
Dental education in the 21st century: A comprehensive approach for new generations
Submitted: 17 September 2021
Accepted: 4 October 2021
Published online: 5 April, TAPS 2022, 7(2), 61-62
https://doi.org/10.29060/TAPS.2022-7-2/LE2691
Gabriela González & Mildred Lopez
Tecnologico de Monterrey, Escuela de Medicina y Ciencias de la Salud, Mexico
Although there have been many calls for dental education to move to comprehensive training, many have remained in rhetoric. However, recently the strategic analysis of the American Dental Association of Education recommended a curriculum transformation to engage students in life-long learning and nurturing an educational community with well-qualified teachers to mentor students and model the values of the profession (Formicola et al., 2018).
Reimagining dental education demands a curriculum that considers the unique characteristics of learners. The generation to come has grown in a globalised world where information about what is happening in remote geographical places is quickly available, which has shaped their cultural and political points of view. Their idealism and advocacy have marked how they relate to patients. As part of the inherent characteristics, students thrive in experiential learning and rely on the internet and multimedia content. Therefore, incorporating technology is a must for engaging them in meaningful learning activities.
Instead of theory-oriented education, institutions should foster learning environments that depict the immediate community’s health challenges, for example, childhood caries, poor access to dental care, and the increase in the number of people with untreated oral conditions. A starting point is to transition to context-rich educational experiences where students can make a positive social impact. While doing so, they honour their social commitment to patients and families and transform into health advocates.
Additionally, this comprehensive approach needs to nurture a professional that can work within a health system. Dentists that are successful in practice are immersed in a community and have an interdisciplinary approach to deliver quality care. To achieve this competence undergraduates, need more opportunities to develop critical thinking skills, engage in self-assessment of performance, provide, and receive feedback to spark growth, and practice evidence-based decision-making (Kornegay et al., 2021).
Considering the evolution of technologies and the emergence of diseases, it is impossible to think that dental training has not changed. However, the unique profile of the new generation of students demands that we accelerate the change process. Learners have raised to the challenge and have demonstrated their will to positively impact their communities and society. The call for action for educational institutions is to embrace a new vision for a wide comprehensive dental education model where students learn from dental sciences and medicine to advocacy and ethics.
Notes on Contributors
Gabriela Gonzalez prepared first draft; literature review; writing and Mildred Lopez revised the final version of the manuscript. ML wrote and revised the final version of the manuscript.
Funding
There is no funding for this study.
Declaration of Interest
Authors declare no conflict of interest.
References
Formicola, A. J., Bailit, H. L., Weintraub, J. A., Fried, J. L., & Polverini, P. J. (2018). Advancing dental education in the 21st century: Phase 2 report on strategic analysis and recommendations. Journal of Dental Education, 82(10), eS1–eS32. https://doi.org/10.21815/JDE.018.109
Kornegay, E. C., Jackson, T. H., LaGarry‐Cahoon, A., Reside, J. M., Wolcott, M. D., & Quinonez, R. B. (2021). “I don’t think the problem’s the student… I think it’s us”: Engaging faculty in curriculum innovation. Journal of Dental Education, 85(4), 582-588. https://doi.org/10.1002/jdd.12495
*Gabriela González
Tecnologico de Monterrey,
Escuela de Medicina y Ciencias de la Salud
Av. Morones Prieto 3000 Pte
64710 Monterrey, N.L. México
Tel: 52/81 8888 2254
Email: dra.gabrielaglzl@gmail.com
Submitted: 23 August 2021
Accepted: 28 October 2021
Published online: 5 April, TAPS 2022, 7(2), 56-60
https://doi.org/10.29060/TAPS.2022-7-2/SC2686
Mae Yue Tan, Nicholas Beng Hui Ng, Marion Margaret Aw & Jeremy Bingyuan Lin
Khoo Teck Puat -National University Children’s Medical Institute, National University Health System, Singapore
Abstract
Introduction: The transition from medical student to houseman is well recognised as a stressful period for newly qualified doctors. This stress is likely to be heightened when the transition occurs during a pandemic. We aimed to evaluate the perceived stress levels of housemen as they begin housemanship and explore their sentiments and preparedness in starting work amidst the coronavirus disease 2019 (COVID-19) pandemic.
Methods: Housemen starting work at a tertiary institution in Singapore in May 2020 completed the following: (1) Perceived Stress Scale, (2) open-ended questions on perceived challenges and concerns and (3) questionnaire on preparedness and confidence in starting work. Descriptive statistics were used to analyse quantitative data and modified thematic analysis performed for qualitative data.
Results: Sixty-one housemen participated. Thirty-five (57.4%) reported high perceived stress. The themes for perceived challenges in this transition included coping with constant change, lack of reliable information from authorities, dealing with disappointment, physical fatigue, and loss of autonomy. The themes for concerns in beginning housemanship elicited relate to clinical competence, transitioning into new responsibilities, risk of infection with COVID-19, senior expectations, physical fatigue and training-related concerns. Despite these challenges and concerns, housemen were prepared to begin work during this pandemic.
Conclusion: Housemen transitioning during this pandemic experienced additional stressors and unique challenges pertaining to working in a pandemic. Encouragingly, they remain prepared to start work. Institutions and departments should be mindful of the specific concerns and challenges so that appropriate support can be put in place to support these junior doctors.
Keywords: COVID-19, Junior Doctor, Intern, Pandemic, Challenges, Preparedness
I. INTRODUCTION
Newly graduated doctors are a particularly vulnerable group of healthcare workers as they start work as housemen amidst the COVID-19 pandemic. The transition from student to doctor is already notorious for steep learning curves and increased stress (Sturman et al., 2017). Moreover, housemen in Singapore experienced drastic changes during their final year of medical school, a time which coincided with the surge of the pandemic in Singapore. Not only was clinical training was disrupted, this batch also experienced a modified form of final examinations, an earlier start to housemanship, and changes to posting selections, as manpower allocation was done centrally based on manpower demands. With that, we aimed to evaluate the perceived stress among housemen and explore their perceived challenges, concerns and preparedness just before they started work.
II. METHODS
We performed a cross-sectional anonymous survey on housemen at our institution on their first day of housemanship, in May 2020. The survey was administered before the hospital orientation by an independent institutional representative not part of the investigating team. Consent was implied through voluntary participation.
The Perceived Stress Scale (PSS) (Cohen et al., 1983) was used as a measure of stress. This tool is designed to assess how unpredictable, uncontrollable, and overloaded respondents find their lives. We also administered structured open-ended questions to elicit perceived challenges and major concerns while transitioning from medical school to starting work as a houseman. Participants also completed 7-point Likert rating scale modelled after an existing military instrument (Zagelbaum et al., 2014) to evaluate perceived preparedness and confidence in starting work.
Quantitative data was analysed using IBM SPSS (Version 23.0), with descriptive analysis. The qualitative data was analysed using modified thematic analysis, with NVivo software. All transcripts were coded independently by three authors. The coding method involved an inductive (ground up) method, looking at generating the unit of meanings, categorising the data and developing themes until data saturation was achieved. The kappa coefficient score for the qualitative data analysis was 0.87, indicating good agreement.
III. RESULTS
Sixty-one housemen participated (response rate 100%). A significant proportion (57.4%) rated high stress on the PSS.
Key themes of perceived challenges reported by the housemen transitioning from medical school to the workforce during the COVID-19 pandemic included: (1) coping with constant change, (2) lack of timely reliable information, (3) dealing with disappointment, (4) physical fatigue, (5) loss of autonomy (Fig 1). Examples of last-minute changes to examinations, work commencement and posting-related information were quoted as a major cause for significant uncertainties. Additionally, some had quoted the lack of timely nor reliable dissemination of the information, coming from third-party sources rather than relevant authorities. The shortened break between end of examinations and housemanship meant that typical traditions of personal and post-graduation plans, had to be cancelled, resulting in disappointment and reduced rest. Many also felt that the central distribution of manpower with increased rotations to pandemic heavy departments meant a loss of autonomy in selecting a posting or institution of choice.
The themes for perceived concerns about starting work during the pandemic included (1) clinical competence as a junior doctor, (2) transitioning into new responsibilities, (3) risk of infection, (4) failing to meet expectations of seniors, (5) physical fatigue and (6) training-related concerns. The lack of competence in patient management, “call” duties, and managing emergencies were a huge concern. This extended from concerns of manpower constraints and reduced supervision during pandemic times. Navigating the new job as a doctor with new responsibilities were also raised, with concerns on the long hours and overnight “calls” leading to burnout. There were also examples given on failing to meet the expectations of senior colleagues. Pandemic-specific concerns included the risk of contracting and transmitting COVID-19 to loved ones. Many had also expressed apprehension about the possible impact that the pandemic may have on their clinical training and career progression.
In terms of preparedness to start work amidst a pandemic, 82.0% (n = 50) housemen shared that they were mentally prepared to start work. Majority (86.8%) felt that their medical school had prepared them adequately to be a junior doctor. Three-quarters (75.4%) agreed that their medical school has prepared them adequately to deal with the pandemic and its related clinical demands. Majority (83.6%) felt confident in their clinical competency to effectively work as a junior doctor, and 77.0% felt confident in their clinical competency in dealing with the pandemic as a junior doctor. Interestingly, when asked about their confidence in managing stress, 80.3% reported being confident of dealing with stressors faced by a junior doctor while 77.0% felt confident in managing pandemic-related stress.

Figure 1. Perceived challenges in the transition period, and perceived concerns of new housemen just before starting their housemanship. The size of the boxes corresponds to the frequencies of the themes with examples of verbatim responses transcribed.
IV. DISCUSSION
Our results show that a significant proportion of housemen starting work in the current pandemic have high perceived stress; this appeared to be higher than what is reported in literature for medical students and house officers in non-pandemic settings (Drachev et al., 2020), and higher than healthcare workers during this pandemic (Chen et al., 2020). As such, we believe that this is a significant finding warranting attention.
The challenges of transitioning from medical school to housemanship is well established: not only do housemen have to cope with the responsibility of being a full-fledged doctor, there is also increased physical fatigue and professional expectations that need to be met. Some of these challenges specific to transitioning have also been raised by our housemen.
The sentiments of housemen transitioning during a pandemic are not unique to this group alone: dealing with frequent and constant change and the lack of reliable and timely information are challenges that have also been reported among other healthcare workers. However, there were specific points unique to this group of junior doctors we had studied, particularly the perceived insecurity over their qualifications due to disrupted student clinical training and modified final examinations. This we feel is an important point that medical schools should be aware of; in the event of disruptions or sudden changes to the process of assessment or accreditation, it is important that these be conveyed clearly to the student body, with appropriate engagement, opportunities for clarification and reassurance on any insecurities which they may result from these changes.
Significant pandemic-specific concerns included fears of contracting the COVID-19 infection and transmitting this to others. This fear is not uncommon among healthcare workers and has been reported in recent literature. There was also the additional concern of postgraduate training disruption, which was not unexpected given the disruptions to teaching, deployment to pandemic areas and the lack of choices in the selection of their postings.
We were encouraged to find that despite the higher perceived stress, reported challenges and concerns shared, the majority had felt that their medical schools had prepared them adequately to be a junior doctor, and to deal with pandemic related demands. Additionally, despite the concerns about starting work earlier, majority still reported being ready to start work and felt confident to work effectively – their response to readiness meant that they were not shying away from the call of duty during this pandemic.
Our study is not without limitations. Open-ended questions instead of interviews that were done in line with social distancing restrictions limited the depth of the qualitative data. That said, the 100% response rate provided us which rich data that could be analysed. Additionally, the use the modified questionnaire on preparedness not only lacked external validation; we are also aware that self-reported preparedness may not correlate with actual readiness.
We believe that the key sentiments we have reported on housemen starting work in a pandemic are likely to be universal and not unique to our institution alone. These data would be informative for institutions to provide targeted support for new housemen amidst the pandemic. These include:
- Providing clear and effective information transfer particularly on rapidly changing protocols.
- Emphasis on training on personal protection and infection prevention throughout their postings.
- If manpower resources permit, institutions may consider first deploying housemen to non-pandemic services with initial job-shadowing before sending them to pandemic areas.
- Close clinical supervision from immediate seniors.
- Specific teaching program catering to the learning needs of housemen during the pandemic.
- Enforcing strict work-rest cycles to ensure adequate rest.
- Dedicated mentors for housemen to share concerns and grievances. These mentors have the responsibility of identifying housemen who are struggling such that early support can be rendered.
- Appropriate resources for housemen who require additional support.
V. CONCLUSION
Newly qualified doctors beginning their housemanship during the COVID-19 pandemic have high perceived stress with specific pandemic-related concerns and challenges on top of the usual stressors in transitioning. That said, there is encouraging data on housemen preparedness in starting work during this time. Institutions should ensure that support systems are in place to support junior doctors in these likely protracted extraordinary times. A successful transition from medical school to workplace is the cornerstone that allows these junior doctors to integrate effectively to contribute to the workforce in the pandemic, and the long journey beyond.
Notes on Contributors
Mae Yue Tan contributed to analysis and interpretation of data, drafting and critical revising of the article.
Nicholas BH Ng contributed to analysis and interpretation of data, drafting and critical revising of the article.
Marion M Aw contributed to interpretation of data, drafting and critical revising of the article.
Jeremy BY Lin contributed to conception and design, interpretation of data, drafting and critical revising of the article.
All authors gave final approval of the version to be published.
Ethical Approval
Ethics approval was obtained from from the NHG Domain Specific Review Board (DSRB), with NHG DSRB reference number of 2020/00392.
Data Availability
The data for this study can be found at https://doi.org/10.6084/m9.figshare.16399107 and https://doi.org/10.6084/m9.figshare.16399419. The access to these datasets are available for use subject to approval of the authors of this article.
Acknowledgement
The authors would like to thank the housemen who participated in this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Interest
All authors have no conflict of interest to declare.
References
Chen, B., Li, Q. X., Zhang, H., Zhu, J. Y., Yang, X., Wu, Y. H., Xiong, J., Li, F., Wang, H., & Chen, Z. T. (2020). The psychological impact of COVID-19 outbreak on medical staff and the general public. Current Psychology, 1–9. https://doi.org/10.1007/s12144-020-01109-0
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behaviour, 24(4), 385-396.
Drachev, S. N., Stangvaltaite-Mouhat, L., Bolstad, N. L., Johnsen, J. K., Yushmanova, T. N., & Trovik, T. A. (2020). Perceived stress and associated factors in Russian medical and dental students: A cross-sectional study in North-West Russia. International Journal of Environmental Research and Public Health, 17(15), 5390. https://doi.org/10.3390/ijerph17155390
Sturman, N., Tan, Z., & Turner, J. (2017). “A steep learning curve”: Junior doctor perspectives on the transition from medical student to the health-care workplace. BMC Medical Education, 17(1), Article 92. https://doi.org/10.1186/s12909-017-0931-2
Zagelbaum, N. K., Heslin, K. C., Stein, J. A., Ruzek, J., Smith, R. E., Nyugen, T., & Dobalian, A. (2014). Factors influencing readiness to deploy in disaster response: Findings from a cross-sectional survey of the department of veterans affairs disaster emergency medical personnel system. BMC Emergency Medicine, 14, Article 16. https://doi.org/10.1186/1471-227X-14-16
*Tan Mae Yue
1E Kent Ridge Road,
NUHS Tower Block Level 12,
Singapore 119228
Tel: +65 6772 5555
Email: mae_yue_tan@nuhs.edu.sg
Submitted: 11 November 2021
Accepted: 27 January 2022
Published online: 5 April, TAPS 2022, 7(2), 51-55
https://doi.org/10.29060/TAPS.2022-7-2/SC2710
Rintaro Imafuku, Kaho Hayakawa & Takuya Saiki
Medical Education Development Center, Gifu University, Japan
Abstract
Introduction: Personal statements are important documents in the admission and programme application processes, including international elective programmes, in medical education. However, writing these is challenging for international applicants not only because of their unfamiliarity with this genre but also their English academic writing skills. This study aims to explore the organisation and elaboration of text in personal statements written by Japanese medical students for international elective programme application.
Methods: Drawing on genre analysis, the first draft of personal statements written by eight fifth-year medical students at a Japanese university were analysed. The text data were deductively classified into moves and steps, using Chiu’s framework of the personal statement genre.
Results: In the introduction, Japanese medical students commonly described the context and issues of healthcare in Japan and the future goals for physicians. In the move of the relevant background, it was notable that six out of eight personal statements showed personality. Although a range of moves was covered when writing about the reasons for applying, only two students described their understanding of programmes and institutional attributes. In the move of conclusion, they focused more on writing their goals of future success and contribution to the course. Furthermore, no applicant expressed self-promotion and praise for academics, programmes, and institutions.
Conclusion: The findings of this study can provide a springboard for the development of support for Japanese students’ academic writing in English in medical education across cultures.
Keywords: Medical Education, International Electives, Personal Statement, Genre Analysis, Discourse, Rhetorical Patterns, Written Communication
I. INTRODUCTION
The personal statement, as a promotional academic genre, is an important document in the admission process for higher education. However, numerous applicants face difficulties while preparing application materials because of their unfamiliarity with the genre of discourse and audience expectations (Ding, 2007). In medical education, particularly institutions in Western countries, several instances require the submission of personal statements for application to, for instance, medical schools, international electives, residency programmes, and research programmes.
Globalisation in medical education has promoted worldwide student mobility. Currently, many Asian medical students, including Japanese students, participate in international electives in Western countries. International electives provide several benefits to medical students, including cultural competence, communication skills, and clinical reasoning (Imafuku et al., 2021). However, because some institutions require the submission of personal statements for application to the international elective programme, it can be challenging for international applicants not only because of their unfamiliarity with the genre of discourse but also their English academic writing skills.
As the preparation of application materials, including personal statements, can be challenging for Asian medical students, educators must facilitate a more comprehensive pre-departure course, along with providing support for composing such documents. Specifically, a better understanding of the linguistic features of their personal statements is fundamental for developing academic writing support for their application documents. Therefore, this study used the genre analysis framework (Swales, 1990) to explore the organisation and elaboration of text in personal statements written by Japanese medical students for the international elective programme application. Specifically, the following research question was developed: What are the rhetorical characteristics of Japanese medical students’ personal statements written in English?
II. METHODS
A. Setting
International electives, which allow the students at the Gifu University School of Medicine to study overseas, are optional modules of either four or eight weeks in the final year of the clinical clerkship programme with the goals of observation, understanding and experiencing clinical practices in different cultural contexts. Through this programme, every year, 10–15 medical students study clinical medicine in a foreign country and gain cross-cultural experience in a clinical setting. As some highly competitive overseas institutions require the submission of personal statements, letters of recommendation, and curriculum vitae during the application, faculty members of the medical education division provide some support for their preparation, if required by the students. Although the guidebook for international electives briefly explains the definition and role of personal statements, the students are not officially given any sample or format of English personal statements.
B. Data Collection and Analysis
This study collected personal statements written in English by fifth-year medical students (n=8; Student A-H) at a Japanese university, from 2013 to 2017, as part of the application documents for international electives in institutions in the United Kingdom (UK) or the United States (US). Their TOEFL (Test of English as a Foreign Language) (iBT) score ranges from 90 to 101. Written informed consent to participate was obtained from them. Their first drafts were analysed through the lens of move analysis as an element of genre analysis (Swales, 1990) to reveal rhetorical patterns from a cultural perspective. The first draft, which has not been revised using feedback from others, directly reflects their cultural and linguistical influences regarding the rhetorical patterns. Text data were analysed by the first author, who has a background in applied linguistics and medical education. Subsequently, the preliminary findings of the text analysis were discussed by all the research team members to establish the credibility and dependability of the data analysis.
Genre analysis aims to describe the organisational patterns of text in a specific context, and genres are viewed as staged goal-oriented social processes of the written or spoken practice. For example, in written communication, reader expectations, document structure, and rhetoric development vary depending on the genre, such as research articles, invitation letters, and reminder emails. A move is an analytical unit defined as a rhetorical component shifting from one part of a text to another that performs a specific communicative function (Swales, 1990, p.140). Each move is subcategorised into one or more functional units called steps.
Specifically, this study applied Chiu’s (2016) framework of moves and steps in the context of personal statements for graduate school application to medical education. Drawing on this analytical framework that comprises five moves: introduction, relevant background, reasons for applying, extra-curricular information, and conclusion, the text data were deductively classified into moves and steps.
Ethical approval was obtained from the Gifu University Ethics Committee (No. 25–367). Students were assured of the confidentiality of the contents.
III. RESULTS
The average length of the personal statements was 535.5 words (range: 314–873 words). The deidentified data of personal statements by some participants who gave their consent to share the whole text that support the findings of this study are available in Figshare at http://doi.org/10.6084/m9.figshare.17030705. All the data set can be available from the corresponding author on reasonable request. Table 1 indicates the total number of personal statements that consists of any step of each move and shows the representative text in each move.
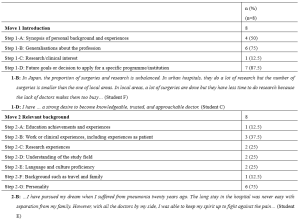

Table 1. Moves and steps of the personal statements for international electives written in English by Japanese medical students
As can be seen from Table 1, in the introduction, Japanese medical students commonly described the context and issues of healthcare in Japan (1-B) and future goals for physicians (1-D). Expressions of their research and clinical interests (1-C) were made the least in the introduction move. In the relevant background move, it is notable that six out of eight personal statements in this study showed personality (2-G), which is much higher than the rest of the other steps. In the reasons for applying move, six Japanese medical students made the rhetorical step of personal development and ambition, whereas only two students described their understanding of programmes and institutional attributes (3-C) and disciplinary and research reasons (3-E). Extra-curricular information (Move 4) was not provided by the applicants in this study. In the move of conclusion, Japanese medical students focused only on their future success goals (5-A) and contribution to the course (5-E). Furthermore, no applicant expressed self-promotion (5-B) and praise for academics, programmes, and institutions (5-D) in this study.
IV. DISCUSSION
Drawing on genre analysis (Swales, 1990), this study revealed the rhetorical patterns of personal statements written by Japanese medical students. Although the participants had high or adequate English proficiency, they seemed to struggle with personal statement writing due to the unfamiliar genre of discourse. Imafuku et al. (2021) found that the participants faced several difficulties related to linguistic, sociolinguistic, and sociocultural aspects during the international electives, whereas this study showed that the applicants had already experienced difficulties of cross-cultural communication at the pre-departure stage.
Genre analysis offers a useful theoretical framework and an analytical perspective of people’s communicative practices in a cultural context, especially allowing educators or researchers to examine how language is used in specific contexts for particular purposes, thus contributing to the knowledge of specific writing instructions (Ding, 2007). Writing a personal statement is a common issue not only in medical education but also in higher education. Personal statements are a type of promotional academic genre in admissions to higher education institutions or programmes that expects textual self-aggrandisement by applicants. Chiu (2016), who examined personal statements in the areas of educational policy, language and literacy, and higher education, demonstrated that self-promotion or evaluation is an important step in the conclusion move for graduate school applications in the UK and the US. As a response to Chiu’s (2016) study, the finding of this study that self-promotion or evaluation is not indicated in the move of conclusion by Japanese medical students suggests their need to learn not only the rhetorical structure and reader expectations but also ways of logically and effectively expressing their own strengths. The results of this study can be a useful learning resource to understand what rhetorically characterises a personal statement.
Reflecting on the rhetorical patterns of the students in a given genre is pivotal to communicative achievement in intercultural settings. In this sense, contrastive rhetoric studies have provided useful implications for a better understanding of writing patterns from a cross-cultural viewpoint. For example, contrastive rhetoric studies of Japanese and English to date have shown different discourse organisations of and approaches to writing in a variety of genres, such as newspaper columns, doctoral dissertations, and narrative essays (Connor, 1996). In the previous studies reviewed by Connor (1996), Japanese writing was characterised by a reader-responsible language and a deductive rhetorical pattern. Furthermore, the Japanese are oriented to share values of indirectness, and the reader is expected to interpret what the writer intended to convey. This study suggests that understanding the rhetorical features in the writer’s own cultural context is essential to writing in the target genre of discourse in different cultural contexts.
Although this study illuminates written communication across cultures through the text analysis of personal statements, investigation should be undertaken continuously for further data collection, as the sample size of text data from eight students is limited to a particular institution. Furthermore, follow-up interviews are worthwhile to explore students’ writer identity and cognitive process during writing.
V. CONCLUSION
There are increased opportunities for cross-cultural communication, including both spoken and written formats, in globalised contexts, such as medicine. For written communication, in the genre of personal statements in medical education, this study found that Japanese students shared limited information about the relevant background (Move 2) and did not express adequate self-promotion (Move 5). The findings can act as a springboard for the development of support for Japanese students’ academic writing in English in medical education across cultures.
Notes on Contributors
Rintaro Imafuku reviewed the literature, designed the study, conducted text analysis, and wrote the manuscript.
Kaho Hayakawa was involved in data collection and analysis of the text.
Takuya Saiki was involved in data collection and analysis of the text.
All the authors have read and approved the final manuscript.
Ethical Approval
This study was approved by the Gifu University Ethics Committees (No. 25–367). Consent was obtained from all participants for the research study. Confidentiality was assured for the contents of students’ writing. All participants have given written consent for their data to be used in the research and for publication.
Data Availability
Deidentified data of personal statements by the participants who gave their consent to share the whole text are openly available at http://doi.org/10.6084 /m9.figshare.17030705. The data are available from the corresponding author on reasonable request.
Funding
This work was supported by the JSPS KAKENHI [Grant number 20K10374].
Declaration of Interest
The authors report no conflicts of interest.
References
Chiu, Y.-L. T. (2016). ‘Singing your tune’: Genre structure and writer identity in personal statements for doctoral applications. Journal of English for Academic Purposes, 21, 48-59. https://doi.org/10.1016/j.jeap.2015.11.001
Connor, U. (1996). Contrastive rhetoric: Cross-cultural aspects of second language writing. Cambridge University Press.
Ding, H. (2007). Genre analysis of personal statements: Analysis of moves in application essays to medical and dental schools. English for Specific Purposes, 26(3), 368-392. https://doi.org/10.1016/j.esp.2006.09.004
Imafuku, R., Saiki, T., Hayakawa, K., Sakashita, K., & Suzuki, Y. (2021). Rewarding journeys: Exploring medical students’ learning experiences in international electives. Medical Education Online, 26(1), 1913784. https://doi.org/10.1080/10872981.2021.1913784
Swales, J. (1990). Genre analysis: English in academic and research settings. Cambridge University Press.
*Rintaro Imafuku
1-1 Yanagido, Gifu, Gifu, 501-1194
Email: rimafuku@gifu-u.ac.jp
Submitted: 30 July 2021
Accepted: 17 January 2022
Published online: 5 April, TAPS 2022, 7(2), 46-50
https://doi.org/10.29060/TAPS.2022-7-2/SC2662
Kheng Tian Lim1 & Bao Yun Koh2
1Department of General Surgery, Khoo Teck Puat Hospital, Singapore; 2Education Development Office, Khoo Teck Puat Hospital, Singapore
Abstract
Introduction: Medical students (MS) may lack the knowledge and experience in performing basic surgical skills (BSS) when they first commence their postgraduate surgical training. We conducted a pilot BSS workshop with specific learning outcomes for MS.
Methods: Our BSS workshop program consisted of reading the pre-workshop online modules, watching the instructional videos of skills demonstration, and completing the pre-workshop multiple-choice questions (MCQ). MS attended the onsite workshop a week later, which consisted of a basic surgical theory lecture, live demonstration of the skills by the teaching faculty and, supervised skills training coupled with feedback. Surgical skills taught were knot tying, suturing techniques, laparoscopic peg transfer, precision cutting, application of endoloop ties. A standardised surgical skills rubric was used to assess the competency and safety of BSS. A post-workshop MCQ was administered to assess the knowledge learned. The criteria for successful completion of BSS were a satisfactory grade in the surgical skills assessment and a pass score in the MCQ.
Results: All the participating MS achieved a satisfactory grade in the surgical skills assessment and passed the MCQ. Several pedagogical methods were used to enhance knowledge learning and practical skills competency including a flipped classroom in blended learning, technology-enhanced learning, kinesthetic learning, and providing effective feedback.
Conclusion: MS taught in BSS workshop can achieve competency in knowledge, skills, safe attitude and prepare them for future postgraduate surgical training. In the current COVID-19 pandemic, our challenge is to develop similar BSS in a safe environment using technology-enhanced tools such as online instructional videos and online feedback.
Keywords: Assessment, Basic Surgical Skills, Competency, Feedback, Medical Students, Outcome-based Education
I. INTRODUCTION
Medical students (MS) may lack the knowledge and experience in performing certain basic surgical skills (BSS) when they first commence their postgraduate surgical training in hospitals. Traditionally, BSS are usually not taught formally in the undergraduate medical curriculum until much later in the postgraduate level. The opportunity for teachers to teach BSS and for MS to learn is much dependent on the situation in operating rooms during assigned core surgical postings or student selective postings.
In Singapore, Yong Loo Lin School of Medicine, National University of Singapore (NUS) provides basic and advanced clinical procedural simulation training to undergraduate MS. Skills taught include gowning, scrubbing techniques, suturing, and knot-tying. Lee Kong Chian School of Medicine, Nanyang Technological University (NTU) teaches suturing and knot-tying skills in dry laboratory to undergraduate MS. All these stimulated practical skills and experience acquired by MS are transferrable to real patients’ environments. In addition, SingHealth Academy, an educational arm of SingHealth, provides BSS workshop training at the postgraduate level for interested learners. In the United Kingdom and Ireland, the BSS course is a curriculum-mandated course for postgraduate Core Surgical Training programmes.
Healthcare institution partners such as Khoo Teck Puat Hospital (KTPH), provide clinical training for MS of NUS and NTU. Our Department of General Surgery (GS) identifies the need in the learning outcomes for the graduating MS, to equip them with the competent foundation of BSS for postgraduate surgical training, although not a graduating competency requirement set by Singapore Medical Council. We conducted a small pilot workshop at our institution, aiming at educational quality improvement for our MS in three learning domains, namely surgical knowledge, practical surgical skills, and attitudes in safety that are common to all forms of surgery.
II. METHODS
A. Workshop organization, MS and Teaching Faculty, Teaching Materials
The Department of GS and Education Development Office (EDO), KTPH organised a 1-day BSS workshop for MS with the request from MS and was scheduled on 20th December 2019. Planning over three months was required to prepare the learning objectives and outcomes, workshop programme schedule, venue, teaching materials, surgical scrubs, sustenance, and coordination by the workshop director and EDO. Both the local and overseas MS were invited and recruited for training. Experienced local teaching faculty members were invited and briefed on the teaching methodology, feedback provision, and assessment criteria.
MS who agreed to participate were given instructions to read the pre-workshop fundamentals of the BSS document, watch the instructional video clips of the BSS demonstration and, complete pre-workshop multiple-choice questions (MCQ), all of which were provided online 1 week before the workshop. These pre-workshop activities may help to motivate the MS and provide an opportunity for self-assessment of their understanding of the BSS topics. MS were allowed to post questions to the workshop director for guidance. The course content and MCQ were prepared by the course director to be appropriate to the MS level.
The workshop was divided into morning and afternoon sessions to cater to a larger group of interested MS coming from overseas. The onsite workshop consisted of a short basic theory lecture, a live demonstration of the practical BSS, MS performing the practical BSS with direct supervision and corrective feedback. BSS taught were knot tying using one-hand, two-hand, and instrumental techniques. Suturing techniques taught included simple, mattress, interrupted, continuous suture. More advanced laparoscopic skills such as laparoscopic peg transfer, precision cutting, and application of endoloop ties were taught. A post-workshop MCQ was administered.
B. Assessment in Knowledge, Skills, and Attitudes
The surgical knowledge was assessed using the pre-and post-workshop MCQ, based on the course content prepared for MS.
The surgical skills assessment was carried out by direct observation of procedural skills (DOPS) using a standardised surgical skills rubric. Open surgery skills assessment included instrument selection and handling, knotting techniques, tissue handling, and suturing techniques. Laparoscopic surgery skills assessment included instrument selection and handling, peg transfer, precision cutting, and ligating loop. The overall summative assessment of global grading in the surgical skills domain by the teaching faculty was either satisfactory or unsatisfactory.
MS were assigned to work in pairs with the ratio of MS: teaching faculty as 2:1. Assessment in the attitude and behavior domain was based on direct observation in the safe handling of sharps and needles, general assisting, and laparoscopic camera assisting skills.
C. Feedback and Competency
The teaching faculty used DOPS to provide feedback on the practical BSS performed by the MS which allowed the MS to improve and progress from a novice to a competent learner level in the skills and attitude domains. The specific, timely, and purposeful feedback served as a channel for MS to improve and reflect on their learning outcomes in these domains.
The competency criteria for successful completion of the BSS workshop were set as a pass mark of 60% in the summative MCQ test and a satisfactory grade in the summative skills assessment by the teaching faculty. A Certificate of Attendance would be awarded to MS who have acquired the competency criteria.
III. RESULTS
Assessment and evaluation data gathered for this workshop and pre-workshop MCQ questions were uploaded to an online repository for archiving and validation purposes. It may be assessed through the following Digital Object Identifier (DOI): https://doi.org/10.6084/m9.figshare.16884877.v2 (Lim & Koh, 2021).
A total of 38 MS signed up for the BSS workshop with 1 dropout. Thirty-seven MS attended the workshop of which 25 were from overseas medical schools. Thirty-six MS attempted the pre-workshop MCQ (10 questions). Thirty-seven MS passed the post-workshop MCQ (15 questions). All MS achieved satisfactory grades in practical skills. There was no needle stick injury reported.
The BSS workshop program evaluation form was administered and completed anonymously for the quality improvement process after verbal consent was taken from the participants. (Table 1).
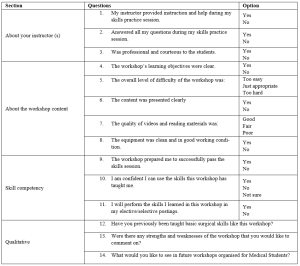
Table 1. BSS Workshop for MS Program Evaluation
IV. DISCUSSION
Bloom’s Taxonomy comprises three learning domains known as cognitive (knowledge), affective (attitude), and psychomotor (skills). Each domain has a hierarchy that corresponds to distinct levels of learning which is important for students to develop holistically. The learning objectives of the BSS workshop for MS are thus designed to fulfil these three domains, specifically to: 1) acquire the fundamental knowledge of BSS (knowledge), 2) demonstrate a variety of surgical knots and suturing skills effectively (skills) and, 3) handle and use of surgical instruments and tissue safely (attitude).
Harden et al. (1999) described an outcome-based education framework that comprises six levels of training to achieve the outcomes. These six levels of training are: 1) awareness of the procedure, 2) full theoretical understanding of the procedure, 3) observation of the procedure, 4) carrying out part of the procedure, 5) undertaking the procedure under the supervision and, 6) undertaking the procedure unsupervised. Similarly, the programme activities of the BSS workshop for MS were developed to cover these six levels of training. The learning outcomes of this workshop are to equip the MS with the competency of BSS for postgraduate surgical training. The teaching faculty members share their knowledge, demonstrate their expertise, advise MS, and provide feedback to improve technical skills and promote learning.
Effective feedback is necessary to enhance learning. Pendleton et al. (2003) described a four-step process for carrying out a feedback session. Ramani and Krackov (2012) described twelve tips for clinical teachers to provide effective feedback to undergraduate and graduate medical trainees. Our teaching faculty members were able to provide effective feedback to MS using these frameworks to establish a respectful learning environment, feedback on direct observation, make feedback timely, reinforce and correct observed behaviors, use specific language to focus on performance, confirm the learner’s understanding and conclude with an action plan.
The assessment for learning in the BSS workshop for MS was designed to align with the three learning domains using: 1) pre-and post-workshop MCQ to test surgical knowledge, 2) DOPS by the teaching faculty to test surgical skills and, 3) DOPS in the safe handling of sharps and needles, general assisting and laparoscopic camera assisting skills to test the attitude and behavior. A standardised surgical skills rubric was used for DOPS.
Technology-enhanced learning (TEL) intervention and enhancement can be characterised by 1) replicating existing teaching practices, 2) supplementing existing teaching or, 3) transforming teaching, learning processes, and outcomes (Kirkwood & Price, 2014). Several pedagogical methods were used in this BSS workshop to enhance knowledge learning and skills acquisition such as flipped classroom in blended learning, a mixture of the three characteristics of TEL, kinesthetic learning, and providing effective feedback. In the current COVID-19 pandemic, there are challenges to conducting such a practical workshop. TEL tools that combine online educational materials, instructional videos, feedback, and face-to-face online interaction such as Zoom, and Microsoft Teams are the new norm.
The limitation of this workshop includes the lack of MCQ standardisation process and the quality of the video clips which we intend to improve in the next workshop.
V. CONCLUSION
Conducting a BSS workshop for MS with specific learning outcomes is feasible where the MS can achieve competency in knowledge, skills, safe attitude and prepare them for postgraduate surgical training. In the current COVID-19 pandemic, our challenge is to develop similar BSS in a safe environment using TEL tools.
Notes on Contributors
Dr. Lim Kheng Tian designed the work, reviewed the literature, drafted the work, revised the content critically, and wrote the manuscript. Ms. Koh Bao Yun contributed to the design and administration of the work, gave critical feedback to the content, and revised the manuscript. All authors have read and approved the final manuscript.
Ethical Approval
This 1-day workshop program was conducted for educational quality improvement (QI) with approval from the Department of GS and EDO, KTPH. This article was submitted with Institutional Review Board/Ethical approval for exemption from full review. We have attached the local IRB waiver document NHG DSRB Ref: 2021/00888.
Data Availability
Inline to make research available to the scientific community for data replication and scientific progress, the dataset of this workshop may be found for free through the Figshare website: https://doi.org/10.6084/m9. figshare.16884877.v2
Acknowledgement
The authors want to thank all the MS and teaching faculty who participated in the workshop. We would like to acknowledge Dr. Lee Yao Zong, Associate Consultant of the Department of GS, KTPH for providing help in the laparoscopic educational content. We would like to acknowledge the technical help of Mr. Mohamad Sean Abdullah, former Experimental Surgical Services Development Executive of the Department of GS, KTPH. We would like to acknowledge equipment support from KARL STORZ Endoscopy Singapore Sales Pte Ltd for providing the reusable laparoscopic trainer and laparoscopic instruments. We also like to acknowledge NHG Education for linking up EDO, KTPH with the Singapore Medical Society of Australia and New Zealand (SMSANZ).
Funding
There is no funding for this paper. The suturing materials used in the workshop were funded by the Pre-Employment Clinical Training (PECT) Funds received by KTPH for local MS whilst overseas MS were self-funded. The funder was not involved in the design, delivery of the workshop, or submission of the paper.
Declaration of Interest
All authors declare no conflicts of interest, including financial, consultant, institutional, and other relationships that might lead to bias or a conflict of interest.
References
Harden, R. M., Crosby, J. R., Davis, M. H., & Friedman, M. (1999). AMEE Guide No. 14: Outcome-based education: Part 5-From competency to meta-competency: A model for the specification of learning outcomes. Medical Teacher, 21(6), 546–552. https://doi.org/10.1080/01421599978951
Kirkwood, A., & Price, L. (2014). Technology-enhanced learning and teaching in higher education: What is ‘enhanced’ and how do we know? A critical literature review. Learning, Media and Technology, 39(1), 6–36. https://doi.org/10.1080/17439884.2013.770404
Lim, K. T., & Koh, B. Y. (2021). Start small and aim big in conducting a basic surgical skills workshop for medical students—Repository data (p. 11710 Bytes) [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.16884877.v2
Pendleton, D., Schofield, T., Tate, P., & Havelock, P. (2003). The New Consultation. Oxford University Press.
Ramani, S., & Krackov, S. K. (2012). Twelve tips for giving feedback effectively in the clinical environment. Medical Teacher, 34(10), 787–791. https://doi.org/10.3109/0142159X.2012.684916
*Lim Kheng Tian
Department of General Surgery,
Khoo Teck Puat Hospital,
90 Yishun Central,
Singapore 768828.
Tel: +65 65558000
Email: lim.kheng.tian@ktph.com.sg
Submitted: 22 August 2021
Accepted: 28 December 2021
Published online: 5 April, TAPS 2022, 7(2), 42-45
https://doi.org/10.29060/TAPS.2022-7-2/SC2682
Lee Man Xin1*, Zhang Yuan Helen2* & Fatimah Lateef2,3
1Changi General Hospital Emergency Department, Singapore; 2Singapore General Hospital Emergency Department, Singapore; 3Singhealth Duke-NUS Institute of Medical Simulation (SIMS) Education Office, Singapore
*Joint first authors
Abstract
Introduction: Advanced Cardiac Life Support (ACLS) course is one of the mandatory certifications for the majority of medical as well as some nursing professionals. There are, however, multiple variations in its instruction model worldwide. We aim to evaluate the efficacy of traditional ACLS course versus a hybrid ACLS course utilised during the COVID-19 pandemic.
Methods: This retrospective study was carried out at SingHealth Duke-NUS Institute of Medical Simulation using course results of participants in the centre’s ACLS course between May to October 2019 for the traditional course were compared with participants attending the hybrid course from February to June 2021.
Results: A total of 925 participants were recruited during the study period. Of these, 626 participants were from the traditional group and 299 participants were from the hybrid learning group. There is no statistically significant difference between the two group (χ2=1.02 p = 0.313) in terms of first pass attempts; first pass attempt at MCQ (p=0.805) and first pass attempt at practical stations (p=0.408). However, there was statistically significant difference between the mean difference in results of traditional vs hybrid MCQ score, -0.29 (95% CI: -0.57 to -0.01, p=0.0409). Finally, senior doctors were also found to perform better than junior doctors in both traditional (p=0.0235) and hybrid courses (p=0.0309) at the first pass attempt of ACLS certification.
Conclusion: Participants in the hybrid ACLS course demonstrated at least equal overall proficiency in certification of ACLS as compared to the traditional instruction.
Keywords: Advanced Cardiac Life Support, Teaching Model, COVID-19, Hybrid Learning
I. INTRODUCTION
Cardiopulmonary resuscitation (CPR) represents an emergency lifesaving procedure for cardiac arrest patients. It is a core skillset for every licensed physician, graduating medical students and paramedics. It provides evidence-based algorithms to be executed to optimise the likelihood of survival in cardiac arrest patients. Cardiac arrest poses a major public health challenge. Worldwide, sudden and unexpected cardiac death is one of the most common causes of death. Given such a substantial disease burden, structured and continued training of physicians and first responders on advanced cardiac life support (ACLS) is extremely crucial. In Singapore, about 3000 people have a sudden cardiac arrest every year (Ong, 2020).
The first Advanced Cardiac Life Support (ACLS) course in Singapore, was started in late 1985 and traditionally it has been conducted over two days. It comprises of pre-reading from a manual outlining the procedure algorithms, a combination of face-to-face didactics and hands-on skills stations conducted by licensed providers and instructors, followed by multiple-choice theory and practical certification tests. It mainly focuses on technical knowledge and skills which needs to be recertified every two years (Anantharaman, 2017). Since the implementation of social distancing measures under DORSCON Orange in Singapore in response to the COVID-19 disease outbreak on 7th February 2020, ACLS teaching model has since been modified to multimedia lectures followed by small-group (maximum 5 people) practical lessons, which was further adjusted to include an online self-administered pre-lecture quiz from 18th February 2021 onwards. Limited evidence has shown that written evaluation is not a predictor for skills performance in an ACLS course and there is now, a growing body of advocates for high-fidelity mannequin-based simulation supplementing ACLS curricula. Multiple research studies have focused on the efficacy of various educational and instructional methods for ACLS teaching in terms of improvement to the resuscitation knowledge and clinical skills (Thorne et al., 2017).
We aim to retrospectively evaluate the efficacy of our new hybrid ACLS teaching model based on participants passing rate of both theory and practical tests as compared to the traditional ACLS instruction model. The primary goal is to provide enhanced insights into the way ACLS training should be conducted and further refine our courses as we evolve in the new norm of living with the COVID-19 pandemic. Institutional Review Board waiver has been obtained through Singapore Health Service (CIRB: 2021/2499).
II. METHODS
A. Study design and participants
This retrospective study was carried out at SingHealth Duke-NUS Institute of Medical Simulation (SIMS) using the course results of participants in the centre’s Advanced Cardiac Life Support (ACLS) course. A waiver of consent was approved by the institute’s CRIB committee as the results were anonymised.
The ACLS course traditionally comprises face-to-face didactic lecture components and practical skills stations culminating in MCQ and practical assessment. Successful completion of both MCQ and practical assessment results in certification or recertification for the participants.
In the hybrid ACLS learning model, the didactic lecture component has been replaced with an interactive online learning platform while maintaining the same practical skills stations with reduced instructor to student ratio because of safe distancing measures. To facilitate learning, a pre- and post-lesson quiz, with 25 MCQ questions, was administered on the online learning platform.
Course results of participants attending the traditional course from May to October 2019 were compared with participants attending the hybrid course from February to June 2021. No participants were found to have attended both the traditional and hybrid ACLS courses, to date. We did not differentiate between recertification and certification courses since there are no differences in assessments.
B. Outcome measures
Our primary outcome measure was the proportion of participants with successful first pass attempt at course certification between traditional and hybrid ACLS courses.
For secondary outcomes, we analysed the mean difference in MCQ scores and first pass attempts at practical stations between traditional and hybrid ACLS instructions. We also compared differences between pre- and post-lesson quiz scores administered during the hybrid learning to assess retention of theoretical knowledge. Lastly, we conducted a sub-group analysis comparing the proportion of senior doctors and junior doctors who pass the course at the first attempt, in both the traditional and hybrid learning groups. Here, senior doctors refer to individuals with specialist registration while junior doctors refer to all other registered medical practitioners.
C. Statistical analysis
A priori sample size estimation was carried out with the assumption that 90% of participants will pass with the first attempt in both traditional and hybrid ACLS teaching models. We used a non-inferiority margin of 10%. Taking α = 0.05 and a statistical power of 80%, we determined that would require at least 155 participants per group.
Statistical analysis was performed using Microsoft Excel 2019. T-test was used when comparing means, Chi-square test was used when comparing categorical variables.
III. RESULTS
A total of 925 participants were recruited during the study period. Of these, 626 participants were from the traditional group and 299 participants, from the hybrid learning group. No participants were excluded from the study. Table 1 shows the characteristics of both groups. The data supporting this study are openly available at https://doi.org/10.6084/m9.figshare.15131664.v1 (Lee et al., 2021).
For the traditional group, 87.7% (549 of 626) passed at the first attempt, whilst for the hybrid group, 90.0% (269 of 299) passed at first attempt (See Table 1). There was no statistically significant difference between the two groups (p = 0.313).
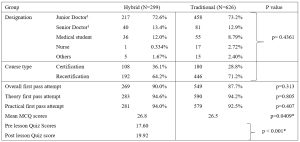
Table 1. Baseline Demographics of Participants for the ACLS Courses and comparison of primary and secondary outcome measures between the Hybrid and Traditional ACLS courses participants
1 Senior doctors are registered specialists under Singapore Medical Council. Junior doctors are all other registered medical practitioners under Singapore Medical Council.
There were no statistically significant differences between the two groups in terms of proportion of first pass attempt at MCQ (p=0.805) and first pass attempt at practical stations (p=0.408). There was however, a statistically significant difference, but with a very small effect size, between the mean difference in results of traditional vs hybrid MCQ score, -0.29 (95% CI: -0.57 to -0.01, p=0.0409).
We also compared the pre- and post-lesson quiz scores in the hybrid learning group. 21 participants were excluded from the analysis due to incomplete pre- or post- test results. We found a mean score difference of 2.32 (95% CI: 1.84 to 2.80, p < 0.001), out of a maximum score of 25, which was higher in post-test group.
Lastly, we compared the proportion of first pass test attempts between senior and junior doctors in both traditional and hybrid learning groups. Senior doctors consistently performed better than junior doctors in both traditional (96.3% vs 87.8% p=0.0235) and hybrid settings (100% vs 89.4% p=0.0309).
IV. DISCUSSION
ACLS is one of the most basic yet crucial skills of medical practitioners worldwide receiving special attention in the framework of various international and national resuscitation councils and societies (Thorne et al., 2017). Clinical educators must explore modalities and evolving technologies that can overcome the barriers of cost, access, and frequency of exposure, while balancing flexibility and applicability that follow deliverable sequelae. Thus far, participants of blended e-learning ACLS courses are known to demonstrate similar scores on the knowledge test, skills test and their final passing rate. The e-learning ACLS course also demonstrates equivalence to traditional face-to-face learning in equipping participants with ACLS skills when compared to the traditional course. This was demonstrated in our results as well. This is a value-added benefit, especially when considering factors such as increased autonomy, cost-effectiveness, decreased instructor burden and improved standardisation of course material (Thorne et al., 2017).
As we shift more towards andragogy among adult professionals, the principles for ACLS instruction should also focus more on self-directed, self-motivated and experiential instruction. Evidence does support that the form and content of these highly structured/model courses are important to transfer the clinical competence that is needed, especially in unstructured, emergencies (Rasmussen et al., 2013). Hence, exploring a sustainable model of ACLS knowledge translation is another important point since further research is needed to develop the optimal evaluation system for the ACLS training program which includes evaluation of the participants, the instructors, and the overall program. The goal should be to assess the degree to which the ACLS program is meeting its objective: to educate medical practitioners, first responders and rescuers.
The COVID-19 pandemic has affected simulation centres where ACLS courses are routinely held. Alternative education modalities have been employed, which include computer-based simulation where technology is used to enhance, augment or even at times, replace real-life simulation. It not only offers the professionals convenience but, complies with safe-distancing or ‘work-from-home’ restrictions put forth by regulatory bodies in many countries. Online modules of virtual reality have also been explored as these can be accessed anywhere electronically and can reduce the amount of face-to-face time that routine training normally requires.
V. CONCLUSION
Hybrid instruction of ACLS training for certification should be recommended as one of the main formats of course delivery as it is as effective compared to the traditional face-to-face training program. From our results it has performed well enough to allow for the safe transition and application of ACLS training in this new era.
Notes on Contributors
Lee Man Xin is involved in conceptualising the study, analysing and interpreting the data, drafting the above manuscript and approving the version to be published. He agrees to be accountable for all aspects of the work.
Zhang Yuan Helen is involved in conceptualising the study, interpreting the data, drafting the above manuscript and approving the version to be published. She agrees to be accountable for all aspects of the work.
Lateef Fatimah is involved in finalising the study conceptualisation and determining key elements for analysis. She is involved in the revision and final approval of the version to be published. She agrees to be accountable for all aspects of the work.
Ethical Approval
Institutional Review Board waiver has been obtained through Singapore Health Service (CIRB: 2021/2499).
Data Availability
The data supporting this study are openly available at figshare repository: https://doi.org/10.6084/m9.figshare.15131664.v1
Acknowledgement
The authors would like to thank Mr Billy Tee, Ms Suppiah Madhavi and Ms Angeline Ng from Singhealth Duke-NUS Institute of Medical Simulation (SIMS) Singapore for providing the data sets.
Funding
This paper receives no funding from outside sources.
Declaration of Interest
Authors have nothing to declare, nor any conflict of interests.
References
Anantharaman, V. (2017). The National Resuscitation Council, Singapore, and 34 years of resuscitation training: 1983 to 2017. Singapore Medical Journal, 58(7), 418–423. https://doi.org/10.11622/smedj.2017069
Lee, M. X., Lateef, F., & Zhang, H. Y. (2021). Hybrid ACLS model (version 1). [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.15131664.v1
Ong, M. E. (2020, October 2). Improving outcomes for Out-of-Hospital cardiac arrest victims. The Straits Times. https://www.singhealth.com.sg/rhs/news/research/improving-outcomes-for-out-of-hospital-cardiac-arrest-victims
Rasmussen, M. B., Dieckmann, P., Barry Issenberg, S., Østergaard, D., Søreide, E., & Ringsted, C. V. (2013). Long-term intended and unintended experiences after Advanced Life Support training. Resuscitation, 84(3), 373–377. https://doi.org/10.1016/j.resuscitation.2012.07.030
Thorne, C. J., Lockey, A. S., Kimani, P. K., Bullock, I., Hampshire, S., Begum-Ali, S., & Perkins, G. D. (2017). e-Learning in Advanced Life Support-What factors influence assessment outcome? Resuscitation, 114, 83–91. https://doi.org/10.1016/j.resuscitation.2017.02.014
*Lee Man Xin
Changi General Hospital Emergency Department
2 Simei Street 3, Singapore 529889
Email: Lee.Man.Xin@singhealth.com.sg
Submitted: 10 August 2021
Accepted: 28 October 2022
Published online: 5 April, TAPS 2022, 7(2), 37-41
https://doi.org/10.29060/TAPS.2022-7-2/SC2670
Qianhui Cheng1, Joanna Pearly Ti1,2, Wai Yung Yu1,2, Hui Ping Oh1, Yih Yian Sitoh1,2
1Department of Neuroradiology, National Neuroscience Institute, Singapore; 2Duke NUS Graduate Medical School, Singapore
Abstract
Introduction: Magnetic Resonance (MR) safety is critically important in any Radiology Department, and MR-related accidents are preventable. Serious games provide opportunities for learners to build MR safety awareness through play in an immersive learning environment by using simulated scenarios such as screening virtual patients and managing an MR-related accident.
Methods: We developed a serious game, in partnership with a game developer, introducing MR safety concepts to learners as they navigate through a virtual 3D Radiology department. Drag-and-drop minigames are incorporated to aid the learner to identify hazards in and around the MR environment. Virtual patients are placed in waiting areas to provide realism, and learners are tasked to screen them as part of MR Safety Screening checks. A simulation of an MR-related accident prompts learners to make decisions or take actions to ensure safety and mitigate further risks during the accident. The learner also role-plays as a Risk Officer to identify the multiple key incidents that led to the accident. These formative assessments, with instantaneous feedback, assesses the learners’ knowledge of MR safety.
Results: Pilot feedback of this serious game revealed that it is realistic, engaging and relatable. The instructions within the game were clear and aided learning. The game has also been scaled up and customised for the radiology departments of 3 other healthcare institutions.
Conclusion: Serious games provide a training solution to raise MR safety awareness by simulating real-life scenarios in an immersive learning environment. It supplements face-to-face training and is scalable to other healthcare institutions.
Keywords: Medical Education, Technology-Enhanced Learning, Gamification, MR Safety, Workplace Safety, Simulation
I. INTRODUCTION
Magnetic Resonance (MR) safety plays a critical role in any Radiology Department to ensure the safety of patients and healthcare workers. MR is an imaging tool that uses a magnetic field to acquire detailed images of the body for the investigation of diseases.
MR-related incidents are prevalent; for instance, the US Food and Drug Administration (US FDA) received 1568 adverse events reports for MR-related incidents over 10 years between 2008 and 2017 (Delfino et al., 2019). These reported adverse events included mechanical events (eg. crushed injuries) and projectiles that are caused by objects pulled in by the magnetic field.
Hence, caution must be taken as the MR scanner’s magnetic field is always on and poses safety risks when MR safety protocols are not adhered to. Ferromagnetic objects can become projectiles within or near the magnetic field and pose a danger to patients and staff members present within it. MR-related accidents are preventable and are caused by MR safety lapses, occasionally resulting in deadly outcomes. Hence, building MR safety awareness for all levels of healthcare staff, from ward staff to those who work in the radiology department, is crucial.
Today’s generation of learners, coined as ‘digital natives’ are accustomed and receptive to the digital world and game-based learning (Girard et al., 2013). Serious games refer to digital games with the specific purpose of training learners to meet an educational objective (Girard et al., 2013). It has been used as an educational tool to realistically simulate incidents for disaster risk management (DRM) and to raise awareness (Solinska-Nowak et al., 2018). Similarly, it has also been used as training tools in health professional education for patient safety (Ricciardi & De Paolis, 2014).
Serious games can virtually replicate the MR environment and simulate MR incidents that are too dangerous to re-enact in the real world, thus preparing the healthcare professionals for such scenarios. The serious game is an ideal training solution to complement face-to-face training of healthcare professionals on MR safety and can be incorporated into the standardised curriculum design. The intended learning outcomes can be achieved through the constructive alignment of learning activities (within the game and on-the-job) and coupled with assessment and in-game feedback.
Using a learner-centric approach, serious games provide learners with risk-free decision-making opportunities, enhancing MR safety competency through play within an immersive, yet safe, virtual learning environment. These allow learners to exercise the safety behaviours and actions required at the workplace to handle situations that they may encounter.
This short communication aims to describe how this serious game was developed and how the game was evaluated at the pilot stage.
II. METHODS
The team was awarded the Learning Technology Adoption Grant in January 2020 offered by SkillsFuture Singapore (SSG). It is a grant to fund medical education serious games in SingHealth. SingHealth Academy partnered the team with game developers, including instructional designers who helped with the game development.
MR safety lapses can be deadly, and the learning outcomes of the game are to gain knowledge of MR safety and accident risk management, and to be able to demonstrate understanding of these concepts by application of knowledge in the application scenarios within the game and at the workplace.
The target audience for this game includes radiology staff, healthcare staff or ancillary staff, such as housekeeping personnel, who may enter the MR environment and thus, are required to ensure MR safety in their line of work.
The game sets out in a virtual radiology department, modelled after the Neuroradiology department at the National Neuroscience Institute. The virtual world includes virtual patients, staff as player and non-player characters in institutional uniforms, and medical devices that mirror real-life equipment in the radiology department.
Two games were created in the MR safety series. In the first game, learners navigate as an avatar to interact with objects in the MR environment, such as medical devices and virtual patients. The learning outcome of the first game is to understand the key MR safety concepts which follow the American College of Radiology (ACR) guidelines (American College of Radiology, 2020).
The second game was modelled on an MR-related accident. Learners assess the accident scenario (Fig 1a) and consider strategies for risk management, evaluating their options within the game. Critical wrong decisions or actions made during the gameplay may trigger an abrupt end to the game. This emphasises the urgency of actions required in an MR-related accident when a life is in danger and the immediate steps required to be taken to reduce the risk for further injuries. Beyond the virtual accident, the learner role-plays as a Risk Officer to assess and identify several key incidents that led to the accident as part of a root cause analysis investigation.

Figure 1a (left): MR accident scenario within the serious game
Figure 1b (right): Application of MR safety labelling near the MR scanner
Minigames are used as formative assessments, and learners receive instantaneous in-game feedback from their attempts. By screening virtual patients and placement of medical devices in their appropriate location, as part of the MR safety screening checks, the game assesses learners’ ability to identify hazards in and around the MR environment (Fig 1b), with correct placement demonstrating their learning.
For the purpose of game development, beta testers from the Neuroradiology department were included to gather preliminary feedback about the game through implied consent. A survey was administered, and responses ranged on a Likert scale (1=Strongly disagree to 5= Strongly agree).
III. RESULTS
In the initial phase of game development, beta testing of the game was conducted on 11 staff, including radiographers, radiologists, radiography assistants, radiology nurses and administrative staff with differing years of MR work experience. Beta-testers were also selected for their experiences in playing games, ranging from none to some experience. Data reported below as ‘agreed’ is aggregated to reflect ‘agreed’ and ‘strongly agree’ responses (Cheng et al., 2021).
In terms of the learning instructions, all respondents (100%) were aware of the learning outcomes. 81.82% found the instructions clear, and they knew what to do at every stage.
In terms of the virtual game environment, respondents generally felt the game has realistic engagement regarding the design. All respondents (100%) agreed that the game environment was realistic; the avatars (player characters) and objects in the game resembled those at the workplace (100%), and the background sound aided the engagement with the game (81.82%). 90.91% of respondents could also relate to the main player character within the game.
On the contrary, some respondents had trouble operationalising the game mechanics; 27.27% had trouble using the controls, and 36.36% found it difficult navigating within the game.
Overall, 90.91% found the game was fun, and engaging (100%). 81.82% agreed that their past experience helped them to overcome some of the obstacles in the game. Furthermore, 81.82% agreed that the results are a fair reflection of their skill and competency in MR safety.
Arising from the positive preliminary feedback of this serious game, the game has been shared and further adopted by radiology departments from three other healthcare institutions [Singapore General Hospital (SGH), KK Women’s and Children’s Hospital (KKH) and Sengkang General Hospital (SKH)]. The respective teams are working with the game developers to customise and adapt the environment to the local site, including medical devices and safety labels in their local settings for MR safety education.
IV. DISCUSSION
The MR safety game is an educational tool to assess and align MR safety competency for healthcare staff. Furthermore, the game can be incorporated into the orientation curriculum of radiographers as part of a competency checklist onboarding package, supplementing face-to-face training.
Being accustomed to the digital games, ‘digital natives’ as the target generation of learners would find this mode of delivery more relatable, engaging and realistic (Girard et al., 2013). At the same time, it also incorporates a structured learning design, constructively aligned with clear learning outcomes, learning activities and assessment coupled with instantaneous in-game feedback.
However, we acknowledge that some learners may experience difficulties with navigation in a virtual world. Hence, clear instructions by the facilitator on gaming instructions need to be incorporated in the pre-briefing to learners for more effective engagement and outcomes.
As learners navigate the virtual environment, they pick up MR safety knowledge and apply them to game scenarios as part of active learning. Role-playing as a Risk Officer also makes them more aware of the possible safety lapses that may occur and lead to an MR-related accident. Post-game play feedback should also be incorporated for learners to align the behaviours expected of learners at the workplace.
Beyond the institution, it is scalable to staff from other radiology departments and hospital ward staff, such as nurses and doctors who have no prior knowledge of MR safety but would have adhoc opportunity to be in the MR environment, for example, accompanying a patient to the radiology department for an MR scan.
Finally, through experiential learning, the game emphasises that everyone plays a critical role in MR safety and that safety lapses can lead to accidents.
V. CONCLUSION
Purpose-built simulation serious games that mimic a virtual radiology department provide an ideal training solution for MR safety education. Serious games provide an immersive learning environment where simulated scenarios such as safety screening of virtual patients and MR-related accidents is made possible. Simulation of dangerous scenarios that are impossible to recreate in the real world provides opportunities to raise MR safety awareness and is also scalable to the wider healthcare community.
Notes on Contributors
Cheng Qianhui contributed to the conceptualisation and design of this serious game, drafting the manuscript and approved the final version to be published.
Joanna Pearly Ti contributed to the conceptualisation and design of this serious game, revised the manuscript for intellectual content and approved the final version to be published.
Yu Wai-Yung is a mentor to the team, revised the manuscript for intellectual content and approved the final version to be published.
Oh Hui Ping contributed to the conceptualisation and design of this serious game, revised the manuscript for intellectual content and approved the final version to be published.
Sitoh Yih Yian is a mentor to the team, revised the manuscript for intellectual content and approved the final version to be published.
Ethical Approval
Review not required as stipulated by CIRB (CIRB Reference No.: 2021/2397).
Data Availability
The beta testing evaluation data presented in this manuscript is available in the Figshare data repository: https://doi.org/10.6084/m9.figshare.14473074.v1
Acknowledgement
We would like to thank SingHealth Academy and Playware Studios for their tremendous contribution for the creation of this serious game. We are also thankful to NNI neuroradiology staff for their help with the pre-testing of the game, contributing to the game development through honest feedback. We are thankful to Serious Games Asia and Singapore University of Technology and Design (SUTD) for co-developing the survey evaluation. We sincerely thank our scale-up teams, the radiology departments from Singapore General Hospital (SGH), Sengkang General Hospital (SKH) and KK Women’s and Children’s Hospital (KKH) so that more staff across SingHealth can benefit from MR safety training through this serious game.
This project has been presented as Free Communication at the Asia Pacific Medical Education Conference 2021, and the author was awarded the Young Scholar Award Runner-up.
Funding
The game development and scale-up is funded by Learning Technology Adoption Grant (LTAG) offered under SkillsFuture Singapore (SSG), which SingHealth Academy has applied to jumpstart medical education serious games in SingHealth institutions. SingHealth Academy is the education arm in SingHealth to coordinate the application with SSG.
Declaration of Interest
The authors declare no conflict of interest.
References
American College of Radiology. (2020). ACR manual on MR safety. https://www.acr.org/-/media/ACR/Files/RadiologySafety/MRSafety/Manual-on-MR-Safety.pdf
Cheng, Q., Ti, J. P., Yu, W.-Y., Oh, H. P., & Sitoh, Y. Y. (2021). MR safety beta testing data [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.14473074.v1
Delfino, J. G., Krainak, D. M., Flesher, S. A., & Miller, D. L. (2019). MRI‐related FDA adverse event reports: A 10‐yr review. Medical Physics, 46(12), 5562–5571. https://doi.org/10.1002/mp.13768
Girard, C., Ecalle, J., & Magnan, A. (2013). Serious games as new educational tools: How effective are they? A meta-analysis of recent studies. Journal of Computer Assisted Learning, 29(3), 207–219. https://doi.org/10.1111/j.1365-2729.2012.00489.x
Ricciardi, F., & De Paolis, L. T. (2014). A comprehensive review of serious games in health professions. International Journal of Computer Games Technology, 2014, Article 787968. https://doi.org/10.1155/2014/787968
Solinska-Nowak, A., Magnuszewski, P., Curl, M., French, A., Keating, A., Mochizuki, J., Liu, W., Mechler, R., Kulakowska, M., & Jarzabek, L. (2018). An overview of serious games for disaster risk management – Prospects and limitations for informing actions to arrest increasing risk. International Journal of Disaster Risk Reduction, 31, 1013–1029. https://doi.org/10.1016/j.ijdrr.2018.09.001
*Cheng Qianhui
National Neuroscience Institution
11 Jalan Tan Tock Seng,
Singapore 308433
Singapore 117593
Email: qianhui_cheng@nni.com.sg
Submitted: 7 December 2021
Accepted: 8 February 2022
Published online: 5 April, TAPS 2022, 7(2), 27-36
https://doi.org/10.29060/TAPS.2022-7-2/OA2718
Tan Charmaine1 & Ivan Cherh Chiet Low1,2
1Department of Physiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Human Potential Translational Research Programme, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: Practicals are core components of an undergraduate health sciences curriculum to promote experiential learning and motivation in students. With restrictions on traditional forms of face-to-face practicals during the COVID-19 pandemic, we designed and investigated the efficacy of remote practicals as a viable learning strategy in exercise physiology teaching.
Methods: Student volunteers were instructed to perform a graded exercise test in a remote setting and provide their collected data for subsequent discussion in an online lecture. The effectiveness of this remote practical in promoting students’ motivation and learning outcomes achievement was assessed via an anonymous questionnaire containing 29 closed-ended and 2 open-ended items. Continual Assessment (CA) results were also investigated. Unpaired student’s t-tests were performed for comparisons between interventions with significance level set at P<0.05.
Results: Sixty-one (out of 81; 75%) students responded to the questionnaires and 49 (60%) consented to the use of their CA results for this study. Results revealed that students were moderately motivated and attained strong achievement of learning outcomes. When compared to students who did not volunteer for the hands-on component of the remote practical, students who participated in the hands-on component reported significantly higher self-efficacy (P<0.05) in explaining the practical procedures to their peers. Qualitative analysis further revealed that experiential learning and real-life data analysis were the central reasons supporting the effectiveness of the remote practical. Students were generally satisfied and would recommend the remote practical to future students.
Conclusion: Our study highlights the potential of remote practicals as viable alternatives to traditional practicals.
Keywords: Remote Practical, Experiential Learning, Student Motivation, Learning Outcomes
Practice Highlights
- Remote practical aids in promoting experiential learning in exercise physiology teaching.
- Remote practical can promote motivation by enabling students to see the relevance of their learning.
- Students perceived that they could achieve the necessary learning outcomes via remote practicals.
I. INTRODUCTION
Laboratory work or practical classes are considered as core components of health sciences curriculum in higher education (Colthorpe & Ainscough, 2021; Dohn et al., 2016; Hofstein & Lunetta, 2004). Past studies have revealed the strong educational value of practical classes in promoting student motivation (Bruce, 1988; Dohn et al., 2016), student learning outcomes achievement (Brinson, 2015) as well as the ability to draw theory to practical applications (Neves et al., 2017).
One of the key subjects in undergraduate health sciences education is human physiology, a discipline seeking to understand the underlying mechanisms and dynamics of the human body (Lellis-Santos & Abdulkader, 2020). The role of practical classes in the teaching and learning of physiology is highly valued by educators and students alike (Dohn et al., 2016; Neves et al., 2017). Experiential learning in physiology practicals commonly takes the form of interactive hands-on activities, real-time data collection and analysis of physiological responses. When such practicals are carried out in a traditional face-to-face manner, students are able to utilise laboratory equipment in an authentic experimental setting and generate real-time data from their peers and/or themselves (Colthorpe & Ainscough, 2021). Data analysis and discussion following the hands-on component of practicals can further promote contextualised learning and facilitate the understanding of the theoretical content (Lewis & Williams, 1994). It has been reported that such an interactive learning approach in physiology enhances the achievement of learning outcomes and increases the level of motivation for students (Dohn et al., 2016).
The emergence of the COVID-19 pandemic has led to increasing safety management restrictions being imposed on physical classes in higher education institutes around the world (Ali, 2020). As such, educators were faced with the sudden need to switch from face-to-face lessons to online and remote teaching (Ali, 2020; Lellis-Santos & Abdulkader, 2020). Amidst the uncertainty of this transition, traditional face-to-face practicals have seen a sharp decline (Ray & Srivastava, 2020; Vasiliadou, 2020). As we examine these educational trends during crises, it becomes apparent that harnessing creativity to adapt and invent novel solutions is vital to maintain and even advance current standards of teaching and learning. Lellis-Santos and Abdulkader (2020) rightfully exemplify this notion by proposing the use of smartphone applications as a creative teaching approach to enable scientific data collection and practical learning from home even during social isolation. Along similar lines, we have designed a remote practical for students to carry out hands-on experiments outside of a traditional laboratory environment as an innovative alternative to circumvent the restrictions on face-to-face practicals and to provide them with experiential learning opportunities on cardiovascular concepts in exercise physiology.
To the best of our knowledge, there are few studies conducted to date regarding the efficacy of such remote practicals, particularly in the field of life sciences and exercise physiology. Therefore, our study aims to address this research gap by evaluating the effectiveness of our remote exercise physiology practical on (1) student learning outcomes, (2) student motivation and (3) students’ perceptions on the effectiveness and relevance of the remote practical. In addition, we also compared the quantitative and qualitative responses between students who participated and did not participate in the hands-on component of the remote practical. The Continual Assessment (CA) results from these two groups of students were also compared to assess if differences in academic performance existed between the two groups.
II. METHODS
A. Description of the Module
LSM3212 Human Physiology: Cardiopulmonary System is a third-year module in Life Sciences conducted by the Department of Physiology, Yong Loo Lin School of Medicine at the National University of Singapore. A total of 81 undergraduate Life Sciences students were enrolled in the module in the Academic Year 2020/2021, Semester 2. Traditionally, both lectures and practicals are carried out in a face-to-face manner for this module. However, due to restrictions imposed by the COVID-19 pandemic, lessons were forced to go online. As a result, a remote practical was designed and conducted as an innovative alternative for this batch of students.
B. Description of the Remote Practical
The remote practical was designed to provide students with experiential learning on cardiovascular concepts in exercise physiology. Conventionally, the practical involved a treadmill-based graded exercise test performed by a student volunteer equipped with specialised electrocardiogram-based heart rate monitors to illustrate how the cardiovascular system changes with increasing exercise stress. For the remote practical, however, students were given a set of practical handouts comprising a novel graded exercise protocol developed by the authors and could choose to perform it in their own time asynchronously, or not carry it out at all. In the graded exercise protocol, students were instructed to carry out a series of graded knee raise exercises and record their heart rate measured via a smartphone application together with other subjective exercise prescription ratings (ratings of perceived exertion and talk test ratings) after each set of exercise. The graded exercise protocol was developed with the intent to encourage contextualised learning from the practical content to real-life exercise routines. The consolidated data was subsequently used for discussion in a virtual lecture to illustrate how heart rate responses and cardiovascular adaptations may differ across individuals, as well as how the consolidated data may serve to guide exercise prescription. Participation in the hands-on component (knee raise exercises) of the remote practical was optional. However, participation in the analysis and discussion of the collated data in the virtual lecture conducted after the graded exercise was made compulsory. Via this design, the remote practical (comprising both the graded exercise and post-exercise discussion) not only replicated the pedagogy of the original in-class practical, but also augmented the opportunity for students to volunteer and take part in the graded exercise component of the practical.
C. Instruments
After the virtual lecture, students completed an anonymous (no informed consent required) questionnaire containing 29 closed-ended and 2 open-ended items. The purpose of this self-report questionnaire was to evaluate students’ perceived effectiveness of the remote practical on their motivation and achievement of learning outcomes of the virtual lecture.
Student motivation was measured by the Lab Motivation Scale (Dohn et al., 2016) containing 21 closed-ended statements based on three aspects – student interest, effort and self-efficacy. Multiple instruments had previously been employed to assess dimensionality and reliability of the validated Lab Motivation Scale (Dohn et al., 2016). A set of six closed-ended items were employed to measure students’ perception on whether they had achieved the intended learning outcomes of the remote practical. Lastly, two closed-ended items were included to elicit a general satisfaction score from students regarding the remote practical and/or the virtual lecture. All the closed-ended statements in the questionnaire were scored on a 5-point Likert Scale, ranging from 5 (strongly agree) to 1 (strongly disagree).
Furthermore, there were two open-ended questions focusing on the effectiveness of the remote practical and the relevance of the remote practical to students’ daily lives. The first question was posed to uncover specific reasons supporting the analysis of the closed-ended items, while the second question aimed to encourage contextualisation of concepts learnt through the remote practical in students’ daily lives.
Finally, the CA results of students who participated in the hands-on component of the remote practical were compared with students who did not participate. To ensure a fair comparison, we took into consideration only the CA result from the questions corresponding to the content covered in the remote practical and virtual lecture. The questions taken into consideration made up 40% of the entire examination score.
D. Analysis
A mixed method approach was employed in analysing the questionnaire responses. An initial 66 questionnaire responses were collected but five incomplete responses were excluded, leaving a total of 61 responses that were included in the final analysis. Responses to the closed-ended items were coded accordingly to a 5-point Likert scale, ranging from strongly agree (5) to strongly disagree (1). Scores were reversed for statements phrased in a negative manner (items 9, 15 and 18). All closed-ended responses were presented in the form of mean ± standard deviation. As a measure of internal consistency, Cronbach’s α was used as an instrument and measured across all scales. Unpaired student’s t-tests were carried out to find out if differences between students who participated and did not participate in the hands-on exercise component were significant with significance level set at P < 0.05. All data analysis and statistical tests were performed using Microsoft Excel 2016.
Open-ended responses were analysed in a 3-part process: informal reviewing, open coding and thematic analysis. Firstly, all responses were informally reviewed to familiarise with general ideas and main themes were identified. Next, open coding was performed where each response was analysed in detail and coded to the most appropriate theme (Braun & Clarke, 2006). Finally, thematic analysis was carried out through ranking themes according to frequency and analysing the results (Braun & Clarke, 2006). The open-ended questions were made optional, and all responses collected were subsequently analysed.
III. RESULTS
Out of the 61 participants, 29 (48%) participated in the hands-on exercise component of the remote practical while 32 (52%) did not participate. Both groups attended the compulsory virtual lecture conducted after the remote practical, where the data collected from the remote practical was consolidated and discussed with the entire class.
Internal consistency was calculated using Cronbach’s α and the reliability coefficient was found to be 0.95 across all closed-ended items, indicating an excellent level of interrelatedness across the overall scale (Cronbach, 1951). Individual scales of learning outcomes and motivation were also subjected to the analyses of Cronbach’s α. The alpha coefficient value was calculated to be 0.86 for perceived achievement of learning outcomes and 0.94 for motivation (Tables 1 & 2). Motivation was further divided into three individual subscales assessing student interest, effort and self-efficacy, with the reliability coefficients returning 0.85, 0.88 and 0.88 respectively (Table 1). These reliability coefficients correlate strongly with those of Dohn et al. (2016), hence providing support for the internal consistency of the Lab Motivation Scale. Data supporting these findings is openly available via Figshare at https://doi.org/10.6084/m9. figshare. 17170 964 (Low, 2021).
A. Remote Practical and Learning Outcomes
In general, students rated between “Agree” and “Strongly Agree” for perceived achievement of learning outcomes, with an overall mean score of 4.16 ± 0.68 on a 5-point Likert scale (Table 1). Students who participated in the hands-on component reported a mean score of 4.20 ± 0.54, which was similar to that rated by students who did not participate in the hands-on component (4.13 ± 0.68, P = 0.567; Table 1). For the first closed-ended statement: I have gained a stronger understanding of how heart rate responds to increasing exercise intensity, students who participated indicated a higher mean score of 4.52 ± 0.51 as compared to the lower mean score of 4.09 ± 0.59 (P = 0.004) for students who did not participate in the hands-on exercise component (Table 1).
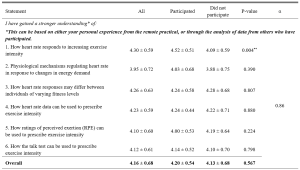
Table 1. Students’ perceived achievement of learning outcomes in cardiovascular physiology
n = 61. Responses were coded from 1 (Strongly Disagree) to 5 (Strongly Agree). All means are shown with ±SD of the mean. **P < 0.01.
B. Remote Practical and Student Motivation
Students generally rated between “Agree” and “Somewhat Agree/Somewhat Disagree” for student motivation, with an overall mean score of 3.66 ± 0.71 (Table 2). Students who participated in the hands-on component reported a mean score of 3.70 ± 0.64, which was similar to that rated by students who did not participate in the hands-on component (3.62 ± 0.78, P = 0.187; Table 2). Students rated between “Agree” and “Somewhat Agree/Somewhat Disagree” regarding the three aspects of student motivation, with a score of 3.92 ± 0.69 for interest, 3.66 ± 0.75 for effort and 3.50 ± 0.68 for self-efficacy respectively (Table 2). For statement 23, students who participated indicated a higher mean score of 3.68 ± 0.61 as compared to the lower mean score of 3.29 ± 0.71 (P = 0.031) for students who did not participate in the hands-on component (Table 2).
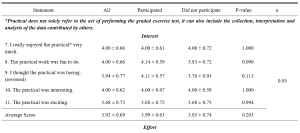
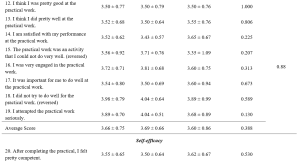
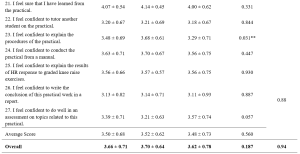
Table 2. Students’ perceived motivation towards the remote practical
n = 61. Adapted from the Lab Motivation Scale (Dohn et al., 2016). Responses were coded from 1 (Strongly Disagree) to 5 (Strongly Agree). Scores were reversed for statements phrased in a negative manner. All means are shown with ± SD of the mean. **P < 0.05.
C. Qualitative Explanations on Perceived Effectiveness and Relevance of Remote Practical
The first open-ended item sought to investigate the reasons underlying the perceived effectiveness or ineffectiveness of the remote practical in enhancing students’ learning. Of the 37 responses, 34 (92%) felt that the remote practical was effective while 3 (8%) felt it was ineffective and of little to no added value to them (Table 3). Experiential learning and real-life data emerged as the most common themes cited across all responses (n = 12), followed by reinforc(ing) concepts taught in lecture (n = 10; Table 3). Experiential learning was reflected as the most common response among students who participated in the hands-on component (n = 10) in comparison to real-life data indicated by students who did not participate in the hands-on component (n = 8; Table 3).
The aim of the second open-ended item was to investigate the relevance and application of the remote practical to students’ daily lives. Of the 36 responses, 29 (81%) felt the remote practical was relevant while 7 (19%) felt that it was irrelevant to their daily lives (Table 3). Overall, the remote practical was found to be most relevant in improving current exercise routine (n = 12), followed by understanding one’s own fitness level (n = 10) and understanding the importance of exercise (n = 7; Table 3). This trend was similar for both students who participated and did not participate in the hands-on component of the remote practical (Table 3).
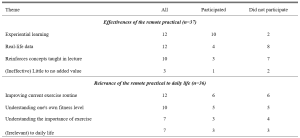
Table 3. Themes identified from the open-ended responses, ranked by frequency
D. Remote Practical and Satisfaction Score
Students rated close to “Agree” for satisfaction, with an overall mean score of 3.95 ± 0.75 (Table 4). Those who participated in the hands-on component reported a mean score of 4.11 ± 0.70, which was similar to that rated by students who did not participate in the hands-on component (3.81 ± 0.77, P = 0.054; Table 4).

Table 4. Students’ satisfaction score
n = 61. Responses were coded from 1 (Strongly Disagree) to 5 (Strongly Agree). All means are shown with ± SD of the mean. **P < 0.05.
E. Remote Practical and Academic Performance
Out of the 49 students who consented to the use of their CA results for this research study, 30 (61%) participated in the hands-on component of the remote practical while 19 (39%) did not (Table 5). Only the questions corresponding to the content covered in the remote practical and relevant virtual lecture were taken into consideration for this study. The overall mean mark was 7.3 ± 1.64 out of 10 (Table 5). Students who participated in the hands-on component (7.3 ± 1.84) and did not participate in the hands-on component (7.3 ± 1.32) exhibited similar mean marks as well (P = 0.940; Table 5).

Table 5. Students’ CA results
n = 49. CA scores are shown as mean ± SD, with *P < 0.05 considered significant.
IV. DISCUSSION
This study sought to evaluate if remote physiology practicals could be viable alternatives to traditional face-to-face practicals, especially during emergency remote teaching in a pandemic. Our results demonstrated that the students who participated in the remote practical perceived that they could achieve the learning outcomes in cardiovascular and exercise physiology teaching with reasonable satisfaction, regardless of whether they participated in the hands-on component of the remote practical. However, students who had actively participated in the hands-on component (graded exercise) reported that the remote practical had particularly benefitted them in better achieving certain learning outcomes as compared to their classmates who did not participate in the graded exercise. Specifically, students indicated that their participation in the graded exercise allowed them to have a better grasp of the concepts concerning heart rate response to increasing exercise intensity. This finding was not unexpected as the remote graded exercise was specifically designed to provide experiential learning opportunities to better comprehend the concepts underlying this particular learning outcome.
Perceived scores for the achievement of learning outcomes were otherwise similar between the participated and non-participated group. This could be attributed to the fact that the remote practical was used as a complement to the virtual lecture, wherein the interpretation and analysis of data collected from the optional graded exercise was discussed with the whole class during the compulsory virtual lecture. The perception scores of learning outcome achievement were well supported by the students’ academic performance as all of them shared similar mean CA marks regardless of their participation in the remote practical. This similarity is especially prominent as the CA questions were set based on the principle of constructive alignment (Biggs, 1996; Bloom, 1956; Stamov Roßnagel et al., 2020).
Interestingly, open-ended responses revealed “experiential learning” as the key reason supporting the efficacy of the remote practical in students who participated in the graded exercise while “having real-life data which reinforces concepts taught in lecture” were key reasons indicated by students who did not participate in the hands-on component of the remote practical. These findings are in line with studies recommending experiential learning as one of the seven “principles of good practice” to achieve excellence in higher education (Chickering & Gamson, 2006). This is accomplished by generating real-life data to allow students to draw the link between theoretical content and practical applications, before applying it to analyse real-life situations in view of course material (Lewis & Williams, 1994). This suggests that the remote practical is able to foster environments which could encourage hands-on learning and real-time data generation to enhance student learning, even if not conducted in a traditional laboratory setting.
Overall, students were satisfied with the remote practical and/or virtual lecture, with those who participated in the hands-on component generally being more satisfied. Even though the remote practical was not compulsory, those who took part in the hands-on component generally did not view it as an additional academic burden and instead would recommend it to future batches of students. This reinforces the potential of such remote practicals in helping students to achieve learning outcomes without imposing unnecessary pressure on them.
With motivation being a strong indicator of self-directed learning and academic achievement (Cortright et al., 2013), it is crucial for educators to assess and understand the importance of motivating students. In fact, educators play a critical role in determining the motivation levels of their students through the nature of their classes and assignments (Cortright et al., 2013). Specifically, Dohn et al. (2016) states that students’ motivation could be negatively impacted by limited equipment or restricted time for practicals. Majority of students face similar limitations for a graded exercise test carried out in a traditional face-to-face practical. Typically, only one volunteer would carry out the actual exercise experimental protocol due to equipment and time constraints, while other students would passively watch and learn from the data collected. The novel remote practical proposed in this study could potentially overcome these limitations as students are able to personally experience the hands-on exercise component within their own spaces at home and at their own convenience, thereby possibly enhancing their motivation levels.
Our results indicated that overall motivation towards the remote practical and/or the virtual lecture ranged from 3 to 5, corresponding to “somewhat agree” and “strongly agree”, with a mean value of 3.62 ± 0.78. This is comparable to the motivation scores previously reported by Dohn et al. (2016) for in-class biomedical laboratory classes. The positive motivation score could be explained by the fact that majority of students (81%) could see the relevance (Table 3) of the remote practical in their daily lives. Learning activities which guide students towards finding ‘personal meaning and value’ in the educational content is known to positively influence their motivation levels (Cortright et al., 2013). By providing opportunities for students to reflect on, find meaning and draw relevance to their personal lives, such remote practicals can potentially address common limitations of traditional practicals and boost student motivation and learning.
Delving further into the three aspects of student motivation – interest, effort and self-efficacy, students rated the highest scores for interest, followed by effort and lastly self-efficacy. The score for effort placed into the practical could have been understandably affected due to the non-compulsory nature of the graded exercise. The exercise component of the practical could not be made compulsory as not all students were medically/physically fit enough to undergo a graded exercise test. Nonetheless, the similarity in perceived learning outcomes and academic results between students who did and did not participate in the graded exercise suggests that the follow up analysis and peer-based discussion of the tabulated data involving the entire class was sufficient to bridge the learning gap between the two groups of students. Overall, the favourable perceived learning outcomes (ranging from “agree” to “strongly agree”) and academic scores (corresponding to a grade of “A-” to “A”) reinforces the value of the remote practical as a teaching strategy to promote learning in exercise physiology, regardless of the students’ ability or interest to participate in strenuous physical activity. However, whether the remote practical is more effective than a conventional face-to-face practical or no practical at all remains an interesting question which necessitates future research as this cannot be addressed given the limitations of our current study design.
Notably, self-efficacy scores were rated the lowest amongst the three aspects of motivation. This could be due to the fact that students are not closely supervised during a remote practical, unlike face-to-face practicals. Without the physical presence and continuous guidance of an instructor, students could have faced uncertainty as to whether instructions were properly executed. Thus, strategies to enhance pre-practical instructions using asynchronous video instructions or the incorporation of remote supervision methods may aid to further enhance the effectiveness of the remote practical. Interestingly, participation in the hands-on component of the remote practical appeared to have nonetheless enhanced the confidence of students in explaining the procedures of the practical to their peers (Table 2). This finding is of particular importance, as the ability to teach and explain is an indication of higher order learning corresponding to the second and third levels of the Bloom’s taxonomy (Bloom, 1956).
A. Limitations
Our study sought to evaluate the effectiveness of a remote exercise physiology practical in promoting student motivation and learning in a cohort of Life Sciences undergraduates. However, the current study design does not permit immediate comparison with conventional face-to-face practicals as students could not be randomly allocated into different comparison groups (remote or face-to-face) owing to pandemic restrictions and ethical reasons. Also, we could only investigate the effects of practical participation on the effectiveness of the remote practical in enhancing student motivation and learning outcomes achievement using a quasi-experimental approach. This is so, for we were unable to randomly allocate students into two comparison groups given that not all students were medically/physically fit enough to undergo a graded exercise test for the hands-on component of the remote practical. Based on this study design, some degree of self-selection bias could have been present as physically active students who had volunteered to take part in the exercise component of the remote practical could have seen greater relevance to their daily lives and could have been more intrinsically motivated to partake and learn from the practical session. In spite of that, the overall student motivation score appeared comparable between the two groups of students who participated and did not participate in the exercise component of the practical, suggesting that the degree of self-selection bias may not be of significant concern in the present study.
V. CONCLUSION
Overall, students reported that experiential learning and real-life data were the main reasons supporting the effectiveness of the remote practical. With experiential learning and real-life data as key components of traditional practicals (Dohn et al., 2016; Randall & Burkholder, 1990), the present study demonstrates the potential of remote practicals as viable and innovative alternatives for face-to-face practicals in exercise physiology teaching. In cases of sudden shifts to emergency remote education, such alternatives offer the possibility of incorporating experiential learning even during social isolation.
Notes on Contributors
Tan conducted the study, analysed and interpreted the data, and drafted the manuscript. I.C.C. Low was involved in experimental conception and design, as well as critically reviewed and revised the manuscript. All authors have read and approved the final version of the manuscript.
Ethical Approval
All students were provided with a participant information sheet containing the purpose and details of the research study. The questionnaire was made completely anonymous. Informed consent was obtained from students for use of their CA results only after the release and confirmation of their results. Circulation of research materials was done virtually and students were never approached directly for recruitment. The study was approved by the National University of Singapore – Institutional Review Board (NUS-IRB) with study code NUS-IRB-2020-631.
Data Availability
Data supporting these findings is openly available via Figshare at DOI: https://doi.org/10.6084/m9.figshare. 17170964.
Acknowledgements
We greatly appreciate the study participants who have spent their time and effort to complete the questionnaires and have provided consent in the use of their results for research purposes.
Funding
There was no funding support accorded for this study.
Declaration of Interest
No potential conflict of interest was reported by the authors.
References
Ali, W. (2020). Online and remote learning in higher education institutes: A necessity in light of COVID-19 pandemic. Higher Education Studies, 10(3), 16-25. https://doi.org/10.5539/hes.v10n3p16
Biggs, J. (1996). Enhancing teaching through constructive alignment. Higher Education, 32(3), 347-364. https://doi.org/10.1007/BF00138871
Bloom, B. S. (1956). Taxonomy of educational objectives. Vol. 1: Cognitive domain. David McKay.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101. https://doi.org/10.1191/1478088706qp063oa
Brinson, J. R. (2015). Learning outcome achievement in non-traditional (virtual and remote) versus traditional (hands-on) laboratories: A review of the empirical research. Computers & Education, 87, 218-237. https://doi.org/10.1016/j.compedu.2015.07.003
Bruce, R. H. (1988). Enhancing student motivation and learning: Experiences with a simple simulation. Higher Education Research & Development, 7(2), 103-110. https://doi.org/10.1080/0729436880070201
Chickering, A., & Gamson, Z. (2006). Seven principles of good practice in undergraduate education. New Directions for Teaching and Learning, 1991, 63-69. https://doi.org/10.1002/tl.37219914708
Colthorpe, K., & Ainscough, L. (2021). Do-it-yourself physiology labs: Can hands-on laboratory classes be effectively replicated online? Advances in Physiology Education, 45(1), 95-102. https://doi.org/10.1152/advan.00205.2020
Cortright, R. N., Lujan, H. L., Blumberg, A. J., Cox, J. H., & DiCarlo, S. E. (2013). Higher levels of intrinsic motivation are related to higher levels of class performance for male but not female students. Advances in Physiology Education, 37(3), 227-232. https://doi.org/10.1152/advan.00018.2013
Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika, 16(3), 297-334. https://doi.org/10.1007/BF02310555
Dohn, N. B., Fago, A., Overgaard, J., Madsen, P. T., & Malte, H. (2016). Students’ motivation toward laboratory work in physiology teaching. Advances in Physiology Education, 40(3), 313-318. https://doi.org/10.1152/advan.00029.2016
Hofstein, A., & Lunetta, V. N. (2004). The laboratory in science education: Foundations for the twenty‐first century. Science education, 88(1), 28-54. https://doi.org/10.1002/sce.10106
Lellis-Santos, C., & Abdulkader, F. (2020). Smartphone-assisted experimentation as a didactic strategy to maintain practical lessons in remote education: Alternatives for physiology education during the COVID-19 pandemic. Advances in Physiology Education, 44(4), 579-586. https://doi.org/10.1152/advan.00066.2020
Lewis, L. H., & Williams, C. J. (1994). Experiential learning: Past and present. New Directions for Adult and Continuing Education, 1994(62), 5-16. https://doi.org/10.1002/ace.36719946203
Low, I. C. C. (2021). Remote physiology practical: Viable alternative to in-person practical in health sciences education? [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.17170964
Neves, B. S., Altermann, C., Goncalves, R., Lara, M. V., & Mello-Carpes, P. B. (2017). Home-based vs. laboratory-based practical activities in the learning of human physiology: The perception of students. Advances in Physiology Education, 41(1), 89-93. https://doi.org/10.1152/advan.00018.2016
Randall, W. C., & Burkholder, T. (1990). Hands-on laboratory experience in teaching-learning physiology. Advances in Physiology Education, 259(6), S4-S7. https://doi.org/10.1152/advances.1990.259.6.s4
Ray, S., & Srivastava, S. (2020). Virtualization of science education: A lesson from the COVID-19 pandemic. Journal of proteins and proteomics, 11, 77-80. https://doi.org/10.1007%2Fs42485-020-00038-7
Stamov Roßnagel, C., Fitzallen, N., & Lo Baido, K. (2020). Constructive alignment and the learning experience: Relationships with student motivation and perceived learning demands. Higher Education Research & Development, 40(4), 838-851. https://doi.org/10.1080/07294360.2020.1787956
Vasiliadou, R. (2020). Virtual laboratories during coronavirus (COVID‐19) pandemic. Biochemistry and Molecular Biology Education, 48(5), 482-483. https://doi.org/10.1002/bmb.21407
*Ivan Cherh Chiet LOW
Department of Physiology,
Yong Loo Lin School of Medicine
Block MD9, 2 Medical Drive Level 4
Singapore 117593
Email: phsilcc@nus.edu.sg
Submitted: 6 April 2021
Accepted: 2 December 2021
Published online: 5 April, TAPS 2022, 7(2), 17-26
https://doi.org/10.29060/TAPS.2022-7-2/OA2510
Nicola Ngiam1,2, Kristy X Fu1,3 & Jacqueline SM Ong1,3
1Khoo Teck Puat- National University Children’s Medical Institute, National University Health System, Singapore; 2Centre for Healthcare Simulation, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 3Department of Paediatrics, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: Personal protection in aerosol-generating procedures is an important skill to safely deliver care to patients in the COVID-19 pandemic. This aim of this study was to evaluate the impact of “just-in-time” simulation training for airway management in a suspected COVID-19 patient.
Methods: This was a prospective mixed-method cohort study in a tertiary paediatric department. A mandatory “just-in-time” simulation training session for intubation of a suspected COVID-19 patient was conducted. Pre- and post-simulation questionnaires were administered. Participants were invited to attend focus group interviews to further delineate their experience. Quantitative and qualitative methods were employed to analyse the data.
Results: Thirty-three participants, including doctors, nurses and respiratory therapists attended the training. Self-confidence in intubation, managing and leading a resuscitation team and dealing with problems with intubation significantly improved. Simulation was valued for the experiential learning as well as for increasing confidence and awareness. Process improvement suggestions from both participants and trainers were raised. There was a small signal of skill translation to real life scenarios.
Conclusion: Simulation-based training is a useful tool for infectious disease outbreak preparedness. Further research will need to be done to determine the impact on actual clinical practice in pandemics.
Keywords: Simulation, COVID-19, Pandemic Preparedness, Training, Intubation
Practice Highlights
- The authors report their experience with “just-in-time” in situ simulation training for emergency preparedness in the face of an infectious disease outbreak.
- Simulation training was well received and improved the confidence as well as awareness of frontline staff in managing intubation and resuscitation in a suspected COVID-19 paediatric patient.
- Process improvement suggestions from participants and trainers was a useful by-product of the simulation training activity.
I. INTRODUCTION
Since the World Health Organization (WHO) declared the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) outbreak a public health emergency of international concern on 30 January 2020 (World Health Organization, 2020), the COVID-19 pandemic has now affected millions of people worldwide, with a wide range of case fatality rates amongst the 210 countries and territories affected (The Centre for Evidence-Based Medicine Nuffield Department of Primary Care Health Sciences University of Oxford, 2020). In Wuhan, China, one of the first epicentres of this international pandemic, out of 44672 confirmed cases of COVID-19, 1716 were healthcare workers (HCWs) (Wu & McGoogan, 2020). Of the confirmed cases among HCWs, 14.6% were classified as severe or critical, and 5 deaths were observed (The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team, 2020). Early reports suggest that modes of transmission of SARS-CoV-2 include droplet and contact (via the fecal-oral route and fomites); airborne transmission may occur during aerosol-generating procedures (World Health Organization, 2020).
During the 2003 SARS-CoV outbreak, despite the presence of existing safety protocols, up to half of the SARS-CoV cases in some centers were HCWs as a result of transmission within hospital units (Booth et al., 2003). Critical care and emergency care providers are often involved in high-risk aerosol-generating procedures such as oronasal suctioning, bag-valve-mask ventilation, non-invasive positive pressure ventilation, and endotracheal intubation in patients with COVID-19 with respiratory failure, and so must be prepared (Caputo et al., 2006; Wax & Christian, 2020; Zuo et al., 2020). The challenge for providers would be to provide high-quality and timely care to infected patients, without compromising their own safety. Apart from having adequate supplies of personal protective equipment (PPE), a safe environment for HCWs requires the provision of up-to-date information regarding the disease, smooth dissemination of protocols, and easy accessibility to portals reinforcing education and training in infection control procedures. Lau et al. (2004) reported that HCWs who underwent more than 2 hours of training were far less likely to be infected with SARS-CoV during the 2003 SARS-CoV outbreak in Hong Kong. In addition to PPE training, we felt that a simulated airway management scenario in a suspected COVID-19 patient was a vital component of training in order for staff to experience the profound challenges of performing high risk aerosol-generating procedures while in PPE and in isolation facilities. During the recent 2014 to 2016 West Africa Ebola outbreak, Grillet et al. (2015) with the use of simulation, found that commonly performed procedures in the intensive care unit becomes more complicated, more stressful and less comfortable in appropriate PPE. We were fortunate to find a window of opportunity close to the beginning of the COVID-19 outbreak in Singapore to prepare our healthcare teams using “just-in-time” in-situ simulation. The main objective of this study was to evaluate the impact of this training on our resuscitation teams when managing a respiratory emergency of a suspected COVID-19 pediatric patient.
II. METHODS
This was a prospective mixed-method cohort study in a paediatric department of a tertiary university hospital. Residents were put through a mandatory “just-in-time” simulation training session to prepare them for intubation of a suspected COVID-19 patient. The doctors involved were senior paediatric residents who regularly manage emergencies on call. Nurses and respiratory therapists were rostered to participate whenever available on shift. Participants worked in teams of 5 to 6 to manage a simulation scenario involving a patient with bronchiolitis who was suspected to have COVID-19. Each team comprised of participants from each of the healthcare professional groups listed above. Actual personal protective equipment (PPE) including powered air-purifying respirators (PAPR) were used in the simulation. Participants received training in the use of PPE and PAPR prior to the simulation session. The simulation was conducted in-situ in the paediatric intensive care unit (PICU) using a SimBaby (Laerdal). The scenario used can be found in the appendix. Each group participated in one scenario. Each scenario lasted 30 to 40 minutes. The end point was successful intubation of the patient. There were 2 instructors (paediatric intensive care clinicians) present, one in the anteroom and one in the patient’s room. Debriefing was conducted as a group by both instructors immediately after every simulation. Each debriefing session lasted 30 to 45 minutes and focused on technical and non-technical skills.
Anonymous pre-simulation and post-simulation questionnaires were administered. Questions focused on confidence levels with managing intubation in a COVID-19 suspect patient, using the PAPR, and anxiety levels. Responses were rated on a Likert scale of 1 to 5. Quantitative data was analysed using Microsoft EXCEL, 2016. Pre and post responses on the Likert scale were analysed using the paired t-test.
After the simulation and debriefing, participants were invited via email to attend focus group interviews to gain better insight into their responses and attitudes towards the simulation sessions. The format and logistics of the interviews were included in a participant information sheet in the email. Participation was voluntary. We aimed for maximal representation from the various groups of healthcare professionals who participated in the simulation. A semi-structured interview was conducted by 2 researchers (NN, JO) in groups of 3 to 5 and interviews were audio-recorded. Two focus group interviews were conducted. Participants were asked questions regarding how they felt, what they learnt and what the benefits of the simulation experience were. Each interview lasted 30 to 40 minutes and were conducted in a quiet room in the PICU. Audio recordings were transcribed verbatim and anonymised at the point of transcription. Participants were only identified by role in the transcript.
Thematic analysis of the transcripts was performed by the 2 interviewers using an inductive approach. Each interviewer coded the data independently, after which both interviewers discussed the codes and generated common themes together. Data was reviewed for commonality in responses, degree of specificity (detailed explanation), and extensiveness (number of different people who had similar responses). Where there was disagreement, review of the data and existing literature was used for resolution. Descriptive summaries were developed for each theme, and participant quotes provided further evidence for interpretation and recommendations made.
This study was approved by the institutional review board (National Healthcare Group, Domain Specific Review Board, NHG DSRB Ref. 2020/00234) and waiver of consent was obtained.
III. RESULTS
A. Pre- and Post-Simulation Questionnaire Responses
A total of 33 participants took part in the training and completed the pre- and post-simulation questionnaires. There were 19 doctors, 12 nurses and 2 respiratory therapists. Confidence, as assessed by the questionnaire, increased significantly after the simulation in the areas of intubation, use of the PAPR, airway management in a COVID-suspect patient, leading a team and dealing with problems that arise during resuscitation (p < 0.05). Regarding anxiety over intubating a COVID-suspect patient, most participants were less anxious after the simulation (p < 0.05). Interestingly, on looking more closely at the responses, 9% (n=3) of participants were more anxious after the simulation than before they started. 42% (n=14) reported no change in their level of anxiety. Table 1 shows the mean scores of the questions asked in the pre- and post-simulation questionnaire.

Table 1: Pre- and post-simulation responses
After the simulation training, 96% of participants agreed or strongly agreed that they were more aware of who to call for help and how to communicate effectively when wearing PPE or PAPR while in an isolation room and 93% agreed or strongly agreed that they were more able to anticipate problems. All participants agreed that simulation training was useful in preparing to deal with a similar situation while on call and in fact, 23% disagreed or strongly disagreed that 1 simulation session was sufficient. Figure 1 illustrates the perceived effectiveness of simulation training by participants.
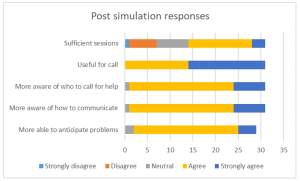
Figure 1: Post-simulation responses on effectiveness of simulation training
B. Focus Group Interviews
Eight participants agreed to focus group interviews, 4 doctors, 3 nurses and 1 respiratory therapist. Comments from the focus group interviews helped to further delineate the benefits and lessons learnt from this simulation exercise. Key benefits were grouped into the following themes:
1) Experiential learning: Participants commented that getting to put theory into practice during the simulation was key to understanding what to expect. Being able to practice before an actual patient encounter helped them to be more prepared. Even simple things like setting an intravenous cannula could not be accomplished with ease. Participants stated that they had to rethink the way that things needed to be done as how they were done previously would not work in this situation. This led to a paradigm shift in the clinical processes and also the application of knowledge. For example, a lesson learnt was that there is a lower threshold for intubation in COVID-19 patients. In the words of a participant about his experience:
“But the fact that you actually go through it, firstly you realize that it takes 3 times the length of the duration of what you would do, and the difficulties in communicating with the people around. So I thought that was the most…an awakening…. the most beneficial part.”
Participants appreciated that this was a complex scenario that was high stakes for the healthcare team as well as for the patient. Getting to practice this, even though it was likely to be an infrequent occurrence, helped with familiarity with protocols and equipment used. Participants also felt that more people should attend this training and that they needed more practice.
2) Increasing confidence: Participants felt that the simulation training was a timely intervention in light of the developing COVID-19 situation. This experience took away the “first-time” feeling and made the participants feel more comfortable with the protective equipment. This took away some of the anxiety and fear about their own safety and the safety of their COVID-19 patients. One participant stated that more practice in simulations may reduce the resistance to wearing the PAPR, which may in itself pose a safety issue if PAPRs are not used when required. They felt that this experience made them a more valuable member to the resuscitation team.
3) Increasing awareness: Participants appreciated the feedback and debriefing that came after the simulation. Experiencing the simulation made taught them to anticipate problems, plan ahead and to prioritize as resources were less accessible than usual. They developed insight into a possible “unconscious incompetence” as they expressed that if they had not gone through the simulation, they would not have known what they did not know and would be inappropriately confident in a real situation. Exploring resource management and considering aspects of waste reduction were thought to be beneficial for future encounters with similar situations. Some of our participants said:
“It really gives you…. the best kind of idea of what to expect in a real life scenario.”
“I would feel quite…. in a sense, bad for the patient that I was doing it for the first time on that patient. So I do feel that it is a responsible thing to do, as healthcare providers that we… that this was actually undertaken.”
“If we had not had this, I probably won’t even have that fear of how terrible it could have been……… But if I had not known, I would still be confident not knowing what I’m expecting.”
Some participants mentioned developing more empathy for colleagues caring for COVID-19 patients through this experience. However, one participant found herself more frustrated after going through the simulation as the experience of managing a resuscitation in this situation was worse than she had thought it would be.
4) Process improvement: In the focus group discussions, participants mentioned the need for process improvement that was discovered while encountering difficulties during the simulation scenario. Communication challenges were brought up multiple times and participants suggested making laminated signs for communication with staff outside the room when assistance was required, having pen, paper and drug labels in the room, as well as using intercoms or walkie-talkies for more efficient communication.
5) Translation: A couple of participants encountered a real subsequent clinical situation which required them to apply skills that they had learnt during the simulation training. The fact that they had gone through the training made them less anxious and more able to take control of the emergency situation. The respiratory therapist in the group expressed more confidence in the nurses that had gone through the simulation training when compared to those who had not when managing a COVID-19 patient. Participants also commented that the skills learnt could be translated to a different institution in the future and perhaps also to a different infective agent. Participants expressed the following:
“And so it would make you, I think… more valuable as a team member in providing care for a COVD patient or any other sort of respiratory pathogen X anywhere.”
“Because I observe that those nurses that attended the simulation, in the actual scenario or in the actual patient handling, they are more confident and competent in doing their PPE and flow of the sequence inside.”
“Because for me, for example, I actually had to initiate and help…coordinate initiation of ECMO for a COVID suspect patient and so I think if not for that…that mock… I would probably have been much more nervous and unsure.”
Key challenges encountered during the simulation were related to the simulation scenario and to the process of simulation itself. The most emphasised challenges encountered during the simulation were cognitive overload and communication barriers. Not only did the team have to deal with a deteriorating patient who was suspected to have COVID-19, they also had to deal with infection control protocols and the inherent challenges that it posed to the resuscitation process. As many tasks needed to be coordinated in a stressful situation, prioritisation was key. Communication barriers came in the form of restricted movement in and out of the isolation room, not being able to use their mobile devices, hearing impairment with the PAPR on and not being able to be heard clearly while wearing the N95 mask. Other challenges raised relating to the scenario were unfamiliarity with the safety equipment as it was not used frequently and having to wait a long time for orders to be carried out. An interesting challenge brought up was a tension between the patient’s safety or well-being and healthcare worker’s own safety. Healthcare professionals frequently put their patients first and in this unique situation, the need for donning personal protective equipment before entering the patient’s environment does not allow for as rapid a response to a deteriorating patient as they are used to:
“I feel like I need to go in as soon as possible but donning the PAPR takes some…. more time than I thought.”
Logistical challenges in planning for this simulation training included the availability and timely attendance of all frontline healthcare workers. With the developing crisis, healthcare professionals were kept busy with their clinical responsibilities, therefore this simulation training was seen as an unwelcome interruption. There was also a perceived resistance to participating by the nurses although the reasons are unclear.
Participants also commented on the design of this simulation training. Prior training in the process of intubation and use of PPE and PAPR were deemed necessary to optimize the benefits of this exercise. Participants appreciated that there were 2 trainers, 1 in the ante-room and 1 in the patient’s room, who were observing different processes and able to give valuable feedback during the debriefing. They also appreciated that the simulation exercise was done in-situ, and therefore was realistic in design.
Suggestions for improvement included providing a variety of clinical scenarios, training junior physicians so that the whole medical team is familiar with the processes, mimicking the typical manpower available on-call in the simulation exercise, and increasing the complexity of the scenarios to address resource allocation issues faced in a pandemic.
IV. DISCUSSION
With the development of the COVID-19 outbreak and patients requiring intensive care, our unit thought it would be imperative to train our frontline staff to be prepared to manage airway emergencies and to be able to resuscitate infected patients. Simulation provides a safe environment for mistakes to be made without compromising patient safety (Ziv et al., 2000). It also provides a platform for deliberate practice (Ericsson, 2004) and not allow for a chance clinical encounter to develop expertise in an area. Simulation has also been utilised in high consequence infectious outbreak training, resulting in improved self-efficacy, reduced anxiety and improved inter-professional teamwork (Marrs et al., 2019; O’Keeffe et al., 2016). As the consequences for patient and individual safety were high in the COVID-19 outbreak, we felt it was prudent to use simulation-based education as a platform for upskilling our staff.
Despite training in the use of personal protection equipment (PPE), including the powered air-purifying respirator (PAPR), Watson et al found that there was an inadequate adherence to the use of PPE and resuscitation guidelines in simulated cardiac arrest in paediatric influenza (H1N1) patients (Watson et al., 2011). Intensive care procedures have been found to be more difficult, stressful and uncomfortable when performed in PPE (Grillet et al., 2015). Simulation training has also been able to detect breaches in infection control procedures (Seet et al., 2009) and potentially improve compliance with infection prevention measures (Tan et al., 2021).
For the above reasons, healthcare professionals who worked in the paediatric intensive care unit were put through a mandatory simulation-based training session on airway management of a deteriorating patient who was suspected to have COVID-19 infection. An in-situ model was chosen as it could be used to evaluate system competence and identify latent conditions that predispose to medical error (Patterson et al., 2013). In this study, in situ simulation provided a means to identify areas for process improvement and knowledge gaps. It provided the ability to test the actual clinical care system, including equipment, processes, and staff response. This form of “just-in-time” training takes place in close proximity to the clinical encounter in a focused concise manner (Itoh et al., 2019). This provides the participants with contextually relevant hands-on experience in dealing with an impending low-frequency event before it actually happens. This has shown to improve confidence levels and clinical skills (Sam et al., 2012).
As expected, there was improvement in self-efficacy as shown in the improvement in pre- and post-simulation responses for all questions relating to management of the patient and clinical team. This has been shown in many previous studies using simulation as a methodology (McLaughlin et al., 2019; Secheresse et al., 2020). Evidence does suggest that clinicians have a limited ability for self-assessment of competence (Davis et al., 2006) and self-assessment. From the Kirkpatrick levels of evaluation, this would be a level 2 evaluation of knowledge, skills and attitudes (Kirkpatrick & Kirkpatrick, 2006). From the qualitative data, the benefits that were emphasised where related to experiential learning and increasing confidence as well as awareness. Kolb’s framework of experiential learning includes the phases of concrete experience and reflective observation (Kolb, 1984). These phases were evident in the simulation experience. Participants reflected that theoretical knowledge does not guarantee perfect execution in real life. The cognitive load of managing a high consequence, low incidence event along with the concomitant risk of exposure to a highly infectious agent makes clinical decision making harder. Although the participants underwent prior PPE training, they appreciated the opportunity to put it all into practice.
There was a definite signal for increased self-efficacy and confidence. This is seen in the literature on simulation-based healthcare education across disciplines (Bragard et al., 2018; Cohen et al., 2013; Fisher et al., 2011; Fouilloux et al., 2019). A study on influenza pandemic preparedness showed that simulation improved staff confidence and also demonstrated that many tasks and procedures took longer to complete with the implementation of guidelines (Phin et al., 2009). This was similarly evident in our participants as they became more aware of the challenges and the additional time needed for most resuscitative actions due to infection control requirements. Going through the simulated scenario and debriefing made them feel more prepared for an actual emergency. In addition, participants highlighted that the simulation experience alleviated anxiety as it successfully removed the “first-time” feeling for them, and felt that it was the responsible thing to do for healthcare workers in the midst a public health crisis. Lessons learnt by the participants included anticipatory planning, prioritisation and resource management. We had a small signal that the skills learnt translated to real life as one participant had a clinical encounter that required initiating extracorporeal life support in a patient with suspected COVID-19. She reported feeling relieved that she had the simulation experience before the real-life clinical encounter, and felt she was less nervous because of her prior stimulated experience. A respiratory therapist also observed that the nurses who he worked with in the PICU who had gone through the simulation seemed more confident and more aware of the necessary processes when intubating suspected COVID-19 patients.
An interesting phenomenon was the signal that there was an increase in anxiety levels after participants went through the simulation as seen in the pre- and post-simulation response. A possible explanation could be what participants brought up in the interviews about the simulation and debriefing revealing their “unconscious incompetence”. This made them more aware of the complexity and so increased their anxiety with dealing with intubation in a COVID-19 patient. Other studies in the literature generally report a reduction in anxiety after simulation (Bragard et al., 2019; Shrestha et al., 2019, 2020). This may not be a negative impact arising from the simulation experience itself as it may reflect increased awareness in an uncommon, yet stressful and complex clinical situation for our healthcare workers. Anxiety levels in frontline healthcare workers in a pandemic may also be due to other factors such as being at higher risk of exposure to COVID-19 at work and the possibility of bringing the infection home to their family (Holmes et al., 2020; Shanafelt et al., 2020).
Another benefit derived from running this simulation-based training is the process improvement suggestions made by the participants. This is a known benefit of simulation (Paige et al., 2018) and was utilised during the 2003 SARS-CoV outbreak (Abrahamson et al., 2005). The main challenge faced by participants during this scenario was the communication barrier which arose from not being able to communicate with personnel outside the room and the presence of the PPE and PAPR physically obstructing hearing and clarity of speech. Also, restriction of movement in and out of the patient’s room experienced during simulation highlighted the need to rethink resuscitation practices when dealing with COIVD patients. These systemic issues surfaced allowed us to brainstorm for practical solutions as a unit, and some have been implemented in our PICU. We have trialled the use of infant monitors as a 2-way communication device. Pre-packed resuscitation drug kits containing intravenous adrenaline and intravenous atropine as well as pre-packed intravenous cannulation disposables have been put in every isolation room so that these would be easily accessible in an emergency. As suggested by the participants, we have also extended the simulation training to include all junior doctors in the department, more nurses and all respiratory therapists in the PICU to facilitate better teamwork. We are also exploring the provision of a dedicated COVID-19 crash cart to minimise waste and prevent cross-contamination.
There are several limitations to this study. Firstly, the sample size is small and selection bias is possible due to the study design. Next, focus group interviews were conducted with a small subset of the participants who agreed to participate, and therefore our findings may not have been representative of the entire cohort. However, we are reassured by the fact that each healthcare professional group that took part in the simulation training was represented in the focus groups. As this simulation exercise was designed to be “just in time” training and we were limited by the urgency of the situation as well as the need to train as many staff in the shortest amount of time, we could only conduct a one-time simulation scenario specific to the highest risk procedure in resuscitating a suspected COVID-19 patient. We were therefore not able to assess the impact of this training on the subsequent performance of the participants either in another simulated scenario or a real life one.
V. CONCLUSION
Simulation-based training is a useful tool for infectious disease outbreak preparedness for the healthcare team. It improves confidence and awareness around managing emergencies while maintaining personal protection through deliberate practice in a safe environment. It also provides an opportunity for process improvement in a new and evolving pandemic situation. It was well-received by the participants and perhaps more sessions are needed for adequate practice. This is limited by the resource-intensive nature of in-situ simulation and the heavy clinical workload at this time of crisis. Further research will need to be done to determine if simulation-based training has a significant impact on actual clinical practice
Notes on Contributors
Nicola Ngiam conceptualised and designed the study, collected data, analysed and interpreted it, drafted the manuscript and approved the final version submitted.
Kristy X Fu did the background work and literature review, assisted in drafting the manuscript and critically revised the manuscript for important intellectual content and approved the final version submitted.
Jacqueline SM Ong designed the study, collected data, interpreted it, critically revised the manuscript for important intellectual content and approved the final version submitted.
Ethical Approval
Ethical approval has been granted by National Healthcare Group Domain Specific Review Board (Ref: NHG DSRB Ref. 2020/00234)
Data Availability
Transcripts from the interviews are confidential and the authors do not have consent to upload onto a repository. Data from questionnaires can be made available on request.
Acknowledgement
We would like to thank Dr Dimple Rajgor for helping with formatting, and submission of the manuscript for publication.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Interest
The Authors declare that there is no conflict of interest.
References
Abrahamson, S. D., Canzian, S., & Brunet, F. (2005). Using simulation for training and to change protocol during the outbreak of severe acute respiratory syndrome. Critical Care, 10(1), R3. https://doi.org/10.1186/cc3916
Booth, C. M., Matukas, L. M., Tomlinson, G. A., Rachlis, A. R., Rose, D. B., Dwosh, H. A., Walmsley, S. L., Mazzulli, T., Avendano, M., Derkach, P., Ephtimios, I. E., Kitai, I., Mederski, B. D., Shadowitz, S. B., Gold, W. L., Hawryluck, L. A., Rea, E., Chenkin, J. S., Cescon, D. W., Poutenan, S.M. & Detsky, A. S. (2003). Clinical features and short-term outcomes of 144 patients with SARS in the greater Toronto area. JAMA, 289(21), 2801-2809. https://doi.org/10.1001/jama.289.21.JOC30885
Bragard, I., Farhat, N., Seghaye, M.-C., Karam, O., Neuschwander, A., Shayan, Y., & Schumacher, K. (2019). Effectiveness of a high-fidelity simulation-based training program in managing cardiac arrhythmias in children: A randomized pilot study. Pediatric Emergency Care, 35(6), 412-418. https://doi.org/10.1097/PEC.0000000000000931
Bragard, I., Seghaye, M.-C., Farhat, N., Solowianiuk, M., Saliba, M., Etienne, A.-M., & Schumacher, K. (2018). Implementation of a 2-day simulation-based course to prepare medical graduates on their first year of residency. Pediatric Emergency Care, 34(12), 857-861. https://doi.org/10.1097/PEC.0000000000000930
Caputo, K., Byrick, R., Chapman, M., Orser, B., & Orser, B. (2006). Intubation of SARS patients: Infection and perspectives of healthcare workers. Canadian Journal of Anaesthesia, 53(2), 122-129. https://doi.org/10.1007/BF03021815
Cohen, E. R., Barsuk, J. H., Moazed, F., Caprio, T., Didwania, A., McGaghie, W. C., & Wayne, D. B. (2013). Making July safer: Simulation-based mastery learning during intern boot camp. Academic Medicine, 88(2), 233-239. https://doi.org/10.1097/ACM.0b013e31827bfc0a
Davis, D. A., Mazmanian, P. E., Fordis, M., Van Harrison, R., Thorpe, K. E., & Perrier, L. (2006). Accuracy of physician self-assessment compared with observed measures of competence: A systematic review. JAMA, 296(9), 1094-1102. https://doi.org/10.1001/jama.296.9.1094
Ericsson, K. A. (2004). Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Academic Medicine, 79(10), S70-S81. https://doi.org/10.1097/00001888-200410001-00022
Fisher, N., Eisen, L. A., Bayya, J. V., Dulu, A., Bernstein, P. S., Merkatz, I. R., & Goffman, D. (2011). Improved performance of maternal-fetal medicine staff after maternal cardiac arrest simulation-based training. American Journal of Obstetrics and Gynecology, 205(3), e1-e5. https://doi.org/10.1016/j.ajog.2011.06.012
Fouilloux, V., Gran, C., Guervilly, C., Breaud, J., El Louali, F., & Rostini, P. (2019). Impact of education and training course for ECMO patients based on high-fidelity simulation: A pilot study dedicated to ICU nurses. Perfusion, 34(1), 29-34. https://doi.org/10.1177/0267659118789824
Grillet, G., Marjanovic, N., Diverrez, J., Tattevin, P., Tadié, J., & L’Her, E. (2015). Intensive care medical procedures are more complicated, more stressful, and less comfortable with Ebola personal protective equipment: A simulation study. The Journal of Infection, 71(6), 703-706. https://doi.org/10.1016/j.jinf.2015.09.003
Holmes, E. A., O’Connor, R. C., Perry, V. H., Tracey, I., Wessely, S., Arseneault, L., Ballard, C., Christensen, H., Silver, R. C., & Everall, I. (2020). Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. The Lancet Psychiatry, 7(6), 547-560. https://doi.org/10.1016/S2215-0366(20)30168-1
Itoh, T., Lee-Jayaram, J., Fang, R., Hong, T., & Berg, B. (2019). Just-in-Time Training for Intraosseous Needle Placement and Defibrillator Use in a Pediatric Emergency Department. Pediatric Emergency Care, 35(10), 712-715. https://doi.org/10.1097/PEC.0000000000001516
Kirkpatrick, D., & Kirkpatrick, J. (2006). Evaluating training programs: The four levels (3rd ed.). Berrett-Koehler Publishers.
Kolb, D. (1984). The experiential learning theory of development. Experiential Learning: Experience as the Source of Learning and Development (pp. 132-160). Prentice Hall, Englewood Cliffs, NJ, 132-160.
Lau, J., Fung, K., Wong, T., Kim, J., Wong, E., Chung, S., Ho, D., Chan, L., Lui, S., & Cheng, A. (2004). SARS transmission among hospital workers in Hong Kong. Emerging Infectious Diseases, 10(2), 280-286. https://doi.org/10.3201/eid1002.030534
Marrs, R., Horsley, T. L., Hackbarth, D., & Landon, E. (2019). High consequence infectious diseases training using interprofessional simulation and TeamSTEPPS. American Journal of Infection Control, 48(6), 615-620. https://doi.org/10.1016/j.ajic.2019.10.007
McLaughlin, C., Barry, W., Barin, E., Kysh, L., Auerbach, M. A., Upperman, J. S., Burd, R. S., & Jensen, A. R. (2019). Multidisciplinary simulation-based team training for trauma resuscitation: A scoping review. Journal of Surgical Education, 76(6), 1669-1680. https://doi.org/10.1016/j.jsurg.2019.05.002
O’Keeffe, D., Bradley, D., Evans, L., Bustamante, N., Timmel, M., Akkineni, R., Mulloy, D., Goralnick, E., & Pozner, C. (2016). Ebola Emergency Preparedness: Simulation Training for Frontline Health Care Professionals. MedEdPORTAL, 12, 10433-10433. https://doi.org/10.15766/mep_2374-8265.10433
Paige, J. T., Fairbanks, R. J. T., & Gaba, D. M. (2018). Priorities related to improving healthcare safety through simulation. Simulation in Healthcare, 13(3S), S41-S50. https://doi.org/10.1097/SIH.0000000000000295
Patterson, M., Geis, G., Falcone, R., LeMaster, T., & Wears, R. (2013). In situ simulation: detection of safety threats and teamwork training in a high risk emergency department. BMJ Quality & Safety, 22(6), 468-477. https://doi.org/10.1136/bmjqs-2012-000942
Phin, N., Rylands, A., Allan, J., Edwards, C., Enstone, J., & Nguyen-Van-Tam, J. (2009). Personal protective equipment in an influenza pandemic: a UK simulation exercise. Journal of Hospital Infection, 71(1), 15-21. https://doi.org/10.1016/j.jhin.2008.09.005
Sam, J., Pierse, M., Al-Qahtani, A., & Cheng, A. (2012). Implementation and evaluation of a simulation curriculum for paediatric residency programs including just-in-time in situ mock codes. Paediatrics & Child Health, 17(2), e16-20. https://doi.org/10.1093/pch/17.2.e16
Secheresse, T., Pansu, P., & Lima, L. (2020). The impact of full-scale simulation training based on Kolb’s learning cycle on medical prehospital emergency teams: A multilevel assessment study. Simulation in Healthcare, 15(5), 335-340. https://doi.org/10.1097/SIH.0000000000000461
Seet, R., Lim, E., Oh, V., Ong, B., Goh, K., Fisher, D., Ho, K., & Yeoh, K. (2009). Readiness exercise to combat avian influenza. QJM : Monthly Journal of the Association of Physicians, 102(2), 133-137. https://doi.org/10.1093/qjmed/hcn159
Shanafelt, T., Ripp, J., & Trockel, M. (2020). Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA, 323(21), 2133-2134. https://doi.org/10.1001/jama.2020.5893
Shrestha, R., Badyal, D., Shrestha, A., & Shrestha, A. (2020). In-situ simulation-based module to train interns in resuscitation skills during cardiac arrest. Advances in Medical education and Practice, 11, 271-285. https://doi.org/10.2147/AMEP.S246920
Shrestha, R., Shrestha, A. P., Shrestha, S. K., Basnet, S., & Pradhan, A. (2019). Interdisciplinary in situ simulation-based medical education in the emergency department of a teaching hospital in Nepal. International Journal of Emergency Medicine, 12(1), 19. https://doi.org/10.1186/s12245-019-0235-x
Tan, K. W., Ong, H. K., & Mok, U. S. (2021). Using simulation and inter-professional education to teach infection prevention during resuscitation. The Asia Pacific Scholar, 6(1), 93-108. https://doi.org/10.29060/TAPS.2021-6-1/OA2229
The Centre for Evidence-Based Medicine Nuffield Department of Primary Care Health Sciences University of Oxford. (2020). Global Covid-19 case fatality rates. https://www.cebm.net/covid-19/global-covid-19-case-fatality-rates/. Accessed April 26, 2020.
The Novel Coronavirus Pnuemonia Emergency Response Epidemiology Team. (2020). The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. China CDC Weekly, 2(8), 113-122. https://doi.org/10.46234/ccdcw2020.032
Watson, C., Duval-Arnould, J., McCrory, M., Froz, S., Connors, C., Perl, T., & Hunt, E. (2011). Simulated pediatric resuscitation use for personal protective equipment adherence measurement and training during the 2009 influenza (H1N1) pandemic. The Joint Commission Journal on Quality and Patient Safety, 37(11), 515-523. https://doi.org/10.1016/S1553-7250(11)37066-3
Wax, R. S., & Christian, M. D. (2020). Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Canadian Journal of Anesthesia/Journal canadien d’anesthésie, 67(5), 568–576. https://doi.org/10.1007/s12630-020-01591-x
World Health Organization. (2020). Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019- nCoV). Retrieved 6 April, 2021, from https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov)
Wu, Z., & McGoogan, J. (2020). Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA, 323(13), 1239-1242. https://doi.org/10.1001/jama.2020.2648
Ziv, A., Small, S. D., & Wolpe, P. R. (2000). Patient safety and simulation-based medical education. Medical Teacher, 22(5), 489-495. https://doi.org/10.1080/01421590050110777
Zuo, M., Huang, Y., Ma, W., Xue, Z., Zhang, J., Gong, Y., & Che, L. (2020). Expert recommendations for tracheal intubation in critically ill patients with Noval Coronavirus Disease 2019. Chinese Medical Sciences Journal, 35(2), 105–109. https://doi.org/10.24920/003724
*Nicola Ngiam
Centre for Healthcare Simulation,
National University of Singapore,
14 Medical Dr,
Singapore 117599
Email: nicola_ngiam@nuhs.edu.sg
Submitted: 5 July 2021
Accepted: 13 September 2021
Published online: 5 April, TAPS 2022, 7(2), 6-16
https://doi.org/10.29060/TAPS.2022-7-2/OA2654
Ming-Jung Ho1,2, Yu-Che Chang3,4,5 & Steven L. Kanter6
1Center for Innovations and Leadership in Education, Georgetown University Medical Center (CENTILE), Washington, D.C., United States; 2Department of Family Medicine, Georgetown University School of Medicine, Washington D.C., United States; 3Chang Gung Medical Education Research Centre (CG-MERC), Chang Gung Medical Foundation, Taoyuan, Taiwan; 4Chang Gung University College of Medicine, Taoyuan, Taiwan; 5Department of Emergency Medicine, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan; 6Association of Academic Health Centers, Washington, D.C., United States.
Abstract
Introduction: The COVID-19 pandemic forced medical schools worldwide to transition online. While there are ample reports about medical education adaptations to this crisis, there are limited studies evaluating the impact.
Methods: This study includes a case study of how Taiwanese medical school deans maintained in-person education during the COVID-19 pandemic. Additionally, it demonstrates how SWOT analyses can help medical educators reflect on adaptations during the COVID-19 pandemic and future crises. This study employed two online surveys and a semi-structured interview regarding curricular adaptations. Eligible participants were deans or associate deans of all medical schools in Taiwan.
Results: Through a SWOT analysis, this study identified Strengths as strong leadership, prior experience with SARS, and ability to promptly adapt curriculum; Weaknesses as lack of faculty confidence in online education, limited numbers of administrative staff, and inability to rapidly add new topics; Opportunities as centralised anti-epidemic policies, inter-institutional collaborations, and educational innovations; and Threats as concerns from parents, patients, and teaching hospitals. It is reported that the quality of education was maintained as students’ evaluations of courses, performances in written exams, clerkship supervisors’ assessments, national OSCE, and national board exams remained comparable to pre-COVID times. Strengths and Opportunities such as strong leadership and centralised anti-epidemic policies can overcome Weaknesses and Threats, such as lack of confidence in online education and familial pressure to suspend hospital-based education.
Conclusion: This study recommends that medical school leaders conduct SWOT analyses as early as possible to plan strategies to continue safe and quality medical education during COVID-19 and future crises.
Keywords: SWOT Analysis, Adaptation, Medical School, COVID-19, Pandemic, National Survey, Medical Education, Taiwan
Practice Highlights
- Medical school deans in Taiwan documented critical observations made during a global pandemic.
- SWOT analysis can help us reflect on medical education adaptations during the pandemic and crises.
- Strong leadership and centralised anti-epidemic policies can aid in overcoming weaknesses/threats.
- Schools can benefit from using SWOT analyses to plan for continuing education during emergent crises.
I. INTRODUCTION
The novel coronavirus disease 2019 (COVID-19) outbreak in Wuhan, China at the end of December 2019 evolved rapidly into a global pandemic and upended almost every aspect of our lives, including school closures across the world (UNICEF, 2021; Zhu et al., 2020). Medical schools are no exception (B. Choi et al., 2020; Harries et al., 2021). Almost all medical schools in the United States transitioned to online teaching by mid-March 2020 and tried to restart teaching on campuses and in hospitals safely in Fall 2020 (Frieden, 2020) . There is a growing literature on how to transition medical education online during the COVID-19 pandemic (Ahmed et al., 2020; Al-Balas et al., 2020; Journal of the Association of American Medical Colleges, 2021; Keegan & Bannister, 2021; Medical Education, 2020). Medical education associations also developed websites and offered webinars to share best practices and innovations focused on online education rather than in-person education (Association for Medical Education in Europe, 2020; Association of American Medical Colleges, 2021; International Association of Medical Science Educators, 2020). Most of the literature reflects the important perspectives of teachers and students with voices from medical school leadership and the forces impacting their decisions relatively limited (Abbas et al., 2020; Al-Balas et al., 2020; Compton et al., 2020; Gordon & Cleland, 2021; Lazarus et al., 2021; Soled et al., 2020). Furthermore, most of the publications are based on lessons learned from English-speaking countries. As non-English-speaking countries encountered COVID-19 and started to reopen medical schools earlier than English-speaking countries, lessons from non-English-speaking medical schools can be valuable to the global medical education community. This study addresses the above gaps in literature by surveying Taiwanese medical school deans on how they adapted their curricula and continued face-to-face medical education on campus and in hospitals amid this historical moment.
Located 81 miles from mainland China, and with over a hundred daily flights in between, Taiwan was predicted to have the second highest number of COVID-19 cases according to early modeling in January 2020 (Gardner, 2020). Having learnt a hard lesson from the severe acute respiratory syndrome (SARS) epidemic in 2003, the Taiwanese government, health system, general public, and medical educators were better prepared to respond to this new pandemic early and proactively (Wang et al., 2020). Before the first confirmed case in Taiwan, the Taiwan Centers for Disease Control began to monitor passengers returning from Wuhan, China, since on January 21, 2020 and set up the Central Epidemic Command Center to coordinate responses to COVID-19, including surveillance and testing, border control, community transmission control, medical system response, personal protective equipment (PPE) and other medical supplies stockpile and distribution, as well as health education and disinformation management (Taiwan Center for Disease Control, 2020).
In contrast to medical schools around world closing campus in the spring semester due to the COVID-19 pandemic, Taiwanese medical schools stayed open except for delaying the start of spring semester one or two weeks later than the originally scheduled date of February 17, 2020.
In addition to exploring how Taiwanese medical schools adapted their curriculum to continue on-campus and workplace-based education at the program level during the COVID-19 pandemic, this study addresses the gap in the literature regarding evaluation of these programmatic changes (Reid & Sam, 2021). This study employed a SWOT analysis (Ghazinoorya et al., 2011; Topor et al., 2018), a method widely used to analyse an organisation’s internal strengths and weaknesses, as well as external opportunities and threats in the environment to examine what medical education leaders critically consider in order to maintain in-person medical education amid the COVID-19 pandemic. This study surveyed and interviewed Taiwanese medical school deans in order to answer the following four research questions:
1. What curricular adaptations have been made in response to the COVID-19 pandemic?
2. What were the impacts of the curricular adaptations?
3. What were the strengths, weaknesses, opportunities, and threats of the curricular adaptations?
4. What are the lessons learned to be applied to the future?
II. METHODS
This study consists of two online surveys and a follow-up individual semi-structured interview. Eligible participants were deans or associate deans of all 13 medical schools in Taiwan. To encourage participation, we emailed invitations with information about study purpose, data confidentiality, and a weblink to the online survey. Participation was voluntary without incentives offered. Following the initial email, reminders were sent periodically. If the dean of a medical school was not available to complete the survey, we invited the associate dean to do so. We collected survey responses and conducted interviews about curricular adaptations between April 29 and May 18, 2020. A follow up survey on the impacts of curricular adaptation was conducted between August 27 and September 10. The online written surveys and follow-up semi-structured interviews were conducted in Chinese (written) and Mandarin (spoken) and translated to English by the first author (MJH). This study was approved as exempt by the Georgetown University Institutional Review Board (STUDY00002812). Since the study poses no greater than minimal risk to subjects, a waiver of written consent was granted, and verbal consent was obtained before data collection began. All methods were carried out in accordance with relevant guidelines and regulations.
A. Study Design
The survey questions were developed based on a review of relevant literature and consultations with international research collaborators in Italy, Japan and Korea, where similar surveys will be conducted. Open-ended survey questions can be found in Supplemental Digital Appendix 1.
In addition to the online survey, each participant was offered an opportunity to be interviewed by the first author (MJH) videoconference in the ensuing two weeks to provide further details about their survey responses. If a participant accepted the interview invitation, a semi-structured interview was conducted, in which the participant was prompted to elaborate on their answers in the surveys. Clarifying questions were asked for survey responses as needed. For example, a participant responded to a survey question by stating that an OSCE exam had been cancelled. During the ensuing interview, the interviewer asked “In the survey, you wrote that an OSCE was cancelled. What was the OSCE for? How did you make up for the cancelled OSCE?”
B. Data Analysis
The free text responses to the open-ended questions in the survey, as well as recordings of the interviews, were analysed by the researchers using a qualitative thematic analysis approach (Braun & Clarke, 2006). One researcher identified themes that emerged from the qualitative data; then, a second researcher determined if they agree or disagree with the analysis. For each point of disagreement, the two researchers discussed the data and reached consensus. Data analysis was initially inductive. After the themes emerged, we used a SWOT analysis framework to group themes into four categories: strengths internal to the institution, weaknesses internal to the institution, opportunities external to the institution, and threats external to the institution (Ghazinoorya et al., 2011; Topor et al., 2018).
III. RESULTS
All 13 medical schools in Taiwan completed the survey for a response rate of 100%. Eleven deans and two associate deans filled out the survey. Three deans and one associate dean agreed to participate in a follow-up interview by videoconference. Characteristics of the medical schools are listed in Table 1. In the first part of results, we will describe curricular adaptations and present themes with representative quotes of curricular adaptations in Table 2. Then Table 3 will summarise the SWOT analysis followed by descriptions of key themes in strengths, weaknesses, opportunities, and threats.
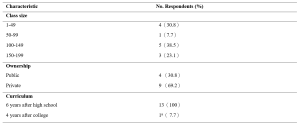
Table 1. Characteristics of Survey Schools
aOne medical school had both 6-year program for high school graduates and 4-year program for college graduates.
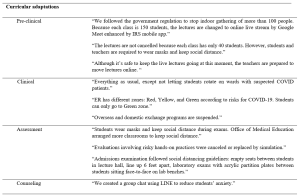
Table 2. Themes and quotes of curriculum adaptations
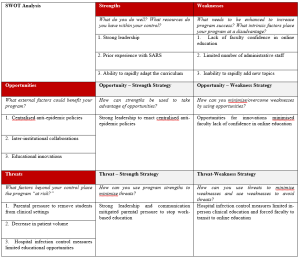
Table 3. SWOT Analysisb
b This table is created using the blank SWOT form from Topor et al.21
A. Curricular Adaptations
1) Pre-clinical curriculum adaptations:
Taiwanese medical schools rapidly adapted their curricula to comply with government policy on social distancing prohibiting indoor gatherings of more than 100 individuals. Whereas a school with a small student body and sufficient classroom capacity did not have to transition online, a school with a large student body and insufficient classroom capacity moved almost all pre-clinical classes online. Some schools went partially online, converting only lectures with more than 100 students to online learning and capping the number of students in the classroom, with live stream available for those not in the classroom. While schools adapted different modalities for lecture-based courses, all schools made efforts to keep laboratory courses face-to-face. Some schools shared how they adjusted laboratory sessions to maintain social distance, including simultaneously using more lab rooms or holding lab sessions in different time slots.
2) Clinical curriculum adaptations:
In contrast to approaches in the United States suspending clinical rotations in spring semester recommended by AAMC (Association of American Medical Colleges, 2021), all medical schools in Taiwan continued clinical rotations while protecting the safety of students. Several strategies were implemented rapidly: Orientation to clinical rotations articulated pandemic prevention and included online modules required by the hospital. Clinical students were provided with surgical masks. In the emergency room, students were given N95 respirators each day. Exposure to suspected and confirmed COVID-19 cases was avoided for students replacing rotations in specialties with high risk of COVID-19 exposure. To prevent cross infection, inter-institutional and overseas exchange programs were cancelled. Students rotated in only one of the affiliated hospitals. Social distancing is also mentioned in clinical rotation adjustments. Several respondents mentioned that the number of students in outpatient clinics, in classrooms, and in conferences was reduced. One school reported an increase of clinical teachers to meet social distancing demands.
3) Assessment adaptations:
Eight schools replied that they did not change the assessment of students by written examinations in classrooms but arranged empty seats between students to keep social distance and protected students from airborne droplet transmissions by requiring everyone to wear a mask. Some schools decreased the use of written exams in classrooms by substituting reports, reflections, online exams, online presentations, and other approaches. Some evaluations involving hands-on practices were cancelled or replaced by simulation. One school reported that their admission exams included tests in laboratories. To prevent face-to-face transmission of airborne droplets, transparent acrylic partitions were installed on the benches in front of each student.
B. Impact of curricular adaptations
Medical school deans tried to evaluate the impact of curricular adaptions by comparing student performance in the 2020 spring semester with previous years. Most deans reviewed the passing rate of courses and reported no statistical differences. They also reported monitoring students’ performances in national board exams in July and national OSCE clinical skills exam held before graduation. The deans were relieved to see that the national exam scores were comparable to previous years and felt that curricular adaptations didn’t impact student competencies negatively.
C. Strengths
The strengths of Taiwanese medical schools’ responses to COVID-19 can be summarised into three themes: strong leadership, prior experience with SARS, and ability to rapidly adapt the curriculum.
1) Strong leadership: The key strength most Taiwanese deans cited in their medical schools’ response to COVID-19 is the strong leadership in the early deployment of epidemic prevention measures. The guidelines from the Central Epidemic Command Center were implemented on each campus, including requiring students to wear masks, to maintain social distance, to monitor temperature and symptoms of COVID-19, and to quarantine international students in separate dormitory areas. Communication also was highlighted by respondents as manifesting strong leadership. Furthermore, two deans made videos in collaboration with students to promote anti-epidemic measures (Chang Gung University, 2020; Fu Jen Catholic University, 2020).
2) Prior experience with SARS: Another strength most respondents noted was the experience of SARS. When COVID-19 spread to Taiwan, most clinical teachers had experienced SARS and were able to share critical lessons to face new emerging infectious diseases with the younger generation. The experience of SARS also prepared medical educators to deal with professionalism and ethics issues such as distribution of limited medical resources. Many participants mentioned that SARS had a great impact on the medical education system in Taiwan because it exposed the lack of primary care workforce with medical school graduates entering specialty training directly after medical school. After SARS, a postgraduate year program was established with one year of required general medicine training prior to specialty training programs with the goal of producing more physicians competent in general medicine to respond to emergent infectious diseases.
3) Ability to rapidly adapt the curriculum: All schools reported rapid curricular adaptations when spring semester started one or two weeks later than the scheduled time. Different strategies were employed in pre-clinical and clinical curricula to prevent and control the spread of COVID-19 as described in 3.1 curricular adaptation.
D. Weaknesses
The weaknesses of Taiwanese medical schools’ responses to COVID-19 can be summarised into three themes: lack of faculty confidence in online education, limited number of administrative staff, and inability to rapidly add new topics.
1) Lack of faculty confidence in online education: All respondents mentioned online teaching as challenging to teachers. Many voiced concerns about the effectiveness of online learning and found assessment of online learning challenging. Online learning is also considered challenging to students. Some respondents mentioned that online learning requires self-directed learning, which is not a strength of Taiwanese students since didactic teaching and rote memorisation is the norm of the K-12 education system.
2) Limited number of administrative staff: In response to the question about weaknesses of their medical schools’ responses to the COVID-19 pandemic, administrative challenges were mentioned frequently. Although Taiwan did not experience high burdens of COVID-19, all schools were preparing for large-scale outbreaks with frequent scenario planning, describing these planning activities using the military metaphor of “military sand table planning” and “early deployment.”
3) Inability to rapidly add new topics: The pandemic also revealed the need for medical educators to engage in some topics traditionally not articulated in medical curricula. It was challenging to add new topics in the ongoing 2020 spring semester curricula but respondents suggested to add the following topics in the future: infectious disease control, emergent infectious disease, crisis management and communication, public policy and ethical issues related to pandemics such as distribution of medical resources, and government control and restrictions on human rights vs quarantine policy.
E. Opportunities
Taiwanese medical school deans highlighted three opportunities which enabled them to continue to open medical schools during the COVID-19 pandemic: centralised anti-epidemic policies, collaborations among medical schools, and educational innovations.
1) Centralised anti-epidemic policies: Taiwanese deans all reported that the policies from the central government are helpful in their implementation of anti-epidemic measures. Several deans shared the policy guidelines issued by the Ministry of Education with clear guidelines to follow the principles of infection containment. Although each university has the flexibility to decide how to comply with the guidelines, there was external oversight to ensure compliance. For example, when a teaching hospital had an intra-hospital transmission of COVID-19, the medical school had to work with the Central Epidemic Command Center and Ministry of Education in its response.
2) Inter-institutional collaborations: Collaborations among medical schools through the Taiwan Association of Medical Education (TAME) also helped Taiwanese medical school deans to adapt to COVID-19. For instance, the deans worked together at TAME to ensure that final-year students graduated on time. Every year, TAME organises a national OSCE examination required for graduation for final year Taiwanese medical students. Medical schools and teaching hospitals collaborated to administer these exams at OSCE centers in selected teaching hospitals with infection mitigating measures.
3) Educational innovations: All respondents mentioned that the COVID-19 pandemic provided opportunities to engage in innovations in medical education, especially online education. Online education was quickly implemented in some schools because access to internet is prevalent in Taiwan and they utilised the technology developed before the pandemic. One school reported an innovation using the Interactive Response System (IRS) developed three years ago and is now applied to enhance online teaching amid COVID-19. Another school adapted communication software instead of face-to-face counseling meetings. One school reported using “LINE” (a messaging app widely used in Taiwan) for a group chat for students to reduce student anxiety related to COVID-19.
F. Threats
Three themes were identified during the COVID-19 pandemic as threats to medical education, but external to medical schools: parental pressure to remove students from clinical settings, decrease in patient volume, and hospital infection control measures limited educational opportunities.
1) Parental pressure to remove students from clinical settings: Several deans mentioned that students’ parents reached out to them, pressuring them to discontinue clinical rotations. One respondent stated, “Parents are more worried than teachers and students. They are concerned that clinical rotations in the hospitals are risky for students. However, parents accepted our explanation that clinical rotations will not proceed unless there is adequate PPE and infection control measures.”
2) Decrease in patient volume: Another threat commonly mentioned was the decrease in patient volume. A participant explained, “Our hospital experienced a 30% decrease in patient volume. It is inconvenient for patients to come to the hospital due to tightened entrance control. The restriction on patients’ family visits is another factor. We are not letting students rotate on wards with suspected COVID-19 patients.” The limited patient encounters are perceived as potential threat to students’ clinical competence.
3) Hospital infection control measures limited educational opportunities: Finally, another threat reported was associated with infection control measures by the teaching hospitals. Deans expressed concerns that students’ clinical learning opportunities were compromised during the pandemic due to cancelled bedside teaching in high-risk specialties, cancelled presentations in conferences, cancelled interdepartmental grand rounds, and suspension of exchange programs both domestically and internationally. Some mentioned that reduced clinical exposures might result in less role modeling.
IV. DISCUSSION
During this historical event, medical schools around the world are challenged to navigate a path forward to meet missions of education, research, and patient care during an ongoing pandemic. As many countries are loosening or tightening restrictions after their curves of infection have flattened or resurged, medical schools globally are at various stages of deliberating when and how to resume campus-based and hospital-based medical education (Blaaza et al., 2020; Cleland et al., 2020; Tolsgaard et al., 2020). A systematic rapid review of published reports of medical educational developments in response to the COVID-19 pandemic concluded that most papers lacked evaluation data and focused on transitioning online and removing students from the clinical contexts (Gordon et al., 2020). The review suggested that medical schools learn from a few postgraduate papers reporting how face-to-face patient contact could be maintained while mitigating risk using PPE and social distancing (G. Choi et al., 2020; Hanel et al., 2020; Kang et al., 2020). Our study of medical school deans in Taiwan on how they continued in-person medical education throughout the COVID-19 pandemic offers lessons for the medical education community to engage medical students in campus-based and workplace-based learning with evaluation of impacts.
This study offers a conceptual advance by demonstrating how SWOT analysis can help us reflect on medical education adaptations to COVID-19 pandemic and future crises. Our analysis of the strengths, weaknesses, opportunities and threats in Taiwanese medical school adaptations to COVID-19 highlights certain strategies to leverage strengths and opportunities to overcome weaknesses and threats. A critical factor in the decision to continue face-to-face medical education, clearly identified by the opportunity-strength strategy in Table 3, was the early deployment of epidemic prevention measures under centralised government policies and strong medical school leadership. Epidemic prevention measures were deployed at all levels of schools in Taiwan as students returned to campus for spring semester in February 2020. To enact anti-epidemic policies in different contexts, this study presented various preventive measures to keep the recommended social distance in classrooms, laboratories, and teaching hospitals. To implement these measures, transparent communication and administrative support from medical school leadership are essential.
SWOT analysis on opportunity-weakness and threat-weakness strategies offers lessons on how to overcome the weakness of lack of faculty confidence in online education. Although online education is an important curricular adaptation to maintain social distance in campus-based medical education, our survey shows that respondents found online teaching challenging to faculty and are concerned about the effectiveness of online education. Strategies identified to overcome this weakness is to take advantage of the educational technology readily available and to transform the threats from hospital infection control to suspend hospital-based education into opportunities for integrating innovative online education. It is important to leverage innovative online education in workplace learning in the context of reduced patient case exposures before the pandemic subsides (B. Choi et al., 2020; Lo et al., 2020). There is sufficient evidence in the education literature that well-designed online education is as effective as traditional classroom teaching and shows equivalent or better learning outcomes (George et al., 2014; Jung & Rha, 2000; Khalil et al., 2020). We hope that the evaluations reported in the fall semester survey showing equivalent outcomes of online adaptations during COVID-19 would encourage medical educators to take advantage of innovations reported by this study, existing literature on online education in general, and the growing literature about innovative online medical education (Ahmed et al., 2020; Medical Education, 2020).
This study highlighted that another enabling factor for Taiwanese medical educators to continue face-to-face medical education was the experience of SARS. The Taiwanese population became accustomed to anti-epidemic measures, including wearing masks after SARS, which facilitated the implementation of anti-epidemic measures in schools during COVID-19. Taiwanese health providers were severely challenged during the 2003 SARS epidemic. 103 of 318 confirmed cases (Centers for Disease Control and Prevention, 2003) and 11 of 60 deaths (including two first-year residents) (Taiwan Centers for Disease Control, 2013) were healthcare workers. Medical education leaders had a difficult decision to make regarding the final year students who were working as interns in hospitals (Lai, 2020). Following closures of clinics and resignation of healthcare providers, there were heated debates about physician duties to treat patients while being at risk of exposure to a deadly infectious disease and of being stigmatised by society (Lee, 2003). After SARS, not only were curricula on ethics and infection control strengthened, but the medical education system was reformed to convert the final-year of medical school to a formal post-graduate year program (Ho et al., 2017). In addition, as articulated by the respondents of the survey, SARS prepared Taiwanese medical educators and clinical teachers to be confident and competent to perform their educational and clinical duties in the time of COVID-19.
Although this study has many lessons to offer both conceptually and practically, there are some limitations to be considered. We conducted the survey with open-ended questions to explore diverse perspectives. The reported theme frequencies should be considered with caution since some respondents record more comprehensive answers than others. While the most frequently mentioned themes might be most important to the respondents, the least frequently given answer might be valuable due to its innovative nature. Another limitation of an open-ended questionnaire is that respondents might not have the time to enter answers in detail. To overcome this limitation, we invited the respondents to participate in a follow-up interview. However, only about one-third of deans were available to be interviewed during the study period. The four interviews conducted nonetheless enriched the study with more context and details. Finally, this study only surveyed medical school deans. It would be interesting to conduct further studies comparing these results to the perspectives of students and faculty members.
V. CONCLUSION
This nationwide study of all medical schools in Taiwan documents critical observations of top medical school leaders during an active pandemic. This case study demonstrated that strengths and opportunities such as strong leadership and centralised anti-epidemic policies can overcome weaknesses and threats such as faculty lack of confidence in online education and parental pressure to stop hospital-based education. We recommend that medical school leaders conduct SWOT analyses as early as possible to plan strategies to continue safe and quality medical education during COVID-19 and forthcoming emergencies. Similar to the impact of SARS, which led to reform of the Taiwanese postgraduate training system, there is hope that thoughtful reflection on medical education adaptations to the COVID-19 pandemic will improve medical education in general and lead to better preparation for future crises.
Notes on Contributors
MH contributed to the conception, acquisition and analysis of data, drafted the article, and approved the final version; YC contributed to the design, acquisition and analysis of data, drafted the article, and approved the final version; SK contributed to analysis and interpretation of data, revised the article critically, and approved the final version.
Ethical Approval
This study was approved as exempt by the Georgetown University Institutional Review Board (STUDY00002812). Since the study poses no greater than minimal risk to subjects, a waiver of written consent was granted. . We emailed invitations with information about study purpose, data confidentiality, and a weblink to the online survey. A verbal consent was obtained before data collection began. Participation was voluntary without incentives offered. All methods were carried out in accordance with relevant guidelines and regulations.
Data Availability
It is not possible to share data since we did not get consent from participants to share all data collected. They agreed to have results reported in a summary format with selected quotes.
Acknowledgement
The authors wish to thank survey respondents and interviewees for providing insights on the research topic. Fred Hafferty and Carrie Chen provided useful feedback to improve the manuscript.
Funding
This study did not receive any funding.
Declaration of Interest
The authors declare that they have no competing interests.
References
Abbas, M., Dhane, M., Beniey, M., Meloche-Dumas, L., Eissa, M., Guerard-Poirier, N., El-Raheb, M., Lebel-Guay, F., Dubrowski, A., & Patocskai, E. (2020). Repercussions of the COVID-19 pandemic on the well-being and training of medical clerks: A pan-Canadian survey. BMC Medical Education, 20(1), 385. https://doi.org/10.1186/s12909-020-02293-0
Ahmed, S. A., Hegazy, N. N., Abdel Malak, H. W., Cliff Kayser, W., 3rd, Elrafie, N. M., Hassanien, M., Al-Hayani, A. A., El Saadany, S. A., Ai-Youbi, A. O., & Shehata, M. H. (2020). Model for utilizing distance learning post COVID-19 using (PACT)TM a cross sectional qualitative study. BMC Medical Education, 20(1), 400. https://doi.org/10.1186/s12909-020-02311-1
Al-Balas, M., Al-Balas, H. I., Jaber, H. M., Obeidat, K., Al-Balas, H., Aborajooh, E. A., Al-Taher, R., & Al-Balas, B. (2020). Distance learning in clinical medical education amid COVID-19 pandemic in Jordan: Current situation, challenges, and perspectives. BMC Medical Education, 20(1), 341. https://doi.org/10.1186/s12909-020-02257-4
Association for Medical Education in Europe. (2020). COVID-19. Retrieved April 1, 2021, from https://amee.org/covid-19
Association of American Medical Colleges. (2021). Coronavirus (COVID-19) resource hub. Retrieved April 1, 2021, from https://www.aamc.org/coronavirus-covid-19-resource-hub
Blaaza, M., Akhtar, H. N., & Tanzim, U. (2020). Returning to clinics amidst COVID-19: A student response to Compton et al. Medical Education, 54(12), 1193. https://doi.org/10.1111/medu.14282
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative research in psychology, 3(2), 77-101.
Centers for Disease Control and Prevention. (2003). Severe acute respiratory syndrome–Taiwan, 2003. Morbidity and mortality weekly report, 52(20), 461‐466.
Chang Gung University. (2020, March 16). Chang Gung University COVID-19 anti-epidemic advanced adaptation measures [Video]. YouTube. https://www.youtube.com/watch?v=WyoOoShXVa8
Choi, B., Jegatheeswaran, L., Minocha, A., Alhilani, M., Nakhoul, M., & Mutengesa, E. (2020). The impact of the COVID-19 pandemic on final year medical students in the United Kingdom: a national survey. BMC medical education, 20(1), 206. https://doi.org/10.1186/s12909-020-02117-1
Choi, G., Wan, W., Chan, A., Tong, S., Poon, S., & Joynt, G. (2020). Preparedness for COVID-19: In situ simulation to enhance infection control systems in the intensive care unit. British Journal of Anaesthesia, 125(2), e236-e239. https://doi.org/10.1016/j.bja.2020.04.001
Cleland, J., McKimm, J., Fuller, R., Taylor, D., Janczukowicz, J., & Gibbs, T. (2020). Adapting to the impact of COVID-19: Sharing stories, sharing practice. Medical Teacher, 42(7), 772-775. https://doi.org/10.1080/0142159X.2020.1757635
Compton, S., Sarraf-Yazdi, S., Rustandy, F., & Radha Krishna, L. K. (2020). Medical students’ preference for returning to the clinical setting during the COVID-19 pandemic. Medical Education, 54(10), 943-950. https://doi.org/10.1111/medu.14268
Frieden, J. (2020, May 9). Medical schools grapple with challenges for the coming year— Three-quarters hope to have students back by the end of July. MedPage Today. Retrieved April 1 fromhttps://www.medpagetoday.com/publichealthpolicy/medicaleducation/86416
Fu Jen Catholic University. (2020, February 16). COVID-19: Fu Jen Catholic University anti-epidemic promotion video. [Video]. YouTube. https://youtu.be/-n3KvlVHpzY
Gardner, L. (2020, January 31). Update January 31: Modeling the spreading risk of 2019-nCoV. Johns Hopkins University Center for Systems Science and Engineering. Retrieved April 1 from https://systems.jhu.edu/research/public-health/ncov-model-2/
George, P. P., Papachristou, N., Belisario, J. M., Wang, W., Wark, P. A., Cotic, Z., Rasmussen, K., Sluiter, R., Riboli-Sasco, E., Tudor Car, L., Musulanov, E. M., Molina, J. A., Heng, B. H., Zhang, Y., Wheeler, E. L., Al Shorbaji, N., Majeed, A., & Car, J. (2014). Online eLearning for undergraduates in health professions: A systematic review of the impact on knowledge, skills, attitudes and satisfaction. Journal of Global Health, 4(1), 010406. https://doi.org/10.7189/jogh.04.010406
Ghazinoorya, S., Abdia, M., & Azadegan-Mehr, M. (2011). SWOT methodology: A state-of-the-art review for the past, a framework for the future. Journal of Business Economics and Management, 12(1), 24-48. https://doi.org/10.3846/16111699.2011.555358
Gordon, L., & Cleland, J. A. (2021). Change is never easy: How management theories can help operationalise change in medical education. Medical Education, 55(1), 55-64. https://doi.org/10.1111/medu.14297
Gordon, M., Patricio, M., Horne, L., Muston, A., Alston, S. R., Pammi, M., Thammasitboon, S., Park, S., Pawlikowska, T., Rees, E. L., Doyle, A. J., & Daniel, M. (2020). Developments in medical education in response to the COVID-19 pandemic: A rapid BEME systematic review: BEME Guide No. 63. Medical Teacher, 42(11), 1202-1215. https://doi.org/10.1080/0142159X.2020.1807484
Hanel, E., Bilic, M., Hassall, K., Hastings, M., Jazuli, F., Ha, M., Trotter, B., Fraser, C., & Rutledge, G. (2020). Virtual application of in situ simulation during a pandemic. Canadian Journal of Eemergency Medicine, 22(5), 563-566. https://doi.org/10.1017/cem.2020.375
Harries, A. J., Lee, C., Jones, L., Rodriguez, R. M., Davis, J. A., Boysen-Osborn, M., Kashima, K. J., Krane, N. K., Rae, G., Kman, N., Langsfeld, J. M., & Juarez, M. (2021). Effects of the COVID-19 pandemic on medical students: A multicenter quantitative study. BMC Medical Education, 21(1), 14. https://doi.org/10.1186/s12909-020-02462-1
Ho, M.-J., Shaw, K., Shih, J., & Chiu, Y.-T. (2017). Mission and modernity: The history and development of medical education in Taiwan. In L. C. Chen, M. R. Reich, & J. Ryan (Eds.), Medical Education in East Asia: Past and Future (pp. 84-111). Indiana University press.
International Association of Medical Science Educators. (2020, April 22). #IAMSECafe Archives & COVID-19 resources for medical science educators. Retrieved April 1 from http://www.iamse.org/covid-19-resources-for-medical-science-educators/
Journal of the Association of American Medical Colleges. (2021). COVID-19 and medical education. Retrieved April 1 from https://journals.lww.com/academicmedicine/pages/collectiondetails.aspx?TopicalCollectionId=68
Jung, I., & Rha, I. (2000). Effectiveness and cost-effectiveness of online education: A review of the literature. Educational Technology, 40(4), 57-60.
Kang, Y., Deng, L., Zhang, D., Wang, Y., Wang, G., Mei, L., Zhou, G., & Shu, H. (2020). A practice of anesthesia scenario design for emergency cesarean section in patients with COVID-19 infection based on the role of standard patient. BioScience Trends, 14(3), 222-226. https://doi.org/10.5582/bst.2020.03066
Keegan, D. A., & Bannister, S. L. (2021). More than moving online: Implications of the COVID-19 pandemic on curriculum development. Medical Education, 55(1), 101-103. https://doi.org/10.1111/medu.14389
Khalil, R., Mansour, A. E., Fadda, W. A., Almisnid, K., Aldamegh, M., Al-Nafeesah, A., Alkhalifah, A., & Al-Wutayd, O. (2020). The sudden transition to synchronized online learning during the COVID-19 pandemic in Saudi Arabia: A qualitative study exploring medical students’ perspectives. BMC Medical Education, 20(1), 285. https://doi.org/10.1186/s12909-020-02208-z
Lai, C. (2020, March 20). 2003 SARS: Reflections on Taiwanese medical education. UDN. https://health.udn.com/health/story/6631/4421448
Lazarus, G., Findyartini, A., Putera, A. M., Gamalliel, N., Nugraha, D., Adli, I., Phowira, J., Azzahra, L., Ariffandi, B., & Widyahening, I. S. (2021). Willingness to volunteer and readiness to practice of undergraduate medical students during the COVID-19 pandemic: A cross-sectional survey in Indonesia. BMC Medical Education, 21(1), 138. https://doi.org/10.1186/s12909-021-02576-0
Lee, M. (2003). SARS 風暴的啟示[Learning from the SARS event] [Editorial]. Journal of Medical Education, 7(1), 1-2.
Lo, H.-Y., Lin, S.-C., Chaou, C.-H., Chang, Y.-C., Ng, C.-J., & Chen, S.-Y. (2020). What is the impact of the COVID-19 pandemic on emergency medicine residency training: An observational study. BMC Medical Education, 20(1), 348. https://doi.org/10.1186/s12909-020-02267-2
Medical Education. (2020, May 7). Medical education adaptations. Retrieved April 1, 2020, from https://onlinelibrary.wiley.com/doi/toc/10.1002/(ISSN)1365-2923.med.adaptations.vi
Reid, M. D., & Sam, A. H. (2021). Reflections on assessment in the wake of change from the COVID-19 pandemic. Medical Education, 55(1), 128-130. https://doi.org/10.1111/medu.14368
Soled, D., Goel, S., Barry, D., Erfani, P., Joseph, N., Kochis, M., Uppal, N., Velasquez, D., Vora, K., & Scott, K. W. (2020). Medical student mobilization during a crisis: Lessons from a COVID-19 medical student response team. Academic Medicine, 95(9), 1384-1387. https://doi.org/10.1097/ACM.0000000000003401
Taiwan Center for Disease Control. (2020). Prevention and control of COVID-19 in Taiwan. Retrieved April 1, 2021, from https://www.cdc.gov.tw/Category/Page/0vq8rsAob_9HCi5GQ5jH1Q
Taiwan Centers for Disease Control. (2013). Severe acute respiratory syndrome (SARS). Retrieved April 1, 2021 from https://www.cdc.gov.tw/File/Get/InG8jagjxffXBDW1UexnrA
Tolsgaard, M. G., Cleland, J., Wilkinson, T., & Ellaway, R. H. (2020). How we make choices and sacrifices in medical education during the COVID-19 pandemic. Medical Teacher, 42(7), 741-743. https://doi.org/10.1080/0142159X.2020.1767769
Topor, D. R., Dickey, C., Stonestreet, L., Wendt, J., Woolley, A., & Budson, A. (2018). Interprofessional health care education at academic medical centers: Using a SWOT analysis to develop and implement programming. MedEdPORTAL, 14, 10766. https://doi.org/10.15766/mep_2374-8265.10766
UNICEF. (2021). COVID-19 Education: From disruption to recovery. Retrieved April 1, 2021, from https://en.unesco.org/covid19/educationresponse
Wang, C. J., Ng, C. Y., & Brook, R. H. (2020). Response to COVID-19 in Taiwan: Big data analytics, new technology, and proactive testing. The Journal of the American Medical Association, 323(14), 1341-1342. https://doi.org/10.1001/jama.2020.3151
Zhu, N., Zhang, D., Wang, W., Li, X., Yang, B., Song, J., Zhao, X., Huang, B., Shi, W., Lu, R., Niu, P., Zhan, F., Ma, X., Wang, D., Xu, W., Wu, G., Gao, G. F., & Tan, W. (2020). A novel coronavirus from patients with pneumonia in China, 2019. The New England Journal of Medicine, 382(8), 727-733. https://doi.org/10.1056/NEJMoa2001017
*Yu-Che Chang
No. 5, Fuxing St.,
Guishan Dist.,
Taoyuan City 333012,
Taiwan (R.O.C.)
Tel: +886-33281200 ext 3807
Email: changyuche@gmail.com
Submitted: 30 July 2021
Accepted: 4 October 2021
Published online: 5 April, TAPS 2022, 7(2), 1-5
https://doi.org/10.29060/TAPS.2022-7-2/GP2663
Mary Anne Reid1 & Kirsty Forrest2
1Senior Policy Officer, Medical Deans Australia and New Zealand, Australia; 2Dean of Medicine, Faculty of Health Sciences and Medicine, Bond University, Australia
Abstract
Introduction: This article summarises a report published in July 2021 by Medical Deans Australia and New Zealand (Medical Deans), the peak body representing the 23 medical programs in Australia and New Zealand. It explores how medical schools responded to the early impacts of COVID-19 in 2020, and how they might build on some of the changes to achieve fundamental improvements in medical education in Australia and New Zealand.
Methods: The Medical Deans report was based on: Responses to a survey midway through 2020 of its member schools about their experiences during the initial lockdowns; the contributions of presenters at the Medical Deans 2020 Annual Conference; subsequent discussions among communities of practice.
Results: Innovations introduced in response to the pandemic, included greater equity of learning opportunities across geographical locations; health services taking more responsibility for clinical placements; greater emphasis on competencies and less on clinical rotations in specific disciplines; strong collaboration between medical schools, and with providers in the medical training and research pipeline. Challenges include balancing the benefits of online learning with the need for human connection and a chronic lack of clinical training opportunities in community-based care.
Conclusion: While the impact of the pandemic on medical education and training was costly for all involved – both financially and personally – the scale of disruption provided a unique opportunity for step change. To fully realise this potential moving forward, medical schools will need to work in partnership with all those involved: students, health services, prevocational training, specialist colleges, regulators and governments.
Practice Highlights
- Equity of learning opportunities across rural, regional and urban locations using digital technology.
- Enhanced learning outcomes through a blend of remote and face-to-face teaching and assessment.
- Shared responsibility for medical students’ clinical placements as an essential part of the health system.
- More emphasis on student competencies and less on clinical rotations in specific disciplines.
- Strong collaboration between medical schools and across the training pipeline.
I. INTRODUCTION
Medical schools in Australia and New Zealand graduated close to the anticipated number of new doctors (3,800) at the end of 2020 – a significant feat given the size and number of shockwaves sent through the sector by the pandemic. Despite the immense stress COVID-19 placed on the sector, it was also the catalyst for significant innovation.
This article summarises the findings of a report published in July 2021 by the peak body representing the 23 medical schools in the two countries, Medical Deans Australia and New Zealand (Medical Deans). The report, Changing for good: What we learned in 2020 (Medical Deans Australia and New Zealand, 2021a), explored those innovations which occurred during the pandemic that medical schools want to retain and build on in the future. It also identified some critical gaps and problems highlighted by the pandemic that must be addressed moving forward.
II. METHODS
The report was authored on the basis of: responses to a survey run by Medical Deans Australia and New Zealand (MDANZ) midway through 2020; the contributions of presenters at the Medical Deans’ 2020 Annual Conference; subsequent discussions among Medical Deans’ communities of practice.
Where quotes are attributed to a particular person, they are drawn largely from the Annual Conference. Where quotes are attributed to a medical school rather than a person, they are drawn from the Medical Deans survey.
III. RESULTS
A. Innovation through Online Learning
As campuses closed early in 2020, schools employed a combination of pre-recorded sessions and interactive online lessons to deliver much of the non-clinical, and a small part of the clinical, medical curriculum to students. This created a sense of unity amongst students in different geographical locations as they all accessed the same lessons online – reducing disparities sometimes faced by those in regional and rural areas.
- University of Auckland: We have done much more synchronous learning across sites – we have eight sites in each clinical year across the north island – and we’re going to keep that.
- University of Newcastle: We’ve found that the expert facilitating a learning session can now be based anywhere and it works well.
- University of New South Wales: We have students at five metro hospitals and at least five rural ones, plus those in GP placements, who can now join each other in learning activities online. Prior to this, the rural students often felt left out of tutorials and activities that the metro students could get to.
The move out of the lecture theatre also allowed more flexibility for students in accessing lessons and interactivity, through online chat functions, and encouraged the use of advanced digital learning platforms. Small group tutorials used online tools to imitate some aspects of face-to-face clinical teaching and assessment, for example, Zoom rooms for interactions with actors or Objective Structured Clinical Examinations (OSCES).
- Sydney: The live Zoom component of the flipped classroom, with two experts (one monitoring chat), has proven very interactive and popular compared to a large lecture theatre. It also allows for more polling, which the students enjoy. With a cohort of 270, we saw increases from an average of 60-80 participants [25%] in lecture theatre mode to up to 210 participants on Zoom [75%].
However, there were also significant problems associated with delivering so much of the curriculum remotely. Online fatigue and the loss by students of a human connection with their peers and teachers was extremely stressful for many, particularly for international students, some of whom were far away from home for the first time. Another cohort at a particular disadvantage were the first-year students who did not get the chance to attend their university campus or make friends in this new phase of their life before the COVID lockdown.
Another issue for students was that access to adequate technology and learning space offsite was not always adequate, despite schools’ best efforts.
“The presumption in delivering medical training online is that all students have equal access to the technology, and that presumption is not correct,” said Professor John Fraser, University of Auckland’s Executive Dean of Medicine and Health Sciences. “Technology comes at a cost and not all students have enough resources to meet their technological needs. Also, the idea that each student has a space of their own to do their online learning is not always the case.”
Finally, medicine uses a very hands-on, apprentice-based educational approach, and there was only so much that could be done remotely.
Professor Fraser “There is so much subtlety in the way you learn in a clinical environment that it cannot be properly replicated online.”
The future of medical education lies in developing and refining the optimal blend of face-to-face and remote learning and assessment. Getting the balance right will be an ongoing priority for medical schools. By comparing approaches, medical schools have the best chance to determine the optimum mix of remote learning for their individual medical programs. This will be a continuing focus for medical schools, through the Medical Deans’ Medical Education Collaborative Committee (MECC). The University of Notre Dame Australia’s Dean of Medicine, Gervase Chaney, told the 2020 MDANZ Annual Conference that there was an opportunity to implement long-lasting change: “I think we’ve learned that if we are going to get value, we’re not going to be bringing our students on to campus four or five days every week. We’ll be looking at a more flexible learning approach and they can still be doing some clinical skills training – like the history-taking over Zoom or other online platforms. It’s a case of how we normalise this so that when students step into the clinical space, it’s a natural step for them.”
B. New Approaches to Clinical Learning
After an initial halt during the onset of the pandemic, clinical placements for later-year medical students were largely re-instated in 2020.
In Australia, one of the defining features of these new-style placements was the emphasis on shared responsibility between medical schools and health services. Medical schools collaborated as never before with each other and with health services on a range of clinical placement models and paid positions for medical students as part of the surge workforce. While remunerated roles already existed for final year students and pre-interns in other countries, including New Zealand, they were a first for Australia.
These new approaches to clinical placements and paid positions had the following features in common:
- the learning needs of the student were explicit and central
- the role of the student, and their scope of practice within the healthcare team, was more clearly defined and articulated
- medical schools and health services shared core responsibilities for students and the success of their placements
There was strong and widespread support from Australian medical schools for the benefits brought by this shared responsibility for medical students on placement or working within healthcare environments.
Another key shift in clinical training came about due to the need to minimise patient exposure to multiple healthcare workers: in many cases, students were placed for longer periods of time in general wards caring for patients with a range of medical conditions, and their rotations in some medical specialties were cancelled (e.g. obstetrics and gynaecology, intensive care). Students reported feeling more connected to the other health professionals they worked alongside during these longer placements and more able to make a valuable work contribution to patient care.
The Deputy Vice Chancellor, Tropical Health and Medicine at James Cook University, Richard Murray, believes this provided greater exposure for students to whole-of-patient care: “The clinical phase of medical education has traditionally been carved into different rotational experiences across medical disciplines and cemented in place through departments, budgets and staffing. COVID-19 has driven more learning around the integrated experience of patients. Rather than curriculum by a set of rotations, you have curriculum according to people of all ages and with all sorts of problems, which are often complex and interrelated. Learning is more integrated now.”
This discussion is furthered in the Medical Deans advocacy document Training tomorrow’s doctors – All pulling in the right direction (Medical Deans Australia and New Zealand, 2021b), with a number of recommendations for change. One of these is for regulators, medical schools and jurisdictional health service providers to build on the insights from the evaluation of the Assistants in Medicine role piloted in response to the pandemic in NSW in 2020 (New South Wales Health, 2021) and the New Zealand Trainee Intern model, to develop a shared and explicit understanding of what is needed to be prepared for practice; and to strengthen arrangements for students’ transition from medical school to employment.
C. Collaboration on Core Competencies
Also supporting this more generalist approach was the co-development by schools of an agreed set of core competencies needed for final-year medical students to progress to graduation.
This unprecedented collaboration between universities saw medical schools co-develop the common core competencies needed to graduate as a means of quality assuring the rapid and extensive changes made to their programs and placements due to the pandemic. Developed through the Medical Deans’ MECC, these core competencies were based on the schools’ own course outcomes and aligned with those required by the Australian Medical Council.
- Deakin University: We now have clear competencies mapped for internship – extended to the penultimate year. It is now less about the rotation and more about the competencies.
- University of Auckland: Based on our local graduate learning outcomes, we are emphasising core competencies over disciplinary learning outcomes. We are emphasising generic skills and capabilities.
The collaboration between medical schools during 2020 – culminating in the collaboration on core competencies – was amongst the most ranked highly ranked innovations of period which resulted in the Guidance statement: Clinical practice core competencies for graduating medical students (Medical Deans of Australia and New Zealand, 2020).
“The challenges of COVID made us create these dynamic and interactive education teams consisting of students, academics, professional support, design and IT staff all working together on re-developing format, content and assessments,” said University of NSW’s Associate Professor Torda. “At university level we did this across faculties; nationally, we worked more closely together, through Medical Deans in particular, to share and solve problems.” (Medical Deans Australia and New Zealand, 2021a)
D. Lack of Opportunities in Community-Based Care
A pre-existing lack of clinical training opportunities for medical students in community settings – in aged care in particular and, in some places, in general practice – only worsened during the COVID-19 pandemic.
National and international studies show that health systems which provide strong primary care are more cost-effective and associated with a more equitable distribution of healthcare across the population (Australian Department of Health, 2019). Yet GPs are not resourced in the same way as hospitals to provide clinical training for medical students, which fuels an over-emphasis on clinical training in hospitals. COVID-19 highlighted this problem, with GP placements becoming variable in 2020, as practices scrambled to secure the Personal Protective Equipment needed to provide patient services and tended to view medical students as an additional burden rather than as part of the health workforce response.
In the case of aged care, the limited training opportunities for clinical training that existed prior to the pandemic were lost completely in 2020, as facilities moved to shield their vulnerable elderly residents from COVID-19.
We know that the aging populations of Australia and New Zealand will increasingly require non-hospital-based care to manage the chronic and comorbidity conditions that typically occur in older populations (Australian Department of Health, 2019). Medical schools and health services must work together and with governments to ensure that more quality clinical training opportunities are available for students in both community-based aged care and general practice. In addition, to develop and implement solutions effectively there has to be continued and stronger collaboration right along the medical training and research pipeline, from medical schools to specialist training.
No single strategy will address this problem; it will require a coordinated effort. Medical Deans is advocating for Australian and New Zealand governments to establish a taskforce comprising the key stakeholders responsible for designing and delivering medical education and training across all stages of the continuum to:
- co-develop future training models that target the priority areas of workforce need; and
- explore the possibility of a “flipped” model for community-based PGY1 and PGY2 doctors where the majority of their experience occurs in a community-based setting, rotating into hospitals for training as required.
IV. CONCLUSION
While the impact of the pandemic on medical education and training in 2020 was costly – both financially and personally – the scale of disruption provided a unique opportunity for step change. In many cases, the sudden and massive changes created strong potential for lasting improvement. In other areas, the pandemic highlighted cracks that already existed within the health sector (e.g. lack of clinical placements in community healthcare settings), which will require coordinated effort beyond the medical education sector to fix.
Medical Deans has incorporated and built on these key learnings with the development of a number of advocacy positions and documents. In addition to those reports already mentioned, the learning has informed the student support document Creating a culture of support – For medical students transitioning to practice (Medical Deans Australia and New Zealand, 2021c), as well as the Medical Deans’ submission to the consultation for the Australian Medical Council’s Review of the Accreditation Standards for Primary Medical Programs.
Medical schools are looking to capitalise on the resourcefulness and innovation of 2020 in all the ways highlighted in this article and the full report by Medical Deans. To fully realise this potential, they will need to work in partnership with all those involved: students, health services, prevocational training, specialist colleges, regulators, and governments.
Notes on Contributors
Mary Anne Reid developed the Medical Deans survey of members schools and collated its findings. She integrated these with elements of the presentations made at the 2020 Annual Conference, and other member discussions, to develop the structure and write the text.
Kirsty Forrest provided key editorial and supervisory input as the member of the Medical Deans Executive supporting the report.
Acknowledgement
The authors acknowledge the support of Helen Craig, Chief Executive Officer of Medical Deans, who came up with the idea for the report and provided guidance throughout.
Funding
There are no funding sources to declare.
Declaration of Interest
The authors declare that there is no conflict of interest related to this manuscript.
References
Australian Department of Health. (2019). National Medical Workforce Strategy Scoping Framework.
Medical Deans Australia and New Zealand. (2020). Guidance statement: Clinical practice core competencies for graduating medical students. Unpublished. Please contact Medical Deans to request a copy at admin@medicaldeans.org.au
Medical Deans Australia and New Zealand. (2021a, July). Changing for good: What we learned in 2020. https://medicaldeans.org.au/md/2021/07/Changing-for-Good-What-We-Learned-in-2020-Medical-Deans-report-July-2021.pdf
Medical Deans Australia and New Zealand. (2021b, September). Training tomorrow’s doctors – All pulling in the right direction. https://medicaldeans.org.au/resource/training-tomorrows-doctors-all-pulling-in-the-right-direction/
Medical Deans Australia and New Zealand. (2021c, October). Creating a culture of support – For medical students transitioning to practice.
New South Wales Health. (2021). Assistant in Medicine Evaluation Report.
https://www.health.nsw.gov.au/workforce/medical/Publications/aim-evaluation-report.pdf
*Mary Anne Reid
Medical Deans Australia and New Zealand,
19 Kent Street, Sydney, NSW 2000
Email: mreid@medicaldeans.org.au
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
