
The emotions, coping strategies and learning behaviours of medical students during quarantine period of COVID-19
Submitted: 30 April 2024
Accepted: 25 September 2024
Published online: 1 April, TAPS 2025, 10(2), 86-90
https://doi.org/10.29060/TAPS.2025-10-2/SC3551
Ozlem Tanriover1, Sukran Peker2, Seyhan Hidiroglu2, Dilek Kitapcioglu3 & M. Ali Gülpınar1
1Department of Medical Education, School of Medicine, Marmara University, Türkiye; 2Department of Public Health, School of Medicine, Marmara University, Türkiye; 3Department of Medical Education, School of Medicine, Acibadem Mehmet Ali Aydinlar University, Türkiye
Abstract
Introduction: This study aimed to identify the emotions experienced by medical students during the quarantine period, explore their coping strategies, and determine whether the pandemic affected their learning behaviours.
Methods: In this descriptive study, data were collected through an online questionnaire. The study included quarantined medical students enrolled in a distance education program at a medical school during the pandemic. The Positive and Negative Affect Scale was used to assess the emotional spectrum of the participants.
Results: The majority of medical students in the sample experienced predominantly negative emotions. Students with higher negative affect scores struggled with stress management and were less able to employ emotional regulation strategies, which adversely affected their learning behaviours.
Conclusion: Emotions should be explicitly addressed in medical education, and students should be supported in managing their emotions as part of their professional development and well-being.
Keywords: Coping, Emotions, Emotion Regulation, Medical Student, Pandemic, Stress
I. INTRODUCTION
Medical education has long been a significant source of stress for students. The COVID-19 pandemic introduced additional challenges with social distancing, home confinement, and online learning, further intensifying this burden (Fegert et al., 2020). In Turkey, the Council of Higher Education suspended face-to-face education on March 26, 2020, shifting all theoretical and some practical medical courses online. This move removed students from campuses and hospital settings to protect public health. As a result, medical students from all years, including those close to graduation, were quarantined and separated from their academic routines.
Quarantine, a measure to prevent disease spread, often leads to frustration, boredom, and heightened distress (Brooks et al., 2020). Medical education is already emotionally taxing, and the pandemic amplified these challenges. While many studies have explored the emotions of healthcare workers and students on the front lines, little is known about how medical students in Turkey, confined at home, experienced and coped with this period. This study aims to explore their emotional experiences, coping mechanisms, and changes in learning behaviours during quarantine.
II. METHODS
This descriptive study utilised an online questionnaire sent via Microsoft Forms to medical students from a university in Istanbul. Participants included both preclinical and clinical students, all engaged in distance learning due to the pandemic. The survey was distributed in June 2020, with participation being voluntary and anonymous. The study ran from mid-June to the end of July 2020.
A. Ethical Approval
The study was approved by the School of Medicine Ethical Committee (No. 09.2020.657). Consent was obtained from all participants before data collection.
B. Data Collection
The questionnaire gathered sociodemographic data and inquired about online education experiences. The Positive and Negative Affect Scale (PANAS), developed by Watson et al. (1988) and adapted to Turkish by Gençöz (2000), was used to assess emotions. The PANAS contains 20 adjectives rated on a five-point Likert scale, with scores ranging from 10 to 50 for both positive and negative emotions. High positive scores reflect engagement and energy, while high negative scores indicate distress.
C. Statistics
Statistical analysis was conducted using SPSS 20.0. Normality was tested with Kolmogorov-Smirnov and Shapiro-Wilk tests. Descriptive statistics were presented as medians (IQR) for non-normal data and frequencies for categorical data. The Mann-Whitney U test was used for two-group comparisons, and the Kruskal-Wallis test for comparisons across more than two groups. A p-value < 0.05 was considered statistically significant.
III. RESULTS
A total of 145 students participated in the survey, with a slight female majority (57%, n=83). The participants’ ages ranged from 20 to 27 years (mean=21.4, SD=1.99), and most (93%, n=135) lived at home with their families. Students attended an average of 4-6 hours of online lectures per day during quarantine. Emotions such as “interested,” “alert,” and “enthusiastic” had low scores, while 63.4% reported feeling distressed, followed by 40.7% upset and 39.3% irritable.
The PANAS total score comparison showed that students aged 22-25 scored significantly higher than those aged 18-21 (51.7 vs 48.1, p=0.028). Similarly, positive affect (PA) scores were higher in older students (p<0.001). Students living alone had higher total PANAS scores (59 vs 49, p=0.008) and PA scores (31.7 vs 23.6, p<0.001) than those living with their families.
A. Coping Strategies
Most students (65.5%) coped with stress using distraction activities like watching TV, while 8.3% sought emotional support. A minority engaged in substance use or denial (4.9%), and 8.3% reported being unable to cope. Those who made an effort to cope had higher PA scores (24.6 vs 21.2, p=0.036) and lower negative affect (NA) scores (25.3 vs 29.5, p=0.01).
B. Changes in Learning Behaviour
About 74.5% of students reported changes in their study methods during the pandemic, though no significant differences in PANAS scores were observed. When asked about adapting to online learning, 33.7% of students reported difficulty adjusting, while 17.3% used self-motivation, and 11.5% created study programs with peers.
C. Emotion Regulation
Cognitive reappraisal was the most common strategy used by 65.5% of students to manage emotions, while 8.3% used expressive suppression. Nearly 25% reported no effective emotion regulation strategy, and 1.4% felt they didn’t need one. Those who used emotion regulation strategies had significantly lower NA scores (p=0.017).
|
Variables |
PA TOTAL |
NA TOTAL |
|||
|
Median (IQR) |
p |
Median (IQR) |
p |
||
|
Gender |
Women |
23 (7) |
0.69 |
24(13) |
0.39 |
|
Men |
24 (12.25) |
24.5(12.25) |
|||
|
Age |
18-21 y |
21(6.5) |
<0.01 |
25(13) |
0.28 |
|
22-25 y |
26(10.75) |
24(9.75) |
|||
|
Class |
Basic Sciences |
21(7) |
<0.001 |
25(12) |
>0.05 |
|
Clinical Sciences |
28.5(10.5) |
24(13.25) |
|||
|
Living Arrangement |
At home |
23(8) |
>0.05 |
25(11.75) |
>0.05 |
|
Dormitory |
23(5.5) |
20(8.5) |
|||
|
Who do you live with? |
With family |
23(8.25) |
<0.001 |
24(12.5) |
0.639 |
|
With friends |
23(7) |
24(8) |
|||
|
Alone |
33(10) |
25(12) |
|||
|
Volunteered During Pandemic |
Yes |
26.5(9.25) |
>0.05 |
23.5(21) |
>0.05 |
|
No |
23(8.5) |
24(11.5) |
|||
|
Distance Education Experience |
Yes |
23(8) |
>0.05 |
27(12) |
>0.05 |
|
No |
24(9.25) |
24(12.25) |
|||
|
Infrastructure Suitability |
Yes |
23(8.75) |
>0.05 |
24(12) |
>0.05 |
|
No |
22(10.5) |
28 (13) |
|||
|
Training Management System Usage |
Yes |
23(9) |
p>0.05 |
24(12) |
p>0.05 |
|
No |
25(7.55) |
27(15.75) |
|||
Table 1. The comparison of the sociodemographic data of the participants with the PANAS median scores
IV. DISCUSSION
This study is the first to explore the emotional experiences of medical students in Turkey during the COVID-19 quarantine period, offering critical insights into how students coped with stress and adapted to the rapid shift to online education. Our findings suggest that medical students predominantly experienced negative affect, with emotions such as distress, irritability, and nervousness being highly prevalent. This aligns with global research during the pandemic, which reported heightened levels of anxiety, stress, and emotional dysregulation among students (Kostic et al., 2021).
One of the most striking findings of our study is the significant role of positive affect (PA) in students’ ability to cope with stress. Students with higher PA scores were more likely to report engaging in adaptive coping strategies, such as cognitive reappraisal and self-motivation. Cognitive reappraisal, in particular, was the most frequently used emotion regulation strategy among the students, highlighting the importance of reframing challenging situations in a more positive light. This ability to change one’s perspective is a valuable skill, especially in stressful academic environments like medical school. It allows students to manage their emotional responses more effectively, thereby reducing the likelihood of burnout and enhancing their capacity for professional growth.
In contrast, students who reported higher levels of negative affect (NA) were more likely to struggle with stress management and adaptation to online education. This is consistent with existing research that links negative emotional states, such as anxiety and distress, with poorer academic performance and lower motivation (Tanriover et al., 2023). Additionally, students with high NA scores were more likely to rely on maladaptive coping strategies or, in some cases, to exhibit no effort to cope with stress at all. This highlights a key area for intervention, as students who are unable to regulate their emotions are at greater risk of developing mental health issues, which can impede their academic and professional development.
Our findings also revealed interesting differences based on living arrangements. Students living alone had higher PA scores compared to those living with their families, possibly due to the greater autonomy and control they experienced over their environments. In contrast, students living with their families reported more stress, potentially due to concerns about the health and safety of their family members or financial pressures exacerbated by the pandemic. These results suggest that the home environment plays a crucial role in shaping students’ emotional well-being during periods of crisis. Medical schools should consider these contextual factors when designing support systems for students, particularly in situations where they may be confined to their homes for extended periods, as was the case during the pandemic.
The shift to online education posed additional challenges for medical students, many of whom struggled to adapt their study methods to the new format. The vast majority (74.5%) of students in our study reported that their study methods had changed during the pandemic, but there was no significant difference in PANAS scores based on these changes. However, it is worth noting that a sizable proportion of students (33.7%) stated that they could not adapt to the new learning environment. This highlights the need for more structured guidance and support from educational institutions to help students navigate the transition to online learning. Studies have shown that students benefit from peer collaboration, instructor support, and a clear organisational structure when adapting to new learning methods (Dhawan, 2020). In this regard, medical schools should invest in developing comprehensive online education strategies that not only address the technical aspects of remote learning but also support students’ emotional and motivational needs.
The findings of this study underscore the importance of emotional regulation in medical education. Emotional awareness and the ability to regulate one’s emotions are essential skills for medical students, not only for their academic success but also for their long-term professional well-being. The high prevalence of negative affect among the students in our study suggests that more attention needs to be paid to the emotional aspects of medical training. Medical education programs should incorporate training on emotional regulation and coping strategies into their curricula. Such training can help students manage the emotional challenges they face, both in their academic pursuits and in their future careers as healthcare professionals.
Moreover, peer support programs, which encourage students to share their experiences and coping strategies with one another, could foster a sense of community and reduce feelings of isolation. Our study found that students who engaged in collaborative learning methods, such as studying with peers, were better able to adapt to the new online education environment. This suggests that creating opportunities for social connection and peer support is critical, especially during times of crisis when traditional forms of social interaction may be limited.
V. CONCLUSION
These findings highlight the critical role of emotional awareness and regulation in medical students’ well-being, especially in times of crisis. Addressing emotions explicitly in medical education curricula and providing support for students to manage stress and regulate their emotions should be integral to fostering their professional growth and resilience.
Notes on Contributors
OT designed the study; interpretated the data, wrote the draft of the manuscript and approved the final version to be published.
SP collected and analysed the data, interpretated the data and approved the final version to be published.
SH collected and analysed the data, interpretated the data and approved the final version to be published.
DK made critical revisions to the paper for important intellectual content and approved the final version to be published.
M.A.G contributed to the conception, made critical revisions to the paper for important intellectual content and approved the final version to be published.
Ethical Approval
The study was approved by the Marmara University School of Medicine Ethical Committee (No. 09.2020.657). Consent was obtained from all participants before data collection.
Data Availability
Based on the ethics approval, data will not be shared on a repository. The anonymised dataset can be obtained from the corresponding author with request. A preprint of our manuscript, which is not peer-reviewed, is available at https://www.researchsquare.com/article/rs-2849167/v1
Acknowledgement
We are grateful to all the medical students who participated in this study.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of Interest
Possible conflicts of interest, sources of financial support, corporate involvement, patent holdings, consultant, institutional and other relationships that might lead to bias or a conflict of interest do not exist.
References
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet, 395(10227), 912-920. https://doi.org/10.1016/S0140-6736(20)30460-8
Dhawan, S. (2020). Online learning: A panacea in the time of COVID-19 crisis. Journal of Educational Technology Systems, 49(1), 5-22. https://doi.org/10.1177/0047239520934018
Fegert, J. M., Vitiello, B., Plener, P. L., & Clemens, V. (2020). Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child and Adolescent Psychiatry and Mental Health, 14(1), 20. https://doi.org/10.1186/s13034-020-00329-3
Kostic, J., Zikic, O., Dordevic, V., & Krivokapic, Z. (2021). Perceived stress among university students in south-east Serbia during the COVID-19 outbreak. Annals of General Psychiatry, 20(1), 25. https://doi.org/10.1186/s12991-021-00346-2
Tanriover, O., Peker, S., Hidiroglu, S., Kitapcioglu, D., Inanici, S. Y., Karamustafalioglu, N., & Gulpinar, M. A. (2023). The emotions experienced by family medicine residents and interns during their clinical trainings: A qualitative study. Primary Health Care Research & Development, 24(e25), 1-8. https://doi.org/10.1017/S1463423623000051
*Prof. Ozlem Tanriover
Marmara University School of Medicine
Department of Medical Education
Marmara Universitesi Tıp Fakültesi
Başıbüyük Mah Maltepe Başıbüyük Yolu Sok
No:9/2 Maltepe – İstanbul/Türkiye
+90 216 777 55 39
Email: drozlemtan56@gmail.com
Submitted: 14 March 2024
Accepted: 13 November 2024
Published online: 1 April, TAPS 2025, 10(2), 91-93
https://doi.org/10.29060/TAPS.2025-10-2/II3264
Han Ting Jillian Yeo & Dujeepa D. Samarasekera
Centre for Medical Education (CenMED), Yong Loo Lin School of Medicine, National University of Singapore, Singapore
I. INTRODUCTION
Assessment is an important component of training in ensuring that graduating students are competent to provide safe and effective medical care to patients. Typically, the passing score is set as a fixed mark, but this approach does not account for the varying difficulty of exams. As a result, students who have achieved the required level of competence might fail if the exam items are particularly challenging (false negative), while students who have not attained the necessary competence might pass if the items are unusually easy (false positive). Hence, deciding on the right pass mark is important for each assessment. To mitigate this issue, criterion referenced standard setting was adopted in medical education (Norcini, 2003). It determines the minimum competence level expected of a candidate and whether a candidate would pass or fail the assessments (Norcini, 2003). The Angoff method is one of the more commonly used standard setting techniques. It is an examinee centred method and requires a panel of judges to estimate the probability that a borderline candidate would get the item correct.
Literature have questioned the reliability of the Angoff method. Variations in pass mark have been reported when the different panels of judges were engaged (Tavakol & Dennick, 2017; Taylor et al., 2017). Judges reportedly faced challenges in visualising and defining the knowledge and skills required of borderline students and hence have difficulty estimating the probability that a borderline student would answer an item correctly (Tavakol & Dennick, 2017). A study by Yeates et al. (2019) also reported the complexity judges faced in the standard setting process due to interaction between the environment, individual judgments, and interaction between the judges. Such variations in pass marks might lead to unfairness to students who were meant to pass but did not due to a higher pass mark. It is of a greater concern to patient safety if students who were meant to fail passed the examination due to a lowered pass mark. To assist the judges, a guide was developed to set standards for medical and health professions examinations using a probability estimate.
II. DEVELOPING A GUIDE
Judges were to rate each item based on three criteria: relevance, frequency, and difficulty. The guide focused on these areas to assist the judges in their evaluations. The relevance of an item was rated on a 5-point scale ranging from “1 – not knowing will not harm a patient” to “5 – not knowing will cause possible death to the patient”. A highly relevant item was one which assessed a foundational knowledge or a core skill. A less relevant item assessed on knowledge or skill which was good to know or acquire but not required for progression to the next level of education. The difficulty of an item was rated on a 5-point scale ranging from “1 – very easy” to “5 – very difficult”. The difficulty of the item was dependent on the ease of understanding the item construction or the difficulty of the disease condition assessed. For instance, the inclusion of multiple comorbidities in the item stem, as opposed to one comorbidity, required the student to synthesise information before responding. The difficulty of the item was also associated with the level of learning that was assessed. Hence, an item which was assessed on application would be more challenging to the student compared to an item assessing recall. The frequency of an item was rated on a 4-point scale from “1 – very rarely seen in practice of a basic doctor” to “4 – seen very often in practice of a basic doctor”. For example, in the local context, influenza is a clinical condition commonly seen in clinical practice while tetanus is a rarer clinical condition.
Judge’s ratings of each criterion were converted into a probability estimate that a borderline candidate would get the item correct ranging from 0 to 100 percent for each item. An item with a low relevance and frequency but a high difficulty would be assigned a probability estimate between 0 to 30 percent suggesting that a borderline candidate was less likely to get the item correct. An item with a high relevance and frequency but a low difficulty would be assigned a probability estimate between 70 to 100 percent suggesting that there was a high probability a borderline candidate would get this item correct. Judges were given the freedom to assign an estimate from the range provided in the guide or to assign a probability estimate based on their own judgement or expertise.
III. IMPLEMENTATION
To date, the guide was shared with judges during the Angoff standard setting sessions for the medical undergraduate assessments. The guide was given at the start of the session when calibrating judges to a similar mental model on what a borderline candidate was. Judges were free to use the guide in the decision-making process when providing a probability estimate for each item. During the calibration phase and discussion phase of the Angoff standard setting session, we observed that judges provided justifications for their probability estimates by referring to the three criteria. This was more prevalent among judges who were new to the Angoff method. We believed that the well-defined and objective criteria provided in the guide served as a useful framework for judges to develop a mental model on what a borderline candidate was.
IV. LIMITATIONS AND FUTURE DIRECTIONS
Several limitations have been identified. While we have attempted to implement the guide, judge’s ratings remained influenced by their own criteria set by their personal experiences and beliefs which were often deeprooted and independent of the three identified criteria. This is especially so for judges who had prior experience in standard setting with Angoff method and had formed their own set of criteria. We see greater value in the use of the guide for training judges who were participating in Angoff standard setting for the first time.
The guide was developed within a specific medical school in Southeast Asia with its own unique curriculum and learning objectives. Its applicability and effectiveness may be limited in different educational contexts with varying curricula and assessment methods. These limitations highlighted the need for ongoing evaluation and adaptation of the guide and standard-setting methods to ensure they meet the needs of diverse educational settings and provide reliable assessment outcomes. The team is working on validating the use of the guide in our own local context. This would be conducted by quantifying the level of agreement between judges’ ratings, correlating with other standard setting methods and soliciting feedback from judges on the utility of the guide.
V. CONCLUSION
As more medical schools begin to adopt criterion referenced standard setting methods to set a defensible pass mark for assessments and given the complex process judges face when rating items, there is value in the provision of a guide to judges with defined criteria to facilitate the process of rating items.
By focusing on criteria such as relevance, frequency, and difficulty, the guide aimed to provide a structured framework for judges to make more consistent and objective probability estimates of a borderline candidate’s performance. Preliminary observations suggested that the guide has been useful in standardising judges’ evaluations and aligning them with the intended competence levels of a borderline candidate. However, variability in judges’ personal criteria and context-specific development posed potential issues. Pilot testing, inter-rater reliability studies, and expert reviews were essential in evaluating the guide’s impact on the pass marks. Ultimately, a well-validated guide has the potential to improve the fairness and reliability of assessments in medical and health professions education, ensuring that graduating students are competently prepared to provide safe and effective patient care.
Notes on Contributors
Han Ting Jillian Yeo contributed to writing and editing the manuscript.
Dujeepa Samarasekera contributed to the concept and development of the manuscript.
Ethical Approval
No ethical approval was required for this study as no data were collected.
Funding
No funding sources are associated with this paper.
Declaration of Interest
There are no conflicts of interests related to the content presented in the paper.
References
Norcini J. J. (2003). Setting standards on educational tests. Medical Education, 37(5), 464–469. https://doi.org/10.1046/j.1365-2923. 2003.01495.x
Tavakol, M., & Dennick, R. (2017). The foundations of measurement and assessment in medical education. Medical Teacher, 39(10), 1010–1015. https://doi.org/10.1080/0142159X. 2017.1359521
Taylor, C. A., Gurnell, M., Melville, C. R., Kluth, D. C., Johnson, N., & Wass, V. (2017). Variation in passing standards for graduation-level knowledge items at UK medical schools. Medical Education, 51(6), 612–620. https://doi.org/10.1111/medu.13240
Yeates, P., Cope, N., Luksaite, E., Hassell, A., & Dikomitis, L. (2019). Exploring differences in individual and group judgements in standard setting. Medical Education, 53(9), 941–952. https://doi.org/10.1111/medu.13915
*Han Ting Jillian Yeo
10 Medical Drive
Singapore 117597
Email: jillyeo@nus.edu.sg
Submitted: 27 June 2024
Accepted: 14 October 2024
Published online: 1 April, TAPS 2025, 10(2), 94-96
https://doi.org/10.29060/TAPS.2025-10-2/II3451
Sulthan Al Rashid
Department of Pharmacology, Saveetha Medical College and Hospital, Saveetha Institute of Medical and Technical Sciences (SIMATS), India
I. INTRODUCTION
In response to the evolving landscape of medical education, this personal view article explores the integration of advanced digital tools into the curriculum for medical students. As the field of medicine continues to advance rapidly, leveraging technologies such as Google Lens, WhatsApp, Microsoft Word (MS Word), Coggle mapping software, and artificial intelligence (AI)-driven assistants like Chat Generative Pre-Trained Transformer (ChatGPT) can significantly enhance the learning experience. This article outlines strategies for creating impactful PowerPoint presentations, developing comprehensive concept maps, and extending class hours to foster active engagement and a deeper understanding of medical concepts. The integration of these digital tools is increasingly recognised as essential in contemporary medical education. Digital tools can offer interactive and personalised learning experiences, providing medical students with innovative ways to grasp complex concepts and apply them in clinical scenarios. For instance, Google Lens can facilitate quick access to medical references and visual aids, while WhatsApp can enable real-time communication and collaboration among students and educators. MS Word is a versatile tool for drafting and organising written content, and Coggle mapping software can assist in visualising and connecting intricate medical concepts. Meanwhile, AI-driven assistants like ChatGPT offer opportunities for interactive learning and immediate support. Contemporary medical education must continuously evolve to effectively harness these technological advancements. Extending class hours and incorporating digital tools can provide students with more opportunities for engagement and learning, thus enhancing their preparedness for modern healthcare challenges. As medical education adapts to incorporate personalised learning and evidence-based practices, it is crucial to integrate these digital tools to navigate complex clinical scenarios effectively (Park et al., 2021). The subsequent sections of this manuscript will delve into the specific ways in which these digital tools can be utilised to improve medical education, ensuring a consistent and impactful learning experience for students.
II. INTEGRATION OF AI TOOLS IN MEDICAL EDUCATION
AI tools like Google Lens and ChatGPT are transforming how students retrieve, process, and present information in medical education. Google Lens allows students to extract information from textbooks and clinical images, aiding in the understanding of disease pathogenesis. For instance, it can scan textbooks to pull relevant content for study notes or presentations. PowerPoint is effective for delivering concise information (Seth et al., 2010), and its impact can be further enhanced by using AI tools to automate content extraction.” The author’s recommendation of using bold 40-point Calibri font for single-sentence slides is suggested to further improve student engagement and focus during lectures. In addition to ChatGPT, tools like Quizlet and Cortana support personalised learning. Quizlet helps create tailored flashcards based on individual learning needs, while Cortana can assist in scheduling study sessions. IBM Watson for Health further revolutionises education by aiding in the interpretation of clinical data, providing real-time analysis and treatment recommendations. AI-driven tools, such as chatbots and intelligent tutoring systems (ITS), play a crucial role in modernising medical education. Chatbots offer instant support, while ITS create customised learning paths, enhancing outcomes through adaptive learning experiences. Gamification and virtual reality (VR) further boost student engagement by making learning interactive and immersive, allowing for realistic practice in clinical scenarios (Narayanan et al., 2023).
III. ENHANCING MEDICAL EDUCATION THROUGH DIGITAL COMMUNICATION AND WORD PROCESSING TOOLS
Additionally, WhatsApp groups can promote Digital communication platforms like WhatsApp and word processing tools like MS Word have become integral to modern medical education, significantly enhancing content distribution and student engagement.
A. WhatsApp in Medical Education
WhatsApp facilitates structured communication within medical education. For instance, medical schools can create dedicated groups for subjects or cohorts, enabling the exchange of vital information. Faculty can share updates on guidelines, fostering discussions about implications and applications. WhatsApp’s voice messaging and video call capabilities allow for immediate feedback and consultations, enhancing student support awareness of current medical issues. During disease outbreaks, for example, specialised groups can disseminate updates and discuss clinical strategies. Educational challenges, such as a “case of the week,” encourage peer interaction and collaborative analysis, reinforcing learning.
B. MS Word in Medical Education
MS Word is widely used for organised note-taking, which aids students in systematically recording lecture content. For instance, during pharmacology lectures, students can create structured notes with headings for different topics and use bullet points for key concepts. The software also allows for annotating texts and research documents, enabling students to clarify and deepen their understanding.
Furthermore, MS Word supports detailed exploration of medical concepts through documentation and conceptual mapping. Students can create outlines or concept maps, integrating diagrams and linking to additional resources. Custom templates for clinical reports ensure consistency and enhance the overall learning experience.
IV CONCEPT MAPPING
Concept mapping is a powerful tool for visualising relationships between medical topics, facilitating deeper understanding and retention (Baliga et al., 2021). Coggle software is an example of a tool that helps illustrate the connections between risk factors and disease outcomes.
A. Expanding on AI-driven Tools for Concept Mapping
While Coggle is useful, several AI-driven tools offer enhanced features for concept mapping. ChatGPT can generate textual descriptions for relationships, which can then be visualised using software like Coggle. Other platforms, such as MindMeister, Lucidchart, and Xmind, provide advanced functionalities for creating dynamic and interactive concept maps, including collaborative features and automated suggestions.
Detailed examples of concept maps can demonstrate their application in medical education. For instance, a map showing the relationship between lifestyle factors and chronic diseases can visually represent how different elements influence disease progression. Incorporating concept maps at the end of sessions can reinforce key points, aiding retention and comprehension.
V. EXTENDED CLASS HOURS FOR ACTIVE ENGAGEMENT
Extending class hours offers opportunities for immersive learning experiences and practical application of medical knowledge. By increasing lecture durations, students can engage more deeply with content through interactive methods such as case-based discussions and clinical simulations. For example, additional time may be allocated for simulating patient consultations, enhancing both practical skills and theoretical knowledge. Research supports the benefits of extended instruction time, particularly when coupled with a high-quality learning environment, fostering individualised learning essential for mastering complex medical concepts (Rivkin & Schiman, 2015).
VI. IMPLEMENTATION CONSIDERATIONS
Successful integration of digital tools and extended class hours requires meticulous planning and consideration. Ensuring equitable access to digital tools among students and faculty, providing technology through university-provided devices, and offering professional development to enhance faculty digital literacy and instructional effectiveness are crucial. Implementing effective assessment methods to evaluate learning outcomes and measure the impact of digital tools on educational efficacy, such as online quizzes using AI-generated questions simulating clinical decision-making scenarios, is essential.
VII. FUTURE DIRECTIONS & CONCLUSION
Summarising the transformative potential of integrating digital tools and extended class hours in medical education, this section highlights the benefits for medical students in terms of enhanced learning, preparation for modern healthcare challenges, and future career readiness. Equipping medical graduates with skills in digital tool utilisation prepares them for evidence-based practice and lifelong learning in clinical settings. Recommendations for future research focus on advancing AI technologies, conducting longitudinal studies on educational outcomes, and expanding digital integration across medical disciplines. Proposing avenues for further research and development in digital-enhanced medical education, this section explores advancements in AI tools to personalise learning experiences and improve adaptive educational technologies. It discusses potential applications of AI-driven learning modules across medical specialties to enhance interdisciplinary collaboration in patient care and research. Curriculum development should continually evolve to integrate digital tools and extend class hours, framed by ongoing research into their efficacy and impact on medical education.
Notes on Contributors
Sulthan Al Rashid contributed to the concept, scientific content, data collection, and manuscript preparation.
Acknowledgement
ChatGPT has been employed for manuscript preparation, encompassing tasks such as preparing, drafting, or editing text, without receiving authorship credit.
Ethical Approval
No ethical approval was required for this study as no data were collected.
Funding
The author did not receive any financial support for this study.
Declaration of Interest
The author asserts that he has no conflict of interest.
References
Baliga, S. S., Walvekar, P. R., & Mahantshetti, G. J. (2021). Concept map as a teaching and learning tool for medical students. Journal of Education and Health Promotion, 10, 35. https://doi.org/10.4103/jehp.jehp_146_20
Narayanan, S., Ramakrishnan, R., Durairaj, E., & Das, A. (2023). Artificial intelligence revolutionizing the field of medical education. Cureus, 15(11), e49604. https://doi.org/10.7759/cureus.49604
Park, J. C., Kwon, H. E., & Chung, C. W. (2021). Innovative digital tools for new trends in teaching and assessment methods in medical and dental education. Journal of Educational Evaluation for Health Professions, 18, 13. https://doi.org/10.3352/jeehp.2021.18.13
Rivkin, S. G., & Schiman, J. C. (2015). Instruction time, classroom quality, and academic achievement. The Economic Journal, 125(588), F425–F448. https://doi.org/10.1111/ecoj.12315
Seth, V., Upadhyaya, P., Ahmad, M., & Moghe, V. (2010). PowerPoint or chalk and talk: Perceptions of medical students versus dental students in a medical college in India. Advances in Medical Education and Practice, 1, 11-16. https://doi.org/10.2147/AMEP.S12154
*Sulthan Al Rashid
Department of Pharmacology
Saveetha Medical College and Hospital,
Saveetha Institute of Medical & Technical Sciences (SIMATS),
Chennai, Tamil Nadu, India
+919629696523
Email: sulthanalrashid@gmail.com
Submitted: 21 May 2024
Accepted: 4 February 2025
Published online: 1 April, TAPS 2025, 10(2), 97-100
https://doi.org/10.29060/TAPS.2025-10-2/II3367
Prabanjini Rajkumar & Lucy Victoria Everett Wilding
Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore
I. INTRODUCTION
The transition from pre-university education to medical school marks the first significant change medical professionals face in the medical education continuum, and is deemed as a remarkable stressor (Sá et al., 2021). This paper seeks to explore the experiences of incoming students in further detail, noting that current literature focuses predominantly on the transition from pre-clinical to clinical years instead. These findings may offer valuable insight for medical educators to incite change in the current medical curriculum that would foster a smoother transition.
II. METHODS
This study employed a qualitative approach in obtaining data to capture expressive information. Individual semi-structured interviews were conducted (Appendix 1) with 11 first-year medical students with voluntary sampling. Informed consent was obtained from all participants to gather information surrounding predetermined questions while also allowing for exploration of new topics, in an individual setting that would allow participants to express themselves freely. Thematic analysis was then used to analyse the transcribed data deductively with the Westerman framework. Other frameworks considered include Tinto’s Model of Student Integration and Mezirow’s Transformative Learning Theory, but these were ultimately not chosen due to their dated nature and lack of direct applicability to the medical context. Furthermore, the Westerman framework uniquely provides clear guidelines on how to incite future change. Westerman’s conceptual framework describes how “novel disruptive elements (first theme) due to the transition from pre-university to undergraduate medical school are perceived and acted on (second theme), and how this directs new medical students’ personal development (third theme)” (Westerman et al., 2010).
III. RESULTS
The themes that surfaced from the data are presented in alignment with the transitional context and the related tasks students encountered (Table 1).
|
Domain |
Challenge |
New Task/Adaptation |
|
Disruptive novel elements (First Theme) |
Adapting to a new pedagogy |
Self-directed learning, dealing with increased workload |
|
Increased number of social activities |
Balancing work and social life |
|
|
Perceptions and coping strategies (Second Theme) |
Perceived inadequate preparation |
Seeking support/guidance |
|
Personal development and outcomes (Third theme) |
Accepting the new reality: gradual process |
Building resilience, finding a community |
Table 1. Overview of the challenges and adaptations identified by the participants
IV. DISCUSSION
A. Theme One: Disruptive Novel Elements
Firstly, participants described their experiences in adapting to a new pedagogy, from Conventional Didactic Learning (CDL) to Team-Based Learning (TBL). While numerous studies confirm TBL’s superior effectiveness and engagement over CDL, participants in this study faced hurdles in adjusting their learning methods.
Participants discovered that a lot of the learning had to be self-directed, with little to no guidance from the school. This left them uncertain about expectations and the ‘proper’ way to prepare for the TBLs. This feeling is similar to other studies performed in Western societies (Malau-Aduli et al., 2020).
“I also didn’t know how to prepare because, the lessons are completely new. It was quite overwhelming.”
Male #1
Participants also expressed that the sheer volume of content was quite overwhelming, marking a significant leap from their experience in secondary education.
Secondly, participants discussed how the increased number of social activities influenced their transition experience. Some found it tough to balance their academic commitments and social life, a challenge exacerbated by the lack of structured timetables and the influx of social events.
Naturally, participants felt some apprehension upon entering medical school, aware that each year it attracts the nation’s most intelligent. However, they experienced a sense of solidarity when they realised that their peers were not markedly smarter or more skilled than they were. It is natural for individuals to unite and support one another during such challenging times, which is mirrored in studies analysing the transition from pre-clinical to clinical years of training.
B. Theme Two: Perceptions and Coping Strategies
First-year medical students often bring preconceptions shaped by prior life experiences into university (Kang et al., 2021) and this influences both their self-perception and their transition experience. Participants with family members who are doctors, seemed better mentally prepared for the rigours of medical education and career while first-in-family doctors were more surprised by the intensity of the workload.
To navigate these changes, participants began to seek avenues for support and guidance, and found that they were readily able to do so within both the school and the broader medical community. While trust among healthcare workers is a cornerstone of efficient interprofessional collaboration and teamwork there is limited literature on how this can be nurtured.
“If I approach my seniors they are really nice about it, even those who are 3 years into being a doctor… it’s cool.”
Female #1
C. Theme Three: Personal Development and Outcomes
Despite being in the early stages of their medical journey, participants already feel driven to excel and manage this significant change in their lives. They exhibit a clear endeavour to cultivate resilience, which mirrors the typical profile of students medical school tends to attract: those fuelled by a deep sense of purpose in the profession, and who are thus willing to invest the necessary effort to succeed.
Transitional periods within the medical education continuum invariably come with heightened stress levels as students experience constant evolutions of their professional roles and identities. Considering that stress can hinder learning, educators are advised to better educate and prepare students for these shifts, thereby facilitating a smoother transition. Even if students do not raise their concerns to the teaching faculty, it might stem from placing trust in the educational system, even within suboptimal learning environments. This can lead to cognitive dissonance, which students might resolve through rationalisation. Recognising that the transition into medical school carries significant mental health implications for students is something educators must consider (Nyquist, 2011).
D. Strengths and Limitations
There is a noticeable lack of research focusing on the transition from pre-university to undergraduate medical education. This report begins to bridge this gap. Additionally, by incorporating the distinct cultural context of Singapore, it offers an Asian perspective in the field of medical education that has been predominantly influenced by Western viewpoints.
The sample size for this study is limited, and the perspectives gathered may not comprehensively represent the broader Year 1 undergraduate medical school population. Further studies may look into gathering data from other local medical schools in Singapore or Southeast Asia or explore clinical educator’s perspectives on balancing altering the curriculum to ease the transition period with meeting the demands of the universities in producing competent doctors.
V. CONCLUSION
For most, studying medicine is a cherished dream. Although the transition presents many challenges, it also offers enriching and positive experiences. Students have their own motivations and coping strategies to navigate this phase, but no matter how adeptly they seem to handle the transition, there remains an ever-present role for educators to improve this process.
Notes on Contributors
Prabanjini Rajkumar is a fourth year medical student at the Lee Kong Chian School of Medicine. She carried out the review of literature, conduction of interviews, analysis and coding of transcripts and the writing of the manuscript.
Dr. Lucy Wilding is a Senior Lecturer in Medical Education and serves as the Assistant Dean for Years 1 and 2 at the Lee Kong Chian School of Medicine. Dr. Wilding conceived the topic and nature of this study. She has provided invaluable expertise and guidance in shaping its direction.
Ethical Approval
The study was approved and IRB number for this paper is IRB-2023-348, with the Review Board being NTU (Nanyang Technological University) Institutional Review Board.
Acknowledgement
I would like to acknowledge the Year 1 Medical Students who graciously took part in this study without any incentives and would like to thank them for sharing their experiences with me.
Funding
This is an unfunded study.
Declaration of Interest
All authors have no potential conflicts of interest.
References
Kang, Y. J., Hwang, J. S., Lin, Y., Lee, H. J., Han, S. Y., & Kim, D. H. (2021). Exploring the preconception of the first year of medical students on medicine before entering medical school. Korean Journal of Medical Education, 33(4), 369–379. https://doi.org/10.3946/kjme.2021.205
Malau-Aduli, B. S., Roche, P., Adu, M., Jones, K., Alele, F., & Drovandi, A. (2020). Perceptions and processes influencing the transition of medical students from pre-clinical to clinical training. BMC Medical Education, 20(1). https://doi.org/10.1186/s12909-020-02186-2
Nyquist, J. G. (2011). Educating physicians: A call for reform of medical school and residency. The Journal of Chiropractic Education, 25(2), 193–195.
Sá, J., Strand, P., Hawthorne, K., Da Silva, A., & Kitto, S. (2021). Transitions in medical education: Filling in the blanks. Educacion Medica, 22(6), 346-351. https://doi.org/10.1016/j.edumed.2021.07.001
Westerman, M., Teunissen, P. W., van der Vleuten, C. P., Scherpbier, A. J., Siegert, C. E., van der Lee, N., & Scheele, F. (2010). Understanding the transition from resident to attending physician: A transdisciplinary, qualitative study. Academic Medicine, 85(12), 1914–1919. https://doi.org/10.1097/ACM.0b013e3181fa2913
*Prabanjini Rajkumar
50 Nanyang Ave
Singapore 639798
82330803
Email: m200068@e.ntu.edu.sg
Submitted: 16 August 2024
Accepted: 12 September 2025
Published online: 1 April, TAPS 2025, 10(2), 104-105
https://doi.org/10.29060/TAPS.2025-10-2/LE3494
Thazin Han1, Tun Tun Win2, Zaw Phyo1 & Zin Min Htike1
1Department of Medical Education, Defence Services Medical Academy, Myanmar; 2Department of Preventive & Social Medicine, Defence Services Medical Academy, Myanmar
Dear Editor,
The Department of Radiology, Defence Services Medical Academy reports the results on the impact of a 2-week radiology program on year 4 medical students’ perception of radiology. Advances in imaging modalities has led to almost every patient getting a scan prior to any planned management making it essential for medical students to understand the importance of radiology’s role in clinical practice. Limited exposure to radiology can perpetuate negative stereotypes by perceiving radiology as providing no significant contribution to patient care (Grimm et al., 2021). In the academic year of 2020/2021, we piloted a 2-week radiology program for 4th year medical students and conducted a qualitative, experiential, and phenomenological study design using Focus Group Interviews (FGIs) from January to July 2022 after obtaining ethical approval to find out the effectiveness of exposure to radiology impacts on 4th year medical students’ opinions and views on radiology. Eighteen out of 20 4th year medical students volunteered to participate. FGIs can be used to gather rich data through participant exchange of ideas or comments on each other’s views (Stalmeijer et al., 2014). We found that students who were hesitant to express their views individually were willing to do so in small groups.
The thematic analysis of the coded transcripts produced 6 themes which are (1) Earlier exposure to radiology-; (2) Integration of radiology into the undergraduate curriculum-; (3) Collaborative learning and practice-; (4) Motivation to learn radiology-; (5) Genuine interest in radiology and (6) Importance of radiology in clinical practice. Students reflected during FGIs that the radiology program provided meaningful learning when correlating radiology images to clinical findings. Learning is a continuous process grounded in experience and the educator’s job is to dispose, modify or implant new ideas as propounded by Kolb. This study showed that the 2-week radiology program disposed of the idea that radiology did not have any significant role on clinical management and implanted new ideas concerning the importance and appropriate use of radiology. The study is evaluated up to Kirkpatrick’s level 3 whereby there is change of students’ behavior as they now appreciated the importance of the role of radiology in clinical practice as evidenced by theme 6.
In conclusion, the radiology program was impactful in changing 4th year medical students’ perceptions regarding the role of radiology in clinical practice and provided justification to roll out the 2-week radiology program for consecutive academic years.
Notes on Contributors
Thazin Han developed the conceptual framework and piloted the radiology program. Tun Tun Win did data sampling, acquisition and analysis. Zaw Phyo recorded the FGIs. Zin Min Htike did member checking and data transcribing. All 4 took turns to conduct and moderate the FGIs and review the data.
Acknowledgement
We wish to express our gratitude and thanks to the Rector of the Defense Services Medical Academy for allowing us to conduct this research. We would like to express special thanks to the Head of the Medical Education Department for providing us with the logistic support. Finally, thanks to the study team members without whom this research would not have been achieved.
Funding
No funding is involved for this research. The research was conducted based on situation analysis of the undergraduate curriculum regarding radiology.
Declaration of Interest
There is no conflict of interest for the current research.
References
Grimm, L. J., Fish, L. J., Carrico. C. WT., Martin, J. G., Nwankwo, V. C., Farley, S., Meltzer, C. C. & Maxfield, C. M. (2022). Radiology stereotypes, application barriers, hospital integration: A mixed methods study of medical student perceptions of radiology. Academic Radiology, 29(7), 1108-1115. https://doi.org/10.1016/j.acra.2021.08.020
Stalmeijer, R. E., Mcnaughton, N. & Van Mook, W. N. (2014). Using focus groups in medical education research: AMEE Guide No. 91. Medical Teacher, 36(11), 923-939. https://doi.org/10.3109/0142159X.2014.917165
*Thazin Han
No. 94, D-1, Pyay Road
Mingaladon Township
Yangon, Myanmar
Postal code – 11021
Email: thazinhn@gmail.com
Submitted: 30 May 2024
Accepted: 21 October 2025
Published online: 1 April, TAPS 2025, 10(2), 101-103
https://doi.org/10.29060/TAPS.2025-10-2/II3420
Nadhee Peries, Nadeeja Samarasekara, Inuka Gooneratne, Niroshan Lokunarangoda, Ushani Wariyapperuma, Senaka Pilapitiya, Mihara Silva & Nandalal Gunaratne
Faculty of Medicine, University of Moratuwa, Sri Lanka
I. THE EARLY CLINICAL EXPOSURE PROGRAM
According to a large body of research, early clinical exposure and simulation-based learning are beneficial for medical students in many ways, hence the University of Moratuwa has used these concepts together in the MBBS program (Peries et al, 2024). It allows students to develop their thinking, communication, clinical reasoning, and room for trial and error (Krajic, 2003). The faculty has developed a spirally integrated, simulation-based program named Early Clinical Exposure (ECE) for students from 1st year onwards to facilitate step-by-step, yet continuous mastering of concepts and skills of history-taking and examination.
5-year MBBS program of the university consists of three phases: Phase 1 (1st / 2nd years), Phase 2 (3rd / 4th years), Phase 3 (Final year). During phase 1, students learn basic sciences integrated into body system-based modules; in phase 2, students learn applied sciences integrated into clinical subjects in body system-based modules, simultaneously ward-based clinical training. Phase 3 consists of full-time clinical training. The article describes how the ECE program was designed and exposed students of phase 1 and the early stage of phase 2 to early clinical skill training via various methods, in which, simulation-based history taking, and examination were major components.
II. DESIGN OF THE PROGRAM
The ECE program was pre-tested to see the content, timing, necessity of resources, and efficacy of teaching tools. We identified the limited number of staff as a challenge at the time, and we trained demonstrators to couple with lecturers ensuring the program ran smoothly until more academics were available. In phase 1, students learned history taking and examination concerning building a rapport and gathering information using communication skills while appreciating patient privacy and concerns. The scenarios were developed and integrated into relevant modules, to cover the applicability of basic sciences in clinical practice and the basics of the ‘clinical method’.
During phase 2 which spanned over 8 weeks, history-taking and examination sessions were revisited where learning outcomes were designed to reach higher skill levels. At this stage, the scenarios were designed to introduce concepts such as identifying problems, critical thinking, and clinical reasoning. Students were taught a holistic approach to medicine and to recognise patients as ‘whole human beings’ rather than health issues/disease entities. These scenarios were developed to ensure students follow a basic history-taking framework and stepwise method to system examination to gather relevant information on symptoms, aetiology, complications, systemic inquiry, compliance, family history, drug history, allergies, co-morbidities, patient concerns, impact on life and fears, etc.
III. DELIVERY OF THE PROGRAM
The program was delivered via small group role-playing between students and lecturers as a series of blended learning activities. The sessions were sequenced just after the relevant basic sciences teaching session to help students understand the relevance and applicability of the knowledge into practice as early as possible. Every student was given adequate time to practice with constructive feedback from teachers and observers.
Furthermore, students were encouraged to relate the most applicable components of the history concerning the patient and his/her presentation appreciating they have different concerns, either related to or not related to the main complaint that needs to be considered. As an example, a scenario developed in the respiratory module on ‘tuberculosis’, allowed students to be involved in a comprehensive information gathering and examination. Further, it also allowed students to evaluate the associated stigma affecting mental status, compliance with drugs, family support, effects on occupation, income, social interaction etc.
At the end of each examination session, videos of body system examinations were posted on Moodle followed by a small discussion forum on common abnormal signs.
IV. DISCUSSION
The ECE program allowed the students to engage in the basics of the ‘clinical method’ at the early stage of their training. It is well noted that early clinical exposure is widely used across Europe (80% of medical schools) (Basak et al., 2009). Even though the medical faculty of the University of Moratuwa is newly developed in a developing country, this program has assisted in targeting high standards in the quality of medical education.
ECE program also aligned with the MBBS program learning outcomes by teaching; clinical skills, patient management, communication skills, information management, critical thinking, professional values, and attitudes. This is similar to the suggestions given by Ottenheijm et al. (2008), that ECE activities should be well-planned with clear learning goals. Many ECE programs in Europe are unstructured, using real patients in ward settings and observation as the main teaching tool (Basak et al., 2009). In contrast, this program uses simulation patients, blended learning methods, hands-on experience, and direct feedback.
Even though the objectives were achieved, the program is currently in the middle of an evaluation. Therefore, the exact evidence is lacking to claim that this program has achieved the intended learning outcomes. On the other hand, a study done in Iran in 2016 shows, that early clinical exposure has allowed medical students to understand the value and the integration of the subjects they learn during their early years and also has provided an opportunity to get motivated regarding their role as future doctors (Mafinejad et al., 2016). It should be noted that the program needs feedback from students and resource persons to improve it further. Additionally, data should be collected from the students after they have completed the ECE program to investigate whether the program has contributed to achieving program learning outcomes.
V. CONCLUSION
Simulation is used in the Faculty of Medicine, University of Moratuwa to teach skills needed for students to take a proper history and to examine a patient before commencing ward-based learning. This spirally-integrated early clinical exposure with specially selected important case scenarios incorporated into body system-based modules in basic and applied sciences improves student preparedness for ward-based clinical training. It also provides an opportunity to improve soft skills, which contributes to achieving program learning outcomes of the degree. We plan to review and then expand and develop the program in the future with proper feedback taken at different levels.
Notes on Contributors
Nadhee Peries has planned this curriculum component, developed the program, and contributed to executing it. As the first author, she has drafted, edited, and finalised the paper. Nadeeja Samarasekara, Inuka Gooneratne, Niroshan Lokunarangoda, Ushani Wariyapperuma, and Senaka Pilapitiya contributed to developing the program to improve it further with relates to the content. They were involved in planning the program, writing the simulation scenarios, and conducting sessions. They also reviewed and improved the drafted paper. Mihara Silva contributed to arranging logistics at the planning stage and provided inputs on delivery methods. She also supported writing the paper by formatting and proofreading. Nandalal Guneratne was involved as a supervisor who conceptualised the idea of simulation-based learning in our MBBS program and guided the execution of the lessons in several steps: writing up the lesson plan, developing learning outcomes, and executing the teaching-learning method. All the authors have read and approved the drafted paper.
Ethical Approval
Specific ethical approval was not applicable as this was a part of the routine curriculum development process of the MBBS program which was approved and expected to be executed by the faculty. There is no data collection involved.
Acknowledgement
We would like to acknowledge the Faculty Board, Curriculum Development Committee, and the Medical Education Department for the guidance, support, approval, and recognition of the developed activity.
Funding
The project is funded neither by any person nor institute.
Declaration of Interest
There are no conflicts of interest, specially regarding financial, consultant, institutional, and other relationships that might lead to bias or a conflict of interest.
References
Başak, O., Yaphe, J., Spiegel, W., Wilm, S., Carelli, F., & Metsemakers, J.F.M. (2009). Early clinical exposure in medical curricula across Europe: An overview. European Journal of General Practice, 15(1), 4–10. https://doi.org/10.1080/13814780 902745930
Krajic, K. E. (2003). Observation during early clinical exposure – An effective instructional tool or a bore. Medical Education, 37(2), 88–89. https://doi.org/10.1046/j.1365-2923.2003.01421.x
Mafinejad, K. M., Mirazazadeh, A., Peiman, S., Hazaveh, M. M., Khajavirad, N., Edalatifars, M., Allameh, S., Naderi, N., Forounmandi, M., Afshari, A., & Asghari, F. (2016). Medical students’ attitudes towards early clinical exposure in Iran. International Journal of Medical Education, 7, 195–199. https://doi.org/10.5116/ijme.5749.78af
Ottenheijm, R. P., Zwietering, P. J., Scherpbier, A. J., & Metsemakers, J. F. (2008). Early student-patient contacts in general practice: An approach based on educational principles. Medical Teacher, 30(8), 802–808. https://doi.org/10.1080/01421 590802047265
Peries, N., Samarasekara, N., Gooneratne, I., Lokunarangoda, N., Wariyapperuma, U., Pilapitiya, S., Silva, M., & Gunaratne, N. (2024, January 15-21). Simulated History Taking and Examination as a Part of Early Clinical Exposure in Undergraduate Medical Education of Faculty of Medicine, University of Moratuwa [Conference presentation abstract]. Asia Pacific Medical Education Conference 2024, Colombo, Sri Lanka.
*Nadhee Peries
Department of Medical Education
Faculty of Medicine, University of Moratuwa,
Bandaranayake Mawatha, Moratuwa,
Sri Lanka, 10400
0094772003061
Email: nnperies@gmail.com, nadheep@uom.lk
https://doi.org/10.29060/TAPS.2025-10-2/TT002
Neil Osheroff
Department of Biochemistry, Vanderbilt University School of Medicine, United States of America; Department of Medicine (Hematology/Oncology), Vanderbilt University School of Medicine, United States of America
Since the time of the Flexner report, it has been accepted that science is the foundation of clinical practice (Finnerty et al., 2010; Flexner, 1910; Grande, 2009; Haramati et al., 2024; Lindsley et al., 2024; Slivkoff et al., 2019; Weston, 2018; Woods et al., 2006). However, the methods traditionally used to teach sciences to medical students have been questioned in the post-Flexner era (AAMC-HHMI Committee, 2009; Cooke et al., 2010; Fulton et al., 2012; Slivkoff et al., 2019). For nearly 100 years, the foundational sciences were taught in a discipline-oriented fashion, primarily through passive learning approaches (lectures), and largely separated from clinical practice (AAMC-HHMI Committee, 2009; Flexner, 1910). Consequently, in the pre-clerkship phase, scientific details were often overtaught and disconnected from clinical applications. This approach frequently required students to “re-learn” their foundational sciences in the setting of patient care. The disconnect between science and medicine was further exacerbated in the later phases of medical training by physicians who taught in a manner that emphasized pattern recognition over scientific underpinnings. We have come to understand that these pedagogical approaches to medical education were neither efficient nor optimal.
Adult learning theory has provided strong evidence that medical trainees are better at learning, applying information to new circumstances, and making informed clinical decisions when the foundational and clinical sciences are taught side-by-side in an integrated fashion (Bandiera et al., 2018; Bucklin et al., 2021; Kulasegaram et al., 2015; Kulasegaram et al., 2013; Lisk et al., 2016; Mylopoulos & Woods, 2014). Learning is also heighted when active rather than passive approaches are employed. In the pre-clerkship phase, small group active learning sessions (problem-based learning, team-based learning, case-based learning, etc.) provide outstanding platforms for integrating foundational and clinical sciences (Bucklin et al., 2021). Similarly, in the clinical workplace, practitioners can integrate science and medicine by probing or explaining the underlying basis of disease and treatment or employing other forms of active learning (Dahlman et al., 2018; Daniel et al., 2021; Hashmi et al., 2024; Spencer et al., 2008).
Some have questioned the need for pre-clerkship science education in medical schools, professing that the heart of medical education is the clinical experience (Emanuel, 2020). However, in the post-genomic era, this perspective would seem to be the antithesis of modern medical practice (AAMC-HHMI Committee, 2009; Haramati et al., 2024). Now more than ever, to ensure the best quality of care for their patients, physicians need to understand the scientific underpinnings of their actions.
If we truly believe that science is the foundation of clinical practice, we should not teach either in isolation. As a first step, we need to stop thinking about foundational and clinical sciences as being separate. I would argue that they are both on the spectrum of “biomedical sciences,” represent two sides of the same coin, and should be taught in an integrated fashion across the entirety of the medical school curriculum. Although this integration has been (or is being) addressed in the pre-clerkship phases at most medical schools, it has proven more challenging in the clinical phases (Brauer & Ferguson, 2015; Pettepher et al., 2016; White & Ghobadi, 2022). While science and medicine are inherently intertwined, interactions between the two in the latter phases of training are often more casual than causal. It is time for the foundational and clinical sciences to be integrated across the continuum of medical training to ensure that future physicians have the skills necessary to provide the highest caliber of care for their patients.
Acknowledgements
Work in the author’s laboratory is funded in part by NIH grants R01 GM126363 and R01 AI170546. The author is grateful to Dr. Emily Bird for critical reading of the manuscript and insightful comments.
Declaration of Interest
The author declares no conflict of interest.
References
Bandiera, G., Kuper, A., Mylopoulos, M., Whitehead, C., Ruetalo, M., Kulasegaram, K., & Woods, N. N. (2018). Back from basics: integration of science and practice in medical education. Medical Education, 52(1), 78-85. https://doi.org/10.1111/medu.13386
Brauer, D. G., & Ferguson, K. J. (2015). The integrated curriculum in medical education: AMEE Guide No. 96. Medical Teacher, 37(4), 312-322. https://doi.org/10.3109/0142159X.20 14.970998
Bucklin, B. A., Asdigian, N. L., Hawkins, J. L., & Klein, U. (2021). Making it stick: Use of active learning strategies in continuing medical education. BMC Medical Education, 21(1), Article 44. https://doi.org/10.1186/s12909-020-02447-0
AAMC-HHMI Committee (2009). Scientific foundations for future physicians.
Cooke, M., Irby, D. M., & B’Brien, B. C. (2010). Educating physicians: A call for reform of medical school and residency. Jossey-Bass.
Dahlman, K. B., Weinger, M. B., Lomis, K. D., Nanney, L., Osheroff, N., Moore, D. E., Jr., Estrada, L., & Cutrer, W. B. (2018). Integrating foundational sciences in a clinical context in the post-clerkship curriculum. Medical Science Educator, 28(1), 145-154.
Daniel, M., Morrison, G., Hauer, K. E., Pock, A., Seibert, C., Amiel, J., Poag, M., Ismail, N., Dalrymple, J. L., Esposito, K., Pettepher, C., & Santen, S. A. (2021). Strategies from 11 U.S. medical schools for integrating basic science into core clerkships. Academic Medicine, 96(8), 1125-1130. https://doi.org/10.1097/ACM.0000000000003908
Emanuel, E. J. (2020). The inevitable reimagining of medical education. JAMA, 323(12), 1127-1128. https://doi.org/10.1001/ jama.2020.1227
Finnerty, E. P., Chauvin, S., Bonaminio, G., Andrews, M., Carroll, R. G., & Pangaro, L. N. (2010). Flexner revisited: The role and value of the basic sciences in medical education. Academic Medicine, 85(2), 349-355. https://doi.org/10.1097/ACM.0b013e3181c88b09
Flexner, A. (1910). Medical education in the United States and Canada: A report to the Carnegie Foundation for the Advancement of Teaching. The Carnegie Foundation for the Advancement of Teaching.
Fulton, T. B., Ronner, P., & Lindsley, J. E. (2012). Medical biochemistry in the era of competencies: Is it time for the Krebs cycle to go? Medical Science Educator, 22(1), 29-32. https://doi.org/10.1007/BF03341749
Grande, J. P. (2009). Training of physicians for the twenty-first century: Role of the basic sciences. Medical Teacher, 31(9), 802-806. https://doi.org/10.1080/01421590903137049
Haramati, A., Bonaminio, G., & Osheroff, N. (2024). Professional identity formation of medical science educators: An imperative for academic medicine. Medical Science Educator, 34(1), 209-214. https://doi.org/10.1007/s40670-023-01922-9
Hashmi, S., Riaz, Q., Qaiser, H., & Bukhari, S. (2024). Integrating basic sciences into clerkship rotation utilising Kern’s six-step model of instructional design: Lessons learned. BMC Medical Education, 24(1), Article 68. https://doi.org/10.1186/ s12909-024-05030-z
Kulasegaram, K., Manzone, J. C., Ku, C., Skye, A., Wadey, V., & Woods, N. N. (2015). Cause and effect: Testing a mechanism and method for the cognitive integration of basic science. Academic Medicine, 90(11 Suppl), S63-S69. https://doi.org/10.1097/ACM.0000000000000896
Kulasegaram, K. M., Martimianakis, M. A., Mylopoulos, M., Whitehead, C. R., & Woods, N. N. (2013). Cognition before curriculum: Rethinking the integration of basic science and clinical learning. Academic Medicine, 88(10), 1578-1585. https://doi.org/10.1097/ACM.0b013e3182a45def
Lindsley, J. E., Abali, E. E., Asare, E. A., Chow, C. J., Cluff, C., Hernandez, M., Jamieson, S., Kaushal, A., & Woods, N. N. (2024). Contribution of basic science eeducation to the professional identity development of medical learners: A critical scoping review. Academic Medicine, 99(11), 1191-1198. https://doi.org/10.1097/ACM.0000000000005833
Lisk, K., Agur, A. M. R., & Woods, N. N. (2016). Exploring cognitive integration of basic science and its effect on diagnostic reasoning in novices. Perspectives on Medical Education, 5(3), 147-153. https://doi.org/10.1007/s40037-016-0268-2
Mylopoulos, M., & Woods, N. (2014). Preparing medical students for future learning using basic science instruction. Medical Education, 48(7), 667-673. https://doi.org/10.1111/medu.12426
Pettepher, C. C., Lomis, K. D., & Osheroff, N. (2016). From theory to practice: Utilising competency-based milestones to assess professional growth and development in the foundational science blocks of a pre-clerkship medical school curriculum. Medical Science Educator, 26(3), 491-497. https://doi.org/10.1007/s40670-016-0262-7
Slivkoff, M. D., Bahner, I., Bonaminio, G., Brenneman, A., Brooks, W. S., Chinn, C., El-Sawi, N., Haight, M., Hurtubise, L., McAuley, R. J., Michaelsen, V., Rowe, B., Vari, R. C., & Yoon, M. (2019). The role of basic science in 21st century medical education. Medical Science Educator, 29(3), 881-883.
Spencer, A. L., Brosenitsch, T., Levine, A. S., & Kanter, S. L. (2008). Back to the basic sciences: An innovative approach to teaching senior medical students how best to integrate basic science and clinical medicine. Academic Medicine, 83(7), 662-669. https://doi.org/10.1097/ACM.0b013e318178356b
Weston, W. W. (2018). Do we pay enough attention to science in medical education? Canadian Medical Education Journal, 9(3), e109-e114.
White, B., & Ghobadi, A. (2022). Models of clinical integration into basic science education for first-year medical students. Medical Teacher, 45(3), 333-335. https://doi.org/10.1080/ 0142159X.2022.2134002
Woods, N. N., Neville, A. J., Levinson, A. J., Howey, E. H., Oczkowski, W. J., & Norman, G. R. (2006). The value of basic science in clinical diagnosis. Academic Medicine, 81(10 Suppl), S124-S127. https://doi.org/10.1097/00001888-200610001-00031
Submitted: 25 January 2024
Accepted: 20 December 2025
Published online: 1 April, TAPS 2025, 10(2), 46-56
https://doi.org/10.29060/TAPS.2025-10-2/OA3228
Chhaya Divecha1, Miriam Simon2 & Ciraj Mohammed3
1Department of Paediatrics, College of Medicine and Health Sciences, National University of Science and Technology, Oman; 2Department of Psychiatry and Behavioural Science, College of Medicine and Health Sciences, National University of Science and Technology, Oman; 3Department of Medical Education, College of Medicine and Health Sciences, National University of Science and Technology, Oman
Abstract
Introduction: Paediatric milestones provide a structured method for observing and monitoring a child’s progress and should be part of core paediatric curriculum. However, a literature review reveals that primary care physicians and pediatricians feel inadequate about their knowledge and practice of developmental paediatrics, thus exposing the lacunae in training.
Methods: An intervention was planned amongst final-year medical undergraduate students in Oman during their paediatric rotation. A 90-minute multimodal active learning module incorporating diverse learning orientations was planned and administered as a skill-lab session. Its effectiveness in learner motivation, engagement, and faculty participation was evaluated using a questionnaire based on the ICAP (Interactive, Constructive, Active, and Passive) framework, administered to students at the end of the session.
Results: Responses of the 62 participants indicated a significant association between their overall experience and tasks related to the active, constructive, and interactive elements of the module (p=0.001). The faculty’s role in facilitating the session significantly contributed to students’ overall experience (p=0.000). On linear regression, active, constructive, and interactive components of the module were moderate to high predictors of the participants’ overall learning experience.
Conclusion: It was beneficial to base the teaching module on established learning theories. Active learning strategies proactively fostered student engagement and self-directed learning during the session. Faculty played an important role in planning and customising the content, flow, and delivery to maximise meaningful learning. Such interactive collaboration, especially for theoretical concepts in medicine, enables better student engagement, providing enhanced opportunities for learning, practice, and feedback.
Keywords: Active Learning, Child Development, Undergraduate Medical Education, Student Engagement, ICAP Framework
Practice Highlights
- Active learning strategies can foster student engagement in teaching paediatrics.
- The use of interactive collaboration for theoretical concepts in medicine is effective.
- The role of faculty is crucial to maximise meaningful student learning.
- Utilisation of learning theories to design modules is beneficial for successful content delivery.
I. INTRODUCTION
Clinical curriculum while preparing students for patient care frequently focuses on abnormal pathologies with normal development or physiology often being neglected or underemphasised (Densen, 2011). Developmental and behavioral paediatrics are integral components of pediatric clinical practice. Paediatric milestones provide a structured method to monitor a child’s progress with a comprehensive understanding of development across all domains (gross motor, fine motor, language, and social) and thus must be adequately addressed in the core paediatrics curriculum. However, review of literature reveals that primary care physicians and paediatricians feel inadequate about their knowledge and practice of developmental paediatrics, thus exposing the gaps in education and training (Bauer et al., 2009; Beggs et al., 2005; Bright et al., 2019; Chödrön et al., 2021; Comley et al., 2008; Honigfeld et al., 2012).
Large group didactic classrooms often involve passive reception, leading to lack of engagement among learners (Huggett & Jeffries, 2021). Undergraduate medical curriculum is transitioning from a passive, teacher-centered approach to a learner-centered, active learning strategy, which has demonstrated enhanced students’ understanding, retention of complex concepts, improved student motivation, and overall course satisfaction (McCoy et al., 2018; O’Sullivan et al., 2022). Innovative active learning approaches on developmental milestones largely employ live visits to community resource sites along with instructional videos, reflective reports, observing live parent-child pairs, and use of short video clips (Clark et al., 2012; Comley et al., 2008). In addition, interactive DVDs containing animated cartoons and questions, live interviews, case vignettes, case write-ups, stimulus videos, observation experiences, discussion groups, field trips, and personal experiences have been documented as teaching-learning strategies (Fox et al., 2007; Leiner et al., 2011). Digital resources such as “Beyond Milestones”, developed as free online material for medical professionals using real-life developmental assessments, have shown improved scores on knowledge, observational expertise, confidence, and learner satisfaction (Connolly et al., 2014).
Though observing children in real-life scenarios (including wards, outpatient departments, well-baby clinics, schools, community centers, etc.) creates opportunities for interactive and authentic learning, restrictions in availability of exposure, time, and faculty, especially during the COVID pandemic have compounded the woes of clinical training. The aforementioned reasons prompted us to develop an active learning module using the ICAP framework to introduce developmental milestones in the paediatric curriculum. This framework identifies four modes of cognitive engagement in active learning: Interactive (I), Constructive (C), Active (A), and Passive (P). Passive modes of cognitive engagement involve receipt of information, compared to active modes which require learners to physically manipulate information provided (Chi & Wylie, 2014). Engagement further increases in the constructive mode as students generate diagrams, questions, etc., and is maximum in the interactive mode where peers collaborate and co-construct knowledge through the process of questioning and responding during a conversation. Research reveals that learning achievement is lowest at P and increases in the order of A, C, and I (Chi & Wylie, 2014). Given that the ICAP framework involves both interactive and active learning, we hypothesised that its application to the education of developmental milestones would further promote and expand learning and performance of undergraduate medical students. Additionally, it would help identify and address gaps in their knowledge and understanding of developmental milestones.
In this study, we developed an innovative learning module for developmental milestones using the ICAP model. The module was active, interactive, experiential, and grounded in the major theories of learning (behaviorism, cognitivism, constructivism, humanism, and social learning theories) to maximise opportunities for learning. This pilot study aimed at testing the effectiveness of the module in terms of learner motivation, engagement, and faculty participation.
II. METHODS
The current study was conducted at a private medical college in Oman. It was a cohort study with a quantitative survey and qualitative component. Final-year undergraduate medical students doing their 6-week clinical rotation in Paediatrics were introduced to the teaching module during their skill-lab session (in groups of 6 to 8 students). Verbal consent was obtained for learner feedback.
The learning session was planned and conducted by faculty researchers with expertise in paediatrics, developmental psychology, and medical education. The learning outcomes of this module on developmental milestones were:
- To identify age-appropriate milestones in children from birth to 5 years of age.
- To apply knowledge of milestones for various domains (gross motor, fine motor, language, and social/cognitive) to assess development in various age groups (birth to 5 years).
- To differentiate between normal and delayed development in children.
The specific learning outcomes were addressed through various strategies as summarised in Figure 1.

Figure 1. Flow chart depicting the sequence of activities mapped with specific learning objectives
The module was planned for 90 minutes and included learning activities based on principles of active and adult learning. Pre-reading material for the multimodal active learning session on developmental milestones was provided (https://aqmedia.org/filestore/2/0/3/6_83bcb34c55b2770/6302_012d2ba650720b8.pdf). Various constructs that underpin major learning theories were adopted while designing the learning approaches which are detailed here:
A. Lid Opener and Think Pair Share
Having a child with a disability can profoundly affect family dynamics, resulting in psychosocial challenges like parental stress, social isolation, mobility limitations, child behavioral issues, and difficulties in coping and adjustment (Woolfson, 2004). Students were shown a short video of a child with developmental delay and its psychosocial impact on the child and family. They were then divided into pairs/groups and asked to reflect on the video in terms of how watching the video made them feel, what they believed the child and family might be going through, and why an awareness of typical developmental milestones is important. Following group discussion, one representative from each group shared the pertinent points that emerged with the larger group.
B. Discourse
The session covered fundamentals related to detection of milestones in children from birth to 5 years of age through a lecturette by faculty from the Paediatrics Department.
C. Exploration via Self-directed Learning Activity
During this section, students were briefed about the interactive activity and divided into two sub-groups (3 to 4 members per group). An instruction sheet explaining the activity was provided. A group leader for each sub-group was identified to monitor group dynamics and ensure active participation. The ‘Paediatric Developmental Milestones Interactive Table’ from Aquifer Pediatrics website’s free student resources was shown on a smart board. The table involved a grid of milestones (gross motor, fine motor, communication/social, cognitive/adaptive) against ages (2 months, 4 months, 6 months, 9 months, 12 months, 15 months, 18 months, 24 months, 2 years, 3 years, 4 years, 5 years). Students explored their knowledge of the milestones by clicking on each square and further reinforced it by double clicking (which would show appropriate video clips of 2 to 8 seconds). During this activity, learners engaged in self-directed learning through the use of the interactive table to compare milestones in various domains across age groups.
D. Case-Based Learning (CBL)-Trigger and Buzz Groups
Following the SDL activity, students were led into Case-Based learning, where they were shown a video of a child undergoing developmental assessment by a doctor. They were asked to identify milestones and estimate the developmental age of the child. To prompt further discussion, a buzz group format in small groups was employed to discuss their findings. The facilitator moved around to help and encourage participation in group discussions. After that, the sub-groups presented their findings to the entire group, which sparked additional discussion and feedback.
E. Game-Based Learning
The acquired knowledge of milestones was further intensified through gamification. A game of BINGO was played, where each student received a bingo ticket with pictures of milestones (sample in Figure 2). The facilitator drew cards from the bingo pile (with age and domain) and students were asked to identify the appropriate milestone picture for that age/domain on their ticket. The first one to get a line of 5 pictures (horizontal/vertical/ diagonal) was declared the winner.

Figure 2. Sample of bingo ticket with milestones
F. Scaffolding
The faculty would wrap up the case and summarise major learning points thus consolidating the knowledge about milestones. Throughout the learning session, the facilitator provided cognitive scaffolding by leading the students through different questions, prompts, tasks, and structured interactions enabling them to learn more about developmental milestones. Students had opportunities to work with their existing knowledge and build further on it through the various learning activities, group discussions and faculty-led facilitation.
G. Reflection on Action
Students were divided into groups (2 or 3 students per group) to reflect on their entire learning experience using Borton’s model of reflection (Rolfe, 2014). Their reflections elucidated the “what”- their experience of the activities, “so what”- how the module improved on their prior knowledge and understanding about the topics and “now what”- providing suggestions for improvement and preference for similar active learning strategies in future sessions. Individual sharing within groups was followed by sharing between groups via their representatives.
H. Data Collection and Analysis
Students were asked to complete a feedback form about their learning experience during the activity via an anonymised electronic feedback form administered at the end of the session. The form had 15 items evaluating their learning experience – 11 quantitative (Likert scale-based) and 4 qualitative questions. The quantitative feedback responses were analysed based on the four domains of the ICAP model- questions were framed for Interactive, Constructive, Active, and Passive engagement of students during the active learning strategies. There were 4 items (Max score=20) about the interactive components of the module, 3 items (Max score=15) based on constructive elements, and two items each (Max score=10) on the active and passive engagement of students during the module. In addition, 4 quantitative items assessed feedback on faculty involvement and students’ overall experience.
Data was analysed using IBM’s Statistical Package for Social Studies (SPSS 22; IBM Corp., Armonk, NY, USA). Descriptive statistical methods such as percentages, mean and standard deviation were employed. Cronbach’s alpha method was used to assess internal consistency/test reliability. The Shapiro-Wilk method was used to test normality. Inferential statistical methods such as the Spearman’s correlation analysis and Chi-square test were used to explore significant associations between variables. Linear regression was also used to explore various predictors of the participants’ learning experience. Thematic analysis was performed for qualitative feedback.
III. RESULTS
A. Overview of Study Participants
A total of 62 students from the final clinical year of the MD program participated in this study; 91% were females and 9% were males. The average age of participants was 24.4 years (SD=0.707).
Results indicate high internal consistency for the survey items developed. Full scale (15 items) Cronbach’s alpha value of 0.808 was obtained. Results of the Shapiro-Wilk test of normality for all survey items (p=0.000) indicate that participant’s responses were not normally distributed. Non-parametric tests were thus employed for data analyses.
B. Analysis of Learner Feedback
In general, participants agreed that the session on developmental milestones was enjoyable.
The preference for game-based interactive/collaborative learning was high. The learner responses categorised item wise are provided in Table 1.
|
Item |
Strongly Agree |
Agree |
Can’t say |
Disagree |
Strongly Disagree |
Mean |
SD |
|
The pre-reading material on developmental milestones was easily understandable
|
59.7% |
35.5% |
4.8% |
0 |
0 |
4.548 |
0.591 |
|
The session established clear learning outcomes and objectives.
|
91.9% |
8.1% |
0 |
0 |
0 |
4.919 |
0.274 |
|
The case-based activity on developmental milestones provided relevant opportunity to witness theory in practice.
|
83.9% |
16.1% |
0 |
0 |
0 |
4.839 |
0.370 |
|
Presentation of real-world contexts followed by discussion in groups helped me learn better.
|
88.7% |
9.7% |
1.6% |
0 |
0 |
4.871 |
0.383 |
|
The game-based activity enabled me to build an emotional connection to learning and the subject matter.
|
82.3% |
16.1% |
0 |
1.6% |
|
4.790 |
0.516 |
|
This session provided me opportunities for feedback and practice
|
83.9% |
16.1% |
0 |
0 |
0 |
4.839 |
0.370 |
|
I enjoyed the session on developmental milestones as it actively engaged me with the course material through case study and discussion.
|
87.1% |
12.9% |
0 |
0 |
0 |
4.871 |
0.338 |
|
The session assisted us in organising our thoughts, reflecting on our understanding, and finding gaps in our reasoning.
|
74.2% |
21% |
4.8% |
0 |
0 |
4.694 |
0.560 |
|
I prefer similar sessions to learn theoretical concepts in paediatrics and medicine.
|
88.7% |
9.7% |
1.6% |
0 |
0 |
4.871 |
0.383 |
|
Today’s session was well-planned and helped me work on my own to accomplish learning goals independently.
|
82.3% |
17.7% |
0 |
0 |
0 |
4.823 |
0.385 |
|
The faculty supported students in the learning process during the session.
|
98.4% |
1.6% |
0 |
0 |
0 |
4.984 |
0.127 |
|
The faculty regulated the level of information and maintained my ability to be responsible for my learning.
|
87.1% |
11.3% |
1.6% |
0 |
0 |
4.855 |
0.398 |
|
The session made me identify psychosocial issues associated with developmental delays
|
69.4% |
21% |
8.1% |
1.6% |
0 |
4.581 |
0.714 |
|
I found myself motivated, engaged and self-directed during the entire session.
|
82.3% |
14.5% |
3.2% |
0 |
0 |
4.790 |
0.483 |
|
Using the interactive online module to explore developmental milestones helped improve my learning in this area. |
66.1% |
25.8% |
6.5% |
1.6% |
0 |
4.565 |
0.692 |
Table 1. Analysis of survey responses based on dimensions of the ICAP Model
C. Analysis of Feedback on Faculty Involvement and Overall Experience
The mean score on the participants’ feedback on the involvement of faculty members during the session was 9.839 (SD=0.450) and their overall experience was 9.710 (SD=0.686).
D. Association among Various Survey Dimensions
Results indicated significant associations between learner’s overall experience and tasks related to the active component of the session (p=0.000), constructive engagement (p=.000), and interactive collaboration with peers (p=0.001). Results also indicated significant associations between the interactive and constructive components of the session (p=0.000), faculty’s role in facilitating the session and students’ overall experience (p=0.000), and faculty involvement with the passive component (designing the initial reading material) (p=0.000).
E. Spearman’s Correlation
Spearman’s correlation across the various survey dimensions based on the ICAP model indicated high positive inter-dimension correlation. A significant correlation was also seen between the survey dimensions and the full-scale scores.
F. Linear Regression
Linear regression analysis was carried out to explore various predictors of the participants’ learning experience. The active (R2=0.438), constructive (R2=0.718), and interactive components (R2=0.644) are moderate to high predictors of the participants’ overall learning experience.
G. Thematic Analysis of Qualitative Items
The following themes and elaborations emerged on analysis of student feedback relating to their experience during the active learning module on developmental milestones which are summarised in Table 2.
|
Themes |
Elaboration of theme |
Samples of students’ feedback |
|
(i) Elevated learning experience
|
Participants expressed positive feedback regarding all components of the active learning session. They enjoyed the game-based activities, technology-integrated tasks, while at the same time enhancing their knowledge on developmental disorders from a clinical perspective.
|
“The bingo game brought a surprisingly fun twist to a boring topic and the competitiveness of the group as well as the doctors fun proctoring made it an overall pleasant and enjoyable experience. In short, this was a session I’m glad I got out of bed for.” “The smart board table was an active way of remembering.” “Encourage us to learn more and attend to skill lab. It was wonderful.” “A lot better than what I thought I would feel compared to a normal session. Confident to answer any questions related to developmental milestones.” |
|
(ii) Efficacious collaborative interactions
|
Students reported increased interest in learning as the session involved working together with their peers. Participants felt that continual interaction throughout the session strengthened learning.
|
“The group interactions really helped me retain the information. It was a fun experience and something new and out of the ordinary.” “Interactions made the information much easier to understand.” “It was interactive which made it interesting.” “I interacted throughout the session, learned quite a lot of information, very helpful.” |
|
(iii) Reflective outlook to patient care
|
Participants appreciated the inclusion of humanism in the learning experience. The incorporation of reflective practice in patient and caregiver experiences is a vital component that may impact future outcomes related to patient care. |
“Playing the video which wasn’t pure scientific as usual, it is emotional also, so it touches both the doctor and the human inside me.” “Watching the video of cerebral palsy and then reflecting over why development is very important.” |
|
(iv) Supportive learning environment
|
Student feedback highlighted the presence of a positive, non-judgmental environment that ensured improvement of learning in a relaxed/ stress-free setting. |
“We were able to make mistakes and learn from them without the fear of being criticised” “It was very fun and interactive. No pressure was there and not scary.” “It was interactive and very useful and most important comfortable and didn’t feel like we were being pressured and that surely helped us learn way better.” “Very happy and I enjoyed it a lot. My favourite session since the beginning of the year… no pressure was put on us, so we were able to actually learn instead of being terrified.” |
Table 2. Thematic analysis of qualitative feedback
IV. DISCUSSION
Monitoring a child’s development over time via milestones is a core part of paediatric curriculum and practice, as it enables early identification of delay or atypical progress, allowing timely referral. As an alternative to traditional learning through lectures as practiced routinely, we utilised active learning strategies that addressed multiple learning orientations for enhanced student engagement and learning.
A. Designing the Module and Active Learning Strategies based on Learning Theories
The developmental milestone module designed to involve multimodal active learning strategies has been described in the methods section. The session began with a novel “lid-opener” showing a real-life video of a child with developmental delay and the psychosocial impact of the disability on the child and family, followed by an active learning strategy; think pair and share (TPS). We explored the utility of “cognitive” orientations to learning by positioning learners to seek and understand the structure of knowledge for meaningful learning. TPS has been known to enhance the process of clinical learning by allowing students to experience different viewpoints on a particular problem and express as well as to listen to others as compared to a traditional classroom lecture (Ganatra et al., 2021; Linsenmeyer, 2021).
A significant proportion (91%) of students agreed that using the interactive module to explore milestones helped improve their learning on the topic which is also reflected in the qualitative feedback (Table 2). The interactive smart board allowed students to explore milestones in a self-directed activity and enabled higher-order cognition through active engagement with the course content. Technology in learning is stimulating for millennial learners and allows them to use online novel educational tools to maneuver their learning process (George & Dreibelbis, 2021). The wide availability of mobile devices, laptops, smart boards, etc. provides the teacher opportunities to use these new technologies effectively to transform learning into a more collaborative, personalised, and empowering experience that is rooted in connectivism- the learning theory of the digital era. We employed a multimodal approach integrating diverse activities such as videos, interactive smart boards, and gamification (via the BINGO game). Integrating many information sources nurtures the learner’s ability to reflect on connections between fields, ideas, and concepts, a core skill linked to the theory of connectivism. (Goldie, 2016).
Case-based learning (CBL) effectively links theory and practice and prepares students for actual clinical application of knowledge through inquiry (Thistlethwaite et al., 2012). The hypothetico-deductive reasoning inherent to a “constructivist” framework was applied while designing this approach (Kalinowski & Pelakh, 2024). It increases the learner’s engagement and motivation for learning through creativity, challenge, interest, and enjoyment afforded through the case-study method. An important part of CBL involves problem-solving through free discussions and with often no correct or incorrect answers, thus broadening the students’ reasoning process (Thistlethwaite et al., 2012). We used a CBL trigger in the form of a video demonstrating an assessment of a child’s development, allowed students analyse the video individually followed by buzz group discussions to share their understanding. All our students unanimously agreed that the case-based activity gave them ample opportunity to witness theory in practice. Buzz groups also provide an opportunity to apply contextual thinking to actual practice and develop collaborative skills. Studies have shown that buzz groups improve clinical reasoning and learning, promote teamwork, increase motivation to learn, improve academic performance through a conducive learning environment, and provide a chance for all members to participate and share their opinions within their sub-group (Abbasi et al., 2017; Balslev et al., 2015; Shrivastava, & Shrivastava, 2018). The elements of exploration and experimentation ensured that the theory of constructivism rooted in the connection of new knowledge to pre-existing knowledge was effectively utilised in the CBL process. Co-creation of this knowledge with peer interactions can be attributed to social learning theories of cognitivism and constructivism.
Selective and purposeful gamification has been known to increase learner motivation and engagement and, ultimately, learning (Rutledge et al., 2018). This was evident in our study where a vast majority (98%) of students agreed that the game-based activity helped them build an emotional connection with the process of learning and concepts being learned, which is also reflected in the qualitative feedback (Table 2). Game-based learning (GBL) builds emotional connections by immersing learners in engaging and interactive environments. These environments evoke emotions such as curiosity, excitement, and empathy, which enhance motivation and deepen the learning experience (Loderer et al., 2020). Based on constructivist theory, the game-based activity integrated their knowledge of age-appropriate milestones with a fun-based BINGO theme. The instant feedback that served as formative assessment in this segment had a behaviorist orientation that is specific and quantifiable.
B. Student Engagement using Multimodal Active Learning Strategies
Studies have noted a preference for multi-modal learning strategies by medical students which have been shown to improve academic performance, and promote deeper learning and enquiry (Alkhasawneh et al., 2008; James et al., 2011; Lujan & DiCarlo, 2006; Nicholson et al., 2016). Different learners have different learning styles and use of a variety of strategies can engage learners synergistically. We used various active learning strategies to facilitate student engagement as shown in Figure 3 which incorporated the ICAP framework of Interactive, Constructive, Active, and Passive activities. In addition, the use of learning theories to rationalise the framing of learning objectives, selection of specific teaching-learning methods/strategies, and design of appropriate evaluation strategies ensured student engagement and meaningful learning.
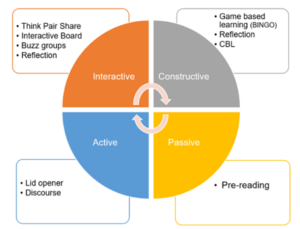
Figure 3. Summary of active learning strategies used in the module based on ICAP framework
The module had more activities involving interactive and constructive domains as compared to the active and passive modes. It is known that student learning and engagement improve as they move from passive to active to constructive to interactive modes (Chi & Wylie, 2014). Significant association between overall experience and interactive collaboration with peers (p=0.001) as well as constructive engagement (p=0.000) was observed. The feedback was also structured to measure student engagement in all four behaviors. We observed high mean scores in interactive and constructive domains. Learners agreed on enough opportunities for feedback, and practice and appreciated the engagement through case studies and discussions. Effective use of multiple active learning strategies thus enabled self-directed learning and students felt that they could accomplish the learning goals independently. The results underpin the utility of behaviorism and humanism as orientations for the learning process in such activities.
C. Individual and Collaborative Learning
The combination of active learning strategies facilitated engagement at both individual and collaborative levels. Students were involved in individual learning through pre-reading, lid-opener, discourse on development, case-based learning, and game (BINGO). These activities provided opportunities to self-regulate and moderate their learning. It also allowed them to organise their thoughts and reflect on their understanding. Active learning has a positive impact on memory and knowledge transfer and hence, individual self-studying before discussion improves the effectiveness of collaboration (Beggs et al., 2005). Activities initiated with an individual thinking process were balanced by subsequent group discussions. Collaborative activities in the form of Think pair share (TPS) after lid-opener, Buzz groups after CBL learning, and interactive table enabled constructive interaction among students and exchange of information and concepts. The collaborative activities helped students work together towards problem-solving, observe both their own and another’s learning process, discover different ways of approaching a situation, and find gaps in their reasoning. It also helped to build on their team skills, leadership, clinical competence, and interpersonal communication which are core attributes of professionalism in our curriculum (Branch, 2015).
D. Faculty Involvement
Though activities in the module were planned to encourage self-directedness, faculty role in the preparation and implementation of these strategies cannot be undermined. We adopted an amalgamation of humanistic and social cognitive orientation to strengthen the relationship between quality of instructional design and outcomes, thereby influencing learning directly. Perhaps for the same reasons we found a significant association between faculty facilitation with overall learning experience (p=.000). Students felt that the faculty supported them through the learning process throughout the session (100%) and regulated information besides allowing students to be responsible for their learning (98%). There was also a significant association between faculty involvement and the passive component (pre-reading material, discourse) (p=0.00); students agreed that pre-reading material was easily understandable (95%) and clear objectives and outcomes laid down before the session facilitated their understanding (100%). It must be noted that faculty can personalise the module based on the strengths, interests, cultural competencies, and time restraints of the student. Thus, rather than delivering a “one size fits all” module, the faculty can customise the content based on the student’s needs and limitations.
Involving various sensory processes enables better processing and retention of information; thus, enhancing the learning process (Friedlander et al., 2011). As more methods are employed, they are likely to engage more senses thus improving learning. Neuroscientific rationale for constructivist cognition may be seen as a possible explanation (Dennick, 2016).
While the use of active learning techniques in undergraduate medical education is not entirely novel, our approach is distinctive in that we’ve designed an entirely active learning module addressing various orientations to student learning, which ensures individual and collaborative student engagement. The study’s primary advantage is the creation and application of a targeted educational resource to teach developmental paediatrics to undergraduate students. This not only addresses the gap in effectively integrating developmental paediatrics into the core paediatrics curriculum but also demonstrates the feasibility of using a fully active learning approach in other clinical topics. Our detailed methodology aims to assist other educators in transforming their content into interactive teaching modules. The module not only meets the institutional requirement for increasing active learning sessions in the clinical years but also addresses a broader need by offering a framework and learning strategies that can be effectively applied to different topics and courses.
We could only assess student engagement based on their perception, i.e. level 1 of the New World Kirkpatrick Model (reaction), and have not quantified their ability to learn, understand, and apply their learning which constitutes higher levels of the model (Liao & Hsu, 2019). Additional limitations include the fact that this is a pilot study, tailored to a specific context and curriculum, which may restrict its generalisability. It also does not directly compare with other learning methods and lacks long-term tracking of students.
V. CONCLUSION
Paediatric topics such as developmental paediatrics are delivered mainly through didactic orientations and fail to capture student engagement leading to poor comprehension. Our study demonstrates that medical students enjoy sessions involving multimodal active learning strategies, particularly while discussing theoretical concepts that provide opportunities for practice and feedback. Heterogeneous learning strategies which underpin various learning theories and constructs have been shown to increase student motivation and engagement, thus contributing towards retention and deep learning. The faculty have an important role in planning such modules to customise the content and delivery for successful student engagement and effective learning thereafter. The framework and active learning strategies presented in the module can be applied more broadly to other subjects adapting to the needs of other undergraduate faculty in their teaching, thus making active teaching strategies easily transferable. We recommend future research be planned to include pre- and post-session assessments or a crossover study with a control group for comprehensive evaluation. Furthermore, the implementation of active learning strategies to create entirely active modules in other courses within the undergraduate medical program can be explored to assess its potential for broader applicability.
Notes on Contributors
Dr. Chhaya Divecha, Associate Professor of Paediatrics was involved in the conceptualisation and design of the study, literature search, data collection and drafting the manuscript.
Dr. Miriam Simon, Associate Professor of Behavioral Science was involved in the design of the study, analysis, interpretation of results and drafting the manuscript.
Dr. Ciraj Mohammed, Professor of Medical Education was involved in the design of the study and revised the manuscript for scientific content.
All authors have read and approved the final manuscript.
Ethical Approval
Approval to conduct this study was obtained from the institution’s Ethics and Biosafety Committee (NU/COMHS/EBC0036/2022).
Data Availability
Data will be made available by the authors on acceptance of the manuscript.
Acknowledgement
The authors wish to thank the participants for their cooperation in the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interests.
References
Abbasi, F., Mofrad, M. N., Borhani, F., & Nasiri, M. (2017). Evaluation of the effect of training by buzz group method on nursing diagnostic skills of nursing students. Research Journal of Pharmacy and Technology, 10(1), 213-218. https://doi.org/10.5958/0974-360x.2017.00045.2
Alkhasawneh, I. M., Mrayyan, M. T., Docherty, C., Alashram, S., & Yousef, H. Y. (2008). Problem-based learning (PBL): Assessing students’ learning preferences using VARK. Nurse Education Today, 28(5), 572–579. https://doi.org/10.1016/j.nedt.2007.09.012
Balslev, T., Rasmussen, A. B., Skajaa, T., Nielsen, J. P., Muijtjens, A., De Grave, W., & Van Merriënboer, J. (2015). Combining bimodal presentation schemes and buzz groups improves clinical reasoning and learning at morning report. Medical Teacher, 37(8), 759–766. https://doi.org/10.3109/0142159X.2014.986445
Bauer, S. C., Smith, P. J., Chien, A. T., Berry, A. D., & Msall, M. (2009). Educating pediatric residents about developmental and social–emotional health. Infants & Young Children, 22(4), 309-320. https://doi.org/10.1097/IYC.0b013e3181bc4da0
Beggs, S., Sewell, J., Efron, D., & Orkin, C. (2005). Developmental assessment of children: A survey of Australian and New Zealand paediatricians. Journal of Paediatrics and Child Health, 41(8), 444–448. https://doi.org/10.1111/j.1440-1754.2005.00664.x
Branch, W. T. (2015). Teaching professional and humanistic values: Suggestion for a practical and theoretical model. Patient Education and Counseling, 98(2), 162–167. https://doi.org/10.1016/j.pec.2014.10.022
Bright, M. A., Zubler, J., Boothby, C., & Whitaker, T. M. (2019). Improving developmental screening, discussion, and referral in pediatric practice. Clinical Pediatrics, 58(9), 941–948. https://doi.org/10.1177/0009922819841017
Chi, M. T. H., & Wylie, R. (2014). The ICAP framework: Linking cognitive engagement to active learning outcomes. Educational Psychologist, 49(4), 219–243. https://doi.org/10.1080/00461520 .2014.965823
Chödrön, G., Barger, B., Pizur-Barnekow, K., Viehweg, S., & Puk-Ament, A. (2021). “Watch Me!” Training increases knowledge and impacts attitudes related to developmental monitoring and referral among childcare providers. Maternal and Child Health Journal, 25(6), 980–990. https://doi.org/10.1007/s10995-020-03097-w
Clark, B., Andrews, D., Taghaddos, S., & Dinu, I. (2012). Teaching child development to medical students. The Clinical Teacher, 9(6), 368–372. https://doi.org/10.1111/j.1743-498X.2012.00581.x
Comley, L., Janus, M., Marshall, D., & Niccols, A. (2008). The early years: Child development in undergraduate medical school training. Canadian Family Physician, 54(6), 876.e1-4.
Connolly, A. M., Cunningham, C., Sinclair, A. J., Rao, A., Lonergan, A., & Bye, A. M. (2014). ‘Beyond Milestones’: A randomised controlled trial evaluating an innovative digital resource teaching quality observation of normal child development. Journal of Paediatrics and Child Health, 50(5), 393–398. https://doi.org/10.1111/jpc.12485
Dennick, R. (2016). Constructivism: Reflections on twenty-five years teaching the constructivist approach in medical education. International Journal of Medical Education, 7, 200–205. https://doi.org/10.5116/ijme.5763.de11
Densen, P. (2011). Challenges and opportunities facing medical education. Transactions of the American Clinical and Climatological Association, 122, 48–58.
Fox, G., Katz, D. A., Eddins-Folensbee, F. F., & Folensbee, R. W. (2007). Teaching development in undergraduate and graduate medical education. Child and Adolescent Psychiatric Clinics of North America, 16(1), 67-94. https://doi.org/10.1016/j.chc.2006.07.006
Friedlander, M. J., Andrews, L., Armstrong, E. G., Aschenbrenner, C., Kass, J. S., Ogden, P., Schwartzstein, R., & Viggiano, T. R. (2011). What can medical education learn from the neurobiology of learning? Academic Medicine, 86(4), 415–420. https://doi.org/10.1097/ACM.0b013e31820dc197
Ganatra, S., Doblanko, T., Rasmussen, K., Green, J., Kebbe, M., Amin, M., & Perez, A. (2021). Perceived effectiveness and applicability of Think-Pair-Share including storytelling (TPS-S) to enhance clinical learning. Teaching and Learning in Medicine, 33(2), 184–195. https://doi.org/10.1080/10401334.2020.1811094
George, D. R., & Dreibelbis, T. D. (2021). Active learning in ‘The cloud’: Using “social” technologies to expand the medical classroom. In A. Fornari & A. Poznanski (Eds.), How-to guide for active learning (pp. 85-99). Springer.
Goldie, J. G. (2016). Connectivism: A knowledge learning theory for the digital age? Medical Teacher, 38(10), 1064–1069. https://doi.org/10.3109/0142159X.2016.1173661
Honigfeld, L., Chandhok, L., & Spiegelman, K. (2012). Engaging pediatricians in developmental screening: The effectiveness of academic detailing. Journal of Autism and Developmental Disorders, 42(6), 1175–1182. https://doi.org/10.1007/s10803-011-1344-4
Huggett, K. N., & Jeffries, W. B. (2021). Overview of active learning research and rationale for active learning. In A. Fornari & A. Poznanski (Eds.), How-to guide for active learning (pp. 1-7). Springer.
James, S., D’Amore, A., & Thomas, T. (2011). Learning preferences of first year nursing and midwifery students: Utilising VARK. Nurse Education Today, 31(4), 417–423. https://doi.org/10.1016/j.nedt.2010.08.008
Kalinowski, S. T., & Pelakh, A. (2024). A hypothetico-deductive theory of science and learning. Journal of Research in Science Teaching, 61(6), 1362–1388. https://doi.org/10.1002/tea.21892
Leiner, M., Krishnamurthy, G. P., Blanc, O., Castillo, B., & Medina, I. (2011). Comparison of methods for teaching developmental milestones to pediatric residents. World Journal of Paediatrics, 7(2), 161–166. https://doi.org/10.1007/s12519-011-0269-5
Liao, S. C., & Hsu, S. Y. (2019). Evaluating a continuing medical education program: New world Kirkpatrick model approach. International Journal of Management, Economics and Social Sciences, 8(4), 266-279.
Linsenmeyer, M. (2021). Brief activities: Questioning, brainstorming, think-pair-share, jigsaw, and clinical case discussions. In A. Fornari & A. Poznanski (Eds.), How-to guide for active learning (pp. 39-66). Springer.
Loderer, K., Pekrun, R., & Plass, J. L. (2020). Emotional foundations of game-based learning. In J. L. Plass, R. E. Mayer, & B. D. Homer (Eds.), Handbook of game-based learning (pp. 111–151). MIT Press.
Lujan, H. L., & DiCarlo, S. E. (2006). First-year medical students prefer multiple learning styles. Advances in Physiology Education, 30(1), 13–16. https://doi.org/10.1152/advan.00045.2005
McCoy, L., Pettit, R. K., Kellar, C., & Morgan, C. (2018). Tracking active learning in the medical school curriculum: A learning-centered approach. Journal of Medical Education and Curricular Development, 5, 2382120518765135. https://doi.org/10.1177/2382120518765135
Nicholson, L. L., Reed, D., & Chan, C. (2016). An interactive, multi-modal anatomy workshop improves academic performance in the health sciences: A cohort study. BMC Medical Education, 16, Article 7. https://doi.org/10.1186/s12909-016-0541-4
O’Sullivan, S., Campos, L. A., & Baltatu, O. C. (2022). “Involve Me and I Learn”: Active learning in a hybrid medical biochemistry first year course on an American-style MD program in the UAE. Medical Science Educator, 32(3), 703–709. https://doi.org/10.1007/s40670-022-01545-6
Rolfe, G. (2014). Reach touch and teach: Terry Borton. Nurse Education Today, 34(4), 488–489. https://doi.org/10.1016/j.nedt.2013.11.003
Rutledge, C., Walsh, C. M., Swinger, N., Auerbach, M., Castro, D., Dewan, M., Khattab, M., Rake, A., Harwayne-Gidansky, I., Raymond, T. T., Maa, T., & Chang, T. P. (2018). Gamification in action: Theoretical and practical considerations for medical educators. Academic Medicine, 93(7), 1014–1020. https://doi.org/10.1097/ACM.0000000000002183
Shrivastava, S. R., & Shrivastava, P. S. (2018). Exploring the scope of introducing buzz group in teaching community medicine to undergraduate medical students. MAMC Journal of Medical Sciences, 4(2), 109.
Thistlethwaite, J. E., Davies, D., Ekeocha, S., Kidd, J. M., MacDougall, C., Matthews, P., Purkis, J., & Clay, D. (2012). The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME Guide No. 23. Medical Teacher, 34(6), e421–e444. https://doi.org/10.3109/0142159X.2012.680939
Woolfson, L. (2004). Family well-being and disabled children: A psychosocial model of disability-related child behaviour problems. British Journal of Health Psychology, 9(1), 1–13. https://doi.org/10.1348/135910704322778687
*Dr. Miriam Simon
Department of Psychiatry and Behavioral Science
College of Medicine and Health Sciences
National University of Science and Technology
PO Box 391; PC 321
Sohar, Sultanate of Oman
+96826852039
Email: miriamsimon@nu.edu.om
Published online: 7 January, TAPS 2025, 10(1), 1-3
https://doi.org/10.29060/TAPS.2025-10-1/EV10N1
The present healthcare environment requires practitioners who are not only technically proficient but also compassionate, empathetic, and fully committed to a patient-centred approach. These professionals can be best described as “holistic practitioners,” given their emphasis on supporting the complete well-being of patients, as well as addressing patients’ physical, emotional, social, and spiritual needs. Our editorial explores strategies for nurturing such practitioners who focus on the person as a whole, rather than merely treating individual diseases.
Building Competence Through Integrated Knowledge and Skills
Competence in healthcare now requires more than a strong grounding in biomedical and clinical sciences. It requires blending knowledge and skills across various disciplines with a focus on a patient-centred approach. This holistic approach involves embracing interprofessional education, which allows students to learn alongside other healthcare roles, while fostering the teamwork essential for comprehensive care (Samarasekera et al., 2024).
Cultivating Empathy and Compassion
Empathy and compassion are key qualities that distinguish a healthcare provider as a genuine healer. Developing empathy involves understanding the patient’s perspective and their unique experiences. Techniques like role-playing, patient storytelling, and reflective exercises can help practitioners view health issues from the patient’s viewpoint. This approach nurtures true empathy that goes beyond simply recognising a patient’s emotions to fostering authentic concern. A medical education culture that values compassion as much as the technical skill underlying clinical practice creates and cultivates practitioners who truly care about the person behind the diagnosis (Samarasekera et al., 2022).
Promoting Efficient, Patient-Centred Care
While efficiency in healthcare is crucial, it must not overshadow patient attentiveness. Holistic practice prioritises streamlining processes to enhance outcomes without compromising empathy or care quality. Training in time management, communication, and systems-based approaches can help practitioners balance effectiveness with patient-centredness. This approach is aptly described by Groopman (2007), who highlights the need for practitioners to deeply listen to the patient narrative. The requirement for attentive listening can be augmented using digital tools, such as electronic health records and telemedicine, which can improve efficiency while supporting personalised care. Furthermore, emerging technologies like AI and wearable health devices offer proactive insights for practitioners, enhancing preventive care and lightening practitioner workload. In telemedicine, training in empathetic communication ensures patients feel genuinely heard, even during virtual appointments.
Recognising cultural diversity is essential in delivering patient-centred care. Cultural competency training helps practitioners respect and understand diverse healthcare beliefs and practices (Vella et al., 2022). Providing the groundwork for holistic patient interaction will likely require medical education to embrace role-play and simulations with diverse patient scenarios, which leads to preparing practitioners to meet the unique needs of various communities and facilitate more inclusive care.
The Role of Self-Care and Well-being in Clinical Practice
The phrase “Physician, heal thyself” highlights the importance of self-care for healthcare practitioners, emphasising the importance of professionals themselves initiating, promoting and cultivating personal health and wellbeing (Mills et al., 2018). Maintaining strong physical, mental, and emotional health enables practitioners to provide the highest quality of care. Self-care directly impacts patient care by building resilience, empathy, and sound decision-making, especially under pressure. Accentuating self-care among clinicians fosters a sustainable healthcare environment, preparing practitioners to meet the challenges of their roles more effectively and to minimise the occurrence of burnout, moral distress, and compassion fatigue (Sanchez-Reilly et al., 2013).
Resilience, often described as “grit”, is vital in healthcare, where professionals face high-stakes and emotionally taxing situations (Samarasekera & Gwee, 2020). This trait supports practitioners in maintaining focus and motivation, even under prolonged stress. When practitioners engage in holistic practices, such as prioritising their own well-being through regular exercise, mindfulness, and ensuring quality sleep, they can bolster resilience and adapt better to challenges, avoiding burnout (Rich et al., 2020). Practitioners with strong self-care habits not only enhance their own lives but also improve their ability to connect with patients meaningfully.
It is likely that holistic practitioners are better able to communicate, display empathy, and build trust with patients (Mills et al., 2018). They also maintain better focus and emotional balance, which are critical for accurate diagnoses and effective clinical decisions. Practitioners experiencing stress or burnout risk adversely impacting care quality, potentially leading to increased errors and reduced patient satisfaction (Sanchez-Reilly et al., 2013).
By modelling healthy behaviours, clinicians set an example for patients, subtly encouraging positive lifestyle choices. When practitioners view their own wellness as integral to patient care, they embody a holistic approach that values both practitioner and patient well-being. Promoting self-care within the curriculum is also essential. Institutions can support this by embedding wellness programmes, resilience training, and mindfulness practices, helping students value their own well-being. Mentorship programmes with experienced clinicians provide support, fostering a model of work-life balance, resilience, and self-care.
Addressing Holistic Skills Gaps
One major challenge in holistic training is the intensive academic and clinical workload, which often overshadows the human aspects of care (Mills et al., 2018). Medical education tends to focus heavily on medical knowledge, diagnostic and procedural skills, at times de-emphasising empathy, communication, and emotional intelligence. This can inadvertently lead practitioners to prioritise efficiency over patient connection. Furthermore, the rigorous demands of medical training may lead to a culture where self-care is undervalued, affecting practitioners’ overall well-being.
Another obstacle is the limited opportunity for interprofessional learning. Holistic care relies on collaboration across healthcare roles, yet many training programmes work in isolation, reducing exposure to real-world teamwork. This will likely limit understanding the interconnected nature of healthcare roles, making it difficult to deliver fully integrated care.
Healthcare practitioners practising holistic care may face ethical challenges, such as maintaining boundaries while showing empathy. Dedicated ethics training, with case studies on boundary management and unbiased care, can prepare practitioners to meet these challenges. Ethical frameworks, like the “Four Principles” of medical ethics namely autonomy, beneficence, non-maleficence, and justice—serve as valuable guidelines for balanced, patient-centred decision-making. Interprofessional education should be prioritised, allowing students to work alongside those from other healthcare disciplines and develop respect for each role’s contributions. Such collaboration enhances communication skills and prepares practitioners to deliver comprehensive, patient-centred care.
Conclusion
Creating a healthcare workforce that is competent, compassionate, and efficient begins with focusing on the practitioners themselves. By embracing self-care, healthcare providers build the resilience and empathy needed to face the demands of clinical practice while improving patient outcomes. Holistic practitioners not only treat patients but embody wellness, showing compassion, commitment, and integrity. Emphasising practitioner well-being as essential to holistic care strengthens the healthcare system, fostering a culture of respect, trust, and shared commitment to patient-centred health.
Dujeepa D. Samarasekera
Centre for Medical Education (CenMED), NUS Yong Loo Lin School of Medicine,
National University Health System, Singapore
Marcus A. Henning
Centre for Medical and Health Sciences Education, Faculty of Medical and Health Sciences,
University of Auckland, New Zealand
Shuh Shing Lee & Han Ting Jillian Yeo
Centre for Medical Education (CenMED), NUS Yong Loo Lin School of Medicine,
National University Health System, Singapore
Groopman, J. (2007). How doctors think. Houghton Mifflin. https://doi.org/10.1172/jci33149
Mills, J., Wand, T., & Fraser, J. A. (2018). Exploring the meaning and practice of self-care among palliative care nurses and doctors: A qualitative study. BMC Palliative Care, 17, Article 63. https://doi.org/10.1186/s12904-018-0318-0
Rich, A., Aly, A., Cecchinato, M. E., Lascau, L., Baker, M., Viney, R., & Cox, A. L. (2020). Evaluation of a novel intervention to reduce burnout in doctors-in-training using self-care and digital wellbeing strategies: A mixed-methods pilot. BMC Medical Education, 20, Article 294. https://doi.org/10.1186/s12909-020-02160-y
Samarasekera, D. D., Chong, Y. S., Ban, K., Lau, L. S. T., Gallagher, P. J., Chen, Z. X., Müller, A. M., Ngiam, N. S., Wong, M. L., Lau, T. C., Dunn, M. C., & Lee, S. S. (2024). Transforming healthcare with integrated inter-professional education in a research-driven medical school. Medical Teacher, 1-8. https://doi.org/10.1080/0142159x.2024.2409293
Samarasekera, D. D., & Gwee, M. C. (2020). Grit in healthcare education and practice. The Asia Pacific Scholar, 5(1), 1. https://doi.org/10.29060/TAPS.2020-5-1/EV5N1
Samarasekera, D. D., Lee, S. S., Yeo, J. H. T., Yeo, S. P., & Ponnamperuma, G. (2022). Empathy in health professions education: What works, gaps and areas for improvement. Medical Education, 57(1), 86-101. https://doi.org/10.1111/medu.14865
Sanchez-Reilly, S., Morrison, L., Carey, E., Bernacki, R., O’Neill, L., Kapo, J., Periyakoil, V., & Thomas, J. (2013). Caring for oneself to care for others: Physicians and their self-care. The Journal of Supportive Oncology, 11(2), 75-81. https://doi.org/10.12788/j.suponc.0003
Vella, E., White, V. M., & Livingston, P. (2022). Does cultural competence training for health professionals impact culturally and linguistically diverse patient outcomes? A systematic review of the literature. Nurse Education Today, 118, Article 105500. https://doi.org/10.1016/j.nedt.2022.105500
Submitted: 6 June 2024
Accepted: 3 September 2024
Published online: 7 January, TAPS 2025, 10(1), 10-16
https://doi.org/10.29060/TAPS.2025-10-1/RA3430
Han Ting Jillian Yeo, Dujeepa D. Samarasekera & Shuh Shing Lee
Centre for Medical Education (CenMED), Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: Despite significant efforts to address gender equality in medical education, the issue persists. The narrative review aimed to address the research question: What are the strategies implemented to address issues of gender inequality in medical education and what were their outcomes?
Methods: Seven major electronic databases of CINAHL, Embase, ERIC, PsyInfo, PubMed, SCOPUS and Web of Science were reviewed. Search phrases used were (Medical education) AND (Gender equality) OR (Gender bias) OR (Gender diversity) OR (Gender discrimination). Original research articles were included, together with systematic reviews with outcomes reporting on strategies to address gender equality.
Results: Articles unrelated to medical education (e.g. allied health and nursing education) and non-English articles were excluded from the study. A total of 1248 articles were identified, and 23 articles met the inclusion criteria. Training programs (n=14; 60.8%) for medical students and faculty have successfully increased awareness on the issues of gender equality and boost confidence in handling cases on gender inequality, yet implicit bias remains with leadership continuing to be associated more strongly with males.
Conclusion: Leadership bodies in Institutions of Higher Education and policymakers would be in an ideal position to address these issues through shaping policies and provision of training for hiring bodies and faculty.
Keywords: Medical Education, Gender Equality, Strategies
Practice Highlights
- Training programs for medical students and faculty can increase awareness of gender equality.
- Structural and cultural barriers preventing women from attaining leadership roles remain entrenched.
- Targeted training for hiring committees and faculty can help mitigate implicit biases.
I. INTRODUCTION
There has been significant progress in the landscape of medical education since 2000 as women’s representation in health professions has increased steadily across the globe. In 2019, nearly half of all doctors in countries in the Organisation for Economic Co-operation and Development were women (Organisation for Economic Co-operation and Development, 2022). However, beneath the surface of this endeavor lies a persistent and pervasive issue concerning gender equality. The World Health Organisation (WHO) (2007) defines gender equality as the absence of discrimination in the allocation of benefits or resources, access to services, or the provision of opportunities based on a person’s sex, thereby enabling individuals to achieve their full potential. Efforts have been made towards achieving gender equality and inclusivity. Changes in the recruitment processes of residency programs in the United States and Canada have shown an increasing ratio of females among residents and faculty (Jain et al., 2022; Ying et al., 2023). Studies evaluating the assessments of medical students and residents have suggested reduced biases in scorings of examinees based on gender (Hannon et al., 2021; Jacques et al., 2016).
Yet, gender inequality remains prevalent in other aspects of medical education. Sexual harassment in the form of sexist behavior or comments were commonly reported among females in the workplace during residency trainings (DeWane et al., 2020; Ellis et al., 2019; Jackson & Drolet, 2021). Learning opportunities were unequal as female residents performed disproportionately lesser number of procedures (Olson et al., 2023; Sobel et al., 2023) and were given less operative autonomy as compared to their male counterparts hence affecting their preparedness for practice (Joh et al., 2020; Meyerson et al., 2019). The impact of gender inequality is far-reaching. Negative emotions, such as helplessness, and lowered self-esteem, were often described by students or residents who had experienced or observed gender inequality (Kristoffersson et al., 2016; Madeeh Hashmi et al., 2013). Additionally, lowered job satisfaction, feelings of burnout and an increased risk of attrition were reported among those who have experienced or observed gender inequality (Bruce et al., 2015; Ellis et al., 2019; Jackson & Drolet, 2021).
Achieving gender equality in medical education is critical, however, literature highlighted that it continues to persist despite various interventions. Numerous studies have documented progress in gender equality following the implementation of specific interventions, but there is a scarcity of comprehensive reviews consolidating these efforts. Hence, this narrative review aimed to address the research question: What are the strategies implemented to address issues of gender inequality in medical education and what were their outcomes?
II. METHODS
A narrative review was conducted based on the framework proposed by Ferrari (2015). Two researchers (SSL and JYHT) searched seven major electronic databases of CINAHL, Embase, ERIC, PsyInfo, PubMed, SCOPUS and Web of Science for the English-language articles or articles which were translated to English and published between 2013 to 2023. The search terms were broadened using the Boolean operator (“OR/AND”) to search the ‘medical’ subject heading (MeSH) to recognise the significance of the study. As a result, the search phrases were (Medical education) AND (Gender equality) OR (Gender bias) OR (Gender diversity) OR (Gender discrimination).
Original research articles were included into the study, together with systematic reviews with outcomes reporting on strategies to address gender equality. Articles unrelated to medical education (e.g. allied health and nursing education) and non-English articles were excluded from the study. Figure 1 showed a flow chart of the process of literature selection for the narrative review.
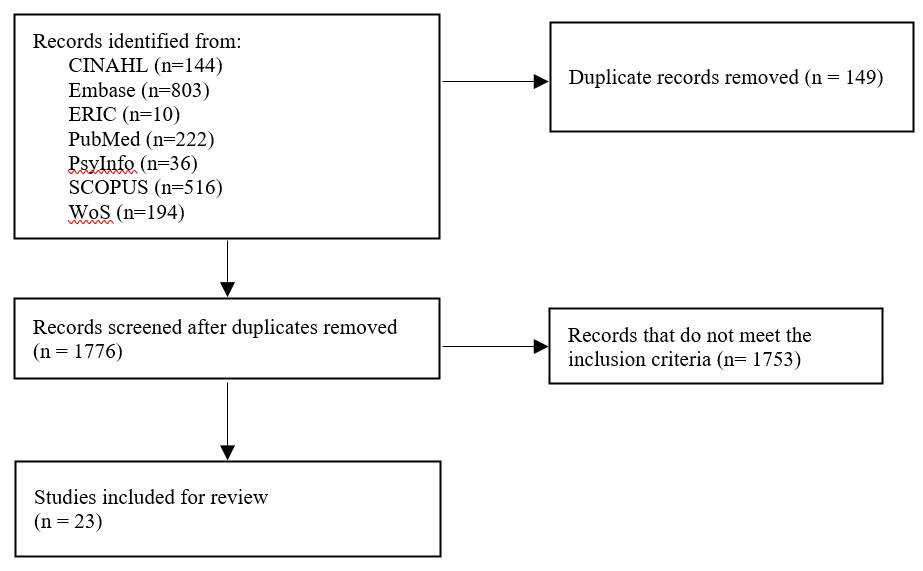
Figure 1. Flow diagram showing the selection of articles
Based on the inclusion and exclusion criteria outlined, both researchers (SSL and JYHT) independently reviewed the title and abstracts of all articles and reviewed the full article when necessary. Articles were categorised based on the types of strategies that were implemented, target audient, method of evaluation and evaluation findings.
III. RESULTS
After removing duplicate articles, a total of 1248 articles were identified through the literature search strategy. Following a thorough examination of the titles and abstracts as well as a review of the articles’ references lists, 23 articles met the review criteria (Table 1). Articles were published between 2015 to 2022. Majority of studies were conducted in the United States (n=16), Canada (n=1), United States and Canada (n=1), Germany (n=1), Sweden (n=1), Switzerland (n=1), Taiwan (n=1), and United Kingdom (n=1).
The findings from this narrative review were divided into two sections: (1) an overview of the interventions implemented to address gender equality and (2) an evaluation of the interventions implemented.
A. Interventions Implemented to Address Gender Equality
Interventions implemented could be divided into micro, meso and macro levels interventions to address gender equality. Micro levels interventions focused on supporting individuals in understanding concepts on gender bias and diversity, its impact on the workplace and strategies to overcome gender bias. These aims could be achieved through training programs for faculty and medical students (n=14; 60.8%). Other micro level interventions described in the articles included giving doctors labelled badges and empowering residents to nominate their chief resident (Olson et al., 2022).
Meso level interventions focused on improving the institutions’ systems, structures, and procedures. Two articles described the formation of task forces in medical societies and higher education institutions (HEIs) to monitor trends and address gender issues (Kandi et al., 2022; Lieberman et al., 2018). Holding a public symposium as a platform to discuss issues on gender equality and enforcing guidelines on writing letter recommendations for medical residency applications were other meso level interventions (Sakowski et al., 2020; Zhang et al., 2021).
Macro level interventions involved shaping policies on a broader, national, or international scale. One study by Chang et al. (2020) shared on three national career developments program aimed at increasing women faculty professional effectiveness. Another macro level intervention involved awarding institutions with Bronze, Silver, and Gold for efforts in addressing gender equity (Caffrey et al., 2016).
The target audience for most interventions were medical students (n=7), these included interventions tailored for women medical students. Other main target audiences included faculty (n=4), residents (n=3) and HEIs (n=2).
B. Addressing Gender Inequality through Training Programs
The duration of the 15 training programmes specified spanned from 15 minutes to 15 weeks long. Seven training programs targeted medical students, 4 training programs targeted faculty, 2 training programs targeted internal medical residents.
Training programs primarily focused on creating an awareness of gender inequality in the workplace through defining terminologies surrounding gender inequality, showing data on gender inequality and its impact on the workplace (Carnes et al., 2015; Driscoll et al., 2019; Farkas et al., 2022; Girod et al., 2016; Jacobs et al., 2022; Kisiel et al., 2020; Lattanza et al., 2016; Sabin et al., 2022). Five programs shared strategies and frameworks to handle situations insinuating gender inequality in the workplace and provided opportunities for practice (Bromberg et al., 2022; Carnes et al., 2015; Farkas et al., 2022; Jacobs et al., 2022; Sabin et al., 2022). Five training programs incorporated elements to guide participants on their career progression through networking opportunities, mentorship programs and leadership training (Chang et al., 2020; Deng et al., 2021; Gaida et al., 2020; Harbold et al., 2021; Lattanza et al., 2016). Training programs developed as part of the Perry’s Initiative for women medical students provided hands-on opportunities to engage in operative procedures to encourage more females to enter the field of orthopaedic surgery (Harbold et al., 2021; Lattanza et al., 2016). Two training programs adopted the approach of engaging in reflexivity with a gendered perspective into one’s own practice and literature materials (Geiser et al., 2022; Liao & Wang, 2020).
C. Evaluation and Findings on the Strategies Implemented
The Kirkpatrick model was adopted to categorise how evaluation of interventions was conducted and the findings.
1) Kirkpatrick Level 1 – Reaction: Participants’ reactions were evaluated for the following strategies: workshops, public symposium, recognition of efforts and empowerment to nominate chief residents (Bromberg et al., 2022; Jacobs et al., 2022; Klein et al., 2020; Sakowski et al., 2020). Participant satisfaction surveys were the main tool adopted to determine if participants found the strategies useful and identify areas for improvement (Bromberg et al., 2022; Jacobs et al., 2022; Klein et al., 2020; Sakowski et al., 2020). One qualitative study by Caffrey et al. (2016) used semi-structured interviews. In general, the interventions were perceived positively in all articles (Bromberg et al., 2022; Jacobs et al., 2022; Klein et al., 2020; Sakowski et al., 2020). However, one study by Caffrey et al. (2016) focusing on recognising institutions which promote gender equity had reported a higher and disproportionate workload on women who were involved in the application process.
2) Kirkpatrick Level 2 – Learning: Participants in 6 studies reported an increased awareness of gender bias after workshops were conducted (Caffrey et al., 2016; Carnes et al., 2015; Deng et al., 2021; Girod et al., 2016; Liao & Wang, 2020; Sabin et al., 2022). Awareness of gender bias can be described in different facets: (1) having an understanding that society has yet to provide equal opportunities for all regardless of their backgrounds; and (2) gaining awareness on the presence of socially constructed gender norms. Two workshops had reported an increase in internal medicine residents’ confidence in responding to incidences related to gender inequality (Bromberg et al., 2022; Farkas et al., 2022).
While strategies had largely positive outcomes with regards to learning, Carnes et al. (2015) and Girod et al. (2016) revealed that workshops on gender bias led to no significant differences in gender/ leadership Implicit Association Test scores suggesting that there remains a persistent association of leadership with males more than females. Gaida, Kujumdshiev and Stengler (2020) shared that low numbers of medical students were able to identify gender sensitive topics despite a week-long elective course on issues of gender equality supported by a mentorship program.
3) Kirkpatrick Level 3 – Behaviour: Reviewed literature revealed conflicting findings on the impact of the interventions on participants’ behaviour. Interventions made to medical assessments (unconscious bias training of examiners, structured interview formats for interviewers and guidelines for writing letter of recommendations) observed no changes in scores and biased language used (Driscoll et al., 2019; Langhan et al., 2022; Zhang et al., 2021).While Olson et al. (2022) had shown a reduction in reported events on gender bias, Kisiel et al. (2020) reported an increase in sexual harassment and gender discrimination events attributing it to an increased awareness in such behaviours.
4) Kirkpatrick Level 4 – Results: Studies which evaluated the overall impact of the interventions on organizational structure showed optimistic results. Articles introducing the Perry’s Initiative to increase women medical students’ exposure to orthopaedic surgery and engineering reported an increased match rates of alumni students to orthopaedics (Harbold et al., 2021; Lattanza et al., 2016). Training of faculty search committee member yielded an increase in number of female candidates throughout the entire hiring process and eventually positions offered to them (Jacobs et al., 2022). Chang et al. (2020) also reported higher rates of promotion for women faculty who had participated in national career development programs.
IV. DISCUSSION
The review highlighted that training programs for students and faculty were not only positively received by students and faculty but were able to create awareness on gender inequality and boost confidence in handling cases on gender inequality. Yet faculty training programs failed to address the implicit bias among faculty who tend to associate leadership with male more than female. This was concurred by more recently published literature reporting that females hold fewer leadership positions in academia or residency programs and hence having potential implications on their career advancement opportunities (Dhingra et al., 2021; Sethi et al., 2022). Achieving gender equality in leadership body is important. The presence of female in any leadership position was correlated with an increase in the number of female faculty or female fellows (Sethi et al., 2022; Sulibhavi et al., 2021). One study also suggested that an increase in the number of female surgical faculty was correlated a decrease in attrition among residents (Saberi et al., 2021).
Macro and meso level interventions via implementation of career development programs and training of recruitment committee showed far reaching impacts on increasing diversity of hires and promotional rates of female faculty. This could serve as a guidance to the leadership bodies in HEIs that the engagement of targeted interventions on training hiring bodies and the provision of faculty development to women faculty can they level the playing field for both genders. Till date few studies reviewed the impact of macro level intervention, and perhaps by sharing the policies in place for training faculty and hiring bodies can the society see an exponential impact on addressing the issues of gender equality.
Lastly, it was evident from the review of selected literature that most research in the areas of gender quality was conducted in the Global North. Given that issues on gender equality tend to be contextual and cultural in nature, there would be a need for medical educators in the Global South to engage in scholarly work in this domain to identify the issues on the ground and identify targeted ways to address the issues on hand.
V. CONCLUSION
While training programs for medical students and faculty have successfully increased awareness of gender equality issues, implicit bias persists, particularly concerning female representation in leadership positions. Despite heightened awareness, the structural and cultural barriers preventing women from attaining leadership roles remain firmly entrenched. Leadership bodies within HEIs and policymakers are uniquely positioned to address these persistent issues. By shaping and implementing equitable policies, they can foster an environment that actively promotes gender diversity. Additionally, targeted training for hiring committees and faculty can help mitigate implicit biases, ensuring a more inclusive and representative leadership. Addressing these challenges requires a multifaceted approach, combining policy reform, education, and continuous evaluation to create lasting change in gender equality within medical education.
Notes on Contributors
Ms. Jillian Yeo was involved in writing the manuscript, conducting the literature search, reviewing the literature retrieved and synthesising the data. Dr Lee Shuh Shing was involved in conducting the literature search, reviewing the literature retrieved and synthesising the data. Dr Dujeepa was involved in the conceptual development of the study and reviewing the manuscript.
Ethical Approval
As this study was a narrative review, ethical approval and IRB application was not required.
Data Availability
The list of articles included in the narrative review can be accessed here:
https://doi.org/10.6084/m9.figshare.25980352.v1 (Yeo, 2024)
Funding
No funding sources are associated with this paper.
Declaration of Interest
There are no conflicts of interests related to the content presented in the paper.
References
Bromberg, G. K., Gay, E. A., Hills-Dunlap, K., & Burnett-Bowie, S. M. (2022). Using a virtual platform to teach residents how to respond to bias. Journal of General Intern Medicine, 37(11), 2871-2872. https://doi.org/10.1007/s11606-021-07156-y
Bruce, A. N., Battista, A., Plankey, M. W., Johnson, L. B., & Marshall, M. B. (2015). Perceptions of gender-based discrimination during surgical training and practice. Med Education Online, 20, 25923. https://doi.org/10.3402/meo.v20.259 23
Caffrey, L., Wyatt, D., Fudge, N., Mattingley, H., Williamson, C., & McKevitt, C. (2016). Gender equity programmes in academic medicine: A realist evaluation approach to Athena SWAN processes. BMJ Open, 6(9), e012090. https://doi.org/10.1136/bmjopen-2016-012090
Carnes, M., Devine, P. G., Baier Manwell, L., Byars-Winston, A., Fine, E., Ford, C. E., Forscher, P., Isaac, C., Kaatz, A., Magua, W., Palta, M., & Sheridan, J. (2015). The effect of an intervention to break the gender bias habit for faculty at one institution: A cluster randomised, controlled trial. Academic Medicine, 90(2), 221-230. https://doi.org/10.1097/acm.0000000000000552
Chang, S., Guindani, M., Morahan, P., Magrane, D., Newbill, S., & Helitzer, D. (2020). Increasing promotion of women faculty in academic medicine: Impact of National Career Development Programs. Journal of Women’s Health (Larchmt), 29(6), 837-846. https://doi.org/10.1089/jwh.2019.8044
Deng, M., Nham, E., Malvea, A., Ramsay, T., Seabrook, C., & Watterson, J. (2021). Exploring the impact of the surgical exploration and discovery (SEAD) program on medical students’ perceptions of gender biases in surgery: A mixed-method evaluation. Journal of Surgical Education, 78(4), 1236-1249. https://doi.org/10.1016/j.jsurg.2020.11.016
DeWane, M. E., Mattessich, S., Wu, R., & Whitaker-Worth, D. (2020). A survey study of resident experiences of sexual harassment during dermatology training. Journal of the American Academy of Dermatology, 83(2), 594-596. https://doi.org/10.1016/j.jaad.2019.07.023
Dhingra, S., Killaspy, H., & Dowling, S. (2021). Gender equality in academic psychiatry in the UK in 2019. BJPsych Bulletin, 45(3), 153-158. https://doi.org/10.1192/bjb.2020.116
Driscoll, S. W., Robinson, L. R., Raddatz, M. M., & Kinney, C. L. (2019). Is there evidence of gender bias in the oral examination for initial certification by the American Board of Physical Medicine & Rehabilitation? American Journal of Physical Medicine & Rehabilitation, 98(6), 512-515. https://doi.org/10.1097/phm.0000000000001126
Ellis, R. J., Hewitt, D. B., Hu, Y. Y., Johnson, J. K., Merkow, R. P., Yang, A. D., Potts, J. R., 3rd, Hoyt, D. B., Buyske, J., & Bilimoria, K. Y. (2019). An empirical national assessment of the learning environment and factors associated with program culture. Annals of Surgery, 270(4), 585-592. https://doi.org/10.1097/sla.0000000000003545
Farkas, A. H., Scholcoff, C., Lamberg, M., Shah, H., Fletcher, K., & Yecies, E. (2022). Preparing residents to respond to incidences of gender discrimination and sexual harassment: An interactive workshop. Southern Medical Journal, 115(10), 740-744. https://doi.org/10.14423/smj.0000000000001459
Ferrari, R. (2015). Writing narrative style literature reviews. Medical Writing, 24(4), 230-235. https://doi.org/10.1179/20474 80615Z.000000000329
Gaida, P., Kujumdshiev, S., & Stengler, K. (2020). Gender sensitivity in career mentoring – A project report from the medical faculty of Leipzig University. GMS Journal for Medical Education, 37(2), Doc24. https://doi.org/10.3205/zma001317
Geiser, E., Schilter, L. V., Carrier, J.-M., Clair, C., & Schwarz, J. (2022). Reflexivity as a tool for medical students to identify and address gender bias in clinical practice: A qualitative study. Patient Education Counselling, 105(12), 3521-3528. https://doi.org/10.10 16/j.pec.2022.08.017
Girod, S., Fassiotto, M., Grewal, D., Ku, M. C., Sriram, N., Nosek, B. A., & Valantine, H. (2016). Reducing implicit gender leadership bias in academic medicine with an educational intervention. Academic Medicine, 91(8), 1143-1150. https://doi.org/10.1097/acm.0000000000001099
Hannon, M., Duffey, K., Bharel, S., Redfield, R., Greidinger, A., Stewart, E., & Diemer, G. (2021). Investigating gender disparities in internal medicine residency awards. The American Journal of Medicine, 134(3), 405-409. https://doi.org/10.1016/j.amjmed.2020.11.003
Harbold, D., Dearolf, L., Buckley, J., & Lattanza, L. (2021). The Perry Initiative’s impact on gender diversity within orthopedic education. Current Reviews in Musculoskeletal Medicine, 14(6), 429-433. https://doi.org/10.1007/s12178-021-09717-4
Jackson, K. R., & Drolet, B. C. (2021). #MedicineToo – Gender bias in medical training: A national survey of residents. Journal of General Internal Medicine, 36(12), 3894-3896. https://doi.org/10.1007/s11606-021-06613-y
Jacobs, N. N., Esquierdo-Leal, J., Smith, G. S., Piasecki, M., & Houmanfar, R. A. (2022). Diversifying academic medicine: One search committee at a time. Front Public Health, 10, 854450. https://doi.org/10.3389/fpubh.2022.854450
Jacques, L., Kaljo, K., Treat, R., Davis, J., Farez, R., & Lund, M. (2016). Intersecting gender, evaluations, and examinations: Averting gender bias in an obstetrics and gynecology clerkship in the United States. Education for Health (Abingdon, England), 29(1), 25-29. https://doi.org/10.4103/1357-6283.178926
Jain, A., Nichols, G., Tarabishy, S., Scomacao, I., & Herrera, F. A. (2022). A comparison of applicant and resident physician demographics among surgical subspecialties from 2009 to 2019: Trends in gender and underrepresented minorities in medicine. Annals of Plastic Surgery, 88(4), 451-459. https://doi.org/10.1097/sap.0000000000003041
Joh, D. B., van der Werf, B., Watson, B. J., French, R., Bann, S., Dennet, E., & Loveday, B. P. T. (2020). Assessment of autonomy in operative procedures among female and male New Zealand general surgery trainees. Journal of the American Medical Association Surgery, 155(11), 1019-1026. https://doi.org/10.1001/jamasurg.2020.3021
Kandi, L. A., Jarvis, T. L., Movtchan, N. V., Hammond, J. B., Teven, C. M., & Rebecca, A. M. (2022). Characterization of national medical societies’ accessible resources to support underrepresented minority and female trainees. Journal of the American Medical Association Network Open, 5(9), Article e2230243. https://doi.org/10.1001/jamanetworkopen.2022.30243
Kisiel, M. A., Kühner, S., Stolare, K., Lampa, E., Wohlin, M., Johnston, N., & Rask-Andersen, A. (2020). Medical students’ self-reported gender discrimination and sexual harassment over time. BioMed Central Medical Education, 20(1), Article 503. https://doi.org/10.1186/s12909-020-02422-9
Klein, R., Law, K., & Koch, J. (2020). Gender representation matters: Intervention to solicit medical resident input to enable equity in leadership in graduate medical education. Academic Medicine, 95(12S), S93-S97. https://doi.org/10.1097/acm.0000000000003698
Kristoffersson, E., Andersson, J., Bengs, C., & Hamberg, K. (2016). Experiences of the gender climate in clinical training – a focus group study among Swedish medical students. BioMed Central Medical Education, 16(1), Article 283. https://doi.org/10.1186/s12909-016-0803-1
Langhan, M. L., Goldman, M. P., & Tiyyagura, G. (2022). Can behavior-based interviews reduce bias in fellowship applicant assessment? Academic Pediatrics, 22(3), 478-485. https://doi.org/10.1016/j.acap.2021.12.017
Lattanza, L. L., Meszaros-Dearolf, L., O’Connor, M. I., Ladd, A., Bucha, A., Trauth-Nare, A., & Buckley, J. M. (2016). The Perry Initiative’s medical student outreach program recruits women into orthopaedic residency. Clinical Orthopaedics and Related Research, 474(9), 1962-1966. https://doi.org/10.1007/s11999-016-4908-y
Liao, H. C., & Wang, Y. H. (2020). Integrating the gender perspective into literature studies to enhance medical university students’ gender awareness and critical thinking. International Journal of Environmental Research and Public Health, 17(24). https://doi.org/10.3390/ijerph17249245
Lieberman, J. A., Ehrhardt, A. A., Simpson, H. B., Arbuckle, M. R., Fyer, A. J., & Essock, S. M. (2018). Eliminating the glass ceiling in academic psychiatry. Academic Psychiatry, 42(4), 523-528. https://doi.org/10.1007/s40596-017-0810-5
Madeeh Hashmi, A., Rehman, A., Butt, Z., Awais Aftab, M., Shahid, A., & Abbas Khan, S. (2013). Gender discrimination among medical students in Pakistan: A cross sectional survey. Pakistan Journal of Medical Sciences, 29(2), 449-453. https://doi.org/10.12669/pjms.292.3256
Meyerson, S. L., Odell, D. D., Zwischenberger, J. B., Schuller, M., Williams, R. G., Bohnen, J. D., Dunnington, G. L., Torbeck, L., Mullen, J. T., Mandell, S. P., Choti, M. A., Foley, E., Are, C., Auyang, E., Chipman, J., Choi, J., Meier, A. H., Smink, D. S., Terhune, K. P., . . . George, B. C. (2019). The effect of gender on operative autonomy in general surgery residents. Surgery, 166(5), 738-743. https://doi.org/10.1016/j.surg.2019.06.006
Organisation for Economic Co-operation and Development. (2022). The proportion of female doctors has increased in all OECD countries over the past two decades. https://www.oecd.org/gender/data/the-proportion-of-female-doctors-hasincreased-in-all-oecd-countries-over-the-past-two-decades.htm
Olson, E. M., Dines, V. A., Ryan, S. M., Halvorsen, A. J., Long, T. R., Price, D. L., Thompson, R. H., Tollefson, M. M., Van Gompel, J. J., & Oxentenko, A. S. (2022). Physician identification badges: A multispecialty quality improvement study to address Professional misidentification and bias. Mayo Clinic Proceedings, 97(4), 658-667. https://doi.org/10.1016/j.mayocp.2022.01.007
Olson, E. M., Sanborn, D. M., Dyster, T. G., Kelm, D. J., Murray, S. G., Santhosh, L., & DesJardin, J. T. (2023). Gender disparities in critical care procedure training of internal medicine residents. American Thoracic Society Scholar, 4(2), 164-176. https://doi.org/10.34197/ats-scholar.2022-0025OC
Saberi, R. A., Herrera Gomez, L. C., Brady, A. C., Sola, J. E., Velazquez, O. C., & Neville, H. L. (2021). AAMC data shows effect of surgery faculty diversity on general surgery resident attrition rate at programs sponsored by LCME-accredited medical schools. Journal of Surgical Education, 78(4), 1123-1126. https://doi.org/10.1016/j.jsurg.2020.11.015
Sabin, J., Guenther, G., Ornelas, I. J., Patterson, D. G., Andrilla, C. H. A., Morales, L., Gurjal, K., & Frogner, B. K. (2022). Brief online implicit bias education increases bias awareness among clinical teaching faculty. Medical Education Online, 27(1), Article 2025307. https://doi.org/10.1080/10872981.2021.2025307
Sakowski, S. A., Feldman, E. L., Jagsi, R., & Singer, K. (2020). Energizing the conversation: How to identify and overcome gender inequalities in academic medicine. Journal of Continuing Education in the Health Professions, 40(4), 274-278. https://doi.org/10.1097/ceh.0000000000000296
Sethi, S., Edwards, J., Webb, A., Mendoza, S., Kumar, A., & Chae, S. (2022). Addressing gender disparity: Increase in female leadership increases gender equality in program director and fellow ranks. Digestive Diseases and Sciences, 67(2), 357-363. https://doi.org/10.1007/s10620-020-06686-5
Sobel, A. D., Lavorgna, T. R., Ames, S. E., Templeton, K. J., & Mulcahey, M. K. (2023). Interpersonal interactions and biases in orthopaedic surgery residency: Do experiences differ based on gender? Clinical Orthopaedics and Related Research, 481(2), 369-378. https://doi.org/10.1097/corr.0000000000002457
Sulibhavi, A., Kaufmann, M. R., Shetty, K. R., Wulu, J. A., Tracy, L. F., & Levi, J. R. (2021). Factors associated with distribution of female otolaryngology residents in United States. Laryngoscope, 131(2), E367-E372. https://doi.org/10.1002/lary.28746
Yeo, J. (2024). Gender equality Data and flow chart.docx (Version 1). Figshare. https://doi.org/10.6084/m9.figshare.25980352.v1
Ying, Y., Dupre, J., & Bhanji, F. (2023). Female surgical trainee recruitment and attrition – A 10-year national retrospective review. The American Journal of Surgery, 225(2), 282-286. https://doi.org/10.1016/j.amjsurg.2022.07.020
Zhang, N., Blissett, S., Anderson, D., O’Sullivan, P., & Qasim, A. (2021). Race and gender bias in internal medicine program director letters of recommendation. Journal of Graduate Medical Education, 13(3), 335-344. https://doi.org/10.4300/jgme-d-20-00929.1
*Han Ting Jillian Yeo
10 Medical Drive,
Singapore 117597
Email: jillyeo@nus.edu.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
