
Promoting medical students’ reflection through feedback interaction: The RAISE model
Submitted: 2 April 2024
Accepted: 12 September 2024
Published online: 7 January, TAPS 2025, 10(1), 27-35
https://doi.org/10.29060/TAPS.2025-10-1/OA3247
Estivana Felaza1, Ardi Findyartini1,2, Rita Mustika1, Jenny Bashiruddin1, Joedo Prihartono3, Lucia RM Royanto4 & Subha Ramani5
1Department of Medical Education, Faculty of Medicine Universitas Indonesia, Indonesia; 2Medical Education Centre, Indonesia Medical Education and Research Institute (IMERI), Faculty of Medicine Universitas Indonesia, Indonesia; 3Department of Public Health, Faculty of Medicine Universitas Indonesia, Indonesia; 4Faculty of Psychology Universitas Indonesia, Indonesia; 5Brigham Women and Child Hospital, Harvard Medical School, USA
Abstract
Introduction: Professional identity formation requires students’ ability to reflect, which can be supported by constructive feedback from teachers. Feedback practice faces many challenges, including those related to sociocultural aspects. Feedback can be optimised by implementing a model suitable to the attributes of students, teachers, and the clinical environment. This study aimed to develop a suitable feedback model and test its effectiveness in promoting reflection.
Methods: The model was designed based on the theoretical framework and identified feedback-related attributes in FMUI. Expert reviews and cognitive interviews were conducted before the model was tested. The model’s effectiveness was tested using a quasi-experimental design involving 74 students in the Paediatric Module. Students were asked to reflect on their mini-CEX experience after receiving feedback from teachers, and the depth of reflection was compared between students in the intervention and control group. The depth of reflection was measured using Kember scoring, and bivariate analysis was conducted using SPSS 20.0.
Results: The model consists of 5 steps including: Rapport building, Acknowledge students’ strengths, Identify aspect(s) that need improvement, Share teachers’ experiences, and Establish a plan to improve. Deep reflection was more frequently found in the intervention group. Mann-Whitney test showed that the difference between groups was statistically significant (Z=2.964, p=0.003), indicating that reflection in the intervention group was deeper than the control group.
Conclusion: The feedback model formulated based on feedback-related attributes in FMUI was named the RAISE model. Upon testing, students receiving the model could reflect more deeply compared to those receiving the standard model.
Keywords: Feedback, Clinical, Reflection, Sociocultural
Practice Highlights
- Constructive feedback is needed for medical students to optimally form their professional identity, especially in clinical settings
- The RAISE model which was developed based on feedback-related attributes can be implemented in clinical education
- The RAISE model consists of five steps: Building rapport, Acknowledge students’ strengths, Identify aspect(s) to improve, Share teachers’ experience, and Establish a plan to improve
- The RAISE model promotes students’ ability to reflect on their experiences
I. INTRODUCTION
Medical students’ professional identity is mostly formed during their clinical education (Cruess et al., 2015). Professional identity formation is a long and complex process that occurs through the integration of values and norms of the profession. Socio-constructivist theory can explain how learning occurs in clinical settings through the involvement of students in a medical community of practice. As students immerse themselves in the clinical environment, they engage in numerous interactions with their surroundings. The interactions expose them to professional values, which are gradually internalised as students develop their new identity as medical doctors (Cruess et al., 2015).
Optimal professional identity formation requires students’ ability to reflect on their experiences. Reflection enables students to extract meaning from their hectic day-to-day activities, and create plans to continuously improve themselves (Mann et al., 2009). The ability to reflect is also essential in their future profession as doctors. Reflection was defined as critically analysing one’s own experience to reach new and deeper comprehension and insight. Experience become the object to reflect, and the process of recalling and analysing the experience was conducted with the intention of improving future performance (Mann et al., 2009). Reflection also becomes the media to process feelings and emotions, and create plans to improve performance, which leads to improved clinical decision-making ability (Rozental et al., 2021). The importance of reflective practice made it necessary to provide students with opportunity to become skilful in conducting reflection.
The analysis of reflection should include many perspectives to get comprehensive views and insights. One of the ways to support reflection is through the provision of constructive feedback (Husebo et al., 2015; Sandars, 2009). Feedback has been shown to be beneficial in helping students improve their performance (Choi et al., 2020; Johnson et al., 2020; Trehan et al., 2015). Information given through feedback assists students in identifying the improvement needed and the strategies they can use. Feedback can initiate reflections by pointing out the gap between the intended outcome and the current performance; and it can also strengthen reflection by confirming students’ judgment and promoting insights into their performance (Nicol & MacFarlane-Dick, 2006).
Many problems are still found in the practice of feedback in clinical settings, such as the message not being specific enough and the limited time available for interaction. In addition, the Indonesian culture adds certain unique challenges to feedback practice, as identified in our previous study (Felaza et al., 2023). These challenges can be associated with the cultural dimensions of high-power distance and collectivism in Indonesian society. Teachers, experienced and have expertise, are believed by students to know what is best. In a busy clinical environment, the hierarchical gap creates a preference of both teachers and students to engage in directive feedback. In receiving feedback, students tend to appear receptive even when not fully agreeing with the feedback. Being a collectivistic society, group approaches in seeking, providing, and processing feedback practices were commonly found. Students share their feedback experiences with their peers, resulting in collective perception of teacher that they had interacted with (Felaza et al., 2023). Similar challenges have been reported in other studies conducted in Indonesia and Thailand (Areemit et al., 2020; Suhoyo et al., 2018).
Considering the importance of feedback in facilitating students’ professional identity formation, and the way feedback practice is affected by sociocultural aspects, there is a need to develop a feedback model suitable to the attributes of students, teachers, and the clinical environment in Indonesia. This study aims to develop a feedback model relevant to our setting and assess its effectiveness in supporting students’ reflective ability. This study proposes two research aims:
- To develop a feedback model suitable for the Indonesian clinical education setting.
- To evaluate the effectiveness of the feedback model in supporting students’ reflective ability.
II. METHODS
This quantitative research was conducted using a design-based research (DBR) approach, comprising the following steps of identifying the problem, designing a solution, evaluating its effectiveness in a real-life setting, and reflecting on the outcomes (Scott et al., 2020). The first step of our DBR was the identification of feedback-related attributes in FMUI, in a study conducted in September 2023. The next steps, described in detail below, included development of a feedback model within our institution based on data from the previous study, followed by evaluation of its effectiveness in promoting reflection.
A. Feedback model development
The development of the model was guided by a theoretical framework from literature and findings of students’, teachers’, and environmental attributes in our setting. Socio-constructivism, as the theoretical framework, perceives learning as a process of making meanings from experiences through social interactions. Discourses between teacher and students exposes students to thought process and professional norms and values which later can be internalised within themselves. The attributes identified were environmental attributes (limited time, collectivistic, hierarchical, and the need for a safe environment), teachers’ attributes (busy, expert, and having the skill to provide feedback), and students’ attributes (dependent on feedback, less able to read between the lines, perceived to be less resilient, appear to be receptive of feedback, critical, and values teacher’s experience). These findings have been published on September 2023 (Felaza et al., 2023). Along with the socio-constructivist approach as the theoretical framework, these attributes would become the foundation in the development of the model.
Review by experts and cognitive interviews were conducted to ensure the model’s readiness for implementation. Review panel included experts on medical education and communication, program coordinator, and module coordinators. The model was sent via e-mail, and experts were asked to provide feedback on each step and the overall applicability of the model. Cognitive interviews involved clinical teachers from surgery-related and non-surgery-related specialties as future users of the model. After receiving explanation of the model, the teachers practiced the model on their clinical teaching activities. Interviews were held with each teacher to gain input on the experience. Inputs from expert review and cognitive interviews were used to refine the model. The final version of the model was taught to clinical teachers in Paediatric Module as a preparation to test the model. The model was tested during Mini-Clinical Evaluation Exercise (Mini-CEX) by comparing its effectiveness with the Feedback Sandwich method as the standard model being used in FMUI. Mini-CEX is a workplace-based assessment which evaluate students’ performance of clinical skills in real setting. The assessment was originally intended for formative purposes as the clinical teacher observes the performance and provide feedback for students (Hejri et al., 2019). The sandwich model was found to be the common method used for feedback provision in FMUI, and it starts with informing students of the positive aspects of their performance, followed by the negative ones, and closed with another positive aspect (Jug et al., 2019).
B. Testing the effectiveness of the model
The design used was quasi-experimental, involving 5th-year FMUI medical students during their clinical rotation in Paediatric Module. There were 37 students in each group and the data collection took place in May 2022–March 2023. Students in the intervention group received feedback using the new model, while their peers in the control group received feedback using the Sandwich model (Jug et al., 2019). Upon completing data collection in the control group, authors conducted training for teachers on how to utilise the new model, followed by data collection in the intervention group.
Data was collected by asking students to record their voices as they reflect by thinking out loud. FMUI students have been introduced to reflection since the beginning of their academic years, and have experienced completing reflective writing assignments in several modules. For this study, they were instructed to reflect on their experience during mini-CEX. The depth of the reflection was then scored using Kember’s scoring. The scoring was developed by Kember based on Mezirow’s four levels of reflection, and it has been adapted to Bahasa Indonesia (Soemantri et al., 2022). Mezirow divided reflection to 4 levels based on its depth, starting from habitual action which showed no reflection, thoughtful action/understanding, reflection, and critical reflection (Kember et al., 2000). The scoring process was conducted separately by the first author (EF) and two co-authors (AF & RM) and later compared in team discussions to reach an agreed score. Bivariate analysis to test to compare the depth of the reflection between the intervention and the control group was conducted using SPSS 20.0.
III. RESULTS
The criteria for the feedback model were developed based on attributes found from the previous stage (as shown in Table 1 and Table 2).
|
|
Attributes |
Criteria of the Feedback Model |
|
Feedback environment |
|
Can be conducted in a limited time Utilise the high-power distance and collectivism to strengthen the importance of feedback Conducted in a safe environment
|
|
Teachers |
|
Practical Utilise the high-power distance to strengthen Using the faculty development program to strengthen feedback
|
|
Students |
|
Conducted consistently Delivered clearly Avoiding belittlement and sarcasm Conducted in a safe environment Accommodate discussions Enable teachers to share experiences
|
Table 1. Attributes of Factors Affecting Feedback and The Criteria of the Feedback Model
|
Step Proposed |
Criteria of the Feedback Model |
|
Rapport Building |
Develop safe environment
|
|
Acknowledge student’s strengths |
Avoid belittlement and sarcasm Accommodate discussions
|
|
Invite student to reflect |
Avoid belittlement and sarcasm Accommodate discussions
|
|
Share teacher’s experience and tips |
Enable teachers to share experiences Utilise the high power distance to strengthen the importance of feedback
|
|
Establish a plan to improve |
Accommodate discussions
|
Table 2. Steps Proposed and How it Accommodates the Criteria of the Feedback Model
The model was named RAISE as an abbreviation of the first letter in each step. The RAISE model was reviewed by an expert panel, consisting of 3 experts in medical education, 2 experts in communication, and 4 clinical program coordinators. Overall, the RAISE model was perceived as suitable to be implemented in the clinical settings by the expert panel (Figure 1). The crucial aspects that needed to be ensured were teachers’ comprehension of the reasoning behind each step, and the adjustability of the model to be applied in limited time and variability of contexts. Rapport building was considered an essential initial step to start feedback interaction. For the second step, it was advised that teachers ask the student to state positive aspects of performance first before confirmation based on their judgment. The focus of the third step was the areas for improvement, a term that experts emphasised. The step which was initially named ‘invite student to reflect’ was changed into ‘identify aspect that needs improvement’. This revision was made to prevent the misconception that reflection was exclusively covered in the 3rd step. In the fourth step, teachers share their experiences from which students can learn and develop ideas to improve their performance. The information shared should be relevant and can be delivered in a manner that is non-threatening and relevant for the students. The final step in the RAISE model focuses on the action plan for improvement. The agreed plan should be feasible and ready to be implemented.
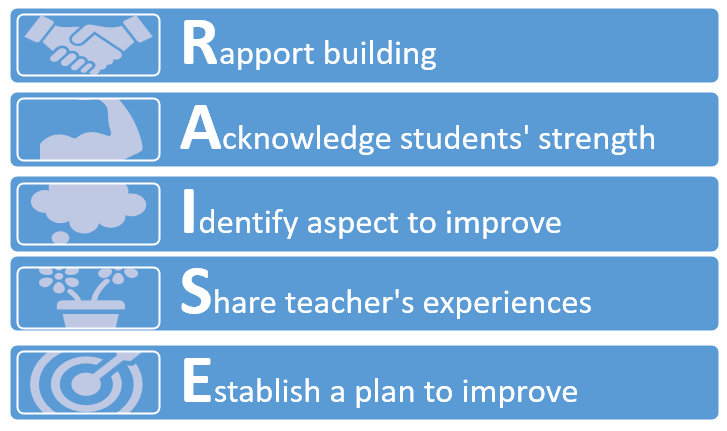
Figure 1. RAISE Model After Expert Review
The model was then utilised by four clinical teachers in various teaching sessions, and cognitive interviews were conducted to gain insight into the experiences. They reported that the model was relatively easy to implement and able to accommodate the limited time available. The model helped develop rapport between teacher and students and enable the two of them to interact more effectively. Continuation between each step was seamless and the conversation did not have to be interrupted due to the movement from one step to another.
The final version was then taught to 22 clinical teachers in August 2022. The training was organised by the first author and two of the co-authors, who had expertise in medical education and experience in conducting faculty development. Various activities were held in the training (video appraisal, discussions, role play, and reflection) to ensure teachers’ ability to perform feedback provision using the RAISE model.
The final version was compared with the Sandwich model, the standard model being used in FMUI, to evaluate its effectiveness. The comparison between the steps of the two models can be seen in Table 3. As shown in the comparison, the strength of the RAISE model lies in its effort to establish rapport from the start of the feedback conversation, its way of facilitating reflection, and the opportunity it provides for teachers to share their experiences.
|
RAISE Model |
Standard Model |
|
Build rapport |
|
|
Discussing positive aspects of performance |
Delivering positive aspects of performance |
|
Discussing negative aspects of performance |
Delivering negative aspects of performance |
|
|
Delivering positive aspects of performance |
|
Sharing teacher’s experience |
|
|
Establishing improvement plan |
|
Table 3. Comparison Between the RAISE Model and the Standard Model
The effectiveness of the model was then tested during mini-CEX in Paediatric Module by comparing the depth of reflection in the experimental and control group. There were 37 students in each group with majority of students in experimental and control groups (30 and 28 students respectively) were female and belonged in the year 2018 batch.
Students reflected on the feedback they received, and the depth of the reflection was rated using the Kember score with the score ranging from 1-4 (1: no reflection; to 4: deep reflection). The distribution of the depth of students’ reflection is shown in Table 4.
|
Kember Score |
Intervention Group (%) |
Control Group (%) |
|
1 (no reflection) |
|
|
|
2 (comprehension) |
2 (5.4%) |
16 (43.2%) |
|
3 (reflection) |
26 (70.2%) |
17 (45.9%) |
|
4 (deep reflection) |
9 (24.4%) |
4 (11.9%) |
Table 4. Distribution of the Depth of Students’ Reflection
The distribution showed most of the students’ reflections in the intervention group were scored 3 based on the Kember score (26 students or 70.2%); while the score in the control group was almost evenly divided between 2 (16 students or 43.2%) and 3 (17 students or 45.9%). Deep reflection was more frequently found in the intervention group (9 students or 24.4%) compared to the control group (4 students or 11.9%).
Mann-Whitney test was used to compare the depth of students’ reflection between the intervention and the control group. The test showed that the mean rank in the intervention group was 30.61 and in the control group was 44.39. The difference between the two groups was statistically significant (Z = 2.964, p = 0.003), indicating that students’ reflections in the intervention group were deeper than their peers in the control group.
IV. DISCUSSION
This study aimed to develop a culturally relevant feedback model that nurtured reflective ability of medical students and to evaluate its effectiveness. The results indicated that students receiving feedback using the RAISE model could reflect more deeply compared to their peers receiving feedback using the standard model. The RAISE model was designed to enable feedback practice in an interactive manner, while feedback using Sandwich model was more directive. The RAISE model starts by building rapport between teacher and student in order to create a safe environment which helps student to optimally conduct reflection. The 2nd and 3rd steps of the model guide students’ reflection systematically, covering both the positive and negative aspects of the performance. On the 4th step, teachers’ sharing of their experiences helps to enrich students’ reflection, enabling them to learn from the experience, as well as strengthening and further maintaining the rapport between them. The final step concludes the interaction with a plan that students can implement to improve. Each of these steps portrays how reflection is guided and supported by the teacher through the feedback interaction.
The RAISE model was developed based on the socio-constructivist theory that describes learning as a way of constructing meaning from experiences. In clinical settings, students are exposed to a variety of experiences to build comprehension, acquire skill proficiency, and integrate professional norms and values. Effective feedback interactions between teachers and students facilitate students’ reflective process and support them in identifying effective ways to improve their performance (Wenger, 2020). Through these interactions, students are exposed to the teacher’s thought process, as well as their professional norms and values. The process that starts as inter-mental between teacher and student gradually becomes internalised into intra-mental within the student (Amineh & Asl, 2015; Tappan, 2010). This process enables teachers to guide students to reach their zone of proximal development (ZPD). Students are supported at each stage of their performance through the concept of scaffolding, and the level of support given would be decreased gradually as students gain the ability for independent clinical practice (Fani & Ghaemi, 2011).
Our previous study highlighted the need for rapport development and the act of sharing teachers’ own experiences in developing the feedback model (Felaza et al., 2023). Rapport was considered essential to create a safe environment for students. Interactions that empowered students in an authentic and safe environment, and teachers as role models in practicing reflection, were needed for creating reflective habits among students (Gathu, 2022; Mann et al., 2009). A sense of safety in feedback interaction was built upon a good relationship between teacher and students, mutual goals, and students’ perception of the teacher’s credibility (Sargeant et al., 2017). In the RAISE model, the safe environment has been developed since the beginning by building rapport between teacher and students. When students reflect, they would need to be open in analysing their experience. Destructive feedback would create reluctance for students to share their reflections (Chan & Lee, 2021; Khoiriyati & Sari, 2021). The model started by asking students’ perceptions of their performance, and their previous experience with similar situations; encouraging them to be open and reflective. The questions were relatively easy to answer and able to lighten the situation. Safety was continuously built through constructive dialogue between teachers and students which created an environment that was safe for reflection (MacNeil et al., 2020; Telio et al., 2015). Mutual goals also can implicitly be seen in students’ perception of the teacher’s intention. When the students believe that feedback was given to help them improve, they would be more willing to openly reflect (Blakey et al., 2019; Eva et al., 2012).
The reflection process is initiated when the condition cannot be handled simply by the automatic action the individual usually conducts or habitual act (Mann et al., 2009). The initiation of reflection might also be triggered by feedback. The feedback information made the individuals realise the quality of their performance, highlighting the strength and weaknesses that requires improvement (Husebo et al., 2015; Mann et al., 2009). When students receive feedback that is aligned with their perception regarding the quality of their performance, reflection usually occurs faster. However, for feedback information that is not aligned, students need to first manage the negative emotion it might evoke, analyse the message, and contemplate what action plan should be taken (Sargeant et al., 2009).
Teachers, perceived as knowledgeable figures, have numerous valuable experiences they can share. By incorporating the act of sharing experience, every feedback interaction would provide lessons from which students can extract meaningful understanding. This particular approach has not been seen explicitly in other feedback models. Other than enriching students’ comprehension, the sharing also provides a sense of relatedness with the teacher, and a role model on how to become reflective (Burgess et al., 2020). A role model in practicing reflection was an important aspect of strengthening students’ motivation. Teachers who practice self-reflection confirm to students that such practice can be done in their profession as doctors. Teachers’ reflective behaviour also showed the students that admitting weaknesses was not an embarrassing act, and on the contrary, it was an important skill to master to improve (Gishen & Chakrabarti, 2022). In the RAISE model, the opportunity for teachers to demonstrate reflection was mostly done in the 4th step. In this step, teachers can share their experiences that was relevant to the situation the students faced. Upon sharing the experience, the teacher can explain the lesson learned from that experience. Students receiving feedback using the RAISE model claimed that this step exposed them to teachers’ openness and minimised the power distance between them. Students also felt more motivated by listening to the experiences. Sense of relatedness was one of the factors that increased intrinsic motivation. The teachers’ willingness to share their experiences creates a connection between them and students, and strengthens students’ internal motivation (Kusurkar et al., 2011).
Other than being influenced on a systemic level by cultural aspects, such as power distance and collectivism; reflection is also affected in individual level by students’ and teachers’ reflective ability, teachers’ ability in facilitating reflection, and the relationship between teacher and students (Chan & Lee, 2021). The RAISE model supports teachers in facilitating students’ reflection through the use of reflective questions and the opportunity to show students how reflection was practiced by themselves as they shared their experiences. The rapport built during the interactions also strengthens the teacher-student relationship which further enables students to be more open and trusting in conducting their reflection.
Students’ reflective ability was crucial in their education process and later as they became member of the medical profession. Experiences in the clinical learning environment, which depicts the authentic professional world that students would enter, expose students to norms and values. Through reflection, students create meanings from these experiences which facilitate the formation of their professional identity as medical doctors (Winkel et al., 2017).
This study showed that implementation of the RAISE model, a feedback model developed based on the feedback-related attributes in Indonesian settings, enabled students to reflect more deeply on their performance. Findings from the study suggested that the RAISE model was suitable for supporting students’ reflection in a setting with high power distance and collectivistic background. However, it should be noted as a limitation of this study that reflection was an internal process and the effect might not be visible immediately. The changes in comprehension, perspectives, and even students’ attitude occurs gradually along the reflection process that was taking place. Therefore, further research is needed to observe the effect of reflection which might require longitudinal observation of students’ performance. The study involved a single institution in Jakarta, and therefore research and certain adjustments might be needed before the model can be implemented in different settings.
V. CONCLUSION
The feedback model formulated based on the feedback-related attributes in our clinical setting was named the RAISE model. It consists of 5 steps, which are Rapport building, Acknowledge student’s strengths, Identify aspects that need improvement, Share teacher’s experience and tips, and Establish a plan to improve. Our data indicate that students receiving feedback using the RAISE model were able to reflect more deeply compared to their peers receiving the standard model. We conclude that the model’s ability to create a safe environment, build rapport between teachers and learners, and teachers’ role-modelling of reflective practice can encourage students to be more self-reflective of their clinical performance.
Notes on Contributors
Estivana Felaza, Ardi Findyartini, Rita Mustika, Jenny Bashiruddin, Joedo Prihartono, Lucia RM Royanto, and Subha Ramani contributed to all processes of this research, and have read and approved this manuscript.
Dr. dr. Estivana Felaza, MPdKed is a Lecturer in Faculty of Medicine, Universitas Indonesia. She reviewed the literatures, designed the study, performed data collection and analysis, and wrote the manuscript.
Prof. dr. Ardi Findyartini, PhD is a Professor of Medical Education in the Faculty of Medicine, Universitas Indonesia. She developed the methodological framework for this research, involved in scoring the students’ reflections (data), provided feedback on the data collection, data analysis, and the manuscript writing process.
Dr. dr. Rita Mustika, M.Epid is an expert in Medical Education and a Lecturer in the Faculty of Medicine, Universitas Indonesia. She developed the methodological framework for this research, was involved in scoring the students’ reflections (data), provided feedback on the data collection, data analysis, and manuscript writing process.
Prof. Dr. dr. Jenny Bashiruddin, SpTHT-KL(K) is a Professor in Otolaryngology and an expert in Medical Education. She provided feedback on the theoretical and methodological framework of this research, data collection, data analysis, and the manuscript writing process.
Dr. dr. Joedo Prihartono, MPH is an expert in Statistics and a Senior Lecturer in Community Medicine, Faculty of Medicine, Universitas Indonesia. He provided feedback on the methodological framework of this research, data collection, data analysis, and the manuscript writing process.
Dr. Lucia RM Royanto, M.Si, Sp.Ed is an expert in Educational Psychology and a Senior Lecturer in the Faculty of Psychology, Universitas Indonesia. She provided feedback on the theoretical framework of this research, data collection, data analysis, and the manuscript writing process.
Dr. Subha Ramani, MBBS, MPH, PhD, FAMEE is an expert in Medical Education and an Associate Professor of Medicine in Harvard Medical School. She provided feedback on the theoretical and methodological framework of this research, data collection, data analysis, and the manuscript writing process.
Ethical Approval
The study was approved by the Research Ethics Review Committee of the Faculty of Medicine, Universitas Indonesia (approval number: KET-1114/UN2.F1/ETIK/ PPM.00.02/2021). The subjects of this study were informed verbally and in writing of the purpose, the methods, and the confidentiality of the data being collected. Each subjects’ involvement in this research were voluntary, and consent were signed upon receiving the necessary information.
Data Availability
Datasets generated and/or analysed in this study are available upon request via electronic mail to the corresponding author.
Acknowledgement
The authors would like to acknowledge the contributions of the students and clinical teachers who willingly involved and cooperated in this study.
Funding
No funding was obtained for this study.
Declaration of Interest
All authors have no declaration of interest.
References
Amineh, R. J., & Asl, H. D. (2015). Review of constructivism and social constructivism. Journal of Social Science, Literature & Language, 1(1), 9–16.
Areemit, R. S., Cooper, C. N., Wirasorn, K., Paopongsawan, P., Panthongviriyakul, C., & Ramani, S. (2020). Hierarchy, “Kreng Jai”, and feedback: A grounded theory study exploring perspectives of clinical faculty and medical students in Thailand. Teaching and Learning in Medicine, 33(3), 235–244. https://doi.org/10.1080/10401334.2020.1813584
Blakey, A. G., Smith-Han, K., Anderson, L., Collins, E., Berryman, E., & Wilkinson, T. (2019). “They cared about us students”: Learning from exemplar clinical teaching environments. BMC Medical Education, 19, 119–128. https://doi.org/10.1186/ s12909-019-1551-9
Burgess, A., van Diggele, C., Roberts, C., & Mellis, C. (2020). Feedback in the clinical settings. BMC Medical Education, 20(Suppl 2), 458–463. https://doi.org/10.1186/s12909-020-02280-5
Chan, C. K. Y., & Lee, K. K. W. (2021). Reflection literacy: A multilevel perspective on the challenges of using reflections in higher education through a comprehensive literature review. Educational Research Review, 32(2), Article 100376. https://doi.org/10.1016/j.edurev.2020.100376
Choi, S., Oh, S., Lee, D. H., & Yoon, H. S. (2020). Effects of reflection and immediate feedback to improve clinical reasoning of medical students in the assessment of dermatologic conditions: A randomized controlled trial. BMC Medical Education, 20, 146–154. https://doi.org/10.1186/s12909-020-02063-y
Cruess, R. L., Cruess, S. R., Boudreau, J. D., Snell, L., & Steinert, Y. (2015). A schematic representation of the professional identity formation and socialization of medical students and residents: A guide for medical educators. Academic Medicine, 90(6), 718–725. https://doi.org/10.1097/acm.0000000000000700
Eva, K. W., Armson, H., Holmboe, E., Lockyer, J., Loney, E., Mann, K., & Sargeant, J. (2012). Factors influencing responsiveness to feedback: On the interplay between fear, confidence, and reasoning process. Advance in Health Science Education, 17, 15–26. https://doi.org/10.1007/s10459-011-9290-7
Fani, T., & Ghaemi, F. (2011). Implications of Vygotsky’s zone of proximal development in teacher education. Social Behavioral Science, 29, 1549–1554. https://doi.org/10.1016/j.sbspro.2011.11. 396
Felaza, E., Findyartini, A., Mustika, R., Bashiruddin, J., Royanto, L. R. M., Prihartono, J., & Ramani, S. (2023). Deeper look into feedback practice in an Indonesian context: Exploration of factors in undergraduate clinical setting. Korean Journal of Medical Education, 35(3), 263–273. https://doi.org/10.3946/kjme.2023.264
Gathu, C. (2022). Facilitators and barriers of reflective learning in postgraduate medical education: A narrative review. Journal of Medical Education and Curriculum Development, 9, 1–8. https://doi.org/10.1177/23821205221096106
Gishen, F., & Chakrabarti, R. (2022). Medical students’ perceptions of reflective practice in the undergraduate curriculum. MedEd Publish, 12, 53–67. https://doi.org/10.12688/mep.19211.3
Hejri, S. M., Jalili, M., Masoomi, R., Shirazi, M., Nedjat, S., & Norcini, J. (2019). The utility of mini clinical examination exercise in undergraduate and postgraduate medical education: A BEME review: BEME guide no. 59. Medical Teacher, 42(2), 1–18. https://doi.org/10.1080/0142159x.2019.1652732
Husebo, S. E., O’Reagen, S., & Nestel, D. (2015). Reflective practice and its role in simulation. Clinical Simulation in Nursing, 11, 368–375. http://doi.org/10.1016/j.ecns.2015.04.005
Johnson, C. E., Weerasuria, M. P., & Keating, J. L. (2020). Effect of face-to-face verbal feedback compared with no alternative feedback on the objective workplace task performance of health professionals: A meta-analysis and systematic review. BMJ Open, 10(3), Article e030672. https://doi.org/10.1136/bmjopen-2019-030672
Jug, R., Jiang, X., & Bean, S. M. (2019). Giving and receiving effective feedback. Archives of Pathology and Laboratory Medicine, 143, 244–250. https://doi.org/10.5858/arpa.2018-0058-RA
Kember, D., Leung, D. Y. P., Jones, A., Loke, A. Y., MacKay, J., Sinclair, K., Tse, H., Webb, C., Wong, F. K. Y., Wong, M., & Yeung, E. (2000). Development of a questionnaire to measure the level of reflective thinking. Assessment and Evaluation in Higher Education, 25(4), 381–395. http://doi.org/10.1080/713611442
Khoiriyati, A., & Sari, N. K. (2021). Reflective practice on nursing students: A qualitative study. Indonesian Nursing Journal of Education and Clinic, 6(2), 201–209. http://doi.org/10.24990/in jec.v6i2.391
Kusurkar, R., Croiset, G., & Ten Cate, O. (2011). Twelve tips to stimulate intrinsic motivation in students through autonomy-supportive classroom teaching derived from self-determination theory. Medical Teacher, 33, 978–982. https://doi.org/10.3109/01 42159x.2011.599896
MacNeil, K., Cuncic, C., Voyer, S., Butler, D., & Hatala, R. (2020). Necessary but not sufficient: Identifying conditions for effective feedback during internal medicine residents’ clinical education. Advances in Health Science Education, 25, 641–654. https://doi.org/10.1007/s10459-019-09948-8
Mann, K., Gordon, J., & MacLeod, A. (2009). Reflection and reflective practice in health professions education: A systematic review. Advances in Health Science Education, 14, 595–621. https://doi.org/10.1007/s10459-007-9090-2
Nicol, D., & MacFarlane-Dick, D. (2006). Formative assessment and self-regulated learning: A model and seven principles of good feedback practice. Studies in Higher Education, 31(2), 199–218. https://doi.org/10.1080/03075070600572090
Rozental, L., Meitar, D., & Karnielli-Miller, O. (2021). Medical students’ experiences and needs from written reflective journal feedback. Medical Education, 55, 505–517. https://doi.org/10.1111/medu.14406
Sandars, J. (2009). The use of reflection in medical education: AMEE Guide no 44. Medical Teacher, 31, 685–695. https://doi.org/10.1080/01421590903050374
Sargeant, J. M., Mann, K. V., van der Vleuten, C. P., & Metsemakers, J. F. (2009). Reflection: A link between receiving and using assessment feedback. Advances in Health Science Education, 14, 399–410. https://doi.org/10.1007/s10459-008-9124-4
Scott, E. E., Wenderoth, M. P., & Doherty, J. H. (2020). Design-based research: A methodology to extend and enrich biology education research. CBE Life Science Education, 19(3), 1–12. https://doi.org/10.1187/cbe.19-11-0245
Soemantri, D., Mustika, R., & Greviana, N. (2022). Inter-rater reliability of reflective writing assessment in an undergraduate professionalism course in medical education. Education in Medicine Journal, 14(1), 87–97. http://doi.org/10.21315/eimj2022.14.1.8
Suhoyo, Y., Schönrock-Adema, J., Emilia, O., Kuks, J. B. M., & Cohen-Schotanus, J. (2018). Clinical workplace learning: Perceived learning value of individual and group feedback in a collectivistic culture. BMC Medical Education, 18, 79–84. https://doi.org/10.1186/s12909-018-1188-0
Tappan, M. (2010). Sociocultural psychology and caring pedagogy: Exploring Vygotsky’s hidden curriculum. Educational Psychology, 33(1), 23–33. http://doi.org/10.1207/s15326985ep3301_2
Telio, S., Ajjawi, R., & Regehr, G. (2015). The “Educational Alliance” as a framework for reconceptualizing feedback in medical education. Academic Medicine, 90(5), 609–614. https://doi.org/10.1097/acm.0000000000000560
Trehan, A., Barton-Vaness, A., Carty, M. J., McCulloch, P., & Maruthappu, M. (2015). The impact of feedback of intraoperative technical performance in surgery: A systematic review. BMJ Open, 5, Article e006759. http://doi.org/10.1136/bmjopen-2014-006759
Wenger, E. (2020). Communities of practice and social learning systems: The career of a concept. Organization, 7(2), 225–246. http://doi.org/10.1177/135050840072002
Winkel, A. F., Yingling, F., Jones, A. A., & Nicholson, J. (2017). Reflection as a learning tool in graduate medical education: A systematic review. Journal of Graduate Medical Education, 5, 430–439. https://doi.org/10.4300/jgme-d-16-00500.1
*Estivana Felaza
Faculty of Medicine Universitas Indonesia,
Jalan Salemba Raya No 6,
Jakarta 10430, Indonesia
Email: estivanafelaza@gmail.com;
estivana.felaza01@ui.ac.id
Submitted: 24 December 2023
Accepted: 31 July 2024
Published online: 7 January, TAPS 2025, 10(1), 4-9
https://doi.org/10.29060/TAPS.2025-10-1/GP3201
Muhamad Saiful Bahri Yusoff1,2
1Department of Medical Education, School of Medical Sciences, Universiti Sains Malaysia, Malaysia; 2Centre for the Development of Academic Excellence, Universiti Sains Malaysia, Malaysia
Abstract
Introduction: This article explores the dynamic relationship between the Scholarship of Teaching and Learning (SoTL) and the well-being of students and educators within the context of medical education.
Methods: The author critically reviewed the salient views and knowledge at the intersection of SoTL, well-being, and resilience. By critically examining literature, insights from various studies were synthesised, offering a detailed overview of the current state of knowledge in this field. This review guided the identification of key practices and recommendations.
Results: SoTL emerges as a transformative force, enhancing well-being for both students and educator through evidence-based practices and innovative teaching methods. The article explores the crucial role of SoTL in fostering resilience, not only among students but also among educators. Despite promising evidence, challenges in implementing SoTL for well-being persist, requiring strategic approaches to overcome traditional paradigms. The discussion extends to the global implications of SoTL, emphasising the need for collaborative efforts to foster better educational practices and establish inclusive learning environments.
Conclusion: As we assess the evidence for transformative change, a call-to-action echoes, urging global collaboration, research endeavors, and institutional support to realise the full potential of SoTL, ultimately creating environments where both learners and educators thrive.
Practice Highlights
- Employ evidence-based teaching methods derived from SoTL practices.
- Prioritise individuals’ mental, emotional, and social growth through SoTL practices.
- Cultivate adaptive learning approaches to enhance student resilience through SoTL practices.
- Acknowledge and bolster the well-being of educators through SoTL practices.
- Embrace cross-cultural collaboration within the realm of SOTL practices.
I. INTRODUCTION
The Scholarship of Teaching and Learning (SoTL) involves a systematic examination of teaching practices and their impact on student outcomes, aiming to achieve optimal educational results and contribute to societal enhancement (Luan et al., 2019). Rooted in research, evidence, and critical reflection, SoTL enhances practices within specific disciplines and professions (Coleman et al., 2023). Typically led by discipline-specific teachers, SoTL-based projects focus on improving both teaching methods and students’ learning experiences (Coleman et al., 2023). In the evolving educational landscape, including advancements in technology and shifts in learning methods, SoTL is essential for improving instructional techniques and evaluating their impact on both academic success and the well-being of students and educators. Wellbeing signifies the state of positive emotions, effective functioning, the realisation of one’s potential, a sense of control, purpose, and positive relationships (Ruggeri et al., 2020). Within traditional teaching methods, a pivotal research question arises: Do we have enough evidence to advocate for a significant change acknowledging the diverse experiences of educators and learners? This prompts a close examination of the current educational landscape, evolving roles of educators and learners, and the urgent need for a comprehensive understanding of well-being and resilience in the context of SoTL.
II. METHODS
The author critically reviewed the salient views and knowledge at the intersection of SoTL, well-being, and resilience. By critically examining selected literature from diverse studies, insights were synthesised to present a detailed overview of the current state of knowledge in this field. The approach allowed for an in-depth exploration of how SoTL principles are implemented and their impact on the well-being of students and educator. The synthesis of study findings resulted in a comprehensive understanding and practical recommendations for transformative educational practices.
III. RESULTS
A. Current Landscape of Teaching and Learning
The current way we teach relies heavily on traditional methods, often involving direct instruction and focusing on course content. While these methods have traditionally aimed at spreading knowledge, we are now questioning their impact on the well-being of students and educator (Coleman et al., 2023; Khairul Anhar Holder et al., 2023). Conventional teaching, with its emphasis on standardised assessments and delivering content, might unintentionally lead to increased stress and reduced resilience among learners. It’s clear that education is changing, and there is a growing call for a more comprehensive approach to teaching and learning. This means exploring methods that not only promote academic success but also prioritising the well-being and resilience of everyone involved in education.
B. Current Concept of Scholar of Teaching and Learning (SoTL)
SoTL is a dynamic approach to education, dedicated to improving teaching methods and enhancing student learning experiences (Coleman et al., 2023; Luan et al., 2019). It employs transformative teaching methods that connect academic content with real-world contexts, fostering critical thinking skills. SoTL involves reflective practice, where educators systematically assess and improve teaching using evidence-based research and educational theory. SoTL promotes knowledge sharing among educators, encouraging collaboration and professional development. Through educational inquiry, SoTL engages educators in thorough investigations, contributing to knowledge creation that enhances teaching practices. Ultimately, SoTL serves as a catalyst for transforming education by advocating for experiential learning, innovative teaching methods, and inclusive strategies, preparing students for success in a changing global landscape. SoTL encompasses transformative pedagogy, reflective practice, teacher dissemination, educational inquiry, and educational transformation (see Figure 1).
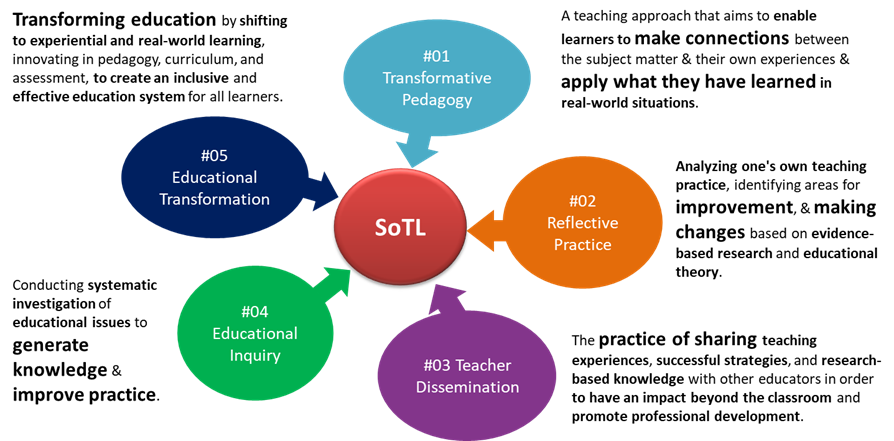
Figure 1. The key characteristics of SoTL
C. Defining Well-being and Resilience in Medical Education
In medical education, well-being goes beyond simply being stress-free (Roslan et al., 2022; Ruggeri et al., 2020). Alongside well-being, resilience becomes essential for overcoming challenges since it is the ability to recover from setbacks, adapt to changing circumstances, and thrive in adversity (Khairul Anhar Holder et al., 2023; Roslan et al., 2022). Figure 2 illustrates the interconnected components and outcomes of well-being in medical education. The left side highlights factors contributing to well-being such as resilience, while the right side shows the outcomes of enhanced well-being, such as better patient care, and reduced burnout.
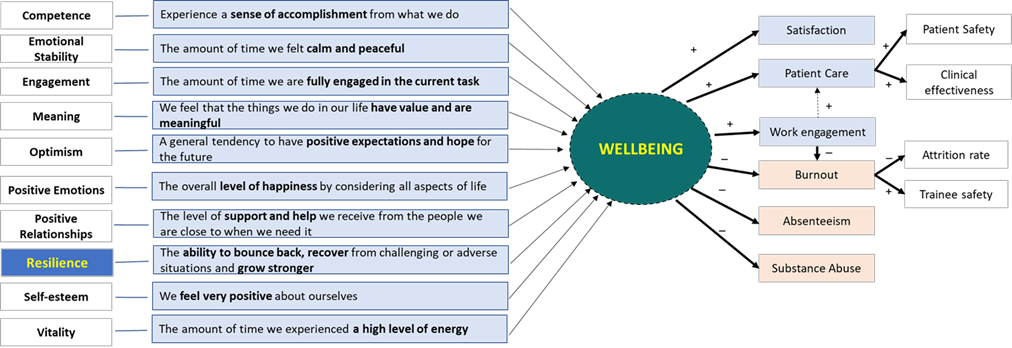
Figure 2. The interconnectedness of wellbeing and resilience in medical education
D. Roles of SoTL in Enhancing Well-being and Resilience
SoTL proves to influence student well-being enhancement within educational environments (Coleman et al., 2023; Luan et al., 2019). As educators embrace evidence-based practices, the imperative of prioritising well-being in pedagogical discourse becomes evident. SoTL, employing rigorous research and reflective teaching, seeks strategies that not only elevate academic success but also positively contributes to the student experience. Research findings highlight the substantial impact of teaching practices guided by SoTL principles on student engagement, motivation, and satisfaction (Coleman et al., 2023; Khairul Anhar Holder et al., 2023). This intertwining of SoTL with well-being underscores its pivotal role in shaping a more comprehensive and enriching educational experience (Coleman et al., 2023).
E. Educator Well-being
Teaching, with its inherent demands and complexities, can significantly influence educators’ well-being. SoTL recognises the critical role of supporting educator well-being as essential for sustainable and effective teaching practices. Educator well-being extends beyond workload management to encompass the emotional and intellectual dimensions of teaching. Institutions embracing SoTL principles prioritise initiatives such as professional development, mentorship programs, and fostering a conducive work environment (Coleman et al., 2023; Luan et al., 2019). These endeavors not only elevate teaching quality but also contribute to the personal and professional growth of educators, leading to their well-being.
F. Student Well-being
The core of SoTL lies in its significant impact on students’ well-being, surpassing traditional measures of academic success by recognising the intricate connection between a student’s educational success and their overall well-being (Khairul Anhar Holder et al., 2023). The implementation of evidence-based teaching practices, guided by SoTL principles, establishes an environment conducive to positive mental, emotional, and social development among students. Research indicates that students exposed to such approaches report higher levels of satisfaction, motivation, and a sense of belonging within the academic setting (Coleman et al., 2023). Through innovative teaching methods, SoTL fosters holistic student development, addressing diverse needs and serve as a catalyst for student well-being, cultivating a rewarding and supportive educational experience (Coleman et al., 2023; Luan et al., 2019).
G. Challenges in Implementing SoTL for Well-being
Despite the potential of SoTL to improve student and educator well-being, its implementation faces challenges, notably overcoming traditional teaching paradigms. Resistance to change within academic institutions, often rooted in institutional cultures and ingrained beliefs, can hinder the integration of SoTL-informed practices. Cultural and institutional barriers may also manifest in the allocation of resources and recognition. SoTL demands time, collaboration, and institutional support for meaningful implementation, posing challenges for institutions in prioritising these aspects over more traditional academic pursuits (Luan et al., 2019). The complex challenges associated with integrating SoTL for well-being underscore the necessity for strategic approaches to overcome these obstacles and pave the way for transformative changes in educational practices (Coleman et al., 2023).
H. The Need for Resilience in Learning Environments
In the ever-evolving field of education, resilience stands out as a crucial quality for navigating the complexities of learning environments (Khairul Anhar Holder et al., 2023; Roslan et al., 2022; Ruggeri et al., 2020). Students who develop resilience not only excel academically but also build a mindset that prepares them for uncertainties in the future. SoTL plays a vital role in fostering resilience by promoting pedagogical strategies that encourage adaptive learning. Through experiential approaches, collaborative projects, and real-world applications of knowledge, SoTL contributes to the development of resilient learners (Coleman et al., 2023). SoTL emphasises the transformative potential of educational practices that not only convey knowledge but also equip learners with the resilience needed to thrive in an ever-changing world (Coleman et al., 2023; Luan et al., 2019).
I. Evaluating the Evidence for Transformational Change
Do we have enough evidence to support a transformative change in educational practices? Recent studies indicate a strong connection between SoTL-informed teaching practices and positive outcomes, both academically and well-being (Coleman et al., 2023). However, challenges exist due to variability in methodologies, research scope, and the need for longitudinal studies to assess sustained effects. The evidence is promising, showing improved student engagement, increased educator satisfaction, and positive learning environments (Coleman et al., 2023). Further research is needed to establish causal relationships and identify specific SoTL elements contributing significantly to well-being. A global perspective is crucial, requiring collaborative, cross-cultural research efforts to enrich the evidence base and ensure global applicability of transformative changes.
J. Implications for Global Medical Education
Exploring SoTL’s impact on student and educator well-being has profound implications for global medical education. Applied globally, SoTL principles can transcend cultural and institutional boundaries, fostering a more inclusive and responsive educational landscape (Roslan et al., 2022; Ruggeri et al., 2020). Successful SoTL implementations globally offer insights for transformative changes in education (Coleman et al., 2023; Luan et al., 2019). However, addressing cultural nuances, regional differences, and institutional variations requires a careful global approach to applying SoTL principles. Global medical education benefits from collective efforts, fostering cross-cultural exchanges of SoTL best practices (Coleman et al., 2023). The wide-reaching implications of SoTL, underscored by a system-learner-oriented framework for well-being (Figure 3), highlight the need for collaborative endeavors to shape a more equitable global educational experience. SoTL should be reimagined as an emerging practice for researchers to impact teaching, learning, and assessment, promoting well-being (Coleman et al., 2023).

Figure 3. A System-Learner-Oriented SoTL for Wellbeing Framework
IV. DISCUSSION
The current education landscape is undergoing a significant shift away from traditional teaching practices due to their potential unwanted impact on student and educator well-being (Coleman et al., 2023; Khairul Anhar Holder et al., 2023). This recognition has led to a growing urgency for transformative changes aligned with global academic needs. SoTL, encompassing transformative pedagogy, reflective practice, teacher dissemination, educational inquiry, and transformation, emerges as a guiding light in this educational shift, committing to enhancing teaching methodologies and student learning experiences despite facing challenges (Coleman et al., 2023; Luan et al., 2019).
Implementing SoTL for well-being faces many challenges, including resistance to change, institutional cultures, and fixed beliefs (Coleman et al., 2023; Luan et al., 2019). The need for resources, time, collaboration, and institutional support becomes apparent for meaningful implementation. This highlight potential lack of awareness amongst educator regarding SoTL practices, emphasising the importance of strategic approaches. Additionally, resilience in learning environments is vital for maintaining well-being and achieving academic success (Roslan et al., 2022; Ruggeri et al., 2020). In medical education, building resilience among students and educator is essential for coping with challenges (Khairul Anhar Holder et al., 2023) and recovering from setbacks effectively (Roslan et al., 2022).
Evaluating the current evidence on SoTL and its impact on well-being reveals promising connections but shows up the need for further research (Coleman et al., 2023). Recognising the variability in methodologies, research scope, and the necessity for longitudinal studies is crucial. Comprehensive evaluations and robust evidence are needed to validate the effectiveness of SoTL practices and their long-term impact on both student and educator well-being. This includes an in-depth examination of SoTL’s potential benefits and challenges to ensure that its implementation leads to meaningful and sustainable improvements in educational practices.
Advocating for a global perspective highlight diverse educational contexts worldwide. Collaborative, cross-cultural research efforts are vital to enrich the evidence base and ensure the global applicability of transformative changes. The extension of educational experiences and innovations through sharing practices and policies will be crucial. By integrating SoTL principles, fostering a culture of continuous improvement, and prioritising well-being, global medical education can create supportive, resilient, and effective learning environments that cater to the holistic development of students and educator.
V. CONCLUSION
Integrating SoTL with student and educator well-being signifies a transformative shift in global education. The evidence reveals that adoption of SoTL principles as a pathway to comprehensive educational experiences, emphasising the connection between teaching methods and well-being. A resounding call to action emphasises the essential need for global collaboration, dedicated research, and institutional support to unlock SoTL’s full potential. Only through these collective efforts can educational environments foster the flourishing of student and educator, marking a paradigm shift worldwide.
Notes on Contributors
MSBY contributes to the conception of the work, the acquisition of data for the work, drafts the work or revising it critically for important intellectual content, approves the final version to be published, and agrees to be accountable for all aspects of the work.
Acknowledgement
The content of this article is mainly based on a presentation titled “SOTL in Student and Faculty Well-being and Resilience – Do We Have Enough Evidence for a Transformational Change?” given by the author at the 20th Asia Pacific Medical Education Conference in Singapore. This article has undergone language editing by ChatGPT 3.5 to enhance its syntax and improve overall clarity.
Funding
This paper has not received any fundings.
Declaration of Interest
The author declared no conflict of interests.
References
Coleman, K., Uzhegova, D., Blaher, B., & Arkoudis, S. (2023). The educational turn: Rethinking the scholarship of teaching and learning in higher education. Springer Nature, Singapore. https://doi.org/10.1007/978-981-19-8951-3
Luan, W. S., Khambari, M. N. M., Razali, A. B. M., Rashid, S. A. & Ching, F. T. H. (2019). Scholarship of teaching and learning @UPM. Centre for Academic Development (CADe), Universiti Putra Malaysia, Malaysia. https://cade.upm.edu.my/upload/doku men/20220624103811eBook_-_SoTL@UPM_(Complete).pdf
Ruggeri, K., Garcia-Garzon, E., Maguire, Á., Matz, S., & Huppert, F. A. (2020). Well-being is more than happiness and life satisfaction: A multidimensional analysis of 21 countries. Health and Quality of Life Outcomes, 18(1), 1-16. https://doi.org/10.1186/ s12955-020-01423-y
Roslan, N. S., Yusoff, M. S. B., Morgan, K., Razak, A. A., & Shauki, N. I. A. (2022). Evolution of resilience construct, its distinction with hardiness, mental toughness, work engagement and grit, and implications to future healthcare research. Education in Medicine Journal, 14(1), 99-114. https://doi.org/10.21315/eimj 2022.14.1.9
Khairul Anhar Holder, N. A., Pallath, V., Vadivelu, J., & Foong C. C. (2023). Using document phenomenology to investigate academic failure among year 1 undergraduate Malaysian medical students. BMC Medical Education, 23(310), 1-19. https://doi.org/10.1186/s12909-023-04285-2
*Assoc. Prof. Dr Muhamad Saiful Bahri Bin Yusoff
Department of Medical Education,
School of Medical Sciences,
Universiti Sains Malaysia,
Kelantan, Malaysia
+60169629640
Email: msaiful_bahri@usm.my
Submitted: 13 June 2024
Accepted: 14 October 2024
Published online: 7 January, TAPS 2025, 10(1), 36-47
https://doi.org/10.29060/TAPS.2025-10-1/OA3438
Sivapalan Sanchayan1, Sisira Dharmaratne2, Shalika Pathirana3, Pavithra Godamunne3 & Madawa Chandratilake3
1Department of Medical Education, Faculty of Medicine, University of Jaffna, Sri Lanka; 2Translational Health Research Institute, Western Sydney University, Australia; Department of Medical Education, Faculty of Medicine, University of Kelaniya, Sri Lanka
Abstract
Introduction: Selection for basic medical training is highly contextual. The use of cognitive aptitude tests, which commonly supplement measures of prior academic achievement in the selection process of medical schools internationally, is rarely reported from resource-constrained settings in South Asia. We report on the psychometric properties of an aptitude test designed based on the UCAT format, administered to first-year medical undergraduates to determine its utility.
Methods: The aptitude test was administered online to first-year medical students shortly after their admission to two medical faculties in Sri Lanka (n=328). The reliability of the test was determined using Cronbach’s alpha. Overall and subtest scores were computed, and the scores of different demographic groups were compared using the t-test. Factor analysis of the subtests was performed.
Results: The internal consistency of the test was 0.63. The difficulty and discrimination indices were within the acceptable range. The mean score of the aptitude test (AT) was 70.9/100 (SD 8.88). The mean score for females was higher than for males (p=0.04). No statistically significant differences in AT scores were observed between different ethnicities or religions. The entry academic scores demonstrated a weak correlation with the overall AT score (Pearson’s correlation coefficient r=0.27), verbal reasoning (r=0.24), the human body (r=0.19), quantitative reasoning (r=0.18), and situational judgement (r=0.128). Factor analysis indicated items that need revision.
Conclusion: The results indicate the potential value of aptitude tests in Sri Lanka and in similar jurisdictions where selection criteria have yet to expand beyond prior academic performance. A way forward in introducing such tests has been outlined.
Keywords: Medical Student Selection, Medical Student Admission, Selection Criteria
Practice Highlights
- Aptitude tests assess cognitive and non-cognitive attributes desirable for healthcare professionals.
- The use of aptitude tests is rarely reported from resource constrained settings in South Asia.
- Sri Lanka uses only the national high school examination performance for medical school admission.
- This study indicates the potential value of aptitude tests in Sri Lanka and in similar jurisdictions.
I. INTRODUCTION
Selection for basic medical training is highly contextual and influenced by educational, geographical, socioeconomic, and political factors (Dharmaratne & Ponnamperuma, 2020; Patterson et al., 2018). High academic achievement has long been considered an appropriate criterion for ranking candidates for medical school (McManus et al., 2013; Patterson et al., 2017). However, this approach has been contested due to the low predictive validity of pre-university performance for medical school success (McManus et al., 2013; Prideaux et al., 2011).
Aptitude tests have emerged to assess cognitive and non-cognitive traits desirable for medical and healthcare professions (Gliatto et al., 2016; Greatrix & Dowell, 2020; Powis et al., 2021). Despite evidence on their potential to improve selection processes (Bala et al., 2022; Greatrix et al., 2021), most resource-constrained jurisdictions, including Sri Lanka, rely solely on prior academic achievement (Soemantri et al., 2020; University Grants Commission, 2023). This study represents an initial step in Sri Lanka toward introducing aptitude tests and reports on the psychometric properties of a test developed to measure cognitive attributes.
The Sri Lankan medical school admission system uses national high school examination results (G.C.E. AL) as the only criterion for admission (Dharmaratne & Ponnamperuma, 2020; University Grants Commission, 2023). The results of three AL subjects (Chemistry, Physics, and Biology) are considered, and an average Z score is used to rank individuals (University Grants Commission, 2023). A minimum of two credit passes and one simple pass is required for eligibility. A few candidates with foreign examination results equivalent to the G.C.E. AL Examination and meeting equitable minimum requirements are also admitted (University Grants Commission, 2023).
G.C.E. AL examination results have shown a mild correlation with subsequent undergraduate performance, with a maximum predictive correlation coefficient of 0.37 (de Silva et al., 2004, 2006; Hewage et al., 2011; Mettananda et al., 2006). These low figures may underestimate the true relationship, as range restriction among high-achieving candidates can affect the statistical accuracy of predictive validity measures (Zimmermann et al., 2017). Studies in the UK, addressing range restriction, found that prior academic performance is the best predictor of subsequent performance, accounting for 65% of the variance in undergraduate performance (McManus et al., 2013). However, this leaves 35% of the variance unexplained.
Aptitude tests are used worldwide to support medical student selection. The United Kingdom Clinical Aptitude Test (UKCAT), now named UCAT, has been used for nearly two decades (Greatrix & Dowell, 2020). The UCAT consists of 200 items in five subtests delivered over two hours (Paton et al., 2022). Results of the UKCAT and UCAT have been used to discriminate between high-achieving students during selection and predict undergraduate and postgraduate performance (Bala et al., 2022; MacKenzie et al., 2016; McManus et al., 2013; Paton et al., 2022).
However, there are additional qualities beyond academic readiness (prior academic performance and cognitive traits) that are necessary qualities of medical professionals that include desirable behaviours and attitudes that could indicate successful development as healthcare practitioners in the future (Patterson et al., 2018). The Ottawa consensus statement recommends that best practice selection should involve the use of selection criteria based on multi-source multi-method job analysis studies (Patterson et al., 2018). This necessitates the use of other selection processes such as structured interviews or multiple mini interviews (MMI).
This study aims to evaluate the psychometric properties of an aptitude test based on the UCAT format, administered to first-year medical undergraduates at two medical faculties in Sri Lanka. Specifically, the objectives are to evaluate the psychometric properties of the test, determine the relationship between Z scores at the AL examination and aptitude test scores, and compare the performance of different demographic groups in the aptitude test.
II. METHODS
A cross-sectional observational study was conducted in the faculties of medicine at the universities of Kelaniya and Jaffna, Sri Lanka. Including these two faculties allowed for the recruitment of an adequate number of students from the three main ethnic groups (Sinhala, Tamil, and Sri Lankan Moors) and a wider range of Z scores. All first-year students in 2023 from these faculties were invited to participate. Students admitted through selection criteria other than Sri Lankan advanced level performance were excluded. We obtained a sample size of 328 students who consented to participated in the study (response rate of 80.8%).
The aptitude test comprised 50 items across six subtests: abstract reasoning (8 items), the human body (8 items), quantitative reasoning (8 items), decision-making (8 items), verbal reasoning (8 items), and situational judgment (10 items). Except for the “the human body” subtest, all others were modelled after the UKCAT examination. The “human body” subtest was designed to assess advanced-level knowledge of human biology from the Sri Lankan school curriculum. Test items were selected by a panel of experts in psychology and medical education from the Faculty of Medicine, University of Kelaniya with the help of disability studies experts who use a similar test for selection to their course. These experts, being native Sri Lankans, ensured the items were culturally relevant and conceptually and semantically equivalent (Hambleton & Zenisky, 2010). Similar methods were used to finalise the Sinhala and Tamil versions of the test, translated by competent translators. Appendix 1 shows sample test items from each subtest. The test was piloted on 15 students and identified issues were corrected.
The test was administered via the online learning management system (LMS) of the respective faculties under examination conditions, with invigilators ensuring adherence to university examination protocols. Students had one hour to complete the test, available in English, Sinhala, and Tamil. Participants could choose the language they were most comfortable with to simulate AL examination conditions and to minimise interpretation errors.
Descriptive statistics and internal consistency (Cronbach’s alpha) were calculated for the test and each subtest and item analysis (Paniagua & Swygert, 2016) was performed. Correlations between the aptitude test score, subtest scores, and Z scores were calculated using Pearson’s correlation coefficient, and relationships to other demographic factors were analysed using Student’s t-test. Factor analysis was performed using R statistical package.
Written informed consent was obtained from the students before the test administration. Ethics approval was granted by the ethics review committee of the Faculty of Medicine, University of Kelaniya, and permission for the study was obtained from the deans of the respective medical faculties.
III. RESULTS
328 students participated in the study, yielding an overall response rate of 80.8%. The descriptive statistics of these students are presented in Table 1. The male-to-female ratio of the sample (31.7% to 68.3%) closely mirrors the demographics of the national cohort of medical undergraduates from the previous academic year (34% to 66%), as reported by the University Grants Commission, Sri Lanka (University Grants Commission, 2022).
|
Total group n=328 |
n |
(%) |
|
Gender |
|
|
|
Male |
104 |
(31.7) |
|
Female |
224 |
(68.3) |
|
Ethnicity |
|
|
|
Sinhala |
161 |
(49.1) |
|
Tamil |
123 |
(37.5) |
|
Moor |
43 |
(13.1) |
|
Other |
1 |
(0.3) |
|
Religion |
|
|
|
Buddhism |
143 |
(43.6) |
|
Hinduism |
108 |
(32.9) |
|
Islam |
43 |
(13.1) |
|
Christianity |
34 |
(10.4) |
|
University |
|
|
|
Jaffna (response rate) |
186 |
(90.7) |
|
Kelaniya (response rate) |
142 |
(70.6) |
Table 1. Descriptive statistics of the demographic variables of the sample
The overall mean aptitude test (AT) score was 70.9 (SD 8.88), with a median of 72. Female students had a higher mean AT score than male students (p=0.044, Table 2), while there was no statistically significant difference in the Z scores between genders (p=0.122). No significant differences in mean AT scores were found between ethnicities and religions. The Faculty of Medicine, University of Kelaniya, had a higher mean AT score (73.7, SD 8.7) than the Faculty of Medicine, Jaffna (68.8, SD 8.4, p=0.000). Similarly, the mean Z score at Faculty of Medicine, University of Kelaniya (2.10, SD 0.07) was higher than at Jaffna (1.89, SD 0.13, p=0.000).
|
AT score |
Z score |
|||
|
Female |
Male |
Female |
Male |
|
|
Mean |
71.6 |
69.4 |
1.99 |
1.96 |
|
Median |
72.0 |
72.0 |
2.06 |
1.99 |
|
Standard Deviation |
8.4 |
9.7 |
0.15 |
0.16 |
Table 2. Comparison of means of AT scores and Z scores between males and females
The internal consistency of the test was 0.628 and the subscales ranged between 0.2 to 0.47 (Table 3).
|
|
Mean |
SD |
Cronbach’s alpha |
|
Abstract Reasoning |
13.4 |
2.32 |
0.339 |
|
The Human Body |
14.6 |
1.72 |
0.248 |
|
Quantitative Reasoning |
13.5 |
2.31 |
0.411 |
|
Decision Making |
10.3 |
2.61 |
0.197 |
|
Verbal Reasoning |
10.2 |
3.17 |
0.433 |
|
Situational Judgment |
8.8 |
3.93 |
0.473 |
Table 3. Data regarding the subtests of the aptitude test
Difficulty and discrimination indices for each test item were calculated (Table 4). The difficulty index represents the proportion of students who answered each item correctly (Paniagua & Swygert, 2016). The mean difficulty index was 70.9% (SD 23.5), ranging from 19.2% to 99.4%. The discrimination index was calculated as the difference between the proportion of students who answered an item correctly in the top group (those who obtained the top 27% in the overall score) and bottom group (bottom 27% scorers) and measures an item’s ability to differentiate between students who performed best and those who performed worst on the test (Paniagua & Swygert, 2016). The mean discrimination index was 19% (SD 12) and ranged from 0 to 50%. There was only one item with the lowest discrimination index of 0. It had a difficulty index of 99.4% indicating that most students had scored it correctly. Items that adversely affected the reliability of the subtests were identified (Appendix 2).
|
Difficulty Index |
Proportion of questions (%) |
|
0 – ≤ 30 |
8 |
|
30 – ≤ 70 |
32 |
|
> 70 |
60 |
Table 4. Distribution of the difficulty indices of the aptitude test questions
The correlation analysis revealed several key findings regarding the relationship between Z and AT scores. The correlation coefficient between Z score and AT score was 0.268 (p=0.000), indicating a weak correlation. The coefficient of determination (r²) was calculated to be 0.072, suggesting that only 7.2% of the variability in AT scores could be explained by Z scores. This signifies a limited association between Z scores and overall AT performance. Further analysis was conducted on the correlation between Z scores and subtest scores. There was a weak but statistically significant correlation between Z scores and the subtests of verbal reasoning (r=0.24, p=0.000), human body (r=0.19, p=0.001), quantitative reasoning (r=0.18, p=0.001), and situational judgment (r=0.128, p=0.021). However, the correlations between Z scores and the subtests of abstract reasoning and decision-making were not statistically significant.
Factor analysis was performed using the most prominent two factors of each of the six subtests separately as they each measure well defined and different cognitive domains. The factor loading of abstract reasoning subtest is shown in figure 1. “Question 3” shows a strong positive loading on Factor 1, suggesting that this item heavily measures the trait most represented by this factor whilst “Question 5” shows a slight negative loading on Factor 1, indicating it measures a trait that is perhaps inversely related to what is captured by this factor. “Question 1” and “Question 2” are both located positively on Factor 2 but with minimal loading on Factor 1. This suggests that they are measuring traits more aligned with Factor 2. The items “Question 1”, “Question 2″ and “Question 3”, appear to be critical for measuring distinct aspects of abstract reasoning as shown by their stronger loadings. “Question 5” shows a strong negative loading on Factor 2, suggesting that it measures a trait that contrasts with what Factor 2 represents. “Question 4”, ” Question 6″, “Question 7”, and “Question 8” are clustered around the origin. This indicates that these items have weaker loadings on both factors, meaning they may not strongly measure the traits represented by either factor, or they could be measuring a balanced mix of both traits. While these questions contribute to the test, they might need to be reviewed to enhance their discriminative power or clarity in measuring specific abstract reasoning skills.
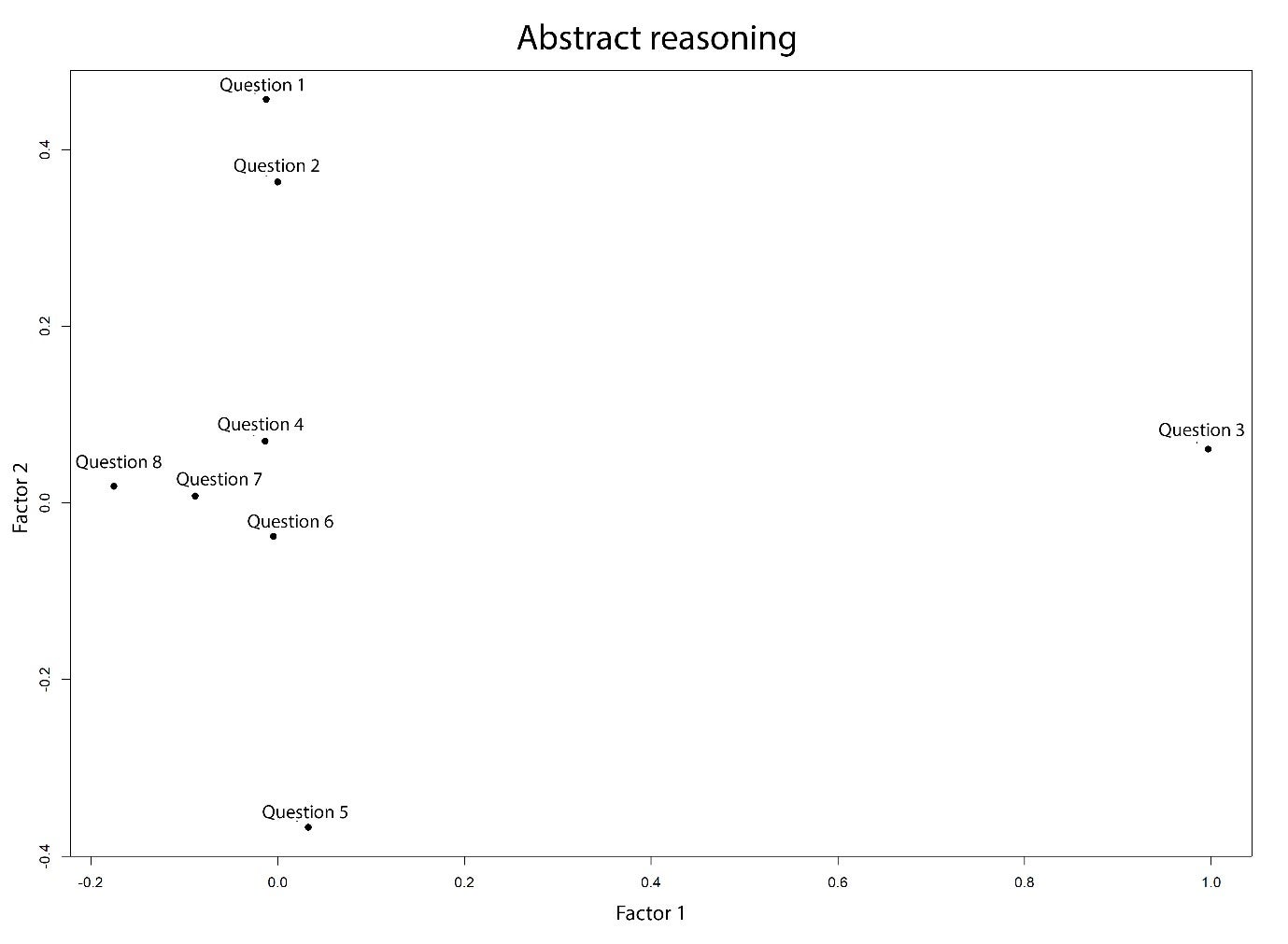
Figure 1. Two factor loading of the abstract reasoning subtest
The factor loadings of the other five subtests are shown in Appendix 3. Regarding the human body subtest, Factor 1 might represent knowledge or understanding of structural aspects of the human body, given the strong loading by “Question 11” and reasonable loading by other items. This factor could reflect knowledge regarding human biology whilst Factor 2 seems to capture a different dimension, suggested by the negative loading of “Question 15”. In quantitative reasoning, most questions are clustered near the centre with a slight spread along Factor 1, indicating moderate influence by this factor across the items. “Question 19” and “Question 22” are slightly farther along Factor 1 suggesting a stronger influence by the trait measured by this factor. Regarding the subtests of decision making, verbal reasoning and situational judgment, Factor 1 and Factor 2 seemed to be capturing different dimension of these subtests thereby suggesting the need for revision of their items.
IV. DISCUSSION
This study aimed to design an aptitude test and investigate its psychometric properties among first-year medical students from two selected faculties of Medicine in Sri Lanka. The results indicate that overall internal reliability of the aptitude test was marginal (Cohen et al., 2018). However, the reliability of the UKCAT has been 0.86 or above overall and between 0.58 – 0.86 for the subtests (MacKenzie et al., 2016). These findings demonstrate the value of evaluating and reviewing aptitude tests locally. Further, reviewing test items that adversely affected the internal consistency of the subtests for clarity and improved alignment with the construct, could improve the overall validity. It is likely that the low number of test items has further contributed to the low-reliability score (Taber, 2018). The UKCAT consists of 200 test items, as opposed to the 50 items in the aptitude test employed by the current study. The item analysis indicated that most of the questions were easy, with 60% having a difficulty index of more than 70%. The discriminating capacity of the items was low (mean discrimination index was 19%). This could be attributed to the aptitude test being administered to students who have performed well in the advanced level examination and already have been selected to medical school.
There was a weak correlation between the aptitude test score and the Z score (0.27), indicating that the test assessed a significantly different aspect of cognitive skills compared to traditional AL examinations. This observation encourages exploring how the aptitude test may be incorporated into the selection process. Different selection authorities use aptitude scores differently (Greatrix & Dowell, 2020). Overall, among the universities which employ UKCAT, the weightage given for school leaver level academic performance in the selection process has increased, while the use of aptitude test scores as an absolute or relative cutoff to be achieved also has increased over the period of 2008-2015 (Greatrix & Dowell, 2020). However, empirical evidence on a best way of using UKCAT or UCAT in the selection process is not available (Greatrix & Dowell, 2020). Therefore, implementing a valid aptitude test as a supplementary test and exploring predictive validities of such a test across a national sample is likely to provide more robust evidence of the utility of aptitude tests in the Sri Lankan context.
This study used an aptitude test developed and deployed systematically and modelled on a widely tested international aptitude test format for medical school selection. The sample was representative of demographics of the national cohort of medical students and included all three major ethnic groups and students with a wide range of Z scores. However, the limited number of test items may have offset these strengths. The authors did not have access to participants’ raw scores at the advanced level examination, which may have provided a more appropriate measure of performance for statistical manipulation. In addition, the aptitude test was administered to students who have already been selected to medical school, whereas ideally, it should have been administered to medical school applicants. Despite the limitations, the aptitude test returned an acceptable internal reliability score, and further analysis demonstrated a way forward.
V. CONCLUSION
This study was the first time in the literature that an aptitude test was evaluated in medical education settings in the Sri Lankan context. Using an aptitude test to select students for medical school in Sri Lanka and similar settings, where admission processes have not diversified, is potentially valuable. However, further studies are necessary to establish evidence to support the adoption of such a test in the Sri Lankan and other similar resource-constrained contexts where prior educational achievement primarily informs selection decisions. In the Sri Lankan context, further evaluating the psychometric properties and the predictive validity of an improved aptitude test using a national cohort is recommended as the way forward.
Notes on Contributors
Dr. Sivapalan Sanchayan contributed to the development of the aptitude test, administering the test, collection of data, analysis and writing of the manuscript.
Dr. Sisira Dharmaratne contributed to the conceptualisation, study design, development of the aptitude test, data analysis and writing of the manuscript.
Ms. Shalika Pathirana took part in developing and administering the test, data collection and reviewing the manuscript.
Dr. Pavithra Godamunne contributed to the conceptualisation, study design, development of the aptitude test, data collection, analysis and revision of the manuscript.
Prof. Madawa Chandratilake took part in the conceptualisation, study design, data analysis and revision of the manuscript
Ethical Approval
Ethical clearance (P/223/12/2018) was obtained from the Faculty of Medicine, University of Kelaniya, Sri Lanka.
Data Availability
The datasets generated and/or analysed during the current study are not publicly available to preserve the confidentiality of the participants in this study but are available from the corresponding author on reasonable request.
Acknowledgement
We acknowledge the contribution of Ms. B. N. Jayasena (former lecturer, Department of Disability Studies, Faculty of Medicine, University of Kelaniya) and Ms. L. K. E. Chathurika (former lecturer, Department of Disability Studies, Faculty of Medicine, University of Kelaniya) in the development of the aptitude test. We also acknowledge the contribution of Dr. Rasiah Thayakaran (Research fellow in Health Informatics, Institute of Applied Health Research, University of Birmingham) in performing factor analysis.
Funding
The research received no specific grant from any funding agency.
Declaration of Interest
The authors have no conflicts of interest to disclose.
References
Bala, L., Pedder, S., Sam, A. H., & Brown, C. (2022). Assessing the predictive validity of the UCAT-A systematic review and narrative synthesis. Medical Teacher, 44(4), 401–409. https://doi.org/10.1080/0142159X.2021.1998401
Cohen, L., Manion, L., & Morrison, K. (2018). Research Methods in Education. Routledge.
de Silva, N. R., Pathmeswaran, A., & de Silva, H. J. (2004). Selection of students for admission to a medical school in Sri Lanka. The Ceylon Medical Journal, 49(3), 81–85. https://doi.org/10.4038/cmj.v49i3.3245
de Silva, N. R., Pathmeswaran, A., de Silva, N., Edirisinghe, J. S., Kumarasiri, P. V., Parameswaran, S. V., Seneviratne, R., Warnasuriya, N., & de Silva, H. J. (2006). Admission to medical schools in Sri Lanka: Predictive validity of selection criteria. The Ceylon Medical Journal, 51(1), 17–21. https://doi.org/10.4038/cmj.v51i1.1371
Dharmaratne, S., & Ponnamperuma, G. (2020). Selection for health professions education. In M. Chandratilake & A. Olupeliyawa (Eds.), 14 topics in health professions education (pp. 120–132). College of Medical Educationists, Sri Lanka.
Gliatto, P., Leitman, I. M., & Muller, D. (2016). Scylla and charybdis: The MCAT, USMLE, and degrees of freedom in undergraduate medical education. Academic Medicine, 91(11), 1498–1500. https://journals.lww.com/academicmedicine/Fulltext/ 2016/11000/Scylla_and_Charybdis__The_MCAT,_USMLE,_and_Degrees.16.aspx
Greatrix, R., & Dowell, J. (2020). UKCAT and medical student selection in the UK – what has changed since 2006? BMC Medical Education, 20(1), 1–12. https://doi.org/10.1186/s12909-020-02214-1
Greatrix, R., Nicholson, S., & Anderson, S. (2021). Does the UKCAT predict performance in medical and dental school? A systematic review. BMJ Open, 11, Article e040128. https://doi.org/10.1136/BMJOPEN-2020-040128
Hambleton, R. K., & Zenisky, A. L. (2010). Translating and adapting tests for cross-cultural assessments. In D. Matsumoto, F. J. R. van de Vijver (Eds.), Cross-cultural research methods in psychology (pp. 46–70). Cambridge University Press.
Hewage, S. N., Salgado, L. S. S., Fernando, G. M. O., Liyanage, P., Pathmeswaran, A., & De Silva, N. R. (2011). Selection of medical students in Sri Lanka: Time to re-think criteria? Ceylon Medical Journal, 56(1), 22–28.
MacKenzie, R. K., Cleland, J. A., Ayansina, D., & Nicholson, S. (2016). Does the UKCAT predict performance on exit from medical school? A national cohort study. BMJ Open, 6, Article e011313. https://doi.org/10.1136/BMJOPEN-2016-011313
McManus, I. C., Dewberry, C., Nicholson, S., & Dowell, J. S. (2013). The UKCAT-12 study: Educational attainment, aptitude test performance, demographic and socio-economic contextual factors as predictors of first year outcome in a cross-sectional collaborative study of 12 UK medical schools. BMC Medicine, 11, Article 244. https://doi.org/10.1186/1741-7015-11-244
McManus, I. C., Dewberry, C., Nicholson, S., Dowell, J. S., Woolf, K., & Potts, H. W. W. (2013). Construct-level predictive validity of educational attainment and intellectual aptitude tests in medical student selection: Meta-regression of six UK longitudinal studies. BMC Medicine, 11, Article 243. https://doi.org/10.1186/1741-701 5-11-243
Mettananda, D. S. G., Wickramasinghe, V. P., Kudolugoda Arachchi, J., Lamabadusuriya, S. P., Ajanthan, R., & Kottahachchi, D. (2006). Suitability of selection criteria as a measure of outcome of medical graduates: University of Colombo. The Ceylon Journal of Medical Science 49, 1–12.
Paniagua, M. A., & Swygert, K. A. (2016). Constructing written test questions for the basic and clinical sciences (4th ed.). National Board of Medical Examiners.
Paton, L. W., McManus, I. C., Cheung, K. Y. F., Smith, D. T., & Tiffin, P. A. (2022). Can achievement at medical admission tests predict future performance in postgraduate clinical assessments? A UK-based national cohort study. BMJ Open, 12, Article e056129. https://doi.org/10.1136/bmjopen-2021-056129
Patterson, F., Cousans, F., Edwards, H., Rosselli, A., Nicholson, S., & Wright, B. (2017). The predictive validity of a text-based situational judgment test in undergraduate medical and dental school admissions. Academic Medicine, 92(9), 1250–1253. https://doi.org/10.1097/ACM.0000000000001630
Patterson, F., Roberts, C., Hanson, M. D., Hampe, W., Eva, K., Ponnamperuma, G., Magzoub, M., Tekian, A., & Cleland, J. (2018). 2018 Ottawa consensus statement: Selection and recruitment to the healthcare professions. Medical Teacher, 40(11), 1091–1101. https://doi.org/10.1080/0142159X.2018.149 8589
Powis, D. A., Munro, D., & Bore, M. R. (2021). Is the UCAT appropriate for selecting undergraduate medical students? Medical Journal of Australia, 214(2), 77–78. https://doi.org/10.5694/mja2.50906
Prideaux, D., Roberts, C., Eva, K., Centeno, A., Mccrorie, P., Mcmanus, C., Patterson, F., Powis, D., Tekian, A., & Wilkinson, D. (2011). Assessment for selection for the health care professions and specialty training: Consensus statement and recommendations from the Ottawa 2010 conference. Medical Teacher, 33(3), 215–223. https://doi.org/10.3109/0142159X.2011.551560
Soemantri, D., Karunathilake, I., Yang, J. H., Chang, S. C., Lin, C. H., Nadarajah, V. D., Nishigori, H., Samarasekera, D. D., Lee, S. S., Tanchoco, L. R., & Ponnamperuma, G. (2020). Admission policies and methods at crossroads: A review of medical school admission policies and methods in seven Asian countries. Korean Journal of Medical Education, 32(3), 243–256. https://doi.org/10.3946/KJME.2020.169
Taber, K. S. (2018). The use of Cronbach’s Alpha when developing and reporting research instruments in science education. Research in Science Education, 48(6), 1273–1296. https://doi.org/10.1007/ s11165-016-9602-2
University Grants Commission. (2022). Sri Lanka university statistics 2022. Ministry of Higher Education. https://www.ugc.ac.lk/downloads/statistics/stat_2022/Chapter%202.pdf
University Grants Commission. (2023). Admission to undergraduate courses of the universities in Sri Lanka – 2022/2023. Ministry of Higher Education. https://www.ugc.ac.lk/downloads/admissions/Handbook_2022_23/student_handbook_english.pdf
Zimmermann, S., Klusmann, D., & Hampe, W. (2017). Correcting the predictive validity of a selection test for the effect of indirect range restriction. BMC Medical Education, 17, Article 246. https://doi.org/10.1186/s12909-017-1070-5
*S. Sanchayan
Faculty of Medicine,
University of Jaffna,
Adiyapatham Road,
Kokuvil West, Kokuvil, Sri Lanka
Email: sanch.s6@gmail.com,
sanchayan@univ.jfn.ac.lk
Submitted: 6 May 2024
Accepted: 12 September 2024
Published online: 7 January, TAPS 2025, 10(1), 48-52
https://doi.org/10.29060/TAPS.2025-10-1/SC3349
Craig S. Webster1,2, Antonia Verstappen1, Jennifer M. Weller1 & Marcus A. Henning1
1Centre for Medical and Health Sciences Education, School of Medicine, University of Auckland, Auckland, New Zealand; 2Department of Anaesthesiology, Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand
Abstract
Introduction: We aimed to determine the extent to which non-technical skills and attitudes acquired during undergraduate interprofessional simulation in an Advanced Cardiac Life Support (ACLS) course translated into clinical work.
Methods: Following ACLS simulation training for final-year nursing and medical students, we conducted a 1-year follow-up survey, when graduates were in clinical practice. We used the Readiness for Interprofessional Learning Scale (RIPLS – higher scores indicate better attitudes to interprofessional practice), and nine contextual questions with prompts for free-form comments. RIPLS scores underwent repeated-measures between-groups (nurses vs doctors) analysis at three timepoints (pre-course, post-course and 1-year).
Results: Forty-two surveys (58% response) were received, demonstrating translation of non-technical skills and attitudes to clinical practice, including insights into the skills and roles of others, the importance of communication, and improved perceptions of preparedness for clinical work. However, RIPLS scores for doctors decreased significantly upon beginning clinical work, while scores for nurses continued to increase, demonstrating a significant interaction effect (reduction of 5.7 points to 75.7 versus an increase of 1.3 points to 78.1 respectively – ANOVA, F(2,76)=5.827, p=0.004). Responses to contextual questions suggested that reductions in RIPLS scores for doctors were due to a realisation that dealing with emergency life support was only a small part of their practice. However, the prevailing work cultures of nurses and doctors in the workplace may also play a part.
Conclusion: We demonstrated the translation of non-technical skills and attitudes acquired in undergraduate simulation to the clinical workplace. However, results are tempered for junior doctors beginning practice.
Keywords: Work Culture, Translation, RIPLS, Simulation, Advanced Cardiac Life Support, Undergraduate Education, Skills and Attitudes, Patient Safety
I. INTRODUCTION
Preparing undergraduate healthcare students for their future roles in the clinical workplace is a central concern for modern healthcare educators and is of critical importance for the maintenance of adequate healthcare services throughout the world (Barnes et al., 2021). Modern healthcare is inherently multidisciplinary, yet much of the training received by healthcare practitioners remains siloed within professional groups, and this is particularly the case at the undergraduate level. The use of simulation in healthcare has become increasingly important in recent years as a way to offer safe and immersive training. Conducting simulation with interprofessional healthcare teams allows those who will work together to be trained together, and can have the double benefit of promoting the acquisition of technical and non-technical skills in participants, while also allowing insight into the skills, roles and knowledge of other team members from different professional groups (Jowsey et al., 2020).
We previously reported on the development and evaluation of an interprofessional Advanced Cardiac Life Support (ACLS) course for undergraduate nursing and medical students in their final year at the University of Auckland, aimed at increasing technical resuscitation and non-technical teamwork skills (Webster et al., 2018). The evaluation study, using a mixed-methods design and recruiting 69% of the entire year’s student cohort, demonstrated significant improvements in scores on the Readiness for Interprofessional Learning Scale (RIPLS) over the course of the training day, and important interprofessional and attitudinal insights into the skills and knowledge of other team members related to communication, teamwork, leadership, realism, and professional roles. Medical and nursing students both reported that such insights would not have occurred during uniprofessional simulation and felt that the course had better prepared them for work in the clinical context. At the end of the training day we invited participants to take part in a further follow-up survey timed to occur approximately one year later, at a time when participants would typically be working clinically.
Our aim in the present study was to determine the extent to which the non-technical skills and attitudes acquired during the undergraduate interprofessional ACLS simulation course translated into the clinical work of the former course participants.
II. METHODS
We conducted a 1-year follow-up survey comprising a further RIPLS questionnaire and nine additional contextual questions, with quantitative response scales and prompts for explanatory free-form comments (see Supplementary Table 1). The survey was mailed to participants who had elected to supply their contact information, along with a post-paid return envelope. All participants gave written informed consent to participate. One postal and one email reminder was also sent if a reply was not forthcoming.
The RIPLS is a validated questionnaire comprising 19 questions using 5-point Likert response scales (anchors, 1=strongly disagree to 5=strongly agree), and yielding a possible total score from 19 to 95 points where higher scores indicate a greater willingness to engage in interprofessional practice (Parsell & Bligh, 1999). In the present analysis, RIPLS responses from each participant in the 1-year follow-up survey were paired with their own corresponding RIPLS scores at two previous time points and underwent repeated-measures between-groups (nurses vs doctors) analysis at three timepoints (pre-course, post-course and 1-year). Responses to quantitative ratings on contextual questions used identical 5-point Likert scales and were summarised along with exemplar quotations from the free-form comments (Supplementary Table 1).
III. RESULTS
Between August 2014 and November 2015, 42 survey responses were received, representing a 58% response rate from the 73 participants who elected to give contact information for the follow-up survey. Two nurses were not working clinically at the time of the survey, and their responses were excluded from analysis – resulting in a total of 14 nurses and 26 doctors being included in the present study. All doctors were working in hospitals at the time of the 1-year survey, as were 71% of nurses. The remaining nurses were working in primary healthcare or general practice. RIPLS data did not significantly depart from a normal distribution (Shapiro-Wilk test, p=0.22), therefore parametric analysis was conducted using SPSS v.27 (IBM SPSS Statistics, Armonk, New York).
A one-way repeated measures ANOVA demonstrated a significant interaction effect between time point and professional group (F(2, 76)=5.827, p=0.004), demonstrating that at the 1-year time point mean RIPLS scores for doctors fell significantly by 5.7 points, while mean RIPLS scores for nurses continued to increase by 1.3 points (Figure 1).
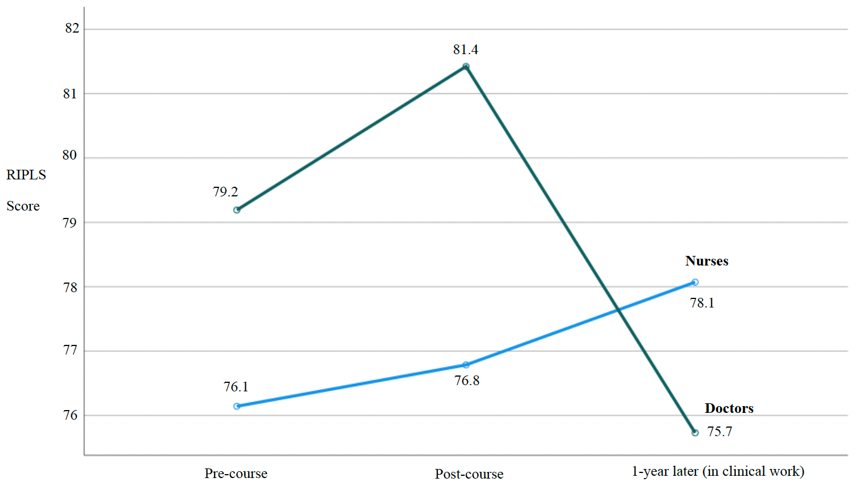
Figure 1. RIPLS scores for nurses and doctors paired over three time points
The results of the contextual questions in the present study (1-year time point) demonstrated strong support by nurses and doctors for the value of the interprofessional ACLS course in general terms and more specifically in terms of feeling part of the team, better understanding the skills and roles of others, and feeling more confident in clinical practice – with all mean responses ranging from high 3’s to >4 (see Supplementary Table 1 for complete summary). Participants strongly agreed that the interprofessional ACLS course should continue to be offered (with an overall mean score of 4.68 out of 5). The single reverse-scored question asking whether ACLS training would have been more effective if conducted uniprofessionally demonstrated strong disagreement with an overall mean score of 1.65. Exemplar quotations from free-form comments provided a context for the quantitative results in terms of demonstrating that the ACLS training better prepared doctors and nurses for emergencies, helped to improve their communication, and was a realistic form of training – for example, stating “Much more ‘real life’ when other professions involved” (doctor) and “Interdisciplinary teamwork is huge in the real world…” (nurse).
Despite the largely positive findings, exemplar quotations also allowed some insight into why doctors’ RIPLS scores were high at the end of the ACLS course, but then fell significantly upon entry into clinical practice at the 1-year time point. Exemplar quotations suggested that once in the clinical workplace junior doctors better appreciated that the technical skills in the ACLS course made up only a small part of their scope of practice, stating that there “are many things… you are unable to do and it is important to know what level of knowledge and ability other individuals may have” and that ACLS “does not make up a large part of my clinical practice” (Supplementary Table 1).
IV. DISCUSSION
Our results demonstrate the translation of non-technical skills and attitudes acquired during undergraduate interprofessional simulation training to the clinical workplace. Our findings show particular benefits for nurses, and reinforce the value of the interprofessional ACLS course as an important part of the undergraduate curriculum. While the overall evaluation of the ACLS course was positive, the differential response in RIPLS scores between nurses and doctors upon entry into the clinical workplace is an intriguing result which clearly warrants further research.
We know of no previous study that has followed the same cohort of undergraduate participants after an interprofessional simulation course up to the point where they have entered the clinical workplace. The ability to pair responses for the same participants across all three time points in our study is a strength, as this avoids the variability that would be present if there were different participants at each time point, and so gives us more confidence in our findings.
Our results suggest that the significant reduction in RIPLS scores upon entry into the clinical workplace for junior doctors may be due to a realisation that the technical skills learnt in the ACLS course make up only a small part of a doctor’s domain of practice. However, recent research into the experiences of junior doctors during interprofessional collaboration suggests that the interaction effect in RIPLS scores across professional groups may also be a consequence of the different work cultures of nurses and doctors. Evidence suggests, including from our own University, that doctors typically believe that they should take individual responsibility for their clinical work, while nurses have a more collective view of patient care (Horsburgh et al., 2006; van Duin et al., 2022). Thus, the prevailing workplace cultures could reinforce and promote nurses’ willingness to work interprofessionally (hence explaining the increase in their RIPLS scores), while for doctors the prevailing individualistic work culture may reduce their willingness to work interprofessionally (hence contributing to the reduction in their RIPLS scores, Figure 1).
Further work to investigate this intriguing interaction effect, and the dynamics of work cultures and professional identity formation, would likely involve mixed-method research, perhaps using observation, interviews or focus groups and quantitative measures such as RIPLS (Jowsey et al., 2020). In addition, such studies conducted with clinicians at various levels of experience within a hospital could potentially yield insight into the state of the prevailing clinical work cultures and may allow some estimate of whether incoming graduates with interprofessional training could change these cultures, and when a critical mass of such graduates may allow this to happen. In the meantime, our results suggest that prevailing work cultures may represent a challenge for interprofessional teamwork initiatives, at least in medicine.
V. CONCLUSION
Our follow-up study demonstrated the translation of the non-technical skills and attitudes acquired during undergraduate interprofessional simulation training to the clinical workplace in terms of insights into the skills and roles of others, the importance of communication, and perceptions of preparedness to deal with emergencies. However, these results appear to be tempered for junior doctors beginning clinical work likely due to realisations around the applicability of ACLS training to their scope of practice and the influences of their prevailing workplace culture.
Notes on Contributors
Craig S. Webster was involved in the conceptualisation of this study, data analysis, writing and revision.
Antonia Verstappen was involved in data collection and analysis, writing and revision.
Jennifer M. Weller was involved in the conceptualisation of this study, writing and revision.
Marcus A. Henning was involved in the writing and revision of this paper.
Ethical Approval
This study was carried out in accordance with all regulations of the host organisation and with the approval of the Human Participants Ethics Committee of the University of Auckland (reference number 9073). All participants gave written informed consent to participate.
Data Availability
The complete data set for this study is openly available on the Figshare repository, https://doi.org/10.6084/m9.figshare.25750230
Funding
This study was conducted without funding.
Declaration of Interest
All authors have no potential conflicts of interest.
References
Barnes, T., Yu, T. W., & Webster, C. S. (2021). Are we preparing medical students for their transition to clinical leaders? A national survey. Medical Science Educator, 31(1), 91-99. https://doi.org/10.1007/s40670-020-01122-9
Horsburgh, M., Perkins, R., Coyle, B., & Degeling, P. (2006). The professional subcultures of students entering medicine, nursing and pharmacy programmes. Journal of Interprofessional Care, 20(4), 425-431. https://doi.org/10.1080/13561820600805233
Jowsey, T., Petersen, L., Mysko, C., Cooper-Ioelu, P., Herbst, P., Webster, C. S., Wearn, A., Marshall, D., Torrie, J., Lin, M. P., Beaver, P., Egan, J., Bacal, K., O’Callaghan, A., & Weller, J. (2020). Performativity, identity formation and professionalism: Ethnographic research to explore student experiences of clinical simulation training. PLoS One, 15(7), e0236085. https://doi.org/10.1371/journal.pone.0236085
Parsell, G., & Bligh, J. (1999). The development of a questionnaire to assess the readiness of health care students for interprofessional learning (RIPLS). Medical Education, 33(2), 95-100. https://doi.org/10.1046/j.1365-2923.1999.00298.x
van Duin, T. S., de Carvalho Filho, M. A., Pype, P. F., Borgmann, S., Olovsson, M. H., Jaarsma, A. D. C., & Versluis, M. A. C. (2022). Junior doctors’ experiences with interprofessional collaboration: Wandering the landscape. Medical Education, 56(4), 418-431. https://doi.org/10.1111/medu.14711
Webster, C. S., Hallett, C., Torrie, J., Verstappen, A., Barrow, M., Moharib, M. M., & Weller, J. M. (2018). Advanced cardiac life support training in interprofessional teams of undergraduate nursing and medical students using mannequin-based simulation. Medical Science Educator, 28(1), 155-163. https://doi.org/10.1007/s40670-017-0523-0
*Craig Webster
Centre for Medical and Health Sciences Education
School of Medicine, University of Auckland
Private Bag 92-019
Auckland 1142, New Zealand.
Email: c.webster@auckland.ac.nz
Submitted: 31 January 2024
Accepted: 3 September 2024
Published online: 7 January, TAPS 2025, 10(1), 56-58
https://doi.org/10.29060/TAPS.2025-10-1/PV3239
Chan Choong Foong1, Mohamad Nabil Mohd Noor1 & Galvin Sim Siang Lin2
1Medical Education and Research Development Unit, Faculty of Medicine, Universiti Malaya, Malaysia; 2Department of Restorative Dentistry, Kulliyyah of Dentistry, International Islamic University Malaysia, Malaysia
I. INTRODUCTION
Contemporary undergraduate medical education is increasingly emphasising the cultivation of student ownership and autonomy, entrusting learners with the responsibility to take charge of their own studies. Across Asian countries, high school graduates embark on their medical education journey at the age of 19 to 20 years, stepping into the realm of adulthood and assuming accountability for their academic pursuits. As the landscape of medical education undergoes transformative shifts propelled by technological advancements and evolving pedagogical approaches, one enduring tradition faces scrutiny: the imposition of compulsory lecture attendance.
Intriguingly, amid the broader trend toward fostering student autonomy, some Asian medical schools grapple with concerns about low lecture attendance. Rather than embracing the prevailing ethos of adult learning, these institutions respond by adopting autocratic measures to enforce mandatory attendance. This perplexing approach begs the question: Why, in an era of educational evolution and empowerment, do certain medical schools resort to rigid mandates to address the issue of diminished lecture participation?
This article does not engage in a debate about the efficacy of lectures; instead, it delves into the heart of the matter — the compulsory attendance. Considering medical teachers’ dissatisfaction with students’ lecture attendance rates, it becomes imperative to explore the underlying frustrations that lead institutions toward autocratic measures. What lies at the core of this apparent contradiction between the shift toward learner autonomy and the persistence of compulsory lecture attendance?
II. THE FRUSTRATIONS AND OUR ARGUMENTS
1. Some medical teachers may argue that frustration lies in the association between lecture attendance and academic performance.
Our arguments are as follows. First, research data show a mixture of supporting and opposing evidence (Doggrell, 2020b). Second, if this association holds true, it implies that high-achieving students should be afforded the freedom to forego lectures. Alternatively, medical students who acquire lecture content from other media, such as recorded lectures or online resources (e.g. YouTube videos), and offline resources (e.g. reference books) should also have the freedom to skip lectures. Third, it appears more rational to correlate academic performance with students’ active engagement during lectures rather than their mere physical attendance. Students who attend lectures to avoid punishment may be reluctant to become involved. Despite their outward presence, if these students remain preoccupied with internet-connected devices, does their mere attendance satisfy the expectations of medical teachers? The scenario becomes even more poignant when considering the time medical teachers spend managing students who are not engaged in lectures. This time could otherwise have been meaningfully invested in students genuinely seeking to absorb and engage with the lecture content.
2. Some medical teachers contend that the crux of the frustration lies within professionalism, positing that attending lectures is an integral aspect of student professionalism.
Our arguments are as follows. First, a systematic review discussing unprofessional behaviours among medical students does not identify lecture attendance as a dimension of professionalism (mak-Van der Vossen et al., 2017). Second, even if one were to categorise lecture absenteeism as unprofessional, the AMEE Guide No. 61, titled “Integrating professionalism into the curriculum”, does not advocate for compulsory attendance as a prescribed professional solution (O’Sullivan et al., 2012).
Some medical teachers draw parallels by likening student absenteeism to the unacceptable conduct of on-duty medical practitioners. However, this analogy lacks validity. The execution of medical duties by practitioners necessitates a specific venue, such as a clinic, and adherence to fixed working hours. In contrast, medical students can fulfil their learning responsibilities at any time and from any location, exemplified by the ability to engage with recorded lectures. For the analogy to be valid, lectures must be proven irreplaceable in delivering certain medical content.
3. Some medical teachers contend that their frustration lies in low lecture attendance, adversely affecting their morale for teaching (Emahiser et al., 2021).
Our arguments are as follows. First, although low attendance can be upsetting and disappointing, medical teachers should not request compulsory attendance to appease their emotional and moral demands. While commenting on student absenteeism as unprofessional, do these teachers, in turn, project a more professional image by demanding mandatory attendance? Second, the variability in audience size for different lectures or lecturers warrants the teachers’ self-reflections on their teaching methods (Emahiser et al., 2021). Third, there is perhaps no downside to the teaching styles employed by medical teachers; however, some medical students have preferences for different learning methods (Emahiser et al., 2021). Alternatively, the characteristics of Generation Z learners, marked by a limited attention span and a preference for online learning environments, may not align with the assumptions underlying compulsory lectures. Mandating attendance presupposes a one-size-fits-all approach, and debatably, lectures might not be the panacea for optimal academic performance among medical students.
4. Some medical teachers may argue that the frustration stems from the perception that many Asian high school leavers are not mature enough to make decisions.
Our central argument posits that, irrespective of the potential benefits of lectures, they should not be mandated. How can medical students cultivate maturity if they are not afforded the opportunity to exercise decision-making in the first place? It is ironic that, while Asian medical schools try to promote adult learning principles into their curriculum, they endorse paternalism in conditioning student behaviours. Our stance is not a discouragement of lecture attendance; rather, we oppose the imposition of paternalism in moulding the physicians of tomorrow.
III. OUR PROPOSALS
To address the challenge of low lecture attendance, our proposal for medical teachers is to reconsider the delivery method of lectures. Let us acknowledge the need for our teaching methods to evolve in response to technological advancements and the distinctive learning preferences of Generation Z. Following is an actual reason for absence – “I don’t consider the lecturer adds to the material given on the PowerPoints” and a reason for attending – “It allows for interaction with course staff and/or students” (Doggrell, 2020a). Thus, it becomes imperative for medical institutions to train educators with interactive strategies (e.g., inquiry activities) that complement lectures and motivate students to actively participate in the learning process. Consequently, faculty development programs that are in line with evolving learning science and the changing needs of learners are deemed necessary.
Next, we should reconsider the emotional need to see students physically. Theoretical and empirical evidence suggests that recorded lectures work effectively, as students can pause and play the recordings, which enables them to learn at their own pace. Medical teachers must accept that, with the tremendous amount of available teaching and learning materials online, attending lectures is no longer the sole source of knowledge. Considering flexible attendance policies that accommodate students’ individual needs and recognising the importance of adapting to evolving educational practices and preferences are equally essential.
For medical students, our suggestion is to foster ownership and autonomy in their studies, predicated on an understanding of the potential repercussions on their academic performance. Medical students should be empowered to make informed choices, cognisant that each choice carries consequences. This approach aligns with the principles observed in medicine, where patients retain the autonomy to continue or discontinue treatment at their own risk. If adult learning is deemed fundamental to the future medical curriculum, Asian medical teachers ought to relinquish paternalistic tendencies.
This shift does not imply a cessation of support for student learning. Instead, we shift to help students “learning to learn”, for instance, to promote the understanding of (including but not limited to) andragogy and self-regulated learning. It may not be the lecture attendance that some low-achieving medical students have missed; rather, it could be the cultivation of appropriate mindsets about learning, including aspects like time management and motivation.
IV. CONCLUSION
In conclusion, our scrutiny of compulsory lecture attendance reveals that it neither serves as a panacea for academic performance nor aligns seamlessly with the principles of professionalism or the preferred learning styles of Generation Z. Rather than acting as an antidote, the imposition of compulsory attendance manifests as a form of paternalism within Asian medical schools. This paternalistic approach, rather than nurturing, acts as a toxic element for aspiring medical professionals, hindering the cultivation of autonomy and adult learning principles in the trajectory of futuristic medical education. To remedy this issue, delivery method of lectures should consider state-of-the-art learning science, matched with the changing needs of students.
Notes on Contributors
Chan Choong Foong conceptualised and designed the work, and drafted the manuscript. Mohamad Nabil Mohd Noor conceptualised and designed the work, and drafted the manuscript. Galvin Sim Siang Lin interpreted the findings from past studies for the work, and revised the manuscript critically. All authors have read and approved the submitted manuscript.
Funding
The authors did not receive support from any organisation for the submitted work.
Declaration of Interest
The author declares that there is no conflict of interest.
References
Doggrell, S. A. (2020a). No apparent association between lecture attendance or accessing lecture recordings and academic outcomes in a medical laboratory science course. BMC Medical Education, 20, Article 207. https://doi.org/10.1186/s12909-020-02066-9
Doggrell, S. (2020b). A systematic review of the relationship between lecture attendance and academic outcomes for students studying the human biosciences. International Journal of Innovation in Science and Mathematics Education, 28(1), 60-76. https://doi.org/10.30722/IJISME.28.01.005
Emahiser, J., Nguyen, J., Vanier, C., & Sadik, A. (2021). Study of live lecture attendance, student perceptions and expectations. Medical Science Educator, 31, 697-707. https://doi.org/10.1007/s40670-021-01236-8
Mak-van Der Vossen, M., van Mook, W., van Der Burgt, S., Kors, J., Ket, J. C., Croiset, G., & Kusurkar, R. (2017). Descriptors for unprofessional behaviours of medical students: A systematic review and categorisation. BMC Medical Education, 17, Article 164. https://doi.org/10.1186/s12909-017-0997-x
O’Sullivan, H., van Mook, W., Fewtrell, R., & Wass, V. (2012). Integrating professionalism into the curriculum: AMEE Guide No. 61. Medical Teacher, 34(2), e64-e77. https://doi.org/10.3109/0142159X.2012.655610
*Chan Choong Foong
Medical Education and Research Development Unit,
Faculty of Medicine, Universiti Malaya,
50603 Kuala Lumpur, Malaysia
Email: foongchanchoong@um.edu.my
Submitted: 6 May 2024
Accepted: 23 September 2024
Published online: 7 January, TAPS 2025, 10(1), 59-61
https://doi.org/10.29060/TAPS.2025-10-1/CS3339
Kye Mon Min Swe1, Amit Bhardwaj2 & Hnin Pwint Phyu3
1School of Medicine, Newcastle University Medicine Malaysia, Malaysia; 2Department of Orthopaedics, Sengkang General Hospital, Singapore; 3M Kandiah Faculty of Medical and Health Science, University Tunku Abdul Rahman, Malaysia
I. INTRODUCTION
Telemedicine is defined as delivering healthcare services across distances using telecommunication technology (Waseh & Dicker, 2019). It helps ensure continuity of care for vulnerable patients to address the unique demands on our health system, especially in times of crisis, such as the COVID-19 pandemic, via virtual follow-up. It is also helpful in engaging medical students in training and patient care (Aron et al., 2020).
During the pandemic, virtual follow-up (VF) home visits were introduced in the integrated family medicine curriculum for Year 4 students. The family medicine curriculum for Year 4 students highlights the significance of comprehending chronic illnesses within the broader framework of the patient’s family and environment via the Follow-up Study of Patients with Chronic Illnesses programme, traditionally conducted through in-person patient visits. This study investigated the challenges faced while conducting virtual follow-up (VF) patient visits amidst the COVID-19 pandemic.
II. METHODS
A cross-sectional study was conducted via online survey questionnaires upon completing the family medicine posting. The online feedback questionnaires were used to explore the challenges of virtual follow-up (VF) via open-ended questionnaires. All participants were duly informed about the study and obtained their consent. The ethical approval was obtained from the Scientific Ethical Review Committee of the University Tunku Abdul Rahman.
III. RESULTS
In this study, among 49 students from year 4 MBBS, 47 year-four medical students participated in the research, and all the students were aged between 20-24. The students were grouped into 18 groups for VF home visits, each containing 2-3 students. A total of 18 chronic illness patients were virtually followed during the COVID-19 pandemic. The challenges and benefits faced by the students during virtual patient follow-up visits were explored via the open-ended questions and shown in Table 1.
|
Challenges |
|
I. Challenges related to follow-up consultation. “Patient refused to have clerked, and we had to clerk family members instead.” “Difficult to obtain updates on the patient’s condition.” “Not really interactive, more like a Q&A session.” “Difficult to express concern for the patient over video conferencing too.” “Cannot observe patient hard to assess patient current condition, hard to assess patient current condition.” “Unable to assess patient’s full motor function through video call as we could not perform physical examination.” “Difficult to access the physical environment.” “Cannot know the patient’s living condition.” |
|
II. Challenges in making appointments with the patients. “Patient didn’t pick up the phone; Patient was not very responsive.” “We could not contact her sometimes.” “Patient no reply to my text, the patient refuses to have a virtual call, and it is hard to conduct the visit.” “The patient kept postponing the virtual visit, and it was difficult to arrange a time with the patient.” |
|
III. Challenges related to technical problems. “The unclear or low video call quality during the virtual follow-up” “We can listen to the patients clearly, but the image or the video was not that clear.” “Blur voice call” “Patient is unable to use video calls such as WhatsApp calls.” “Difficulty arranging a virtual visit with the elderly patient as he is unfamiliar with the gadgets.” “Difficulty in video calling patient as she doesn’t know how to use WhatsApp video or other social platforms.” “Patient does not have access to a smartphone.” |
|
Benefits |
|
I. The benefit of a virtual follow-up visit “It’s a new experience”. “Convenient” “Time is more flexible.” “No need to travel, less travelling and saving cost” “Virtual home visit has reduced risk of transmission.” |
|
II. The benefit of a follow-up visit to a patient with chronic illness. “Teamwork makes working easier and enjoyable.” “Teamwork helped us plan and conduct virtual home visits before the deadline.” “I learnt the importance of home visits.” “Patient is a better teacher than the textbook”. “Delightful, enjoyed learning other people’s culture.” “Learnt interacting with the patient, sharing information with the patient.” “Learnt about real-life follow-up with patients who are not compliant with medical treatment.” |
Table 1. The Challenges and Benefits When Conducting Virtual Follow-up Home Visits
IV. DISCUSSION
Although the experiences of VF visits are challenging, medical students found the experiences valuable. The students found the importance of VF for chronic illness, which made them aware of the challenges and benefits of telemedicine. The challenges were similar to the studies from literature, such as technological difficulties, lack of familiarity with telehealth platforms, lack of access to internet or devices and sufficient internet connection speed, especially with patients with low socioeconomic status, which hinder effective communication and assessment. Moreover, patients with physical, cognitive, and language disabilities may find it hard to use the technology. Another challenge was the inability to perform an in-person clinical examination, and the students found less confidence in evaluating patient conditions through a screen, which impacted the quality of care delivered (Cheng et al., 2022; Pathipati et al., 2016).
To overcome these challenges, it is essential to provide comprehensive training focused on telehealth skills to familiarise students with virtual platforms and their functionalities. Additionally, implementing a mentorship programme or clinical attachment with telehealth practitioners guiding medical students during VF visits can foster confidence and communication skills. Encouraging regular feedback sessions will allow students to improve their techniques and address specific concerns in real-time.
As medical education shifts toward integrating telehealth, understanding the challenges students encounter is essential in preparing the next generation of healthcare professionals. The study identified a range of challenges, including technological barriers, such as unfamiliarity with telemedicine platforms, as well as issues related to patient engagement and communication. Medical students reported difficulties building rapport with patients, which is essential for effective follow-up, and expressed concerns regarding their ability to conduct comprehensive assessments virtually.
By documenting these challenges, this study contributes to the existing literature by highlighting medical students’ specific hurdles in the VF context. While experiencing the challenges, the VF visits allowed students exposed to various acute and chronic patient cases to learn about a holistic approach to managing chronic illness, work with teamwork, and have the opportunity to communicate with the patient and their family members. (Cheng et al., 2022; Iancu et al., 2020).
The findings inform educators and curriculum developers of the need for enhanced training programmes focusing on telehealth competencies. Physical follow-up visits have resumed following the pandemic, and a hybrid approach has been embraced to nurture telemedicine concepts and overcome challenges. It recommended medical institutions integrate telemedicine into curricula, ensuring today’s students are prepared for the evolving landscape of medical practice.
V. CONCLUSION
In conclusion, challenges exist in conducting virtual follow-up visits for chronic illness patients, targeting educational strategies to mitigate these difficulties. By equipping medical students with the necessary skills and support, healthcare institutions can enhance the effectiveness of virtual follow-ups, ultimately improving patient care and outcomes in a digital healthcare environment.
Notes on Contributors
Dr Kye is the corresponding author for this paper. She designed the study, analysed the data, and prepared the manuscript, working with the co-author.
Dr Amit and Dr Hnin contributed substantially to the final manuscript’s design, editing and preparation.
Ethical Approval
The research study was approved by Universiti Tunku Abdul Rahman Scientific and Ethical Review Committee on 20th April 2021 (Approval number: UTAR/SERC/92/2021).
Acknowledgement
We would like to acknowledge the Year 4 medical students of UTAR (Academic Year 2020/2021) for voluntary participation in this study.
Funding
There was no funding for this research study.
Declaration of Interest
The authors declare no conflicts of interest, including financial, consultant, institutional or other relationships.
References
Aron, J. A., Bulteel, A. J. B., Clayman, K. A., Cornett, J. A., Filtz, K., Heneghan, L., Hubbell, K. T., Huff, R., Richter, A. J., Yu, K., & Weil, H. F. (2020). A role for telemedicine in medical education during the COVID-19 pandemic. Academic Medicine, 95(11), e4-e5. https://doi.org/10.1097/ACM.0000000000003572
Cheng, C., Humphreys, H., & Kane, B. (2022). Transition to telehealth: Engaging medical students in telemedicine healthcare delivery. Irish Journal of Medical Science, 191, 2405-2422. https://doi.org/10.1007/s11845-021-02720-1
Iancu, A. M., Kemp, M. T., & Alam, H. B. (2020). Unmuting medical students’ education: Utilizing telemedicine during the COVID-19 pandemic and beyond. Journal of Medical Internet Research, 22(7), e19667. https://doi.org/10.2196/19667
Pathipati, A. S., Azad, T. D., & Jethwani, K. (2016). Telemedical education: Training digital natives in telemedicine. Journal of Medical Internet Research, 18(7), e193. https://doi.org/10.2196/ jmir.5534
Waseh, S., & Dicker, A. P. (2019). Telemedicine training in undergraduate medical education: Mixed methods review. JMIR Medical Education, 5(1), e12515. https://doi.org/10.2196/12515
*Dr Kye Mon Min Swe
Newcastle University Medicine Malaysia,
No 1, Jalan Sarjana 1,
Kota Ilmu, Educity@Iskandar,
Nusajaya, 79200, Johor, Malaysia
601115133799
Email: drkyemonfms@gmail.com
Submitted: 13 May 2024
Accepted: 26 August 2024
Published online: 7 January, TAPS 2025, 10(1), 62-64
https://doi.org/10.29060/TAPS.2025-10-1/CS3346
Daniel Ardian Soeselo1,2, Rennie Yolanda3, Gisella Anastasia1, Dwi Jani Juliawati1 & Natalia Puspadewi1
1Medical Education Unit and 2Department of Surgery, School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, Indonesia; 3School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, Indonesia
I. INTRODUCTION
Providing comprehensive palliative care is a global challenge, particularly in resource-limited settings like Indonesia (Putranto et al., 2017). Palliative care education in Indonesia is often underrepresented in medical curricula, leading to gaps in understanding and application among future healthcare professionals. This issue is compounded by the dominance of lecture-based classrooms from elementary to high school in Southeast Asia, including most medical education in Indonesia. Implementing a flipped classroom approach, which reverses traditional lecture-based and promotes active learning, could transform the education of healthcare professionals by effectively integrating surgery and palliative care within the Indonesian context (Hew & Lo, 2018).
The flipped classroom has rapidly developed in recent years, proving effective in medical education by enhancing learning performance and student satisfaction (Hew & Lo, 2018). While widely adopted in parts of Asia, particularly in Taiwan, Korea, and China (Ha et al., 2019), it remains less common in Southeast Asia, especially within medical education.
This study introduces a flipped classroom model to promote active learning and better knowledge retention, shifting the focus from traditional lecture-based teaching to student-centered learning. We aim to enhance the comprehension and application of palliative care principles among pre-clinical students.
II. METHODS
This study explores the novel use of a flipped classroom method to teach the role of surgery in palliative care, and assessed using the Kirkpatrick model (Heydari et al., 2019). Participants were preclinical students in the palliative care elective module at the School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia.
In the asynchronous stage, students were divided into four groups and given two medical journals and four trigger questions (Supplementary) one week before the synchronous class. They independently studied the material and discussed the questions in groups, submitting their answers to the facilitator a day before the synchronous session. During the synchronous stage, each group had 15 minutes to present their answers, followed by 45 minutes of interactive discussions with the facilitator using case simulations and videos. The facilitator is an experienced educator in palliative surgery.
Kirkpatrick level 1 evaluates student reactions to the learning experience at the end of class sessions using a questionnaire with a Likert scale and open-ended questions on learning materials (journals and trigger questions), learning time, active participation of students, and facilitators. Kirkpatrick level 2 evaluates student learning outcomes through five multiple-choice questions (MCQs). Questionnaires are available in Supplementary. The flipped classroom effectiveness was assessed based on multiple criteria, specifically the student’s interest in attending classes, encouragement to seek additional knowledge sources, active involvement, and motivation to study the material more deeply.
III. RESULTS
Thirty-three out of 37 students who attended the learning agreed to be included in the study. Each group comprises 9 to 10 people with a similar mean GPA (3.21 to 3.33). We assumed identical average GPA scores to mitigate any bias in the study toward students’ learning abilities. Table 1 shows students’ reactions to the learning experience (Kirkpatrick level 1).
|
Statement |
Mean* ± SD |
|
The flipped classroom method makes me interested in attending classes |
4.54 ± 0.56 |
|
Flipped classroom makes me want to study the material more deeply |
4.84 ± 0.36 |
|
The journal provided triggers me to seek other sources of knowledge |
4.45 ± 0.83 |
|
Trigger questions help me understand the material |
4.78 ± 0.48 |
|
I am actively involved in the learning process |
3.90 ± 1.07 |
|
The time given for the learning process is sufficient |
4.81 ± 0.46 |
|
The instructor facilitates my active participation in class |
4.81 ± 0.39 |
Table 1. Student reactions evaluation (Kirkpatrick level 1) towards the flipped classroom method
*Mean Likert scale
SD = Standard Deviation
Most students spend 1 to 2 hours reading journals (19 students; 57.6%) and discussing in groups (20 students; 60.6%) respectively. Kirkpatrick level 2 evaluation was conducted using five multiple-choice questions administered at the end of the class. The difficulty levels of the questions were assessed, comprising 80% moderate and 20% easy questions. The evaluation results indicated that the average percentage of correct answers was 43.76%, reflecting an unsatisfactory outcome. Specifically, four out of the five questions had correct answer rates below 50%. These results suggest that the learning objectives were not effectively met, highlighting the need for further refinement of the flipped classroom approach and instructional methods to improve comprehension and retention of the material. The data of this study are openly available at https://doi.org/10.6084/m9.figshare.25594335.
IV. DISCUSSION
The flipped classroom method increased student interest in attending classes and deepened their study of the material. The learning materials encouraged students to seek additional knowledge, enhancing understanding and active participation. Most students strongly agreed that the trigger questions helped them understand the material and were satisfied with both the time given and the facilitators. However, active participation in the learning process was scored the lowest (3.90 ± 1.07 SD), with some students citing embarrassment, fear, and difficulty expressing opinions. Additionally, group discussions during the asynchronous stage, which were conducted online, made it difficult for students to unite ideas and draw conclusions from the discussions.
The learning outcome evaluation (Kirkpatrick level 2) revealed that most students answered four of five questions incorrectly, likely due to a lack of clinical experience. Interestingly, question number 2 was the most accurately answered, likely because it aligned with the theoretical principles of palliative learning.
These findings align with other studies demonstrating the flipped classroom enhances medical students’ learning outcomes and experiences (Nichat et al., 2023). Nichat et al. (2023) found that the flipped classroom promotes active learning by allowing students to study foundational concepts independently during the asynchronous stage and use class time for interactive discussions and collaborative activities, fostering critical thinking and collective analysis.
The challenges observed, such as the low active participation and difficulties in online group discussions, align with findings from Ha et al. (2019). Ha et al. (2019) highlighting that students in flipped classrooms may initially struggle with active engagement and online collaboration due to a lack of experience and confidence. Providing structured guidance during the asynchronous phase, such as online forums and regular check-ins with facilitators, could enhance student participation and collaboration.
The need for clinical experience to answer certain questions suggests that incorporating practical, scenario-based learning activities, such as simulations and role-playing exercises, could bridge this gap. This approach can help students apply theoretical knowledge in a clinical context, improving their readiness for practical evaluations (Hew & Lo, 2018; Nichat et al., 2023).
V. CONCLUSION
The flipped classroom method enhances critical thinking, communication, and reasoning skills, leading to higher student satisfaction and engagement. These findings highlight flipped classroom potential impact in Indonesian medical education. Addressing challenges through targeted interventions, such as clinical simulations and improved online collaboration, can further optimise its effectiveness for preclinical students.
Notes on Contributors
Daniel Ardian Soeselo designed the study, reviewed the literature, analysed the data, and gave feedback during manuscript writing.
Rennie Yolanda participated in data analysis and coding of the qualitative data, reviewed the literature, and wrote the manuscript.
Gisella Anastasia, Dwi Jani Juliawati, and Natalia Puspadewi reviewed the literature, provided input at all stages of the study, and reviewed the manuscript.
Ethical Approval
This research has received ethical approval from the Research Ethics Commission of the Atma Jaya Catholic University of Indonesia No. 13/10/KEP-FKIKUAJ/2022.
Acknowledgement
We would like to thank all the medical students who willingly cooperated in the study.
Funding
No funding was obtained for this study.
Declaration of Interest
All authors have no declaration of interest.
References
Ha, A. S., O’Reilly, J., Ng, J. Y. Y., & Zhang, J. H. (2019). Evaluating the flipped classroom approach in Asian higher education: Perspectives from students and teachers. Cogent Education, 6(1), Article 1638147. https://doi.org/10.1080/2331186X.2019.1638147
Hew, K. F., & Lo, C. K. (2018). Flipped classroom improves student learning in health professions education: A meta-analysis. BMC Medical Education, 18(1), 38. https://doi.org/10.1186/s12909-018-1144-z
Heydari, M. R., Taghva, F., Amini, M., & Delavari, S. (2019). Using Kirkpatrick’s model to measure the effect of a new teaching and learning methods workshop for health care staff. BMC Research Notes, 12(1), 388. https://doi.org/10.1186/s13104-019-4421-y
Nichat, A., Gajbe, U., Bankar, N. J., Singh, B. R., & Badge, A. K. (2023). Flipped classrooms in medical education: Improving learning outcomes and engaging students in critical thinking skills. Cureus, 15(11), Article e48199. https://doi.org/10.7759/cureus.48199
Putranto, R., Mudjaddid, E., Shatri, H., Adli, M., & Martina, D. (2017). Development and challenges of palliative care in Indonesia: Role of psychosomatic medicine. BioPsychoSocial Medicine, 11(1), 29. https://doi.org/10.1186/s13030-017-0114-8
*Daniel Ardian Soeselo
Atma Jaya Catholic University of Indonesia,
Jakarta, Indonesia
+62 813 8193 7250
E-mail: daniel.ardian@atmajaya.ac.id
Submitted: 5 June 2024
Accepted: 24 July 2024
Published online: 7 January, TAPS 2025, 10(1), 65-66
https://doi.org/10.29060/TAPS.2025-10-1/LE3428
Sulthan Al Rashid1 & Mohmed Isaqali Karobari2
1Department of Pharmacology, Saveetha Medical College and Hospital, Saveetha Institute of Medical and Technical Sciences (SIMATS), India; 2Department of Dental Research, Centre for Global Health Research, Saveetha Medical College and Hospital, Saveetha Institute of Medical and Technical Sciences (SIMATS), India
Dear Editor,
Comprehensive review articles require more than just gathering information; they require careful synthesis, analysis, and effective communication (Dhillon, 2022). Benjamin Bloom’s Taxonomy offers a systematic framework, guiding authors through remembering, understanding, applying, analysing, evaluating, and creating (Adams, 2015). Leveraging Bloom’s Taxonomy enriches writing, ensuring impactful and thorough reviews.
At the foundational level of remembering, authors embark on a meticulous literature search to gather pertinent studies. For instance, in a review exploring “Innovative Pedagogical Approaches in Medical Education,” authors meticulously scour databases such as PubMed and ERIC using keywords like “medical education” and “innovative teaching methods.”
In transitioning to Understanding, the authors synthesise the literature, identifying key concepts such as problem-based learning and simulation-based training. This enables a more profound comprehension of fundamental principles, such as how active learning strategies enhance student engagement and knowledge retention.
Applying involves contextualising synthesised information within broader educational frameworks. By referencing theories such as cognitive load theory, the authors elucidate how instructional design principles can optimise learning outcomes in medical education.
Analysis necessitates evaluating the strengths and weaknesses of existing educational practices. Despite the prevalent use of lecture-based teaching, the review highlights the benefits of active learning approaches in improving critical thinking skills and clinical reasoning among medical students.
During evaluation, authors assess the overall quality and significance of synthesised literature. While some studies demonstrate the effectiveness of flipped classroom models in medical education, others yield mixed results, underscoring the need for further research with rigorous methodologies.
Lastly, creating involves synthesising information to propose innovative educational interventions. Drawing insights from the review, the authors propose a comprehensive model illustrating the integration of technology-enhanced learning tools and interprofessional education strategies. Future research recommendations include exploring virtual reality simulations’ impact on clinical skill acquisition.
By embracing Bloom’s Taxonomy, writers adeptly navigate the complexities of review article writing with clarity and depth. This systematic approach empowers scholars to recapitulate existing literature and assess, integrate, and expand knowledge within the field, thereby enhancing the credibility and significance of scholarly endeavours in any educational field.
Notes on Contributors
Sulthan Al Rashid contributed to the concept, scientific content, data collection, and manuscript preparation.
Mohmed Isaqali Karobari helped with the review and editing of the manuscript.
The final manuscript has been read and approved by all the authors.
Acknowledgement
The authors would like to acknowledge the director of Saveetha Medical College and Hospital for support in this educational research.
Funding
For this study, the authors were not given any funding.
Declaration of Interest
The authors claim to have no conflicts of interest.
References
Adams, N. E. (2015). Bloom’s taxonomy of cognitive learning objectives. Journal of the Medical Library Association, 103(3), 152-153. https://doi.org/10.3163/1536-5050.103.3.010
Dhillon, P. (2022). How to write a good scientific review article. The FEBS Journal, 289(13), 3592-3602. https://doi.org/10.1111/febs.16565
*Sulthan Al Rashid
Department of Pharmacology,
Saveetha Medical College and Hospital,
Saveetha Institute of Medical & Technical Sciences (SIMATS),
Chennai, Tamil Nadu, India
+919629696523
Email: sulthanalrashid@gmail.com
https://doi.org/10.29060/TAPS.2025-10-1/TT001
Marcus A. Henning
Centre for Medical and Health Sciences Education, Faculty of Medical and Health Sciences, University of Auckland, New Zealand
Whenever I think about student and faculty wellness, I am reminded of two sayings. Firstly, a Taoist saying that recommends we should always “look close, not far” (Wee Kee Jin, personal communication, August 25, 2012). And secondly, William Osler’s saying, “Our main business is not to see what lies dimly in the distance but to do what lies clearly at hand” (Bryan, 1997). Both quotes suggest that the most prudent course of action for students and faculty is to always reflect on one’s own actions and focus on the tasks at hand.
There is also a strong sense of reflecting in- and on-action, whereby students and faculty need to reflect on their experiences in a timely manner to optimise the opportunity for constructive transformation (Schon, 1983). With this in mind, monitoring wellbeing engenders the prospect of the cultivation of wellbeing. To engage this mindset, it is crucial that students and faculty are aware of, and honest about, what is happening in their minds and bodies and accept that mistakes can happen, but these experiences can lead to transformation, i.e., that they invest in loss (Buchanan, 2024).
Therefore, the core principle is to solve problems and be task-oriented on what needs to be done to solve any issues as they arise, rather than attributing blame and creating a shame and blame cycle. It is further crucial that students and faculty embrace help-seeking strategies to mitigate emotional exhaustion and proactively engage health professionals when things go awry (Dyrbye et al., 2015). The earlier this engagement occurs, the more likely the outcome will be positive.
Help-seeking strategies have attitudinal components but need to be seen as an essential part of developing common-sense wellbeing strategies that enable wellbeing. Other factors include healthy eating, living in favourable accommodation, exercising regularly, and ensuring optimal sleep patterns (Trockel et al., 2000). It is also crucial that students and faculty allow for a recovery period after experiencing stress-provoking incidents to allow them to return to a healthy state. If this recovery period is not initiated, it may lay the foundation for a worsening response to future adversarial stress incidents (Sisley et al., 2010).
To summarise, students and faculty need to monitor their health status on a daily basis, create strategies that will enhance their wellbeing, and be open to seeking help if things go awry.
Bryan, C. S. (1997). Osler: Inspirations from a great physician. New York: Oxford University Press. http://ci.nii.ac.jp/ncid/BA34173998
Buchanan, M. (2024, March 17). The Chinese secret of investing in loss (with Professor Cheng Man Ching). https://morganbuchanan.substack.com/p/the-chinese-secret-of-investing-in
Dyrbye, L. N., Eacker, A., Durning, S. J., Brazeau, C., Moutier, C., Massie, F. S., Satele, D., Sloan, J. A., & Shanafelt, T. D. (2015). The impact of stigma and personal experiences on the help-seeking behaviors of medical students with burnout. Academic Medicine, 90(7), 961-969. https://doi.org/10.1097/acm.0000000000000655
Schon, D. A. (1983). The reflective practitioner: How professionals think in action. New York: Basic Books. https://stars.library.ucf.edu/cirs/1748/
Sisley, R., Henning, M. A., Hawken, S. J., & Moir, F. (2010). A conceptual model of workplace stress: The issue of accumulation and recovery and the health professional. New Zealand Journal of Employment Relations, 35(2), 3-15. https://aut.researchgateway.ac.nz/handle/10292/3011
Trockel, M. T., Barnes, M. D., & Egget, D. L. (2000). Health-related variables and academic performance among first-year college students: Implications for sleep and other behaviors. Journal of American College Health, 49(3), 125-131. https://doi.org/10.1080/07448480009596294
Submitted: 20 December 2023
Accepted: 22 July 2024
Published online: 7 January, TAPS 2025, 10(1), 53-55
https://doi.org/10.29060/TAPS.2025-10-1/PV3196
Galvin Sim Siang Lin1 & Chan Choong Foong2
1Department of Restorative Dentistry, Kulliyyah of Dentistry, International Islamic University Malaysia, Kuantan Campus, Malaysia; 2Medical Education and Research Development Unit (MERDU), Faculty of Medicine, Universiti Malaya, Malaysia
We are writing to express our strong support for a crucial initiative aimed at improving health profession education, particularly in dental education. Dental education, like all healthcare fields, evolves continuously due to advances in research, technology, and patient expectations (Wong et al., 2020). Dental schools have a pivotal role in shaping the future of oral healthcare professionals, and the absence of such departments may hinder their ability to prepare competent, patient-focused dental professionals. Currently, curriculum development in dental education often faces challenges in keeping pace with the rapidly evolving landscape of oral healthcare. While dental schools are renowned for their rigorous curriculum and comprehensive clinical training, the development of effective teaching methods, curriculum enhancement, appropriate assessment, and faculty development often receive insufficient attention. This can lead to a gap between the skills and knowledge imparted to students and the demands of modern dental practice. Similarly, assessment practices may lack the sophistication needed to adequately evaluate students’ competence in areas beyond technical proficiency, such as communication skills, ethical considerations, and understanding of diversity, equity, and inclusion. Moreover, faculty development initiatives, while crucial for ensuring teaching quality and staying abreast of advancements in educational techniques, may be sporadic and lack a coordinated approach. In most countries, obtaining a professional dental qualification is a prerequisite for becoming a dental lecturer, without the need for an academic qualification in education. Therefore, it is essential to establish dedicated dental education departments with full-time academic members and to define job scopes (Nafea, 2021).
Historically, dental education may have been perceived as a part-time commitment for full-time dental academicians or dental specialists in the teaching fraternities. Some dental schools also established dental education committees comprising representatives from various departments within the dental schools. However, it has become increasingly evident that the dedication to progress within these committees is in jeopardy. This is mainly because each staff member carries their own teaching and administrative duties within their respective dental disciplines. The effective functioning of a dental education department necessitates a multidisciplinary team comprising individuals with diverse expertise and academic qualifications, encompassing dental sciences, educational sciences, and information technology. This diverse team is fundamental to the department’s ability to undertake various responsibilities, including curriculum development, assessment, evaluation, and faculty development. While the responsibilities of dental education departments may involve academic roles such as serving as workshop trainers and providing guidance to dental specialists in module design, it is crucial to distinguish their primarily academic nature from administrative functions. Unlike administrative roles that involve managing events for other trainers or handling paperwork for modules, dental education departments primarily contribute to the academic advancement of dental professionals.
Undeniably, establishing dental education departments within dental schools will foster innovation in teaching and learning methodologies. These departments can serve as hubs for researching and implementing effective pedagogical approaches, ensuring students receive the most up-to-date knowledge and skills. By integrating evidence-based educational techniques, dental schools can improve education quality, encourage active student engagement, and cultivate more competent and compassionate dental professionals. For instance, consider the implementation of team-based and case-based learning in dental education. A specialised department could spearhead research into the effectiveness of this methodology, develop protocols for its integration into the curriculum, and assess its impact on student outcomes. By doing so, the department contributes not only to the enrichment of teaching methods but also to the optimisation of the learning experience.
Furthermore, the dental education department can serve as a cornerstone for supporting faculty development. Recognising the indispensable role of faculty in educational excellence, these departments can facilitate tailored training programs, workshops, and collaborative research endeavours which would have a direct impact on the teaching quality (Irby et al., 2015). They empower educators to stay abreast of the latest teaching methods and scientific advancements. This, in turn, translates into an enriched student learning experience, with educators equipped to effectively inspire and guide the next generation of dental professionals. Consider a scenario where a dental education department collaborates with faculty to implement a novel assessment tool that evaluates not only technical proficiency but also communication skills and ethical considerations. This multidimensional approach not only aligns with the evolving expectations of the dental profession but also contributes to the holistic development of future dental practitioners.
Curriculum development and evaluation represent another critical sphere that stands to benefit profoundly from the establishment of dental education departments. In an era marked by transformative trends, dental schools must adapt to changing healthcare landscapes, incorporating digital dentistry, teledentistry, and cultural competence into their curricula. Dental education departments can lead curriculum reform efforts, ensuring graduates are not only well-versed in traditional dental practices but also adept in navigating the complexities of modern oral healthcare. For instance, envision a dental education department driving the integration of artificial intelligence applications into the dental curriculum. This would prepare students to leverage cutting-edge technologies, ensuring their readiness for a technologically advanced dental landscape (Islam et al., 2022).
In addition, these departments can also play an essential role in assessment and accreditation. In maintaining high education standards and ensuring that graduates are adequately prepared for licensure, dental education departments become custodians of public safety. They serve as a quality assurance mechanism, safeguarding the integrity of dental education and, by extension, the well-being of patients. Consider a scenario where a dental education department collaborates with accreditation bodies to develop robust assessment criteria that encompass not only clinical competence but also ethical considerations, cultural sensitivity, and effective communication skills. This holistic approach not only ensures the competency of graduates but also aligns dental education with the broader goals of promoting patient-centred care.
Dental education departments can also catalyse interdisciplinary research initiatives, fostering collaboration between dental and other healthcare disciplines. This approach encourages the development of holistic healthcare professionals who can work seamlessly within multidisciplinary teams (Yusoff et al., 2014). For example, the department can initiate research projects exploring the intersection of oral and systemic health, thereby promoting a more comprehensive understanding of the impact of dental care on overall well-being. Establishing these departments also encourages global collaboration with dental institutions, benefiting students and the wider dental community by sharing and exchanging knowledge and best practices. This exchange benefits students and the wider dental community by providing exposure to diverse perspectives and approaches to dental education. For example, international partnerships between dental education departments, lead to collaborative research projects, student exchange programs, and shared educational resources, enriching the educational experience for all involved.
The dental education department can lead educational initiatives by actively engaging in student enhancement programs. Through strategic leadership, the department can orchestrate initiatives beyond dental schools, collaborating with the broader university and healthcare communities to address learning issues among dental students. For instance, the department can organise learning-to-learn or peer-assisted learning workshops, providing diagnostic and interventional programs to academically at-risk students. By forging partnerships with external organisations, dental education departments can contribute to the development of outreach programmes that broaden dental training initiatives. This leadership includes advocating policy changes that prioritise the affective domain of dental training agendas and fostering a more comprehensive and inclusive approach to dentists’ professionalism. Hence, dental education departments not only enhance the visibility of dental training within the community but also contribute significantly to society’s overall well-being.
Nonetheless, establishing dental education departments necessitates collaboration among various stakeholders, including governments, dental associations, and educational institutions. Adequate funding, infrastructure, and faculty support are imperative for the successful realisation of these departments. This is not merely an investment in dental education; it is an investment in the future of dentistry itself. To underscore the urgency and significance of this proposal, it is essential for relevant authorities and stakeholders to engage in earnest deliberations and collaborative efforts. Dental education departments with a multidisciplinary team of full-time and academically qualified members should be considered as a requirement for accreditation. The establishment of specialised dental education departments is not a mere augmentation of existing structures; it is a forward-thinking move towards aligning dental education with society’s changing needs. It represents a collective commitment to nurturing a generation of dental professionals who are not only technically proficient but also adaptable, empathetic, and attuned to the complexities of modern healthcare. By customising dental programmes to include modules such as diversity, equity, and inclusion in dentistry as well as communication skills, this department can instil in future dental professionals a greater understanding of patient experiences, fostering empathy and comprehension within the dental profession.
In conclusion, the establishment of specialised dental education departments within dental schools is a transformative initiative that holds the potential to reshape the landscape of dental education. One approach is to send academic staff within the dental schools for postgraduate training in health profession education. By addressing the nuanced aspects of teaching, curriculum development, assessment, and faculty development, these departments can contribute to the holistic preparation of dental professionals. This is not just a need; it is a strategic imperative for championing progress in dental education and ensuring the delivery of high-quality oral healthcare to communities worldwide.
Notes on Contributors
Galvin Sim Siang Lin conceptualised and wrote the manuscript. Chan Choong Foong edited and revised the manuscript.
Funding
The authors received no financial support for the authorship or publication of this article.
Declaration of Interest
There is no conflict of interest.
References
Irby, D. M., O’Sullivan P, S., & Steinert, Y. (2015). Is it time to recognize excellence in faculty development programs? Medical Teacher, 37(8), 705-706. https://doi.org/10.3109/0142159X.2015.1044954
Islam, N. M., Laughter, L., Sadid-Zadeh, R., Smith, C., Dolan, T. A., Crain, G., & Squarize, C. H. (2022). Adopting artificial intelligence in dental education: A model for academic leadership and innovation. Journal of Dental Education, 86(11), 1545-1551. https://doi.org/10.1002/jdd.13010
Nafea, E. T. (2021). The dental education specialism in KSA: Are we there yet? Journal of Taibah University Medical Sciences, 16(2), 217-223.
Wong, M. L., Lee, T. W. O., Allen, P. F., & Foong, K. W. C. (2020). Dental education in Singapore: A journey of 90 years and beyond. The Asia Pacific Scholar, 5(1), 3-7. https://doi.org/10.29060/taps.2020-5-1/gp1086
Yusoff, M. S. B., Abdul Rahim, A. F., & Jaa’far, R. (2014). Medical education department roles and initiatives towards achieving APEX agenda. Education in Medicine Journal, 6(2), e1-e7. https://doi.org/10.5959/eimj.v6i2.261
*Galvin Sim Siang Lin
International Islamic University Malaysia,
Kuantan Campus, 25200,
Pahang, Malaysia
Email: galvin@iium.edu.my
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
