
A third wave in medical education
During the years preceding 1910, the education and training of physicians (doctors)-to-be was based mainly on a master-apprentice model; the primary focus then was on the teaching and development of clinical skills.
In 1910, however, Flexner submitted a highly influential report to the American medical authorities: in it he recommended that all medical schools should be university-based and that, importantly, medical practice should have a scientific basis strongly underpinned by the basic medical sciences such as anatomy, biochemistry and physiology. Flexner’s1 recommendation was readily accepted, not only in the USA, but also globally- including Asia.
The recommendation of Flexner1 provided the impetus for the design of medical education that begins with a pre-clinical phase in which student learning will focus mainly on the acquisition of content knowledge derived from the basic medical sciences to provide the strong scientific foundation for the clinical phase that follows. During the clinical phase, student learning will focus primarily on the clinical sciences relating to the diagnosis, treatment and management of patient care.
Thus, two key ‘pillars’ (the basic sciences and the clinical sciences) of medical education were established; this two pillar model of medical education persisted for many decades thereafter and remained so till today. The two pillar model of medical education, as strongly advocated in the recommendation of Flexner1, has served medical practice well as “…the reforms equipped health professionals with the knowledge that contributed to the doubling of life span during the 20th century.” 2 and all seemed well.
However, in order to optimise patient care today, health care delivery must be viewed as an ‘eco-system’, i.e. within an entire health system in which the patient is linked to as the central figure. Such a ‘health system’ has been clearly recognised by the Education Consortium of the American Medical Association (AMA) which recently published the textbook ‘Health Systems Science’ (2017). In the ‘Preface’ of the textbook, it has been firmly expressed that “Even if basic and clinical sciences are expertly learned and executed, without health systems science, physicians cannot realize their full potential on patients’ health or on the population.” 3
In the ‘Foreword’ James L. Madara, executive vice president and CEO of the AMA, has also expressed that: “The emergence of health systems science will be a key component of the medical school of the future, bridging the study of basic and clinical sciences and giving new physicians a broad view of the societal influences and administrative challenges that sometimes complicate patient care. Health systems science is that window into the lives of our patients and our communities that makes us more effective, compassionate, and knowledgeable doctors.”
The Education Consortium of the AMA has therefore proposed ‘Health Systems Science’ as a “third pillar” in medical education, thus leading the charge for a new wave in 21st century medical education.
January edition features several important areas in Health Professions Education such as ways to promote excellence in medical education, team work and interprofessional learning. The student led, faculty supported Tri-Generational Homecare project highlight the importance of encouraging students outside their curriculum to develop innovative community centric projects.
Dujeepa D. Samarasekera & Matthew C.E. Gwee
Centre for Medical Education (CenMED), NUS Yong Loo Lin School of Medicine,
National University Health System, Singapore
1 Flexner A. (1910). Medical Education in the United States and Canada: A Report To the Carnegie Foundation For the Advancement of Teaching (Bulletin Number Four). New York, USA: The Carnegie Foundation for the Advancement of Teaching.
2 Frenk, J., Chen, L., Bhutta, Z. A., Cohen, J., Crisp, N., Evans, T., … Zurayk H. (2010). Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. The Lancet, 376 (9756), 1923-1958.
3 Susan E. S., Richard, H., Luan, L., Stephanie, S., Jeffrey, B. & Jed, G. (2016). Health Systems Science. American Medical Association Education Consortium: Elsevier Canada.
Published online: 7 January, TAPS 2020, 5(1), 1-2
DOI: https://doi.org/10.29060/TAPS.2020-5-1/EV5N1
What we eventually accomplish may depend more on passion and perseverance than on our innate talent.
—Angela Duckworth, Grit: The power of passion and perseverance, 2016
There is now strong and compelling research evidence that individual grit (i.e. the combination of passion and perseverance of an individual for a given task—independent of the domain) is a better predictor of an individual’s potential for success in the future work environment (and, therefore, presumably one’s lifetime achievements as well) than just one’s innate talent. For example, cadets who gain admission into prestigious military institutions like West Point and the Army Special Operation Forces in the USA, are often selected from student cohorts with high scholastic achievements and excellent sportsmen: thus, acceptance into these prestigious institutions is highly competitive—requiring, both, intense physical endurance and high mental agility. However, in spite of such competitiveness, a small percentage of cadets selected often ‘drop-out’ prematurely from the training programme. The ‘dropouts’ often constitute an ‘economic waste’ to the organisation concerned, especially when candidates have been specially selected over many others with similar qualifications. The ability to predict such ‘potential dropouts’, even before the candidates undertake the training programme, will help in the selection of more suitable candidates for the training course, with consequent cost-savings to the organisation concerned. Moreover, if selected candidates are deemed “more suitable” for the training course, then it probably can also be assumed that such candidates will also perform well in their future work environment.
The “Grit Scale” was developed, designed and tested in several cohorts of individuals from different organisations (Duckworth, 2016). The grit scale is essentially a questionnaire designed to include “50% of statements” relating to “passion” and “50%” relating to “perseverance”. The Grit Scale is “… a test that, when taken honestly, measures the extent to which you approach life with grit” (Duckworth, 2016, p. 9); the total “grit score” will then determine how “gritty” an individual is and, therefore, an individual’s passion and perseverance for a given task. When the grit scale was tested in several cohorts of cadets who had gained admission into West Point, Grit turned out to be an astoundingly reliable predictor of who made it through and who did not. In fact, interestingly, it was found that “… stayers and leavers had indistinguishable Whole Candidate Scores [consisting of SAT scores, high school rank, leadership experience and athletic ability]”. The study clearly showed that “What matters is grit.” (Duckworth, 2016, p. 10)
Angela Duckworth (2016) was able to conclude, from the results of her studies in the military, education and business, that “Regardless of specific attributes and advantages that help someone succeed in each of these diverse domains of challenge, grit matters in all of them.” (p. 12)
USING ‘GRIT’ TO SELECT STUDENTS FOR ADMISSION INTO MEDICAL SCHOOL
Medical students often represent student cohorts with high scholastic achievements. Consequently, especially in the past, the selection of students for admission into medical school was based mainly on their scholastic achievements. However, such a practice was later found to be unsatisfactory and unreliable, as many graduates (the future medical practitioners) were often unable to deliver optimum healthcare to patients, and many were unable to cope with the rigours of the tasks ahead. This, of course, prompted medical authorities responsible for the selection of students for admission into medical school to expand the selection process through the inclusion of psychological tests such as the Multiple Mini Interviews (Eva, Macala, & Fleming, 2019).
In view of the high predictive value of ‘grit’ we would like to propose that all students, who aspire to become future medical practitioners, take the ‘grit test’ to first determine their individual grit scores and, therefore, their suitability for selection and admission into medical school. After all, the individual grit scores have been confirmed to be highly reliable predictors of the suitability of students for admission into an organisation’s training programme.
More recently, Thomas H. Lee, an experienced “clinician and health care leader”, and Angela L. Duckworth, a distinguished researcher on ‘grit’, have combined their expertise to write the article Organizational Grit in which the authors have highlighted,
contemporary perspectives on organizational and health care cultures [and] … the new model of grit in healthcare—exemplified by leading institutions like Mayo Clinic and Cleveland Clinic—passion for patient well-being and perseverance in the pursuit of that goal [i.e. Grit] become social norms at the individual, team, and institutional levels. (2018, para. 4)
DEVELOPING THE NEW MODEL OF GRIT IN HEALTHCARE
If a health care provider wishes to pursue and develop “the new model of grit in healthcare”, what approach should the organisation adopt? Based on the discussions of Lee and Duckworth (2018), the health care provider should ensure that all participants [i.e. all personnel within the system] “are committed to pursuing a shared high-level goal. Putting patients first is a common and effective objective.” A useful approach, therefore, is for the organisation to develop grit so that “Grit become social norms at the individual, team, and institutional levels” (Lee & Duckworth, 2018, para. 4) with “clear communication of [institutional] values by [the] leadership [within the organisation.]” (Duckworth, 2016, Chapter 12).
“For leaders, building a gritty culture begins with selecting and developing gritty individuals.” (Lee & Duckworth, 2018, para. 5)
Thus, a new model of grit in health care must ensure passion for patient well-being, and perseverance in the pursuit of that goal become social norms at the individual, team and institutional levels- as exemplified by leading institutions such as Mayo Clinic and Cleveland Clinic. Should healthcare organisations in Asia adopt the new model of grit in healthcare in view of the global paradigm shift from individual to team care of patients?
Dujeepa D. Samarasekera & Matthew C. E. Gwee
Centre for Medical Education (CenMED), NUS Yong Loo Lin School of Medicine,
National University Health System, Singapore
Duckworth, A. (2016). Grit: The power of passion and perseverance. United Kingdom: Ebury Publishing.
Eva, K. W., Macala, C., & Fleming, B. (2019). Twelve tips for constructing a multiple mini-interview. Medical Teacher, 41(5), 510-516. https://doi.org/10.1080/0142159X.2018.1429586
Lee, T. H. & Duckworth, A. L. (2018). Organizational grit. Retrieved from Harvard Business Review, https://hbr.org/2018/09/organizational-grit
“Curiosity…is the spark that can lead to breakthrough innovation. … it helps
produce more than new ideas.” (A. Ignatius, 2018).
We believe that curiosity is vital to learning. Many studies have shown that if a student is curious or the subject matter generates learners’ curiosity, then the student learning is deeper and that they remember better (Dyche & Epstein, 2011; Yuhas, 2014).
The quotation cited above is the editorial by Ignatius (2018) in a current issue of the Harvard Business Review. Ignatius, as the Editor-in-Chief, was drawing attention to the recent research “The Business Case for Curiosity” published in the same issue of HBR, by his colleague Francesca Gino (2018). According to Ignatius (2018), the “Recent research … points to several surprisingly practical benefits for business: … . In short, curiosity boosts business performance.”
There is also an interesting link between the ‘curiosity for learning’ and ‘lifelong learning’, as reported by Yang (2018): “In Finland, lifelong learning is fast becoming a way of life. Schools start kids young by nurturing their curiosity for learning… .” Indeed, one of the major aims of medical and health professions education is to equip learners with lifelong learning skills so that, as the end-products of education (i.e. as learners become the new generation of healthcare practitioners upon graduation), they would already possess the skills and motivation for lifelong learning to ensure, firstly, their professional competence throughout their respective professional lives and, for a smaller cohort, to acquire new knowledge and skills to become discipline experts.
A learning design commonly used in the 21st century is interactive teaching- learning in which the teacher interacts with learners and the latter also interact among themselves. The teacher merely guides the learning process through ‘QUESTIONING–Listening and Responding’; learners also interact in like manner as they learn (with – from) each other (see figure 1, below). In such active learning situations, the power of questioning will induce learners need to think deeply, critically and creatively about likely answers to the questions posed! This should arouse the curiosity of learners about what they are learning (i.e. arouse the curiosity for learning) which should become habit-forming with time! Thus, ultimately, the power of habit should lead to the systematic development of lifelong learning skills.
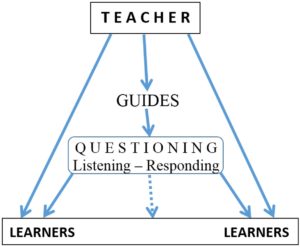
Figure 1. Interactive Teaching-Learning. A useful learning design to nurture, firstly, curiosity for learning through the power of questioning (i.e. by asking ‘smart’ questions like “why…”, “what if…”, “how might we…”) and, ultimately, to systematically develop lifelong learning skills through the power of habit.
Teachers will need a major role change to engage effectively in interactive teaching-learning: in particular, teachers need to undertake a major educational paradigm shift from “just informing” to “involving students actively” in the teaching-learning process. When our role as teachers is mainly that of “just informing” (as in didactic lectures), then the primary focus of student learning will be on factual content i.e. learning will be focused mainly on fact memorisation.
However, when learning is focused on involving students actively, then students need to engage in peer to peer learning, i.e. the students learn (with-from) each other through social learning that involves active social interaction; such learning will require intellectual as well as interpersonal inputs from learners, as they need to think and collaborate in their search for likely answers to the questions posed.
“Most of the breakthrough discoveries and remarkable inventions throughout history from flints for starting a fire to self-driving cars, have something in common: they are the result of curiosity.” (Gino, 2018).
Teachers should, therefore, exploit the phenomenon of curiosity (an innate human quality) to enhance student learning! But what is curiosity? There is a common saying that curiosity kills the cat! However, curiosity has been defined as “The impulse to seek new information and experiences and explore novel possibilities… . [It is] a basic human attribute.” (Gino, 2018), and also as “… a penchant for seeking new experiences, knowledge, and feedback and an openness to change.” (Fernandez-Araoz, Roscoe, & Aramaki, 2018).
After all, there is a close link between curiosity for learning and lifelong learning, as discussed above. So curiosity should be the spark for learning, and nature has endowed all of us with the special gift, curiosity, to ensure our very own survival in this world.
Dujeepa D. Samarasekera & Matthew C.E. Gwee
Centre for Medical Education (CenMED), NUS Yong Loo Lin School of Medicine,
National University Health System, Singapore
Fernández-Aráoz, C., Roscoe, A., & Aramaki, K. (2018). From curious to competent. Harvard Business Review, September-October 2018. Retrieved on November 1st, 2018 from https://hbr.org/2018/09/curiosity#from-curious-to-competent.
Dyche, L., & Epstein, R. M. (2011). Curiosity and medical education. Medical education, 45(7), 663-668.
Gino, F. (2018). The business case for curiosity. Harvard Business Review, September-October 2018. Retrieved on November 1st, 2018 from https://hbr.org/2018/09/curiosity.
Ignatius, A. (2018). Cultivate curiosity. Harvard Business Review, September-October 2018. Retrieved on November 1st, 2018 from https://hbr.org/2018/09/cultivate-curiosity.
Yang, C. (2018, October 15). Lifelong learning is a big thing for Finns. The Straits Times. Retrieved on November 1st, 2018 from https://www.straitstimes.com/world/lifelong-learning-is-a-big-thing-for-finns.
Yuhas, D. (2014, October 2). Curiosity prepares the brain for better learning: Neuroimaging reveals how the brain’s reward and memory pathways prime inquiring minds for knowledge. Scientific American, 311(4), 6-100. Retrieved on November 1st, 2018 from www.scientificamerican.com/article/curiosity-prepares-the-brain-for-better-learning.
Published online: 3 September, TAPS 2019, 4(3), 1-2
DOI: https://doi.org/10.29060/TAPS.2019-4-3/EV4N3
1Judy McKimm & 2Hiroshi Nishigori
1Strategic Educational Development, Swansea University Medical School, Swansea University, United Kingdom; 2Center for Medical Education, Nagoya University Graduate School of Medicine, Japan
It has been a pleasure for us to act as guest editors for this themed issue on the Implications of Culture in the Education and Practice of Healthcare Professionals. We thank the TAPS Editorial team, our reviewers, and authors for all their hard work and patience and we hope you enjoy this varied issue with articles from around the region, and the world.
The Lancet Commission’s Report on Health Professionals for a New Century (Bhutta et al 2010) emphasised the interconnectedness between education and health systems and that we live and work in a ‘global village’. This is highlighted in the paper considering the cross-cultural implications of a ’transnational’ faculty providing clinical teacher training. Many factors affect the education and practice of healthcare professionals, including the resources available, however tradition, language and culture are hugely influential, whatever the resource setting. Understanding the cultural contexts in which we work is vital as, without this, we may be misunderstood, unable to influence change, or cause offence. ‘Culture’ is a broad term, referring to the society and its subcultures, cultural influences, organisational culture, the sub-cultures of professions (tribes and territories), and of students (the ‘hidden curriculum’). The impact of the ‘hidden curriculum’ is explored in a Thai context, with an article looking at cultural influences on peer-assisted learning. And of course, culture(s) are located in both the past (the influence of history, legacy and tradition) as well as being influenced by internal and external forces and events.
‘The needs of the global community are best served by practitioners who can function effectively and flexibly in an ever-changing and unpredictable world, across cultures and under different social conditions and who are social and environmental advocates for all communities, not just for those in which they live and work’ (McKimm & McLean 2011). It is important therefore that we try to develop ‘cultural intelligence and competency’ in our students, practitioners and faculty, and this theme runs throughout this issue. Two articles focus on specific educational initiatives designed to develop cultural competency in residents (doctors in training) and General Practitioners (family doctors), considering what might work and whether these skills are generalizable or need to be contextually situated. Individual and group identity is closely tied to the cultures from which people come, in which they live and with which they identify. However, the way individuals or groups might perceive themselves might be very different to how they are perceived by others, or how society portrays and represents them through stereotypes, language, images and stories. This theme is explored in two ways in a New Zealand context, one paper considering how Māori are characterised in health professions’ education, and another exploring the cultural motivating factors that lead students to apply to medical school.
Language is also important, reflecting, constructing and shaping meaning, and helping to explain behaviours and events within their cultural context. This issue is explored in the article from Sri Lanka, in which the authors consider the potential impact on students when they are learning in a second language. Cultural issues and potential for poor or miscommunications can also impact greatly on the doctor-patient relationship. Two interesting articles, one from Japan regarding cultural perceptions of doctors’ competency and another, from Indonesia, exploring cultural factors influencing informed consent and patient empowerment, shed light on these issues and suggest strategies for improving communication and minimising the impact of cultural factors, such as traditional dominance and deference.
So, what can we learn from these articles to inform and improve our practice? As educators and practitioners, we are (directly and indirectly, positively and negatively) role models for colleagues and learners, so it is essential that we try our best to develop our own cultural intelligence and competency. As part of this, it is vital that we learn to identify and acknowledge our own cultural and unconscious biases, we all have these, and the more we can surface them, and learn to manage them, the better. We all have a responsibility for creating and sustaining a culture that welcomes and promotes diversity and inclusivity, whether that is in the classroom, in clinical practice or in everyday conversations with colleagues, patients and students. This involves learning to safely challenge behaviours that are not culturally competent or intelligent, being an ‘active bystander’. Alongside this is to continue to be curious about the wide range of cultural issues and how they impact on everyday conversations, on relationships, and on educational and care practices, but in a values-based and respectful way.
Finally, we would like to note that, in the international convention of medical education, these articles are written in English, many by non-native speakers of English. However, social anthropologists, experts in culture, often learn the native languages of the countries they visit so they can understand the nuances of those cultures. A limitation of this special issue on ‘Culture’ is therefore that some of these nuances may literally have been ‘lost in translation’ but, even so, these articles provide much food for thought, interesting ideas and promote cross-cultural learning. There is a lot more research to be carried out in this area however, and we hope this issue of TAPS has stimulated you to think more about cultural influences, and perhaps consider carrying out some research or innovation in your own context.
Judy McKimm & Hiroshi Nishigori
Guest Editors &
International Editorial Board Members
The Asia Pacific Scholar (TAPS)
Bhutta, Z. A., Chen, L., Cohen, J., Crisp, N., Evans, T., Fineberg, H., … Kelley, P. (2010). Education of health professionals for the 21st century: A global independent commission. The Lancet, 375(9721), 1137-1138.
Mckimm, J., & McLean, M. (2011). Developing a global health practitioner: Time to act? Medical Teacher, 33(8), 626-631.
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
