
Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters
Submitted: 5 August 2022
Accepted: 2 November 2022
Published online: 4 April, TAPS 2023, 8(2), 76-79
https://doi.org/10.29060/TAPS.2023-8-2/SC2861
Poh-Sun Goh1 & Elisabeth Frieda Maria Schlegel2
1Department of Diagnostic Radiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Department of Science Education, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hofstra University, United States
Abstract
Introduction: The aim of this short communication is to examine the journey of scholarship in health professions education (HPE).
Methods: We will focus on tangible small steps to start, sustain, and succeed along this journey. Through a proposed innovation in scholarship – micro-scholarship – we will describe how this is similar to and an extension of bite-size or micro-learning, and workplace micro-practice related to just-in-time (JiT) learning settings.
Results: We will demonstrate how the small steps for generating and engaging with micro-content can be similarly applied to micro-scholarship. Then, progressive and iterative refinement of output and practice of micro-scholarship can be combined and result in macro-scholarship after cycles of public engagement for final digital or print publication. This stepwise approach creates an accessible, sustainable strategy to achieve success as a scholar in HPE. We will elaborate on micro, macro, and meta matters and celebrate how these small steps encourage and allow broad participation in the creation, critique, and progressive refinement of scholarship.
Conclusion: Small, sustainable, steps leads to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Keywords: Micro-Scholarship, Micro-Learning, Just-In-Time (JiT) Learning, Community of Practice (CoP), Technology, Network Effects, Post-Publication Peer Review (PPPR)
I. INTRODUCTION
Modern changes in the pace and way we conduct and experience teaching and learning have resulted in production and consumption of smaller chunks of content. Succinct, bite-size content is easier to remember and consumes less cognitive bandwidth with reduced cognitive load. In addition, it is also significantly easier to share and engage with within a professional community of practice (CoP). Compact modular, bite-size content is also ideal for just-in-time (JiT) micro-learning and workplace micro-practice (Yilmaz et al., 2022), or on-demand learning and practice, with which we are all familiar. In this paper, we will extend this idea of micro-learning and micro-practice to scholarship, by examining the “new” idea of micro-scholarship – defined as “the process of making visible the smallest accessible and assessable steps that document a scholarly journey, which can then be assembled and presented as an outcome of academic scholarship” (Goh et al., 2021). Mobile technology tools and platforms support open display, access to, and iterative engagement with this content by a community of practice (CoP), both in learning and scholarship (Goh et al., 2021; Goh & Sandars, 2020; Schlegel, 2021).
II. MICRO-MATTERS
Just as a musical composition is made up of individual notes, a construction from its individual parts, and a meal of its individual ingredients, commonly accepted and acknowledged finished works of scholarship in HPE are composed of its individual parts. A conference presentation or journal paper, peer reviewed, read by and engaged with by a CoP, contains core components – e.g., the title (which includes key ideas); key words (which are defined and illustrated in the presentation or paper); and cited published work by earlier authors (from a review of the field, including takeaways from the author(s) that are relevant and that the authors intend to discuss, elaborate, and build upon). However, a close examination and reflection of these core parts of finished works of scholarship show that they not only form the ingredients of the final work, but that they also fall within the categories of scholarship proposed by Boyer, with evaluation criteria described by Hutchings and Shulman; (Goh et al., 2021; Goh & Sandars, 2020). Boyer’s model for scholarship includes (1) integration, (2) application, (3) teaching and learning, and (4) discovery.
Innovative JiT micro-content on mobile platforms is easily accessible for members of a CoP to engage with, evaluate, critique, and build upon. All online content, including, e.g., on Twitter, blogs, or modular courses, is subject to creative reader collectives, which post comments, repost, reshare, and create new meaning and value from individual posts of content, contributing to group engagement, which has many of the characteristics of scholarship (Schlegel & Primacio, 2021). We propose that these artefacts and activities illustrate examples of Boyer’s Scholarship categories, including demonstrating the Scholarship of Teaching and Learning SoTL. Digital and online content and platforms support and scale our efforts as learners and scholars, no different yet more facile as compared to in-person activities, with increased importance placed on being a public professional, and respecting intellectual property, shown by proper citation of digital content, and use of this content with permission where applicable, followed by data-driven dissemination (Arrington & Cohen, 2015; Kern et al., 2015). This public reaction and appraisal of content compares to wide audience post-publication peer review (PPPR) with the added value of a feedback-loop through responses on comments. Just as developing bite-size, short format, JiT digital, online content, has transformed and continues to transform our educational and professional practices, a similar process can now facilitate and support granular, open digital display and engagement of both our initial and subsequent steps when engaging in scholarship in HPE, similar to and an extension of micro-learning. Practicing micro-scholarship involves encountering a “new idea”; researching its meaning; adding relevance to specific discussion themes and takeaways; discovering key published and presented work; and then both taking note of and making notes on these findings during reflection and discussions within a local CoP. This micro-scholarship is subsequently made open and visible to a global readership or a CoP, through private, semi-private, and public engagement platforms. Micro-scholarship content gets progressively refined through iterative engagement with members of a CoP, through discussion, feedback, critique, and personal reflection. The relevance and usefulness of this content, as well as confidence in the authors of this micro- scholarship content, is progressively enhanced. We also learn how and where this content is best disseminated and presented, and best ways this might be combined and stacked. The iterative in- person and scalable digital conversations amplifying the spread and engagement with this material to create meaning, in step-by-step fashion, form the core practices of both micro-scholarship (Goh et al., 2021) and bite-size engagement with material (Schlegel, 2021). After refinement, these pieces can be combined into larger pieces of finished work of macro-scholarship. Thus, activities undertaken as part of micro-learning or micro-scholarship are accessible, independent, and sustainable small, step-wise efforts that can and do add-up. Progression along the developmental path of a scholar will include a variety of conversations within a CoP, such as the supportive networks of peers, senior practitioners, mentors and coaches, including collaborative (team)work and initially supervised instruction as part of a successful scholar’s journey. Conversations and engagement within a CoP do range from positive and helpful to (those that are or perceived to be) occasionally provocative and challenging. However, professional and good-natured discussion generally guide scholarly development similar to trial and error, and progressive improvement and iterative steps enable learning and growth.
III. MACRO-MATTERS
Simply put, a finished larger work is made up small pieces that have been selected and refined, through an iterative process of reflection and feedback, by engaging with a CoP or specialised collective of readers. Open (digital) practice from an early stage, the platforms (places and readers) we engage in, and our active participation in professional CoP of global specialised readers provide both “informed” and “critical” feedback – and review of these “early” and “small” or “micro” pieces of work – from a (much wider) audience. The key distinction is who engages with this work, from as wide a spectrum of professional practice, experience, and expertise as possible, and from a diversity of points of view. Digital tools and practices facilitate and scale this process. This is similar to the work of artists, who engage in open sketching, including showcasing early drafts and ideas, prototyping, drawing, and artistic creation in open studios. When members of a CoP engage through digital platforms the impact from their individual and collective input can scale exponentially through network effects (Azhar, 2021).
IV. META-MATTERS
The process of scholarship mirrors the stepwise, sequential, cumulative process of learning, and training for proficiency and mastery in any area of practice. Our roles as practitioners, educators and scholars are all informed by learning science. Digital devices, tools, platforms, and practices exponentially scale up the impact of our efforts through applied network theory and interactions. Ultimately, we live and practice professionally within our CoP, which provides both the audience and peer reviewers of our public work, thus driving a fruitful evolution of our profession. Our ultimate aim is to engage a CoP in conversations, including broader participation in the production, refinement, and consumption of products of scholarship, in form and format, and through processes accessible for all. Micro-scholarship is a starting point that allows wider participation and engagement in the process of scholarship. The components of micro-scholarship, when refined and confidently presented, are contained within published finished macro-scholarship outputs. Then, micro-scholarship and macro-scholarship add collaboration and value within a larger scholarship ecosystem and professional CoP, a meta-level practice or meta-system, within which micro- and macro- level activities occur. An explicit example of the outputs and process of moving from micro, through macro, to meta practice illustrated https://www.slideshare.net/dnrgohps/illustrated-stacked-microscholarship-steps-along-academic-path-of-educational-scholar.
Another example of enhancing scholarship of teaching and learning SoTL across different levels might include, e.g. a remote consultation with members of scholarly project teams, prompting to publish a themed blog post, which, in return, becomes now a generalizable, transferrable offering to the global CoP, moving from the meta-system to the macro-level, as evidenced by comments from different institutions and subsequent implementation of ideas (Arrington & Cohen, 2015).
V. CONCLUSION
In this paper, we have examined, showcased, and celebrated the small sustainable steps to success as a scholar in HPE, describing micro, macro, and meta matters and illustrating how combining small components of scholarship is an effective strategy for dissemination, access, engagement, conversation and collaboration within a CoP in HPE.
Notes on Contributors
Poh-Sun Goh pitched initial idea, was involved in active discussion and brainstormed with co-author iterative refinement of core message(s), wrote first draft, and actively revised series of subsequent drafts, and submitted final draft. This manuscript built on previous collaborative work, cited in article on Micro-Scholarship and Digital Scholarship.
Elisabeth Schlegel was involved in active discussion and brainstormed with co-author iterative refinement of core message(s), and actively revised series of subsequent drafts, and including and approving final draft. This manuscript built on previous work, cited in article including on bite-sized learning.
Ethical Approval
As this manuscript is a description of an innovative approach to scholarship, ethical approval and IRB application was not required.
Data Availability
There is no additional data separate from available in cited references.
Acknowledgement
No technical help and/or financial and material support or contributions was received in preparation of this manuscript.
Funding
Both authors have no funding source to declare.
Declaration of Interest
Both authors declare that there are no possible conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
Arrington, N. M., & Cohen, A. L. (2015). Enhancing scholarship of teaching and learning through micro-level collaboration across two disciplines. International Journal of Teaching and Learning in Higher Education, 27(2), 194.
Azhar, A. (2021). The exponential age: How accelerating technology is transforming business, politics and society. Diversion Books.
Goh, P. S., Roberts-Lieb, S., & Sandars, J. (2021). Definition of Micro-Scholarship. https://microscholarship.blogspot.com/
Goh, P. S., & Sandars, J. (2020). Rethinking scholarship in medical education during the era of the COVID-19 pandemic. MedEdPublish, 9(97). https://doi.org/10.15694/mep.2020.000097.1
Kern, B., Mettetal, G., Dixson, M., & Morgan, R. K. (2015). The role of SoTL in the academy: Upon the 25th anniversary of Boyer’s scholarship reconsidered. Journal of the Scholarship of Teaching and Learning, 15(3), 1-14. https://doi.org/10.14434/josotl.v15i3.13623
Schlegel, E. (2021). (Not only) for medical students: Get involved in medical education research & scholarship. https://elisabeth-fm-schlegel.weebly.com/elearning-bites/not-only-for-medical-students-get-involved-in-medical-education-research-scholarship
Schlegel, E., & Primacio, J. (2021). Blogging for the continuum of medical education: Engaging diverse communities of learners. MedEdPublish, 10, Article 136. https://doi.org/10.15694/mep.2021.000136.1
Yilmaz, Y., Papanagnou, D., Fornari, A., & Chan, T. M. (2022). The learning loop: Conceptualizing Just-in-Time faculty development. AEM Education and Training, 6(1), e10722. https://doi.org/10.1002/aet2.10722
*Poh-Sun Goh
Department of Diagnostic Radiology
National University Hospital,
Main Building, Lobby F, Level 4
#04-398, DDI Library
5 Lower Kent Ridge Road, Singapore 119074
+6567724211
Email: dnrgohps@nus.edu.sg
Submitted: 28 April 2022
Accepted: 19 August 2022
Published online: 4 April, TAPS 2023, 8(2), 70-75
https://doi.org/10.29060/TAPS.2023-8-2/SC2802
Sok Mui Lim, Ramesh Shahdadpuri & Ching Yee Pua
Centre for Learning Environment and Assessment Development (CoLEAD), Singapore Institute of Technology, Singapore
Abstract
Introduction: Coaching has gained acceptance in the education field as a way to enable learners to achieve their fullest potential. In the endeavor to set up a coaching ecosystem in our university, we started by equipping our educators with fundamental coaching skills and techniques. Our training workshop, Coaching As An SIT Educator, covers the key coaching competencies and is highly practice focused. Participants get hands-on skills practice using contextualised scenarios that are based on realistic academic, workplace and clinical placement settings.
Methods: To address concerns on time-effectiveness, we adopt a solution-focused approach to coaching. We want to create a mindset shift for educators, from subject experts providing advice and solutions, to coaches asking powerful coaching questions that help students make discoveries and work towards their goals. We encourage our educators to engage students holistically by finding coachable moments in their daily student interactions.
Results: Competency-based assessments are conducted to determine achievement of the learning outcomes, articulated by the knowledge, attitude, and demonstration of coaching skills with students. Assessments consist of a reflection, multiple-choice question (MCQ) quiz, and scenario-based coaching role plays. Participants achieved the learning outcomes as demonstrated from the assessments.
Conclusion: The coach training workshop is the major pillar of our coaching initiative. Beyond the workshop, ongoing coaching development is supported through other activities and resources, including community of practice, coaching circle and knowledge repository. Opportunities for continuous learning and conversation platforms for sharing coaching experiences are part of the growing coaching ecosystem at SIT.
Keywords: Assessments, Coaching Competencies, Coaching Conversations, Coaching Ecosystem, Coachable Moments, Faculty Development, Feedback, Holistic Development, Solution-Focused
I. INTRODUCTION
Coaching has gained greater awareness and wider acceptance in the education field in the past decade, led by the efforts of innovative educators and more evidence-based research. Coaching has been described as a very powerful approach that facilitates personal and professional change through deep level listening, questioning, setting the right challenges and providing support along the process (Griffiths, 2005). More specifically, academic coaching is defined as individualised practice of asking students reflective, motivation-based questions, providing opportunities for formal self-assessment, sharing effective strategies, and co-creating a tangible plan that promotes accountability (Deiorio et al., 2017).
In traditional educational settings, communication tends to be mostly directive, where the educator is the subject expert who gives instructions, solutions or advice to students. From this “telling” or “pushing” stance where the focus is on problem solving and advice giving, shifting to coaching conversations requires an “asking” or “pulling” communication approach. Engaging in coaching conversations involves the educator coaching students through powerful questioning, active listening and guiding them to explore possibilities so as to discover new ideas and find solutions for themselves.
In 2020, Singapore Institute of Technology (SIT) introduced internal coach training for all academic staff with the aim to build educators’ capability to work with students at a deeper level. This highly contextualised academic coaching training was made mandatory for all educators. This was essential for the creation of a strong coaching ecosystem in the university and adopting coaching practices across a variety of learning contexts, such as providing assignment feedback, consultations on projects and supervising students at the workplace. In working with students towards their preferred futures, SIT educators can help the students develop confidence and self-efficacy, enabling them to achieve their fullest potential.
II. METHODS
This section highlights the critical elements of the faculty development programme.
A. Solution-focused Approach
One of the top concerns of many educators is time. There are underlying concerns on whether coaching students will take up too much time, and what happens if they uncover student issues that they cannot deal with. A solution-focused coaching approach alleviates some of these concerns. The basic principle of the solution-focused approach is to help coachees reflect and design their solutions, rather than go down the path of root cause analysis. Its forward-oriented solution approach contrasts with other traditional psychological techniques, which tend to look back at the past or are problem-focused (Grant & Gerrard, 2020).
The solution-focused approach is known for its simplicity, attention to language and time effectiveness. The conversation is steered to a preferred future of the issue at hand without dwelling on the troubled past. The coach encourages the coachee to focus on their strengths and positive resources, to think about their resourceful past, and to draw on positive lessons from when they have been at their best. After identifying their desired outcomes and considering their options in the context of present realities, the coach guides the coachee to think about the next steps to progress towards their preferred future.
B. Mindset Shift
In higher education, many coachable opportunities outside the formal contact hours can be easily missed. For example, instead of merely deducting marks for repeated late submissions of assignments, the educator could coach the student on improving time management. In clinical fieldwork, when a student complains about limited interaction with the busy clinical educator, the university supervisor can coach the student on how best to schedule time for feedback. Our daily encounters and interactions with students present many coachable moments that offer just-in-time and authentic learning opportunities to support students in their development to become work-ready graduates.
Students may initially find coaching sessions difficult as it is easier to just ask for solutions than to discover solutions for oneself. However, with time, students will realise the value of coaching as they witness their progress. In an Asian context, where many students are respectful and value advice from authoritative figures, such as professors, coaching can require a mindset shift for both students and faculty (Lim, 2021).
C. Tailoring the Coaching Training to Education Context
The Coaching As An SIT Educator workshop is an in-house designed 2-day program. It is highly contextualised for the needs of SIT academic staff, to equip them to be versatile and agile educators, performing the role of Teacher-Coach-Mentor. The workshop covers the key coaching fundamentals and is highly practice-oriented. The programme design was intended for participants to develop hands-on coaching skills with contextualised role play scenarios (see Appendix A for an example), so that they can apply what they have learnt with their students immediately after the workshop.
While we do not intend to train credentialed professional coaches, the key International Coaching Federation (ICF) coaching competencies were referenced to guide the design of the SIT workshop. The GROW model (Whitmore, 2019) was introduced as a framework for the participants to organise and manage the flow of the coaching conversation. Drawing on inputs from academic staff, realistic student-centric scenarios were created for class discussions and role plays. The coaching practice sessions are conducted in dyad, triad, and hot seat formats. The workshop design and facilitation ensure that there is psychological safety, providing a trusting space for constructive debriefing, feedback sharing and open questions and answers to take place.
To manage the workshop time and resources effectively, e-learning content was developed in-house, specifically to complement the interactive classroom session. A week before the start of the workshop, the participants can access materials in the form of an asynchronous pre-recorded webinar. The webinar consists of five micromodules, covering topics such as Mindset, Motivation, Emotional Intelligence, and Feedback Skills (refer to Appendix B for more details). As many participants may already be familiar with these topics, this self-learning component serves as a good refresher to prepare participants for the coaching workshop.
Please refer to Table 1 for details of the Coaching as An SIT Educator workshop.
|
Workshop: Coaching As An SIT Educator |
|
|
Learning Outcomes By the end of this course, participants will be able to:
|
|
|
Topics Covered |
|
|
Pre-Workshop: eLearning
|
Workshop Day 1:
Workshop Day 2:
|
|
Assessments (Day 2) |
|
|
Role Plays: Standardised Students & Assessors Scenarios (each – 20 minutes):
|
Quiz: Multiple Choice Questions (MCQs)
|
Table 1. Coaching As An SIT Educator Workshop
III. EVALUATION OF COACHING COMPETENCY
To assess the attainment of the learning outcomes and development of the participants’ coaching competence (knowledge, skills, attitude), assessments and reflection exercises are incorporated into the workshop. As this is not a certification program, assessments are formative in nature, with focus on providing the educators quality feedback. Coaching knowledge is assessed through a multiple-choice question (MCQ) quiz. Attitude and mindset shift is evaluated through pre- and post- workshop surveys, and reflection questions.
Coaching skills are assessed via role plays (with standardised students). The role play format involves two 20-minute coaching sessions with the participant (playing the role of an educator) having a coaching conversation with standardised students (who act as coachees) and are conducted virtually in real time over the Zoom platform, using breakout rooms. The role plays that are based on common scenarios in university and workplace supervision settings. An invaluable part of the learning in this assessment comes from the feedback conversation between the participant (coach) and assessor, who observes the coaching conversation. Many participants regard the skills assessment and individualised feedback on their coaching skills as the highlight of the training programme.
IV. DISCUSSION
Many readily available coaching materials or vendor-run workshops are geared towards executive or corporate scenarios. While the skills of coaching may be transferable, it is difficult for educators to draw relevance to student engagement. Therefore, Coaching As An SIT Educator workshop focuses on case studies of university scenarios, and supervision for work-integrated learning (e.g., internship, clinical placement). Participants get to work with fellow learners in group work and discussions, to engage in personal reflection, and takeaway practical knowledge and skills on their learnings in a safe space.
For a sustained effort to practice coaching and build an on-going coaching culture, a mandatory workshop is inadequate. Other coaching resources are available to support coaching practice and promote continuous learning in SIT:
- Community of Practice: Coaching Conversations @SIT (offered to any interested academic staff)
- Coaching Circle (offered to all alumni of the coaching workshop)
- Coach Academy (knowledge repository with academic and coaching industry resources).
V. CONCLUSION
In coaching, there lies great potential for students to be developed holistically if we tap on coachable moments in higher education. A contextualised, well-developed coaching development programme is an enabler for this potential to be fulfilled. Drawing on evidence-based research from academia and professional practice, a practice-oriented programme which focuses on developing hands-on coaching skills will be impactful, as educators can put these skills into action in their interaction with students.
Notes on Contributors
Associate Professor Lim Sok Mui (May) led the Center for Learning Environment and Assessment Development (CoLEAD) and spearheaded the coaching initiative in the university, contributed to the conception, drafted and critically revised the manuscript.
Ramesh Shahdadpuri is the senior educational developer in CoLEAD and plays the role of the coaching trainer for the faculty training program. reviewed the literature, contributed to the conception and assisted in revising the manuscript.
Pua Ching Yee is the learning analyst in CoLEAD and plays the role of coordinating the coaching training and assessment of the participants. She assisted in critically reviewing, revising and formatting the manuscript.
All authors gave their final approval and agree to be accountable for all aspects of the work.
Ethical Approval
This is a narrative review related to coaching training program with no data presented and no ethical approval is required.
Data Availability
This paper is a narrative review with no data analysis.
Acknowledgement
The authors would like to thank Miss Cherine Foo for her significant contribution of the coaching program.
Funding
There is no funding involved in the preparation of the manuscript.
Declaration of Interest
The authors declare no conflict of interest.
References
Deiorio, N. M., Skye, E., & Sheu, L. (2017). Introduction and definition of academic coaching. In N. M. Deiorio & M. M. Hammoud (Eds.), Coaching in medical education: A faculty handbook (pp. 1-5). American Medical Association.
Grant, A. M., & Gerrard, B. (2020). Comparing problem-focused, solution-focused and combined problem-focused/solution-focused coaching approach: solution-focused coaching questions mitigate the negative impact of dysfunctional attitudes. Coaching: An International Journal of Theory, Research and Practice, 13(1), 61-77. https://doi.org/10.1080/17521882.2019.1599030
Griffiths, K. (2005). Personal coaching: A model for effective learning. Journal of Learning Design, 1(2), 55–65. http://dx.doi.org/10.5204/jld.v1i2.17
Lim, S. M. (2021, May 27). The answer is not always the solution: using coaching in higher education. Times Higher Education. https://www.timeshighereducation.com/campus/answer-not-always-solution-using-coaching-higher-education
Whitmore, J. (2019). Coaching for performance: The principles and practice of coaching and leadership (5th ed.). Nicholas Brealey Publishing.
*Lim Sok Mui
Singapore Institute of Technology,
10 Dover Drive, Singapore 138683
+65 65921171
Email: may.lim@singaporetech.edu.sg
Submitted: 4 October 2022
Accepted: 5 December 2022
Published online: 4 April, TAPS 2023, 8(2), 66-69
https://doi.org/10.29060/TAPS.2023-8-2/SC2894
Simon Field1, Pat Croskerry2, Susan Love3, & Peggy Alexiadis Brown4
1Undergraduate Medical Education and Emergency Medicine, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 2Critical Thinking Program, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 3Faculty Development, Continuing Professional Development, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 4Dalhousie Medicine New Brunswick, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada
Abstract
Introduction: For all clinical providers in healthcare, decision-making is a critical feature of everything they do. Every day physicians engage in clinical decision-making where knowledge, evidence, experience, and interpretation of clinical data are used to produce decisions, yet, it is fair to say that most do not have an explicit insight or understanding of this complex process. In particular, few will have training in teaching and assessing the cognitive and affective factors that underlie clinical decision-making.
Methods: To foster an increased awareness and understanding of these factors, the Dalhousie Critical Thinking Program was established with the mandate to develop and deliver curriculum for critical thinking in the 4-year undergraduate program. To assist teaching faculty with the goal and objectives of the program, the Teaching and Assessing Critical Thinking Program (TACT) was introduced.
Results: Using the dual process model as a platform for decision-making, this program introduces general principles of critical thinking and provides tools to teach learners how to strengthen their critical thinking skills. To offer flexible learning, an online approach was chosen for delivery of the program.
Conclusion: To date, we have offered eleven iterations of Part 1 to a total of 261 participants and six iterations of Part 2 to a total of 89 participants. Evaluations show the online approach to content delivery was well received and the content to be of practical use.
Keywords: Critical Thinking, Clinical Decision-Making, Faculty Development, Asynchronous Learning
I. INTRODUCTION
This paper provides a review of a two-part Teaching and Assessing Critical Thinking (TACT) program which was developed to help faculty understand vulnerability to bias and the role of metacognitive processes in clinical decision-making. The objective of the TACT program is to better prepare faculty to teach learners these important skills. In this paper, we describe how it was implemented, how participants perceived the program, and what changes were needed to address this important hidden ‘soft’ skill within the clinical setting.
II. METHODS
Physicians are constantly required to interpret information when they interact with patients, communicate with colleagues, review medical histories and laboratory reports, conduct physical exams, review the medical literature, and attend rounds. All of these clinical activities demand a sustained level of accuracy, clarity, and especially rationality. Critical thinking (CT) does not guarantee rationality but is one of its more important features and is essential for the role of physician.
Reliable and accurate diagnosis is the barometer of good clinical decision-making and will have a direct impact on treatment outcomes and patient safety. One in 20 (or roughly 12 million) American adult outpatients are affected by diagnostic errors every year. The overall number of fatalities associated with diagnostic failure is not known, but it is estimated that 40,000 – 80,000 deaths occur annually in hospitalised patients in the USA due to diagnostic failure.
A number of studies have shown that training in the development of CT skills in undergraduate students is effective. (Abrami et al., 2015) However, given that most faculty in medical schools today will not have had explicit CT training, specific initiatives in teaching it seem appropriate, not only for the faculty themselves but, importantly, for the students they teach.
To better prepare learners, Dalhousie’s Faculty of Medicine established the Critical Thinking Program in 2012. The program incorporated principles from the Foundation for Critical Thinking into a general model of clinical reasoning (Croskerry, 2018). The Dalhousie critical thinking curriculum reflects a consensus in the current medical literature that the dual process model (System 1 and System 2) is the most appropriate platform for reviewing the clinical decision-making process (See Figure 1).
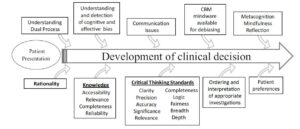
Figure 1. The Dalhousie University model for clinical decision making. (Reproduced with Permission)
A key component in the delivery of this curriculum is helping faculty develop the skills they will need to teach and mentor critical thinking in the clinical environment. Most educators have limited understanding of the advances in medical decision-making and how to best teach critical thinking and clinical reasoning.
The TACT Program comprises two distinct courses: TACT 1 and TACT 2. The program is structured to develop a sound knowledge of critical thinking principles in TACT 1, followed by a focus on teaching and learning in TACT 2. TACT 1 centres on three main themes: How Physicians Make Decisions, Cognitive and Affective Biases, and Cognitive Debiasing Strategies. TACT 2 centres on two main themes: Fundamentals of Medical Education and Strategies for Teaching and Assessing CT. In TACT 2, participants choose one of four elective options: Evidence Based Medicine, Competency Based Medical Education, Medical Humanities, or Curriculum Development.
The TACT Program uses an asynchronous online approach to reach Dalhousie faculty who are distributed across the Canadian Maritime Provinces. This approach mediates potential barriers for participation such as distance and time constraints and allows for individualised learning experiences while building an interactive online community of practice experience (Cook & Steinert, 2013). We use a combination of curricular tools including online didactic lectures, independent study activities, webinars, and discussion boards.
To date (Winter 2022), we have held 11 iterations of TACT 1 and 6 iterations of TACT 2, with 163 of 261 participants completing TACT 1 and 78 of 89 registrants completing TACT 2.
Of those who completed TACT 1, 55 % went on to enrol in TACT 2.
We initially developed the TACT Program for Dalhousie faculty (primarily physicians); however, due to growing interest in the topic, we have opened enrolment to include participants from around the world, including the United States, Mexico, United Kingdom, Australia, New Zealand, Turkey and Brazil. We also opened enrolment to participants from a variety of health professions and other fields of study. By opening the program to participants with diverse backgrounds in practice and location we have increased the diversity of perspectives and the richness of reflections posted to the discussion boards.
Prior to starting the TACT Program, we asked participants to complete a survey measuring their current knowledge of teaching and assessing CT, and motivation for taking the course.
Participants reported little satisfaction with previous knowledge in CT (Mean: 2.67 ± 0.84 on a Likert Scale of 1 (not at all satisfied) to 5 (very satisfied)). The following themes were identified as motivators for taking the TACT Program — a desire to: learn, improve clinical reasoning by increasing knowledge, understand the impact of critical thinking, provide better clinical care, decrease diagnostic error, and become a better educator.
We administered a summative evaluation following both TACT 1 and TACT 2. For TACT 1, 75% (121/162) completed the final evaluation and for TACT 2, 90% (63/70). In the summative evaluation, we asked participants to rate their course in a number of areas from course delivery to the effectiveness of increasing their knowledge and comfort in teaching critical thinking. Consent to data collection was implied as part of the administration of the evaluation. We found that participants were very satisfied with delivery methods.
III. RESULTS
A. What Did We Learn about the Participants?
All participants taking the TACT Program shared a similar motivation: the intent to improve their critical thinking skills and to teaching others. Steinert et al. (2002) found that faculty are more likely to enrol in an online program if they believe it would meet a perceived need. Our participants identified a desire to improve their own practice, confidence and awareness, to make the unconscious conscious, and to develop the language to name, identify and act on cognitive biases and those circumstances that create biases. This enabled them to better teach and mentor CT.
Participants also identified the value of communicating with others who offered a different perspective on clinical work and life experiences.
Physicians may not readily share/disclose mistakes they make in the clinical setting. In medical training environments, overconfidence and reluctance to admit mistakes are often the norm, which may work against fostering a culture of reflection (Brezis et al., 2016). Due to the confidentiality of the discussion boards, our participants could freely reflect on what factors contribute to errors they have made/seen and share those lessons with peers without fear of loss of reputation and embarrassment.
B. What Did We Learn about the Delivery?
We found that the online delivery was successful in reaching a broad base of participants. Some participants appreciated the mode of delivery as well.
A benefit of online courses is the ease with which faculty can control their pace of instruction. When asked, we found that 97.4% of respondents identified they would do more faculty development programs online.
When we reviewed the online tracking statistics, we found that our participants were accessing materials at all hours. Participants, each with their own learning style, appreciated the mix of interactivity and self-study the online format offered.
IV. DISCUSSION
Ideally, we would like to know how effectively participants in the TACT program incorporated the teaching principles into their own practices in the real clinical world. However, it is very challenging methodologically to do this, and it appears the best we can do is to ask about participant impressions and insight into their experience.
It appeared that the TACT program provided a rich opportunity for participants to interact and share their quest to understand and refine the metacognitive aspects associated with their clinical decision-making and critical thinking processes. It also provided our participants with the language to describe and teach these processes to trainees.
V. CONCLUSION
In summary, the TACT program shows promise in engaging distributed faculty to further their curiosity and interest in how to improve, teach and foster critical thinking skills within medical education and in their own practice. We recognise that although this online asynchronous mode of delivery may not be appropriate to meet the diverse learning styles of all potential participants, the favourable reviews we have received from our program graduates highlighted that the flexible interactivity with the content contributed to the success of the TACT program.
Notes on Contributor
Simon Field assisted in the initial development of the TACT program and contributed to the data analysis and writing of the article.
Pat Croskerry was a founding member of the Critical Thinking Advisory Group, and contributed to the development of the TACT program and to the writing of the article.
Susan Love has been an active contributor to the running of the TACT program, designed the survey tools, collected and analyzed qualitative and quantitative data from the program evaluation, and contributed to the writing of the article.
Peggy Alexiadis Brown collected and analyzed qualitative and quantitative data from the program evaluation survey tools, and contributed to the writing of the article.
All authors have reviewed and approved the final manuscript.
Ethical Approval
The data gathered for this article was collected anonymously as part of Program Evaluation, and a written waiver has been obtained stating that it is exempt from full institutional Research Ethics approval.
Acknowledgement
We acknowledge the valuable support and contribution of Deirdre Harvey and other members of the Critical Thinking Advisory Group. For further information on how to implement a similar program in your region, please feel free to contact us.
Funding
There is no funding associated with this project.
Declaration of Interest
None of the authors have any conflicts of interest to declare, and they do not receive any financial assistance or funding for their participation in the TACT program.
References
Abrami, P. C., Bernard, R. M., Borokhovski, E., Waddington, D. I., Wade, C. A., & Persson, T. (2015). Strategies for teaching students to think critically: A meta-analysis. Review of Educational Research, 85(2), 275-314. https://doi.org/10.3102%2F0034654314551063
Brezis, M., Orkin-Bedolach, Y., Fink, D., & Kiderman, A. (2016). Does physician’s training induce overconfidence that hampers disclosing errors? Journal of Patient Safety, 15(4) 296-298. https://doi.org/10.1097/pts.0000000000000255
Cook, D. A., & Steinert, Y. (2013). Online learning for faculty development: a review of the literature. Medical Teacher, 35(11), 930-937. https://doi.org/10.3109/0142159X.2013.827328
Croskerry, P. (2018). A model for clinical decision-making in medicine. Medical Science Educator, 27(Suppl 1), S9-S13. https://doi.org/10.1007/s40670-017-0499-9
Steinert, Y. L., McLeod, P. J., Conochie, L., & Nasmith, L. (2002). An online discussion for medical faculty: An experiment that failed. Academic Medicine., 77(9), 939-940. https://doi.org/10.1097/00001888-200209000-00046
*Simon Field
Dept of Emergency Medicine,
Dalhousie University, Halifax,
Nova Scotia, Canada
Email: simonfield@dal.ca
Submitted: 16 March 2022
Accepted: 26 May 2022
Published online: 4 April, TAPS 2023, 8(2), 57-65
https://doi.org/10.29060/TAPS.2023-8-2/OA2778
Vijay Kautilya Dayanidhi1, Arijit Datta2, Shruti P Hegde3 & Preeti Tiwari4
1Department of Forensic Medicine, Medicine, Manipal Tata Medical College, MAHE, India; 2Department of Forensic Medicine, Medicine, Pramukhswamy Medical college, India; 3Department of Ophthalmology, Medicine, Manipal Tata Medical College, MAHE, India; 4Department of Community Medicine, Medicine, Pramukhswamy Medical college, India
Abstract
Introduction: Summative assessments play a major role in shaping the student’s learning. There is little literature available on validity of summative assessment question papers in Forensic Medicine & Toxicology. This study analyses 30 question papers from 6 reputed universities for content validity.
Methods: A retrospective cross-sectional record-based observational study was conducted where 30 university summative question papers in Forensic Medicine & Toxicology from 6 universities across India were evaluated for content validity. The learning domain assessed, the type of questions asked, and sampling of the content was compared and presented in the results.
Results: From the results of the study, it was noted that 80% weightage was allotted to recall in most papers and only one paper tested for application. 70 to 80% of the marks were allotted to Forensic Pathology leading to disproportionate sampling. Core areas in Toxicology and Medical Jurisprudence were sparsely assessed.
Conclusion: The content validity of the summative question papers in Forensic Medicine and Toxicology was unsatisfactory, emphasising the need for evaluation of the clarity and efficacy of the blueprints being used by the universities. Faculty training to motivate and influence a change in the mindset is necessary to bring about a course correction.
Keywords: Forensic Medicine & Toxicology, Summative Assessments, University Assessments, Blueprint, Content Validity, Learning Domains
Practice Highlights
- Content validity of the Forensic Medicine & Toxicology university exam question papers form six universities was studied.
- It was observed that certain subtopics like Forensic Pathology over time have been over value (80% Weightage).
- Core areas in Medical Jurisprudence and toxicology like substance abuse, environmental toxicology, and pharmaceutical toxicity have been undervalued.
- None of the QPs analysed tested for application. Most items in the assessment tested only recall.
- The blueprints for the paper setters, considering the competencies to be assessed must be designed and validated.
I. INTRODUCTION
Reflecting on our learning experience during MBBS, we realised that we have always had issues with the examination system. The questions are vague and clustered around few important topics. Undergraduate students look up to previous examination question papers as references to decide the stake to be allotted to the topics while preparing for examination. Invariable all students attempt to predict the examination pattern and allot appropriate time and efforts to different subjects, skills, and topics. This reiterates George E Miller’s quote “Assessment drives Learning”. Summative assessments need to be planned appropriately as medicine has high stakes (Amin et al., 2006). Properly designed and executed assessments are known to have a “positive steering effect on the student’s learning. They are also needed to evaluate the programs. Improper assessments can drive a hidden curriculum leading to a completely unintended outcomes (Amin & Khoo, 2003, pp. 260).
Competency Based Medical Education (CBME) model being adopted in India as per the new Graduate Medical Education Regulations 2019, has attempted to bring about a radical change in the educational process. Undergraduate examinations in India are shifting towards a criteria-based process (Aggarwal & Agarwal., 2017; Bhattacharya et al., 2017; Mehta & Kikani, 2019). Outcome based education demands that the examinations be designed to sample and evaluate specific competencies prescribed. The success of these models strongly depended on the validity of the examination process. Summative assessments require that the assessment tool be validated. Key outcomes need to be tested (Amin & Khoo, 2003, pp. 260; McAleer, 2001). Content validity and construct validity are two very important aspect that support the effectiveness of an assessment. Content validity tests the representativeness of the learning objectives in the assessment tool and construct validity represents the congruence of the assessment tool with the intended purpose (Amin & Khoo, 2003, pp. 260).
Forensic Medicine and Toxicology in India, trains the undergraduate to apply their knowledge gained in Medicine for the benefit of law. It is a culmination of Forensic Pathology, Medical Jurisprudence and Toxicology put together. Its key objective is to empower Indian Medical Graduates in handling Medical Legal issues and critically apply their medical skills in delivering justice. Emphasis is also placed on training in etiology, identification, and management of Poisoning ( Sharma et al., 2005). Studies on student perception suggest that teaching is significantly teacher centric and theory oriented. Skill training in Medical Jurisprudence and Toxicology is significantly neglected. Students allege though they value the subject, they spend less time as only select concepts are emphasised (Gupta et al., 2017; Parmar, 2018; Sharma et al., 2005; Sudhan & Raj, 2019). As the new CBME UG curriculum 2019 is being rolled out it is necessary that deficiencies in the traditional curriculum be identified in order to deliver an efficient and effective Forensic Medicine & Toxicology curriculum (National Medical Commission, 2018).
Summative theory exams inherently have a challenge with distribution of the items being tested (Aggarwal & Agarwal, 2017; Amin et al., 2006; Amin & Khoo, 2003, pp. 260; Bhattacharya et al., 2017). Validity of the content being tested in examination is always in question. Selecting appropriate questions, question types and domain can make all the difference in the validity of the examination (Amin et al., 2006; Amin & Khoo, 2003, pp. 260; McAleer, 2001). Particularly in Forensic Medicine which is purely application-based course, testing critical thinking and synthesis is necessary. This is found wanting in the traditional curriculum (Parmar, 2018; Sharma et al., 2005; Sudhan & Raj, 2019). Published literature on systematic analysis of summative assessment question papers in Forensic Medicine & Toxicology are sparsely available. In this study, we have analysed and compared undergraduate summative examination question papers of Forensic Medicine & Toxicology from six reputed universities all over India for the distribution of content tested, Domain of learning and Construct of the question.
II. METHODS
A retrospective cross-sectional record-based observational study was conduct at Government Medical College, Bharatpur after obtaining ethical approval from the Institutional Ethics Committee between October to December 2020. For the study, 30 summative exam question papers from six reputed medical universities were selected based on the availability of the University question papers in public domain. The last five-year (2016-20) undergraduate question papers in Forensic Medicine & Toxicology were collected from the university websites and the college records from constituent colleges after thorough web search. The names of the universities have been kept anonymous during the analysis of results. All the data was collected form sources in public domain hence explicit consent was not taken. Two of the selected universities were based in North India and four universities were based in South India. The identity of the Medical Universities was kept confidential during the analysis of the question papers.
The Summative theory examination in Forensic Medicine & Toxicology as per the Medical Council of India (MCI) regulations consists of one theory paper of minimum 40 marks. The question paper consists of essay type questions and objective questions like very short answer questions or Multiple-choice questions depending on the universities (National Medical Commission, 2018).
For analysis, the questions were categorised based on the question type as LEQ (Long Essay Question), SAQ (Short Answer Question) & VSAQ (Very Short Answer Question including MCQs). The Questions were also categorised based on the domain of learning as Recall Based, Comprehension Based and Application Based Questions.
The Topics in Forensic Medicine & Toxicology can be broadly subdivided into Medical Jurisprudence, Forensic Pathology and Toxicology. These were further subdivided as Six Categories as Legal Procedure, Medical jurisprudence, Forensic Pathology, Forensic Psychiatry, Lab Technique, emerging trends, and Toxicology (Medical Council of India, 1997). Percentage of marks allotted to each of these topics was analysed in each of the papers.
Further, Forensic Pathology was Sub divided into Subtopics like Identification, Postmortem Changes, Mechanical Injuries, Mechanical Asphyxia, Thermal Deaths, Sexual Offences and Medico Legal issues related to Pregnancy, Delivery, Abortion. Toxicology was Sub divided into General Toxicology, Chemical Toxicology, Drug, Pharmacy & Substance abuse Toxicology, Bio toxicology (Medical Council of India, 1997). Percentage allotment of Marks in each of the question papers was analysed for each of the subtopics.
The data thus collected was tabulated in an Excel Sheet and the percentage distribution of marks in various subtopics noted. The SPSS Statistical Software (IBM SPSS Statistics for Windows, Version 23.0) was used to analyse the data. Radar Graphs and line graphs were plotted to represent and compare pattern of distribution of marks in various topics in each question paper. The type of questions asked, the weightage allotted to the subtopics were compared keeping in mind the expected outcomes in the Forensic Medicine & Toxicology curriculum proposed by National Medical Commission and Medical Council of India for content validity (Medical Council of India, 1997; National Medical Commission, 2018). The learning domain targeted in the questions was compared for construct validity of the question papers.
III. RESULTS
In this study, five question papers(n=30) from each university(n=6) were analysed and compared. The data that supports the findings of this study are openly available in Figshare at https://doi.org/10.6084/m9.Fig share.19367864 (Kautilya et al., 2022).
As regulated the university Summative examination in Forensic Medicine & Toxicology consists of one theory assessment and one practical assessment (Medical Council of India, 1997; National Medical Commission, 2018). The theory paper is allotted a minimum of 40 marks. Five universities conducted exam for 40 marks and one university paper was of 100 marks. All question papers had three types of questions, namely Essay questions (Long Answer Questions-LAQs) of 8 to 10 marks each, short essays (Short Answer questions-SAQs) of 3-5 marks each and Objective questions (like Multiple choice questions-MCQs or Very short answer questions- VSAQs) of 1-2 marks each. Table 1 presents the percentage distribution of the marks allotted to each question type.
|
University
|
% Marks LAQ |
% Marks SAQ |
% Marks VSAQ/ MCQ |
|
U1 |
43 |
49.5 |
7.5 |
|
U2 |
25 |
50 |
25 |
|
U3 |
20.4 |
51.2 |
28.4 |
|
U4 |
25 |
50 |
25 |
|
U5 |
25 |
56 |
19 |
|
U6 |
42 |
40.5 |
17.5 |
Table 1. University vice distribution marks in the question papers based on the type of questions
Nearly 50% of the marks in all universities is allotted to Short Essay or Short Answer question types. This was followed by Long Answer questions and very short answer questions respectively. Relative to the number of marks allotted to each question type the university question papers consisted of 11 to 22 items or questions in every question paper.
A. Domain of the Learning Tested
Theory questions papers attempt to test the knowledge/ cognition of the students. Limiting the questions to just recall type affects the quality of the question paper. Medicine and Forensic Medicine, requires application of knowledge. Testing of higher order cognition is necessary for the assessment to be Valid. To evaluate this the questions were categorised into Recall type, Comprehension type and application type. The percentage distribution of marks in each question paper was also analysed and presented in the Line graph (Figure 1).
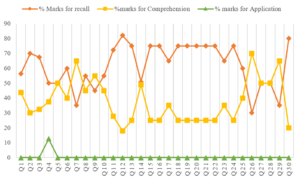
Figure 1. Comparison of percentage mark distribution based on the domain of learning
B. Distribution of Marks Based on the Subtopics
The Graduate Medical education regulation- 2019 further divide the subject of Forensic Medicine and Toxicology into Forensic Pathology, General Information and legal procedures, medical jurisprudence, Forensic Psychiatry, Toxicology, Lab investigations and general trends. The question papers were further analysed for the percentage distribution of marks among these six subtopics and presented in a radar graph in Figure 2.
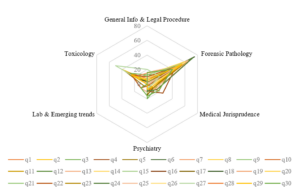
Figure 2. Topic wise distribution of marks (%) in the question papers
From the graph it is noted that Forensic Pathology receives the most attention in almost all the question papers from all the universities. Forensic pathology can further be divided into seven subtopics. From the total marks allotted in each paper for forensic Pathology, percentage marks allotted for each of these subtopics was calculated and presented as a separate radar graph in Figure 3.
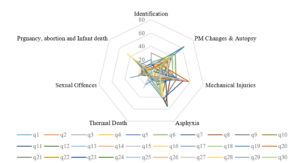
Figure 3. Percentage distribution of marks in Forensic Pathology in the question papers
Toxicology can further be divided into subtopics like General Toxicology dealing with management of poisons, Chemical Toxicology, drug-pharmacy, and substance abuse dealing with pharmaceutical agents and banned substances, Bio and environmental toxicology dealing with snakebite, venomous stings, mushrooms, Food poisoning and plant toxicology etc. From the total marks allotted to toxicology, the percentage distribution of marks allotted to each of these subtopics was analysed and presented in Figure 4.
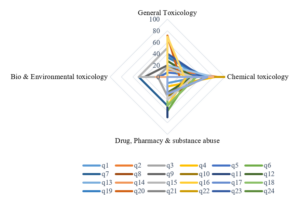
Figure 4. Percentage distribution of marks in Toxicology in the question papers
IV. DISCUSSION
The undergraduate medical education curriculum has been governed by the Graduate Medical Education Rule- GMR 1997 (Medical Council of India, 1997) framed by the Medical Council of India over the last two decades and in 2019, the National Medical Commission adopted a competency-based training model to revamp the medical education in India. The National Medical Commission in its series of reports and documents has attempted to identify the lacuna in the old curriculum. To be able to successfully implement this radically new proposal it is necessary that we understand the limitations of the current curriculum. The Graduate Medical Education Rules 1997, like the newer GMER 2019 provides a clear framework of the Undergraduate curriculum. It lays down guidelines on the standards of implementation. The curriculum framework is designed in a manner that there is significant room for the colleges and the Universities to plan and implement the same as they deem best suits them. This however is not the case always. It has been observed in various previous studies that universities and colleges sometimes fall short of the expectations (Medical Council of India, 1997; National Medical Commission, 2018; Sharma et al., 2005).
Previous studies attempting to gauge the student’s perception on the implementation of Forensic Medicine and Toxicology curriculum have raised serious doubts among the academicians. Kumar et al. (2018) in their study of student’s perception revealed that 20% of the students felt that autopsy was a mere formality and 64% felt the need for student involvement during the autopsy training. Mardikar and Kasulkar (2015) revealed that 89% of the Interns and 41% of the residents didn’t have any exposure to handling medico-legal cases. It was noted that only 14% of the Interns and 21% of the residents were aware of the proper preservatives to be used for body fluids in poisoning. Only 32% of the interns and 46% of the residents were aware of Medical Indemnity Insurance. Only 13% of the interns were aware of the consumer protection act. There is a serious disconnect between the proposed and the implemented curriculum in forensic medicine.
As per the guidelines framed by the Medical Council of India in the GMER-1997, a variety of essay questions and short answer questions are permitted. Objective question like Very Short Answer questions and MCQs are permitted to the extent of 20 % only (Medical Council of India, 1997). Most of the question papers analysed in this study conformed to this regulation. From the Table 1 it can be noted that nearly 50% of the marks were allotted for short essay/Answer questions (SAQ) requiring a descriptive answer. Long Answer Questions (LAQ) requiring an elaborate explanation of the concepts represented about 20% to 42 % of the question paper. The total marks allotted for the individual questions also varied with the LAQs being allotted between 8 to 10 marks each, SAQs being allotted 3 to 5 marks and VSAQs being allotted 1- 2 marks each. Thus, the Number of Items included in each question paper ranged from 11 to 22. This distribution is similar to the analysis published in papers of other subjects like microbiology, Pharmacology, anatomy, Physiology etc (Aggarwal & Agarwal , 2017; Ayub et al., 2013; Bhattacharya et al., 2017; Choudhary et al., 2012; Chowdhury et al., 2017; Mehta & Kikani, 2019; Pichholiya et al., 2021).
With the number of items being limited the chance of certain areas being missed increases. This has a profound influence on the sampling while making the blueprint (Raymond & Grande, 2019). In papers with only 11 Items, there is a definite probability of certain topics being left out compared to papers having 22 items. As Forensic Medicine and Toxicology has only one paper compared to other subjects which have two papers in the second year MBBS, some key topics get left out, adversely effecting its content validity.
A. Analysis of the Domain of Learning Tested
From the Figure No 1, it can be observed that in about 10 of the 30 papers, more than 75% of the questions/ Items tested recall. In only 7 of the 30 papers, more than 50% of the marks were allotted to comprehension. In only one paper the application was assessed to an extant of 12.5%. This is similar studies done in Anatomy, Physiology, Pharmacology, and microbiology (Aggarwal & Agarwal., 2017; Bhattacharya et al., 2017; Choudhary et al., 2012; Chowdhury et al., 2017; Mehta & Kikani, 2019).
This raises a serious doubt on the construct validity of the question papers. Forensic Medicine and Toxicology, an application-based course requires that higher order cognition like application is tested. The current papers fall short of assessing the right competency domains. The Regulations prescribed by the GMER-1997 require that the at least one long answer question (LAQ) of 10 marks (i.e., 25% of the Marks) testing application is asked in the theory question paper (Medical Council of India, 1997). The newer Competency based medical education Regulations prescribed in the GMER- 2019 document also reiterate this fact and in addition suggest that an application based question including Attitude, Ethics and communication skills module be included in every paper (National Medical Commission, 2018). This needs serious introspection in the times to come.
B. Content Validity of the Question Papers
The content validity of a test depends strongly on how well the sample is spread across the syllabus. From the analysis of the percentage distribution of marks allotted to different subtopics presented in figure no 2, it is very clear that in majority of the question papers the bulk of the questions asked are from forensic pathology. There is distinct skewing of the graph toward forensic pathology with an average allocation of 60% of the marks.
This is like studies in physiology with over 42% of the marks being allotted to Cardiovascular system. The observations in the figure no 2 classically suggest that the forensic medicine and toxicology curriculum is a victim of “Carcinoma of the Curriculum” (Abrahamson, 1978). Over a period, certain section of the curriculum takes precedence and are valued more than other equally relevant sections. Core areas like Toxicology and Medical Jurisprudence which are clinically more relevant to the undergraduate students, considering their role as a physician of the first contact, seem to have been blatantly missed and neglected. Faculty should reflect on the factors that might have caused this drift which over time has led to this dangerous disease of the curriculum.
The New Competency based UG curriculum being implemented by the National Medical Commission wonderfully provides a framework of competencies in forensic medicine and toxicology (National Medical Commission, 2018). They serve as guiding milestones to reorient and redistribute the weightage, time and value allotted to certain topics.
From the Percentage marks allotted to each of these subtopics in forensic pathology in Figure no 3 it clearly shows that over 60 to 70% of the marks allotted were distributed among just 3 key topics i.e., Post-Mortem Changes, Mechanical Injuries and Asphyxia. The source of the error in the assessment is this high value allotted to theoretical aspects related to Autopsy and Medical examination. The faculty and the student’s attention have shifted towards the conduct of postmortem examination which is generally a high stakes scenario. But only a handful of undergraduates end up doing autopsies in their career. The ability to do autopsy is no doubt an important competency for the Undergraduates but the competencies related to Medical Jurisprudence and Toxicology are equally Important. The competencies related to handling Medico- legal issues related to patient care are encountered more frequently by an undergraduate thus requiring additional attention in the undergraduate curriculum than Forensic Pathology which is a rare or chance encounter for an MBBS graduate in India (Kumar et al., 2018; Medical Council of India, 1997; National Medical Commission, 2018; Sharma et al., 2005).
An Indian Medical graduate needs to make accurate observation, logical deductions and take critical decisions applying medical ethics in patient care. He should be able to diagnose and manage the common cases of poisoning as a physician of the first contact (Kumar et al., 2018; Medical Council of India, 1997; National Medical Commission, 2018; Sharma et al., 2005).
Most of the competencies in Toxicology are covered in the Forensic Medicine curriculum rather than in General Medicine. Hence, the percentage marks allotted for various subtopics of toxicology was also analysed in figure no 4. From figure no 2 it can be noted that about 20% of the marks were allotted to toxicology. Further considering figure no 4 it can be observed that 60-80% of the marks for toxicology was allotted to general toxicology and chemical toxicology showing a skewing in the distribution of marks.
Assessments must complement the roles of the undergraduate after completion of the course. Snake bite, an occupational disease in India, is an emergency frequently encountered by physicians of first contact (Vijay & Hegde, 2019). Substance abuse and pharmaceutical toxicity are also some of the most encountered cases in clinical practice following pesticide abuse (Basu & Mattoo, 1999). As a curriculum planner it is imperative that these factors considered as core in the curriculum (Amin et al., 2006; Amin & Khoo, 2003, pp. 260; McAleer, 2001). The current UG curriculum is deficient as certain areas have been undervalued leading to poor perception about the subject. Students undervalue the subject as the core competencies tested are not relevant considering their role as physician of the first contact. Students allot little time to study as most assessments cover few topics leading deterioration in the quality of teaching and learning in the course (Sharma et al., 2005).
Adult learners value learning bases on its immediate applicability and its use in problem solving. Curriculum must value topic and skill that complement the roles the learner after the training. Medical jurisprudence and toxicology have not been sufficiently assessed in this curriculum.
V. CONCLUSION
From the above discussion, it is reiterated that the university assessments in Forensic Medicine and Toxicology need to be realigned with the curricular needs. Certain subtopics like Forensic Pathology have been over valued compared to Medical Jurisprudence and Toxicology which have been undervalued. The sampling in Forensic Medicine and Toxicology assessment is not ideal. Application must be tested instead of just recall.
Universities need to periodically Assess their question papers for validity and chalk down clear guidelines for the paper setters. The current blueprints being used must be revalidated to check if there is clarity and scope of improvement. Most importantly, training the faculty and the question paper setters to use the blueprint and value the competencies mandated by the Curriculum lies at the heart of the solution to this problem. Overtime, this curricular malignancy observed, has had a profound effect on the mindsets of the faculty trainers. Faculty Developments activities to motivate and influence these mindsets to bring change is indispensable. The Application centered regulations prescribed by the National Medical Commission provides an excellent opportunity to motivate positive changes leading to the required course correction.
Notes on Contributors
Dr Vijay Kautilya was instrumental in conseptualising the idea, designing the study, data collection, data analysis, drafting and reviewing the manuscript.
Dr Arijit Datta contributed in designing the study, data collection, data analysis, drafting and reviewing the manuscript.
Dr Shruti P Hegde was instrumental in designing the study, data analysis, drafting and reviewing portions of the manuscript.
Dr Preethi Tiwari, contributed in data collection, data analysis, drafting and reviewing portions of the manuscript.
Ethical Approval
Institutional Ethics committee approval was received from the IEC, Government Medical College, Bharatpur where the study was conducted (GMCB/IEC/2020/009 dated 26th September 2020).
Data Availability
Datasets generated and/or analysed during the current study are available from the following DOI.
https://doi.org/10.6084/m9.figshare.19367864
Acknowledgement
We wish to acknowledge the Faculty of Forensic Medicine and Toxicology at MTMC, Jamshedpur for assisting in procurement of the question papers.
Funding
No external funding was received for the conduct of this study.
Declaration of Interest
There is no conflict of Interests to the best of our knowledge.
References
Abrahamson, S. (1978). Diseases of the curriculum. Academic Medicine, 53(12), 951-957. https://doi.org/10.1097/00001888-197812000-00001
Aggarwal, M., & Agarwal, S. (2017). Analysis of undergraduate pharmacology annual written examination papers at Pt. B. D. Sharma University of health sciences Rohtak. National Journal of Physiology, Pharmacy and Pharmacology, 7(5), 509. https://doi.org/10.5455/njppp.2017.7.1236224012017
Amin, Z., Chong, Y. S., & Khoo, H. E. (2006). Practical guide to medical student assessment. World Scientific. https://doi.org/10.1142/6109
Amin, Z., & Khoo, H. E. (2003). Basics in Medical Education. World Scientific.
Ayub, M., Habib, M., Huq, A., Manara, A., Begum, N., & Hossain, S. (2013). Trends in covering different aspects of anatomy in written undergraduate MBBS course. Journal of Armed Forces Medical College, Bangladesh, 9(1), 75-83. https://doi.org/10.3329/jafmc.v9i1.18729
Basu, D., & Mattoo, S. K. (1999). Epidemiology of substance abuse in India: Methodological issues and future perspectives. Indian Journal of Psychiatry, 41(2), 145-153.
Bhattacharya, S., Wagh, R., Malgaonkar, A., & Kartikeyan, S. (2017). Analysis of content of theory question papers in preliminary examinations and marks obtained by first-year MBBS students in physiology. International Journal of Physiology, Nutrition and Physical Education, 2(2), 856-868.
Choudhary, R., Chawla, V. K., Choudhary, K., Choudhary, S., & Choudhary, U. (2012). Content validity of first MBBS Physiology examinations and its comparison with teaching hours devoted for different sub-divisions of physiology. Journal of Physiology and Pathophysiology, 3(1), 8-11.
Chowdhury, D. K., Saha, D., Talukder, M. H., Habib, M. A., Islam, A. S., Ahmad, M. R., & Hossin, M. I. (2017). Evaluation of pharmacology written question papers of MBBS professional examinations. Bangladesh Journal of Medical Education, 8(2), 12-17. https://doi.org/10.3329/bjme.v8i2.33331
Gupta, S., Parekh, U. N., & Ganjiwale, J. D. (2017). Student’s perception about innovative teaching learning practices in forensic medicine. Journal of Forensic and Legal Medicine, 52, 137-142. https://doi.org/10.1016/j.jflm.2017.09.007
Kumar, A., Kumar, S., Goel, N., Ranjan, S. K., Prasad, M., & Kumari, P. (2018). Attitude of undergraduate medical students towards medico-legal autopsies at IGIMS, Patna, Bihar. International Journal of Medical Research Professionals, 4(6), 132-135.
Kautilya, D. V., Datta, A., Hegde, S. P., & Tiwari, P. (2022). Evaluating the content validity of the undergraduate summative exam question papers of forensic medicine & toxicology from 6 medical universities in India. [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.19367864
Mardikar, P. A., & Kasulkar, A. A. (2015). To assess the need of medicolegal education in interns and residents in medical institution. Journal of Evolution of Medical and Dental Sciences, 4(17), 2885-2889. https://doi.org/10.14260/jemds/2015/417
McAleer, S. (2001). Formative and Sumative assessment. In J. A. Dent, & R. M. Harden, A Practical Guide to Medical teachers (pp. 293-302). Edinbergh Churchill Livingstone.
Medical Council of India. (1997). Regulations on Graduate medical education, 1997. https://www.nmc.org.in/wp-content/uploads/2017/10/GME_REGULATIONS-1.pdf
Mehta, S., & Kikani, K. (2019). Descriptive analysis of II – MBBS university question papers of microbiology subject. Journal of Education Technology in Health Sciences, 6(2), 44-47. https://doi.org/10.18231/j.jeths.2019.011
National Medical Commission. (2018). Competency based undergraduate curriculum for the indian medical graduate. https://www.nmc.org.in/information-desk/for-colleges/ug-curriculum/
Parmar, P. (2018). Study of students’ perceptions towards case based learning in forensic medicine. Indian Journal of Forensic Medicine & Toxicology, 12(1), 154-160.
Pichholiya, M., Yadav, A., Gupta, S., Kamlekar, S., & Singh, S. (2021). Blueprint for summative theory assessment in pharmacology – A tool to increase the validity as per the new competency based medical education. National Journal of Physiology, Pharmacy and Pharmacology, 11(12), 1345-1355. https://doi.org/10.5455/njppp.2021.11.06170202107072021
Raymond, M. R., & Grande, J. P. (2019). A practical guide to test blueprinting. Medical Teacher, 41(8), 854-861. https://doi.org/10.1080/0142159x.2019.1595556
Sharma, B., Harish, D., & Chavali, S. (2005). Teaching, training and practice of forensic medicine in India-An overview. Indian Journal of Forensic medicine & Toxicology 27(4), 247-251.
Sudhan, S. M., & Raj, M. N. (2019). Current status of knowledge, attitude and awareness of medical students on forensic autopsy in Tumkur district of Karnataka. Indian Journal of Forensic Medicine & Toxicology, 13(1), 131-141.
Vijay, D. K., & Hegde, S. P. (2019). Study of snake bite and factors influencing snake bite among the rural population of Kancheepuram district. Journal of Punjab Academy of Forensic Medicine & Toxicology, 19(2), 142-146.
*Vijay Kautilya D
Kadani Road, Baridih,
Jamshedpur-831017
Jharkhand, India.
+919448651848
Email: kautilya.dacroo@gmail.com
Submitted: 19 August 2022
Accepted: 5 December 2022
Published online: 4 April, TAPS 2023, 8(2), 47-56
https://doi.org/10.29060/TAPS.2023-8-2/OA2869
Edyta Truskowska1, Yvonne Emmett2 & Allys Guerandel1
1Department of Psychiatry, Faculty of Medicine, University College Dublin, Ireland; 2National College of Ireland, Ireland
Abstract
Introduction: Digital Badges have emerged as an alternative credentialing mechanism in higher education. They have data embedded in them and can be displayed online. Research in education suggests that they can facilitate student motivation and engagement. The authors introduced digital badges in a Psychiatry module in an Irish University. Completion of clinical tasks during the student’s clinical placements, which were previously recorded on a paper logbook, now triggers digital badges. The hope was to increase students’ engagement with the learning and assessment requirements of the module.
Methods: The badges – gold, silver and bronze level – were acquired on completion of specific clinical tasks and an MCQ. This was done online and student progress was monitored remotely. Data was collected from the students at the end of the module using a questionnaire adapted from validated questionnaires used in educational research.
Results: The response rate was 68%. 64% of students reported that badges helped them achieve learning outcomes. 68% agreed that digital badges helped them to meet the assessment requirements. 61% thought badges helped them to understand their performance. 61% were in favour of the continuing use of badges. Qualitative comments suggested that badges should contribute to a higher proportion of the summative mark, and identified that badges helped students to structure their work.
Conclusions: The findings are in keeping with the literature in that engagement and motivation have been facilitated. Further evaluation is required but the use of badges as an educational tool is promising.
Keywords: Medical Education, Digital Badges, Students’ Engagement, Continuous Assessment Gamification, Health Profession Education
Practice Highlights
- Digital badges may enhance student engagement.
- Digital badges may promote motivation for learning.
- Evaluation of digital badges using a questionnaire with ordinal analysis of data and coding of free comments.
- Majority of students reported working harder than in a non-gamified module.
- Digital badges provided structure and direction to the student’s learning.
I. INTRODUCTION
Educational research recognises student engagement as valuable and as having significant impact on their learning (Mandernach, 2015). While searching for tools impacting on engagement, educators observed that games have been good at engaging players for decades, through their ability to sustain players’ attention and keep them motivated throughout the games (Przybylski et al., 2010). This level of engagement is desirable to both students and educators. This achievable level of engagement in gaming strategies has led to the exploration of its use in education. Elements from game design applied in non-game contexts to influence, engage and motivate individuals and groups have resulted in the development of a new field known as gamification (Deterding et al., 2011).
Digital badges are common tools of gamification (Barata et al., 2013). They are frequently used by game designers and in recent years also by educators. A digital badge used in education can be a validated symbol of academic achievement, accomplishment, skill, quality or interest (HASTAC, n.d.). Digital badges are digital images obtained through the completion of some pre-specified goals that are annotated with metadata and that can be displayed online (Hensiek et al., 2017). In higher education badges have been used to recognise a student’s participation in a learning activity, to help students explicitly and visually capture and monitor progress made on learning tasks, to recognise the achievement of skills and competencies and to serve as a means of certifying these achievements. They are reported to have a positive effect on the learners’ motivation if they are considered as awards or if they trigger competition among peers (Yildirim et al., 2016).
It appears that the value of digital badges depends on their design (when awarded, for what, and what they mean). For example, the use of badges as credentials only, has been criticised for focusing exclusively on extrinsic motivating factors, which have less impact on engagement than intrinsic ones (Seaborn & Fels, 2015). This is why combining the use of badges, as credentials as well as using them within the assessment process appears to be a better idea. Considering, that assessment has proven to have the most impact on effective learning, the use of badges during structured assessment has been favoured by educators (Abramovich, 2016; Rolfe & McPherson, 1995). The assessments that have potential to generate formative and summative feedback are presented as particularly useful (Armour-Thomas & Gordon, 2013). Digital Badges represent a viable alternative to existing methods of assessment in educational institutions and in the work environment (Dowling-Hetherington & Glowatz, 2017). It was also noted that access to regular feedback (broadly available in games) is helpful to learners. Students that are given opportunities to complete a task and learn from their mistakes do better in overall assessment. Games are a great example of the design where a player learns through feedback, gets better and eventually becomes successful (McGonigal, 2011). Similarly, the literature states that the use of badges has potential to offer a sort of “covert assessment”, meaning that students can approach a task as if it was a game. This helps to maintain the benefits of assessment while minimizing the potential for unhelpful levels of test anxiety (McGonigal, 2011) (Abramovich et al., 2013).
Another advantage given for the use of digital badges is their potential for remote monitoring of students’ progress and their difficulties by instructors and tutors (Huang & Soman, 2013). There is a growing momentum for the use of digital badges as an innovative instruction and credentialling strategy in higher education (Noyes et al., 2020).
In our University, Psychiatry is taught as a 10-credit module to both undergraduate and graduate entry students in the final stage of their degree in medicine. Typically, approximately 240 students are taught the module in four different groups: two groups in the spring and two groups in autumn, for six weeks at a time. Face to face teaching is centralized on Mondays and Fridays. Clinical teaching is delivered during the rest of the week and takes place in multiple different clinical centres. The overall assessment of this module comprised a continuous assessment with specific formative and summative tasks recorded in a paper logbook. The summative tasks were worth 20% of their overall assessment.
Standardising the student clinical experience, engaging them in their clinical placements and monitoring their attendance and progress can be challenging. The paper logbook/portfolio we were using was inadequate in that it did not allow for central monitoring of progress and often the difficulties students were encountering came to the attention of the teaching staff only when the logbook was handed over at the end of the module. Provision of feedback on progress was also limited. We felt that, in particular, students that were slow to progress were missing potential remediation before the summative assessments. We also encountered practical difficulties such as lost logbooks that affected the continuous assessment process.
We felt that digital badges offered a way of monitoring attendance and participation in tasks remotely, providing feedback, facilitating remediation and allowing students’ gauge how they are doing in relation to their peers while optimizing engagement in the clinical placements and structuring the learning to sustain progress through the module. We introduced and piloted the use of digital badges in the Psychiatry module as part of the continuous assessment. We carried out a descriptive study to appraise the potential usefulness of digital badges as part of our teaching strategy.
II. METHODS
A. Course Design
Students taking the 6-week Psychiatry module start their clinical placement on day 2 of the Module. Each week, students participate in their continuous assessment in order to collect their weekly badge. To acquire a badge, they need to complete and upload specific clinical tasks including formative clinical cases scheduled for them, to upload a Clinical Placement Form signed by the consultant on the team they are attached to and do an online multiple-choice question test at the end of the week. As all of this is done online their progress can be monitored remotely by the teaching team independent of the location of their clinical placement. Collecting their weekly badges provides them with 5% of their continuous assessment mark. The other marks for continuous assessment come from a summative clinical case (90%) and a reflective assignment (5%). Continuous assessment contributes to 20% of overall assessment mark.
B. Badges Design
Tutors in Psychiatry in conjunction with the University’s Teaching and Learning Department created Badges. It was part of an institution-wide digital badging pilot project (UCD Teaching and learning, 2017). It was agreed that there would be three types of badges -bronze, silver and gold – obtained and displayed on the university’s virtual learning environment (currently, Brightspace). As noted above students receive a digital badge on completion of assigned tasks, which are part of their continuous assessment. The type of badge awarded depends on the MCQ score and it is displayed on the student’s Blackboard profile. Figure 1 depicts the process. It shows that all badges are contributing to 5% of the module continuous assessment. Every week students receive information as to what percentage of the group has acquired a bronze, silver or gold badge so they have an idea of their performance in relation to that of the rest of the group.
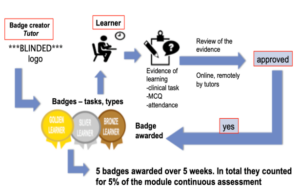
Figure 1. Step-by-step the process of getting/awarding a badge
C. Questionnaire
The ‘Digital Badges Experience Survey’ questionnaire was designed based on previously described surveys: the ARCS Badge Motivation Survey (Foli et al., 2016) and the Badge Opinion Survey (Abramovich et al., 2013) with some additional questions suggested by the literature on digital badges. The authors and faculty members identified and agreed on the following constructs as being relevant to our teaching delivery and our study: previous knowledge of digital badges (items 1 & 2), their meaning and relevance to students (items 22, 13, 14, 12, 8 & 5) motivation and engagement (items 3, 4 & 23), relevance to assessment and feedback (items 11, 9, 10, 24, 18 & 19), their use in structuring learning (items 15, 6, 7 & 16), self-efficacy (items 17, 20, 21 & 25), social context implication (items 26, 27 & 28). Under each construct, items from the above questionnaires were discussed and agreement reached on the ones to be used, altered or added assessing relevance and acceptability for our aims and teaching context.
Our survey consisted of 30 items with answers displayed on a seven-point Likert Scale. The 31st (final) question required dichotomous (yes/no) answer with space for respondents to explain their reasons for it. We also provided for free commenting from students (Questionnaire is available in Table 1).
Please rate your agreement with each of the statements using the following scale:
|
Strongly Agree |
Agree |
Somewhat Agree |
Neutral |
Somewhat Disagree |
Disagree |
Strongly Disagree |
||
|
+3 |
+2 |
+1 |
0 |
– 1 |
-2 |
-3 |
||
|
Please circle one number for each statement |
Strongly Agree |
|
|
Strongly Disagree |
||||
|
1. I knew what digital badges were before I began this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
2. I have earned digital badges before beginning this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
3. I felt motivated to complete the module because I was earning digital badges. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
4. Compared to other modules on my programme, the digital badges motivated me to work harder. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
5. The digital badges helped me to understand the learning outcomes for this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
6. The digital badges helped me to achieve the learning outcomes for this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
7. The badge helped draw my attention to the clinical seminars. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
8. The digital badges helped me to understand the content of this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
9. The digital badges helped me to understand the assessment requirements for this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
10. I was more aware of the module continuous assessment requirements because I would be earning digital badges. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
11. Because I was earning digital badges, I knew the continuous assessment requirements were important. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
12. Earning digital badges made a difference in how I viewed completing the continuous assessment requirements. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
13. Earning badges made the assignments more significant to me. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
14. The badges increased how relevant the assignments were. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
15. The digital badges helped me to structure my work in this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
16. The digital badges helped me to meet the assessment requirements of this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
17. The badges increased my confidence that I could demonstrate the content of my knowledge. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
18. The digital badges helped me to understand my performance in this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
19. The digital badges helped me to understand my progress through the module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
20. The badges were symbols that I had mastered content. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
21. The badges increased my overall level of satisfaction with completing the continuous assessment requirements. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
22. By earning the badges I was more fulfilled as a student by completing the assessment requirements. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
23. The digital badges made me want to keep on working. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
24. I understand why I earned all of my badges. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
25. The badges I earned represent what I learned on this module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
26. I talked to others about the badges I earned. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
27. I compared the badges I earned with others’ on the module. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
28. The potential to earn digital badges at gold, silver and bronze levels made me feel competitive. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
29. I think digital badges are a good addition to the programme. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
30. I would like to earn digital badges in other modules on my programme. |
+3 |
+2 |
+1 |
0 |
-1 |
-2 |
-3 |
|
|
31. I think the badges are helpful and should be used in the coming years: tick as appropriate and give 3 reasons why |
Yes ☐ |
No ☐ |
||||||
|
32. Any other comments |
||||||||
Thank you for your participation
Table 1. Digital Badges Experience Survey
D. Participants
The questionnaires were distributed to all the students of final year of Medicine in our university at the beginning of the final or sixth week of the module and collected by their tutors. Informed verbal consent was obtained from study participants. As described above, the course was run four times in one academic year, and we collected data from all four groups of students: two in the spring and two in the autumn.
E. Data Collection and Analysis
As noted above, questionnaires were distributed and collected by tutors at the beginning of the sixth (last) week of the Psychiatry Course. The level of student’s agreement with various statements was marked on the 7-point Likert-type scale. Those data were uploaded to Excel. Data from Likert scales can be analysed as ordinal as well as interval data (Sullivan & Artino 2013), (Norman, G. 2010) and we have considered both options. We concluded that using descriptive statistics such as the mean in relation to students’ opinions had limited value (Sullivan & Artino 2013), (Knapp 1990). This is why we decided to analyse our data as ordinal. To simplify the answers, we organised them into three groups: “agreed”, “neutral”, “disagreed”.
Students’ comments were entered into an excel sheet and analysed by two independent researchers. The comments relating to the use of badges in teaching of Psychiatry were coded according to topics, which were identified and agreed upon by the two independent researchers (Johnson & LaMontagne, 1993), (Sundler et al., 2019). Topics were further codified as positive or negative. This way of coding is described and performed in more details in other studies (Quesenberry et al., 2011).
III. RESULTS
A. Demographics
161 out of 237 students completed questionnaires giving a 68% response rate. The response rate was 75% in the first half (from springtime) of the students and 61% in the second (autumn rotation).
B. Analysis of Answers
65% of students had no previous knowledge of digital badges and 93% had never earned a badge before the module as per items 1 & 2 of questionnaire.
1) Meaning and relevance: Item 22: 48% of respondents agreed that by earning the badges they felt more fulfilled as a student when completing the assessment requirements. 31% disagreed. 45% agreed and 39% disagreed that earning badges made the assignments more significant to them (item 13) and similarly only 42% felt the badges increased the sense of how relevant the assignments were, while 40 % disagreed with this view as per item 14.
Earning digital badges made a difference in how 59% of students viewed completing the continuous assessment requirements, (item 12). 29% disagreed with this. 68% students felt that the digital badges helped them to understand the content of this module and 18% disagreed, (item 8). 66% students agreed and 24% disagreed about the fact that digital badges helped them to understand the learning outcomes for this module (item 5).
2) Motivation and engagement: 51% of students that responded felt motivated to complete the module because they earned a digital badge (item 3). 33% did not agree with this. The possibility of earning a digital badge motivated 43% of respondents to work harder (item 4). 39% disagreed with this. The digital badges made 45% of students want to keep on working, while 29% were not impacted (item 23).
3) Assessment and feedback: Item 11: 50% felt that because they were earning digital badges, they knew that the continuous assessment requirements were important. 36% disagreed. The digital badges also helped 69% respondents to understand the assessment requirements for this module but not so for the 15% respondents (item 9). Out of all respondents, 78% were more aware of the module continuous assessment requirements because of the digital badges, and only 15% disagreed with that (item 10). Item 24: As many as 74% of all respondents did and 14% did not understand why they earned their badges. The digital badges helped 61% of students to understand their performance in this module (item18). 27% did not find that badges helped in that way. Similarly, the digital badges helped 61% of students to understand their progress through the module. 22% disagreed with this (item 19).
4) Structure: Out of all respondents 50% agreed and 33% disagreed that the digital badges helped them to structure their work in the module (item 15). 64% of respondents agreed and 21% disagreed that the digital badges helped them to achieve the learning outcomes for this module (item 6). Similarly, the badge helped draw attention to the clinical seminars for 57% of respondents, but not so for 25%. 68% of students (vs 19% who have disagreed) felt that the digital badges helped them to meet the assessment requirements of this module (item 16).
5) Self-efficacy: Item 17: 48% of students agreed (vs 33% who disagreed) that earning the digital badges made them more confident that they could demonstrate the content of their knowledge. Item 20: 41% of all respondents agreed that the badges were symbols of mastering the content of the module. A similar number (40%) of students disagreed and 17% stayed neutral. 59% found the badges increased their overall level of satisfaction with completing the continuous assessment requirements (item 21). 27% disagreed with this. 44% of students agreed and 41% disagreed with the statement that the badges they earned represented their learning in the module (item 25).
6) Social context and competitiveness: 42% of students did and 44% did not talk to others about the badges they earned (item 26). The potential to earn digital badges at gold, silver and bronze levels made 49% of students more competitive (item 28). 39% disagreed with this. 29% of students did and 56% did not compare the badges they earned with others on the module (item 27).
7) Overall: 56% agreed that digital badges were a good addition to the program. 61% of students found digital badges helpful and felt that they should be used in the future. 31% did not agree with the statement and 8% did not answer.
Students’ opinions: 136 students did and 25 students did not write any comment. Students’ comments related either to one or to several topics. Students were positive about the use of badges (in various topics) 134 times (See Figure 1) and negative/critical 106 times (See Figure 2). It is important to note however that as many as 67 out of the 106 negative comments related to the low value of the badges.
Figure 2 depicts information about positive topics included in students’ comments. 50 students liked the structure and focus that the badge system provided. Twenty-eight students found badges motivating and 24 valued feedback they received in the process. A number of students found the whole process enjoyable, rewarding and fun (See Figure 2). Figure 3 indicates the negative opinions. The most frequent topic of all was repeated 67 times as was related to the value of badges (See Figure 3). Figure 4 shows some comments made by students in the free comment box provided on the survey (See Figure 4).
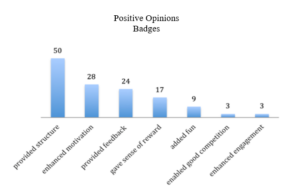
Figure 2. Frequency of positive comment grouped by topic
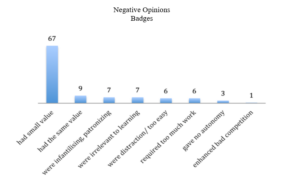
Figure 3. Frequency of negative comment grouped by topic
Figure 4. Comments written by students
In summary, the majority of the students liked the way Digital Badges were used in the teaching of Psychiatry, however both groups (those that liked and those that dislike badges) criticized them for their low value of the overall assessment.
IV. DISCUSSION
Students met digital Badges piloted in the teaching of Psychiatry to Medical Students of our university originally with apprehension. The majority of the students had never heard of digital badges and have never earned a digital badge before this module. However, data from the study looking at students’ perception of the use of digital badges in medical education provided encouraging results.
A. Sense of Reward
Students found badges rewarding yet complained about the small value of the badges. This reflected our design intention in which we wanted to support and engage students rather than focus on extrinsic motivating factors such as sense of reward.
As mentioned above the badge was awarded for completion of weekly tasks, and the acquisition of a badge was functioning more as a method of feedback to students rather than for grading. However, a number of students complained about this, and reported a sense of frustration and a lack of motivation to try harder when the assessment value of the badge was so low.
Nevertheless, our design was supported by other studies. One such study concluded that achievement of badges could influence students’ behaviour even if they do not interfere with grading (Hakulinen & Auvinen, 2014). It seems that competitiveness was triggered in those who wanted to do better anyway.
We were pleased to see learners’ comments about reduced stress during the module. We wanted our award system to potentiate a sense of safety around assessment, giving participants freedom to learn from their mistakes without influencing their final grade. This is a well-recognized principle in gamification as a facilitator of students’ engagement (De Byl & Hooper, 2013).
In addition, our design was guided by the fact that the best use of badges was linked with the recognition of already occurred learning, therefore more viewed as an assessment tool, providing feedback and possibly self-reflection (Reid et al., 2015).
B. Impact on Structure, Assessment and Feedback
We were pleased to note that students in our study felt that digital badges provided direction and structure to their learning. This was also reflected in their comments: students mentioned how badges impacted on their study structure, helping them to focus attention on important aspects of the seminars. These findings are consistent with a study that reported that students who enjoyed badges, found them helpful in giving them the direction they needed to work in (Abramovich et al., 2013). These students also praised the alignment between badge topics and course content (Abramovich et al., 2013).
We were also hoping that badges designed, as part of an assessment that generates formative feedback would help students know if they are progressing enough to meet the requirements of their class (HASTAC n.d.). Based on responses to items 24, 18 and 19 it appeared that students benefited somewhat from the potential guidance and feedback provided by the digital badges system.
It is important to remember that students were asked about the badges at their review seminar and few days prior to their exams. This timing could have influenced their answers. For example, students’ opinion was divided on the statement that earning a badge gave them a sense that they have mastered the course content. Similarly, opinion was divided on whether badges increased students’ confidence that they could demonstrate their knowledge, nevertheless more students felt that they had an impact. It would be interesting to see if students’ responses had been different after their exams. We know gamification has already been described as a powerful strategy that can help achieve learning objectives by affecting the way students behave (Huang & Soman, 2013).
C. Impact on Motivation and Engagement
In our study, a majority of students responded that they worked harder in this module compared to non-gamified modules. Similarly, about 30% more students stated that they were more motivated to work harder through the module because they were earning digital badges. Interestingly when they were given space to provide free comment, many have noted that they did feel more motivated, and a few felt more engaged. Previous studies also reported that students were more likely to engage in the game-like tasks providing rapid feedback (Thamvichai & Supanakorn-Davila, 2012). In other publications students also considered gamified courses to be more motivating, interesting and easier to learn as compared to other courses (Barata et al., 2013), (Dicheva et al., 2015), (Hakulinen & Auvinen, 2014). It is suggested that badges are most valued by learners who are extrinsically motivated and value external validation (Foli et al., 2016).
D. Impact on Outcomes
We did not compare outcomes in overall performance in assessment between students before and after implementation of badges. Having considered this, we decided against it. We felt there were too many variables influencing students’ performance and it would be difficult to definitely attribute potential change to the implementation of digital badges.
E. View of Badges and Learner Type
The impact of an educational tool could also depend on characteristics of the student as a learner. It is reported that students with high expectation for learning and those that value their learning tasks may view the badge as validating if designed as a performance assessment (having impact on intrinsic motivation), but it may devalue their learning if it was viewed as an external reward (Reid et al., 2015). On the other hand, badges used as an assessment model can have a negative impact on students with low expectancy values (Reid et al., 2015). Another study concluded that engagement in the gamified classroom was dependent on students’ playfulness (De Byl & Hooper, 2013). In this study, we have not addressed the learner types and other such specifications of the individuals in our group of students.
In a systematic review of digital badges in health care education, it is mentioned that digital badges represent an innovative approach to learning and assessment and evidence in further education literature demonstrates that their use increases knowledge, retention and motivation to learn. However, they also report a lack of empirical research investigating digital badges within the health care education context (Noyes et al., 2020).
F. Limitations
Our study is limited by the lack of demographic data from all participants. This reduces the potential for comparison between genders and undergraduate vs postgraduate students. As mentioned above, we have not addressed learner characteristics and types (intrinsic versus extrinsic motivation, playfulness). The timing of the data collection (students completed questionnaires before their exams, rather than after) may also be limiting factors. It is also important to remember that this study allowed only for assessment of subjective impact (via students’ opinions and experience) of the badges on students learning and did not perform objective measures of students’ overall performance.
V. CONCLUSION
This study was performed at the start of the implementation of the digital badges in the module and at the time, it was the only module with elements of gamification throughout the whole undergraduate medical curriculum in our university. Like most changes in the assessment process, the students greeted this with a level of apprehension. It would be interesting to see if students’ opinion has evolved after a few years of digital badges being integrated in the module and when other modules are using them. Nevertheless, our data shows that our group of students felt, that they benefited from the learning structure provided by the digital badges. The online process of obtaining the badges enabled tutors to provide timely feedback and monitor students’ progress. In addition, our findings are in keeping with the literature in that engagement and motivation have been facilitated by introducing the digital badges and as such, they indicate that the use of digital badges is a promising tool in education.
The use of digital badges in Medical Education is only starting and would benefit from more research in its judicious integration in higher education curriculum as appropriate.
Notes on Contributors
Dr Edyta Truszkowska did the literature search, collected and analysed the data and gave feedback on methodology and questionaire developed and wrote paper.
Dr Yvonne Emmett designed the methodology and developed questionaire. She gave feedback on the data analysis and edited the writing of the paper.
Prof Allys Guerandel suggested the implementation of digital badges and research project. She gave feedback on data analysis and wrting of paper making revisions to same.
All three authors have read and approved the final manuscript.
Ethical Approval
Our project has been exempted by ethics committee of our institution Human Research Ethics Committee – Sciences (Exemption number LS-E-17-56).
Data Availability
Data is available on reasonable request and data is shared in the institution.
Acknowledgement
We would like to acknowledge our institution psychiatry teaching team for their support in the implementation of the digital badges.
Funding
There are no sources of funding.
Declaration of Interest
There is no conflict of interest for any of the authors.
References
Abramovich, S. (2016). Understanding digital badges in higher education through assessment. On the Horizon, 24(1), 126-131. https://doi.org/10.1108/OTH-08-2015-0044
Abramovich, S., Schunn, C., & Higashi, R. M. (2013). Are badges useful in education? It depends upon the type of badge and expertise of learner. Educational Technology Research and Development, 61(2), 217-232. https://doi.org/10.1007/s11423-013-9289-2
Armour-Thomas, E., & Gordon, E. (2013). Toward an Understanding of Assessment as a Dynamic Component of Pedagogy. https://www.ets.org/Media/Research/pdf/armour_thomas_gordon_understanding_assessment.pdf
Barata, G., Gama, S., Jorge, J., & Gonçalves, D. (2013, September). Engaging engineering students with gamification. In 2013 5th International Conference on Games and Virtual Worlds for Serious Applications IEEE, UK (VS-GAMES) (pp. 1-8). https://doi.org/10.1109/VS-GAMES.2013.6624228
De Byl, P., & Hooper, J. (2013). Key attributes of engagement in a gamified learning environment. In ASCILITE-Australian Society for Computers in Learning in Tertiary Education Annual Conference, Australia (221-230). https://www.learntechlib.org/p/171232/
Deterding, S., Dixon, D., Khaled, R., & Nacke, L. (2011, September). From game design elements to gamefulness: defining” gamification”. In Proceedings of the 15th international academic MindTrek conference: Envisioning future media environments (pp. 9-15). https://doi.org/10.1145/2181037.2181040
Dicheva, D., Dichev, C., Agre, G., & Angelova, G. (2015). Gamification in education: A systematic mapping study. Journal of Educational Technology & Society, 18(3), 75-88. https://www.jstor.org/stable/jeductechsoci.18.3.75
Dowling-Hetherington, L., & Glowatz, M. (2017). The usefulness of digital badges in higher education: Exploring the student perspectives. Irish Journal of Academic Practice, 6(1), 1-28. https://researchrepository.ucd.ie/handle/10197/9691
Foli, K. J., Karagory, P., & Kirby, K. (2016). An exploratory study of undergraduate nursing students’ perceptions of digital badges. Journal of Nursing Education, 55(11), 640-644. https://doi.org/10.3928/01484834-20161011-06
Hakulinen, L., & Auvinen, T. (2014, April). The effect of gamification on students with different achievement goal orientations. In 2014 international conference on teaching and learning in computing and engineering, Malaysia (pp. 9-16). IEEE. https://doi.org/10.1109/LaTiCE.2014.10
HASTAC. (n.d.). Digital Badges. http://www.hastac.org/digital-badges
Hensiek, S., DeKorver, B. K., Harwood, C. J., Fish, J., O’Shea, K., & Towns, M. (2017). Digital badges in science: A novel approach to the assessment of student learning. Journal of College Science Teaching, 46(3), 28. https://www.proquest.com/scholarly-journals/digital-badges-science-novel-approach-assessment/docview/1854234735/se-2
Huang, W. H. Y., & Soman, D. (2013). Gamification of education. Report Series: Behavioural Economics in Action, 29, 11 -12.
Johnson, L. J., & LaMontagne, M. J. (1993). Research methods using content analysis to examine the verbal or written communication of stakeholders within early intervention. Journal of Early Intervention, 17(1), 73-79.
Knapp, T. R. (1990). Treating ordinal scales as interval scales: An attempt to resolve the controversy. Nursing Research, 39(2), 121-123.
Mandernach, B. J. (2015). Assessment of student engagement in higher education: A synthesis of literature and assessment tools. International Journal of Learning, Teaching and Educational Research, 12(2), 1-14.
McGonigal, J. (2011). Reality is broken: Why games make us better and how they can change the world. Penguin.
Norman, G. (2010). Likert scales, levels of measurement and the “laws” of statistics. Advances in health sciences education, 15(5), 625-632.
Noyes, J. A., Welch, P. A., Johnson, J. W., & Carbonneau, K. J. (2020). A systematic review of digital badges in health care education Medical Education, 54(7), 600-615. https://doi.org/10.1111/medu.14060
Przybylski, A. K., Rigby, C. S., & Ryan, R. M. (2010). A motivational model of video game engagement. Review of General Psychology, 14(2), 154. https://doi.org/10.1037/a0019440
Quesenberry, A. C., Hemmeter, M. L., & Ostrosky, M. M. (2011). Addressing challenging behaviors in Head Start: A closer look at program policies and procedures. Topics in Early Childhood Special Education, 30(4), 209-220. https://doi.org/10.1177/0271121410371985
Reid, A. J., Paster, D., & Abramovich, S. (2015). Digital Badges in undergraduate composition courses: effects on intrinsic motivation. Journal of Computers in Education, 2(4), 377-98. https://doi.org/10.1007/s40692-015-0042-1
Rolfe, I., & McPherson, J. (1995). Formative assessment: How am I doing? The Lancet, 345(8953), 837-839. https://doi.org/10.1016/S0140-6736(95)92968-1
Seaborn, K., & Fels, D. I. (2015). Gamification in theory and action: A survey. International Journal of Human Computer Studies, 1(74), 14-31. https://doi.org/10.1016/j.ijhcs.2014.09.006
Sullivan, G. M., & Artino, A. R. (2013). Analyzing and interpreting data from likert-type scales. Journal of Graduate Medical Education, 5(4), 541-542 https://doi.org/10.4300/JGME-5-4-18
Sundler, A. J., Lindberg, E., Nilssonn, C., & Palmer, L. (2019). Qualitative thematic analysis based on descriptive phenomenology. Nursing Open, 6(3), 733-739. https://doi.org/10.1002/nop2.275
Thamvichai, R., & Supanakorn-Davila, S. (2012). A pilot study: Motivating students to engage in programming using game-like instruction. Proceedings of Active Learning in Engineering Education. St Cloud University. https://nms.asee.org/wp-content/uploads/sites/47/2020/02/St_Cloud_2012_Conference_Proceedings.pdf#page=18
UCD Teaching and learning. (2017). UCD digital/open badges pilot 2016/2017. Implementation and evaluation report. UCD Teaching and Learning, 1-23. https://www.ucd.ie/t4cms/UCD%20Digital%20Badges%20Pilot%20Report.pdf
Yildirim, S., Kaban, A., Yildirim, G., & Celik, E. (2016). The effect of digital badges specialization level of the subject on the achievement, satisfaction and motivation levels of the students. Turkish Online Journal of Educational Technology- TOJET, 15(3), 169-182. https://eric.ed.gov/?id=EJ1106420
*Allys Guerandel
University College Dublin,
School of Medicine and Medical Sciences,
Belfield, Dublin 4, Ireland D04V1W8.
00353868590063
Email: allys.guerandel@ucd.ie
Submitted: 1 August 2022
Accepted: 1 November 2022
Published online: 4 April, TAPS 2023, 8(2), 36-46
https://doi.org/10.29060/TAPS.2023-8-2/OA2855
Marina C. Jenkins1, Caroline R. Paul2, Shobhina Chheda1 & Janice L. Hanson3
1School of Medicine and Public Health, University of Wisconsin-Madison, United States; 2Langone Health, Grossman School of Medicine, New York University, United States; 3School of Medicine, Washington University in St. Louis, United States
Abstract
Introduction: Increases in vaccine hesitancy continue to threaten the landscape of public health. Literature provides recommendations for vaccine communication and highlights the importance of patient trust, yet few studies have examined medical student perspectives on vaccine hesitancy in clinical settings. Therefore, we aimed to explore medical student experiences encountering vaccine hesitancy, mistrust, and personal biases, with the goal of informing medical student education.
Methods: A health disparities course including simulated clinical scenarios required students to complete a written reflection. We sorted reflections written in 2014-2016 to identify common topics and used inductive thematic analysis to identify themes relevant to vaccine hesitancy by group consensus.
Results: Our sample included 84 de-identified essays sorted into three non-exclusive topics: vaccine hesitancy (n=42), mistrust (n=34), and personal bias (n=39). We identified four themes within medical students’ reflections: 1) Building a Relationship, including emphasis on patient-centred approaches; 2) Preparedness and Need to Prepare for Future Encounters, including highlighting gaps in medical education; 3) Reactions to Encountering Hesitant Patients, including frustration; 4) Insights for Providing Information and Developing a Plan with Hesitant Patients, including approaches to presenting knowledge.
Conclusion: Reflections in the context of simulated encounters and discussion are useful in students identifying their preparedness for vaccine discussion with patients. Student reflections can assist educators in identifying missing educational frameworks for particular scenarios such as vaccine hesitancy. Without a structured framework regarding addressing vaccine hesitancy, students draw upon other skills that may contradict recommended practices.
Keywords: Medical Education, Vaccine Hesitancy, Reflective Writing, Bias, Mistrust
Practice Highlights
- Reflective writing can be a useful tool in medical education toward addressing vaccine hesitancy.
- Medical student reflective writing can be used to demonstrate curricular gaps.
- Medical students expressed feeling unprepared to care for vaccine hesitant patients.
- Without a framework for vaccine communication, students may draw on other inappropriate skills.
I. INTRODUCTION
Increases in vaccine hesitancy and refusal threaten public health (He et al., 2022; Hough-Telford et al., 2016; Kempe et al., 2020; Santibanez et al., 2020), especially with the COVID-19 pandemic introducing a need for quick and widespread uptake of a new vaccine (Hamel et al., 2022; Ognyanova et al., 2022). Patients, especially parents, are increasingly seeking alternative forms of health information, such as online sources that can include misinformation (Broniatowski et al., 2018; Hara & Sanfilippo, 2016; Jenkins & Moreno, 2020; Meleo-Erwin et al., 2017). Patient trust in their clinician and the health care system delivering the vaccine strongly influence vaccination decisions (Goldenberg, 2016; Kennedy et al., 2011; Larson, 2016). Trust remains the most important barrier to acceptance and uptake of the COVID-19 vaccine, with mistrust of government, medicine, and science presenting major barriers to vaccine uptake (Ognyanova et al., 2022). Vaccine hesitant patients may bring preconceptions and concerns from their own research to in-clinic vaccine communication. Thus, it is important for clinicians to be well-prepared to work with vaccine-hesitant patients and parents.
Existing recommendations for clinicians encountering vaccine hesitancy emphasise centring patient views and voice instead of a medical, academic perspective (Holt et al., 2016; Koski et al., 2019). Approaches including motivational interviewing, presumptive language around vaccine recommendations, and persistent vaccine reminders without pressuring or dismissing patients have been shown to be effective in addressing vaccine hesitancy in medical practice (Dempsey et al., 2018; Gagneur et al., 2018; Hofstetter et al., 2017), while correcting misinformation and offering evidence to patients have been found to be counterproductive (Holt et al., 2016; Koski et al., 2019). These pre-COVID recommendations remain the same for addressing COVID-19 vaccine hesitancy, and lack of physician preparedness for encountering these patients is still an important issue (Centres for Disease Control and Prevention, 2021). Physicians may have misconceptions about patients’ reasons for vaccine hesitancy, often assuming lack of understanding or information on the safety, effectiveness, and necessity of vaccines (Hough-Telford et al., 2016), rather than recognising the more central roles of trust and validation of concerns. If physicians do not learn approaches for centring patient voices in vaccine communication, these pre-conceived biases may present a barrier to vaccine uptake and patient-physician trust.
While valuable recommendations for addressing vaccine hesitancy in the clinical setting exist, current efforts center around informing practicing clinicians on these approaches and providing more educational resources to patients (Centres for Disease Control and Prevention, 2021). These may not represent a sufficient, long-term solution. Furthermore, resources available for healthcare workers may be inaccessible or overwhelming for physicians independently seeking tools (Karras et al., 2019). Incorporating vaccine hesitancy-centred curriculum into medical education may be the optimal, long-term solution to the lack of physician preparedness for these encounters, especially in the face of future pandemics and introduction of new vaccines. With curriculum renewal efforts incorporating early clinical experiences, students could encounter patients for whom vaccines are recommended, including vaccine hesitant patients, early in medical school. It would provide a better educational experience for students and a better health care experience for patients if students receive education to prepare them for these conversations. However, few studies have examined medical student perspectives on vaccine hesitancy in the clinical setting. Existing studies have found mixed findings around medical students’ reflections on their preparedness for encountering vaccine hesitant patients and highlight the need for expansion of related curriculum in medical education (Brown et al., 2017; Kernéis et al., 2017). While COVID vaccine hesitancy literature lacks exploration of medical student perspectives and preparedness, recent studies have highlighted an additional barrier of vaccine hesitancy among medical students in some settings (Lucia et al., 2021). These findings provide additional motivation for including vaccine hesitancy-specific curriculum in medical education.
Understanding medical students’ reactions to vaccine hesitancy is critical in preparing students to address vaccine hesitancy while maintaining patient trust. In the present study, which used a scholarship-of-teaching approach, we aimed to expand on existing research on medical student preparedness for encountering vaccine hesitancy to examine written reflections on mistrust and personal bias in clinical encounters more broadly and use a larger sample of student narratives. We analysed students’ structured reflections regarding assigned reading, simulated patient encounters, peer discussions, and faculty-facilitated discussions to evaluate medical students’ learning during a health disparities curriculum. Structured reflection on simulated encounters has been shown to be a useful tool for understanding student perspectives (Koski et al., 2018); this approach can inform development of medical curriculum for addressing vaccine hesitancy and may be a useful teaching tool as well for students to practice, discuss, and reflect on their own biases in an educational setting. Therefore, the purpose of this study was to explore medical student reflections on encountering vaccine hesitancy, patient mistrust, and personal biases, with the goal of informing medical student education.
II. METHODS
In this qualitative study, we analysed written reflections from a third-year medical student Skills to Impact Health Disparities course, to evaluate their learning about interacting with vaccine-hesitant patients and parents. This study was determined to be exempt by the relevant institutional review boards, including a waiver of informed consent.
From 2006-2018, a medical school at a U.S., Midwestern university required a one-day core session with the goal of developing learner skills to impact health disparities. Small groups of approximately six students went through five to six standardized patient scenarios, each designed to generate discussion and reflection about clinician bias that can unintentionally influence patient care. During the learning activity, each student spent 3-5 minutes interacting with a standardized patient who presented a challenge designed to provoke a level of discomfort in the learners to allow for discussion and reflection. One of these six scenarios included a parent with a history of vaccine refusal for their child expressing concerns about a recommended vaccine.
Following each case, students engaged in a 15-minute, non-facilitated discussion based on a list of focused questions. After all cases, students joined another group of six students for a 75-minute faculty-facilitated debrief. In addition, students were required to complete a brief critical reflection based on a theme of the core day activity using the LeAP framework (Aronson et al., 2012). This framework is modelled on a clinical framework, the SOAP note (Chief complaint, Subjective, Objective, Assessment, and Plan). Students were asked to consider a specific experience that led to concern or questions; describe the experience as fully as possible; reconsider the experience by getting other perspectives; synthesize learning; and make a plan to address future similar challenges. Students could choose to reflect on simulated or real clinical experiences.
Written reflective essays were available for analysis from years 2014-2016, providing qualitative data about students’ observations and experiences with health disparities and health equity. All available essays (n=292) from 2014, 2015, and 2016 that were submitted as a course requirement for the Skills to Impact Health Disparities Core Day required course were de-identified and organized by year.
To ascertain the topics that the students addressed, three investigators (two involved in this study and one from another study using the larger set of all essays) read all essays. Each investigator then designated each essay to a topic from a jointly-developed list of non-exclusive topics derived from the data. After individually assigning topics for a sample of essays, the investigators met to compare their sorting and reconcile any differences before they went on to sort through another set of essays. This process continued until all essays were assigned to one or more topics. Most topic labels matched topics of the simulated scenarios that the students encountered in the course, while others related to broader issues highlighted across scenarios. With the goal of selecting reflections relevant to the issue of vaccine hesitancy, all reflections designated under the topics of vaccine hesitancy, mistrust, and personal bias were gathered for qualitative data analysis. Literature review and initial reading of essays suggested essays on encountering mistrust and bias relate to students’ experiences when encountering vaccine hesitant patients, despite not all essays relating directly to vaccine hesitancy. Each essay was assigned an identifier with cohort year and an essay number. Individual essays were excluded based on group consensus on lack of relevance to vaccine hesitancy.
Inductive thematic analysis was used to identify codes and themes in the reflection data using a semantic, realist approach to identify explicit reactions from students grounded in clinical experiences to identify themes that could be directly applied to clinical practice (Braun & Clarke, 2006). Four investigators, including two involved in topic assignment (CRP, SC) and two additional investigators (MCJ, JLH), read and discussed six essays to develop a preliminary codebook, applied these codes to the same six essays, then met to discuss and revise the codebook. Subsequently, investigators coded the remaining essays in pairs using the revised codebook through four rounds of coding, making further iterative changes to the codebook and reconciling differences within pairs. The full team then met to discuss the coding, revise code descriptions, refine the grouping of the codes, and agree on descriptions of the groups. Any changes made to the codebook during the analysis process were retrospectively updated in all previous coding, so that all coding data reflected the final version of the codebook. Data were organized with qualitative analysis software (HyperResearch version 4.5.4). After all data were coded, investigators discussed and reached consensus on the themes.
III. RESULTS
A total of 90 reflections were collected from the Skills to Impact Health Disparities course across three cohorts of third-year medical students from 2014-2016 at one U.S., Midwestern university. Based on investigator consensus on lack of content relevance, six reflections were excluded from our study sample. Our final study sample included 84 de-identified reflections across three, non-exclusive topics: 42 categorized as relating to vaccine hesitancy, 34 as mistrust, and 39 as personal bias. We identified four major themes in medical students’ reflections on encountering vaccine hesitancy, mistrust and personal bias: 1) Building a Relationship, 2) Preparedness and Need to Prepare for Future Encounters, 3) Reactions to Encountering Hesitant Patients, and 4) Insights for Providing Information and Developing a Plan with Hesitant Patients. Representative quotes for each theme can be found in Table 1. Supplemental Table 1 lists each theme with the codes that informed the theme.
A. Building a Relationship
In our first theme, medical students recognized the importance of Building a Relationship with hesitant parents or patients as the foundation for discussions about vaccines or other care about which patients expressed hesitance. They focused on approaches such as building rapport, centring the parent/patient’s views during the discussion, acknowledging their efforts to gather information about their health decisions, expressing empathy, and avoiding direct confrontation of the patient’s viewpoint during the discussion. Many of these observations occurred during the core day experience. For example, one student wrote:
“I learned the importance of letting the patient try to teach the doctor what they know rather than the doctor jumping in and lecturing to the patient. In the future I will try to talk less and let the patient explain more about why they oppose vaccinations to better gauge what they understand about the literature before I try to explain why vaccinations are important and the facts about vaccinations.”
[Year3_61]
The students saw the importance of finding points of commonality between their perspectives and those of the patient and moving the conversation toward establishing goals that they could work together with the patient to accomplish.
One student described, “I learned that a big part of approaching this difficult conversation is establishing the correct approach: common goal, shared decision making.”
[Year3_65]
B. Preparedness and Need to Prepare for Future Encounters
Another major theme identified in medical student reflections on encountering hesitant patients was Preparedness and Need to Prepare for Future Encounters. This theme included discussion of whether the student expressed feeling ready for the encounter or whether they thought it was successful, as well as specific plans for preparing for similar encounters in the future. One way that students discussed their own feelings of preparedness was by recognizing their own biases upon reflection of the encounter. For example, one student wrote:
“I realized my own prejudices influenced my care of my patients more than I would have liked. … It was an eye opener that I am not as impartial as I would like to be and that it takes a lot more self-reflection and awareness to be the best care provider I can be.
[Year3_16]
When discussing a need to prepare for future encounters, many students referenced plans to independently seek additional resources, especially those referenced by patients in encounters.
Other students mentioned plans to practice patient interactions related to the reflection encounter; including, “For me, practicing acknowledging a patient’s views and concerns without endorsing or validating false information is paramount.”
[Year1_07]
Some students also referenced plans to request feedback or advice from more senior clinicians. Additionally, several students identified gaps in their medical school curriculum that contributed to their lack of preparedness or that needed to be filled to support future preparedness. Students specifically referred to needing more resources, support, and training for encountering hesitant patients. They sometimes called for system-wide changes to address this gap in knowledge.
C. Reactions to Encountering Hesitant Patients
One of the themes identified in the students’ self-reflection was related to their own and others’ Reactions to Encountering Hesitant Patients. While some students expressed frustration with patients/parents who expressed hesitance about vaccines, they acknowledged that they can be passionate about the topic of vaccines in their patient care, but ultimately, patients and parents make their own decisions.
One student shared, “I have always found it quite distressing when an otherwise healthy child goes unvaccinated, given the enormous amount of evidence in favour of vaccination efficacy and its effect on public health.”
[Year2_86]
Another student shared, “I knew I could not force the patient, and I knew that she ultimately was in control of what she would do.”
[Year3_78]
In some reflections patient and parents were labelled, for example, as “anti-vaxxers.” Some reflections described parents’ and patients’ bias towards the physician or clear messaging of a desire for a different doctor. In encountering standardized patients in our scenarios or in reflecting on patients seen in clinical settings, students acknowledged that these conversations were difficult, and they were able to self-assess their level of comfort with conversations.
This was well-summarized in one reflection: “It was remarkable to me how such a strong reaction from this patient’s mother elicited an equally strong reaction in me.”
[Year2_34]
At times students recognized a point where these difficult conversations could reach a dead end. One student stated, “No matter how hard I would try, nothing seemed to work.”
[Year2_03]
Especially in this context, students reflected ambivalence towards the patient’s decision. For example:
“I personally feel that providers allowing for healthy children on their patient panels to remain unvaccinated indirectly reinforces non-vaccination as being acceptable by the medical establishment. That said, I also see and appreciate that turning a child away from one’s practice because their parents refuse to vaccinate them not only does not solve the problem at hand, but it also leaves a child at a very critical developmental age with no health care at all until an alternative provider can be found. Ultimately, I found attempting to reconcile these seemingly incompatible sides of the issue of dealing with anti-vaccination quite confusing and uncomfortable.”
[Year2_86]
D. Insights for Providing Information and Developing a Plan with Hesitant Patients
A fourth theme centred on students’ insights regarding how to provide information appropriately to patients and how to create a plan with patients who were hesitant regarding the medical recommendations given to them. Medical students suggested a variety of ways to provide information to patients who were hesitant. They noted the importance of contributing relevant facts and evidence, stressing that such information and knowledge in general needed to be presented in an understandable manner.
As one student described, “Finding the appropriate words to use in such conversations with a patient is essential.”
[Year1_44]
Students often wrote that they needed to provide reputable information to inform the patient’s decision-making. Some suggested strategies for how to present information to patients, including the sharing of stories and the use of scary information to convey the level of seriousness of the medical recommendation and advice.
One student referenced storytelling in the literature, “…the use of storytelling, the same method used by the anti-vaccination movement, [can be] a way to counteract the barrage of misinformation regarding vaccines.”
[Year1_90]
Sharing these insights about how to present information, students also moved towards how to develop a plan with their patients with some deliberate suggestions. Some students felt they needed to be persistent in their recommendations for vaccines. Some students explained how intentional discussions on the risks and benefits of their recommendations can help in their negotiation about a care plan with their patients.
One student noted, “This draws along the line of patient autonomy, and as long as we are clear about the risks and benefits with the patient, then ultimately, it’s up to the patient to make the decision about which medications she will take.”
[Year1_52]
|
Medical Students’ Experiences with Vaccine Hesitancy, Mistrust, and Bias |
|
|
Themes |
Exemplar Quotes |
|
Building a relationship |
“I felt it was most important that I listen to his story as much as I possibly could, before I spoke. So I let him talk. I said, ‘tell me your concerns.’” [Year3_18] “My feelings during this situation were somewhat of frustration but more of just desire for the patient to feel as though I was there to care for her child above all else and to come alongside her rather than combat with her.” [Year3_03] “One suggestion that my classmate said was to start out the conversation by validating how they are feeling more and that you understand that they are a good parent rather than jumping into facts about vaccinations which caused the patient to become defensive.” [Year3_61] |
|
Preparedness and need to prepare for future encounters
|
“I need more tools for dealing with these situations in the future.” [Year1_04] “My plan is to educate myself more on the materials available for parents regarding immunizations.” [Year3_03] “Ultimately it would be nice to see EMRs advance to the point where they can track a patient’s problem, not just on a list, but through stages of management and onto completion, with a provider responsible for follow-up.” [Year2_33] “I will seek feedback from my attendings and residents so that I can improve my motivational interviewing skills.” [Year3_81] |
|
Reactions to encounter-ing hesitant patients |
“Ultimately this is a decision of the parent and I can only offer my professional advice…I learned that this topic did elicit some emotion which I was surprised about.” [Year3_79] “I learned that I need to work on my bluntness (what I consider to be honesty), as well as increasing affirmation of patients’ fears, since telling someone they are wrong (in any facet of life) typically doesn’t work out that well.” [Year2_34] “I felt uncomfortable and offended at times during the conversation. The patient clearly was not interested in negotiating vaccination, and when I tried to discuss the validity of some of the studies and articles she had read, she became very defensive.” [Year2_82] “I dealt with a mother who had embraced the anti-vaccination movement. This is an issue that I have thought about a lot but despite my reflections, it is an issue that I do not know how to address well. This filled me with fear because I honestly didn’t know what the best approach was.” [Year1_90] |
|
Insights for providing information and creating a plan with hesitant patients
|
“From the debriefing session I learned that a promising approach for the anti-vaccine population is to continue to offer the vaccines at each well-child check-up without intensive counsel on the risks/benefits of vaccines.” [Year1_13] “I also learned about using pictures to get a visceral response from the parent which hopefully would change their mind about not getting a vaccine.” [Year3_69] “When I encounter this scenario in the future, as I’m sure I will, I will begin by teasing out whether the patient is interested in more information, in which case I can have resources and studies available, or if they have already made up their mind and at that point I need to negotiate the visit to ensure that they continue to see me for whatever care they are willing to receive, even if that doesn’t include all the preventive measures I would like.” [Year2_82] |
Table 1. Medical students’ experiences with vaccine hesitancy, mistrust, and bias—Themes and exemplar quotes
IV. DISCUSSION
In this qualitative study of a curricular activity designed to build medical students’ skills for interacting with patients toward reducing health disparities, we explored medical student reflections on real and simulated patient care encounters related to vaccine hesitancy, mistrust and personal bias, with the overall goal of informing medical student education. This allowed for evaluation of the utility of this curriculum framework, as well as highlighting gaps in medical curriculum around addressing vaccine hesitancy. Our analysis supports that medical student reflections across the areas of vaccine hesitancy, mistrust and personal bias share thematic structure and implications for informing medical curriculum regarding encounters with patients who resist medical advice, as well as recommendations for teaching approaches to communication with patients and parents who express hesitancy about vaccines.
This study highlights the benefits of reflections on simulated clinical encounters in the context of a Skills to Impact Health Disparities course. Reflections in the context of simulated encounters and discussion were successful in encouraging students assess their preparedness for vaccine discussions with patients. Review of written reflections, like those analysed in this study, can assist educators in identifying missing educational frameworks for particular patient care scenarios such as vaccine hesitancy. While efforts are growing to incorporate vaccine hesitancy information into medical curricula, especially now, in response to the COVID-19 pandemic (Kelekar et al., 2022; Onello et al., 2020; Real et al., 2017; Schnaith et al., 2018), there is little focus on recommending or evaluating these efforts on a large scale in the U.S. However, recent efforts to establish innovative curriculum of this kind have shown it to be feasible and effective for improving medical student preparedness in addressing vaccine hesitancy (Kelekar et al., 2022; Onello et al., 2020; Real et al., 2017; Schnaith et al., 2018). The curriculum structure assessed in this study may offer a strong approach to teach students valuable lessons related to vaccine hesitancy and evaluate existing progress in this area.
Findings from this study also highlight gaps in existing medical curriculum for preparing students to encounter hesitant patients. We found that without a structured and deliberate learning framework for addressing vaccine hesitancy, students will draw upon other skills that may not be appropriate and may be counterproductive. Students in this study often expressed feeling unprepared, aligning with prior studies (Brown et al., 2017; Kernéis et al., 2017). However, we found that using a structured framework for reflection encouraged planning future preparation for similar encounters. This included calling for system-wide changes to curriculum and availability of resources. Additionally, discussion with peers and reflection were cited as helping students to feel more prepared for future encounters with hesitant patients.
While discussion with peers as a learning strategy was widely recognized as helpful, outcomes of these discussions varied greatly and were directly related to the student’s overall reflection and plan for future preparation. This sometimes led to misguided solutions, highlighting the need for aligning education and training around similar encounters with evidence-informed recommendations. Many students referenced using an approach of centring patient views, either during the clinical encounter or after peer discussion and reflection, which aligns with recommendations (Centres for Disease Control and Prevention, 2021; Holt et al., 2016; Jarrett et al., 2015; Koski et al., 2019). However, many others referenced using only facts to correct knowledge, which is advised against in the vaccine hesitancy literature (Holt et al., 2016; Koski et al., 2019). In the context of these reflections, there would not be a space for students who came to misguided conclusions about approaching vaccine hesitancy to have this knowledge corrected based on recommended practices. Additional support and curriculum around vaccine hesitancy should be implemented alongside this framework of practice, peer discussion and reflection.
Previous research has shown that written reflections provide an effective tool for students to acknowledge their biases and the potential impact on patient care, as was seen in this study (Ross & Lypson, 2014). Physician biases related to perceptions of patient education, lifestyle, and identity have been documented and found to impact patient care and rapport (Forhan & Salas, 2013; Franz et al., 2021; Verbrugge & Steiner, 1981; Walls et al., 2015). There are concerns of physicians’ dismissal of patients expressing vaccine hesitancy from their care and physicians’ beliefs that patient hesitancy is due to lack of reliable information (Hough-Telford et al., 2016). Physician frustration may contribute to lack of willingness to bridge communication with hesitant patients; this has been seen even at the student-level, in this study and in previous research (Koski et al., 2018). Preparing students for these types of encounters by promoting reflection on frustrations and biases is important for addressing vaccine hesitancy.
Limitations of this study include that data were collected from a single institution. However, detailed, written reflections allowed for in-depth thematic analysis that may transfer to medical students more broadly. Additionally, reflections were from a course required for all medical students at the institution from cohorts over three years. Students’ reflections were written in 2014-2016, prior to the COVID-19 pandemic. However, vaccine hesitancy is an even more relevant topic now and reasons for vaccine hesitancy as well as strategies for addressing it are largely unchanged (Centres for Disease Control and Prevention, 2021). Indeed, vaccine hesitancy to the COVID-19 vaccine highlights the need for deliberate curricular efforts. Another limitation is that our sample only includes students who chose to discuss vaccine hesitancy, mistrust and bias in their reflections. However, this allowed us to analyse a fairly large sample of student reflections for a qualitative study, aiding in robust thematic saturation and providing insights that are relevant beyond vaccine hesitancy cases.
V. CONCLUSION
There are several meaningful implications of this study for medical education. Our findings illustrate benefits of learner reflection to build insights about communicating and building relationships to address vaccine hesitancy in medical education. Students found encounters with vaccine hesitant patients challenging, in part due to lack of preparedness, highlighting a gap in curriculum. Findings demonstrate varied familiarity with existing recommendations for addressing vaccine hesitancy, emphasizing the need to incorporate specific training into medical curriculum regarding specific skills gaps such as with communication. By focusing on mistrust and personal bias beyond vaccine hesitancy-specific cases, medical curriculum can better prepare students to approach these underlying issues with vaccine hesitant patients and patients expressing hesitancy to other medical recommendations in their future clinical practice. Finally, comprehensive efforts to improve vaccine hesitancy preparedness amongst learners are needed in our current climate of medical mistrust, given the prominence of vaccine hesitancy not just in paediatrics but also throughout clinical care in the context of the current COVID-19 pandemic. To improve vaccine confidence and decrease mistrust in the physician-patient relationship, medical educators must address medical student preparedness for encounters with vaccine-hesitant patients and parents through intentional learning strategies incorporated into medical school curriculum. We recommend that medical schools explore incorporating simulated patient encounters or role-play scenarios with structured reflection and discussion activities in response to encounters with hesitant patients, alongside didactic curriculum on evidence-based vaccine communication strategies, as research continues to evaluate best practices for preparing medical students to encounter vaccine hesitancy.
Notes on Contributors
Marina C. Jenkins BA was involved in the conceptual development of this qualitative analysis; analysis of reflective writings for development of themes; writing of introduction, results, methods and discussion and editing all sections and final approval of the manuscript.
Caroline R. Paul MD was involved in the original curriculum, the original sorting process of student reflective writing; the conceptual development of this qualitative analysis; analysis of reflective writings for development of themes; writing of results section and editing of all sections and final approval of the manuscript.
Shobhina Chheda MD MPH was involved in the original curriculum, the original sorting process of student reflective writing; analysis of reflective writings for development of themes; writing of results section and editing of all sections and final approval of the manuscript.
Janice L. Hanson PhD EdS MH was lead in the conceptual development of this qualitative analysis and organization of qualitative data; analysis of reflective writing; writing of results; writing of methods; and primary mentor to first author on writing of introduction and discussion; editing of all sections and final approval.
Ethical Approval
This study received exemption status from the Institutional Review Boards from the University of Wisconsin-Madison and the Washington University in St. Louis.
Data Availability
We do not have IRB permission to share our data in a data repository. The data are essays written by medical students during a required university course. While the essays are de-identified, it could be possible for someone who wrote an essay or participated in discussion groups with those who wrote the essays to identify an individual who wrote an essay.
Acknowledgement
We would like to acknowledge Andrea Maser, MS for her assistance in de-identifying student reflections and organization of student reflections from various student cohorts.
We would like to acknowledge Roberta Rusch, MPH for assistance in the original sorting of student reflections.
Funding
There is no funding source for this study.
Declaration of Interest
The authors have no conflicts of interest to disclose.
References
Aronson, L., Kruidering, M., Niehaus, B., & O’Sullivan, P. (2012). UCSF LEaP (Learning from your experiences as a professional): guidelines for critical reflection. MedEdPORTAL, 8, 9073. https://doi.org/10.15766/mep_2374-8265.9073
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101. https://doi.org/10.1191/1478088706qp063oa
Broniatowski, D. A., Jamison, A. M., Qi, S. H., AlKulaib, L., Chen, T., Benton, A., Quinn, S. C., & Dredze, M. (2018). Weaponized health communication: Twitter bots and russian trolls amplify the vaccine debate. American Journal of Public Health, 108(10), 1378-1384. https://doi.org/10.2105/ajph.2018.304567
Brown, A. E. C., Suryadevara, M., Welch, T. R., & Botash, A. S. (2017). “Being persistent without being pushy”: Student reflections on vaccine hesitancy. Narrative Inquiry in Bioethics, 7(1), 59-70. https://doi.org/10.1353/nib.2017.0018
Centres for Disease Control and Prevention. (2021). COVID-19 vaccination field guide: 12 strategies for your community. United States Department of Health and Human Services. https://www.cdc.gov/vaccines/covid-19/downloads/vaccination-strategies.pdf.
Dempsey, A. F., Pyrznawoski, J., Lockhart, S., Barnard, J., Campagna, E. J., Garrett, K., Fisher, A., Dickinson, L. M., & O’Leary, S. T. (2018). Effect of a health care professional communication training intervention on adolescent human papillomavirus vaccination: A cluster randomized clinical trial. JAMA Pediatrics, 172(5), e180016. https://doi.org/10.1001/jamapediatrics.2018.0016
Forhan, M., & Salas, X. R. (2013). Inequities in healthcare: A review of bias and discrimination in obesity treatment. Canadian Journal of Diabetes, 37(3), 205-209. https://doi.org/10.1016/j.jcjd.2013.03.362
Franz, B., Dhanani, L. Y., & Miller, W. C. (2021). Rural-urban differences in physician bias toward patients with opioid use disorder. Psychiatric services, 72(8), 874-879. https://doi.org/10.1176/appi.ps.202000529
Gagneur, A., Gosselin, V., & Dubé, È. (2018). Motivational interviewing: A promising tool to address vaccine hesitancy. Vaccine, 36(44), 6553-6555. https://doi.org/10.1016/j.vaccine.2017.10.049
Goldenberg, M. J. (2016). Public misunderstanding of science? Reframing the problem of vaccine hesitancy. Perspectives on Science, 24(5), 552-581. https://doi-org/10.1162/POSC_a_00223
Hamel, L., Sparks, G., Lopes, L., Stokes, M., & Brodie, M. (2022). KFF COVID-19 Vaccine Monitor: January 2022 Parents And Kids Update. K. F. Foundation. https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-january-2022-parents-and-kids-update/
Hara, N., & Sanfilippo, M. R. (2016). Co-constructing controversy: Content analysis of collaborative knowledge negotiation in online communities. Information Communication & Society, 19(11), 1587-1604. https://doi.org/10.1080/1369118x.2016.1142595
He, K., Mack, W. J., Neely, M., Lewis, L., & Anand, V. (2022). Parental perspectives on immunizations: Impact of the COVID-19 pandemic on childhood vaccine hesitancy. Journal of Community Health, 47(1), 39-52. https://doi.org/10.1007/s10900-021-01017-9
Hofstetter, A. M., Robinson, J. D., Lepere, K., Cunningham, M., Etsekson, N., & Opel, D. J. (2017). Clinician-parent discussions about influenza vaccination of children and their association with vaccine acceptance. Vaccine, 35(20), 2709-2715. https://doi.org/10.1016/j.vaccine.2017.03.077
Holt, D., Bouder, F., Elemuwa, C., Gaedicke, G., Khamesipour, A., Kisler, B., Kochhar, S., Kutalek, R., Maurer, W., Obermeier, P., & Seeber, L. (2016). The importance of the patient voice in vaccination and vaccine safety—Are we listening? Clinical Microbiology and Infection, 22, S146-S153. https://doi.org/10.1016/j.cmi.2016.09.027
Hough-Telford, C., Kimberlin, D. W., Aban, I., Hitchcock, W. P., Almquist, J., Kratz, R., & O’Connor, K. G. (2016). Vaccine delays, refusals, and patient dismissals: A survey of pediatricians. Pediatrics, 138(3), 9, Article e20162127.https://doi.org/10.1542/peds.2016-2127
Jarrett, C., Wilson, R., O’Leary, M., Eckersberger, E., & Larson, H. J. (2015). Strategies for addressing vaccine hesitancy–A systematic review. Vaccine, 33(34), 4180-4190. https://doi.org/10.1016/j.vaccine.2015.04.040
Jenkins, M. C., & Moreno, M. A. (2020). Vaccination discussion among parents on social media: A content analysis of comments on parenting blogs. Journal of Health Communication, 25(3), 232-242. https://doi.org/10.1080/10810730.2020.1737761
Karras, J., Dubé, E., Danchin, M., Kaufman, J., & Seale, H. (2019). A scoping review examining the availability of dialogue-based resources to support healthcare providers engagement with vaccine hesitant individuals. Vaccine, 37(44), 6594-6600. https://doi.org/10.1016/j.vaccine.2019.09.039
Kelekar, A., Rubino, I., Kavanagh, M., Lewis-Bedz, R., LeClerc, G., Pedell, L., & Afonso, N. (2022). Vaccine hesitancy counseling—an educational intervention to teach a critical skill to preclinical medical students. Medical Science Educator, 32(1), 141-147. https://doi.org/10.1007/s40670-021-01495-5
Kempe, A., Saville, A. W., Albertin, C., Zimet, G., Breck, A., Helmkamp, L., Vangala, S., Dickinson, L. M., Rand, C., & Humiston, S. (2020). Parental hesitancy about routine childhood and influenza vaccinations: A national survey. Pediatrics, 146(1). https://doi.org/10.1542/peds.2019-3852
Kennedy, A., LaVail, K., Nowak, G., Basket, M., & Landry, S. (2011). Confidence about vaccines in the United States: Understanding parents’ perceptions. Health Affairs, 30(6), 1151-1159. https://doi.org/10.1377/hltaff.2011.0396
Kernéis, S., Jacquet, C., Bannay, A., May, T., Launay, O., Verger, P., Pulcini, C., Abgueguen, P., Ansart, S., Bani-Sadr, F., Bannay, A., Bernard, L., Botelho-Nevers, E., Boutoille, D., Cassir, N., Cazanave, C., Demonchy, E., Epaulard, O., Etienne, M., & Wyplosz, B. (2017). Vaccine education of medical students: A nationwide cross-sectional survey. American Journal of Preventive Medicine, 53(3), e97-e104. https://doi.org/10.1016/j.amepre.2017.01.014
Koski, K., Lehto, J. T., & Hakkarainen, K. (2018). Simulated encounters with vaccine-hesitant parents: Arts-based video scenario and a writing exercise. Journal of Medical Education and Curricular Development, 5, 2382120518790257. https://doi.org/10.1177/2382120518790257
Koski, K., Lehto, J. T., & Hakkarainen, K. (2019). Physician self-disclosure and vaccine-critical parents׳ trust: Preparing medical students for parents׳ difficult questions. Health Professions Education, 5(3), 253-258. https://doi.org/10.1016/j.hpe.2018.09.005
Larson, H. J. (2016). Vaccine trust and the limits of information. Science, 353(6305), 1207-1208. https://doi.org/10.1126/science.aah6190
Lucia, V. C., Kelekar, A., & Afonso, N. M. (2021). COVID-19 vaccine hesitancy among medical students. Journal of Public Health, 43(3), 445-449. https://doi.org/10.1093/pubmed/fdaa230
Meleo-Erwin, Z., Basch, C., MacLean, S. A., Scheibner, C., & Cadorett, V. (2017). “To each his own”: Discussions of vaccine decision-making in top parenting blogs. Human Vaccines & Immunotherapeutics, 13(8), 1895-1901. https://doi.org/10.1080/21645515.2017.1321182
Ognyanova, K., Lazer, D., Baum, M., Perlis, R. H., Druckman, J., Santillana, M., Qu, H., Trujillo, K. L., Safarpour, A., Uslu, A., Quintana, A., Green, J., Pippert, C. H., & Shere, A. (2022). The COVID States Project# 82: COVID-19 vaccine misinformation trends, awareness of expert consensus, and trust in social institutions. Open Science Framework. https://doi.org/10.31219/osf.io/9ua2x
Onello, E., Friedrichsen, S., Krafts, K., Simmons, G., Jr., & Diebel, K. (2020). First year allopathic medical student attitudes about vaccination and vaccine hesitancy. Vaccine, 38(4), 808-814. https://doi.org/10.1016/j.vaccine.2019.10.094
Real, F. J., DeBlasio, D., Beck, A. F., Ollberding, N. J., Davis, D., Cruse, B., Samaan, Z., McLinden, D., & Klein, M. D. (2017). A virtual reality curriculum for pediatric residents decreases rates of influenza vaccine refusal. Academic Pediatrics, 17(4), 431-435. https://doi.org/10.1016/j.acap.2017.01.01
Ross, P. T., & Lypson, M. L. (2014). Using artistic-narrative to stimulate reflection on physician bias. Teaching and Learning in Medicine, 26(4), 344-349. https://doi.org/10.1080/10401334.2014.945032
Santibanez, T. A., Nguyen, K. H., Greby, S. M., Fisher, A., Scanlon, P., Bhatt, A., Srivastav, A., & Singleton, J. A. (2020). Parental vaccine hesitancy and childhood influenza vaccination. Pediatrics, 146(6), Article e2020007609. https://doi.org/10.1542/peds.2020-007609
Schnaith, A. M., Evans, E. M., Vogt, C., Tinsay, A. M., Schmidt, T. E., Tessier, K. M., & Erickson, B. K. (2018). An innovative medical school curriculum to address human papillomavirus vaccine hesitancy. Vaccine, 36(26), 3830-3835. https://doi.org/10.1016/j.vaccine.2018.05.014
Verbrugge, L. M., & Steiner, R. P. (1981). Physician treatment of men and women patients: Sex bias or appropriate care? Medical Care, 19(6), 609-632. https://doi.org/10.1097/00005650-198106000-00005
Walls, M. L., Gonzalez, J., Gladney, T., & Onello, E. (2015). Unconscious biases: Racial microaggressions in American Indian health care. The Journal of the American Board of Family Medicine, 28(2), 231-239. https://doi.org/10.3122/jabfm.2015.02.140194
*Marina C. Jenkins
Department of Paediatrics
University of Wisconsin-Madison
2870 University Ave., Suite 200
Madison, WI 53703
Email address: mcjenkins@wisc.edu
Submitted: 11 March 2022
Accepted: 28 June 2022
Published online: 4 April, TAPS 2023, 8(2), 14-35
https://doi.org/10.29060/TAPS.2023-8-2/OA2762
Sayaka Oikawa1, Ruri Ashida2 & Satoshi Takeda3
1Center for Medical Education and Career Development, Fukushima Medical University, Fukushima, Japan; 2Center for International Education and Research, Tokyo Medical University, Tokyo, Japan; 3Department of Emergency Medicine, The Jikei University School of Medicine, Tokyo, Japan
Abstract
Introduction: There are various difficulties in treating foreign patients; however, the existing educational programs are still insufficient for addressing this issue. The purpose of this study is to investigate what difficulties are encountered in the treatment of foreigners in emergency departments, and to create scenarios for simulation-based education using real-life cases.
Methods: A cross-sectional anonymous survey to 457 emergency departments was conducted in 2018. Additionally, we conducted a survey of 46 foreign residents who had visited hospitals for treatment in Japan. The data was analysed quantitatively, and the narrative responses were thematically analysed.
Results: Of the 141 hospitals that responded (response rate: 30.9%), 136 (96.5%) answered that they had treated foreign patients. There were 51 and 66 cases with cultural and linguistic difficulties, respectively. In the qualitative analysis, different ideas/beliefs towards treatments or examinations (51.0%) and communication with non-English speaking patients (65.2%) were most common categories in the cases with cultural and linguistic difficulties, respectively. The survey of 46 foreign residents on the surprising aspects of Japanese healthcare showed, 14% mentioned difference in treatment plans between own country and Japan, 12% each mentioned a lack of explanation by medical staff, and a lack of privacy in the examination room. Based on the survey results, we created 2 scenarios of simulation.
Conclusions: Scenarios of simulation-based education using real-life cases may be effective materials for cultivating cultural awareness of medical staff.
Keywords: Cultural Awareness, Cultural Humility, Emergency Department, Foreign Patients, Simulation-based Education
I. INTRODUCTION
According to the Japan Tourism Agency (JTA), the number of foreign visitors to Japan was increasing every year in the midst of the recent rapid globalisation (Japan Tourism Agency, 2021). Although it is currently on the decline due to COVID-19 infection, a survey of foreign visitors to Japan conducted by the JTA in 2018 revealed that 5% of 3,000 visitors had suffered injuries or illnesses while visiting Japan (Japan Tourism Agency, 2019). When visiting a medical institution in an unfamiliar country, patients have anxiety due to language and cultural differences. Various measures are being taken around the world to prevent patients with different cultural backgrounds from being disadvantaged in medical care (NHS England, 2016; Office of Disease Prevention and Health Promotion, 2021), such as training medical staff to recognise factors impeding cultural awareness (Hobgood et al., 2006).
Due to its nature, prompt treatment is required in emergency departments (EDs). Previous reports showed that among 97 EDs in Japan, 84 had some difficulties in treating foreign patients (Kubo et al., 2014), and medical staff faced complex cultural and social problems with foreign patients (Osegawa et al., 2002). According to the reports of Japanese government, health care institutions in Japan organise English conversation training or lectures on cultural differences by foreign lecturers for medical staff to improve treatment of foreign patients (Japan Ministry of Economy, Trade and Industry, 2019; Japan Ministry of Health, Labour and Welfare, 2021). However, a training for cultivating cultural awareness among medical staff who take care of foreign patients is still insufficient (Osegawa et al., 2002; Serizawa, 2007).
Simulation-based education (SBE) is a practical learning method which enables mastery learning (Kelly et al., 2018; Motola et al., 2013), and in Japan, English-speaking simulated patients are increasingly introduced in medical education (Ashida & Otaki, 2022). Simulated patients enhance reflective learning which improves cultural awareness of learners (Leake et al., 2010; Paroz et al., 2016). However, according to a survey of emergency training programs, less than 10% of the programs used SBE as a training method for cultivating cultural awareness (Mechanic et al., 2017).
The purposes of this study were to investigate what difficulties are encountered in the treatment of foreigners in EDs, and to create scenarios of SBE using real-life cases.
II. METHODS
In January 2018, we sent a questionnaire to 457 EDs of residency training hospitals in the top 10 prefectures with the highest number of foreign visitors, Hokkaido, Chiba, Tokyo, Kanagawa, Shizuoka, Aichi, Kyoto, Osaka, Fukuoka, and Okinawa (Japan Tourism Agency, 2016), by postal mail. In an anonymous survey, we asked about the hospital readiness for treating foreign patients and about difficult cases of foreign patients with linguistic or cultural differences in medical care (Appendix 1). The questions about readiness on treating foreign patients were analysed by simple percentages, and descriptive statistics were used for the questions about number of patients visiting ED per day. The narrative responses were collated and thematic analysis was performed. First, two authors created codes, generated several categories based on the codes, and sorted each case into categories independently as an investigator triangulation. Following that, we merged categories that were similar and revised categories that were different in interpretation through discussion. We repeated the member checking until we built our consensus, and the final categorisation was confirmed by all authors. The number of cases in each category was also calculated.
As a sub study, we also conducted a survey of 46 foreigners who were residing in Japan and had visited the hospital for treatment in Japan (hereafter foreign residents) to find patients’ perspectives on medical care in Japan (Appendix 2). The questionnaire was initially sent to those who were recruited by the authors via email using Google form from January to May in 2018, and data were collected by snowball sampling. The data were analysed by simple percentages, and for narrative responses, we created codes and sorted the responses into categories. The number of responses in each category was also calculated. Both questionnaires stated that the participants’ responses would be considered as their consent to the study, and the answers would be used anonymously for educational research.
Following the survey analysis, we selected cases suitable for scenario creation from an educational perspective with focus on the following points: 1) cases which were noted by multiple facilities, 2) difficulties that can be demonstrated by simulated patients; and 3) cases which had teaching points for multiple professions. The scenarios were composed following the Scenario Folder Sections by Seropian (2003) and included case description, manual for simulated patients, and teaching guide for the instructors. The scenarios were reviewed by an experienced medical English communication teacher from a linguistic and cultural standpoint, and by 2 experienced emergency medicine physicians from a medical standpoint. All 3 experts co-reviewed the final scenarios.
III. RESULTS
A. Survey of the EDs
1) Characteristics of the responding EDs: We received responses to the questionnaire from 141 EDs (response rate: 30.9%). Of these, 136 (96.5%) answered that they had accepted foreign patients, 116 (82.3%) had English-speaking staff, and 76 (53.9%) used translation tools or manuals. On the other hand, only 13 (9.2%) answered that they had a full-time English interpreter, and 27 (19.1%) had a website in English. The median number of overall outpatients visiting the ED per day was 30 (1–135), and the median number of foreign patients visiting the ED per day was 0.5 (0–8.3) (Table 1). As for translation method, a variety of methods were used. Of the 76 EDs, 36 (47.4%) answered that they used translation applications on tablet/PC or smartphone (Appendix 3).
|
Total Responded Hospitals |
141 |
|
|
|
|
Readiness on treating foreign patients |
n |
( % ) |
||
|
Have accepted foreign patients |
136 |
( |
96.5 |
) |
|
Have an English-speaking staff |
116 |
( |
82.3 |
) |
|
Use translation tools or manuals |
76 |
( |
53.9 |
) |
|
Have English medical history forms |
52 |
( |
36.9 |
) |
|
Have English medical certificates |
50 |
( |
35.5 |
) |
|
Have English signs for patients |
46 |
( |
32.6 |
) |
|
Have English medical explanation / consent forms |
27 |
( |
19.1 |
) |
|
Have a hospital website in English |
27 |
( |
19.1 |
) |
|
Have a full-time English interpreter |
13 |
( |
9.2 |
) |
|
No. of patients visiting emergency department per day |
Median |
|
Range |
|
|
Total |
30 |
( |
1-135 |
) |
|
Foreign patients |
0.5 |
( |
0-8.3 |
) |
Table 1: Characteristics of the responding hospitals.
2) Cases with cultural / linguistic difficulties: Cultural difficulties were encountered in 51 cases, and linguistic difficulties were encountered in 66 cases. In the thematic analysis, the cultural difficulties were classified into 4 categories: different ideas/beliefs towards treatments or examinations, medical fees, patients’ lifestyle, and others. The linguistic difficulties were classified into 4 categories: communication with non-English-speaking patients, communication with English-speaking patients, communication with interpreters or using translation tools, and others. Different ideas/beliefs towards treatments or examinations (51.0%), and communication with non-English-speaking patients (65.2%) were the most common, respectively. Case examples in each category and how the hospital handled to the cases are shown in Table 2.
|
Cases with cultural difficulties (51 cases) |
|||
|
Categories |
n (%) |
Examples and ways they were handled |
|
|
1 |
Different ideas/beliefs towards treatments or examinations |
26 (51.0) |
The patient’s husband requested that only female medical staff be allowed to examine the patient. -Initially, the doctor in charge was a male, but he was switched to a female doctor. |
|
2 |
Medical fees |
10 (19.6) |
The patient’s credit card was over its limit and he/she could not pay for the hospitalisation. -They asked the embassy of his/her country to handle the international money transfer.
|
|
3
|
Patients’ lifestyle
|
7 (13.7)
|
The patient complained about the predominantly rice-based diet during his/her hospitalisation. -They changed his/her diet to the bread-based one during the hospitalisation. |
|
4 |
Others |
8 (15.7) |
The patient had a low threshold for pain and was very assertive about the pain. -They confirmed that the complaint was due to pain and prescribed adequate painkillers.
|
|
Cases with linguistic difficulties (66 cases) |
|||
|
Categories |
n (%) |
Examples and ways they were handled |
|
|
1 |
Communication with non-English-speaking patients |
43 (65.2) |
The medical staff could not communicate with the patient in either English or Japanese. -They used a translation tool to communicate. |
|
2 |
Communication with English-speaking patients |
10 (15.2) |
The medical staff could understand ordinary conversation, but it was difficult for them to explain medical terms in English. -The English-speaking staff helped them. |
|
3 |
Communication with interpreters or translation tools |
9 (13.6) |
The patient brought in an interpreter, but it was unclear if the interpreter was able to understand the details. -They asked an interpreter to support. |
|
4 |
Others |
4 (6.1) |
The patient asked to provide a medical certificate in his/her native language. -They could not provide a medical certificate in the patient’s native language, so we provided one in English. |
Table 2: Categories of cultural and linguistic difficulties, their examples and ways handled
B. A Survey of the Foreign Residents
As regards the questionnaire sent to the foreign residents, we received 46 responses. Of those, 11 (23.9%) had lived in Japan for more than 30 years. In the multiple-answer questions regarding the reasons for visiting the hospital, 11 (8.2%) answered acute illness treated in the ED (The demographic data of foreigners responded to the survey is shown in Appendix 4). In terms of interpretation in the hospital, 10 (21.7%) answered that they have had some means of interpretation. For the question “What aspects of your medical care in Japan were most surprising or different from those in your country?”, of a total of 50 responses with multiple answers, 7 (14%) answered “difference in treatment plans between own country and Japan ” while 6 respondents (12%) each answered “a lack of explanation by medical staff” and “a lack of privacy in the examination room” (Table 3).
|
Questions about the medical care/staff |
Answer |
No. (%) in total respondents |
|||||
|
Q1 |
Did you have any means of interpretation in the hospital? |
Yes |
10 (21.7) |
||||
|
No |
36 (78.3) |
||||||
|
Q2 |
Could you tell the doctor/nurse about your concerns in history taking? |
Yes |
27 (58.7) |
||||
|
Somewhat |
18 (39.1) |
||||||
|
No |
1 (2.2) |
||||||
|
|
|||||||
|
Q3 |
Did you feel the doctor/nurse really cared for your ideas and culture during the history taking? |
Yes |
23 (50.0) |
||||
|
Somewhat |
17 (37.0) |
||||||
|
No |
6 (13.0) |
||||||
|
Q4 |
Did you feel that you were sincerely cared for during the physical exam? |
Yes |
29 (63.0) |
||||
|
Somewhat |
16 (34.8) |
||||||
|
No |
1 (2.2) |
||||||
|
Q5 |
Could you tell the doctor/nurse about your true concerns about treatment? |
Yes |
29 (63.0) |
||||
|
Somewhat |
12 (26.1) |
||||||
|
No |
5 (10.9) |
||||||
|
Q6 |
Did the doctor/nurse explain the diagnosis and treatment plan clearly? |
Yes |
29 (63.0) |
||||
|
Somewhat |
12 (26.1) |
||||||
|
No |
5 (10.9) |
||||||
|
|
|
|
|||||
|
Q7 |
Were you satisfied with the medical care you received? |
Yes |
32 (69.6) |
||||
|
Somewhat |
12 (26.1) |
||||||
|
No |
2 (4.3) |
||||||
|
Questions about surprising points |
|||||||
|
Q8 |
What aspects of your medical care in Japan was most surprising or different from your country? |
Top 3 Answers |
No. (%) |
||||
|
|
Different treatment plan |
7 (14.0) |
|||||
|
|
Lack of explanation by medical staffs |
6 (12.0) |
|||||
|
|
No privacy in the examination room |
6 (12.0) |
|||||
Table 3: Result of the survey of foreign residents
C. Scenario Development
Based on the survey results, we decided the main topic of the scenarios based on the contents overlapped in multiple cases. “Gender restriction of doctors who treated patients” and “communication difficulty in languages other than Japanese or English” were the most frequent topics in cultural and linguistic difficulties respectively. Following the selection of topics, we synthesised the similar responses to create a scenario that could occur in any size of ED setting. We developed the settings including patient age, sex, language, and backgrounds, regarding that the patient characteristics can be demonstrated by simulated patients. As a result, we developed two scenarios: a scenario of abdominal pain in a Muslim female patient and a scenario of forearm fracture in a Chinese male patient (Appendices 5 and 6). In the abdominal pain scenario, no female doctor was available, and a learner, a male doctor, had to examine and treat a simulated patient who refused to be seen by a male doctor. In the forearm fracture scenario, no interpreter was available, and a learner had to communicate with a simulated patient who spoke Chinese only. The learning objective for the learners was to communicate appropriately with patients with different cultural and linguistic backgrounds. Based on the results of the survey for foreign residents, we indicated the importance of listening to the patient’s concerns carefully as a teaching point. Also, we reflected the survey results of how each hospital handled the cases on the information for instructors and teaching points.
IV. DISCUSSION
At the time of writing this paper, 96.5% of the EDs had accepted foreign patients; and 82.3% had English-speaking staff. However, only 32.6% of the EDs had multilingual signs for patients, which is listed as actions to be taken in the manual for treating foreign patients (Japan Ministry of Health, Labour and Welfare, 2021).
In the present study, most of the EDs used translation tools when treating foreign patients. Various types of translation methods were found to be used in the EDs, the use of which is consistent with the manual for treating foreign patients (Japan Ministry of Health, Labour and Welfare, 2021). However, we found that the EDs still encountered a significant number of cases with linguistic difficulties. This suggests that even though the EDs own the translation tools, medical staff are not able to utilise them in communicating with foreign patients. According to our survey result, it was revealed that more than half of the cases with linguistic difficulties were of non-English speaking patients. To overcome the linguistic difficulties, medical staff need to be capable of using them enough to communicate with patients of various native languages. In addition to the use of translation tools, multilingual medical explanation/consent forms or signs in hospitals may be effectively used in the aim of communication with foreign patients.
Regarding culturally difficult cases, our survey showed the various issues caused by differences of religious background, lifestyles, and ideas and beliefs on treatment and testing between medical staff and patients. This result is consistent with the reports which elaborated difficulties in treating foreign patients in Japan (Tatsumi et al., 2016). Our study showed that different ideas/beliefs towards treatments or examinations was most common theme in the cases with cultural difficulties in EDs. Knowing beliefs of other culture is one of individual’s capabilities to manage effectively in culturally diverse settings (Ang et al., 2007), and a report on psychiatric hospitals showed that medical staff adapted to hospitalised foreign patients’ culture and religion as they built the relationships with the patients over a long period of time (Kobayashi et al., 2014). Whereas, it is difficult to build relationships with foreign patients in the acute ED setting. Thus, we realised that practical training of communication with foreign patients provide knowledge about their cultures and religions in limited time and is critically important for medical staff in EDs.
SBE is an effective educational format which makes learners’ unconscious incompetence to conscious incompetence (Morell et al., 2002), in other words, medical staff may be able to recognise their unconscious biases towards foreign patients by participating in SBE. As consistent with the previous survey by the MHLW (2021), the culturally difficult cases included complicated issues that require the cooperation of administrative staff and full-time English interpreters in the hospital. In the present study, we created the two scenarios targeting medical staff as learners based on the real-life cases with the many responses in the survey. However, we need to create more varieties of scenarios that can involve other professions than health care professionals. Furthermore, the acquisition and retention of learners’ skills in a single training session of SBE is limited (Legoux et al., 2021). SBE aimed at cultivating cultural awareness cannot be completed in a single session but in continuous sessions with multiple scenarios.
The results of our survey of foreign residents showed that they had been surprised at the differences in treatment plans between their country and Japan, a lack of explanation by medical staff, and a lack of privacy in the examination room. We found that it is important to investigate the opinions of those who receive medical care in a country different from their home because their perspectives allow us to recognise the things taken for granted among medical staff. Medical staff’s unconscious biases about patients of different cultural backgrounds or national origins influence their decision-making (Tervalon & Murray-Garcia, 1998), and implicit bias can contribute to miscommunication (Bartlett et al., 2019). Therefore, listening to the concerns of foreign patients is important in order to avoid providing treatment based solely on medical staff’s biases. Furthermore, in creating scenarios, referring to the survey results of multiple stakeholders made the contents more multi-dimensional and relevant. This study was conducted in the contexts of EDs in Japan, however, scenarios created with perspectives of both medical staff and patients who have various cultural backgrounds may effectively address to the real-life problems triggered by unconscious biases, even in other contexts.
In Emergency situations, we often focus on the patients’ cultural backgrounds, national origins, languages, and religious background in order to provide effective treatments. However, recognising our own bias is not achieved by only focusing on the patients’ culture. Self-reflection is necessary to recognise one’s own cultural biases. The process of self-reflection of our own culture is important for cultivating cultural awareness. Furthermore, the importance of cultural humility – discovering one’s own values toward other cultures through continuous self-reflection and becoming aware of one’s own relationship to the world – has been recently noted in medical education (Chang et al., 2012). As a further research, the development of scenarios that include the study guide which ensure the learners’ self-reflection is required for SBE in emergency settings.
There are several limitations in this study. The response rate of a survey for EDs was 30.9%, which is unable to deny sampling bias. We conducted a survey for EDs with a focus on English, however, it is necessary to conduct surveys on languages other than English. In addition, the survey was only for the EDs of training hospitals in the top 10 prefectures with the most foreign tourists. We may consider expanding the number of hospitals to collect more information about difficulties they encounter in treating foreign patients. For the sub study, the snowball sampling had a methodological limitation in calculating total number the survey sent. As a further research, impacts of SBE using these scenarios on the treatment of foreign patients is less clear. To assess whether foreign patients’ satisfaction of medical care will change, and whether unconscious bias towards foreign patients among medical staff will decrease by conducting these scenarios are necessary.
V. CONCLUSION
In the current study, we were able to clarify linguistic and cultural difficulties in treating foreign patients in the EDs. We developed the scenarios for SBE using the real-life difficult cases of foreign patients with linguistic or cultural differences in medical care in Japan. The simulation training using these scenarios may be useful for promoting cultural awareness of medical staff in EDs. In future, more varieties of scenarios of SBE need to be created and shared in order to treat foreign patients safely and adequately.
Notes on Contributors
SO contributed to the design of the study and conducted data collection and analysis. RA devised the project, the main conceptual ideas, and conducted data collection and analysis. ST contributed to the design of the study and the interpretation of the data.
Ethical Approval
This study was approved by the Institutional Review Board of The Jikei University School of Medicine Japan (Approval No. 28-211(8454), 28-276(8519)). An informed consent was obtained from all the participants responded to the survey.
Data Availability
The data that support the findings of this study are not openly available due to privacy. The materials are available from the corresponding author on reasonable request.
Acknowledgement
The authors would like to acknowledge the respondents at the EDs of training hospitals, the foreigners living in Japan, and the young clinicians at The Jikei University School of Medicine for their cooperation in the study.
Funding
This work has been supported by JSPS KAKENHI, grant number 16K08883.
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content of the article.
References
Ang, S., Van Dyne, L., Koh, C., Ng, K. Y., Templer, K. J., Tay, C., & Chandrasekar, N. A. (2007). Cultural intelligence: Its measurement and effects on cultural judgment and decision making, cultural adaptation and task performance. Management and Organization Review, 3(3), 335-371. https://doi.org/10.1111/j.1740-8784.2007.00082.x
Ashida, R., & Otaki, J. (2022). Survey of Japanese medical schools on involvement of English-speaking simulated patients to improve students’ patient communication skills. Teaching and Learning in Medicine, 34(1), 13-20. https://doi.org/10.1080/10401334.2021.1915789
Bartlett, K., Strelitz, P., Hawley, J., Sloane, R., & Staples, B. (2019). Explicitly addressing implicit bias in a cultural competence curriculum for pediatric trainees. MedEdPublish, 8. https://doi.org/10.15694/mep.2019.000102.1
Chang, E. S., Simon, M., & Dong, X. (2012). Integrating cultural humility into health care professional education and training. Advances in Health Sciences Education, 17(2), 269–278. https://doi.org/10.1007/s10459-010-9264-1
Hobgood, C., Sawning, S., Bowen, J., & Savage, K. (2006). Teaching culturally appropriate care: a review of educational models and methods. Academic Emergency Medicine, 13(12), 1288-1295. https://doi.org/10.1197/j.aem.2006.07.031
Japan Ministry of Economy, Trade and Industry. (2019, January). Kokunai iryokikan ni okeru gaikokujin kanja no ukeire jittai chosa [Survey on the actual conditions of foreign patients accepted at domestic medical institutions in Japan]. https://www.meti.go.jp/policy/mono_info_service/healthcare/iryou/inbound/activity/survey_report.html
Japan Ministry of Health, Labour and Welfare. (2021, March). Gaikokujin kanja no ukeire no tameno iryokikan muke manyuaru [A manual for medical institutions to accept foreign patients]. https://www.mhlw.go.jp/content/10800000/000795505.pdf
Japan Tourism Agency. (2018, February). Shukuhakuryoko tokeichosa hokokusho [Report on the survey of accommodations and travel statistics]. Ministry of Land, Infrastructure, Transport and Tourism. https://www.mlit.go.jp/common/001220398.pdf
Japan Tourism Agency. (2019, March). Honichi gaikokujin ryokosha no iryo ni kansuru jittaichosa ukeire kankyo no seibikyoka wo okonaimashita [Conducted a survey on the actual conditions of medical care for foreign visitors to Japan and strengthened the development of the receiving environment]. Ministry of Land, Infrastructure, Transport and Tourism. https://www.mlit.go.jp/kankocho/news08_000272.html
Japan Tourism Agency. (2021, June). Shukuhakuryoko tokeichosa [Survey of accommodations and travel statistics]. Ministry of Land, Infrastructure, Transport and Tourism. https://www.mlit.go.jp/kankocho/siryou/toukei/content/001413644.pdf
Kelly, M. A., Balakrishnan, A., & Naren, K. (2018). Cultural considerations in simulation-based education. The Asia Pacific Scholar, 3(3), 1-4. https://doi.org/10.29060/TAPS.2018-3-3/GP10 70
Kobayashi, Y., Yoshimitsu, Y., & Kato, S. (2014). Super kyukyu ni okeru kangoshi no gaikokujinkanja nitaishite ninshiki suru mondai to taio no jissai [Nurses’ perceptions of and responses to foreign patients in a super emergency hospitals]. Nihon Seishinka Kango Gakujutsu Shukaishi [The Japanese Psychiatric Nursing Society], 57(3), 379 383.
Kubo, Y., Takaki, S., Nomoto, Y., Maeno, Y., & Kawaguchi, Y. (2014). Nihon no byoin ni okeru kyukyugairai deno gaikokujinkanja heno kango no genjo ni kansuru chosa. [A survey on the current status of nursing care for foreign patients in emergency departments in Japanese jospitals]. Kosei no shihyo [Journal of Health and Welfare Statistics], 61(1), 17-25.
Leake, R., Holt, K., Potter, C., & Ortega, D. M. (2010). Using simulation training to improve culturally responsive child welfare practice. Journal of Public Child Welfare, 4(3), 325-346. https://doi.org/10.1080/15548732.2010.496080
Legoux, C., Gerein, R., Boutis, K., Barrowman, N., & Plint, A. (2021). Retention of critical procedural skills after simulation training: a systematic review. AEM Education and Training, 5(3), e10536. https://doi.org/10.1002/aet2.10536
Mechanic, O. J., Dubosh, N. M., Rosen, C. L., & Landry, A. M. (2017). Cultural competency training in emergency medicine. The Journal of Emergency Medicine, 53(3), 391-396. https://doi.org/10.1016/j.jemermed.2017.04.019
Morell, V. W., Sharp, P. C., & Crandall, S. J. (2002). Creating student awareness to improve cultural competence: creating the critical incident. Medical Teacher, 24(5), 532-534. https://doi.org/10.1080/0142159021000012577
Motola, I., Devine, L. A., Chung, H. S., Sullivan, J. E., & Issenberg, S. B. (2013). Simulation in healthcare education: a best evidence practical guide. AMEE Guide No. 82. Medical Teacher, 35(10), e1511-e1530. https://doi.org/10.3109/0142159X.2013.818632
NHS England. (2016). NHS England response to the specific duties of the Equality Act. Equality information relating to public facing functions. https://www.england.nhs.uk/wp-content/uploads/2016/02/nhse-specific-duties-equality-act.pdf
Office of Disease Prevention and Health Promotion. (2021, August). Disparities. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities
Osegawa, M., Morio, H., Nomoto, K., Nishizawa, M., & Sadahiro, T. (2002). Present medical practice and problems in emergency disease in foreign travelers requiring hospital admission. Nihon Kyukyu Igakukai Zasshi [Journal of Japanese Association for Acute Medicine], 13(11), 703-710. https://doi.org/10.3893/jjaam.13.703
Paroz, S., Daele, A., Viret, F., Vadot, S., Bonvin, R., & Bodenmann, P. (2016). Cultural competence and simulated patients. The Clinical Teacher, 13(5), 369-373. https://doi.org/10.1111/tct.12466
Serizawa, A. (2007). Developing a culturally competent health care workforce in Japan: implications for education. Nursing education perspectives, 28(3), 140-144.
Seropian, M. A. (2003). General concepts in full scale simulation: getting started. Anesthesia & Analgesia, 97(6), 1695-1705. https://doi.org/10.1213/01.ane.0000090152.91261.d9
Tatsumi, Y., Sasaki-Otomaru, A., & Kanoya, Y. (2016). The actual situation and issues of emergency medical services for foreigners staying in Japan extracted by systematic review. Nihon Kenko Igakukai Zasshi [Journal of Japan Health Medicine Association], 25(2), 91-97.
Tervalon, M., & Murray-Garcia, J. (1998). Cultural humility versus cultural competence: A critical distinction in defining physician training outcomes in multicultural education. Journal of Health Care for the Poor and Underserved, 9(2), 117-125. https://doi.org/10.1353/hpu.2010.0233
*Sayaka Oikawa
Center for Medical Education and Career Development,
Fukushima Medical University,
1 Hikarigaoka, Fukushima, 960-1295, Japan
Email: sayaka9@fmu.ac.jp
Submitted: 11 February 2022
Accepted: 21 July 2022
Published online: 4 April, TAPS 2023, 8(2), 4-13
https://doi.org/10.29060/TAPS.2023-8-2/OA2755
Tri Nur Kristina1, Fatikhu Yatuni Asmara2, Sudaryanto Sudaryanto1, Nuryanto Nuryanto3 & Saekhol Bakri1
1Department of Medicine, Faculty of Medicine, Universitas Diponegoro, Indonesia; 2Department of Nursing, Faculty of Medicine, Universitas Diponegoro, Indonesia; 3Department of Nutrition, Faculty of Medicine, Universitas Diponegoro, Indonesia
Abstract
Introduction: This study aimed to examine the usefulness of Community Based-Education (CBE) and Interprofessional Education (IPE) to community health outcomes.
Methods: The design was a mixed-method study. Each small group worked together to identify family health problems, implement interventions, and evaluate the results. The Readiness for Interprofessional Learning Scale (RIPLS) questionnaire was applied to compare students’ perceptions before and after the implementation. In addition, qualitative data were acquired from students’ comments on the questionnaire, interviews with community representatives, and FGDs with instructors at the end of the program.
Results: Three hundred and sixty-seven out of 465 students returned the completed paired questionnaire (78.9 % response rate). Paired t-test showed that student perception of responsibility slightly increased, whereas teamwork and collaboration, negative and positive professional identity decreased somewhat. However, most pre-post students’ responses already trended to the positive side (scales 4 and 5). Moreover, the Chi-square test showed that pre-post students’ confidence levels significantly increased. Most small groups of students successfully empowered the community to solve health problems. Students, instructors, and representatives of community members appreciated the program. However, several students felt their instructors were not motivated to mentor their tasks, and sometimes they had difficulty conducting home visits together.
Conclusion: This study showed that the combination of CBE-IPE contributes to more favourable community health outcomes. However, it was challenging in several aspects of preparation, including highly motivated instructors. Nevertheless, pre and post-implementation students’ attitudes are still positive.
Keywords: Interprofessional Education (IPE), Community Based Education (CBE), Health Profession Students, Readiness
I. INTRODUCTION
Community-based education (CBE) programs for medical and other health professionals expose students to community health problems, in which they will work in the future as health professionals. However, the CBE program is usually implemented within a single discipline, whereas community health problems must be solved collaboratively among a health care team (Housley et al., 2018).
Interprofessional Education (IPE) has been identified as a valuable method of learning experiences to increase the collaboration and communication of health professionals in healthcare settings. Several studies have reported positive student perceptions of IPE, including improved patient and community outcomes (Dynes et al., 2013). For example, the Leicester Model of IPE demonstrated that students and healthcare professionals gain valuable insights into the balance task of patient-related issues and offer clarity about the effectiveness of collaborative opportunities in addressing patients’ needs (Lennox & Anderson, 2012). Carr (2015) also reported that after the IPE experience, students perceived strong confidence in communication with other professions, increased knowledge of the importance of teamwork and collaboration, learning professional roles, respecting other professional points of view, and improved communication skills.
The goal of undergraduate education for students in the health professions is mainly to produce graduates who can solve community health problems and increase community health, particularly in primary health care. Moreover, community health problems should be solved collaboratively. Thus, Community Based Education (CBE) combined with IPE is needed to be implemented in health professions schools. Several studies have implemented IPE in the community and positively affected students. For example, a study in the Philippines showed the usefulness of the IPE in the community, such as: learning about collaboration, appreciation of roles, holistic care, service to the community, and unique learning experience (Opina-Tan, 2013). A qualitative study in Australia also concluded that students who were voluntarily involved in an IPE program appreciate the opportunity to have direct practice experience in a community context and see this as a valuable way of engaging in interprofessional learning (Stewart et al., 2015). Furthermore, Wagner et al. (2011) stated that IPE in the community improved teamwork.
However, the IPE implementation in community-setting in Indonesia is not yet promising. Lestari et al. (2020) reported that communication and mutual support were problems faced by students. Furthermore, Randita et al. (2019) also stated that collaborative patient-centred competence has a moderate effect when IPE is implemented in the community setting. Therefore, IPE in Indonesia needs further exploration, especially when it is implemented in the community setting with a large number of students who are not volunteers but are obliged to be involved in such programs. In addition, it is anticipated that a learning model combining CBE and IPE will have additional benefits in supporting community health. Thus, the research question of this study was, is the combination of CBE-IPE valuable on community health outcomes, and what are the students’ attitudes and perceptions towards the new program?
II. METHODS
A. The Combination CBE-IPE Model
Before implementation, we matched the curricula of three health professions study programs (Medicine, Nursing, and Nutrition) at the Faculty of Medicine Universitas Diponegoro (a government medical school in Semarang, Indonesia). Based on the acquired competencies and timing possibility, we agreed that the new CBE-IPE program should be implemented for students in the 6th semester. In the 6th semester, all 465 health professions students (212 medical students, 127 nursing students, and 126 nutrition students) participated in this program during one semester.
Before implementation, we discussed with the head of the district health office and the director of the community health centre (CHC) to receive suggestions related to this program, especially in conjunction with the population health situation. As a result, we agreed that students should be assigned to families with pregnant women to support the local government health program in reducing maternal mortality. Thirty-six cadres (voluntary community members) were requested to participate in the project by the director of the CHC and agreed to help them in the program implementation. All cadres had been trained to conduct simple health promotion by the CHC.
A total of 465 health professions students were divided into 126 small groups consisting of 1-2 medical and nursing students and one nutrition student. One small group was attached to one family with a pregnant woman. To have experiences with a continuum of care, small groups of students added one other family if the first family had no children or elderly. Students had to work together to measure the health status of all family members, identify health problems, and propose a solution for identified health problems in discussions with their instructors. Based on those discussions, the students worked collaboratively with the cadres to implement collaborative interventions and eventually evaluated the result of their interventions. During this implementation, groups of students presented their work three times in seminars attended by all instructors and coordinators from three departments. The head of CHC received final reports for follow-up.
B. Study Design and Subjects
The design of this study was a mixed-method study to combine quantitative and qualitative data, in which the qualitative data was used to enrich the quantitative ones. Quantitative data was acquired by asking all students (465 health professions students) to fill out questionnaires before and after implementing the CBE-IPE program. We used the Readiness for Interprofessional Learning Scale (RIPLS) to evaluate students’ perceptions. This questionnaire has been widely used to collect students’ attitudes and perceptions to measure the readiness of healthcare professional students to undertake shared learning activities (Hertweck et al., 2012; Parsell & Bligh, 1999). Negative professional identity items represented negative statements regarding the value of working with other healthcare students. Therefore, this study reversed scored items so that high scores indicated IPE readiness (McFadyen et al., 2006). We used RIPLS in the Indonesian language version, which was developed by Tyastuti et al. (2014). It used exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). The EFA accounted for 59.9% of the total variance, while the alpha coefficient of CFA was > 0.7. Furthermore, construct validity was acceptable goodness of fit. Thus, the RIPLS in the Indonesian language version is a valid tool to assess students’ attitudes toward IPE.
The qualitative data were gained by collecting student comments in the questionnaire by asking: “Please write your words regarding this new program.” Moreover, TNK conducted interviews one by one with representatives of community members: two housewives and three cadres. At the end of the program, we conducted a workshop, including two times FGD conducted by TNK, FYA, and SB with 16 instructor’s representatives. Verbatim of all qualitative data was completed by TNK. The result of students’ intervention for patients and families was identified from students’ reports.
C. Data Analyses
We described the student’s characteristics and the result of student intervention on community outcomes. Paired-sample t-tests were used to compare the pre-post students’ responses to RIPLS. In addition, students’ perceptions related to self-confidence before and after the implementation were compared using chi-square. SPSS v22 was used to analyse the quantitative data. The students’ comments and interviews with community member representatives and instructors were analysed using content analysis according to Braun and Clarke (2006). First, keywords were identified as codes, and we used a matrix consisted three columns, namely keywords, categories, and themes. TNK and FYA conducted qualitative data analysis. Different coding was discussed to reach a consensus.
D. Ethical Consideration
We verbally explained this study to all participants before collecting the data. Especially for students, we guaranteed that their perceptions would not affect their scores. Then, we asked for participants’ agreement to join this study by signing the informed consent. The author would confidentially keep their identity.
III. RESULTS
Three hundred and sixty-seven out of 465 students returned the completed paired questionnaire (78.9 % response rate). Table 1 shows the subject’s characteristics of this study.
|
No |
Subject’s characteristics |
Categories |
Quantity |
Percentage |
|
1. |
Students (n= 367) |
|||
|
The study program |
Medicine |
167 |
45.4 |
|
|
Nursing |
100 |
27.3 |
||
|
Nutrition |
100 |
27.3 |
||
|
Gender |
Male |
73 |
20 |
|
|
Female |
294 |
80 |
||
|
2. |
Instructors (n: 16) |
|||
|
The study program |
Medicine |
6 |
38 |
|
|
Nursing |
5 |
31 |
||
|
Nutrition |
5 |
31 |
||
|
Gender |
Male |
4 |
25 |
|
|
Female |
12 |
75 |
||
|
Age |
31-40 |
6 |
37 |
|
|
41-50 |
10 |
63 |
||
|
3 |
Representative of community members |
|||
|
Age |
30-40 |
3 |
60 |
|
|
41-50 |
2 |
40 |
||
|
Gender |
Male |
0 |
0 |
|
|
Female |
5 |
100 |
||
Table 1. Characteristics of study subjects
A. The Result of Students’ Intervention in the Community Outcomes
Various health problems were identified and successfully managed by the students in collaboration with cadres (Table 2 and 3). Students also recognised that most families with low social-economic status and little education did not have health insurance. The head of the CHC agreed to follow up on some parts of the identified health problems, such as visiting pregnant women with high risk to ensure that they will deliver in the hospital, giving intervention for malnutrition toddlers, and vitalizing the post-health for the elderly.
|
No |
Problems identified |
Students’ interventions |
Results
|
|
1 |
One pregnant woman with an abortion |
Students and cadre provided education and accompanied the mother to the hospital. |
a. The mother should be curettage by the doctor in the hospital. b. The mother healthy and agrees to postpone the next pregnancy. |
|
2 |
Only 20% of pregnant women without risk factors who follow gymnastic program in CHC |
Motivation to follow gymnastic for pregnant women |
Moderate-high compliance
|
|
3 |
About 40% of pregnant women have low knowledge about monitoring of pregnancy and low compliance with routine ANC |
Direct education and gave motivation |
Increasing knowledge and compliance for ANC |
|
4 |
25.4% of pregnant women with risk factors according to the standard of WHO and 0.04% with high risk |
Motivation to routinely ANC and monitoring |
High compliance |
|
5 |
42.1% of pregnant women do not have health insurance |
Education to apply government health insurance |
25% have insured key person agrees to follow up |
|
6 |
Social and cultural problem (do not want to eat fish) |
Direct education |
Moderate-high compliance |
|
7 |
83.3% of pregnant women not enough nutrition in their daily diet (2 days recall) |
Gave leaflet and an example of healthy food |
Moderate-high compliance |
|
8 |
20% of pregnant women with anemia)
|
Gave Fe from CHC or midwives. |
Low compliance (reason: not good taste and felt nausea) |
Table 2. Students’ work-related pregnant women in the community
|
No |
Problems identified |
Students’ interventions |
Results
|
|
Baby and Toddlers |
|||
|
1 |
10% with malnutrition |
Education to mother and giving an example of healthy food |
Head of CHC followed up based on student’s report |
|
2 |
Acute Respiratory Infection |
Education and Suggested to CHC |
Cured |
|
3 |
Diarrhoea |
Education and Suggested to CHC |
Cured |
|
4 |
Motoric low development |
Education and Suggested to CHC |
Still to be followed up |
|
5 |
Difficult to eat, low knowledge of mother about healthy food |
Education to mother and give an example of healthy food |
Increasing knowledge |
|
6 |
One child with hydrocephalus |
Motivation to go to the hospital and finding the agency of hydrocephalus |
Has been tackled by the agency of hydrocephalus |
|
Puberty |
|||
|
1 |
Low knowledge about reproductive health |
Direct education |
Increasing knowledge and Head of CHC agree to follow up |
|
2 |
Smoking habit & Narcotic consumption |
Direct education |
|
|
3 |
Anemia among girl |
Direct education |
|
|
Adult |
|||
|
1 |
Low knowledge of occupational accident |
Direct education |
Increasing knowledge |
|
2 |
Low knowledge about family planning |
Direct education |
Increasing knowledge |
|
Elderly |
|||
|
1 |
Hypertension, Knee osteoarthritis, DM type II, Low Back Pain, Stroke, Low quality of life due to osteoarthritis and LBP |
Education and Suggestion to routinely to CHC |
Have been followed up by CHC
|
|
2 |
Only 15% routinely come to the integrative post health for elderly |
Education and Motivation |
Low compliance
|
Table 3. Students’ work with other family members
B. Pre-post Comparison of Students’ Perceptions
Students’ perceptions using RIPLS (5-point Likert scale) from all study programs showed a slight decrease in team collaboration, professional identity, and the cumulative sub-scale. Only student perception of responsibility slightly increased (Table 4). However, most pre-post students’ responses to the RIPLS questionnaire already trended to the positive side (scales 4 and 5). Comparison of pre-post students’ self-assessment of their confidence level significantly increased (Table 5).
|
No |
Subscale |
Pre Mean ± SD |
Post Mean ± SD |
P |
|
1 |
Teamwork & Collaboration |
38.96 ± 3.2 |
36.93 ± 4.0 |
< 0.001* |
|
2 |
Negative professional identity |
6.01 ± 2.4 |
5.29 ± 1.9 |
< 0.001* |
|
3 |
Positive Professional identity |
20.91 ± 1.9 |
20.23 ± 2.5 |
< 0.001* |
|
4 |
Role of responsibility |
5.38 ± 1.3 |
5.56 ± 1.5 |
0.07 |
|
5 |
Total subscale |
70.57 ± 5.0 |
68.74 ± 5.9 |
< 0.001* |
Table 4. Comparison of all students’ perception using RIPLS pre and post implementation (n: 367)
*Significance (p < 0.05) with paired t test
|
No |
Level of Confidence |
Pre |
Post |
Sig |
|
1 |
Not so confident |
69 (18.8%) |
3 (0.8%) |
< 0.00* |
|
2 |
Confident |
272 (74.1%) |
281 (76.6%) |
|
|
3 |
Very confident |
26 (7.1%) |
83 (22.6%) |
Table 5. Level of students’ Confidence (N: 367)
*Significance (p < 0.05) with chi-square test
C. Students’ Comments
Only 141/367 (38%) students wrote their comments in the questionnaire. However, most students (94% of 141 students) appreciated this program and suggested it be continued.
“The program is good; it can help community member to solve their health problem”
F23Nurs
“I agree if the program will be continued”
F50Nurs
Positive aspects raised by the students were:
- Opportunity to have direct communication with the community member (68%),
“I have the opportunity to communicate directly with patients and family, which is difficult to do when I’m only studying in the class”
M13Med
- Understanding each other when exploring and sharing knowledge to solve the identified health problems (32%),
“I feel amazed that each of us has our roles in solving health problems”
F67Med
- Learning about health team collaboration in the actual situation (40%),
“I learn a lot about how to collaborate with other health students in the real situation”
F90Nut
- Feeling proud that they had the opportunity to contribute to managing community health problems (69%).
“This program gives me an opportunity to collaborate with other professions to solve community health problems”
F44Nurs
The student’s complaints were as follows:
- Their task of working with a continuum of care was too heavy and exhausting.
“Focus on one family problem for one small team would be more useful.”
F57Med
- Several students (13%) also felt that their instructors were not motivated to mentor their tasks.
“It is difficult to make an appointment with the instructors, so we don’t have enough time to get feedback from him”
F21Med
- They had difficulty conducting home visits together (73%).
“Our biggest problem is matching the schedule to do a home visit.”
M98Nut
D. Interviews with Representatives of Community Members (two housewives, three cadres)
Both housewives and cadres appreciated the students’ work. They believed the students already had enough competencies to help their health problems. Cadres were still committed to participating in the following program and working with the students to implement, monitor, and evaluate the intervention.
“We are so happy that students help us a lot to identify and to solve our health problems”
F01HW
“Yes, of course, we will help students to communicate with the family as well as report the result of students’ intervention to Community Health Centre”
F03C
Community members thought they were not receiving enough information about the students’ purpose for visiting their house. They suggested that the cadre should have explained to them this program. However, they welcomed the students and told them to make an appointment before the home visit.
“There was no information from cadres of CHC that students will come to our house, but we still welcoming the students because it gives many benefits for us”
FHW02
E. FGD with Instructors at the End of the Program
Most instructors (94,5%) appreciated the value of this program. However, they needed more detailed information about the program, especially assessing students. They also thought it was too hard for students to add one family after already concentrating on one family’s health problem. They agreed that a tiny group should only be attached to one family with a pregnant woman. To strengthen collaboration competencies, all groups of students should implement a “collaborative intervention” that involves all disciplines.
“Sometimes students implemented their intervention within a single discipline that they thought more appropriate to solve the specified health problem.”
F05Inst
The instructors suggested that the assessment include peer assessment to increase students’ attitudes toward valuing each other. It was finally agreed that in the next implementation, various types of assessment would be implemented, namely students’ activities, presentation and discussion, peer assessment, and students’ assessment by the family members.
“Various assessment methods are preferable to capture students’ performance from the different side”
M09Inst
IV. DISCUSSION
This study aimed to examine the impact of implementing the CBE-IPE model on the outcomes of student intervention in the community and students’ attitudes and perceptions towards the new program. Within the CBE-IPE program, the health professions students successfully worked together to empower the community to solve most community health problems. The CBE-IPE program aims to give health profession students direct experiences in working as a health team in dealing with community health problems that might correlate with the social and economic backgrounds of community members. In this study, students identified several health problems in the family with low financial status, low education, and did not have any health insurance. Hence, the health profession students within this program also had an opportunity to learn several principles, including the level of education and economic aspects when implementing their interventions. It is in line with the study by Ngo et al. (2021), who reported that hypertension and cardiovascular risk could be identified by conducting CBE-IPE in homeless adults.
We implemented the CBE-IPE program without any serious obstacles due to the support from the local health government and the director of CHC. Cadres and representatives of community members also commented that the students’ presence and work were beneficial. They stated that they would be involved in the program and work with students to implement, monitor, and evaluate the result. It is important to involve cadres in this program because they will handle the follow-up under the supervision of CHC. Some studies also involved non-health workers in IPE implementation, such as Akter et al. (2016), who involved lay health workers, and Dynes et al. (2013), that involved health extension workers and community health promoters in improving maternal and neonatal health outcomes.
A. Students’ Attitudes and Perceptions Toward the CBE-IPE Program
This study showed that students’ attitudes and perceptions toward this program have improved, especially regarding the role of responsibility and confidence level. In this study, students have tasks to implement health intervention after discussing health problems identified with their instructor, which might increase their commitment and confidence. Tan et al. (2021) also demonstrated the importance of feedback and discussion, in which IPE participants noted that the debriefing process improves their compliance and teamwork.
Students’ perceptions as assessed by the RIPLS in aspects of team collaboration and interprofessional identity were slightly lower, although statistically significant. These statistically significant differences might result from the large sample size of this study. Several studies have shown that one-time IPE implementation is unlikely to change attitudes, whereas multiple or longitudinal IPE experiences elicit attitudinal change with a more positive response (Hammick et al., 2007; Pollard et al., 2006). Hind et al. (2003) reported little to no change in the health professions students’ perception of the RIPLS between pre-and post-implementation. Schreiber et al. (2014) also reported a slight increase and no statistically significant differences in the pre-post response to the RIPLS because the students already had positive attitudes toward IPE. Torsvik et al. (2021) reported that RIPLS tends to have a ceiling effect. Therefore, RIPLS no longer seems suitable for measuring and evaluating the impact of interprofessional learning. In this study, “most pre-post students’ responses to the RIPLS questionnaire already trended to the positive side.” Thus, the RIPLS also possibly has a ceiling effect in this study.
B. Wrapped up CBE-IPE Program Evaluation
Evaluation of this initial program demonstrates that students felt favourable toward the CBE-IPE program and felt more confident when dealing with community health problems. In line with Wong et al. (2018) study, the final students of six health programs have a positive attitude towards working together in an interprofessional health care team.
Nevertheless, students also complained that their tasks in working within a continuum of care were too heavy. As a result, they felt exhausted and less motivated to identify other health problems in another family. This complaint was in line with the instructors’ opinion. It concurred that students could learn from each other when they presented and discussed their work in the seminar. The recommendations included an adjustment in the tasks, scheduling, and improvements in the communication and quality of supervision. Therefore, the students’ tasks must be adjusted to accommodate these suggestions in the following implementation. Sunguya et al. (2014) reported that curriculum is an essential challenge in implementing IPE, which is in line with the study conducted by Thistlethwaite (2012) and Herath et al. (2017), which states that teaching methods and learning activities can be problems faced when implementing IPE. Furthermore, scheduling is one of the problems faced by faculty who implement the IPE program (Ngabonzima et al., 2020)
The instructors mentioned that the students’ interventions were not always “collaborative disciplines” since sometimes only a single discipline intervention for some health problems, and very little content was contributed by the other students in the specified group. Therefore, these circumstances might influence the lower perception of negative professional identity after the program implementation (Hind et al., 2003). Milot et al. (2015) also reported that it could sometimes be challenging to combine heterogeneous student teams during the learning together phase, where every discipline should be represented.
Understanding the attitudes of health professional students and the factors that influence their perceptions, including the situation they face during implementation, may help implement the program in several stages. There are four levels for the students to join the interprofessional collaborative practice. These include level 1: intra-professional education: the foundation of group skills, level 2: introduction to interprofessional education and collaboration: exposure to the healthcare team, level 3: interprofessional collaboration, and level 4: becoming an influential member of the healthcare team (Salfi et al., 2012).
C. Limitations
This study’s limitation lies in the type of data collection that only uses a closed-ended questionnaire and asks the students to write their comments on the program. Although the students raised several positive attributes, this study did not obtain sufficient information about what happened during the implementation and what was behind the students’ rated aspects. Therefore, FGDs with students are still needed to understand program implementation in-depth. Further, direct participation in program implementation might identify obstacles regarding when students should collaborate in their intervention program. Additionally, limitations in this study are acknowledged as data were collected from less than 80% of students participating in the program. Finally, no formal feedback was collected from the community members, although verbal input in the interview was positive. A collection of more detailed data would have provided a deeper understanding of the program’s impact on community perceptions.
We realize that implementing the CBE-IPE program in the community, which involves many students, was challenging and needed more careful preparation. Moreover, the lecturers’ motivation might be increased by encouraging and facilitating them to include field epidemiology research in the same area, with research funding from the faculty. Several changes should be made based on this evaluation, including more detailed guidance for the students and instructors.
V. CONCLUSION
This study revealed that the combination of CBE-IPE for 6th-semester health profession students had been perceived as a valuable learning experience to build community health. Nevertheless, it was challenging for many students in several aspects of the preparation. Moreover, highly motivated lecturers are required, which might be increased by encouraging and facilitating field epidemiology research in the same area. Finally, further research is needed to explore students’ experiences during implementation, primarily how they work as a team and their belief in professional identity. It is also important to identify the result of a combination of CBE-IPE implementation in terms of the satisfaction of students, instructors, and family members.
Notes on Contributors
Tri Nur Kristina conceptualised and designed the research, participated in the analysis and intepretation of data, drafted and revised the manuscript, and giving final approval of the version to be published.
Fatikhu Yatuni Asmara conceptualised of the program implementation, participated in the data collection, and revised the manuscript.
Sudaryanto conceptualised of the program implementation.
Nuryanto conceptualised of the program implementation and participated in the data collection.
Saekhol Bakri conception of the program implementation and participated in the data collection.
Ethical Approval
The Medical and Health Research Ethics Committee (MHREC), Faculty of Medicine Diponegoro University-Dr. Kariadi General Hospital had approved this study (No. 519/EC/FK/2020).
Data Availability
Author could not share the data of this study widely because of its privacy. It also contains qualitative data.
Acknowledgement
The authors would like to thank the Faculty of Medicine Universitas Diponegoro for providing the funding for this study.
Funding
This work supported by Faculty of Medicine Universitas Diponegoro (Grant number: 233-71/UN7.6.1/PP/2020).
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
References
Akter, T., Sibbritt, D., & Dawson, A. (2016). Workforce interventions to deliver postnatal care to improve neonatal outcomes in low- and lower-middle-income countries: A narrative synthesis. Asia-Pacific Journal of Public Health, 28(8), 659–681. https://doi.org/10.1177/1010539516656435
Braun, V., & Clarke, V. (2006). Qualitative research in psychology using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101.
Carr, S. (2015). Examining health professional students’ attitudes on interprofessional education. (Publication no. 309) [Doctoral Dissertations, University of Rhode Island]. DigitalCommons@URI. http://digitalcommons.uri.edu/oa_diss/309
Dynes, M., Buffington, S. T., Carpenter, M., Handley, A., Kelley, M., Tadesse, L., Beyene, H. T., & Sibley, L. (2013). Strengthening maternal and newborn health in rural Ethiopia: Early results from frontline health worker community maternal and newborn health training. Midwifery, 29(3), 251–259. https://doi.org/10.1016/j.midw.2012.01.006
Hammick, M., Freeth, D., Koppel, I., Reeves, S., & Barr, H. A. (2007). A best evidence systematic review of interprofessional education. BEME guide no.9. Medical Teacher, 29(8), 735-751. https://doi.org/10.1080/01421590701682576
Herath, C., Zhou, Y., Gan, Y., Nakandawire, N., Gong, Y., & Lu, Z. (2017). A comparative study of interprofessional education in global health care: A systematic review. Medicine, 96(38), 1-7. https://doi.org/10.1097/MD.0000000000007336
Hertweck, M., Hawkins, S., Bednarek, M., Goreczny, A., Schreiber, J., & Sterrett, S. (2012). Attitudes towards interprofessional education: Comparing physician assistant and other health care professions students. The Journal of Physician Assistant Education, 23(2), 8-15.
Hind, M., Norman, I., Cooper, S., Gill, E., Hilton, R., Judd, P., & Jones, S. (2003). Interprofessional perceptions of health care students. Journal of Interprofessional Care, 17(1), 21-34. https://doi.org/10.1080/1356182021000044120
Housley, C. L., Neill, K. K., White, L. S., Tedder, A. T., & Castleberry, A. N. (2018). An evaluation of an interprofessional practice-based learning environment using student reflections. Journal of Interprofessional Care, 32(1), 108–110. http://doi.org/10.1080/13561820.2017.1356808
Lennox, A., & Anderson, E. S. (2012). Delivering quality improvements in patient care: the application of the Leicester Model of interprofessional education. Quality in Primary Care, 20(3), 219–226.
Lestari, E., Scherpbier, A., & Stalmeijer, R. (2020). Stimulating students’ interprofessional teamwork skills through community-based education: A mixed methods evaluation. Journal of Multidisciplinary Healthcare, 13, 1143–1155. http://doi.org/10.2147/JMDH.S267732
McFadyen, A. K., Webster, V. S., & Maclaren, W. M. (2006). The test-retest reliability of a revised version of the Readiness for Interprofessional Learning Scale (RIPLS). Journal of Interprofessional Care, 20(6), 633-639. https://doi.org/10.1080/13561820600991181
Milot, E., Dumont, S., Aubin, M., Bourdeau, G., Azizah, G. M., Picard, L., & St‑Germain, D. (2015). Building an interfaculty interprofessional education curriculum: What can we learn from the Université Laval Experience? Education for Health, 28(1), 58-63. https://doi.org/10.4103/1357-6283.161896
Ngabonzima, A., Kenyon, C., Hategeka, C., Utuza, A. J., Banguti, P. R., Luginaah, I., & F Cechetto, D. (2020). Developing and implementing a novel mentorship model (4+1) for maternal, newborn and child health in Rwanda. BMC Health Services Research, 20(1), Article 924. https://doi.org/10.1186/s12913-020-05789-z
Ngo, A. N., Islam, M. A., Aoyagi, J., Sandor, Z., & Sandor, S. (2021). Prevalence of hypertension in homeless adults: An interprofessional education community-based health fairs cross-sectional study in urban long beach, California. High Blood Pressure and Cardiovascular Prevention, 28(1), 63-68. https://doi.org/ doi: 10.1007/s40292-020-00424-8
Opina-Tan, L. A. (2013). A pilot implementation of interprofessional education in a community‑academy partnership in the Philippines. Education for Health, 26(3), 164-171. https://doi.org/10.4103/1357-6283.125992
Parsell, G., & Bligh, J. (1999). The development of a questionnaire to assess the readiness of healthcare students for interprofessional learning (RIPLS). Medical Education, 33(2), 95-100. https://doi.org/10.1046/j.1365-2923.1999.00298.x
Pollard, K. C., Miers, M. E., Gilchrist, M., & Sayers, A. (2006). A comparison of interprofessional perception and working relationship among health and social care students: The results of a 3-year intervention. Health and Social Care in the Community, 14(6), 541-552. https://doi.org/10.1111/j.1365-2524.2006.00642.x
Randita, A. B. T., Widyandana, W., & Claramita, M. (2019). IPE-COM: A pilot study on interprofessional learning design for medical and midwifery students. Journal of Multidiscipline Health Care, 12, 767–775. http://doi.org/10.2147/JMDH.S202522
Salfi, J., Solomon, P., Allen, D., Mohaupt, J., & Patterson, C. (2012). Overcoming all obstacles: A framework for embedding interprofessional education into a large, multisite bachelor of science nursing program. Journal of Nursing Education, 51(2), 106-110. https://doi.org/10.3928/01484834-20111230-05
Schreiber, J., Goreczny, A., Bednarek, M. L., Hawkins, S. R., Hertweck, M. L., & Sterret, S. E. (2014). The effects of single event interprofessional education (IPE) experience on occupational therapy students’ attitude toward IPE. The Internet Journal of Allied Health Sciences and Practice, 12(1), 1-8. https://doi.org/10.46743/1540-580X/2014.1467
Stewart, V., Betts, H., Chee, P., & Ingamells, A. (2015). Interprofessional learning: Health and allied health students in a community context. Advance in Social Work & Welfare Education, 17(2), 70-85.
Sunguya, B. F., Hinthong, W., Jimba, M., & Yasuoka, J. (2014). Interprofessional education for whom? – Challenges and lessons learned from its implementation in developed countries and their application to developing countries: A systematic review. PLoS ONE, 9(5), e96724. https://doi.org/10.1371/journal.pone.0096724
Tan, K. W., Ong, H. K., & Mok, U. S. (2021). Using simulation and inter-professional education to teach infection prevention during resuscitation. The Asia Pacific Scholar, 6(1), 93-108. https://doi.org/10.29060/TAPS.2021-6-1/OA2229
Thistlethwaite, J. (2012). Interprofessional education: a review of context, learning and the research agenda. Medical Education, 46(1), 58–70. https://doi.org/10.1111/j.1365-2923.2011.04143.x
Torsvik, M., Johnsen, H. C., Lillebo, B., Reinaas, L. O., & Vaag, J. R. (2021). Has “the ceiling” rendered the readiness for interprofessional learning scale (RIPLS) outdated? Journal of Multidisciplinary Healthcare, 14, 523–531. https://doi.org/10.2147/JMDH.S296418
Tyastuti, D., Onishi, H., Ekayanti, F., & Kitamura, K. (2014). Psychometric item analysis and validation of the Indonesian version of the Readiness for Interprofessional Learning Scale (RIPLS). Journal of Interprofessional Care, 28(5), 426-432. https://doi.org/10.3109/13561820.2014.907778
Wagner, J., Liston, B., & Miller, J. (2011). Developing interprofessional communication skills. Teaching and Learning in Nursing, 6(3), 97-101. https://doi.org/10.1016/j.teln.2010.12.003
Wong, P. S., Hasan, S. S., Ooi, J., Lim, L. S. H., & Nadarajah, V. D. (2018). Assessment of attitude for interprofessional team working and knowledge of health professions competencies for final year health professional students. The Asia Pacific Scholar, 3(1), 27-37. https://doi.org/10.29060/TAPS.2018-3-1/OA1064
*Fatikhu Yatuni Asmara
Department of Nursing, Faculty Medicine,
Universitas Diponegoro
Jl. Prof Soedarto, SH, Tembalang,
Semarang, Indonesia
+6281229495962
Email: f.y.asmara@fk.undip.ac.id
Published online: 4 April, TAPS 2023, 8(2), 1-3
https://doi.org/10.29060/TAPS.2023-8-2/EV8N2
Shuh Shing Lee1 & John Norcini2
1Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Foundation for Advancement of International Medical Education and Research, United States of America
It has been almost three decades since Boyer (1990) introduced the concept of the Scholarship of Teaching and Learning (SoTL). In their own disciplines, faculty members are required to stay abreast of emerging knowledge and to contribute to the literature so that they advance their field through well-informed inquiry and disseminated work. Although they also have educational responsibilities, faculty are neither similarly motivated nor are they incentivised to participate in educational scholarship. Consequently, their efforts in this regard are often based on personal belief and opinion rather evidence and scientific inquiry. This problem persists despite a growing body of evidence that adopting sound instructional practices and pursuing scholarly work related to teaching, will increase the quality of the institution’s educational processes. In turn, this will enhance student learning and ultimately lead to better patient care. To achieve this end, teaching and learning must be scrutinised in terms of theory, methods, evidence, and outcomes. And faculty members who engage in teaching need to be rewarded for their participation in educational scholarship just as they are for efforts in their own disciplines.
In supporting educators’ SoTL journey and enhancing the quality of their teaching, this special issue “Celebrating Excellence in Scholarship of Teaching and Learning” aims to demonstrate how educators adopt a scholarly approach and how they collect and present rigorous evidence of their effectiveness. It encompasses much of current health professions education, touching on topics such as interprofessional education, the globalisation of healthcare, the impact of COVID-19, vaccine hesitancy, and digital badges.
Educators from Indonesia shared their strategy for enhancing interprofessional education through community-based education (Kristina et al., 2023). Teams of students developed solutions to family health issues together. The authors found implementation challenges when applying this model, especially in terms of scheduling home visits. However, through this experience the students learned the value of teamwork and the roles of each of the representatives.
As a result of globalisation, there is a significant increase in the number of patients being admitted to hospitals outside of their home countries. The Emergency Department is often the first point of contact for these foreign patients and cultural differences naturally pose challenges. To address this issue and to help patients with different backgrounds obtain high quality care, some hospitals in Japan have initiated cultural awareness training for their doctors. While this is a positive step, doctors in the Emergency Department in Japan still face difficulties in this area. To address these challenges going forward, educators from Japan would like to identify the difficulties still encountered and eventually design scenarios, based on real life cases, for use in simulations (Oikawa et al., 2023).
COVID-19 has changed the way teaching has occurred and it has accelerated the use of technology in all phases of education. This special edition contains two Case Studies related to this issue. The report by Kushare et al. (2023) takes on the use of blended learning that occurred synchronously at different campuses in Malaysia. The report by Lim et al. (2023) focuses on student perspectives on the prohibition of direct patient contact during pandemic. It will be important to follow future developments in these areas as restrictions are lifted.
COVID-19 has not only affected teaching, but it has also had a profound influence on the practice of medicine. Vaccine hesitancy among patients is a growing phenomenon for which not all health care providers are prepared. Physicians may have misconceptions about what drives patient behaviour leading to the less effective provision of information and counselling. To better understand this issue and design a relevant curriculum to create awareness, Jenkins et al. (2023) explored medical students’ reactions to vaccine hesitancy and their reflections on their own biases in patient interactions. The qualitative analysis of students’ reflections offered by the authors is a useful basis for working with students around this issue.
In recent years, digital badges have increasingly become a part of the educational landscape. They constitute an innovative instructional strategy combing the teaching and credentialing of competencies to provide evidence for achievement. However, research in this area is scare. Truskowska et al. (2023) introduced a pilot project regarding the use of digital badges in a Psychiatry module offered as part of a continuous assessment programme. They evaluated the effectiveness of the digital badges based on students’ perspectives of their utility, their level of engagement with the module, and their motivation to study. Students found the badges rewarding but noted that their value was unclear which would eventually lead to a loss of motivation.
Assessment has been a main topic of discussion in SoTL because it shapes how student learn and informs teachers about the effectiveness of their own work. Dayanidhi et al. (2023) present information about a radical curriculum and assessment reform that has been taken place in India. Forensic Medicine and Toxicology, a major competence, is often underrepresented in assessment. The authors established this through an analysis and comparison of the distribution of content tested, domain of learning and construct of the questions derived from undergraduate summative examination question papers on the topic from six universities across India. Also focused on assessment, Lim and Lim (2023) share an innovative assessment method – oral interactive assessment– which they have implemented among the occupational therapy students. Instead of multiple-choice questions or short written answers, each student was assessed with a standardised actor who simulate concerned parents, asking questions about their children’s development. While students are more anxious with this format, an interactive oral assessment has real world relevance.
There are several articles discussing initiatives that were conducted for faculty members in this special issue. For example, Lim et al. (2023) described a coaching programme aimed at providing educators a framework that helps students make discoveries and work towards their goals and training them how to question students. Field et al. (2023) offered a study in training their faculty members to teach and assess students’ clinical thinking skills using a model. Goh and Schlegal (2023) examined the journey of scholarship in health professions education and suggested tangible small steps to start, sustain, and succeed along the SoTL journey.
Felten (2013) in his paper “Principles of Good Practice in SoTL” mentioned that good scholarship should be grounded in context because it takes place in a particular classroom, institution, organisation, and education system where the culture is bounded. Tan et al. (2023) elaborated this aspect in his article using Bronfenbrenner’s Ecological Systems theory (EST). Grant (2023), similarly, highlighted the notion that the practice of teaching is socially bound and highly dependent on the culture, content and context. She further described the relationship between medical educationalists and teachers in the entire SoTL journey.
Good teaching is multidimensional, challenging, and contextual as demonstrated by all the authors in this special issue. However, this is an excellent place to start and it encourages all of us to apply the same thoughts processes to our teaching as we do in our discipline-specific research. Teaching is a process of reflection on our practice and if we follow this dictum, more scholarly teaching will result in higher quality in learning among our students.
Shuh Shing Lee & John Norcini
Guest Editors
The Asia Pacific Scholar (TAPS)
Boyer, E. L. (1990). Scholarship revisited: Priorities of the professionals. Carnegie Foundation for the Advancement of Teaching.
Dayanidhi, V. K., Datta, A., Hegde, S. P., & Tiwari, P. (2023). Evaluating the content validity of the undergraduate summative exam question papers of Forensic Medicine & Toxicology from 6 medical universities in India. The Asia Pacific Scholar, 8(2), 57-65. https://doi.org/10.29060/TAPS.2023-8-2/OA2778
Felten, P. (2013). Principles of Good Practice in SoTL. Teaching & Learning Inquiry: The ISSOTL Journal, 1(1), 121-125. https://doi.org/10.2979/teachlearninqu.1.1.121
Field, S., Croskerry, P., Love, S., & Alexiadis Brown, P. (2023). An online programme in teaching and assessing critical thinking for medical faculty. The Asia Pacific Scholar, 8(2), 66-69. https://doi.org/10.29060/TAPS.2023-8-2/SC2894
Goh, P. S., & Schlegal, E. F. M. (2023). Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters. The Asia Pacific Scholar, 8(2), 76-79. https://doi.org/10.29060/TAPS.2023-8-2/SC2861
Grant, J. (2023). The Scholarship of teaching: Who is the truth teller? The Asia Pacific Scholar, 8(2), 83-85. https://doi.org/10.29060/TAPS.2023-8-2/PV2874
Jenkins, M. C., Paul, C. R., Chheda, S., & Hanson, J. L. (2023). Qualitative analysis of reflective writing examines medical student learning about vaccine hesitancy. The Asia Pacific Scholar, 8(2), 36-46. https://doi.org/10.29060/TAPS.2023-8-2/OA2855
Kristina, T. N., Asmara, F. Y., Sudaryanto, S., Nuryanto, N., & Bakri, S. (2023). Increasing the value of Community-Based Education through Interprofessional Education. The Asia Pacific Scholar, 8(2), 4-13. https://doi.org/10.29060/TAPS.2023-8-2/OA2755
Kushare, V., MK., B., Pamidi, N., Selvaratnam, L., Sen, A., & Dominic, N. A. (2023). Vertical integration of anatomy and women’s health: Cross campus blended learning. The Asia Pacific Scholar, 8(2), 89-92. https://doi.org/10.29060/TAPS.2023-8-2/CS2806
Lim, M. J., Wee, J. C. P., Han, D. X. T., & Wong, E. (2023). Perspectives of medical students towards the prohibition of direct patient contact during a pandemic. The Asia Pacific Scholar, 8(2), 93-96. https://doi.org/10.29060/TAPS.2023-8-2/CS2849
Lim, S. M., & Lim, C. Y. (2023). Use of interactive oral assessment to increase workplace readiness of occupational therapy students. The Asia Pacific Scholar, 8(2), 86-88. https://doi.org/10.29060/TAPS.2023-8-2/SC2804
Lim, S. M., Shahdadpuri, R., & Pua, C. Y. (2023). Coaching as an educator: Critical elements in a faculty development program. The Asia Pacific Scholar, 8(2), 70-75. https://doi.org/10.29060/TAPS.2023-8-2/SC2802
Oikawa, S., Ashida, R., & Takeda, S. (2023). Increasing cultural awareness in emergency departments with simulation scenarios created through a survey. The Asia Pacific Scholar, 8(2), 14-35. https://doi.org/10.29060/TAPS.2023-8-2/OA2762
Tan, K., Foo, Y. Y., & Tan, N. C. K. (2023). Refocusing SoTL – Myopia, context lenses and ecological systems theory. The Asia Pacific Scholar, 8(2), 80-82. https://doi.org/10.29060/TAPS.2023-8-2/PV2842
Truskowska, E., Emmett, Y., & Guerandel, A. (2023). Digital badges: An evaluation of their use in a Psychiatry module. The Asia Pacific Scholar, 8(2), 47-56. https://doi.org/10.29060/TAPS.2023-8-2/OA2869
Published online: 3 January, TAPS 2023, 8(1), 1-2
https://doi.org/10.29060/TAPS.2023-8-1/EV8N1
COVID pandemic created worldwide disruptions to all services and had profound impact on training of health professionals, posing serious challenges to maintaining essential healthcare services. During the height of the pandemic, most of the undergraduate learners were prevented from clinical training sites, restricted intra, inter-institutional and overseas learning opportunities and in many institutions, there were termination of onsite learner-educator engagements (Ng et al., 2021; Renaud et al., 2021; Samarasekera et al., 2020). Less face to face, peer and faculty interactions and restricted mobility of learners led to some of them facing poor mental wellbeing and health issues. The learning activities were mostly restricted to online platforms during the pandemic for students following health professional programs. During the latter part of the pandemic, however, there were changes when better preventive measures and immunisation were developed. The students were also allowed to provide limited care services to assist the practitioners who were providing critical services (Lau et al., 2021).
The silver lining, however, was that several new curricular designs, teaching-learning and assessment modalities were developed due to the sheer necessity. The faculty members and students were forced to adapt and adopt these new measures, mostly online systems and processes, to continue the training and provide that much needed support to the healthcare services (Shorey et al., 2022). This became critical when it was apparent that the pandemic would continue for several years. There are some such innovations in teaching-learning highlighting not only the innovation and their impact but also the challenges faced by students and faculty members. Most of these changes to student learning environment were done hurriedly and, unfortunately, without the proper grounding in best evidence practices or taking a systematic approach to incorporate changes to a curriculum. Another reason was the lack of knowledge and support of educators to develop impactful curricula and learning environments leveraging on technology (Popa, 2022).
We are now emerging from the pandemic and many lessons have been learnt from this experience. We now have an opportunity to leapfrog from these experiences. The key to creating an impactful and sustainable post-pandemic learning environment lies with the faculty members. There are several important areas we need to focus on if we want to sustain and further improve the education based on our past experience.
As part of faculty development, it is necessary to engage our faculty members to share best practices and assist them to co-create with their learners teaching-learning activities. For faculty leadership, it is critical to create that safe practice environment for all stakeholders to reflect on and improve what they have developed. Through these collaborative activities, not only the faculty members learn about what works and what to avoid, but also build trust with other stakeholders including the students. Furthermore, it supports them to critically analyse the learning and assessment activities with regard to their relevance in one’s context. Providing a structured and timely faculty support with the necessary resources will augment the building of trust (Connolly et al., 2022).
Another important area we learnt especially during the pandemic and as we currently emerge from the pandemic is the necessity to modify the existing policies and guidelines. These should support systematic and rapid development of learning environments. What worked in the past may not be appropriate now, and even hinder the development of innovative strategies. We need to relook at how we evaluate an educator’s performance and the learning impact from traditional matrixes in place at present in health professional training institutions. Aligned to the performance evaluations, there needs to be supportive schemes to incentivise and reward faculty members who contributed to enhance the learning environment for students and residents.
Medical education is very much context-based and situation-focused. What worked in one setting may not be appropriate in another learning context. The leadership, planners, and educators must be aware of this and carefully design and incorporate innovations and new approaches to learning that have worked in another setting to one’s own. This is especially true when one is incorporating technology-enhanced learning activities such as simulation based or remote distance online learning formats. Finally, the quality improvement and quality assurance processes in health professions education must be aligned to the local context needs. These standards, however, should be benchmarked to internationally accepted best practices, but situated very much on the local needs and promoting impactful changes to student learning environments (Samarasekera & Gwee, 2021).
A quick literature search at present will demonstrate large number of innovations and changes that were incorporated to medical and health professional training curricula over the pandemic period (Ng et al., 2021). It is an opportune time now to focus on developing these changes, based on best evidence practices., The impact of these changes need to be subsequently evaluated to further enhance student learning. At the end of it all, what is most vital is to provide quality care to our patients by competent, caring, and empathetic health professionals.
Dujeepa D. Samarasekera
Centre for Medical Education (CenMED), NUS Yong Loo Lin School of Medicine,
National University Health System, Singapore
Connolly, K. K., Olson, H. L., & Buenconsejo-Lum, L. E. (2022). Medical school faculty development post-pandemic – Opportunities in the digital shift. Hawai’I Journal of Health & Social Welfare, 81(11), 316-318.
Lau, T. C., Chong, Y. S., Loo, B. K. G., Ganapathy, S., Ho, J. M. D., Lee, S. S., Yeo, J., Samarasekera, D. D., & Goh, D. L. M. (2021). Adapting undergraduate paediatric medical education to the challenges of COVID-19 pandemic: Perspective of NUS medicine. Singapore Medical Journal, 62(1 Supp), S39-S42. https://doi.org/10.11622/smedj.2021075
Ng, N. B. H., Chiong, T., Lau, P. Y. W., & Aw, M. A. (2021). Delivering medical education amidst COVID-19: Responding to change during a time of crisis. The Asia Pacific Scholar, 6(3), 111-113. https://doi.org/10.29060/TAPS.2021-6-3/PV2375
Popa, S. (2022). Taking stock: Impacts of the Covid-19 pandemic on curriculum, education, and learning. PROSPECTS, 51, 541-546. https://doi.org/10.1007/s11125-022-09616-7
Renaud, C. J., Chen, Z. X., Yuen, H.-W., Tan, L. L., Pan, T. L. T., & Samarasekera, D. D. (2021). Impact of COVID-19 on health profession education in Singapore: Adoption of innovative strategies and contingencies across the educational continuum. The Asia Pacific Scholar, 6(3), 14-23. https://doi.org/10.29060/TAPS.2021-6-3/RA2346
Samarasekera, D. D., Goh, D. L. M., & Lau, T. C. (2020). Medical school approach to manage the current COVID-19 crisis. Academic Medicine, 95(8), 1126-1127. https://doi.org/10.1097/ACM.0000000000003425
Samarasekera, D. D., & Gwee, M. C. E. (Eds.). (2021). Educate, train and transform: Toolkit on medical and health professions education. World Scientific.
Shorey, S., Pereira, T. L.-B., Teo, W. Z., Ang, E., Lau, T. C., & Samarasekera, D. D. (2022). Navigating nursing curriculum change during COVID-19 pandemic: A systematic review and meta-synthesis. Nurse Education in Practice. 65, Article 103483. https://doi.org/10.1016/j.nepr.2022.103483
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
