
Involving stakeholders in postgraduate health professions education programmes
Submitted: 10 April 2023
Accepted: 15 May 2023
Published online: 3 October, TAPS 2023, 8(4), 59-60
https://doi.org/10.29060/TAPS.2023-8-4/LE3036
Siti Suriani Abd Razak, Bhavani Veasuvalingam, Pathiyil Ravi Shankar & Norul Hidayah Mamat
IMU Centre for Education, International Medical University, Malaysia
Dear Editor,
We read the article titled ‘Involving stakeholders in re-imagining a medical curriculum’ (Foster, 2022) with great interest. We would like to share our experiences and extend the importance of stakeholder involvement in postgraduate health professions education programmes (PGHPE). These programmes are utilised by educators for skills development, career progressions and advancement of health professions education across various health professions. Our institution started accredited PGHPE programmes in 2018 to equip health professional educators within and outside our institution with competencies to deliver evidence-based education and impact graduate outcomes positively. Our curriculum review conducted in early 2023, began with a stakeholder engagement meeting involving students, facilitators, alumni, employers, and ‘institutional partners’ (national and international HPE experts). Focus group discussions were held on four areas: (1) HPE ‘Industry’ institutional Needs and Graduate Competencies, (2) Student Experience, (3) Scholarship in HPE, and (4) Inter-Institutional Partnership and Collaboration.
Four key outcomes emerged from the engagement. The four outcomes were increased educators’ competency, digitalisation in health profession education, supporting scholarly work and publication and widening the scope of learning with global engagement.
The first theme of increased educators’ competency is related to the value of our PGHPE programmes. Our alumni strongly felt their teaching and learning competencies were enhanced and they were more confident in accepting leadership roles. Greater emphasis on contextualisation was requested for example local and regional accreditation frameworks. Stakeholders jointly highlighted the increasing use of artificial intelligence (AI) in HPE and emphasised that both awareness of and being able to work with digital tools is important. The use of AI in curriculum design, review and assessment may need greater emphasis. Greater HPE student engagement with online learning tools and assessments to promote deep learning was firmly echoed by our stakeholders.
The need for greater support to facilitate educational research and the possible formation of research consortiums was widely agreed upon by participants. The team has identified and initiated Health Professional Educational Research Clusters to facilitate HPE students achieve this goal. The final theme focused on widening engagement and collaboration. The centre’s strong international collaboration provides opportunities for HPE students to share ideas and thoughts and enhances networking and collaboration.
As a postgraduate programme, the number of alumni is more limited, and are educators with work experience, hence stakeholder involvement becomes more valuable to programme developers. Importantly, postgraduate programmes provider can utilise stakeholder engagement and feedback during different stages in a developmental manner.
Notes on Contributors
Siti Suriani Abd Razak organised and conducted the stakeholders’ engagement meeting, conceptualised and wrote the manuscript and approved the final version.
Bhavani Veasuvalingam organised and conducted the stakeholders’ engagement meeting, conceptualised, revised the manuscript and approved the final version.
Pathiyil Ravi Shankar organised and conducted the stakeholders’ engagement meeting, conceptualised, revised the manuscript and approved the final version
Norul Hidayah Mamat organised and conducted the stakeholders’ engagement meeting, revised the manuscript and approved the final version.
Acknowledgement
We would like to thank Professor Vishna Devi Nadarajah and Professor Er Hui Meng for their support and feedback in the process of conducting the stakeholders engagement meeting and writing this letter.
Funding
No funds, grants, or other support were received.
Declaration of Interest
No conflicts of interest are associated with this paper.
References
Foster, K. (2023). Involving stakeholders in re-imagining a medical curriculum. The Asia Pacific Scholar, 8(1), 43-46. https://doi.org/10.29060/TAPS.2023-8-1/SC2807
*Siti Suriani binti Abd Razak
No 126, Jalan Jalil Perkasa 19
Bukit Jalil, 47000
Kuala Lumpur, Malaysia
+6019-4429985
Email: sitisuriani@imu.edu.my
Submitted: 14 March 2023
Accepted: 31 March 2023
Published online: 3 October, TAPS 2023, 8(4), 57-58
https://doi.org/10.29060/TAPS.2023-8-4/LE3021
Tomoko Miyoshi1, Mikiko Iwatani2 & Fumio Otsuka1
1Department of General Medicine, Faculty of Medicine, Dentistry and Pharmaceutical Sciences, Okayama University, Japan; 2Department of Nursing, Okayama University Hospital, Japan
It was found that the excess mortality rate for U.S. physicians was considerably lower during the COVID-19 pandemic than in the general population, but more physicians died than expected when compared to pre-pandemic levels. These results suggest that appropriate infection control measures can reduce mortality; however, additional measures are needed.
During the COVID-19 pandemic, there have been many reports of burnout among healthcare professionals (HCPs). Although no causal relationship has been established, it is acknowledged that it would be difficult to pay attention to mental health issues and the creation of a healthy work environment during a pandemic.
Globally, the COVID-19 pandemic has subsided, but what have we learned from this COVID-19 pandemic?
We conducted six online significant event analyses (SEAs) in collaboration with facilities providing administrative support, nursing care, and medical care for COVID-19-infected individuals in March 2022. The participants were limited to HCPs and healthcare students. The presentations were based on actual cases of COVID-19-infected patients, focusing on the struggles of their positions and efforts to overcome them. Seventy-three people participated, and 38 responded to the post-event survey (52.1% response rate). Twenty respondents (52.6%) were satisfied, and 16 (42.1%) were very satisfied with this initiative, with gratitude for having the reflection.
SEA, a method of reflection, is a learning process in which recognition of one’s feelings is important (Henderson et al., 2002). HCPs are always considered to be engaged in reflective practices. However, during the COVID-19 pandemic, there were issues that were insufficient to transfer previous experiences. However, in the case of the COVID-19 pandemic, “reflection in action” was not sufficient to overcome the challenges, and the SEA may have served as a place for “reflection on action” to prepare for the next stage of the COVID-19 pandemic.
Furthermore, this SEA provided an opportunity to recognise the existence of “common humanity,” which is one of the three elements of self-compassion (the ability to understand that people other than oneself are also suffering). It is believed that, through the SEA, the HCPs were able to become aware of the feelings of other HCPs. It has been reported that increased self-compassion increases compassion for others (Neff & Germer, 2013), and the increased self-compassion of HCPs may increase their compassion for other HCPs and patients.
In the COVID-19 pandemic, reflection among healthcare providers beyond the facility may enhance self-compassion and compassion for others in preparation for the next pandemic, which may lead to HCPs’ well-being.
Notes on Contributors
T Miyoshi conceptualised and wrote the manuscript and approved the final version.
M Iwatani conceptualised and approved the manuscript.
F Otsuka supervised and edited the manuscript.
Funding
There is no funding provided.
Declaration of Interest
There is no conflict of interest, including financial, consultant, institutional or otherwise for the author.
References
Henderson, E., Berlin, A., Freeman, G., & Fuller, J. (2002). Twelve tips for promoting significant event analysis to enhance reflection in undergraduate medical students. Medical Teacher, 24(2),121–124. https://doi.org/10.1080/01421590220125240
Neff, K. D., & Germer, C. K. (2013). A pilot study and randomized controlled trial of the mindful self-compassion program. Journal of Clinical Psychology. 69(1), 28–44. https://doi.org/10.1002/jclp.21923
*Tomoko Miyoshi
2-5-1 Shikata-cho, Kita-ku
Okayama, 700-8558, Japan
+81-86-235-7342
Email: tmiyoshi@md.okayama-u.ac.jp
Submitted: 4 February 2023
Accepted: 19 April 2023
Published online: 3 October, TAPS 2023, 8(4), 53-56
https://doi.org/10.29060/TAPS.2023-8-4/CS3003
Maximilian Andreas Storz1 & Rintaro Imafuku2
1Department of Internal Medicine II, Center for Complementary Medicine, Faculty of Medicine, Freiburg University Hospital, University of Freiburg, Germany; 2Medical Education Development Center, Gifu University, Japan
I. INTRODUCTION
International medical electives are a central component of the academic curriculum in many medical schools and universities worldwide (Storz, 2022). As short-term clinical immersion experiences, abroad electives are essential in connecting medical faculties and academic hospitals around the globe. They foster cross-cultural exchange, medical skill training, as well as professional identity formation (Imafuku et al., 2021; Storz, 2022). From a global health perspective, abroad electives provide medical students with an opportunity to gain a better understanding of healthcare and medical education in an international context.
Historically, some countries cultivate close relationships in this regard. One example is the bilateral relation between Japan and Germany, which is characterised by a strong economic cooperation and close political dialogue (Hook et al., 2011). As pluralistic democracies, both share fundamental values and are closely tied in many socioeconomic aspects. Traditionally, there has also been a strong partnership in medical sciences between both countries (Horowski, 2018).
Japan is traditionally a popular destination for German-speaking medical students (Storz et al., 2021), and the most frequently reported elective destination in Asia. Nevertheless, little is known about student’s elective experiences in Japan. To address this gap, we reviewed four German open-access online-databases cataloguing elective testimonies and extrapolated key elective characteristics that may allow for a better understanding of abroad elective experience in Japan.
II. METHODS
The employed analysis method with its strengths and drawbacks has been described elsewhere (Storz et al., 2021). In brief, we analysed the 4 largest German open-access clinical elective reports databases called “Famulatur-Ranking” (www.famulaturranking.de), “PJ-Ranking” (www.pj-ranking.de), “ViaMedici” (https:// www.thieme. de/viamedici/medizin-im-ausland-ausland saufenthalt-allgemein-1627.htm), and “Medizinernach-wuchs” (www.medizinernachwuchs.de). Databases allow students to anonymously rate medical electives and to share their experience by uploading reports on a voluntary basis. Key information necessary to upload a report include the precise elective destination (e.g. country, city, hospital name), the elective year, the elective discipline and duration, a subjective elective rating (ranging from 1 to 6, whereby 1 is the best and 6 is the worst grade), and a short comment allowing a brief narrative summary of the elective experience. Generally, elective ratings refer exclusively to a subjective “overall elective experience”, and are not based on a clear rubric to guide students in their rating process. The databases’ search function was used to filter Japan-specific electives. For this particular analysis, all electives from 2005 onwards were considered. Databases were reviewed in September 2022 and data pertaining to any kind of clinical elective experience in Japan was then extrapolated to a Microsoft Excel-File.
III. RESULTS
We extrapolated n=36 Japan elective reports uploaded until 2020. Tokyo was the most frequently reported elective destination, accounting for 47% of reports (n=17), followed by Kyoto (11%, n=4). The remaining elective destinations are shown in Figure 1, which displays regions (coloured) and prefectures of Japan.

Figure 1. Elective destinations in Japan: An overview. Modified from TUBS (https://commons.wikimedia.org/wiki/File:Regions_and_Prefectures_of_Japan_no_labels.svg), based on a license under the Creative Commons Attribution-Share Alike 4.0 International license.
General surgery was the most frequently reported discipline (30.56%, n=11), followed by internal medicine (22.22%, n=8). Surgical disciplines accounted for 45% of reported electives (n=16), whereas internal medicine (including subspecialties) accounted for 1/3 of reports (n=12). The following disciplines accounted for n=3 reports each: Gastroenterology, Gynaecology, Neurology and Radiology.
Thirty-three students shared organisational details of their electives. More than 60% of electives were self-organised (n=20). Thirty-nine percent of electives (n=13) were organised through a bilateral international elective exchange program where a Japanese university partnered with a German university based on a signed memorandum of understanding.
Eight students possessed Japanese language skills to a varying degree (22.22%). Three students reported learning Japanese for one year, while one student learned Japanese for more than two years. The remaining four students did not share any information about their level of Japanese language skills. Despite the rather low percentage of students speaking Japanese, the vast majority of students rated their overall experience in Japan as excellent (grade: A, n=26). Of 28 students, two students rated their elective with the grade B.
Students reported a diverse set of gratifying elective experiences. The large majority of reports (n=33, 97.22%) highly appreciated the Japanese hospitality and the high level of social manners. More than half of students (n=19, 52.78%) reported the impression that students were generally highly respected in Japan. Frequent high-quality teaching and a thorough elective organisation were frequently mentioned (n=27 and n=29 mentions, respectively). Students also valued that they received clear instructions on the first elective day, often receiving in the form of a timetable or schedule, detailing their assignments, classes and teaching opportunities. Fourteen reports explicitly mentioned that a contact person at the international office was always available for questions, and reported their elective to be first-class in terms of organisation and structure.
Many students were surprised that students are denied hands-on experience in Japan by law prior to graduation, although this is usually explicitly mentioned on the elective program homepages. Almost 42% of students (n=15) valued that their hosting institution organised social and cultural events, including get-togethers and language courses. Eating-out after work with other hospital staff was considered an important and highly appreciated team-building strategy.
One third of students (n=12) stated that they received enough free time to explore the Japanese culture. Finally, n=5 students (13.89%) expressed their appreciation for the high technical standard in Japanese hospitals, particularly in terms of medical equipment and workflow.
IV. DISCUSSION
Our descriptive analysis allows for various helpful insights into German medical students’ destinations and experiences during their Japan elective. Students reported gratifying experiences and emphasised the very good organisation of electives in Japan.
Such information may be of paramount importance for host institutions because incoming students may be a double-edged sword. Hosting elective students is time-consuming and requires human resources. In some cases, international elective students may negatively impact the local community in terms of patient care and resource allocation (Storz et al., 2021), Then again, well-structured electives may also increase the reputation of hosting institutions and help foster bidirectional and transnational academic exchange.
As in most cases, benefits and downsides of electives are context-specific, and depend on local elective program structures. Here, students valued their electives and reported a substantial amount of gratifying experiences. Several students explicitly mentioned that their Japan elective was the “best elective during [their] entire time at medical school”. Understanding incoming students’ perspectives is vital for host institutions, and may benefit them in multiple dimensions, e.g. when tailoring elective programs. This may apply in particular to the post-COVID-19 era, where an increase in international student mobility is expected (Storz, 2022). In this context, it is worthy to mention that the majority of electives in our sample was self-organised. Host institutions should be prepared for receiving an increasing amount of elective applications in the post-pandemic years, where the elective landscape will likely be characterised by a more competitive seat-to-applicant ratio.
The reservation must be made that our analysis builds on a small convenience sample (n=36) that is not representative of German medical students in general (Storz et al., 2021). Additional interesting aspects, for example as to whether clinical experiences in Japan affected students’ career or future goals, were not ascertainable from our data. In addition, we were unable to measure whether Japan electives strengthened student’s clinical skills. Our data predominately suggested an increase in cultural competences but due to the cross-sectional nature of our data no reliable statementa can be made. For this, an interview-based approach utilising focused interviews with returnee students would have been more suitable. Regrettably, such an approach was hardly realisable during the past pandemic years.
V. CONCLUSION
Our results enable hosts to understand why foreign students seek electives at their institutions. Said information might be of paramount importance for elective organisers, since well-structured electives may increase the reputation of hosting institutions and help fostering transnational academic exchange.
Notes on Contributors
Maximilian Andreas Storz conceputalised the study, collected the data, performed the formal analysis, wrote the first draft of the manuscript, and approved the final version submitted.
Rintaro Imafuku contributed to the project administratition, supported the visualisation and criticially revised the manuscript for important intellectual content and approved the the final version submitted.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Interest
The authors declare that they have no competing interests.
References
Hook, G. D., Gilson, J., Hughes, C. W., & Dobson, H. (2011). Japan’s International Relations: Politics, economics and security (3rd ed.). Routledge. https://doi.org/10.4324/9780203804056
Horowski, R. (2018). Japanese medicine and Berlin: A very special and successful relationship. Journal of Neural Transmission, 125(1), 3–7. https://doi.org/10.1007/s00702-017-1800-1
Imafuku, R., Saiki, T., Hayakawa, K., Sakashita, K., & Suzuki, Y. (2021). Rewarding journeys: Exploring medical students’ learning experiences in international electives. Medical Education Online, 26(1), Article 1913784. https://doi.org/10.1080/10872981.2021.1913784
Storz, M. A., Lederer, A.-K., & Heymann, E. P. (2021). German-speaking medical students on international electives: An analysis of popular elective destinations and disciplines. Globalization and Health, 17(1), Article 90. https://doi.org/10.1186/s12992-021-00742-z
Storz, M. A. (2022). International medical electives during and after the COVID-19 pandemic – current state and future scenarios: A narrative review. Globalization and Health, 18(1), Article 44. https://doi.org/10.1186/s12992-022-00838-0
*Maximilian Andreas Storz
Hugstetter Str. 55
79106 Freiburg im Breisgau, Germany
+49 15754543852
Email: maximilian.storz@uniklinik-freiburg.de
Submitted: 19 February 2023
Accepted: 10 July 2023
Published online: 3 October, TAPS 2023, 8(4), 50-52
https://doi.org/10.29060/TAPS.2023-8-4/PV3007
Nathasha Luke1, Reshma Taneja1, Kenneth Ban2, Dujeepa Samarasekera3 & Celestial T Yap1
1Department of Physiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Department of Biochemistry, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 3Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Health Professional Education has considerably evolved over the years. Traditional classroom teaching has shifted to blended learning modalities, and clinical teaching has embraced virtual reality and simulation-based learning.
Education is poised for another major change with the development of artificial intelligence (AI) models that can emulate human-like intelligent behaviour, particularly in the field of large language models (LLM) that are capable of generating text in response to user input. There has been remarkable progress in the development of these models, with each iteration having an increasing ability to generate human-like responses to user input.
In November 2022, Open AI released ChatGPT. This marked a major milestone in the ability of LLMs. This leap in performance was driven in part by the training of the model on large text datasets from various sources such as books, articles, and websites. It was combined with supervised learning and reinforcement learning to fine-tune the model based on human feedback about the quality of the output. This was further augmented by the release of GPT-4, a further advanced version in early 2023.
A study demonstrated that ChatGPT was able to pass or preform at near parsing threshold in the United States Medical Licensing Examination (USMLE) (Kung et al., 2023). Also, ChatGPT passed a law entrance examination at a level equivalent to a C+ grade (Kelly, 2023). These studies highlight the potential of modern LLMs to impact education.
Despite its impressive performance, LLMs have limitations. These caveats notwithstanding, when educators and students are aware of the capabilities and limitations, LLM tools could provide opportunities to improve the way we teach and the way students learn. More evidence is needed to depict a specific model as if how this technology could be incorporated. This article particularly focuses on capabilities and limitations of LLMs in the context of medical education with suggestions on how this technology might be used. There is a huge scope for discussion on the impact of LLMs in various dimensions of medical education. However, we limit this discussion to commonest domains pertaining undergraduate medical education.
Being widely available and accessible to educators and students around the world including resource poor settings, LLMs promote equity in medical education. Certain educational institutes have customised learning platforms to support student learning while such amenities are not accessible in resource poor settings. On the contrary, the technology of LLMs could at least partially counterbalance such shortages promoting equity.
In addition, Universities in resource-poor settings often find inadequate number of educators as a barrier to implement new teaching strategies and curriculum reformation, particularly with the shifting paradigms to competency based medical education (Ramanathan et al., 2022). Effective incorporation of LLM tools could ease their workload to some extent, providing more time to explore new teaching pedagogies and scope for curricular reformations.
LLM tools are being adopted in medical education, and assistive in both clinical and non-clinical settings, as discussed below. In non-clinical settings, the following are some areas where LLMs are helpful.
From an educator’s perspective, LLM tools are helpful in generating summaries, quizzes, and flashcards to make the learning interesting.
From learners’ perspective, LLM tools can generate customised information within a short span of time. For example, we may ask the LLM tool to answer a question ‘at a level of a medical student’ or ‘at the level of a resident’, to generate distinct responses. This will assist students in self-learning and understanding difficult concepts. LLM tools are also helpful in generating mnemonics, poems, and flashcards. Students who are not native English speakers will have the added advantage of AI tools being assistive in improving language skills.
Additionally, LLMs are assistive tools in many stages of research including design and development, implementation, literature survey and data analysis.
There is emerging literature illustrating capabilities of LLMs as useful tools in medical practice (Lee et al., 2023). Though there aren’t many publications evaluating implications of current LLM technology in the domain of clinical education per -se, this technology is likely to be helpful in the development of skills such as history-taking and doctor-patient communication. Customized chatbots have been used by some medical schools to improve history-taking skills. Development of such tools are not affordable in resource-poor settings. LLM tools such as ChatGPT are not capable of ‘acting’ as a model patient to practice history taking. However, they can guide students to formulate relevant questions for effective history-taking in specific scenarios. Students should not be encouraged to use AI tools as the sole reference to guide the task, rather use it as an adjunct to ones’ thought process. For instance, if a student encounters a patient with palpitations, he or she should brainstorm based on theoretical knowledge to formulate relevant questions to be asked in history taking. An LLM tool can be an adjunct to ‘cross-check’ if all salient points were captured.
LLMs could potentially be assistive in improving patient communication skills among students and junior doctors.AI systems could aid in generating facts that are comprehensible to non-medical personnel. This ability is particularly helpful for students in generating content to practice patient communication skills. Accuracy and suitability of such information should be objectively assessed, before recommending LLM tool use for this purpose.
The LLM technology is a tool that can augment the process of multi- dimensional education, encompassing competency-based approaches to education, in addition to discipline-based education. This multidimensional approach comprises knowledge along with various other skills including professionalism, communication, practice-based learning, and patient care. This approach demands more commitment from students and educators and requires more learning resources. With the emergence of more sophisticated AI technologies, harnessing of LLM capabilities could be explored as future learning resources to be developed.
Unbundling and rebundling the curriculum is a concept that emphasizes revising the existing curricula by combining various educational resources including textbooks, lectures and web-based resources (Morris et al., 2018). This is pertinent to the multi-dimensional approach discussed above. The advances in current LLM tools have the potential to become an integral component of the curriculum bundle to meet the demands of reformations in modern medical education.
Potential negative implications of LLM tools have caused anxiety among educators. Firstly, the content generated may not be accurate at all times. LLMs generate responses from language patterns learnt from the training data and not from a deeper understanding of a subject. This is also compounded by the inability of some LLMs to link to external resources to gauge the validity of the output. Another limitation of the current LLM technology is ‘hallucination’ to create non-existent or wrong information in a convincing manner. (Lee et al., 2023) Consequences of such information could cause huge impact particularly in patient safety in medical education.
LLMs have potential negative implications on the evaluation of students’ learning. In modern-day multidimensional education, assessments have moved a long way from traditional examinations to include projects, assignments, and research. Certain assignments are designed to foster the development of critical thinking and analytical skills. AI tools may direct students to take an easier path in completing these tasks, impeding the accomplishment of intended learning outcomes.
There is no consensus on how this technology should be adopted in higher education. At the start, certain educational institutes banned the use of LLMs, and software was developed to detect work done by AI. These approaches are not sustainable in the long run.
Users should have a clear understanding on potentials and imitations of current LLM technology, in order to use LLMs effectively.
LLM technology is improving rapidly, and efficacious compared to many other sources of education. However they are not yet at a standpoint to be recommended as the primary source in education, rather, they could be adjuncts to standard resources like lectures, textbooks, peer-reviewed literature, and online materials. Students should know when and when not to use it, and the content should be critically and cautiously looked into.
Educators have a crucial role in guiding the students on using AI effectively. Navigating students to experience the limitations of LLMs through practical scenarios is a potential strategy. An example would be to assign students to critically analyse a draft answer generated through an LLM platform. This will allow both the students and tutors identify the capabilities and limitations of LLMs.
In the context of evolving LLMs educators have to re look into the existing assessment modalities and implement changes to ensure the potential objectives of the assessment are met. The policies regarding LLM use for the particular task should be clearly communicated to the students on contextual basis.
Impacts of LLMs on educational development is yet another area warranting discussion. This encompasses exploring the role of LLMS in instructor, instructional and organizational development. We didn’t include it within the scope of this write up.
In summary, generative AI could be harnessed to potentiate students’ learning, in knowledge acquisition as well as application. Even though LLM tools may pose challenges, we foresee a larger potential for the betterment of medical education, ultimately leading to the overall goal of better patient care.
Notes on Contributors
WANVL, CTY, RT, DS and KB were involved in planning of the article.
WANVL drafted the initial version of the mauscript.
WANVL, CTY, RT, DS and KB revised and edited the initial draft manuscript and approved the final version of the manuscript for submission.
Funding
The authors received no financial support for the authorship or publication of this article.
Declaration of Interest
The authors do not have any conflicts of interest to disclose.
References
Kelly, S. M. (2023, January 26). ChatGPT passes exams from law and business schools. CNN Business. https://edition.cnn.com/2023/01/26/tech/chatgpt-passes-exams/index.html
Kung, T. H., Cheatham, M., Medenilla, A., Sillos, C., De Leon, L., Elepaño, C., Madriaga, M., Aggabao, R., Diaz-Candido, G., Maningo, J., & Tseng, V. (2023). Performance of ChatGPT on USMLE: Potential for AI-assisted medical education using large language models. PLOS Digital Health, 2(2), Article e0000198. https://doi.org/10.1371/journal.pdig.0000198
Lee, P., Bubeck, S., & Petro, J. (2023). Benefits, Limits, and Risks of GPT-4 as an AI Chatbot for Medicine. The New England Journal of Medicine, 388(13), 1233–1239. https://doi.org/10.1056/NEJMsr2214184
Morris, N., Ivancheva, M., Swinnerton, B., Coop, T., & Czerniewicz, L. (2018, September 11-13). Critical perspectives on unbundling and rebundling higher education provision online [Research session]. [18-97]. ALT Annual Conference, Manchester, UK. https://www.youtube.com/watch?v=F2FS0n3Dr0k
Ramanathan, R., Shanmugam, J., Gopalakrishnan, S. M., Palanisamy, K. T., & Narayanan, S. (2022). Challenges in the Implementation of Competency-Based Medical Curriculum: Perspectives of Prospective Academicians. Cureus. https://doi.org/10.7759/cureus.32838
*Celestial T Yap
Department of Physiology
Yong Loo Lin School of Medicine
National University of Singapore
+6590560468
Email: phsyapc@nus.edu.sg
Submitted: 21 December 2023
Accepted: 3 July 2023
Published online: 3 October, TAPS 2023, 8(4), 46-49
https://doi.org/10.29060/TAPS.2023-8-4/PV2934
Dhivya Subramanian
School of Medicine, University of Dundee, United Kingdom
Portfolio has been used since the early 15th century to showcase designs, and folders of work for architectural, artistic and financial purposes. Though the method of delivering a portfolio has shifted over the years from a “folder of loose papers” to “electronic portfolios” with the advent of technology; the crux of portfolios has remained the same. The purpose of portfolio to allow for a personalised approach for each individual to showcase their knowledge, professional values and skills has remained constant over the past hundreds of years. (Buckley et al., 2009) The usage of portfolio in medical education has been thought to give students more responsibilities for their own learning and development and aid in stimulating the reflective thought process (Driessen et al., 2003). Moreover, portfolio has been considered being a more holistic approach to assessing students in medicine, which allows a broader method in assessment rather than a ‘snap-shot’ examination (Van Tartwijk & Driessen, 2009).
Portfolio was first introduced in the University of Dundee in 1997 and the first portfolio assessment occurred in 1999. Portfolios are formatively assessed from 1st to 4th year and are a summative assessment in 5th, the final year (Davis et al., 2009). As a final year Singaporean student from the University of Dundee, I was introduced to the new concept of portfolio during my medical course (MBChB) and its importance was emphasised from the very beginning in Year 1. Appendix 1 underlines the portfolio requirements for the respective years. These requirements are regularly updated in our portfolio section on Medblogs (medical school website for students and staff), allowing us to check deadlines and ensure we are up to date with tasks required.
The portfolio in the University of Dundee and all universities in the United Kingdom is based on the 3 Outcomes of Graduates 2018 set by the General Medical Council (Outcome 1–Professional values and behaviours, Outcome 2–Professional skills, Outcome 3–Professional knowledge) (Monrouxe et al., 2018). All portfolios are uploaded on to the system known as “NHS e-portfolios” which provides a platform for all students throughout the nation to upload their works.
Four years ago, as a 1st year medical student, I found it hard to understand the importance of portfolio. The medical school organised lectures to inform us about the purpose of portfolio and its significance to aid our professional development. However, it appeared more of an abstract concept. Since the school gave information on what we needed to submit and when, it seemed more of a checklist of things we needed to finish. It was difficult to appreciate the holistic picture of portfolio and its purpose in our development as a medical professional.
Growing up in Singapore, practicing reflections was not part of our culture. A more difficult task-oriented environment is what most of us are used to during our schooling and work life in Singapore. The concept of reflections was new and seemed redundant, however as years went by and when I entered the clinical years of medicine (year 4 and year 5), I began to understand why the emphasis on reflection was so strong.
The reflective essays we add in our portfolio can be chosen from a list provided to us but also can be done on topics we choose ourselves to reflect on. This gives us freedom to decide what we felt was impactful during our placements and does not constrain us to write about certain issues, thus avoiding the ‘checklist-like’ feeling that can often be felt during the initial stages of developing a portfolio. The University of Dundee encourages the use of either Gibb’s cycle, Rolfe et al, or John’s model as reflective writing models to aid the reflection process.
Often my peers including myself would debate that reflections are things we do regularly, such as thinking about how the day went before we sleep or reflecting on action such as recognising a patients’ emotions while speaking to them and reacting appropriately. However, I recognised the importance of writing down reflections as we can look back at it in the future and learn from the past.
During my paediatric placement in 4th year, I had the opportunity to reflect on a case I found myself getting emotionally involved. A two-year old child was vigorously shaken by his parents which led to a hypoxic brain injury and consequently cerebral palsy. Seeing the patient every day on ward rounds was disheartening as I could witness the stark difference between the neglected, immobile child and another child playing happily in the next bed. Upon reflecting, I could appreciate that there will be circumstances in the future where I encounter similar situations, and the practice of reflecting and debriefing with colleagues can aid in alleviating the emotional weight we take back home. This served as a turning point in appreciating the value of reflections as a medical student.
Even though portfolio assessments are summative in final year, the process of developing the portfolio became more genuine nearing the end of the course. On reflection, I would think this is mainly due to the realisation that the reflective process required in building a portfolio helped me become a better medical professional; with not only arming myself with the right skills but also enabling the confidence to perform well once we set foot into the clinical world as a Foundation Doctor / House Officer.
It is important to emphasise that it is not only reflective questions that use the skill of reflection. Reflections for feedback given for case discussions and clerkings allow us to reflect on the process of writing the essays and how we could improve in the future. The reflection serves as a critical interrogation which creates meaning from an event and urges us to act. I realised that only if one identifies their limitations and develops an action plan, they can work towards a target in mind. Setting an action plan paves path to avidly look for opportunities in order to gain more practice in those areas. This made me realise that it is truly up to an individual’s initiative whether they want to gain something useful from building a portfolio.
If I had the opportunity to tell my year 1 self something, I would advise to regularly update her portfolio rather than leaving it to the very end and to approach it as something she does for herself rather than to impress a supervisor or faculty member. Even if one does not understand the purpose of portfolio at the initial stages, completing reflections and small pieces of work are valuable as the skill is slowly starting to develop. Ultimately “every expert was once a beginner”.
Looking back at my portfolio and seeing all my achievements collated in one area fills me with a sense of pride and fulfilment. After all, portfolio is something you develop throughout your life; from the first year you start working till the day you retire. So why not start early if you can!
Notes on Contributors
Dhivya Subramanian is a final year medical student at the University of Dundee, UK. The author based this personal view from past experiences in developing a portfolio during the period of undergratudate medical school.
Acknowledgement
Thanks to Dr. Shuh Shing Lee for her support and guidance.
Funding
No funding has been received for this article.
Declaration of Interest
No conflicts of interest, including financial, consultant, institutional, and other relationships that might lead to bias or a conflict of interest.
References
Buckley, S., Coleman, J., Davison, I., Khan, K. S., Zamora, J., Malick, S., Morley, D., Pollard, D., Ashcroft, T., Popovic, C., & Sayers, J. (2009). The educational effects of portfolios on undergraduate student learning: A Best Evidence Medical Education (BEME) systematic review. BEME Guide No. 11. Medical Teacher, 31(4), 282–298. https://doi.org/10.1080/01421590902889897
Davis, M. H., Ponnamperuma, G. G., & Ker, J. S. (2009). Student perceptions of a portfolio assessment process. Medical Educa- tion, 43(1), 89–98. https://doi.org/10.1111/j.1365-2923.2008.03250.x
Driessen, E., Van Tartwijk, J., Vermunt, J., & van der Vleuten, C. (2003). Use of portfolios in early undergraduate medical training. Medical Teacher, 25(1), 18–23. https://doi.org/10.1080/0142159021000061378
Monrouxe, L. V., Bullock, A., Gormley, G., Kaufhold, K., Kelly, N., Roberts, C. C., Mattick, K., & Rees, C. E. (2018). New graduate doctors’ preparedness for practice: a multistakeholder, multicentre narrative study. BMJ Open, 8(8), 1–15. https://doi.org/10.1136/bmjopen-2018-023146
Van Tartwijk, J., & Driessen, E. W. (2009). Portfolios for assessment and learning: AMEE Guide no. 45. Medical Teacher, 31(9), 790–801. https://doi.org/10.1080/01421590903139201
*Dhivya Subramanian
University of Dundee, Nethergate,
Dundee DD1 4HN, United Kingdom
Email: sdhivya1509@gmail.com
Submitted: 18 February 2023
Accepted: 28 March 2023
Published online: 3 October, TAPS 2023, 8(4), 40-45
https://doi.org/10.29060/TAPS.2023-8-4/SC3010
Kit Mun Tan1, Chan Choong Foong2, Donnie Adams3, Wei Han Hong2, Yew Kong Lee4 & Vinod Pallath2
1Department of Medicine, Faculty of Medicine, Universiti Malaya, Malaysia; 2Medical Education and Research Development Unit (MERDU), Faculty of Medicine, Universiti Malaya, Malaysia; 3Department of Educational Management, Planning and Policy, Faculty of Education, Universiti Malaya, Malaysia; 4Department of Primary Care, Faculty of Medicine, Universiti Malaya, Malaysia
Abstract
Introduction: The global COVID-19 pandemic had greatly affected the delivery of medical education, where institutions had to convert to remote learning almost immediately. This study aimed to measure undergraduate medical students’ readiness and factors associated with readiness for remote learning.
Methods: A cross-sectional quantitative study was conducted amongst undergraduate medical students using the Blended Learning Readiness Engagement Questionnaire, during the pandemic where lessons had to be delivered fully online in 2020.
Results: 329 students participated in the study. Mean scores for remote learning readiness were 3.61/4.00 (technology availability), 3.60 (technology skills), 3.50 (technology usage), 3.35 (computer and internet efficacy), and 3.03 (self-directed learning). Male students appeared more ready for remote learning than females, in the dimensions of self-directed learning and computer and internet efficacy. Students in the pre-clinical years showed a lower level of readiness in the technology availability domain compared to clinical students. The lowest score however was in the self-directed learning dimension regardless of the students’ year of studies.
Conclusion: The pandemic had created a paradigm shift in the delivery of the medical program which is likely to remain despite resumption of daily activities post-pandemic. Support for student readiness in transition from instructor-driven learning models to self-directed learning models is crucial and requires attention by institutions of higher learning. Exploring methods to improve self-directed learning and increase availability of technology and conducting sessions to improve computer and internet efficacy can be considered in the early stages of pre-clinical years to ensure equitable access for all students.
Keywords: Remote Learning, Student’s Readiness, Medical Education
I. INTRODUCTION
The COVID-19 pandemic and global emergency from the end of January 2020 had greatly affected the education sector, with many institutions including undergraduate medical schools converting to remote learning within a short timeframe.
Previous studies have shown that e-learning methods were effective and acceptable among medical undergraduate students (Chen et al., 2020). Studies have also suggested that students may struggle in adapting to a self-directed learning process (Vaughan, 2007), prefer traditional face-to-face lectures and possibly lacking the technological skills and infrastructure for a satisfactory remote learning experience.
It is important to determine the remote learning readiness of undergraduate medical students to facilitate the adaptation of these practices to maximise student competencies. Therefore, the primary objective of this study was to determine the readiness for remote learning in undergraduate medical students in a South-East Asian university and the secondary objective was to identify factors associated with their remote learning readiness.
II. METHODS
This was a cross-sectional quantitative study to measure medical students’ readiness towards remote learning using the BLREQ questionnaire. This study was approved by the Research Ethics Committee (Reference UM.TNC2/UMREC-889) of the university.
In the Covid-19 enforced scenario at that time, the physical face-to-face teaching in our institution was moved to online almost immediately, requiring the students to adapt their learning approaches rapidly to suit the needs of a virtual learning environment.
The duration of the study was one month, from the 19th of June to the 19th of July 2020. Our country implemented a national lockdown (and emergency remote learning) due to COVID-19 on the 18th of March 2020. Thus, data collection occurred in the first few months of the remote learning situation and represented students’ experiences and readiness during the early phase of the change.
The students were from all five years of study in the medical undergraduate program. They were contacted via their online educational platform and WhatsApp group chats with details of the study, participant’s consent form, link to the online self-administered questionnaire and weekly reminders to encourage participation. Participation was voluntary and consent was obtained from the students. Data were anonymised and not traceable to a particular individual.
This study utilised Section A and B of the BLREQ questionnaire which is a validated questionnaire on the readiness and engagement of students in blended learning (Adams et al., 2018). Although ‘Blended Learning’ is defined as a combination of e-learning (online) and traditional education (face-to-face) approaches, the BLREQ is appropriate for this study as it primarily measures students’ readiness for remote learning. Section A contained basic demographic questions (i.e., age, gender, year of study). Section B had 37 items in five dimensions which addressed various aspects of students’ readiness for remote learning. A 4-point Likert-type scale ranging from strongly disagree (1) to strongly agree (4) was provided with only one response allowed per item.
The data was analysed using IBM SPSS version 25. The data was non-normally distributed; hence the Mann-Whitney U test was used to test for significant difference in scores between gender and stages of study.
III. RESULTS
There were 329 complete responses out of 734 invited participants (44.8% response rate). Most respondents were aged between 20 to 24 years old (Mean=21.9; SD=1.8). Approximately 59% were female and 59% were clinical students.
The total dimension and individual item mean scores are reported in Table I with the highest and lowest scores of each dimension annotated. The dimensions of remote learning readiness arranged in descending order of total mean score are Technology Availability (3.61+50), Technology Skills (3.60+.43), Technology Usage (3.50+.44), Computer and Internet Efficacy (3.35+.49), and Self-directed Learning (3.03+.51) (Table 1). Research data of this study are available at https://doi.org/10.6084/m9.figshare.21443100
Analysed by gender, the mean scores of male students were significantly higher than female students in the dimensions of Self-directed Learning; 3.13 vs 2.96 (U=10354.5, z=-3.18, p=.001), and Computer and Internet Efficacy; 3.39 vs 3.32 (U=11332.5, z=-2.02, p=.044). Individual items in which male students scored significantly higher in each dimension were [SDL1], [SDL4], [CIE2] and [CIE3].
When comparing between stages of study, the mean score of clinical students was significantly higher than pre-clinical students only in the Technology Availability dimension; 3.65 vs 3.55 (U=11376.0, z=-2.13, p=.034) An individual item which clinical students scored significantly higher in Technology Availability dimension was [TA3].
|
Dimensions and items |
Mean |
SD |
|
[TS] Technology Skills dimension |
3.60 |
.43 |
|
[TS1] I know the basic functions of a computer/laptop and its peripherals like the printer, speaker, keyboard, mouse etc.** |
3.76 |
.45 |
|
[TS2] I know how to save and open documents from a hard disk or other removable storage device. |
3.67 |
.52 |
|
[TS3] I know how to open and send email with file attachments. |
3.72 |
.48 |
|
[TS4] I know how to log on to Wi-Fi |
3.74 |
.46 |
|
[TS5] I know how to navigate web pages (go to next or previous page). |
3.68 |
.50 |
|
[TS6] I know how to download files using browsers (e.g., Google Chrome, Internet Explorer, Firefox) and view them. |
3.67 |
.51 |
|
[TS7] I know how to access an online library or database.* |
3.19 |
.78 |
|
[TS8] I know how to use Word processing software (e.g., Microsoft (MS) Word). |
3.62 |
.53 |
|
[TS9] I know how to use Presentation software (e.g., MS PowerPoint). |
3.60 |
.53 |
|
[TS10] I know how to use Spreadsheet software (e.g., MS Excel). |
3.30 |
.75 |
|
[TS11] I know how to open several applications at the same time and move easily between them. |
3.60 |
.60 |
|
[TU] Technology Usage [TU] dimension |
3.50 |
.44 |
|
[TU1] I often use the internet to find information.** |
3.86 |
.37 |
|
[TU2] I often use e-mail to communicate.* |
2.93 |
.93 |
|
[TU3] I often use office software (e.g., MS Word, PowerPoint, Excel). |
3.62 |
.56 |
|
[TU4] I often use social networking sites to share information (e.g., Facebook, Twitter, Instagram, Snapchat). |
3.39 |
.83 |
|
[TU5] I often use instant messaging (e.g., WhatsApp, Viber, WeChat, Line, Telegram). |
3.72 |
.54 |
|
[TU6] I often use cloud-based file hosting services to store or share documents (e.g., Google Drive, Dropbox, One drive). |
3.44 |
.69 |
|
[TU7] I often use learning management systems (e.g., Blackboard, Moodle). |
3.28 |
.69 |
|
[TU8] I often use mobile technologies (e.g., Smartphone, Tablet) to communicate. |
3.72 |
.51 |
|
[TA] Technology Availability dimension |
3.61 |
.50 |
|
[TA1] I have a computer/laptop with an internet connection.** |
3.74 |
.53 |
|
[TA2] I have a computer/laptop with adequate software for learning (e.g., Microsoft (MS) Office). |
3.63 |
.57 |
|
[TA3] I have speakers for courses with video presentations.* |
3.50 |
.72 |
|
[TA4] I have a computer/laptop and its peripherals like the printer, speaker, keyboard, mouse etc. |
3.57 |
.66 |
|
[SDL] Self-directed Learning dimension |
3.03 |
.51 |
|
[SDL1] I am a highly independent learner. |
3.12 |
.69 |
|
[SDL2] I am able to learn new technologies.** |
3.60 |
.55 |
|
[SDL3] I do not need direct lectures to understand materials.* |
2.36 |
.92 |
|
[SDL4] I would describe myself as a self-starter in learning using technology. |
3.18 |
.79 |
|
[SDL5] I am not distracted by other online activities when learning online (e.g., Facebook, Gaming, Internet surfing). |
2.42 |
1.04 |
|
[SDL6] I can read the online instructional materials on the basis of my needs. |
3.49 |
.58 |
|
[CIE] Computer and Internet Efficacy dimension |
3.35 |
.49 |
|
[CIE1] I feel confident in using online tools (e.g., email, internet chat, instant messenger) to communicate effectively with others. |
3.48 |
.65 |
|
[CIE2] I feel confident in expressing myself (e.g., emotions and humour) in my university’s learning management systems (e.g., Blackboard, Moodle) |
2.89 |
.83 |
|
[CIE3] I feel confident in posting questions in online discussions.* |
2.87 |
.82 |
|
[CIE4] I feel confident in performing the basic functions of Word processing software (e.g., MS Word). |
3.59 |
.55 |
|
[CIE5] I feel confident in performing the basic functions of Presentation software (e.g., MS PowerPoint). |
3.48 |
.62 |
|
[CIE6] I feel confident in performing the basic functions of Spread sheet (e.g., MS Excel). |
3.26 |
.78 |
|
[CIE7] I feel confident in using web browsers (e.g., Google Chrome, Mozilla Firefox) to find or gather information for online learning.** |
3.67 |
.53 |
|
[CIE8] I feel confident in using computer or tablet or mobile phone for online learning. |
3.56 |
.63 |
Table 1. Dimension and individual item mean scores of student readiness to engage in remote learning
** highest score in the dimension
*lowest score in the dimension
IV. DISCUSSION
This study aimed to identify medical students’ readiness for remote learning across five dimensions and to identify factors associated with their readiness during the early months of the COVID-19 online learning transition period. Although there is significant resumption of usual activities post-COVID-19 pandemic, many of the online and self-directed components of learning are likely to remain as the way forward in the medical curriculum. Therefore, we feel that this study still has relevance currently.
All mean scores of the subscales Technology Availability (TA), Technology Skills (TS), Technology Usage (TU), Computer and Internet Efficacy (CIE) and Self-directed Learning (SDL), were above 3 on a scale of 1 to 4. The mean scores in our study were much higher and have less deviation than Adams et al’s study conducted in a similar setting before the COVID-19 pandemic, in which the five dimensions scored lower than 3.00, with SDL scoring the lowest mean in the other study at 1.25+1.55 (Adams et al., 2018). Adams et al’s study also did not show much difference when comparing between medicine, social science, science and engineering students (Adams et al., 2018), indicating that readiness for online learning was much lower overall pre-COVID-19.
Despite the increase compared to Adams et al’s study, SDL still scored the lowest in our study out of the five dimensions. An implication of this is that universities need to help learners transition from facilitator/ instructor-driven learning models to self-directed learning models. This can be done by making training in ‘learning to learn’ (L2L) an essential component of student support. In our setting, this training should address items which scored lowest in SDL as these indicate areas of struggle for students; [SDL3] and [SDL5]. It is also possible that some facilitators are not aware of what SDL is, therefore facilitators can also benefit from training for SDL methods.
Our study demonstrated significantly higher readiness for remote learning among male students in comparison to female students in the domains of SDL and CIE. While some studies indicate no gender differences in e-Learning readiness, other studies also report gender differences such as males having more positive attitudes toward online learning; males being more ready for online learning (Adams et al., 2018) and males using more learning strategies and having better technical skills than females (Alghamdi et al., 2020). In the CIE domain, males scored higher in the items [CIE2] and [CIE3] which are both related to communication through a virtual platform. This resulted in males scoring higher in the CIE domain in general. The gender disparity in remote learning readiness needs to be addressed as female students are increasingly the majority (and therefore primary stakeholders) in medical schools worldwide.
The mean score of clinical students was significantly higher than pre-clinical students only in the Technology Availability domain with clinical students reporting better hardware and infrastructure access compared to pre-clinical students. It is likely that as the learners progress through a course, they become more aware of the technological requirements of the course and invest in better devices and internet access. It is also possible that the students’ socioeconomic status at the beginning of their course may not have been good, for example if they were awaiting scholarships to be processed, which subsequently became available later in their course of study. This may have then enabled the students to purchase better hardware and infrastructure further on in their course, during the clinical years. However, this financial aspect was not included our study. It is still worth considering future programs early in the course, where there could be subsidies for students to purchase necessary technological equipment for their studies.
A. Limitations and Recommendations
One limitation of this study was that it looked at remote learning in general and did not look at clinical elements such as using online simulated patients for history taking classes, or procedural skills videos. The study also only looked at student perspectives, and not faculty perspectives to get a complete picture of the online learning experiences. Future studies should explore student readiness for clinical online learning as this would be a struggle for students even if the transition was under normal circumstances (Vaughan, 2007). The perspectives of faculty members on readiness to move towards online learning also need to be explored. The strength of this study was that it used a previously validated questionnaire which allowed some comparison on students’ remote learning readiness with pre-COVID-19 studies.
V. CONCLUSION
In conclusion, the study explored medical undergraduates’ remote learning readiness in a public medical school in Malaysia during the COVID-19 pandemic. In general, students were found to be ready for remote learning. However, the lowest scores were for the domain of self-directed learning and computer and internet efficacy. Based on our findings, we feel that support for student readiness in transition from instructor-driven learning models to self-directed learning models is crucial and requires attention by institutions of higher learning. Exploring methods to improve self-directed learning and increase availability of technology and conducting sessions to improve computer and internet efficacy can be considered in the early stages of pre-clinical years to ensure equitable access for all students. There should also be efforts to train the educators to develop online learning activities which incorporate the socio-relational aspects of learning into the remote learning experience.
Notes on Contributors
Kit Mun, Tan is the first author and person who initiated the study, contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Chan Choong, Foong contributed to the design of study, data collection and analysis, writing and approval of the final version of the manuscript.
Donnie, Adams is the creator of the original Blended Learning Readiness Questionnaire (BLREQ) and contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Wei Han, Hong contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Yew Kong, Lee contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Vinod, Pallath is the corresponding author and contributed to the design of the study, data collection and analysis, writing and approval of the final version of the manuscript.
Ethical Approval
This study received ethical approval from the Universiti Malaya Ethics Review Committee with the approval number of UM.TNC2/UMREC-889.
Data Availability
Research data of this study are available at https://doi.org/10.6084/m9.figshare.21443100.
Readers may access the anonymised data freely with the above URL. Kindly contact the authors for permission if you wish to use the data for a subsequent study or collaboration.
Acknowledgement
We would like to acknowledge and express gratitude to the undergraduate medical students who took the time to participate in this study.
Funding
There was no external funding for this study.
Declaration of Interest
All the authors do not have a conflict of interest to declare.
References
Adams, D., Sumintono, B., Mohamed, A., & Mohamad Noor, N. S. (2018). E-learning readiness among students of diverse backgrounds in a leading Malaysian higher education institution. Malaysian Journal of Learning and Instruction, 15(2), 227-256. https://doi.org/10.32890/mjli2018.15.2.9
Alghamdi, A., Karpinski, A. C., Lepp, A., & Barkley, J. (2020). Online and face-to-face classroom multitasking and academic performance: Moderated mediation with self-efficacy for self-regulated learning and gender. Computers in Human Behavior, 102, 214-222. https://doi.org/10.1016/j.chb.2019.08.018
Chen, J., Zhou, J., Wang, Y., Qi, G., Xia, C., Mo, G., & Zhang, Z. (2020). Blended learning in basic medical laboratory courses improves medical students’ abilities in self-learning, understanding, and problem solving. Advances in Physiology Education, 44(1), 9-14.
Vaughan, N. (2007). Perspectives on blended learning in higher education. International Journal on E-Learning, 6(1), 81-94. https://www.learntechlib.org/primary/p/6310/
*Associate Professor Dr Vinod Pallath
Medical Education Research and Development Unit,
Faculty of Medicine, Universiti Malaya,
50603 Kuala Lumpur
Email: vinodpallath@um.edu.my
Submitted: 9 February 2023
Accepted: 22 March 2023
Published online: 3 October, TAPS 2023, 8(4), 36-39
https://doi.org/10.29060/TAPS.2023-8-4/SC3000
Komson Wannasai1, Wisanu Rottuntikarn1, Atiporn Sae-ung2, Kwankamol Limsopatham2, Wiyada Dankai1
1Department of Pathology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 2Department of Parasitology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
Abstract
Introduction: Global medical and healthcare education systems are increasingly adopting team-based learning (TBL). TBL is an interactive teaching programme for improving the performance, clinical knowledge, and communication skills of students. The aim of this study is to report the learning experience and satisfaction of participants with the TBL programme in the preclinical years of the Faculty of Medicine, Chiang Mai University.
Methods: Following the implementation of TBL in the academic year 2022, we asked 387 preclinical medical students, consisting of 222 Year 2 and 165 Year 3 medical students who attended the TBL class to voluntarily complete a self-assessment survey.
Results: Overall, 95.35% of the students were satisfied with the structure of the TBL course and agreed to attend the next TBL class. The overall satisfaction score was also high (4.44 ± 0.627). In addition, the students strongly agreed that the TBL programme improved their communication skills (4.50 ± 0.796), learning improvement (4.41 ± 0.781), and enthusiasm for learning (4.46 ± 0.795).
Conclusion: The survey findings indicated that students valued TBL-based learning since it enabled them to collaborate and embrace learning while perhaps enhancing their study abilities. However, since this is a pilot study, further investigations are warranted.
Keywords: Team-based Learning, Small Group Interaction, Medical Education, Implementation
I. INTRODUCTION
Team-based learning (TBL) is a form of small-group teaching which can improve student performance, clinical knowledge, and communication skills. It has been employed in medical and healthcare education in the US, Australia, Austria, Japan, South Korea, and Singapore (Burgess et al., 2014; Michaelsen & Sweet, 2008). Since 2000s, this model has been used in medical education to foster deep learning across a variety of subjects and educational contexts, benefiting teachers and helping academically weak and strong students achieve the same or better results than with conventional methods (Parmelee et al., 2012). In addition, it is more effective for engaging students than lecturing in a large class with few teachers (Burgess et al., 2020b).
The key elements of TBL include pre-class preparation to encourage self-study, teamwork, and instant feedback. These key elements promote active learning and critical thinking (Burgess et al., 2020a; Parmelee et al., 2012). The steps in TBL include pre-class preparation, individual readiness assurance test (iRAT), team readiness assurance test (tRAT), feedback, and team application (Burgess et al., 2014). In the tRAT and team application phase, students work in small groups to demonstrate the use of teamwork for problem-solving. Clinical problem-solving exercises by students lead to class discussions and instructor comments (Burgess et al., 2020a; Michaelsen & Sweet, 2008). The teacher’s feedback can help clarify students’ responses by discussing their answers. In the academic year 2022, TBL was implemented on second- and third-year medical students in the Faculty of Medicine, Chiang Mai University, and self-assessment questionnaires were used to assess students’ satisfaction with the TBL model. This research aims to examine the impact of team-based learning on whether or not students were able to build their own learning processes, as well as to measure student satisfaction with teaching and learning in the TBL paradigm in order to improve further TBL classrooms in the faculty.
II. METHODS
A. Sampling and Participants
In 2022, 387 pre-clinic medical students from Chiang Mai University’s Faculty of Medicine were studied (222 from Year 2 and 165 from Year 3). Year 2 medical students studied human skin and the connective tissue system, while Year 3 medical students studied human haematology. Each TBL class consisted of 50 teams of mixed-gender and grades. Each team contained five members.
B. Structure and Components of TBL
The TBL programme was first implemented in the 2022 academic year, covering preclinical academic Years 2 and 3 at the Faculty of Medicine, Chiang Mai University. The TBL structure comprised two major phases: pre-class and in-class. The TBL topics included automated haematology and venomous snakes for Year 3 medical students. The skin infection topic was selected for Year 2 medical students.
After TBL, the non-researcher academic team informed medical students about the study and sought volunteers to avoid a conflict of interest between the instructors and the medical students. The non-researchers urged students interested in the experiment to complete a Google Forms questionnaire outlining the study’s relevance, including an explanation of the topic, data gathering, and the pros and cons of participation. If participants agreed to answer the questionnaire, they could complete the Google Form to consent and submit the questionnaire, with their personal information remaining anonymous.
For validity, a questionnaire to explore students’ views on TBL was prepared via a literature study, student review (two students), peer review (faculty members from two departments), and expert opinion (a TBL expert). It also examined students’ perceptions of teams and their beliefs and values in collaboration. The outcomes of the different years of student were then compared.
C. Data Collection and Analysis
Upon completing the TBL class, participant students were invited to voluntarily take the self-assessment survey to explore their thoughts on the assertions made in the TBL literature. The questionnaire was in Thai and we used a five-point Likert scale (1 = strongly dissatisfied, 2 = unsatisfied, 3 = neither satisfied nor dissatisfied, 4 = satisfied, 5 = strongly satisfied). Students were asked about the preparation for the TBL class, including student material, classroom, teaching content, self-preparation, orientation programme, class material, and the overall programme. The self-assessment survey also asked about promoting self-understanding, including communication skills, learning improvement, and enthusiasm in learning using a five-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = strongly agree).
The TBL self-assessment survey data were analysed according to mean and standard deviation (SD) using STATA version 16 (STATA Corp., Texas, USA). The Pearson’s Chi-square test was used to analyze the difference between second- and third-year medical students’ percentages of satisfaction or agreement in each aspect. Statistical significance was accepted at p < 0.05. The reliability of the questionnaire was calculated using Cronbach’s alpha.
III. RESULTS
In years 2 and 3, Cronbach’s alpha of the medical students’ questionnaire was 0.869. In total, 369/387 (95.35%) participants appreciated the course structure and agreed to attend the next TBL session. Students rated the TBL class 4.44 ± 0.627 on a five-point Likert scale, with 1 being severely dissatisfied and 5 very pleased. Students also liked the classroom (4.48 ± 0.738), TBL structure (4.41 ± 0.771), and self-preparation (4.28 ± 0.780). The orientation programme, instructional material, pre-recorded video, and handouts were also well-received. Most students (69.25%, 268/387) spent 1–2 days self-preparing before the TBL class, followed by 3–4 days (24.55%, 95/387) and 5–7 days (5.43%, 21/387), while 0.78% (3/387) did not self-prepare.
On a five-point Likert scale from 1 to 5, students assessed their self-understanding progress, stating that TBL increased their communication, learning, and enthusiasm (4.50 ± 0.796, 4.41 ± 0.781, 4.46 ± 0.795).
The student t-tests revealed no significant differences between students in years 2 and 3. Except time for preparation (Pearson’s Chi-square test; p < 0.005), medical students in years 2 and 3 had similar self-assessment survey scores. In addition, Year 3 medical students also scored better in enthusiasm for studying than Year 2 medical students in increasing self-understanding (Student t-test; p = 0.023) (Table 1).
|
|
Year 2 |
Year 3 |
p-value |
|
Student satisfaction towards the TBL class |
|||
|
Agree to attend the next TBL class: % (n) |
95.95% (213/222) |
94.55% (156/165) |
0.519 |
|
Classroom: mean (SD) |
4.49 (0.671) |
4.47 (0.823) |
0.903 |
|
TBL structure: mean (SD) |
4.38 (0.73) |
4.45 (0.822) |
0.377 |
|
Orientation programme: mean (SD) |
4.46 (0.628) |
4.40 (0.810) |
0.417 |
|
Teaching material: mean (SD) |
4.67 (0.568) |
4.56 (0.578) |
0.064 |
|
Student preparation time: mean (SD) |
4.20 (0.788) |
4.40 (0.755) |
0.012 |
|
Time for preparation: % (n) 1–2 days 3–4 days 5–7 days No preparation |
80.18% (178/222) 14.41% (32/222) 4.50% (10/222) 0.90% (2/222) |
54.55% (90/165) 38.18% (63/165) 6.67% (11/165) 0.61% (1/165) |
< 0.005 |
|
Promotion of learning skills |
|||
|
Communication skills: mean (SD) |
4.46 (0.734) |
4.56 (0.674) |
0.154 |
|
Understanding of the topics: mean (SD) |
4.36 (0.729) |
4.47 (0.845) |
0.180 |
|
Enthusiasm for learning: mean (SD) |
4.38 (0.797) |
4.56 (0.783) |
0.023 |
|
Cronbach’s alpha |
0.869 |
0.869 |
|
Table 1. Comparison between the satisfaction of medical students in years 2 and 3 towards the TBL class and agreement to the promotion of self-understanding
IV. DISCUSSION
TBL changes how students learn by encouraging them to become more accountable by preparing for the team assurance test and application exercise (Burgess et al., 2020a). Teacher-directed pre-class preparation for advanced tasks may involve reading textbooks, reference articles, or instructor-created material while the readiness assurance test enhances students’ enthusiasm for TBL (Parmelee et al., 2012). However, students may resist TBL or active learning because it varies from passive lecture-based learning. Teachers must be aware of this and advocate TBL-style learning to improve ability and encourage students to be more prepared. This research examines the attitudes of medical students towards the two courses post-TBL and provides valuable input on TBL strategies, regardless of the course schedule.
Student feedback can improve teaching and student satisfaction. Students agreed that TBL can improve communication, learning, and passion. Second-year medical students were less motivated than third-year (p = 0.023), implying they need to focus on the core content of the preclinical module rather than TBL preparation, while third years have more time management experience for pre-class self-study. Students liked the teaching material because, in addition to textbooks, the instructors prepared PowerPoint presentations, recorded VDOs, and documentation, allowing those with different learning styles to make the appropriate choice.
Interestingly, both classes found the TBL structure and location less satisfying, possibly because first-time students could not comprehend group activities. Students can further grasp the TBL framework and enjoy the structured process with a revamped instructional layout and additional classes. As for the classroom, the seat layout may prevent suitable group conversations, with a small-group or smart classroom being more appropriate for TBL.
The preparation time satisfaction results are significantly difference, with Year 2 students being considerably less satisfied than Year 3 (p = 0.012). Most second-year medical students spent one to two days planning, and third years one to four (p = 0.005), primarily because the third-year course was longer. Second-year medical students attended a two-week course on human skin and the connective tissue system with a TBL class in the second week, whereas third years took a five-week haematological system course with a TBL class in the fourth week. Both classes received course material on Mondays, while the TBL was on Fridays in the same week. Second-year medical students may need to study the basic science aspects and be unable to independently assess the pre-class material, whereas third-year students had more time. Accordingly, a TBL course should last at least three to four weeks to allow medical students to understand the basic TBL instructional material and independently assess it.
This study has limitations. The questionnaire was expert-evaluated without instructor facilitation. In addition, our study focused on students’ satisfaction with TBL, hence we didn’t include academic outcomes to prove the value of TBL.
V. CONCLUSION
The survey showed that students appreciated TBL-based learning since it helped them to work together and embrace learning, while potentially improving their study skills. A diversity of pre-class material allows students to choose learning tactics depending on their individual abilities. Students found the activity venue inadequate and classroom improvements would boost their satisfaction level.
Notes on Contributors
KW reviewed the literature, designed the study, analysed data, co-wrote the manuscript, critically reviewed and edited the manuscript, and then read it through prior to final approval.
WD reviewed the literature, analysed the data, co-wrote the manuscript, and critically reviewed and edited the manuscript.
WR gave critical feedback on the writing of the manuscript.
AS and KL provided scientific insight and advice, and critically reviewed and edited the manuscript.
Ethical Approval
This research was approved by the institutional ethics committee of the Faculty of Medicine at Chiang Mai University (Study code: PAT-2565-09243).
Data Availability
On reasonable request, the corresponding author will provide data to support the conclusions of this study. Due to privacy and ethical considerations, the data cannot be made public.
Acknowledgement
The authors wish to express their sincere appreciation to Ms. Naorn Sriwangdang for assisting with the preparation of the research proposal.
Funding
This study was supported by the Faculty of Medicine, Chiang Mai University, grant no. 062-2566.
Declaration of Interest
The authors confirm they have no potential conflicts of interest.
References
Burgess, A., Bleasel, J., Hickson, J., Guler, C., Kalman, E., & Haq, I. (2020a). Team-based learning replaces problem-based learning at a large medical school. BMC Medical Education, 20, Article 492. https://doi.org/10.1186/s12909-020-02362-4
Burgess, A., van Diggele, C., Roberts, C., & Mellis, C. (2020b). Team-based learning: Design, facilitation and participation. BMC Medical Education, 20(Suppl 2), Article 461. https://doi.org/10.1186/s12909-020-02287-y
Burgess, A. W., McGregor, D. M., & Mellis, C. M. (2014). Applying established guidelines to team-based learning programs in medical schools: A systematic review. Academic Medicine, 89(4), 678–688. https://doi.org/10.1097/ACM.0000000000000162
Michaelsen, L. K., & Sweet, M. (2008). The essential elements of team-based learning. New Directions for Teaching and Learning, 2008(116), 7–27. https://doi.org/10.1002/tl.330
Parmelee, D., Michaelsen, L. K., Cook, S., & Hudes, P. D. (2012). Team-based learning: A practical guide: AMEE Guide No. 65. Medical Teacher, 34(5), e275–e287. https://doi.org/10.3109/0142159X.2012.651179
*Komson Wannasai
Department of Pathology,
Faculty of Medicine,
Chiang Mai University,
110 Inthavaroros road, Sriphume
Meaung, Chiang Mai, 50200
+6653935442
Email: komson.wanna@gmail.com
Submitted: 9 February 2023
Accepted: 15 May 2023
Published online: 3 October, TAPS 2023, 8(4), 23-35
https://doi.org/10.29060/TAPS.2023-8-4/OA3006
Sethapong Lertsakulbunlue1, Kaophiphat Thammasoon2, Kanlaya Jongcherdchootrakul3, Boonsub Sakboonyarat3 & Anupong Kantiwong1
1Department of Pharmacology, Phramongkutklao College of Medicine, Thailand; 2Department of Personnel Administration Division, Phramongkutklao College of Medicine, Thailand; 3Department of Military and Community Medicine, Phramongkutklao College of Medicine, Thailand
Abstract
Introduction: Although medical research (MR) is constantly promoted, a global deficit of medical researchers has been noted. We aimed to explore the relationship among practice, perceptions, attitudes, barriers and motivation toward MR and its impacts on MR publication.
Methods: A cross-sectional study included 262 senior medical students and interns. An electronic, standardised Likert scale questionnaire was used to collect the data. Binary logistic regression was used to determine the odds ratio between characteristics and MR publication. Confirmatory factor analysis was used to confirm the loading factor of each question, and structural equation modeling (SEM) was used to investigate the relationship between latent variables and MR publication.
Results: Cronbach’s alpha revealed a good internal reliability of 0.93. The accumulated grade point average did not differ between those who had published and those who had not. MR presentations were strongly associated with MR publication. SEM showed that attitudes (0.71, p<0.001) and perceptions (0.27, p<0.001) had a direct effect on practices. Practices (0.49, p<0.001) and attitudes (0.30, p<0.001) had a direct effect on motivation, while motivation had a total effect = 0.36, p<0.001 on MR publication through MR presentation as a mediator.
Conclusion: Positive attitudes and perceptions might lead to positivity in the intention to practice MR, which would lead to motivation and finally increase the odds of MR publication. Different approaches to promote excitement and perceptions in MR learning should be encouraged by teachers and faculty members.
Keywords: Medical Research, Students, Perceptions, Attitudes, Barriers, Motivation
Practice Highlights
- Enjoyment and excitement should be promoted while learning medical research.
- Medical research experiences enhanced publication, particularly medical research presentations.
- Extracurricular medical research activities should be routinely promoted.
- Facilitators in medical research might be tailor-made for each individual.
- Regular meetings regarding medical research with mentors or role models should be held.
I. INTRODUCTION
Health-related research is constantly promoted and has gained great importance over time (Sobczuk et al., 2022). However, a global shortage of medical researchers was noted despite an increasing demand for them (Funston et al., 2016). For example, in the US, the proportion of medical researchers has declined from approximately 4.7% to 1.5% in the 1980s and 2014, respectively (Carberry et al., 2021; Davila, 2016; Puljak, 2007). Several barriers toward conducting medical research (MR) have been reported among undergrads and postgraduates. For instance, lack of allotted time, lack of physician engagement in research early during medical students’ training, and lack of mentoring and guidance (Bonilla-Escobar et al., 2017; El Achi et al., 2020; Habineza et al., 2019; Okoduwa et al., 2018). To resolve these problems, medical education has globally incorporated research methods and epidemiology into its curriculum (Carberry et al., 2021). Nevertheless, only a minority of medical students had reached the primary goal of research, namely publishing (Bonilla-Escobar et al., 2017; Carberry et al., 2021; Laidlaw et al., 2012).
Factors associated with MR publication have been identified. Students from highly ranked undergraduate institutions were more likely to achieve publication. Mentors also played an important role in increasing the likelihood of publication. For example, a student working with a mentor with a PhD degree or a mentor with prior publication(s) with prior mentee(s) increases the chance of achieving publication (Parker et al., 2021). Medical students participating in an extracurricular scientific activity, such as the Scientific Society of Medical Students, or who take a scientific writing skills course, were also associated with greater odds of producing a scientific publication (Valladares-Garrido et al., 2022).
One of the main reasons researchers conduct a study is because of what they believe (Lev et al., 2010). Attitudes toward and barriers against health research influence research success (Lev et al., 2010; Memarpour et al., 2015; Osman, 2016). Attitudes and motivations toward a particular type of study also showed a positive relationship with achievement (Ma & Xu, 2004; Özer, 2020; Simpson & Oliver, 1990). Furthermore, a theory of success describes perception leading to passion, and the continuation of passion leading to obsession, which drives an individual to succeed (Dange, 2016; Schellenberg et al., 2022).
Previously, several studies reported descriptive data on attitudes, practices, knowledge levels, perceptions, motivation and barriers involving research among medical and science students (AlGhamdi et al., 2014; Al-Shalawy & Haleem, 2015; Arif et al., 2018; El Achi et al., 2020; Habineza et al., 2019; Memarpour et al., 2015; Osman, 2016; Pallamparthy & Basavareddy, 2019). Even though these factors are known to affect one’s behaviour, to our knowledge, research on whether these factors are associated with research publications among medical students is scarce.
Without research, no breakthroughs can be achieved in managing disease. Therefore, strategies to enhance medical students’ appreciation of research and publication should be promoted. As a step toward this goal, our study aimed to determine the relations between MR practices, perceptions, attitudes, barriers and motivation toward medical research and their effect on MR publications among senior medical students and internists graduated from Phramongkutklao College of Medicine, Thailand. Furthermore, we also explore the differences in the characteristics and MR experiences of the participants between the publishing group and the non-publishing group. The goal involved influencing future research and actions to increase research publications among physicians in the country and contribute to medical practices.
II. METHODS
A. Study Design and Subjects
A cross-sectional study based on a self-administered survey was conducted at Phramongkutklao College of Medicine (PCM), Bangkok, Thailand. The survey was distributed among senior medical students, including fourth-, fifth-, and sixth-year students and internists who graduated from PCM. The total number of senior medical students and internists was 292 and approximately 250 interns, respectively. The curriculum at PCM is spread out over six years, with the first three being pre-clinical years spent studying basic science and the last three being clinical years spent developing clinical experiences. An introductory module about MR is mandatory in three years of the curriculum in the third, fourth, and sixth years of medical school. Firstly, third-year medical students learn the basics of MR, such as basic study designs focusing on quantitative methods, data analysis, and research proposal development. Furthermore, students learn about public health aspects, including community participation. Secondly, fourth-year medical students learn more about advanced study designs and are more focused on conducting a study and multivariate analysis. Fourth-year students were divided into eight groups of approximately twelve to conduct a community-based research proposal before finalizing their project as a report. Finally, sixth-year medical students were divided into pairs or a group of three to conduct medical research to improve medical care in a community hospital setting. Then the research is presented, and a manuscript report is submitted. However, an MR publication was not mandatory. After they graduated, the students were sent to both Thai Army hospitals and government hospitals run by the Ministry of Public Health to work as interns.
The present study included senior medical students and internists due to their similar MR experiences. First, both groups were enrolled within the same curriculum paradigm. Second, the MR presentation and publications are according to the willingness of the student, as MR publications and presentations are not mundane. Finally, almost all the published research among the population is from projects developed during their fourth and sixth years as medical students. Therefore, several projects were published during the internship.
B. Data Collection
We used an electronic standardised questionnaire, including six parts: short answer questions for obtaining demographic data; a 5-score Likert scale questionnaire on practice, perceptions, attitudes, barriers, and motivation toward MR. The questionnaire was translated using related published work that is relevant to this paper, as well as the investigators’ experience and context of PCM (El Achi et al., 2020; Funston et al., 2016; Habineza et al., 2019; Ichsan et al., 2018; Kamwendo, 2002; Okoduwa et al., 2018; Pallamparthy & Basavareddy, 2019). In addition, five expert professors examinedthe content validity and reliability of the questionnaire; pilot testing was conducted among 66 first year medical students and Cronbach’s alpha score ranged from 0.74-0.93.Then the questionnaire was launched in November and December of 2022 as a Google Form and advertised via social media to the study population. Information sheets, objectives, and methods of the study were provided on the first page of the Google Form, which participants were asked to read carefully before agreeing to participate. The questionnaire was then self-completed and took, on average, about 10–15 minutes to complete. The finalised Cronbach’s alphas were 0.83, 0.84, 0.74, 0.89, 0.88, and 0.93 for practices, perceptions, attitudes, barriers, motivation and overall questions, respectively.
Practice was defined as their willingness or intention to practice MR (El Achi et al., 2020). Perceptions are how the student perceives the importance of MR, while attitude is how they feel about conducting MR (El Achi et al., 2020; Funston et al., 2016). Barriers are defined as what the students perceive as being resistant to conducting MR; on the other hand, motivations are what they perceive as facilitating conducting MR (Habineza et al., 2019; Okoduwa et al., 2018).
C. Statistical Analysis
All data were downloaded from Google Forms, and data analyses were performed using StataCorp, 2021, Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC. A frequency distribution of demographic characteristics was performed to describe the study subjects. Categorical data were presented as percentages, and continuous variables were presented as means and standard deviations (SD). Univariable and multivariable logistic regression analysis was used to determine the odds ratio (OR) and adjusted odds ratio (AOR) with a 95% confidence interval (CI) of the association between the characteristics and MR experiences of the participants and the MR publication. All statistical tests were two-sided, and a p-value less than 0.05 was considered statistically significant.
The structural equation modeling (SEM) using maximum likelihood extraction was done to find out how the latent variables, including practice, perceptions, attitudes, barriers, and motivation, were related and what effect it had on MR publications. The procedure is comprised of two steps. The first is validating the measurement model, which is carried out primarily using confirmatory factor analysis (CFA), and the other is fitting the structural model, which is achieved primarily through path analysis of latent variables. CFA was applied to demonstrate the impact of each question (observed variable) on different beliefs toward MR (latent variable) and presented as a lambda. Questions with a low factor loading (below 0.60) were excluded from the SEM. During the SEM construction, questions with factor loadings below 0.60 were also removed. In the final model, there are 17 observed variables included within the SEM. The samples/observed variable were 15.41, which is more than 10, indicating adequate sample size for SEM (Wolf et al., 2013). The SEM was carried out to investigate the relationship among latent variables and their impact on MR publication in our study population.The six following indices were used to evaluate model fit: (1) the chi-square test, χ2; (2) the chi-square test over degree of freedom (df), χ2/df (3) the comparative fit index, CFI; (4) the Tucker–Lewis index, TLI (5) the root-mean square error of approximation, RMSEA; and (6) the root-mean square residual, (SRMR). All these indices indicated a proposed fit for SEM data. A χ2/df lower than 2, CFI greater than 0.95, TLI greater than 0.95, RMSEA less than 0.06 and SRMR less than 0.06 each indicated a good fit between the data and the hypothesised model.
III. RESULTS
A. Characteristic of Participants
Table 1 demonstrates the characteristics of participants stratified by MR publishing. A total of 139 senior medical students and 123 interns participated in the survey. The response rate was 47.6% and 49.2% for senior medical students and interns, respectively. Over one-fifth (22.1%) of the participants had published MR and were mostly internists (81.0%). Approximately 60% of the participants were male, corresponding to an enrolment at PCM of 60 male and 40 female students. The accumulated grade point average (GPAX) was approximately the same at 3.4±0.3 among both published and those who had not published. Regarding, MR experience or roles served during medical student years, being a group leader (AOR: 2.12, 95% CI: 0.97 to 4.64, p=0.06) was associated with MR publishing. Finally, those having experience in MR presentation, whether oral or poster, and international or national presentation, were strongly associated with MR publishing, with adjusted odds ratios of 4.34 (p<0.001) shown in Table 2.
|
Characteristics |
Non-Published |
Published |
|
n (% of 204) |
n (% of 58) |
|
|
Demographics |
||
|
Sex |
||
|
Male |
119 (58.3) |
37 (63.8) |
|
Female |
85 (41.7) |
21 (36.2) |
|
Educational level |
||
|
Clinical year |
128 (62.7) |
11 (19.0) |
|
Intern |
76 (37.3) |
47 (81.0) |
|
Accumulated grade point average (GPAX) |
||
|
Mean ± SD |
3.4±0.3 |
3.4±0.3 |
|
Medical research participation |
||
|
MR elective |
59 (28.9) |
15 (25.9) |
|
Time spent on MR (hours/week) |
||
|
<1 |
119 (58.3) |
27 (46.6) |
|
1-5 |
56 (27.5) |
17 (29.3) |
|
5-10 |
15 (7.4) |
7 (12.1) |
|
>10 |
14 (6.9) |
7 (12.0) |
|
Extra curriculum research activity |
39 (19.1) |
23 (39.7) |
|
Academic club activity |
30 (14.7) |
13 (22.4) |
|
MR experience during medical student |
||
|
Group leader |
45 (22.1) |
24 (41.4) |
|
Design MR |
89 (43.6) |
34 (58.6) |
|
Proposal writing |
142 (69.6) |
45 (77.6) |
|
Data enter |
126 (51.5) |
41 (70.7) |
|
Data analysis |
99 (48.5) |
34 (58.6) |
|
Literature review |
125 (61.3) |
42 (72.4) |
|
Manuscript writing |
76 (37.3) |
33 (56.9) |
|
None |
7 (3.4) |
2 (3.4) |
|
National MR presentation |
||
|
Oral presentation |
23 (11.3) |
22 (37.9) |
|
Poster presentation |
22 (10.8) |
22 (37.9) |
|
International MR presentation |
||
|
Oral presentation |
7 (3.4) |
8 (13.8) |
|
Poster presentation |
9 (4.4) |
15 (25.9) |
|
Published national MR |
0 (0) |
29 (50.0) |
|
Published international MR |
0 (0) |
37 (63.8) |
MR: Medical Research
Table 1. Characteristics of participants stratified by medical research publishing experience (N=262)
|
Characteristics |
Non-Published |
Published |
OR |
95% CI |
p-value |
AOR |
95% CI |
p-value |
|
n (% of 204) |
n (% of 58) |
|||||||
|
Sex |
||||||||
|
Male |
119 (58.3) |
37 (63.8) |
ref |
ref |
||||
|
Female |
85 (41.7) |
21 (36.2) |
0.79 |
0.43-1.45 |
0.455 |
0.76 |
0.37-1.56 |
0.458 |
|
Educational level |
||||||||
|
Clinical year |
128 (62.7) |
11 (19.0) |
ref |
ref |
||||
|
Intern |
76 (37.3) |
47 (81.0) |
3.09 |
1.74-5.50 |
<0.001 |
6.67 |
3.12-14.28 |
<0.001 |
|
Accumulated grade point average (GPAX) |
||||||||
|
Mean±SD |
3.4±0.3 |
3.4±0.3 |
1.02 |
0.40-2.59 |
0.971 |
0.417 |
0.12-1.41 |
0.159 |
|
Extra curriculum research activity |
39 (19.1) |
23 (39.7) |
2.78 |
1.48-5.23 |
0.002 |
1.47 |
0.62-3.46 |
0.379 |
|
MR experience during medical student |
||||||||
|
Group Leader |
45 (22.1) |
24 (41.4) |
2.49 |
1.34-4.63 |
0.004 |
2.12 |
0.97-4.64 |
0.060 |
|
MR presentation |
||||||||
|
No |
170 (83.3) |
27 (46.6) |
ref |
ref |
||||
|
Yes |
34 (16.7) |
31 (53.5) |
5.74 |
3.05-10.82 |
<0.001 |
4.34 |
1.99-9.47 |
<0.001 |
MR: Medical Research, OR: Odds Ratio, AOR: Adjusted Odds Ratio, CI: Confidence interval
Table 2. Univariable and multivariable analysis of characteristics and medical research experiences by medical research publishing experience (N=262)
B. Confirmatory Factor Analysis of Practices, Perceptions, Attitudes, Barriers and Motivation toward Medical Research
Table 3 demonstrates the confirmatory factor analysis (CFA) of practices, perceptions, attitudes, barriers and motivation Likert scores and MR publishing experience. In the practice section, all questions had a loading factor of approximately 0.80. The loading factors for perception range from 0.74 to 0.79, except for two questions: (1) research or publication should be mandatory and (2) research experience should be a criterion for residency training. For the attitude section, the CFA found that MR is exciting and MR is enjoyable, with high impacts of 0.89 and 0.87, respectively, followed by MR being valuable and essential for the medical profession, with loading factors of 0.58 and 0.54, respectively. However, for the questions where MR is complicated and time-consuming, the loading factor was relatively low, under 0.30. Regarding barriers, lack of exposure and opportunities, training and support, mentoring and guidance, and lack of personal knowledge of the research process all had a high loading factor of over 0.70. Lack of statistical support, funding, and lack of rewards or motivations had relatively lower loading factors between 0.60 and 0.69. For motivation, pursuit of further education, pursuit of personal interest, improving their potential in research skills, having mentor guidance/role model and to be a part of solving medical problems in society had high loading factors over 0.70.
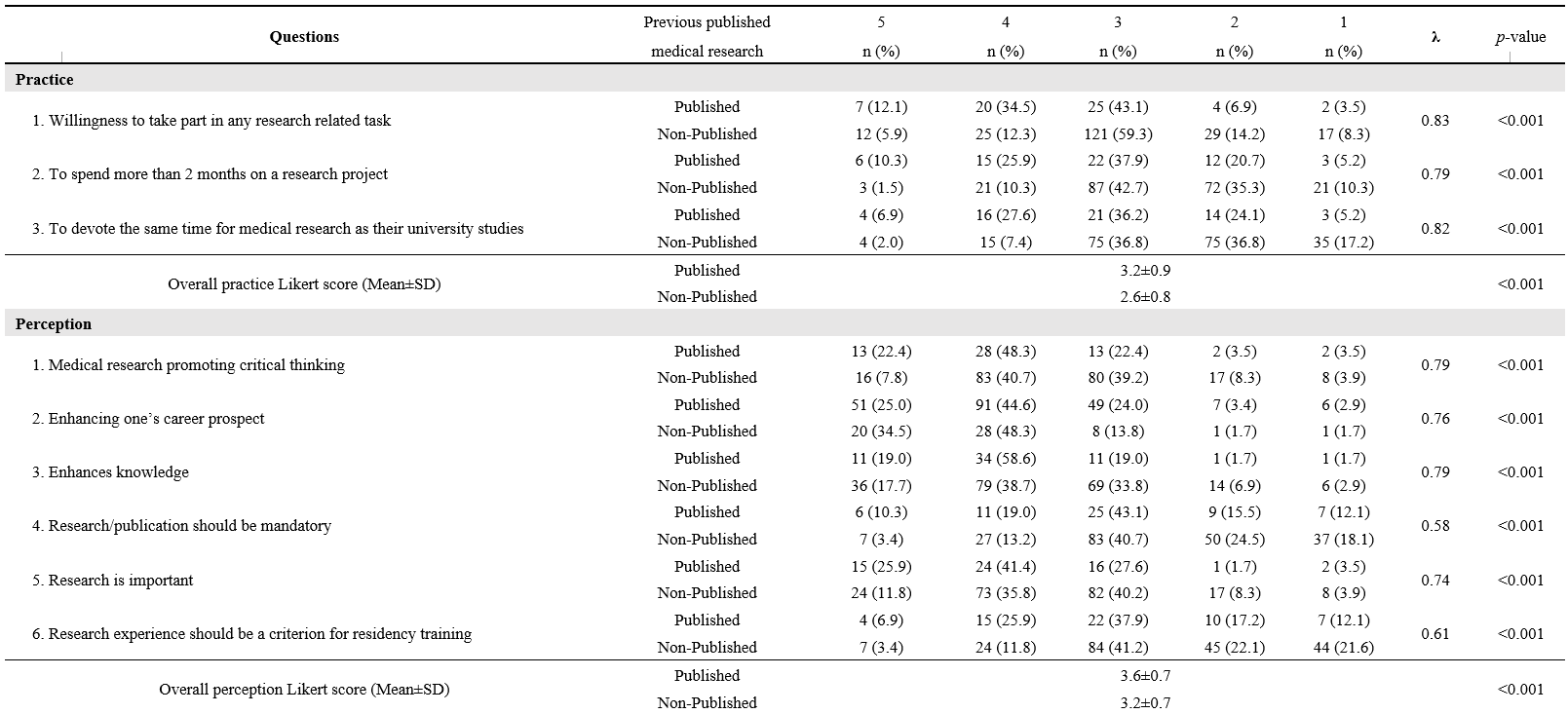

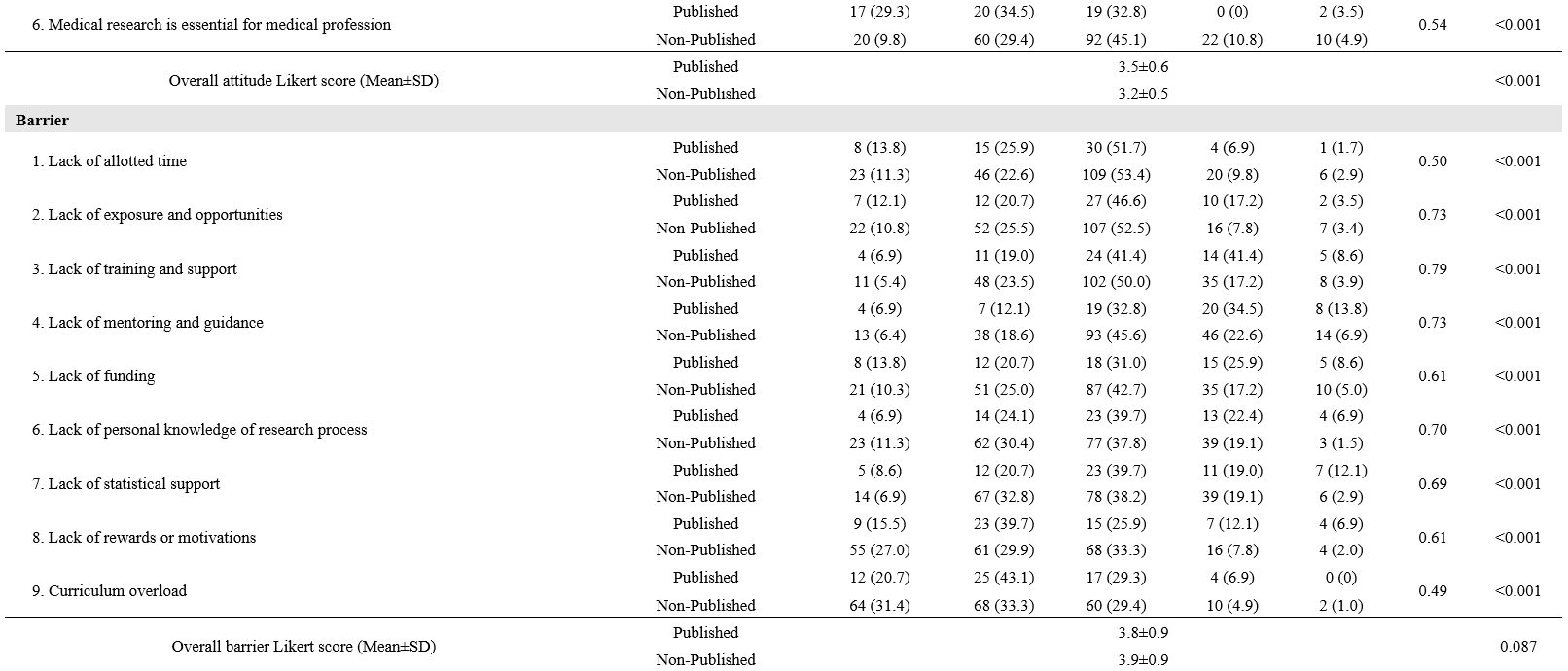


Table 3. Confirmatory factor analysis of practice, perception, attitude, barrier and motivation Likert-score and medical research publishing experience
C. SEM of Practices, Perceptions, Attitudes, Barriers and Motivation and MR Publishing
The SEM is developed from five latent variables, leading to the outcome, including medical research presentation and publication (Figure 1). We found that perception has a direct effect on both practices (0.27, p<0.001) and motivation (0.12, p= 0.087). Perceptions and attitudes also correlated (0.57, p<0.001). Practices and attitudes have a direct effect on motivation, 0.49 and 0.30, respectively (p<0.001 for both). The indirect effect of attitudes through practices on motivation was 0.71 * 0.49 = 0.35, all coefficients p<0.001. Practices also exhibited a direct negative effect on barriers (-0.13, p= 0.072). Regarding our primary outcome, both motivation and, surprisingly, barriers also revealed a positive direct effect on MR publishing (0.28, p<0.001 for motivation and 0.15, p= 0.014 for barriers). The MR presentation experience also showed a direct effect on MR publication (0.26, p<0.001). Furthermore, MR presentation also acted as a mediator for motivation, with an indirect effect of 0.08 and a total effect of motivation on MR publication of 0.36. The SEM model provided a good fit for the data (χ²/df= 1.67, CFI= 0.96, TLI= 0.95, RMSEA= 0.05, SRMR= 0.05).
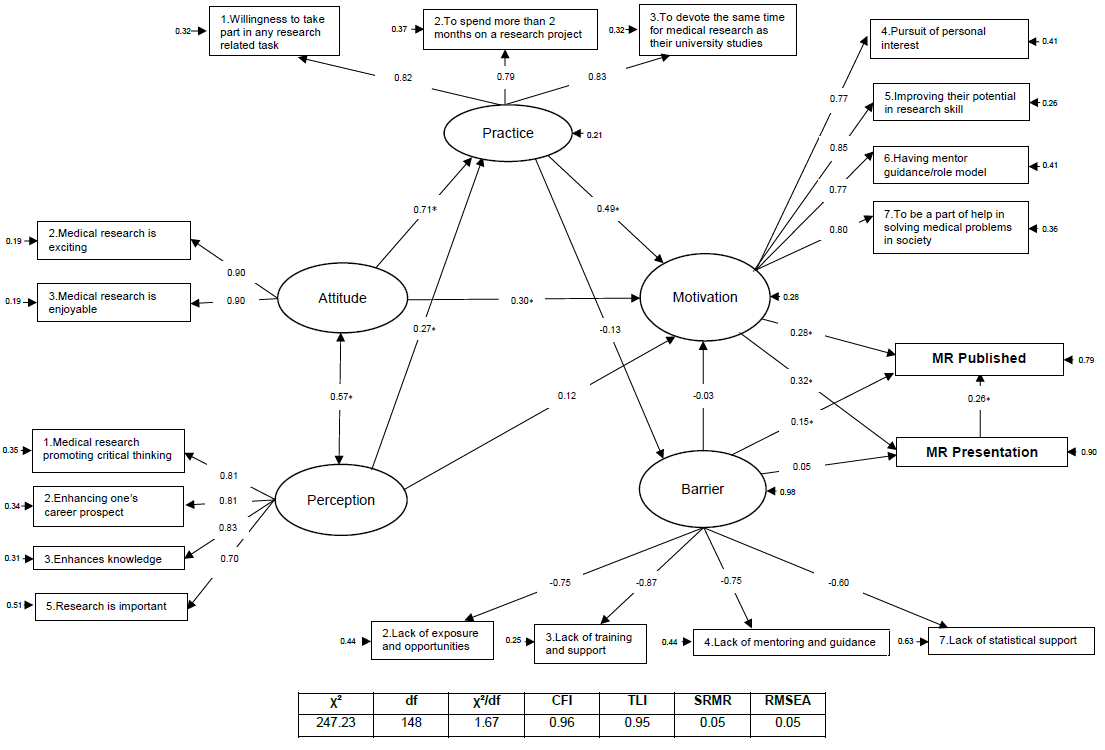
*= P<0.05
Figure 1. SEM of practices, perceptions, attitudes, barriers and motivation and MR publishing
IV. DISCUSSION
We successfully enrolled 139 PCM senior medical students, and 123 interns graduated from PCM. This study is the first to formulate a SEM on the relationship between practices, perceptions, attitudes, motivation and barriers to MR publication and presentation. We found that attitudes, practices and motivation significantly contribute to MR publication and presentation. The roles and experiences that medical students have in medical research during their medical student years are also important to the success of MR publications. However, because our population only includes those who have studied or are studying at PCM, additional external validation may be required.
This study described how baseline characteristics and MR experiences were associated with MR publication. Unsurprisingly, a higher proportion of interns had published MR. GPAX, on the other hand, were not associated with MR publication, which is a common factor in a relative study with positive associations toward perceptions, attitudes and practices (El Achi et al., 2020). A large study in China also reported that research engagement was associated with improving overall learning outcomes (Zhang et al., 2022). This controversy may be explained by two reasons. First, the time required for developing MR and publications is large and might interfere with normal curriculum activity. A study in Colombia noted that their students believed that they could obtain higher GPAs if they were not involved in research (Bonilla-Escobar et al., 2017). The latter is that MR skills and academic skills might not completely overlap. While MR engagement might improve science, scholarship, and professionalism, other domains, such as clinical practice, require more time and effort to learn (Zhang et al., 2022).
MR experiences and roles during MR learning also play an important part in MR publication. Experience in MR presentation was strongly associated with MR publication. This may be partially explained by the student’s readiness before the research presentation; students need to be highly knowledgeable about their own research, and knowledge is a key to success and behavioural change (Bettinghaus, 1986; Pengpid et al., 2016). Furthermore, presentation requires planning, preparation, creating visual aids, and practicing one’s presentation skills. The effort and time spent on this process might be motivation to achieve a higher goal, namely publication. Our study demonstrates that MR presentations, whether nationally, internationally, oral, or poster, are highly associated with MR publication. Thus, MR presentations should be promoted.
Those who had been group leaders had a higher chance of MR publication. During the PCM curriculum, the group leader for MR conduct was never assigned and was elected in each group. Northouse mentioned two forms of leadership: assigned and emergent. Those assigned leadership positions were given the role of group leader. When an individual is perceived as one of the most influential members of a group or organization, that person is exhibiting emergent leadership (Northouse, 2021). Medical leadership development was seen to improve outcomes at the individual, organizational and clinical levels (Lyons et al., 2021). Several leadership training programs in medicine and clinical practices were widely visible. However, to our knowledge, no curriculum focusing on medical research leadership was available.
Perception is described as a method for identifying and interpreting the environment and the meaning of sensual motivations. Cognition may influence perception, which can also occur subconsciously and without cognizance (Saini et al., 2020). Some literature has been carried out showing perceptions, attitudes, and motivation toward research among medical students, in which those with positive perceptions mostly had positive attitudes and motivation (AlGhamdi et al., 2014; El Achi et al., 2020; Osman, 2016). These were similar to our research showing that perception impacts positively on practices and motivation.
In line with the current study, the theory of planned behaviour describes that one’s attitude and how they perceive the behaviour directly affect their intention to perform the behaviour (Bosnjak et al., 2020). The SEM also demonstrated that perception and attitude directly affect the population’s intention to conduct MR (practice). Moreover, a study in Turkey on the predictiveness of attitude and motivation on achievement (vocational English course scores) found a significant positive relationship between attitude and motivation, attitude and achievement, and motivation and achievement (Özer, 2020). Therefore, a positive attitude may positively impact their motivation and their willingness to practice MR. The feeling that MR is exciting and enjoyable had the greatest impact on the attitude domain. Hence, activities that increase the excitement and joy of conducting MR should be encouraged.
The main factors impacting MR publication are motivation, practices, attitudes and perceived barriers. Based on the health-belief model (HBM), providing motivation as needed might help students overcome the triggers of MR barriers so that correct thoughts and perceptions about MR will arise. Thus, techniques derived from motivational interviews might be a useful option for encouraging students toward MR publication (Tober, 2013). One of the most important motivations in our study is having a mentor or role model, and the lack of a mentor constitutes a high-impact barrier. Therefore, mentors should play an important role in guiding their students toward research success. Based on motivational interview techniques, active listening might be the key skill for mentors to better understand their students’ motivations and empower them toward success (Rollnick et al., 2010).
Surprisingly, our study showed that perceived barriers had a positive impact on MR publication. The perception of a barrier greatly influences the likelihood of an individual’s uptake of that behaviour (Becker & Maiman, 1975). Usually, a barrier is a resistance to achieving a goal, which negatively affects achievement. However, the barriers included in our study consisted of a lack of exposure and opportunities, training and support, mentoring and guidance, and statistical support. As a result, those who had not yet published any medical research may not have had the prestige of encountering these barriers, which is why they are perceived as insignificant.
The practice domain included three questions: (1) willingness to participate in any research-related task; (2) willingness to spend more than two months on a research project; and (3) willingness to devote the same amount of time to medical research as they did to their university studies, indicating a willingness to practice medical research. Willingness is the quality or state of being prepared to accomplish something. A study in China about speaking English demonstrated that the willingness to communicate is directly related to motivation and mastery approach (Turner et al., 2021). Furthermore, passion and obsession are what drive an individual to succeed (Dange, 2016).
In view of all the factors presented, mentors have an important role to play in guiding and facilitating the students’ acquisition of adequate experience in medical research during their medical school years. A good extracurricular MR learning environment might be needed to ensure statistical confidence and exposure to conducting research. Actively listening to students and empowering and motivating them to break through barriers may result in successful MR publications. In addition, a different approach to learning MR might be needed to promote attitudes, perceptions and motivations toward MR. According to Self-Determination Theory (SDT), when students perceive that the primary purpose of learning is to obtain external rewards, such as exam grades, they may perform less well due to a detrimental effect on their intrinsic motivation (Deci et al., 1999).
SDT revealed that three basic needs must be fulfilled to empower one’s attitude and motivation, including autonomy, competence, and a feeling of belonging (Deci et al., 1999). To promote these basic needs, faculty members could provide extracurricular research time, give choice to research topics and mentors, and hire students to be research assistants, if possible, to promote their autonomy (Rosenkranz et al., 2015). Competence could be enhanced by early research skills introduction and practical training (Rosenkranz et al., 2015). Research mentors may play a crucial role in fostering a sense of belonging toward MR by promoting well-functioning group work through guidance and evaluation (Dorrance et al., 2008). Furthermore, portfolios, logbooks and reflective journals are particularly useful to improve the students’ attitude and motivation (Taylor & Hamdy, 2013). Constant positive feedback from mentors during MR activities is encouraged to improve the learning environment (Peifer et al., 2020). A different approach to learning MR might also benefits the MR learning environment, for example, through game-based learning and other collaborative learning models (Blakely et al., 2009).
The present study encountered several limitations. First, the study included only senior medical students and interns who graduated from PCM, so the model might not be accurately applied to other universities with different curricula and further validation might be needed. Even though most participants who had published a MR were interns (81%), the medical research published was composed while they were medical students. Second, the study was a cross-sectional study, and causal relationships were unavailable. However, according to PCM curricula, for most participants, the MR presentation and their experience with medical research came before the MR publication. Furthermore, personal beliefs change over time, and recall bias might have affected the study results. (Seitz et al., 2017). The beliefs elicited by the questionnaire comprised the participants’ current beliefs, rather than beliefs formed during their participation in medical research publications. As a result, our study investigated only the participants’ current beliefs and their impact on the publication of medical research. A further prospective cohort or qualitative study on whether the students’ current beliefs toward MR are related to successful MR publication is encouraged. Finally, because only participants who volunteered to take part in the study were included, selection bias may also be a significant limitation of this study. Our study had considerable strengths, there had been no reports describing practices, perceptions, attitudes, motivation and barriers toward medical research. However, this is the first study to formulate a SEM model displaying factors related to MR publication.
V. CONCLUSION
Medical research experience and positive practices or willingness, perception, attitude, and motivation in medical research might pave the road to a successful MR publication. Medical research experience and extracurricular activities should be supported by both teachers and faculties through active policies. A different approach to medical research learning might also be needed to promote enjoyment and excitement. Finally, external validation needs to be explored to generalise the model.
Notes on Contributors
SL reviewed the literature, designed the study, collected the data, data analysis and wrote the manuscript. KT, KJ and BS collected the data, developed the methodology framework and developed the manuscript. AK reviewed the literature, designed the study, data analysis and wrote the first draft.
Ethical Approval
The study was approved by the Medical Department Ethics Review Committee for Research in Human Subjects, Institutional Review Board, Royal Thai Army (Approval no. S060q/65_Exp), according to the international guidelines including the Declaration of Helsinki, the Belmont Report, CIOMS Guidelines, and the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use – Good Clinical Practice (ICH-GCP). A documentation of informed consent was used, and was granted permission by the Institutional Review Board, RTA Medical Department.
Data Availability
The datasets used and/or analysed during the current are available from https://doi.org/10.6084/m9.figshare.22128725
Acknowledgement
We thank professors Mathirut Mungthin, Ram Rangsin Panadda Hattachote, Phunlerd Piyaraj and Picha Suwannahitatorn for validating our questionnaire and providing support. This work would not have been possible without the active support of Phramongkutklao College of Medicine and its academic leaders.
Funding
The authors report that there is no funding associated with the work featured in this article.
Declaration of Interest
The authors declare they have no competing interests.
References
AlGhamdi, K. M., Moussa, N. A., AlEssa, D. S., AlOthimeen, N., & Al–Saud, A. S. (2014). Perceptions, attitudes and practices toward research among senior medical students. Saudi Pharma- ceutical Journal, 22(2), 113–117. https://doi.org/10.1016/j.jsps.2013.02.006
Al–Shalawy, F. A.-N., & Haleem, A. (2015). Knowledge, attitudes and perceived barriers towards scientific research among undergraduate health sciences students in the central province of Saudi Arabia. Education in Medicine Journal, 7(1), e16-e21. https://doi.org/10.5959/eimj.v7i1.266
Arif, A., Siddiqui, M. A., Aziz, K., Shahid, G., Shiekh, A., & Fahim, M.F. (2018). Perception towards research among undergraduate physical therapy students. Biometrics & Biostatistics International Journal, 7(3), 171–175. https://doi.org/10.15406/bbij.2018.07.00206
Becker, M. H., & Maiman, L. A. (1975). Sociobehavioral determinants of compliance with health and medical care recommendations. Medical Care, 13(1), 10–24. https://doi.org/10.1097/00005650–197501000–00002
Bettinghaus, E. P. (1986). Health promotion and the knowledge–attitude–behavior continuum. Preventive Medicine, 15(5), 475–491. https://doi.org/10.1016/0091–7435(86)90025–3
Blakely, G., Skirton, H., Cooper, S., Allum, P., & Nelmes, P. (2009). Educational gaming in the health sciences: Systematic review. Journal of Advanced Nursing, 65(2), 259–269. https://doi.org/10.1111/j.1365-2648.2008.04843.x
Bonilla–Escobar, F. J., Bonilla–Velez, J., Tobón–García, D., & Ángel–Isaza, A. M. (2017). Medical student researchers in Colombia and associated factors with publication: A cross–sectional study. BMC Medical Education, 17(1), Article 254. https://doi.org/10.1186/s12909–017–1087–9
Bosnjak, M., Ajzen, I., & Schmidt, P. (2020). The theory of planned behavior: Selected recent advances and applications. Europe’s Journal of Psychology, 16(3), 352–356. https://doi.org/10.5964/ejop.v16i3.3107
Carberry, C., McCombe, G., Tobin, H., Stokes, D., Last, J., Bury, G., & Cullen, W. (2021). Curriculum initiatives to enhance research skills acquisition by medical students: A scoping review. BMC Medical Education, 21(1), Article 312. https://doi.org/10.1186/s12909–021–02754–0
Dange, J. K. (2016). Perception, passion and obsession: The three elements of theory of success. International Journal of Advanced Education and Research, 1(7), 1–3.
Davila, J. R. (2016). The physician–scientist: Past trends and future directions. Michigan Journal of Medicine, 1(1), 66-73. https://doi.org/10.3998/mjm.13761231.0001.112
Deci, E. L., Koestner, R., & Ryan, R. M. (1999). A meta-analytic review of experiments examining the effects of extrinsic rewards on intrinsic motivation. Psychological Bulletin, 125(6), 627–668. https://doi.org/10.1037/0033-2909.125.6.627
Dorrance, K. A., Denton, G. D., Proemba, J., La Rochelle, J., Nasir, J., Argyros, G., & Durning, S. J. (2008). An internal medicine interest group research program can improve scholarly productivity of medical students and foster mentoring relationships with internists. Teaching and Learning in Medicine,20(2), 163–167. https://doi.org/10.1080/10401330801991857
El Achi, D., Al Hakim, L., Makki, M., Mokaddem, M., Khalil, P. A., Kaafarani, B. R., & Tamim, H. (2020). Perception, attitude, practice and barriers towards medical research among undergraduate students. BMC Medical Education, 20(1), Article 195. https://doi.org/10.1186/s12909–020–02104–6
Funston, G., Piper, R. J., Connell, C., Foden, P., Young, A. M. H., & O’Neill, P. (2016). Medical student perceptions of research and research–orientated careers: An international questionnaire study. Medical Teacher, 38(10), 1041–1048. https://doi.org/10.3109/0142159X.2016.1150981
Habineza, H., Nsanzabaganwa, C., Nyirimanzi, N., Umuhoza, C., Cartledge, K., Conard, C., & Cartledge, P. (2019). Perceived attitudes of the importance and barriers to research amongst Rwandan interns and pediatric residents – A cross–sectional study. BMC Medical Education, 19(1), Article 4. https://doi.org/10.1186/s12909–018–1425–6
Ichsan, I., Wahyuniati, N., McKee, R., Lobo, L., Lancaster, K., & Redwood–Campbell, L. (2018). Attitudes, barriers, and enablers towards conducting primary care research in Banda Aceh, Indonesia: A qualitative research study. Asia Pacific Family Medicine, 17(1), Article 8. https://doi.org/10.1186/s12930–018–0045–y
Kamwendo, K. (2002). What do Swedish physiotherapists feel about research? A survey of perceptions, attitudes, intentions and engagement. Physiotherapy Research International, 7(1), 23–34. https://doi.org/10.1002/pri.238
Laidlaw, A., Aiton, J., Struthers, J., & Guild, S. (2012). Developing research skills in medical students: AMEE Guide No. 69. Medical Teacher, 34(9), 754–771. https://doi.org/10.3109/0142159X.2012.704438
Lev, E. L., Kolassa, J., & Bakken, L. L. (2010). Faculty mentors’ and students’ perceptions of students’ research self-efficacy. Nurse Education Today, 30(2), 169–174. https://doi.org/10.1016/j.nedt.2009.07.007
Lyons, O., George, R., Galante, J. R., Mafi, A., Fordwoh, T., Frich, J., & Geerts, J. M. (2021). Evidence–based medical leadership development: A systematic review. BMJ Leader, 5(3), 206–213. https://doi.org/10.1136/leader–2020–000360
Ma, X., & Xu, J. (2004). Determining the causal ordering between attitude toward mathematics and achievement in mathematics. American Journal of Education, 110(3), 256–280. https://doi.org/10.1086/383074
Memarpour, M., Fard, A. P., & Ghasemi, R. (2015). Evaluation of attitude to, knowledge of and barriers toward research among medical science students. Asia Pacific Family Medicine, 14(1), Article 1. https://doi.org/10.1186/s12930–015–0019–2
Northouse, P. G. (2021). Leadership: Theory and practice (9th ed.). SAGE publications.
Okoduwa, S. I. R., Abe, J. O., Samuel, B. I., Chris, A. O., Oladimeji, R. A., Idowu, O. O., & Okoduwa, U. J. (2018). Attitudes, perceptions, and barriers to research and publishing among research and teaching staff in a Nigerian research institute. Frontiers in Research Metrics and Analytics, 3, Article 26. https://doi.org/10.3389/frma.2018.00026
Osman, T. (2016). Medical students’ perceptions towards research at a Sudanese University. BMC Medical Education, 16(1), Article 253. https://doi.org/10.1186/s12909–016–0776–0
Özer, S. (2020). The predictiveness of attitude and motivation on achievement in ESP: The mediating role of anxiety. International Journal of Curriculum and Instruction, 12(2), 25-41.
Pallamparthy, S., & Basavareddy, A. (2019). Knowledge, attitude, practice, and barriers toward research among medical students: A cross–sectional questionnaire–based survey. Perspectives in Clinical Research, 10(2), 73.
Parker, S. M., Vona-Davis, L. C., & Mattes, M. D. (2021). Factors predictive of publication among medical students participating in school-sponsored research programs. Cureus, 13(9), e18176. https://doi.org/10.7759/cureus.18176
Peifer, C., Schönfeld, P., Wolters, G., Aust, F., & Margraf, J. (2020). Well done! Effects of positive feedback on perceived self-efficacy, flow and performance in a mental arithmetic task. Frontiers in Psychology,11, Article 1008. https://doi.org/10.3389/fpsyg.2020.01008
Pengpid, S., Peltzer, K., Puckpinyo, A., Tiraphat, S., Viripiromgool, S., Apidechkul, T., Sathirapanya, C., Leethongdee, S., Chompikul, J., & Mongkolchati, A. (2016). Knowledge, attitudes, and practices about tuberculosis and choice of communication channels in Thailand. Journal of Infection in Developing Countries, 10(7), 694-703. https://doi.org/10.3855/jidc.6963
Puljak, L. (2007). An overlooked source of physician–scientists. Journal of Investigative Medicine, 55(8), 402–405. https://doi.org/10.2310/6650.2007.00029
Rollnick, S., Butler, C. C., Kinnersley, P., Gregory, J., & Mash, B. (2010). Motivational interviewing. BMJ, 340, c1900. https://doi.org/10.1136/bmj.c1900
Rosenkranz, S. K., Wang, S., & Hu, W. (2015). Motivating medical students to do research: A mixed methods study using self-determination theory. BMC Medical Education, 15, Article 95. https://doi.org/10.1186/s12909-015-0379-1
Saini, M., Kumar, A., & Kaur, G. (2020). Research perception, motivation and attitude among undergraduate students: A factor analysis approach. Procedia Computer Science, 167, 185–192. https://doi.org/10.1016/j.procs.2020.03.210
Schellenberg, B. J. I., Gaudreau, P., & Bailis, D. S. (2022). Lay theories of obsessive passion and performance: It all depends on the bottom line. Personality and Individual Differences, 190, Article 111528. https://doi.org/10.1016/j.paid.2022.111528
Seitz, R. J., Paloutzian, R. F., & Angel, H.-F. (2017). Processes of believing: Where do they come from? What are they good for? F1000Research, 5, Article 2573. https://doi.org/10.12688/f1000research.9773.2
Simpson, R. D., & Oliver, J. S. (1990). A summary of major influences on attitude toward and achievement in science among adolescent students. Science Education, 74(1), 1–18. https://doi.org/10.1002/sce.3730740102
Sobczuk, P., Dziedziak, J., Bierezowicz, N., Kiziak, M., Znajdek, Z., Puchalska, L., Mirowska–Guzel, D., & Cudnoch–Jędrzejewska, A. (2022). Are medical students interested in research? – Students’ attitudes towards research. Annals of Medicine, 54(1), 1538–1547. https://doi.org/10.1080/07853890.2022.2076900
Taylor, D. C. M., & Hamdy, H. (2013). Adult learning theories: Implications for learning and teaching in medical education: AMEE Guide No. 83. Medical Teacher, 35(11), e1561–e1572. https://doi.org/10.3109/0142159X.2013.828153
Tober, G. (2013). Motivational interviewing: Helping people change. Alcohol and Alcoholism, 48(3), 376–377. https://doi.org/10.1093/alcalc/agt010
Turner, J. E., Li, B., & Wei, M. (2021). Exploring effects of culture on students’ achievement motives and goals, self–efficacy, and willingness for public performances: The case of Chinese students’ speaking English in class. Learning and Individual Differences, 85, Article 101943. https://doi.org/10.1016/j.lindif.2020.101943
Valladares–Garrido, M. J., Mejia, C. R., Rojas–Alvarado, A. B., Araujo–Chumacero, M. M., Córdova–Agurto, J. S., Fiestas, J., Rojas–Vilar, F. J., & Culquichicón, C. (2022). Factors associated with producing a scientific publication during medical training: Evidence from a cross–sectional study of 40 medical schools in Latin America. F1000Research, 9, Article 1365. https://doi.org/10.12688/f1000research.26596.2
Wolf, E. J., Harrington, K. M., Clark, S. L., & Miller, M. W. (2013). Sample size requirements for structural equation models: An evaluation of power, bias, and solution propriety. Educational and Psychological Measurement, 76(6), 913–934. https://doi.org/10.1177/0013164413495237
Zhang, G., Wu, H., Xie, A., & Cheng, H. (2022). The association between medical student research engagement with learning outcomes. Medical Education Online, 27(1), Article 2100039. https://doi.org/10.1080/10872981.2022.2100039
*Anupong Kantiwong
317 Ratchawithi Rd,
Thung Phaya Thai,
Ratchathewi, Bangkok 10400
+66909838338
E-mail: anupongpcm31@gmail.com
Submitted: 2 December 2022
Accepted: 24 July 2023
Published online: 3 October, TAPS 2023, 8(4), 13-22
https://doi.org/10.29060/TAPS.2023-8-4/OA3093
Julie Yun Chen1,2, Tai Pong Lam1, Ivan Fan Ngai Hung3, Albert Chi Yan Chan4, Weng-Yee Chin1, Christopher See5 & Joyce Pui Yan Tsang1
1Department of Family Medicine and Primary Care, University of Hong Kong, Hong Kong; 2Bau Institute of Medical and Health Sciences Education, University of Hong Kong, Hong Kong; 3Department of Medicine, University of Hong Kong, Hong Kong; 4Department of Surgery, University of Hong Kong, Hong Kong; 5School of Biomedical Sciences, The Chinese University of Hong Kong, Hong Kong
Abstract
Introduction: Medical students have long provided informal, structured academic support for their peers in parallel with the institution’s formal curriculum, demonstrating a high degree of motivation and engagement for peer teaching. This qualitative descriptive study aimed to examine the perspectives of participants in a pilot peer teaching programme on the effectiveness and feasibility of adapting existing student-initiated peer bedside teaching into formal bedside teaching.
Methods: Study participants were senior medical students who were already providing self-initiated peer-led bedside clinical teaching, clinicians who co-taught bedside clinical skills teaching sessions with the peer teachers and junior students allocated to the bedside teaching sessions led by peer teachers. Qualitative data were gathered via evaluation form, peer teacher and clinician interviews, as well as the observational field notes made by the research assistant who attended the teaching sessions as an independent observer. Additionally, a single Likert-scale question on the evaluation form was used to rate teaching effectiveness.
Results: All three peer teachers, three clinicians and 12 students completed the interviews and/or questionnaires. The main themes identified were teaching effectiveness, teaching competency and feasibility. Teaching effectiveness related to the creation of a positive learning environment and a tailored approach. Teaching competency reflected confidence or doubts about peer-teaching, and feasibility subthemes comprised barriers and facilitators.
Conclusion: Students perceived peer teaching effectiveness to be comparable to clinicians’ teaching. Clinical peer teaching in the formal curriculum may be most feasible in a hybrid curriculum that includes both peer teaching and clinician-led teaching with structured training and coordinated timetabling.
Keywords: Peer Teaching, Undergraduate Medical Education, Bedside Teaching, Medical Students
Practice Highlights
- Peer-led teaching environment facilitates questions and answers from learners to strengthen learning.
- Training on specific skills and pre-case preparation can help improve peer teacher effectiveness.
- Clear understanding of the logistics and expectations is necessary to optimise the process.
- Formal peer teacher training may help quality assurance and encourage more participation.
I. INTRODUCTION
In accordance with the longstanding apprenticeship model of medical training, senior doctors and trainees have been responsible for teaching their junior colleagues across the continuum of medical education. Despite this accepted practice, peer teaching has not become widely formalised in undergraduate medical curricula.
Peer teaching has been shown to be beneficial at multiple levels. For students who are being taught by peers, learning is enabled by social and cognitive congruence because of the near-peer demographic which allows for a more comfortable learning environment for free flow of discussion and better understanding of the learner’s challenges including awareness of the primacy for exam success (Benè & Bergus, 2014; Rees et al., 2016). The peer teacher develops and hones teaching skills that will be useful in internship (Haber et al., 2006) and through teaching, develops higher motivation and deeper understanding of concepts and perhaps also improve their own exam performance (Burgess et al., 2014). The institution derives some practical benefit from the supplementary manpower (Tayler et al., 2015) due to the comparable effectiveness of peer teachers in teaching in certain areas such as physical examination and communication skills (Rees et al., 2016) but perhaps most importantly, it benefits from building a collaborative relationship with students in their learning process. Though the benefits of peer teaching have been noted, students remain an untapped resource as training provided for students to serve as teachers is inconsistent (Soriano et al., 2010).
Undergraduate medical curricula aim to provide a foundation for future training and the framework for such curricula are guided by the recognition that medical students must achieve certain outcomes, including being able to teach, to be prepared for future practice. Well-accepted frameworks such as the ‘Outcomes for Graduates’, from the UK General Medical Council (2015) and the ‘CanMEDS Framework’ from the Royal College of Physicians and Surgeons of Canada (2015) expect medical graduate to teach others. In Hong Kong, similar guidance is provided in the document ‘Hong Kong Doctors’ published by the Medical Council of Hong Kong, which states that undergraduate medical education must prepare graduates to fulfil the roles of ‘medical practitioner, communicator, educator…’ (Medical Council of Hong Kong, 2017).
It is common in medical schools to have informal peer teaching, where senior students coach junior students on an ad hoc basis or organise revision sessions before exams. Zhang et al. (2011) revealed that a majority of medical students believed that informal learning approaches, including the use of past student notes, and participation in self-organised study groups and peer-led tutorials, helped them pass examinations and be a good doctor. Similarly, in our institution, these kinds of informal peer teaching are popular among students and include sharing sessions on study and exam tips, bedside sessions, and sharing of organised study notes. These activities are not subject to any formal oversight.
With the documented benefits of peer teaching, the availability of enthusiastic senior students who are willing to coach their junior peers, and the demand from junior students to learn from their seniors, there is an opportunity to harness the potential peer teaching that is already taking place. This pilot project is important as it aimed to adapt existing student-initiated peer bedside teaching into the formal bedside teaching curriculum and to examine the perspectives of participants on the effectiveness and feasibility of this initiative. It will be helpful to understand the benefits and drawbacks of formal peer bedside teaching in order to further develop this pedagogical approach in medical education.
II. METHODS
This was a descriptive qualitative study of participants in a pilot peer-teaching initiative for bedside teaching implemented in the first clinical year of study for medical students.
A. Setting
1) Small group bedside teaching for Year 4 medical students in the Clinical Foundation Block: The 11-week Clinical Foundation Block (CFB) of the MBBS Year 4 curriculum at The University of Hong Kong runs from August to October and is the first block of the first clinical year of study. It serves to prepare students for the ward- and clinic-based teaching to follow in the clinical clerkships (Figure 1). Year 4 medical students were selected for the study because it is the first clinical year of study when clinical bedside teaching begins. In addition, as the most junior clinical students, they would benefit most from learning from their senior peers. During the CFB, all Year 4 students learn basic history taking, physical examination and clinical skills as well as common clinical problems of 10 key specialty disciplines. In internal medicine, students attend whole class sessions in which the proper clinical examination of each body system is demonstrated followed by seven small group sessions at the bedside for hands-on practice led by a clinician.
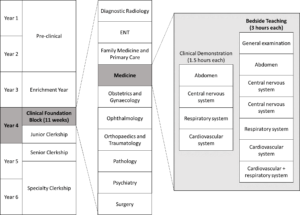
Figure 1. Teaching activities under Medicine within the Clinical Foundation Block in the medical curriculum
Each small group bedside teaching session is comprised of six to eight CFB students who follow the same clinical teacher to examine 3 pre-selected ward patients over a two-hour period. In this pilot study, a peer teacher joined the clinical teacher for the bedside teaching with the first patient case taught by the clinician, the second case taught by the peer teacher under the supervision of the clinician and the final case taught by the peer teacher alone.
2) Peer teaching recruitment and training: Over the years, medical students have been organising bedside peer-teaching on their own and we identified these peer-teaching leaders to help recruit peer teachers for this initiative. Peer teachers recruited in July 2018 and comprised Year 5 students in Senior Clerkship, who were enthusiastic in teaching, and were available to join the training tutorial and take up a subsequent Year 4 CFB bedside teaching session. During the 2.5-hour tutorial, the CFB Coordinator explained the project, and three clinicians then provided a briefing on cardiovascular, neurological, respiratory and abdominal physical examination, common pitfalls, and how to give feedback. There was also time for students to raise questions both on the project and bedside teaching techniques.
B. Participants
The target participants included the three peer teachers who were recruited for this study, together with the three clinician partners and the 24 CFB students in the corresponding three bedside teaching groups. Written informed consent was obtained from all participants before data collection.
C. Data Collection
The qualitative data were collected using a dual subjective (peer teachers, clinicians and students) and objective (independent observer) approach was taken to provide a more holistic perspective of the peer teaching experience. A research assistant not involved in the teaching followed one (of the three) peer teachers as the independent observer. All peer teachers and clinicians were interviewed in-person, by phone or by email, using an interview guide (Appendix 1) by the research assistant after the session where field notes were taken and transcribed. CFB students were invited to complete an evaluation form comprised of open-ended questions and a single Likert-scale question (Appendix 2) immediately after the bedside session, to rate effectiveness and to give general feedback about the peer teaching session.
D. Data Analysis
The qualitative data comprising interview field notes, interview transcripts, email transcripts and open-ended questions from the evaluation form collected from CFB students were analysed thematically by the authors JC and JPYT. The Likert-scale question from the evaluation form was analysed using descriptive statistics. All data were anonymised.
III. RESULTS
All three peer teachers and three clinicians who participated in the pilot peer teaching sessions were interviewed. Eighteen out of 24 CFB students consented to participate and 12 completed questionnaires were collected. Three main themes were identified with two corresponding subthemes for each.
A. Teaching Effectiveness
Peer teachers were rated favourably in terms of their teaching effectiveness. From the evaluation form completed by CFB students, the mean peer teaching effectiveness rating was 4.5/5. While a few students felt the teaching effectiveness of clinicians and peer teachers was comparable, many of them felt less intimidated being taught by the peer teachers. Students also appreciated that the peer teachers understood their current level of understanding and therefore were able to make the teaching more effective by tailoring it to their needs. Students found the experience-sharing by the peer teachers an added-value as shown in Table 1 (Item 1-4). All clinicians agreed that the CFB students appeared more relaxed while the peer teachers were teaching, and the peer teachers met their standard of professionalism as shown in Table 1 (Item 3).
|
Subtheme: Learning environment |
|
1. ‘I was more willing to ask questions.’ – CFB Student 8 |
|
2. ‘I felt more comfortable and less intimidate[ed] with the peer teacher.’ – CFB Student 12 |
|
3.‘I think it is pretty well received among the CFB students – they looked like they are more comfortable and less stressed.’ – Clinician B |
|
Subtheme: Tailoring to needs |
|
4.‘We were told her past experience.’ – CFB Student 9 |
|
5.‘More exam advice from peer tutor.’ – CFB student 10 |
Table 1. Exemplar quotes from participants on teaching effectiveness
These comments were congruent with the observations of the independent observer. When the clinician was teaching, students appeared to be cautious when performing physical examination and answering questions from the clinician. On the other hand, when the peer teacher was teaching, students were asking for reassurance while performing physical examination, and appeared less hesitant when attempting to answer the questions. The peer teacher sometimes also asked the students how they would do a certain examination before they actually performed it. He also shared his own bedside experience. After the clinician ended the bedside session and left, the peer teachers stayed behind and answered further questions from the students regarding physical examination skills and examination tips.
B. Teaching Competence
For students, the teaching on physical examination skills by peer teacher appeared to be comparable to that by clinicians, with the perceived benefit of tailored instructions to student’s current level, and additional personal experience sharing as shown in Table 2 (Item 1-2).
After co-teaching with the peer teacher, clinicians had different opinions about the competency of an undergraduate student as a formal peer teacher. Two stated that it was more appropriate for senior students to do sharing instead of teaching, while the other was satisfied with the ability of the peer teachers to teach, and appreciate the opportunity to exchange ideas with peer teachers. One clinician also suggested that peer teachers might need more practice on teaching to build up confidence as shown in Table 2 (Item 3, 6 and 7).
On the other hand, all the peer teachers expressed that they felt stressed being observed by the clinicians. Two of them felt confident to teach, while one was less confident and prefer to co-teach with a clinician as shown in Table 2 (Item 4, 5 and 8).
The peer teachers also questioned their role as a peer teacher in the regular curriculum. They were unsure to teach in place of clinicians in the regular bedside sessions for the CFB students, yet were more comfortable to co-teach with the clinicians, or to teach in unofficial or supplementary peer-led sessions as shown in Table 2 (Item 4, 8 and 9).
|
Subtheme: Confidence in teaching competence |
|
1. ‘Very comprehensive teaching; detailed explanation on how to report findings.’ – CFB Student 1 |
|
2. ‘Senior students know what we need to know and what we don’t know at this stage.’ – CFB Student 5 |
|
3. ‘The peer teacher was sufficiently prepared on content knowledge and teaching skills.’ – Clinician A |
|
4. ‘I am confident with my knowledge and teaching skills. The CFB cases were easy enough for me to handle. I have been teaching student-initiated sessions anyway.’ – Peer Teacher A |
|
5. ‘Are we going to replace the clinicians? The student-initiated sessions worked just fine.’ – Peer Teacher B |
|
Subtheme: Doubts on teaching competence |
|
1. ‘It is too early for the current peer teachers to teach as they lack competency and confidence in teaching.’ – Clinician B |
|
2. ‘Tutors should be at least medical graduates who have shown evidence of proficiency and knowledge in the areas that they teach. Senior students can share their experience of learning, but not to teach.’ – Clinician C |
|
3. ‘The clinicians are definitely better at teaching and has better skills… It would work better if I was to co-teach with a clinician but not to teach solo.’ – Peer Teacher C |
|
4. ‘It isn’t appropriate to take away the proper learning opportunity to be taught by clinicians from the students.’ – Peer Teacher C |
Table 2. Exemplar quotes from participants on teaching competency
C. Feasibility
1) Barriers: One of the peer teachers was disappointed that the session did not go as planned. He suspected that the clinicians may not truly understand the purpose and the plan for the project, and hence sometimes took the lead when the peer teachers were supposed to be teaching as shown in Table 3 (Item 1).
They also mentioned that timetabling conflicts between CFB and Senior Clerkship were also an issue. For all groups, the session overran and resulted in peer teachers missing their own class, which was scheduled immediately following the intended finishing time of this bedside session.
Peer teachers also commented that there was no concrete incentive for them to join the project. With the added pressure of being observed by clinicians, most peer teachers were hesitant to volunteer again.
2) Facilitators: One peer teacher considered it as an extra learning opportunity as shown in Table 3 (Item 2). Clinicians also believed that the peer teachers could benefit since these were essentially extra tutorials and bedside exposure for them outside of the regular curriculum although students thought that the cases used for CFB were too easy for them to learn anything new. Both peer teachers and clinicians agreed that more practical training on physical examination would be beneficial to boost the confidence and competence of the peer teachers in teaching. Peer teachers suggested that to make the session more efficient, they would prefer to clerk the case themselves before the session, to be better prepared to recognise abnormal physical signs shown in Table 3 (Item 3). A pre-meeting between the peer teacher and the partner clinician would be helpful to clarify expectations and understanding of the process since the training tutorial was conducted by a different clinician. A clinician pointed out that an open call should be made for the recruitment to allow all interested students to participate.
|
Barriers |
|
1. ‘I felt like the clinician did not want to let me teach solo. Maybe he did not understand the project.’ – Peer Teacher A |
|
Facilitators |
|
2. ‘The organisation of the curriculum is weird – there were a lot to learn in the Medicine Block of the Junior Clerkship, but not much in that of Senior Clerkship. There was also a large gap of time where there was no supervised physical examination at bedside. This is a good refresher session for me.’ – Peer Teacher C |
|
3. The students and I all saw the case for the first time during the session. I felt a bit unprepared and can only comment on the physical examination skills of the students. There is no way to tell if they reported the correct findings. It would help if the peer tutors can clerk the case before the session.’ – Peer Teacher C |
Table 3. Exemplar quotes from participants on barriers and facilitators
IV. DISCUSSION
This pilot project aimed to examine the effectiveness and feasibility of adapting peer bedside teaching into the formal curriculum. Student rating has been used as the primary measure of teaching effectiveness in many schools (Chen & Hoshower, 2003). In this project, we triangulated student ratings with clinician viewpoint and also that of an independent observer to assess teaching effectiveness. All found the teaching by the peer teachers was professional and comparable to clinicians.
Their views were also congruent to the observation that peer teaching provided a more relaxed learning environment as cited in the literature (Tai et al., 2016). This is reflected in a study on problem-based learning (PBL) that showed student tutor-led tutorials were rated more highly in group functioning and supportive atmosphere, compared with faculty-led sessions (Kassab et al., 2005).
Sharing from peer teachers was also identified as a bonus feature of bedside peer teaching in our study. Sharing from senior students not only provide junior student with practical exam and ward survival tips, but also served as inspiration and motivation for students to learn. Again this has also been observed in other studies such as one in which students whose peer teachers shared real life experiences performed better in a post-training CPR knowledge test, and demonstrated more confidence and learning motivation (Souza et al., 2022).
In the next incarnation of peer teaching the barriers and facilitators noted by stakeholders need to be addressed. The difficulty in scheduling can be overcome by engaging senior students who are already on the ward to teach by embedding this requirement as part of their usual work. A clinical peer-assisted learning programme by Nikendei, et al. (Nikendei et al., 2009) had demonstrated a successful peer teaching programme at the bedside with final year medical students who were working in the wards as tutors. The comment among peer teachers that there is no ‘concrete incentive’ to being a peer teacher may be due a lack of awareness of the appreciation from peer learners as well as from faculty teachers. More regular and deliberate sharing of learner feedback and role modelling the enjoyment of teaching by teachers and experienced peer teachers can help. Reflecting on the benefits of the learning process undertaken through the preparation and ‘paying forward’ the efforts from other teachers are also less tangible (but important!) factors to emphasise to encourage future students to undertake peer-teaching.
Peer teachers and clinicians should meet before the teaching session to clarify aims and logistics, and match their expectations. To improve peer teacher confidence and to alleviate clinician concern about their competency to teach, more extensive and formal training can be provided to peer teachers, including both theoretical and practical training on physical examination, and on teaching skills. Burgess et al. (2017) had developed and implemented an interprofessional Peer Teaching Training (PTT) programme for medicine, pharmacy and health sciences students, which aimed to develop students’ skills in teaching, assessment and feedback for peer assisted learning and future practice. The PTT course design was adapted by Karia et al. (Karia et al., 2020) for medical students only. Both programmes were shown to be effective in improving students’ confidence and competence in peer teaching, and increasing intention to participate in teaching. This is encouraging and we are also developing a structured peer teaching training programme to fill this gap. Nevertheless, when attempting to include peer teachers in the formal curriculum as a complement to formal teaching by the faculty care must be taken to not over-formalise the process which may undermine the unique benefits of peer teaching (Tong & See, 2020).
A. Strengths and Limitations
This was a small-scale pilot study and the evaluation of the impact was limited to perceptions and feedback from stakeholders and did not include tangible outcomes such as academic performance and clinical competency of participants. However, the objective contemporaneous observations made during the teaching sessions by a third-party researcher strengthened the trustworthiness of the data. A 360-degree evaluation including feedback from patients and ward staff could also provide a more comprehensive evaluation.
V. CONCLUSION
This study examined the perspectives of clinicians, peer teachers and students on the effectiveness and feasibility of peer-led bedside teaching in the formal curriculum and the benefits are encouraging. Peer teaching effectiveness was comparable to clinicians with the added benefit that peer-teachers are better able to understand and meet students’ needs while creating a friendlier environment conducive to constructive learning. Concerns about peer teaching competency were expressed by clinicians and peer-teachers and all participants did not wish to have peer-teaching replace clinician-led teaching. Clinical peer teaching in the formal curriculum may be most feasible in a hybrid curriculum that includes both peer teaching and clinician-led teaching. It can be accomplished with more structured training and overcoming practical barriers of timetabling and preparation. The benefits of peer teaching and promising responses from all stakeholders support further initiatives in clinical peer teaching.
Notes on Contributors
JY Chen designed the study, performed data collection and data analysis, drafted the manuscript and approved the final manuscript.
TP Lam designed the study, gave critical feedback, read and approved the final manuscript.
IFN Hung designed the study, gave critical feedback, read and approved the final manuscript.
ACY Chan designed the study, gave critical feedback, read and approved the final manuscript.
WY Chin designed the study, gave critical feedback, read and approved the final manuscript.
JPY Tsang performed data collection and data analysis, drafted the manuscript and approved the final manuscript.
C See designed the study, gave critical feedback, read and approved the final manuscript.
Ethical Approval
This study was approved by the Institutional Review Board of the University of Hong Kong/ Hospital Authority Hong Kong West Cluster (Reference number: UW 18-439).
Data Availability
The data of this qualitative study are not publicly available due to confidentiality agreements with the participants.
Acknowledgement
We would like to thank the peer teachers, students and clinicians of HKUMed for participating in the study.
Funding
This work was supported by a Teaching Development Grant funded by The University of Hong Kong (Ref No:. N/A).
Declaration of Interest
The authors declare that there is no conflict of interest.
References
Benè, K. L., & Bergus, G. (2014). When learners become teachers: A review of peer teaching in medical student education. Family Medicine, 46(10), 783-787.
Burgess, A., McGregor, D., & Mellis, C. (2014). Medical students as peer tutors: A systematic review. BMC Medical Education, 14(1), 115.
Burgess, A., Roberts, C., van Diggele, C., & Mellis, C. (2017). Peer teacher training (PTT) program for health professional students: Interprofessional and flipped learning. BMC Medical Education, 17(1), Article 239.
Chen, Y., & Hoshower, L. B. (2003). Student evaluation of teaching effectiveness: An assessment of student perception and motivation. Assessment Evaluation in Higher Education, 28(1), 71-88.
General Medical Council. (2015). Outcomes for graduates (Tomorrow’s Doctors). Retrieved July 18, 2022 from https://www.gmc-uk.org/-/media/documents/Outcomes_for_graduates_jul_15_1216.pdf_61408029.pdf
Haber, R. J., Bardach, N. S., Vedanthan, R., Gillum, L. A., Haber, L. A., & Dhaliwal, G. S. (2006). Preparing fourth‐year medical students to teach during internship. Journal of General Internal Medicine, 21(5), 518-520. https://doi.org/10.1111/j.1525-1497. 2006.00441.x
Karia, C., Anderson, E., Hughes, A., West, J., Lakhani, D., Kirtley, J., Burgess, A., & Carr, S. (2020). Peer teacher training (PTT) in action. Clinical Teacher, 17(5), 531-537.
Kassab, S., Abu-Hijleh, M. F., Al-Shboul, Q., & Hamdy, H. (2005). Student-led tutorials in problem-based learning: Educational outcomes and students’ perceptions. Medical Teacher, 27(6), 521-526.
Medical Council of Hong Kong. (2017). Hong Kong Doctors. Retrieved July 18, 2022 from https://www.mchk.org.hk/english/publications/hk_doctors.html
Nikendei, C., Andreesen, S., Hoffmann, K., & Jünger, J. (2009). Cross-year peer tutoring on internal medicine wards: Effects on self-assessed clinical competencies–A group control design study. Medical Teacher, 31(2), e32-e35.
Rees, E. L., Quinn, P. J., Davies, B., & Fotheringham, V. (2016). How does peer teaching compare to faculty teaching? A systematic review and meta-analysis. Medical Teacher, 38(8), 829-837.
Royal College of Physicians and Surgeons of Canada. (2015). CanMEDS Framework. Retrieved July 18, 2022 from http://www.royalcollege.ca/rcsite/canmeds/canmeds-framework-e
Soriano, R. P., Blatt, B., Coplit, L., CichoskiKelly, E., Kosowicz, L., Newman, L., Pasquale, S. J., Pretorius, R., Rosen, J. M., & Saks, N. S. (2010). Teaching medical students how to teach: a national survey of students-as-teachers programs in US medical schools. Academic Medicine, 85(11), 1725-1731.
Souza, A. D., Punja, D., Prabhath, S., & Pandey, A. K. (2022). Influence of pretesting and a near peer sharing real life experiences on CPR training outcomes in first year medical students: A non-randomized quasi-experimental study. BMC Medical Education, 22(1), 1-11.
Tai, J., Molloy, E., Haines, T., & Canny, B. (2016). Same‐level peer‐assisted learning in medical clinical placements: A narrative systematic review. Medical Education, 50(4), 469-484.
Tayler, N., Hall, S., Carr, N. J., Stephens, J. R., & Border, S. (2015). Near peer teaching in medical curricula: Integrating student teachers in pathology tutorials. Medical Education Online, 20(1), 27921.
Tong, A. H. K., & See, C. (2020). Informal and formal peer teaching in the medical school ecosystem: Perspectives from a student-teacher team. JMIR Medical Education, 6(2), e21869.
Zhang, J., Peterson, R. F., & Ozolins, I. Z. (2011). Student approaches for learning in medicine: What does it tell us about the informal curriculum? BMC Medical Education, 11(1), Article 87.
*Julie Chen
4/F William MW Mong Block
Faculty of Medicine Building
21 Sassoon RoadMarrakesh, Marrakesh-Safi,
Pokfulam, Hong Kong
Email address: juliechen@hku.hk
Submitted: 28 September 2022
Accepted: 2 March 2023
Published online: 3 October, TAPS 2023, 8(4), 5-12
https://doi.org/10.29060/TAPS.2023-8-4/OA2883
Soumia Merrou1, Abdellah Idrissi Jouicha2, Abdelmounaim Baslam3, Zakaria Ouhaz3 & Ahmed Rhassane El Adib1
1Health Sciences Research Centre (HSRC), Faculty of Medicine and Pharmacy of Marrakech, Cadi Ayyad University, Morocco; 2Health Sciences Research Centre (HSRC), Faculty of Science Semlalia, Cadi Ayyad University, Morocco; 3Pharmacology, neurobiology and behaviour Lab, Faculty of Science Semlalia, Cadi Ayyad University, Morocco
Abstract
Introduction: A deep understanding of physiology, physiopathology, pharmacology, and the management of pain is crucial for nurse anaesthetists to ensure the well-being of their patients. Thus, the teaching strategies should enhance the transition from acquiring the fundamental pain phenomena, to developing translational and critical thinking. The aim of the study is to determine if the flipped classroom that is considered an active learning approach is most effective compared to the traditional method in teaching pain management and if it improves students’ academic performance.
Methods: This study was quasi experimental, at a higher institute of nursing professions, among third-year anaesthesia resuscitation nursing students. participants were randomly allocated into either: the flipped classroom group where PBL was used (FG, n = 19), or the traditional lecture-based classroom group (TG, n = 19). The results and impact of the above approach were appreciated via the analysis of the summative assessment of the class group and from the questionnaire submitted to students.
Results: The present study revealed that in the midterm exam, the mean score of the flipped classroom group (14.0) which is significantly higher (p<0.01) than the traditional lecture group (11.9). Moreover, the standard deviation of this latter is slightly higher (2.41) which indicates scores far from the average. Also, a significant difference between the averages of the two approaches in favor of flipped classroom Group was revealed (p<0.01).
Conclusion: The assessment of student’s grades and their appreciation of both teaching approaches showed a preference for the PBL.
Keywords: Flipped Classroom, Nursing Education, Pain Management, Problem-Based Learning
Practice Highlights
- Flipped classroom showed advantageous results on nursing students’ grades.
- Flipped classroom endorsed positive results on course comprehension by nursing students.
- Flipped classroom has shown to effectively support content learning.
I. INTRODUCTION
Flipped classroom is a pedagogical approach defined as: “What was previously completed as homework is now finished in class, and what was previously completed in class is now completed at home” (Dong, 2016). Using this approach, traditional classroom time is spent on active learning strategies such as problem-based learning, games, or practice questions to allow teachers to guide students in developing strategies. critical thinking (Dong, 2016). Flipped classrooms are used as the main teaching method in the courses of health professions such as nursing theory, statistics and pharmacology (Hanson, 2016; Immekus, 2019; Peisachovich et al., 2016). In fact, there is evidence that students’ academic performance improved in midterm exams while using flipped classroom approach (Geist et al., 2015).
Despite feeling that this method increased their knowledge, nursing students said they preferred traditional lectures to the use of a flipped classroom (Hanson, 2016). It is not uncommon for students to prefer lectures to the flipped classroom method, which may be related to how much work they feel they have to do or insecurity of exam preparation or both of them (Dong, 2016; Tune et al., 2013). The use of the flipped classroom in nursing was supported by evidence that showed lecturers were enthusiastic about this method. The most effective method for implementing and assessing this strategy in nursing education, though, is not consistently supported by the available data (Barranquero-Herbosa et al., 2022; Dong, 2016; Njie-Carr et al., 2017).
Contextual learning can encourage the growth of critical reasoning, which enables students to pick out the top nursing concerns for patients from a long list of problems, ultimately fostering the development of problem-based nursing analysis in line with Benner’s model (Dong, 2016). Problem-based learning (PBL) uses problem scenarios to develop knowledge and understanding learning objectives (Wood, 2003). Among the strategies used in a flipped classroom, the PBL has been used in nursing education, in courses such as pharmacology, mental health nursing and critical care nursing (Alton, 2016; Gholami et al., 2016). Any teaching strategy that involves students in the learning process is considered to be an active learning strategy, which includes PBL (Peisachovich et al., 2016).
Despite the introduction of pain management in health professions education, pain is still undertreated. It affects 80%-90% of patients in medicine, surgery, and cancer units (Gerbershagen et al., 2009; Gianni et al., 2010). Previous research also highlighted that 43% to 51% of patients received inadequate or insufficient analgesic treatment and only 14% of patients who received analgesia benefit from reassessment (Deandrea et al., 2008; Manias et al., 2005). To effectively manage pain, nurses are crucial. Therefore, it is crucial that they receive effective training to ensure better pain management (Teike Lüthi et al., 2015).
In this direction, in order to encourage students’ acquisition strategies, nursing science professors must implement effective teaching techniques. Training typically aims to increase knowledge, which is insufficient in this case; as a result, skills development is a top priority (Kerner et al., 2013). While prior research emphasised the value of nurse-patient interactions in pain management, it undervalued the impact of nurses’ scientific knowledge of pain mechanisms and pharmacology. It is interesting to note that a recent study highlighted the significance of the classroom setting and instructional methods in approaching pain management in a novel manner (Teike Lüthi et al., 2015).
However, a need for a rigorous evaluation of learning strategies is crucial for best practices in nursing education (Barranquero-Herbosa et al., 2022; Njie-Carr et al., 2017). The present study provides an assessment of PBL as a model of applied learning in a flipped classroom of anesthesia nursing students in the context of a pain management course.
The main purpose of the study was to determine if the flipped classroom is more effective than traditional learning in teaching pain management by assessing students’ academic performance and determine their perceptions about the flipped classroom approach. In that capacity, the research questions of the study are:
- Is there a significant difference in students’ academic performance between the traditional and flipped classroom approaches on declarative knowledge?
- Is there a significant difference in students’ academic performance between the traditional and flipped classroom approaches on conditional knowledge?
- What are anesthesia and resuscitation nursing students’ perceptions of PBL impact on the acquisition and application of pain management knowledge?
- What are anesthesia and resuscitation nursing students’ perceptions of PBL as a model for learning in pain management?
II. METHODS
A. Research Design and Samples
This study is quasi experimental, and was conducted from September at a higher institute of nursing professions. The participants are third-year anaesthesia resuscitation nursing students. Participation in the study was voluntary and anonymous. Oral consent of all participants was obtained. These participants were randomly allocated into either: The flipped classroom group where PBL was used (FG, n = 19), or the traditional lecture-based classroom group (TG, n = 19). Both classroom groups had the same professor.
B. Curriculum Description
The “pain management” course (50h) is taught during the third year of nursing studies in the institute. It is composed of three parts: the pathophysiology of pain; the evaluation of pain, and the pain management.
C. Problem Based Learning on Flipped Classroom Approach
The problem-based template was designed by the professor who teaches the course, by using small groups of 5 to 6 students. The students were the facilitators of the discussion; they meet in group work to discuss a case for an hour. The objective is to identify the type of pain or to choose the best pain assessment tool for the case. The group must then suggest a drug treatment protocol and design appropriate nursing interventions. The role of the professor was to provide immediate and specific feedback during the discussion.
All cases were written by the professor. The objectives were the acquisition of knowledge and the development of clinical reasoning. Each case contained 300 words and included key patient data. Each of these cases included information that could be analysed to provide priority elements to the discussed case.
D. Data Collection and Statistical Analyses
The results and impact of the above approach were extracted via an analysis of the summative assessment of the class group and from the questionnaire submitted to students.
1) Summative assessment (exam):
Students in both groups went through two exams: midterm exam (ME) which took place in the middle of the course in the 6th week in order to assess the students’ declarative knowledge, and a final exam (FE) which took place at the end of the course, to assess conditional knowledge. The tests were graded from zero to twenty. The final score (FS) was obtained by the following equation:
FS=(ME+FE)/2
2) Questionnaire:
At the end of the course, the FG students were asked to fill out an anonymous questionnaire divided into two sections. The questions were developed in the first section of the questionnaire to determine students’ perceptions of knowledge acquisition. Elements evoked in the questionnaire were created with a language that demonstrates perceived ability and related to self-efficacy (Tune et al., 2013). The second set of items was created to determine students’ perceptions of the cases used in the course. The statements began, for example, with “Participating in the group discussions made me more confident for…”. Likert scale was used to measure the responses. The scale is presented as follows:
1 = Strongly disagree, 2 = Disagree, 3 = Neither agree nor disagree, 4 = Agree, and 5 = Strongly agree.
3) Statistical analyses:
Data analysis was performed using MS Excel (21), background variables of the study participants were calculated, and the results are presented as frequency distribution, percentages, mean, and standard deviation, statistical significance when p <0.05.
III. RESULTS
The data that support the findings of this RCT study are openly available at https://doi.org/10.6084/m9.figshare.22639279 (Merrou et al., 2023).
A. Demographics
The number of participants in the study was 38 students, 19 per group. Female students represented 79% of the study participants, whereas 21% were male.
B. Students’ Grades
Based on the data obtained, statistical analysis was done to analyse the influence of the teaching approach and the type of examination on learners’ results. The obtained findings have been presented in Tables 1 and 2. They indicate the average performance of learners in both exams: midterm (ME) and final exam (FE) where conditional knowledge is measured for both teaching approaches.
|
Type of exam |
Teaching approach |
M |
Sd |
Inf born |
Sup born |
P value |
|
ME |
TG |
11.9 |
2.41 |
7.38 |
16.1 |
<0.01 |
|
FG |
14.0 |
1.94 |
9.0 |
16.5 |
||
|
FE |
TG |
11.9 |
3.28 |
6.09 |
16 |
<0.01 |
|
FG |
14.1 |
1.96 |
10 |
16 |
Table 1. Descriptive statistics by exam type for each teaching approach.
According to Table 1, it is noted that in the midterm exam (ME), the mean score is significantly higher (p<0.01) in the FG (14.0) compared to the TG (11.9), also, with this latter, there is a slightly high standard deviation of 2.41 which indicates scores far from the average. FG, on the other hand, dressed a lower standard deviation (1.94) which indicates that the scores are more grouped around the mean (14.0). The application of the PBL on flipped classroom approach has, as it appears, improved the grades and reduced the gap between them.
For the final exam, with the traditional approach, the dispersion increased (Sd=3.28). On the other hand, PBL approach has improved student outcomes and widened the gap between them compared to TG (p<0.01). Figure 1 highlights the dispersion of the continuous and final control data (before for the traditional approach and after for PBL).
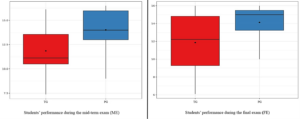
Figure 1. Students’ performance during the midterm exam (ME) and final exam (FE)
The ME grades were improved using PBL. As the number of compared participants is limited, a nonparametric test was carried out (Paired Mann-Whitney test) which revealed that the average grade of MEs is significantly different (p <0.01), between the traditional approach and the PBL. Similarly, an improvement in FE grades is observed when using the PBL approach. This approach allowed an improvement in the means as well as the dispersion. This leads us to state that the teaching approach based on case studies in the context of a flipped classroom (PBL), may improve both declarative and conditional knowledge on students’ outcomes.
|
Teaching approach |
N |
M |
Standard deviation |
Δ mean |
p |
|
TG |
19 |
11.9 |
3.30 |
2.21
|
0.01
|
|
FG |
19 |
14.1 |
1.95 |
Table 2: Descriptive statistics by teaching approach for the different types of controls.
From Table 2, there is a difference between the averages of the two approaches in favor of FG (p<0.01). This means that students who have taken the PBL approach had increased grades compared to those who have taken the traditional approach. To check if these differences are significant, a Paired Mann-Whitney test was used. This one demonstrated that the average rank of the grades is significantly different between the two studied approaches (p = 0.01).
The mean score and the standard deviation for each question in the questionnaire was determined. Average responses to the 12 items that referred to acquisition and application of knowledge related to the pain management ranged from 3.8 to 4.5 (See Table 3).
|
Statements |
Average score (Sd) |
|
1. I am confident in my ability to read a case and select the patient’s key factors that may impact their care. |
4.3 (0.7) |
|
2. I am confident in my ability to identify the presence of pain in a given patient. |
4.1 (0.6) |
|
3. I feel confident in determining the type of pain from the etiology involved. |
4.2 (0.6) |
|
4. I feel confident in determining the type of pain from the descriptive semiology used by a patient. |
4.2 (0.7) |
|
5. I am confident in my ability to choose the right pain assessment test for a given patient. |
4.5 (0.5) |
|
6. I am confident in my ability to use pain assessment tests with a given patient. |
4.3 (0.6) |
|
7. I am confident in my ability to understand the mechanism of action of an analgesic according to its pharmacological class. |
4.1 (0.6) |
|
8. I feel confident in my ability to relate the therapeutic benefit of a drug to its mechanism of action. |
4.1 (0.5) |
|
9. I am confident in my ability to determine the oxidative, supra-additive, or sub-additive effects of painkillers. |
4.1 (0.8) |
|
10. I feel more sensitive to the importance of pain management. |
4 (0.7) |
|
11. I feel better prepared at the clinic after participating in clinical case discussions as part of the flipped classroom. |
4.1 (0.5) |
|
12. I feel better prepared to act as an advocate for my patient’s interests to ensure comfort. |
3.8 (0.8) |
Table 3. Acquisition and application of knowledge
The statement “I feel better prepared to act as an advocate for my patient’s interests to ensure comfort” received a response rate of 3.8. This statement has the least satisfaction rate compared to all statements in the corresponding section.
|
Statements |
Average score (Sd) |
P value |
|
1. The cases were relevant and interesting. |
4.7 (0.4) |
Ns* |
|
2. I was nervous at the beginning of the module, but I gained confidence in myself as the course progressed. |
4.3 (0.8) |
|
|
3. Participating in the group discussions made me more confident in analysing key pain-related data. |
4.1 (0.9) |
|
|
4. I find that discussions have helped me learn more effectively than lectures. |
4.5 (0.6) |
|
|
5. I found that the group discussions helped my learning more effectively than the manual (handout). |
4.6 (0.7) |
|
|
6. I would recommend case-based seminar discussions as a tool for other courses. |
4 (0.9) |
*mean comparison of each item
Table 4. Perception of LPLs as a teaching/learning model
Average responses to the six questionnaire items that referred to cases as a learning model ranged from 4 to 4.7. None of the average responses differed significantly (p>0.05) from the other responses in this section of the questionnaire. The average response to the question “Were the cases relevant and interesting?” was 4.7, which was higher than all other answers. The statement “I would recommend the PBL format (no lectures, only case studies with assigned readings) as a tool for other courses” has a response average of 4, which is lower than all other responses in the corresponding category.
IV. DISCUSSION
Nursing students must grasp intricate concepts of basic physiology, pathophysiology, pharmacology, and more. Employing effective teaching methods with active learning can foster critical thinking abilities and uphold patient safety in complex care scenarios (Dong, 2016; Forsgren et al., 2014; Wood, 2003). Nowadays, nursing education has embraced the use of the flipped classroom as it offers a rich learning environment (Dong, 2016; Hanson, 2016; Immekus, 2019; Missildine et al., 2013; Ndosi & Newell, 2009; Peisachovich et al., 2016; Wood, 2003). Problem-based learning (PBL) is a frequently employed active learning approach in flipped classroom scenarios (Dong, 2016; Geist et al., 2015). PBL has been demonstrated to enhance the capacity of nursing students to evaluate patient information and arrive at more contemplative clinical judgments (Forsgren et al., 2014; Njie-Carr et al., 2017). When nursing students engage in discussions within small groups, they open themselves up to a wealth of interactive learning opportunities that are guided by their professor. This active learning situation is far more advantageous than the traditional lecture format as it promotes critical thinking skills and fosters independent learning. By participating in small group discussions, nursing students are able to delve deeper into the subject matter, ask questions, and engage in meaningful dialogue with their peers and instructor. This type of collaborative learning environment encourages students to take ownership of their education and empowers them to become more confident and competent healthcare professionals. Therefore, it is crucial that nursing programs prioritise small group discussions as a key component of their curriculum (Bailey, 2017; Carvalho et al., 2017; Kong et al., 2014; Teike Lüthi et al., 2015; Wood, 2003). High-level thinking and independent learning are enhanced with the use of interactive small groups (Alton, 2016; Gholami et al., 2016). We note from a review of the literature that a limited number of studies have examined the use of PBL in nursing (Bailey, 2017; Forsgren et al., 2014).
The current study revealed that regardless of the nature of the exam, student learning outcomes significantly improved with the flipped classroom method. Furthermore, the students participating in this study consider this method as a useful model to improve their learning and be more engaging. In fact, active learning allows effective knowledge acquisition (Arrue et al., 2017) and the development of critical thinking skills on nursing students as well as the improvement of metacognitive skills (Bailey, 2017; Carvalho et al., 2017; Domínguez, 2012). Furthermore, the students participating in this study consider this method as a useful model to improve their learning and be more engaging (Schlairet et al., 2014). Consequently, alternating between lectures and PBL approach may be a better option for health science courses (Alexandre & Wright, 2013). Greater confidence is demonstrated in acquiring and applying knowledge (practice) related to pain management.
Participation in this approach was considered a positive learning strategy, regardless of course content, the flipped classroom has shown to effectively support content learning (Hanson, 2016). When students were asked to consider whether it helped them learn more effectively than lectures, a higher response was obtained, and the response was very positive. This conclusion is in line with one from a study conducted in Portugal, which found that using this method in a second-year pathophysiology course led to higher levels of student satisfaction (Marques & Correia, 2017). Although some discomfort may be reported students are uncertain about the content and will attend classes on the assumption that it will help them understand exactly what they need to do and what they hope to achieve. This result confirms that student satisfaction does not always accurately reflect their learning (Dong, 2016). Further evaluation of this strategy and other learning tools is needed to establish best practices in nursing education (Barranquero-Herbosa et al., 2022; Njie-Carr et al., 2017).
A. Limitations
The small number of participants may affect the validity of the study. The results of this study cannot be generalised because participants belonged to one track only, so they are not representative to all nursing students. In addition, the small sample size of the study participants and the small number of available academic levels covered by the study.
B. Implications for Teaching and Future Research
Future studies could be considered to compare different learning strategies (e.g., games, medication card design, and practice problems) to determine the best practices for active learning strategies that support learning in a professional education setting and support flipped classroom learnings in nursing education.
V. CONCLUSION
Nursing education is about the development of professional skills; hence it is important to adopt active teaching strategies that promote critical thinking and knowledge transfer. However, the time constraint often pushes teachers to adopt the magistral lectures, the traditional form of knowledge delivery which mostly lacks the element of interactivity which is an issue recognised among many researchers worldwide.
The flipped classroom, in our case, is a solution to the time management problem. It allowed us to free up time in class which was beneficial to give space for interactive activities and active animation techniques such as case studies. In addition, in this study, we were able to compare the impact of the flipped classroom with the traditional model on two groups of students enrolled to the same course: pain management. The comparison results were mainly based on the acquisition of knowledge by students. We also measured students’ satisfaction with the proposed model as well as their sense of self-efficacy.
Students’ grades were clearly in favour of the PBL model in the flipped classroom. The students were also mostly satisfied with the proposed model and confirmed the development of their sense of self-efficacy regarding the pain management course.
Our perspective is the improvement of our teaching which, in our opinion, must be constantly corrected and enriched to face new conditions and situations. In this direction, the present study could constitute a roadmap for further in-depth studies to bring more to the PBL-based teaching model in the flipped classroom.
Notes on Contributors
Soumia Merrou is involved in the conceptualisation, methodology, data curation, writing and original draft preparation.
Abdellah Idrissi Jouicha helped in the methodology, participated in data curation and software, helped in writing – reviewing and editing.
Baslam Abdelmounaim participated in writing the original draft preparation, performed statistical analyses, helped in reviewing and editing corrections.
Zakaria Ouhaz was involved in visualisation, participated in data collection, helped writing and reviewed the manuscript.
Ahmed Rhassane El Adib was central to the conceptualisation and methodology, validated the design study, and supervised work progress. All authors have read and approved the final manuscript.
Ethical Approval
Participation in the study was voluntary and anonymous. Oral consent of all participants was obtained and the research was approved by the Institutional Ethical committee (CCBE-FSA Ref. No: ER-CS-10/2022-000).
Data Availability
The data that support the findings of this study are openly available in Figshare repository, https://doi.org/10.6084/m9.figshare.21385446.
Acknowledgement
We acknowledge the efforts of both professor and participants.
Funding
The study received no funding.
Declaration of Interest
The authors declare that they have no conflict of interest.
References
Alexandre, M. S., & Wright, R. R. (2013). Flipping the classroom for student engagement. International Journal of Nursing Care, 1(2), 100.
Alton, S. (2016). Learning how to learn: Meta-learning strategies for the challenges of learning pharmacology. Nurse Education Today, 38, 2–4. https://doi.org/10.1016/j.nedt.2016.01.003
Arrue, M., Ruiz de Alegría, B., Zarandona, J., & Hoyos Cillero, I. (2017). Effect of a PBL teaching method on learning about nursing care for patients with depression. Nurse Education Today, 52, 109–115. https://doi.org/10.1016/j.nedt.2017.02.016
Bailey, L. A. (2017). Adaptation of know, want to know, and learned chart for problem-based learning. Journal of Nursing Education, 56(8), 506–508. https://doi.org/10.3928/01484834-20170712-11
Barranquero-Herbosa, M., Abajas-Bustillo, R., & Ortego-Maté, C. (2022). Effectiveness of flipped classroom in nursing education: A systematic review of systematic and integrative reviews. International Journal of Nursing Studies, 105, Article 104327. https://doi.org/10.1016/j.ijnurstu.2022.104327
Carvalho, D. P. S. R. P., Azevedo, I. C., Cruz, G. K. P., Mafra, G. A. C., Rego, A. L. C., Vitor, A. F., Santos, V. E. P., Cogo, A. L. P., & Ferreira Júnior, M. A. (2017). Strategies used for the promotion of critical thinking in nursing undergraduate education: A systematic review. Nurse Education Today, 57, 103–107. https://doi.org/10.1016/j.nedt.2017.07.010
Deandrea, S., Montanari, M., Moja, L., & Apolone, G. (2008). Prevalence of undertreatment in cancer pain. A review of published literature. Annals of Oncology, 19(12), 1985–1991. https://doi.org/10.1093/annonc/mdn419
Domínguez, R. G. (2012). Participatory Learning. In N. M. Seel (Ed.), Encyclopedia of the Sciences of Learning (pp. 2556–2560). Springer.
Dong, X. (2016). Application of flipped classroom in college english teaching. Creative Education, 7(9), 1335–1339. https://doi.org/10.4236/ce.2016.79138
Forsgren, S., Christensen, T., & Hedemalm, A. (2014). Evaluation of the case method in nursing education. Nurse Education in Practice, 14(2), 164–169. https://doi.org/10.1016/j.nepr.2013.08.003
Geist, M. J., Larimore, D., Rawiszer, H., & Al Sager, A. W. (2015). Flipped versus traditional instruction and achievement in a baccalaureate nursing pharmacology course. Nursing Education Perspectives, 36(2), 114-115. https://doi.org/10.5480/13-1292
Gerbershagen, K., Gerbershagen, H. J., Lutz, J., Cooper-Mahkorn, D., Wappler, F., Limmroth, V., & Gerbershagen, M. (2009). Pain prevalence and risk distribution among inpatients in a German teaching hospital. The Clinical Journal of Pain, 25(5), 431–437.
Gholami, M., Moghadam, P. K., Mohammadipoor, F., Tarahi, M. J., Sak, M., Toulabi, T., & Pour, A. H. H. (2016). Comparing the effects of problem-based learning and the traditional lecture method on critical thinking skills and metacognitive awareness in nursing students in a critical care nursing course. Nurse Education Today, 45, 16–21. https://doi.org/10.1016/j.nedt.2016.06.007
Gianni, W., Madaio, R., Cioccio, L., D’Amico, F., Policicchio, D., Postacchini, D., Franchi, F., Ceci, M., Benincasa, E., Gentili, M., & Zuccaro, S. (2010). Prevalence of pain in elderly hospitalized patients. Archives of Gerontology and Geriatrics, 51(3), 273-276. https://doi.org/10.1016/j.archger.2009.11.016
Hanson, J. (2016). Surveying the experiences and perceptions of undergraduate nursing students of a flipped classroom approach to increase understanding of drug science and its application to clinical practice. Nurse Education in Practice, 16(1), 79–85. https://doi.org/10.1016/j.nepr.2015.09.001
Immekus, J. C. (2019). Flipping statistics courses in graduate education: Integration of cognitive psychology and technology. Journal of Statistics Education, 27(2), 79–89. https://doi.org/10.1080/10691898.2019.1629852
Kerner, Y., Plakht, Y., Shiyovich, A., & Schlaeffer, P. (2013). Adherence to guidelines of pain assessment and intervention in internal medicine wards. Pain Management Nursing, 14(4), 302–309. https://doi.org/10.1016/j.pmn.2011.06.005
Kong, L.-N., Qin, B., Zhou, Y., Mou, S., & Gao, H.-M. (2014). The effectiveness of problem-based learning on development of nursing students’ critical thinking: A systematic review and meta-analysis. International Journal of Nursing Studies, 51(3), 458–469. https://doi.org/10.1016/j.ijnurstu.2013.06.009
Manias, E., Bucknall, T., & Botti, M. (2005). Nurses’ strategies for managing pain in the postoperative setting. Pain Management Nursing: Official Journal of the American Society of Pain Management Nurses, 6(1), 18–29. https://doi.org/10.1016/j.pmn.2004.12.004
Marques, P. A. O., & Correia, N. C. M. (2017). Nursing education based on “hybrid” problem-based learning: The impact of PBL-based clinical cases on a pathophysiology course. Journal of Nursing Education, 56(1), 60. https://doi.org/10.3928/01484834-20161219-12
Merrou, S., Jouicha, A. I., Baslam, A., Ouhaz, Z., & El Adib, A. R. (2023). Problem-based learning method in the context of a flipped classroom: Outcomes on pain management course acquisition [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.22639279
Missildine, K., Fountain, R., Summers, L., & Gosselin, K. (2013). Flipping the classroom to improve student performance and satisfaction. Journal of Nursing Education, 52(10), 597-599.
Ndosi, M. E., & Newell, R. (2009). Nurses’ knowledge of pharmacology behind drugs they commonly administer. Journal of Clinical Nursing, 18(4), 570–580. https://doi.org/10.1111/j.1365-2702.2008.02290.x
Njie-Carr, V. P. S., Ludeman, E., Lee, M. C., Dordunoo, D., Trocky, N. M., & Jenkins, L. S. (2017). An integrative review of flipped classroom teaching models in nursing education. Journal of Professional Nursing, 33(2), 133–144. https://doi.org/10.1016/j.profnurs.2016.07.001
Peisachovich, E. H., Murtha, S., Phillips, A., & Messinger, G. (2016). Flipping the classroom: a pedagogical approach to applying clinical judgment by engaging, interacting, and collaborating with nursing students. International Journal of Higher Education, 5(4), 114. https://doi.org/10.5430/ijhe.v5n4p114
Schlairet, M. C., Green, R., & Benton, M. J. (2014). The flipped classroom. Nurse Educator, 39(6), 321–325. https://doi.org/10.1097/nne.0000000000000096
Teike Lüthi, F., Gueniat, C., Nicolas, F., Thomas, P., & Ramelet, A.-S. (2015). Les obstacles à la gestion de la douleur perçus par les infirmières: Étude descriptive au sein d’un hôpital universitaire Suisse. [Barriers to pain management as perceived by nurses: A descriptive study in a Swiss University Hospital.] Douleur et Analgesie [Douleur & Analgésie], 28, 93-99. https://doi.org/10.1007/s11724-015-0414-3
Tune, J. D., Sturek, M., & Basile, D. P. (2013). Flipped classroom model improves graduate student performance in cardiovascular, respiratory, and renal physiology. Advances in Physiology Education, 37(4), 316–320. https://doi.org/10.1152/advan.00091.2013
Wood, D. (2003). Problem based learning. British Medical Journal, 326, 328–330. https://doi.org/10.1136/bmj.326.7384.328
*Abdellah Idrissi Jouicha
Marrakesh, Marrakesh-Safi,
40000, Morocco
Email: abdellah.idrissi@ced.uca.ac.ma
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
