
Indonesian medical students’ strategies to strengthen resilience: Among self, others, and faith
Submitted: 31 January 2025
Accepted: 16 June 2025
Published online: 6 January, TAPS 2026, 11(1), 74-78
https://doi.org/10.29060/TAPS.2026-11-1/SC3658
Astrid Pratidina Susilo1, Ervin Dyah Ayu Masita Dewi1, Satrio Utomo2 & Jasmine Aulia Sabrina2
1Department of Medical Education and Bioethics, Faculty of Medicine, Universitas Surabaya, Indonesia; 2Bachelor Program of Medical Education, Faculty of Medicine, Universitas Surabaya, Indonesia
Abstract
Introduction: Limited resources have caused many challenges in health care. Health workers faced dilemmas that potentially cause burnout. Medical students must be strengthened with resilience when facing dilemmas. This study aimed to investigate Indonesian students’ strategies for strengthening resilience after participating in a bioethics workshop based on reflective and collaborative principles.
Methods: A bioethics workshop based on reflective and collaborative principles without didactic elements was conducted with 30 medical students. We collected quantitative data from the Adapted Version of the Adult Personal Resilience Questionnaire and qualitative data from the students’ reflections on strategies to strengthen resilience. Descriptive statistics and thematic analysis were used to analyse the quantitative and qualitative data, respectively.
Results: Thirty students participated in the study. The total score of the resilience questionnaire was 4.28 (SD 0.39), indicating that the students perceived themselves as having a moderate-to-high level of resilience for all items. The following four themes from the qualitative analysis were identified: faith, adaptation, self-management, and relationships.
Conclusion: Indonesian students’ strategies for strengthening resilience are related to faith, adaptation, self-management, and relationships. Although without a didactic approach, the reflective and collaborative learning in this workshop can raise medical students’ awareness of strategies for building resilience and provided an opportunity for students to reflect on their resilience level.
Keywords: Resilience, Reflective Learning, Collaborative Learning, Self-Management, Relationships, Faith, Mixed-Method Approach
I. INTRODUCTION
During the corona virus disease 2019 (COVID-19) pandemic, many healthcare professionals worldwide experienced burnout for several reasons, such as a high workload, fear of getting infected, and passing on the infection to family members. They also faced ethical dilemmas, were compelled to make challenging decisions about which patients to focus on during resource scarcity, and experienced hopelessness about not being able to help all the patients. They had to “play God without God’s power,” determine who could be admitted for care, and who had to be left behind. Previous studies have shown that the situation was overwhelming, and healthcare professionals were unprepared to face it (Ningrum & Missel, 2023).
Beyond the COVID-19 pandemic, healthcare resource scarcity is a reality that healthcare professionals frequently encounter. Therefore, it is essential to prepare future healthcare professionals to be able to decide on resource allocation during resource scarcity and build their resilience to face unpredictable situations (Dewi et al., 2023). Resilience refers to one’s ability to “spring back into shape,” that is, recover quickly from challenges by using a positive coping mechanism. Resilience is multidimensional and can be learned. Nurturing resilience is more than a mere one-point process. It is a longitudinal process that requires practice and perseverance (Calo et al., 2024).
Most resilience education includes didactic content that introduces theories and strategies related to resilience, such as mindfulness or meditation practices (Calo et al., 2024).As students naturally have coping mechanisms and can learn from each other, we developed a workshop to raise awareness of resilience based on reflective (Calo et al., 2024) and collaborative learning principles (Yang, 2023). We asked the students to complete a questionnaire to reflect on their resilience levels and subsequently engage in discussions with peers. To investigate whether this educational approach can raise students’ awareness of resilience, we explored the students’ key takeaways from this workshop using the following research question: what are the students’ strategies to strengthen resilience after attending a workshop based on reflective and collaborative principles?
II. METHODS
This study was conducted in a private medical school in East Java, Indonesia. We developed a one-day bioethics workshop tailored to address the gaps highlighted by previous study (Dewi et al., 2023) with three objectives. First, we aimed to improve students’ decision-making skills in ethical decisions. Second, we introduced the communication skills necessary to discuss with patients and their families. Third, we attempted to raise students’ awareness of developing resilience. This study focuses on the third objective. The participants were third- and fourth-year pre-clinical phase medical students who were selected using a random sampling approach. Although they have not yet experienced significant real-patient encounters, they had a basic understanding of bioethics and doctor-patient communication skills, while modules on resilience were not yet included in the curriculum. All participants were informed about the study goals and procedures and signed written consent forms.
During the session on resilience, which lasted one hour, the students engaged in several activities. They reflected on their resilience levels by completing a questionnaire. This activity was based on the principle of reflective learning. Subsequently, considering the ethical dilemma of resource scarcity, the students discussed in pairs how to mitigate burnout due to such a dilemmatic situation and how to strengthen their resilience. The method was based on the collaborative learning principle. Finally, the students shared their strategies to strengthen their resilience as medical students.
We collected the quantitative and qualitative data from the questionnaire and students’ reflections, respectively. This study used the Adapted Version of Adult Personal Resilience Questionnaire, translated to Indonesian, and used in a study to explore physicians’ resilience in remote areas (Handoyo et al., 2021). The questionnaire had a 5-point Likert scale (1=strongly disagree, 2=disagree, 3=neutral, 4=agree, 5=strongly agree). We modified the Indonesian version and validated the content with three experts (two medical educationalists and one psychiatrist). The experts scored the relevance of each item to measure resilience (1=highly irrelevant, 2=irrelevant, 3=relevant, and 4=highly relevant). Only those items for which all experts scored 4 were included. The final questionnaire consisted of 19 items, with a Cronbach’s alpha of 0.848. Data from the questionnaire were descriptively analysed using SPSS 26 while the qualitative data were analysed using a thematic analysis approach. Two researchers independently coded and developed themes and discussed them until a consensus was achieved.
III. RESULTS
Thirty students (11 male and 19 female) participated in the study. The total score of the resilience questionnaire was 4.28 (SD 0.39), indicating that the students perceived themselves as having a moderate-to-high level of resilience for all items.
|
No. |
Item |
Mean |
Standard Deviation (SD) |
|
Determination |
|||
|
1 |
Once I set a goal, I am determined to achieve it. |
4.10 |
0.89 |
|
2 |
I persevere at the things I decide, despite difficulties. |
4.27 |
0.69 |
|
3 |
Being determined is an important part of my character. |
4.23 |
0.86 |
|
4 |
I keep trying for the things I want until I reach them. |
4.37 |
0.62 |
|
|
Subtotal |
4.24 |
0.54 |
|
Endurance |
|||
|
5 |
I am able to live through difficult times |
4.23 |
0.77 |
|
6 |
I can withstand difficult situations. |
4.30 |
0.84 |
|
7 |
I can endure the problems that life brings. |
4.23 |
0.86 |
|
8 |
I can endure even when I am attacked |
4.00 |
0.87 |
|
|
Subtotal |
4.19 |
0.69 |
|
Adaptability |
|||
|
9 |
I have the ability to adapt to difficult situations. |
3.73 |
1.02 |
|
10 |
I can change to fit into many kinds of circumstances |
3.90 |
0.80 |
|
11 |
I can find ways to adapt to unexpected conditions. |
3.97 |
0.62 |
|
|
Subtotal |
3.87 |
0.67 |
|
Recuperability |
|||
|
12 |
I recover from any misfortune that happens to me. |
3.93 |
0.74 |
|
13 |
I am able to bounce back from any kind of adversity. |
3.93 |
0.74 |
|
14 |
I can recover from any type of problem. |
3.97 |
1.00 |
|
|
Subtotal |
3.94 |
0.66 |
|
Life Calling |
|||
|
15 |
I believe that God has a purpose in placing me here. |
4.80 |
0.48 |
|
16 |
God has always guided me through my life. |
4.73 |
0.58 |
|
17 |
God would never allow me to walk through life alone. |
4.77 |
0.68 |
|
18 |
Even in difficult situations, God has been there to guide me. |
4.83 |
0.46 |
|
19 |
I believe that God is ever-present, in everything I do |
4.93 |
0.25 |
|
|
Subtotal |
4.81 |
0.36 |
|
Total |
4.28 |
0.39 |
Table 1. Participants’ Resilience as Measured in the Adapted Version of the Adult Personal Resilience Questionnaire
Four themes emerged from the qualitative analysis: faith, adaptation, self-management, and relationships. Each theme was described and relevant examples of quotes to illustrate them are provided below.
A. Faith
The participants implied that resilience was related to their faith in God. They believed that God would not give them a “test” that was more difficult than their ability to handle it. The importance of believing that God will give the strength to deal with every problem was strongly emphasised. Additionally, the participants mentioned striving to be “Ikhlas” (sincere) and repeatedly accepting their reality as strategies to improve resilience. For example, Student 3 wrote, “I will accept the reality and handle every situation with sincerity.”
B. Adaptation
Participants believed that they could increase their resilience through ongoing practice. Thus, self-motivation and self-confidence were essential factors. They mentioned strategies, such as stepping out of their comfort zones, trying new things, and improving their perseverance and recoverability. For instance, Student 25 mentioned “Practice to challenge oneself toward change” as a strategy for resilience.
C. Self-Management
Participants reported that self-management is important in achieving resilience. They need to understand their limits as well as learn how to manage stress, emotions, and time. Students also mentioned meditation, journal writing, and rest as self-management strategies that improved resilience. They argued that a balance between logic and feelings increases one’s resilience.
D. Relationship
Students were aware of the fact that they need friends and colleagues to share, collaborate with, and make decisions. They need to have friends with a positive attitude, surround themselves with individuals with a positive outlook, and participate in volunteering activities. Student 8 shared, “Do not push yourself; try to share your problems with your friends.”
IV. DISCUSSION
The study findings revealed that the workshop based on reflective and collaborative learning principles can raise students’ awareness of effective strategies to strengthen their resilience. Two themes were in line with the constructs in the questionnaire: “faith” and “adaptation”. “Faith” is a fairly similar concept to “life calling” while “adaption” reflected other subscales in the questionnaire, such as “determination” and “recuperability” (Handoyo et al., 2021). This resemblance suggested that students were inspired when they reflected on the questionnaire in which they scored themselves on a relatively high scale of 3 or above for all items. The reflection process exposed them to the concept of resilience.
However, “self-management” and “relationships” were not reflected in the questionnaire responses, but found in pair discussions and personal reflections. Beyond what they learned while completing the questionnaire, the students gained new ideas through discussions with their peers. Collaborative learning raised the students’ awareness, as they learned from each other’s perspectives during the discussion (Yang, 2023).
Overall, the students’ ideas were in line with the findings of previous research on strengthening resilience (Calo et al., 2024) and covered diverse aspects. In their writing, they could indicate the dynamics of the strengthening resilience through internal adaptation, relationships with others, and views from a faith perspective. “Adaptation” and “self-management” reflected the strategies for improving resilience which comes from within. The “relationship” aspect suggested the students’ need for other people in their lives as a critical support system in strengthening resilience. Finally, “faith” showed that the students viewed God’s influence as essential for nurturing resilience.
This study has certain limitations. First, the workshop focusing on resilience was short (only one hour) as it was embedded in a larger workshop aimed at enhancing the students’ decision-making skills in ethical dilemmas. A longitudinal workshop may yield different results. Second, the qualitative data were based on the students’ writing, which was influenced by their ability to express themselves. Interviews may have yielded different results.
Despite this constraint, the findings showed that a workshop based on reflective and collaborative learning, without a didactic approach, could raise medical students’ awareness of strategies to build resilience. This finding is important in providing alternative strategies to strengthen resilience in medical education, particularly when time is constrained. Future studies need to explore the transfer of learning, that is, to what extent students apply what they are aware of in actual practice and how it can improve their resilience levels. Additionally, it is essential to examine whether improved awareness of resilience will enhance medical students’ abilities to face ethical dilemmas in future clinical practice.
V. CONCLUSION
Although without a lecture, a workshop based on reflective and collaborative learning could raise medical students’ awareness of strategies to build resilience. Students’ have ideas of strategies which fall into four categories: faith, adaptation, self-management, and relationship.
Notes on Contributors
Astrid Pratidina Susilo conceptualised the study, organised the workshop, collected and analysed the data, and drafted the manuscript.
Ervin Dyah Ayu Masita Dewi conceptualised the study, organised the workshop, analysed the data, and drafted the manuscript.
Satrio Utomo organised the workshop, collected the data, and reviewed the manuscript.
Jasmine Aulia Sabrina organised the workshop, collected the data, and reviewed the manuscript.
Ethical Approval
Ethical approval was obtained from the University Surabaya Ethical Committee (approval no.297/KE/I/2024).
Data Availability
Data were in Indonesian and can be made available upon personal request.
Acknowledgement
We would to thank all the students who participated in the workshops and the experts who validated the questionnaire. We would like to thank Editage (www.editage.com) for English language editing.
Funding
This study was supported by a research grant from the Universitas Surabaya (N0.165/SP-Lit/LPPM-01/Int/FK/XI/2023).
Declaration of Interest
The authors declare no conflicts of interest.
References
Calo, M., Judd, B., & Peiris, C. (2024). Grit, resilience and growth-mindset interventions in health professional students: A systematic review and meta-analysis. Medical Education, 58(8), 902–919. https://doi.org/10.1111/medu.15391
Dewi, E. D. A. M., Matter, L., Susilo, A. P., & Krumeich, A. (2023). A qualitative study on patients’ selection in the scarcity of resources in the COVID-19 pandemic in a communal culture. Developing World Bioethics, 10, 84–92. https://doi.org/10.1111/dewb.12438
Handoyo, N. E., Rahayu, G. R., Claramita, M., Keraf, M. K. P. A., Octrisdey, K., Yuniarti, K. W., Ash, J., & Schuwirth, L. (2021). Developing personal resilience questionnaire for rural doctors: An indigenous approach study in Indonesia. BMC Psychology, 9(158). https://doi.org/10.1186/s40359-021-00666-8
Ningrum, A. P., & Missel, M. (2023). Urip iku urup (life is lit) by service to others: A qualitative study of frontline healthcare workers’ lived experiences providing patient care in Indonesia’s COVID-19-designated hospital. BMC Health Services Research, 23(262). https://doi.org/10.1186/s12913-023-09257-2
Yang, X. (2023). A historical review of collaborative learning and cooperative learning. TechTrends, 67(4), 718–728. https://doi.org/10.1007/s11528-022-00823-9
*Ervin Dyah Ayu Masita Dewi
Faculty of Medicine, Universitas Surabaya
Jalan Raya Kalirungkut, Surabaya,
60293, Indonesia
+62-85865256147
Email: ervin_dyah@staff.ubaya.ac.id
Submitted: 25 February 2025
Accepted: 9 September 2025
Published online: 6 January, TAPS 2026, 11(1), 79-81
https://doi.org/10.29060/TAPS.2026-11-1/II3679
Gaik Kin Teoh1 & Darlina Hani Fadil Azim2
1Department of Psychology and Counselling, School of Psychology and Social Science, IMU University, Malaysia; 2Department of Psychology and Counselling, School of Psychology and Social Science, IMU University, Malaysia
I. WHERE THE STORY STARTED…
Climate change and health tractions have loudly cumulated at the recent Asian Pacific Medical Education Conference, APMEC 2025. This has alerted us, the mental health professionals in Malaysia, to reflect and to wonder what has been put in place to address the mental health issues while climate change is impending in our country. Thus, this paper aims to skim through the websites of global and Malaysian mental health governing organisations and advocates for climate change and mental health information. The keywords used for searching the official websites were “mental health” and “climate change.” The official websites selected were those that discuss and outline action plans for both mental health and climate change.
II. HIGHLIGHTS ON THE GLOBAL STATUS OF CLIMATE CHANGE
According to the Climate Change 2023 Synthesis Report: Summary for Policymakers,
- About 3.3 to 3.6 billion people live in conditions that are highly vulnerable to climate change.
- Increasing climate change events have caused millions of people to live with the threat of acute shortages of food and water security. These communities are found in Africa, Asia, Central and South America, Least Developed Countries, small islands and the Arctic. Meanwhile, in developing countries, the current global financial flows for adaptation are lacking.
- Between 2010 and 2020, the death toll due to floods, droughts and storms was 15 times higher in highly vulnerable areas.
- In the near term, every region of the world is predicted to face further escalation in climate hazards, increasing multiple risks to ecosystems and humans. The hazards and associated risks are – an increase in heat-related human mortality and morbidity, food-borne, water-borne, and vector-borne diseases and mental health challenges, floods, biodiversity loss in land, freshwater, and ocean ecosystems and a decrease in food production.
- The choices and actions taken in this decade will influence the situation now and for thousands of years to come. Thus, deep, rapid, and sustained mitigation and accelerated implementation of changes in this decade would decrease future losses and damages. Delayed mitigation will further increase global warming and damage.
The threat of climate change to health has been highlighted by the World Health Organization (WHO) for many years. In 2008, WHO published a comprehensive report on the health impacts of climate change. In 2021, a survey conducted by WHO, among the 95 participating countries, only 9% included mental health and psychosocial support in national health and climate change plans. In 2022, a new WHO policy brief was put in place to underscore the serious risks of climate change to mental health. One of the most concerning mental health outcomes related to climate change is suicidal risk (Chen et al., 2025).
III. GLIMPSES OF CLIMATE CHANGE AND MENTAL HEALTH AMONG THE MENTAL HEALTH ORGANISATIONS IN THE WESTERN DEVELOPED COUNTRIES
On the other side of the coin, the American Psychological Association [APA] (2017) published Mental Health and Changing Climate: Impacts, Implications and Guidance. In 2020, the American Counseling Association’s task force disseminated a Climate Change Fact Sheet, to familiarise counselors to facts, actions and resources that help to address the needs of clients and communities based on climate change. In 2022, the American Psychological Association (APA) published Addressing Climate Crisis: An Action Plan for Psychologists. The British Psychological Society issued two Clinical Psychology Forum within a year and repeating the same theme – the climate and ecological emergency. This indicated the urgency to take actions and to come together to address the issues of climate change. The Australian Psychological Society [APS] (2024) spotlighted that 94% of its members are concerned about the upcoming impact of climate change on mental health. Particularly, psychological distress has risen from 18.4% in 2011 to 42.30% in 2021 among the 15-24 year old, due to climate change. The New Zealand government underscored climate change and well-being in New Zealand’s Environmental Reporting Series: Our Atmosphere and Climate 2020. In 2024, the Ministry of Health of New Zealand launched the Health National Adaptation Plan 2024-2027, where mental health is embedded to be part of the action plan. In Europe, Climate Change Impacts on Mental Health in Europe was published in 2022. This shows that information on mental health issues associated with climate change is apparent among mental health advocates, particularly, from most Western developed countries.
IV. GLIMPSES OF CLIMATE CHANGE AND MENTAL HEALTH IN SOME ASIAN COUNTRIES
In Asian countries, India has called for action plans for climate change and mental health. Japan and Taiwan have established initiatives focused on mental health and disaster management. Many Asian countries are prioritising net-zero emissions and carbon neutrality. Information and discussions on mental health associated with climate change are not readily available on the official websites of most mental health organisations. Eliciting information from official websites among Asian countries proved challenging due to language differences.
V. CLIMATE CHANGE AND MENTAL HEALTH IN MALAYSIA
Skimming through the websites of the mental health associations in Malaysia, such as the Malaysian Society of Clinical Psychology, the Malaysian Board of Counsellors (Lembaga Kaunselor Malaysia), the International Counselling Association of Malaysia (PERKAMA International) and the Malaysian Psychiatric Association, no information was found pertaining to climate change and mental health.
Although climate change and health were highlighted in NEHAP Malaysia (National Environmental Health Action Plan) official website, mental health was only mentioned in the context of post-disaster recovery and Post-Traumatic Stress Disorder (PTSD). In reality, mental health issues caused by climate change can also manifest in daily activities. The Ministry of Natural Resources and Environmental Sustainability (NRES) published the National Climate Change Policy 2.0 in 2024, but addressing mental health concerns was not stated in the policy.
Mahmood and Guinto (2022) have highlighted the seriousness of the climate crisis in Malaysia, including how mental health associated with climate change can further complicate the nascent mental healthcare systems. Besides, Pandya-Wood et al. (2024) underscored that no study was conducted pertaining to mental health and climate change. Urgent attention and investment into climate change-related studies, particularly equitable initiatives, are urged. The readiness to curb the subtle and looming “2nd pandemic” seems to be dubious.
VI. POSSIBLE ACTIONABLE SOLUTIONS FOR MALAYSIA
Firstly, mental health challenges related to climate change should be integrated into the National Climate Change Policy. In addition to the existing stakeholders (such as the Ministry of Health, the Ministry of Natural Resources and Environmental Sustainability etc), forming new partnerships with the Ministry of Communications and Ministry of Women, Family and Community Development and NEHAP will play a crucial role in enhancing public awareness towards the issue, as well as implementing targeted health initiatives to uphold the safety, health and mental health of the high risk groups (i.e. pregnant, breastfeeding, postpartum and menopausal women, older people, children under 18, outdoor workers, indigenous communities, low-income populations, people with disabilities and chronic medical conditions). In addition to mass media, information on mental health and climate change should be widely disseminated across the websites and digital platforms of health and mental health-related organisations. In other words, mental health should be given equal prominence as physical health in policy planning. Innovative technology research is crucial for sustainable development; however, there is a pressing need for more community-based research initiatives that actively seek to understand, involve, and empower the public to contribute to sustainable solutions. Nevertheless, more research grants should be offered to directly address the link between mental health and climate change.
VII. CONCLUSION
We acknowledge that the information retrieved is only limited to publicly available website content. We might also have a bias towards what we consider global mental health organisations. Meanwhile, we have observed that the priorities and initiatives to address mental health and climate change differ by country. Mental health concerns could be addressed by various ministries rather than solely mental health organisations. Achieving carbon neutrality is prioritised over solving mental health concerns in many Asian countries, including Malaysia. Rapid, explicit and organised concerted efforts among the governing bodies are pivotal to curb the subtle and approaching pandemic such as climate change. Forthcoming top-down and bottom-up initiatives are imperative, especially the choices and actions we make in this decade will bear enduring effects for years to come.
Notes on Contributors
GKT initiated, conceptualised, analysed the literature and wrote the paper.
DHFA echoed the significance of the issue, conceptualised, cross-checked the literature, and revised the paper.
Ethical Approval
There is no data presented in this paper, and thus ethical approval is not required.
Acknowledgement
We would like to thank the Dean of the School of Psychology and Social Sciences, in IMU University, Professor Haslee Sharil Lim Bin Abdullah, for supporting our participation in this conference. We also would like to thank Professor Nilesh Kumar Mitra for inviting us to participate in conducting the pre-conference workshop.
Funding
IMU University, Malaysia, funded our participation in this conference.
Declaration of Interest
All authors have no conflict of interest to declare.
References
Australian Psychological Society. (2024, April 24). 94% of psychologists are concerned about the impact of climate change on mental health. https://psychology.org.au/insights/94-of-psychologists-are-concerned-about-the-impact
Chen, D. D., Tu, J. H., Ling, K. N., Jin, X. H., & Huang, H. Y. (2025). Climate change and suicide epidemiology: A systematic review and meta-analysis of gender variations in global suicide rates. Frontiers in Public Health, 12, 1463676. https://doi.org/10.3389/fpubh.2024.1463676
IPCC, 2023: Climate change 2023: Synthesis report, summary for policymakers. Contribution of working groups I, II and III to the sixth assessment report of the Intergovernmental Panel on Climate Change [Core Writing Team, H. Lee and J. Romero (eds.)]. IPCC, Geneva, Switzerland. 1-34. https://doi.org/10.59327/IPCC/AR6-9789291691647.001
Mahmood, J., & Guinto, R. R. (2022). Lessons from climate reports for the Malaysian medical community. The Malaysian Journal of Medical Sciences: MJMS, 29(3), 1-4. https://doi.org/10.21315/mjms2022.29.3.1
Pandya-Wood, R., Azhari, A., Johar, H., Johns-Putra, A., Muhamad, N., & Su, T. T. (2024). Systematic review of climate change induced health impacts facing Malaysia: Gaps in research. Environmental Research: Health, 2(3), 032002. https://doi.org/10.1088/2752-5309/ad6208
*Teoh Gaik Kin
IMU University,
126, Jalan Jalil Perkasa 19, Bukit Jalil,
5700 Kuala Lumpur, Malaysia
60126714766
Email: GaikKinTeoh@imu.edu.my
Submitted: 19 September 2024
Accepted: 16 April 2025
Published online: 6 January, TAPS 2026, 11(1), 69-73
https://doi.org/10.29060/TAPS.2026-11-1/SC3524
Eng-Koon Ong1-4,7, April Thant Aung3,8, Min Chiam3, Lalit Kumar Radha Krishna1,3,4, Yingxuan Chen10, Filomar Cortezano Tariao9, Faith Ng11, Jamie Zhou1,4 & Wen-Shan Sim4-6
1Division of Supportive and Palliative Care, National Cancer Centre Singapore, Singapore; 2Office of Medical Humanities, SingHealth Medicine Academic Clinical Programme, Singapore; 3Division of Cancer Education, National Cancer Centre Singapore, Singapore; 4Duke-NUS Graduate Medical School, Singapore; 5Maternal Fetal Medicine, KK Women’s and Children’s Hospital, Singapore; 6PGY1 Programme, SingHealth, Singapore; 7Assisi Hospice, Singapore; 8School of Humanities, Nanyang Technological University, Singapore; 9School of Dance, Nanyang Academy of Fine Arts, Singapore; 10Shaw Heritage Arts and Wellbeing Studios, Singapore; 11Checkpoint Theatre, Singapore
Abstract
Introduction: Through collaborative pedagogical initiatives, the medical humanities (MH) have the potential to support healthcare professionals in developing various competencies in medical education (ME). However, there is a lack of data on faculty development programmes specific to this field.
Methods: Based on our experience in designing a medical humanities workshop for medical students, we conducted two faculty development (FD) workshops that adopted an interdisciplinary approach towards faculty training. These FD workshops served to train fellow clinician educators in the integration of the MH in ME.
Results: A total of 17 participants completed two workshops over two years, with seven participants in 2023 and 6 in 2024 completing pre- and post-workshop surveys that evaluated their experience, knowledge and skills. The survey consisted of six self-rated questions based on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree) with an open-ended question embedded in the post-workshop survey. A paired t-test evaluation of the results suggests that there was an increase in awareness, knowledge, and confidence.
Conclusion: Our MH-based FD programme is limited by the lack of qualitative data and further studies are needed. Similar programmes should include an introduction to the medical humanities and its methodologies so that a train-the-trainers approach is adopted. Programmes should also look beyond teaching effectiveness to include developing systemic awareness and support, assess outcomes such as professional identity formation, and build communities of practice for faculty members.
Keywords: Faculty Development, Medical Humanities, Medical Education, Health Professions Education
I. INTRODUCTION
The role of the medical humanities (MH) in healthcare is multifaceted, supported by its methodologies from the arts and humanities in promoting perspective-taking, reflective practice, and professional identity formation. Specifically, its relevance in aspects of medical education (ME) such as professionalism, communications, and humanistic care has rallied healthcare educators exploring the field to achieve educational goals in developing empathy, improving patient experience, and preventing burnout (Ong et al. 2024).
A vision to integrate MH within ME has gained prominence over the past decade, with articles describing its epistemological functions, guidelines on programme development, and emerging evidence of acceptability and effectiveness of pilot programmes. Despite this, there is a disproportionate lack of data on faculty development (FD) to support this vision. A white paper by Howley et al. (2020) advocates for interdisciplinary collaboration between clinician educators, humanities scholars and creative arts practitioners. However, little guidance was provided on the type of effort, support, and considerations needed to nurture an interdisciplinary team of faculty members to design, implement, and sustain MH programmes.
II. CONTEXT AND PROGRAMME
Since 2022, a one-day theatre-based MH workshop has been conducted for all medical students from Duke-NUS Graduate Medical School (Singapore) rotating through the Division of Supportive and Palliative Care at the National Cancer Centre Singapore. During the workshop held on the final day of their one-week clinical rotation, students watch a full recording of a local theatre play, A Good Death by the playwright Faith Ng, and participate in small group discussions on scenarios that depict pain crises experienced by oncology and hospice patients, difficult conversations about end-of-life care, and moral distress faced by palliative care practitioners and its impact on their mental wellbeing. Students also participate in a “hot-seating” activity where they embody the different characters of the play, and respond to questions from the class while in character. Prior to this core clinical rotation, most students had little prior exposure to end-of-life care and the activities were intended to promote perspective-taking, self-awareness, and professional identity formation through the use of theatre. The workshop is co-facilitated by a specialist palliative care physician with a master’s degree in medical education, a medical humanities doctorate fellow, a medical social worker trained in counselling and narrative therapy, and the director of the play. This interdisciplinary faculty team facilitated dynamic discussions and generated new insights for the students.
Based on our positive experience in developing this programme, we decided to conduct a yearly faculty development (FD) workshop for other educators who were keen on designing arts and humanities programmes within their specialities and settings. The workshop consisted of three segments. Firstly, an introduction to conceptual frameworks and principles within both MH and ME was presented by EKO and YC, listing frameworks such as adult learning, community of practice, and reflective practice. Principles such as the need to create a sense of agency, establish common goals, validate values of faculty members, and promote reflective processes were also identified. Secondly, YC described and explained theatre-based facilitation methods such as improvisation and applied theatre techniques. This provided refreshing insight on how MH programmes could be designed and conducted by arts practitioners like herself. The choice of teaching materials that considered learners’ receptivity, appropriateness to achieve learning objectives, and ease of access were also explored. Lastly, the team demonstrated how learning objectives and lesson plans could be written based on Bloom’s taxonomy and Gagne’s model of instruction respectively. The educators were then asked to practice doing the same in groups of three for an existing or potential MH-based ME programme.
We applied the conceptual framework of adult learning in the design of the FD workshop and the relevance of medical humanities in medical education was regularly alluded to in all three segments. This promoted a sense of agency towards self-directed learning. All staff from the SingHealth Academic Medicine Centre, the largest healthcare cluster in Singapore, were invited to participate in the FD workshops in 2023 and 2024. The same team of faculty members from the original medical students’ workshops conducted the FD workshops.
III. METHODS / RESULTS
A total of 17 participants completed the FD workshops over two years. We found a lack of validated evaluation methods for MH-based ME programmes and thus designed a questionnaire guided by Bloom’s taxonomy for our programme. This was similarly done by Kumagai et al. (2007) who investigated the effects of a forum theatre-based workshop for 29 medical school faculty members that facilitated discussions on race and gender through a self-designed survey pre- and post-workshop that assessed self-awareness and “critical consciousness”.
All 17 participants were invited to complete an online survey within one week before and after the FD workshops. The survey consisted of six self-rated questions based on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree) that alluded to the participants’ experience, knowledge, and skills gained from the workshop.
In total, 7 participants in 2023 and 6 in 2024 consented to and completed the surveys (Ong et al., 2024). The group consisted of seven doctors, a clinical psychologist, a clinical pastoral counsellor, a healthcare education executive, two pharmacists, and an assistant director of community outreach and philanthropy. Table 1 lists the questions and the outcomes of the survey. A paired t-test evaluation of the results suggests that there was an increase in awareness, knowledge, and confidence.
|
|
Questions |
Mean score (n=13) |
t-score difference |
p-value |
|
|
Pre-workshop |
Post-workshop |
||||
|
1. |
I would recommend this workshop to my fellow colleagues. |
3.62 |
4.23 |
2.309 |
0.04 |
|
2. |
I am keen to attend similar workshops again in the future. |
3.85 |
4.62 |
2.993 |
0.011 |
|
3. |
I agree that the arts and humanities have valuable knowledge to offer to medical education. |
4.38 |
4.62 |
0.478 |
0.641 |
|
4. |
I can identify potential content, materials and facilitation needed for medical education programs involving the arts and humanities. |
2.54 |
3.92 |
4.454 |
<0.001 |
|
5. |
I am able to pursue the design and implementation of a medical education program involving the arts and humanities confidently as part of a team. |
2.46 |
3.69 |
6.121 |
<0.001 |
|
6. |
I am able to pursue the design and implementation of a medical education program involving the arts and humanities confidently as an education lead, alongside arts practitioners. |
1.92 |
2.77 |
4.430 |
<0.001 |
Table 1. Survey questions and results
IV. LIMITATIONS
Programme evaluation is limited by the small number of participants and lack of a validated measure. While there may be apparent statistical significance to the improvement of the scores collected, a solely quantitative outcome measure may not be adequate to provide insight on the success of the programme. Future programme evaluations with bigger cohorts coupled with qualitative data are needed.
V. DISCUSSION
Existing publications in FD focus on broader teaching competencies such as facilitation and communication skills, curriculum development, education leadership, and scholarship (Steinert et al. 2016), suggesting that faculty members could translate what they have learnt into individual fields of interest. Based on our experience, we posit that further considerations are needed for FD programmes in the field of the medical humanities.
Firstly, a low awareness of the relevance of the MH in ME (Ong, 2021), the need for faculty members to achieve basic understanding of content from diverse theoretical and practical frameworks from both fields, distinct but complementary roles of co-faculty members from medicine and the arts and humanities (Ong et al. 2024), and a lack of agreement on how teaching effectiveness is defined can affect faculty members’ decision to enrol in FD workshops and subsequently how they experience FD in MH. Thus, equipping faculty members with teaching skills may not be adequate. A “train-the-trainers” approach where teaching competencies are complemented with knowledge about MH’s content, methodologies, theoretical frameworks, and assessment tools may be preferable. This approach ensures that faculty members not only develop the skills required to co-facilitate MH programmes, but also reinforces the value of MH when employed within ME.
Secondly, Steinert et al.’s (2016) Best Evidence Medical Education (BEME) guide on faculty development in ME concludes that the outcomes of FD programmes should include the development of a community of practice that can affect organisational and cultural change towards education. In countries such as Singapore where the field of MH within ME is still in its nascent stage, building a community of practice (COP) is essential. A COP can increase awareness and promote endorsement by both senior leadership and peer educators, ensuring programme sustainability beyond initial “pilot” programmes. We hope that this study can inspire like-minded educators to develop FD programmes in tandem to the novel MH programmes that they implement.
Finally, we would also like to remind readers that with its unique methodologies like narrative inquiry, close reading, and experiential learning frameworks, the FD programmes for MH for medical educators have the potential to contribute to professional identity formation and foster wellbeing (Ong et al., 2024). These outcomes though not listed as the learning objectives of our study, have been consistently expressed by the participants during our workshops.
VI. CONCLUSION
In summary, we have described and presented the quantitative outcomes of a faculty development (FD) workshop specific to the field of medical humanities. Qualitative data is still needed for programme evaluation. Addressing gaps in the current literature, we recommend that all MH FD programmes incorporate an introduction to MH and its methodologies, look beyond teaching effectiveness to include systemic awareness and support, assess outcomes such as professional identity formation, and build communities of practice. Future research into these aspects and the development of validated learning outcome measures that include qualitative data will enhance current insight on FD and support the call for integrating MH within the medical education landscape.
Notes on Contributors
OEK conceptualised the outline of the paper and focused mainly on the perspectives from clinicians and clinician educators. He also designed and taught at the faculty development workshops, reviewed and approved the final draft of the manuscript, and agree to be accountable for all aspects of the paper.
LKRK conceptualised the outline of the paper and focused mainly on the perspectives from clinicians and clinician educators. He also designed and taught at the faculty development workshops, reviewed and approved the final draft of the manuscript, and agree to be accountable for all aspects of the paper.
JZ conceptualised the outline of the paper and focused mainly on the perspectives from clinicians and clinician educators. She also designed and taught at the faculty development workshops, reviewed and approved the final draft of the manuscript, and agree to be accountable for all aspects of the paper.
SWS conceptualised the outline of the paper and focused mainly on the perspectives from clinicians and clinician educators. She also reviewed and approved the final draft of the manuscript, and agree to be accountable for all aspects of the paper.
ATA contributed to the layout of the paper and focused on perspectives as medical humanities scholars and teachers. She also designed and taught at the faculty development workshops, reviewed and approved the final draft of the manuscript, and agree to be accountable for all aspects of the paper.
CM contributed to the layout of the paper and focused on perspectives as medical humanities scholars and teachers. She also designed and taught at the faculty development workshops, reviewed and approved the final draft of the manuscript, and agree to be accountable for all aspects of the paper.
FCT contributed to the layout of the paper and focused on perspectives as performing arts practitioners and tutors. He also designed and taught at the faculty development workshops, reviewed and approved the final draft of the manuscript, and agree to be accountable for all aspects of the paper.
CYX contributed to the layout of the paper and focused on perspectives as performing arts practitioners and tutors. She also designed and taught at the faculty development workshops, reviewed and approved the final draft of the manuscript, and agree to be accountable for all aspects of the paper.
NF contributed to the layout of the paper and focused on perspectives as performing arts practitioners and tutors. She also designed and taught at the faculty development workshops, reviewed and approved the final draft of the manuscript, and agree to be accountable for all aspects of the paper.
Ethical Approval
The project was submitted to the SingHealth centralised institutional review board (IRB) but exempted from review due to its nature as a medical education programme evaluation (CIRB number 2023/2036).
Data Availability
The data that support the findings of this study are openly available in the Figshare repository https://doi.org/10.6084/m9.figshare.27038086 (Ong et al. 2024).
Acknowledgement
We would like to thank Ms Eve Seraphina Low for setting up the online survey form and correspondence with the participants, and logistical support of the conduct of the workshop.
Funding
The faculty development workshop was supported by the SingHealth Oncology Academic Clinical Programme Education Support Grant (project number 08/FY2022/P2/09-A75).
Declaration of Interest
All of the authors state no conflicts of interest.
References
Howley, L., Gaufberg, E., & King, B. (2020). The fundamental role of the arts and humanities in medical education. Washington, DC: AAMC.
Kumagai, A. K., White, C. B., Ross, P., Purkiss, J. A., O’Neal, C. M., & Steiger, J. A. (2007). Use of interactive theater for faculty development in multicultural medical education. Medical Teacher, 29(4), 335-340. https://doi.org/10.1080/01421590701378662
Ong, E. K. (2021). HAPPE – A pilot programme using humanities to teach junior doctors empathy in a palliative medicine posting. The Asia Pacific Scholar, 6(1), 83-92. https://doi.org/10.29060/TAPS.2021-6-1/OA2251
Ong, E. K., Tan, E. U., Min, C., & Sim, W. S. (2024). The employment of art therapy to develop empathy and foster wellbeing for junior doctors in a palliative medicine rotation – A qualitative exploratory study on acceptability. BMC Palliative Care, 23(1), 84. https://doi.org/10.1186/s12904-024-01414-6
Ong, E. K., Aung, A. T., Min, C., Krishna, L. K. R., Chen, Y., Tariao, F. C., Ng, F., Zhou, J., & Sim, W. S. (2024). Data from pre- and post-surveys of participants [Dataset]. Figshare. https://doi.org/10.6084/m9.figshare.27038086
Steinert, Y., Mann, K., Anderson, B., Barnett, B.M., Angel., C., Naismith, L., Prideaux, D., Spencer, J., Tullo, E., Viggiano, T., Ward, H., & Dolmans, D. (2016). A systematic review of faculty development initiatives designed to enhance teaching effectiveness: A 10-year update: BEME Guide No. 40. Medical Teacher, 38(8), 769-786. https://doi.org/10.1080/0142159X.2016.1181851
*Ong Eng Koon
National Cancer Centre Singapore
30 Hospital Blvd, Singapore 168583
Email: ong.eng.koon@assisihospice.org.sg
Submitted: 3 January 2025
Accepted: 14 May 2025
Published online: 6 January, TAPS 2026, 11(1), 82-85
https://doi.org/10.29060/TAPS.2026-11-1/II3600
Sulthan Al Rashid1 & Pubalan Rajagopalan2
1Department of Pharmacology, Saveetha Medical College and Hospital, Saveetha Institute of Medical and Technical Sciences (SIMATS), India; 2Medical Surgical Department, Farrer Park Hospital, Singapore
I. INTRODUCTION
Medical education is transforming to nurture not just clinical expertise and theoretical understanding but also the holistic development of healthcare clinicians. In an era where sustainability in healthcare demands adaptable, resilient, and empathetic professionals, Personal Development Programs (PDPs) have emerged as vital tools. These programs aim to equip healthcare clinicians —doctors, nurses, and allied professionals—with essential skills like communication, empathy, and resilience while fostering lifelong learning and personal well-being. This personal view explores the critical role of PDPs in shaping healthcare clinicians who are prepared to meet the physical, psychological, and social challenges of their roles, thereby contributing to a sustainable future in healthcare. We highlight the benefits, current frameworks, challenges, and strategies necessary for effectively integrating PDPs into medical education to cultivate a holistic, future-ready workforce.
II. THE RATIONALE FOR PERSONAL DEVELOPMENT
The healthcare profession is synonymous with high-pressure work environments that challenge even the most seasoned professionals. As such, equipping healthcare clinicians with resources for self-improvement and mental well-being is not just desirable—it is crucial. Healthcare clinicians regularly contend with issues like burnout, compassion fatigue, and work-life imbalance. The ripple effects of these challenges extend beyond the individual to affect the quality of patient care. Hence, incorporating personal development into medical education is more than a value-added option; it is a foundational component that addresses the holistic training needs of healthcare clinicians.
III. EMOTIONAL INTELLIGENCE AND COMMUNICATION SKILLS
Emotional intelligence (EI) and strong communication skills are essential for effective patient interaction and care. According to research, healthcare clinicians with high EI are more adept at understanding patient concerns, managing personal emotions and potential biases (Webster et al., 2022), and handling complex interpersonal dynamics (Giménez-Espert et al., 2023). Programs focused on EI employ hands-on exercises, role-playing, and workshops that allow healthcare clinicians to develop these skills in real-world scenarios. For instance, simulation labs can recreate patient encounters that test and improve healthcare clinicians’ emotional responses, making them better communicators and more empathetic caregivers.
Moreover, EI training is associated with tangible benefits like higher patient satisfaction and lower medical error rates. In a clinical setting, the ability to manage stress and maintain clear, empathetic communication can significantly affect patient outcomes. Thus, by integrating EI training into the medical curriculum, educators are nurturing a new generation of healthcare clinicians who prioritise both technical precision and human connection.
IV. BUILDING RESILIENCE AND MANAGING STRESS
The healthcare profession is notorious for its physical and emotional demands, making resilience a crucial attribute for survival and success. PDPs that focus on resilience-building often include mindfulness practices, stress management techniques, and guided self-reflection. For example, mindfulness training has been shown to lower levels of burnout among healthcare workers. Programs like these teach healthcare clinicians to manage stress, recover from setbacks, and foster a supportive work culture. This approach benefits both individual well-being and professional performance, ultimately enhancing patient care.
Additionally, stress management workshops can be designed to simulate high-pressure scenarios, helping healthcare clinicians develop coping mechanisms they can use in real clinical environments. Practical training sessions, such as mock emergency simulations, prepare healthcare clinicians to think critically and remain composed under pressure. By equipping future healthcare clinicians with these skills, educational institutions are ensuring that healthcare clinicians can thrive in the demanding healthcare fields.
V. CURRENT MODELS OF PERSONAL DEVELOPMENT IN MEDICAL EDUCATION
A. Reflective Learning and Mentorship
Reflective practices are key components of many personal development programs, allowing healthcare clinicians to analyse their experiences, learn from them, and adjust their behaviour or thinking accordingly. Journaling, in particular, is a powerful tool for self-reflection. By regularly documenting their experiences, thoughts, and emotions, healthcare clinicians can gain a deeper understanding of their learning processes and emotional responses. This habit helps them identify patterns, recognise areas for improvement, and appreciate personal growth over time. Journaling also serves as a therapeutic outlet, reducing stress and fostering self-awareness.
Techniques like case-based discussions and guided reflections complement journaling by encouraging active engagement and peer learning. For instance, healthcare clinicians may write about a challenging patient encounter and later discuss it in a group setting, exploring different perspectives and potential strategies for improvement. These reflective exercises promote a culture of continuous self-improvement and emotional resilience (Hagrass et al., 2023).
Mentorship is another cornerstone of personal development in medical education. Structured mentorship programs provide a platform for healthcare clinicians to discuss both professional and personal challenges. A mentor can offer guidance, emotional support, and career advice, fostering a nurturing relationship that promotes growth and emotional well-being. Through regular discussions, mentees can share insights from their journaling or reflect on professional challenges, receiving valuable feedback and support from experienced practitioners. These mentorship relationships not only guide healthcare clinicians in their academic and clinical journeys but also offer a supportive network that contributes to their overall well-being.
B. Wellness and Achieving Work-Life Balance
Maintaining a healthy work-life balance is vital for healthcare clinicians, who often face long hours and emotionally taxing work (Mitra et al., 2024). Medical education programs that emphasise wellness strategies—such as exercise, nutrition, and self-care—can equip healthcare clinicians with tools to manage stress and sustain their energy levels. Some schools offer wellness electives or modules focusing on self-care and practical life skills, such as time and financial management; for instance, Hackensack Meridian School of Medicine provides a financial wellness elective titled ‘Dollars and Sense for Medical Students,’ which focuses on practical budgeting and saving strategies (Schiavone et al., n.d.).
Practical courses can also prepare healthcare clinicians for the unique challenges of a medical career. Time management workshops, for example, can help healthcare clinicians learn to prioritise tasks and maintain productivity without sacrificing their well-being. Financial literacy courses could teach them how to manage their finances, easing the stress associated with economic pressures during residency and early practice. A holistic curriculum addresses physical, mental, and emotional health, ensuring that healthcare clinicians are well-rounded and resilient.
VI. OVERCOMING CHALLENGES IN IMPLEMENTATION
Despite the numerous advantages of PDPs, integrating them into an already rigorous medical curriculum is fraught with challenges. Heavy academic schedules leave little room for additional content, and there is often scepticism among both faculty and students about the value of PDPs compared to traditional clinical training. However, these hurdles can be surmounted with thoughtful strategies.
VII. EFFECTIVE STRATEGIES FOR INTEGRATION
A. Embedding PDPs into Existing Courses
Instead of introducing separate modules, personal development content can be seamlessly integrated into clinical courses. For instance, stress management techniques can be taught as part of clinical skills training, making it easier for healthcare clinicians to apply these lessons in practical settings.
B. Offering Flexible Learning Options
Workshops or online modules provide flexibility, accommodating diverse schedules and learning preferences. This approach ensures that healthcare clinicians can benefit from PDPs, regardless of their time constraints.
C. Leveraging E-Learning Platforms
Online resources can make personal development topics more engaging and accessible. Interactive e-learning modules on resilience, time management, and communication can be tailored to fit into the existing curriculum without overloading healthcare clinicians.
D. Evidence-Based Customisation
Programs should be tailored to the specific needs of healthcare clinicians and backed by research. Continuous evaluation and feedback loops can refine these programs, ensuring they remain effective and relevant. Institutions should commit to ongoing research to evaluate the long-term impact of PDPs on healthcare clinicians’ professional success and personal well-being.
VIII. THE INFLUENCE ON PATIENT CARE
The ultimate goal of medical education is to produce healthcare clinicians who are not only clinically skilled but also compassionate, resilient, and emotionally intelligent. PDPs that focus on active listening, empathy, and teamwork have a direct, positive impact on patient care. Healthcare providers who are emotionally healthy and well-rounded offer more patient-centered care, communicate better, and work more effectively within teams. For example, a healthcare clinician who can manage their own stress is less likely to make hasty decisions, reducing the risk of medical errors.
Emotionally intelligent practitioners are also better equipped to handle complex clinical scenarios, contributing to lower malpractice claims and improved patient safety. Furthermore, a workforce trained in empathy and effective communication fosters a more compassionate healthcare environment, benefiting patients and professionals alike.
IX. LOOKING TO THE FUTURE
As the healthcare landscape evolves, so too must the training of future professionals. Medical educators, healthcare leaders, and policymakers must collaborate to create curricula that prepare healthcare clinicians for the multifaceted realities of medical practice. The future of effective healthcare delivery depends on the well-being of its providers, making personal development programs a vital component of medical education. Research should continue to explore innovative methods to embed personal growth into medical training, measuring the outcomes on both a personal and professional level.
X. CONCLUSION
Integrating personal development programs into medical education is essential for cultivating healthcare practitioners who are not only clinically proficient but also emotionally intelligent and resilient. These programs empower healthcare clinicians to navigate the challenges of their field with empathy, adaptability, and a strong sense of well-being, aligning their personal growth with professional excellence. Medical educators play a pivotal role in shaping a generation of practitioners who prioritise both their own holistic development and the sustainable delivery of compassionate, high-quality care. By embracing this approach, the medical community can ensure a future where healthcare clinicians are equipped to contribute meaningfully to a sustainable and patient-centered healthcare system.
Notes on Contributors
Sulthan Al Rashid was responsible for the conceptualisation, development of scientific content, data collection, manuscript preparation, editing, and proofreading. Pubalan Rajagopalan contributed significantly to drafting the manuscript and provided critical revisions for important intellectual content. He reviewed and approved the final version of the manuscript and agrees to be accountable for all aspects of the work to ensure its accuracy and integrity.
Ethical Approval
Ethical approval is not required as no human participant data was collected.
Acknowledgement
ChatGPT has been utilised in manuscript preparation, including tasks like drafting, editing, and refining text, without being credited as an author.
Funding
The authors did not receive any funding for this study.
Declaration of Interest
The authors declare that they have no conflicts of interest.
References
Giménez-Espert, M. D. C., Maldonado, S., & Prado-Gascó, V. (2023). Influence of emotional skills on attitudes towards communication: Nursing students vs. nurses. International Journal of Environmental Research and Public Health, 20(6), 4798. https://doi.org/10.3390/ijerph20064798
Hagrass, H. M., Ibrahim, S. A. E. A., Anany, R. I. E. S., & El-Sayed, H. A. (2023). Effect of an educational program about mentorship competencies on nurse mentors’ performance: A quasi-experimental study. BMC Nursing, 22, 429. https://doi.org/10.1186/s12912-023-01597-y
Mitra, L. G., Sharma, J., & Walia, H. S. (2024). Improving work-life balance and satisfaction to improve patient care. Indian Journal of Critical Care Medicine, 28(4), 326–328. https://doi.org/10.5005/jp-journals-10071-24689
Schiavone, J., Ambalu, N., Cheriyan, J., & Josephs, J. (n.d.). Financial wellness for medical students: Practical budgeting and saving tips. AAMC. Retrieved April 4, 2025, from https://students-residents.aamc.org/medical-student-well-being/financial-wellness-medical-students-practical-budgeting-and-saving-tips
Webster, C. S., Taylor, S., Thomas, C., & Weller, J. M. (2022). Social bias, discrimination and inequity in healthcare: Mechanisms, implications and recommendations. BJA Education, 22(4), 131–137. https://doi.org/10.1016/j.bjae.2021.11.011
*Mr Pubalan Rajagopalan
Farrer Park Hospital
1 Farrer Park Station Rd Singapore 217562
+6591050751
Email: pubalan83@outlook.sg
Submitted: 14 October 2024
Accepted: 4 March 2025
Published online: 6 January, TAPS 2026, 11(1), 86-88
https://doi.org/10.29060/TAPS.2026-11-1/II3542
Craig Hassed
Department of Medical Education, Faculty of Medicine, Nursing and Health Sciences, Monash University, Australia
I. INTRODUCTION
In this article I will outline some of the personal and clinical challenges faced by medical and allied health professionals. Mindfulness will be proposed as a necessary skill to be taught in under and postgraduate training to address a number of these challenges. To provide some insights into how this can be done effectively, I will share our experience from Monash University where we have successfully integrated the mindfulness-based Health Enhancement Program (HEP) into medical and allied health professional training for over 20 years. The case will be made for why other medical schools around the world can benefit from adopting similar curriculum.
II. DISCUSSION
It is well documented that medical and allied health professionals face many challenges in their working life including high rates of burnout, stress, alcohol and substance use, and poor mental health. Furthermore, in the complex work environments that health professionals work in, they need to make many decisions throughout the day which have major implications for patients’ health. The complexity is further complicated by the fast-paced modern world where the misuse and overuse of technology is leading to high levels of distraction and clinical errors.
The job-ready health professional needs practical skills to help them navigate such challenges. Unfortunately, these skills are often seen as optional ‘soft’ and are rarely part of the core-curriculum, but without these skills being taught in a comprehensive way, history keeps repeating itself.
One generic skill which can help address many specific challenges outlined above is mindfulness. The most widely used definition by Jon Kabat-Zinn is, “paying attention in a particular way: on purpose, in the present moment, and nonjudgmentally.” In its broadest sense, mindfulness is a practice in training attention and attitude. It can be practiced formally as in mindfulness meditation, and informally by being present and engaged as one goes about daily life.
Before introducing such training into the medical and allied health curriculum one needs a rationale for doing it supported by a sound evidence-base. The exponential growth of research into mindfulness for health professionals has confirmed its efficacy in managing stress and anxiety, reducing relapse rates from depression, lowering burnout, and reducing addictive behaviours. Importantly, the modern doctor also needs to be equipped with non-pharmaceutical options or adjuncts for their patients in the management of stress and mental health problems, chronic pain, and coping with chronic illness.
Because of the enhanced attentional, situational awareness and self-monitoring capacities that mindfulness provides, there is evidence that it enhances clinical decision making, reduces the impact of cognitive biases and helps prevent clinical errors, in part because doctors can learn to be alert to the negative impact of practices like complex multitasking or the distracting effect of technology.
Also important is the evidence from Krasner and Epstein (Krasner et al., 2009) showing that mindfulness not only enhances physician wellbeing but also conscientiousness, emotional intelligence, communication and compassion leading to better clinical interactions with patients.
Mindfulness training has been a part of the core curriculum for medical students at Monash University since 1992. Initially it was on a small scale and then in 2002 the program grew into what we call the Health Enhancement Program. Monash was the first university in the world to integrate mindfulness as core-curriculum and soon after Rochester University introduced a mindfulness program into its curriculum (Dobkin & Hutchinson, 2013).
The HEP is a mindfulness-based healthy lifestyle program delivered in the first semester of the first year of Monash’s five-year undergraduate medical curriculum. It is underpinned by mindfulness training alongside content on lifestyle including the benefits of healthy diet, exercise, environment, connectedness and spirituality, as well as behaviour change strategies and goal setting.
A lecture series providing the evidence and clinical rationale for learning about mindfulness and other elements of the HEP followed by a series of five two-hour tutorials where the students learn to apply mindfulness and lifestyle-focused behaviour change skills in their own lives.
This experiential and deep learning model helps students to foster their own wellbeing, be better manage their stress, and to build an understanding of how these approaches can be used with patients in future medical practice. To assist in the reflective learning approach, students are very actively engaged in group discussions during tutorials. They also keep a weekly reflective journal sharing their reflections, insights, challenges and questions in applying mindfulness and healthy lifestyle change in their own lives. These journals are read by the tutor who provides personalised feedback and encouragement to the students.
The authenticity, credibility and motivation of the tutoring team is crucial for the effectiveness of the program. All tutors are working health professionals – nearly all doctors and psychologists – who personally and professionally use the mindfulness skills they are teaching.
The HEP is core-curriculum and, like any other part of core-curriculum, is assessable and students are required to attend tutorials and learn the content, but we are very clear in communicating to the students that what they practice or apply outside of the tutorial room in their personal life is very much their own personal choice. Students are invited to explore the techniques and apply them in ways that are meaningful for them, but mindfulness is not being imposed on them.
Contextualisation of mindfulness to fit with students’ studies, lives and future work is vital otherwise it won’t be seen as being relevant in the medical curriculum. If this is done well then students receive mindfulness very positively and they apply it in meaningful ways. We have found that over 90% of students report personally applying the formal and informal mindfulness practices in their own lives outside of tutorials (Hassed et al., 2009). If it’s done poorly then the opposite will happen. Contextualisation is further reinforced with mindfulness-based experiments like exploring the effects of complex multitasking, mindful communication, dealing with distractors, and a mindful eating and exercise.
Students need to understand that mindfulness is a transferable skill relevant to their work and life generally, and it is not just seen as a superfluous addition to the ‘serious’ medical curriculum. It is therefore important that mindfulness is horizontally and vertically integrated with other relevant curriculum such as being more present in communication skills training, better focus when learning medical procedures like venepuncture, learning how to manage exam anxiety and, in later years, being more self-aware in clinical decision-making. One method of increasing integration and giving the content a clinical focus is through weekly role-plays similar to the kinds of cases students might meet in OSCE exams.
For the students to take any part of the curriculum seriously and to engage with it, it needs to be assessable. If the mindfulness content is not assessable students will not think it’s important because, in their perception, if it was important, it would be assessed. The journal is marked by the tutors based on the insights students glean and the authenticity and quality of their self-reflection. The knowledgebase and science covered in the HEP lectures is assessed in written exams. Students’ understanding of how to communicate the principles of what mindfulness is about, and what kinds of clinical applications would be appropriate for its use is assessed in OSCE exams. We do not expect the students to reach a point where they could teach mindfulness skills to patients. Further training would be required to reach this objective.
The HEP has become an integral and distinctive part of the Monash medical curriculum. As core-curriculum we have never had the option of performing a randomised control trial on the program outcomes, but we have performed a series of pre-post studies. Our findings that students report improvements in mental health, perceived stress, study engagement, and mindfulness from pre- to post-intervention, even though pre-intervention measures were taken in a low stress period of semester and the post-intervention measures were taken in the period immediately prior to mid-year exams, is very encouraging and counter to evidence showing medical student wellbeing inevitably declines as the semester progresses and students approach assessment (Hassed et al., 2009; Kakoschke et al., 2021).
III. CONCLUSION
Deficiencies in medical education in providing job-ready health professional do not generally lie with a lack of biomedical knowledge and clinical teaching in undergraduate years. The main deficit in training relates to necessary personal skills like attentional control, emotional regulation, stress management, resilience, self-awareness and self-care. One generic skill that has the potential to meet these diverse needs is mindfulness. There is much to be gained by giving all medical and allied health professional students contextualised, relevant, and evidence-based training in mindfulness to help them meet the personal and professional demands that come with increasingly complex and demanding careers in healthcare. A more extensive discussion of the why and how of doing that successfully can be found in a discussion paper in the journal, Mindfulness (Hassed, 2021).
Notes on Contributors
Craig Hassed was the sole author, responsible for the conceptual development and writing of this article.
Funding
There was no funding source for this paper.
Declaration of Interest
The author declares to have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
Dobkin, P. L., & Hutchinson, T. A. (2013). Teaching mindfulness in medical school: Where are we now and where are we going? Medical education, 47(8), 768–779. https://doi.org/10.1111/medu.12200
Hassed, C., de Lisle, S., Sullivan, G., & Pier, C. (2009). Enhancing the health of medical students: Outcomes of an integrated mindfulness and lifestyle program. Advances in Health Sciences Education, 14(3), 387–398. https://doi.org/10.1007/s10459-008-9125-3
Hassed, C. (2021). The art of introducing mindfulness into medical and allied health curricula. Mindfulness, 12, 1909–1919. https://doi.org/10.1007/s12671-021-01647-z
Kakoschke, N., Hassed, C., Chambers, R., & Lee, K. (2021). The importance of formal versus informal mindfulness practice for enhancing psychological wellbeing and study engagement in a medical student cohort with a 5-week mindfulness-based lifestyle program. PloS one, 16(10), e0258999. https://doi.org/10.1371/journal.pone.0258999
Krasner, M. S., Epstein, R. M., Beckman, H., Suchman, A. L., Chapman, B., Mooney, C. J., & Quill, T. E. (2009). Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA, 302(12), 1284–1293. https://doi.org/10.1001/jama.2009.1384
*Craig Hassed
Faculty of Medicine, Nursing and Health Sciences
Monash University
Wellington Road, Clayton,
Victoria, Australia
Email: craig.hassed@monash.edu
Submitted: 28 January 2025
Accepted: 5 July 2025
Published online: 6 January, TAPS 2026, 11(1), 89-91
https://doi.org/10.29060/TAPS.2026-11-1/II3646
Darlina Hani Fadil Azim1, Gaik Kin Teoh1 & Nilesh Kumar Mitra2
1Department of Psychology & Counselling, School of Psychology & Social Sciences, IMU University, Malaysia; 2Human Biology Division, School of Medicine, IMU University, Malaysia
I. INTRODUCTION
Sustainability was the key topic at APMEC 2025. However, how can we maintain care quality when patient demands overshadow healthcare workers’ well-being? The mental health challenges faced by medical students and healthcare professionals – including high workload, burnout, and the emotional toll of the second victim phenomenon, which is the emotional and psychological distress healthcare professionals experience after being involved in or witnessing an adverse patient event or medical error – are well-documented yet often insufficiently addressed (Busch et al., 2021). Despite growing awareness, existing institutional policies for managing and monitoring mental well-being remain fragmented and unsustainable (Kuhlmann et al., 2024). In the Conference workshop session, “Promoting Mental Health in HPE and Healthcare: Partnering for Change”, we were able to create a safe space in which sincere and honest experiences were shared among the participants, who were medical doctors, medical educators, and support staff for medical students and they were able to learn from one another. Therefore, the aim of this paper is to share our insights and recommendations that can be helpful for medical educators and policymakers in ensuring that the healthcare workers well-being is maintained for a sustainable future.
II. STRESSORS OF STUDENTS AND RESIDENTS
The participants highlighted in the small group discussions that the stressors among residents are quite different from those faced by medical students. While students tend to be more concerned about academic pressures and uncertainties about their future careers, residents are more concerned about the high workload and challenging work demands, including patient care responsibilities and personal factors such as managing a young family.
The participants also expressed their concerns about providing the necessary support for both students and residents under their care. They have observed that they tend not to reach out for help when they need it, and for those who do, participant X mentioned that “they are not as forthcoming in sharing about the core of the problem and instead tend to keep it at a superficial level”. Several participants hypothesised that this could be due to the stigma surrounding mental health and the limited time to consult with a senior or superior. This is supported by the study by Hawsawi et al. (2024) who also found other factors such as no or minimal access to mental health support, as well as the normalisation of stress and burnout in the medical field.
To address this, participant Y shared his strategy of “approaching students during informal settings such as class break time or lunch breaks” to make the interaction less formal and a more congenial interaction. He also prefers to “just listen and support, instead of trying to change or correct the student”. Another participant who works in a teaching hospital found that “my students were more willing to open up when I shared my own struggles from when I was a junior doctor”. These practices can help encourage more open communications from the medical students and residents.
III. COPING STRATEGIES OF MEDICAL EDUCATORS
To explore the participants’ coping strategies in managing their own stressors, each participant was requested to list both internal and external supports that are available to them and to share with the whole group. Internal coping mechanisms such as turning to religion offer comfort, meaning, and community support. Positive self-talk and acceptance promote self-compassion and reduce negative thinking. Distraction techniques, such as engaging in hobbies, practicing mindfulness, or exercising, provide temporary relief and improve mood. In terms of external support, most of the participants have a strong support system from family, colleagues and mentors who provide emotional support, understanding, and a sense of belonging. Having a safe space to vent frustrations and anxieties without judgment offers crucial emotional release. One participant found this workshop activity of self-disclosure and sharing helped her to see that she is not alone in her own struggles with mental health issues. Interestingly, none of the participants mentioned systemic support as one of the coping factors. Could this imply systemic support is beyond their capacity, or are they not aware of its availability or significance? The participants highlighted that while there are efforts in their institutions to promote mental health and well-being, these tend to be more focused on the students, rather than on staff. Two of the participants also discussed how their institutions have made available third-party digital therapeutics companies that includes access to mental health professionals and also AI chatbots that can provide online support. This could be a more accessible option for those who are hesitant to reach out for help.
IV. PROPOSED SOLUTIONS
Considering the input from the workshop participants, we recommend the following:
1) To reduce the stigma of seeking formal mental health support that are provided by the institutions, incorporate in the medical curriculum the provision of a safe platform for sharing personal stories from senior staff or alumni that showcase their mental health challenges in different stages of their career and how they managed it. This fosters a work culture that powerfully conveys mental health challenges are not signs of weakness, but rather that understanding how and where to seek help is an essential component of professional practice.
2) To further harness the support that staff are already providing informally to their peers and students, a mandatory training programme on Mental Health First Aid focusing on recognising signs of distress, basic active listening skills, motivational interviewing skills and appropriate referral pathways can be implemented. This can be made available to the students as well.
3) To address the perceived lack of systemic support for staff, a mandatory wellness program is recommended. This may include regular and dedicated mental health check-ins with independent mental health professionals who are familiar with the unique stressors and challenges faced by healthcare professionals and students including the second victim phenomenon. These check-ins can be in an informal setting like during coffee breaks or gym sessions to encourage open and non-judgmental conversations, reduce stigma, and normalise seeking psychological support as a routine part of professional well-being. Using AI chatbots could also be an alternative approach. These conversations can provide valuable opportunities to identify early warning signs and offer timely support.
V. CONCLUSION
The format of this APMEC 2025 workshop can serve as a model for fostering collaborative mental health discussions, thus making it a replicable innovation. The insight from the workshop clearly shows that more needs to be done to address healthcare workers’ well-being at the systemic level. This is a direct call to action for HPE institutions to prioritise and implement strong, dedicated mental health support systems. Furthermore, HPEs must equip all staff and students with the essential skills to proactively offer mental health support to their peers and colleagues, fostering a truly supportive academic and professional environment.
Notes on Contributors
DHFA conceptualised the core idea, developed the argument and wrote the paper.
GKT initiated, conceptualised, analysed the literature and revised the paper.
NKM analysed the literature and revised the paper.
Ethical Approval
There is no data presented in this paper, and thus ethical approval is not required.
Acknowledgement
We would like to thank the Deans of the School of Psychology and Social Sciences and the School of Medicine at IMU University, for supporting our participation in this conference.
Funding
IMU University, Malaysia, funded our participation in this conference.
Declaration of Interest
All authors have no conflict of interest to declare.
References
Busch, I. M., Moretti, F., Campagna, I., Benoni, R., Tardivo, S., Wu, A. W., & Rimondini, M. (2021). Promoting the psychological well-being of healthcare providers facing the burden of adverse events: A systematic review of second victim support resources. International Journal of Environmental Research and Public Health, 18(10), 5080. https://doi.org/10.3390/ijerph18105080
Hawsawi, A. A., Nixon, N., Stewart, E., & Nixon, E. (2024). Exploring access to support services for medical students: Recommendations for enhancing wellbeing support. BMC Medical Education, 24(1), 671. https://doi.org/10.1186/s12909-024-05492-1
Kuhlmann, E., Falkenbach, M., Brînzac, M. G., Correia, T., Panagioti, M., & Ungureanu, M. I. (2024). The mental health needs of healthcare workers: When evidence does not guide policy. A comparative assessment of selected European countries. The International Journal of Health Planning and Management, 39(3), 614-636. https://doi.org/10.1002/hpm.3752
*Darlina Hani Fadil Azim
126, Jalan Jalil Perkasa 19, Bukit Jalil,
57000 Kuala Lumpur, Malaysia
+60122846675
Email: darlinahani@imu.edu.my
https://doi.org/10.29060/TAPS.2026-11-1/TT005
Tim Wilkinson
Professor of Medicine and Medical Education,
Dean’s Department (Christchurch),
University of Otago, New Zealand
“My student is not very professional.”
“They failed their OSCE station because they need to be more professional.”
“What’s the best tool to assess professionalism?”
These kinds of comments and questions are common in medical education – and they reflect an unhelpful tendency to treat professionalism as a singular, all-encompassing trait. In reality, professionalism is not one thing. It’s many things. It’s time we started talking about professionalisms – plural.
A student might be honest but disorganised. Another might communicate beautifully with patients but struggle to take feedback from colleagues. Being professional in one domain doesn’t mean being professional in all. Just as we wouldn’t assess clinical knowledge with a single multiple-choice test, we can’t evaluate or develop professionalism with a single lens.
In my systematic review (Wilkinson et al., 2009), I found that while definitions of professionalism vary, most can be clustered into five broad domains:
- Ethical practice – Honesty, integrity, and respect for confidentiality.
- Interpersonal behaviour with patients and families – Empathy, rapport, communication.
- Teamwork and collaboration – Collegiality, accountability to the wider health system.
- Reliability – Following through, being prepared, respecting deadlines.
- Commitment to improvement – Reflectiveness, lifelong learning, system contributions.
Different cultures, institutions, and disciplines may emphasise some of these more than others, but none of them captures professionalism alone. What matters most is not drawing hard boundaries, but being clear and specific – with ourselves, our colleagues, and our students – about which dimensions we are referring to in a given context.
When we shift from thinking about professionalism as a singular trait to seeing it as a set of behaviours and commitments that evolve over time, we create more space for growth.
Here are some useful questions to ask ourselves:
- What specific behaviour or value am I referring to when I talk about “professionalism”?
- How can I name and model that behaviour clearly for learners?
- What would the learner need to do to convince me the concern about professionalism has resolved?
- Where might I be expecting students to “just know” what’s expected?
By embracing professionalism in the plural, we make it more meaningful, teachable, and explicit.
Reference
Wilkinson, T. J., Wade, W. B., & Knock, L. D. (2009). A blueprint to assess professionalism: Results of a systematic review. Academic Medicine, 84(5), 551-558. https://doi.org/10.1097/acm.0b013e31819fbaa2
Submitted: 24 September 2024
Accepted: 3 June 2025
Published online: 7 October, TAPS 2025, 10(4), 81-83
https://doi.org/10.29060/TAPS.2025-10-4/II3527
Nathasha Luke, Shing Chuan Hooi & Celestial T. Yap
Department of Physiology, Yong Loo Ling School of Medicine, National University of Singapore, Singapore
I. INTRODUCTION
Lifelong learning is an essential skill for a successful medical practitioner to keep pace with rapidly advancing medical knowledge and technologies. Artificial intelligence(AI) has a potential in developing and promoting the skill of lifelong learning among medical undergraduates. AI can facilitate adaptive learning, collaborative learning, coaching, and incorporating evidence-based learning in undergraduate education as measures promoting lifelong learning. Users should be aware of the capabilities and limitations of the technology to promote effective incorporation in education. Medical undergraduates should receive a basic AI education to harness its’ potential in the best possible ways in lifelong learning.
Modern-day medical practice is rapidly revolutionising. The increasing content and complexity of medical knowledge are often beyond the human capacity to process and synthesise. A study in 2019 revealed there was an overall 2620% increase in the number of knowledge syntheses published over 20 years, from 1999 to 2019 (Maggio et al., 2020). Medical students and doctors struggle to stay updated with the expanding knowledge and find it difficult to cope with information overload. A successful practitioner should have excellent foundational knowledge, be up-to-date, know when and where to seek additional information, and understand optimal practices in the work environment. Such practitioners will adopt technologies to make their lifelong learning more effective and targeted toward improving patient care.
Artificial intelligence (AI) is at exponential growth, particularly in the field of medicine. AI inventions span across multiple dimensions such as AI-aided diagnostic systems, image interpretation, medical records, patient communication, and community-based care. Future practice environments are likely to be heavily AI-integrated. AI-based knowledge management systems and search engines will streamline the process of practitioners keeping themselves up to date with evolving medicine.
Developing lifelong learning among students is an important domain of medical education, that will them to keep abreast of rapid advances in medicine. Medical schools foster the development of lifelong learning habits through strategies such as (1) adaptive learning (2) collaborative learning (3) coaching and (4) incorporating evidence-based learning into the curriculum. This article focuses on how AI could be harnessed to facilitate and enhance these strategies to inculcate lifelong learning among medical undergraduates.
II. HOW COULD AI ENHANCE THE PROCESS OF ADAPTIVE LEARNING?
Adaptive learning is a process that customises individual learning experiences by determining an individual’s strengths and weaknesses and specifically addressing them. The concept of adaptive learning has become popular in recent years. However, this concept was originally highlighted more than a century ago. In 1912, Edward Thorndike introduced the idea of the learning machine, where the machine could ask questions from the learner and suggest areas that need improvement. With the rise of Generative AI, this concept is coming to reality. Generative AI, which produced content like text, videos and music in response to user prompts, powers adaptive learning tools that assess student knowledge, offer personalised feedback, and pinpoint areas for improvement to help guide their learning process toward mastery (Luke & Hooi, 2024).
Rapid advancements in generative AI have made this technology accessible to many users, allowing learning institutions to customise adaptive AI platforms at a relatively lower cost. Such tools may not only facilitate the learning journey of medical students but also make them strive for continuous feedback-driven improvement as practitioners. In the future, AI-driven adaptive learning may revolutionise continuous professional development (CPD) to pinpoint and address learning gaps, allowing efficient and relevant learning for busy clinicians.
III. WILL AI-DRIVEN LEARNING ENVIRONMENTS PROMOTE COLLABORATION?
Collaboration is defined as the mutual engagement of participants in a coordinated effort to solve the problem together (Roschelle & Teasley, 1995). Collaborative learning by means of peer learning, interdisciplinary learning, and interprofessional learning should be promoted to ensure students develop the skills and confidence to collaborate as clinicians in the future. In clinical environments, doctors learn from each other in both formal and informal ways. This type of learning is particularly important in learning new skills and encourages self-learning behaviours in individuals. In medical school, collaborative learning skills are enhanced through group work, simulations, and collaborative activities among students from different related streams such as medicine, nursing, and pharmacy. These approaches strengthen interprofessional communication, knowledge sharing, and enhance learning.
AI-based virtual reality simulated clinical environments are adopted by multiple medical schools to promote experiential learning. Promoting collaboration should be incorporated as a learning outcome when possible into such simulations. For example, simulations can focus on students’ decision-making skills as what team members are to be activated in a simulated encounter and developing communication skills for effective collaboration. In addition, in the future, AI-based platforms may allow more widespread collaboration crossing boundaries, such as enabling clinicians to find the ‘expert’ to seek opinions on a particular condition, where AI-based systems can facilitate collaboration.
IV. COACHING FOR LIFE-LONG LEARNING – CAN AI DO THIS?
Coaching is a development process that enables a person to identify and enhance their own capabilities to reach personal and professional goals. This process has been demonstrated to be beneficial for students in educational settings (Breslin et al., 2023). How does coaching promote lifelong learning? Coaching, which allows the person to learn about self, enables one to identify own impediments towards learning. This will enhance behaviours facilitating learning. AI coaching or virtual coaching is now being explored. The advantages of AI coaching are accessibility, lack of bias, and convenience. Human coaching is still believed to be superior due to the aspects of the ability to express empathy, pick up non-verbal cues during conversation, and be more adaptive. Though the current technology of AI is unable to surpass an experienced human coach (Terblanche et al., 2022), these hurdles may be overcome with future advancements of the technology.
V. EMPHASISE EVIDENCE-BASED APPROACHES WITHIN THE CURRICULUM
Reading journals, critically appraising relevant publications, and adopting them in one’s own practice are essential elements of the lifelong learning process for doctors, which should be developed from undergraduate days themselves. The main hurdle for such incorporations is the tight schedule within the curriculum and the content load. Despite traditional teaching being replaced by integrated teaching, the content load covered within the curriculum remains substantial. The depth and breadth of the content taught in medical school have not proportionately evolved over the years, despite major changes happening in clinical environments with AI integration. AI acts as an instant source of knowledge, aiding clinical decision-making and patient care. Bearing this in mind, educators should revise their curricula to reduce the depth of certain elements that could be easily retrieved digitally. However, students should have a sound knowledge on foundational principles on which advanced concepts can build on.
Re-evaluating the curriculum to reduce the content load would free more time in the schedule to promote critical appraisal of scientific literature, enabling students to wisely use scientific literature to stay up to date. A thoughtful and pragmatic approach to curriculum revaluation for lifelong learning involves embedding core competencies such as critical thinking, adaptability, self-directed learning, and interdisciplinary collaboration instead of overloading content.
VI. EQUIP UNDERGRADUATES WITH BASIC AI KNOWLEDGE AND SKILLS
Some medical schools, including NUS Medicine, have incorporated AI into the curricula. Exposing medical undergraduates to the foundations of AI technology can help them foresee the revolutionisation of future practice and equip themselves to embrace the technology. In addition, this will enable them to pursue new career pathways combining AI and Medicine. With regards to lifelong learning, clinicians may be equipped with AI-based tools to learn from real-time patient data for clinical decision-making, rather than waiting for prospective clinical trials or research. For example, students with foundational knowledge of AI will be able to use AI analytical skills to draw conclusions based on real-time and latest clinical data, as well as to detect trends of emerging diseases and antibiotic resistance, promoting early intervention.
Equipping future generations with AI knowledge will improve the quality of care and reduce diagnostic errors. Also, AI knowledge will guide practitioners to remain vigilant about data privacy and algorithmic bias when using AI. A future-ready curriculum will not only prepare students to use AI responsibly but also to question and enhance the tools.
AI comes with challenges and opportunities. The risk of bias, data quality and security issues, risk of over-reliance, AI relying on historical rather than real-time data, and lack of transparency in decision-making processes are some of the limitations. Still, AI has a vast potential to augment healthcare and health professions’ education as discussed above. AI should augment clinical decision making, and not replace. Ethical considerations, including patient consent, data security, and accountability, must remain central to any AI integration in healthcare practice.
In summary, AI has huge potential to enhance the strategies implemented in medical education to promote lifelong learning in medical undergraduates. The users should be aware of the limitations of the technology, and incorporate it cautiously to harness the maximum benefit of the technology in the process of transforming our undergraduates to better clinicians and lifelong learners.
Notes on Contributors
NL conceptualised the article, created the first draft, and revised subsequent versions. In addition, approved the final version of the article for submission.
HSC conceptualised the article, revised the draft versions, and approved the final version of the article for submission.
CTY conceptualised the article, revised the draft versions, and approved the final version of the article for submission.
Funding
We did not receive any funding for this publication.
Declaration of Interest
We do not have any conflicts of interest, including financial, consultant, institutional, or other relationships that might lead to bias or a conflict of interest.
References
Luke, W. N. V., & Hooi, S. C. (2024). The role of artificial intelligence in knowledge management for medical students and doctors. Medical Teacher, 1–2. https://doi.org/10.1080/0142159x.2024.2336065
Maggio, L. A., Costello, J. A., Norton, C., Driessen, E. W., & Artino, A. R., Jr. (2020). Knowledge syntheses in medical education: A bibliometric analysis. Perspectives on Medical Education, 10(2), 79–87. https://doi.org/10.1007/s40037-020-00626-9
Roschelle, J., & Teasley, S. D. (1995). The construction of shared knowledge in collaborative problem solving (pp. 69–97). Springer eBooks. https://doi.org/10.1007/978-3-642-85098-1_5
Terblanche, N., Molyn, J., De Haan, E., & Nilsson, V. O. (2022). Comparing artificial intelligence and human coaching goal attainment efficacy. PLoS ONE, 17(6), e0270255. https://doi.org/10.1371/journal.pone.0270255
*Nathasha Luke
2 Medical Drive, MD 9,
National University of Singapore, 117593
+6596204104, +6566013506
Email: nathasha@nus.edu.sg
Submitted: 6 February 2025
Accepted: 14 May 2025
Published online: 7 October, TAPS 2025, 10(4), 94-96
https://doi.org/10.29060/TAPS.2025-10-4/II3664
Charlene Tan1 & Ruth Neo2
1College of Arts, Humanities and Languages, Life University, Cambodia; 2UNSW Medicine & Health, University of New South Wales, Australia
I. INTRODUCTION
This article proposes a Chinese philosophical approach to well-being for medical education by drawing on the thought of Mencius (372-289 B.C.E.). As it is not possible to cover all areas of Mencius’ philosophy within this short essay, our focus is on Mencius’ idea of interpersonal joy, as recorded in the classic Mengzi. This paper shall explain how interpersonal joy, from a Mencian perspective, centres on the shared delight from benefiting others while cultivating personal virtue.
II. MENCIUS ON WELL-BEING AND INTERPERSONAL JOY
Well-being is used synonymously or in conjunction with related terms such as welfare, happiness, prudential value, the good life, prudential good life, quality of life, flourishing, self-interest, fulfilment, utility and pastoral care (Fletcher, 2016). Mencius’ approach to well-being is encapsulated in his idea of interpersonal joy, which harmonises personal and communal delight. A representative passage is 7A20.1 in the Mengzi:
Mengzi said, “An exemplary person [Junzi] takes joy in three things, and being King of the world is not one of them. The person’s first joy is that one’s parents are both alive and one’s siblings have no difficulties. The second joy is that looking up one is not disgraced before Heaven, and looking down on one is not ashamed before humans. The third joy is getting assistance and cultivating the brave and talented people of the world. An exemplary person takes joy in three things, and being King of the world is not one of them (Van Norden, 2008, p. 176).
This passage is about a Junzi which literally means ‘son of a noble’. Confucius appropriated this historical term and infused it with moral import, thereby changing its meaning to denote an exemplary person. That the exemplary person embodies Confucian well-being is evidenced by passages in the Mengzi that describe such a person as having “no anxieties” (4B28.7) and experiencing “joy” (7A20.1, 7A21.2).
With respect to 7A20.1, the passage begins by stating that an exemplary person does not derive joy from being King of the world. Mencius is not asserting that holding political power is wrong or detrimental to one’s well-being. On the contrary, he acknowledges in the next passage that an exemplary person, like all rulers, “desires a large territory and numerous people” (7A21.1). Mencius’ point is that Kingship, in itself, does not give satisfaction to an exemplary person; instead, such a person “takes joy in taking one’s place in the middle of the world and making all the people within the Four Seas settled” (7A21.1) (Van Norden, 2008, p. 176). We see here how an exemplary person obtains personal joy by bringing joy to others (“making all the people within the Four Seas settled”).
All people can become exemplary people by developing the four sprouts within them, namely the mind-and-heart of compassion, the shame of evil in oneself and hatred of evil in others, humility and deference, and right and wrong (2A.6). These four sprouts, when consistently cultivated, will grow into the virtues of benevolence, propriety, righteousness and wisdom, all of which contribute to interpersonal joy. Retuning to 7A20.1, Mencius’ message is that an exemplary person does not obtain pleasures and life satisfaction from prudential desires, which are manifested in egoistic ambitions with little regard for others. Instead, joy is felt when a person immerses oneself in social interactions and builds strong connections with others. An exemplary person also derives delight by treating others well and developing their potential for the common good. The end result is “making all the people within the Four Seas settled” (7A21.1) (Van Norden, 2008, p. 176).
To sum up, Mencian well-being is indicated by interpersonal joy which integrates individual and collective happiness, as demonstrated by the exemplary person. Communal joy engenders collective well-being, illustrated by the King “sharing the same delight as the people” (1B1.4) (Van Norden, 2008, p. 16).
III. RECOMMENDATIONS FOR MEDICAL EDUCATION
A major implication of Mencian well-being is for medical schools to promote interpersonal joy in the curriculum and assessment. Two suggestions are elaborated in this section: a shift from summative assessment and competition to formative assessment and collaboration; and the introduction of a wellness curriculum that pivots on interpersonal joy.
First, medical schools need to review their curriculum and assessment so as to remove any hindrances to the realisation of interpersonal joy in their students. A specific recommendation is to replace summative assessment and competition with formative assessment and collaboration. Mencius’ call for collective well-being is difficult to achieve if students are fixated with outperforming one another due to the pressures of high-stakes exams. Kachel et al. (2020) report that “during medical school interpersonal skills linked to being an active member of an institution are underrepresented in curricula” (p. 11). It is a challenge for medical students to care for the well-being of others and be open about their mental health needs if they are circumscribed by a culture of competition, distrust and judgement (Canadian Federation of Medical Students, 2021). Cooperation and interdependence can be enhanced by reducing or removing pen-and-paper examination and norm-referenced assessments, and introducing (more) collaborative projects and criterion-referenced assessments. The assessment mode for the cultivation of interpersonal joy should be formative, where students are given continuous feedback and find enjoyment in learning and sharing.
A pedagogical approach to foster interpersonal joy is group projects, where students collaborate for shared success. Anchored upon the principles of cooperation and harmony, group projects foreground interpersonal joy and competencies that are underrepresented in the curricula (Kachel et al., 2020). Termly group projects nurture communication and teamwork skills, spanning a wide range of topics from the basic clinical sciences to medical ethics and public health. The group projects can be evaluated via negotiated assignment, where students develop their own research questions and set their own assessment criteria that are aligned with the course themes. The goal is to foster student-driven learning that gives students the opportunity to explore common topics of interest beyond the confines of standard, end-of-course examinations. A related pedagogical approach is encouraging students to participate in service learning, community involvement as well as local and overseas volunteer projects, so as to generate communal interactions and bonding. By serving others, the students’ sprout of compassion is cultivated and manifested through empathy, beneficence and concern for others (Van Norden, 2008).
The second recommendation is for medical schools to enact a wellness curriculum that pivots on interpersonal joy. Medical schools could adapt the wellness curriculum for medical students in a Canadian university; students there were asked to “define their core values and beliefs while respecting those of others, and apply them in the context of their developing physician identity and that of the medical profession” (Canadian Federation of Medical Students, 2021, p. 22). Mencian ideas can be integrated into the before-mentioned wellness curriculum through reflective questions such as: What does an exemplary person (junzi) mean to me? How can Mencian interpersonal joy be part of my core values as a medical professional? How can I obtain interpersonal joy through interacting with and serving others? The self-reflection activity can be undertaken in various formats such as group discussions, journalling and multi-media presentations.
Mencian ideas of well-being and related suggestions may face challenges in medical schools where individualism and competition are often culturally entrenched. In this regard, Mencian well-being may be more appropriate for medical education in Confucian heritage cultures. Significantly, studies have shown that Asian adolescents experience a strong sense of well-being when they partake in collective activities; in contrast, adolescents in Anglo-American societies typically enjoy higher well-being when they engage in more individualistic activities (Chue, 2023). Relatedly, Mencian well-being’s focus on moral cultivation sets it apart from two dominant models in Anglophone societies, namely Seligman’s PERMA (Positive emotions, Engagement, Relationships, Meaning & Accomplishment) and Ryff’s six aspects of psychological well-being, which are autonomy, environmental mastery, personal growth, positive relations with others, purpose in life, and self-acceptance. As noted earlier, Mencius advocates for the development of our innate goodness in the form of the four sprouts, which in turn contributes to interpersonal joy. In contrast, the theories of Seligman and Ryff generally de-emphasise moral education.
In individualistic societies, interpersonal joy can complement the existing wellness frameworks by underscoring collaborative learning, such as group projects and service learning (Bourcier et al., 2021). Staff development is also critical, where faculty members are introduced to Mencian principles and practical ways to promote them, such as organising service learning and designing wellness curricula. Ultimately, the successful implementation of interpersonal joy necessitates faculty development, which should be strategically incorporated into the staff training programmes (Canadian Federation of Medical Students, 2021).
IV. CONCLUSION
Mencius’ approach to well-being is encapsulated in his idea of interpersonal joy, which harmonises personal and communal delight. Mencian well-being supports collective well-being by twinning self-interests and other interests. This paper has also suggested that medical schools revamp the curriculum and assessment modes to shift from summative assessment and competition to formative assessment and collaboration. Medical schools should also explore pedagogical methods that incorporate Mencian idea of interpersonal joy into the curriculum.
Notes on Contributors
Charlene Tan conceptualised the topic, provided philosophical ideas and drafted the manuscript. Ruth Neo gave inputs that pertained to medical student well-being and co-drafted the manuscript.
Ethical Approval
Ethical approval is not relevant as this is a conceptual paper that does not involve human participants and/or animals.
Acknowledgement
The authors thank the anonymous reviewers for valuable suggestions to earlier drafts.
Funding
The authors did not receive support from any organisation for the submitted work.
Declaration of Interest
No potential competing interest was reported by the authors. The authors have no relevant financial or non-financial interests to disclose.
References
Canadian Federation of Medical Students. (2021). Canadian federation of medical students wellness curriculum framework. https://www.cfms.org/files/wellness-resources/CFMS-Wellness-Curriculum-Framework_FINAL.pdf
Chue, K. L. (2023). Cultural issues in measuring flourishing of adolescents. In R. B. King, I. S. Caleon, & A. B. I. Bernardo (Eds.), Positive psychology and positive education in Asia: Understanding and fostering well-being in schools (pp. 329-342). Springer.
Fletcher, G. (Ed.). (2016). The Routledge handbook of philosophy of well-being. Routledge.
Kachel, T., Huber, A., Strecker, C., Höge, T., & Höfer, S. (2020). Development of cynicism in medical students: Exploring the role of signature character strengths and well-being. Frontiers in Psychology, 11(328), 1-16. https://doi.org/10.3389/fpsyg.2020.00328
Van Norden, B. W. (2008). Mengzi. With selections from traditional commentaries. Hackett Publishing Company, Inc.
*Charlene Tan
Life University, Phreah Sihanouk,
Sihanoukville, Cambodia
Email: chptan@u.nus.edu
Submitted: 18 November 2024
Accepted: 14 May 2025
Published online: 7 October, TAPS 2025, 10(4), 5-25
https://doi.org/10.29060/TAPS.2025-10-4/RA3572
Matthew Jian Wen Low1, Han Ting Jillian Yeo2, Dujeepa D. Samarasekera2, Gene Wai Han Chan1 & Lee Shuh Shing2
1Department of Emergency Medicine, National University Hospital, Singapore; 2Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: Effective and actionable instructional design features improve return on investment in Technology enhanced simulation (TES). Previous reviews on instructional design features for TES that improve clinical outcomes covered studies up to 2011, but updated, consolidated guidance has been lacking since then. This review aims to provide such updated guidance to inform educators and researchers.
Methods: A narrative review was conducted on instructional design features in TES in medical education. Original research articles published between 2011 to 2022 that examined outcomes at Kirkpatrick level three and above were included.
Results: A total of 30,491 citations were identified. After screening, 31 articles were included in this review. Most instructional design features had a limited evidence base with only one to four studies each, except 11 studies for simulator modality. Improved outcomes were observed with error management training, distributed practice, dyad training, and in situ training. Mixed results were seen with different simulation modalities, isolated components of mastery learning, just-in-time training, and part versus whole task practice.
Conclusion: There is limited evidence for instructional design features in TES that improve clinical outcomes. Within these limits, error management training, distributed practice, dyad training, and in situ training appear beneficial. Further research is needed to assess the effectiveness and generalisability of these features.
Keywords: Simulation, Instructional Design, Clinical Outcomes, Review
Practice Highlights
- This review pinpoints additional beneficial instructional design features emerging since 2011.
- These include error management training, distributed practice, dyad training, and in situ training.
- Further evidence from diverse task and learner contexts is needed to establish generalisability.
- Current evidence continues to suggest no clear superiority of one simulator modality over the other.
I. INTRODUCTION
Technology enhanced simulation (TES) training has been shown to be effective for skills, behaviour, and patient-related outcomes (Cook et al., 2011; McGaghie et al., 2011). Instructional design features in simulation refer to variations in aspects of simulation design that act as active ingredients or mechanisms that make simulation effective, with examples including distributed practice, mastery learning, and range of difficulty (Cook, Hamstra, et al., 2013). Effective instructional design features for TES are actionable for educators because they offer specific, implementable guidance, and an area of research interest (Issenberg et al., 2005; Nestel et al., 2011; Schaefer et al., 2011), including those that lead to transfer to authentic clinical practice (Frerejean et al., 2023; Zendejas et al., 2013).
While it is acknowledged that conducting a study to establish a causal relationship between an educational intervention and subsequent patient and clinical process outcomes is challenging (Cook & West, 2013), such studies become particularly valuable when appropriately executed (Dauphinee, 2012). These studies represent the apex of impact in Kirkpatrick’s model for program evaluation (Kirkpatrick & Kirkpatrick, 2006), holding the highest clinical significance and representing the ultimate goal of health professions education which is to enhance patient outcomes by equipping the healthcare workforce to effectively address societal needs (Carraccio et al., 2016). Additionally, the examination of clinical outcomes, when coupled with a consideration of costs, contributes to the informed allocation of limited institutional resources to such educational approaches (Lin et al., 2018).
In prior reviews of TES including studies up to 2011, the vast majority of studies examined outcomes at the levels of reaction and learning demonstrated in written or simulation tests, with only a small body of evidence studying outcomes in workplace contexts (Cook, Hamstra, et al., 2013; Nestel et al., 2011; Zendejas et al., 2013) suggesting that clinical variation, multiple learning strategies, and increased time learning are beneficial variations. This limited evidence base for transfer to workplace contexts hinders educators in fully harnessing the potential of TES to improve patient and system outcomes and obtain the best returns on investments in simulation technology. Given the time interval since these prior reviews, further evidence would have accrued regarding these and other instructional design features.
Given the time elapsed since the last comprehensive review of TES instructional design features, the scarcity of prior studies on clinical outcomes, and the importance of these outcomes, we conducted this narrative review. The objective was to provide an updated understanding of the instructional design features in TES that are associated with enhanced clinical outcomes, thereby addressing a significant gap in the existing literature, to guide educators seeking to optimise instructional design, and provide researchers with an overview of the current state of this literature and guide further inquiry.
II. METHODS
We conducted a narrative review based on the framework proposed by Ferrari (2015). We searched MEDLINE, ERIC, Embase, Scopus and Web of Science databases for articles published from 2012 January 01 to 2022 December 06. We translated abstracts and articles not in English into English using Google Translate.
The following search terms were used: (Medical education) AND (Simulation OR Cadaver OR Simulator OR Augmented Reality OR Virtual reality OR Mixed reality).
Studies were included if they were original research articles examining instructional design variations in TES with at least one outcome at Kirkpatrick levels three or above, as described and utilised by the Best Evidence Medical Education Collaboration (Steinert et al., 2006). We included a broad range of TES modalities, such as computer based virtual reality simulators, high fidelity and static mannequins, plastic models, live animals, inert animal products, and human cadavers as stipulated in the review by Cook et al. (2011). We included augmented reality and mixed reality as they satisfied the prior definition of “materials and devices created or adapted to solve practical problems” in simulation established by Cook et al (2011). Studies where TES was utilised together with human patient actors were included. We included studies with observational, experimental, and qualitative designs.
Studies were excluded if they involved only human patient actors as the sole modality of simulation, used simulation outside of health professions education, used simulation for noneducation purposes such as procedural planning or patient education, or only compared simulation with no simulation. We excluded studies involving only nurses given that there are recent and ongoing reviews addressing a similar research question (El Hussein & Cuncannon, 2022; Jackson et al., 2022), but included interprofessional studies. Figure 1 shows the flow of studies through the review and selection process.
Three researchers (MJWL, SSL, JHTY) independently read the full text of articles that met the inclusion criteria and extracted study information including geographical origin, specialty context, type of skill studied, level of the learner, simulation modalities used, instructional design variations studied, and outcomes categorised into the highest Kirkpatrick level studied. Any differences were resolved by a discussion among researchers to arrive at a consensus.
III. RESULTS
A total of 30,491 records were identified using the search strategy. From these, 31 eligible studies were identified and reviewed (Figure 1 and Table 1). Figure 2 summarises basic information on these studies. The number of studies from each geographic region were 13 from North America (42%), 11 from Europe (35%), three from Asia (10%), two from Africa (6%), and one from South America (3%). One study did not clearly state the countries involved.
28 out of 31 (90%) of the studies adopted a quantitative research design focusing on experimental design. Most simulation interventions were conducted among residents/fellows/interns, followed by medical students.
The results reported in the studies are divided into two groups:
- Evidence suggests improved outcomes
- Evidence shows mixed results
A. Improved Outcomes
Error management training was associated with improved obstetric ultrasound skills compared to error avoidance training in novices (Dyre et al., 2017). Frequent brief on-site simulation, at 40 minutes a month and three minutes a week, was associated with reduced infant mortality compared to a single day course (Mduma et al., 2015). Integrating non-technical skills (NTS) training into a colonoscopy skills curriculum with TES, without increasing time spent teaching, improved observed performance during colonoscopies on real patients, although it was unclear whether this was driven by changes in observed NTS only, or both NTS and technical skills (Walsh et al., 2020).
One qualitative study found that in situ training had greater organisational impact and provided more information for practical organisational changes (Sørensen et al., 2015). One qualitative study found that multi-professional training led to improved communication, leadership, and clinical management of post-partum haemorrhage (Egenberg et al., 2017).
1. Dyad Training
In one study of obstetric ultrasound skills (Tolsgaard et al., 2015) a larger proportion of the dyad training group (71%) scored above the criterion referenced pass fail level than the individual training group (30%) on the objective structured assessment of ultrasound skills, though the difference in mean scores on did not reach statistical significance. Other benefits included increased efficiency from greater faculty to learner ratios.
2. Complex Bundles
Three studies found improvements with complex bundles comprising multiple instructional design variations.
Medical students performed the correct sequence of steps for endotracheal intubation measured by a checklist more often when practice with a mannequin was augmented by a 10-question pre-test, hand held tablets containing scenarios, checklists, and learning algorithms, 24-hour access to the simulation laboratory, and remote review of practice recordings with feedback from teachers via email (Mankute et al., 2022).
Residents had improved observed performance in laparoscopic salpingectomy with lectures, videos, reading materials, a box trainer with pre-set proficiency benchmarks, a VR simulator for technical skills, and non-technical skills training with scripted confederates, compared to a conventional curriculum including simulation with minimal further description (Shore et al., 2016).
In one qualitative study of obstetric residents, there was improved transfer of communication and team work skills and situational awareness with simulation aligned to multiple principles including authenticity, psychological fidelity, engineering fidelity, Paivio’s dual coding, feedback, variability, and increasing complexity (de Melo et al., 2018).
B. Mixed Results
1. Simulation Modality
Eleven studies examined whether outcomes differed when different simulation modalities were used. Examples include higher versus lower technological complexity in a physical simulator (DeStephano et al., 2015; Sharara-Chami et al., 2014), cadaveric versus synthetic models (Lal et al., 2022; Tan et al., 2018; Tchorz et al., 2015), virtual reality (VR) versus physical simulators (Daly et al., 2013; Gomez et al., 2015; Orzech et al., 2012; O’Sullivan et al., 2014), and a computer based versus physical simulated operating room for student orientation (Patel et al., 2012).
Overall, there no clear pattern of superiority of a particular type of simulator. Most studies found no difference, with three exceptions: Gomez et al (2012) found that VR alone, and VR with physical simulator, led to superior performance in observed colonoscopic skills in real patients, compared to physical simulator alone; Chunharas et al (2013) found that adding practice on fellow students on top of mannequin practice improved observed performance in subcutaneous and intramuscular injection skills; Patel et al (2012) found that using a physical simulated operating room was superior to an online computer based operating room for training novice medical students in appropriate behaviour in the operating room.
To view Table 1 click here.
Abbreviations. ACS/APDS: American College of Surgeons / Association of Program Directors in Surgery; EAT: Error avoidance training; EMT: Error management training; GAGES-C: Global Assessment of Gastrointestinal Endoscopic Skills-Colonoscopy; GOALS: Global Operative Assessment of Laparoscopic Skills; ISS: In situ simulation; JAG DOPS: Joint Advisory Group Direct Observation of Procedural Skills; JIT: Just in time; OSA-LS: objective structured assessment of laparoscopic salpingectomy; NTS: Non-technical skills. OSAUS: objective structured assessment of ultrasound; OSS: Off-site simulation; PGY: Post graduate year; UK: United Kingdom; USA: United States of America; VR: Virtual reality.
Kirkpatrick levels. 1: Reaction e.g. participants’ views on learning experience; 2a: Learning – Change in attitudes; 2b: Learning – Modification of knowledge or skills; 3: Behaviour – Change in behaviours; 4a: Results – Change in the system/organisational practice; 4b: Results – Change in patient outcomes.
Table 1. List of included studies and skills, instructional design variations and outcomes examined
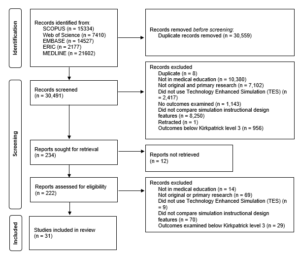
Figure 1. Flow of studies through identification process
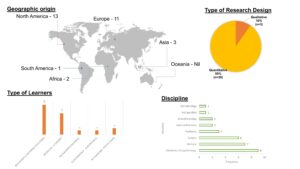
Figure 2. Summary of geographical origin, type of research, type of learners and disciplines studied
2. Components of Mastery Learning
Four studies examined components of mastery learning, such as progressive task difficulty and proficiency-based progression. Progressive task difficulty for TES was associated with improved rater observed colonoscopic performance on real patients (Grover et al., 2017), while the evidence was mixed for proficiency-based progression for TES, with studies finding reduced epidural failure rates (Srinivasan et al., 2018) and fewer adverse events in laparoscopic cholecystectomy (De Win et al., 2016), while another found no difference in operative performance for bowel anastomosis in real patients (Naples et al., 2022).
3. Part Versus Whole Task
Two studies compared part versus whole task training. Both found no difference, in rater observed performance in laparoscopic inguinal hernia repair (Hernández-Irizarry et al., 2016), and intraoperative camera navigation skills (Nilsson et al., 2017), though randomised part task training led to faster skills mastery with greater cost effectiveness compared to whole task training.
4. Increased Time Spent in Simulation Training
Two studies examined amount of time spent in simulation training. One study showed reduced incidence of malpractice claims (Schaffer et al., 2021), while another study found no difference in successful deep biliary cannulation during endoscopic retrograde cholangiopancreatography (Liao et al., 2013).
5. Just in Time (JIT) Training
Overall, there was mostly no benefit seen with JIT training with TES, across three studies. One study examined the addition of JIT video after prior TES (Todsen et al., 2013), and one study compared JIT practice alone, JIT practice with feedback from this practice, and feedback alone derived from baseline testing (Kroft et al., 2017). JIT and just-in-place physical simulator training did not improve first pass lumbar puncture success, but improved mean number of attempts and process measures such as early stylet removal (Kessler et al., 2015).
IV. DISCUSSION
We sought to provide an updated synthesis on effective instructional design features in simulation in medical education, focusing on those that produce higher level outcomes at Kirkpatrick levels three and above. A prior review searching until 2011 identified only 18 studies that examined outcomes at Kirkpatrick level three and above, out of their pool of 10,297 studies. Our review reveals a notable rise in the number of studies over the past ten years, exploring instructional design and clinical outcomes. In the discussion that follows, we synthesise the findings with existing literature and theory to extract valuable insights for medical educators.
A. Implications for Current Practice
This review underscores the necessity of directing resources towards effective instructional design features, emphasising that these need not be strictly tied to specific simulator types, as advocated by Norman. Despite the ongoing evolution and incorporation of an expanding array of TES modalities, including Virtual Reality (VR) in this review, we observed mixed results concerning simulation modality as an instructional design variation. Upon closer examination of interventions outlined in studies comparing simulation modalities, it becomes evident that confounding factors may arise due to variations in the application of training to proficiency criteria (a characteristic of mastery learning) or differences in the quality of measurement.
In the study conducted by Gomez et al (2015), training to proficiency criteria was incorporated in study arms demonstrating benefit (VR and VR plus physical simulator) and not incorporated in the remaining arm (physical simulator alone). Similarly, in the study by Orzech et al (2012) where training until proficiency criteria were reached was a shared feature of both arms, no significant difference between groups was observed. It remains unclear whether observed differences were attributable to the application of training until proficiency criteria were met or to the varied simulation modalities.
Chunharas et al (2013) and Patel et al (2012) also noted outcome differences when comparing different simulation modalities. However, the robustness of these findings is constrained using a checklist observation scale developed for individual studies with minimal validity evidence. Clinical and task variations, recognised as beneficial in prior reviews (Zendejas et al., 2013), may elucidate the advantages identified by Chunharas et al and the VR plus physical simulator arm in the study by Gomez et al.
Components of mastery learning appear mostly effective, although isolated implementation of a component without the whole may erode effectiveness. The inconsistent evidence for effectiveness of components of mastery learning in this review is surprising, given prior evidence for the effectiveness of mastery learning for translational outcomes (Griswold-Theodorson et al., 2015). The difference may lie in piecemeal rather than holistic implementation of mastery learning as a complex intervention, with seven complementary components working together (McGaghie, 2015).
Another difference is that our review only included studies comparing different TES interventions, while the review by Griswold-Theodorson et al included studies that compared mastery learning with a wider range of comparators, including no TES. Notably, a separate systematic review and meta-analysis of mastery learning found only three studies from 1984-2010 comparing mastery learning to other TES interventions for patient outcomes, with no statistically significant benefit overall and substantial heterogeneity (Cook, Brydges, et al., 2013).
Methodological issues may be another contributory factor. Naples et al (2022) postulate in their study the reasons for the lack of observed difference, including a long duration between intervention and outcome assessment, which was longer in the intervention group than the control group, biasing towards the null, and surprisingly high baseline performance with an insufficiently sensitive rater observation tool. This study had only nine participants, limiting statistical power. These represent important methodological considerations for researchers designing educational intervention studies.
The effectiveness of increased time spent in simulation training is associated with incorporation of learning conversations. Discrepancies in outcomes between the two studies assessing the impact of time spent in simulation training may be attributed to the presence of debriefing in the study conducted by Schaffer et al (2021), as opposed to un-coached practice without feedback in the study by Liao et al (2013). It is crucial to note that the advantages derived from extended training periods are not solely attributed to prolonged duration but are also influenced by the integration of learning conversations. These conversations encompass both debriefing and feedback (Tavares et al., 2020), both of which have demonstrated efficacy, as supported by existing research (Cheng et al., 2014; Hattie & Timperley, 2007).
In a systematic review by Hatala and colleagues (Hatala et al., 2014), feedback emerged as moderately effective for procedural skills simulation training. Notably, feedback from multiple sources, including instructors, proved more effective than feedback from a single source.
Distributed practice is preferred over blocked practice for TES. Frequent brief simulation (Mduma et al., 2015) essentially describes distributed rather than blocked practice. The increased effectiveness seen with distributed practice here is consistent with existing literature within (Cecilio-Fernandes et al., 2023) and outside (Dunlosky et al., 2013) of health professions education.
Dyad training is notable for being efficient with similar or better outcomes, and is consistent with existing literature on motor skills learning (Wulf et al., 2010). The optimal group size has not been clearly determined, beyond single versus dyad, and would be a productive avenue of inquiry for evidence-based determination of learner to faculty ratios, accounting for contextual factors such as task complexity and stage of learner’s development.
In situ simulation may be beneficial in generating participant insights that feed into systems-based improvements through quality improvement mechanisms (Calhoun et al., 2024; Nickson et al., 2021). This combines multiple mechanisms by which TES can produce meaningful impact: through changing individual learner behaviour and changing systems processes.
Error management training appears beneficial for transfer outcomes in novices. This is congruent with literature outside of medical education (Keith & Frese, 2008). The limited evidence base within medical education makes this ripe for further study across task and learner types.
In summary, the features mentioned above are predominantly drawn from previous studies, primarily conducted at Kirkpatrick level two. This review contributes by offering an updated synthesis of evidence, outlining the extent to which this evidence can be extrapolated to higher Kirkpatrick levels, and highlighting features that were previously unexplored at clinical process and outcome levels. Collectively, evidence spanning these levels serves as a guide for those designing TES with the goal of achieving educational and clinical impact.
B. Limitations and Implications for Future Research
Studies that examine Kirkpatrick levels three and above continue to constitute a relatively small fraction of the overall research landscape. Furthermore, this limited body of research is dispersed among various instructional design features, with only a small number of studies investigating each specific feature. Consequently, drawing definitive conclusions about effectiveness becomes challenging, representing a primary constraint of this review. Despite these limitations, we have tried to extract valuable insights for health professions educators by synthesising the findings with existing literature and theory.
The limited evidence bases for most individual instructional design features, especially those demonstrating benefits at Kirkpatrick levels three and four, limits the strength of conclusions that can be drawn about their effectiveness. Further studies replicating these results would strengthen the argument that a particular instructional design feature is able to achieve clinical impact. The evidence base is also limited in the variety of task and learner contexts studied for each individual instructional design feature. Determining the generalisability of these findings requires further research applying these features across diverse TES contexts with different skills and learner groups. Future research should also continue to explore novel and promising instructional design features, such as hybrid simulations where mannequins are overlayed with animal tissue or gel-based phantoms (Balakrishnan et al., 2025).
V. CONCLUSION
There is limited evidence for instructional design features in TES that translate to improved clinical outcomes. Within these limits, error management training, distributed practice, dyad training, and in situ training appear beneficial. Given the limited evidence base for these individual features, definitive determination of effectiveness and generalisability requires further research applying promising target features across different task and learner contexts.
Notes on Contributors
Matthew Low is an emergency physician at National University Hospital, Singapore, and adjunct assistant professor at the Yong Loo Lin School of Medicine, National University of Singapore.
Jillian Yeo is a medical educationalist at the Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore.
Dujeepa Samarasekera is senior director at the Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore.
Gene Chan is an emergency physician at National University Hospital, Singapore, and adjunct assistant professor at the Yong Loo Lin School of Medicine, National University of Singapore.
Shuh Shing Lee is a medical educationalist at the Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore.
Matthew Low, Jillian Yeo and Shuh Shing Lee conceived of the work, collected and analysed data, and drafted the work. Gene Chan and Dujeepa Samarasekera conceived of the work and reviewed it critically for important intellectual content. All contributors gave final approval of the version to be published and are agreeable to be accountable for all aspects of the work.
Ethical Approval
Ethical approval was not applicable as this is a review paper.
Funding
There was no funding for this paper.
Declaration of Interest
The authors report no conflicts of interest.
References
Balakrishnan, A., Law, L. S.-C., Areti, A., Burckett-St Laurent, D., Zuercher, R. O., Chin, K.-J., & Ramlogan, R. (2025). Educational outcomes of simulation-based training in regional anaesthesia: A scoping review. British Journal of Anaesthesia, 134(2), 523–534. https://doi.org/10.1016/j.bja.2024.07.037
Calhoun, A. W., Cook, D. A., Genova, G., Motamedi, S. M. K., Waseem, M., Carey, R., Hanson, A., Chan, J. C. K., Camacho, C., Harwayne-Gidansky, I., Walsh, B., White, M., Geis, G., Monachino, A. M., Maa, T., Posner, G., Li, D. L., & Lin, Y. (2024). Educational and patient care impacts of in situ simulation in healthcare: A systematic review. Simulation in Healthcare, 19(1S), S23–S31. https://doi.org/10.1097/SIH.0000000000000773
Carraccio, C., Englander, R., Van Melle, E., Ten Cate, O., Lockyer, J., Chan, M.-K., Frank, J. R., Snell, L. S., & International Competency-Based Medical Education Collaborators. (2016). Advancing competency-based medical education: A charter for clinician-educators. Academic Medicine, 91(5), 645–649. https://doi.org/10.1097/ACM.0000000000001048
Cecilio-Fernandes, D., Patel, R., & Sandars, J. (2023). Using insights from cognitive science for the teaching of clinical skills: AMEE Guide No. 155. Medical Teacher, 45(11), 1214–1223. https://doi.org/10.1080/0142159X.2023.2168528
Cheng, A., Eppich, W., Grant, V., Sherbino, J., Zendejas, B., & Cook, D. A. (2014). Debriefing for technology-enhanced simulation: A systematic review and meta-analysis. Medical Education, 48(7), 657–666. https://doi.org/10.1111/medu.12432
Chunharas, A., Hetrakul, P., Boonyobol, R., Udomkitti, T., Tassanapitikul, T., & Wattanasirichaigoon, D. (2013). Medical students themselves as surrogate patients increased satisfaction, confidence, and performance in practicing injection skill. Medical Teacher, 35(4), 308–313. https://doi.org/10.3109/0142159X.2012.746453
Cook, D. A., Brydges, R., Zendejas, B., Hamstra, S. J., & Hatala, R. (2013). Mastery learning for health professionals using technology-enhanced simulation: A systematic review and meta-analysis. Academic Medicine, 88(8), 1178–1186. https://doi.org/10.1097/ACM.0b013e31829a365d
Cook, D. A., Hamstra, S. J., Brydges, R., Zendejas, B., Szostek, J. H., Wang, A. T., Erwin, P. J., & Hatala, R. (2013). Comparative effectiveness of instructional design features in simulation-based education: Systematic review and meta-analysis. Medical Teacher, 35(1), e867-898. https://doi.org/10.3109/0142159X.2012.714886
Cook, D. A., Hatala, R., Brydges, R., Zendejas, B., Szostek, J. H., Wang, A. T., Erwin, P. J., & Hamstra, S. J. (2011). Technology-enhanced simulation for health professions education: A systematic review and meta-analysis. JAMA, 306(9), 978–988. https://doi.org/10.1001/jama.2011.1234
Cook, D. A., & West, C. P. (2013). Perspective: Reconsidering the focus on “outcomes research” in medical education: A cautionary note. Academic Medicine, 88(2), 162–167. https://doi.org/10.1097/ACM.0b013e31827c3d78
Daly, M. K., Gonzalez, E., Siracuse-Lee, D., & Legutko, P. A. (2013). Efficacy of surgical simulator training versus traditional wet-lab training on operating room performance of ophthalmology residents during the capsulorhexis in cataract surgery. Journal of Cataract and Refractive Surgery, 39(11), 1734–1741. https://doi.org/10.1016/j.jcrs.2013.05.044
Dauphinee, W. D. (2012). Educators must consider patient outcomes when assessing the impact of clinical training. Medical Education, 46(1), 13–20. https://doi.org/10.1111/j.1365-2923.2011.04144.x
de Melo, B. C. P., Rodrigues Falbo, A., Sorensen, J. L., van Merriënboer, J. J. G., & van der Vleuten, C. (2018). Self-perceived long-term transfer of learning after postpartum haemorrhage simulation training. International Journal of Gynaecology and Obstetrics, 141(2), 261–267. https://doi.org/10.1002/ijgo.12442
De Win, G., Van Bruwaene, S., Kulkarni, J., Van Calster, B., Aggarwal, R., Allen, C., Lissens, A., De Ridder, D., & Miserez, M. (2016). An evidence-based laparoscopic simulation curriculum shortens the clinical learning curve and reduces surgical adverse events. Advances in Medical Education and Practice, 7, 357–370. https://doi.org/10.2147/AMEP.S102000
DeStephano, C. C., Chou, B., Patel, S., Slattery, R., & Hueppchen, N. (2015). A randomized controlled trial of birth simulation for medical students. American Journal of Obstetrics and Gynaecology, 213(1), 91.e1-91.e7. https://doi.org/10.1016/j.ajog.2015.03.024
Dunlosky, J., Rawson, K. A., Marsh, E. J., Nathan, M. J., & Willingham, D. T. (2013). Improving students’ learning with effective learning techniques: Promising directions from cognitive and educational psychology. Psychological Science in the Public Interest, 14(1), 4–58. https://doi.org/10.1177/1529100612453266
Dyre, L., Tabor, A., Ringsted, C., & Tolsgaard, M. G. (2017). Imperfect practice makes perfect: Error management training improves transfer of learning. Medical Education, 51(2), 196–206. https://doi.org/10.1111/medu.13208
Egenberg, S., Karlsen, B., Massay, D., Kimaro, H., & Bru, L. E. (2017). “No patient should die of PPH just for the lack of training!” Experiences from multi-professional simulation training on postpartum haemorrhage in northern Tanzania: A qualitative study. BMC Medical Education, 17(1), 119. https://doi.org/10.1186/s12909-017-0957-5
El Hussein, M. T., & Cuncannon, A. (2022). Nursing students’ transfer of learning from simulated clinical experiences into clinical practice: A scoping review. Nurse Education Today, 116, 105449. https://doi.org/10.1016/j.nedt.2022.105449
Ferrari, R. (2015). Writing narrative style literature reviews. Medical Writing, 24(4), 230–235. https://doi.org/10.1179/2047480615Z.000000000329
Frerejean, J., van Merriënboer, J. J. G., Condron, C., Strauch, U., & Eppich, W. (2023). Critical design choices in healthcare simulation education: A 4C/ID perspective on design that leads to transfer. Advances in Simulation (London, England), 8(1), 5. https://doi.org/10.1186/s41077-023-00242-7
Gomez, P. P., Willis, R. E., & Van Sickle, K. (2015). Evaluation of two flexible colonoscopy simulators and transfer of skills into clinical practice. Journal of Surgical Education, 72(2), 220–227. https://doi.org/10.1016/j.jsurg.2014.08.010
Griswold-Theodorson, S., Ponnuru, S., Dong, C., Szyld, D., Reed, T., & McGaghie, W. C. (2015). Beyond the simulation laboratory: A realist synthesis review of clinical outcomes of simulation-based mastery learning. Academic Medicine, 90(11), 1553–1560. https://doi.org/10.1097/ACM.0000000000000938
Grover, S. C., Scaffidi, M. A., Khan, R., Garg, A., Al-Mazroui, A., Alomani, T., Yu, J. J., Plener, I. S., Al-Awamy, M., Yong, E. L., Cino, M., Ravindran, N. C., Zasowski, M., Grantcharov, T. P., & Walsh, C. M. (2017). Progressive learning in endoscopy simulation training improves clinical performance: A blinded randomized trial. Gastrointestinal Endoscopy, 86(5), 881–889. https://doi.org/10.1016/j.gie.2017.03.1529
Hatala, R., Cook, D. A., Zendejas, B., Hamstra, S. J., & Brydges, R. (2014). Feedback for simulation-based procedural skills training: A meta-analysis and critical narrative synthesis. Advances in Health Sciences Education, 19(2), 251–272. https://doi.org/10.1007/s10459-013-9462-8
Hattie, J., & Timperley, H. (2007). The power of feedback. Review of Educational Research, 77(1), 81–112. https://doi.org/10.3102/003465430298487
Hernández-Irizarry, R., Zendejas, B., Ali, S. M., & Farley, D. R. (2016). Optimizing training cost-effectiveness of simulation-based laparoscopic inguinal hernia repairs. American Journal of Surgery, 211(2), 326–335. https://doi.org/10.1016/j.amjsurg.2015.07.027
Issenberg, S. B., McGaghie, W. C., Petrusa, E. R., Lee Gordon, D., & Scalese, R. J. (2005). Features and uses of high-fidelity medical simulations that lead to effective learning: A BEME systematic review. Medical Teacher, 27(1), 10–28. https://doi.org/10.1080/01421590500046924
Jackson, M., McTier, L., Brooks, L. A., & Wynne, R. (2022). The impact of design elements on undergraduate nursing students’ educational outcomes in simulation education: Protocol for a systematic review. Systematic Reviews, 11(1), 52. https://doi.org/10.1186/s13643-022-01926-3
Keith, N., & Frese, M. (2008). Effectiveness of error management training: A meta-analysis. Journal of Applied Psychology, 93(1), 59–69. https://doi.org/10.1037/0021-9010.93.1.59
Kessler, D., Pusic, M., Chang, T. P., Fein, D. M., Grossman, D., Mehta, R., White, M., Jang, J., Whitfill, T., Auerbach, M., & INSPIRE LP investigators. (2015). Impact of just-in-time and just-in-place simulation on intern success with infant lumbar puncture. Pediatrics, 135(5), e1237-1246. https://doi.org/10.1542/peds.2014 -1911
Kirkpatrick, D., & Kirkpatrick, J. (2006). Evaluating training programs: The four levels. Berrett-Koehler Publishers.
Kroft, J., Ordon, M., Po, L., Zwingerman, N., Waters, K., Lee, J. Y., & Pittini, R. (2017). Preoperative practice paired with instructor feedback may not improve obstetrics-gynaecology residents’ operative performance. Journal of Graduate Medical Education, 9(2), 190–194. https://doi.org/10.4300/JGME-D-16-00238.1
Lal, B. K., Cambria, R., Moore, W., Mayorga-Carlin, M., Shutze, W., Stout, C. L., Broussard, H., Garrett, H. E., Nelson, W., Titus, J. M., Macdonald, S., Lake, R., & Sorkin, J. D. (2022). Evaluating the optimal training paradigm for transcarotid artery revascularization based on worldwide experience. Journal of Vascular Surgery, 75(2), 581-589.e1. https://doi.org/10.1016/j.jvs.2021.08.085
Liao, W.-C., Leung, J. W., Wang, H.-P., Chang, W.-H., Chu, C.-H., Lin, J.-T., Wilson, R. E., Lim, B. S., & Leung, F. W. (2013). Coached practice using ERCP mechanical simulator improves trainees’ ERCP performance: A randomized controlled trial. Endoscopy, 45(10), 799–805. https://doi.org/10.1055/s-0033-1344224
Lin, Y., Cheng, A., Hecker, K., Grant, V., & Currie, G. R. (2018). Implementing economic evaluation in simulation-based medical education: Challenges and opportunities. Medical Education, 52(2), 150–160. https://doi.org/10.1111/medu.13411
Mankute, A., Juozapaviciene, L., Stucinskas, J., Dambrauskas, Z., Dobozinskas, P., Sinz, E., Rodgers, D. L., Giedraitis, M., & Vaitkaitis, D. (2022). A novel algorithm-driven hybrid simulation learning method to improve acquisition of endotracheal intubation skills: A randomized controlled study. BMC Anaesthesiology, 22(1), 42. https://doi.org/10.1186/s12871-021-01557-6
McGaghie, W. C. (2015). Mastery learning: It is time for medical education to join the 21st century. Academic Medicine, 90(11), 1438–1441. https://doi.org/10.1097/ACM.0000000000000911
McGaghie, W. C., Issenberg, S. B., Cohen, E. R., Barsuk, J. H., & Wayne, D. B. (2011). Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Academic Medicine, 86(6), 706–711. https://doi.org/10.1097/ACM.0b013e318217e119
Mduma, E., Ersdal, H., Svensen, E., Kidanto, H., Auestad, B., & Perlman, J. (2015). Frequent brief on-site simulation training and reduction in 24-h neonatal mortality—An educational intervention study. Resuscitation, 93, 1–7. https://doi.org/10.1016/j.resuscitation.2015.04.019
Naples, R., French, J. C., Han, A. Y., Lipman, J. M., & Awad, M. M. (2022). The impact of simulation training on operative performance in general surgery: Lessons learned from a prospective randomized trial. Journal of Surgical Research, 270, 513–521. https://doi.org/10.1016/j.jss.2021.10.003
Nestel, D., Groom, J., Eikeland-Husebø, S., & O’Donnell, J. M. (2011). Simulation for learning and teaching procedural skills: The state of the science. Simulation in Healthcare, 6 Suppl, S10-13. https://doi.org/10.1097/SIH.0b013e318227ce96
Nickson, C. P., Petrosoniak, A., Barwick, S., & Brazil, V. (2021). Translational simulation: From description to action. Advances in Simulation (London, England), 6(1), 6. https://doi.org/10.1186/s41077-021-00160-6
Nilsson, C., Sorensen, J. L., Konge, L., Westen, M., Stadeager, M., Ottesen, B., & Bjerrum, F. (2017). Simulation-based camera navigation training in laparoscopy—A randomized trial. Surgical Endoscopy, 31(5), 2131–2139. https://doi.org/10.1007/s00464-016-5210-5
Orzech, N., Palter, V. N., Reznick, R. K., Aggarwal, R., & Grantcharov, T. P. (2012). A comparison of 2 ex vivo training curricula for advanced laparoscopic skills: A randomized controlled trial. Annals of Surgery, 255(5), 833–839. https://doi.org/10.1097/SLA.0b013e31824aca09
O’Sullivan, O., Iohom, G., O’Donnell, B. D., & Shorten, G. D. (2014). The effect of simulation-based training on initial performance of ultrasound-guided axillary brachial plexus blockade in a clinical setting—A pilot study. BMC Anaesthesiology, 14, 110. https://doi.org/10.1186/1471-2253-14-110
Patel, V., Aggarwal, R., Osinibi, E., Taylor, D., Arora, S., & Darzi, A. (2012). Operating room introduction for the novice. American Journal of Surgery, 203(2), 266–275. https://doi.org/10.1016/j.amjsurg.2011.03.003
Schaefer, J. J., Vanderbilt, A. A., Cason, C. L., Bauman, E. B., Glavin, R. J., Lee, F. W., & Navedo, D. D. (2011). Literature review: Instructional design and pedagogy science in healthcare simulation. Simulation in Healthcare, 6 Suppl, S30-41. https://doi.org/10.1097/SIH.0b013e31822237b4
Schaffer, A. C., Babayan, A., Einbinder, J. S., Sato, L., & Gardner, R. (2021). Association of simulation training with rates of medical malpractice claims among obstetrician-gynaecologists. Obstetrics and Gynaecology, 138(2), 246–252. https://doi.org/10.1097/AOG.0000000000004464
Sharara-Chami, R., Taher, S., Kaddoum, R., Tamim, H., & Charafeddine, L. (2014). Simulation training in endotracheal intubation in a paediatric residency. Middle East Journal of Anaesthesiology, 22(5), 477–485.
Shore, E. M., Grantcharov, T. P., Husslein, H., Shirreff, L., Dedy, N. J., McDermott, C. D., & Lefebvre, G. G. (2016). Validating a standardized laparoscopy curriculum for gynaecology residents: A randomized controlled trial. American Journal of Obstetrics and Gynaecology, 215(2), 204.e1-204.e11. https://doi.org/10.1016/j.ajog.2016.04.037
Sørensen, J. L., Navne, L. E., Martin, H. M., Ottesen, B., Albrecthsen, C. K., Pedersen, B. W., Kjærgaard, H., & van der Vleuten, C. (2015). Clarifying the learning experiences of healthcare professionals with in situ and off-site simulation-based medical education: A qualitative study. BMJ Open, 5(10), e008345. https://doi.org/10.1136/bmjopen-2015-008345
Srinivasan, K. K., Gallagher, A., O’Brien, N., Sudir, V., Barrett, N., O’Connor, R., Holt, F., Lee, P., O’Donnell, B., & Shorten, G. (2018). Proficiency-based progression training: An “end to end” model for decreasing error applied to achievement of effective epidural analgesia during labour: A randomised control study. BMJ Open, 8(10), e020099. https://doi.org/10.1136/bmjopen-2017-020099
Steinert, Y., Mann, K., Centeno, A., Dolmans, D., Spencer, J., Gelula, M., & Prideaux, D. (2006). A systematic review of faculty development initiatives designed to improve teaching effectiveness in medical education: BEME Guide No. 8. Medical Teacher, 28(6), 497–526. https://doi.org/10.1080/01421590600902976
Tan, T. X., Buchanan, P., & Quattromani, E. (2018). Teaching residents chest tubes: Simulation task trainer or cadaver model? Emergency Medicine International, 2018, 9179042. https://doi.org/10.1155/2018/9179042
Tavares, W., Eppich, W., Cheng, A., Miller, S., Teunissen, P. W., Watling, C. J., & Sargeant, J. (2020). Learning conversations: An analysis of the theoretical roots and their manifestations of feedback and debriefing in medical education. Academic Medicine, 95(7), 1020–1025. https://doi.org/10.1097/ACM.0000000000002932
Tchorz, J. P., Brandl, M., Ganter, P. A., Karygianni, L., Polydorou, O., Vach, K., Hellwig, E., & Altenburger, M. J. (2015). Pre-clinical endodontic training with artificial instead of extracted human teeth: Does the type of exercise have an influence on clinical endodontic outcomes? International Endodontic Journal, 48(9), 888–893. https://doi.org/10.1111/iej.12385
Todsen, T., Henriksen, M. V., Kromann, C. B., Konge, L., Eldrup, J., & Ringsted, C. (2013). Short- and long-term transfer of urethral catheterization skills from simulation training to performance on patients. BMC Medical Education, 13, 29. https://doi.org/10.1186/1472-6920-13-29
Tolsgaard, M. G., Madsen, M. E., Ringsted, C., Oxlund, B. S., Oldenburg, A., Sorensen, J. L., Ottesen, B., & Tabor, A. (2015). The effect of dyad versus individual simulation-based ultrasound training on skills transfer. Medical Education, 49(3), 286–295. https://doi.org/10.1111/medu.12624
Walsh, C. M., Scaffidi, M. A., Khan, R., Arora, A., Gimpaya, N., Lin, P., Satchwell, J., Al-Mazroui, A., Zarghom, O., Sharma, S., Kamani, A., Genis, S., Kalaichandran, R., & Grover, S. C. (2020). Non-technical skills curriculum incorporating simulation-based training improves performance in colonoscopy among novice endoscopists: Randomized controlled trial. Digestive Endoscopy, 32(6), 940–948. https://doi.org/10.1111/den.13623
Wulf, G., Shea, C., & Lewthwaite, R. (2010). Motor skill learning and performance: A review of influential factors. Medical Education, 44(1), 75–84. https://doi.org/10.1111/j.1365-2923.2009.03421.x
Zendejas, B., Brydges, R., Wang, A. T., & Cook, D. A. (2013). Patient outcomes in simulation-based medical education: A systematic review. Journal of General Internal Medicine, 28(8), 1078–1089. https://doi.org/10.1007/s11606-012-2264-5
*Matthew Low
Emergency Medicine Department,
National University Hospital
9 Lower Kent Ridge Road, Level 4,
Singapore 119085
Email: mlow@nus.edu.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
