
From conflict zones to classrooms: Humanitarian deployments as catalysts for medical education

Submitted: 17 December 2025
Accepted: 6 April 2026
Published online: 7 July, TAPS 2026, 11(3), 1-7
https://doi.org/10.29060/TAPS.2026-11-3/GP3968
Mohamad Hamim Mohamad Hanifah1 & Jubaida Paraja2
1Department of Emergency Medicine and 2Department of Pathology and Microbiology, Faculty of Medicine and Health Sciences, Universiti Malaysia Sabah, Kota Kinabalu, Sabah, Malaysia
Abstract
Introduction: Medical education increasingly values experiential learning, yet the profound pedagogical potential of humanitarian deployments remains underexplored. This narrative review, based on a clinician-educator’s first-hand field experiences, argues that humanitarian fieldwork in conflict and resource-limited settings serves as a powerful catalyst for innovation in medical education, offering unique lessons that can transform teaching and learning.
Methods: Drawing on the author’s humanitarian missions in Bangladesh, Myanmar, Afghanistan, and Lebanon, this paper employs a reflective, practice-based analysis from a clinician-educator’s perspective. Key experiences are examined and systematically aligned with established educational theories, including transformative and experiential learning, to extract transferable educational principles and pedagogical strategies.
Results: The analysis identifies four critical themes from humanitarian fieldwork: ethics-in-action, cultural humility, resilience, and clinical improvisation. These themes were translated into concrete educational strategies–low-resource simulation, narrative medicine, case-based ethics, and train-the-trainer models–when integrated into formal curricula, significantly enrich student learning. They foster not only clinical competence but also empathy, ethical reasoning, and a sense of global citizenship.
Conclusion: Humanitarian medicine represents a powerful form of transformative professional development, where discomfort becomes a catalyst for growth. Integrating these field-derived lessons enhances teaching effectiveness, deepens reflective practice, and strengthens institutional capacity for global health education. These insights highlight the educational value of humanitarian experiences in cultivating resilient, ethical, and compassionate educators–qualities essential for preparing future-ready healthcare professionals.
Practice Highlights
- Humanitarian fieldwork generates critical educational themes.
- Low-resource simulation is a powerful, transferable pedagogical tool.
- Integrating authentic field narratives and ethical dilemmas into curricula.
- The “Train-the-Trainer” model empowers learners and builds sustainable capacity.
- Humanitarian deployments should be recognised as valuable faculty development.
I. INTRODUCTION
Modern medical education prioritises experiential learning to shape competent and compassionate healthcare professionals (Taylor & Hamdy, 2013). Among the most potent yet underutilised sources of this learning are humanitarian deployments. These missions place clinicians in conflict zones, disaster areas, and resource-limited settings, demanding not only clinical skill but also ethical sensitivity, cultural awareness, and logistical adaptability. For educators, they offer a transformative lens through which to re-examine teaching and curriculum design.
This narrative review is grounded in my first-hand experiences with humanitarian organisations in Bangladesh, Myanmar, Afghanistan, and Lebanon. Each mission, set against a backdrop of crisis, provided unique insights into healthcare delivery under extreme duress. More importantly, they revealed the essential competencies for humane and effective practice–skills increasingly vital in today’s unpredictable global health landscape.
I argue that humanitarian fieldwork, when critically reflected upon, is a powerful engine for educational innovation. By aligning field-based lessons with established educational frameworks, I demonstrate how these experiences can enrich mainstream medical education. My aim is to advocate their structured integration to foster a new standard of clinical excellence, empathy, resilience, and global citizenship.
II. FIELD-BASED LEARNING: THE WORLD AS A CLASSROOM
Humanitarian deployments are immersive, high stakes learning environments where conventional medical training is both tested and transcended. Far from the structured confines of academia, these missions unfold in unpredictable and resource-constrained contexts. They demand real-time clinical decision-making, deep cultural sensitivity, and the ability to improvise–skills often peripheral in standard curricula. My experiences across four distinct settings illustrate how such environments become unparalleled classrooms.
A. Bangladesh-Myanmar Food Flotilla (2017): Learning through Adaptability
During a maritime aid mission, bureaucratic delays in port clearance were inevitable. Instead of idling, we transformed this time into a training opportunity. Onboard the vessel, we conducted capacity-building sessions for volunteers, using realistic simulation drills for man-overboard and mass casualty scenarios. This was not abstract theory; it was essential preparation for potential emergencies at sea. The core educational insight was clear: when original plans fail, meaningful learning can still thrive if we reimagine our objectives with flexibility and purpose.
B. Afghanistan (2024): Education Amidst Extreme Scarcity
A mission to a high-volume maternity hospital in Kabul presented a starkly different challenge: profound resource scarcity. With only two CTG monitors for hundreds of high-risk patients, the constraint was omnipresent. Yet, the commitment of local staff was extraordinary.
Despite exhausting clinical shifts, they engaged deeply in hands-on workshops on basic life support (BLS), advanced life support (ALS), neonatal resuscitation, obstetric emergencies, and point-of-care ultrasound (POCUS). Navigating Dari and Pashto language barriers through interpreters and translated materials embedded inclusivity into our teaching. The most powerful validation came hours into the training, when a resident successfully revived a newborn using the techniques just practiced–a direct testament to the life-saving impact of contextually relevant education.
C. Lebanon (2025): Building Community Capacity
In Beirut’s Shatila refugee camp, the focus shifted to sustainable, community-based learning. Within the camp’s dense and fragile infrastructure, we delivered interactive simulation workshops on BLS, ALS, trauma care, and pain management to Palestinian healthcare providers. Physical space was limited, necessitating creative scheduling and use of communal areas. A pivotal moment occurred when a volunteer physiotherapist excelled in an ALS simulation. Recognising her potential, we empowered her to become a trainer herself. This outcome embodies a core educational principle: sustainable capacity is built by identifying and empowering talent within the community.
Collectively, these missions reveal field-based learning as a multidimensional crucible. It forges not only clinical competence but also emotional intelligence, cultural humility, and emergent leadership. This process aligns perfectly with Kolb’s (1984) experiential learning cycle, where concrete experience sparks reflection, conceptualisation, and active experimentation. In each setting, the field itself–with all its challenges–became the most authentic and relevant curriculum. A summary of these missions, their challenges, and derived educational themes is provided in Table 1.
|
Mission Location |
Context |
Key Challenges |
Educational Themes |
Pedagogical Translation |
|
Bangladesh (2017) |
Maritime humanitarian aid |
Restricted clinical access |
Flexibility, resilience |
Emergency drills, BLS training |
|
Afghanistan (2024) |
Maternity hospital |
Resource scarcity, language barriers |
Ethics-in-action, cultural humility |
Low-resource simulation, translated materials |
|
Lebanon (2025) |
Refugee camp |
Infrastructure limitations |
Empowerment, improvisation |
Train-the-Trainer model, peer teaching |
Table 1. Summary of Humanitarian Missions and Educational Insights
III. CORE EDUCATIONAL THEMES FROM THE FIELD
Beyond technical skills, humanitarian deployments expose broader, transformative themes that are difficult to replicate in a traditional classroom. From my missions, four essential themes emerge as critical for holistic physician development.
A. Ethics in Action
Medical ethics are often taught as abstract principles. In Kabul’s maternity hospital, they became urgent, daily dilemmas. With only two CTG monitors, deciding which high-risk patient received monitoring was a matter of distributive justice in real time. Allocating the last ICU bed or final dose of a critical drug required instant ethical reasoning rooted in clinical urgency and compassion. These experiences underscore that ethics must be taught as a dynamic, context-sensitive process, not a detached philosophical debate.
B. Cultural Humility and Linguistic Sensitivity
Effective cross-cultural practice requires cultural humility–an ongoing openness to self-reflection and acknowledgment of one’s limitations. In Kabul, this meant adapting all materials and using interpreters for Dari and Pashto speakers. In Shatila, it involved localising content into Arabic and framing it within the Palestinian refugee experience. These efforts shift the paradigm from one-way knowledge transfer to building collaborative learning partnerships that respect and integrate linguistic and cultural realities.
C. Resilience and Emotional Intelligence
The emotional weight of humanitarian work is profound. In Bangladesh, our team faced moral distress when logistical barriers prevented direct clinical care. Pivoting our role from healers to educators required significant emotional resilience and a reframing of purpose. Witnessing local providers in Lebanon continue to offer dignified care amidst overwhelming adversity highlighted the indispensable role of emotional intelligence–self-awareness, empathy, and peer support–as a core clinical competency.
D. Improvisation and Clinical Agility
Each mission demanded creative problem-solving. On a ship’s rolling deck in Myanmar, we adapted emergency drills to the moving environment. In Afghanistan, we taught ALS using minimal equipment, relying on inventive substitutions. In Lebanon’s cramped spaces, we redesigned schedules and used community resources innovatively. These experiences cement the value of “thinking on one’s feet”–maintaining safety and efficacy despite severe constraints, a skill of increasing relevance in all healthcare settings.
IV. PEDAGOGICAL TRANSLATION: FROM FIELD TO CURRICULUM
Transforming the raw lessons of humanitarian fieldwork into structured medical education requires more than storytelling–it demands intentional pedagogical design (Milota et al., 2019). My experiences have been translated into educational strategies, simulations, and reflective exercises that enrich clinical teaching and professional identity formation. These core strategies, their origins, and their educational benefits are outlined in Table 2.
|
Strategy |
Origin |
Educational Benefit |
Classroom Application |
|
Low resource simulation |
Afghanistan, Myanmar |
Adaptability, teamwork |
Emergency medicine modules |
|
Narrative medicine |
Lebanon, Bangladesh |
Empathy, identity formation |
Reflective writing assignments |
|
Train-the-Trainer |
Lebanon |
Leadership, sustainability |
Peer-led BLS/ALS sessions |
|
Case-based ethics |
Kabul |
Ethical reasoning |
Tutorials on distributive justice |
Table 2. Pedagogical Strategies Derived from Humanitarian Deployments
A. Simulation-Based Learning in Low-Resource Contexts
Simulation was a cornerstone of all field missions, proving that high-fidelity learning doesn’t require advanced technology. Inspired by maritime drills in Myanmar and low-equipment ALS simulations in Afghanistan, I developed low-resource simulation modules for students. These exercises challenge learners to manage emergencies with limited personnel and tools, emphasising adaptability, teamwork, and clinical reasoning over technical dependence.
B. Ethics and Cultural Humility through Case-Based Discussion
The ethical dilemmas of Kabul and the cultural adaptations of Shatila have been transformed into compelling case studies. Students now grapple with scenarios like triaging the last ICU bed, sparking deep discussions on justice in resource-poor settings. Cases involving language barriers prompt reflection on informed consent and cross-cultural trust-building, grounding abstract ethical principles in tangible complexity.
C. Narrative Medicine and Reflective Writing
Authentic field stories are powerful catalysts for discussion. The journey of the Shatila physiotherapist who became a trainer sparks conversations about identity, potential, and medicine’s social mission. Reflections on the pivot from clinical care to training in Bangladesh form the basis of writing assignments that help students process concepts of frustration, failure, and purpose, humanising their own educational journey.
D. Train-the-Trainer and Peer Teaching Models
The success of empowering local providers in Lebanon inspired the adoption of peer-teaching models in my home institution. Senior medical students now co-facilitate BLS and trauma sessions for their juniors. This reinforces their knowledge while developing essential skills in leadership, communication, and mentorship, creating a self-sustaining educational culture.
These translations are rooted in Mezirow’s (1991) transformative learning theory. The “disorienting dilemmas” faced in the field–ethical, cultural, logistical–act as powerful triggers for critical reflection. When imported into the classroom via simulation and narrative, they disrupt students’ assumptions about healthcare and their role within it, fostering the perspective shift essential for transformative growth. The complete model for translating humanitarian fieldwork into curricular innovation is illustrated in Figure 1.
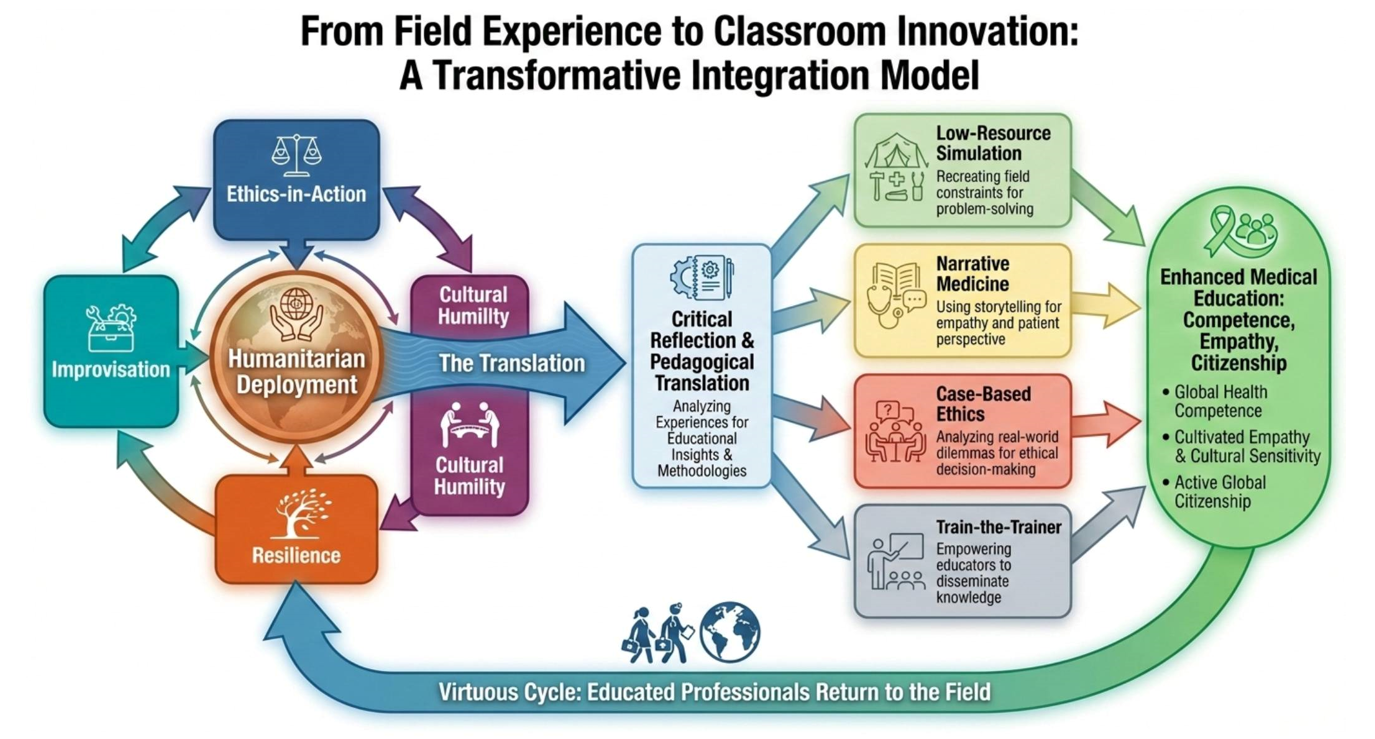
Figure 1: From Humanitarian Fieldwork to Curricular Innovation: A Model for Transformative Integration in Medical Education
(Note: This diagram illustrates the authors’ original conceptual framework and was visually rendered using OpenAI’s DALL-E 3 image generation tool on 17 December 2025.)
V. DISCUSSION: THEORETICAL ALIGNMENT AND INSTITUTIONAL IMPLICATIONS
The case for integrating humanitarian field experiences into medical education is strengthened by its firm grounding in foundational learning theories. This alignment provides a robust rationale for formal inclusion in faculty development and curriculum design.
A. Transformative Learning in Practice
Mezirow’s (1991) theory finds vivid expression in these missions. The discomfort and dissonance encountered are not impediments but the essential catalysts for deep learning. When educators model the vulnerability of grappling with ethical ambiguity or logistical failure, they give students permission to engage in the critical self-reflection necessary for their own transformative professional development.
B. Enacting the Experiential Cycle
These deployments perfectly illustrate Kolb’s (1984) experiential learning cycle. The concrete experience of teaching neonatal resuscitation in Kabul leads to reflective observation (debriefing), then to abstract conceptualisation (understanding the power of low-resource simulation), and finally to active experimentation (designing and implementing a new curriculum module). This cycle ensures field learning is an active, iterative process of knowledge creation, not a passive event.
C. Building Communities of Practice
The Train-the-Trainer model’s success in Lebanon is a direct embodiment of Lave and Wenger’s (1991) situated learning theory. By progressing from peripheral participant to central trainer, local volunteers fully entered their community of practice. Similarly, when students engage with these global health narratives, they begin to envision themselves as part of an international community of healthcare providers, fostering a sense of shared responsibility and belonging.
To harness this potential, institutions must act. Humanitarian work should be formally recognised as valuable Continuing Professional Development (CPD) for educators. Faculty development programs should incorporate modules on “contextual pedagogy,” teaching in low-resource settings, and using narrative and simulation drawn from global health. Creating structured platforms–such as dedicated grand rounds or digital story repositories–for faculty to share field-based insights can enrich an institution’s entire educational ecosystem.
Ultimately, humanitarian medicine teaches us to reframe discomfort. The field’s unpredictability, emotional intensity, and ethical complexity create a fertile ground for the deepest form of learning. By embracing these experiences as central to our educational mission, we can prepare a generation of physicians who are not only clinically expert but also emotionally intelligent, culturally humble, and equipped to lead in an uncertain future.
VI. CONCLUSION
Humanitarian medicine is more than service; it is a transformative educational journey. Stepping beyond institutional comfort zones fosters profound growth. These missions demanded a synthesis of clinical expertise, emotional resilience, cultural humility, and ethical clarity–the very qualities that define a compassionate, globally minded physician.
Challenges like language barriers, scarcity, and human suffering were not obstacles but essential catalysts for learning. These “disorienting dilemmas” prompted deep reflection, reshaped my professional identity, and inspired innovative approaches to teaching.
By integrating humanitarian narratives, low-resource simulations, and real-world ethical dilemmas into curricula, we bridge the gap between theoretical knowledge and practical wisdom. We invite learners to explore not just how to treat disease, but what it means to serve, lead, and care in adversity. These lessons cultivate empathy, global citizenship, and a service-oriented mindset–qualities indispensable in our interconnected world.
For educators, humanitarian deployments are unparalleled faculty development. They refine pedagogy, deepen reflective practice, and foster knowledge co-creation with diverse communities. Academic institutions must recognise and support these experiences not as extracurricular, but as essential to health professions education.
The most powerful education occurs in the messiness of real life–in refugee camps, on ships, in under-equipped hospitals, in moments of shared humanity. Here, textbook knowledge meets compassion, theory is tested by reality, and both learners and educators grow. Humanitarian medicine must be embraced not only as service but as a transformative force that teaches with both knowledge and heart.
Notes on Contributors
Mohamad Hamim Mohamad Hanifah conceived the work based on firsthand field experiences; acquired and interpreted the narrative data and drafted the initial manuscript and its critical intellectual content.
Jubaida Paraja contributed to the conceptual design of the pedagogical translation framework and critically revised the manuscript for important intellectual content.
All Authors provided final approval of the version to be published and agree to be accountable for all aspects of the work.
Acknowledgement
We are deeply grateful to the humanitarian partners and the dedicated local health teams in each field location for their partnership, resilience, and shared commitment to care under extreme conditions. Their work is the foundation of this reflection. We also thank our peers for their insightful comments during the development of this article.
Funding
No specific grant was received from any funding agency for the writing of this manuscript. The humanitarian deployments described were conducted in a voluntary capacity with various non-governmental organisations.
Declaration of Interest
The authors declare no conflicts of interest related to the research, authorship, or publication of this article.
Declaration of AI and AI-assisted Technologies in the Writing Process
All structural mapping, pedagogical pathways, and textual content were defined solely by the authors. Figure 1 illustrates the authors’ original conceptual framework and was visually rendered using OpenAI’s DALL-E 3 image generation tool on 17 December 2025.
References
Kolb, D. A. (1984). Experiential learning: Experience as the source of learning and development. Prentice-Hall.
Lave, J., & Wenger, E. (1991). Situated learning: Legitimate peripheral participation. Cambridge University Press. https://doi.org/10.1017/CBO9780511815355
Mezirow, J. (1991). Transformative dimensions of adult learning. Jossey-Bass.
Milota, M. M., van Thiel, G. J. M. W., & van Delden, J. J. M. (2019). Narrative medicine as a medical education tool: A systematic review. Medical Teacher, 41(7), 802–810. https://doi.org/10.1080/0142159X.2019.1584274
Taylor, D. C. M., & Hamdy, H. (2013). Adult learning theories: Implications for learning and teaching in medical education: AMEE Guide No. 83. Medical Teacher, 35(11), e1561–e1572. https://doi.org/10.3109/0142159X.2013.828153
*Assoc. Prof. Dr. Jubaida Paraja
Faculty of Medicine and Health Sciences,
Universiti Malaysia Sabah,
88400 Kota Kinabalu,
Sabah, Malaysia
Email: jubaida@ums.edu.my
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
