and constructive feedback, which are essential for fostering a collaborative and supportive work environment.
D. Pillar 4 – Data Literacy for Healthcare
In an era of data-driven healthcare, this pillar equips students with the skills to evaluate clinical evidence, understand study designs, and recognise sources of bias in data analysis. Students learn to calculate and interpret basic statistical tests, enabling them to make informed decisions based on data. This pillar is particularly relevant in Singapore, where the integration of data and technology is a key component of the Healthier SG initiative.
E. Pillar 5 – Digital Literacy for Healthcare
The final pillar focuses on developing students’ ability to apply computational thinking and use digital tools safely and effectively. In a rapidly digitising healthcare landscape, this pillar prepares students to leverage technology to improve practice and outcomes. It aligns with Singapore’s vision of becoming a global leader in healthcare innovation, as outlined in the Healthcare 2020 Masterplan.
III. METHODS
NUS Medicine employs several strategies to ensure that its curriculum fosters effective collaboration among healthcare professionals:
A. Interprofessional Education (IPE) Initiatives
Students from medicine, nursing, pharmacy, and allied health programs participate in joint training sessions and collaborative projects. These activities are designed to break down silos and promote mutual respect among disciplines (Reeves et al., 2019).
B. Longitudinal Patient Experience (LPE)
As part of their interdisciplinary experiential learning, students from the four healthcare professions are grouped together to visit patients in their homes and living environments over a one-year period. This program allows students to apply concepts learned in class to real-world situations, fostering a person-centered approach to care.
C. Technology and Digital Tools
NUS Medicine leverages digital platforms to facilitate collaborative learning. Virtual case discussions and online modules allow students to engage with peers from different disciplines, even outside the classroom (Masters et al., 2020).
D. Assessment and Feedback
Students receive regular feedback on their teamwork and communication skills, helping them identify areas for improvement. Reflective practices, such as reflective writing and debriefing sessions, further enhance learning (Ramani & Krackov, 2019).
The CCHPE is likely to have a profound impact on NUS Medicine graduates and the broader healthcare system. Studies have shown that interprofessional education improves teamwork, communication, and patient outcomes (Reeves et al., 2019). In Singapore, graduates of NUS Medicine are known for their ability to work effectively in multi-disciplinary teams, contributing to the high standards of care that the country is renowned for.
IV. STRATEGIES AND RESULTS
Implementing a multi-disciplinary curriculum like the CCHPE is not without its challenges. However, NUS Medicine has identified key strategies to address these obstacles:
A. Building Relationships and Trust Among Faculties and Administrators
- Challenge: Different faculties and departments may have varying priorities and teaching styles, which can hinder collaboration.
- Solution: NUS Medicine emphasises relationship-building and trust among educators and administrators. Regular communication and mutual support are key to ensuring the success of the curriculum.
B. Ensuring Senior Leadership Support
- Challenge: Without strong support from senior leadership, it can be difficult to align resources and priorities across disciplines.
- Solution: NUS Medicine has secured strong backing from senior leadership, which has been instrumental in driving the curriculum forward and ensuring its sustainability.
C. Adapting to Evolving Needs
- Challenge: The healthcare landscape is constantly evolving, requiring the curriculum to adapt to new challenges and technologies.
- Solution: The curriculum is designed to be agile, with regular reviews and updates to ensure it remains relevant. Faculty members are encouraged to be flexible and responsive to emerging needs.
D. Integrating Evaluation and Research
- Challenge: Measuring the effectiveness of a multi-disciplinary curriculum can be complex.
- Solution: NUS Medicine has built evaluation and research into the curriculum from the outset, allowing for continuous improvement based on data-driven insights.
V. CONCLUSION
Looking ahead, NUS Medicine aims to expand its interprofessional training opportunities and strengthen partnerships with healthcare institutions. By doing so, it will continue to produce graduates who are not only skilled clinicians but also effective collaborators and innovators.
The NUS Yong Loo Lin School of Medicine’s Common Curriculum for Healthcare Professional Education (CCHPE) represents a forward-thinking approach to medical education, emphasising the importance of collaboration in modern healthcare. By integrating multi-disciplinary learning into every aspect of the curriculum, NUS Medicine is preparing its students to meet the challenges of an increasingly complex healthcare system. In Singapore, where the demand for high-quality, team-based care is greater than ever, this approach is not just beneficial—it is essential. As other institutions look to NUS Medicine as a model, the school’s commitment to innovation and collaboration will continue to shape the future of healthcare education.
Notes on Contributors
Adjunct Professor Lau Tang Ching contributes to the conception and writing of the initial draft, and revising it critically for important intellectual content, approves the final version to be published, and agrees to be accountable for all aspects of the work.
Funding
No funding was received.
Declaration of Interest
The author has no conflict of interest, including financial, consultant, institutional and other relationships that might lead to bias.
References
Brandt, B., Lutfiyya, M. N., King, J. A., & Chioreso, C. (2019). A scoping review of interprofessional collaborative practice and education using the lens of the Triple Aim. Journal of Interprofessional Care, 28(5), 393-399. https://doi.org/10.3109/13561820.2014.906391
Motola, I., Devine, L. A., Chung, H. S., Sullivan, J. E., & Issenberg, S. B. (2020). Simulation in healthcare education: A best evidence practical guide. AMEE Guide No. 82. Medical Teacher, 35(10), e1511-e1530. https://doi.org/10.3109/0142159X.2013.818632
Masters, K., Ellaway, R. H., Topps, D., Archibald, D., & Hogue, R. J. (2020). Mobile technologies in medical education: AMEE Guide No. 105. Medical Teacher, 38(6), 537-549. https://doi.org/10.3109/0142159X.2016.1141190
Ramani, S., & Krackov, S. K. (2019). Twelve tips for giving feedback effectively in the clinical environment. Medical Teacher, 34(10), 787-791. https://doi.org/10.3109/0142159x.2012.684916
Reeves, S., Fletcher, S., Barr, H., Birch, I., Boet, S., Davies, N., McFayden, A., Rivera, J., & Kitto, S. (2019). A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Medical Teacher, 38(7), 656-668. https://doi.org/10.3109/0142159x.2016.1173663
*Lau Tang Ching
1E Kent Ridge Road
NUHS Tower Block, Level 11,
NUS Yong Loo Lin School of Medicine,
Singapore 119228
Email: mdcltc@nus.edu.sg
Submitted: 16 November 2024
Accepted: 7 February 2025
Published online: 6 January, TAPS 2026, 11(1), 18-21
https://doi.org/10.29060/TAPS.2026-11-1/GP3573
Dayo Rotimi Omotoso1 & Joy Oyiza Peter2
1Department of Human Anatomy, Faculty of Basic Medical Sciences, Redeemer’s University, Ede, Nigeria; 2Department of Educational Technology, Faculty of Education, University of Ilorin, Ilorin, Nigeria
Abstract
Introduction: The application of modern and innovative technology into anatomical science education has been on a rapid increase globally in recent years with the anatomy tutors and students playing important and complementary roles in the process of the integration.
Methods: This narrative perspective presents the current state of technological applications adopted in anatomy education in medical colleges in Africa and the roles of the anatomy tutors and students in the process.
Results: The role of the anatomy tutors in African medical colleges include facilitation of technological integration into anatomy education and curriculum, promotion of active learning in anatomy, design of innovative assessment strategies, provision of relevant technological support, and advocate for provision of resources and infrastructure. Similarly, the trainees played important roles in the process of technological integration into anatomy education in Africa which include increased acceptability of technology for anatomy learning, utilisation and validation of innovative assessment methods, peer-advocacy for technology-driven learning, and bridging the technological gap.
Conclusion: The active participation of both the tutors and students in the adoption of technological solutions and tools will continue to enhance the quality of anatomical science pedagogy across African medical colleges.
Practice Highlights
- Application of technology in anatomy education has been on a rapid increase globally.
- Technology applications are used in anatomy education to complement traditional methods.
- Tutors and students in Africa have played vital roles in the adoption of technology for anatomy education.
- Technological applications are currently re-shaping anatomy education landscape to improve learning outcomes.
- Application of technology in anatomy education should be promoted to further enhance learning.
I. INTRODUCTION
Anatomy is a foundational discipline in medical education which is required in the training of medical and allied health students in order to gain requisite knowledge and professional competence. Hence, anatomical science content remains a pivotal component of the academic curricula of all sub-disciplines of the medical sciences (Hildebrandt, 2019). The provision of quality education (including medical education) is one (number 4) of the United Nations’ sustainable development goals (SDGs) targeted at ensuring equitable and inclusive quality education for all. Technological advancements of the past decade have been applied to facilitate educational processes. Hence, digital technologies have been identified as important tools that would facilitate the achievement of the SDG 4.
The integration of technology has resulted in major evolution in anatomical pedagogy leading to a wide array of positive outcomes. In essence, the use of modern and innovative technological applications by the anatomy tutors and students for teaching and learning processes has resulted in satisfactory outcomes (Patra et al., 2022). In several African medical colleges, the characteristic cadaveric-based learning is being augmented with technological applications in order to improve learning outcomes and to prepare the students for the emerging medical professional practice (Owolabi et al., 2022). Additionally, technology-driven interactive learning strategies that ensure online delivery of learning resources are being explored for histology education. These strategies, which have enabled the trainees to complete learning outcomes while not physically present in classrooms or laboratories, have further helped to solve associated cognitive challenges of histology learning (Meyer, 2023).
The transition from the conventional classroom to technological-driven anatomy teaching and learning became prevalent during the coronavirus disease 19 (COVID-19) pandemic when medical colleges were shut down around the world (Omotoso, 2023). In essence, both the anatomy tutors and students necessarily played a complementary role in the adoption of the technological applications to sustain anatomy education. The current study presents the perspective on the role of the anatomy tutors and students in the application of technology for anatomy education in medical colleges across Africa.
II. METHODS
Based on the appraisal of the current practices and existing literature, the authors have developed the narrative perspective on the role of tutors and students in the emerging process of application of technology for anatomy education in African medical colleges.
III. RESULTS
The anatomy tutors and students are the most important stakeholders at the centre of the process of application of technology for anatomy education in African medical colleges. Regardless of the identified beneficial impact of technological adoption in anatomy education, the acceptability and successful integration of technology into anatomical science pedagogy in African medical colleges largely depend on the roles of the anatomy tutors and students in the process.
IV. DISCUSSION
A. Roles of African Tutors in the Application of Technology into Anatomy Education
Anatomy tutors in medical colleges across Africa have played the following crucial roles in the integration of technology into anatomical science pedagogy:
1) Facilitate technological integration into anatomy education: Anatomy tutors are the key players in facilitating the adoption of technology into anatomical science pedagogy. In essence, anatomy tutors in African medical colleges act the crucial linkages that connect the students to technology-based learning strategies as a complement to the conventional cadaver-based anatomy learning. In addition, technological applications such as virtual microscopy are being explored in the delivery of histology education to enhance the teaching and learning process by enabling continuous interaction with unlimited numbers of high-quality, digitised histological sections. In essence, the African anatomists are generally technology inclined and are helping to facilitate the integration of technology into anatomy education in African medical colleges.
2) Design of innovative anatomy curriculum: The incorporation of technology into anatomy pedagogy entails an integration of innovative and technological-based strategies into the conventional anatomy curriculum for health profession students. This process is currently driven by the anatomy tutors in African medical colleges by ensuring that digital technological applications are tailored to achieve the learning objectives and expected outcomes of anatomy modules. The tutors further drive the students’ knowledge of emerging anatomy education concepts in the updated curriculum through digital applications in complement to conventional physical learning.
3) Promote active learning and student engagement: Active learning, which emphasises students’ participation and interaction, is a key pedagogical strategy which is currently enabled by technology in anatomical education. Anatomy tutors encourage the students to engage with digital applications like virtual reality (VR)-based anatomy models or interactive anatomy applications, thereby fostering more hands-on approach to anatomy learning in order to improve learning experiences and satisfaction.
4) Design and utilise innovative assessment strategies: The strategies for students’ assessment in anatomical science are steadily evolving due to integration of technological-enhanced methods with the utilisation of these innovative methods essentially dependent on the tutors to drive the process. Technology-driven assessments such as computer-based test (CBT), conducted on online platforms or learning management systems (LMS), have been adopted to execute the conventional assessments including short answer questions, multiple choice questions, and objective structured practical examination (OSPE) with comparable or improved outcomes and satisfaction.
5) Provide mentorship and technological support: Due to the socio-economic background, some students in African medical colleges may not be compliant with the modern digital technologies used for educational purposes. The anatomy tutors act as mentors and instructors that provide support for the students to overcome the barriers associated with technological literacy. In this role, anatomy tutors offer both academic and technological support to help the students use modern technological applications for anatomy learning.
6) Advocate for provision of infrastructure and resources: The application of technology in anatomical science pedagogy requires robust infrastructure such as regular internet connectivity, computer laboratories, VR laboratory, virtual platforms such LMS and so on. Anatomy tutors play a crucial role in advocating for institutional support toward the provision of requisite infrastructure and resources to drive the technology-based anatomy learning environment. In many African medical colleges, infrastructural deficits pose significant barriers to technological integration.
7) Act as technology advocates and change agents: Another role of the anatomy tutors is the promotion of paradigm shift towards acceptability of technology as an effective tool for anatomical science education. Essentially, the African medical colleges have always adopted the conventional cadaver-based anatomy learning. The recent application of technology in anatomy pedagogy has attracted some concerns, especially the uncertainty of its effectiveness and efficiency compared to the conventional methods. However, with the scientific findings of comparable effectiveness of technological-driven anatomy learning, advocacy now revolves around its adoption as a complement and not replacement to conventional methods of learning.
B. Roles of African Students in Application of Technology for Anatomy Education
Anatomy trainees are the major end-users of the technological applications and hence, positioned as the key determinants of how the applications would be utilised in classrooms, laboratories, or clinical settings for anatomy learning. Therefore, the roles of the African trainees in driving the technological-based anatomical science pedagogy include:
1) Adoption of digital applications for improved anatomy learning outcomes: Students in African medical colleges act as early adopters of technological applications that could enhance anatomy learning. Virtual anatomy platforms like the Visible Body and Complete Anatomy are currently used to complement the traditional cadaver-based learning and technological tools such as 3D anatomy apps, virtual dissection tables, and online simulations have become increasingly popular in medical schools across the continent.
2) Utilisation and validation of innovative assessment methods: The advancement of digital technology has enabled the development of more interactive and objective assessments strategies in anatomy pedagogy. Essentially, the anatomy trainees are central to the pilot testing and deployment of these technology-driven assessment strategies for anatomical science. In addition, the anatomy trainees provide critical feedback on the effectiveness and efficiency of the technology-driven assessment tools. This feedback is required for their improvement and validation for consequent integration into the overall assessment strategies.
3) Peer-advocacy for technology-driven learning: Recent technological advancements have further impacted anatomy education due to the more technological-compliance of the emerging trainees. As such, anatomy trainees have become more inclined to online learning than conventional classroom learning with reported satisfactory or even improved outcomes. The trainees actively learn through online anatomy resources or virtual dissection simulations in order to sustain anatomy education when the physical classroom learning was not accessible.
4) Bridging the technology gap: Despite the growing availability of digital tools, there remain challenges in accessing technological resources in many African medical colleges, particularly in remote and under-funded institutions. The anatomy trainees have risen to the responsibility of bridging this gap by setting-up initiatives to share access to digital anatomy tools through shared devices or group licenses for online platforms.
V. CONCLUSION
Technology applications applied in anatomical science learning and assessment are actively complementing the traditional methods in Africa medical colleges thereby gradually transforming the anatomy education landscape in Africa. Anatomy tutors play crucial roles in the utilisation of the technology for facilitation and learning to complement the traditional method of delivering anatomy education. The students have similarly adopted innovative technological tools to achieve self-directed and flexible anatomy learning. The active participation of both the tutors and students in the adoption of technological solutions and tools will continue to enhance the quality of anatomical science pedagogy across African medical colleges.
Notes on Contributors
DRO conceptualised the study, participated in literature search, manuscript drafting, manuscript editing, final review and approval of the manuscript.
JOP participated in literature search, manuscript drafting, manuscript editing, final review and approval of the manuscript.
Acknowledgement
The authors would like to acknowledge the support from the staff of Department of Human Anatomy, Faculty of Basic Medical Sciences, Redeemer’s University, Ede, Nigeria.
Funding
This work has not received any external funding.
Declaration of Interest
The authors declare no conflict of interest for this study.
References
Hildebrandt, S. (2019). The role of history and ethics of anatomy in medical education. Anatomical Science Education, 12(4), 425-431. https://doi.org/10.1002/ase.1852
Meyer, G. T. (2023). Online, interactive, digital visualisation resources that enhance histology education. In: S. Border, P. M. Rea, & I. D. Keenan (Eds.), Biomedical Visualisation: Advances in Experimental Medicine and Biology (vol 1421., pp. 125-160). Springer. https://doi.org/10.1007/978-3-031-30379-1_6
Omotoso, D. R. (2023). Adoption of online classes for anatomy learning during coronavirus disease 2019 pandemic – participation, perception and preference of basic medical students of a Nigerian University. National Journal of Clinical Anatomy, 12, 121-126. https://doi.org/10.4103/NJCA.NJCA_48_23
Owolabi, J., Ojiambo, R., Seifu, D., Nishimwe, A., Masimbi, O., Okorie, C. E., Ineza, D., & Bekele, A. (2022). African medical educators and anatomy teachers’ perceptions and acceptance of the anatomage table as an edtech and innovation: a qualitative study. Advances in Medical Education and Practice, 12, 619-625. https://doi.org/10.2147/AMEP.S358702
Patra, A., Asghar, A., Chaudhary, P., & Ravi, K. S. (2022). Integration of innovative educational technologies in anatomy teaching: New normal in anatomy education. Surgical and Radiological Anatomy, 44(1), 25-32. https://doi.org/10.1007/s00276-021-02868-6
*Dayo Rotimi Omotoso
Department of Human Anatomy,
Faculty of Basic Medical Sciences,
Redeemer’s University, Ede,
Nigeria.
+2348034779886
dayohmts@gmail.com
Submitted: 19 August 2025
Accepted: 30 September 2025
Published online: 7 October, TAPS 2025, 10(4), 1-4
https://doi.org/10.29060/TAPS.2025-10-4/GP3858
Dujeepa D. Samarasekera1, Gominda Ponnamperuma2, Lee Shuh Shing1 & Han Ting Jillian Yeo1
1Centre for Medical Education (CenMED), Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Faculty of Medicine, University of Colombo, Sri Lanka
Abstract
Introduction: Medical education aims to produce healthcare professionals who are not only competent, but also able to perform effectively in clinical practice settings. Assessment systems are critical to achieving this by guiding learning, ensuring competence, and certifying readiness for independent practice. This article proposes a staged assessment approach that integrates both competence and performance to ensure safe and empathetic healthcare practice.
Methods: First, we analysed the strengths and limitations of the existing assessment methods and their roles in medical education. Then, we explored strategies to integrate diverse assessment tools into a cohesive assessment system capable of effectively and reliably evaluating the competencies required for developing holistic practitioners.
Results: Competence is assessed via structured assessment tools such as written assessments. Clinical performance in real-world settings relies on Supervised in-practice assessments (SuPs), including tools like Direct Observation of Procedural Skills (DOPS) and Mini-Clinical Evaluation Exercises (mini-CEXs). Assessment tools used to evaluate performance rely on expert judgement, which, although subjective, is essential for evaluating non-cognitive skills such as empathy and professionalism.
Conclusion: This article outlines the design of a progressive assessment system, transitioning from objective assessment methods such as Multiple-Choice Questions (MCQs) to performance-focused methods, anchored by Entrustable Professional Activities (EPAs), using Workplace-Based Assessment tools and portfolios. The progression from early objective assessment tools to those which leverage expert judgement and situational specificity are highlighted as essential for preparing safe, effective, and empathetic healthcare practitioners.
Practice Highlights
- Modern assessment systems focus on both competence in non-practice settings and performance in authentic clinical practice settings.
- A combination of tools is required to assess from “knows” to “is” level of clinical performance.
- Expert evaluations provide qualitative insights into candidate performance.
I. INTRODUCTION
Traditionally, assessments in clinical education strived for standardisation, structuredness and objectivity. A single quantitative method, such as paper-based Multiple-Choice Questions (MCQs), was often used to assess a student’s competence in knowledge. Similarly, the Objective Structured Clinical Examinations (OSCEs) or long/short clinical cases were used for assessing psychomotor and affective domains related to clinical skills. To deliver healthcare effectively and empathetically, a broad range of skills must be cultivated. Over the years, there has been a gradual yet noteworthy transition from exclusively focusing on the development and assessment of one’s competence in clinical skills to placing greater emphasis on enhancing clinical performance within specific clinical contexts (Hays et al,2024).
Miller’s Pyramid (1990) of Clinical Competence illustrates this progression: from “knows” to “knows how”, “shows how”, and finally “is” as proposed by Cruess et al. (2016). At present, medical and health professional training programs judiciously select a combination of assessment methods to ensure learners are task-ready, empathetic, and safe for clinical practice. This article proposes and elaborates on the use of a staged assessment approach in health professional training, progressing from the development of competence to the refinement of clinical performance within specific practice contexts. The core idea is that competence alone does not ensure effective clinical practice. Both competence and performance must be developed to ensure safe and compassionate care.

Figure 1: The diagram adapted from Cruess et al (2016) article on “Amending Miller’s Pyramid to Include Professional Identity Formation”, to illustrate a shift in focus as trainees progress to the later stages of training from assessment of competence to assessment of performance.
II. COMPETENCE AND ITS ASSESSMENT
As illustrated in Figure 1, competence or “Readiness to Practice” refers to an individual’s “ability”, encompassing knowledge, psychomotor or clinical skills, and attitudes, which together form the foundation of medical practice. Knowledge-based skills include problem-solving and clinical reasoning, psychomotor skills involve physical examinations and procedural techniques, while affective skills pertain to empathetic communication. Historically, our assessments have primarily focused on evaluating competence, employing a range of assessment tools as the following.
Written assessments, such as MCQs and Modified Essay Questions (MEQs), are designed to evaluate the “knows” and “knows how” levels of Miller’s Pyramid. These assessments primarily focus on theoretical knowledge, including understanding disease pathophysiology, as well as the procedural steps involved in performing clinical skills and managing medical conditions.
In contrast, practical and competence-based assessments, such as OSCEs, evaluate psychomotor and affective competencies, including procedural skills, diagnostic reasoning, patient interaction and communication in a controlled environment. Long and short cases, on the other hand, assess the same abilities within semi-controlled environments. These assessment formats target the “shows” level of Miller’s Pyramid, emphasising the development and demonstration of clinical skills in structured, controlled testing settings.
The feature of “shows” assessment methods is that they promote standardisation and assessment based on a rubric. Hence, they are “objective” and fairly reliable for assessing specific aspects of competence.
III. PERFORMANCE AND THE ROLE OF SUPERVISED IN-PRACTICE ASSESSMENTS (SuPs)
As illustrated in Figure 1, as learners progressed from early stages to later or final stages of learning, the focus shifts from assessment of competence to assessment of performance. While the assessment of knowledge continues to play an important role, the focus increasingly shifts towards ensuring that graduates are ready for clinical practice. Performance or “Quality in Practice” requires learners to apply their competence in dynamic, high-pressure clinical settings. These situations are both context-specific and situation-specific. In modern medical education, Entrustable Professional Activities (EPAs) anchor these authentic clinical tasks. EPAs focus on specific professional responsibilities, such as managing acute care or conducting patient handovers. These tasks are assessed by an “expert” using professional judgement. Entrustment decisions are based on evaluations from multiple experts (Cate & Schumacher, 2022).
Common tools used during SuPs include Direct Observation of Procedural Skills (DOPS), Case-Based Discussions (CBDs), multi-rater or 360 assessments, and Mini-Clinical Evaluation Exercises (mini-CEXs). These tools provide real-time feedback on a student’s or resident’s clinical performance in specific contexts. Collectively, they are also known as Workplace-Based Assessment tools (WBAs).
As students’ progress through clinical rotations or clerkships, these SuPs are compiled into an assessment portfolio. This portfolio includes case logs, feedback from supervisors and learner reflections. Together, these elements document the student’s longitudinal development. At certain time points, the portfolio is assessed by a Committee of Experts (CoE), and an Entrustment Decision is given. SuP assessments immerse learners in authentic clinical environments, enabling them to demonstrate how they apply competence gained in clinical practice. Final judgement of a student or a trainee’s performance and fitness for clinical practice then should be based on the CoE’s value judgement based on the portfolio.
IV. ADVOCATING FOR EXPERT JUDGEMENT: HOLISTIC EVALUATION OF A LEARNER
Expert judgement by assessors when conducting SuP assessments is commonly perceived to be subjective and bias-laden as it shifts away from quantitative to qualitative measures. However, we offer a different insight on how SuP assessments can triangulate with other more “objective” assessment tools to formulate a complete evaluation of a learner.
Expert judgement made by assessors can synthesise multiple facets of performance of a task such as that involving clinical reasoning, empathy and professionalism, in a specific context, into an interconnected evaluation, something that an objective assessment is unable to measure authentically. Multiple ‘subjective’ evaluations by many experts often provide richer, more personalised feedback that helps learners understand their strengths and areas for improvement, promoting deeper learning and growth. At the same time, in WBA, if multiple cases (i.e., patients with varying disease conditions) in many situations/contexts are assessed by multiple expert assessors, both validity and reliability of such assessment are not compromised.
Expert judgement is essential for performance assessments. While often viewed as subjective, expert judgement is vital for evaluating attributes like clinical reasoning, empathy, and professionalism. For example, in EPA-based assessments, experts determine whether learners can perform specific tasks independently, considering not just technical skills but also communication, prioritisation, and adaptability (Cate & Regehr, 2018). To ensure consistency, assessors require thorough calibration through training. Standardised tools, rating scales, and regular discussions among assessors enhance reliability and minimise bias.
Non-cognitive skills such as empathy and professionalism are essential for safe practice but challenging to assess. Portfolios which incorporate Multi-Source Feedback (MSF) provide avenues to evaluate these qualities, incorporating input from patients, peers, and supervisors. Reflective exercises encourage learners to explore biases, communication styles, and values, fostering self-awareness and empathy, and continued learning.
V. PRACTICAL CONSIDERATIONS
A. Balancing Objectivity and Subjectivity
The challenge lies in balancing “objective” assessments with “subjective” evaluations of performance. While MCQs and OSCEs provide standardised measures, expert judgement is crucial for situational assessments. Safeguards need to be in place to maximise the value of subjectivity while ensuring fairness and reliability. These include developing a structured rating scale, calibrating assessors on the scale through vocalising their thought process, discussion on biases, and using judgements from many assessors and contexts before an assessment decision is made.
B. Resource Allocations
SuP assessments demand significant resources, including trained assessors, robust documentation systems, and protected time for feedback as well as the transience of the judgement. Institutions must prioritise these investments to sustain an effective assessment system.
C. Prioritising Transparency
Ensuring transparency of expectations and standards for all assessment tools for educators and learners is important. This involves clearly defining and effectively communicating the criteria for both “objective and subjective” components of the assessment process. Judgements should be documented and explained, with a clear linkage to observable behaviours or outcomes, to foster understanding and trust in the assessment process.
VI. COMPETENCE AND ITS ASSESSMENT
Designing an assessment system to develop a safe, effective, and empathetic practitioners requires a staged, integrated approach. Competency-based assessments build foundational skills, while SuP assessments evaluate task-specific performance through expert judgement. The gradual shift from competence to performance ensures learners are prepared for the complexities of clinical practice. By incorporating EPAs, expert feedback and portfolios, the system prepares graduates to deliver patient-centred, professional, and safe care.
Future innovations like simulation-based assessments, AI-driven capture of assessor comments and feedback systems hold promise for further improving the credibility, transferability, dependability and confirmability of assessments processes for health professional programmes. The ultimate goal is to prepare practitioners for high-quality, empathetic care in an evolving healthcare landscape.
Notes on Contributors
Dujeepa Samarasekera contributed to the concept and writing of the manuscript.
Lee Shuh Shing and Han Ting Jillian Yeo contributed to writing and editing the manuscript.
Gominda Ponnamperuma contributed to reviewing the manuscript.
Funding
This study has not received any funding.
Declaration of Interest
There are no conflicts of interests related to the content presented in the paper.
References
Cate, O. T., & Regehr, G. (2018). The power of subjectivity in the assessment of medical trainees. Academic Medicine, 94(3), 333–337. https://doi.org/10.1097/ACM.0000000000002495
Cate, O. T., & Schumacher, D. J. (2022). Entrustable professional activities versus competencies and skills: Exploring why different concepts are often conflated. Advances in Health Sciences Education, 27(2), 491–499. https://doi.org/10.1007/s10459-022-10098-7
Cruess, R. L., Cruess, S. R., & Steinert, Y. (2016). Amending Miller’s Pyramid to Include Professional Identity Formation. Academic medicine: Journal of the Association of American Medical Colleges, 91(2), 180–185. https://doi.org/10.1097/ACM.0000000000000913
Hays, R.B., Wilkinson, T., Green-Thompson, L., McCrorie, P., Bollela, V., Nadarajah, V.D., Anderson, M.B., Norcini, J., Samarasekera, D.D., Boursicot, K. and Malau-Aduli, B.S. (2024). Managing assessment during curriculum change: Ottawa consensus statement. Medical Teacher, 1-11. https://doi.org/10.1080/0142159X.2024.2350522
Miller, G. E. (1990). The assessment of clinical skills/competence/performance. Academic Medicine, 65(9), S63-7. https://doi.org/10.1097/00001888-199009000-00045
*Dujeepa D. Samarasekera
Yong Loo Lin School of Medicine,
National University of Singapore,
Block MD 11, #01-11,
Clinical Research Centre 10 Medical Drive,
Singapore 117597
Email: dujeepa@nus.edu.sg
Submitted: 27 November 2024
Accepted: 28 April 2025
Published online: 1 July, TAPS 2025, 10(3), 10-14
https://doi.org/10.29060/TAPS.2025-10-3/GP3589
Thilanka Seneviratne, Wathsala Edirisingha & Wathsala Palpola
Department of Pharmacology, Faculty of Medicine, University of Peradeniya, Sri Lanka
Abstract
Introduction: Pharmacology, though challenging, is fundamental in medical practice, necessitating effective knowledge acquisition and retention for future application. This study aims to analyse student perceptions of the newly introduced teaching method, peer assessment, to enhance pharmacology teaching.
Method: Eighty-six third-year medical students of the Faculty of Medicine, University of Peradeniya participated in the peer assessment. They were divided into two groups of 40-45 and a case scenario in pharmacology was given to answer. Three volunteers from each group presented the answers. Peers evaluated the answers using provided criteria and gave feedback. The teacher then facilitated discussions, highlighting key points. Assessors and assesses perceptions on the teaching learning method was assessed using questionnaire and focus group discussions (FGD).
Results: The majority of students (n=64) (74.41%) enjoyed the task of assessing their peers. 80.23% (n=69) acknowledged the value of peer assessment for student engagement. However, 34.88% (n=30) mentioned that they did not feel they had the skills and knowledge to assess their peers. 17.43% (n=15) mentioned that they were reluctant to be critical of their peers. In the FGD students mentioned that in this student-centered learning method all students actively participated than the usual small group discussion sessions. They could compare peers’ knowledge with their own knowledge and preferred the teacher grading to be combined with peer grading.
Conclusion: Peer assessment for enhancing pharmacology teaching was well received by the students. Also, students emphasise the importance of lecturer guidance and advocate for a combined assessment approach to improve engagement and learning outcomes.
Practice Highlights
- Peer assessment keeps the students more focused during teaching learning process.
- Peer assessment enhances critical thinking and allows student centered learning.
- Combined assessment approach improves engagement and learning outcomes.
- Peer assessment for enhancing pharmacology teaching is well received by the students.
I. INTRODUCTION
The focus in higher education has shifted from conventional teaching methods to a more learner-centric approach, moving away from teacher-centered management toward fostering student self-direction (Arnold et al., 2005). This transition has sparked a growing interest in the educational benefits associated with students evaluating both their own work (self-assessment) and that of their peers (peer assessment).
Peer assessment is defined as assessment by and of individuals who have attained the same general level of training or expertise, exercise no formal authority over each other, and share the same hierarchic status in an institution (Arnold et al., 2005).
Peer assessment can be summative or formative. This focuses on the formative side, helping students plan learning, identify strengths and weaknesses, improve, and build metacognitive and professional skills. Traditional teacher-centered assessments often limit such growth. Educators valuing dialogue and collaboration should actively involve students in assessments.
Evidence is scarce regarding the utilisation of peer assessment methods for undergraduate formative assessments of a particular subject.
Pharmacology is often perceived as challenging to remember and thus, less engaging for students. Consequently, there’s reduced enthusiasm for participation in lectures. However, pharmacology serves as a fundamental aspect of medical practice, necessitating students to acquire and retain knowledge effectively for future application. Interactive teaching offer distinct advantages over traditional, teacher-centered methods by facilitating long-term retention, contextual learning, and the development of essential skills and attitudes. Thus, we introduced this teaching and learning method related to the peer assessment that integrates student centered learning within the classroom setting.
II. METHODS
A. Study Setting
The study was conducted at the Faculty of Medicine, University of Peradeniya, Sri Lanka.
B. Informed Consent
Informed written consent was obtained from the students who volunteered to the study.
C. Participants
The study involved third-year medical students from the Faculty of Medicine, University of Peradeniya, Sri Lanka. These students participated in small group discussions, each consisting of 40-45 members.
D. Peer Assessment Process
Each group was assigned short essay questions on pharmacology and students encouraged to draft written answers. Three volunteers from each group presented their answers to the class, and peers assessed them gave feedback based on criteria set by the lecturer. The teacher then facilitated discussions, highlighting key points.
E. Gathering Student Perceptions
1) Using Questionnaires: All students, except the three who presented, were provided with a self-administered Likert scale questionnaire to capture their perspectives as “assessors,” drawing from McGarr and Clifford (2013). The students who presented their answers completed a different Likert scale questionnaire, designed to capture their viewpoints as “assesses,” referencing Tahir (2012).
2) Focus Group Discussions: Nineteen students volunteered. They were divided into 3 groups. Focus group discussions, using a structured interview guide led by one investigator, lasted 30 to 40 minutes each, continued until data saturation was reached. The discussions were recorded for transcription. Participants were assured of confidentiality, and their views were anonymised. During transcription, all identifying features were removed.
F. Analysis
Quantitative data from the questionnaires were analysed using percentages. Qualitative data from the focus group discussions were analysed separately by identifying common themes in the responses.
Transcribed data were analysed using inductive content analysis. The researchers first read the transcripts to familiarise themselves with the data. Then, each transcript was coded into broad content categories. The transcripts were reread sentence by sentence and further coded into categories and subcategories.
G. Ethical Considerations
Ethical clearance was obtained from the ethics review committee of the Faculty of Medicine, University of Peradeniya. (2024/EC/25).
III. RESULTS
Eighty-six students participated as assessors. Six students participated as assesses. The results from students who assessed their peers showed mixed perceptions. A significant portion (74.41%) enjoyed the task. 44.17% agreed they were nervous about the peer assessment at the start of the module, while 29.07% were neutral (Table 1).
The comments from students assessed by their peers were generally positive. 66.67% felt they received sufficient comments, while the rest remained neutral. All participants noted that peer assessment offered more opportunities for discussion and practice. Peer assessment is recognised as a valuable exercise for students shown in Table 2.
|
Questions |
Agree (%) |
Neutral (%) |
Disagree (%) |
Total responses (%) |
|
1. nervous about the peer assessment |
38 (44.17) |
25 (29.07) |
21 (24.41) |
84 (97.67) |
|
2. limited educational values |
6 (6.97) |
25 (29.7) |
53 (61.62) |
84 (97.67) |
|
3. reluctant to be critical |
15 (17.43) |
45 (52.32) |
21 (24.41) |
81 (94.19) |
|
4. fairer assessment approach |
54 (62.78) |
20 (23.25) |
7 (8.13) |
81 (94.19) |
|
5. enjoyed assessing peers |
64 (74.41) |
10 (11.62) |
4 (4.64) |
78 (90.70) |
|
6. difficult to remove personal feelings |
19 (22.08) |
24 (27.9) |
43 (50.00) |
86 (100.00) |
|
7. I did not feel I had the skills and knowledge to assess my peers |
30 (34.88) |
23 (26.44) |
32 (37.2) |
85 (98.84) |
|
8. reluctant to give low marks |
33 (38.36) |
19 (22.09) |
31 (36.04) |
83 (96.51) |
|
9. Including peer assessment in our course made the assessment more accurate |
54 (62.79) |
27 (31.39) |
4 (4.64) |
85 (98.84) |
|
10. prefer tutor grading over peer grading |
37 (43.02) |
28 (32.55) |
19 (22.08) |
84 (97.67) |
|
11. course assessments were inaccurate |
13 (15.11) |
38 (44.18) |
30 (34.88) |
81 (94.19) |
|
12. Assessing peers was difficult |
24 (27.9) |
20 (23.25) |
40 (46.5) |
84 (97.67) |
|
13. unfair |
4 (4.64) |
17 (19.76) |
64 (74.41) |
85 (98.84) |
|
14. valuable exercise |
69 (80.23) |
10 (11.63) |
7 (8.13) |
86 (100.00) |
Table 1. Assessors’ perception regarding the peer assessment method
|
Question |
Agree (%) |
Neutral (%) |
Disagree (%) |
|
1. Evaluation and comments are fair |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
2. Comments are useful for making improvement |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
3. Comments are sufficient |
4 (66.67) |
2 (33.33) |
0 (0.00) |
|
4. Chance to practice and discuss |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
5. Less pressure and more relaxed |
3 (50.00) |
3 (50.00) |
0 (0.00) |
|
6. Who review my essays are nice |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
7. Overestimate me |
3 (50.00) |
2 (33.33) |
1 (16.67) |
|
8. Underestimate me |
0 (0.00) |
1 (16.67) |
5 (88.33) |
|
9. The quality of comments given by my peers is low |
1 (16.67) |
3 (50.00) |
2 (33.33) |
|
10. I did not like being assessed by my peers |
0 (0.00) |
1 (16.67) |
5 (88.33) |
|
11. Comments were beneficial for identifying errors in content and ideas |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
12. Comments were beneficial for identifying errors in the organisation |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
13. Prefer my tutor to grade me rather than my peers |
1 (16.67) |
5 (83.33) |
0 (0.00) |
|
14. I did not feel my peers assessed the content accurately |
1 (16.67) |
1 (16.67) |
4 (66.67) |
|
15. Unfair |
0 (0.00) |
0 (0.00) |
6 (100.00) |
|
16. A valuable exercise |
6 (100.00) |
0 (0.00) |
0 (0.00) |
Table 2. Perception of the students who got assessed by peers
Several key themes were identified by the focus group discussion.
A. Benefits of the Peer Assessment
1) Less stressful: Students mentioned that being assessed by their peers was less stressful than being assessed by a lecturer. They also noted that this method encouraged active participation in the assessment process due to its more convenient and relaxed nature.
“No nervousness at all. Because I just assesses my colleagues”
2) Kept students focused: Students commented that peer assessment is fairer than the traditional method as it kept them focused on work more than usual.
“When students have to assess their peers, they have to focus on the presenting answer. So, all students fully focus on the process. The lecturer will discuss the given scenario again. So, I think we do not miss any subject content, we can learn effectively.”
3) Peers are more accessible than lecturers: They accepted this method as a good alternative to traditional assessment methods as lecturers are not always available for the assessment.
“It’s unable to assess students by lecturers all the time, so peer assessment is a good approach to assess students.”
4) Improved understanding: Being able to know how their peers answer a question was found as a good way of comparing their knowledge and improving themselves.
“Can compare our knowledge with peers”
5) Confidence building: Another advantage they pointed out was an improvement in the level of confidence in facing an assessment as they felt more comfortable when they are assessed by peers.
“Improved confidence”
B. Challenges of Peer Assessment
1) Peers are not knowledgeable enough: Some students identified being assessed by the lecturers is better than the peer assessment as lecturers are more knowledgeable than the peers.
“Lecturers are more knowledgeable than students, so being assessed by them is essential.”
“We didn’t have deep, fine knowledge to assess peers, but we had superficial knowledge to assess them.”
C. Suggestions
A larger proportion of participants expressed appreciation for both traditional assessment methods and peer assessment, stating that using both simultaneously would be ideal.
“I think the lecturer grading is the best because we are not very experienced. However, with the time limitation, it is hard to assess students by lecturer frequently. In that case, peer assessment will be beneficial if it is combined with lecturer grading.”
Many participants expressed preference for using this in other courses.
IV. DISCUSSION
While superior assessment has been the traditional and more prevalent approach, it faces challenges due to increasing student numbers, limited lecturer availability, and time constraints. This study aims to explore students’ perceptions of peer assessment as a complementary evaluation method, addressing some of the limitations of superior assessment. The findings reveal several advantages and challenges of peer assessment.
A. Less Stressful, More Focused Learning Environment
One of the key advantages of peer assessment is its ability to create a less stressful and more focused learning environment. The results indicate that students feel more comfortable being evaluated by their peers, which allows them to engage more deeply in the learning process.
Presenters and assessors both noted that the peer assessment structure promoted active engagement, as assessors remained attentive throughout the session to provide meaningful feedback, and those not presenting felt more relaxed and focused compared to traditional SGD formats. This shows that peer assessment method enhances student focus in learning environment.
B. Increased Availability and Accessibility
Given the time constraints and growing student populations, continuous evaluation by lecturers is challenging. However, well-prepared peer groups can effectively bridge this gap, providing timely feedback and support. This aspect of peer assessment enhances students’ opportunities for formative feedback, which is critical for their learning process.
C. Improves the Assessor’s Understanding of the Subject/Confidence Building
Students gain valuable insights and deepen their understanding by evaluating and providing feedback on their peers’ written work, as this process enhances their critical thinking and analytical skills (Topping, 2009). This fact was noted by the participants of our study also. They appreciated the chance to analyse their peers’ answers.
The supportive environment of peer assessment enabled students to share and compare their knowledge openly, which in turn helped them refine their answers and learn better organisational techniques, which improve their confidence.
D. Addressing Knowledge Gaps
One challenge identified in peer assessment is the limited expertise of peers in accurately assessing their classmates. However, this challenge can be mitigated with proper preparation and guidance from lecturers. Topping (2009) has highlighted that training students to provide constructive feedback is a challenging process. However, the benefits it yields outweigh the burden of training peer assessors.
Literature also gives evidence regarding the doubt about the validity level of peer assessment among teachers and students (Holroyd, 2000). This attitude has been identified as a major barrier to the use of peer assessment as a standard method of evaluating students.
Fry (1990) highlighted that, when it is implemented in the right way, peer evaluation demonstrates results, which are comparable with lecturer evaluation.
E. Overcoming Personal Bias
A drawback noted by students was the difficulty of remaining objective when assessing their peers. Many students found it challenging to give low marks or critically evaluate their friends’ work as a lecturer might. This concern highlights the need for students to be properly trained as an assessor.
Several published studies shows that peer evaluation can be affected by negative social factors like peer pressure, favoritism, or fear of criticism, especially when done face-to-face. To address these issues, it’s important to use methods that ensure anonymity in peer reviews.
F. Recommendations for Future Application
Overall, students in this study expressed a positive view of peer assessment and suggested its use in other courses. They acknowledged that combining peer assessment with superior assessment could enhance learning outcomes. To ensure the effectiveness of peer assessment, students recommended conducting it under the supervision and guidance of lecturers. This combined approach would offer the benefits of peer-to-peer engagement while maintaining the academic rigor provided by expert feedback.
V. CONCLUSION
While peer assessment presents certain challenges, it offers substantial advantages in creating a more accessible, engaging, and confidence-building learning environment. With proper training and lecturer involvement, peer assessment can serve as a valuable complement to traditional assessment methods in higher education.
Notes on Contributors
Thilanka Seneviratne led the study’s conception, design, and implementation, contributed to data analysis and interpretation, drafted and critically revised the manuscript. Wathsala Edirisingha was involved in the implementation of the study and contributed to data acquisition and analysis. Himali Palpola contributed to the study’s implementation, data analysis, and manuscript drafting. All the authors have read and approved the final manuscript.
Ethical Approval
Ethical clearance was obtained from the ethics review committee of the Faculty of Medicine, University of Peradeniya, (2024/EC/25).
Acknowledgement
We acknowledge the staff of the department of Pharmacology, Faculty of Medicine, University of Peradeniya for their valuable contribution in material and organisational support.
Funding
No funding sources are associated with this paper.
Declaration of Interest
All authors declare no conflict of interest.
References
Arnold, L., Shue, C. K., Kritt, B., Ginsburg, S., & Stern, D. T. (2005). Medical students’ views on peer assessment of professionalism. Journal of General Internal Medicine, 20(9), 819–824. https://doi.org/10.1111/j.1525-1497.2005.0162.x
Fry, S. A. (1990). Implementation and evaluation of peer marking in higher education. Assessment & Evaluation in Higher Education, 15(3), 177–189. https://doi.org/10.1080/0260293900150301
Holroyd, C. (2000). Are assessors professional? Student assessment and the professionalism of academics. Active Learning in Higher Education, 1(1), 28–44. https://doi.org/10.1177/1469787400001001003
McGarr, O., & Clifford, A. M. (2013). ‘Just enough to make you take it seriously’: exploring students’ attitudes towards peer assessment. Higher education, 65, 677-693. https://doi.org/10.1007/s10734-012-9570-z
Tahir, I. H. (2012). A study on peer evaluation and its influence on college ESL students. Procedia-Social and Behavioral Sciences, 68, 192-201. https://doi.org/10.1016/j.sbspro.2012.12.219
Topping, K. J. (2009). Peer assessment. Theory Into Practice, 48(1), 20–27. https://doi.org/10.1080/00405840802577569
*Thilanka Seneviratne
Faculty of Medicine,
University of Peradeniya, Sri Lanka, 20400
Email: thilanka.medi@gmail.com
Submitted: 26 September 2024
Accepted: 25 March 2025
Published online: 1 July, TAPS 2025, 10(3), 5-9
https://doi.org/10.29060/TAPS.2025-10-3/GP3504
Shihoko Yamakawa1, Olga Razvina2, Fumiko Okazaki2, Hiroshi Hibino3, Toshiyuki Someya4 & Tatsuo Ushiki4
1Niigata University Institute of Global Affairs, Japan; 2Niigata University Medical Education Centre, Niigata University Graduate School of Medical and Dental Sciences, Japan; 3Department of Pharmacology, Osaka University Graduate School of Medicine, Japan; 4Niigata University, Japan
Abstract
Introduction: Niigata University School of Medicine and Niigata University Graduate School of Medical and Dental Sciences have been engaging in medical exchanges with Russian medical universities for over 30 years. In 2015, a double-degree program with Russian medical universities was initiated, leading to a multi-layered education project that included short-term undergraduate student exchange programs and graduate-level double-degree programs, resulting in the circulation of human resources.
Methods: The program was conducted in English, and a maximum of 15 credits could be transferred based on the universities’ regulations. Degree examinations were conducted independently, and successful candidates were awarded degrees from both Niigata University and their home university in Russia. The project was overseen by the G-MedEx Centre at Niigata University, which included staff with international experience.
Results: The difference in standard study duration between Japan and Russia was eliminated by using a four-year system in the graduate school doctoral programs. Three study models were proposed by Russian universities, considering each university’s regulations and various circumstances. The curriculum was determined based on the rules of the universities in Russia and the circumstances of the students. Agreements were made with each university in supplementary documents.
Conclusion: Despite the differences in educational standards and the lack of a common educational framework between Japan and Russia, the difficulties can be overcome, and educational compatibility can be increased.
Practice Highlights
- Thanks to a long history of interaction with Russia, we were able to organise a large educational project, which included multi-layered programs, one of which was a double degree program.
- As part of the project, we established a coordination centre (G-MedEx Centre) that effectively engaged with students, teachers, and university administration to address challenges and tasks as they arose.
- We successfully navigated the differences in educational standards between Russia and Japan and developed effective mechanisms for collaboration.
- Despite the challenges of the double degree program, we have two successful examples of students who completed their double degrees.
- We were able to train doctors and scientists who gained unique international experience and will be able to make significant contributions on the world stage in the future.
I. INTRODUCTION
Since 2014, Russia and Japan have started to actively cooperate in the academic sphere, particularly after the Ministry of Education, Culture, Sports, Science, and Technology (MEXT) adopted two programs “Special Program for Priority Placement of Japanese Government Scholarship International Students” and “Re-inventing Japan Program for Strengthening Universities’ Globalisation”. These programs were designed to promote interaction with Russia and continued until 2018. Prior to this project, interactions with Russian universities were decentralised, with each university managing its exchange programs. Niigata University School of Medicine and Niigata University Graduate School of Medical and Dental Sciences have also conducted bi-directional medical exchanges with Russian universities since 1993. However, it was in 2014 that the exchange program received a significant boost due to a decision made by the Japanese and Russian governments. Niigata University merged these two programs into one initiative called the G-MedEx (Globalization and Medical Exchange) project (Yamakawa et al., 2018). As a result, the Japan-Russia exchanges made significant progress. The project aimed to expand Niigata University’s educational programs and enhance research collaboration (Obst & Kuder, 2012), leading to the establishment of the Double Degree Program (DDP) to advance medical care and develop skilled human resources in Japan and Russia (Teplyashina et al., 2017). DDP allows universities to award degrees to students who meet their graduation requirements. The number of public universities in Japan implementing DDPs has increased from 47 to 56 out of a total of 85 public universities over the past ten years, though only a few have partnered with Russian universities. Intrinsic differences in education and credit systems between Japanese and Russian universities have become an obstacle to student exchange and the establishment of joint educational programs (Jargin, 2024; Sitnikov & Bizunkov, 2016).
This paper reports on specific issues such as the graduate school curriculum, credit system, degree examination requirements, and solutions to help overcome these differences.
II. METHODS
A. Implementation Method
The DDP at the Graduate School of Medical and Dental Sciences admitted up to two students annually from three Russian partner universities. Candidates, recommended by their home institutions, enrolled concurrently at NU and their respective universities upon passing NU’s entrance exam. The program was conducted in English.
B. Credit Transfer and Grade Evaluation
Under the DDP agreement, up to 15 of the 30 required credits were transferable. A standardised Japanese-Russian grading system (A–E) was implemented to ensure educational quality.
C. Degree Examination and Conferral of Degrees
Degree examinations were conducted independently per each university’s standards. Graduates were awarded a PhD from both NU and their home university. A joint DDP certificate was also conferred.
D. Implementation System
The G-MedEx Centre at NU managed the program. A Russian physician and administrative staff oversaw the program on their end, while liaison professors from partner universities facilitated coordination. Support structures for international students were established in collaboration with university committees. In Figure 1, we compare the credit standards of the Russian Federation with those of our university’s doctoral program in medical and dental sciences, which serves as a benchmark in Japan. Russia’s ECTS model defines one credit as 36 hours, with doctoral programs needing 180 credits, compared to Japan’s 45 credits.

Figure 1. Credits and study hours (Niigata University and Russian Partner Universities)
III. RESULTS
A. Education Reform and DDP in Russia
The European Credit Transfer System (ECTS) and the UMAP Credit Transfer Scheme (UCTS) have enhanced international education quality. Russia, undergoing education reforms since 1991, joined the Bologna Process in 2003 and enacted a federal law on networked education in 2012. Its credit system aligns with ECTS. However, when NU launched the DDP in 2015, faculty-level understanding and overseas credit recognition were insufficient. Japanese and Russian faculty collaboratively developed a compliant curriculum through trial and error.
B. Graduate School Curriculum and Credit Transfer
Completing two dissertations within the study period required curricular alignment. Figure 2 illustrates the Russian doctoral curriculum which includes general courses (9 credits) and specialised subjects (21 credits) in the first year, advanced coursework (7 credits) and clinical practice in the second year, and research (48 credits) in the third year, culminating in a final evaluation. A structured course mapping and unified grading system aided in credit transfer.

Figure 2. Basic course curriculum and number of credits, Russian Graduate School doctoral program
We developed a group of courses for specialised classes to streamline the collation process. A unified evaluation standard based on Japan and Russia’s systems was adopted, significantly speeding up credit transfers.
C. Eliminating Differences in the Standard Study Period and Creating a Study Model
We have worked on eliminating the difference in standard study duration between Japan and Russia, which is a structural problem. Although undergraduate education in the medical field is six years both in Japan and Russia, the duration of graduate school doctoral programs differs. In Japan, it is four years, and in Russia, it is usually three years. Although DDP allows credits to be transferred, it is quite difficult to complete study programs at both universities and write two dissertations in three years. Therefore, we decided to use a four-year system.
The extra one-year study period in Russia has been an ongoing academic issue. After discussions between Japan and Russia, Russian universities proposed three study models based on regulations and circumstances. It was suggested that students spend the first two years in Russia and the remaining two at their home university. They also noted that compulsory subjects are concentrated in the first year, making it appropriate for students to start research and gain basic skills in their native language.
The three study models proposed were as follows:
– Model 1: After completing two years, the student takes a one-year leave at a Russian university. Then the student returns to school for the fourth year and completes the Japanese and Russian programs at the same time.
– Model 2: Establishing a new four-year doctoral course program at Russian universities. This is a special curriculum in which the 180 credits that should be earned over three years are distributed evenly over four years, resulting in 45 credits earned in one year.
– Model 3: At the end of the third year, all completion requirements except for thesis defense should be completed, and graduation is suspended. After it is confirmed that the students are expected to graduate from the university in their fourth year, they will proceed to the examination and officially complete their studies in Japan and Russia at the same time.
In the case of models 2 and 3, students have to pay tuition fees for four years in Russia based on the length of study. Additionally, in the case of model 3, upon completion of the third year, students are required to return to Japan temporarily for up to one month for graduation exams and related procedures. The curriculum was determined based on the rules of the universities in Russia and the circumstances of the students. The agreements were made with each university in supplementary documents.

Figure 3. DDP Models
D. Thesis Defense
Russia and Japan have different systems for evaluating theses. In Russia, dissertations are typically 100 to 150 pages long and are written in Russian. They are reviewed by the Higher Accreditation Commission. In contrast, in Japan, dissertations must be written in English and be published in an international journal. Because of these regulatory differences, a single-thesis evaluation approach was not feasible, resulting in separate reviews for each thesis. While foreign examiners can attend public hearings for dissertations in Russia, they are not allowed to serve on examination committees due to government restrictions.
E. Building a Network with a Dedicated Project Team
Since the G-MedEx Centre’s establishment, its international network has expanded across Russia, with exchange agreements established with nine universities. Appointing liaison professors at Russian universities significantly motivated local faculties and had an unexpected positive impact. Regular information exchange enabled the swift identification and resolution of issues, contributing to the project’s success and improvements in the study environment and safety management for international students.
IV. DISCUSSION
This paper highlights the challenges faced in implementing the Double Degree Program (DDP) and the measures taken to address them. Six students were enrolled in the program, and two of them have already obtained their degrees. While most of the academic and curricular challenges have been resolved, some issues still need to be addressed. Although credit transfer can reduce some duplication of study content, fulfilling the graduation requirements of two universities within the standard study period is challenging. After gathering feedback from students participating in the program, we learned that many found it very challenging, particularly those conducting research that required wet experiments. In contrast, students focused on statistical research did not express similar concerns.
Another factor contributing to the program’s complexity was that the research topics at the two universities often had no connection, forcing students to manage two entirely unrelated projects. This increased their workload and sometimes hindered their ability to complete the program successfully.
Consequently, we concluded that for future programs, it is essential to choose departments that can coordinate their projects, ensuring they engage in collaborative research. This approach would make it easier for students to complete both projects on time. Regarding the credit system, a transfer method based on the “competency-based” approach is being considered, where students are evaluated based on the acquired results of comprehensive and specialised abilities and skills required for the subject, rather than assigning academic training per credit by the time spent in it. To speed up the process, we have limited credit transfer to specialised subjects at our university. However, as the number of students increases and the scale of projects grows, it will be essential to systemise credit transfer and simplify administrative procedures further. Therefore, we need to build a system that guarantees a higher level of educational quality between the two countries while referring to the framework provided by ECTS and the Erasmus Project (European Community Action Scheme for the Mobility of University Students), which are the standard in Russia. From the viewpoint of human resource circulation, some graduates have become post-doctoral fellows or faculty members at Niigata University, while others have returned to their home countries to work as doctors.
V. CONCLUSION
Witnessing young medical scientists grow and start playing active roles in both countries is the greatest joy of international collaboration in education. Russia recently withdrew from the Bologna Process. As a result, the country may develop its own education system that does not depend on the European framework. Russian students may face challenges in integrating into the European education system and accessing European educational grants.
However, interactions with countries not part of the Bologna process—such as Japan, India, and China—will remain unaffected, since these countries operate according to their own independent systems. The key will be finding common ground and promoting academic mobility, though this won’t be straightforward based on our past experiences.
Thus, cooperation with these countries will require careful attention. It is essential to focus on the future effects on education and ensure the educational environment’s protection for students, drawing on the knowledge and experience gained so far.
Notes on Contributors
SY, the first author, contributed significantly to the design, wrote and edited the paper, and reviewed the literature. OR was responsible for data collection, resource verification, reviewing and editing the manuscript. FO conducted resource verification, reviewed and edited the manuscript. HH provided critical feedback during the writing process, analysed the data, implemented and supervised the project. TS led the project, interpreted the data, and provided guidance. TU, the lead conceptualiser, designed the study, was responsible for conceptualisationand obtaining funding.
Acknowledgement
We would like to express our sincere gratitude to professors of Krasnoyarsk State Medical University, Far Eastern State Medical University, and Pacific State Medical University for their cooperation in conducting this study.
Funding
This research was supported by JSPS Grant-in-Aid for Scientific Research 20K02936.
Declaration of Interest
The authors declare that they have no conflict of interest.
References
Jargin, S. (2024). Medical education and postgraduate training in Russia: An update. Journal of Integrative Medicine & Therapy, 7(1), 1. https://doi.org/10.13188/2378-1343.1000019
Obst, D., & Kuder, M. (2012). International joint- and double-degree programs. International Higher Education, 66, 5-7. https://doi.org/10.6017/ihe.2012.66.8585
Sitnikov, V., & Bizunkov, A. (2016). The higher education at the post-Soviet territories: The long echo of the Bologna process. Vestnik Otorinolaringologii, 81(4), 72-77. https://doi.org/10.17116/otorino201681472-77
Teplyashina E., Petrova M., Salmina A., & Razvina O. (2017) The experience of networking postgraduate training programmes. The Education and Science Journal, 19, 4. https://doi.org/10.17853/1994-5639-2017-4-118-129
Yamakawa, S., Razvina, O., Ito, M., Hibino, H., Someya, T., & Ushiki, T. (2018) Medical exchange project for students and young doctors between Japan and Russia. Medical University, 1, 32-39. https://doi.org/10.2478/medu-2018-0005
*Shihoko Yamakawa
1-757, Asahimacho-dori, Chuo-ku,
Niigata, Japan 951-8510
-81 (025) -227-2063
Email: yamakawa@med.niigata-u.ac.jp
Submitted: 29 July 2024
Accepted: 24 February 2025
Published online: 1 July, TAPS 2025, 10(3), 1-4
https://doi.org/10.29060/TAPS.2025-10-3/GP3478
Tayzar Hein1, Ye Phyo Aung1, Khin Aung Htun1 & Tin Tun2
1Department of Medical Education, Defence Services Medical Academy, Myanmar; 2Department of Human Resources for Health, Ministry of Health, Myanmar
Abstract
Introduction: The medical education system of Myanmar has evolved through a dynamic history influenced by colonial legacies, national development efforts, and global collaborations. This article explores the progression of medical education in Myanmar, focusing on its historical milestones, challenges, and advancements in response to societal and healthcare needs.
Method: This study is based on a comprehensive review of historical records, policy documents, and academic literature, with “A Concise History of Medical Education in Myanmar” by Aung Than Batu as a primary reference. Key milestones, collaborations, and innovations were analysed to trace the evolution of medical education from the colonial period (1907) to the present day. Quantitative data, including the number of medical universities, training durations, and infrastructure developments, were included for a clearer perspective.
Results: The analysis highlights transformative milestones, including the establishment of the first medical school in 1907 and Rangoon Medical College in 1927. Over time, Myanmar has adapted to challenges such as resource constraints and political instability by fostering international collaborations and leveraging technology. Teaching methods have evolved significantly, integrating modern technologies alongside traditional pedagogies.
Conclusion: Myanmar’s medical education exemplifies resilience and adaptability. By aligning its system with global standards, fostering research, and leveraging international expertise, the nation continues to contribute to global medical education and healthcare. This narrative serves as an inspiration for countries navigating similar challenges in medical education.
Practice Highlights
- Myanmar’s medical education journey began in 1907, blending indigenous practices with Western methodologies, and expanded post-independence with the establishment of multiple medical universities.
- Myanmar overcame challenges like resource limitations and political instability by fostering global collaborations and integrating modern technologies into medical education.
- The MBBS program combines robust theoretical knowledge with clinical training, while postgraduate education emphasises research, making Myanmar a contributor to global medical advancements.
I. INTRODUCTION
Myanmar, a nation of profound cultural richness and historical depth, unfolds a narrative that intricately intertwines with the evolution of its medical education system. This comprehensive overview embarks on a journey through the diverse facets of Myanmar’s medical education landscape (Batu, 2015). Beyond a mere chronological exploration of historical administrative periods, it endeavors to unravel the intricate threads woven into policy development, the establishment of medical universities, and the ceaseless pursuit of addressing challenges and seizing opportunities within the nation’s healthcare and educational sectors. The journey begins in 1927, with the establishment of the Rangoon (Yangon) Medical College, a milestone in introducing formal medical education during the British colonial era (Batu, 2015). This marked the fusion of indigenous healing traditions with Western medicine, laying the foundation for a unique and dynamic approach to healthcare education (Coderey, 2021). After independence in 1948, the nation’s commitment to advancing medical education became evident with the expansion of medical facilities and the development of policies aimed at addressing the healthcare needs of its population. By the 1960s, the establishment of additional institutions, such as the Institute of Medicine (I), reflected Myanmar’s growing emphasis on training a competent cadre of healthcare professionals. In 1970, the establishment of the University of Medicine 2 in Yangon further demonstrated this dedication to expanding medical education access (Batu, 2015). Infrastructure development and facility expansions in subsequent decades signaled foresight that extended beyond immediate requirements, highlighting a long-term vision for excellence and capacity-building in medical education (Batu, 2015).
Amidst challenges such as resource limitations and periods of political instability during the 1980s and 1990s, the story Myanmar of took a resilient turn, transforming obstacles into opportunities. International collaborations, such as partnerships initiated in the 2000s, and the adoption of technological advancements emerged as beacons of progress, underscoring the adaptability and determination of Myanmar to elevate the standards of its medical education (Saw et al., 2019). As Myanmar enters the 21st century, it not only continues to address its domestic healthcare needs but also contributes to the global context. Its influence reverberates through research contributions, milestones in undergraduate and postgraduate medical education, and a commitment to integrating public health perspectives (Saw et al., 2019). Myanmar emerges not just as a nation shaping its healthcare narrative but also as a participant in the broader discourse on global health, contributing to the collective effort to address worldwide health challenges (Proserpio, 2022).
II. ADMINISTRATIVE PERIODS IN MYANMAR
Colonial Era (1824–1948): Under the shadow of British rule, the colonial period of Myanmar bore witness to the initial introduction of Western medicine. The 1860s marked the beginnings of formal medical education when the British established training programs for healthcare workers to address the needs of colonial administration and military personnel. In 1927, the foundation of the Rangoon (Yangon) Medical College became a pivotal moment in the integration of Western methodologies into Myanmar’s medical education system. This era marked the confluence of indigenous healing practices with the methodologies imported during colonial occupation (Coderey, 2021).
Post-Independence Era (1948 onwards): The post-independence period signaled a fervent drive by Myanmar to shape its own destiny. The establishment of the Institute of Medicine (I) in the 1960s marked a significant step toward creating specialised medical education institutions to cater to the nation’s healthcare needs. This commitment was further exemplified by the opening of the University of Medicine 2 in Yangon in 1970, ensuring broader access to medical education. In 1992, the Defence Services Medical Academy (DSMA) was established as the nation’s sole military medical university, dedicated to training medical professionals for the armed forces. With six medical universities in total five civil institutions and one military. The country has demonstrated a sustained effort to expand medical education. This era also saw the formulation of policies aimed at strengthening public health systems and addressing resource limitations, particularly during the politically turbulent 1980s and 1990s. These efforts laid a strong foundation for Myanmar’s aspiration to build a healthcare system reflective of its cultural identity and societal requirements (Coderey, 2021).
III. MEDICAL EDUCATION POLICY IN MYANMAR AND DEVELOPMENT OF MEDICAL UNIVERSITIES
The evolution of medical education policies in Myanmar from 1950 onwards has been a dynamic and adaptive process. Over the years, these policies have responded to societal needs, embraced technological advancements, and aligned with global standards in medical education. A key focus has been the alignment with international benchmarks, ensuring that the education imparted equips Myanmar’s medical graduates to meet and exceed global standards in healthcare delivery. Myanmar’s journey in medical education began in 1907, with the establishment of the Government Medical School in Yangon, which laid the groundwork for structured medical training. The pivotal moment came in 1927, with the establishment of the Rangoon (Yangon) Medical College, formalising Western medical education. Following independence in 1948, the nation prioritised medical education policy development, leading to the creation of the Institute of Medicine (I) in the 1960s and the University of Medicine 2 in 1970 (Batu, 2015). The subsequent decades witnessed the growth of additional medical universities, including the University of Medicine, Mandalay, and the University of Medicine, Magway, which were established to decentralise medical education and improve access. Infrastructure development and the expansion of facilities became pivotal strategies, particularly during the 1980s and 1990s, to accommodate the surging demand for medical education and enhance the overall quality of healthcare provision. These initiatives reflect the commitment of Myanmar to fostering a robust and sustainable healthcare system (Batu, 2015).
IV. CHALLENGES, OPPORTUNTIES AND MEDICAL EDUCATION RESEARCH
Throughout its history, the medical education system of Myanmar has faced formidable challenges, ranging from resource limitations to periods of political instability, such as during the politically turbulent 1980s and 1990s (Saw et al., 2019). Despite these adversities, these challenges have served as crucibles for transformation, providing opportunities for resilience and innovation. By the 2000s, Myanmar actively embraced international collaborations, partnering with global institutions to strengthen its medical education framework. These collaborations have acted as catalysts for overcoming structural and educational challenges, fostering knowledge exchange, and enhancing training methodologies (Proserpio, 2022). In recent decades, technological advancements have presented unprecedented opportunities to bridge gaps in medical education delivery. For instance, the integration of e-learning platforms and simulation-based training since the 2010s has improved both accessibility and quality, enabling students across Myanmar to benefit from innovative educational tools (Saw et al., 2019). This dual narrative of challenges and opportunities paints a dynamic picture of Myanmar’s medical education landscape one that is continuously evolving and adapting to the shifting sands of the global healthcare arena.
Myanmar’s indelible mark on medical education research is a testament to its commitment to academic excellence. The country has emerged as a significant contributor to the global knowledge base in medical education, particularly since the early 2000s, fostering an environment where researchers explore innovative methodologies and address critical questions within the field in 1990s (Saw et al., 2019). Myanmar’s researchers, often collaborating across borders, have played a pivotal role in advancing educational practices worldwide. The research landscape in Myanmar is characterised by a diverse array of studies, including pedagogical approaches, curriculum development, and assessments of educational outcomes. Researchers have delved into the effectiveness of various teaching methods, the impact of cultural nuances on medical education, and the integration of technology into learning strategies (Coderey, 2021). These endeavors not only enhance the quality of medical education within Myanmar but also contribute valuable insights to the broader international community. the commitment of Myanmar to medical education research extends beyond national boundaries, with researchers actively engaging in cross-cultural studies and collaborative projects. Examples include partnerships with institutions in Southeast Asia and beyond, leading to impactful studies on public health education and global health challenges (Proserpio, 2022). This collaborative spirit enriches the local research landscape and fosters a global exchange of ideas, ultimately elevating the standards of medical education on an international scale.
V. UNDERGRADUATE MEDICAL EDUCATION AND POSTGRADUATE MEDICAL EDUCATION
Undergraduate Medical Education in Myanmar: The structure of undergraduate medical education in Myanmar has undergone a transformative journey, evolving into a robust system that imparts a comprehensive understanding of medical science. The curriculum, meticulously developed over the decades, strikes a balance between theoretical knowledge and practical application, ensuring that graduates are well-equipped to navigate the complexities of healthcare. Milestones in curriculum development have played a pivotal role in shaping an adaptable and rigorous educational framework. Since the establishment of the Government Medical School in 1907 and the introduction of formal undergraduate medical training at Rangoon Medical College in 1927, Myanmar has continually refined its approach to align with global standards while addressing local healthcare needs (Batu, 2015). The integration of foundational medical sciences with clinical training, particularly from the 1960s onward, has created a holistic educational experience.
Clinical Training: Clinical training is a cornerstone of undergraduate medical education, offering students invaluable exposure to patient care, medical decision-making, and collaborative healthcare practices. From the 1970s, rotations in diverse medical specialties were formalised, enabling students to gain insights into the multifaceted nature of healthcare delivery. This hands-on approach fosters the development of critical thinking, diagnostic acumen, and a patient-centered mindset. Despite challenges such as resource constraints and political instability during the 1980s and 1990s, the resilience of Myanmar has been evident. By the 2000s, international collaborations and advancements in technology allowed for significant improvements in medical education delivery (Batu, 2015). Initiatives such as e-learning platforms and virtual simulations have enhanced accessibility and quality, ensuring a dynamic learning environment.
Outcomes and Global Impact: Graduates of Myanmar undergraduate programs emerge with a blend of strong theoretical knowledge, practical skills, ethical grounding, and communication proficiency. Many contribute to the global medical community, bringing cultural understanding and internationally recognised expertise to diverse healthcare settings.
Postgraduate Medical Education in Myanmar: Myanmar postgraduate medical education system has witnessed substantial transformation, adapting to the increasing demand for specialised expertise in healthcare (Saw et al., 2019). The diversification of postgraduate programs since the 1980s reflects a commitment to align with global standards while addressing the unique challenges of the nation’s healthcare system.
Specialised Training and Research: Postgraduate training emphasises advanced clinical skills and specialisation across medical disciplines. From the 1990s, research became an integral part of postgraduate education, fostering innovation and addressing critical healthcare gaps. Myanmar postgraduate students actively contribute to cutting-edge research, positioning the nation as a hub for medical advancements (Batu, 2015). This dual focus on research and clinical expertise ensures the preparation of professionals capable of tackling evolving healthcare challenges.
Collaborative Endeavors: International collaborations have played a pivotal role in enhancing postgraduate medical education. Partnerships with regional and global institutions have facilitated the exchange of expertise and best practices, enriching both training programs and research initiatives (Proserpio, 2022). These efforts underscore Myanmar’s commitment to participating in and contributing to the global medical community.
Outcomes and Ethical Practice: Myanmar postgraduate medical education is characterised by a dynamic interplay of specialised training, collaborative research, and a steadfast commitment to ethical medical practice (Rosenbaum et al., 2021). This multifaceted approach elevates the capabilities of healthcare professionals and enhances the overall standard of healthcare delivery, both nationally and internationally.
VI. CONCLUSION
Myanmar’s history of medical education is a dynamic narrative marked by resilience, adaptability, and the ability to turn challenges into opportunities. From its early adoption of Western medical practices during the colonial era to the establishment of a robust and evolving educational framework, Myanmar has consistently demonstrated a commitment to excellence. This global perspective highlights Myanmar’s efforts to align its medical education system with international benchmarks, contribute substantively to medical research, and actively engage in global public health initiatives. As Myanmar continues to shape its medical education landscape, it stands poised to make lasting contributions to global healthcare. Myanmar’s unwavering dedication to excellence not only enhances its own healthcare system but also enriches the global discourse on medical education and public health, positioning the nation as a vital contributor to the collective effort of improving global health outcomes.
Notes on Contributors
Tayzar Hein contributed to this manuscript’s first draft version , and revised its subsequent draft. Ye Phyo Aung, Khin Aung Htun, and Tin Tun contributed to the manuscript and critically revised the first draft. All the authors discussed and contributed to the final manuscript.
Funding
The activity is undertaken for the sake of personal and professional growth, and does not require any financial support.
Declaration of Interest
There is no conflict of interest in the current research.
References
Batu, A. T. (2015). The history of medical education in Myanmar (1886 to 2010). Myanmar Academy of Medical Science.
Coderey, C. (2021). Myanmar Traditional Medicine: The making of a national heritage. Modern Asian Studies, 55(2), 514-551. https://doi.org/10.1017/S0026749X19000283
Proserpio, L. (2022). Myanmar higher education in transition: the interplay between state authority, student politics and international actors.
Rosenbaum, S. A., Tushaus, D., Hubbard, B., & Sharp-Bauer, K. (2021). The Myanmar Shwe: Empowering law students, teachers, and the community through clinical education and the rule of law. Indiana Journal of Global Legal Studies, 28(1), 153-230.
Saw, Y. M., Than, T. M., Thaung, Y., Aung, S., Shiao, L. W.-S., Win, E. M., Khaing, M., Tun, N. A., Iriyama, S., & Win, H. H. (2019). Myanmar’s human resources for health: Current situation and its challenges. Heliyon, 5(3), e1390. https://doi.org/10.1016/j.heliyon.2019.e01390
*Tayzar Hein
No.94, D-1, Pyay Road, Mingaladon Township,
Yangon, Myanmar Postal code – 11021
+95 95188093
Email: dr.tayzarhein@gmail.com
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
