
Advanced Cardiac Life Support instruction in the new norm: Evaluating the hybrid versus the traditional model

Submitted: 22 August 2021
Accepted: 28 December 2021
Published online: 5 April, TAPS 2022, 7(2), 42-45
https://doi.org/10.29060/TAPS.2022-7-2/SC2682
Lee Man Xin1*, Zhang Yuan Helen2* & Fatimah Lateef2,3
1Changi General Hospital Emergency Department, Singapore; 2Singapore General Hospital Emergency Department, Singapore; 3Singhealth Duke-NUS Institute of Medical Simulation (SIMS) Education Office, Singapore
*Joint first authors
Abstract
Introduction: Advanced Cardiac Life Support (ACLS) course is one of the mandatory certifications for the majority of medical as well as some nursing professionals. There are, however, multiple variations in its instruction model worldwide. We aim to evaluate the efficacy of traditional ACLS course versus a hybrid ACLS course utilised during the COVID-19 pandemic.
Methods: This retrospective study was carried out at SingHealth Duke-NUS Institute of Medical Simulation using course results of participants in the centre’s ACLS course between May to October 2019 for the traditional course were compared with participants attending the hybrid course from February to June 2021.
Results: A total of 925 participants were recruited during the study period. Of these, 626 participants were from the traditional group and 299 participants were from the hybrid learning group. There is no statistically significant difference between the two group (χ2=1.02 p = 0.313) in terms of first pass attempts; first pass attempt at MCQ (p=0.805) and first pass attempt at practical stations (p=0.408). However, there was statistically significant difference between the mean difference in results of traditional vs hybrid MCQ score, -0.29 (95% CI: -0.57 to -0.01, p=0.0409). Finally, senior doctors were also found to perform better than junior doctors in both traditional (p=0.0235) and hybrid courses (p=0.0309) at the first pass attempt of ACLS certification.
Conclusion: Participants in the hybrid ACLS course demonstrated at least equal overall proficiency in certification of ACLS as compared to the traditional instruction.
Keywords: Advanced Cardiac Life Support, Teaching Model, COVID-19, Hybrid Learning
I. INTRODUCTION
Cardiopulmonary resuscitation (CPR) represents an emergency lifesaving procedure for cardiac arrest patients. It is a core skillset for every licensed physician, graduating medical students and paramedics. It provides evidence-based algorithms to be executed to optimise the likelihood of survival in cardiac arrest patients. Cardiac arrest poses a major public health challenge. Worldwide, sudden and unexpected cardiac death is one of the most common causes of death. Given such a substantial disease burden, structured and continued training of physicians and first responders on advanced cardiac life support (ACLS) is extremely crucial. In Singapore, about 3000 people have a sudden cardiac arrest every year (Ong, 2020).
The first Advanced Cardiac Life Support (ACLS) course in Singapore, was started in late 1985 and traditionally it has been conducted over two days. It comprises of pre-reading from a manual outlining the procedure algorithms, a combination of face-to-face didactics and hands-on skills stations conducted by licensed providers and instructors, followed by multiple-choice theory and practical certification tests. It mainly focuses on technical knowledge and skills which needs to be recertified every two years (Anantharaman, 2017). Since the implementation of social distancing measures under DORSCON Orange in Singapore in response to the COVID-19 disease outbreak on 7th February 2020, ACLS teaching model has since been modified to multimedia lectures followed by small-group (maximum 5 people) practical lessons, which was further adjusted to include an online self-administered pre-lecture quiz from 18th February 2021 onwards. Limited evidence has shown that written evaluation is not a predictor for skills performance in an ACLS course and there is now, a growing body of advocates for high-fidelity mannequin-based simulation supplementing ACLS curricula. Multiple research studies have focused on the efficacy of various educational and instructional methods for ACLS teaching in terms of improvement to the resuscitation knowledge and clinical skills (Thorne et al., 2017).
We aim to retrospectively evaluate the efficacy of our new hybrid ACLS teaching model based on participants passing rate of both theory and practical tests as compared to the traditional ACLS instruction model. The primary goal is to provide enhanced insights into the way ACLS training should be conducted and further refine our courses as we evolve in the new norm of living with the COVID-19 pandemic. Institutional Review Board waiver has been obtained through Singapore Health Service (CIRB: 2021/2499).
II. METHODS
A. Study design and participants
This retrospective study was carried out at SingHealth Duke-NUS Institute of Medical Simulation (SIMS) using the course results of participants in the centre’s Advanced Cardiac Life Support (ACLS) course. A waiver of consent was approved by the institute’s CRIB committee as the results were anonymised.
The ACLS course traditionally comprises face-to-face didactic lecture components and practical skills stations culminating in MCQ and practical assessment. Successful completion of both MCQ and practical assessment results in certification or recertification for the participants.
In the hybrid ACLS learning model, the didactic lecture component has been replaced with an interactive online learning platform while maintaining the same practical skills stations with reduced instructor to student ratio because of safe distancing measures. To facilitate learning, a pre- and post-lesson quiz, with 25 MCQ questions, was administered on the online learning platform.
Course results of participants attending the traditional course from May to October 2019 were compared with participants attending the hybrid course from February to June 2021. No participants were found to have attended both the traditional and hybrid ACLS courses, to date. We did not differentiate between recertification and certification courses since there are no differences in assessments.
B. Outcome measures
Our primary outcome measure was the proportion of participants with successful first pass attempt at course certification between traditional and hybrid ACLS courses.
For secondary outcomes, we analysed the mean difference in MCQ scores and first pass attempts at practical stations between traditional and hybrid ACLS instructions. We also compared differences between pre- and post-lesson quiz scores administered during the hybrid learning to assess retention of theoretical knowledge. Lastly, we conducted a sub-group analysis comparing the proportion of senior doctors and junior doctors who pass the course at the first attempt, in both the traditional and hybrid learning groups. Here, senior doctors refer to individuals with specialist registration while junior doctors refer to all other registered medical practitioners.
C. Statistical analysis
A priori sample size estimation was carried out with the assumption that 90% of participants will pass with the first attempt in both traditional and hybrid ACLS teaching models. We used a non-inferiority margin of 10%. Taking α = 0.05 and a statistical power of 80%, we determined that would require at least 155 participants per group.
Statistical analysis was performed using Microsoft Excel 2019. T-test was used when comparing means, Chi-square test was used when comparing categorical variables.
III. RESULTS
A total of 925 participants were recruited during the study period. Of these, 626 participants were from the traditional group and 299 participants, from the hybrid learning group. No participants were excluded from the study. Table 1 shows the characteristics of both groups. The data supporting this study are openly available at https://doi.org/10.6084/m9.figshare.15131664.v1 (Lee et al., 2021).
For the traditional group, 87.7% (549 of 626) passed at the first attempt, whilst for the hybrid group, 90.0% (269 of 299) passed at first attempt (See Table 1). There was no statistically significant difference between the two groups (p = 0.313).
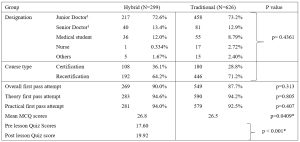
Table 1. Baseline Demographics of Participants for the ACLS Courses and comparison of primary and secondary outcome measures between the Hybrid and Traditional ACLS courses participants
1 Senior doctors are registered specialists under Singapore Medical Council. Junior doctors are all other registered medical practitioners under Singapore Medical Council.
There were no statistically significant differences between the two groups in terms of proportion of first pass attempt at MCQ (p=0.805) and first pass attempt at practical stations (p=0.408). There was however, a statistically significant difference, but with a very small effect size, between the mean difference in results of traditional vs hybrid MCQ score, -0.29 (95% CI: -0.57 to -0.01, p=0.0409).
We also compared the pre- and post-lesson quiz scores in the hybrid learning group. 21 participants were excluded from the analysis due to incomplete pre- or post- test results. We found a mean score difference of 2.32 (95% CI: 1.84 to 2.80, p < 0.001), out of a maximum score of 25, which was higher in post-test group.
Lastly, we compared the proportion of first pass test attempts between senior and junior doctors in both traditional and hybrid learning groups. Senior doctors consistently performed better than junior doctors in both traditional (96.3% vs 87.8% p=0.0235) and hybrid settings (100% vs 89.4% p=0.0309).
IV. DISCUSSION
ACLS is one of the most basic yet crucial skills of medical practitioners worldwide receiving special attention in the framework of various international and national resuscitation councils and societies (Thorne et al., 2017). Clinical educators must explore modalities and evolving technologies that can overcome the barriers of cost, access, and frequency of exposure, while balancing flexibility and applicability that follow deliverable sequelae. Thus far, participants of blended e-learning ACLS courses are known to demonstrate similar scores on the knowledge test, skills test and their final passing rate. The e-learning ACLS course also demonstrates equivalence to traditional face-to-face learning in equipping participants with ACLS skills when compared to the traditional course. This was demonstrated in our results as well. This is a value-added benefit, especially when considering factors such as increased autonomy, cost-effectiveness, decreased instructor burden and improved standardisation of course material (Thorne et al., 2017).
As we shift more towards andragogy among adult professionals, the principles for ACLS instruction should also focus more on self-directed, self-motivated and experiential instruction. Evidence does support that the form and content of these highly structured/model courses are important to transfer the clinical competence that is needed, especially in unstructured, emergencies (Rasmussen et al., 2013). Hence, exploring a sustainable model of ACLS knowledge translation is another important point since further research is needed to develop the optimal evaluation system for the ACLS training program which includes evaluation of the participants, the instructors, and the overall program. The goal should be to assess the degree to which the ACLS program is meeting its objective: to educate medical practitioners, first responders and rescuers.
The COVID-19 pandemic has affected simulation centres where ACLS courses are routinely held. Alternative education modalities have been employed, which include computer-based simulation where technology is used to enhance, augment or even at times, replace real-life simulation. It not only offers the professionals convenience but, complies with safe-distancing or ‘work-from-home’ restrictions put forth by regulatory bodies in many countries. Online modules of virtual reality have also been explored as these can be accessed anywhere electronically and can reduce the amount of face-to-face time that routine training normally requires.
V. CONCLUSION
Hybrid instruction of ACLS training for certification should be recommended as one of the main formats of course delivery as it is as effective compared to the traditional face-to-face training program. From our results it has performed well enough to allow for the safe transition and application of ACLS training in this new era.
Notes on Contributors
Lee Man Xin is involved in conceptualising the study, analysing and interpreting the data, drafting the above manuscript and approving the version to be published. He agrees to be accountable for all aspects of the work.
Zhang Yuan Helen is involved in conceptualising the study, interpreting the data, drafting the above manuscript and approving the version to be published. She agrees to be accountable for all aspects of the work.
Lateef Fatimah is involved in finalising the study conceptualisation and determining key elements for analysis. She is involved in the revision and final approval of the version to be published. She agrees to be accountable for all aspects of the work.
Ethical Approval
Institutional Review Board waiver has been obtained through Singapore Health Service (CIRB: 2021/2499).
Data Availability
The data supporting this study are openly available at figshare repository: https://doi.org/10.6084/m9.figshare.15131664.v1
Acknowledgement
The authors would like to thank Mr Billy Tee, Ms Suppiah Madhavi and Ms Angeline Ng from Singhealth Duke-NUS Institute of Medical Simulation (SIMS) Singapore for providing the data sets.
Funding
This paper receives no funding from outside sources.
Declaration of Interest
Authors have nothing to declare, nor any conflict of interests.
References
Anantharaman, V. (2017). The National Resuscitation Council, Singapore, and 34 years of resuscitation training: 1983 to 2017. Singapore Medical Journal, 58(7), 418–423. https://doi.org/10.11622/smedj.2017069
Lee, M. X., Lateef, F., & Zhang, H. Y. (2021). Hybrid ACLS model (version 1). [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.15131664.v1
Ong, M. E. (2020, October 2). Improving outcomes for Out-of-Hospital cardiac arrest victims. The Straits Times. https://www.singhealth.com.sg/rhs/news/research/improving-outcomes-for-out-of-hospital-cardiac-arrest-victims
Rasmussen, M. B., Dieckmann, P., Barry Issenberg, S., Østergaard, D., Søreide, E., & Ringsted, C. V. (2013). Long-term intended and unintended experiences after Advanced Life Support training. Resuscitation, 84(3), 373–377. https://doi.org/10.1016/j.resuscitation.2012.07.030
Thorne, C. J., Lockey, A. S., Kimani, P. K., Bullock, I., Hampshire, S., Begum-Ali, S., & Perkins, G. D. (2017). e-Learning in Advanced Life Support-What factors influence assessment outcome? Resuscitation, 114, 83–91. https://doi.org/10.1016/j.resuscitation.2017.02.014
*Lee Man Xin
Changi General Hospital Emergency Department
2 Simei Street 3, Singapore 529889
Email: Lee.Man.Xin@singhealth.com.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
