
Impact of intimate relationships on medical undergraduate performance and extracurricular activities
Submitted: 21 June 2024
Accepted: 18 November 2025
Published online: 7 April, TAPS 2026, 11(2), 32-39
https://doi.org/10.29060/TAPS.2026-11-2/OA3446
Prabodha De Silva1, Kavishan De Silva1, Supun Deshapriya1, Sachini Dewagiri1, Uthpali Dhammadinna1, Kasun Bandara Ekanayake2 & Amal Nishantha Vadysinghe2
1Faculty of Medicine, University of Peradeniya, Sri Lanka; 2Department of Forensic Medicine, Faculty of Medicine, University of Peradeniya, Sri Lanka
Abstract
Introduction: University students may be influenced by intimate relationships (IR) and extracurricular activities (EA), which can impact academic performance (AP). This study assessed the effects of IR and EA on the AP of medical undergraduates.
Methods: A cross-sectional study was conducted among 253 medical undergraduates at the University of Peradeniya, Sri Lanka. Data was collected using an online self-administered questionnaire. AP was evaluated using the cumulative grade point average (cGPA) from the previous semester.
Results: Of the 253 participants, 110 (43.5%) were involved in IR and 143 (56.5%) were single; 56.9% were female. Among participants in relationships, 44.5% had partners within the same faculty. There was no significant association between involving in an IR and AP (p=0.651), regardless of the other variables of IR. Most participants (51.8%) believed EA had no impact on AP, and analysis showed no significant association between EA and AP (p=0.394). Economic status of participants was positively associated with their AP (p=0.015). The prevalence of IPV in IR was 18.2% (7.9% of the total sample), with psychological type being the most prominent. Out of those in relationships, 18.2% reported experiencing IPV, of whom 75.0% were male and 25.0% were female, possibly due to underreporting by females. However, there was no significant association between experiencing IPV and AP (p=0.534).
Conclusions: Although involvement in IR and EA did not significantly affect AP, the presence of IPV highlights the need for targeted interventions. Males were more likely to report IPV than females, emphasising the importance of support programs.
Keywords: Academic Performance, Demographic Data, Intimate Relationships, Extracurricular Activities, Medical Education, Medical Undergraduates
Practice Highlights
- There was no significant association between academic performances and intimate relationships.
- Extracurricular activities didn’t show any impact on academic performances.
- No significant association was observed between intimate partner violence and academic performance.
- Males were more likely to experience intimate partner violence than females.
I. INTRODUCTION
Intimate relationships (IR) include, but are not limited to, heterosexual/homosexual romantic relationships. IR can have a significant impact on the university life of medical students. Medical undergraduates represent a unique population because their training requires them to fulfil high academic demands. Unlike many other undergraduate groups, medical students have limited time for leisure or personal life. These challenges make them particularly vulnerable to stressors arising from balancing IR with academic commitments.
Studies have shown that medical students in IR often experience higher levels of stress, anxiety, and depression than their single counterparts (Dyrbye et al., 2006). This is likely due to the demanding nature of medical school and the pressure to balance academic and personal responsibilities. Additionally, medical students in IR may have a harder time maintaining boundaries and achieving work-life balance. They may also have difficulty finding time for their relationship due to the demands of medical school and clinical rotations.
However, some studies suggest that healthy IRs shown to have a positive impact on students in healthcare professions (Avci et al., 2022). Being in a relationship can provide emotional support, which can be beneficial for coping with the stress of medical education. Additionally, having a partner can provide a sense of social support, which can help medical students feel less isolated and lonely. Despite the potential challenges, many medical students can successfully navigate IR while in medical school. Even so, to prevent the potential harmful impact of IRs, medical schools need to provide support and resources for students in relationships, such as counselling services and relationship awareness programs.
A Sri Lankan study found that 52% of the participants who were university students were engaged in romantic relationships (Gunawardena et al., 2012). Therefore, it’s crucial to understand how these relationships impact their university experience. The majority of studies regarding IRs were focused on violence towards intimate partners, and there was an overall lack of relevant literature when it came to the effects of IRs as general on academic performances (AP). Previous studies have identified vulnerabilities among university students, particularly young women, who are at increased risk of experiencing unwanted sexual attention (Forke et al., 2008) and unhealthy or stressful IRs (Hayden et al., 2016). These findings highlight the importance of further research into how such relational factors may influence AP. A study from the United States involving over 6800 female undergraduates revealed that there is an indirect link between physical and psychological intimate partner violence (IPV) and academic disengagement via depression symptoms (Schrag et al., 2020). Furthermore, American studies involving over 84,000 subjects found that undergraduates experiencing IPV were more likely to have increased academic difficulties (N. Brewer et al., 2018) as well as health impairments (N. Q. Brewer & Thomas, 2019).
These findings suggest that IPV and its consequences may be particularly relevant for medical students, who already face high academic stress. Therefore, exploring not only the general influence of IRs but also the potential academic impact of IPV is essential in understanding the relationship between students’ personal and academic lives. The University of Peradeniya, being one of the largest public universities in Sri Lanka, attracts students from diverse regions and socioeconomic backgrounds. Its academically rigorous environment provides a suitable context to study how interpersonal and extracurricular factors relate to AP. The objective of this study was to examine the association between involvement in IR, AP and extracurricular activities (EA) among the medical undergraduates of the University of Peradeniya, Sri Lanka.
II. METHODS
A descriptive cross-sectional study with an analytical component was conducted with the participation of 2018/19 (3rd year), 2019/20 (2nd year) and 2020/21 (2nd year) batches enrolled at the Faculty of Medicine, University of Peradeniya, Sri Lanka. The senior-most batches were excluded because they were engaged in clinical rotations at external hospitals, making it logistically difficult to ensure their participation. The sample size was calculated based on a total population of 707 students from the 2018/19, 2019/20, and 2020/21 batches. Using a conservative proportion (p=0.5), a 95% confidence level (z=1.96), and a 5% margin of error (e=0.05), the minimum required sample size was 249.
A self-administered questionnaire was newly developed to assess the study objectives. It included sections on demographic factors (age, gender, economic status), IR status, partner characteristics, AP, and EA. Items related to IPV assessed physical, psychological, and combined abuse using Yes/No questions. The questionnaire was pilot tested to ensure clarity and reliability. Economic status was self-reported by participants and categorised as less than 50,000 LKR (1 USD = 323 LKR at the time of data collection in August 2023), between 50,000–100,000 LKR and above 100,000 LKR. IR included romantic relationships, heterosexual or homosexual, in the duration of the last semester’s work. IPV types were specified as physical, mental or both. EA were defined as participation in university clubs, sports, arts or other organised student activities.
Data collected using the questionnaire, via Google Forms, was entered into a Microsoft Excel spreadsheet and analysed using IBM SPSS Statistics 26. Normality of the data collected was assessed, and non-parametric tests (Chi-square tests) were used accordingly. Microsoft Excel was used to calculate a cumulative Grade Point Average (cGPA) value for examination results up to the last semester, based on the university’s 0.000 to 4.000 grading scale. Before administering the questionnaire, written informed consent was obtained from each participant. The ethical approval for the study was obtained from the Ethics Review Committee (2023/EC/SP/38) of the Faculty of Medicine, University of Peradeniya, Sri Lanka.
III. RESULTS
Data was collected from 253 medical undergraduates enrolled in 2018/19, 2019/20 and 2020/21 batches of the Faculty of Medicine, University of Peradeniya, Sri Lanka.
A. Socio-Demographic Profile
The age of the sample ranged from 19 to 26 years, with a mean age of 23.2 years. The sample included 144 females (56.9%) while males accounted for 43.1% (n=109) respondents. Among the 3 batches considered, the 2018/19 batch had the highest number of responses, which amounted to 33.9% (n=86). Respondents from the 2020/21 batch amounted to 33.2% (n=84) while the 2019/20 batch had 32.8% (n=83) respondents. When considering the economic background of the family, 58 subjects (22.9%) represented the group earning less than 50,000 LKR per month, followed by 90 subjects (35.6%) earning 50,000-100,000 LKR per month and 105 subjects (41.5%) earning more than 100,000 LKR per month.
Out of 253 respondents, 110 respondents (43.5%) claimed that they were involved in IR during the last semester. Out of the females in the sample, 58 subjects (40.3%) were involved in an IR during the last semester. Among the 110 subjects who were involved in IR, 67 respondents (60.1%) had their partners in the same university, and 49 of them (44.5%) in the same medical faculty as the subjects. Only 43 (39.0%) claimed to have partners outside the university, including in other universities (34, 30.9%), another residential area (8, 7.2%) and in the health training sector (1, 0.9%).
B. Academic Performance
When the Shapiro-Wilk test was applied to the total sample of 253, the distribution of cGPA significantly deviated from a normal distribution (p<0.001). Therefore, the median (3.200) of the cGPA of respondents was used as a cut-point for assessing AP, differentiating between high-performing and low-performing, instead of the mean (3.065). More than half of the samples (58.1%) had a cGPA of 3.000 or more, while only 7.9% had a cGPA of less than 1.500.
Of the 110 respondents involved in IR, 57 (51.8%) scored lower than a cGPA of 3.200, while 73 (51.0%) of the respondents who were not involved in any IRs scored at or above a cGPA of 3.200 (Table 1). However, this finding was not statistically significant (p=0.651, OR=1.12, 95% CI: 0.68–1.84). The mean cGPA for respondents involved/not involved in IRs was calculated, and respondents who were in an IR had a mean cGPA of 3.05, in contrast to a mean cGPA of 3.08 of the respondents with no involvement in IRs.
|
Relationship Status |
Low performing (cGPA<3.200) |
High performing (cGPA>=3.200) |
Total |
|
Involved in IR |
57 (51.8%) |
53 (48.2%) |
110 |
|
Not involved in IR |
70 (49.0%) |
73 (51.0%) |
143 |
|
Total |
127 (50.2%) |
126 (49.8%) |
253 |
Table 1. Impact of IR on AP
Considering the 144 female respondents, 31 performed low in academics whilst being in a relationship, and 40 female students who weren’t involved in IRs performed relatively low in academics. Among high performing females, the majority (63.0%) were not involved in IRs during the last semester. In contrast, high-performing males were more evenly distributed, with 49.1% not in IRs and 50.9% involved in IRs (Table 2). However, the association of AP with gender and IR was not statistically significant (p=0.275; OR=1.45, 95% CI: 0.74–2.84). Economic status was also analysed in relation to AP, and a statistically significant positive association was observed (p=0.015), indicating that students from higher economic backgrounds were more likely to achieve higher cGPA scores.
|
Relationship Status |
Low performing (cGPA<3.200) |
High performing (cGPA>=3.200) |
Total |
||
|
Male |
Female |
Male |
Female |
||
|
Involved in IR |
24 (44.4%) |
31 (43.7%) |
28 (50.9%) |
27 (37.0%) |
110 |
|
Not involved in IR |
30 (55.6%) |
40 (56.3%) |
27 (49.1%) |
46 (63.0%) |
143 |
|
Total |
54 |
71 |
55 |
73 |
253 |
Table 2. AP according to gender and relationship status
Out of the 110 participants who were involved in an IR, the majority (63, 57.3%) of respondents believed it to have a positive impact on their AP, while 8 (7.3%) believed that it had negatively affected their AP and 39 subjects (35.5%) believed that there is no significant impact. Among the 110 respondents with an intimate partner, 54 (49.1%) stated that they do not miss any academic work in their coursework, and 49 (44.5%) respondents stated that they have missed academic work due to their relationship. There was no significant association between missing academic work and AP (p=0.226; OR=1.67, 95% CI: 0.76–3.64) (Table 3).
|
|
Academic Performance |
Total |
||
|
Low performing |
High performing |
|||
|
Have you ever missed a lecture/clinical appointment/practical/tutorial due to the relationship? |
No |
30 |
24 |
54 (49.1%) |
|
Yes, about 1-4 |
15 |
22 |
49 (44.5%) |
|
|
Yes, about 5-9 |
5 |
5 |
||
|
Yes, more than 10 |
1 |
1 |
||
|
Don’t know |
6 |
1 |
7 (6.3%) |
|
|
Total |
57 |
53 |
110 |
|
Table 3. Number of academic work sessions missed due to IR
C. Extracurricular Activities
Among the participants who were involved in IR, 58 (52.7%) had engaged in EA before the relationship started, and 65 (59.1%) were currently engaged in EA during the duration of the relationship. In the sample, 8 subjects (7.3%) stated that they have stopped EA due to the current IR. The subjects have claimed that 44 (40.0%) have a positive impact, 9 (8.2%) have a negative impact and no impact on 57 (51.8%) from IR on EA.
Among the 65 respondents involved in both IR and EA, 25.5% were academically performing better while being engaged in EA, whereas 33.6% were performing lower academically while being engaged in EA (Table 4). There was no significant impact between participating in EA and AP (p=0.394; OR=0.61, 95% CI: 0.28–1.30).
|
Participated in extracurricular activities |
Academic Performance |
Total |
|
|
Low performing |
High performing |
||
|
No |
20 (18.2%) |
25 (22.7%) |
45 (40.9%) |
|
Yes |
37 (33.6%) |
28 (25.5%) |
65 (59.1%) |
|
Total |
57 (51.8%) |
53 (48.2%) |
110 |
Table 4. Impact of EA on AP
D. Intimate Partner Violence
Out of the 110 respondents who were involved in relationships, 20 subjects (18.2%) had experienced some form of IPV, which included 15 males (75.0% of IPV victims) and 5 females (25.0% of IPV victims) (Table 5). This was 7.9% of the original sample of 253 students. Among the 20 victims of IPV, mental IPV was the most prevalent single type, with 15 respondents (75.0%) being victims. Only 2 respondents (10.0%) stated that they had experienced physical IPV, while 3 respondents (15.0%) had experienced both physical and mental IPV. Out of the 20 respondents who experienced IPV, 8 (40.0%) were high performers. There was no statistically significant association between IPV and AP (p=0.534, OR=0.54, 95% CI: 0.17–1.77). These findings, particularly the higher proportion of male IPV victims, should be interpreted with caution and reported sensitively, as they challenge common gender-related assumptions about IPV.
|
Have you ever experienced IPV within your relationship? |
Frequency |
Total |
|
|
Male |
Female |
||
|
Yes |
15 (13.6%) |
5 (4.5%) |
20 (18.2%) |
|
No |
37 (33.6%) |
53 (48.2%) |
90 (81.8%) |
|
Total |
52 (47.3%) |
58 (52.7%) |
110 |
Table 5. Incidence of IPV in IR
A summary of the main analyses is shown in Appendix 1.
IV. DISCUSSION
The current study compares AP and EA of Sri Lankan medical undergraduates involved in IR. Compared with previous studies in South Asia, the mean age and gender distribution of this cohort were generally consistent, with a majority of female students, aligning with regional trends (Nawaz, Hussain, Sarwar, Afzal, & Gilani, 2018; Rashid, Hassan, Bhat, & Bhat, 2021; Wijekoon et al., 2017). Socioeconomic distribution was also comparable, with over 40% of participants coming from families with urban-level income (Department of Census and Statistics, 2022).
Only 43.5% of respondents reported being in a relationship during the previous semester, slightly lower than reported in some university studies internationally (McLaughlin, 2015). Regarding EA, no significant association with AP was found, consistent with findings from a Nigerian study (Umar et al., 2010). EA encompasses a broad spectrum of activities, and its impact may vary: sports may enhance time management and stress reduction, whereas social engagements may aid networking but reduce study time. In the present study, most participants believed that EA did not influence their AP, suggesting that either their engagement in a level that does not affect AP or that medical students can maintain AP regardless of EA involvement in EA. While no significant association was found between involvement in IR and AP, relationships can provide emotional support and stress relief, which may benefit AP and EA (Avci et al., 2022).
Mental IPV was the most prevalent type among those reporting any IPV (75.0% of IPV victims; 7.9% of the total sample), which is lower than figures reported in studies from the USA and Iraq (Al-Atrushi et al., 2013; Wood et al., 2020). Interestingly, the majority of IPV victims in this study were male, which contrasts with common assumptions and previous research where females are often reported as the primary victims. This finding should be interpreted with caution, as cultural and social factors may contribute to underreporting among females due to stigma, fear, or social desirability bias. Conversely, male victims may feel more comfortable reporting IPV in anonymous surveys. No significant association was found between IPV and AP, possibly because medical undergraduates are relatively homogenous regarding age, academic motivation, and coping strategies (Kötter et al., 2017). Cultural and methodological differences likely account for discrepancies in IPV prevalence across studies.
When comparing the findings of this study with previous studies, contextual and methodological differences may have accounted for observed discrepancies. As an example, the prevalence of IPV in this sample was lower than that of studies in the USA and Iraq (Al-Atrushi et al., 2013; Wood et al., 2020) which may reflect differences in cultural norms regarding reporting and social acceptability. Furthermore, the cited studies often included larger or more heterogeneous student populations, including non-medical undergraduates, limiting the variability in academic outcomes and relationship experiences.
A Scottish study found that their female participants performed better academically than males (Lumsden et al., 2005). The same finding was reported in single studies from Sri Lanka, Germany, Turkey, Scotland and Saudi Arabia (Dayioğlu & Türüt-Aşik, 2007; De Silva et al., 2004; De Silva et al., 2006; Haidinger et al., 2005). There was no significant association between one’s gender and their AP within this study. This may be due to selection bias inherent in medical school admissions, as students are already filtered through competitive examinations and represent a relatively homogenous group of high achievers. Additionally, coping strategies and time management skills may be well-developed in both male and female medical students, further reducing gender-related variation in performance.
A. Limitations
This study evaluated heterosexual and homosexual romantic relationships but not the other types of interpersonal relationships, which may have different impacts on AP and EA. Although only current relationships during the previous semester were considered, the lasting effects of past relationships were not considered, which may have a long-term psychological impact on AP. This study excluded the two senior-most batches enrolled in the Faculty of Medicine, University of Peradeniya. Therefore, this study could not compare whether the gravity of the effect of IR had any difference between the most senior batches who could have more stable or long-term IRs and different levels of AP. This study also could not evaluate the level of involvement in EA in an objective manner using a proper grading system for various competitive levels. This limits the ability to detect associations between the level of commitment in EA and AP. Lack of validated techniques for the evaluation of the impact of IR on EA was one of the limitations faced in the study, which could have underestimated such impacts. The questionnaire used in this study was not formally validated, which may affect the reliability and generalisability of the responses. This study did not assess the participants’ English language proficiency, which could influence AP, since many undergraduates receive their pre-university education in their native language, and the transition to English can be a considerable challenge.
Additionally, the small subsample for IPV (n=20) may have underpowered the detection of associations between IPV and AP. Future studies could address these limitations by including all batches of students to capture variations in IR and AP, employing validated questionnaires to assess IPV, IR dynamics, and EA involvement.
V. CONCLUSION
This study highlights the importance of supporting the psychosocial well-being of medical undergraduates, particularly in relation to IR and IPV. Implementing counselling services, peer-support networks, and stress management programs can help students navigate IR-related challenges while maintaining AP. The findings also highlight the need for awareness and prevention strategies addressing IPV among young adults. Expanding similar research to other faculties and universities could support evidence-based interventions, contributing to a better understanding of how interpersonal relationships affect student well-being and academic success worldwide.
Notes on Contributors
Prabodha De Silva contributed to the conception and design of the work; the acquisition, analysis, and interpretation of data for the work; drafting the work and revising it critically for important intellectual content and approved the final manuscript submission.
Kavishan De Silva contributed to the conception and design of the work; the acquisition, analysis, and interpretation of data for the work; drafting the work and revising it critically for important intellectual content and approved the final manuscript submission.
Supun Deshapriya contributed to the conception and design of the work; the acquisition, analysis, interpretation of data for the work; drafting the work and revising it critically for important intellectual content and approved the final manuscript submission.
Sachini Dewagiri contributed to the conception and design of the work; the acquisition, analysis, interpretation of data for the work; drafting the work and revising it critically for important intellectual content and approved the final manuscript submission.
Uthpali Dhammadinna contributed to the conception and design of the work; the acquisition, analysis, interpretation of data for the work; drafting the work and revising it critically for important intellectual content and approved the final manuscript submission.
Kasun Bandara Ekanayake contributed to the conception and design of the work; the acquisition, analysis, interpretation of data for the work; drafting the work and revising it critically for important intellectual content and approved the final manuscript submission.
Amal Nishantha Vadysinghe contributed to the conception and design of the work; the acquisition, analysis, interpretation of data for the work; drafting the work and revising it critically for important intellectual content and approved the final manuscript submission.
Ethical Approval
All procedures performed in the study were in accordance with the ethical standards of the institution and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Before data collection, written informed consent was obtained from each participant. Ethical approval (2023/EC/SP/38) for this project was granted by the Ethics Review Committee, Faculty of Medicine, University of Peradeniya, Sri Lanka.
Data Availability
The data that supports the findings of this study are available from the corresponding author, ANV, upon reasonable request.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of Interest
The authors declare that they have no competing interests.
References
Al-Atrushi, H. H., Al-Tawil, N. G., Shabila, N. P., & Al-Hadithi, T. S. (2013). Intimate partner violence against women in the Erbil city of the Kurdistan region, Iraq. BMC Women’s Health, 13, 1-9. https://doi.org/10.1186/1472-6874-13-37
Avci, N., Gursoy, Z., & Murat, M. (2022). Violence responsibility, attitudes toward violence, and factors affecting violence: Examining the intimate relationships of university students. Journal of Psychiatric Nursing, 13(4), 352-362. https://doi.org/10.14744/phd.2022.11129
Brewer, N., Thomas, K. A., & Higdon, J. (2018). Intimate partner violence, health, sexuality, and academic performance among a national sample of undergraduates. Journal of American College Health, 66(7), 683-692. https://doi.org/10.1080/07448481.2018.1454929
Brewer, N. Q., & Thomas, K. A. (2019). Intimate partner violence and academic performance: The role of physical, mental, behavioral, and financial health. Social Work in Health Care, 58(9), 854-869. https://doi.org/10.1080/00981389.2019.1659905
Dayioğlu, M., & Türüt-Aşik, S. (2007). Gender differences in academic performance in a large public university in Turkey. Higher Education, 53, 255-277. https://doi.org/10.1007/s10734-005-2464-6
De Silva, N. R., Pathmeswaran, A., & De Silva, H. J. (2004). Selection of students for admission to a medical school in Sri Lanka. Ceylon Medical Journal, 49(3), 81-85. http://dx.doi.org/10.4038/cmj.v49i3.3245
De Silva, N. R., Pathmeswaran, A., De Silva, N., Edirisinghe, J. S., Kumarasiri, P. V. R., Parameswaran, S. V., . . . De Silva, H. J. (2006). Admission to medical schools in Sri Lanka: Predictive validity of selection criteria. Ceylon Medical Journal, 51(1), 17-21. https://doi.org/10.4038/cmj.v51i1.1371
Department of Census and Statistics. (2022). The household income and expenditure survey – 2019. Ministry of Economic Policies and Plan Implementation. http://www.statistics.gov.lk/Resource/en/IncomeAndExpenditure/HouseholdIncomeandExpenditureSurvey2019FinalResults.pdf
Dyrbye, L. N., Thomas, M. R., Huntington, J. L., Lawson, K. L., Novotny, P. J., Sloan, J. A., & Shanafelt, T. D. (2006). Personal life events and medical student burnout: A multicenter study. Academic Medicine, 81(4), 374-384. https://doi.org/10.1097/00001888-200604000-00010
Forke, C. M., Myers, R. K., Catallozzi, M., & Schwarz, D. F. (2008). Relationship violence among female and male college undergraduate students. Archives of Pediatrics & Adolescent Medicine, 162(7), 634-641. https://doi.org/10.1001/archpedi.162.7.634
Gunawardena, N., Weerasinghe, M., Rajapaksa, L., Wijesekara, P., & Chathurangana, P. W. P. (2012). Romance, sex and coercion: Insights into undergraduate relationships. Sri Lanka Journal of Psychiatry, 2(2). https://doi.org/10.4038/sljpsyc.v2i2.4042
Haidinger, G., Frischenschlager, O., & Mitterauer, L. (2005). Prediction of success in the first-year exam in the study of medicine – A prospective survey. Wiener Klinische Wochenschrift, 117, 827-832. https://doi.org/10.1007/s00508-005-0477-x
Hayden, K., Graham, M., & Lamaro, G. (2016). A cross-sectional study examining the extent of unwanted sexual attention and unhealthy intimate relationships among female university students. Health Promotion Journal of Australia, 27(2), 134-139. https://doi.org/10.1071/HE15113
Kötter, T., Wagner, J., Brüheim, L., & Voltmer, E. (2017). Perceived medical school stress of undergraduate medical students predicts academic performance: An observational study. BMC Medical Education, 17, 256. https://doi.org/10.1186/s12909-017-1091-0
Lumsden, M. A., Bore, M., Millar, K., Jack, R., & Powis, D. (2005). Assessment of personal qualities in relation to admission to medical school. Medical Education, 39(3), 258-265. https://doi.org/10.1111/j.1365-2929.2005.02087.x
McLaughlin, N. (2015). An analysis of the effect of relationship status on self-esteem and academic performance. Scholars: Journal of Undergraduate Research, 25. https://www.mckendree.edu/academics/scholars/mclaughlin-issue-25.pdf
Nawaz, K., Hussain, M., Sarwar, H., Afzal, M., & Gilani, S. A. (2018). Determine the factors influencing absenteeism among nursing students. Journal of Health, Medicine and Nursing, 50(7), 64-72.
Rashid, S., Hassan, A. U., Bhat, I. H., & Bhat, G. M. (2021). Analyzing the attitude of medical students toward class absenteeism. National Journal of Clinical Anatomy, 10(4), 226-231. https://doi.org/10.4103/NJCA.NJCA_52_20
Schrag, R. V., Wood, L., & Busch-Armendariz, N. (2020). Pathways from intimate partner violence to academic disengagement among women university students. Violence and Victims, 35(2), 227-245. http://dx.doi.org/10.1891/%20VV-D-18-00173
Umar, S. S., Shaib, I. O., Aituisi, D. N., Yakubu, N. A., & Bada, O. (2010). The effect of social factors on students’ academic performance in Nigerian tertiary institutions. Library Philosophy and Practice, 2010, 1-19. https://digitalcommons.unl.edu/cgi/viewcontent.cgi?article=1342&context=libphilprac
Wijekoon, C. N., Amaratunge, H., de Silva, Y., Senanayake, S., Jayawardane, P., & Senarath, U. (2017). Emotional intelligence and academic performance of medical undergraduates: A cross-sectional study in a selected university in Sri Lanka. BMC Medical Education, 17(1), 1-11. https://doi.org/10.1186/s12909-017-1018-9
Wood, L., Voth Schrag, R., & Busch-Armendariz, N. (2020). Mental health and academic impacts of intimate partner violence among IHE-attending women. Journal of American College Health, 68(3), 286-293. https://doi.org/10.1080/07448481.2018.1546710
*Amal Nishantha Vadysinghe
Department of Forensic Medicine,
Faculty of Medicine, University of Peradeniya,
Peradeniya, Sri Lanka
+94779117011
Email: amal_vadysinghe@yahoo.com
Submitted: 2 May 2025
Accepted: 8 September 2025
Published online: 7 April, TAPS 2026, 11(2), 89-101
https://doi.org/10.29060/TAPS.2026-11-2/OA3735
Ardo Sanjaya1,2, Ray Sebastian3, Kevin Gunawan3, Christian Edwin4, Nathanael Andry Mianto1 & Cindra Paskaria5
1Department of Anatomy, Faculty of Medicine, Maranatha Christian University, Indonesia; 2Maranatha Biomedical Research Laboratory, Faculty of Medicine, Maranatha Christian University, Indonesia; 3Undergraduate Program in Medicine, Faculty of Medicine, Maranatha Christian University, Indonesia; 4Medical Education Unit, Faculty of Medicine, Maranatha Christian University, Indonesia; 5Department of Public Health, Faculty of Medicine, Maranatha Christian University, Indonesia
Abstract
Introduction: Medical students often face psychological distress affecting their academic performance and well-being. While coping and resilience may buffer this stress, their roles in academic outcomes across different training stages are poorly understood. This study explored how distress, coping, resilience, and learning perception relate to academic performance across semesters.
Methods: A cross-sectional study of 677 pre-clinical medical students was conducted in 2024 across Semesters 1, 3, 5, and 7. Standardised instruments measured psychological distress, burnout, resilience, coping, and perceptions of the learning environment. Data were analysed using ANCOVA to compare constructs across semesters. Principal Component Analysis (PCA) and Structural Equation Modeling (SEM) assessed the direct and indirect pathways linking distress to Grade Point Average (GPA).
Results: Psychological distress and burnout increased during mid-training while resilience traits such as perseverance and help-seeking consistently decreased. Coping styles remained stable. PCA identified three latent constructs: distress, coping, and resilience. SEM revealed that distress negatively predicted GPA both directly (β = –0.186, p < .001) and indirectly via resilience (β = 0.052, p = .003). Coping was positively associated with resilience (β = 0.412, p < .001), but its effect on GPA was marginal. A multi-group SEM confirmed a consistent relationship across academic semesters.
Conclusion: Although the effects were small, psychological distress significantly influenced academic performance, partially mediated by resilience. While coping remained stable, resilience declined and did not recover, highlighting the need for support. Interventions to enhance coping may bolster resilience and improve academic outcomes.
Keywords: Medical Students, Resilience, Coping Strategies, Academic Performance, Psychological Distress
Practice Highlights
- Distress and resilience vary by semester, supporting tailored interventions in medical training.
- Psychological factors weakly predict GPA; wellness should target broader student outcomes.
- Adaptive coping links to greater resilience, underscoring its role in early medical training.
- Early-semester students report more distress, marking a window for mental health support.
- Structural modeling reveals psychological pathways for targeted interventions in education.
I. INTRODUCTION
The medical profession demands lifelong learning and commitment to high standards of care, requiring academic proficiency and a strong foundation of psychological well-being, resilience, and work-life balance (Braquehais & Vargas-Cáceres, 2023; Fares et al., 2016). However, increasing pressures within medical education have led to a mismatch between academic and clinical expectations with available personal resources, placing these students at risk for stress and burnout (Shanafelt, 2021; Siddiqui & Malik, 2019). These challenges are compounded by an often competitive and high-pressure environment that lacks adequate support (Almansour et al., 2024; Kassab et al., 2024; Wasson et al., 2016). Research has shown that the early years are often marked by adjustment difficulties, which heighten stress levels. Reports indicate that the prevalence of stress in medical students ranges from 20.9% to 90%, with burnout affecting up to 75% (Fares et al., 2016). Some students cope through constructive mechanisms like time management, help-seeking, and emotional regulation (van der Merwe et al., 2020), while others turn to avoidance, denial, or emotional withdrawal (Neufeld & Malin, 2021).
Stress and burnout are two related constructs that originated from distinct sources. Stress arises from outside demands exceeding personal resources, while burnout is typically defined as a prolonged response to chronic stress, manifesting as emotional exhaustion and depersonalisation (Bayram Deger, 2024; Dyrbye et al., 2008). Both are influenced by external factors such as academic load, social expectations, and institutional support, as well as internal factors like coping styles and resilience (Dyrbye et al., 2009; Findyartini et al., 2021). According to Lazarus and Folkman’s transactional stress model, individuals experience stress when their perceived demands outweigh their coping resources (Ben-Zur, 2019; Folkman, 2013). Coping mechanisms are broadly categorised into problem-focused, emotion-focused, and avoidant coping. Adaptive coping using problem-focused and emotion-focused strategies is associated with better academic and mental health outcomes (O. Ogoma, 2020; Simons et al., 1999), while avoidant or maladaptive forms of emotion-focused coping are linked to increased distress, poorer performance, and higher dropout risk (Abreu Alves et al., 2022; Ding et al., 2021; Holahan et al., 2005). Resilience, the capacity to recover from adversity, is a protective buffer against stress and burnout. It encompasses traits like perseverance, optimism, and help-seeking behavior (Lin et al., 2019). Resilience is dynamic, and changes are made in response to stressors and interventions (Wang et al., 2022). Programmes that incorporate cognitive, behavioral, and mindfulness strategies have demonstrated success in bolstering resilience and adaptive coping in medical students (Liu & Cao, 2022; Nguyen et al., 2023).
Although stress, coping, and resilience have been widely studied among medical students, most research has focused on these constructs independently and within a single academic stage. Few have examined how these psychological factors evolve across different phases of training or how they interact to influence academic performance. To address this gap, the present study compares levels of psychological distress, coping styles, resilience, and learning perceptions across semesters. Additionally, it integrates these constructs into a structural framework to explore their direct and indirect effects on academic performance, aiming to identify periods and mechanisms for intervention.
II. METHODS
This was a cross-sectional, single-center study involving medical students enrolled in four academic semesters (1, 3, 5, and 7), representing the pre-clinical years, conducted in 2024. The target population comprised 1,012 students, all invited to participate in an on-site survey administered via the SurveyMonkey platform using their electronic devices. 862 students responded, yielding an 85.2% response rate, with 726 students completing the survey. Students who had retaken any semesters were excluded from subsequent analyses to minimise potential confounding effects. Following these exclusions, the final sample consisted of 677 participants.
A. Instruments & GPA Calculations
This study initially gathered data using a set of standardised, validated instruments translated into Indonesian. The full details regarding the instruments and GPA calculations can be found in Appendix 1.
B. Demographics
Descriptive statistics were used to summarise the demographic and contextual characteristics of the participants across the four academic levels. Continuous variables were assessed for normality and were described using either means and standard deviations or medians with interquartile ranges. Categorical variables were reported as frequencies and percentages.
C. Analysis of Covariance
A series of ANCOVA models were conducted to examine differences in psychological and academic variables across semesters, using validated instrument scores as dependent variables (Appendix 1). Assumptions were checked prior to analysis. Minor non-normality was accepted, but models with robust standard errors were used when heteroscedasticity was detected.
Bivariate analyses identified significant demographic and lifestyle covariates, which were included in the models. For significant ANCOVA results, pairwise comparisons with Holm’s correction were performed. Analyses and visualisations were conducted in Python (v3.10.15) using seaborn (v0.13.2) and statsmodels (v0.14.4).
D. Structural Equation Modeling Analysis
A two-step approach was used to develop the Structural Equation Model (SEM). First, Principal Component Analysis (PCA) was performed on nine normalised psychological variables to address conceptual overlap and identify latent components. Variables were grouped, and composite scores were calculated by averaging items within each component for use in the SEM as observed variables.
The SEM tested the hypothesised relationships between psychological stress, coping, resilience, and learning environment perception, with GPA as the primary outcome. The model was guided by theories suggesting that stress negatively impacts academic outcomes (Almarzouki, 2024) and that this effect may be buffered through adaptive responses and psychological resources (Masten, 2001). The models were estimated using maximum likelihood (ML) estimation with bootstrapping (1,000 draws) and evaluated using multiple fit indices. A multi-group SEM was also conducted by semester to assess whether these relationships varied across academic stages. Constrained and unconstrained models were compared using a chi-square difference test. Analyses were conducted in R (v4.4.2) using the lavaan package (v0.6-19) for SEM and psych (v2.4.6.26) for PCA.
III. RESULTS
677 medical students were included in the final analysis. The demographic characteristics of the sample are summarised in Table 1. The majority of the participants are females (71.2%), and a considerable proportion (15.95%) reported having received formal mental health diagnoses. Daily routines such as average sleep duration and social media usage remained relatively stable across groups. However, some variability was observed in study-related behaviors. Similarly, involvement in extracurricular activities was more common among students in semesters 3 and 5, with participation rates exceeding 47% and 50%, respectively, reflecting higher engagement. A series of ANCOVAs were conducted to examine the influence of semester progression, and the full results are available on Figshare.
|
Semesters |
|||||
|
|
|
1 |
3 |
5 |
7 |
|
Age (years) |
17.85 ± 0.63 |
19.00 (0) |
20.00 (0) |
21.00 (0) |
|
|
Average Sleep Time per Day (Hours) |
5.00 (2) |
5.00 (1) |
5.00 (1) |
5.00 (1) |
|
|
Average Social Media Time per Day (Hours) |
3.00 (3) |
4.00 (3) |
4.00 (2) |
4.00 (3) |
|
|
Average Study Time per Day (Hours) |
3.00 (2.75) |
4.00 (5.75) |
3.00 (3) |
3.00 (2) |
|
|
Alcohol Consumptiona |
Yes |
4 (2.9%) |
11 (6.36%) |
5 (2.72%) |
15 (8.29%) |
|
No |
134 (97.1%) |
162 (93.64%) |
179 (97.28%) |
166 (91.71%) |
|
|
Chronic Diseases |
Yes |
5 (3.62%) |
4 (2.3%) |
10 (5.43%) |
9 (4.97%) |
|
No |
133 (96.38%) |
170 (97.7%) |
174 (94.57%) |
172 (95.03%) |
|
|
Gender |
Male |
37 (26.81%) |
52 (29.89%) |
50 (27.17%) |
56 (30.94%) |
|
Female |
101 (73.19%) |
122 (70.11%) |
134 (72.83%) |
125 (69.06%) |
|
|
Mental Health Diagnosis |
Yes |
19 (13.77%) |
33 (18.86%) |
34 (18.48%) |
23 (12.71%) |
|
No |
119 (86.23%) |
142 (81.14%) |
150 (81.52%) |
158 (87.29%) |
|
|
Extracurricular Activities |
Yes |
33 (23.91%) |
82 (47.13%) |
92 (50.0%) |
80 (44.2%) |
|
No |
105 (76.09%) |
92 (52.87%) |
92 (50.0%) |
101 (55.8%) |
|
|
Smoking |
Yes |
2 (1.45%) |
9 (5.17%) |
16 (8.7%) |
18 (9.94%) |
|
No |
136 (98.55%) |
165 (94.83%) |
168 (91.3%) |
163 (90.06%) |
|
|
Tuition Source |
Scholarship / Grants |
2 (1.45%) |
3 (1.72%) |
2 (1.09%) |
4 (2.21%) |
|
Parents / Family Members |
135 (97.83%) |
169 (97.13%) |
182 (98.91%) |
176 (97.24%) |
|
|
|
Others |
1 (0.72%) |
2 (1.14%) |
0 (0.0%) |
1 (0.55%) |
Table 1. Demographic Characteristics of the Research Participants
A. Psychological Distress and Burnout are Affected by Academic Progression
Semester progression had a significant effect on DASS-21 scores (F [3, 663] = 8.35, p < .001, η² = .036). Post-hoc comparisons (Figure 1) revealed that students in Semester 1 reported significantly lower distress compared to those in Semester 3 (adjusted mean difference = –0.27, 95% CI [–0.43, –0.11], p = .006) and Semester 5 ( –0.26, 95% CI [–0.42, –0.09], p = .010), suggesting a rise in psychological burden as students progressed. However, distress levels declined by Semester 7, possibly reflecting increased adaptation and adjustment over time. Mental health diagnosis was an even stronger predictor (p < .001, η² = .057), followed by gender (p < .001, η² = .043) and average sleep and social media time. The full post hoc results are available on Figshare.
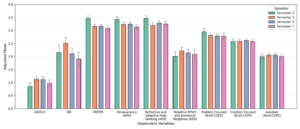
Figure 1. Adjusted Mean Scores of Measured Variables Across Academic Semesters
Barplot displays adjusted means from ANCOVA analyses across four academic stages (Semesters 1, 3, 5, and 7) after adjustment for relevant covariates. Variables include psychological distress (DASS-21), school burnout (SBI), educational environment perception (DREEM), resilience traits (ARS-24), and coping strategies (Brief-COPE). Note that students in Semester 1 showed the most favorable characteristics, with lower distress and burnout and higher DREEM and positive resilience traits. In the middle of their training (particularly Semester 3), students were characterised by high distress, burnout, and low positive resilience traits. Error bars denote the 95% confidence intervals.
Student progression also influenced School Burnout Inventory scores (F [3, 663] = 5.33, p = .001, η² = .024). Post-hoc comparisons revealed that Semester 3 students reported the highest levels of burnout, with greater scores than those in Semester 7 (0.60, 95% CI [0.24, 0.96], p = .006) and a marginally significant difference than those in Semester 5 (0.40, 95% CI [0.08, 0.72], p = .075). These findings suggest a pattern of increased stress during the early-to-mid stages of medical training, which appears to taper off in later semesters. Like DASS-21, students with a mental health diagnosis and more time on social media reported higher burnout (p = .009, η² = .010 and p < .001, η² = .024, respectively).
B. Academic Progression and Lifestyle Factors Influenced Students’ Perception of the Learning Environment
DREEM scores differed significantly by semester (F [3, 663] = 14.53, p < .001, η² = .062) and represent one of the strongest effects observed in this study. These suggest that students’ perceptions are influenced by their stage of training. Post-hoc comparisons revealed that students in Semester 1 reported significantly higher DREEM scores compared to those in Semester 3 (0.31, 95% CI [0.20, 0.43]), Semester 5 (0.30, 95% CI [0.18, 0.42]), and Semester 7 (0.38, 95% CI [0.25, 0.51]). All pairwise comparisons were statistically significant at p < .001. These consistent declines in the perceived learning environment across semesters may reflect growing academic pressures and a gradual expectation shift, although we did not explore these potential causes. DREEM scores were also significantly influenced by chronic illness, sleep duration, daily social media use, and time spent studying (p < .05 for all), suggesting that these factors influence students’ perceptions of the learning environment.
C. Resilience Evolves with Academic Progression, while Coping Styles Remain Stable
Perseverance and Adaptive Help-Seeking differed significantly across semesters (F [3, 663] = 6.09, p < .001, η² = .027 and F [3, 663] = 6.92, p < .001, η² = .030, respectively). Post-hoc analysis revealed a consistent decline from Semester 1 compared to Semester 3 (0.20, 95% CI [0.07, 0.33], p = .013), Semester 5 (0.19, 95% CI [0.06, 0.31], p = .013), and Semester 7 (0.30, 95% CI [0.17, 0.44], p < .001). A similar pattern was observed for Adaptive Help-Seeking, with statistically significant declines in Semester 3 (0.27, 95% CI [0.13, 0.41], p = .002) and Semester 7 (0.22, 95% CI [0.07, 0.37], p = .023), and a marginally significant decline in Semester 5 (0.17, 95% CI [0.03, 0.32], p = .069). These findings suggest that these two resilience traits diminish as students progress through medical school, potentially due to academic fatigue or limited support. Both traits were associated with longer average study time (p < .001, η² = .025 and p < .001, η² = .022, respectively), reflecting a bi-directional relationship between them. In contrast, Negative Affect and Emotional Response did not differ significantly by semester (F [3, 663] = 2.21, p = .086, η² = .010). However, it was strongly associated with a history of mental health diagnosis (p < .001) and greater social media use (p < .001, η² = .026). These findings suggest that positive resilience traits like perseverance and help-seeking change dynamically with academic progression and reflect greater study effort. In contrast, negative emotional responses may reflect underlying mental health challenges and lifestyle factors.
Problem-focused, emotion-focused, and avoidant coping demonstrated non-significant effects during the semester. However, avoidant coping was significantly more prevalent among students with a history of mental health diagnosis (p < .001, η² = .038). The influence may be bidirectional as avoidant coping may exacerbate psychological distress, and vice versa. (Holahan et al., 2005) Additional factors such as chronic illness (p = .018), alcohol consumption (p = .004), and gender (p = .001) also showed small but statistically significant associations with avoidant coping. These findings suggest that coping styles are likely shaped more by individual characteristics and previous experiences than by semester progression.
D. Principal Component Analysis (PCA) Identified Distress, Coping, and Resilience as Latent Constructs
A PCA was conducted on the nine standardised variables to address conceptual overlap among psychological variables and improve model stability. Several prerequisites were tested, indicating that the data were suitable for subsequent PCA (Kaiser-Meyer-Olkin test = 0.77; Bartlett’s test of sphericity = p < .001). As shown in Figure 2A, the scree plot supports a three-component solution, which explains approximately 74.3% of the total variance. The component matrix (Figure 2B) showed the pattern of loadings. We interpret component 1 (RC1) as Distress with strong loadings from DASS-21, SBI, avoidant coping, and negative affect. Component 2 (RC2) was interpreted as Coping, haracterized by loadings from problem-focused and emotion-focused coping strategies. Lastly, Component 3 (RC3) was interpreted as Resilience with loadings from perseverance, adaptive help-seeking, and DREEM. Model fit was adequate, with a root mean square residual (RMSR) of 0.065 and an off-diagonal values fit of 0.969.
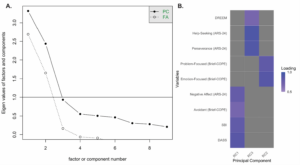 A. Scree plot showing eigenvalues from principal component analysis across component numbers. Note that the inflection point supports a three-component solution.
A. Scree plot showing eigenvalues from principal component analysis across component numbers. Note that the inflection point supports a three-component solution.
B. Heatmap of loadings for the three retained principal components. Component 1 (RC1) has strong loadings from DASS-21, SBI, avoidant coping, and negative affect. Component 2 (RC2) has loadings from emotion- and problem-focused coping. Component 3 (RC3) includes loading from perseverance, adaptive help-seeking resilience traits, and DREEM. Loadings below 0.5 are not shown
Figure 2. Dimensional Reduction Using Principal Component Analysis for the Measured Variables
E. Direct and Indirect Pathways Linked Distress to Academic Performance
A structural equation model (SEM) was tested to examine distress’s direct and indirect effects on GPA, with coping and resilience mediating variables (Table 2). The model was just-identified, and global fit indices indicated perfect fit (CFI = 1.000, TLI = 1.000, RMSEA = 0.000). Our interpretation centers on the theoretical basis and the significance of the individual path estimates. Figure 3 shows that distress significantly negatively affected resilience (β = –0.34, p < .001) and weakly positively affected coping (β = 0.08, p = .045). Coping was positively associated with resilience (β = 0.41, p < .001), suggesting that students using more adaptive coping reported higher resilience. Distress also negatively predicted GPA (β = –0.19, p < .001), while resilience (β = –0.15, p = .002) and coping (β = 0.18, p < .001) were also associated with GPA. Mediation analysis revealed a significant indirect effect of distress on GPA via resilience (β = 0.05, p = .003), while the path through coping was not significant (β = 0.02, p = .069). The total indirect effect was significant (β = 0.06, p < .001), supporting the role of coping and resilience as partial mediators. Note that indirect paths are not shown in Figure 3.
|
Paths |
Std. Estimate |
95% CI |
p-value |
|
Direct Effects |
|||
|
Distress → Coping |
0.084 |
[0.00, 0.16] |
0.045 |
|
Distress → Resilience |
-0.341 |
[-0.40, -0.28] |
< .001 |
|
Distress → GPA |
-0.186 |
[-0.21, -0.08] |
< .001 |
|
Coping → Resilience |
0.412 |
[0.34, 0.49] |
< .001 |
|
Coping → GPA |
0.182 |
[0.08, 0.21] |
< .001 |
|
Resilience → GPA |
-0.153 |
[-0.20, -0.04] |
0.002 |
|
Indirect Effects |
|||
|
Distress → Coping → GPA |
0.015 |
[0.00, 0.03] |
0.069 |
|
Distress → Resilience → GPA |
0.052 |
[0.01, 0.07] |
0.003 |
|
Distress → Coping → Resilience → GPA |
-0.005 |
[-0.01, -0.00] |
0.11 |
|
Total Indirect |
0.062 |
[0.02, 0.08] |
< .001 |
Table 2. Direct and Indirect Effects from the Structural Equation Modeling Analysis
The model explains 0.7% of coping, 26.3% of resilience, and 4.7% of GPA variance. While distress and coping predict resilience, they explain little of academic performance and coping, suggesting other factors remain unmeasured and warrant further exploration.
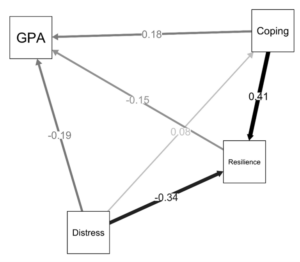
Figure 3. Structural Equation Model Demonstrating the Relationships Between Distress, Coping, Resilience and Academic Performance
Standardised path coefficients are displayed along each arrow. GPA represents academic performance. Distress negatively predicted both resilience (β = -0.34) and GPA (β = -0.19) and had a small positive effect on coping (β = 0.08). Coping was positively associated with resilience (β = 0.41) and GPA (β = 0.18), while resilience negatively predicted GPA (β = -0.15). Arrow thickness reflects the strength of the relationship. All coefficients shown are statistically significant (p < .05). GPA = grade point average. Note that indirect effects are not shown.
F. Psychological Influences on Academic Performance are Stable Across Semesters
A multi-group SEM was conducted using semester as the grouping variable to examine whether the structural relationships in the SEM differed across academic stages. A constrained model was compared to an unconstrained model. This approach allowed us to compare whether the groups’ structural pathways were statistically similar. The chi-square difference test revealed no statistically significant difference between the two models, χ² (18) = 26.75, p = .084. We can conclude that the relationships between psychological predictors and academic performance remained relatively stable throughout the different stages of medical training.
IV. DISCUSSION
This study explored the relationship between psychological distress, coping, resilience, and academic performance among medical students, as well as how these constructs evolved across different stages of training using a pseudo-longitudinal approach. To examine temporal trends, we conducted ANCOVA to compare key variables across academic semesters. We then applied PCA to identify underlying latent constructs, followed by SEM to assess these psychosocial factors’ direct and indirect effects on academic performance. While our findings provide insights into the psychological well-being of medical students, the cross-sectional nature of this study limits our ability to draw causal relationships among distress, coping, resilience, and academic performance.
ANCOVA revealed that psychological distress (DASS-21) and burnout (SBI) varied by semester, following a U-shaped pattern. Distress was lowest in Semester 1, peaked in Semesters 3 and 5, then subsided by Semester 7, reflecting mid‐phase stress during the shift from basic sciences to complex integrated human systems, consistent with prior reports of heightened stress at major curricular transitions (Boni et al., 2018; Hansell et al., 2019; Prendergast et al., 2024; Voltmer et al., 2021). Our results reinforce the importance of implementing preventive mental health measures early in the curriculum to support students during this transition.
Positive resilience traits, including perseverance and help-seeking, declined across semesters and did not recover by Semester 7, unlike distress and burnout. This suggests a lasting impact, likely due to early academic stress. Resilience is known to be dynamic and sensitive to environmental stressors (Köhne et al., 2023; Ollis et al., 2022; Thompson et al., 2016). Wang et al. (2022) longitudinal analysis identified a bidirectional relationship between resilience and burnout, showing that high burnout can degrade resilience over time and vice versa. Our findings support the idea that early distress may weaken resilience, though causality cannot be confirmed due to the study’s cross-sectional design. Perceptions of the learning environment declined steadily across semesters, with Semester 1 students reporting the most positive views. This may reflect rising stress or disillusionment. Prior studies link poor learning climate to burnout, lower academic performance, and reduced quality of life (Edgerton & McKechnie, 2023; Esquerda et al., 2024; Shahzad & Wajid, 2024), highlighting the need for targeted support strategies.
Unlike resilience, coping styles remained stable throughout the semester, supporting their view as enduring personality traits (Kardum & Krapić, 2001). However, avoidant coping was more common in students with mental health diagnoses, chronic illness, or alcohol use, supporting earlier findings linking avoidant strategies with poor psychological outcomes (Thompson et al., 2016; Villasana et al., 2016; Wang et al., 2022). These associations suggest that although coping styles are stable, they may become independent risk factors over time. Since resilience is environmentally influenced and were shown to be modifiable (Rosas-Santiago, 2019), targeting maladaptive coping early may be a viable preventive action. Identifying avoidant patterns and offering structured interventions, especially during curricular transitions, could support well-being, resilience, and academic success.
We employed PCA to combine the nine variables to reduce redundancy and increase stability. PCA analysis identified three main components that explained 74.3% of the total variance. The three interpretable components are distress, coping, and resilience. The conceptual grouping is grounded in established theoretical frameworks and supported by statistical analysis. The distress component, comprising psychological distress, burnout, negative affect, and avoidant coping, captures a multidimensional construct of distress as interactions between demands and coping resources, aligning with Lazarus and Folkman’s transactional model (Folkman, 2013). Avoidant coping and negative affect were factors affecting and causing distress (Holahan et al., 2005; Kardum & Krapić, 2001; Thompson et al., 2016), reinforcing their role as core components.
The resilience component, perseverance, adaptive help-seeking, and perceptions of the learning environment reflect resilience as a positive resource that interacts with students’ perceptions within their learning environment. This aligns with models that conceptualise resilience not as a fixed trait but as a dynamic construct shaped by both the individual and the social and environmental context they are currently in (Béné et al., 2016; Waxman et al., 1997). The coping component, emotion-focused and problem-focused strategies, captures the adaptive behavioral and cognitive responses to stress (Kardum & Krapić, 2001; Thompson et al., 2016). This contrasts with avoidant coping, which was viewed as maladaptive and had a higher association with distress (Holahan et al., 2005). According to Lazarus and Folkman’s model, these strategies serve as the primary means through which individuals attempt to manage stress and maintain psychological equilibrium (Folkman, 2013). The constructs we defined were statistically distinct and theoretically sound, supporting their use as latent constructs in subsequent SEM analysis.
Structural equation modeling supported the framework linking distress, coping, and resilience to academic performance. In line with Lazarus and Folkman’s model (Folkman, 2013), distress negatively affected GPA directly and indirectly via reduced resilience. This highlights how psychological burden can impair concentration and motivation (Almarzouki, 2024). The model confirmed resilience as a buffer that mitigates distress’s impact on performance, aligning with studies showing its protective role against burnout and stress both in academic and work contexts (de la Fuente et al., 2021; Herrero & Díaz, 2025, 2025; Zhang et al., 2024, 2024; Zhu et al., 2024, 2024). While coping had a marginal indirect effect, its strong link to resilience suggests that enhancing adaptive coping may improve both resilience and academic outcomes. Promoting effective coping as an intervention target may boost resilience and, in turn, academic performance.
An unexpected finding of this study was that resilience negatively predicted GPA, a result that contrasts with the literature suggesting resilience supports academic success (Calo et al., 2019, 2024; Ho & Kwek, 2022; Jumat et al., 2020; Sanjaya et al., 2024). Possible explanations include measurement artifacts due to how resilience was defined and its overlap with burnout, and reference bias in self‐ratings. West et al. showed that students in demanding environments judge non‐cognitive traits like grit using their peers as standards, which can obscure their relationship with GPA (West et al., 2016). Future studies should account for this bias by using methods like external observer ratings or vignettes to improve measurement validity.
Although most SEM effect sizes were small, they were significant and consistent with prior research linking distress, resilience, and coping to student well-being and performance. Small effects, when sustained or combined with other stressors, can undermine engagement and outcomes. This highlights the need for early psychological interventions to prevent cumulative impacts throughout medical school. Given the fluctuating mean levels across semesters, we conducted a multi-group SEM using semester as the grouping variable to test whether relationships among distress, coping, resilience, and performance varied across training stages. The non-significant chi-square difference indicates stable structural pathways, suggesting that interventions targeting coping and resilience may be effective across all semesters.
This study helps us understand how distress, coping, and resilience relate to academic performance throughout medical school. One of its strengths is its local setting in Indonesia, offering insight into how unique factors in Southeast Asia, like education systems, cultural expectations, and health care environments, shape students’ mental health and academic experience. These findings add to the limited research from the Asia-Pacific region and point to the need for tailored support and policies.
There are some limitations to this study. Other important factors that could affect stress and performance were not measured. Students’ sense of belonging, which recent studies have shown plays a key role in helping students stay engaged, avoid burnout, and do well academically, was not measured (Aker & Şahin, 2022; Leep Hunderfund et al., 2025). Similarly, impostor syndrome, which affects up to half of medical students (Sotiropoulos, 2021; Villwock et al., 2016) and is linked to burnout, low self-esteem, and poorer academic outcomes (Diaconescu et al., 2024; Faizan Siddiqui & Azaroual, 2024; Villwock et al., 2016), was not assessed. The absence of these constructs may account for unexplained variance in our models and represents important directions for future research.
Additionally, while the tuition source was collected, it was not analysed as a proxy for socio-economic status, and we acknowledge that it may not fully reflect students’ financial circumstances. This is a notable limitation, as socioeconomic status has been consistently linked to academic success (Tan, 2024). Future studies should incorporate measurements, such as parental income or education.
Other limitations regarding the study design are also acknowledged. First, the cross-sectional design of our study prevents causal inferences regarding the relationships among distress, coping, resilience, and academic performance. Although we used a pseudo-longitudinal approach by comparing semester groups, longitudinal data would be needed to confirm how these constructs evolve over time. Second, reliance on self-reported measures introduces potential bias, such as recall and social desirability. Psychological and behavioural data, including alcohol, smoking, and mental health history, were self-reported, which may lead to underreporting, especially among those with higher use (Davis et al., 2010). Future studies should consider objective or multi-source reporting. Third, although PCA and SEM reduced redundancy and improved model stability, they may oversimplify complex psychological constructs. The relatively low explained variance in GPA also suggests other key predictors were not captured. Finally, as this was a single-institution study, generalisability is limited. Future research should adopt a multi-center, longitudinal design to improve validity and capture differences across educational and cultural contexts in the Asia-Pacific region.
V. CONCLUSION
This study presents a robust, theory-driven model that directly and indirectly defines how distress impacts GPA through coping and resilience. Notably, resilience declined over time and did not recover to baseline, even without high psychological stress and burnout, while coping styles remained relatively stable. This suggests that interventions should not focus solely on resilience but also on enhancing coping strategies. Embedding such interventions during academic transition periods may help preserve psychological resources and improve academic outcomes.
Notes on Contributors
Ardo Sanjaya contributed to concept, analysis, and writing. Ray Sebastian helped collect data and draft the paper. Kevin Gunawan assisted in drafting and data collection. Christian Edwin led concept, analysis, and revisions. Nathanael A. Mianto worked on analysis and revisions. Cindra Paskaria contributed to concept and revisions. All authors have read and approved the final version of the manuscript.
Ethical Approval
This study followed the Declaration of Helsinki and received ethical approval from the Research Ethics Committee of Maranatha Christian University (Approval Number: 089/KEP/VII/2024). Electronic informed consent was obtained from all participants before their inclusion, with the consent form presented at the start of the online survey. Participants’ registration numbers, names, and email addresses were initially collected to facilitate accurate data matching and communication. However, all identifiable information was removed, and the dataset was fully anonymised before analysis to ensure confidentiality. Participants were informed that their responses would remain confidential and be used exclusively for research. All data collection and analysis procedures complied with institutional and national ethical standards to safeguard participant privacy and well-being.
Data Availability
The datasets generated during the study are available from the corresponding author upon reasonable request and are subject to ethical considerations. Supplementary materials, including the complete statistical results, complementing the articles, are available on Figshare: https://doi.org/10.6084/m9.figshare.28916246 (Sanjaya, 2025).
Acknowledgement
The authors thank Maranatha Christian University for providing the facilities to create this research.
Funding
This research was supported by an Internal Research Grant from Maranatha Christian University, under grant number 020/SK/AK/UKM/III/2025.
Declaration of Interest
The authors declare no conflict of interest.
References
Abreu Alves, S., Sinval, J., Lucas Neto, L., Marôco, J., Gonçalves Ferreira, A., & Oliveira, P. (2022). Burnout and dropout intention in medical students: The protective role of academic engagement. BMC Medical Education, 22(1), 83. https://doi.org/10.1186/s12909-021-03094-9
Aker, S., & Şahin, M. K. (2022). The relationship between school burnout, sense of school belonging and academic achievement in preclinical medical students. Advances in Health Sciences Education, 27(4), 949–963. https://doi.org/10.1007/s10459-022-10121-x
Almansour, M., Abouammoh, N., Idris, R. Bin, Alsuliman, O. A., Alhomaidi, R. A., Alhumud, M. H., & Alghamdi, H. A. (2024). Exploring medical students’ experience of the learning environment: A mixed methods study in Saudi medical college. BMC Medical Education, 24(1), 723. https://doi.org/10.1186/s12909-024-05716-4
Almarzouki, A. F. (2024). Stress, working memory, and academic performance: A neuroscience perspective. Stress, 27(1). https://doi.org/10.1080/10253890.2024.2364333
Bayram Deger, V. (2024). Editorial: Anxiety, burnout, and stress among healthcare professionals. Frontiers in Psychology, 14. https://doi.org/10.3389/fpsyg.2023.1348250
Béné, C., Al-Hassan, R. M., Amarasinghe, O., Fong, P., Ocran, J., Onumah, E., Ratuniata, R., Tuyen, T. Van, McGregor, J. A., & Mills, D. J. (2016). Is resilience socially constructed? Empirical evidence from Fiji, Ghana, Sri Lanka, and Vietnam. Global Environmental Change, 38, 153–170. https://doi.org/10.1016/j.gloenvcha.2016.03.005
Ben-Zur, H. (2019). Transactional model of stress and coping. In V. Zeigler-Hill & T. Shackelford (Eds.), Encyclopedia of personality and individual differences (pp. 1–4). Springer International Publishing. https://doi.org/10.1007/978-3-319-28099-8_2128-1
Boni, R. A. dos S., Paiva, C. E., de Oliveira, M. A., Lucchetti, G., Fregnani, J. H. T. G., & Paiva, B. S. R. (2018). Burnout among medical students during the first years of undergraduate school: Prevalence and associated factors. PLOS ONE, 13(3), e0191746. https://doi.org/10.1371/journal.pone.0191746
Braquehais, M. D., & Vargas-Cáceres, S. (2023). Psychiatric issues among health professionals. Medical Clinics of North America, 107(1), 131–142. https://doi.org/10.1016/j.mcna.2022.04.004
Calo, M., Judd, B., & Peiris, C. (2024). Grit, resilience and growth‐mindset interventions in health professional students: A systematic review and meta‐analysis. Medical Education, 58(8), 902–919. https://doi.org/10.1111/medu.15391
Calo, M., Peiris, C., Chipchase, L., Blackstock, F., & Judd, B. (2019). Grit, resilience and mindset in health students. The Clinical Teacher, 16(4), 317–322. https://doi.org/10.1111/tct.13056
Davis, C. G., Thake, J., & Vilhena, N. (2010). Social desirability biases in self-reported alcohol consumption and harms. Addictive Behaviors, 35(4), 302–311. https://doi.org/10.1016/j.addbeh.2009.11.001
de la Fuente, J., González-Torres, M. C., Artuch-Garde, R., Vera-Martínez, M. M., Martínez-Vicente, J. M., & Peralta-S’anchez, F. J. (2021). Resilience as a buffering variable between the big five components and factors and symptoms of academic stress at university. Frontiers in Psychiatry, 12. https://doi.org/10.3389/fpsyt.2021.600240
Diaconescu, L. V., Mihăilescu, A. I., Stoian-Bălăşoiu, I. R., Cosma, A.-N., Drakou, A., & Popa-Velea, O. (2024). The predictive value of burnout and impostor syndrome on medical students’ self-esteem and academic performance: A cross-sectional study. Education Sciences, 14(12), 1318. https://doi.org/10.3390/educsci14121318
Ding, Y., Fu, X., Liu, R., Hwang, J., Hong, W., & Wang, J. (2021). The impact of different coping styles on psychological distress during the COVID-19: The mediating role of perceived stress. International Journal of Environmental Research and Public Health, 18(20), 10947. https://doi.org/10.3390/ijerph182010947
Dyrbye, L. N., Thomas, M. R., Harper, W., Massie, F. S., Power, D. V, Eacker, A., Szydlo, D. W., Novotny, P. J., Sloan, J. A., & Shanafelt, T. D. (2009). The learning environment and medical student burnout: A multicentre study. Medical Education, 43(3), 274–282. https://doi.org/10.1111/j.1365-2923.2008.03282.x
Dyrbye, L. N., Thomas, M. R., Massie, F. S., Power, D. V, Eacker, A., Harper, W., Durning, S., Moutier, C., Szydlo, D. W., Novotny, P. J., Sloan, J. A., & Shanafelt, T. D. (2008). Burnout and suicidal ideation among U.S. medical students. Annals of Internal Medicine, 149(5), 334–341. https://doi.org/10.7326/0003-4819-149-5-200809020-00008
Edgerton, E., & McKechnie, J. (2023). The relationship between student’s perceptions of their school environment and academic achievement. Frontiers in Psychology, 13. https://doi.org/10.3389/fpsyg.2022.959259
Esquerda, M., Garcia-Estañ, J., Ruiz-Rosales, A., Garcia-Abajo, J. M., & Millan, J. (2024). Relationship between academic climate and burnout in Spanish medical schools. Educación Médica, 25(6), 100955. https://doi.org/10.1016/j.edumed.2024.100955
Faizan Siddiqui, M., & Azaroual, M. (2024). Combatting burnout culture and imposter syndrome in medical students and healthcare professionals: A future perspective. Journal of Medical Education and Curricular Development, 11. https://doi.org/10.1177/23821205241285601
Fares, J., Al Tabosh, H., Saadeddin, Z., El Mouhayyar, C., & Aridi, H. (2016). Stress, burnout and coping strategies in preclinical medical students. North American Journal of Medical Sciences, 8(2), 75. https://doi.org/10.4103/1947-2714.177299
Findyartini, A., Greviana, N., Putera, A. M., Sutanto, R. L., Saki, V. Y., & Felaza, E. (2021). The relationships between resilience and student personal factors in an undergraduate medical program. BMC Medical Education, 21(1), 113. https://doi.org/10.1186/s12909-021-02547-5
Folkman, S. (2013). Stress: Appraisal and coping. In M. D. Gellman & J. R. Turner (Eds.), Encyclopedia of behavioral medicine (pp. 1913–1915). Springer New York. https://doi.org/10.1007/978-1-4419-1005-9_215
Hansell, M. W., Ungerleider, R. M., Brooks, C. A., Knudson, M. P., Kirk, J. K., & Ungerleider, J. D. (2019). Temporal trends in medical student burnout. Family Medicine, 51(5), 399–404. https://doi.org/10.22454/FamMed.2019.270753
Herrero, R., & Díaz, A. (2025). The role of resilience as a buffer for burden and psychological distress in ads caregivers: A cross-sectional study. Sci, 7(2), 38. https://doi.org/10.3390/sci7020038
Ho, S. W., & Kwek, E. B. (2022). Levels of burnout and its association with resilience and coping mechanisms among orthopaedic surgery residents: A single institution experience from Singapore. Singapore Medical Journal, 63(7), 381–387. https://doi.org/10.11622/smedj.2021010
Holahan, C. J., Moos, R. H., Holahan, C. K., Brennan, P. L., & Schutte, K. K. (2005). Stress generation, avoidance coping, and depressive symptoms: A 10-year model. Journal of Consulting and Clinical Psychology, 73(4), 658–666. https://doi.org/10.1037/0022-006X.73.4.658
Jumat, M. R., Chow, P. K.-H., Allen, J. C., Lai, S. H., Hwang, N.-C., Iqbal, J., Mok, M. U. S., Rapisarda, A., Velkey, J. M., Engle, D. L., & Compton, S. (2020). Grit protects medical students from burnout: A longitudinal study. BMC Medical Education, 20(1), 266. https://doi.org/10.1186/s12909-020-02187-1
Kardum, I., & Krapić, N. (2001). Personality traits, stressful life events, and coping styles in early adolescence. Personality and Individual Differences, 30(3), 503–515. https://doi.org/10.1016/S0191-8869(00)00041-6
Kassab, S. E., Rathan, R., Taylor, D. C. M., & Hamdy, H. (2024). The impact of the educational environment on student engagement and academic performance in health professions education. BMC Medical Education, 24(1), 1278. https://doi.org/10.1186/s12909-024-06270-9
Köhne, S., Engert, V., & Rosendahl, J. (2023). Stability of resilience in times of the COVID-19 pandemic. Personality and Mental Health, 17(1), 55–66. https://doi.org/10.1002/pmh.1560
Leep Hunderfund, A. N., Saberzadeh Ardestani, B., Laughlin-Tommaso, S. K., Jordan, B. L., Melson, V. A., Montenegro, M. M., Brushaber, D. E., West, C. P., & Dyrbye, L. N. (2025). Sense of belonging among medical students, residents, and fellows: Associations with burnout, recruitment retention, and learning environment. Academic Medicine, 100(2), 191–202. https://doi.org/10.1097/ACM.0000000000005892
Lin, Y. K., Lin, C.-D., Lin, B. Y.-J., & Chen, D.-Y. (2019). Medical students’ resilience: A protective role on stress and quality of life in clerkship. BMC Medical Education, 19(1), 473. https://doi.org/10.1186/s12909-019-1912-4
Liu, Y., & Cao, Z. (2022). The impact of social support and stress on academic burnout among medical students in online learning: The mediating role of resilience. Frontiers in Public Health, 10. https://doi.org/10.3389/fpubh.2022.938132
Masten, A. S. (2001). Ordinary magic: Resilience processes in development. American Psychologist, 56(3), 227–238. https://doi.org/10.1037/0003-066X.56.3.227
Neufeld, A., & Malin, G. (2021). How medical students cope with stress: A cross-sectional look at strategies and their sociodemographic antecedents. BMC Medical Education, 21(1), 299. https://doi.org/10.1186/s12909-021-02734-4
Nguyen, T., Pu, C., Waits, A., Tran, T. D., Ngo, T. H., Huynh, Q. T. V., & Huang, S.-L. (2023). Transforming stress program on medical students’ stress mindset and coping strategies: A quasi-experimental study. BMC Medical Education, 23(1), 587. https://doi.org/10.1186/s12909-023-04559-9
O. Ogoma, S. (2020). Problem-focused coping controls burnout in medical students: The case of a selected medical school in Kenya. Journal of Psychology and Behavioural Science, 8(1), 69–79. https://jpbs.thebrpi.org/journals/jpbs/Vol_8_No_1_June_2020/8.pdf
Ollis, L., Cropley, M., Plans, D., & Cogo-Moreira, H. (2022). Disentangling change across the time and true stability of employees’ resilience using latent state model. BMC Psychiatry, 22, 651. https://doi.org/10.1186/s12888-022-04294-3
Prendergast, M., Cardoso Pinto, A. M., Harvey, C.-J., & Muir, E. (2024). Burnout in early year medical students: Experiences, drivers and the perceived value of a reflection-based intervention. BMC Medical Education, 24, 7. https://doi.org/10.1186/s12909-023-04948-0
Rosas-Santiago, F. J. (2019). Cognitive behavioral and psychoeducational intervention to modify coping styles and burnout syndrome in civil servants: An experimental study. Ansiedad y Estrés, 25(2), 91–96. https://doi.org/10.1016/j.anyes.2019.09.001
Sanjaya, A. (2025). A cross-sectional study of distress, coping, resilience, and academic performance in medical students [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.28916246
Sanjaya, A., Mianto, N. A., Wijayanto, K. R., & Edwin, C. (2024). Resilience: A panacea for burnout in medical students during clinical training?: A narrative review. Medicine, 103(49), e40794. https://doi.org/10.1097/MD.0000000000040794
Shahzad, S., & Wajid, G. (2024). Learning environment and its relationship with quality of life and burn-out among undergraduate medical students in Pakistan: A cross-sectional study. BMJ Open, 14(8), e080440. https://doi.org/10.1136/bmjopen-2023-080440
Shanafelt, T. D. (2021). Physician well-being 2.0: Where are we and where are we going? Mayo Clinic Proceedings, 96(10), 2682–2693. https://doi.org/10.1016/j.mayocp.2021.06.005
Siddiqui, F., & Malik, A. A. (2019). Promoting self-regulated learning skills in medical students is the need of time. Journal of Taibah University Medical Sciences, 14(3), 277–281. https://doi.org/10.1016/j.jtumed.2019.03.003
Simons, C. T., Dessirier, J. M., Carstens, M. I., O’Mahony, M., & Carstens, E. (1999). Neurobiological and psychophysical mechanisms underlying the oral sensation produced by carbonated water. The Journal of Neuroscience: The Official Journal of the Society for Neuroscience, 19(18), 8134–8144. https://doi.org/10.1523/JNEUROSCI.19-18-08134.1999
Sotiropoulos, M. G. (2021). Impostor syndrome: A calling for a career in medical education? Postgraduate Medical Journal, 97(1146), 264–265. https://doi.org/10.1136/postgradmedj-2020-138360
Tan, C. Y. (2024). Socioeconomic status and student learning: Insights from an umbrella review. Educational Psychology Review, 36(4), 100. https://doi.org/10.1007/s10648-024-09929-3
Thompson, G., McBride, R. B., Hosford, C. C., & Halaas, G. (2016). Resilience among medical students: The role of coping style and social support. Teaching and Learning in Medicine, 28(2), 174–182. https://doi.org/10.1080/10401334.2016.1146611
van der Merwe, L. J., Botha, A., & Joubert, G. (2020). Resilience and coping strategies of undergraduate medical students at the University of the Free State. South African Journal of Psychiatry, 26, a1471. https://doi.org/10.4102/sajpsychiatry.v26i0.1471
Villasana, M., Alonso-Tapia, J., & Ruiz, M. (2016). A model for assessing coping and its relation to resilience in adolescence from the perspective of “person–situation interaction”. Personality and Individual Differences, 98, 250–256. https://doi.org/10.1016/j.paid.2016.04.053
Villwock, J. A., Sobin, L. B., Koester, L. A., & Harris, T. M. (2016). Impostor syndrome and burnout among American medical students: A pilot study. International Journal of Medical Education, 7, 364–369. https://doi.org/10.5116/ijme.5801.eac4
Voltmer, E., Köslich-Strumann, S., Voltmer, J.-B., & Kötter, T. (2021). Stress and behavior patterns throughout medical education – A six year longitudinal study. BMC Medical Education, 21(1), 454. https://doi.org/10.1186/s12909-021-02862-x
Wang, Q., Sun, W., & Wu, H. (2022). Associations between academic burnout, resilience and life satisfaction among medical students: A three-wave longitudinal study. BMC Medical Education, 22(1), 248. https://doi.org/10.1186/s12909-022-03326-6
Wasson, L. T., Cusmano, A., Meli, L., Louh, I., Falzon, L., Hampsey, M., Young, G., Shaffer, J., & Davidson, K. W. (2016). Association between learning environment interventions and medical student well-being. JAMA, 316(21), 2237. https://doi.org/10.1001/jama.2016.17573
Waxman, H. C., Huang, S.-Y. L., & Wang, M. C. (1997). Investigating the classroom learning environment of resilient and non-resilient students from inner-city elementary schools. International Journal of Educational Research, 27(4), 343–353. https://doi.org/10.1016/S0883-0355(97)90016-1
West, M. R., Kraft, M. A., Finn, A. S., Martin, R. E., Duckworth, A. L., Gabrieli, C. F. O., & Gabrieli, J. D. E. (2016). Promise and paradox: Measuring students’ non-cognitive skills and the impact of schooling. Educational Evaluation and Policy Analysis, 38(1), 148–170. https://doi.org/10.3102/0162373715597298
Zhang, X., Tian, W., Tang, X., Jia, L., Meng, X., Shi, T., & Zhao, J. (2024). Mediating role of resilience on burnout to well-being for hospital nursing staff in Northeast China: A cross-sectional study. BMJ Open, 14(11), e081718. https://doi.org/10.1136/bmjopen-2023-081718
Zhu, Z., Hu, X., & Zhang, B. (2024). The role of resilience in navigating work stress and achieving daily work goals. Journal of Organizational Behavior, 46(8), 1107–1119. https://doi.org/10.1002/job.2839
*Ardo Sanjaya
Maranatha Biomedical Research Laboratory,
Faculty of Medicine,
Maranatha Christian University
Jl. Surya Sumantri No. 65
Bandung, Indonesia, 40164
+62 859 1066 09851
ardo.sanjaya@med.maranatha.edu
https://doi.org/10.29060/TAPS.2026-11-2/TT006
Craig S. Webster
Centre for Medical and Health Sciences Education,
School of Medicine, University of Auckland,
Auckland, New Zealand
LLMs are a powerful new tool, and like any other technology introduced into healthcare, clinicians must carefully consider the risks, and use LLMs in a way that leverages and augments clinical knowledge and skill, rather than outsourcing tasks to LLMs in an uncritical way.
Large Language Models (LLMs), such as ChatGPT (Open AI), are a prominent form of Artificial Intelligence (AI) currently capturing the imagination of millions of people around the world. Although not conscious, LLMs comprise artificial neural networks trained on vast datasets of human language. This allows the LLM to identify statistical patterns in language, and to generate coherent and contextually appropriate responses to a wide range of prompts, yielding impressive conversational abilities. ChatGPT has even gained a pass grade on the United States Medical Licensing Examination (Gilson et al., 2023).
In healthcare, LLMs may assist with tasks such as transcribing medical notes, offering clinical decision support, or generating teaching materials. However, the statistical patterns and rules learnt by the LLM during training are entirely dependent on the training data, and so are not equivalent to known causal mechanisms of disease or evidence-based medicine (Webster, 2025). Hence the introduction of LLMs to healthcare without careful consideration carries substantial risk.
LLMs can generate plausible but incorrect or misleading information, known as hallucinations, which could have dangerous consequences in a medical context. Because LLMs are trained on historical and internet-based texts, they may inherit and even amplify existing societal biases, including those based on race, gender, or socioeconomic status (Webster & Jowsey, 2025; Webster et al., 2022). The use of LLMs in healthcare may therefore perpetuate or worsen health disparities.
In a high-stakes field like healthcare, accountability and trust are crucial, but LLMs are not morally or legally bound agents. Misplaced trust in an AI-generated recommendation without proper oversight could result in harm, and this includes the possibility of inappropriate disclosure of confidential patient information. Unlike regulated clinical decision support systems, LLMs lack transparent mechanisms for verifying the validity of their output.
However, LLMs excel at summarising large domains of knowledge, and if used in conjunction with appropriate human oversight, can save considerable time in many teaching and research activities (Topol, 2019). For example, in research LLMs make excellent sounding boards for the development of new ideas or hypotheses, and can very quickly generate patient vignettes useful for teaching.
We have a strong tendency to anthropomorphise LLMs and to see them as all-knowing. However, an understanding of the risks inherent in this technology is critical. LLMs are a powerful new tool, and like any other technology introduced into healthcare, clinicians must carefully consider the risks, and use LLMs in a way that leverages and augments clinical knowledge and skill, rather than outsourcing tasks to LLMs in an uncritical way.
References
Gilson, A., Safranek, C. W., Huang, T., Socrates, V., Chi, L., Taylor, R. A., & Chartash, D. (2023). How does
ChatGPT perform on the United States Medical Licensing Examination (USMLE)? The implications of large language
models for medical education and knowledge assessment. JMIR Medical Education, 9, e45312.
https://doi.org/10.2196/45312
Topol, E. J. (2019). High-performance medicine: The convergence of human and artificial intelligence. Nature
Medicine, 25, 44-56. https://doi.org/10.1038/s41591-018-0300-7
Webster, C. S. (2025). Natural and artificial intelligence – The psychotechnical agenda of the 21st century. Journal of
Psychology and AI, 1(1), 2491445. https://doi.org/10.1080/29974100.2025.2491445
Webster, C. S., & Jowsey, T. (2025). Artificial intelligence must operate ethically in health care and not be prone to
racist or sexist biases. Anesthesia and Analgesia, 140(5), 1099-1104. https://doi.org/10.1213/ane.0000000000007140
Webster, C. S., Taylor, S., Thomas, C., & Weller, J. M. (2022). Social bias, discrimination and inequity in healthcare:
Mechanisms, implications and recommendations. BJA Education, 22(4), 131-137. https://doi.org/10.1016/j.bjae.2021.11.011
Submitted: 6 March 2025
Accepted: 27 August 2025
Published online: 7 April, TAPS 2026, 11(2), 114-117
https://doi.org/10.29060/TAPS.2026-11-2/SC3684
Kye Mon Min Swe1,2, Amit Bhardwaj3 & Hnin Pwint Phyu4
1Faculty of Medical Sciences, Newcastle University, United Kingdom; 2Newcastle University Medicine Malaysia (NUMed), Malaysia; 3Sengkang General Hospital, Singapore; 4M Kandiah Faculty of Medicine and Health Science, University Abdul Rahman, Malaysia
Abstract
Introduction: Student motivation in teaching-learning is pivotal in promoting overall well-being, enhancing performance, and nurturing skilled professionals. Knowledge about student motivation allows educators to broaden their understanding, and this study investigates the levels of student motivation at different phases of their medical education.
Methods: A quantitative study explored medical students’ academic motivation using the validated Academic Motivation Scale AMS-C 28, with a rating on a 7-point Likert Scale. IBM-SPSS was used to analyse the data.
Results: A total of 105 students participated in the study. The results indicated that students exhibited higher levels of intrinsic motivation compared to extrinsic motivation. The mean score for intrinsic motivation (M=5.13, SD=0.91) surpassed that of extrinsic motivation (M=4.63, SD=1.00). Regarding the association between academic year and student motivation, second-year and fourth-year medical students exhibited the highest intrinsic motivation (M=5.36, SD=0.8) and (M=5.36, SD=0.68), respectively, and second-year medical students showed the highest extrinsic motivation (M=4.87, SD=0.96) compared to other academic years, but this difference was statistically not significant.
Conclusion: The findings exhibited higher levels of intrinsic motivation, indicating active involvement in learning activities and deriving satisfaction from the course. The MBBS students in the second year displayed more intrinsic motivation, influenced by the challenging nature of successfully completing the first year, which is historically associated with a high failure rate.
Keywords: Motivation, Medical Student, Academic Motivation Scale
I. INTRODUCTION
Student motivation is a critical component of the educational process, significantly influencing academic achievement, retention, and overall student well-being (Ryan & Deci, 2000). Particularly in demanding fields, such as medical education, the quality of motivation can vary substantially among students due to various internal and external factors. Medical education poses unique challenges, necessitating effective strategies to sustain students’ motivation through the rigors of their training.
Prior research highlights the distinction between intrinsic and extrinsic motivation and their different impacts on academic performance. Intrinsic motivation refers to engaging in a task for its inherent satisfaction, while extrinsic motivation involves external rewards or pressures (Ryan & Deci, 2000). Studies have shown that stronger intrinsic motivation is associated with greater persistence, improved learning outcomes, and higher satisfaction (Schunk et al., 2014).
In medical education, motivation can profoundly influence students’ engagement with their coursework and clinical practices. For instance, intrinsic factors such as a passion for medicine and a desire to help others can actively drive students to seek knowledge (Ryan & Deci, 2000). Conversely, extrinsic factors, such as grades and external validation, can enhance motivation to a certain extent but may lead to burnout or disengagement if overemphasised.
A crucial aspect of the student experience in medical education is the transition through various academic years. Each stage presents unique challenges affecting motivation. Understanding these stages and their impact on student motivation is vital for fostering an enriching educational environment (Nadel & Rosenberg, 2020). Exploring the academic motivations of medical students is essential for informing educators and administrators about the various factors affecting student engagement and success. Understanding these motivations can help target interventions for students struggling or disinterested in their studies.
This study aims to explore the levels of student motivation throughout different phases of medical education, utilising a quantitative framework that assesses both intrinsic and extrinsic motivations. By understanding how motivation fluctuates with educational years, educators and administrators can better tailor student interventions and support systems.
II. METHODS
A descriptive quantitative research design was employed to measure academic motivation among medical students. Participants were recruited through classroom announcements, and voluntary consent was obtained.
A. Instrument
The Academic Motivation Scale (AMS-C 28) was used to measure students’ academic motivation levels. The AMS scale (Vallerand et al., 1992) contains 28 items, three domains, further subdivided into seven subscales:
1) Intrinsic motivation:
- Intrinsic motivation—to know
- Intrinsic motivation—toward accomplishment
- Intrinsic motivation—to experience stimulation
2) Extrinsic motivation:
- Extrinsic motivation—Identified
- Extrinsic motivation—Introjected
- Extrinsic motivation—external regulation
3) Amotivation:
Each item was rated on a 7-point Likert scale ranging from 1 (not at all true) to 7 (very true).
The AMS has demonstrated robust internal consistency (Cronbach’s alpha = .81). This scale provides valuable insights into students’ motivations in various educational contexts.
Data were analysed using IBM-SPSS version 25. Descriptive statistics (means and standard deviations) were calculated for each subscale. ANOVA tests were employed to compare intrinsic and extrinsic motivation levels across different academic years. A significance level of p<0.05 was considered statistically significant.
III. RESULTS
A total of 105 MBBS students from years 1 to 5 participated in the study, with a response rate of 47.5%. The majority were aged between 21-25 years, and female participants constituted a significant portion (n=74), (70.5%).
A. Academic Motivation
The data demonstrated that students had higher internal than external motivation, with the “intrinsic motivation to know” achieving the highest mean score (M = 5.58, SD = 1.01). The aggregate score for intrinsic motivation (M = 5.13, SD = 0.91) was significantly higher than the external motivation score (M = 4.36, SD = 1.10). Moreover, the average score for amotivation was (M = 2.5, SD = 1.14). The statement “Because I think that medical education will help me better prepare for the career I have chosen” received the highest mean score (M = 6.07, SD = 0.953).
B. Comparisons of the Academic Motivation Scale Among Different Academic Years
Regarding the association between academic year and student motivation, Analysis of variance (ANOVA) revealed significant differences in amotivation levels across academic years (F = 4.688, p = .002). Post-hoc Tukey HSD tests identified significant differences between MBBS Year 3 and Year 4 (mean difference = 1.54583, p = .003), and between MBBS Year 4 and Year 5 (mean difference = -1.25417, p = .005). MBBS Year 4 students exhibited the lowest amotivation (M = 1.60), while Year 3 students demonstrated the highest (M = 3.15).
Regarding intrinsic motivation, MBBS Year 2 students (M = 5.36, SD = 0.8) and MBBS Year 4 students (M = 5.36, SD = 0.68) displayed the highest levels, whereas MBBS Year 3 students showed the lowest (M = 4.75, SD = 1.28). However, no statistically significant differences in intrinsic motivation were observed across academic years (F = 2.312, p = .063).
For extrinsic motivation, MBBS Year 2 students demonstrated the highest levels (M = 4.87, SD = 0.96), while MBBS Year 4 students exhibited the lowest (M = 4.1333). Nevertheless, no statistically significant differences in extrinsic motivation were found across academic years (F = 2.295, p = .064).
These findings suggest that motivation, particularly amotivation, can fluctuate significantly as students progress through their medical education. While intrinsic and extrinsic motivation levels varied across years, these differences did not reach statistical significance.
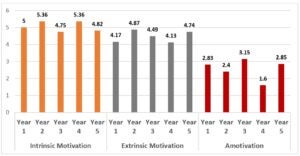
Figure 1. The relation between the academic year and subscales of AMS
IV. DISCUSSION
The findings of this study align with previous research, highlighting the importance of intrinsic motivation as a driver of academic success (Ryan & Deci, 2000). The higher intrinsic motivation among second-year medical students may be attributed to their positive experiences after successfully completing a challenging first year, and the same for the fourth-year medical students who had successfully completed a challenging clinical year 3. This transitional phase often acts as a motivational catalyst, increasing engagement and satisfaction in their studies (Nadel & Rosenberg, 2020).
Conversely, the lower motivation levels observed among third-year students may suggest a possible decline in intrinsic motivation due to the increasing pressures and clinical responsibilities accompanying their first year in clinical training at the hospital setting and clinical campus. This transitional period is often marked by numerous challenges, including stress from clinical evaluations and the need for adaptive learning strategies (Schunk et al., 2014). The study by Lyndon et al. (2023) found that academic motivation indeed fluctuates across different academic years, and several factors contribute to these changes. Changes in the curriculum structure from classroom-based learning to more clinical experiences can affect motivation levels, with some students finding clinical work more engaging and others struggling to adapt. The study emphasises the importance of understanding these fluctuations in academic motivation to develop targeted interventions and support systems for medical students.
A. Limitations
This study has a moderate response rate (47.5%), which may introduce response bias and potentially limit generalisability. The single institution may not represent diverse educational settings or geographical locations. The cross-sectional design prevents the examination of longitudinal changes in student motivation, and potential gender imbalances in the sample could limit generalisability across genders.
B. Implications
This study highlights the importance of medical educators recognising fluctuations in motivation across academic years. Medical schools should implement regular assessments of student motivation and well-being and develop targeted interventions to sustain students’ enthusiasm and engagement. For instance, mentorship programmes, peer support groups, and structured feedback sessions can provide tailored support to help students maintain their motivation throughout their academic journey.
These initiatives can help foster an environment conducive to maintaining high motivation levels.
C. Recommendations
Future research should aim to explore the qualitative aspects of motivation, diving deeper into individual experiences and the psychological factors influencing students’ intrinsic and extrinsic motivation. Additionally, comparing motivation levels with academic performance can provide useful insight into how motivation affects learning outcomes.
A more rigorous randomised approach with a larger sample size is advisable for future research endeavours. Additionally, exploring qualitative approaches to student-faculty interaction, student engagement, and student performance should be included in the investigation.
V. CONCLUSION
In conclusion, this preliminary study reveals that medical students display higher intrinsic than extrinsic motivation, particularly in their second year. Recognising these trends is essential for developing effective educational interventions to support student success throughout their medical education journey. Cultivating an environment that promotes and sustains motivation may lead to better academic performance and enhanced well-being among medical students.
Notes on Contributors
Dr Kye MMS is the corresponding author for this paper. She designed the study, analysed the data, and prepared the manuscript, working with the co-author.
Dr. Amit B. and Dr. Hnin PP contributed substantially to the design, editing, and preparation of the final manuscript.
Ethical Approval
The research study was approved by the Universiti Tunku Abdul Rahman Scientific and Ethical Review Committee on 4 November 2022 (Approval number: U/SERC/228/2022).
Data Availability
The data that support the findings of the study are openly available at https://doi.org/10.6084/m9.figshare.28544321.
Acknowledgment
We would like to acknowledge Newcastle University Medicine Malaysia for the support, and we also would like to acknowledge the students for their voluntary participation in this study.
Funding
There was no funding for this research study.
Declaration of Interest
The authors declare no conflicts of interest, including financial, consultant, institutional, or other relationships.
References
Nadel, B., & Rosenberg, A. (2020). The role of motivation in medical education. Medical Education Journal, 54(9), 883-890. https://doi.org/10.1111/medu.14205
Lyndon, M. P., Henning, M. A., Alyami, H., Krishna, S., Yu, T. C., & Hill, A. G. (2023). Changes in motivation and burnout in medical students over time: A longitudinal study. BMC Medical Education, 23(1), 1-9. https://doi.org/10.1186/s12909-023-04127-1
Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist, 55(1), 68-78. https://doi.org/10.1037/0003-066X.55.1.68
Schunk, D. H., Pintrich, P. R., & Meece, J. L. (2014). Motivation in education: Theory, research, and applications (4th ed.). Pearson. https://api.pageplace.de/preview/DT0400.9781292055251_A24621767/preview-9781292055251_A24621767.pdf
Vallerand, R. J., Pelletier, L. G., & Blais, M. R. (1992). The academic motivation scale: A measure of intrinsic, extrinsic, and amotivation in education. Educational and Psychological Measurement, 52(1), 1003-1017. https://doi.org/10.1177/0013164492052004014
*Dr Kye Mon Min Swe
Faculty of Medical Sciences, Newcastle University,
Newcastle upon Tyne, NE1 7RU, United Kingdom;
Newcastle University Medicine Malaysia (NUMed),
1, Jalan Sarjana 1, Kota Ilmu, Educity@Iskandar,
79200 Iskandar Puteri, Johor, Malaysia
601115133799
Email: kye-mon.min-swe@newcastle.edu.my
Submitted: 8 January 2025
Accepted: 25 August 2025
Published online: 7 April, TAPS 2026, 11(2), 54-63
https://doi.org/10.29060/TAPS.2026-11-2/OA3622
Zaw Phyo, Ye Phyo Aung, Tun Tun Naing & Tayzar Hein
Department of Medical Education, Defence Services Medical Academy, Myanmar
Abstract
Introduction: This study evaluates military medicine education at the Defence Services Medical Academy (DSMA) in Myanmar, focusing on curriculum structure, practical training quality, and alignment with evolving military and civilian healthcare needs. Despite a comprehensive approach, identified gaps in practical training (e.g., trauma care, CBRN management) and curriculum continuity hinder student preparedness for modern military medicine.
Methods: This qualitative study used Focused Group Discussions (FGDs) with 24 participants (12 students, 12 faculty) to explore themes like time constraints, practical training, curriculum integration, and modern technology integration. Data were analysed using MAXQDA 24 to identify key themes related to the curriculum’s content and effectiveness.
Results: Findings indicate that while the military medicine module of DSMA covers a broad range of topics, practical training remains inadequate, especially in critical areas such as trauma care, CBRN management, and digital health technologies. Furthermore, curriculum continuity issues, marked by disconnected annual topics, impede clear progression. The study recommends revising the module to include modern warfare medicine, expanding hands-on training, and incorporating mobile learning platforms. It also suggests increasing simulation-based training, restructuring the module to enhance its practical application, and establishing a dedicated military medicine department.
Conclusion: The study identifies critical gaps in DSMA’s curriculum, particularly in practical training (e.g., trauma, CBRN) and coherence. These must be addressed to better prepare students for the challenges of modern military and civilian healthcare. Proposed improvements will ensure DSMA graduates are equipped to handle contemporary healthcare demands, reinforcing the academy’s role as a leader in military medical education.
Keywords: Military Medicine, Curriculum Development, Practical Training, Outcome-Based Education, Tactical Combat Casualty Care, Qualitative Analysis
Practice Highlights
- Extending the duration of military medicine training will provide more hands-on practice, ensuring students are better equipped to handle high-pressure medical situations.
- Making “THAMAR ZARNI” field exercises mandatory and increasing their frequency will offer students the essential real-world medical experience necessary for operational readiness.
- Updating the curriculum to incorporate modern medical technologies and advanced trauma care will prepare students to effectively address the challenges posed by modern warfare.
- Improving resource allocation, including the integration of mobile learning platforms and high-fidelity simulations, will enhance the overall training experience and increase student engagement.
- Establishing a dedicated military medicine department at DSMA will centralise education, improve curriculum coherence, and provide students with a focused space for more in-depth learning.
I. INTRODUCTION
Military medicine is a vital branch of healthcare that ensures the operational readiness of armed forces personnel in high-stakes environments such as combat zones, disaster areas, and peacekeeping missions (van der Wal et al., 2024). Unlike traditional civilian healthcare, military medicine integrates clinical expertise with operational skills, including trauma care, medical logistics, crisis management, and adaptability under resource-constrained conditions (Woolley et al., 2017). Given the complexity and high-pressure nature of military operations, it is essential that healthcare professionals are trained to handle rapidly evolving situations (McGraw, 2023).
As global security landscapes evolve, with rapid advancements in warfare technologies and the rise of hybrid threats, military medicine has adapted to meet new challenges. Training programs worldwide now integrate contemporary medical practices to address the shifting dynamics of military operations. For example, the Tactical Combat Casualty Care (TCCC) guidelines have significantly reduced battlefield fatalities, demonstrating how modern medical education can improve outcomes (Butler Jr et al., 2007). Additionally, NATO’s initiatives to standardise medical practices across member states have emphasised the importance of interoperability in multinational military operations (Onderková et al., 2024). While studies like Butler Jr et al. (2007) and Kollek et al. (2009) establish best practices in TCCC and CBRN training, few explore their integration into OBE curricula in resource-constrained regions like Southeast Asia, where there are significant gaps in practical training.
Military medicine programs in NATO aligned countries and U.S. based institutions also face similar gaps in training, particularly in areas such as trauma care and the management of chemical, biological, radiological, and nuclear (CBRN) incidents. However, what sets the Defence Services Medical Academy (DSMA) in Myanmar apart is the unique context within Southeast Asia, where resource constraints are more pronounced, necessitating tailored strategies for integrating modern military medical practices. This underscores the challenges DSMA faces compared to other institutions and highlights the need for resource-sensitive solutions in military medical education.
DSMA in Myanmar has played a significant role in shaping military medicine education in Southeast Asia since 1992. The academy’s curriculum combines traditional medical education with specialised military training, equipping graduates with skills in combat casualty care, medical logistics, disease prevention, and trauma management (Naing et al., 2022). Since 2017, DSMA has implemented an Outcome-Based Education (OBE) curriculum, which aligns with global standards set by the World Federation for Medical Education. This approach focuses on measurable outcomes and competency-based learning, marking a shift from traditional teacher-centred methods to student-centred learning. Despite these advances, integrating a comprehensive military medicine module remains a challenge due to the need for specialised skills and faculty development (Garg et al., 2017).
DSMA employs innovative teaching strategies, such as case-based learning (CBL), problem-based learning, and simulation exercises to equip students with high-pressure competencies. However, the academy continues to face significant gaps in practical training, particularly in trauma care, CBRN incident management, and the application of digital health technologies. These gaps indicate a misalignment between the academy’s training programs and the evolving demands of modern military medicine. While CBRN preparedness and digital health solutions are critical for addressing military and civilian crises, these areas remain underdeveloped within military medicine module of DSMA’s curriculum (Kollek et al., 2009).
This study aims to assess how military medicine is integrated into DSMA’s OBE curriculum, focusing on aligning it with essential military medical competencies. By evaluating the effectiveness of current teaching methods and identifying areas for improvement, this research seeks actionable insights to enhance military medicine module of DSMA’s curriculum and offer a model for other countries with similar resource constraints. The ultimate goal is to ensure DSMA graduates are prepared to meet the multifaceted demands of both military and civilian healthcare sectors, particularly in the context of modern warfare and global health challenges. Furthermore, this research will highlight how countries facing resource limitations can adapt military medical education strategies to overcome gaps and improve operational readiness.
II. METHODS
A. Research Design
This study utilised a qualitative research design to examine the military medicine module of DSMA’s curriculum and identify areas for improvement. A qualitative approach was chosen to capture participants’ perspectives, particularly on practical training, integration of modern warfare knowledge, and the curriculum’s effectiveness in preparing students for both military and civilian medical roles. Data were primarily collected through Focused Group Discussions (FGDs) to gain in-depth insights into participants’ experiences and perceptions.
B. Interview Guide Development
The interview guide for military medicine education was developed through a review of literature and consultations with the DSMA curriculum committee. It focused on key aspects such as practical training, curriculum continuity, modern warfare strategies, and simulation effectiveness. The guide began with broad open-ended questions and gradually moved to specific ones. Pilot testing provided feedback that helped refine the guide before the main study.
C. Validity and Reliability
To ensure the validity and reliability of the data collection instruments, the interview guide was reviewed by three expert researchers in the field of military medicine education. These experts provided feedback on the relevance and comprehensiveness of the questions, which enhanced the study’s overall rigor. Additionally, all FGDs and interviews were conducted in a controlled environment to minimise external influences and ensure consistency across data collection sessions.
D. Participant Selection and Data Saturation
Data collection for this study was conducted over a three-month period. A total of 24 participants, comprising 12 students and 12 teachers, were organised into two main groups. These groups were further divided into four FGDs, with six participants in each. Participants were selected using a purposeful sampling method to ensure a representative mix of perspectives from both students and faculty across various academic years.
Each session was led by the principal investigator, who ensured a conducive environment for open dialogue, encouraging active participation and ensuring all voices were heard. Data collection continued until thematic saturation was achieved, meaning no new themes or significant insights emerged from the discussions.
E. Data Analysis
The data were transcribed and analysed using MAXQDA 24. A codebook was created to guide the analysis, and themes were identified both deductively (based on research objectives) and inductively (emerging from the data). To ensure consistency, intercoder agreement was checked by comparing codes with a second researcher. While MAXQDA was used for systematic analysis, manual coding could have been sufficient given the small dataset.
F. Informed Consent
Prior to participation, informed verbal consent was obtained from all respondents, ensuring that they understood their autonomy in deciding whether to participate in the study. Participants were also made aware that they could withdraw from the study at any time without consequence.
G. Ethical Considerations
Ethics approval was obtained from DSMA ethical Committee, and participant confidentiality and anonymity were ensured by assigning unique identifiers and securely storing personal data, accessible only to the research team. The Principal Investigator (PI), a lecturer at the Defence Services Medical Academy, conducted the FGDs. To mitigate the potential power imbalance and encourage open dialogue, several measures were implemented.
Participants were assured of complete anonymity and confidentiality, and informed consent was obtained with the explicit understanding that they could withdraw at any time without consequence. The PI began each session by emphasising that the research’s sole purpose was to improve the curriculum, fostering a non-judgmental environment where all feedback was valued, regardless of its critical nature. These steps were crucial to ensure participants felt safe to speak their minds freely.
III. RESULTS
This qualitative study explores the military medicine module at DSMA, focusing on the perspectives of both students and faculty. By examining their experiences, perceptions, and suggestions, the study identifies critical gaps and areas for improvement in the integration of military and civilian medical education. The findings reveal that the current military medicine module struggles to meet the practical and theoretical needs of students preparing for both military and civilian medical roles.
The results are categorised into two primary areas of focus:
- Table 1: Challenges and Relevance of Military Medicine Education – Summarises concerns regarding insufficient training time, lack of curriculum cohesion, and the relevance of military medicine education.
- Table 2: Curriculum Structure, Practical Training, and Improvement Strategies – Proposes strategies for improving curriculum integration, expanding practical training, and enhancing resource availability.
These findings underscore the urgent need for strategic reforms to improve DSMA’s curriculum, better preparing students for the multifaceted challenges of both military and civilian healthcare.
A. Challenges and Relevance of Military Medicine Education
The following table presents the challenges and relevance of military medicine education, as viewed by both students and teachers. It outlines key concerns regarding time constraints, curriculum integration, and the importance of military medicine across different sectors, particularly in response to real-world scenarios such as national disasters.
|
|
Theme |
Sub-Theme |
Student Perspectives |
Teacher Perspectives |
|
1. |
Challenges in Military Medicine |
Time Constraints and Practical Exposure |
“We only spend one to two weeks per year learning about military medicine, insufficient for crisis management.”
“Field training, like ‘THAMAR ZARNI,’ should be extended to a minimum of two weeks during the internship.” |
“The military medicine module lasts around 150 hours from Year 1 to internship, with a need for more time during internships to develop essential skills for future military doctor duties.” |
|
Curriculum Integration |
“Annual topics aren’t connected, making it feel like starting from scratch.” |
“Curriculum needs real time, relevant topics with more hands-on training.” |
||
|
2. |
Relevance of Military Medicine |
Importance Across Sectors |
“Military medicine is important not just for military doctors, but also for civilian doctors, especially given the current situation in our country, Myanmar.” |
“Essential knowledge for all medical students, regardless of future sectors.”
“Given the current situation in our country, military medicine is crucial for supporting both military personnel and civilians during times of crisis.” |
|
Real World Application |
“Crucial for work in the military and responding to national disasters.”
“Military medicine is essential for both military operations and providing critical healthcare during national disasters, ensuring support for civilians in times of crisis.” |
“In recent years, our country has faced numerous crises, including the COVID-19 pandemic, natural disasters, and ongoing conflicts. Military doctors have played a crucial role in responding to these challenges, providing essential healthcare not only to military personnel but also to civilians in need.” |
Table 1. Challenges and Relevance of Military Medicine Education
The study found that the limited time for military medicine training at DSMA—only two to three weeks each year—impedes students’ crisis management development. The academic year structure, with time allocated to commemoration parade training and national holidays, further reduces training opportunities. The study recommends restructuring the military medicine module of the curriculum to allocate more time for military medicine.
The study also highlighted a need for more practical training. Despite the introduction of OBE, faculty resistance limits its impact. Increasing field exercises and internships, such as “THAMAR ZARNI”, would better prepare students for real-world military medical challenges.
B. Curriculum Structure, Practical Training, and Improvement Strategies
This table highlights student and teacher views on military medicine education, emphasising the need for a more focused curriculum, modern warfare updates, and increased practical training. Both groups called for better resource allocation, use of technology, and consistent assessments, with students suggesting mobile platforms and teachers recommending a dedicated department.
|
No. |
Theme |
Sub-Theme |
Student Perspectives |
Teacher Perspectives |
|
1. |
Curriculum Structure and Integration |
Overlap and Redundancy |
“I suggest reviewing and reorganising these areas to eliminate overlap, making the curriculum more focused and efficient for better learning outcomes” |
“Beneficial to remove overlapping topics to focus on practical aspects.”
|
|
Modern Warfare Updates |
“As a medical student, I suggest incorporating updates on modern warfare into the curriculum, focusing on new medical technologies, advanced trauma care, and the evolving challenges of treating injuries in current conflicts.” |
“Need updates to include relevant modern warfare information.”
“It is important to update our curriculum to reflect on the current national and global situations.” |
||
|
2. |
Practical Training and Hands-On Learning |
Increased Field Exercises |
“Annual field training like ‘THAMAR ZARNI’ should be mandatory.” |
“Strong need for more practical learning opportunities.” |
|
Hands-on Experience during Internship |
“Opportunities like ‘THAMAR ZARNI’ are crucial for practicing essential skills.” |
“Hands-on experience is vital for building competence for real world situations.” |
||
|
3. |
Improvement and Evaluation |
Use of Technology in Learning |
” If there are no limitations on using mobile devices, we can learn more effectively, not just in military medicine but across all modules” |
“While the Learning Management System (LMS) is currently running, it is not fully activated.” |
|
Need for Resources |
“There is a significant limitation of resources for military medicine training.” |
“Limited resources means students can only see, not use, items like first aid kits and other essential tools during internships.” |
||
|
Curriculum Assessments |
“It’s important to assess these topics across all years, not just in Year 4, to ensure consistent learning and engagement throughout the program.” |
“We conduct formative assessments in Years 1, 2, 3, 5, and during internships, with a summative assessment in Year 4.” |
||
|
Establish a Dedicated Department |
“If a military medicine department is established, we would have a dedicated space to learn more and ask questions about any unclear concepts, ensuring a deeper understanding of the field.” |
“No dedicated department at our university; coordinators come from other departments specialising in relevant fields.” “The plan to establish a military medicine department is still ongoing, but once it’s in place, it will provide students with a dedicated space to deepen their knowledge and address any uncertainties in the field.” |
Table 2. Curriculum Structure, Practical Training, and Improvement Strategies
This table highlighted key insights from both students and teachers regarding the DSMA military medical curriculum. Both groups agreed on the need to eliminate military medicine module of the DSMA’s curriculum overlap and incorporate updates on modern warfare, such as new medical technologies and advanced trauma care to keep pace with global needs.
Regarding practical training, both students and teachers emphasised the importance of increasing field exercises, particularly “THAMAR ZARNI”, and providing more hands-on experience during internships to improve real-world competence. Both groups also noted resource limitations, including a lack of access to essential tools like first aid kits. Lastly, the creation of a dedicated military medicine department was supported to facilitate deeper learning and address any gaps in knowledge.
IV. DISCUSSION
The research analyses DSMA’s military medical curriculum, focusing on its strengths and areas for improvement. This study emphasises the importance of specialised training, the quality of practical training, curriculum continuity, the relevance of military medical education to civilian healthcare, and the need for updates reflecting modern technologies. The study concludes with evidence-based recommendations to improve DSMA’s military medical education and better prepare students for real-world healthcare challenges.
A. Time Constraints in Military Medicine Education
A significant limitation identified in the study is the insufficient time allocated to military medicine within the DSMA curriculum. The time spent on military medicine—no more than two or three weeks per academic year—is inadequate for developing the necessary skills for effective crisis management. Furthermore, the academic structure of DSMA consists of a ten-month academic year, in addition to approximately 30 national holidays within that year. Each year, students undergo one month of commemoration parade training, followed by an additional month off. This schedule is consistently followed each calendar year as part of the academic calendar. These time constraints exacerbate the gap in students’ preparedness for real-world military medical challenges. This aligns with findings from Ellington and Farrukh (2020), who argue that time constraints are a major obstacle in military medicine education. To address this, this study suggests a restructuring of the curriculum to emphasise military medicine. Extending the duration of military medicine training would provide students with the necessary time to gain hands-on experience and develop critical competencies for high-pressure situations, ultimately enhancing their operational readiness and ability to respond effectively to emergencies (Watson et al., 2025).
B. Enhancement of Practical Training
The study finds consensus among both students and faculty on the need to enhance the practical training components of the DSMA curriculum. While the OBE curriculum introduced in 2017 aims to foster better learning outcomes, faculty resistance remains due to their familiarity with previous teaching methods. Increasing hands-on experiences, such as field exercises and internships, is crucial for developing the competencies required for real-world medical challenges. This finding is consistent with Vogel and Harendza (2016), who emphasise that practical training directly impacts clinical competence, especially in military environments.
The study also highlights the importance of mandatory field exercises like “THAMAR ZARNI”, which are essential for preparing students for emergency situations. Increasing the frequency and intensity of such training will significantly enhance the competence and confidence of DSMA graduates, aligning with Dieck-Assad et al. (2021)’s recommendation for more frequent high-stakes training to improve real-world emergency response skills.
C. Curriculum Disjointedness and Continuity
The study reveals a critical issue in the lack of continuity and integration within the military medicine of DSMA’s curriculum. The curriculum does not progressively build upon itself from year to year, leading to fragmentation in the educational experience. This finding mirrors the research by Brauer and Ferguson (2015), who argue that fragmented curricula hinder the development of cohesive medical knowledge.
The study contributes to the growing body of literature by identifying this issue as not unique to DSMA but prevalent in military medical education programs worldwide. Vertical integration of the curriculum is proposed as a solution to this problem. By ensuring that content from earlier years builds upon that of subsequent years, students will be able to better understand military medicine as a cohesive discipline and apply their theoretical knowledge in practice. A unified curriculum will improve both learning outcomes and operational readiness, enabling students to apply what they have learned in real-world scenarios (O’Connell et al., 2021).
While both students and faculty acknowledged the disjointedness, their perspectives on its impact differed. Students, such as Student 1, described it as “starting from scratch” annually, highlighting the learning burden and lack of a foundational understanding. In contrast, faculty members, like Teacher 4, focused more on the need for “real-time, relevant topics,” which suggests a priority on content relevance over the structural flow of the curriculum. This nuanced finding is a significant contribution to the literature, showing that even with a shared concern, the specific priorities of stakeholders can vary significantly. This requires a dual approach that not only updates the content but also ensures its logical progression throughout the academic years. The current structure, which dedicates a few weeks each year to isolated topics, prevents students from developing a deep and cumulative understanding of military medicine as a cohesive discipline.
Vertical integration of the curriculum is proposed as a solution to this problem. By ensuring that content from earlier years builds upon that of subsequent years, students will be able to better understand military medicine as a cohesive discipline and apply their theoretical knowledge in practice.
A unified curriculum will improve both learning outcomes and operational readiness, enabling students to apply what they have learned in real-world scenarios (O’Connell et al., 2021).
Furthermore, the study highlighted a subtle but important divergence in views on resource limitations. Both groups agreed on the lack of resources, but their specific concerns differed. Students focused on the lack of hands-on access to essential tools like first aid kits, which directly impacts their ability to practice skills. In contrast, teachers’ concerns centred more on the overall resource allocation, including the need for a dedicated department and functional digital platforms, which they see as necessary for institutional-level improvement. This highlights the need for a two-pronged strategy: addressing the immediate, practical needs of students while simultaneously working towards the long-term, structural improvements advocated by the faculty.
D. Relevance to Civilian Roles
Another key finding of the study is the relevance of military medicine training to civilian healthcare. Both students and faculty agree that skills acquired in military medicine, such as triage, emergency response, and disaster management, are increasingly relevant in civilian healthcare systems. The integration of military medical knowledge into civilian contexts is beneficial not only for DSMA graduates but also as a model for global healthcare systems, where military and civilian medical teams often collaborate during disasters and public health crises.
The study suggests that DSMA should incorporate more dual-use military medical knowledge, such as trauma treatment and public health strategies, into its curriculum. These additions would better prepare students for both military and civilian healthcare roles, improving the overall military medicine module of DSMA’s curriculum and ensuring that DSMA graduates can transition seamlessly between the two sectors (Cole et al., 2024; Michaud et al., 2019).
E. Curricular Updates for Modern Warfare
The study also identifies the need for curricular updates to include modern military and medical technologies. DSMA’s current module of the curriculum fails to adequately cover emerging topics such as drones, cyber warfare, and modern medical technologies used in combat situations. As Lewis et al. (2024) note, outdated curricula do not prepare students for the evolving complexities of modern medical practice in conflict zones.
To address this, the study recommends that DSMA regularly update its curriculum to include the latest advancements in battlefield medicine. For example, training on medical drone operations could enhance the ability of military medical teams to deliver supplies to remote areas under combat conditions. Furthermore, training in cyber warfare would ensure that students understand how to protect military medical infrastructure from digital threats. Incorporating such cutting-edge technologies would ensure that DSMA graduates are prepared to handle the future challenges of military medicine (Fuentes, 2021).
F. Practical Training and Hands-On Learning
As noted earlier, field exercises and internships are essential for bridging the gap between theoretical knowledge and real-world application. However, the limited frequency and scope of these opportunities hinder effective training. While the “THAMAR ZARNI” exercise is a valuable learning tool, its infrequency limits students’ exposure to real-world complexities (McGraw, 2023).
To improve this, the study suggests expanding opportunities for hands-on learning through more frequent and diverse field exercises. Kolb’s Experiential Learning Theory suggests that learners best acquire skills through reflection on experience. The lack of hands-on training at DSMA limits opportunities for reflective learning, which may hinder students’ development in real-world medical scenarios (Kolb et al., 2014). Additionally, the integration of virtual simulations and augmented reality (AR) platforms could create simulated combat medical environments, allowing students to practice trauma care and disaster response in a controlled, virtual setting, thus overcoming logistical constraints of traditional field exercises.
G. Improvement and Evaluation
The study highlights the underuse of the Learning Management System (LMS) at DSMA, which remains a missed opportunity for self-directed learning. Mobile platforms and real-time feedback through LMS could significantly enhance the training experience, creating a more dynamic and responsive learning environment. This challenge is mirrored in other military medical institutions worldwide, where underutilisation of technology limits students’ ability to engage with learning materials outside of the classroom.
The study also suggests that increasing the frequency of formative assessments could help reinforce key concepts and improve knowledge retention over time. By providing more consistent feedback, DSMA could better prepare students for military medical practice. Furthermore, the lack of a dedicated department for military medicine education results in a fragmented approach to military medicine module delivery. A specialised department would ensure better curriculum coherence and oversight, ultimately improving the quality of military medical education.
V. CONCLUSION
This research identifies key areas for improvement in the DSMA military medical curriculum, focusing on time management, practical training, curriculum integration, and content modernisation. Findings show that limited training time, insufficient practical opportunities, and a lack of curriculum continuity hinder students’ preparedness for real-world military medical challenges. Recommendations include extending training durations, increasing hands-on experiences like field exercises, and reorganising the military medicine module for better integration.
The study also stresses the need for military medicine module updates to include emerging medical technologies and dual-use knowledge relevant to both military and civilian healthcare. Enhancing technology use and improving assessment structures are also proposed to create a more dynamic learning environment. Implementing these changes will better prepare students to meet the evolving demands of military and civilian healthcare.
These recommendations have global relevance, offering valuable insights for institutions in resource-constrained regions to bridge the gap between military medicine and civilian healthcare. By adopting new technologies and integrating dual-use knowledge, military medical education can better equip students for modern warfare and global health challenges.
A clear action plan for restructuring the module of the DSMA’s curriculum includes extending practical training time, integrating simulation-based learning, and establishing a dedicated military medicine department. However, barriers such as budget constraints and faculty resistance to new teaching methods must be addressed for successful implementation.
To address the identified gaps, a phased implementation strategy is recommended, acknowledging the budget constraints and potential faculty resistance.
Phase 1 (Immediate & Low-Cost): Focus on quick, resource-efficient changes. This includes making “THAMAR ZARNI” field exercises mandatory and increasing their frequency to provide more hands-on practice, as noted by both students and teachers. Additionally, the underutilised Learning Management System (LMS) can be fully activated to support mobile learning and self-directed study, a cost-effective solution to improve access to materials. These measures can be implemented quickly with minimal budget impact and will show immediate benefits.
Phase 2 (Mid-Term & Moderate-Cost): This phase involves curriculum restructuring and targeted faculty development. The curriculum should be reorganised to eliminate overlapping topics and vertically integrate content from year to year, a key recommendation from both students and faculty to improve learning continuity. Investment in faculty training is also crucial to ensure they adopt the Outcome-Based Education (OBE) model effectively and embrace modern teaching methods like simulation. This phase requires a moderate investment but will build the necessary institutional capacity for long-term change.
Phase 3 (Long-Term & High-Cost): The final and most impactful change is the establishment of a dedicated military medicine department at DSMA. While this requires significant budget allocation, it is essential for centralising education, ensuring curriculum coherence, and providing a focused space for in-depth learning and expertise development. This step should be pursued after the foundational improvements from the first two phases are successfully implemented, demonstrating the academy’s commitment to prioritising military medical education and justifying the necessary financial investment.
By adopting this strategic, phased approach, DSMA can systematically address its curriculum’s shortcomings while managing resource constraints and garnering buy-in from all stakeholders. This plan offers a clear path forward, ensuring that DSMA graduates are not only prepared for the challenges of modern warfare but also equipped to serve as leaders in both military and civilian healthcare contexts.
Notes on Contributors
Dr Zaw Phyo is the Principal Investigator. As a lecturer at Myanmar’s Defence Services Medical Academy, he played a significant role in the development of the manuscript. His contributions included a thorough review of the existing literature, identification of research gaps, and clarification of the study’s objectives and questions. Additionally, he was involved in drafting and revising the manuscript, ensuring that the content was both relevant and of significant value to the field of medical education.
Dr Ye Phyo Aung, serving as a mentor, played a crucial role during the methodology phase of the study. He endorsed the chosen research design, sampling strategies, and data collection techniques, providing valuable insights that greatly enhanced the research execution.
Dr Tayzar Hein contributed by assisting in the meticulous proofreading of the article, ensuring that it met clarity, coherence, and strict academic standards.
Dr Tun Tun Naing was instrumental in analysing the collected data. He applied statistical techniques to ensure the research findings were robust and reliable, further enriching the manuscript’s quality and academic integrity.
Ethical Approval
The Ethical Review Committee of the Defence Services Medical Academy, Yangon, Myanmar, granted ethical approval (2/Ethics/2024).
Data Availability
The data that support the findings of this study are openly available in Figshare repository, https://doi.org/10.6084/m9.figshare.28245230.v1.
Acknowledgement
The author would like to thank his supervisor, the head of the medical education department (DSMA), and his colleagues. Without their help, the author would not have been able to conduct the research. The author is grateful to all the curriculum committee members and students from DSMA, Myanmar, who helped to complete the survey and provide valuable opinions and experiences.
Funding
No financing is associated with this publication; it is produced for personal and professional advancement.
Declaration of Interest
There is no conflict of interest in the current research.
References
Brauer, D. G., & Ferguson, K. J. (2015). The integrated curriculum in medical education: AMEE Guide No. 96. Medical Teacher, 37(4), 312-322. https://doi.org/10.3109/0142159X.2014.970998
Butler Jr., F. K., Holcomb, J. B., Giebner, S. D., McSwain, N. E., & Bagian, J. (2007). Tactical combat casualty care 2007: Evolving concepts and battlefield experience. Military Medicine, 172(suppl_1), 1-19. https://doi.org/10.7205/MILMED.172.Supplement_1.1
Cole, R., Durning, S. J., Shen, C., Reamy, B. V., & Rudinsky, S. L. (2024). Civilian and military medical school graduates’ readiness for deployment: Areas of strength and opportunities for growth. Military Medicine, 189(9), e2220-e2228. https://doi.org/10.1093/milmed/usae167
Dieck-Assad, G., González Peña, O. I., & Rodríguez-Delgado, J. M. (2021). Evaluation of emergency first response’s competency in undergraduate college students: Enhancing sustainable medical education in the community for work occupational safety. International Journal of Environmental Research Public Health, 18(15), 7814. https://doi.org/10.3390/ijerph18157814
Ellington, M., & Farrukh, S. (2020). Are battlefield and prehospital trauma scenarios an effective educational tool to teach leadership and crisis resource management skills to undergraduate medical students? BMJ Military Health, 166, e34-e37. https://doi.org/10.1136/jramc-2018-001146
Fuentes, M. R. W. C. (2021). Operational curriculum and research initiatives: Shaping the future of military medicine. Federal Practitioner, 38(10), 474. https://doi.org/10.12788/fp.0192
Garg, M., Peck, G. L., Arquilla, B., Miller, A. C., Soghoian, S. E., Anderson, H. L., Bloem, C., Firstenberg, M. S., Galwankar, S. C., Guo, W. A., Izurieta, R., Krebs, E., Hansoti, B., Nanda, S., Nwachuku, C. O., Nwomeh, B., Paladino, L., Papadimos, T. J., Sharpe, R. P., . . . Stawicki, S. P. (2017). A comprehensive framework for international medical programs: A 2017 consensus statement from the American College of Academic International Medicine. International Journal of Critical Illness, 7(4), 188-200. https://doi.org/10.4103/IJCIIS.IJCIIS_65_17
Kolb, D. A., Boyatzis, R. E., & Mainemelis, C. (2014). Experiential learning theory: Previous research and new directions. In Perspectives on thinking, learning, and cognitive styles (pp. 227-247). Routledge.
Kollek, D., Welsford, M., & Wanger, K. (2009). Chemical, biological, radiological and nuclear preparedness training for emergency medical services providers. Canadian Journal of Emergency Medicine, 11(4), 337-342. https://doi.org/10.1017/S1481803500011386
Lewis, K. O., Popov, V., & Fatima, S. S. (2024). From static web to metaverse: Reinventing medical education in the postpandemic era. Annals of Medicine, 56(1), 2305694. https://doi.org/10.1080/07853890.2024.2305694
McGraw, A. P. (2023). “Train like you fight”: A literature review of best practices for training marines to perform in stressful combat situations. North Carolina State University.
Michaud, J., Moss, K., Licina, D., Waldman, R., Kamradt-Scott, A., Bartee, M., Lim, M., Williamson, J., Burkle, F., Polyak, C. S., Thomson, N., Heymann, D. L., & Lillywhite, L. (2019). Militaries and global health: Peace, conflict, and disaster response. The Lancet, 393(10168), 276-286. https://doi.org/10.1016/s0140-6736(18)32838-1
Naing, T. T., Minamoto, Y., Aung, Y. P., & Than, M. (2022). Faculty development of medical educators: Training evaluation and key challenges. The Asia Pacific Scholar, 7(3), 23-32. https://doi.org/10.29060/TAPS.2022-7-3/OA2742
O’Connell, K., Hoke, K., Berkowitz, A., Branchaw, J., & Storksdieck, M. (2021). Undergraduate learning in the field: Designing experiences, assessing outcomes, and exploring future opportunities. Journal of Geoscience Education, 69(4), 387-400. https://doi.org/10.1080/10899995.2020.1779567
Onderková, A., Quinn, J., Meoli, M., Taylor, D., Nesterenko, S., Schramm, J. M., Gimpelson, A. J., O’Kelly, A., Parks, S., Rizek, J., Davis, T., Surkov, D., Cherniawski, B., & Fernando, R. (2024). Enhancing prehospital care during the conflict in Ukraine: NATO’s role in global health engagement. Military Medicine, 190(3), 86-94. https://doi.org/10.1093/milmed/usae380
van der Wal, H., Duijnkerke, D., Engel, M. F., Hoencamp, R., & Hazelzet, J. A. (2024). Value-based healthcare from a military health system perspective: A systematic review. BMJ Open, 14(11), e085880. https://doi.org/10.1136/bmjopen-2024-085880
Vogel, D., & Harendza, S. (2016). Basic practical skills teaching and learning in undergraduate medical education – A review on methodological evidence. GMS Journal for Medical Education, 33(4). https://doi.org/10.3205/zma001063
Watson, A. L., Anderson, M., Drake, J., Heaston, S., Schmutz, P., Rasmussen, R., & Reed, C. (2025). Nursing and emergency medical technician students’ perspectives on mass casualty simulation training: A phenomenological study. Nursing and Health Sciences, 27(2), e70104. https://doi.org/10.1111/nhs.70104
Woolley, T., Round, J., & Ingram, M. (2017). Global lessons: Developing military trauma care and lessons for civilian practice. BJA: British Journal of Anaesthesia, 119(suppl_1), I135-I142. https://doi.org/10.1093/bja/aex382
*Dr Zaw Phyo
Department of Medical Education,
Defence Services Medical Academy (DSMA),
Yangon, Myanmar
No. 94, Pyay Road, Mingaladon Township,
Yangon, Myanmar Postal code – 1102
+95 92032754
Email: dr.zawphyoo@gmail.com
Submitted: 10 February 2025
Accepted: 17 October 2025
Published online: 7 April, TAPS 2026, 11(2), 64-72
https://doi.org/10.29060/TAPS.2026-11-2/OA3666
Sameera Anuruddha Gunawardena, Rovindu Sandul Hettige, Yap Hui Nee & Tai Suyee Sophia
School of Medicine, IMU University, Kuala Lumpur, Malaysia
Abstract
Introduction: English is the main medium of medical education in many institutions worldwide. However, several terms in the medical lexicon carry colonial, cultural, or linguistic origins that may be outdated or confusing for students from non-English-speaking backgrounds. This study explores culturally exclusive and outdated metaphorical terms in medicine and debates their continued usage.
Methods: A two-stage protocol was followed. First, textbooks and teaching material from the pre-clinical phase of the medical curriculum at the authors’ institution were screened for metaphorical medical terms with outdated concepts or Anglo-European cultural elements. Next, the definitions and origins of each term were explored using open-source etymological resources and peer-reviewed literature from PubMed and Google Scholar. Terms were then thematically grouped and narratively analysed.
Results: Twenty Anglo-European references were identified and categorised into sub-themes: Western food (e.g., “port-wine stain,” “maple syrup urine disease”), fiction (e.g., “Alice-in-Wonderland syndrome”), religion (e.g., “Hand of Benediction”), and foreign languages (e.g., “café-au-lait spots,” “tache noire”). These may be unrelatable to students from diverse cultural or religious backgrounds. In addition, ten obsolete societal references were noted (e.g., “Washerwoman’s hands,” “rugger jersey spine,” “Indian file pattern”), which are no longer part of common knowledge.
Conclusion: While such terms aided understanding for Anglo-European learners, they may now burden today’s diverse student population. Medical educators should reassess their continued use to ensure clarity and equity in global medical education. This review, based on single institutional findings, provides a foundation for broader, multi-institutional studies to explore the prevalence and impact of these terms across curricula.
Keywords: Medical Terminology, Equity in Medical Education, Colonialism in Medicine, Obsolete Medical Terms, Global Medical Education
Practice Highlights
- Several medical metaphors are based on culturally exclusive and outdated references.
- Many metaphorical terms require knowledge of Anglo-European history, culture, or religion.
- Some metaphors refer to societal elements or occurrences that are no longer common knowledge.
- Such metaphors would be meaningless to students who do not understand their relevance.
- Learning these outdated terms intended to simplify medicine would now be an additional burden.
I. INTRODUCTION
Medicine is an extremely challenging and complex program of study (Davis & Harden, 2003; Ogden et al, 2023; Woodruff, 2019) and many medical undergraduates face numerous difficulties in mastering the program, especially during the early years of the course (Kirtchuk et al, 2022; Malau-Aduli BS et al, 2020). Amidst the countless hours of study, clinical rotations, and immersive learning experiences, medical students are also expected to acquire a robust vocabulary of medical terms that enables them to comprehend, communicate, and apply complex medical concepts. Language has been identified as one of the main challenges in medical education programs. (Tayem et al, 2020) Since most institutions deliver their medical programs in English, there is a high expectation of English language proficiency among medical entrants (Chan et al, 2022; Hayes & Farnill, 1993; McLean et al, 2013). English has been considered as a barrier for understanding basic medical disciplines among non-native English-speaking students (Bendriss & Bendriss, 2015; Lucas et al., 1997) and interviews with trainers have found that the deficiencies in the figurative and colloquial language affected the performance of international students even at the graduate level (Henderson et al., 2017). Although studies like Jain & Krieger (2010) and Byrne et al. (2019) highlight the linguistic and cultural adaptation struggles among medical students, they do not specifically address the difficulties in comprehending medical language.
Medical lingo is as complex as the science itself and is rife with idiosyncrasies and irregularities that can confound even native English speakers. Modern English has evolved through the influence of Greco-Roman, French, and Germanic languages. (Van der Auwera & Genee, 2002) Many medical terms, therefore, have etymological roots in Latin, Greek or French (Banay, 1948; Faure, 2018). Some terms are often shaped by scientific advancements and technological innovations, and quite a number of them are eponymous references to a person or persons who described a particular phenomenon. (Thomas, 2016; Whitworth, 2007) Similarly, some terms originate from specific cultural and linguistic nuances to English folklore, literature, and society while some others have an archaic origin or are metaphors representing a phenomenon that is non-existent or inapplicable in today’s context. Many clinicians and lecturers continue to use these terms in medical education and in the authors’ experience, students from non-English speaking backgrounds, tend to learn these terms without truly understanding their relevance. Although there have been concerns raised over the authenticity and appropriateness of use of eponyms in medical literature (Strous & Edelman, 2007; Whitworth, 2007; Woywodt & Matteson, 2007), however, there is very little attention given to the propriety of culturally specific and obsolete metaphorical terms in the medical lexicon. This study explores culturally exclusive or outdated metaphorical medical terms and traces their meanings and etymological origins with the aim of stimulating dialogue on whether their continued use in contemporary medical education is justifiable. Except for a few articles (Cohen et al., 2013; Gheewala et al., 2022; Torrey, 2023), no published study has systematically undertaken an exploration of the historical and cultural context of these terms.
II. METHODOLOGY
We followed a two-stage qualitative approach that combined a document analysis with an exploratory targeted search to identify and contextualise terms that were metaphors, figurative labels, or colloquial descriptions of a medical condition. This approach followed previously published strategies for mapping and contextualising terminology from medical documents (Bearman et al., 2021; Bowen, 2009; Dalglish et al., 2020).
A. Stage 1: Document Analysis
During the period from November 2023 to November 2024, all four authors screened the teaching-learning material and textbooks within the pre-clinical medical program at the authors’ university. The pre-clinical curriculum is distributed within 12 modules over four semesters and delivered in the form of synchronous and asynchronous lectures, practical’s, team-based learning, problem-based learning, case-based learning, and self-directed learning. Teaching-learning material for all lessons are uploaded and accessible via the university’s e-learning portal, either in document form, voice-over narrations, microlearning videos, or interactive SCORM packages. We also identified the most frequently borrowed textbook within each of the six main pre-clinical disciplines through the institutional library resource utilisation data. The indices of the textbooks in anatomy (Agur et al., 2019), pathology (Rubin & Reisner, 2019), and pharmacology (Whalen, 2019) were screened by the first and second authors while physiology (Widmaier et al., 2019), biochemistry (Abali et al., 2022), and microbiology (Bauman, 2015) were screened by the other two authors.
The terms were eligible for inclusion if they met at least one of the two following criteria: 1) Anglo-European connotations – terms including Latin and French words and terms requiring knowledge of Western culture, literature or history. 2) Outdated terms – references to phenomena or practices that used to be common knowledge during previous times but are no longer present or rarely encountered in modern-day living. We did not collect data on the frequency of the use of the terms. We also did not screen any formative or summative assessment documents.
B. Stage 2: Contextualisation of Identified Terms
We then conducted an exploratory targeted search of the definitions, etymological origins and medical relevance of each term. We did not intend to conduct an exhaustive review based on any systematic protocol but instead focused on gathering sufficient contextual information using the term itself as a key word, or where necessary, combining them with words such as ‘origin’, ‘history’ or ‘etymology’. Our sources included online open-source etymological databases, such as the online etymology dictionary (https://www.etymonline.com), Oxford reference (https://www.oxfordreference.com), the Oxford concise medical dictionary and peer reviewed publications indexed in PubMed and Google Scholar.
Terms were grouped into subcategories, and each term was then charted according to definition, medical usage, historical or etymological context and justification for inclusion. Any disagreements on the meaning of the terms or the justification for their inclusion in this study were resolved through mutual consensus among the authors.
III. RESULTS AND DISCUSSION
We identified 20 terms as Anglo-European references and 10 terms as obsolete phenomena. A summary of the terms and their medical context is given in Table 1 and is discussed in more detail below.
|
Category |
Sub-category |
Term |
Medical context and Etymology |
|
ANGLO EUROPEAN REFERENCES |
Westernised Food |
Maple syrup urine disease |
The sweet smell of maple syrup is present in the urine of infants who have inherited deficiency in metabolising amino acids. |
|
Port-wine stain |
Cutaneous haemangiomas which are the same colour as port wine. |
||
|
Red currant jelly stools |
Stools in babies with intussusception have the same appearance and colour as red-currant jelly. |
||
|
Literary Works |
Alice in Wonderland syndrome |
A neurological condition with abnormal visual perceptions. It is named after Lewis Carroll’s Alice in Adventures where Alice, the central character, sees surrounding objects in distorted shapes and sizes. |
|
|
Mad-hatter disease |
Psycho-behavioural abnormalities due to chronic mercury poisoning. Such behaviours were seen in persons engaged in the manufacturing of top hats leading to the term ‘as mad as a hatter’. This was also the basis for the character Mad Hatter in Alice in Wonderland. |
||
|
Lilliputian syndrome |
Hallucinations where objects or people appear smaller than usual. From Jonathan Swift’s Gulliver’s Travels where Gulliver finds the land of miniature people who are called Lilliputians. |
||
|
Miss Havisham syndrome/ Plyushkin syndrome (also called Diogenes syndrome) |
A neuropathological state of hoarding, neglect, and social withdrawal. This is based on the character Miss Havisham in Charles Dickens’ Great Expectations. |
||
|
Pickwickian syndrome |
Obesity-hyperventilation syndrome is based on the character of a fat and excessively sleepy coachman in Charles Dickens’ Pickwick Papers. |
||
|
Rapunzel syndrome |
Psychiatric abnormality of ingesting hair is based on the fairy tale character of Rapunzel who had extremely long hair. |
||
|
Othello syndrome |
A state of morbid jealousy is named after the central character in William Shakespeare’s play, Othello, who murders his wife due to unfound suspicions of his wife’s infidelity. |
||
|
Mythology & Religion |
Caput medusae |
Dilated umbilical vessels in portal hypertension resembling the Greek mythological character Medusa’s head. |
|
|
Hand of Benediction |
Median or Ulnar nerve neuropathy of the hand giving the appearance of a Catholic priest’s hand gesture during blessing. |
||
|
St. Vitus dance |
Rhythmic dance-like movements seen in rheumatic chorea are named after the medieval tradition of dancing in homage to Saint Vitus. |
||
|
Rachitic rosary |
Also known as ‘string of beads’ appearance where the enlarged costochondral junctions are seen as a series of rounded shadows on the chest X-ray of a child with Ricketts. The rosary is a string of prayer beads used in the Christian and Catholic religions. |
||
|
Non-English Terms |
Café-au-lait spots |
Meaning Coffee with milk (French) given to the light-tanned skin lesions typically seen in neurofibromatosis. |
|
|
Peau d’orange appearance |
Meaning Orange peel (French) – the appearance of skin manifestations in breast carcinoma. |
||
|
Tache noire |
Black spot (French) – the discolouration of sclera after death. |
||
|
Linitis plastica |
Meaning linen-like and non-pliable (etymology unclear) diffuse thickening of the stomach wall in gastric cancer also known as leather bottle stomach. |
||
|
Rigor mortis |
Meaning stiffening after death (Latin). |
||
|
Cutis anserina |
Meaning goose skin (Latin) appearance of the skin in immersed bodies. |
||
|
OBSOLETE PHENOMENA |
Lead pipe rigidity |
Muscle tone in upper motor neuropathies resembling the feeling of bending a lead pipe. |
|
|
Rugger Jersey spine |
Horizontal radio dense lines of the vertebrae resemble horizontal lines of the rugger jersey. |
||
|
Washerwoman’s sign |
Macerated palms and soles in immersed bodies like the appearance of the hands in a laundress. |
||
|
Indian file pattern |
Lining of nuclei in invasive breast carcinoma resembling the pattern of Red Indians moving one behind another. |
||
|
Pugilistic attitude |
Postmortem flexing of arms and legs after burning or putrefaction that resembles the posture of a boxer (pugilist). |
||
|
Rodent ulcer |
Chronic enlarging ulcer in basal cell carcinoma that resembles a rodent bite. |
||
|
Signet ring cell carcinoma |
Carcinoma of mucin-producing glandular epithelial cells where the excessive mucin pushes the nucleus to a periphery giving the appearance of a signet ring. |
||
|
Coal miner’s lung |
Pneumoconiosis used to be common among coal miners. |
||
|
Hay fever |
Allergic rhinitis is believed to be due to exposure to hay. |
||
|
Farmer’s lung/ Bird fancier’s lung |
Hypersensitive pneumonitis is common among farmers and bird breeders. |
||
Table 1. Metaphors or figurative labels in medicine that are exclusively Anglo-European or refer to obsolete phenomena
A. Exclusively Anglo-European References
Among the many pathological terms that are linked to common food items, some are analogies to Western food items that are rarely consumed elsewhere. It is very unlikely that students coming from non-Anglo-European backgrounds would have seen or tasted these food items. Notable terms include, ‘maple syrup urine’ which refers to the specific ketotic odor of maple syrup in urine in babies with inherited deficiencies in amino acid metabolism or ‘port wine stain’ which refers to the colour of congenital capillary malformations in the skin. Another example is the ‘red currant jelly’, which is almost exclusive to English cuisine, being linked to the colour of stools in intussusception or sputum in Klebsiella. Interestingly, the term ‘red currant jelly stools’, although taught as a characteristic feature of intussusception, appears to have very little value in actual clinical practice (Yamamoto et al., 1997).
Metaphorical references to literary works are also quite common in medicine. Mad-hatter disease is a term referring to neuropsychiatric manifestations seen in people regularly exposed to mercuric fumes. This occupational hazard was particularly common in the top hat industry during the 16-18th century which was the basis for the common English simile, ‘as mad as a hatter’. The manufacturing of top-hats using Mercury is almost nonexistent today (Crean, 1962; Martin & Kite, 2006). Therefore, this term could be considered under the obsolete category as well. Those who have read Lewis Carroll’s Alice in Wonderland might probably understand its relevance better through the character of Mad Hatter. This novel is featured in another context, based on the unusual experiences of the protagonist. The term ‘Alice in Wonderland Syndrome’ is given to a neurological disorder that causes distorted visual perception. Similarly, Lilliputian hallucinations’, a term that was coined from Jonathan Swift’s Gulliver’s Travels, refers to the complex visual perception of objects or people greatly reduced in size (Chand & Murthy, 2007). Several other fictional characters from Anglo-European literature have found their way into medicine. The terms, ‘Miss Havisham syndrome’, ‘Plyushkin syndrome’, ‘Diogenes syndrome’ all refer to a neurological condition that manifests with social withdrawal, extreme hoarding, self-neglect and squalor. Miss Havisham is a character in Charles Dickens’ Great Expectations and Plyushkin is a character in Nikolai Gogol’s novel Dead Souls. Both these fictional characters were portrayed as having social isolation and hoarding tendencies. Diogenes on the other hand was a Greek philosopher who lived in the 4th Century BC and the use of his name for this condition has been criticised as his desire was to live contentedly with minimal possessions and did not display any characteristics of this syndrome (Cooney & Hamid, 1995). Several other eponyms based on fiction, such as Rapunzel, Othello, Pickwickian syndrome were identified during our search but were excluded from further exploration considering the rarity of their usage.
Aligned to fiction were numerous references to mythological characters, predominantly from Greek mythology, such as the anatomical terms, Achilles’ tendon, atlas vertebra, hymen, iris, labyrinth or diseases such as nymphomania, hermaphroditism, narcissism (Lysanets & Bieliaieva, 2023). These do not require any comparative imagery for comprehension whereas, using terms like ‘caput medusae’ to denote the appearance of dilated veins around the umbilicus in liver failure would be meaningless to students unfamiliar with the mythological creature, Medusa. The ‘Hand of Benediction’ which is the neuropathological effect of hyperextension of the lateral three fingers and flexion of the medial two fingers is termed after the gesture made by Catholic priests during blessing. Similarly, the ‘Rachitic rosary’ refers to the rosary or string of beads used in prayer. The abnormal rhythmic movements in rheumatic chorea, now popularly known as Sydenham chorea, was given the term ‘St. Vitus dance’ by Sydenham himself, who compared them to the maniacal dancing epidemics in medieval Europe that were miraculously cured in the chapel of St Vitus (Park & Park, 1990). These metaphors have an exclusively Christian or Catholic origin and understanding the relevance of these terms to the clinical and radiological features would be difficult for students from other religious backgrounds.
It is well known that many scientific terms in medicine originate from Greek, Latin and other European languages. However, some metaphors and terms are distinct from these foreign languages. The terms included here are only those that intend to evoke imagery but require knowledge of the respective language to do so. Only a student who understands that café-au-lait means coffee mixed with milk could visualise the light, tan-coloured spots in neurofibromatosis. A student unfamiliar with Latin would not be able to relate the term cutis anserina to a goose skin to visualise the sign of immersion or that the French term ‘tache noire’ relates to a black spot. To students growing up in the UK or Europe, these terms would still be meaningful but would be too much to expect of students coming from other regions. A peculiar term that deserves mention in this category is ‘linitis plastica’. This term is used interchangeably with the relatively older term ‘leather bottle stomach’ to denote a diffuse thickening of the stomach wall characteristically seen in signet ring cell carcinoma (Armstrong, 1914). The term has a confusing and obscure origin, which some scholars believe was coined to indicate sheets of filaments like linen (linitis) that were non-pliable (plastica) (Agnes et al., 2017).
B. References to Obsolete Phenomena
This category holds terms that refer to material or sociocultural elements that no longer exist in society. A good example of a reference to obsolete material is the ‘lead pipe rigidity’ described as the uniform spastic muscle tone found in upper motor neuron disorders analogous to bending a lead pipe. In the past, domestic plumbing used lead pipes and the feeling of bending such a pipe would have been common knowledge. However, in today’s context, with the use of polyvinyl chloride (PVC) pipes, students would not be able to relate to this experience at all. Similarly, the ‘signet ring’ which used to be a commonly worn item by kings and nobles to stamp their authentication on sealed correspondence and legal transactions during early civilisations and medieval periods has only a historical and heirloom value today. Students need to be shown the image of a signet ring to help them understand the resemblance. The game of rugger or rugby football is quite popular, albeit in a few countries and the ‘rugger-jersey spine’ seen as horizontal radio-dense lines in the upper and lower margins of the vertebral bodies in X-rays of patients with renal osteodystrophy, refers to the horizontally striped jersey typically worn by players in the game. However, this characteristic pattern is no longer seen in the attire of rugby players and while the game itself is only known to a few, the relevance of the pattern of the jersey would also be confusing to those who do.
A reference to an obsolete sociocultural element is the sodden, macerated postmortem appearance of palms and soles in bodies immersed for a long time in water, called the ‘washer-woman’s sign’. This is because the washerwoman, whose occupation was to wash people’s clothes, had palms that were softened and wrinkled due to constant washing. This profession hardly exists today as washing, even on a commercial scale, is now automated in most regions. Another noteworthy mention is the ‘pill-rolling tremor’ in Parkinson disease. The term pill-rolling is meant to evoke imagery of the ancient art of dispensing pills in the era of apothecaries, where the medicinal paste was rolled into small spherical masses between the fingers and thumb (Yu, 2015). Some other occupation-related conditions that existed in the past such as the ‘coal miner’s lung’ in pneumoconiosis, farmer’s lung or bird fancier’s lung for hypersensitivity pneumonitis, and athlete’s foot for ringworm infection of the toes are still being used despite the decline in their prevalence due to improved occupational health strategies and hygiene. The term ‘pugilistic attitude’ refers to an artefactual change in body posture seen in cases of burning or advanced putrefaction and is meant to resemble the flexing of the upper limbs into a posture that resembles a boxer’s (pugilist) stance. Scrutiny of the postmortem posture shows that the arms are partially flexed and partially abducted at the shoulder joint, flexed, and pronated at the elbow joint while the hands are partially clenched and flexed at the wrist. This posture certainly does not resemble the stance in modern-day boxing and is only like stances depicted in paintings and murals of boxers during Roman times (Vivonia, 2020).
Misnomers are a frequent occurrence in medicine (Manikat & Chopra, 2023). Two terms that we felt were relevant in this regard were ‘hay fever’ and ‘rodent ulcer’. It is now quite well known that hay is not the cause for seasonal allergic rhinitis as once believed. The term ‘rodent ulcer’ is frequently used to indicate the chronic invasive ulcer of basal cell carcinoma. The term has its origins in the mid-1800s (Paul, 1885) when rodent bites were a common occurrence due to poorer housing and sanitary conditions. However, in today’s context where rodent bites are a rarity, understanding its relevance is quite challenging.
The characteristic description of the single file pattern of nuclei in many tumors, typically seen in invasive lobular breast carcinoma, has been popular as the ‘Indian file pattern’ since the mid-1960s (Pai, 2025). This phrase which originates from the European settlers’ descriptions of how the Red Indians move in a line behind one another when hunting or warring is irrelevant now, as the current lifestyles of these native American Indians are quite different and conflicts with the current principle of moving away from ethnically or racially charged references in medical terminology (Magguilli et al. 2024).
C. Rethinking Medical Terminology for a More Equitable Medical Education
Some scholars view the use of exclusively Anglo-European terms in medical education in non-English-speaking countries as a continuation of colonialism in Western allopathic medicine (Jayasinghe, 2021; Shankar, 2024; Supe, 2016). Considerable inequities have been identified in health professions education between the global north and the global south (Rashid & Grant, 2024) which include the slow update cycle of medical textbooks, the comparative dearth of medical textbooks from the global south, and the need for medical educational institutions to align with Western models for accreditation and employability.
While it is understandable that certain metaphors and eponyms simplify medical concepts and make the study of medicine more interesting and colourful, care should be taken to ensure that they do not become added burdens to the student. If medical eponyms and metaphors intend to enhance memory and understanding then, these unfamiliar terms would create a paradoxical effect to a significantly large population of medical students who come from Asian, African or South American countries. An interesting point to note was that many of the learning resources we screened did not explain the meaning of these terms. This problem is likely to be aggravated among future generations of medical students as their teachers may be unfamiliar with the terms themselves.
A proposed strategy would be to avoid eponyms and metaphors and use more descriptive terminology instead. Recommendations have been made to streamline the use of medical eponyms and reduce confusion, especially considering the globalisation of the medical fraternity (Jana et al., 2009), and possibly as a response, there has been a reduced usage of eponyms in scientific papers since the early 90s (Thomas, 2016). However, this is likely to make medicine even more monotonous to the student and possibly, complicate communication among medical professionals. Like the debate on the use of eponyms (Fargen & Hoh, 2014) there would be those who value the continued use of these metaphors and figurative labels despite their obscurity and colonialist links. However, in the context of providing equitable medical training to the vast numbers of students from non-English speaking backgrounds, the continued use of such unfamiliar and obscure terms needs re-evaluation.
D. Limitations and Recommendations
The terms generated through this study are limited to the teaching and learning resources available within our institution which restricts the generalisability of the significance of using these terms in medical education. Although we used the most recent editions of textbooks, some of them had not been editorially revised within recent times. We did not use any structured systematic protocol to explore the definitions of these terms. We do not have any data related to how frequently these terms were used or the actual context of how they were taught within the curriculum. Therefore, we are unable to indicate the actual impact of these terms on student learning nor any strategies to minimise them. Further studies should incorporate a wider variety of sources and attempt to quantify their use within teaching and assessments in medical curricula in different institutions. We also propose focus group discussions and interviews with students and educators to explore their understanding and perceptions of these terms. While the value of using these unfamiliar terms to teach medicine to non-English speaking medical students is debatable, their inclusion in assessments would be less justifiable. If such terms are to be used, teachers should ensure that their etymological relevance is also clearly explained in the teaching-learning material, and we believe that this article would be a useful resource in that regard.
IV. CONCLUSION
We identified several outdated, culturally exclusive metaphors, eponyms, and historical references which would have once served as vivid teaching-aids in medicine, but could now pose a challenge to medical students, particularly from non-English-speaking backgrounds. Although the variability of teaching practices across institutions limits their generalisability, these findings reveal a tension between historical shorthand and modern inclusivity, urging a rethink of medical language. Future research across multiple institutions and different cultural contexts would provide a clearer understanding of the prevalence, educational impact, and cultural resonance of metaphorical medical terms in contemporary medical education. This would, however, need strong collaborative approaches as access to institutional material is often restricted.
As an initial exploration, this study lays the groundwork for global dialogue and provides some practical implications for medical educators to either contextualise these terms explicitly or replace them with more universally acceptable terminology. Educators could consider piloting a more descriptive, standardised medical lexicon that transcends cultural and linguistic barriers, especially in the pre-clinical disciplines and evaluate their outcomes. Although such endeavours would require consensus and efforts from numerous experts, it would make the learning experience more equitable and effective for students worldwide.
Notes on Contributors
Author SAG designed the study and the methodological framework and was involved in data collection, data analysis and final revision and formatting of the manuscript. Author RSH was involved in data collection, data analysis, drafting and revising the manuscript and is the corresponding author. Author YHN was involved in data collection, data analysis and drafting of the manuscript. Author TSS was involved in data collection and drafting of the manuscript. All authors have read and approved the final manuscript.
Ethical Approval
University approval for the use of teaching learning materials was granted, and as it was a review of terms, no further ethical issues were considered.
Data Availability
The extracted data can be made available if needed.
Funding
There is no funding available for this paper.
Declaration of Interest
All authors confirm that they have no conflict of interest in conducting this study.
References
Abali, E. E., Cline, S. D., Franklin, D. S., & Viselli, S. M. (2022). Lippincott® illustrated reviews: Biochemistry (8th ed.). Wolters Kluwer.
Agnes, A., Estrella, J. S., & Badgwell, B. (2017). The significance of a nineteenth century definition in the era of genomics: Linitis plastica. World Journal of Surgical Oncology, 15(1), 123. https://doi.org/10.1186/s12957-017-1187-3
Agur, A. M. R., Dalley, A. F., & Moore, K. L. (2019). Moore’s essential clinical anatomy (6th ed.). Wolters Kluwer.
Armstrong, G. E. (1914). Linitis Plastica. The Canadian Medical Association Journal, 4(9), 770–775. https://pmc.ncbi.nlm.nih.gov/articles/PMC406735/pdf/canmedaj00244-0028.pdf
Bauman, R. W. (2015). Microbiology: With diseases by body system (4th ed.). Pearson.
Banay, G. L. (1948). An introduction to medical terminology I. Greek and Latin derivations. Bulletin of the Medical Library Association, 36(1), 1–27. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC194697/pdf/mlab00247-0013.pdf
Bendriss, G., & Bendriss, R. (2015). Raising awareness among health educators and educational institutions of the need to overcome the language barrier among non-native English speaking students of health sciences in Qatar: A needs analysis and solutions. Journal of Local and Global Health Science, 2015(1), 1. https://doi.org/10.5339/jlghs.2015.1
Bearman, M., Mahoney, P., Tai, J., Castanelli, D., & Watling, C. (2021). Invoking culture in medical education research: A critical review and metaphor analysis. Medical Education, 55(8), 903–911. https://doi.org/10.1111/medu.14464
Bowen, G. A. (2009). Document analysis as a qualitative research method. Qualitative Research Journal, 9(2), 27–40. https://doi.org/10.3316/QRJ0902027
Byrne, E., Brugha, R., & McGarvey, A. (2019). ‘A melting pot of cultures’ – Challenges in social adaptation and interactions amongst international medical students. BMC Medical Education, 19(1). https://doi.org/10.1186/s12909-019-1514-1
Chan, S. M. H., Mamat, N. H., & Nadarajah, V. D. (2022). Mind your language: The importance of English language skills in an International Medical Programme (IMP). BMC Medical Education, 22(1), 405. https://doi.org/10.1186/s12909-022-03481-w
Chand, P. K., & Murthy, P. (2007). Understanding a strange phenomenon: Lilliputian hallucinations. German Journal of Psychiatry, 10(1), 21–24. https://www.researchgate.net/publication/286497468_Understanding_a_Strange_Phenomenon_Lilliputian_Hallucinations
Cohen, H. K. S., Luther, A., & Hart, C. A. (2013). Confusing medical terms: Disease that may or may not exist. QJM: An International Journal of Medicine, 106(7), 617–621. https://doi.org/10.1093/qjmed/hct076
Cooney, C., & Hamid, W. (1995). Review: Diogenes syndrome. Age and Ageing, 24(5), 451–453. https://doi.org/10.1093/ageing/24.5.451
Crean, J. F. (1962). Hats and the fur trade. The Canadian Journal of Economics and Political Science, 28(3), 373–386. https://doi.org/10.2307/139669
Dalglish, S. L., Khalid, H., & McMahon, S. A. (2021). Document analysis in health policy research: The READ approach. Health Policy and Planning, 35(10), 1424–1431. https://doi.org/10.1093/heapol/czaa064
Davis, M. H., & Harden, R. M. (2003). Planning and implementing an undergraduate medical curriculum: The lessons learned. Medical Teacher, 25(6), 596–608. https://doi.org/10.1080/0142159032000144383
Fargen, K. M., & Hoh, B. L. (2014). The debate over eponyms. Clinical Anatomy, 27(8), 1137–1140. https://doi.org/10.1002/ca.22409
Faure, P. (2018). From accouchement to agony: A lexicological analysis of words of French origin in the modern English language of medicine. Lexis, 11. https://doi.org/10.4000/lexis.1171
Gheewala, R., Carrillo-Castro, J. M., & Bowden, S. (2022). Outdated medical terminology – A guide for medical students, educators and providers. Oregon Health & Science University. https://www.ohsu.edu/school-of-medicine/diversity-equity/diversity-resources
Hayes, S. C., & Farnill, D. (1993). Medical training and English language proficiency. Medical Education, 27(1), 6–14. https://doi.org/10.1111/j.1365-2923.1993.tb00222.
Henderson, D., McGrath, P. D., & Patton, M. A. (2017). Experience of clinical supervisors of international medical graduates in an Australian district hospital. Australian Health Review, 41(4), 365–371. https://doi.org/10.1071/AH15094
Jain, P., & Krieger, J. L. (2010). Moving beyond the language barrier: The communication strategies used by international medical graduates in intercultural medical encounters. Patient Education and Counseling, 84(1), 98–104. https://doi.org/10.1016/j.pec.2010.06.022
Jana, N., Barik, S., & Arora, N. (2009). Current use of medical eponyms – A need for global uniformity in scientific publications. BMC Medical Research Methodology, 9(1), 18. https://doi.org/10.1186/1471-2288-9-18
Jayasinghe, S. (2021). Ethics and health communication in English: Tackling the consequences of colonial era linguicism and racism. Asian Bioethics Review, 13(2), 245–253. https://doi.org/10.1007/s41649-021-00172-4
Kirtchuk, D., Wells, G., Levett, T., Castledine, C., & De Visser, R. (2021). Understanding the impact of academic difficulties among medical students: A scoping review. Medical Education, 56(3), 262–269. https://doi.org/10.1111/medu.14624
Lucas, P., Lenstrup, M., Prinz, J., Williamson, D., Yip, H., & Tipoe, G. (1997). Language as a barrier to the acquisition of anatomical knowledge. Medical Education, 31(2), 81–86. https://doi.org/10.1111/j.1365-2923.1997.tb02463.x
Lysanets, Y., & Bieliaieva, O. (2023). The use of eponyms in medical case reports: Etymological, quantitative, and structural analysis. Journal of Medical Case Reports, 17, 151. https://doi.org/10.1186/s13256-023-03895-0
Magguilli, M., Thomas, C., & Fowle, E. (2024). What’s in a name? Replacing pejorative terminology in anatomic pathology. International Journal of Surgical Pathology, 33(1). https://doi.org/10.1177/10668969241236700
Malau-Aduli, B. S., Ray, R. A., O’Connor, T., Van Der Kruk, Y., Alele, F. O., & Bellingan, M. (2020). Dealing with academic difficulty in medical school: A pilot study. Education Sciences, 10(3), 83. https://doi.org/10.3390/educsci10030083
Manikat, R., & Chopra, S. (2023). Medical misnomers are murky: Time to memorialize and rename. The American Journal of Medicine, 136(12), 1160–1164. https://doi.org/10.1016/j.amjmed.2023.08.021
Martin, G., & Kite, M. (2006). Potential for human exposure to mercury and mercury compounds from hat collections. AICCM Bulletin, 30(1), 12–16. https://doi.org/10.1179/bac.2006.30.1.002
McLean, M., Murdoch-Eaton, D., & Shaban, S. (2012). Poor English language proficiency hinders generic skills development: A qualitative study of the perspectives of first-year medical students. Journal of Further and Higher Education, 37(4), 462–481. https://doi.org/10.1080/0309877x.2011.645461
Ogden, K., Kilpatrick, S., & Elmer, S. (2023). Examining the nexus between medical education and complexity: A systematic review to inform practice and research. BMC Medical Education, 23(1). https://doi.org/10.1186/s12909-023-04471-2
Pai, S. A. (2025). Medical origin of the phrase “Indian File” in lobular carcinoma of the breast. International Journal of Surgical Pathology, 33(1), 254–255. https://doi.org/10.1177/10668969241283491
Park, R. H., & Park, M. P. (1990). Saint Vitus’ dance: Vital misconceptions by Sydenham and Bruegel. Journal of the Royal Society of Medicine, 83(8), 512–515. https://doi.org/10.1177/014107689008300814
Paul, F. T. (1885). The pathology of rodent ulcer. British Medical Journal, 1(1270), 881–884. https://doi.org/10.1136/bmj.1.1270.881
Rashid, M. A., & Grant, J. (2024). Power and place: Uncovering the politics of global medical education. Medical Education, 58(8), 930–938. https://doi.org/10.1111/medu.15459
Rubin, E., & Reisner, H. M. (2019). Principles of Rubin’s pathology (7th ed.). Wolters Kluwer.
Shankar, P. R. (2024). “Colonialism” in modern allopathic medical education. Archives of Medicine and Health Sciences, 12(3), 436–437. https://doi.org/10.4103/amhs.amhs_148_24
Strous, R. D., & Edelman, M. C. (2007). Eponyms and the Nazi era: Time to remember and time for change. The Israel Medical Association Journal, 9(3), 207–214. https://pubmed.ncbi.nlm.nih.gov/17402342
Supe, A. (2016). Evolution of medical education in India. Journal of Postgraduate Medicine, 62(4), 255–259. https://doi.org/10.4103/0022-3859.191011
Tayem, Y., AlShammari, A., Albalawi, N., & Shareef, M. (2020). Language barriers to studying medicine in English: Perceptions of final-year medical students at the Arabian Gulf University. Eastern Mediterranean Health Journal, 26(2), 233–238. https://doi.org/10.26719/2020.26.2.233
Thomas, P. (2016). Are medical eponyms really dying out? A study of their usage in the historical biomedical literature. The Journal of the Royal College of Physicians of Edinburgh, 46(4), 295–299. https://doi.org/10.4997/jrcpe.2016.417
Torrey, T. (2023, October 9). Historical names of diseases and conditions. Verywell Health. https://www.verywellhealth.com/outdated-disease-names-2615295
Van Der Auwera, J., & Genee, I. (2002). English do: On the convergence of languages and linguists. English Language and Linguistics, 6(2), 283–307. https://doi.org/10.1017/s1360674302000242
Vivonia, M. (2020). Boxing in the Roman empire. World History Encyclopedia. https://www.worldhistory.org/article/1641/boxing-in-the-roman-empire
Whalen, K. (2019). Pharmacology (7th ed., International ed.). Wolters Kluwer.
Whitworth, J. A. (2007). Should eponyms be abandoned? No. British Medical Journal, 335(7617), 425. https://doi.org/10.1136/bmj.39308.380567.ad
Widmaier, E. P., Vander, A. J., & Strang, K. T. (2018). Vander’s human physiology: The mechanisms of body function. Ingram.
Woodruff, J. N. (2019). Accounting for complexity in medical education: A model of adaptive behaviour in medicine. Medical Education, 53(9), 861–873. https://doi.org/10.1111/medu.13905
Woywodt, A., & Matteson, E. (2007). Should eponyms be abandoned? Yes. British Medical Journal, 335(7617), 424. https://doi.org/10.1136/bmj.39308.342639.ad
Yamamoto, L. G., Morita, S. Y., Boychuk, R. B., Inaba, A. S., Rosen, L. M., Yee, L. L., & Young, L. L. (1997). Stool appearance in intussusception: Assessing the value of the term “currant jelly”. The American Journal of Emergency Medicine, 15(3), 293–298. https://doi.org/10.1016/s0735-6757(97)90019-x
Yu, E. C. L. (2015). The pill rolling machine. Hong Kong Medical Journal, 21(3), 290–291. https://www.hkmj.org/abstracts/v21n3/290.htm
*Rovindu Sandul Hettige
School of Medicine, IMU University,
No. 126, Jln Jalil Perkasa 19, Bukit Jalil, 57000,
Kuala Lumpur, Malaysia
Email: rovindu.h@gmail.com
Submitted: 11 February 2025
Accepted: 6 October 2025
Published online: 7 April, TAPS 2026, 11(2), 22-31
https://doi.org/10.29060/TAPS.2026-11-2/RA3871
Leonaldo Lukito Nagaria1, Sri Linuwih Menaldi2 & Diantha Soemantri1
1Department of Medical Education, 2Department of Dermatology and Venereology, Faculty of Medicine, University of Indonesia, Indonesia
Abstract
Introduction: The culture of respect is a crucial aspect of medical learning environments. It has many positive impacts on learning, inclusivity, healthcare collaboration, and healthcare quality. Since it has not been specifically described in previous studies, this review aimed to describe the nature of respect cultivation in medical education (including its definition, assessment, exemplary actions, actors, impacts, and barriers) and thus identify the potential gaps therein.
Methods: This scoping review adapted Arksey and O’Malley’s steps for scoping reviews. Five databases (PubMed, Medline, Science Direct, Google Scholar, and Wiley) were searched, using combinations of related keywords and Boolean operators. The publication year was limited to within the last 15 years. The data analysis was performed using descriptive charting and thematic analysis.
Results: Out of 3,900 articles searched, 169 were full text screened, and 23 were included for further analysis. Six discussed themes were (1) the definition of respect, (2) assessment methods of respect, (3) exemplary actions of respect, (4) contributing actors of respect, (5) the impacts of respect, and (6) barriers to cultivating respect.
Conclusion: The nature of respect in medical education was described diversely in the studies, which lacked specific assessment instruments. Barriers to cultivating respect were reported on multiple levels (personal, interpersonal, and institutional), thus requiring multilevel-based approaches. Further studies are required to explore the theoretical framework of respect in various medical educational settings and strategic approaches for cultivating respect in each context.
Keywords: Respect, Professionalism, Learning Environment, Culture, Medical Education
Practice Highlights
- Practices of respect might vary according to the medical education sociocultural context.
- No valid instrument to assess the culture of respect in medical education yet exists.
- Respect could enhance professionalism, trust, healthcare collaboration, and patient safety.
- Cultivating respect is challenging and should incorporate multilevel-based approaches.
I. INTRODUCTION
The learning environment comprises a complex interplay between the psychosocial, personal, and organizational aspects surrounding the educational setting (Gruppen, 2014). A supportive learning environment creates a safe learning climate, enhances professional identity formation, and nurtures students’ academic achievement (Alotiby et al., 2021). Conversely, a negative learning environment has been associated with medical students’ burnout, psychological distress, and suboptimal learning outcomes. Of all aspects, educational norms and cultures play a significant role in constructing the medical environment (Karani, 2015).
Medical educational culture is still perceived as hierarchical, with a disequilibrium in the distribution of power. In such a culture, individuals with higher social status have a better chance of gaining respect and becoming more influential toward others (Claramita et al., 2022). From the medical education perspective, the hierarchical culture has tended to produce a disrespectful culture and behaviours from faculty toward students, perceived as the inferior group (Lim et al., 2021). For instance, 85% of surveyed Indonesian medical students had experienced disrespectful behaviours from faculty, senior peers, or other health professionals (Rozaliyani et al., 2019).
In extreme cases, disrespectful actions might lead to negative consequences regarding patient care delivery, commonly termed disruptive behaviours (Leape et al., 2012). Dabekaussen et al. (2023) reported that 63% of 388 healthcare workers had experienced disruptive behaviours, such as humiliation, shaming, angry outbursts, insensitive comments, threats, and uncooperative behaviours. These behaviours might result in burnout, moral distress, workflow disengagement, and loss of trust among health professionals. More specifically, the loss of trust and workflow disorganization could contribute to higher risks of miscommunication, false decision-making, and medical errors, which threaten patient safety (Leape et al., 2012).
To foster safety in healthcare settings, respect should be cultivated from the training stage. Medical students who feel respected by their colleagues will treat patients in the same manner (Leape et al., 2012). However, the nature of respect in medical education has been expressed variously across studies. For instance, Karnieli-Miller et al. (2010) described respect as an intrinsic value of being non-judgmental to students and patients. Subramani and Biller-Andorno (2022) broadened the concept to describe attitudes and behaviours that reflect physician bioethics codes. This lack of agreement regarding the nature of respect might prevent us from deeply understanding this topic and subsequently recommending a plausible approach to cultivating respect in medical contexts.
A standardized tool to assess respect in medical education has also not been formulated yet (Karnieli-Miller et al., 2010). Numerous previous studies have attempted to measure expressed respect from a patient perspective, using the Patient Dignity Inventory tool (Aboumatar et al., 2015). Another study by Karnieli-Miller et al. (2010) used qualitative assessment to describe the culture of respect. Considering the wide range of descriptions, this study focused on describing the nature of respect in medical education and identifying the potential gaps in cultivating it. The study findings should provide new insights for medical institutions on how to more appropriately cultivate respect.
II. METHODS
This study adapted the Arksey and O’Malley (2005) scoping review protocol as its methodological guidance. The study method is divided into five appropriate steps, consecutively described below.
A. Identifying Research Questions and Relevant Studies
This scoping review aimed to address the nature of the cultivation of respect in medical education. Through prior literature scanning, we agreed on six leading research questions:
- What are the definitions of respect throughout studies?
- What instruments were used to assess respect throughout studies?
- Who are the contributing actors in cultivating respect throughout studies?
- What are the exemplary actions of respect throughout studies?
- What are the impacts of cultivating respect throughout studies?
- What are the barriers to cultivating respect throughout studies?
The PCC (population, concept, and context) framework was used as guidance for the literature searching and screening. The descriptors were as follows:
- Population: Any individual involved in medical education
- Concept: The nature of respect culture (definitions, assessment instruments, actors, exemplary actions, impacts, and barriers)
- Context: Medical educational settings.
B. Identifying Relevant Studies
Five online databases were used for the literature search: PubMed, Medline, Science Direct, Google Scholar, and Wiley. The search used synonymous terms (such as “respect,” “respectful,” and “dignity”), along with Boolean operators (“AND” and “OR”). The detailed search terms are described in Table 1.
The inclusion criteria were (1) studies conducted in medical education settings, (2) published during 2009–2024, and (3) written in English. The timeframe limit was selected considering that studies specifically discussing “respect” were rarely retrieved before then. The exclusion criteria comprised (1) studies that were not full-text accessible, (2) secondary studies (including reviews, commentaries, and books), and (3) studies that did not empirically assess respect. The publication years were pre-determined using the journals’ automatic search filters.
|
Database(s) |
Searching keywords |
Hits |
|
Medline |
((respect[Title/Abstract] OR respectful[Title/Abstract] OR dignity [Title/Abstract]) AND (“medical student”[Title/Abstract] OR preclinical[Title/Abstract] OR “clinical education”[Title/Abstract] OR “medical school”[Title/Abstract] OR “resident”[Title/Abstract])) AND (“learning environment”[Title/Abstract] OR culture [Title/Abstract] OR interaction [Title/Abstract] OR relationship[Title/Abstract]) |
1001 |
|
Science Direct |
(“medical education” OR “medical student” OR “medical school” OR “resident”) Year: 2004-2024 Title, abstract, keywords: (respect OR respectful OR dignity) AND (learning environment OR culture OR relationship OR interaction) |
1254 |
|
Wiley |
“respect OR respectful OR dignity” in Abstract AND “medical education OR medical student OR clinical education OR medical undergraduate OR resident” in Abstract AND “interaction OR culture OR relationship OR learning environment” anywhere |
652 |
|
Google scholar |
Allin title: (“medical student” OR medical training) AND (“respect” OR |
486 |
|
PubMed Central |
(((respect[Abstract] OR respectful[Abstract] OR dignity[abstract])) AND (medical education[Abstract] OR medical student[Abstract] OR medical undergraduate[Abstract] OR residency[Abstract] OR learning environment [Abstract])) AND (interaction OR culture OR value OR relationship) |
507 |
Table 1. Search Strategy and Keyword Combinations
C. Study Selection
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) diagram is shown in Figure 1. The initial search of the five databases extracted 3,900 articles. After excluding duplicate articles, 2,963 were screened based on their abstracts, and 169 full-text articles underwent full-text eligibility screening. Finally, 23 articles were included.
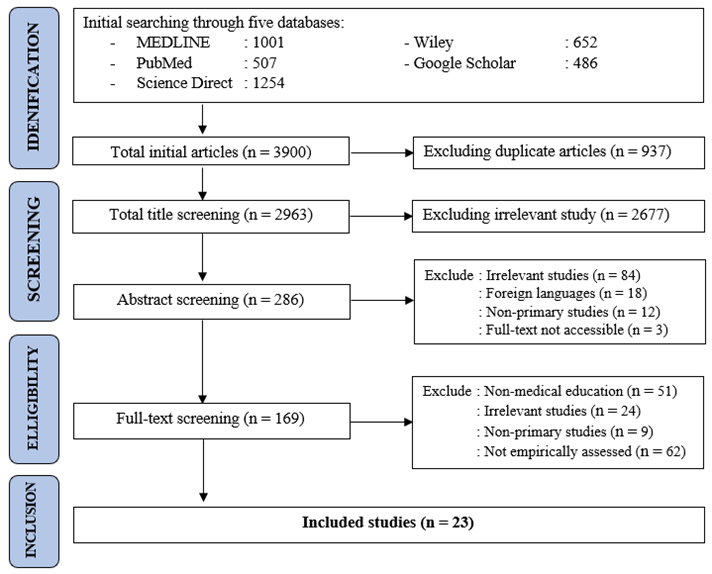
Figure 1. PRISMA-ScR Flow Chart
D. Charting the Data
The methodological characteristics of all the studies included were visualized. Several elements were recorded, such as the authors, publication year, study type, study setting, and study population. As needed, the data were visualized using tables and appropriate graphics.
E. Collecting, Summarising and Reporting
Data regarding the culture of respect in medical education were thematically analyzed into several themes in concordance with the research questions. Then, all studies’ findings were summarized using a narrative approach, manually performed by all authors (LLN, SLM, DS).
III. RESULTS
A. Study Charting Results
23 studies were considered eligible according to the study criteria. The dataset is available in Figshare (https://doi.org/10.6084/m9.figshare.28479062). Most were published in either 2021 or 2024 (three studies each). On average, fewer than three related articles were published annually during the last 15 years. Based on geographical distribution, 21 out of 23 studies were published in Western countries, of which 14 originated from the United States. Two studies originated from Eastern countries: Malaysia (Haque et al., 2016) and Iran (Hazrati et al., 2020). One study compared cultural perspectives in Canada and Thailand (Wong, 2011).
By methodology, most (nine) studies used a cross-sectional design with a self-made survey. The others comprised six mixed-methods studies, five qualitative studies, two retrospective cohort studies, and one interventional study. The interventional study evaluated pediatric residents’ skills after they underwent focused communication training (Howell et al., 2022). The study settings were either the pre-clinical (five studies) or clinical phase (18 studies). The study details are provided in Supplementary Table 1.
1. What are the definitions of “respect” throughout studies?
Five out of the 23 studies stated the definition of respect. Klinner et al. (2024) explained that respect is a multidimensional concept, projected as three distinct concepts: (1) individual intrinsic value, (2) interpersonal relationship, and (3) organizational culture or norms. Respect is a basic humanistic value, encouraging every person to treat others the way they want to be treated (Hazrati et al., 2020). Karnieli-Miller et al. (2010) believed that every individual is worthy of respect and dignity. Klinner et al. (2024) also highlighted the importance of dignity, the universal conscience implying that every person is worthy of respect.
From interpersonal perspectives, respect was defined as attitudes of upholding adversity (Weiss et al., 2021). Respectful relationships could be expressed through politeness and kindness toward others (Curry et al., 2011). Referring to the educational environment, medical staff should appropriately perceive students as individuals who are growing and hence deserving of respectful treatment during their learning (Klinner et al., 2024). One study referred to a “respectful culture” as a supportive educational environment that embraces diversity (Weiss et al, 2021).
2. What instruments were used to assess respect throughout studies?
All studies assessed respect using either questionnaires (15 studies) or qualitative interviews (eight studies). All surveys were self-made, consisting of various questions. For example, DiBrito et al. (2024) used three questions to assess the respectful behaviours of clinical mentors toward patients, learners, and other healthcare members. Haque et al. (2016) used six questions regarding self-respect. Jauregui et al. (2016) used two questions, addressing equal treatment and respect toward healthcare coworkers.
In other studies, respect was assessed as a part of other assessed aspects, such as humanism (Hazrati et al., 2020), professionalism (Gillespie et al., 2009; Haque et al., 2016; O’Flynn et al., 2014), learning environment (Gillespie et al., 2009), communication (Verhagen et al., 2024), or healthcare collaboration (Nagraj et al., 2018). No specific instruments were developed to assess the culture of respect in medical education settings.
3. Who are the contributing actors for cultivating the culture of respect?
Figure 2 conveys the contributing actors for cultivating a culture of respect in medical education. The relevant individuals consist of medical students (Curry et al., 2011), residents (Gonzalo et al., 2014), faculty (DiBrito et al., 2024; Marquardt et al., 2022), patients (Elfassy et al., 2020), senior / peers (Haque et al., 2016), and other health professionals such as nurses (Gillespie et al., 2009). Faculty, medical students, and patients were the most reported contributors to respectful actions. Three studies also showed that respectful interactions could be mutually given by students and faculty (Hazrati et al., 2020; Verhagen et al., 2024; Wong, 2011).
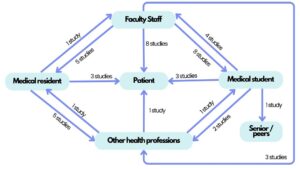
Figure 2. Respectful Relationships in Medical Education
4. What are exemplary actions of respect throughout studies?
Respect in medical education can be expressed by various actions. For instance, respect might be given to students by responding to questions properly (Marquardt et al., 2022), appreciating students’ work (Ekenze et al., 2013), and giving constructive feedback (Jung et al., 2021). On the other hand, respect toward residents was shown by providing autonomous clinical guidance (Wong, 2011) and acknowledging difficulties (Verhagen et al., 2024).
Several studies also described concrete forms of respect toward faculty staff, including polite communication and active engagement during teaching (Haque et al., 2016). The details are provided in Table 2. In medical education, respect could also be regulated by the faculty or institution in the form of targeted policies, such as workload restriction and mistreatment prevention policies. Institutions could also implement specific development programmes for students or faculty as needed (Ekenze et al., 2013).
5. What are the impacts of cultivating respect throughout studies?
Sociocultural impact was the most frequently mentioned effect of a culture of respect. Respect also enhanced trust among healthcare team members and minimized hierarchical gaps (Hazrati et al., 2020). For instance, respect could be portrayed by allowing discussion regarding medical errors and dilemmatic cases (Nagraj et al., 2018), which might foster interprofessional collaboration and improve patient care quality (Klinner et al., 2024).
A culture of respect also positively impacts psychological status. With the cultivation of respect in educational settings, students and residents might develop empathy, trust, inclusivity, and a sense of belonging in the learning process. They would be less afraid of making mistakes while learning and thus feel safer expressing their opinions in such environments (Howell et al., 2022; Karnieli-Miller et al., 2010; Klinner et al., 2024). Conversely, disrespectful culture might lead to psychological stress (Weiss et al., 2021), negativity (Karnieli-Miller et al., 2010), and moral distress (DiBrito et al., 2024).
A culture of respect might boost the academic outcomes of medical students and residents by providing more learning opportunities and clinical experiences (Gillespie et al., 2009; Klinner et al., 2024). Medical teachers also played significant roles as positive role models by giving constructive feedback to foster students’ confidence, motivation, and professionalism (Raikhel et al., 2024).
6. What are the barriers to cultivating respect throughout studies?
Extracting from 11 studies, challenges in cultivating respect involved several layers, including at the personal, interpersonal, and institutional levels. The most frequent challenge to cultivating respect was related to organizational aspects, particularly due to hierarchical cultures (Abedini et al., 2015; DiBrito et al., 2024; Klinner et al., 2024; Marquardt et al., 2022; Wong, 2011) and stressful workloads (Abedini et al., 2015; Elfassy et al., 2020; Marquardt et al., 2022; Verhagen et al., 2024).
From an interpersonal perspective, negative role models (Haque et al., 2016; Weiss et al., 2021), could also hinder the cultivation of respect because they tend to portray disrespectful behaviours toward others. In one study from Western countries, racial microaggressions also represented a barrier to health professionals’ respectful interaction.
Personal barriers derived from a lack of specific skills, namely cultural sensitivity (Weiss et al., 2021) and respectful communication. Some individuals could also perceive respect differently, seeing the same behaviours as mistreatment or disrespect. For instance, some faculty might unconsciously involve certain students less in clinical experience, for which these students might feel disrespected (Ekenze et al., 2013).
|
Orientation |
Study Count |
Exemplary Actions of Respect |
References |
|
|
Respect toward students and residents |
7 |
Acknowledging student/residents’ concerns Accepting sociocultural diversity among students |
(Ekenze et al., 2013; Gordon et al., 2012; Haque et al., 2016; Klinner et al., 2024; Marquardt et al., 2022; Raikhel et al., 2024; Weiss et al., 2021) |
|
|
Showing a respectful manner |
||||
|
Rejecting any form of bullying |
||||
|
Accepting questions from students/residents |
||||
|
Involvement in real clinical experiences |
||||
|
Appreciating students’ work and achievements |
||||
|
Giving feedback with polite language |
||||
|
Respect toward faculty |
4 |
Communicating politely |
(Ekenze et al., 2013; Haque et al., 2016; O′Flynn et al., 2014; Wong, 2011) |
|
|
Active engagement in teaching sessions |
||||
|
Greeting staff politely |
||||
|
Respect toward other health professionals |
7 |
Collaborating with other health professionals |
(Curry et al., 2011; Gillespie et al., 2009; Haque et al., 2016; Jauregui et al., 2016; Nagraj et al., 2018; Palvic et al., 2018; Verhagen et al., 2024) |
|
|
Giving clear briefings to healthcare teams |
||||
|
Respectfully resolving interdisciplinary conflict |
||||
|
Acknowledging other professionals’ contributions |
||||
|
Considering suggestions regarding patient care |
||||
|
Actively listening to other professionals’ concerns |
||||
|
Being willing to help with patient care |
||||
|
Showing gratitude for other professionals’ work |
||||
|
Courageously apologizing if necessary |
||||
|
Establishing rapport with healthcare teams |
||||
|
Respect toward patients |
12 |
Upholding patient privacy and dignity |
(Abedini et al., 2015; Curry et al., 2011; DiBrito et al., 2024; Elfassy et al., 2020; Gillespie et al., 2009; Haque et al., 2016; Howell et al., 2022; Jauregui et al., 2016; Jung et al., 2021; Karnieli-Miller et al., 2010; Klinner et al., 2024; Palvic et al., 2018) |
|
|
Treating patients equally |
||||
|
Being considerate of patients’ decisions |
||||
|
Respecting patients’ boundaries while teaching |
||||
|
Acknowledging patients’ feelings sincerely |
||||
|
Showing empathy |
||||
|
Giving compassionate care |
||||
|
Actively listening to patients’ stories |
||||
|
Showing professionalism in patient care |
||||
|
Taking history with appropriate questions |
||||
|
Communicating politely |
||||
|
Involving patients’ family members Respecting others’ time (being on time) |
||||
|
Respect for the learning environment |
1 |
Setting clear expectations for learning |
(Clay et al., 2022) |
|
|
Maintaining positivity for learning |
||||
|
Reinforcing constructive feedback |
||||
|
Respecting others’ time (being on time) |
||||
Table 2. Respectful Relationships in Medical Education
IV. DISCUSSION
Fundamentally, respect is a basic moral value that applies to all. Treating other people how we would like to be treated is a basic human obligation (Hazrati et al., 2020; Subramani & Biller-Andorno, 2022). According to Darwell, respect can be generated by valuing individuals’ merit (appraisal respect) or simply by human moral conscience (recognition respect) (Subramani & Biller-Andorno, 2022). Both concepts resonate well with the humanism concept in medical education, which depends on the “respect for others” principle (Karnieli-Miller et al., 2010). Nevertheless, the theoretical framework of respect in medical education settings is still lacking.
The unique sociocultural aspects of medical education might impact how respect should be conveyed (Subramani & Biller-Andorno, 2022). For instance, respect toward medical residents could be specifically demonstrated by giving autonomy to their clinical work (Wong, 2011), which might be irrelevant in other educational settings (Subramani & Biller-Andorno, 2022). Additionally, respect toward patients could be specifically portrayed by ensuring their confidentiality, involving their beliefs in decision-making, and delivering compassionate care (Elfassy et al., 2020; Hazrati et al., 2020; Karnieli-Miller et al., 2010). For students, respect could be portrayed by delivering constructive feedback (Jung et al., 2021) and involving them in relevant clinical work (Elfassy et al., 2020).
The authors believed that cultivating respect in medical education was important for several reasons. First, medical doctors treat patients with diverse conditions and sociocultural backgrounds (Subramani & Biller-Andorno, 2022). Internalizing respect could enhance their clinical skills, particularly in effective communication, active listening, empathy, and cultural awareness (Hazrati et al., 2020), which may benefit the quality of patient care. Second, medical doctors must collaborate with other health professionals, who have their own roles and perspectives in managing patients (Nagraj et al., 2018). In terms of mutual respect, health professionals must actively recognize others’ roles and capabilities, hence promoting mutual trust and interprofessional collaboration (Croker et al., 2016).
Generally, fostering respect could nurture students’ academic outcomes and professionalism, thus creating a supportive learning environment (Klinner et al., 2024; Raikhel et al., 2024). However, this review revealed multilevel barriers to cultivating respect in medical education. Consequently, due to hierarchical cultures, many of these disrespectful behaviours were skeptically reported or even misperceived as common culture in medical education (Claramita et al., 2022; DiBrito et al., 2024; Klinner et al., 2024). Work-related stress might also be associated with a high risk of moral distress and unprofessional behavior by fellow students or faculty. Moreover, Palvic et al. (2018) reported that some health professionals might be seen as negative role models, tending to feel superior to others, which might break the sense of teamwork and respectful interaction.
Another concerning issue was that, even with a presumably less hierarchical culture (Wong, 2011), disrespectful actions were still reported in Western medical education (DiBrito et al., 2024; Weiss et al., 2021). This might be due to individualism and a lack of social communalism in Western cultures, which leads to cynicism. Cynical people express much negativity and distrust towards others, which is the core of many disrespectful acts (Stavrova et al., 2020). Some also reported that residents from Western cultures tended to show professional arrogance, which might be another challenge to cultivating respect (Wong, 2011).
Concerning practical implications, the authors proposed that respect should be cultivated using multilevel interventional approaches. At the individual level, medical institutions should promote skills that enhance respect through various approaches, such as promoting cultural sensitivity (Weiss et al., 2021) and respectful communication skills (Elfassy et al., 2020). At the interpersonal level, the sense of interprofessional collaboration should be more emphasized, especially when encountering role conflicts. Medical faculty development programme is also warranted, particularly in developing positive role-modelling and respectful feedback delivery skills.
Lastly, at the institutional level, leaders should arrange a code of conduct for respectful interactions and promote policies of respect toward students and faculty (e.g., working hour restrictions, formal reporting system for disrespectful behaviours etc.). Concrete exemplary actions and commitments from educational leaders should be mandatory; otherwise, all codes and policies would work only on paper (Leape et al., 2012; Raikhel et al., 2024).
This scoping review also highlighted several research gaps that could be further explored. The current research lacked a theoretical framework for respect cultivation in medical education, which could be different from many perspectives. For instance, respect between faculty and medical students could be different from respect toward residents or other health professionals. Secondly, no valid instrument existed to properly assess respect culture in medical educational settings. Most studies used either self-made questionnaires or other constructs containing respect as one of their indicators (Ekenze et al., 2013; Gillespie et al., 2009). This could raise an issue regarding external validity. By comparison, other studies used more standardized assessment tools, such as the Perceived Workplace Civility Climate Scale and Nursing Civility Scale (Peng, 2023).
To the best of the authors’ knowledge, this is the first scoping review to summarize the nature of respect in the medical education context. Previous reviews have mentioned respect, but not as a single entity. Respect was more likely to be integrated with broader concepts such as professionalism (Desain et al., 2022) or cultural competence (Constantinou & Nikitara, 2023). By placing more attention on respect itself, we could further explore both the theoretical construct and practical aspects to cultivating respect in medical educational contexts. While the role of organizational-level leadership has been previously highlighted (Sokol-Hessner et al, 2021), this scoping review also emphasized the roles of personal, interpersonal, and sociocultural barriers to cultivating respect.
Several limitations are acknowledged in this study. First, the literature search and thematic analysis were performed manually by the authors, which might contribute to subjectivity. Second, studies written in non-English languages were excluded due to language barriers. Consequently, some studies discussing respect, especially from local Eastern journals, might be under-reported. Much room exists for further studies, particularly discussing the theoretical framework of respect in various medical education settings and developing specific approaches to cultivate respect in such contexts.
V. CONCLUSION
Respect in medical education is a multifaceted concept. Theoretical frameworks and specific instruments to assess the culture of respect in such settings were lacking. Therefore, medical education should focus on cultivating a culture of respect because it likely enhances academic outcomes, professional development, sense of trust, healthcare collaboration, and patient safety.
Notes on Contributors
Dr Leonaldo Lukito Nagaria developed ideas and methodology, conducted literature searching, synthesized the included data, wrote the initial draft, and finalized the manuscript.
Prof Dr Sri Linuwih Menaldi, Sp.D.V.E, Subsp.D.T, FINSDV, FAADV developed the ideas and methodology, synthesized the included data, and finalized the manuscript.
Prof Dr Diantha Soemantri, M.Med.Ed, Ph.D developed the ideas and methodology, synthesized the included data, and finalized the manuscript.
Ethical Approval
Ethical approval is not necessary as no human subjects or data were involved.
Data Availability
Extracted datasets are freely accessible at (https://doi.org/10.6084/m9.figshare.28479062).
Acknowledgement
We would like to thank all the staff from the Medical Education Department, Faculty of Medicine, University of Indonesia who also contributed to giving valuable feedback and support throughout the entire process.
Funding
This research received no specific funding or grant from any agencies in any sector.
Declaration of Interest
All authors confirmed no affiliation or conflict of interest with any related institutions regarding the study materials or issues.
References
Abedini, N. C., Danso-Bamfo, S., Kolars, J. C., Danso, K. A., Donkor, P., Johnson, T. R. B., & Moyer, C. A. (2015). Cross-cultural perspectives on the patient-provider relationship: A qualitative study exploring reflections from Ghanaian medical students following a clinical rotation in the United States. BMC Medical Education, 15(1), 161. https://doi.org/10.1186/s12909-015-0444-9
Aboumatar, H., Beach, M. C., Yang, T., Branyon, E., Forbes, L., & Sugarman, J. (2015). Measuring patients’ experiences of respect and dignity in the intensive care unit: A pilot study. Narrative Inquiry in Bioethics, 5(1A), 69A-84A. https://doi.org/10.1353/nib.2015.0005
Alotiby, A., Almaghrabi, M., Alosaimy, R., Alharthi, A., Khawandanah, B., Alansari, R., Basahal, A., & Zamil, G. (2021). Learning environment quality for medical students at umm al-qura university: A comprehensive study on stressors, sources, and solutions after introduction of a new Bachelor of Medicine and Bachelor of Surgery (MBBS) curriculum. Advances in Medical Education and Practice, 12, 1487–1497. https://doi.org/10.2147/AMEP.S343792
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19-32. https://doi.org/10.1080/1364557032000119616
Claramita, M., Findyartini, A., Samarasekera, D., & Nishigori, H. (2022). Challenges and opportunities in health professions education (1st ed). Springer. https://doi.org/10.1007/978-981-16-7232-3_14
Clay, A. S., Leiman, E. R., Theiling, B. J., Song, Y., Padilla, B. B. I., Hudak, N. M., Hartman, A. M., Hoder, J. M., Waite, K. A., Lee, H.-J., & Buckley, E. G. (2022). Creating a win-win for the health system and health profession’s education: A direct observation clinical experience with feedback in real-time (DOCENT) for low acuity patients in the emergency department. BMC Medical Education, 22(1), 66. https://doi.org/10.1186/s12909-022-03133-z
Constantinou, C. S., & Nikitara, M. (2023). The culturally competent healthcare professional: The RESPECT competencies from a systematic review of delphi studies. MDPI, 13(5), 127. https://doi.org/10.3390/soc13050127
Croker, A., Higgs, J., & Trede, F. (2016). Collaborating in healthcare: Reinterpreting therapeutic relationships (1st ed). Sense Publishers. https://doi.org/10.1007/978-94-6300-806-8
Curry, S. E., Cortland, C. I., & Graham, M. J. (2011). Role-modelling in the operating room: Medical student observations of exemplary behaviour. Medical Education, 45(9), 946–957. https://doi.org/10.1111/j.1365-2923.2011.04014.x
Dabekaussen, K. F. A. A., Scheepers, R. A., Heineman, E., Haber, A. L., Lombarts, K. M. J. M. H., Jaarsma, D. A. D. C., & Shapiro, J. (2023). Health care professionals’ perceptions of unprofessional behaviour in the clinical workplace. PLOS ONE, 18(1), Article e0280444. https://doi.org/10.1371/journal.pone.0280444
Desai, M. K., Kapadia, J. D. (2022). Medical professionalism and ethics. Journal of Pharmacology and Pharmacotherapeutics, 13(2), 113-118. https://doi.org/10.1177/0976500X221111448
DiBrito, S., Mago, J., Reczek, A., Suresh, D., Kim, D., Jacoby, L., & Shelton, W. (2024). Medical student perspectives on professionalism in a third-year surgery clerkship – A mixed methods study. Journal of Surgical Education, 81(11), 1720–1729. https://doi.org/10.1016/j.jsurg.2024.08.018
Ekenze, S. O., Ugwumba, F. O., Obi, U. M., & Ekenze, O. S. (2013). Undergraduate surgery clerkship and the choice of surgery as a career: Perspective from a developing country. World Journal of Surgery, 37(9), 2094–2100. https://doi.org/10.1007/s00268-013-2073-y
Elfassy, M. D., Duncan, L., Green, A., Sun, H., Guimond, T., Tzanetos, K., & Nyhof-Young, J. (2020). Patients as teachers: Evaluating the experiences of volunteer inpatients during medical student clinical skills training. Canadian Medical Education Journal, 11(6), e8-16. https://doi.org/10.36834/cmej.70158
Gillespie, C., Paik, S., Ark, T., Zabar, S., & Kalet, A. (2009). Residents’ perceptions of their own professionalism and the professionalism of their learning environment. Journal of Graduate Medical Education, 1(2), 208–215. https://doi.org/10.4300/JGME-D-09-00018.1
Gonzalo, J. D., Heist, B. S., Duffy, B. L., Dyrbye, L., Fagan, M. J., Ferenchick, G., Harrell, H., Hemmer, P. A., Kernan, W. N., Kogan, J. R., Rafferty, C., Wong, R., & Elnicki, D. M. (2014). Identifying and overcoming the barriers to bedside rounds: A multicenter qualitative study. Academic Medicine, 89(2), 326–334. https://doi.org/10.1097/ACM.0000000000000100
Gordon, J., Markham, P., Lipworth, W., Kerridge, I., & Little, M. (2012). The dual nature of medical enculturation in postgraduate medical training and practice. Medical Education, 46(9), 894–902. https://doi.org/10.1111/j.1365-2923.2012.04301.x
Gruppen, L. D. (2014). Humility and respect: Core values in medical education. Medical Education, 48(1), 53–58. https://doi.org/10.1111/medu.12269
Haque, M., Zulkifi, Z., Zohurul Haque, S., Kamal, Z., Salam, A., Bhagat, V., Ghazi Alattraqchi, A., & A Rahman, N. I. (2016). Professionalism perspectives among medical students of a novel medical graduate school in Malaysia. Advances in Medical Education and Practice, 7, 407–422. https://doi.org/10.2147/AMEP.S90737
Hazrati, H., Bigdeli, S., Gavgani, V. Z., Soltani Arabshahi, S. K., Behshid, M., & Sohrabi, Z. (2020). Humanism in clinical education: A mixed methods study on the experiences of clinical instructors in Iran. Philosophy, Ethics, and Humanities in Medicine, 15(1), 5. https://doi.org/10.1186/s13010-020-00088-1
Howell, H. B., Desai, P. V., Altshuler, L., McGrath, M., Ramsey, R., Vrablik, L., Levy, F. H., & Zabar, S. (2022). Teaching and assessing communication skills in pediatric residents: How do parents think we are doing? Academic Pediatrics, 22(2), 179–183. https://doi.org/10.1016/j.acap.2021.06.011
Jauregui, J., Gatewood, M., Ilgen, J., Schaninger, C., & Strote, J. (2016). Emergency medicine resident perceptions of medical professionalism. Western Journal of Emergency Medicine, 17(3), 355–361. https://doi.org/10.5811/westjem.2016.2.29102
Jung, S., Greenberg, J., O’Rourke, A. P., Minter, R. M., Foley, E., & Voils, C. I. (2021). Comparison of the perspectives of medical students and residents on the surgery learning environment. Journal of Surgical Research, 258, 187–194. https://doi.org/10.1016/j.jss.2020.08.070
Karani, R. (2015). Enhancing the medical school learning environment: A complex challenge. Journal of General Internal Medicine, 30(9), 1235–1236. https://doi.org/10.1007/s11606-015-3422-3
Karnieli-Miller, O., Taylor, A. C., Cottingham, A. H., Inui, T. S., Vu, T. R., & Frankel, R. M. (2010). Exploring the meaning of respect in medical student education: An analysis of student narratives. Journal of General Internal Medicine, 25(12), 1309–1314. https://doi.org/10.1007/s11606-010-1471-1
Klinner, C., Dario, A. B., Bell, A., Nisbet, G., Penman, M., & Monrouxe, L. V. (2024). Beyond mere respect: New perspectives on dignity for healthcare workplace learning. Frontiers in Medicine, 10, Article 1274364. https://doi.org/10.3389/fmed.2023.1274364
Leape, L. L., Shore, M. F., Dienstag, J. L., Mayer, R. J., Edgman-Levitan, S., Meyer, G. S., & Healy, G. B. (2012). Perspective: A culture of respect, part 2: Creating a culture of respect. Academic Medicine: Journal of the Association of American Medical Colleges, 87(7), 853–858. https://doi.org/10.1097/ACM.0b013e3182583536
Lim, S., Goh, E. Y., Tay, E., Tong, Y. K., Chung, D., Devi, K., Tan, C. H., & Indran, I. R. (2022). Disruptive behavior in a high-power distance culture and a three-dimensional framework for curbing it. Health Care Management Review, 47(2), 133–143. https://doi.org/10.1097/HMR.0000000000000315
Marquardt, D., Langdale, L., Kim, S., Leroux, B., Friedrich, J., Schreuder, A. B., & Wood, D. E. (2022). Closing the gap: Triangulation of surgeons’ respectful behaviours perceived by medical students, residents, and patients. Surgery, 172(1), 96–101. https://doi.org/10.1016/j.surg.2021.11.036
Nagraj, S., Harrison, J., Hill, L., Bowker, L., & Lindqvist, S. (2018). Promoting collaboration in emergency medicine. The Clinical Teacher, 15(6), 500–505. https://doi.org/10.1111/tct.12762
O′Flynn, S., Power, S., Horgan, M., & O′Tuathaigh, C. M. P. (2014). Attitudes towards professionalism in graduate and non-graduate entrants to medical school. Education for Health, 27(2), 200–204. https://doi.org/10.4103/1357-6283.143770
Pavlic, A., Liu, D., Baker, K., House, J., Byrd, M., Martinek, T., O’Leary, D., & Santen, S. (2018). Behind the curtain: The nurse’s voice in assessment of residents in the emergency department. Western Journal of Emergency Medicine, 20(1), 23–28. https://doi.org/10.5811/westjem.2018.10.39821
Peng, X. (2023). Advancing workplace civility: A systematic review and meta-analysis of definitions, measurements, and associated factors. Frontiers in Psychology, 14, Article 1277188. https://doi.org/10.3389/fpsyg.2023.1277188
Raikhel, A. V., Starks, H., Berger, G., & Redinger, J. (2024). Through the looking glass: Comparing hospitalists’ and internal medicine residents’ perceptions of feedback. Cureus, 16(6), Article e63459. https://doi.org/10.7759/cureus.63459
Rozaliyani, A., Wasisto, B., Santosa, F., Sjamsuhidajat, R., & Setiabudy, R. (2019). Bullying (perundungan) di lingkungan pendidikan kedokteran [Bullying in medical education]. Jurnal Etika Kedokteran Indonesia, 3(2), 56–60.
Sokol-Hessner, L., Folcarelli, P. H., Annas, C. L., Brown, S. M., Fernandez, L., Roche, S. D., Lee, B. S., & Sands, K. E. (2018). A road map for advancing the practice of respect in health care: The results of an interdisciplinary modified delphi consensus study. The Joint Commission Journal on Quality and Patient Safety, 44(8), 463-476. https://doi.org/10.1016/j.jcjq.2018.02.003
Stavrova, O., Ehlebracht, D., & Vohs, K. D. (2020). Victims, perpetrators, or both? The vicious cycle of disrespect and cynical beliefs about human nature. Journal of Experimental Psychology: General, 149(9), 1736–1754. https://doi.org/10.1037/xge0000738
Subramani, S., & Biller-Andorno, N. (2022). Revisiting respect for persons: Conceptual analysis and implications for clinical practice. Medicine, Health Care and Philosophy, 25(3), 351–360. https://doi.org/10.1007/s11019-022-10079-y
Verhagen, M. J., Frouws, M. A., Timmer, R. A., Schepers, A., Brunsveld-Reinders, A. H., De Vos, M. S., & Hamming, J. F. (2024). How to support communication between nurses and residents during shift work: A mixed-methods study into local practices and perceptions. Journal of Surgical Education, 81(8), 1034–1043. https://doi.org/10.1016/j.jsurg.2024.05.017
Weiss, J., Balasuriya, L., Cramer, L. D., Nunez-Smith, M., Genao, I., Gonzalez-Colaso, R., Wong, A. H., Samuels, E. A., Latimore, D., Boatright, D., & Sharifi, M. (2021). Medical students’ demographic characteristics and their perceptions of faculty role modeling of respect for diversity. JAMA Network Open, 4(6), e2112795. https://doi.org/10.1001/jamanetworkopen.2021.12795
Wong, A. K. (2011). Culture in medical education: Comparing a thai and a canadian residency programme. Medical Education, 45(12), 1209–1219. https://doi.org/10.1111/j.1365-2923.2011.04059.x
*Leonaldo Lukito Nagaria
Department of Medical Education
Faculty of Medicine, University of Indonesia
Jalan Salemba Raya No 6,
Jakarta 10430, Indonesia
Email: leonaldo.lukito@ui.ac.id
Submitted: 26 March 2025
Accepted: 5 November 2025
Published online: 7 April, TAPS 2026, 11(2), 73-80
https://doi.org/10.29060/TAPS.2026-11-2/OA3702
Maheen Zulfiqar, Muhammad Khalil ur Rahman, Behram Khayyam, Naeem Sarwar, Ashbil Malik, Ayesha Mazhar Khan & Hassan Saleem
Department of Surgery, Arif Memorial Teaching Hospital/Rashid Latif Medical College, Lahore, Pakistan
Abstract
Introduction: Absenteeism during clinical rotations among medical students is on the rise, adversely affecting both patient care and the development of essential clinical skills. Factors such as inadequate learning resources, exhaustion, and disengagement contribute to this trend, which must be addressed to safeguard the quality of medical training and future healthcare quality. This study aimed to identify the underlying causes of absenteeism among undergraduate medical students and to propose strategies to improve attendance and learning outcomes.
Methods: A cross-sectional study was conducted on third, fourth, and final-year students of primary medical qualification at Rashid Latif Medical College, Lahore, Punjab, Pakistan, from June 2024 to July 2024. A validated, self-structured questionnaire was distributed during clinical rotations. Data were analysed using SPSS version 25. Frequencies and percentages were calculated to summarise attendance patterns and perceived barriers. Pearson’s correlation was used to examine associations between absenteeism factors—personal health, family obligations, academic workload, perceived relevance of rotations and academic year, with statistical significance set at p ≤ 0.05.
Results: Out of 450 surveys, 270 students responded: 31% third year, 27% fourth year, and 43% final year students. Faculty-related barriers included poor feedback (3.2), ineffective communication (3.2), lack of preparation (3.3), and unprofessional attitude (3.3). Personal obstacles included personal health (3.2), lack of learning resources (3.4), and family obligations (3.3). Additionally, 41% of the students believed that non-exam-specific rotations were irrelevant.
Conclusion: Faculty dissatisfaction, peer pressure and downplaying non-exam specific rotations cause clinical rotation absenteeism. Systemic reforms and enhanced faculty engagement are essential to improve students’ professional development and clinical engagement.
Keywords: Medical Education, Absenteeism, Faculty, Clinical Rotations
Practice Highlights
- Many students do not find non-exam-specific rotations valuable due to the heavy workload.
- Students often feel demotivated to attend rotations because of uncooperative and unprofessional behaviour from faculty members.
- It is recommended that institutions implement policies to manage student workload, uphold professional conduct, and create a more motivating environment for clinical rotations.
I. INTRODUCTION
Absenteeism refers to the habitual absence from classes/ clinical rotations without a valid or justifiable reason (Qureshi & Ahmad, 2019). Student absenteeism is a common issue observed globally across all academic fields, and medicine is no exception (Gul et al., 2016). However, in the field of medicine, absenteeism has several negative consequences. It impacts students not only academically but also in terms of their professional development (Shenawi et al., 2021). Absenteeism, especially during clinical rotations, hinders both academic learning and patient care as well (Qureshi &
Ahmad, 2019).
Despite strict policies regarding attendance at clinical rotations and lectures, absenteeism remains prevalent among students (Sharmin & Azim, 2017). In Pakistan, there is a growing trend where medical students primarily attend clinical rotations for subjects that carry weight in their current year of study. According to student feedback and informal discussions, many students tend to skip ward rounds, following the example of their seniors, who claim that the material will be thoroughly covered the following year when the subject becomes compulsory. Even those who wish to attend non-compulsory wards often feel pressured by their peers to do otherwise. Additionally, a lack of professionalism among some faculty members and the overall ward environment can diminish students’ morale and motivation (Khan et al., 2019; Mitra et al., 2022).
Despite being a widespread issue, there is no valid justification for the absence of undergraduate medical students from their clinical rotations. To date, no study has been published that thoroughly investigates the key factors contributing to student absenteeism from clinical rotations, particularly at Rashid Latif Medical College and Arif Memorial Teaching Hospital in Lahore. Therefore, this study was undertaken to explore the primary reasons for low attendance among third year, fourth year and final year students of primary medical qualification (PMQ) at Rashid Latif Medical College and to identify initiatives that could improve their participation in clinical rotations.
II. METHODS
This cross-sectional study was conducted from June 2024 to July 2024 on 450 students after taking approval from the Institutional Review Board (RLMC/IRB/2024/153). The aim was to explore the factors influencing attendance in clinical rotations among undergraduate medical students. A self-designed, validated questionnaire was used. The study targeted 3rd, 4th and final year students of primary medical qualification (PMQ) at Rashid Latif Medical College, Lahore, Punjab, Pakistan.
Non-probability purposive sampling was used to recruit students. A total of 450 students were approached during their ward rotations. Out of those, 270 completed the survey, yielding a response rate of 60%. The inclusion criteria were students who were currently enrolled in the clinical years and attending rotations during the study period. Students in pre-clinical years (namely first and second year), those on academic leave or suspension, or those who declined participation were excluded. While purposive sampling allows access to students in relevant clinical settings, it does, however, carry the inherent limitation of selection bias, potentially over-representing students with better attendance or stronger academic engagement.
Data were collected using a self-designed, validated questionnaire. A thorough analysis of the body of research on medical school absenteeism and suggestions from three senior medical education specialists guided the development process. The questionnaire underwent content validation by the expert panel to assess clarity, relevance, and alignment with study objectives. There were both closed-ended and open-ended questions on the finished form.
Closed-ended questions included demographic variables, frequency of clinical attendance, and 5-point Likert scale items evaluating perceived faculty behaviours, personal and academic barriers, and attitudes toward clinical teaching. Preliminary reliability testing using pilot data yielded a Cronbach’s alpha of 0.779, indicating moderate internal consistency. Factor analysis revealed that the questionnaire could be sub-grouped into eight distinct domains, collectively accounting for 97% of the variance in responses.
Participation was entirely voluntary, and informed consent was implied through the completion and return of the questionnaire. Anonymity and confidentiality were ensured to encourage honest and uninfluenced responses. Questionnaires were distributed in printed form during each academic year’s scheduled ward rotations, with responses collected immediately to minimise non-response and preserve the context of clinical learning environments. Data were entered and analysed using IBM SPSS version 25.
Quantitative variables were presented as mean ± standard deviation (SD). For qualitative variables, mean scores were used to assess correlations between causes of absenteeism among third, fourth, and final year MBBS students. Frequencies and percentages were calculated to summarise attendance patterns, causes of absenteeism, and deficiencies in clinical faculty impacting attendance. Pearson’s correlation was employed to assess the relationships between absenteeism factors (such as personal health, family responsibilities, workload, perceived relevance of rotations) and academic year, with significance set at p ≤ 0.05.
III. RESULTS
This study explores the factors influencing attendance in clinical rotations among medical students. The data supporting the finding is available at Figshare (https://doi.org/10.6084/m9.figshare.28602041.v1) (Mazhar Khan, 2025).
Evaluating responses from 450 students we found that 270 students participated in the survey, representing diverse academic years: 31% from the third year, 27%
from the fourth year, and 43% from the fifth year. Notably, gender distribution among respondents included 133 males (49.1%) and 137 females (50.9%).
A. Regularity of Attendance
The attendance at clinical rotations was recorded as follows: 29% of third-year students, 40% of fourth-year students, and 36% of final-year students reported attending all required rotations in their third and fourth academic years (Figure 1).
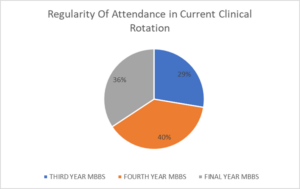
Figure 1. Regularity of Attendance in Clinical Wards
Among these students, a significant proportion missed their clinical wards sometimes (3–4 times per month; 24%) and often (5–6 times per month; 20%), respectively (Table 1). Further analysis of exam-specific and non-exam-specific rotations showed that only 18.5% of students attended both rotations equally, whereas 40.7% reported attending exam-specific rotations more frequently. The most important reasons for attending exam specific rotation were because it was required for their course completion (63%) and was directly related to their assessments and exam (56%).
|
Academic Year |
All (100%) |
Most (75–99%) |
Some (50–74%) |
Few (25–49%) |
None (0–24%) |
|
Third Year |
25 (29.4%) |
20 (23.5%) |
15 (17.6%) |
15 (17.6%) |
10 (11.8%) |
|
Fourth Year |
28 (40.0%) |
18 (25.7%) |
15 (21.4%) |
5 (7.1%) |
4 (5.7%) |
|
Final Year |
35 (30.4%) |
40 (34.8%) |
20 (17.4%) |
15 (13.0%) |
5 (4.3%) |
|
Total |
88 (33%) |
78 (29%) |
50 (19%) |
35 (13%) |
19 (7%) |
Table 1. Regularity of Attendance in Current Clinical Rotations (Third to Final Year)
B. Causes of Absenteeism
Furthermore, students expressed that discouragement from attending clinical rotations stemmed primarily from faculty behaviours. The mean scores for these factors were as follows: unprofessional behaviour (3.3), lack of preparation for teaching sessions (3.2), inadequate feedback on performance (3.2), ineffective communication (3.2), overemphasis on rote learning over critical thinking (3.1), and lack of enthusiasm in teaching (3.1) (Table 2). Specifically, Barriers to attending non-examination-specific rotations were identified, with 41% of students citing a lack of perceived value, 30% referring to heavy workloads as a limiting factor.
|
Factor |
Mean Score |
1 (Not at all) |
2 |
3 |
4 |
5 (Extremely) |
|
Personal Health Issues |
3.2 |
40 (15%) |
50 |
55 |
80 |
45 (17%) |
|
Family Responsibilities |
3.3 |
35 (13%) |
45 |
60 |
80 |
50 (19%) |
|
Financial Difficulties |
3.0 |
60 (22%) |
40 |
50 |
70 |
50 (19%) |
|
Workload from Other Courses |
3.1 |
50 (19%) |
45 |
60 |
65 |
50 (19%) |
|
Perceived Irrelevance of Rotations |
2.8 |
70 (26%) |
55 |
45 |
60 |
40 (15%) |
|
Timing of Clinical Rotations |
3.1 |
45 (17%) |
50 |
70 |
65 |
40 (15%) |
|
Transportation Issues |
3.0 |
55 (20%) |
50 |
55 |
70 |
40 (15%) |
|
Quality of Teaching |
3.2 |
40 (15%) |
60 |
60 |
65 |
45 (17%) |
|
Poor Relationships with Staff |
3.3 |
50 (19%) |
45 |
60 |
60 |
55 (20%) |
|
Lack of Learning Resources |
3.4 |
45 (17%) |
40 |
50 |
70 |
65 (24%) |
|
Personal Safety Concerns |
3.0 |
60 (22%) |
40 |
45 |
65 |
60 (22%) |
|
Influence of Seniors’ Opinions |
3.0 |
55 (20%) |
60 |
55 |
50 |
50 (19%) |
|
Personal Health Issues |
3.2 |
40 (15%) |
50 |
55 |
80 |
45 (17%) |
Table 2. Causes of Absenteeism (Combined Data for All Years)
Additional barriers identified included the lack of learning resources (mean score 3.4), strained relationships with clinical staff (mean score 3.3), family obligations (mean score 3.3), perceived quality of teaching during rotations (mean score 3.2), and personal health issues (mean score 3.2) (Table 3).
|
Faculty Deficiency |
Mean Score |
1 (Not at all) |
2 |
3 |
4 |
5 (Extremely) |
|
Lack of Preparation for Teaching Sessions |
3.3 |
40 (15%) |
45 |
60 |
75 |
50 (18%) |
|
Inability to Effectively Communicate |
3.2 |
45 (17%) |
50 |
65 |
60 |
50 (18%) |
|
Lack of Enthusiasm in Teaching |
3.1 |
50 (19%) |
60 |
55 |
55 |
50 (18%) |
|
Unavailability of Additional Support |
3.0 |
55 (20%) |
50 |
60 |
55 |
50 (18%) |
|
Unprofessional Behaviour |
3.3 |
50 (19%) |
45 |
55 |
55 |
65 (24%) |
|
Lack of Constructive Feedback |
3.2 |
45 (17%) |
50 |
65 |
55 |
55 (20%) |
|
Inconsistent or Unfair Assessments |
3.0 |
60 (22%) |
45 |
50 |
65 |
50 (19%) |
|
Overemphasis on Rote Learning |
3.1 |
50 (19%) |
55 |
60 |
55 |
50 (18%) |
|
Poor Integration of Theory and Clinical Work |
3.1 |
55 (20%) |
50 |
60 |
55 |
50 (18%) |
Table 3. Deficiencies in Clinical Faculty Impacting Attendance (All Years)
C. Correlation Between Professional Years and Causes of Absenteeism
The table below summarises the correlation between professional years and various factors affecting absenteeism in medical students (Table 4). It helps to identify which factors are perceived differently across different years of study. A p-value less than 0.05 indicates a statistically significant correlation. It reveals that there is a significant correlation among quality of teaching during rotations (p-value=0.012), lack of learning resources (p-value=0.025), family responsibilities (p-value=0.02), workload from other courses (p-value=0.036) and personal health issues (p-value=0.045) across the different academic years.
|
Factor |
Mean Score |
Correlation with Professional Year |
p-value |
Interpretation |
|
Personal Health Issues |
3.2 |
0.25 |
0.045 |
Statistically significant |
|
Family Responsibilities |
3.3 |
0.32 |
0.020 |
Statistically significant |
|
Financial Difficulties |
3.0 |
0.10 |
0.310 |
Not significant |
|
Workload from Other Courses |
3.1 |
0.28 |
0.036 |
Statistically significant |
|
Perceived Irrelevance of Rotations |
2.8 |
-0.15 |
0.215 |
Not significant |
|
Timing of Clinical Rotations |
3.1 |
0.22 |
0.056 |
Borderline (Not statistically significant) |
|
Transportation Issues |
3.0 |
0.05 |
0.750 |
Not significant |
|
Quality of Teaching During Rotations |
3.2 |
0.38 |
0.012 |
Statistically significant |
|
Poor Relationships with Clinical Staff |
3.3 |
0.20 |
0.067 |
Not statistically significant |
|
Lack of Learning Resources |
3.4 |
0.30 |
0.025 |
Statistically significant |
|
Personal Safety Concerns |
3.0 |
0.15 |
0.180 |
Not significant |
|
Influence of Seniors’ Opinions |
3.0 |
0.05 |
0.800 |
Not significant |
Table 4. Correlation Results Table
IV. DISCUSSION
Clinical Rotations are an important aspect of undergraduate medical education, giving students an opportunity to apply their theoretical knowledge, develop core clinical principals and prepare for professional responsibilities of the future. Attendance during these rotations correlates with academic performance, patient safety and readiness for medical practice (Bamuhair et al., 2016). This cross-sectional study involving 270 students, highlights an alarming pattern of absenteeism with attendance rates of only 29%, 40% and 36% among third-year, fourth year and final year students, respectively. A trend like this, if unaddressed can have a negative impact on the competencies of medical graduates.
One of the most frequently cited reasons for absenteeism in this study was discontentment with faculty behaviour and teaching methods. Students frequently referred to inadequate communication, absence of constructive feedback, lack of interest in teaching, and instances of unprofessional conduct as major drivers of their disengagement. These findings are in line with those of Bahadori et al. (2021), who outlined that unprofessional conduct and poor interaction between student and faculty served as key reasons for absenteeism during clinical rotations. Similarly, Desalegn et al. (2014), reported that faculty performance and student discipline were significant determinants of attendance habits.
A lack of faculty engagement not only discourages student participation but also contributes to a disconnection between theoretical instruction and its clinical application, thereby reinforcing surface learning strategies such as rote memorisation. This perception is reinforced by Nevins et al. (2016) who observed substantial improvement in attendance when sessions were made more clinically relevant in a medical school based in the United Kingdom (UK). Hence, these findings highlight the pivotal role of faculty in moulding students’ motivation and engagement with clinical training.
An inflexible and poorly structured curriculum appears to be a significant deterrent to clinical attendance. The participants of this study lay emphasis on the burden of excessive academic workload, especially during non-exam-specific rotations, which were often perceived as less valuable. These concerns align with findings by Hafeez et al. (2014) and Massingham and Herrington (2006), who reported that students are likely to prioritise independent study over attendance when clinical rotations are not directly assessed. Similarly, a Nigerian study by Olorunfemi et al. (2021) found that the absence of structured feedback and ineffective curriculum delivery led to a drop in engagement with clinical training.
Interestingly, Simcock et al. (2017) found that while students increasingly used recorded lectures for exam preparations, those who attended live, interactive sessions showed better academic performance. These findings underscore the importance of in-person, interactive learning experiences despite the growing availability of digital alternatives.
A range of personal factors emerged as contributors to absenteeism. These included mental health concerns, such as anxiety and stress, physical illness and family responsibilities. The findings of this study are consistent with Massingham and Herrington (2006), who noted that student well-being has a significant impact on attendance. Although the cross-sectional nature of the current study captures these concerns at a particular point in time, longitudinal research may offer deeper insights into health-related absenteeism. The concept of “sickness presenteeism” is of particular relevance here, whereby students continue to attend lectures despite illness due to fears of academic disadvantage. This phenomenon, discussed by Desalegn et al. (2014), highlights the importance of ensuring adequate access to healthcare and mental health support within educational institutions.
Family responsibilities, especially among students from joint families or low socio-economic backgrounds, were also found to negatively affect attendance. Furthermore, peer influence was recognised as a notable social factor; numerous students admitted to missing non-examination-based sessions due to collective absenteeism within their peer group. This observation aligns with the findings of Khatoon et al. (2024) who observed that peer pressure played a major role in determining attendance trajectories. Notably, although Stenberg and Carlson, (2015) in a Swedish cohort, found that peer learning enhanced confidence and clinical competence, they also noted the presence of competitive stress. These findings suggest that peer dynamics can contribute as both motivating or inhibiting factor in clinical attendance, depending on the nature of the interactions.
Students displayed markedly higher attendance during exam-specific rotations, primarily driven by examination pressure and mandatory completion requirements. While this behaviour is understandable, it undermines the broader educational aims of clinical training, which extend beyond exam preparation. The perception that certain rotations are less valuable unless directly linked to assessments reflects a strategic learning approach, whereby students prioritise immediate academic performance over long-term skill development. This trend, which was also observed by Hafeez et al. (2014), appears to be a response to cope with the extensive academic workload faced by medical students.
Such findings suggest that the current structure of clinical education may inadvertently reinforce surface learning behaviours. The tendency to devalue non-exam-specific rotations indicates a misalignment between students’ learning priorities and the intended outcomes of clinical education. It is crucial to address this disconnect by devising curricular strategies that foster intrinsic motivation and emphasise the enduring clinical relevance of all rotations.
From a global perspective, patterns of absenteeism appear to be context-dependent, shaped by institutional culture and pedagogical frameworks. For example, Simcock et al. (2017), in a study conducted across Australia and New Zealand, highlighted the limitations of recorded lectures, noting that their substitution for live teaching sessions negatively impacted student engagement. In contrast, Stenberg and Carlson, (2015) demonstrated that peer-led teaching models positively influenced student participation in clinical settings.
On the contrary, Marburger (2006) presented evidence that traditional, structured, lecture-based teaching methods were associated with improved academic performance in certain settings. This divergence underscores the importance of accounting for local educational cultures, student learning preferences, and institutional dynamics when developing interventions aimed at improving attendance.
Although the present study did not identify significant differences in attendance rates between male and female students, certain gender-based academic disparities were observed. Hakami (2021) reported that increased absenteeism was more strongly associated with academic decline among male students compared to their female counterparts. This disparity may reflect variations in learning styles, coping strategies, or resilience across genders, suggesting that male and female students may respond differently to academic pressures and absenteeism. These findings point to the potential value of adopting a more nuanced, gender-informed perspective when analysing academic outcomes in relation to attendance behaviour.
Despite numerous studies addressing absenteeism in medical education, there remains a notable lack of focus on attendance during clinical rotations, particularly within South Asian institutions (Bahadori et al. 2021; Hafeez et al. 2014). Much of the existing research is centred on preclinical or lecture-based settings, which do not fully capture the distinct challenges faced by students in clinical environments. By focusing on clinical rotations within this regional context, the present study helps to fill this gap and offers insights that are underrepresented in current literature. However, given the complexity of factors influencing attendance and their evolution over time, further longitudinal and multi-institutional research is warranted to better understand these dynamics and inform targeted interventions.
However, this study is not without limitations. As it is a cross-sectional study, it only captures student behaviour at single point in time, thereby limiting its ability to shed light on evolving patterns or long term trends in clinical attendance. The use of self-reported data introduces the possibility of response bias. Moreover, the study was conducted within a single institution, which may restrict the generalisability of the findings to other medical colleges with differing academic cultures, policies, or student demographics. The absence of qualitative interviews or focus groups also constrained a deeper exploration of underlying motivations and interpersonal dynamics influencing absenteeism. Future research could benefit from adopting a longitudinal, multi-centre design incorporating both quantitative and qualitative methodologies for better understanding.
V. CONCLUSION
This study highlights a multifaceted set of factors contributing to absenteeism among medical students during clinical rotations, including dissatisfaction with faculty engagement, inflexible curricular structures, mental health challenges, peer influence, and the strategic devaluation of non-exam-specific sessions. These findings point towards systemic and cultural gaps in clinical education that may compromise the quality of learning and long-term professional development.
In light of these findings, several policy-level interventions are recommended. Medical institutions should ensure that all clinical rotations—regardless of examination linkage—are regarded as essential and are integrated into structured assessment frameworks. Attendance policies should be applied uniformly and accompanied by transparent accountability mechanisms. Faculty development programmes must be prioritised, with particular emphasis on improving communication skills, delivering constructive feedback, and maintaining professional conduct. These efforts could help restore trust and motivation among students while strengthening the link between theoretical knowledge and clinical practice.
In addition, educational institutions should provide accessible mental health services to support students coping with stress, anxiety, and illness, thereby reducing both absenteeism and the phenomenon of sickness presenteeism. Awareness sessions on peer influence and group dynamics could transform peer pressure from a deterrent into a positive, motivating force. Lastly, curricular reforms that balance academic workload and reinforce the clinical relevance of all rotations are essential to promote consistent student engagement and long-term competence.
Notes on Contributors
Maheen Zulfiqar led the conceptualisation of the study and was responsible for drafting the original manuscript. She also played a key role in reviewing and editing the final version.
Muhammad Khalilur Rahman contributed to both the conceptual development and project administration, ensuring coordination across the team. He was also actively involved in reviewing and refining the manuscript.
Behram Khayyam handled the methodological design, formal analysis, and validation of results. He also participated in the review and editing process, enhancing the technical rigour of the study.
Ayesha Mazhar Khan supported the methodological and validation efforts, contributing to data analysis and manuscript revisions.
Naeem Sarwar oversaw project administration and contributed to the manuscript’s review and editing, ensuring smooth project execution.
Ashbil Malik was responsible for data curation and participated in the review process, offering insights based on her data expertise.
Hassan Saleem co-managed data curation with Ashbil Malik and assisted in reviewing and editing the manuscript for data-related accuracy.
Ethical Approval
This cross-sectional study was conducted after taking approval from the Institutional Review Board (RLMC/IRB/2024/153). IRB approval letter has been provided in the attached documents.
Data Availability
Our dataset is publicly accessible through the referenced repository and is available under the CC BY 4.0 license, ensuring open usage and attribution (https://doi.org/10.6084/m9.figshare.28602041.v1).
Funding
The authors declare that no financial support or funding was received from any organisation or institution for the research, authorship, or publication of this article.
Declaration of Interest
No potential conflict of interest relevant to this article was reported.
References
Al Shenawi, H., Yaghan, R., Amer, H., & Shenawi, M. (2021). The relationship between attendance and academic performance of undergraduate medical students during surgical clerkship. BMC Medical Education, 21(1), Article 287. https://doi.org/10.1186/s12909-021-02833-2
Bahadori, M., Salari, S., Alizadeh, M., Moaddab, F., Balasi, L. R., & Soodmand, E. (2020). The root causes of absenteeism in medical students: Challenges and strategies ahead. Educational Research in Medical Sciences, 19(2), 1–8. https://doi.org/10.5812/erms.107120
Bamuhair, S. S., Farhan, A. I., Althubaiti, A., Rahman, S. U., & Al-Kadri, H. M. (2021). Class attendance and cardiology examination performance: A study in problem-based medical curriculum. International Journal of General Medicine, 14, 613–619. https://doi.org/10.2147/IJGM.S96627
Desalegn, A. A., Berhan, Y., & Berhan, A. (2014). Absenteeism among medical and health science undergraduate students at Hawassa University, Ethiopia. BMC Medical Education, 14, Article 81. https://doi.org/10.1186/1472-6920-14-81
Gul, R., Khan, S., Alam, M., Luqman, M., Shahab, M., & Sohail, M. (2016). Absenteeism among medical undergraduate students. Journal of Medical Sciences (Peshawar), 24(1), 16–18. https://jmedsci.com/index.php/Jmedsci/article/view/177
Hafeez, K., Khan, Z., Jawaid, M., & Haroon, S. (2019). Low attendance in lectures at medical colleges of Karachi: A cross-sectional survey. Journal of Postgraduate Medical Institute, 33(2), 123–128. https://jpmi.org.pk/index.php/jpmi/article/view/1565
Hakami, A. (2021). Effect of absenteeism on the performance of medical sciences students: Gender differences. Medical Education Online, 25(1), Article 1875531. https://doi.org/10.1080/10872981.2021.1875531
Khan, A. M. (2025). Absence of undergraduate medical students from clinical rotations [Dataset]. Figshare. https://doi.org/10.6084/m9.figshare.28602041.v1
Khan, M. J., Lodhi, F. S., Bhatti, A., & Ali, S. (2019). Does absenteeism affect academic performance among undergraduate medical students? Evidence from Rashid Latif Medical College. Advances in Medical Education and Practice, 10, 999–1008. https://doi.org/10.2147/AMEP.S226255
Khatoon, S., Khan, M. A., Nadeem, M., & Majeed, I. (2024). Demographic characteristics and perceived absenteeism among students in government secondary schools. Asian Journal of Integrated Social and Behavioural Sciences, 1(1), 23–28. https://journals.uol.edu.pk/AJISB/article/view/3627/1579
Marburger, D. R. (2006). Does mandatory attendance improve student performance? Journal of Economic Education, 37(2), 148–155. https://doi.org/10.3200/JECE.37.2.148-155
Massingham, P., & Herrington, T. (2006). Does attendance matter? An examination of student attitudes, participation, performance, and attendance. Journal of University Teaching & Learning Practice, 3(2), 82–103. https://files.eric.ed.gov/fulltext/EJ1105382.pdf
Mitra, S., Sarkar, P., Bhattacharyya, S., & Basu, R. (2022). Absenteeism among undergraduate medical students and its impact on academic performance: A record-based study. Journal of education and health promotion, 11, 414. https://doi.org/10.4103/jehp.jehp_638_21
Nevins, E. J., Moori, P. L., Alexander, L., Richards, B., Bleasdale, V., & Sharma, A. K. (2016). Could attendance at medical school be improved? A prospective study of medical education at the University of Liverpool: Study of attendance at a UK medical school. MedEdPublish, 5(2), Article 78. https://doi.org/10.15694/mep.2016.000078
Olorunfemi, O., Oduyemi, R. O., Sowunmi, C. O., Okafor, V., Chukwuka, L. O., Osunde, N. R., & Ezinne, A. F. (2021). Clinical instructors’ motivational roles and perceived effect on absenteeism among student nurses in a tertiary hospital, Benin‑City, Nigeria. Journal of Education and Health Promotion, 10, 203. https://doi.org/10.4103/jehp.jehp_1048_20
Qureshi, M. A., & Ahmad, F. (2019). Medical students’ perspective on absenteeism and its remedies. Pakistan Armed Forces Medical Journal, 69(2), 332–339. https://pafmj.org/index.php/PAFMJ/article/view/2749
Sharmin, T., & Azim, E. (2017). Reasons of absenteeism among undergraduate medical students: A review. Anwer Khan Modern Medical College Journal, 8(1), 60–66. https://doi.org/10.3329/akmmcj.v8i1.31660
Simcock, D. C., Chua, W. H., Hekman, M., Levin, M. T., & Brown, S. (2017). A survey of first-year biology student opinions regarding live lectures and recorded lectures as learning tools. Advances in Physiology Education, 41(1), 129–137. https://doi.org/10.1152/advan.00117.2016
Stenberg, M., & Carlson, E. (2015). Swedish student nurses’ perception of peer learning as an educational model during clinical practice in a hospital setting—an evaluation study. BMC Nursing, 14, Article 48. https://doi.org/10.1186/s12912-015-0098-2
*Ayesha Mazhar Khan
Department of Surgery,
Arif Memorial Teaching Hospital/Rashid Latif Medical College,
Lahore, Pakistan
+92 3009494461
Email: ayeshamazharkhan.amk@gmail.com
Submitted: 16 July 2024
Accepted: 27 August 2025
Published online: 7 April, TAPS 2026, 11(2), 40-48
https://doi.org/10.29060/TAPS.2026-11-2/OA3458
Siti Suhailah Zahari1, Roshan Peiris1,3,4, Ruhaya Hasan2, Nik Aloesnisa Nik Mohd Alwi1 & Nurhafizah Ghani1
1Medical & Basic Dental Sciences Unit, School of Dental Sciences, Universiti Sains Malaysia, Malaysia; 2Dental Public Health Unit, School of Dental Sciences, Universiti Sains Malaysia, Malaysia; 3Department of Basic Sciences, Faculty of Dental Sciences, University of Peradeniya, Sri Lanka; 4College of Health Sciences, VinUniversity, Vietnam
Abstract
Introduction: The growing use of social media among students offers educators in dental education enhanced opportunities for student-teacher interaction and improved access to learning materials. This study aims to examine the patterns of social media usage for learning purposes among undergraduate dental students at Universiti Sains Malaysia.
Methods: A cross-sectional questionnaire-based study was conducted involving 222 undergraduate dental students from all academic years, excluding those without social media accounts or who declined participation. A validated questionnaire was distributed online via Google Forms and WhatsApp, collecting data on socio-demographics, smartphone ownership and internet access, preferred social media platforms, and the use of social media for academic purposes.
Results: All 222 respondents completed the survey. The majority (65.8%) were iPhone users, and 95.0% reported access to internet data via Wi-Fi or 4G networks. Almost all participants used social media to connect with friends (99.1%), while 10.4% used it for business. Instagram (99.1%), WhatsApp (97.7%), and YouTube (91.9%) were the most commonly used platforms, with WhatsApp being the most frequently used (86.0%). Gender showed a significant association with academic use, particularly for inquiries and consultations, with female students engaging more than males. No significant differences were found across academic years. Google (91.0%) and YouTube (84.2%) were the preferred platforms for academic content.
Conclusion: Social media presents valuable opportunities to support dental education by enhancing learning engagement and communication. However, as the study focuses on a single institution, broader research involving multiple dental schools is recommended to achieve more generalisable findings.
Keywords: Dental Education, Dental Undergraduate, Learning, Malaysia, Social Media
Practice Highlights
- Widespread social media usage indicates the extensive integration of social media into their daily lives.
- Gender was significantly associated with the use of social media for academic purposes.
- Google and YouTube platforms are key resources for dental education.
I. INTRODUCTION
The world is in a state of perpetual evolution, particularly in relation to the internet and its various impacts, both positive and negative (Al-Dayyeni, 2021). Acquiring information has never been easier, with social media playing a crucial role in communication and information retrieval (Uma et al., 2021). According to Uma et al. (2021), professional and personal lives have become intertwined as a result of numerous interactions they have with each other on various issues. They elaborated those social media platforms facilitate users in generating and distributing information or engaging in social networking. This includes social networking platforms such as Facebook, YouTube and Instagram (Uma et al., 2021). According to Giroux and Moreau (2022), social media platforms serve both formal and informal learning purposes in health professions education (HPE). Formal learning pertains to structured educational activities like classes or assignments, while informal learning involves knowledge gained from other extracurricular activities.
Social media has become widespread in society and significantly impacts personal and professional aspects, including dentistry (Uma et al., 2021). Social media has been crucial for communication and education throughout the COVID-19 pandemic (Giroux & Moreau, 2022). Amid the pandemic, medical and dentistry education relied on digital tools and social media platforms for information retrieval, sharing learning resources, and conducting virtual meetings. Students and lecturers frequently used these technologies for academic and non-academic activities (Uma et al., 2021).
Currently, more dentists are using social media to share and acquire knowledge, advertise their professional practice, and offer online consultations (Ghandhi et al., 2022). Affendi et al. (2020) investigated the utilisation of social media for advertising by dentists in Malaysia and found that most respondents believe that social media marketing could gain popularity in the field of dentistry, despite its current primary use for personal reasons (Affendi et al., 2020). Meanwhile, Rani et al. (2020) detailed how Malaysian dental undergraduates are educated to utilise social media to advocate for oral health in the community. Social media also plays roles in dental education outcomes. Platforms such as YouTube and Instagram are increasingly used by dental students to access clinical demonstrations, case discussions, and peer-shared learning resources, which can enhance clinical reasoning and practical understanding (Acosta et al., 2025; Khanagar et al., 2022). This growing use of social media shows its expanding role in dentistry, not only for professional promotion and health education, but also as a helpful tool for dental students to support their own learning.
Undergraduate dental students in Malaysia, typically aged 20–27, belong to Generation Z (born 1997–2012), the largest generational group in the country, comprising 27% of the population (DOSM, 2024). Gen Z is known for being digitally connected, well-educated, entrepreneurial, and empowered (Tjiptono et al., 2020). They rely heavily on technology, using the internet and smartphones for communication, news, education, and social interactions (Slepian et al., 2024). Education integrated with social media enhances learning for Gen Z, promoting engagement, collaboration, and the development of critical skills for the digital era. This tech-savvy nature shapes their learning preferences and readiness for modern professional challenges.
Incorporating social media into education has been shown to enhance learning and promote positive behavioral changes in health profession students (Hamid & Jaafar, 2021). Undergraduate dental students reported enjoying online learning more than conventional lectures (Jayasinghe et al., 2021). However, excessive social media use may cause distractions and unethical online behavior (Nieminen et al., 2022). Students with poor social skills and internet usage exceeding 40 hours weekly are at greater risk of internet addiction (Radeef & Faisal, 2019). Thus, while social media offers educational benefits, its overuse poses potential challenges to student well-being and professionalism.
Numerous social media platforms have proven to be effective for educational reasons (Spallek et al., 2015). With reference to the COVID-19 epidemic, technological advancements have radically revolutionised teaching and learning activities. Previous studies had identified social media has been seen as a mean for connection and a substitute for information distribution (Hamid & Jaafar, 2021; Jayasinghe et al., 2021; Nieminen et al., 2022). In Malaysia’s educational context, there has been a strong national push toward digital learning and technology integration across universities, including in dental education (Kathirveloo, 2024). Given these global trends, understanding social media’s role in Malaysian dental education is critical.
Despite these developments, the use of social media for academic purposes among dental undergraduates in Malaysia has not been firmly established.
Therefore, this study intends to investigate the utilisation of social media platforms for educational purposes in Malaysia. The current study aims to establish the prevalence and characteristics of social media usage for educational purposes among dental undergraduates and to identify the association between the type of social media platforms and its educational purposes. Furthermore, this study could offer essential foundational data for further studies on the advantages of integrating social media into education and this data will help educators to determine which platform and engagement strategies will be most effective with the current generation of learners.
II. METHODS
A. Study Design
A questionnaire-based online cross-sectional survey was conducted from April to October 2023 with participation of all dental undergraduates from Year 1 – Year 5 academic session 2022/2023 in Universiti Sains Malaysia (USM). The validated google form questionnaire used was adapted from a previous similar study (Alshuaibi et al., 2015). The questionnaire developed by Alshuaibi et al. (2015) was designed for a similar sample group which are undergraduate students in Malaysia. This justifies its suitability for the current study. This study was approved by the Human Research Ethics Committee USM (HREC) (Ref. No.: USM/JEPeM/KK/23040324). Data were collected via a Google Form link shared through WhatsApp and email to student representatives, who forwarded it to peers. Participation was voluntary, with informed consent obtained by ticking an agreement box. The questionnaire contained no sensitive information, ensuring anonymity, and all responses were kept strictly confidential.
B. Questionnaire Form
The questionnaire, adapted from Alshuaibi et al. (2015) with permission, had a content and face validity index > 0.80 (Hamid & Jaafar, 2021), indicating strong expert agreement on its content and clarity. It comprised four sections: (1) Socio-Demographic Factors: age, gender, year of study, and other relevant details to contextualise findings; (2) Smartphone Ownership and Connection: smartphone usage, features, and preferred internet connection; (3) Social Media Applications: frequently used platforms and purposes; (4) Social Media for Academic Purposes: use of social media for learning, including information exchange, consultations, and educational queries.
A five-point Likert-type frequency scale was used to assess the respondents’ frequency of behaviour, with response options ranging from “Never” to “Almost always”: Never, Seldom, Sometimes, Often, and Almost always. This scale was employed for all questionnaire items, with response options ranging from Never (1) to Almost Always (5). Items were organised into specific domains. To generate a domain score for each respondent, individual item responses within the same domain were numerically coded and then averaged. This method ensured standardisation across domains.
This structured approach provides a holistic understanding of students’ interaction with technology and social media, particularly in academic settings, while ensuring the findings are relevant and actionable for improving educational practices.
C. Sample Size Determination
The outcome variable selected for estimating sample sizes was the use of social media for academic purposes. Finite population correction formula was utilised to estimate the minimum sample sizes at Universiti Sains Malaysia:
Where n= required minimum sample size, P= 95.1% which is proportion of the outcome variable (Hamid & Jaafar, 2021), p(1−p) = variance of the outcome variable, Z= 1.96 for 95% confidence limit with absolute precision (Δ)= ± 5%. For anticipated 10% of non-response rate, the minimum number of participants required is 80.
For the gender variable, a priori power analysis was performed with G*Power version 3.1.9.7 to establish the required sample size for testing the study hypothesis. The study found that a sample size of N=128 is needed to have an 80% power of detecting a medium effect size with a significance level of α=0.05 when comparing two independent means (male and female). The overall sample size of N=128 was sufficient to test the study hypothesis.
For the years of study variable, a priori power analysis is performed with G*Power version 3.1.9.7 to establish the appropriate sample size for testing the study hypothesis. It was found that a sample size of N=200 was needed to have an 80% power of detecting a medium effect in a one-way ANOVA test at a significance level of α=0.05. Therefore, the sample size of N=200 was sufficient to test the study hypothesis. Since the calculated sample size for the difference in social media use among dental undergraduates between years of study was the highest (200), this number was used for the study.
D. Data Analysis
IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA) was used for data entry and analysis. Data was presented using tables and graphs. Descriptive analysis included frequencies and percentages for categorical variables and mean with standard deviation or median with interquartile range for continuous variables, depending on normality. An independent t-test assessed differences in social media use between male and female dental undergraduates at Universiti Sains Malaysia.
A one-way ANOVA test was utilised to assess the use of social media for learning in different undergraduate years of study and to differentiate the type of internet access. A multiple logistic regression analysis was also applied to provide insight into how various factors impact learning outcomes. The independent variables are influencing factors (ResearchGate, Google, YouTube, Skype, LinkedIn, WhatsApp, Instagram, Twitter, Facebook, and TikTok). These platforms were selected based on their popularity among the target population, relevance to academic and social communication. Multicollinearity among the independent variables was assessed using Variance Inflation Factor (VIF) and Pearson correlation coefficients. The dependent variable is the outcome (Never, Seldom, Sometimes, Often, and Almost always). The outcome tested in the study significance level was set at p ≤ 0.05. at 95% confidence intervals.
III. RESULTS
A. Demographic Characteristics
There were 222 dental undergraduates who participated in the study. The mean age of the participants was 22.1 ± 1.50 years. The vast majority of the participants were female, accounting for 79.7% of the total sample (n = 177). 20.7% (n = 46) in the first year, 19.4% (n = 43) in the second year, 23.0% (n = 51) in the third year, 14.0% (n = 31) in the fourth year, and 23.0% (n = 51) in the fifth year. While all academic years were represented, the distribution was not exactly even, with slightly lower participation from fourth-year students and slightly higher representation from third- and fifth-year students. This variation reflects natural variation in voluntary participation across cohorts.
B. Smartphone Ownership and Connection
The majority of dental undergraduates were iPhone users (65.8%) while the other respondents were android smartphone users. Particularly, 95.0% (n = 211) of the participants were able to connect to the internet through a fourth generation (4G) mobile carrier and Wi-Fi.
C. Social Media Application
Most participants utilised social media for connecting with friends (99.1%), communicating with family members (92.8%), and acquiring new skills or information (85.1%). About 74.8% of individuals engage with their lecturers through these communication channels. About 67.1% of participants use these tools to build professional or social connections and only 10.4% of respondents focus on promoting their business through these platforms. Most participants had accounts on Instagram (99.1%), WhatsApp (97.7%), and YouTube (91.9%). The most frequently used platforms were WhatsApp (86.0%), Instagram (81.1%), and YouTube (61.7%) (Figure 1).
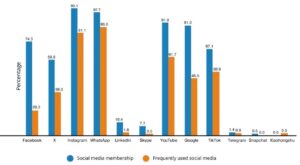
Figure 1. Social media membership accounts and the most frequently utilised social media accounts by the respondents (n=222)
D. Social Media for Academic Purposes
The social media apps that assist respondents in their education are shown in Figure 2. Participants chose Google (91.0%), YouTube (84.2%), WhatsApp (53.2%), ResearchGate (48.6%), and Instagram (25.2%) as their top five social networking applications. Google was the most popular application.
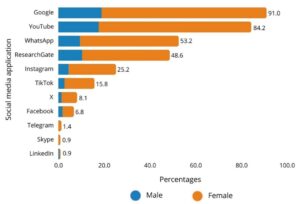
Figure 2. Social media applications that assist the respondents in the course of their studies
Table 1 displays the respondents’ utilisation of social media for academic purposes. Most respondents selected “often” for the exchange of information, consulting, and queries domains. About 46.4% of respondents prefer to stay updated on a subject/course “almost always,” while 33.3% chose to consult teachers “sometimes” to clarify challenging subjects. The domain of exchange of information, consultation, and queries had a grand mean score of 2.94 (SD = 0.67), 2.81 (SD = 0.75), and 3.09 (SD = 0.74), respectively.
|
Domain |
Survey question: In relation with use social media for academic purposes. I use social media… |
Overall number and percentage of students |
Mean (SD) |
Grand mean (SD) |
||||
|
Never n (%) |
Seldom n (%) |
Sometimes n (%) |
Often n (%) |
Almost always n (%) |
||||
|
Exchange information |
To join in the group project discussions. |
6 (2.7) |
17 (7.7) |
53 (23.9) |
89 (40.1) |
57 (25.7) |
2.78 (1.00) |
2.94 (0.67) |
|
To do coursework. |
3 (1.4) |
7 (3.2) |
40 (18.0) |
88 (39.6) |
84 (37.8) |
3.09 (0.89) |
|
|
|
To exchange useful documentation and resources of the subject/course. |
2 (0.9) |
3 (1.4) |
38 (17.1) |
98 (44.1) |
81 (36.5) |
3.14 (0.81) |
|
|
|
To remain updated on what is happening in a subject/course (changes, unforeseen events). |
1 (0.5) |
6 (2.7) |
25 (11.3) |
87 (39.2) |
103 (46.4) |
3.28 (0.81) |
|
|
|
To find out about activities organised by my university. |
2 (0.9) |
14 (6.3) |
59 (26.6) |
80 (36.0) |
67 (30.2) |
2.88 (0.94) |
|
|
|
To organise extracurricular activities. |
7 (3.2) |
44 (19.8) |
57 (25.7) |
68 (30.6) |
46 (20.7) |
2.46 (1.12) |
|
|
|
Consultation |
To search books and resources recommended by the teacher. |
1 (0.5) |
8 (3.6) |
42 (18.9) |
89 (40.1) |
82 (36.9) |
3.09 (0.86) |
2.81 (0.75) |
|
To resolve doubts about my life at university. |
1 (0.5) |
10 (4.5) |
62 (27.9) |
78 (35.1) |
71 (32.0) |
2.94 (0.91) |
|
|
|
To contact experts on the topics of the study. |
7 (3.2) |
24 (10.8) |
65 (29.3) |
80 (36.0) |
46 (20.7) |
2.60 (1.03) |
|
|
|
To consult teachers to clarify difficult areas of the subject/course. |
4 (1.8) |
25 (11.3) |
74 (33.3) |
68 (30.6) |
51 (23.0) |
2.61 (1.02) |
|
|
|
Queries |
To resolve queries about content or exams with other students. |
0 (0.0) |
6 (2.7) |
44 (19.8) |
90 (40.5) |
82 (36.9) |
3.12 (0.82) |
3.09 (0.74) |
|
To find out what has been covered in class during non-attendance. |
0 (0.0) |
9 (4.1) |
44 (19.8) |
93 (41.9) |
76 (34.2) |
3.06 (0.84) |
|
|
Table 1. Utilisation of social media for academic purposes by the respondents
Among the respondents, the mean values of gender, year of study, and type of internet connection are displayed in Table 2. These values pertain to the utilisation of social media for academic inquiry, information exchange, and consultation. For statistical analysis, a one-way analysis of variance (ANOVA) was carried out with a significance level of p ≤ 0.05. There was a significant association between gender and the use of social media for academic purposes, with a greater number of females engaging in inquiries and consultations compared to males. In contrast, there was no significant difference found between the academic year indicating relatively consistent use patterns across academic levels. The use of social media for academic purposes, as well as the form of internet connection and the usage of social media for academic purposes was not significantly related, suggesting that mode of connectivity had minimal influence on students’ usage patterns.
|
Variables |
Queries |
p value |
Exchange of Information |
p value |
Consultation |
p value |
|
Mean (SD) |
Mean (SD) |
Mean (SD) |
||||
|
Gender |
|
|
|
|
|
|
|
Male |
5.64 (1.32) |
0.007 |
16.69 (3.64) |
0.076 |
10.27 (2.98) |
0.013 |
|
Female |
6.32 (1.50) |
|
17.89 (4.12) |
|
11.50 (2.97) |
|
|
Year of study |
|
|
|
|
|
|
|
First year |
6.02 (1.39) |
0.760 |
18.35 (3.65) |
0.611 |
11.10 (3.07) |
0.869 |
|
Second year |
6.02 (1.44) |
|
17.40 (4.59) |
|
10.95 (3.11) |
|
|
Third year |
6.22 (1.42) |
|
17.33 (3.72) |
|
11.59 (2.87) |
|
|
Fourth year |
6.29 (1.79) |
|
18.10 (3.87) |
|
11.29 (2.78) |
|
|
Fifth year |
6.35 (1.51) |
|
17.25 (4.36) |
|
11.31 (3.20) |
|
|
Internet access |
|
|
|
|
|
|
|
4G only |
6.44 (1.24) |
0.243 |
17.67 (2.18) |
0.992 |
11.22 (2.49) |
0.133 |
|
Wi-Fi |
4.50 (2.12) |
|
18.00 (0.00) |
|
7.00 (1.42) |
|
|
4G and Wi-Fi |
6.18 (1.49) |
|
17.64 (4.05) |
|
11.29 (3.02) |
|
The significance level was set at p ≤ 0.05 at 95% confidence intervals. Note: Mean shown is the total mean.
Table 2. The mean values of gender, year of study, and type of internet access among the respondents regarding the usage of social media for academic inquiry, information exchange, and consultation
A multiple logistic regression analysis was conducted to examine the influence of various social media platforms on learning-related factors, with the results presented in Table 3. The analysis included 10 platforms: ResearchGate, Google, YouTube, Skype, LinkedIn, WhatsApp, Instagram, Twitter, Facebook, and TikTok. To perform binary logistic regression, the responses were grouped into two categories: Often and Almost Always were coded as “1” (frequent use), while Never, Seldom, and Sometimes were coded as “0” (infrequent use). This helped to clearly separate high and low levels of social media influence on learning activities. The significant platforms identified were ResearchGate, Instagram, and Twitter. In ResearchGate, a significant positive coefficient is observed for searching books and resources (0.645), while negative coefficients are found for exchanging useful documentation (-0.467) and contacting experts (-0.394). The negative association in exchange useful documentation may suggest that this platform is less effective or less frequently used for peer-to-peer document sharing among students compared to other tools. Similarly, the negative association for contacting experts could reflect limited interactivity or response rates from professionals, making it a less reliable platform for interactive communication with experts. In Instagram, the significant positive coefficients are for finding out what has been covered (0.517) and resolving doubts (0.507), while the negative coefficient is for doing coursework (-0.427) possibly because it lacks the right tools or easy access to materials, making it less useful for doing coursework. In Twitter, the significant positive coefficient is for organising extracurricular activities (0.8).
Another multiple logistic regression analysis was conducted to explore the relationship between various factors, academic year, and learning outcomes. Resolving doubts has a significant positive (p = 0.014), indicating that resolving doubts is significantly associated with academic year progression.
|
95% C.I. for EXP(B) |
||||||||
|
Domain |
Variables in the Equation |
B |
S.E. |
Wald |
Sig. |
Exp(B) |
Lower |
Upper |
|
*ResearchGate |
To exchange useful documentation |
-0.467 |
0.216 |
4.686 |
0.030 |
0.627 |
0.410 |
0.957 |
|
To search books and resources |
0.645 |
0.212 |
9.268 |
0.002 |
1.906 |
1.258 |
2.887 |
|
|
To contact experts |
-0.392 |
0.181 |
4.695 |
0.030 |
0.676 |
0.474 |
0.963 |
|
|
To find out what has been covered |
0.394 |
0.217 |
3.299 |
0.069 |
1.483 |
0.969 |
2.269 |
|
|
Constant |
-0.767 |
0.719 |
1.140 |
0.286 |
0.464 |
|||
|
|
To find out what has been covered |
0.517 |
0.237 |
4.744 |
0.029 |
1.676 |
1.053 |
2.668 |
|
To do coursework |
-0.427 |
0.205 |
4.349 |
0.037 |
0.652 |
0.437 |
0.975 |
|
|
To resolve doubts |
0.507 |
0.224 |
5.116 |
0.024 |
1.660 |
1.070 |
2.576 |
|
|
Constant |
-2.942 |
0.795 |
13.683 |
0.000 |
0.053 |
|||
|
|
To organise extracurricular activities |
0.800 |
0.280 |
8.175 |
0.004 |
2.225 |
1.286 |
3.850 |
|
Constant |
-4.698 |
0.921 |
26.047 |
0.000 |
0.009 |
|||
Notes:
* Hosmer and Lemeshow Test: Chi-square=6.193, p>0.05, Classification table = 60.8%, Area Under Curve: 0.659, p<0.05, (95% CI:0.588, 0.730)
** Hosmer and Lemeshow Test: Chi-square=5.392, p>0.05, Classification table = 74.3 %, Area Under Curve:0.665, p<0.05, (95% CI:0.588, 0.742)
*** Hosmer and Lemeshow Test: Chi-square=2.661, p>0.05, Classification table = 91.9%, Area Under Curve:.713, p<0.05, (95% CI:0.606,0 .819)
Table 3. Multiple logistic regression analysis of social media platform uses for educational purposes.
IV. DISCUSSION
A. Socio-Demographic Factors: Female Students Show Greater Use of Social Media for Educational Purposes
The study found that females were more likely than males to use social media for academic queries and discussions, reflecting their preference for interactive, collaborative learning (Ansari & Khan, 2020). Social media supports group discussions, resource sharing, and seeking assistance, aligning with these preferences. Women may also have stronger peer networks and norms encouraging educational dialogue. In contrast, females show greater interest in learning via social media, while males are more inclined toward activities such as video gaming (Leonhardt & Overå, 2021).
B. Smartphone Ownership and Connection: Strong Connectivity Enable Student to Access Online Resources
The study found that 65.8% of dental undergraduates used iPhones, with the rest using Android devices, possibly reflecting brand popularity, user experience, or socioeconomic factors. Most participants (95.0%) had reliable internet access via 4G and Wi-Fi, facilitating engagement with educational resources, social media, and communication tools. Such connectivity supports real-time interaction with peers and instructors, enhancing collaboration and information access (Guo et al., 2021). The widespread availability of high-speed internet highlights the vital role of technology infrastructure in enabling academic activities, especially where digital tools and online platforms are integral to learning.
C. Social Media Application: Benefits, Challenges, and the Role of Platforms like WhatsApp, Instagram, and YouTube
Dental undergraduates mainly use WhatsApp, Instagram, and YouTube for communication and learning. WhatsApp emerged as the most popular platform, consistent with studies from Malaysia, Finland, and Saudi Arabia (Aboalshamat et al., 2019; Hamid & Jaafar, 2021; Naguib et al., 2018; Rajeh et al., 2021; Uma et al., 2021). It is widely preferred for academic purposes, allowing students to easily share information, ask lecturers questions, and resolve issues through group discussions without needing personal interaction (Amanullah & Ali, 2014; Baishya & Maheshwari, 2019). Nevertheless, these results differ from some study (United States and United Kingdom) that found Facebook as the most often used platform (Arnett et al., 2014; Kenny & Johnson, 2016). The cause of this difference is uncertain, but it could be linked to cultural variances (Rajeh et al., 2021). Malaysia is known as a collectivist society, where people value working together, supporting each other, and maintaining group harmony. In this culture, learning is often seen as a shared activity rather than something done alone. This may help explain why students in Malaysia prefer using social media platforms that support group work and collaboration (Rahman et al., 2020).
Instagram is another popular platform among undergraduate students. Many universities use social media platforms like Instagram to share information alongside websites or email (Stuart et al., 2017). Information related to both academic and extracurricular events and activities relevant to dental education can be effectively communicated among students via Instagram to keep them updated. Social media also helps graduate students stay connected with their institutions (Irfan et al., 2018).
Social media significantly influences educational outcomes, including skill development, critical thinking, and clinical practice. Platforms like YouTube and WhatsApp offer valuable tools for learning and collaboration but can also lead to distractions and time-wasting (Shousha & Abdelgawad, 2021). Constant notifications, unrelated content, and easy socialising may reduce focus, affecting productivity and academic performance (Sundaram, 2017). A balanced discussion of both benefits and drawbacks is essential to fully understand social media’s educational impact. Effective management of its use is crucial to maximise learning potential while minimising distractions, ensuring it serves as a supportive rather than disruptive tool for students.
D. Social Media for Academic Purposes: The Popularity of Google and YouTube among Dental Students
Students preferred Google and YouTube for studying. YouTube was used to deliver pre-class micro-lecture videos, helping link theoretical concepts to clinical procedures (Knösel et al., 2011). Unlike static slides, YouTube provides interactive videos and multimedia, enhancing learning (Hamid & Jaafar, 2021). For accessing journal papers unavailable through library subscriptions, students used ResearchGate, mainly for finding books and resources, but less for contacting experts or exchanging documents (Hamid & Jaafar, 2021; Muscanell & Utz, 2017). Thus, ResearchGate can be a valuable tool for undergraduates conducting research projects.
Social media offers dental students free access to diverse academic materials worldwide, expanding learning opportunities and introducing varied educational approaches (Bhola & Hellyer, 2016). It provides flexibility in when and where learning occurs (Henderson et al., 2017; Jankauskaite, 2015). Instagram is useful for resolving doubts and finding information, though less used for coursework. Integrating social media into dental education enhances traditional teaching and is well-received globally (Katzman et al., 2024; Knösel et al., 2011; Turkyilmaz et al., 2019). Its educational role gained official recognition when ministries of education began leveraging technology to improve learning, even before COVID-19. For example, Saudi Arabia’s Ministry of Education streams lessons via YouTube (Rajeh et al., 2021). The pandemic accelerated online learning adoption, making platforms like WebEx, Google Meet, Skype, and Zoom essential for virtual lectures, offering chatrooms, recordings, and breakout rooms for collaborative problem-solving (Hamid & Jaafar, 2021; Hung et al., 2021). Twitter plays a significant role in organising extracurricular activities, showing strong user preference for this purpose, underscoring social media’s value in fostering engagement beyond academics. Collectively, these platforms support both academic and extracurricular development, highlighting the central role of digital tools in modern dental education.
The use of social media in dental education can lead to some challenges. Many dental students may not be aware of the ethical and professional guidelines governing social media use, which can result in unprofessional behavior and negative outcomes (Aboalshamat et al., 2019; Kenny & Johnson, 2016). For example, sharing patients’ information online without using proper guidelines, risk of sharing unnecessary/inappropriate information, risk of passing the information to a third party, etc. To address this, dental curricula should include guidelines on professional conduct for social media use to raise awareness among students (Kenny & Johnson, 2016). Several countries, including the UK, USA, and Australia, have already implemented policies on social media use for healthcare professionals (Agency, 2014; Council, 2024; Kind, 2015). The UK’s General Dental Council (GDC) guidelines emphasise confidentiality, privacy, and appropriate boundaries, advising against sharing personal views or patient information on social media (Council, 2024).
Additionally, clinical year students may be concerned about online education, as lectures and case studies cannot replace essential hands-on experience with patients (Hamid & Jaafar, 2021). This underscores the need to combine online learning with methods like faculty-reviewed video cases, simulations, demonstrations, and tele-dentistry to support practical skill development (Hung et al., 2021).
Lack of academic year differences: social media usage across academic years is the uniform exposure to digital tools throughout the dental curriculum. Many Malaysian universities have introduced digital learning resources such as online lectures, virtual simulations, and e-learning platforms, early in the academic programme (Ismail et al., 2022). Therefore, students across all academic levels may have similar levels of familiarity and engagement with social media for academic purposes. Additionally, the availability of smartphones and internet access, combined with a shared digital learning environment, may contribute to consistent patterns of usage among students regardless of their year of study. This suggests that digital literacy and the adoption of educational technologies are being implemented uniformly across the dental education.
V. CONCLUSION
In conclusion, this study highlights the significant role of social media in dental education, particularly in communication and academic purposes. Female students demonstrate a greater use of social media for educational activities, emphasising the need to consider gender-based differences in technology integration. Strong smartphone ownership and reliable connectivity are essential for accessing online resources, enabling students to engage with educational content more effectively. Social media platforms like WhatsApp, Instagram, and YouTube offer both opportunities and challenges in enhancing the learning experience. The popularity of Google and YouTube among dental students further underscores the importance of these platforms in supporting learning and collaboration. Educators should be encouraged to develop curated YouTube playlists for dental procedures. ResearchGate, Instagram, and Twitter each play distinct roles in educational and professional contexts. ResearchGate is mainly used for finding books and resources, not for contacting experts or sharing documents. Instagram helps with resolving doubts and finding information but is less useful for coursework. Twitter is popular for organising extracurricular activities, showing its strength in coordination and communication. The present study further emphasises the importance of incorporating social media ethics training in the dental curriculum. Overall, integrating social media into dental education can enrich the learning process, but it requires thoughtful implementation to maximise benefits while addressing potential challenges. Meanwhile, health related faculties should consider maintaining the balance online and hands-on learning, especially in clinical training in order to sustain the quality of teaching. Future longitudinal studies are also recommended to assess the social media impact on clinical skill development.
A. Limitation and Recommendation
This study has limitations. Using an online self-completed questionnaire in a single Malaysian dental school may not represent all dental students or future graduates nationwide. A more accurate understanding requires inclusion of all dental schools through systematic sampling. Similar studies in other countries could estimate social media use prevalence across diverse educational settings, offering insights into its global benefits in dental education. Furthermore, exploring innovative ways to integrate social media into curricula could enhance learning and engagement (Zupanic et al., 2019). Such efforts would provide broader perspectives on their role and potential in improving dental education worldwide.
Notes on Contributors
NG designed and supervised the research project and contribute to data analysis and manuscript development.
RP designed and supervised the research project and contributed to data analysis and manuscript development.
RH supervised the research project and contribute to data analysis.
NANA contribute to manuscript development.
SS a key role in the development, conducted the survey and data analysis of this research project, and drafted the manuscript.
Ethical Approval
Formal ethical approval (Reference No.: USM/JEPeM/KK/23040324) was obtained from the Human Research Ethics Committee USM (HREC), Universiti Sains Malaysia, Kelantan, Malaysia (Approval date: 8th June 2023).
Data Availability
As per institutional policy, research dataset is available on reasonable request to the corresponding author.
Acknowledgement
We want to express our gratitude to research project coordinator, Assoc. Prof. Ts. Dr. Wan Nazatul Shima Shahidan from School of Dental Sciences, Universiti Sains Malaysia, Dr Nor Faharina Abdul Hamid from Universiti Teknologi MARA, Dr Mohammad Alshuaibi Dubai Business School, University of Dubai and team for sharing their research instrument. Finally, for all those who contributed to the data collection.
Funding
The funding agencies in the public sector, the commercial sector, and the not-for-profit sector weren’t funding this research with any specific grants.
Declaration of Interest
The authors have no potential conflicts to disclose.
References
Aboalshamat, K., Alkiyadi, S., Alsaleh, S., Reda, R., Alkhaldi, S., Badeeb, A., & Gabb, N. (2019). Attitudes toward social media among practicing dentists and dental students in clinical years in Saudi Arabia. The Open Dentistry Journal, 13(1), 143-149. https://doi.org/10.2174/1874210601913010143
Acosta, J. M., Detsomboonrat, P., Pisarnturakit, P. P., & Urwannachotima, N. (2025). The use of social media on enhancing dental care and practice among dental professionals: Cross-sectional survey study. JMIR Formative Research, 9, e66121. https://doi.org/10.2196/66121
Affendi, N. H. K., Hamid, N. F. A., Razak, M. S. A., & Nudin, I. I. I. (2020). The pattern of social media marketing by dentist in Malaysia. Malaysian Dental Journal, 1(2020), 24-42. https://web.mda.org.my/wp-content/uploads/2020/06/mdj-2020-01-03-Dr-Hafizah.pdf
Al-Dayyeni, H. H. R. (2021). The use of social media by dental students as a learning resource. Universidad Europea. http://hdl.handle.net/20.500.12880/587
Amanullah, A. N. A. A., & Ali, N. A. M. (2014). The most favourable mobile messaging apps among IIUM students. International Journal of Science and Research, 3(12), 2497-2502. http://irep.iium.edu.my/40515/
Alshuaibi, M. S. I., Alshuaibi, A. S., & Mohd Shamsudin, F. (2015). Exploring the patterns of social media use among business students in Malaysia. Proceedings of the Asia Pacific Conference on Business and Social Sciences 2015, Kuala Lumpur. https://repo.uum.edu.my/id/eprint/16722/
Ansari, J. A. N., & Khan, N. A. (2020). Exploring the role of social media in collaborative learning the new domain of learning. Smart Learning Environments, 7(1), 9. https://doi.org/10.1186/s40561-020-00118-7
Arnett, M. R., Christensen, H. L., & Nelson, B. A. (2014). A school-wide assessment of social media usage by students in a US dental school. British Dental Journal, 217(9), 531-535. https://doi.org/10.1038/sj.bdj.2014.956
Australian Health Practitioner Regulation Agency. (2014). Social media: How to meet your obligations under the National Law. https://www.ahpra.gov.au/Resources/Social-media-guidance.aspx
Baishya, D., & Maheshwari, S. (2019). WhatsApp groups in academic context: Exploring the academic uses of WhatsApp groups among the students. Contemporary Educational Technology, 11(1), 31-46. https://doi.org/10.30935/cet.641765
Bhola, S., & Hellyer, P. (2016). The risks and benefits of social media in dental foundation training. British Dental Journal, 221(10), 609-613. https://doi.org/10.1038/sj.bdj.2016.854
General Dental Council. (2024). Guidance on using social media. https://www.gdc-uk.org/docs/default-source/guidance-documents/guidance-on-using-social-media
Ghandhi, D., Bodani, N., Lal, A., Maqsood, A., Ahmed, N., Basha, S., Assiry, A. A., Heboyan, A., & Karobari, M. I. (2022). Evaluation of social media usage by dental practitioners of Pakistan for professional purposes – A cross-sectional study. Clinical Cosmetic And Investigation Dentistry, 14, 245-252. https://doi.org/10.2147/ccide.S374111
Giroux, C. M., & Moreau, K. A. (2022). Nursing students’ use of social media in their learning: A case study of a Canadian School of Nursing. BMC Nursing, 21(1), 195. https://doi.org/10.1186/s12912-022-00977-0
Guo, F., Yu, F. R., Zhang, H., Li, X., Ji, H., & Leung, V. C. M. (2021). Enabling massive IoT toward 6G: A comprehensive survey. IEEE Internet of Things Journal, 8(15), 11891-11915. https://doi.org/10.1109/JIOT.2021.3063686
Hamid, N. F. A., & Jaafar, A. (2021). Use of social media in dental education: A single institutional study. Archives of Orofacial Sciences, 16(2), 141-152. https://doi.org/10.21315/aos2021.16.2.5
Henderson, M., Selwyn, N., & Aston, R. (2017). What works and why? Student perceptions of ‘useful’ digital technology in university teaching and learning. Studies in Higher Education, 42(8), 1567-1579. https://doi.org/10.1080/03075079.2015.1007946
Hung, M., Licari, F. W., Hon, E. S., Lauren, E., Su, S., Birmingham, W. C., Wadsworth, L. L., Lassetter, J. H., Graff, T. C., Harman, W., Carroll, W. B., & Lipsky, M. S. (2021). In an era of uncertainty: Impact of COVID-19 on dental education. Journal of Dental Education, 85(2), 148-156. https://doi.org/10.1002/jdd.12404
Irfan, A., Rasli, A., Sulaiman, Z., Sami, A., & Qureshi, M. I. (2018). Use of social media sites by Malaysian universities and its impact on university ranking. International Journal of Engineering and Technology, 7(4.28), 67-71. https://doi.org/10.14419/ijet.v7i4.28.22393
Ismail, A., Syakir, A. H. A., Bahrudin, I. A., Samsudin, N. A., & Shafieek, M. S. M. (2022). Implementation of distance and digital learning during pandemic Covid-19 in Malaysia. Online Journal for TVET Practitioners, 7(1), 8-19. https://doi.org/10.30880/ojtp.2022.07.01.002
Jankauskaite, D. (2015). Social media as a tool for improving teaching and learning experience. Journal of Research in Pedagogy and Psychology / Signum Temporis, 7(1), 54. https://doi.org/10.1515/sigtem-2016-0008
Jayasinghe, R. M., Thilakumara, I. P., Bandara, D. L., Edirisinghe, G., Fonseka, M. C. N., Attygalla, M., & Jayasinghe, R. D. (2021). Sri Lankan dental students’ perspective on the effectiveness of e-learning. The Asia Pacific Scholar, 6(4), 7-16. https://doi.org/10.29060/TAPS.2021-6-4/OA2415
Kathirveloo, P. (2024). Assessing institutional readiness for blended learning management and implementation in Malaysian higher education. Management Research Journal, 13(2), 55-67. https://doi.org/10.37134/mrj.vol13.2.5.2024
Katzman, B. D., Farshait, N., & Patlas, M. N. (2024). The role of Twitter in radiology medical education and research: A review of current practices and drawbacks. Canadian Association of Radiologists Journal, 75(2), 245-252. https://doi.org/10.1177/08465371231180643
Kenny, P., & Johnson, I. G. (2016). Social media use, attitudes, behaviours and perceptions of online professionalism amongst dental students. British Dental Journal, 221(10), 651-655. https://doi.org/10.1038/sj.bdj.2016.864
Khanagar, S. B., Alolayan, L. S., Alobaid, T. A., Alharbi, A. A., Alazaz, N. N., & Alanazi, M. H. (2022). Use of YouTube as a learning modality for clinical procedures among dental students in Riyadh, Saudi Arabia – A cross-sectional study. Applied Sciences, 12(23), 11977. https://doi.org/10.3390/app122311977
Kind, T. (2015). Professional guidelines for social media use: A starting point. AMA Journal of Ethics, 17(5), 441-447. https://doi.org/10.1001/journalofethics.2015.17.5.nlit1-1505
Knösel, M., Jung, K., & Bleckmann, A. (2011). YouTube, dentistry, and dental education. Journal of Dental Education, 75(12), 1558-1568. https://doi.org/10.1002/j.0022-0337.2011.75.12.tb05215.x
Leonhardt, M., & Overå, S. (2021). Are there differences in video gaming and use of social media among boys and girls? – A mixed methods approach. International Journal of Environmental Research and Public Health, 18(11), 6085. https://doi.org/10.3390/ijerph18116085
Muscanell, N., & Utz, S. (2017). Social networking for scientists: An analysis on how and why academics use ResearchGate. Online Information Review, 41(5), 744-759. https://doi.org/10.1108/OIR-07-2016-0185
Naguib, G. H., Alyamani, I., Alnowaiser, A. M., & Hamed, M. T. (2018). Social media usage and self perception among dental students at King Abdulaziz University, Saudi Arabia. Journal of Medical Education, 17(2), e105614. https://doi.org/10.3390%2Fhealthcare9111408
Nieminen, P., Uma, E., Mani, S. A., John, J., Laitala, M. L., & Lappalainen, O. P. (2022). E-professionalism among dental students from Malaysia and Finland. International Journal of Environmental Research and Public Health, 19(6), 3234. https://doi.org/10.3390/ijerph19063234
OpenDOSM. (2024). Current population estimate.https://open.dosm.gov.my/dashboard/population
Radeef, A. S., & Faisal, G. G. (2019). Internet addiction among dental students in Malaysia. Journal of International Dental and Medical Research, 12(4), 1452-1456. https://www.jidmr.com/journal/wp-content/uploads/2019/12/35.D19_876_Ghasak_Ghazi_Faisal.pdf
Rahman, N. S. A., Handayani, L., Othman, M. S., Al-Rahmi, W. M., Kasim, S., & Sutikno, T. (2020). Social media for collaborative learning. International Journal of Electrical and Computer Engineering, 10(1), 1070. https://doi.org/10.11591/ijece.v10i1.pp1070-1078
Rajeh, M. T., Sembawa, S. N., Nassar, A. A., Al Hebshi, S. A., Aboalshamat, K. T., & Badri, M. K. (2021). Social media as a learning tool: Dental students’ perspectives. Journal of Dental Education, 85(4), 513-520. https://doi.org/10.1002/jdd.12478
Rani, H., Yahya, N. A., Rosli, T. I., & Mohd-Dom, T. N. (2020). Preparing dental students to use social media as a platform to promote oral health. Journal of Dental Education, 85(S1), 1152-1153. https://doi.org/10.1002/jdd.12349
Shousha, N. M., & Abdelgawad, L. R. (2021). Down in minutes, out for six hours: A brief report on feelings during the outage of WhatsApp, Instagram, and Facebook. British Journal of Psychology Research, 9(2), 38-44. https://doi.org/https://tudr.org/id/eprint/43
Slepian, R. C., Vincent, A. C., Patterson, H., & Furman, H. (2024). 4.02 – “Social media, wearables, telemedicine and digital health,” – A Gen Y and Z perspective. In K. S. Ramos (Ed.), Comprehensive precision medicine (first edition) (pp. 524-544). Elsevier. https://doi.org/10.1016/B978-0-12-824010-6.00072-1
Spallek, H., Turner, S. P., Donate-Bartfield, E., Chambers, D., McAndrew, M., Zarkowski, P., & Karimbux, N. (2015). Social media in the dental school environment, part A: Benefits, challenges, and recommendations for use. Journal of Dental Education, 79(10), 1140-1152. https://doi.org/10.1002/jdd.13310
Stuart, E., Stuart, D., & Thelwall, M. A. (2017). An investigation of the online presence of UK universities on Instagram. Online Information Review, 41, 582-597. https://doi.org/10.1108/OIR-02-2016-0057
Sundaram, A. (2017). The dark side of social media: A reality becoming more contemporary by the day. Asian Social Science, 14(1), 23. https://doi.org/10.5539/ass.v14n1p23
Tjiptono, F., Khan, G., Yeong, E. S., & Kunchamboo, V. (2020). Generation Z in Malaysia: The four ‘E’ generation. In E. Gentina & E. Parry (Eds.), The new Generation Z in Asia: Dynamics, differences, digitalisation (pp. 149-163). Emerald Publishing Limited. https://doi.org/10.1108/978-1-80043-220-820201015
Turkyilmaz, I., Hariri, N. H., & Jahangiri, L. (2019). Student’s perception of the impact of e-learning on dental education. The Journal of Contemporary Dental Practice, 20(5), 616-621. https://doi.org/10.5005/jp-journals-10024-2568
Uma, E., Nieminen, P., Mani, S. A., John, J., Haapanen, E., Laitala, M. L., Lappalainen, O. P., Varghase, E., Arora, A., & Kaur, K. (2021). Social media usage among dental undergraduate students – A comparative study. Healthcare (Basel), 9(11), 1408. https://doi.org/10.3390/healthcare9111408
Zupanic, M., Rebacz, P., & Ehlers, J. P. (2019). Media use among students from different health curricula: Survey study. JMIR Medical Education, 5(2), e12809. https://doi.org/10.2196/12809
*Nurhafizah Ghani
Basic Sciences Unit, School of Dental Sciences,
Universiti Sains Malaysia, Health Campus,
16150 Kubang Kerian, Kelantan, Malaysia
+6097675857
Email: drnurha@usm.my
Submitted: 22 February 2025
Accepted: 6 October 2025
Published online: 7 April, TAPS 2026, 11(2), 9-21
https://doi.org/10.29060/TAPS.2026-11-2/RA3677
Jyoti M. Benni & Anupama M. Gudadappanavar
Department of Pharmacology, Jawaharlal Nehru Medical College, KLE Academy of Higher Education and Research (KAHER), Deemed-to-be-University, Belagavi, India
Abstract
Introduction: Medical education is continuously adapting to new challenges. Cinemeducation, the use of films in teaching, provides contextualised learning experiences, yet its role in pharmacology has not been systematically reviewed. This systematic review synthesises the reported applications and outcomes of cinemeducation in pharmacology education.
Methods: A systematic review (PROSPERO ID: CRD42024568417) was conducted following PRISMA 2020 guidelines. PubMed, Scopus, and Google Scholar were searched for studies published up to June 2024. Eligible studies included healthcare undergraduates where films were used as teaching interventions in pharmacology. Methodological quality was assessed using the QuADS (Quality Assessment with Diverse Studies) tool. Data extracted included study characteristics, teaching approaches, and reported educational outcomes (e.g., test performance, reflections, feedback, and student perceptions).
Results: A total of 77 records were identified; 22 full texts were assessed, and 9 studies met inclusion criteria. Most involved medical undergraduates, using qualitative, longitudinal, or cross-sectional designs. Key details are summarized in Table 1. Reported outcomes included improved post-test scores, better knowledge retention, enhanced engagement, and deeper understanding of pharmacological concepts, ethics, and palliative care. Students also reported greater motivation and confidence in decision-making.
Conclusion: Cinemeducation is an engaging adjunct to conventional pharmacology teaching, supporting cognitive, affective, and ethical learning. However, the lack of control groups and heterogeneous methodologies limit the strength of conclusions. Short, thematically relevant film clips integrated into lectures are recommended to enhance comprehension and engagement.
Keywords: Cinemeducation, Movies, Pharmacology, Medical Education, Systematic Review
Practice Highlights
- Medical education continues to evolve to address changing needs and expectations.
- Cinemeducation refers to the use of movies or video clips as a tool for teaching medical education.
- Movies can bring dry concepts to life, make them more comprehensible, and support diverse types of learning.
- Cinemeducation is an effective approach for teaching pharmacology, as it makes classes more interactive, improves learning, supports knowledge retention, and adds enjoyment to the process.
I. INTRODUCTION
Pharmacology, the study of drugs, is a crucial component of the medical curriculum. It serves as the cornerstone of medical science and lays the groundwork for clinical practice among physicians. The applied aspects of pharmacology strengthen rational therapeutic approaches in clinical settings. However, teaching pharmacology presents challenges. The principal objective is to prepare undergraduate medical students to make informed therapeutic decisions in clinical contexts (Parimala et al., 2013). Given the vast scope of the pharmacology syllabus, students often struggle to remember and recall concepts and drug names. This challenge can be addressed by making pharmacology education more engaging and relevant.
Traditional didactic lectures, utilising either “chalk and board” or PowerPoint presentations, have long been the predominant teaching methods in pharmacology (Agarwal & Sankdia, 2016; Sahu & Supe, 2000). The integration of audio-visual aids enhances the appeal and effectiveness of these lectures (Priyadarshini et al., 2012; Roy & Saha, 2015). In recent years, pharmacology education for undergraduates has undergone significant transformation with the adoption of innovative teaching approaches such as computer-assisted learning, advanced audio-visual tools, mannequins, role-playing, and clinical pharmacology practices (Seth et al., 2010). Additionally, clinical pharmacology and problem-based learning (PBL) methods are now employed in many universities (Burrows & Tamlyn, 1989; Sim, 2004). As pharmacology remains a dynamic and ever-evolving discipline, its complexity and need for contextual learning it’s essential for educators to regularly review and adapt their teaching and evaluation strategies to meet contemporary educational needs (Jayakaran et al., 2010; Padmanabha et al., 2016).
Medical education continues to evolve to address changing needs and expectations. In modern society, television and movies have become deeply ingrained in daily life, presenting diverse life situations and addressing a variety of issues. This versatility makes movies a valuable tool in medical education. The first recorded usage of videos in medical education was at a 1979 psychiatry session (Fritz & Poe, 1979). Cinema, through its combination of sight and sound, engages viewers by encouraging interaction with audio-visual media. It stimulates the affective domain, connects learning with real-life experiences, enhances observational learning, fosters reflection, and boosts motivation. In 1994, Matthew Alexander introduced the term “Cinemeducation” to describe the integration of movies into medical education (Alexander et al., 1994).
The concept of “Cinema + Medicine + Education” refers to the use of movies or video clips as a tool for teaching medical education (Lumlertgul et al., 2009). Recent studies in medical literature highlight videos as an effective and innovative teaching method (Alexander, 2002). Movies offer several advantages: they can bring abstract and dry concepts to life, make them more comprehensible, and support diverse types of learning. They can also explore the emotional, social, and ethical dimensions of diseases, such as suffering, emotions, conflicts, and dilemmas. Films have been utilised as teaching aids in various fields, including clinical research, medical ethics, pharmacology, microbiology, doctor–patient relationships, professionalism, mental health, and psychosocial topics like breaking bad news or dealing with terminal illnesses (Blasco et al., 2016; Farre et al., 2004; Saab et al., 2005; Bhaskara & Shelley, 2016). The profound emotional impact of movies can be leveraged to teach vital qualities such as empathy, self-reflection, compassion, and altruism, and medical professionalism – areas often overlooked in traditional medical training (Shankar, 2019).
Cinemeducation is a globally adaptable teaching approach, capable of exceeding verbal and cultural boundaries. Films, whether local or international, offer universally relatable themes such as ethical dilemmas, patient care, and human behavior, making them effective across diverse educational and cultural settings. This global relevance justifies the inclusion of studies from diverse regions, providing a broader perspective on the application of cinemeducation in pharmacology education. The Medical Council of India, in its 2019 curriculum revision for “Competency-Based Medical Education,” recommended incorporating short films and videos as teaching tools (Medical Council of India, 2019). Published data indicate that cinemeducation is increasingly being used to train healthcare professionals across undergraduate, postgraduate, and continuing medical education programs in diverse clinical settings (Swanwick, 2018). To our knowledge, no prior systematic reviews have focused exclusively on the application of cinemeducation in the teaching of pharmacology. Therefore, this review aims to evaluate the use of cinemeducation in pharmacology education, examining its applications and reported outcomes. Furthermore, it will explore the perceptions of educators and students regarding the integration of cinemeducation into pharmacology teaching.
II. METHODS
A. Search Strategy
Our review was conducted and reported in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines, which are widely recognised for systematic review reporting (Page et al., 2021). With registration number CRD42024568417, the study protocol was pre-registered in PROSPERO: International Prospective Register of Systematic Reviews. A comprehensive literature search on the use of movies in pharmacology education was independently carried out by both authors, covering publications from inception up to June 2024. The primary databases used for the search were PubMed and SCOPUS. In order to find further pertinent research, Google Scholar was also used, and the reference lists of the publications that were retrieved were reviewed.
B. Search Terms
The search utilised the following keywords:
(“Cinemeducation”[All Fields] OR “Cinemedicine”[All Fields] OR “movies”[MeSH] OR “films”[MeSH] OR “motion pictures”[MeSH] OR “audiovisual aids”[MeSH] OR “TV series”[All Fields]) AND (“Pharmacology/education”[MeSH] OR “Pharmacology/ethics”[MeSH] OR “Pharmacology/methods”[MeSH] OR “Pharmacology/research”[MeSH] OR “Pharmacology/clinical trials”[MeSH]). Free-text terms were searched in the title, abstract, and keywords, while MeSH terms were used to capture indexed articles. Database full search strategy details are provided in Appendix 1.
C. Selection Criteria
The articles that were included in this review were chosen because they satisfied the following selection criteria, and those that did not were excluded.
D. Inclusion Criteria
- Peer-reviewed scholarly research articles were taken into consideration.
- Articles that addressed the use of motion pictures, television shows, and cinema as teaching resources in pharmacology.
- Studies describing teaching experiences in pharmacology within medical, dental, pharmacy, or nursing degree programs were eligible.
- Only articles published in English were included.
- All types of articles, from randomised controlled trials to letters, were considered, with no restrictions on publication date.
E. Exclusion Criteria
- Articles that weren’t entirely available in the selected databases.
- Research that is not fully translated into English.
- Book reviews, review articles and editorials were not included.
F. Study Selection
The search strategy (PRISMA flow chart) is illustrated in Figure 1. The reviewers independently screened all article titles. Once the findings were retrieved from the chosen databases, irrelevant research and duplicates, including conference papers and publications written in languages other than English, were eliminated. We evaluated the remaining papers’ abstracts for initial eligibility. Full articles that were deemed eligible were examined to make sure they satisfied the requirements for inclusion. All articles were assessed by both authors, who discussed and resolved any disagreements to improve the validity and reliability of the selection process.
G. Data Extraction, Quality Assessment (Risk of Bias) and Data Synthesis
This study aims to explore the role of cinema and motion pictures in medical education. The research team reviewed and collected data aligned with the keywords in the research questions, results, and discussions of the selected publications. Quality Assessment of Diverse Studies (QuADS) technique, both authors independently assessed every study that was involved (Albert et al., 2024; Harrison, et al., 2021). This tool provides a straightforward scoring system for assessing study quality in systematic reviews. It consists of 13 items, with each study receiving a score between 0 and 3, where ‘0’ indicates no mention, ‘1’ signifies minimal detail, ‘2’ represents moderate detail, and ‘3’ denotes complete information, resulting in a maximum possible score of 39. For the purpose of this review, studies were grouped descriptively into three categories of methodological quality: low (≤17), moderate (18–28), and high (≥29). These categorisations were used solely for summarising study quality and not for excluding any studies from the review. All studies that met the inclusion criteria were retained, and the quality appraisal results were used to inform the interpretation of the findings rather than as an exclusion criterion.
A standardised data extraction form was designed to collect predefined data points from each study. Extracted data included study authors, year, country, participant characteristics, study design, intervention details (e.g., film used, duration, pre/post-tests, group discussion, reflection writing), and results. In order to ensure a comprehensive and uniform assessment, disagreements during the review were settled through a consensus meeting. When analysing results and drawing conclusions, the significance of the findings was taken into account rather than the quality scores of the studies. In order to improve the validity and reliability of the review findings, the research team also addressed any difficulties or ambiguities that arose during the selection and data extraction procedure.
III. RESULTS
The search process is depicted in the PRISMA flow diagram (Figure 1). A total of 77 publications were found through the search method. After removing duplicates and irrelevant studies, 22 publications were selected for preliminary eligibility screening. Of these, 13 were excluded for studies not pertaining to pharmacology teaching, or absence of a cinema-based intervention, and review articles or editorials. Finally, 09 publications were included in the study after they fully satisfied the selection criteria. Every member of the study team developed a consensus to address any possible ambiguities in meeting the inclusion criteria.
A. Study Characteristics
Table 1 provides a detailed summary of the study characteristics, which were published between 2000 and 2024 and conducted in Spain, India, Brazil, Iran, Netherlands, Slovenia, and Thailand. Most studies employed qualitative approaches, while a few used longitudinal or cross-sectional quantitative designs. Importantly, none of the studies included a control group for comparison.
B. Study Participants
Most of the research involved medical undergraduate students and were carried out in academic institutions such medical colleges and universities (Cambra-Badii, 2020; Kadivar et al., 2018; Kersnik & Klemenc-Ketiš, 2011; Lumlertgul et al., 2009; Patel et al., 2022; Picanço et al., 2019; Shankar et al., 2016). One study focused on pharmacy undergraduate students in a pharmacy college (Desai & Kakodkar, 2022). An alternative study included students from medical, human biology and pharmaceutical and biotechnological industry (Cambra-Badii, 2020). Another study was carried out in a hospital setting to assess patient safety in the hospital environment (Cambra-Badii, 2024). Of the included studies, six used films or movies (Cambra-Badii, 2020; Kadivar et al., 2018; Kersnik & Klemenc-Ketiš, 2011; Lumlertgul et al., 2009; Patel et al., 2022; Picanço et al., 2019; Shankar et al., 2016), one employed TV series (Cambra-Badii, 2024), and two studies incorporated both films and TV series in their methodology (Desai & Kakodkar, 2022; Lumlertgul et al., 2009).
C. Cognitive Outcomes
Three studies employed pre- and post-intervention questionnaires to assess baseline knowledge and subsequent changes after the intervention (Cambra-Badii, 2020; Cambra-Badii, 2024; Patel et al., 2022). Knowledge was typically measured using multiple-choice or open-ended questions, and all three reported improved post-test scores, indicating enhanced understanding of pharmacology concepts.
D. Affective Outcomes
Most studies used post-intervention questionnaires to evaluate students’ perceptions and attitudes toward cinemeducation (Cambra-Badii, 2020; Desai & Kakodkar, 2022; Kadivar et al., 2018; Lumlertgul et al., 2009; Picanço et al., 2019; ShaJnkar et al., 2016). Students consistently reported that incorporating movies or TV shows increased their motivation, attention, and concentration, while adding entertainment value to learning. They also felt that they understood more compared to conventional lecture-based teaching.
E. Ethical Understanding
Several studies addressed the role of cinema-based learning in enhancing awareness of ethical and professional issues such as informed consent (Patel et al., 2022), clinical trial enrolment (Shankar et al., 2016), adverse drug reactions (Cambra-Badii, 2020), error management (Lumlertgul et al., 2009), and ethical considerations in medical and palliative care (Kadivar et al., 2018; Kersnik & Klemenc-Ketiš, 2011). Student reflections indicated that cinematic narratives helped them better appreciate the complexity and importance of these issues in real-world clinical practice.
F. Quality Appraisal of Studies
The QuADS scores for the included studies are shown in Table 2. Scores ranged from 24 to 34 out of a maximum of 39. Four studies were rated as high quality, and five received a moderate quality rating; none were classified as low quality. The studies performed well in clearly stating aims and objectives, describing the research setting and target population, outlining data collection procedures, selecting appropriate study designs, and using analytical methods that matched the research aims. However, there were limitations in explaining conceptual or theoretical frameworks and justifying the chosen analytical methods. Most studies scored zero for involving research stakeholders in the planning or conduct of the study. This underscores the importance of enhancing stakeholder engagement and participant collaboration in the co-creation of research.
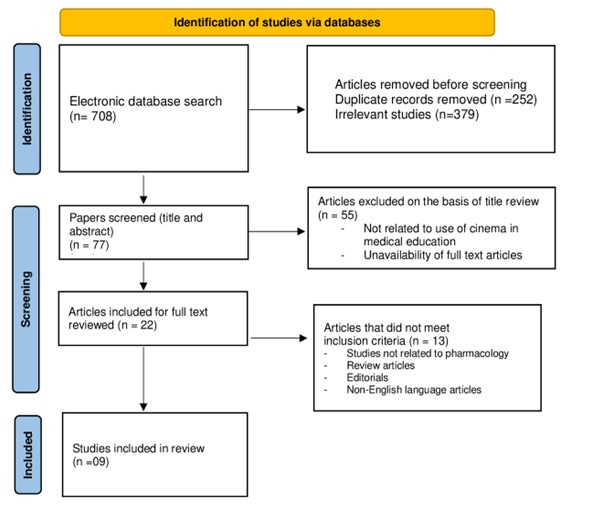
Figure 1. Study selection flow diagram (Prisma Flow diagram)
A quantitative synthesis of pre/post-test data was not undertaken due to substantial heterogeneity in outcome measures, assessment tools, scoring systems, and reporting formats. Only three studies (Cambra-Badii, 2020; Cambra-Badii, 2024; Patel et al., 2022) provided pre/post-intervention knowledge data, but variations in question types, item numbers, and scoring methods precluded meaningful pooling. The results are therefore narratively presented with an emphasis on ethical, affective, and cognitive outcomes. Most of the included studies had post-test, pre/post-test, or single-group designs without a control arm. The lack of comparator groups makes it challenging to attribute improvements to the intervention alone, even though these designs show that cinemeducation has positive effects. This is because confounding factors, such as related coursework, cannot be completely ruled out. The formats of the interventions also differed, ranging from short clips incorporated into lectures to full-length film screenings. Shorter clips were more focused on particular pharmacology or patient management concepts, whereas full films tended to offer richer narratives that encouraged ethical reflection and empathy. These variations probably affected the scope of learning objectives and added to limited quantitative synthesis.
|
Sl. No. |
Authors, Year, Country |
Study design / settings |
Participants |
Intervention |
Result |
|
1 |
Cambra-Badii 2024, Spain |
Qualitative study, pre & post-test questionnaire |
70 medical students, 2nd year |
TV series ‘The Resident’ centred on patient safety, focused on adverse events during hospitalisation and error management. Pre and post intervention scores, 10 questions on patient safety, single best answer. Also, 2 open ended questions were used. |
Cinemeducation significantly improve learning on patient safety in complex situations.
|
|
2 |
Desai & Kakodkar, 2022, India |
Qualitative study, pre & post-test questionnaire |
111 students, from 3rd year Bachelor of Pharmacy |
Movie/ web series were used. Presentation of topics related to pharmacology of drugs like ephedrine, cocaine, alcohol, beta blockers, digitalis. Pedagogy notes to be written and Fill feedback google form, 8 closed ended questionnaire using Likert scale. |
Movies are an effective academic method for learning pharmacology. It makes learning interesting, increases enthusiasm and motivation for learning, piques students’ curiosity, accelerates learning, helps them retain information, and aids in understanding the subject through visual imaging. |
|
3 |
Patel et al., 2022, India |
Qualitative study prospective, longitudinal, interventional study |
139 second professional year medical students
|
Watch movie clips à divided into groups à presentation and Individual reflection writing done. Feedback was taken. Pre & post-test questionnaire to test baseline & change in knowledge about the ethics (informed consent, clinical trial enrolment & details about, inform drugs) and right to choose treatment available. |
The students said they would treat patients with respect, honour their choices of treatment, follow ethics and professionalism, respect co-workers. |
|
4 |
Picanço et al., 2019, Brazil |
An exploratory, cross-sectional, quantitative study was conducted |
107 students, first- to sixth-year students from the Medicine course
|
Two Movies were screened. The psychometric scale (questionnaire) with Likert scale responses, included the primary health care, physician’s role and importance of research were utilised. |
The preclinical series of the medical course uses films as an effective teaching tool to develop humanistic attitudes.
|
|
5 |
Kadivar et al., 2018, Iran |
Quantitative and qualitative data analysis |
270 medical students participated in this study |
Student viewed 09 movies in different sessions, related to biopsychosocial topics like palliative care, managing terminal illness and ethics in medical care, palliative care and mental illness. Group discussion and post-test questionnaire with 11 questions with Likert scale and one open ended question about perception & attitude were used. |
Through watching and analysing films, medical students can gain knowledge on psychosocial topics related to medicine through cinemedicine.
|
|
6 |
Shankar et al., 2016, Netherlands |
Qualitative data analysis |
60 basic science undergraduate medical students |
Two Movies were screened and student presented on findings related to enrolling a patient in clinical trials, process of obtaining written informed consent, treatment modalities. Later student presentation and feedback was obtained through questionnaire. |
The session received great reviews from the students. Movies help medical students learn about humanistic issues, improve their comprehension of death and dying, and promote professionalism. |
|
7 |
Kersnik & Klemenc-Ketiš, 2011, Slovenia
|
Qualitative data analysis
|
Group of eleven fourth year medical students |
Students watch movie, followed by discussion and reflection writing & presentations on the topics. Topics chosen were (doctor/patient communication, ethical issues and the role of doctor and nurse in palliative care). |
Students understood that physicians should respect patients’ ability to select their own treatments and offer palliative care.
|
|
8 |
Lumlertgul et al., 2009, Thailand |
Qualitative study |
26 second-year (preclinical) medical students
|
Five movies were chosen for the project and ethical issues were depicted as main themes for group discussion, which included the doctor–patient relationship, informed consent and clinical trials in patients, management of genetic disorders, patient management, and brain death and organ transplantation. Movie screening followed by discussion. Questionnaire and reflection writing were used. |
Movies have proven to be an effective and entertaining method of facilitating students with learning on professionalism. |
|
9 |
Cambra-Badii, 2020, Spain |
Exploratory comparative analysis |
237 students participated in the study |
Movie clips were used to study the pharmacovigilance processes and adverse drug effects. Also, the film shows about the importance of a signal alert, the studies needed to confirm/reject causality of an adverse drug event, and the roles of the pharmaceutical industry and public health agencies. Pre & post-test questionnaire were used. |
The teaching activity used in this study helped students learn about adverse drug reactions and the process of pharmacovigilance. |
Table 1. Characteristics of the included studies in the review
|
QuADS criteria |
Author & year |
||||||||
|
Cambra-Badii, 2024 |
Desai & Kakodkar, 2022 |
Patel et al., 2022 |
Picanço et al., 2019 |
Kadivar et al., 2018 |
Shankar et al., 2016 |
Kersnik & Klemenc-Ketiš, 2011 |
Lumlertgul et al., 2009 |
Cambra-Badii, 2020 |
|
|
Theoretical or conceptual underpinning to the research |
2 |
2 |
1 |
1 |
1 |
1 |
2 |
3 |
2 |
|
Statement of research aim/s |
3 |
2 |
2 |
2 |
3 |
2 |
3 |
3 |
2 |
|
Clear description of research setting and target population |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
|
The study design is appropriate to address the stated research aim/s |
3 |
2 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
|
Appropriate sampling to address the research aim/s |
2 |
2 |
3 |
2 |
3 |
1 |
1 |
1 |
3 |
|
Rationale for choice of data collection tool/s |
2 |
2 |
3 |
3 |
2 |
2 |
2 |
3 |
3 |
|
The format and content of data collection tool is appropriate to address the stated research aim/s |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
|
Description of data collection procedure |
3 |
3 |
3 |
3 |
2 |
3 |
3 |
3 |
3 |
|
Recruitment data provided |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
|
Justification for analytic method selected |
2 |
2 |
3 |
3 |
1 |
0 |
0 |
0 |
3 |
|
The method of analysis was appropriate to answer the research aim/s |
3 |
3 |
2 |
3 |
2 |
1 |
2 |
3 |
3 |
|
Evidence that the research stakeholders have been considered in research design or conduct. |
2 |
0 |
0 |
0 |
1 |
0 |
0 |
0 |
0 |
|
Strengths and limitations critically discussed |
2 |
1 |
1 |
1 |
1 |
2 |
2 |
1 |
3 |
|
Total score (%) |
33/39 (85%) |
28/39 (72%) |
30/39 (77%) |
30/39 (77%) |
29/39 (74%) |
24/39 (62%) |
27/39 (69%) |
29/39 (74%) |
34/39 (87%) |
|
Quality of study |
High |
Moderate |
High |
High |
Moderate |
Moderate |
Moderate |
Moderate |
High |
Table 2. Quality assessment of reviewed studies using the Quality Assessment of Diverse Studies (QuADS) criteria
IV. DISCUSSION
This study aimed to explore the applications and reported outcomes of incorporating movies/films into pharmacology teaching and their impact on enhancing knowledge and skills among undergraduate students. A qualitative review of nine eligible studies revealed various cinemeducation strategies employed as teaching tool in undergraduate pharmacology education. These studies demonstrated that using movie clips are a promising tool for enhancing engagement and understanding in pharmacology. It makes classes more engaging, sparks student interest, enhances learning, aids knowledge retention, and makes the process enjoyable. Additionally, it fosters greater interest and motivation, helps students grasp concepts through visual representation, and improves understanding of empathy, research ethics, patient care, palliative care, error management in complex scenarios, and autonomy in treatment choices. The findings strongly support cinemeducation as a valuable tool for medical education, effectively enhancing both knowledge and skills.
Medical education is encountering new and evolving challenges. Over the past few decades, the field of pharmacology has significantly expanded its scope. Traditional teaching methods, such as lectures and practical sessions, are increasingly being replaced by innovative pedagogical approaches to enhance the conceptual understanding of pharmacology. A recent systematic review of these methods highlighted the positive impact of using movies in pharmacology education across various health disciplines (Baños et al., 2024). Films have been utilised to teach diverse topics, including pharmacology concepts, preclinical and clinical research, pharmacovigilance, medical ethics, the doctor-patient relationship, microbiology, mental health, drug addiction, palliative care, pain management, medical professionalism, and social conflicts in healthcare (Baños et al., 2024; Cambra-Badii, 2020; Darbyshire & Baker, 2012; Farre et al., 2004; Icart Isern, 2012). Historically, the movie Awakenings was among the first to be used in pharmacology education, with Koren employing it to teach principles of clinical pharmacology to medical students. This approach proved to be a valuable tool for improving pharmacology instruction (Koren, 1993).
Movies serve as an excellent tool to boost students’ motivation to grasp clinical pharmacology principles and can inspire a stronger desire to learn (Farre et al., 2004). A recent systematic review highlights several popular films that are particularly effective for teaching topics such as basic and clinical pharmacology, drug research, and bioethics. These include Awakenings, Lorenzo’s Oil, Miss Evers’ Boys, The Fugitive, Wit, The Constant Gardener, Side Effects, and Dallas Buyers Club (Baños et al., 2024). Additionally, various TV series, such as House MD, Emergency Room (ER), Grey’s Anatomy, The Resident, and New Amsterdam have been employed to teach concepts like pharmacovigilance, drug abuse, pharmacological classifications, and the doctor-patient relationship, which can influence therapeutic compliance (Baños et al., 2024; Cambra-Badii, 2024; Desai & Kakodkar, 2022; Williams et al., 2015). Notably, House MD episodes have proven effective for teaching clinical pharmacology (Wicclair, 2008). Another example of cinemeducation is the film Wit, which portrays pain management in a woman undergoing chemotherapy for late-stage ovarian cancer. This movie helped students understand approaches to pain management and the importance of professionalism in patient care (Carpenter et al., 2008). A study demonstrated that incorporating the TV series The Resident into teaching effectively enhanced students’ understanding of patient safety strategies in complex situations. Students reported gaining valuable insights into identifying, preventing, and managing adverse events, showcasing learning progression from Level 1 to Level 5 of Bloom’s Taxonomy (Cambra-Badii, 2024).
Movies have been utilised effectively to teach medical students ethics and professionalism in countries such as the USA, Brazil, Israel, and Korea (Shankar, 2019). Given that Indian Medical Graduates (IMGs) are frequently seen to be less competent in comprehending the moral implications of informed consent in clinical research, a study was carried out to use cinemeducation to teach second-year medical students about ethics (Patel et al., 2022). Most participants thought this approach was a good way to teach ethics and professionalism. The study revealed strong agreement among students on the importance of obtaining informed consent, thoroughly explaining clinical trials, and discussing potential adverse drug reactions with patients before their enrolment (Patel et al., 2022). Additionally, students emphasised the significance of informing patients about their treatment options. It was also discovered that using fictional audio-visual materials encouraged students to think critically and morally, pushing them to consider ethical issues outside of the scope of textbooks (Piqué-Buisan, Sorribes, & Cambra-Badii, 2024).
Palliative care, an evolving medical field, often highlights the limitations of modern medical technologies and is fraught with ethical dilemmas, communication challenges, and professional behaviour issues (Meier & Morrison, 2004). Through the movie Wit, students identified several key aspects of palliative medicine and began to understand their significance. They recognised that doctors should incorporate palliative care as a legitimate form of treatment, emphasising that managing symptoms is just as crucial as addressing pain and providing psychological support. Additionally, students believed that palliative care planning should be done in collaboration with patients, particularly regarding critical decisions such as resuscitation (Kersnik & Klemenc-Ketiš, 2011).
The articles reviewed indicate that most experiences with movies lead to increased knowledge and higher student satisfaction. In this review, some authors suggested that a traditional lecture prior to viewing these materials is essential to help students retain key theoretical concepts and terminology afterward. They provided a brief lecture about the process, to clear concepts and hands on training was conducted for the participants, which primarily helped them to develop their rational thinking and cognitive skills and aided to write reflections at the end of the project (Kersnik & Klemenc-Ketiš, 2011; Lumlertgul et al., 2009; Patel et al., 2022), Similar results were found with previous studies, where they suggested that using cinematic resources alone may not significantly augment students’ acquaintance and should be complemented with didactic classes to reinforce core concepts (Aboul-Fotouh & Asghar-Ali, 2010; Self, 1993). Thus, finding a balance between this creative approach and conventional teaching techniques might be the most effective way to promote learning.
In our review, some studies utilised entire movies (Kadivar et al., 2018; Lumlertgul et al., 2009; Picanço et al., 2019; Shankar et al., 2016) while others relied on selected video clips (Baños et al., 2024; Cambra-Badii, 2024; Lumlertgul et al., 2009). While authors acknowledged that watching an entire movie could be time-consuming, they noted it provided valuable context for each character and helped students better understand the complex and controversial issues presented. Similarly, earlier studies have recommended viewing the full movie (Masters, 2005; Silk & Weber, 2007) as part of the learning process, whereas others argue that a few carefully selected clips are sufficient to achieve the desired educational outcomes (Alexander, 2002; Blasco, 2006; Onsman & Ventura, 2009). Some authors recommended adding one to two-minute movie clips that referenced the topic being covered to power point presentations in pharmacology lectures. These clips received positive feedback because they allowed students to connect theory to simulated practice, encouraged them to attend lectures, and served as a sectioning break that kept them interested throughout the entire lecture (Onsman & Ventura, 2009). According to encouraging faculty input, students’ attention spans, retention of the material, and engagement were all enhanced by cinemeducation, which also helps to associate the films with real-life situations. Faculty pointed out that this approach has several shortcomings, including the possibility of pupils misinterpreting the situation, the need for extensive technical assistance, and the fact that it can only cover a limited number of topics (Patel et al., 2022).
To sum up, incorporating films alongside traditional teaching methods has received positive feedback from students, as it helps review and enhances the retention of theoretical concepts. These films promote lively debates on difficult pharmacology subjects, like the difficulties of organising and carrying out clinical trials on novel medications, the significance of following bioethical guidelines in human subjects’ research, Pharmacovigilance, and the psychological and social facets of medication treatment. Still, others contend that engaging with actual patients or taking part in bedside rounds can offer more worthwhile educational opportunities.
A significant disadvantage of using films is the time required for preparation and scheduling during the academic calendar. Furthermore, films may sometimes exaggerate medical or pharmacological information for dramatic effect. The main limitation of our systematic review is the selection of databases, which may have excluded publications in other languages. The primary drawback is the lack of a comparison group employing alternative teaching methods in the included studies. Furthermore, these studies focused only on immediate knowledge gains, without exploring long-term knowledge retention or evaluating the impact on the clinical application of that knowledge. Additional restrictions that could restrict the findings’ generalisability include the diversity of medical programs, English language bias, and the prevalence of cross-sectional studies. Although they draw attention to important gaps in the literature, the comparatively small number of studies on some fields may also limit interpretation. Lastly, publication bias may have influenced the findings of this review, as most included studies reported favorable outcomes. Negative or neutral findings may be underrepresented in the literature, thereby skewing the overall perception of cinemeducation’s usefulness.
Few practical recommendations for teachers include, educators can select films or clips that match the learning objectives, are relevant to the topic, and are of suitable length. Short clips (5–10 minutes) that clearly show key concepts work best. These can be combined with traditional teaching methods and followed by discussions or reflection activities to deepen understanding.
V. CONCLUSION
Cinemeducation emerges as a valuable adjunct in pharmacology education, with reported benefits in enhancing student engagement, contextual understanding, and reflective thinking. Integrating short, thematically relevant film clips – addressing issues such as drug use, side effects, ethical dilemmas, and informed consent – into lectures, followed by guided discussions or reflection activities, can enrich the learning experience. Current evidence primarily highlights short-term gains; further studies are needed to explore its influence on long-term knowledge retention, professional attitudes, and clinical practice. Beyond pharmacology, cinemeducation holds potential for wider application in fields such as public health, physiotherapy, and nursing, thereby extending its educational impact.
Notes on Contributors
Dr Jyoti M. benni contributed to conceptual development of the study, conducting the literature search, reviewing the literature retrieved, synthesising the data, data analysis, writing and reviewing the manuscript.
Dr Anupama M. Gudadappanavar contributed to conducting the literature search, reviewing the literature retrieved, synthesising the data and reviewing the manuscript.
Ethical Approval
As this study is a systematic review, ethical approval is not required. The review is registered in PROSPERO – The International Prospective Register of Systematic Reviews, with the registration number CRD42024568417.
Data Availability
All reviewed articles reported in this systematic review are listed in the References section for readers to access.
Funding
The study was not funded by any funding agencies.
Declaration of Interest
The author declares no conflict of interest.
References
Aboul-Fotouh, F., & Asghar-Ali, A. A. (2010). Therapy 101: A psychotherapy curriculum for medical students. Academic Psychiatry, 34(4), 248-252. https://doi.org/10.1176/appi.ap.34.4.248
Agrawal, M., & Sankdia, R. K. (2016). Attitude of medical students towards the use of audio-visual aids during didactic lectures in pharmacology in a medical college of central India. International Journal of Basic & Clinical Pharmacology, 5(2), 416-422. http://dx.doi.org/10.18203/2319-2003.ijbcp20160755
Albert, F. A., Seidu, A. A., Mason, H. M., Anderson, E., Alele, F. O., Heggarty, P., Hollins, A., Gupta, T. S., Hays, R. B., McArthur, L., & Malau-Aduli, B. S. (2024). A systematic review of medical practitioners’ retention and application of basic sciences to clinical practice. BMC Medical Education, 24, 997. https://doi.org/10.1186/s12909-024-05952-8
Alexander, M., Hall, M. N., & Pettice, Y. J. (1994). Cinemeducation: An innovative approach to teaching psychosocial medical care. Family Medicine, 26(7), 430-433.
Alexander, M. (2002). The doctor: A seminal video for Cinemeducation. Family Medicine, 34, 92-94.
Baños, J. E., Blanco-Reina, E., Bellido-Estévez, I., Bosch F., Cabello, M. R., Cambra-Badii, I., De la Cruz, J. P., D’Ocón, P., Ivorra, M. D., Ferrándiz, M., González-Correa, J. A., Martín-Montañez, E., Martos, F., Pavía, J. & Sanz, E. (2024). Beyond lectures and practical courses: Teaching pharmacology using imaginative pedagogical tools. Pharmacological Research, 202, 107130. https://doi.org/10.1016/j.phrs.2024.107130
Blasco, P. G., Moreto, G., Roncoletta, A. F., Levites, M. R., & Janaudis, M. A. (2006). Using movie clips to foster learners’ reflection: Improving education in the affective domain. Family Medicine, 38(2), 94-96.
Burrows, H. S., & Tamlyn, R. N. (1989). Problem-based learning: An approach to medical education. Springer.
Cambra-Badii, I., Francés, M. L., Videla, S., Farré, M., Montané, E., Blázquez, F., & Baños, J. E. (2020). Cinemeducation in clinical pharmacology: Using cinema to help students learn about pharmacovigilance and adverse drug reactions. European Journal of Clinical Pharmacology, 76(12), 1653-1658. https://doi.org/10.1007/s00228-020-02985-y
Cambra-Badii, I., Gomar-Sancho, C., Mastandrea, P. B., Arrebola-Trias, X., Baños, J. E., Farriols, R. P., & Gonzalez-Caminal, G. (2024). Cinemeducation to teach patient safety: An experience in medical students. Humanities and Social Sciences Communications, 11, 561. https://doi.org/10.1057/s41599-024-03054-w
Carpenter, J., Stevenson, B., & Carson, E. (2008). Creating a shared experience: Using movies in nursing education. Nurse Educator, 33, 103-104. https://doi.org/10.1097/01.NNE.0000312182.98023.86
Darbyshire, D., & Baker, P. (2012). A systematic review and thematic analysis of cinema in medical education. Medical Humanities, 38(1), 28-33. https://doi.org/10.1136/medhum-2011-010026
Desai, S. M., & Kakodkar, P. V. (2022). Using clips from movies and web series as a pedagogic method for learning pharmacology. Pharmacy Education, 22(1), 445-449. https://doi.org/10.46542/pe.2022.221.445449
Farre, M., Bosch, F., Roset, P. N., & Baños, J. E. (2004). Putting clinical pharmacology in context: The use of popular movies. Journal of Clinical Pharmacology, 44(1), 30-36. http://dx.doi.org/10.1177/0091270003260679
Fritz, G. K., & Poe, R. O. (1979). The role of a cinema seminar in psychiatric education. American Journal of Psychiatry, 136(2), 207-210. http://dx.doi.org/10.1176/ajp.136.2.207
Harrison, R., Jones, B., Gardener, P., & Lawton, R. (2021). Quality Assessment with Diverse studies (QuADS): An appraisal tool for methodological and reporting quality in systematic reviews of mixed- or multi-method studies. BMC Health Services Research, 21, 144. https://doi.org/10.1186/s12913-021-06122-y
Icart Isern, M. T., & Donaghy, K. (2012). Films in health sciences education: Learning through moving images. Ediciones Universitat de Barcelona.
Jayakaran, S., Chavda, N., Yadav, P., & Kantharia, N. D. (2010). Intern doctors’ feedback on teaching methodology in pharmacology. Journal of Pharmacology & Pharmacotherapeutics, 1(2), 114-116. https://doi.org/10.4103/0976-500X.72359
Kadivar, M., Mafinejad, M. K., Bazzaz, J. T., Mirzazadeh, A., & Jannat, Z. (2018). Cinemedicine: Using movies to improve students’ understanding of psychosocial aspects of medicine. Annals of Medicine and Surgery, 21(28), 23-27. https://doi.org/10.1016/j.amsu.2018.02.005
Klemenc-Ketiš, Z., & Kersnik, J. (2011). Using movies to teach professionalism to medical students. BMC Medical Education, 11, 60. https://doi.org/10.1186/1472-6920-11-60
Koren, G. (1993). Awakenings: Using a popular movie to teach clinical pharmacology. Clinical Pharmacology & Therapeutics, 53(1), 3-5. https://doi.org/10.1038/clpt.1993.2
Lumlertgul, N., Kijpaisalratana, N., Pityaratstian, N., & Wangsaturaka, D. (2009). Cinemeducation: A pilot student project using movies to help students learn medical professionalism. Medical Teacher, 31(7), e327-e332. https://doi.org/10.1080/01421590802637941
Masters, J. C. (2005). Hollywood in the classroom. Nurse Educator, 30(3), 113-116. https://doi.org/10.1097/00006223-200505000-00013
Medical Council of India. (2019). Foundation course for the undergraduate medical education program. Medical Council of India. https://www.nmc.org.in/wp-content/uploads/2020/08/FOUNDATION-COURSE-MBBS-17.07.2019.pdf
Morrison, R. S., & Meier, D. E. (2004). Clinical practice: Palliative care. New England Journal of Medicine, 350, 2582-2590. https://doi.org/10.1056/NEJMcp035232
Roy, M., & Saha, N. (2015). Medical students and the use of mixed audio-visual aids in lecture classes. IOSR Journal of Dental and Medical Sciences, 14(12), 1-4. http://dx.doi.org/10.9790/0853-141256870
Padmanabha, T. S., Manu, G., Kulkarni, G. P., Chandrakantha, T., & Neha, K. (2016). Second year medical student’s feedback and perspective on teaching methodology in pharmacology in a tertiary care teaching hospital from India. Scholars Journal of Applied Medical Sciences, 4(6C), 2089-2094. https://doi.org/10.21276/SJAMS.2016.4.6.45
Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … McKenzie, J. E. (2021). PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. British Medical Journal, 372, n160. https://doi.org/10.1136/bmj.n160
Parimala, K., Subash, K. R., Jagan, N., Vijay Kumar, S., Vishwanath, S., & Chandrashekar, M. (2013). Assessment of pharmacology teaching – A critical appraisal by medical school learners. International Journal of Medical Research & Health Sciences, 2(2), 124-129. https://dx.doi.org/10.5958/j.2319-5886.2.2.001
Patel, P. P., Gandhi, A. M., & Desai, C. K. (2022). Cinemeducation: A teaching-learning tool to teach professionalism and ethics in medical undergraduates. International Journal of Basic & Clinical Pharmacology, 11, 91-96. https://dx.doi.org/10.18203/2319-2003.ijbcp20220405
Picanço, T., Nazima, M., Santos, B., Júnior, O., Cambraia, M., Morais, L., Pena, L., & Costa, K. (2019). Films as an educational resource in the teaching of humanistic attitudes to medicine students. Revista Brasileira de Educação Médica, 43(Suppl.1), 57-68. https://doi.org/10.1590/1981-5271v43suplemento1-20180164.ing
Piqué-Buisan, J., Sorribes, E., & Cambra-Badii, I. (2024). Exploring the impact of using cinema and TV series in medical education: A systematic review. Medicina Clínica Práctica, 2, 100421. https://doi.org/10.1016/j.mcpsp.2023.100421
Priyadarshini, K. S., Shetty, H. V., Reena, R. (2012). Assessment of different teaching aids and teaching methods for the better perception of biochemistry by 1st MBBS students. Journal of Evolution of Medical and Dental Sciences, 1(6), 1159-1165. http://dx.doi.org/10.21276/sijap.2019.2.3.11
Saab, B. R., Usta, J., Major, S., Musharrafieh, U., & Ashkar, K. (2005). Communication skills in a Lebanese medical school: From movie theaters to medical classrooms. Family Medicine, 37(2), 90-92. https://pubmed.ncbi.nlm.nih.gov/15690245/
Sahu, D. R., & Supe, A. N. (2000). The art and science of presentation: 35-mm slides. Journal of Postgraduate Medicine, 46(4), 280-285. https://pubmed.ncbi.nlm.nih.gov/11435658/
Self, D. J., Baldwin, D. C. Jr., & Olivarez, M. (1993). Teaching medical ethics to first-year students by using film discussion to develop their moral reasoning. Academic Medicine, 68(5), 383-385.
Seth, V., Upadhyaya, P., Ahmad, M., & Kumar, V. (2010). Impact of various lecture delivery methods in pharmacology. EXCLI Journal, 9, 96-101. https://pubmed.ncbi.nlm.nih.gov/29255392/
Shankar, P. R., Rose, C., Balasubramanium, R., Nandy, A., & Friedmann, A. (2016). Using movies to strengthen learning of the humanistic aspects of medicine. Journal of Clinical and Diagnostic Research, 10(1), JC05-JC07. https://doi.org/10.7860/JCDR/2016/16264.7066
Shankar, P. R. (2019). Cinemeducation: Facilitating educational sessions for medical students using the power of movies. Archives of Medicine and Health Sciences, 7, 96-103. http://dx.doi.org/10.4103/amhs.amhs_30_19
Shelley, B. P. (2016). Re-humanizing “high-tech, no touch” medicine: Narrative medicine and cinemeducation perspectives. Archives of Medicine and Health Sciences, 4(1), 1-5. http://dx.doi.org/10.4103/2321-4848.183367
Sim, S. M. (2004). Teaching of pharmacology in Universiti Malaya and the other medical schools in Malaysia – A historical perspective. Acta Pharmacologica Sinica, 25(9), 1209-1219. https://pubmed.ncbi.nlm.nih.gov/15339399/
Swanwick, T. (2018). Understanding medical education. In T. Swanwick, K. Forrest, & B. C. O’Brien (Eds.), Understanding medical education: Evidence, theory, and practice (pp. 1-6). Wiley-Blackwell. https://doi.org/10.1002/9781119373780.ch1
Ventura, S., & Onsman, A. (2009). The use of popular movies during lectures to aid the teaching and learning of undergraduate pharmacology. Medical Teacher, 31(7), 662-664. https://doi.org/10.1080/01421590802641489
Weber, C. M., & Silk, H. (2007). Movies and medicine: An elective using film to reflect on the patient, family, and illness. Family Medicine, 39(5), 317-319. https://pubmed.ncbi.nlm.nih.gov/17476603/
Wicclair, M. R. (2008). The pedagogical value of House, M.D.: Can a fictional unethical physician be used to teach ethics? American Journal of Bioethics, 8, 16-17. https://doi.org/10.1080/15265160802478503
Williams, R., Evans, L., & Alshareef, N. T. (2015). Using TV dramas in medical education. Education for Primary Care, 26(1), 48-49. https://doi.org/10.1080/14739879.2015.11494308
*Dr Jyoti M. Benni
Department of Pharmacology,
Jawaharlal Nehru Medical College,
KLE Academy of Higher Education and Research (KAHER),
Deemed-to-be-University, Belagavi-590010. Karnataka. India
Email: benni_jyoti@yahoo.co.in
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
