
Flipped Classroom Model for teaching and learning medical microbiology

Published online: 2 May, TAPS 2017, 2(2), 24-29
DOI: https://doi.org/10.29060/TAPS.2017-2-2/OA1006
Vindya Perera & Nelun de Silva
South Asian Institute of Technology and Medicine (SAITM), Malabe, Sri Lanka
Abstract
Flipped Classroom Model (FCM) is a method that was introduced to the educational system during the past decade which had shown substantial evidence of changing the traditional classroom learning to a more student centred learning environment. This method offers both students and the faculty, flexibility in teaching leaning activities that encourages a deeper approach to learning. This study was conducted to introduce FCM to undergraduates, to compare its effectiveness in learning clinical microbiology with lectures done in the traditional manner and to evaluate this system through student feedback. Power point presentations of 5 lectures were made accessible to students online and five lectures were done in a traditional manner. Freed lecture time was utilized to conduct discussions on clinical cases and problems. The effectiveness of this approach was determined by comparing the average marks students obtained for answers to questions covering the topics delivered by two methods. Questionnaires were given to students to evaluate their perceptions, effectiveness and experience of FCM versus traditional lectures for learning. Flipped classroom model was shown to be more effective than traditional lectures when the average marks in the final assessment were compared. More than 50% of students agreed on the benefits of FCM. Majority suggested a combination of FCM and traditional lectures followed by small group discussions would be more beneficial. Newer models of teaching and learning such as FCM would enable teaching and learning in pre and para clinical subjects in a medical curriculum to be more students centred and encourage deep learning.
Keywords: Flipped Classroom Model; Medical Education; Microbiology
Practice Highlights
- FCM can be adopted as a strategy to implement higher order teaching learning activities without increasing class time.
- This study shows that students performed better in the clinical microbiology assessment given from the topics covered by FCM than traditional lectures.
- Taking into consideration the perceptions of students, a combination model of FCM and traditional lectures is the best option for teaching and learning in clinical microbiology in our institution.
I. INTRODUCTION
Effectiveness of teaching methods that depends on lectures has been a questioned among educators involved in adult education (Barr & Tagg, 1995). For centuries teaching and learning pedagogy has mainly depended on lectures (Bligh, 2000). Even though these traditional face to face lectures provide an efficient method of transferring knowledge, it does not engage students in active learning. Educators are searching for techniques that move learners away from ‘superficial learning’ towards ‘deep learning’ that occur by being involved actively in the learning process (Ritchhart, Church & Morrison, 2011). To encourage the active participation of learners that leads to deep learning, educators use different techniques to shift the teacher centred paradigm towards a learner centred paradigm. One such technique that has become popular in the past decade is the ‘Flipped Classroom’ Model (Roehl, Reddy & Shannon, 2013).
Flipped Classroom model (FCM) is a technique that was introduced by Jonathan Bergmann and Aaron Sams in early 2000 where they delivered their lectures as video records for students to watch at home and the students did more constructive activities during freed class time (Siegle, 2014). According to Bergman and Sams, students need assistance of teachers to answer questions and when solving problems in an assignment but not when listening to a lecture. With the advancement of technology in the new millennium, where students have access to information at the tip of their fingers, the importance of lectures keep diminishing in adult education. Newer technologies like Learning Management System (LMS) software, allow educators to manage their teaching materials in a manner where students can read or listen to lectures whenever and wherever they want. These technologies make it easier for educators to adopt innovative ideas such as flipping the classroom that allow students to access and study lectures at their own pace. Freed class time would allow teachers to engage in techniques that involve students in higher order cognitive work.
Medical education can be improved without increasing the time it takes to earn a medical degree, if lessons are made more comprehensible and memorable and use a learning strategy that is student centred to encourage deep engagement in learning (Heath & Heath, 2007). If the FCM can be applied to teaching and learning in the pre and para clinical sciences in medical schools, class time would be freed up for more interactive lessons. Using LMS to deliver lectures also makes it possible for teachers to monitor each student’s access to the system and to use that knowledge to conduct focused interactions with students using freed lecture time. Students would also welcome more opportunities for case-based, problem based, and team-based exercises; strategies that activate prior knowledge. Teachers would be able to actually teach, rather than merely make a speech (Prober & Heath, 2012). A meta-analysis published by the Department of Education, USA has concluded that “on average, students in online learning conditions performed modestly better than those receiving face-to-face instruction,” with larger effects if the online learning was combined with face-to face instruction (<http://www2.ed.gov 2010>).
This study was conducted to introduce FCM to undergraduates learning clinical microbiology, to compare its effectiveness with traditional lectures and to evaluate this system through student feedback.
II. OBJECTIVES
A. General Objective:
To compare the effectiveness of FCM with lecture based traditional method of learning in Microbiology.
B. Specific Objectives:
- To obtain and analyse the perceptions of students about FCM
- To compare the effectiveness of FCM in learning clinical microbiology with lecture based traditional teaching
- To compare changes in student performance before and after introducing FCM
III. METHODS
The Department of Microbiology, Faculty of Medicine, South Asian Institute of Technology and Medicine (SAITM) introduced this new model in the last six weeks of semester five, when students learn Clinical Microbiology. Of the ten lectures scheduled during this time period, five were randomly selected to be conducted as FCM. Power point presentations (with detailed explanatory notes in the notes section of each slide) of the selected five lectures and relevant quizzes were uploaded on a learning management system, one per week, for students to view, learn and assess themselves. The students were not given curricular time to view the slides, since they were available online throughout the week for them to learn by themselves at their own pace and time. During the freed curricular time in the semester, clinical cases and problems relevant to the lectures given on line were discussed by students in small groups with teachers acting as facilitators. The other half of the lectures were done in the traditional manner face to face. Here too these lectures were followed by student led small group discussion of clinical cases and problems in the same manner. Therefore, to ensure that students were not deprived of equal opportunities for learning in the two methods, both the online and traditional lectures were followed by student led small group discussions. The contents of the clinical cases and their discussions were organized and conducted in a similar manner following online lectures and traditional lectures to prevent any bias that would have arisen due to the research. The only difference in the two methods was that the students were allowed to learn the content on their own in the FCM rather than listening to a didactic lecture. The lecture topics covered by the FCM and by the traditional method were selected randomly. The degree of difficulty of the contents in each lecture topic was similar since they covered the general objectives of the microbiology course and the specific objectives developed for each topic in clinical microbiology. The same teachers were involved for the lectures and the small group discussion during the study period. Ethical clearance was obtained from the Ethical Review Committee of the Faculty of Medicine, SAITM.
A. Analysis of perception of students on FCM
Questionnaires were given to students to evaluate their perceptions on the importance, effectiveness and their experience of the new model versus the traditional model for learning. Feedback from students was collected anonymously at the end of the course in microbiology but before the final examination. This was done with a questionnaire containing pre-prepared options for students to select, together with a few open ended questions to find out the reasons for their selected options. The responses given were analysed by descriptive statistics.
B. Comparison of the effectiveness of FCM in learning clinical microbiology with lecture based traditional teaching
The performance of students in the final examination in microbiology was analysed. The final examination consisted of a theory paper which included 20 true false MCQ, 4 EMI and 4 SEQ. The practical component consisted of 20 OSPE questions. The questions set for the examination were designed to cover course content in clinical microbiology as well as general and systematic microbiology. MCQ were made to assess mainly the students’ knowledge on general and systematic microbiology, while EMI and SEQ were used to assess the application of their knowledge on clinical microbiology case scenarios and situations. OSPE questions were also made to assess mainly the application of their knowledge on infectious diseases. The setting of questions for the final examination was not done with the intention of covering topics done by the two methods. It was done in the usual manner according to a blue print and taking into consideration past examination questions.
Of the 20 MCQ, 5 questions covered the clinical microbiology lectures and of these, 3 covered topics done by FCM and 2 covered topics done by traditional lectures. Of the 4 EMI with 20 leading questions (5 scenarios for each EMI), 4 scenarios were from clinical microbiology topics done by FCM and 6 scenarios from lecture topics done in the traditional method. Six of the OSPE questions were from topics done by FCM and 8 OSPE questions from topics done traditionally. Of the 4 SEQ given in the theory paper, 1 question was from a topic done by FCM and 1 was by a topic covered by traditional method. The marks obtained for answers to questions set on topics covered by FCM were compared to the marks obtained for answers to questions set on topics delivered as traditional lectures. The mean marks of students for the questions covered by FCM and traditional learning was compared using paired student t test.
C. Comparison of changes in student performance before and after introducing FCM
The average scores of SEQ and OSPE components in the microbiology final examination of the present study batch was compared with the scores obtained in the final examination of the previous batch. In the previous batch all the topics were done by traditional lecture based teaching methods. (Scores obtained for MCQ and EMI were not compared since the formats of these two tools were different between the batches in the two examinations).
IV. RESULTS
A. Analysis of perception of students on FCM
Quantitative feedback was obtained from 50 students by using a questionnaire with pre -prepared options. All the options were analysed independently. Fifty-six percent agreed that FCM was important in medical education while forty-two percent stated it was not important. Fifty-four percent preferred a combination of FCM and traditional lectures followed by small group discussions. Fifty-four percent said their experience in the new model was good and forty percent said it was a waste of time. From the responses given by 50 students, factors that the students pointed out as important for the success of innovative models like FCM were analysed separately. Of the 50 students 28% pointed out that competency in the use of information technology of students was important for the success of FCM. Students’ preference for innovative techniques (18%) and student centred learning methods (18%) were the other factors that were pointed out by the students as factors that contributed to the success of the FCM. The factors that contributed to the failure of FCM were, conventional ideas they have regarding learning (12%); learning as they would have done in school where the teacher is the centre of information and learning is centred around lectures. In addition, 6% of students attributed the failure of FCM to their limited knowledge on information technology hindering them from actively engaging with learning on line and their unwillingness to engage in extra learning activities at home.
B. Comparison of the effectiveness of FCM in learning clinical microbiology with lecture based traditional teaching
In the final assessment in microbiology, the performance of students in areas covered by FCM and traditional learning was compared using a paired student t test. T-test results (p < 0.05) showed a significant difference in the marks obtained for answers to questions covered by FCM compared to those done in the traditional way. The average score of the questions covered by FCM was significantly higher than the average score of the questions covered by traditional lectures.
The difference between the mean score for the Extended Matching Items (EMI) in the final examination that were covered by FCM (mean = 6.85, sd = 1.9) and from the conventional lectures (mean = 5.4, sd = 2.6) was significant (p < 0.001). (Fig. 1)
There was also a significant difference (p < 0.001) between mean marks of answers to Structured Essay Questions (SEQ) covered by FCM (mean = 57.6, sd = 17.5) and from traditional lectures (mean = 41.6, sd = 21.3). (Fig. 2)
The difference between mean marks of Objective Structured Practical Examination (OSPE) covered by FCM (mean = 7.1, sd = 2.851) and conventional lectures (mean= 5.3, sd= 3.5) was also significant (p < 0.001). (Fig. 3)
However, there was no remarkable difference between the true false response MCQ’s asked from FCM (mean = 4.6, sd = 1.4) and from traditional lectures. (mean = 4.5, sd =1.5).
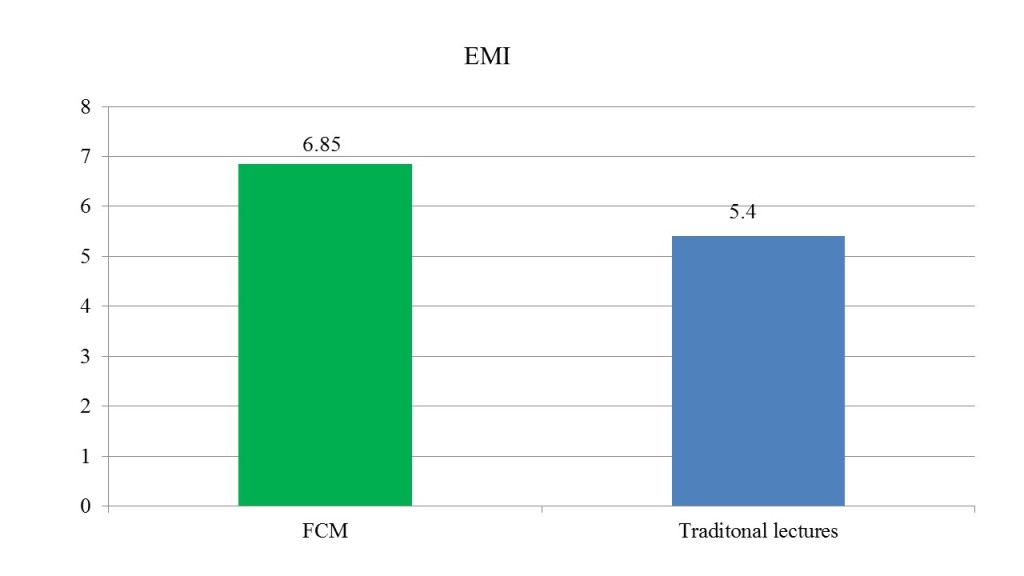 Figure 1. Bar chart shows the mean marks of answers to EMI from lectures covered by FCM and traditional lectures
Figure 1. Bar chart shows the mean marks of answers to EMI from lectures covered by FCM and traditional lectures
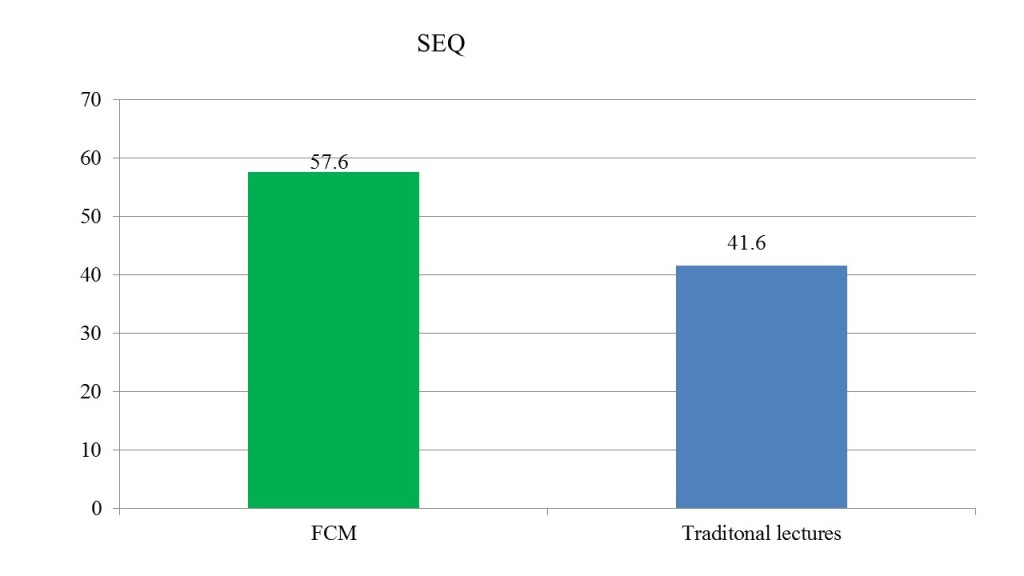 Figure 2. Bar chart shows the mean marks of answers to SEQ from lectures covered by FCM and traditional lectures
Figure 2. Bar chart shows the mean marks of answers to SEQ from lectures covered by FCM and traditional lectures
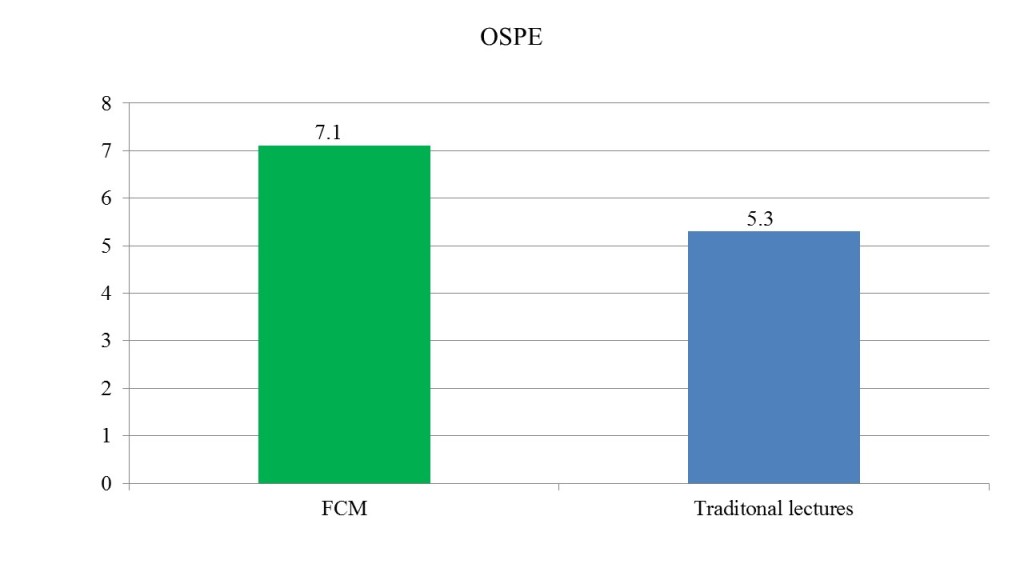 Figure 3. Bar chart shows the mean marks of answers to OSPE from lectures covered by FCM and traditional lectures
Figure 3. Bar chart shows the mean marks of answers to OSPE from lectures covered by FCM and traditional lectures
| Exam component | Topics covered by traditional lectures in the study | Topics covered by FCM in the study | ||
| Average Score of Previous Batch | Average Score of Study Batch | Average Score of Previous Batch | Average Score of Study Batch | |
| SEQ | 0.52 | 0.41 | 0.42 | 0.57 |
| OSPE | 6.27 | 5.3 | 5.06 | 7.1 |
Table 1. Table shows the comparison of average scores of SEQ & OSPE, of the previous batch and the present study population for lectures covered by traditional lectures & FCM in the study
C. Comparison of the changes in student performance before and after introducing FCM
A difference was observed, when comparing students’ average scores of the present study batch with the previous batch where all the topics were covered by lecture based teaching methods. The average score for topics covered by traditional lectures in the present study batch had not improved when compared to the previous batch (scores were higher in the previous batch) (Table 1). The average score for topics covered by the FCM in the present study batch had improved when compared to the previous batch (Table 1).
V. DISCUSSION AND CONCLUSIONS
Introducing FCM produced a mixed reaction from the students. While appreciating the importance of a novel method, the students in this batch preferred a combination of traditional lectures and FCM. Overall the marks obtained in the majority of the components of the final examination in microbiology indicated that students performed better in areas covered by FCM. Perhaps learning on their own encouraged them to participate actively in the small group discussions that followed during the freed lecture hours in FCM, enabling them to learn more effectively and perform better in these areas. However, noting the students’ preferences, it would be best if the combination model of FCM and traditional lectures are done for learning in clinical microbiology.
In countries like Sri Lanka where students are used to a teacher centred environment for learning in schools with little exposure to student centred learning, introducing novel techniques such as FCM in higher education may be difficult. However, if students had been exposed to student centred learning and information technology courses during their school years or the first year in higher education, educators would have found it easier to implement student centred teaching and learning activities and students would have coped better and welcomed new strategies like FCM.
Innovative techniques such as the Flipped Classroom Model is more likely to address issues that higher education institutes face in the current context of increased demand for higher education and increase of student numbers in medical schools. However, when introducing models like FCM it is important to consider the other factors such as students’ IT knowledge that can influence the success of these models. Especially in countries like Sri Lanka, few students in a batch may not be competent in IT. In such instances the introduction of IT into a foundation course in the medical schools will enhance the usefulness of novel methods of learning dependent on IT and students too will be more willing to use such techniques when they can handle such methods with ease and comfortably. These factors have been rectified to some extent in the medical faculty of SAITM where a foundation course for medicine has been introduced to the new entrants which include IT among other aspects.
In this study although 56% is not an impressive number to show students acceptance of FCM, adopting different strategies like uploading video lectures, including online discussion forums may improve the model and make it more acceptable to the students.
In the study there was no significant difference in the students’ performance with MCQ questions. This may be due to the fact that MCQ are developed purely to assess the lower level of cognitive domain (knowledge component). Perhaps the increase of interactive learning with application based deep learning that was covered by FCM may improve the students’ performance in examination components that were assessing higher levels in the cognitive domain (SEQ and OSPE).
A difference was observed, when comparing students’ average scores of the present study batch and the previous batch. The improvement of the average score for topics covered by the FCM in the study population can be a result of batch to batch variations. However, since the performance of the study batch for the topics covered by traditional lectures did not show any improvement when compared to the previous batch, the batch to batch variation may be minimal.
Considering that the lectures were done by the same tutors for the two batches and questions given covered the same objectives in the two examinations, the change in the delivery of the lectures could also be a factor that influences the change in the performance of the two batches in the topics covered by FCM.
The study could not confirm that FCM was the sole contributory factor for improvement of students’ performance. However, if students can be introduced to different pedagogical approaches like FCM, the limited time allocated for teaching and learning activities could be used to improve higher order knowledge and skills of students.
Notes on Contributors
Vindya Perera- BVSc (Pera.)- Lecturer in microbiology in the Department of Microbiology, Faculty of Medicine, SAITM with three years of teaching and research. Registered for MPhil in Faculty of Medicine, University of Colombo, Registered Veterinary surgeon in Sri Lanka Veterinary Council.
Nelun de Silva- MBBS. (Patna) MD Medical Micro (Col.)- Professor and consultant in microbiology, Department of Microbiology, Faculty of Medicine, SAITM and Neville Fernando Teaching Hospital, Malabe, Sri Lanka. Accredited Senior Teacher in Higher Education (ASTHE) University of Colombo with accreditation from Staff and Educational Development Association (SEDA) UK.
Acknowledgments
The authors acknowledge the cooperation and commitment of 5th batch of medical students, especially those of Sachitra Wijetunga and Ammar M. Jawfer.
Declaration of Interest
All the authors declared no competing interests.
References
Barr, R., & Tagg, J. (1995). From Teaching to Learning — A New Paradigm For Undergraduate Education. Change: The Magazine of Higher Learning, 27(6), 12-26.
Bligh, D.A. (2000). What’s the use of lectures? San Francisco, CA: Jossey-Bass
Heath, C., & Heath, D. (2007). Made to stick: why some ideas survive and others die. New York: Random House.
Means, B., Toyama, Y., Murphy, R., Bakia, M., & Jones, K. (2010). Evaluation of evidence-based practices in online learning: a meta-analysis and review of online learning studies. Retrieved from http://www2.ed.gov/rschstat/eval/tech/evidence-based-practices /final report
Prober, C.G., & Heath, C. (2012). Lecture halls without lectures—a proposal for medical education. New England Journal of Medicine, 366(18), 1657-1659.
Ritchhart, R., Church, M., & Morrison, K. (2011). Making thinking visible: How to promote engagement, understanding, and independence for all learners. San Francisco, CA: Jossey-Bass.
Roehl, A., Reddy, S., & Shannon, G. (2013). The flipped classroom: an opportunity to engage millennial students through active learning strategies. (Strategies). Journal of Family and Consumer Sciences, 105(2), 44-49.
Siegle, D. (2014). Technology: Differentiating instruction by flipping the classroom. Gifted Child Today, 37(1), 51-55.
*Vindya Perera
South Asian Institute of Technology and Medicine (SAITM), Malabe, Sri Lanka
Tel: +(94) 11 241 3351, +(94) 11 241 3331
Fax: +(94) 11 241 3332
Email:v.perera83@yahoo.com
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
