
Head-mounted display-based (HMD) vs desktop-based (DB) virtual reality anatomy: A preliminary usability study
Submitted: 22 July 2024
Accepted: 4 February 2025
Published online: 1 July, TAPS 2025, 10(3), 80-83
https://doi.org/10.29060/TAPS.2025-10-3/SC3470
Zaitunnatakhin Zamli1, Rohaini Ramli2, Hidayah Sulaiman2, Mohd Zulfaezal Che Azemin3, Wan Muhamad Salahudin Wan Salleh4, Nurul Asyiqin Yusof5, Imran Mahalil2 & Azmi Mohd. Yusof2
1Department of Biomedical Science, Kulliyyah of Allied Health Sciences, International Islamic University Malaysia, Malaysia; 2Department of Informatics, College of Computing & Informatics, Universiti Tenaga Nasional, Malaysia; 3Department of Optometry and Visual Sciences, Kulliyyah of Allied Health Sciences, International Islamic University Malaysia, Malaysia; 4Department of Basic Medical Sciences, Kulliyyah of Medicine, International Islamic University Malaysia, Malaysia; 5Department of Basic Medical Sciences, Kulliyyah of Pharmacy, International Islamic University Malaysia, Malaysia
Abstract
Introduction: Virtual reality (VR) has been widely used in medical and health sciences education since the late twentieth century. VR complements the conventional teaching and learning (T&L) approach by providing an engaging and immersive 3D spatial learning environment, especially for understanding the orientation of anatomical structures. Despite these advantages, the usability and student preference of highly immersive head-mounted display-based (HMD) and less immersive desktop-based (DB) VR in human anatomy courses have yet to be determined.
Methods: In a cross-sectional study, 49 Year-2 medical students were recruited through a convenient sampling. The participants were asked to identify 15 skeletal system components using the HMD and DB platform with human anatomy VR application. Both applications’ System Usability Scale (SUS) and preference scores were obtained via a self-administered questionnaire. The data were expressed as median [IQR] and statistically analysed using MATLAB R2022b.
Results: Most participants preferred the HMD over the DB platform (p=0.04), especially the male participants (p=0.01). There was no significant difference in overall SUS scores between both platforms (p=0.14). However, when compared within and between genders, females scored significantly higher in the DB than HMD (p=0.02) and higher than males’ DB SUS scores (p=0.03).
Conclusion: The overall usability of HMD was comparable with the DB platform for learning human anatomy. Although most participants prefer to use the HMD, further exploration of why females prefer the DB is needed. Subsequently, VR application developers must consider gender-related adaptions to promote the equitability and inclusivity of the technology for all users.
Keywords: Human Anatomy, Virtual Reality, Head-mounted Display, Desktop-based Application, Usability, Preference
I. INTRODUCTION
Virtual reality (VR) is a simulated three-dimensional (3D) environment that enables users to explore and interact with virtual surroundings, perceiving them through their senses as if they were in the real world. It has been widely used in various fields, including education, to provide users with immersive, engaging, and experiential learning experiences.
In medical education, VR allows students to manipulate anatomical structures into different planes, sections and orientations in a simulated environment, benefiting learners with low-spatial ability. VR also helps students better grasp the relative size differences of organs and allows students to relate the location and position of the organs with their surroundings, resulting in better memorisation and learning outcomes, with VR groups outperforming control groups in post-test assessments (Kurul et al., 2020). As the current generation is more digitally savvy, most students are easily adapted to VR simulation, which enables them to grasp knowledge from a new perspective. For instance, students can dissect a muscle from the human body, gaining insight into the interaction and innervation of individual muscles during exercise.
However, despite the high acceptability of use in anatomy courses among students, some participants reported simulator sickness symptoms like headaches, dizziness, and blurred vision. These symptoms are more pronounced in females, who tend to experience discomfort in a VR environment (Stanney et al., 2020), potentially due to differences in spatial awareness, sensitivity to sensory stimuli, or physiological responses. In addition, regardless of gender, the mismatch between visual motion and the body’s sensory feedback in VR environments can lead to sensory conflict and an increased likelihood of discomfort.
While VR modalities show great potential in anatomy education, research comparing highly immersive head-mounted display-based (HMD) with less immersive desktop-based (DB) VR platforms, particularly regarding gender differences in usability and preferences, remains limited. In addition, considering the high cost of VR applications for HMD, addressing this knowledge gap before its development is crucial to ensuring optimal and cost-effective learning outcomes for a diverse student population. Therefore, this study aimed to compare the usability and preferences between DB and HMD platforms in exploring the VR anatomy applications, within and between genders, among medical students.
II. METHODS
Upon their written consent, forty-nine undergraduate medical students (23 males and 26 females, aged 19-21 years) were recruited through a convenience sampling. They were second-year medical students and participated in this study in two sessions. The participants were asked to identify 15 skeletal components (i.e. skull, vertebrae, hyoid bone, sternum, ribs, scapula, clavicle, humerus, radius, ulna, hip bone, femur, patella, tibia, and fibula) using two platforms: a head-mounted display-based (HMD) virtual reality system with the human anatomy VR application (BodyMap v3.2, https://www.mai.ai/bodymap), and a desktop-based (DB) application (Zygote Body, https://www.zygotebody.com/). BodyMap v3.2 is a VR application for exploring the human body in 3D using the Oculus Quest 2 headset, which provides an immersive and interactive experience for anatomy education. Meanwhile, Zygote Body is a web-based platform that offers detailed 3D anatomical models for desktop or laptop exploration.
Each platform was given a time limit of 15 minutes for the participants to complete the task. After completing the task, the participants completed the System Usability Scale (SUS), a 10-item questionnaire designed to measure the perceived usability of both platforms. The SUS score ranges from 0 (very poor usability) to 100 (perfect usability). In addition, the participants were also asked to rate their preference for using each platform on a scale from 1 (do not prefer at all) to 10 (most preferred). The data were expressed as median (interquartile range, IQR), which best represents the central tendency for non-normally distributed data. Normality was assessed using the Kolmogorov-Smirnov test, and the Wilcoxon signed-rank tests were used to compare the median scores of SUS / Preferences within and between genders. All statistical analyses were performed using MATLAB R2022b, with a p-value < 0.05 considered statistically significant.
III. RESULTS
A. Demographic Data
Forty-nine Year-2 IIUM medical students participated in this study. Most of the students were female (n=26, 53%), with a mean age of 20.10 ± 0.37 years old.
B. Comparison of SUS and Preference Scores between the HMD and DB
There was no significant difference between the median SUS scores between the HMD and DB applications (p=0.14). However, most students preferred the HMD (90, IQR 80.0-100.0) rather than the DB (80, IQR 75.0-90.0) applications (p=0.04).
C. Comparison of SUS and Preference Scores of the HMD and DB within and between Gender
The SUS and preference scores of the HMD and DB applications within and between genders are shown in Figure 1, and individual scores are accessible at https://doi.org/10.6084/m9.figshare.26711965. Based on gender, significantly higher median SUS scores were observed for the DB (85, IQR 77.5-95.0) than the HMD application (75, IQR 59.4-85.6) among the female students (p=0.02). In contrast, the male students had a significantly higher preference score for the HMD (100, IQR 85.0-100.0) than the DB application (80, IQR 70.0-90.0) (p=0.01). A significant difference between gender was only observed in the SUS score, in which the female students scored 85 (IQR, 77.5 – 95.0), and the male students scored 75 (IQR, 58.1 – 86.9; p=0.03) for the DB application.
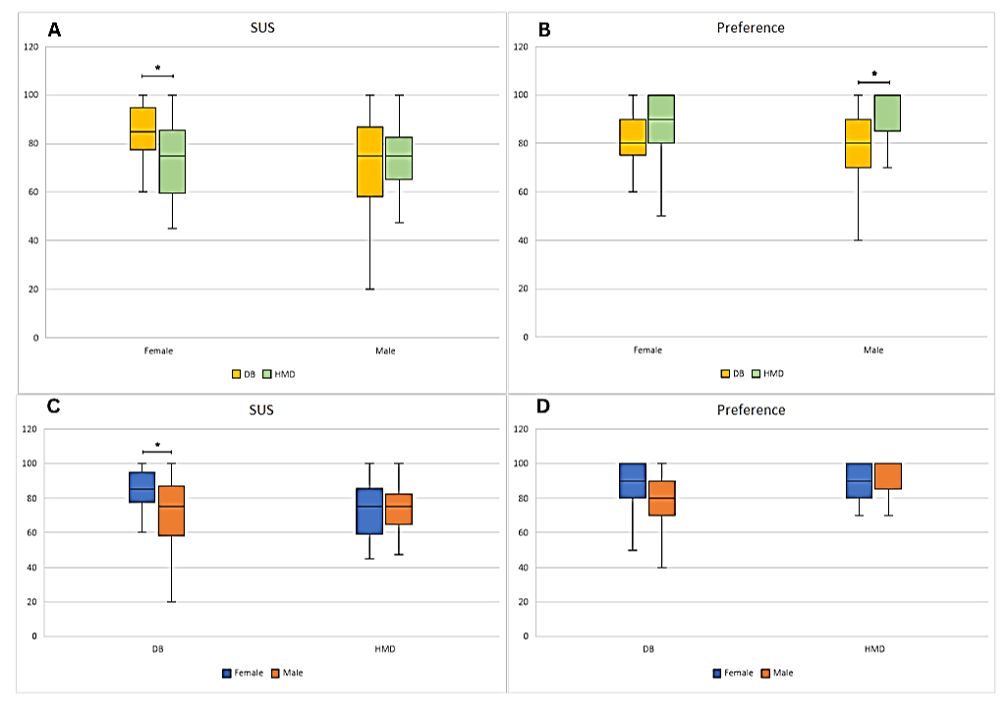
Figure 1. Comparison of SUS and Preference median scores of the HMD and DB application within (A-B) and between genders (C-D). A significant difference of p≤0.05 is denoted as *.
IV. DISCUSSION
This study found that the overall usability scores of the head-mounted display-based (HMD) and the desktop-based (DB) in human anatomy VR applications are comparable. However, a significant gender-related difference was observed in the reported usability scores of the HMD. Female participants reported significantly better usability with the DB than the HMD, likely due to their unfamiliarity with the HMD modality and disadvantage in the 3D spatial ability than males in visualising and manipulating objects in the navigating space. While traditional explanations link these gender differences to brain lateralisation, Bartlett and Camba (2023) challenge this view, suggesting societal expectations and gender roles may shape spatial skills.
Despite this, the study also found that most participants, especially males, prefer the HMD over the DB. This preference might be due to males’ active engagement and early adaptation to the technology, particularly in online gaming, making it more intuitive. This aligns with Deisinger et al. (1997), who found that inexperienced users favoured screen-based projection due to their familiarity with the conventional technology over the HMD. Interestingly, although females perceived DB as more usable, this did not significantly affect their preference for HMD. Many females acknowledged needing more technical help with the HMD but believed they would quickly adapt and prefer it over time. The study’s findings resonate with prior research in medical education, where HMDs are favoured for their immersive experience, enhancing spatial or physical presence and interaction as compared to DB (Yamazaki et al., 2021). However, the effectiveness of HMDs in improving learning outcomes compared to traditional methods remains inconclusive.
Given HMDs’ potential to enhance anatomy education, further research is crucial, especially in complex topics like embryology and neuroanatomy. Developers must focus on high content quality, intuitive user interfaces, and user comfort to ensure a positive learning experience. Gender-related adaptations can promote inclusivity, ensuring that the educational benefits of HMDs are accessible to all users.
Three main limitations of the present study also warrant mention. First, we used the available human anatomy VR applications from two developers, which may have different image quality of VR. However, both VR applications are comparable in terms of content quality. Second, we have not explored their reasons for high preference for utilising HMD when exploring human anatomy VR, potentially limiting our understanding of the user experience (e.g. comfort, immersion, satisfaction, and overall interaction) related to HMD usage. Third, participants’ previous experience using HMD in other platforms, such as gaming, virtual tours, etc, was not determined. Future studies should consider these limitations to understand user experiences with the HMD platform better and identify factors influencing user preferences.
V. CONCLUSION
In summary, this study concluded that the usability of both HMD and DB in exploring the human anatomy VR application is almost similar. As seen in other studies, students tend to favour HMD over DB because of its immersive, interactive, and engaging features. However, at an individual level, gender may influence their perception of its usability and preference. Therefore, it is essential to take gender-related adaptations into account when developing VR applications.
Notes on Contributors
Zaitunnatakhin Zamli reviewed the literature, designed the study, performed data collection and analysis, and developed the manuscript. The author has read, given critical feedback and approved the final manuscript.
Nurul Asyiqin Yusof reviewed the literature, designed the study, performed data collection and analysis, and developed the manuscript. The author has read, given critical feedback and approved the final manuscript.
Azmi Mohd Yusof reviewed the literature, designed the study, performed data collection and analysis, and developed the manuscript. The author has read, given critical feedback and approved the final manuscript.
Wan Muhamad Salahudin Wan Salleh designed the study and performed data collection, analysis and interpretation. The author has read, given critical feedback and approved the final manuscript.
Mohd Zulfaezal Che Azemin designed the study and performed data collection, analysis and interpretation. The author has read, given critical feedback and approved the final manuscript.
Rohaini Ramli advised on study design and data interpretation. The author has read, given critical feedback and approved the final manuscript.
Hidayah Sulaiman advised on study design and data interpretation. The author has read, given critical feedback and approved the final manuscript.
Imran Mahalil facilitated the data collection process. The author has read, given critical feedback and approved the final manuscript.
Ethical Approval
Ethical approval of this study was granted by the Kulliyyah Postgraduate and Research Committee (IIUM/305/20/4/1/7) and IIUM Research Ethics Committee (IREC) (IIUM/504/14/11/2/IREC2022-194). All participants involved in the study had given their written consent, and their participation was voluntary.
Data Availability
The data of this study data are available at a Figshare repository, https://doi.org/10.6084/m9.figshare.26711965
Acknowledgement
The authors would like to thank the Department of Informatics, College of Computing & Informatics, Universiti Tenaga Nasional, Selangor, Malaysia, for providing equipment, software and logistics support.
Funding
This study did not receive any funding or financial support.
Declaration of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
Bartlett, K. A., & Camba, J. D. (2023). Gender differences in spatial ability: A critical review. Educational Psychology Review, 35(1), Article 8. https://doi.org/10.1007/s10648-023-09728-2
Deisinger, J., Cruz-Neira, C., Riedel, O., & Symanzik, J. (1997). The effect of different viewing devices for the sense of presence of immersion in virtual environments: A comparison of stereoprojections based on monitors, HMDs and screens. Proceedings of the Seventh International Conference on Human-Interaction Computer, (2), 881-884. https://www.usu.edu/math/symanzik/papers/1997_HCI_Int.html
Kurul, R., Ögün, M. N., Narin, A. N., Avci, Ş., & Yazgan, B. (2020). An alternative method for anatomy training: Immersive virtual reality. Anatomical Sciences Education, 13(5), 648-656. https://doi.org/10.1002/ase.1959
Stanney, K., Fidopiastis, C., & Foster, L. (2020). Virtual reality is sexist: But it does not have to be. Frontiers in Robotics and AI, 7, 476417 https://doi.org/10.3389/frobt.2020.00004
Yamazaki, A., Ito, T., Sugimoto, M., Yoshida, S., Honda, K., Kawashima, Y., Fujikawa, T., Fujii, Y., & Tsutsumi, T. (2021). Patient-specific virtual and mixed reality for immersive, experiential anatomy education and for surgical planning in temporal bone surgery. Auris Nasus Larynx, 48(6), 1081-1091. https://doi.org/10.1016/j.anl.2021.03.009
*Azmi Mohd. Yusof
Jalan IKRAM-UNITEN,
43000 Kajang,
Selangor, Malaysia
Email: azmiy@uniten.edu.my
Submitted: 17 February 2024
Accepted: 25 March 2025
Published online: 1 July, TAPS 2025, 10(3), 65-74
https://doi.org/10.29060/TAPS.2025-10-3/SC3251
Dani R Firman1,2, Friedo W Dekker2,3, Eriska Riyanti1, Sunardhi Widyaputra1 & Peter GM de Jong2
1Faculty of Dentistry, Universitas Padjadjaran, Indonesia; 2Center for Innovation in Medical Education, Leiden University Medical Center, the Netherlands; 3Department of Clinical Epidemiology, Leiden University Medical Center, the Netherlands
Abstract
Introduction: To explore the current situation regarding teaching evidence-based practice (EBP) in Indonesian dental schools as a low-middle-income country (LMIC) setting.
Methods: Two nation-wide surveys were administered to all Indonesian dental schools (N=32) to capture the perceived value of the deans about EBP skills and teaching with its resource-related situation, as well as the actual teaching implementation and its challenges by their curriculum teams. The analysis was performed descriptively as national aggregate data.
Results: The response rates were 96.9% and 90.6%, respectively. The deans considered EBP skills to be very important (61.3%) or important (38.7%). However, only 16.1% of deans reported that the implementation of teaching EBP met their expectations. Most schools (75.9%) considered providing training for teachers as the priority plan. Most schools (62.1%) had an independent EBP course in their curriculum, while 86.2% incorporated EBP teaching (also) into other courses. All dental schools employed a lecture strategy for teaching EBP topics, but also used other strategies such as interactive strategies with a wide range of percentages being utilised (10.3 – 89.7%). EBP-specific topics were generally taught with a level of implementation varying from 34.5% to 96.6% in the pre-clinical and from 10.3% to 62.1% in the clinical programme.
Conclusion: The used approach can be considered an effective strategy to provide opportunities for schools to reflect their EBP teaching. This study confirmed the necessity for improvement, especially the need to support faculty development. The deans and their curriculum teams highly value collaborative improvement plans.
Keywords: National Survey, Evidence-based Practice, Faculty Perception, Low-middle-income Country
I. INTRODUCTION
Evidence-based practice (EBP) is emerging as the standard in clinical dentistry. It integrates the best research evidence with patients’ values, preferences, and clinical experiences (Young et al., 2014). The EBP process involves five key steps in sequence (ask, acquire, appraise, apply, and evaluate). The appraise or critical appraisal skill as part of the steps is related to research capacity still considered as crucial gaps in the LMIC setting compared to high-income country (HIC) setting, and known to hinder EBP development and implementation (Gill et al., 2021). Furthermore, the suboptimal practice of EBP among dental professionals in lower and middle-income countries (LMIC) was suspected due to limited access of web-based subscription database and scarcity of experts as mentor (Minja & Lwoga, 2021).
Potentially, dental schools can play a significant role in promoting EBP implementation in dentistry of such setting by providing the access to evidence, supporting professional development and integrate the EBP teaching and learning in the curriculum. However, institutionalising EBP requires consistent policy and strong administrative support. To understand the current situation of EBP teaching in Indonesian dental schools, we conducted a study exploring the deans’ perceptions about its importance and the need for improvement. We also determined the actual level of implementation as reported by their curriculum teams. The study’s outcomes could inform future interventions to enhance EBP teaching in Indonesian dental schools.
II. METHODS
At the time of the study, in September 2022, there were 32 dental schools in Indonesia, all of which ran a bachelor’s programme (year 1-4) and a clinical programme (year 5-6). A descriptive survey study was conducted online using two sets of Indonesian-language questionnaires in sequence.
The first survey was launched during an in-person national meeting in Surabaya. Only the principal investigator himself participated via Zoom. This first survey aimed to gauge deans’ perceived importance of EBP skills and teaching, along with necessary resource improvements. The questionnaire included demographic items, five-point of Likert-scale questions on EBP teaching value, resources-related, an open-ended item on EBP teaching challenges, and a section for additional comments. Most deans completed the first online survey during that meeting, while those who did not attend the meeting were received the survey’s link via email.
Upon completion for each school by the deans, a second survey was sent to vice dean for academic affairs as corresponding contact using the email address provided by the deans in the previous survey. In the introduction letter, we specifically requested the involvement of their curriculum team of the bachelor and clinical programme as a group response for each school. This second survey gathered data on EBP teaching implementation and challenges more in details. It was translated and adapted from a previous survey used by Gorgon et al. (2013) which was considered relevant to all health professions, including dentistry. The adaptation included a pilot test beforehand to ensure its relevance and clarity.
The study protocol was approved by the Educational Research Review Board of the LUMC (Registry number: OEC/ERRB/20220913/1). Participants electronically consented to both surveys after reviewing the provided information. Respondents with missing or unclear data were contacted for clarification. Five-point Likert scale items, checklist items, and multiple-choice items were analysed descriptively. The open-ended item responses and additional comments were analysed thematically.
III. RESULTS
The first survey’s responses were received from 31 dental schools across Indonesia (96.9%). The schools were located on Java (18), Sumatera (6), Sulawesi (3), and Kalimantan and Bali (2 each). For the second survey, which targeted the curriculum team for each school, the responses were received from 29 schools (90.6%).
A. The Perceived Value of EBP Teaching (The 1st Survey, n=31)
The deans perceived EBP skills as very important/essential (61.3%) or important (38.7%) for students. Incorporating EBP in the curriculum was seen as very important/essential (51.6%) or important (48.4%). Improving teachers’ EBP teaching expertise was deemed very necessary (54.8%) or necessary (38.7%). Five deans (16.1%) felt their schools met faculty expectations for EBP teaching, while others observed room for improvement (64.5% necessary, 19.4% very necessary). Resources like database access and librarian expertise varied in satisfaction. Most respondents (71%) valued collaboration with other schools on EBP training and implementation (See Appendix 1).
B. The Implementation of EBP Teaching (The 2nd Survey, n=29)
Over half (62.1%) of participated schools have a standalone EBP course, and 86.2% incorporate EBP in other courses. Lecture-based teaching is the most common EBP strategy, followed by thesis discussions, journal readings, colloquiums, and seminars. Small group discussions and problem-based tutorials are also used. “Critically appraised topics” (CATs) are least used, with only three schools employing this active learning method. Both summative and formative assessments are used. Most schools use a blended approach for EBP courses, with one school offering a fully online course (See Appendix 2.a).
C. Available Resources for EBP Teaching (The 1st and 2nd Survey, n=31 and n=29)
Of the participating institutions, only 8 out of 29 dental schools have teachers formally-trained in EBP. Most schools have access to scientific databases, with ScienceDirect being the most accessible (58.6%). Other databases include Web of Science, Cochrane Library, EBSCO Host, CINAHL, and UpToDate, with some schools also subscribing to Springer Link, Wiley, Emerald, and SAGE (See Appendix 2.b). Database access is mostly provided by the university (80.6%), with some funded by faculty budgets (29%) or government institutions (9.7%). Only one school lack subscribed database access (See Appendix 3.a).
D. The EBP Specific Topics Coverage (The 2nd Survey, n=29)
The five EBP steps (ask, acquire, appraise, apply, evaluate) are taught in Indonesian dental schools, with varying implementation levels from 34.5% to 96.6% in pre-clinic programmes and 10.3% to 62.1% in clinic programmes. The ‘apply’ and ‘evaluate’ steps are least taught in pre-clinic programmes. Interpreting forest plots in systematic reviews is the least covered topic, with only 10 out of 29 schools teaching it in pre-clinic levels, 3 in clinical levels, and 19 not covering it at all. Over a third of the schools (37.9%) do not teach critical appraisal of a systematic review. See Table 1 below for details.
|
Pre-clinic |
Clinic |
Not taught in both programme** |
|||
|
EBP steps and its specific topics coverage (n=29) |
Taught* |
Not taught* |
Taught* |
Not taught* |
|
|
I. Asking clinical question |
|||||
|
(1) Formulating clinically questions using the PICO format |
22 (75.9) |
7 (24.1) |
12 (41.4) |
17 (58.6) |
5 (17.2) |
|
(2) Guided literature search by the clinical questions |
20 (69.0) |
9 (31.0) |
18 (62.1) |
11 (37.9) |
5 (17.2) |
|
II. Search the evidence |
|||||
|
(3) Constructing a focused search with Boolean operator in a database |
23 (79.3) |
6 (20.7) |
7 (24.1) |
22 (75.9) |
6 (20.7) |
|
(4) Locating clinical evidence using electronic databases |
26 (89.7) |
3 (10.3) |
8 (27.6) |
21 (72.4) |
3 (10.3) |
|
(5) Utilising a reference manager software |
25 (86.2) |
4 (13.8) |
9 (31.0) |
20 (69.0) |
4 (13.8) |
|
III. Critically appraising evidence |
|||||
|
(6) Study designs and their major strength and limitations |
27 (93.1) |
2 (6.9) |
7 (24.1) |
22 (75.9) |
2 (6.9) |
|
(7) Assessing the relevance of study design to the question asked |
22 (75.9) |
7 (24.1) |
5 (17.2) |
24 (82.8) |
7 (24.1) |
|
(8) Hierarchy or levels of evidence |
23 (79.3) |
6 (20.7) |
6 (20.7) |
23 (79.3) |
5 (17.2) |
|
(9) Difference between narrative, systematic review, and meta-analysis |
21 (72.4) |
8 (27.6) |
4 (13.8) |
25 (86.2) |
7 (24.1) |
|
(10) Difference between clinical and statistical significance |
22 (75.9) |
7 (24.1) |
9 (31.0) |
20 (69.0) |
6 (20.7) |
|
(11) Interpreting t tests, chi-square tests |
28 (96.6) |
1 (3.4) |
6 (20.7) |
23 (79.3) |
1 (3.4) |
|
(12) Interpreting p-value, confidence interval |
28 (96.6) |
1 (3.4) |
6 (20.7) |
23 (79.3) |
1 (3.4) |
|
(13) Understanding sensitivity and specificity, number needed to treat, odds ratio |
28 (96.6) |
1 (3.4) |
6 (20.7) |
23 (79.3) |
1 (3.4) |
|
(14) Understanding intention to treat analysis and power calculation |
20 (69.0) |
9 (31.0) |
3 (10.3) |
26 (89.7) |
9 (31.0) |
|
(15) Use of appraisal tool(s) to assess validity |
22 (75.9) |
7 (24.1) |
7 (24.1) |
22 (75.9) |
7 (24.1) |
|
(16) Ways in which study validity can be threatened |
25 (86.2) |
4 (13.8) |
5 (17.2) |
24 (82.8) |
4 (13.8) |
|
(17) Difference between internal and external validity |
21 (72.4) |
8 (27.6) |
3 (10.3) |
26 (89.7) |
8 (27.6) |
|
(18) Critical appraisal of systematic reviews |
18 (62.1) |
11 (37.9) |
6 (20.7) |
23 (79.3) |
11 (37.9) |
|
(19) Interpreting forest plots in systematic reviews |
10 (34.5) |
19 (65.5) |
3 (10.3) |
26 (89.7) |
19 (65.5) |
|
(20) Critical appraisal of studies about intervention (RCTs and clinical trials) |
18 (62.1) |
11 (37.9) |
7 (24.1) |
22 (75.9) |
9 (31.0) |
|
(21) Critical appraisal of studies about diagnosis (cohort, case-control studies) |
21 (72.4) |
8 (27.6) |
5 (17.2) |
24 (82.8) |
7 (24.1) |
|
(22) Critical appraisal of studies about prognosis (longitudinal studies) |
18 (62.1) |
11 (37.9) |
5 (17.2) |
24 (82.8) |
10 (34.5) |
|
IV. Implementation and communication |
|||||
|
(23) Communicating the recommendation from EBP process to the patient |
14 (48.3) |
15 (51.7) |
9 (31.0) |
20 (69.0) |
12 (41.4) |
|
(24) Deciding the clinical decision considering the patient’s value |
12 (41.4) |
17 (58.6) |
11 (37.9) |
18 (62.1) |
11 (37.9) |
|
V. Evaluation |
|||||
|
(25) Evaluation of the EBP implementation (The patient’s outcome and student’s performance through self-reflection) |
13 (44.8) |
16 (55.2) |
9 (31.0) |
20 (69.0) |
13 (44.8) |
Table 1. EBP steps and its specific topics coverage for each programme level (n=29)b
* n (%)
** n (%) Overlap calculation with the number of not taught on each programme
b From the 2nd survey to the curriculum teams
E. Challenges (The 1st Survey, n=31 and The 2nd Survey, n=29)
The top three challenges in Indonesian dental schools, as reported by curriculum teams, are a lack of EBP experts (72.4%), insufficient accessible EBP courses for faculty (69%), and students’ inadequate knowledge of statistics and research methodology (65.5%) (See appendix 4). In the open-ended item section, most of the deans expressed the challenges of EBP teaching. Teachers-related factors were considered the most challenging, such as limitation in knowledge and skills, and an overloaded work situation.
F. Action Plans (The 2nd Survey, n=29)
Most respondents (75.9%) highly valued teacher training. They also preferred incorporating EBP skills into the curriculum (48.3%) and holding faculty meetings to discuss EBP programme development (44.8%) (See appendix 3.b).
IV. DISCUSSION
To our knowledge, this is the first nation-wide survey with very high response rate to report insights of EBP teaching in the South-east Asia region, more specifically in Indonesian dental education setting. Targeting both deans and curriculum teams yielded rich data and stakeholder involvement, potentially fostering acceptance of future EBP improvements at institutional or national levels.
There is a slight gap between the perceived importance of EBP skills for students and the importance of incorporating such skills into the curriculum, which may be related to limited resources. The deans considering room for improvement, especially in teacher expertise. This is echoed by curriculum teams, as less than a third of Indonesian dental schools’ teachers have formal training experience, i.e. training from a well-known academic-based institution or recognised training organisation. This lack of EBP teachers is a top challenge identified by respondents. Deans and curriculum teams agree on the need for improved teacher skills.
The majority of Indonesian dental schools are teaching EBP topics in stand-alone EBP courses as well as incorporated in other regular courses using both face-to-face and online delivery. Lecture-based is the most used teaching strategy among the schools. Our findings suggest that there is room for enhancing the teaching strategy of EBP in Indonesian dental schools towards a more multi-facet, interactive and more authentic setting in the clinical environment as suggested by Howard et al. (2022).
Regarding critical appraisal topics based on the study design (See Table 1, item 18, 19-21), there were very few schools implementing a Critically Appraised Topics (CATs) teaching strategy (See Appendix 2.a). CATs, one-page summaries of evidence on a clinical question, offer active, authentic learning and being recommended in the literature to provide both a critique of the research and a statement of the clinical relevance of its findings. It is crucial to teach critical appraisal skills using the teaching strategy that is supported by the evidence to ensure sufficient development of EBP skills. Many Indonesian dental educators may not be familiar with this CATs teaching method.
The survey reveals that the ‘apply’ and ‘evaluate’ steps of EBP are less addressed than the ‘ask’, ‘acquire’, and ‘appraise’ steps. These five-steps, identical to those in Evidence-Based Medicine (EBM), form the basis of clinical practice and teaching. Key EBM developments like shared-decision making skills, part of the ‘apply’ step, are often overlooked. Hence, it’s vital to teach all EBP steps, ideally in a more authentic clinical setting.
The need for more EBP-trained faculty in most schools highlights the importance of a faculty development programme supported by national collaboration. As a lower-resource country, Indonesia faces challenges in dental education, including limited access to databases and librarian expertise, primarily due to financial constraints, inadequate institutional support, and the absence of national policies prioritising scientific resources. These limitations hinder faculty and students from fully implementing evidence-based practices, widening disparities with high-income countries. To address these issues, a policy brief should be directed to high-level stakeholders, advocating for essential infrastructure, more funding and resource investments for both private and government-funded schools.
This study has limitations. Due to the five-point Likert scale in the first questionnaire were not constructed on the same concept, the reliability test was not feasible. This is also applied for the second questionnaire, which adapted from a previous study, was mostly factual and checklist-based. The value of EBP teaching, reported by deans and curriculum teams, might be socially desirable. However, the results underscore the importance of EBP teaching and the need for improvement. It is worth noting that after the data collection was completed, Indonesia formally transitioned from a lower-middle-income to an upper-middle-income country as of July 2023. This transition suggests a more promising future, with potential improvements in the financial capacity, but it will require the national policy support to be fully implemented.
V. CONCLUSION
This first national survey reveals the state of EBP teaching in Indonesian dental schools, representing Southeast Asian countries. It highlights the need for faculty development and more active, authentic learning experiences but further analysis is required to adopt and adapt these interventions for lower-resource settings. The deans and their curriculum teams highly value collaborative improvement plans. This supports EBP’s vision of using current research to improve Indonesian oral healthcare.
Notes on Contributors
DF is the principal investigator. He designed, analysed, prepared and wrote the manuscript collaboratively with co-authors.
SW and ER made substantial contributions to preparation of the instruments, data collection and editing the final manuscript.
FD and PJ made substantial contribution to the design, analysis, preparation and editing the final manuscript.
All authors read and approved the final version.
Ethical Approval
The study protocol was approved by the Educational Research Review Board of the LUMC (Registry number: OEC/ERRB/20220913/1).
Data Availability
Due to confidentiality of the responses and commitments made with the study participants, also considering the small size data set with its unique data for some variables that might still be traceable to the respondent. Data are available on reasonable request by email to the corresponding author.
Acknowledgement
The authors express gratitude to all participants and schools involved in this study, AFDOKGI and its members for their support and data access, the Research group at the OEC LUMC for their constructive feedback, Universitas Padjadjaran for sponsoring the first author’s PhD scholarship, and Edward Gorgon for permitting the modification and use of the questionnaire.
Funding
This research is part of the first author’s (DF) PhD study, funded by a scholarship from Universitas Padjadjaran, Indonesia (Registry number 3781/UN.6.WR2/KP.10/2021).
Declaration of Interest
The first author (DF), an assistant professor at the Faculty of Dentistry, Universitas Padjadjaran, which participated in this study. DF also had ties until 2020 with AFDOKGI, the association of Indonesian dental schools, as a dental education consultant.
References
Gill, P. J., Ali, S. M., Elsobky, Y., Okechukwu, R. C., Ribeiro, T. B., Soares dos Santos Junior, A. C., Umpierre, D., & Richards, G. C. (2021). Building capacity in evidence-based medicine in low-income and middle-income countries: Problems and potential solutions. BMJ Evidence-Based Medicine, 26(3), 82–84. https://doi.org/10.1136/bmjebm-2019-111272
Gorgon, E. J. R., Basco, M. D. S., & Manuel, A. T. (2013). Teaching evidence-based practice in physical therapy in a developing country: A national survey of Philippine schools. BMC Medical Education, 13(1), Article 154. https://doi.org/10.1186/1472-6920-13-154
Howard, B., Diug, B., & Ilic, D. (2022). Methods of teaching evidence-based practice: A systematic review. BMC Medical Education, 22(1), Article 742. https://doi.org/10.1186/s12909-022-03812-x
Minja, I. K., & Lwoga, E. T. (2021). Evidence based dentistry among dentists in low- and middle-income countries: A systematic review. The East African Health Research Journal, 5(2), 129–136. https://doi.org/10.24248/eahrj.v5i2.662
Young, T., Rohwer, A., Volmink, J., & Clarke, M. (2014). What are the effects of teaching evidence-based health care (EBHC)? Overview of systematic reviews. PLOS ONE, 9(1), e86706. https://doi.org/10.1371/journal.pone.0086706
*Dani R Firman
Jalan Sekeloa Selatan I,
Kota Bandung, Jawa Barat 40132,
Indonesia
+62222534985
Email: dani.firman@unpad.ac.id / d.r.firman@lumc.nl
Submitted: 6 November 2024
Accepted: 11 April 2025
Published online: 1 July, TAPS 2025, 10(3), 58-64
https://doi.org/10.29060/TAPS.2025-10-3/OA3567
Nathania Nishida Tan1, Daniel Ardian Soeselo2,3, Natalia Puspadewi2, V. Dwi Jani Juliawati2 & Gisella Anastasia2
1Faculty of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, Indonesia; 2Medical Education Unit and 3Department of Surgery, Faculty of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, Indonesia
Abstract
Introduction: Career selection is a critical decision influenced by various factors, including media exposure. As a popular genre among adolescents, medical dramas may shape perceptions of the medical profession. This study explores the impact of medical dramas on medical students’ motivation to pursue a career in medicine.
Methods: This study was conducted at the School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, between February and March 2024, using a mixed-method approach. Quantitative data were gathered through a questionnaire, followed by qualitative insights from in-depth interviews. A two-stage sampling strategy was employed, initially identifying first-year students influenced by medical dramas through screening, followed by purposive sampling to select participants for in-depth interviews.
Results: Analysis identified six key motivational aspects through which medical dramas influence students’ decision to pursue medicine. These include the detailed portrayal of doctors’ roles, their daily lives, and the reinforcement of a positive perception of the profession. Notably, emotional engagement- such as inspiring doctor characters- and the realistic depiction of challenges, including the dedication and hardships of becoming a doctor, emerged as significant factors.
Conclusion: Medical dramas play a significant role in shaping students’ motivation and perception of the medical profession. This study highlights six key motivational aspects influencing career decisions, offering new insights into media-driven career choices and their potential implications for medical education.
Keywords: Medical Dramas, Medical Education, Medical Students, Student Motivation, Career Choice
Practice Highlights
- Medical dramas serve as informal educational tools through entertainment for the public.
- Television influences adolescents’ career aspirations by shaping their interests.
- Medical dramas shape public perceptions of the medical profession and may inspire viewers.
I. INTRODUCTION
Medical dramas have remained a widely popular television genre since their emergence in the 1960s, continuously evolving to portray healthcare professionals’ professional and personal lives within hospital settings (14th Media Mutations International Conference, 2023; Sonego & Rocchi, 2024).
Communication theorist Marshall McLuhan had predicted the success of medical dramas as early as 1964 in his book Understanding Media: The Extensions of Man, attributing their appeal to the immersive experience viewers have when witnessing medical procedures, which fosters an “obsession with bodily well-being” (Aboud, 2012; Levine & McLuhan, 1964).
Beyond entertainment, medical dramas serve as informal educational tools illustrating medical practices, bioethical dilemmas, and professional conduct (Cambra-Badii et al., 2021; Zago et al., 2024). Research suggests that these dramas reinforce key principles of medical ethics and professionalism, including communication skills, patient confidentiality, and empathetic bedside manner (Aboud, 2012). By portraying both the challenges and rewards of medical practice, these narratives may also shape viewers’ perceptions of the profession, inspiring people to pursue careers in healthcare (Alahmari, 2023).
Research indicates a correlation between specific television programs and career aspirations, suggesting that the content adolescents consume can shape vocational interests and goals (Gehrau et al., 2016). As an accessible informal educational resource, television provides insight into professional responsibilities and challenges (Mendick & Williams, 2022). Within this context, medical dramas may play a significant role in shaping students’ motivation to enter the medical field. Unlike prior studies that broadly examine media influence over career perceptions, this study focuses on first-year medical students, analysing their motivational drive. By integrating quantitative and qualitative data, this study provides deeper insight into how medical dramas influence medical students’ motivation to pursue a career in medicine.
II. METHODS
This study was conducted at the School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, from February to March 2024, using a mixed-method approach. A two-stage sampling method was employed, beginning with a questionnaire to identify eligible participants, followed by purposive sampling to select individuals for in-depth interviews. The target population consisted of first-year medical students enrolled in the 2023 academic year who acknowledged that medical dramas had influenced their motivation to pursue a medical degree.
A. Participant Selection
Out of 210 first-year students, 114 reported watching medical dramas. These students completed a demographic questionnaire, which gathered information on gender, parents’ profession, and their viewing habits related to medical dramas. Additionally, they completed the Strength of Motivation for Medical School Revised (SMMS-R) Questionnaire, a validated self-report instrument consisting of 15 items rated on a 5-point Likert scale (ranging from “strongly disagree” to “strongly agree”), with possible scores ranging from 15 to 75, indicating the strength of motivation for medical school.
B. Qualitative Phase Sampling
Purposive sampling was used to ensure an accurate representation of the study population based on key demographic factors, specifically the profession of participants’ parents. The selection process identified respondents from diverse parental backgrounds in the medical field: those with both parents as physicians, those with one parent in medicine, and those with no parental medical background. To ensure gender diversity, one male and one female were selected from each category, all of whom had high motivation scores based on their SMMS-R results. Six participants were selected to achieve thematic saturation, as preliminary analysis showed no new themes emerging beyond this point. Although not statistically representative, this sample captures diverse perspectives on medical career motivation based on different childhood backgrounds.
C. Data Collection
The in-depth interviews, conducted by the researcher (NNT), explored participants’ perceptions of how medical dramas influenced their motivation to pursue a career in medicine. The interview guide addressed various aspects of this influence on their decision-making process. One key question asked was “How have medical dramas influenced your decision to pursue medicine?” All participants provided written informed consent, including permission for audio recording. The interviews were then transcribed verbatim for further analysis.
D. Data Analysis
The transcribed interviews were analysed using thematic analysis with an inductive coding approach, facilitated by Atlas.Ti software. Initial coding was conducted by NNT, who identified key patterns and concepts. These were then systematically categorised into themes and subthemes to capture broader meanings and insights emerging from the interviews. To ensure coding reliability, DAS and NP reviewed the preliminary codes and analysis results. Through thorough discussions and iterative revisions, the team resolved discrepancies and achieved near-total agreement on the coding structure. To maintain participant confidentiality, each transcript was assigned a unique identification code.
III. RESULTS
A total of 114 respondents participated in this study, consisting of 26 males and 88 females, reflecting a possible gender disparity in medical drama viewership. Among them, 93 students (81.6%) reported that medical dramas significantly impacted their decision to pursue a medical career, while 21 students indicated no such impact.
|
Characteristic |
Respondents (n) |
Percentage (%) |
|
|
Parental Background |
|
|
|
|
|
Both parents are doctors |
8 |
7.0 |
|
|
Only one parent is a doctor |
18 |
15.8 |
|
|
Neither parent is a doctor |
88 |
77.2 |
|
|
|
||
|
Reports Motivation to Enter Medical Field Due to Medical Dramas |
|||
|
|
Yes |
93 |
81.6 |
|
|
No |
21 |
18.4 |
|
|
Total Respondents |
114 |
100.0 |
Table 1. Distribution of Respondent Demographic Characteristics
A. Various Dimensions of the Impact of Medical Dramas on Motivation
The following table presents the themes and subthemes derived from the in-depth interview analysis, which has been discussed and approved by each inter-rater.
|
No. |
Theme |
Subtheme |
|
1. |
Medical dramas provide an in-depth portrayal of the roles and responsibilities of doctors. |
Medical dramas shape public perceptions of the medical profession and doctors’ roles. |
|
Medical dramas depict the challenges and rewards of doctors’ daily work. |
||
|
Medical dramas highlight doctors’ lives beyond their profession. |
||
|
2. |
Medical dramas depict both the professional and personal aspects of doctors’ lives. |
Medical dramas reveal lesser-known aspects of doctors’ personal experiences. |
|
Medical dramas provide an authentic portrayal of doctors’ daily lives. |
||
|
Medical dramas depict ethical dilemmas, emphasising doctors’ professional integrity. |
||
|
3. |
Medical dramas contribute to a positive public perception of the medical profession. |
Medical dramas portray impressive doctors, evoking admiration, and inspiration in viewers. |
|
Doctors’ life-saving actions in medical dramas evoke deep emotions and motivation. |
||
|
Medical dramas illustrate doctors’ perseverance and resilience in their profession. |
||
|
Medical dramas spark curiosity about medical procedures and treatments. |
||
|
4. |
Medical dramas evoke emotional responses that may inspire viewers to pursue a medical career. |
Medical dramas evoke empathy by portraying patients in distress. |
|
5. |
Medical dramas showcase inspiring doctor characters, motivating viewers to follow in their footsteps. |
|
|
6. |
Medical dramas illustrate the challenges and dedication required to become a doctor. |
|
Table 2. Table of Themes and Subthemes
B. Medical Dramas Provide an In-Depth Portrayal of the Roles and Responsibilities of Doctors
Medical dramas frequently portray various medical scenarios using specialised terminology, offering viewers insight into the daily responsibilities of doctors. As medical settings are generally inaccessible to the public, these dramas provide a unique perspective on the profession. Among the key influences explored in this study, this aspect resonated most with respondents, with four out of six students emphasising its significance.
One participant explained how watching medical dramas sparked their interest in the field, as they previously had limited information about medicine.
“Grey’s Anatomy offered me insight into the medical field and sparked my interest, as reliable information is not easily accessible to those outside the profession” (V1_H3_B19)
Another respondent shared how their perception of doctors shifted from fear to admiration after watching medical dramas, recognising the profession’s vital role in society:
“As a child, I perceived doctors as intimidating due to painful medical visits, such as dental appointments. However, after watching Grey’s Anatomy, I realised that medicine extends beyond that and saw how doctors can positively impact many lives.” (V1_H2_B27)
Beyond hospital settings, medical dramas also depict the role of doctors in broader societal contexts. Through diverse narratives, these dramas offer multiple perspectives on the medical profession. For example, Doc Martin illustrates the role of a doctor in a rural community, showcasing their involvement in local issues, such as water problems and education (V2_H4_B21). This highlights how doctors contribute beyond clinical practice, reinforcing their role in public health and community development.
Additionally, medical dramas influence students’ motivation to pursue medicine by portraying the realities of medical work, including complex procedures and life-saving interventions. More than half of the respondents identified this as a significant factor in their decision to study medicine. As one participant stated:
“The scenes depicting doctors helping others, particularly during surgeries, inspired me to study medicine. I wanted to experience performing surgeries and learn how to help others.” (V4_H7_B19)
These findings suggest that medical dramas not only enhance public understanding of the profession but also play a role in inspiring future medical students.
C. Medical Dramas Depict Both the Professional and Personal Aspects of Doctors’ Lives
Medical dramas depict not only medical procedures but also the personal lives of doctors, including their relationships, friendships, and personal struggles. By presenting doctors as multidimensional individuals beyond their professional roles, these narratives contribute to a more relatable and humanised portrayal of the profession. Notably, four out of six highlighted the importance of this aspect in shaping their motivation. One respondent noted that their interest in medical dramas stemmed primarily from the blend of romantic elements, rather than the medical content alone (V3_H6_B1).
The public often has limited insight into the personal experiences of doctors, making it difficult to relate to them. However, medical dramas help bridge this gap by shedding light on aspects of doctors’ lives that are not commonly shared. This increased visibility fosters a sense of closeness and enhances a deeper understanding of the profession, which may, in turn, inspire career interest. As one participant expressed:
“Medical dramas reveal stories that doctors seldom share, providing an effective way to convey these experiences to the general public.” (V5_H11_B4)
By offering a representation of doctors’ daily lives, medical dramas provide viewers with a deeper understanding of what a career in medicine entails. This additional perspective can be a key factor in the decision-making process for those considering entering the field (V2_H4_B28).
D. Medical Dramas Contribute to a Positive Public Perception of the Medical Profession
Three out of six respondents emphasised that medical dramas portray the ethical dilemmas faced by doctors, reinforcing professional values that shape viewers’ perceptions of the medical field. One respondent noted that the depiction of doctors’ strong work ethic in these dramas increased their interest in pursuing a career in medicine (V3_H6_B4).
Additionally, medical dramas present compelling and admirable doctor characters, which can serve as a source of inspiration for viewers. As one respondent shared:
“The dramatised portrayal made it inspiring for my younger self, leading me to think, ‘Doctors are cool.’” (V5_H11_B2)
The depiction of medical procedures, particularly surgeries, also left a strong impression on some respondents, reinforcing their motivation to enter the medical field. One participant stated:
“Medical dramas provide insight into a doctor’s work, including various surgeries, highlighting the fascinating ability to help many people.” (V4_H7_B33)
Furthermore, the portrayal of doctors saving lives in medical dramas can evoke strong emotional responses, fostering admiration and a desire to pursue medicine. One respondent expressed how these scenes encouraged them to consider a career in medicine (V5_H11_B2). Medical dramas also emphasise the perseverance and resilience of doctors in the face of various pressures and stress, further reinforcing the appeal of the profession for aspiring medical students (V5_H9_B11).
E. Medical Dramas Evoke Emotional Responses that may Inspire Viewers to Pursue a Medical Career
Medical dramas can spark viewers’ curiosity about medical procedures, motivating them to explore the medical field further and increase their interest in the profession. One respondent noted that medical dramas played a role in their initial motivation for pursuing medicine, as the cases depicted often align with real-world medical scenarios, piquing their interest to learn more:
“I believe the medical procedures shown in Grey’s Anatomy exist in real life and are up to date. For example, an episode featured an abdominal wall transplant, which piqued my curiosity. After researching it, I discovered that the procedure had only recently been developed, showing how the show connects to world medicine.” (V1_H2_B14)
Beyond fostering curiosity, medical dramas also evoke strong emotional responses, such as sadness and empathy, particularly when portraying patients in need of medical care. One respondent shared that such portrayals heightened their awareness of the number of people requiring medical assistance. The emotions they experienced, combined with this awareness, ultimately served as an inspiration to pursue medicine (V1_H2_B31).
F. Medical Dramas Showcase Inspiring Doctor Characters, Motivating Viewers to Follow in their Footsteps
Medical dramas can inspire viewers through uplifting scenes and compelling portrayals of doctor characters. These representations serve as role models, fostering admiration and desire to follow in their footsteps. Notably, three out of six respondents indicated that such portrayals influenced their decision to pursue a medical career. As one participant shared:
“In ‘New Amsterdam’, there is a doctor who stands out from others – someone who wants to create change and has a unique vision. I found him quite inspiring.” (V3_H6_B5)
G. Medical Dramas Illustrate the Challenges and Dedication Required to Become a Doctor
Medical dramas not only portray the professional responsibilities of doctors but also illustrate the journey of becoming one, highlighting the challenges and obstacles along the way. Two out of six students emphasised the significance of this theme, noting that the depiction of medical interns’ experience in these dramas played a crucial role in their motivation to pursue medicine. As one participant shared:
“Medical dramas often depict doctors under immense stress, highlighting the challenges of the profession. However, rather than discouraging me, witnessing their struggles made the career even more appealing.” (V5_H10_B28)
IV. DISCUSSION
The in-depth interviews revealed that medical students felt more mentally prepared and motivated to pursue medicine after watching medical dramas. These shows provided insight into both the professional and personal lives of doctors, reinforcing previous studies on their educational influence in shaping viewers’ perceptions of the medical field. This aligns with the Media Effect Theory, introduced by Gerbner in 1960, which suggests that television shapes individuals’ perceptions of reality, particularly among frequent viewers (Stacks et al., 2015). Hoffman and colleagues further applied this theory to medical dramas, highlighting their role in influencing viewers’ perception of the medical profession (Arias, 2018).
Beyond depicting technical medical procedures, medical dramas also emphasise ethical principles and professional values, contributing to a favourable image of the profession. Research indicates that medical and nursing students often use these shows as supplementary learning tools for bioethics and professionalism (Cambra-Badii et al., 2021). Similarly, these portrayals may inspire high school students to consider careers in medicine by offering an engaging introduction to the field.
Emotional engagement is another key factor in the influence of medical dramas. Strong emotional responses- such as curiosity, empathy, and excitement- can enhance motivation, as emotions play a crucial role in learning, achievement, and psychological well-being, particularly in adolescents (Pekrun, 2017). Positive emotions make tasks more appealing, fostering inner motivation that arises after the initial external excitement provided by medical dramas (Legault, 2016).
Furthermore, medical dramas often depict the challenges of medical training, including long working hours and emotional strain, providing a more nuanced perspective on the profession. While these portrayals may initially present an idealised view of medicine, they also serve as a reality check, reinforcing the dedication required to pursue a medical career. This dual representation may deter less committed individuals while strengthening the resolve of those deeply passionate about the field (Tedeschi, 2024).
However, the potential for misinformation in medical dramas must also be considered. The oversimplifications or dramatisation of medical practice may create discrepancies between fictional portrayals and real-world medicine, leading to misconceptions among viewers (Alismail et al., 2018). One notable bias is the tendency to depict doctors as infallible heroes performing miraculous saves amidst dramatic emergencies, often intertwined with personal achievements and romantic subplots. This portrayal fosters unrealistic expectations, potentially leading to disillusionment when aspiring medical students encounter the demanding and less glamorous realities of medical education and practice (Tedeschi, 2024).
These findings highlight the complex role of medical dramas in shaping career motivation, offering both inspiration and potential misconceptions. Their influence appears particularly significant for students without a familial background in medicine, as most respondents came from non-medical families. This trend may suggest that medical dramas serve as an accessible source of insight into the profession for those without direct exposure. However, the possibility of sampling bias should be considered, as students already interested in medicine may be more likely to engage in medical dramas. While these dramas may serve as informal educational tools, their impact should be critically assessed to ensure they provide a balanced and realistic portrayal of the medical profession.
V. CONCLUSION
Medical dramas play a significant role in shaping students’ motivation to pursue a medical career by providing an engaging portrayal of the profession. These shows offer insight into the roles and responsibilities of doctors, their daily challenges, and the emotional rewards of the profession. Additionally, they influence public perceptions of medicine and evoke strong emotional responses through inspiring characters and narratives. By depicting both the struggles and triumphs of medical training, medical dramas contribute to students’ understanding of the dedication required to become a doctor. This study highlights six key aspects through which medical dramas impact students’ decision to pursue medical education, highlighting their role as both an informational and motivational tool.
Notes on Contributors
Nathania Nishida Tan participated in data collection, data analysis, review, the writing of the paper, and the formatting for publication.
dr. Daniel Ardian Soeselo, Sp.B, MSi.Med. participated in the data analysis, review, and direction of the paper.
dr. Natalia Puspadewi, M.Med.Ed, Ph.D participated in the data analysis, review, and direction of the paper.
dr. Gisella Anastasia, MHPE participated in the review of the paper.
dr. V. Dwi Jani Juliawati, M.PD, Sp.KKLP participated in the review of the paper.
Ethical Approval
This study received ethical clearance from the Research Ethics Commission of the Faculty of Medicine and Health Sciences Atma Jaya Catholic University of Indonesia under the ethical approval code 13/02/KEP-FKIKUAJ/2024. To ensure confidentiality and data security, all interview transcripts were anonymised and securely stored in password-protected files, accessible only to the research team.
Data Availability
The data of this qualitative study are not publicly available due to confidentiality agreements with the participants.
Acknowledgement
The authors would like to thank all the students who participated in this study.
Funding
There was no funding for this article.
Declaration of Interest
The authors have no conflicts of interest in connection with this article.
References
Aboud, K. A. (2012). Medical dramas – The pros and the cons. Dermatology Practical & Conceptual, 2(1), 75–77. https://doi.org/10.5826/dpc.0201a14
Alahmari, A. A. (2023). Professionalism, ethics, and realism of television medical dramas as perceived by Saudi medical students. Journal of Medical Education and Curricular Development, 10. https://doi.org/10.1177/23821205231175037
Alismail, A., Meyer, N. C., Almutairi, W., & Daher, N. S. (2018). CPR in medical TV shows: Non-health care student perspective. Advances in Medical Education and Practice, 9, 85–91. https://doi.org/10.2147/AMEP.S146149
Arias, E. (2018). How does media influence social norms? Experimental evidence on the role of common knowledge. Political Science Research and Methods, 7(3), 561–578. https://doi.org/10.1017/psrm.2018.1
Cambra-Badii, I., Moyano, E., Ortega, I., Baños, J., & Sentí, M. (2021). TV medical dramas: Health sciences students’ viewing habits and potential for teaching issues related to bioethics and professionalism. BMC Medical Education, 21, Article 509. https://doi.org/10.1186/s12909-021-02947-7
Gehrau, V., Brüggemann, T., & Handrup, J. (2016). Media and occupational aspirations: The effect of television on career aspirations of adolescents. Journal of Broadcasting & Electronic Media, 60(3), 465–483. https://doi.org/10.1080/08838151.2016.1203319
14th Media Mutations International Conference. (2023). Investigating medical drama TV series: Approaches and perspectives.
Legault, L. (2016). Intrinsic and extrinsic motivation. Springer eBooks. https://doi.org/10.1007/978-3-319-28099-8_1139-1
Levine, S., & McLuhan, M. (1964). Understanding media: The extensions of man. American Quarterly, 16(4), 646. https://doi.org/10.2307/2711172
Mendick, H., & Williams, K. (2022). Does television influence young people’s career choices? Journal of the National Institute for Career Education and Counselling, 21(1), 18–22. https://doi.org/10.20856/jnicec.2103
Pekrun, R. (2017). Emotion and achievement during adolescence. Child Development Perspectives, 11(3), 215–221. https://doi.org/10.1111/cdep.12237
Sonego, A., & Rocchi, M. (2024). Medical drama TV series: A semi-systematic literature review. Online Journal of Communication and Media Technologies, 14(4), Article e202459. https://doi.org/10.30935/ojcmt/15268
Stacks, D. W., Li, Z. C., & Spaulding, C. (2015). Media effects. Elsevier eBooks. https://doi.org/10.1016/B978-0-08-0970868.95045-1
Tedeschi, R. (2024). The paradox of medical dramas: Global aspirations versus realities. BJPsych Advances, 31(1), 62–64. https://doi.org/10.1192/bja.2024.56
Zago, D., Cautero, P., Scarpis, E., Pompili, E., Voglino, G., Siliquini, R., Brusaferro, S., & Brunelli, L. (2024). TV medical dramas: Assessing the portrayal of public health in primetime. Frontiers in Public Health, 12. https://doi.org/10.3389/fpubh.2024.1432528
*Daniel Ardian Soeselo
Medical Education Unit and Department of Surgery,
Faculty of Medicine and Health Sciences,
Atma Jaya Catholic University of Indonesia
Jl. Pluit Raya No.2 21, RT.21/RW.8,
Penjaringan, Kec. Penjaringan, Jakarta Utara,
Daerah Khusus Ibukota Jakarta, Indonesia 14440
Email: daniel.ardian@atmajaya.ac.id
Submitted: 16 August 2024
Accepted: 23 December 2024
Published online: 1 July, TAPS 2025, 10(3), 49-57
https://doi.org/10.29060/TAPS.2025-10-3/OA3495
Shuh Shing Lee1, Shefaly Shorey2, Tang Ching Lau3 & Dujeepa D. Samarasekera1
1Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Alice Lee Centre for Nursing Studies, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 3Dean’s Office, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: Numerous studies have been conducted on COVID-19, with the majority focusing on interventions involving students and teachers. However, limited research has delved into the pandemic’s impact on the wellness of various stakeholders and how they have adapted to the challenges it presented. This study aims to fill this gap by exploring these neglected areas.
Methods: This study employs a sequential mixed-method approach to study these areas. The quantitative data collection was carried out using a combination of validated surveys (ranging between 63-88 items) for students, faculty and administrators. Subsequently, qualitative data collection was gathered via semi-structured interview using a convenient sampling method.
Results: Seventeen faculty, 18 administrators and 369 students responded to the survey. The quantitative data indicated faculty (teachers) exhibited the lowest stress levels and the highest resilience during the pandemic. In comparison, administrators and students experienced moderate levels of stress, with students scoring slightly higher on the stress level. The themes that emerged from the qualitative data were personal endurance, emotional reaction, cognitive-behavioural reaction and social support.
Conclusion: Our study highlighted that, apart from personal endurance, the tension arises from emotional and cognitive-behavioural responses of students, teachers, and administrators can be mitigated based on the presence or absence of support mechanisms.
Keywords: Wellbeing, Change, Stakeholders, Educational Environment, Culture
Practice Highlights
- Students experienced the highest stress levels compared to administrators and teachers.
- However, students and administrators demonstrated resilience, bouncing back quickly after challenging times.
- Students and administrators tolerated for uncertainty and displayed cognitive flexibility to enable them to adapt and seek opportunities.
- Teachers and administrators initially experienced negative emotions, but their emotional resilience facilitated quick recovery.
- Coming from a culture emphasising collectivism, the sense of belonging and social connection served as a protective factor against psychological distress.
I. INTRODUCTION
The foundation of any education system rests upon the harmonious collaboration of three essential elements: teachers, students, and administrators. Each of these components play a vital role in ensuring the smooth functioning of the educational ecosystem and this symbiotic relationship becomes even more evident during challenging times, such as the COVID-19 pandemic. Together, they navigated the complexities of remote learning, ensuring that the pursuit of knowledge remained uninterrupted. In essence, it is the collaborative synergy of these three integral components that propels the educational journey forward. The strength of an education system lies in the seamless interplay of these elements, fostering a holistic and empowering learning experience for all.
Nevertheless, numerous studies have studied the impact of pandemic such as SARS, COVID-19, with a predominant focus on students and teachers. A significant portion of these studies, approximately 50%, has highlighted the insights and innovations from health professions educators in response to the pandemic, particularly at the undergraduate level (Daniel et al., 2021; Eva & Anderson, 2020; Gordon et al., 2020). The majority of these investigations have primarily collected data on student reactions, satisfaction levels, shifts in attitudes, and changes in knowledge and skills. The review conducted by Best Evidence Medical Education (BEME) revealed that almost half of the studies centred on the transition from traditional in-person teaching to online education, only a meagre 6% of the research primarily focused on aspects related to well-being, mental health, or learner support (Daniel et al., 2021). Amid the widespread concern about the well-being of individuals during the pandemic, much attention has been given to medical students (Jia et al., 2022; Paz et al., 2022; Wilcha, 2020) and frontline healthcare workers (Danet, 2021; Muller et al., 2020; Xiong et al., 2022) in the published articles. The reactions of teachers and administrators to the changes brought about by the pandemic, and how these changes have impacted their well-being, have been largely overlooked in the existing literature.
Hence, the principal objective of this research is to investigate the impact of the initiatives implemented during the pandemic on the well-being of students, teachers, and administrators. This study aims to explore how these key stakeholders reacted and adapted to the changes, shedding light on a vital aspect that has been underrepresented in the current body of literature.
II. METHODS
We employed a sequential explanatory mixed-methods design to assess the adaptation and impact of the pandemic on the well-being of administrators, teachers, and students within the specific context of the Yong Loo Lin School of Medicine (YLLSoM) at the National University of Singapore. This design involved collecting and analysing both quantitative and qualitative data in two consecutive phases within a single study. In the quantitative phase, data were gathered through a comprehensive survey/questionnaire, allowing us to capture a broad spectrum of responses from the participants. Subsequently, in the qualitative phase, we employed the phenomenological approach, conducting in-depth interviews with participants representing various categories. Phenomenology, as an approach in qualitative research, enables us to delve deeply into the shared experiences within a specific group. The primary objective of this approach is to develop a detailed description of the nature of the phenomenon under investigation (Creswell, 2013). The details of this methodological approach are elaborated in the subsequent sections.
A. Phase I Quantitative Data Collection
The quantitative data collection was carried out using a survey. The survey was adapted from Landis’s and Bradley’s (2003) work on The Impact of the 2003 SARS Outbreak on Medical Students at the University of Toronto, The Brief Resilience Scale (Smith et al., 2008), Perceived Stress Scale (Cohen et al., 1983) and Teachers’/Students’ Self-Efficacy towards Technology Integration (Kiili et al., 2016). Table 1 shows the sections of the surveys for administrators, teachers and students.
|
Section |
Items in each section |
||
|
Student |
Teacher |
Administrator |
|
|
A: Demographic Information |
5 |
8 |
7 |
|
B: The psychological impact of COVID-19 |
7 |
||
|
C: Perception of medical students on the restriction of clinical activities and the impact of COVID-19 on their medical/nursing education |
15 (13 5-point likert scale items & 2 open-ended questions) |
2 (open-ended questions) |
2 (open-ended questions) |
|
D: Perceived quality of information received by respondents about COVID-19 from specific groups |
8 |
||
|
E: The source and level of psycho-social support that medical students rely on during the COVID-19 outbreak |
26 |
19 |
|
|
F: Brief Resilience Scale |
6 |
||
|
G: Perceived Stress Scale |
10 |
||
|
H: Teachers’/Students’ Self-Efficacy towards Technology Integration |
11 |
4 |
|
|
Total Items |
88 |
71 |
63 |
Table 1. Sections of the Surveys for Administrators, Teachers and Students
The survey was validated by 10 medical educators from various departments (Paediatrics, Surgery, Centre for Medical Education, Nursing). After the validation, the survey was administered to medical (Year 1 – 5) and nursing (Year 1 – 4) students, administrators and faculty members in Yong Loo Lin School of Medicine and Alice Lee Centre for Nursing Studies using convenient sampling. It took about 20-30 minutes to complete the survey and the data was collected between Jan – June 2021.
B. Phase II Qualitative Data Collection
The qualitative data collection was gathered via semi-structured interview. The interview was conducted for about 60-90 minutes among the medical/nursing students, administrators and faculty members (teachers). Followed up from the data collected from the quantitative data, the questions were revolved around teaching and learning, content, assessment, policies, guidelines, communication, environment (safety)/support and wellness.
From July 2021 – Nov 2022, we used convenient sampling method to recruit of students, administrators and faculty members. The interviews were carried out by 2 trained interviewers with no power relationship with the interviewees. Interviews were carried out after getting consent from the volunteer interviewees. All digital audio recordings made during the interviews were transcribed and member-checked with the interviewees to ensure transparency and trustworthiness of the data.
Data collection ceased when the data reached saturation stage.
C. Data Analysis
The quantitative data was analysed using descriptive statistics (such as mean, frequency and percentage) using Microsoft Excel for the data collected from students, administrators and teachers.
The interviews were thematically analysed by 2 researchers in the team. The two researchers coded the transcripts independently and came together to resolve any discrepancy or disagreement on the coding. Subsequently, they continued to code and form categories and eventually themes. There were multiple discussions that took place among the researchers and the team before the themes were crystalised.
III. RESULTS
A. Phase I Quantitative Data
The demographic information was illustrated in Table 2. Majority of the participants were not quarantined during the pandemic and more than 80% of them did not have a family member tested positive for COVID when this study was conducted. The teachers from the school of medicine were mainly from Family Medicine, Paediatrics, Physiology, Pathology, Public Health, Medicine, Anatomy and Anaesthesia departments. They are educators for postgraduate and undergraduate students. As for administrators, their roles in the departments are educational related such as instructional design, learning analytics, planning and execution of education, managing project and training.
|
|
|
|
Teachers |
Administrators |
Students |
|||
|
0 |
Finished |
Completed |
17 |
65.4% |
18 |
54.5% |
369 |
73.8% |
|
Did not complete |
9 |
34.6% |
15 |
45.5% |
131 |
26.2% |
||
|
Total Responses |
26 |
33 |
|
500 |
|
|||
|
1 |
Faculty |
Medicine |
12 |
70.6% |
16 |
88.9% |
305 |
83.0% |
|
Nursing |
5 |
29.4% |
2 |
11.1% |
64 |
17.0% |
||
|
2 |
Gender |
Male |
6 |
35.3% |
3 |
16.7% |
140 |
37.9% |
|
Female |
11 |
64.7% |
15 |
83.3% |
229 |
62.1% |
||
|
6 |
Living arrangement |
Alone |
1 |
5.9% |
1 |
5.6% |
17 |
4.6% |
|
With Parents |
2 |
11.8% |
7 |
38.9% |
338 |
91.6% |
||
|
With Partners (married, common-law, etc.) |
14 |
82.4% |
9 |
50.0% |
1 |
0.3% |
||
|
With Room-mates |
0 |
0.0% |
1 |
5.6% |
13 |
3.5% |
||
|
7 |
Status during COVID-19 Outbreak |
Non-Quarantined |
17 |
100.0% |
18 |
100.0% |
355 |
96.2% |
|
Quarantined |
0 |
0.0% |
0 |
0.0% |
7 |
1.9% |
||
|
Stay-Home-Notice (SHN) |
0 |
0.0% |
0 |
0.0% |
7 |
1.9% |
||
|
8 |
I have family member(s), relative or friend(s) who tested positive for COVID-19 |
Yes |
2 |
11.8% |
1 |
5.6% |
29 |
7.9% |
|
No |
15 |
88.2% |
17 |
94.4% |
340 |
92.1% |
||
Table 2. Demographic Information of the Respondents
For each section, the summary was illustrated in Table 3. The mean for different sections was quite close for the 3 groups. Likewise, the items that were scored low and high were quite similar for all the sections. For example, Section B The psychological impact of COVID-19, The sleep quality and concentration in all three groups were not affected by the pandemic, but they are more worries about their family members contracted with COVID-19.
|
Section |
Administrator |
Teacher |
Student |
|
B: The psychological impact of COVID-19 (7 items) |
Mean ranging between 2.39-3.67 |
Mean ranging between 1.71 – 3.29 |
Mean ranging between 2.14 – 3.85 |
|
C: Perception of medical students on the restriction of clinical activities and the impact of COVID-19 on their medical/nursing education (15 items) |
Mean ranging between 1.77 – 3.78 |
Not relevant |
|
|
D: Perceived quality of information received by respondents about COVID-19 from specific groups |
Mean ranging between 3.33 – 4.17 |
Mean ranging between 3.47 – 4.19 |
Mean ranging between 3.17 – 4.14
|
|
E: The source and level of psycho-social support that medical students rely on during the COVID-19 outbreak |
Mean ranging between 2.78 – 4.11 |
Mean ranging between 2.47 – 4.47 |
Mean ranging between 2.65 – 4.36
|
|
F: Brief Resilience Scale |
Mean 3.4 |
Mean 4.01 |
Mean 3.3 |
|
G: Perceived Stress Scale |
Mean: 16.6 (Moderately stress) |
Mean 11.7 (Low stress) |
Mean 18.7 (Moderately stress) |
|
H: Teachers’/Students’ Self-Efficacy towards Technology Integration |
Mean ranging between 3.83-4.06 |
Mean ranging between 3.47 – 4.12 |
Mean ranging between 3.68 – 4.22 |
Table 3. Summary of the Mean for Different Sections for the 3 Groups
During the pandemic, students expressed significant concerns about the adequacy of their training, particularly due to reduced patient contact, raising apprehensions about their preparedness for exams. This concern will be elaborated upon in the qualitative data section, shedding light on the depth of their worries. All three groups shared the view that information originating from the government and hospitals was the most reliable, with friends and family scoring the lowest mean among all sources. Despite this, the participants unanimously agreed that the support from friends and family, in terms of both source and level of assistance, was the most substantial. Conversely, organisational support from entities such as the University Wellness Centre, Dean’s office, community, and social media was perceived as unreliable and lacking during the pandemic.
Furthermore, our observations revealed that teachers exhibited the lowest stress levels and the highest resilience during the pandemic, showcasing their ability to cope effectively. In comparison, administrators and students experienced moderate levels of stress, with students scoring slightly higher on the Perceived Stress Scale. Although students acknowledged challenges, as indicated by their agreement with statements such as “I have a hard time making it through stressful events” (mean: 2.93), they also exhibited resilience, agreeing with the statement “I tend to bounce back quickly after hard times” (mean: 3.76). Additionally, concerning self-efficacy towards technology integration, students reported the highest mean score, indicating confidence in their ability to navigate various Internet applications. While teachers felt competent in using technology for teaching and learning, their confidence wavered when it came to resolving technical issues, as reflected in their mean score of 3.47. This nuanced understanding underscores the complex interplay of stress, resilience, and technological proficiency among the different groups during the challenging circumstances of the pandemic.
B. Phase II Qualitative Data
As for the qualitative data collection, we have recruited 7 administrators, 17 teachers (12 from Yong Loo Lin School of Medicine and 5 from Alice Lee Centre for Nursing Studies) and 9 undergraduate students (6 from Yong Loo Lin School of Medicine and 3 from Alice Lee Centre for Nursing Studies). The themes and subthemes that emerged were depicted in the Figure 1.
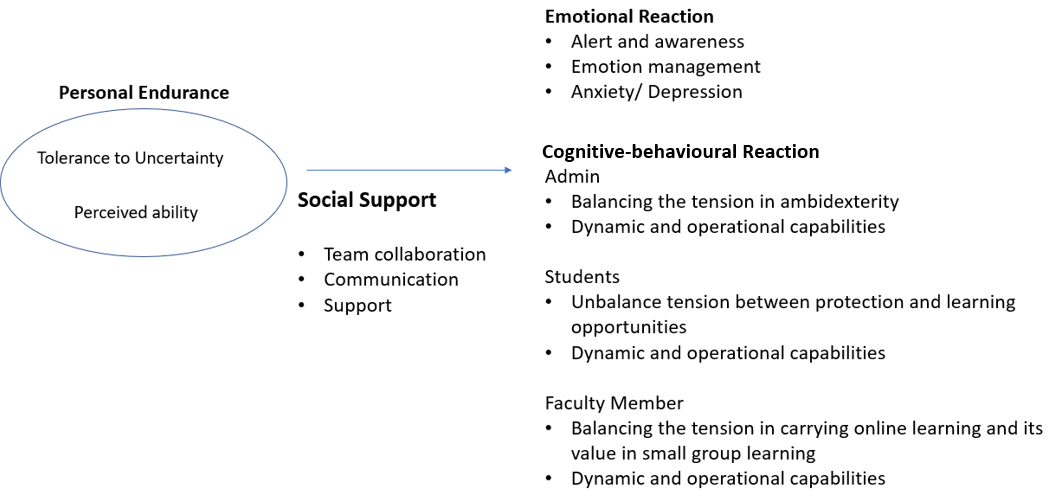
Figure 1. Themes and Subthemes of the Qualitative Data
1) Theme 1: Personal Endurance
Personal endurance depends on perceived ability and tolerance to uncertainty. For administrators, they felt that it was quite stressful and frustrated during the pandemic as the situation was unclear. However, they were able to manage and there was a sense of relief after they had gone through the critical phase.
“It was very intense, stressful but looking back now, it is not that bad. We have gone through the worse” (Admin 5)
While administrators’ contribution to the education system is crucial, some of the administrators perceived their contribution was minor as compared to medical front liner.
“We are not front liner, our contribution is limited.” (Admin 3)
Although the situation was stressful in the beginning, we noticed a positive endurance among the teachers and perceived the pandemic as an opportunity instead of a threat.
“Overall, I think the predominant mood was of a challenge that needs to be overcome and that brought a certain amount of excitement.” (Teacher 7)
On the other hand, the students felt that they were being too protected and perceived themselves as having the ability to manage the situation themselves.
“I understood that they wanted to protect us but I felt that eventually, they can’t protect us anymore” (Student 3)
The students also perceived that the teachers lacked ability in using technology in teaching and learning especially in remote learning.
“A lot of professors are not familiar with the technology.” (Student 5)
2) Theme 2: Emotional Reaction
There were a lot of negative emotions illustrated by the students, administrators and teachers due to various reasons. Students were worried, frustrated and anxious that they may not learn since the contact with the patients was less during the pandemic. Too much protection from the school and the system put in place has heightened these negative emotions.
“We feel quite unconfident because we feel we have not seen enough patients”/ “..fear that we are not as good as the previous batch” (Students 1 & 2)
Administrators were frustrated mainly because they need to manage the family and work at the same time when working from home system was implemented. However, some of them shared that they are able to regulate and get used to the situation after a while.
“Everybody was under pressure at that time…while I have to juggling with work, my kids were at home because school close.” (Admin 4)
“I usually regulate my own emotion.” (Admin 7)
While there were some positive emotions state in Theme 1 for teachers, they did feel stressful in the early stage of the pandemic due to the change of the approaches in teaching and learning and they are unsure of the outcomes when the teaching was entirely online.
“…stressful in the beginning… I even have nightmares…dreaming students get lost in the virtual room.” (Teacher 17)
“It was a bit stressful in the beginning because you did not know how is going to turn out…” (Teacher 5)
3) Theme 3: Cognitive-Behavioural Reaction
Amidst the challenges posed by the pandemic, administrators, students, and teachers made concerted efforts to adapt their cognition and behavior in response to various initiatives, including social distancing measures, reduced patient contact, and a shift to virtual teaching environments. Throughout this period, interviewees shared both positive and negative reactions to these changes.
Administrators and teachers found themselves navigating the delicate balance between the need to innovate and the need to maintain productivity (ambidexterity). Administrators, in particular, faced the challenge of fostering creativity in coordinating and delivering the curriculum, which involved tasks such as timetabling, resource management, and providing IT support for online learning. These adjustments were made within a short timeframe, reflecting their resilience and adaptability. However, amid these innovative efforts, administrators were also keen on upholding the quality of their work, highlighting the complexity of their role in managing these rapid changes.
“We have to deliver in a short time but also the content has to be rigorous” (Administrator 3)
Similarly, teachers tried to be creative in an online teaching environment and ensure the student learned at the same time especially in small group teaching. However, they find it challenging.
“…there is an urgency to find a way around this small group teaching…we kind of lose the whole power of collaboration.” (Teacher 5)
There is also a tension arose among the students for being too protected by the school and compromised with their learning as shared in the quotes below. This was repeatedly mentioned by the students, and they felt they have to face the situation eventually.
“I am not very interested in surgery, but this is like once in a lifetime and after I go out of medical school I won’t have the chance to see surgery” (Students 3)
“There’s a culture… in the society in general…protect my child from COVID. But once day we are going to deal with COVID” (Students 6)
Notwithstanding the aforementioned tensions, it’s worth noting that administrators, students, and teachers exhibited remarkable innovativeness and adaptability during the pandemic. All three groups demonstrated evidence of both Operational Capabilities, which encompass the efficient and effective use of resources, and Dynamic Capabilities, which involve the continuous development of competencies to align with the evolving environment.
With the predominant shift in communication from face-to-face to virtual platforms, administrators found themselves assuming the role of intermediaries responsible for conveying information to various stakeholders. In this new virtual setting, where body language cues were less apparent, administrators recognised the need to be more attuned and sensitive to subtle nuances in communication compared to traditional face-to-face interactions. This adaptation reflected their ability to pivot and operate effectively within the changing landscape of remote communication.
“We play the middleman role because we have to speak administrative language to certain people and be sensitive when communicate with faculty members” (Admin 3)
“We have to start thinking about (what kind of information needed) before the faculty member even ask those questions” (Admin 7)
Teachers utilised different resources to innovate in their teaching as well as learning from different others.
“I break it up my lectures into smaller bits and disperse it with PollEverywhere” (Teacher 5)
“We formed a group we called a brown bag meeting – basically we meet at lunchtime with technologically savvy administrators to introduce to the staff on how to make online learning more interactive.” (Teacher 10)
Likewise, since there was less patient contact time, students tried to make use of their time for other learning sessions.
“Since there’s little time in the hospital, I had read up a lot” (Students 1)
“It allows us to have some processing time and have time to consolidate our knowledge” (Students 5)
4) Theme 4: Social Support Mechanism
Social support mechanism has been mentioned by the 3 groups as one of the prominent mechanisms in adapting the changes during pandemic. It includes transparent communication, team collaboration and support from various stakeholders. For example, administrators shared that they all came together and supported each other during the hard times.
“All different teams come together, I think that was very precious” (Administrator 2)
Students sought seniors’ help to provide additional sessions to compensate their learning.
“What my group would do is we call our seniors to give us extra tutorials” (Student 2)
However, there was also lack of support mechanism brought up by the teachers which led to negative emotion (such as frustration).
“Educational technology team are overworked…if the school would really want to be the best or world class, I think we need a very good support from the IT.” (Teacher 9)
IV. DISCUSSION
The impact of the COVID-19 pandemic on both our educational systems and personal lives has been profound. This unprecedented disruption has been keenly observed by various stakeholders, including administrators, teachers, many of whom were also frontline workers, and students in medical schools. Swift adaptation to the ever-changing situation became imperative, particularly in response to the government’s new guidelines. The abrupt alterations in social interactions and extracurricular activities routines compelled a shift towards a heightened emphasis on family life, accompanied by the necessity to work and learn from home due to lockdown measures. These changes had profound physical and psychological effects on our lives.
Our study revealed that students experienced the highest stress levels compared to administrators and teachers, a finding consistent with previous research indicating that medical students often have higher baseline anxiety than their peers studying other disciplines (Dyrbye et al., 2006; Lasheras et al., 2020). Qualitative data highlighted that students’ stress levels were primarily attributed to the lack of patient contact and inadequate training, potentially impacting their future practice. Additionally, students expressed feelings overly protected due to initiatives like stay-at-home learning. The altered learning environment, combined with a lack of guidance on learning strategies and interpersonal relationships, left students vulnerable to intense emotional fluctuations and strained family relationships (Zhang et al., 2020). Similarly, for administrators, the shift to remote work and social isolation policies posed challenges in balancing work and family responsibilities, as evident from their qualitative comments.
However, students and administrators demonstrated resilience, bouncing back quickly after challenging times. According to Del Carmen Pérez Fuentes et al.’s (2020) Adaptability to Change framework, a sense of control, tolerance for uncertainty, and cognitive flexibility are crucial in coping with adverse situations. Despite feeling anxious and frustrated due to the inability to control the study-from-home or working-from-home policy, student and administrator tolerated for uncertainty and display cognitive flexibility to enable them to adapt and seek opportunities. Emotional resilience, the ability to generate positive emotions and recover swiftly from negative emotional experiences, played a pivotal role in psychological resilience (Zhang et al., 2020). This emotional resilience led to diverse emotional responses, influencing the cognitive processing of emotional information. Teachers and administrators initially experienced negative emotions, but their emotional resilience facilitated quick recovery, evident from their transcripts.
Emotional and cognitive-behavioural responses were further shaped by social support mechanisms within peer groups, colleagues, organisational leaders, and the government. While studies have shown that social media can heighten anxiety due to misinformation and distressing news (Gao et al., 2020), our research indicated that students, teachers, and administrators placed significant trust in information provided by the government and institutions. This trust in government intentions and capabilities fosters adherence to health regulations, essential in crisis management (Siegrist & Zingg, 2014).
Coming from a culture emphasising collectivism, our society values interdependence and family connections highly. This sense of belonging and social connection served as a protective factor against psychological distress, aligning with previous research findings (Xiao, 2021; Yu et al., 2020) . Conversely, a lack of social support within a collectivist culture, as reported by teachers and students, contributed to psychological distress. Our qualitative and quantitative data in this study support this observation, emphasising the significance of social support structures in mitigating the adverse effects of challenging circumstances. The importance of fostering a supportive environment, both within institutions and at a societal level, cannot be overstated in times of crisis.
V. LIMITATIONS
This study has some potential limitations. The study was carried out in a single medical school; hence, the results can only be transferable to the same context. The number of respondents was quite small (especially for nursing respondents) despite multiple reminders sent to the various groups. Therefore, they may not be representative of the entire student, teachers and administrator’s population. Third, the survey was a self-reported survey and may have inherent biases while answering the questions. While rigor is more challenging to achieve in qualitative data collection and analysis, the researchers adhere to the trustworthiness principles as much as possible in analysing and presenting the results in this paper.
VI. CONCLUSION
In conclusion, achieving wellness during a pandemic is indeed possible, but it hinges not only on the resources that organisations and governments can marshal but also on individual resilience in navigating uncertainty, cultural factors, trust, and support systems. Our study highlights the importance of familial and peer connections within our cultural context, underscoring how these bonds facilitate adaptation and innovation amid the challenges posed by the pandemic. The emotional and cognitive-behavioural responses of students, teachers, and administrators are depending on their personal endurance. However, the tension that arises in these individuals can be mitigated or exacerbated based on the presence or absence of adequate support mechanisms. Sufficient support can act as a buffer, helping individuals cope effectively with the challenges they face. Conversely, insufficient support can exacerbate stress and strain, hindering their ability to adapt and respond positively to the situation at hand.
Therefore, fostering a strong support network, both within organisations and communities, is crucial. This support not only alleviates the immediate challenges faced by individuals but also empowers them to build emotional resilience, enabling them to navigate uncertainties and adversities with greater ease. In this way, the collective endurance of individuals, coupled with robust support systems, becomes the cornerstone of achieving wellness and fostering positive responses in the face of a pandemic.
Notes on Contributors
DDS developed the research idea and design with SSL, SR & LTC. The data collection was performed by SSL. The data were analysed by SSL & DDS. DDS, SSL, SR & LTC performed the data interpretation. DDS, SSL & SR wrote the article with revision by LTC. All the authors read and agreed with the final manuscript.
Ethical Approval
Ethics approval was sought from the National University of Singapore (NUS) Institutional Review Board (NUS-IRB-2020-216). Written informed consent was obtained from all participants.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available as the participants of this study did not give written consent for their data to be shared publicly.
Acknowledgement
We would like to express our heartfelt gratitude to Jillian Yeo and Lilusha Kaludewa for helping in data collection and analysis.
Funding
No funding is available for this research.
Declaration of Interest
The authors report that there are no conflict of interests to declare.
References
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385. https://doi.org/10.2307/2136404
Creswell, J. W. (2013, January 1). Steps in conducting a scholarly mixed methods study [Slide show]. https://digitalcommons.unl.edu/cgi/viewcontent.cgi?article=1047&context=dberspeakers
Danet, A. D. (2021). Psychological impact of COVID-19 pandemic in Western frontline healthcare professionals. A systematic review. Medicina Clínica (English Edition), 156(9), 449–458. https://doi.org/10.1016/j.medcle.2020.11.003
Daniel, M., Gordon, M., Patricio, M., Hider, A., Pawlik, C., Bhagdev, R., Ahmad, S., Alston, S., Park, S., Pawlikowska, T., Rees, E., Doyle, A. J., Pammi, M., Thammasitboon, S., Haas, M., Peterson, W., Lew, M., Khamees, D., Spadafore, M., . . . Stojan, J. (2021). An update on developments in medical education in response to the COVID-19 pandemic: A BEME scoping review: BEME guide no. 64. Medical Teacher, 43(3), 253–271. https://doi.org/10.1080/0142159x.2020.1864310
Del Carmen Pérez-Fuentes, M., Del Mar Molero Jurado, M., Martínez, Á. M., Fernández-Martínez, E., Valenzuela, R. F., Herrera-Peco, I., Jiménez-Rodríguez, D., Mateo, I. M., García, A. S., Del Mar Simón Márquez, M., & Linares, J. J. G. (2020). Design and validation of the adaptation to change questionnaire: New realities in times of COVID-19. International Journal of Environmental Research and Public Health, 17(15), 5612. https://doi.org/10.3390/ijerph17155612
Dyrbye, L. N., Thomas, M. R., & Shanafelt, T. D. (2006). Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Academic Medicine, 81(4), 354–373. https://doi.org/10.1097/00001888-200604000-00009
Eva, K. W., & Anderson, M. B. (2020). Medical education adaptations: Really good stuff for educational transition during a pandemic. Medical Education, 54(6), 494. https://doi.org/10.1111/medu.14172
Gao, J., Zheng, P., Jia, Y., Chen, H., Mao, Y., Chen, S., Wang, Y., Fu, H., & Dai, J. (2020). Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE, 15(4), Article e0231924. https://doi.org/10.1371/journal.pone.0231924
Gordon, M., Patricio, M., Horne, L., Muston, A., Alston, S. R., Pammi, M., Thammasitboon, S., Park, S., Pawlikowska, T., Rees, E. L., Doyle, A. J., & Daniel, M. (2020). Developments in medical education in response to the COVID-19 pandemic: A rapid BEME systematic review: BEME guide no. 63. Medical Teacher, 42(11), 1202–1215. https://doi.org/10.1080/0142159x.2020.1807484
Jia, Q., Qu, Y., Sun, H., Huo, H., Yin, H., & You, D. (2022). Mental health among medical students during COVID-19: A systematic review and meta-analysis. Frontiers in Psychology, 13, Article 846789. https://doi.org/10.3389/fpsyg.2022.846789
Kiili, C., Kauppinen, M., Coiro, J., & Utriainen, J. (2016). Measuring and supporting pre-service teachers’ self-efficacy towards computers, teaching, and technology integration. The Journal of Technology and Teacher Education, 24(4), 443–469. https://jyx.jyu.fi/bitstream/123456789/53087/1/kiilikauppinencoiroutriainen.pdf
Lasheras, I., Gracia-García, P., Lipnicki, D., Bueno-Notivol, J., López-Antón, R., De La Cámara, C., Lobo, A., & Santabárbara, J. (2020). Prevalence of anxiety in medical students during the COVID-19 pandemic: A rapid systematic review with meta-analysis. International Journal of Environmental Research and Public Health, 17(18), 6603. https://doi.org/10.3390/ijerph17186603
Mark, L., & John, B. (2003). The impact of the 2003 SARS outbreak on medical students at the University of Toronto. University of Toronto Medical Journal, 82, 158–164. https://api.semanticscholar.org/CorpusID:59193656
Muller, A. E., Hafstad, E. V., Himmels, J. P. W., Smedslund, G., Flottorp, S., Stensland, S. Ø., Stroobants, S., Van De Velde, S., & Vist, G. E. (2020). The mental health impact of the COVID-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Research, 293, Article 113441. https://doi.org/10.1016/j.psychres.2020.113441
Paz, D. C., Bains, M. S., Zueger, M. L., Bandi, V. R., Kuo, V. Y., Cook, K., & Ryznar, R. (2022). COVID-19 and mental health: A systematic review of international medical student surveys. Frontiers in Psychology, 13, Article 1028559. https://doi.org/10.3389/fpsyg.2022.1028559
Siegrist, M., & Zingg, A. (2014). The role of public trust during pandemics. European Psychologist, 19(1), 23–32. https://doi.org/10.1027/1016-9040/a000169
Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The brief resilience scale: Assessing the ability to bounce back. International Journal of Behavioral Medicine, 15(3), 194–200. https://doi.org/10.1080/10705500802222972
Wilcha, R. (2020). Effectiveness of virtual medical teaching during the COVID-19 Crisis: Systematic review. JMIR Medical Education, 6(2), Article e20963. https://doi.org/10.2196/20963
Xiao, W. S. (2021). The role of Collectivism–Individualism in attitudes toward compliance and psychological responses during the COVID-19 Pandemic. Frontiers in Psychology, 12, Article 600826. https://doi.org/10.3389/fpsyg.2021.600826
Xiong, N., Fritzsche, K., Pan, Y., Löhlein, J., & Leonhart, R. (2022). The psychological impact of COVID-19 on Chinese healthcare workers: A systematic review and meta-analysis. Social Psychiatry and Psychiatric Epidemiology, 57(8), 1515–1529. https://doi.org/10.1007/s00127-022-02264-4
Yu, H., Li, M., Li, Z., Xiang, W., Yuan, Y., Liu, Y., Li, Z., & Xiong, Z. (2020). Coping style, social support and psychological distress in the general Chinese population in the early stages of the COVID-19 epidemic. BMC Psychiatry, 20, Article 426. https://doi.org/10.1186/s12888-020-02826-3
Zhang, Q., Zhou, L., & Xia, J. (2020). Impact of COVID-19 on emotional resilience and learning management of middle school students. Medical Science Monitor, 26, Article e924994. https://doi.org/10.12659/msm.924994
*Lee Shuh Shing
Centre for Medical Education,
Yong Loo Lin School of Medicine,
National University of Singapore, Singapore
10 Medical Dr, Singapore 117597
Email: medlss@nus.edu.sg
Submitted: 31 July 2024
Accepted: 24 February 2025
Published online: 1 July, TAPS 2025, 10(3), 37-48
https://doi.org/10.29060/TAPS.2025-10-3/OA3473
Kevin Xuan Hong Tang1, Koon Kee Teo1 & Kye Mon Min Swe2
1Department of Medicine, Faculty of Medicine, Newcastle University Medicine Malaysia (NUMed), Malaysia; 2Department of Research, Faculty of Medicine, Newcastle University Medicine Malaysia (NUMed), Malaysia
Abstract
Introduction: Every medical graduate is expected to fulfil the teaching responsibilities stated by the General Medical Council (GMC). It is beneficial to nurture both teaching motivation and skills early in the undergraduate program. This study aims to evaluate the outcomes of final-year medical students as near-peer teachers in a student-led near-peer teaching program and their fulfilment of the educational responsibilities stated by the GMC.
Methods: A cross-sectional study was conducted among the year 5 medical students who participated in the Peer Teaching Program. A structured post-participation 6-point Likert scale questionnaire with written consent was distributed to the near-peer teachers to assess their perspectives on skills enhancement, motivation, and career direction. Additionally, the Peer Tutor Assessment Instrument questionnaires were distributed to the near-peer students to evaluate the performance of the near-peer teachers in five areas: responsibility and respect, information processing, communication, critical analysis, and self-awareness.
Results: There were 28 near-peer teachers, and 49 near-peer students participated in the study. The near-peer teachers score the highest in skills (5.36 ± 0.53), followed by motivation (5.16 ± 0.60) and career direction (4.79 ± 0.82). Three quarters of the near-peer teachers considered teaching to be their future primary career path after experiencing this teaching experience (4.36 ±1.34). Generally, the near-peer teachers were highly evaluated by the near-peer students across all domains (5.06 ± 0.51).
Conclusion: Overall, the near-peer teaching programme likely improved the final-year medical students in fulfilling the “Doctors as Teachers” responsibilities outlined by the GMC.
Keywords: Near-peer Teaching, Medical Students, Undergraduate Medical Education, General Medical Council, Doctors as Teachers
Practice Highlights
- Near-peer teachers are likely improved in skills enhancement, motivation and career direction.
- Sex and students’ background are not associated with the perceived outcomes of near-peer teachers.
I. INTRODUCTION
One of the aspects of Good Medical Practice outlined by the General Medical Council (GMC) for all medical professionals is to “be willing to offer professional support to colleagues, including students, through teaching” (General Medical Council, 2023). The role of doctors as teachers has been widely recognised as they need to teach and educate juniors, students and even patients (General Medical Council, 2011, 2015, 2023). On average, junior doctors spend around 80 minutes per day teaching medical students (Busari et al., 2002). This task is daunting for every new medical graduate who has just begun their UK foundation programme. They need to assume this responsibility with minimal formal training and preparations (Pierce et al., 2024; Qureshi et al., 2013).
Therefore, it is beneficial to motivate medical graduates to teach and equip them with appropriate teaching skills as early as their undergraduate programme (General Medical Council, 2011; Knobloch et al., 2018). Near-peer teaching involves students one or more academic years ahead teaching their peers or junior students (De Menezes & Premnath, 2016; Ten Cate & Durning, 2007; Yu et al., 2011). This has long been thought of as a programme to be incorporated into the medical curriculum to optimise teaching qualities and to produce more competent and knowledgeable doctors in the future (Botelho et al., 2022; Burgess et al., 2014; Zheng & Wang, 2022). Generally, medical schools provide a safe space for medical students to practice, correct and improve their teaching and pedagogical skills (Hardie et al., 2022). Most medical students feel less daunted and more supported involved in teaching their near-peer students (Yu et al., 2011).
To address this gap of insufficient teaching opportunities, most medical schools provide near-peer teaching programmes for their medical student (Frearson & Gale, 2017). However, most of the near-peer teaching programmes are carried out formally with structured guidance and training (General Medical Council, 2011), be it in the form of the Peer Assisted Learning Scheme (PALS) student-selected components (SSC) (Furmedge et al., 2014; Hettle & Morgan, 2019; Ross & Cameron, 2007; Ten Cate & Durning, 2007) or Doctors as Teachers and Educators training course (Cook et al., 2010; General Medical Council, 2011). Little is known about the outcomes of the student-led, student-run, near-peer teaching (NPT) programme in medical schools.
In the academic year 2023/2024, the Newcastle University Medicine Malaysia (NUMed) final-year medical students were involved as near-pear teachers in an NPT programme. This study thus aims to evaluate the outcomes of participation of the final year medical students as near-peer teachers in the student-led near-peer teaching programme and to determine whether the soon-to-be medical graduates can fulfil the “Doctors as Teachers” responsibilities stated by the GMC.
II. METHODS
The NPT Programme was a purely student-led, student-run 3-month teaching programme which provided additional focus on the learning outcomes of the third-year medical curriculum. This programme functioned as an adjunct to the formal curriculum and provided precious opportunities for final-year medical students to improve their teaching skills.
Before the academic year started, invitation email was sent out to recruit final-year medical students to participate voluntarily as the near-peer teachers and the year 3 medical students as the near-peer students. A total of 51 final-year medical students and 100 year 3 medical students signed up for this programme. The near-peer students were randomly assigned to groups of 5 to 6 each, and each group was guided by 3 near-peer teachers. Before the programme commenced, all near-peer teachers were required to attend a mandatory online training course conducted by the lecturers to enhance their presentation and teaching skills.
This programme comprised a total of twelve teaching sessions spanning twelve weeks, covering four sessions of Essential Clinical Placement teaching sessions, four sessions of Case-Based Discussion, one surgical teaching topic and case-based session, one Single Best Answer practice session, one Written Prescribing Exam (WRISKE) session and one Objective Structural Clinical Examination (OSCE) session. Most sessions were delivered virtually (Zoom) or physically, depending on students’ preferences, except for the OSCE session, which was always conducted physically. The teaching materials were prepared by the near-peer teachers beforehand and distributed to the students after each teaching session. The NPT programme coordinator supervised and provided necessary support to both near-peer teachers and near-peer students throughout the entire programme.
The near-peer teachers and near-peer students consented to participate in this study via written consent. A structured post-participation Likert 6-point scale “Peer Tutors Own Assessment” questionnaire with written consent, which was adopted from Liew et al. (2015), was sent to the near-peer teachers after this Near-Peer Teaching Programme via Google form to explore their perceived benefits in three components which are 1) Skills Enhancement, 2) Motivation and 3) Career Direction [Expectation]. This questionnaire (Appendix 1) contains 14 items, with responses scale from strongly disagree (1) to strongly agree (6). Cronbach’s alpha was 0.801, 0.714, and 0.814 for the domains of skills enhancement, motivation, and career direction.
Similarly, all the near-peer students who participated in this near-peer teaching programme were given the Peer Tutor Assessment questionnaire adopted from Liew et al. (2015), to fill in via Google form (Appendix 2). This questionnaire is to assess the acceptability of the teachings of the near-peer teachers. It contains 16 items that evaluate five domains: (1) Responsibility and Respect, (2) Information Processing, (3) Communication, (4) Critical Analysis, and (5) Self-Awareness. Subgroup analyses were conducted to evaluate whether sex and student background affect self-perceived outcomes of near-peer teachers using independent T-test. Each participant was given 3 weeks to complete the questionnaire. Several reminders were sent via email throughout these 3 weeks to each participant to encourage them to fill in the questionnaire. Both near-peer teachers and near-peer students’ data were checked for normality. The asymmetry fell between -1 and +1 and assumed relatively symmetrical and mesokurtic.
III. RESULTS
A total of 51 medical students in their final year signed up as near-peer teachers. Of these, 28 near-peer teachers completed the questionnaire (response rate 54.9%), while 49 out of 100 near-peer students who joined this NPT programme responded in this study (response rate 49.0%). Among those near-peer teachers who responded, there were 9 (32.1%) males and 19 (67.9%) females. More local students responded in this study than international students (75% vs 25%). The overall mean age ± SD of the near-peer teachers is 23.75 ±1.21 years old. For the near-peer students, the overall mean age ± SD is 21.69 ± 0.74 years old. The number of international and local near-peer students who responded was similar. The data of the responses of both near-peer teachers and near-peer students that supports the findings of this study is openly available at Figshare https://doi.org/10.6084/m9.figshare.26886517.v1 (Tang et al., 2024a) and https://doi.org/10.6084/m9.figshare.26886514.v1 (Tang et al., 2024b).
Table 1 showed peer review findings to ensure their voices were represented. To ensure the trustworthiness of the findings, actions were taken to address credibility, dependability, confirmability, transferability, and reflexitivity are outlined in Table 2. Figure 1 indicates the near-peer teachers view of the benefits of involving in the student-led near-peer teaching program.
|
Demographic |
Near-peer Teachers (n,%) |
Near-peer Students (n,%) |
|
Sex |
||
|
Male |
9 (32.1) |
27 (55.1) |
|
Female |
19 (67.9) |
22 (44.9) |
|
Age (Mean ± SD) |
23.75 ±1.21 |
21.69 ± 0.74 |
|
Student background |
||
|
Local |
21 (75) |
28 (57.1) |
|
International |
7 (25) |
21 (42.9) |
Table 1. Demographic data of the near-peer teachers
|
Skills Enhancement |
Mean score +/- SD |
|
Improved own learning skills |
5.21 ± 0.63 |
|
Improved practical teaching skills |
5.39 ± 0.69 |
|
Improved understanding of educational principles |
5.14 ± 0.93 |
|
Increased confidence in speaking to groups |
5.54 ± 0.58 |
|
Improved organisation/planning skills |
5.50 ± 0.64 |
|
Total Mean Score |
5.36 ± 0.53 |
|
Motivation |
|
|
Increased my desire to help fellow students |
4.96 ± 1.14 |
|
Helped me to focus on practical skills |
5.07 ± 0.60 |
|
Revised my own clinical skills |
5.36 ± 0.56 |
|
Increased my desire to emulate good teaching I have had |
5.32 ± 0.61 |
|
Encouraged me to do more |
5.11 ± 0.92 |
|
Total Mean Score |
5.16 ± 0.60 |
|
Career Direction (Expectation) |
|
|
Motivated me to undertake more teaching trainings |
4.96 ± 1.04 |
|
Helped me to decide on my career direction |
4.71 ± 0.94 |
|
Teaching will be a major part of my career |
4.36 ± 1.34 |
|
Enhanced my curriculum vitae |
5.14 ± 0.65 |
|
Total Mean Score |
4.79 ± 0.82 |
|
Total mean score for all domains |
5.11± 0.58 |
Table 2. The mean score (± SD) for the self-evaluation of near-peer teachers in relation to (1) skills enhancement, (2) motivation and (3) career direction (expectation)
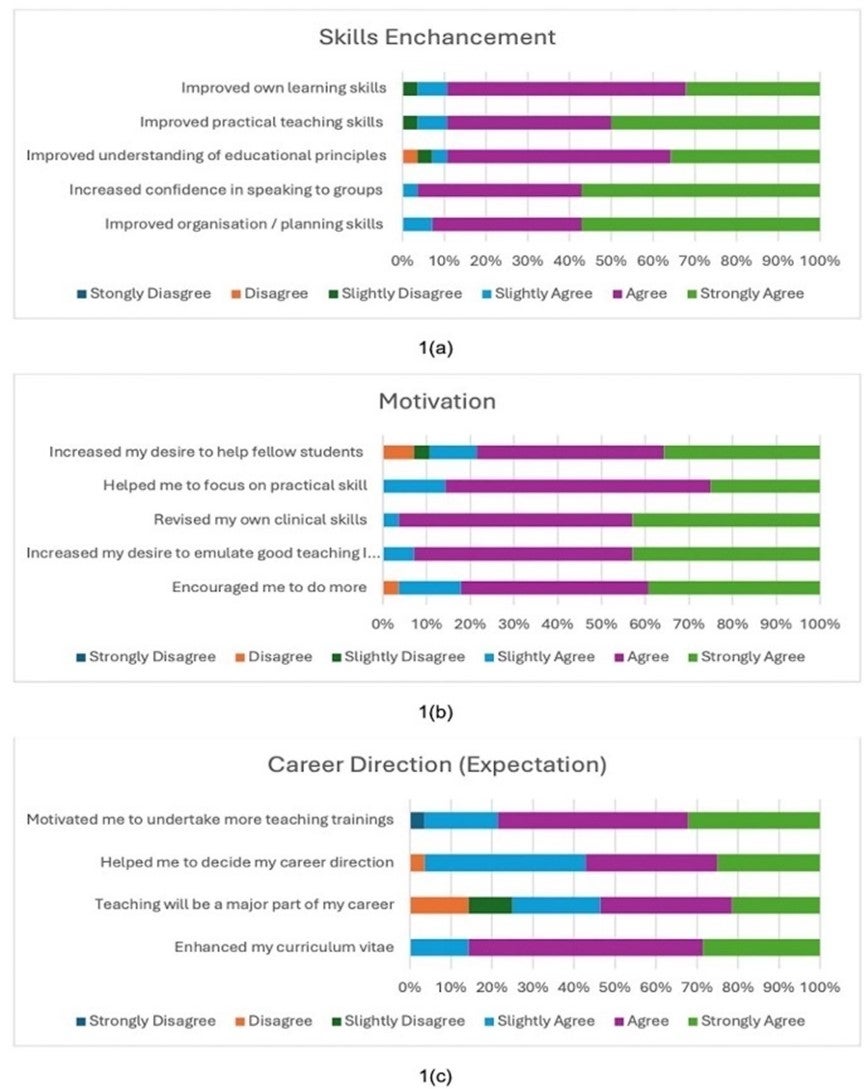
Figure 1. Near-peer teachers view of the benefits of involving in the student-led NPT program: Analysis of post-participation questions responses (n=28) in Likert 6-point scale in relation to (a) skills enhancement, (b) motivation and (c) career direction (expectation)
Based on the responses to the questionnaire, the near-pear teachers widely agreed that the NPT programme positively impacted them (5.11 ± 0.58), with the highest score in the domain of skills enhancement (5.36 ± 0.53), followed by motivation (5.16 ± 0.60) and career direction (4.79 ± 0.82). Most of the near-peer teachers considered this programme improved their skills in terms of teaching, organising, communicating and understanding educational principles (Table 2). 100% of them agreed that this NPT programme increased their confidence in speaking to groups and enhanced their planning and organising skills. Furthermore, all 28 respondents (100%) reported being more motivated to revise their own clinical skills and focus more on their practical skills after teaching near-peer students to address the
knowledge gap. A significant proportion of near-peer teachers felt more encouraged to participate in more teaching programmes in the future (n=27, 96.43%) and more inclined to help fellow students next time (n=25, 89.28%). It is noteworthy that 96.43% of near-peer teachers agreeing that this NPT programme helped in deciding their career direction and motivated them to undertake more trainings. Besides, three quarters of them would consider teaching as their major career pathway in the future, with a mean score of 4.36 ± 1.34. Lastly, all 28 respondents (100%) agreed that joining the NPT programme had enhanced their curriculum vitae (100%).
Table 3 shows the mean score of near-peer students’ evaluation of near-peer teachers in five domains after joining the near-peer teaching programme.
|
Responsibility and Respect |
Mean Score +/- SD |
|
Completed all assigned tasks to the appropriate level |
5.27 ± 0.73 |
|
Completed all assigned tasks on time |
5.08 ± 0.67 |
|
Participated actively in the session |
5.14 ± 0.76 |
|
Showed behaviour and input that facilitated learning |
5.16 ± 0.66 |
|
Was punctual to the session |
5.08 ± 0.89 |
|
Listened and showed respect for the opinions of others |
5.16 ± 0.66 |
|
Total Mean Score |
5.15 ± 0.57 |
|
Information Processing |
|
|
Brought in new information to share with the group |
5.16 ± 0.71 |
|
Provided information that was relevant and helpful |
5.10 ± 0.77 |
|
Seemed to use a variety of resources to obtain the information |
5.10 ± 0.82 |
|
Total Mean Score |
5.12 ± 0.66 |
|
Communication |
|
|
Was able to communicate ideas clearly |
5.10 ± 0.68 |
|
Made comments and responses that were not confusing |
4.92 ± 0.84 |
|
Total Mean Score |
5.01 ± 0.65 |
|
Critical analysis |
|
|
Gave input that was focused and relevant to the case |
4.94 ± 0.75 |
|
Gave a summary of the session |
4.90 ± 0.82 |
|
Gave a summary of the session that showed evidence of reflection and evaluation |
4.94 ± 0.83 |
|
Total Mean Score |
4.93 ± 0.66 |
|
Self-awareness |
|
|
Appeared to be able to acknowledge his/her own strengths and weaknesses |
5.12 ± 0.73 |
|
Accepted and responded to criticism gracefully |
5.10 ± 0.74 |
|
Total Mean Score |
5.11 ± 0.62 |
|
Total mean score for all domains |
5.06 ± 0.51 |
Table 3. The mean score (± SD) for the near-peer students’ evaluation of near-peer teachers after the NPT programme in relation to (1) responsibility and respect, (2) information processing, (3) communication, (4) critical analysis and (5) self-awareness
When asked to evaluate the teaching of their near-peer teachers, the near-peer students considered the near-peer teachers demonstrating positive outcomes in all five domains (5.06 ± 0.51). The near-peer teachers were thought to have a high degree of professionalism in terms of responsibility and respect (5.15 ± 0.57) and self-awareness (5.11 ± 0.62). The most outstanding attribute demonstrated was the ability to complete assigned tasks appropriately (5.27 ± 0.73). Besides, the near-peer teachers performed satisfactorily to process information (5.12± 0.66), communicate (5.01± 0.65) and analyse critically (4.93 ± 0.66). However, the near-peer teachers were identified to score slightly lower in making non-confusing comments and responses (4.92 ± 0.84) as well as giving a summary of the session (4.90 ± 0.82).
|
Variables |
Independent T- test |
|
|
Mean difference (95% CI) |
P-value |
|
|
Sex (Male vs Female) |
||
|
Skills |
-0.101 (-0.549, 0.348) |
0.649 |
|
Motivation |
0.118 (-0.385, 0.621) |
0.634 |
|
Career Direction (Expectation) |
0.507 (-0.154, 1.169) |
0.127 |
|
Students’ background (Local vs International) |
||
|
Skills |
-0.210 (-0.688, 0.268) |
0.376 |
|
Motivation |
-0.276 (-0.810, 0.258) |
0.297 |
|
Career Direction (Expectation) |
0.280 (-0.439, 1.034) |
0.414 |
Table 4. Comparison of self-perceived outcomes of near-peer teachers between male and female, local and international students (Independent t-test)
The independent t-test were performed to find out the association between sex and perceived outcomes of the near-peer teachers. Our study revealed that it is statistically insignificant between male and female in the perceived benefits for skills (P = 0.649), motivation (P = 0.549) and career direction (P = 0.127).
Besides, there is no correlation between students’ background and the three measured outcomes. There is statistically insignificant between local and international students in term of skills (P = 0.376), motivation (P = 0.397) and career direction (P = 0.414).
IV. DISCUSSION
This study provides valuable insights into the background and characteristics of the final-year medical students who voluntarily participated in a student-led, student-run NPT programme. The outcomes of their participation concerning their perceived benefits in terms of skills, motivation, and expectations were investigated. Overall, the near-peer teachers reported that this NPT programme helped them tremendously to improve their skills in terms of learning and teaching, which might be driven by their primary motive for joining this programme. This finding was similar to previous studies, which showed skills enhancement in volunteer near-peer teachers (Buckley & Zamora, 2007; Liew et al., 2015). Our study further reaffirms the plausibility of a student-run NPT programme to enhance teaching and learning skills. However, due to the voluntary nature of participation in this near-peer teaching programme, the students who are likely most in need of skill enhancement may have been omitted from this programme, and they might be less equipped to teach after they graduate. Some studies recommended more incentives to be given to such students to encourage them to make use of the opportunities offered (Buckley & Zamora, 2007).
The motivation evaluated includes both self-actualising inner motivations to improve their clinical and practical skills and the external, tangible desire to help fellow students. The high motivation score suggests the reinforcement of a desirable attitude towards future educational and teaching responsibilities, which matches the GMC’s emphasis on the teaching role of doctors (General Medical Council, 2015). A couple of reasons may explain this: firstly, the near-peer teachers are final-year medical students, who will sit for their final examinations very soon and are desperately finding ways to improve their learning. The process of teaching, which requires extensive preparation, a comprehensive understanding of the content, dynamic synthesis, and anticipation of the questions that may be asked of them, forms an efficient learning strategy. Secondly, the near-peer teachers, inspired by the excellent teaching they once had, wish to impart good teaching to the near-peer students going through the same journey.
Although many near-peer teachers are more motivated to be involved in more teaching and even take up teaching training courses in the future, the influence is not apparent in the long-term career direction. This could be explained well by the brief intervention of this NPT programme that lasted 3 months. However, the lucrative income opportunities in other medical specialities and the limited exposure to medical education pathways in undergraduate medical schools are some factors that may sway them away from considering medical education as their primary career pathway (Puri et al., 2021; Sarikhani et al., 2021). Therefore, more effort should be directed to increase teaching opportunities and to raise awareness of medical education career options in the undergraduate medical school programme. This includes developing Student Selected Components focusing on medical education and giving opportunities to shadow clinical teaching staff (Liew et al., 2015; Wilson et al., 2008).
After participating in this study, the near-peer students evaluated the near-peer teachers highly in all the domains. This provides a strong indication of the recognition and acceptance of the teaching skills of the near-peer teachers. In addition, the ability of the near-peer teachers to demonstrate responsibility and respect throughout this programme shows their preparedness to work under the GMC with desirable attitudes and professionalism. Previous studies have also shown that near-peer teachers gain more subjectively and objectively than students (Liew et al., 2015; Ten Cate & Durning, 2007). This can be related to the underpinning of the psychological and social theories behind the dynamics between near-peer teachers and near-peer students (Loda et al., 2019). The theoretical model of cognitive and social congruence explains the positive evaluation of the near-peer teachers (Loda et al., 2019; Rollmann et al., 2023). The proximity of age between the near-peer teachers and the near-peer students enables them to share similar knowledge frameworks, language and social roles. Besides, near-peer teachers are perceived to be more approachable and understanding of the needs and struggles of the near-peer students. This may be because the near-peer teachers have had similar experiences themselves. Therefore, near-peer teachers are better able to process difficult concepts and frameworks, emphasize the key points, and communicate the information using familiar and non-confusing language to ensure that near-peer students comprehend better (Loda et al., 2019; Loda et al., 2020). The perceived barrier to providing feedback to near-peer teachers is also lower compared to faculty-led staff, as the age difference between them is much smaller. This might suggest why near-peer teachers feel less offended by criticism and are more likely to accept and respond to criticism gracefully (Loda et al., 2019). Nevertheless, the near-peer students thought that some near-peer teachers experienced some difficulties in giving relevant input and summary of the sessions, thus necessitating more structured pedagogical training for near-peer teachers in this aspect. Mastering these teaching skills would allow the near-peer students to appreciate better the big picture and key takeaway points of each lesson (Khaw & Raw, 2016).
One of the focuses of this study is to analyse the sex-specific difference of the perceived outcomes of the near-peer teachers. Although there is an appropriate twice female near-peer teachers who responded to this study compared to male near-peer teachers, the results shows that the sex-specific difference in the perceived improvement in motivation, skills and career direction is not significant. There is no sex-specific difference in term of enthusiasm and motivation to involve in near-peer teaching (Messerer et al., 2021). Throughout the whole process, they receive similar gender-equitable support and guidance without any discrimination.
V. LIMITATIONS AND RECOMMENDATIONS
As few studies have reported outcomes for a purely student-led student-run NPT programme, this study offers valuable insights concerning the perceived benefits for near-peer teachers. However, this study has several limitations. Firstly, given the relatively small sample size of the near-peer teachers and the subjective nature of the self-reported questionnaire, the results may benefit from further objective testing, such as correlation with examination results. Secondly, this study is only carried out in a single medical school, with a slight variation in the implementation of the NPT compared to other institutions. Verification of these results across various medical schools would strengthen these findings. This study thus calls for more structured student-led peer teaching programmes to be implemented in more medical schools and to be assessed longitudinally to evaluate the association between the student-led peer teaching programme and the outcomes of participation of the near-peer teachers. It may also be worthwhile to investigate and assess the perspective of near-pear teachers who demonstrated interest in medical education, as well as to evaluate the long-term outcomes in career direction for medical graduates who once participated in near-peer teaching programmes.
VI. CONCLUSION
In conclusion, this purely student-led, student-run near-peer teaching programme likely improved the final-year medical students in fulfilling the “Doctors as Teachers” responsibilities outlined by the GMC. Besides, the near-peer teachers also reported having positive outcomes in their skills and career direction. Likewise, from the perspective of the near-peer students, the near-peer teachers demonstrated outstanding skills and professionalism in all five domains: responsibility and respect, information processing, communication, critical analysis and self-awareness. Possessing the skills and professionalism fulfils the expectations of GMC for healthcare professionals to provide the right care at the right time with the right skills for the good of patients.
Notes on Contributors
Kevin Xuan Hong Tang was a final year medical student who conceptualised and designed the study, reviwed the literature, conducted the data collection and analysis, prepared the figures and wrote the manuscript.
Koon Kee Teo was a final year medical student who reviewed the literature, collected and analysed the data, prepared the figures and helped in writing the manuscript.
Kye Mon Min Swe is an Associate Professor in Education Research in NUMed. She participated in conceptualising the study, performed statistical analysis and drafted, reviewed and edited the manuscript. All the authors have read and approved the final manusript.
Ethical Approval
This study titled “Embracing Doctors as Teachers: Evaluating the Student-led Near-Peer Teaching at Transnational Campus” was approved by the Research Management Committee and the Newcastle University Ethics Committee (Approval number 45070/2023).
Data Availability
The data that support the findings of this study are openly available in Figshare repository, as below,
https://doi.org/10.6084/m9.figshare.26886517.v1 (Tang et al., 2024a) and
https://doi.org/10.6084/m9.figshare.26886514.v1 (Tang et al., 2024b).
Acknowledgement
The authors would like to thank the NUMed Medical Education Society for carrying out this programme. The authors are grateful for Professor Vishna Devi Nadarajah for her support and feedback in this research.
Funding
The authors declare that there is no funding received in this study.
Declaration of Interest
The authors declare that there is no conflict of interest.
References
Botelho, M. G., Boubaker, B., & Wong, I. B. (2022). Near‐peer teaching for learning clinical photography skills: Perceptions of students. European Journal of Dental Education, 27(3), 477–488. https://doi.org/10.1111/eje.12831
Buckley, S., & Zamora, J. (2007). Effects of participation in a cross year peer tutoring programme in clinical examination skills on volunteer tutors’ skills and attitudes towards teachers and teaching. BMC Medical Education, 7(1), Article 20. https://doi.org/10.1186/1472-6920-7-20
Burgess, A., McGregor, D., & Mellis, C. (2014). Medical students as peer tutors: A systematic review. BMC Medical Education, 14(1), Article 115. https://doi.org/10.1186/1472-6920-14-115
Busari, J. O., Prince, K. J., Scherpbier, A. J., Van Der Vleuten, C. P., & Essed, G. G. (2002). How residents perceive their teaching role in the clinical setting: A qualitative study. Medical Teacher, 24(1), 57-61. https://doi.org/10.1080/00034980120103496
Cook, V., Fuller, J. H., & Evans, D. E. (2010). Helping students become the medical teachers of the future – The Doctors as Teachers and Educators (DATE) programme of Barts and the London School of Medicine and Dentistry, London. Education for Health, 23(2), 415. https://doi.org/10.4103/1357-6283.101487
De Menezes, S., & Premnath, D. (2016). Near-peer education: A novel teaching program. International Journal of Medical Education, 7, 160–167. https://doi.org/10.5116/ijme.5738.3c28
Frearson, S., & Gale, S. (2017). Educational opportunities on a ward round; utilising near-peer teaching. Future Healthcare Journal, 4(1), 19–22. https://doi.org/10.7861/futurehosp.4-1-19
Furmedge, D. S., Iwata, K., & Gill, D. (2014). Peer-assisted learning – Beyond teaching: How can medical students contribute to the undergraduate curriculum? Medical Teacher, 36(9), 812–817. https://doi.org/10.3109/0142159x.2014.917158
General Medical Council. (2011, February). Developing teachers and trainers in undergraduate medical education. Retrieved June 2, 2024, from https://www.gmc-uk.org/-/media/documents/developing-teachers-and-trainers-in-undergraduate-medical-education—guidance-0815_pdf-56440721.pdf
General Medical Council. (2015, July). Outcomes for graduate (Tomorrow’s doctors). Retrieved June 2, 2024, from https://www.gmcuk.org//media/documents/Outcomes_for_graduates_ Jul_15_1216.pdf_61408029.pdf
General Medical Council. (2023, August 22). Good medical practice. Retrieved June 2, 2024, from https://www.gmc-uk.org/-/media/documents/good-medical-practice-2024—english-102607294.pdf
Hardie, P., O’Donovan, R., Jarvis, S., & Redmond, C. (2022). Key tips to providing a psychologically safe learning environment in the clinical setting. BMC Medical Education, 22(1), Article 816. https://doi.org/10.1186/s12909-022-03892-9
Hettle, D., & Morgan, J. (2019 December 2-3). “Teaching and Training for the future”: Final-year students’ perspectives on their role as near-peer teachers” [Conference presentation abstract]. Developing Excellence in Medical Education, Manchester. https://www.researchgate.net/publication/344439487_Teaching_and_Training_for_the_future_Finalyear_students’_perspectives_on_their_role_as_near-peer_teachers
Khaw, C., & Raw, L. (2016). The outcomes and acceptability of near-peer teaching among medical students in clinical skills. International Journal of Medical Education, 7, 189–195. https://doi.org/10.5116/ijme.5749.7b8b
Knobloch, A. C., Ledford, C. J., Wilkes, S., & Saperstein, A. K. (2018). The impact of near-peer teaching on medical students’ transition to clerkships. Family Medicine, 50(1), 58–62. https://doi.org/10.22454/fammed.2018.745428
Liew, S., Sow, C., Sidhu, J., & Nadarajah, V. D. (2015). The near-peer tutoring programme: embracing the ‘doctors-to-teach’ philosophy – A comparison of the effects of participation between the senior and junior near-peer tutors. Medical Education Online, 20(1), 27959. https://doi.org/10.3402/meo.v20.27959
Loda, T., Erschens, R., Loenneker, H., Keifenheim, K. E., Nikendei, C., Junne, F., Zipfel, S., & Herrmann-Werner, A. (2019). Cognitive and social congruence in peer-assisted learning – A scoping review. PloS One, 14(9), e0222224. https://doi.org/10.1371/journal.pone.0222224
Loda, T., Erschens, R., Nikendei, C., Giel, K., Junne, F., Zipfel, S., & Herrmann-Werner, A. (2020). A novel instrument of cognitive and social congruence within peer-assisted learning in medical training: construction of a questionnaire by factor analyses. BMC Medical Education, 20(1), Article 214. https://doi.org/10.1186/s12909-020-02129-x
Messerer, D. A. C., Kraft, S. F., Horneffer, A., Messerer, L. A. S., Böckers, T. M., & Böckers, A. (2021). What factors motivate male and female Generation Z students to become engaged as peer teachers? A mixed‐method study among medical and dental students in the gross anatomy course. Anatomical Sciences Education, 15(4), 650–662. https://doi.org/10.1002/ase.2114
Pierce, H., Kermack, A., & Foley, V. (2024). What training do foundation doctors feel they require to develop as clinical teachers? Journal of Education and Training Studies, 12(2), 106–113. https://doi.org/10.11114/jets.v12i2.6714
Puri, P., Landman, N., Smoldt, R. K., & Cortese, D. (2021). Quantifying the financial value of clinical specialty choice and its association with competitiveness of admissions. Curēus, 13(2), e13272. https://doi.org/10.7759/cureus.13272
Qureshi, Z., Gibson, K., Ross, M., & Maxwell, S. (2013). Perceived tutor benefits of teaching near peers: Insights from two near peer teaching programmes in South East Scotland. Scottish Medical Journal, 58(3), 188–192. https://doi.org/10.1177/0036933013496935
Rollmann, I., Lauter, J., Kuner, C., Herrmann-Werner, A., Bugaj, T. J., Friederich, H., & Nikendei, C. (2023). Tutors ́ and students’ agreement on social and cognitive congruence in a Sonography peer-assisted-learning scenario. Medical Science Educator, 33(4), 903–911. https://doi.org/10.1007/s40670-023-01814-y
Ross, M. T., & Cameron, H. S. (2007). Peer assisted learning: A planning and implementation framework: AMEE Guide no. 30. Medical Teacher, 29(6), 527–545. https://doi.org/10.1080/01421590701665886
Sarikhani, Y., Ghahramani, S., Bayati, M., Lotfi, F., & Bastani, P. (2021). A thematic network for factors affecting the choice of specialty education by medical students: A scoping study in low-and middle-income countries. BMC Medical Education, 21(1), Article 99. https://doi.org/10.1186/s12909-021-02539-5
Tang, K. X. H., Teo, K. K., & Swe, K. M. M. (2024a). The evaluation of near-peer teachers in five domains completed by near-peer students after joining peer teaching program (Version 1) [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.26886517.v1
Tang, K. X. H., Teo, K. K., & Swe, K. M. M. (2024b). Near-peer teachers self-evaluation data after joining peer teaching program (Version 1) [Data set]. Figshare. https://doi.org/10.6084/m9.fig share.26886514.v1
Ten Cate, O., & Durning, S. (2007). Dimensions and psychology of peer teaching in medical education. Medical Teacher, 29(6), 546–552. https://doi.org/10.1080/01421590701583816
Wilson, S., Denison, A. R., & McKenzie, H. (2008). A survey of clinical teaching fellowships in UK medical schools. Medical Education, 42(2), 170–175. https://doi.org/10.1111/j.1365-2923.2007.02933.x
Yu, T. C., Wilson, N. C., Singh, P. P., Lemanu, D. P., Hawken, S. J., & Hill, A. G. (2011). Medical students-as-teachers: A systematic review of peer-assisted teaching during medical school. Advances in Medical Education and Practice, 2, 157–172. https://doi.org/10.2147/amep.s14383
Zheng, B., & Wang, Z. (2022). Near-peer teaching in problem-based learning: Perspectives from tutors and tutees. PloS One, 17(12), e0278256. https://doi.org/10.1371/journal.pone.0278256
*Kye Mon Min Swe
1, Jalan Sarjana 1, Educity,
79200 Iskandar Puteri, Johor, Malaysia
Email: kye-mon.min-swe@newcastle.edu.my
Submitted: 13 June 2024
Accepted: 4 February 2025
Published online: 1 July, TAPS 2025, 10(3), 26-36
https://doi.org/10.29060/TAPS.2025-10-3/OA3439
Humairah Zainal1, Xin Xiaohui1, Julian Thumboo1,2,3 & Fong Kok Yong2,3
1Health Services Research Unit, Singapore General Hospital, Singapore; 2Department of Rheumatology and Immunology, Singapore General Hospital, Singapore, 3Duke-NUS Medical School, National University of Singapore, Singapore
Abstract
Introduction: As healthcare becomes increasingly digital, undergraduate medical students receive limited formal training in digital healthcare technologies (DHTs). Additionally, stakeholders’ perspectives on essential digital health competencies (DHCs) across generations remain underexplored. This comparative study aims to identify knowledge gaps, inform evolving expectations, and promote continuous learning by comparing medical students’ and senior clinicians’ views on essential DHCs in Singapore.
Methods: Individual semi-structured interviews were conducted with medical students, clinical educators, and clinical teachers. Clinical-year medical students from all three local medical schools were recruited using convenience and snowball sampling, while purposive sampling ensured diverse representation of clinicians across Singapore’s public healthcare organisations, focusing on those engaged in education-related activities. Data were collected from September 2020 to February 2023 until thematic saturation was achieved, and analysed using qualitative thematic analysis.
Results: Sixty-three participants took part, including 30 medical students, 12 clinical educators and 21 clinical teachers. All clinicians had more than 10 years of clinical experience and came from 24 different disciplines and 12 healthcare institutions. The findings showed unanimous support for integrating electronic health records in patient communication, and training in DHTs like telemedicine and point-of-care ultrasound. Discrepancies emerged; clinicians prioritised physical examination, while students viewed it as potentially replaceable by DHTs. Furthermore, while students valued healthcare-related smartphone applications in patient care, few clinicians shared this view, citing privacy and security concerns.
Conclusion: Evaluating stakeholders’ perspectives highlights evolving clinical skills and essential DHCs for medical students, potentially informing global DHC training programmes.
Keywords: Technology, Medical Education, Curriculum, Clinical Competence, Digital Competence, Qualitative, Singapore
Practice Highlights
- An inter-generational perspective in medical education leverages the strengths of both medical students and senior clinicians, ensuring a balanced approach that keeps pace with technological advancements while maintaining the core principles of patient care.
- The digital health competencies deemed essential for future clinical practice are consistent across all stakeholders.
- The study highlights the emerging need for additional competencies among medical trainees so as to meet the evolving demands of healthcare delivery.
- Regularly comparing the perspectives of various stakeholders in the healthcare system enables educational institutions to adapt and refine their curricula continuously.
I. INTRODUCTION
Digital healthcare, which leverages advanced technologies to enhance, complement, or replace traditional healthcare services, is becoming increasingly common in clinical practice (Alkire (née Nasr) et al., 2020). Digital healthcare technologies (DHTs) such as electronic health records (EHR), telemedicine, and Artificial Intelligence (AI) have significantly improved data management, diagnostics, and patient care (Clay-Williams et al., 2023; Food and Drug Administration, 2019; Welcher et al., 2018;). However, many studies and reviews have highlighted a global lack of formal and systematic training in DHTs for undergraduate medical students (Aungst & Patel, 2020; Edirippulige et al., 2018; Tudor Car et al., 2021). While recommendations for integrating digital health education (DHE) exist, they often propose standalone courses focused on specific DHTs rather than embedding DHE into the core medical curriculum (Tudor Car et al., 2021; Zainal et al., 2023a; Zainal et al., 2023b). Barriers to consistently incorporating DHE into medical curricula, as reported in countries such as Canada, Germany, the United Kingdom (U.K.), and the United States (U.S.) include limited faculty expertise, curriculum overload and fragmented implementation efforts (Gillissen et al., 2022; Hurley et al., 2011; Machleid et al., 2020; Sit el al., 2020; Sorg et al., 2022).
Furthermore, there is limited research exploring the perspectives of both medical students and senior clinicians on the relevant digital health competencies (DHCs) required for clinical care. DHCs encompass the knowledge, skills, and attitudes essential for assessing, diagnosing, and treating patients in the digital age. An inter-generational comparison of these perspectives is crucial for identifying gaps in the existing curricula and ensuring medical education aligns with the rapidly evolving healthcare landscape. Medical students can offer fresh insights into emerging tools and platforms while senior clinicians can contribute perspectives on clinical skills given their wealth of clinical experience.
Despite Singapore’s advanced digitalisation, challenges remain in standardising DHE across its three medical schools: Yong Loo Lin School of Medicine at National University of Singapore (NUS), Lee Kong Chian School of Medicine at Nanyang Technological University (NTU) and Duke-NUS Medical School (Duke-NUS) (Zainal et al., 2023a). Although these institutions boast state-of-the-art facilities, a disconnect persists between medical training and clinical practice due to various institutional and structural barriers (Zainal et al., 2023a). While efforts to integrate DHE, such as virtual reality courses, have been initiated, there are variations in content and duration across institutions, underscoring the lack of a standardised approach (Zainal et al., 2023a).
This study uses Singapore as a case study to explore the perceptions of medical students, clinical educators, and teachers regarding DHCs, with the aim of improving DHE integration into undergraduate medical curricula. Specifically, it compares the views of these stakeholders in identifying any digital competencies that may be relevant for clinical practice in an increasingly digital healthcare landscape. By focusing on Singapore, this study not only sheds light on gaps in the local curricula but also provides insights that can inform global efforts to strengthen DHE integration in medical education.
II. METHODS
A. Setting and Sample
A qualitative study was conducted using individual semi-structured interviews with medical students, clinical educators, and clinical teachers. Participants were identified by Principal Investigator (P.I.) FKY, based on their year of study and clinical roles respectively, ensuring relevant knowledge and experience.
The study employed a combination of convenience sampling and snowballing technique to recruit students from all three local medical schools. Clinical-year students (third to fifth years) were included due to their potential exposure to DHTs during clinical rotations, while pre-clinical students were excluded. Convenience sampling was initially used for ease of access, and snowballing technique was subsequently employed to expand participation and capture diverse perspectives.
To ensure diverse representation among clinicians, purposive sampling was applied across Singapore’s three public healthcare organisations. Clinical educators dedicating over 20 per cent of their time to education-related activities (e.g., teaching, curriculum planning, research, and administration) and clinical teachers contributing less than 20 per cent of their time to such roles were included. Clinicians not involved in educational roles were excluded from the study.
This study was classified as a quality improvement (QI) project on medical education curricula by the SingHealth Research Integrity, Compliance, and Ethics (RICE) committee. As such, it did not meet the criteria for human subject research and was granted an ethical waiver by SingHealth Institutional Review Board (Reference Number: 2020/2880). Nonetheless, this research adhered strictly to the ethical principles of the Declaration of Helsinki and institutional guidelines.
Data collection occurred from September 2020 to February 2023. Participants were invited by the P.I. via email detailing the study’s purpose, procedures, potential risks, and benefits, with consent obtained before the interviews. To address potential biases due to the P.I.’s professional relationships, interviews were conducted by a research fellow without prior connections to participants. Verbal consent was recorded at the start of each Zoom session, and participants were reminded of their right to withdraw, with pre-withdrawal data retained for comprehensive analysis.
To ensure anonymity, participants were assigned coded identifiers (‘MS’ for medical students, ‘CL’ for clinicians). Identifying information and audio recordings were securely stored and separated from the main dataset. Results were reported with care to avoid identifying individuals, and the data was exclusively used for curriculum development.
B. Data Collection
The interview guide followed Kallio et al.’s (2016) framework, including pre-requisites for semi-structured interviews, literature review, expert consultation, preliminary guide development, pilot testing with five participants, and finalisation. Questions addressed clinical competencies, their relevance to digital healthcare, and ways medical schools can better prepare students for digitalisation (Tables 1 and 2). Interviews included medical students and clinicians across specialties to ensure diverse perspectives.
The study involved 63 participants, with sample size guided by theoretical and practical considerations. Data collection continued until thematic saturation was reached, ensuring all relevant perspectives were captured. Practical constraints like time and resources influenced the participant number, but the focus remained on data richness and diversity for a comprehensive exploration of the research questions.
Sixty interviews were conducted via Zoom due to COVID-19 restrictions, with three in-person interviews held under local health guidelines. Each session lasted about 40 minutes and was audio-recorded. Transcriptions were generated using Otter AI and reviewed for accuracy by the P.I. and research fellow.
|
No. |
Topics |
Questions and prompts |
|
1. |
Clinical skills that doctors should have |
In general, what are the clinical skills that a medical doctor should have? Are there any clinical skills that have become less essential or relevant in this digital age? Are there any other clinical skills that have been fulfilled or transformed by digital technology? What new skills, clinical or otherwise, should a medical doctor have today and in the future especially in light of the digital age? |
|
2. |
Medical school curriculum |
Do you think the clinical skills taught in your medical school have adequately prepared you for clinical practice, especially in today’s modern setting? Prompts: – Are there any modules in your formal curriculum that might have exposed you to the digital aspects of medicine, such as telemedicine, AI or healthcare informatics? – Are you aware of any elective courses or programmes that might have done the same? |
|
3. |
Exposure to digital technologies in clinical practice |
Have you ever adopted or come across any forms of digital technology such as robotics surgery, AI or big data in your clinical practice yet? Prompts: – If yes, where did you encounter this? – What digital healthcare technologies would you be interested in learning if given the opportunity, and why? |
|
4. |
Experience with digital technologies |
Have you ever encountered any recurring challenges in clinical practice that you foresee could be overcome by digital technologies? |
|
5. |
Role of various stakeholders |
What do you think medical schools can do to help doctors optimise the use of digital healthcare technologies in the future? What do you think professional bodies such as Singapore Medical Association (SMA) and Academy of Medicine can do to help doctors make full use of digital healthcare technologies in the future? What do you think the government can do to help doctors optimise the use of digital healthcare technologies in the future? |
|
6. |
Other thoughts on how the medical school curriculum can better prepare students |
Do you have any other comments on how the medical school curriculum can better prepare you for future clinical practice? Any other comments on digital transformations of medicine or healthcare before we end this interview? |
Table 2. Interview questions for clinical educators and teachers
C. Data Analysis
Thematic analysis followed Braun and Clarke’s six-step framework to explore curricular gaps (Braun & Clarke, 2006). Two researchers independently coded the data, resolving discrepancies through discussion to refine the codebook and ensure consistency. Credibility was enhanced by triangulating findings across participants from various medical schools and healthcare clusters, capturing diverse perspectives and minimising bias.
To contextualise the findings, comparisons were made with studies from other high-income countries undergoing similar healthcare digitalisation. Additionally, recent data from stakeholders, including medical school leaders, were analysed to understand the digital competencies needed for future clinical practice. Reporting adhered to the Standards for Reporting Qualitative Research (O’Brien et al. 2014).
III. RESULTS
Sixty-three participants took part in our study. Thirty of them were medical students who were undergoing clinical rotations in various disciplines, with 10 coming from each school. Twelve were clinical educators and 21 were clinical teachers. The clinicians were aged between 44 and 70 years. All had more than 10 years of clinical experience and came from 24 different disciplines and 12 healthcare institutions. A summary of their demographics is reported in Table 3 and illustrative excerpts are found in Table 4.
|
Profile |
Number of participants |
||||||||||||
|
Gender |
|
||||||||||||
|
Medical students: Male Female |
15 (50%) 15 (50%) |
||||||||||||
|
Clinical educators and teachers: Male Female |
26 (78.8%) 7 (21.2%) |
||||||||||||
|
Year of study/ specialty |
|
||||||||||||
|
Medical students: Third year Fourth year Fifth year |
8 (26.7%) 14 (46.7%) 8 (26.7%) |
||||||||||||
|
Clinical educators and teachers:
|
|||||||||||||
Table 3. Demographics of participants
Four major themes were derived from the data.
A. Limited and Inconsistent Exposure to DHTs
Students reported limited exposure to DHTs in core medical curricula, with training mainly through electives, select programmes, and student-driven initiatives. Exposure to health informatics and telemedicine was brief, with telemedicine training primarily prompted by the COVID-19 pandemic. Other DHTs like robotic surgery, virtual reality, and POCUS were inconsistently incorporated across medical schools. Some clinicians also reiterated the need for DHT exposure in public healthcare institutions, as doing so could inspire medical students to engage in innovation, research, and development in cutting-edge fields like robotics.
B. Unified Views among Clinicians and Students on Essential Competencies
Clinicians and students shared unified perspectives on incorporating key DHCs like EHR, telemedicine, and POCUS into medical curricula. These competencies are viewed as crucial for preparing students for contemporary clinical practice.
Participants emphasised the need to balance EHR use with effective patient interaction. M25, a third-year student, highlighted the importance of maintaining empathy and humanistic values, while CL27, a rheumatologist, stressed integrating EHR data into patient discussions to improve engagement and understanding of health conditions.
All groups also agreed on the importance of telemedicine training. Students expressed interest in learning how to identify conditions suitable for virtual consultations, build patient rapport, and conduct comprehensive assessments via tele-platforms. MS5 noted the challenges of teleconsultation, such as interpreting body language and addressing legal responsibilities. Clinicians like CL14 underscored the need to teach students how to select patients for teleconsultation and identify red flags effectively.
Additionally, both clinicians and students strongly supported incorporating POCUS into the curriculum. Students acknowledged its utility in bedside diagnostics, while clinicians like CL9 and CL18 highlighted its value in resource-limited settings and its role in enhancing diagnostic accuracy. They advocated for routine training in ultrasound, considering its increasing use in general practice and as a critical tool in diverse healthcare settings. These unified views suggest the need to prioritise these DHCs in medical education to meet the evolving demands of healthcare delivery.
C. Divergent Opinions on Traditional Clinical Skills
Discrepancies in opinions emerged regarding traditional clinical skills, particularly physical examination. Students often viewed diagnostic imaging and tests as superior to these skills, perceiving physical exams as less critical. For instance, M11, a Year 4 student, argued that ultrasonography provides more precise diagnoses, making physical examination less relevant.
Clinicians, however, emphasised preserving traditional skills like history-taking and physical examination, especially for resource-limited settings. CL3, an ophthalmologist, expressed concern that reliance on diagnostic tools has led to the erosion of these essential skills.
D. Emerging Technologies and Concerns
The perceived competencies for medical education varied between students and senior clinicians. Students valued wearables and healthcare apps for patient empowerment, personalised care, and strengthening doctor-patient trust. For instance, MS30, a fourth-year student, suggested that wearable data could help create personalised care plans and enhance clinical practice.
Clinicians, however, expressed concerns about the privacy and security of patient data in these apps. They emphasised the responsibility to protect patient information and were cautious about using apps that did not meet security standards. These differing opinions highlight the need for a DHE curriculum that addresses both student interests and clinician concerns.
In our sample selection, we included both clinical educators and clinical teachers to capture a range of perspectives on the integration of DHCs into medical education. However, our analysis did not reveal significant differences in the views expressed by these two groups. Both shared similar opinions on the importance of teaching DHCs such as EHR, telemedicine and POCUS. This alignment may be attributed to their shared roles in preparing medical students for clinical practice, regardless of their specific titles or responsibilities. As such, the findings reflect a unified perspective among clinicians involved in medical education, despite the initial distinction made in the sample selection.
|
Themes |
Quotes from Participants |
|
Limited and inconsistent exposure to DHTs |
In private practice, particularly in Family Medicine, telemedicine is fairly common. But I don’t think it is a model that has been adopted in public hospitals or tertiary settings yet… Telemedicine is a new thing that only came up because of COVID. (MS10, Year 4) In Korea, medical students are already exposed to advanced medical robots, with 40 robots used in operating theaters. Introducing a robotics module for medical students could spark interest and lead to innovations in robotics and research. (CL20, Otorhinolaryngology) |
|
Essential competencies for clinical practice |
EHR: A skill that should be taught to students is the ability to strike a balance between facing the screen and interacting with patients. In clinics, you need to face the computer to scribe your notes while talking to the patient. (MS8, Year 5). In the United States, students are trained in communication skills that incorporate electronic medical records into patient interactions. This training is lacking here, which is why patients often complain that doctors focus too much on the computer screen during consultations. (CL27, Rheumatology) Telemedicine: I wish to be adept at performing teleconsultation, as this seems to be the up-and-coming practice. But with this comes many ambiguities such as reading body language, building rapport, and with that comes legal liabilities and responsibilities, like what exactly are the conditions that are suitable for teleconsultation, what are the ways to circumvent issues with teleconsultation and how to best integrate it into a patient’s individualized care. (MS5, Year 5) A skill students need to learn is how to interact well in a non-face-to-face context, like in a tele-setting. They need to learn how to select patients appropriately and spot red flags. (CL14, Respiratory Medicine) POCUS: Ultrasound is currently not taught routinely to students. It is important to know ultrasound because a lot of GPs are now using it in their clinics as an adjunct to diagnosing conditions and confirm clinical examinations. (CL9, General Surgery) Every medical student should learn ultrasound. It’s a useful skill for those who may work in developing countries, where they may need to provide treatment directly at the point of care. (CL18, Orthopaedic Surgery) |
|
Divergent opinions on traditional clinical skills |
Students’ perspective: When it comes to clinical signs, if a patient has a mildly enlarged liver, if we are able to feel it, we can actually do tests like ultrasound or further testing to know exactly the length, size or span of the liver. So, it doesn’t actually matter whether you feel it on the physical examination or not. (M11, Year 4) When assessing heart murmurs in patients with heart conditions, it is not always important to precisely diagnose the type of murmur, as an echocardiogram will ultimately provide the exact diagnosis. Similarly, for cases like detecting abdominal masses, even if physical examination is challenging, such as with obese patients, an ultrasound can be readily ordered to confirm the findings. (MS11, Year 4) Clinicians’ perspective: As doctors become more dependent on investigation findings and diagnostic tests, I do see basic skills such as history-taking and physical examination skills have eroded. (CL3, Ophthalmology) Imaging has somewhat replaced traditional clinical examination skills, but these skills remain important and relevant. I still emphasise teaching clinical examination as a fundamental component before turning to imaging. However, most schools now default to imaging, which might be a drawback of technological advances. We need to strike a balance by ensuring clinical examination skills are adequately taught alongside imaging. (CL9, General Surgery) |
|
Emerging technologies and concerns · Wearables and healthcare apps |
We should empower patients by improving their access to reliable medical knowledge. In this modern era, trustworthy and accurate apps can be valuable tools for disseminating information, such as red flags patients should be aware of. Apps offering verified and relevant information could greatly benefit patients by providing better guidance than what they might find through general online searches. (MS17, Year 3) Health trackers, like wearable devices for cardiovascular or gynaecological health, hold great potential. If doctors are equipped with the knowledge to interpret the data generated by these devices—many of which patients already use voluntarily—it could significantly enhance clinical practice. (MS30, Year 4) |
Table 4. Illustrative quotes from interviews with participants
IV. DISCUSSION
This study contributes to the literature by comparing the views of medical students, clinical educators, and clinical teachers on essential competencies for medical school curricula. It highlights a consensus on the need for training in EHR, telemedicine, and POCUS, while also identifying emerging needs like interpreting data from healthcare devices and engaging patients with this data. Unlike previous studies that focused on either clinicians or students (Blacketer et al., 2021; Foadi et al., 2021; Gillissen et al., 2022; Hersh et al., 2017; Liu et al., 2022; Machleid et al., 2020; Pontefract & Wilson, 2019), this research explores inter-generational differences, revealing that younger trainees prioritise patient-centred care and digital health literacy. This emphasis on inclusivity and data literacy is crucial given the global challenge of inadequate health literacy, particularly among older populations (Sørensen et al., 2021; Wittink & Oosterhaven, 2018). Integrating these competencies into curricula can foster ongoing improvement in medical education.
In comparing the views of medical students and senior clinicians regarding DHCs, it is important to acknowledge that the latter group represents a diverse range of roles within the clinical environment. While this study focused specifically on clinicians involved in medical education, senior clinicians may also take on roles as clinical researchers, administrators, or leaders in healthcare innovation. These differing responsibilities could shape their perspectives on the DHCs that should be emphasised in medical curricula. The results of this study should be interpreted within the context of the clinical educators’ primary role in teaching medical students, which may prioritise practical and immediate clinical skills over broader administrative or research-based digital competencies.
The integration of EHR systems into medical education has been recognised as essential. Successful models in the U.S. and U.K. have embedded EHR systems into training, such as allowing students to write notes at primary clinical sites or use de-identified patient data for practice (Pereira et al., 2018; Pontefract & Wilson, 2019; Welcher et al., 2018). These approaches ensure hands-on learning and prepare students for modern healthcare environments. For broader applicability, partnerships with local healthcare institutions and technology providers can enable the development of localised EHR modules tailored to different healthcare contexts. However, over-reliance on EHR systems may reduce critical thinking or direct patient interaction. Mitigation strategies include embedding reflective practices into training and balancing EHR use with patient engagement activities. When successfully implemented, EHR training enhances data management skills and promotes patient interaction.
Telemedicine training varies globally, often focusing on rural healthcare placements, as seen in Australia and the U.K. (Rienits et al., 2016; Wootton, 1999). In Singapore, telemedicine exposure arose mainly during the COVID-19 pandemic’s social distancing requirements, highlighting its potential in urban healthcare. To ensure comprehensive telemedicine training, curricula should include simulated consultations, role-playing exercises, and coverage of diverse scenarios, such as breaking bad news over digital platforms. To address the challenge of interpreting body language, medical schools should incorporate modules that focus on interpreting non-verbal cues, such as facial expressions and gestures, which are essential for building rapport and understanding patients’ concerns. Courses that address the legal responsibilities in telemedicine, including patient confidentiality, informed consent, and documentation requirements, should also be integrated to ensure students are aware of the regulatory frameworks guiding virtual care. Case studies and real-life examples that discuss the legal implications of telemedicine can also help students navigate potential legal challenges. With regard to patient selection, it is crucial for professional bodies to develop frameworks that guide clinicians in determining when in-person care is more appropriate, especially for complex or high-risk cases. Additionally, the curricula should provide guidance on how to recognise red flags such as signs of mental health distress, urgent medical conditions, or patient non-compliance with digital tools, and escalate them appropriately. Providing continuing education opportunities for practising clinicians is also important to keep them updated on telemedicine advancements. The healthcare system can then pair students with experienced telemedicine practitioners who can provide the necessary mentorship and guidance.
POCUS has become an essential component of undergraduate medical education (Glass et al., 2021; Sheppard et al., 2023). However, its application is often limited to specific specialties, such as emergency medicine, obstetrics and gynaecology, and radiology (Glass et al., 2021). In contrast, our study advocates for a longitudinal POCUS curriculum spanning all years and specialties. Integrating POCUS training into medical curricula improves diagnostic accuracy, enhances bedside decision-making, and builds clinical confidence. A structured approach, such as Kern’s six-step model, provides a robust framework for designing and implementing a standardised curriculum with consistent competency assessments (Kern, 1998). Innovative teaching methods, including handheld devices and near-peer instruction, have been shown to improve ultrasound proficiency and student performance, as evidenced by successful implementations at the University of Connecticut School of Medicine (Boivin et al., 2022). While improper use of POCUS can result in diagnostic errors, these risks can be mitigated through routine competency evaluations and guided practice, ensuring students develop the necessary skills safely and effectively.
Addressing differing opinions regarding DHC priorities in schools requires collaboration among medical educators, technology developers, and healthcare providers. Medical curricula should include training on the responsible use of DHTs, and evaluating the reliability of apps. Developers should design apps that address clinicians’ data security concerns. Moreover, healthcare organisations should establish guidelines and protocols for healthcare-related app use to ensure patient safety and privacy. Integrating these competencies into medical curricula will better prepare future healthcare professionals for evolving demands of healthcare delivery.
Implementing DHC also requires consideration of diverse healthcare systems and resource availability. Local adaptations, coupled with ongoing evaluation and feedback, ensure curricula remain relevant and scalable. Training programmes must balance global standards with local needs, enabling students to navigate evolving healthcare landscapes effectively. By addressing the implementation strategies, risks, and benefits of DHTs, this study provides actionable insights for advancing DHE.
A. Strengths and Limitations
This qualitative study highlights the DHCs needed in the core medical curricula from the perspectives of students, clinical educators and teachers. The diverse sample of institutions and specialties enriched the data. Student feedback provided up-to-date information on curricula gaps, while senior clinicians’ experience enhanced credibility. Interviewing participants from different generations ensured medical education remains relevant to current and future healthcare needs.
A perceived limitation of this study is its small sample size, which may affect its generalisability, validity and reliability. With a small sample, the findings might not represent the broader population and could miss the population’s diversity (Sandelowski, 1995). Additionally, small sample sizes may not adequately capture the diversity within the population of interest (Sandelowski, 1995). Moreover, the unique socio-political, cultural and economic context of Singapore may limit the generalisability of our findings to other settings. Singapore’s relatively small population and centralised governance create conditions that may differ from other countries. Consequently, while the insights from our study provide valuable lessons, they should be interpreted with caution when applying them to contexts with different governance structures or cultural dynamics.
Despite the limitations, this qualitative study provides a contextualised understanding of participants’ expectations and concerns through in-depth narrative analysis. While not entirely generalisable, the findings have significant implications for medical curricula in other developed countries. They highlight valued competencies, informing curriculum design, training programmes and continuing education initiatives.
Furthermore, this study focused on clinicians from public healthcare institutions, which may influence their perspectives on DHCs. Public sector clinicians often work within more structured systems that prioritise certain competencies differently than in the private sector. While this focus provides insights specific to public healthcare education, it is important to note that the views of private-sector clinicians, who may face different digital health challenges, were not captured in this study. Future work comparing clinicians across both sectors could provide a more comprehensive view. The perspectives of clinicians from the private healthcare sector may also differ due to the distinct operational and financial frameworks in which they practise.
Moreover, future research could explore the perspectives of clinicians in various roles beyond medical education, such as clinical researchers, healthcare administrators, or those involved in clinical governance. By comparing these viewpoints with those of clinical educators, a more comprehensive understanding of the DHCs required across different professional pathways in healthcare can be developed. Such studies could further inform curriculum development to ensure that medical students are adequately prepared not only for clinical practice but also for the evolving demands of digital health in research, administration, and leadership.
V. CONCLUSION
In conclusion, an inter-generational perspective in medical education leverages the strengths of both medical students and senior clinicians, ensuring a balanced approach that keeps pace with technological advancements while maintaining the core principles of patient care. This collaborative model prepares future healthcare professionals to navigate the evolving landscape of healthcare technology effectively. As the findings have shown, despite their varying levels of experience and diverse medical backgrounds, the DHCs deemed essential for future clinical practice are consistent across all stakeholders. While all stakeholder groups considered most basic clinical skills important, medical students viewed physical examination as replaceable by DHTs. In contrast, the clinical educators and teachers thought otherwise. To address the needs and concerns of all groups, DHCs should complement instead of replace traditional clinical skills.
We acknowledge that the DHTs deemed important in other countries may vary from those reported in this study. However, the type of DHTs to be introduced should not distract us from the main goal of ensuring that the curricula of medical schools around the world remain updated and relevant to current and future healthcare needs. Regularly comparing the perspectives of various stakeholders in the healthcare system is crucial, as it enables educational institutions to adapt and refine their curricula continuously. This iterative process ensures that the curricula remain responsive to the dynamic nature of clinical work.
Notes on Contributors
Humairah Zainal collected and analysed the data, wrote the initial drafts, revised the manuscript for publication and approved the submitted copy of the manuscript.
Xin Xiaohui reviewed, edited, read and approved the submitted copy of the manuscript.
Julian Thumboo reviewed, edited, read and approved the submitted copy of the manuscript.
Fong Kok Yong was involved in the conception and design of the study, reviewed, edited, read and approved the submitted copy of the manuscript.
Ethical Approval
Waiver for ethical approval was granted by SingHealth Institutional Review Board (Reference Number: 2020/2880).
Data Availability
The data that support the findings of this study are available from the first author upon reasonable request. The data cannot be uploaded to the repository as it contains some confidential views of participants.
Acknowledgements
The authors extend their gratitude to the reviewers for their insightful feedback on the manuscript drafts. Special thanks go to Anisa Muhammad for transcribing the interviews, as well as to Dr. Warren Fong Weng Seng and Dr. Ng Qin Xiang for their assistance in recruiting some of the medical students. The authors also deeply appreciate the invaluable contributions of the study participants.
Funding Statement
This study was supported by SingHealth Duke-NUS Medicine Academic Clinical Programme under Seah Cheng Siang Distinguished Professorship in Medicine.
Declaration of Interest
There are no relevant financial or non-financial competing interests to report.
References
Alkire (née Nasr), L., O’Connor, G. E., Myrden, S., & Köcher, S. (2020). Patient experience in the digital age: An investigation into the effect of generational cohorts. Journal of Retailing and Consumer Services, 57, Article 102221. https://doi.org/10.1016/j.jretconser.2020.102221
Aungst, T. D., & Patel, R. (2020). Integrating digital health into the curriculum – Considerations on the current landscape and future developments. Journal of Medical Education and Curriculum Development, 7, Article 2382120519901275. https://doi.org/10.1177/2382120519901275
Blacketer, C., Parnis, R., B. Franke, K., Wagner, M., Wang, D., Tan, Y., Oakden-Rayner, L., Gallagher, S., Perry, S. W., Licinio, J., Symonds, I., Thomas, J., Duggan, P., & Bacchi, S. (2021). Medical student knowledge and critical appraisal of machine learning: A multicentre international cross-sectional study. Internal Medicine Journal, 51(9), 1539-1542. https://doi.org/10.1111/imj.15479
Boivin, Z., Carpenter, S., Lee, G., Chimileski, B., Harrison, J., Choudhary, D., & Herbst, M. (2022). Evaluation of a required vertical point-of-care ultrasound curriculum for undergraduate medical students. Cureus, 14(10), e30002. https://doi.org/10.7759/cureus.30002
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Clay-Williams, R., Hibbert, P., Carrigan, A., Roberts, N., Austin, E., Fajardo Pulido, D., Meulenbroeks, I., Nguyen, H. M., Sarkies, M., Hatem, S., Maka, K., Loy, G., & Braithwaite, J. (2023). The diversity of providers’ and consumers’ views of virtual versus inpatient care provision: A qualitative study. BMC Health Services Research, 23(1), 724. https://doi.org/10.1186/s12913-023-09715-x
Edirippulige, S., Brooks, P., Carati, C., Wade, V. A., Smith, A.C., Wickramasinghe, S., & Armfield, N. (2018). It’s important, but not important enough: eHealth as a curriculum priority in medical education in Australia. Journal of Telemedicine and Telecare, 24(10), 697-702. https://doi.org/10.1177/1357633×18793282
Food and Drug Administration. (2019). Digital health center of excellence. https://www.fda.gov/medical-devices/digital-health-center-excellence
Foadi, N., Koop, C., Mikuteit, M., Paulmann, V., Steffens, S., & Behrends, M. (2021). Defining learning outcomes as a prerequisite of implementing a longitudinal and transdisciplinary curriculum with regard to digital competencies at Hannover Medical School. Journal of Medical Education and Curricular Development, 8, 23821205211028347. https://doi.org/10.1177/23821205211028347
Gillissen, A., Kochanek, T., Zupanic, M., & Ehlers, J. (2022). Medical students’ perceptions towards digitization and Artificial Intelligence: A mixed-methods study, Healthcare (Basel), 10(4), 723-737. https://doi.org/10.3390/healthcare10040723
Glass, C., Sarwal, A., Zavitz, J., Nitsche, J., Joyner, J., Johnson, L. L., Garcia-Vargas, J., & O’Brien, M. C. (2021). Scoping review of implementing a longitudinal curriculum in undergraduate medical education: The wake forest experience. The Ultrasound Journal, 13(1), 23. https://doi.org/10.1186/s13089-021-00206-w
Hersh, W., Biagioli, F., Scholl, G., Gold, J., Mohan, V., Kassakian, S., Kerns, S., & Gorman, P. (2017). From competencies to competence: Model, approach, and lessons learned from implementing a clinical informatics curriculum for medical students. In Shachak, A., Borycki, E.M., & Reis, S.P. (Eds.), Health professionals’ education in the age of clinical information systems, mobile computing and social networks (pp. 269-287). Academic Press. https://doi.org/10.1016/B978-0-12-805362-1.00013-9
Hurley, K. F., Taylor, B., Postuma, P., & Paterson, G. (2011). What are Canadian medical students learning about health informatics. Electronic Journal of Health Informatics, 6(4), np.
Kallio, H., Pietilä, A.-M., Johnson, M., & Kangasniemi, M. (2016). Systematic methodological review: Developing a framework for a qualitative semi-structured interview guide. Journal of Advanced Nursing., 72(12), 2954–2965. https://doi.org/10.1111/jan.13031
Kern, D. E. (1998). Overview: A six-step approach to curriculum development. In P.A., Thomas, D.E., Kern, M.T., Hughes & B.Y. Chen (Eds.), Curriculum Development for Medical Education: A Six-Step Approach (pp. 5-10). Johns Hopkins University Press.
Liu, D. S., Sawyer, J., Luna, A., Aoun, J., Wang, J., Boachie, L., Halabi S., & Joe B. (2022). Perceptions of US medical students on Artificial Intelligence in medicine: Mixed methods survey study. JMIR Medical Education, 8(4), e38325. https://doi.org/10.2196/38325
Machleid, F., Kaczmarczyk, R., Johann, D., Balčiūnas, J., Atienza-Carbonell, B., von Maltzahn, F., & Mosch, L. (2020). Perceptions of digital health education among european medical students: Mixed methods survey. Journal of Medical Internet Research, 22(8), e19827. https://doi.org/10.2196/19827
O’Brien, B. C., Harris, I. B., Beckman, T. J., Reed, D. A., & Cook, D. A. (2014). Standards for reporting qualitative research: A synthesis of recommendations. Academic Medicine, 89(9), 1245–1251. https://doi.org/10.1097/ACM.0000000000000388
Pereira, A. G., Kim, M., Seywerd, M., Nesbitt, B., & Pitt, M. B. (2018). Collaborating for competency – A model for single electronic health record onboarding for medical students rotating among separate health systems. Applied Clinical Informatics, 9(1), 199-204. https://doi.org/10.1055/s-0038-1635096
Pontefract, S. K., & Wilson, K. (2019). Using electronic patient records: Defining learning outcomes for undergraduate education. BMC Medical Education, 19(1), 30. https://doi.org/10.1186/s12909-019-1466-5
Rienits, H., Teuss, G., & Bonney, A. (2016). Teaching telehealth consultation skills. The Clinical Teacher, 13(2), 119–123. https://doi.org/10.1111/tct.12378
Sandelowski, M. (1995). Sample size in qualitative research. Research in Nursing & Health, 18(2), 179–183. https://doi.org/10.1002/nur.4770180211
Sheppard, G., Williams, K.-L., Metcalfe, B., Clark, M., Bromley, M., Pageau, P., Woo, M., Yi, Y., Devasahayam, A. J., & Dubrowski, A. (2023). Using Kane’s framework to build an assessment tool for undergraduate medical student’s clinical competency with point of care ultrasound. BMC Medical Education, 23(1), 43. https://doi.org/10.1186/s12909-023-04030-9
Sørensen, K., Levin-Zamir, D., Duong, T. V., Okan, O., Brasil, V. V., & Nutbeam, D. (2021). Building health literacy system capacity: A framework for health literate systems. Health Promotion International, 36(Supp 1), i13–i23. https://doi.org/10.1093/heapro/daab153
Tudor Car, L., Kyaw, B. M., Panday, R. S. N., van der Kleij, R., Chavannes, N., Majeed, A., & Car, J. (2021). Digital health training programs for medical students: Scoping review. JMIR Medical Education, 7(3), e28275. https://doi.org/10.2196/28275
Welcher, C. M., Hersh, W., Takesue, B., Stagg Elliott, V., & Hawkins, R. E. (2018). Barriers to medical students’ electronic health record access can impede their preparedness for practice. Academic Medicine, 93(1), 48–53. https://doi.org/10.1097/ACM.0000000000001829
Wittink, H., & Oosterhaven, J. (2018). Patient education and health literacy. Musculoskeletal Science and Practice, 38, 120–127. https://doi.org/10.1016/j.msksp.2018.06.004
Wootton, R. (1999). Telemedicine and isolated communities: A UK perspective. Journal of Telemedicine and Telecare, 5(2), 27–34. https://doi.org/10.1258/1357633991933495
Zainal, H., Xiaohui, X., Thumboo, J., & Kok Yong, F. (2023a). Digital competencies for Singapore’s national medical school curriculum: A qualitative study. Medical Education Online, 28(1), 2211820. https://doi.org/10.1080/10872981.2023.2211820
Zainal, H., Xiaohui, X., Thumboo, J., & Kok Yong, F. (2023b). Exploring the views of Singapore junior doctors on medical curricula for the digital age: A case study. PLOS ONE, 18(3), e0281108. https://doi.org/10.1371/journal.pone.0281108
*Fong Kok Yong
10 Hospital Boulevard
Singapore 168582
+65 6908 8949
Email: fong.kok.yong@singhealth.com.sg
Submitted: 29 February 2024
Accepted: 5 February 2025
Published online: 1 July, TAPS 2025, 10(3), 15-25
https://doi.org/10.29060/TAPS.2025-10-3/OA3259
Zaw Phyo¹, Titi Savitri Prihatiningsih2, Ye Phyo Aung¹ & Tun Tun Naing¹
1Department of Medical Education, Defence Services Medical Academy, Yangon, Myanmar; 2Public Health and Nursing Universitas Gadjah Mada, Yogyakarta, Indonesia
Abstract
Introduction: The effective implementation of changes in medical school curricula requires modifications to assessments alongside teaching strategies. The World Federation for Medical Education emphasises the need for assessment policies to align with educational outcomes. In Myanmar, the Defence Services Medical Academy (DSMA) has adopted an outcome-based curriculum since 2017, but the standard setting in assessments remains pending. This study explores concerns and challenges for enhancing assessment practices.
Methods: An explanatory sequential design was used. For a quantitative approach, 36 assessment committee members were surveyed using questionnaires, and pre-and post-test analyses were conducted using SPSS Statistics Version 25. Qualitatively, eight committee members were selected through purposive sampling for in-depth interviews using interpretative methodology with thematic analysis by MAXQDA Software 2022.
Results: It shows that most committee members acknowledge the advantages of standard settings, such as improved teaching and learning defect identification, staff knowledge application, enhanced educational programs, and personal contributions to education quality. Half of the committee members expressed concerns about the increased workload and administrative burden, while another half-supported standard-setting implementation. They all appreciate the integration of standard setting in the outcome-based curriculum, recognising its positive impact on student quality and accreditation standards. Challenges include limited human resources, resistance to change, time-consuming, and an increased workload.
Conclusion: Committee members suggested that targeted interventions are needed to improve awareness, collaboration, and successful implementation. These should consider perspectives, enhance understanding, define roles, and address resources and resistance. This will optimise standard setting, ensure educational quality, and meet accreditation standards.
Keywords: Assessment, Standard Setting, Integrated Curriculum, Awareness, Perception, Attitude, Lifelong Learning
Practice Highlights
- Members of the committee think that having standards in DSMA’s curriculum is essential for raising the quality of students and the school’s standards.
- Most members know how important it is to set standards, especially for pass/fail exams, and stress how important it is to consider culture and institutional factors.
- Setting standards is thought to help with aligning the curriculum, giving students relevant tests, and meeting accreditation requirements.
- For implementation to go well, all stakeholders must be involved, the process must be in line with real evaluation principles, and teachers must continue to learn and grow.
- Not enough resources, resistance to change, limited time, and more work to do are problems that need solutions based on educational ideas.
I. INTRODUCTION
In the last 30 years, there have been many suggestions for changing the curriculum, but only a few medical schools have made significant changes (Supe & Burdick, 2006). Without altering assessments, modifying curricula or teaching strategies will be ineffective. In the global standards for quality improvement area of the World Federation for Medical Education (WFME), there are clear rules about primary medical education in chapter 3.1 of Assessment Policy and System:
“An assessment policy with a centralised system that guides and supports its implementation will entail using multiple summative and formative methods to acquire the knowledge, clinical skills, and behaviors needed to be a doctor. The policy and the system should be responsive to the school’s mission, specified educational outcomes, available resources, and the context” (World Federation for Medical Education, 2020).
In current Medical Education, with competency-based education becoming more popular, healthcare educational institutions and assessment bodies are being looked at more closely than ever before to make sure they are fair, transparent, and defensible when setting the expected level of performance and rating students’ performance to make decisions about their next steps (Lane et al., 2020). With competency-based assessment, the way the test is done must align with what the student has learned (Crespo et al., 2010).
Regularly setting, keeping, and evaluating assessment standards is essential in medical education. It is not an exact science to set standards. Most educational test validity arguments focus on how well the test matches the curriculum and how valuable the test’s content is (Barman, 2008).
Standards are an expression of values, so the ways to set them are systematic ways to gather people’s opinions on values, make agreements, and show that agreement as a single score on a test (Norcini, 2003). “Standard Setting” is a process used to make precise lines between things like “pass” and “fail” or “honors,” “proficient,” and “needs improvement.” Setting standards is “central to giving meaning to test results and, as such, is at the heart of validity arguments” (Wiliam, 1996).
There are two primary methods in which standards are set: (1) criterion-referenced or absolute methods, in which standards setting is not based on test results, and (2) norm-referenced or relative methods, in which setting standards is based on test results. No golden rule exists (Cohen-Schotanus & Van Der Vleuten, 2010). In health professions education, it can be challenging to develop credible, defendable, and acceptable passing or cut-off scores for exams (Norcini & Guille, 2002).
In Myanmar, there are currently no private medical schools, although there are five public medical schools and one military medical school (Defence Services Medical Academy). Myanmar medical schools have used traditional lecture-based teaching methods, and many eminent physicians have emerged from teacher-centered educational programs (Myint, 2020).
Defence Services Medical Academy (DSMA), listed in the World Directory of Medical Schools, was founded in Mingalardon, Yangon, on November 19, 1992 (Naing et al., 2022). Since 2017, DSMA has been the first medical school in Myanmar to implement an outcome-based, integrated curriculum. According to the Dundee three circle models, the graduates of DSMA are supposed to be scholars and scientists, as well as practitioners and practitioners professionals (Harden et al., 1999). The new DSMA curriculum is meant to encourage students to keep learning and give them more responsibility for their learning. It is presently focusing on meeting the criteria of WFME accreditation.
In DSMA, the assessment methods (written, practical, oral, and structured and unstructured observations) include accurate and standardised patients, objective structured clinical examination, patient management problems or simulations, etc. The assessments include continuous assessment, formative assessment, and summative assessment. However, there is no Standard Setting in DSMA, and it will be implemented soon (after training standard setting experts) to set the required basic minimum standards.
Even though accrediting organisations advise medical schools in general what the curriculum should cover and how it should be tested, most medical schools decide how and what to test (Epstein, 2007). There are five ways to figure out how valuable a method of assessment is: reliability (how accurate and repeatable the measurement is), validity (whether the assessment measures what it says it measures), impact on future learning and practice, acceptability to students and teachers, and costs (Van Der Vleuten, 1996). Therefore, the Assessment Committee’s DSMA meetings establish the process and procedures for conducting assessments throughout the undergraduate medical program. The Assessment committee must collect and evaluate feedback regularly, and faculty feedback revealed issues with the assessment process in DSMA.
For a successful, acceptable, and feasible assessment to implement an outcome-based, integrated curriculum, it is essential to explore how students, faculty, and assessment committee members perceive the implication of the standard setting for the assessment. Therefore, this study investigated what the Assessment Committee members think about setting standards in medical education and the most significant problems.
II. METHODS
A. Research Design
Figure 1 shows explanatory sequential mixed methods design (also called a two-phase model (Creswell & Clark, 2017)): Quantitative followed by qualitative was used to explore the views, opinions, beliefs, and feelings of the assessment committee members (Ivankova & Stick, 2007). For the quantitative, all assessment committee members were asked using questionnaires (Likert scale), and qualitatively, Individual In-depth Interviews (IDI) were asked of the selected assessment committee members.

Figure 1. Explanatory sequential mixed methods design
The main benefit of mixed methods research is that they make a potent mix when quantitative and qualitative data are combined (Miles & Huberman, 1994). In addition, a “complex” image of a social phenomenon might be created, for instance, by evaluating both the quantitative and qualitative aspects of a study’s results (Greene, 2006).
B. Data Collection
For Phase 1 (Quantitative): The survey consists of four parts: (1) Collecting demographic information; (2) Investigating people’s perception of standard-setting procedures; (3) Examining attitudes towards these procedures; and (4) Evaluating these procedures using five-point Likert scale items ranging from 5 (strongly agree) to 1 (strongly disagree).
For Phase 2 (Qualitative): An in-depth interview (IDI) with semi-structured questions was used to collect the data. The researcher made an interview guide, which helped shape the interview and get detailed comments from the assessment committee members. The IDIs lasted 30-45 minutes, and the researcher informed participants that their names and information would be kept private.
The researcher performed all the interviews in the participants’ local language (Myanmar). The IDI explored the themes of the conceptual framework. A video recording was made for continuous recording in a quiet, private section of the medical education department office. The researcher conducted open discussions with the assessment committee members and kept them confidential, especially the students. Each interviewer uses a different set of questions (10–12), and the sessions last between 45 and 60 minutes. The researcher kept doing interviews until it became clear that the stories, themes, and problems had been covered to saturation point. The researchers utilised constructivist reflexivity throughout the entire study procedure, as advised by Alvesson and Sköldberg (2017).
C. Sampling Procedure
In DSMA, there are 38 members of the assessment committee. The assessment committee comprises three groups: Discussant members, voting members, and secretariat.
For Phase 1 (Quantitative): All the assessment committee members of DSMA were recruited. Among the 38 eligible persons who met eligibility, approximately 95% of the population (36 participants) responded to the evaluation survey.
For Phase 2 (Qualitative): By using the purposes sampling methods, individual in-depth interviews (IDIs) with semi-structured questions were given to the selected eight members of the assessment committee who are information-rich persons (two discussant Members, five voting members, and one secretariat) to find out what they thought, what they had done, and how they did it.
D. Data Analysis
The survey data was stored in an Excel file and processed using SPSS software (version 25). Descriptive analysis explored assessment committee members’ perceptions, attitudes, and practices.
The MAXQDA 2022 program extracted themes and sub-themes (Côté & Turgeon, 2005). The recorded interviews were transcribed to do content analysis. First, the data were summarised, proofread, and translated into English. Second, for the data analysis, themes, sub-themes, and clusters were identified (Cresswell, 2012). Finally, conceptualisation and explanation throughout the later stages led to the development of concrete abstracts. Analytic coding was done while reading the transcripts, and emerging issues were thought to be included in the thematic statements.
E. Ethical Considerations
The study was done according to the guidelines published by the Ethical and Research Committee of DSMA. Participation in this study is entirely voluntary.
F. Informed Consent
Before conducting the study, informed verbal consent was obtained for respondents’ autonomy to participate in this study.
III. RESULTS
Quantitatively, thirty-seven questions were asked about each participant’s background, knowledge, perception, attitude, and practices regarding the standard-setting. The survey received responses from 36 participants. The data supporting this study’s findings are openly available in the Figshare repository, https://doi.org/10.6084/m9.figshare.25657875.v1 (Phyo et al., 2024).
A. Demographic Characteristics
According to an analysis of the committee’s demography (see Table 1), two-thirds of the members were older than 25, and males dominated. Faculty members (64%) were primarily doctoral holders on the evaluation committee. More than ten years of teaching experience can be found among half of the assessment committee members.
|
No |
Personal Background Information |
Total (n = 36) |
||
|
Frequency |
Percentage |
|||
|
1 |
Age Group |
less than 25 |
10 |
27.8 |
|
26-40 |
4 |
11.1 |
||
|
above 40 |
22 |
61.1 |
||
|
2 |
Gender |
Male |
26 |
72.2 |
|
Female |
10 |
27.8 |
||
|
3 |
Level of Education |
Undergraduate |
10 |
27.7 |
|
Master’s degree |
3 |
8.3 |
||
|
Doctoral |
23 |
63.8 |
||
|
4 |
Current Position |
Assistant Lecturer |
3 |
8.3 |
|
Lecturer |
9 |
25.0 |
||
|
Assistant Professor |
4 |
11.1 |
||
|
Professor |
9 |
25.0 |
||
|
Students |
10 |
27.8 |
||
|
Others |
1 |
2.8 |
||
|
5 |
Time in the teaching profession |
less than five years |
12 |
33.3 |
|
5 – 10 years |
6 |
16.7 |
||
|
More than ten years |
18 |
50.0 |
||
|
6 |
Served in Current Position |
less than five years |
20 |
55.6 |
|
5 – 10 years |
11 |
30.6 |
||
|
More than ten years |
5 |
13.9 |
||
Table 1. Personal background information of the assessment committee members
B. Awareness of Standard Setting
In Table 2, most assessment committee members believe that DSMA has been implementing a standard setting in the assessment process, but it is still in the process of being fully implemented. However, 75% know the purpose behind establishing standard settings in DSMA. Furthermore, faculty members are debating whether DSMA is a precise standard-setting approach for standardisation and how DSMA intends to implement whatever assessment model.
|
No |
Question |
Answers |
Total (n=36) |
|
|
Frequency |
Percentage |
|||
|
1 |
Does DSMA have a standard Setting in the MBBS Programme? |
Yes |
23 |
63.9 |
|
No |
11 |
30.6 |
||
|
Uncertain |
2 |
5.6 |
||
|
2 |
Who Is the most Responsible person in the Implementation standard setting within DSMA? |
Rector |
9 |
25.0 |
|
Assessment Committee |
6 |
16.7 |
||
|
All Staff |
20 |
55.6 |
||
|
Uncertain |
1 |
2.8 |
||
|
3 |
Why did DSMA introduce a Standard setting? |
Rector’s foresight and planning |
8 |
22.2 |
|
Requirement of MMCAC guideline |
27 |
75.0 |
||
|
Uncertain |
1 |
2.8 |
||
|
4 |
How many types of standard settings? |
One |
6 |
16.7 |
|
Two |
22 |
61.1 |
||
|
Three |
8 |
22.2 |
||
|
5 |
The assessment system of the DSMA is designed by applying a ready-made model like programmatic assessment. |
Yes |
12 |
33.3 |
|
No |
12 |
33.3 |
||
|
Uncertain |
12 |
33.3 |
||
|
6 |
Does DSMA have an exact standard-setting method to standardise the assessment system? |
Yes |
17 |
47.2 |
|
No |
10 |
27.8 |
||
|
Uncertain |
9 |
25.0 |
||
Table 2. Awareness of standard setting
C. Perception, Attitude, and Practice towards Standard Setting
Table 3 shows the mean scores above 4.0 indicate a positive perspective on the effects of standard setting, suggesting that it can aid in problem identification, improve educational programs, and raise the standard of education. Lower scores (3.6) and agreement percentages (71%–72%) on items related to the regularity and straightforwardness of the process in regular process implementation suggest improving how standard setting is carried out and perceived.
|
No |
Questions |
Total (n=36) |
|
|
Mean ± SD |
Agreement percent |
||
|
Perception towards Standard Setting |
|||
|
1 |
Standard setting stimulates the identification of defects in the teaching and learning process. |
4.0 ± 0.8 |
80 |
|
2 |
The standard-setting process helps staff members apply their academic lives. |
4.1 ± 0.6 |
82 |
|
3 |
Standard setting can improve the development of educational programs. |
4.3 ± 0.9 |
85 |
|
4 |
The standard setting enables staff members to contribute to the quality of education. |
4.1 ± 0.6 |
82 |
|
5 |
Standard setting can ensure borderline candidates to make pass/fail decisions. |
3.9 ± 0.6 |
79 |
|
6 |
In DSMA, standard-setting development is processed regularly. |
3.6 ± 0.7 |
71 |
|
7 |
DSMA has been initiating a straightforward standard-setting process for the undergraduate program. |
3.6 ± 0.9 |
72 |
|
8 |
In DSMA, standard-setting processes are planned by the Assessment Committee. |
4.0 ± 0.7 |
79 |
|
9 |
Standard-setting development is regularly monitored and improved. |
3.8 ± 0.9 |
76 |
|
10 |
There is a process for monitoring individual students’ progression. |
3.6 ± 0.9 |
72 |
|
Attitude towards Standard Setting |
|||
|
1 |
I often have negative attitudes about Standard setting. |
2.0 ± 0.7 |
39 |
|
2 |
The standard setting is the job of institution administrators only. |
2.1 ± 0.8 |
43 |
|
3 |
Implementation of Standard setting makes me an uncomfortable environment for academic activities |
1.9 ± 0.7 |
38 |
|
4 |
I am still determining the work of standard setting and its outcomes. |
2.0 ± 0.7 |
41 |
|
5 |
Implementation of Standard setting contributes to the increased workload. |
3.0 ± 1.0 |
59 |
|
6 |
I get nervous that I am not able to handle changes introduced by standard setting |
2.2 ± 0.7 |
44 |
|
7 |
Implementation of Standard setting contributes to administrative burden. |
2.8 ± 0.8 |
56 |
|
8 |
Overall, the process of standard setting is effective. |
4.0 ± 0.7 |
81 |
|
9 |
Implementing the standard setting can improve pass/fail decisions for the progression of next year. |
4.0 ± 0.7 |
79 |
|
Practice towards Standard Setting |
|||
|
1 |
I support the implementation of Standard setting. |
4.4 ± 0.7 |
88 |
|
2 |
I have been involved in some discussions about Standard setting. |
3.8 ± 1.0 |
76 |
|
3 |
I am encouraging my colleague to adopt the Standard setting. |
3.9 ± 0.9 |
79 |
|
4 |
I am doubtful that I will work longer hours to implement standards set standard-setting successfully |
3.8 ± 1.0 |
76 |
|
5 |
I have been involved in setting up processes in my department |
4.0 ± 1.3 |
82 |
|
6 |
I have been involved in the standard-setting process at my institution. |
4.3 ± 1.1 |
85 |
Table 3. Perception, attitude, and practice towards standard setting
The attitudes section indicates lower ratings (2.0–3.0) with worries about increasing workload (59% agreement) and administrative burden (56% agreement), revealing resistance or uncertainty among some staff members towards the practical implications of standard setting. They also feel that implementing standards creates an uncomfortable academic environment, but 81% think the standard-setting process is successful (4.0 ± 0.7).
The high mean scores (4.0–4.4) and agreement percentages (up to 88%) in sections on perceptions and practices indicate strong support for standard setting among respondents. This suggests a recognition of its value in improving educational quality.
The data suggests that standard settings are supported, but there’s a need for more engagement and clear communication about its processes. Apprehension about workload and administrative tasks may stem from a lack of understanding or poor implementation strategies. Institutions could benefit from transparent, inclusive, and efficient management of standard-setting processes, including regular updates, training sessions, and support systems. A balanced approach is needed to address apprehensions and ensure positive outcomes for educational quality and student success.
D. Thematic Analysis Outcomes
The participants were Assessment Committee Members (n=8) from the Assessment Committee of the DSMA who were involved in developing the Standard setting for the Assessment. The data collected from IDIs were organised into five themes and 19 sub-themes in Figure 2.

Figure 2. Showing the main themes and sub-themes
1) Perceptions of the assessment committee members: The assessment committee members expressed appreciation for the incorporation of standard setting in the Outcome-based Integrated curriculum at our university. Most committee members showed enthusiasm for using this method, which they believed was fitting for assessing students in this program. Additionally, the committee aimed to enhance the assessment techniques used in the Outcome-based Integrated curriculum. They were convinced that implementing standard settings would improve student and DSMA quality.
“An outcome-based integrated curriculum has replaced DSMA’s old curriculum. The product of an outcome-based curriculum is not produced. So, we must prepare for that product to be assessed using the standard setting. It is a transitional period for our DSMA from the old curriculum to the outcome-based curriculum. So, the state holders and teachers from DSMA must understand the standard setting. We must set the standard for the assessment of DSMA, but slowly and steadily.”
(Participant 1)
“If the integrated curriculum is changed and outcomes are improved, the quality of the university will improve. Local or international qualifications will be enhanced, not only by students but also by the quality of the DSMA.”
(Participant 3)
2) Understanding of standard settings: It was evident that members emphasised the importance of standard setting, particularly in the context of Pass/Fail exams for students. Furthermore, committee members demonstrated knowledge regarding various types of standard setting. They were able to identify the most suitable method for DSMA, taking into consideration factors such as cultural context and institutional requirements.
“The standard setting is a method designed to determine a student’s pass or fail scores, and it is also a technique for determining whether students will pass or fail a test.”
(Participant 4)
“DSMA has to set standards for the assessment according to our culture, values, and conditions. We have taken the standard setting of another prestigious university as a reference. It is not suitable to apply the ready-made model.”
(Participant 1)
3) Benefits of implementing standard settings: The assessment committee members recognised Standard Settings are essential for effective curriculum alignment, meaningful student assessment, and accreditation. DSMA can demonstrate its commitment to delivering high-quality education and meeting accreditation standards by aligning the curriculum, teaching practices, and assessments through Standard Settings. The committee members believe Standard Settings play a crucial role in enhancing the quality of education DSMA provides.
“It is beneficial for constructive alignment. So, we adopted and prepared the standard setting for assessing DSMA for accreditation. It is also essential for the teaching and learning process and method. We can check the teaching and learning process, and if errors occur, we can fix them and circle again for the following year.”
(Participant 1)
“I think the outcomes that come out improve not only the student’s quality but also the DSMA’s quality. If the integrated curriculum is changed and outcomes are improved, the quality of the university will improve. Local or international qualifications will be enhanced, not only by students but also by the quality of the DSMA.”
(Participant 3)
4) Roles and responsibilities while implementing standard setting in DSMA: The Assessment Committee members recognised the critical roles and responsibilities of implementing standard setting. They emphasised the need for an inclusive approach involving all stakeholders. Furthermore, they highlighted the importance of aligning standard setting with authentic assessment principles and providing continuous professional development for faculty members. By considering these factors, the committee members aimed to enhance the quality of assessment and promote meaningful learning outcomes for students.
“The standard setting must be built with support; all teachers at DSMA are responsible for it because only the medical education department knows about the standard setting, which is ineffective. Teachers in all departments, including professors, must know about the standard setting. That’s why all the teachers at the university need to understand when setting standards.”
(Participant 2)
“The assessment committee is in charge of the standard setting in DSMA, including the medical education committee, the curriculum committee, the quality assurance committee, the assessment committee, etc. The assessment committee can emphasise its role and responsibility, including implementing the standard setting. Thus, it is more reasonable and practical.”
(Participant 6)
5) Challenges and weaknesses of implementing the standard-setting: The Assessment committee members identified several challenges in implementing standard setting. These challenges include limited human resources, resistance to change, time-consuming processes, and increased workload. Understanding these challenges through the lens of educational theories can guide the development of strategies to address them effectively and ensure the successful implementation of standard-setting practices.
“Human resources are our main weakness. There are very few human resources in DSMA to apply the standard setting. Time-consuming is another area for improvement.”
(Participant 1)
“Most importantly, students don’t know what a “standard” setting is, and some teachers don’t know either. They need to know what a “standard” setting is.”
(Participant 7)
IV. DISCUSSION
The outcomes from the study at the Defence Service Medical Academy (DSMA) assessment committee shed light on essential aspects of standard-setting in medical education. In institutions like DSMA, which implement the outcome-based integrated curriculum, medical students must remember what they learned in their preclinical training to make sound clinical decisions based on reliable scientific principles (Lazić et al., 2006). In medical education, it is crucial to establish, maintain, and frequently review assessment criteria (Senanayake & Mettananda, 2005).
The study revealed a predominantly male composition within the assessment committee, highlighting the need for diversity and expertise among committee members. While increasing the diversity of academic medical leadership to address the underrepresentation of minorities and women in medicine has been proposed, there has been limited investigation into this topic (Meadows et al., 2023). Encouraging diversity can contribute to robust discussions and decision-making processes related to standard-setting. While committee members demonstrate a solid grasp of standard-setting, the results indicate a requirement for continual education to translate this knowledge into practical application (Norcini & McKinley, 2007). Therefore, targeted interventions and professional development programs must enhance their knowledge and awareness.
Committee members show favorable attitudes towards standard-setting, but there is a discrepancy between their perceptions and actual practices. Implementing open communication strategies consistent with Downing’s (2005) emphasis on the value of clarity in assessment practices could close this gap. Moreover, the lack of active participation in the implementation process may indicate a more significant engagement problem within academic committees (Van der Vleuten et al., 2010).
The study highlights issues that align with existing literature on medical education reform, citing resource limitations and reluctance to change as typical obstacles to adopting innovative instructional approaches (Swing, 2007). The committee’s alignment with constructivist and cognitive theories advocates for a transition to more interactive and participatory learning methods, which a parallel change in evaluation methods should accompany (Harden & Crosby, 2000). Committee members emphasised the need for an inclusive approach involving all stakeholders and aligning standard-setting with authentic assessment principles, resonating with sociocultural theories emphasising social interaction and collaboration in the learning process.
The findings offer crucial insights into the committee’s perceptions and experiences with standard-setting in the integrated outcome-based curriculum. Aligned with educational theories, these insights underscore the importance of lifelong learning and can guide future research and targeted interventions to continuously enhance standard-setting practices.
V. CONCLUSION
In conclusion, the findings from both the quantitative and qualitative research provide valuable insights into the assessment committee’s knowledge, perceptions, attitudes, and practices regarding standard-setting in medical education at the Defence Service Medical Academy (DSMA). While there is a positive attitude towards the potential benefits of standard-setting, there are also concerns and doubts among some committee members.
The study emphasises the importance of targeted interventions in medical education to improve awareness, address concerns, foster collaboration, and support the successful implementation of standard-setting. The Assessment Committee Members appreciate the incorporation of standard setting in the outcome-based integrated curriculum and recognise its importance during the transitional period. They demonstrate a strong understanding of standard settings, particularly in Pass/Fail exams, and emphasise the need to consider cultural and institutional requirements. Standard settings can enhance curriculum alignment, meaningful student assessment, and accreditation purposes.
The committee members emphasise the roles and responsibilities associated with implementing standard setting, including an inclusive approach, continuous professional development for faculty members, and addressing challenges such as limited human resources, resistance to change, time-consuming processes, and increased workload. Strategies informed by educational theories are needed to improve human resource capacity, provide training on standard setting, and create awareness among students and teachers.
These findings underscore the importance of supporting the assessment committee in their understanding, implementation, and continuous improvement of standard-setting practices. By addressing concerns, providing necessary resources, and promoting collaboration, DSMA can optimise the benefits of standard-setting in medical education and ensure the quality of its educational programs. Incorporating lifelong learning fosters continuous professional development, keeping DSMA at the forefront of educational excellence and adaptability.
Notes on Contributors
Dr. Zaw Phyo contributed significantly to the manuscript development process, including reviewing existing literature, identifying research gaps, and addressing questions and goals. He helped draft and revise the manuscript, emphasising its importance for medical education.
Titi Savitri Prihatiningsih contributed to shaping the research question and framework, ensuring a systematic approach. She applied her expertise in evaluation to refine the research tools and meticulously reviewed the thesis and manuscript for accuracy.
Dr. Ye Phyo Aung engaged in the study’s methodology phase, endorsing the chosen research design, sampling strategies, and data collection techniques, adding valuable insights to the research execution.
Dr. Tun Tun Naing assisted in the meticulous proofreading of the article, ensuring clarity, coherence, and compliance with academic standards.
Ethical Approval
The Ethical Review Committee of the Defence Services Medical Academy, Yangon, Myanmar, granted ethical approval. (2 / Ethics/ 2021).
Data Availability
The data supporting this study’s findings are openly available in the Figshare repository, https://doi.org/10.6084/m9.figshare.25657875.v1 (Phyo et al., 2024).
Acknowledgment
I would also like to thank the FAIMER Regional Institute of Indonesia for Educational Development and Leadership (FRIENDSHIP) for helping me finish this research project at the Faculty of Medicine, Public Health, and Nursing at Universitas Gadjah Mada (Indonesia).
I would also like to thank my supervisor, the head of the medical education department (DSMA), and my colleagues. Without their help, I would not have been able to survey my research. I am grateful to all the assessment committee members from DSMA, Myanmar, who helped me complete my survey by giving me their valuable opinions and experiences.
Funding
The research was carried out during the study period at the FRIENDSHIP-FAIMER Regional Institute of Indonesia for Educational Development and Leadership. No financing is associated with this publication.
Declaration of Interest
There is no conflict of interest in the current research.
References
Alvesson, M., & Sköldberg, K. (2017). Reflexive methodology: New vistas for qualitative research. Sage publications.
Barman, A. (2008). Standard setting in student assessment: Is a defensible method yet to come? Annals Academy of Medicine Singapore, 37(11), 957-963. https://doi.org/10.47102/annals-acadmedsg.V37N11p957
Cohen-Schotanus, J., & Van Der Vleuten, C. P. (2010). A standard-setting method with the best-performing students as a point of reference: Practical and affordable. Medical Teacher, 32(2), 154-160. https://doi.org/10.3109/01421590903196979
Côté, L., & Turgeon, J. (2005). Appraising qualitative research articles in medicine and medical education. Medical Teacher, 27(1), 71–75. https://doi.org/10.1080/01421590400016308
Crespo, R. M., Najjar, J., Derntl, M., Leony, D., Neumann, S., Oberhuemer, P., Totschnig, M., Simon, B., Gutierrez, I., & Delgado Kloos, C. (2010). Aligning assessment with learning outcomes in outcome-based education. Proceedings of the IEEE International Engineering Education Conference (EDUCON) 2010. https://doi.org/10.1109/EDUCON.2010.5492385
Cresswell, J. W. (2012). Educational research: Planning, conducting, and evaluating quantitative and qualitative research (4th ed.). Pearson.
Creswell, J. W., & Clark, V. L. P. (2017). Designing and conducting mixed methods research (3rd ed.). Sage.
Downing, S. M. (2005). The effects of violating standard item writing principles on tests and students: The consequences of using flawed test items on achievement examinations in medical education. Advances in Health Sciences Education, 10(2), 133-143. https://doi.org/10.1007/s10459-004-4019-5
Epstein, R. M. (2007). Assessment in medical education. New England Journal of Medicine, 356(4), 387-396. https://doi.org/10.1056/nejmra054784
Greene, J. C. (2006). Toward a methodology of mixed methods social inquiry. Research in the Schools, 13(1), 93-98. https://www.researchgate.net/publication/228968099
Harden, R. M., & Crosby, J. (2000). AMEE Guide No 20: The good teacher is more than a lecturer – The twelve roles of the teacher. Medical Teacher, 22(4), 334–347. https://doi.org/10.1080/014215900409429
Harden, R. M., Crosby, J., Davis, M., & Friedman, R. M. (1999). AMEE Guide No. 14: Outcome-based education: Part 5-From competency to meta-competency: A model for the specification of learning outcomes. Medical Teacher, 21(6), 546–552. https://doi.org/10.1080/01421599978951
Ivankova, N. V., & Stick, S. L. (2007). Students’ persistence in a distributed doctoral program in educational leadership in higher education: A mixed methods study. Research in Higher Education, 48(1), 93-135. https://doi.org/10.1007/s11162-006-9025-4
Lane, A. S., Roberts, C., & Khanna, P. (2020). Do we know who the person with the borderline score is, in standard-setting and decision-making. Health Professions Education, 6(4), 617-625. http://doi.org/10.1016/j.hpe.2020.07.001
Lazić, E., Dujmović, J., & Hren, D. (2006). Retention of basic sciences knowledge at clinical years of medical curriculum. Croatian medical journal, 47(6), 880-882. https://pubmed.ncbi. nlm.nih.gov/17167861
Meadows, A. M., Skinner, M. M., Hazime, A. A., Day, R. G., Fore, J. A., & Day, C. S. (2023). Racial, ethnic, and sex diversity in academic medical leadership. JAMA Network Open, 6(9), e2335529. https://doi.org/10.1001/jamanetworkopen.2023.35529
Miles, M. B., & Huberman, A. M. (1994). Qualitative data analysis: An expanded sourcebook (2nd ed.) Sage Publications.
Myint, K. M. (2020). Curriculum reform and teaching methodologies: A survey on teachers’ perspectives in the university of medicine 1, Yangon. Myanmar Medical Journal, 62(1), 27-33.
Naing, T. T., Minamoto, Y., Aung, Y. P., & Than, M. (2022). Faculty development of medical educators: Training evaluation and key challenges. The Asia Pacific Scholar, 7(3), 23-32. https://doi.org/10.29060/TAPS.2022-7-3/OA2742
Norcini, J. J. (2003). Setting standards on educational tests. Medical Education, 37(5), 464-469. https://doi.org/10.1046/j.1365-2923.2003.01495.x
Norcini, J. J., & Guille, R. (2002). Combining tests and setting standards. In G. R. Norman, C. P. M. van der Vleuten, D. I. Newble, D. H. J. M. Dolmans, K. V. Mann, A. Rothman, & L. Curry (Eds.), International Handbook of Research in Medical Education (pp. 811-834). Springer. https://doi.org/10.1007/978-94-010-0462-6_30
Norcini, J. J., & McKinley, D. W. (2007). Assessment methods in medical education. Teaching and teacher education, 23(3), 239-250. https://doi.org/10.1016/j.tate.2006.12.021
Phyo, Z., Aung, Y, P., Naing, T. T., & Prihatiningsih, T. S. (2024). Perception of the assessment committee on the standard setting in medical education [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.25657875.v1
Senanayake, M. P., & Mettananda, D. S. (2005). Standards medical students set for themselves when preparing for the final MBBS examination. Annals of the Academy of Medicine, Singapore, 34(8), 483–485.
Supe, A., & Burdick, W. (2006). Challenges and issues in medical education in India. Academic Medicine, 81(12), 1076-1080. https://doi.org/10.1097/01.acm.0000246699.94234.ab
Swing, S. R. (2007). The ACGME outcome project: Retrospective and prospective. Medical Teacher, 29(7), 648–654. https://doi.org/10.1080/01421590701392903
Van der Vleuten, C., Schuwirth, L., Scheele, F., Driessen, E., & Hodges, B. (2010). The assessment of professional competence: Building blocks for theory development. Best Practice & Research Clinical Obstetrics & Gynaecology, 24(6), 703-719. https://doi.org/10.1016/j.bpobgyn.2010.04.001
Van Der Vleuten, C. P. M. (1996). The assessment of professional competence: Developments, research and practical implications. Advances in Health Sciences Education, 1(1), 41-67. https://doi.org/10.1007/bf00596229
Wiliam, D. (1996). Meanings and consequences in standard setting. Assessment in Education: Principles, Policy & Practice, 3(3), 287-308. https://doi.org/10.1080/0969594960030303
World Federation for Medical Education. (2020). Basic medical education WFME global standards for quality improvement – The 2020 revision. https://wfme.org/wp-content/uploads/2022/03/WFME-BME-Standards-2020.pdf
*Zaw Phyo
No.94, Pyay Road, Mingaladon Township,
Postal code – 1102
Yangon, Myanmar
Phone: 95 92032754
Email: dr.zawphyoo@gmail.com
Submitted: 27 November 2024
Accepted: 28 April 2025
Published online: 1 July, TAPS 2025, 10(3), 10-14
https://doi.org/10.29060/TAPS.2025-10-3/GP3589
Thilanka Seneviratne, Wathsala Edirisingha & Wathsala Palpola
Department of Pharmacology, Faculty of Medicine, University of Peradeniya, Sri Lanka
Abstract
Introduction: Pharmacology, though challenging, is fundamental in medical practice, necessitating effective knowledge acquisition and retention for future application. This study aims to analyse student perceptions of the newly introduced teaching method, peer assessment, to enhance pharmacology teaching.
Method: Eighty-six third-year medical students of the Faculty of Medicine, University of Peradeniya participated in the peer assessment. They were divided into two groups of 40-45 and a case scenario in pharmacology was given to answer. Three volunteers from each group presented the answers. Peers evaluated the answers using provided criteria and gave feedback. The teacher then facilitated discussions, highlighting key points. Assessors and assesses perceptions on the teaching learning method was assessed using questionnaire and focus group discussions (FGD).
Results: The majority of students (n=64) (74.41%) enjoyed the task of assessing their peers. 80.23% (n=69) acknowledged the value of peer assessment for student engagement. However, 34.88% (n=30) mentioned that they did not feel they had the skills and knowledge to assess their peers. 17.43% (n=15) mentioned that they were reluctant to be critical of their peers. In the FGD students mentioned that in this student-centered learning method all students actively participated than the usual small group discussion sessions. They could compare peers’ knowledge with their own knowledge and preferred the teacher grading to be combined with peer grading.
Conclusion: Peer assessment for enhancing pharmacology teaching was well received by the students. Also, students emphasise the importance of lecturer guidance and advocate for a combined assessment approach to improve engagement and learning outcomes.
Practice Highlights
- Peer assessment keeps the students more focused during teaching learning process.
- Peer assessment enhances critical thinking and allows student centered learning.
- Combined assessment approach improves engagement and learning outcomes.
- Peer assessment for enhancing pharmacology teaching is well received by the students.
I. INTRODUCTION
The focus in higher education has shifted from conventional teaching methods to a more learner-centric approach, moving away from teacher-centered management toward fostering student self-direction (Arnold et al., 2005). This transition has sparked a growing interest in the educational benefits associated with students evaluating both their own work (self-assessment) and that of their peers (peer assessment).
Peer assessment is defined as assessment by and of individuals who have attained the same general level of training or expertise, exercise no formal authority over each other, and share the same hierarchic status in an institution (Arnold et al., 2005).
Peer assessment can be summative or formative. This focuses on the formative side, helping students plan learning, identify strengths and weaknesses, improve, and build metacognitive and professional skills. Traditional teacher-centered assessments often limit such growth. Educators valuing dialogue and collaboration should actively involve students in assessments.
Evidence is scarce regarding the utilisation of peer assessment methods for undergraduate formative assessments of a particular subject.
Pharmacology is often perceived as challenging to remember and thus, less engaging for students. Consequently, there’s reduced enthusiasm for participation in lectures. However, pharmacology serves as a fundamental aspect of medical practice, necessitating students to acquire and retain knowledge effectively for future application. Interactive teaching offer distinct advantages over traditional, teacher-centered methods by facilitating long-term retention, contextual learning, and the development of essential skills and attitudes. Thus, we introduced this teaching and learning method related to the peer assessment that integrates student centered learning within the classroom setting.
II. METHODS
A. Study Setting
The study was conducted at the Faculty of Medicine, University of Peradeniya, Sri Lanka.
B. Informed Consent
Informed written consent was obtained from the students who volunteered to the study.
C. Participants
The study involved third-year medical students from the Faculty of Medicine, University of Peradeniya, Sri Lanka. These students participated in small group discussions, each consisting of 40-45 members.
D. Peer Assessment Process
Each group was assigned short essay questions on pharmacology and students encouraged to draft written answers. Three volunteers from each group presented their answers to the class, and peers assessed them gave feedback based on criteria set by the lecturer. The teacher then facilitated discussions, highlighting key points.
E. Gathering Student Perceptions
1) Using Questionnaires: All students, except the three who presented, were provided with a self-administered Likert scale questionnaire to capture their perspectives as “assessors,” drawing from McGarr and Clifford (2013). The students who presented their answers completed a different Likert scale questionnaire, designed to capture their viewpoints as “assesses,” referencing Tahir (2012).
2) Focus Group Discussions: Nineteen students volunteered. They were divided into 3 groups. Focus group discussions, using a structured interview guide led by one investigator, lasted 30 to 40 minutes each, continued until data saturation was reached. The discussions were recorded for transcription. Participants were assured of confidentiality, and their views were anonymised. During transcription, all identifying features were removed.
F. Analysis
Quantitative data from the questionnaires were analysed using percentages. Qualitative data from the focus group discussions were analysed separately by identifying common themes in the responses.
Transcribed data were analysed using inductive content analysis. The researchers first read the transcripts to familiarise themselves with the data. Then, each transcript was coded into broad content categories. The transcripts were reread sentence by sentence and further coded into categories and subcategories.
G. Ethical Considerations
Ethical clearance was obtained from the ethics review committee of the Faculty of Medicine, University of Peradeniya. (2024/EC/25).
III. RESULTS
Eighty-six students participated as assessors. Six students participated as assesses. The results from students who assessed their peers showed mixed perceptions. A significant portion (74.41%) enjoyed the task. 44.17% agreed they were nervous about the peer assessment at the start of the module, while 29.07% were neutral (Table 1).
The comments from students assessed by their peers were generally positive. 66.67% felt they received sufficient comments, while the rest remained neutral. All participants noted that peer assessment offered more opportunities for discussion and practice. Peer assessment is recognised as a valuable exercise for students shown in Table 2.
|
Questions |
Agree (%) |
Neutral (%) |
Disagree (%) |
Total responses (%) |
|
1. nervous about the peer assessment |
38 (44.17) |
25 (29.07) |
21 (24.41) |
84 (97.67) |
|
2. limited educational values |
6 (6.97) |
25 (29.7) |
53 (61.62) |
84 (97.67) |
|
3. reluctant to be critical |
15 (17.43) |
45 (52.32) |
21 (24.41) |
81 (94.19) |
|
4. fairer assessment approach |
54 (62.78) |
20 (23.25) |
7 (8.13) |
81 (94.19) |
|
5. enjoyed assessing peers |
64 (74.41) |
10 (11.62) |
4 (4.64) |
78 (90.70) |
|
6. difficult to remove personal feelings |
19 (22.08) |
24 (27.9) |
43 (50.00) |
86 (100.00) |
|
7. I did not feel I had the skills and knowledge to assess my peers |
30 (34.88) |
23 (26.44) |
32 (37.2) |
85 (98.84) |
|
8. reluctant to give low marks |
33 (38.36) |
19 (22.09) |
31 (36.04) |
83 (96.51) |
|
9. Including peer assessment in our course made the assessment more accurate |
54 (62.79) |
27 (31.39) |
4 (4.64) |
85 (98.84) |
|
10. prefer tutor grading over peer grading |
37 (43.02) |
28 (32.55) |
19 (22.08) |
84 (97.67) |
|
11. course assessments were inaccurate |
13 (15.11) |
38 (44.18) |
30 (34.88) |
81 (94.19) |
|
12. Assessing peers was difficult |
24 (27.9) |
20 (23.25) |
40 (46.5) |
84 (97.67) |
|
13. unfair |
4 (4.64) |
17 (19.76) |
64 (74.41) |
85 (98.84) |
|
14. valuable exercise |
69 (80.23) |
10 (11.63) |
7 (8.13) |
86 (100.00) |
Table 1. Assessors’ perception regarding the peer assessment method
|
Question |
Agree (%) |
Neutral (%) |
Disagree (%) |
|
1. Evaluation and comments are fair |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
2. Comments are useful for making improvement |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
3. Comments are sufficient |
4 (66.67) |
2 (33.33) |
0 (0.00) |
|
4. Chance to practice and discuss |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
5. Less pressure and more relaxed |
3 (50.00) |
3 (50.00) |
0 (0.00) |
|
6. Who review my essays are nice |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
7. Overestimate me |
3 (50.00) |
2 (33.33) |
1 (16.67) |
|
8. Underestimate me |
0 (0.00) |
1 (16.67) |
5 (88.33) |
|
9. The quality of comments given by my peers is low |
1 (16.67) |
3 (50.00) |
2 (33.33) |
|
10. I did not like being assessed by my peers |
0 (0.00) |
1 (16.67) |
5 (88.33) |
|
11. Comments were beneficial for identifying errors in content and ideas |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
12. Comments were beneficial for identifying errors in the organisation |
6 (100.00) |
0 (0.00) |
0 (0.00) |
|
13. Prefer my tutor to grade me rather than my peers |
1 (16.67) |
5 (83.33) |
0 (0.00) |
|
14. I did not feel my peers assessed the content accurately |
1 (16.67) |
1 (16.67) |
4 (66.67) |
|
15. Unfair |
0 (0.00) |
0 (0.00) |
6 (100.00) |
|
16. A valuable exercise |
6 (100.00) |
0 (0.00) |
0 (0.00) |
Table 2. Perception of the students who got assessed by peers
Several key themes were identified by the focus group discussion.
A. Benefits of the Peer Assessment
1) Less stressful: Students mentioned that being assessed by their peers was less stressful than being assessed by a lecturer. They also noted that this method encouraged active participation in the assessment process due to its more convenient and relaxed nature.
“No nervousness at all. Because I just assesses my colleagues”
2) Kept students focused: Students commented that peer assessment is fairer than the traditional method as it kept them focused on work more than usual.
“When students have to assess their peers, they have to focus on the presenting answer. So, all students fully focus on the process. The lecturer will discuss the given scenario again. So, I think we do not miss any subject content, we can learn effectively.”
3) Peers are more accessible than lecturers: They accepted this method as a good alternative to traditional assessment methods as lecturers are not always available for the assessment.
“It’s unable to assess students by lecturers all the time, so peer assessment is a good approach to assess students.”
4) Improved understanding: Being able to know how their peers answer a question was found as a good way of comparing their knowledge and improving themselves.
“Can compare our knowledge with peers”
5) Confidence building: Another advantage they pointed out was an improvement in the level of confidence in facing an assessment as they felt more comfortable when they are assessed by peers.
“Improved confidence”
B. Challenges of Peer Assessment
1) Peers are not knowledgeable enough: Some students identified being assessed by the lecturers is better than the peer assessment as lecturers are more knowledgeable than the peers.
“Lecturers are more knowledgeable than students, so being assessed by them is essential.”
“We didn’t have deep, fine knowledge to assess peers, but we had superficial knowledge to assess them.”
C. Suggestions
A larger proportion of participants expressed appreciation for both traditional assessment methods and peer assessment, stating that using both simultaneously would be ideal.
“I think the lecturer grading is the best because we are not very experienced. However, with the time limitation, it is hard to assess students by lecturer frequently. In that case, peer assessment will be beneficial if it is combined with lecturer grading.”
Many participants expressed preference for using this in other courses.
IV. DISCUSSION
While superior assessment has been the traditional and more prevalent approach, it faces challenges due to increasing student numbers, limited lecturer availability, and time constraints. This study aims to explore students’ perceptions of peer assessment as a complementary evaluation method, addressing some of the limitations of superior assessment. The findings reveal several advantages and challenges of peer assessment.
A. Less Stressful, More Focused Learning Environment
One of the key advantages of peer assessment is its ability to create a less stressful and more focused learning environment. The results indicate that students feel more comfortable being evaluated by their peers, which allows them to engage more deeply in the learning process.
Presenters and assessors both noted that the peer assessment structure promoted active engagement, as assessors remained attentive throughout the session to provide meaningful feedback, and those not presenting felt more relaxed and focused compared to traditional SGD formats. This shows that peer assessment method enhances student focus in learning environment.
B. Increased Availability and Accessibility
Given the time constraints and growing student populations, continuous evaluation by lecturers is challenging. However, well-prepared peer groups can effectively bridge this gap, providing timely feedback and support. This aspect of peer assessment enhances students’ opportunities for formative feedback, which is critical for their learning process.
C. Improves the Assessor’s Understanding of the Subject/Confidence Building
Students gain valuable insights and deepen their understanding by evaluating and providing feedback on their peers’ written work, as this process enhances their critical thinking and analytical skills (Topping, 2009). This fact was noted by the participants of our study also. They appreciated the chance to analyse their peers’ answers.
The supportive environment of peer assessment enabled students to share and compare their knowledge openly, which in turn helped them refine their answers and learn better organisational techniques, which improve their confidence.
D. Addressing Knowledge Gaps
One challenge identified in peer assessment is the limited expertise of peers in accurately assessing their classmates. However, this challenge can be mitigated with proper preparation and guidance from lecturers. Topping (2009) has highlighted that training students to provide constructive feedback is a challenging process. However, the benefits it yields outweigh the burden of training peer assessors.
Literature also gives evidence regarding the doubt about the validity level of peer assessment among teachers and students (Holroyd, 2000). This attitude has been identified as a major barrier to the use of peer assessment as a standard method of evaluating students.
Fry (1990) highlighted that, when it is implemented in the right way, peer evaluation demonstrates results, which are comparable with lecturer evaluation.
E. Overcoming Personal Bias
A drawback noted by students was the difficulty of remaining objective when assessing their peers. Many students found it challenging to give low marks or critically evaluate their friends’ work as a lecturer might. This concern highlights the need for students to be properly trained as an assessor.
Several published studies shows that peer evaluation can be affected by negative social factors like peer pressure, favoritism, or fear of criticism, especially when done face-to-face. To address these issues, it’s important to use methods that ensure anonymity in peer reviews.
F. Recommendations for Future Application
Overall, students in this study expressed a positive view of peer assessment and suggested its use in other courses. They acknowledged that combining peer assessment with superior assessment could enhance learning outcomes. To ensure the effectiveness of peer assessment, students recommended conducting it under the supervision and guidance of lecturers. This combined approach would offer the benefits of peer-to-peer engagement while maintaining the academic rigor provided by expert feedback.
V. CONCLUSION
While peer assessment presents certain challenges, it offers substantial advantages in creating a more accessible, engaging, and confidence-building learning environment. With proper training and lecturer involvement, peer assessment can serve as a valuable complement to traditional assessment methods in higher education.
Notes on Contributors
Thilanka Seneviratne led the study’s conception, design, and implementation, contributed to data analysis and interpretation, drafted and critically revised the manuscript. Wathsala Edirisingha was involved in the implementation of the study and contributed to data acquisition and analysis. Himali Palpola contributed to the study’s implementation, data analysis, and manuscript drafting. All the authors have read and approved the final manuscript.
Ethical Approval
Ethical clearance was obtained from the ethics review committee of the Faculty of Medicine, University of Peradeniya, (2024/EC/25).
Acknowledgement
We acknowledge the staff of the department of Pharmacology, Faculty of Medicine, University of Peradeniya for their valuable contribution in material and organisational support.
Funding
No funding sources are associated with this paper.
Declaration of Interest
All authors declare no conflict of interest.
References
Arnold, L., Shue, C. K., Kritt, B., Ginsburg, S., & Stern, D. T. (2005). Medical students’ views on peer assessment of professionalism. Journal of General Internal Medicine, 20(9), 819–824. https://doi.org/10.1111/j.1525-1497.2005.0162.x
Fry, S. A. (1990). Implementation and evaluation of peer marking in higher education. Assessment & Evaluation in Higher Education, 15(3), 177–189. https://doi.org/10.1080/0260293900150301
Holroyd, C. (2000). Are assessors professional? Student assessment and the professionalism of academics. Active Learning in Higher Education, 1(1), 28–44. https://doi.org/10.1177/1469787400001001003
McGarr, O., & Clifford, A. M. (2013). ‘Just enough to make you take it seriously’: exploring students’ attitudes towards peer assessment. Higher education, 65, 677-693. https://doi.org/10.1007/s10734-012-9570-z
Tahir, I. H. (2012). A study on peer evaluation and its influence on college ESL students. Procedia-Social and Behavioral Sciences, 68, 192-201. https://doi.org/10.1016/j.sbspro.2012.12.219
Topping, K. J. (2009). Peer assessment. Theory Into Practice, 48(1), 20–27. https://doi.org/10.1080/00405840802577569
*Thilanka Seneviratne
Faculty of Medicine,
University of Peradeniya, Sri Lanka, 20400
Email: thilanka.medi@gmail.com
Submitted: 26 September 2024
Accepted: 25 March 2025
Published online: 1 July, TAPS 2025, 10(3), 5-9
https://doi.org/10.29060/TAPS.2025-10-3/GP3504
Shihoko Yamakawa1, Olga Razvina2, Fumiko Okazaki2, Hiroshi Hibino3, Toshiyuki Someya4 & Tatsuo Ushiki4
1Niigata University Institute of Global Affairs, Japan; 2Niigata University Medical Education Centre, Niigata University Graduate School of Medical and Dental Sciences, Japan; 3Department of Pharmacology, Osaka University Graduate School of Medicine, Japan; 4Niigata University, Japan
Abstract
Introduction: Niigata University School of Medicine and Niigata University Graduate School of Medical and Dental Sciences have been engaging in medical exchanges with Russian medical universities for over 30 years. In 2015, a double-degree program with Russian medical universities was initiated, leading to a multi-layered education project that included short-term undergraduate student exchange programs and graduate-level double-degree programs, resulting in the circulation of human resources.
Methods: The program was conducted in English, and a maximum of 15 credits could be transferred based on the universities’ regulations. Degree examinations were conducted independently, and successful candidates were awarded degrees from both Niigata University and their home university in Russia. The project was overseen by the G-MedEx Centre at Niigata University, which included staff with international experience.
Results: The difference in standard study duration between Japan and Russia was eliminated by using a four-year system in the graduate school doctoral programs. Three study models were proposed by Russian universities, considering each university’s regulations and various circumstances. The curriculum was determined based on the rules of the universities in Russia and the circumstances of the students. Agreements were made with each university in supplementary documents.
Conclusion: Despite the differences in educational standards and the lack of a common educational framework between Japan and Russia, the difficulties can be overcome, and educational compatibility can be increased.
Practice Highlights
- Thanks to a long history of interaction with Russia, we were able to organise a large educational project, which included multi-layered programs, one of which was a double degree program.
- As part of the project, we established a coordination centre (G-MedEx Centre) that effectively engaged with students, teachers, and university administration to address challenges and tasks as they arose.
- We successfully navigated the differences in educational standards between Russia and Japan and developed effective mechanisms for collaboration.
- Despite the challenges of the double degree program, we have two successful examples of students who completed their double degrees.
- We were able to train doctors and scientists who gained unique international experience and will be able to make significant contributions on the world stage in the future.
I. INTRODUCTION
Since 2014, Russia and Japan have started to actively cooperate in the academic sphere, particularly after the Ministry of Education, Culture, Sports, Science, and Technology (MEXT) adopted two programs “Special Program for Priority Placement of Japanese Government Scholarship International Students” and “Re-inventing Japan Program for Strengthening Universities’ Globalisation”. These programs were designed to promote interaction with Russia and continued until 2018. Prior to this project, interactions with Russian universities were decentralised, with each university managing its exchange programs. Niigata University School of Medicine and Niigata University Graduate School of Medical and Dental Sciences have also conducted bi-directional medical exchanges with Russian universities since 1993. However, it was in 2014 that the exchange program received a significant boost due to a decision made by the Japanese and Russian governments. Niigata University merged these two programs into one initiative called the G-MedEx (Globalization and Medical Exchange) project (Yamakawa et al., 2018). As a result, the Japan-Russia exchanges made significant progress. The project aimed to expand Niigata University’s educational programs and enhance research collaboration (Obst & Kuder, 2012), leading to the establishment of the Double Degree Program (DDP) to advance medical care and develop skilled human resources in Japan and Russia (Teplyashina et al., 2017). DDP allows universities to award degrees to students who meet their graduation requirements. The number of public universities in Japan implementing DDPs has increased from 47 to 56 out of a total of 85 public universities over the past ten years, though only a few have partnered with Russian universities. Intrinsic differences in education and credit systems between Japanese and Russian universities have become an obstacle to student exchange and the establishment of joint educational programs (Jargin, 2024; Sitnikov & Bizunkov, 2016).
This paper reports on specific issues such as the graduate school curriculum, credit system, degree examination requirements, and solutions to help overcome these differences.
II. METHODS
A. Implementation Method
The DDP at the Graduate School of Medical and Dental Sciences admitted up to two students annually from three Russian partner universities. Candidates, recommended by their home institutions, enrolled concurrently at NU and their respective universities upon passing NU’s entrance exam. The program was conducted in English.
B. Credit Transfer and Grade Evaluation
Under the DDP agreement, up to 15 of the 30 required credits were transferable. A standardised Japanese-Russian grading system (A–E) was implemented to ensure educational quality.
C. Degree Examination and Conferral of Degrees
Degree examinations were conducted independently per each university’s standards. Graduates were awarded a PhD from both NU and their home university. A joint DDP certificate was also conferred.
D. Implementation System
The G-MedEx Centre at NU managed the program. A Russian physician and administrative staff oversaw the program on their end, while liaison professors from partner universities facilitated coordination. Support structures for international students were established in collaboration with university committees. In Figure 1, we compare the credit standards of the Russian Federation with those of our university’s doctoral program in medical and dental sciences, which serves as a benchmark in Japan. Russia’s ECTS model defines one credit as 36 hours, with doctoral programs needing 180 credits, compared to Japan’s 45 credits.

Figure 1. Credits and study hours (Niigata University and Russian Partner Universities)
III. RESULTS
A. Education Reform and DDP in Russia
The European Credit Transfer System (ECTS) and the UMAP Credit Transfer Scheme (UCTS) have enhanced international education quality. Russia, undergoing education reforms since 1991, joined the Bologna Process in 2003 and enacted a federal law on networked education in 2012. Its credit system aligns with ECTS. However, when NU launched the DDP in 2015, faculty-level understanding and overseas credit recognition were insufficient. Japanese and Russian faculty collaboratively developed a compliant curriculum through trial and error.
B. Graduate School Curriculum and Credit Transfer
Completing two dissertations within the study period required curricular alignment. Figure 2 illustrates the Russian doctoral curriculum which includes general courses (9 credits) and specialised subjects (21 credits) in the first year, advanced coursework (7 credits) and clinical practice in the second year, and research (48 credits) in the third year, culminating in a final evaluation. A structured course mapping and unified grading system aided in credit transfer.

Figure 2. Basic course curriculum and number of credits, Russian Graduate School doctoral program
We developed a group of courses for specialised classes to streamline the collation process. A unified evaluation standard based on Japan and Russia’s systems was adopted, significantly speeding up credit transfers.
C. Eliminating Differences in the Standard Study Period and Creating a Study Model
We have worked on eliminating the difference in standard study duration between Japan and Russia, which is a structural problem. Although undergraduate education in the medical field is six years both in Japan and Russia, the duration of graduate school doctoral programs differs. In Japan, it is four years, and in Russia, it is usually three years. Although DDP allows credits to be transferred, it is quite difficult to complete study programs at both universities and write two dissertations in three years. Therefore, we decided to use a four-year system.
The extra one-year study period in Russia has been an ongoing academic issue. After discussions between Japan and Russia, Russian universities proposed three study models based on regulations and circumstances. It was suggested that students spend the first two years in Russia and the remaining two at their home university. They also noted that compulsory subjects are concentrated in the first year, making it appropriate for students to start research and gain basic skills in their native language.
The three study models proposed were as follows:
– Model 1: After completing two years, the student takes a one-year leave at a Russian university. Then the student returns to school for the fourth year and completes the Japanese and Russian programs at the same time.
– Model 2: Establishing a new four-year doctoral course program at Russian universities. This is a special curriculum in which the 180 credits that should be earned over three years are distributed evenly over four years, resulting in 45 credits earned in one year.
– Model 3: At the end of the third year, all completion requirements except for thesis defense should be completed, and graduation is suspended. After it is confirmed that the students are expected to graduate from the university in their fourth year, they will proceed to the examination and officially complete their studies in Japan and Russia at the same time.
In the case of models 2 and 3, students have to pay tuition fees for four years in Russia based on the length of study. Additionally, in the case of model 3, upon completion of the third year, students are required to return to Japan temporarily for up to one month for graduation exams and related procedures. The curriculum was determined based on the rules of the universities in Russia and the circumstances of the students. The agreements were made with each university in supplementary documents.

Figure 3. DDP Models
D. Thesis Defense
Russia and Japan have different systems for evaluating theses. In Russia, dissertations are typically 100 to 150 pages long and are written in Russian. They are reviewed by the Higher Accreditation Commission. In contrast, in Japan, dissertations must be written in English and be published in an international journal. Because of these regulatory differences, a single-thesis evaluation approach was not feasible, resulting in separate reviews for each thesis. While foreign examiners can attend public hearings for dissertations in Russia, they are not allowed to serve on examination committees due to government restrictions.
E. Building a Network with a Dedicated Project Team
Since the G-MedEx Centre’s establishment, its international network has expanded across Russia, with exchange agreements established with nine universities. Appointing liaison professors at Russian universities significantly motivated local faculties and had an unexpected positive impact. Regular information exchange enabled the swift identification and resolution of issues, contributing to the project’s success and improvements in the study environment and safety management for international students.
IV. DISCUSSION
This paper highlights the challenges faced in implementing the Double Degree Program (DDP) and the measures taken to address them. Six students were enrolled in the program, and two of them have already obtained their degrees. While most of the academic and curricular challenges have been resolved, some issues still need to be addressed. Although credit transfer can reduce some duplication of study content, fulfilling the graduation requirements of two universities within the standard study period is challenging. After gathering feedback from students participating in the program, we learned that many found it very challenging, particularly those conducting research that required wet experiments. In contrast, students focused on statistical research did not express similar concerns.
Another factor contributing to the program’s complexity was that the research topics at the two universities often had no connection, forcing students to manage two entirely unrelated projects. This increased their workload and sometimes hindered their ability to complete the program successfully.
Consequently, we concluded that for future programs, it is essential to choose departments that can coordinate their projects, ensuring they engage in collaborative research. This approach would make it easier for students to complete both projects on time. Regarding the credit system, a transfer method based on the “competency-based” approach is being considered, where students are evaluated based on the acquired results of comprehensive and specialised abilities and skills required for the subject, rather than assigning academic training per credit by the time spent in it. To speed up the process, we have limited credit transfer to specialised subjects at our university. However, as the number of students increases and the scale of projects grows, it will be essential to systemise credit transfer and simplify administrative procedures further. Therefore, we need to build a system that guarantees a higher level of educational quality between the two countries while referring to the framework provided by ECTS and the Erasmus Project (European Community Action Scheme for the Mobility of University Students), which are the standard in Russia. From the viewpoint of human resource circulation, some graduates have become post-doctoral fellows or faculty members at Niigata University, while others have returned to their home countries to work as doctors.
V. CONCLUSION
Witnessing young medical scientists grow and start playing active roles in both countries is the greatest joy of international collaboration in education. Russia recently withdrew from the Bologna Process. As a result, the country may develop its own education system that does not depend on the European framework. Russian students may face challenges in integrating into the European education system and accessing European educational grants.
However, interactions with countries not part of the Bologna process—such as Japan, India, and China—will remain unaffected, since these countries operate according to their own independent systems. The key will be finding common ground and promoting academic mobility, though this won’t be straightforward based on our past experiences.
Thus, cooperation with these countries will require careful attention. It is essential to focus on the future effects on education and ensure the educational environment’s protection for students, drawing on the knowledge and experience gained so far.
Notes on Contributors
SY, the first author, contributed significantly to the design, wrote and edited the paper, and reviewed the literature. OR was responsible for data collection, resource verification, reviewing and editing the manuscript. FO conducted resource verification, reviewed and edited the manuscript. HH provided critical feedback during the writing process, analysed the data, implemented and supervised the project. TS led the project, interpreted the data, and provided guidance. TU, the lead conceptualiser, designed the study, was responsible for conceptualisationand obtaining funding.
Acknowledgement
We would like to express our sincere gratitude to professors of Krasnoyarsk State Medical University, Far Eastern State Medical University, and Pacific State Medical University for their cooperation in conducting this study.
Funding
This research was supported by JSPS Grant-in-Aid for Scientific Research 20K02936.
Declaration of Interest
The authors declare that they have no conflict of interest.
References
Jargin, S. (2024). Medical education and postgraduate training in Russia: An update. Journal of Integrative Medicine & Therapy, 7(1), 1. https://doi.org/10.13188/2378-1343.1000019
Obst, D., & Kuder, M. (2012). International joint- and double-degree programs. International Higher Education, 66, 5-7. https://doi.org/10.6017/ihe.2012.66.8585
Sitnikov, V., & Bizunkov, A. (2016). The higher education at the post-Soviet territories: The long echo of the Bologna process. Vestnik Otorinolaringologii, 81(4), 72-77. https://doi.org/10.17116/otorino201681472-77
Teplyashina E., Petrova M., Salmina A., & Razvina O. (2017) The experience of networking postgraduate training programmes. The Education and Science Journal, 19, 4. https://doi.org/10.17853/1994-5639-2017-4-118-129
Yamakawa, S., Razvina, O., Ito, M., Hibino, H., Someya, T., & Ushiki, T. (2018) Medical exchange project for students and young doctors between Japan and Russia. Medical University, 1, 32-39. https://doi.org/10.2478/medu-2018-0005
*Shihoko Yamakawa
1-757, Asahimacho-dori, Chuo-ku,
Niigata, Japan 951-8510
-81 (025) -227-2063
Email: yamakawa@med.niigata-u.ac.jp
Submitted: 29 July 2024
Accepted: 24 February 2025
Published online: 1 July, TAPS 2025, 10(3), 1-4
https://doi.org/10.29060/TAPS.2025-10-3/GP3478
Tayzar Hein1, Ye Phyo Aung1, Khin Aung Htun1 & Tin Tun2
1Department of Medical Education, Defence Services Medical Academy, Myanmar; 2Department of Human Resources for Health, Ministry of Health, Myanmar
Abstract
Introduction: The medical education system of Myanmar has evolved through a dynamic history influenced by colonial legacies, national development efforts, and global collaborations. This article explores the progression of medical education in Myanmar, focusing on its historical milestones, challenges, and advancements in response to societal and healthcare needs.
Method: This study is based on a comprehensive review of historical records, policy documents, and academic literature, with “A Concise History of Medical Education in Myanmar” by Aung Than Batu as a primary reference. Key milestones, collaborations, and innovations were analysed to trace the evolution of medical education from the colonial period (1907) to the present day. Quantitative data, including the number of medical universities, training durations, and infrastructure developments, were included for a clearer perspective.
Results: The analysis highlights transformative milestones, including the establishment of the first medical school in 1907 and Rangoon Medical College in 1927. Over time, Myanmar has adapted to challenges such as resource constraints and political instability by fostering international collaborations and leveraging technology. Teaching methods have evolved significantly, integrating modern technologies alongside traditional pedagogies.
Conclusion: Myanmar’s medical education exemplifies resilience and adaptability. By aligning its system with global standards, fostering research, and leveraging international expertise, the nation continues to contribute to global medical education and healthcare. This narrative serves as an inspiration for countries navigating similar challenges in medical education.
Practice Highlights
- Myanmar’s medical education journey began in 1907, blending indigenous practices with Western methodologies, and expanded post-independence with the establishment of multiple medical universities.
- Myanmar overcame challenges like resource limitations and political instability by fostering global collaborations and integrating modern technologies into medical education.
- The MBBS program combines robust theoretical knowledge with clinical training, while postgraduate education emphasises research, making Myanmar a contributor to global medical advancements.
I. INTRODUCTION
Myanmar, a nation of profound cultural richness and historical depth, unfolds a narrative that intricately intertwines with the evolution of its medical education system. This comprehensive overview embarks on a journey through the diverse facets of Myanmar’s medical education landscape (Batu, 2015). Beyond a mere chronological exploration of historical administrative periods, it endeavors to unravel the intricate threads woven into policy development, the establishment of medical universities, and the ceaseless pursuit of addressing challenges and seizing opportunities within the nation’s healthcare and educational sectors. The journey begins in 1927, with the establishment of the Rangoon (Yangon) Medical College, a milestone in introducing formal medical education during the British colonial era (Batu, 2015). This marked the fusion of indigenous healing traditions with Western medicine, laying the foundation for a unique and dynamic approach to healthcare education (Coderey, 2021). After independence in 1948, the nation’s commitment to advancing medical education became evident with the expansion of medical facilities and the development of policies aimed at addressing the healthcare needs of its population. By the 1960s, the establishment of additional institutions, such as the Institute of Medicine (I), reflected Myanmar’s growing emphasis on training a competent cadre of healthcare professionals. In 1970, the establishment of the University of Medicine 2 in Yangon further demonstrated this dedication to expanding medical education access (Batu, 2015). Infrastructure development and facility expansions in subsequent decades signaled foresight that extended beyond immediate requirements, highlighting a long-term vision for excellence and capacity-building in medical education (Batu, 2015).
Amidst challenges such as resource limitations and periods of political instability during the 1980s and 1990s, the story Myanmar of took a resilient turn, transforming obstacles into opportunities. International collaborations, such as partnerships initiated in the 2000s, and the adoption of technological advancements emerged as beacons of progress, underscoring the adaptability and determination of Myanmar to elevate the standards of its medical education (Saw et al., 2019). As Myanmar enters the 21st century, it not only continues to address its domestic healthcare needs but also contributes to the global context. Its influence reverberates through research contributions, milestones in undergraduate and postgraduate medical education, and a commitment to integrating public health perspectives (Saw et al., 2019). Myanmar emerges not just as a nation shaping its healthcare narrative but also as a participant in the broader discourse on global health, contributing to the collective effort to address worldwide health challenges (Proserpio, 2022).
II. ADMINISTRATIVE PERIODS IN MYANMAR
Colonial Era (1824–1948): Under the shadow of British rule, the colonial period of Myanmar bore witness to the initial introduction of Western medicine. The 1860s marked the beginnings of formal medical education when the British established training programs for healthcare workers to address the needs of colonial administration and military personnel. In 1927, the foundation of the Rangoon (Yangon) Medical College became a pivotal moment in the integration of Western methodologies into Myanmar’s medical education system. This era marked the confluence of indigenous healing practices with the methodologies imported during colonial occupation (Coderey, 2021).
Post-Independence Era (1948 onwards): The post-independence period signaled a fervent drive by Myanmar to shape its own destiny. The establishment of the Institute of Medicine (I) in the 1960s marked a significant step toward creating specialised medical education institutions to cater to the nation’s healthcare needs. This commitment was further exemplified by the opening of the University of Medicine 2 in Yangon in 1970, ensuring broader access to medical education. In 1992, the Defence Services Medical Academy (DSMA) was established as the nation’s sole military medical university, dedicated to training medical professionals for the armed forces. With six medical universities in total five civil institutions and one military. The country has demonstrated a sustained effort to expand medical education. This era also saw the formulation of policies aimed at strengthening public health systems and addressing resource limitations, particularly during the politically turbulent 1980s and 1990s. These efforts laid a strong foundation for Myanmar’s aspiration to build a healthcare system reflective of its cultural identity and societal requirements (Coderey, 2021).
III. MEDICAL EDUCATION POLICY IN MYANMAR AND DEVELOPMENT OF MEDICAL UNIVERSITIES
The evolution of medical education policies in Myanmar from 1950 onwards has been a dynamic and adaptive process. Over the years, these policies have responded to societal needs, embraced technological advancements, and aligned with global standards in medical education. A key focus has been the alignment with international benchmarks, ensuring that the education imparted equips Myanmar’s medical graduates to meet and exceed global standards in healthcare delivery. Myanmar’s journey in medical education began in 1907, with the establishment of the Government Medical School in Yangon, which laid the groundwork for structured medical training. The pivotal moment came in 1927, with the establishment of the Rangoon (Yangon) Medical College, formalising Western medical education. Following independence in 1948, the nation prioritised medical education policy development, leading to the creation of the Institute of Medicine (I) in the 1960s and the University of Medicine 2 in 1970 (Batu, 2015). The subsequent decades witnessed the growth of additional medical universities, including the University of Medicine, Mandalay, and the University of Medicine, Magway, which were established to decentralise medical education and improve access. Infrastructure development and the expansion of facilities became pivotal strategies, particularly during the 1980s and 1990s, to accommodate the surging demand for medical education and enhance the overall quality of healthcare provision. These initiatives reflect the commitment of Myanmar to fostering a robust and sustainable healthcare system (Batu, 2015).
IV. CHALLENGES, OPPORTUNTIES AND MEDICAL EDUCATION RESEARCH
Throughout its history, the medical education system of Myanmar has faced formidable challenges, ranging from resource limitations to periods of political instability, such as during the politically turbulent 1980s and 1990s (Saw et al., 2019). Despite these adversities, these challenges have served as crucibles for transformation, providing opportunities for resilience and innovation. By the 2000s, Myanmar actively embraced international collaborations, partnering with global institutions to strengthen its medical education framework. These collaborations have acted as catalysts for overcoming structural and educational challenges, fostering knowledge exchange, and enhancing training methodologies (Proserpio, 2022). In recent decades, technological advancements have presented unprecedented opportunities to bridge gaps in medical education delivery. For instance, the integration of e-learning platforms and simulation-based training since the 2010s has improved both accessibility and quality, enabling students across Myanmar to benefit from innovative educational tools (Saw et al., 2019). This dual narrative of challenges and opportunities paints a dynamic picture of Myanmar’s medical education landscape one that is continuously evolving and adapting to the shifting sands of the global healthcare arena.
Myanmar’s indelible mark on medical education research is a testament to its commitment to academic excellence. The country has emerged as a significant contributor to the global knowledge base in medical education, particularly since the early 2000s, fostering an environment where researchers explore innovative methodologies and address critical questions within the field in 1990s (Saw et al., 2019). Myanmar’s researchers, often collaborating across borders, have played a pivotal role in advancing educational practices worldwide. The research landscape in Myanmar is characterised by a diverse array of studies, including pedagogical approaches, curriculum development, and assessments of educational outcomes. Researchers have delved into the effectiveness of various teaching methods, the impact of cultural nuances on medical education, and the integration of technology into learning strategies (Coderey, 2021). These endeavors not only enhance the quality of medical education within Myanmar but also contribute valuable insights to the broader international community. the commitment of Myanmar to medical education research extends beyond national boundaries, with researchers actively engaging in cross-cultural studies and collaborative projects. Examples include partnerships with institutions in Southeast Asia and beyond, leading to impactful studies on public health education and global health challenges (Proserpio, 2022). This collaborative spirit enriches the local research landscape and fosters a global exchange of ideas, ultimately elevating the standards of medical education on an international scale.
V. UNDERGRADUATE MEDICAL EDUCATION AND POSTGRADUATE MEDICAL EDUCATION
Undergraduate Medical Education in Myanmar: The structure of undergraduate medical education in Myanmar has undergone a transformative journey, evolving into a robust system that imparts a comprehensive understanding of medical science. The curriculum, meticulously developed over the decades, strikes a balance between theoretical knowledge and practical application, ensuring that graduates are well-equipped to navigate the complexities of healthcare. Milestones in curriculum development have played a pivotal role in shaping an adaptable and rigorous educational framework. Since the establishment of the Government Medical School in 1907 and the introduction of formal undergraduate medical training at Rangoon Medical College in 1927, Myanmar has continually refined its approach to align with global standards while addressing local healthcare needs (Batu, 2015). The integration of foundational medical sciences with clinical training, particularly from the 1960s onward, has created a holistic educational experience.
Clinical Training: Clinical training is a cornerstone of undergraduate medical education, offering students invaluable exposure to patient care, medical decision-making, and collaborative healthcare practices. From the 1970s, rotations in diverse medical specialties were formalised, enabling students to gain insights into the multifaceted nature of healthcare delivery. This hands-on approach fosters the development of critical thinking, diagnostic acumen, and a patient-centered mindset. Despite challenges such as resource constraints and political instability during the 1980s and 1990s, the resilience of Myanmar has been evident. By the 2000s, international collaborations and advancements in technology allowed for significant improvements in medical education delivery (Batu, 2015). Initiatives such as e-learning platforms and virtual simulations have enhanced accessibility and quality, ensuring a dynamic learning environment.
Outcomes and Global Impact: Graduates of Myanmar undergraduate programs emerge with a blend of strong theoretical knowledge, practical skills, ethical grounding, and communication proficiency. Many contribute to the global medical community, bringing cultural understanding and internationally recognised expertise to diverse healthcare settings.
Postgraduate Medical Education in Myanmar: Myanmar postgraduate medical education system has witnessed substantial transformation, adapting to the increasing demand for specialised expertise in healthcare (Saw et al., 2019). The diversification of postgraduate programs since the 1980s reflects a commitment to align with global standards while addressing the unique challenges of the nation’s healthcare system.
Specialised Training and Research: Postgraduate training emphasises advanced clinical skills and specialisation across medical disciplines. From the 1990s, research became an integral part of postgraduate education, fostering innovation and addressing critical healthcare gaps. Myanmar postgraduate students actively contribute to cutting-edge research, positioning the nation as a hub for medical advancements (Batu, 2015). This dual focus on research and clinical expertise ensures the preparation of professionals capable of tackling evolving healthcare challenges.
Collaborative Endeavors: International collaborations have played a pivotal role in enhancing postgraduate medical education. Partnerships with regional and global institutions have facilitated the exchange of expertise and best practices, enriching both training programs and research initiatives (Proserpio, 2022). These efforts underscore Myanmar’s commitment to participating in and contributing to the global medical community.
Outcomes and Ethical Practice: Myanmar postgraduate medical education is characterised by a dynamic interplay of specialised training, collaborative research, and a steadfast commitment to ethical medical practice (Rosenbaum et al., 2021). This multifaceted approach elevates the capabilities of healthcare professionals and enhances the overall standard of healthcare delivery, both nationally and internationally.
VI. CONCLUSION
Myanmar’s history of medical education is a dynamic narrative marked by resilience, adaptability, and the ability to turn challenges into opportunities. From its early adoption of Western medical practices during the colonial era to the establishment of a robust and evolving educational framework, Myanmar has consistently demonstrated a commitment to excellence. This global perspective highlights Myanmar’s efforts to align its medical education system with international benchmarks, contribute substantively to medical research, and actively engage in global public health initiatives. As Myanmar continues to shape its medical education landscape, it stands poised to make lasting contributions to global healthcare. Myanmar’s unwavering dedication to excellence not only enhances its own healthcare system but also enriches the global discourse on medical education and public health, positioning the nation as a vital contributor to the collective effort of improving global health outcomes.
Notes on Contributors
Tayzar Hein contributed to this manuscript’s first draft version , and revised its subsequent draft. Ye Phyo Aung, Khin Aung Htun, and Tin Tun contributed to the manuscript and critically revised the first draft. All the authors discussed and contributed to the final manuscript.
Funding
The activity is undertaken for the sake of personal and professional growth, and does not require any financial support.
Declaration of Interest
There is no conflict of interest in the current research.
References
Batu, A. T. (2015). The history of medical education in Myanmar (1886 to 2010). Myanmar Academy of Medical Science.
Coderey, C. (2021). Myanmar Traditional Medicine: The making of a national heritage. Modern Asian Studies, 55(2), 514-551. https://doi.org/10.1017/S0026749X19000283
Proserpio, L. (2022). Myanmar higher education in transition: the interplay between state authority, student politics and international actors.
Rosenbaum, S. A., Tushaus, D., Hubbard, B., & Sharp-Bauer, K. (2021). The Myanmar Shwe: Empowering law students, teachers, and the community through clinical education and the rule of law. Indiana Journal of Global Legal Studies, 28(1), 153-230.
Saw, Y. M., Than, T. M., Thaung, Y., Aung, S., Shiao, L. W.-S., Win, E. M., Khaing, M., Tun, N. A., Iriyama, S., & Win, H. H. (2019). Myanmar’s human resources for health: Current situation and its challenges. Heliyon, 5(3), e1390. https://doi.org/10.1016/j.heliyon.2019.e01390
*Tayzar Hein
No.94, D-1, Pyay Road, Mingaladon Township,
Yangon, Myanmar Postal code – 11021
+95 95188093
Email: dr.tayzarhein@gmail.com
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
