
Medical education adaptation in South Korea during the COVID-19 pandemic
Submitted: 24 December 2020
Accepted: 10 March 2021
Published online: 13 July, TAPS 2021, 6(3), 10-13
https://doi.org/10.29060/TAPS.2021-6-3/GP2455
Young-Mee Lee1 & Hyunmi Park1,2
1Department of Medical Education, Korea University College of Medicine, Seoul, South Korea; 2Department of Brain Convergence Research Center, Korea University College of Medicine, Seoul, South Korea
Abstract
Introduction: We describe the circumstances and adaptations in the South Korean medical education during the COVID-19 pandemic and discuss areas in need of improvement in preparation of a worsening situation or for similar future public health crises.
Methods: Literature reviews, focusing on research papers about medical educational changes in South Korea during the COVID-19 pandemic were performed. Selective data collected from a nationwide online survey by the Korean Association of Medical Colleges on the status of curricular changes in medical schools during the COVID-19 was presented.
Results: All lectures have moved online, but clinical students continued their hospital placements during the pandemic, except for the first 3-5 weeks during the first surge in 2020. Initial technical naivety of the faculty and lack of technical resources were short-lived and the medical students settled well showing a much higher than expected student satisfaction level over online education. Practical skills sessions which benefit most from onsite hands-on experiences such as anatomy dissection, were delivered through a blended approach in some medical school. Student evaluation is the area of least change, mainly due to the students’ lack of trust in online assessments.
Conclusion: South Korea’ underwent major changes in medical education brought upon COVID-19 and the readiness of the technology adoption has been much increased. Student evaluation is the area of least transformation. Adoption of a programmatic assessment system should be considered to enhance not only learning but also improve trust among stakeholders of medical schools.
Practice Highlights
- Medical education in South Korea has evolved rapidly due to COVID-19.
- Korea’s medical schools moved all its lectures online with positive student responses.
- Clinical placements continued under strict personal protection equipment.
- The readiness of technology adoption in education bore fruit during the current pandemic.
- Assessment is the area of least change, but to prepare for the future, adaptations are necessary.
I. INTRODUCTION
However, from the beginning of December 2020, the daily positive COVID-19 patients have steadily increased reaching the new 1,000 mark by mid-December. The government having raised its social distancing level up to 2.5 in the Seoul metropolitan area, is contemplating raising it to the maximum, which will become akin to the European lockdown with most non-essential businesses and institutions shutting down. At the time of writing this paper in the middle of December the whole country is trying hard to avoid lockdown.
In this paper, the authors described the circumstances and adaptations in the South Korean medical education during the COVID-19 pandemic with some specific examples and discuss areas in need of improvement in preparation of a worsening situation or for similar future public health crises.
II. OVERALL ADAPTATIONS IN MEDICAL SCHOOL WITH SPECIFIC EXAMPLES
On the 30th of January 2020, the Korean government, via the Central Disease Control Headquarters, raised the infectious disease alert level to three out of the four-tier system, and the Korean Association of Medical Colleges (KAMC) produced its first recommendation for its 40 medical schools. This recommendation included advice to medical schools to enhance its infection control measures, augment communication with the students and hospitals, and provide adequate personal protective equipment (PPE) to all students in the clinical hospital rotation. On the 23rd of February 2020, the Korean government raised its infectious disease alert to the highest level. On the 24th of February 2020, KAMC released its second guidance to all medical schools, relaying the advice from the ministry of education on delaying the school opening date for 2 weeks and suspending all clinical rotations.
To explore the overall adaptations in medical schools by the mid-May 2020, KAMC conducted a nationwide online survey which 37 deans out of the 40 medical schools in South Korea participated in. This survey showed that all 37 medical schools had changed to online education for their preclinical courses. Laboratory skills in basic science subjects moved online, but anatomy dissection laboratory varied: online e-Anatomy replaced them in 11 schools, and 14 schools delayed it to the end of semester, and 10 schools proceeded with on-campus cadaveric dissection under strict infection control measures when the government social distancing level decreased to level 2 (the daily new positive COVID-19 patient fell under 100). The early glitches derived from the technical naivety of the faculty and lack of technical resources did not last long, and all students, faculty and institutions adapted rapidly, which resulted in a much higher than expected student satisfaction level on online education. The area of least change was in the student assessment. The student assessment was mostly delayed, and held later in face-to-face format at the end of the semester.
The suspension of clinical rotations varied widely between schools, from the first week of March to the last week of May 2020, with a median of 21 days. 14 schools provided online teaching and one school provided alternative simulation lessons but without patient contact during the closure or delay of clinical rotations. Before making the decision on restarting clinical rotations, there were high tensions between medical schools and students and even parents who were concerned and nervous on the potential infection risk to students that the hospital rotations potentially posed. To reduce this anxiety, medical schools held a series of meetings with student representatives and after putting in place safeguards against the risk of COVID-19 infection including PPE, the clerkships restarted. KAMC’s great efforts in the procurement of masks for medical students was critical for restarting clinical rotations, and medical schools were able to provide five masks per student per week even during the period of extreme masks shortage (Park et al., 2020).
A. Blended Anatomy Learning: Does Students’ Satisfaction Equal Achievement of Intended Learning Outcomes?
In the authors’ medical school, the COVID-19 pandemic forced the anatomy course to change from the traditional large group lectures and cadaveric dissection to blended anatomy courses. The theory lectures were delivered entirely online and the anatomy dissection course, resulted in an inadvertent flipped learning effect. The e-Anatomyâ videos (Panmun Education, Seoul, Republic of Korea), and Complete Anatomyâ (Elsevier, Amsterdam, Netherlands) online platform were provided to students as home assignment while on-campus dissection sessions were suspended. At the end of April, face-to-face cadaver dissections recommenced following the infection prevention measures guidelines with the use of proper PPE.
Although the students’ responses to the online anatomy teaching were remarkably positive, the anatomy department faculty at the authors’ school were concerned about the effectiveness of the altered teaching methods in achieving the intended learning outcomes. Therefore, Yoo et al. (2021) examined the educational outcomes of the online and blended learning approach in anatomy, and the results showed the anatomy achievement scores of the blended learning group (the 2020 class) being higher than those of traditional lectures (2019 class). The authors of this study interpreted that in-advance self-study at home using online learning videos before the actual on-campus dissection labs induced a flipped learning effect, and online education let the students to achieve more self-study time and individual tailored learning.
B. Adaptations in Paediatric Clerkship Education
As described earlier, most university-based hospital rotations restarted around March 16th with limited patient contact in respiratory and primary community clinics. Although the reduced patient volume which students could come into contact was inevitable, this situation was most serious in paediatric clinical clerkships. Paediatric patients visiting primary clinics and even tertiary university hospitals drastically decreased down in South Korea during the COVID-19 pandemic. In addition, the paediatric parents’ refusal or complaints on being seen by medical students worsened and the number of medical students allowed into hospital rotations were restricted in some hospitals.
To overcome the shortcomings of paediatric clerkship education, the authors of the study (Lee, K. D. Park et al., 2020) created an actual patient encounter-based role play. One student within the student group (usually 3-4 students in one group) performed a history taking and physical examination of a hospitalised child with a guardian, who later played the role of the parent, with another student in the same group taking the doctor’s role, interacting with each other in front of faculty physicians, residents, and the rest of the peer students. This role play session facilitated the provision of feedback and discussion. The students’ responses to the alternative educational approaches were positive, but the students required more discussion, and detailed feedback from the faculty physicians on their performance.
C. Online Medical Education Seminar for Faculty
Although the advantages of webinars in higher education and professional training have already been proven, they have not been widely used in South Korea before the COVID-19 pandemic. However, currently webinars and online academic conferences have almost totally replaced onsite gatherings. The COVID-19 pandemic has forced the Faculty Academy of Medical Education (FAME) seminars at Korea University College of Medicine (KUCM) to go online (Lee, H. Park et al., 2020). The authors of this study reported that FAME was established to enhance the teacher’s educational competency and promote a positive educational culture, but the participation of faculty members in this seminar has not been very active. When FAME had to be abruptly changed to online, the authors moved the seminar format online with pessimistic expectations of further decrease in the number of participants. However, such expectations were thoroughly shattered on April 8th by the login attendance of 210 faculty members on the first webinar which was the highest attendance since its inception in 2012. Although the webinar for faculty development was launched successfully and received positive reviews, further studies should follow to examine its educational effectiveness.
D. Medical Licensing Examination
The Korean Medical licensing exam consists of two parts; the written test takes place annually in January and the clinical skills test is held the previous year usually between September and October. During the span of 35 days 3,100 participants are examined in one examination centre. This year, the clinical exam was planned to be held between September 1st and October 27th, at its usual centre under strict infection control measures. However, another unprecedented crisis was added on the present COVID-19 pandemic in South Korea. In August 2020 Korean doctors held a series of national strikes as the government tried to push new policies amidst a pandemic where healthcare workers have been working tirelessly over the previous half a year to maintain the COVID-19 cases at bay and protecting the public. The doctors’ national protest was triggered by a sudden governmental announcement on critical policy changes without any previous discussion or consultation to medical associations or medical education authorities. The policies included the foundation of a ‘public medical school’ funded by taxpayers’ money with a non-transparent admission criterion and an exemption from the standard accreditation process to accelerate its building. This policy only focused on increasing the total number of doctors with the hope to fill the currently essential specialties which residents undersupply without dealing with the core underlying problem.
The national doctors strike resulted in 86% of medical students forfeiting their application for the national licensing exams (Kim & Choi, 2020) with only around 400 students undertaking the clinical exam on site wearing masks. All the stations were carried out as before with only the oral cavity examination being replaced for a verbal explanation.
III. DISCUSSION
Korea has managed the COVID-19 situation relatively well and only the lectures were moved online, whilst exams were carried face-to-face, and almost near-normal clinical practice training ensued in medical education. This double edge sword situation might not have prepared us as a nation in the event of a worse pandemic in the future. Fortunately, we can learn from the published experiences of other countries such as virtual rounds, virtual patient encounters, clinical skills simulations through the use of information technology (IT), and from virtual or augmented reality experiences used in resident skills training.
Remarkable advances in the Korean medical education in recent decades, especially, the readiness of technology adoption in education bore fruit during the current pandemic. More importantly, the experiences gained by educators during COVID-19 have consolidated student-centred education which was previously a concept rather than an actioned need. Nevertheless, student evaluation is the area of least transformation. The main reason for the resistance by the students towards online assessments is the lack of trust in the security and fairness of such method. The students’ negative perceptions over online assessments are mainly due to their belief that no technical method can 100% prevent cheating. Some medical educators pointed out that having to consider using various devices to prevent cheating during online exams is born out of the schools’ mistrust towards students, a non-educational behaviour in need of reconsideration. However, in Korea, the distrust among student peers is a bigger issue than the mistrust between the schools and students. To reduce the distrust surrounding examination, we should reconsider the current competitive summative assessment system. We could aspire for a better model, which can promote student learning instead of focusing on achieving good grades only. It is time to discuss a transition to a programmatic assessment and investigate ways on its adaptation and incorporation in medical education.
The authors of this article described major changes in medical education brought upon COVID-19 and the lessons what we’ve learned in South Korea. Since each country has faced differing levels of the COVID-19 crisis, our experience in South Korea may not be directly transferrable to other countries or contexts. However, sharing eclectic experiences from differing countries the mounting literature that can be tapped into by countries who find themselves in similar situations as ours in the future. Medical educators should actively share their novel ideas, experiences and hardships encountered on medical education through the current health crisis, as such cooperation will prepare us all against the uncertain medical future.
Notes on Contributors
Young-Mee Lee is a professor at the Department of Medical Education, Korea University College of Medicine, Seoul, South Korea, reviewed the literature, developed the methodological framework for the study, performed data analysis and developed the manuscript, gave critical feedback to the writing of the manuscript.
Hyunmi Park, MBChB, FRCS, PhD, is a research professor at the Department of Brain Convergence Research Center, Korea University, Seoul, South Korea, reviewed the literature, analysed the data and was involved in the writing of the draft, review and editing of the manuscript.
Both authors have read and approved the final manuscript.
Acknowledgments
We, authors of this study, are very grateful to KAMC for sharing the national survey data so we could perform the analysis and interpretation of such data. We wish to show our deepest gratitude to every single one of the Korean medical school deans, who not only have taken their time to participate in our study, but have tirelessly worked during the worst pandemic in living memory to ensure the safety of students and staff whilst maintaining the highest of standards in medical education.
Funding
There are no funding sources to declare.
Declaration of Interest
No conflicts of interest to declare.
References
Kim, M., & Choi, H. (2020). S. Korean government to not let over 2,700 medical students another shot at medical licensing exam. Hankyoreh. http://english.hani.co.kr/arti/english_edition/e_national/961515.html
Lee, Y. -M., Park, H., Pyun, S. B., & Yoon, Y. W. (2020). Enforced format change to medical education webinar during the coronavirus disease 2019 pandemic. Korean Journal of Medical Education, 32(2), 101–102. https://doi.org/10.3946/KJME.2020.158
Lee, Y. – M., Park, K. D., & Seo, J. H. (2020). New paradigm of pediatric clinical clerkship during the epidemic of COVID-19. Journal of Korean Medical Science, 35(38), 1–5. https://doi.org/10.3346/JKMS.2020.35.E344
Park, J., Park, H., Lim, J. E., Rhim, H. C., & Lee, Y. -M. (2020). Medical students’ perspectives on recommencing clinical rotations during coronavirus disease 2019 at one institution in South Korea. Korean Journal of Medical Education, 32(2), 223–229. https://doi.org/10.3946/KJME.2020.170
Yoo, H., Kim, D., Lee, Y. -M., & Rhyu, I. J. (2021). Adaptations in anatomy education during COVID-19. Journal of Korean Medical Science, 36(1), e13. https://doi.org/10.3346/jkms.2021.36.e13
*Young-Mee Lee
Department of Medical Education,
Korea University College of Medicine,
73 Goryodae-ro, Seongbuk-gu,
Seoul, 02841, Republic of Korea
Email: ymleehj@korea.ac.kr
Submitted: 28 July 2020
Accepted: 3 December 2020
Published online: 13 July, TAPS 2021, 6(3), 75-82
https://doi.org/10.29060/TAPS.2021-6-3/OA2366
Kirsty J Freeman1 & Brid Phillips2
1Office of Education, Duke-NUS Medical School, Singapore; 2Health Professions Education Unit, The University of Western Australia, Australia
Abstract
Introduction: Healthcare requires its practitioners, policymakers, stakeholders, and critics to have empathetic awareness and skills in critical thinking. Often these skills are neglected or lost in current educational programs aimed at those interested in the field of health. Health humanities and, in particular narrative medicine, aim to redress this omission.
Methods: We used a mixed methods approach to explore the experience of health humanities students in creative writing and staged readings to foster empathic awareness and critical thinking. Data was collected from 20 second-year students enrolled in an undergraduate health humanities unit via a post-assessment survey, and thematic analysis of a reflective paper.
Results: 92.9% of the students felt that writing a creative piece helped them to understand the health topic from a different perspective, with 85.7% reporting that the use of creative writing helped to create emotional connections. From the reflective paper, six themes were elicited through the thematic data analysis: (1) The value of language; (2) Insights into the patient experience; (3) Giving voice to the patient; (4) Creating empathic exchanges; (5) Illness and emotion; and (6) Reflective practice.
Conclusion: By offering a mode of experiential learning involving both creative writing and staged readings, students develop empathic ways of thinking and being while deepening their critical engagement with a range of health topics. Students were able to understand the need to make humanistic sense of the health and well-being narrative, providing them with a range of transferable skills which will be an asset in any workplace.
Keywords: Narrative Medicine, Empathy, Critical Thinking, Staged Reading, Health Humanities
Practice Highlights
- Creative writing and staged readings are effective in fostering empathetic awareness and critical thinking.
- Narrative medicine techniques result in greater understanding about the perspectives of others.
- Developing creative language leads to enhanced communication skills and nuanced ways of thinking.
- Staged readings delivered online provide effective teaching and learning opportunities.
I. INTRODUCTION
Health humanities, and the attendant field of medical humanities, refer to the application of the creative or fine arts (visual arts, performing arts etc.) and humanities disciplines (literary studies, law, history, philosophy, etc.) to discussions and explorations on the nature of human health and well-being (Crawford et al., 2010). Within this broad umbrella lies the discipline of narrative medicine. The application of humanities to health has had a long pedigree, but the distinct disciplines of both narrative medicine and health humanities only began to emerge over the first decade of the 21st Century. In part, they emerged from a growing concern about an increasing lack of empathy in health professionals (Dean & McAllister, 2018; Lai, 2020). Narrative medicine with its interest in creativity and ambiguity strives to address this concern. Through narrative medicine, skills in thinking reflectively, listening actively, observing more closely and writing creatively can be developed. It has been shown that there is a positive impact on empathy and communication following narrative medicine education (Barber & Moreno-Leguizamon, 2017). This is important as the empathy conveying physician is more successful in promoting better clinical outcomes for patients. However, ‘[d]espite the centrality of stories to many of the tasks that clinicians perform it remains that explicit and formal teaching of knowledge and methods in narrative is relatively novel’ (Boudreau et al., 2012, p. 152).
One of the educational techniques embraced in narrative medicine is staged readings. A staged reading is an event which may have some rehearsal time, but the readers use scripts on stage. There is minimal staging, costuming, and props. This is pertinent as the use of theatre in academic teaching represents a new model of education that reminds students of the humanity of people (Baker et al., 2019). This form of engagement involves an emotional transaction through the spectacle of theatre which, as the Greeks understood it, was an occasion that provided recognition, catharsis, and release for both the individual and the wider community (Shapiro & Hunt, 2003). Health topics are also more easily understood through the medium of performance (Ünalan et al., 2009). Ünalan et al. (2009) also surmised that theatrical performance could increase empathy levels. There are similar benefits to be had from staged medical readings which foster introspection and reflection (Matharu et al., 2011). The purpose of this study was to determine whether the use of creative writing and staged readings could develop empathy and critical thinking in second year university students enrolled in an undergraduate health humanities unit of study. Student enrolment information confirms majority of students are on a pathway to studying medicine, pharmacy, dentistry, ophthalmology, or global health.
A. Context
In semester one of 2020, 20 second-year students were enrolled in a narrative medicine unit, as part of their undergraduate bachelor’s degree. By delivering an undergraduate unit in narrative medicine, the goal is to give students the opportunity:
- To dip their toes into the world of literary fiction.
- To present their own creative pieces relating to health topics.
- To gain an understanding of health issues from the perspective of others as this increases empathetic awareness.
Through a series of scaffolded assessments, students have a unique opportunity to develop empathetic awareness and critical thinking skills through creative presentations mimicking staged readings.
Two of the three assessments related to the staged reading, the second assessment was a creative piece and the third was a reflection on process of creating the piece and the health topic to which it related. The purpose of these assessments was to demonstrate different modes of narrative writing. This was achieved through the construction of a creative piece that explored a health topic using narrative medicine techniques including but not limited to short story writing, poetry, and play writing.
The unit involved supporting students to devise a short creative writing piece. Within the piece, themes of empathy, communication, cultural difference, and societal biases and assumptions around the students’ chosen health topics were explored. The piece was then to be presented as a staged reading by the students for an invited audience. The audience would include the wider university community of undergraduate and postgraduate students, staff, and invited guests such as health professionals to the reading. Immediately following their reading, the students, supported by academic staff, were to hold a guided discussion on the significance of health topics in the piece. This discussion would bring biases and assumptions into focus and heighten the individual’s awareness of emotional dynamics at work in the healthcare context while also offering insights into the perspective of others. Similar programs have been used to educate bioethical students, help them to develop discussion questions, and enhance their critical self-reflection (Kerr et al., 2020; Robeson & King, 2017).
Students were required to read a literary fiction novel, Extinctions (Wilson, 2020). The act of reading itself has demonstrated benefits of improving processing of experiences and developing empathy. Reading literature also improves our social awareness and our ability to see the perspectives of others (Fennelly, 2020; Kaptein et al., 2018). In the novel Extinctions, there are many discernible health topics such as traumatic brain injury, drug use, ageing, mobility issues, death and dying, and loss of independence. There is also a range of characters involved in these issues from a young girl with a drug problem to the protagonist, Fred, a man in his declining years. It was important to foster student engagement with the project by offering a fully scaffolded experience to allay performance anxieties. Scaffolding has been shown to support students as they negotiate a challenging environment and allow them to make meaning for themselves rather than have it imposed on them from an autocratic perspective (Wilson, 2016). Each week from the first week of semester, the seminar included both a close reading exercise and a creative writing exercise. The scaffolding also included several resource folders addressing the main genres the students were encouraged to explore – short story, poetry, drama. The folders contained videos, book chapters, blog posts, and journal articles that introduced the students to ways of writing creatively. There was also a dedicated workshop which explored these techniques and answered any questions the students had on creative writing.
Due to COVID-19 restrictions on social gatherings and the cancellation of face-to-face interactions, the presentation aspect had to be cancelled at short notice and instead, presentations took place online without the wider audience participation. The creative pieces were read in an online forum limited to students and the unit coordinator. The students had the opportunity to read their work to other participating students and to lead a short discussion on their health topic. This sharing is important as ‘representation is always a dialogue, in which, the receiver of the work contributes a necessary response to the creator of the work’ (Charon et al., 2016, p. 347). As the students based their pieces on fully rounded characters from the novel, this process shares similarities with verbatim theatre. Verbatim theatre has been shown to allow positive exploration of emotional behaviours (Scott et al., 2017). After this process, students were encouraged to incorporate feedback from the presentations into their pieces before submission of the creative piece.
The third assessment component of the unit required the students to submit a reflective essay on the experience where they discuss the creative process and their representation of the health topic which they had chosen. They had to discuss the significance of the health topic and examine their personal responses to the topic and how it was influenced by their research, the creative process, and the discussions which took place following the presentation of the piece. To support the reflective process, we developed a reflective writing toolkit which illustrates both the process and its importance.
II. METHODS
A cross-sectional mixed methods design was used to evaluate the experience of health humanities students in creative writing and staged readings to foster empathic awareness and critical thinking. 20 second-year students who were enrolled in a narrative medicine unit between January and June 2020 were invited to participate.
A. Data Collection and Analysis
Data was collected at two points over the semester, an online survey in week 10, and a reflective paper at the end of semester in week 13.
1) Creative writing and staged reading assessment student experience survey: All 20 undergraduate students enrolled in the unit in semester one, 2020, were invited to participate in an online survey examining the student experience of participating in the creative writing and staged reading assessment. The survey tool curated by author one (KF) was designed to collect basic demographic data about the student, along with information about their current enrolment. The survey was designed to evaluate the first two level of Kirkpatrick’s model of program evaluation, level one being reaction and level two learning (Frye & Hemmer, 2012). Given that this is the first time the program had been offered, the authors felt that the data collected would provide a baseline upon which further detailed evaluations can build upon. Students were asked to rate their experience with the staged reading project using a five-point Likert scale, as well as responding to open-ended questions designed to further expand on the students’ experience. A statement of voluntary consent was included at the start of the survey and the participant had to agree to the consent before the survey could commence. Thus participation in the anonymized online evaluation indicates consent. Descriptive statistics were calculated for the demographic data. Categorical data are presented as number and percentage. The analyses were performed using IBM SPSS Statistics Version 25.0. Thematic analysis of the open-ended questions was then undertaken. Researcher bias was minimised by having author one (KF), who was not involved in delivering the course, undertake the analysis of the survey data.
2) Staged reading reflective essay: The second data collection point was a reflective essay (n=20). Thematic analysis of the text was undertaken by both authors. Each author reviewed the transcripts separately, making note of key phrases, outline possible categories or themes. Discussion of our interpretations took place over teleconference, as we then jointly rearranged and renamed the codes, developing higher order themes. NVivo 12™ was used to manage the qualitative data (QSR International., 2018). This mixed methods design combines quantitative and qualitative data to provide a richer source of information about the experience of staged readings.
III. RESULTS
A. Creative Writing and Staged Reading Assessment Student Experience Survey
Of the 20 students enrolled in the unit, 14 completed the student experience survey, a response rate of 70%. Table 1 summarises the demographic characteristics of the respondents. As can be seen in Table 1, the students were enrolled in one of three bachelor degrees. The degree enrolled by majority of students in is science based, with only 1 respondent studying an Arts based degree. 92.8% of respondents had not previously completed an undergraduate degree. Three respondents spoke languages other than English at home.
When asked to rate their experience in the staged reading project 92.9% of the respondents felt that writing a creative piece helped them to understand the health topic from a different perspective; with 85.7% reporting that the use of creative writing helped to create emotional connections (Table 2).
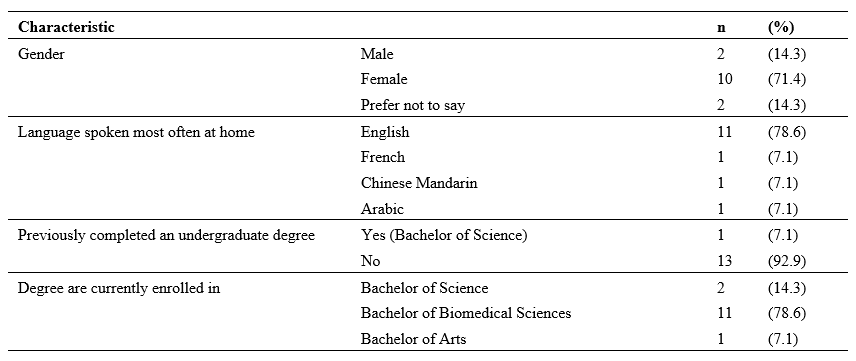
Table 1. Summary of demographic characteristics of respondents
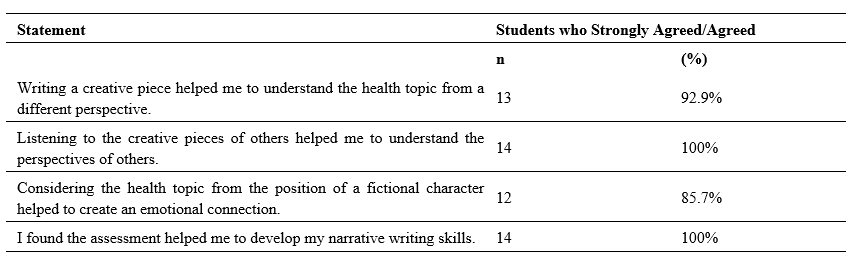
Table 2. Student rating of creative writing and staged reading assessment
When asked to describe their experience of the staged reading assessment in the free text survey questions students reported feeling daunted, nervous and apprehensive about the prospect of writing a creative piece, as many of them shared that they had little or no experience with creative writing. With several students describing to task as challenging, on reflection they expressed feeling fulfilled, enriched, sharing that they found the task rewarding.
A. Staged Reading Reflective Essay
The qualitative data analysis resulted in six themes being identified: (1) The value of language; (2) Insights into the patient experience; (3) Giving voice to the patient; (4) Creating empathic exchanges; (5) Illness and emotion; and (6) Reflective practice (Figure 2). These themes are described in this section, illustrated with representative quotes.
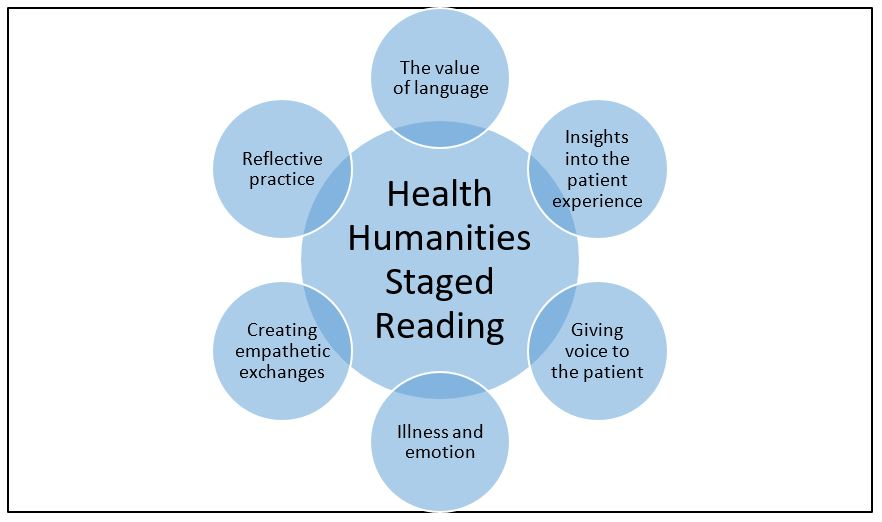
Figure 1. Overview of the staged reading themes
1) The value of language: as they worked through their creative piece, students discovered the value and power of language as a tool for expression and communication. Students commented on their appreciation of language:
Since I wanted to create a powerful and emotional piece, I experimented using literacy techniques to achieve a desperate and anxious tone.
Student 2
I learnt that the use of language is also vital in writing a creative piece, emphasising the importance of communication between the author and readers.
Student 14
2) Insights into the patient experience: Students developed an awareness of the value of research when trying to understand the issues surrounding health topics. Better equipped with quality knowledge and research, they were able to give more nuanced accounts of health experiences. Students learned the value of looking beyond the symptom to see the whole person and, thus the value and importance of person-centred care:
Acknowledging that my research and reflections had resulted in greater understandings of both the health topic and the importance of seeing a patient beyond their physical disease.
Student 2
It is very important to take into consideration all aspects of what a person is experiencing in order to make the best assessment and to come up with the best route of action to help the patient overcome whatever it is they are suffering from.
Student 1
3) Giving voice to the patient: Students gained an insight into the need to give a voice to patients in order to gain better understanding of the perspectives of others. They reflected on the powerlessness and silence that often surrounds certain conditions and situations:
I felt that I was able to give Katie an authentic voice, through which readers were then able to empathise with, and better understand, her struggles.
Student 4
Furthermore, the narratives of victims can empower them by giving them a voice in times when they are often silenced.
Student 7
4) Creating empathetic exchanges: Students gained an understanding of empathetic exchanges and in some instances understood the need to create opportunities for the development of empathy. The students did not always articulate the word empathy but instead alluded to the concept by talking about experiencing and understanding the emotions and perspectives of others:
I felt increased levels of empathy towards individuals dealing with the disorder as I now understand the many other challenges and hurdles that accompany eating disorders that I didn’t know prior to this assignment.
Student 8
When using these descriptions, I felt that I was able to build an emotional connection with Katie’s character, thus encouraging readers to also empathise with her situation.
Student 4
5) Illness and emotion: Students discovered that emotional transactions and states are intertwined with health and illness. They understood, through their work, the interconnectiveness of emotional responses and illness. Some of their observations included:
I have become more sensitive to the idea that human beings are inherently emotional and can be affectively moved when provided with an impetus.
Student 3
The purpose of the piece was unearthing the complex thoughts and emotions individuals with eating disorders and substance abuse go through.
Student 8
6) Reflective Practice: On topics where students previously had felt knowledgeable, deeper reflection and considerations revealed their own misconceptions and lack of knowledge. Within this paradigm, they also showed a maturation of habits and behaviours. Their comments were insightful:
I entered a phase of reflection where I realised that I would have previously contributed to these harmful views.
Student 2
I learnt and later researched further the differences in the perception of STEM women in both Western and Asian populations. This is something I would attempt to change. It was really interesting for me to discover that I had this unconscious bias forcing me to further expand my learning and knowledge in the area.
Student 18
IV. DISCUSSION
While the use of creative writing and staged readings is a developing area in health humanities, the findings of this study suggest that they are effective in fostering emotional awareness and critical thinking. McDonald et al. (2015) found that ‘[a]nalysis of the student’s writing showed that they demonstrated the ability to “stand in another’s shoes” and, interestingly, the students’ comments on their own writing showed that their ability to relate to characters they initially felt little affinity for deepened’ (McDonald et al., 2015, p. 9).
By taking part in the creative writing project and the accompanying reflection piece, students were exposed to an innovative and experiential form of learning that provided a unique pedagogical experience. Whilst the students reported being daunted at the thought of constructing a creative piece, the self-reflective processes and actively engaging with the perspectives of others, ensured students were able to enhance their critical thinking skills. In the creative writing and staged reading assessment student experience survey, 100% of students agreed, “Listening to the creative pieces of others helped me to understand the perspectives of others”. This accords with the work of Deloney and Graham who note “[e]xperiential learning activities increase student engagement and are a helpful tool to connect abstract ideas with concrete knowledge” (Deloney & Graham, 2003, p. 249).
The findings of this study highlight the value of language as a tool for expression and communication. Educators need to be mindful of their student population when contemplating incorporating creative writing and staged readings into their programs. For students to be accepted for enrolment at The University of Western Australia they must demonstrate a minimum level of English language proficiency necessary for academic studies. Whilst there has been several studies examining what Hyland calls “linguistics disadvantage in terms of a Native/non-Native divide” (Hyland, 2016, p. 61) in academic writing (Badenhorst et al., 2015; Bocanegra-Valle, 2014; Zhao, 2017), the impact of this linguistic divide in creative writing and staged readings has not been fully explored.
The students gained insights into holistic care relating to both themselves and others. As these are undergraduate students, many on a pathway to a career in health, insights into holistic care and self-care are valuable life lessons. There was also an indication that the process contributed to the social and cultural well-being of themselves and others. Nagji et al. (2013) note that theatre based programs/novel humanities based curriculum items contribute to student well-being, an increasingly important area for universities to address particularly during a pandemic. Although the student population participating in this unit are studying science-based degrees where creative writing is not commonplace, the learning strategies were structured in a way that enabled development of narrative writing skills.
By integrating the narrative medicine techniques of creative writing and staged readings the students were able to give more nuanced accounts of health experiences. Students learned the value of looking beyond the symptom to see the whole person and, thus the value and importance of person-centred care. This gave them valuable insights into the patient experience. During this process, students gained an insight into the need to give a voice to patients in order to gain better understanding of the perspectives of others. They learnt about the powerlessness and silence that often surrounds certain conditions and situations. In their responses, the students did not always articulate the word empathy but instead alluded to the concept by talking about experiencing and understanding the emotions and perspectives of others. Students gained an understanding of the power of empathetic exchanges and in some instances understood the importance of creating empathetic exchanges opportunities. Another important theme which was uncovered, was a growing awareness amongst students that emotional transactions and states are intertwined with health and illness. They understood, through their work, the interconnectiveness of illness and emotion. On topics where students previously had felt knowledgeable, deeper reflection and considerations revealed their own misconceptions and lack of knowledge. Within this paradigm, they also showed a maturation of habits and behaviours leading to improved reflective practices.
There were limitations with the project as we had to move from face-to-face to online teaching due to constraints placed upon teaching during the COVID-19 pandemic. However, the online format did have some unexpected benefits, with a number of students feeling less intimidated when presenting online compared to a face-to-face workshop. Despite the move to online teaching, the cohort remained present and engaged in the project. Many expressed regrets at losing physical contact and the incidental discussions that happen before and after classes but overall with support they adapted well.
V. CONCLUSION
This study has described the experience of students engaging in creative writing and staged readings as part of a narrative medicine unit. Students completing the unit and its attendant assessments developed useful life skills including critical thinking, understanding the perspectives of others, and the positive use of narrative in appreciating the experiences of others. The work engaged them in new and innovative ways evidenced by some statements which noted that their experience in this unit was unique in their university journey. Having autonomy over the health topic they chose, the character they explored, and the creative medium they used to express their thinking, enhanced the learning experience and allowed them to meet the learning outcomes of the unit.
Notes on Contributors
Kirsty J Freeman crafted the paper with her co-author, performed the data collection and analysis of the survey, and undertook thematic analysis of the reflective essays. Dr Brid Phillips crafted the paper with her co-author, conducted the literature search, and undertook thematic analysis of the reflective essays. All the authors have read and approved the final manuscript.
Ethical Approval
Ethics approval was granted by The University of Western Australia Human Research Ethics Committee: HREC RA/4/20/5254.
Data Availability
All relevant quantitative data are within the manuscript. The qualitative data collected for this manuscript originates from assessment items submitted as part of the participants’ academic studies. The authors do not have consent to upload this data into a data repository.
Acknowledgement
We would like to thanks the students who participated in this unit and their willingness to adapt to the online platform with grace and enthusiasm.
Funding
This work has not received any external funding.
Declaration of Interest
All authors declare that there are no conflicts of interest.
References
Badenhorst, C., Moloney, C., Rosales, J., Dyer, J., & Ru, L. (2015). Beyond deficit: Graduate student research-writing pedagogies. Teaching in Higher Education, 20(1), 1-11. https://doi.org/10.1080/13562517.2014.945160
Baker, H. F., Moreland, P. J., Thompson, L. M., Clark-Youngblood, E. M., Solell-Knepler, P. R., Palmietto, N. L., & Gossett, N. A. (2019). Building empathy and professional skills in global health nursing through theatre monologues. The Journal of Nursing Education, 58(11), 653-656. https://doi.org/10.3928/01484834-20191021-07
Barber, S., & Moreno-Leguizamon, C. J. (2017). Can narrative medicine education contribute to the delivery of compassionate care? A review of the literature. Medical Humanities, 43(3), 199-203. https://doi.org/10.1136/medhum-2017-011242
Bocanegra-Valle, A. (2014). ‘English is my default academic language’: Voices from LSP scholars publishing in a multilingual journal. Journal of English for Academic Purposes, 13(1), 65-77. https://doi.org/10.1016/j.jeap.2013.10.010
Boudreau, J. D., Liben, S., & Fuks, A. (2012). A faculty development workshop in narrative-based reflective writing. Perspectives on Medical Education, 1(3), 143-154. https://doi.org/10.1007/s40037-012-0021-4
Charon, R., Hermann, N., & Devlin, M. J. (2016). Close reading and creative writing in clinical education: Teaching attention, representation, and affiliation. Academic Medicine, 91(3), 345-350. https://doi.org/10.1097/ACM.0000000000000827
Crawford, P., Brown, B., Tischler, V., & Baker, C. (2010). Health humanities: The future of medical humanities? Mental Health Review Journal, 15(3), 4-10. https://doi.org/10.5042/mhrj.2010.0654
Dean, S., & McAllister, M. (2018). How education must reawaken empathy. Journal of Advanced Nursing, 74(2), 233-234. https://doi.org/10.1111/jan.13239
Deloney, L. A., & Graham, C. J. (2003). Wit: Using drama to teach first-year medical students about empathy and compassion. Teaching and Learning in Medicine, 15(4), 247-251. https://doi.org/10.1207/S15328015TLM1504_06
Fennelly, B. A. (2020, May 15). What’s the use of reading? Literature and empathy [Video] . https://youtu.be/9nJv8sxpUKU
Frye, A. W., & Hemmer, P. A. (2012). Program evaluation models and related theories: AMEE guide no. 67. Medical Teacher, 34(5), e288-299. https://doi.org/10.3109/0142159x.2012.668637
Hyland, K. (2016). Academic publishing and the myth of linguistic injustice. Journal of Second Language Writing, 31, 58-69. https://doi.org/10.1016/j.jslw.2016.01.005
Kaptein, A., Hughes, B., Murray, M., & Smyth, J. (2018). Start making sense: Art informing health psychology. Health Psychology Open, 5(1), 205510291876004. https://doi.org/10.1177/2055102918760042
Kerr, A., Biechler, M., Kachmar, U., Palocko, B., & Shaub, T. (2020). Confessions of a reluctant caregiver palliative educational program: Using readers’ theater to teach end-of-life communication in undergraduate medical education. Health Communication, 35(2), 192-200. https://doi.org/10.1080/10410236.2018.1550471
Lai, C.-W. (2020). “Booster shots” of humanism at bedside teaching. The Asia Pacific Scholar, 5(2), 45-47. https://doi.org/10.29060/TAPS.2020-5-2/PV1085
Matharu, K. S., Howell, J., & Fitzgerald, F. (2011). Drama and empathy in medical education: Drama and empathy. Literature Compass, 8(7), 443-454. https://doi.org/10.1111/j.1741-4113.2011.00778.x
McDonald, P., Ashton, K., Barratt, R., Doyle, S., Imeson, D., Meir, A., & Risser, G. (2015). Clinical realism: A new literary genre and a potential tool for encouraging empathy in medical students. BMC Medical Education, 15(1), 112-112. https://doi.org/10.1186/s12909-015-0372-8
Nagji, A., Brett-MacLean, P., & Breault, L. (2013). Exploring the benefits of an optional theatre module on medical student well-being. Teaching and Learning in Medicine, 25(3), 201-206. https://doi.org/10.1080/10401334.2013.801774
QSR International. (2018). NVivo 12 [Software]. In https://qsrinternational.com/nvivo/nvivo-products/
Robeson, R., & King, N. (2017). Performable case studies in ethics education. Healthcare, 5(3), 57. https://doi.org/10.3390/healthcare5030057
Scott, K. M., Berlec, Š., Nash, L., Hooker, L., Dwyer, P., Macneill, P., River, J., & Ivory, K. (2017). Grace under pressure: A drama-based approach to tackling mistreatment of medical students. Medical Humanities, 43(1), 68. https://doi.org/10.1136/medhum-2016-011031
Shapiro, J., & Hunt, L. (2003). All the world’s a stage: The use of theatrical performance in medical education. Medical Education, 37(10), 922-927. https://doi.org/10.1046/j.1365-2923.2003.01634.x
Ünalan, P. C., Uzuner, A., Ifçili, S., Akman, M., Hancolu, S., & Thulesius, H. O. (2009). Using theatre in education in a traditional lecture oriented medical curriculum. BMC Medical Education, 9(1), 73-73. https://doi.org/10.1186/1472-6920-9-73
Wilson, J. (2020). Extinctions. UWA Publishing.
Wilson, K. (2016). Critical reading, critical thinking: Delicate scaffolding in english for academic purposes (EAP). Thinking Skills and Creativity, 22, 256-265. https://doi.org/10.1016/j.tsc.2016.10.002
Zhao, J. (2017). Native speaker advantage in academic writing? Conjunctive realizations in EAP writing by four groups of writers. Ampersand, 4, 47-57. https://doi.org/10.1016/j.amper.2017.07.001
*Kirsty J Freeman
Duke-NUS Medical School
8 College Road, Singapore 169857
Tel:+65 89219676
Email: kirsty.freeman@duke-nus.edu.sg
Submitted: 15 October 2020
Accepted: 17 February 2021
Published online: 13 July, TAPS 2021, 6(3), 5-9
https://doi.org/10.29060/TAPS.2021-6-3/GP2430
Wei-Han Hong1a, Vinod Pallath1b, Chan Choong Foong1, Christina Phoay Lay Tan2, Mary Joseph Marret3, Yang Faridah Abdul Aziz4 & Jamuna Vadivelu1
1Medical Education Research and Education Unit, Faculty of Medicine, Universiti Malaya, Malaysia; 2Department of Primary Care Medicine, Faculty of Medicine, Universiti Malaya, Malaysia; 3Department of Paediatrics, Faculty of Medicine, Universiti Malaya, Malaysia; 4Department of Biomedical Imaging, Faculty of Medicine, Universiti Malaya, Malaysia
a,bJoint first author
Abstract
Introduction: The article is a succinct summary of events and process for emergency digitisation and transition to remote teaching during the COVID- 19 pandemic. The challenges of such transition included the need for enhanced infrastructure facilities, compliance to directives from regulatory bodies, providing an equivalent learning experience in the virtual learning environment (VLE) and ensuring the end user capacity to utilise the VLE created.
Methods: To accomplish this task a suitable instructional design and transition model was utilised to create an integrated Moodle and Microsoft Teams platform as the VLE. The curriculum was recreated in the VLE through review of existing infrastructure and resources, deconstructing the demands of the curriculum, reconstructing the learning experiences of curriculum in VLE and innovating to improve. The end user training was also provided using the same VLE created, which ensured capacity building. Virtual Clinical Assessments (VCA) were created to ensure the completion of assessment tasks.
Results: The utilisation of the ACTIONS transition model resulted in the evolution of instructional delivery from a Web Enhanced approach to a customised Web Centric approach and implementation of Virtual Clinical Assessments. Students expressed their satisfaction in the learning experience through VLE, but were anxious about their clinical training and connectivity issues.
Conclusion: This transition demonstrated the need of future directions in terms of learner readiness to be more self-directed and self-determined, design thinking for transformation to a Web Centric curriculum, faculty readiness to change and develop the competency of Technological Pedagogical Content Knowledge (TPACK).
Practice Highlights
- ACTIONS model is an appropriate design and transition model.
- Exigent transition is an opportunity to augment the capabilities of VLE and innovate.
- Ensure the recreation of an equivalent virtual learning experience to the onsite learning experience
- TPACK has emerged as an essential trainer competency.
I. INTRODUCTION
The COVID-19 pandemic has been a catalyst for extraordinary transformation in medical education. Malaysia underwent a form of lockdown under the Movement Control Order (MCO). The MCO was initiated on 18th March 2020 for two weeks and extended several times until 9th June 2020, with changing levels of restrictions in phases. With the designation of their usual clinical learning environment as a COVID Hospital, it was inevitable that medical students at the Universiti Malaya experienced major disruptions in clinical teaching.
The exodus of all students to their hometowns at the start of the MCO necessitated overnight conversion of teaching and learning processes into online delivery. With the emergence of the initial four weeks of the MCO as a fluid, unpredictable and undefined landscape, the medical faculty formulated a range of teaching and learning modalities adaptable to different conditions.
These adaptations were made while maintaining compliance with requirements of various regulatory bodies and policy makers, including the Ministry of Higher Education, Malaysian Medical Council, the Malaysian Qualifying Agency and university governance. This process of assimilation within a rapidly evolving milieu was a formidable challenge. This article aims to provide a succinct summary of events and processes for emergency digitisation and transition to remote teaching during the COVID-19 pandemic. This summary will function as a model for transformation on the run to manage the implementation and delivery of higher education programme during a major crisis or disaster.
II. METHODS
As events preceding the implementation of the MCO unfolded, sequential meetings were held to brainstorm on the safety, mode of delivery in emergency transition, preparation for training of students and staff, and evaluation of the changes. The faculty of medicine seized the opportunity to plan and implement a comprehensive online learning experience during the MCO period. Designated teams explored the various technologies available to support learning and shared best practices in an explosion of webinars. It became evident that dedicated teamwork to deal with sudden and enforced changes was crucial for this transition to be effective.
A. Theoretical Framework to Support the Digital Transition
An exigent digital transition like this required an instructional design model to affect a transition that was sustainable and future-ready. There was also a need to ensure that learning objectives envisaged for a physical face-to-face curriculum delivery model could be achieved with digital transition. The most practical model for such a transition was the ACTIONS model by Tony Bates (as cited in Boettcher & Conrad, 1999). ACTIONS is an acronym for Access, Costs, Teaching and learning, Interaction and user friendliness, Organisational issues, Operational and implementation expenses, Novelty and Speed.
B. The Development Approach – Review, Deconstruct, Reconstruct and Innovate
Recreating the entire learning experience in the VLE required the following steps
1) Review of existing e-resources and mapping them to curriculum: The existing e-resources available at Faculty of Medicine and Library were reviewed to analyse the need for additional resources. Contents of the e- resources were also mapped to the curriculum to understand the alignment of available resources with topics covered in different stages.
2) Deconstruct the existing curriculum and detailing its demands: The Universiti Malaya Medical Programme (UMMP) comprises five stages. Stages 1 and 2 (years 1 and 2) provide the preclinical and Stages 3. 1, 3.2 and 3.3 (years 3 to 5) provide the clinical learning experiences to students. The unique instructional demands of each stage were carefully analysed to clarify the possibilities and limitations of the VLE created. This step enabled categorisation of learning experiences which were suitable for delivery in the VLE and learning experiences which were not suited to a VLE with regard to the achievement of learning outcomes.
3) Reconstruct the learning experiences of curriculum in VLE: While contents of the curriculum were already available on a university learning management system (LMS) called Student Powered e- Collaborative Transforming UM (SPeCTRUM), the Moodle-based segment of the VLE, learning spaces had to be created within the Microsoft Teams segment to enable synchronous collaboration. The design principle adopted was to replicate physical facilities of Faculty of Medicine as closely as possible by providing virtual large and small group learning spaces (virtual classrooms) within Microsoft Teams. Each stage was denoted as a team. Designated channels were then created within each team for system-based blocks in preclinical stages and specialty-based postings in clinical stages. Small group teaching activity spaces including PBL rooms were created as separate channels within respective teams.
4) Innovate and improve: Although it was an exigent digital transition, the opportunity to innovate and improve could not be missed. Through deep linking of Moodle-based SPeCTRUM and Microsoft Teams, a seamless login and navigation experience was created. The learning spaces created in Microsoft Teams were provided with direct access to e-resources in the forms of ‘tabs’, simulating the existence of resource libraries within the learning spaces. OneNote was made available in these tabs as potential ‘white boards’. A complete transition to ‘flipped classes’ was also adopted by the faculty, replacing the traditional lectures.
C. Ensuring the Effective Utilisation of the VLE and Digital Instructional Delivery – The End User Training
Effective digital transition was enabled through utilisation of the VLE itself as the learning space for training of end-users. Detailed user guides were prepared. A series of synchronous hands-on sessions were also provided. All training sessions were recorded and accessible in the VLE for future reference. Continuous one-to-one support was provided on request for end-users. This dynamic transition support became an opportunity for upskilling faculty members and administrators.
D. Evaluation of Learning Experiences of the Students
A 13-item questionnaire was developed to examine learning experiences of students. The development considered existing institutional expectations of teaching, standards for problem-based learning and online learning, and generic criteria for learning environments. In addition, two open-ended questions were created for students to express what they liked and what did not work well. One week after commencement of the VLE, students were invited to relate their learning experiences via this questionnaire. This early feedback from the perspective of end-users was vital to identify aspects of the newly-constructed VLE which required adjustments.
III. RESULTS
A. The Challenge Made into an Opportunity – The Digital Transition
The school faced a huge hurdle as these sudden changes required augmented capabilities, stretching the existing connectivity infrastructure to its limits. As Information Technology (IT) professionals addressed the obvious task of ensuring good connectivity for all faculty members, administrators and students, others worked to transform mindsets of the eager and less-willing to adapt to the new norm of providing emergency online teaching to the students.
Universiti Malaya had an existing web-enhanced blended learning approach which utilised SPeCTRUM to support e-learning. The pandemic compelled transition from a Web-Enhanced approach with a physical classroom as the primary site of instruction to a web-centric approach with a virtual online platform as the primary site of instruction. To effect this change, capabilities of the existing LMS were enhanced to provide experiences of asynchronous and synchronous communication together with collaboration possibilities in a robust Virtual Learning Environment (VLE).
The ACTIONS model facilitated the evaluation of issues including uniform access to the selected web-based tools, adaptability of existing teaching learning methods to the VLE, organisational constraints and support needed for implementation, reliability and future-readiness of the VLE platform as well as the speed or ease with which the curriculum could be fully transitioned to a Web-Centric mode. Such planning resulted in the decision of deep linking and combining the capabilities of Moodle-based SPeCTRUM and Microsoft Teams as a VLE solution for the instantaneous digital transition.
B. Transition in Assessments
Assessment activities also had to be aligned with teaching and learning, taking into account guidelines of various regulatory bodies. During the MCO, existing written assessment components, which were in the form of single best answer (SBA) and extended matching type questions, were administered using online software in the SBA format.
Clinical end-of-rotations examinations posed a greater challenge. During the MCO, it was not possible to conduct examinations in the clinical environment with actual patients or a simulated clinical environment where both examiners and students could have face-to-face interaction with standardised patients. We therefore created Virtual Clinical Assessments (VCAs), writing clinical scenarios which could be used in a format similar to a structured oral examination online. Each VCA lasted 30 minutes with components of history-taking, physical examination, differential diagnoses, investigations and management along the lines of an “observed long case” clinical examination. Examiners or standardised patients were trained to role play for history-taking. De-identified clinical photographs were used for the physical examination component. Investigations such as biomedical images and laboratory results provided data for interpretation. An existing final-year examiner clinical assessment mark sheet with reference rubric was adapted for use, with components of history-taking, examination, clinical reasoning, management, knowledge, communication skills and professionalism. Specific trigger questions to assess these components were incorporated into each scenario. This assessment format could be utilised on a totally virtual platform or in a partially virtual assessment, combining face-to-face interaction with simulated patients/caregivers and clinical photographs or videos, complying with prevailing restrictions at different phases of the MCO.
C. Students’ Experiences of the Virtual Learning Environment
Students recognised and appreciated the Faculty’s efforts in establishing the online learning system for them to continue their studies. Students reported several aspects that worked well. These included pre-recorded teaching materials which allowed students to learn at their own pace. Students were also able to obtain adequate information and understood the information delivered during the virtual problem-based learning sessions. They were also less inhibited to ask questions from behind the screen during synchronous sessions.
However, there were also some areas of concern. Some students encountered internet stability issues. They needed time to adapt to the online learning platform, such as learning how to avoid speaking at the same time during the problem-based learning sessions. While acknowledging the usefulness of videos for some clinical exposure, they yearned to return to hands-on practice of clinical skills and receive feedback on their performance.
D. Prioritising Safety
With the relaxation of MCO restrictions in June to a “recovery MCO” when final year medical students were allowed back, guidelines and protocols were established to ensure safety of students, staff as well as patients. Students returned in batches and were provided with instructions to self-assess their risks before travelling. Subsequent orientation was given to perform risk assessments whenever they checked into their hostel, other buildings within the university campus, and into the hospital. The Occupational Safety, Health and Environment (OSHE) and hospital infection control teams developed a software application for the purpose of tracking the entry of patients, students and staff into the hospital premises. Students were placed on a staggered schedule within their clinical rotation to avoid overcrowding of wards and clinics. Students and staff were constantly reminded to adhere to social distancing and safety guidelines from the Ministry of Health.
IV. CONCLUSION- FUTURE DIRECTIONS
The COVID-19 pandemic has enhanced the use of technology-enhanced learning and instructional delivery as a medium for education. To adapt to this paradigm shift and ensure future readiness, the following areas require immediate attention:
A. Student Readiness
Ensuring readiness of learners to become self-directed and self-determined as they move from higher secondary/ high school to University education. Students should also be supported to develop effective online learning approaches.
B. Academic Faculty Readiness and TPACK as a competency
Academic faculty readiness to facilitate learning among the generation Z learners needs to be ensured. This essentially means that faculty members need to develop Technological Pedagogical Content Knowledge (TPACK, Figure 1) (Koehler & Mishra, 2009), as an essential competency to be effective in technology integration to facilitate learning. TPACK essentially represents the fundamental understanding of faculty members on effectively facilitating the learning process using technology, using appropriate pedagogical approaches to meet the instructional demands of each discipline/ specialty. The importance of up-skilling and re-skilling academic faculty members to equip them with latest tools available for teaching and learning is getting emphasised here.
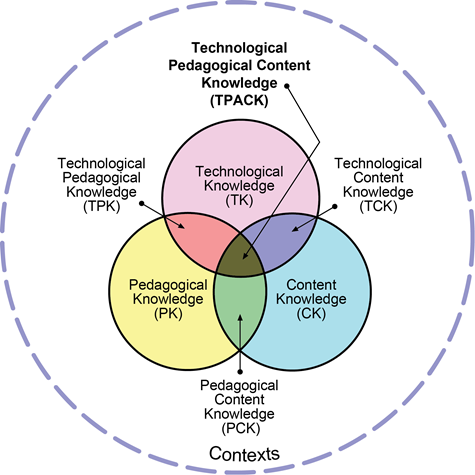
Figure 1: Technological Pedagogical Content Knowledge (TPACK). Reproduced by permission of the publisher (Koehler, 2011)
C. Infrastructure Development
Infrastructure planning, development and resource allocation to meet the future needs of technology-enhanced learning becomes a necessity to ensure the implementation of curriculum.
Notes on Contributors
Dr. Wei Han Hong involved in development of the concept, contributed to the creation of VLE through the inputs of curriculum requirements and ensured implementation, participated in the trials and troubleshooting of VLE, coordinated and contributed to the manuscript writing and approved the final version.
Associate Professor Dr. Vinod Pallath involved in conceptualising and development of the VLE, coordinated the development of VLE and lead the training of the faculty members through the VLE, contributed to manuscript writing and performed critical revisions to make the final version and approved the final version.
Dr. Chan Choong Foong involved in development of the concept, ensured the integration of quality requirements in the VLE, participated in the trials and troubleshooting of VLE, contributed to the manuscript and approved the final version.
Professor Dr. Christina Tan Phoay Lay involved in development of the concept, coordinated and contributed to development of assessments in the VLE, participated in the training, contributed to the manuscript and approved the final version.
Professor Dr. Mary Joseph Marret involved in development of the concept, coordinated and contributed to development of assessments in the VLE, participated in the training, contributed to the manuscript and approved the final version.
Professor Dr. Yang Faridah binti Abdul Aziz involved in development of the concept, supported the development of VLE in the capacity of Deputy Dean (undergraduate), ensured the demands of the curriculum are met through the VLE, contributed and critically reviewed the manuscript and approved the final version.
Professor Dr. Jamuna Vadivelu involved in development of the concept, supported the development of VLE in the capacity of Head of Unit, ensured the demands of the curriculum are met through the VLE, contributed and critically reviewed the manuscript and approved the final version.
Acknowledgement
Authors acknowledge the technical contributions and administrative support received from Medical Education and Research Development Unit and Dean’s Office, Faculty of Medicine, Universiti Malaya.
Funding Statement
There was no funding for the process described in the manuscript.
Declaration of Interest
The authors declare that there is no conflict of interest related to this manuscript.
References
Boettcher, J. V., & Conrad, R. M. (1999). Faculty guide for moving teaching and learning to the web. League for Innovation in the Community College.
Koehler, M. (2011, May 11). Using the TPACK image. TPACK.ORG. http://matt-koehler.com/tpack2/using-the-tpack-image/
Koehler, M., & Mishra, P. (2009). What is technological pedagogical content knowledge (TPACK)? Contemporary Issues in Technology and Teacher Education, 9(1), 60-70. https://doi.org/10.1177/002205741319300303
*Jamuna Vadivelu
Medical Education and Research Development Unit,
Faculty of Medicine,
University of Malaya,
50603 Kuala Lumpur, Malaysia.
Email: jamuna@ummc.edu.my
Published online: 13 July May, TAPS 2021, 6(3), 1-4
https://doi.org/10.29060/TAPS.2021-6-3/EV6N3
Lambert Schuwirth1 & Ardi Findyartini2
1Prideaux Centre for Research in Health Professions Education, College of Medicine and Public Health, Flinders University, Australia; 2Department of Medical Education, Faculty of Medicine, Universitas Indonesia, Indonesia
This quote is attributed to Nicolo Machiavelli, an Italian Renaissance political philosopher. And it may sound reasonable, but at a time where the Covid-19 pandemic is still very active around the world it is also callous to think of a crisis as an opportunity. We want to acknowledge this and we want to send our deepest sympathy to all those who have been personally affected by this pandemic.
Nevertheless, it is also fair to say that in many places in the world the pandemic has served as a catalyst for changes in a variety of human domains–not in the least in health professions education. When we say catalyst, we use the word very purposefully, because there are many developments that were already taking place prior to 2020 and which have already produced quite disruptive changes in society. This crisis is a catalyst, therefore, in the sense that it has heightened the awareness that such fundamental changes will be very soon have an impact on the way we educate future health professionals.
We could easily fill 20 thematic issues with examples of how medical schools around the world have rapidly adapted their educational processes to allow them to continue whilst complying with Covid-19 related restrictions. These changes were necessary and often quite successful. However, it also has to be stated that they were often merely the proverbial Plan B rather than really fundamental innovations. And while Plan B is a good solution for the short term it also has to be a steppingstone for more fundamental innovations. In other words, our attention should not only focus on ‘what where the changes and how were they made, but also ‘why did the changes take place and in what ways can they improve education’.
So, let us quickly reflect on what are these changes that are taking place in the world around us and conjecture about what they could mean for health professions education. Not surprisingly, many of these changes have to do with the rapid development in information and communication technology. These have opened up completely new ways of dealing with the important aspects of society and those in health professions education.
The first example concerns the way we conceptualise knowledge. This is quite different to what it was 50 years ago. Fifty years ago, knowledge was typically seen as the possession of the experts, and out of altruism or for a tuition fee, the expert was willing to share their knowledge with the learner. The typical business equivalent of this was the traditional encyclopaedia. In an encyclopaedia the knowledge of the group of experts is laid down and sold to clients. Nowadays, in contrast, knowledge/information is seen as something that can or even must be constructed collaboratively, by a community of people each adding small pieces to the whole ‘puzzle’. Such a re-conceptualisation has found its crystallisation in wikis, with Wikipedia as the most well-known example. There was a time when businesses tried to put the traditional encyclopaedia on a CD-ROM and made it more feasible to use. However, an encyclopaedia on a CD-ROM is just still a traditional encyclopaedia, just a technical delivery differs. Needless to state that this wasn’t a profitable business development; it wasn’t a real innovation but rather a sort of Plan B. It is therefore, plausible to assume that online lectures are a similar form of Plan B in health professions education.
Another important development concerns the way we manage trust. From a society that has institutionalised trust we are gradually moving into a society that relies on distributed trust (Botsman, 2017). In an institutionalised trust society, important transactions and the trust in those transactions are managed by a trusted institution. For example, we transfer large sums of money preferably via a bank, we negotiate house sales through a conveyancer, and so on. Many of these still exist, but increasingly trust is distributed. Previously, if you wanted to go out for fine dining and spend a lot of money on a fancy restaurant, you could consult the Michelin guide. In fact, this means that you ‘outsourced’ your trust in finding a good quality restaurant to a trusted organisation. Most people no longer used this guide; they just go online and read the long list of customer reviews and evaluate the way the restaurant has dealt with the reviews. This is an example of distributed trust, as a community with direct experience we collectively construct ‘quality’. Our universities still operate as trusted institutions, they provide the transaction–education–and the trust and transaction–academic degrees–in one. Of course, recognition of prior learning are early steps to disconnect the educational transaction from the management of trust, but there is still a long way to go.
For instance, in order to organise recognition of prior learning and the disentanglement of trust and transaction effectively, there is a need of a trusted dossier/portfolio that can be managed across educational phases and by different stakeholders in a fully authenticated way. Open ledger or block chain technology is very likely able to provide such systems, although much may still be under development (Mikroyannidis et al., 2018, June). It is not a huge leap of faith to imagine what this would mean for future employers. Instead of having to trust an academic transcript with only a few numbers or grades and with seals and signatures, an employer would have the opportunity to ‘interrogate’ an applicant’s whole dossier of learning, improvement and achievements. Such developments are likely to also severely disrupt the way accreditation works and probably influence how learners engage in more meaningful way to achieve competence in health professions education.
For the learner this means that they would easily be able to fill such a portfolio with a combination of course material, micro credentialing and elements obtained from the cognitive surplus (Shirky, 2010). ‘Cognitive surplus’ refers to the fact that, increasingly, knowledge is provided or shared for free in the Internet. The probably most well-known example of this is the Khan Academy (Khan Academy, n.d.). Tuition and learning that were previously only available to feepaying students, is now available for free. Of course, not all that is offered in the cognitive surplus is of high quality and there is a challenge for learners to distinguish between offerings of poor and of good quality, but it does mean that most modern learners are increasingly used and expecting to be able to access knowledge for free or for a negligible fee. This will place an increasing burden on universities to demonstrate their added value to a feepaying student’s learning, including in instilling students’ ability to critically think and reflect on the abundant information they can access freely. One could argue that the higher education industry is still highly regulated in most countries and the only way to achieve a credible degree in the health professions is by going through a university. Such industry which has to rely purely on a regulatory framework is vulnerable.
Finally, the development that most people are talking about are artificial intelligence and machine learning. It is very difficult to predict what the future will hold, but it is likely that artificial intelligence and machine learning will significantly augment or even substitute what currently is most doctors’ specific expertise; making a diagnosis and deciding on therapeutic management plans. The former is generally a categorisation task, something at which artificial intelligence is becoming better and better. The latter is becoming ever more patient specific, especially with the emergence of precision medicine, which will increasingly require decision support systems. This does not automatically mean that patients will not be needing somebody to care for them, to partner with them or to help them make meaning in periods of illness, angst and uncertainty. Obviously, this will require health professionals with more elaborate so-called ‘soft’ skills which enable them to develop empathetic and professional connections with their patients either for better cure or care.
Such changes to what makes a ‘good’ doctor will require changes to health professions education. On the one hand, education should equip students with data and technology literacies, but on the other, it should allocate sufficient resources for the development of human literacy (Aoun, 2017). Development of soft skills means the training of doctors who can partner with their patients, who can nurture them and help them make meaning. It also requires students who eventually will be able to embrace uncertainty and who will be equally comfortable with ‘knowing’ and with ‘not knowing’; which further highlights the importance of creativity and innovations, self-awareness, and lifelong learning skills.
Obviously, there are implications for health professions education. Firstly, a purely transactional process of passing on knowledge may not need to take a central role in a curriculum. The traditional lecture was an educational ‘technology’ that was designed to cater to students who did not have access to books. The lecturer, the reader, read the knowledge to the students who either were able to write it down or had to memorise it. The purely transactional process of passing on knowledge should no longer have a central role in the learning process, and it has implications for assessment as well. The assessment arm of it is the typical structured and standardised knowledge test in which the candidates reproduce the knowledge that they’ve been provided with. This no longer seems current nor relevant one of which because of a lot of changes and uncertainties this pandemic has taught us. Modern students, through their laptops, tablets or smart phones, have accesses to a whole world of information. This is quite recent because even in the early days of problem-based learning, the university had control over the quality of the resources students could use for their learning. Nowadays, there is a whole Internet of information–some relevant and some absolutely incorrect nonsense–that is absolutely not under the control of the University. It is under the control of the students, though, and they will use that information. In order to manage this huge affordance educationally, changes will have to be made to develop curricula that incorporate both the formal and informal educational spaces. To successfully combine those spaces, curricula may have to give more room to students and teachers to develop a dialogue in such a positive relationship that it better facilitates students’ critical thinking and professional identity formation.
Such changes cannot happen in an educational context in which the students are not allowed or supported to exhibit agency over their own learning, and as a consequence, over their own assessment. But changing this organisational mindset culture is probably the biggest challenge ahead of us. It requires a culture shift from distrust and control to one of trust and empowerment. Thinking about trust and empowerment is not idealism but we think it is pure necessity. The dramatic events in the world of online proctoring are a clear demonstration that the choice to go further down the pathway of distrust and control has not been the best use of what technology affords.
Furthermore, trust and empowerment are not only needed during training but also after graduation. Where in our time as students it could still be reasonably expected that upon graduation we were equipped with all the knowledge, skills, problem-solving ability and attitudes to last us for the rest of our career–bar some updating through Continuing Medical Education (CME)–it is now clear that the world, the healthcare environment and the expectations of patients are changing rapidly. No longer can we assume that upon graduation our students will be a complete ‘product’. Instead, they will have to continue to learn, to develop and probably to reinvent themselves continually. But if we as universities have never empowered them or allowed them to take agency over their own learning and assessment, it is implausible that our graduates would suddenly and magically be capable to do this after graduation. The implication for assessment is obvious. The notion of single moment assessments of final examinations is not in alignment with these views. Assessment will have to take on a more longitudinal and integrated form to be aligned with more than educational processes and the lifelong learning requirements.
A final point relates to the so-called affordances modern students have (Friedman & Friedman, 2008). There are several listed in the literature, but some are most pertinent in the short run. Through their laptops, tablets or smart phones, students are able to be in multiple communities and entertain multiple communications at the same time. They can be in a practical session working with one group of peers, but also texting to other members of the student cohort or more general friends about what they currently learning or even about completely unrelated issues. There are numerous examples of Information and Communications Technology (ICT) afforded learners–or academics for that matter–who entertain to communications with two communities at the same time. Everyone who has been in an online meeting and has used the chat function at the same time, has had experience with this. Of course, this rapid switching between communities and communications, this time slicing, comes at the expense of cognitive load, but it can also be used in a very enriching way for learning. The same applies to collaborations. Any student who is a tutorial group or even in a lecture hall and accesses the cognitive surplus or Wikipedia is in fact in two knowledge creation collaboratives at the same time.
Unfortunately, our students are not yet very well experienced in how to use these affordances well, but also most educational designers or curriculum developers are not able to incorporate them and take maximum advantage of what they enable the learner to do.
The challenge that lies ahead of us is to bring these developments to health professions education. One ramification is already inevitable, ICT in most contexts has dramatically reduced power asymmetries. In the example of the restaurant and the reviews, any customer now has the power to publicise their experience and restaurant owner would be wise to respond appropriately, in healthcare patients come to the consulting room prepared with Dr Google and whether what they found is relevant or not, they do have knowledge that the doctor will have to deal with, and finally in education students have point of care access to a whole world of information which will make them more equal partners in their education. Students who are well prepared for lectures are able to disagree with their lecturers or even be better informed on details than the lecturer. Universities may need to increase efforts to better engage students and to facilitate their personalised learning needs, as well as to enable more co-creation in knowledge development. Universities that do not acknowledge these changes run the risk of quickly becoming obsolete. But acknowledging this also means better preparation of teachers through more comprehensive faculty development programmes.
However, this editorial is not about doom and gloom or risks, it is about opportunities. All the affordances that are already or could be incorporated in modern health professions education make it possible to educate even better health professionals for the future, who are agile and optimally positioned to an ever-changing healthcare system and align better with their patients. The potential and opportunities are vast. Whether or not these disruptive changes give us those opportunities, will depend both on how we adapt for the short-term needs and how we prepare to embrace substantial and necessary changes in our health professions education for the future.
Lambert Schuwirth & Ardi Findyartini
Guest Editors &
International Editorial Board Members
The Asia Pacific Scholar (TAPS)
Botsman, R. (2017). Who can you trust?: How technology brought us together and why it might drive us apart. Hachette.
Mikroyannidis, A., Domingue, J., Bachler, M., & Quick, K. (2018, June 25-29). A learner-centred approach for lifelong learning powered by the blockchain. EdMedia+ Innovate Learning, Amsterdam, Netherlands.
Shirky, C. (2010). Cognitive surplus: Creativity and generosity in a connected age. Penguin Books.
Khan Academy. (n.d.). https://en.khanacademy.org/
Aoun, J. E. (2017). Robot-proof: Higher education in the age of artificial intelligence. The MIT Press.
Friedman, L. W. & Friedman, H. H. (2008). The new media technologies: Overview and research framework. Social Science Research Network. http://dx.doi.org/10.2139/ssrn.1116771
Submitted: 17 May 2020
Accepted: 2 September 2020
Published online: 4 May, TAPS 2021, 6(2), 91-93
https://doi.org/10.29060/TAPS.2021-6-2/CS2263
K. Anbarasi1 & Kasim Mohamed2
1Department of Dental Education, Sri Ramachandra Institute of Higher Education and Research, Chennai, India; 2Department of Maxillofacial Prosthodontics, Sri Ramachandra Institute of Higher Education and Research, Chennai, India
I. INTRODUCTION
Dental practitioners often encounter situations that require customising the prosthesis to satisfy the needs of patients. Artificial devices called dental appliances or prosthesis is custom fabricated for the functional, aesthetic, and psychological wellbeing of patients (Chu et al. 2013). The patient’s complaints may vary from missing natural teeth to extensive maxillofacial defects, and there is no single best rehabilitative therapy for these conditions. Designing our product is the choice, and this demands adaptive expertise, i.e., the ability to generate potential solutions (Mylopoulos et al. 2018). Maxillofacial Prosthodontics applies a variety of learning methods like systematic simulation laboratory exercises, See One, Do One, Teach One (SODOTO method), and supervised clinical practice to train the routine technical skills and clinical practice. To maximise the outcomes in the complex prosthetic treatment, the course specialists designed an “Interdisciplinary Device Development program (IDDP)”—a value-added course for the postgraduates in collaboration with the Biomedical Instrumentation Engineering Faculty of our Institution. IDDP is the first of its kind challenge-based learning model in Dentistry that uses innovations to deal with rehabilitation care beyond routine practice. This paper aims to present our IDDP model and programme outcomes.
II. METHODS
IDDP is structured in three stages referring to problem determination, design, and development. An abstract idea about the essential requirements and intellectual property protection is also included and is scheduled for 3 hours per week for 10 weeks’ (Table 1). The IDDP concept and curriculum were presented in the College Council meeting and subsequently in the Board of Studies and Academic Council. The proposal was approved and permitted implementation.
Table 1: IDDP curriculum framework
Participation in IDDP is mandatory for all postgraduates (PGs) of Maxillofacial Prosthodontics, but knowledge translation into practice is expected only when patients present with unique/challenging conditions. Chances of treating these patients are given for all PGs, but priority is given to those who showed valuable accomplishments in their regular clinical works. Once get allotted with such cases, the PG needs to work with their faculty in-charge, the primary consultant, a faculty member from biomedical engineering, and laboratory technicians.
The device designing demands advanced prosthodontic techniques and the attainment of competency depends on repeated practice. Skill assessment before accustoming it is not a safe practice hence the IDDP is not emphasising on assessments that reflect on summative grade, but performance assessment was made for the postgraduates who have undertaken the task to appraise their diligence, completeness, and problem-solving ability in a standard template, and supporting them to improve their learning.
III. INVENTIONS IN THE CLINICAL GROUNDS
A. Cheek Bumper
A Von Recklinghausen’s disease patient reported with a nodule on the left buccal mucosa and chewing difficulty. The patient expected non-surgical management, and there was a need for invention. Relieving the contact between the mucosal nodule and teeth was suggested as a solution and one PG student turned out the novel idea as an acrylic cheek bumper, an intraoral device that separated the growth 5mm away from the teeth surface. Wearing this appliance at mealtime solved the patient’s problem.
B. Training Pad for Jaw Reposition
A patient has undergone hemimandibulectomy on the right side. After a month, he reported aesthetic concern because of the deviation of the lower third of the face during jaw movements. Denture rehabilitation with a flange is a routine treatment to improve aesthetics. In our discussion, a PG student proposed to reposition the jaws before denture treatment to achieve the jaw compatibility for receiving the denture, hence optimising the success. The team accepted to transform the vision into reality. A prototype was prepared, and an intraoral acrylic pad with retainers was developed. Later the patient was treated with a prosthesis and he expressed his happiness in gaining back the chewing efficiency and confidence
C. Modified Impression Tray to Make Ear Prosthesis
To avoid the shape distortion and to get the adequate fine details in the replica, a postgraduate student in the existing tray pattern did a design modification and got an excellent result.
D. Compression Stent
A patient was referred for the management of a hypertrophic scar following ear piercing. The literature search revealed a solution of stent fabrication to cover the affected ear completely and wearing it full time for a year. The drawbacks like patient discomfort and long-time follow-up were highlighted and a PG student suggested redesigning the compression sent to cover only the scar region using claw type hair clip model. The patient was instructed to wear the stent for 10 to 12 hours per day. At the end of the fifth month, the scar was completely disappeared and she regained the ear lobe shape.
The devices in the process include:
- Mouth opening assisting device to treat trismus.
- Impression tray with size adjustable screws.
- Custom designed intraoral radio-productive device for patients receiving radiotherapy.
IV. STRENGTHS AND LIMITATIONS
A supportive curriculum always opens an avenue for innovation. Integration of Biomedical engineering solved the clinical problem by applying engineering principles, formulas, and materials in device designing as the dental specialty lacks the potential to practice the engineering domain. IDDP inspired our postgraduates to take part actively in treatment planning sessions. There is a positive shift in their clinical reasoning skill, describing the treatment options with their pros and cons, and finally specifying the target device by solving the limitations on the existing model or developing an alternative model.
The unresolved factors of IDDP include the struggle to tap the inventive potential of graduate students, their level of commitment, and time allocation. Formal assessment, patient satisfaction survey, student perception, and feedback should be considered.
V. MOVING FORWARD
Incorporating IDDP in the dental curriculum at the national level is the way forward.
VI. CONCLUSION
Our experience in IDDP evidences the innovation that happened on academic grounds. The structured training and opportunity to transform the learning into practice enhanced the confidence level of the clinicians to think out of the box, act as problem solvers, and shape the future health care industry.
Notes on Contributors
Dr. K. Anbarasi, MDS, PhD, devised the presented concept, framed the theoretical framework, wrote the manuscript, and agreed on its final form for submission.
Dr. Kasim Mohamed, MDS, involved in curriculum planning, conducted the programme, contributed to the final version of the manuscript, and agreed to its final form for submission.
Acknowledgment
The authors like to acknowledge the programme coordinators of IDDP.
Funding
The program was supported by the authors’ institution as an academic event.
Declaration of Interest
The authors have no conflict of interest.
References
Chu, K. Y., Yang, N. P., Chou, P., Chi, L. Y., & Chiu, H. J. (2013). Dental prosthetic treatment needs of inpatients with schizophrenia in Taiwan: A cross-sectional study. BMC Oral Health, 13(1), 8. https://doi.org/10.1186/1471-2458-10-482
Mylopoulos, M., Kulasegaram, K., & Woods, N. N. (2018). Developing the experts we need: Fostering adaptive expertise through education. Journal of Evaluation in Clinical Practice, 24(3), 674-677. https://doi.org/10.1111/medu.12893
*K. Anbarasi
Faculty of Dental Sciences,
Sri Ramachandra Institute of
Higher Education and Research,
Chennai, India.
Email: anbarasi815@gmail.com
Submitted:5 September 2020
Accepted: 11 January 2021
Published online: 4 May, TAPS 2021, 6(2), 94-96
https://doi.org/10.29060/TAPS.2021-6-2/CS2449
Y.G. Shamalee Wasana Jayarathne1,2, Riitta Partanen2 & Jules Bennet2
1Medical Education Unit, Faculty of Medicine and Allied Sciences, Rajarata University of Sri Lanka, Sri Lanka; 2Rural Clinical School, Faculty of Medicine, University of Queensland, Australia
I. INTRODUCTION
The mal-distributed Australian medical workforce continues to result in rural medical workforce shortages. In an attempt to increase rural medical workforce, the Australian Government has invested in the Rural Health Multidisciplinary Training (RHMT) program, involving 21 medical schools (RHMT program, 2020). This funding requires participating universities to ensure at least 25% of domestic students attend a year-long rural placement during their clinical years and 50% of domestic students experience a short-term rural clinical placement for at least four weeks.
Multiple factors influence selecting a rural medical career pathway. Four basic truths presented by Talley (1990) USA on successful medical career pathways are still pertinent today.
1. Students from rural origin are more likely to return to rural areas of practice.
2. Medical graduates who trained in rural areas are more likely to choose rural practice.
3. General practice is the key discipline of rural health care.
4. Doctors practice close to where they train.
The evidence shows the longer a student spends training in rural area, the more likely they are to work in a rural
area (Kwan et al., 2017; Talley, 1990). Repeated exposure of rural clinical practice promotes rural living and practice, enabling the development of professional and social networks within rural communities (Eley et al., 2008). However, there is a dearth of empirical data on whether brief rural clinical learning experiences increases medical students’ rural medical career intent.
We report a case study on the pilot project of Objective Simulated Bush Engagement Experience (OSBEE), a novel approach to promote rural medical careers to medical students, where second year (of a four year program) medical students participated in a series of rurally themed scenarios and skills stations set in a rural location, with near peer supervisors (The term bush in OSBEE refers to the forested setting where the stations were undertaken).
II. OBJECTIVE AND METHODS
The objective was to evaluate the introduction of a one day immersive rural clinical learning experience in the form of the OSBEE. Metropolitan-based students travelled 280km to attend OSBEE, set in a forested area on a large farm. The students rotated through a series of simulated rural emergency scenarios and skills stations with predominantly third and fourth year medical students as supervisors.
The participants of the study were second year medical students of The University of Queensland (UQ). These students would all be attending a UQ Rural Clinical School (UQRCS) for their third year. To evaluate the influence of this program on their rural medical career intent, on peer-assisted learning and the program itself, a mixed study using a focus group and questionnaire. A focus group discussion conducted by the principal investigator, where informed written consent was obtained from all participants, was audio recorded, verbatim transcribed and thematically analysed. All correspondence was anonymous, and confidentiality maintained. The online questionnaire was administered two weeks after the OSBEE. Frequencies were calculated for questionnaire items. Themes were identified for open ended questions.
III. RESULTS
Identified key themes and quotes from the focus group and open-ended questionnaire questions are presented in Table 1.
|
Key Themes |
Quotes |
|
“Overall a positive impression on OSBEE program”
|
“Awesome learning environment, everyone was so positive and enthusiastic” “I really liked – overall it was good, …” “I think this today is quite eye-opening for me to see what approaches to take when it comes to different scenarios” “For me it was a very collaborative, We could ask questions, it was very friendly” “It kind of was an exam scenario I suppose. But not in a bad way” |
|
About the OSBEE stations |
“I think it’s a lot of real-life scenarios that you could potentially face out in the bush,” “Snake bite was pretty fun” “I don’t know if you guys have heard, where students are actually thrown into these scenarios and they can actually practice their skills.” “There was a lot of clinical practice, but not much clinical reasoning” |
|
“Positive learning during OSBEE”
|
“So I think that really – the most useful part of the day was the similar-ish things but different problems and different contexts and different patients to facilitate memory retention…” “Supervisors were very supportive. Learned a lot from them.” “I feel like the debrief session is enough of a learning. Just enough to know what to do.” |
|
“Positive impression of rural practice” |
“Yeah, it really paints a picture of the typical things, the different situations you might find in a rural scenario.” |
Table 1: Key themes with quotes
The questionnaire response rate by the six study participants was 100 %. All students agreed: “OSBEE was a positive learning experience” and “enjoyed the program”. And 2/3 (4 students) felt “OSBEE encouraged them to consider working in rural context”.
IV. DISCUSSION
Maldistribution of medical workforce is a global concern. Different strategies to address this have been implemented and described in the global literature. Medical schools play an important role in implementing initiatives that best promote rural medical career to grow the rural medical workforce. The OSBEE program provided an enjoyable peer-assisted rural contextualised learning experience and inspired participants to consider rural practice. Although brief rural clinical immersions alone are unlikely to significantly increase rural practice intent, they may enhance the impact of short-term and year-long rural clinical placements on future rural medical workforce.
V. MOVING FORWARD
Whilst our study group was small, and limits the generalisability of our findings, we believe our findings infer brief immersive clinical learning experiences play a role in the promotion of rural medical careers, thus have continued to offer the OSBEE program to early program medical students. However further evaluations of brief (and frequent or repeated) immersive rural clinical learning experiences, on student perceptions of rural medical careers would be useful. Tracking of students involved in these brief rural experiences, as well as short-term and year-long clinical placements would provide valuable insights, to see if participants of the various rural learning experiences do subsequently work in rural areas. Our program and findings may help other medical schools focused on increasing rural medical workforce.
Notes on Contributors
YGSW Jayarathne, MBBS, PG Dip in MEd, MD in MEd was involved the conceptual development, ethics application, data collection including focus group facilitator for the OSBEE evaluation, analysis of the quantitative data, thematic analysis of the qualitative data and the development of the manuscript, including the final approval.
Riitta Partanen, MBBS, FRACGP, DRACOG, General Practitioner, Head of UQRCS was involved in the conceptual development, ethics application, data collection including focus group facilitator for the near peer supervisors, analysis of the quantitative data, thematic analysis of the qualitative data and the development of the manuscript, including the final approval.
Jules Bennet, RN, Masters of Clin Ed, Grad Cert Emerg Nursing, Grad Cert Healthcare Simulation, Lead Clinical Educator – Clinical Skills & Simulation, UQRCS Hervey Bay was involved the conceptual development, ethics application, quantitative data collection, analysis of the quantitative data and the development of the manuscript and final approval.
Funding
This study was supported by funding received from the RHMT grant.
Declaration of Interest
There are no conflicts of interests related to the content presented in the paper.
References
Australian Government Department of Health. Rural Health Multidisciplinary Training (RHMT) Program. Retrieved February 20, 2020, from https://www1.health.gov.au/internet/main/publishing.nsf/Content/rural-health-multidisciplinary-training
Eley, D. S., Young, L., Wilkinson, D., Chater, A. B., & Baker, P. G. (2008). Coping with increasing numbers of medical students in rural clinical schools: Options and opportunities. Medical Journal of Australia, 188(11), 669-671.
Kwan, M. M., Kondalsamy-Chennakesavan, S., Ranmuthugala, G., Toombs, M. R., & Nicholson, G. C. (2017). The rural pipeline to longer-term rural practice: General practitioners and specialists. PLoS One, 12(7), e0180394
Talley, R. C. (1990). Graduate medical education and rural health care. Academic Medicine: Journal of the Association of American Medical Colleges, 65(12 Suppl), S22-5.
*Y G Shamalee Wasana Jayarathne
Medical Education Unit,
Faculty of Medicine and Allied Sciences,
Rajarata University of Sri Lanka
Email: wasana@med.rjt.ac.lk
Submitted:4 August 2020
Accepted: 29 October 2020
Published online: 4 May, TAPS 2021, 6(2), 97
https://doi.org/10.29060/TAPS.2021-6-2/MA1601
Piyanjali de Zoysa1, G. A. Chathra Erandi2, D. B. Umaya Wijayaratne2, K. P. Navodya Shavindi Jinani2, Piumi Kavindya Kandanaarachchi2
1Department of Psychiatry, University of Colombo, Sri Lanka; 2University of Colombo, Sri Lanka
Video Player
Submitted:6 November 2020
Accepted: 10 March 2021
Published online: 4 May, TAPS 2021, 6(2), 98
https://doi.org/10.29060/TAPS.2021-6-2/MA1602
Dujeepa D Samarasekera1, Bettina Lieske2, Derrick Aw3, Shuh Shing Lee1, Yih Lin Lim1, Chee Yen Ang1, Su Ping Yeo1, Dow Rhoon Koh4
1Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Division of Colorectal Surgery, Department of Surgery, National University Hospital, Singapore; 3Department of General Medicine, Sengkang General Hospital, Singapore; 4Department of Physiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Video Player
Submitted: 30 September 2020
Accepted: 18 November 2020
Published online: 4 May, TAPS 2021, 6(2), 88-90
https://doi.org/10.29060/TAPS.2021-6-2/PV2407
Teng Chun Koh1, Eugene Zhi Jie Lee1, Charlene Jie Lin Yak1, Jack Botao Sun1, Joshua Ren Wei Tay1, Ann Chong Hui Fong2 & Clara Yuen Pun Mok3
1Faculty of Dentistry, National University of Singapore, Singapore; 2Office of Undergraduate Education and Student Affairs, Faculty of Dentistry, National University of Singapore, Singapore; 3Discipline of Endodontics, Operative Dentistry and Prosthodontics, Faculty of Dentistry, National University of Singapore, Singapore
I. INTRODUCTION
Freshmen orientation programmes are important milestones of university life. In Dentistry, orientation helps build camaraderie and friendship among the small undergraduate student enrolment. Before the COVID-19 pandemic, freshmen orientation featured overnight camps, mass games and group activities which involved face-to-face interactions. With the pandemic, precautionary measures were put in place to curb the spread of the virus. A key measure was the radical move away from face-to-face activities. This had a profound impact on the conduct of the orientation programme in Dentistry. The authors share their experiences as student organisers of a first-ever online freshmen orientation programme (involving 72 freshmen and 60 seniors), and highlight key lessons gleaned from the experience.
II. E-ORIENTATION – CHALLENGING THE STATUS QUO
Planning and implementing an e-Orientation programme is vastly different from that of a conventional face-to-face one. While the latter leverages physical space, infrastructure, resources, and interactions to create a conducive environment to achieve the goals of Orientation, e-Orientation operates in the online space and relies heavily on technology. However, the ongoing COVID-19 pandemic necessitated a turn towards online platforms and tools for the execution of university orientation programmes worldwide (Ullman, 2020), and it was no different for students in the Faculty of Dentistry. As the organisers and planners of the programme, the lack of prior experience with such an online approach proved daunting for us and the challenges we faced included:
A. Managing Unfamiliar Online Tools
While technology was widely available to support the e-Orientation, familiarity with it was lacking. It was therefore necessary to overcome a steep learning curve and get acquainted with the use of new tools such as Zoom, the video-conferencing tool.
B. Security, Privacy and Safety Concerns
A key concern with the e-Orientation revolved around security and privacy of the freshmen and seniors facilitating the online activities. Zoom was the platform of choice for our e-Orientation, due to its numerous security features, such as the usage of end-to-end encryption to secure meetings and the utilisation of meeting passcodes to ensure that only designated participants could access and enter meetings for e-Orientation (Zoom Communications Inc., n.d.). Additionally, with many of the activities taking place remotely online, the physical safety of the participants was also a concern if any of them injured themselves during the activities.
C. Sustaining Engagement of Freshmen
The long hours spent in front of the camera, coupled with the difficulty in engaging their peers over a virtual setting, resulted in participants quickly losing interest within a short time. The remote nature of the engagement also made it more difficult for the participants to deepen their interactions. The participants’ focus could be easily lost with them disengaging from the activities going on online. There was a need for the seniors to constantly exude high levels of energy and enthusiasm needed to keep the freshmen engaged. The lack of reciprocation from the freshmen did little to encourage the seniors.
D. Grappling with Technological Difficulties
An online orientation opened the possibility of technological difficulties presenting a stumbling block to the smooth flow of the entire programme. While the impromptu nature of these occurrences meant these problems could not be entirely headed off beforehand, proper planning for contingencies allowed us to deal with these issues swiftly and effectively when they arose.
III. RISING ABOVE THE CHALLENGES
The e-Orientation was organised primarily using Zoom with each Orientation group comprising 10 freshmen and 2 Orientation Group Leaders (OGLs). This helped to optimise the group size and maximise the online interactions. Over a two-week period, the activities were rolled out for two to three hours on alternate days. The longer duration and shorter engagement each day was deliberate to avoid online fatigue and provide ample opportunity to informally catch up online in smaller groups after the official programme ended each day. The following strategies contributed to the success of organising the e-Orientation.
A. Drawing from the Familiar and Conventional
Traditional games were creatively adapted for adoption online. An example was Human Cluedo where the freshmen messaged their group mates an assigned word to initiate conversations on their own. In the classic game of Cluedo, players attempt to deduce words that are hidden in an envelope, with the player who guesses right winning. In our version of Human Cluedo, every freshman was assigned a word, and had to complete a “murder” by making 2 other freshmen, their “victims”, say this word in their day-to-day conversations over text. If they did so successfully without arousing suspicion, they got a point for completing the “murder”! The “victims” on the other hand had to be wary and deduce the word that the murderer was trying to get them to say – the component of the game that was inspired by the original game. Inspiration was also sought from online games which the participants would be familiar with.
B. Experimenting with Newer Methods of Information Dissemination
While instructions could be given out efficiently through briefings in a face-to-face setting, this was not possible online. To reach out to the participants more effectively and expediently, an Instagram page was used to disseminate information quickly among the participants.
C. Empowering and equipping Orientation Group Leaders
An Orientation Group Leader (OGL) handbook was developed to guide the student leaders in running the programme independently. It accorded them the flexibility to make adaptations to some of the activities if it was necessary. Zoom meetings were organised to familiarise the OGLs with the use of Zoom and dry runs proved quintessential in foreseeing and eradicating potential technical difficulties.
IV. GOING VIRTUAL – A REALITY CHECK
Looking back on the e-Orientation, its success was the result of several values. First, the need to be open to new ideas and not discount any suggestions. The e-Orientation experience required new ideas to be tested to make sure these would still achieve the objectives of the Freshmen Orientation programme. Second, the need to see change as fresh opportunities. This also meant that any unexpected twists and turns to the original plans had to be embraced positively and recognised as opportunities to do something differently but with the potential to be better. Thirdly, perseverance proved an important ingredient in the recipe for success. With a major change to the original plans and being thrust into new unknowns, an easy way out would have been to cancel the orientation programme. This would have been an easier option, but not necessarily the correct one. The seniors persisted and rallied together to overcome the difficulties and eventually they succeeded in their foray into an online orientation programme. These values will go a long way in our training to become oral healthcare professionals of the future.
V. CONCLUSION
There was a palpable sense of apprehension and fear in the beginning. There were many unknowns – would the camp proceed smoothly? Would the juniors enjoy themselves? Would it be overly awkward? Many thought that an online orientation programme would not be as fun and would not achieve the intended objectives.
The willingness to be open to new ideas; a positive attitude towards changes and uncertainty, and a spirit of perseverance helped to overcome the initial fear and scepticism. While this e-Orientation was definitely not on the agenda, its successful conduct has opened our eyes to how it could offer a viable alternative to the tried and tested conventional face-to-face programme. The convenience, accessibility and flexibility of the online platform, together with suitably designed online activities differentiated this Orientation into a unique experience, and possibly resulting in high participation rates among the freshmen.
With an eye on the future, the knowledge learnt through this experience can be passed on to the next batch of junior Orientation leaders, and may also come in helpful should we be involved in the organisation of online versions of regional events, such as the Asia-Pacific Dental Students Association (APDSA) conference, in the future. On a more personal note, this experience has also made each one of us more cognisant of pertinent issues inextricably linked to the use of social media, such as security and privacy, and will shape our behaviour on online platforms in the future as well.
If asked whether we would do this all over again, we would gladly step forth with a resounding Yess!!!
Notes on Contributors
Teng Chun Koh directed the project, reviewed literature and took the lead in writing and editing the manuscript.
Eugene Zhi Jie Lee contributed to the design of the project and ideas for this manuscript.
Charlene Jie Lin Yak contributed to the design of the project and ideas for this manuscript.
Jack Botao Sun contributed to the ideas for the project and this manuscript.
Joshua Ren Wei Tay was invited to make some brief corrections to the manuscript.
Ann Chong Hui Fong advised and provided feedback on the manuscript, aiding development of the manuscript.
Clara Yuen Pun Mok advised and provided feedback on the manuscript, aiding development of the manuscript.
All authors discussed and contributed to the final manuscript.
Acknowledgement
This e-Orientation could not have been successfully carried out without the support and encouragement from fellow classmates and friends, who hosted the e-Orientation games and activities with enthusiasm and passion. Their hard work indubitably contributed to the success of the event.
Funding
The authors have no funding to report.
Declaration of Interest
The authors have no conflict of interest to declare.
References
Ullman, E. (2020, October 27). How to take college orientation online. https://www.techlearninguniversity.com/how-to/how-to-take-college-orientation-online
Zoom Communications Inc. (n.d.). Security: Zoom trust center. Retrieved January 26, 2021, from https://explore.zoom.us/en-us/trust/security.html
*Teng Chun Koh
9 Lower Kent Ridge Road, #10-01,
National University Centre for Oral Health,
Singapore 119085
Email: e0405935@u.nus.edu
Submitted: 1 October 2020
Accepted: 3 December 2020
Published online: 4 May, TAPS 2021, 6(2), 78-87
https://doi.org/10.29060/TAPS.2021-6-2/OA2406
Yoshitaka Maeda1, Yoshikazu Asada2, Yoshihiko Suzuki1, Akihiro Watanabe3, Satoshi Suzuki3 & Hiroshi Kawahira1
1Medical Simulation Center, Jichi Medical University, Japan; 2Center for Information, Jichi Medical University, Japan; 3Faculty of Health and Medical Sciences, Kanagawa Institute of Technology, Japan
Abstract
Introduction: Students in the early years of medical school should learn clinical site risk assessment skills. However, the effect of this training on clinically inexperienced students is not clear, and it is difficult for students to predict risks from a wide range of perspectives. This study aims to develop and implement three patterns of safety walk rounds (SWR) in a class of students with no clinical experience.
Methods: Three types of SWR were conducted: (A) 37 students observed a familiar classroom and predicted safety risks; (B) 39 students created a profile of a fictitious student in advance and then used Type A parameters; (C) 100 students participated. First, Type A was conducted as a practice. Next, students observed a hospital and predicted risks. All participants in Types A to C had no clinical experience. We classified all risks into perception, comprehension, and action.
Results: For each safety walk-round, there were two types of risk prediction. In Type A, risks such as perception and comprehension were more than 80%. In Types B and C, action risks were 60%. Students had little experience in observing facilities and none at finding safety risks.
Conclusion: Each method had a different risk prediction tendency. Combining the methods could enable students to acquire comprehensive skills in assessing hidden environmental patient safety risks.
Keywords: Patient Safety Education, Undergraduate Education, Risk Assessment Skill, Safety Walk-Rounds
Practice Highlights
- Proposes a patient safety education method incorporating safety walk rounds (SWR).
- Clarifies the risk prediction tendency of clinically inexperienced students in each SWR pattern.
- Students conducting SWR in familiar classrooms tend to predict certain risks.
- Creating fictitious user profiles before SWR enables prediction of action risks.
- Combining different SWR types could enable comprehensive risk assessment skills.
I. INTRODUCTION
In Japan, first-year medical students are recent high school graduates. 60% of universities that train medical professionals provide patient safety education to fourth year medical students at the start of clinical training (Ishikawa et al., 2008). Further, lower grade educational methods do not include specific guidelines for patient safety education, and students in lower grades do not have sufficient medical knowledge to immediately apply their patient safety knowledge in clinical practice. This problem has been pointed out not only in Japan but also in the US and Canada (Alper et al., 2009). Conversely, the Telluride Interdisciplinary Roundtable (Mayer et al., 2009) and Lucian Leape Institute (2010) showed that patient safety education should be included in the curriculum of all grades. This would enable students to learn the necessity and importance of patient safety knowledge and consider patient safety as an implementation science while continuously practising patient safety skills (Nakajima, 2012).
However, many medical schools teach basic patient safety knowledge through lectures on accident analysis tools, legal responsibility knowledge, ethics, and infection (Mayer et al., 2009); however, students lack education on non-technical skills (Mayer et al., 2009; Nakajima, 2012; Walton et al., 2010). Students should be trained in awareness of safety weaknesses, threats (risks) in the workplace or operations, and how to avoid these risks (Doi et al., 2012). Topic 6 of the World Health Organization’s (WHO’s) Patient Safety Curriculum Guide indicates that students need to take appropriate corrective action when they see an unsafe situation or environment (Walton et al., 2010). However, the WHO guidelines do not explain how these risk assessment skills can be taught to students. Literature that examines the effectiveness of risk assessment skills training for early-year medical students is deficient.
To address these issues, we focused on Safety walk rounds (SWR), in which a safety manager goes to a workplace, listens to staff opinions on safety, and observes the workplace to identify safety issues before an accident (Hafey, 2017; Womack, 2013). Singer and Tucker (2014) pointed out that SWR enhances safety culture. The effects of SWR in the radiology department have reduced the number of unsafe events by half (Donnelly et al., 2008). Additionally, other studies reported that safety managers grow more sensitive to safety issues using SWR and that motivation regarding safety is increased (Frankel et al., 2003; Singer & Tucker, 2014). However, its educational effect and applicability to educating clinically inexperienced students are not clear since SWR has not been used for education.
This study aims to develop and implement three patterns of SWR in a class of students with no clinical experience. We clarify the risk prediction tendency of students in each SWR pattern and discuss the effects.
II. METHODS
A. Development Process of Three Types of SWR
We developed three patterns of SWRs to help clinically inexperienced students predict risk and considered what motivates students to learn. We used the ARCS model proposed by J. M. Keller in 1983, which is a framework using four elements: Attention (stimulating the learner’s interest, intellectual curiosity, and inquisitiveness); Relevance (making the content familiar and meaningful); Confidence (encouraging learners to learn); and Satisfaction (giving the learner a sense of satisfaction and motivation to learn more) (Keller, 1987). ARCS is an acronym for these elements.
· SWR in daily situations (SWR-D): Experts are better at predicting risks than novices as the latter has limited knowledge of important aspects of each situation (Murata et al., 2009). Hence, clinically inexperienced students might find it difficult to predict risks in clinical situations. Using the ARCS model, students need to be given Attention, Confidence and Satisfaction. Therefore, we developed SWR in daily situations (SWR-D). Students observe daily situations in classrooms and school buildings for instances of safety risk and take pictures. We use daily situations as classrooms and school buildings are familiar environments for students, and there are many safety risks for educating students.
· SWR in daily situations using the Persona method (SWR-DP): It may be difficult for students who have never performed SWR to observe safety risks in daily situations, and students’ Confidence should be high. Therefore, we combined the persona method with SWR to create a virtual profile of a virtual user, including name, gender, age, and information about the system (e.g., technological literacy). The Persona method has been used to examine the safety of driving support systems (Lindgren et al., 2007). We hypothesize that the Persona method would help students to predict risk from the perspective of a specific user. The student considers the problems the virtual user will face and their behaviour (Cooper, 2004; Mulder & Yaar, 2006). Students created fictitious student profiles (personas) and conducted SWR assuming that the persona students would spend one day in school buildings and classrooms.
· SWR in clinical situations (SWR-C): It may be difficult for students to associate SWR with patient safety in clinical practice, as SWR in daily situations were not related to clinical practice conducted. Further, students might not be motivated to learn—using the ARCS model, students need to see Relevance and Satisfaction. Therefore, we developed the SWR in clinical situations (SWR-C). First, to practice SWR, students performed SWR-D. After SWR-D, they observed clinical situations in hospitals to predict risks (SWR-C).
B. Description of Participants and SWR Implementation Process
This study involved first-year medical students and third-year students in the medical engineer training courses who had no clinical experience. After participating in each SWR pattern, students were asked for their opinions.
1) SWR-D: The participants included 37 students in the third-year medical engineer training course and 100 students who had been in medical school for one month. SWR-D was administered to the third-year (2018) medical engineer training students in one session. SWR-D was implemented as one of the required general education courses for first-year medical students in 2019. An exercise using SWR-D was given to all participants who worked in groups of four to five. Students photographed incidences of safety risk (30 minutes) and collaborated to identify the risks in each photo (20 minutes).
2) SWR-DP: The participants included 39 students (different from SWR-D) in the third-year medical engineer training course. SWR-DP was administered to the third-year (2019) medical engineering students in one session and conducted in groups of four to five. Each group considered one persona (virtual student profile) for the first 20 minutes, and SWR-D was conducted as before.
3) SWR-C: The participants included 100 students (same as SWR-D) who had been in medical school for one month. Each student was assigned one clinical department in advance. Two weeks after the SWR-D, early exposure training was conducted. During training, students found safety risks in clinical situations and outlined the identified risks in reports as photography was not allowed for confidentiality.
C. Statistical Analysis
The risks predicted by students in each SWR pattern were counted and classified into the following: perception—difficulty perceiving something that exists in the outside world (e.g., signs that are difficult to read); comprehension—difficulty understanding the meaning of something that exists in the outside world and in planning what action to take (e.g., signs that are difficult to understand); and action—difficulty performing the intended action (e.g., places where it is difficult to walk).
These classifications are based on Norman’s seven stages of action (Norman & Draper, 1986) where human actions are classified into seven stages: forming the goal, forming the intention, specifying an action, executing the action, perceiving the state of the world, interpreting the perception, and evaluating the outcome (Norman, 1988). This is a representative model widely used for the design evaluation of man-machine systems such as computers (Fleming & Koman, 1998) to understand human cognitive behaviour that leads to human error in medical treatment (Zhang et al., 2002; Zhang et al., 2004).
D. Ethical Considerations in This Research
The ethical requirements in this study are in accord with the Declaration of Helsinki. We emphasized and explained to students that participation was voluntary and that declining to cooperate would have no influence on their grades. We also explained that consent to participate could be withdrawn at any time, that the results of this study may be published after processing, and that the students’ personal information would not be revealed. The students entered their consent in the e-learning system Moodle. This study was considered exempt by the Jichi Medical University Review Board (Number 18-014).
III. RESULTS
The total number of perception, comprehension, and action risks in each SWR is shown in Figure 1. Table 1 shows typical predicted risks and some of the images taken by students. The data that support the findings of this study are openly available in Figshare at <http://doi.org/10.6084/m9.figshare.13012664 (Maeda et al., 2021)>.
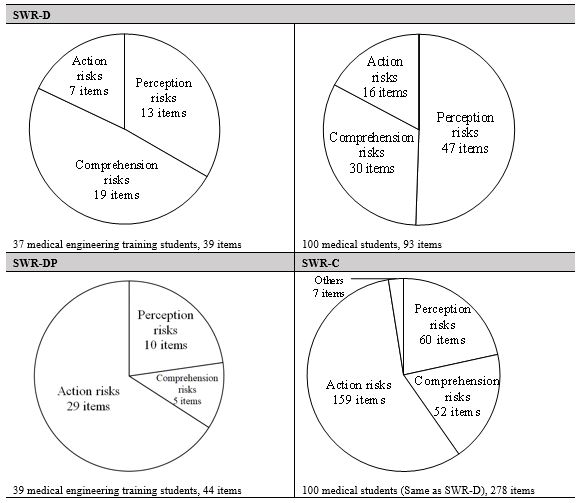
Figure 1. Classification results of risks predicted by students in each SWR pattern
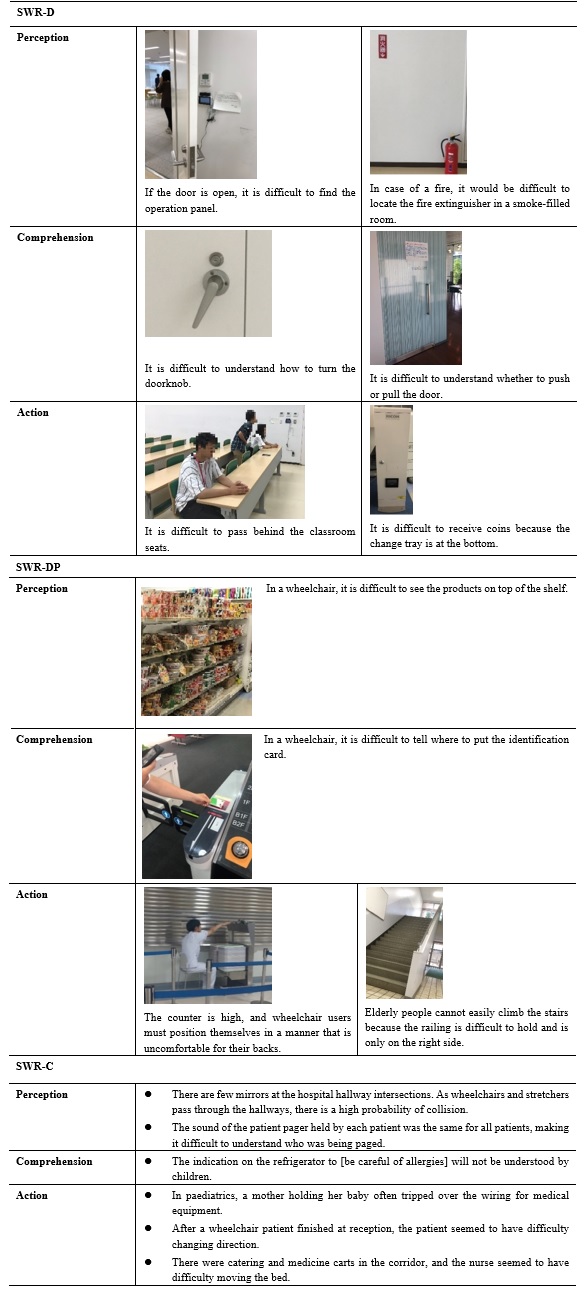
Table 1. Typical risks and captured images for each SWR pattern
In SWR-D, the number of action risks was lower than that of perception and comprehension risks. Risks related to guidance signs for school buildings and classrooms, signs, maps, doors, and operation panels for electric lights were predicted. Also, for example, a group of students who pointed out that it was difficult to find a fire extinguisher did not simply point out the problem of perception, but pointed out that “in the case of a fire, it would have been difficult to find the fire extinguisher in a room filled with smoke”. In other words, they imagined a fire situation that differed from the current conditions of the site they observed.
In SWR-DP, students created the persona shown in Table 2. Many students created fictitious profiles of students who had disabilities or who were elderly. Despite observing the same school building as SWR-D, the number of action risks is almost 70% of the total number (Figure 1). Table 1 shows that many students made extensive predictions from the same perspective as the persona—the risks associated with persons with some kind of disability. For example, from the height of the eyes of a person in a wheelchair, students predicted problems with the visibility of products in a shop, the height of a counter in a cafeteria, and with the routes, the persona would be likely to take within a building. Most identified problems pertained to a lack of easy access to the environment. In one image (Table 1), a student is seen simulating being in a wheelchair at the cafeteria counter.
|
Male, 70 years old, 160 cm, 55 kg, using a cane, hearing loss, narrow vision. He entered college to re-learn after retirement. He goes to school by bus. He is worried about being able to see the whiteboard. He is worried that he will be late for class because he moves more slowly. |
|
Male, 18 years old, 141 cm, 85 kg. He uses a wheelchair because he lost his left leg in a traffic accident. He is apprehensive about moving between classrooms. |
Table 2. Example of a persona (fictitious student profile) created by SWR-DP students
In SWR-C, action risks were the most frequent (Figure 1). Of the total 251 risks, approximately 90% were risks to patients and approximately 10% to healthcare professionals. From Table 1, regarding action, we can see that students observed the behaviour and embarrassment of patients at hospitals and predicted risks based on them (e.g., “The mother holding her baby was almost stumbling”; “Patients in wheelchairs were difficult to move”). In perception and comprehension, students brainstormed risks from the patients’ perspective (e.g., “The indication on the refrigerator to [be careful of allergies] will not be understood by children”). The students identified risks from the child’s perspective.
Table 3 shows the students’ opinions of each SWR. In all SWRs, students had little experience in observing the facilities they usually used, and finding safety risks was new to them. In SWR-DP, students said that although they were able-bodied, they could notice accessibility problems by observing the environments from the persona’s perspectives. For SWR-C, students noticed that there were many problems in the design and environment of the hospital facilities and that various safety measures had already been implemented.
|
SWR-D
SWR-DP
SWR-C
|
Table 3. Student opinion on SWR
IV. DISCUSSION
A. Student Risk Predicting Tendency in Each SWR Pattern
The importance of institutional design in patient safety has been pointed out in many publications. For example, environmental design is being considered to avoid various risks, such as falls and patient suicides, mixing up patients, and improper handling of tubes and connectors (Joseph & Rashid, 2007; Michalska & Szewieczek, 2007; Reiling, 2006; Reiling et al., 2003; Reiling et al., 2008). In particular, it has been pointed out that the indoor environment (e.g., noise and lighting) and interior design (e.g., furniture and materials) are important (Joseph & Rashid, 2007). When considering the design, it is necessary to predict both the direct impact risks and the indirect impact risks of accidents as points of view when predicting onsite risks. Direct impact risks are the aspects of hospital design that can directly impact safety outcomes, such as patient falls and medical errors (Joseph & Rashid, 2007). This is considered to correspond to “action” in this study. For example, a tall counter design is directly linked to the undesirable consequence of a wheelchair user being unable to receive a meal. Indirect impact risks are the aspects of hospital design that can cause users to make incorrect decisions that lead to accidents and errors (Joseph & Rashid, 2007). This is considered to correspond to “perception” and “comprehension” in this study. For example, a paediatric refrigerator’s “be careful of allergies” poster does not directly lead to an unsafe outcome; however, if a child is unable to understand, then an incorrect decision to eat food to which the child is allergic may lead to an unsafe outcome.
In SWR-D, many indirect impact risks (perception and comprehension) were predicted. Conversely, few action risks (direct impact risks) were predicted. SWR-DP and SWR-C results were the opposite to SWR-D; many direct impact risks and few indirect impact risks were identified.
In SWR, it is necessary to identify risks through brainstorming and simulation using the operators’ experience and reasoning (Okubo et al., 2014). However, different techniques identify different risk types. Indirect impact risks such as perception and comprehension are related to human internal thinking, such as incorrect decisions. To identify these risks, students need to observe from the perspective of the person concerned and brainstorm the risks. Conversely, the action is observable—a risk that students can predict by observing the actions of the concerned person or simulating behaviour as the concerned person. Subsequently, what caused each SWR to favour predicting one type of risk over another?
In SWR-D, most students observed a familiar daily situation from their (able-bodied) perspective. In SWR-DP, students observed a familiar daily situation from a persona’s point of view that differed from that of an able-bodied person. In SWR-C, they observed unfamiliar clinical situations from the patients’ perspective (it is unknown whether this perspective was different from their own). This suggests that when students observe a familiar environment from their own perspective, they concentrate on brainstorming about risks but do not conduct much action simulation (acting on a simulated basis and identifying risks). Consequently, the risks related to action were few.
Conversely, if students observe risk from others’ perspective, they may not be able to brainstorm well, and they may tend to predict risks by performing action simulations. In SWR-DP, many images of simulations, such as trying to use a cafeteria as a persona (for example, a wheelchair user), were recorded. Notably, novice nurses tend to observe bedsides without being able to imagine the patient’s condition or behaviour (Daikoku & Saito, 2017); it seems difficult to predict risks associated with unfamiliar subjects (people/environment) only by brainstorming.
However, during SWR-C, we asked students to predict risks only by observation to avoid interference with patient care, and students were unable to perform action simulations. Nevertheless, the risks associated with actions were the most predicted. According to the risks predicted by the students (Table 1), students likely found patients who were confused and observed their behaviour. In the clinical situation, there were several observable patients that students could predict many risks based on observable actions.
In summary, for clinically inexperienced students to predict many indirect impact risks (perception, comprehension), it is better for them to make observations from their own perspectives in a daily situation where brainstorming can be easily conducted. It is better to ask students to observe an unfamiliar person and environment to identify more direct impact risks (actions). It would be better to create a fictitious user profile (persona) and conduct SWR (SWR-DP) or conduct SWR in a clinical situation unfamiliar to students (SWR-C). In any case, if each SWR is implemented independently, the predicted risks are biased. Therefore, by combining each SWR, it may be possible to develop skills that enable students to find direct impact and indirect impact risks in a well-balanced manner.
B. Limitations
This study evaluates the educational benefits of three SWR patterns and discusses their effectiveness. We could not compare the three patterns of SWR for the following aspects. First, we could not examine the relationship between participants’ background and SWR. This study targeted first-year medical students (SWR-C) and third-year students in the medical engineer training course (SWR-D, SWR-DP). Each student’s age and expertise were different. Therefore, the background of each participant could have affected the participant’s risk prediction tendency. However, all students shared the common background of having no clinical experience and had basic education on patient safety and conducted SWR with a basic knowledge of human factors, such as medical accident analysis methods. Second, we could not conduct a comparative study of each SWR by statistical analysis as there were differences in the way each SWR was conducted. SWR-D and SWR-DP were administered as a group, while SWR-C was administered individually because of restrictions in clinical practice. We could not calculate the average number of hazard predictions per student.
Further, each SWR was conducted in a compulsory class; therefore, there were a large number of students per faculty member. Consequently, we could not observe all students. Therefore, we have little record of how students predicted risks, especially in SWR-C. This is because the simulation actions in clinical situations and photography were restricted.
Additionally, when examining the safety of facility design, it is important to predict risks to healthcare professionals as well as patients (Reiling et al., 2003). However, in SWR-C, 90% of the risks were related to patients. Future studies should examine training methods that enable clinically inexperienced students to predict risks to healthcare professionals.
V. CONCLUSION
In this study, we proposed a patient safety education method incorporating SWR. We conducted SWR-D, SWR-DP, and SWR-C sessions and clarified the risk assessment tendency of students in each SWR pattern. For students to predict many indirect impact risks (perception comprehension), it is better to have students observe a daily situation in which it is easy to identify risks from their own points of view (SWR-D). To find many direct impact risks (action), it is better for students to create a persona and observe a daily situation (SWR-DP) or clinical situation (SWR-C). This suggests that a combination of these SWRs would provide students with the skills to comprehensively predict the patient safety risks in facilities and the environment. By continuously conducting all SWR session types starting at lower grade levels, it is expected that skills related to risk assessment will be effectively acquired. It is expected that SWR education from pre-graduates will increase the number of medical professionals who can conduct an appropriate risk assessment in the field, resulting in improved quality and safety of healthcare.
Notes on Contributors
Yoshitaka Maeda, PhD, a Research Associate at the Medical Simulation Center at Jichi Medical University, Japan, contributed to the conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing (original draft, review, and editing), and visualization.
Yoshikazu Asada, PhD, an Assistant Professor at the Center for Information at Jichi Medical University, Japan, contributed to the methodology, validation, formal analysis, and visualization.
Yoshihiko Suzuki, MD, an Assistant Professor at the Medical Simulation Center at Jichi Medical University, Japan, contributed to the conceptualization and methodology.
Akihiro Watanabe, MS, a Research Associate at the Faculty of Health and Medical Sciences at Kanagawa Institute of Technology, Japan, contributed to the validation and investigation.
Satoshi Suzuki, PhD, a Professor at the Faculty of Health and Medical Sciences at Kanagawa Institute of Technology, Japan, contributed to the data curation, writing (review and editing), and visualization.
Hiroshi Kawahira, MD, PhD, FACS, a Professor at the Medical Simulation Center at Jichi Medical University, Japan, contributed to the writing (review and editing), supervision, and project administration.
All the authors have read and approved the final manuscript.
Ethical Approval
This study was approved by the Jichi Medical University Institutional Review Board (protocol number 18-014).
Data Availability
The data that support the findings of this study are openly available in Figshare repository, http://doi.org/10.6084/m9.figshare.13012664
Funding
There is no funder for this study.
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
Alper, E., Rosenberg, E. I., O’Brien, K. E., Fischer, M., & Durning, S. J. (2009). Patient safety education at US and Canadian medical schools: Results from the 2006 clerkship directors in internal medicine survey. Academic Medicine, 84(12), 1672-1676. https://doi.org/10.1097/acm.0b013e3181bf98a4
Cooper, A. (2004). The inmates are running the asylum: Why high-tech products drive us crazy and how to restore the sanity (Vol. 2). Sams Publishing.
Daikoku, R., & Saito, Y. (2017). Characteristics of gaze in expert nurses during observation at the bedside. Japanese Journal of Nursing Art and Science, 15(3), 218-226. https://doi.org/10.18892/jsnas.15.3_218
Doi, T., Kawamoto, K., & Yamaguchi, K. (2012). Difference by level of awareness and the years of experience to patient treatment safety. Japanese Journal of Radiological Technology, 68(5), 608-616. https://doi.org/10.6009/jjrt.2012_JSRT_68.5.608
Donnelly, L. F., Dickerson, J. M., Lehkamp, T. W., Gessner, K. E., Moskovitz, J., & Hutchinson, S. (2008). IRQN award paper: Operational rounds: A practical administrative process to improve safety and clinical services in radiology. Journal of the American College of Radiology, 5(11), 1142-1149. https://doi.org/10.1016/j.jacr.2008.05.017
Fleming, J., & Koman, R. (1998). Web navigation: Designing the user experience. O’Reilly Media.
Frankel, A., Gandhi, T. K., & Bates, D. W. (2003). Improving patient safety across a large integrated health care delivery system. International Journal for Quality in Health Care, 15(suppl_1), i31-i40. https://doi.org/10.1093/intqhc/mzg075
Hafey, R. B. (2017). Lean safety gemba walks: A methodology for workforce engagement and culture change. Productivity Press.
Ishikawa, M., Hirao, T., & Maezawa, M. (2008). Study of patient safety education for undergraduates. Medical Education, 39(2), 115-119. https://doi.org/10.11307/mededjapan1970.39.115
Joseph, A., & Rashid, M. (2007). The architecture of safety: Hospital design. Current Opinion in Critical Care, 13(6), 714-719. https://doi.org/10.1097/mcc.0b013e3282f1be6e
Keller, J. M. (1987). Development and use of the ARCS model of instructional design. Journal of Instructional Development, 10(3), 2-10. https://doi.org/10.1007/BF02905780
Lindgren, A., Chen, F., Amdahl, P., & Chaikiat, P. (2007). Using personas and scenarios as an interface design tool for advanced driver assistance systems. In: Stephanidis C. (eds) Universal Access in Human-Computer Interaction. Ambient Interaction. UAHCI 2007. Lecture Notes in Computer Science, vol 4555. Springer. https://doi.org/10.1007/978-3-540-73281-5_49
Lucian Leape Institute. (Eds.). (2010). Unmet needs: Teaching physicians to provide safe patient care. National Patient Safety Foundation.
Maeda, Y., Asada, Y., Suzuki, Y., Watanabe, A., Suzuki, S., & Kawahira, H. (2021). Proposal for safety walk-round education to develop risk prediction skills of novice health professional students [Data set]. Figshare. http://doi.org/10.6084/m9.figshare.13012664
Mayer, D., Klamen, D. L., Gunderson, A., & Barach, P. (2009). Designing a patient safety undergraduate medical curriculum: The Telluride interdisciplinary roundtable experience. Teaching and Learning in Medicine, 21(1), 52-58. https://doi.org/10.1080/10401330802574090
Michalska, J., & Szewieczek, D. (2007). The 5S methodology as a tool for improving the organization. Journal of Achievements in Materials and Manufacturing Engineering, 24(2), 211-214.
Mulder, S., & Yaar, Z. (2006). The user is always right: A practical guide to creating and using personas for the web. New Riders.
Murata, A., Hayami, T., & Moriwaka, M. (2009). Visual information processing characteristics of drivers in prediction of dangerous situation-Comparison among novice, expert and non-licensed person. In IEEE SMC Hiroshima Chapter (Eds.), Proceedings of Fifth International Workshop on Computational Intelligence & Applications, (pp. 254-257). IEEE SMC Hiroshima Chapter.
Nakajima, K. (2012). Patient safety and quality of medical care. Topics: III. Management of patient safety and quality of medical care: Theory and practice; 4. Patient safety and quality improvement education for undergraduate medical students. Nihon Naika Gakkai zasshi. The Journal of the Japanese Society of Internal Medicine, 101(12), 3477. https://doi.org/10.2169/naika.101.3477
Norman, D. A. (1988). The psychology of everyday things. Basic Books.
Norman, D. A., & Draper, S. W. (1986). User centered system design: New perspectives on human-computer interaction. L. Erlbaum Associates.
Okubo, Y., Kuroda, R., & Yamamoto, K. (2014). Health and safety patrol in universities. Journal of Environment and Safety, 5(3), 169-175. https://doi.org/10.11162/daikankyo.14C0702
Reiling, J. (2006). Safe design of healthcare facilities. BMJ Quality & Safety, 15(suppl 1), i34-i40. https://dx.doi.org/10.1136%2Fqshc.2006.019422
Reiling, J., Breckbill, C., Murphy, M., McCullough, S., & Chernos, S. (2003). Facility designing around patient safety and its effect on nursing. Nursing Economics, 21(3), 143.
Reiling, J., Hughes, R. G., & Murphy, M. R. (2008). The impact of facility design on patient safety. In Hughes, R. G (Ed.), Patient safety and quality: An evidence-based handbook for nurses. Agency for Healthcare Research and Quality.
Singer, S. J., & Tucker, A. L. (2014). The evolving literature on Safety walkrounds: Emerging themes and practical messages. BMJ Quality & Safety, 23(10), 789–800. http://dx.doi.org/10.1136/bmjqs-2014-003416
Walton, M., Woodward, H., Van Staalduinen, S., Lemer, C., Greaves, F., Noble, D., Ellis, B., Donaldson, L., & Barraclough, B. (2010). The WHO patient safety curriculum guide for medical schools. BMJ Quality & Safety, 19(6), 542-546. http://dx.doi.org/10.1136/qshc.2009.036970
Womack, J. (2013). Gemba walks: Expanded 2nd edition. Lean Enterprise Institute.
Zhang, J., Patel, V. L., & Johnson, T. R. (2002). Medical error: Is the solution medical or cognitive? Journal of American Medical Informatics Association, 9(6 Suppl 1), s75-77. https://dx.doi.org/10.1197%2Fjamia.M1232
Zhang, J., Patel, V. L., Johnson, T. R., & Shortliffe, E. H. (2004). A cognitive taxonomy of medical errors. Journal of Biomedical Informatics, 37(3), 193-204. https://doi.org/10.1016/j.jbi.2004.04.004
*Yoshitaka Maeda, PhD
3311-1, Yakushiji, Shimotsuke-shi,
(Kinen-tou 7th floor),
Tochigi,Japan, 329-0498
Tel: +81-285-58-7455
Email: y-maeda@jichi.ac.jp
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
