
Learners’ report and perceptions concerning undergraduate paediatric endocrinology curriculum content and delivery across Southern Nigeria

Submitted: 23 August 2022
Accepted: 3 January 2023
Published online: 4 July, TAPS 2023, 8(3), 15-25
https://doi.org/10.29060/TAPS.2023-8-3/OA2871
Iroro Enameguolo Yarhere1, Tudor Chinnah2 & Uche Chineze3
1Department of Paediatrics, College of Health Sciences, University of Port Harcourt, Nigeria; 2Department of Anatomy, University of Exeter, United Kingdom; 3Department of Education and Curriculum studies, University of Port Harcourt, Nigeria
Abstract
Introduction: This study aimed to compare the paediatric endocrinology curriculum across Southern Nigeria medical schools, using reports from learners. It also checked the learners’ perceptions about different learning patterns and competency in some expected core skills.
Methods: This mixed (quantitative and qualitative) study was conducted with 7 medical schools in Southern Nigeria. A multi-staged randomized selection of schools and respondents, was adopted for a focus group discussion (FGD), and the information derived was used to develop a semi-structured questionnaire, which 314 doctors submitted. The FGD discussed rotation patterns, completion rates of topics and perceptions for some skills. These themes were included in the forms for general survey, and Likert scale was used to assess competency in skills. Data generated was analysed using statistical package for social sciences, SPSS 24, and p values < 0.05 were considered significant
Results: Lectures and topics had various completion rates, 42.6% – 98%, highest being “diabetes mellitus”. Endocrinology rotation was completed by 58.6% of respondents, and 58 – 78 % perceived competency in growth measurement and charting. Significantly more learners, 46.6% who had staggered posting got correct matching of Tanner staging, versus learners who had block posting, 33.3%, p = 0.018.
Conclusion: Respondents reported high variability in the implementation of the recommended guidelines for paediatric endocrinology curriculum between schools in Southern Nigeria. Variabilities were in the courses’ completion, learners’ skills exposure and how much hands-on were allowed in various skills acquisitions. This variability will hamper the core objectives of human capital development should the trend continue.
Keywords: Paediatric Endocrinology Curriculum, Perception, Compliance, Completion Rate, Learners
Practice Highlights
- Medical and dental council of Nigeria has a recommended benchmark for minimum academic standards in all medical schools to which total compliance is expected.
- Evaluation of paediatric endocrinology curriculum content and training methods was conducted using reports from learners.
- Variability in the content, and training methods of the intended competency were reported across medical schools.
- Compliance rate of the recommended curriculum was less than 50% in some contents and some learners reported low skill performance training.
- The lack of uniformity can prevent achievement of the overarching objective of the curriculum in Nigeria with wide variations in competence among graduating doctors.
I. INTRODUCTION
The primary aim of the Medical and Dental council of Nigeria (MDCN) undergraduate curriculum is “to train doctors and dentists who can work effectively in a health team to provide comprehensive health care to individuals in any community in the nation, and keep up to date on issues of global health” (Federal Ministry of Health of Nigeria, 2012). In Nigeria today, there are 49 federal, 59 states and 111 private universities, and 44 of these have full or partially accredited medical schools and while these schools have a prescribed curriculum, some are not following explicitly (Federal Ministry of Health of Nigeria, 2012). This curriculum advocates for universities to develop syllabus to meet the benchmark for minimum academic standards (BMAS) across schools, however there is no uniform template developed for assessing graduates to know how their competence converge as is applicable in United States of America (USA), Canada and United Kingdom (UK) (Santen et al., 2019; Shah et al., 2020; Sosna et al., 2021). Diabetes mellitus, thyroid disorders, puberty, rickets and growth abnormalities are topics included in the MDCN paediatric curriculum under endocrinology which learners are expected to acquire competence in cognitive and psychomotor skills to diagnose and treat or refer appropriately children presenting with these diseases.
A. Problem
Most deaths from diseases in Nigeria and other resource-limited countries are consequent upon general public ignorance of disease, late presentation to the health care systems, poverty and lack of funds to access healthcare facilities and reduced knowledge of some disease patterns by the healthcare providers (Yarhere & Nte, 2018). Addressing the gaps in reduced knowledge can be done by developing competency-based curriculum for all graduating doctors to have as near-similar competence as possible but achieving this may not be feasible. Training activities are not uniform throughout medical schools in Nigeria and elsewhere, and depend on schools’ vision, mission and objectives, and the structures and processes put in place. There are barriers to positive implementation across schools including but not limited to individual school’s determination of what is relevant in the curriculum, access to the materials needed to teach the curriculum content and getting trainers to use these curriculums (Polikoff, 2018). The lack of uniformity of curriculum across universities may not be contending issues, but when the graduating doctors have varying degree of competencies in skills and cognition, then a template for imparting uniform and up to date knowledge and to evaluate this is needed to find ways of reducing the variability (McManus, 2003; McManus et al., 2020; Rimmer, 2014).
The curriculum uniformity across schools is one way of improving competency and thus, healthcare standards, and there is need to explore this uniformity or diversity within the paediatric undergraduate training. In some countries, there is a uniform board certification examination before doctors can practice and this is also done for doctors immigrating into these countries (Hohmann & Tetsworth, 2018; Puri et al., 2021; Tiffin et al., 2017; van Zanten et al., 2022) but Nigeria is exempt from this uniform exit examination. This uniform exit board examination makes these schools align course contents, and therefore reduces the variabilities between medical schools and undergraduate training.
B. Curriculum Evaluation for Change or Improvement
Curriculum evaluation is a means by which educators understand whether the curriculum used to train learners is working as intended, and whether there is need to change the entire programme or redesign aspects (Burton & McDonald, 2001; Ornstein & Hunkins, 2009). It is also a way of identifying deficiencies in training syllabus across universities, (Rufai et al., 2016) or whether compliance to a curriculum is being achieved (Grant, 2014; Olson et al., 2000). Kirkpatrick’s curriculum evaluation method is widely acceptable in medical education using the 4 steps; learners’ reaction or satisfaction, knowledge, behavioural changes and results or impact, and in Nigeria, for paediatric endocrinology, this has not been done (Alsalamah, 2021; Bates, 2004).
Universities have variabilities in organisation, students’ numbers in classes, duration of specific posting, posting types and whether the courses are elective or core. In medical schools in Nigeria, paediatric postings are undertaken in the 5th or 6th year of a 6-year programme. While some stagger the posting to be done within the last 2 years, others do theirs in the 5th or the 6th year exclusively, and the extent of these variabilities and how they affect the training processes and products has not been evaluated in Nigeria and this can be done using learners’ or graduates’ perceptions.
The aim of this research was to evaluate learners’ report and perception of some aspects of the paediatric endocrinology curriculum contents and learning methods across Southern Nigeria medical schools. Endocrinology was taken from the paediatric course to reduce the volume of information to be analysed.
II. METHODS
This was a cross sectional study design with qualitative and quantitative data analyses, evaluating learners’ report and their perception of the curriculum being used by various medical schools in Southern Nigeria to deliver the MDCN paediatric endocrinology curriculum. Survey was conducted across 10 medical schools in Southern Nigeria that have learners who have either completed their final year, or are doing their internship. Two steps were used to retrieve the information needed; a focus group discussion of sampled learners, and a questionnaire survey sent out to randomly selected respondents and these 2 methods complemented each other. The focus group discussion was used to explore in depth, the minds of the respondents and what they perceived was being done well and what needed to be changed in the syllabus in their respective schools. The questionnaire survey was then used to collect reports and perceptions from a wider set of learners who had completed their paediatric posting within the past 6 – 12 months. Some of these were already doing their internship and others were in their final year in preparation for their final examinations.
Sample size for respondents will be calculated using the formula:
N = (Z score)2 x SD x (1 – SD)
(CI)2
Z score = 1.96, SD (standard deviation of the mean) = estimated at ± 0.5, Confidence interval = 0.05
= 384 respondents, with an attrition rate of 10% will be added 10% of 384 = 38
384 + 38 = 422 respondents.
A. Sampling Technique
Multi-staged sampling technique was used to determine the schools, and respondents that participated in the study. There are 29 Southern Universities with medical / health colleges and 16 of these had more than 50 learners in their final year or had graduated. Ten schools were randomly selected using the excel formula [= rand ()], and a proportionate stratified sampling was done using the matriculation numbers of the students in each school to arrive at 422 respondents. Total number of learners that studied paediatrics in various institutions was 800; Ibadan 150, Port Harcourt, 128, Lagos 128, Niger delta University 69, UNN Enugu 128, University of Benin 128, Others 69. From the total number of learners in each school, selected learners and interns were sent the questionnaire using their email addresses. Selection for the FGD was done using simple random sampling from each school and these were sent separate emails with details for the meeting.
B. Focus Group Discussions Process
Focus group discussion was conducted with the respondents using zoom video platform, and the process lasted for 2 hours, 30 minutes. Ten learners’ representatives from the selected schools were contacted for this FGD, however, 7 (70%) agreed to participate after several email reminders. The interview was semi-structured with a flexible topic guide, which covered issues relating to the respondents’ views and opinions on the curriculum in paediatric endocrinology; description of posting type in each school, whether block, or staggered, topics received and/or completed, perception of their competence in a key psychomotor skill. The focus group interview discussions were recorded in the zoom meeting platform and transcribed verbatim. The data were analysed using the thematic framework content analyses method. The themes generated were categorised into; 1. Lecture contents and completion rate, 2. Types of paediatric rotation and posting, 3. Skill competence acquisition and clinical postings. Their perceptions about these themes were also sought and discussed. The transcription of the groups’ discussions was reviewed by IY and TC to help categorise the data and pull-out important quotes used.
C. Questionnaire Survey
Following thematic analyses of the FGD, the themes generated were converted to questions in a survey for a larger sample population. Themes generated were the type of paediatric posting, rotations through units in the departments and paediatric endocrinology topics, training methods and competency acquired. Demographic characteristics of responders such as level/year of study, age, gender and university of study were collected. The respondents were also asked to select topics from a poll, included in their paediatric endocrinology syllabus, with result in Figure 1, and to state the various methods used to learn growth and growth disorders in their schools. A means of assessing cognitive (recall) skills of the learners was conducted using animated pictures of Tanner staging and matching-type multiple choice, and the responses were crossmatched with the type of posting learners were exposed to, i.e. block posting or staggered posting. Tanner staging was chosen as it cuts across general paediatrics and endocrinology as part of growth and puberty (endocrinology).
Data retrieved were analysed statistically by using chi-square test, and Pearson correlation for categorical variables. The level of competence perceived by learners in height measurement and charting on growth chart was retrieved using 5-point Likert scale (where 1 = not competent; 2 = low competence; 3 = neutral; 4 = competent; and 5 = proficient). The association between level of competence and whether learners rotated through paediatric endocrinology was checked using Pearson’s correlation test. For all statistics, p value < 0.05 was considered significant.
D. Ethics
The research commenced after the Research Ethics committee of the University of Port Harcourt granted approval (UPH/CEREMAD/REC/MM80/056). Verbal informed consent was obtained from the participants during the focus group discussion, who also gave consent for video and recording of the process. Informed consent was also obtained from all participants who filled and submitted the online survey. The focus group discussants received N3,000 ($10) for internet data only as monetary compensation.
III. RESULTS
There were 314 learners from the 422 calculated sample size, responded to the questionnaire survey, giving a response rate of 74.4%. There were more final year respondents than early career doctors and more of the respondents were in the age bracket 20 – 24 years, with a mean of 25.02 ±2.71 years. The male: female ratio was 1:1.01, and the data that support the findings of this study are available in Figshare at https://doi.org/10.6084 /m9.figshare.20730937.v1 (Yarhere et al., 2022).
|
RESPONDENTS |
Frequency |
Percentage |
|
|
Year of study |
|
|
|
|
Early career doctor (graduate/intern) |
130 |
41.4 |
p = 0.002 |
|
Final year |
184 |
58.6 |
|
|
University attended (calculated cohort) |
|
|
|
|
University of Port Harcourt (63) |
62 |
19.7 |
|
|
Niger Delta University (54) |
54 |
17.2 |
|
|
University of Ibadan (76) |
50 |
15.9 |
|
|
University of Benin (65) |
44 |
14.0 |
|
|
University of Lagos (65) |
40 |
12.7 |
|
|
University of Nigeria (65) |
42 |
13.4 |
|
|
Other western Universities (34) |
22 |
7.0 |
|
|
Age |
|
|
|
|
20-24 |
140 |
44.6 |
|
|
25-29 |
162 |
51.6 |
|
|
>=30 |
12 |
3.8 |
|
|
Mean |
25.02 ± 2.71 |
|
|
|
Gender |
|
|
|
|
Male |
152 |
48.4 |
p = 0.612 |
|
Female |
162 |
51.6 |
|
Table 1. Demographic characteristics of all respondents and the universities attended
A. Evaluating Contents of Lecture Topics and Completion of Lectures
The syllabus lecturers use to teach courses are supposed to be descriptive with all learning outcomes stated in the handbook or in the log books given to them before the start of the academic year. The prescribed topics for paediatric endocrinology as stated below were not completely taught to learners or learners did not attend the lectures. In the discussion, some agreed that they did not have the full complement of lectures suggested by the BMAS. One respondent said she and her group mates did not receive diabetes mellitus lectures in their final paediatric posting. This fact was corroborated in the questionnaire survey as 2% of the respondents revealed not having diabetes mellitus lectures, and more than 40% did not learn genetics in their paediatric endocrinology training as shown in Figure 1.
Diabetes had almost 100% lecture recipient while genetic had the least. In some schools, genetics were placed under endocrine disorders while in others, genetics were left for the pathology and basic medicine classes.
“I was taught, I personally received 4 lectures in Paed Endo including ambiguous genitalia, “CAH” congenital adrenal hyperplasia, hypothyroidism, and puberty.”
Participant 3
“So, you did not get to do calcium and rickets?”
Facilitator
“No, I was not taught calcium and rickets.”
Participant 3
“What about growth and short stature?”
Facilitator
“Yes, I received introductory lectures in my young (sic), junior posting, yes I did in my 400 level, but not in my senior posting and it was not part of endocrinology but general paediatrics.”
Participant 3
“I did not take lectures in diabetes mellitus because it was rescheduled several times until we finally had to sit for our exams. In the end, many of us just took notes from our seniors and other students who had theirs when it was scheduled.”
Participant 2
“Why were the classes rescheduled? I mean what did the lecturer tell you?”
Facilitator
“The lecturer kept traveling or was indisposed most of our time in the senior posting.”
Participant 2
Participant 4 shared:
Dr. xxxxxx taught us diabetes mellitus and the topic was quite extensive. We learnt the different types, pathophysiology, aetiology, DKA, precipitating factors, risk factors, management. Our lecturers even made us do presentations on DKA, we monitored patients that were being managed for DKA, checking their urine samples for ketones, glucose and their blood pressure.
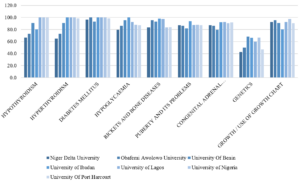
Figure 1: Percentage of learners in various schools who received/attended specific endocrinology lectures in their universities
B. Types of Paediatric Posting and Rotation and Perception of Learners Relating to Task Completion
There were basically 2 modes of paediatric posting in the institutions sampled; 4-months block posting where respondents have a month of didactic lectures and 3 months of clinical rotations through various units in the Paediatric departments, and 4 months of staggered rotations with junior and senior postings in the clinical classes. While some learners rotated through all the units (core and electives) in the departments, some went through core units, emergency and neonatal units, and 2 other units randomly selected for the respondents by the departments.
C. Learners’ Responses to Rotation through Paediatrics and Posting Types
Participant 2 shared:
The way it works in University of xxxx, we rotate through 2 elective postings with core (CHEW and SCBU) postings in the junior and senior postings. These elective postings are randomly selected by the department (meaning heads or coordinators). I did neurology and gastroenterology in my junior posting and haemato-oncology and I really can’t remember the other one in my senior posting.
“Will I be wrong to say you did not see a patient with Diabetic keto acidosis?”
Facilitator
“I saw a child with diabetic keto acidosis in the ward but it wasn’t my unit managing the patient. I only went to the ward to do some other thing.”
Participant 2
“If you were given the opportunity to design a curriculum or programme for your university, will you prefer what is being practiced now, or will you rather have every student go through every unit and get titbits from each unit?”
Facilitator
Participant 2 responded:
Yes, I will prefer that situation where you get to be exposed to every unit in the department but …. emmm, that creates a problem because you may be in a unit for a week, and no patient comes in but the next group rotating to the unit gets to see many patients. I would want to suggest that perhaps, instead of focusing on more of clinical posting, that a unified tutorial class which will expose everyone to the core diseases in the various disciplines.
Table 2 corroborates the information given by the focus group discussants. Testing the competency outcome in either method can give some estimated guess as to which is better, however, there are several confounding factors that will not allow fair comparison (See Table 3).
|
Variable |
Frequency |
Percent (%) |
|
|
Paediatric posting in your university |
|
|
|
|
Staggered posting into Junior and senior paediatrics |
176 |
56.1 |
c2 = 4.59, |
|
Block posting of 4 months total |
138 |
43.9 |
p = 0.032 |
|
Paediatric rotations through various units in universities |
|
|
|
|
I rotated through all units in the department |
162 |
51.6 |
c2 = 0.318, |
|
I rotated through CHEW, neonatal unit, and 2/3 other units |
152 |
48.4 |
p = 0.573 |
|
Rotate through paediatric endocrinology unit in your university |
|
|
|
|
Yes |
184 |
58.6 |
c2 = 7.48, |
|
No |
130 |
41.4 |
p = 0.006 |
Table 2. Paediatric posting and unit rotations in the departments (n=314)
Though there were differences in the mode of paediatric postings where staggered or block, c2 = 4.59, p = 0.032. the difference in proportion of respondents who had core and selected elective posting as against all units posting was not significant, c2 = 0.318, p = 0.573.
|
|
Block posting of 4 months |
Staggered junior and senior paediatrics |
|
|
Correct |
Count |
46 |
82 |
|
% within paediatric posting |
33.3% |
46.6% |
|
|
% of Total |
14.6% |
26.1% |
|
|
Wrong |
Count |
92 |
94 |
|
% within paediatric posting |
66.7% |
53.4% |
|
|
% of Total |
29.3% |
29.9% |
|
|
Total |
Count |
138 |
176 |
|
% within correct response |
43.9% |
56.1% |
|
|
% of Total |
43.9% |
56.1% |
|
Table 3: Comparing correct response to animated picture of Tanner stage (pubic hair) in females, and the type of paediatric rotation learners were exposed to
In the 2×2 table above where recall was tested in the learners based on their paediatric posting type, higher percentage of those who had staggered posting got the correct matching of Tanner stage, and the difference was significant, c2 = 5.630, p = 0.018. However, the total number of respondents with the correct response was low.
D. Perception of Core Competency Skill in Growth Measurement and Charting by Learners
One of the most important courses in paediatrics is growth and development and training future medical doctor to acquire skills and competence in growth and management is a key component of the BMAS. While growth measurement may seem easy to the uninformed, the whole task is daunting especially in children with complex growth abnormalities and malformation, and for more complex skills like arm span. Which of the more complex skills should the learner be expected to be competent in, will be debated in an expert forum of trainers.
“So, did you do anthropometric measures?”
Facilitator
Participant 1 shared:
Yes, anytime we clerk a patient, we must check the weight and height and interpret using age-appropriate charts, but we did not plot them in the charts. We carry the age-appropriate chart and interpreted our patients, as this is a requirement.
Using the chart may not be emphasised by all paediatric lecturers, so learners can be smart to know those lecturers who will request this skill from them during the clerkship period or the unit rotations.
“We did not quite get the concept of mid parental height, height percentile, it was just mentioned in passing. I never saw a severely short child that needed growth hormone. I was only told by a classmate of mine.”
Participant 3
The charting and interpretation of weight and height measurements of children was not done in all schools as shown in Table 4 below, which tells that only 65.8% of total respondents were taught interpretation of measured and charted growth parameters. The level of competence in these tasks will also be varied as seen in Appendix 1. Two hundred and thirty-eight (75.8%) learners perceived they had competency/ proficiency in height measures using stadiometer, and 44.6 % of the learners with these perceptions actually had paediatric endocrinology clinical rotation (Appendix 1).
|
Variable |
Frequency n = 314 |
Percent (%) |
|
How was growth and growth disorders taught in your school (Multiple response applicable) |
|
|
|
Didactic lectures |
272 |
86.6 |
|
Measurement of children using standardised stadiometer |
230 |
73.2 |
|
Charting of growth measurements in CDC/WHO growth charts |
203 |
64.6 |
|
Measurement of children using improvised height rules |
157 |
50.0 |
|
Interpretation of measured and charted growth parameters |
203 |
64.6 |
|
Ward clerkship and presentation |
230 |
73.2 |
|
Measurements of children using bathroom spring balance |
140 |
44.6 |
|
Use of bone age X radiographs |
78 |
24.8 |
|
Use of orchidometer |
90 |
28.6 |
Table 4: Methods used to teach growth and growth disorders in various institutions
Bone age and orchidometers are used to assess skeletal maturation and puberty, which are advanced for the undergraduate learners and certainly not compulsory, but some respondents were taught with the tools showing the variabilities in contents and skills delivery between these schools. From Table 4 above, framers of the syllabus for endocrinology aspect of paediatrics curriculum are unlikely to include use of orchidometer and bone age during the undergraduate paediatric endocrinology rotation as the skill is complex, and not necessary for their level of development.
IV. DISCUSSION
This study has highlighted differences in course contents and training methods across medical schools in Southern Nigeria. While many schools have used the BMAS prescribed by the MDCN, the syllabus used are different and the intended learning outcomes are diverse based on the respondents’ reports. Some learners reported not having diabetes lectures in their school through no fault of theirs, as lecturer rescheduled the lectures and never gave them. While learners have the responsibility to attend lectures, trainers are also obligated to be present at their scheduled lectures or transfer this to their teacher-assistants, or use technologies (Grant, 2014; Ruiz et al., 2006). Some learners had little participation in the Emergency Room, others participated fully in DKA management, learning empathy, specialised skills and communication. The intended competencies to be acquired can be achieved through shadowing and participation, bed-side teaching, and tutorial to improve the cognitive and psychomotor skill, and these opportunities must be created for them in experiential settings (Ryan et al., 2020; Shah et al., 2020).
More learners had staggered postings, going through junior and senior paediatric postings in what may be considered as integrated learning departing from the traditional method (Patel et al., 2005; Watmough et al., 2006, 2009). In the staggered posting type of rotation, we noticed that not all learners went through paediatric endocrinology unit posting, and like one of the discussants said, they would rather everyone went through each unit getting bits of everything and having opportunity to study specific and prevalent diseases in paediatric units rather than leaving them with the possibility of not learning important disorders. As it is not always possible to encounter specific diseases like DKA during entire posting in the schools that use staggered posting types, the likelihood of exposure was higher in schools that had block posting from the FGD conducted, but this did not translate to better retention of skills or cognitions as depicted in the Tanner staging matching question.
Having learners train in all special postings may not be the best approach in undergraduate medicine because the specialised skills may not be utilised in general practice and even in general paediatrics should the learners plan paediatric specialisation (Bindal et al., 2011). While some trainers may argue that all information and skill should be taught to the learners, the time to acquire and achieve mastery may be short for the learners (Jensen et al., 2018; Offiah et al., 2019). This study can be referenced in curriculum designing and implementation so the framers understand what society needs should be filled at any time. The concept of cognitive overload has actually reduced the duration of core specialty in clinical medicine while increasing the duration for others with emphasis on psychomotor, affective skills and professionalism. Some medical schools have core paediatric posting of 7 – 8 weeks, but Nigeria is still fixed with the traditional 3 – 4 months. In some schools in South Africa, the clinical posting is run as modular block for 3 years, with paediatric curriculum running from year 4 through year 6 (Dudley & Rohwer, 2015). With the long duration in the Nigeria curriculum, skills competencies are still deficient, so there is need to revamp the curriculum to make it more competency driven. It is excusable that more sophisticated competence like use of orchidometer were not known by more than half the learners, but if some were taught, the level of confidence in these skills at this stage of their learning should also be assessed as was done for diabetes by George et al. (2008).
Medical schools in Nigeria and other countries will have to continually evolve and produce curricula that are competency based, using problem-based learning, simulations, mannikin training for skills as is done in other countries (Watmough et al., 2006). Diabetes, thyroid, ambiguous genitalia with congenital adrenal hyperplasia, short stature and calcium disorders are common in Nigeria and should be taught in structured and integrated formats. Integrated curriculum where skills are graded from simple to complex can also be tested e g, skills of height measurements and charting using the stadiometer and growth charts can be taught in the 1st clinical year, and then the mid parental heights, target height calculation and bone age may be taught in the 2nd and 3rd clinical years. (Brauer & Ferguson, 2015; Grant, 2014).
A. Strength of the Research
Articulating the perceptions of learners is not always easy as they are varied and subjective, but getting them to come together, discuss and give suggestions on how curriculum can be designed and achieved increases the strength of this research. There was no sense of victimisation of the learners as many had already graduated from their schools, and the discussants admitted to not missing classes, or clinical learning. They spoke freely, with courtesy to others and there was little or no argument among them.
B. Limitations of the Research
As this research is based on past experiences of the cognitive and psychomotor skills achieved during the learners’ training period, the possibility of recall bias is high, and respondents may underestimate or exaggerate their skills. Using respondents who had just concluded their paediatric postings was an attempt at reducing this limitation. The best time to evaluate a programme is usually soon after the programme has been concluded however, as there has been no report of this type of evaluation, there was need to embark on it and make recommendations.
V. CONCLUSION
Respondents reported high variability in the implementation of the recommended guidelines for paediatric endocrinology curriculum between schools in Southern Nigeria. Variabilities were in the courses’ completion, learners’ skills exposure and how much hands-on were allowed in various skills acquisitions. This variability will hamper the core objectives of human capital development should the trend continue.
A. Area of Future Research
Noting the differences exist between schools, curriculum strategists and implementation teams in universities should commission a DELPHI study by experts, where core competencies and objectives for paediatric endocrinology will be agreed on and sent to the regulatory bodies for endorsement and implementation.
Notes on Contributors
IY conceived, designed, planned, executed and conducted interviews and the research. He also collected the data, analysed it and wrote the manuscript.
TC helped in designing the methodology for the data colllection and analyses, and reviewed the manuscript.
CU gave critical appraisal of the manuscript and all authors have approved the final manuscript.
Ethical Approval
The research ethics committee of the Univeristy of Port Harcourt gave ethical approval before the start of the study with the number: UPH/CEREMAD/REC/MM80/056.
Data Availability
The data supporting this research is available for publication purposes, without editing. Data can be shared only with express permission from the corresponding author as deposited in Figshare repository, using the private url:
https://figshare.com/articles/dataset/Copy_of_CURRICULUM_STUDENTS_xls/21154396
Acknowledgement
We acknowledge the early career doctors and final year students who participated in the online survey especially the selected ones who took part in the focus group discussion.
Declaration of Interest
Authors declare that there are no conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
Funding
There was no funding for this survey.
References
Alsalamah, A., & Callinan, C. (2021). Adaptation of Kirkpatrick’s four level model of training criteria to evaluate training programmes for head teachers. Education Science, 11(116), 1-25. https://doi.org/10.3390/educsci11030116
Bates, R. (2004). A critical analysis of evaluation practice: The Kirkpatrick model and the principle of beneficence. Evaluation and Program Planning, 27, 341-347. https://doi.org/10.1016/j.evalprogplan.2004.04.011
Bindal, T., Wall, D., & Goodyear, H. M. (2011). Medical students’ views on selecting paediatrics as a career choice. European Journal of Pediatrics, 170(9), 1193-1199. https://doi.org/10.1007/s00431-011-1467-9
Brauer, D. G., & Ferguson, K. J. (2015). The integrated curriculum in medical education: AMEE Guide No. 96. Medical Teacher, 37(4), 312-322. https://doi.org/10.3109/0142159X.2014.970998
Burton, J. L., & McDonald, S. (2001). Curriculum or syllabus: Which are we reforming? Medical Teacher, 23(2), 187-191. https://doi.org/10.1080/01421590020031110
Dudley, L. D., Young, T. N., Rohwer, A. C., Willems, B., Dramowski, A., Goliath, C., Mukinda, F. K., Marais, F., Mehtar, S., & Cameron, N. A. (2015). Fit for purpose? A review of a medical curriculum and its contribution to strengthening health systems in South Africa. African Journal Health Profession Education, 7(1), 81-84. https://doi.org/10.7196/AJHPE.512
Federal Ministry of Health of Nigeria, Health Systems 20/20Project. (2012). Nigeria undergraduate medical and dental curriculum template. Health systems 20/20 Project, Abt Associates Inc.
George, J. T., Warriner, D. A., Anthony, J., Rozario, K. S., Xavier, S., Jude, E. B., & Mckay, G. A. (2008). Training tomorrow’s doctors in diabetes: Self-reported confidence levels, practice and perceived training needs of post-graduate trainee doctors in the UK. A multi-centre survey. BMC Medical Education, 8, Article 22. https://doi.org/10.1186/1472-6920-8-22
Grant, J. (2014). Principles of curriculum design. In T. Swanwick, K. Forrest, B. C. O’Brien (Eds.), Understanding medical education evidence, theory and practice Sussex, UK: Wiley Blackwell, 31-46.
Hohmann, E., & Tetsworth, K. (2018). Fellowship exit examination in orthopaedic surgery in the commonwealth countries of Australia, UK, South Africa and Canada. Are they comparable and equivalent? A perspective on the requirements for medical migration. Medical Education Online, 23(1), Article 1537429. https://doi.org/10.1080/10872981.2018.1537429
Jensen, J. K., Dyre, L., Jørgensen, M. E., Andreasen, L. A., & Tolsgaard, M. G. (2018). Simulation-based point-of-care ultrasound training: a matter of competency rather than volume. Acta Anaesthesiology Scandanavia, 62(6), 811-819. https://doi.org/10.1111/aas.13083
McManus, I. C. (2003). Medical school differences: beneficial diversity or harmful deviations. BMJ Quality and Safety in Health Care, 12(5), 324-325. https://doi.org/10.1136/qhc.12.5.324
McManus, I. C., Harborne, A. C., Horsfall, H. L., Joseph, T., Smith, D. T., Marshall-Andon, T., Samuels, R., Kearsley, J. W., Abbas, N., Baig, H., Beecham, J., Benons, N., Caird, C., Clark, R., Cope, T., Coultas, J., Debenham, L., Douglas, S., Eldridge, J., . . . Devine, O. P. (2020). Exploring UK medical school differences: the MedDifs study of selection, teaching, student and F1 perceptions, postgraduate outcomes and fitness to practise. BMC Medicine, 18(1), Article 136. https://doi.org/10.1186/s12916-020-01572-3
Offiah, G., Ekpotu, L. P., Murphy, S., Kane, D., Gordon, A., O’Sullivan, M., Sharifuddin, S. F., Hill, A. D. K., & Condron, C. M. (2019). Evaluation of medical student retention of clinical skills following simulation training. BMC Medical Education, 19(1), Article 263. https://doi.org/10.1186/s12909-019-1663-2
Olson, A. L., Woodhead, J., Bekow, R., Kaufman, N., & Marshal, S. (2000). A national general pediatric clerkship curriculum: The process of development and implementation. Pediatrics, 160(S1), 216 -222. https://doi.org/10.1542/peds.106.S1.216
Ornstein A, H. F., & Hunkins, F. P. (2009). Curriculum: Foundations, principles and issues (5th Ed.). Pearson.
Patel, V. L., Arocha, J. F., Chaudhari, S., Karlin, D. R., & Briedis, D. J. (2005). Knowledge integration and reasoning as a function of instruction in a hybrid medical curriculum. Journal of Dental Education, 69(11), 1186-1211. https://www.ncbi.nlm.nih.gov/pubmed/16275683
Polikoff, M. S. (2018). The challenges of curriculum materials as a reform lever Evidence Speaks Reports, 2, 58
Puri, N., McCarthy, M., & Miller, B. (2021). Validity and reliability of pre-matriculation and institutional assessments in predicting USMLE STEP 1 success: Lessons from a traditional 2 x 2 curricular model. Frontiers in Medicine (Lausanne), 8, Article 798876. https://doi.org/10.3389/fmed.2021.798876
Rimmer, A. (2014). GMC will develop single exam for all medical graduates wishing to practise in UK. BMJ, 349, g5896. https://doi.org/10.1136/bmj.g5896
Rufai, S. R., Holland, L. C., Dimovska, E. O., Bing Chuo, C., Tilley, S., & Ellis, H. (2016). A national survey of undergraduate suture and local anesthetic training in the United Kingdom. Journal of Surgical Education, 73(2), 181-184. https://doi.org/10.1016/j.jsurg.2015.09.017
Ruiz, J. G., Mintzer, M. J., & Leipzig, R. M. (2006). The impact of E-learning in medical education. Academic Medicine, 81(3), 207-212. https://doi.org/10.1097/00001888-200603000-00002
Ryan, A., Hatala, R., Brydges, R., & Molloy, E. (2020). Learning with patients, students, and peers: Continuing professional development in the solo practitioner workplace. Journal of Continuing Education in the Health Profession, 40(4), 283-288. https://doi.org/10.1097/CEH.0000000000000307
Santen, S. A., Feldman, M., Weir, S., Blondino, C., Rawls, M., & DiGiovanni, S. (2019). Developing comprehensive strategies to evaluate medical school curricula. Medical Science Educator, 29(1), 291-298. https://doi.org/10.1007/s40670-018-00640-x
Shah, S., McCann, M., & Yu, C. (2020). Developing a national competency-based diabetes curriculum in undergraduate medical education: A Delphi study. Canadian Journal of Diabetes, 44(1), 30-36. https://doi.org/10.1016/j.jcjd.2019.04.019
Sosna, J., Pyatigorskaya, N., Krestin, G., Denton, E., Stanislav, K., Morozov, S., Kumamaru, K. K., Jankharia, B., Mildenberger, P., Forster, B., Schouman-Clayes, E., Bradey, A., Akata, D., Brkljacic, B., Grassi, R., Plako, A., Papanagiotou, H., Maksimović, R., & Lexa, F. (2021). International survey on residency programs in radiology: similarities and differences among 17 countries. Clinical Imaging, 79, 230-234. https://doi.org/10.1016/j.clinimag.2021.05.011
Tiffin, P. A., Paton, L. W., Mwandigha, L. M., McLachlan, J. C., & Illing, J. (2017). Predicting fitness to practise events in international medical graduates who registered as UK doctors via the Professional and Linguistic Assessments Board (PLAB) system: a national cohort study. BMC Medicine, 15(1), Article 66. https://doi.org/10.1186/s12916-017-0829-1
van Zanten, M., Boulet, J. R., & Shiffer, C. D. (2022). Making the grade: licensing examination performance by medical school accreditation status. BMC Medical Education, 22(1), Article 36. https://doi.org/10.1186/s12909-022-03101-7
Watmough, S., Garden, A., & Taylor, D. (2006). Does a new integrated PBL curriculum with specific communication skills classes produce Pre Registration House Officers (PRHOs) with improved communication skills. Medical Teachers, 28(3), 264-269. https://doi.org/10.1080/01421590600605173
Watmough, S., O’Sullivan, H., & Taylor, D. (2009). Graduates from a traditional medical curriculum evaluate the effectiveness of their medical curriculum through interviews. BMC Medical Education, 9, Article 64. https://doi.org/10.1186/1472-6920-9-64
Yarhere, I., Chinnah, T., & Uche, C. (2022). Learners’ report and perception of differences in undergraduate paediatric endocrinology curriculum content and delivery across Southern Nigeria. [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.20730937.v1
Yarhere, I. E., & Nte, A. R. (2018) A ten-year review of all cause paediatric mortality in University of Port Harcourt Teaching Hospital, Nigeria (2006–2015). Nigerian Journal of Paediatrics, 45(4), 185-91.
*Iroro Enameguolo Yarhere
East/West Road,
PMB 5323 Choba,
Rivers State, Nigeria
+2347067987148
Email: iroro.yarhere@uniport.edu.ng
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
