
Absence of Undergraduate Medical Students from Clinical Rotations; Its Causes and Way Forward

Submitted: 26 March 2025
Accepted: 5 November 2025
Published online: 7 April, TAPS 2026, 11(2), 73-80
https://doi.org/10.29060/TAPS.2026-11-2/OA3702
Maheen Zulfiqar, Muhammad Khalil ur Rahman, Behram Khayyam, Naeem Sarwar, Ashbil Malik, Ayesha Mazhar Khan & Hassan Saleem
Department of Surgery, Arif Memorial Teaching Hospital/Rashid Latif Medical College, Lahore, Pakistan
Abstract
Introduction: Absenteeism during clinical rotations among medical students is on the rise, adversely affecting both patient care and the development of essential clinical skills. Factors such as inadequate learning resources, exhaustion, and disengagement contribute to this trend, which must be addressed to safeguard the quality of medical training and future healthcare quality. This study aimed to identify the underlying causes of absenteeism among undergraduate medical students and to propose strategies to improve attendance and learning outcomes.
Methods: A cross-sectional study was conducted on third, fourth, and final-year students of primary medical qualification at Rashid Latif Medical College, Lahore, Punjab, Pakistan, from June 2024 to July 2024. A validated, self-structured questionnaire was distributed during clinical rotations. Data were analysed using SPSS version 25. Frequencies and percentages were calculated to summarise attendance patterns and perceived barriers. Pearson’s correlation was used to examine associations between absenteeism factors—personal health, family obligations, academic workload, perceived relevance of rotations and academic year, with statistical significance set at p ≤ 0.05.
Results: Out of 450 surveys, 270 students responded: 31% third year, 27% fourth year, and 43% final year students. Faculty-related barriers included poor feedback (3.2), ineffective communication (3.2), lack of preparation (3.3), and unprofessional attitude (3.3). Personal obstacles included personal health (3.2), lack of learning resources (3.4), and family obligations (3.3). Additionally, 41% of the students believed that non-exam-specific rotations were irrelevant.
Conclusion: Faculty dissatisfaction, peer pressure and downplaying non-exam specific rotations cause clinical rotation absenteeism. Systemic reforms and enhanced faculty engagement are essential to improve students’ professional development and clinical engagement.
Keywords: Medical Education, Absenteeism, Faculty, Clinical Rotations
Practice Highlights
- Many students do not find non-exam-specific rotations valuable due to the heavy workload.
- Students often feel demotivated to attend rotations because of uncooperative and unprofessional behaviour from faculty members.
- It is recommended that institutions implement policies to manage student workload, uphold professional conduct, and create a more motivating environment for clinical rotations.
I. INTRODUCTION
Absenteeism refers to the habitual absence from classes/ clinical rotations without a valid or justifiable reason (Qureshi & Ahmad, 2019). Student absenteeism is a common issue observed globally across all academic fields, and medicine is no exception (Gul et al., 2016). However, in the field of medicine, absenteeism has several negative consequences. It impacts students not only academically but also in terms of their professional development (Shenawi et al., 2021). Absenteeism, especially during clinical rotations, hinders both academic learning and patient care as well (Qureshi &
Ahmad, 2019).
Despite strict policies regarding attendance at clinical rotations and lectures, absenteeism remains prevalent among students (Sharmin & Azim, 2017). In Pakistan, there is a growing trend where medical students primarily attend clinical rotations for subjects that carry weight in their current year of study. According to student feedback and informal discussions, many students tend to skip ward rounds, following the example of their seniors, who claim that the material will be thoroughly covered the following year when the subject becomes compulsory. Even those who wish to attend non-compulsory wards often feel pressured by their peers to do otherwise. Additionally, a lack of professionalism among some faculty members and the overall ward environment can diminish students’ morale and motivation (Khan et al., 2019; Mitra et al., 2022).
Despite being a widespread issue, there is no valid justification for the absence of undergraduate medical students from their clinical rotations. To date, no study has been published that thoroughly investigates the key factors contributing to student absenteeism from clinical rotations, particularly at Rashid Latif Medical College and Arif Memorial Teaching Hospital in Lahore. Therefore, this study was undertaken to explore the primary reasons for low attendance among third year, fourth year and final year students of primary medical qualification (PMQ) at Rashid Latif Medical College and to identify initiatives that could improve their participation in clinical rotations.
II. METHODS
This cross-sectional study was conducted from June 2024 to July 2024 on 450 students after taking approval from the Institutional Review Board (RLMC/IRB/2024/153). The aim was to explore the factors influencing attendance in clinical rotations among undergraduate medical students. A self-designed, validated questionnaire was used. The study targeted 3rd, 4th and final year students of primary medical qualification (PMQ) at Rashid Latif Medical College, Lahore, Punjab, Pakistan.
Non-probability purposive sampling was used to recruit students. A total of 450 students were approached during their ward rotations. Out of those, 270 completed the survey, yielding a response rate of 60%. The inclusion criteria were students who were currently enrolled in the clinical years and attending rotations during the study period. Students in pre-clinical years (namely first and second year), those on academic leave or suspension, or those who declined participation were excluded. While purposive sampling allows access to students in relevant clinical settings, it does, however, carry the inherent limitation of selection bias, potentially over-representing students with better attendance or stronger academic engagement.
Data were collected using a self-designed, validated questionnaire. A thorough analysis of the body of research on medical school absenteeism and suggestions from three senior medical education specialists guided the development process. The questionnaire underwent content validation by the expert panel to assess clarity, relevance, and alignment with study objectives. There were both closed-ended and open-ended questions on the finished form.
Closed-ended questions included demographic variables, frequency of clinical attendance, and 5-point Likert scale items evaluating perceived faculty behaviours, personal and academic barriers, and attitudes toward clinical teaching. Preliminary reliability testing using pilot data yielded a Cronbach’s alpha of 0.779, indicating moderate internal consistency. Factor analysis revealed that the questionnaire could be sub-grouped into eight distinct domains, collectively accounting for 97% of the variance in responses.
Participation was entirely voluntary, and informed consent was implied through the completion and return of the questionnaire. Anonymity and confidentiality were ensured to encourage honest and uninfluenced responses. Questionnaires were distributed in printed form during each academic year’s scheduled ward rotations, with responses collected immediately to minimise non-response and preserve the context of clinical learning environments. Data were entered and analysed using IBM SPSS version 25.
Quantitative variables were presented as mean ± standard deviation (SD). For qualitative variables, mean scores were used to assess correlations between causes of absenteeism among third, fourth, and final year MBBS students. Frequencies and percentages were calculated to summarise attendance patterns, causes of absenteeism, and deficiencies in clinical faculty impacting attendance. Pearson’s correlation was employed to assess the relationships between absenteeism factors (such as personal health, family responsibilities, workload, perceived relevance of rotations) and academic year, with significance set at p ≤ 0.05.
III. RESULTS
This study explores the factors influencing attendance in clinical rotations among medical students. The data supporting the finding is available at Figshare (https://doi.org/10.6084/m9.figshare.28602041.v1) (Mazhar Khan, 2025).
Evaluating responses from 450 students we found that 270 students participated in the survey, representing diverse academic years: 31% from the third year, 27%
from the fourth year, and 43% from the fifth year. Notably, gender distribution among respondents included 133 males (49.1%) and 137 females (50.9%).
A. Regularity of Attendance
The attendance at clinical rotations was recorded as follows: 29% of third-year students, 40% of fourth-year students, and 36% of final-year students reported attending all required rotations in their third and fourth academic years (Figure 1).
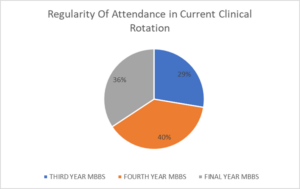
Figure 1. Regularity of Attendance in Clinical Wards
Among these students, a significant proportion missed their clinical wards sometimes (3–4 times per month; 24%) and often (5–6 times per month; 20%), respectively (Table 1). Further analysis of exam-specific and non-exam-specific rotations showed that only 18.5% of students attended both rotations equally, whereas 40.7% reported attending exam-specific rotations more frequently. The most important reasons for attending exam specific rotation were because it was required for their course completion (63%) and was directly related to their assessments and exam (56%).
|
Academic Year |
All (100%) |
Most (75–99%) |
Some (50–74%) |
Few (25–49%) |
None (0–24%) |
|
Third Year |
25 (29.4%) |
20 (23.5%) |
15 (17.6%) |
15 (17.6%) |
10 (11.8%) |
|
Fourth Year |
28 (40.0%) |
18 (25.7%) |
15 (21.4%) |
5 (7.1%) |
4 (5.7%) |
|
Final Year |
35 (30.4%) |
40 (34.8%) |
20 (17.4%) |
15 (13.0%) |
5 (4.3%) |
|
Total |
88 (33%) |
78 (29%) |
50 (19%) |
35 (13%) |
19 (7%) |
Table 1. Regularity of Attendance in Current Clinical Rotations (Third to Final Year)
B. Causes of Absenteeism
Furthermore, students expressed that discouragement from attending clinical rotations stemmed primarily from faculty behaviours. The mean scores for these factors were as follows: unprofessional behaviour (3.3), lack of preparation for teaching sessions (3.2), inadequate feedback on performance (3.2), ineffective communication (3.2), overemphasis on rote learning over critical thinking (3.1), and lack of enthusiasm in teaching (3.1) (Table 2). Specifically, Barriers to attending non-examination-specific rotations were identified, with 41% of students citing a lack of perceived value, 30% referring to heavy workloads as a limiting factor.
|
Factor |
Mean Score |
1 (Not at all) |
2 |
3 |
4 |
5 (Extremely) |
|
Personal Health Issues |
3.2 |
40 (15%) |
50 |
55 |
80 |
45 (17%) |
|
Family Responsibilities |
3.3 |
35 (13%) |
45 |
60 |
80 |
50 (19%) |
|
Financial Difficulties |
3.0 |
60 (22%) |
40 |
50 |
70 |
50 (19%) |
|
Workload from Other Courses |
3.1 |
50 (19%) |
45 |
60 |
65 |
50 (19%) |
|
Perceived Irrelevance of Rotations |
2.8 |
70 (26%) |
55 |
45 |
60 |
40 (15%) |
|
Timing of Clinical Rotations |
3.1 |
45 (17%) |
50 |
70 |
65 |
40 (15%) |
|
Transportation Issues |
3.0 |
55 (20%) |
50 |
55 |
70 |
40 (15%) |
|
Quality of Teaching |
3.2 |
40 (15%) |
60 |
60 |
65 |
45 (17%) |
|
Poor Relationships with Staff |
3.3 |
50 (19%) |
45 |
60 |
60 |
55 (20%) |
|
Lack of Learning Resources |
3.4 |
45 (17%) |
40 |
50 |
70 |
65 (24%) |
|
Personal Safety Concerns |
3.0 |
60 (22%) |
40 |
45 |
65 |
60 (22%) |
|
Influence of Seniors’ Opinions |
3.0 |
55 (20%) |
60 |
55 |
50 |
50 (19%) |
|
Personal Health Issues |
3.2 |
40 (15%) |
50 |
55 |
80 |
45 (17%) |
Table 2. Causes of Absenteeism (Combined Data for All Years)
Additional barriers identified included the lack of learning resources (mean score 3.4), strained relationships with clinical staff (mean score 3.3), family obligations (mean score 3.3), perceived quality of teaching during rotations (mean score 3.2), and personal health issues (mean score 3.2) (Table 3).
|
Faculty Deficiency |
Mean Score |
1 (Not at all) |
2 |
3 |
4 |
5 (Extremely) |
|
Lack of Preparation for Teaching Sessions |
3.3 |
40 (15%) |
45 |
60 |
75 |
50 (18%) |
|
Inability to Effectively Communicate |
3.2 |
45 (17%) |
50 |
65 |
60 |
50 (18%) |
|
Lack of Enthusiasm in Teaching |
3.1 |
50 (19%) |
60 |
55 |
55 |
50 (18%) |
|
Unavailability of Additional Support |
3.0 |
55 (20%) |
50 |
60 |
55 |
50 (18%) |
|
Unprofessional Behaviour |
3.3 |
50 (19%) |
45 |
55 |
55 |
65 (24%) |
|
Lack of Constructive Feedback |
3.2 |
45 (17%) |
50 |
65 |
55 |
55 (20%) |
|
Inconsistent or Unfair Assessments |
3.0 |
60 (22%) |
45 |
50 |
65 |
50 (19%) |
|
Overemphasis on Rote Learning |
3.1 |
50 (19%) |
55 |
60 |
55 |
50 (18%) |
|
Poor Integration of Theory and Clinical Work |
3.1 |
55 (20%) |
50 |
60 |
55 |
50 (18%) |
Table 3. Deficiencies in Clinical Faculty Impacting Attendance (All Years)
C. Correlation Between Professional Years and Causes of Absenteeism
The table below summarises the correlation between professional years and various factors affecting absenteeism in medical students (Table 4). It helps to identify which factors are perceived differently across different years of study. A p-value less than 0.05 indicates a statistically significant correlation. It reveals that there is a significant correlation among quality of teaching during rotations (p-value=0.012), lack of learning resources (p-value=0.025), family responsibilities (p-value=0.02), workload from other courses (p-value=0.036) and personal health issues (p-value=0.045) across the different academic years.
|
Factor |
Mean Score |
Correlation with Professional Year |
p-value |
Interpretation |
|
Personal Health Issues |
3.2 |
0.25 |
0.045 |
Statistically significant |
|
Family Responsibilities |
3.3 |
0.32 |
0.020 |
Statistically significant |
|
Financial Difficulties |
3.0 |
0.10 |
0.310 |
Not significant |
|
Workload from Other Courses |
3.1 |
0.28 |
0.036 |
Statistically significant |
|
Perceived Irrelevance of Rotations |
2.8 |
-0.15 |
0.215 |
Not significant |
|
Timing of Clinical Rotations |
3.1 |
0.22 |
0.056 |
Borderline (Not statistically significant) |
|
Transportation Issues |
3.0 |
0.05 |
0.750 |
Not significant |
|
Quality of Teaching During Rotations |
3.2 |
0.38 |
0.012 |
Statistically significant |
|
Poor Relationships with Clinical Staff |
3.3 |
0.20 |
0.067 |
Not statistically significant |
|
Lack of Learning Resources |
3.4 |
0.30 |
0.025 |
Statistically significant |
|
Personal Safety Concerns |
3.0 |
0.15 |
0.180 |
Not significant |
|
Influence of Seniors’ Opinions |
3.0 |
0.05 |
0.800 |
Not significant |
Table 4. Correlation Results Table
IV. DISCUSSION
Clinical Rotations are an important aspect of undergraduate medical education, giving students an opportunity to apply their theoretical knowledge, develop core clinical principals and prepare for professional responsibilities of the future. Attendance during these rotations correlates with academic performance, patient safety and readiness for medical practice (Bamuhair et al., 2016). This cross-sectional study involving 270 students, highlights an alarming pattern of absenteeism with attendance rates of only 29%, 40% and 36% among third-year, fourth year and final year students, respectively. A trend like this, if unaddressed can have a negative impact on the competencies of medical graduates.
One of the most frequently cited reasons for absenteeism in this study was discontentment with faculty behaviour and teaching methods. Students frequently referred to inadequate communication, absence of constructive feedback, lack of interest in teaching, and instances of unprofessional conduct as major drivers of their disengagement. These findings are in line with those of Bahadori et al. (2021), who outlined that unprofessional conduct and poor interaction between student and faculty served as key reasons for absenteeism during clinical rotations. Similarly, Desalegn et al. (2014), reported that faculty performance and student discipline were significant determinants of attendance habits.
A lack of faculty engagement not only discourages student participation but also contributes to a disconnection between theoretical instruction and its clinical application, thereby reinforcing surface learning strategies such as rote memorisation. This perception is reinforced by Nevins et al. (2016) who observed substantial improvement in attendance when sessions were made more clinically relevant in a medical school based in the United Kingdom (UK). Hence, these findings highlight the pivotal role of faculty in moulding students’ motivation and engagement with clinical training.
An inflexible and poorly structured curriculum appears to be a significant deterrent to clinical attendance. The participants of this study lay emphasis on the burden of excessive academic workload, especially during non-exam-specific rotations, which were often perceived as less valuable. These concerns align with findings by Hafeez et al. (2014) and Massingham and Herrington (2006), who reported that students are likely to prioritise independent study over attendance when clinical rotations are not directly assessed. Similarly, a Nigerian study by Olorunfemi et al. (2021) found that the absence of structured feedback and ineffective curriculum delivery led to a drop in engagement with clinical training.
Interestingly, Simcock et al. (2017) found that while students increasingly used recorded lectures for exam preparations, those who attended live, interactive sessions showed better academic performance. These findings underscore the importance of in-person, interactive learning experiences despite the growing availability of digital alternatives.
A range of personal factors emerged as contributors to absenteeism. These included mental health concerns, such as anxiety and stress, physical illness and family responsibilities. The findings of this study are consistent with Massingham and Herrington (2006), who noted that student well-being has a significant impact on attendance. Although the cross-sectional nature of the current study captures these concerns at a particular point in time, longitudinal research may offer deeper insights into health-related absenteeism. The concept of “sickness presenteeism” is of particular relevance here, whereby students continue to attend lectures despite illness due to fears of academic disadvantage. This phenomenon, discussed by Desalegn et al. (2014), highlights the importance of ensuring adequate access to healthcare and mental health support within educational institutions.
Family responsibilities, especially among students from joint families or low socio-economic backgrounds, were also found to negatively affect attendance. Furthermore, peer influence was recognised as a notable social factor; numerous students admitted to missing non-examination-based sessions due to collective absenteeism within their peer group. This observation aligns with the findings of Khatoon et al. (2024) who observed that peer pressure played a major role in determining attendance trajectories. Notably, although Stenberg and Carlson, (2015) in a Swedish cohort, found that peer learning enhanced confidence and clinical competence, they also noted the presence of competitive stress. These findings suggest that peer dynamics can contribute as both motivating or inhibiting factor in clinical attendance, depending on the nature of the interactions.
Students displayed markedly higher attendance during exam-specific rotations, primarily driven by examination pressure and mandatory completion requirements. While this behaviour is understandable, it undermines the broader educational aims of clinical training, which extend beyond exam preparation. The perception that certain rotations are less valuable unless directly linked to assessments reflects a strategic learning approach, whereby students prioritise immediate academic performance over long-term skill development. This trend, which was also observed by Hafeez et al. (2014), appears to be a response to cope with the extensive academic workload faced by medical students.
Such findings suggest that the current structure of clinical education may inadvertently reinforce surface learning behaviours. The tendency to devalue non-exam-specific rotations indicates a misalignment between students’ learning priorities and the intended outcomes of clinical education. It is crucial to address this disconnect by devising curricular strategies that foster intrinsic motivation and emphasise the enduring clinical relevance of all rotations.
From a global perspective, patterns of absenteeism appear to be context-dependent, shaped by institutional culture and pedagogical frameworks. For example, Simcock et al. (2017), in a study conducted across Australia and New Zealand, highlighted the limitations of recorded lectures, noting that their substitution for live teaching sessions negatively impacted student engagement. In contrast, Stenberg and Carlson, (2015) demonstrated that peer-led teaching models positively influenced student participation in clinical settings.
On the contrary, Marburger (2006) presented evidence that traditional, structured, lecture-based teaching methods were associated with improved academic performance in certain settings. This divergence underscores the importance of accounting for local educational cultures, student learning preferences, and institutional dynamics when developing interventions aimed at improving attendance.
Although the present study did not identify significant differences in attendance rates between male and female students, certain gender-based academic disparities were observed. Hakami (2021) reported that increased absenteeism was more strongly associated with academic decline among male students compared to their female counterparts. This disparity may reflect variations in learning styles, coping strategies, or resilience across genders, suggesting that male and female students may respond differently to academic pressures and absenteeism. These findings point to the potential value of adopting a more nuanced, gender-informed perspective when analysing academic outcomes in relation to attendance behaviour.
Despite numerous studies addressing absenteeism in medical education, there remains a notable lack of focus on attendance during clinical rotations, particularly within South Asian institutions (Bahadori et al. 2021; Hafeez et al. 2014). Much of the existing research is centred on preclinical or lecture-based settings, which do not fully capture the distinct challenges faced by students in clinical environments. By focusing on clinical rotations within this regional context, the present study helps to fill this gap and offers insights that are underrepresented in current literature. However, given the complexity of factors influencing attendance and their evolution over time, further longitudinal and multi-institutional research is warranted to better understand these dynamics and inform targeted interventions.
However, this study is not without limitations. As it is a cross-sectional study, it only captures student behaviour at single point in time, thereby limiting its ability to shed light on evolving patterns or long term trends in clinical attendance. The use of self-reported data introduces the possibility of response bias. Moreover, the study was conducted within a single institution, which may restrict the generalisability of the findings to other medical colleges with differing academic cultures, policies, or student demographics. The absence of qualitative interviews or focus groups also constrained a deeper exploration of underlying motivations and interpersonal dynamics influencing absenteeism. Future research could benefit from adopting a longitudinal, multi-centre design incorporating both quantitative and qualitative methodologies for better understanding.
V. CONCLUSION
This study highlights a multifaceted set of factors contributing to absenteeism among medical students during clinical rotations, including dissatisfaction with faculty engagement, inflexible curricular structures, mental health challenges, peer influence, and the strategic devaluation of non-exam-specific sessions. These findings point towards systemic and cultural gaps in clinical education that may compromise the quality of learning and long-term professional development.
In light of these findings, several policy-level interventions are recommended. Medical institutions should ensure that all clinical rotations—regardless of examination linkage—are regarded as essential and are integrated into structured assessment frameworks. Attendance policies should be applied uniformly and accompanied by transparent accountability mechanisms. Faculty development programmes must be prioritised, with particular emphasis on improving communication skills, delivering constructive feedback, and maintaining professional conduct. These efforts could help restore trust and motivation among students while strengthening the link between theoretical knowledge and clinical practice.
In addition, educational institutions should provide accessible mental health services to support students coping with stress, anxiety, and illness, thereby reducing both absenteeism and the phenomenon of sickness presenteeism. Awareness sessions on peer influence and group dynamics could transform peer pressure from a deterrent into a positive, motivating force. Lastly, curricular reforms that balance academic workload and reinforce the clinical relevance of all rotations are essential to promote consistent student engagement and long-term competence.
Notes on Contributors
Maheen Zulfiqar led the conceptualisation of the study and was responsible for drafting the original manuscript. She also played a key role in reviewing and editing the final version.
Muhammad Khalilur Rahman contributed to both the conceptual development and project administration, ensuring coordination across the team. He was also actively involved in reviewing and refining the manuscript.
Behram Khayyam handled the methodological design, formal analysis, and validation of results. He also participated in the review and editing process, enhancing the technical rigour of the study.
Ayesha Mazhar Khan supported the methodological and validation efforts, contributing to data analysis and manuscript revisions.
Naeem Sarwar oversaw project administration and contributed to the manuscript’s review and editing, ensuring smooth project execution.
Ashbil Malik was responsible for data curation and participated in the review process, offering insights based on her data expertise.
Hassan Saleem co-managed data curation with Ashbil Malik and assisted in reviewing and editing the manuscript for data-related accuracy.
Ethical Approval
This cross-sectional study was conducted after taking approval from the Institutional Review Board (RLMC/IRB/2024/153). IRB approval letter has been provided in the attached documents.
Data Availability
Our dataset is publicly accessible through the referenced repository and is available under the CC BY 4.0 license, ensuring open usage and attribution (https://doi.org/10.6084/m9.figshare.28602041.v1).
Funding
The authors declare that no financial support or funding was received from any organisation or institution for the research, authorship, or publication of this article.
Declaration of Interest
No potential conflict of interest relevant to this article was reported.
References
Al Shenawi, H., Yaghan, R., Amer, H., & Shenawi, M. (2021). The relationship between attendance and academic performance of undergraduate medical students during surgical clerkship. BMC Medical Education, 21(1), Article 287. https://doi.org/10.1186/s12909-021-02833-2
Bahadori, M., Salari, S., Alizadeh, M., Moaddab, F., Balasi, L. R., & Soodmand, E. (2020). The root causes of absenteeism in medical students: Challenges and strategies ahead. Educational Research in Medical Sciences, 19(2), 1–8. https://doi.org/10.5812/erms.107120
Bamuhair, S. S., Farhan, A. I., Althubaiti, A., Rahman, S. U., & Al-Kadri, H. M. (2021). Class attendance and cardiology examination performance: A study in problem-based medical curriculum. International Journal of General Medicine, 14, 613–619. https://doi.org/10.2147/IJGM.S96627
Desalegn, A. A., Berhan, Y., & Berhan, A. (2014). Absenteeism among medical and health science undergraduate students at Hawassa University, Ethiopia. BMC Medical Education, 14, Article 81. https://doi.org/10.1186/1472-6920-14-81
Gul, R., Khan, S., Alam, M., Luqman, M., Shahab, M., & Sohail, M. (2016). Absenteeism among medical undergraduate students. Journal of Medical Sciences (Peshawar), 24(1), 16–18. https://jmedsci.com/index.php/Jmedsci/article/view/177
Hafeez, K., Khan, Z., Jawaid, M., & Haroon, S. (2019). Low attendance in lectures at medical colleges of Karachi: A cross-sectional survey. Journal of Postgraduate Medical Institute, 33(2), 123–128. https://jpmi.org.pk/index.php/jpmi/article/view/1565
Hakami, A. (2021). Effect of absenteeism on the performance of medical sciences students: Gender differences. Medical Education Online, 25(1), Article 1875531. https://doi.org/10.1080/10872981.2021.1875531
Khan, A. M. (2025). Absence of undergraduate medical students from clinical rotations [Dataset]. Figshare. https://doi.org/10.6084/m9.figshare.28602041.v1
Khan, M. J., Lodhi, F. S., Bhatti, A., & Ali, S. (2019). Does absenteeism affect academic performance among undergraduate medical students? Evidence from Rashid Latif Medical College. Advances in Medical Education and Practice, 10, 999–1008. https://doi.org/10.2147/AMEP.S226255
Khatoon, S., Khan, M. A., Nadeem, M., & Majeed, I. (2024). Demographic characteristics and perceived absenteeism among students in government secondary schools. Asian Journal of Integrated Social and Behavioural Sciences, 1(1), 23–28. https://journals.uol.edu.pk/AJISB/article/view/3627/1579
Marburger, D. R. (2006). Does mandatory attendance improve student performance? Journal of Economic Education, 37(2), 148–155. https://doi.org/10.3200/JECE.37.2.148-155
Massingham, P., & Herrington, T. (2006). Does attendance matter? An examination of student attitudes, participation, performance, and attendance. Journal of University Teaching & Learning Practice, 3(2), 82–103. https://files.eric.ed.gov/fulltext/EJ1105382.pdf
Mitra, S., Sarkar, P., Bhattacharyya, S., & Basu, R. (2022). Absenteeism among undergraduate medical students and its impact on academic performance: A record-based study. Journal of education and health promotion, 11, 414. https://doi.org/10.4103/jehp.jehp_638_21
Nevins, E. J., Moori, P. L., Alexander, L., Richards, B., Bleasdale, V., & Sharma, A. K. (2016). Could attendance at medical school be improved? A prospective study of medical education at the University of Liverpool: Study of attendance at a UK medical school. MedEdPublish, 5(2), Article 78. https://doi.org/10.15694/mep.2016.000078
Olorunfemi, O., Oduyemi, R. O., Sowunmi, C. O., Okafor, V., Chukwuka, L. O., Osunde, N. R., & Ezinne, A. F. (2021). Clinical instructors’ motivational roles and perceived effect on absenteeism among student nurses in a tertiary hospital, Benin‑City, Nigeria. Journal of Education and Health Promotion, 10, 203. https://doi.org/10.4103/jehp.jehp_1048_20
Qureshi, M. A., & Ahmad, F. (2019). Medical students’ perspective on absenteeism and its remedies. Pakistan Armed Forces Medical Journal, 69(2), 332–339. https://pafmj.org/index.php/PAFMJ/article/view/2749
Sharmin, T., & Azim, E. (2017). Reasons of absenteeism among undergraduate medical students: A review. Anwer Khan Modern Medical College Journal, 8(1), 60–66. https://doi.org/10.3329/akmmcj.v8i1.31660
Simcock, D. C., Chua, W. H., Hekman, M., Levin, M. T., & Brown, S. (2017). A survey of first-year biology student opinions regarding live lectures and recorded lectures as learning tools. Advances in Physiology Education, 41(1), 129–137. https://doi.org/10.1152/advan.00117.2016
Stenberg, M., & Carlson, E. (2015). Swedish student nurses’ perception of peer learning as an educational model during clinical practice in a hospital setting—an evaluation study. BMC Nursing, 14, Article 48. https://doi.org/10.1186/s12912-015-0098-2
*Ayesha Mazhar Khan
Department of Surgery,
Arif Memorial Teaching Hospital/Rashid Latif Medical College,
Lahore, Pakistan
+92 3009494461
Email: ayeshamazharkhan.amk@gmail.com
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
