
Impact of International Trends on Medical Education Curriculum
Submitted: 11 February 2025
Accepted: 11 July 2025
Published online: 7 October, TAPS 2025, 10(4), 97-99
https://doi.org/10.29060/TAPS.2025-10-4/II3669
Suryanti Chan1, Hamzah Hamzah2 & Insan Sosiawan Tunru3
1Department of Medical Education, Faculty of Medicine, Universitas Dian Nuswantoro, Indonesia; 2Airlangga Teaching Hospital, Airlangga University, Indonesia; 3Faculty of Medicine, University Yarsi, Indonesia
I. INTRODUCTION
Medical education is a cornerstone of effective healthcare delivery, directly shaping professionals responsible for addressing the complex and evolving needs of patients, families, and communities. Over the last few decades, medical education has undergone significant transformations due to global trends that have influenced curricula structures, learning methodologies, and competency requirements for healthcare professionals. These shifts reflect broader societal, technological, and policy changes, necessitating adaptable and forward-thinking medical education systems.
One key driver of change is globalisation, fostering interconnected healthcare systems and necessitating curricula that emphasise global health perspectives, cultural competence, and cross-disciplinary collaboration.
Additionally, technological advancements, such as simulation-based learning, virtual reality (VR), augmented reality (AR), and telemedicine training, have revolutionised medical education, improving accessibility and enhancing learning experiences.
The increasing importance of accreditation and quality assurance frameworks ensures standardisation in medical education across regions, promoting transparency and continuous improvement (Bedoll et al., 2021). Simultaneously, the shift towards outcome-based education (OBE) prioritise competency-driven frameworks over traditional content-heavy curricula, aligning medical training with healthcare needs. Furthermore, cultural and contextual adaptations are crucial in tailoring curricula to regional healthcare priorities while maintaining global standards.
This paper examines how these international trends, globalisation, technological advancements, accreditation, outcome-based education, and cultural contextualisation, are shaping the future of medical education and influencing curricula to remain responsive to evolving healthcare demands.
II. APPROACH TO SYNTHESIS
Drawing on peer-reviewed articles, academic texts, and authoritative reports published over the past decade, this paper explores key international trends influencing medical education curricula. Sources were identified through a purposive review of major databases, such as PubMed, Scopus, and Web of Science, using keywords including “medical education curriculum,” “globalisation,” “technological change in education,” and “outcome-based education.” Selection was guided by relevance, conceptual contribution, and alignment with contemporary educational discourse. Through interpretive synthesis, the emerging themes were organised to highlight the evolving priorities and challenges in curriculum development across diverse global settings.
III. GLOBAL TRENDS SHAPING MEDICAL EDUCATION
Synthesising insights from the existing literature, several key themes emerge, including globalisation, technological advancement, accreditation and quality assurance, and the shift toward outcome-based education, each significantly shaping curriculum design in medical education.
A. Globalisation and Medical Education
Globalisation necessitates the integration of global health perspectives in medical curricula, enhancing students’ cultural competence, global awareness, and adaptability in diverse clinical settings. Imafuku et al. (2021) report that international electives and exposure to various healthcare systems foster a broader understanding of global health challenges. Rukadikar et al. (2022) emphasise embedding cultural competence longitudinally rather than as isolated modules. However, integrating global content can be hampered by linguistic, ethical, and logistical barriers, particularly in low-resource regions. There is also a risk of curricular homogenisation that overlooks local relevance. Initiatives such as the ASEAN Medical Schools Network attempt to address this tension by fostering regional collaboration while maintaining context-sensitive design. Ultimately, globalisation challenges medical educators to balance international standards with localised priorities, cultivating graduates who are both globally minded and locally responsive.
B. Technological Advancements
The digital transformation of medical education, catalysed by the COVID-19 pandemic, has reshaped how knowledge and clinical skills are imparted. Simulation-based learning, virtual patients, high-fidelity manikins, and telemedicine platforms offer realistic, risk-free environments for students to practise complex procedures (Castro et al., 2021). Virtual and augmented reality hold immense promise, especially in underserved areas where traditional clinical exposure is limited (Li et al., 2024). Nevertheless, adoption remains uneven. Barriers such as digital illiteracy, inadequate infrastructure, and resistance to change among faculty hinder optimal implementation. Furthermore, technological integration demands a pedagogical shift towards student-centred, self-directed learning models that not all institutions are prepared to adopt. Addressing these challenges requires systemic investment in digital infrastructure, faculty development, and curriculum redesign to fully harness the potential of educational technology.
C. Accreditation and Quality Assurance
Global accreditation standards, such as those set by the WFME, aim to enhance comparability and mobility of medical graduates by ensuring a baseline of quality and accountability (Bedoll et al., 2021). These frameworks advocate for continuous self-evaluation, peer review, and outcome monitoring. However, rigid adherence to international benchmarks may marginalise unique local needs and strain under-resourced institutions. For example, some Southeast Asian medical schools struggle to meet standards due to shortages in qualified faculty, simulation resources, or research infrastructure. Regional mechanisms like the ASEAN-QA (Asian University Network-Quality Assurance) Framework provide a more flexible model, supporting capacity-building and mutual recognition of quality. Moving forward, accreditation should not be seen solely as a compliance mechanism but as a catalyst for meaningful institutional improvement rooted in contextual realities.
D. Outcome-Based Education
OBE represents a fundamental paradigm shift, placing student competencies at the heart of curriculum design and assessment. Instead of focusing on the amount of content delivered, OBE emphasises the achievement of predefined clinical, ethical, and interpersonal outcomes. The model supports accountability and alignment between educational outcomes and healthcare needs. Ten Cate advocates for the use of Entrustable Professional Activities (EPAs) to operationalise OBE, offering a structured way to assess readiness for clinical practice. However, the practical implementation of OBE remains challenging. Many institutions lack robust tools for assessing soft skills, professional attitudes, and interprofessional collaboration. Furthermore, faculty may be unfamiliar with the principles of formative, feedback-oriented assessment that OBE requires. Successful implementation demands long-term commitment to faculty development, curriculum mapping, and resource allocation, as well as a cultural shift toward continuous quality improvement.
IV. CONCLUSION
The evolution of medical education is shaped by globalisation, technological advancements, accreditation, cultural adaptation, and outcome-based education. These trends emphasise the need for medical curricula that are adaptable, inclusive, and aligned with global healthcare challenges. Moving forward, medical education must remain dynamic and forward-thinking to prepare graduates for both current and future healthcare landscapes.
Notes on Contributors
Suryanti Chan (SC) contributed to the study design, data collection, and manuscript writing. She was responsible for analysing the findings and drafting the discussion.
Hamzah Hamzah (HH) contributed to the study design, literature review, and manuscript revision. He provided insights on the impact of international trends on medical education curriculum, particularly from the perspective of clinical training and healthcare service management in teaching hospitals.
Insan Sosiawan Tunru (IST) contributed to the study design, literature review, and manuscript revision. He provided insights on the impact of international trends on medical education curriculum, particularly from the perspective of accreditation regulation in Indonesia.
Ethical Approval
This manuscript is a literature review based on existing published studies and does not involve any original data collection or interaction with human participants.
Acknowledgement
Authors would like to express their deepest gratitude and appreciation to Prof. Ir Edi Noersasongko, M.Kom, Prof. Pulung Nurtantio Andono, S.T., M.Kom, Dr. Abdul Syukur, M.M, Dr. Hendriani Selina, Sp. A (K), MARS which has supported during this review.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Interest
The authors declare that there are no conflicts of interest related to this study.
References
Bedoll, D., Van Zanten, M., & McKinley, D. (2021). Global trends in medical education accreditation. Human Resources for Health, 19(70), 1–15. https://doi.org/10.1186/s12960-021-00588-x
Castro, M. R. H., Calthorpe, L. M., Fogh, S. E., McAllister, S., Johnson, C. L., Isaacs, E. D., Ishizaki, A., Kozas, A., Lo, D., Rennke, S., Davis, J., & Chang, A. (2021). Lessons from learners: Adapting medical student education during and post COVID-19. Academic Medicine, 96(12), 1671–1679. https://doi.org/10.1097/ACM.0000000000004148
Imafuku, R., Saiki, T., Hayakawa, K., Sakashita, K., & Suzuki, Y. (2021). Rewarding journeys: Exploring medical students’ learning experiences in international electives. Medical Education Online, 26(1), 1913784. https://doi.org/10.1080/10872981.2021.1913784
Li, X., Elnagar, D., Song, G., & Ghannam, R. (2024). Advancing medical education using virtual and augmented reality in low- and middle-income countries: A systematic and critical review. Virtual Worlds, 3(3), 384–403. https://doi.org/10.3390/virtualworlds3030021
Rukadikar, C., Mali, S., Bajpai, R., Rukadikar, A., & Singh, A. K. (2022). A review on cultural competency in medical education. Journal of Family Medicine and Primary Care, 11(8), 4319–4329. https://doi.org/10.4103/jfmpc.jfmpc_2503_21
*Suryanti Chan
MD, MPH, MMed, PhD (Health Sciences), FIHFAA
Universitas Dian Nuswantoro,
Pendrikan Kidul Number 184,
Semarang, Central Java Province, Indonesia
(62)851-011-56248
Email: suryanti83@yahoo.com
Submitted: 11 January 2025
Accepted: 11 August 2025
Published online: 7 October, TAPS 2025, 10(4), 77-80
https://doi.org/10.29060/TAPS.2025-10-4/SC3818
Yassar Alamri
Department of Medicine, University of Otago, Christchurch, New Zealand
Abstract
Introduction: Response rates to surveys of medical students and junior doctors have not previously been explicitly examined. Reasons for the observed response rates have not been scrutinised. The aims of the present study were to establish an expected response rate to electronic survey among medical students and junior doctors, and to explore reasons behind non-response.
Methods: A follow-up online survey was sent to 93 medical students and junior doctors. The primary method for participants to complete the survey was via the Internet using a well-known and established survey tool. Descriptive and inferential statistics were used to assess response rates and reasons for non-response.
Results: Out of 93 invited medical students and junior doctors, 47 returned the follow-up survey (response rate = 50.5%). The main reasons for non-response were: there were too many surveys (74.4%), lack of time (25.5%), and the original survey being too long (10.6%).
Conclusion: We found a mediocre response rate (50.5%) to electronic surveys by medical students and junior doctors included in this study. Several factors that may impede response to surveys (survey-related, and participant-related) have been identified, and these may be specifically targeted to improve survey response rates.
Keywords: Medical Student, Survey, Response Rate, Research, Methodology
I. INTRODUCTION
Surveys offer an important method of collecting quantitative data from physicians and medical students on various aspects of medical and clinical research. The ease and convenience of online and web-based surveys (compared with telephone or face-to-face interviews) should theoretically enhance response rates. However, the ideal method of surveying the medical workforce (which would yield a high rate of and representative responses) is yet to be identified.
Physicians have traditionally been reported to have poor response rates to surveys in general. Studies that have specifically assessed response rates to surveys among physicians revealed overall rates of 35–50% (Cunningham et al., 2015). Response rates to surveys and reasons for non-response by medical students and junior doctors have seldom been specifically examined. Previous response rates to the National Physician Survey in Canada reported response rates of approximately 28–35% by medical students and junior doctors (Grava-Gubins & Scott, 2008), although these data are almost two decades old now.
Several reasons for non-response emerge from reviewing the pertinent literature; these can be divided into: survey-factors, and respondent-factors. Survey-factors include the length of the questionnaire (Grava-Gubins & Scott, 2008), perceived interest in and sensitivity of the surveyed topic (Cunningham et al., 2015), and the mode of survey delivery (i.e., electronic, telephone or face-to-face) (Grava-Gubins & Scott, 2008; Weaver et al., 2019). Several incentives have been instigated in order to improve response rates by addressing some of these survey-factors, including utilising electronic surveys that can be completed in more than one setting (at the participants’ convenience)(Weaver et al., 2019), monetary gifts or “educational credit” for participation (Grava-Gubins & Scott, 2008; Viera & Edwards, 2012), and employing internal “buy in” from a respected member of the intended sample (e.g., senior clinician or head of department) (Akl et al., 2011). Respondent-factors for non-response include lack of time, demographic differences, and the specialty of the respondent.
The aims of the present study were to establish an expected response rate to electronic survey among medical students and junior doctors, and to explore reasons behind non-response. No previous study has focused on medical students and junior doctors (i.e., junior medical workforce); therefore, addressing these issues would help fill several gaps in our knowledge.
II. METHODS
A. Study Setting
A previous study (Alamri et al, in press) invited all medical students at the University of Otago, and junior doctors at the Christchurch Hospital (both in Christchurch, New Zealand), to complete an electronic ‘index questionnaire’ on their research activities. The overall response rate of the original survey was 36% despite employing an online survey, several reminders and monetary gift vouchers.
B. Study Participants and Instrument
For the present study, eligible participants were medical student and junior doctor who had started the ‘index questionnaire’, but never completed it. The identified ‘non-responders’ were then invited to a secondary follow-up survey which was sent after the allotted time-period for the index questionnaire had lapsed (August–September 2018).
The follow-up survey was intentionally designed to be very brief, and based upon previous similar surveys (Cunningham et al., 2015). It only included four questions: participant age and sex, current career, and “what were the reasons for not completing [the index questionnaire]?”.
C. Statistical Analysis
Descriptive statistics (means ± standard deviations, and percentages) were used to analyse most of the data. Comparisons between medical students and junior doctors (two sub-populations with different responsibilities and time commitments) were conducted using Chi-square analyses for categorical values (e.g., sex, and entry to medical school), and Mann-Whitney U test for nonparametric continuous variables (e.g., age). Statistical significance was determined if type I error rate was < 5% (p-value < 0.05). All analyses were performed using the Statistical Package for Social Sciences software (SPSS Statistics®, version 22.0.0.0).
III. RESULTS
A. Study Participants
A total of 93 eligible participants were identified as potential participants. Following electronic invitation, 47 returned the follow-up survey (response rate: 47/93 = 50.5%). Two thirds (31/47; 66%) of the respondents were female. The median age was 23 years (range, 19–42). Most of the respondents (40/47, 85.1%) were medical students (see Table 1).
|
|
Medical students |
Junior doctors |
p value |
|
N |
40 |
7 |
|
|
Sex (% male, standard error) |
40% (0.08) |
22% (0.09) |
0.15 |
|
Age (mean, SD) |
21.2 ± 3.7 |
24.9 ± 5.5 |
0.01 |
|
Entry to medical school (% post-graduate) |
71.8% |
59.1% |
0.33 |
Table 1. Summary of participant data
B. Non-Response Survey Findings
Reasons for non-response varied among the participants. The most common reasons included: there were too many surveys (74.4%), lack of time (25.5%), the original survey was too long (10.6%), participant erroneously thought they had completed the survey (8.4%), and participant did not think they were eligible (2.1%). Of note, two of the participants (4.3%) responded unfavourably to the offer of the follow-up survey, finding it annoying and offensive.
IV. DISCUSSION
The response rate to the follow-up survey was 50.5% which was lower than anticipated. Non-responders to the index questionnaire were re-contacted to explore reasons behind the observed low response rate. The most common cited reasons were there were too many surveys requests (‘survey fatigue’), and lack of time. Just under 10% of participants had genuinely thought that they completed the original survey, which may indicate an underlying technical problem/lack of clarity. These reasons generally echo those voiced by physician specialists when asked about their response rates (Cunningham et al., 2015), although no studies have examined these reasons in medical students or junior doctors.
Only a handful of previous studies have specifically examined the rates of survey response by medical students and junior doctors. Canadian medical students had response rates of 30.8–31.2% to an electronic version of the Canadian National Physician Surveys in 2004 and 2007 (Grava-Gubins & Scott, 2008). From our experience over several studies in New Zealand, the average response rate from medical students seems to be around 30–35% (Alamri et al, in press). Response rates from junior doctors seem to be even lower, with 27.9–35.6% response rates in Canada (Grava-Gubins & Scott, 2008), and 24.9% in New Zealand (Alamri et al, in press). The range of response rates to surveys by junior doctors varies significantly—at least in part due to the fact that some of the surveys were compulsory to complete (thus, resulting in very high response rates).
Whilst a survey’s response rate ought not be the sole judge of the study’s validity (Cunningham et al., 2015), it is important to understand the reasons behind low survey response rates. We are unaware of any studies that have examined reasons for students’ survey non-response, or factors that would influence them. On the other hand, several randomised trials examined the effect of various factors on the response rates by physicians. Factors that increased response rates by physicians included: contact by regular mail (Akl et al., 2011) (although this finding was inconsistent among studies (Viera & Edwards, 2012), and the availability of the survey in several local languages (Grava-Gubins & Scott, 2008). Factors that worsened response rates included: offering continuing medical education credits for completing a survey (Viera & Edwards, 2012), and surveys on sensitive topics (Cunningham et al., 2015). Finally, factors that had no influence on response rates included: length of the survey (Akl et al., 2011), the day of invitation to the survey (Akl et al., 2011), and monetary compensation for participation (Akl et al., 2011).
V. CONCLUSION
Our findings generally reflect those reported in the literature of the response rates to research surveys by medical professionals; these seem to vary between 25 and 50% (usually at the lower end for junior doctors/medical students, and the higher end for specialists). Several factors that impede response to surveys (survey-related, and participant-related) have been identified, including the number of surveys sent to medical professionals, and the general lack of time.
The current study was limited by the relatively small number of participants, and by the fact that it originates from a single centre in New Zealand which may limit its generalisability. However, it provides a unique perspective by targeting survey non-responders (i.e., the population of interest), offers recent and updated data, and corroborates findings from previous studies in other settings/countries.
Finally, it is imperative to acknowledge that a high response rate may not necessarily be the panacea to the perfect survey study. How factors can be manipulated in order to yield higher response rates remains to be answered. One solution could be the implementation of an advisory body that provides guidance to researchers about how to design surveys, and regulates the number of survey invitations received by medical professionals in order to avoid ‘survey fatigue’.
Notes on Contributors
The sole author conceived the idea, collected and analysed the data and wrote the manuscript.
Ethical Approval
This study was approved by the University of Otago Human Ethics Committee (reference D18/207). All participants provided consent on the electronic survey form.
Data Availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request after completion of data publication as this remains a work in progress.
Acknowledgement
The authors would like to extend their gratitude to the Department of Psychological Medicine, University of Otago, Christchurch, for their financial assistance with participant compensation. The Department had no involvement in the study otherwise.
Funding
The author received financial assistances (NZ $1,500) from the Department of Psychological Medicine, University of Otago, Christchurch in the form of gift vouchers in order to reimburse participants in our study.
Declaration of Interest
The author declares no conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
Akl, E. A., Gaddam, S., Mustafa, R., Wilson, M. C., Symons, A., Grifasi, A., McGuigan, D., & Schünemann, H. J. (2011). The effects of tracking responses and the day of mailing on physician survey response rate: Three randomized trials. PLoS One, 6(2), e16942. https://doi.org/10.1371/journal.pone.0016942
Cunningham, C. T., Quan, H., Hemmelgarn, B., Noseworthy, T., Beck, C. A., Dixon, E., Samuel, S., Ghali, W. A., Sykes, L. L., & Jette, N. (2015). Exploring physician specialist response rates to web-based surveys. BMC Medical Research Methodology, 15, 32. https://doi.org/10.1186/s12874-015-0016-z
Grava-Gubins, I., & Scott, S. (2008). Effects of various methodologic strategies: Survey response rates among Canadian physicians and physicians-in-training. Canadian Family Physician, 54(10), 1424-1430. https://www.cfp.ca/content/54/10/1424.long
Viera, A. J., & Edwards, T. (2012). Does an offer for a free on-line continuing medical education (CME) activity increase physician survey response rate? A randomized trial. BMC Research Notes, 5, 129. https://doi.org/10.1186/1756-0500-5-129
Weaver, L., Beebe, T. J., & Rockwood, T. (2019). The impact of survey mode on the response rate in a survey of the factors that influence Minnesota physicians’ disclosure practices. BMC Medical Research Methodology, 19(1), 73. https://doi.org/10.1186/s12874-019-0719-7
*Yassar Alamri
Department of Medicine, Christchurch Hospital,
2 Riccarton Avenue, Christchurch 8011,
New Zealand
Email: yassar.alamri@nzbri.org
Submitted: 13 February 2024
Accepted: 28 April 2025
Published online: 1 July, TAPS 2025, 10(3), 75-79
https://doi.org/10.29060/TAPS.2025-10-3/SC3235
Tayzar Hein1 & Susan Somerville2
1Department of Medical Education, Defence Services Medical Academy, Myanmar; 2University of Dundee, Scotland
Abstract
Introduction: Case-Based Learning (CBL) is increasingly used in modern medical schools to improve students’ critical thinking and problem-solving skills. While CBL is established in Western Resource-Structured (WRS) educational settings, its use in Asian-Pacific regions like Myanmar is under explored. This research studied the integration of CBL at the Defence Services Medical Academy (DSMA) in Myanmar, focusing on the perspectives of both students and faculty involved in curriculum reforms.
Methods: This study used constructivist grounded theory to gather data from 24 DSMA participants through four focus group discussions. Twelve students and twelve faculty members, were invited a subgroup of six, and after providing informed consent discussed their experiences of CBL, aiming to assess its effectiveness and relevance in their specific educational and cultural context.
Result: Analysis shows that students valued CBL for enhancing group discussions, reflecting upon real-world situations, and building critical thinking abilities. Faculty members also appreciated CBL for its capacity to create realistic applications and its support for student-centered learning and interpersonal skills development. Both groups acknowledged CBL as an effective method for simulating the complexities of medical practice.
Conclusion: This study found that CBL is well-regarded at DSMA for preparing students competence and confidence for clinical encounters. However, faculty indicated that the extensive time required in preparation of this teaching modality was a significant challenge for the wider adoption of CBL. These insights highlight the adaptability and potential challenges of implementing CBL in non-Western educational settings and suggest possible areas for development for its broader application in the Asia-Pacific region.
Keywords: Medical Education, Case-based Learning, Perceptions, Grounded Theory, Focus Group Discussion
I. INTRODUCTION
In 2017, Defence Services Medical Academy (DSMA) in Yangon, Myanmar, introduced an outcome-based integrated curriculum incorporating Case-Based Learning (CBL) as a key pedagogical approach. This shift from teacher-centered to student-centered learning was aimed at encouraging students to take greater responsibility for their education. However, CBL’s widespread adoption across all subjects at DSMA remains uncertain, highlighting the need for further research. CBL has been established in Western Resource-Structured (WRS) medical education, where it fosters critical thinking, active learning, and problem-solving skills (Thistlethwaite et al., 2012). However, its adoption in the Asian-Pacific context, including Myanmar, has been limited. Cultural and institutional challenges such as insufficient faculty training, resource constraints, and resistance to pedagogical change present unique barriers (McLean, 2016; Yoo & Park, 2015). These challenges underline the importance of research to adapt CBL to resource-constrained settings.
At DSMA, CBL is relatively new, and while the institution can be considered an early adopter within the local context, faculty have faced challenges transitioning from traditional teaching methods due to inadequate training and support (Thistlethwaite et al., 2012). This study aimed to explore how students and faculty perceive the implementation of CBL and to assess the opportunities and challenges of CBL in a resource-constrained, Asian-Pacific context. By addressing gaps in the CBL literature, this research contributes valuable insights for adapting pedagogical practices to diverse cultural and educational settings.
This study aimed to explore:
- How students and faculty at DSMA perceive the implementation of CBL.
- The opportunities and challenges associated with implementing CBL in a resource-constrained, Asian-Pacific context.
By addressing gaps in the CBL literature, particularly in non-WRS settings, this research contributes to a better understanding of how pedagogical practices can be adapted to diverse cultural and educational contexts, offering insights for both early and late adopters within similar settings.
II. METHODS
This qualitative study used a constructivist grounded theory approach, focusing on the experiences and meanings constructed by participants engaged with CBL in the DSMA integrated curriculum.
A. Sampling and Focus Group Composition
Purposive sampling (Patton, 2014) was used to select participants with direct involvement in CBL activities, either as facilitators or active learners. The study included 24 participants, evenly split between 12 students and 12 faculty members. Four focus groups, each containing six participants, were conducted. To reduce power dynamics, the focus groups were divided by role, with separate groups for students and faculty.
B. Participant Demographics
Table 1 below shows the demographic breakdown of participants is for understanding the responses and receptivity to CBL.
|
Participant Type |
Year |
Medicine |
Surgery |
Pediatrics |
Obstetrics and Gynaecology |
Years Study |
|
|
Students (n=12) |
Year 3 |
2 |
1 |
1 |
0 |
4 |
|
|
|
Year 4 |
2 |
1 |
0 |
1 |
4 |
|
|
|
Year 5 |
1 |
0 |
2 |
1 |
4 |
|
|
Faculty (n=12) |
Years of experience |
||||||
|
0-4 years |
3 |
||||||
|
5-9 years |
2 |
||||||
|
10-14 years |
3 |
||||||
|
15-19 years |
2 |
||||||
|
20+ years |
2 |
||||||
Table 1. Participant demographic
C. Theoretical Framework
The constructivist grounded theory approach guided both data collection and analysis. This approach emphasises the co-construction of knowledge, meaning participants not only shared their experiences but actively engaged in interpreting them. The analysis followed a constant comparative method (Patton, 2014), allowing key themes to emerge from the data.
D. Data Analysis
Data were analysed using MAXQDA software, and the constant comparative method was applied to identify recurring themes and refine categories as new insights developed.
E. Ethical Considerations
Ethical approval was granted by the DSMA Ethical Review Board. Informed consent was obtained from all participants, ensuring they were aware of the study’s aims and their rights. Confidentiality and anonymity were maintained throughout the study, and all focus group discussions were audio-recorded with consent.
III. RESULTS
The core category identified in the study was that CBL is a student-centered approach that develops critical thinking, simulates discussion about real-world scenarios, and enhances interpersonal skills, making it a key facet of modern medical education. These findings emphasise the role of CBL in bridging theoretical knowledge with practical application and supporting the development of essential skills for clinical encounters. Both students and faculty members offered different but aligned perspectives, providing valuable insights into the opportunities and challenges associated with CBL.
A. Students’ Perceptions of CBL
1) Theme 1: CBL as group discussion: Students welcomed the collaborative nature of CBL, emphasising the shared learning experience it offers. One student stated, “It’s like a team effort where we learn from each other while solving problems.” This highlights the significance of peer interaction in CBL, which is consistent with research indicating that collaborative learning enhances problem-solving skills.
2) Theme 2: Real-World Relevance: Students appreciated the practical aspects of CBL, particularly its similarity to real-life clinical scenarios. A participant remarked, “It feels like we are preparing for actual hospital situations.” This theme aligns with studies showing how CBL effectively bridges the gap between theoretical knowledge and clinical practice, preparing students for real-world medical challenges.
3) Theme 3: Fostering Critical Thinking: Students frequently mentioned the role of CBL in promoting deeper analytical skills. One student shared, “CBL makes us analyse why things happen instead of just memorising.” This observation reflects the literature that highlights critical thinking as a fundamental outcome of CBL, encouraging students to engage more deeply with the material.
B. Faculty Perceptions of CBL
1) Theme 1: Preparation for Clinical Practice: Faculty members emphasised the effectiveness of CBL in preparing students for real-world medical contexts. One faculty member noted, “CBL allows students to apply their knowledge in realistic medical contexts.” This highlights the need for carefully designed scenarios that accurately mimic clinical challenges, supporting students in applying theoretical knowledge.
2) Theme 2: The Role of Facilitator: Faculty highlighted the critical role of facilitators in guiding effective CBL sessions. A faculty member stated, “Guiding discussions and asking the right questions is key to effective CBL sessions.” This underscores the importance of facilitator training, as their competence significantly impacts the success of CBL in achieving its objectives.
3) Theme 3: Development of Personal Skills: Faculty also emphasised the role of CBL in cultivating essential personal skills for medical practice, such as communication and empathy. One faculty member remarked, “CBL is instrumental in teaching students how to communicate effectively and empathise with patients, which are essential skills in medicine.” This theme reflects a structured focus on skill development, complementing students’ emphasis on the experiential aspects of learning.
IV. DISCUSSION
This study identified both the opportunities and challenges of adopting CBL in a resource-constrained, Asian-Pacific context. Students recognised CBL’s role in fostering teamwork and critical thinking, consistent with previous research (Ferguson & Lee, 2012; Thistlethwaite et al., 2012). Faculty highlighted its effectiveness in preparing students for clinical practice and developing essential interpersonal skills. However, both groups noted challenges, such as the time-intensive nature of CBL and the varying levels of facilitator preparedness.
A. Student Perspectives
Students appreciated the collaborative nature of CBL, noting that it enhanced communication and problem-solving skills. They also valued its practical relevance, which bridged the gap between theory and clinical practice. However, challenges related to the time commitment and inconsistent preparation for case studies were identified.
B. Faculty Perspectives
Faculty acknowledged the value of CBL in preparing students for real-world challenges but emphasised the importance of facilitator training. Inconsistent facilitation was cited as a barrier to effective implementation, suggesting the need for structured training programs focusing on communication and group management skills.
C. Adapting CBL for the Asian-Pacific Context
Cultural dynamics at DSMA, including hierarchical relationships, were seen as barriers to open dialogue and peer-led activities. Strategies such as peer-led activities and anonymous feedback could help mitigate these issues, creating a more inclusive and collaborative environment. Although hierarchical relationships are common across educational settings, these challenges may be viewed as institutional factors rather than unique cultural issues. Thus, the solutions proposed peer-led activities and feedback are relevant for various contexts beyond Asian-Pacific.
D. Core Category and Future Directions
The findings underscore the need for ongoing research to explore facilitation models and cultural adaptations that can optimise CBL in diverse settings. Future studies should examine how CBL can be further refined to address institutional factors like hierarchical relationships, and how these adaptations can be applied in resource-limited settings.
V. CONCLUSION
This study highlights both the strengths and challenges of implementing CBL at DSMA. Students valued CBL for its relevance to clinical scenarios and its emphasis on clinical reasoning, while faculty recognised its potential in fostering interpersonal skills. However, challenges such as inconsistent facilitation, insufficient faculty training, and the lack of localised case studies were identified. Moving forward, DSMA should focus on enhancing faculty development, particularly in facilitation skills, and integrate case studies that reflect local clinical realities. Additionally, leveraging technology to support CBL in resource-limited settings could improve access and engagement.
For the broader health education community, this study underscores the importance of adapting CBL to local contexts, considering cultural dynamics and institutional constraints. Successful implementation of CBL in resource-constrained settings requires flexibility in adapting global pedagogical methods to meet the needs of local learners and educators. Expanding CBL at DSMA, with a focus on faculty training, case study development, and the use of technology, will better prepare students for the challenges of medical practice. This study contributes to the growing body of literature on CBL and provides actionable recommendations for institutions in similar settings.
Notes on Contributors
Dr. Tayzar Hein contributed significantly to the manuscript’s conception, design, and writing, leveraging his expertise to shape its content.
Dr. Susan Somerville provided essential support during the research process, particularly in data collection and analysis, contributing to the manuscript’s presentation.
Ethical Approval
Ethics approval was granted by the Ethical Review Committee of the DSMA, Ethical Review Board (2/ ERB/ 2022).
Data Availability
The data that support the findings of this study are openly available in https://doi.org/10.6084/m9.figshare.26550262.v1.
Acknowledgement
The author would like to express sincere gratitude to their supervisor, Dr Susan Somerville, for her thoughtful guidance throughout the research project. Dr Susan Somerville provided invaluable suggestions, constant encouragement, and generously dedicated her time during video chats, despite being on the other side of the world. The support of the Ethical Review Committee at DSMA is also deeply appreciated. Their rigorous adherence to ethical standards ensured that the study met the highest research ethics guidelines, which is essential to both advancing medical knowledge and protecting human subjects.
Special thanks are extended to the Phase II medical students and faculty members who participated in interviews and provided honest, insightful discussions that significantly contributed to the research. Phase II students, typically in the years of medical education, engage in more clinical-based learning and were crucial in offering perspectives on applying Case-Based Learning (CBL) to real-world medical scenarios. Faculty members from both basic science and clinical practice domains also played an integral role in facilitating these discussions. The assistance of the Medical Education Department faculty in facilitating these interviews was also instrumental, and their support is gratefully acknowledged.
Finally, the author wishes to express heartfelt thanks to his wife and son for their unwavering support and encouragement throughout the academic journey. Without their constant love and understanding, this research project would not have been possible.
Funding
This research is entirely self-funded, as there is currently no external financial support available for the project, necessitating the coverage of all expenses independently.
Declaration of Interest
The author conducted original research and wrote this dissertation, which was not previously submitted for a degree. The author has the copyright to the dissertation according to UK Copyright Acts and University of Dundee’s rules. Any use of material from this thesis should be acknowledged.
References
Ferguson, A., & Lee, E. (2012). Desperately seeking… relevant assessment? A case study on the potential for using online simulated group based learning to create sustainable assessment practices. Legal Education Review, 22(1), Article 6. https://doi.org/10.53300/001c.6258
McLean, S. F. (2016). Case-based learning and its application in medical and health-care fields: A review of worldwide literature. Journal of Medical Education and Curricular Development, 3, S20377.
Patton, M. Q. (2014). Qualitative research & evaluation methods: Integrating theory and practice (4th ed.). SAGE Publications.
Thistlethwaite, J. E., Davies, D., Ekeocha, S., Kidd, J. M., MacDougall, C., Matthews, P., Purkis, J., & Clay, D. J. (2012). The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME Guide No. 23. Medical Teacher, 34(6), e421-e444. https://doi.org/10.3109/0142159X.2012.680939
Yoo, M. S., & Park, H. R. (2015). Effects of case‐based learning on communication skills, problem‐solving ability, and learning motivation in nursing students. Nursing & Health Sciences, 17(2), 166-172. https://doi.org/10.1111/nhs.12151
*Tayzar Hein
Defence Services Medical Academy,
Pyay Road, Mingalardon Township,
Yangon, Myanmar
+9595188093
Email: dr.tayzarhein@gmail.com
https://doi.org/10.29060/TAPS.2025-10-3/TT003
Gominda Ponnamperuma
MBBS, MMEd, PhD
Professor in Medical Education
Faculty of Medicine, University of Colombo, Sri Lanka
Standard setting is the process of deciding the boundary or standard that separates the candidates into two (e.g. pass and fail) or more groups, based on their ability shown at an assessment. Standard setting methods can be broadly grouped into four clusters (see table below).
When to use which method, though a crucial decision for any Board of Examiners, is inadequately explored in the literature. The following brief guide attempts to bridge this literature gap.
|
Cluster of methods |
Key features |
Issues |
When to use |
|
Arbitrary standards and norm-referenced standards |
|
The pass mark is unrelated to the difficulty of assessment items. |
|
|
Test-centred methods |
|
Although the pass mark is directly related to the difficulty of test items,
Due to the above difficulties, the pass mark can be unrealistic. |
|
|
Partially results-based methods-I: Examinee-centred methods |
|
Although judgements are realistic, the introduction of actual test results tends to make the standard cohort-dependent, i.e., norm-referencing features influence the standard. |
|
|
Partially results-based methods-II: Compromise methods |
|
|
|
|
Results-based methods |
|
Due to the norm-referencing |
These methods should be used in high-stakes assessment only when an adequate evidence base is built by conducting them parallelly with another more established method. |
References
Angoff, W. H. (1971). Scales, norms, and equivalent scores. In R. L. Thorndike (Ed.), Educational measurement (2nd ed., pp. 508-600). American Council on Education.
Ebel, R. L. (1972). Essentials of educational measurement. Prentice Hall.
Nedelsky, L. (1954). Absolute grading standards for objective tests. Educational and Psychological Measurement, 14(1), 3-19. https://doi.org/10.1177/001316445401400101
Karantonis, A., & Sireci, S. G. (2006). The bookmark standard-setting method: A literature review. Educational Measurement Issues and Practice, 25(1), 4-12. https://doi.org/10.1111/j.1745-3992.2006.00047.x
Jaeger, R. M. (1982). An iterative structured judgment process for establishing standards on competency test: Theory and application. Educational Evaluation and Policy Analysis, 4(4), 461-476. https://doi.org/10.3102/01623737004004461
Smee, S. M., & Blackmore, D. E. (2001). Setting standards for an Objective Structured Clinical Examination: The borderline group method gains ground on Angoff. Medical Education, 35(11), 1009-1010. https://doi.org/10.1111/j.1365-2923.2001.01047.x
Kramer, A., Muijtjens, A., Jansen, K., Dusman, H., Tan, L., & van der Vleuten, C. (2003) Comparison of a rational and an empirical standard setting procedure for an OSCE. Medical Education, 37(2), 132-139. https://doi.org/10.1046/j.1365-2923.2003.01429.x
Livingston, S. A., & Zieky, M. J. (1982). Passing scores: A manual for setting standards of performance on educational and occupational tests. Educational Testing Service.
Hofstee, W. K. B. (1973). Een alternatief voor normhandhaving bij toetsen. Nederlands Tijdschrift voor de Psychologie, 28, 215-227.
Cohen-Schotanus, J., & van der Vleuten, C. P. M. (2010). A standard setting method with the best performing students as point of reference: Practical and affordable. Medical Teacher, 32(2), 154-160. https://doi.org/10.3109/01421590903196979
Wijnen, W. H. F. W. (1971). Onder of boven de maat. Amsterdam: Swets & Zeitlinger.
Submitted: 30 October 2024
Accepted: 8 April 2025
Published online: 1 July, TAPS 2025, 10(3), 89-92
https://doi.org/10.29060/TAPS.2025-10-3/SC3562
Shanya Shanmugam1, Rajeswari Kathirvel1,2, Kayda Soh2 & Xinyi Li1,2
1Lee Kong Chian School of Medicine, Singapore; 2Division of Obstetrics and Gynaecology, KK Women’s and Children’s Hospital, Singapore
Abstract
Introduction: The Objective Structured Clinical Examination (OSCE) is a popular method for assessing medical students’ clinical proficiency. Mock OSCEs are often incorporated into medical curricula to help students familiarise themselves with the examination format. While the impact of mock OSCEs on academic performance has been studied, their perceived utility remains less explored. This study aimed to assess the effectiveness of a mock OSCE in preparing medical students for their final examinations.
Methods: A prospective study was conducted at a tertiary hospital in Singapore, involving medical students undergoing their Obstetrics and Gynaecology posting. The mock OSCE consisted of five stations and included immediate feedback from examiners. Students completed three questionnaires: pre-mock OSCE, post-mock OSCE and post final examinations, rating the utility of the session and their confidence levels.
Results: Of the cohort of 147 students, 121 responded to the pre-mock OSCE survey, 132 responded to the post-mock OSCE survey, and 105 to the survey after their final examinations. The percentage of students who found the mock OSCE useful/very useful increased significantly from 97.5% before to 98.5% after the session, and significantly decreased to 96.2% after the examinations. Confidence levels rose significantly from a mean score of 2.34/5 pre-mock to 3.89/5 post-mock, to 4.67/5 post-exam. Qualitative feedback was positive, highlighting the benefit of familiarisation with examination mark schemes.
Conclusion: The mock OSCE was well-received by students and perceived as a valuable tool in preparation for examinations. Despite the limited sample size, these findings support the implementation of mock OSCEs to enhance students’ learning and exam preparedness.
Keywords: OSCE, Undergraduate, Medical Education, Medicine, Students’ Perception
I. INTRODUCTION
The Objective Structured Clinical Examination (OSCE) is a well-established, widely utilised method for assessing the clinical proficiency of medical students. This format comprises multiple stations where students perform clinical tasks, including history taking, physical examination, and discussing clinical management. Despite being a crucial assessment tool, OSCEs can be a daunting experience for medical students. Educational institutions often incorporate mock OSCEs into curricula to alleviate this stress, allowing students to familiarise themselves with the format and receive feedback. These sessions aim to mimic the actual OSCE, allowing students to familiarise themselves with the format and requirements, and offer an opportunity to receive feedback.
The correlation between mock OSCE practice and performance in the actual OSCE has yielded mixed results in literature. Studies on medical students (Townsend et al., 2001), and residents from internal medicine (Pugh et al., 2016), paediatrics (Hilliard et al., 1998), and emergency medicine (Lee et al., 2021) have established positive correlations between mock OSCE scores and final examination scores. Conversely, a study on second-year medical students concluded that while the mock OSCE led to improved performance in individual stations, it did not cause a significant change in the pass rate of the final examinations (Chisnall et al., 2015).
While the impact of mock OSCEs on students’ academic performance has been examined, the perception of their utility among participants has not been extensively analysed. As OSCE is viewed as a stressful component of medical assessments, the introduction of mock OSCE sessions is thought to mitigate this stress by fostering confidence and familiarity among students (Chisnall et al., 2015).
We performed a study to determine the perceived effectiveness of a mock OSCE in preparing its participants for their final examinations. More specifically, the study aimed to assess whether participation in the mock OSCEs improved students’ understanding of the domain-based exam scoring system employed by markers, enhanced their time management skills, delivered valuable content, helped them develop effective approaches to OSCE stations, and boosted their confidence levels.
II. METHODS
This prospective study evaluated students’ perceptions of the mock OSCE’s utility. This was conducted at KK Women’s and Children’s Hospital (KKH), which is a tertiary hospital in Singapore. KKH caters to students from the three different medical schools in Singapore including Lee Kong Chian School of Medicine (LKC), Yong Loo Lin School of Medicine and Duke-NUS Medical school.
A mock OSCE programme was organised by the Obstetrics and Gynaecology (O&G) department for the fourth-year medical students from LKC during their O&G posting from 2022-2023. The mock OSCE was conducted three times as the students attended in three streams. This is the first of such a programme in the O&G curriculum and was introduced as this cohort had reduced clinical exposure due to COVID-19 restrictions during their clinical years.
The mock OSCE included five 10-minute stations covering history taking, physical examination, and clinical management in O&G. Students were evaluated according to the domain-based scoring system used by LKC for their final examinations. The assessment was designed to be formative in nature and the students received immediate feedback at the conclusion of each station.
The students were asked to complete anonymous questionnaires before and after participating in the mock OSCE, and after completing their final year examinations. A 4-point Likert scale was used to gauge the usefulness of the mock OSCE session, with 1 being “not useful at all” and 4 being “very useful” and a 5-point Likert scale was used to gauge confidence for final examinations, where 1 represented “not confident” and 5 represented “very confident”. The responses collected before and after the mock OSCE session were compared. The study also examined the impact of the mock OSCE on insight into exam scoring system, time management, and content relevance through Likert scale questions. Qualitative feedback was obtained through open-text responses. The data obtained through the Likert scales were combined into nominal categories. Statistical significance was determined by performing Chi-square tests, with p<0.05 being considered significant. Informed consent was implied through the voluntary participation of individuals in the questionnaires.
The study was approved and given exempt status by the Nanyang Technological University Institutional Review Board for research (IRB 2023-677).
III. RESULTS
There were 147 fourth-year medical students for the academic year 2022–2023. 121 students responded to the questionnaire prior to the mock OSCE (82.3%), 122 (83.0%) after the mock OSCE, and 105 (71.4%) after their final examinations.
Before the mock OSCE, 97 (80.8%) students believed that it would be very useful for their exam preparation, while 20 (16.7%) believed it would be useful, and 3 (2.5%) were unsure. After the mock OSCE, 120 (91.6%) students thought it was very useful for their exam preparation, with 9 (6.9%) believing it was useful, 1 (0.8%) being unsure, and 1 (0.8%) believing it was not useful. After the final examinations, 77 (74.8%) students found it to be very useful for their exam preparation, 22 (21.4%) found it was useful, 3 (2.9%) were unsure, and 1 (1.0%) found it was not useful (Figure 1). Overall, the percentage of students who found the mock OSCE useful/very useful increased from 97.5% before to 98.5% after the session and decreased to 96.2% after the examinations. The difference in perceived utility of the mock OSCE, as determined by the combining “very useful” and “useful” into one category and “unsure” and “not useful” into another, from before the OSCE, after the OSCE, and after the examinations, was statistically significant at p<0.05, with a p-value of 0.0147.

Figure 1. Comparison of perceived utility of mock OSCE
When asked to rate their confidence regarding their final examinations, the overall score improved from 2.34/5 before the mock OSCE to 3.89/5 after, to 4.67/5 after the examinations. This rise in confidence levels was statistically significant, with a p-value of <0.00001.
We asked the students to rate the domain that they found the mock OSCE helped them with the most, including improved insight into domain-based exam scoring system, improved time management, useful content, prepare an approach for OSCE stations, and improved confidence. Almost a third (n = 32, 30.5%) of the students found that the mock OSCE helped them to prepare an approach for OSCE stations the most. This was followed by improved confidence (28, 26.7%), improved insight into exam scoring system (21, 20.0%), useful content (15, 14.3%), and lastly, time management (9, 8.6%). Furthermore, a majority of students (n=70, 66.7%) felt that the O&G mock OSCE was helpful not only for the O&G component, but for the entire OSCE examination.
Qualitative feedback obtained from the students was largely positive. The common theme that surfaced was how the mock OSCE allowed students to familiarise themselves with what to expect from the final examination. Examples include:
“Helped to give us a broader understanding of how 1) clinician thinks and how 2) an examiner grades.”
“It was a great opportunity for medical students to learn about history taking and physical examination in a controlled environment.”
IV. DISCUSSION
Overall, the mock OSCE was well-received by students as a useful tool in preparation for final examinations. The differences in the perceived utility of the mock OSCE from before the OSCE, after the OSCE, and after their final examinations was statistically significant. This supports the value of the mock OSCE programme, given the students’ lack of exposure to clinical scenarios and examination structure as previously outlined. Interestingly, the proportion of students who found the mock OSCE programme useful/very useful decreased from 98.5% after the OSCE to 96.2% after final examinations. This drop can be explained by the qualitative feedback obtained, which cites the examination’s increased complexity and variations in content.
Most students felt that the mock OSCE helped them prepare their approach to OSCE stations, consistent with previous studies showing that mock OSCEs help students familiarise themselves with the format. (Lee et al., 2021, Chisnall et al., 2015) These sentiments are echoed in the qualitative feedback obtained. Furthermore, the difference in confidence levels before and after the mock OSCE was statistically significant.
This study is limited by its small sample size, ranging from 105 to 132 students. As participation was voluntary and the questions were not compulsory, some students did not complete the survey, leading to discrepancies in response rates. Furthermore, due to the anonymous nature of the surveys, we are unable to monitor for survey drop-offs. Using Likert scales to assess the utility of the mock OSCE may not fully capture participants’ opinions. Students may have interpreted the scales differently, as utility is subjective to the individuals’ standards for themselves. This could have resulted in less reliable data due to the diversity in how participants understood the scales.
V. CONCLUSION
The results of this study indicate that a mock OSCE is perceived to be an important part of examination preparation for medical students. Despite being a single-specialty mock OSCE, most students felt it was useful for preparing for their entire final exam.
These findings suggest that there is great potential in using mock OSCEs as a revision tool for medical students and support the implementation of such programmes to guide students in their learning and examination preparation.
Notes on Contributors
Shanya Shanmugam is a medical student at Lee Kong Chian School of Medicine, who is interested in medical education. She reviewed the literature, analysed data and wrote the manuscript.
Dr Rajeswari Kathirvel is a senior consultant at KK Women’s and Children’s Hospital and the principal lead for Obstetrics and Gynaecology at Lee Kong Chian School of Medicine. She, alongside with Dr Li Xinyi, designed the study, developed the questionnaire, and developed the manuscript.
Kayda Soh is an executive in KK Women’s and Children’s Hospital OBGYN Academic Clinical Programme. She was involved in administering the questionnaires and collating the data.
Dr Li Xinyi is a consultant at KK Women’s and Children’s Hospital and the posting lead for Obstetrics and Gynaecology at Lee Kong Chian School of Medicine. She, alongside with Dr Rajeswari Kathirvel, designed the study, developed the questionnaire, and developed the manuscript.
Ethical Approval
The study was approved and given exempt status by the Nanyang Technological University Institutional Review Board for research (IRB 2023-677).
Data Availability
The data that support the findings of this study are openly available in the Figshare repository, at https://doi.org/10.6084/m9.figshare.25903786.
Acknowledgement
We would like to thank the students at Lee Kong Chian School of Medicine who participated in this study.
Funding
The authors report that there is no funding associated with the work featured in this article.
Declaration of Interest
The authors report there are no competing interests to declare.
References
Chisnall, B., Vince, T., Hall, S., & Tribe, R. (2015). Evaluation of outcomes of a formative objective structured clinical examination for second-year UK medical students. International Journal of Medical Education, 6, 76–83. https://doi.org/10.5116/ijme.5572.a534
Hilliard, R. I., & Tallett, S. E. (1998). The use of an objective structured clinical examination with postgraduate residents in Pediatrics. Archives of Pediatrics & Adolescent Medicine, 152(1). https://doi.org/10.1001/archpedi.152.1.74
Lee, M. H., Phua, D. H., & Heng, K. W. (2021). The use of a formative OSCE to prepare emergency medicine residents for summative OSCE: A mixed-methods cohort study. Research Square. https://doi.org/10.21203/rs.3.rs-495003/v1
Pugh, D., Bhanji, F., Cole, G., Dupre, J., Hatala, R., Humphrey-Murto, S., Touchie, C., & Wood, T. J. (2016). Do OSCE progress test scores predict performance in a national high-stakes examination? Medical Education, 50(3), 351–358. https://doi.org/10.1111/medu.12942
Townsend, A. H., Mcllvenny, S., Miller, C. J., & Dunn, E. V. (2001). The use of an objective structured clinical examination (OSCE) for formative and summative assessment in a general practice clinical attachment and its relationship to final medical school examination performance. Medical Education, 35(9), 841–846. https://doi.org/10.1046/j.1365-2923.2001.00957.x
*Shanya Shanmugam
Lee Kong Chian School of Medicine,
11 Mandalay Road,
Singapore
Email: shanya001@e.ntu.edu.sg
Submitted: 19 October 2024
Accepted: 28 April 2025
Published online: 1 July, TAPS 2025, 10(3), 84-88
https://doi.org/10.29060/TAPS.2025-10-3/SC3547
Eranthi Weeratunga, Shashika Karunanayaka, Pramudika Kariyawasam & Bimba Wickramarachchi
Department of Nursing, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka
Abstract
Introduction: Palliative care nursing (PCN) supports individuals with life-threatening illnesses, aiming to improve the quality of life (QoL) for patients and families. The objective was to assess the necessity of establishing an Advanced Certificate Course in PCN at University of Ruhuna, Sri Lanka.
Methods: A descriptive cross-sectional study was conducted among 220 registered nurses (RNs) using purposive sampling, working at National Hospital Galle. A pre-tested, interviewer-administered questionnaire was used, including questions on prior education or training experiences on palliative care (PC), and its principles, services, and management. Descriptive statistics and the chi-square test were used to analyse.
Results: The majority of the RNs were aged 31-40 years (45.2%), females (86.0%), and married (55.7%). A higher proportion of RNs were nursing diploma holders (67.4%), with 55.7% having less than ten years of nursing experience. Only 11.3% of the RNs had formal additional training on PC, such as workshops and a few training hours. Most RNs correctly identified PC aims: improving survival (59.7%), improving QoL of patients and their families (91.4%), providing relief and pain (93.7%), understanding PC (80.1%), etc. The majority (84.6%) had a good attitude toward palliative caregiving, though only 20.4% had average knowledge of PC. Formal PCN training was significantly associated with PC knowledge (p=0.004).
Conclusion: Limited educational exposure, average knowledge levels, and good attitudes toward PC suggest the need for a PCN course for nurses. Providing a special education programme reduces the current gaps in PC by equipping RNs with the respective knowledge, skills, and attitudes to deliver complex management for patients requiring PC.
Keywords: Palliative Care Nursing, Sri Lanka, Educational Needs, Registered Nurse
I. INTRODUCTION
Palliative care (PC) is an approach that aims to improve the quality of life (QoL) of patients and their families facing the physical, psychosocial, and spiritual problems associated with life-threatening illnesses (World Health Organization [WHO], 2022). About forty million people need a PC every year in the world, but the majority are from lower-middle-income countries (LMICs) (WHO, 2022). PC is offered by a range of professionals comprising physicians, nurses, support workers, etc., who are equally important, in addition to family members (WHO, 2022).
The major obstacle to improving PC among healthcare professionals (HCPs) and policymakers in LMICs is a lack of education/training (WHO, 2022) and a need for knowledge on PC for nursing professionals, which emphasised in previous findings in Sri Lanka (Meegoda et al., 2018) in addition to less PC content in the undergraduate curriculum (Pesut & Greig, 2018). Further, less awareness of PC, cultural/social barriers, and misconceptions was found among HCPs; PC education improved nurses’ knowledge, confidence, attitudes, and communication abilities (WHO, 2022). In Sri Lanka, there is a growing number of non-communicable diseases (NCDs), such as cancers, end-stage renal disease, HIV/AIDS, motor neuron disease, etc., that require comprehensive PC at every stage of the disease process in addition to the rapidly aging population.
PC services in Sri Lanka remain limited due to a shortage of trained HCPs. In response to the rising burden of NCDs, the Ministry of Health has emphasised the need to strengthen PC across all levels of the healthcare system. However, gaps in knowledge, skills, and attitudes among HCPs hinder effective implementation. While universities have introduced theoretical PC education, nursing undergraduates receive minimal practical exposure. Although a one-year post-basic diploma in palliative care nursing (PCN) has been launched for registered nurses (RNs), it is insufficient to meet the growing national demand. The initiation of a new course is of paramount importance, as specialisation in PCN has become an urgent necessity both nationally and internationally. The rising number of patients requiring PC, driven by demographic transitions, underscores this need. In developed countries such as Japan and Australia, the demand for PCN is expected to increase due to aging populations. Nationwide studies in Japan estimated that PC needs will continue to rise. Evidence suggests a growing demand for PC services in Australia, in particular, as the number of Australians aged over 85 continues to increase, the need for PC services has also surged. As a result, the demand for Sri Lankan RNs specialising in PC is expected to rise in these developed countries.
To address the existing gaps in PC knowledge and skills among RNs, we sought to quantify RN’s readiness for specialisation in PCN. The key objective was to assess the necessity of establishing an Advanced Certificate Course in PCN at the Department of Nursing, Faculty of Allied Health Sciences (FAHS), University of Ruhuna (UoR), Sri Lanka, to enhance professional competency and meet the growing demand for PC services.
II. METHODS
This descriptive cross-sectional study was conducted at the National Hospital Galle (NGH), Sri Lanka. The study participants were 220 RNs purposively selected based on having at least one year of experience, surveyed from June to December 2023. Data were collected using a content-validated and pre-tested questionnaire, which had been previously utilised in a Sri Lankan study (Fernando & Prathapan, 2019). The questionnaire comprised sections designed to assess socio-demographic characteristics and knowledge of four distinct domains: basic principles, service organisation, clinical management, and ethical considerations. Additionally, participants’ attitudes were evaluated after obtaining written informed consent. Statistical Package for Social Science (SPSS) 26 software was used; the descriptive statistics, frequencies, and percentages were checked. Further, a chi-square test was used. All results were regarded as statistically significant at p < 0.05.
III. RESULTS
The majority of the RNs were aged 31-40 years (45.2%). The mean±SD age was 36.61 ± 7.47 years. The majority were female (86.0%) and married (55.7%). Of the RNs, 35.7% had a monthly income between Sri Lankan Rupees 50,000 and 74,999. A higher proportion of RNs were nursing diploma holders (67.4%), with 55.7% having less than ten years of nursing experience. Emergency trauma care was the special training received by the RNs (4.5%). Only 11.3% of the RNs had formal additional training on PCN, such as workshops and a few training hours. Most RNs correctly identified PC aims (Table. 1). However, the majority gave incorrect answers regarding general knowledge/concepts of PC principles, such as increasing the life expectancy of terminally ill patients (59.7%) and consultants as ideal coordinators for PC (87.8%). Most RNs agreed that PC offers hope to patients (47.1%) and considered it a basic human right (79.6%). The majority (84.6%) had a good attitude toward PC, though only 20.4% had average knowledge of PC. Knowledge of PC was significantly associated with formal PCN training (p=0.004).
|
No. |
Statements on General Principles of PC among RNs |
Correct option |
True % |
False % |
Do not know % |
|
1 |
It is aimed at increasing the life expectancy of terminally ill patients. |
F |
57.9 |
40.3 |
1.8 |
|
2 |
It may improve survival. |
T |
59.7 |
37.1 |
3.2 |
|
3 |
PC was provided for patients of any age. |
T |
85.1 |
10 |
5.0 |
|
4 |
Aims to improve the QoL of patients. |
T |
91.4 |
6.3 |
2.3 |
|
5 |
Aims to increase the QoL of their families facing the physical, psychosocial, and spiritual problems associated with life-threatening illnesses. |
T |
91.4 |
5.0 |
3.6 |
|
6 |
Aim to provide relief from pain and control symptoms in patients. |
T |
93.7 |
5.0 |
1.4 |
|
7 |
Aim to provide psycho-social and spiritual care for patients and families. |
T |
95.0 |
2.7 |
2.3 |
|
8 |
The goal of PC is to help people better understand their treatment options. |
T |
72.4 |
20.4 |
7.2 |
|
9 |
PC could be provided together with other treatments aimed at prolonging life. |
T |
58.4 |
33.5 |
8.1 |
|
10 |
PC could be provided early in the course of illness. |
F |
34.8 |
48.9 |
16.3 |
|
11 |
Bereavement support to the loved ones following the death of the patient concerned comes under the purview of PC. |
T |
64.3 |
9.0 |
26.7 |
|
12 |
Patients with cancer, cardiovascular diseases, chronic respiratory diseases, Acquired Immune Deficiency Syndrome/AIDS, and diabetes may need PC. |
T |
81.4 |
13.6 |
5.0 |
|
13 |
Other diseases are major organ failure (kidney failure), chronic liver disease, multiple sclerosis, Parkinson’s disease, rheumatoid arthritis, neurological disease, dementia, congenital anomalies, drug-resistant tuberculosis, severe burns, extreme frailty of old age, and chronic obstructive pulmonary disease. |
T |
74.7 |
12.2 |
13.1 |
|
No. |
Statements on Service Organisation |
Correct option |
True % |
False % |
Do not know % |
|
1 |
The relevant consultant is the ideal coordinator of the multidisciplinary team involved. |
F |
87.8 |
7.7 |
4.5 |
|
2 |
PC is provided exclusively in hospices and not in tertiary healthcare institutions. |
F |
39.4 |
48.4 |
12.2 |
|
3 |
Include inpatient centers or hospice, hospital-based, community-based, and homecare. |
T |
80.1 |
8.1 |
11.8 |
|
4 |
The main duty of the “Lasting Power of Attorney” is to construct the “Advanced Care Directive”. |
F |
46.6 |
10.4 |
43.0 |
|
5 |
Pastoral caregivers are involved with the social domain of palliation. |
F |
51.6 |
12.2 |
36.2 |
|
No. |
Statements on Drugs and Management Aspects |
Correct option |
True % |
False % |
Do not know % |
|
1 |
The preferred routes of administration of drugs in the most terminal stages of life are “oral” and “rectal” (non-invasive). |
F |
60.6 |
29.4 |
10.0 |
|
2 |
Steroids improve the QoL of palliative patients. |
T |
48.9 |
34.4 |
16.7 |
|
3 |
Anti-convulsants may be added to step one of the WHO analgesic ladder. |
T |
36.2 |
30.8 |
33.0 |
|
4 |
Hyperkalaemia is the most common life-threatening metabolic emergency in palliative patients. |
T |
52.5 |
25.8 |
21.7 |
|
5 |
Due to the development of tolerance, the dosage of morphine for otherwise healthy adults is allowed up to a maximum of 600mg per day. |
F |
34.8 |
31.2 |
33.9 |
|
No. |
Statements on Ethical Concerns |
Correct option |
True % |
False % |
Do not know % |
|
1 |
PC should be incorporated into the care plan of a patient with a terminal diagnosis only after treatments with curative intent have failed. |
F |
55.7 |
27.6 |
16.7 |
|
2 |
Although “Palliative Sedation” usually hastens death, it is not considered a serious issue in the terminal stages of a patient’s life. |
F |
44.3 |
31.2 |
24.4 |
|
3 |
“Death rattle” (noisy respiratory secretions), noticed closer to the patient’s death, is one of the most distressing symptoms suffered by the patient. |
F |
59.3 |
15.8 |
24.9 |
|
4 |
Evidence shows that most patients with terminal diagnoses wish that only their next-of-kin/family understands the prognosis. |
F |
61.1 |
19.0 |
19.9 |
|
Ethical principles are concerned when applying the following PC practices. |
|
|
|
|
|
|
5 |
Have you heard about Do Not Resuscitate? (DNR) |
T |
80.1 |
7.7 |
12.2 |
|
6 |
Understanding advanced care planning in PC |
T |
62.9 |
16.3 |
20.8 |
Table 1. General principles of PC among RNs, service organisation, drug management aspects, and ethical concerns
IV. DISCUSSION
This study assessed PC knowledge, management, ethical concerns, and attitudes among RNs in the NHG, Sri Lanka. RNs reported average knowledge and satisfactory attitudes, with age and prior PC training significantly influencing knowledge levels. Compared to the current study, Fernando and Prathapan (2019) reported higher satisfactory scores.
Sri Lankan medical graduates showed limited PC knowledge (37.23%), lower than RNs (20.4%), likely due to curriculum gaps (Fernando & Prathapan, 2019; Prem et al., 2012). While young medical graduates had adequate knowledge of general principles (63%), ethics was the weakest area (19.55%), mirroring findings among RNs.
PC is a relatively new discipline in Sri Lanka, contributing to limited ethical awareness. Cultural norms favor “hiding bitter truths” over transparency rather than “telling the truth,” which is a fundamental principle in Western healthcare practices, influencing attitudes and ethical concerns (Fernando & Prathapan, 2019).
The medical graduates studied by Fernando and Prathapan (2019) were younger than the RNs in this study. Despite some PC exposure, RNs had fewer opportunities for specialised training, impacting knowledge levels. Nevertheless, their positive attitudes likely stem from empathy-based patient care within the Asian context.
A previous study highlighted insufficient PC preparedness among nurses, attributing it to curriculum deficiencies and inadequate training in pain management (Prem et al., 2012). Female RNs performed better than males, but knowledge gaps remain a global issue. Student nurses and new RNs often feel inadequately prepared to discuss end-of-life issues, death, and other ethical concerns.
Meegoda et al. (2018) emphasised the need for adequate PC knowledge among nurses, as limited PC services worsen cancer care challenges. Heavy workloads and time constraints hinder learning, and 96% of RNs had not attended PC training. In-service programmes were considered beneficial, but specialised training is mainly available in Colombo, restricting accessibility. Distance learning could bridge this gap.
Nurses are vital in PC across various healthcare settings. Skilled PCNs provide essential support to patients and families. WHO (2022) stresses PC’s role in alleviating suffering and advocates its integration into national healthcare. However, LMICs face educational and awareness barriers.
Although Sri Lankan nurses have access to higher education, PC specialisation remains limited, especially in remote areas. With rising NCDs and aging populations, introducing PCN courses is crucial. Establishing a PCN programme aligned with national priorities would enhance patient care and improve career opportunities, particularly for nurses seeking employment abroad. A PCN course at FAHS, UoR, outside Colombo, could improve access to PC education.
A. Limitations
This study highlights the need for PC training, but it has limitations. Sampling bias may affect validity, and self-reported data could introduce response bias.
V. CONCLUSION
Limited educational exposure, average knowledge, and positive attitudes toward PC indicate a need for PCN courses to address existing gaps. RNs at NHG support an Advanced Certificate Course in PCN, emphasising the necessity for specialised training. Expanding PC education will enhance patient care and create new professional opportunities. Future research should assess the impact of PC training on HCP competencies and patient outcomes. Collaboration between the University of Ruhuna and the Ministry of Health is essential for establishing a sustainable PCN course.
Notes on Contributors
EW was involved in conceptual development, data collection/entry/analysis, manuscript drafting, editing, and final correction. SK was incorporated into conceptual development, data collection/entry/analysis, and editing. Data entry/analysis, editing, and final correction were done by PK, and BW was involved in manuscript draft editing.
Ethical Approval
Ethical approval (Ref. No. 83.11.2021) and institutional approval were obtained from the Ethics Review Committee of the FAHS, UoR, and the relevant institutions/authorities.
Data Availability
Data analysed during the current study will be available from the corresponding author upon reasonable request.
Acknowledgment
The authors are grateful to the Dean, FAHS, UoR, Galle, Sri Lanka, and the Head, Department of Nursing, FAHS, UoR, Galle, Sri Lanka. The Director, Chief Grade Nursing Officer, and all in-charge nursing sisters of the National Hospital Galle are acknowledged for their permission. Ms. Nimesha and Mr. Dilan (11th batch/nursing graduates) are appreciated for their enormous contribution while collecting data despite their busy schedules. All consented RNs were further acknowledged for giving their true opinions and great support to uplift nursing education in the PCN field.
Funding
The authors received no funding for this study.
Declaration of Interest
The authors declare that they have no competing interests.
References
Fernando, G. V. M. C., & Prathapan, S. (2019). What do young doctors know of palliative care; How do they expect the concept to work? BMC Research Notes, 12(1), 1–6. https://doi.org/10.1186/s13104-019-4462-2
Meegoda, D. L., Fernando, D. M. S., Atulomah, N., Sivayogan, S., & Marasinghe, R. B. (2018). Improvement of nurses’ skills following a hybrid model educational intervention on cancer palliative care. International Journal of Health Sciences & Research, 8(5), 196–203. http://www.ijhsr.org/IJHSR_Vol.8_Issue.5_May2018/IJHSR_Abstract.031.html
Pesut, B., & Greig, M. (2018). Resources for educating, training, and mentoring nurses and unregulated nursing care providers in palliative care: A review and expert consultation. Journal of Palliative Medicine, 21(S1), S50–S56. https://doi.org/10.1089/jpm.2017.0395
Prem, V., Karvannan, H., Kumar, S. P., Karthikbabu, S., Syed, N., Sisodia, V., & Jaykumar, S. (2012). Study of nurses’ knowledge about palliative care: A quantitative cross-sectional survey. Indian Journal of Palliative Care, 18(2), 122–127. https://doi.org/10.4103/0973-1075.100832
World Health Organization. (2022). Palliative care. https://www.who.int/news-room/fact-sheets/detail/palliative-care
*Eranthi Weeratunga
Department of Nursing,
Faculty of Allied Health Sciences,
University of Ruhuna
Galle, 80 000, Sri Lanka
+94 71 440 2662, +94 77 225 8519
Email: eranthiw@ahs.ruh.ac.lk,
eranthiweeratunga@yahoo.com
Submitted: 22 July 2024
Accepted: 4 February 2025
Published online: 1 July, TAPS 2025, 10(3), 80-83
https://doi.org/10.29060/TAPS.2025-10-3/SC3470
Zaitunnatakhin Zamli1, Rohaini Ramli2, Hidayah Sulaiman2, Mohd Zulfaezal Che Azemin3, Wan Muhamad Salahudin Wan Salleh4, Nurul Asyiqin Yusof5, Imran Mahalil2 & Azmi Mohd. Yusof2
1Department of Biomedical Science, Kulliyyah of Allied Health Sciences, International Islamic University Malaysia, Malaysia; 2Department of Informatics, College of Computing & Informatics, Universiti Tenaga Nasional, Malaysia; 3Department of Optometry and Visual Sciences, Kulliyyah of Allied Health Sciences, International Islamic University Malaysia, Malaysia; 4Department of Basic Medical Sciences, Kulliyyah of Medicine, International Islamic University Malaysia, Malaysia; 5Department of Basic Medical Sciences, Kulliyyah of Pharmacy, International Islamic University Malaysia, Malaysia
Abstract
Introduction: Virtual reality (VR) has been widely used in medical and health sciences education since the late twentieth century. VR complements the conventional teaching and learning (T&L) approach by providing an engaging and immersive 3D spatial learning environment, especially for understanding the orientation of anatomical structures. Despite these advantages, the usability and student preference of highly immersive head-mounted display-based (HMD) and less immersive desktop-based (DB) VR in human anatomy courses have yet to be determined.
Methods: In a cross-sectional study, 49 Year-2 medical students were recruited through a convenient sampling. The participants were asked to identify 15 skeletal system components using the HMD and DB platform with human anatomy VR application. Both applications’ System Usability Scale (SUS) and preference scores were obtained via a self-administered questionnaire. The data were expressed as median [IQR] and statistically analysed using MATLAB R2022b.
Results: Most participants preferred the HMD over the DB platform (p=0.04), especially the male participants (p=0.01). There was no significant difference in overall SUS scores between both platforms (p=0.14). However, when compared within and between genders, females scored significantly higher in the DB than HMD (p=0.02) and higher than males’ DB SUS scores (p=0.03).
Conclusion: The overall usability of HMD was comparable with the DB platform for learning human anatomy. Although most participants prefer to use the HMD, further exploration of why females prefer the DB is needed. Subsequently, VR application developers must consider gender-related adaptions to promote the equitability and inclusivity of the technology for all users.
Keywords: Human Anatomy, Virtual Reality, Head-mounted Display, Desktop-based Application, Usability, Preference
I. INTRODUCTION
Virtual reality (VR) is a simulated three-dimensional (3D) environment that enables users to explore and interact with virtual surroundings, perceiving them through their senses as if they were in the real world. It has been widely used in various fields, including education, to provide users with immersive, engaging, and experiential learning experiences.
In medical education, VR allows students to manipulate anatomical structures into different planes, sections and orientations in a simulated environment, benefiting learners with low-spatial ability. VR also helps students better grasp the relative size differences of organs and allows students to relate the location and position of the organs with their surroundings, resulting in better memorisation and learning outcomes, with VR groups outperforming control groups in post-test assessments (Kurul et al., 2020). As the current generation is more digitally savvy, most students are easily adapted to VR simulation, which enables them to grasp knowledge from a new perspective. For instance, students can dissect a muscle from the human body, gaining insight into the interaction and innervation of individual muscles during exercise.
However, despite the high acceptability of use in anatomy courses among students, some participants reported simulator sickness symptoms like headaches, dizziness, and blurred vision. These symptoms are more pronounced in females, who tend to experience discomfort in a VR environment (Stanney et al., 2020), potentially due to differences in spatial awareness, sensitivity to sensory stimuli, or physiological responses. In addition, regardless of gender, the mismatch between visual motion and the body’s sensory feedback in VR environments can lead to sensory conflict and an increased likelihood of discomfort.
While VR modalities show great potential in anatomy education, research comparing highly immersive head-mounted display-based (HMD) with less immersive desktop-based (DB) VR platforms, particularly regarding gender differences in usability and preferences, remains limited. In addition, considering the high cost of VR applications for HMD, addressing this knowledge gap before its development is crucial to ensuring optimal and cost-effective learning outcomes for a diverse student population. Therefore, this study aimed to compare the usability and preferences between DB and HMD platforms in exploring the VR anatomy applications, within and between genders, among medical students.
II. METHODS
Upon their written consent, forty-nine undergraduate medical students (23 males and 26 females, aged 19-21 years) were recruited through a convenience sampling. They were second-year medical students and participated in this study in two sessions. The participants were asked to identify 15 skeletal components (i.e. skull, vertebrae, hyoid bone, sternum, ribs, scapula, clavicle, humerus, radius, ulna, hip bone, femur, patella, tibia, and fibula) using two platforms: a head-mounted display-based (HMD) virtual reality system with the human anatomy VR application (BodyMap v3.2, https://www.mai.ai/bodymap), and a desktop-based (DB) application (Zygote Body, https://www.zygotebody.com/). BodyMap v3.2 is a VR application for exploring the human body in 3D using the Oculus Quest 2 headset, which provides an immersive and interactive experience for anatomy education. Meanwhile, Zygote Body is a web-based platform that offers detailed 3D anatomical models for desktop or laptop exploration.
Each platform was given a time limit of 15 minutes for the participants to complete the task. After completing the task, the participants completed the System Usability Scale (SUS), a 10-item questionnaire designed to measure the perceived usability of both platforms. The SUS score ranges from 0 (very poor usability) to 100 (perfect usability). In addition, the participants were also asked to rate their preference for using each platform on a scale from 1 (do not prefer at all) to 10 (most preferred). The data were expressed as median (interquartile range, IQR), which best represents the central tendency for non-normally distributed data. Normality was assessed using the Kolmogorov-Smirnov test, and the Wilcoxon signed-rank tests were used to compare the median scores of SUS / Preferences within and between genders. All statistical analyses were performed using MATLAB R2022b, with a p-value < 0.05 considered statistically significant.
III. RESULTS
A. Demographic Data
Forty-nine Year-2 IIUM medical students participated in this study. Most of the students were female (n=26, 53%), with a mean age of 20.10 ± 0.37 years old.
B. Comparison of SUS and Preference Scores between the HMD and DB
There was no significant difference between the median SUS scores between the HMD and DB applications (p=0.14). However, most students preferred the HMD (90, IQR 80.0-100.0) rather than the DB (80, IQR 75.0-90.0) applications (p=0.04).
C. Comparison of SUS and Preference Scores of the HMD and DB within and between Gender
The SUS and preference scores of the HMD and DB applications within and between genders are shown in Figure 1, and individual scores are accessible at https://doi.org/10.6084/m9.figshare.26711965. Based on gender, significantly higher median SUS scores were observed for the DB (85, IQR 77.5-95.0) than the HMD application (75, IQR 59.4-85.6) among the female students (p=0.02). In contrast, the male students had a significantly higher preference score for the HMD (100, IQR 85.0-100.0) than the DB application (80, IQR 70.0-90.0) (p=0.01). A significant difference between gender was only observed in the SUS score, in which the female students scored 85 (IQR, 77.5 – 95.0), and the male students scored 75 (IQR, 58.1 – 86.9; p=0.03) for the DB application.
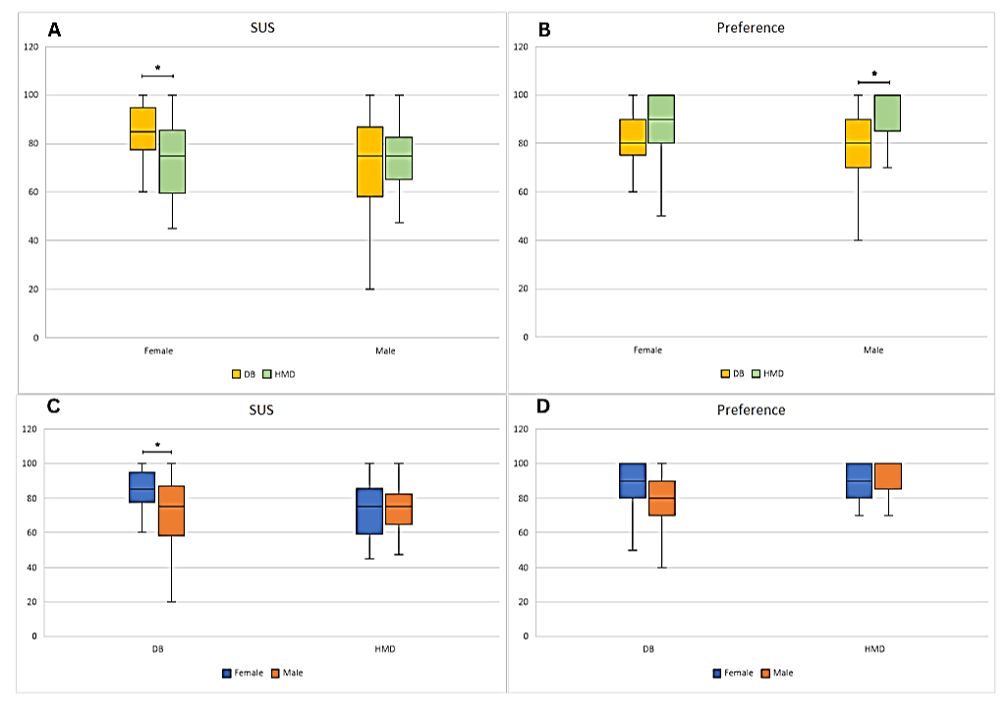
Figure 1. Comparison of SUS and Preference median scores of the HMD and DB application within (A-B) and between genders (C-D). A significant difference of p≤0.05 is denoted as *.
IV. DISCUSSION
This study found that the overall usability scores of the head-mounted display-based (HMD) and the desktop-based (DB) in human anatomy VR applications are comparable. However, a significant gender-related difference was observed in the reported usability scores of the HMD. Female participants reported significantly better usability with the DB than the HMD, likely due to their unfamiliarity with the HMD modality and disadvantage in the 3D spatial ability than males in visualising and manipulating objects in the navigating space. While traditional explanations link these gender differences to brain lateralisation, Bartlett and Camba (2023) challenge this view, suggesting societal expectations and gender roles may shape spatial skills.
Despite this, the study also found that most participants, especially males, prefer the HMD over the DB. This preference might be due to males’ active engagement and early adaptation to the technology, particularly in online gaming, making it more intuitive. This aligns with Deisinger et al. (1997), who found that inexperienced users favoured screen-based projection due to their familiarity with the conventional technology over the HMD. Interestingly, although females perceived DB as more usable, this did not significantly affect their preference for HMD. Many females acknowledged needing more technical help with the HMD but believed they would quickly adapt and prefer it over time. The study’s findings resonate with prior research in medical education, where HMDs are favoured for their immersive experience, enhancing spatial or physical presence and interaction as compared to DB (Yamazaki et al., 2021). However, the effectiveness of HMDs in improving learning outcomes compared to traditional methods remains inconclusive.
Given HMDs’ potential to enhance anatomy education, further research is crucial, especially in complex topics like embryology and neuroanatomy. Developers must focus on high content quality, intuitive user interfaces, and user comfort to ensure a positive learning experience. Gender-related adaptations can promote inclusivity, ensuring that the educational benefits of HMDs are accessible to all users.
Three main limitations of the present study also warrant mention. First, we used the available human anatomy VR applications from two developers, which may have different image quality of VR. However, both VR applications are comparable in terms of content quality. Second, we have not explored their reasons for high preference for utilising HMD when exploring human anatomy VR, potentially limiting our understanding of the user experience (e.g. comfort, immersion, satisfaction, and overall interaction) related to HMD usage. Third, participants’ previous experience using HMD in other platforms, such as gaming, virtual tours, etc, was not determined. Future studies should consider these limitations to understand user experiences with the HMD platform better and identify factors influencing user preferences.
V. CONCLUSION
In summary, this study concluded that the usability of both HMD and DB in exploring the human anatomy VR application is almost similar. As seen in other studies, students tend to favour HMD over DB because of its immersive, interactive, and engaging features. However, at an individual level, gender may influence their perception of its usability and preference. Therefore, it is essential to take gender-related adaptations into account when developing VR applications.
Notes on Contributors
Zaitunnatakhin Zamli reviewed the literature, designed the study, performed data collection and analysis, and developed the manuscript. The author has read, given critical feedback and approved the final manuscript.
Nurul Asyiqin Yusof reviewed the literature, designed the study, performed data collection and analysis, and developed the manuscript. The author has read, given critical feedback and approved the final manuscript.
Azmi Mohd Yusof reviewed the literature, designed the study, performed data collection and analysis, and developed the manuscript. The author has read, given critical feedback and approved the final manuscript.
Wan Muhamad Salahudin Wan Salleh designed the study and performed data collection, analysis and interpretation. The author has read, given critical feedback and approved the final manuscript.
Mohd Zulfaezal Che Azemin designed the study and performed data collection, analysis and interpretation. The author has read, given critical feedback and approved the final manuscript.
Rohaini Ramli advised on study design and data interpretation. The author has read, given critical feedback and approved the final manuscript.
Hidayah Sulaiman advised on study design and data interpretation. The author has read, given critical feedback and approved the final manuscript.
Imran Mahalil facilitated the data collection process. The author has read, given critical feedback and approved the final manuscript.
Ethical Approval
Ethical approval of this study was granted by the Kulliyyah Postgraduate and Research Committee (IIUM/305/20/4/1/7) and IIUM Research Ethics Committee (IREC) (IIUM/504/14/11/2/IREC2022-194). All participants involved in the study had given their written consent, and their participation was voluntary.
Data Availability
The data of this study data are available at a Figshare repository, https://doi.org/10.6084/m9.figshare.26711965
Acknowledgement
The authors would like to thank the Department of Informatics, College of Computing & Informatics, Universiti Tenaga Nasional, Selangor, Malaysia, for providing equipment, software and logistics support.
Funding
This study did not receive any funding or financial support.
Declaration of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
Bartlett, K. A., & Camba, J. D. (2023). Gender differences in spatial ability: A critical review. Educational Psychology Review, 35(1), Article 8. https://doi.org/10.1007/s10648-023-09728-2
Deisinger, J., Cruz-Neira, C., Riedel, O., & Symanzik, J. (1997). The effect of different viewing devices for the sense of presence of immersion in virtual environments: A comparison of stereoprojections based on monitors, HMDs and screens. Proceedings of the Seventh International Conference on Human-Interaction Computer, (2), 881-884. https://www.usu.edu/math/symanzik/papers/1997_HCI_Int.html
Kurul, R., Ögün, M. N., Narin, A. N., Avci, Ş., & Yazgan, B. (2020). An alternative method for anatomy training: Immersive virtual reality. Anatomical Sciences Education, 13(5), 648-656. https://doi.org/10.1002/ase.1959
Stanney, K., Fidopiastis, C., & Foster, L. (2020). Virtual reality is sexist: But it does not have to be. Frontiers in Robotics and AI, 7, 476417 https://doi.org/10.3389/frobt.2020.00004
Yamazaki, A., Ito, T., Sugimoto, M., Yoshida, S., Honda, K., Kawashima, Y., Fujikawa, T., Fujii, Y., & Tsutsumi, T. (2021). Patient-specific virtual and mixed reality for immersive, experiential anatomy education and for surgical planning in temporal bone surgery. Auris Nasus Larynx, 48(6), 1081-1091. https://doi.org/10.1016/j.anl.2021.03.009
*Azmi Mohd. Yusof
Jalan IKRAM-UNITEN,
43000 Kajang,
Selangor, Malaysia
Email: azmiy@uniten.edu.my
Submitted: 17 February 2024
Accepted: 25 March 2025
Published online: 1 July, TAPS 2025, 10(3), 65-74
https://doi.org/10.29060/TAPS.2025-10-3/SC3251
Dani R Firman1,2, Friedo W Dekker2,3, Eriska Riyanti1, Sunardhi Widyaputra1 & Peter GM de Jong2
1Faculty of Dentistry, Universitas Padjadjaran, Indonesia; 2Center for Innovation in Medical Education, Leiden University Medical Center, the Netherlands; 3Department of Clinical Epidemiology, Leiden University Medical Center, the Netherlands
Abstract
Introduction: To explore the current situation regarding teaching evidence-based practice (EBP) in Indonesian dental schools as a low-middle-income country (LMIC) setting.
Methods: Two nation-wide surveys were administered to all Indonesian dental schools (N=32) to capture the perceived value of the deans about EBP skills and teaching with its resource-related situation, as well as the actual teaching implementation and its challenges by their curriculum teams. The analysis was performed descriptively as national aggregate data.
Results: The response rates were 96.9% and 90.6%, respectively. The deans considered EBP skills to be very important (61.3%) or important (38.7%). However, only 16.1% of deans reported that the implementation of teaching EBP met their expectations. Most schools (75.9%) considered providing training for teachers as the priority plan. Most schools (62.1%) had an independent EBP course in their curriculum, while 86.2% incorporated EBP teaching (also) into other courses. All dental schools employed a lecture strategy for teaching EBP topics, but also used other strategies such as interactive strategies with a wide range of percentages being utilised (10.3 – 89.7%). EBP-specific topics were generally taught with a level of implementation varying from 34.5% to 96.6% in the pre-clinical and from 10.3% to 62.1% in the clinical programme.
Conclusion: The used approach can be considered an effective strategy to provide opportunities for schools to reflect their EBP teaching. This study confirmed the necessity for improvement, especially the need to support faculty development. The deans and their curriculum teams highly value collaborative improvement plans.
Keywords: National Survey, Evidence-based Practice, Faculty Perception, Low-middle-income Country
I. INTRODUCTION
Evidence-based practice (EBP) is emerging as the standard in clinical dentistry. It integrates the best research evidence with patients’ values, preferences, and clinical experiences (Young et al., 2014). The EBP process involves five key steps in sequence (ask, acquire, appraise, apply, and evaluate). The appraise or critical appraisal skill as part of the steps is related to research capacity still considered as crucial gaps in the LMIC setting compared to high-income country (HIC) setting, and known to hinder EBP development and implementation (Gill et al., 2021). Furthermore, the suboptimal practice of EBP among dental professionals in lower and middle-income countries (LMIC) was suspected due to limited access of web-based subscription database and scarcity of experts as mentor (Minja & Lwoga, 2021).
Potentially, dental schools can play a significant role in promoting EBP implementation in dentistry of such setting by providing the access to evidence, supporting professional development and integrate the EBP teaching and learning in the curriculum. However, institutionalising EBP requires consistent policy and strong administrative support. To understand the current situation of EBP teaching in Indonesian dental schools, we conducted a study exploring the deans’ perceptions about its importance and the need for improvement. We also determined the actual level of implementation as reported by their curriculum teams. The study’s outcomes could inform future interventions to enhance EBP teaching in Indonesian dental schools.
II. METHODS
At the time of the study, in September 2022, there were 32 dental schools in Indonesia, all of which ran a bachelor’s programme (year 1-4) and a clinical programme (year 5-6). A descriptive survey study was conducted online using two sets of Indonesian-language questionnaires in sequence.
The first survey was launched during an in-person national meeting in Surabaya. Only the principal investigator himself participated via Zoom. This first survey aimed to gauge deans’ perceived importance of EBP skills and teaching, along with necessary resource improvements. The questionnaire included demographic items, five-point of Likert-scale questions on EBP teaching value, resources-related, an open-ended item on EBP teaching challenges, and a section for additional comments. Most deans completed the first online survey during that meeting, while those who did not attend the meeting were received the survey’s link via email.
Upon completion for each school by the deans, a second survey was sent to vice dean for academic affairs as corresponding contact using the email address provided by the deans in the previous survey. In the introduction letter, we specifically requested the involvement of their curriculum team of the bachelor and clinical programme as a group response for each school. This second survey gathered data on EBP teaching implementation and challenges more in details. It was translated and adapted from a previous survey used by Gorgon et al. (2013) which was considered relevant to all health professions, including dentistry. The adaptation included a pilot test beforehand to ensure its relevance and clarity.
The study protocol was approved by the Educational Research Review Board of the LUMC (Registry number: OEC/ERRB/20220913/1). Participants electronically consented to both surveys after reviewing the provided information. Respondents with missing or unclear data were contacted for clarification. Five-point Likert scale items, checklist items, and multiple-choice items were analysed descriptively. The open-ended item responses and additional comments were analysed thematically.
III. RESULTS
The first survey’s responses were received from 31 dental schools across Indonesia (96.9%). The schools were located on Java (18), Sumatera (6), Sulawesi (3), and Kalimantan and Bali (2 each). For the second survey, which targeted the curriculum team for each school, the responses were received from 29 schools (90.6%).
A. The Perceived Value of EBP Teaching (The 1st Survey, n=31)
The deans perceived EBP skills as very important/essential (61.3%) or important (38.7%) for students. Incorporating EBP in the curriculum was seen as very important/essential (51.6%) or important (48.4%). Improving teachers’ EBP teaching expertise was deemed very necessary (54.8%) or necessary (38.7%). Five deans (16.1%) felt their schools met faculty expectations for EBP teaching, while others observed room for improvement (64.5% necessary, 19.4% very necessary). Resources like database access and librarian expertise varied in satisfaction. Most respondents (71%) valued collaboration with other schools on EBP training and implementation (See Appendix 1).
B. The Implementation of EBP Teaching (The 2nd Survey, n=29)
Over half (62.1%) of participated schools have a standalone EBP course, and 86.2% incorporate EBP in other courses. Lecture-based teaching is the most common EBP strategy, followed by thesis discussions, journal readings, colloquiums, and seminars. Small group discussions and problem-based tutorials are also used. “Critically appraised topics” (CATs) are least used, with only three schools employing this active learning method. Both summative and formative assessments are used. Most schools use a blended approach for EBP courses, with one school offering a fully online course (See Appendix 2.a).
C. Available Resources for EBP Teaching (The 1st and 2nd Survey, n=31 and n=29)
Of the participating institutions, only 8 out of 29 dental schools have teachers formally-trained in EBP. Most schools have access to scientific databases, with ScienceDirect being the most accessible (58.6%). Other databases include Web of Science, Cochrane Library, EBSCO Host, CINAHL, and UpToDate, with some schools also subscribing to Springer Link, Wiley, Emerald, and SAGE (See Appendix 2.b). Database access is mostly provided by the university (80.6%), with some funded by faculty budgets (29%) or government institutions (9.7%). Only one school lack subscribed database access (See Appendix 3.a).
D. The EBP Specific Topics Coverage (The 2nd Survey, n=29)
The five EBP steps (ask, acquire, appraise, apply, evaluate) are taught in Indonesian dental schools, with varying implementation levels from 34.5% to 96.6% in pre-clinic programmes and 10.3% to 62.1% in clinic programmes. The ‘apply’ and ‘evaluate’ steps are least taught in pre-clinic programmes. Interpreting forest plots in systematic reviews is the least covered topic, with only 10 out of 29 schools teaching it in pre-clinic levels, 3 in clinical levels, and 19 not covering it at all. Over a third of the schools (37.9%) do not teach critical appraisal of a systematic review. See Table 1 below for details.
|
Pre-clinic |
Clinic |
Not taught in both programme** |
|||
|
EBP steps and its specific topics coverage (n=29) |
Taught* |
Not taught* |
Taught* |
Not taught* |
|
|
I. Asking clinical question |
|||||
|
(1) Formulating clinically questions using the PICO format |
22 (75.9) |
7 (24.1) |
12 (41.4) |
17 (58.6) |
5 (17.2) |
|
(2) Guided literature search by the clinical questions |
20 (69.0) |
9 (31.0) |
18 (62.1) |
11 (37.9) |
5 (17.2) |
|
II. Search the evidence |
|||||
|
(3) Constructing a focused search with Boolean operator in a database |
23 (79.3) |
6 (20.7) |
7 (24.1) |
22 (75.9) |
6 (20.7) |
|
(4) Locating clinical evidence using electronic databases |
26 (89.7) |
3 (10.3) |
8 (27.6) |
21 (72.4) |
3 (10.3) |
|
(5) Utilising a reference manager software |
25 (86.2) |
4 (13.8) |
9 (31.0) |
20 (69.0) |
4 (13.8) |
|
III. Critically appraising evidence |
|||||
|
(6) Study designs and their major strength and limitations |
27 (93.1) |
2 (6.9) |
7 (24.1) |
22 (75.9) |
2 (6.9) |
|
(7) Assessing the relevance of study design to the question asked |
22 (75.9) |
7 (24.1) |
5 (17.2) |
24 (82.8) |
7 (24.1) |
|
(8) Hierarchy or levels of evidence |
23 (79.3) |
6 (20.7) |
6 (20.7) |
23 (79.3) |
5 (17.2) |
|
(9) Difference between narrative, systematic review, and meta-analysis |
21 (72.4) |
8 (27.6) |
4 (13.8) |
25 (86.2) |
7 (24.1) |
|
(10) Difference between clinical and statistical significance |
22 (75.9) |
7 (24.1) |
9 (31.0) |
20 (69.0) |
6 (20.7) |
|
(11) Interpreting t tests, chi-square tests |
28 (96.6) |
1 (3.4) |
6 (20.7) |
23 (79.3) |
1 (3.4) |
|
(12) Interpreting p-value, confidence interval |
28 (96.6) |
1 (3.4) |
6 (20.7) |
23 (79.3) |
1 (3.4) |
|
(13) Understanding sensitivity and specificity, number needed to treat, odds ratio |
28 (96.6) |
1 (3.4) |
6 (20.7) |
23 (79.3) |
1 (3.4) |
|
(14) Understanding intention to treat analysis and power calculation |
20 (69.0) |
9 (31.0) |
3 (10.3) |
26 (89.7) |
9 (31.0) |
|
(15) Use of appraisal tool(s) to assess validity |
22 (75.9) |
7 (24.1) |
7 (24.1) |
22 (75.9) |
7 (24.1) |
|
(16) Ways in which study validity can be threatened |
25 (86.2) |
4 (13.8) |
5 (17.2) |
24 (82.8) |
4 (13.8) |
|
(17) Difference between internal and external validity |
21 (72.4) |
8 (27.6) |
3 (10.3) |
26 (89.7) |
8 (27.6) |
|
(18) Critical appraisal of systematic reviews |
18 (62.1) |
11 (37.9) |
6 (20.7) |
23 (79.3) |
11 (37.9) |
|
(19) Interpreting forest plots in systematic reviews |
10 (34.5) |
19 (65.5) |
3 (10.3) |
26 (89.7) |
19 (65.5) |
|
(20) Critical appraisal of studies about intervention (RCTs and clinical trials) |
18 (62.1) |
11 (37.9) |
7 (24.1) |
22 (75.9) |
9 (31.0) |
|
(21) Critical appraisal of studies about diagnosis (cohort, case-control studies) |
21 (72.4) |
8 (27.6) |
5 (17.2) |
24 (82.8) |
7 (24.1) |
|
(22) Critical appraisal of studies about prognosis (longitudinal studies) |
18 (62.1) |
11 (37.9) |
5 (17.2) |
24 (82.8) |
10 (34.5) |
|
IV. Implementation and communication |
|||||
|
(23) Communicating the recommendation from EBP process to the patient |
14 (48.3) |
15 (51.7) |
9 (31.0) |
20 (69.0) |
12 (41.4) |
|
(24) Deciding the clinical decision considering the patient’s value |
12 (41.4) |
17 (58.6) |
11 (37.9) |
18 (62.1) |
11 (37.9) |
|
V. Evaluation |
|||||
|
(25) Evaluation of the EBP implementation (The patient’s outcome and student’s performance through self-reflection) |
13 (44.8) |
16 (55.2) |
9 (31.0) |
20 (69.0) |
13 (44.8) |
Table 1. EBP steps and its specific topics coverage for each programme level (n=29)b
* n (%)
** n (%) Overlap calculation with the number of not taught on each programme
b From the 2nd survey to the curriculum teams
E. Challenges (The 1st Survey, n=31 and The 2nd Survey, n=29)
The top three challenges in Indonesian dental schools, as reported by curriculum teams, are a lack of EBP experts (72.4%), insufficient accessible EBP courses for faculty (69%), and students’ inadequate knowledge of statistics and research methodology (65.5%) (See appendix 4). In the open-ended item section, most of the deans expressed the challenges of EBP teaching. Teachers-related factors were considered the most challenging, such as limitation in knowledge and skills, and an overloaded work situation.
F. Action Plans (The 2nd Survey, n=29)
Most respondents (75.9%) highly valued teacher training. They also preferred incorporating EBP skills into the curriculum (48.3%) and holding faculty meetings to discuss EBP programme development (44.8%) (See appendix 3.b).
IV. DISCUSSION
To our knowledge, this is the first nation-wide survey with very high response rate to report insights of EBP teaching in the South-east Asia region, more specifically in Indonesian dental education setting. Targeting both deans and curriculum teams yielded rich data and stakeholder involvement, potentially fostering acceptance of future EBP improvements at institutional or national levels.
There is a slight gap between the perceived importance of EBP skills for students and the importance of incorporating such skills into the curriculum, which may be related to limited resources. The deans considering room for improvement, especially in teacher expertise. This is echoed by curriculum teams, as less than a third of Indonesian dental schools’ teachers have formal training experience, i.e. training from a well-known academic-based institution or recognised training organisation. This lack of EBP teachers is a top challenge identified by respondents. Deans and curriculum teams agree on the need for improved teacher skills.
The majority of Indonesian dental schools are teaching EBP topics in stand-alone EBP courses as well as incorporated in other regular courses using both face-to-face and online delivery. Lecture-based is the most used teaching strategy among the schools. Our findings suggest that there is room for enhancing the teaching strategy of EBP in Indonesian dental schools towards a more multi-facet, interactive and more authentic setting in the clinical environment as suggested by Howard et al. (2022).
Regarding critical appraisal topics based on the study design (See Table 1, item 18, 19-21), there were very few schools implementing a Critically Appraised Topics (CATs) teaching strategy (See Appendix 2.a). CATs, one-page summaries of evidence on a clinical question, offer active, authentic learning and being recommended in the literature to provide both a critique of the research and a statement of the clinical relevance of its findings. It is crucial to teach critical appraisal skills using the teaching strategy that is supported by the evidence to ensure sufficient development of EBP skills. Many Indonesian dental educators may not be familiar with this CATs teaching method.
The survey reveals that the ‘apply’ and ‘evaluate’ steps of EBP are less addressed than the ‘ask’, ‘acquire’, and ‘appraise’ steps. These five-steps, identical to those in Evidence-Based Medicine (EBM), form the basis of clinical practice and teaching. Key EBM developments like shared-decision making skills, part of the ‘apply’ step, are often overlooked. Hence, it’s vital to teach all EBP steps, ideally in a more authentic clinical setting.
The need for more EBP-trained faculty in most schools highlights the importance of a faculty development programme supported by national collaboration. As a lower-resource country, Indonesia faces challenges in dental education, including limited access to databases and librarian expertise, primarily due to financial constraints, inadequate institutional support, and the absence of national policies prioritising scientific resources. These limitations hinder faculty and students from fully implementing evidence-based practices, widening disparities with high-income countries. To address these issues, a policy brief should be directed to high-level stakeholders, advocating for essential infrastructure, more funding and resource investments for both private and government-funded schools.
This study has limitations. Due to the five-point Likert scale in the first questionnaire were not constructed on the same concept, the reliability test was not feasible. This is also applied for the second questionnaire, which adapted from a previous study, was mostly factual and checklist-based. The value of EBP teaching, reported by deans and curriculum teams, might be socially desirable. However, the results underscore the importance of EBP teaching and the need for improvement. It is worth noting that after the data collection was completed, Indonesia formally transitioned from a lower-middle-income to an upper-middle-income country as of July 2023. This transition suggests a more promising future, with potential improvements in the financial capacity, but it will require the national policy support to be fully implemented.
V. CONCLUSION
This first national survey reveals the state of EBP teaching in Indonesian dental schools, representing Southeast Asian countries. It highlights the need for faculty development and more active, authentic learning experiences but further analysis is required to adopt and adapt these interventions for lower-resource settings. The deans and their curriculum teams highly value collaborative improvement plans. This supports EBP’s vision of using current research to improve Indonesian oral healthcare.
Notes on Contributors
DF is the principal investigator. He designed, analysed, prepared and wrote the manuscript collaboratively with co-authors.
SW and ER made substantial contributions to preparation of the instruments, data collection and editing the final manuscript.
FD and PJ made substantial contribution to the design, analysis, preparation and editing the final manuscript.
All authors read and approved the final version.
Ethical Approval
The study protocol was approved by the Educational Research Review Board of the LUMC (Registry number: OEC/ERRB/20220913/1).
Data Availability
Due to confidentiality of the responses and commitments made with the study participants, also considering the small size data set with its unique data for some variables that might still be traceable to the respondent. Data are available on reasonable request by email to the corresponding author.
Acknowledgement
The authors express gratitude to all participants and schools involved in this study, AFDOKGI and its members for their support and data access, the Research group at the OEC LUMC for their constructive feedback, Universitas Padjadjaran for sponsoring the first author’s PhD scholarship, and Edward Gorgon for permitting the modification and use of the questionnaire.
Funding
This research is part of the first author’s (DF) PhD study, funded by a scholarship from Universitas Padjadjaran, Indonesia (Registry number 3781/UN.6.WR2/KP.10/2021).
Declaration of Interest
The first author (DF), an assistant professor at the Faculty of Dentistry, Universitas Padjadjaran, which participated in this study. DF also had ties until 2020 with AFDOKGI, the association of Indonesian dental schools, as a dental education consultant.
References
Gill, P. J., Ali, S. M., Elsobky, Y., Okechukwu, R. C., Ribeiro, T. B., Soares dos Santos Junior, A. C., Umpierre, D., & Richards, G. C. (2021). Building capacity in evidence-based medicine in low-income and middle-income countries: Problems and potential solutions. BMJ Evidence-Based Medicine, 26(3), 82–84. https://doi.org/10.1136/bmjebm-2019-111272
Gorgon, E. J. R., Basco, M. D. S., & Manuel, A. T. (2013). Teaching evidence-based practice in physical therapy in a developing country: A national survey of Philippine schools. BMC Medical Education, 13(1), Article 154. https://doi.org/10.1186/1472-6920-13-154
Howard, B., Diug, B., & Ilic, D. (2022). Methods of teaching evidence-based practice: A systematic review. BMC Medical Education, 22(1), Article 742. https://doi.org/10.1186/s12909-022-03812-x
Minja, I. K., & Lwoga, E. T. (2021). Evidence based dentistry among dentists in low- and middle-income countries: A systematic review. The East African Health Research Journal, 5(2), 129–136. https://doi.org/10.24248/eahrj.v5i2.662
Young, T., Rohwer, A., Volmink, J., & Clarke, M. (2014). What are the effects of teaching evidence-based health care (EBHC)? Overview of systematic reviews. PLOS ONE, 9(1), e86706. https://doi.org/10.1371/journal.pone.0086706
*Dani R Firman
Jalan Sekeloa Selatan I,
Kota Bandung, Jawa Barat 40132,
Indonesia
+62222534985
Email: dani.firman@unpad.ac.id / d.r.firman@lumc.nl
Submitted: 6 November 2024
Accepted: 11 April 2025
Published online: 1 July, TAPS 2025, 10(3), 58-64
https://doi.org/10.29060/TAPS.2025-10-3/OA3567
Nathania Nishida Tan1, Daniel Ardian Soeselo2,3, Natalia Puspadewi2, V. Dwi Jani Juliawati2 & Gisella Anastasia2
1Faculty of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, Indonesia; 2Medical Education Unit and 3Department of Surgery, Faculty of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, Indonesia
Abstract
Introduction: Career selection is a critical decision influenced by various factors, including media exposure. As a popular genre among adolescents, medical dramas may shape perceptions of the medical profession. This study explores the impact of medical dramas on medical students’ motivation to pursue a career in medicine.
Methods: This study was conducted at the School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, between February and March 2024, using a mixed-method approach. Quantitative data were gathered through a questionnaire, followed by qualitative insights from in-depth interviews. A two-stage sampling strategy was employed, initially identifying first-year students influenced by medical dramas through screening, followed by purposive sampling to select participants for in-depth interviews.
Results: Analysis identified six key motivational aspects through which medical dramas influence students’ decision to pursue medicine. These include the detailed portrayal of doctors’ roles, their daily lives, and the reinforcement of a positive perception of the profession. Notably, emotional engagement- such as inspiring doctor characters- and the realistic depiction of challenges, including the dedication and hardships of becoming a doctor, emerged as significant factors.
Conclusion: Medical dramas play a significant role in shaping students’ motivation and perception of the medical profession. This study highlights six key motivational aspects influencing career decisions, offering new insights into media-driven career choices and their potential implications for medical education.
Keywords: Medical Dramas, Medical Education, Medical Students, Student Motivation, Career Choice
Practice Highlights
- Medical dramas serve as informal educational tools through entertainment for the public.
- Television influences adolescents’ career aspirations by shaping their interests.
- Medical dramas shape public perceptions of the medical profession and may inspire viewers.
I. INTRODUCTION
Medical dramas have remained a widely popular television genre since their emergence in the 1960s, continuously evolving to portray healthcare professionals’ professional and personal lives within hospital settings (14th Media Mutations International Conference, 2023; Sonego & Rocchi, 2024).
Communication theorist Marshall McLuhan had predicted the success of medical dramas as early as 1964 in his book Understanding Media: The Extensions of Man, attributing their appeal to the immersive experience viewers have when witnessing medical procedures, which fosters an “obsession with bodily well-being” (Aboud, 2012; Levine & McLuhan, 1964).
Beyond entertainment, medical dramas serve as informal educational tools illustrating medical practices, bioethical dilemmas, and professional conduct (Cambra-Badii et al., 2021; Zago et al., 2024). Research suggests that these dramas reinforce key principles of medical ethics and professionalism, including communication skills, patient confidentiality, and empathetic bedside manner (Aboud, 2012). By portraying both the challenges and rewards of medical practice, these narratives may also shape viewers’ perceptions of the profession, inspiring people to pursue careers in healthcare (Alahmari, 2023).
Research indicates a correlation between specific television programs and career aspirations, suggesting that the content adolescents consume can shape vocational interests and goals (Gehrau et al., 2016). As an accessible informal educational resource, television provides insight into professional responsibilities and challenges (Mendick & Williams, 2022). Within this context, medical dramas may play a significant role in shaping students’ motivation to enter the medical field. Unlike prior studies that broadly examine media influence over career perceptions, this study focuses on first-year medical students, analysing their motivational drive. By integrating quantitative and qualitative data, this study provides deeper insight into how medical dramas influence medical students’ motivation to pursue a career in medicine.
II. METHODS
This study was conducted at the School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, from February to March 2024, using a mixed-method approach. A two-stage sampling method was employed, beginning with a questionnaire to identify eligible participants, followed by purposive sampling to select individuals for in-depth interviews. The target population consisted of first-year medical students enrolled in the 2023 academic year who acknowledged that medical dramas had influenced their motivation to pursue a medical degree.
A. Participant Selection
Out of 210 first-year students, 114 reported watching medical dramas. These students completed a demographic questionnaire, which gathered information on gender, parents’ profession, and their viewing habits related to medical dramas. Additionally, they completed the Strength of Motivation for Medical School Revised (SMMS-R) Questionnaire, a validated self-report instrument consisting of 15 items rated on a 5-point Likert scale (ranging from “strongly disagree” to “strongly agree”), with possible scores ranging from 15 to 75, indicating the strength of motivation for medical school.
B. Qualitative Phase Sampling
Purposive sampling was used to ensure an accurate representation of the study population based on key demographic factors, specifically the profession of participants’ parents. The selection process identified respondents from diverse parental backgrounds in the medical field: those with both parents as physicians, those with one parent in medicine, and those with no parental medical background. To ensure gender diversity, one male and one female were selected from each category, all of whom had high motivation scores based on their SMMS-R results. Six participants were selected to achieve thematic saturation, as preliminary analysis showed no new themes emerging beyond this point. Although not statistically representative, this sample captures diverse perspectives on medical career motivation based on different childhood backgrounds.
C. Data Collection
The in-depth interviews, conducted by the researcher (NNT), explored participants’ perceptions of how medical dramas influenced their motivation to pursue a career in medicine. The interview guide addressed various aspects of this influence on their decision-making process. One key question asked was “How have medical dramas influenced your decision to pursue medicine?” All participants provided written informed consent, including permission for audio recording. The interviews were then transcribed verbatim for further analysis.
D. Data Analysis
The transcribed interviews were analysed using thematic analysis with an inductive coding approach, facilitated by Atlas.Ti software. Initial coding was conducted by NNT, who identified key patterns and concepts. These were then systematically categorised into themes and subthemes to capture broader meanings and insights emerging from the interviews. To ensure coding reliability, DAS and NP reviewed the preliminary codes and analysis results. Through thorough discussions and iterative revisions, the team resolved discrepancies and achieved near-total agreement on the coding structure. To maintain participant confidentiality, each transcript was assigned a unique identification code.
III. RESULTS
A total of 114 respondents participated in this study, consisting of 26 males and 88 females, reflecting a possible gender disparity in medical drama viewership. Among them, 93 students (81.6%) reported that medical dramas significantly impacted their decision to pursue a medical career, while 21 students indicated no such impact.
|
Characteristic |
Respondents (n) |
Percentage (%) |
|
|
Parental Background |
|
|
|
|
|
Both parents are doctors |
8 |
7.0 |
|
|
Only one parent is a doctor |
18 |
15.8 |
|
|
Neither parent is a doctor |
88 |
77.2 |
|
|
|
||
|
Reports Motivation to Enter Medical Field Due to Medical Dramas |
|||
|
|
Yes |
93 |
81.6 |
|
|
No |
21 |
18.4 |
|
|
Total Respondents |
114 |
100.0 |
Table 1. Distribution of Respondent Demographic Characteristics
A. Various Dimensions of the Impact of Medical Dramas on Motivation
The following table presents the themes and subthemes derived from the in-depth interview analysis, which has been discussed and approved by each inter-rater.
|
No. |
Theme |
Subtheme |
|
1. |
Medical dramas provide an in-depth portrayal of the roles and responsibilities of doctors. |
Medical dramas shape public perceptions of the medical profession and doctors’ roles. |
|
Medical dramas depict the challenges and rewards of doctors’ daily work. |
||
|
Medical dramas highlight doctors’ lives beyond their profession. |
||
|
2. |
Medical dramas depict both the professional and personal aspects of doctors’ lives. |
Medical dramas reveal lesser-known aspects of doctors’ personal experiences. |
|
Medical dramas provide an authentic portrayal of doctors’ daily lives. |
||
|
Medical dramas depict ethical dilemmas, emphasising doctors’ professional integrity. |
||
|
3. |
Medical dramas contribute to a positive public perception of the medical profession. |
Medical dramas portray impressive doctors, evoking admiration, and inspiration in viewers. |
|
Doctors’ life-saving actions in medical dramas evoke deep emotions and motivation. |
||
|
Medical dramas illustrate doctors’ perseverance and resilience in their profession. |
||
|
Medical dramas spark curiosity about medical procedures and treatments. |
||
|
4. |
Medical dramas evoke emotional responses that may inspire viewers to pursue a medical career. |
Medical dramas evoke empathy by portraying patients in distress. |
|
5. |
Medical dramas showcase inspiring doctor characters, motivating viewers to follow in their footsteps. |
|
|
6. |
Medical dramas illustrate the challenges and dedication required to become a doctor. |
|
Table 2. Table of Themes and Subthemes
B. Medical Dramas Provide an In-Depth Portrayal of the Roles and Responsibilities of Doctors
Medical dramas frequently portray various medical scenarios using specialised terminology, offering viewers insight into the daily responsibilities of doctors. As medical settings are generally inaccessible to the public, these dramas provide a unique perspective on the profession. Among the key influences explored in this study, this aspect resonated most with respondents, with four out of six students emphasising its significance.
One participant explained how watching medical dramas sparked their interest in the field, as they previously had limited information about medicine.
“Grey’s Anatomy offered me insight into the medical field and sparked my interest, as reliable information is not easily accessible to those outside the profession” (V1_H3_B19)
Another respondent shared how their perception of doctors shifted from fear to admiration after watching medical dramas, recognising the profession’s vital role in society:
“As a child, I perceived doctors as intimidating due to painful medical visits, such as dental appointments. However, after watching Grey’s Anatomy, I realised that medicine extends beyond that and saw how doctors can positively impact many lives.” (V1_H2_B27)
Beyond hospital settings, medical dramas also depict the role of doctors in broader societal contexts. Through diverse narratives, these dramas offer multiple perspectives on the medical profession. For example, Doc Martin illustrates the role of a doctor in a rural community, showcasing their involvement in local issues, such as water problems and education (V2_H4_B21). This highlights how doctors contribute beyond clinical practice, reinforcing their role in public health and community development.
Additionally, medical dramas influence students’ motivation to pursue medicine by portraying the realities of medical work, including complex procedures and life-saving interventions. More than half of the respondents identified this as a significant factor in their decision to study medicine. As one participant stated:
“The scenes depicting doctors helping others, particularly during surgeries, inspired me to study medicine. I wanted to experience performing surgeries and learn how to help others.” (V4_H7_B19)
These findings suggest that medical dramas not only enhance public understanding of the profession but also play a role in inspiring future medical students.
C. Medical Dramas Depict Both the Professional and Personal Aspects of Doctors’ Lives
Medical dramas depict not only medical procedures but also the personal lives of doctors, including their relationships, friendships, and personal struggles. By presenting doctors as multidimensional individuals beyond their professional roles, these narratives contribute to a more relatable and humanised portrayal of the profession. Notably, four out of six highlighted the importance of this aspect in shaping their motivation. One respondent noted that their interest in medical dramas stemmed primarily from the blend of romantic elements, rather than the medical content alone (V3_H6_B1).
The public often has limited insight into the personal experiences of doctors, making it difficult to relate to them. However, medical dramas help bridge this gap by shedding light on aspects of doctors’ lives that are not commonly shared. This increased visibility fosters a sense of closeness and enhances a deeper understanding of the profession, which may, in turn, inspire career interest. As one participant expressed:
“Medical dramas reveal stories that doctors seldom share, providing an effective way to convey these experiences to the general public.” (V5_H11_B4)
By offering a representation of doctors’ daily lives, medical dramas provide viewers with a deeper understanding of what a career in medicine entails. This additional perspective can be a key factor in the decision-making process for those considering entering the field (V2_H4_B28).
D. Medical Dramas Contribute to a Positive Public Perception of the Medical Profession
Three out of six respondents emphasised that medical dramas portray the ethical dilemmas faced by doctors, reinforcing professional values that shape viewers’ perceptions of the medical field. One respondent noted that the depiction of doctors’ strong work ethic in these dramas increased their interest in pursuing a career in medicine (V3_H6_B4).
Additionally, medical dramas present compelling and admirable doctor characters, which can serve as a source of inspiration for viewers. As one respondent shared:
“The dramatised portrayal made it inspiring for my younger self, leading me to think, ‘Doctors are cool.’” (V5_H11_B2)
The depiction of medical procedures, particularly surgeries, also left a strong impression on some respondents, reinforcing their motivation to enter the medical field. One participant stated:
“Medical dramas provide insight into a doctor’s work, including various surgeries, highlighting the fascinating ability to help many people.” (V4_H7_B33)
Furthermore, the portrayal of doctors saving lives in medical dramas can evoke strong emotional responses, fostering admiration and a desire to pursue medicine. One respondent expressed how these scenes encouraged them to consider a career in medicine (V5_H11_B2). Medical dramas also emphasise the perseverance and resilience of doctors in the face of various pressures and stress, further reinforcing the appeal of the profession for aspiring medical students (V5_H9_B11).
E. Medical Dramas Evoke Emotional Responses that may Inspire Viewers to Pursue a Medical Career
Medical dramas can spark viewers’ curiosity about medical procedures, motivating them to explore the medical field further and increase their interest in the profession. One respondent noted that medical dramas played a role in their initial motivation for pursuing medicine, as the cases depicted often align with real-world medical scenarios, piquing their interest to learn more:
“I believe the medical procedures shown in Grey’s Anatomy exist in real life and are up to date. For example, an episode featured an abdominal wall transplant, which piqued my curiosity. After researching it, I discovered that the procedure had only recently been developed, showing how the show connects to world medicine.” (V1_H2_B14)
Beyond fostering curiosity, medical dramas also evoke strong emotional responses, such as sadness and empathy, particularly when portraying patients in need of medical care. One respondent shared that such portrayals heightened their awareness of the number of people requiring medical assistance. The emotions they experienced, combined with this awareness, ultimately served as an inspiration to pursue medicine (V1_H2_B31).
F. Medical Dramas Showcase Inspiring Doctor Characters, Motivating Viewers to Follow in their Footsteps
Medical dramas can inspire viewers through uplifting scenes and compelling portrayals of doctor characters. These representations serve as role models, fostering admiration and desire to follow in their footsteps. Notably, three out of six respondents indicated that such portrayals influenced their decision to pursue a medical career. As one participant shared:
“In ‘New Amsterdam’, there is a doctor who stands out from others – someone who wants to create change and has a unique vision. I found him quite inspiring.” (V3_H6_B5)
G. Medical Dramas Illustrate the Challenges and Dedication Required to Become a Doctor
Medical dramas not only portray the professional responsibilities of doctors but also illustrate the journey of becoming one, highlighting the challenges and obstacles along the way. Two out of six students emphasised the significance of this theme, noting that the depiction of medical interns’ experience in these dramas played a crucial role in their motivation to pursue medicine. As one participant shared:
“Medical dramas often depict doctors under immense stress, highlighting the challenges of the profession. However, rather than discouraging me, witnessing their struggles made the career even more appealing.” (V5_H10_B28)
IV. DISCUSSION
The in-depth interviews revealed that medical students felt more mentally prepared and motivated to pursue medicine after watching medical dramas. These shows provided insight into both the professional and personal lives of doctors, reinforcing previous studies on their educational influence in shaping viewers’ perceptions of the medical field. This aligns with the Media Effect Theory, introduced by Gerbner in 1960, which suggests that television shapes individuals’ perceptions of reality, particularly among frequent viewers (Stacks et al., 2015). Hoffman and colleagues further applied this theory to medical dramas, highlighting their role in influencing viewers’ perception of the medical profession (Arias, 2018).
Beyond depicting technical medical procedures, medical dramas also emphasise ethical principles and professional values, contributing to a favourable image of the profession. Research indicates that medical and nursing students often use these shows as supplementary learning tools for bioethics and professionalism (Cambra-Badii et al., 2021). Similarly, these portrayals may inspire high school students to consider careers in medicine by offering an engaging introduction to the field.
Emotional engagement is another key factor in the influence of medical dramas. Strong emotional responses- such as curiosity, empathy, and excitement- can enhance motivation, as emotions play a crucial role in learning, achievement, and psychological well-being, particularly in adolescents (Pekrun, 2017). Positive emotions make tasks more appealing, fostering inner motivation that arises after the initial external excitement provided by medical dramas (Legault, 2016).
Furthermore, medical dramas often depict the challenges of medical training, including long working hours and emotional strain, providing a more nuanced perspective on the profession. While these portrayals may initially present an idealised view of medicine, they also serve as a reality check, reinforcing the dedication required to pursue a medical career. This dual representation may deter less committed individuals while strengthening the resolve of those deeply passionate about the field (Tedeschi, 2024).
However, the potential for misinformation in medical dramas must also be considered. The oversimplifications or dramatisation of medical practice may create discrepancies between fictional portrayals and real-world medicine, leading to misconceptions among viewers (Alismail et al., 2018). One notable bias is the tendency to depict doctors as infallible heroes performing miraculous saves amidst dramatic emergencies, often intertwined with personal achievements and romantic subplots. This portrayal fosters unrealistic expectations, potentially leading to disillusionment when aspiring medical students encounter the demanding and less glamorous realities of medical education and practice (Tedeschi, 2024).
These findings highlight the complex role of medical dramas in shaping career motivation, offering both inspiration and potential misconceptions. Their influence appears particularly significant for students without a familial background in medicine, as most respondents came from non-medical families. This trend may suggest that medical dramas serve as an accessible source of insight into the profession for those without direct exposure. However, the possibility of sampling bias should be considered, as students already interested in medicine may be more likely to engage in medical dramas. While these dramas may serve as informal educational tools, their impact should be critically assessed to ensure they provide a balanced and realistic portrayal of the medical profession.
V. CONCLUSION
Medical dramas play a significant role in shaping students’ motivation to pursue a medical career by providing an engaging portrayal of the profession. These shows offer insight into the roles and responsibilities of doctors, their daily challenges, and the emotional rewards of the profession. Additionally, they influence public perceptions of medicine and evoke strong emotional responses through inspiring characters and narratives. By depicting both the struggles and triumphs of medical training, medical dramas contribute to students’ understanding of the dedication required to become a doctor. This study highlights six key aspects through which medical dramas impact students’ decision to pursue medical education, highlighting their role as both an informational and motivational tool.
Notes on Contributors
Nathania Nishida Tan participated in data collection, data analysis, review, the writing of the paper, and the formatting for publication.
dr. Daniel Ardian Soeselo, Sp.B, MSi.Med. participated in the data analysis, review, and direction of the paper.
dr. Natalia Puspadewi, M.Med.Ed, Ph.D participated in the data analysis, review, and direction of the paper.
dr. Gisella Anastasia, MHPE participated in the review of the paper.
dr. V. Dwi Jani Juliawati, M.PD, Sp.KKLP participated in the review of the paper.
Ethical Approval
This study received ethical clearance from the Research Ethics Commission of the Faculty of Medicine and Health Sciences Atma Jaya Catholic University of Indonesia under the ethical approval code 13/02/KEP-FKIKUAJ/2024. To ensure confidentiality and data security, all interview transcripts were anonymised and securely stored in password-protected files, accessible only to the research team.
Data Availability
The data of this qualitative study are not publicly available due to confidentiality agreements with the participants.
Acknowledgement
The authors would like to thank all the students who participated in this study.
Funding
There was no funding for this article.
Declaration of Interest
The authors have no conflicts of interest in connection with this article.
References
Aboud, K. A. (2012). Medical dramas – The pros and the cons. Dermatology Practical & Conceptual, 2(1), 75–77. https://doi.org/10.5826/dpc.0201a14
Alahmari, A. A. (2023). Professionalism, ethics, and realism of television medical dramas as perceived by Saudi medical students. Journal of Medical Education and Curricular Development, 10. https://doi.org/10.1177/23821205231175037
Alismail, A., Meyer, N. C., Almutairi, W., & Daher, N. S. (2018). CPR in medical TV shows: Non-health care student perspective. Advances in Medical Education and Practice, 9, 85–91. https://doi.org/10.2147/AMEP.S146149
Arias, E. (2018). How does media influence social norms? Experimental evidence on the role of common knowledge. Political Science Research and Methods, 7(3), 561–578. https://doi.org/10.1017/psrm.2018.1
Cambra-Badii, I., Moyano, E., Ortega, I., Baños, J., & Sentí, M. (2021). TV medical dramas: Health sciences students’ viewing habits and potential for teaching issues related to bioethics and professionalism. BMC Medical Education, 21, Article 509. https://doi.org/10.1186/s12909-021-02947-7
Gehrau, V., Brüggemann, T., & Handrup, J. (2016). Media and occupational aspirations: The effect of television on career aspirations of adolescents. Journal of Broadcasting & Electronic Media, 60(3), 465–483. https://doi.org/10.1080/08838151.2016.1203319
14th Media Mutations International Conference. (2023). Investigating medical drama TV series: Approaches and perspectives.
Legault, L. (2016). Intrinsic and extrinsic motivation. Springer eBooks. https://doi.org/10.1007/978-3-319-28099-8_1139-1
Levine, S., & McLuhan, M. (1964). Understanding media: The extensions of man. American Quarterly, 16(4), 646. https://doi.org/10.2307/2711172
Mendick, H., & Williams, K. (2022). Does television influence young people’s career choices? Journal of the National Institute for Career Education and Counselling, 21(1), 18–22. https://doi.org/10.20856/jnicec.2103
Pekrun, R. (2017). Emotion and achievement during adolescence. Child Development Perspectives, 11(3), 215–221. https://doi.org/10.1111/cdep.12237
Sonego, A., & Rocchi, M. (2024). Medical drama TV series: A semi-systematic literature review. Online Journal of Communication and Media Technologies, 14(4), Article e202459. https://doi.org/10.30935/ojcmt/15268
Stacks, D. W., Li, Z. C., & Spaulding, C. (2015). Media effects. Elsevier eBooks. https://doi.org/10.1016/B978-0-08-0970868.95045-1
Tedeschi, R. (2024). The paradox of medical dramas: Global aspirations versus realities. BJPsych Advances, 31(1), 62–64. https://doi.org/10.1192/bja.2024.56
Zago, D., Cautero, P., Scarpis, E., Pompili, E., Voglino, G., Siliquini, R., Brusaferro, S., & Brunelli, L. (2024). TV medical dramas: Assessing the portrayal of public health in primetime. Frontiers in Public Health, 12. https://doi.org/10.3389/fpubh.2024.1432528
*Daniel Ardian Soeselo
Medical Education Unit and Department of Surgery,
Faculty of Medicine and Health Sciences,
Atma Jaya Catholic University of Indonesia
Jl. Pluit Raya No.2 21, RT.21/RW.8,
Penjaringan, Kec. Penjaringan, Jakarta Utara,
Daerah Khusus Ibukota Jakarta, Indonesia 14440
Email: daniel.ardian@atmajaya.ac.id
Submitted: 16 August 2024
Accepted: 23 December 2024
Published online: 1 July, TAPS 2025, 10(3), 49-57
https://doi.org/10.29060/TAPS.2025-10-3/OA3495
Shuh Shing Lee1, Shefaly Shorey2, Tang Ching Lau3 & Dujeepa D. Samarasekera1
1Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Alice Lee Centre for Nursing Studies, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 3Dean’s Office, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: Numerous studies have been conducted on COVID-19, with the majority focusing on interventions involving students and teachers. However, limited research has delved into the pandemic’s impact on the wellness of various stakeholders and how they have adapted to the challenges it presented. This study aims to fill this gap by exploring these neglected areas.
Methods: This study employs a sequential mixed-method approach to study these areas. The quantitative data collection was carried out using a combination of validated surveys (ranging between 63-88 items) for students, faculty and administrators. Subsequently, qualitative data collection was gathered via semi-structured interview using a convenient sampling method.
Results: Seventeen faculty, 18 administrators and 369 students responded to the survey. The quantitative data indicated faculty (teachers) exhibited the lowest stress levels and the highest resilience during the pandemic. In comparison, administrators and students experienced moderate levels of stress, with students scoring slightly higher on the stress level. The themes that emerged from the qualitative data were personal endurance, emotional reaction, cognitive-behavioural reaction and social support.
Conclusion: Our study highlighted that, apart from personal endurance, the tension arises from emotional and cognitive-behavioural responses of students, teachers, and administrators can be mitigated based on the presence or absence of support mechanisms.
Keywords: Wellbeing, Change, Stakeholders, Educational Environment, Culture
Practice Highlights
- Students experienced the highest stress levels compared to administrators and teachers.
- However, students and administrators demonstrated resilience, bouncing back quickly after challenging times.
- Students and administrators tolerated for uncertainty and displayed cognitive flexibility to enable them to adapt and seek opportunities.
- Teachers and administrators initially experienced negative emotions, but their emotional resilience facilitated quick recovery.
- Coming from a culture emphasising collectivism, the sense of belonging and social connection served as a protective factor against psychological distress.
I. INTRODUCTION
The foundation of any education system rests upon the harmonious collaboration of three essential elements: teachers, students, and administrators. Each of these components play a vital role in ensuring the smooth functioning of the educational ecosystem and this symbiotic relationship becomes even more evident during challenging times, such as the COVID-19 pandemic. Together, they navigated the complexities of remote learning, ensuring that the pursuit of knowledge remained uninterrupted. In essence, it is the collaborative synergy of these three integral components that propels the educational journey forward. The strength of an education system lies in the seamless interplay of these elements, fostering a holistic and empowering learning experience for all.
Nevertheless, numerous studies have studied the impact of pandemic such as SARS, COVID-19, with a predominant focus on students and teachers. A significant portion of these studies, approximately 50%, has highlighted the insights and innovations from health professions educators in response to the pandemic, particularly at the undergraduate level (Daniel et al., 2021; Eva & Anderson, 2020; Gordon et al., 2020). The majority of these investigations have primarily collected data on student reactions, satisfaction levels, shifts in attitudes, and changes in knowledge and skills. The review conducted by Best Evidence Medical Education (BEME) revealed that almost half of the studies centred on the transition from traditional in-person teaching to online education, only a meagre 6% of the research primarily focused on aspects related to well-being, mental health, or learner support (Daniel et al., 2021). Amid the widespread concern about the well-being of individuals during the pandemic, much attention has been given to medical students (Jia et al., 2022; Paz et al., 2022; Wilcha, 2020) and frontline healthcare workers (Danet, 2021; Muller et al., 2020; Xiong et al., 2022) in the published articles. The reactions of teachers and administrators to the changes brought about by the pandemic, and how these changes have impacted their well-being, have been largely overlooked in the existing literature.
Hence, the principal objective of this research is to investigate the impact of the initiatives implemented during the pandemic on the well-being of students, teachers, and administrators. This study aims to explore how these key stakeholders reacted and adapted to the changes, shedding light on a vital aspect that has been underrepresented in the current body of literature.
II. METHODS
We employed a sequential explanatory mixed-methods design to assess the adaptation and impact of the pandemic on the well-being of administrators, teachers, and students within the specific context of the Yong Loo Lin School of Medicine (YLLSoM) at the National University of Singapore. This design involved collecting and analysing both quantitative and qualitative data in two consecutive phases within a single study. In the quantitative phase, data were gathered through a comprehensive survey/questionnaire, allowing us to capture a broad spectrum of responses from the participants. Subsequently, in the qualitative phase, we employed the phenomenological approach, conducting in-depth interviews with participants representing various categories. Phenomenology, as an approach in qualitative research, enables us to delve deeply into the shared experiences within a specific group. The primary objective of this approach is to develop a detailed description of the nature of the phenomenon under investigation (Creswell, 2013). The details of this methodological approach are elaborated in the subsequent sections.
A. Phase I Quantitative Data Collection
The quantitative data collection was carried out using a survey. The survey was adapted from Landis’s and Bradley’s (2003) work on The Impact of the 2003 SARS Outbreak on Medical Students at the University of Toronto, The Brief Resilience Scale (Smith et al., 2008), Perceived Stress Scale (Cohen et al., 1983) and Teachers’/Students’ Self-Efficacy towards Technology Integration (Kiili et al., 2016). Table 1 shows the sections of the surveys for administrators, teachers and students.
|
Section |
Items in each section |
||
|
Student |
Teacher |
Administrator |
|
|
A: Demographic Information |
5 |
8 |
7 |
|
B: The psychological impact of COVID-19 |
7 |
||
|
C: Perception of medical students on the restriction of clinical activities and the impact of COVID-19 on their medical/nursing education |
15 (13 5-point likert scale items & 2 open-ended questions) |
2 (open-ended questions) |
2 (open-ended questions) |
|
D: Perceived quality of information received by respondents about COVID-19 from specific groups |
8 |
||
|
E: The source and level of psycho-social support that medical students rely on during the COVID-19 outbreak |
26 |
19 |
|
|
F: Brief Resilience Scale |
6 |
||
|
G: Perceived Stress Scale |
10 |
||
|
H: Teachers’/Students’ Self-Efficacy towards Technology Integration |
11 |
4 |
|
|
Total Items |
88 |
71 |
63 |
Table 1. Sections of the Surveys for Administrators, Teachers and Students
The survey was validated by 10 medical educators from various departments (Paediatrics, Surgery, Centre for Medical Education, Nursing). After the validation, the survey was administered to medical (Year 1 – 5) and nursing (Year 1 – 4) students, administrators and faculty members in Yong Loo Lin School of Medicine and Alice Lee Centre for Nursing Studies using convenient sampling. It took about 20-30 minutes to complete the survey and the data was collected between Jan – June 2021.
B. Phase II Qualitative Data Collection
The qualitative data collection was gathered via semi-structured interview. The interview was conducted for about 60-90 minutes among the medical/nursing students, administrators and faculty members (teachers). Followed up from the data collected from the quantitative data, the questions were revolved around teaching and learning, content, assessment, policies, guidelines, communication, environment (safety)/support and wellness.
From July 2021 – Nov 2022, we used convenient sampling method to recruit of students, administrators and faculty members. The interviews were carried out by 2 trained interviewers with no power relationship with the interviewees. Interviews were carried out after getting consent from the volunteer interviewees. All digital audio recordings made during the interviews were transcribed and member-checked with the interviewees to ensure transparency and trustworthiness of the data.
Data collection ceased when the data reached saturation stage.
C. Data Analysis
The quantitative data was analysed using descriptive statistics (such as mean, frequency and percentage) using Microsoft Excel for the data collected from students, administrators and teachers.
The interviews were thematically analysed by 2 researchers in the team. The two researchers coded the transcripts independently and came together to resolve any discrepancy or disagreement on the coding. Subsequently, they continued to code and form categories and eventually themes. There were multiple discussions that took place among the researchers and the team before the themes were crystalised.
III. RESULTS
A. Phase I Quantitative Data
The demographic information was illustrated in Table 2. Majority of the participants were not quarantined during the pandemic and more than 80% of them did not have a family member tested positive for COVID when this study was conducted. The teachers from the school of medicine were mainly from Family Medicine, Paediatrics, Physiology, Pathology, Public Health, Medicine, Anatomy and Anaesthesia departments. They are educators for postgraduate and undergraduate students. As for administrators, their roles in the departments are educational related such as instructional design, learning analytics, planning and execution of education, managing project and training.
|
|
|
|
Teachers |
Administrators |
Students |
|||
|
0 |
Finished |
Completed |
17 |
65.4% |
18 |
54.5% |
369 |
73.8% |
|
Did not complete |
9 |
34.6% |
15 |
45.5% |
131 |
26.2% |
||
|
Total Responses |
26 |
33 |
|
500 |
|
|||
|
1 |
Faculty |
Medicine |
12 |
70.6% |
16 |
88.9% |
305 |
83.0% |
|
Nursing |
5 |
29.4% |
2 |
11.1% |
64 |
17.0% |
||
|
2 |
Gender |
Male |
6 |
35.3% |
3 |
16.7% |
140 |
37.9% |
|
Female |
11 |
64.7% |
15 |
83.3% |
229 |
62.1% |
||
|
6 |
Living arrangement |
Alone |
1 |
5.9% |
1 |
5.6% |
17 |
4.6% |
|
With Parents |
2 |
11.8% |
7 |
38.9% |
338 |
91.6% |
||
|
With Partners (married, common-law, etc.) |
14 |
82.4% |
9 |
50.0% |
1 |
0.3% |
||
|
With Room-mates |
0 |
0.0% |
1 |
5.6% |
13 |
3.5% |
||
|
7 |
Status during COVID-19 Outbreak |
Non-Quarantined |
17 |
100.0% |
18 |
100.0% |
355 |
96.2% |
|
Quarantined |
0 |
0.0% |
0 |
0.0% |
7 |
1.9% |
||
|
Stay-Home-Notice (SHN) |
0 |
0.0% |
0 |
0.0% |
7 |
1.9% |
||
|
8 |
I have family member(s), relative or friend(s) who tested positive for COVID-19 |
Yes |
2 |
11.8% |
1 |
5.6% |
29 |
7.9% |
|
No |
15 |
88.2% |
17 |
94.4% |
340 |
92.1% |
||
Table 2. Demographic Information of the Respondents
For each section, the summary was illustrated in Table 3. The mean for different sections was quite close for the 3 groups. Likewise, the items that were scored low and high were quite similar for all the sections. For example, Section B The psychological impact of COVID-19, The sleep quality and concentration in all three groups were not affected by the pandemic, but they are more worries about their family members contracted with COVID-19.
|
Section |
Administrator |
Teacher |
Student |
|
B: The psychological impact of COVID-19 (7 items) |
Mean ranging between 2.39-3.67 |
Mean ranging between 1.71 – 3.29 |
Mean ranging between 2.14 – 3.85 |
|
C: Perception of medical students on the restriction of clinical activities and the impact of COVID-19 on their medical/nursing education (15 items) |
Mean ranging between 1.77 – 3.78 |
Not relevant |
|
|
D: Perceived quality of information received by respondents about COVID-19 from specific groups |
Mean ranging between 3.33 – 4.17 |
Mean ranging between 3.47 – 4.19 |
Mean ranging between 3.17 – 4.14
|
|
E: The source and level of psycho-social support that medical students rely on during the COVID-19 outbreak |
Mean ranging between 2.78 – 4.11 |
Mean ranging between 2.47 – 4.47 |
Mean ranging between 2.65 – 4.36
|
|
F: Brief Resilience Scale |
Mean 3.4 |
Mean 4.01 |
Mean 3.3 |
|
G: Perceived Stress Scale |
Mean: 16.6 (Moderately stress) |
Mean 11.7 (Low stress) |
Mean 18.7 (Moderately stress) |
|
H: Teachers’/Students’ Self-Efficacy towards Technology Integration |
Mean ranging between 3.83-4.06 |
Mean ranging between 3.47 – 4.12 |
Mean ranging between 3.68 – 4.22 |
Table 3. Summary of the Mean for Different Sections for the 3 Groups
During the pandemic, students expressed significant concerns about the adequacy of their training, particularly due to reduced patient contact, raising apprehensions about their preparedness for exams. This concern will be elaborated upon in the qualitative data section, shedding light on the depth of their worries. All three groups shared the view that information originating from the government and hospitals was the most reliable, with friends and family scoring the lowest mean among all sources. Despite this, the participants unanimously agreed that the support from friends and family, in terms of both source and level of assistance, was the most substantial. Conversely, organisational support from entities such as the University Wellness Centre, Dean’s office, community, and social media was perceived as unreliable and lacking during the pandemic.
Furthermore, our observations revealed that teachers exhibited the lowest stress levels and the highest resilience during the pandemic, showcasing their ability to cope effectively. In comparison, administrators and students experienced moderate levels of stress, with students scoring slightly higher on the Perceived Stress Scale. Although students acknowledged challenges, as indicated by their agreement with statements such as “I have a hard time making it through stressful events” (mean: 2.93), they also exhibited resilience, agreeing with the statement “I tend to bounce back quickly after hard times” (mean: 3.76). Additionally, concerning self-efficacy towards technology integration, students reported the highest mean score, indicating confidence in their ability to navigate various Internet applications. While teachers felt competent in using technology for teaching and learning, their confidence wavered when it came to resolving technical issues, as reflected in their mean score of 3.47. This nuanced understanding underscores the complex interplay of stress, resilience, and technological proficiency among the different groups during the challenging circumstances of the pandemic.
B. Phase II Qualitative Data
As for the qualitative data collection, we have recruited 7 administrators, 17 teachers (12 from Yong Loo Lin School of Medicine and 5 from Alice Lee Centre for Nursing Studies) and 9 undergraduate students (6 from Yong Loo Lin School of Medicine and 3 from Alice Lee Centre for Nursing Studies). The themes and subthemes that emerged were depicted in the Figure 1.
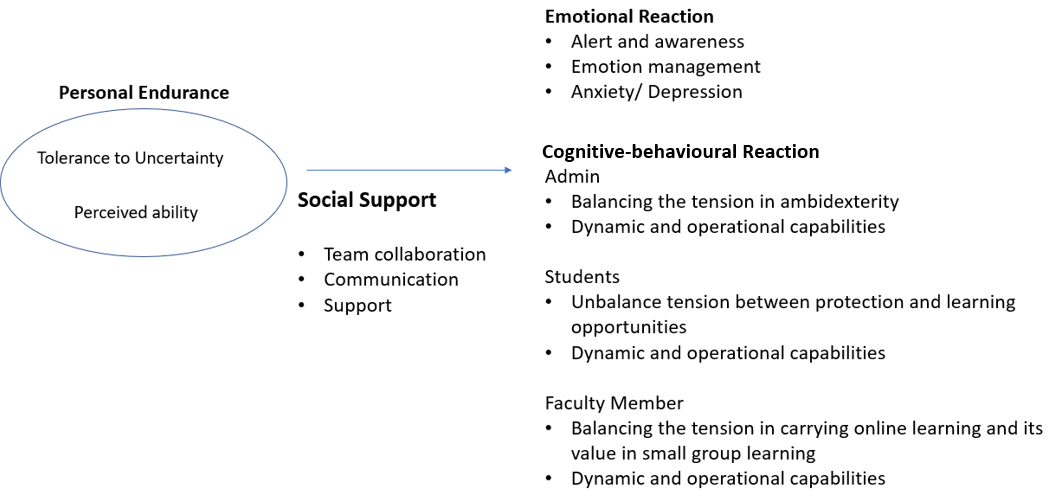
Figure 1. Themes and Subthemes of the Qualitative Data
1) Theme 1: Personal Endurance
Personal endurance depends on perceived ability and tolerance to uncertainty. For administrators, they felt that it was quite stressful and frustrated during the pandemic as the situation was unclear. However, they were able to manage and there was a sense of relief after they had gone through the critical phase.
“It was very intense, stressful but looking back now, it is not that bad. We have gone through the worse” (Admin 5)
While administrators’ contribution to the education system is crucial, some of the administrators perceived their contribution was minor as compared to medical front liner.
“We are not front liner, our contribution is limited.” (Admin 3)
Although the situation was stressful in the beginning, we noticed a positive endurance among the teachers and perceived the pandemic as an opportunity instead of a threat.
“Overall, I think the predominant mood was of a challenge that needs to be overcome and that brought a certain amount of excitement.” (Teacher 7)
On the other hand, the students felt that they were being too protected and perceived themselves as having the ability to manage the situation themselves.
“I understood that they wanted to protect us but I felt that eventually, they can’t protect us anymore” (Student 3)
The students also perceived that the teachers lacked ability in using technology in teaching and learning especially in remote learning.
“A lot of professors are not familiar with the technology.” (Student 5)
2) Theme 2: Emotional Reaction
There were a lot of negative emotions illustrated by the students, administrators and teachers due to various reasons. Students were worried, frustrated and anxious that they may not learn since the contact with the patients was less during the pandemic. Too much protection from the school and the system put in place has heightened these negative emotions.
“We feel quite unconfident because we feel we have not seen enough patients”/ “..fear that we are not as good as the previous batch” (Students 1 & 2)
Administrators were frustrated mainly because they need to manage the family and work at the same time when working from home system was implemented. However, some of them shared that they are able to regulate and get used to the situation after a while.
“Everybody was under pressure at that time…while I have to juggling with work, my kids were at home because school close.” (Admin 4)
“I usually regulate my own emotion.” (Admin 7)
While there were some positive emotions state in Theme 1 for teachers, they did feel stressful in the early stage of the pandemic due to the change of the approaches in teaching and learning and they are unsure of the outcomes when the teaching was entirely online.
“…stressful in the beginning… I even have nightmares…dreaming students get lost in the virtual room.” (Teacher 17)
“It was a bit stressful in the beginning because you did not know how is going to turn out…” (Teacher 5)
3) Theme 3: Cognitive-Behavioural Reaction
Amidst the challenges posed by the pandemic, administrators, students, and teachers made concerted efforts to adapt their cognition and behavior in response to various initiatives, including social distancing measures, reduced patient contact, and a shift to virtual teaching environments. Throughout this period, interviewees shared both positive and negative reactions to these changes.
Administrators and teachers found themselves navigating the delicate balance between the need to innovate and the need to maintain productivity (ambidexterity). Administrators, in particular, faced the challenge of fostering creativity in coordinating and delivering the curriculum, which involved tasks such as timetabling, resource management, and providing IT support for online learning. These adjustments were made within a short timeframe, reflecting their resilience and adaptability. However, amid these innovative efforts, administrators were also keen on upholding the quality of their work, highlighting the complexity of their role in managing these rapid changes.
“We have to deliver in a short time but also the content has to be rigorous” (Administrator 3)
Similarly, teachers tried to be creative in an online teaching environment and ensure the student learned at the same time especially in small group teaching. However, they find it challenging.
“…there is an urgency to find a way around this small group teaching…we kind of lose the whole power of collaboration.” (Teacher 5)
There is also a tension arose among the students for being too protected by the school and compromised with their learning as shared in the quotes below. This was repeatedly mentioned by the students, and they felt they have to face the situation eventually.
“I am not very interested in surgery, but this is like once in a lifetime and after I go out of medical school I won’t have the chance to see surgery” (Students 3)
“There’s a culture… in the society in general…protect my child from COVID. But once day we are going to deal with COVID” (Students 6)
Notwithstanding the aforementioned tensions, it’s worth noting that administrators, students, and teachers exhibited remarkable innovativeness and adaptability during the pandemic. All three groups demonstrated evidence of both Operational Capabilities, which encompass the efficient and effective use of resources, and Dynamic Capabilities, which involve the continuous development of competencies to align with the evolving environment.
With the predominant shift in communication from face-to-face to virtual platforms, administrators found themselves assuming the role of intermediaries responsible for conveying information to various stakeholders. In this new virtual setting, where body language cues were less apparent, administrators recognised the need to be more attuned and sensitive to subtle nuances in communication compared to traditional face-to-face interactions. This adaptation reflected their ability to pivot and operate effectively within the changing landscape of remote communication.
“We play the middleman role because we have to speak administrative language to certain people and be sensitive when communicate with faculty members” (Admin 3)
“We have to start thinking about (what kind of information needed) before the faculty member even ask those questions” (Admin 7)
Teachers utilised different resources to innovate in their teaching as well as learning from different others.
“I break it up my lectures into smaller bits and disperse it with PollEverywhere” (Teacher 5)
“We formed a group we called a brown bag meeting – basically we meet at lunchtime with technologically savvy administrators to introduce to the staff on how to make online learning more interactive.” (Teacher 10)
Likewise, since there was less patient contact time, students tried to make use of their time for other learning sessions.
“Since there’s little time in the hospital, I had read up a lot” (Students 1)
“It allows us to have some processing time and have time to consolidate our knowledge” (Students 5)
4) Theme 4: Social Support Mechanism
Social support mechanism has been mentioned by the 3 groups as one of the prominent mechanisms in adapting the changes during pandemic. It includes transparent communication, team collaboration and support from various stakeholders. For example, administrators shared that they all came together and supported each other during the hard times.
“All different teams come together, I think that was very precious” (Administrator 2)
Students sought seniors’ help to provide additional sessions to compensate their learning.
“What my group would do is we call our seniors to give us extra tutorials” (Student 2)
However, there was also lack of support mechanism brought up by the teachers which led to negative emotion (such as frustration).
“Educational technology team are overworked…if the school would really want to be the best or world class, I think we need a very good support from the IT.” (Teacher 9)
IV. DISCUSSION
The impact of the COVID-19 pandemic on both our educational systems and personal lives has been profound. This unprecedented disruption has been keenly observed by various stakeholders, including administrators, teachers, many of whom were also frontline workers, and students in medical schools. Swift adaptation to the ever-changing situation became imperative, particularly in response to the government’s new guidelines. The abrupt alterations in social interactions and extracurricular activities routines compelled a shift towards a heightened emphasis on family life, accompanied by the necessity to work and learn from home due to lockdown measures. These changes had profound physical and psychological effects on our lives.
Our study revealed that students experienced the highest stress levels compared to administrators and teachers, a finding consistent with previous research indicating that medical students often have higher baseline anxiety than their peers studying other disciplines (Dyrbye et al., 2006; Lasheras et al., 2020). Qualitative data highlighted that students’ stress levels were primarily attributed to the lack of patient contact and inadequate training, potentially impacting their future practice. Additionally, students expressed feelings overly protected due to initiatives like stay-at-home learning. The altered learning environment, combined with a lack of guidance on learning strategies and interpersonal relationships, left students vulnerable to intense emotional fluctuations and strained family relationships (Zhang et al., 2020). Similarly, for administrators, the shift to remote work and social isolation policies posed challenges in balancing work and family responsibilities, as evident from their qualitative comments.
However, students and administrators demonstrated resilience, bouncing back quickly after challenging times. According to Del Carmen Pérez Fuentes et al.’s (2020) Adaptability to Change framework, a sense of control, tolerance for uncertainty, and cognitive flexibility are crucial in coping with adverse situations. Despite feeling anxious and frustrated due to the inability to control the study-from-home or working-from-home policy, student and administrator tolerated for uncertainty and display cognitive flexibility to enable them to adapt and seek opportunities. Emotional resilience, the ability to generate positive emotions and recover swiftly from negative emotional experiences, played a pivotal role in psychological resilience (Zhang et al., 2020). This emotional resilience led to diverse emotional responses, influencing the cognitive processing of emotional information. Teachers and administrators initially experienced negative emotions, but their emotional resilience facilitated quick recovery, evident from their transcripts.
Emotional and cognitive-behavioural responses were further shaped by social support mechanisms within peer groups, colleagues, organisational leaders, and the government. While studies have shown that social media can heighten anxiety due to misinformation and distressing news (Gao et al., 2020), our research indicated that students, teachers, and administrators placed significant trust in information provided by the government and institutions. This trust in government intentions and capabilities fosters adherence to health regulations, essential in crisis management (Siegrist & Zingg, 2014).
Coming from a culture emphasising collectivism, our society values interdependence and family connections highly. This sense of belonging and social connection served as a protective factor against psychological distress, aligning with previous research findings (Xiao, 2021; Yu et al., 2020) . Conversely, a lack of social support within a collectivist culture, as reported by teachers and students, contributed to psychological distress. Our qualitative and quantitative data in this study support this observation, emphasising the significance of social support structures in mitigating the adverse effects of challenging circumstances. The importance of fostering a supportive environment, both within institutions and at a societal level, cannot be overstated in times of crisis.
V. LIMITATIONS
This study has some potential limitations. The study was carried out in a single medical school; hence, the results can only be transferable to the same context. The number of respondents was quite small (especially for nursing respondents) despite multiple reminders sent to the various groups. Therefore, they may not be representative of the entire student, teachers and administrator’s population. Third, the survey was a self-reported survey and may have inherent biases while answering the questions. While rigor is more challenging to achieve in qualitative data collection and analysis, the researchers adhere to the trustworthiness principles as much as possible in analysing and presenting the results in this paper.
VI. CONCLUSION
In conclusion, achieving wellness during a pandemic is indeed possible, but it hinges not only on the resources that organisations and governments can marshal but also on individual resilience in navigating uncertainty, cultural factors, trust, and support systems. Our study highlights the importance of familial and peer connections within our cultural context, underscoring how these bonds facilitate adaptation and innovation amid the challenges posed by the pandemic. The emotional and cognitive-behavioural responses of students, teachers, and administrators are depending on their personal endurance. However, the tension that arises in these individuals can be mitigated or exacerbated based on the presence or absence of adequate support mechanisms. Sufficient support can act as a buffer, helping individuals cope effectively with the challenges they face. Conversely, insufficient support can exacerbate stress and strain, hindering their ability to adapt and respond positively to the situation at hand.
Therefore, fostering a strong support network, both within organisations and communities, is crucial. This support not only alleviates the immediate challenges faced by individuals but also empowers them to build emotional resilience, enabling them to navigate uncertainties and adversities with greater ease. In this way, the collective endurance of individuals, coupled with robust support systems, becomes the cornerstone of achieving wellness and fostering positive responses in the face of a pandemic.
Notes on Contributors
DDS developed the research idea and design with SSL, SR & LTC. The data collection was performed by SSL. The data were analysed by SSL & DDS. DDS, SSL, SR & LTC performed the data interpretation. DDS, SSL & SR wrote the article with revision by LTC. All the authors read and agreed with the final manuscript.
Ethical Approval
Ethics approval was sought from the National University of Singapore (NUS) Institutional Review Board (NUS-IRB-2020-216). Written informed consent was obtained from all participants.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available as the participants of this study did not give written consent for their data to be shared publicly.
Acknowledgement
We would like to express our heartfelt gratitude to Jillian Yeo and Lilusha Kaludewa for helping in data collection and analysis.
Funding
No funding is available for this research.
Declaration of Interest
The authors report that there are no conflict of interests to declare.
References
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385. https://doi.org/10.2307/2136404
Creswell, J. W. (2013, January 1). Steps in conducting a scholarly mixed methods study [Slide show]. https://digitalcommons.unl.edu/cgi/viewcontent.cgi?article=1047&context=dberspeakers
Danet, A. D. (2021). Psychological impact of COVID-19 pandemic in Western frontline healthcare professionals. A systematic review. Medicina Clínica (English Edition), 156(9), 449–458. https://doi.org/10.1016/j.medcle.2020.11.003
Daniel, M., Gordon, M., Patricio, M., Hider, A., Pawlik, C., Bhagdev, R., Ahmad, S., Alston, S., Park, S., Pawlikowska, T., Rees, E., Doyle, A. J., Pammi, M., Thammasitboon, S., Haas, M., Peterson, W., Lew, M., Khamees, D., Spadafore, M., . . . Stojan, J. (2021). An update on developments in medical education in response to the COVID-19 pandemic: A BEME scoping review: BEME guide no. 64. Medical Teacher, 43(3), 253–271. https://doi.org/10.1080/0142159x.2020.1864310
Del Carmen Pérez-Fuentes, M., Del Mar Molero Jurado, M., Martínez, Á. M., Fernández-Martínez, E., Valenzuela, R. F., Herrera-Peco, I., Jiménez-Rodríguez, D., Mateo, I. M., García, A. S., Del Mar Simón Márquez, M., & Linares, J. J. G. (2020). Design and validation of the adaptation to change questionnaire: New realities in times of COVID-19. International Journal of Environmental Research and Public Health, 17(15), 5612. https://doi.org/10.3390/ijerph17155612
Dyrbye, L. N., Thomas, M. R., & Shanafelt, T. D. (2006). Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Academic Medicine, 81(4), 354–373. https://doi.org/10.1097/00001888-200604000-00009
Eva, K. W., & Anderson, M. B. (2020). Medical education adaptations: Really good stuff for educational transition during a pandemic. Medical Education, 54(6), 494. https://doi.org/10.1111/medu.14172
Gao, J., Zheng, P., Jia, Y., Chen, H., Mao, Y., Chen, S., Wang, Y., Fu, H., & Dai, J. (2020). Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE, 15(4), Article e0231924. https://doi.org/10.1371/journal.pone.0231924
Gordon, M., Patricio, M., Horne, L., Muston, A., Alston, S. R., Pammi, M., Thammasitboon, S., Park, S., Pawlikowska, T., Rees, E. L., Doyle, A. J., & Daniel, M. (2020). Developments in medical education in response to the COVID-19 pandemic: A rapid BEME systematic review: BEME guide no. 63. Medical Teacher, 42(11), 1202–1215. https://doi.org/10.1080/0142159x.2020.1807484
Jia, Q., Qu, Y., Sun, H., Huo, H., Yin, H., & You, D. (2022). Mental health among medical students during COVID-19: A systematic review and meta-analysis. Frontiers in Psychology, 13, Article 846789. https://doi.org/10.3389/fpsyg.2022.846789
Kiili, C., Kauppinen, M., Coiro, J., & Utriainen, J. (2016). Measuring and supporting pre-service teachers’ self-efficacy towards computers, teaching, and technology integration. The Journal of Technology and Teacher Education, 24(4), 443–469. https://jyx.jyu.fi/bitstream/123456789/53087/1/kiilikauppinencoiroutriainen.pdf
Lasheras, I., Gracia-García, P., Lipnicki, D., Bueno-Notivol, J., López-Antón, R., De La Cámara, C., Lobo, A., & Santabárbara, J. (2020). Prevalence of anxiety in medical students during the COVID-19 pandemic: A rapid systematic review with meta-analysis. International Journal of Environmental Research and Public Health, 17(18), 6603. https://doi.org/10.3390/ijerph17186603
Mark, L., & John, B. (2003). The impact of the 2003 SARS outbreak on medical students at the University of Toronto. University of Toronto Medical Journal, 82, 158–164. https://api.semanticscholar.org/CorpusID:59193656
Muller, A. E., Hafstad, E. V., Himmels, J. P. W., Smedslund, G., Flottorp, S., Stensland, S. Ø., Stroobants, S., Van De Velde, S., & Vist, G. E. (2020). The mental health impact of the COVID-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Research, 293, Article 113441. https://doi.org/10.1016/j.psychres.2020.113441
Paz, D. C., Bains, M. S., Zueger, M. L., Bandi, V. R., Kuo, V. Y., Cook, K., & Ryznar, R. (2022). COVID-19 and mental health: A systematic review of international medical student surveys. Frontiers in Psychology, 13, Article 1028559. https://doi.org/10.3389/fpsyg.2022.1028559
Siegrist, M., & Zingg, A. (2014). The role of public trust during pandemics. European Psychologist, 19(1), 23–32. https://doi.org/10.1027/1016-9040/a000169
Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The brief resilience scale: Assessing the ability to bounce back. International Journal of Behavioral Medicine, 15(3), 194–200. https://doi.org/10.1080/10705500802222972
Wilcha, R. (2020). Effectiveness of virtual medical teaching during the COVID-19 Crisis: Systematic review. JMIR Medical Education, 6(2), Article e20963. https://doi.org/10.2196/20963
Xiao, W. S. (2021). The role of Collectivism–Individualism in attitudes toward compliance and psychological responses during the COVID-19 Pandemic. Frontiers in Psychology, 12, Article 600826. https://doi.org/10.3389/fpsyg.2021.600826
Xiong, N., Fritzsche, K., Pan, Y., Löhlein, J., & Leonhart, R. (2022). The psychological impact of COVID-19 on Chinese healthcare workers: A systematic review and meta-analysis. Social Psychiatry and Psychiatric Epidemiology, 57(8), 1515–1529. https://doi.org/10.1007/s00127-022-02264-4
Yu, H., Li, M., Li, Z., Xiang, W., Yuan, Y., Liu, Y., Li, Z., & Xiong, Z. (2020). Coping style, social support and psychological distress in the general Chinese population in the early stages of the COVID-19 epidemic. BMC Psychiatry, 20, Article 426. https://doi.org/10.1186/s12888-020-02826-3
Zhang, Q., Zhou, L., & Xia, J. (2020). Impact of COVID-19 on emotional resilience and learning management of middle school students. Medical Science Monitor, 26, Article e924994. https://doi.org/10.12659/msm.924994
*Lee Shuh Shing
Centre for Medical Education,
Yong Loo Lin School of Medicine,
National University of Singapore, Singapore
10 Medical Dr, Singapore 117597
Email: medlss@nus.edu.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
