
Developments in medical humanities in Sri Lanka: A call for regional and global action
Submitted: 6 September 2022
Accepted: 1 March 2023
Published online: 3 October, TAPS 2023, 8(4), 1-4
https://doi.org/10.29060/TAPS.2023-8-4/GP2878
Saroj Jayasinghe1, Santhushya Fernando2
1Department of Clinical Medicine, Faculty of Medicine, University of Colombo, Sri Lanka; 2Department of Medical Humanities, Faculty of Medicine, University of Colombo, Sri Lanka
Abstract
Introduction: Medical Humanities is the interface of health sciences and humanities and an emerging field of interest. Several papers have outlined the status of this field in the Asian region where a diversity of teaching and learning approaches have been used. We share developments initiated in a Sri Lankan medical school and discuss its relevance to the southern Asian region, especially in using arts in medical humanities.
Methods: Historical records, narratives, grey literature, and published resources were collated to describe the initiative in the Faculty of Medicine, University of Colombo. The data was collected, synthesized and described especially in the context of the region.
Results: We observe a structured development of medical humanities in the curriculum. The novelty of the curriculum is that it evolving to include wider experiences from the visual and performance arts, in order to achieve the goal of promoting humaneness. The contents were locally developed, based on needs with an indigenous cultural bias giving rise to a unique southern Asian perspective of medical humanities.
Conclusion: There are diverse experiences and initiatives in medical humanities in Asian, and some are not captured in published literature. It is challenging to follow these diverse trends in different locations, share experiences and learn from each other, and place medical humanities in the regional and global maps of health professional education.
Practice Highlights
- Asia has seen several developments in the field of medical humanities.
- Sri Lanka has made significant progress and introduced it to medical education.
- One key innovation is the integration of arts to its teaching-learning.
- Southern Asia has rich and diverse religious, cultural and artistic traditions.
- The region could give a unique perspective to medical humanities.
I. INTRODUCTION
A recent scoping review traced the history of developments in the teaching / learning of humane care and recognition of its importance in medical training (Zhu et al., 2021). This paper also outlined the need to develop culturally relevant, effective, and integrative curricula that would promote humanistic attitudes and behaviours among medical students and physicians in Asia. There were developments of this field in Nepal that were shared in a subsequent correspondence (Shankar, 2022). These papers and several other publications have highlighted the developments in the field with a diversity of experiences.
We share a few developments from Sri Lanka that demonstrate a widening interest in the field in southern Asia and opportunities to use its unique heritage to move forward.
II. SCOPE AND BACKGROUND INFORMATION
The Faculty of Medicine, University of Colombo is one of the oldest continuously functioning medical schools in Asia (from 1870). It has the distinction of pioneering an integrated curriculum in the country in 1995 and establishing the first Department of Medical Humanities in 2016.
For decades, the curriculum was based on Flexner’s structures and was a conventional discipline-based curriculum with little inputs from the humanities. The reforms in 1995 led to a more integrated modular system with a longitudinal input from Behavioural Sciences (BS). The BS program had modules that focused on teaching / learning in topics related to personal development, communication skills, medical ethics, health management and professionalism (Jayasinghe, 2017). It was organized by appointing a group of academics to a Behavioural Science Stream (BSS) to coordinate the teaching / learning programs through the 5-year MBBS course.
However, inputs from the arts were minimal though it flourished outside the formal curriculum in the form of concerts, art festivals, photography exhibitions and musical events organized by the student body. These activities were heavily influenced by the urbanized Western culture and activities such as ball-room dancing, predominantly British literature, and Western models of theatre played a predominant role.
A qualitative change in the range of activities was observed around 1974 with the establishment of an Arts Circle in the Faculty of Medicine that promoted infusion of local culture. Interestingly, this coincided with changes in the admission criteria to universities that resulted in student intakes from diverse of social groups and a significant increase in entry from a wider range of districts and more rural schools.
In 2011, the BSS began to organize internal workshops to review its curriculum and propose future developments. During these discussions, participants expressed the need to promote more humaneness, empathy and compassion among students (Jayasinghe, 2017). This led to discussions on the potential role of the arts to meet these needs. The first lecture on “Illness from the perspective of humanities” was introduced in 2012. Soon a consensus view emerged to establish a Department of Medical Humanities in order to deliver a heavier educational input from humanities and thereby promote humane values in students. In August 2016, the Faculty of Medicine, University of Colombo, formally established the first Department of Medical Humanities in the country. In 2020 the BSS was renamed Humanities, Society and Professionalism Stream (HSPS) to reflect the introduction of new content to the curriculum.
III. EDUCATIONAL STRATEGIES
In order to identify contents for its new curriculum, the Department organized a series of invited lectures and discussions targeting the academic staff. It was titled “Exploring the Role of Humanities in Health”. The resource persons were experts on medical humanities and a diverse range of topics included “Role of Arts in Medicine”; “Approaches to teaching humanities to medical students”; “Medical narratives”; “Using poetry to inculcate attitudes”; and “Humanities in medicine: The Ruhuna Experiment”. Other opportunities, such as invitations to deliver guest lectures in conferences, were used by the authors to stimulate discussions on the potential role of the arts in health professional education (Jayasinghe, 2018).
The series of lectures culminated in the First International Conference on Medical Humanities held in 2018, on the theme “Learning to be more humane: The role of Medical Humanities” (Colombo Medical Humanities News, 2019). It included a half-day workshop on “Arts in Health Professional Education”. There was wide participation by experts in the field and the conference and workshop were used to refine the curriculum on medical humanities, especially on how to effectively introduce the arts to health professional education. This issue was further debated and discussed during seminars on Medical Humanities at the Colombo Medical Congress (in 2020) and orations dedicated to Medical Humanities (from 2021).
The knowledge gained from the above activities, were used to design an innovative curriculum that included a wider infusion from the arts and narrative-based learning. The main goals of the latter were to promote humaneness, encourage learners to develop a person-centred approach to clinical practice, and appreciate patient perspectives of illness. A range of educational strategies were used: assignment on appreciation of the arts and its relevance to empathy in care; student seminar to reflect on personal experiences of kind and unkind health professional behaviours, obtaining narratives from patients to highlight the humane and person-centered issues of illness; large-group lectures on topics such as “The Arts in Health and Illness” and “Empathy and Compassion”. The latter focused on research evidence from neurophysiology to demonstrate links between art appreciation and traits such as compassion and empathy.
In 2021, during the COVID pandemic, the HSPS and the Department of Medical Humanities introduced an innovative programme aimed at the students. A series of interactive multi-disciplinary webinars termed Humanitas were organied to explore contemporary issues connected to health and have continued as part of the teaching-learning programme. They have been held approximately at bi-monthly intervals and addressed a wide range of issues: life-experiences amidst environmental disasters, linguicism and decolonizing tertiary education, the world of animal welfare, lives of workers in the apparel industry, social and psychological issues faced by those with different sexual identities and orientations, and the emotional journey of a parent who lost her child to cancer.
Interviews from affected groups of people, artists, academics and intellectuals were creatively juxtaposed with short films, extracts from movies, selected musical scores. Examples of the latter included songs of peace sung during non-violent protests organised by Mahatma Gandhi and Martin Luther King Sr., and extracts of poetry and literature that drew attention to contemporary issues such as the plight of garment factory workers. Contributions were predominantly from Sri Lankan commentators reflecting our own historical and cultural context and local experiences.
Since the pandemic ended, Humanitas will be conducted in-person. The first for 2023 was titled ‘Dance and Life’, featuring live Indian and traditional Sri Lankan dance recitals by professional dancers. These performances were accompanied by commentaries by dancers on the emotions they felt while dancing, and the mechanisms of evoking feelings in the audience described by medical experts. These emotions and feelings were in turn linked to the ability of certain dances to generate compassion and empathy. The session ended with an expert dancer performing and describing how certain traditional dances of the Sinhalese (e.g. ‘Thovil’) were used as therapy for a diversity of illnesses.
The second recent innovation relates to activities on medical humanities organized for the 3rd Colombo Medical Congress in November 2022, an annual event in the University calendar and open to students. We organised a symposium exploring the neurophysiological correlates of music, poetry, and dance and complemented the academic program with a series of activities throughout the conference: free exhibitions of art, sculptures and photography, open-air musical events by students, and live sculpture and portrait sessions by professional artists. The latter live sessions enabled students and attendees to experience and interact with the process of artistic creations.
IV. DISCUSSION
Medical Humanities is an emerging field of interest in the interface of health sciences and humanities. The diversity of experiences in the Asian region has led to several initiatives. The initiative in Colombo used contemporary topics with contributions mainly from Sri Lankan commentators reflecting on our own historical and cultural contexts. We believe this enriched a field that is dominated by an allopathic or modern medical system that are predominantly Eurocentric and based on ‘Western’ values and culture.
We hope our experiences would diffuse in the Asian region. Southern Asia has a rich, historical and cultural heritage based predominantly from the Indian religions and include Hinduism, Sikhism, Jainism, Buddhism, and Islam that came from the Middle East and spread to the Indian sub-continent. The philosophical, cultural and religious foundations of this region give us a unique opportunity to give a novel perspective to the field. This will require a process of decolonizing our values and beliefs, and reconnecting to our own cultures and heritages. We also need to follow these trends in different locations, share experiences and learn from each other, often a difficult task because these initiatives may fail to reach mainstream journals or remain unpublished.
V. CONCLUSION
The paper highlights the need to have more collaborations within the southern Asian region and share knowledge that would be mutually beneficial. Southern Asia has a rich historical and cultural heritage. These roots could help develop a unique southern Asian version of Medical Humanities and place our version of medical humanities in the global maps of health professional education.
Notes on Contributors
Saroj Jayasinghe conceptualised and wrote the initial draft.
It was revised and expanded by Santhushya Fernando.
Both authors read and approved the manuscript.
Funding
The study was funded by personal funds.
Declaration of Interest
The authors have no conflicts of interest, including financial, consultant, institutional and other relationships that might lead to bias.
References
Our beginnings. (2019). Colombo Medical Humanities News, 1(1). https://med.cmb.ac.lk/medical-humanities/
Jayasinghe, S. (2017). Of course! We must look at the Arts… in its widest sense! Journal of the Ruhunu Clinical Society, 22(1), 4-5. http://doi.org/10.4038/jrcs.v22i1.26
Jayasinghe, S. (2018). Can the arts promote more humane health professionals? Exploring evidence from the neurosciences. Ceylon Journal of Medical Science, 55(1), 1-2. http://doi.org/10.4038/cjms.v55i1.4938
Shankar, P. R. (2022). Learning humanistic values in Nepal. The Asia Pacific Scholar, 7(3), 63-64. https://doi.org/10.29060/TAPS.2022-7-3/LE2777
Zhu, C. S., Yap, R. K. F., Lim, S. Y. S., Toh, Y. P., & Loh, V. W. K. (2021). Humanism in Asian medical education – A scoping review. The Asia Pacific Scholar, 7(1), 9-20. https://doi.org/10.29060/TAPS.2022-7-1/RA2460
*Saroj Jayasinghe
Faculty of Medicine,
University of Colombo,
No 25, Kinsey Road,
Colombo 8, Sri Lanka
+94718619331
Email: saroj@clinmed.cmb.ac.lk
Submitted: 19 August 2022
Accepted: 1 February 2023
Published online: 4 July, TAPS 2023, 8(3), 72
https://doi.org/10.29060/TAPS.2023-8-3/MA1603
Christopher See1*, Cynthia Sin Nga Lam2* & Yalsin Yik Sum Li2
1School of Biomedical Sciences, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong; 2Hospital Authority, Hong Kong
*Authors contributed equally
References
Chang, C. Y., Hwang, G. J., & Gau, M. L. (2022). Promoting students’ learning achievement and self‐efficacy: A mobile chatbot approach for nursing training. British Journal of Educational Technology, 53(1), 171-188. https://doi.org/10.1111/bjet.13158
Huang, W., Hew, K. F., & Gonda, D. E. (2019). Designing and evaluating three chatbot-enhanced activities for a flipped graduate course. International Journal of Mechanical Engineering and Robotics Research, 8(5), 813-818. https://doi.org/10.18178/ijmerr.8.5.813-818
Inkster, B., Sarda, S., & Subramanian, V. (2018). An empathy-driven, conversational artificial intelligence agent (Wysa) for digital mental well-being: Real-world data evaluation mixed-methods study. JMIR mHealth and uHealth, 6(11), e12106. http://doi.org/10.2196/12106
Lam, C. S. N., Li, Y. S., Chan, L. K., & See, C. (2019, November 11). Can the A.I.natomy chatbot teach anatomy? [Poster presentation]. 2nd Korea University International Medical Student Conference, Korea University, Seoul, Korea.
Li, C., Zhang, X., Chrysostomou, D., & Yang, H. (2022). ToD4IR: A humanised task-oriented dialogue system for industrial robots. IEEE Access, 10, 91631-91649. https://doi.org/10.1109/ACCESS.2022.3202554
Schlögl, S., Doherty, G., & Luz, S. (2015). Wizard of Oz experimentation for language technology applications: Challenges and tools. Interacting with Computers, 27(6), 592-615. https://doi.org/10.1093/iwc/iwu016
See, C., Lam, C. S. N., Li, Y. S., & Chan, L. K. (2019, May 31). Methods for training an AI for Higher Education [Poster presentation]. Centre for Information Technology in Education Research Symposium 2019, Faculty of Education, the University of Hong Kong, Hong Kong.
Suleman, R. M., Mizoguchi, R., & Ikeda, M. (2016). A new perspective of negotiation-based dialog to enhance metacognitive skills in the context of open learner models. International Journal of Artificial Intelligence in Education, 26, 1069-1115. https://doi.org/10.1007/s40593-016-0118-8
Kron, F. W., Fetters, M. D., Scerbo, M. W., White, C. B., Lypson, M. L., Padilla, M. A., Gliva-McConvey, G. A., Belfore II, L. A., West, T., Wallace, A.M., Guetterman, T. C., Schleicher, L. S., Kennedy, R. A., Mangrulkar, R. S., Cleary, J. F., Marsella, S. C., Becker, D. M. (2017). Using a computer simulation for teaching communication skills: A blinded multisite mixed methods randomized controlled trial. Patient Education and Counseling, 100(4), 748-759. https://doi.org/10.1016/j.pec.2016.10.024
Ward, T., Falconer, L., Frutos-Perez, M., Williams, B., Johns, J., & Harold, S. (2016). Using virtual online simulations in Second Life® to engage undergraduate psychology students with employability issues. British Journal of Educational Technology, 47(5), 918-931. https://doi.org/10.1111/bjet.12307
Weizenbaum, J. (1966). ELIZA – A computer program for the study of natural language communication between man and machine. Communications of the ACM, 9(1), 36-45.
*Christopher See
Rm 610S, 6/F, Choh-Ming Li Basic Medical Sciences Building,
The Chinese University of Hong Kong, Shatin, New Territories,
Hong Kong Special Administrative Region, China
+852 3943 0465
Email: christophersee@cuhk.edu.hk
Submitted: 16 December 2022
Accepted: 3 January 2023
Published online: 4 July, TAPS 2023, 8(3), 68-69
https://doi.org/10.29060/TAPS.2023-8-3/LE2930
David Mathew
Department of Anaesthesia, Khoo Teck Puat Hospital, Singapore
Dear Editor,
I read with great interest the article entitled “The associates of Emotional Intelligence in medical students: A systematic review” (Edussuriya et al., 2022) in your journal published in October 2022. The association of Emotional Intelligence (EI) with wellbeing cannot be underestimated, especially with the plethora of positive effects it has on mental health and academic performance. In fact, I think this can be extended beyond students, to all healthcare professionals.
In my opinion, humanities in medicine provide a potentially novel way of improving emotional intelligence. The writer of a piece acknowledges the scientific experience that has moved him/her, and subsequently reflects on the entire experience through the arts and writing. The process of writing can be cathartic as it presents an avenue for the writer to release emotions that might have been pent-up or hidden as we provide a brave front to our patients. Once written, the piece can be shared, and reach out to other healthcare professionals who might have encountered similar experiences. Some may find comfort in reading such pieces, as they realise they are not alone in experiencing the roller-coaster of emotions in their daily lives.
I have appended a piece I wrote regarding my experience with an obstetrics patient and how sometimes the lesser said, the more it means. The process of writing and sharing this piece helped me better understand and appreciate what I went through and I hope it can do the same for fellow readers.
Cry
The day I saw her cry
was when her baby’s heart
slowed.
She needed the Caesarean
quickly.
Her eyes conceived tears
crawling down her cheeks
shaping into an anxious cry.
I counted the tears
and spoke more words
comforting, reassuring.
I saw her cry
one week later,
this time her littlest bundle
the greatest joy.
Tears of happiness
dancing muted screams of relief
I counted the tears
but spoke nothing
comforting, reassuring.
Tears
instead of words,
won wars of emotions.
And staying silent
might be the most reassuring cry
of comfort.
Note on Contributor
DM came up with the concept of the manuscript, and wrote the entirety of its contents.
Funding
There was no funding for this paper.
Declaration of Interest
There is no conflict of interest declared.
References
Edussuriya, D., Perera, S., Marambe, K., Wijesiriwardena, Y., & Ekanayake, K. (2022). The associates of Emotional Intelligence in medical students: A systematic review. The Asia Pacific Scholar, 7(4), 59–70. https://doi.org/10.29060/taps.2022-7-4/oa2714
*David Mathew
Khoo Teck Puat Hospital,
90 Yishun Central, Singapore
Email: davidmathew3142@gmail.com
Submitted: 20 October 2022
Accepted: 3 January 2023
Published online: 4 July, TAPS 2023, 8(3), 65-67
https://doi.org/10.29060/TAPS.2023-8-3/CS2906
Hiroshi Kawahira1, Yoshitaka Maeda1, Yoshihiko Suzuki1, Yuji Kaneda1, Yoshikazu Asada2, Yasushi Matsuyama2, Alan Kawarai Lefor3 & Naohiro Sata3
1Medical Simulation Center, Jichi Medical University, Japan; 2Medical Education Center, Jichi Medical University, Japan; 3Department of Surgery, Jichi Medical University, Japan
I. INTRODUCTION
The ongoing COVID-19 pandemic has a significant impact on medical education, forcing changes in the curriculum (Rose, 2020). Since the COVID-19 pandemic began, governments and authorities in many countries have imposed online learning on medical students and in many institutions, medical students were not permitted to participate in in-person clinical clerkships or other practical training at university hospitals (Mian & Khan, 2020). Although the surgical clerkship is an important contributing factor to nurture student interest in a surgical career (Khan & Mian, 2020), medical students were excluded from the operating room due to lack of personal protective equipment, and participation in ward duties and training facilities were restricted (Calhoun, et al., 2020).
The purpose of this study is to analyse how the lack of in-person surgical experience and ward duties (online clerkship), among the most important components of a surgical clerkship, affected student interest in a career in surgery. The impact on student perceptions of surgery comparing online learning and onsite clinical clerkship (typical in-person clerkship) was assessed by comparing student satisfaction with the surgical clerkship, changes in interest in a career in surgery, and changes in the image of surgery at the beginning and end of rotations for online and onsite training groups.
II. METHODS
This study was reviewed by the Ethical Review Committee of Jichi Medical University, and no ethical review was required (Reference No. 20-186). A total of 133 fifth-year medical students, all in the same academic year, participated in surgery clerkships from April 2020 to February 2021. All 133 medical students completed clerkships in internal medicine during the previous academic year. The 133 students were divided into eight groups, with 16 or 17 students per group, rotating in surgery every three weeks. The first five groups of that academic year had online lectures only and the last three groups had onsite practice (typical clerkship experience).
Of the 133 students, 124 who provided consent were included in this study. Of these, 79 received online training from April through September 2020, and 45 received onsite clerkship training from October 2020 through February 2021. Moodle, an online learning management system, was used as the platform for online learning, and designed content to be studied on demand. An orientation and lecture with a comprehensive explanation of each aspect of surgical training were synchronous, and online communication with individual students was also conducted. Faculty also communicated online with individual students using Moodle, and individual questions were answered via email as appropriate.
Questionnaires for students in the clerkship were administered using the Moodle platform regardless of whether the clerkship was onsite or online. Questionnaire items addressed: 1. anxiety about surgery, 2. Opinion about difficulty of surgery compared to internal medicine, and 3. interest in surgery. Responses were given as a single choice and were scored using a four-point scale: 1: disagree, 2: somewhat disagree, 3: somewhat agree, and 4: agree.
Comparisons between responses at the beginning and end of the three-week clerkship for all participants were made with the Wilcoxon signed rank test. After calculating differences between the beginning and end of the clerkship, the online and onsite groups were compared using the Mann-Whitney U test. A p < 0.05 was considered statistically significant. Cohen’s d was used as an index of effect size, with 0.2 as a small effect size, 0.5 as a medium effect size, and 0.8 as a large effect size. The statistical software used was R 3.6.1 with GUI 1.70 (The R Project for Statistical Computing, Vienna).
III. RESULTS
The results for the 124 students enrolled in this study showed that after three weeks of practice compared to the beginning of the study, they were less anxious about surgery (p<0.00001, effect size 0.43), less likely to find surgery difficult compared to study in other departments (p<0.00001, effect size 0.57), and were more interested in surgery as a career (p<0.0001 and effect size 0.38) (See Table 1).
The onsite clinical clerkship resulted in less anxiety about surgery (p = 0.017, effect size 0.41) compared with the online clerkship. There was no significant difference in change of the image of surgery as hard compared to other departments (p = 0.293, effect size 0.21) or change of interest in surgery (p = 0.407, effect size 0.09) in comparing the onsite and the online groups, and the effect size on change of image and interest were also small (See Table 1).
|
|
|
Average |
p* |
p# |
Cohen’s d |
||
|
|
|
Beginning |
Ending |
Beginning – End |
|||
|
How anxious are you about the surgery rotation? |
Total (n=124) |
3.31 |
2.99 |
– |
< 0.00001 |
– |
0.43 |
|
online clerkship (n=79) |
3.38 |
3.19 |
0.19 |
– |
0.017 |
0.41 |
|
|
onsite clerkship (n=45) |
3.20 |
2.64 |
0.56 |
||||
|
How difficult is the surgery rotation compared to other departments? |
Total (n=124) |
3.40 |
2.99 |
– |
< 0.00001 |
– |
0.57 |
|
online clerkship (n=79) |
3.62 |
2.99 |
0.63 |
– |
0.293 |
0.21 |
|
|
onsite clerkship (n=45) |
3.53 |
3.00 |
0.53 |
||||
|
How interested do you feel in surgery as a career? |
Total (n=124) |
3.06 |
3.32 |
– |
< 0.0001 |
– |
0.38 |
|
online clerkship (n=79) |
3.00 |
3.29 |
-0.29 |
– |
0.407 |
0.09 |
|
|
onsite clerkship (n=45) |
3.16 |
3.38 |
-0.22 |
||||
Table 1. Changes in the results of responses at the beginning and end of online and onsite clerkships
p*: Wilcoxon signed rank test, p#: Mann-Whitney U test
IV. DISCUSSION
During the COVID-19 pandemic, medical schools have established integrating digital technology and novel pedagogy (Tan, et al., 2022). Regardless of the clerkship format, three weeks of surgical clinical clerkship resulted in less anxiety about surgery than initially felt, a less daunting image of surgery in comparison to other departments, and significantly higher interest in surgery. However, the effect sizes were moderate (0.43, 0.57, and 0.38), suggesting a positive change in the image of surgery, especially in comparison with other departments. The onsite clinical clerkship group showed a greater decrease in change in anxiety about surgery than the online clinical clerkship at the end of the surgical clinical clerkship (effect size 0.41). The effect size was moderate, suggesting the effectiveness of the onsite clinical clerkship. This study also shows that there were no statistical differences in the feeling of difficulty or interest in a surgical career between the onsite and the online groups. We believe that online content via Moodle was attractive for medical students. Also, medical students could feel the realism of the surgical workplace using Moodle.
V. CONCLUSION
Face-to-face communications with senior physicians are essential to foster an image of the role of physicians to medical students. It is desirable to develop a hybrid type of clinical clerkship that takes advantage of the advantages of the realism of surgery provided by an onsite clinical clerkship and the easy accessibility of educational content of an online clinical clerkship.
Notes on Contributors
Kawahira, Maeda and Suzuki designed the study. Asada and Kawahira constructed the Moodle platform. Kaneda, Lefor and Sata conducted surgical clinical practice. Kawahira and Maeda analyzed data. Kawahira and Lefor wrote the manuscript.
Acknowledgement
The authors would like to acknowledge Ms. Yasuko Saikai who did the administrative contact for the students, and all the staffs and surgeons of the Department of Surgery for instructing the students on the clinical clerkship.
Funding
This research was funded by the education and research expenses from Jichi Medical University.
Declaration of Interest
The authors declare that they have no competing interests.
References
Rose, S. (2020). Medical student education in the time of COVID-19. JAMA, 323(21), 2131-2132. https://doi.org/10.1001/jama.2020.5227
Mian, A., & Khan, S. (2020). Medical education during pandemics: a UK perspective. BMC Medicine, 18, Article 100. https://doi.org/10.1186/s12916-020-01577-y
Khan, S., & Mian, A. (2020). Medical education: COVID-19 and surgery. British Journal of Surgery, 107(8), Article e269. https://doi.org/10.1002/bjs.11740
Calhoun, K. E., Yale, L. A., Whipple, M. E., Allen, S. M., Wood, D. E., & Tatum, R. P. (2020). The impact of COVID-19 on medical student surgical education: Implementing extreme pandemic response measures in a widely distributed surgical clerkship experience. American Journal of Surgery, 220(1), 44-47. https://doi.org/10.1016/j.amjsurg.2020.04.024
Tan, C. J., Cai, C., Ithnin, F., & Eileen, L. (2022). Challenges and innovations in undergraduate medical education during the COVID-19 pandemic – A systematic review. The Asia Pacific Scholar, 7(3), 1-9. https://doi.org/10.29060/TAPS.2022-7-3/OA2722
*Hiroshi Kawahira
Medical Simulation Center
Jichi Medical University
3311-1 Yakushiji, Shimotsuke, Tochigi
Japan 329-0498
Email: kawahira@jichi.ac.jp
Submitted: 14 December 2022
Accepted: 22 March 2023
Published online: 4 July, TAPS 2023, 8(3), 62-64
https://doi.org/10.29060/TAPS.2023-8-3/PV2926
Sachiko Kasamo, Satoshi Ozeki, Hiroyasu Inoue & Seiji Matsumoto
Institutional Research Office, Asahikawa Medical University, Japan
I. INTRODUCTION
There is growing interest in social responsibility around the world in order to accomplish a sustainable society. Indeed, modern universities cannot be ivory towers unrelated to society. It would not be an overstatement to say that without interaction and contribution to society, the university’s survival and development are unlikely.
It is frequently said that the university fulfils three different missions: education, research, and social contribution. J. A. Perkins, the eminent theoretician of higher education in the 1960s, proposed there are three aspects of knowledge that must be understood as they have their institutional reflections in the university’s three missions (Perkins, 2016). For knowledge itself to have significant power, there must be communication and interaction between the newly acquired knowledge, its transmission, and its application. The above concept began in the United States and has since been widely adopted as three major missions in many universities worldwide. Despite these three missions, however, depending on the university’s expertise and readiness, and the resources and support received from external organisations and individuals, the university may be more active on some missions and less active on others.
Some with a conventional conception of “social contribution” may wonder “why now?”, as the results of both “education and research” are ultimately returned to society. However, the major difference is that while the conventional efforts of the university were at the level of individual responses by faculty members and others, the current “social contribution” is positioned as the essential function of the university. Expectations for universities have changed significantly, and universities have changed in a variety of ways; universities are now required to use knowledge for society from various perspectives. The greater the need to contribute to society and the greater its role, the more we need to question the meaning of “social contribution” in relation to the traditional roles of “education and research” in the university.
II. GLOBAL CONCEPTS OF SOCIAL ACCOUNTABILITY IN MEDICAL SCHOOLS
The concept of social contribution is embedded in the social accountability of medical schools. The World Health Organization defined it as “the obligation to direct their education, research and service activities towards addressing the priority health concerns of the community, region, and/or nation they have a mandate to serve” (Boelen & Heck, 1995). Following this, the Global Consensus for Social Accountability of Medical Schools defined a socially accountable medical school as one that “responds to current and future health needs and challenges in society, re-orientates its education, research and service priorities accordingly, strengthens governance and partnerships with other stakeholders and use evaluation and accreditation to assess their performance and impact” (Global Consensus for Social Accountability of Medical Schools [GCSA], 2010). This document also emphasised the significance of enhancing medical schools’ ability to address the demands and difficulties of providing healthcare for citizens and society at large, in accordance with the fundamental principles of quality, equity, relevance, and effectiveness. In addition, the criteria for ASPIRE-to-Excellence Award for Social Accountability by Association for Medical Education in Europe provide a practical framework for medical schools to consider when examining their own social contribution. This award itself gives schools the opportunity to be acknowledged globally for their excellence in education, which also covers social accountability (Mori et al., 2022). These internationally accepted concepts should always be kept in mind when promoting social contribution activities in medical schools.
III. SOCIAL CONTRIBUTIONS IN JAPANESE MEDICAL SCHOOLS
Japan might be one of the unique countries to set clear objectives regarding the university’s social contribution in legislation. There are two revisions that have pushed the idea of social contribution forward as a fundamental function of the university (Hosono, 2014). First, the 2006 Revision of Basic Act on Education, Article 7 stated, “Universities, as the core of scholarly activities, are to contribute to the development of society by cultivating advanced knowledge and specialised skills, inquiring deeply into the truth to create new knowledge, and broadly offering the fruits of these endeavours to society.” Second, 2007 Revision of School Education Act, Article 83(2) stated, “Universities shall contribute to the development of society by conducting education and research to achieve their objectives and by providing the results widely to the society.” In light of these key statement revisions, the mission of the universities has changed along with the social trends, and more direct social contributions are being sought.
The importance of social contribution is also emphasised by Japanese medical schools. The recent study has analysed the Japan Accreditation Council for Medical Education accreditation documents of 45 medical schools against a global framework, and revealed that social contribution is identified to be one of the key components in the main category of “issues in society” for social accountability (Mori et al., 2022). As an essential aspect of social contribution, the need for an individual’s lifelong learning has increased by an accumulation of factors, such as disaster-related disruptions, pandemics, and the ageing population with longevity. Medical schools can certainly use their strengths as health experts to assist in health literacy and well-being for the members of communities. In addition, the government has long been prioritising, promoting, and advancing lifelong learning in Japan, in recognition of global challenges and social changes. Therefore, social contribution activities by medical schools can come into play to satisfy the need of individuals, society, and the country.
IV. SOCIAL CONTRIBUTION THROUGH COMMUNITY LECTURES: A CASE FROM A REGIONAL MEDICAL UNIVERSITY
Here, we share an example of ongoing direct social contribution activity at our university. The university positions social contribution as a significant role and mission in Educational Philosophy, and our “Community Lectures (haken kouza)” constitutes one of the essential elements in this role. This activity began in 2002 to meet the local community’s lifelong learning needs, and the university’s members have been giving lectures at the request of local public organisations. There are over 350 different topics offered to date. The lecture themes are not limited to medical and nursing topics, but also include educational and cultural topics. Between 2016 and 2019, we provided over 600 lectures to the local and regional communities. As the northernmost medical university in Japan, it is necessary to devise something unique to the region that makes the best use of the regional characteristics, and we firmly believe that there is a stage for the university to play an active role.
V. WHAT, THEN, IS THE SOCIAL CONTRIBUTION OF UNIVERSITIES
We acknowledge that the above Community Lecture is just one example, and in fact, social contribution can take many forms and shapes and be offered at various levels. The social contribution made by universities must not be merely the provision of free labour or lending facilities, but should fully utilise the characteristics of the university as the base for intellectual creative activities. In other words, the knowledge acquired and transmitted through the university’s education and research activities should be returned to the local community by the mechanism of social contribution with the aim of improving the lives and welfare of the local population. The ideal relationship between the university and the community should not be a one-way relationship but should be a reciprocal one; where the community benefits from the intellectual and human resources of the university through community cooperation, and the university makes effective use of the region as part of its education and research.
In addition, activities such as international collaboration, regional collaboration, industry-academia-government collaboration, and training programs are all solid initiatives aimed at giving back to society in a more direct way. The university faculty and staff have been independently engaged in these activities as experts in their respective fields. These include serving on committees of administrative agencies, supporting science education in schools, joint research with industries, and public lectures for non-students. They voluntarily carry out these social contribution activities (without even recognising them as such) alongside their busy daily clinical duties, teaching and research. However, these activities are often missed or not subject to systematic evaluation by the universities. In the future, these activities should be highlighted and evaluated as important activities that play a role in the functions of universities. We hope this article will stimulate interest in expanding social contribution in the university context. For future work, we plan to review other areas of social contribution activities conducted at the university.
Notes on Contributors
Sachiko Kasamo reviewed the literature, conceptualised and took the lead in writing and editing the manuscript.
Satoshi Ozeki contributed to the conception and revision of the manuscript critically.
Hiroyasu Inoue contributed to the conception and theoretical ideas of the manuscript.
Seiji Matsumoto supervised and gave critical feedback on the intellectual content of the manuscript.
All the authors have read and approved the final manuscript.
Acknowledgement
We sincerely thank Ms Misako Sato (Institutional Research Office’s administrative staff) and the Research Support Section of Asahikawa Medical University for their support.
Funding
There is no funding source required for this study.
Declaration of Interest
All authors have no conflicts of interest to disclose.
References
Boelen, C., & Heck, J. E. (1995). Defining and measuring the social accountability of medical schools. Geneva: World Health Organization.
Global Consensus for Social Accountability of Medical Schools (GCSA). (2010). Global census for social accountability of medical schools. https://healthsocialaccountability.sites.olt.ubc.ca/files/2011/06/11-06-07-GCSA-English-pdf-style.pdf
Hosono, M. (2014). Kokuritsu daigaku niokeru syakaikoukenkatsudouno genjyou to kadai. [Current Status and Issues of Social Contribution Activities at National Universities]. The Journal of Science Policy and Research Management, 29(1), 44-49. https://doi.org/10.20801/jsrpim.29.1_44
Mori, H., Izumiya, M., Hayashi, M., & Eto, M. (2022). Current perception of social accountability of medical schools in Japan: A qualitative content analysis. Medical Teacher, 1-8. https://doi.org/10.1080/0142159X.2022.2140033
Perkins, J. A. (2016). The university in transition. Princeton University Press.
*Seiji Matsumoto
Institutional Research Office,
Asahikawa Medical University,
2-1-1-1, Midorigaoka-Higashi,
Asahikawa, Hokkaido,
078-8510, Japan
Email: matsums@asahikawa-med.ac.jp
Submitted: 11 September 2021
Accepted: 22 March 2023
Published online: 4 July, TAPS 2023, 8(3), 58-61
https://doi.org/10.29060/TAPS.2023-8-3/SC2694
Maria Isabel Atienza & Noel Atienza
San Beda University College of Medicine, Philippines
Abstract
Introduction: An evaluation of the online medical course was conducted to assess student readiness, engagement, and satisfaction at the San Beda University College of Medicine in Manila during the COVID-19 pandemic.
Methodology: A convergent mixed methods approach was done with a quantitative online survey and a qualitative thematic analysis of focus group discussions (FGD) with medical students. A total of 440 students participated in the survey while 20 students participated in the FGDs.
Results: The medical students were sufficiently equipped with computers and internet connections that allowed them to access the online medical course from their homes. The 5 themes identified during the study that were relevant to education were: Student readiness for online learning, Learning Management System (LMS) and internet connectivity, teaching and learning activities, the value of engagements, and teaching effectiveness of the faculty. The combined quantitative and qualitative analysis revealed vital issues that affect student learning. This included the need for students to interact with fellow students and to be engaged with their faculty. The issues that affect teaching included the need for continuing faculty training and management skills in delivering the full online course.
Conclusion: The success of online education rests heavily on the interactions of the students, the teachers, and the knowledge. Student interactions, managerial and skills training for the faculty, and providing students with a mix of synchronous and asynchronous activities are the most effective means to ensure the effective delivery of online medical courses.
Keywords: Medical Curricular Revision, Formative Evaluation, Student Engagement, Synchronous and Asynchronous Online Learning, Cognitive Overload
I. INTRODUCTION
The COVID-19 pandemic necessitated a shift to online teaching and a revision of the medical curriculum with synchronous and asynchronous online activities. Medical schools worldwide adapted teaching strategies utilising Video Conferencing and Learning Management Systems.
This program evaluation of the online medical course aimed to evaluate the effectiveness of instruction using the various components of online learning. The study centered on the perspectives of students using a mixed methods design (Fitzpatrick et al., 2011). The study focused on the interplay of digital capabilities, students’ perceptions and satisfaction with the interactions and engagements during the online course.
II. METHODS
The mixed methods research protocol was approved by the Institutional Ethics Board of San Beda University. The study utilised a convergent mixed method design with a quantitative online survey that was conducted on 440 respondent students representing each of the four-year levels of the medical school. Six focus group discussion (FGD) sessions were conducted on 20 students. All student participants provided a signed informed consent form to participate in the survey and in the FGDs. The 25-item online survey questionnaire included a 5-point Likert scale for items on readiness for the online course, overall satisfaction, and engagement. The online FGD sessions were conducted using an open-ended questionnaire guide on student capabilities for the online course, student satisfaction, and student engagement.
The FGD recordings were transcribed and subjected to thematic analysis to identify major themes. Quantitative and qualitative data were analysed simultaneously through a joint display of the two sets of results. A joint display using pillar integration was done to demonstrate the themes where the data corroborated or validated each other. The conceptual framework, data collection tools, the data results, and the pillar integration table are posted in a data repository file for this study can be accessed through a repository at: https://doi.org/10.6084/m9.figshare.16682569.v2 (Atienza & Atienza, 2021).
III. RESULTS
The survey revealed that students were adequately equipped with the necessary computers and smartphones needed to access the online course. Only 50% of the students were taking the online course from their homes within the same city as the medical school. While 72% encountered internet connectivity problems, 88% of students were successful in the use of the LMS and the videoconferencing platform to access the course and take online examinations.
Seventy-eight percent of students found online student-to-student and faculty-to-class interactions to be beneficial to student learning. Among the synchronous activities, 63% of students preferred live online lectures. Among the asynchronous activities, 52% of students preferred uploaded video lectures. Overall, around 52% of students experienced being overloaded with study requirements while 48% of students felt there was sufficient time for independent study.
The results of the survey and the thematic analysis of the FGDs were organised into themes and subthemes. These themes were generated from the integration of the quantitative and qualitative data. The schematic diagram (Figure 1) demonstrates how the themes are related to the effectiveness of learning based on the perspective of the students.
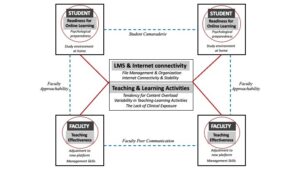
Figure 1. Schematic diagram of themes and subthemes identified in a mixed methods analysis of a fully online medical course at SBU-COM during the COVID pandemic
A. Student Readiness
The first theme that surfaced from the results was Student Readiness to engage in online learning. Students found their readiness to be dependent on two subthemes:
1) Study environment at home: Students expressed that the sudden shift to studying from home required that they designate sufficient time and space for studying. Students recognised that responsibilities at home and to the family could be distractions if not managed properly.
2) Psychological preparedness: The students also expressed the value of psychological preparedness as essential in dealing with stress and fatigue resulting from the unexpected shift to the online learning mode.
B. LMS and Internet Connectivity
The second theme highlights the importance of having computers and a stable internet connection as major determinants of student satisfaction with the online course. The introduction of an LMS for the medical course required immediate training for both the students and the faculty. While 81% of the students had the necessary gadgets and a good internet signal, 17% experienced major connection problems that disrupted up to 50% of live lectures and offline recorded videos. Student satisfaction with online learning was dependent on how timely and how organised the learning materials were uploaded into the LMS.
C. Teaching and Learning Activities
The third theme refers to the blend of online and offline activities for the different courses. The major subthemes included cognitive overload, variability of teaching and learning activities across courses, and the lack of clinical exposure.
1) Cognitive overload: Students had a perception of being overloaded by the volume of information delivered through the online course. The introduction of new forms of assessments such as video assignments, group reports, and research outputs contributed to the perceived cognitive overload.
2) Variability of teaching and learning activities: The variability in the blend of online and offline activities across the different courses required varying degrees of adjustments from the students. The students expressed their preference for live or recorded lectures over small group discussions and live laboratory demonstrations.
3) Lack of clinical exposure: Students in the 3rd and 4th year levels were apprehensive about the lack of clinical exposure in the actual medical environment due to the restrictions brought about by the pandemic. They recognise that they may not have the necessary skills training needed for internship.
D. The Value of Engagements
Unexpectedly, the fourth theme that students found important in the shift to online learning was the value of engagements.
1) Student-to-student online interactions: Up to 78% of students found support through interactions with other students. These interactions were useful not only for sharing the academic workload but also for mental and emotional support highlighting the value of student camaraderie despite being limited to virtual interactions.
2) Faculty-to-class interactions: Up to 80% of students expressed appreciation for the efforts of the faculty to get student feedback, answer clarificatory questions, and provide explanations when necessary. The students also expressed greater satisfaction with courses delivered online. Both faculty interactions with the class and with individual students were recognised as faculty approachability.
E. Teaching Effectiveness of The Faculty
The fifth theme Teaching pertains to the ability of the faculty to manage the online platform for teaching.
1) Faculty management skills: Teaching effectiveness is facilitated by the ease by which the faculty manages virtual teaching.
2) Faculty peer communication: Students recommend that the faculty within and across different courses coordinate their activities so that students can more easily manage their time and learning.
IV. DISCUSSION
The experience of delivering the medical course online has been very limited in the past. The teaching and learning strategies for medical courses to be delivered fully online require extensive preparation of the three main points in the transaction of learning: the learners, the teachers, and the course content. Learner readiness entails a clear delineation of the study environment in terms of time and space for study. Proper orientation to the online learning environment and psychological support should be made available to the students before the course begins. An inventory of the students’ computers and internet connectivity should also be done to ensure readiness for the course.
Delivering the course online necessitates faculty training on teaching and learning strategies for synchronous and asynchronous delivery as well as the proper navigation of the LMS and its available features. The faculty must maximise the benefits of technology as well as pedagogy in the online learning environment.
This study showed that in the shift of medical education to an online mode during the pandemic, student learning relies heavily on interactions between the learners, the teachers, and the course content. In an online course that relies so much on technology as a means of course delivery and integration, teaching and learning success depends on how well the interactions are established among these three points (Ifinedo & Rikala, 2019).
The design of courses must facilitate student-to-student interactions while faculty-to-class interactions using both synchronous and asynchronous activities would provide a good learning experience for students (Rhim & Han, 2020; Seymour-Walsh et al., 2020).
V. CONCLUSION
To succeed in the delivery of the online medical course, sufficient time must be given for faculty-to-student interactions during synchronous sessions and after the online classes. The faculty must demonstrate approachability by being open to continuing interactions with students outside the synchronous sessions. The coordination of faculty members within and across different courses must be enhanced to reflect efficiency in delivering their respective courses.
This study was performed during the early phase after the shift to full online delivery of the medical course. While the study is based on the perceptions of the students, the results of this study may be valuable in planning for continuing the online delivery of the medical course. The results of this study may be more robust with the inclusion of faculty perceptions and indicators of student academic performance.
Notes on Contributors
Dr. Maria Isabel Atienza conceptualised, designed, and implemented this study. She conducted the focus group discussions, prepared the thematic analysis, and wrote the manuscript for this study.
Dr. Noel Atienza helped in the design and conduct of the online survey and was involved in the data processing and data analysis of the survey. He was also involved in the preparation and editing of the final manuscript.
Ethical Approval
The research protocol SBU-REB # 2020-028 for this study was reviewed and approved by the San Beda University Research Ethics Board on November 28, 2020.
Data Availability
Data collection tools and research data are available and can be accessed by any interested reader through a repository at: https://doi.org/10.6084/m9.figshare.16682569.v2. The data in the repository may not be copied or cited without written permission from the authors.
Acknowledgment
The authors would like to acknowledge the support provided by the Alumni of San Beda and their commitment to promoting faculty research activities.
Funding
This study was funded by the Jesus P. Francisco Distinguished Professorial Chair Research Grant from the San Beda College Alumni Foundation, Inc.
Declaration of Interest
There are no conflicts of interest in this study.
References
Atienza, M., & Atienza, N. (2021). An online medical course during the COVID-19 pandemic: A mixed methods analysis. [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.16682569.v2
Fitzpatrick, J., Sanders, J., & Worthen, B. (2011). Program evaluation: Alternative approaches and practical guidelines 4th Edition. Pearson Education, Inc.
Ifinedo, E., & Rikala, J. (2019). TPACK and educational interactions: Pillars of successful technology integration. World Conference on E-Learning. Association for the Advancement of Computing in Education, 295-305. https://www.learntechlib.org/primary/p/211094/
Rhim, H., & Han, H. (2020). Teaching online: Foundational concepts of online learning and practical guidelines. Korean Journal of Medical Education, 32(3), 175-183. https://doi.org/10.3946/kjme.2020.171
Seymour-Walsh, A., Bell, A., Weber, A., & Smith, T. (2020). Adapting to a new reality: COVID-19 coronavirus and online education in the health professions. Rural and Remote Health, 20, 6000. https://doi.org/10.22605/RRH6000
*Maria Isabel Maniego Atienza
San Beda University, Mendiola Street,
Barangay San Miguel,
City of Manila, Philippines
+639178668751
Email: mimatienza@yahoo.com
Submitted: 15 August 2022
Accepted: 20 December 2022
Published online: 4 July, TAPS 2023, 8(3), 54-57
https://doi.org/10.29060/TAPS.2023-8-3/SC2867
Seow Chong Lee & Foong May Yeong
Department of Biochemistry, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: In the first weeks of medical school, students learn fundamental cell biology in a series of lectures taught by five lecturers, followed by a mass tutorial session. In this exploratory study, we examined students’ perceptions of the mass tutorial session over two academic years to find out if they viewed the tutorials differently after minor tweaks were introduced.
Methods: Reflective questions were posted to the undergraduate Year 1 Medical students at the end of each mass tutorial session in 2019 and 2020. Content analysis was conducted on students’ anonymous responses, using each response as the unit of analysis. The responses were categorised under the learning objectives, with responses coded under multiple categories where appropriate. The distribution of the counts from responses in 2019 and 2020 was compared, and the tutorial slides used over the two years were reviewed in conjunction with students’ perceptions to identify changes.
Results: In 2019, we collected 122 responses which coded into 127 unique counts, while in 2020, 119 responses coded into 143 unique counts. Compared to 2019, we noted increases in the percentage of counts under “Link concepts” and “Apply knowledge”, with concomitant decreases in percentage of counts in “Recall contents”. We also found that the 2020 tutorial contained additional slides, including a summary slide and lecture slides in their explanations of answers to the tutorial questions.
Conclusion: Minor tweaks in the tutorial presentation could improve students’ perceptions of our mass tutorials.
Keywords: Mass Tutorials, Students’ Reflections, Apply Knowledge, Link Concepts, Minor Tweaks
I. INTRODUCTION
In the first few weeks of medical school, students learn about cell biology which is fundamental to what they need to know about tissues, organs, and the whole body in a series of lectures co-taught by five lecturers. In the lectures, efforts are made to highlight basic cellular processes, and illustrate how these are inter-connected in a cell. Where appropriate, how knowledge in the biomedical sciences underpins applications in clinical settings is also illustrated by the lecturers. At the end of the series of lectures, the lecturers will co-facilitate a mass tutorial session aimed at summing up the topics.
The mass tutorial session has several learning objectives. These include basic levels of learning such as recalling concepts, preparing for assessments, and building knowledge on topics, to higher levels of learning such as applying concepts to solve real life problems, and linking concepts between topics. Being the only teaching and learning activity that all lecturers co-teach, the mass tutorial provides the best opportunity to demonstrate links and apply the consolidated knowledge learnt during the different lectures.
Once the teaching and learning activities are completed, the coordinator of the lectures Foong May Yeong (YFM) reviews the curriculum to ensure that the teaching and learning activities delivered the intended learning objectives. Such reviews include students’ experiences of the curriculum (Erickson et al., 2008), which the coordinator (YFM) routinely collect through posting reflective questions at the end of the tutorial. In this exploratory study, we analysed students’ reflections from 2019 and 2020, and categorised them under different learning objectives of the tutorial. We noted an increase in percentage counts under “Apply knowledge” and “Link concepts” in 2020 compared to 2019. A review of the tutorial slides revealed the addition of summary and lecture slides in 2020. Our results suggest that minor tweaks to the tutorial presentation are sufficient to help students see the intended usefulness and relevance of tutorials.
II. METHODS
A. Format of Mass Tutorials
The mass tutorial was conducted after completion of the cell lectures. For 2019, this was a face-to-face session. For 2020, due to the COVID-19 pandemic, the tutorial was conducted online via Microsoft Teams. The class size was 281 for 2019, and 280 for 2020. Four out of five lecturers taught the same topics for both years. For both years, during the mass tutorial, each lecturer used Poll Everywhere to pose a mix of five to six recall and application questions linked to their topic. Identical questions were used in 2019 and 2020. Students discussed among themselves before answering these questions. The class responses were then revealed, after which the lecturer explained the solutions to their questions. The cycle was repeated until all the lecturers completed their parts.
B. Collection of Student Reflections
After each tutorial, the coordinator (YFM) posted two reflection questions on Poll Everywhere. The two questions were: 1. “What were the key points you learned in this session?”, 2. “Any questions?”. Answering these reflection questions were voluntary and anonymous. A waiver of informed consent was approved by Yong Loo Lin School of Medicine Medical Sciences Departmental Ethics Review Committee. The responses to question 1 obtained from students in 2019 and 2020 were analysed in this study.
C. Content Analysis
The responses to question 1 were coded and categorized into the different learning objectives of the mass tutorial, using each response as a unit of analysis. Each response could be coded into multiple categories when appropriate. The counts under each category were represented as a percentage of all counts coded from the responses. The tutorial slides used in 2019 and 2020 were also reviewed to understand students’ perceptions.
III. RESULTS
In 2019, we collected 122 responses which were coded into 127 unique counts. In 2020, we collected 119 responses which were coded into 143 unique counts. The number of responses and unique counts coded were largely similar between the two years. The unique counts were categorised into the five learning objectives and their percentage counts were presented in Figure 1. Supplemental data containing an overview of the categories and samples of students’ responses, as well as the counts under each category, are openly available in Tables 1 and 2 shared at Figshare at http://doi.org/10.6084/m9.figshare.20484498 (Lee & Yeong, 2022). The distribution of the counts differed between the two years. In 2019, majority of the counts were categorized to “Recall contents” (37.0%), with low numbers categorized as “Apply knowledge” and “Link concepts” (15.0% and 3.1% respectively). In comparison, in 2020, we observed a decrease in percentage of counts in “Recall contents” (to 21.0%), with an increased percentage in counts in “Apply knowledge” and “Link concepts” (to 22.4% and 15.4% respectively). Overall, there is a shift in distribution of counts, from a skewed distribution in 2019, to an even distribution in 2020.
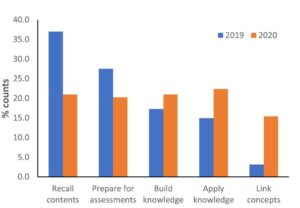
Figure 1. Categorisation of students’ responses into the learning objectives
Given that tutorial questions used in the two years were largely identical, we reviewed the tutorial slides used in these two years to look for possible differences. In 2020, firstly, a summary slide detailing the different aspects of the cell was added to the start of the tutorial slides. Secondly, lecture slides were included in the tutorial slides to explain the answers to the tutorial questions. The lecture slides could come from the lecturer teaching the topic of interest, or from other lecturers if connections across topics were important. These additions could have altered students’ perceptions of the mass tutorial session in 2020.
IV. DISCUSSION
In this study, we examined students’ reflections collected across two academic years to understand their perceptions of the mass tutorial sessions that capped the teaching of cell biology. One of the intentions of the lecturers when designing the tutorial questions was to demonstrate links across topics, and illustrate how questions can be solved using connections across topics. The decrease in percentage of counts under “Recall contents” in 2020 suggested an increase in students’ awareness of the usefulness and relevance of the tutorial sessions when minor changes were made in the presentation of the overview of the cell biology topic and the answers to the tutorial questions.
Both lecture and summary slides likely promoted links in different ways. The lecture slides represent theoretical knowledge for each topic, and also add visuals to the explanations of tutorial questions. Inclusion of lecture slides allow students to use both visual and audio channels to process the explanations, instead of using only the audio channel to listen to explanations when they were delivered verbally without visuals (Mayer, 2014). Using both channels could lower the cognitive load for students to learn and construct meaningful frameworks to solve problems. Summary slides juxtaposed different topics within a slide, allowing students to visualize connections between topics in the proper functioning of a cell (Bae & Watson, 2014). Adding these slides require little effort from the lecturers as the slides are readily available. Such small changes in improving the instructional approach could result in improvements in student learning (Lang, 2016).
There are several limitations to our study. Firstly, we only reviewed the tutorial slides, which covers part of the enacted curriculum. Secondly, the tutorial in 2019 was conducted face-to-face while the one in 2020 was conducted online. Online learning normally is not something students view positively, hence the improvements in student perceptions was surprising. Students prefer the social aspects of learning, which is abundant in face-to-face learning but greatly diminished in online learning (Siah et al., 2022). However, the diminished opportunities for peer-learning in online environment might contribute to increased attention diverted to lecturers for explanations.
V. CONCLUSION
Surveying and analysing students’ reflections at the end of mass tutorial proved to be informative in evaluating and improving our tutorials. In our preliminary analysis, a change in students’ perceptions of the tutorial from recalling of concepts to application of knowledge and linking concepts corresponded to minor tweaks in our tutorial presentation slides. Such minor tweaks, requiring little time, but yet are effective in helping students see the usefulness and relevance of tutorials, is an approach that even busy academics can do.
Notes on Contributors
Seow Chong Lee contributed to the analysis and interpretation of data, drafting and revising of the manuscript.
Foong May Yeong contributed to the conception and design of the study, interpretation of data, drafting and revising of the manuscript.
Ethical Approval
Ethics approval was obtained from Yong Loo Lin School of Medicine Medical Sciences Departmental Ethics Review Committee (Reference code: MSDERC-2022-006).
Data Availability
An overview of the categorization of responses into categories and samples of students’ responses, as well as the counts under each category are openly available in Figshare at https://doi.org/10.6084/m9.figshare.20484498.
Funding
This paper receives no funding from outside sources.
Declaration of Interest
The authors have no conflict of interest to declare.
References
Bae, J., & Watson, B. (2014). Toward a better understanding and application of the principles of visual communication. In W. Huang (Ed.), Handbook of Human Centric Visualization (pp. 179-201). Springer. https://doi.org/10.1007/978-1-4614-7485-2_7
Erickson, F., Bagrodia, R., Gook-Sather, A., Espinoza, M., Jurow, S., Shultz, J. J., & Spencer, J. (2008). Students’ experience of school curriculum: the everyday circumstances of granting and withholding assent to learn. In F. M. Connelly, M. F. He, & J. Phillion. (Eds.), The SAGE Handbook of Curriculum and Instruction (pp. 198-218). https://doi.org/10.4135/9781412976572.n10
Lang, J. M. (2016). Small Teaching: Everyday Lessons from the Science of Learning (1st ed.). Jossey-Bass.
Lee, S. C., & Yeong, F. M. (2022). Minor tweaks to tutorial presentation improved students’ perceptions of our mass tutorial. https://doi.org/10.6084/m9.figshare.20484498
Mayer, R. E. (2014). Multimedia instruction. In M. Spector, D. Merrill, J. Elen, & M. J. Bishop (Eds.), Handbook of Research on Educational Communications and Technology (pp. 385-399). https://doi.org/10.1007/978-1-4614-3185-5_31
Siah, C. R., Huang, C. M., Poon, Y. S. R., & Koh, S. S. (2022). Nursing students’ perceptions of online learning and its impact on knowledge level. Nurse Education Today, 112, Article 105327. https://doi.org/10.1016/j.nedt.2022.105327
*Foong May Yeong
MD4, 5 Science Drive 2,
S117545
+65 6516 8866
Email: bchyfm@nus.edu.sg
Submitted: 28 April 2022
Accepted: 9 February 2023
Published online: 4 July, TAPS 2023, 8(3), 50-53
https://doi.org/10.29060/TAPS.2023-8-3/SC2798
Olivia MY Ngan1,2, Jasmine YN Hui3 & Sihan Sun4
1Medical Ethics and Humanities Unit, School of Clinical Medicine, LKS Faculty of Medicine, The University of Hong Kong, HKSAR; 2Centre for Medical Ethics and Law, Faculty of Law and LKS School of Medicine, The University of Hong Kong; 3Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR; 4CUHK Centre for Bioethics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR
Abstract
Introduction: Didactic pedagogy and passive learning in bioethics and medical humanities teaching are ineffective in engaging students and gauging learning interests. As a result, medical students are unaware of why and how bioethics and medical humanities relate to their learning and thus prioritising acquiring clinical knowledge in their medical education.
Methods: This project involves a teacher-student collaboration to develop a teaching approach, which bridges historical events and contemporary issues, acknowledging how ethics and humanities are interwoven in clinical and everyday life. The objectives are to (1) highlight landmark historical events in bioethics and medical humanities and (2) recognise the evolving nature of values and social norms that inform current practice.
Results: The three activities include the use of historical narratives, annual newsletter publications, and social media to augment didactic classroom teaching and learning. Video narratives of landmark events in bioethics were developed to strengthen historical knowledge and encourage self-reflection. The newsletter invited students to write about any topic in bioethics and medical humanities and enabled them to experience a peer-review process. It allowed students to critically appraise everyday issues. Social media engagement via Instagram offered a flexible and informal medium to diversify the traditional bioethics content taught in the classroom. The advantages and obstacles of each element are discussed.
Conclusion: A holistic approach using historical narratives, newsletters, and social media engages students’ learning and allows students to become conscious of how past events shape the present.
Keywords: Bioethics, Medical Ethics, Medical Humanities, Education, History, Curriculum Development, Social Media, Student as Partner, Newsletter
I. INTRODUCTION
With modern bioethics taking shape in the late 1960s, the introduction of formal bioethics teaching in medical schools developed slowly in Europe and Northern America over the subsequent decades. It was recognised that professional ability not only encompassed scientific knowledge and clinical skills, but also embodied a high standard of professional ethics, values, and moral conduct. A paradigm shift in how medical education shaped students’ moral compasses and holistic decision-making abilities was needed. In 1987, the Liaison Committee on Medical Education stated that medical schools must incorporate bioethics and medical humanities teaching into their curricula (Carrese et al., 2015). In 1993, the British General Medical Council published a white paper, Tomorrow’s Doctors, which outlined a blueprint for reforming the curriculum and affirmed that teaching ethics and law was an integral part of medical education (Mattick & Bligh, 2006).
Bioethics teaching started relatively late in Asia-Pacific and is strategically less developed in its teaching content, methodology, and assessment (Qian et al., 2018; Sim et al., 2019). There is little discussion on how to best deliver bioethics education through a multidisciplinary lens, as the disciplines of humanities (e.g., philosophy, history, and law), social sciences (e.g., anthropology and sociology), and arts (e.g., literature) are extensive. Our team recognised that passive learning using conventional pedagogy (e.g., didactic lectures and tutorials) had significant drawbacks. Earlier studies showed that teachers adopting these methods struggled to engage and stimulate students’ reception to ethics learning (Ganguly et al., 2022; Ngan & Sim, 2021). They were unaware of why and how bioethics and medical humanities were related to their science background, called them “soft” subject, and thus prioritised acquiring clinical knowledge (Leo & Eagen, 2008).
This paper describes a new teaching approach that draws reference from the philosophy of history teaching, using the past to understand and predict present and future actions. We describe three activities, including using historical narratives, annual newsletter publications, and social media to augment classroom teaching and learning in hopes of promoting ethical sensitivity to students’ clinical and everyday life experiences. Our learners are medical students undertaking a six-year undergraduate medical degree programme. These activities were implemented to support pre-clinical year teaching, though also applicable to clinical year students.
II. DESCRIPTIONS OF THREE TEACHING ACTIVITIES
A. Historical Narratives
The adoption of historical narratives in bioethics teaching draws reference from the philosophy of history teaching, using the past to appreciate the present and the future. But its history is often neglected in the curriculum due to time constraints. Students perceived a disconnection between themselves and unethical events, struggling to understand the significance and effects specific past events may have had on present society (Ngan & Sim, 2021). Gerald L. Gutek (1995), History Educator, advocated that “[teaching] should illuminate the past in order to provide the perspective in time and place that we need to make reflective decisions on the [medical] education choices that face us today. Understanding the importance of bioethics history reminds ourselves about the wrongdoings in science, either due to procedural insensitivity or limited guidelines, and may also improve individual behaviour and organisational culture, re-enforcing a high standard of professional conduct. The video narratives reinforce historical knowledge and the ability to discern and scrutinize the similarities and differences between the past and present.
In this pilot project supported by the faculty’s teaching development grant, landmark historical events were developed as short video narratives that complemented the teaching curriculum topic. Table 1 is a non-exhaustive list of examples describing key events in ethics and how they relate to contemporary issues. In our experience, the video productions were well-received by students’ feedback evaluation. The high cost, however, would be a concern. Should the video improve students’ sensitivity towards bioethics, a comprehensive development of bioethics history video should be invested as an educational media to support teaching.
|
Historical Events |
Related Ethical Concerns |
Contemporary Issues |
|
Eugenics measures in the United States (1896- 1940), Germany (1933-45), and Japan (1948-1996) |
Eugenics |
Emerging technologies (e.g., gene-editing technologies, preimplantation diagnosis, and prenatal diagnosis) |
|
The “God” Committee: Rationing dialysis machines (1961) |
Equity, fair allocation approach, transplantation ethics |
Allocation of scarce resources (e.g., vaccine, ICU bed, funds) |
|
Tuskegee Syphilis Study, (1972) |
Research ethics (e.g., informed consent, exploitation of vulnerable populations) |
Research involving vulnerable populations (e.g., homeless, inmates) |
|
Stanford Prison Experiment (1971)
Milgram’s “destructive obedience” Study (1974) |
Unethical research conduct was uncovered (e.g., psychological harms, deception) |
Social and behaviour research illuminates the need for participant protection beyond the scope of biomedical studies. |
|
Table 1. Implications of Landmark Events on Present-day |
||
B. Bioethics Newsletter
In this pilot project, our team incepted a student-led bioethics newsletter aiming to draw ethical sensitivity in everyday life. Medical students were invited to contribute and write a commentary based on a topical issue of their interest; stimuli may have ranged from the news, movies, dramas, documentaries, plays, clinical ward experiences, and overseas observations. The opportunity provided students with a platform to voice and elucidate their opinions. It also allowed students to be more receptive to opposing ideas, developing a greater awareness of ethical dilemmas.
We published three annual newsletters and reflected on our experience. In the first issue, there was no peer-review process. We felt that the absence of a communication medium between the student writers and student editors hindered the quality of submissions. A peer-review process was implemented starting from the second issue, which was perceived to be beneficial as students were able to receive feedback and enhance intellectual rigour. More importantly, students were also exposed to the peer-reviewing process, which is useful for their future professional career development in academia.
Several obstacles relating to the submission process and the future sustainability of the newsletter were also met. In the first issue, interest was generated primarily through word-of-mouth and promotion on social media. In the second issue, prize incentives were given to best-written submissions. Participation gained momentum in the second and third issues, where we saw an average of 15-20 submissions. Sustainability was also a concern in terms of reader engagement and recruiting altruistic junior students to take over the project. To encourage multidisciplinary engagement, we aim to call for submissions in both written Chinese and English and accept entries from all students within the medicine faculty. We have a long-term goal of fostering a multidisciplinary collaboration across the Faculties.
C. Social Media
Given the generational influx of physicians and medical educators, the use of social media in medical education has seen rising popularity in recent years. Platforms like Twitter, Instagram, YouTube, and LinkedIn are easily accessible, user-friendly and encourage users’ interaction in a local and international setting. The flexibility of social media may also promote active learning pedagogies and personalised education, allowing students to build upon the knowledge they perceive to be interesting.
We started an Instagram page (IG: cubioethics) in June 2020 and curated content on a monthly basis. Content covered a broad range of bioethical topics, including several themed series: a news roundup named “Ethics in the News” and a series based on biotechnology seen in the sci-fi television series, Black Mirror. Each post consisted of a short synopsis on the topic and multiple discussion points were raised to incite critical thinking and reflection.
The flexibility and informal nature of Instagram allowed us to diversify the traditional bioethics content taught in the classroom. For example, it offered an experimental opportunity to teach through television and film. Moreover, the Instagram page allowed us to connect with students and professionals from local and international institutes. Engagement was reflected in post shares, likes, comments, and page follows. As the bioethics community on Instagram remains relatively small, it was easy to establish rapport. This community was able to help expand our audience via mutual post sharing and furthered the ethical debate raised in our posts.
Maintaining an Instagram page was not easy – content creation, the design process, and engaging with readers required careful planning and time. Also, from a cultural standpoint, it seemed as if there was a stronger tendency for international users to publicly participate in the conversation by commenting rather than local students. This may be due to worries about online criticism or the pervasive nature of social media and how it may no longer be viewed as a “safe space” for controversial discourse.
III. CONCLUSION
We reflected on our experience refining traditional didactic pedagogy by adopting three activities: historical narratives, newsletters, and social media. Each component presents unique educational benefits (e.g., recounting the evolution of today’s achievements, exposing students to peer-review publishing experience, cultivating sensitivities to everyday life) and operational barriers (e.g., budget constraints, altruistic students’ recruitment, time- and labour-intensive). Our teaching pedagogy may also be adopted in bioethics teaching in other disciplines, including biomedical and life sciences.
Notes on Contributors
OMYN conceived the study, developed the narration scripts, facilitated the newsletter peer-review as a teacher editor, reviewed the literature, and drafted the intellectual content of the manuscript.
JYNH led the newsletter peer-review as a student editor, managed the social media platform, and drafted the intellectual content of the manuscript.
SS reviewed newsletter entries and critically revised the manuscript for intellectual content. All authors are accountable for all aspects of the work and approve the final manuscript.
Ethical Approval
This study involves a theoretical discussion only and does not require ethical approval.
Data Availability
The data that support the findings of this study are openly available in the Figshare repository. http://doi.org/10.6084/m9.figshare.19768264
Funding
The study is supported by the Teaching Development and Language Enhancement Grant (TDLEG) for the 2019-22 Triennium. The funders had no role in the content review of the manuscript.
Declaration of Interest
The authors declare no conflict of interest.
References
Carrese, J. A., Malek, J., Watson, K., Lehmann, L. S., Green, M. J., McCullough, L. B., Geller, G., Braddock III, C. H., & Doukas, D. J. (2015). The essential role of medical ethics education in achieving professionalism: The Romanell Report. Academic Medicine, 90(6), 744–752. http://doi.org/10.1097/ACM.0000000000000715
Ganguly, B., D’Souza, R., & Nunes, R. (2022). Challenges in the teaching–learning process of the newly implemented module on bioethics in the undergraduate medical curriculum in India. Asian Bioethics Review. https://doi.org/10.1007/s41649-022-00225-2
Gutek, G. L. (1995). A history of the western educational experience (2nd ed.). Waveland Press, Inc.
Leo, T., & Eagen, K. (2008). Professionalism education: The medical student response. Perspectives in Biology and Medicine, 51(4), 508–516. https://doi.org/10.1353/pbm.0.0058
Mattick, K., & Bligh, J. (2006). Teaching and assessing medical ethics: Where are we now? Journal of Medical Ethics, 32(3), 181–185. http://doi.org/10.1136/jme.2005.014597
Ngan, O. M. Y., & Sim, J. H. (2021). Evolution of bioethics education in the medical programme: A tale of two medical schools. International Journal of Ethics Education, 6, 37–50. https://doi.org/10.1007/s40889-020-00112-0
Qian, Y., Han, Q., Yuan, W., & Fan, C. (2018). Insights into medical humanities education in China and the West. Journal of International Medical Research, 46(9), 3507–3517.
Sim, J. H., Ngan, O. M. Y., & Ng, H. K. (2019). Bioethics education in the medical programme among Malaysian medical schools: Where are we now? Journal of Medical Education and Curricular Development, 6.
*Olivia M.Y Ngan
Medical Ethics and Humanities Unit,
School of Clinical Medicine,
Li Ka Shing Faculty of Medicine,
The University of Hong Kong, Pokfulam,
Hong Kong Island, Hong Kong SAR
Email: olivian1@hku.hk
Submitted: 30 Nov 2022
Accepted: 30 Jan 2023
Published online: 4 July, TAPS 2023, 8(3), 45-49
https://doi.org/10.29060/TAPS.2023-8-3/SC2921
Sasikala Devi Amirthalingam1, Shamala Ramasamy2 & Sharifah Sulaiha Hj Syed Aznal3
1Department of Family Medicine, International Medical University, Kuala Lumpur, Malaysia; 2Department for Psychology, International Medical University, Kuala Lumpur, Malaysia; 3Department of Obstetrics and Gynaecology, International Medical University, Kuala Lumpur, Malaysia
Abstract
Introduction: Introduction to Health Profession (IHP) was designed to teach first-year medical students the importance of self-directed learning, accountability, and teamwork in healthcare. Due to the COVID 19 pandemic, the course was delivered virtually, incorporating elements of gamification.
Methods: Gamification features included collaborative teamwork to simulate and record the roleplay for assignments based on crisis management scenarios. The syllabus involves knowledge checks to promote self-directed learning and personal accountability as well as online questionnaires to identify personality traits followed by discussion. Games like Chinese whispers and charades were introduced to identify listening skills. Additional gamification features include progress mechanics for collecting badges upon successful completion of knowledge checks / assessments and completing collaborative teamwork activities.
Results: Results from the descriptive study on the educational usefulness of the IHP module was found to be satisfactory. The feedback was encouraging as >95% of students gave positive feedback that the IHP activities enabled them to understand the value of teamwork, effective communication, professional behavior and enabled them to be resilient and adaptable. 92% agreed that the IHP activities helped to make connections and network with their peers during the pandemic
Conclusion: Gamification of IHP course was successful in terms of practicality and usefulness in promoting communication, collaborative work, experiential learning, and teamwork. Students were empowered to take charge of their own learning of both content and development of interpersonal skills and teamwork through gamification. The isolation caused by the pandemic was alleviated by the networking that occurred during collaborative group activities.
Keywords: Gamification, Self-directed Learning, Collaborative Learning
I. INTRODUCTION
Introduction to Health Profession (IHP) course was initiated during Covid-19 pandemic and conducted at the beginning of our medical program enrolment to introduce freshmen to the real world and value systems of health professional. The learning activities were designed to provide real life experiences, exposing to communication skills within the community and peers, professionalism including teamwork and ethics, and the value of self-reflecting practice. The isolation caused by the pandemic was alleviated by networking that occurred during collaborative group activities and online interactive discussion with invited speakers of health professionals. The group activities were gamified to make learning fun, memorable, engaging and motivating. It is designed to promote a sense of accomplishment while learning through discovery and during the social interaction.
Gamification in education has existed since time immemorial but with the advent of wireless technology, it has given rise to unique ways to improve student engagement (Dodson, 2021) in learning. Gamification is defined as “the craft of deriving all the fun and addicting elements found in games and applying them to real-world or productive activities” (Chou, 2012). There is growing evidence for gamification in a wider pedagogical context and the concept is gaining traction within the medical education community. These “fun and addicting elements” include progress mechanics such as badges, narrative structure and immediate feedback. The gamification features introduced in the IHP module are badges, immediate feedback, challenges in the form of knowledge checks and roleplay in virtual reality in crisis management scenarios.
II. METHODS
Collaborative group activities were conducted by dividing 171 first year students into 16 small groups. Activities were carried out using synchronous and asynchronous virtual platforms to accommodate about 40 % of international students who were still in their home countries. Lessons in IHP consisted of recognising personality traits, application of communication skills, ethics and professionalism and recognising teamwork as intrinsic requirements for delivery of effective healthcare.
Asynchronous sessions required students to individually go through the prepared learning materials followed by knowledge checks. Test repetition without penalty is allowed within an allotted time frame until learners reach a satisfactory result. Following successful completion of knowledge check, students would earn their badge of completion.
Activities like ‘discovering personality traits’ are conducted as online synchronous workshops and facilitated by a group of psychologists. Self-administered questionnaire was administered to determine personality traits, followed by a psychologist-led group discussion to share feedback and reflection. Having the session on a virtual platform provided the students with a degree of anonymity, which enabled them to share profound reflections and feedback. Through the questionnaire responses, the psychologists were able to identify red flags and reach out to the students.
During the online ‘communication skills’ workshop, games such as Chinese whispers and charades were used to cultivate active listening skills and understand nonverbal communication. Students were assigned to group works comprising of preparing oral presentations on scenarios involving ethics and professionalism. In addition, they were tasked to solve issues in selected crisis management scenarios using role-plays and virtual reality. Creativity is highly encouraged and weighted with high percentage. This encourages social interaction and influences learning by creating a subjective sense of presence to facilitate virtual experiential learning.
Upon completion of the IHP activities, students are required to complete a self-administered questionnaire to feedback on the efficacy of the module, hence implied consent is given. The questionnaire measured whether the gamification of IHP achieved the learning outcomes of enabling the understanding of the value of teamwork, effective communication, professional behaviour and to be adaptable and resilient. In addition, the questionnaire inquired if participation in IHP activities helped them create contacts and network with their peers. Open comments are sought after for thematic analysis.
III. RESULTS
51.4% of the cohort responded to the self-administered online questionnaire. Feedback was encouraging as >95% of students gave positive feedback. They felt IHP activities enabled them to understand the value of teamwork, effective communication, professional behaviour and being resilient and adaptable. Most agreed IHP activities helped to make connections and network with peers during the pandemic. Many agreed they developed some insight about themselves during IHP activities. Several themes were drawn from the collected feedback. The primary theme is teamwork where students demonstrate co-operation in working together in teams to attain mutual goals and learn leadership qualities. Majority felt they developed skills in active listening, organisation, patience, self-confidence, and showing empathy. Other characteristics learnt were resilience building, controlling emotions, adaptation, overcoming challenges, professionalism and ethical behaviour.
Common comments on areas to improve are their lack of confidence and discomfort in expressing one’s thoughts. Both being too rigid and overly flexible were commented. Other comments were not feeling at ease with working in a team, becoming overwhelmed, paying excessive attention to detail, and becoming frustrated. Being shy and quiet as well as not being assertive were among the constructive feedback (See Table 1). A copy of the survey questions and the additional tables of survey results are openly available at https://doi.org/10.6084/m9.figshare.21656864.
|
Student Feedback for the Introduction to Health Profession (IHP) module Total number of respondents: 88 |
|||
|
NO. |
THEMES |
OPEN FEEDBACK FROM STUDENTS |
|
|
Majority of the positive responses are as follows: |
Common comments on areas to improve self: |
||
|
1 |
Teamwork |
|
|
|
2 |
Effective Communication |
|
|
|
3 |
Professional Behavior |
|
|
|
4 |
Adaptability and resilience |
|
|
|
5 |
Making connections and networking with peers |
|
|
|
6 |
Insight to self |
|
|
|
Table 1. Student Feedback from IHP Cohort ME121 |
|||
IV. DISCUSSION
IHP is a new course with the objectives of introducing students to the real world and value systems of the health professional, focusing on communication skills, medical ethics, teamwork, and the importance of self-reflective practice. The learning is mainly facilitated by group work and formative assessment through immediate provision of feedback and self-reflection. Due to pandemic-related restrictions, the initial plans for real life experience and exposure in IHP course had to be converted to the online platform. An instructional method such as gamification was selected to help retain student engagement and encourage participation (Chou, 2012). Applying the design elements and principles found in games to education was useful in sparking student interest and motivation (Chou, 2012).
Knowledge checks challenged the minds, improved cognition and knowledge retention (Singhal et al., 2019). Progress mechanics in the form of earning ‘a badge on completion’ of assigned activities, going through the provided learning material and completing the knowledge check to an acceptable level, promoted self-directed learning, created a sense of achievement and retained student engagement. This reward system fosters student participation, as it is a tangible reward (Dodson, 2021).
The seclusion from real life interaction is feared to mentally and psychologically affect students. A study in Switzerland has shown a significant impact on the mental health of learners due to the lockdown in 2020 (Elmer et al., 2020). In another study, social interaction is recognised as an important factor for enhancing learning especially in areas of critical thinking and problem solving (Hurst et al., 2013). The group works in the IHP course, though set virtually, have assisted students in networking and socialising during the pandemic. This was agreed by majority of the students who participated in IHP activities.
Effective leadership is essential in delivering high standards of clinical practice. The students learnt leadership skills through organising group work, delegating roles and responsibilities among team members. Among the examples of group work are problem- solving scenarios like managing a fire in CCU or multiple vehicle accident on the highway. The instructional content was related to the teamwork and roles and responsibilities of the different health professionals involved in managing the crisis and it was gamified by adding elements of game fiction such as the different themes, settings and characters. As students had to self- produce scripts after some brief research of relevant contents, they had some autonomy over the depth and breadth of their learning. Working in teams towards common goals lead to improved productivity and self-esteem and created supportive relationships during the collaborative learning (Singhal et al., 2019). Narrative synthesis and role playing in scenarios managing crisis situations stimulated reflective practice whilst integration of cause and effect enabled experiential learning.
Overall feedback was encouraging as almost all students enjoyed the activities and found them both educational and engaging. They discovered characteristics in themselves that helped them to improve team spirit and communication. The groupwork on the various projects developed learning communities and promoted interpersonal skills, integrating diverse learner types with a wide range of knowledge, skills, past experiences and personal attributes. This was effectively utilized in the groupwork and collaborative learning.
Some setbacks occurred when both the faculty and students were unfamiliar with online gamification. The synchronous sessions with international students in different time zones, made group discussions challenging. Support from the Information Technology team is valuable but poses an exorbitant cost. Students having expectations of medical school learning to be more didactive, instead had to adapt to being adult learners, for more extensive self- directed learning and reflective practice.
V. CONCLUSION
In conclusion, gamification of IHP module encouraged student engagement, teamwork and collaborative learning. IHP course was accessible virtually, which was a boon for our international students who could interact virtually with peers and access and take part in the lessons. The gamification features used were reproducible. Gamification is useful in medical education and can be pursued as a method to deliver lessons and engage students. It is a tool to allow learning in depth and for experiential learning on the virtual platform.
Notes on Contributors
Dr Sasikala Devi Amirthalingam is the first author, contributing to the abstract, introduction, discussion and literature review. She agrees to be accountable for all aspects of the work.
Dr Shamala Ramasamy is the second author, contributing to methodology, results and literature review. She agrees to be accountable for all aspects of the work.
Prof Sharifah Sulaiha Hj Syed Aznal is the third author, contributing to abstract, introduction, discussion and revising it critically for important intellectual content. She agrees to be accountable for all aspects of the work.
Ethical Approval
The dean of School of Medicine, International Medical University has given a letter to say that there is no objection to sharing of findings for educational purpose.
Data Availability
The data that support the finding are openly available in the Figshare repository. https://doi.org/10.6084/m9.figshare.21656864
Acknowledgement
We would like to acknowledge Fareeza Marican Bt Abu Backer and Norhasliza Binti Hashim from E Learning Department from International Medical University for the technical assistance in the gamification features to the module.
Funding
There is no financial support or any financial relationships that may pose a conflict of interest.
Declaration of Interest
There is no conflicting interest to any parties concerned.
References
Chou, Y. K. (2012). What is gamification. Yukai Chou: Gamification and Behavioral Design. https://yukaichou.com/gamification-examples/what-is-gamification/
Dodson, K. R. (2021). Can gamification drive increased student engagement? Educause Review. https://er.educause.edu/articles/sponsored/2021/10/can-gamification-drive-increased-student-engagement
Elmer, T., Mepham, K., & Stadtfeld, C. (2020). Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE, 15(7), Article e0236337. https://doi.org/10.1371/journal.pone.0236337
Hurst, B., Wallace, R., & Nixon, S. B. (2013). The impact of social interaction on student learning. Reading Horizons: A Journal of Literacy and Language Arts, 52(4), Article 5. https://scholarworks.wmich.edu/reading_horizons/vol52/iss4/5
Singhal, S., Hough, J., & Cripps, D. (2019). Twelve tips for incorporating gamification into medical education. MedEdPublish, 8(3), Article 216.
*Sasikala Devi Amirthalingam
International Medical University,
Kuala Lumpur, Malaysia
+60133513435
Email: SasikalaDevi@imu.edu.my
Submitted: 30 May 2022
Accepted: 7 December 2022
Published online: 4 July, TAPS 2023, 8(3), 35-44
https://doi.org/10.29060/TAPS.2023-8-3/OA2876
Rachel Jiayu Lee1*, Jeannie Jing Yi Yap1*, Abhiram Kanneganti1, Carly Yanlin Wu1, Grace Ming Fen Chan1, Citra Nurfarah Zaini Mattar1,2, Pearl Shuang Ye Tong1,2, Susan Jane Sinclair Logan1,2
1Department of Obstetrics and Gynaecology, National University Hospital, Singapore; 2Department of Obstetrics and Gynaecology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
*Co-first authors
Abstract
Introduction: Disruptions of the postgraduate (PG) teaching programmes by COVID-19 have encouraged a transition to virtual methods of content delivery. This provided an impetus to evaluate the coverage of key learning goals by a pre-existing PG didactic programme in an Obstetrics and Gynaecology Specialty Training Programme. We describe a three-phase audit methodology that was developed for this
Methods: We performed a retrospective audit of the PG programme conducted by the Department of Obstetrics and Gynaecology at National University Hospital, Singapore between January and December 2019 utilising a ten-step Training Needs Analysis (TNA). Content of each session was reviewed and mapped against components of the 15 core Knowledge Areas (KA) of the Royal College of Obstetrics & Gynaecology membership (MRCOG) examination syllabus.
Results: Out of 71 PG sessions, there was a 64.9% coverage of the MRCOG syllabus. Four out of the 15 KAs were inadequately covered, achieving less than 50% of knowledge requirements. More procedural KAs such as “Gynaecological Problems” and those related to labour were poorly (less than 30%) covered. Following the audit, these identified gaps were addressed with targeted strategies.
Conclusion: Our audit demonstrated that our pre-pandemic PG programme poorly covered core educational objectives i.e. the MRCOG syllabus, and required a systematic realignment. The COVID-19 pandemic, while disruptive to our PG programme, created an opportunity to analyse our training needs and revamp our virtual PG programme.
Keywords: Medical Education; Residency; Postgraduate Education; Obstetrics and Gynaecology; Training Needs Analysis; COVID-19; Auditing Medical Education
Practice Highlights
- Regular audits of PG programmes ensure relevance to key educational objectives.
- Training Needs Analysis facilitates identification of learning goals, deficits & corrective change.
- Mapping against a milestone examination syllabus & using Delphi technique helps identify learning gaps.
- Procedural-heavy learning goals are poorly served by didactic PG and need individualised assessment.
- A central committee is needed to balance the learning needs of all departmental CME participants.
I. INTRODUCTION
Postgraduate medical education (PG) programmes are an important aspect in meeting core Specialty Trainees’ (ST) learning goals in addition to other modalities of instruction such as practical training (e.g. supervised patient-care or simulator-based training) (Bryant‐Smith et al., 2019) and workplace-based assessments (e.g. case-based discussions and Objective Structured Clinical Examinations [OSCEs] (Chan et al., 2020; Parry-Smith et al., 2014). In academic medical centres, PG education may often be nestled within a wider departmental or hospital Continuing Medical Education (CME) programme. While both PG and CME programmes indirectly improve patient outcomes by keeping clinicians abreast with the latest updates, reinforcing important concepts, and changing practice (Burr & Johanson, 1998; Forsetlund et al., 2021; Marinopoulos et al., 2007; Norman et al., 2004; Raza et al., 2009; Sibley et al., 1982), it is important to balance the learning needs of STs with that of other learners (E.g. senior clinicians, scientists and allied healthcare professionals). This can be challenging as multiple objectives need be fulfilled amongst various learners. Nevertheless, just as with any other component of good quality patient care, it is amenable to audit and quality improvement initiatives (Davies, 1981; Norman et al., 2004; Palmer & Brackwell, 2014).
The protracted COVID-19 pandemic has disrupted the way we deliver healthcare and conduct non-clinical services (Lim et al., 2009; Wong & Bandello, 2020). In response, the academic medical community has globally embraced the use of teleconferencing platforms such as ZoomⓇ, Microsoft TeamsⓇ and WebexⓇ (Kanneganti, Sia, et al., 2020; Renaud et al., 2021) as well as other custom-built solutions for the synchronous delivery of didactics and group discourse (Khamees et al., 2022). While surgical disciplines have suffered a decline in the quality of “hands-on” training due to reduced elective surgical load and safe distancing (English et al., 2020), the use of simulators (Bienstock & Heuer, 2022; Chan et al., 2020; Hoopes et al., 2020; Xu et al., 2022), remote surgical preceptorship, and teaching through surgical videos (Chick et al., 2020; Juprasert et al., 2020; Mishra et al., 2020) have helped mitigate some of these. Virtual options that that have been reproducibly utilised during the pandemic and will be a part of the regular armamentarium of post-graduate medical educationists include online didactic lectures, livestreaming or video repositories of surgical procedures, (Grafton-Clarke et al., 2022) and virtual case discussions and grand ward rounds (Sparkes et al., 2021). Notably, they facilitate the inclusion of a physically wider audience, be it trainer or trainee, and allow participants to tune in from different geographical locations.
At the Department of Obstetrics and Gynaecology, National University Hospital, Singapore, the forced, rapid transition to a virtual CME format (vCME) (Chan et al., 2020; Kanneganti, Lim, et al., 2020) provided an impetus to critically review and revamp the didactic component of our PG programmes. A large component of this had been traditionally baked into our departmental CME programme which comprises daily morning meetings covering recent specialty and scientific updates, journal clubs, guideline reviews, grand round presentations, surgical videos, exam preparation, topic modular series, and research and quality improvement presentations. The schedule and topics were previously arbitrarily decided by a lead consultant one month prior and were presented by a supervised ST or invited speaker. While attendance by STs at these sessions was mandatory and comprised the bulk of protected ST teaching time, no prior attempt had been made to assess its coverage of core ST learning objectives and in particular, the syllabus for milestone ST exams.
Our main aim was to conduct an audit on the coverage of our previous PG didactic sessions on the most important learning goals with the aim of subsequently restructuring them to better meet these goals.
II. METHODS
We audited and assessed our departmental CME programme’s relevance to the core learning goals of our STs by utilising a Training Needs Analysis (TNA) methodology. While there are various types of TNA used in healthcare and management (Donovan & Townsend, 2019; Gould et al., 2004; Hicks & Hennessy, 1996, 1997; Johnston et al., 2018; Markaki et al., 2021), in general they represent systematic approaches towards developing and implementing a training plan. The common attributes can be distilled into three common phases (Figure 1). Importantly for surgical and procedurally-heavy disciplines, an dimension that is not well covered by didactic sessions alone are assessments for procedural skill competency. These require separate attention that is beyond the scope of this audit.
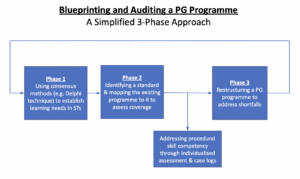
Figure 1. A simplified three phase approach to blueprinting, mapping, and auditing a Postgraduate (PG) Education Programme
A. Phase 1: Identifying Organisational Goals and Specific Objectives
The overarching goal of a specialty PG education programme is to produce well-balanced clinicians with a strong knowledge base. Singapore’s Obstetrics and Gynaecology specialty training programmes have adopted the membership examinations for the Royal College of Obstetricians and Gynaecologists (MRCOG) (Royal College of Obstetricians and Gynaecologists, 2021) of the United Kingdom as the milestone examination for progression from junior to senior ST.
First, we adapted a ten-step TNA proposed by Donovan & Townsend (Table 1) to crystallise our our core learning goals, identify deficiencies, and subsequently propose steps to address these gaps in a systematic fashion that is catered to our specific context. While most aspects were followed without change, we adapted the last aspect i.e. Cost Benefit Analysis. As a general organisational and management tool, the original TNA primarily looked at the financial costs of implementing a training programme. At an academic medical institution, the “cost” is mainly non-financial and mainly refers to time taken away from important clinical service roles.
As part of formulating what were deemed to be core learning goals of an ideal PG programme (i.e. Steps 1 to 4), we had a focused group discussion comprising key stakeholders in postgraduate education, including core faculty (CF), physician faculty (PF), and representative STs. The discussions identified 18 goals specific to our department. We then used a modified Delphi method (Hasson et al., 2000; Humphrey-Murto et al., 2017) to distil what CF, PFs, and STs felt were important priorities for grooming future specialists. Three rounds of priority ranking were undertaken via an anonymised online voting form. At each round, these 18 goals were progressively ranked and distilled until five remained. These were then ranked from highest to lowest priority and comprised 1) exam preparedness, 2) clinical competency, 3) in-depth understanding of professional clinical guidelines, 4) interpretation of medical research literature, and 5) ability to conduct basic clinical research and audits.
|
Training Needs Analysis |
||
|
1 |
Strategic objectives |
|
|
2 |
Operational outcome |
|
|
3 |
Employee Behaviours |
|
|
4 |
Learnable Capabilities |
|
|
5 |
Gap Assessment |
|
|
6 |
Prioritise Learning and Training Needs |
|
|
7 |
Learning Approaches |
|
|
8 |
Roll-out Plan |
|
|
9 |
Evaluation Criteria |
|
|
10 |
Cost Benefit Analysis |
|
Table 1. 10-step Training Needs Analysis
Table adapted from Donovan, Paul and Townsend, John, Learning Needs Analysis (United Kingdom, Management Pocketbooks, 2019)
MRCOG: Member of the Royal College of Obstetricians and Gynaecologists, O&G: Obstetrics and Gynaecology
CREOG: Council on Resident Education in Obstetrics and Gynecology
ACGME: Accreditation Council for Graduate Medical Education,
PG: Post-Graduate Education
B. Phase 2: Identifying a Standard and Assessing for Coverage against This Standard
As with any audit, a “gold-standard” should be identified. As the focus group discussion and Delphi method identified exam preparedness as the highest priority, we created a “blueprint” based on the syllabus of the MRCOG examination (Royal College of Obstetricians and Gynaecologists, 2019). This comprised more than 200 Knowledge Requirements organised more than 200 knowledge requirements into 15 Knowledge Areas (KAs) (Table 2). We mapped the old CME programme against this blueprint to understand the extent of coverage of these KAs. We analyse the session contents between January and December 2019. We felt the best way to ensure systematic coverage of these KAs would be through sessions with pre-identified areas of topical focus conducted during protected teaching time as opposed to opportunistic and voluntary learning opportunities that may not be widely available to all STs. In our department, this applied to morning CME sessions which indeed formed the bulk of protected teaching time for STs, required mandatory attendance, and comprised sessions covering pre-defined topics. Thus, we excluded didactic sessions where 1) the content of the presentations was unavailable for audit, 2) they covered administrative aspects and did not have a pre-identified topical focus where learning was opportunistic (e.g. risk management meetings, labour ward audits), and 3) where the attendance was optional.
Mapping was conducted independently by two members of the study team (JJYY and CYW) with conflict resolved by a third member (RJL). The number of knowledge requirements fulfilled within a KA were expressed as a percentage.
|
Core knowledge areas |
|
Clinical skills |
|
Teaching and research |
|
Core surgical skills |
|
Post operative care |
|
Antenatal care |
|
Maternal Medicine |
|
Management of Labour |
|
Management of delivery |
|
Postpartum problems |
|
Gynaecological problems |
|
Subfertility |
|
Sexual and reproductive health |
|
Early pregnancy care |
|
Gynaecological Oncology |
|
Urogynaecology & pelvic floor problems |
Table 2. RCOG Core Knowledge Areas (Royal College of Obstetricians and Gynaecologists, 2019)
C. Phase 3: Restructuring a PG Programme
The final phase i.e. the restructuring of a PG programme, is directed by responses to Steps 7-10 of the 10-step TNA (Table 1). As the focus of our article is on the methodology of auditing the extent of coverage of our departmental didactic sessions over our core ST learning goals i.e. the MRCOG KAs, these subsequent efforts are detailed in the discussion section.
III. RESULTS
Altogether, 71 presentations were identified (Table 3) of which 12 CME sessions (16.9%) were unavailable and, thus, excluded from the mapping exercise. The most common types of CME sessions presented clinical updates (31.0%), original research (29.6%), journal clubs (16.9%), and exam-preparation sessions (e.g. Case Based Discussion and OSCE simulations) (12.6%). The overall coverage of the entire syllabus was 64.9% (Figure 2). The KAs demonstrating complete coverage (i.e. 100% of all requirements) were “Teaching and Research”, “Postoperative Care” and “Early Pregnancy Care”. Three KAs had a coverage of 75-100% in the CME programme i.e. “Clinical Skills” (89%), “Urogynaecology and Pelvic Floor” (82%), and “Subfertility” (77%) while three were covered below 50% i.e. “Management of Labour”, “Management of Delivery”, “Postpartum Problems”, and “Gynaecological Problems”. These were more practical KAs that were usually covered during ward covers, operating theatre, clinics, and labour ward as well as during practical skills training workshops and grand ward rounds where clinical vignettes were opportunistically discussed depending on in-patient case mix. Nevertheless, this “on-the-ground” training is often unplanned, unstructured and ‘bite-sized’, thus complicating integration with the deep and broad guideline and knowledge proficiency that may be needed to train STs to adapt to complex situations.
|
Type of presentation |
Number of sessions |
Percentage breakdown |
|
Clinical Updates |
22 |
31.0% |
|
Presentation of Original Research |
21 |
29.6% |
|
Journal Club |
12 |
16.9% |
|
Case Based Discussion |
5 |
7.0% |
|
OSCE practice |
4 |
5.6% |
|
Others* |
2 |
2.8% |
|
Audit |
2 |
2.8% |
|
Workshops |
3 |
3.0% |
|
Total |
71 |
100% |
|
*Others: ST Sharing of Overseas Experiences and Trainee Wellbeing |
||
Table 3. Type of CME presentations
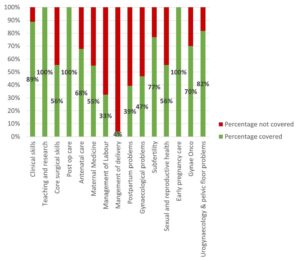
Figure 2. Graph showing the percentage coverage of knowledge areas
IV. DISCUSSION
Our audit revealed a relatively low coverage of the MRCOG KAs with only 64.9% of the syllabus covered. While the morning CME programme caters to all members of the department, the sessions are an important didactic component for ST education and exam preparation as they are deemed “protected” teaching time. There had been no prior formal review assessing whether it catered to this very important section of the department’s workforce. We were also able to recognise those KAs which had exceptionally low coverage were those with a large amount of practical and “hands-on” skills (i.e. “Gynaecological Problems”, “Management of Labour”, “Management of Delivery”, and “Postpartum Problems”). As a surgical discipline, this highlighted that these areas needed directed solutions through other forms of practical instruction and evaluation. In the pandemic environment, this may involve virtual or home-based means (Hoopes et al., 2020). These “hands-on” KAs likely require at least semi-annual individualised assessment by the CF through verified case logs, Objective Structured Assessment of Technical Skills, Direct Observation of Procedural Skills, and Non-Technical Skills for Surgeons (NOTSS) (Bisson et al., 2006; Parry-Smith et al., 2014). This targeted assessment was even more crucial during the recovery “catch-up” phase due to de-skilling because of reduced elective surgical caseload (Amparore et al., 2020; Chan et al., 2020) and facilitated the redistributing of surgical training material to cover training deficits.
While there is significant literature on how to organise a robust PG didactic programme (Colman et al., 2020; Harden, 2001; Willett, 2008), little has been published on how to evaluate an established didactic programme’s coverage of its learner’s educational requirements (Davies, 1981). Most studies evaluating the efficacy of such programmes typically assess the effects of individual CME sessions on physician knowledge or performance and patient outcomes after a suitable interval (Davis et al., 1992; Mansouri & Lockyer, 2007), with most citing a small to medium effect. We believe, however, that our audit process permits a more holistic, reproducible, and structured means of evaluating an existing didactic programme and finding deficits that can be improve upon to brings value to any specialty training programme.
At our institution, safe distancing requirements brought on by the COVID-19 pandemic required a rapid transition to a video-conferencing-based approach i.e. vCME. As milestone examinations were still being held, the first six months were primarily focused on STs as examination preparation remained a high and undisputed priority and learning opportunities had been significantly disrupted by the pandemic. During this phase, our vCME programme was re-organised into three to four sessions per week which were peer-led and supervised by a faculty member. Video-conferencing platforms encouraged audience participation through live feedback, questions posed via the chat box, instantaneous online polling, and directed case-based discussions with ST participants. These facilitated real time feedback to the presenter in a way that was not possible in previous face-to-face sessions due to reasons such as shyness and difficulty conducting polls. Other useful features included being able to record presentations for digital storage in a hospital-based server for access on-demand for revision purposes by STs.
A previously published anonymised questionnaire within our department (Chan et al., 2020) found very favourable opinions of vCME as an effective mode of learning amongst 28 junior doctors (85.7%) and nine presenters (100%) with 75% hoping for it to continue even after normalisation of social distancing policies. Nevertheless, common issues reported included a lack of personal interaction, difficulties in engaging with speakers, technical difficulties, and inaccurate attendance confirmation as shared devices for participating on these vCME sessions sometimes failed to identify who was present. While there is altered teacher and learner engagement due to physical separation across a digital medium, studies have also found that the virtual platform provided a useful means of communication and feedback and created a psychologically safe learning environment (Dong et al., 2021; Wasfy et al., 2021).
While our audit focused primarily on STs, departmental CME programmes need to find balanced in catering to the educational outcome of various groups of participants within a clinical department (e.g. senior clinicians, nursing staff, allied healthcare professionals, clinical scientists). Indeed, as these groups started to return to the CME programme after about six months following the vCME transition, we created a core postgraduate committee comprising members representing the learning interests of each party i.e. Department research director, ST Programme Director and Assistant Director, and a representative senior ST in the fifth or sixth year of training, so that we could continue to meet the recommendations set in our TNA while rebalancing the programme to meet the needs of all participants. Out of an average of 20 CME sessions per month, four were dedicated to departmental and hospital grand rounds each. Of the remaining 12 sessions, two were dedicated towards covering KAs, four scientific presentations, three clinical governance aspects, and one journal club. The remaining two sessions would be “faculty wildcard” sessions to be used at the committee’s discretion of the committee to cover poorly covered, more contemporary, “breaking news” topics, or serve as a buffer in the event of cancellations of other topics. Indeed, the same TNA-based audit methodology can be employed any other group of CME participants.
A key limitation in our audit method is that it focused on the breadth of coverage of learning objectives, but not the quality of the teaching and its depth. Teaching efficacy is also important in the delivery of learning objectives (Bakar et al., 2012) and needs more specific assessment tools (Metheny et al., 2005). Evaluating the quality of PG training could take several forms and may be direct e.g. an evaluation by the learner (Gillan et al., 2011), or could be indirect e.g. charting the learner’s progress through OSCEs and CEXs, scheduled competency reviews, and ST examination pass rates (Pinnell et al., 2021). Importantly, despite the rise of virtual learning platforms, there is little consensus on the best way to evaluate e-learning methods (De Leeuw et al., 2019). Nevertheless, our main audit goal was to assess the extent of coverage of the MRCOG syllabus which is a key training outcome. Future audits, however, should incorporate this element to provide additional qualitative feedback to assess this dimension as well. Further research should be carried out in terms of evaluating the effects of optimising a PG didactic programme on key outcomes such as ST behaviour, perceptions, and objective outcomes such as examination results.
Finally, while these were the results of an audit conducted in a single hospital department and used a morning CME programme as a basis for evaluation, we believe that this audit methodology based on a ten-step TNA and also utilising the Delphi method and syllabus mapping techniques (Harden, 2001) can be reproduced to any academic department that has a regular didactic programme as long as a suitable standard is selected. The Delphi method can easily be conducted via online survey platforms (e.g. Google Forms) to crystallise the PG programme goals. Our audit shows that without a systematic evaluation of past didactic sessions, it is possible for even mature CME programme to fall significantly short of ameeting the needs of its learners and that PG didactic sessions need deliberate planning.
V. CONCLUSION
Just as any other aspect of healthcare delivery, CME and PG programmes are amenable to audits and must adjust to an ever-changing delivery landscape. Rather than curse the darkness during the COVID-19 pandemic, we explored the potential of reformatting the PG programme and adjusting course to better suit the needs of our STs. We demonstrate a method of auditing an existing programme, distilling important learning goals, comparing it against an appropriate standard (i.e. coverage of the MRCOG KAs), and implementing changes utilising reproducible techniques such as the Delphi method (Humphrey-Murto et al., 2017). This process should be a regular mainstay of any mature ST programme to ensure continued relevancy. As continual outbreaks, even amongst vaccinated populations (Amit et al., 2021; Bar-On et al., 2021; Bergwerk et al., 2021) auger a future of COVID-19 endemicity, we must accept a “new-normal” comprising of intermittent workplace infection control policies such as segregation, shift work, and restrictions for in-person meetings (Kwon et al., 2020; Liang et al., 2020). Through our experience, we have shown that this auditing methodology can also be applied to vCME programmes.
Notes on Contributors
Rachel Jiayu Lee participated in the data collection and review, the writing of the paper, and the formatting for publication.
Jeannie Jing Yi Yap participated in the data collection and review, the writing of the paper, and the formatting for publication.
Carly Yanlin Wu participated in data collection and review.
Grace Chan Ming Fen participated in data collection and review.
Abhiram Kanneganti was involved in the writing of the paper, editing, and formatting for publication. Citra Nurfarah Zaini Mattar participated in the editing and direction of the paper.
Pearl Shuang Ye Tong participated in the editing and direction of the paper.
Susan Jane Sinclair Logan participated in the editing and direction of the paper.
Ethical Approval
IRB approval for waiver of consent (National Healthcare Group DSRB 2020/00360) was obtained for the questionnaire assessing attitudes towards vCME.
Data Availability
There is no relevant data available for sharing in this paper.
Acknowledgement
We would like to acknowledge the roles of Mr Xiu Cai Wong Edwin, Mr Lee Boon Kai and Ms Teo Xin Yue in the administrative roles behind auditing and reformatting the PG medical education programme.
Funding
There was no funding for this article.
Declaration of Interest
The authors have no conflicts of interest in connection with this article.
References
Amit, S., Beni, S. A., Biber, A., Grinberg, A., Leshem, E., & Regev-Yochay, G. (2021). Postvaccination COVID-19 among healthcare workers, Israel. Emerging Infectious Diseases, 27(4), 1220. https://doi.org/10.3201/eid2704.210016
Amparore, D., Claps, F., Cacciamani, G. E., Esperto, F., Fiori, C., Liguori, G., Serni, S., Trombetta, C., Carini, M., Porpiglia, F., Checcucci, E., & Campi, R. (2020). Impact of the COVID-19 pandemic on urology residency training in Italy. Minerva Urologica e Nefrologica, 72(4), 505-509. https://doi.org/10.23736/s0393-2249.20.03868-0
Bakar, A. R., Mohamed, S., & Zakaria, N. S. (2012). They are trained to teach, but how confident are they? A study of student teachers’ sense of efficacy. Journal of Social Sciences, 8(4), 497-504. https://doi.org/10.3844/jssp.2012.497.504
Bar-On, Y. M., Goldberg, Y., Mandel, M., Bodenheimer, O., Freedman, L., Kalkstein, N., Mizrahi, B., Alroy-Preis, S., Ash, N., Milo, R., & Huppert, A. (2021). Protection of BNT162b2 vaccine booster against Covid-19 in Israel. New England Journal of Medicine, 385(15), 1393-1400. https://doi.org/10.1056/NEJMoa2114255
Bergwerk, M., Gonen, T., Lustig, Y., Amit, S., Lipsitch, M., Cohen, C., Mandelboim, M., Levin, E. G., Rubin, C., Indenbaum, V., Tal, I., Zavitan, M., Zuckerman, N., Bar-Chaim, A., Kreiss, Y., & Regev-Yochay, G. (2021). Covid-19 breakthrough infections in vaccinated health care workers. New England Journal of Medicine, 385(16), 1474-1484. https://doi.org/10.1056/NEJMoa2109072
Bienstock, J., & Heuer, A. (2022). A review on the evolution of simulation-based training to help build a safer future. Medicine, 101(25), Article e29503. https://doi.org/10.1097/MD.0000000000029503
Bisson, D. L., Hyde, J. P., & Mears, J. E. (2006). Assessing practical skills in obstetrics and gynaecology: Educational issues and practical implications. The Obstetrician & Gynaecologist, 8(2), 107-112. https://doi.org/10.1576/toag.8.2.107.27230
Bryant‐Smith, A., Rymer, J., Holland, T., & Brincat, M. (2019). ‘Perfect practice makes perfect’: The role of laparoscopic simulation training in modern gynaecological training. The Obstetrician & Gynaecologist, 22(1), 69-74. https://doi.org/10.1111/tog.12619
Burr, R., & Johanson, R. (1998). Continuing medical education: An opportunity for bringing about change in clinical practice. British Journal of Obstetrics and Gynaecology, 105(9), 940-945. https://doi.org/10.1111/j.1471-0528.1998.tb10255.x
Chan, G. M. F., Kanneganti, A., Yasin, N., Ismail-Pratt, I., & Logan, S. J. S. (2020). Well-being, obstetrics and gynaecology and COVID-19: Leaving no trainee behind. Australian and New Zealand Journal of Obstetrics and Gynaecology, 60(6), 983-986. https://doi.org/10.1111/ajo.13249
Chick, R. C., Clifton, G. T., Peace, K. M., Propper, B. W., Hale, D. F., Alseidi, A. A., & Vreeland, T. J. (2020). Using technology to maintain the education of residents during the COVID-19 pandemic. Journal of Surgical Education, 77(4), 729-732. https://doi.org/10.1016/j.jsurg.2020.03.018
Colman, S., Wong, L., Wong, A. H. C., Agrawal, S., Darani, S. A., Beder, M., Sharpe, K., & Soklaridis, S. (2020). Curriculum mapping: an innovative approach to mapping the didactic lecture series at the University of Toronto postgraduate psychiatry. Academic Psychiatry, 44(3), 335-339. https://doi.org/10.1007/s40596-020-01186-0
Davies, I. J. T. (1981). The assessment of continuing medical education. Scottish Medical Journal, 26(2), 125-134. https://doi.org/10.1177/003693308102600208
Davis, D. A., Thomson, M. A., Oxman, A. D., & Haynes, R. B. (1992). Evidence for the effectiveness of CME: A Rreview of 50 randomized controlled trials. Journal of the American Medical Association, 268(9), 1111-1117. https://doi.org/10.1001/jama.1992.03490090053014
De Leeuw, R., De Soet, A., Van Der Horst, S., Walsh, K., Westerman, M., & Scheele, F. (2019). How we evaluate postgraduate medical e-learning: systematic review. JMIR medical education, 5(1), e13128.
Dong, C., Lee, D. W.-C., & Aw, D. C.-W. (2021). Tips for medical educators on how to conduct effective online teaching in times of social distancing. Proceedings of Singapore Healthcare, 30(1), 59-63. https://doi.org/10.1177/2010105820943907
Donovan, P., & Townsend, J. (2019). Learning Needs Analysis. Management Pocketbooks.
English, W., Vulliamy, P., Banerjee, S., & Arya, S. (2020). Surgical training during the COVID-19 pandemic – The cloud with a silver lining? British Journal of Surgery, 107(9), e343-e344. https://doi.org/10.1002/bjs.11801
Forsetlund, L., O’Brien, M. A., Forsén, L., Mwai, L., Reinar, L. M., Okwen, M. P., Horsley, T., & Rose, C. J. (2021). Continuing education meetings and workshops: Effects on professional practice and healthcare outcomes. Cochrane Database of Systematic Reviews, 9(9), CD003030. https://doi.org/10.1002/14651858.CD003030.pub3
Gillan, C., Lovrics, E., Halpern, E., Wiljer, D., & Harnett, N. (2011). The evaluation of learner outcomes in interprofessional continuing education: A literature review and an analysis of survey instruments. Medical Teacher, 33(9), e461-e470. https://doi.org/10.3109/0142159X.2011.587915
Gould, D., Kelly, D., White, I., & Chidgey, J. (2004). Training needs analysis. A literature review and reappraisal. International Journal of Nursing Studies, 41(5), 471-486. https://doi.org/10.1016/j.ijnurstu.2003.12.003
Grafton-Clarke, C., Uraiby, H., Gordon, M., Clarke, N., Rees, E., Park, S., Pammi, M., Alston, S., Khamees, D., Peterson, W., Stojan, J., Pawlik, C., Hider, A., & Daniel, M. (2022). Pivot to online learning for adapting or continuing workplace-based clinical learning in medical education following the COVID-19 pandemic: A BEME systematic review: BEME Guide No. 70. Medical Teacher, 44(3), 227-243. https://doi.org/10.1080/0142159X.2021.1992372
Harden, R. M. (2001). AMEE Guide No. 21: Curriculum mapping: A tool for transparent and authentic teaching and learning. Medical Teacher, 23(2), 123-137. https://doi.org/10.1080/01421590120036547
Hasson, F., Keeney, S., & McKenna, H. (2000). Research guidelines for the Delphi survey technique. Journal of Advanced Nursing, 32(4), 1008-1015. https://doi.org/10.1046/j.1365-2648.2000.t01-1-01567.x
Hicks, C., & Hennessy, D. (1996). Applying psychometric principles to the development of a training needs analysis questionnaire for use with health visitors, district and practice nurses. NT Research, 1(6), 442-454. https://doi.org/10.1177/174498719600100608
Hicks, C., & Hennessy, D. (1997). The use of a customized training needs analysis tool for nurse practitioner development. Journal of Advanced Nursing, 26(2), 389-398. https://doi.org/https://doi.org/10.1046/j.1365-2648.1997.199702 6389.x
Hoopes, S., Pham, T., Lindo, F. M., & Antosh, D. D. (2020). Home surgical skill training resources for obstetrics and gynecology trainees during a pandemic. Obstetrics and Gynecology 136(1), 56-64. https://doi.org/10.1097/aog.0000000000003931
Humphrey-Murto, S., Varpio, L., Wood, T. J., Gonsalves, C., Ufholz, L.-A., Mascioli, K., Wang, C., & Foth, T. (2017). The use of the Delphi and other consensus group Methods in medical education research: A review. Academic Medicine, 92(10), 1491-1498. https://doi.org/10.1097/ACM.0000000000001812
Johnston, S., Coyer, F. M., & Nash, R. (2018). Kirkpatrick’s evaluation of simulation and debriefing in health care education: a systematic review. Journal of Nursing Education, 57(7), 393-398. https://doi.org/10.3928/01484834-20180618-03
Juprasert, J. M., Gray, K. D., Moore, M. D., Obeid, L., Peters, A. W., Fehling, D., Fahey, T. J., III, & Yeo, H. L. (2020). Restructuring of a general surgery residency program in an epicenter of the Coronavirus Disease 2019 pandemic: Lessons from New York City. JAMA Surgery, 155(9), 870-875. https://doi.org/10.1001/jamasurg.2020.3107
Kanneganti, A., Lim, K. M. X., Chan, G. M. F., Choo, S.-N., Choolani, M., Ismail-Pratt, I., & Logan, S. J. S. (2020). Pedagogy in a pandemic – COVID-19 and virtual continuing medical education (vCME) in obstetrics and gynecology. Acta Obstetricia et Gynecologica Scandinavica, 99(6), 692-695. https://doi.org/10.1111/aogs.13885
Kanneganti, A., Sia, C.-H., Ashokka, B., & Ooi, S. B. S. (2020). Continuing medical education during a pandemic: An academic institution’s experience. Postgraduate Medical Journal, 96, 384-386. https://doi.org/10.1136/postgradmedj-2020-137840
Khamees, D., Peterson, W., Patricio, M., Pawlikowska, T., Commissaris, C., Austin, A., Davis, M., Spadafore, M., Griffith, M., Hider, A., Pawlik, C., Stojan, J., Grafton-Clarke, C., Uraiby, H., Thammasitboon, S., Gordon, M., & Daniel, M. (2022). Remote learning developments in postgraduate medical education in response to the COVID-19 pandemic – A BEME systematic review: BEME Guide No. 71. Medical Teacher, 44(5), 466-485. https://doi.org/10.1080/0142159X.2022.2040732
Kwon, Y. S., Tabakin, A. L., Patel, H. V., Backstrand, J. R., Jang, T. L., Kim, I. Y., & Singer, E. A. (2020). Adapting urology residency training in the COVID-19 era. Urology, 141, 15-19. https://doi.org/10.1016/j.urology.2020.04.065
Liang, Z. C., Ooi, S. B. S., & Wang, W. (2020). Pandemics and their impact on medical training: Lessons from Singapore. Academic Medicine, 95(9), 1359-1361. https://doi.org/10.1097/ACM.0000000000003441
Lim, E. C., Oh, V. M., Koh, D. R., & Seet, R. C. (2009). The challenges of “continuing medical education” in a pandemic era. Annals Academy of Medicine Singapore, 38(8), 724-726. https://www.ncbi.nlm.nih.gov/pubmed/19736579
Mansouri, M., & Lockyer, J. (2007). A meta-analysis of continuing medical education effectiveness. Journal of Continuing Education in the Health Professions, 27(1), 6-15. https://doi.org/10.1002/chp.88
Marinopoulos, S. S., Dorman, T., Ratanawongsa, N., Wilson, L. M., Ashar, B. H., Magaziner, J. L., Miller, R. G., Thomas, P. A., Prokopowicz, G. P., Qayyum, R., & Bass, E. B. (2007). Effectiveness of continuing medical education. Evid Rep Technol Assess (Full Rep), 149, 1-69. https://www.ncbi.nlm.nih.gov/pubmed/17764217
Markaki, A., Malhotra, S., Billings, R., & Theus, L. (2021). Training needs assessment: Tool utilization and global impact. BMC Medical Education, 21(1), Article 310. https://doi.org/10.1186/s12909-021-02748-y
Metheny, W. P., Espey, E. L., Bienstock, J., Cox, S. M., Erickson, S. S., Goepfert, A. R., Hammoud, M. M., Hartmann, D. M., Krueger, P. M., Neutens, J. J., & Puscheck, E. (2005). To the point: Medical education reviews evaluation in context: Assessing learners, teachers, and training programs. American Journal of Obstetrics and Gynecology, 192(1), 34-37. https://doi.org/10.1016/j.ajog.2004.07.036
Mishra, K., Boland, M. V., & Woreta, F. A. (2020). Incorporating a virtual curriculum into ophthalmology education in the coronavirus disease-2019 era. Current Opinion in Ophthalmology, 31(5), 380-385. https://doi.org/10.1097/icu.0000000000000681
Norman, G. R., Shannon, S. I., & Marrin, M. L. (2004). The need for needs assessment in continuing medical education. BMJ (Clinical research ed.), 328(7446), 999-1001. https://doi.org/10.1136/bmj.328.7446.999
Palmer, W., & Brackwell, L. (2014). A national audit of maternity services in England. BJOG, 121(12), 1458-1461. https://doi.org/10.1111/1471-0528.12973
Parry-Smith, W., Mahmud, A., Landau, A., & Hayes, K. (2014). Workplace-based assessment: A new approach to existing tools. The Obstetrician & Gynaecologist, 16(4), 281-285. https://doi.org/10.1111/tog.12133
Pinnell, J., Tranter, A., Cooper, S., & Whallett, A. (2021). Postgraduate medical education quality metrics panels can be enhanced by including learner outcomes. Postgraduate Medical Journal, 97(1153), 690-694. https://doi.org/10.1136/postgradmedj-2020-138669
Raza, A., Coomarasamy, A., & Khan, K. S. (2009). Best evidence continuous medical education. Archives of Gynecology and Obstetrics, 280(4), 683-687. https://doi.org/10.1007/s00404-009-1128-7
Renaud, C. J., Chen, Z. X., Yuen, H.-W., Tan, L. L., Pan, T. L. T., & Samarasekera, D. D. (2021). Impact of COVID-19 on health profession education in Singapore: Adoption of innovative strategies and contingencies across the educational continuum. The Asia Pacific Scholar, 6(3), 14-23. https://doi.org/10.29060/TAPS.2021-6-3/RA2346
Royal College of Obstetricians and Gynaecologists. (2019). Core Curriculum for Obstetrics & Gynaecology: Definitive Document 2019. https://www.rcog.org.uk/media/j3do0i1i/core-curriculum-2019-definitive-document-may-2021.pdf
Sibley, J. C., Sackett, D. L., Neufeld, V., Gerrard, B., Rudnick, K. V., & Fraser, W. (1982). A randomized trial of continuing medical education. New England Journal of Medicine, 306(9), 511-515. https://doi.org/10.1056/NEJM198203043060904
Sparkes, D., Leong, C., Sharrocks, K., Wilson, M., Moore, E., & Matheson, N. J. (2021). Rebooting medical education with virtual grand rounds during the COVID-19 pandemic. Future Healthc J, 8(1), e11-e14. https://doi.org/10.7861/fhj.2020-0180
Wasfy, N. F., Abouzeid, E., Nasser, A. A., Ahmed, S. A., Youssry, I., Hegazy, N. N., Shehata, M. H. K., Kamal, D., & Atwa, H. (2021). A guide for evaluation of online learning in medical education: A qualitative reflective analysis. BMC Medical Education, 21(1), Article 339. https://doi.org/10.1186/s12909-021-02752-2
Willett, T. G. (2008). Current status of curriculum mapping in Canada and the UK. Medical Education, 42(8), 786-793. https://doi.org/10.1111/j.1365-2923.2008.03093.x
Wong, T. Y., & Bandello, F. (2020). Academic ophthalmology during and after the COVID-19 pandemic. Ophthalmology, 127(8), e51-e52. https://doi.org/10.1016/j.ophtha.2020.04.029
Xu, J., Zhou, Z., Chen, K., Ding, Y., Hua, Y., Ren, M., & Shen, Y. (2022). How to minimize the impact of COVID-19 on laparoendoscopic single-site surgery training? ANZ Journal of Surgery, 92, 2102-2108. https://doi.org/10.1111/ans.17819
*Abhiram Kanneganti
Department of Obstetrics and Gynaecology,
NUHS Tower Block, Level 12,
1E Kent Ridge Road,
Singapore 119228
Email: abhiramkanneganti@gmail.com
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
