
Opinions on the impact of COVID-19 on undergraduate students from diverse backgrounds and health needs
Submitted: 28 July 2020
Accepted: 23 December 2020
Published online: 13 July, TAPS 2021, 6(3), 104-107
https://doi.org/10.29060/TAPS.2021-6-3/PV2363
Tushar Hari1, Dennis Hathey1, Sonia Kumar2, Ilona Blee2, Rachel Browne3 & Simon Tso3
1Buckingham Medical School, United Kingdom; 2South Warwickshire National Health Service Foundation Trust, United Kingdom; 3Jephson Dermatology Centre, South Warwickshire National Health Service Foundation Trust, United Kingdom
I. INTRODUCTION
We live in unprecedented times with the COVID-19 pandemic disrupting our normal way of life. First identified in December 2019, the novel SARS-CoV-2 strain has brought about vast devastation. According to the World Health Organisation (WHO), as of 21st November 2020, there are 56.9 million confirmed cases and 1.3 million deaths worldwide. The government approach to control the spread of COVID-19 in the United Kingdom (UK) is underpinned by social distancing measures; to limit the spread and prevent the inundation of National Health Service (NHS).
Social distancing impacts society on both an individual and population level. Across the country, virtual learning has become the new normal. It is our experience at Buckingham Medical School that students saw their clinical placements suspended. Educational resources were shared via online platforms and final year examinations done remotely to fast-track the transition to newly qualified doctors with an interim registration with the UK General Medical Council (GMC).
In this opinion piece, a diverse panel of two medical students, two doctors-in-training and two educators, including individuals with international student status, learning and sensory difficulties, chronic diseases, and dependents, discussed the impact on undergraduate medical education for individuals who may risk being left behind if efforts towards widening participation are not considered amidst this crisis and its aftermath. The focus group was held as an online asynchronous unstructured discussion through emails over a three-month period, moderated by a consultant, who regularly posted questions for the groups to discuss. This was supplemented by face-to-face discussion between the participants to summarise key outcomes and then circulated the conclusions to the panel before manuscript inclusion. Verbal consent was obtained from participants.
II. OVERVIEW: THE CHANGING LANDSCAPE OF UNDERGRADUATE MEDICAL TRAINING IN THE UK
What was once a curriculum encompassing face-to-face clinical teaching to deliver a degree in medicine, has now become reliant on the virtual learning environment (VLE).
In the UK, medical teaching methods vary between institutions. Under such unprecedented times, these long-established methods of education have required immediate reform, with VLE taking over and clinical teaching being significantly reduced or temporarily paused (Taha et al., 2020).
The use of VLE in UK medical schools has increased within the last decade. Many already utilise VLE for lecture recording, uploading learning materials, or online assessments. Challenges with virtual teaching existed before COVID-19, particularly the lack of time for educators to become familiar with and implement online learning. Some educators view virtual teaching negatively and thus engage poorly with these platforms (O’Doherty et al., 2018). These learning platforms may also be perceived as expensive. However, need is a big driver for change. With the COVID-19 pandemic forcing the need for socially distant learning, many institutions have become more receptive to this change and many students are benefitting from the flexibility of engaging with the material remotely.
Since the start of the pandemic, medical schools have begun to disseminate pre-recorded or live lectures using online platforms such as Microsoft Teams or Zoom. Simulations of the clinical setting are being recreated to accommodate for the loss of practical experience and provide medical students in the early stages an introduction to the clinical environment. Reduced opportunity for workplace-based clinical learning, suspension of rotational training and medical electives could also potentially impact on career choices due to a lack of exposure.
Student pastoral care is vital during this pandemic, with new anxieties and stresses arising daily. This can be continued on these virtual platforms, either as one-to-one sessions or in tutorial groups. However, members of our focus group expressed how they found video conferencing less personal, and difficulty with internet connections can make it hard to discuss personal problems.
III. INCLUSIVITY AND WIDENING PARTICIPATION CONSIDERATIONS
The GMC states that: “a diverse population is better served by a diverse workforce” (General Medical Council, 2018). Much effort has gone into widening access to medicine and focusing on inclusivity and diversity within medicine. This work must not be forgotten amidst this crisis.
A. Our International Community of Medical Students in the UK
An international UK medical student from our focus group explained that governments are advising their citizens abroad to return home. COVID-19 has impacted countries to varying degrees and many students have been recalled to help with national efforts such as volunteer work and contact tracing. With medical school teaching resuming via VLE in the UK, the challenge of now balancing voluntary commitments at home, family life and university work is made more difficult by differing time zones. Educators in the UK should bear in mind that these factors could impact on students’ level of engagement and learner satisfaction with online synchronous learning opportunities. Furthermore, access to certain learning resources such as the electronic British National Formulary and NICE (National Institute for Health & Care Excellence) guidelines is restricted outside the UK, causing difficulties with revision for some. Many have expressed concern regarding the future of their degrees; with questions around when respective governments will change travel advice so that they can return to the UK, and implications of the pandemic on their visas and degree duration. This uncertainty and stress are impacting some international students’ focus on their degrees. International students have also found positives to the new methods of teaching. Many students shared that online learning is more engaging compared to live classes and easier to access, ensuring standardised availability of resources for all, regardless of location. Also, many are content to be home with family support during a time of international crisis.
B. Students with Sensory Disability, Learning Differences and Chronic Diseases
In 2016/2017 the proportion of students with a declared disability was 9.3%, rising to 10.4% in 2017/2018 (General Medical Council, 2021). In the time of COVID-19, having a disability or chronic disease presents an additional barrier to effective workplace-based learning. Specific learning differences could impact on students’ ability to assist on ward round activities such as documentation. Documentation in medical notes at our institution is now performed away from patients’ bedside following completion of daily ward rounds due to infection control considerations. This presents student scribers with difficulties in working memory or other specific learning differences, the additional challenge of recalling large volumes of complex information after an event. In our real-life example, the clinician supported and debriefed the student after the ward round, and ensured the student had adequate time to document the plan in the patient notes, demonstrating a positive example of inclusivity.
Medical students with hearing impairment require lip-reading as a communication adjunct. Unfortunately, implementation of using face masks in the clinical setting limits this and there is a lack of availability of medical grade transparent face masks. Therefore, considerations on using appropriate debriefing and non-verbal communication skills such as hand gestures and written forms of expression can be vital in delivering a complete learning experience for students.
Many vulnerable students are concerned about their risks of contracting COVID-19 and thus their ability to complete their degree in the original timeframe. High-risk individuals have been advised to avoid clinical areas or even isolate at home. Students must fulfil time-based and performance-based criteria to be awarded a GMC-recognised medical degree, but the loss of time and clinical experience in a compact degree programme could put into question their ability to complete on time.
C. Students with Dependents
Students with dependents and those balancing part-time work with medicine to ease the financial burden of their degree could also require additional support. Universities and Colleges Admissions Service (UCAS) guidelines state, a student who holds responsibility for a child aged 17 or younger, should have access to additional support with studies (Universities and Colleges Admissions Service [UCAS], 2021). Students with dependents face many challenges during their degree due to personal obligations. The VLE offers students with dependents an opportunity to maintain their learning at a time when access to schools and care facilities are restricted during the lockdown, but this also presents the challenge of learning and completing coursework while simultaneously caring for their dependents. For some, a distinction between the place of study and the home environment was key to maintaining an effective work-life balance. The availability of care facilities, financial health of students and access to university hardship grants and support systems, would be key to maintaining this group of students’ participation in studying medicine.
IV. CONCLUSION
From our experience, the COVID-19 pandemic has changed the delivery of undergraduate medical education at the current time – whether these changes persist remains to be seen. Educators should be considerate about student support in this new way of working, to benefit all students. This applies especially to those with undeclared or undiagnosed learning difficulties, disability, chronic disease, and those with dependents, to encourage their full participation in all available workplace and online-based learning activities and integrate them into the clinical team. It is also important to implement the perceived advantages of VLE in future medical curricula. Further literature is required to see if these changes have truly made a positive impact on learning. Such inclusion is crucial to not deter students from continuing medicine. Neglecting the demands for these groups can hinder our previous efforts at widening participation within the NHS.
Notes on Contributors
Tushar Hari was involved mainly with creating the first draft of the paper and leading the focus group. He contributed some of his experiences as an international student. He participated in revising the paper prior to submission.
Dennis Hathey was involved with initially drafting the paper and helped organise the focus group. He was involved with designing the focus group questions and gathering various perspectives. He took part in final approval of the published version as did all the other authors.
Dr Sonia Kumar contributed to shaping the paper in the later stages and added input on all aspects of the paper. She helped with data collection and critical appraisal of the final draft of the submitted paper.
Dr Ilona Blee added input into the needs of disabled students and overall shaped the paper to its final draft. She played an important role in approving the final copy and contributed to data analysis and interpretation.
Dr Rachel Browne contributed to final changes made to the draft and made final approval of the paper along with the other authors.
Dr Simon Tso contributed to the final approval of the paper and helped supervise the conception and progression of the paper and focus group.
In summary, all authors fulfill the four criteria stated for authorship.
Acknowledgement
We would like to express our gratitude to our focus group participants for their contributions.
Funding
No funds were required for this paper.
Declaration of Interest
We have no conflicts of interest to disclose.
References
General Medical Council. (2018). Medical school reports. https://www.gmc-uk.org/education/reports-and-reviews/medical-school-reports.
General Medical Council. (2021). Who is a disabled person. https://www.gmc-uk.org/education/standards-guidance-and-curricula/guidance/welcomed-and-valued/health-and-disability-in-medicine/who-is-a-disabled-person.
O’Doherty, D., Dromey, M., Lougheed, J., Hannigan, A., Last, J., & McGrath, D. (2018). Barriers and solutions to online learning in medical education – An integrative review. BMC Medical Education, 18(1), 130. https://doi.org/10.1186/s12909-018-1240-0
Taha, M., Abdalla, M., Wadi, M., & Khalafalla, H. (2020). Curriculum delivery in Medical Education during an emergency: A guide based on the responses to the COVID-19 pandemic. MedEdPublish, 9(1), 69. https://doi.org/10.15694/mep.2020.000069.1
Universities and Colleges Admissions Service. (2021). Students with parenting responsibilities. https://www.ucas.com/undergraduate/applying-university/individual-needs/students-parenting-responsibilities
*Tushar Hari
Buckingham Medical School
Yeomanry House, Hunter Street,
University of Buckingham
Buckinghamshire, UK, MK181EG
Email: 1606656@buckingham.ac.uk
Submitted: 14 August 2020
Accepted: 6 November 2020
Published online: 13 July, TAPS 2021, 6(3), 45-55
https://doi.org/10.29060/TAPS.2021-6-3/OA2377
Nathalie Khoueiry Zgheib1, Ahmed Ali2 & Ramzi Sabra1
1Department of Pharmacology and Toxicology, American University of Beirut Faculty of Medicine, Beirut, Lebanon; 2Medical Education Unit, American University of Beirut Faculty of Medicine, Beirut, Lebanon
Abstract
Introduction: The forced transition to online learning due to the COVID-19 pandemic has impacted medical education significantly.
Methods: In this paper, the authors compare the performance of Year 1 and 2 classes of medical students who took the same courses either online (2019-2020) or face-to-face (2018-2019), and compare their evaluation of these courses. The authors also present results of three survey questions delivered to current Year 1 medical students on the perceived advantages and disadvantages of online learning and suggestions for improvement.
Results: Performance and evaluation scores of Year 1 and 2 classes was similar irrespective of the mode of delivery of the course in question. 30 current (2019-2020) Year 1 students responded to the survey questions with a response rate of 25.4%. Some of the cited disadvantages had to do with technical, infrastructural and faculty know-how and support. But the more challenging limitations had to do with the process of learning and what facilitates it, the students’ ability to self-regulate and to motivate themselves, the negative impact of isolation, loss of socialisation and interaction with peers and faculty, and the almost total lack of hands-on experiences.
Conclusion: Rapid transition to online learning did not affect student knowledge acquisition negatively. As such, the sudden shift to online education might not be a totally negative development and can be harnessed to drive a more progressive medical education agenda. These results are particularly important considering the several disadvantages that the students cited in relation to the online delivery of the courses.
Keywords: Online Learning, COVID-19 Pandemic, Medical Students
Practice Highlights
- The authors report on the forced transition to online learning due to the COVID-19 pandemic.
- The performance and evaluation scores were similar in online delivery vs face-to face.
- The sudden shift to online education might not be a totally negative development despite the several disadvantages that students cited.
I. INTRODUCTION
The COVID-19 pandemic has impacted medical education significantly. Students were sent home and many schools were forced to shift their teaching, almost overnight, from face-to-face encounters to virtual, online delivery, in many cases without having had substantial previous experience with this mode of delivery. This disruption spanned the clinical and preclinical years. In previous events, researchers prioritised the synthesis of available evidence in terms of training medical students to respond and mitigate the effects of different types of disasters (Ashcroft et al., 2020). While there was more attention to find solutions for medical education in difficult settings (McKimm et al., 2019), including few examples that came to light after the outbreaks of H1N1 and H5N1 influenza, the severe acute respiratory syndrome (SARS) (Patil et al., 2003), and most recently, Ebola (Woodward & McLernon-Billows, 2018), there is paucity of literature that could inform adaptations of medical education methods during or post disasters, conflicts, or outbreaks. Recent articles have reflected on these changes and challenges and have suggested means of responding to the new reality, and offered advice on adopting new tools to ensure the best possible delivery of the curriculum (Daniel, 2020; Fawn et al., 2020; Liang et al., 2020; Ross, 2020; Sandars et al., 2020).
A recent meta-analysis that compared offline and online undergraduate medical education (under normal circumstances) revealed either no difference in outcomes on knowledge tests or a slightly higher performance for those who received online learning (Pei & Wu, 2019). In addition, a review of the literature showed that the adoption of E-Learning, in comparison with mostly traditional and other means of learning, expands access to education and increases the pool of faculty, in low resource settings (Frehywot et al., 2013). These data suggest that for preclinical education, there might not be a major negative impact of moving to online learning. It should be noted, however, that the situation brought about by the COVID-19 pandemic, which necessitated an abrupt transition to online education, may not be identical to that in which online delivery was a, planned and well-designed method to deliver at least part of the curriculum of the medical school; thus, the outcomes in knowledge acquisition during the recent COVID-19- forced transition to online teaching cannot be confidently predicted (Lim et al., 2009).
The American University of Beirut Faculty of Medicine (AUBFM), which follows the American model of medical education, suspended all in-person physical classes and assessments for years 1 and 2 on March 12, 2020. Thus, faculty, students and staff had to shift to online learning practically immediately. In this paper, we report our experience with this forced transition to online learning, specifically addressing Year 1 and 2 students’ perceptions of and response to it, and examining whether this transition affected their knowledge acquisition as reflected by their performance on written examinations.
II. METHODS
This is not a research study, as confirmed by our Institutional Review Board (IRB), since our purpose was to describe our experience with the delivery of the medical school curriculum after the sudden shift to online education, and whether that affected the students’ performance on their examinations and their evaluation of the courses. This was neither a planned intervention nor a systematic approach to test a specific hypothesis.
A. Setting
We analysed data from Year 1 and 2 classes of medical students who took the same courses either online (2019-2020) or face-to-face (2018-2019). We examined student performance in two courses, one for first year medical students (115 Class of 2022 students as face-to-face in 2018-2019 versus 118 Class of 2023 students as online in 2019-2020) entitled The Blood, and the other for second year medical students (114 Class of 2021 students as face-to-face in 2018-2019 versus 115 Class of 2022 students as online in 2019-2020) entitled Human Development and Psychopathology. Both courses are integrated modules that cover the histology, pathology, physiology, biochemistry, pathophysiology, pharmacology of the blood and lymphatic system and of neuropsychiatry, as well as the clinical, social, ethical, and behavioural aspects of related disorders.
Both courses extend over four weeks and end with a final summative examination. The main teaching activities consist of lectures and team-based learning (TBL) sessions, along with other small or large group discussions sessions dealing with epidemiology, evidence-based medicine, medical ethics, and social determinants of health relevant to the medical topics being covered.
The transition to online learning with the current medical students (2019-2020) was as follows: The didactic lectures were delivered either as asynchronous Voice-Over-PowerPoint (VOP) recordings or synchronous live lectures using Webex, which were recorded live. These recordings were made available to students on Moodle, the learning management system used at AUBFM. Faculty chose which of the two modes best suited them. As for the TBLs and group discussion sessions, they were run live using either Webex or Zoom applications. The latter was particularly appropriate for TBL sessions as it allowed virtual breakout rooms for team discussions.
The Respondus lockdown browser, with camera recordings serving as a virtual proctor, was adopted for written assessments, which included the individual Readiness Assurance Tests (i-RAT) of the TBLs as well as the final examinations. All these assessments utilise single-best answer multiple choice questions. Previous to the transition to online learning in 2018-2019, all i-RATs and group-RATs (g-RATs) were paper-based with physical proctoring, while the final course examinations, which used single best answer multiple choice questions, were computer-based, and were run on American University of Beirut (AUB) secure computers, also with physical proctoring.
Prior to COVID-19, final examinations were a hybrid of locally generated questions and National Board of Medical Examiners (NBME) customised examinations. During the COVID-19 pandemic, NBME examinations were not available and final examinations were totally locally generated. With regard to TBL’s, during the online transition, no g-RATs were performed due to our inability to ensure their security; thus, automatic feedback, which was an integral part of the TBL process, was not possible, and was replaced by a brief review of the questions by the TBL preceptor.
In addition, and in order to reduce the potential for cheating and communication among students, we reduced the time allotted for final examinations from 1.2 minutes per question to 1 minute per question. Reducing the on-line time during examinations was also done in order to minimise connectivity problems that arise due to the poor internet infrastructure in Lebanon and due to the frequent cuts in electricity.
B. Students’ Attitudes
At AUBFM, at the end of every course, students are expected to anonymously fill an online course evaluation form. This form includes twelve statements on various aspects of the course with which the students express a level of agreement (Sup. Table 1). Scores are assigned to their responses as follows: 1: Strongly disagree, 2: Disagree, 3: Neither agree nor disagree, 4: Agree, 5: Strongly agree. One of the items on that form (# 4) addresses the effectiveness of the teaching methods. An overall course rating is calculated as the average score for all 12 items. We compared the scores on both item #4 and the overall rating for the course given online (2019-2020) for both Year 1 and 2 medical students with the scores for the same course when delivered face-to-face (2018-2019).
Due to the lack of survey items that are specifically tailored to online teaching in the regular course evaluation forms, we asked the students to respond to 3 additional open-ended questions. This part was administered only to the current (2019-2010) first year medical students who had completed the Blood course and were the following:
1) In your opinion, what are the advantages of online teaching and learning over face-to-face teaching and learning?
2) In your opinion, what are the disadvantages of online teaching and learning over face-to-face teaching and learning?
3) Please provide suggestions for improvement of the online teaching and learning process.
C. Performance on the Final Examinations
Overall performance in the same courses was compared between the current classes (online) and the previous year’s classes (face-to-face). Thus, for the current Year 1 class (Class of 2023) the comparator class was the current Year 2 class (Class of 2022), and for the latter the comparator class was the current Year 3 class (Class of 2021). We restricted the comparisons of final examination grades to performance of the various classes on the locally generated questions.
In order to ensure that any two classes being compared did not differ in terms of academic or cognitive abilities, we also compared the performance of the current and the previous year’s classes according to: 1) their scores on the Medical College Admissions Test (MCAT) taken prior to admission to medical school; and 2) their overall grades in other courses that were given face-to-face during the current year (i.e. in the earlier part of the 2019-2020 academic year); these courses included one entitled Cellular and Molecular Basis of Medicine (CMM) given during year 1, and another entitled The Kidney and Urinary System given during year 2; these were the first courses to be delivered during the current year.
In comparing grades and scores on courses and examinations, we took into account the passing standards set for each. At AUBFM, we use criterion based absolute passing grades for every assessment. For written assessments such as final examinations using multiple choice questions, the Angoff method is utilised to set the passing grade. Similarly, the passing grade for a course is calculated based on the weighting of the individual assessment tools in that course. Thus, for any two courses or examinations that we compared, we first did the analysis using the raw grades, and then, when needed, we also compared the adjusted grades after equalising the passing grades.
D. Data Analysis
For the three survey questions, answers were downloaded on excel for systematic and iterative thematic analysis. Answers were manually coded by one of the authors. The compiled codes were then discussed, compared and consolidated into themes by two of the authors over 3 meetings. The focus was on main themes, commonalities and conflicting views of participants, and relationships between themes. Findings were tabulated with relevant quotes. For the evaluation scores and performance on exam, data were available on excel and statistical comparisons were conducted using the Student’s unpaired t-test.
III. RESULTS
A. Students’ Attitudes
Twenty-six of the 118 current medicine one student filled the survey, and four more sent an email to the course coordinator, the response rate is hence 24.5%. Several themes emanated for each of the three questions especially concerning disadvantages of online learning; these are tabulated in Table 1 with representative quotes. The main advantages of online learning were the time flexibility with asynchronous learning coupled with better overall well-being as a result of staying at home. VOPs were valued because they allowed students to control their learning pace.
As for disadvantages, there were several. These included: the loss of motivation, the potential for procrastination, the problems arising from a bad internet connection leading to greater internet costs, inadequacy of the home environment for learning, less interaction with teachers and students, paucity of immediate feedback, loss of hands on experiences, and struggles because of the faculty’s deficiencies in the area of information technology in general, and in online teaching, in particular.
The students made several suggestions to improve the process, and these included proposals for faculty development, and provision of better technical support and knowhow. In addition, they proposed to decrease or cancel synchronous lectures and provide all didactic lectures as VOPs, to be followed by synchronous online sessions for questions and feedback. They also proposed to imbed questions within the VOPs to stimulate students to think (akin to audience response polls used in live lectures), as well as forum discussions to increase interactions with peers and faculty. Students also insisted that they receive more detailed feedback on their performance on examinations and i-RAT questions.
Despite the many disadvantages cited and the clear room for improvement for online teaching and learning, the overall course ratings as well as the evaluation of teaching for the online courses were not different from their face-to-face counterparts (Tables 2 and 3).
|
Survey question |
Theme |
Quote |
|
Advantages of online teaching and learning in comparison to face to face teaching and learning |
Time flexibility with asynchronous learning |
“Better scheduling that allows us to sleep and rest at night in order to wake up better prepared to ace those PowerPoints” (S9) “Easier to manage our time” (S18) |
|
Control of learning pace with VOP |
“Being able to speed through slides/concepts we already understood and pausing and replaying concepts that we have trouble with makes the whole learning process a lot more efficient and focused” (S27) |
|
|
More wellbeing |
“Less time to commute which allows more time to rest and take care of oneself” (S9) “Having a very healthy diet with my family in the village” (S12) “The [exam] performance is better and stress in minimal” (S23) |
|
|
Disadvantages of online teaching and learning in comparison to face to face teaching and learning |
Potential for procrastination and loss of motivation |
“Less motivation, harder to follow the schedule, requires strong time management skills” (S5) “Face to face teaching helps me organize my day better” (S4) “Being at university with other students around studying during the day motivated me” (S26) |
|
Bad internet connection |
“Internet connection in our country is not stable to hold a class or an exam, so we are resorting to 3g/4g. This leads to a lot of extra expense” (S3) “Time consuming” (S2) and “Sessions would run for more than their original allocated time” (S3) “Longer exams might coincide with the times of the electricity shut offs. This would automatically freeze Respondus and the student will have to restart their computer and so on. Although we are given extra time this adds a lot of stress to an already stressful situation” (S19) “Asking questions are much more difficult and needs much more time” (S7) “WebEx needed a stronger Wi-Fi in some sessions which leads to a harder way to grasp the information” (S18) “The internet connection everywhere in Lebanon is not the best, sometimes we have trouble listening. Sometimes it also gets really crowded when everyone wants to talk at the at the same” (S21) |
|
|
Home environment less conducive to learning |
“Not everybody has the privilege of adjusting their environments to their liking, whether that be because of their dog barking or their family members not respecting their study time” (S28) “This experience helped my appreciate how much I concentrate better in the library” (S9)
|
|
|
Loss of interaction with teachers |
“No direct interaction, harder to communicate directly with professors” (S2) “Face to face interaction was lost: no clues to non-verbal clues, no gestures seen” (S17) “It is true that we can always email the doctors for any additional questions but that does not compare to in person interactions” (S19)
|
|
|
Loss of interaction with students |
“not being able to interact with my friends” (S12) “Students lose their social skills as they interact less with each other-more into introversion” (S17) “You feel there is a barrier between you and the students” (S17) |
|
|
Lack of immediate feedback |
“One problem is during exams not being able to see my mistakes” (S15) “Not correcting our exam and not seeing our mistakes was a huge disadvantage for the online learning” (S18) “Restricting questions to only emails” (S11) and “some professors don’t respond to emails” (S16) and “the response may be delayed” (S29) |
|
|
Loss of hands on experiences |
“No hands-on experience for courses like clinical skills” (S3) “Mainly missing out on clinical skills” (S22) |
|
|
Faculty’s lack of IT knowhow or experience |
“Professors have different abilities and effectiveness in knowing how to do a VOP/online lecture” (S11) “Most Drs. don’t know how to use zoom or WebEx” (S6) “Many instructors are not technically inclined or are outright aversive to it” (S13) “So much time is wasted on technical issues” (S19) “Professors sometimes don’t see the raised hands and sometimes it doesn’t even work. In some lectures we had to wait for the professor to give us access, so we spent time waiting while they didn’t see that some people are trying to access the lecture” (S21) “One of the disadvantages is using the live WebEx sessions. Some professors are losing their recordings, others have a poor connection” (S23) |
|
|
Effect on faculty’s teaching skills |
“Some professors …just read instead of teaching” (S7) “Many professors are not exactly cooperative in terms of explaining mainly because they read their PowerPoints” (S23) “Can’t explain a topic and be passionate about it if talking to a screen or microphone” (S23) |
|
|
Suggestions to improve the current online teaching |
Technical support and knowhow |
“Train the staff on the proper way of utilising the platforms” (S2) “Make IT staff more readily available to help instructors” (S16) “Agree on one way to give the lecture via WebEx as some professors used WebEx team, where we had to ask permission for access, and it was kind of chaotic. It would also be better if the professor agreed on one way to have the questions asked to avoid interruptions and multiple people talking at the same time” (S21) |
|
More VOPs and less WebEx for lectures |
“I think VOP is a much safer option and a less tiring one” (S23) “Revert from live WebEx sessions to VOP” (S3) |
|
|
More interaction and immediate feedback |
“Open forums for discussion” (S3) “Adding analytical questions in PowerPoints” (S9) “See exams and mistakes” (S15) “If the professors want to use WebEx … then they should allow questions at all times and not only at the end of the session” (S11) “Include small assessment questions (clicker like questions) at the end of each major concept so that the students can assess their understanding” (S19) “Recording voice over PowerPoint for lectures, with every group of lectures followed by a WebEx session where the professor answers questions” (S24) “Review/Q&A session once a week” (S25) |
Table 1. Themes Generated from the Three Survey Questions with Selected Representative Quotes
VOP: Voice Over PowerPoint
|
Medicine class of |
2022 |
2023 |
P-value |
|
Academic Year 1 |
2018-2019 |
2019-2020 |
|
|
Number of students |
115 |
118 |
|
|
|
Baseline performance |
||
|
MCAT scores |
509±6 |
510±6 |
0.119 |
|
Class average on the final exam of the CMM course |
82.6±6.1 |
84.3±7.4 |
0.011 |
|
Passing grade for the final exam of the CMM course |
64.1 |
64.7 |
|
|
Adjusted grade for the final exam of the CMM coursea |
83.2±6.1 |
84.3±7.4 |
0.065 |
|
|
Performance in The Blood course |
||
|
Course delivery |
Face to Face |
Online |
|
|
Number of questions on the final exam |
50 |
77 |
|
|
Class average on the final exam |
83±9 |
81±9 |
0.043 |
|
Passing grade for the final exam |
65 |
61 |
|
|
Adjusted grade for the final exama |
83±9 |
85±9 |
0.091 |
|
|
Student Evaluation of The Blood Course |
||
|
Rating of teaching methods |
4.0±0.8 |
4.0±1.0 |
0.920 |
|
Overall course rating |
4.0±0.7 |
4.1±0.8 |
0.754 |
Table 2. Comparison of Performance of Year 1 Students in Various Courses and Examinations and Their Evaluation of the Blood Course
Data are presented as Mean ± Standard Deviation
P-values were generated by Student’s unpaired t-test
MCAT: Medical College Admissions Test; CMM: Cellular and Molecular Basis of Medicine
aadjusted after equalizing the passing grades on the examinations in the 2 different years
|
Medicine class of |
2021 |
2022 |
P-value |
|
Academic Year 2 |
2018-2019 |
2019-2020 |
|
|
Number of students |
114 |
115 |
|
|
|
Baseline performance |
||
|
MCAT scores |
509±5 |
509±6 |
0.842 |
|
Class average on the final exam of the CMM course |
83.8±6.4 |
82.6±6.1 |
0.156 |
|
Passing grade for the final exam of the CMM course |
65.3 |
64.1 |
|
|
Adjusted grade for the final exam of the CMM coursea |
82.6±6.4 |
82.6±6.1 |
0.455 |
|
Performance on the final exam of The Kidney course |
78.1±7.9 |
78.7±7.2 |
0.558 |
|
Passing grade for the final exam of The Kidney course |
62.2 |
62.3 |
|
|
|
Performance in the Human Development and Psychopathology course |
||
|
Course delivery |
Face to Face |
Online |
|
|
Number of questions on the final exam |
45 |
75 |
|
|
Class average on the final exam |
83.7±7.4 |
83.5±6.8 |
0.892 |
|
Passing grade for the final exam |
68.0 |
64.8 |
|
|
Adjusted grade for the final exama |
83.7±7.4 |
86.7±6.8 |
0.002 |
|
|
Student evaluation of the Human Development and Psychopathology course |
||
|
Rating of teaching methods |
4.2±0.9 |
4.1±0.9 |
0.426 |
|
Overall course rating |
4.3±0.7 |
4.1±0.8 |
0.251 |
Table 3. Comparison of Performance of Year 2 Students in Various Courses and Examinations and Their Evaluation of the Human Development and Psychopathology Course
Data are presented as Mean ± Standard Deviation
P-values were generated by Student’s unpaired t-test
MCAT: Medical College Admissions Test; CMM: Cellular and Molecular Basis of Medicine
aadjusted after equalizing the passing grades on the examinations in the 2 different years
B. Performance of Students in the Courses and Examinations
As shown in Tables 2 and 3, there were no statistically significant differences in the MCAT scores between any two classes that were compared. The performance of the Year 1 students on the CMM course during the current academic year (online) was higher than that of students during the previous year (face-to-face); however, the passing grade for the two courses was slightly different. When the passing grades were equalised, there was no longer a difference between the two classes. Similarly, there was no difference in the performance of the Year 2 students on either the CMM course they took in Year 1, or on The Kidney and Urinary System course between the current class and the previous year’s class (all face-to-face).
With regard to The Blood course, the grade on the final examination was significantly lower for current students (online) relative to their predecessors (face-to-face); however, the passing grades on these examinations were different, with the current year’s examination having a lower passing grade than last year’s. When the passing grades were equalised, there was no longer a difference in the performance on the final examination.
The performance of the students in the Human Development and Psychopathology course’s final examination was almost identical in the online group compared with their predecessors (all face-to-face). Interestingly, the passing grade on this year’s examination was lower than that on last year’s examination, such that when the passing scores were equalized, the current class had better performance on the final examination than last year’s class.
IV. DISCUSSION
Medical education scholars have been increasingly disseminating opinions about sudden transitioning to online education to COVID-19 and the adaptations that are being implemented. Few studies have documented the actual institutional experiences, the perspectives of students, and the lessons learned in different medical courses or curricula such as TBL (Gaber et al., 2020), anatomy (Srinivasan, 2020) and continuing medical education in obstetrics and gynaecology (Kanneganti et al., 2020). Only one report from Wuhan, China, evaluated nursing interns’ outcomes on emergency medicine theoretical and practical examination scores (Zhou et al., 2020). The current paper is the first to examine the impact of this abrupt transition to online learning, which occurred in numerous countries worldwide, on the performance of our medical students in knowledge-based examinations. It reveals that the sudden shift to full online learning that our medical school had to adopt did not have a negative influence on the students’ knowledge acquisition as judged by their performance on final examinations. It also did not affect their overall reception and evaluation of the courses. These results are particularly interesting and important considering the many disadvantages that the students cited in relation to the online delivery of the courses.
Many of the limitations and disadvantages of online education cited by students had to do with technical and infrastructural matters and with faculty know-how and IT support. These are problems that can, theoretically, be easily remedied. The more challenging, however, limitations had to do with the process of learning, what facilitates or hampers it, the students’ ability to self-regulate and to motivate themselves, the negative impact of isolation, loss of socialisation and interaction with peers and faculty, and the almost total lack of hands-on experiences.
These limitations did not affect the students’ ability to achieve learning, at least in the domain of knowledge acquisition and application. It is clear that students in the three classes that were examined had, at baseline, a similar level of achievement meaning that any differences in student performance in the courses that were given online this year cannot be ascribed to differences in the academic performance or ability of the students. Therefore, the lack of difference in performance between classes taking the course online versus those taking it face-to-face suggests a consistency in performance that was not affected adversely by the sudden transition to online learning.
One reason for this lack of difference in performance between online and face-to-face delivery of the courses may be that the outcomes that were being sought and assessed were essentially knowledge acquisition and knowledge application. This agrees with the overall results of multiple studies that compared online vs offline learning in medical school, and which, in fact, tended to favour online learning (Pei & Wu, 2019). Indeed, even before our sudden shift to total online education, many of our students had adopted their own approaches to achieve the knowledge learning outcomes. Even though lectures were not available online, attendance at face-to-face lectures (which was not mandatory) was never complete, and for the majority of students, the rate of attendance ranged between 25% and 75% (unpublished data). In fact, the students indicated that they depended instead on notes and voice recordings made during the lecture that were shared by their classmates or predecessors, and that they used several Web-based resources. In contrast, attendance at TBL exercises and other interactive and small group sessions is mandatory at our school, and students uniformly participated in them, as they did in the online Zoom-based sessions. Thus, our students were probably well prepared for this sudden shift. In line with this view, Ferrel and Ryan (2020), in a recent editorial on the impact of COVID-19 on medical education, predicted that many medical students in their didactic years may perceive little change in their study schedule, since many of them already use outside resources and watch school lectures after they have been presented.
The lack of significant differences in scores and attitudes may also attest to our – and indeed all – medical students’ resilience and adaptability to difficult situations, for they are high-achieving and resourceful students who have been selected from among an exceedingly competitive group of applicants, and likely have the cognitive powers and non-cognitive qualities to meet such challenges. Ferrel and Ryan (2020) also emphasised the need for medical students to adapt and be innovative during the pandemic, and to devise ways by which they can exhibit their skills, work ethics and teamwork. In fact, one of the advantages of the online shift that our students cited was the flexibility this approach afforded them in managing their time, setting their schedules, controlling their pace of learning and achieving better self-care. Nevertheless, some of them found it challenging to do so, and to regulate their environment and motivate themselves; rather, they seemed to require external cues or assistance to get into a learning mode, and found difficulty in establishing boundaries between work and home, as suggested recently by Rose (2020). In this context, it is noteworthy that our students preferred asynchronous to synchronous learning, and this is consistent with Daniel’s recommendation to use this approach because it gives teachers “flexibility in preparing learning materials and enables students to juggle the demands of home and study” (Daniel, 2020).
Our findings also raise questions about certain assumptions regarding student learning and the optimal teaching approaches for knowledge-based objectives, such as the value and benefits of face-to-face interactions among students and with faculty in a didactic context. Our results suggest that students can achieve these knowledge objectives without the personal interaction and contact with faculty. This, of course, does not address the non-cognitive learning outcomes that might be negatively affected by pure online learning. As summarised by Fawn et al. (2020), while content may be covered well in such abrupt transitions to online learning, we cannot be sure that the valuable non-cognitive learning that happens as a result of the “social activity, the relationship-building, the problem-solving, the dialogue and generation of ideas and the students’ own discovery of other content that has not been pre-defined by the teacher” has been achieved.
We cannot make definite, long-term conclusions from this single account that is restricted to 2 courses in the preclinical years, a brief period of time, and one institution, and a low response rate for the survey questions, but the results are encouraging, and may have implications for educational practice. The lack of decline in cognitive performance may suggest that the sudden shift to online education might not be a totally negative development. If our findings are reproduced or generalised, one can use them to validate what progressive medical educators have been advocating for years, that: online educational technology must change the way we educate our students; didactic lecturing should give way to flipped classrooms; and valuable teacher time must be expended to help students apply knowledge rather than to simply transfer information in scheduled lectures. Quoting Ezekiel Emanuel (2020), who in a recent article stated that the reconfiguration of medical education, fuelled by online educational technology, seemed inevitable, Wolanskyj-Spinner (2020) suggested that the coronavirus epidemic appears to be an inflection point that is forcing a disruption in how we teach medicine. At AUBFM, we have long pressed the faculty who teach medical students to record their lectures and use the scheduled class time thus saved to implement flipped classrooms, employing small-group-based, problem-solving and interactive sessions. While many responded, many also hesitated, objected, and even resisted. The following two additional comments provided by two students illustrate their frustration with the resistance of faculty and their hopes to move in that direction:
“I really hope we can make online learning standard coming out of this phase … There was an attempt a few years ago but many instructors refused to be recorded or to fiddle with computers; we must seize the opportunity now.”
“Please never stop recording lectures, regardless of the status of live classes!”
Ahmed et al. (2020) recently reported that during the 2003 SARS epidemic in China, novel online problem-based learning techniques had to be implemented in one medical school that proved to be so popular that they were applied as part of the regular curriculum in later years. We believe that medical educators can harness the current disruption in how we teach medical students, and make use of to implement novel and sound educational practices and adopt a wide variety of valid approaches and tools that, otherwise, might have been resisted by unwilling individuals with entrenched ideas.
V. CONCLUSION
In conclusion, rapid transition to online learning did not affect student knowledge acquisition negatively. As such, the sudden shift to online education might not be a totally negative development and can be harnessed to drive a more progressive medical education agenda. These results are particularly important considering the several disadvantages that the students cited in relation to the online delivery of the courses.
Notes on Contributors
Nathalie Zgheib developed the concept, collected and analysed data, and wrote the first draft of the manuscript. Ahmed Ali also developed the concept, performed the literature review, and revised the manuscript write-up. Ramzi Sabra also developed the concept, collected and analysed data, and revised the manuscript write-up. The three authors read and approved the final version of the manuscript.
Data Availability
The data that support the findings of this manuscript are available from the corresponding author upon reasonable request.
Ethical Approval
This is a report of experience with educational practices. It was confirmed by our Institutional Review Board (IRB) that the activities described in this article do not constitute human subject research.
Acknowledgments
The authors wish to thank AUBFM faculty and medical students for their support, diligence and flexibility during the COVID-19 pandemic.
Funding
This study did not receive any funding.
Declaration of interest
The authors do not have any conflict of interest to declare.
References
Ahmed, H., Allaf, M., & Elghazaly, H. (2020). COVID-19 and medical education. The Lancet Infectious Diseases, 20(7), 777-778. https://doi.org/10.1016/S1473-3099(20)30226-7
Ashcroft, J., Byrne, M. H. V., Brennan, P. A., & Davies, R. J. (2020). Preparing medical students for a pandemic: A systematic review of student disaster training programmes. Postgraduate Medical Journal, Advance online publication. https://doi.org/10.1136/postgradmedj-2020-137906
Daniel, S. J. (2020). Education and the COVID-19 pandemic. Prospects, 49, 91-96. https://doi.org/10.1007/s11125-020-09464-3
Emanuel, E. J. (2020). The inevitable reimagining of medical education. Journal of the American Medical Association, 323(12), 1127-1128. https://doi.org/10.1001/jama.2020.1227
Fawn, T., Jones, D., & Aitken, G. (2020). Challenging assumptions about “moving online” in response to COVID-19, and some practical advice. MedEdPublish, 9(1), 83. https://doi.org/10.15694/mep.2020.000083.1
Ferrel, M. N., & Ryan, J. J. (2020). The impact of COVID-19 on medical education. Cureus, 12(3), e7492. https://doi.org/10.7759/cureus.7492
Frehywot, S., Vovides, Y., Talib, Z., Mikhail, N., Ross, H., Wohltjen, H., Koumare, A. K., & Scott, J. (2013). E-learning in medical education in resource constrained low- and middle-income countries. Human Resources for Health, 4(11), 4. https://doi.org/10.1186/1478-4491-11-4
Gaber, D. A., Shehata, M. H., & Amin, H. A. A. (2020). Online team-based learning sessions as interactive methodologies during the pandemic. Medical Education, 54(7), 666-667. https://doi.org/10.1111/medu.14198
Kanneganti, A., Lim, K. M. X., Chan, G. M. F., Choo, S. N., Choolani, M., Ismail-Pratt, I., & Logan, S. J. S. (2020). Pedagogy in a pandemic – COVID-19 and virtual continuing medical education (vCME) in obstetrics and gynecology. Acta Obstetetricia et Gynecologica Scandinavica, 99(6), 692-695. https://doi.org/10.1111/aogs.13885
Liang, Z. C., Ooi, S. B. S., & Wang, W. (2020). Pandemics and their impact on medical training: Lessons from Singapore. Academic Medicine, 95(9), 1359-1361. https://doi.org/10.1097/ACM.0000000000003441
Lim, E. C., Oh, V. M., Koh, D. R., & Seet, R. C. (2009). The challenges of “continuing medical education” in a pandemic era. Annals of Academic Medicine Singapore, 38(8), 724-726.
McKimm, J., Mclean, M., Gibbs, T., & Pawlowicz, E. (2019). Sharing stories about medical education in difficult circumstances: Conceptualizing issues, strategies, and solutions. Medical Teacher, 41(1), 83-90. https://doi.org/10.1080/0142159X.2018.1442566
Patil, N. G., Chan, Y., & Yan, H. (2003). SARS and its effect on medical education in Hong Kong. Medical Education, 37(12), 1127-1128. https://doi.org/10.1046/j.1365-2923.2003.01723.x
Pei, L., & Wu, H. (2019). Does online learning work better than offline learning in undergraduate medical education? A systematic review and meta-analysis. Medical Education Online, 24(1), 1666538. https://doi.org/10.1080/10872981.2019.1666538
Rose, S. (2020). Medical student education in the time of COVID-19. Journal of the American Medical Association, 323(21), 2131-2132. https://doi.org/10.1001/jama.2020.5227
Ross, D. (2020). Creating a “quarantine curriculum” to enhance teaching and learning during the COVID-19 pandemic. Academic Medicine, 95(8), 1125-1126.
Sandars, J., Correia, R., Dankbaar, M., de Jong, P., Sun Goh, P., Hege, I., Oh, S., Patel, R., Premkumar, K., Webb, A., & Pusic, M. (2020). Twelve tips for rapidly migrating to online learning during the COVID-19 pandemic. MedEdPublish, 9(1), 82. https://doi.org/10.15694/mep.2020.000082.1
Srinivasan, D. K. (2020). Medical students’ perceptions and an Anatomy teacher’s personal experience using an e-learning platform for tutorials during the Covid-19 crisis. Anatomical Sciences Education, 13(3), 318-319. https://doi.org/10.1002/ase.1970
Wolanskyj-Spinner, A. (2020). COVID-19: The global disrupter of medical education. ASH Clinical News, https://www.ashclinicalnews.org/viewpoints/editors-corner/covid-19-global-disrupter-medical-education/
Woodward, A., & McLernon-Billows, D. (2018). Undergraduate medical education in Sierra Leone: A qualitative study of the student experience. BMC Medical Education, 18(1), 298. https://doi.org/10.1186/s12909-018-1397-6
Zhou, T., Huang, S., Cheng, J., & Xiao, Y. (2020). The distance teaching practice of combined mode of massive open online course micro-video for interns in emergency department during the COVID-19 epidemic period. Telemedicine Journal and E-Health, 26(5), 584-588. https://doi.org/10.1089/tmj.2020.0079
*Ramzi Sabra
Department of Pharmacology and Toxicology,
Faculty of Medicine,
American University of Beirut,
PO. Box 11-0236, Riad El Solh,
Beirut, Lebanon
Tel: +961-1-350000 Ext: 4848
Email: rsabra@aub.edu.lb
Submitted: 20 July 2020
Accepted: 30 September 2020
Published online: 13 July, TAPS 2021, 6(3), 108-110
https://doi.org/10.29060/TAPS.2021-6-3/PV2369
Kimberly Hires1 & Colleen Davis2
1Lewis College of Nursing and Health Professions, Georgia State University, United States of America; 2Leadership Development, Vuselela Davis, South Africa
I. INTRODUCTION
Historically, health professional education has focused on the development of clinical expertise over leadership skills that enable practitioners to lead dynamic teams who can adapt and pivot rapidly in a crisis. Clinical acumen and the ability to lead effectively are not mutually exclusive within healthcare systems. Leadership development is vital for health professionals as it allows them to lead patients and health systems, adapt to rapidly changing healthcare environments, and elicit optimal performance from their teams—all of which lead to improved health outcomes. The COVID-19 crisis highlights an opportunity to innovate health professional education to create practitioners who can treat and lead with excellence.
In December 2019, the Wuhan Municipal Health Commission reported four cases of pneumonia of an unknown origin. The cluster of cases were the first sign of COVID-19. COVID-19 is caused by a novel coronavirus that can spread from person to person. Within six months, the virus spread to 231 countries and infected over 13 million people worldwide. In attempts to slow the spread of the virus, countries issued emergency shutdowns, schools were closed, global travel was prohibited, and every industry was affected. One industry most affected by COVID-19 is the healthcare industry. Healthcare infrastructures are facing unprecedented challenges to meet the demands for care related to COVID-19. Providers are battling burnout, insufficient supply of personal protective equipment, depression, anxiety, job dissatisfaction and in some cases increased rates of suicide (Greenberg et al., 2020). To identify the contributing factors to challenges faced by health professionals during COVID-19, leaders must go to the root: health professional education.
Current health professional education competencies prioritize the development of hard skills that focus on clinical performance or evidence-based practice over the development of soft skills that facilitate building healthy interpersonal relationships, self-awareness, communication, leadership skills and effective coping (Albarqouni et al., 2018). Health professions encompass art and science. Current health professional education rewards the science of healthcare but starves the art of leadership. The COVID-19 pandemic, has created a collective trauma within the global community for which current leaders are not equipped to respond (Greenberg et al., 2020). The evidence for COVID-19 is constantly changing and leaders do not have the confidence and care algorithms to which they have grown accustomed. Due to COVID-19, health care workers worldwide have experienced an increase in depression, anxiety, and other forms of psychological distress. Health professionals already experience higher levels of burnout and job dissatisfaction than other professions; COVID-19 has amplified existing challenges for healthcare leaders who were struggling with employee recruitment and retention prior to the global pandemic.
As COVID-19 becomes a critical component of the world’s new normal, this is the optimal time for health professional education to innovate and prepare graduates who can lead in the midst of the new normal. This paper draws on experience of the two authors and their work with students enrolled in health professional programmes at the initial level and the specialist level, as well as the post-academic level in the United States and South Africa. This paper aims to introduce a new model of leadership development informed by over three decades of observations from combined experiences in health professional education, hospital learning and development, and leadership coaching.
II. DISCUSSION
Top down, traditional styles of leadership with an emphasis on self-sacrifice do not have a future in 21st century healthcare leadership. Leaders who are highly aware, connected, and genuinely compassionate experience success in productivity, high performing teams, cost effectiveness, strategy, innovation and employee retention. Just as health professional education relies on evidence-based practice, the Human-based leader (HBL) Model was developed to explain how effective leadership skills are developed. The HBL model utilizes an ecological framework. Ecological systems theory was developed by Urie Bronfenbrenner and posits that development is guided by interactions between an individual and the surrounding environment; this interaction populates a system (Bronfenbrenner, 1979). Bronfenbrenner’s original system is comprised of four systems represented as four concentric circles: the individual/microsystem (the core), mesosystem (second sphere), exosystem (third sphere), and macrosystem (fourth sphere) (Bronfenbrenner, 1995).
The HBL is comprised of three concentric circles. At the core is phase I. The goal of phase I is the development of self-awareness. The microsystem (the individual/leader) is housed within this sphere. The next sphere is phase II which houses the mesosystem (relationships with others such as family, friends, team members, peers) and the exosphere (additional factors related to the organization including patients and the community). In phase II leaders develop an awareness of others. The third sphere, phase III, houses the macrosystem (factors related to the profession, population, values, and cultural customs). Development of this phase allows the health professional leader to contribute to the building of a global community. The HBL makes the following assumptions: (1) Leadership development is a dynamic process that is influenced by exchanges between the individual (the leader) and the environment. (2) Leadership development is a continuous process. (3) Leadership success is not limited to job related competencies. Success includes healthy organizational culture, employee job satisfaction, recruitment, retention, customer/client satisfaction, and work-life balance as well as profit and loss.
Historically, health professional education focuses on team development and neglects teaching students how to understand their own experiences and worldview. Engaging in reflective practices are vital for professional identity development, however, current practices limit the reflection to clinical experiences (Wald, 2015). This approach ignores the very rich and varying life experiences students bring with them into a health professional programme. These life experiences follow students well into practice. Healthcare leaders with decades of experience are often surprised to find how influential their worldview is on patient care and working within teams. In this phase, it is vital for the individual to be able to answer, “Who am I?” beyond the professional identity. As individuals reflect on who they are, they can identify triggers, motivators and fears. Seeing the Self and helping a leader understand the Why behind behaviour is fundamental to healing and growth for the leader and the organization. Leaders who are self-aware in a crisis, such as a pandemic, can move dynamically as the environmental norms shift.
Current practices in health professional education emphasizes teamwork, however, by ignoring phase I, health professional educators make a fallible assumption that self-awareness is not vital to working effectively in teams. If individuals are unable to see the humanness in themselves (self-awareness) to value their own stories, challenges, and uniqueness, then they will fail to see it in others (peers, staff). In this phase, leaders gain a clear understanding of how to connect with and motivate each member of the team for optimal performance and retention. Failure to successfully achieve this phase results in poor performance, increased risk for medical errors, and high turnover.
Once leaders have an awareness of self and an appreciation for others, then they can graduate to the macrosystem or global sphere. The COVID-19 pandemic has illustrated the power of globalization. Within six months, healthcare systems experienced a global rate of infection that needed a swift, fluid, innovative and agile response. It is imperative that health professional education helps students and future leaders develop a global paradigm that sees beyond local hospitals and communities. A healthy worldview facilitates an easier transition into a global macrosystem.
The HBL can be adapted and implemented at various levels of health professional education and practice. It can be incorporated as learning modules in existing courses at the initial level and as a formal coaching programme at the specialist and post-academic levels. At the initial level of health professional education, the HBL was implemented with students in their final semester of a health professional (baccalaureate) programme at a research institution in the United States. The model was integrated into a leadership and management course as learning modules, case-studies, and self-development activities to equip students with skills needed to successfully progress through phases I, II, and III. At the specialist level, health professional students in the United States benefited from a formal coaching programme comprised of individual and group coaching sessions delivered over 12 weeks. At the post-academic level, the HBL model was implemented with practitioners in the United States and South Africa. At the post-academic level, practitioners benefit from a formal, customised coaching programme comprised of individual coaching sessions or a combination of individual and group coaching sessions delivered over 12 to 16 weeks. The greatest challenge with implementing the HBL at the specialist and post-academic levels is facilitating the unlearning of maladaptive leadership behaviours that lead to unhealthy organizational culture.
III. CONCLUSION
As demands for quality health care increase, health professional education is charged with meeting the supply. COVID-19 has provided a unique disruption for global health professional education to pivot from a rigid, process-driven and task-oriented model towards a model of a self-aware, empathetic leader. The Asia Pacific health care market was significantly impacted by COVID-19. Building this model into health professional education curriculums now will result in increased resilience and retention among providers. The HBL model can be adapted to regional needs to provide guidance for health professional educators to help students embrace their unique worldview and experience, teach lifelong reflective processes, be effective members of teams, and significantly contribute to improving population health.
Notes on Contributors
Assistant Professor Kimberly Hires reviewed the literature, designed the manuscript, developed the conceptual framework, and wrote the manuscript. Colleen Davis developed the conceptual framework, developed the manuscript, gave critical feedback to the writing of the manuscript. All the authors have read and approved the final manuscript.
Acknowledgements
The authors thank all students, faculty, colleagues, and clients who have informed our model.
Funding
No funding was used for the development of this personal view.
Declaration of Interest
The authors declare no conflict of interest concerning any aspect of this research.
References
Albarqouni, L., Hoffmann, T., Straus, S., Olsen, N. R., Young, T., Dragan, I., Shaneyfelt, T., Haynes, R., Guyatt, G., & Glasziou, P. (2018). Core competencies in evidence-based practice for health professionals: Consensus statement based on a systematic review and Delphi Survey. Journal of the American Medical Association Network Open, 1(2), e180281. https://doi.org/10.1001/jamanetworkopen.2018.0281
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Harvard university press.
Bronfenbrenner, U. (1995). Developmental ecology through space and time: A future perspective. In P. Moen, G. H. Elder, Jr., & K. Lüscher (Eds.), Examining lives in context: Perspectives on the ecology of human development. (pp. 619–647). American Psychological Association. https://doi.org/10.1037/10176-018
Greenberg, N., Docherty, M., Gnanapragasam, S., & Wesseley, S. (2020). Managing mental health challenges faced by healthcare workers during COVID-19 pandemic. British Medical Journal, 368, m1211. https://doi.org/10.1136/bmj.m1211
Wald, H. S. (2015). Professional identity (trans)formation in medical education: Reflection, relationship, resilience. Academic Medicine, 90(6), 701-706. https://doi.org/10.1097/ACM.0000000000000731
*Kimberly A. Hires
Georgia State University
Atlanta, GA 30302,
United States
Email: khires@gsu.edu
Submitted: 28 August 2020
Accepted: 3 March 2021
Published online: 13 July, TAPS 2021, 6(3), 32-44
https://doi.org/10.29060/TAPS.2021-6-3/OA2385
Judy McKimm1, Subha Ramani2 & Vishna Devi Nadarajah3
1Swansea University Medical School, United Kingdom; 2Harvard Medical School, United States of America; 3International Medical University, Malaysia
Abstract
Introduction: The COVID-19 pandemic has caused huge change and uncertainty for universities, faculty, and students around the world. For many health professions’ education (HPE) leaders, the pandemic has caused unforeseen crises, such as closure of campuses, uncertainty over student numbers and finances and an almost overnight shift to online learning and assessment.
Methods: In this article, we explore a range of leadership approaches, some of which are more applicable to times of crisis, and others which will be required to take forward a vision for an uncertain future. We focus on leadership and change, crisis and uncertainty, conceptualising ‘leadership’ as comprising the three interrelated elements of leadership, management and followership. These elements operate at various levels – intrapersonal, interpersonal, organisational and global systems levels.
Results: Effective leaders are often seen as being able to thrive in times of crisis – the traditional ‘hero leader’ – however, leadership in rapidly changing, complex and uncertain situations needs to be much more nuanced, adaptive and flexible.
Conclusion: From the many leadership theories and approaches available, we suggest some specific approaches that leaders might choose in order to work with their teams and organisations through these rapidly changing and challenging times.
Keywords: Leadership, Followership, Management, Health Professions Education, Change, Crisis, Uncertainty, Emotional Intelligence, COVID-19 Pandemic, Universities
Practice Highlights
- In rapid change and uncertainty, different leadership approaches are needed.
- Primal leadership and emotional intelligence are essential.
- Followers need to feel safe, physically and psychologically.
- Authentic and inclusive leadership draws from diverse views.
- Adaptive and regenerative leadership acknowledges interrelated systems.
I. INTRODUCTION
The COVID-19 pandemic has caused huge change and uncertainty for universities and their stakeholders around the world. For many health professions education (HPE) leaders, the pandemic has caused an unforeseen crisis, the ripples from which will probably be felt for years to come. Effective leaders are often seen as being able to thrive in times of crisis – the traditional ‘hero leader’ – however, leadership in rapidly changing, complex and uncertain situations need to be much more nuanced and flexible. In this article we explore leadership approaches, some of which are more applicable to times of crisis, and others which will be required to take forward a vision for the ‘new normal’ to ensure that we learn from our experiences during the pandemic.
In this article we focus on leadership and change. We start with an overview of the leadership triad, a discussion of the educational challenges imposed by the COVID-19 pandemic, followed by detailed discussion of effective leadership styles and competencies during challenging situations, approaching these through three lenses: Intrapersonal, referring to characteristics that successful leaders possess; interpersonal, referring to leadership styles and approaches leaders can adopt when they interact with others; and system level, which refers to leadership attributes to effectively lead organisations during a crisis. We conceptualise ‘leadership’ as comprising three interrelated elements: leadership, management, and followership (see Figure 1), which we call the ‘leadership triad’ (McKimm & O’Sullivan, 2016).

Figure 1: The Leadership Triad
Note: From “When I say … leadership,” by J. McKimm, and H. O’Sullivan, 2016, Medical Education, 50(9), 896–897. https://doi.org/10.1111/medu.13119
Leadership is about change and movement, putting the power and energy into a system or initiative, whereas management provides the means of enacting the leadership vision and making change happen. Leadership is always about ‘people’ (motivating them towards goals or activities) whereas management is about systems, processes and policies and we structure the article around this approach (Scouller, 2011). Followership provides the leadership with the ‘people power’ to enact the change; without followers, leadership cannot happen as leaders cannot do everything themselves. Even the most senior leaders do not ‘lead’ all the time, in ‘real life’ we move around these three elements as we lead, manage, and follow in various situations.
As leaders in HPE ourselves (Refer to Appendix A), we reflect and ask, what can a leader do during this period to ensure the best interest of all stakeholders? What lessons can we offer from our own experiences and the experiences of other leaders to those who need guidance to weather and even thrive after the crisis? The approach we have taken is to first examine the major challenges facing health professions’ leaders during this crisis, we then offer specific leadership approaches that can effectively address these challenges, concluding with change management approaches required to prepare and sustain the new normal.
II. CRISIS AND CHALLENGES FOR HEALTH PROFESSIONS EDUCATION
2020 has been a hugely challenging year for all higher education leaders across the world. From managing the rapid switch to online learning, answering student calls for some form of refund or reduction in fees, to expanded support for students and staff including emotional support, the COVID-19 pandemic has forced educational leaders to manage a different type of crisis altogether.
HPE leadership has been hugely tested during the pandemic ‘crisis’ which is very different from leading in ‘normal’ times. How do we define a crisis? A crisis is any event that could lead to an unstable, difficult and/or dangerous situation affecting an individual, group, community, or whole society. It means that difficult or important decisions must be made amidst great uncertainty and lack of information about what the future might hold. In the middle of a crisis everything can feel like it is failing or impossible. The pandemic accelerated and exacerbated many of the challenges already being experienced in HPE, including the rising costs of operating universities, increase in tuition fees and accessibility to higher education, and competition from commercial and online learning providers. Leaders in HPE face additional and different sets of challenges, as they service and are dependent on both the education and health care sectors for student education and postgraduate training. The crisis is not only experienced at organisational or team level, but the pandemic has also impacted individuals (students, academic faculty, clinical teachers, and healthcare staff) whose normal coping mechanisms may be insufficient.
However, this is not all negative and leaders need to tap into a growth mind-set, which has been defined as one that views failure and challenges as learning opportunities (Dweck, 2016). For example, Kanter (2020) suggests that it is possible to come out of a crisis stronger than before if leaders operate with a ‘people first culture’ and pay ‘attention to three things: establish clear accountability in the leadership ranks; develop a nuts-and-bolts, collaborative plan for getting through the crisis; and appoint a separate group in charge of defining the “new normal,” when the worst is over’.
It is also important to recognise that the pandemic (set alongside climate change and causes related to systemic social injustices) has foregrounded and increased awareness on inequalities across the globe in many areas, including HPE. Leadership in these times needs to pay close attention to this and seize the moment to facilitate and mobilise real change within their institutions or communities. Perhaps more so when such institutions train future health professionals and develop future leaders, who need to believe that a positive change is possible and that their own cultural context can be celebrated.
III. WHAT SORT OF LEADERSHIP IS NEEDED TO ADDRESS THESE CHALLENGES?
Inevitably changes are to be expected as the impact of the pandemic is unprecedented and is a matter of national security and public health. In most countries, governance and decision making during this crisis will be by National security councils with advisories or guidelines offered by ministries of health higher education, home affairs, or other relevant bodies. This means that universities and educational leaders who usually have autonomy in decision making are subject to stricter controls and frequent changes from authorities who are understandably making decisions at national and international levels. For people in leadership positions, this is unchartered territory and given the ‘traditional’ power and authority hierarchies and processes in higher education and health professions education, it is unsurprising that leaders may feel helpless during a crisis such as this. In Figure 2, we list four levels along which leadership needs to be enacted, and some suggested approaches to help leaders move out of this feeling of helplessness so that they can lead the people for whom they are responsible.
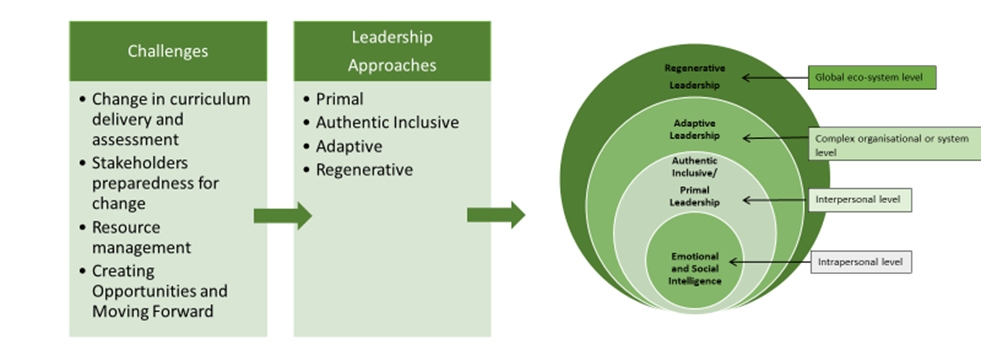
Figure 2: Four levels of leadership for addressing challenges during a crisis
Note: Drawing from “ABC of clinical leadership,” by T. Swanwick and J. McKimm, 2017, John Wiley & Sons.
A. The Intrapersonal Level: Working with Emotional and Social Intelligence
Challenging circumstances which force change, such as the COVID-19 pandemic, result in a range of emotional responses among leaders and all those for whom they are responsible.
In 1998, Daniel Goleman proposed that leadership skills such as toughness, vision, determination, and intelligence alone are insufficient. He stated that the most successful leaders also possess a high degree of emotional intelligence (EI) which includes the traits of self-awareness, self-regulation, motivation, empathy, and social skills (Goleman, 1998). Boyatzis and Goleman went to analyse the core attributes that were present in those identified by a variety of companies as their most successful leaders. As a result, twelve competencies of emotional and social intelligence were described under four domains and depicted in Figure 3. The four domains include: Self-awareness, self-management, social awareness, and relationship management; these are critical attributes for leaders to operate effectively through own and others’ emotions during challenging circumstances such as the COVID-19 pandemic. These competencies and behaviours help to simplify a complex construct such as EI and can facilitate leadership development in this area.
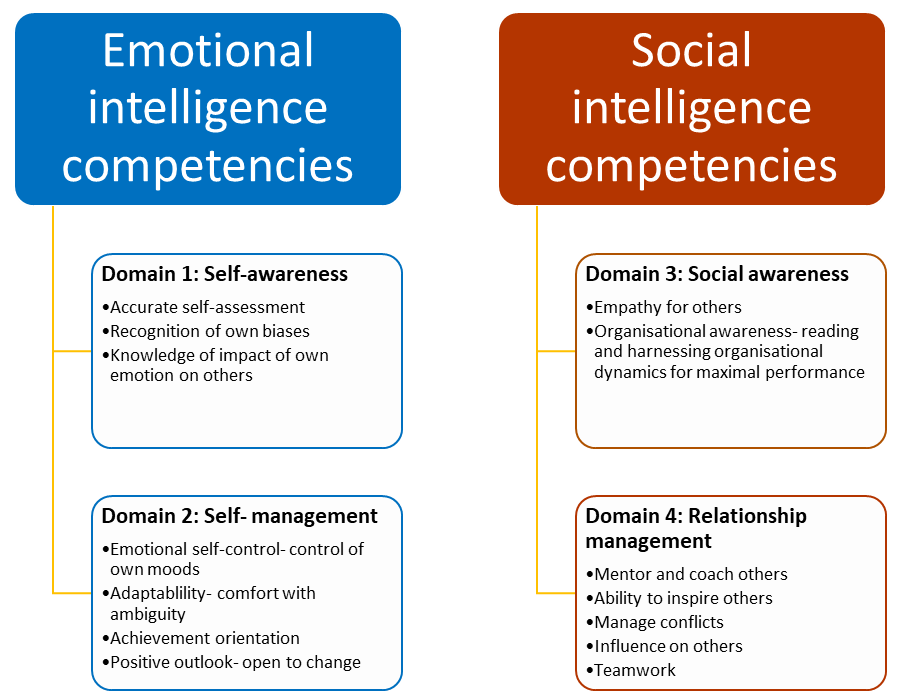
Figure 3: Intrapersonal leadership attributes: Emotional and social intelligence competencies essential to lead and manage change during challenging circumstances.
Note: Adapted from “Competencies as a behavioral approach to emotional intelligence,” by R. E. Boyatzis, 2009, Journal of Management Development, 28(9), 749–770. https://doi.org/10.1108/02621710910987647
While the construct of EI and competencies can serve as a useful guide to leaders in leading and managing change, the actual behaviours that are most effective depend on the organisational culture and the societal culture within which an organisation is situated. Moreover, at institutions which feature diversity in the composition of its leaders, staff and learners, leaders should recognise that individuals on a team might have different emotional reactions even when working towards a common goal. All four domains of EI competencies are essential for leaders to manage the groups of people they lead (See Table 1).
|
1. Self-awareness allows leaders to recognise their assumptions and biases, and how they affect their worldview. 2. Self-management promotes thought before action and ability to manage own emotions and reactions, important in reigning in negative emotion. 3. Social awareness allows leaders to understand the individuals who make up their team and recognise differences in viewpoints and personalities. 4. Relationship management is essential to welcome a variety of perspectives, nurture talent, and maximise the potential and productivity of individuals, teams, and the organisation. Mentoring and coaching skills fall under this domain.
|
Table 1: The impact of the four EI domains
A. The Interpersonal Level: Influencing Others and Drawing on Their Individual and Collective Strengths
In rapid change and uncertainty, what people want from their leaders is an authentic voice and to feel that leaders are listening, taking their concerns seriously and that they have the expertise and authority to lead and manage change. Leaders are created and maintained by how their followers see, relate to, and trust them (Uhl-Bien & Carsten, 2018). Simon Sinek talks about how followers will follow their leaders into highly unsafe situations (such as war) if they feel their leaders can keep them safe and that they are ‘in it’ together (Sinek, 2014). Whilst internally, leaders may feel as lost and at sea as those for whom they are responsible, they must draw on their own resilience and ‘grit’ (Duckworth & Duckworth, 2016) to step up and provide effective leadership. This involves displaying courage, putting personal interests aside to achieve what needs to be done and acting on convictions and principles even when it requires personal risk-taking. In crisis or uncertainty, followers need leaders who can communicate clearly, transparently, and regularly, who can make decisions (even if these are unpopular or later change) and who look out for and care for them (Paixão et al., 2020).
Primal leadership, described by EI experts, emphasises that leaders’ emotional affect and mood is a major driver of the mood and behaviours of others around them (Goleman et al., 2001). Thus, during a crisis, leaders need to be optimistic, yet, authentic and realistic. Positive emotion or resonance is critical to motivate people, allow them to be productive amidst chaos and preserve their wellbeing. As the pandemic spread around the world, some academic leaders demonstrated a highly person-centred approach in relation to staff and students, recognising their fears and anxieties, encouraging virtual education and work whenever possible, thus demonstrating primal leadership as well as cultural intelligence (Liao & Thomas, 2020; Velarde et al., 2020). If we want people to work interprofessional, pay attention to well-being and motivation, and work together to meet organisational goals, then flattening hierarchies is essential to generate ideas and functional collaboration (Barrow et al., 2011; Barrow et al., 2014) (Refer to Appendix B).
Whilst leaders may need to take a ‘command and control’ type of leadership in times of great crisis because important decisions must be taken and communicated quickly, after the immediate crisis other approaches will be helpful. For example, authentic, altruistic, person-centred, and inclusive leadership (Avolio & Gardner, 2005; Cardiff et al., 2018; Hollander, 2012; Sosik et al., 2009) approaches are very much focussed on the leader drawing from their own strengths and, through awareness and acknowledgement of their own weaknesses and biases, proactively seeking a range of perspectives on issues and demonstrating that they value and listen to those around them. When leaders are trying to make impactful decisions in times of uncertainty, having a range of views and ideas is essential. Leaders may also need to show intellectual humility – admitting mistakes, learning from criticism and different points of view, and acknowledging and seeking contributions of others to overcome limitations. As tasks are defined, leaders need to empower and demonstrate their confidence in people by delegating and holding them responsible for activities they can control.
B. The Complex Organisation or System Level: Adaptive Leadership
While conventional approaches to leadership and management have their place, as the pandemic elapsed around the world leaders needed to be highly adaptive and flexible, adjusting their outcomes and approaches based on rapidly changing information. Because we live in a VUCA (Volatile, Uncertain, Complex, Ambiguous)
(Worley & Jules, 2020) and RUPT (Rapid, Uncertain, Paradoxical, Tangled) (Till, Dutta, McKimm, 2016) world, leadership is needed that is flexible and agile enough to adapt to circumstances which most HPEs have not experienced before.
Adaptive leadership (Heifetz et al., 2009; Randall & Coakley, 2007) is specifically focussed on leadership in complex systems or situations and is helpful when thinking about how to respond to change, uncertainty, and crisis. Adaptive leaders do not simply work in a technical way (by just applying familiar management processes and ways of working) but involve people throughout the organisation to help solve ‘wicked’ problems, which may not have a clear solution and may require new ways of working. Adaptive leaders create the organisational conditions that enable dynamic networks and environments to achieve agreed goals in uncertain environments. Adaptive leadership focuses on four dimensions: Navigating organisational/system environments; leading with empathy; learning through self-correction and reflection and creating win-win solutions. These dimensions have many parallels with EI competencies. One of the most useful concepts in adaptive leadership which helps leaders to make decisions, is the ability to diagnose the ‘precious’ from the ‘expendable’ (Heifetz et al., 2009). What do we mean by this? The ‘precious’ is what is vitally important to the organisation; in education this is the learners themselves, the faculty, and the quality of educational provision – you do not want to lose the focus on these as you respond to crisis and change. What is ‘expendable’? Because of campus closures due to the pandemic, suddenly the large lecture theatres, shiny new buildings, and campuses that many universities see as artefacts of success and prestige, were expendable. Once the ‘new normal’ emerges, we will no doubt see a return to campuses and utilisation of buildings again, but adaptive leaders recognise what is precious and make sure that this is looked after and nurtured. We must remember this once the immediate crises are past (Refer to Appendix C).
C. The Global Eco-System Level: A Focus on Healing and Regeneration
The pandemic has highlighted starkly that the world, its countries, people, and structures are highly interconnected. In such times what affects one country, and actions (or inactions) cause ripples across the globe. We have already alluded to the need for leaders to work collaboratively and share practices, and during the pandemic we have seen multiple examples of international collaboration and the sharing of practice by HPEs everywhere. When we are all in the same boat, we need to sail in the same direction.
As well as being willing and proactive in collaborating on finding solutions to common challenges, leaders in HPE also need to consider the wider implications of the impact of climate change and human activities on health and health care. McKimm and McLean (2020) make the case for an ‘eco-ethical’ leadership approach which focuses leaders’ minds on the need for sustainable health professions’ education and practices. Another approach that is very relevant to HPE and its response to the pandemic is that of ‘regenerative’ leadership (Hutchins & Storm, 2019). In stimulating the recovery of health professions’ education and the organisations that provide it, leaders will need to pay attention to ensuring the conditions for healing, regeneration and thriving are present, so that people (faculty and students) feel safe to return to campuses and a more ‘normal’ way of working.
IV. PREPARING FOR A ‘NEW NORMAL’
A. Planning and Implementing Change
As countries, organisations and individuals start to look forward and prepare for mass returns to campus, leaders will need to support students and faculty for a ‘new normal’. This requires managing expectations as well as physical and psychological safety as discussed above. Management is all about maintaining stability and order (as Drucker (2007) says: ‘doing the thing right’) therefore, in addition to choosing appropriate leadership approaches, leaders will need to utilise a range of management tools to help plan how universities and their research, education programmes and other activities will function.
B. Risk Assessment
In an ideal world, all changes would be able to be planned for and there would be no surprises. However, successful organisations (and individuals) also plan for unforeseen circumstances to stay resilient and help mitigate risk. There are a few ways of assessing risks, with one of the most widely used being a ‘risk matrix’ (Ni et al., 2010). This is used during risk assessment to define the level of risk by considering the category of probability or likelihood against the category of consequence severity. This simple tool helps to increase the visibility of risks and assist management decision making. At university level as well as departmental and programme levels, a risk analysis should be carried out and updated regularly. In stable times, risk analysis helps the organisation keep aware of external and internal risk factors and put plans in place, but during the pandemic it is essential.
C. Managing Change
A widely used tool to lead, accelerate and manage change is Kotter’s (2007) eight-stage process (Refer to Appendix D).
The pandemic itself provided a sense of urgency as universities and teachers scrambled to respond, and leaders needed a good understanding of organisational resources, the external environment, and educational responses worldwide to develop meaningful and realistic strategies (Schwartzstein et al., 2008). The fluidity and volatility of the pandemic situation early on made any progress along Kotter’s steps difficult to see at either individual or institutional level. Whilst it can feel very unsettling to have to return to an earlier Step, after moving a few steps forward, it is often necessary to do so and Kotter’s model acknowledges that change is iterative, not linear. Kotter’s and similar models are very useful both for planning the changes needed as well as offering a framework for analysis of where change efforts are faltering or failing. A formal communications strategy is essential which provides consistent messages, opportunities for questions to be answered for all key stakeholders and celebrates ‘quick visible wins’, such as learners returning to their studies or a successfully run online assessment or graduation ceremony.
D. Focus on Outcomes
Across the world, universities (many of which had never provided online learning or assessment) suddenly had to decide how (or whether) they would (or could) provide educational opportunities for their students. Cameron and Green (2019) suggest that leaders responding to or stimulating change need to balance their efforts across three dimensions of any change: outcomes, interests, and emotions. In terms of ‘outcomes’, they stress that clear outcomes (deliverables) must be developed and implemented. Outcomes (goals, targets or objectives) need to be SMART (specific, measurable, achievable, realistic and time bound). In times of immediate crisis, some goals will need to be very short-term (e.g. ‘ensure all faculty are able and prepared to work from home by the end of next week’), whereas strategically, senior leaders have the responsibility to keep the longer terms outcomes in mind, e.g. ‘ensure that the university remains financially viable’. In terms of ‘emotions’, Cameron and Green (2019) suggest that the role of the leader is to enable people and the culture to adapt to the change and leaders also need to pay attention to (what may be competing) interests, here they need to mobilize their influence, authority and power to enact the change.
E. Planning and Implementation
McKimm and Jones (2018) suggest using project management techniques for operational planning and implementation. During the pandemic, plans will need to be devised and aligned in a range of areas (learning and teaching, student and faculty wellbeing, research, estates, finance etc.) and at many levels: whole university, department, and programme.
A project management approach sees activities as temporary, non-routine, acknowledging uncertainty and with a defined end point. Techniques taking a ‘linear’ view of change such as Lewin’s ‘freeze/unfreeze’ model (Cummings et al., 2016; Lewin, 1951) can be useful in framing the response into simple terms rather than getting bogged down in complexity. These look at the change process as comprising three steps: current state (how the university, schools and programmes ran pre-pandemic) – transitional state (how the university runs during the pandemic) – desired state (how might everything run after the pandemic, in the ‘new normal’). Once the broad elements and strategy have been agreed, then the detailed planning and implementation stages begin.
F. Sustaining Change
1) Recognising the dynamism of change: While crisis can bring about opportunities for real change, realistically there will be challenges sustaining the change. Buchanan et al. (2005) suggests organisational sustainability is contextual and dependent of various factors, including changes in market demands, financial viability, or political decisions. The drivers of sustainability will also differ based on organisational levels for example whether at the individual, managerial or leadership role. Given the uncertainties that leaders will face, an important step in sustaining change with positive outcomes would be an awareness that change, and sustainability is not static but is instead dynamic, requiring an improvement trajectory over time. This concept can also be described as dynamic stability: a process of continual, small, and possibly innovative changes that involve the modification or enhancement existing practices and business models (Hodges & Gill, 2014). When translated into practice, sustaining change requires as much attention from leaders as when developing and implementing change.
2) Supporting individuals at multiple levels: As sustainability of change is also dependent at the individual level, leaders should strongly promote and support initiatives that promote both individual professional and personal development. In the context of HPE, staff support is often interpreted as faculty development activities and more often is the form of workshops or, more recently, webinars. It is important for institutions to broaden the support activities to include non-faculty staff, provide activities other than workshops and implement initiatives for wellness and mental health wellbeing at the workplace. Another example of staff supports activities that has gained traction during this crisis are global community of practices. Given the similar challenges faced, global community of practices offer an opportunity to share strategies of mutual interest and benefit and build networks of educators across socio-cultural contexts (Thampy et al., 2020). As health professions’ leaders and educational organisations brace for the financial impact of the crisis, the case to reduce funding for staff support and investment in people maybe put forward. Leaders need to reflect and balance the impact reducing operating costs with enhancing the skills of staff to embrace, work with and sustain change.
3) Exchanging and co-creating global solutions: Sustaining change requires a vision for a new way of leadership and ways of working (McKimm & McLean, 2020). The recent COVID-19 crisis has highlighted that solutions to manage and sustain positive outcomes may not come from familiar local sources or authorities. The crisis also challenged the previously held assumptions of standards and readiness of healthcare systems and governance of it in some countries, suggesting much can be learned from successful approaches taken across the globe. Leaders in HPE should work collaboratively to acknowledge that solutions can come from across boundaries and draw from it lessons and guidelines for a global approach in the training of health professionals.
V. CONCLUSION
Although this paper provides a roadmap and suggested approaches for HPE leaders and followers alike to reflect on as they work through various waves of the pandemic, it is critical for leaders to be flexible and adaptive and adopt an emotionally intelligent and person-centred approach. Psychological safety is integral for professionals at all levels to successfully accomplish individual and institutional goals during challenging circumstances, along with leaders who provide stability and vision. What has become abundantly clear during the pandemic is that health professions’ educators from around the world have common as well as unique challenges and are increasingly seeking a diverse, multicultural global community of practice, sharing best practices and seeking to understand other cultural, regional and national educational context. These insights emphasise that health professions educators, regardless of their geographical location, cannot succeed in their leadership roles without a culturally sensitive, competent and grounded approach. No longer can experts from one group of countries impose their best practices on another region of the world without opening themselves to learning from other cultures and contexts.
Notes on Contributors
Judy McKimm conceptualised the idea for the article, wrote specific sections, and reviewed and edited the full article prior to submission.
Subha Ramani helped design the structure for this perspective, wrote content sections, edited, read and approved the final manuscript.
Vishna Devi Nadarajah helped design the structure for this perspective, wrote content sections, edited, read and approved the final manuscript.
Ethical Approval
No ethics approval was required as this is an opinion piece supported by a literature review and does not relate to primary research.
Funding
No funding sources are associated with this paper.
Declaration of Interest
I confirm that the manuscript is original work of authors which has not been previously published or under review with another journal.
I confirm that all research meets the legal and ethical guidelines.
I confirm that I have stated all possible conflicts of interest in my manuscript and explicitly stated even if there is no conflict of interest.
I am not using third-party material that requires formal permission.
References
Ashokka, B., Ong, S. Y., Tay, K. H., Loh, N. H. W., Gee, C. F., & Samarasekera, D. D. (2020). Coordinated responses of academic medical centres to pandemics: Sustaining medical education during COVID-19. Medical Teacher, 42(7), 762–771. https://doi.org/10.1080/0142159x.2020.1757634
Avolio, B. J., & Gardner, W. L. (2005). Authentic leadership development: Getting to the root of positive forms of leadership. The Leadership Quarterly, 16(3), 315–338. https://doi.org/10.1016/j.leaqua.2005.03.001
Barrow, M., McKimm, J., & Gasquoine, S. (2011). The policy and the practice: early-career doctors and nurses as leaders and followers in the delivery of health care. Advances in Health Sciences Education, 16(1), 17–29. https://doi.org/10.1007/s10459-010-9239-2
Barrow, M., McKimm, J., Gasquoine, S., & Rowe, D. (2014). Collaborating in healthcare delivery: Exploring conceptual differences at the “bedside.” Journal of Interprofessional Care, 29(2), 119–124. https://doi.org/10.3109/13561820.2014.955911
Boyatzis, R. E. (2009). Competencies as a behavioral approach to emotional intelligence. Journal of Management Development, 28(9), 749–770. https://doi.org/10.1108/02621710910987647
Buchanan, D., Ketley, D., Gollop, R., Jones, J. L., Lamont, S. S., Neath, A., & Whitby, E. (2005). No going back: A review of the literature on sustaining strategic change. International Journal of Management Review, 7 (3). https://doi.org/10.1111/j.1468-2370.2005.00111.x
Cameron, E., & Green, M. (2019). Making sense of change management: A complete guide to the models, tools, and techniques of organizational change. Kogan Page Publishers.
Cardiff, S., McCormack, B., & McCance, T. (2018). Person-centred leadership: A relational approach to leadership derived through action research. Journal of Clinical Nursing, 27(15–16), 3056–3069. https://doi.org/10.1111/jocn.14492
Cummings, S., Bridgman, T., & Brown, K. G. (2016). Unfreezing change as three steps: Rethinking Kurt Lewin’s legacy for change management. Human Relations, 69(1), 33-60.
Duckworth, A. (2016). Grit: The power of passion and perseverance (Vol. 234), Scribner. https://doi.org/10.1111/peps.12198
Dweck, C. (2016). What having a “growth mindset” actually means. Harvard Business Review, 13, 213-226.
Goleman, D. (1998). The emotionally competent leader. The Healthcare Forum Journal, 41(2), 36-38.
Goleman, D., Boyatzis, R., & McKee, A. (2001). Primal leadership: The hidden driver of great performance. Harvard Business Review, 79(11), 42-53.
Heifetz, R. A., Heifetz, R., Grashow, A., & Linsky, M. (2009). The practice of adaptive leadership: Tools and tactics for changing your organization and the world. Harvard Business Press.
Hodges, J., & Gill, R. (2014). Sustaining change in organizations (1st ed.). SAGE Publications.
Hollander, E. P. (2012). Inclusive leadership: The essential leader-follower relationship (Applied Psychology Series) (1st ed.). Routledge.
Hutchins, G., & Storm, L. (2019). Regenerative Leadership: The DNA of life-affirming 21st century organizations. Wordzworth Publishing.
Kanter, R. M. (2020). Leading your team past the peak of a crisis. Harvard Business Review
Kotter, J. (2007). Leading change: Why transformation efforts fail. Harvard Business Review, 86, 97-103.
Lazarus, G., Mangkuliguna, G., & Findyartini, A. (2020). Medical students in Indonesia: An invaluable living gemstone during coronavirus disease 2019 pandemic. Korean Journal of Medical Education, 32(3), 237–241. https://doi.org/10.3946/kjme.2020.165
Lewin, K. (1951). Field theory in social science: Selected theoretical papers (D. Cartwright, Ed.). Harpers.
Liao, Y., & Thomas, D. C. (2020). Conceptualizing Cultural Intelligence. In Cultural Intelligence in the World of Work (pp. 17-30). Springer.
McKimm, J., & Jones, P. K. (2018). Twelve tips for applying change models to curriculum design, development and delivery. Medical Teacher, 40(5), 520-526.
McKimm, J., & McLean, M. (2020). Rethinking health professions’ education leadership: Developing ‘eco-ethical’leaders for a more sustainable world and future. Medical Teacher, 42(8), 855-860.
McKimm, J., & O’Sullivan, H. (2016). When I say … leadership. Medical Education, 50(9), 896–897. https://doi.org/10.1111/medu.13119
Nadarajah, V. D., Er, H. M., & Lilley, P. (2020). Turning around a medical education conference: Ottawa 2020 in the time of COVID‐19. Medical Education, 54(8), 760–761. https://doi.org/10.1111/medu.14197
Ni, H., Chen, A., & Chen, N. (2010). Some extensions on risk matrix approach. Safety Science, 48(10), 1269–1278. https://doi.org/10.1016/j.ssci.2010.04.005
Paixão, G., Mills, C., McKimm, J., Hassanien, M. A., & Al-Hayani, A. A. (2020). Leadership in a crisis: Doing things differently, doing different things. British Journal of Hospital Medicine, 81(11), 1–9. https://doi.org/10.12968/hmed.2020.0611
Randall, L. M., & Coakley, L. A. (2007). Applying adaptive leadership to successful change initiatives in academia. Leadership & Organization Development Journal, 28(4), 325–335. https://doi.org/10.1108/01437730710752201
Schwartzstein, R. M., Huang, G. C., & Coughlin, C. M. (2008). Development and implementation of a comprehensive strategic plan for medical education at an academic medical center. Academic Medicine, 83(6), 550–559. https://doi.org/10.1097/acm.0b013e3181722c7c
Scouller, J. (2011). The three levels of leadership: How to develop your leadership presence, knowhow, and skill. Management Books 2000.
Sinek, S. (2014). Leaders eat last: Why some teams pull together and others don’t. Penguin.
Sosik, J. J., Jung, D., & Dinger, S. L. (2009). Values in authentic action. Group & Organization Management, 34(4), 395–431. https://doi.org/10.1177/1059601108329212
Swanwick, T., & McKimm, J. (2017). ABC of clinical leadership. John Wiley & Sons.
Thampy, H. K., Ramani, S., McKimm, J., & Nadarajah, V. D. (2020). Virtual speed mentoring in challenging times. The Clinical Teacher, 17(4), 430–432. https://doi.org/10.1111/tct.13216
Till, A., Dutta, N., & McKimm, J. (2016). Vertical leadership in highly complex and unpredictable health systems. British Journal of Hospital Medicine, 77(8), 471–475. https://doi.org/10.12968/hmed.2016.77.8.471
Uhl-Bien, M., & Carsten, M. (2018). Reversing the lens in leadership: Positioning followership in the leadership construct. In Leadership now: Reflections on the legacy of Boas Shamir. Emerald Publishing Limited.
Velarde, J. M., Ghani, M. F., Adams, D., & Cheah, J.-H. (2020). Towards a healthy school climate: The mediating effect of transformational leadership on cultural intelligence and organisational health. Educational Management Administration & Leadership. https://doi.org/10.1177/1741143220937311
Worley, C. G., & Jules, C. (2020). COVID-19’s uncomfortable revelations about agile and sustainable organizations in a VUCA world. The Journal of Applied Behavioral Science, 56(3), 279–283. https://doi.org/10.1177/0021886320936263
*Judy McKimm
Swansea University Medical School,
Swansea University
Swansea, UK, SA1 8PP
Email: j.mckimm@swansea.ac.uk
Submitted: 14 August 2020
Accepted: 14 October 2020
Published online: 13 July, TAPS 2021, 6(3), 114-117
https://doi.org/10.29060/TAPS.2021-6-3/PV2376
Meredith T. Yeung1, Melissa Y. Chan1, Clement C. Yan1,2 & Katherin S. Huang1
1Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore; 2Department of Physiotherapy, Sengkang General Hospital, Singapore
I. INTRODUCTION
Coronavirus Disease 2019 (COVID-19), which requires no introduction, is transmitted through droplet transmission and is highly contagious (del Rio & Malani, 2020; Guan et al., 2020; Sohrabi et al., 2020). After it was declared a pandemic on 11 March 2020, the Singapore government implemented a “circuit breaker” period, or partial lockdown, on 7 April 2020 (Ministry of Health, 2020). In spite of numerous initiatives for faculty to embrace technology-enhanced learning over the past years, it was a steep take-off for most programmes at institutes of higher learning. This short personal view intends to share our experience from the sole entry-level physiotherapy programme in Singapore.
II. ONLINE LESSONS
During the preliminary stages of the pandemic, faculty proactively switched all face-to-face lectures and tutorials that involved 50 or more students to online lessons. As the academic timetable had already been established, there was little to no disruption to lesson scheduling. Synchronous methods of e-learning occurred via video-conferencing software, such as Zoom and Microsoft Teams, and was used for lectures and tutorials. The virtual classroom allowed live interaction, and was especially useful for small group case study discussions when students were allocated into breakout rooms. Asynchronous methods of e-learning took the form of pre-recorded lectures, predominantly via Microsoft PowerPoint or iSpring, or recordings of live lectures. This promoted ubiquitous learning where the learner could learn at a time and place of their convenience, and which garnered positive feedback of over 60% from an unofficial survey of students. One student commented that “the online lectures were very useful, especially those that are pre-recorded so [that we] won’t miss out on what the professor is saying”.
While the move to online teaching was essential, it certainly had its challenges. Many of the faculty were not proficient with the advanced features of Zoom, resulting in initial hiccups in organising multiple lessons for over a hundred students. For example, being unfamiliar with the software, lack of stable Wi-Fi off-campus, and insufficient software accounts were some teething problems. Training workshops for the use of Zoom were initially planned prior to the pandemic, however these could not be realised due to sudden time constraints. Training and troubleshooting manuals were thus made available for all educators and students via an online portal, in addition to a phone helpdesk for further assistance. Furthermore, the other challenge we faced was the short amount of time available to produce and upload enough e-learning material, such as filming of teaching videos, organising self-directed packages, and modifying lecture material to suit live online or pre-recorded delivery. Students also faced challenges due to the multiple modules they were enrolled in during the academic term, having to keep track of up to five randomly-generated meeting identification numbers (ID) each day. The use of one meeting ID per module, set at a regular occurrence, was implemented to alleviate this burden.
One concern we had was over “Zoom fatigue” and general lack of engagement from students. One strategy we implemented was to insert stretching exercises and a rest period after each hour of lesson. Quiz apps, such as Kahoot and Socrative, was also used to poll content-specific questions, to promote student engagement and active participation. These strategies helped to sustain attention span and was deemed successful as reflected by near-100% participant responses and structured module feedback. One student commented that she was “quite happy that we can still continue lessons, although it is modified…and not have to worry about the uncertainty of lessons being cancelled”.
III. BLENDED FORMAT FOR PRACTICAL LESSONS
Physiotherapy students are highly dependent on skills-based learning and hands-on practice, which equips them with competencies to treat real patients in the clinical setting. Conducting practical lessons was met with additional challenges due to the strict rules on safe distancing, restrictions on human movement, and limits on class size and frequency. We approached this using video-augmented practicum. A pre-recorded demonstration of physiotherapy skills was disseminated to students via the learning management system (LMS) before each hands-on lesson. This strategy was useful for teaching of skills which require physical space and simulation, such as performing auscultation, manual handling, patient positioning and transfers, airway suctioning, or walking tests. To illustrate, in the teaching of cardiopulmonary exercise testing (CPET), we divided the content into several components: an introductory video and stepwise guide on how to conduct the exercise test; a self-directed learning package on CPET results interpretation with self-evaluation; and a hands-on practical session of performing the full CPET with peers in the human performance laboratory on university campus. Faculty then utilised the face-to-face practical sessions to provide critical feedback and correct students’ techniques. Students were further able to consult with faculty and receive real-time feedback on their performance of skills via video-conferencing, if requested.
IV. CONDUCTING ASSESSMENT DURING A PANDEMIC
Following the declaration of the pandemic, our programme converted all physical paper examinations to online examinations. Commercially available remote proctoring systems, such as Respondus® and Proctortrack by Verificient, allowed us to mitigate cheating in the virtual environment. The three-point identity check in these systems ensures that authentication is vigorous, while the manual or artificial intelligence proctoring technology enables remote invigilation. ‘Browser lock’ disables platform-sharing functions such as screen-sharing or remote desktop control that would otherwise allow a proxy to take the examination.
V. ONLINE VIVA VOCE
To assess the “thinking” portion of patient management, we conducted online viva examinations in lieu of physical examinations. To prepare for the large volume of online assessments, we underwent several trials of Zoom, tinkering with features such as the waiting room and breakout rooms. These trials enabled us to familiarise ourselves with the logistic flow, as well as troubleshoot issues such as interruptions during entrance and exit, transfer of host rights, and audio-visual glitches. Administrative coordinators were designated to manually allocate students into the breakout rooms, which was preferred over pre-allocation in order to reduce errors. In anticipation of potential lapses, we used a separate chat messaging software for assessors and coordinators to flag and resolve technical issues. A spreadsheet was used to schedule detailed information about switchover times and room allocation for each candidate, ensuring smooth transition from main room to breakout rooms, as well as to resolve any scheduling conflict. Advance dissemination of the examination schedule and login details was crucial in minimising technical issues. Marking rubrics with clear descriptors were developed, with time set aside for pre- and post-viva calibration amongst assessors. Students had access to the marking rubrics, and a mock run was held to familiarise students with the logistic flow of the assessment. With these preparations in place, we were able to conduct online viva examinations for over a hundred students successfully and efficiently.
VI. VIDEO SUBMISSION FOR SKILLS ASSESSMENT
To assess the “doing” portion of patient management, we utilised video-based assessment. The evidence for video-based assessment in healthcare education is at its infancy, with most evidence evolving around the idea of video-based peer feedback, assessment for communication skills, or the assessment of surgical skills. We tested this method in a final-year elective module that required learners to demonstrate manually-assisted cough—a skill that would traditionally be performed in front of an assessor and marked against a checklist. Casually dubbed the ‘open-book practical assessment’, faculty listed detailed requirements of the assessment, which gave students time to practise skills before recording and submission. The use of student-generated video assessment (mean marks 77.84 ± 4.59, class size of 30) to replace traditional skills assessment (mean marks 80 ± 3.88, class size of 25) was considered a success as there was no significant difference in the pass-fail ratio between the affected cohort and prior cohorts. In addition, we observed some unintentional benefits, such as the demonstration of digital capability and communication skills by the students, while aligned with the learning and assessment objectives – a finding consistent with the available literature (Walters et al., 2015).
The assessment of skills may also be performed real-time through video-conferencing. However, the logistics and time required to assess such a large number of students within a relatively short timeframe made it a task too immense for us to undertake. Nonetheless, with adequate manpower and resources, it could undoubtedly be feasible, perhaps even superior, as a form of video assessment.
VII. CONCLUSION
The unprecedented COVID-19 pandemic has forced us to refashion pedagogical approaches to our curriculum and to embrace positive changes for the future of physiotherapy education. Utilising aforementioned strategies, we were able to deliver our teaching effectively and almost entirely virtually, despite initial hiccups. Pragmatically, it would be ideal to formally evaluate the impact of a virtual curriculum on established learning outcomes, as well as the general acceptability of such a programme for both students and faculty. In the event of future similar state of emergencies, it may even be prudent to develop a blueprint of and stepwise approach to pedagogy escalating along the spectrum of face-to-face methods versus virtual technology. We hope that this short personal view will provide other educators with some solutions to coping with the challenges of teaching surrounding this exigent time.
Notes on Contributors
Meredith T. Yeung is an Associate Professor at the Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore. She contributed to the conception and revision of the manuscript critically for important intellectual content.
Melissa Y. Chan is an Associate Faculty at the Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore. She contributed to the conception and revision of the manuscript critically for important intellectual content.
Clement C. Yan is an Associate Professor at the Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore and Senior Principal Physiotherapist at the Department of Physiotherapy, Sengkang General Hospital, Singapore. He contributed to the conception and revision of the manuscript critically for important intellectual content.
Katherin S. Huang is an Associate Faculty at the Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore. She contributed to the conception and revision of the manuscript critically for important intellectual content.
Acknowledgements
The authors wish to thank all students and staff members from the Singapore Institute of Technology and the physiotherapy programme for all the support during this challenging time of COVID-19. All comments and module feedback referred to in this article were willingly and voluntarily provided by students.
Funding
This personal view did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Interest
The authors declare no form of possible conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
del Rio, C., & Malani, P. N. (2020). 2019 Novel coronavirus – Important information for clinicians. Journal of the American Medical Association, 323(11), 1039-1040. https://doi.org/10.1001/jama.2020.1490
Guan, W., Ni, Z., Hu, Y., Liang, W., Ou, C., He, J., Liu, L., Shan, H., Lei, C., Hui, D. S. C., Du, B., Li, L., Zeng, G., Yuen, K.-Y., Chen, R., Tang, C., Wang, T., Chen, P., Xiang, J., … Zhong, N. (2020). Clinical characteristics of Coronavirus Disease 2019 in China. New England Journal of Medicine, 382(18), 1708–1720. https://doi.org/10.1056/NEJMoa2002032
Ministry of Health (2020, April 7). Speech by Mr Gan Kim Yong, Minister for Health, at the second reading of COVID-19 (temporary measures) Bill, 7 April 2020 [Press release]. https://www.moh.gov.sg/news-highlights/details/speech-by-mr-gan-kim-yong-minister-for-health-at-the-second-reading-of-covid-19-(temporary-measures)-bill-7-april-2020
Sohrabi, C., Alsafi, Z., O’Neill, N., Khan, M., Kerwan, A., Al-Jabir, A., Iosifidis, C., & Agha, R. (2020). World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). International Journal of Surgery, 76, 71–76. https://doi.org/10.1016/j.ijsu.2020.02.034
Walters, S. R., Hallas, J., Phelps, S., & Ikeda, E. (2015). Enhancing the ability of students to engage with theoretical concepts through the creation of learner-generated video assessment. Sport Management Education Journal, 9(2), 102-112. https://doi.org/10.1123/smej.2014-0041
*Meredith T. Yeung
Singapore Institute of Technology,
10 Dover Drive,
Singapore 138683
Tel: +65 65928671
Email: Meredith.Yeung@SingaporeTech.edu.sg
Submitted: 16 July 2020
Accepted: 4 November 2020
Published online: 13 July, TAPS 2021, 6(3), 118-120
https://doi.org/10.29060/TAPS.2021-6-3/CS2392
Wai Keung Chui, Han Kiat Ho, Li Lin Christina Chai & Paul J. Gallagher
Department of Pharmacy, Faculty of Science, National University of Singapore, Singapore
I. THE CHANGING LANDSCAPE IN PHARMACY PRACTICE
Pharmacy practice in Singapore is rapidly evolving with the advent of technological innovations and changes in patient demographics. For instance, the dispensing process in hospitals have been automated; telepharmacy has made access to pharmaceutical services more convenient in the community; an aging population has brought along complex co-morbidities, chronic diseases, polypharmacy and community-based pharmaceutical care services that will require clinical interventions by pharmacists. These examples have raised the question of the “relevance of pharmacists” in the evolving health system. To stay relevant, pharmacists must move from the traditional medication supply (product focus) role to curating the optimal use of medicines by patients (patient focus) in a technology and informatics driven health system. This paradigm shift can only be enabled if the education of pharmacists is suitably re-constructed with outcomes that will future-roof their capabilities in the new healthcare ecosystem. This prompted the Department of Pharmacy at the National University of Singapore (NUS) to make a commitment to review its present programme thereby turning the threats into opportunities for its future pharmacy graduates. This case study reports the approach taken by the Department to re-engineer its curriculum for modern pharmacy practice in the twenty-first century.
II. NEEDS ANALYSIS AND RECOMMENDATIONS
In late 2018, a needs analysis was conducted by the Department to inform the design strategies. This was done through structured interviews by informed consent of key opinion leaders, and focused group discussions with alumni and students. The data collected were coded and analysed thematically. Some main themes about the graduates that came through were the weakness in applying their knowledge, their lack of an understanding of the health system and their reluctance to take leadership role. Feedback on the present curriculum included a lack of connectivity between modules that were taught in silos and the structured experiential learning was scheduled too late in the curriculum. It was recommended that a competency-based and integrated curriculum (Husband et al., 2014; Pearson & Hubball, 2012) would help students achieve the necessary competence as a health professional and apply the multidisciplinary knowledge holistically to problem solve. An introduction of systems thinking, and a longitudinal experiential learning programme across the four years will help students understand their future work environment better.
III. PROGRAMME DESIGN
Based on these recommendations, the department had to deconstruct and re-organise the current traditional teaching approach where basic sciences are taught in separate modules in years 1 to 2 while topics in pharmacy practice and therapeutics are introduced from years 3 to 4; with work-place learning happening only after year three. A Curriculum Design Group (CDG) was established to dissect and develop the curriculum. The CDG adapted the key competencies listed in the Association of Faculties of Pharmacy in Canada Educational Outcomes for First Professional Degree Programs in Pharmacy (Association of Faculties of Pharmacy of Canada, 2017) as the basis for the competency-based curriculum. The students will learn to approach pharmacy practice by skilfully integrating sub-competencies of communicator, collaborator, leader-manager, scholar-innovator, health advocate and professional roles into an overarching care provider role. The scholar role is expanded to scholar-innovator role as innovation aligns well with the core value of NUS and is also a critical attribute to safeguard against future disruptions. The key competencies under each role are carefully mapped onto the learning outcomes of themed modules. The themed modules (based on physiological systems) are designed using a theoretical framework of integrating basic, clinical and systems sciences (Gonzalo et al., 2017) (Figure 1). To help students make sense of what they learn, experiential learning is incorporated longitudinally across the four years so that students can apply their theoretical studies at the workplace when they go on clinical placements (Figure 1). This 3-pillar educational framework has been successfully applied in medical education in the US to develop medical competencies and systems thinking among the physicians (Gonzalo et al., 2017); the CDG believed that the same framework would work for pharmacists in Singapore.
Pharmacy graduates must be prepared for a health system that is driven by informatics and technology. Joseph Aoun in his book “Robot-Proof: Higher Education in the Age of Artificial Intelligence” (Aoun, 2017) recommended undergraduate students to acquire technical, data and human literacies, which he collectively refers to as the “humanics”, for them to stay ahead of the technological revolution. Therefore, subjects such as medical sociology, computational thinking, health informatics are included to cultivate the humanics in the pharmacy students. It is envisaged that this approach can better prepare the graduates to work with patients, co-workers, data and technologies in providing quality care. Furthermore, instilling characteristics of a transformational leader and familiarising students to implementation science will take a step closer to grooming the student pharmacists into future leaders.
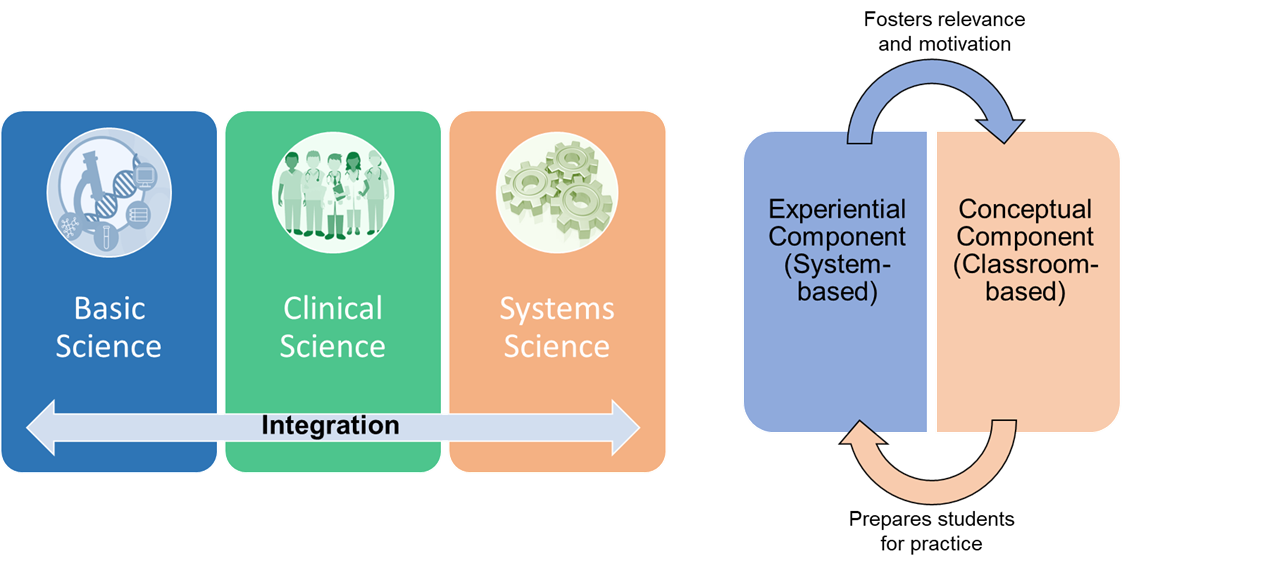
Figure 1: The theoretical framework of curricular integration. Adapted from Gonzalo et al. (2017) and Pearson and Hubball (2012).
In the new programme, students are made accountable of their own learning through pre-class preparations and interactive team-based learning (TBL) in the classroom. TBL sessions are facilitated by a scientist and a clinician who help students to use integrative thinking to solve the cases. In the laboratory, students will also work in teams to gather scientific data for inquiry-based learning. The impact of the new educational approach will be evaluated against all the four levels of the new world Kirkpatrick Model to determine the effectiveness of the curriculum.
IV. TRANSFORMING PHARMACY EDUCATION IN RESPONSE TO THREATS
The fourth industrial revolution has indeed caused disruptions to pharmacy practice. Pharmacists will have to step forward and be leaders of change when it comes to any matter related to medicines, be it optimising drug use, identifying drug-related problems or recommending cost-effective therapy. Therefore, it is the mission of NUS Department of Pharmacy to respond to the threats by transforming its professional pharmacy programme to one that can future proof its graduates who will be ready to seize new opportunities in a dynamic health system.
Notes on Contributors
Professor Christina Chai is the Head of the Pharmacy Department at NUS. She initiated the EduRx project by calling for the need to redesign the professional pharmacy degree curriculum to better prepare the graduates for the evolving healthcare landscape in Singapore.
Associate Professor Ho Han Kiat, in the capacity of the Deputy Head (Education), supported the curriculum design group in ensuring that the new pharmacy curriculum is closely aligned to both the NUS educational philosophy and the educational outcomes for pharmacy graduates.
Professor Paul Gallagher and Associate Professor Chui Wai Keung are co-leaders of the EduRx project who under their co-leadership worked with the curriculum design group to develop the competency-based and integrative pharmacy programme.
Acknowledgements
The authors would like to acknowledge the contributions made by the curriculum design group that comprises the following members: Chng Hui Ting, Fan Wenjie, Han Zhe, Priscilla How, Law Hwa Lin, Eugene Lim Zi Jie, Anson Lim Zong Neng, Tan Bee Jen, Matthias Gerhard Wacker, and Yeo Shao Jie.
Funding
There is no research funding source for the programme review project.
Declaration of Interest
The authors declare no conflict of interest concerning any aspect of this case study.
References
Aoun, J. (2017). Robot-proof: Higher education in the age of artificial intelligence. The MIT Press.
Association of Faculties of Pharmacy of Canada. (2017). AFPC educational outcomes for first professional degree programs in pharmacy in Canada 2017. https://afpc.info/system/files/public/AFPC-Educational%20Outcomes%202017_final%20Jun2017.pdf
Gonzalo, J. D., Haidet, P., Papp, K. K., Wolpaw, D. R., Moser, E., Wittenstein, R., & Wolpaw, T. (2017). Educating for the 21st-century healthcare system: An interdependent framework of basic, clinical and systems sciences. Academic Medicine, 92 (1), 35-39. https://doi.org/10.1097/ACM.0000000000000951
Husband, A. K., Todd, A., & Fulton, J. (2014). Integrating science and practice in pharmacy curricula. American Journal of Pharmaceutical Education, 78 (3), 63. https://doi.org/10.5688/ajpe78363
Pearson, M. L., & Hubball, H. T. (2012). Curricular Integration in Pharmacy Education. American Journal of Pharmaceutical Education, 76 (10), 204. https://doi.org/10.5688/ajpe7610204
*Wai Keung Chui
Department of Pharmacy,
Faculty of Science,
Block S4A, 18 Science Drive 4,
Singapore 117543.
Tel: +65 6516 2933
Email: phacwk@nus.edu.sg
Submitted: 25 May 2020
Accepted: 30 December 2020
Published online: 13 July, TAPS 2021, 6(3), 24-31
https://doi.org/10.29060/TAPS.2021-6-3/RA2314
Maria Isabel Atienza
Curriculum and Instruction, College of Medicine, San Beda University, Philippines
Institute of Pediatrics & Child Health, St. Luke’s Medical Center, Global City, Philippines
Abstract
Introduction: The prevailing consensus is that medical professionalism must be formally included as a programme in the undergraduate medical curriculum.
Methods: A literature search was conducted to identify institutions that can serve as models for incorporating professionalism in medical education. Differences and similarities were highlighted based on a framework for the comparison which included the following features: Definition of professionalism, curricular design, student selection, teaching and learning innovations, role modelling and methods of assessment.
Results: Four models for integrating professionalism in medical education were chosen: Vanderbilt University School of Medicine (VUSM), University of Washington School of Medicine (UWSOM), University of Queensland (UQ) School of Medicine, and Mayo Clinic and Mayo Medical School. The task of preparing a programme on medical professionalism requires a well-described definition to set the direction for planning, implementing, and institutionalising professionalism. The programmes are best woven in all levels of medical education from the pre-clinical to the clinical years. The faculty physicians and the rest of the institution’s staff must also undergo a similar programme for professionalism.
Conclusion: The development of all scopes of professionalism requires constant planning, feedback and remediation. The students’ ability to handle professionalism challenges are related to how much learning situations the students encounter during medical school. The learning situations must be adjusted according to the level of responsibilities given to students. The goal of learning is to enable students to grow from a novice to a competent level and afterwards to a proficient and expert level handling professionalism challenges in medicine.
Keywords: Medical Professionalism, Medical Curriculum, Role Modelling in Medical Education, Culture of Medical Professionalism
Practice Highlights
- A programme on medical professionalism in education starts with a working definition of the term.
- The culture of professionalism must be articulated in the school’s vision and mission.
- The professionalism programme must be woven through the four years of medical education.
- Role models are essential in teaching medical professionalism.
- For teaching medical professionalism, a nurturing environment is preferable over punitive actions.
I. INTRODUCTION
There is a prevailing sentiment that professionalism must be taught formally and explicitly in all medical schools (Cruess & Cruess, 2006). This review aims to highlight some exceptional models for incorporating professionalism in the curriculum of medical education. The models were chosen based on the consensus among medical educators that medical schools need to respond to the following observations and recommendations from the vast literature on this subject:
1. Society expects physicians to act professionally (Lynch et al., 2004; Mueller, 2009; O’Sullivan et al., 2012).
2. There is a link between unprofessional behaviour in medical school and subsequent practice (Mueller, 2009; O’Sullivan et al., 2012; Parker et al., 2008).
3. Professionalism is associated with improved medical outcomes (Mueller, 2009).
4. Professionalism needs to be taught in the undergraduate medical institutions (O’Sullivan et al., 2012).
5. The teaching and learning must be coupled with a carefully constructed means of assessment of professionalism and professional behaviour (O’Sullivan et al., 2012).
6.Students must be supported in developing the skills for continuing professional development throughout their career (O’Sullivan et al., 2012).
This review aims to utilise these assumptions as a framework for reviewing and comparing models for the incorporation of medical professionalism in the curriculum of medical schools. This paper aims to provide answers to this question: Among medical schools that have incorporated professionalism in the medical curriculum, what are the salient features of the programmes that may be adopted by other institutions in need of such curricular innovations?
II. METHODOLOGY
A literature search was conducted to search for relevant institutions that have established a programme for incorporating professionalism in their medical schools. There was no attempt to review all published reports but to focus on the schools that can serve as models for other institutions in need of such curricular innovations. All information concerning the programmes were taken from the published journal articles which were authored by the faculty members in charge of the respective programmes on professionalism. An independent appraisal was done using a framework adopted from a systematic review by Passi and co-workers which included the following criteria: institutional definition of professionalism, curricular design, student selection, teaching and learning innovations, role modelling and assessment (Passi et al., 2010).
III. RESULTS
The review of literature on undergraduate medical programmes on professionalism revealed four notable models that describe how their institutions have integrated the teaching and assessment of professionalism among medical students, namely, Vanderbilt University School of Medicine (VUSM), University of Washington School of Medicine (UWSOM), University of Queensland (UQ) School of Medicine, and Mayo Clinic School of Medicine.
A. Vanderbilt University School of Medicine (VUSM)
A model applied at the VUSM focused on an Academic Leadership Programme (ALP) established to address unprofessional and disruptive behaviours of students (Hickson et al., 2007). The ALP is a programme designed for leaders and administrators tasked to identify and tackle unprofessional behaviours. A four-level graduated intervention programme was designed to deal with the incident cases occurring in the school. The tenets of professionalism are introduced to the medical students through a discussion of case vignettes dealing with unprofessional behaviour. The faculty are also asked to sign a creed and a commitment to be role models of professional behaviour for graduates and medical students.
A so-called “disruptive behaviour pyramid” serves as a guide for identifying and assessing variable degrees of unprofessional behaviour with their corresponding intervention. Surveillance systems have also been put in place to detect unprofessional behaviour of students and physicians from patients, visitors, and health care team members (Hickson et al., 2007).
B. University of Washington School of Medicine (UWSOM)
The UWSOM introduced their professionalism curriculum through the development of the Colleges programme for the preclinical medical students. Outstanding faculty-clinicians are selected and trained to teach and model clinical skills with small groups of students at the bedside from the second-year level until the time of their graduation. The institution recognises these faculty as role model physicians working closely with students in the care of patients (Goldstein et al., 2006).
The school promotes an “ecology of professionalism” in the campus and provides an environment for group discussions, role modelling and reflection among the different year levels of medical education. Professionalism is an institution wide concern such that both students and the faculty are required to undergo training on professionalism. In order to make the programme more meaningful, the institution added the “Patients as Teachers” project whereby the patients are asked to provide feedback and to offer advice to the medical students. The loop of learning involving the faculty, the students, and the patient is deemed as a “safe” and respectful educational environment that encourages professionalism as an institutional-wide responsibility (Goldstein et al., 2006).
C. University of Queensland (UQ) School of Medicine
The programme of the University of Queensland integrates medical ethics, law and the professionalism curriculum with a “Personal and Professional Development” process (Parker et al., 2008). Throughout the four-year levels of undergraduate medical education, topics of ethics and professional development are taught and assessed through written tests and objective structured clinical examinations. A document called “Commitment to Professionalism” is signed by every student at the start of their first-year level to reinforce the principles and their acceptance of the expectations of the school, including attendance.
A “Pyramid of Professionalism” serves as a model to identify the students that require supervision and eventually pass or fail the programme. Students are assessed at several levels with a committee providing support, feedback and remediation. Professional conduct ultimately affects the student’s promotion to the next year level (Parker et al., 2008).
D. Mayo Clinic School of Medicine
The Mayo Clinic incorporated professionalism into medical education by first articulating its culture through a statement of the institution’s primary value: “The needs of the patient come first”. Their mission statement declares that “Mayo will provide the best care to every patient every day through integrated clinical practice, education, and research.” This culture is expressed in all the institution’s policies and procedures (Mueller, 2009).
Mayo has adopted a framework for professionalism which places clinical competence, communication skills and sound understanding of ethics at its foundation (Mueller, 2015). Built on this foundation are the pillars or the key attributes of accountability, altruism, excellence and humanism. With this framework and the culture that Mayo promotes, professionalism teaching and assessment programmes have been implemented involving all levels of learners of the Mayo Clinic School of Medicine. An intensive bioethics courses and a leadership and professionalism course is given to the first-year medical students. For the second-year level, the “Advance Doctoring” professionalism reflective writing programme is given. For the third-year level, the “Safe Harbor” professionalism programme and an intensive bioethics course is applied (Mueller, 2009; Mueller, 2015).
More professionalism and ethics teaching are incorporated into different courses and clinical rotations throughout the four-year curriculum. Other interesting features include an elective course in Professionalism and Ethics related to the students’ career interest. Professionalism assessments are carried out by way of formative and summative feedback and professionalism “portfolios” which are summarized for their future applications for further training (Mueller, 2009; Mueller, 2015).
The Mayo Clinic faculty physicians also have their share of professionalism modules. The new physician staff are required to attend a complete series of professionalism courses. All faculty physicians have to take a complete web-based, interactive module on professionalism in order to maintain their status as practicing physicians. They also undergo a 360-degree review to identify and address lapses in professionalism. The non-physician allied healthcare staff of the institution also have their own professionalism programme to support Mayo’s service philosophy (Mueller, 2009; Mueller, 2015).
The core value of professionalism continues to guide the clinic in its leadership practices and management strategies. The value-based culture serves as a positive hidden curriculum that promotes the achievement of desired educational outcomes among the health care professionals (Viggiano et al., 2007).
E. Institutional Definitions of Medical Professionalism
The lack of a universal definition of medical professionalism has resulted in medical schools formulating what is suitable to their context (O’Sullivan et al., 2012). Among the four curricular models, Mayo clearly expounded on their definition of medical professionalism. This institution defined professionalism by embracing seven patient care-related and seven practice environment-related attributes as summarised in the Mayo Clinic Model of Care (Mueller, 2009).
In the case of UQ, while no clear-cut definition of professionalism was described in the journal article, the institution instead presented a list of topics of medical ethics and professional development for formal training and instruction. A review of the UQ listing shows that most of the elements of professionalism covered were related to the theme of public or societal professionalism, such as Medical Practice and the Law, Accountability and Self-Regulation, Inappropriate Practice and Medical Over servicing, and Commercialization of Medicine (Parker et al., 2008).
A second list of elements of professionalism was prepared by the UQ faculty, and this list contained attributes related to intrapersonal and interpersonal professionalism. This list served as their guide to identify students who required support, feedback or remediation through the process called the Pyramid of Professionalism (Parker et al., 2008).
The VUSM also did not state the elements of professionalism in their model. Instead, the institution focused on defining the unprofessional or disruptive behaviours that required case discussions in particular year levels of medical education. These were the same unacceptable behaviours that were used to identify students who needed immediate intervention ranging from non-punitive interventions up to the imposition of disciplinary processes if needed (Hickson et al., 2007).
The UWSOM developed a list of elements of professionalism that served as benchmarks for preclinical students, namely, the principles of altruism, honour and integrity, compassion, communication, respect, accountability and responsibility, scholarship, excellence and leadership. Despite this listing, the faculty received feedback from the students that the idea of professionalism and cultural competency remained unclear to them. This feedback came with a request from the students that the teaching of professionalism should be “more specific, clinically relevant, and challenging” (Goldstein et al., 2006).
F. Comparison of Programme Implementation
A systematic review (Passi et al., 2010) was done with the aim to summarise the evidence on methods used by medical schools to promote medical professionalism. Five main strategic areas to promote the development of professionalism in medical education were identified from the review: Curriculum design, student selection, teaching and learning methods, role modelling and assessment methods. These five areas can be used as guideposts in reviewing school programmes on professionalism. Table 1 shows a comparison of the four models presented earlier.
G. Similar Features in the Four Models
These are the features common to all four models: (1) Commitment of the leadership of the institution to embark on integrating professionalism into the curriculum, (2) Built-in programme for training of faculty for teaching and modelling of clinical skills, and (3) Vertical integration of the programme of professionalism from preclinical to clinical years.
These features are significant means to heighten the attention of both students and faculty to the need for growth in the area of professionalism. This will also help institutionalize professionalism. The journals on the models did not mention any policy regarding the screening for unprofessional behaviour during the student selection process.
H. Differences in the Four Models
Major differences are evident in the approach to teaching professionalism in the four curricular models.
1) The formal teaching and learning experience of the students of the four schools were varied in terms of duration and delivery of instruction: UWSOM and Mayo incorporates a formal course throughout the four years of medical education. In Mayo, all faculty physicians are trained and involved in the training of students for professionalism. UWSOM, on the other hand, has a select group of thirty faculty assigned for this purpose. UQ described a formal course on professionalism in the first two years of medical education. After the first 2 years, UQ proceeds to the clinical years of medical education using the personal and professional development (PPD) process of identifying personal and professional shortcomings among the students.
The approach taken by VUSM is more interventional in nature. Although short problem-based discussions are provided in the four-year levels of medical education, the main thrust of the programme is on identifying and rectifying incident cases of unprofessional behaviour. Its basis rests on the idea that “failing to address unprofessional behaviour simply promotes more of it.” The VUSM model mentions four graduated interventions as a disciplinary measure to address unprofessional behaviour.
2) The four schools also differed in their assessment methods: VUSM focuses on immediate recognition and grading using the “disruptive behaviour pyramid” to determine the appropriate intervention. UWSOM uses reflection and feedback in the preclinical years followed by a “closed loop” system of obtaining feedback from patients and faculty. Deficiencies in professional behaviour are identified so that remediation may be provided to ensure that only students who are ready will graduate or advance to the next year (Hickson et al., 2007).
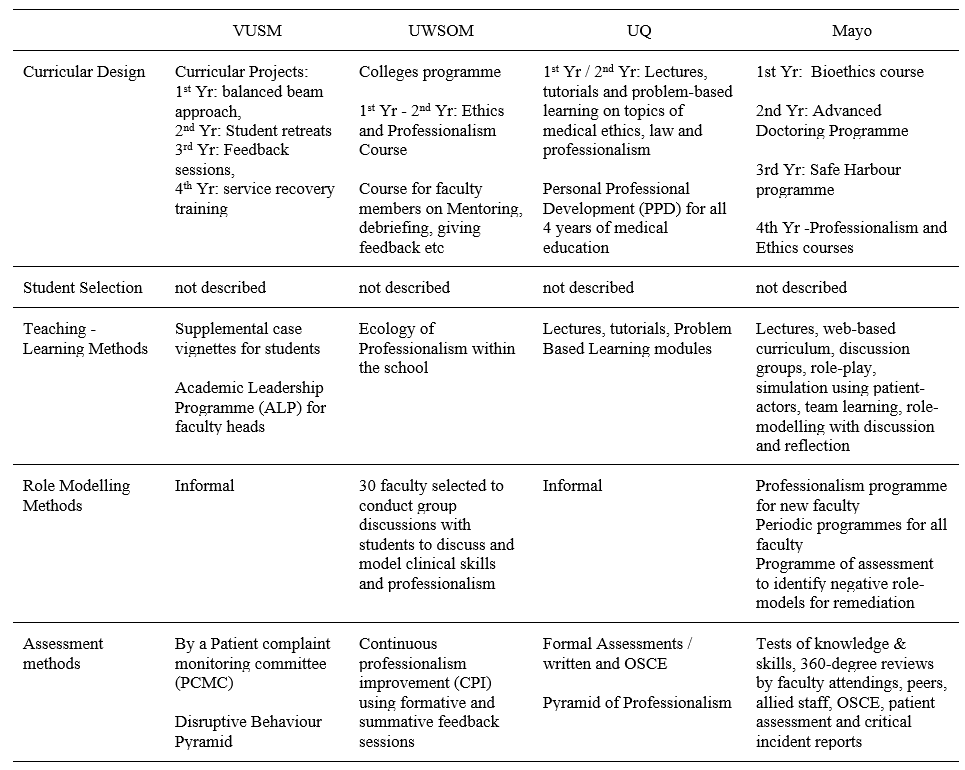
(Goldstein et al., 2006; Hickson et al., 2007; Mueller, 2009; Mueller, 2015; Parker et al., 2008)Table 1. Comparative Summary of Four Models of Educational Programme for Teaching Medical Professionalism
UQ focuses more on written tests and objective structured clinical examinations (OSCE) in the preclinical years. Because the school recognises that these assessment methods may not necessarily measure actual attitudes, the personal and professional development (PPD) process serves as a means directed towards identifying students with problems who are then referred to a committee for support and remediation (Parker et al., 2008).
Mayo has a more comprehensive assessment method by including a 360-degree review from faculty attendings, peers, allied staff and patients to complement the written tests and OSCE (Mueller, 2009).
3) Role modelling: On the area of role modelling, UWSOM has developed a formal programme to train select faculty members to promote role modelling as a means of teaching students. The programme to promote an “ecology of professionalism” within the institution is unique to UWSOM. This is the school’s way of making professionalism an institution-wide responsibility and yet maintains a “safe” educational environment for learning and improvement (Goldstein et al., 2006).
Mayo, on the other hand, has required all faculty and staff physicians to attend and successfully complete a series of modules on professionalism, physician-patient communication, self-awareness, and diversity. Maintaining the culture of professionalism in the Mayo Clinic is a result of a continuing process of allowing ethics and professionalism to be woven into the courses and clinical rotations (Mueller, 2009).
I. Professionalism in Medical Education in the Future
Much progress has been attained in the last decade when various models for incorporating professionalism in medical education have been disseminated in various journals. The Bioethics Core Curriculum introduced by the UNESCO also declared that bioethical principles and human rights must be taught early to medical students and that Medical Ethics, which is a branch of Bioethics, must be taught in all levels of education (United Nations Educational, Scientific and Cultural Organization, 2008).
The Medical Ethics Manual released by the World Medical Association (WMA) provided a basic and universally used curriculum for the teaching of medical ethics. The WMA curriculum includes professionalism as a key component needed for the inclusion of Medical Ethics and Human Rights as an obligatory course for medical schools worldwide (Williams, 2015).
It has been observed that professionalism taught through time-based training might not be sufficient to address the changing healthcare environment and new learners. For the current generation of learners, specialty training must now be aligned with global standards such as that of Accreditation Council for Graduate Medical Education (ACGME). The ACGME standards incorporates professionalism and system-based practice as core components of the curriculum that begins with acquisition of medical knowledge and clinical skills.
Moving forward to the future necessitates the development of methods of assessment of professionalism as a means to successfully teach these professional behaviours (Chay, 2019).
Another key step in the future includes the teaching of professionalism as part of health professions education. Future academic health centres will need more medical educators who can pursue further education and help foster an environment that supports educator development. This key step will help in the attainment of long-term goals and to adapt to the changes in medical education (Dickinson et al., 2020).
Providing doctors with professional models as they move from novice to expert in their professional career will be instrumental as a framework for education. One clear example is the professional identity model that incorporated leadership, followership and team-working roles A more rounded and mature professional identity eventually develops that would set these doctors as models of professionalism for other health workers (McKimm et al., 2017).
IV. CONCLUSION
The unresolved definition of medical professionalism has made the incorporation of programmes on professionalism quite challenging. Any programme that will be implemented must be well thought of and tailored to the needs of the institution and all stakeholders. Analysing unique contexts of the curricular programme will be the key to keep any programme on professionalism relevant and viable.
The fact is that there are few curricular models for the incorporation of medical professionalism into the medical curriculum. This process is not an easy task and needs a strong institutional commitment and resolve for it to be successfully implemented. The four models were amazing attempts to incorporate professionalism in medical education. No formal evaluation has been published concerning this. Based on the comparative analysis of the four models, certain aspects should be highlighted so that we could possibly learn from them:
1. The task of preparing a programme on medical professionalism would be more systematic if the institution starts with a working definition of professionalism. This was seen in Mayo where a well-described definition set the direction for planning, implementing and institutionalising professionalism.
2. The culture of professionalism needs to be articulated institutionally and incorporated in the institution’s vision, mission, goals and policies. Mayo’s declaration of its primary value that “the needs of the patient come first” sets the stage for an atmosphere that is conducive to serving with professionalism.
UWSOM also opened its door to a culture of professionalism by declaring an “ecology of professionalism”. However, its implementation may have been limited when the Colleges programme for the purpose of institutionalising professionalism was limited to thirty designated faculty and role models.
3. The professionalism programme must be woven in all levels of medical education from the pre-clinical to the clinical years. Just like any competency, acquiring the values and skills and putting it into practice requires constant learning and reinforcement throughout the years of education.
Mayo and VUSM have prepared programmes for all the four years of medical education. Both institutions have crafted programmes for the pre-clinical years and have provided teaching and learning activities such as lectures, problem-based learning, small group discussions and feedback. Mayo engaged their students in the clinical years in elective experiences in professionalism and ethics and a “professionalism portfolio” for all students. VUSM designed a programme for the clinical year that was limited to a service recovery training for the purpose of addressing actual patient complaints.
4. Role models are essential in teaching professionalism because they can greatly influence attitudes and behaviours. Unprofessional physician behaviours such as disrespect and abuse of medical personnel, and refusal to complete duties must be corrected. If left unchecked, the observing medical students may consider such behaviours as normal (Mueller, 2009). These are among the ill effects of a hidden curriculum that occurs when an institution lacks role models. For a programme on professionalism to be successful, the faculty physicians and the rest of the healthcare team and institution’s staff need to undergo professionalism programmes applicable to their needs and roles.
In the case of UWSOM, a group of 30 selected faculty underwent training while in Mayo, all faculty underwent a professionalism programme.
5. Based on the curricular models described, it appears that a nurturing environment is preferable over punitive actions. The development of all scopes of professionalism from the intrapersonal to interpersonal to societal professionalism requires constant discussion, feedback and remediation. Although repetitive unprofessional behaviours may have consequences, the medical trainee will need to go through the nurturing process in order to fully imbibe the heart and soul of a medical professional.
6. The ability to handle professionalism challenges follows a learning curve as well. The levels of difficulty of professionalism challenges are related to how much learning situations a student may have encountered. The goal is to move from novice to competent to proficient and hopefully to an expert level of handling professionalism challenges just like all other aspects of learning in medicine.
The ability of the future generation of physicians to serve society ultimately rests on how professionalism has been woven into the curriculum in medical education. How to incorporate professionalism will be a continuing challenge for all medical educators.
Note on Contributor
Dr. Maria Isabel M. Atienza, Professor, San Beda University College of Medicine, Philippines and Head, Institute of Pediatrics & Child Health, St. Luke’s Medical Center, Global City developed the methodological framework for the study and performed data collection and data analysis as part of her PhD research, and wrote and approved the manuscript.
Ethical Approval
This review article was not submitted for IRB/ethical approval.
Acknowledgement
The author would like to acknowledge the insightful suggestions of the Vice Dean of San Beda University College of Medicine: Dr Noel Atienza.
Funding
This review article did not receive any funding.
Declaration of Interest
There are no conflicts of interest to declare.
References
Chay, O. M. (2019). Transformation of medical education over the years – A personal view. The Asia Pacific Scholar, 4(1), 59-61. https://doi.org/10.29060/taps.2019-4-1/pv1076
Cruess, R. L., & Cruess, S. R. (2006). Teaching professionalism: General principles. Medical Teacher, 28(3), 205-208. https://doi.org/10.1080/01421590600643653
Dickinson, B. L., Chen, Z. X., & Haramati, A. (2020). Supporting medical science educators: A matter of self-esteem, identity, and promotion opportunities. The Asia Pacific Scholar, 5(3), 1-4. https://doi.org/10.29060/taps.2020-5-3/pv2164
Goldstein, E. A., Maestas, R. R., Fryer-Edwards, K., Wenrich, M. D., Oelschlager, A.-M. A., Baernstein, A., & Kimball, H. R. (2006). Professionalism in medical education: An institutional challenge. Academic Medicine, 81(10), 871-876. https://doi.org/10.1097/01.acm.0000238199.37217.68
Hickson, G. B., Pichert, J. W., Webb, L. E., & Gabbe, S. G. (2007). A complementary approach to promoting professionalism: Identifying, measuring, and addressing unprofessional behaviors. Academic Medicine, 82(11), 1040-1048. https://doi.org/10.1097/acm.0b013e3185761ee
Lynch, D. C., Surdyk, P. M., & Eiser, A. R. (2004). Assessing professionalism: A review of literature. Medical Teacher, 26(4), 366-373. https://doi.org/10.1080/01421590410001696434
McKimm, J., Vogan, C., & Mannion, H. (2017). Implicit leadership theories and followership informs understanding of doctors’ professional identity formation: A new model. The Asia Pacific Scholar, 2(2), 18-23. https://doi.org/10.29060/taps.2017-2-2/oa1022
Mueller, P. S. (2009). Incorporating professionalism into medical education: The Mayo clinic experience. The Keio Journal of Medicine, 58(3), 133-143. https://doi.org/10.2302/kjm.58.133
Mueller, P. S. (2015). Teaching and assessing professionalism in medical learners and practicing physicians. Ramban Maimonides Medical Journal, 6(2), e0011. https://doi.org/10.5041/rmmj.10195
O’Sullivan, H., van Mook, W., Fewtrell, R., & Wass, V. (2012). Integrating professionalism into the curriculum. Medical Teacher, 34(2), 155-157. https://doi.org/10/3109/0142159x.2011.595600
Parker, M., Luke, H., Zhang, J., Wilkinson, D., Peterson, R., & Ozolins, I. (2008). The pyramid of professionalism: Seven years of experience with an integrated program of teaching, developing, and assessing professionalism among medical students. Academic Medicine, 83(8), 733–741. https://doi.org/10.1097/acm.0b013e31817ec5e4
Passi, V., Doug, M., Peile, E., Thistlewaite, J., & Johnson, N. (2010). Developing medical professionalism in future doctors: A systematic review. International Journal of Medical Education, 1, 19-29. https://doi.org/10.5116/ijme.4bda.ca2a
United Nations Educational, Scientific and Cultural Organization. (2008). Bioethics core curriculum. Syllabus section 1: Ethics education programme. UNESCO. http://www.unesco-chair-bioethics.org/?mbt_book=bioethics-core-curriculum
Viggiano, T. R., Pawlina, W., Lindor, K. D., Olsen, K. D., & Cortese, D. A. (2007). Putting the needs of the patient first: Mayo clinic’s core value, institutional culture, and professionalism covenant. Academic Medicine, 82(11), 1089-93. https://doi.org/10.1097/acm.0b013e3181575dcd
Williams, J. R. (2015). Medical ethics manual (3rd ed.). World Medical Association. https://www.wma.net/what-we-do/education/medical-ethics-manual/
*Maria Isabel Maniego Atienza
San Beda University
College of Medicine,
Mendiola Street,
City of Manila,
Philippines 1005
Tel: 6329178668751
Email: mmatienza@sanbeda.edu.ph
Submitted: 23 July 2020
Accepted: 21 October 2020
Published online: 13 July, TAPS 2021, 6(3), 121-123
https://doi.org/10.29060/TAPS.2021-6-3/CS2361
Sandra E Carr, Katrine Nehyba & Bríd Phillips
Division of Health Professions Education, School of Allied Health, The University of Western Australia, Australia
I. INTRODUCTION
COVID-19 has caused a major disruption to medical education with many educators making rapid shifts to online teaching (Sandars et al., 2020). Many have had to make critical changes in their instructional delivery (Ferrel & Ryan, 2020; Perkins et al., 2020). These changes may have lasting effects on the shape of educational delivery impacting generations to come (Ferrel & Ryan, 2020). It is important to share these changes and innovations as “Students and educators can help document and analyse the effects of current changes to learn and apply new principles and practices to the future” (Rose, 2020, p. 2132). Our case study examined the transition of small group teaching from blended learning to an emergency remote teaching environment.
II. CONTEXT
At the University of Western Australia, medical students undertake a scholarly activity during the third and final years of their Doctor of Medicine that enables specialisations in research or coursework. Of these students, 27% (n=65) choose a specialisation in Medical Education and graduate having completed 75% of a graduate certificate in health professions education. The first unit, Principles of Teaching and Learning offers an introduction to educational theory, curriculum design, teaching and assessment with a focus on developing teaching skills in small and large group settings and applies blended learning strategies. The final assignment assesses small group teaching techniques and the application of peer assisted learning and feedback. This group assignment requires students to:
a. Develop, plan and deliver a face to face small group teaching activity.
b. Describe and assess the group work processes using an audio journal and group assessment rating.
c. Engage in Peer Observation of Teaching.
With the advent of COVID-19 a change in the assessment was required. The 65 students were informed that the group work would have to occur on line and the small group teaching activity would now be an online Video Presentation. Within the Blackboard learning management system, each group had access to a Discussion Board and a virtual meeting tool to support collaboration and teamwork. The marking rubric was not adjusted so the focus on application of small group teaching techniques remained. The video of the developed small group teaching activity was uploaded along with the audio journal and peer observation of teaching components of the assessment.
III. STUDENT EXPERIENCE
We undertook a thematic analysis of students’ audio journals and written responses to describe their experience in five broad themes (see Figure 1).
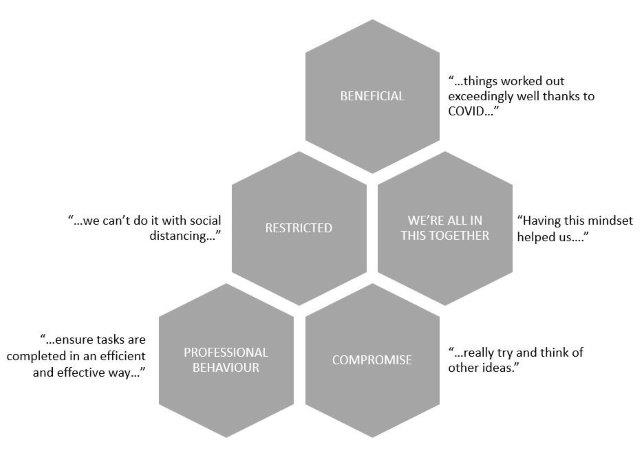
Figure 1. Student experiences of an online group assignment
Thirty percent of students reported aspects of working online as beneficial, and in some ways an improvement on face-to-face contact. For example, students who otherwise could have experienced difficulty meeting in person were able communicate and meet more easily:
“…we have already managed to organise our first meeting quite swiftly and with ease…”
(S1)
They also reported learning new skills:
“This group project taught me valuable skills when working in an online environment, including how to utilise and contribute in video meetings, share resources and regularly update the group…”
(S25)
“I have also learnt that filming or video is a great medium to communicate messages…once it is done, it can be a very effective tool.”
(S5)
However, not unexpectedly, some of the changes were seen as restrictions. The students talked of being “…banned from entering the hospital…” and of “…having no access…” to equipment or rooms, and “…we can’t do it with social distancing…” This led to feelings of disappointment and frustration, as they tried to find feasible options for the assignment.
“…all four of us were trying to actively brainstorm for an hour, trying to think of something…”
(S60)
“…we had fantastic plans…but unfortunately we didn’t have any of these options…”
(S25)
The perceived restrictions challenged the students’ persistence and adaptability (Ferrel & Ryan, 2020) and led them to compromise. One student, after their group changed their assignment idea from venepuncture to handwashing, said “…we…decided to try and make this idea work the best we could.” (S18). This adjustment and negotiation of ideas led to some innovative and varied submissions, using, for example, dolls; online role-plays; on-screen debate and custom virtual backgrounds.
Another theme that emerged was that of a shared experience, and a sense of we’re all in this together. The use of online communication platforms such as Zoom and Facebook Chat, and the use of shared documents meant that “…everyone could be involved, regardless…” There was evidence of a supportive environment and shared accountability, to ensure that they were “…giving everyone a chance…” and “…everyone seemed equally invested…”
Finally, despite the changes, restrictions and compromise, the students remained task-focussed and were able to plan, allocate, collaborate and communicate in their new online environment. The spread of grades for this assignment was consistent with previous cohorts, suggesting that the change in method was not detrimental to their performance. They were aware of potential dangers of working in this new, unknown way.
“…it will be important for us to be mindful of the risk of losing a professional mindset during our meetings, and divert away from the task at hand.”
(S1)
However, they described the same professional behaviours that would be expected in a face-to-face assignment, such as planning; delegation; effective communication; setting and meeting deadlines; and providing constructive feedback to other team members.
“…our team worked really well together. I suspect things worked out exceedingly well thanks to COVID and lockdown, which forced us to work online.”
(S8)
IV. CONCLUSION
Sklar states that during these unprecedented times “…it is important that our voices are loud about what we have experienced and learned” (Sklar, 2020, p. 9). In this case study we have described an experience of emergency remote teaching, in which a face-to-face small group teaching assignment was moved online. Our experience suggests that, even with its challenges, it was a success. Despite restrictions and compromise the students reported beneficial aspects to working online, and demonstrated a sense of comradery and professionalism while developing digital learning skills that are proving essential for learners and applicable for health professionals in the 21st century.
Notes on Contributors
Sandra Carr conceived the idea of the case study and contributed to the design of the work, gathered the qualitative data and interpretation of the findings. Katrine Nehyba contributed to the design of the case study, searched the supporting and relevant literature, undertook the thematic analysis of the data and constructed the Figure. Bríd Phillips contributed to the design of the work, searched the supporting and relevant literature to construct the rationale and introduction and contributed to the interpretation of the findings. All contributed to confirmation of the themes, the Discussion and Conclusion. All reviewed and contributed to each draft of the paper and approval the final submission.
Acknowledgement
This project was subject to ethical approval by the human ethics committee of the University of Western Australia. Consent was waived in line with the ethical approval obtained.
Funding
This work has not received any external funding.
Declaration of Interest
All authors declare that there are no conflicts of interest.
References
Ferrel, M., & Ryan, J. (2020). The Impact of COVID-19 on Medical Education. Curēus, 12(3), e7492–e7492. https://doi.org/10.7759/cureus.7492
Perkins, A., Kelly, S., Dumbleton, H., & Whitfield, S. (2020). Pandemic pupils: COVID-19 and the impact on student paramedics. Australasian Journal of Paramedicine, 17(1), 1-4. https://doi.org/10.33151/ajp.17.811
Rose, S. (2020). Medical student education in the time of COVID-19. Journal of the American Medical Association, 323(21), 2131–2132. https://doi.org/10.1001/jama.2020.5227
Sandars, J., Correia, R., Dankbaar, M., de Jong, P., Goh, P., Hege, I., Masters, K., Oh, S., Patel, R., Premkumar, K., Webb, A., & Pusic, M. (2020). Twelve tips for rapidly migrating to online learning during the COVID-19 pandemic. MedEdPublish, 9(1), 82. https://doi.org/10.15694/mep.2020.000082.1
Sklar, D. (2020). COVID-19: Lessons from the disaster that can improve health professions education. Academic Medicine, 95(11), 1631–1633. https://doi.org/10.1097/ACM.0000000000003547
*Sandra Carr
Division of Health Professions Education
The University of Western Australia
35 Stirling Hwy,
Crawley WA 6009, Australia
Tel: +61 64886892
Email: Sandra.carr@uwa.edu.au
Submitted: 20 July 2020
Accepted: 6 November 2020
Published online: 13 July, TAPS 2021, 6(3), 14-23
https://doi.org/10.29060/TAPS.2021-6-3/RA2346
Claude Jeffrey Renaud1, Zhi Xiong Chen2,6, Heng-Wai Yuen3, Lay Ling Tan4, Terry Ling Te Pan5 & Dujeepa D. Samarasekera6
1Department of Medicine, Khoo Teck Puat Hospital, Singapore; 2Department of Physiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 3Department of Otorhinolaryngology-Head & Neck Surgery, Changi General Hospital, Singapore; 4Department of Psychological Medicine, Changi General Hospital, Singapore; 5Department of Anaesthesiology, National University Health System, Singapore; 6Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: The Coronavirus-19 pandemic has had profound effects on health professions education (HPE) posing serious challenges to the continued provision and implementation of undergraduate, postgraduate and continuing medical education (CME). Across these HPE domains, the major disruptions included the exclusion of undergraduate learners from clinical learning environments, restricted intra-, inter-institutional and overseas movement of medical professionals, termination of face-to-face learner-educator interactions, deployment of postgraduate learners into non-scope service settings, and CME postponement.
Methods: In this review we report on how in Singapore various adaptive measures were instituted across the 3 HPE domains at institutional and national level to maintain adequate resources at the frontline to meet service exigencies, promote healthcare professionals’ wellbeing and safety as well as mitigate the spread of the pandemic.
Results: We identified several strategies and contingencies developed to address these challenges. These involved the use of online learning platforms, distributed and asynchronous learning, an undergraduate Pathway Programme, and use of innovative hands-on technology like simulation. Robust, well pre-planned pandemic preparedness, effective communication, as well as provision of psychological support resources ensured maintenance of service and academic continuity, trust and resilience within HPE. However, several challenges remain, namely the timing and manner of conducting formative and summative assessments, cybersecurity, and the indispensable hands-on, in-person experiential learning for surgical training.
Conclusion: Strong leadership with vision and planning, good communication, prioritising learners’ and educators’ wellbeing and safety, and harnessing existing and emerging online learning technologies are crucial elements for effective contingencies for HPE disruption during pandemics.
Keywords: Pandemic Preparedness, COVID-19, Curriculum Development, Online Learning and Assessment, Learner Wellbeing and Safety, Health Profession Education
Practice Highlights
- COVID-19 pandemic has caused profound disruption to medical education and Singapore is no exception.
- Health professions education community (undergraduate, residency and continuous professional development) had to rethink traditional learning approaches.
- There is a need for contingencies that integrate service and academic continuity and safety.
- Implementing contingencies requires coordinated national and institutional pandemic pre-preparedness.
- There remain uncertainties as to the long-term effectiveness of these contingencies on learning.
I. INTRODUCTION
Singapore had its first case of Coronavirus 19 (COVID-19) on 23rd January 2020 and scaled up its response from DORSCON (Disease Outbreak Response System Condition) Yellow to Orange 2 weeks later as the crisis evolved to pandemic proportion (Ashokka et al., 2020; J.E.L. Wong et al., 2020). This involved setting up a suite of strategies aimed at containing community transmission (Lee et al., 2020).
At the healthcare service and health profession education (HPE) level, these strategies centred on mobilising adequate resources at the frontline, mandating use of personal protective equipment (PPE) in high-risk areas and restricting healthcare workers’ movement (Ashokka et al., 2020; Lee et al., 2020; Liang et al., 2020; C. Wong et al., 2020; J.E.L. Wong et al., 2020). In addition, undergraduate medical education put a stop to clinical clerkships and large and small on-campus learning and restructured formative and summative assessments.
As the very stakeholders and resources required for HPE were diverted to fighting the pandemic, HPE faced extraordinary disruption. Educators and learners had to delicately balance service continuity, patients’ and learners’ wellbeing and safety versus maintaining a business-as-usual approach to learning. Moreso, the entire HPE community had to critically relook at the applicability of competency-based learning which is traditionally predicated on the principles of authentic supervised patient experience, programmatic assessment, learners as part of a community of practice and continuous professional development (CPD) (Harris et al., 2010; Iobst et al., 2010).
Previous public health emergencies like Severe Acute Respiratory Syndrome (SARS) have taught that such disruptions can provide unique opportunities for contingency planning in HPE especially when there is little time for wholesale programme redesign (Lim et al., 2009; Patil & Yan, 2003). This report thus describes the experience of 3 HPE domains in Singapore in mitigating the dissonance between optimal pandemic preparedness, unconstrained academic continuity and learners’ and educators’ well-being.
II. METHODS
A comprehensive review of the adaptive contingency strategies adopted at 1 undergraduate (Yong Loo Lin School of Medicine), Singapore residency programmes and across the CPD was made by looking at institutional and governmental programmes during the early phase of the pandemic and prevalent COVID-19 related literature on HPE. As this research is a description of events that have already happened and did not involve HPE stakeholders’ directly and interventionally, participants’ informed consent and internal review board approval were not required for its conduct.
III. RESULTS
Herein, is a detailed outline of the contingencies implemented across the 3 HPE domains which are also summarised in Table 1.
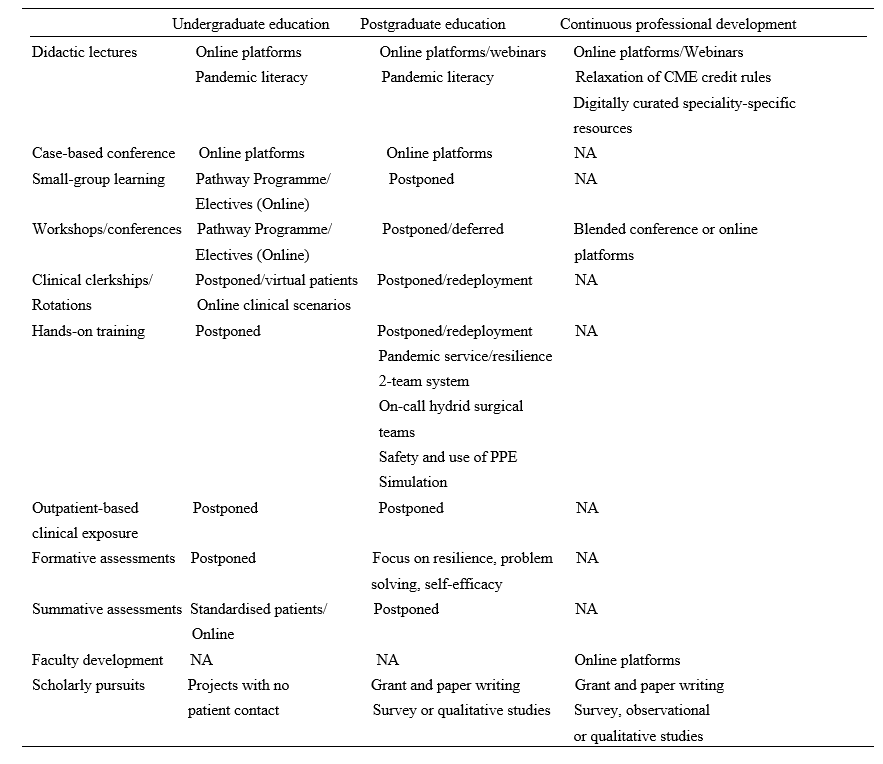
Table 1. Summary of disruptions and contingences across the health profession education spectrum during COVID-19 pandemic in Singapore.
Note: NA=not applicable; PPE= personal protective equipment
A. Contingencies in Undergraduate Medical Education: Experience of Yong Loo Lin School of Medicine
At the Yong Loo Lin School of Medicine which is the largest of the three medical schools in Singapore, the Education Team led by the Vice Dean (Education) started preparing in February 2020 for the possibility of loss of clinical teaching. Those most affected would be Phase 3 and 4 (Year 3 and 4) medical students. Phase 5 (Year 5) students were preparing for their Final Professional Examinations even though assessment was significantly disrupted across all Phases. Phase 1 and 2 (Year 1 and 2) students have relatively less clinical learning exposure and assessments, and were finishing their curricula and preparing for exams. Focusing on the Phase 3 and 4 students, first, their vacation and elective periods were brought forward respectively. Next, to give students meaningful learning opportunities that do not require patient contact, the Pathway Programme which had been launched before the pandemic was paced up (National University Singapore, Yong Yoo Lin School of Medicine, 2020).
The Pathway Programme consists of six Pathways. They are Health and Humanity, Health Informatics, Inquiry and Thinking, Medical Education and Medical Innovation and Entrepreneurship all led by a team of trained educationists. In addition, a non-Pathway initiative called Education Innovation completed the suite of new education offerings for the students. The sixth Pathway Behavioural and Implementation Science was partially offered under Inquiry and Thinking through a series of lectures on Health Economics. Below we describe what each Pathway is about.
1) Behavioral and implementation science: This pathway exposes medical students to principles of behavioural and implementation science, and applies this knowledge to effectively design and deliver healthcare in real-world settings, and lays the foundation for them to become active agents of change in clinical practice.
2) Health and humanity: This pathway aims to nurture emotionally resilient, socially conscious and globally minded health leaders through rekindling one’s love for medicine and humanity. Through experiential activities, inspirational workshops and hands-on project work in the community, students develop critical thinking skills in global health, teamwork and leadership skills to inspire health for all.
3) Health informatics: This pathway aims to enable students to gather and critically evaluate research and health informatics data, equipping them with the skills necessary to apply the principles of health informatics, summarise and visualise datasets to perform basic analyses, so they become data-science competent clinicians who can identify and analyse medical data to address clinical issues.
4) Inquiry and thinking: This pathway aims to inspire and motivate our medical students to develop a sense of curiosity so as to foster a habit of inquiry that is able to dynamically utilise a range of thinking methods, processes and skillsets to tackle questions and problems. The end goal of this pathway is to groom a pipeline of thinking doctors who can advance healthcare in any aspect they desire.
5) Medical education: This pathway exposes medical students to concepts and principles in HPE, to equip them with foundational skills in HPE, with a focus on educational innovation and scholarship of teaching and learning, so as to groom future clinical educators.
6) Medical innovation and entrepreneurship: This pathway aims to nurture medical students with the 6Cs attributes: Curiosity, Creativity, Compassion, Collegiality, Collaboration, and Commercial Intelligence. The programme gradually exposes medical students to concepts and principles in innovation, and the selective elements equip students with foundational skills in innovation and entrepreneurship.
With the elective period brought forward, Phase 4 students were exposed to the Pathway Programme from early-March to early-May 2020 through two weeks of front-loading online lectures, followed by four to eight weeks of projects. Most Pathways followed the general structure with slight variations between them. For Phase 3 students, they enjoyed an early vacation before encountering a shortened Pathway Programme from early-April to early-May 2020, comprising of 2 weeks of front-loading online lectures and 2 weeks of projects, which students had the option of continuing into Phase 4.
Using Inquiry and Thinking Pathway as an example, topics of front-loading online lectures included ‘Complexity and Systems Thinking’, ‘Habits of Inquiry and Critical Thinking’ and ‘Evidence-based Medicine and Search Methods’. More than 80 projects were offered by prospective supervisors with more than 70 students getting involved in projects. Each student was guided in the project by the supervisor as well as engaged in a one to two-hour weekly reflection sessions with a separate mentor or the supervisor who doubled up as a mentor. Students were required to submit a weekly reflection write-up of 50 words or more. At the end of the Pathway Programme, students submitted a single slide of their projects for evaluation. Top two projects from each Pathway were selected to present and compete in a Grand Finale on 8 May 2020 before the School’s leadership, a panel of judges, their peers and overseas observers. The Grand Finale attracted over 200 participants. Single slides of all projects were compiled into an e-book to be shared with students and faculty members.
B. Postgraduate Training: Experience of Residency Programmes across Singapore Three Sponsoring Institutions (SIs)
Since SARS, Singapore has steadily been bolstering critical resource reserves and expertise in pandemic preparedness, culminating in the setup of the 330-bed purpose-built National Centre for Infectious Diseases (NCID) at the National Healthcare Group (NHG) Novena campus (Lee et al., 2020; Seah, 2020). Concurrently, postgraduate medical education underwent significant transformation with the adoption of Accreditation Council for Graduate Medical Education (ACGME) styled competency-based learning, culminating in the setup of three residency SIs of which NHG is one (Huggan et al., 2012; Khoo et al., 2014). Thus during the build-up to COVID-19 pandemic, NCID, residents and faculty at NHG 27 residency programmes formed the initial frontliners in managing the pandemic before being later joined by the other two SIs (C. Wong et al., 2020).
Care delivery and learning had to be restructured so that adequate manpower could be redeployed at screening centres, emergency departments, outbreak wards and critical care units. Frontline residents had to endure long and exhausting shifts wearing PPEs and prolonged time away from family, not to mention postponed leaves. Residents and faculty also had to be segregated into independent two-team system with phased two-weekly rotations to avoid manpower attrition and service disruption as a result of staff infection, quarantine or burnout. Elective surgeries, continuity clinics, grand rounds, face-to-face case conferences, cross-institutional elective rotations, in-person programme selection interviews as well as summative assessment had to be deferred. Postgraduate specialty conferences, courses and workshops, whether local or international, also had to be postponed or cancelled due to travel restrictions, further limiting opportunities for learning.
As a result of these changes several resourceful strategies were implemented to balance the palpable tensions between service, wellbeing and learning.
The first was maintaining open and transparent communication between institutional and academic leaders, faculty and residents so that the rationale for a pandemic-mode centralised command-control leadership model could be accepted. This allowed residents to grasp the real sense of urgency brought in by COVID-19, thus facilitating speedier buy-in and compliance to ever changing human resource and education policies. In addition, this strategy helped build up trust in the institutional support structure and contain the spread of parallel distracting infodemics, allowing residents to focus on service delivery, learning and well-being.
The second strategy was the promotion of residents’ physical and psychological safety and wellbeing. This entailed ensuring all residents had adequate orientation to the proper use of PPEs and could easily access them. Well-being and resilience support resources like in-person or anonymous virtual outreach psychological crisis intervention counselling and peer support through online debriefing and feedback were put in place across all hospitals under the three SIs. The ancillary effect was that residents felt their safety, their families’ and patients’ was valued and that there was fair and equitable work and rest allocation. Further, ACGME cancelled all accreditation and Clinical Learning Environment Review site visits and took steps to reframe and relax some accreditation criteria (Nasca, 2020). This went a long way in allaying residents’ anxieties regarding clinical progression.
The third strategy was leveraging existing online tools to maintain some element of learning continuity without the need to invest in significantly expensive technologies, curricular redesign or faculty re-development. Programmes transferred their core didactic lectures, journal clubs and case-based discussions onto distributed learning platforms such as Zoom, Go to meeting, Google meet or WebEx for synchronous learning. Access to Webinars had the added advantage of providing opportunities for asynchronous learning. Zoom teleconferencing in particular, remains the most popular due to its affordable subscription, large participant capacity and easier accessible collaborative interface and a breakout feature that enables mounting learning models like team-based learning.
Residents from surgical residency programmes who rely on direct-patient encounter and hands-on experience for learning were more significantly impacted. Importantly, because non-emergency visits to hospitals were halted, elective procedures and surgeries were postponed or cancelled and, the number of patients and learning opportunities was thus greatly reduced. This was further aggravated by the shift of many training institutions and teaching hospitals to pandemic service (Liang et al., 2020). In many instances, surgical residents were redeployed to frontline areas, like screening centres, which are beyond their usual scope of practice (C. Wong et al., 2020).
Curriculum development contingencies thus went beyond online didactic content dissemination to embrace enhanced distributed learning approaches like videos, podcasts, virtual reality and simulated learning (C. Wong et al., 2020). Some programmes improvised by forming on-call hybrid surgical teams, which allowed surgical residents some measure of hands-on exposure to generic emergency or semi-elective cases during on calls but not necessarily within the scope of their area of interest.
C. Contingencies for Continuous Professional Development (CPD)
The disruption brought on by closure of higher educational institutions, scaling down of healthcare organisations and travel restrictions, compelled educators and health care professionals to adapt and embrace curricular changes and transition to virtual learning and use of technology for simulated learning.
Continuing medical education (CME) and CPD are integral parts of the development of a healthcare professional in providing optimal clinical care for his/her patient. CME is aimed at maintaining or updating the requisite knowledge, skills, professional performance and relationships and crucially, is a requirement for maintenance of certification in the discipline or specialty of the healthcare profession (Davis et al., 2008). CPD on the other hand caters to a broader range of competencies that reflect the healthcare profession attitudes towards learning and learning needs (Filipe et al., 2018). Every specialty and governing medical body has its stipulated requirements. In Singapore, the Singapore Medical Council (SMC) states that all fully and conditionally registered doctors are required to meet the compulsory CME requirements of 50 core points for the qualifying period before their practising certificate can be renewed (Singapore Medical Council, 2020a). While most CME activities involve attendance at local, regional or international scientific meetings or conferences, self-study, review and authorship of articles are also considered core CME points. Most hospitals hold regular Grand Ward Rounds, journal clubs and peer review learning sessions at departmental and institutional levels, which also contribute towards core CME points.
However, with Singapore moving to DORSCON Orange, many of these learning activities were immediately suspended as staff scrambled to reorganise clinical services amidst the pandemic imperative for team separation and safe distancing. Thus, traditional face-to-face meetings were replaced by online meetings and webinars facilitated by virtual platforms mentioned previously. In tandem the SMC relaxed requirements for CME credits by allowing healthcare professionals to log in attendance to online sessions, including webinars (Singapore Medical Council, 2020b). There was also an increase in allocation of CME credits for self-study (e.g., reading of referenced journals listed in PubMed). COVID-19-related CME activities were also considered core points for all doctors (Singapore Medical Council, 2020b).
While, much of the recent global CME content has primarily focused on increasing understanding of COVID-19 and its infectious nature across various medical disciplines, there has been lesser emphasis on its medical and psychological impact to health. It has nonetheless enabled healthcare professionals to better provide optimal care for patients while adopting best available evidenced practice relating to all aspects of this rapidly contagious disease. Thus, online information dissemination has been at an unprecedented high with multiple local, regional and international webinars and resource websites being made readily accessible. Professional societies have also made available to their members regularly curated digital speciality-specific resources on best practices pertaining to COVID-19 management (Academy of Medicine Singapore, 2020).
In addition to CME, healthcare professionals have traditionally relied on annual live face-to-face local, regional and international scientific conferences, symposiums, and educational workshops to network as a learning community and keep abreast of domain-specific advances. With strict travel restrictions these have been cancelled, postponed or moved online as webinars, interactive content, forums and chats.
Some conference organisers decided to still proceed to issue notices of acceptance of abstract submissions as ‘proof’ of scholarly work or allowed online presentation. Other creative ways of continuing with international conferences have included a “blended conference” approach with a mix of face-to-face and online content to support those attending onsite and online (Nadarajah et al., 2020). With careful attention paid to safe distancing for onsite participants, such “blended conferences” provide the all-important human face-to-face interactions which online webinars and conferences, though functional in most parts, sorely lack. They also provide the best of both worlds and may indeed be the new normal in the foreseeable future as COVID-19 further changes the HPE landscape relating to international travel and social interaction.
Similarly, Singapore’s three medical school curriculum development centres rapidly transited in-person to virtual faculty development sessions. This allowed educators openly dispersed by social distancing and clinical exigencies to continue tapping on the best pedagogic practices, interact and engage in interprofessional learning.
IV. DISCUSSION
The COVID-19 pandemic disruptions have reinforced the need for agency and adaptation in HPE. We have shown that through well-coordinated, multisectoral efforts, solutions can be harnessed to minimise their negative impact on learning. However COVID-19, unlike other recent coronavirus epidemics like SARS and Middle East Respiratory Syndrome (MERS) seems a more formidable crisis (Jones, 2020; Peeri et al., 2020). It may not go away quickly without the advent of effective vaccines and sustained infection control measures. These contingencies are therefore aimed at promoting service and academic continuity, safety and resilience. Whilst they are useful blueprints for pandemic preparedness and responsiveness in the short term, they may not be applicable in all contexts or in a crisis of attrition. Further, they have their own strengths and limitations.
A major strength is institutional and academic leaders’ sense of long-term planning and commitment to educators’ and learners’ safety through effective communication, being visible and providing programme and system support. In a rapidly evolving disruptive environment, this is crucial, as stakeholders remain engaged and trusting without having to anguish over under-resourcing or abandonment. Recent publications have alluded to the social capital returns of such an “integrative resilience approach” that amplifies individual and system wellbeing and minimises burn-out and contagion (Neufeld & Malin, 2020; Samarasekera et al., 2020; Schwartz et al., 2020; Wald, 2020).
Another strength is the adoption of adaptive online technologies which not only ensures academic continuity but also allows a smooth and rapid quarantine and pandemic curriculum development. Large virtual communities of learners can thus be rapidly mobilised without fundamentally affecting content, quality and institutional bottom lines. Indeed, this may have had the unintended consequences of unprecedentedly boosting attendance rates in medical schools, residency programmes and CPD sessions. Online migration also facilitates quick and mass standardised training and deployment of untrained or returning retired healthcare professionals in general and critical care medicine, allowing healthcare institutions to boost capacity in those critical areas during pandemics (Brunner et al., 2020; Li et al., 2020). More so, these emergent technologies hold a lot of promise for post-pandemic medical education and replication of authentic patient experiences. It is envisioned that they can be interfaced onto learning management systems (LMS) and into areas like virtual patient consults, telemedicine, adaptive learning and extended reality or avatar-like high fidelity simulation (Goh & Sandars, 2020). They are also important as a source of asynchronous learning whereby learners who are too busy with clinical duties or for surgical residents when there is a lack of critical hands- on training (Tolu et al., 2020).
A third strength, is that such crisis can open unintended opportunities for learners to develop competencies outside the core curricular knowledge and procedural skills sphere. For instance, the mere exposure of undergraduate learners not directly involved in patient care to pandemic-related content, volunteering in contact tracing or public awareness centres or restructuring of learning experiences like the Pathway Programme can nurture professional identity, pandemic literacy and doctor-ready qualities like service prioritisation, altruism and resilience (Bauchner & Sharfstein, 2020; Rose, 2020; Stetson et al., 2020). Indeed, the Pathway Programme succeeded in meaningfully engaging medical students at a time when clinical teaching and clinical elective opportunities were frozen. It gave time for the medical school to work out a safe and calibrated approach to resume clinical training in consultation with the relevant government bodies. The fact that it was conceptualised pre-pandemic demonstrates an extraordinary sense of prescience by the academic leadership. The advent of COVID-19 served to accelerate its implementation. It thus not only helped undergraduate medical education to cope with the pandemic but enrich the medical curriculum by catering to the diverse strengths and interests of each learner in order to nurture future-ready doctors for a post-COVID world.
As to residents’ learning, negotiating challenging pandemic duty rosters, making personal choices and sacrifices, navigating processes like resource allocation and public health measures and being deployed into non-core areas, can be just-in-time learning platforms for more nuanced ACGME competencies like professionalism, interpersonal and communication skills, system-based practice and practice-based learning (Hall et al., 2020; Nasca, 2020; Schwartz et al., 2020; Tolu et al., 2020; C. Wong et al., 2020). For surgical residents, there is also an added learning and safety benefit when hitherto straightforward surgical procedures like tracheostomy suddenly come with a myriad of precautions, criteria, and protocols (Givi et al., 2020). Clinic and elective surgery postponement can provide ample opportunities for self-directed learning, exit exams preparation and scholarly pursuits like grant, research ventures and quality improvement projects writing (Schwartz et al., 2020; Tolu et al., 2020). Additionally, prioritisation of public health emergency response training across the HPE spectrum can render healthcare institutions better prepared at handling future pandemics and burn-out (Yang et al., 2020).
Nevertheless, these contingencies have a number of limitations. Namely, moving medical education from the bedside to the ‘web-side’ cannot replace the real patient-centred clinical experience and case-mix learners derive from ward rounds, grand rounds and continuity clinics. Even the Pathway Programme was not without its challenges. With Singapore entering into Circuit Breaker phase of DORSCON Orange on 3rd April 2020, some projects were disrupted as access and movement became more limited (Ministry of Health Singapore, 2020).
Secondly, the utility of online learning is very much predicated on the vagaries of internet penetration and connectivity which makes this approach not always transferable to all socio-economic contexts (Cecilio-Fernandes et al., 2020). More so, for surgical residents, online learning or high-fidelity simulation cannot substitute for in-person learning. The technical skills, haptic feedback, the realism of live surgery, the experiential and contextual learning of ‘being there’ in a surgical team, and the non-cognitive domain skills like collaboration and resilience can be hard to simulate. Reduced contact time between residents and faculty also impacts adversely on opportunities for mentoring, role modelling and supervision. There is also always a danger of breaching learning principles such as cognitive overload when online content design is outside the hands of curriculum developers and programme directors (Kachra & Ma, 2020). As to health professionals, most of these online CME resources represent rather an amalgam of available information that may not have been well curated and pre-approved by accreditation organisations for relevancy.
Thirdly, the contingencies fail to address the enormous challenges in conducting clinical workplace-based assessments, without compromising their validity, reliability, defensibility and educational impact. Although high-stakes OSCE can be successfully conducted in a pandemic environment, its implementation comes with tremendous logistical and political manoeuvring to ensure students’, examiners’ and patients’ safety and assessment integrity are preserved (Boursicot et al., 2020). Cancelling both formative and summative assessments can delay learners’ progression or completion unless adjustments are made to previously established competency criteria. Undergraduates may fail to graduate on time to join the vital pool of medical workforce and residents may not be able to practise as independent practitioners. This can create anxiety and concern to both learners and educators about how to catch up post-pandemic with piling assessment and case and portfolio backlogs.
Lastly, reliance on third party software entities for online content dissemination contrary to institution-designed LMS or whole-sale programme information technology infrastructure redesign carries cybersecurity, privacy and data ownership risks (Fawns et al., 2020; Sandars et al., 2020). Not all faculty are tech savvy to handle the technical intricacies and the many options in the market. Predatory providers may thus seek to peddle behaviourist tactics onto users for their own corporate gains.
V. CONCLUSION
In summary, the COVID-19 pandemic has been a major threat to HPE in Singapore but it has also created opportunities for adaptive and flexible contingencies so that learning goes on safely with minimum constraints. While there is a need to celebrate these early successes, it is also imperative that we assess and learn from their limitations so that we can further refine and more successfully, collaboratively and iteratively apply them in a prolonged crisis. Furthermore, these experiences can serve as templates for adaptive and value-added learning at both regional and international HPE settings beset by larger service and academic disruption. But most importantly they foreshadow the resilience, reimagining and resourcefulness that are expected of HPE as it transits from the new normal of pandemic crisis management to the post-pandemic next normal of innovative technology-based learning.
Notes on Contributors
Adj Associate Professor Claude J Renaud is a senior consultant nephrologist at Khoo Teck Puat hospital Singapre and Associate Programme Director at the National Healthcare Group Renal Residency Programme. He conceptualised, drafted and revised article and wrote introduction, postgraduate medical education (PGME), discussion and conclusion sections.
Dr Zhi Xiong Chen is a Senior Lecturer in Physiology and Assistant Dean for Education at Yong Loo Lin School of Medicine, National University of Singapore. He conceptualised article and wrote the undergraduate medical education section.
Adj Associate Professor Heng Wai Yuen is senior consultant in the Department of Otorhinolaryngology-Head & Neck Surgery, Changi General Hospital, Singapore and Campus Director, SingHealth Duke-NUS Institute for Medical Simulation (SIMS). He wrote abstract and post graduate medical education sections and revised article.
Adj Associate Professor Tan Lay Ling is senior consultant in the Department of Psychological Medicine, Psychogeriatric Service, at Changi General Hospital (CGH). She wrote the section on continuous professional development and revised article overall.
Dr Terry Ling Te Pan is a Senior Consultant, Department of Anaesthesia, National University Hospital and Advisor, Education Technology Unit, Yong Loo Lin School of Medicine, National University of Singapore. He co-wrote the section on continuous professional development and revised article overall.
Dr Dujeepa D. Samarasekera, director at Centre for Medical Education (CenMED) Yong Loo Lin School of Medicine, National University of Singapore. conceptualised and revised article.
Ethical Approval
This study is a description of events and practices and therefore did not require approval from institutional review boards.
Funding
There is no external funding involved in this study.
Declaration of Interest
Other than Dr Dujeepa D Samarasekera who is Editor of TAPS, all authors have no conflict of interest, including financial, consultant, institutional and other relationships that might lead to bias.
References
Academy of Medicine Singapore (AMS) (2020, June 2). Resource site on COVID-19. https://www.ams.edu.sg/policy-advocacy/covid-19-resource-page
Ashokka, B., Ong, S. Y., Tay, K. H., Loh, N. H. W., Gee, C. F., & Samarasekera, D. D. (2020). Coordinated responses of academic medical centres to pandemics: Sustaining medical education during COVID-19. Medical Teacher, 42(7), 717-720. https://doi.org/10.1080/0142159X.2020.1757634
Bauchner, H., & Sharfstein, J. (2020). A bold response to the COVID-19 pandemic: Medical students, national service, and public health. The Journal of the American Medical Association, 323(18), 1790-1791, https://doi.org/10.1001/jama.2020.6166
Boursicot, K., Kemp, S., Ong, T. H., Wijaya, L., Goh, S. H., Freeman, K., & Curran, I. (2020). Conducting a high-stakes OSCE in a COVID-19 environment. MedEdPublish, 9(1), 54. https://doi.org/10.15694/mep.2020.000054.1
Brunner, M., Vogelman, B., & Smith, J. (2020). Rapid development of an outpatient‐to‐inpatient crash curriculum for COVID providers. Medical Education. Advanced online publication. https://doi.org/10.1111/medu.14244
Cecilio-Fernandes, D., Parisi, M. C. R., Santos, T. M., & Sandars, J. (2020). The COVID-19 pandemic and the challenge of using technology for medical education in low and middle income countries. MedEdPublish, 9(1), 74. https://doi.org/10.15694/mep.2020.000074.1
Davis, N., Davis, D., & Bloch, R. (2008). Continuing medical education: AMEE education guide No 35. Medical Teacher, 30(7), 652–666. https://doi.org/10.1080/01421590802108323
Fawns, T., Jones, D., & Aitken, G. (2020). Challenging assumptions about “moving online” in response to COVID-19, and some practical advice. MedEdPublish, 9(1), 83. https://doi.org/10.15694/mep.2020.000083.1
Filipe, H. P., Golnik, K. C., & Mack, H. G. (2018). CPD? What happened to CME? CME and beyond. Medical Teacher, 40(9), 914–916. https://doi.org/10.1080/0142159X.2018.1471200
Givi, B., Schiff, B. A., Chinn, S. B., Clayburgh, D., Iyer, N. G., Jalisi, S., Moore, M. G., Nathan, C. A., Orloff, L. A., O’Neill, J. P., Parker, N., Zender, C., Morris, L., & Davies, L. (2020). Safety Recommendations for evaluation and surgery of the head and neck during the COVID-19 pandemic. The Journal of the American Medical Association Otolaryngology-Head & Neck Surgery, 146(6),579-584. https://doi:10.1001/jamaoto.2020.0780
Goh, P. S., & Sandars, J. (2020). A vision of the use of technology in medical education after the COVID-19 pandemic. MedEdPublish, 9(1), 49. https://doi.org/10.15694/mep.2020.000049.1
Hall, A. K., Nousiainen, M. T., Campisi, P., Dagnone, J. D., Frank, J. R., Kroeker, K. I., Brzezina, S., Purdy, E., & Oswald, A. (2020). Training disrupted: Practical tips for supporting competency-based medical education during the COVID-19 pandemic. Medical Teacher, 42(7), 756-761. https://doi.org/10.1080/0142159X.2020.1766669
Harris, P., Snell, L., Talbot, M., & Harden, R. M. (2010). Competency-based medical education: Implications for undergraduate programs. Medical Teacher, 32(8), 646–650. https://doi.org/10.3109/0142159X.2010.500703
Huggan, P. J., Samarasekara, D. D., Archuleta, S., Khoo, S. M., Sim, J. H. J., Sin, C. S. P., & Ooi, S. B. S. (2012). The successful, rapid transition to a new model of graduate medical education in Singapore: Academic Medicine, 87(9), 1268–1273. https://doi.org/10.1097/ACM.0b013e3182621aec
Iobst, W. F., Sherbino, J., Cate, O. T., Richardson, D. L., Dath, D., Swing, S. R., Harris, P., Mungroo, R., Holmboe, E. S., & Frank, J. R. (2010). Competency-based medical education in postgraduate medical education. Medical Teacher, 32(8), 651–656. https://doi.org/10.3109/0142159X.2010.500709
Jones, D. S. (2020). History in a crisis—Lessons for Covid-19. New England Journal of Medicine, 382(18), 1681–1683. https://doi.org/10.1056/NEJMp2004361
Kachra, R., & Ma, I. W. Y. (2020). Practical tips for faculty development workforce training under pressure in the time of COVID-19 pandemic. MedEdPublish, 9(1), 81. https://doi.org/10.15694/mep.2020.000081.1
Khoo, S. M., Lahiri, M., Huggan, P. J., Archuleta, S., Olszyna, D. P., Goh, W. P., Chua, S. W., & Ho, K. Y. (2014). When traditional model meets competencies in Singapore: Beyond conflict resolution. Annals of the Academy of Medicine Singapore, 43, 544–549.
Lee, V. J., Chiew, C. J., & Khong, W. X. (2020). Interrupting transmission of COVID-19: Lessons from containment efforts in Singapore. Journal of Travel Medicine, 27(3), 1-5. https://doi.org/10.1093/jtm/taaa039
Li, L., Xv, Q., & Yan, J. (2020). COVID-19: The need for continuous medical education and training. The Lancet Respiratory Medicine, 8(4), e23. https://doi.org/10.1016/S2213-2600(20)30125-9
Liang, Z. C., Ooi, S. B. S., & Wang, W. (2020). Pandemics and their impact on medical training: Lessons from Singapore. Academic Medicine, 95(9), 1359-1361. https://doi.org/10.1097/ACM.0000000000003441
Lim, E. C., Oh, V. M., Koh, D. R., & Seet, R. C. (2009). The challenges of “continuing medical education” in a pandemic era. Annals of the Academy of Medicine, Singapore, 38(8), 724–726.
Ministry of Health Singapore. (2020, June 1). Circuit breaker to minimise further spread of COVID-19. https://www.moh.gov.sg/news-highlights/details/circuit-breaker-to-minimise-further-spread-of-covid-19
Nadarajah, V. D., Er, H. M., & Lilley, P. (2020). Turning around a medical education conference: Ottawa 2020 in the time of COVID‐19. Medical Education, 54(8), 760-67. https://doi.org/10.1111/medu.14197
Nasca, T. J. (2020). ACGME’s early adaptation to the COVID-19 pandemic: Principles and lessons learned. Journal of Graduate Medical Education, 12(3), 375-378. https://doi.org/10.4300/JGME-D-20-00302.1
National University of Singapore, Yong Yoo Lin School of Medicine. (2020, June 30). Curriculum structure and requirements. https://www.nus.edu.sg/nusbulletin/yong-loo-lin-school-of-medicine/undergraduate-education/degree-requirements/bachelor-of-medicine-and-bachelor-of-surgery-m-b-b-s/curriculum-structure-and-requirements
Neufeld, A., & Malin, G. (2020). Twelve tips to combat ill-being during the COVID-19 pandemic: A guide for health professionals & educators. MedEdPublish, 9(1), 70. https://doi.org/10.15694/mep.2020.000070.1
Patil, N. G., & Yan, Y. C. H. (2003). SARS and its effect on medical education in Hong Kong. Medical Education, 37(12), 1127–1128. https://doi.org/10.1046/j.1365-2923.2003.01723.x
Peeri, N. C., Shrestha, N., Rahman, M. S., Zaki, R., Tan, Z., Bibi, S., Baghbanzadeh, M., Aghamohammadi, N., Zhang, W., & Haque, U. (2020). The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? International Journal of Epidemiolology, 49(3), 717-720. https://doi.org/10.1093/ije/dyaa033
Rose, S. (2020). Medical student education in the time of COVID-19. The Journal of the American Medical Association, 323(21), 2131-2132. https://doi.org/10.1001/jama.2020.5227
Samarasekera, D. D., Goh, D., & Lau, T. C. (2020). Medical school approach to manage the current COVID-19 crisis. Academic Medicine: Journal of the Association of American Medical Colleges, 95(8), 1126–1127. https://doi.org/10.1097/ACM.0000000000003425
Sandars, J., Correia, R., Dankbaar, M., de Jong, P., Goh, P. S., Hege, I., Masters, K., Oh, S.-Y., Patel, R., Premkumar, K., Webb, A., & Pusic, M. (2020). Twelve tips for rapidly migrating to online learning during the COVID-19 pandemic. MedEdPublish, 9(1), 82. https://doi.org/10.15694/mep.2020.000082.1
Schwartz, A. M., Wilson, J. M., Boden, S. D., Moore, T. J., Bradbury, T. L., & Fletcher, N. D. (2020). Managing resident workforce and education during the COVID-19 pandemic: Evolving strategies and lessons learned. Journal of Bone & Joint Surgery Open Access, 5(2), 1-5. https://doi.org/10.2106/JBJS.OA.20.00045
Seah, I. (2020). Striving as a nation to become an academic leader in the COVID-19 crisis. Singapore Medical Journal, 61(7), 370-372. https://doi.org/10.11622/smedj.2020059
Singapore Medical Council (2020a, May 29). Continuing medical education (CME) for doctors. https://www.healthprofessionals.gov.sg/smc/continuing-medical-education-(cme)-for-doctors
Singapore Medical Council (SMC) (2020b, May 29). Fulfilling continuing medical education (CME) requirements via online platforms. https://www.healthprofessionals.gov.sg/docs/librariesprovider2/continuing-medical-education-(cme)-for-doctors/circular—fulfilling-cme-requirements-via-online-platforms.pdf
Stetson, G. V., Kryzhanovskaya, I. V., Lomen‐Hoerth, C., & Hauer, K. E. (2020). Professional identity formation in disorienting times. Medical Education, 54(8), 765-766. https://doi.org/10.1111/medu.14202
Tolu, L. B., Feyissa, G. T., Ezeh, A., & Gudu, W. (2020). Managing Resident Workforce and residency training during COVID-19 pandemic: Scoping review of adaptive approaches. Advances in Medical Education and Practice, 11, 527–535. https://doi.org/10.3171/2020.4.JNS201012
Wald, H. S. (2020). Optimizing resilience and wellbeing for healthcare professions trainees and healthcare professionals during public health crises—Practical tips for an ‘integrative resilience’ approach. Medical Teacher, 42(7), 744-755. https://doi.org/10.1080/0142159X.2020.1768230
Wong, C., Tay, W., Hap, X., & Chia, F. (2020). Love in the time of coronavirus: Training and service during COVID-19. Singapore Medical Journal, 61(7), 384-386. https://doi.org/10.11622/smedj.2020053
Wong, J. E. L., Leo, Y. S., & Tan, C. C. (2020). COVID-19 in Singapore—current experience: Critical global issues that require attention and action. The Journal of the American Medical Association, 323(13), 1243. https://doi.org/10.1001/jama.2020.2467
Yang, D.-Y., Cheng, S.-Y., Wang, S.-Z., Wang, J.-S., Kuang, M., Wang, T.-H., & Xiao, H.-P. (2020). Preparedness of medical education in China: Lessons from the COVID-19 outbreak. Medical Teacher, 42(7), 787-790. https://doi.org/10.1080/0142159X.2020.1770713
*Claude J Renaud
Department of Medicine,
Division of Renal Medicine,
Khoo Teck Puat Hospital,
90 Yishun Central, Singapore 768828
Email: jeffrey.renaud@ktph.com.sg
Submitted: 16 July 2020
Accepted: 12 August 2020
Published online: 13 July, TAPS 2021, 6(3), 124-127
https://doi.org/10.29060/TAPS.2021-6-3/CS2344
Kirsty J Freeman, Weiren Wilson Xin & Claire Ann Canning
Office of Education, Duke-NUS Medical School, Singapore
I. INTRODUCTION
The Duke-NUS Medical School Simulated Patient programme is instrumental in the development of clinical and behavioural skills in the future medical workforce of Singapore. Starting with a group of 20 passionate individuals in 2007, the Simulated Patient programme currently engages over 100 individuals, of which 58% are Female, 42% are Male; with 46% over 50 years of age. Simulated Patients (SPs) are individuals who are trained to portray a real patient in order to simulate a set of symptoms or problems used for healthcare education, evaluation, and research (Lioce et al., 2020). The SPs are engaged across the curriculum and are specifically trained to provide realistic and convincing patient-centred encounters, as well as identify and give feedback on key elements of interpersonal and communication skills in face-to-face interactions for a unique educational experience.
Medical students at Duke-NUS engage with SPs from their first year, as they learn the fundamental skills of clinical practice (FOCP), the skill of history taking being one of the cornerstones of the programme. Keifenheim et al. (2015) define history taking as “a way of eliciting relevant personal, psychosocial and symptom information from a patient with the aim of obtaining information useful in formulating a diagnosis and providing medical care to the patient”. Several studies have reported on the impact of engaging SPs to teach history taking (Hulsman et al., 2009; Nestel & Kidd, 2003).
The COVID-19 pandemic dramatically impacted the delivery of on-campus education, requiring medical educators to adapt teaching methods to reflect governmental and institutional restrictions. Whilst journals have been expedient in their ability to publish the experience of educators and students during the COVID-19 pandemic, the experience of other stakeholders are lacking. This paper will describe the experience of simulated patients in adopting telesimulation during a pandemic.
II. ADOPTING TELESIMULATION DURING A PANDEMIC
McCoy et al. (2017) define telesimulation as “a process by which telecommunication and simulation resources are utilised to provide education, training, and/or assessment to learners at an off-site location” (McCoy et al., 2017, p. 133). With staff, students and SPs in numerous off-site locations (their own homes), the telecommunication platform adopted for this experience was Zoom. The main reason behind this was it was the platform of choice by the institution when face-to-face teaching was shifted to e-learning, therefore staff and students were familiar with the functionality. To effectively engage our simulation resources, i.e. our SPs, it was essential that we provide an orientation programme that would educate them on the use of telesimulation. Through an online training session, seen in Figure 1, the SPs were introduced to the rationale behind the adoption of telesimulation and the functionality of the Zoom platform. Topics such as how to use the video and audio effectively to build rapport during the interaction as well as functions such as moving between breakout rooms were covered. A telesimulation orientation manual was emailed to all SPs after the session, summarising the online training session, with step by step instructions and screenshot examples on how to use Zoom. See Figure 2 for summary of the orientation programme.

Figure 1. Simulated patient large group telesimulation training
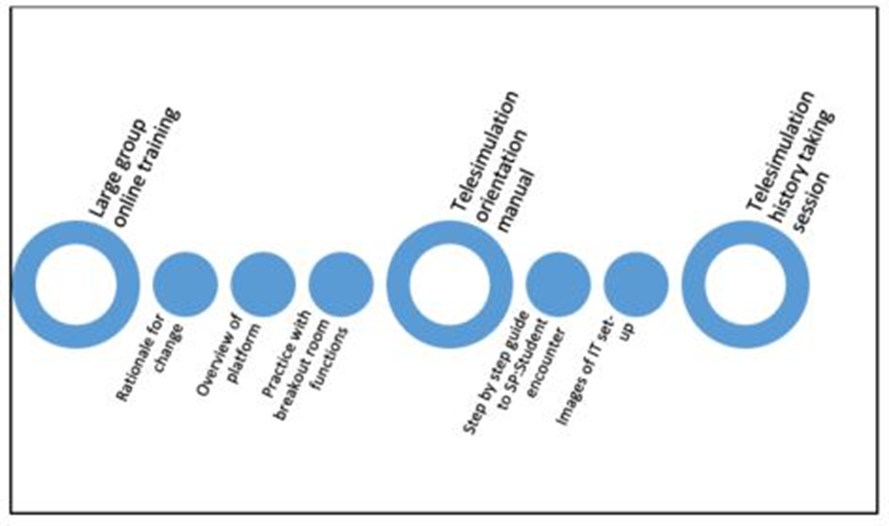
Figure 2. Summary of SP orientation to history taking telesimulation encounter
45 SPs participated in a series of tele-simulated history taking encounters for the class of 82 students. All SPs were invited to participate in a post tele-simulation history taking electronic questionnaire. Using a 5-point Likert scale SPs were asked to indicate their agreement on 13 items as seen in Table 1.
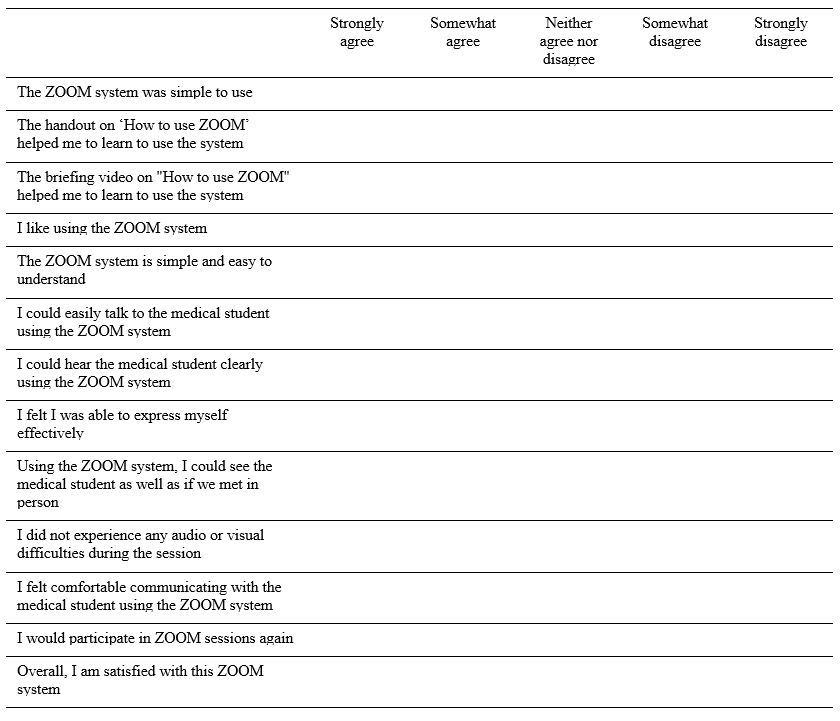
Table 1: Likert scale items form post-telesimulation evaluation questionnaire
III. THE SP EXPERIENCE
Of the 45 respondents 64% were male, 36% were female, with 93% stating that they had participated in previous face-to-face sessions with students. Aged between 21 and 71 years, half of the respondents were over 50. To participate in the telesimulation the majority of SPs (67%) utilised a laptop or desktop computer, with 71% reporting that they used a headset. 80% of the SPs had previous experience with video-based calls prior to this session.
Key to the history taking encounters is the ability to communicate clearly. While 11% of SPs did report some technical difficulties related to Wi-Fi connectivity, the majority of SPs (91%) could hear the student clearly and 89% felt they could express themselves effectively. 96% felt they could communicate easily with the student. On whether they could see the medical student as well as they would in a face-to-face interaction, responses were mixed, with SPs acknowledging that the limitations of the telesimulation experience is the non-verbal communication component of the interaction:
“Sometimes, the lighting is not good enough to see the expression on the student’s face”, and “I was not able to observe students’ body posture via zoom as such, I was unable to comment fully on students’ non-verbal communication skills”.
One of the themes that arose in the written feedback was that many SPs appreciated the travelling time saved by being off-site during the telesimulation:
“I used to take 45-60mins to arrive/return at/from a SP rehearsal/session. Now it only takes 15mins to be in the meeting – saves a lot of traveling time; and all is done in the comfort of my home :)”.
Whilst it was acknowledged that telesimulation could not replace the authenticity of face-to-face interactions, the SPs overwhelmingly rated the experience as extremely positive, noting that the online training session and handout helped in learning how to negotiate the online platform. An unexpected benefit that was shared was the sense of connection that the telesimulation experience provided the SPs during a time of lockdown, as they “got to see other SPs”. One respondent shared how they were able to integrate these new skills to maintain social connections:
“…even it has broadened my experience and now been using this app for communication with friends during this CB (circuit breaker)”.
IV. CONCLUSION
As the restrictions around face-to-face teaching due to COVID-19 continues to impact how health professional educators engage SPs in teaching and assessing, this paper demonstrates how to safely and effectively engage the SP workforce during a pandemic. By describing the experience of SPs in adopting telesimulation to teach history taking, we hope that fellow educators across the region can continue to engage SPs in their curriculum.
Notes on Contributors
Kirsty J Freeman is the main author, conceptualised, wrote and revised the manuscript based on comments and suggestions from the other authors. She contributed to the development and facilitation of the simulated patient telesimulation training programme, and conducted the data collection.
Xin Weiren Wilson developed and conducted the simulated patient telesimulation training programme, assisted with data collection, performed the data analysis, and developed the manuscript.
Claire Ann Canning assisted with data collection, and contributed to the conceptualisation of the manuscript, reviewed and revised drafts.
All the authors have read and approved the final manuscript.
Acknowledgements
We would like to thank all the simulated patients who took part in the telesimulation programme and were willing to share their experiences. We also wish to acknowledge the Clinical Faculty and Administrative Coordinators of the FOCP programme for adopting telesimulation into the programme.
Funding
This work has not received any external funding.
Declaration of Interest
All authors declare that there are no conflicts of interest.
References
Hulsman, R. L., Harmsen, A. B., & Fabriek, M. (2009). Reflective teaching of medical communication skills with DiViDU: Assessing the level of student reflection on recorded consultations with simulated patients. Patient Education and Counseling, 74(2), 142-149. https://doi.org/10.1016/j.pec.2008.10.009
Keifenheim, K., Teufel, M., Ip, J., Speiser, N., Leehr, E., Zipfel, S., & Herrmann-Werner, A. (2015). Teaching history taking to medical students: A systematic review. BMC Medical Education, 15(159), 1-12. https://doi.org/10.1186/s12909-015-0443-x
Lioce L., Lopreiato J., Downing D., Chang T.P., Robertson J.M., Anderson M., Diaz D.A., Spain A.E., & Terminology and Concepts Working Group (2020). Healthcare Simulation Dictionary (2nd Ed.). Agency for Healthcare Research and Quality. https://doi.org/10.23970/simulationv2
McCoy, C. E., Sayegh, J., Alrabah, R., & Yarris, L. M. (2017). Telesimulation: An innovative tool for health professions education. Academic Emergency Medicine Education and Training, 1(2), 132-136. https://doi.org/10.1002/aet2.10015
Nestel, D., & Kidd, J. (2003). Peer tutoring in patient-centred interviewing skills: Experience of a project for first-year students. Medical Teacher, 25(4), 398-403. https://doi.org/10.1080/0142159031000136752
*Kirsty J Freeman
Duke-NUS Medical School
8 College Rd,
Singapore 169857
Email: kirsty.freeman@duke-nus.edu.sg
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
