
LOTTE Transdisciplinary medical education promotes interprofessional collaboration and independent learning in medical undergraduates
Submitted: 2 June 2021
Accepted: 21 June 2021
Published online: 4 January, TAPS 2022, 7(1), 115-116
https://doi.org/10.29060/TAPS.2022-7-1/LE2546
Clement Luck Khng Chia1, Shaun Wen Yang Chan1, Priscilla Ng2 & Chee Chew Yip3
1Department of General Surgery, Khoo Teck Puat Hospital, Singapore; 2Department of Geriatrics, Khoo Teck Puat Hospital, Singapore; 3Department of Ophthalmology, Khoo Teck Puat Hospital, Singapore
Dear Editor,
Khoo Teck Puat Hospital held its first LOTTE (Learning Oriented Teaching in Transdisciplinary Education) elective program for Yong Loo Lin School of Medicine students in April 2021. The four-week program focuses on undergraduate medical education in an inter-professional collaborative setting through observation and presentation of complex clinical cases. Its teaching-learning activities are underpinned by the Learning Oriented Teaching (LOT) theory (ten Cate et al., 2004) to improve learning at the cognitive, affective and metacognitive levels with shared guidance between students and faculty.
At the cognitive level, students were encouraged to take ownership of learning, do literature review and present cases. Faculty critiqued and helped students to refine learning objectives and identify pertinent clinical aspects for elaboration and learning.
At the affective level, students were motivated to present cases on Zoom videoconferencing to classmates as they learned through active doing and attained peer recognition of their good effort. The teacher highlighted the importance of peer learning through discussing authentic, complex cases that required transdisciplinary holistic patient care.
At an interactive self and peer learning level, students used tools such as the Kahoot! game-based app for peer teaching to optimise learning and increase participation.
With a greying population, there is a need for transdisciplinary education to improve patient outcomes in the geriatric population (Chia et al., 2016). LOTTE provided an introduction to transdisciplinary education and highlighted importance of integrating competencies from various disciplines in preparation for future practice.
The first run of LOTTE consisted of seven transdisciplinary themes. An example of a transdisciplinary theme would be “Palliative Surgery” offered by both a palliative physician and an oncology surgeon. LOTTE differed from traditional “single discipline” electives as it emphasised inter-professional collaboration and collective learning involving the surgeon, physician and students. Students divided their time equally in both subspecialties, attending ward rounds, clinics, operating theatres and home visits. They encapsulated their learnings by presenting real-life complex cases via Zoom in the last week to their peers and faculty. Learning opportunities in two subspecialties were maximised with the student following through the patient journey from ‘Start to Finish’ (Chia et al., 2016).
Medical graduates face an increasingly complex healthcare landscape where management of co-morbidities may be beyond one’s expertise. LOTTE may be helpful to promote transdisciplinary collaboration for holistic management of complex geriatric patients and nurture the development of independent learning in medical undergraduates.
Notes on Contributors
Dr Clement Chia conceptualised and designed LOTTE framework, was a faculty in LOTTE and wrote the manuscript and approved the final version.
Dr Shaun Chan conceptualised and designed LOTTE framework, helped coordinate students, was a faculty in LOTTE and revised and approved the manuscript.
Dr Priscilla Ng conceptualised and designed LOTTE framework, was a faculty in LOTTE, revised and approved the manuscript.
A/Prof Yip Chee Chew conceptualised and designed LOTTE, revised and approved the manuscript.
Acknowledgement
We would like to thank all the transdisciplinary educators who made this inaugural run of LOTTE possible. They include A/Prof Tan Kok Yang, A/Prof Toh Hong Chuen, A/Prof Tavintharan Subramaniam, Dr Desmond Ooi, Dr Tan Mingyuan, Dr Tan Bo Chuan, Dr Ruth Chua, Dr Benjamin Lam, Dr Visnja Baksa Reynolds and Dr Gabriel Cher.
Funding
There is no funding for this study.
Declaration of Interest
Authors declare no conflict of interest.
References
ten Cate, O., Snell, L., Mann, K., & Vermunt, J. (2004). Orienting teaching toward the learning process. Academic Medicine, 79(3), 219-228. https://doi.org/10.1097/00001888-200403000-00005
Chia, C. L. K., Mantoo, S. K., & Tan, K. Y. (2016). ‘Start to finish trans-institutional transdisciplinary care’: A novel approach improves colorectal surgical results in frail elderly patients. Colorectal Disease, 18(1), O43–O50. https://doi.org/10.1111/codi.13166
*Clement Chia
Khoo Teck Puat Hospital,
90 Yishun Central,
Singapore 768828
Department of General Surgery
Tel: +6566022207
Email: chia.clement.lk@ktph.com.sg
Submitted: 28 May 2021
Accepted: 25 August 2021
Published online: 4 January, TAPS 2022, 7(1), 112-114
https://doi.org/10.29060/TAPS.2022-7-1/PV2544
Sok Ying Liaw & Siew Tiang Lau
Alice Lee Centre for Nursing Studies, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
I. BACKGROUND
The coronavirus disease 2019 (COVID-19) has been declared as a pandemic. On 7 February 2020, the Ministry of Health (MOH), announced the suspension of all clinical postings. All healthcare students were ordered to withdraw from hospitals within hours after the announcement. Graduating year nursing students from the National University of Singapore (NUS) were into their final phases of clinical postings. The suspension of clinical postings greatly disrupted the students’ preparations in developing clinical competencies critical to their future nursing professions.
Across the world, healthcare policymakers and institutions have responded to nursing students’ clinical education in a variety of ways. One compelling argument for continuing the clinical education of graduating nursing students is to treat them as part of the healthcare teams and leverage their clinical skills to boost the capacity of care teams. However, as our nursing students were at an earlier stage of their final year clinical practicum and have yet to acquire the knowledge, skills and clinical experience of a qualified nurse, it may be argued that their involvement in patient care delivery would have primarily been for educational purposes. Thus, the potential of compromising patient safety due to lack of supervision by the overwhelmed trained staff, the risks of contracting the contagion and giving rise to psychological concerns might not overweigh their educational benefits.
In Singapore, healthcare policymakers and institutions face the challenge of balancing education, healthcare service and potential risks for students in the healthcare settings. The main reasons for the suspension of clinical postings were the unknown risk of COVID-19 at that timepoint and the need for hospitals to manage their resources to transform their facilities and manpower to care for infectious patients. The suspension of clinical postings affected the nursing students’ abilities to fulfil the required number of clinical hours set out by the Singapore Nursing Board (SNB) to be registered as a registered nurse. Academic nurses at the NUS had to react quickly by employing simulation strategies to replace clinical hours. This gave rise to a debate around evidence-based practice versus practicalities in designing simulation as a substitute for clinical practice in nursing clinical education.
II. SIMULATION TO REPLACE CLINICAL PRACTICE HOURS
In light of the suspension of clinical placements, the SNB has permitted the substitution of 160 out of 400 clinical hours (40%) of the final year students’ clinical practicums with simulation. This can be supported by existing evidences on the use of simulation as a substitute for clinical placement in prelicensure nursing programmes (Curl et al., 2016). In our plan to replace 160 clinical hours, we initially assumed a ratio of one hour of simulation to one hour of clinical time. However, we recognised the challenges to implement this 1:1 ratio for the training of 300 nursing students using the existing simulation facilities, along with the need to adhere to the safe distancing measures initiated by the university. We had to plan a class size of not more than ten persons in a simulation laboratory, including a facilitator and a simulated patient, in order to keep everyone at a safe distance of at least two metres apart. Given these resource implications, we equated a ratio of one hour of simulation to two hours of clinical practice.
There is no clear evidence on the substitution ratio for simulation hours to clinical placement hours. A study by Curl et al., (2016) evaluated the use of simulation experiences to replace 50% of clinical experiences by employing a ratio of a substitute of one hour of simulation to two hours of clinical experience. Bogossian et al. (2019) postulated that as a simulation can be both controlled and time-compressed, it should draw more than parity in clinical practice hours, which is an aspect worth future investigation.
III. TYPES OF SIMULATION MODALITIES
We had to work out different types of simulation modalities to meet the 80 hours of simulation learning as well as to achieve the learning outcomes based on the SNB’s competency domains for registered nurses. The 80 hours also included the simulation-based assessment on clinical performance and post simulation activities on reflective writing to provide evidence to SNB on the achievement of learning outcomes. Earlier studies focused mainly on the use of high-fidelity simulations to replace clinical practices (Bogossian et al., 2019; Curl et al., 2016). The adequacy of existing simulation facilities and their accesses were constraints that led us to explore a variety of simulation modalities, including simulated clinical immersion using high-fidelity simulations, procedural simulations and computer-based simulations.
We adopted and expanded our earlier developed evidence-based simulation program, known as SIMulated Professional Learning Environment (SIMPLE) to create simulated clinical immersion learning and assessments in the NUS Centre for Healthcare Simulation. The availability of the SIMPLE guide, which included learning objectives, details of scenarios, debriefing guides and scripts for simulated patient, prompted our quick planning and implementation of the facilitators’ briefing and simulation learning. A total of six simulation sessions were implemented based on themes related to common ward nursing practices. In each simulation session, we incorporated two patients (one high-fidelity simulator and one simulated patient) in a simulated general ward setting. Our earlier study provided evidence on the benefits of the SIMPLE programme in promoting nursing students’ transition-to-practice experiences (Liaw et al., 2015). We also put in place a contingency plan on the use of video-based simulations in case we could not conduct face-to-face simulations. The video-based simulations were conducted via video conferencing for a small group of students who were unable to attend face-to-face simulations.
In the simulated clinical immersion scenarios, the students were required to perform a set of clinical procedures related to patient care. Thus, we incorporated procedural simulations to provide opportunities for the students to revise the procedures and practise the technical skills that they had acquired in years one and two. As a result of a lack of simulation facilities and faculty resources, the self-direct practice approach was adopted for procedure simulation learning. The students were given case scenarios and a set of requisites, including a wound dressing set, an intravenous priming set and an indwelling catheterization set, to practise the clinical procedures innovatively at home. They were also instructed to develop and submit video recordings of their best ten performed procedures, selected from a list of core skills for registered nurses, to provide evidence of their time (e.g. 20 hours) in engaging self-directed learning as well as for instructor feedback. Apart from procedural simulation learning, we managed to implement procedural simulation assessments on donning and doffing personal protection equipment (PPE) at remote locations by leveraging telecommunication resources using Zoom’s video conference calls. This approach enabled direct observations of performance and feedback between a student and an assessor.
Earlier, we developed two computer-based simulations, e-RAPIDS (Rescuing A Patient In Deteriorating Situation) and CREATIVE (Create Real-time Experience And Teamwork In Virtual Environment), to allow the students to participate in experiential learning. These were considered valuable resources for students’ off-site learning for the development of non-technical skills. Using experiential learning approach, the e-RAPIDS provided a self-directed learning resource for students to develop clinical reasoning skills through the application of knowledge to problem solve deteriorating virtual patients with feedback from multiple scenarios. The CREATIVE provided nursing students opportunities to undertake simulation-based interprofessional education with medical students on nurse-doctor communication skills training. We evaluated the effectiveness of these computer-based screen simulations on students’ learning outcomes performance by comparing with high-fidelity simulation in the previous studies (Liaw et al., 2014, 2020). The non-inferiority outcomes of these simulations to high-fidelity simulations may justify the use of these computer-based screen simulations to replace some clinical hours.
IV. CONCLUSION
The COVID-19 outbreak posed a unique challenge to nursing clinical education. The cessation of clinical placements led to immediate concerns on nursing students’ clinical competencies, which necessitated the adoption of various simulation resources as an alternative means of delivering clinical education. The inadequacy of existing simulation resources and their limited accessibilities posed challenges in the replacement of clinical hours. Nonetheless, this COVID-19 pandemic has prompted us to embrace more innovative simulation initiatives, including video-based simulations and tele-simulations. These innovations inevitably gave rise to a debate around evidence-based practice versus practicalities for designing simulation as a replacement for nursing clinical practice. More evidence is warranted to justify the use of different types of simulation modalities to replace clinical practices in terms of learning outcomes and cost-effectiveness. Such evidence can inform future implementations and policy development on the regulation of using simulations to replace clinical practices to ensure student competency for the nursing workforce. We look forward to seeing more simulation innovations along with evaluation research for simulation technology amid the COVID-19 pandemic.
Notes on Contributors
Sok Ying Liaw designed and implemented the simulation and took the lead in writing the manuscript.
Siew Tiang Lau contributed to the planning of the simulation and aided the development of the manuscript.
Acknowledgement
The authors would like to thank the faculty staff of Alice Lee Centre for Nursing Studies for supporting the implementation of simulation. The authors would like to thank the National University Health System, Research Support Unit, for providing editing services to this manuscript.
Funding
The authors have no funding to report.
Declaration of Interest
The authors have no conflict of interests to declare.
References
Bogossian, F. E., Cant, R. P., Ballard, E. L., Cooper, S. J., Levett-Jones, T. L., McKenna, L. G., Ng, L. C., & Seaton, P. C. (2019). Locating “gold standard” evidence for simulation as a substitute for clinical practice in prelicensure health professional education: A systematic review. Journal of Clinical Nursing, 28(21-22), 3759-3775. https://doi.org/10.1111/jocn.14965
Curl, E. D., Smith, S., Chisholm, L. A., McGee, L. A., & Das, K. (2016). Effectiveness of integrated simulation and clinical experiences compared to traditional clinical experiences for nursing. Nursing Education Perspectives, 37(2), 72-77. https://doi.org/10.5480/15-1647
Liaw, S. Y., Chan, S. W.-C., Chen, F.-G., Hooi, S. C., & Siau, C. (2014). Comparison of virtual patient simulation with mannequin-based simulation for improving clinical performances in assessing and managing clinical deterioration: Randomized controlled trial. Journal of Medical Internet Research, 16(9), e214. https://doi.org/10.2196/jmir.3322
Liaw, S. Y., Ooi, S. W., Rusli, K. D. B., Lau, T. C., Tam, W. W. S., & Chua, W. L. (2020). Nurse-physician communication team training in virtual reality versus live simulations: Randomized controlled trial on team communication and teamwork attitudes. Journal of Medical Internet Research, 22(4), e17279. https://doi.org/10.2196/17279
Liaw, S. Y., Palham, S., Chan, S. W.-C., Wong, L. F., & Lim, F. P. (2015). Using simulation learning through academic-practice partnership to promote transition to clinical practice: A qualitative evaluation. Journal of Advanced Nursing, 71(5), 1044-1054. https://doi.org/10.1111/jan.12585
*Sok Ying Liaw
Alice Lee Centre for Nursing Studies,
Yong Loo Lin School of Medicine,
National University of Singapore
Level 2, Clinical Research Centre, Block MD11
Singapore 117597
Email: nurliaw@nus.edu.sg
Submitted: 8 June 2021
Accepted: 11 August 2021
Published online: 4 January, TAPS 2022, 7(1), 109-111
https://doi.org/10.29060/TAPS.2022-7-1/PV2558
Jimmie Leppink
Hospital virtual Valdecilla, Spain
I. INTRODUCTION
Single case designs (SCDs) comprise repeated measurements (time series) of the same variables of interest (Van de Schoot & Miocevic, 2020) to understand changes in knowledge, skill, attitude or other constructs in a defined time period that includes one or more events or developments that may affect that change. Possible units of analysis include individuals (e.g., individual skill development), teams (e.g., team dynamics), or settings (e.g., situational-contextual change). Whether the outcome variables are quantitative (e.g., time-on-task), qualitative (e.g., changes in habits or preferences), or some combination of the two (e.g., test scores and transitions in practice strategy), a range of parametric and nonparametric statistical models are available for analysis at the level of N = 1, and the outcomes of multiple N = 1 analyses can be combined using multilevel and meta-analytic models (for reviews and examples, see: Leppink, 2020; Van de Schoot & Miocevic, 2020). This makes SCDs useful for any sample size and, contrary to traditional randomised controlled experiments and other group comparison studies, can help health professions education (HPE) researchers and practitioners to (1) Respect the dynamic nature of learning, (2) Use no more resources than needed, (3) Bridge the research-practice gap, and (4) Appreciate diversity and approach challenges in the sector accordingly. Each of these advantages is explained in the following.
II. RESPECT THE DYNAMIC NATURE OF LEARNING
Although learning by definition involves time, the vast majority of traditional randomised controlled experiments and other group comparison studies focus on performance at a single occasion or at best at two occasions. SCDs can incorporate quantitative and qualitative information to understand the longitudinal and non-linear nature of learning, effects of interventions or events, and possibly the temporal order of changes. For example, in a five-year medicine program in which we assess knowledge, skill and attitude every 3-4 months in each year of the program, we can monitor change in each of these variables and study possible temporal orders in changes at the level of the individual student as well as – through multilevel and meta-analytic models that combine individual outcomes – at the level of a larger group (e.g., changes in attitude tending to precede changes in knowledge, or the other way around). Although a commonly perceived limitation of SCDs is a lack of generalisability to larger populations, generalisability is not always of interest in our field (e.g., ‘what is the level of competence of this resident at this point?’, or ‘does this simulation session contribute to more effective communication in this team in this hospital?’), and where it is of interest (e.g., under which conditions can the use of virtual reality games help to improve communication skills?), it can be increased through replication studies from different settings the findings of which are combined in multilevel and meta-analytic models.
III. USE NO MORE RESOURCES THAN NEEDED
While traditional randomised controlled experiments and other group comparison studies with a limited number of measurements (usually one or two) often require more than 100 participants, SCDs – through their use of series of repeated measurements – allow researchers and practitioners to investigate educationally interesting phenomena with any number of individuals, teams or situations including one (i.e., N = 1). This is great for example for institutions that do not have large numbers of students or residents (e.g., eleven students or six residents) and do not pretend that the outcomes of their study can be generalised to all of the rest of the world, and is one of the reasons why in some clinical areas (Van de Schoot & Miocevic, 2020) and some areas in education (Leppink, 2020) SCDs have already been used successfully for a while. In addition, not using more resources than needed is always important and even more so in times of enormous pressure on healthcare systems across the world. To use an example from assessment practice, decisions about the progression of individuals or teams usually require longer exams when performance is borderline (i.e., almost at the expected level with minor lapses that would not cause concerns for patient outcomes) compared to where performance is good or poor. In this context, SCDs can help us determine when we have sufficient information about the knowledge (how many questions?), techniques (how many tasks?), skills (how many stations?) or attitudes (how many portfolio reflections?) of a specific individual or team being assessed in order to make informed and confident decisions.
IV. BRIDGE THE RESEARCH-PRACTICE GAP
Most group comparison studies include the unethical and often practically nonsensical action of withholding an educational intervention from some participants (control group), whereas in SCDs the question is not if but when that intervention takes place. Just like in a study on skydiving one would never include a ‘control’ condition in which participants are not allowed to open their parachute (the question should be when not if one should open that parachute), in an educational context in which the use of for instance virtual reality technology which allows students or residents to practice with complex anatomy structures in 3D is an inherent part of an anatomy training programme, including a condition in which no virtual reality technology is offered does not make sense. A more appropriate question in this context is when to use the virtual reality technology. On a related note, in complex domains such as medicine, we tend to move from simple to complex because more complex tasks require one to be able to complete a series of simpler tasks. Sticking with simple tasks only or moving from complex to simple does not make sense in this practice, and it is therefore pointless to design experiments which incorporate such conditions (i.e., a no-complex-tasks control group or a group in which we start with complex and end with simple). SCDs which introduce (more) complexity at different points in time for different participants or teams make more sense, and if that starting point is randomised for different participants, we speak of a single case experimental design (SCED; Van de Schoot & Miocevic, 2020); experimental because like in traditional experiments we have both manipulation (here: simple vs. more complex) and randomisation. SCEDs can facilitate causal inference, although where effects of several interventions are considered the complexity of the design as well as the number (generally a higher demand) and timing of measurements (sufficient measurements in each of several stages of the study) will require very careful thought. Finally, HPE is ultimately about contributing to the best possible healthcare, hence research questions on possible effects of training on future healthcare performance (e.g., are we delivering good doctors?) are key (Nickson et al., 2021; Prideaux, 2019), and the longitudinal character of SCDs allows us to study these questions.
V. APPRECIATE DIVERSITY AND ACT ACCORDINGLY
As eloquently formulated by Prideaux (2019), medical schools must “direct their activities to local priorities and to serving local health systems” (p. 25) and at the same time healthcare systems across the world share many challenges and can all benefit from solid theory on what works in which circumstances. SCD (or in experimental form called SCED) findings from different institutions or settings can be combined into meta-analyses (Van de Schoot & Miocevic, 2020) and systematic reviews, helping us to understand commonalities and diversity across institutions, to develop existing and new theory, and to approach sector challenges accordingly. Although where generalisability is of interest smaller samples tend to provide substantially less information than larger samples, many carefully performed smaller sample studies combined in meta-analyses and systematic reviews can make a more powerful and, in our field, much more useful end result than small numbers of larger sample studies. Besides, although the number of measurements needed depends on what we are measuring and not all models require large numbers of measurements (e.g., 10 measurements of the same individual for relatively simple conclusions about that individual), larger numbers of measurements – where that it is possible and makes sense in the context at hand – generally provide more information and allow for a study of more complex relations than smaller numbers of measurements.
VI. CONCLUSION
Nearly 17 years ago, Johnson and Onwuegbuzie (2004) published their immensely popular article “Mixed methods research: A research paradigm whose time has come”. SCDs allow researchers to adopt that mixed methods lens by integrating qualitative and quantitative information on complex phenomena such as learning and other types of development, to address the needs of educational and healthcare practice while using no more resources than what is needed (no more statistical power calculations for group experiments of more than 100 participants that include conditions that would never occur in educational practice), and to appreciate diversity (rather than to average where things should not be averaged). SCDs constitute a wonderful tool for research and practice in specific institutions as well as for multi-institution studies that are part of national or international collaborative projects. Recent years have resulted in parametric and nonparametric models for different types of data, which make SCDs useful regardless of the type of data we are considering. These questions and developments in combination make that the time for SCDs in HPE has come. Institutions and centres should be encouraged to use SCDs to answer local questions and serve local needs, and to document and publish findings arising from such SCDs so others can learn from these findings and design similar studies in their local contexts. Additionally, institutions and centres should consider the use of SCDs in multi-institution or multi-centre collaborations. Both ways can facilitate generalisability through meta-analysis and systematic review.
Note on Contributor
This manuscript has one author who wrote the full letter and meets all four criteria of authorship listed under International Committee of Medical Journal Editors (ICMJE); there were no other authors contributing to this letter.
Funding
No funds, grants or other support was received.
Declaration of Interest
No conflicts of interest are associated with this paper.
References
Johnson, R. B., & Onwuegbuzie, A. J. (2004). Mixed methods research: A research paradigm whose time has come. Educational Researcher, 33(7), 14-26. https://doi.org/10.3102/0013189X033007014
Leppink, J. (2020). The art of modelling the learning process: Uniting educational research and practice. Springer. https://doi.org/10.1007/978-3-030-21241-4
Nickson, C. P., Petrosoniak, A., Barwick, S., & Brazil, V. (2021). Translational simulation: From description to action. BMC Advances in Simulation, 6(6), 1-11. https://doi.org/10.1186/s41077-021-00160-6
Prideaux, D. (2019). The global-local tension in medical education: Turning ‘think global, act local’ on its head? Medical Education, 53(1), 25-31. https://doi.org/10.1111/medu.13630
Van de Schoot, R., & Miocevic, M. (2020). Small sample size solutions: A guide for applied researchers and practitioners. Routledge. https://doi.org/10.4324/9780429273872
*Jimmie Leppink
Avenida de Valdecilla,
s/n, 39008, Santander, Spain
Email: jleppink@hvvaldecilla.es
Submitted: 4 May 2021
Accepted: 22 July 2021
Published online: 4 January, TAPS 2022, 7(1), 106-108
https://doi.org/10.29060/TAPS.2022-7-1/PV2532
Shamalee Wasana Jayarathne1 & Lambert Schuwirth2
1Medical Education Unit, Faculty of Medicine and Allied Sciences, Rajarata University of Sri Lanka, Sri Lanka; 2Prideaux Centre for Research in Health Professions Education, Flinders University, Australia
Medical Professional Identity Formation (PIF) has been suggested as a fundamental outcome in medical education (Cruess et al., 2014). Medical professional identity is development of both personal and professional identity as a physician. PIF achieved in stages over time during which the characteristics, values, and norms of the medical profession are internalised, resulting in individual thinking, acting, and feeling like a physician (Cruess et al., 2014). It is basically not a process of learning to demonstrate professional behaviour but of change into a “professional being” or professional physician. Throughout the journey of PIF, moments of dissonance between personal values and professional values are likely to occur. So logically, there will be phases of learning and unlearning. Learning is generally well-defined, but unlearning has been conceptualised through different lenses both on the process of unlearning and the unlearnt content, leading to conflicting views.
Unlearning has been conceptualised through different lenses. Hislop et al. (2014) have described unlearning as “abandoning or giving up knowledge or behaviours without making any judgement on the status of the knowledge or behaviours being unlearned”. In addition, Macdonald (2002) has explained unlearning in terms of transformative unlearning, which is as a process of questioning, reflecting and giving up some core values, assumptions, knowledge and practices. On the other hand, some authors have given subjective value to unlearnt knowledge and practices. Srithika and Bhattacharyya (2009) have defined unlearning as a process that includes judging the knowledge, values or practices with current knowledge. If current knowledge is superior to previous knowledge, individuals do unlearn previous knowledge. In this background, we hypothesise unlearning to be a meta-cognitive process and not as a permanent loss of something. Instead, we recognise it as a person consciously discarding, abandoning, or giving up particular values, knowledge, or behaviour and consciously choosing not to continue using them; a meta-cognitive process.
Several authors have categorised unlearning in various ways, which leads to sometimes conflicting views on the characteristics of the process of unlearning. Rushmer and Davies (2004) have categorised unlearning into three categories namely, ‘fading’, ‘wiping’ and ‘deep unlearning’. Fading occurs due to lack of use and it occurs over time. Wiping is deliberate process, occurs due to external change or due to an experience. Wiping is a process in which unlearning of behaviours and complex social learning (beliefs, values, attitudes, assumptions, and interpersonal skills) happens. Deep unlearning was defined as a “sudden, unexpected, and potentially painful event that ruptures part of our way of being or deeply held understanding of the world” (Rushmer & Davies, 2004). They further explained that deep unlearning occurs in an unpredictable, disruptive way and it is less planned and less deliberate. It trigged by a sudden action or an event (Rushmer & Davies, 2004). Although, transformative unlearning is defined similar to the concept of deep unlearning, the characteristics of the process of unlearning are rather conflicting in deep unlearning and transformative unlearning. Transformative unlearning is conceptualised as a process of reflecting upon, questioning and giving up some values, assumptions and practices (Macdonald, 2002). This transformative unlearning process has three phases which are “receptiveness, recognition and grieving”. Hence, during this process a “person loses prior ways of seeing [which] until now had brought certainty and security”. However, this is a slow process.
There is a scarcity of empirical studies found in relation to individual unlearning process. One study in the UK explored health care managers’ engagement in unlearning and the impact of unlearning in decision making (Coombs et al., 2013). Authors distinguished two types of unlearning based on these health care managers’ experiences: “behavioural unlearning” and “cognitive unlearning”. Behavioural unlearning has similarities with wiping, whereas cognitive unlearning has similarities with deep unlearning. Behavioural unlearning is triggered by a deliberate process of change that had been externally imposed, while deep unlearning is triggered by questioning individuals’ basic assumptions due to an external event. Hence, the descriptions on characteristics of process of unlearning is conflicting in deep unlearning, transformative unlearning and cognitive unlearning and it is worth further exploration.
It is important to recognise the similarities and differences between to forgetting and unlearning. Some researchers tend to use unlearning and forgetting interchangeably (Rushmer & Davies, 2004). According to Rushmer and Davies (2004) fading occurs due to lack of use and it occurs over time. This is not an intentional action and it equals to forgetting. However, they have conceptualised fading under the concept of unlearning, which is questionable. Equally, several authors observed the contrasting nature of unlearning and forgetting. They distinguish the deliberate, conscious nature of unlearning (Coombs et al., 2013) from unintentional nature of forgetting. Our stance is that forgetting as loss of knowledge not necessarily planned or intended, which is distinct from unlearning.
Although there is conflicting conceptual literature, the concept of unlearning is worthwhile to explore; especially the different conceptual models of ‘transformative unlearning’ (Macdonald, 2002) ‘deep unlearning’ (Rushmer & Davies, 2004) and cognitive unlearning (Coombs et al., 2013) in relation to PIF in physicians. Unlearning is important in PIF process, because an inability to give up values, norms, practices when they no longer match the demand of one’s current perspectives inevitably leads to rigidity in thinking and lack of flexibility. It is plausible that individuals who enter into the career of medicine have their own personal values and assumptions or specific world views. But professional values of medicine are often a set of values defined by society and public. It is proven that, professional attributes are contextually depended. Physicians need to keep to these professional values based on the context in which they work. During the journey of PIF moments of dissonance between personal values and professional values are likely to occur. These can be struggling points for both medical students and physicians while they unlearn their worldviews and replace them by new or adapted ones. Also, there are still many unclear areas concerning PIF and unlearning. For instance, can individuals unlearn deep values and assumptions? would that process really entail deep unlearning or merely wiping? Why is this unlearning cognitively and emotionally challenging for some individuals? Exactly how does unlearning of deep values and assumptions of individuals occur during PIF of physicians is currently under-researched. Thus, understanding the process of professional identity formation in the light of unlearning of deep values and assumptions of individuals is important in medical education to support journey of PIF of physicians and medical students.
Notes on Contributors
YGSW Jayarathne, MBBS, PG Dip in MEd, MD in MEd is a Senior Lecturer in Medical Education and was involved the conceptual development, argument building, ethics application and the development of the manuscript.
Lambert Schuwirth, MBBS, MD, PhD, FANZHPE is a Professor of Medical Education and Director Prideaux Centre for Research in Health Professions Education, College of Medicine and Public Health, Flinders University and was involved the conceptual development, argument building and the development of the manuscript.
Acknowledgement
No acknowledgement is associated with this paper.
Funding
No funding sources are associated with this paper.
Declaration of Interest
There are no conflicts of interests related to the content presented in the paper.
References
Coombs, C. R., Hislop, D., Holland, J., Bosley, S. L. C., & Manful, E. (2013). Exploring types of individual unlearning by local health-care managers: An original empirical approach. Health Services and Delivery Research, 1(2), 1–146.
Cruess, R. L., Cruess, S. R., Boudreau, J. D., Snell, L., & Steinert, Y. (2014). Reframing medical education to support professional identity formation. Academic Medicine, 89(11), 1446-1451. https://doi.org/10.1097/ACM.0000000000000427
Hislop, D., Bosley, S., Coombs, C. R., & Holland, J. (2014). The process of individual unlearning: A neglected topic in an under-researched field. Management Learning, 45(5), 540-560. https://doi.org/10.1177/1350507613486423
Macdonald, G. (2002). Transformative unlearning: Safety, discernment and communities of learning. Nursing Inquiry, 9(3), 170-178. https://doi.org/10.1046/j.1440-1800.2002.00150.x
Rushmer, R., & Davies, H. T. (2004). Unlearning in health care. BMJ Quality and Safety, 13(Suppl 2), 10-15. https://doi.org/10.1136/qshc.2003.009506
Srithika, T. M., & Bhattacharyya, S. (2009). Facilitating organizational unlearning using appreciative inquiry as an intervention. Vikalpa, 34(4), 67-78. https://doi.org/10.1177/0256090920090406
*YG Shamalee Wasana Jayarathne
Medical Education Unit,
Faculty of Medicine and Allied Sciences,
Rajarata University of Sri Lanka
Email: wasana@med.rjt.ac.lk, wjayaratna@yahoo.com
Submitted: 21 April 2021
Accepted: 7 October 2021
Published online: 4 January, TAPS 2022, 7(1), 87-97
https://doi.org/10.29060/TAPS.2022-7-1/OA2519
Nisakorn Deesaen1, Kongpop Sutantikorn1, Punyanuch Phonngoenchai1, Sakchai Chaiyamahapruk2 & Patcharada Amatyakul3
1Faculty of Medicine, Naresuan University, Thailand; 2Department of Community Medicine, Faculty of Medicine, Naresuan University, Thailand; 3Department of Obstetrics and Gynaecology, Faculty of Medicine, Naresuan University, Thailand
Abstract
Introduction: Pelvic examination of patients in the department of obstetrics and gynaecology (Ob–Gyn) is an important skill for medical students. Because it involves a physical assessment of the patients’ genitalia, patients may refuse medical students to participate in the examination, affecting the medical students’ clinical skills.
Methods: This cross–sectional study was conducted at Naresuan University Hospital to determine the factors that influence the acceptance of medical student participation in the pelvic examinations. A total of 198 out–patients from the Ob–Gyn department were included. A Likert scale questionnaire was designed which featured topics on patients’ attitudes and circumstances related to medical student involvement in gynaecological procedures.
Results: The majority of outpatients (71.7%) accepted the participation of medical students in pelvic examinations. Patients with prior experiences in physical and pelvic examination by medical students had a significant impact on the patients’ acceptance (P–value<0.001). The patients’ impressions had an influence on the decision to accept students in pelvic exam participation. Approximately 40% of patients were concerned about the breach of confidentiality. However, most patients strongly agreed that allowing medical students to perform pelvic examination would benefit their medical education.
Conclusion: Most of the participants permitted medical students to participate in pelvic examinations and preferred that the medical instructor be the one to request permission. The patients’ impressions of medical students were crucial factors that significantly influence their decision whether to allow or deny them to participate in the procedure. Disclosure of confidentiality was found to be matters of concern to most patients.
Keywords: Pelvic Examination, Medical Students, Acceptance, Performance, Clinical Teaching
Practice Highlights
- Most of the patients consent to a medical student participating in a pelvic examination.
- Medical instructors should ask for patients’ permission.
- Confidentiality and privacy of patients are critical issues that must be addressed.
- Patients’ impressions and prior examination experiences by medical students influence patients’ decisions.
I. INTRODUCTION
Medical students should learn how to perform pelvic examinations on patients during clinical years. History taking, physical examination, and pelvic examination are taught during the fourth to sixth year of medical training in our curriculum. Pelvic examination is defined as the assessment of external genitalia, speculum examination of the vagina and cervix, bimanual palpation of the uterus, adnexa and sometimes rectovaginal examination. This procedure is used to screen for gynaecological diseases and cancers in asymptomatic women and to diagnose gynaecological diseases in symptomatic women. Pelvic examination differs from other physical examinations because it involves an inspection of the genitalia, which, according to studies, commonly causes anxiety, fear, embarrassment (10–80% of women), pain, and discomfort (11–60% of women) (Bloomfield et al., 2014). Some factors why patients feel uncomfortable during a physical examination by medical students are concerns about privacy, confidentiality, and embarrassment (Rizk et al., 2002). As a result, patients may refuse to allow medical students to participate in the pelvic examination, affecting the learning experience and clinical skills of medical students. Furthermore, factors related to age, race, religion, cross–cultural differences, marital status, and previous delivery may also influence the patients’ decision to allow medical students in conducting pelvic examination (Anfinan et al., 2014; McLean et al., 2010). Compared to other ethnic and religious groups, Muslim women had a higher rate of refusing medical students, particularly male students (Nicum & Karoo, 1998). During intrapartum care, approximately 50% of Hindu and Muslim patients refused to accept medical students. Sikh and Muslim patients accepted only female medical students, 41% and 40%, respectively, whereas 59% of Christian patients accepted both female and male medical students (Nicum & Karoo, 1998). However, patients’ reasons for accepting and refusing medical student participation in pelvic examination have not been established in Southeast Asia because of limited investigation.
According to the patient’s bill of rights, patients have a right to accept or refuse the medical students’ participation. They should have the opportunity to decide if they want to contribute to the medical education or decline care from medical students (Teunissen, 2018). Approximately 26% of the patients refused to have a medical student perform a pelvic examination (Fortier et al., 2006). Previous study reported that the refusal rate increased as the level of student involvement increased, from observation to history taking to examinations and procedure, particularly with digital vaginal and rectal examination (Salah et al., 2015). In contrast, some patients accepted the medical students’ participation because they wanted to contribute to the clinical training in medical education. Because of the training process, the patients felt more confident that they would receive appropriate treatments. From the literature review, most studies were conducted in developed and some Arab countries. There are limited data from women in Southeast Asia countries on the factors and attitudes that influence their decision whether they allow or refuse medical students to participate in a pelvic examination. This research aimed at studying the patients’ characteristics, influencing factors and correlation with the acceptance of medical students, which may increase the Ob–Gyn patients to participate in clinical education.
II. METHODS
This cross–sectional descriptive study was conducted at the out–patient unit of the Department (OPD) of Obstetrics and Gynaecology, Naresuan University Hospital. Patients who visited Ob–Gyn department between November 2018 and May 2019 were included in the study. Patients under 20 years old, mentally or critically ill and unable to understand the questionnaire in Thai language were excluded in this study. All the participants were able to complete the consent forms and questionnaires independently, and were guaranteed anonymity.
The questionnaire was developed to evaluate 4 domains, as follows: (1) demographic and socio–economic data (age, gender, educational level, occupation and parity), (2) patient preference, (3) factors influencing patient receptivity of medical student involvement in pelvic examination (gender, hygiene, manner and demeanour, patients’ impressions of the medical students, prior experience in physical and pelvic examination), and (4) patients’ attitudes toward accepting medical students to conduct pelvic examination under supervision of medical instructors. Influencing factors and attitudes included in the questionnaire were modified based on a literature review. A 5–point Likert scale was used to determine the level of agreement (1= strongly agree; 2= agree; 3= neutral; 4= disagree; and 5= strongly disagree). The questionnaire was initially tested for content validity using the item-objective congruence (IOC) index, and then used in a pilot study on 30 patients who were not included in the study to ensure clarity and reliability.
A. Statistical Analysis
A Microsoft Excel spreadsheet was created for data entry and statistical analysis. Descriptive data was presented in the form of frequency, mode, and percentage. Chi-square test was calculated for proportions. The p–value of less than 0.05 was considered statistically significant.
B. Ethical Considerations
All collected data was kept confidential, and the information was used for research only. This study was approved by Naresuan University Institutional Review Board in compliance with the principles of the Helsinki Declaration.
III. RESULTS
During the study period, 236 participants were recruited from the out–patient department of Ob–Gyn, but only 198 completed the questionnaire. Most of them (99.0%) were aware that Naresuan University Hospital is a primary teaching hospital of the Faculty of Medicine, Naresuan University which provides clinical training for medical students and residents. The socio–demographic data of the study population are shown in Table 1. The data that supports the findings of this study are openly available at http://doi.org/10.17605/OSF.IO/HBV68 (Amatyakul, 2021).
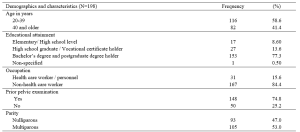
Table 1. Demographics and characteristics of the study population
From 198 participants, 71.7% accepted the medical students to participate in pelvic examination. Fifty–seven percent of the participants in the acceptor group allowed both male and female medical students, while 42.9% in the same group allowed only female medical students. The correlation between patients’ acceptance and refusal for the medical students to participate in pelvic examination showed that age, occupation and parity of the patients were not statistically different (p> 0.05). Thirty–one percent of bachelor’s degree holders and 37% of postgraduate degree holders refused the participation of medical students. The higher the patient’s educational attainment, the more likely they are to refuse a pelvic examination performed by medical students, as observed in this study. In the conduct of pelvic exam procedure, 69.3% of the patients in the acceptor group and 53.6% of the patients in the non-acceptor group felt comfortable with students present as observers. Before the students participate in a pelvic examination, most of the participants (81.4%) preferred that the medical instructors (56.6%) ask permission rather than the medical students (21.7%) or nurses (21.7%).
This research recorded 52.7% of the patients with prior experience of physical examination by medical students from other departments in Naresuan University Hospital. Thirty–two percent of the patients previously received pelvic examination by medical students (from our department or other medical training hospitals). Patients who had their physical examinations performed by medical students from other departments or had pelvic examinations performed by medical students had a statistically significant increase in allowing medical students to participate in pelvic examinations under the supervision of a medical instructor (Table 2).
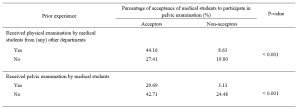
Table 2. The correlation between the acceptance of medical student participation in pelvic examination and prior experience of pelvic examination performed by medical students.
The participants’ decisions were influenced by their impressions of medical students. More than 90% of the participants believed that characteristics like manner, demeanour, cleanliness, hygiene, trustworthiness, and respect had a substantial impact on their attitudes and acceptance. Similarly, the gender of the medical students also influenced the decision of the participants (69.2%), which female students were preferred. The negative and positive attitudes of the patients related to medical student participation in pelvic examination are shown in Table 3.
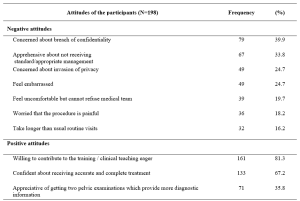
Table 3. The positive and negative attitudes of the participants about medical students’ participation in pelvic examination under the supervision of medical instructors.
IV. DISCUSSION
Our study demonstrated that 71.7% of the participants agreed to have their pelvic examinations performed by medical students. This result was comparable to the study of Western women that reported an acceptance rate ranging from 58 to 77% (Nicum & Karoo, 1998). Conversely, our acceptance rate was lower when compared to a study conducted in United Arab Emirates by Rizk et al. (2002), in which 87.1% of the out-patients in Ob-Gyn accepted the involvement of medical students. According to the results of our study, there were no statistically significant differences between acceptors and non-acceptors in terms of age, educational level, occupation, parity, or prior pelvic examination. Hartz and Beal (2000) also reported similar findings, stating that the age and education of the patients were not statistically different between the two groups. However, Rizk et al. (2002) stated that the acceptance of the patients with older age, higher parity, and higher education was statistically significant. Interestingly, there was a trend discovered in our research that patients who are highly educated were more reluctant to allow medical students in performing pelvic examination, even when supervised by medical instructors. This reluctance could be because of a strong concern for their privacy, which should be investigated further through an in-depth interview.
Prior experience of the patients receiving physical examination by medical students from other departments, and prior experience of the patients receiving pelvic examination performed by medical students significantly increased the rate of acceptance. These findings are consistent with those of Ghobain et al. (2016) who reported that a positive prior experience with a medical student was significantly related to giving medical students permission to perform a physical examination. This can be explained by the fact that these patients were already aware of the medical student involvement in performing physical examinations. Therefore, they are more likely to accept medical student participation in subsequent Ob-Gyn consultations.
One interesting finding from our study was the positive patient receptivity of medical students acting as observers during pelvic examination. Patients in approximately 70% of the acceptor group allowed other medical students to observe the examination process. Remarkably, 53.6% in the non-acceptor group was comfortable with medical students observing a pelvic examination performed by medical instructor. This would imply that even if students cannot perform pelvic examinations, they can still gain clinical knowledge through observation, and clinical instructors can take advantage of this valuable opportunity to educate their students.
Other major concern of patients is the requirement for students to obtain permission before participating in any procedures. The majority of the participants prefer that medical instructors be in charge of obtaining patient permission to allow students to perform physical examinations on their behalf. This tendency may lead to a higher rate of acceptance of student participation.
The characteristics and performance of the medical students in our study had a significant impact on patients’ decision. The external part of the female reproductive organ is a sensitive and the most private area for every woman, and patients would only allow medical students who practice good hygiene and cleanliness to participate in the examination. Furthermore, the appropriate manner and demeanour, including respectfulness and politeness toward patients, and trustworthiness of the medical students during the clinical procedure may increase the patients’ receptivity of medical students to conduct pelvic examination. Professional appearance reflecting cultural backgrounds also impacts patient preference and acceptance; therefore, medical students should dress properly (Aljoudi et al., 2016).
Several studies, including ours, found that participants felt more at ease with female students than with male students (Salah et al., 2015; Subki et al., 2018). Chang et al. (2010) reported that male students were refused by patients to participate in clinical interviews and physical examinations, including pelvic examinations. In a study conducted at Taibah University in India (Shetty et al., 2021), women significantly preferred female students during abdominal and genital examinations. As a result, it is difficult for obstetrics and gynaecology educators to consider methods of encouraging patients to accept participation of medical students, regardless of their genders.
Patients’ positive attitudes toward medical students’ participation contributed to clinical teaching, which is an important process for professional development. The patients agreed that they would receive more accurate and comprehensive treatment if they had two pelvic examinations. These details are consistent with the findings of a study conducted by Rizk et al. (2002), which revealed that 69.7% of the participants were willing to contribute to the education of students. Most participants were satisfied with the overall service because they were well informed about their care by the health care team and were actively involved in the treatment decision-making process. Like other literature (Nicum & Karoo, 1998), medical students also provided patients with useful medical information and support. Furthermore, patients strongly supported the idea that real patient encounters and practices under clinical supervision are more effective methods for improving student’s clinical skills than just mere observation or skill laboratory practice (Subki et al., 2018).
Patients’ main reasons for refusing medical students’ participation in pelvic examination were concerns about breaching their confidentiality and privacy, which were similar to a study conducted in London. According to the findings, the common reasons for patients’ uneasiness with participation of the medical students were related to privacy, receiving lower standard of care, examinations, lack of control over the student’s level of involvement, and a longer consultation time (Ryder et al., 2005). The participants in our study were also concerned about taking a longer than usual routine visit. Not only applicable in Ob-Gyn department, patients’ perceptions of students’ professionalism and respect for privacy were significantly related to the acceptance of medical students’ participation in surgical ward (Ghobain et al., 2016). Thus, all medical students must be informed about the doctor-patient relationship and the importance of maintaining patient confidentiality. Medical instructors must inform and reassure patients about their confidentiality. Before participating in any clinical teachings, medical instructors should explain to students their roles and responsibilities. To minimise patients’ feeling of discomfort, these roles and responsibilities should be conveyed and explained to them before asking for their approval.
This paper has highlighted the significance of patients’ attitudes toward medical students’ manner and demeanor, which greatly influences patients’ decision-making process. However, some limitations should be considered, such as the fact that all participants were Thai, and that the study was carried out in one of the Southeast Asia countries where data on the attitudes of female patients had not been thoroughly investigated. Since socio-demographic factors and cultural issues vary across Southeast Asia, the results of this research only represent the characteristics of the Thai population and not the entire region. Additionally, this cross-sectional study could not establish the reasons for patients’ negative attitudes toward student involvement in pelvic examination. Therefore, it is suggested that future research use in-depth interview methodology to gather more information from both the acceptor and non-acceptor groups.
V. CONCLUSION
Most of patients agreed to medical students participating in pelvic examinations and preferred medical instructors to be the persons to ask patients for permission. Essentially, patients’ confidentiality and privacy must always be safeguarded. The performance of medical students, and their observance of patient privacy and confidentiality are crucial factors in gaining the patient’s approval. Furthermore, the gender of the medical student influences the patient’s acceptance and comfort level in student’s involvement. Clinical instructors must effectively convince patients in gynaecology department to allow male medical students to perform gynaecologic procedures.
Notes on Contributors
Nisakorn Deesaen, Punyanuch Phonngoenchai, and Kongpop Sutantikorn contributed to the literature review, concept development, questionaire design, data collection, data analysis, and manuscript finalisation. Sakchai Chaiyamahapruk was involved in the study design, data analysis, and manuscript finalisation. Patcharada Amatyakul contributed to the literature review, concept development, study design, data analysis, and manuscript writing and finalisation.
Ethical Approval
Ethical approval for this study was obtained from the Naresuan University Institutional Review Board, Naresuan University, Thailand (Ethics approval number IRB 0653/60).
Data Availability
The data that support the findings of this study are publicly available in Open Science Framework repository, http://doi.org/10.17605/OSF.IO/HBV68.
Acknowledgement
The authors would like to express their gratitude to the nurses at the out-patient unit of the Department of Obstetrics and Gynaecology, Naresuan University Hospital, for their help in distributing and collecting questionnaires from the patients.
Funding
This research received no specific grant from any funding agency.
Declaration of Interest
The authors declare no conflict of interest.
References
Aljoudi, S. B., Alsolami, S. S., Farahat, F. M., Alsaywid, B., & Abuznadah, W. (2016). Patients’ attitudes towards the participation of medical students in clinical examination and care in Western Saudi Arabia. Journal of Family and Community Medicine, 23(3), 172‑178. https://doi.org/10.4103/2230-8229.189133
Amatyakul, P. (2021). Proposal for patients’ attitude and factors influencing the acceptance of medical students’ participation in pelvic examination. [Data set]. Open Science Framework. http://doi.org/10.17605/OSF.IO/HBV68
Anfinan, N., Alghunaim, N., Boker, A., Hussain, A., Almarstani, A., Basalamah, H., Sait, H., Arif, R., & Sait, K. (2014). Obstetric and gynecologic patients’ attitudes and perceptions toward medical students in Saudi Arabia. Oman Medical Journal, 29(2), 106-109. https://doi.org/10.5001/omj.2014.26
Bloomfield, H. E., Olson, A., Greer, N., Cantor, A., MacDonald, R., Rutks, I., & Wilt, T. J. (2014). Screening pelvic examinations in asymptomatic, average-risk adult women: An evidence report for a clinical practice guideline from the American College of Physicians. Annals of Internal Medicine, 161(1), 46–53. https://doi.org/10.7326/M13-2881
Chang, J. C., Odrobina, M. R., & McIntyre-Seltman, K. (2010). The effect of student gender on the obstetrics and gynecology clerkship experience. Journal of Women’s Health, 19(1), 87-92. https://doi.org/10.1089/jwh.2009.1357
Fortier, A. M., Hahn, P. M., Trueman, J., & Reid, R. L. (2006). The acceptance of medical students by women with gynaecology appointments. Journal of Obstetrics and Gynaecology Canada, 28(6), 526-530. https://doi.org/10.1016/S1701-2163(16)32179-X
Ghobain, M. A., Alghamdi, A., Arab, A., Alaem, N., Aldress, T., & Ruhyiem, M. (2016). Patients’ perceptions towards the participation of medical students in their care. Sultan Qaboos University Medical Journal, 16(2), 224–229. https://doi.org/10.18295/squmj.2016.16.02.014
Hartz, M. B., & Beal, J. R. (2000). Patients’ attitudes and comfort levels regarding medical students’ involvement in Obstetrics–Gynecology outpatient clinics. Academic Medicine, 75(10), 1010-1014. https://doi.org/10.1097/00001888-200010000-00018
McLean, M., Al Ahbabi, S., Al Ameri, M., Al Mansoori, M., Al Yahyaei, F., & Bernsen, R. (2010). Muslim women and medical students in the clinical encounter. Medical Education, 44(3), 306-315. https://doi.org/10.1111/j.1365-2923.2009.03599.x.
Nicum, R., & Karoo, R. (1998). Expectations and opinions of pregnant women about medical students being involved in care at the time of delivery. Medical Education, 32(3), 320-324. https://doi.org/10.1046/j.1365-2923.1998.00205.x.
Rizk, D. E. E., Al-Shebah, A., El-Zubeir, M. A., Thomas, L. B., Hassan, M. Y., & Ezimokhai, M. (2002). Women’s perceptions of and experiences with medical student involvement in outpatient obstetric and gynecologic care in the United Arab Emirates. American Journal of Obstetrics and Gynecololgy, 187(4), 1091-1100. https://doi.org/10.1067/mob.2002.126284.
Ryder, N., Ivens, D., & Sabin, C. (2005). The attitude of patients towards medical students in a sexual health clinic. Sexually Transmitted Infection, 81(5), 437–439. https://doi.org/10.1136/sti.2004.014332.
Salah, A. B., Mhamdi, S. E., Bouanene, I., Sriha, A., & Soltani, M. (2015). Patients’ attitude towards bedside teaching in Tunisia. International Journal of Medical Education, 6, 201-207. https://doi.org/10.5116/ijme.5669.ea24.
Shetty, P. A., Magazine, R., & Chogtu, B. (2021). Patient outlook on bedside teaching in a medical school. Journal of Taibah University Medical Sciences, 16(1), 50-56. https://doi.org/10.1016/j.jtumed.2020.10.002
Subki, A. H., Algethami, M. R., Addas, F. A., Alnefaie, M. N., Hindi, M. M., & Abduljabbar, H. S. (2018). Women’s perception and attitude to medical students’ participation in obstetrics and gynecology care. Saudi Medical Journal, 39(9), 902-909. https://doi.org/10.15537/smj.2018.9.22668
Teunissen, P. W. (2018). An inconvenient discussion. Medical education, 52(11), 1104-1110. https://doi.org/10.1111/medu.13689
*Patcharada Amatyakul
Department of Obstetrics and Gynaecology,
Faculty of Medicine, Naresuan University,
99 Thaphoe District, Muang,
Phitsanulok, 65000 Thailand
Tel: 66-86-397-3455
Email: pamatyakul@hotmail.com
Submitted: 14 April 2021
Accepted: 24 June 2021
Published online: 4 January, TAPS 2022, 7(1), 98-101
https://doi.org/10.29060/TAPS.2022-7-1/SC2517
Lean Heong Foo & Marianne Meng Ann Ong
Department of Restorative Dentistry, National Dental Centre Singapore, Singapore
Abstract
Introduction: Team-based learning (TBL) pedagogy is a structured, flipped classroom approach to promote active learning. In April 2019, we designed a TBL workshop to introduce the New Classification of Periodontal Diseases 2017 to a group of general dental practitioners (GDPs). We aimed to investigate GDPs feedback on learning this new classification using TBL pedagogy.
Methods: Two articles related to the 2017 classification were sent to 22 GDPs 2 weeks prior to a 3-hour workshop. During the face-to-face session, they were randomly assigned to five groups. They participated in individual and group readiness assurance tests. Subsequently, the GDPs had inter- and intragroup facilitated discussions on three simulated clinical cases. They then provided feedback using a pen-to-paper survey. Based on a 5-point Likert scale (1-strongly disagree to 5-strongly agree), they indicated their level of agreement on items related to the workshop and their learning experience.
Results: Majority (94.7%, 18 out of 19 GDPs) agreed the session improved their understanding of the new classification and they preferred this TBL pedagogy compared to a conventional lecture. All learners agreed they can apply the knowledge to their work and there was a high degree of participation and involvement during the session. They found the group discussion and the simulated clinical cases useful.
Conclusion: A TBL workshop is suitable for clinical teaching of the New Classification of Periodontal Diseases 2017 for GDPs. Its structure promotes interaction among learners with the opportunity to provide feedback and reflection during the group discussions. This model might be a good pedagogy for continuing dental education.
Keywords: Team-based Learning, General Dental Practitioners, New Classification of Periodontal Diseases
I. INTRODUCTION
Team-based learning (TBL) is a flipped classroom, structured learning pedagogy that was introduced by Larry Michaelsen and has gained popularity among healthcare educators recently. TBL is learner-centric and dialectic based, and practices logical discussion used for determining the truth of a theory or opinion (Michaelsen et al., 2008). It provides the opportunity for peer-teaching by group members and can assist weaker students in understanding course materials.
Several dental educators have utilised TBL in undergraduate dentistry programmes and observed higher engagement among learners, less student contact time and faculty time, and higher course grades (Haj-Ali & Al Quran, 2013). General dental practitioners (GDPs), unlike undergraduate dental students, juggle between busy dental practice and family life. Hence, GDPs might seek active learning with direct knowledge application to manage their continuing dental education needs efficiently. The World Workshop of Periodontology recently revamped the diagnosis of periodontal diseases and proposed a new classification of staging (Stage I-IV; based on severity of disease) and grading (Grade A-C; based on disease progression) for periodontitis (Tonetti et al., 2018). We aimed to investigate GDP feedback on learning this new classification using TBL pedagogy.
II. METHODS
This is a descriptive study on GDPs’ feedback on learning the New Classification of Periodontal Diseases 2017 using a TBL approach. 22 GDPs attended the TBL workshop in April 2019.
Two articles related to the new classification were sent to the GDPs 2 weeks prior to the 3-hour workshop. Five multiple-choice questions were crafted from the two articles (Individual Readiness Assurance Test, IRAT) to assess learners’ basic understanding of the new classification. Learners were divided into five groups to discuss IRAT and provide answers using the immediate feedback assessment technique card (Group Readiness Assurance Test, GRAT). Faculty then highlighted key elements of the new classification. Three clinical periodontal cases crafted based on the 4S framework principles i.e. same problem, significant problem, specific choice, and simultaneous reporting, were used in the application process (Michaelsen et al., 2008). The key question was to diagnose the periodontal condition based on the staging and grading criteria. Lastly, learners provided implied consent by answering an anonymous pen-to-paper survey voluntarily. They answered based on their level of agreement on a 5-point Likert scale (5 indicating strongly agree, 1 indicating strongly disagree). The survey comprising 13 education-related statements: two statements related to programme content, two to presentation, six to learning experience, and three about the workshop. Three qualitative questions in the survey were: “What do you like most about the workshop?”, “What aspects of the session could be improved?” and “Other comments and feedback”.
III. RESULTS
Nineteen out of the 22 GDPs who attended the TBL workshop responded to the survey (response rate 86.4%). Results are summarised in Figure 1. We conducted a reliability analysis on the perceived task values scale comprising two subscales (learning experience and workshop) with at least three items.
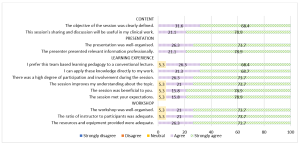
Figure 1. Learners’ feedback about the workshop
A. Content (Two items)
During the workshop, we highlighted the staging and grading criteria for the new classification. Learners provided a mean score of 4.74 (standard deviation, SD, 0.446; median 5) in two statements related to content. In general, 68.4% of them strongly agreed and 31.6% agreed the objective of the workshop was clearly defined. There were 78.9% and 21.1% of learners who strongly agreed and agreed respectively that the sharing and discussion during the workshop was useful to their clinical work.
B. Presentation (Two items)
Learners gave a mean score of 4.76 for presentation (SD 0.431; median 5). There were 73.7% learners who strongly agreed and 26.3% who agreed that the presentation was well-organised. In addition, 78.9% and 21.1% of the learners strongly agreed and agreed respectively that the presenter presented relevant information professionally.
C. Learning Experience (Six items)
Cronbach’s alpha for the learning experience subscale reached acceptable reliability at α = 0.81. The mean score for learning experience was 4.70 (SD 0.531; median 5). There were 68.4% learners who strongly agreed and 26.3% who agreed that they prefer TBL pedagogy to a conventional lecture. Also, 68.7% of the learners strongly agreed and 31.3% agreed they could apply the knowledge directly to their work. All learners agreed that there was a high degree of participation and involvement during the session. 18 learners (94.7%) agreed that the session met their expectations and improved their understanding about the topic.
D. Workshop (Three items)
The mean score for learners’ feedback on the workshop was 4.71 (SD 0.533; median 5). 18 learners (94.7%) agreed that the workshop was well organised with an adequate ratio of instructor to participants (2:22). There were 73.7% learners who strongly agreed and 26.3% who agreed that resources and equipment provided were adequate. Cronbach’s alpha for the workshop subscale reached acceptable reliability at α = 0.75.
E. Qualitative Feedback
The learners cited the following themes as their favourite component of the workshop: “group interaction and discussion” (4), “clinical case discussion” (3), “useful and relevant clinical cases” (1), “interesting readiness assurance test” (1), and “pre-reading material” (1). They also cited “active learning” (1), “correct wrong understanding” (1), “discussion improves my understanding” (1), and “great information and lecturer” (1) as positive learning experiences. Three different learners provided feedback of “best workshop ever attended”, “well done”, and “very good” respectively. One learner commented that the air-conditioning in the room was cold. One learner commented on small font size in dental charting and another learner suggested “less tests at the start”.
IV. DISCUSSION
The flipped classroom concept in TBL was suitable for GDPs to study the pre-reading articles at their own pace. The structured workshop enabled them to correct any misconception immediately and deepen their understanding about the new classification. This observation concurs with the finding that all GDPs agreed they could apply the knowledge to their work and preferred this pedagogy over a traditional lecture. This active learning process differs from a conventional didactic lecture, which is faculty-centric with less feedback and interaction. Hence, this pedagogy can be applied for some continuing dental education programmes by improving the delivery and application of new concepts. The 4S framework in the application cases are key elements to promote productive and logical discussion similar to a debate facilitated by faculty. The problem-solving aspect of TBL, along with the scaffolding and guidance by faculty, can enhance the metacognition process among learners (Hrynchak & Batty, 2012). Almost all learners agreed there was an adequate ratio of faculty to participants, emphasising the benefit of using TBL workshops to teach a large group of learners with less faculty. However, faculty needs to work more in planning and preparing the teaching materials, executing, and facilitating the session following the TBL structure and process. In addition, hurdles in conducting TBL include acceptance from faculty and learners, difficulty in supervising a large group, the customisation of the course content, and adequate training and expertise to conduct TBL effectively.
The learners also cited “group interaction and discussion” as their favourite component of the workshop. The learning theory underpinning TBL is the constructivist learning theory where the faculty exposes knowledge inconsistency during group discussion, subsequently allowing a new mental framework to be built upon the new understanding (Hrynchak & Batty, 2012). TBL is useful in healthcare education since it can promote good critical thinking and teamwork. In addition, the intra- and intergroup formal discussion provides the opportunity to reflect, give feedback, and enable peer-teaching. Self-reflection enables learners to make a judgement when modifying their existing knowledge. Peer-to-peer teaching in TBL enhances learning and aids weaker learners to understand the course material (Park et al., 2014).
Some limitations of our study were that the sample size was small, reporting participants’ self-perception on how they felt after attending the workshop and the lack of longitudinal follow-up on retention of knowledge. In addition, we did not have a separate didactic lecture on the new classification as a control group to truly compare the two different modes of teaching. Future recommendation includes having two groups of GDPs to collate their perceptions as well as include a pre and post assessment to investigate the difference in improvement and in knowledge retention comparing TBL workshop and traditional didactic lecture, and include peer evaluation in TBL to increase accountability among learners. Besides, ethnographic research method can be explored to provide insight to researchers to understand the essence of how dental professionals learn during TBL. It would be meaningful to follow up this group of GDPs to assess the accuracy of their periodontal diagnoses based on the new classification to investigate the effectiveness of the TBL workshop. Of note, TBL workshops can be adapted into an online format; this is particularly useful during the current COVID-19 pandemic to engage learners and promote active learning in an online setting.
V. CONCLUSION
In conclusion, TBL pedagogy may be another mode of teaching for GDPs in continuing dental education where participants are actively engaged, and direct application of knowledge gained can be made. During this pandemic, where face-to-face sessions are minimised, educators can consider adopting TBL pedagogy on an online platform to improve learning experience and engagement of their learners.
Notes on Contributors
Dr Lean Heong Foo is a Consultant Periodontist in Department of Restorative Dentistry and Head to the Dental Surgery Assistant Certification Programme in National Dental Centre Singapore. FLH reviewed the literature, contributed to study conception, data acquisition, data analysis, drafted and critically revised the manuscript.
Dr Marianne M. A. Ong is a Senior Consultant Periodontist & Director of Education in National Dental Centre Singapore. MO contributed to study conception, data acquisition and critically revised the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Ethical Approval
This study was exempted from formal Centralised Institutional Review Broad review by SingHealth Institutional Review Board (CIRB Ref: 2021/2133).
Data Availability
Data is deposited at Figshare. https://doi.org/10.6084/m9.figshare.14411858
Acknowledgement
The authors would like to thank Ms Safiyya Mohamed Ali for providing editorial support.
Funding
There was no funding involved in the preparation of the manuscript.
Declaration of Interest
The authors declare no conflict of interest.
References
Haj-Ali, R., & Al Quran, F. (2013). Team-based learning in a preclinical removable denture prosthesis module in a United Arab Emirates dental school. Journal of Dental Education, 77(3), 351–357.
Hrynchak, P., & Batty, H. (2012). The educational theory basis of team-based learning. Medical Teacher, 34(10), 796–801.https://doi.org/10.3109/0142159X.2012.687120
Michaelsen, L. K., Parmelee, D. X., McMahon, K. K., & Levine, R. E. (2008). Team-based learning for health professions education: A guide to using small groups to improving learning. Stylus.
Park, S. E., Kim, J., & Anderson, N. K. (2014). Evaluating a team-based learning method for detecting dental caries in dental students. Journal of Curriculum and Teaching, 3(2), 100-105. https://doi.org/10.5430/jct.v3n2p100
Tonetti, M. S., Greenwell, H., & Kornman, K. S. (2018). Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. Journal of Periodontology, 89(Suppl 1), S159–S172. https://doi.org/10.1002/JPER.18-0006
*Foo Lean Heong
National Dental Centre Singapore,
5, Second Hospital Avenue,
168938 Singapore
Email: foo.lean.heong@singhealth.com
Submitted: 29 March 2021
Accepted: 28 September 2021
Published online: 4 January, TAPS 2022, 7(1), 102-105
https://doi.org/10.29060/TAPS.2022-7-1/SC2508
Mairi Scott & Susie Schofield
Centre for Medical Education (CME), School of Medicine, University of Dundee, Scotland, United Kingdom
Abstract
Introduction: The switch to online off-campus teaching for universities worldwide due to COVID-19 will transform into more sustainable and predictable delivery models where virtual and local student contact will continue to be combined. Institutions must do more to replace the full student experience and benefits of learners and educators being together.
Methods: Our centre has been delivering distance blended and online learning for more than 40 years and has over 4000 alumni across five continents. Our students and alumni come from varied healthcare disciplines and are at different stages of their career as educators and practitioners. Whilst studying on the programme students work together flexibly in randomly arranged peer groups designed to allow the establishment of Communities of Practice (CoP) through the use of online Discussion Boards.
Results: We found Discussion Boards encouraged reflection on learning, sharing of ideas with peers and tutors, reduce anxiety, support progression, and enable benchmarking. This led to a highly effective student sense of belonging to each other, our educators, and the wider University, with many highlighting an excellent student experience and maintaining a thriving CoP within the alumni body.
Conclusion: Despite being based on one large postgraduate programme in medical education, our CoP approach is relevant to any undergraduate programme, particularly those that lead to professional qualification. With our mix of nationalities, we can ‘model the way’ for enabling strong CoP’s to share ideas about best practice with a strong student and alumni network which can be shared across the international healthcare community.
Keywords: Communities of Practice, Sense of Belonging, Student Experience
I. INTRODUCTION
The sudden switch to online, dual delivery and on-campus/off-campus teaching for Universities worldwide will not be reversed at the end of the current COVID-19 crisis but will transform into a more sustainable and predictable delivery model where virtual and local student contact will continue to be combined. The switch, known as Emergency Remote Teaching (ERT) (Hodges et al., 2020) achieved much in a short timeframe but institutions need to do more to truly replace the full student experience and benefits of learners and educators being together on-site. The need for this new approach is acute in professional-based courses such as medicine where students need to learn complex skills within the context of healthcare delivery. These skills are acquired through multiple interactions with clinical colleagues in the workplace which, although often brief, are focused in real-time.
Given that the learning environment is dependent on the institutional ‘personality, spirit, and culture’ (Holt & Roff, 2004, pp. 553), human interaction is necessary to create that culture. We must develop new approaches to delivering medical education by merging established educational technologies with virtual approaches to establish on-line interaction with peers and senior colleagues such as can be achieved in Communities of Practice (CoPs) (Lave & Wenger, 1991). CoPs are social structures where people can share ideas, stories, and experiences relevant to the community’s activities. They help participants make sense of new knowledge and enable novices to benefit from working with experts, thus reducing anxiety, supporting progression, and enabling benchmarking. These components lead to the creation of a rich environment for information-sharing which has become increasingly important within healthcare delivery organisations during the COVID-19 pandemic.
We have built on over 40 years’ experience of delivering distance, blended and online Masters-level accredited medical education learning across five continents to ‘model the way’ to providing a strong student experience for online learners. Our students and alumni come from various interdisciplinary healthcare disciplines, at different stages of their career as educators and practitioners.
II. METHODS
Several Discussion Boards (DBs), usually one per study week plus one for assignment questions are created in each 12-week Moodle-based module. Students are randomly assigned to groups to work together flexibly within these peer groups. Each discussion has a ‘prompt’ linked to that week’s work, designed to create CoPs and a highly effective student sense of belonging (SoB) to each other and programme educators. In the first module students are actively encouraged to participate, with emphasis being on the ‘safe space’ created that allows them to learn effectively from and with each other. DB comments are used as part of programme enhancement and quality assurance. Students give informed consent to their evaluation comments within DBs being extracted for overall programme review.
III. RESULTS
As students move from legitimate peripheral participant to experienced member, they often express increased confidence that their posts will allow them to share their view and help colleagues. The forum posts have been analysed as part of a much larger study; the following diagram (Figure 1) highlights some of the benefits.
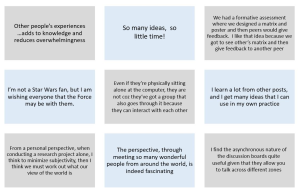
Figure 1. Sample of comments in DBs posts
Our experience over the last four years is that student levels of interaction increase the further into the programme they go, suggesting that they value and enjoy it. Overall, when asked specifically if that assumption is correct, feedback from students is exceptionally positive and they comment on their achievement of a SoB through engagement with the DBs. Many highlight the excellent student experience. Another indirect indication of success is that student module success rate averages 93% across the modules, which is high for an online learning programme.
The benefits of using DBs are threefold:
- They allow for reflection on learning in real-time due to regular module-specific weekly activities requiring students to reflect on that week’s educational materials and post their thoughts on the DBs.
- They allow sharing with peers and tutors, establishing CoPs: The DB posts create peer-to-peer dialogue, encouraging students to practise the language of the discipline in a safe, supported environment. Learning activities are based on the principle of linking previous experience with the interpretation of new knowledge, thus enabling an escalation of the complexity of questions to enhance deeper connection and dialogue. Although essentially (and importantly) it is the students as peers who are encouraged to respond to each other’s questions and comments, the tutors do monitor posts, providing input when necessary and desirable. In some modules, students are required to give peer feedback on draft assignments using a 1:4 ratio to encourage a range of views and expertise, increasing the depth and extent of their critical thinking and analysis. This also gives them practice in giving and receiving feedback, an essential skill for future medical educators.
- CoPs build trust in colleagues and a SoB within the learning environment, leading to an excellent learning experience. Students state that they value the tutor contribution as this increases the confidence they have in their own online comments, sometimes shifting the discussion to a more profitable area for new learning in a way that was not pre-planned or even at times expected.
IV. DISCUSSION
Our approach to the creation of CoPs is based on the principle that in order to establish student trust and a SoB DBs are an essential tool. Management research describes trust within organisations as being multifaceted, with the main components being capability, well-meaning intent, and integrity (Ridings et al., 2002). It is accepted that within our programmes both tutor and student capabilities have been established. Integrity is established by clearly explaining the expected mode of student behaviour at the outset and demonstrated as students work through the programme. Well-meaning intent is demonstrated by acts of positive reciprocation built up over time by asking students to give peer feedback frequently and around increasingly complex activities. Both integrity and well-meaning intent therefore need to have a continued focus during module design and delivery and throughout the assessment process.
Now that medical education has been forced to re-evaluate the place of online learning as a consequence of the COVID-19 crisis, it seems inevitable that many of the discovered benefits will lead to significant changes in the way we teach and learn. Davis (2018) explored a future medical school being one ‘without walls’ by which he meant that the artificial separation of the ‘classroom and the clinic’ would inevitably diminish as we embraced flipped classrooms and online collaborative learning.
If we adopt this approach for student learning it may also change the way we think about faculty development, as we could create extensive networks of faculty development special interest grouped CoPs beyond the ‘walls’ of our own schools. A recent study by Chan et al. (2018) in McMaster describes the creation of a Faculty Incubator – a virtual CoP which uses a longitudinal, asynchronous, online platform to deliver a one-year curriculum to support early-to mid-career educators from 30 different locations with their professional development. This widespread (geographically) collaborative approach was found to be well received, with lively interactions which broke down some of the boundaries that normally prevent early career academics from approaching unknown colleagues in different locations, colleagues they would normally never have met in person.
An additional challenge created by the COVID-19 pandemic was the necessity for healthcare professionals to make clinical decisions in an ‘evidence-poor’ disease by gathering emerging data (often by word-of-mouth) and treating patients without the certainty of a knowledge base built up over decades of robust randomised controlled trial (RCT) evidence. This is described by Rosenquist (2021, pp. 8) as a kind of “Bayesian fatigue”: a stress-induced dysphoria experienced when the corpus of knowledge that is the foundation of one’s work acquired over decades, becomes less important than information being gathered from disparate sources in real time.’ The ‘disparate sources’ referred to here are groups of widely dispersed practitioners (within current and new CoPs) who are sharing individual and collective rapid learning by experience that has become necessary when treating patients with COVID-19. These CoPs are based on the collective trust healthcare professionals express in valuing the views of colleagues struggling with similar challenges. This helps reduce that ‘Bayesian’ impact when it comes to making difficult clinical decisions in real time with limited evidence. However, trust within a CoP also comes from previous positive experience of being within other CoPs, and so it is important that we as medical educators enable our students to have experience of the value of sustainable CoPs in their own learning. Despite the limitations of the range of the study comments, we believe that given the extent of the sudden switch to ERT our findings of use of DBs to establish much appreciated CoPs justifies early dissemination through this short communication.
V. CONCLUSION
As medical educators we must have the skills necessary to establish strong and sustainable CoPs to educate current and future healthcare professionals in this effective way of learning from each other. This can be done as effectively with online learning as with on-campus interaction, allowing the possibility of the widespread creation of truly effective international CoPs sustainable for years to come.
Notes on Contributors
Professor Mairi Scott reviewed the literature, selected the data, wrote the manuscript, created the presentation and presented the materials virtually to the Conference. Dr Susie Schofield reviewed the literature, advised on the selection of the data and gave critical feedback on the manuscript. Both authors have read and approved the final manuscript.
Ethical Approval
Ethics approved was granted by School of Medicine & School of Life Sciences Research Ethics Committee, University of Dundee, Dundee, DD1 4HN on 03/05/19. Application Number: 19/41.
Data Availability
Ethical approval specified that raw data would not be made available for others out with the Centre ‘beyond the anonymised published or reported versions within the dissemination strategy’.
Acknowledgement
The authors would like to thank Dr Thillainathan Sathaananthan (PhD student) and Dr Linda Jones (PhD supervisor, Senior Lecturer) CME, University of Dundee, who produced some of the outcomes as part of research into student experiences with online learning and the use of Discussion Boards.
Funding
No grant or external funding was received for this work.
Declaration of Interest
Both authors have no conflict of interest to declare.
References
Chan, T. M., Gottlieb, M., Sherbino, J., Cooney, R., Boysen-Osborn, M., Swaminathan, A., Ankel, F., & Yarris, L. M. (2018). The ALiEM faculty incubator: A novel online approach to faculty development in education scholarship. Academic Medicine, 93(10), 1497–1502. https://doi.org/10.1097/ACM.0000000000002309
Davis, D. (2018). The medical school without walls: Reflections on the future of medical education. Medical Teacher, 40(10), 1004–1009. https://doi.org/10.1080/0142159X.2018.1507263
Hodges, C., Moore, S., Lockee, B., Trust, T., & Bond, A. (2020). The difference between emergency remote teaching and online learning. EDUCAUSE Review. https://er.educause.edu/%20articles/2020/3/the-difference-between-emergency-remote-teaching-and-online-learning
Holt, M. C., & Roff, S. (2004). Development and validation of the Anaesthetic Theatre Educational Environment Measure (ATEEM). Medical Teacher, 26(6), 553-558. https://doi.org/10.1080/01421590410001711599
Lave, J., & Wenger, E. (1991). Situated learning: Legitimate peripheral participation. Cambridge University Press.
Ridings, C. M., Gefen, D., & Arinze, B. (2002). Some antecedents and effects of trust in virtual communities: The Journal of Strategic Information Systems, 11(3-4), 271–295. https://doi.org/10.1016/S0963-8687(02)00021-5
Rosenquist, J. N. (2021). The stress of Bayesian medicine—Uncomfortable uncertainty in the face of COVID-19. New England Journal of Medicine, 384(1), 7-9. https://doi.org/10.1056/NEJMp2018857
*Mairi Scott
Centre for Medical Education,
University of Dundee
Email: m.z.scott@dundee.ac.uk
Submitted: 3 June 2021
Accepted: 4 October 2021
Published online: 4 January, TAPS 2022, 7(1), 76-86
https://doi.org/10.29060/TAPS.2022-7-1/OA2547
Nadia Greviana1,2, Dewi Anggraeni Kusumoningrum2, Ardi Findyartini1,2, Chaina Hanum1 & Garry Soloan1,3
1Medical Education Center, Indonesian Medical Education & Research Institute (IMERI) Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 2Department of Medical Education, Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 3Undergraduate Program in Medicine, Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia
Abstract
Introduction: As significant autonomy is given in a Massive Open Online Course (MOOC), online self-regulated learning (SRL) ability is crucial in such courses. We aim to measure the online SRL abilities of early-career medical doctors enrolled in a MOOC.
Methods: We performed a cross-sectional study using the Self-Regulated Online Learning Questionnaire-revised version (SOL-Qr). We conducted a three-stage cross-cultural validation of the SOL-Qr, followed by Confirmatory Factor Analysis (CFA). The online SRL ability of 5,432 medical doctors enrolled in a MOOC was measured using the validated SOL-Qr.
Results: The CFA of the cross-translated SOL-Qr confirmed its comparability to the original version, with excellent validity & reliability. Participants showed high levels of online SRL during their early careers. Despite high online SRL scores, MOOC completion rate was low. Male participants showed slightly better time management ability than female participants. Participants working in the primary epicentrum for COVID-19 in the country showed lower online SRL scores, while participants who graduated from higher accreditation levels showed better time management ability.
Conclusion: The SOL-Qr and its subscales are suitable and valid for measuring the online SRL abilities of medical doctors in a MOOC during their early-career period. Time management ability was associated with previous experience during the medical education period, while other online SRL subscales were mostly associated with workload. However, as the scores did not correlate with the time spent for learning in MOOC, the corresponding learning effort or time spent may be beyond just the commitment to the described MOOC.
Keywords: Self-Regulated Learning, MOOC, Online Learning
Practice Highlights
- It is important to take into account learners’ online SRL ability in MOOCs as it is dynamic across online learning contexts.
- The use of the SOL-Qr is beneficial for providing learners’ online SRL profiles in MOOC during medical doctors’ early career period.
- Understanding online SRL abilities helps MOOC developers to evaluate learning activities in MOOC and support learners’ online SRL ability.
I. INTRODUCTION
Massive Open Online Courses (MOOCs) are open academic platforms in which students can access learning resources interactively. The self-paced nature of MOOCs provides time-flexibility, facilitating deeper learning (Bullock & De Jong, 2013). MOOCs are useful for replacing direct interaction for knowledge transfer and learning processes during the ongoing pandemic because they utilise various formats, such as video lectures, reading resources, assignments, tests, and asynchronous discussion within the platform (Sandars & Patel, 2020). Because MOOC’s aim to give learners useful resources and empower teachers to provide vital knowledge, curation of the platform, with its copious information, it is beneficial for achieving high-quality content that fits the learning objectives and learners’ characteristics (Asarbakhsh & Sandars, 2013). As demand for technological solutions in education rise during the COVID-19 pandemic, MOOCs have been promoted as forms of disruption that accelerate adaptation to balance safety with the achievement of competencies by medical students and graduates (Hall et al., 2020; Liang et al., 2020).
MOOCs have generally been designed as open in access, location, pace, and time of completion; therefore, learners must control their learning process. Learning goals are usually set less strictly in MOOCs than in other courses. Unlike traditional, face-to-face teaching, MOOCs require highly engaged & strategic students. Learners must plan their study, set goals, evaluate their knowledge related to the course material, adapt their learning strategies, and assess their performance. They are solely responsible for managing their time and study environment (Jansen et al., 2017).
With high enrollment rates, the majority of learners fail to complete MOOCs, for various reasons: lack of time, insufficient prior knowledge, inadequate supervision, and difficulties in understanding the course materials (Hew & Cheung, 2014). Time management, effort regulation, metacognition, and critical thinking as part of Self-Regulated Learning (SRL) relate to success in online academic activities (Broadbent & Poon, 2015). Because MOOCs give students significant autonomy in completing the course, SRL is crucial for successful completion of MOOCs (Chung, 2015; Wong et al., 2018).
SRL encompasses a student’s ability to actively and constructively control their thoughts, acts, and emotions towards learning objectives (Jouhari et al., 2015), using the cycle of forethought, performance, and self-reflection phases, which should be implemented in an online learning environment (Panadero, 2017). Various external factors may interplay and affect self-regulated learning among students. This underscores the importance of a supportive family, helpful peers, and motivational, feedback-centered instruction methods; together, these factors support SRL (Jouhari et al., 2015).
Virtanen and Nevgi (2010) recognised gender as a factor affecting how SRL is perceived by students, especially during the forethought stage; they found that male students scored slightly higher on the sub-scale for self-efficacy, while female students demonstrated greater help-seeking strategies, performance anxiety, and beliefs in the value of studying. Bembenutty (2009) also found that female students perceive learning as a more valuable task in SRL than male students do.
Several instruments were developed to measure SRL, including structured interviews like the Self-Regulation Interview Schedule (SRLIS), questionnaires, teachers’ judgments, think-aloud techniques, and performance observations (Magno, 2011). The Motivated Strategies for Learning Questionnaire (MSLQ) is a common measure of SRL. It assesses two aspects: motivational orientation—encompassing values, expectations, and affective components—and the use of different learning strategies, e.g. cognitive and metacognitive strategies or resource management strategies (Pintrich et al., 1993). Another instrument for measuring students’ SRL in higher education is the Academic Self-Regulated Learning Scale (A-SRL-S), evaluating memory strategy, goal-setting, self-evaluation, seeking assistance, environmental structuring, learning responsibility, and planning and organising (Magno, 2011).
In the context of online learning, several instruments have been developed to measure students’ SRL, such as the Online Self-regulated Learning Questionnaire (OSLQ) and the Self-regulated Online Learning Questionnaire (SOL-Q). The OSLQ consists of six subscales: environment structuring, goal-setting, time management, help-seeking, task strategies, and self-evaluation (Barnard et al., 2009). However, this questionnaire cannot measure SRL activities in the appraisal or self-reflection phase. Meanwhile, the SOL-Q was developed by Jansen et al. (2017), using other existing SRL questionnaires to measure SRL activities, specifically in MOOCs, for all three SRL phases: preparatory, performance, and appraisal. The SOL-Q consists of five sub-scales: metacognitive skills, environmental structuring, help-seeking, time management, and persistence (Jansen et al., 2017). In 2018, a revision was made to split the metacognitive skills scale into three subscales: metacognitive activities before, during, and after a learning task. The revised questionnaire (SOL-Qr) demonstrated improved validity, usability, and reliability (Jansen et al., 2018).
Recognising the importance of learners’ during the use of MOOCs—and that SRL is affected by various factors—we attempted to measure the online self-regulated learning of early-career medical doctors enrolled in a MOOC that provides essential knowledge about COVID-19 to support medical doctors’ early careers during the COVID-19 pandemic. We seek to answer the following questions in this study:
- Is the Self-Regulated Online Learning Question (SOL-Qr) valid for use in our setting?
- What is the profile of students’ SRL scores, and are there any relationships between the SRL score, course completion, gender, respondents’ former medical school, and internship location
II. METHODS
A. Context
With approximately 270 million inhabitants across 34 provinces, Indonesia is one of the largest archipelagos in the world. According to a recent report, there is one medical doctor per 2500 people across the country (National Ministry of Health, 2020). Recently graduated medical doctors must undergo a one-year compulsory internship program upon graduation, where they serve as front-liners in primary health care settings across the country to serve in societies in very diverse sociocultural contexts and ethnicities. Those who graduated in 2020, mostly finished high school and entered medical schools in 2013–2014, completed their clinical stages and graduated from different medical schools in Indonesia at the beginning of the COVID-19 pandemic, during which some of the clinical duties in teaching hospitals were suspended and amended for safety reasons (Findyartini et al., 2020). A total of 93 public and private medical schools are distributed across Indonesia, all accredited by the National Accreditation Agency for Higher Education in Health with A-level as the highest accreditation indicating that the medical school has reached an established quality in teaching-learning processes and faculty members.
Considering the need for the newly graduated medical doctors serving as front liners to learn about the current pandemic situation and the importance of safety for both patients and healthcare workers, the Ministry of Health equipped these new graduates with essential COVID-19 knowledge before their involvement in patient management during the ongoing pandemic. Given the geographical reality of the country’s archipelago and the nature of the workplace setting during the internship program, the use of a Massive Open Online Course (MOOC) was preferred.
Little was known about COVID-19 at the beginning of the pandemic. Guidelines created by organisations (such as the CDC and WHO) are mostly amended living documents based on newly published articles, data, and clinical expertise. Studies on COVID-19 are being conducted on a massive scale worldwide, which may create information overload and overwhelm learners, especially those serving as front–liners (Poonia & Rajasekaran, 2020). A MOOC approach would facilitate a prompt response for equipping medical and health students, professionals, and the broader community to learn about the pandemic situation and prepare them to contribute to the pandemic response in community and hospital settings (Ortiz-Martìnez et al., 2021).
B. The COVID-19 MOOC Description
All internship doctors in Indonesia batch 3 and 4 in 2020, were compulsorily enrolled in an open course on COVID-19 at the beginning of their internship period. The open course was sequenced into two, sequentially accessed parts. The mandatory part A consists of fundamental knowledge on COVID-19 (such as COVID-19 screening, triage, infection control, management of patients, preventive strategy, etc); Part B consists of supplemental knowledge about COVID-19 (such as management of patients with comorbidity, ethics, and medicolegal aspects, perioperative management, etc); it is optional for participants to choose which topics to learn based on their interests and needs. Participants were encouraged to complete Part A during the first two weeks of their internship program to ensure sufficient knowledge before their service. However, participants were given full access to revisit the MOOC for up to 9–12 months of their internship programs. More details on the online course are reported elsewhere (Findyartini et al., 2021).
C. Study Design and Instruments
Our cross-sectional study uses the SOL-Qr (Jansen et al., 2018), which was adapted to Bahasa Indonesia, to assess online self-regulated learning ability in a Massive Open Online Course. Secondary data were obtained from the Moodle-based MOOC platform, including the total number of respondents, gender, internship location, former medical school, and course completion.
SOL-Qr measures seven aspects of SRL as mentioned in Table 1. Respondents answer each item on a 7-point Likert scale (1 for “not at all true for me” and 7 for “very true for me”). This questionnaire was translated to Bahasa Indonesia and back-translated to English to ensure similarity in meaning. Cognitive interviews with four respondents resembling the study participants were also conducted to obtain clarity of the items. The two respondents in this phase were final year medical school students from the authors’ institution (prospective participants of the national internship program) and the other two respondents were medical doctors who have just completed the national internship program.
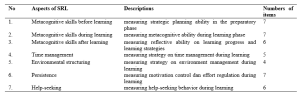
Table 1. Descriptions of SOL-Qr (Jansen et al., 2018)
Course completion, as analysed in this study, refers to the completion rate (in percentage) of the optional topics in part B that were accessed and completed by study participants in the open course.
D. Data Collection
Data were collected from the Moodle-based MOOC platform of the COVID-19 module from January to February 2021, two months after each course had started. This study uses a total sampling approach, with a minimum sample size of 204 respondents, calculated from standard deviation of 3.43 (Yen et al., 2016) and alpha (type I error) of 0.05 and beta (type II error) of 0.20 and 10% estimated drop out level.
All study participants were National Internship Medical Doctors in the year 2020 who were enrolled in the COVID-19 Open Course on the MOOC platform.
The SOL-Qr questionnaire was embedded in the evaluation questionnaire placed at the end of Part A, before participants moved forward to Part B. The questionnaire was completed voluntarily by participants who agreed to participate in this study. They were given adequate written information about the study and assured that there were no consequences of participation in regards to the course or the internship program evaluation. All data included in this study were collected from participants who signed and agreed upon the written consent embedded in the questionnaire. This study obtained ethical clearance from Faculty of Medicine Universitas Indonesia/ dr. Cipto Mangunkusumo General Hospital Research Ethics Committee Board (KET-1395/UN2.F1/ETIK/PPM.00.02/2020) in 2020.
E. Data Analysis
We conducted a three-stage validation process for the SOL-Qr, including the process of translation to Bahasa Indonesia by the research investigator, the back-translation process, and a review process by four newly graduated medical doctors who represented the characteristics of the study participants. This process ensured that the Bahasa Indonesia version of SOL-Qr was comparable to the original version. Furthermore, a Confirmatory Factor Analysis (CFA) was performed to confirm the model proposed by Jansen et al. (2018) as a fit model in the Bahasa Indonesia version compared to the original version. The fit model of CFA analysis determined whether normality, multicollinearity, residual values, and multivariate outliers were met. Furthermore, the Two-Index Presentation Strategy, the fit index combination of at least two indicators among the root mean square error of approximation (RMSEA), the standardised root mean square residual (SRMR), and the comparative fit index (CFI) all indicated the fit model of CFA analysis (Hu & Bentler, 1999; Schreiber et al., 2006). Internal consistency analysis of the Bahasa Indonesia version of SOL-Qr was also completed. Items were concluded as valid if the corrected item-total item correlation value was higher than 0.3. The questionnaire was considered reliable if alpha Cronbach ≥ 0.700; an alpha value higher than 0.900 indicates excellent internal consistency (Blunch, 2008).
All survey data obtained from the questionnaire were statistically analysed using IBM SPSS Statistic version 21. Demographic data were processed using descriptive statistics (proportion, mean, and standard deviation). Study participants were classified into two groups according to their internship location:
- Medical doctors who serve in Java- Bali Region, which was the primary epicenter of COVID-19 in the country in 2020.
- Medical doctors who serve in Outside Java- Bali Region.
We also classified participants according to their former medical school accreditation.
Bivariate analysis using the t-independent test was used to find relationships between the online self-regulated learning scores and gender, internship location, the former medical school, and the course completion. The Pearson correlation test was also used to analyse correlations between online SRL subscales and the course completion rate.
III. RESULTS
A. Validation of the SOL-Qr
The three stages of validation were conducted in the SOL-Qr instrument to ensure the content validity of the Bahasa Indonesia version of SOL-Qr. CFA was performed on the Bahasa Indonesia version of SOL-Qr, with the results showing the goodness-of-fit according to Hu and Bentler’s Two Index Presentation; the SRMR value was 0.056 (<0.08) while RMSEA value was 0.078 (<0.08). Meanwhile, the χ2/df value was < 0.001; the CFI value was 0.874 (Hu & Bentler, 1999). The model (Figure 1) also confirms the comparability of the subscales to the original SOL-Qr.
The Bahasa Indonesia version of SOL-Qr also shows excellent validity and reliability, with a Cronbach’s alpha of 0.974. The reliability of each subscale ranges from 0.971 to 0.975.
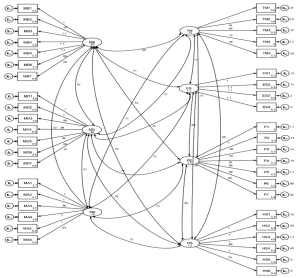
Figure 1. CFA results of the National Language Version of SOL-Qr (MB: Metacognitive Before, MD: Metacognitive During, MA: Metacognitive After, TM: Time Management, ES: Environmental Structuring, P: Persistence, and HS: Help Seeking)
B. Profile of Participants’ Online SRL Scores
A total of 5,846 internship doctors from all 34 provinces in Indonesia were enrolled and accessed the MOOC; as many as 5,432 participants, graduated from 74 medical schools (of which 46% are A-accredited while 54% are B-accredited), agreed to participate in the study (response rate of 92.9%). Details on the study participants are presented in Table 2.
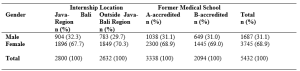
Table 2. Study participants (N = 5,432)
C. Relationship Between Online SRL Score, Course Completion, Gender, and Internship Location
Data on the online SRL scores and course completion were analysed according to gender, internship location, and medical school accreditation. The data are described in means and standard deviations, as they were normally distributed, as shown in Table 3.
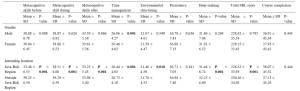

Table 3. Profile of online SRL and course completion according to gender, internship location, and medical school
According to Table 3, the average total scores of participants’ online self-regulated learning in all groups show high levels of online SRL (SRL score > 5). When comparing the male and female participants, the finding suggests that only the Time Management subscale shows a significant difference (p = 0.001). Male participants show higher scores in time management than female participants. Participants from the Outside Java-Bali Region had significantly higher online SRL scores in all subscales, except for the Persistence subscale (p = 0.181), than participants from the Java-Bali Region, which was the primary epicenter of COVID-19 in the country.
Meanwhile, the online SRL scores of participants who graduated from A-level versus B-level accredited medical schools mostly show similar online self-regulated learning scores, except in the time management scale (p = 0.009).
Although Table 3 shows no significant difference regarding course completion across gender, internship region, or former internship location, it does show a low course completion rate. Participants only completed less than approximately 40% of all optional topics in Part B.
The results of the Pearson correlation test show significant differences between the course completion rate and several SRL subscales, with very low correlation values (r < 0.1 in all subscales) for the SOL-Qr in the whole samples, as well as between the internship location and former medical education groups. Only the Time Management score was correlated to Course Completion in the Outside Java-Bali group, with a very low correlation value (r = 0.102). Therefore, the course completion rate does not correlate with the online SRL scores.
IV. DISCUSSION
Self-regulated learning is a dynamic process and may change while learners undergo various learning contexts (Barnard et al., 2009). The rapidly changing pandemic has accelerated the adaptation of new learning approaches and methods worldwide, including MOOCs that had gained popularity. Therefore, the use of the SOL-Qr is beneficial for providing MOOC learners’ SRL profiles (Jansen et al., 2018).
This study represents the first successful attempt to cross-culturally validate the SOL-Qr and determine the suitability of all its subscales for profiling online SRL of medical doctors in their early career. The three-stage validation process for the SOL-Qr was conducted as a form of cross-cultural adaptation of the instrument to facilitate its use in measuring self-regulated learning abilities in an online setting in the context of medical education—specifically in the MOOC used for continuing medical education and professional development programs for early-career, newly graduated medical doctors (Hambleton, 2005). The CFA conducted in this study also demonstrates a good fit, with excellent internal consistencies of the SOL-Qr and its subscales; this demonstrates the comparability of the instrument with the original SOL-Qr (Jansen et al., 2018).
The use of the SOL-Qr in this study demonstrates online SRL abilities during the transition phase in the early careers of medical doctors, from medical students to medical interns. This study demonstrates the high average level of online SRL ability among newly graduated medical doctors (SRL score > 5). Participants’ online SRL may increase due to the positive online learning experience obtained, considering that the knowledge on COVID-19 provided in this particular MOOC was vital and timely knowledge for these recent graduates. While participant perceptions of MOOCs have been reported elsewhere, it is known that positive perceptions of an online learning experience and environments are significantly correlated with the online SRL score (Abouzeid et al., 2021; Findyartini et al., 2020; Liaw & Huang, 2013).
The high scores for online SRL in our study were found in total and in most of the subscales, except for the metacognitive skills before learning (MB) scale in participants from the Java-Bali region. A similar finding on the low level of metacognitive ability was reported during the transition phase from preclinical to clinical learning, which was associated with previous clinical experience (Cho et al., 2017). Albeit being assessed using a different instrument, the decreased level of metacognitive skill in this study may also be affected by a similar factor. Since the Java-Bali Region had been the primary epicenter of COVID-19 in the country, with the greatest number of COVID-19 cases (69.41%) out of all other regions (National Ministry of Health, 2021), most interns in the Java-Bali Region may have experienced being removed from their duties at the beginning of the pandemic for safety reasons during their last clinical rotations as medical students (Findyartini et al., 2020). This may have caused discomfort because they felt useless and unable to contribute to patient care, further affecting their sense of competence and motivation, despite previous clinical experiences. Hence, this may have affected the process of goal-setting and reflecting on their prior knowledge during the transition to becoming medical interns (Dornan et al., 2014; Dubé et al., 2015).
Findings of this study demonstrate no significant correlation between online SRL and the number of optional topics achieved by participants. This result was supported by the fact that, despite the high level of online SRL ability depicted in this study, the duration of which participants accessed the compulsory Part A was lower than the expected minimum duration as estimated by course developers although we did not explore whether participants learned about COVID-19 from any other learning resources (Findyartini et al., 2021). The current study also supports the results of a previous study with similar findings regarding online SRL scores and academic achievement, although this study does report a significant relationship between online discussion and academic achievement (Abouzeid et al., 2021). The MOOC examined in this study does not provide two-way interactions among learners or between learners and instructors, which may affect the low number of optional courses completed.
Our study also shows that the online SRL scores of participants in the Outside Java-Bali Region were significantly higher (p < 0.001) across all scales than those of participants in the Java-Bali Region, except on the Persistence scale (p = 0.181). This suggests that participants in the Outside Java-Bali Region also have better time management, environmental structuring, and help-seeking abilities, which may relate to the workload at the internship locations. Participants in the Java-Bali Region face a higher workload and stress as front-liners in managing patients during the COVID-19 pandemic (as health educators, contact tracers, vaccinators, etc.). This aligns with other findings suggesting that an optimal workload determines the quality of students’ SRL in the early transition and adaptation phases (Barbosa et al., 2018).
Furthermore, the MOOC was given to the participants at the beginning of their internship programs, in which several orientations and patient management also took place. Hence, it is confirmed that the participants’ workload affected the time allocated to learn the MOOC (Eriksson et al., 2017). This study also suggests that the use of the MOOC for knowledge provision would preferably occur with sufficient time before immersion in other workplace-based learning experiences.
Hew and Cheung (2014) report few challenges in MOOC completion, including a lack of time and having other priorities to fulfill the course; therefore, time management ability remains crucial. The results of this study indicate that male participants had slightly better time management abilities than female participants. Although the absolute difference of the scores between groups is small, this study involved 5,432 respondents (much more than the minimum sample size), thus small differences in results can be statistically significant. As newly graduated doctors, study participants were interns who worked in a new environment hence new challenges regarding workplace relationships and workload may be faced. Previous studies show that female and male physicians may perceive these challenges differently (Babaria et al., 2009). Female physicians report that they feel uncertain and stressed when facing different clinical environments. Because they tend to need more time to adapt than male physicians (Malau-Aduli et al., 2020), completing a MOOC may not be their priority. Moreover, with masculinity/femininity level of cultural determinant, Indonesians have a clear cut between gender roles, thus affecting roles of female participants in most settings (Mangundjaya, 2013). Female participants may culturally face different roles in their personal lives, such as the expectation to perform housework and childcare, in addition to their internship obligation resulting in conflicting time and higher stress levels. The conflicting time and higher stress level in both work and personal life (Isaac et al., 2013) may influence female participants’ ability to commit time to learn and work and may explain the lower time management scores among female participants.
This study also highlights that, overall, the online SRL scores of participants graduating from the A-level and B-level of accredited medical schools show similar results, except on the time management scale (p = 0.009), where the participants from the higher level accredited schools show higher scores than the participants from the lower level accredited schools. Prior online learning experience has been reported as an important determinant of online learning success (Vilkova, 2019). For newly graduated doctors completing an internship program, prior online learning experience may be largely attributed to the use of online learning formally in their medical school’s curriculum. Our study suggests that the higher accredited medical schools may provide more online learning experiences, leading to better time management skills among the participants from this group. Furthermore, MOOC completion and the fulfillment of learning outcomes were determined by the forethought phase in the students’ SRL; thus, the goal-setting, self-efficacy, and task values should be emphasised by the participants and facilitated by the MOOC (Vilkova, 2019). Our study further indicates that time management in the use of the MOOC should be considered by learners in the forethought, performance, and self-reflection phases of their SRL; the planning stage of the MOOC development must determine the estimated completion time for the whole course and its sections about the course learning outcomes and the participant’s characteristics (Stracke et al., 2018).
Similar to the SRL ability in offline learning, our findings further imply the importance of accounting for learners’ online SRL abilities, which are dynamic across online learning contexts, including MOOCs. Certain characteristics of MOOCs, such as their open access and self-paced nature, stress the importance of online SRL ability, especially for MOOCs used in the transition phase in the early career of medicine. Therefore, using validated and reliable instruments, such as the SOL-Qr, to measure the online SRL abilities of MOOC participants would help course developers to identify whether the online learning context supports or hinders learners’ SRL abilities, thus helping course administrators further improve MOOC to provide further support for learners’ SRL (Barnard et al., 2009; Sandars & Patel, 2020).
V. LIMITATIONS OF THE STUDY
We identify several limitations of this study. As this study examined online SRL ability of participants using a self-reported questionnaire, it was unable to examine the actual online SRL ability, given the poor correlation with the course completion rate. Furthermore, as the evaluation of online SRL was only conducted once, it was not possible to observe changes in SRL ability throughout the use of the MOOC or in a longer period. With the data that we obtained, we were also unable to analyse whether participants used other online resources to learn about COVID-19 before the internship program or parallel with accessing the provided module as the marker of online SRL nor to explain any causal relationships between online SRL scores and the factors under investigation. However, measurement of online SRL ability using the cross-culturally validated SOL-Qr reveals that this instrument can be used for MOOCs on continuing medical education and professional development in the early-career context.
VI. CONCLUSION
Our study demonstrates the cross-cultural validity of the SOL-Qr and the suitability of its subscales for use in the medical and health fields. The results portray the online SRL ability of medical doctors as participants in a MOOC during the transition phase in their early career. We found that the time management ability was associated with previous experience during the medical education period, while other subscales were mostly associated with workload during the transition phase. However, as the scores did not correlate with the completion rate of MOOC, it can be concluded that the questionnaire is a possible valid tool to assess self-regulated learning in the MOOC environment. Yet, the corresponding learning effort or completion rate may be beyond just the commitment to the described MOOC.
Notes on Contributors
NG designed and led the study, led data collection and analysis, and led manuscript development. AF, DAK, and CH contributed in data collection, completed data analysis, and contributed to manuscript development. GS contributed in the data analysis and manuscript development. All authors approved the final version of the manuscript.
Ethical Approval
This study obtained ethical clearance from Research Ethics Committee of Faculty of Medicine Universitas Indonesia/ dr. Cipto Mangunkusumo General Hospital (KET-1395/UN2.F1/ETIK/PPM.00.02/2020) in 2020.
Data Availability
Data will be available upon request to corresponding author due to conditions of consent provided by respondents in this study and that it should abide data sharing policy from the authors’ institution and the Republic of Indonesia Ministry of Health.
Acknowledgement
The authors would like to acknowledge the Ministry of Health Republic of Indonesia for the trust that has been given to develop and organise the MOOC for the national internship program participants. We would also like to thank all national internship program participants for participation in this study and to Vernonia Yora Saki for assisting the authors with statistical analysis of the study. The preliminary results of this study were presented in Niigata Meeting 2020.
Funding
The development of MOOC and data analysis has been supported by the Ministry of Health Republic of Indonesia through a direct appointment decree to our institution.
Declaration of Interest
All authors state no possible conflicts of interest, including financial, consultant, institutional, and other relationships that might lead to bias or a conflict of interest.
References
Abouzeid, E., O’Rourke, R., El-Wazir, Y., Hassan, N., Ra’oof, R. A., & Roberts, T. (2021). Interactions between learner’s beliefs, behaviour and environment in online learning: Path analysis. The Asia Pacific Scholar, 6(2), 38-47. https://doi.org/10.29060/TAPS.2021-6-2/OA2338
Asarbakhsh, M., & Sandars, J. (2013). E-learning: The essential usability perspective. The Clinical Teacher, 10(1), 47-50. https://doi.org/10.1111/j.1743-498X.2012.00627.x
Babaria, P., Abedin, S., & Nunez-Smith, M. (2009). The effect of gender on the clinical clerkship experiences of female medical students: Results from a qualitative study. Academic Medicine, 84(7), 859-866. https://doi.org/10.1097/ACM.0b013e3181a8130c
Barbosa, J., Silva, Á., Ferreira, M. A., & Severo, M. (2018). Do reciprocal relationships between academic workload and self-regulated learning predict medical freshmen’s achievement? A longitudinal study on the educational transition from secondary school to medical school. Advances in Health Sciences Education, 23, 733-748. https://doi.org/10.1007/s10459-018-9825-2
Barnard, L., Lan, W. Y., To, Y. M., Paton, V. O., & Lai, S.-L. (2009). Measuring self-regulation in online and blended learning environments. The Internet and Higher Education, 12(1), 1-6. https://doi.org/10.1016/j.iheduc.2008.10.005
Bembenutty, H. (2009). Academic delay of gratification, self-regulation of learning, gender differences, and expectancy-value. Personality and Individual Differences, 46(3), 347-352. https://doi.org/10.1016/j.paid.2008.10.028
Blunch, N. J. (2008). Introduction to structural equation modelling using SPSS and AMOS. SAGE.
Broadbent, J., & Poon, W. L. (2015). Self-regulated learning strategies & academic achievement in online higher education learning environments: A systematic review. The Internet and Higher Education, 27, 1–13. https://doi.org/10.1016/j.iheduc.2015.04.007
Bullock, A., & De Jong, P. G. M. (2013). Technology-enhanced learning. In T. Swanwick (Ed.), Understanding medical education: Evidence, theory, and practice (2nd ed., pp. 149-160). Wiley Blackwell. https://doi.org/10.1002/9781118472361.ch11
Cho, K. K., Marjadi, B., Langendyk, V., & Hu, W. (2017). Medical student changes in self-regulated learning during the transition to the clinical environment. BMC Medical Education, 17(59). https://doi.org/10.1186/s12909-017-0902-7
Chung, L.-Y. (2015). Exploring the effectiveness of self-regulated learning in massive open online courses on non-native English speakers. International Journal of Distance Education Technologies, 13(3), 61-73. https://doi.org/10.4018/ijdet.2015070105
Dornan, T., Tan, N., Boshuizen, H., Gick, R., Isba, R., Mann, K., Scherpbier, A., Spencer, J., & Timmins, E. (2014). How and what do medical students learn in clerkships? Experience based learning (ExBL). Advances in Health Sciences Education, 19(5), 721-749. https://doi.org/10.1007/s10459-014-9501-0
Dubé, T. V., Schinke, R. J., Strasser, R., Couper, I., & Lightfoot, N. E. (2015). Transition processes through a longitudinal integrated clerkship: A qualitative study of medical students’ experiences. Medical Education, 49(10), 1028-1037. https://doi.org/10.1111/medu.12797
Eriksson, T., Adawi, T., & Stöhr, C. (2017). “Time is the bottleneck”: A qualitative study exploring why learners drop out of MOOCs. Journal of Computing in Higher Education, 29, 133-146. https://doi.org/10.1007/s12528-016-9127-8
Findyartini, A., Anggraeni, D., Husin, J. M., & Greviana, N. (2020). Exploring medical students’ professional identity formation through written reflections during the COVID-19 pandemic. Journal of Public Health Research, 9(s1). https://doi.org/10.4081/jphr.2020.1918
Findyartini, A., Greviana, N., Hanum, C., Husin, J. M., Sudarsono, N. C., Krisnamurti, D. G. B., & Rahadiani, P. (2021). Supporting newly graduate medical doctors in managing COVID-19: An evaluation of Massive Open Online Course in a limited-resource setting. PLoS ONE, 16(9), e0257039. https://doi.org/10.1371/journal.pone.0257039
Hall, A. K., Nousiainen, M. T., Campisi, P., Dagnone, J. D., Frank, J. R., Kroeker, K. I., Brzezina, S., Purdy, E., & Oswald, A. (2020). Training disrupted: Practical tips for supporting competency-based medical education during the COVID-19 pandemic. Medical Teacher, 42(7), 756-761. https://doi.org/10.1080/0142159X.2020.1766669
Hambleton, R. K. (2005). Issues, designs, and technical guidelines for adapting tests into multiple languages and cultures. In R. K. Hambleton, P. F. Merenda, & C. D. Spielberger (Eds.), Adapting educational and psychological tests for cross-cultural assessment (pp. 3–38). Lawrence Erlbaum.
Hew, K. F., & Cheung, W. S. (2014). Students’ and instructors’ use of massive open online courses (MOOCs): Motivations and challenges. Educational Research Review, 12, 45–58. https://doi.org/10.1016/j.edurev.2014.05.001
Hu, L.-t., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. https://doi.org/10.1080/10705519909540118
Isaac, C., Petrashek, K., Steiner, M., Manwell, L. B., Carnes, M., & Byars-Winston, A. (2013). Male spouses of women physicians: Communication, compromise, and carving out time. The Qualitative Report, 18(52), 1-12. https://doi.org/10.46743/2160-3715/2013.1423
Jansen, R. S., van Leeuwen, A., Janssen, J., & Kester, L. (2018). Validation of the revised self-regulated online learning questionnaire. In V. Pammer-Schindler, M. Pérez-Sanagustín, H. Drachsler, R. Elferink, & M. Scheffel (Eds.), Lifelong Technology-Enhanced Learning (pp. 116-121). Springer. https://doi.org/10.1007/978-3-319-98572-5_9
Jansen, R. S., van Leeuwen, A., Janssen, J., Kester, L., & Kalz, M. (2017). Validation of the self-regulated online learning questionnaire. Journal of Computing in Higher Education, 29, 6-27. https://doi.org/10.1007/s12528-016-9125-x
Jouhari, Z., Haghani, F., & Changiz, T. (2015). Factors affecting self-regulated learning in medical students: A qualitative study. Medical Education Online, 20(1). https://doi.org/10.3402/meo.v20.28694
Liang, Z. C., Ooi, S. B. S., & Wang, W. (2020). Pandemics and their impact on medical training: Lessons from Singapore. Academic Medicine, 95(9), 1359-1361. https://doi.org/10.1097/ACM.0000000000003441
Liaw, S.–S., & Huang, H.–M. (2013). Perceived satisfaction, perceived usefulness and interactive learning environments as predictors to self-regulation in e-Learning environments. Computers & Education, 60(1), 14-24. https://doi.org/10.1016/j.compedu.2012.07.015
Magno, C. (2011). Validating the academic self-regulated learning scale with the Motivated Strategies for Learning Questionnaire (MSLQ) and Learning and Study Strategies Inventory (LASSI). The International Journal of Educational and Psychological Assessment, 7(2), 56-73.
Malau-Aduli, B. S., Roche, P., Adu, M., Jones, K., Alele, F., & Drovandi, A. (2020). Perceptions and processes influencing the transition of medical students from pre-clinical to clinical training. BMC Medical Education, 20, 279. https://doi.org/10.1186/s12909-020-02186-2
Mangundjaya, W. L. H. (2013). Is there cultural change in the national cultures of Indonesia? In Y. Kashima, E. S. Kashima, & R. Beatson (Eds.), Steering the cultural dynamics: Selected papers from the 2010 Congress of the International Association for Cross-Cultural Psychology. https://scholarworks.gvsu.edu/iaccp_papers/105/
National Ministry of Health. (2020, December 31). Health care workforce statistics database in Indonesia. Retrieved May 10, 2021, from http://bppsdmk.kemkes.go.id/info_sdmk/info/index?rumpun=101
National Ministry of Health. (2021, April 23). Current situations of the development of novel coronavirus (COVID-19). Retrieved May 10, 2021, from https://covid19.kemkes.go.id/situasi-infeksi-emerging/situasi-terkini-perkembangan-coronavirus-disease-covid-19-23-april-2021
Ortiz-Martìnez, Y., Castellanos-Mateus, S., Vergara-Retamoza, R., Gaines-Martìnez, B., & Vergel-Torrado, J. A. (2021). Online medical education in times of COVID-19 pandemic: A focus on Massive Open Online Courses (MOOCs), Educación Médica, 22, S40. https://doi.org/10.1016%2Fj.edumed.2020.12.001
Panadero, E. (2017). A review of self-regulated learning: Six models and four directions for research. Frontiers in Psychology, 8, Article 422. https://doi.org/10.3389/fpsyg.2017.00422
Pintrich, P. R., Smith, D. A. F., Garcia, T., & Mckeachie, W. J. (1993). Reliability and predictive validity of the Motivated Strategies for Learning Questionnaire (MLSQ). Educational and Psychological Measurement, 53(3), 801-813. https://doi.org/10.1177%2F0013164493053003024
Poonia, S. K., & Rajasekaran, K. (2020). Information overload: A method to share updates among frontline staff during the COVID-19 pandemic. Otolaryngology-Head and Neck Surgery, 163(1), 60-62. https://doi.org/10.1177%2F0194599820922988
Sandars, J., & Patel, R. (2020). The challenge of online learning for medical education during the COVID-19 pandemic. International Journal of Medical Education, 11, 169-170. https://doi.org/10.5116/ijme.5f20.55f2
Schreiber, J. B., Nora, A., Stage, F. K., Barlow, E. A., & King, J. (2006). Reporting structural equation modelling and confirmatory factor analysis results: A review. The Journal of Educational Research, 99(6), 323–338. https://doi.org/10.3200/JOER.99.6.323-338
Stracke, C. M., Tan, E., Moreira Texeira, A., do Carmo Pinto, M., Vassiliadis, B., Kameas, A., Sgouropoulou, C., & Vidal, G. (2018). Quality Reference Framework (QRF) for the Quality of Massive Open Online Courses (MOOCs): Developed by MOOQ in close collaboration with all interested parties worldwide. MOOQ. http://www.mooc-quality.eu/QRF
Vilkova, K. A. (2019, May 20-22). Self-regulated learning and successful MOOC completion [Europeaan MOOCs Stakeholders Summit 2019 Conference]. Proceedings of EMOOCs: Work in Progress Papers of the Research, Experience and Business Tracks.
Virtanen, P., & Nevgi, A. (2010). Disciplinary and gender differences among higher education students in self-regulated learning strategies. Educational Psychology, 30(3), 323-347. https://doi.org/10.1080/01443411003606391
Wong, J., Baars, M., Davis, D., Van Der Zee, T., Houben, G.-J., & Paas, F. (2018). Supporting self-regulated learning in online learning environments and MOOCs: A systematic review. International Journal of Human-Computer Interaction, 35(4-5), 356-373. https://doi.org/10.1080/10447318.2018.1543084
Yen, C.-J., Tu, C.-H., Sujo-Montes, L., & Sealander, K. (2016). A predictor for PLE management: Impacts of self-regulated online learning on students’ learning skills. Journal of Educational Technology Development and Exchange, 9(1), 29-48. https://doi.org/10.18785/jetde.0901.03
*Nadia Greviana
Faculty of Medicine Universitas Indonesia,
Jalan Salemba 6 Central Jakarta, Indonesia,
Email: nadiagreviana@ui.ac.id/ nadia.greviana@gmail.com
Submitted: 19 May 2021
Accepted: 26 August 2021
Published online: 4 January, TAPS 2022, 7(1), 66-75
https://doi.org/10.29060/TAPS.2022-7-1/OA2521
Lay Ling Tan1, Pim W. Teunissen2, Wee Shiong Lim3, Vanessa Wai Ling Mok1 & Hwa Ling Yap1
1Department of Psychological Medicine, Changi General Hospital, Singapore; 2School of Health Professions Education (SHE), Maastricht University, Netherlands; 3Cognition and Memory Disorders Service, Tan Tock Seng Hospital, Singapore
Abstract
Introduction: Development of expertise and counselling skills in psychiatry can be mastered only with effective supervision and mentoring. The conceptualisations of educational supervision amongst supervisors and residents were explored in this study to understand how supervisory roles may have been affected by the adoption of competency-based psychiatry residency training.
Methods: A qualitative research approach with thematic analysis was adopted. Individual in-depth interviews using a semi-structured interview guide with a purposive sample of six supervisors and six newly graduated residents were conducted. Transcripts of the interview were analysed and coded using the Atlas Ti software.
Results: Four major themes emerged from analysis of the transcripts: (1) Meaning and definition of supervision; (2) Expectations and responsibilities of the educational supervisor; (3) Elusiveness of mentoring elements in educational supervision and (4) Personal and professional development of residents in supervision. Supervisors and residents perceived educational supervision narrowly to be transactional with acquisition of knowledge and skills, but residents yearned for more relational interactions.
Conclusion: This study showed that the roles and functions of supervisors in educational supervision were unclear. It also highlighted the lack of a mentoring orientation in supervision in the psychiatry residency training program. An emphasis on assessment of competencies might have contributed to tension in the supervisory relationship and lack of a mentoring role, with concerns on residents’ personal and professional identity development in their psychiatry training.
Keywords: Psychiatry, Mentoring, Educational Supervision, Competency-Based Medical Education, Professional Identity Development
Practice Highlights
- Supervision in psychiatry has been described to encompass more than just a teaching and learning relationship but also a supportive and mentoring one.
- Educational supervision has been purported to offer the unique opportunity for effective mentoring within supervision.
- This qualitative study highlighted significant differences in definitions, roles and expectations of educational supervision.
- The conflict between mentoring and appraisal of competency needs to be addressed.
- Roles and expectations of the educational supervisor must be articulated clearly to both supervisors and residents.
I. INTRODUCTION
Postgraduate medical education (PGME) in Singapore underwent tremendous changes in the last decade. Before 2009, Singapore’s PGME was structured around time frames and curricular processes, in contrast to competency-based medical education (CBME) (Frank et al., 2017). In 2008, Singapore’s Ministry of Health (MOH) raised concerns of the lack of clear learning objectives and absence of measurable standards of training and outcomes with the medical schools and teaching hospitals. MOH recognised a need to ensure that every PGME graduate is prepared for clinical practice with the necessary competencies. With that vision in mind, MOH collaborated with the United States (US) Accreditation Council for Graduate Medical Education (ACGME) to revamp the PGME structure and accreditation system in 2009 (Chay, 2019). This move has resulted in major changes in the psychiatry postgraduate program. The 5-year National Psychiatry Residency Training Program was launched with a main teaching site and six sponsoring institutions. It also instituted the educational supervision framework where an assigned educational supervisor meets the supervisee regularly during the whole duration of training.
A. Concepts of Supervision
Supervision originated in professions outside of medicine (Launer, 2013) and is a distinct professional practice with specific articulated competence and training (Falender & Shafranske, 2007). It has been considered as a combination of various elements and is not a uniform concept (Carroll, 2006). Supervision is critical for ensuring effective professional practice of the healthcare sector (Tebes et al., 2011), particularly in psychiatry, where counselling skills can be developed only with effective supervision and mentoring.
1) Clinical supervision: Clinical supervision is subcategory to the wider concept of supervision. One definition is “provision of guidance and feedback on matters of personal, professional and educational development in the context of a trainee’s experience of providing safe and appropriate care” (Kilminster et al., 2007). There is consensual acceptance of the basic functions of clinical supervision: formative, supportive and managerial (Kilminster et al., 2007). These functions overlap depending on the context, problems emphasised and supervision goals (Kadushin, 1985).
2) Educational supervision: Educational supervision, on the other hand, has been described as regular supervision occurring in the context of a training program to determine learning needs and review progress of the supervisee (Passi, 2016). There has been extensive research done in clinical supervision (Kilminster et al., 2007; Patel, 2016) but educational supervision is under-researched with very few such studies conducted in psychiatry. It can be considered to be the most complex and challenging form of supervision as there are a number of overlapping and at times conflicting roles which need to be fulfilled (Launer, 2013). Aside from having to facilitate learning, there is also the need to evaluate the supervisee’s performance, which may result in confusion in the supervisory roles. Educational supervision has been purported to offer the unique opportunity for effective mentoring within supervision (Passi, 2016), which ideally should be recognised as an important component of the whole supervisory framework (Driessen et al., 2011).
B. Conceptual Framework for Educational Supervision in Postgraduate Psychiatry Training
Clinical and educational supervision are essential for development of health professionals and widely recognised as crucial for effective learning (Pront et al., 2016) and reflective practice (Schon, 1987). Learning in educational supervision can be conceptualised from experiential and social learning theory. Experiential learning is a key concept of the developmental-educational model of educational supervision (Kolb, 1984/2014). Learning is also a social process, where the supervisee is influenced by the cultural system of social knowledge and learns the trade with the guide of a more experienced colleague (Vec et al., 2014), a particularly important component in the field of psychiatry, a discipline closely related to the social sciences. Thus, there has been frequent reference to this apprenticeship model in supervision, although there is no clear definition of the term in the context of psychiatry training (MacDonald, 2002).
Supervision in psychiatry has its roots in psychoanalysis (Torby et al., 2015). Supervision in the context of general psychiatry training was mentioned infrequently and the concepts of supervision of the psychotherapeutic work of trainees were often transferred directly into the setting of general clinical supervision as if the two situations were identical (MacDonald, 2002). The supervisor can be seen as fulfilling the role of the analyst of the supervisee’s analytic ego (Akhtar, 2009). This necessitates a trusting relationship between the supervisor and supervisee, very much akin to that of informal mentoring, which has been described as psychosocial in nature and serves to enhance the supervisee’s self-esteem through interpersonal dynamics of the relationships, the emotional bonds they form and the work they accomplish together (Hansman, 2001). Supervision has also been frequently conceptualised as a development process or a process of identification (MacDonald, 2002). This is the transformation of a trainee through the acquisition of requisite knowledge, skills, attitudes, values, and attributes; from doing the work of a psychiatrist to being a psychiatrist (Wald, 2015). This active, constructive and transformative process has been referred to as professional identity formation (Wald, 2015). This continuous process requires the fostering of personal and professional growth through mentorship and self-reflection (Holden et al., 2015). The provision of guidance and mentoring with respect to personal and professional identity development would arguably be more critical in supervision in psychiatry. The personal aspects and the development of better self-awareness in the supervisee and the ‘internalised supervisor’ has been considered by some to be the fundamental goal of supervision (Kadushin, 1985). However, this will require the training program to allow sufficient time and opportunity to build and develop the supervisor-supervisee relationship.
With ACGME setting up collaborative initiatives with other countries and a trend towards a competency-based training approach, a better understanding of the impact of CBME on the supervision process and structure will be relevant to our international educators. The mentoring element in educational supervision has the potential to ensure that learning is not guided entirely by assessment and evaluation but is supplemented by the periodic guidance of a trusted mentor and addressing the personal and professional components in clinical supervision (Kilminster et al., 2007). With the implementation of the ACGME training framework, understanding the complexity and barriers of developing a mentoring relationship in educational supervision will be crucial. The research questions which this study aimed to answer were:
1. What are supervisors’ and residents’ perceptions on the educational supervisory role in the psychiatry residency program?
2. How do supervisors and residents perceive the supervisor’s mentoring roles in their educational supervision experience?
II. METHODS
A. Design
This was a qualitative research strategy where individual in-depth interviews with a purposive sample of six supervisors and six residents were conducted, the intent of which was to understand the participants’ meanings of the phenomenon of educational supervision (Creswell, 2014). Ethics approval was sought from the Institutional Review Board (CIRB Ref: 2017/2319) and informed consent was received from all participants.
B. Setting
The residency training program instituted the educational supervision framework by ACGME where an assigned educational supervisor meets the supervisee weekly of at least an hour duration. The educational supervisor is responsible for completion of the resident’s evaluation reports based on feedback gathered from the resident’s clinical supervisors and offer recommendations for the supervisee’s training progress. Clinical supervisors in the residency program are consultants managing patients together with the residents in the ward and clinic settings. Work-placed based assessments in the form of mini-clinical evaluations (mini-cex) and 360-degree feedback evaluations are done by both the educational and clinical supervisors.
There are six teaching sites in the psychiatry residency program and the researcher’s teaching site is one of the largest, with 18 supervisors overseeing nine to 12 residents posted in their various years of training. The setting of the research was the teaching site where the PI (Principal Investigator) served as Associate Program Director (APD).
C. Subjects
Six supervisors with two each from the Associate Consultant, Consultant and Senior Consultant group, and one male and one female from each group were invited to participate. For the residents, those who had just graduated from the residency program were invited. A total of six recently graduated residents (three males and three females) were sampled. This was to minimise biases related to fear of negative evaluation or power differentials while still undergoing residency training. It was hoped that with this purposive sampling, a relevant mix of supervisory experiences from the participants would be achieved.
D. Data collection
One-to-one semi-structured interviews were conducted by the PI using an interview guide (Appendix 1). The interview guide was developed by the PI with inputs from the research team. The interviews were audio-recorded with informed consent of the participants. Due attention was paid to the content of the participants’ sharing and the emerging themes during the interview and analysis process such that consideration of including more participants in the study would be taken if there was a need for further varied views to be elicited (Creswell, 2014).
E. Analysis
A qualitative research approach with thematic analysis was adopted. The Atlas Ti (version 8) software was used to code and analyse the data. Coding of all the data was made by the PI before a coding structure was created. There was a reiterative development and re-development of the coding structure such that all the data were appropriately accounted for. Codes were added and revised as more interviews were conducted. All the data were coded according to the study objectives and were classified into categories that reflected the emerging themes. Based on further readings in medical education literatures, the themes were grouped and sub-grouped in a logical fashion to form a thematic template. The raw data were revisited regularly throughout the analytic process to ascertain that the codes and resulting themes were grounded in the data. To ensure adequate coding and to improve the research reliability, we performed investigators’ triangulation. The co-investigator (LWS) was invited to analyse the first three interviews independently. The PI and co-investigators (TLL, VM, YHL) discussed regarding the main themes developed and differences were addressed and reconciled. To further improve credibility and transferability of the research data and its analysed results, member checking was used and participants’ comments regarding the developed themes were solicited. There was general agreement with the results generated from their interviews.
III. RESULTS
Six supervisors and six supervisees completed the study. As the research progressed, there was the progressive realisation of an overarching pattern emerging around the supervisory process, namely, the heterogeneity of the concept of supervision and the tension and conflicts amongst its various roles and functions.
Four major themes emerged:
- Meaning and definition of supervision
- Expectations and responsibilities
- Elusiveness of mentoring elements in educational supervision
- Personal and professional development in supervision
A. Meaning and Definition of Supervision
1) Supervisor’s perspectives: Supervisors defined supervision as “observing”, “helping”, “guiding”, “teaching”, “grading” and “assessing” the residents such that they could be certified to fulfil the program requirements. These descriptors suggested a supervisor-centric definition.
“Someone in a position of experience or age supervises, in other words…observe…teaches, impact knowledge and skills to the supervisee…is like watching somebody”
(S1)
2) Residents’ perspectives: Residents referred to supervision as an “apprenticeship”, “guiding and checking on progress” and promoting the “maturation as a clinician”. There was the repeated emphasis on the supervisor attending to the resident’s “growth”, “personal well-being” and to “encourage” and “commend”.
“…essentially is in line with the whole practice of medicine where there is apprenticeship, someone has to guide…to encourage, commend, growth…”
(R1)
B. Expectations and Responsibilities
1) Supervisor’s perspectives: Supervisors expected residents to be able to exhibit the attitude of being “able to talk about things and not being afraid of being judged”; “to pay attention to personal development so that the resident is more real as a person”; “to be ready to give feedback about supervision” and “being comfortable, open and trusting of the supervisor’s intentions”.
In practice, however, faculty observed that residents were “not expecting beyond helping them with clinical work”; “does not talk about struggles and frustrations” and were “not used to opening up”. Although engaging the resident with regards to their struggles was identified to be important, it was highlighted as “not the culture or consistently practiced” and that “residents may not appreciate why we want them to talk about their feelings”.
Faculty viewed discussing about resident’s personal issues as intrusive and a violation of the boundaries in supervision.
“We also have to keep some boundaries… we are careful not to go beyond certain boundary especially if it is something which the supervisee is not very comfortable with”
(S1)
Table 1 illustrates our faculty’s understanding of the roles and functions of the educational supervisor.
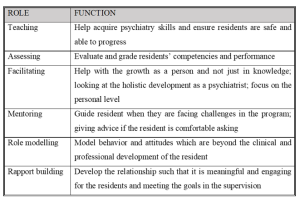
Table 1: Faculty’s understanding of the roles and functions of the educational supervisor
2) Residents’ perspectives: Residents’ expected the educational supervisor to be “approachable and open”, “easy to talk to”, “relaxed”, “able to attend to personal growth”, “helping to reflect” and “build rapport”. Residents thus expected a more relational as opposed to transactional interaction with the supervisor.
“…apart from the bread and butter clinical aspects of work…talk to you a bit more about your personal stage in life, how things are coming along… It is this stuff that I find it hard to find in textbooks or anywhere along the clear training roadmap”
(R1)
Residents tended to see the educational supervisor’s role as conflictual in view of the attendant assessor function, and how boundaries between the two roles are often not clearly delineated.
“Ultimately is quite hierarchical in the system…. so if a supervisee has a lot of problems and come to the supervisor for advice…the supervisor might negatively evaluate the supervisee”
(R2)
C. Elusiveness of Mentoring Elements in Educational Supervision
1) Supervisor’s perspectives: Faculty viewed mentoring as “broader”, “longer term” and “beyond clinical and professional development”. “Trust” and “special” characterised a mentoring relationship but the focus was more on “professional development” rather than “personal development”. Faculty did not see themselves as fulfilling a mentoring role but generally agreed that there could be opportunities in offering elements of mentoring in educational supervision and to “contribute to the growth of residents beyond the short-term focus on clearing examinations”.
“…take about certain other aspects you know…mentorship if possible…beyond the pure clinical and professional development”
(S1)
Supervisors alluded to their roles in educational supervision as “facilitating the growth as a person”; “giving advice” and “role modelling” but they did not consider these as mentoring roles even though these were generally accepted as mentoring in nature.
“…never seen myself in a mentoring position…mentoring goes beyond just the supervisor-supervisee relationship…but I don’t think it has really extended beyond that”
(S3)
2) Residents’ perspectives: There was a similar reference to mentoring as “adopting a broader view of the development of the resident” over “a longer period of time”. Residents described mentoring as having a “deeper emotional connect” and “beyond the clinical development”. The evaluator role was viewed as potentially inhibiting the development of a mentoring relationship.
“So, it muddles the role…when they are so tied up to assess…they may not be able to mentor as much…”
(R1)
D. Personal and Professional Development of Residents
1) Supervisor’s perspectives: Professional development was referred to as the “professional attitudes and motivation”, “duty of care”, “ethical boundaries” and the attributes which are more “formal” as contrasted to personal development. The latter being referred to as “one’s character”, “temperament”, “personality”; “the way we see things”; “development of self-awareness and self-actualisation” and the “need to know yourself and what problems you have in order to be able to help your patients struggling with personal problems”. Faculty also referred to personal development as “developing as a person and handling of stress”, “how to handle complaints”, and “how to juggle various roles to have a work-life balance”. Other views of personal development included “extracurricular activities outside of psychiatry” and “some hobbies” which some faculty opined as “more important in psychiatry because of the importance for self-care”.
However, some faculty held the opposing view that personal development should not be the focus of educational supervision. Lapses in personal development would only be brought up during supervision if there were “negative effects on professional roles and clinical practice and impeding progress” for risk of being accused of “prying into the residents’ personal lives and being nosy”.
“…but I don’t focus so much unless they hinder the work side of things. But maybe we should…”
(S3)
The reluctance of some residents to discuss issues of personal development were interpreted as an “Asian thing”, for instance being “uncomfortable” talking about personal struggles and “residents not expecting it”’.
2) Residents’ perspectives: Residents’ referred to personal developmental aspects as “be as a person”, “religious growth”, “personal well-being”, “how you are getting on with life as a whole”, “finding out about the person’s preferences”, “strengths and weaknesses” and “outside of the career”.
There was the fear of the lack of confidentiality and of being evaluated negatively if residents were to portray themselves as having personal struggles.
“though resident want to grow and develop but exposing these shortcomings could be very sensitive…”
(R1)
Residents considered personal aspects of their development to be “more private”; “should not be covered unless interferes with professional development”; “not so important”; “not fair for the supervisee and supervisor” and “something you should sort out on your own”. They perceived supervision to be formal and mainly moments of assessment for their professional development and so it would be inappropriate to discuss about personal struggles. Some residents also held the view that “personal and professional lives are separate” and the “supervisor may not be interested”.
“…to say that the supervisor should cover personal growth I don’t think that is very fair as well”
(S4)
IV. DISCUSSION
A. Conceptualisation of Educational Supervision
The concept of educational supervision was alien to both residents and supervisors. Supervision was seen mainly as teaching the residents to acquire knowledge and clinical skills with a focus on the transactional aspects. Our residents preferred a more relational supervisory interaction. The finding of psychiatry trainees valuing a supervisor’s emotional supportiveness more highly than clinical competence was also reported in another study (Chur-Hansen & McLean, 2007).
Our results showed that roles of teaching and assessing were more consistently endorsed by the supervisors. Relational roles like facilitating, role modelling, rapport building, and mentoring were considered important but cited less frequently by both groups. Participants tended to attribute this to the training’s emphasis on evaluation and assessment such that the focus of the supervision was more on the transactional rather than the relational components. This might have resulted in tension within the supervisory relationship as expectations for assessment of competencies take precedence (Julyan, 2009). This phenomenon was both ironic and worrying as the original intention for setting up the supervisory framework in the psychiatry residency program was to ensure that the training and learning would be supplemented by the presence of an educational supervisor with a mentoring role, entrusted with the fostering of the personal and professional components in clinical supervision (Kilminster et al., 2007).
B. Assessor Role of Supervisors
Although residency assessments were mainly formative, residents in our study still harbored concerns about the supervisor fulfilling the assessor role and determining their readiness to progress. If assessments were to be perceived as high stake in our examination-oriented training environment, the role of the teacher as helper might be compromised (van der Vleuten et al., 2012). As highlighted by the data in our study, combining the roles of helper and judge could confront the supervisor with a conflict of interest (Cavalcanti & Detsky, 2011). There might be situations either of inflation of judgement (Govaerts et al., 2007) or trivialisation of the assessment process (Dudek et al., 2005), which would potentially impair the professional development of the residents.
C. Personal and Professional Development
There was a common reference by both faculty and residents to the growth of the resident. Based on our data, there appeared to be some overlap of the concept of personal and professional development of residents in psychiatry training. Supervisors viewed the ability to handle stress and developing resilience not only as aspects of personal development but a reflection of the professional competence as well. But supervisors also opined that within the current supervisory framework, they would not be able to support the personal development of the residents. Although residents indicated their desires for supervisors to facilitate their holistic development and growth towards becoming a psychiatrist, they did not expect supervisors to be interested in their personal development but to focus more on the professional development of their clinical competencies.
There was avoidance by supervisors and residents to discuss personal struggles and frustrations in our study. This would be of concern if in the context of educational supervision in psychiatry, the personal aspects and development of better self-awareness could not be achieved, bearing in mind that this had been considered by some to be the fundamental goal of supervision in counselling (Kadushin, 1985). Concerns of boundary violations within the supervision relationship were raised by both groups of participants. In our study, the supervisors’ strict adherence to the boundaries as accustomed to in psychotherapeutic practice might deter self-disclosure. In contrast, our data suggested that sharing of clinical experiences by their supervisors were very much welcomed by the residents. Research has shown that there might be improvement in alliance when supervisors disclosed relevant past clinical experiences (Matazzoni, 2008). Self-disclosure by the supervisor usually normalised clinical struggles experienced by the residents and could enhance the supervision relationship (Knox et al., 2011). In our study, supervisors held fairly rigid boundaries within supervision, which had been shown to hinder the development of authentic emotional relationships or deeper mentoring relationships (Kozlowski et al., 2013).
Supervisors in our study reflected that it might have been cultural or an ‘Asian thing’ for residents to avoid discussion of personal struggles. Eastern cultures were noted to appreciate a larger power distance than Western cultures (Hofstede, 2011). Cultural value theory also opined that Eastern cultures tended to be more conservative and hierarchical and valued mastery to a lesser extent than the West (Schwartz, 1999). In our predominantly Asian context, the perception of a hierarchical training system might result in supervisors maintaining a stricter teacher-student boundary, or residents being more reluctant to share personal frustrations, particularly with the more senior supervisors. The evaluator role of the supervisor might also result in the resident erecting certain boundaries in the supervisory relationship. This would have implications for nurturing the personal and professional growth of the residents, which require guidance through mentorship and self-reflection within a trusting relationship (Holden et al., 2015).
D. Psychological Safety Within a Trusting Supervisory Relationship
Previous research has shown that any feedback which invoked the self potentially carried with it social judgements which might threaten the educational alliance (Pugh & Regehr, 2016; Telio et al., 2015) and there was a tendency for both supervisors and supervisees to interpret performance assessments as part of a judgement of personal worth (Hawe, 2003). The psychological safety within the supervisory relationship would be particularly important as awareness of the residents’ own inadequacies might be unpleasant and threatening as they faced their imperfect understanding and subjective theories (Vec et al., 2014). As such, the goals of supervision would be best attained with a trusting supervisor-supervisee relationship. However, our study showed that residents are unwilling to reveal too much of their inadequacies as this was too threatening for them, considering that their supervisors also evaluated their overall work performance and ability to deal with stress. This had resulted in tension in the supervisory relationship. The failure to pay heed to this, whether it was inherent to the training program or secondary to the supervisors’ lack of awareness, might further hinder and jeopardise the supervisory process.
The tension between assessment for support and assessment for high stakes decision-making will continue to challenge supervisors. The conflict between mentoring and appraisal of competency would need to be addressed. It would be important for residency training programs to create opportunities to allow the fostering of trusting supervisory relationships. Roles and expectations of the educational supervisor would need to be articulated clearly to both supervisors and residents. Supervisor training would need to focus not only on supervisor ability and competencies but more importantly, supervisor motivation. There should be the emphasis on instilling awareness of internal values and beliefs encompassing competency assessment, accountability, potential role conflicts, feedback delivery and “skills for establishing trusting, open and non-defensive yet problem–confronting relationships” (Govaerts et al., 2007).
E. Limitations of the Study
In our study, newly graduated residents who were agreeable to participate were recruited. The views of the ‘unwilling’ participants regarding supervision which might be more diverse and contentious might be inadvertently excluded. The content of the interview guide used was also not validated. Another limitation concerned the dual roles of researcher and APD. The view of the resident group might be subjected to biases and undue influence due to power differentials (Kotter, 2010). The researcher had minimised such potential biases by being reflexive and addressed concerns of imposing on the participants’ views openly during the interview (Creswell & Miller, 2000).
V. CONCLUSION
The mentoring role in supervision was found to be lacking in our current residency training. The residency program structure, with its focus on assessments of competencies and examinations, might have the unintended consequences of encouraging a transactional supervisory structure at the expense of a relational and mentoring relationship. This qualitative study highlighted significant differences in definitions, roles and expectations of educational supervision. It was our intention that this research endeavor contribute towards better appreciation of the dynamics within educational supervision in a competency-based residency training framework and further inform developments in the mentoring component of supervisory practices in the other training programs as well.
Notes on Contributors
Dr Lay Ling Tan formulated the research question and designed the research methodology. She conducted the semi-structured interviews and wrote the first draft of the manuscript.
Prof Pim W. Teunissen provided guidance for the research methodology and data analysis. He was also involved with the revision of the manuscript drafts.
Dr Wee Shiong Lim provided guidance for the research methodology, assisted with the initial analysis of the first three interviews independently as well as the revision of the manuscript drafts.
Both Dr Vanessa Wai Ling Mok and Dr Hwa Ling Yap were involved with recruitment of participants and data analysis.
Ethical Approval
Ethics approval was sought from the Institutional Review Board (CIRB Ref: 2017/2319) and informed consent was received from all participants.
Data Availability
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
Acknowledgement
We would like to acknowledge the contributions of the National Psychiatry Residency Program Supervisors and Residents for their willingness to participate.
Funding
We did not receive any funding for this research study.
Declaration of Interest
Dr Lay Ling Tan is the Associate Program Director and the PI of this research. Dr Hwa Ling Yap and Dr Vanessa Mok are both teaching faculty of the teaching site. They have a vested interest in ensuring the quality of supervision of residents. The other authors have no other conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
Akhtar, S. (2009). Comprehensive dictionary of psychoanalysis. Routledge.
Carroll, M. (2006). Counselling supervision: Theory, skills and practice. SAGE.
Cavalcanti, R. B., & Detsky, A. S. (2011). The education and training of future physicians: Why coaches can’t be judges. JAMA, 306(9), 993-994. https://doi.org/10.1001/jama.2011.1232
Chay, O. M. (2019). Transformation of medical education over the years – A personal view. The Asia Pacific Scholar, 4(1), 59–61. https://doi.org/10.29060/TAPS.2019-4-1/PV1076
Chur-Hansen, A., & McLean, S. (2007). Trainee psychiatrists’ views about their supervisors and supervision. Australasian Psychiatry, 15(4), 269-272.
Creswell, J. W. (2014). Research design: Qualitative, quantitative, and mixed method approaches (4th ed.). SAGE.
Creswell, J. W., & Miller, D. L. (2000). Determining validity in qualitative inquiry. Theory Into practice, 39(3), 124-130. https://doi.org/10.1207/s15430421tip3903_2
Driessen, E. W., Overeem, K., & van der Vleuten, C. P. M. (2011). Get yourself a mentor. Medical Education, 45(5), 438-439. https://doi.org/10.1111/j.1365-2923.2011.03948.x
Dudek, N. L., Marks, M. B., & Regehr, G. (2005). Failure to fail: The perspectives of clinical supervisors. Academic Medicine, 80(10), S84-S87.
Falender, C. A., & Shafranske, E. P. (2007). Competence in competency-based supervision practice: Construct and application. Professional Psychology: Research and Practice, 38(3), 232–240. https://doi.org/10.1037/0735-7028.38.3.232
Frank, J. R., Snell, L., Englander, R., & Holmboe, E. S. (2017). Implementing competency-based medical education: Moving forward. Medical Teacher, 39(6), 568–573. https://doi.org/10.1080/0142159x.2017.1315069.
Govaerts, M. J., van der Vleuten, C. P., Schuwirth, L. W., & Muijtjens, A. M. (2007). Broadening perspectives on clinical performance assessment: rethinking the nature of in-training assessment. Advances in Health Sciences Education Theory Practical, 12(2), 239-260. https://doi.org/10.1007/s10459-006-9043-1
Hansman, C. A. (2001). Mentoring as continuing professional education. Adult learning, 12(1), 7–8. https://doi.org/10.1177/104515950101200104
Hawe, E. (2003). “It’s Pretty Difficult to Fail”: The reluctance of lecturers to award a failing grade. Assessment & Evaluation in Higher Education, 28(4), 371–382. https://doi.org/10.1080/0260293032000066209
Hofstede, G. (2011). Dimensionalizing Cultures: The Hofstede Model in Context. Online Readings in Psychology and Culture, 2(1), 1–26. https://doi.org/10.9707/2307-0919.1014
Holden, M. D., Buck, E., Luk, J., Ambriz, F., Boisaubin, E. V., Clark, M. A., Mihalic, A. P., Sadler, J. Z., Sapire, K. J., Spike, J. P., Vince, A., & Dalrymple, J. L. (2015). Professional identity formation: Creating a longitudinal framework through TIME (Transformation in Medical Education). Academic Medicine, 90(6), 761–767. https://doi.org/10.1097/acm.0000000000000719
Julyan, T. E. (2009). Educational supervision and the impact of workplace-based assessments: a survey of psychiatry trainees and their supervisors. BMC Medical Education, 9(1), 51. https://doi.org/10.1186/1472-6920-9-51
Kadushin, A. (1985). Supervision in social work. Columbia University Press.
Kilminster, S., Cottrell, D., Grant, J., & Jolly, B. (2007). AMEE Guide No. 27: Effective educational and clinical supervision. Medical Teacher, 29(1), 2–19. https://doi.org/10.1080/01421590701210907
Knox, S., Edwards, L. M., Hess, S. A., & Hill, C. E. (2011). Supervisor self-disclosure: Supervisees’ experiences and perspectives. Psychotherapy, 48(4), 336–341. https://doi.org/10.1037/a0022067
Kolb, D. A. (2014). Experiential learning: Experience as the Source of Learning and Development (2nd ed.). Pearson Education, Inc. (Original work published 1984).
Kotter, J. P. (2010). Power and influence. Simon and Schuster.
Kozlowski, J. M., Pruitt, N. T., DeWalt, T. A., & Knox, S. (2013). Can boundary crossings in clinical supervision be beneficial? Counselling Psychology Quarterly, 27(2), 109–126. https://doi.org/10.1080/09515070.2013.870123
Launer, J. (2013). Supervision, mentoring and coaching. In Swanwick. T (Ed.), Understanding medical education. Evidence, theory and practice (2nd ed., pp 111-122). Wiley Blackwell. https://doi.org/10.1002/9781118472361.ch8
MacDonald, J. (2002). Clinical supervision: A review of underlying concepts and developments. Australian & New Zealand Journal of Psychiatry, 36(1), 92-98. https://doi.org/10.1046/j.1440-1614.2002.00974.x
Matazzoni, T. A. (2008). The influence of supervisor self-disclosure on the supervisory working alliance in beginning and advanced therapists-in-training [Doctoral dissertation]. ProQuest.
Passi, V. (2016). The importance of mentoring during educational supervision. Perspectives on Medical Education, 5, 195-196.
Patel, P. (2016). An evaluation of the current patterns and practices of educational supervision in postgraduate medical education in the UK. Perspectives on Medical Education, 5(4), 205-214. https://doi.org/10.1007/s40037-016-0280-6
Pront, L., Gillham, D., & Schuwirth, L. W. (2016). Competencies to enable learning-focused clinical supervision: a thematic analysis of the literature. Medical Education, 50(4), 485–495. https://doi.org/10.1111/medu.12854
Pugh, D., & Regehr, G. (2016). Taking the sting out of assessment: is there a role for progress testing? Medical Education, 50(7), 721-729.
Schon, D. A. (1987). Educating the reflective practitioner: Toward a new design for teaching learning in the professions. John Wiley.
Schwartz, S. H. (1999). A theory of cultural values and some implications for work. Applied psychology, 48(1), 23-47. https://doi.org/10.1111/j.1464-0597.1999.tb00047.x
Tebes, J. K., Matlin, S. L., Migdole, S. J., Farkas, M. S., Money, R. W., Shulman, L., & Hoge, M. A. (2011). Providing competency training to clinical supervisors through an international supervision approach. Research on Social Work Practice, 21(2), 190-199. https://doi.org/10.1177/1049731510385827
Telio, S., Ajjawi, R., & Regehr, G. (2015). The “educational alliance” as a framework for reconceptualizing feedback in medical education. Academic Medicine, 90(5), 609-614. https://doi.org/10.1097/acm.0000000000000560
Torby, A., Turner, M. B., Kinzie, J. M., & Usher, C. (2015). What we talk about when we talk about supervision: The clear and the confusing in graduate psychiatric education. Journal of the American Psychoanalytic Association, 63(5), NP7-NP12. https://doi.org/10.1177/0003065115609724
van der Vleuten, C. P. M., Schuwirth, L. W. T., Driessen, E. W., Dijkstra, J., Tigelaar, D., Baartman, L. K. J., & van Tartwijk, J. (2012). A model for programmatic assessment fit for purpose. Medical Teacher, 34(3), 205-214. https://doi.org/10.3109/0142159X.2012.652239
Vec, T., Rupnik Vec, T., & Žorga, S. (2014). Understanding how supervision works and what it can achieve. In Watkins C. E. &. Milne D. I (Eds.) The Wiley International Handbook of Clinical Supervision (pp 103-127). Wiley. https://doi.org/10.1002/9781118846360.ch5
Wald, H. S. (2015). Professional identity (trans) formation in medical education: Reflection, relationship, resilience. Academic Medicine, 90(6), 701-706.
*Lay Ling Tan
2 Simei Street 3 S529889
Email: tan.lay.ling@singhealth.com.sg
Submitted: 23 January 2021
Accepted: 11 August 2021
Published online: 4 January, TAPS 2022, 7(1), 55-65
https://doi.org/10.29060/TAPS.2022-7-1/OA2475
Marcus A Henning1, Vanamali Joseph1, Roger J Booth2, Christian U Krägeloh3 & Craig S Webster1
1School of Medicine, University of Auckland, New Zealand; 2Department of Medical Science, University of Auckland, New Zealand; 3Department of Psychology and Neuroscience, Auckland University of Technology, New Zealand
Abstract
Introduction: This study investigates psychological distress and quality of life (QoL) amongst first year premedical and health science students. The primary aim of this study was to investigate potential differences in QoL and psychological distress between students who sought entry into a medicine programme when compared to those opting for a non-medicine career.
Methods: We examined participant responses to measures of QoL, psychological distress, and course preference (medicine or other). A structural equation model was conducted to consider the interrelationships among future course preference, gender, QoL, depression, anxiety and stress.
Results: Three hundred and sixty-five students completed the online survey. An a priori conceptual model was developed and then evaluated using a structural equation model. The values obtained for RMSEA (0.027), CFI (0.999), and SRMR (0.016) indicated an excellent model fit. The overall model fit statistic, chi-square (χ2 = 7.626, df=6, p= .267), confirmed a good model fit. Students aiming to enrol in medicine generated higher psychological health and environmental QoL scores compared to their non-medicine oriented peers. In addition, physical QoL and psychological health QoL scores significantly predicted psychological distress measures.
Conclusion: The study raises a potential debate regarding placing students with mixed career intentions into the same course and the potential implications this may have on teaching in interprofessional and large student groups in relation to wellbeing, pedagogy, equity, and expenditure. The findings clearly indicated that medical students are not as adversely impacted upon in terms of QoL and psychological distress compared with their non-medical peers.
Keywords: Medical and Health Science Students, Quality of Life, Psychological Distress, Course Preference
Practice Highlights
- Students focusing on medicine report higher levels of psychological health and environmental QoL.
- Course preference is associated with psychological QoL and psychological distress.
- Issues with psychological QoL are more common among females.
- QoL and learning in large lecture theatres requires further investigation.
I. INTRODUCTION
At the University of Auckland, the Biomedical Common Year or Overlapping Year 1 (BCY) programme is a first-year syllabus and the gateway for many students aiming to enrol into either medicine or other healthcare disciplines (e.g., nursing, optometry, or pharmacy). The requirements for entry into medicine is highly competitive such that approximately 700 students who study in BCY aim to apply for medicine out of which only 250 students are chosen (Henning et al., 2017b). Entry into other healthcare disciplines (e.g., nursing, optometry, or pharmacy) is less competitive and selection is thus likely less distressing (Al Alwan et al., 2013). However, the large class sizes within the pre-medical and health science year (of approximately 1,300 students) containing students applying for either medicine or non-medicine programmes may also create a marginalising learning dynamic that may hinder the motivation and wellbeing of non-medicine students (Henning et al., 2017a). Hence, the aim of this research was to assess whether those students aiming for selection into medicine were more at risk of poor quality of life (QoL) and psychological distress relative to those students aiming for selection into other healthcare disciplines.
Numerous studies have researched the areas of QoL and psychological distress amongst medical students (Lovibond & Lovibond, 1995; Szabó, 2010; Wickramasinghe et al., 2019). In their systematic review, Dyrbye et al. (2006) reported concerning rates of depression, anxiety and general psychological distress among medical students, citing for example in one report that 37% of medical students in their first year of study experienced mental health issues of some kind. The adverse impact of distress among students can contribute to problems associated with academic attainment, professional development, academic honesty, substance abuse, cynicism, humanitarian attitude, and development of empathy. Moreover, psychological distress appears to be more of a concern among female medical students. The implication underlying the research investigating QoL and psychological distress suggests that medical students are more compromised than their non-medical peers.
Our conceptual model for the present study was developed in accordance with self-determination theory (Ryan & Deci, 2000). According to this theory, the act of choosing can positively affect motivation, well-being and learning if the needs for autonomy, relatedness, and competence in the individual are high. In this study, students were free to choose their course of study and hence freedom of choice was perceived as equivalent to the notion of course preference. According to this theory, students can be intrinsically motivated (engaged in their studies because of inherent enjoyment) and extrinsically motivated with a focus on outcome (Vansteenkiste et al., 2006). Extrinsic motivation, however, can be differentiated into aspects of regulation dependent upon the degree of autonomy. Therefore, there are facets of autonomous motivation (which involves volition and choice) versus that of controlled motivation (feeling pressured or coerced) (Vansteenkiste et al., 2006). Hence, intrinsic motivation and well-intentioned aspects of extrinsic motivation are considered autonomous, whilst the poorly internalised form of extrinsic motivation are less well incorporated into an individual’s sense of self. In our proposed model, we suggest features of choice with links to QoL.
We cannot assume that the medical or non-medical students differ in terms of their intrinsic or extrinsic motivation, but we do know that the majority of non-medical students at this university (e.g. nursing and pharmacy) have been given conditional entry into their courses on the proviso that they pass their courses in the BCY. However, medical students do not have this luxury and are in a more competitive mode of action. They are, thus, likely intrinsically and extrinsically motivated, and their extrinsic motivation could be either autonomous or controlled. Our assumption is that the non-medical students are also likely to be intrinsic and extrinsically motivated, but their extrinsic motivation is likely more autonomous as they have conditional entry. Therefore, non-medical students would likely experience more heightened levels of QoL than medical students who are experiencing higher levels of competition (Katz & Assor, 2007; Ryan & Deci, 2000). If this is not true another more pressing variable may be affecting the QoL outcome, such as mixing high numbers of students together from different disciplines into one course (Hornsby & Osman, 2014). In addition, given the established empirical evidence (Haist et al., 2000; Henning et al., 2013; Naylor et al., 2018; Ramsbottom-Lucier et al., 1995), we argued that gender would likely moderate choice and QoL. Therefore, the first stage of our conceptual model proposes that, once students have chosen a particular course of study (medicine or other) this will directly impact their QoL given the increased expectation associated with the decision process (Katz & Assor, 2007). Therefore, those students aiming for a programme (i.e., medicine) requiring higher stakes will likely be more at risk of ill-health.
The next element of our argument proposes that QoL will likely impact psychological distress. For example, if a student experiences good health-related physical QoL they are then likely to have lowered risk of psychological distress (Burris et al., 2009). In their study of first year medical students, Verger et al. (2009) reported that psychological distress was moderated by gender and influenced by wellbeing protective factors, such as social support, coping with academic pressure, and socio-economic factors. Consequently, we suggest that there is likely a follow-on effect such that those students with compromised QoL will likely experience more psychological distress (Dyrbye et al., 2006). Nonetheless, the causes of poor QoL are likely complex and vary substantially between individuals given that some studies have shown that students aiming to study medicine may be more motivated and experience higher levels of QoL (Henning et al., 2017a).
The primary aim of this study was to empirically investigate potential differences in QoL and psychological distress between students who sought entry into a medicine programme when compared to those opting for a non-medicine career. The issue of follow-on effects from QoL to psychological distress has not been studied within this learning context. To illustrate potential differences between the two groups, we scrutinised conceptual links between choice, gender, QoL and psychological distress in reference to students’ course preference (medicine or other) whilst studying in the BCY programme.
II. METHODS
A. Participants
All students (N=1277) studying within the BCY programme were invited to participate in this survey. Students aiming to study in any health-related course at the University of Auckland first enrol in the BCY programme in preparation for formalised entry into degrees for Bachelor of Health Science, Bachelor of Pharmacy, Bachelor of Optometry or Bachelor of Medicine (The University of Auckland, 2019).
B. Procedure
Ethics approval for the collection and use of data was obtained from the University of Auckland Human Participants Ethics Committee (Ref. 021985).
Students were informed about the study by email in late July (2018), and two reminder emails were sent out. The anonymous survey was conducted prior to final course completion in Semester 2 (2018), but after grades for the first semester had been released. Informed consent was implied given that study participants received a participant information sheet prior to the start of the questionnaire. Data were collected online using a Google Forms questionnaire (Google.com, 2015), which requires respondents to fully complete the survey before they are able to submit it.
C. Measures
Demographic and background details were obtained to assess the representativeness of the sample included: (1) Age in years; (2) Gender; (3) Future course preference (medicine or other); (4) Enrolment status (international or domestic); and (5) Ethnicity.
Quality of life was measured using the New Zealand version of the WHOQOL (NZ WHOQOL-BREF) questionnaire (Krägeloh et al., 2016). It has four domains (physical QoL, psychological health QoL, social relationships QoL and the environmental QoL) and contains 31 items. In this study, physical QoL had six items, psychological health QoL had 10 items, social relationships QoL had four items and environmental QoL had eight items (The NZ WHOQOL Group, 2017). Questions 1 and 2 are global QoL and health items and, thus, not included in the scoring of the four quality of life domains. Question 3 was deemed to have little relevance with respect to the research question and had been previously identified as having a ceiling effect in early career medical students (Krägeloh et al., 2011). All items utilised a 5-point Likert scale with varying anchors (the scores for two items were reversed). High scores indicated higher levels of QoL.
Psychological distress was measured using the Depression, Anxiety and Stress Scale (DASS-21), which captures respondents’ emotional states in reference to three domains: depression, anxiety and stress (within the past seven days). Each domain is comprised of seven items. The DASS-21 instrument has been developed from a previous 42-item version (Lovibond & Lovibond, 1995), and has undergone psychometric investigation among a variety of populations (Le et al., 2017; Medvedev et al., 2018; Szabó, 2010; Yıldırım et al., 2018). Each item utilises a 4-item Likert scale. Higher scores indicate more frequency and severity in the experience of negative emotions.
D. Data Analysis
First, the response rate (n/N) was calculated as a percentage measure, and the details of the participants were described. Second, descriptive statistics (means and standard deviations (SDs)) were computed for the two self-reported questionnaires measures (NZ WHOQOL-BREF and DASS-21). These measures were computed for each of the questionnaire domains with respect to course preference (medicine; other) and gender (male; female). A multivariate analysis of variance (ANOVA) approach was used to assess levels of significance for the independent variables, course preference and gender, with respect to the aforementioned dependent variables.
Lastly, one structural equation model (SEM) was developed to consider the interrelationships among course preference, gender, and QoL and DASS-21 domain measures. This SEM was developed using the software AMOS v25 (Arbuckle, 2017). The primary goodness-of-fit indices used to assess the model fit were inspection of the model chi-square value, root mean square error of approximation (RMSEA), comparative fit index (CFI), and standardised root mean square residual (SRMR). Model fits were considered acceptable if they met the following recommendations: (1) RMSEA < 0.06; (2) SRMR < 0.08; and (3) CFI close to 0.95 or higher (Hu & Bentler, 1998). Additionally, using maximum likelihood bootstrapping with 1,000 samples, regression weights were computed, and bias-corrected 95% confidence intervals were determined (Byrne, 2010).
III. RESULTS
A. Response Rate and Participant Data
Three hundred and sixty-five students (n = 365) fully completed the online survey resulting in a response rate of 29%. The average age of participants was 19 years (SD = 1.84) with 75% of respondents being female. Table 1 provides the demographic profile for the sample, and upon examination, the distributions of the sample data appeared representative of the population profile. In this study, more than 75% of participants stated a preference to study medicine as opposed to other non-medicine health options, which is a rate higher than that found elsewhere (Henning et al., 2017b). The data that support the findings of this study are openly available in Figshare at https://figshare.com/articles/dataset/_/1405 0463 (Henning et al., 2021).
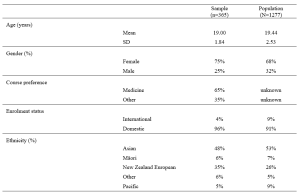
Table 1. Demographic and academic achievement details of the sample versus the population.
The means and standard deviations for the variables of interest are shown in Table 2. The NZ WHOQOL-BREF questionnaire means for these participants are marginally lower than those found elsewhere (Henning et al., 2017b). No comparable New Zealand medical student reference values for the DASS-21 are available for this population. In reference to internal consistency coefficients computed for each of the measures (Table 2), all Cronbach’s alpha values were equal to or greater than 0.70 thus meeting ‘acceptable’ requirements (Field, 2005).
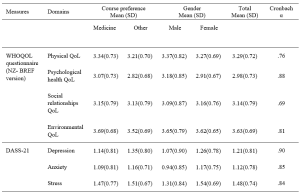
Table 2. Means, standard deviations (SD) and internal consistency scores (Cronbach alpha) of the measures used in the study.
Note: Using a multivariate ANOVA approach, significant differences (p<.05) for course preference (medicine vs. other) were noted for psychological health QoL, environmental QoL, and depression. In addition, significant differences (p<.05) for gender (male vs. female) were noted for psychological health QoL, depression, anxiety and stress.
B. Structured Equation Modelling
Based on previous literature (Dyrbye et al., 2006) and self-determination theory (Katz & Assor, 2007; Ryan & Deci, 2000), an a priori conceptual model was developed and tested using a SEM framework. The primary criterion variable was the students’ course preference (medicine, scored as 1 vs. other, scored as 0). The values obtained for RMSEA, SRMR, and CFI indicated that the model fit was excellent, that is, RMSEA = 0.027, CFI = 0.999, and SRMR = 0.016. As a secondary check, the overall model fit determined by the chi-square (χ2 = 7.626, df=6. p= .267) also indicated the model fitted very well. We noted that some of the error variances within measures of the NZ WHOQOL-BREF and DASS-21 were required to be correlated.
Figure 1 shows the path diagram for all the data collected (n = 365). The path coefficients are shown for significant relationships only (p < .05). The bias-corrected 95% confidence intervals for the regression weights (path coefficients) obtained using the maximum likelihood bootstrapping method were generated (Table 3) to ensure the accuracy and stability of the parameter estimates (Byrne, 2010).
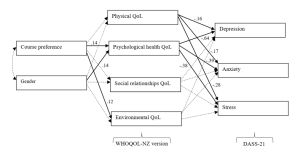
Figure 1. Path diagram of the tested structural equation model for all study participants.
Note. The path standardised regression weight estimates were shown only when statistically significant (p<.05). For non-significant relationships, directive arrows are shown with dashed lines (see Table 3 for details). Errors for all pertinent measures were removed to improve clarity of the figure. Error variances among the WHOQOL- NZ version and DASS-21 domian measures were were allowed to be correlated. No other error variances were correlated. Key fit indices and chi-square calculations were standardised RMR = .016, CFI = .999, RMSEA = .027, χ2 = 7.626, df=6. p= .267
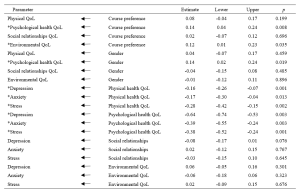
Table 3. Standardised regression weights: Lower and upper ends of bias-corrected 95% confidence intervals of the regression weights of the directional paths of the SEM.
Note. * p<.05
Table 3 and Figure 1 indicated the following relationships. The standardised regression weights determined that course preference significantly predicted psychological health QoL and environmental QoL. More specifically, those students preferring a medical course will likely have higher psychological health QoL and environmental QoL. Gender did not influence course preference but had a significant association with psychological health QoL. In turn, physical QoL and psychological health QoL scores significantly predicted depression, anxiety and stress (DASS-21 measures). The two remaining QoL measures (social relationships QoL and environmental QoL) did not significantly predict the DASS-21 measures.
When inspecting Table 2 and Figure 1, we can make certain assertions related to the differences between the two groups (medical and other students) with respect to QoL and psychological distress. Figure 1 indicates two significant associations between course preference and psychological health QoL and environmental QoL. Therefore, students indicating a preference for enrolling in a medical course were likely to experience greater psychological health QoL and environmental QoL. The findings in Table 2, clarify that students aiming to study medicine have higher levels of QoL in these two domains, compared to students aiming to study in non-medicine courses. In addition, the multivariate analyse indicate that depression is more of a concern for non-medical students than intending medicine students.
IV. DISCUSSION
The known health concerns associated with first year students (Naylor et al., 2018; Tinto, 2009) appear consistent with the current findings. The actual values (Table 2) for three of the four QoL domains from the NZ WHOQOL-BREF -psychological health QoL, social relationships QoL, and environmental QoL – are lower than previously published values for year 4 and 5 students at the same university (Henning et al., 2012), although the physical QoL score was higher. This indicates that year 1 students at this university appear to have relatively lower QoL than their year 4 and 5 peers and are consequently lower than the general population norms, particularly in the areas of psychological health QoL, social relationships QoL, and environmental QoL (Henning et al., 2012). In addition, the values for all domains are lower than those acquired from a 2015 first-year cohort (overall) studying in the same programme (Henning et al., 2017b).
Similarly, the DASS-21 findings (Table 2) show that this group scored higher on the domains of depression and anxiety compared to early career doctors also graduating from the same university (Henning et al., 2014). In comparison to a Malaysian student group, the mean values for the present study show distinct similarity in terms of stress and anxiety scores, but a marked lower score for depression (Yusoff et al., 2013). Therefore, we have provided good evidence to suggest that this group of students, irrespective of choosing either medicine or other as their preferred course option, studying in the BCY programme are experiencing relatively lower levels of QoL and higher levels of psychological distress compared to previous cohorts studying at the same university. However, their experiences may not differ greatly when compared to those students’ psychological distress perceptions in other universities.
In reference to the conceptual model, the findings also confirm that preference for course of study is linked with aspects of QoL. This in turn influences psychological distress, suggesting a feedback loop. Both of these associations were confirmed by the path analysis resulting in an excellent model fit for the SEM (Figure 1). The first part of the model considered how the preferred course option (medicine versus other) could directly impact QoL measures and the second part of the model considered the flow-on (indirect) effects to psychological distress (depression, anxiety and stress).
A. Choosing to Study medicine and Its Impact on Quality of Life
Figure 1 clearly shows that choosing to study medicine has an influence on aspects of QoL, although gender was not found to be significantly correlated with course preference. The decision to choose to study medicine was directly and significantly associated with psychological health QoL and environmental QoL (with higher scores noted for intending medicine students), but did not influence either physical QoL or social relationships QoL. In Table 2, we noted that psychological health QoL and environmental QoL for those vying for a place in the medical programme was higher than students’ scores for other health options (e.g., nursing, pharmacy, or optometry). The direction of the arrows in the model implies that the act of deciding to study medicine is likely influencing QoL on these two domains. These findings can be interpreted in several ways.
First, it is likely that students who aim for admission to medicine may be more psychologically robust to begin with. The psychological health QoL domain of the New Zealand version of the WHOQOL encompasses 10 facets (Krägeloh et al., 2016; WHOQoL Group, 1998). The facets that likely emphasise the difference between those applying for medicine and those applying for another degree are self-esteem, perception of negative or positive feelings, concentration, ability to meet expectation, and management of personal circumstances. In a previous study (Henning et al., 2017b), perceived stress was found to be highly correlated with psychological QoL and also noted to be a strong predictor of course preference (medicine versus other), with potential medical students scoring higher than their other heath professional peers.
Second, the aspects of cognitive capacity, personal management, and mental wellbeing need to be weighed in comparison to environmental QoL (measured in perceived access to resources, i.e., finance, health care, transport, security, technology, and housing) (WHOQoL Group, 1998). The current findings confirm previous research linking course preference to environmental QoL, suggesting that those students who come from affluent and supportive backgrounds will likely have more interest in pursuing a medical degree (Henning et al., 2017b).
B. Impact of Quality of Life on Psychological Distress
The SEM also revealed an interesting flow-on effect suggesting that those students not choosing medicine will have more issues with psychological wellbeing than those choosing to pursue medicine, which translates to greater risk of psychological distress in the form of depression, anxiety and stress for non-medical students. Furthermore, intending medicine students generated significantly lower depression scores than their non-medicine peers. Even though physical QoL is also directly connected with psychological distress factors, this association was not influenced by course preference. Hence, the key issues linked to course preference are related to psychological health QoL, which is incidentally linked to gender. Environmental QoL appears to have no flow-on psychological distress effects.
These findings indicate that some perceptions of QoL are likely linked to choice and ultimately psychological distress factors. The flow-on effect suggests that those students who struggle with psychological health QoL tend to further struggle with psychological distress. The point of difference between the two groups (medical and other) is that the intending medical students appear less affected by depression than their non-medical peers. The concept of choice has been established as a key component in motivation and wellbeing, for example, the perceived expectancies and values regarding a task are influenced by weighing up the benefits and costs associated with the forthcoming task (Katz & Assor, 2007). Hence, in the medical context the preferred choice of medicine likely has a powerful impact on motivation, learning and wellbeing (Katz & Assor, 2007). The current findings indicate that students focussing on medicine have higher psychological health QoL and lower psychological distress (particularly in the area of depression) than non-medicine students in the same year. This may imply that the current programme is more suited to those aiming for a medical career than those heading for a non-medicine health-related vocation, although this proposition requires further investigation.
C. Implications for Learning and Wellbeing
There are two clear implications associated with these results.
First, the findings indicate that intending medical students are more likely to have good access to environmental resources. The elevation of environmental QoL scores for students intending to study medicine as compared to students in other disciplines is consistent with findings reported elsewhere (Collins et al., 1993; Henning et al., 2012; Ng et al., 2009), suggesting that these students likely have better access to the needed resources. Equity arguments regarding selection of medical students is a global concern and impacts areas related to communication, empathetic listening, and shared understandings between clinician and patient (Rao & Flores, 2007). The resources differential suggests a clear argument that students who prefer to study medicine may not equitably mirror the less-resourced population at large and thus may have difficulty relating to large proportions of society. It is important to also emphasise that equity initiatives at the university in which this study was conducted are in place, although the complexity of the issues are multifaceted and may require further development (Curtis et al., 2015; Poole et al., 2009).
Second, the findings in this study clearly indicate that intending medical students are more likely to experience higher levels of psychological health QoL. Therefore, they are more likely to have a different wellbeing outcome than those students who aim for an alternative health sciences career, which may warrant investigating the rationale for placing students aiming for different health professions in one course of study. An argument for placing all health-career students together is likely based on the idea of interprofessional learning (Salamonson et al., 2009). Some of the benefits include improved knowledge gains especially for those students preparing for non-medical courses and positive attitudinal shifts regarding each profession (Carpenter, 1995). The findings in this study revealed that one lecturer was able lecture to 1277 students at one time (using asynchronous technology), suggesting this is a cost effective teaching option. Nonetheless, the findings in this study do indicate that the implication of large classes (or ‘massification’) in reference to wellbeing gains requires further investigation (Hornsby & Osman, 2014).
It has been established that students preferring medicine to other health science options will lead to greater academic attainment. For example, Henning et al. (2017b) reported that those students preferring to pursue medicine attained a bioscience grade average of 6.77 which was significantly higher than the non-medical comparison cohort which attained a grade average of 4.42. Therefore, creating smaller, discipline-specific groups could create more equitable learning, as well as engendering more opportunities for staff-student engagement, more engagement with relevant content, and greater likelihood of motivation for learning (Hornsby & Osman, 2014). However, in the context of pre-medical courses, such as the BCY programme, even though there are clear differences in resulting grade achievement, more research is required to tease out the subtle learning and wellbeing interconnections and to further investigate whether one group is more disadvantaged in their learning than the other (in this case the non-medicine group).
A limitation of this study is the relatively low response rate, although this is comparable with other studies using online questionnaires (Nulty, 2008) and the participants engaged in this study had similar characteristics to the total population (Table 1). Moreover, the response rate is within the range considered acceptable for surveys of representatives of organisations (36%±13%) – a category arguably appropriate for students entering their respective professions (Baruch, 1999). A further limitation of the study is that the research design is cross-sectional suggesting that the links between variables cannot infer temporal causality. Lastly, we acknowledge that it was outside the scope of the study to fully explore some of the speculations raised in this paper, such as whether choice of course of study was influenced by either intrinsic or extrinsic factors (i.e., degree of autonomy).
V. CONCLUSION
The main implication of this study is the direct relationships between course preference (medicine versus other) and psychological health QoL and environmental QoL, as well as the further indirect or flow-on effects to psychological distress via the psychological QoL pathway. Thus, indicating that medical students are not as adversely impacted upon in terms of QoL and psychological distress compared with their non-medicine peers. Lastly, the study findings provide useful debate and scope for further research in the areas of pedagogy, educational equity, career aspiration, and financial cost related to interprofessional education and teaching in large student groups.
Notes on Contributors
Marcus A. Henning is an associate professor in the Centre for Medical and Health Sciences Education at the University of Auckland, New Zealand. MAH was involved in the conceptualisation of the idea, data curation, formal analysis, developing the design of the study, writing the original draft and ongoing editing.
Vanamali Joseph was, at the time of this study, a third year medical student studying in the Faculty of Medical and Health Sciences at the University of Auckland, New Zealand. VJ was involved in the conceptualisation of the idea, data curation, developing the design of the study and ongoing editing.
Roger J. Booth is an associate professor in molecular medicine and pathology, in the Faculty of Medical and Health Sciences at the University of Auckland, New Zealand. RB was involved in the conceptualisation of the idea, data curation, developing the design of the study and ongoing editing.
Christian U. Krägeloh is an associate professor in the Department of Psychology at AUT University, New Zealand. CUK was involved in the conceptualisation of the idea, formal analysis and ongoing editing.
Craig S. Webster is an associate professor in the Centre for Medical and Health Sciences Education at the University of Auckland, New Zealand. CSW was involved in the conceptualisation of the idea, data curation, formal analysis, developing the design of the study, writing the original draft and ongoing editing.
Ethical Approval
Ethics approval for the collection and use of data was obtained from the University of Auckland Human Participants Ethics Committee (Ref. 021985).
Data Availability
The anonymised data that supports the findings of this study are openly available in the Figshare repository, https://figshare.com/articles/dataset/_/14050463
Funding
No funding source required for this study.
Declaration of Interest
The authors declare no conflicts of interest.
References
Al Alwan, I., Al Kushi, M., Tamim, H., Magzoub, M., & Elzubeir, M. (2013). Health sciences and medical college preadmission criteria and prediction of in-course academic performance: A longitudinal cohort study. Advances in Health Sciences Education, 18(3), 427-438. https://doi.org/10.1007/s10459-012-9380-1
Arbuckle, J. L. (2017). IBM® SPSS® Amos™ 25 User’s Guide. https://usermanual.wiki/Document/IBMSPSSAmosUserGuide.2983928102/view
Baruch, Y. (1999). Response rate in academic studies- A comparative analysis. Human Relations, 52(4), 421-438. https://doi.org/10.1177/001872679905200401
Burris, J. L., Brechting, E. H., Salsman, J., & Carlson, C. R. (2009). Factors associated with the psychological well-being and distress of university students. Journal of American College Health, 57(5), 536-544. https://doi.org/10.3200/JACH.57.5.536-544
Byrne, B. M. (2010). Structural Equation Modeling with AMOS: Basic concepts, applications and programming (2nd ed.). Routledge.
Carpenter, J. (1995). Interprofessional education for medical and nursing students: Evaluation of a programme. Medical Education, 29(4), 265-272. https://doi.org/10.1111/j.1365-2923.1995.tb02847.x
Collins, J., Jones, J., & White, G. (1993). Demographic variables in Auckland medical students. New Zealand Medical Journal, 106(960), 306-308.
Curtis, E., Wikaire, E., Jiang, Y., McMillan, L., Loto, R., Airini., & Reid, P. (2015). A tertiary approach to improving equity in health: Quantitative analysis of the Māori and Pacific admission scheme (MAPAS) process, 2008–2012. International Journal for Equity in Health, 14(1), 1-15. https://doi.org/10.1186/s12939-015-0133-7
Dyrbye, L. N., Thomas, M. R., & Shanafelt, T. D. (2006). Systematic review of depression, anxiety, and other indicators of psychological distress among US and Canadian medical students. Academic Medicine, 81(4), 354-373. https://doi.org/10.1097/00001888-200604000-00009
Field, A. P. (2005). Discovering statistics using SPSS : And sex, drugs and rock’n’roll (2nd ed.). SAGE.
Google.com. (2015). Homepage. https://www.google.co.nz/forms/about/
Haist, S. A., Wilson, J. F., Elam, C. L., Blue, A. V., & Fosson, S. E. (2000). The effect of gender and age on medical school performance: An important interaction. Advances in Health Sciences Education: Theory and Practice, 5(3), 197-205. https://doi.org/10.1023/A:1009829611335
Henning, M. A., Joseph, V., Booth, R. J., Krageloh, C. U., & Webster, C. S. (2021). Biomedical students’ course preference and links with quality of life and psychological distress [Data set]. Figshare. https://figshare.com/articles/dataset/_/14050463
Henning, M. A., Krägeloh, C. U., Hawken, S. J., Zhao, Y., & Doherty, I. (2012). The quality of life of medical students studying in New Zealand: A comparison with non-medical students and a general population reference group. Teaching and Learning in Medicine, 24(4), 334-340.https://doi.org/10.1080/10401334.2012.715261
Henning, M. A., Krägeloh, C. U., Booth, R., Hill, E. M., Chen, J., & Webster, C. S. (2017a). Biomedical students in their first year of study: Factors explaining performance in a high stakes examination. Medical Science Educator, 27(4), 633–643. https://doi.org/10.1007/s40670-017-0444-y
Henning, M. A., Krägeloh, C. U., Booth, R., Hill, E. M., Chen, J., & Webster, C. S. (2017b). Profiling potential medical students and exploring determinants of career choice. The Asia Pacific Scholar, 2(1), 7-15. https://doi.org/10.29060/TAPS.2017-2-1/OA1019
Henning, M. A., Krägeloh, C. U., Manalo, E., Doherty, I., Lamdin, R., & Hawken, S. J. (2013). Medical students in early clinical training and achievement motivation: Variations according to gender, enrolment status, and age. Medical Science Educator, 23(1), 6-15. https://doi.org/10.1007/BF03341798
Henning, M. A., Sollers, J., Strom, J. M., Hill, A. G., Lyndon, M. P., Cumin, D., & Hawken, S. J. (2014). Junior doctors in their first year: Mental health, quality of life, burnout and heart rate variability. Perspectives in Medical Education, 3, 136-143. https://doi.org/10.1007/s40037-013-0075-y
Hornsby, D. J., & Osman, R. (2014). Massification in higher education: Large classes and student learning. Higher Education Research & Development, 67(6), 711-719. https://doi.org/10.1007/s10734-014-9733-1
Hu, L.-t., & Bentler, P. M. (1998). Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods, 3(4), 424-453. https://doi.org/10.1037/1082-989X.3.4.424
Katz, I., & Assor, A. (2007). When choice motivates and when it does not. Educational Psychology Review, 19(4), 429. https://doi.org/10.1007/s10648-006-9027-y
Krägeloh, C., Henning, M., Hawken, S., Zhao, Y., Shepherd, D., & Billington, R. (2011). Validation of the WHOQOL-BREF quality of life questionnaire for use with medical students. Eductaion for Health, 24(2), 545.
Krägeloh, C. U., Billington, D. R., Hsu, P. H.-C., Feng, X. J., Medvedev, O. N., Kersten, P., Landon, J., & Siegert, R. J. (2016). Ordinal-to-interval scale conversion tables and national items for the New Zealand version of the WHOQOL-BREF. PLOS ONE, 11(11), e0166065. https://doi.org/10.1371/journal.pone.0166065
Le, M. T. H., Tran, T. D., Holton, S., Nguyen, H. T., Wolfe, R., & Fisher, J. (2017). Reliability, convergent validity and factor structure of the DASS-21 in a sample of Vietnamese adolescents. PLOS ONE, 12(7), e0180557. https://doi.org/10.1371/journal.pone.0180557
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335-343.
Medvedev, O. N., Krägeloh, C. U., Titkova, E. A., & Siegert, R. J. (2018). Rasch analysis and ordinal-to-interval conversion tables for the Depression, Anxiety and Stress Scale. Journal of Health 25(10–11), 1374–1383. https://doi.org/10.1177/1359105318755261
Naylor, R., Baik, C., & Arkoudis, S. (2018). Identifying attrition risk based on the first year experience. Higher Education Research & Development, 37(2), 328-342. https://doi.org/10.1080/07294360.2017.1370438
Ng, C. L., Tambyah, P. A., & Wong, C. Y. (2009). Cost of medical education, financial assistance and medical school demographics in Singapore. Singapore Medical Journal, 50(5), 462-467.
Nulty, D. D. (2008). The adequacy of response rates to online and paper surveys: What can be done? Assessment and Evaluation in Higher Education, 33(3), 301-314. https://doi.org/10.1080/02602930701293231
Poole, P. J., Moriarty, H. J., Wearn, A. M., Wilkinson, T. J., & Weller, J. M. (2009). Medical student selection in New Zealand: looking to the future. New Zealand Medical Journal, 122(1306), 88-100.
Ramsbottom-Lucier, M., Johnson, M. M., & Elam, C. L. (1995). Age and gender differences in students’ preadmission qualifications and medical school performances. Academic Medicine, 70(3), 236-239. https://doi.org/10.1097/00001888-199503000-00016
Rao, V., & Flores, G. (2007). Why aren’t there more African-American physicians? A qualitative study and exploratory inquiry of African-American students’ perspectives on careers in medicine. Journal of the National Medical Association, 99(9), 986-993.
Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist, 55(1), 68-78. https://doi.org/10.1037/0003-066X.55.1.68
Salamonson, Y., Everett, B., Koch, J., Wilson, I., & Davidson, P. M. (2009). Learning strategies of first year nursing and medical students: A comparative study. International Journal of Nursing Studies, 46(12), 1541-1547. https://doi.org/10.1016/j.ijnurstu.2009.05.010
Szabó, M. (2010). The short version of the Depression Anxiety Stress Scales (DASS-21): Factor structure in a young adolescent sample. Journal of Adolescence, 33(1), 1-8. https://doi.org/10.1016/j.adolescence.2009.05.014
The NZ WHOQOL Group. (2017). WHOQOL tools. Auckland University of Technology. https://cpcr.aut.ac.nz/new-zealand-whoqol
The University of Auckland. (2019). Biomedical Science. https://www.auckland.ac.nz/en/study/study-options/find-a-study-option/biomedical-science.html
Tinto, V. (2009). Taking student retention seriously: Rethinking the first year of university. FYE curriculum design symposium. Queensland University of Technology, Australia.
Vansteenkiste, M., Lens, W., & Deci, E. L. (2006). Intrinsic versus extrinsic goal contents in self-determination theory: Another look at the quality of academic motivation. Educational Psychologist, 41(1), 19-31. https://doi.org/10.1207/s15326985ep4101_4
Verger, P., Combes, J.-B., Kovess-Masfety, V., Choquet, M., Guagliardo, V., Rouillon, F., & Peretti-Wattel, P. (2009). Psychological distress in first year university students: Socioeconomic and academic stressors, mastery and social support in young men and women. Social Psychiatry and Psychiatric Epidemiology, 44(8), 643-650. https://doi.org/10.1007/s00127-008-0486-y
WHOQoL Group. (1998). Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychological Medicine, 28(3), 551-558. https://doi.org/10.1017/S0033291798006667
Wickramasinghe, D. P., Almeida, I. S., & Samarasekera, D. N. (2019). Depression and stressful life events among medical students during undergraduate career: Findings from a medical school in South Asia. The Asia Pacific Scholar, 4(1), 42-47. https://doi.org/10.29060/TAPS.2019-4-1/OA2025
Yıldırım, A., Boysan, M., & Kefeli, M. C. (2018). Psychometric properties of the Turkish version of the Depression Anxiety Stress Scale-21 (DASS-21). British Journal of Guidance & Counselling, 46(5), 582-595. https://doi.org/10.1080/03069885.2018.1442558
Yusoff, M. S. B., Rahim, A. F. A., Baba, A. A., Ismail, S. B., Pa, M. N. M., & Esa, A. R. (2013). Prevalence and associated factors of stress, anxiety and depression among prospective medical students. Asian Journal of Psychiatry, 6(2), 128-133. https://doi.org/10.1016/j.ajp.2012.09.012
*Marcus A. Henning
The University of Auckland,
Private Bag 92019,
Auckland 1142, New Zealand
Tel: 0064 923 7392
Email: m.henning@auckland.ac.nz
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
