
Key takeaways from the Asia Pacific Medical Education Conference (APMEC) 2025
Submitted: 13 March 2025
Accepted: 18 March 2025
Published online: 1 April, TAPS 2025, 10(2), 1-3
https://doi.org/10.29060/TAPS.2025-10-2/GP3694
Shuh Shing Lee, Jillian Han Ting Yeo & Dujeepa D Samarasekera
Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: The Asia Pacific Medical Education Conference (APMEC) 2025 focused on evolving medical education amidst global transformations. The theme, “Developing a Holistic Healthcare Practitioner for a Sustainable Future,” emphasised integrating sustainability, inclusivity, and advanced technologies like AI into healthcare education.
Methods: APMEC 2025 featured a comprehensive program including 29 workshops, 1 special course, 2 keynote speeches, 6 plenary sessions, 19 symposia, and 3 panel discussions, with 84 free communications and 107 short communications presented. The conference facilitated dialogues on innovative curriculum design, sustainability in healthcare education, AI integration, and interprofessional education.
Results: Key discussions emphasised incorporating “Possibility Thinking” and student-centered learning, embedding planetary health in curricula, and integrating AI while preserving essential human skills like empathy. The NUS Common Curriculum for Healthcare Professional Education demonstrated significant improvements in empathy and teamwork. The conference highlighted the importance of faculty development and inclusivity, particularly concerning disability in medical education.
Conclusion: APMEC 2025 demonstrated a commitment to transforming medical education through collaboration and innovation. By aligning educational practices with global trends and regional needs, APMEC serves as a catalyst for comprehensive curriculum reforms. Ongoing efforts are needed to translate these insights into actionable strategies, ensuring future healthcare professionals are well-prepared to address dynamic global challenges.
Practice Highlights
- Student involvement in curriculum planning is essential to enhance student-centered learning and competency-based education.
- AI’s role in augmenting healthcare education while ensuring the retention of essential human skills.
- Incorporating planetary health concepts into medical curricula to prepare healthcare professionals for environmentally responsible practice.
- Implementing structured models like NUS’s Common Curriculum to improve empathy and teamwork in healthcare training.
- Enhancing teaching quality and leadership through structured faculty training programs, crucial for sustained educational improvements.
I. INTRODUCTION
The APMEC conference was held this year from January 13th (Monday) to 18th (Saturday) at Yong Loo Lin School of Medicine, National University of Singapore. Medical education is in the midst of a global transformation, influenced by technological advancements, new pedagogical techniques, and a focus on sustainability and inclusivity. The Asia Pacific Medical Education Conference (APMEC) serves as a crucial platform for medical educators, researchers, and policymakers to discuss and shape the future of healthcare education. This year’s theme, “Developing a Holistic Healthcare Practitioner for a Sustainable Future – Trends ● Issues ● Priorities ● Strategies,” highlights the alignment of medical education with sustainable practices, innovative learning, and inclusive policies. The conference featured 29 workshops, 1 special course, 2 keynotes, 6 plenary sessions, 19 symposia, 3 panel discussions, 84 free communications, and 107 short communications, providing a comprehensive platform for exchange and learning.
II. LEARNINGS FROM VARIOUS SESSIONS
The concept of “Possibility Thinking” advocating for a shift beyond disease-focused approaches toward holistic healthcare strategies was shared in Plenary 1 by Professor Ronald Harden. Prof Harden emphasised the need for student engagement in curriculum planning, fostering a more integrated and participatory learning experience. This aligns with global calls for student-centered learning, competency-based education, and the co-creation of curricula with learners. In line with this year’s theme, symposiums explored how to embed sustainability in medical education. Climate change is affecting global health, making sustainability a key focus in health professions education worldwide.
In the opening keynote, Prof Yang Faridah shared practical approaches for resource-poor countries. She gave examples from Malaysia, showing how medical schools are integrating planetary health into their curricula. This prepares future healthcare professionals for environmentally responsible practice. The use of artificial intelligence (AI) is reshaping health professions education. It enhances decision-making, improves efficiency, and boosts diagnostic accuracy. However, panellists stressed the irreplaceable value of human skills like empathy, communication, and ethical judgment. The discussion highlighted a global shift towards integrating AI in healthcare education while ensuring technology complements, not replaces, the human touch. Another key aspect discussed at the conference was how best to restore engagement and joy in learning by revitalising medical. Several sessions focused on applying practical strategies to boost engagement and create supportive learning environments. Key discussions covered creative learning approaches that use playfulness to improve concept retention. Panellists highlighted the importance of teamwork in reducing loneliness and enhancing performance. They also stressed the need for inclusive, psychologically safe spaces that nurture enthusiasm for medical education. The speakers also emphasised mentorship and peer support as critical factors in reducing burnout and increasing overall satisfaction. Participants explored strategies to encourage work-life balance, recognising the importance of self-care and having hobbies outside medicine. Addressing burnout triggers and implementing sustainable changes within medical education institutions were highlighted as necessary steps to prioritise joy and well-being alongside academic excellence.
Interprofessional education (IPE) is gaining global recognition as a key strategy to break down professional silos and prepare healthcare graduates for integrated, patient-centred care. In the opening ceremony speech, the Dean of the Yong Loo Lin School of Medicine, National University of Singapore, Prof Chong Yap Seng, introduced NUS’s Common Curriculum for Healthcare Professional Education, launched in 2023. This structured approach to IPE aims to enhance collaboration. Early evaluations of the program show improvements in empathy, teamwork, and collaborative practice.
Inclusivity, particularly support for students with disabilities in medical and health professions education, was a key focus at APMEC this year. The updated Canadian technical standards were shared by Professor Cheryl Holmes from University of British Columbia defining core competencies based on functional abilities. These standards were developed through collaboration with a diverse group, including learners and physicians with disabilities. This initiative sets a precedent for regional collaboration. It encourages other countries to update educational standards to promote equity, support students with physical challenges, and improve the quality and accessibility of medical education.
Amid these evolving trends, faculty development remains a cornerstone of advancing medical education. Stories shared during the faculty development session illustrated how structured programs empower educators to drive change at institutional, national, and regional levels. Investments in faculty training are critical in ensuring sustained improvements in teaching quality and leadership in health professions education. By exposing participants to global best practices, it encourages the adoption of innovative teaching strategies. These approaches are tailored to address specific regional challenges and opportunities, enhancing the overall quality of medical and health professions education.
III. GLOBAL TRENDS AND IMPACT IN THE ASIA PACIFIC REGION AND BEYOND
The themes discussed at APMEC align with several global trends shaping the future of medical education. One key shift is the growing adoption of competency-based medical education (CBME), which is gradually replacing traditional time-based models. CBME prioritises the acquisition of practical skills and the application of knowledge in real-world settings, ensuring that graduates are better prepared for clinical practice.
Technological advancements are also playing a transformative role. Artificial intelligence (AI), virtual reality (VR), and simulation-based training are becoming more accessible, revolutionising the way medical students learn. These innovations enhance diagnostic accuracy, refine clinical decision-making, and provide immersive, hands-on learning experiences in a risk-free environment.
At the same time, sustainability in healthcare education is gaining momentum. With increasing awareness of environmental challenges, medical schools are integrating planetary health concepts into their curricula. This ensures that future healthcare professionals are equipped to adopt sustainable practices and address the impact of climate change on global health.
These evolving trends reflect a broader movement towards a more adaptive, technology-driven, and socially responsible approach to training the next generation of healthcare practitioners. Another key area of discussion was student and faculty well-being. There is a growing focus on addressing mental health challenges and reducing burnout in medical training. Faculty well-being is especially crucial, as educators play a vital role in shaping future healthcare professionals. Supporting their mental and emotional health ensures they can provide high-quality education while maintaining their own resilience and job satisfaction.
IV. CONCLUSION
APMEC continues to align global trends with regional needs, acting as a hub for advancing medical education. It drives transformation by offering a platform for knowledge exchange, enabling collaboration among educators and policymakers. The conference strengthens connections between institutions across the Asia-Pacific region, promoting shared learning and research. As participants return to their institutions, the focus must shift to translating insights into concrete actions that improve medical and health professions education. Through collaboration, innovation, and inclusivity, APMEC ensures that future healthcare professionals are prepared to tackle the evolving challenges of a dynamic world.
Notes on Contributors
LSS contributes to the conception of the work. LSS, JHTY and DDS drafts the work and revising it, approves the final version to be published, and agrees to be accountable for all aspects of the work.
Acknowledgement
We extend our gratitude to all participants, speakers, and organisers of APMEC for their invaluable contributions to advancing medical education.
Funding
There is no funding for this paper.
Declaration of Interest
The author declared no conflict of interests.
*Lee Shuh Shing
10 Medical Drive,
Singapore 117597
66013452
Email: medlss@nus.edu.sg
Submitted: 18 May 2024
Accepted: 25 November 2024
Published online: 1 April, TAPS 2025, 10(2), 4-7
https://doi.org/10.29060/TAPS.2025-10-2/GP3347
Juliet Mathew1, Hazlina Binti Abu Bakar2 & Shilpa Murthy2
1Clinical Skills & Simulation Centre and School of Medicine, IMU University, Malaysia; 2Department of Clinical Skills and School of Medicine, IMU University, Malaysia
Abstract
Introduction: Medical students are known to have a higher prevalence of psychological distress although they begin medical school with better mental health than their peers. Depression and burnout rates are high among them and many of these students do not seek help due to the associated stigma linked with mental health concerns. At present, there are several known resilience-enhancing modules incorporated within the curriculum to improve students coping skills, however, there are no known modules yet that introduce this concept within the early medical curriculum, especially within the pre-clinical years.
Methods: IMU University introduces a Resilience Workshop within early pre-clinical years to appropriately engage students to recognise and address common challenges. This can be tackled by understanding the various coping mechanisms that can be adopted. This workshop describes four main areas: introduction to resilience, interactive activities, discussions, and reflection platforms. This initiative aligns with the university’s curriculum focus on person-centred care, emphasising personalised care as a priority.
Results: Preliminary results suggest that the Resilience Workshop can aid in developing suggested and self-regulated interventions to manage adversities faced by medical students. Attention to individual students’ coping reservoirs can help promote well-being and minimise burnout. Formal and informal offerings within medical schools can help fill the reservoir.
Conclusion: This article provides a perspective on fostering resilience building within the early medical curriculum to cultivate core strengths among medical students for managing adversities.
Practice Highlights
- Psychological distress is prevalent among medical students.
- Challenges occur in medical students seeking help.
- Resilience strength is vital to medical students to recognise and address common challenges.
- A gap exists in the curriculum to improve medical students’ coping skills in the early years.
- Fostering resilience in early medical curricula can cultivate core strengths among medical students for managing adversities.
I. INTRODUCTION
IMU University’s Resilience Workshop was designed and implemented within the medical curriculum in pre-clinical years to develop students’ core inner strengths to their possible highest growth. This is so that they are fully equipped and ready to meet the challenges of competent care delivery to patients. In line with IMU University’s revised medical curriculum’s direction which focuses on the philosophy of person-centred care with humanistic values, this workshop emphasises self-care as a priority before embarking on to selfless care of patients.
In this revised curriculum, much emphasis is placed on the development of skills, behaviours, and attitudes within the delivery of care to patients, encompassing the basic concepts of human interaction, patient safety, quality improvement, and systems thinking; while enhancing the skills of teamwork, effective communication, leadership, negotiation, and cooperation.
The aim has been to best prepare our graduates to practice within the needs of the health profession in the 21st century. This includes equipping them in communication, clinical, cultural, interpersonal, research, and system thinking competencies. These prepare our students to be ready for any advanced clinical training within local or international institutions.
The curriculum’s goal is also to produce graduates who are person-centred and with humanistic values, with professional attributes of being empathetic, compassionate, responsive, and adaptive besides being a transformative leader, lifelong learner, and professionally competent.
Thus, the new curriculum emphasises graduates’ wellness, person-focus services, effective communication, personalised care, multi-disciplinary collaboration & approach, coordinated, continuous & seamless care delivery manner; & application of system thinking and value-based care.
In aligning with this direction and ensuring that our graduates are fit to practice as global doctors with opportunities to practice internationally, the Resilience Workshop engages and guides students in building their own core coping mechanisms while reviewing the principles of determinants of resilience. It is designed to inspire and empower students to be resilient. The postulation is that the students would have retained a substantial knowledge base which constitutes an increasing resource for coping with the diverse challenges they will be exposed to in their medical journey, and for building core resilience strength.
II. METHODS
A. Structured Workshop Flow
The lesson outcomes from this workshop aim at achieving student’s understanding of the importance of adapting well in the face of adversity, threats, or even significant sources of stress, as well as engaging in resilience throughout medical school. With inspiring themes such as “Bend, But Do Not Break” in semester two and “Be Managing Adversities Delightfully (Be MAD)” in semester four, pre-clinical medical students are exposed to challenging scenarios that they may encounter. These scenarios extend beyond their roles as students, to include their relationships with friends, roommates, peers, and more.
The workshop is designed to engage students in four main areas:
Session 1: Introduction to Resilience
Session 2: Activity on Resilience
Session 3: Discussions on Resilience
Session 4: Reflection on Resilience
At the beginning of the workshop, students are provided with The Brief Resilience Scale adapted from Ohio University. It consists of simple and focused scoring scales. It is concise and has good psychometric properties including strong validity and reliability, capturing resilience effectively. Students can score and gauge their resilience levels with easy-to-follow instructions. This allows them to understand their coping strengths, identify their ability to recover from adversities, focus on areas for improvement, and guide them toward improved performances within medical training.
Subsequently, students are introduced to the concept of resilience. They are then led into small group discussions to engage, brainstorm scenarios presented, and grasp levels of coping and managing difficult scenarios that are commonly encountered. They are also given opportunities to share their experiences and discuss possible solutions to the scenarios and their insights. Debriefing includes discussions based on structured questions that could engage students in their thought processes and emotional experiences. It also focuses on their possible courses of action, ideas, or solutions in managing difficult situations within the scenario presented.
B. Reflection Analysis
Students are encouraged to reflect on their experiences and take-home messages from the workshop. They are required to submit a 500-word essay via e-mail, documenting the challenges and strengths that surfaced for them during the session. This must be submitted within a stipulated time frame after the workshop, via e-mail to facilitators for assessment. These reflection essays are reviewed and students with potential mental health concerns are identified. They are then followed personally or referred to their mentors for appropriate support.
III. RESULTS
The scenarios used exposed students to common issues encountered during their early medical training. It encompassed adjustments to the new environment on campus and hostels, adjustments to a new culture of peers, understanding new subjects, meeting professionalism requirements, and addressing unique and individualised adversities.
These scenarios stimulated discussions in the breakout sessions, where standard questions were posed to ignite the development of possible solutions to the simulated adversities faced: (A) How would you handle this situation? (B) What would you do? (C) How would you feel? (D) Explain.
Students were encouraged to narrate their experiences and explore their thoughts and emotions. This helped students realise that there are common issues that are endured by many. Most students reported that the workshop helped them to understand the various coping mechanisms that can be adopted to solve issues that may arise within their journey and progress in medical school. Verbal responses received include:
“I didn’t realise how important managing stress was until I was hit by a personal issue. It affected my studies. This workshop showed me how I can handle stress better…”
“I didn’t want to attend this workshop at first. But the scenarios discussed were mostly what I had endured. I wish I knew these coping strategies earlier…”
IV. DISCUSSION
Students can establish strong foundations in coping strategies, emotional intelligence, and stress management by introducing resilience throughout the preclinical years. The hurdles are mostly theoretical and academic, making it a less demanding environment to begin honing these talents. Students can study the fundamentals of resilience, through such workshops. The basic ideas from the preclinical years could be modified and built upon to deal with the interpersonal, ethical, and emotional difficulties that may arise in their academic obligations and their clinical practice.
The challenges encountered can be described within the following phases:
A. Pre-workshop Challenges
The lack of facilitators with adequate skills in resilience science and mental health advocacy was the main challenge. As mental health issues require more in-depth management, the deliverance of such workshops had to be done by facilitators who are skilled in strong communication skills, empathy, patience, and compassion. The initial perspective was that all faculty would be well-equipped with these skills, however, it became clear post-workshop, that this was not the case. The selection of such facilitators to deliver the context of this workshop in a non-lecturing but inspiring way posed a challenge. The solution is to include training for faculty before the workshop.
B. Workshop Challenges
During the Malaysian Movement Control Order (M.C.O.) when this workshop was first introduced to help students cope, it was delivered online. Hence, the active involvement of students was limited as being on camera had its challenges. Further, many students considered such a workshop to be non-mainstream and non-exam oriented, thus, needing much encouragement to participate fully. The solution is to introduce face-to-face workshops to better engage students.
C. Post-workshop Challenges
Most students who attended the workshop completed and e-mailed the reflection exercises. However, a certain percentage of them failed to do so. This presents a challenge in identifying any student who may have a serious underlying issue with managing adversities resiliently. The solution is to track attendance when delivering assignments.
A possible way to capture all reflections would be to make attendance marked only upon receiving the assignment. As these are medical students in their early years, this approach may not be effective and can lead to non-genuine or robotic responses. While addressing and reinforcing professionalism may be another goal for obtaining reflective essays, it may seem forced. More self-regulating and motivating strategies should hence be developed and applied.
This two-hour workshop is a brief intervention within the time-limited curriculum within semesters two and four. Moving forward, a half-day workshop with more time for interaction with peers and educators could better engage students. A survey could be conducted post-workshop to assess students’ feedback. Providing progression reports of students’ resilience levels could be a more accurate measure of the workshop’s impact. Also, the BRS could be re-used in semester four, to review recovery or the ability to regain equilibrium after adversity.
The students’ submissions of their reflective essays constitute a dataset that can be analysed for further studies in this field, to address and create various aspects of positive interventions within mental health access and stress-relief resources. The aim is, to create better impacts on students’ learning and experience in medical school.
V. CONCLUSION
Above all, we need to understand that resilience is a lifelong ability that cannot be acquired in a single workshop. It needs to be constantly supported through different educational stages, within challenging and stressful circumstances.
Attention to individual students’ coping reservoirs can help promote well-being and minimise burnout. Formal and informal offerings within medical schools can contribute to this effort. Helping students cultivate the skills to sustain their well-being throughout their careers has important payoffs for the overall medical education enterprise.
IMU University’s Resilience Workshop can aid in the development of suggested as well as self-regulated interventions to manage adversities faced by medical students. A formal study is ongoing to substantiate this. Further to this, the development of a student-led multifaceted approach that promotes not only care-taking behaviours but also focuses on institutional and cultural change to empower students to participate in these resiliency strategies can be considered.
This and other models of coping should be empirically validated, for students to not stumble through medical school, but soar.
Notes on Contributors
Dr Juliet Mathew is the first author who designed and wrote this article. Director of the Clinical Skills & Simulation Centre at IMU University, she teaches simulation concepts to pre-clinical students. She confirms sole responsibility for this article’s conception, design, analysis, interpretation of results of context, and manuscript preparation.
Dr Hazlina Binti Abu Bakar supervised the conception of this project and contributed to the critical review of the manuscript. She is a lecturer teaching clinical skills and simulation concepts at the School of Medicine University, IMU University. She also holds a master’s degree in healthcare and medical simulation.
Dr Shilpa Murthy contributed to the continuous review of the important intellectual content and final version of the manuscript. She also contributed to the conception of this project. She is a senior lecturer teaching clinical skills and simulation concepts to pre-clinical medical students at the School of Medicine, IMU University.
Acknowledgements
The authors would like to express our sincere appreciation to Dr Cheah Xian-Yang for his invaluable assistance in proofreading this article. We also extend our gratitude to Associate Professor Dr Sow Chew Fei for her guidance.
Funding
There is no funding for this paper.
Declaration of Interest
The authors of this paper have no conflicts of interest to declare.
References
Bird, A., Tomescu, O., Oyola, S., Houpy, J., Anderson, I., & Pincavage, A. (2020). A curriculum to teach resilience skills to medical students during clinical training. MedEdPORTAL, 16, Article 10975. https://doi.org/10.15766/mep_2374-8265.10975
Cook, M. C., & Stewart, R. (2023). Resilience and sub-optimal social determinants of health: Fostering organizational resilience in the medical profession. Primary Care: Clinics in Office Practice, 50(4), 689-698. https://doi.org/10.1016/j.pop.2023.04.013
Omari, O. A., Yahyaei, A. A., Wynaden, D., Damra, J., Aljezawi, M., Qaderi, M. A., Ruqaishi, H. A., Shahrour, L. A., & AlBashtawy, M. (2023). Correlates of resilience among university students in Oman: A cross-sectional study. BMC Psychology, 11, Article 2. https://doi.org/10.1186/s40359-022-01035-9
Rotenstein, L. S., Ramos, M. A., Hom, J., & Gardner, A. (2016). Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: A systematic review and meta-analysis. JAMA, 316(21), 2214-2236.https://doi.org/10.1001/jama.2016.17324
Thompson, G., McBride, R. B., Hosford, C. C., & Halaas, G. (2016). Resilience among medical students: The role of coping style and social support. Teaching and Learning in Medicine, 28(2), 174-182. https://doi.org/10.1080/10401334.2016.1146611
*Dr Juliet Mathew
IMU University, 126, Jalan Jalil Perkasa 19,
Bukit Jalil, 57000 Kuala Lumpur
Federal Territory of Kuala Lumpur
+6012 – 574 1723
Email: julietmathew@imu.edu.my
Submitted: 15 June 2024
Accepted: 12 September 2024
Published online: 1 April, TAPS 2025, 10(2), 8-12
https://doi.org/10.29060/TAPS.2025-10-2/GP3440
Galvin Sim Siang Lin1, Tong Wah Lim2 & Mariana Minatel Braga3
1Department of Restorative Dentistry, Kulliyyah of Dentistry, International Islamic University Malaysia, Malaysia; 2Division of Restorative Dental Sciences, Faculty of Dentistry, The University of Hong Kong, Hong Kong S.A.R.; 3Department of Orthodontics and Pediatric Dentistry, School of Dentistry, University of São Paulo, Brazil
Abstract
Introduction: Dental education is undergoing a major transformation due to evolving healthcare needs, technological advancements, and the demand for dental practitioners to meet the diverse needs of a global patient community. Competency-based education (CBE) is at the forefront of this change, focusing on what students are competent in upon graduation. Unlike traditional models, CBE emphasises practical skills, critical thinking, and problem-solving.
Methods: This article explo res the shift towards CBE in dental education, examining frameworks that support CBE like Miller’s Pyramid and guidelines from organisations such as the Accreditation Council for Graduate Medical Education (ACGME) and the American Dental Education Association (ADEA). It also involves a detailed analysis of these frameworks and their application in designing competency-based curricula.
Results: The findings reveal that CBE facilitates a student-centric approach, enhancing critical thinking, problem-solving, and autonomous self-assessment. These frameworks guide the design of curricula including identifying core competencies, defining competency levels, mapping competencies to learning outcomes, selecting effective teaching methods and utilising various assessment strategies. However, implementing CBE faces challenges, including measuring soft skills and resistance from educators and students.
Conclusion: CBE represents a paradigm shift in dental education, ensuring graduates are not only knowledgeable but proficient in practical skills. Future recommendations include incorporating technology-enhanced learning, global health competencies, and sustainability practices into the curriculum. Continuous professional development for educators and robust feedback mechanisms are needed to maintain the curriculum’s relevance and effectiveness, ensuring dental graduates are well-equipped to meet the demands of modern dental practice.
Practice Highlights
- Dental education is evolving to meet global healthcare needs and technological advancements.
- CBE focuses on practical skills, critical thinking, and problem-solving
- CBE ensures dental graduates are competent and ready for modern practice challenges.
- Several frameworks can be used to guide CBE in developing clinical
- Designing CBE curricula involves defining core competencies and using diverse assessment methods.
I. INTRODUCTION
Dental education is at a pivotal moment, facing a profound transformation influenced by the dynamic intersection of changing healthcare needs, technological advancements, and the urgent call for dental practitioners to cater to the diverse requirements of a globalised patient community. Amid this swiftly evolving landscape, traditional approaches to dental education are undergoing a fundamental reimagination. The aim is to nurture a generation of dental professionals not only well-versed in theoretical knowledge but, crucially, equipped with the competencies vital for thriving in modern dental practice. Competency-based education (CBE) emerges as a key player in this educational revolution. This approach to curriculum design and teaching revolves around a central question: What should students be able to do or achieve at the culmination of their course or program? In the realm of dental education, CBE moves beyond the traditional focus on accumulating knowledge and places a spotlight on the practical skills students need to excel in their future roles. It is not just about what students know; it is about what they can proficiently do. Why adopt competency-based education in dentistry? The answer lies in its power to enhance student learning by emphasising hands-on skills, critical thinking, and problem-solving abilities. CBE ensures that graduates are not merely well-informed in dental theory but are also competent practitioners capable of meeting the ever-changing demands of contemporary dental care.
II. THE SHIFT TOWARDS COMPETENCY-BASED DENTAL EDUCATION
In recent years, the field of dental education has undergone a transformative shift, pivoting away from the traditional education models to embrace the principles of competency-based dental education. This evolution is rooted in a fundamental recognition that the mastery of dental skills and knowledge is a dynamic process, necessitating an educational paradigm that transcends mere adherence to a predetermined timeframe (Chuenjitwongsa et al., 2018). While various definitions of competency-based education exist, there is a consensus that it revolves around outcome-based learning, ensuring the production of graduates with the requisite knowledge, skills, and attitudes to serve society effectively, meeting the standards of national qualifications frameworks, stakeholders, and the labour market.
Traditional-based dental education has faced criticisms for its potential to produce graduates who may lack practical proficiency or struggle to adapt to emerging trends in dentistry. It emphasises time spent in the classroom, irrespective of individual mastery. Furthermore, traditional models may sometimes struggle to keep pace with the rapid advancements in dental technology and shifting paradigms in patient care, underscoring the need for a more adaptive and outcomes-focused approach. On the other hand, CBE signifies a departure from traditional education, characterised by its teacher-centred, examination-focused, time-constrained, and discipline-oriented approach. It transitions towards a student-centric educational model using an outcome-based approach that enhances students’ capabilities in critical thinking, problem-solving, and autonomous self-assessment.
Moreover, in CBE, the focus shifts from completing a predefined course of study to ensuring that learners attain proficiency in specific competencies, enabling them to navigate the complexities of dental practice effectively. In a competency-based framework, success is measured by demonstrating specific skills, ensuring that graduates are not merely knowledgeable but possess the practical expertise required for clinical practice. Besides, future professionals tend to be able to make decisions even when ideal/learned circumstances are changed. This paradigm shift promotes a deeper understanding of concepts and fosters a culture of continuous improvement. In CBE, novice dental students commence their training in simulation laboratories, preparing them to progressively attain beginner and competent levels in clinical settings.
III. FRAMEWORK FOR COMPETENCY-BASED DENTAL EDUCATION
A. Miller’s Pyramid
The Miller Pyramid of Competence, introduced by psychologist George Miller in 1990 (Miller, 1990), stands as a foundational framework for evaluating clinical proficiency in healthcare education. This pyramid encapsulates a four-tiered hierarchy, delineating the progressive stages of competence acquisition. At its base, the pyramid begins with “knowledge”, representing the foundational cognitive understanding of concepts typically assessed in classroom-based environments. Moving upwards, the tiers evolve into “competence” and subsequently “performance”, encompassing knowledge translation into practical skills through simulated clinical settings. The higher echelons of the pyramid, namely “action”, signify the culmination of clinical competence in real-world scenarios. Here, learners demonstrate their ability to apply theoretical knowledge and practical skills in authentic clinical environments. The Miller Pyramid’s distinction between cognitive and behavioural components is particularly noteworthy. The lower tiers, focusing on knowledge and competence, mention the importance of classroom-based assessments in gauging cognitive understanding. In contrast, the apex tiers of performance and action underline the significance of evaluating behavioural aspects within simulated and real clinical settings. This hierarchical structure provides a great understanding of competency development, guiding educators in designing competency-based curricula.
B. Accreditation Council for Graduate Medical Education (ACGME)
The ACGME plays a role in shaping the educational standards for healthcare professionals. ACGME has delineated six core competencies, transcending traditional disciplinary boundaries and applicable to various healthcare practitioners (Batalden et al., 2002). These competencies form a holistic approach to evaluating the proficiency of healthcare professionals and are integral to fostering well-rounded practitioners capable of meeting the complex demands of modern healthcare. The six core competencies identified by ACGME are Patient Care, Medical Knowledge, Professionalism, Interpersonal and Communication Skills, Practice-Based Learning and Improvement, and Systems-Based Practice. Patient Care centres on delivering compassionate, effective, evidence-based care to individuals and populations, while medical knowledge encompasses the understanding needed for sound clinical decision-making. Professionalism emphasises ethical behaviour, accountability, and a commitment to the well-being of patients. Interpersonal and Communication Skills are crucial for effective collaboration and patient interaction, whereas practice-Based Learning and Improvement involves the ability to critically assess and improve one’s own clinical practice continuously. Systems-Based Practice involves comprehending healthcare delivery systems and endorsing high-quality and cost-effective patient care within the broader healthcare system context. Customising these competencies for the dental context allows dental educators to align educational objectives, ensuring their curriculum imparts technical skills while cultivating the ethical, communication, and systemic perspectives essential for a well-rounded dental practitioner.
C. American Dental Education Association (ADEA) Competencies for the New General Dentist
The ADEA has crafted the Competencies for the New General Dentist, a set of guidelines tailored specifically for dental education (American Dental Education Association, 2017). Ratified by the ADEA House of Delegates on 2nd April 2008, this framework is a decisive step in defining the essential competencies for individuals entering the dental profession as general dentists., This document reflects a departure from the 1997 competencies, aligned with patient care responsibilities, public oral health needs, and contemporary trends in dental practice and draws inspiration from the 2002 Institute of Medicine’s core competencies with a heightened emphasis on quality patient care and safety. Structured into six domains—Critical Thinking, Professionalism, Communication and Interpersonal Skills, Health Promotion, Practice Management and Informatics, and Patient Care—the competencies are thoughtfully organised, allowing for more flexible and adaptable integration into dental education curricula. This framework serves as a central resource for the ADEA at the national level and individual dental schools at the local level, fostering an environment conducive to innovation in predoctoral dental school curricula. Overall, the ADEA competencies serve as a benchmark, enabling dental educators to design curricula that not only meet but exceed the contemporary expectations and requirements of the dental profession.
D. The Graduating European Dentist Curriculum
The Graduating European Dentist Curriculum, under the auspices of the Association for Dental Education in Europe (ADEE), presents a contemporary framework embodying the optimal academic practices for undergraduate dental education in Europe (Field et al., 2017). This curriculum is structured across five integral domains, each contributing to a comprehensive educational experience: (1) Professionalism, (2) Safe and Effective Clinical Practice, (3) Patient-Centred Care, (4) Dentistry and Society, and (5) Research. Crafted through a collaborative process involving consultation, consensus-building, and collegial learning, this curriculum highlights the importance of patient safety, teamwork, and teaching excellence. Aligned with European Quality in Higher Education benchmarks, “The Graduating European Dentist” introduces an innovative approach reflecting the pinnacle of academic standards in European dental education. The revised framework features a more explicit linkage between “Learning Outcomes” and the defined curriculum, accompanied by detailed guidance specific to each competence domain, encompassing “Methods of Teaching and Learning” and “Methods of Assessment”. It is anticipated that this framework would facilitate an enriched educational experience for dental students across Europe.
IV. DESIGNING A COMPETENCY-BASED DENTAL CURRICULUM
To effectively design and develop a competency-based dental curriculum, educators need a comprehensive framework that aligns with the unique challenges and requirements of dental practice. The following components are some of the basic summarised steps that serve as foundational guides for the implementation of a competency-based curriculum:
A. Identifying Core Competencies
Begin by identifying the core competencies that future dental practitioners must possess. This involves collaboration with practitioners, educators, and stakeholders to ensure that the curriculum reflects the evolving needs of the dental profession. Core competencies might encompass knowledge acquisition, clinical skills, patient communication, ethical practice, and the ability to integrate new research findings into practice.
B. Defining Competency Levels
Once core competencies have been identified, it is crucial to define distinct competency levels for each skill or knowledge area. These levels serve as benchmarks for assessing student progress and proficiency. They facilitate a granular approach to education, where learning and assessment can be tailored to students’ individual needs, recognising that learners progress at different rates and may require differentiated levels of support to achieve competency.
C. Mapping Competencies to Learning Outcomes
Each identified competency should be mapped to specific learning outcomes within the curriculum. This mapping process ensures that the curriculum is logically structured, with a clear progression from foundational knowledge to applying skills in complex clinical scenarios. It allows educators to design courses and modules that systematically build upon each other, guiding students on a clear path towards achieving the essential competencies required for successful dental practice.
D. Selecting Effective Teaching Methods
Adopt diverse and innovative teaching methods that cater to different learning styles and encourage active engagement. Techniques such as problem-based learning (PBL), case-based learning (CBL), team-based learning (TBL), simulation exercises, and hands-on clinical practice are effective in helping students develop critical thinking and practical skills. Incorporating technology, such as virtual reality (VR) and digital simulations, can also enhance learning experiences and prepare students for real-world challenges.
E. Utilising Assessment Strategies
Implement a variety of assessment methods to evaluate students’ competency levels. This may include practical exams, case-based assessments, and objective structured clinical examinations (OSCEs). These should be complemented by regular, formative assessments and feedback, which are instrumental in identifying areas where students may struggle and providing them with the support needed to overcome these challenges. The ultimate goal of assessment within a competency-based curriculum is not merely to test knowledge but to facilitate the development of skilled, reflective, and adaptable dental practitioners.
V. LIMITATIONS AND CHALLENGES IN IMPLEMENTING A COMPETENCY-BASED CURRICULUM
Authenticity and the ability to accurately measure skills have been identified as the primary challenges in CBE for dentistry. In this field, knowledge and skills are often assessed as separate entities, leading to a potential loss of authenticity throughout the learning process. While CBE incorporates a variety of subjective and objective evaluations, measuring certain soft skills, such as clinician-patient communication, ethics, and values, remains a challenge due to their complex and intangible nature. Moreover, implementing CBE in dental education may face additional obstacles, including the limited availability of established theoretical frameworks to guide the teaching-learning process, insufficient training for educators in adapting to this curriculum style, and resistance from both teaching staff and students. Addressing these challenges is essential for ensuring the successful adoption and integration of competency-based education within dental programs.
VI. CONCLUSION
The transition towards competency-based dental education marks a significant paradigm shift aimed at equipping future dental professionals with the practical skills, ethical understanding, and critical thinking abilities necessary for success in the contemporary dental landscape. Future recommendations include the further integration of technology-enhanced learning tools, the development of global health competencies, and the emphasis on sustainability and ethical practices within the curriculum. Additionally, establishing robust feedback mechanisms and promoting continuous professional development among educators will be crucial in maintaining the curriculum’s relevance and effectiveness.
Notes on Contributors
GSSL and TWL were involved in the conception and design of the study. GSSL, TWL and MMB reviewed the literature, collected the data, and wrote the original draft. TWL edited the original draft. All authors have read and approved the final manuscript.
Funding
No funding is required for this paper.
Declaration of Interest
All authors have no conflicts of interest.
References
American Dental Education Association. (2017). ADEA competencies for the new general dentist. Journal of Dental Education, 81(7), 844-847. https://doi.org/10.1002/j.0022-0337.2017.81.7.tb06299.x
Batalden, P., Leach, D., Swing, S., Dreyfus, H., & Dreyfus, S. (2002). General competencies and accreditation in graduate medical education. Health Affairs (Millwood), 21(5), 103-111. https://doi.org/10.1377/hlthaff.21.5.103
Chuenjitwongsa, S., Oliver, R., & Bullock, A. D. (2018). Competence, competency‐based education, and undergraduate dental education: A discussion paper. European Journal of Dental Education, 22(1), 1-8. https://doi.org/10.1111/eje.12213
Field, J. C., Cowpe, J. G., & Walmsley, A. D. (2017). The graduating European dentist: A new undergraduate curriculum framework. European Journal of Dental Education, 21 Suppl 1, 2-10. https://doi.org/10.1111/eje.12307
Miller, G. E. (1990). The assessment of clinical skills /competence/performance. Academic Medicine, 65(9), S63-67. https://doi.org/10.1097/00001888-199009000-00045
*Galvin Sim Siang Lin
Department of Restorative Dentistry,
Kulliyyah of Dentistry,
International Islamic University Malaysia,
Kuantan Campus, Pahang, Malaysia
Email: galvin@iium.edu.my
Submitted: 5 July 2024
Accepted: 25 November 2024
Published online: 1 April, TAPS 2025, 10(2), 13-16
https://doi.org/10.29060/TAPS.2025-10-2/GP3456
Eng Koon Ong1-4,7 & Wen Shan Sim4-6
1Division of Supportive and Palliative Care, National Cancer Centre Singapore, Singapore; 2Office of Medical Humanities, SingHealth Medicine Academic Clinical Programme, Singapore; 3Division of Cancer Education, National Cancer Centre Singapore, Singapore; 4Duke-NUS Graduate Medical School, Singapore; 5Maternal Fetal Medicine, KK Women’s and Children’s Hospital, Singapore; 6PGY1 Programme, SingHealth, Singapore; 7Assisi Hospice, Singapore
Abstract
Introduction: The medical humanities (MH) have the potential to support medical education (ME) by developing observational skills, promote reflective practice and transformative growth. However, contextual content and methods relevant to our local and regional learners and teachers are lacking.
Methods: We describe three MH-based ME programmes within SingHealth to illustrate our considerations in the choice of conceptual frameworks and content selection in programme development and evaluation.
Results: Highlighting pertinent challenges in developing the field due to poor awareness, lack of resources and research capability, we emphasise the importance of interdisciplinarity, engaging leadership, and generating research output. Broad strategies to achieve these goals are then presented.
Conclusion: Highlighting challenges due to the lack of awareness, administrative and funding support, and research capability, we propose strategies to overcome such barriers and hope that readers will be inspired to contribute to this developing landscape where science and art intersect.
Practice Highlights
- Established frameworks and methods should be employed in programme development and evaluation.
- Art, literature, and theatre may be employed in medical humanities-programmes.
- Interdisciplinarity, leadership engagement and development of research capability are essential.
- Alignment with organisational needs and vision will ensure relevance and sustained support.
- The impact of the humanities on fostering wellbeing should not be neglected.
I. INTRODUCTION
The medical humanities (MH) is an interdisciplinary field characterised by critical enquiry and engagement of humanities disciplines. In medical education (ME), content or pedagogy derived from the arts and humanities may be employed to develop observational skills, promote reflective practice and transformative growth, and support humanistic clinical practice and communications (Dennhardt et al., 2016). However, while the integration of the MH in ME in Western countries has been widely supported and reported, a similar movement within Asian countries appears to be lacking and challenging. Educators in Arab-Muslim environments have lamented the lack of culturally-relevant content and concepts that remain predominantly Western-centric (Daher-Nashif & Kane, 2022), while additional challenges cited in China, Hong Kong, and Taiwan include limited awareness exacerbated by conflicting priorities of academic institutions (Tan et al., 2021; Wu & Chen, 2018). These factors result in a lack of impetus for higher education reform and slow research advancement of the field. To address these gaps, we first describe three educational programmes to highlight how local content and methods of co-facilitation may be employed. Next, we list the respective conceptual frameworks, learning objectives and programme evaluation methods selected. Finally, we discuss strategies to increase awareness, maintain leadership and participant interest, secure sustained funding, and promote scholarly efforts. We hope that this article will support and inspire like-minded clinician educators with structurally relevant guidance that is currently lacking in the literature.
II. PROGRAMME DESCRIPTION
One of the first programmes we implemented was the HAPPE (Humanistic Aspirations as a Propellor for Palliative care Education) workshop, a 1.5-hour small group discussion session for junior doctors in a palliative care rotation at the Division of Supportive and Palliative Care, National Cancer Centre Singapore, facilitated by an accredited clinical psychologist and art therapist. Schon’s theory of Reflective Practice defined by reflection-in-action and reflection-on-action guided the discussions that focused on the participants’ experience with challenging clinical encounters that they expressed through readings of literary work and art-based craftwork. Parts of Gagne’s model of lesson planning such as the importance of gaining the learner’s attention, stimulating recall, presenting stimulus, and providing learning guidance were aptly supported by our choice of materials and facilitation. The themes of empathy and wellbeing were discussed and highlighted the importance of reflective practice on past challenging encounters. As a pilot educational intervention started since 2018, we chose to investigate the feasibility and acceptability of the MH-based workshop using self-reported quantitative scales such as the Consultation and Relational Empathy (CARE) Measure and Jefferson Physician Empathy Scale (JPES) pre- and post-workshop. Both scores improved after attendance of the workshop, supporting continual efforts for future runs of the workshop.
One year later, the half-day ADEPT (Arts and Drama to Enable Perspective Taking) workshop was implemented. In contrast to HAPPE, ADEPT was conducted for final year medical students from the Duke-NUS medical school within their core rotation to palliative care. Addressing the lack of adequate clinical exposure and role-modelling due to the brevity of the week-long rotation, a full recording of a local play A Good Death which portrayed theatrical presentations of severe pain, end-of-life conversations, and physician burnout was shown to the students. They then participated in small group discussions about perceptions of palliative care, professional identity formation, clinical communications, and physician wellbeing. These discussions were co-facilitated by a palliative care specialist, trained counsellor, and the director of the play and served to dispel myths about palliative care, promote self-awareness, and introduce coping strategies. The workshop was guided by Knowles’ theory of adult-learning and we ensured that a sense of agency and empowerment was promoted, with the students participating in self-directed reflection and learning. Building on the quantitative results of the HAPPE workshop, ADEPT was evaluated through a qualitative lens where students were invited to participate in individual semi-structured interviews by an independent interviewer to share their experiences of the workshop.
Finally, the full-day HEARTEN (Harnessing Educational approaches with the Arts to encourage End of life Conversations) workshop was started in 2022 and employed theatre-based techniques to address healthcare professionals’ discomfort in initiating advanced care planning (ACP) conversations with patients. The workshop marked our first formal collaboration with a local professional theatre group (ArtsWok) external to the SingHealth Duke-NUS Academic Medicine Centre and was attended by physicians, nurses, and various allied health professionals. This collaboration further cemented our approach of engaging local content and co-facilitators. Together, the team of physicians, social workers, art therapists, humanities researchers, and a theatre director employed Mezirow’s framework of transformational change to design experiential theatre- and acting-based exercises to trigger discussions about deep-seated perceptions and misgivings about initiating ACP discussions. We evaluated participants’ change in confidence levels in ACP discussions pre- and post-workshop through the Self-Competence in Death Work Scale (SC-DWS) survey quantitatively. An open-ended question was also embedded within the post-workshop survey to allow triangulation of the quantitative data collected. Preliminary data analysis showed an improvement in the SC-DWS surveys, with participants reflecting that their pre-existing concerns about triggering unhappiness and anxiety in patients might have been unfounded.
III. CHALLENGES
The HAPPE, ADEPT, and HEARTEN workshops illustrate a spectrum of MH-based ME programmes in terms of scale (5 to 20 participants per workshop; workshop durations of 1.5 to 8 hours), learning objectives, involvement of co-facilitators, choice of materials, and evaluation methods. In addition, all three workshops were supported by local institutional academic research funding, the amount of which increased over the years (SGD$5,000 – $42,000). By clearly enunciating our choice of educational conceptual frameworks and validated scales for programme evaluation, and consistently incorporating local content and engaging local stakeholders, we posit that some of the challenges such as the lack of contextually relevant content and frameworks and rigor in programme development and evaluation may be addressed.
However, several pertinent challenges exist. Firstly, awareness about the MH remains poor, with its integration into ME at a nascent stage compared to Western countries. Competing with other educational programmes that are better established, the small group size and similar pools of participants who enrolled in our programmes risk the case of “preaching to the choir.” This in turn may lead to challenges in garnering leadership support to encourage staff participation. In addition, securing sustained programme funding is challenging as education grants are limited to smaller, project-based programmes. Relative to clinical research, institutional management and administrative teams have less experience and expertise in supporting medical education research. Often, the project team members find themselves overwhelmed with administrative tasks including financial processes and manpower recruitment. These barriers towards research capacity building may deter interested but busy clinician educators from contributing to scholarly work that is crucial to support the growth of the field.
IV. PROPOSED STRATEGIES
We propose three areas of consideration that we have found helpful in navigating challenges in the landscape. While our experience stems from a single local healthcare centre, similar cultural, societal, and systemic factors in other parts of the Asia-Pacific region will allow applicability and relevance to other clinician educators.
A. Promoting Interdisciplinary Teaching and Learning
The MH is defined by an interdisciplinary approach and we adopt a collaborative approach in engaging various stakeholders such as local and regional humanities scholars, creative arts therapists, professional artistes, and community arts organisations. This allows us access to content from diverse subjects including anthropology, literature, history, philosophy, and other social sciences and to methods such as narrative inquiry, close reading, narrative therapy, and conversational analysis which were previously unfamiliar to us. Learners have described our programmes as refreshing and eye-opening. However, we are also mindful that some may not take to the arts and humanities naturally. Thus, co-facilitators take extra care to emphasise that learners need not be experts in the arts to engage in reflective practice, and co-facilitators from the humanities are always paired with a clinician educator to ensure the discussions are balanced and relevant.
B. Alignment with Individual Needs and Organisational Goals
An awareness about existing needs and organisational vision is crucial to ensure relevance of the MH programmes. In the SingHealth Duke-NUS Academic Medicine Centre (AMC), our programmes support pillars of the medical education (ME) masterplan such as interprofessional education, educational excellence, and fostering wellbeing. By including other health professions besides doctors, approaching programme development and evaluation through established educational frameworks and methods, and promoting wellbeing by engaging in the arts, the ADEPT workshops have now been adopted by the SingHealth College of Allied Health and Singapore Institute of Technology for allied health professionals and trainees respectively. Notably, the impact of the arts in fostering wellbeing by providing an avenue for expression of difficult emotions, building a sense of community, and processing grief for healthcare professionals provides further impetus for leadership support of our programmes. While MH programmes are not psychotherapy-based per se, participants have shared that the experience was therapeutic and with an increased awareness about struggles, some have been prompted to seek support from professional mental health professionals after programme attendance. Seeing the value of the MH, various offices of the medical humanities have been set up within the AMC since 2019. In 2023, the SingHealth Duke-NUS Medical Humanities Institute was established to further provide centre-wide administrative and funding support for MH programmes within ME. Supported by social media platforms, these offices have organised webinars, colloquiums, and Medical Humanities conferences that increase the visibility of our endeavours and continue to engage leadership, increase interest, and sustain awareness of MH-based programmes.
C. Developing Research Capability
Despite its rich history and diverse cultural perspectives, research in the medical humanities (MH) in medical education (ME) within Asian countries remains at a nascent stage compared to our Western counterparts. To develop research capability, we adopt a two-pronged approach. Firstly, all of our programmes follow a best practice approach towards development and evaluation guided by established educational theoretical frameworks and methods respectively. Secondly, all of our programmes include a scholarly component, as illustrated above. We are currently analysing qualitative data collected from the ADEPT and HEARTEN workshops and preliminary findings suggest that more data is needed to guide the choice of content, teaching methods, learning objectives, and matching of these aspects to different learner populations. Future funding from the MH offices coupled with national and regional funding on a larger scale made possible by our cross-institutional and interdisciplinary collaborations will allow us to embark on further research to address these gaps.
V. CONCLUSION
The medical humanities (MH) have the potential to impact medical education (ME) learning and teaching outcomes but contextual content and methods relevant to our local and regional learners are lacking. We have described three MH-based ME programmes to illustrate considerations in programme development and evaluation. Highlighting considerations in awareness, administrative and funding support, and research capability, we propose strategies to overcome such challenges and hope that readers will be inspired to contribute to this developing landscape where science and art intersect.
As Carlo Rubbia, Nobel prize winner in physics says,
“Science for me is very close to art. Scientific discovery is an irrational act. It’s an intuition which turns out to be reality at the end of it – and I see no difference between a scientist developing a marvellous discovery and an artist making a painting.”
Notes on Contributors
Both OEK and SWS contributed to the conceptualisation of the paper through their experience and work in both undergraduate and postgraduate training. With repeated discussions, the approach towards explaining the value of the paper and learning points for readers were finalised. Both authors worked on the initial draft of the manuscript, before refining the contents though an iterative process of literature review and discussions with other educators and participants of the various programs. The final draft of the paper was reviewed by both authors who reached the consensus that the paper was ready for submission for publication. Both authors agree to be accountable for all aspects of the paper.
Acknowledgements
We would like to thank Ms Chiam Min and Ms April Thant Aung for proofreading the article.
Funding
No funding was received.
Declaration of Interest
Both OEK and SWS state no conflicts of interest.
References
Daher-Nashif, S., & Kane, T. (2022). A culturally competent approach to teach humanities in international medical school: Potential frameworks and lessons learned. MedEdPublish, 12(6). https://doi.org/10.12688/mep.18938.1
Dennhardt, S., Apramian, T., Lingard, L., Torabi, N., & Amtfield, S. (2016). Rethinking research in the medical humanities: A scoping review and narrative synthesis of quantitative outcome studies. Medical Education, 50(3), 285-299. https://doi.org/10.1111/medu.12812
Ong, E. K., & Anantham, D. (2019). The medical humanities: Reconnecting with the soul of medicine. Annals of the Academy of Medicine Singapore, 48(7), 233-237.
Tan, M. K. B., Tan, C. M., Tan, S. G., Yoong, J., & Gibbons, B. (2021). Connecting the dots: The state of arts and health in Singapore. Arts & Health, 15(2), 119-134. https://doi.org/10.1080/17533015.2021.2005643
Wu, H. Y. J., & Chen, J. Y. (2018). Conundrum between internationalisation and interdisciplinarity: Reflection on the development of medical humanities in Hong Kong, Taiwan and China. MedEdPublish, 7(184). https://doi.org/10.15694/mep.2018.0000184.1
*Ong Eng Koon
National Cancer Centre Singapore
30 Hospital Blvd, Singapore 168583
Email: ong.eng.koon@assisihospice.org.sg
Submitted: 7 April 2024
Accepted: 5 February 2025
Published online: 1 April, TAPS 2025, 10(2), 34-45
https://doi.org/10.29060/TAPS.2025-10-2/RA3272
Jasmin Oezcan1, Marcus A. Henning2 & Craig S. Webster2
1Pediatric Department, Erlangen University Hospital, Erlangen, Germany; 2Centre for Medical and Health Sciences Education, School of Medicine, University of Auckland, New Zealand
Abstract
Introduction: Paediatric practice presents unique challenges for clinical reasoning, including the collection of clinical information from multiple individuals during history taking, often in emotionally charged circumstances, and the variable presentation of signs and symptoms due to the developmental stage of the child. Communication skills are clearly important but the most effective methods of teaching clinical reasoning in paediatrics remains unclear. Our review aimed to examine the existing methods of teaching clinical reasoning in paediatrics, and to consider the evidence for the most effective approaches.
Methods: We performed a scoping review and evidence synthesis drawn from reports found during a systematic search in five major databases. We reviewed 211 reports to include 11.
Results: Students who received explicit training in clinical reasoning showed a significant improvement in their experiential learning, diagnostic ability, and reflective clinical judgement. More specifically, key findings demonstrated frequent student-centered interactive strategies increased awareness of the critical role of communication skills and medical history taking. Real case-based exercises, flipped classrooms, workshops, team-based or/and bed-side teaching, and clinical simulation involving multisource feedback were effective in improving student engagement and performance on multiple outcome measures.
Conclusion: This review provides a structured insight into the advantages of different teaching methods, focusing on the multistep decision process involved in teaching clinical reasoning in paediatrics. Our review demonstrated a relatively small number of studies in paediatrics related to clinical reasoning, underlining the need for further research and curricular developments that may better meet the known unique challenges of the care of paediatric patients.
Keywords: Clinical Reasoning, Paediatrics, Teaching Methods, Medical Students
Practice Highlights
- Clinical reasoning in paediatrics involves unique challenges including the collection of clinical information from multiple people (child, parents and care givers), symptoms that may present differently due to children’s stage of development, and complex pharmacokinetics.
- The efficacy of paediatric training could be increased by combining student-centered methods like flipped-classroom, team-based or bed-side teaching and simulation.
- Low stakes training such as simulation that allows repetition and learning from mistakes is particularly effective and engaging for students.
- Our review demonstrated a relatively small number of studies specifically related to clinical reasoning in paediatrics, underlining the need for further research and curricular developments that may better meet the known unique challenges of the care of paediatric patients.
I. INTRODUCTION
Reflective diagnostic skills, comprising the analyses of symptoms and health issues and the weighing up of alternative explanations, are essential for establishing a correct diagnosis and for successful treatment and patient management. In addition, it is important to acknowledge that conscious and unconscious biases may be associated with human errors underlining clinical decision-making (Croskerry, 2005; Webster, Taylor, et al., 2021). The prevalence of incorrect acute clinical diagnosis has been estimated at 5-15% and emphasises the importance of understanding and minimising reasoning errors (Scott, 2009). It has been estimated that 75% of diagnostic errors may be associated with problems of clinical reasoning, in particular related to failures to elicit, synthesise, decide, or act on clinical information (Graber et al., 2005; Pennaforte et al., 2016).
Clinical reasoning requires a competent and highly developed cognitive process, which can use experiential and formal knowledge to work through a cluster of symptoms to generate a correct diagnosis (Pinnock & Welch, 2014). A general approach should incorporate comprehensive problem-solving and involves the need for clear questioning to discern a set of viable differential diagnoses while remaining mindful of the potential of bias in the decision-making process (Pinnock et al., 2021).
The practice of paediatric medicine, however, presents particular challenges for a careful, question-based process of differential diagnosis. Taking a medical history typically requires the collection of clinical information from multiple individuals, including parents, caregivers and the child themselves, often in emotionally charged circumstances. In addition, symptoms in children and neonates can be subtle and unclear – children often have limited communication abilities, their symptoms may present differently depending on their stage of development, many diagnostic tools and tests are designed for adults and have limited utility in children, and children may have unexpected sensitivities and responses to medications due to having pharmacokinetics that are very different to those of adults (Webster, Anderson, et al., 2021).
Despite these challenges, the teaching and experience of clinical reasoning for trainees in paediatrics is often informal and occurs in an unstructured way throughout clinical attachments. In addition, there is often a lack of opportunity to review performance with an experienced clinician, which hinders the development of insight regarding common causes of errors (Lee et al., 2010; Schmidt & Mamede, 2015). It is well known that quality supervision and feedback leads to better learning in trainees, however, there is often a shortage of appropriately qualified paediatricians able to provide such supervision and feedback (de Jong & Ferguson-Hessler, 1996; Zhang et al., 2019).
The medical curriculum typically focuses on the acquisition of content knowledge, cultivating both theory and practical skills, which culminates in the ability to develop a treatment strategy for the patient (Norman, 2005). Clinical reasoning can be described as a multistep process consisting of: data gathering; the proposal of a diagnosis from a range of possible different hypotheses, and the reevaluation of that proposal in light of new information.
Early approaches to the teaching of diagnostic reasoning included the hypothetico-deductive procedural method that involved establishing a series of hypotheses, which then required the gathering of selective patient data to confirm or rule out the hypotheses being made (Norman, 2005; Schwartz & Elstein, 2008). This approach was intended to promote an understanding of the physical development of a disease or condition, and is also known as the pathophysiological approach, and relies on hypothetico-deductive reasoning and knowledge acquisition (Page et al., 1995). Hence, this approach may not represent the most efficient way to cultivate clinically relevant skills. An alternative approach involves the explanation of an expert’s reasoning as an unconscious and automatic pattern recognition process (Groen & Patel, 1985; Schwartz & Elstein, 2008). This can be linked with the dual-cognition theory (Marcum, 2012). It has been suggested that in 95% of case encounters, expert clinicians use the fast, automatic, and unconscious pattern recognition abilities of system 1, while system 2, which is conscious, slow and effortful, tends to be applied only in unusual and complicated cases (Fabry, 2022; Webster, Taylor, et al., 2021). Studies have underlined that both systems should be used simultaneously to ensure an efficient outcome (Pennaforte et al., 2016). Therefore, the teaching of the awareness of individual unconscious information processing and judgment is a major pedagogical challenge, particularly in potentially difficult practice domains such as paediatrics (Bargh & Chartrand, 1999; Gruppen & Frohna, 2002; Webster et al., 2022).
It takes years to train a qualified paediatrician with accurate perception and judgment, enabling them to work effectively with children and their parents, guardians, or caregivers (Gong et al., 2022). Gathering the medical history appropriately and forming an accurate diagnosis through a reliable clinical reasoning process is a critical professional competency in paediatricians, which may require specific curricular techniques to achieve. Therefore in this review we aimed to examine the existing methods of teaching clinical reasoning and diagnosis in paediatrics, and to consider the evidence for which approaches may be the most effective.
II. METHODS
A. The Search Process
In consideration of the array and typology of available reviews, we choose the scoping review because it is a useful synthesis approach to create an overview of the salient literature and to identify key findings. A preliminary search identified no published review with an equal or comparable research question as the current work, suggesting that our scoping review may allow priorities for future investigations to be outlined, including potentially informing later systematic reviews (Grant & Booth, 2009). The literature search was conducted during the period of March and April 2023, using five major databases (Pubmed, PsychInfo, Scopus, ERIC, and Google Scholar). We aimed to identify studies, without restriction of type or year of publication, reported in English or German, to capture as much of the Western thought on clinical reasoning in paediatrics as possible and to make the most of the language fluency of the authors. The search employed the PICO (Population, Intervention, Comparison and Outcome) framework and the terms listed in Table 1 (Schardt et al., 2007). These search terms were used according to the following structure, for example: “medical-student” AND “clinical-reasoning” AND “paediatrics”. The search included MeSH terms, truncations, subject headings, word variants and incorporated both American and British spellings.
|
Types of participants |
Types of intervention |
Types of comparison |
Types of outcomes |
|
Medical-students, clinic*ians, experts and teachers. |
Clinical-reasoning, paediatric setting, clinical-rotation, medicine |
Types of educational system, study types and teaching methods.
|
Depending on the study type the comparison of assessment and efficacy. |
Table 1. PICO Framework Components
B. Data Analysis
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) was utilised as an evidence-based guideline for the inclusion and exclusion process, as illustrated in the flow diagram (Figure 1) (Moher et al., 2009). Author JO screened reports initially by title and abstract, with uncertainties being resolved at regular meetings with authors MAH and CSW. Those with suitable titles were placed in a citation management program (Vanhecke, 2008). We included studies that focused on teaching methods in clinical reasoning in paediatrics, in particular approaches that were intended to improve the quality of reasoning and decision making (see Figure 1 for inclusion and exclusion criteria). Author JO subsequently reviewed the references of the publications yielded by the search to identify additional relevant articles. Authors JO, MAH and CSW worked collaboratively to review and categorise each publication in terms of its quality of evidence (Eccles et al., 2001; Moher et al., 2009). The included articles were then summarised with reference to: (1) first study author, year, and country; (2) study design; (3) type of curricula; (4) assessment; and (5) key outcomes related to clinical reasoning (Table 2).

Figure 1. Flow diagram used in search strategy: PRISMA flow chart
III. RESULTS
A. Summary of Search Strategy
The primary literature search generated the most results from Pubmed, Scopus and Google Scholar (Pubmed n=129, Scopus n=28 and Google Scholar n=50). Search results after the first 5 pages on Google Scholar were not considered for inclusion as these pages contained no relevant reports. After the exclusion of duplicates and screening at the title and abstract levels, the application of the inclusion and exclusion criteria upon reading the full text of candidate papers resulted in a further 11 reports being excluded on the basis that they did involve
medical students, clinical contexts or had their full texts available. Eleven studies were admitted to the final scoping review (Figure 1).
Table 2 illustrates an overview of each included study. The curriculum was classified based on the teaching methodology described by Fabry et al. (2022), which entailed dividing the typology into group size and didactic principles, i.e., flipped classroom or bed-side teaching. Due to multifaceted teaching concepts, some studies are included under more than one subheading.
|
First author (year, country) |
Study design |
Type of Curriculum |
Assessment |
Key outcome |
|
Gong et al., (2022) China
|
Randomised-Controlled |
Bedside teaching; team-based learning |
Computer-based case simulation; Mini-CEX; Questionnaire |
Creating a role shift to support and develop awareness of diagnostic steps and team-based mutual critical thinking. Significant improvement of satisfaction, clinical judgement, counseling skills in favor of the intervention group.
|
|
Bye et al., (2009) University of Sydney, Australia |
Randomised-Crossover |
Interactive lecture vs. computerised tutorial. |
Expert Observation; Questionnaire |
Interactive lecture was perceived as being more enjoyable, more effective in teaching clinical reasoning than observation. Face-to-face teaching considered critical to maximising the value of computer-assisted self-learning.
|
|
Yousefichaijan et al., (2016) Amir Kabir Hospital, Iran |
Semi-experimental study |
Workshop |
Clinical-reasoning tests (Diagnostic Thinking Inventory (DTI), Key Features and Clinical Reasoning Problems) |
This study emphasises the lack of teaching concepts of medical data acquisition techniques of reasoning steps. Effective example of repeatedly practicing clinical reasoning as a practical skill by working in small groups on illness scenarios of real medical histories.
|
|
Konopasek et al., (2014) New York-Presbyterian Hospital, Graduate Medical Education, New York, NY, USA
|
Experimental study |
Group Objective Structured Clinical Experience (OSCE); practice of communication skills and Multi- Source Feedback (MSF)
|
Questionnaire |
Studies emphasise the relationship between efficient communication skills, diagnostic accuracy, patient adherence, and positive health outcomes. Additionally this approach used problem-solving exercises based on dual-process theory. Students were instructed to consciously work through their first pattern recognition and second hypothesis-data driven clinical assumptions. Significant improvements of self-efficacy, confidence and learning motivation in the post-training scores.
|
|
Rideout & Raszka (2018) University of Vermont Children’s Hospital, USA |
Comparative studies
|
Simulation Case (Hypovolemic Shock in a Child) |
Questionnaire and Evaluation |
Simulation of rapid critical-illness recognition, diagnostic interpretation, decision-making, management, and procedural skills with the motto: learning from your mistakes. Improvements were noted in clinical judgement in critical situations, procedural and team skills.
|
|
Bhardwaj et al., (2022) University of Florida College of Medicine, USA
|
Longitudinal Survey
|
Script Concordance Test (SCT) |
Written Exam: Comparing the SCT to usual clinical assessments |
Significant correlations between SCT, as ambiguous evolving clinical case scenario, and improved decision-making competency and valid assessment items. The SCT facilitated feedback and meaningful conversation about problem-solving insecurities
|
|
Wright et al., (2019) University of Western Australia |
Retrospective study |
Feedback Learning Opportunities (FLO) |
Multi-source feedback |
Prescence of FLOs in complex cases underlines one problem: insufficient clinical information related to clinical reasoning. Advantages shown for systematic feedback-related advice to handle diagnostic and treatment inaccuracies and the learning of alternatives
|
|
Forbes & Foulds (2023) Department of Pediatrics, University of Alberta, Edmonton, Canada
|
Comparative study |
Team-based learning (TBL) with Key Feature Questions (KFQ) |
Written and oral exam involving KFQ, OSCE and MCQ. Anonymous evaluation |
Significant improvement in KFQ scores. Valuable feedback on team-based approach on KFQ to progress clinical reasoning Ability to experience mistakes and identifying “learning gaps”
|
|
Khera et al., (2020) McGovern Medical School at the University of Texas Health Science Center, USA |
Non-experimental descriptive studies |
Skill session on writing patient assessments
|
Written exam involving Pre- and post-written patient assessments |
Introduction and practice of the efficient usage of semantic qualifiers for key problem summaries. Positive effect demonstrated when practicing the formulation, synthesising, and reviewing of potential differential diagnoses and integration of clinical reasoning.
|
|
Lissinna et al., (2022) Department of Pediatrics, University of Alberta, Edmonton Clinic, Canada
|
Qualitative Study |
Pediatric bootcamp using flipped classroom |
Questionnaire and Evaluation |
Positive effects of pre-readings and virtual interactive illness approach on efficiency of clinical data collection, critical-thinking and new mental approach to learning strategies in low stakes environment. Showed possible benefits from the preclinical-clinical transition. |
|
Schmidt & Grigull (2018) Medizinischen Hochschule Hannover (MHH), Germany |
Qualitative Study |
Interactive Serious Game: “Pedagotchi,” for case-based learning; blended learning |
Questionnaire System Usability Scale (SUS) and User Experience Questionnaire (UEQ) |
Motivational and digital additions to traditional lectures. Improved dialogue, real-time feedback and practice of clinical-reasoning in a low-stakes environment. |
Table 2. Overview of reports included in scoping review
B. Source of Studies and Research Design
Included studies came from 6 countries, in general being conducted at university hospitals. The largest group of included studies (n=4) originated in the USA (Bhardwaj et al., 2022; Khera et al., 2020; Konopasek et al., 2014; Rideout & Raszka, 2018). Two articles came from Australia (Bye et al., 2009; Wright et al., 2019) and Canada (Forbes & Foulds, 2023; Lissinna et al., 2022). Single studies were derived from China (Gong et al., 2022), Germany (Schmidt & Grigull, 2018) and Iran (Yousefichaijan et al., 2016).
We categorised the evidence in each publication based on an established evidence hierarchy (Table 3) (Eccles et al., 2001; Jensen et al., 2004). No reviewed study could be aligned to criterion 1a, i.e., evidence from meta-analysis of randomised controlled trials. Two studies employed a randomised-control design, with Bye et al. conducting a crossover controlled design (Bye et al., 2009; Gong et al., 2022). The method of employing a quasi-experimental study was conducted by two included studies (Konopasek et al., 2014; Yousefichaijan et al., 2016). The majority of included studies could be aligned with category III, i.e., evidence from non-experimental descriptive methods, or more specifically longitudinal surveys (Bhardwaj et al., 2022), retrospective studies (Wright et al., 2019) and qualitative approaches (Forbes & Foulds, 2023; Khera et al., 2020; Lissinna et al., 2022; Rideout & Raszka, 2018; Schmidt & Grigull, 2018).
|
Category of evidence |
Number of studies identified on each rank |
|
Ia: evidence from meta-analysis of randomised controlled trials |
|
|
Ib: evidence from at least one randomised controlled trial |
n=2 Gong et al., 2022; Bye et al., 2009 |
|
IIa: evidence from at least one controlled study without randomisation |
|
|
IIb: evidence from at least one other type of quasi-experimental study |
n=2 quasi-experimental Yousefichaijan et al., 2016; Konopasek et al., 2014 |
|
III: evidence from non-experimental descriptive studies, such as comparative studies, correlation studies |
n=7 Longitudinal survey: Bhardwaj et al., 2022 Qualitative study: Lissinna et al., 2022; Khera et al., 2020; Rideout & Raszka, 2018; Forbes & Foulds, 2023; Schmidt & Grigull, 2018. Retrospective study: Wright et al., 2019 |
|
IV: evidence from expert committee reports or opinions and ⁄ or clinical experience of respected authorities |
|
Table 3. Included studies categorised according to levels of evidence defined by Eccles et al. (2001)
C. Summary based on Type of Evidence
The key outcomes derived from the included studies mostly focused on the principle of problem-based learning and can be framed in reference to experiential learning, such as clinical simulation and the acquisition of theoretical reasoning skills (Fabry, 2022; Jensen et al., 2004).
1) Experiential learning: There is evidence, based on the following studies, indicating that a team-based approach of clinical scenarios, with patients or simulated scenarios facilitate the impartation of clinical skills and critical thinking. The role shift towards student-centered learning increases the motivation to actively participate and overcome passive decision-making (Gong et al., 2022). The randomised study by Gong et al. established a division of bedside tasks (i.e., medical history, physical examination, etc.) amongst the case group students. This facilitated knowledge exchange within the team, and enabled both awareness and practice of reasoning steps. Subsequent assessment using computer-based case simulations and the Mini-CEX (Mini Clinical Evaluation Exercise) detected significant improvements in clinical judgment and counselling skills after bedside team-based learning (Gong et al., 2022). In reference to critical thinking, all of the included studies demonstrated a preference for students to encounter and use real cases involving ambiguity, symptom polymorphisms and the possibility of false leads in the context of paediactric practice (Kassirer, 2010).
Forbes and Foulds (Forbes & Foulds, 2023) found that students’ evaluations of team-based learning showed that positive feedback on the ability to use the experiences of mistakes were linked with significant improvements in assessment scores using the Observed Structured Clinical Exam (OSCE).
Similarly, a survey by Rideout and Raszka (Rideout & Raszka, 2018) highlighted that increased team skills can result from feedback exchange and lead to the improvement of communication skills learnt during simulation, including working in intensive ettings and with distressed parents (Konopasek et al., 2014; Rideout & Raszka, 2018). In addition, improved motivation to learn was related to learning in a low-stakes environment (Lissinna et al., 2022; Rideout & Raszka, 2018; Schmidt & Grigull, 2018). Wright et al. reported that student log entries underlined the advantages of feedback-related advice in handling diagnostic and treatment inaccuracies (Wright et al., 2019).
A technique called the Group Objective Structured Clinical Experience used by Konopasek et al. (Konopasek et al., 2014) showed benefits for the learner-centered method through the practice of communication skills in teams during the process of clinical reasoning. This approach brought together experiential learning, multisource feedback and the perspective of dual-process theory in directing students to begin with their recognition of symptoms, then consider hypotheses based on history taking, and information and feedback from multiple parties (Table 2). In a questionnaire-based evaluation such clinical problem solving demonstrated significant increases in self-efficacy and their motivation to learn data gathering techniques (Konopasek et al., 2014).
A further example, Khera et al. (Khera et al., 2020) focused on written patient information prioritisation by using semantic qualifiers to efficiently summarise key problems. Semantic qualifiers are bipolar descriptions of symptoms linked to distil broad medical histories (Norman, 2005). The comparison of pre- and post-intervention evaluation resulted in statistically significant increases in differential diagnosis assessment scores (Khera et al., 2020).
Furthermore, half of the included studies identified multi-source feedback (student, teacher, patient) as being integral to the development of insight into their reasoning and decision-making processes. Feedback itself can proactively influence students’ awareness about their mistakes allowing a meaningful conversation about areas of confusion.
2) Theoretical reasoning skills: Examples of didactic approaches included the use of short-term workshops, flipped classroom teaching, virtual learning experiences, and script-concordance tests. These teaching methods resulted in improved awareness of theory, development of knowledge structures, data prioritisation, and critical thinking (Yousefichaijan et al., 2016). More specifically, half of the studies acknowledged the incorporation of a medical data acquisition technique as being a useful approach to teaching, since diagnostic inaccuracy can be linked with a lack of accurate data gathering (Bye et al., 2009). In reference to these diagnostic techniques, the workshop of Yousefichaijan et al. is an effective example of repeatedly practicing clinical reasoning as a pragmatic skill (Yousefichaijan et al., 2016). Comparing analyses of the Diagnostic Thinking Inventory (DTI) and Clinical Reasoning Problem (CRP) showed significant advantages of working in small groups on illness scenarios (Yousefichaijan et al., 2016). Lissinna et al. (2022) employed a virtual flipped classroom exercise, and then assessed students’ experiences of pre-reading and their practice of efficient sorting of clinically relevant data via semi-structured interviews. The concept of Blended-Learning, as a combination of digital and traditional teaching, embodies the Serious Game approach of Schmidt et al. (2018). The complementary results of Bye et al.’s comparative study, which focused on interactive versus computerised methods of pedagogy, underlines the advantages of the digital addition in the practice of interactive case-based learning with real-time feedback (Bye et al., 2009). In consideration of the aforementioned aspects, the implementation of the Script-Concordance Test that assesses case training, can reveal several advantageous measurements, related to pedagogical techniques using case-based and feedback methods and thus can be regarded as a valid assessment tool (Bhardwaj et al., 2022).
IV. DISCUSSION
A. Clinical Reasoning – A Complex Practical Skill
The findings from this scoping review affirm that clinical reasoning can be described as the mediatory link influencing a clinician’s cognitive multistep process. This process involves knowledge organisation, efficient data gathering, critical data integration culminating in generating a set of reasonable hypotheses, to finally achieve accurate diagnostic interpretation and reflection (Lissinna et al., 2022; Pennaforte et al., 2016; Pinnock et al., 2021). From a data driven perspective, used by novice learners, teaching these reasoning steps separately would likely impair the effectiveness of the reasoning process (Schmidt & Mamede, 2015). At the moment no peer-reviewed paediatric curricula guidelines focus on active educational experience of clinical reasoning. Additionally, short paediatric rotations only allow limited practice of common paediatric diagnoses (Madduri et al., 2024).
Consistent with Miller’s pyramid of clinical competence learning clinical skills effectively, involves promoting practice by doing, along with frequent repetition (Fabry, 2022; Miller, 1990). In reference to the dual-process model, repetition moves much of the cognitive effort involved in understanding the relevant illness presentation from system 2 to the pattern recognition abilities of system 1 (Yazdani et al., 2017). Considering clinical reasoning as a practical skill, student passivity is the reason why it is relatively difficult to attain a high level of competency (Forbes & Foulds, 2023). Ulfa et al. (2021) used a randomised control trial comparing lecture vs. team-based learning of postpartum hemorrhage of midwifery students. The results indicated the superiority of active team-based methods on the development of independent and effective critical-thinking abilities. This suggests substantial benefits for a paediatric curricula configuration that involves implementation of more active learning experiences starting in the pre-clinical years in the form of mixed teaching strategies (Forbes & Foulds, 2023; Jost et al., 2017; Koenemann et al., 2020). Jost and colleagues observed significantly improved clinical reasoning performance with Team-Based Learning groups in an undergraduate neurology course using key-feature examination (Jost et al., 2017).
B. Mix of Teaching Methods
In reference to this scoping review’s aim, we can identify the advantages of combining different teaching styles. Lectures remain the fundamental method used to convey basic scientific knowledge, which can be an essential precondition for using more practical teaching methods. The findings indicated that improvements of the decision-making process were first identified by theory presentation, i.e., teaching dual-process theory and its links to common cognitive pitfalls and the potentially significant adverse consequences for paediatric clinical reasoning (Schmidt & Mamede, 2015). However, lectures also have didactic disadvantages, which include teacher-centered explanations with less activation and linking of previous knowledge and may create cognitive overload in learners (Fabry, 2022). There are different options to overcome this by promoting active pre-class learning and open discussions about information processing ambiguities (Lissinna et al., 2022). For example, the use of the flipped classroom approach can improve clinical understanding and increase the motivation to learn in contrast to lecture-based approaches (Tang et al., 2017). The crossover study of Tan et al. (Tan et al., 2016) also indicated superior problem-solving ability attributed to team-based learning in comparison with interactive lectures. Similarly, Jackson et al. (Jackson et al., 2020) demonstrated a significant increase in satisfaction when using critical thinking and promoting student self-directed learning when attending an online team-based learning module in a family medicine rotation.
C. Clinical Reasoning and Clinical Cases
The simulation of clinical judgment can be enhanced using an evolving clinical scenario (Fabry, 2022). The focus on improvement of clinical judgment in paediatrics can be justified by a unique interaction of fine perception and empathy of the child’s clinical problem. In particular, the practice of effective communication plays a critical role in the analyses of symptoms when in discussion with parents and children. Since both are overlaid with anxiety, this adds to the diagnostic challenge. This requires experiential learning, for example by the careful student-centered bedside practice of communication with anxious and vulnerable families. This can increase students’ awareness of emotional messages and changes in the patient. The link of promoting empathy by teaching problem-solving plays a critical role in paediatrics (Gong et al., 2022). One example, could be the use of Illness scripts, describing an approach to synthesising patient history into a meaningful flowchart. Levin et al. and Konemann et al. showed students’ motivation working on real complex cases embodying a step-by-step information disclosure approach (Koenemann et al., 2020; Levin et al., 2016). Interestingly, Schmidt and Mamede also described these two opposing ways to present clinical cases, calling them “serial-cue” vs. “whole case” methods (Schmidt & Mamede, 2015). The studies included in this review emphasised students’ challenges with obtaining the correct collection of critical information for a stepwise disclosure in paediatrics.
Furthermore, the randomised trial protocol of Pennaforte et al., embodies an example of combining real-environment patient simulation and iterative discussions (Pennaforte et al., 2016). These discussion protocols appear as reminders at three key moments in time, namely data gathering, integration, and confirmation. The reminder and task verbalisation provide better insight into the dynamic systems, based on the dual-process theory. Debriefing thoughts, in the form of thinking aloud and self-explanation, could promote higher performance of active understanding, more accurate symptom correlations, deliberate reflection and especially detecting pitfalls in the reasoning process (Chamberland et al., 2015; Pennaforte et al., 2016).
Studies revealed the important role of appropriate and timely feedback on the overall improvement of a clinical skill (DeLeon et al., 2018; Fabry, 2022; Wright et al., 2019). Torre et al., identifies the contribution of bedside teaching and multi-source feedback (supervisor, students, and patients) as an essential part of enhancing students’ perceptions and understandings of a meaningful teaching experience (Torre et al., 2005). Feedback allows access to different perspectives, which can promote learning capacity; it is clearly regarded as a positive and proactive influence on the personal development required for successful teamwork (Koenemann et al., 2020).
The constant reference to decision making should not be regarded as relevant only to the clinician’s perspective since effective disease management in paediatric care also depends on decisions being made by the patient and the child’s parents and care givers. Consequently, we also need to focus on shared decision-making and communication skills as a crucial part of such deliberation (Gay et al., 2013). Patient-centered communication includes personal factors, like empathy and authenticity, which are essential when building a trusted and authentic clinician-patient relationship. Additionally, these skills can be seen as a tool for efficiently eliciting information and in the communication of treatment information, including medication information, to parents and children (Konopasek et al., 2014; Yousefichaijan et al., 2016). Effective communication skills of this sort increase patient adherence, especially when treatment strategies are planned in consensus with the patient (Amey et al., 2017).
V. CONCLUSION
Our scoping review illustrated a knowledge gap regarding the teaching of clinical reasoning as a practical skill in paediactric practice. The findings indicate that active student-centered repetition involving experiential learning would likely facilitate more effective learning during clinical reasoning in paediatrics as aligned with the following key steps. Firstly, it would facilitate activation of prior knowledge, supporting clinically relevant knowledge structure and ensuring accurate data gathering techniques. Secondly, the simulation of critical thinking is required to improve the process of reflection to reduce cognitive biases and pitfalls. And thirdly, such an approach would promote efficient communication and the development of feedback skills to overcome diagnostic and treatment inaccuracies. Despite our comprehensive search and the international representation present in the evidence-based studies included in our review, the total number of medical education studies in paediatrics related to clinical reasoning was limited, which underlines the need for further research and curricular development in this domain, particularly given the known unique challenges of the care of paediatric patients.
Notes on Contributors
Dr. Jasmin Oezcan was involved in the conceptualisation of the study, review of the literature, analysis of included reports and in the writing and revision of the manuscript.
Associate Professor Marcus A. Henning was involved in the development of the final list of papers considered for the review and in the writing and revision of the manuscript.
Associate Professor Craig S. Webster was involved in the development of the final list of papers considered for the final review, and in the writing and revision of the manuscript.
All authors have read and approved the final version of the manuscript and agree to be accountable for the work and its findings.
Ethical Approval
This manuscript comprises a scoping review of existing published reports and, therefore did not require approval from institutional review boards.
Data Availability
All relevant quantitative data are within the manuscript.
Acknowledgement
This work was conducted by Dr. Jasmin Oezcan as a visiting scholar at the Centre for Medical and Health Science Education, School of Medicine, University of Auckland, New Zealand. The authors also wish to thank Professor Cameron Grant, Head of the Department of Paediatrics, Child and Youth Health, for helpful insights regarding the development of teaching programs for primary care practitioners in child health and paediatrics in New Zealand.
Funding
There is no external funding involved in this study.
Declaration of Interest
Associate Professor Marcus Henning is an Editor of The Asia Pacific Scholar. Other authors have no conflicts of interest.
References
Amey, L., Donald, K. J., & Teodorczuk, A. (2017). Teaching clinical reasoning to medical students. British Journal of Hospital Medicine, 78(7), 399-401. https://doi.org/10.12968/hmed.2017.78.7.399
Bargh, J. A., & Chartrand, T. L. (1999). The unbearable automaticity of being. American Psychologist, 54(7), 462–479. https://doi.org/10.1037/0003-066X.54.7.462
Bhardwaj, P., Black, E. W., Fantone, J. C., Lopez, M., & Kelly, M. (2022). Script concordance tests for formative clinical reasoning and problem-solving assessment in General Pediatrics. MedEdPORTAL, 18, 11274. https://doi.org/10.15766/mep_2374-8265.11274
Bye, A. M., Connolly, A. M., Farrar, M., Lawson, J. A., & Lonergan, A. (2009). Teaching paediatric epilepsy to medical students: A randomised crossover trial. Journal of Paediatrics and Child Health, 45(12), 727-730. https://doi.org/10.1111/j.1440-1754.2009.01602.x
Chamberland, M., Mamede, S., St-Onge, C., Setrakian, J., Bergeron, L., & Schmidt, H. (2015). Self-explanation in learning clinical reasoning: The added value of examples and prompts. Medical Education, 49(2), 193-202. https://doi.org/10.1111/medu.12623
Croskerry, P. (2005). Diagnostic failure: A cognitive and affective approach. In K. Henriksen, J. B. Battles, E. S. Marks, & D. I. Lewin (Eds.), Advances in Patient Safety: From Research to Implementation (Vol. 2, pp. 241-254). PsycEXTRA Dataset. https://doi.org/10.1037/e448242006-001
de Jong, T., & Ferguson-Hessler, M. G. M. (1996). Types and qualities of knowledge. Educational Psychologist, 31(2), 105-113. https://doi.org/10.1207/s15326985ep3102_2
DeLeon, S., Mothner, B., & Middleman, A. (2018). Improving student documentation using a feedback tool. The Clinical Teacher, 15(1), 48-51. https://doi.org/10.1111/tct.12625
Eccles, M., Freemantle, N., & Mason, J. (2001). Using systematic reviews in clinical guideline development. In M. Egger, G. D. Smith, & D. G. Altman (Eds.), Systematic Reviews in Health Care (pp. 400-409). Wiley Online Library. https://doi.org/10.1002/9780470693926.ch21
Fabry, G. (2022). Medical Didactics- A competence-orientated, practical and scientific-funded education. Hogrefe.
Forbes, K. L., & Foulds, J. L. (2023). A team-based learning approach during pediatric clerkship to promote clinical reasoning. Academic Pediatrics, 23(7), 1459-1464. https://doi.org/10.1016/j.acap.2023.04.002
Gay, S., Bartlett, M., & McKinley, R. (2013). Teaching clinical reasoning to medical students. The Clinical Teacher, 10(5), 308-312. https://doi.org/10.1111/tct.12043
Gong, J., Du, J., Hao, J., & Li, L. (2022). Effects of bedside team-based learning on pediatric clinical practice in Chinese medical students. BMC Medical Education, 22(1), Article 264. https://doi.org/10.1186/s12909-022-03328-4
Graber, M. L., Franklin, N., & Gordon, R. (2005). Diagnostic error in internal medicine. Archives of Internal Medicine, 165(13), 1493-1499. https://doi.org/10.1001/archinte.165.13.1493
Grant, M. J., & Booth, A. (2009). A typology of reviews: an analysis of 14 review types and associated methodologies. Health Information & Libraries Journal, 26(2), 91-108. https://doi.org/10.1111/j.1471-1842.2009.00848.x
Groen, G. J., & Patel, V. L. (1985). Medical problem-solving: Some questionable assumptions. Medical Education, 19(2), 95-100. https://doi.org/10.1111/j.1365-2923.1985.tb01148.x
Gruppen, L. D., & Frohna, A. Z. (2002). Clinical Reasoning. In G. R. Norman, C. P. M. van der Vleuten, D. I. Newble, D. H. J. M. Dolmans, K. V. Mann, A. Rothman, & L. Curry (Eds.), International Handbook of Research in Medical Education (pp. 205-230). Springer. https://doi.org/10.1007/978-94-010-0462-6_8
Jackson, L., Otaki, F., Powell, L., Ghiglione, E., & Zary, N. (2020). Study of a COVID-19 induced transition from face-to-face to online team-based learning in undergraduate family medicine. MedEdPublish, 9(1), 232. https://doi.org/10.15694/mep.2020.000232.1
Jensen, L. S., Merry, A. F., Webster, C. S., Weller, J., & Larsson, L. (2004). Evidence-based strategies for preventing drug administration error during anaesthesia. Anaesthesia, 59(5), 493-504. https://doi.org/10.1111/j.1365-2044.2004.03670.x
Jost, M., Brüstle, P., Giesler, M., Rijntjes, M., & Brich, J. (2017). Effects of additional team-based learning on students’ clinical reasoning skills: A pilot study. BMC Research Notes, 10(1), Article 282. https://doi.org/10.1186/s13104-017-2614-9
Kassirer, J. P. (2010). Teaching clinical reasoning: Case-based and coached. Academic Medicine, 85(7), 1118-1124. https://doi.org/10.1097/acm.0b013e3181d5dd0d
Khera, S., Gavvala, S., Parlar-Chun, R., Huh, H., Hsu, J., & Ford, C. (2020). Skill session on writing patient assessments for pediatric clerkship students. MedEdPORTAL, 16. https://doi.org/10.15766/mep_2374-8265.11029
Koenemann, N., Lenzer, B., Zottmann, J. M., Fischer, M. R., & Weidenbusch, M. (2020). Clinical case discussions – A novel, supervised peer-teaching format to promote clinical reasoning in medical students. GMS Journal for Medical Education, 37(5), Doc48. https://doi.org/10.3205/zma001341
Konopasek, L., Kelly, K. V., Bylund, C. L., Wenderoth, S., & Storey-Johnson, C. (2014). The group objective structured clinical experience: building communication skills in the clinical reasoning context. Patient Education and Counseling, 96(1), 79-85. https://doi.org/10.1016/j.pec.2014.04.003
Lee, A., Joynt, G. M., Lee, A. K., Ho, A. M., Groves, M., Vlantis, A. C., Ma, R. C., Fung, C. S., & Aun, C. S. (2010). Using illness scripts to teach clinical reasoning skills to medical students. Family Medicine, 42(4), 255-261.
Levin, M., Cennimo, D., Chen, S., & Lamba, S. (2016). Teaching clinical reasoning to medical students: A case-based illness script worksheet approach. MedEdPORTAL, 12, Article 10445. https://doi.org/10.15766/mep_2374-8265.10445
Lissinna, B., Rashid, M., Foulds, J. L., & Forbes, K. L. (2022). Embracing uncertainty: Medical student perceptions of a pediatric bootcamp developed in response to mandated changes during the pandemic. BMC Medical Education, 22(1), Article 390. https://doi.org/10.1186/s12909-022-03471-y
Madduri, G. B., Torwekar, E. L., Demirel, S., Durham, M., Hauff, K. I., Kaul, R., Nichols, T., Ravid, N. L., Shaner, M. A., & Rassbach, C. E. (2024). CRISP: An inpatient pediatric curriculum for family medicine residents using clinical reasoning and iIllness scripts. MedEdPORTAL, 20, Article 11393. https://doi.org/10.15766/mep_2374-8265.11393
Marcum, J. A. (2012). An integrated model of clinical reasoning: Dual-process theory of cognition and metacognition. Journal of Evaluation in Clinical Practice, 18(5), 954-961. https://doi.org/10.1111/j.1365-2753.2012.01900.x
Miller, G. E. (1990). The assessment of clinical skills/competence/performance. Academic Medicine, 65(9), S63-S67. https://doi.org/10.1097/00001888-199009000-00045
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & The PRISMA Group. (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Medicine, 6(7), e1000097. https://doi.org/10.1371/journal.pmed.1000097
Norman, G. (2005). Research in clinical reasoning: Past history and current trends. Medical Education, 39(4), 418-427. https://doi.org/10.1111/j.1365-2929.2005.02127.x
Page, G., Bordage, G., & Allen, T. (1995). Developing key-feature problems and examinations to assess clinical decision-making skills. Academic Medicine, 70(3), 194-201. https://doi.org/10.1097/00001888-199503000-00009
Pennaforte, T., Moussa, A., Loye, N., Charlin, B., & Audétat, M. C. (2016). Exploring a new simulation approach to improve clinical reasoning teaching and assessment: Randomised trial protocol. MIR Research Protocols, 5(1), e26. https://doi.org/10.2196/resprot.4938
Pinnock, R., Ritchie, D., Gallagher, S., Henning, M. A., & Webster, C. S. (2021). The efficacy of mindful practice in improving diagnosis in healthcare: A systematic review and evidence synthesis. Advances in Health Sciences Education, 26(3), 785-809. https://doi.org/10.1007/s10459-020-10022-x
Pinnock, R., & Welch, P. (2014). Learning clinical reasoning. Journal of Paediatrics and Child Health, 50(4), 253-257. https://doi.org/10.1111/jpc.12455
Rideout, M., & Raszka, W. (2018). Hypovolemic shock in a child: A pediatric simulation case. MedEdPORTAL, 14, Article 10694. https://doi.org/10.15766/mep_2374-8265.10694
Schardt, C., Adams, M. B., Owens, T., Keitz, S., & Fontelo, P. (2007). Utilisation of the PICO framework to improve searching PubMed for clinical questions. BMC Medical Informatics and Decision Making, 7(1), Article 16. https://doi.org/10.1186/1472-6947-7-1
Schmidt, H. G., & Mamede, S. (2015). How to improve the teaching of clinical reasoning: A narrative review and a proposal. Medical Education, 49(10), 961-973. https://doi.org/10.1111/medu.12775
Schmidt, R., & Grigull, L. (2018). Pedagotchi: Entwicklung einer neuartigen Lernanwendung für die Pädiatrie. Monatsschrift Kinderheilkunde, 166(3), 228-235. https://doi.org/10.1007/s00112-017-0253-9
Schwartz, A., & Elstein, A. (2008). Clinical reasoning in medicine. In J. Higgs, M. Jones, S. Loftus, & N. Christensen (Eds.), Clinical Reasoning in the Health Professions (pp. 223-234). Elsevier.
Scott, I. A. (2009). Errors in clinical reasoning: causes and remedial strategies. BMJ, 338, b1860. https://doi.org/10.1136/bmj.b1860
Tan, N., Tan, K., & Ng, C. (2016). Does team-based learning improve clinical reasoning in neurology? Neurology, 86(16_supplement). https://doi.org/10.1212/wnl.86.16_supplement.p2.373
Tang, F., Chen, C., Zhu, Y., Zuo, C., Zhong, Y., Wang, N., Zhou, L., Zou, Y., & Liang, D. (2017). Comparison between flipped classroom and lecture-based classroom in ophthalmology clerkship. Medical Education Online, 22(1), Article 1395679. https://doi.org/10.1080/10872981.2017.1395679
Torre, D. M., Simpson, D., Sebastian, J. L., & Elnicki, D. M. (2005). Learning/feedback activities and high-quality teaching: Perceptions of third-year medical students during an inpatient rotation. Academic Medicine, 80(10), 950-954. https://doi.org/10.1097/00001888-200510000-00016
Ulfa, Y., Igarashi, Y., Takahata, K., Shishido, E., & Horiuchi, S. (2021). A comparison of team-based learning and lecture-based learning on clinical reasoning and classroom engagement: A cluster randomised controlled trial. BMC Medical Education, 21(1), Article 444. https://doi.org/10.1186/s12909-021-02881-8
Vanhecke, T. E. (2008). Zotero. Journal of the Medical Library Association, 96(3), 275.
Webster, C. S., Anderson, B. J., Stabile, M. J., Mitchell, S., Harris, R., & Merry, A. F. (2021). Improving the safety of pediatric sedation: Human error, technology, and clinical microsystems. In K. P. Mason (Ed.), Pediatric Sedation Outside of the Operating Room, 721–752. https://doi.org/10.1007/978-3-030-58406-1_38
Webster, C. S., Taylor, S., Thomas, C., & Weller, J. M. (2022). Social bias, discrimination and inequity in healthcare: Mechanisms, implications and recommendations. BJA Education, 22(4), 131-137. https://doi.org/10.1016/j.bjae.2021.11.011
Webster, C. S., Taylor, S., & Weller, J. M. (2021). Cognitive biases in diagnosis and decision making during anaesthesia and intensive care. BJA Education, 21(11), 420-425. https://doi.org/10.1016/j.bjae.2021.07.004
Wright, H. M., Maley, M. A. L., Playford, D. E., Nicol, P., & Evans, S. F. (2019). Feedback learning opportunities from medical student logs of paediatric patients. BMC Medical Education, 19(1), Article 107. https://doi.org/10.1186/s12909-019-1533-y
Yazdani, S., Hosseinzadeh, M., & Hosseini, F. (2017). Models of clinical reasoning with a focus on general practice: A critical review. Journal of Advances in Medical Education & Professionalism, 5(4), 177-184.
Yousefichaijan, P., Jafari, F., Kahbazi, M., Rafiei, M., & Pakniyat, A. (2016). The effect of short-term workshop on improving clinical reasoning skill of medical students. Medical Journal of the Islamic Republic of Iran, 30, 396.
Zhang, Y., Huang, L., Zhou, X., Zhang, X., Ke, Z., Wang, Z., Chen, Q., Dong, X., Du, L., Fang, J., Feng, X., Fu, J., He, Z., Huang, G., Huang, S., Ju, X., Gao, L., Li, L., Li, T., … Sun, K. (2019). Characteristics and workload of pediatricians in China. Pediatrics, 144(1), e20183532. https://doi.org/10.1542/peds.2018-3532
*Dr. Jasmin Oezcan
Department of Pediatrics Erlangen
University Hospital Erlangen,
Loschgestraße 15, 91054 Erlangen, Germany,
Email: oezcanj@yahoo.de
Submitted: 5 March 2024
Accepted: 14 October 2024
Published online: 1 April, TAPS 2025, 10(2), 17-33
https://doi.org/10.29060/TAPS.2025-10-2/RA3261
Cheng Li & Gunjeong Lee
School of Nursing, Ewha Womans University, Republic of Korea
Abstract
Introduction: This study aims to explore the development of nurse prescribing and identify nurse prescribing implementation and challenges in China.
Methods: Conducted as a systematic review adhering to the PRISMA, this study involved a comprehensive literature search across various databases. A timeline mapping and a region mapping were conducted.
Results: A total of 28 articles from databases were included in the study. The growth of nursing education and research, the emergence of specialty nurses, and the establishment of nurse-led clinics have contributed to the advancement of nurse prescribing in China. Presently, approximately half of the 34 regions in China are either actively researching or preparing for nurse prescribing involving medication.
Conclusion: Based on the findings, several tasks have been identified for the implementation of nurse prescribing in China. Firstly, it is imperative to elevate the overall level of nursing education and revise the existing curriculum to equip nursing students with the necessary knowledge and skills required for prescribing. Secondly, it is crucial to establish a systematic qualification system for prescribing nurses, defining the roles of specialty nurses and advanced practice nurses. Thirdly, the development of nurse prescribing includes scope of nursing practice and prescribing protocols are essential. Lastly, extension of the geographic reach of legislation and pilot projects is needed to realise the nationwide implementation of nurse prescribing.
Keywords: Nursing, Health Professional, Prescribing
Practice Highlights
- Nurse prescribing is fueled by the emergence of specialty nurses and nurse-led clinics.
- There are regional disparities in readiness for nurse prescribing.
- The key tasks are enhancing nursing education, qualification systems, and prescribing protocols.
I. INTRODUCTION
A. Background
Prescribing is a complex process requires deep understanding of pharmacology and disease, clinical judgement on risks and benefits of a treatment under an unpredictable context (Abuzour et al., 2018). The International Council of Nurses (ICN) stated that prescribing is an evolving process involving information gathering, clinical decision-making, communication, and evaluation which results in the initiation, continuation, or cessation of a medication (International Council of Nurses, 2021).
The extension of prescriptive authority to nurses has taken place for several reasons. First, nurse prescribing contributes to efficient and effective patient care and the quality and continuity of care (Gielen et al., 2014). Second, nurse prescribing accommodates nurses’ professional skills, increases nurses’ autonomy, and minimises unnecessary time waste for medical practitioners and patients (Kilańska et al., 2022). Third, the patient outcome of nurse prescribing is indicated as similar or better compared to the prescribing of other healthcare professionals (Ling et al., 2018; McMenamin et al., 2023).
The legislative expansion of prescriptive authority for nurses has taken place in the 1980s in the USA, 1990s in the UK, at the turn of the 21st Century in Canada, Europe, Australia, New Zealand, some countries of Africa, and Spain. As of 2021, 44 countries were reported to have formal laws or regulations that authorise nurse prescribing (International Council of Nurses, 2021; Maier, 2019).
Nurse prescribing is identified by scholars as sensitive to the country’s context and the healthcare culture, defining and implementing of nurse prescribing follows a distinctive pattern in different countries (International Council of Nurses, 2021; Nissen et al., 2010). The common areas of prescription include medications, therapies and therapeutics, durable medical equipment, appliances and certain dressings, foods designated for specific therapeutic purposes, and electrolytes (International Council of Nurses, 2021). Due to its complexity, the following frameworks and models are formed by scholars and institutions to enhance the understanding of nurse prescribing.
The ICN published the ‘Guidelines on Prescriptive Authority for Nurses’ in 2021, suggesting a framework with five components including education, regulation, authorisation,, scope of practice, and continuing professional development. This guideline adopted a four-category prescribing model (Nissen et al., 2010). This model consists of four categories: independent prescribing, supplementary prescribing (dependent), prescribing via a structured prescribing arrangement (protocol), and prescribing to administer. Each of these four categories in order requires increased skill level, decision-making ability, and accountability of prescriber.
The qualification system of prescribing nurses in different countries and regions is diverse (Maier, 2019). ICN differentiates the post-basic level nurse prescribing from the advanced practice level nurse prescribing. Prescribing nurses at the post-basic level are those who have completed their basic nursing education, and practice nursing as registered nurses (RNs). Prescribing nurses at the advanced practice level are those with a certain period of clinical experience, holding higher credentials such as APN (advanced practice nurse), NP (nurse practitioner) or specialty nurse (International Council of Nurses, 2021).
In China, nurse prescribing is defined as nurses diagnosing and making decisions on diet, psychological health, treatment, disease, and care level of the patients (Ma & Ding, 2018). In 2022, Shenzhen of China passed a medical regulation. This is seen as the first legislation in China that grants prescriptive authority to nurses. The growth of nursing education and research, the emergence of specialty nurses, and the establishment of nurse-led clinics have contributed to the advancement of nurse prescribing in China.
B. Nursing in China
By 2021, the number of registered nurses in China doubled in the last decade and exceeded 5.02 million, nurses fill about 45% of the total number of health professionals and the number of registered nurses per 1,000 population reached 3.56 (National Health Commission of the People’s Republic of China, 2022). The number of RN with a bachelor’s degree or higher has steadily grown for decades, nearly 180,000 in 2010 and 1.36 million in 2020 (National Health Commission of the People’s Republic of China, 2022), 30.4% of whom have received a baccalaureate or higher credential. An increased number of nurses with higher education level accelerates the development of nursing research (Wu, 2022).
Referring to advanced practice nursing in some developed countries, specialty nursing in China umbrellas registered nurses who have received specialised training and been certified by the training institutions, appeared first in the 1990s (Wu, 2022). Oncology, wound ostomy, PICC (Peripherally inserted central catheter), and blood purification are the most common and comparably developed specialties (Wang et al., 2018). Around 8000 nurses participated in specialty nurse (专业护士) training programs run by the Chinese Nursing Association in 2021 (Wu, 2022).
Advanced practice nursing, on the other hand, in 2007, the Guangdong Health Commission worked with the Hong Kong Hospital to prepare 614 APNs of 14 specialties over 4 years (Wong, 2018). To attain an APN credential, nurses are suggested to have a bachelor’s degree, a minimum of 8 years of clinical experience, and 2 years of specialised clinical experience (Wong, 2018). Beijing University in 2017 admitted two candidates to an advanced practice nursing program (Zhang et al., 2022).
A nurse-led clinic is defined as a clinical practice facility where nurses have their own formalised and structured standards to address the healthcare needs of patients and their families (Hatchett, 2003). The common NLCs (护理门诊) of China are run as divisions of outpatients by hospitals. NLCs accommodate specialty nurses and are one of the main settings where pilot nurse prescribing takes place in China (Chen & Peng, 2023; Ling et al., 2018). China first initiated NLCs on maternal health in 1995, psychiatric NLCs in 1997. In 2016, over 900 NLCs in 19 provinces were open, an average number of 2.8 NLCs were operated at each hospital, each NLC accommodated 36 clients a day, and 75.5% of these clinics were PICC NLCs (Gao et al., 2017). 69.3% of the NLC nurses reported that the lack of prescriptive authority is a major challenge they face in NLC nursing (Dong et al., 2022).
Given this global and domestic context, the objective of this study is to examine nurse prescribing in China, offering an overview of its development and implementation, identifying the challenges associated with it.
II. METHODS
The aim of this study is to review, identify, and synthesise the evidence presented in the included literature on nurse prescribing, so to
- Track the development of nurse prescribing in China;
- Describe nurse prescribing implementation in China; &
- Identify challenges faced in nurse prescribing of China
A systematic review was conducted in accordance with the procedure of the PRISMA Statement 2020 (Page et al., 2021). The flow diagram was utilised for the literature search and the checklist was followed as an overall guide of this study.
A. Data Collection
The literature search was conducted on Medline (PubMed), CINAHL, CNKI (China National Knowledge Infrastructure), and Wanfang Data. The records with titles or abstracts containing the terms ‘nurs* prescri*’ (护*处方*)and ‘Chin*’ were expected in this process. The database and document search were conducted from 1 January to 17 June 2023. Articles are included when they present nurse prescribing in China and the full text is available in either Chinese or English. Articles are excluded when the focus is nurse prescribing out of China, or is a single group of a client population or a particular medicine.
B. Data Analysis
A quality assessment was conducted after the screening process, using the Mixed Methods Appraisal Tool 2018 (Hong et al., 2018).
For data analysis, timeline and region mapping were used in former studies to approach nurse prescribing of other countries. In this study, a timeline mapping was conducted to chart the progression of nurse prescribing practices over time. A region mapping was performed focusing on the geographical distribution and implementation of nurse prescribing practices. An overall nurse prescribing profile of China was provided and a discussion on the current practice and indicated challenges was applied.
III. RESULTS
A. Search Outcomes
As a result, a total of 441 studies were taken into the identification process (Figure 1). At the end of the screening, a total number of 28 articles from the databases were included for analysis.

Figure 1. Screening Flow Diagram
CINAHL – Cumulative Index to Nursing and Allied Health Literature
CNKI – China National Knowledge Infrastructure
|
No |
Authors |
Origin |
Purpose |
Research design |
Disciplinary home |
Method/ framework |
Major finding |
|
1 |
Chen L. & Peng G. (2023) |
Guangdong |
To describe nurse prescribing at NLCs in Guangdong |
Quantitative |
Nursing |
No |
Detailed nurse prescribing in Guangdong (content focused) |
|
2 |
Wang, X. et al. (2022) |
Shanxi |
To construct general clinical practice training program for drug prescribing applicants of nurses in China |
Qualitative |
Nursing |
Delphi method |
Three-level indexed training program development and comparison with the US, UK and Ireland. |
|
3 |
Zhang, Q. et al. (2022) |
Shanxi |
To interpret ICN guideline to promote common understanding of nurse prescribing in China |
Qualitative |
Nursing |
ICN Guideline |
Analyses nurse prescribing in China providing interpretation of the guide and comparison of other countries |
|
4 |
Han, S. et al. (2022) |
Shanxi |
To review main research results and application on nurse decision making and prescribing |
Qualitative |
Nursing |
No |
Further research and practice in nursing education, APN, nurse prescribing is needed |
|
5 |
Fan, Y. et al. (2022) |
Henan |
To review development of nurse prescribing globally and summarise theory and practice evidence |
Qualitative |
Nursing |
No |
Provides suggestion for the government, nursing institutions and scholars. |
|
6 |
Xing, M. et al. (2022) |
Zhejiang |
To identify nurse prescribing challenges and advantages in China. |
Qualitative |
Nursing |
SWOT analysis |
Summarises internal and external challenges and advantages and provides future strategies. S-O, W-O, S-T, W-T strategies are proposed. |
|
7 |
Han, S. et al. (2021) |
Shanxi |
To further explore nurse prescribing contents |
Qualitative |
Nursing |
Delphi method |
Conducted a list of nurse prescribing medications, suggested forms and training curriculums of nurse prescribing. 348 nurse prescribing medications, 6-unit training |
|
8 |
Wang, L. et al. (2021) |
Zhejiang, Liaoning |
To identify regulatory challenges in nurse prescribing, suggest effort on liability system and institutional mechanism |
Qualitative |
Law |
No |
Redefines nurse prescribing in China, suggests regulatory support and clarification on liability |
|
9 |
Wang, Y. et al. (2021) |
Shanxi |
To construct the general training syllabus for nurses’ prescription right of applicants for prescription right in different clinical specialist nurses |
Qualitative |
Nursing |
Delphi method |
The constructed training syllabus for clinical specialist nurses was reliable, which could provide basis for prescription right training of clinical specialist nurses. A training guide of nurse prescriber is provided. |
|
10 |
Wang, X. et al. (2021) |
Shanxi |
To conduct a global analysis of nurse prescribing training |
Qualitative |
Nursing |
No |
Identifies challenges, provides suggestions on practical training of nurse prescribing |
|
11 |
Hou, X. (2021) |
Sichuan |
To investigate scope and related factors of nurse prescribing in third-level hospitals |
Qualitative |
Nursing |
Phenomenological analysis, Colaizzi |
Nurse prescribing in China is in its infancy. |
|
12 |
Zhong, M. et al. (2020) |
Guangdong |
To understand nurses’ belief in and attitudes towards nurse’s prescription right so as to provide a reference for medical decision makers to formulate relevant policies and expand the scope of nursing service |
Quantitative |
Nursing |
Scale of nurses’ attitudes and belief towards nurse prescribing |
Nurses have positive attitudes and beliefs in nurse’s prescription. A minimum of 10 years’ clinical work experience, a professional title of supervisor nurses and a bachelor’s degree are suggested as entry qualifications for the right |
|
13 |
Wang, Y. et al. (2020) |
Shanxi |
To discuss training in nurse prescribing under global context to provide evidence for domestic application |
Qualitative |
Nursing |
/ |
Standardised trainings to nurses with different education backgrounds are needed |
|
14 |
Wang, S. et al. (2020) |
Shandong |
Discuss the content of the prescription right of nurses and provide references for relevant decision-making |
Qualitative |
Nursing |
Delphi method |
Content table of medical and non-medical nurse prescribing: 27 nursing intervention prescriptions, 15 examination prescriptions, 21 medical device prescriptions and 35 drug prescriptions were identified. |
|
15 |
Wan, Z. & He, Y. (2020) |
Beijing |
To summarise the classification, development data and qualification of nurse prescribing at home and abroad |
Qualitative |
Nursing |
/ |
4 suggestions on nurse prescribing |
|
16 |
Feng, S. et al. (2020) |
Shandong |
To summarise practical exploration and theoretical research of nurse prescribing in China |
Qualitative |
Nursing |
/ |
Stresses both education curriculum and continuing training on prescribing for nurses |
|
17 |
Li, M. (2019) |
Guizhou |
To compare nurse prescribing at home and abroad: the US, Australia, England |
Qualitative |
Medicine |
/ |
Comparison on prescriber qualification, specialization, contents. |
|
18 |
Han, S. & Hou, Y. (2019) |
Shanxi |
Advantages, disadvantages, opportunities and threats of granting prescription rights to clinical nurses in China |
Qualitative |
Nursing |
SWOT analysis |
Construction of nurses team the development of specialist nurses and the training of highly educated personnel in China all should be strengthened |
|
19 |
Tian, Y. et al. (2019) |
Henan |
To investigate the status quo of clinical nurses’ cognition of nurse prescribing |
Quantitative |
Nursing |
/ |
262 nurses lack of knowledge on nurse prescribing while showing a strong will for it. |
|
20 |
Wang, M. et al. (2018) |
Anhui |
To explore attitudes of doctors and nurses towards nurses’ qualification of prescribing |
Quantitative |
Nursing |
/ |
1056 medical staff from 14 hospitals in Anhui |
|
21 |
Li, H. & Ding, P. (2018) |
Anhui |
Overview nurse prescribing under NLC context |
Qualitative |
Nursing |
/ |
NLC nurse prescribing overview and future suggestions |
|
22 |
Ma, D. & Ding, P. (2018) |
Anhui |
To identify the scope of authority on prescription right of nurses in Anhui |
Qualitative |
Nursing |
/ |
Zoom in on Anhui trail |
|
23 |
Cheng, Z. & Xia, H. (2017) |
Shanghai |
To review nurse prescribing in England, Canada, Australia and the US. |
Qualitative |
Nursing |
/ |
Provides details of prescriber qualification, content, format, extension of nurse prescribing, suggests regulations and trials on nurse prescribing in China |
|
24 |
Gong, S. et al. (2016) |
Jilin |
To review nurse prescribing in England, so to provide evidence for domestic application |
Qualitative |
Nursing |
/ |
Provides details of prescriber qualification, content, format, extension of nurse prescribing in England. Identifies 3 challenges of China. |
|
25 |
Wei, X. (2016) |
Gansu |
Explore certain prescriptions that meet nurse’s capability in China |
Qualitative |
Nursing |
/ |
Suggests certain prescriptions nurse should practice within extended prescribing. 11 prescriptions for extended prescribing |
|
26 |
Zhang, G. et al. (2012) |
Shanxi |
To gain opinions on baccalaureate curriculum for nurse prescribing from experts |
Qualitative |
Nursing |
Delphi method |
Provides evidence for baccalaureate curriculum in preparation of nurse prescribing. 3 categories, 11 subjects |
|
27 |
* Zhang, G. et al. (2012) |
Shanxi |
To study on qualification of nurse prescribing applicants |
Qualitative |
Nursing |
Delphi method |
Provides evidence on minimised qualification of nurse prescriber. Baseline of nurse prescribing applicants |
|
28 |
Han, S. & Li, X. (2011) |
Shanxi |
To probe into the promotion factors of nurse prescribing implementation in China |
Qualitative |
Nursing |
Delphi method |
Categorises and lists factors of nurse prescribing in China. 43 promoting factors of nurse prescribing |
Table 1. Summary of included studies
*NLC (Nurse-Led Clinics), Shanxi (山西省), ICN (International Council of Nurses), US (United States), UK (United Kingdom), SWOT (Strengths, Weaknesses, Opportunities, and Threats), AHP (Analytic Hierarchy Process)
The 28 (100%) articles were all in Chinese, published between 2010 and 2023, eleven papers (39.3%) were conducted in the Shanxi (山西) Province. Four (14.3%) studies are designed quantitative and 24 (85.7%) are qualitative. Two articles (7.1%) were conducted in the medicine or law disciplines, the rest 26 (92.9%) were conducted in nursing. Seven studies (25.0%) applied Delphi method and 2 (7.1%) applied SWOT analysis. The studies on nurse prescribing fall mostly into the reviews of nurse prescribing abroad. This research work provides evidence for the qualification of prescribing nurses, the prescription protocols and the challenges in nurse prescribing.
B. Development of Nurse Prescribing in China
Nurse prescribing as well as nurse-led clinic nursing are being practiced since 1996 in Hong Kong (Parker & Hill, 2017; Wong & Chung, 2006). As for the mainland, the realization of nurse prescribing started in 2005 (Han et al., 2022). Research teams formed in 2005 and started research on decision-making in the patient classification system among nurses (Han et al., 2022). In 2007, a research team proposed that nurses should be the decision maker of nursing care, and divided nursing interventions into 16 independent and 11 integrated categories for decision making (Han et al., 2022). In 2020, a list of nurse prescriptions was provided (Wang et al., 2022), it consists of 27 prescriptions for nursing interventions, 15 for tests and examinations, 21 for medical aids and instruments, and 35 for medicine.
For medicine nurse prescribing, starting in 2008, researchers have looked into the contents and forms of prescribing (Han et al., 2022). They identified the contents in 7 acute and 4 chronic illnesses, modified the qualification of prescribing nurses (Han et al., 2022). They also provided a list of nurse prescriptions with 348 medicines and proposed a four-level prescribing model: independent prescribing, supplementary prescribing, extended prescribing, and adjusted prescribing (Han et al., 2022).
As for the qualification of prescribers, prescribing nurses should be those who work at third level hospitals, have bachelor’s degrees in nursing, and have 5 years of clinical work experience after obtaining the intermediate profession rank (Zhang et al., 2012). Researchers also proposed to add courses in nursing education to prepare nurses to prescribe, such as laws and regulations, nursing intervention, dosage calculation and substance abuse (Han et al., 2022).
In July 2017, Anhui Province initiated a trial as the landing of nurse prescribing in China. By the end of 2017, Anhui arranged 78 specialty nurses into 22 community health centers, opened 7 nurse-led clinics, and authorised these nurses limited prescribing (Ma & Ding, 2018). Guangdong Province is known as the first region opened traditional Chinese medicine NLCs in 2006. In 2022, the Shenzhen City of Guangdong Province authorises specialty nurses with the examination, treatment, and external medicine prescribing (Shenzhen Municipal People’s Congress, 2022). A survey conducted in Guangdong indicates 88.54% of the NLC nurses practice independent nurse prescribing (Chen & Peng, 2023).

Figure 2. Nurse Prescribing Timeline in China
*The left presents events in policy and practice, right in education and research.
C. Present Nurse Prescribing in China
Nurses have shown their positive intention in nurse prescribing in several research. A sample of nurses responded with an intermediate to a positive level of faith and attitude toward nurse prescribing (Zhong et al., 2020). The same study also emphasises that higher professional ranking and longer clinical experience led to a stronger intention and faith in nurse prescribing.
In the Anhui trial, the nurse prescribing is limited to non-medicine prescription for hypertension, diabetes, stroke, wound stoma, mental illness, gestational diabetes, and childbirth (Ma & Ding, 2018). Prescribers are limited to a group of nurses who have over 15 years of clinical experience, had received specialty nurse training with certificates, and have advanced communication skills (Ma & Ding, 2018). Prescribers make decisions and provide interventions on dressing changes, general physical examination, health education and consultation, test result and report reading, history taking, and physical or mental examination in chronic diseases (Ma & Ding, 2018).
In Guangdong Province, the NLC nurse prescribing includes medicine, tests and treatments, medical aids and devices, home medical devices, dressings, therapeutic diet prescriptions, and health education (Chen & Peng, 2023). Nurses prescribe several external medicines and limited injected medicines (normal saline solution, heparin injection, peritoneal fluid, etc.) (Chen & Peng, 2023).
In the Shenzhen legislation, specialty nurses are regulated to be the only qualified prescribing nurses, specifically those who have a baccalaureate degree or above in nursing, more than five years of clinical experience and more than two years in relevant specialised departments, meanwhile having intermediate profession ranks or above (Shenzhen Municipal People’s Congress, 2022).
More than half of the 34 provinces run nurse-led clinics and about 70% of nurses at these clinics report independent nursing practice (Gao et al., 2017). Currently, about half of the total 34 regions are recognised in the research or preparation phase for the implementation of nurse prescribing on medicine (Figure 3). Trials and legislative move are seen to take place in regions with intermediate research activity.

Figure 3. Nurse Prescribing Region Mapping of China in 2023
D. Indicated Challenges
Despite the positive intentions, nurses and nursing students lack knowledge of nurse prescribing and lack confidence in it (Hou, 2021; Tian et al., 2019). A percentage 60.7 of registered nurses reported it necessary for nurses to have prescriptive authorization and 58% are willing to have it, but about half, 49.2% of the nurses have not heard about nurse prescribing by the time they were surveyed (Tian et al., 2019). A qualitative study indicates all participated specialty nurses advocated for nurse prescribing (Hou, 2021). Less than 35% of medical and nursing students had heard of nurse prescribing, and less than 5% had heard of the Anhui trial (Tian et al., 2019).
The current nursing education level is a major concern in nurse prescribing (Feng et al., 2020; Y. P. Wang et al., 2020; Zhang et al., 2012). In China, as of 2020 and 2021, respectively, 71.2% and 69.5% of the nurses had credentials below baccalaureate, 28.7% and 30.1% had a baccalaureate degree, 0.2% and 0.3% had a master’s or a higher credential (National Health Commission of the People’s Republic of China, 2022).
For the education curriculum, researchers suggest multi-level prescribing training due to the diversity of current nursing education levels. Researches focus on curriculum design for baccalaureate nursing education (Zhang et al., 2012) or the design for specialty nurse training (Wang et al., 2022), most suggest including pharmacology and related legislation (Zhang et al., 2012).
For the nurse prescribing training, an education program is recommended to reach a performance set standard for the nurse seeking prescriptive authority (International Council of Nurses, 2021). A prescribing-specific training is suggested in some studies (Wang et al., 2021; Wang et al., 2022), most of these studies take the training system of the United Kingdom (UK) as their reference.
The current qualification system for prescribing nurses has been identified as problematic in several studies (Gong et al., 2016; Xing et al., 2022; Zhong et al., 2020). Some studies suggest a combination of a master’s degree and the highest professional rank (Cheng & Xia, 2017). Some suggest specialty nurses (Cheng & Xia, 2017) practice prescribing in their specialties. Some others suggest a baccalaureate degree and 5 years of clinical experience with intermediate profession rank (Wang et al., 2018; Zhang et al., 2012).
The present nurse prescribing implementation is limited within the extended category (Wang et al., 2021) due to the lack of organizational preparation (Han et al., 2022; Hou, 2021). These organizational conditions include the current nursing education level, the lack of systematic qualification of prescribers (Zhang et al., 2012), the clear scope of nursing practice (Fan et al., 2022; Wei, 2016), guidelines and protocols (Han et al., 2021), and solutions on extension and geographic expansion (Wang et al., 2021).
Under the limited pilot practice and the absence of national legislation, current nurse prescribing in China requires both expansion and extension. This session summarised the implementation of nurse prescribing and analysed the indicated challenges. The improvement of nurses’ knowledge of prescribing, the current nursing education level, and the training and qualification of prescribing nurses are indicated as the priorities.
IV. DISCUSSION
Previous studies on nurse prescribing have primarily focused on developed countries, however, it is worth noting that developing countries have shown a slightly higher rate of nurse prescribing authorization, with 38% compared to 31% in developed countries (International Council of Nurses, 2021). This study reviewed the development and implementation of nurse prescribing and identified the challenges China is facing to further practice nursing prescribing.
Unlike other countries that initiated nurse prescribing decades ago, in China, the exploration of nurse prescribing appeared late. Nurse prescribing related regulations can be traced to the 2006 Prescription Administrative Policy, the Article 2 indicates that physicians are the only prescribers of medicine in China. The Nursing Regulation indicates nurses are obliged to implement necessary first aid in emergencies and remain critical on instructions of doctors according to Article 17.
On June 23, 2022, the Municipal People’s Congress of Shenzhen passed the Medical Regulation of Shenzhen Special Economic Zone that came into force on January 1, 2023. This is the first legislation in China that grants prescriptive authority for nurses according to Article 65. It also provides a general qualification guide of specialty nurses, clarified in Article 64.
For the implementation, nurses and nursing students show limited knowledge and confidence in nurse prescribing. This is seen caused by the current nursing education level and the content of the education curriculum. For nursing education level, referring to the nursing education level in the United States, 2016 is reported as the year when all the states in the US practice nurse prescribing. In 2015, an estimated 65% of nurses had obtained a baccalaureate or higher degree (National Council of State Boards of Nursing, 2016). In 2017, the number of RNs with a master’s degree in nursing has increased to 17.1% and 1.1% had a Doctorate in Nursing Practice, 10.0% held an APRN credential (National Council of State Boards of Nursing, 2018).
As for the training of prescribing nurses, the UK applies prescribing-specific training. The training follows a structured framework governed by regulatory bodies such as the Nursing and Midwifery Council (NMC) and involves a combination of theoretical and practical components (Courtenay et al., 2007). The training program typically consists of two parts: the academic component and the clinical component (Nursing and Midwifery Council, 2018).
For qualification of prescribing nurses, thirty-one of the 44 countries authorise nurse prescribing at post-basic levels, to nurses who have completed their basic nursing education; 13 countries at advanced practice levels; 11 countries allow nurses to prescribe at both the post-basic and advanced practice levels (International Council of Nurses, 2021). In the United States by 2016, all 50 states and the District of Columbia authorise certain levels of independent prescribing to APNs (American Nurses Association, 2018). Canada has a broad advanced practice level prescriptive authority for NPs federally and in recent years at a post-basic level for RNs provincially in Alberta and Ontario (Canadian Nurses Association, 2015). In Europe, prescribing by nurses has been recognised legally in 15 countries at a post-basic level (Gielen et al., 2014).
In the UK, the NMC outlines the requirements and standards that nurses must meet to become qualified prescribers. Upon successful completion of an NMC-approved prescribing course delivered by a recognised educational institution, nurses are eligible to apply for the relevant prescribing qualification from the NMC (Nursing and Midwifery Council, 2018). These qualifications determine the scope of prescribing authority for nurses, specifying the range of medications they can prescribe and any limitations or restrictions.
In China, specialty nurses are recognised as prescribing nurses in the Shenzhen legislation. Although prerequisite 2 years of clinical experience, 2 to 3 months training period is seen in most specialty nurse training programs, current evidence shows there is no modified training, qualification, or scope of practice for specialty nurses at a national level (Han & Hou, 2019; Han & Li, 2011).
The confusion in specialty nursing and advanced practice nursing is seen in former studies. The specialty nurse system should be well differentiated from the advanced practice nurse system in China. In a long-term stance either form a linked structure to umbrella both specialty nurses and APNs as equal prescribing nurses or assign respective categories of prescriptive authorities to each group. As a result, the qualifications of prescribing nurses can be modified at a national level.
Evidence on the outcome and evaluation of the current trial practice and the region-specific analysis were rare. The possibility and plan for the expansion of nurse prescribing over the country were not observed in former research. Despite expansion, the extension to other levels of nurse prescribing is needed. In the US, some states allow advanced practice registered nurses (APRNs) to practice independently (independent), some others require APRNs to work within a collaborative agreement with a physician (supplementary), 16 states allow RNs to dispense some medications (protocol) including contraceptives and drugs for sexually transmitted infection care in outpatient settings, such as a health department or a family planning clinic (Guttmacher Institute, 2023).
A. Limitation & Implication
Despite the scarcity of research on nurse prescribing in China and the lack of recent studies addressing the latest updates, this study overviewed nurse prescribing in China through a review of the development, the implementation, and the challenges, provides insights with global relevance. As healthcare systems worldwide face increasing demands and evolving roles for healthcare professionals, understanding diverse implementations of nurse prescribing offers crucial comparative perspectives. This article not only provides evidence on how nurse prescribing is integrated within China’s unique healthcare landscape but also serves as a benchmark for evaluating similar practices across different countries. For researchers and policymakers, these findings contribute to a broader understanding of effective healthcare strategies, policy development, and the global advancement of nursing roles.
As for the limitation, bias might exist in the screening and analysis process as they were conducted by two reviewers. In China, the community healthcare setting is regulated as one of the nurse prescribing settings in the Shenzhen legislation. More investigation on nurse prescribing in community settings seems necessary.
V. CONCLUSION
This systematic review followed the PRISMA 2020 Statement, analysed 28 articles. The 28 articles were assessed by the MMAT 2018 for synthesis. Both a time and a region mapping of nurse prescribing in China were conducted. This study provides an overview of the implementation and challenges of nurse prescribing in China.
Along with the development of specialty nursing, more than half of the province-level regions run hospital-based nurse-led clinics and about 70% of the nurses at these clinics practice independently. As for nurse prescribing, post a long research and preparation period, Anhui Province started a trial in July 2017 and practices non-medicine prescriptions for certain diseases and conditions. In June 2022, the Congress of Shenzhen City passed a medical regulation authorises specialty nurses with examination, treatment, and external medicine such as ointment and dressing prescribing, as the first legislative move in China. About half of the total 34 regions are in research or preparation phase for the implementation of medicine nurse prescribing.
The lack of knowledge and confidence related to nurse prescribing among nurses and nursing students, the current nursing education level and curriculum, and the training and qualification of prescribing nurses are recognised as the major concerns of nurse prescribing in China. Limited research, pilot practice, and legislative move of nurse prescribing are observed.
To meet the growing need for nurse prescribing in China, the following tasks are identified. First, improvement in nursing education level and curriculum is necessary. Second, a systematic qualification system for prescribing nurses should be established based on the clarification of specialty nurses and advanced practice nurses. Third, the scope of nursing practice consists of prescribing and the protocols for prescribing are in need. Fourth, the geographic expansion of legislation and pilot project are expected to reach nurse prescribing implementation at a national level. Last, future research should focus on nurse prescribing in community healthcare settings.
Notes on Contributors
CL performed the literature search and analysis, wrote the original manuscript, prepared the figures and tables, and worked on the review and editing. GJL supervised the conceptualisation and the methodology, provided suggestions on the validation and visualization.
Ethical Approval
As this study is a systematic review, ethical approval and IRB application was not applicable.
Data Availability
Data set that support the findings of this study are openly available in Figshare repository https://doi.org/10.6084/m9.figshare.25310869
Funding
No funding sources are associated with this study.
Declaration of Interest
No conflicts of interest are associated with this paper.
References
Abuzour, A. S., Lewis, P. J., & Tully, M. P. (2018). Practice makes perfect: A systematic review of the expertise development of pharmacist and nurse independent prescribers in the United Kingdom. Research in Social and Administrative Pharmacy, 14(1), 6-17. https://doi.org/10.1016/j.sapharm.2017.02.002
American Nurses Association. (2018). Nursing scope of practice. https://www.nursingworld.org/practice-policy/scope-of-practice/
Canadian Nurses Association. (2015). Framework for Registered Nurse Prescribing in Canada. https://www.cna-aiic.ca/en/nursing/ regulated-nursing-in-canada/rn-prescribing-framework
Chen, L. H., & Peng, G. Y. (2023). Investigation research on nursing outpatient clinics and prescriptive authority for nurses in Guangdong province. Nursing Research, 37(8), 1443-1448. https://doi.org/10.12102/j.issn.1009-6493.2023.08.024
Cheng, Z. H., & Xia, H. O. (2017). Implementation of nurse prescribing rights abroad and its implications for China. Chinese Journal of Nursing, 06, 764-767. http://zh.zhhlzzs.com/CN/Y2017/V52/I6/764
Courtenay, M., Carey, N., & Burke, J. (2007). Independent extended and supplementary nurse prescribing practice in the UK: A national questionnaire survey. International Journal of Nursing Studies, 44(7), 1093-1101. https://doi.org/10.1016/j.ijnurstu. 2006.04.005
Dong, Z., Wei, L., Sun, X., Xiang, J., Hu, Y., Lin, M., & Tan, Y. (2022). Experiences of nurses working in nurse-led clinics in traditional chinese medicine hospitals: A focused ethnographic study. Nursing Open, 10(2), 603-612. https://doi.org/10.1002/nop2.1326
Fan, Y. L., Zhang, Y., Cheng, Q. Y., Zhu, M. Y., Guo, Y. P., Zhao, S. B., & Geng, X. (2022). Management of prescription right of nurses internationally and its application to the practice. Chinese Journal of Nursing Education, 19(02), 187-192. https://doi.org/10.3761/j.issn.1672-9234.2022.02.017
Feng, S. T., Li, X. Z., Li, L., & Zhao, Y. L. (2020). Research progress and advices on nurse prescribing right in China. Chinese Nursing Research, 1, 101-104. https://qikan.cqvip.com/Qikan/Article/Detail?id=7100822761
Gao, F. L., Ding, S., & Huang, J., Dong, L., Wang, S. Q., Lv, Y., Duan, J. M., Li, T. T., Zhang, L. X., & Liu, J. E. (2017). The establishment and advanced nursing practice status of Nurse-Led Clinics in tertiary hospitals in China: findings from a national survey. Chinese Journal of Nursing Management, 17(10), 1297-1302.
Gielen, S. C., Dekker, J., Francke, A. L., Mistiaen, P., & Kroezen, M. (2014). The effects of nurse prescribing: A systematic review. International Journal of Nursing Studies, 51(7), 1048-1061. https://doi.org/10.1016/j.ijnurstu.2013.12.003
Gong, S. S., Lv, J., Wang, S. Y., & Wang, X. (2016). Development of nurse prescribing rights abroad and implementation of nurse prescribing rights in China. Journal of Nursing Continuing Education, 20, 1848-1851. https://doi.org/10.16821/j.cnki.hsjx.2016.20.008
Han, S. F., Duan, Z. G., Han, Q. H., Xue, P., Cheng, J. L., Wang, Y. Q., Zhu, R., Cao, Y., Zhang, Q., Wang, Y., Gao, J., Wang, X., Fan, J., Xue, N., Li, J., Li, X., Han, H., Yang, Y., Zhang, G., … Li, R.(2021). Expert consensus on the scope of nurse prescribing rights for advanced practice nurses in the new era (continuation). Nursing Research, 35(24), 4325-4342. https://doi.org/10.12102/j.issn.1009-6493.2021.24.001
Han, S. F., & Hou, Y. C. (2019). SWOT analysis of granting nurse prescribing rights in China. General Practice Nursing, 17(21), 2574-2578.
Han, S. F., & Li, X. (2011). Application of Delphi method to study the promoting factors of nurse prescribing rights implementation. General Practice Nursing, 19, 1693-1695. https://cqvip.com/doc/journal/967995293
Han, S. F., Zhang, Q., Zhu, R. F., & Cao, Y. (2022). From the decision-making subject of hierarchical nursing to the legislation of nurses’ prescribing authority: A research report. Nursing Research, 36(16), 2821-2826.
Hatchett, R. (2003). The emergence of the modern nurse-led clinic. In R. Hatchett (Ed.), Nurse-led clinics: Practice issues (pp. 1–27). Routledge.
Hong, Q. N., Fàbregues, S., Bartlett, G., Boardman, F., Cargo, M., Dagenais, P., Gagnon, M., Griffiths, F., Nicolau, B., O’Cathain, A., Rousseau, M., Vedel, I., & Pluye, P. (2018). The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Education for Information, 34(4), 285-291. https://doi.org/10.3233/efi-180221
Hou, X. L. (2021). A qualitative study on the cognition and influence of specialist nurses on the prescription right of Chinese nurses. China Academic Journal Electronic Publishing House, 36(7), 655-659. https://doi.org/10.16821/j.cnki.hsjx.2021.07.019
International Council of Nurses. (2021). Guidelines on prescriptive authority for nurses. https://www.icn.ch/sites/default/files/inline-files/PR_45_%20Nurse%20Prescribing_V1_FINAL.pdf
Kilańska, D., Lipert, A., Guzek, M., Engelseth, P., Marczak, M., Sienkiewicz, K., & Kozłowski, R. (2022). Increased accessibility to primary healthcare due to nurse prescribing of medicines. International Journal of Environmental Research and Public Health, 19(1), 292. https://doi.org/10.3390/ijerph19010292
Ling, D. L., Lyu, C. M., Liu, H., Xiao, X., & Yu, H. J. (2018). The necessity and possibility of implementation of nurse prescribing in China: An international perspective. International Journal of Nursing Sciences, 5(1), 72-80. https://doi.org/10.1016/j.ijnss.2017.12.011
Ma, D. H., & Ding, P. (2018). Practical study on scope of authority on prescription right of nurses in Anhui Province. Chinese Nursing Research, 32(1), 6-12. https://doi.org/10.3969/j.issn.1009-6493.2018.01.002
Maier, C. B. (2019). Nurse prescribing of medicines in 13 European countries. Human Resources for Health, 17(95). https://doi.org/10.1186/s12960-019-0429-6
McMenamin, A., Turi, E., Schlak, A., & Poghosyan, L. (2023). A systematic review of outcomes related to nurse practitioner-delivered primary care for multiple chronic conditions. Medical care research and review: MCRR, 80(6), 563–581. https://doi.org/10.1177/10775587231186720
National Health Commission of the People’s Republic of China. (2022). China health statistics yearbook.
Nissen, L., Kyle, G., Stowasser, D., Lum, E., Jones, A., McLean, C., & Gear, C. (2010). Non-medical prescribing: An exploration of likely nature of, and contingencies for, developing a nationally consistent approach to prescribing by non-medical health professionals-Final Report 1 June 2010. https://eprints.qut.edu.au/204992/1/Non_Medical_Prescribing.pdf
Nursing and Midwifery Council. (2018). Part 3: Standards for prescribing programmes – Nursing and midwifery. Retrieved June 12, 2023, from https://www.nmc.org.uk/globalassets/sitedocuments/education-standards/programme-standards-prescribing.pdf
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., . . . Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71
Parker, J. M., & Hill, M. N. (2017). A review of advanced practice nursing in the United States, Canada, Australia and Hong Kong Special Administrative Region (SAR), China. International Journal of Nursing Sciences, 4(2), 196-204. https://doi.org/10.1016/j.ijnss.2017.01.002
Shenzhen Municipal People’s Congress. (2022). Shenzhen Special Economic Zone Medical Regulations. Retrieved from https://www.gd.gov.cn/zwgk/wjk/zcfgk/content/post_2532140.html
National Council of State Boards of Nursing. (2016). The 2015 National Nursing Workforce Survey. Retrieved from https://doi.org/10.1016/S2155-8256(16)31055-9
National Council of State Boards of Nursing. (2018). The 2017 National Nursing Workforce Survey. Retrieved from https://doi.org/10.1016/S2155-8256(18)30131-5
Tian, Y. T., Zhang, Y., Yu, Z. J., Wang, R. H., Zhao, J., Li, H. J., Du, C. C., & Liu, Z. (2019). Survey on nurses’ cognition on prescription right in tertiary hospitals. Chinese Nursing Research, 33(10), 1649-1653. https://doi.org/10.12102/j.issn.1009-6493.2019.10.003
Wang, D., Bo, Y. M., Zhu, J., & Zhong, Q. (2018). Bibliometrics analysis of core competence related literatures of specialist nurses in China. Nursing Research, 32(19), 3107-3110. https://doi.org/10.3969/j.issn.1009-6493.2018.19.030
Wang, L., Kan, K., Shi, Y., & Shi, L. (2021). On legislation on nurse prescribing in China. Journal of Nursing Science, 12, 66-69. http://www.hlxzz.com.cn/hlxzz/article/abstract/20211219
Wang, S. Y., Jiang, W. B., Chen, K., Chen, Q. Q., & Wie, L. L. (2020). Research on the content of the prescription right of nurses based on Delphi method. China Health Standard Management, 11(11), 165-168.https://mqikan.cqvip.com/Article/ArticleDetail?id=7102148196&from=Article_index
Wang, X. J., Han, S. F., Cao, Y., Zhang, Q., & Zhu, R. F. (2022). Construction of general clinical practice training program for drug prescribing applicants of nurses in China. Chinese Nursing Research, 36(23), 4164-4173. https://doi.org/10.12102/j.issn.1009-6493.2022.23.006
Wang, X. J., Han, S. F., Zhang, Q., Zhu, R. F., Wang, Y. P., & Cao, Y. (2021). Current status and implications of clinical practice training for nurse prescribing rights at home and abroad. Nursing Research, 10, 1785-1788. https://doi.org/10.12102/j.issn.10096493.2021.10.016
Wang, Y. P., Han, S. F., Zhu, R. F., Cao, Y., Meng, Y. F., Xu, Z. Y., & Gao, J. P. (2020). Development and enlightenment of education and training of international nurses′ prescription rights. Chinese General Practice Nursing, 18(17), 2069-2073. https://doi.org/10.12104/j.issn.1674-4748.2020.17.005
Wei, X. (2016). Acquisition and content of nurse prescribing rights under specific conditions for clinical nurses. Electronic Journal of Clinical Medical Literature, 40, 8078-8080. https://doi.org/10.16281/j.cnki.jocml.2016.40.132
Wong, F. K. Y., & Chung, L. C. Y. (2006). Establishing a definition for a nurse-led clinic: Structure, process, and outcome. Journal of Advanced Nursing, 53(3), 358-369. https://doi.org/10.1111/j.1365-2648.2006.03730.x
Wong, F. K. Y. (2018). Development of advanced nursing practice in China: Act local and think global. International Journal of Nursing Sciences, 5(2), 101-104. https://doi.org/10.1016/j.ijnss.2018.03.003
Wu, X. J. (2022). Promoting nursing development towards health for all: Overview and prospect of nursing development in China. International Journal of Nursing Sciences, 10(1), 1-4.https://doi.org/10.1016/j.ijnss.2022.12.011
Zhang, G. Z., Han, S. F., & Cheng, J. L., & Wang, Y. J. (2012). Study on expert demonstration for qualification of applicants of nurse prescription right. Chinese Nursing Research, 26(15), 1360-1362.
Zhang, Q., Li, M. Z., Han, S. F., Li, X. P., Zhu, R. F., Wang, X. J., & Zhang, Y. X. (2022). Interpretation of the 2021 International Council of Nurses’ Nurse Prescribing Rights Guidelines. Nursing Research, 16, 2827-2835. https://doi.org/10.12102/j.issn.1009-6493.2022.16.002
Zhong, M. Y., Ling, D. L., Yu, H. J., & Li, W. T. (2020). A survey on nurses’ attitudes towards and belief in nurse’s prescription right. Modern Clinical Nursing, 19(9), 19-25. https://doi.org/10.3969/j.issn.1671-8283.2020.09.004
*Gunjeong Lee
School of Nursing, Ewha Womans University
52, Ewhayeodae-gil, Seodaemun-gu,
Seoul 03760 Republic of Korea
Email: gunjeong@ewha.ac.kr
Submitted: 6 April 2024
Accepted: 10 December 2025
Published online: 1 April, TAPS 2025, 10(2), 57-64
https://doi.org/10.29060/TAPS.2025-10-2/OA3332
Chatchai Kreepala1, Srunwas Thongsombat2, Krittanont Wattanavaekin3, Taechasit Danjittrong4, Nattawut Keeratibharat5 & Thitikorn Juntararuangtong1
1School of Internal Medicine, Institute of Medicine, Suranaree University of Technology, Thailand; 2Department of Orthopedics, Faculty of Medicine, Prince of Songkla University, Thailand; 3Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Thailand; 4Department of Anesthesiology, Chulabhorn Hospital, Thailand; 5School of Surgery, Institute of Medicine, Suranaree University of Technology, Thailand
Abstract
Introduction: Factors affecting decision-making duration in MCQs can enhance assessment effectiveness, ensuring they accurately measure the intended objectives and address issues related to incomplete exams due to time constraints. The authors aimed to explore the aspects of medical student’s perspective regarding the factors influencing their decision making on MCQ assessments.
Methods: A mixed-methods explanatory sequential design was utilised. Initial surveys were conducted using percentages, mean and non-parametric analysis obtained via online questionnaires from the sample group: all 2nd – 5th year medical students from SUT, Thailand. The validity of the questionnaires was verified by three independent reviewers (IOC=0.89). This was followed by semi-structured group interviews to explore student’s perspective on the factors affecting their decision. Qualitative analysis was conducted to explore detailed information until data saturation was achieved.
Results: Data from the quantitative analysis identified four factors that students believe affect the duration of the exam: the total word count of each question, test difficulty, and images in tests. Meanwhile, the qualitative analysis provided additional insights on factors such as the examination atmosphere affecting their decisions.
Conclusion: This report indicated that data acquired from a comprehensive reading question should be distinguished from those requiring decisive reading. Apart from text length, question taxonomy-such as recall or application- and questions with given images and tables should be considered as factors determining time allocation for an MCQ. Future research based on these results should aim to develop a mathematical formula to calculate exam duration, accounting for question difficulty and length.
Keywords: MCQ, Medical Assessment, Medical Education, Testing Time Estimation, Qualitative Research, Students’ Perspective
Practice Highlights
- The multiple-choice question (MCQ) stands as one of the objective assessment methods, widely regarded as the most utilised form of assessment.
- The word-length effect has been proposed to determine the length of each examination.
- Educational theories on decision-making have posited that decision-making is a dynamic process stemming from prior experiences.
- The authors were interested in exploring the aspects of the medical student’s perspective about the factors affecting their decision on MCQs answering.
I. INTRODUCTION
The multiple-choice question (MCQ) stands as one of the available objective assessment methods, widely regarded as the most utilised form of assessment, particularly within the fields of medical sciences and technology. Evidence suggests that the recall of short words often surpasses that of longer words (Tehan & Tolan, 2007). This observation is frequently analysed within the framework of a working memory model and the role of the phonological loop in immediate recall. However, the word-length effect has also been observed in delayed tests and in lists that surpass the memory span, thereby challenging the working memory interpretation of the phenomenon. Three alternative interpretations of the word-length effect have been proposed to explain how an exam length should be determined (Arif & Stuerzlinger, 2009; Kumar et al., 2021).
Educational theories on decision-making have posited that decision-making is a dynamic process stemming from prior experiences (Phillips et al., 2004) and meaningful learning (Foley, 2019). As a result, the ability to comprehend text while reading does not automatically equate to reading for decision-making or answering questions. From the literature, the context of factors influencing medical students’ decisions on MCQs includes 1) Length or number of words: The time students need to read to gather information before making a decision on an answer (Arif & Stuerzlinger, 2009). 2) Difficulty of the questions: analytical thinking, especially calculations are involved, may increase decision-making time. This depends on the students’ prior learning experiences before the exam (González et al., 2008). 3) Language comprehension: since exams in medical schools are often in English, non-native speakers may take longer to read and understand the questions (Schenck, 2020). 4) Visuals and tables: these serve as symbols that help students retrieve information from their prior learning experiences more easily (Ziefle, 1998). It is certain that teachers want academic assessment tests, such as MCQs, to be used to distinguish between high-performing and low-performing students and to assess the knowledge and understanding they have acquired. However, these objectives may be undermined by issues such as students running out of time and resorting to guessing. This inevitably reduces the reliability of the test.
The authors were interested in exploring medical student’s aspect regarding factors affecting their decision on MCQs answering. Previous studies focused on duration required for question comprehension and understanding but not for analysis. These were also mostly done in native Englisher speakers. This study builds upon previous studies but with an emphasis on factors affecting non-native English speakers’ decision making after analysis of the provided questions to answer MCQs in English. This research should be approached from the perspective of the student to obtain appropriate data. Semi-structured qualitative interviews were analysed in conjunction with quantitative data to identify and clarify the reasons and factors that students believe influence their performance on exams.
II. METHODS
A. Study Population
The research participants were second to fifth-year Thai medical students who had taken MCQ tests during their preclinical and clinical years between the academic years 2021-2022. Questionnaires were sent to all students without sampling.
To minimise data artifacts caused by recall bias, the online questionnaires were distributed the first week after each MCQ test before the study to the students who completed the exams. All examinations in this study were computer-based, closed book, single best answer MCQs written in English. The participants were non-native English speakers of Thai nationality (as detailed in Definition of Terms). An online survey or questionnaire-based study was used to collect information from participants in this study. If the data was unsaturated, triangulated data from a group of interviews consisting of students from different rotations was included to receive as much information from students’ perspectives as possible.
B. Study Design and Data Collection
The authors employed a mixed method study comprising a quantitative approach and a sequential, explanatory approach. The literature review unveiled several factors influencing MCQ test duration, including the number of questions, question types (recall or comprehension), subject matter difficulty, calculation items, and picture identification, as outlined in the questionnaire (O’Dwyer, 2012).
An online survey or questionnaire-based study was used to collect information from participants with minimal disruption to their learning activities. The quantitative research section was managed by CK, NK and TJ. Students completed the questionnaire once, based on their experiences in medical school. This, therefore, necessitates the researcher to summarise the responses and, if required, categorise interviews into groups according to their year of study. Open-ended questions were included in the last section of the questionnaire. The open-ended questions about the factors that, in the student’s opinions, were helpful information about the other factors affecting MCQ time (Lertwilaiwittaya et al., 2019). Survey research was employed as a quantitative method, while semi-structured group interviews were utilised in qualitative data collection to gather insights from medical students’ perspectives. The interview questions were designed to investigate whether students possessed any additional insights regarding the factors influencing MCQ test duration (Carnegie Mellon University, 2019; Schenck, 2020; Wang, 2019).
There were three sections in the questionnaire. Part I consisted of the instruction and informed consent. Part II consisted of general information of the participants, including sex, age, and academic year. Part III consisted of the questionnaires covering all four constructive domains previously mentioned (the domains affecting MCQ time from the literature included: 1) the number and total word count, 2) English language questions, 3) calculation questions, 4) the analytical thinking questions and open-ended questions about the factors that, in the students’ opinions, were helpful information about the other factors affecting MCQ time. After the questions in Part One were completed, they would be taken away so that the researchers would not be able to identify whose students have answered Part II and Part III.
To prevent neutral opinions from students, each questionnaire item featured a four-point Likert scale corresponding to levels of agreement: ‘Strongly disagree,’ ‘Disagree,’ ‘Agree,’ and ‘Strongly agree.’ The researcher wanted clear opinion whether the students were trending towards which side, hence the four-point Likert scale to prevent neutral opinion which may complicate statistical analysis. Validity of the questionnaires were verified by three independent reviewers with an Index of Item-Objective Congruence (IOC) value of 0.89.
Semi-structured group interviews were adopted into this study as insufficient flexibility is provided by a structured interview, whereas unstructured interviews would be too flexible. Semi-structured group interviews were the combination of formal and informal interviews focusing on personal experience; this often leads to unexpected results, enhancing the quality of data collected.
These interviews would take place after class by independent interviewers without any conflict of interest. Two facilitators were present in each session, CK facilitated the conversation and NK contributed ideas. The two facilitators were known by the student participants as faculty members, but they were not actively engaged in their academic learning. Audio and written recording would be coded then decoded by the researchers (SK, KW and TD).
The interview would take around 30-45 minutes per group, with each group consisting of five to eight people. Analysis would be done after the first three groups using relevant domain analysis and further analysis done after new interviews until data saturation was achieved. Coding, theme identification, and triangulation would be undertaken following the analysis and evaluation of the quantitative and qualitative data of which the analysis could be extrapolated to form a conclusion of the study. In this study, the open-end question would be analysed, and the semi-structured interview would be done.
Triangulation helped to provide meaning and helped to gain broader and more precise understanding. It could help increase validity. Triangulation was undertaken following the analysis and evaluation of the quantitative and qualitative data of which the analysis was extrapolated to form a conclusion of the study.
C. Definition of Terms
1) Multiple choice question (MCQ): This paper exclusively focused on the Single Best Answer (SBA) Multiple Choice Questions (MCQs), which were structured as questions followed by 4 or 5 potential answers, with only one correct response per question (Coughlin & Featherstone, 2017).
2) Taxonomy MCQ: MCQs were formulated based on two assumptions: that they could be categorised into higher or lower orders according to Bloom’s taxonomy (Stringer et al., 2021). This study sought to comprehend students’ approaches to questions by examining variances in their perceptions of the Bloom’s level of MCQs regarding their knowledge and confidence. The authors employed Bloom’s taxonomy in this study, classifying questions as “recall,” “comprehension,” and “application” (Stringer et al., 2021).
3) Non-native English speakers: The term non-native English speakers was defined as those students who spoke a language other than English domestically. Non-native English speakers were inclusive of both competent bi-literate and limited English proficiency students. In addition, it is also defined as students who learn the language as older children or adults (Cassels & Johnstone, 1984).
D. Statistical Analysis
Statistical analyses were performed for quantitative analysis with SPSS Statistics for Windows, Version 18.0 (SPSS Inc., Chicago, Illinois, USA). Information in the quantitative section was elaborated and displayed in and counts percentage. The qualitative data was analysed by code grouping of text fragments based on content. Subsequently, the codes were reorganised and grouped, main themes and subthemes were identified, and illustrative quotations were selected. The authors assigned other three medical teachers to undertake independent coding of the transcripts for each interview. The final coding and discussions continued until the frameworks were agreed upon and new themes were derived (CK, SK, KW and TD).
III. RESULTS
A. Demographic Information
The questionnaire was done online by the participants from second to fifth-year medical students in the academic year 2021-2022. There were 93 second-year medical students, 92 third-year medical students, 92 fourth-year medical students, and 93 fifth-year medical students, respectively, with 370 participants in total. It was found that there were 298 respondents (a return rate of 81%). 73 second-year medical students (78% response rate) answered the questions, while 70 third year (76%), 75 fourth year (81%), and 80 fifth year medical students (86%) answered the questions respectively as shown in Table 1.
|
General information |
Category |
n (%) |
|
Gender |
Male |
102(34) |
|
Female |
196(66) |
|
|
Age (year) |
Mean ± SD |
21.3 ± 1.23 |
|
Max, Min |
28, 19 |
|
|
College Year |
Second Year |
73(24) |
|
Third Year |
70(23) |
|
|
Fourth Year |
75(25) |
|
|
Fifth Year |
80(27) |
Table 1. Demographic information of student participants in the survey
Abbreviation: n= number, Max=maximum, Min= minimum
B. Students’ Perspective on Examination Time and Number of MCQs
From the questionnaires, it was found that the medical students thought that the suitable number of questions in the 1-hour examinations that consisted of the intermediate level questions was approximately 41.4±15.62 questions (min-max: 20-120 questions). Moreover, students wanted to gain some more points by guessing rather than leaving the answer blank during the final period of the examination. Regardless of the difficulty of the examinations or the time given, the students would rush to finish the examination in time. Most of the students started to guess the answers at the last 5.4±1.11 minutes (min-max: 2-10 minutes).
C. The Information from the Survey and Semi-Structured Interview
The quantitative data also indicated that various factors influenced the examination duration according to the students’ perspectives. The first three factors were identified through quantitative survey research, encompassing 1) the number of tests and total word count, 2) English language questions, and 3) test difficulty influencing time allocation (including calculation questions and analytical thinking questions) (Table 2). Concurrently, the examination environment also impacted students’ concentration during each test. The latter two pieces of information were corroborated through triangulation from the semi-structured group interviews.
|
Question |
Level of Agreement n (%) (total n =298) |
||||
|
Strongly Agree |
Agree |
Moderate |
Disagree |
Strongly disagree |
|
|
1. Number of word count (texts) |
80(27) |
105(35) |
110(37) |
3(1) |
0(0) |
|
2. The English questions |
77(26) |
80(27) |
110(37) |
24(8) |
7(2) |
|
3. The Calculation questions |
131(44) |
60(20) |
92(31) |
11(4) |
4(1) |
|
4 Analytical thinking tests (not a comprehension test) |
105(35) |
105(35) |
77(26) |
11(4) |
0(0) |
Table 2. Evaluating Factors Affecting MCQ Test Time in Student’s Perspectives and the Rating Scores
Abbreviation: n= number
D. The Number Tests and Total Word Count
The exam questions, according to some students, were challenging and time-consuming, and the answer options were likewise lengthy. It was shown that not only the number of tests, but the length of each test item also affected the testing time.
Quote: Student B1F*; “The questions were too long. I can’t complete them in time.”
Quote: Student A2M*; “If there are too many questions in the exam, I wouldn’t be able to finish it”
* student’s code
English Language Questions and Examiners (Native Versus Non-Native English Speakers): The respondents, who were not native English speakers, believed that the English-language test took longer to finish than the Thai-language test. Accordingly, they decided to guess or answer each question slowly since they could not understand the questions. They believed that the English-language tests took longer to finish than the Thai-language tests. Accordingly, they decided to guess or answer each question slowly since they could not fully understand the English questions.
Quote: Student D1F*; “I’m not good at reading English. Sometimes I just have to guess on the exam.”
Quote: Student C1M*; “The language in the test is too hard to understand.”
* student’s code
E. Test Difficulty Determining Time Allocation
For the analysis of coding, grouping, and generating themes, the author found that the medical students paid attention to the difficulty level of the questions which affected the decision to answer the questions.
1) The Calculation and Analytical Thinking: The calculation and analytical thinking tests took students longer to read. Additionally, students believed that examinations they had never taken before or exams that required knowledge application took longer to complete, such as exams that included questions requiring the students to diagnose patients by themselves which occasionally left them unsure of how to respond.
Quote: Student C2M*; “Calculation tests take a long time to get the answers.”
* student’s code
2) Recall Question Leads to Quick Answers: Students commented that recall-type questions, including tests from previous academic years, contained duplicated sentences, pictures, or messages from textbooks that students remembered. This led to students being able to complete the test in a short thinking time.
Quote: Student K1M*; “If the teacher copied the exact words from the course sheet, I would remember and answer questions quickly.”
Quote: Student L1M*; “If the questions are the same as in the sheet provided, I can answer them.”
*student’ code
This information indicated that the taxonomy of the test (recall -compression-application) had a large effect on decision time. Applied questions, not direct or calculated questions, required more attention and time for decision-making when compared to comprehensive questions (questions about knowledge understanding). In contrast, recall questions required the least decision-making time.
F. The Visual Image and Atmosphere of the Examination: the New Derived Domains Recognised by Qualitative Analysis
1) Questions with images, graphs, or tables serve as key guides for decision-making: The students thought that the exams that consisted of graphs and tables helped them understand the questions and were better than the questions that only had descriptions. That would lead to less time consumed.
Quote: Student L2M*; “If the test got the exact same summary table from the book, I could remember and get the answers right away.”
* student’s code
2) The Atmosphere of the Examination: The environment and atmosphere of the exam were also mentioned. The student’s response time was slowed down by the distractions during the exam. The environment such as brightness, temperature, and examination devices affected the concentration of the students.
Quote: Student H1F*; “The atmosphere in the exam venue, noise, and the air quality in the room affect the exam results.”
*student’s code
IV. DISCUSSION
The results revealed that students perceived lengthy exam content or a large number of questions as time-consuming, particularly when exams were conducted in English. Studies indicated that English speakers could read up to 150 words per minute (Trauzettel-Klosinski et al., 2012). However, for non-native English speakers, the expected reading time for exams was longer. Hence, using the English reading rate as a basis for determining exam duration was deemed unsuitable for Thai students, given that English was not their primary language of communication. When compared with a previous study (Trauzettel-Klosinski et al., 2012), the increased duration may result from decision making, thus this implicates reading for decision making requires more time than reading for the context which is cumulatively longer for non-English native speakers.
Qualitative findings indicated that irrespective of the exam duration set by the administering professor, students generally completed exams within the allotted time frame. This often entailed guessing answers towards the end of the exam period, as students might not have adequate time to complete the exam thoroughly. It was observed that students tended to resort to guessing exam questions approximately five minutes before the exam conclusion, thereby minimising threats to validity posed by guessing due to time constraints during exam (Foley, 2019).
There may be limitations if the exam questions contain lengthy content that cannot be comprehended and decided upon within one minute. Furthermore, the difficulty level of the exam questions is often established as a passing criterion, prioritising validity considerations in terms of content format and achieving the intended objectives. Moreover, students naturally desire to obtain the highest possible score on the exam, regardless of the level of difficulty or length of the exam. Therefore, it is important for students to manage their time effectively to ensure they can complete all the exam questions within the given timeframe.
The qualitative results indicated that regardless of the exam duration set by the administering professor, students ultimately would complete the exam within the allotted time frame. Additionally, students agreed that application and calculation questions on the exam require more time to read and decide upon, as opposed to questions with figures and tables that aided in faster decision making. Based on these findings, it could be concluded that comprehensive reading rates may not be a reliable indicator of decision-making reading rates, particularly in the context of medical school exams. Therefore, studying decision-making reading rates within the context of medical school exams was crucial.
The researcher, therefore, examined the domain and specific factors on the characteristics of the MCQ test. Additionally, the study scope was limited to English tests administered to non-native English speakers and onsite computer-based tests, thereby eliminating unrelated factors that could impact exam duration. The analysis yielded the following results: Firstly, factors positively correlated with exam duration (negatively correlated with decision-making) included the number of questions, total word count, calculation questions, and analytical thinking questions. Secondly, factors negatively correlated with exam duration (positively correlated with decision-making) were recall questions, questions with provided images, and tables.
A factor contributing to longer reading times for decision-making purposes was when the exam contained a higher proportion of application or calculation questions, comprising over 33% of the exam questions, as evidenced by qualitative data from students. Therefore, analysing exam completion time based on reading comprehension data for decision-making purposes is not recommended. Moreover, it should be noted that these factors present internal threats to validity, but they can be managed to ensure that examination tools are effectively used and aligned with intended objectives. Incorporating data from research can lead to the identification of new themes related to factors influencing examination time.
Five constructive domains were identified: 1) the number and total word count, 2) positive difficulty factors (application/calculation questions), 3) negative difficulty factors (recall questions), 4) examiners (non-native English speakers or not), and 5) pictures/symbols in tests.
A distinctive aspect of this study was its targeted focus on Thai medical students who were non–native English speakers. While many studies have examined MCQ performance across broad and diverse populations, this research concentrated on a specific demographic, enabling a more in-depth exploration of how cultural and linguistic factors influence test-taking behaviour. The study uniquely combined quantitative survey data with qualitative insights from semi-structured group interviews. While some research utilised either quantitative or qualitative methods, this study’s integration of both provided a more holistic understanding of student perspectives and experiences (Lertwilaiwittaya et al., 2019). This methodological triangulation strengthened the validity of the findings by cross-verifying quantitative data with qualitative insights. In contrast to many existing studies that focused predominantly on performance metrics (such as scores or pass rates), this research examined the cognitive processes and decision-making strategies students employed while answering MCQs. It investigated how elements like question difficulty, language comprehension, and prior experiences shaped students’ approaches to test questions—a dimension less frequently explored in previous literature.
In conjunction with examination-related factors, students also recognised the importance of considering the test environment within the examination room which was a new finding found using qualitative analysis from this research. This was crucial for promoting student concentration and facilitating accurate response selection in line with assessment tool objectives. It aligned with existing literature, which suggested that the test environment poses a construct irrelevant threat to the validity of educational measurement. The findings from this study may have led to future research on developing a mathematical formula to tailor the exam duration for different sets of questions. This would have involved analysing factors such as the number of words, length, difficulty, and the presence of images and tables in the exam. Additionally, the impact of language proficiency on reading and decision-making time should have been considered, as there may have been differences between native and non-native speakers. The study suggested that the future research direction should include diverse populations of non-native English speakers from different countries and educational contexts. This could help identify whether the findings are consistent across various cultural backgrounds and educational systems. Moreover, conducted longitudinal studies should be used to track students’ performance and decision-making processes over time. This approach could provide insights into how experiences and familiarity with MCQs influence their strategies and confidence levels throughout their medical education.
A major limitation of this research was the variation in learning experiences, exam-taking skills, and analytical thinking among medical students at different year levels, which might lead to differing opinions. Therefore, the researcher needed to conduct qualitative analysis to examine the reasons behind these differences. However, the diversity of experiences might also introduce bias due to varying familiarity with different types of exams. The online format restricted the depth of responses, as students often did not fully articulate their thoughts without immediate follow-up questions, which limited the richness of the qualitative data. Additionally, the focus on Thai medical students constrained the applicability of the findings to other populations or contexts, thereby limiting broader conclusions about non-native English speakers in different educational settings.
V. CONCLUSION
Based on the student’s perspective, data showed questions with lengthy content required more time whilst those with tables or diagrams required less time. This report indicated that the data acquired from a comprehensive reading examination should be distinguished from a decisive reading examination.
In addition to the number of questions and the length of text, factors that should be positively correlated with the duration of the exam include the number of questions, word count, calculation-based questions, and analytical thinking questions. These factors should be considered for additional time allocation beyond the regular exam duration, particularly when the proportion of analytical thinking questions exceeds one-third of the total question set. On the other hand, recall questions, as well as questions accompanied by images and tables, should be taken into account to ensure a balanced distribution of exam time, as they can be answered more easily and quickly in terms of decision-making compared to general questions.
Notes on Contributors
CK conceived of the presented idea, developed the theory, and performed the computations and discussed the results and contributed to the final manuscript. ST, KW, and TD. discussed the results and wrote the manuscript with support from CK, NK, and TJ, designed the model and the computational framework and analysed the data.
Ethical Approval
All participants voluntarily signed a consent form prior to participating in the study. The participation protocol was approved by the Human Research Ethics Committee, Suranaree University of Technology (Issue # EC-64-102).
Data Availability
Institutional ethical clearance was given to maintain the data in the secure storage of the principal investigator of the study. The data to this study may be provided upon reasonable request to the corresponding author. A preprint of our manuscript, which is not peer-reviewed, is available at https://www.researchsquare.com/article/rs-3019852/v1
Acknowledgement
The authors would like to thank the participants of this study, the medical students in the Institute of Medicine, Suranaree University of Technology. Without their passionate participation and input, the validation survey could not have been successfully conducted.
Funding
This work was supported by the Grant of Suranaree University of Technology (contract number SUT-602-64-12-08(NEW)).
Declaration of Interest
The authors have no conflicts of interest to disclose.
References
Arif, A. S., & Stuerzlinger, W. (2009). Analysis of text entry performance metrics [Conference presentation]. 2009 IEEE Toronto International Conference Science and Technology for Humanity (TIC-STH), Canada. https://doi.org/10.1109/TIC-STH.2009.5444533
Cassels, J., & Johnstone, A. (1984). The effect of language on student performance on multiple choice tests in chemistry. Journal of Chemical Education, 61(7), 613. https://doi.org/10.1021/ed061p613
Coughlin, P., & Featherstone, C. (2017). How to write a high-quality multiple-choice question (MCQ): A guide for clinicians. European Journal of Vascular and Endovascular Surgery, 54(5), 654-658. https://doi.org/10.1016/j.ejvs.2017.07.012
Carnegie Mellon University. (2019). Creating exams Eberly Center. https://www.cmu.edu/teaching/assessment/assesslearning/creatingexams.html
Foley, B. P. (2019). Getting lucky: How guessing threatens the validity of performance classifications. Practical Assessment, Research, and Evaluation, 21(1), 3. https://doi.org/10.7275/1g6p-4y79
González, H. L., Palencia, A. P., Umaña, L. A., Galindo, L., & Villafrade M, L. A. (2008). Mediated learning experience and concept maps: A pedagogical tool for achieving meaningful learning in medical physiology students. Advances in Physiology Education, 32(4), 312-316. https://doi.org/10.1152/advan.00021.2007
Kumar, D., Jaipurkar, R., Shekhar, A., Sikri, G., & Srinivas, V. (2021). Item analysis of multiple choice questions: A quality assurance test for an assessment tool. Medical Journal Armed Forces India, 77, S85-S89. https://doi.org/10.1016/j.mjafi.2020.11.007
Lertwilaiwittaya, P., Sitticharoon, C., Maikaew, P., & Keadkraichaiwat, I. (2019). Factors influencing the National License Examination step 1 score in preclinical medical students. Advances in Physiology Education, 43(3), 306-316. https://doi.org/10.1152/advan.00197.2018
O’Dwyer, A. (2012). A teaching practice review of the use of multiple-choice questions for formative and summative assessment of student work on advanced undergraduate and postgraduate modules in engineering. All-Ireland Journal of Teaching and Learning in Higher Education, 4(1). https://doi.org/10.21427/D7C03R
Phillips, J. K., Klein, G., & Sieck, W. R. (2004). Expertise in judgment and decision making: A case for training intuitive decision skills. Blackwell Handbook of Judgment and Decision Making, 297, 315. https://doi.org/10.1002/9780470752937.ch15
Schenck, A. (2020). Examining the influence of native and non-native English-speaking teachers on Korean EFL writing. Asian-Pacific Journal of Second and Foreign Language Education, 5(1), 2. https://doi.org/10.1186/s40862-020-00081-3
Stringer, J., Santen, S. A., Lee, E., Rawls, M., Bailey, J., Richards, A., . . . Biskobing, D. (2021). Examining Bloom’s taxonomy in multiple choice questions: Students’ approach to questions. Medical Science Educator, 31(4), 1311-1317. https://doi.org/10.1007/s40670-021-01305-y
Tehan, G., & Tolan, G. A. (2007). Word length effects in long-term memory. Journal of Memory and Language, 56(1), 35-48. https://doi.org/10.1016/j.jml.2006.08.015
Trauzettel-Klosinski, S., Dietz, K., & Group, I. S. (2012). Standardized assessment of reading performance: The new international reading speed texts IReST. Investigative Ophthalmology & Visual Science, 53(9), 5452-5461. https://doi.org/10.1167/iovs.11-8284
Wang, A. (2019, July 15). How to determine the best length for your assessment. Pear Deck Learning. https://www.peardeck.com/blog/how-to-determine-the-best-length-for-your-assessment
Ziefle, M. (1998). Effects of display resolution on visual performance. Human Factors, 40(4), 554-568. https://doi.org/10.1518/001872098779649355
*Assoc. Prof. Chatchai Kreepala, M.D.
Institute of Medicine
Suranaree University of Technology
Thailand
+66(93)3874665
Email: chatchaikree@gmail.com
Submitted: 17 April 2024
Accepted: 18 December 2025
Published online: 1 April, TAPS 2025, 10(2), 65-70
https://doi.org/10.29060/TAPS.2025-10-2/OA3336
Rachael Tufui Masilomani1, Sophaganie Jepsen1, Maria Lourdes Villaruel1, Aying Wang1, Alena Kotoiwasawasa1, Lusiana Naikawakawavesi1, Norman Bartolome1, Claudia Paterson2, Andrew Hill2 & Maria Concepcion Bartolome1
1Basic Clinical Medicine, Fiji National University, Fiji; 2Department of Surgery, Middlemore Hospital, University of Auckland, New Zealand
Abstract
Introduction: The MBBS programme at Fiji National University reduced its teaching weeks from 18 to 14 weeks in 2018. The purpose of this study was to assess student perceptions of learning and teachers following the reduction in the number of teaching weeks from 18 to 14 weeks.
Methods: A questionnaire was created using a modified Dundee Ready Education Environment Measure (mDREEM) tool (23 items). This was comprised of two subscales; Students Perception of Learning (SPL – 12 items) and Students Perception of Teachers (SPT – 11 items). This was circulated to Year 5 MBBS students through an online survey in 2020.
Results: The response rate was 96%. The students regarded their educational environment as positive in both length of teaching weeks, with an overall mDREEM mean score of 63.29 in 18 weeks and 62.03 in 14 weeks. No statistically significant differences were found between 18 week and 14 week scores across mDREEM scores, SPL scores or SPT scores. The highest scoring item over both was ‘teachers are knowledgeable’.
Conclusion: A positive perception was noted for both lengths of teaching weeks. Reducing the teaching weeks from 18 to 14 did not statistically significantly reduce students’ perception of their educational environment. Items identified with low scores will give a window of opportunity for lecturers and to improve these areas. Future studies may explore the use of the five subscales of the DREEM tool and this study can be integrated into further evaluations of educational environment at Fiji National University.
Keywords: Medical Students, Educational Learning Environment, DREEM Tool, Fiji National University, Teaching, Medical Education
Practice Highlights
- mDREEM scores did not significantly differ between 18 weeks and 14 weeks of teaching.
- The highest scoring item over both weeks was ‘teachers are knowledgeable’.
I. INTRODUCTION
The Fiji National University (FNU) was founded in 2010 by the merging of six academic institutions in the Fiji Islands, including the Fiji School of Medicine (FSM). FNU has continued the FSM’s tradition of educating and training a diverse population of students from Fiji and neighbouring Pacific Island nations. The Bachelor of Medicine and Bachelor of Surgery (MBBS) programme is a six-year course at FNU. As part of the academic year, each pre-clinical year group have a teaching week block course. During this time, students receive 2-4 hours of scheduled lectures, 2-hour tutorials twice weekly, as well as 2 hours of clinical skills and 2 hours of anatomy, 2 hours of laboratory sessions and a health centre attachment 4 hours a week.
In 2018, FNU reduced the teaching week block course in the MBBS programme from 18 weeks to 14 weeks. The teaching weeks were shortened due to the decision to move specialty courses such as Psychiatry and Public Health to their respective clinical blocks from Years 4 to 6. This adaptation was challenging for the lecturers, who had to reformat their teaching sessions, in addition to providing resources onto an online Moodle platform. It is well established that the educational environment plays an important role in determining the academic success of medical students (Prosser et al., 1999; Ramsden 2003). Therefore, it is important to evaluate the impact of any major changes to the educational environment, such as a reduction in teaching weeks from 18 weeks to 14 weeks.
Previous research has demonstrated that the duration of clinical rotations has been able to be decreased without adversely affecting the academic success of medical students. For example, one group demonstrated that a shortened four-week clinical rotation in Obstetrics and Gynaecology provided enough opportunity for final year medical students to undertake a quality improvement project in the curriculum (Kool et al., 2017).
The Dundee Ready Education Environment Measure (DREEM) is a quantitative tool used to evaluate students’ perceptions of the educational environment in medical schools. The DREEM tool consists of 50 items, each rated on a scale from 0 to 4. It has five domains, allowing for a maximum score of 200. Higher scores indicate a positive perception of the learning environment (Roff et al., 1997).
A systematic review published in 2012 analysed 40 studies reporting DREEM scores from 20 countries. This review demonstrated that DREEM had been used internationally for various purposes, including diagnostic assessments and comparative studies across different groups (Miles et al., 2012). Five studies focused on investigating the impact of a changed curriculum, which was our area of interest (Demirören et al., 2008, Edgren et al., 2010, O’Brien et al., 2008, Riquelme et al., 2009, Till et al., 2004). We identified three key themes: 1) the DREEM tool was able to highlight areas of concern and/or remediation among students (Riquelme et al., 2009 Till et al., 2004), 2) DREEM scores were different in different phases of medical education, with year 3 students having the highest scores, and year 5 students having the lowest scores (Demirören et al., 2008, Riquelme et al., 2009), and 3) the DREEM tool identified clusters of students based on how positively they perceived the curriculum (O’Brien et al., 2008).
The aim of this research was to compare students’ perception of learning and teachers between 18 weeks and 14 weeks, using a modified DREEM (mDREEM) tool which utilises two of the five domains from the original DREEM tool. The authors’ hypothesis was that students’ perception of learning and teaching would be reduced in with a decrease in teaching weeks to 14 weeks compared to 18 weeks.
II. METHODS
A. Participants
An online survey was developed by the authors. This was distributed via email to eligible participants using Google Forms from 12th December to 17th December 2020. Eligible participants included the Year 5 MBBS cohort of 2021, as this cohort was exposed to both 18 week and 14 week teaching programmes. Participation in the survey was optional and results were anonymous. Submission of a completed survey was taken as providing informed consent to participate in this research. Full ethics approval was provided through FNU’s College Human Health Ethics Committee (ID: 292.20). Facility approval was granted to conduct the research.
B. mDREEM Tool
The authors selected two of the five domains of the DREEM tool to be included in the survey. The selected two domains included students’ perceptions of learning (SPL) and students’ perceptions of teachers (SPT). The rationale for using only these two domains was that they were the two domains of interest for the teachers, and it was thought that a survey with less questions would be more likely to be filled to completion by more of the students. Using a Likert scale, each item was scored from 0 to 4, with 4 = strongly agree, 3 = agree, 2 = not sure, 1 = disagree and 0 = strongly disagree. Six of the 23 statements in the mDREEM tool were negative statements: 1) the teaching over-emphasised factual learning; 2) the teaching is too teacher-centred; 3) teachers ridicule the students; 4) the teachers are authoritarian; 5) teachers get angry in class and 6) the students irritate the teachers. These were scored in a reverse manner.
The mDREEM tool had a maximum score of 92. The SPL domain included 12 items, with a maximum score of 48. The SPT domain included 11 items, with a maximum score of 44. This research used the following guide to interpret the overall scores:
- 0–23 = Very poor environment
- 24 – 46 = A large number of problems in the environment
- 47–69 = More positive than negative environment
- 70–92 = Excellent
C. Statistical Analysis
Analysis of the collected data was by using R version 4.3.1. Mean scores were reported with standard deviations. Paired t-tests were performed to compare aspects of the mDREEM scores over 18 weeks and 14 weeks, with a statistical significance threshold of p<0.05. Reliability analysis of the mDREEM tool was assessed using Cronbach’s Alpha test, where >0.7 was deemed acceptable internal consistency.
III. RESULTS
Seventy-eight out of eighty-one (96%) MBSS Year 5 students participated in the online survey. Fifty-one (65%) were females and 51% of participants were aged between 23 and 25 years old. Fijian of Indian descent students made up the majority of the responders (67%) followed by other ethnicities (18%) and i-Taueki students (15%). The majority of students resided at the FNU Hostel (69%) while 28% lived within Suva and only 3% lived outside Suva.
Table 1 illustrates the 23 individual mDREEM items with mean scores across 18 weeks and 14 weeks. The item ‘the teaching overemphasised factual learning’ scored the lowest for both 18 and 14 weeks. The item ‘teachers are knowledgeable’ scored the highest for both 18 and 14 weeks.
|
Items |
mDREEM item |
Code |
18 weeks |
14 weeks |
||
|
|
Mean |
SD |
Mean |
SD |
||
|
1 |
I am encouraged to participate in class |
SPL |
3.13 |
0.91 |
2.78 |
1.03 |
|
2 |
The teaching is often stimulating |
SPL |
2.79 |
1.02 |
2.65 |
0.94 |
|
3 |
The teaching is student-centred |
SPL |
2.97 |
0.95 |
2.79 |
0.92 |
|
4 |
The teaching helps to develop my competence |
SPL |
3.06 |
0.82 |
2.63 |
0.92 |
|
5 |
The teaching is well focused |
SPL |
2.67 |
1.00 |
2.55 |
1.03 |
|
6 |
The teaching helps to develop my confidence |
SPL |
2.88 |
1.01 |
2.79 |
0.94 |
|
7 |
The teaching time is put to good use |
SPL |
2.81 |
1.12 |
2.60 |
1.00 |
|
8 |
The teaching over-emphasised factual learning |
SPL |
1.85 |
0.92 |
1.91 |
0.79 |
|
9 |
I am clear about the learning objectives of the course |
SPL |
2.77 |
1.02 |
2.78 |
0.98 |
|
10 |
The teaching encourages me to be an active learner |
SPL |
2.86 |
1.16 |
2.97 |
0.88 |
|
11 |
Long term learning is emphasised over short term learning |
SPL |
2.59 |
1.13 |
2.56 |
0.98 |
|
12 |
The teaching is too teacher-centred |
SPL |
2.85 |
0.80 |
2.74 |
0.78 |
|
13 |
The teachers are knowledgeable |
SPT |
3.18 |
0.83 |
3.13 |
0.80 |
|
14 |
The teachers are patient |
SPT |
3.01 |
0.73 |
2.74 |
0.89 |
|
15 |
The teachers ridicule the students |
SPT |
2.49 |
0.97 |
2.56 |
0.97 |
|
16 |
The teachers are authoritarian |
SPT |
2.49 |
0.96 |
2.58 |
0.91 |
|
17 |
The teachers have good communication skills |
SPT |
3.04 |
0.90 |
2.99 |
0.71 |
|
18 |
The teachers are good at providing feedback to students |
SPT |
2.54 |
1.15 |
2.86 |
0.96 |
|
19 |
The teachers provide constructive criticisms |
SPT |
2.85 |
0.90 |
2.92 |
0.84 |
|
20 |
The teachers give clear examples during class |
SPT |
2.78 |
0.91 |
2.79 |
0.84 |
|
21 |
The teachers get angry in class |
SPT |
2.63 |
1.01 |
2.63 |
0.85 |
|
22 |
The teachers are well prepared for their classes |
SPT |
2.87 |
0.90 |
2.92 |
0.81 |
|
23 |
The students irritate the teachers |
SPT |
2.23 |
0.95 |
2.23 |
0.83 |
Table 1. Descriptive statistics of individual item DREEM scores for 18 and 14 teaching weeks
The mean SPL scores over 18 weeks and 14 weeks were 33.23 (SD 7.38) and 31.74 (SD 7.52), respectively, out of a maximum of 48 (SPL 18 weeks: 69.33%; SPL 14 weeks: 66.13%). The mean SPT scores over 18 weeks and 14 weeks were 30.06 (SD 6.34) and 30.28 (SD 5.74), respectively, out of a maximum of 44 (SPT 18 weeks: 68.32%; SPT 14 weeks: 68.82%). The mean mDREEM scores over 18 weeks and 14 weeks were 63.29 (SD 12.58) and 62.03 (SD 12.01), respectively, out of a maximum of 92 (mDREEM 18 weeks: 68.80%; mDREEM 14 weeks: 67.42%). These results are presented in Table 2.
|
|
SPL 18 |
SPL 14 |
SPT 18 |
SPT 14 |
mDREEM 18 |
mDREEM 14 |
|
Mean |
33.23 |
31.74 |
30.06 |
30.28 |
63.29 |
62.03 |
|
SD |
7.38 |
7.52 |
6.34 |
5.74 |
12.58 |
12.01 |
Table 2. Descriptive summary statistics for 18 and 14 teaching weeks
The mean difference in SPL scores between 18 weeks and 14 weeks was 1.48. This difference was not statistically significant (t (77) = 1.61, p = 0.11). The mean difference in SPT scores between 18 weeks and 14 weeks was -0.22, and this was also not statistically significant (t (77) = -0.43, p = 0.67). The mean difference in overall mDREEM scores between 18 weeks and 14 weeks was 1.27, which was also not statistically significant (t (77) = 1.04, p = 0.30).
The reliability analysis for both 18 and 14 teaching weeks found a Cronbach’s Alpha Test of 0.58 for SPL, which was less than the threshold of 0.7 and 0.84 for SPT, which was greater than the threshold of 0.7. For mDREEM, the Cronbach’s Alpha Test was 0.77, which was greater than the threshold of 0.7 and confirmed acceptable internal consistency for the mDREEM tool.
IV. DISCUSSION
This study has demonstrated that a reduction in teaching from 18 to 14 weeks did not result in a significant decrease in mDREEM, SPL or SPT scores among Year 5 MBBS students at FNU in 2020. This finding refuted the authors’ hypothesis of a reduction in teaching weeks leading to student dissatisfaction of the educational environment.
Both 18 weeks and 14 weeks scored within the range of 47 to 69 out of 92, indicating a ‘more positive than negative environment’ based on predefined thresholds outlined in the methods section. The ‘excellent’ threshold of 70+ out of 92 was not obtained, indicating room for improvement. In particular, the item ‘teachers are knowledgeable’ scored the highest for both 18 and 14 weeks indicating that students perceived their teachers to have high levels of knowledge despite the reduction in teaching weeks. In contrast, ‘the teaching overemphasised factual learning’ was identified as the most significant negative statement and provides an area of focus for the lecturers.
One group used the DREEM tool to assess curriculum changes in an Irish medical school and that found that the new curriculum was associated with students reporting higher mean DREEM scores (Finn et al., 2014). While FNU’s curriculum change did not result in higher mDREEM scores, the maintenance of mDREEM scores is encouraging and provides a framework for ongoing work towards improving students’ perception of their educational environment.
This finding was similar to a previous study reviewing shortened medical education rotations previously discussed in the introduction section of this paper (Kool et al., 2017). Given the concordance with other similar research findings, the authors are of the belief that the results from this study are largely generalisable to MBBS students and lecturers worldwide, despite only being a single-centre study.
A major strength of this study was the high response rate of 96%. This ensures that data collected as part of this research is representative of the population of interest as compared to several studies with lower response rates (Al-Ansari et al., 2015; Ali et al., 2012; Hyde et al., 2018). Moreover, the results are comparable to the high response rates of other DREEM studies conducted internationally (Alraawi et al., 2020; Stormon et al., 2019; Till et al., 2004).
One limitation of this study was using only two domains of the DREEM tool, neglecting the three domains of Students’ Academic Self-Perception (SAP), Students’ Perception of Atmosphere (SPA) and Students’ Social Self-Perception (SSP). The authors selected SPT and SPL as the two key domains for this research, and thought that by selecting the two most relevant domains, that this would shorten the questionnaire and improve completion of the questionnaire amongst participants. Future research at FNU should trial the use of all five domains of the DREEM tool to assess whether this provides further insights into how teaching weeks can be improved for MBBS students. It will be of interest to see whether response rates are reduced with the use of the full DREEM tool in a questionnaire. Furthermore, future surveys should investigate perspectives of MBBS students over a range of year groups, given previous research suggesting that Year 3 MBBS students have higher DREEM scores than Year 5 MBBS students. A second limitation of this study was that the alpha value for SPL failed to achieve the threshold of >0.7, making it concerning that this domain was unable to achieve acceptable internal consistency. However, the authors note that SPT and mDREEM both achieved acceptable internal consistency. A final limitation of this study was the fully quantitative nature of the survey – the authors did not provide an option for students to add comments to this survey. Future surveys should provide an option for students to add comments, in order to provide more insights into the perspectives of MBBS students.
V. CONCLUSION
In conclusion, the students rated FNU’s MBBS programme educational environment positively. A reduction in teaching weeks from 18 to 14 did not result in a statistically significant decrease in SPL, SPT or mDREEM scores. This study identified valuable information for the authors regarding the improvement of educational environment for medical students. Utilisation of these results to guide educational development in these areas needing improvement will be of help in shaping the delivery of quality education to medical students. In addition, this research may open a door for further studies to investigate challenges faced by tutors and link it to the perceptions of medical students in their educational environment. Likewise, this study is important for future studies in evaluating the educational climate for FNU and other local and international universities.
Notes on Contributors
Dr Maria Bartolome is the corresponding author for this research. She is a PBL (problem based learning) lecturer at the School of Medicine, Fiji National University. She was involved in conceptualisation, methodology, investigation, formal analysis, and writing the original draft.
Dr Norman Bartolome is a PBL lecturer at the School of Medicine, Fiji National University. He was involved in conceptualisation, methodology, investigation, and writing the original draft.
Dr Alena Kotoiwasawa is a PBL lecturer at the School of Medicine, Fiji National University, and was involved in conceptualisation, methodology, and investigation.
Dr Rachael Masilomani is a former PBL lecturer at the School of Medicine, Fiji National University. She was involved in conceptualisation, methodology, investigation, and formal analysis.
Dr Lusiana Naikawakawavesi is a PBL lecturer at the School of Medicine, Fiji National University, and was involved in conceptualisation, methodology, and investigation.
Dr Maria Villareul is a PBL lecturer at the School of Medicine, Fiji National University. She was involved in conceptualisation, methodology, and investigation.
Dr Sophaganie Jepson is a PBL lecturer at Fiji National University. She was involved in conceptualisation, methodology, investigation.
Dr Aying Wang is a former PBL Lecturer at Fiji National University. He was involved in conceptualisation, methodology, investigation.
Dr Claudia Paterson is a research fellow at The University of Auckland, New Zealand. She was involved in formal analysis, reviewing and editing.
Professor Andrew Hill is a colorectal surgeon and Professor of Surgery at Middlemore Hospital, Auckland, New Zealand. He was involved in supervision, reviewing and editing.
Ethical Approval
Ethical approval was provided through FNU’s College Human Health Ethics Committee (CHHREC) – reference ID: 292.20.
Data Availability
The corresponding author is able to provide researchers access to our anonymised dataset, on reasonable request.
Acknowledgements
The authors acknowledge the efforts of the students in participating in this study.
Funding
No funding was used for this study.
Declaration of Interest
The authors do not have any conflicts of interest to disclose.
References
Al-Ansari, A. A., & El Tantawi, M. M. A. (2015). Predicting academic performance of dental students using perception of educational environment. Journal of Dental Education, 79(3), 337–344. https://doi.org/10.1002/j.00220337.2015.79.3.tb05889.x
Ali, K., Raja, M., Watson, G., Coombes, L., & Heffernan, E. (2012). The dental school learning milieu: Students’ perceptions at five academic dental institutions in Pakistan. Journal of Dental Education, 76(4), 487–494. https://doi.org/10.1002/j.0022-0337.2012.76.4.tb05281.x
Alraawi, M. O., Baris, S. A., Ahmari, N. A., Alshadidi, A. B., Abidi, N. A., & Al Moaleem, M. (2020). Analyzing students’ perceptions of educational environment in new dental colleges, Turkey using DREEM Inventory. Bioscience Biotechnology Research Communications, 13(2), 556–564. http://dx.doi.org/10.21786/bbrc/13.2/29
Demirören, M., Palaoğlu, Ö., Kemahlı, S., Özyurda, F., & Ayhan, İ. H. (2008). Perceptions of students in different phases of medical education of educational environment: Ankara University Faculty of Medicine. Medical Education Online, 13, Article 8. https://doi.org/10.3885/meo.2008.Res00267
Edgren, G., Haffling, A. C., Jakobsson, U., McAleer, S., & Danielsen, N. (2010). Comparing the educational environment (as measured by DREEM) at two different stages of curriculum reform. Medical Teacher, 32(6), e233–e238. https://doi.org/10.3109/01421591003706282
Finn, Y., Avalos, G., & Dunne, F. (2014). Positive changes in the medical educational environment following introduction of a new systems-based curriculum: DREEM or reality? Irish Journal of Medical Science, 183(2), 253–258. https://doi.org/10.1007/s11845-013-1000-4
Hyde, S., Hannigan, A., Dornan, T., & McGrath, D. (2018). Medical school clinical placements – The optimal method for assessing the clinical educational environment from a graduate entry perspective. BMC Medical Education, 18, Article 7. https://doi.org/10.1186/s12909-017-1113-y
Kool, B., Wise, M. R., Peiris-John, R., Sadler, L., Mahony, F., & Wells, S. (2017). Is the delivery of a quality improvement education programme in obstetrics and gynaecology for final year medical students feasible and still effective in a shortened time frame? BMC Medical Education, 17, Article 91. https://doi.org/10.1186/s12909-017-0927-y
Miles, S., Swift, L., & Leinster, S. J. (2012). The Dundee Ready Education Environment Measure (DREEM): A review of its adoption and use. Medical Teacher, 34(9), e620–e634. https://doi.org/10.3109/0142159X.2012.668625
O’Brien, A. P., Chan, T. M. F., & Cho, M. A. A. (2008). Investigating nursing students’ perceptions of the changes in a nursing curriculum by means of the Dundee Ready Education Environment Measure (DREEM) Inventory: Results of a cluster analysis. International Journal of Nursing Education Scholarship, 5(1), Article 25. https://doi.org/10.2202/1548-923X.1503
Prosser, M., & Trigwell, K. (1999). Understanding learning and teaching: The experience in higher education. McGraw-Hill Education.
Ramsden, P. (2003). Learning to teach in higher education (2nd ed.). Routledge.
Riquelme, A., Oporto, M., Oporto, J., Méndez, J. I., Viviani, P., Salech, F., Chianale, J., Moreno, R., & Sánchez, I. (2009). Measuring students’ perceptions of the educational climate of the new curriculum at the Pontificia Universidad Católica de Chile: Performance of the Spanish translation of the Dundee Ready Education Environment Measure (DREEM). Education for Health, 22(1), Article 112.
Roff, S., McAleer, S., Harden, R. M., Al-Qahtani, M., Ahmed, A. U., Deza, H., Groenen, G., & Primparyon, P. (1997). Development and validation of the Dundee Ready Education Environment Measure (DREEM). Medical Teacher, 19(4), 295–299.
Stormon, N., Ford, P. J., & Eley, D. S. (2019). DREEM-ing of dentistry: Students’ perception of the academic learning environment in Australia. European Journal of Dental Education, 23(1), 35–41. https://doi.org/10.1111/eje.12384
Till, H. (2004). Identifying the perceived weaknesses of a new curriculum by means of the Dundee Ready Education Environment Measure (DREEM) Inventory. Medical Teacher, 26(1), 39–45. https://doi.org/10.1080/01421590310001642948
*Dr Maria Concepcion Bartolome
Basic Clinical Medicine Department
School of Medical Sciences (SMS)
College of Medicine, Nursing and Health Sciences (CMNHS),
Fiji National University
Hoodless House, Brown St. Suva, Fiji Islands
+679 3311700
Email: maria.bartolome@fnu.ac.fj
Submitted: 5 June 2024
Accepted: 30 October 2024
Published online: 1 April, TAPS 2025, 10(2), 71-81
https://doi.org/10.29060/TAPS.2025-10-2/OA3424
Mary Xiaorong Chen1, Meredith Tsz Ling Yeung1, Nur Khairuddin Bin Aron2, Joachim Wen Jie Lee3 & Taylor Yutong Liu4
1Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore; 2Rehabilitation Department, Jurong Community Hospital, Singapore; 3Rehabilitation Medicine, Singapore General Hospital, Singapore; 4Clinical Support Services Department, National University Hospital, Singapore
Abstract
Introduction: Transitioning from a novice physiotherapist (NPT) to an independent practitioner presents significant challenges. Burnout becomes a risk if NPTs lack adequate support for learning and coping. Despite the importance of this transition, few studies have explored NPTs’ experiences in Singapore. This study aims to investigate the transitional journey of NPTs within this context.
Methods: Conducted as a descriptive phenomenological study, researchers collected data through semi-structured online interviews with eight NPTs from six acute hospitals across Singapore. Simultaneous data analysis during collection allowed for a reflexive approach, enabling the researchers to explore new facets until data saturation. Thematic analysis was employed and complemented by member triangulation.
Results: The challenges NPTs encountered include seeking guidance from supervisors, managing fast-paced work and patients with complex conditions. Additionally, NPTs grappled with fear of failure, making mistakes and self-doubt. They adopted strategies such as assuming responsibility for learning, developing patient-focused approaches, and emotional resilience. However, a concerning trend emerged with the growing emotional apathy and doubts about their professional choice.
Conclusion: This study provides a nuanced understanding of the challenges faced by NPTs during their transition. The workplace should be viewed as a learning community, where members form mutual relationships and support authentic learning. Recommendations include augmenting learning along work activities, fostering relationships, ensuring psychological safety, and allowing “safe” mistakes for comprehensive learning.
Keywords: Novice Physiotherapist Transition in Practice, Clinical Learning and Supervision, Mentoring, Emotional Resilience and Support, Safe Learning Environment
Practice Highlights
- Gradual assumption of responsibilities helps Novice Physiotherapists (NPTs) build competence.
- Learning should be augmented along with work activities.
- It is important to support NPTs to overcome the fear of failure and self-doubt.
- NPTs’ ability to negotiate learning and emotional resilience are essential.
- Trusting relationships and a safe learning environment are essential to NPTs’ learning.
I. INTRODUCTION
Novice Physiotherapists (NPTs) are physical therapy graduates with two years or less of clinical practice, and during this transition to independent practitioners in clinical settings, they face significant challenges (Martin et al., 2020; Wright et al., 2018). Despite the expectation of competence, concerns persist regarding NPTs’ abilities in various aspects of their practice.
It was reported that the persistent challenges faced by NPTs include managing workload, handling patients with complex conditions, seeking adequate guidance, and navigating relationship dynamics (Latzke et al., 2021; Mulcahy et al., 2010). One critical issue is the oversight of NPTs’ “new” status, leading to their assignment of patient loads comparable to experienced practitioners. Consequently, NPTs find themselves under tremendous stress in managing patients with complex conditions and diverse sociocultural backgrounds beyond their abilities (Stoikov et al., 2021; Wells et al., 2021). Workloads and time constraints hinder the development of meaningful connections between NPTs and supervisors, affecting teaching and coping abilities (Rothwell et al., 2021). In the busy clinical environment, NPTs cannot solely rely on their assigned supervisors, the support from senior colleagues around them along their developmental journey is necessary. Unfortunately, studies suggest that inadequate support and guidance from senior colleagues exacerbate these challenges (Forbes et al., 2021; Jones et al., 2021; Phan et al., 2022; Stoikov et al., 2020; Te et al., 2022).
Additionally, as NPTs are inexperienced, communicating with patients, their families, and other healthcare professionals present a significant hurdle in clinical decision-making (Atkinson & McElroy, 2016). The pressure to make informed clinical decisions, drawing upon extensive knowledge and experience, contributes to job-related stress and feelings of inadequacy among NPTs (Adam et al., 2013).
Job stress-related symptoms, including exhaustion, self-doubt, and depression, further impact NPTs’ well-being. These symptoms, akin to burnout, result from a mismatch between the worker’s performance and job expectations (Brooke et al., 2020; Pustułka-Piwnik et al., 2014). Studies reveal that burnout affects approximately 65% of physiotherapists in Spain (Carmona-Barrientos et al., 2020). This is a concern as burnout was found to be correlated positively with intentions to leave the profession (Cantu et al., 2022), leading to low morale, and compromised patient service quality (Evans et al., 2022; Lau et al., 2016).
Studies suggest that ill-prepared PTs may feel inadequate and lack confidence in making decisions which can negatively influence their clinical management and support for patients’ needs. For example, PTs who lack the ability to adopt a person focused approach might not be able to manage patients with chronic lower back pain effectively (Gardner et al., 2017). Furthermore, such impacts are subtle, difficult to pinpoint, and can result in poor care quality, low patient satisfaction and staff morale (Gardner et al., 2017; Holopainen et al., 2020; Marks et al., 2017).
In Singapore, the healthcare system is bifurcated into public and private sectors. Public hospitals, which fall under government ownership (Ministry of Health, 2023), are pivotal in delivering healthcare services. These hospitals are organised into three distinct clusters, each serving specific regions within the country. Table 1 for a comprehensive list of public hospitals categorised by their respective clusters.
|
Healthcare Clusters |
Hospitals |
|
National Healthcare Group (NHG) |
Tan Tock Seng Hospital |
|
|
Khoo Teck Puat Hospital IMH (Institute of Mental Health) |
|
National University Health System (NUHS) |
National University Hospital |
|
|
Ng Teng Fong General Hospital |
|
|
Alexandra Hospital |
|
SingHealth |
Singapore General Hospital |
|
|
Changi General Hospital |
|
|
Sengkang General Hospital |
|
|
National Heart Centre |
|
|
KK Women’s and Children’s Hospital |
Table 1. Public hospitals in Singapore
At the beginning of 2022, Singapore had 165 physiotherapists under conditional registration, with 97 (59.51%) employed by public hospitals (Allied Health Professions Council, 2022). Novice Physiotherapists (NPTs) require close supervision and guidance from their clinical mentors/supervisors. During their initial phase, all NPTs undergo a 13-month conditional registration before qualifying for a full registration status. With an average 200 PT students graduate from the Singapore Institute of Technology each year, coupled with the NPTs under conditional registration, the supervisory tasks shared by the limited pool of PT Supervisors are tremendous. Besides their supervisory roles, PT supervisors are also clinically responsible to managing patients and workplace administrations.
A recent study conducted in Singapore explored the perspectives of allied health practitioners, including physiotherapists, occupational therapists, and radiographers, regarding clinical supervision in tertiary hospitals (Lim et al., 2022). The findings revealed that newly qualified allied health practitioners often faced challenges related to insufficient clinical supervision, emotional support, and professional guidance from their supervisors. Contributing factors included time constraints and staffing limitations (Lim et al., 2022). These findings underscore the need for a deeper understanding of the experiences encountered by NPTs during their early clinical practice.
Despite the significance of this issue, no further research has specifically explored the clinical experiences of NPTs in Singapore. Among NPTs, those working in acute public hospitals constitute a compelling subgroup, representing 59.51% of the NPT workforce. Additionally, acute public hospitals provide multidisciplinary services, making them ideal settings for studying the challenges faced by NPTs. Therefore, this study aims to delve into the experiences of NPTs within Singapore’s acute public hospitals.
II. METHODS
A. Study Design
The study employed a descriptive phenomenological approach to understand participants’ lived experiences (Neubauer et al., 2019). In this approach, researchers intentionally set aside their preconceptions and assumptions in this method, allowing the data to speak for itself (Shorey & Ng, 2022). Giorgi (1997) highlights that descriptive phenomenology is particularly well-suited for phenomena that lack extensive literature evidence. Given the limited research on NPTs’ transitional experiences in Singapore, adopting descriptive phenomenology is appropriate for this study.
B. Ethical Considerations
Ethical approval was obtained from the University Institutional Review Board (Approval number: 2022033). The participant information sheet was emailed to prospective participants for recruitment. Written informed consent was obtained. All researchers had no authoritative relations with the participants. Participants were assured that their participation was anonymous and voluntary.
C. Participant Recruitment
Adopting a convenient and snowballing sampling approach, the researchers approached NPTs and sought referrals for further recruitment. The inclusion criteria were: (1) NPTs who had less than two years of clinical practice after graduation; (2) NPTs who were working in acute public hospitals. The exclusion criteria were: (1) NPTs who had prior working experience in healthcare; (2) NPTs who were not working in acute public hospitals.
The recruitment email sought voluntary return of information such as place of practice, date of employment, alma mater, and previous work experience in healthcare. A follow-up email was sent to arrange for the online semi-structured interview. Eight participants from six acute public hospitals were included in the study.
|
Participant* |
Gender |
Race |
Age (Years) |
Hospital * |
Length of Employment |
|
Alpha |
Female |
Chinese |
26 |
Hospital G |
348 days |
|
Beta |
Female |
Chinese |
24 |
Hospital E |
419 days |
|
Charlie |
Male |
Malay |
27 |
Hospital I |
310 days |
|
Delta |
Female |
Chinese |
27 |
Hospital K |
432 days |
|
Epsilon |
Female |
Chinese |
24 |
Hospital G |
452 days |
|
Foxtrot |
Female |
Chinese |
24 |
Hospital G |
515 days |
|
Golf |
Female |
Chinese |
24 |
Hospital E |
531 days |
|
Hotel |
Female |
Chinese |
24 |
Hospital A |
531 days |
Table 2. Participant demographic information
* Participants’ names and hospitals are given pseudonyms to maintain anonymity.
D. Data Collection
Data were collected by researchers NK, JL and TL, who were final-year physiotherapy students. The interview guide was developed based on the literature review and validated by MC and MY, both are experienced in clinical supervision. The researchers conducted pilot interviews to test the interview guide and their approaches. The interview guide is presented in Appendix 1.
With the semi-structured approach, the researchers had the flexibility to follow up on questions. Open-ended questions were used to mitigate the potential issues of over-leading the discussion (Green & Thorogood, 2018). MC provided feedback to NK, JL and TL after each interview. The researchers kept a reflexive journal to record their thoughts, feelings, knowledge and perceptions of the research process (Chan et al., 2013).
Interviews were conducted between July and November 2022 over Zoom. The interview recordings were transcribed. The research team reviewed the video recordings and the aspects needed to follow up with the next interview (Ryan et al., 2009). Data saturation was reached by the fifth interview. Three more interviews were done to ensure no new findings. Each interview lasted between 33 to 110 minutes, with a mean duration of 77 minutes.
E. Data Analysis
The data were analysed using an inductive approach with no predetermined structure, framework, or theory simultaneously with data collection (Burnard et al., 2008). The four stages include decontextualisation, recontextualisation, categorisation, and compilation (Bengtsson, 2016) as shown in Figure 1.
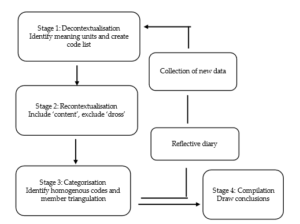
Figure 1. Data analysis process (Adapted from Bengtsson, 2016)
For decontextualisation, NK, JL and TL read interview transcripts and code the text into smaller meaning units independently. A meaningful unit is the smallest unit that can be defined as sentences or paragraphs containing aspects related to one another and addressing the aim of the study (Graneheim & Lundman, 2004) (see Figure 2).
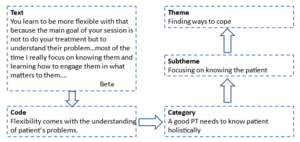
Figure 2. An example of the analysis process
For recontextualisation, the researchers read the original text alongside the final list of codes. The unmarked text was included if it was relevant to the research question. For unrelated text, it was labelled as “dross” and excluded (Bengtsson, 2016). Discrepancies were resolved through consulting MC and MY. Codes were reviewed to identify patterns and similarities and then categorised into themes and sub-themes. The rigor of analysis was ensured through researcher triangulation (Lao et al., 2022). Qualitative data analysis software Quirkos was used to assist with the analysis.
III. RESULTS
From the data analysis based on the dataset (Chen, 2023), two themes were synthesised as shown in Table 3.
|
Themes |
Subthemes |
|
Challenges from multiple aspects |
Challenges in getting guidance from the Supervisors |
|
Challenges from the pace and nature of the work |
|
|
Challenges from patient |
|
|
Fear and self-doubt |
|
|
Finding ways to cope |
Be intentional and responsible in learning |
|
Focusing on knowing the patient and managing time |
|
|
Emotional resilience and emotional apathy |
Table 3. Themes and subthemes
These themes are supported by subthemes depicting the multiple dimensions of challenges and NPTs’ coping strategies.
A. Challenges from Multiple Aspects
This theme is supported by four sub-themes, indicating NPTs encountered challenges from many aspects of their practice context.
1) Challenges in getting guidance from the supervisors: NPTs reported that they were scheduled to manage patients independently soon after their orientation, often at a different location from their supervisors. Working in different locations to manage different groups of patients posed difficulties for NPTs to learn from their supervisors. Even if the clinics were nearby, their supervisors had to stop their clinics temporarily to guide the NPTs, which caused the accumulation of patients on the waiting list and prolonged clinical hours. Knowing this would happen, NPTs were reluctant to consult their supervisors.
Furthermore, NPTs might not be familiar with the patient’s medical conditions, posing challenges for them to ask questions. Some of them had been ridiculed for asking questions deemed “inappropriate”. For example, the supervisor might pass a remark such as “This kind of question you also ask!” or the supervisor ignores their questions. As a result, NPTs felt they were left alone to struggle with the feeling of inadequacy and anxiety.
2) Challenges from the pace and nature of the work: NPTs operated within a tight timeframe, similar to the experienced colleagues’ schedule, with only 20 minutes allocated for each patient. This brevity limited their ability to build rapport with patients and to discuss treatment options. The rapid succession of patients, where one consultation immediately followed another, left NPTs mentally exhausted and hindered effective patient management.
Meanwhile, NPTs were required to record their consultations with patients promptly. However, unfamiliarity with the items on the documentation often led to incomplete records. The accumulation of unfinished document recordings throughout the day left NPTs with a backlog to address during their shifts. By the end of the day, recalling specific patient details became challenging.
Additionally, NPTs as the “gatekeepers”, must assess patients’ fitness for discharge. Balancing medical guidelines, patient readiness and family expectations are delicate. NPTs occasionally found themselves at odds with doctors’ decisions when they believed a patient’s condition was not ready for discharge. This stance can lead to stress and feelings of being disregarded. NPT Hotel shared:
“We do have our reasoning and know why we do certain things. So sometimes it is frustrating when you bring it across for the doctor, and they don’t take you seriously.”
3) Challenges from patients: Many patients, particularly the elderly, communicate primarily in dialects in Singapore. For NPTs who are educated in English, understanding these dialects could be akin to deciphering a foreign language, hindering accurate assessment and treatment planning. This challenge creates another layer of stress for NPTs to understand the patients and tailor the interventions. Understandably patients’ outcomes were not always predictable. However, NPTs could be blamed when patients experience setbacks after discharge. The weight of unjust accusations took a toll on NPTs’ mental well-being. NPT Charlie shared such an encounter:
“I assessed the patient, and he met all the outcome measures for discharge. The day he went home, he fell! The patient’s family was angry and made a complaint. It wasn’t my fault. He didn’t take his medication, and he is suffering from Parkinson’s Disease…it is a very mentally taxing job…You know, when I called the family, they yelled at me… it is emotionally draining…”
4) Fear and self-doubt: NPTs realised that their knowledge was but a drop in the vast ocean of medical expertise and they started to question their abilities. Each patient encounter became a tightrope walk – a delicate balance between thoroughness and efficiency. Fearing they might miss crucial details, NPTs reported to work early and pored over each patient’s medical record to prepare themselves. Yet, despite their diligence, inadequacy gnawed at their confidence.
Practicing under a conditional license, the aim to achieve competence is like a ticking clock, NPTs must prove their worth within a limited timeframe. The fear of failure loomed large and each misstep felt like a step toward the abyss. NPT Golf shared his feeling of inadequacy:
“You take a long time to read the patient’s medical record to screen them, much slower than your seniors, but you will still miss out important things… you see each patient a bit longer…you spend longer time on documentation (recording), then you have many days with extended working hours…”
B. Finding ways to cope
NPTs adopted various approaches to cope with their work demand, some of the methods helped while some were not so.
1) Be intentional and responsible in learning: Recognising the limitations of case scenario-based classroom learning, some NPTs proactively learn through their daily work. NPT Golf shared the importance of such learning:
“Discharge planning and prognostication required a lot of clinical reasoning, which is very difficult to teach in a lecture. You have to see the real patient to know their background and the cause of the condition and to discuss with the patient their rehab potential.”
NPTs learned to present their clinical reasoning when asked questions, to show that they were proactive in learning. Some NPTs maintained a question log throughout the day and negotiated a dedicated time slot to consult their supervisors after work. Another strategy was to review the next day’s patient list, anticipate difficulties they might encounter, and seek opportunities to see the selected patients with supervisors. With this arrangement, NPTs can learn on the job and get immediate feedback.
2) Focusing on knowing the patient and managing time: NPTs acknowledged that patient care extends beyond physical assessment. They delved into patients’ medical records to know the medications the patient is on, their side effects, and the underlying conditions. By meticulously assessing patients, NPTs gained a holistic understanding of their health status. This knowledge informs treatment decisions and ensures patient safety. Delta’s example underscores this approach:
“Knowing a patient’s medication regimen and potential side effects allows us to anticipate complications. For instance, abdominal bloating from a specific medication may impact diaphragm movement, leading to patient agitation.”
Meanwhile, NPTs recognised the pivotal role of families in patient care. They actively sought input from family members to understand cultural nuances and contextual factors. As each patient comes with unique physical limitations and emotional stressors, understanding patients’ goals, fears, and preferences is paramount. Beta emphasises:
“Our sessions aren’t solely about treatments. We invest time in understanding patients’ problems and engaging them and their families in meaningful conversations…most of the time I focus on knowing them and learning how to engage them…(know) what matters to them.”
NPTs recognise that time is a precious resource. They make deliberate choices to maximise their time at work. For example, they shorten their lunch breaks to catch up with workload demands. They took quick notes or used visual reminders (such as photographs) to aid memory in recording. NPTs also learned to quickly jot down relevant details before the next patient consultation to ensure the accuracy of document recording and continuity of care.
3) Emotional resilience and emotional apathy: NPTs need to go through a series of skills competency assessments. When faced with assessment failure, being resilient is helpful. Delta explained:
“I think a good mindset would be to ask myself ‘Why did I fail this competency (assessment)? Was it because I did not maintain sterility? Did I do something wrong?’…the next time I will remember to correct my mistakes…then I realised that ‘oh, it (failure) doesn’t matter. I can learn and do (it) again…”
Some, like NPT Foxtrot, experience sadness and grief when the patients they care for deteriorate and die. To maintain emotional resilience, NPTs used strategies such as “letting go”, “emotional detachment” and “getting enough sleep” to avoid intense emotions. They also get support from peers, friends, and family.
However, some NPTs worried about the loss of enthusiasm and became too detached emotionally by “seeing every patient as a condition or a case” and transformed patient encounters into mechanical routines. They called it “emotional apathy” or “turned off”.
IV. DISCUSSION
This study is the first to explore the experiences of newly graduated physiotherapists (NPTs) during their initial two years of clinical practice in Singapore. The findings indicate that NPTs encounter several challenges during this transition, such as obtaining adequate guidance from supervisors, managing patients with complex conditions, and coping with demanding workloads. These findings align with existing literature evidence, suggesting that the challenges faced by NPTs in Singapore are comparable to those encountered in other countries.
Furthermore, this research provides a nuanced understanding of the factors contributing to NPTs’ transitional challenges. Workplace learning can be difficult due to tight schedules, and multiple members in the process with various roles and responsibilities. According to Billett et al. (2018), the workplace is the most authentic learning place and workplace learning has to be intentional. Firstly, there is a need to set up the curriculum. This happens only when learning is viewed as an integral part of work where the use of knowledge, roles, and processes are continuously negotiated. Therefore, NPTs, their supervisors, and coworkers need to discuss learning opportunities along the pathways of work to plan activities that augment learning.
Secondly, there is a need to enable effective learning facilitated by experts within the workplace. This means the workplace is a learning community where all members share a common purpose and are willing to help one another learn. The responsibility of teaching and guiding the NPTs are shared responsibilities, members can take part in teaching in their expertise.
Thirdly, there is a need to consider individual factors and construct learning according to what learners know, can do and value. For this to happen, clinical experts, such as supervisors and senior members need to have conversations with the NPTs to help them identify learning needs, as NPTs sometimes do not know what they do not know.
However, revealing one’s learning needs can leave one feeling vulnerable; thus, trust relationships and psychological safety are crucial in the workplace. Sellberg et al. (2022) suggested that supervisors can initiate meetings to get to know NPTs and share their own learning experiences as novices. NPTs need to feel safe to share what they know, can do, and need to learn.
Initial placement of NPTs in the same clinic with their supervisors can foster relationships, confidence, and learning. Several clinical supervision strategies, including understanding clinical situations, aligning learning objectives with roles, discussing goals with learners, and actively observing and debriefing learners (Hinkle et al., 2017), can be recommended to NPTs’ supervisors and senior members in the community. Additionally, dedicated time for supervisors and NPTs to discuss and reflect on work and learning, or even engage in social activities, can help boost relationships.
Clinical supervisors should be carefully selected and trained in supervision skills. A research study suggested that they should be knowledgeable, good communicators, approachable, interested in building relationships with learners, and capable of providing feedback and tailored guidance (Alexanders et al., 2020). A meta-analysis by Nienaber et al. (2015) suggests that supervisor attributes, subordinate attributes, interpersonal processes, and organisational characteristics influence relationship building. Therefore, efforts for relationship building should not only be at the individual level but also the organisational level. Organisations can provide targeted training to supervisors to empower them with the knowledge and skills to mentor NPTs.
This study also highlights the dilemma NPTs face between the fear of making mistakes and the responsibility of learning. Such fear is not unique to NPTs as studies suggest novice nurses also report similar anxieties during the transition (Cowen et al., 2016; Ten Hoeve et al., 2018). Singapore studies on novice nurses (Chen et al., 2021) and nursing students (Leong & Crossman, 2016) highlighted similar fear, as making mistakes in healthcare is taboo. In their effort to avoid mistakes, NPTs adopt a “safe” approach and avoid opportunities that could significantly enhance their competence and abilities.
Fear of failure limits learning, while comprehensive learning requires a degree of autonomy and the safety to make mistakes. There is a need to change attitudes towards “safe” mistakes. Harteis et al. (2008) suggested that allowing workers to learn from mistakes at work can maximise learning and cooperativeness. Eskreis-Winkler and Fishbach (2019) reviewed five studies on learning from failure, emphasising that effective learning happens from the feedback of mistakes and such feedback must separate failure from personal judgment. Creating a psychologically safe learning environment, where learners feel safe to ask questions and learn from mistakes, is essential (Edmondson, 2023).
NPTs also faced challenges in their interactions with other healthcare professionals and patients. Patton et al. (2018) highlighted that the clinical setting is a multidimensional learning space where environmental factors, the nature of the work, and member interactions shape clinical learning. Hence educators at higher learning institutes can design learning using role play by engaging students, clinical supervisors, other healthcare professionals, and standardised patients to learn different roles and perspectives.
This study is the first to explore the transitional experiences of newly graduated physiotherapists (NPTs) in Singapore. It is important to note that NPTs from community and private settings were not represented. Future research should investigate the transitional experiences of NPTs in tertiary and community care settings to provide a more comprehensive understanding.
This study highlighted several critical aspects of NPTs’ transition, including fear, emotional apathy, intention in learning, and relationship building with supervisors and patients. However, these areas warrant further exploration to deepen our understanding. Additionally, incorporating the perspectives of clinical supervisors could complement the current findings in facilitating NPTs’ learning in transition.
V. CONCLUSION
This study provides a nuanced understanding of the challenges encountered by newly graduated physiotherapists (NPTs) and their coping strategies during their transition. The findings underscore the necessity for a well-structured clinical supervision setting, a safe learning environment, well-trained clinical supervisors, an emotional support framework for NPTs and clinical roleplay training in schools. It is also crucial to cultivate NPTs’ abilities to learn and to develop meaningful relationships with supervisors and patients.
Notes on Contributors
Author MC provided research conceptualisation and methodology guidance, performed data analysis, validated findings and wrote the manuscript. Author MY provided methodology guidance, validated findings and provided feedback to the writing of the manuscript. Author NK, JL and TL reviewed the literature, developed the methodological framework for the study, and performed data collection and data analysis as their final-year project. All authors have read and agreed to the published version of the manuscript.
Ethical Approval
The study was approved by the Singapore Institute of Technology Ethics Committee (Project 2022033).
Data Availability
The data that support the findings of this study are available at https://figshare.com/s/4f1ecf288001750e72 e4
Acknowledgment
The authors thank the physiotherapists who participated in the study.
Funding
This study received no funding.
Declaration of Interest
The authors do not have any conflicts of interest. Participation in the research was voluntary and anonymous. Novice Physiotherapists were assured that their participation or nonparticipation would not affect their work performance appraisal.
References
Adam, K., Peters, S., & Chipchase, L. (2013). Knowledge, skills and professional behaviours required by occupational therapist and physiotherapist beginning practitioners in work-related practice: A systematic review. Australian Ooccupational Therapy Journal, 60(2), 76-84. https://doi.org/10.1111/1440-1630.12006
Allied Health Professions Council. (2022). Allied Health Professions Council Annual Report 2022. AHPC. https://www.healthprofessionals.gov.sg/docs/librariesprovider5/announcements/2022_ahpc-annual-report_v7-(final).pdf
Alexanders, J., Chesterton, P., Gordon, A., Alexander, J., & Reynolds, C. (2020). Physiotherapy student’s perceptions of the ideal clinical educator [version 1]. MedEdPublish, 9(254). https://doi.org/10.15694/mep.2020.000254.1
Atkinson, R., & McElroy, T. (2016). Preparedness for physiotherapy in private practice: Novices identify key factors in an interpretive description study. Manual Therapy, 22, 116-121. https://doi.org/10.1016/j.math.2015.10.016
Bengtsson, M. (2016). How to plan and perform a qualitative study using content analysis. NursingPlus Open, 2, 8-14. https://doi.org/https://doi.org/10.1016/j.npls.2016.01.001
Billett, S., Harteis, C., & Gruber, H. (2018). Developing occupational expertise through everyday work activities and interactions. In K. A. Ericsson, R. R. Hoffman, A. Kozbelt, & A. M. Williams (Eds.), The Cambridge Handbook of Expertise and Expert Performance (2 ed., pp. 105-126). Cambridge University Press. https://doi.org/10.1017/9781316480748.008
Brooke, T., Brown, M., Orr, R., & Gough, S. (2020). Stress and burnout: Exploring postgraduate physiotherapy students’ experiences and coping strategies. BMC Medical Education, 20(1), Article 433. https://doi.org/10.1186/s12909-020-02360-6
Burnard, P., Gill, P., Stewart, K., Treasure, E., & Chadwick, B. (2008). Analysing and presenting qualitative data. British Dental Journal, 204(8), 429-432. https://doi.org/10.1038/sj.bdj.2008.292
Cantu, R., Carter, L., & Elkins, J. (2022). Burnout and intent-to-leave in physical therapists: A preliminary analysis of factors under organisational control. Physiotherapy Theory and Practice, 38(13), 2988-2997. https://doi.org/10.1080/09593985.2021.1967540
Carmona-Barrientos, I., Gala-León, F. J., Lupiani-Giménez, M., Cruz-Barrientos, A., Lucena-Anton, D., & Moral-Munoz, J. A. (2020). Occupational stress and burnout among physiotherapists: A cross-sectional survey in Cadiz (Spain). Human Resources for Health, 18, 1-10. https://doi.org/10.1186/s12960-020-00537-0
Chan, Z. C. Y., Fung, Y.-l., & Chien, W.-t. (2013). Bracketing in phenomenology: Only undertaken in the data collection and analysis process? Qualitative Report, 18(30), 1-9. https://doi.org/10.46743/2160-3715/2013.1486
Chen, M. X. (2023). Novice physiotherapists’ first-year clinical practice in Singapore [Data set]. Figshare. https://figshare.com/s/4f1ecf288001750e72e4
Chen, M. X., Newman, M., & Park, S. (2021). Becoming a member of a nursing community of practice: Negotiating performance competence and identity. Journal of Vocational Education & Training, 76(1), 164-178. https://doi.org/10.1080/13636820.2021.2015715
Cowen, K. J., Hubbard, L. J., & Hancock, D. C. (2016). Concerns of nursing students beginning clinical courses: A descriptive study. Nurse Education Today, 43, 64-68. https://doi.org/10.1016/j.nedt. 2016.05.001
Edmondson, A. C. (2023). Right Kind of Wrong: The Science of Failing Well. Simon and Schuster.
Eskreis-Winkler, L., & Fishbach, A. (2019). Not learning from failure—the greatest failure of all. Psychological Science, 30(12), 1733-1744. https://doi.org/10.1177/0956797619881133
Evans, K., Papinniemi, A., Vuvan, V., Nicholson, V., Dafny, H., Levy, T., & Chipchase, L. (2022). The first year of private practice – New graduate physiotherapists are highly engaged and satisfied but edging toward burnout. Physiotherapy Theory and Practice, 40(2), 262–275. https://doi.org/10.1080/09593985.2022.2113005
Forbes, R., Lao, A., Wilesmith, S., & Martin, R. (2021). An exploration of workplace mentoring preferences of new‐graduate physiotherapists within Australian practice. Physiotherapy Research International, 26(1), Article e1872. https://doi.org/10.1002/pri.1872
Gardner, T., Refshauge, K., Smith, L., McAuley, J., Hübscher, M., & Goodall, S. (2017). Physiotherapists’ beliefs and attitudes influence clinical practice in chronic low back pain: A systematic review of quantitative and qualitative studies. Journal of Physiotherapy, 63(3), 132-143. https://doi.org/10.1016/j.jphys.20 17.05.017
Giorgi, A. (1997). The theory, practice, and evaluation of the phenomenological method as a qualitative research procedure. Journal of Phenomenological Psychology, 28(2), 235-260. https://doi.org/10.1163/156916297X00103
Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2), 105-112. https://doi.org/10.1016/j.nedt.2003.10.001
Green, J., & Thorogood, N. (2018). Qualitative methods for health research. Sage.
Harteis, C., Bauer, J., & Gruber, H. (2008). The culture of learning from mistakes: How employees handle mistakes in everyday work. International Journal of Educational Research, 47(4), 223-231. https://doi.org/10.1016/j.ijer.2008.07.003
Hinkle, L. J., Fettig, L. P., Carlos, W. G., & Bosslet, G. (2017). Twelve tips for just in time teaching of communication skills for difficult conversations in the clinical setting. Medical Teacher, 39(9), 920-925. https://doi.org/10.1080/0142159X.2017.1333587
Holopainen, R., Simpson, P., Piirainen, A., Karppinen, J., Schütze, R., Smith, A., O’Sullivan, P., & Kent, P. (2020). Physiotherapists’ perceptions of learning and implementing a biopsychosocial intervention to treat musculoskeletal pain conditions: A systematic review and metasynthesis of qualitative studies. Pain, 161(6), 1150-1168. https://journals.lww.com/pain/fulltext/2020/06000/physiotherapists__perceptions_of_learning_and.5.aspx
Jones, A., Ingram, M. E., & Forbes, R. (2021). Physiotherapy new graduate self-efficacy and readiness for interprofessional collaboration: A mixed methods study. Journal of Interprofessional Care, 35(1), 64-73. https://doi.org/10.1080/13 561820.2020.1723508
Lao, A., Wilesmith, S., & Forbes, R. (2022). Exploring the workplace mentorship needs of new-graduate physiotherapists: A qualitative study. Physiotherapy Theory & Practice, 38(12), 2160-2169. https://doi.org/10.1080/09593985.2021.1917023
Latzke, M., Putz, P., Kulnik, S. T., Schlegl, C., Sorge, M., & Mériaux-Kratochvila, S. (2021). Physiotherapists’ job satisfaction according to employment situation: Findings from an online survey in Austria. Physiother Research International, 26(3), e1907. https://doi.org/10.1002/pri.1907
Lau, B., Skinner, E. H., Lo, K., & Bearman, M. (2016). Experiences of physical therapists working in the acute hospital setting: Systematic Review. Physical Therapy, 96(9), 1317-1332. https://doi.org/10.2522/ptj.20150261
Leong, Y. M. J., & Crossman, J. (2016). Tough love or bullying? New nurse transitional experiences. Journal of Clinical Nursing, 25(9-10), 1356-1366. https://doi.org/10.1111/jocn.13225
Lim, B., Cook, K., Sutherland, D., Weathersby, A., & Tillard, G. (2022). Clinical supervision in Singapore: Allied health professional perspectives from a two-round delphi study, 20(1), Article 12. The Internet Journal of Allied Health Sciences and Practice. https://doi.org/10.46743/1540-580X/2022.2103
Marks, D., Comans, T., Bisset, L., & Scuffham, P. A. (2017). Substitution of doctors with physiotherapists in the management of common musculoskeletal disorders: A systematic review. Physiotherapy, 103(4), 341-351. https://doi.org/10.1016/j.physio. 2016.11.006
Martin, R., Mandrusiak, A., Lu, A., & Forbes, R. (2020). New‐graduate physiotherapists’ perceptions of their preparedness for rural practice. The Australian Journal of Rural Health, 28(5), 443-452. https://doi.org/10.1111/ajr.12669
Ministry of Health. (2023). Health Facilities. Ministry of Health. https://www.moh.gov.sg/resources-statistics/singapore-health-facts/health-facilities
Mulcahy, A. J., Jones, S., Strauss, G., & Cooper, I. (2010). The impact of recent physiotherapy graduates in the workforce: A study of Curtin University entry-level physiotherapists 2000-2004. Australian Health Review, 34(2), 252-259. https://doi.org/10.1071/ AH08700
Neubauer, B. E., Witkop, C. T., & Varpio, L. (2019). How phenomenology can help us learn from the experiences of others. Perspectives on Medical Education, 8(2), 90-97. https://doi.org/10.1007/s40037-019-0509-2
Nienaber, A.-M., Romeike, P. D., Searle, R., & Schewe, G. (2015). A qualitative meta-analysis of trust in supervisor-subordinate relationships. Journal of Managerial Psychology, 30(5), 507-534. https://doi.org/10.1108/JMP-06-2013-0187
Patton, N., Higgs, J., & Smith, M. (2018). Clinical learning spaces: Crucibles for practice development in physiotherapy clinical education. Physiother Theory Practice, 34(8), 589-599. https://doi.org/10.1080/09593985.2017.1423144
Phan, A., Tan, S., Martin, R., Mandrusiak, A., & Forbes, R. (2022). Exploring new-graduate physiotherapists’ preparedness for, and experiences working within, Australian acute hospital settings. Physiotherapy Theory and Practice, 39(9), 1918-1928. https://doi.org/10.1080/09593985.2022.2059424
Pustułka-Piwnik, U., Ryn, Z. J., Krzywoszański, Ł., & Stożek, J. (2014). Burnout syndrome in physical therapists – Demographic and organisational factors. Medycyna pracy. Workers’ Health and Safety, 65(4), 453-462. https://doi.org/10.13075/mp.5893.00038
Rothwell, C., Kehoe, A., Farook, S. F., & Illing, J. (2021). Enablers and barriers to effective clinical supervision in the workplace: A rapid evidence review. BMJ open, 11(9), e052929. https://doi.org/10.1136/bmjopen-2021-052929
Ryan, F., Coughlan, M., & Cronin, P. (2009). Interviewing in qualitative research: The one-to-one interview. International Journal of Therapy and Rehabilitation, 16(6), 309-314. https://doi.org/10.12968/ijtr.2009.16.6.42433
Sellberg, M., Halvarsson, A., Nygren-Bonnier, M., Palmgren, P. J., & Möller, R. (2022). Relationships matter: A qualitative study of physiotherapy students’ experiences of their first clinical placement. Physical Therapy Reviews, 27(6), 477-485. https://doi.org/10.1080/10833196.2022.2106671
Shorey, S., & Ng, E. D. (2022). Examining characteristics of descriptive phenomenological nursing studies: A scoping review. Journal of Advanced Nursing, 78(7), 1968-1979. https://doi.org/10.1111/jan.15244
Stoikov, S., Gooding, M., Shardlow, K., Maxwell, L., Butler, J., & Kuys, S. (2021). Changes in direct patient care from physiotherapy student to new graduate. Physiotherapy Theory and Practice, 37(2), 323-330. https://doi.org/10.1080/09593985.2019.1628138
Stoikov, S., Maxwell, L., Butler, J., Shardlow, K., Gooding, M., & Kuys, S. (2020). The transition from physiotherapy student to new graduate: Are they prepared? Physiotherapy Theory and Practice, 38(1), 101-111. https://doi.org/10.1080/09593985.2020.1744206
Te, M., Blackstock, F., Liamputtong, P., & Chipchase, L. (2022). New graduate physiotherapists’ perceptions and experiences working with people from culturally and linguistically diverse communities in Australia: A qualitative study. Physiotherapy Theory and Practice, 38(6), 782-793. https://doi.org/10.1080/09593985.2020.1799459
Ten Hoeve, Y., Kunnen, S., Brouwer, J., & Roodbol, P. F. (2018). The voice of nurses: Novice nurses’ first experiences in a clinical setting. A longitudinal diary study. Journal of Clinical Nursing, 27(7-8), e1612-e1626. https://doi.org/10.1111/jocn.14307
Wells, C., Olson, R., Bialocerkowski, A., Carroll, S., Chipchase, L., Reubenson, A., Scarvell, J. M., & Kent, F. (2021). Work readiness of new graduate physical therapists for private practice in Australia: Academic faculty, employer, and graduate perspectives. Physical Therapy, 101(6), pzab078. https://doi.org/10.1093/ptj/pzab078
Wright, A., Moss, P., Dennis, D. M., Harrold, M., Levy, S., Furness, A. L., & Reubenson, A. (2018). The influence of a full-time, immersive simulation-based clinical placement on physiotherapy student confidence during the transition to clinical practice. Advances in Simulation, 3(1), Article 3. https://doi.org/10.1186/s41077-018-0062-9
*Mary Xiaorong Chen
10 Dover Drive
Singapore 138680
Email: Mary.chen@singaporetech.edu.sg
Submitted: 30 April 2024
Accepted: 25 September 2024
Published online: 1 April, TAPS 2025, 10(2), 82-85
https://doi.org/10.29060/TAPS.2025-10-2/SC3345
Sethapong Lertsakulbunlue & Anupong Kantiwong
Department of Pharmacology, Phramongkutklao College of Medicine, Thailand
Abstract
Introduction: Very Short Answer Questions (VSAQs) minimise cueing and simulate actual clinical practice more accurately than Single Best Answer Questions, as multiple-choice options might not be realistic. Phramongkutklao College of Medicine has developed a Self-Marked VSAQ (SM-VSAQ) for formative assessments. This study determines the validity and reliability of the SM-VSAQs.
Methods: Ninety-four third-year pre-clinical students took two occasions of 10-question SM-VSAQ exams regarding cardiovascular drugs. Each question consisted of two steps: (1) clinical vignettes with questions and (2) expected answers with scores, self-marking, and feedback comprehension. Scores ranged from 0.00 to 1.00 in 0.25 increments, though not every increment was applied to all questions. A distribution of the rating agreement between students’ and teacher’s ratings was presented to determine criterion-related validity and inter-rater reliability.
Results: Criterion-related validity revealed 90.64% and 93.19% of the ratings demonstrated exact agreement between students’ and teachers’ ratings, with an inter-rater reliability of 0.972 and 0.977 for the first and second occasions, respectively (p=0.001). The exact agreement was relatively lower on the first occasion for questions with more diverse expected answers (85.11%, r=0.867, p=0.001) and drugs requiring their specific full names for a perfect mark (74.47%, r=0.849, p=0.001). While questions with specific guides do not require complex answers, they received a higher exact agreement.
Conclusion: The SM-VSAQ format effectively combines guided answers with the VSAQ model. The agreement with teacher-rated is excellent. Marking discrepancies rooted in misconceptions underscores the importance of teacher feedback in improving self-grading in formative assessments. Regular self-assessment practice is recommended to enhance grading accuracy.
Keywords: Very Short Answer Question, Self-assessment, Medical Education, Undergraduate, Pharmacology
I. INTRODUCTION
Very Short Answer Questions (VSAQs) emerge as a relatively novel assessment format, addressing the constraints of traditional examination methods like Single Best Answer Questions (SBAQs), Constructed Response Questions (CRQs), and Modified Essay Questions (MEQs) (Sam et al., 2018). Although SBAQs are widely adopted in medical education globally, they are prone to cueing effects, leading examinees to depend on contextual clues, promoting a recognition-based learning approach (Sam et al., 2018). Moreover, the absence of multiple-choice options in real-life scenarios diminishes the relevance of SBAQs to medical practice.
Conversely, while CRQs and MEQs better mimic real-life situations, they suffer from rater dependency and significant evaluation time. Whereas VSAQs, free-response questions with 1–5 word answers, lessen rater dependency and evaluation time. Evidence indicates that VSAQs outperform SBAQs in discrimination, validity, and reliability in undergraduate assessments. Their open-ended nature prevents recognition-based learning and cueing. Additionally, VSAQs adeptly pinpoint common errors, often missed by SBAQs, and offer valuable feedback opportunities for educators (van Wijk et al., 2023).
Feedback is crucial for supporting and enhancing learning. Despite its longstanding importance in medical education, effective feedback is frequently deemed insufficient (Kuhlmann Lüdeke & Guillén Olaya, 2020). Self-assessment, enabled by formative exams, allows learners to identify their learning needs (Gedye, 2010). To improve feedback in formative assessments, Phramongkutklao College of Medicine (PCM) developed the Self-marked VSAQ (SM-VSAQ) format, which pairs a VSAQ with possible answers and a marking guide. Students may assess their understanding and pinpoint study areas through SM-VSAQ, enhancing feedback. Although VSAQs offer several benefits, challenges remain in grading the tests, as they may require a longer time. The self-graded format could address this issue in low-stakes examinations. This study assesses whether the SM-VSAQ with partial credit format, utilizing the marking guide, would achieve valid and reliable ratings compared with the teachers.
II. METHODS
Ninety-four third-year pre-clinical students participated in two 10-item SM-VSAQ during a cardiovascular pharmacology course. The exams covered antihypertensive, antiarrhythmic, antianginal, antithrombotic drugs, heart failure drugs, rational drug use, dyslipidaemia treatments, and drugs for atherosclerotic cardiovascular disease (ASCVD). The second SM-VSAQ sessions vary by changing the clinical vignette, the question, or both while maintaining the same underlying blueprint as the first session. Difficulty levels align with the Thai Medical Competency Assessment Criteria. Students had attended lectures on these drug groups before the exams. The VSAQ was content-validated by three professors for relevance, difficulty, feasibility, and simplicity using the Item Objective Congruence method with all over 0.67 of 1.00, indicating acceptable content validity. This approach ensured comparable difficulty.
The formative test was administered through Google Forms under examination conditions within a one-hour timeframe. Ethical approval was obtained from the Institutional Review Board, Royal Thai Army, and the waiver of the requirement for participant consent was deemed unnecessary following national regulations. An information sheet was provided on the first page of the Google Form. This initial test was conducted a day after they completed all lectures. After receiving teacher-led feedback and having time to review, students took a second parallel formative test ten days before the summative exam.
The SM-VSAQs featured four components for each question: clinical vignettes and questions on the first page, answers with scoring guidelines on the next page after they’ve answered, and a self-scoring option with feedback on answer comprehension. Scores ranged from 0.00 to 1.00 in 0.25 increments, though not every increment was applied to all questions. After the students completed the exam, they provided open-ended feedback on the pros and cons of the format. Examples of the format are shown in supplementary figures 1 and 2.
The self-rated, according to the marking guide, were exported into a Microsoft Excel spreadsheet to facilitate teacher ratings of the VSAQ answers. Using the ‘filter’ function in Microsoft Excel, the range of answers for each question was examined, and marks were awarded (Sam et al., 2018). Minor misspellings or alternative correct spellings were considered correct. Three pharmacology professors, who assigned scores, reviewed student answers that fell outside the guide. Consensus-determined scores require agreement from at least two of the three professors.
The data analyses were performed using StataCorp, 2021, Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC. Consistency reliability was analysed using Cronbach’s alpha. Criterion-related validity was demonstrated by the distribution of the rating agreement between student and teacher ratings, presented as frequency and percentages. Inter-rater reliability was calculated using Pearson’s correlation.
III. RESULTS
Cronbach’s alpha for the SM-VSAQ was 0.741 and 0.721 on the first and second occasions, respectively. The teacher-rated alpha was 0.766 initially and 0.735 on the second. Criterion-related validity was assessed through agreement analysis (Supplementary Tables 1 and 2). Table 1 summarises the results of the agreement analysis. 90.6% and 93.19% of the ratings showed exact agreement between the students’ and teachers’ ratings, with an inter-rater reliability of 0.972 and 0.977 for the first and second occasions, respectively. The exact agreement is relatively low on the first occasion of Drugs used in heart failure (85.11%) and Anti-angina drugs (74.47%). Conversely, antithrombotics and drugs used in ASCVD received a high exact agreement of 96.81%. Example of questions with high and low agreement is demonstrated in supplementary figures 1 and 2. Additionally, content analysis of student’s feedback revealed that they perceived that the format helps identify knowledge gaps, encourages review of missed topics, and aids in recognizing their current knowledge level (Supplementary Table 3).
|
Item |
First Occasion |
Second Occasion |
||||||||||
|
Exact agreement |
0.25 difference |
0.50 difference |
0.75 difference |
1.00 difference |
r* |
Exact agreement |
0.25 difference |
0.50 difference |
0.75 difference |
1.00 difference |
r* |
|
|
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
|||
|
Q1. Antihypertensive drugs |
86 (91.49) |
0 (0.00) |
8 (8.51) |
0 (0.00) |
0 (0.00) |
0.943 |
90 (95.74) |
0 (0.00) |
4 (4.26) |
0 (0.00) |
0 (0.00) |
0.969 |
|
Q2. Antihypertensive drugs |
87 (92.55) |
4 (4.26) |
3 (3.19) |
0 (0.00) |
0 (0.00) |
0.964 |
91 (96.81) |
0 (0.00) |
3 (3.19) |
0 (0.00) |
0 (0.00) |
0.965 |
|
Q3. Antihypertensive drugs |
91 (96.81) |
2 (2.13) |
1 (1.06) |
0 (0.00) |
0 (0.00) |
0.981 |
90 (95.74) |
1 (1.06) |
1 (1.06) |
2 (2.13) |
0 (0.00) |
0.960 |
|
Q4. Antiarrhythmic drugs |
90 (95.74) |
2 (2.13) |
1 (1.06) |
0 (0.00) |
1 (1.06) |
0.961 |
91 (96.81) |
2 (2.13) |
0 (0.00) |
1 (1.06) |
0 (0.00) |
0.980 |
|
Q5. Drugs used in heart failure |
80 (85.11) |
7 (7.45) |
5 (5.32) |
0 (0.00) |
2 (2.13) |
0.867 |
88 (93.62) |
0 (0.00) |
4 (4.26) |
0 (0.00) |
2 (2.13) |
0.922 |
|
Q6. Anti-angina drugs |
70 (74.47) |
9 (9.57) |
14 (14.89) |
0 (0.00) |
1 (1.06) |
0.849 |
79 (84.04) |
5 (5.32) |
10 (10.64) |
0 (0.00) |
0 (0.00) |
0.918 |
|
Q7. Antithrombotic drugs |
91 (96.81) |
2 (2.13) |
1 (1.06) |
0 (0.00) |
0 (0.00) |
0.983 |
83 (88.30) |
6 (6.38) |
2 (2.13) |
2 (2.13) |
1 (1.06) |
0.880 |
|
Q8. Drugs used in dyslipidemia |
84 (89.36) |
3 (3.19) |
6 (6.38) |
0 (0.00) |
1 (1.06) |
0.915 |
89 (94.68) |
1 (1.06) |
2 (2.13) |
1 (1.06) |
1 (1.06) |
0.936 |
|
Q9. CVS rational drug used |
82 (87.23) |
2 (2.13) |
10 (10.64) |
0 (0.00) |
0 (0.00) |
0.907 |
82 (87.23) |
3 (3.19) |
6 (6.38) |
0 (0.00) |
3 (3.19) |
0.851 |
|
Q10. Drugs used in ASCVD |
91 (96.81) |
2 (2.13) |
1 (1.06) |
0 (0.00) |
0 (0.00) |
0.978 |
93 (98.94) |
0 (0.00) |
0 (0.00) |
0 (0.00) |
1 (1.06) |
0.973 |
|
Total |
852 (90.64) |
33 (3.51) |
50 (5.32) |
0 (0.00) |
5 (0.53) |
0.972 |
876 (93.19) |
18 (1.91) |
32 (3.40) |
6 (0.64) |
8 (0.85) |
0.977 |
*p=0.001 for all items, CVS: Cardiovascular system ASCVD: Atherosclerotic cardiovascular disease
Table 1. Comparison of rater agreement between the teacher and the self-rating on the VSAQ assessment
IV. DISCUSSION
VSAQs have demonstrated their discrimination, validity, and reliability among undergraduate assessments and their capacity to identify errors not detectable by SBAQs. However, the marking process poses challenges, potentially requiring more time than SBAQs, even with computerised marking systems (Bala et al., 2023). Delayed marking results in slower feedback delivery to students regarding their examination performance. Therefore, to our knowledge, the study is the first to demonstrate the reliability of using self-guided marking to provide students with immediate feedback after a formative VSAQ examination.
The inter-rater reliability exceeded 0.90 for nearly every question, suggesting the validity of self-grading compared with teacher grading. Moreover, by furnishing students with a partial credit guide, they were encouraged to analyse their answers to each guided answer, fostering a more profound understanding than the singular correct answer required in SBAQs, and encouraging engagement in higher-order thinking. The content analysis of student comments supports this. They found the partial credit guide helpful in identifying key knowledge areas, analyzing expected answers, and engaging in self-directed learning. Additionally, path analysis showed that the first VSAQ attempt score positively influenced the second VSAQ understanding levels, primarily through the second attempt score, highlighting the benefits of multiple attempts for gaining insights (Supplementary Figure 3).
Discrepancies in ratings with the teacher likely stem from misconceptions. For example, while the correct response involved furosemide acting as a Na+/K+/2Cl– channel inhibitor, some students mistakenly identified it as a “Na+-K+-ATPase” and awarded themselves full marks. Some students gave full marks for partially correct and imprecise responses. For instance, concerning the drug interaction between clarithromycin and warfarin, the answer involves enzyme inhibition by clarithromycin, yet some students merely stated, “Drug interaction between drugs.” Similarly, in the anti-angina question, the correct answer is “sublingual nitroglycerin or sublingual isosorbide dinitrate.” However, those who answered partially correctly still awarded themselves full marks. Additionally, disagreement may also be related to student ability, as those less familiar with the content, which leads to misconceptions, might not rate as well as those who are. To address discrepancies in the ratings, reviewing students’ divergent responses could help refine the marking guide. Furthermore, repeated practice in self-assessment will enhance students’ ability to grade their answers accurately.
Conversely, questions with a high level of agreement provided detailed answers consisting solely of the drug name without asking for additional components such as the route of administration or mechanism of action. However, asking for multiple components helped enrich the knowledge and feedback that students could gain.
The present SM-VSAQ format has several strengths. First, it presents a realistic examination, as multiple-choices might not be available in real life. Second, it is simple, feasible, and adaptable, as perceived by the students. Third, it can be administered as an online formative examination, reducing the burden on teachers and providing immediate feedback to students, which has proven reliable and in high agreement with teachers. Nonetheless, this study has certain limitations. It only included a third-year pre-clinical student from a specific educational context, necessitating further research to assess the external validity of the findings.
V. CONCLUSION
SM-VSAQ approach facilitates engagement in higher-order thinking more effectively than the traditional single-best answer method. The format is also simple, adaptable to other subjects, and can be easily reviewed. The agreement between self-graded and teacher-provided ratings is outstanding. Discrepancies between student and teacher evaluations primarily stem from misconceptions in guided answers, highlighting the crucial need for teacher-led feedback to resolve these misunderstandings. This step is essential before implementing self-grading as an alternative in formative evaluations. Regular practice in self-assessment is advised to refine precision in self-grading. The SM-VSAQ format merges the VSAQ model with guided answers and may be further developed to improve feedback timeliness.
Notes on Contributors
SL reviewed the literature, designed the study, collected the data, conducted data analysis and wrote the manuscript. AK reviewed the literature, supervised, designed the study, performed the data analysis.
Ethical Approval
Ethical approval was obtained from the Medical Department Ethics Review Committee for Research in Human Subjects, Institutional Review Board, Royal Thai Army (IRBRTA) (Approval no. S079q/66_Xmp).
The IRBRTA waived the requirement for participant consent, deeming it unnecessary in accordance with national regulations.
Data Availability
Data sets analysed during the current study would be available from the corresponding author upon reasonable request. The Supplementary file for the current study is available from: https://doi.org/10.6084/m9.figshare.26507170
Acknowledgement
This work would not have been possible without the active support of Phramongkutklao College of Medicine faculty members and its academic leaders, who are too numerous to name individually.
Funding
The authors reported no funding associated with the work featured in this article.
Declaration of Interest
The authors declare no competing interests.
References
Bala, L., Westacott, R. J., Brown, C., & Sam, A. H. (2023). Twelve tips for introducing very short answer questions (VSAQs) into your medical curriculum. Medical Teacher, 45(4), 360–367. https://doi.org/10.1080/0142159X.2022.2093706
Gedye, S. (2010). Formative assessment and feedback: A review. Planet, 23(1), 40–45. https://doi.org/10.11120/plan.2010.002300 40
Kuhlmann Lüdeke, A. B. E., & Guillén Olaya, J. F. (2020). Effective feedback, an essential component of all stages in medical education. Universitas Médica, 61(3). https://doi.org/10.11144/ Javeriana.umed61-3.feed
Sam, A. H., Field, S. M., Collares, C. F., van der Vleuten, C. P. M., Wass, V. J., Melville, C., Harris, J., & Meeran, K. (2018). Very-short-answer questions: Reliability, discrimination and acceptability. Medical Education, 52(4), 447–455. https://doi.org/10.1111/medu.13504
van Wijk, E. V., Janse, R. J., Ruijter, B. N., Rohling, J. H. T., van der Kraan, J., Crobach, S., de Jonge, M., de Beaufort, A. J., Dekker, F. W., & Langers, A. M. J. (2023). Use of very short answer questions compared to multiple choice questions in undergraduate medical students: An external validation study. PLOS ONE, 18(7), e0288558. https://doi.org/10.1371/journal.pone.0288558
*Anupong Kantiwong
Department of Pharmacology
Phramongkutklao College of Medicine, Bangkok, 10400
Email: anupongpcm31@gmail.com
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
