
Micro CEX vs Mini CEX: Less can be more
Submitted: 28 January 2023
Accepted: 17 August 2023
Published online: 2 January, TAPS 2024, 9(1), 3-19
https://doi.org/10.29060/TAPS.2024-9-1/OA2947
Thun How Ong1, Hwee Kuan Ong2, Adrian Chan1, Dujeepa D. Samarasekera3 & Cees Van der Vleuten4
1Department of Respiratory and Critical Care Medicine, Singapore General Hospital, Duke-NUS Medical School, Singapore; 2Department of Physiotherapy, Singapore General Hospital; 3Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 4Department of Educational Development and Research, Maastricht University, Maastricht, The Netherlands
Abstract
Introduction: The mini-Clinical Evaluation Exercise (CEX) is meant to provide on the spot feedback to trainees. We hypothesised that an ultra-short assessment tool with just one global entrustment scale (micro-CEX) would encourage faculty to provide better feedback compared to the traditional multiple domain mini-CEX.
Methods: 59 pairs of faculty and trainees from internal medicine completed both the 7-item mini-CEX and a micro-CEX and were surveyed regarding their perceptions of the 2 forms. Wordcount and specificity of the feedback was assessed. Participants were subsequently interviewed to elicit their views on factors affecting the utility of the CEX.
Results: Quantity and quality of feedback increased with the micro-CEX compared to the mini-CEX. Wordcount increased from 9.5 to 17.5 words, and specificity increased from 1.6 to 2.3 on a 4-point scale, p < 0.05 in both cases. Faculty and residents both felt the micro-CEX provided better assessment and feedback. The micro-CEX, but not the mini-CEX, was able to discriminate between residents in different years of training. The mini-CEX showed a strong halo effect between different domains of scoring. In interviews, ease of administration, immediacy of assessment, clarity of purpose, structuring of desired feedback, assessor-trainee pairing and alignment with trainee learning goals were identified as important features to optimize utility of the (mini or micro or both) CEX.
Conclusions: Simplifying the assessment component of the CEX frees faculty to concentrate on feedback and this improves both quantity and quality of feedback. How the form is administered on the ground impacts its practical utility.
Keywords: Workplace Based Assessment, Mini-CEX, Micro-CEX, Feedback, Assessment
Practice Highlights
- Simplifying the assessment component of the CEX frees faculty to concentrate on feedback.
- A simpler form can result in better and more feedback.
- Making it easy for faculty to use the form is important and increases its utility in providing feedback and assessment.
I. INTRODUCTION
The Mini-CEX is one of the most widely used work-placed based assessment (WBA) tools and is supported by a large body of theoretical and empirical evidence which have shown that when used in the context of repeated sampling, it is both a valid assessment tool and is also an effective education tool in giving feedback to the trainee (Hawkins et al., 2010; Norcini et al., 2003). However, in practice, the educational value of the mini-CEX, as measured chiefly by trainee and faculty perceptions and satisfaction, varied significantly (Lorwald et al., 2018). Factors affecting the educational value have been described by Lorwald et al. and categorised into context of usage, and user, implementation and outcome factors (Lorwald et al., 2018).
Context refers to the situation in which the mini-CEX is executed, and factors which impact its actual usage, such as time needed for conducting the Mini-CEX, or the usability of the tool. Time constraint on the part of both the residents and the assessors is an especially frequent issue across multiple studies (Bindal et al., 2011; Brazil et al., 2012; Castanelli et al., 2016; Lörwald et al., 2018; Morris et al., 2006; Nair et al., 2008; Yanting et al., 2016). The mini-CEX was conceived as a 30-minute exercise of directly observed assessment, and there are 6 or 7 domains which faculty are expected to assess (Norcini et al., 2003). In a busy clinical environment however, what actually occurs is often a brief clinical encounter of 10-15 minutes or even less where only a few of the mini-CEX’s domains were assessed (Berendonk et al., 2018).
User factors refers to trainee and faculty knowledge of the mini-CEX and their perceptions of its use. Studies have found that the mini-CEX is frequently regarded as a check box exercise (Bindal et al., 2011; Sabey & Harris, 2011). Assessor’s and trainee’s training and attitudes, or unfamiliarity with the WBA tools also negatively impact the educational value of the mini-CEX (Lörwald et al., 2018). Reports have shown that educating faculty on the formative intent of mini-CEX can improve feedback provided (Liao et al., 2013).
Implementation factors refer to how the mini-CEX is actually executed on the ground. Some studies have reported that the mini-CEX often occurs without actual direct observation (Lörwald et al., 2018) or feedback provided (Weston & Smith, 2014). Implementation in turn affected outcome, which refers to the trainees appraisal of the feedback received (Lörwald et al., 2018).
One way of improving the educational value of the mini-CEX then might be to improve the context of its usage, by redesigning the mini-CEX to better fit the realities of the clinical workplace. In different clinical encounters, specific domains of performance are more easily and obviously observed and assessed than others (Crossley & Jolly, 2012). Reducing the number of dimensions the assessors are asked to rate was shown to decrease measured cognitive load and improved interobserver reliability (Tavares et al., 2016). It has also been shown that using rating scales that align with the clinician’s cognitive schema perform better, for instance, scales that ask the clinician assessors about the trainees ability to practice safely with decreasing levels of supervision (i.e. entrustability) showed better discrimination and higher reliability (Weller et al., 2014). Compared to multidimension rating scales, global rating scales have greater reliability and validity in assessing candidates in OSCE examinations (Regehr et al., 1998), assessing technical competence in procedures (Walzak et al., 2015) and in simulation-based training (Ilgen et al., 2015).
We proposed therefore to replace the multiple domains with a single rating asking faculty what level of supervision the resident would require in performing a similar task, i.e. a global entrustment scale. The shorter assessment task should refocus the faculty on the feedback component, whilst still retaining the ability to identify trainee progression. One such form has been proposed by Kogan and Holmboe (2018), and we designated this the micro-CEX.
We hypothesised that these changes would improve the usability (“context” as described by Lorwald et al.) and hence improve the educational value of the assessment, measured in this study by the specificity and quality of the feedback given by faculty.
Our study aims to show therefore that the shorter micro-CEX can provide better feedback than the usual mini-CEX. We also sought to find out, from the perspective of the end-users, what other adjustments to the implementation and design of the mini or micro-CEX can be made to improve its acceptability, educational value and validity.
The study focussed on the following questions:
Does the micro-CEX stimulate faculty to provide more specific and actionable feedback compared to the mini-CEX?
Can the micro-CEX provide discriminatory assessment for residents across different years of practice?
What are the perceptions of the faculty and residents regarding the factors affecting utility of the assessment instrument in providing feedback and assessment?
II. METHODS
A. Setting and Subjects
The study was conducted in the division of Internal Medicine in a 1700 bed hospital in Singapore between September and December 2018. All faculty and residents rotating through internal medicine were invited to participate via e-mail, and agreeable faculty and residents paired up. In usual practice, residents must complete at least 2 mini-CEX covering standard inpatient or outpatient encounters during each three-month internal medicine posting, hence both residents and faculty are familiar with the usual mini-CEX.
B. Design
In order to evaluate for any participant reactivity affecting the CEX data (i.e. a Hawthorne effect) (Paradis & Sutkin, 2017), a baseline sample of 30 of the usual mini-CEX performed in the 3 months prior to the study was randomly selected and deidentified (from June to August 2018) . The quantity and specificity of feedback in these was evaluated as detailed below.
For the study itself, faculty and residents used the usual mini-CEX as the first assessment in the first 2 weeks of the month, followed by a second assessment using the micro-CEX in the next 2 weeks. This sequence was chosen as performing the micro-CEX first might affect how the subsequent mini-CEX was performed. Cases chosen for the mini-CEX and micro-CEX were inpatient or outpatient internal medicine encounters, and faculty were simply instructed to choose cases that represented typical cases of average difficulty with no restrictions on the exact cases to be chosen.
Faculty and residents completed an anonymised survey on their experiences at the end of the study and were invited to participate in a semi-structured group interview to elicit their views regarding which aspects of the mini-CEX exercise influenced feedback and assessment (Appendix 2). Both faculty and residents were informed that the survey and interviews were part of this study and participation in either was taken to be implied consent. The workflow of the study is seen in Figure 1.
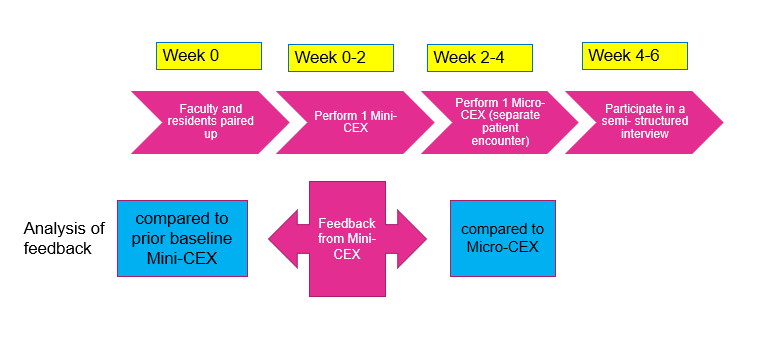
Figure 1. Study workflow
C. Instruments
The mini-CEX used in the program is based on the one described by Norcini (Norcini et al., 2003).This form was hosted on the internet ( New Innovations, Ohio, USA) and could be accessed by faculty from their mobile devices or their email. The micro- CEX was hosted on an opensource online survey tool (LimeSurvey GmbH, Hamburg, Germany) and can be accessed from mobile devices. A copy of both forms is available in Appendix 1.
D. Analysis of Feedback
The quality of feedback was assessed firstly by a word count, and then by grading the specificity of the feedback on a three-point scale (Pelgrim et al., 2012) (Appendix 3) and finally by the presence or absence of an actionable plan for improvement. In order to avoid rater bias, the assessor for the specificity of the feedback was blinded to the source of feedback (mini or Micro CEX). The first 20 forms were independently graded by two separate assessors (OTH and AC) using the above criteria, achieving a kappa coefficient of 0.852; all subsequent forms were graded by OTH, with any uncertainty resolved by discussion between AC and OTH. Word count and specificity, as well as faculty and resident preferences between the forms, were analysed using paired samples T-test. Proportion of Feedback which showed an actionable plan was compared using a Chi-Square test.
E. Semi-structured Interviews
Faculty and residents were interviewed separately. 21 residents and 6 faculty were interviewed over 8 sessions lasting between 20 to 30 minutes each. Interviews were conducted by the investigator (OTH). The interviews were audiotaped and transcribed verbatim. Data collection ended when saturation was reached. Member checking of the transcripts was carried out.
The inductive template analysis as described by Nigel King was used to analyse the interview transcripts (King, 2012). Two transcripts were studied and coded separately by the investigator (OTH) and a collaborator (OHK). A priori themes of assessment, feedback and administration were used to structure the data so that the research question could be answered. Codes were discussed between OTH and OHK until a consensus was reached, and a codebook was created. The subsequent transcripts were coded by OTH. OHK, AC and OTH subsequently met to discuss the categories and emerging themes. NVivo 12 was used to store and manage the codes and transcripts. Results were triangulated with data from the quantitative surveys.
For all quantitative data, an alpha of 0.05 was used as the cut-off for significance. IBM SPSS 25 (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY) was used for calculations.
III. RESULTS
The data that support the findings of this study are openly available in Figshare repository, at https://doi.org/10.60 84/m9.figshare.21862068.v1 (Ong, 2023).
There were 33 internal medicine residents during the study period and 32 (97%) participated in the study; one resident declined to participate. They were paired with 39 different faculty over the three months of the study. 59 unique faculty- resident pairs completed both sets of CEX. 30.5% of the residents were in their first year of residency (R1), 47.9% in second year (R2), and 22.0% were in their third year (R3). The residents completed an average of 1.96 pairs of mini and micro CEX each. Time taken to complete the assessments was estimated by faculty to be 11.33 +/- 6.56 min for mini-CEX vs 9.42 +/-5.51 min for the micro-CEX (p = 0.02).
A. Evaluation of Feedback in the Mini-CEX: Baseline and During Study
30 de-identified mini-CEX were extracted randomly from the 3 months preceding the initiation of the study. These served as a baseline control and were compared to the feedback from the first, traditional mini-CEX done during the study (Table 1). During the period of the study, faculty using the same mini-CEX provided feedback that was more specific. Proportion of actionable feedback provided was much more in the mini-CEX done as part of the study compared to baseline controls (Table 1: 3.3% controls vs 28% study mini-CEX, p = 0.005).
|
|
Mini-CEX vs prior baseline control |
Mini-CEX vs Micro-CEX |
||||
|
Prior baseline control mini-CEX (mean+/-SD) |
Study Mini-CEX (mean +/- SD) |
p value |
Mini-CEX (mean +SD) |
Micro CEX (mean +SD) |
p value |
|
|
Q1 in which areas did the resident do well |
|
|||||
|
Word count |
12.1 +/-14.1 |
9.5 +/- 7.0 |
0.93 |
9.5 +/- 7.0 |
17.5 +/- 10.3 |
<0.001 |
|
Specificity* |
1.2 +/- 1.0 |
1.6 +/- 0.90 |
0.08 |
1.6+/- 0.9 |
2.3 +/- 0.7 |
<0.001 |
|
Q2/3 Areas needing improvement/ recommendations for future improvement |
||||||
|
Word count |
3.8 +/- 6.8 |
5.7 +/- 7.3 |
0.06 |
5.7 +/- 7.3 |
19.3 +/- 15.1 |
<0.001 |
|
Specificity* |
0.5 +/- 0.7 |
1.1 +/-1.1 |
0.01 |
1.1 +/- 1.0 |
1.8 +/- 0.9 |
<0.001 |
|
Actionable |
1/30 (3.3%) |
17/59(28.8%) |
0.005 |
17/59 (28.8%) |
18/59(30.5%) |
0.84 |
Table 1. Quality and quantity of feedback in prior baseline control vs study mini-CEX, and in mini vs Micro-CEX
B. Evaluation of Feedback in the Micro and Mini-CEX During Study
Comparison of the feedback given in the mini and micro-CEX during the study is shown in Table 1. Feedback wordcount increased and was more specific with micro-CEX compared to the contemporaneous mini-CEX done by the same pair. However, there were no differences in the proportion of actionable feedback given in both forms.
C. Discrimination Between Residents in Different Years of Training
The micro-CEX was able to show progression between the years of training, with a significant rise in the resident’s mean score across the three years of training. On a 4 point score the mean entrustment score increased from 2.45 in the first year of training to 3.30 by the third year (p<0.05). (Figure 2)
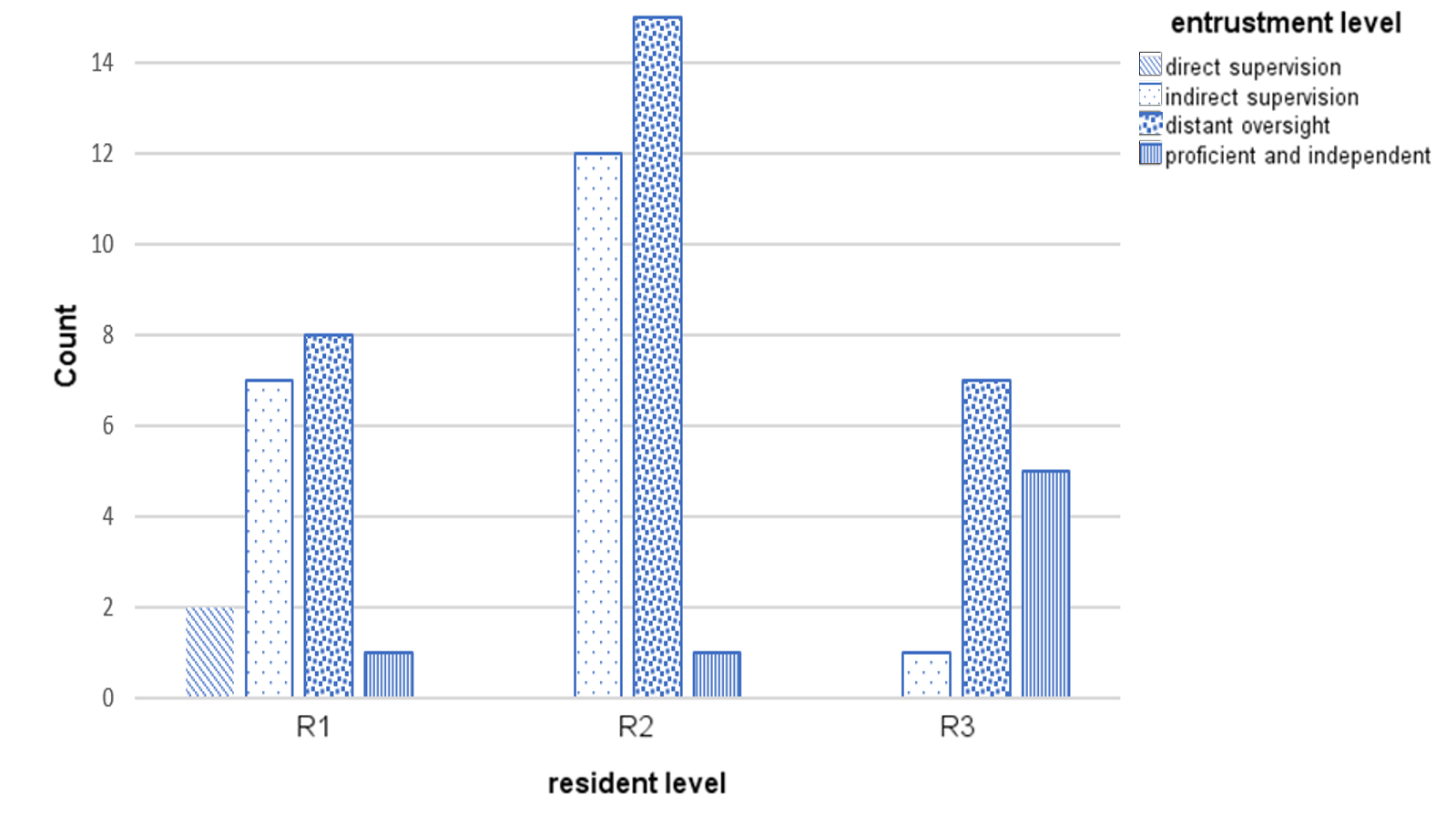
Figure 2. Level of entrustment vs Year of training
Correlation of residents’ year of training and grading of the mini-CEX domains was moderate (kappa 0.39 to 0.60). There was high correlation between all seven questions in the mini-CEX (kappa 0.7 to 0.8) (see appendix 4), implying that the resident’s score in one domain heavily influenced the score in other domains i.e. a halo effect.
D. Faculty and Resident Preferences
21 (out of total 32 participating residents, 65% response rate) residents and 25 (out of total 39 participating faculty, 64.9% response rate) responded to the survey. Faculty and residents felt that the Micro -CEX had better value for both assessment and feedback compared to the Mini-CEX (Table 2).
|
|
Mini-CEX Mean + SD |
Micro CEX Mean + SD |
p value |
t-Stats |
Cohen’s d |
|
Usefulness for assessment |
|||||
|
Faculty |
6.04 +/- 1.34 |
6.57 +/- 0.95 |
0.04 |
2.23 |
0.46 |
|
Residents |
6.00 +/- 1.62 |
6.9 +/- 0.91 |
0.03 |
-2.31 |
0.52 |
|
Usefulness for feedback |
|||||
|
Faculty |
6.00 +/- 1.35 |
6.87 +/- 1.10 |
0.01 |
-3.07 |
0.64 |
|
Residents |
5.43 +/- 1.40 |
6.81 +/- 1.57 |
0.09 |
-3.82 |
0.83 |
Table 2. Perceptions of faculty and residents regarding usefulness of mini and micro-CEX for assessment and feedback
*Scoring is on a 9-point Likert scale, with 1 = not useful at all …. 9 = very useful
E. Qualitative Data
Qualitative data from the semi-structured interviews was analysed to better understand what the features of the micro-CEX driving this preference were, and to look for helpful features in the CEX. Themes from the semi-structured interviews were distilled into 6 themes (Table 3):
1) Make it easy: A recurrent theme was that the micro-CEX was easier to use and the short form could be used by the bedside, on resident or faculty mobile devices.
2) Immediacy is important: Faculty and residents both prized the ability to integrate the assessment into their daily routines, and this immediacy was very important in enhancing the value of the feedback.
3) Tell us what it’s for: Faculty and residents both expressed that the intended purpose of the forms needed to be explicit. Uncertainty in purpose of the form resulted in a perception of redundancy with the other assessments, and confusion about summative vs formative intent of the assessment inhibited honest feedback and assessment.
4) Structure the form so we know what you want: Structuring the form with specific areas to remind them to provide narrative feedback, and what specific areas to provide feedback in, was useful. Faculty and residents both felt that the micro-CEX had better learning value than the mini-CEX.
5) Choice of assessor matters depending on objective of the tool: Faculty and residents agreed that assessments were frequently affected by the prior experiences between the two, impacting the objectivity of assessments via both the micro-and mini- CEX. Prior engagement with the resident facilitated provision of feedback. However, for assessment purposes, residents felt that a faculty with no prior knowledge of the trainee might be more objective.
6) Align assessment with learning goals: Many of the residents were preparing for their postgraduate medical examinations, and they found the mini-CEX exercise especially useful if it was conducted in a way similar to their examinations (the Royal College of Physicians PACES exam) – in other words, the utility of the exercise increased greatly when the assessment was aligned with the residents’ own learning goals.
|
S/N |
Themes |
Quotations |
|
1. |
Make it easy to do |
The micro-CEX was “more succinct. So, it’s, it’s much easier to administer” -F
“If it’s a shorter form, even though the quantity may be less maybe the fact that the quality of whatever feedback we’re given is better because they’re really giving the one or two points that really stood out to them that we need to improve on or the one or two things that we really did well” -R
(Regarding the mini-CEX) “The fact that it’s more detailed actually maybe reduces the quality of the feedback because … if you ask me for additional remarks for every single domain, then they just put nil, nil, nil because there’s no time” -F
|
|
2. |
Immediacy is important |
“Memory is also fresh because you’ve just done the case and so I think the learning value’s a lot better” -R
“I think looking at it in terms of like a learning experience also, um, when we have that micro-CEX on the spot, ah, not only can we address, like all the points immediately, like what the resident should, um, but at the same time, ah, you can kinda go through certain topics at the same setting as well” -F
|
|
3. |
What is this for |
“I think we need clear goals as to why we do these, rather than to simply check boxes.” -R
“The form should come with what is the expectation of this, uh, assessment, whether it’s for assessing, or it’s for a feedback, or it’s …. whether this person can work as a HO. I mean, the intention will drive how I assess” -R
“We have a lot of forms, the 360 and the mini-cex and all. Sometimes maybe I personally don’t really see what the difference is sometimes or how it can help to change assessment. I think it’s just extra admin for everyone and everyone just gets fed up doing it” -R
“I think the assessor, sometimes they’re very nice, they know it affects your, your grading or your, your overall performance in the residency, so they try not to be too strict” -R
|
|
4. |
Be specific about what you want to know |
The micro-CEX had “I think several features currently that are really quite useful. Number one is that there is the mandatory open-ended field, um, for areas that need improvement and areas that need to be reinforced” -F
“I find the comments, uh, quite useful. Maybe not the grades itself, because usually people would just give, like, mod- middle-grade. But, the written comments are actually quite useful” -R
|
|
5. |
Choice of assessor matters depending on objective for the tool |
“It’s quite easy for me to, to, to, remember each of them and give them dedicated feedback” -F
“It should be someone that you don’t really know, but maybe in the same department. So, that it can be like, really, like a proper case scenario, yeah. Instead of grading you based on what their other impressions are” -R
|
|
6. |
Align assessment with learning goals |
“So I had this one particular case, that was a very good PACES case, that I clerked in the morning, and, we impromptu made it into a mini-CEX kind of session and, and we went in quite in depth into the discussion, and PACES that sort of stuff, and I thought that was very useful.” -R
|
Table 3. Themes with supporting quotations
*1 PACES = Membership of Royal Collage Physicians clinical examination, a required exit certification for the residents.
IV. DISCUSSION
The most striking result from this study is that even without specific faculty training or other intervention, simplifying the assessment task alone led faculty to write longer, and more specific feedback. Faculty and residents also perceived that the feedback was better. By simplifying the assessment, the faculty’s attention was shifted from grading the resident in multiple domains toward qualitatively identifying good and bad points in the encounter, providing feedback for the residents.
Proportion of actual actionable feedback in the two forms, however, was not different. This is perhaps because there was no specific faculty training for the study as we felt that the additional training itself would impact results. Specific faculty training may be needed to improve this aspect.
A Hawthorne effect was noticed in the study (Adair, 1984). The proportion of actionable feedback provided was much more in the mini-CEX done as part of the study compared to baseline controls (Table 1: 3.3% controls vs 28% study mini-CEX, p = 0.005). Word count and specificity also increased. However, despite this, we were still able to show that the micro-CEX induced faculty to provide more and better feedback.
From the global entrustment scale used in the micro-CEX, it was possible to demonstrate progression from first year to third year of residency (Figure 2). One potential concern is loss of granularity in assessment of different domains, i.e., that we might lose the ability to identify the specific domain in which the resident is weak if we do not ask faculty to score physical examination, history taking, management etc. separately. However, we found a high correlation between the scores in all domains in the mini-CEX (kappa ranged from 0.7 to 0.8, see appendix 4), indicating a strong halo effect. This suggests that in practice, faculty are making a global assessment anyway rather than a separate assessment of separate domains. Faculty and residents perceived that the single global assessment with the micro-CEX provided better assessment.
The messages from faculty and residents about what they perceive to be important in making the CEX work for them speak for themselves. The importance of making the form easy to administer is very intuitive; the bureaucratic impracticality of paper portfolios was pointed out long ago and e-portfolios were touted as the preferred solution (Van Tartwijk & Driessen, 2009) but the message here is that administrative details have significant impact on the utility of the CEX – many of the issues cited such as the number of assessments an individual assessor has to make, whether the assessor is equipped to do the assessment on the spot, or whether the assessor has prior exposure to the resident or not – are administrative and educational design details that faculty training alone cannot solve.
Our study had several limitations. Variations in the clinical environment such as ward vs ambulatory clinic, variable workload or competing responsibilities of the faculty and residents might have affected how the CEX was administered. However, distractions in the ward do affect the performance of CEX in real life as well.
We also note that in this study design, the mini-CEX was performed before the micro-CEX. This was deliberate as the residents and faculty were used to doing the mini-CEX on an ongoing basis so the first mini-CEX would be a “usual” assessment followed by the new assessment. Performing the micro-CEX first might affect how the subsequent mini-CEX was performed.
In this study, we did not attempt to make judgements about reliability and validity of the micro-CEX as only one specific data point was obtained for each trainee. The mini-CEX is validated to be reliable mainly in the context of repeated tests , and preferably in the context of a coherent program of assessment (van der Vleuten & Schuwirth, 2005). Whether the micro-CEX is able to provide equivalent robust and valid assessment compared to the mini-CEX depends on how it is used and is an area ripe for future study.
V. CONCLUSION
Our study demonstrated that the micro-CEX has a high rate of acceptability amongst faculty and residents, as well as a measurable improvement in feedback characteristics compared to the usual mini-CEX. The context in which the form is administered in actual practice has significant impact on its utility for feedback and assessment.
Ethical Approval
The study protocol was reviewed by the hospital Institutional Review Board, who deemed this as an educational quality improvement project which did not require IRB approval (Singhealth CIRB Ref: 2018/2696).
Notes on Contributors
Thun How Ong conceptualised and designed the study, administered the interviews, analysed the data and wrote the manuscript.
Hwee Kuan Ong participated in data analysis and coding of the qualitative data.
Adrian Chan participated in data analysis and in grading of the feedback specificity.
Dujeepa D. Samarasekera provided input on initial study design and reviewed the manuscript.
C. P. M. van der Vleuten provided guidance and input at all stages of the study, from initial study design to data analysis and manuscript writing.
Data Availability
The data that support the findings of this study are openly available in Figshare repository, at
https://doi.org/10.6084/m9.figshare.21862068.v1
Acknowledgement
The authors would like to acknowledge the contributions of the following:
Tan Shi Hwee and Nur Suhaila who provided the administrative support that made the whole project feasible.
The Faculty and Residents who were willing to do the extra CEX and the interviews, and who labour daily in pursuit of the ultimate goal of providing better care for our patients.
Funding
No funding was obtained for this study.
Declaration of Interest
All authors have no declaration of interest.
References
Adair, J. G. (1984). The Hawthorne effect: A reconsideration of the methodological artifact. Journal of Applied Psychology, 69(2), 334-345. https://doi.org/10.1037/0021-9010.69.2.334
Berendonk, C., Rogausch, A., Gemperli, A., & Himmel, W. (2018). Variability and dimensionality of students’ and supervisors’ mini-CEX scores in undergraduate medical clerkships – A multilevel factor analysis. BMC Medical Education, 18(1), 100. https://doi.org/10.1186/s12909-018-1207-1
Bindal, T., Wall, D., & Goodyear, H. M. (2011). Trainee doctors’ views on workplace-based assessments: Are they just a tick box exercise? Medical Teacher, 33(11), 919-927. https://doi.org/10.3109/0142159X.2011.558140
Brazil, V., Ratcliffe, L., Zhang, J., & Davin, L. (2012). Mini-CEX as a workplace-based assessment tool for interns in an emergency department – Does cost outweigh value? Medical Teacher, 34(12), 1017-1023. https://doi.org/10.3109/0142159X.2012.719653
Castanelli, D. J., Jowsey, T., Chen, Y., & Weller, J. M. (2016). Perceptions of purpose, value, and process of the mini-Clinical Evaluation Exercise in anesthesia training. Canadian Journal of Anaesthesia, 63(12), 1345-1356. https://doi.org/10.1007/s12630-016-0740-9
Crossley, J., & Jolly, B. (2012). Making sense of work-based assessment: Ask the right questions, in the right way, about the right things, of the right people. Medical Education, 46(1), 28-37. https://doi.org/10.1111/j.1365-2923.2011.04166.x
Hawkins, R. E., Margolis, M. J., Durning, S. J., & Norcini, J. J. (2010). Constructing a validity argument for the mini-Clinical Evaluation Exercise: A review of the research. Academic Medicine, 85(9), 1453-1461. https://doi.org/10.1097/ACM.0b013 e3181eac 3e6
Ilgen, J. S., Ma, I. W., Hatala, R., & Cook, D. A. (2015). A systematic review of validity evidence for checklists versus global rating scales in simulation-based assessment. Medical Education, 49(2), 161-173. https://doi.org/10.1111/medu.12621
King, N. (2012). Doing template analysis. Sage Knowledge, 426-450. https://doi.org/10.4135/9781526435620.n24
Kogan, J. R., & Holmboe, E. (2018). Practical guide to the evaluation of clinical competence appendix 4.6 (2nd ed.). Elsevier.
Liao, K. C., Pu, S. J., Liu, M. S., Yang, C. W., & Kuo, H. P. (2013). Development and implementation of a mini-Clinical Evaluation Exercise (mini-CEX) program to assess the clinical competencies of internal medicine residents: From faculty development to curriculum evaluation. BMC Medical Education, 13, 31-31. https://doi.org/10.1186/1472-6920-13-31
Lörwald, A. C., Lahner, F. M., Greif, R., Berendonk, C., Norcini, J., & Huwendiek, S. (2018). Factors influencing the educational impact of Mini-CEX and DOPS: A qualitative synthesis. Medical Teacher, 40(4), 414-420. https://doi.org/10.1080/0142159X.2017 .1408901
Lorwald, A. C., Lahner, F. M., Nouns, Z. M., Berendonk, C., Norcini, J., Greif, R., & Huwendiek, S. (2018). The educational impact of mini-Clinical Evaluation Exercise (mini-CEX) and Direct Observation of Procedural Skills (DOPS) and its association with implementation: A systematic review and meta-analysis. PLoS One, 13(6), Article e0198009. https://doi.org/10.1371/jour nal.pone.0198009
Morris, A., Hewitt, J., & Roberts, C. M. (2006). Practical experience of using directly observed procedures, mini Clinical Evaluation Examinations, and peer observation in pre-registration house officer (FY1) trainees. Postgraduate Medical Journal, 82(966), 285-288. https://doi.org/10.1136/pgmj.2005.040477
Nair, B. R., Alexander, H. G., McGrath, B. P., Parvathy, M. S., Kilsby, E. C., Wenzel, J., Frank, I. B., Pachev, G. S., & Page, G. G. (2008). The mini clinical evaluation exercise (mini-CEX) for assessing clinical performance of international medical graduates. Medical Journal of Australia, 189(3), 159-161.
Norcini, J. J., Blank, L. L., Duffy, F. D., & Fortna, G. S. (2003). The mini-CEX: A method for assessing clinical skills. Annals Internal Medicine, 138(6), 476-481.
Ong, T. H., Ong, H. K., Chan, A., Samarasekera, D. D., van der Vleuten, C. (2023). Micro CEX vs Mini CEX: Less can be more [Dataset]. Figshare. https://doi.org/https://doi.org/10.6084/m9.Fig share.21862068.v3
Paradis, E., & Sutkin, G. (2017). Beyond a good story: From Hawthorne Effect to reactivity in health professions education research. Medical Education, 51(1), 31-39. https://doi.org/10.1111/medu.13122
Pelgrim, E. A. M., Kramer, A. W. M., & Van der Vleuten, P. M. (2012). Quality of written narrative feedback and reflection in a modified mini-Clinical Evaluation Exercise: An observational study. BMC Medical Education, 12(1), 97. https://doi.org/10.1186/1472-6920-12-97
Regehr, G., MacRae, H., Reznick, R. K., & Szalay, D. (1998). Comparing the psychometric properties of checklists and global rating scales for assessing performance on an OSCE-format examination. Academic Medicine, 73(9), 993-997.
Sabey, A., & Harris, M. (2011). Training in hospitals: What do GP specialist trainees think of workplace-based assessments? Education for Primary Care, 22(2), 90-99.
Tavares, W., Ginsburg, S., & Eva, K. W. (2016). Selecting and simplifying: Rater performance and behavior when considering multiple competencies. Teaching and Learning in Medicine, 28(1), 41-51. https://doi.org/10.1080/10401334.2015.1107489
van der Vleuten, C. P., & Schuwirth, L. W. (2005). Assessing professional competence: From methods to programmes. Medical Education, 39(3), 309-317. https://doi.org/10.1111/j.1365-2929. 2005.02094.x
Van Tartwijk, J., & Driessen, E. W. (2009). Portfolios for assessment and learning: AMEE Guide no. 45. Medical Teacher, 31(9), 790-801. https://doi.org/10.1080/01421590903139201
Walzak, A., Bacchus, M., Schaefer, J. P., Zarnke, K., Glow, J., Brass, C., McLaughlin, K., & Ma, I. W. (2015). Diagnosing technical competence in six bedside procedures: Comparing checklists and a global rating scale in the assessment of resident performance. Academic Medicine, 90(8), 1100-1108. https://doi.org/10.1097/acm.0000000000000704
Weller, J. M., Misur, M., Nicolson, S., Morris, J., Ure, S., Crossley, J., & Jolly, B. (2014). Can I leave the theatre? A key to more reliable workplace-based assessment. British Journal of Anaesthesia, 112(6), 1083-1091. https://doi.org/10.1093/bja/aeu052
Weston, P. S. J., & Smith, C. A. (2014). The use of mini-CEX in UK foundation training six years following its introduction: Lessons still to be learned and the benefit of formal teaching regarding its utility. Medical Teacher, 36(2), 155-163. https://doi.org/10.3109/0142159X.2013.836267
Yanting, S. L., Sinnathamby, A., Wang, D., Heng, M. T. M., Hao, J. L. W., Lee, S. S., Yeo, S. P., & Samarasekera, D. D. (2016). Conceptualizing workplace-based assessment in Singapore: Undergraduate mini-Clinical Evaluation Exercise experiences of students and teachers. Tzu-Chi Medical Journal, 28(3), 113-120. https://doi.org/10.1016/j.tcmj.2016.06.001
*Ong Thun How
Academia, 20 College Road,
Singapore 168609
97100638
Email: ong.thun.how@singhealth.com.sg
Published online: 2 January, TAPS 2024, 9(1), 1-2
https://doi.org/10.29060/TAPS.2024-9-1/EV9N1
The practice of medicine and provision of healthcare is evolving rapidly, driven not just by advancements in new treatment modalities but also by the integration of modern technologies in providing precision care to our patients. It is important to understand and embrace, where appropriate, innovative technologies to respond effectively to the evolving needs of a modern society. What will be seen in this transformative wave is how Artificial Intelligence (AI) has the potential to revolutionise various sectors in medicine and healthcare (Yu et al., 2018).
Focusing on health professions education, AI emerges as a pivotal force in training the future healthcare practitioners and preparing them for the multifaceted challenges of the modern medical landscape (Paranjape et al., 2019). There are 3 distinct uses of AI in education which was reported by Baker et al. (2019): Learner-oriented AI, Instructor-oriented AI and Institution-oriented AI. Let’s focus on some of these areas:
A. Enriched Learning Experiences
One of the most significant advantages of integrating AI into health professions education is the enhancement of learning experiences. AI-powered platforms can provide personalised, adaptive learning modules tailored to individual students’ needs and learning paces (Kong et al., 2021). This personalisation not only accelerates the learning process but also ensures that students grasp complex concepts thoroughly, laying a robust foundation for their future careers. Furthermore, AI provides the opportunity for the students as well as for the trainers to use and adapt the best materials from multiple sources. It also enhances their networking through AI search capabilities and the ability to link up with other experts in the field or learning communities (Luke et al., 2021).
B. Simulation and Practical Training
AI-driven simulations are revolutionising practical training in healthcare education. Medical students can now practice patient safety, surgical procedures, diagnose illnesses, and interact with virtual patients in a risk-free environment. These simulations not only refine their technical skills but also improve their decision-making and inter-professional teamwork abilities. By repeatedly engaging in realistic scenarios, students can hone their expertise, fostering confidence and competence before they enter real-world clinical settings, a critical step to ensure patient safety and ethical practice of medicine.
C. Data-Driven Insights
AI’s ability to analyse large amounts of data quickly and efficiently provide an excellent platform to improve systems and processes (American Medical Association [AMA], 2016). In the context of health professions education, this capability translates into valuable insights. Educational institutions can collect data on students’ performance, identify areas where they struggle, and provide targeted interventions. Educators can adapt their teaching methods based on this data, ensuring that their teaching-learning approaches are appropriate and leading to good outcomes. Moreover, AI can predict trends in learning, enabling institutions to proactively address challenges and optimise their curricula. Funding and resource allocations can also be done where it is needed most or areas of future needs to build capacity and relevance of programs.
D. Fostering Research and Innovation
AI-powered tools are accelerating Scholarship of Teaching and Learning in the areas of research and innovation. AI algorithms help to analyse large amounts of data quickly and identify patterns that researchers could potentially miss. This could help us better understand the complex datasets, find relationships between variables faster, and draw appropriate conclusions and recommendations. AI has also reduced the time required to conduct literature review by analysing large amounts of scientific articles, identifying relevant research, and summarising the content in seconds.
E. Addressing Global Health Disparities
Focusing on medical and health professions education, we believe that this is another area AI could assist and enhance the training of healthcare practitioners in resource poor settings. Unbundling of curricula and connecting with the best training materials as well as experts are key advantages of AI capable training environments could support the resource poor settings.
Another area that AI driven knowledge and skills sharing could be addressing the present shortage of skilled healthcare professionals, leading to significant disparities in healthcare access. AI-based education has the potential to bridge this gap. Online platforms and mobile applications powered by AI can deliver high-quality continuous professional development to remote and underserved communities, reaching out to healthcare professionals irrespective of their geographical location. With this unbundling, the present set programs or training, we believe has the potential to significantly reduce global healthcare disparities.
F. Ethical Considerations and Collaboration
While the potential of AI in health professions education is immense, it is crucial to navigate ethical challenges. In the process of developing AI capable environments, we must ensure that the systems are transparent, unbiased and fair. However, we do not see in any medical school or a healthcare training site developing or having conversations on the use of guidelines/protocols on ethical use of AI in health professional education. Educators, policymakers, and technology developers must collaborate to establish ethical guidelines that ensure the responsible use of AI. This collaboration should prioritise transparency, fairness, and equity, safeguarding the integrity of healthcare education and the welfare of future patients (Chan & Zary, 2019).
Artificial Intelligence provides huge benefits to health professions education in many ways. By embracing AI-powered tools and methodologies, educational institutions can produce a generation of healthcare professionals who are not only adept at leveraging advanced technologies, but also compassionate and skilled in delivering patient-centred care. As we advance and evolve, it is clear that we need to channel our efforts into the investment of AI capabilities, aiming to elevate the learning experiences of our students and residents, propel educational scholarship and research forward, and foster enhanced collaboration. This strategic commitment is essential to maximising the potential advantages of this technology, with a primary objective of ultimately enhancing the health and well-being of patients within both local and global communities. The achievement of success in this pursuit necessitates a united front, where educators, institutions, and policymakers collaborate seamlessly. Only through such concerted efforts can we guarantee that AI not only benefits current learners but also ensures future positive impact on the well-being of the patients they will serve.
Dujeepa D. Samarasekera, Shuh Shing Lee & Han Ting Jillian Yeo
Centre for Medical Education (CenMED), NUS Yong Loo Lin School of Medicine,
National University Health System, Singapore
American Medical Association. (2016). Digital Health Study Physicians’ motivations and requirements for adopting digital clinical tools. https://www.ama-assn.org/practice-management/digital
Baker, T., Smith, L., & Anissa, N. (2019). Educ-AI-tion Rebooted? Exploring the future of artificial intelligence in schools and colleges. Nesta. https://www.nesta.org.uk/report/education-rebooted/
Chan, K. S., & Zary, N. (2019). Applications and challenges of implementing artificial intelligence in medical education: Integrative review. JMIR Medical Education, 5(1), Article e13930. https://doi.org/10.2196/13930
Luke, N., Taneja, R., Ban, K., Samarasekera, D., & Yap, C. T. (2021). Large language models (ChatGPT) in medical education: Embrace or abjure? The Asia Pacific Scholar, 8(4), 50-52. https://doi.org/10.29060/TAPS.2023-8-4/PV3007
Paranjape, K., Schinkel, M., Nannan Panday, R., Car, J., & Nanayakkara, P. (2019). Introducing artificial intelligence training in medical education. JMIR Medical Education, 5(2), Article e16048. https://doi.org/10.2196/16048
Yu, K. H., Beam, A. L., & Kohane, I. S. (2018). Artificial intelligence in healthcare. Nature Biomedical Engineering, 2(10), 719-731. https://doi.org/10.1038/s41551-018-0305-z
Submitted: 11 August 2023
Accepted: 23 August 2023
Published online: 2 January, TAPS 2024, 9(1), 64-65
https://doi.org/10.29060/TAPS.2024-9-1/LE3109
Mildred Lopez
Tecnologico de Monterrey, Escuela de Medicina y Ciencias de la Salud, Mexico
Artificial intelligence (AI) in education has raised several ethical questions regarding academic integrity, privacy, and bias in language algorithms (Master, 2023). These concerns have yielded to distrust to the point that several institutions banned chatbots at Campus locations. Still, the discussion should not be about whether we should use them but how fast we can leverage the data-crunching possibilities to address the biggest challenges of medical education. To do so, educators have the task of transforming the generic use of generative AI to a specific task, such as designing an educational case, a grading rubric, or an exam. However, the quality of the designs depends heavily on the clarity of the educational intent and the technological savviness of the user to provide clear instructions for the algorithm to process.
Early experimentation of educators with generative AI, such as ChatGPT, could be an opportunity to refine the technological savviness and the specificity of prompts we supply to make the algorithm produce more effectively. Recently, Rospigliosi (2023) discussed that the challenge is to define what to ask of ChatGPT, as the quality of the prompt makes the quality of the response. In this ideation and creation stage, where early adopters are piloting small-scale interventions and experimenting with the tool’s limits, educators must work collaboratively across continents and among fields to define guidelines and identify effective strategies for large-scale implementations. While doing so, we speed up the developing process of learning resources in medical education and aspire to have more updated content in the curriculum.
Nevertheless, once a recipe to generate a learning resource has been implemented, the quality of the produced content should be assessed by specialists in the field. The definition of that quality level is also a field for discussion but should be closely aligned with the educational intent. In the future, not so far away, we could even have an AI tool to assess the quality of the content that the generative AI created. Then the question remains: What AI prompt would be the best to do what I, as an educator, need to work on?
Notes on Contributors
ML wrote the manuscript and edited it.
Funding
No funding was received for writing this paper.
Declaration of Interest
The author declares that there is no conflict of interest to disclose.
References
Masters, K. (2023). Ethical use of Artificial Intelligence in Health Professions Education: AMEE Guide No. 158, Medical Teacher, 45(6), 574-584. https://doi.org/10.1080/0142159X.2023.2186203
Rospigliosi, P. (2023). Artificial intelligence in teaching and learning: What questions should we ask of ChatGPT? Interactive Learning Environments, 31(1), 1-3. https://doi.org/10.1080/10448 20.2023.2180191
*Mildred Lopez
Ave. Eugenio Garza Sada 2501 Sur. Col Tecnologico,
64710
Monterrey, Mexico
Email: mildredlopez@tec.mx
Submitted: 25 May 2023
Accepted: 27 July 2023
Published online: 2 January, TAPS 2024, 9(1), 61-63
https://doi.org/10.29060/TAPS.2024-9-1/CS3061
Veranja Liyanapathirana
Department of Microbiology, Faculty of Medicine, University of Peradeniya, Sri Lanka
I. INTRODUCTION
Antimicrobial resistance has been considered a “silent” global pandemic of magnitudes similar to climate change. However, just as climate change, awareness and understanding of the public on this needs to be increased. Recent work from Sri Lanka indicates the same (Gunasekera et al., 2022). World Health Organisation (WHO) also recommends that awareness should be increased among those involved in antibiotic prescription as well as consumers and that this should be made part of the core curriculum in professional training (World Health Organisation, 2023). Those studying in health-science related streams and other biology related streams tend to take knowledge on concepts like “microorganisms”, “infectious diseases” and “antibiotics” as granted. As they are taught these concepts, or they revise what they learnt in school once again in the university, they assume that the others may also have an acceptable level of understanding on these key concepts. This leads to a communication gap between the two groups of people, the ones who have formal education on concepts like “microorganisms”, “infectious diseases” and “antibiotics” and the ones who do not have such education. Therefore, we find that health education materials are not targeted to the level of simplicity that is required by the general public.
The target audience for the assignment in this particular course were from a general biology background, with no training in health-sciences in the university. For these students, a course on “Bacteria of Medical Importance” was commenced in the first semester of the third year. This included introductory lectures on antibiotics, antibiotic sensitivity testing and antimicrobial resistance. The course was conducted by the staff of the Department of Microbiology, Faculty of Medicine, University of Peradeniya, Sri Lanka and the given assignment was designed and conducted by the author.
This activity was planned as an assignment with a reflective component, so that the undergraduates who follow the course would get a first-hand experience in the extent of ignorance that is there regarding antibiotics and their use in the community.
II. METHODS
The assignment being described was developed aiming at increasing the awareness among the participants on the ground reality about the public perceptions on antibiotic use and resistance. At the same time, the activity also aimed to develop reflective practices among the students.
The assignment included the following simple instructions as shown in Table 1. Students were given a period of two weeks to complete the task and upload the content to the learner management system. Students were requested to inform the interviewee they had chosen that the assignment was part of their course work and were requested to get verbal consent for participation.
Once the assignments were submitted, evaluation was conducted and students were given feedback on their reflective write up. For this paper, their reflective write ups were coded and thematically analysed.
|
Talk to a family member/friend who has had no formal teaching on microbiology or health sciences and ask the following questions in English or in the language you converse in. Document the answers you get, translate to English. The last two questions are for you to answer.
• Age of the person spoken to • Highest educational qualification of the person you spoke to • Occupation of the person you spoke to (if a university student, state the course) 1.What is an antibiotic (open ended question)? 2.When did you last take an antibiotic?
3. How did you get that antibiotic?
4. What was the antibiotic you took?
5. Name two other antibiotics you know of.
6. Have you ever taken antibiotics when you have had a cold?
7. What group of micro-organisms cause common cold?
8. 8.1 Do you think it is correct to take antibiotics for common cold?
8.2 Why? (Open ended question): ……………………….. •State one more question you would have liked to ask the participant (just state this without asking your informant): ……………………………. •Your reflection on the answers you got in relation to combatting antimicrobial resistance (500 words): …………………………………………….. |
Table 1: The assignment
III. RESULTS
There were 11 students who took the said course and all of them submitted the assignment on time. The common themes and the narrative that emerged from the analysis of the reflections given by the participants follows.
The subjects interviewed by students were from varying backgrounds. And while some knew that viruses cause common cold other did not know or thought it was caused by bacteria. Nine of the eleven participants interviewed had stated that taking antibiotics for common cold was correct. The reasons given by the subjects interviewed were that doctors prescribe; therefore, antibiotics are indicated in common cold, antibiotics are more potent than pain killers, they give faster cure and boost immunity. Students reflected that the knowledge on antibiotics was poor among the subjects interviewed. Students identified that there is a need for education on this among the general public. There was a theme that emerged which queried the reason for medical officers continue to prescribe antibiotics for common cold as they have been equipped for the necessary knowledge.
IV. DISCUSSION
Reflection is a learned skill. This is not formally taught in many undergraduate courses in Sri Lanka or during secondary education. Therefore, some of the students in the course had written accounts on what is correct and incorrect in relation to antibiotic use or accounts on antibiotic resistance instead of writing a reflection as instructed. Some students did write reflections, still their reflections were mostly not in relation to the possible implications on combatting antimicrobial resistance, but on the answers given in general. Students were given feedback on their reflections.
However, from the reflections provided, a narrative could be derived as stated in the results section, which shows that collectively, their reflections do generate a narrative that is useful. Therefore, from the next batch onwards, we plan to get the students to construct a narrative from their collective reflections.
This was the first time this assignment was used. We chose the questions used as in the local context, antibiotic misuse for upper respiratory tract infections is the commonest reason for antibiotic prescription as well as irrational use (Tillekeratne et al., 2017). But, globally too, upper respiratory tract infections are one of the commonest reasons for antibiotic prescriptions.
We plan to modify this assignment slightly and use it on other undergraduates or postgraduates who are following courses on antibiotics and antimicrobial resistance. As pre-activity exercise, we would like to conduct a briefing session on reflective writing, before the assignment is given to the students.
V. CONCLUSION
The given assignment can be modified and used to increase awareness on the ground realities about the understanding on antibiotics among students who are being educated on antibiotics and antibiotic resistance.
Notes on Contributors
The author conceptualised, conducted and evaluated the assignment and drafted the paper.
Acknowledgement
The author would like to acknowledge all the students of the class and the participants they interviewed.
Funding
No funding was received for the activity.
Declaration of Interest
The author does not have any conflict of interest to declare.
References
Gunasekera, Y. D., Kinnison, T., Kottawatta, S. A., Silva-Fletcher, A., & Kalupahana, R. S. (2022). Misconceptions of antibiotics as a potential explanation for their misuse. A survey of the general public in a rural and urban community in Sri Lanka. Antibiotics, 11(4), 454. https://doi.org/10.3390/antibiotics11040454
Tillekeratne, L. G., Bodinayake, C. K., Dabrera, T., Nagahawatte, A., Arachchi, W. K., Sooriyaarachchi, A., Stewart, K., Watt, M., Østbye, T., & Woods, C. W. (2017). Antibiotic overuse for acute respiratory tract infections in Sri Lanka: A qualitative study of outpatients and their physicians. BMC Family Practice, 18(1), Article 37. https://doi.org/10.1186/s12875-017-0619-z
World Health Organisation. (2023, June) Raising awareness and educating on antimicrobial resistance. https://www.who.int/activities/raising-awareness-and-educating-on-antimicrobial-resistance
*Veranja Liyanapathirana
Department of Microbiology,
Faculty of Medicine,
University of Peradeniya,
Galaha Rd, Peradeniya 20400,
Sri Lanka
+94777060887
Email: veranja.liyanapathirana@med.pdn.ac.lk
Submitted: 12 June 2023
Accepted: 2 August 2023
Published online: 2 January, TAPS 2024, 9(1), 58-60
https://doi.org/10.29060/TAPS.2024-9-1/PV3064
Rintaro Imafuku, Chihiro Kwakami, Kaho Hayakawa & Takuya Saiki
Medical Education Development Center, Gifu University, Japan
I. GLOBALISATION IN EAST ASIA
Globalisation, a complex and multifaceted phenomenon, encompasses not merely an increasing people’s mobility and economical trades, but sometimes, their political and ideological struggles, and cultural identity formation issues, too. While North American and European countries have had a long history of accepting a large number of immigrants, while Asia experienced 74% growth of hosting international migrants from 2000 to 2020, which was most remarkable (McAuliffe & Triandafyllidou, 2021). For example, Japan’s proportion of immigrant population increased from 1.3% in 2000 to 2.2% in 2021, with Chinese migrants constituting the largest group, followed by Vietnamese, Koreans, Filipinos, and Brazilians. Similarly, in 2021, immigrants accounted for 3.4% of Korea’s total population in 2021, compared to 0.5% in 2000. These immigrants came from China, Vietnam, Thailand, Uzbekistan and other countries (McAuliffe & Triandafyllidou, 2021).
These changes in culture and population dynamics have significantly impacted on people’s health and healthcare in East Asia. One of the most challenging issues in such globalised Asian societies is managing intercultural communication between health professionals and migrant patients. Given this context, as languages become a key issue, health professionals are expected to accommodate patients’ communication needs. Moreover, while responding to the rapid internationalisation, health professionals in Asia need to embrace the belief that individuals are members of multiple, diverse, local and non-local networks, thus promoting global citizenship. In fact, the question is: How should Asian health professionals address the intercultural communication situations in healthcare?
II. COMMUNICATION STRATEGIES IN INTERCULTURAL SETTINGS
Many previous linguistic studies have discussed that in Asia, English serves as the lingua franca – a common language adopted among people who do not share a native language. Singaporeans, for instance, use English as an intra-national communication medium, while in East Asian countries, somewhat different contexts would have existed, particularly in relatively ‘monolingual’ speech communities. Given that, most immigrants in East Asia are not native English speakers, in many cases where English does not function as their medium of communication for them. In other words, English is not the sole solution for intercultural communication issues, particularly in East Asian countries. However, some health professionals in Japan viewed English as the panacea for intercultural communication issues, regardless of the patients’ native language, which highlighted the need to consider another communication management strategy in an intercultural setting (Imafuku et al., 2022).
A host country’s plain language, which is defined as clear and concise language accommodation, can be an effective medium of communication (Imafuku et al., 2022). For example, a national survey in Japan demonstrated that many immigrants could understand simple Japanese in daily life, even though their proficiency was limited. Assuming that the speakers tailor their communication to the interlocutors’ language proficiency levels and cultural backgrounds, plain language in spoken communication can be achieved by using short and simple sentences, active voice which emphasises the doer of an action, and personal pronouns which makes it easier for the listeners to picture themselves in the message. Furthermore, speakers must avoid ambiguous expressions and fillers that fill pauses with words, such as “um”, “ah”, “er” and so forth. Visual aids, such as charts, pictures and writing down messages, are also helpful for listeners to process the information in conversations.
Language translation devices, application software, and artificial intelligence (AI) technologies can be useful resources for managing intercultural communication in healthcare. For example, ChatGPT has the potential to assist and enhance health communication in hospitals. In particular, as these AI tools rely on patterns in huge amounts of existing text data, they excel at automating routine tasks, generating document summaries and translating simple texts of factual information. However, the users also need to be aware of the potential drawbacks of these tools, which may lack the ability to interpret patients’ communication signals by patients, such as tone, prosody, and non-verbal cues, potentially resulting in misunderstandings and miscommunications, especially with immigrant patients. This absence of human interaction, including the consideration of patients’ thoughts, emotions, patience, and empathy, emphasises the need for health professionals to critically evaluate and appraise the use of these AI tools for use in intercultural communication (Santandreu-Calonge et al., 2023).
In addition to the linguistic and sociolinguistic aspects, different cultural values and religious beliefs may create barriers in intercultural communication between providers and patients (Zhao, 2023). For example, patients may have diverse perspectives on confidentiality, gender, trust in health professionals and privacy concerns, which greatly impact on interactions in healthcare. Zhao (2023) suggests that patients with certain cultural backgrounds view the family as a collective unit, and would trade off their privacy for family support. However, sharing patients’ information with their family members can pose an issue of confidentiality issues for health professionals. In this case, the patients’ beliefs about family support and ties are closely intertwined with confidentiality in healthcare. In other words, effective intercultural communications will be enhanced by health professionals gaining a better socio-cultural understanding of immigrant patients.
III. MOVING FORWARD: EDUCATIONAL DEVELOPMENT
Educational development is key to effectively addressing the challenges faced by health professionals in East Asia’s globalisation wave. English has been taught as an ‘international academic language’ in Asian medical schools and serves as the medium of instruction in certain countries and Asian institutions. In other words, English can be a means of facilitating intercultural communication in Asian healthcare, particularly for foreign visitors from Western countries.
Additionally, for more successful language accommodation, plain language should be systematically taught in health communication courses in East Asia’s medical education. A growing body of evidence from Western countries indicates that incorporating plain language training into medical education has positive implications for oral and written communication skills. By using the host country’s plain language for practical training of intercultural communication in the curriculum, medical students in East Asia should be given more opportunities to interact with migrant citizens with different cultural backgrounds.
In addition to the effective use of plain language as an option of communication management strategies, this opportunity will also broaden the students’ worldviews and cultural understanding in the current globalised societies. Specifically, our institution, Gifu University, has incorporated learning opportunities through interactions with migrant citizens from Vietnam, Philippines and Brazil into first year medical education. This can serve as a springboard to cultivate the medical students’ global citizenship by learning diverse cultural values through conversations with the migrants in Japan.
Translation software and AI technologies are increasingly being utilised in the intercultural communication settings. Although these devices and tools are helpful, they can also be a double-edged sword for healthcare professionals as communicators. Health professionals and educators should recognise that human interaction is the foundation of communication. Relying excessively on such tools without critical evaluation may cause serious communication problems with migrant patients and their family members. In Japan, information technology has been newly set as a learning objective in the 2022 revision of the Model Core Curriculum for Medical Education (Medical Education Model Core Curriculum Expert Research Committee, 2022). Further educational development is necessary to train health professionals to fully understand the principles of the information science and technology, and effectively apply them in clinical practice. Specifically, in the field of health communication education, the educators must address the challenges posed by rapid globalisation by developing programs that enable learners to understand the advantages and disadvantages of AI-mediated communications and effectively utilise the information technologies in the intercultural settings.
Finally, from the perspective of medical education research, more internationally published research on intercultural health communication from Asian countries is necessary. The rich descriptions and analysis of the interactions between healthcare providers and migrant patients in the current globalised Asian countries can offer different perspectives on medical education for an international readership. Additionally, for further educational development, it would be worthwhile to explore AI-mediated communication in intercultural situations, as this is a relatively new research area.
Notes on Contributors
Rintaro Imafuku contributed to this manuscript’s conceptualisation, wrote its first draft, and revised its subsequent draft. Chihiro Kawakami, Kaho Hayakawa and Takuya Saiki contributed to the conceptualisation and critically revised the first draft. All the authors discussed and contributed to the final manuscript.
Funding
This study was supported by the JSPS KAKENHI [Grant number: 20K10374].
Declaration of Interest
The authors declare no competing interests.
References
Imafuku, R., Nagatani, Y., & Shoji, M. (2022). Communication management processes of dentists providing healthcare for migrants with limited Japanese proficiency. International Journal of Environmental Research and Public Health, 19(22), Article 22. https://doi.org/10.3390/ijerph192214672
McAuliffe, M., & Triandafyllidou, A. (2021). World migration report 2022. International Organization for Migration (IOM). https://publications.iom.int/books/world-migration-report-2022
Medical Education Model Core Curriculum Expert Research Committee. (2022). Model core curriculum for medical education in Japan 2022. Ministry of Education, Culture, Sports, Science and Technology. https://www.mext.go.jp/content/20230315-mxtigaku -000026049_00003.pdf
Santandreu-Calonge, D., Medina-Aguerrebere, P., Hultberg, P., & Shah, M.A. (2023). Can ChatGPT improve communication in hospitals? Profesional de la información, 32(2), Article e320219. https://doi.org/10.3145/epi.2023.mar.19
Zhao, X. (2023). Challenges and barriers in intercultural communication between patients with immigration backgrounds and health professionals: A systematic literature review. Health Communication, 38(4), 824–833. https://doi.org/10.1080/10410236.2021.1980188
*Rintaro Imafuku
1-1 Yanagido Gifu, Gifu, Japan
+81-58-230-6469
Email: imafuku.rintaro.f9@f.gifu-u.ac.jp
Submitted: 20 April 2023
Accepted: 23 August 2023
Published online: 2 January, TAPS 2024, 9(1), 54-57
https://doi.org/10.29060/TAPS.2024-9-1/SC3048
Atul Kumar1, Amol Gawande1, Meghana Bhilare2, Vishal Wadajkar2, Indrajit Ghoshal3 & Shirish Raibagkar4
1Dr.D.Y. Patil B-School, Pune, India; 2Dr.D.Y. Patil Institute of Management and Research, Pune, India; 3Faculty of Computer Science and Engineering, Poornima University, Jaipur, India; 4Savitribai Phule Pune University, Pune, India
Abstract
Introduction: The purpose of this study is to carry out a comparative analysis of the job satisfaction of nurses working in India based on the different types of the hospital they are working with. The study tests the null hypothesis that the job satisfaction of nurses from India across different types of hospitals is the same.
Methods: Four hundred nurses divided into 100 each for four popular types of hospitals – (1) Educational; (2) Government; (3) Charitable Trust; and (4) Private, from all over India were surveyed. Two ANOVA tests were performed. The first one was performed, taking overall job satisfaction as the dependent variable. The second ANOVA was performed by taking the monetary and compensation factors, work environment and management support, and job-related factors as the dependent variables.
Results: The overall mean of job satisfaction was -0.73 (SD 0.60). Overall, 65 percent of the variability of the dependent variable, job satisfaction, is explained by the type of hospital and is statistically significant (p<0.0001).
Conclusion: Monetary and compensation factors, work environment and management support, and job-related factors impact nurses’ job satisfaction. These factors vary with the type of hospital, and hence it can be concluded that due to variation in these factors depending on the type of hospital, the job satisfaction of nurses varies. Implications of our study are for the educational, government, and charitable trust hospitals to improve their work culture, management, and work environment so that nurses will have higher job satisfaction.
Keywords: Nurses, Job Satisfaction, India, Hospitals, Government, Private, Charitable Trust, Educational
I. INTRODUCTION
India’s ratio of nurses per 1000 population is only 1.96 as against the WHO norm of 3 per 1000 population. Another 4.3 million more nurses are required by India by the year 2024 to meet the World Health Organization (WHO) standard of 3 nurses per 1000 population (Business Standard, 2021). Job satisfaction of nurses assumes significance given the huge gap between its current ratio of nurses per 1000 and the WHO norm. But studies investigating linkages between types of hospitals (legal structure of the hospital) and their impact on the job satisfaction of nurses are relatively low. Different types of hospitals can be found in India – Educational, Government, Charitable Trust, Private, Military, Missionary, Railway, and a few more. A sizable amount of literature is available which suggests that factors like organisational culture matters in the job satisfaction of nurses (Rahnavard et al., 2018). But there are few studies correlating these factors with the type of hospital. The association between the factors and the type of hospital remains unexplored. This research attempts to provide empirical evidence supporting the association of the factors influencing job satisfaction and the type of hospitals. The study expects to generate valuable insights for nurses and their employers of different types. It is based on a survey of 100 nurses each from the four most popular types of hospitals – (1) Educational; (2) Government; (3) Charitable Trust; and (4) Private owned.
II. METHODS
The size of the Indian population of nurses is more than 3 million. At a 95 percent confidence interval, the sample size for this population works out to 384, which we rounded off to 400, giving an equal representation of 100 nurses each from the four types of hospitals – educational, government, charitable trust, and private owned. The task of collecting 100 responses for each type of hospital was distributed among the authors. Convenience and purposive sampling method were used. However, to make the study group more inclusive, the sample included nurses from all regions and parts of India – urban, semi-urban, and rural. The questionnaire was administered through Google Forms. The survey was conducted in March 2023. Express written consent for participation was obtained from each respondent.
The study got ethics committee approval number DYP202301, from the Dr.D Y Patil (Deemed to be) University, Pune, India, and Dr.Ajeenkya D Y Patil University, Pune, India.
A scale developed by Chang et al. (2017) to measure the job satisfaction of healthcare workers was largely referred to while designing our scale, which was duly tested for validity and reliability (Cronbach Alpha 0.96). We spoke to a few senior nurses who advised us to consider monetary and compensation factors while assessing the job satisfaction of nurses. Monetary benefits are important for any working human in any part of the world. Studies on job satisfaction (conducted in developed, developing, and underdeveloped countries) include monetary benefits as a parameter. Based on our discussion with the senior nurses and the existing literature, we identified three main factors as determinants of job satisfaction for Indian nurses – monetary and compensation factors, work environment and management support, and job-related factors. monetary and compensation Factors included items like “The salary pay-scales are satisfactory”, “Benefits like provident fund, and gratuity are duly given”, and others. work environment and management support included items like “The management of this organization is supportive of me”, “The management makes changes based on my suggestions and feedback”, and others. job-related factors included items like “I receive the right amount of support and guidance from my direct supervisor”, “I am provided with all trainings necessary for me to perform my job”, and others.
III. RESULTS
Some of the distinctive features of the profile information include a relatively high concentration of respondents in the work experience groups of 10-15 years (158 respondents representing 40 percent of the sample), very low representation of postgraduate educational qualification (10 respondents representing 3 percent of the sample); very low representation of hospitals with a standing of <10 years (11 respondents representing 3 percent of the sample). All these 11 hospitals with a standing of <10 years were private hospitals. The data that support the findings of this study are openly available at https://www.openicpsr.org/ openicpsr/project/190042/version/V1/view (Bhilare, 2023).
A. Descriptive Statistics
Table 1 shows descriptive statistics of the sample.
|
Type |
Total |
Monetary |
Work Env. |
Job related |
||||
|
Mean |
SD |
Mean |
SD |
Mean |
SD |
Mean |
SD |
|
|
Educational |
-0.22 |
0.86 |
-0.21 |
0.87 |
-0.27 |
0.89 |
-0.19 |
0.90 |
|
Govt. |
-1.55 |
0.40 |
-1.53 |
0.39 |
-1.60 |
0.47 |
-1.54 |
0.44 |
|
Trust |
-1.57 |
0.46 |
-1.51 |
0.47 |
-1.65 |
0.50 |
-1.53 |
0.50 |
|
Private |
0.42 |
0.68 |
0.39 |
0.74 |
0.39 |
0.68 |
0.48 |
0.71 |
|
Total |
-0.73 |
0.60 |
-0.71 |
1.05 |
-0.78 |
1.09 |
-0.70 |
1.09 |
Table 1. Descriptive statistics of the sample
The overall job satisfaction mean scores of the hospitals were -0.22 (0.86) for educational hospitals, -1.55 (0.40) for Government hospitals, -1.57 (0.46) for Trust hospitals, and 0.42 (0.68) for private hospitals. For all the 400 respondents taken together, the mean job satisfaction score was -0.73 (SD 0.60).
In the case of educational hospitals, all three factors of job satisfaction were negative – monetary and compensation factors (M= -0.21, SD 0.87), work environment and management support (M= -0.27, SD 0.89), and Job-related factors (M= -0.19, SD 0.90). The same was the case with government hospitals which reported negative job satisfaction for all three factors – monetary and compensation factors (M= -1.53, SD 0.39), work environment and management support (M= -1.60, SD 0.47), and Job-related factors (M= -1.54, SD 0.44).
Further, charitable trust hospitals too reported negative job satisfaction for all three factors – monetary and compensation factors (M= -1.51, SD 0.47), work environment and management support (M= -1.65, SD 0.50), and job-related factors (M= -1.53, SD 0.50). However, private hospitals were the only type of hospitals that reported positive job satisfaction for all three factors – monetary and compensation factors (M= 0.39, SD 0.74), Work environment and management support (M= 0.39, SD 0.68), and job-related factors (M= 0.48, SD 0.71).
B. Testing of the Hypotheses
Two ANOVA tests were performed. The first one was performed, taking overall job satisfaction as the dependent variable (R2 0.65, p<0.0001). The second ANOVA was performed by taking the monetary and compensation factors (R2 0.62, p<0.0001), work environment and management support (R2 0.64, p<0.0001), and job-related factors (R2 0.64, p<0.0001) as the dependent variables.
IV. DISCUSSION
The overall job satisfaction score of the entire sample size of 400 respondents is -0.73 (SD 0.60), which is close to -1, indicating somewhat dissatisfied. Thus, on an overall basis, Indian nurses have reported job dissatisfaction. An important reason for this is the mismatch between the guidelines of the Nursing Council about the working conditions and the actual working conditions at the various hospitals. The analysis shows that for all the three factors, namely, the Monetary and compensation factors, the work environment and management support factors, and job-related factors the scores are range-bound. This indicates a close relationship between these three factors.
However, when we look at the analysis by the type of hospitals, major variations are seen. Three out of the four types: educational hospitals, government hospitals, and charitable trust hospitals, show negative job satisfaction, whereas only one type, the private owned hospitals, show positive job satisfaction. This is because private hospitals offer a much better and more professional work culture leading to higher job satisfaction among the nurses (Srimulyani & Hermanto, 2022). Interestingly, there is not much difference between the job satisfaction scores of government hospitals and charitable trust hospitals. The standard deviations associated with these two high negative scores are also similar. Scores of government hospitals and charitable trust hospitals can be taken as lying between somewhat dissatisfied and strongly dissatisfied ratings, pointing out a big gap between the prescribed norms of working conditions and the actual working conditions. The score of -0.22 indicates relatively much lesser job dissatisfaction in the case of educational hospitals (as compared to government and charitable trusts). It indicates that the control over educational hospitals is better as compared to the other two types of hospitals. The positive score of 0.42 in the case of private hospitals lies between neutral and somewhat satisfactory pointing a positive and professional work culture.
An important observation that emerges from the analysis is that for each of the four types of hospitals, there is little variation in the three factors of job satisfaction or dissatisfaction. This is because the three factors are closely related to each other.
V. CONCLUSION
Indian nurses, on an overall basis, are somewhat dissatisfied with their jobs. However, when we look into different types of hospitals, it is concluded that nurses working in private hospitals are moderately satisfied, those working in educational hospitals are moderately dissatisfied, and those working in government and charitable trust hospitals are highly dissatisfied. monetary and compensation factors, work environment and management support, and job-related factors impact nurses’ job satisfaction. These factors vary with the type of hospital, and hence it can be concluded that due to variation in these factors depending on the type of hospital, the job satisfaction of nurses varies. This impact is strong on an overall basis, as well as for the three factors (monetary and compensation Factors, work environment and management support, and job-related factors) separately. Interestingly there is a strong correlation among the three factors that we have used for measuring the job satisfaction of nurses. We conclude that positive and relatively higher job satisfaction among nurses working in private hospitals (Srimulyani & Hermanto, 2022) can be attributed to professional working culture, better monetary and compensation factors, better co-worker relationships, and other factors.
Notes on Contributors
Dr. Atul Kumar contributed to the conceptualization of the entire study. Dr. Amol Gawande contributed in designing methods for the study. Dr. Meghana Bhilare contributed to data collection. Dr. Vishal Wadajkar contributed to data analysis. Dr. lndrajit Ghoshal contributed in deducing findings and writing the discussion. Dr. S S Raibagkar contributed in writing the full paper including the conclusion. All the authors have read and approved the final manuscript.
Ethical Approval
The study got ethics committee approval number DYP202301, from the Institutional Review Boards of Dr.D Y Patil (Deemed to be) University, Pune, India, and Dr.Ajeenkya D Y Patil University, Pune, India.
Data Availability
All 400 responses were collated in a data set that has been deposited in a repository and can be accessed at https://www.openicpsr.org/openicpsr/project/190042/version/V1/view
Funding
No external funding was used for the study.
Declaration of Interest
We declare that there is no conflict of interest or competing interest of any sort with any individual or organization.
References
Bhilare, M. (2023). Data set Nurses Job Satisfaction (ICPSR 190042; Version V1) [Data set]. ICPSR. https://www.openicpsr.org/openicpsr/project/190042/version/V1/view
Business Standard. (2021, September 2). India in need of 4.3 mn more nurses by 2024 to meet who norms: Nurse org. Retrieved March 29, 2023, from https://www.business-standard.com/article/ current-affairs/india-in-need-of-4-3-mn-more-nurses-by-2024-to-meet-who-norms-nurse-org-121090201448_1.html
Chang, E., Cohen, J., Koethe, B., Smith, K., & Bir, A. (2017). Measuring job satisfaction among healthcare staff in the United States: a confirmatory factor analysis of the Satisfaction of Employees in Health Care (SEHC) survey. International Journal for Quality in Health Care, 29(2), 262-268. https://doi.org/10.1093/intqhc/mzx012
Rahnavard, F., Sadati, A. K., Hemmati, S., Ebrahimzade, N., Sarikhani, Y., Heydari, S. T., & Lankarani, K. B. (2018). The impact of environmental and demographic factors on nursing job satisfaction. Electronic Physician, 10(4), 6712. https://doi.org/10.19082%2F6712
Srimulyani, V. A., & Hermanto, Y. B. (2022). Organizational culture as a mediator of credible leadership influence on work engagement: empirical studies in private hospitals in East Java, Indonesia. Humanities and Social Sciences Communications, 9(1), Article 274. https://doi.org/10.1057/s41599-022-01289-z
*Shirish S Raibagkar
Savitribai Phule Pune University,
Ganeshkhind, Pune, India
Email: ssrssr696@gmail.com
Submitted: 5 March 2023
Accepted: 2 August 2023
Published online: 2 January, TAPS 2024, 9(1), 49-53
https://doi.org/10.29060/TAPS.2024-9-1/SC3016
Thamudi D Sundarapperuma1, Eranthi Weeratunga1, Prabhavi Wijesiriwardhana2, Eranga Silva2, Shanika Karunanayaka3, & Kithmini Yasarathne3
1Department of Nursing, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka; 2Department of Medical Laboratory Science, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka; 3Department of Pharmacy, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka
Abstract
Introduction: Several nations around the world had to close schools, colleges, universities, and other educational institutions as they were badly affected by the spread of COVID-19. The purpose of this study was to measure the effectiveness of online vs physical teaching during the COVID-19 pandemic, at the Faculty of Allied Health Sciences (FAHS), University of Ruhuna (UoR) Sri Lanka.
Method: A cross-sectional study was conducted among 200 undergraduates. The data were collected through displayed/approved results sheets of the students of selected batches in the Department of Nursing, Department of Pharmacy, and Medical Laboratory Science (MLS). Paired sample T-test was used to compare the results of undergraduates.
Results: The examination results of 47-54 undergraduates in nursing, 28 in pharmacy, and 22 in MLS were analysed. Significant differences in Psychiatry in Nursing and Nursing Clinical Attachment were identified in the Department of Nursing (p=0.001). In the Department of Pharmacy, only Pharmaceutical Chemistry I (p=0.012) reported a significant difference. The undergraduates of MLS who underwent online theory sessions had scored more in Microbiology and Immunology (p=0.022) and Basic Genetics and Molecular Biology (p=0.000) whereas in Research Methodology and Epidemiology, the undergraduates who participated in physical lectures had scored more marks (p=0.001).
Conclusion: Practical/interactive session-based course units and clinical appointments had a higher impact on the mode of teaching than many theoretical course units. The results might serve as a primer for the creation of an action plan to support the academics and clinical/practical components of undergraduates.
Keywords: Undergraduates, Online Teaching, Physical Teaching, Examination Results, COVID-19
I. INTRODUCTION
The provisional closure of educational institutions during the coronavirus disease-19 (COVID-19) pandemic has unexpectedly transformed the Sri Lankan education landscape in favour of distance learning or online learning. As a result of this, drastic changes in digital platforms and applications i.e., digital learning management systems became common among universities (Ariyananda et al., 2022). These universities used existing modular object-oriented dynamic learning environment-based learning management systems (Moodle) and the Lanka Education and Research Network (LEARN) was connected to university web servers and used for online education to mitigate the effects of disrupted learning (Hayashi et al., 2020).
Online teaching was a novel experience for university lecturers and undergraduates, and it was a huge challenge for both parties. In the beginning, both parties had to face several issues due to the unfamiliarity of these novel methods, the unavailability of basic facilities, and insufficient network coverage in Sri Lanka. Though it would be an effective alternative to conduct Zoom lectures again as physical lectures once the university reopened, we were unable to conduct lectures due to limited time during the semester. Therefore, the need emerged to identify a more effective mode to deliver lectures to undergraduates. This study aims to address the effectiveness of online vs. physical teaching during the COVID-19 pandemic, by analysing the examination results at the Faculty of Allied Health Sciences (FAHS), University of Ruhuna (UoR).
II. METHODS
A cross-sectional study was conducted to measure the effectiveness of online teaching vs. traditional/physical teaching and its impact on the performance of undergraduates. The data were collected through displayed/approved results sheets of the students of selected batches in the Department of Nursing, Pharmacy, MLS, FAHS, UoR. Nursing, though considered as a separate discipline from other para-medical disciplines in other countries, is considered under the Faculties of Allied Health Science in Sri Lanka. The examination results of two batches of undergraduates in a similar semester but who had learned in a different mode (in this group one batch has completely learned online while another batch has learned physically) were purposefully selected from each department. All lectures done via Zoom were recorded and distributed among students. Both groups underwent the same types of examination, mainly multiple-choice questions (MCQs) and short structured questions (SEQ) for theoretical knowledge. Practical and clinical skills were assessed using practical-based examination and patient-based clinical examination respectively. These examinations had been conducted in 2021 and 2022 and results were released in 2022. The analysis of results was conducted in January and February 2023.
Data from approximately 208 proper undergraduates (who sat for the first time) were analysed. The population was composed of nursing (n=108), pharmacy (n=56), and MLS (n=44) students. However, the results of repeat undergraduates were excluded. Six subjects were considered under the Department of Nursing. The number of candidates for the subjects was not equal. To analyse the effectiveness, a comparative analysis of the results of the end-semester examinations was performed by three departments separately. Mainly, in the Department of Nursing and Pharmacy the end semester examination results (two examinations/academic year) were evaluated while in the Department of MLS, the final term results were evaluated (three examinations /academic year).
Statistical Package for Social Science (SPSS) 26 software was used to analyse data. The mean and standard deviation (SD) values of the results sheets were analysed using descriptive statistics. After considering the distribution of the data set, paired sample T-test was used to compare the means of two batches. All results were regarded as statically significant at p < 0.05.
Ethical approval was obtained to analyse the published data from the Ethics Review Committee, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka (Ref. no. 200.01.2023). Consent was obtained from all relevant authorities before taking results from the notice board.
III. RESULTS
Two batches were selected in the nursing department and each batch consisted of 54 undergraduates. An equal number of candidates had not participated in every subject and therefore results were analysed based on students’ attendance for the different subjects. Under the nursing department, there were six subjects for students. Four subjects out of these six subjects consisted only of theory components. One subject had both theory and clinical components and the other subject had only clinical-based examination.
All the subjects had only a theory component in the selected semester in the pharmacy department. Under the department of MLS, all subjects consisted of theory and practical components.
|
Course units |
Component (Theory/ practical/clinical) |
Physical mode |
Virtual mode |
p-value |
||||
|
|
|
n |
Mean value |
+SD |
n |
Mean value |
+SD |
|
|
Nursing (2nd year 1st semester results) |
2016/2017 batch |
2017/2018 batch |
||||||
|
Pharmacology in Nursing |
T |
50 |
55.9 |
15.9 |
50 |
60.16 |
19.14 |
0.24 |
|
Medical Nursing 1 |
T |
50 |
54.9 |
7.8 |
50 |
68.09 |
15.6 |
0.053 |
|
Surgical Nursing 1 |
T |
47 |
57.83 |
8.47 |
47 |
57.61 |
10.08 |
0.914 |
|
Psychiatry in Nursing |
T+C |
51 |
59.53 |
7.38 |
51 |
66.03 |
10.69 |
0.001* |
|
Psychology in Nursing |
T |
54 |
67.41 |
12.88 |
54 |
62.51 |
14.5 |
0.071 |
|
Nursing Clinical Attachment III |
C |
47 |
71.85 |
9.79 |
47 |
66.03 |
10.69 |
0.001* |
|
Pharmacy (1st year 1st semester results) |
2017/2018 batch |
|
The 2019/2020 batch |
|||||
|
Pharmaceutical Chemistry I |
T |
28 |
66.14 |
10.49 |
28 |
69.62 |
12.11 |
0.012* |
|
Pharmaceutics IA |
T |
28 |
76.96 |
9.43 |
28 |
76.56 |
14.50 |
0.412 |
|
Mathematics |
T |
28 |
66.25 |
19.09 |
28 |
62.10 |
16.10 |
0.230 |
|
MLS (2nd year-end examination results) |
2016/2017 batch |
2017/2018 batch |
||||||
|
Microbiology and Immunology |
T+P |
22 |
68.11 |
4.86 |
22 |
72.69 |
7.94 |
0.022* |
|
Statistics, Research Methodology & Epidemiology |
T+P |
22 |
62.01 |
5.28 |
22 |
57.09 |
5.14 |
0.001* |
|
Haematology |
T+P |
22 |
57.22 |
3.58 |
22 |
60.42 |
4.98 |
0.058 |
|
Medical Parasitology |
T+P |
22 |
68.26 |
6.14 |
22 |
70.53 |
5.41 |
0.185 |
|
Basic Genetics, Molecular Genetics & Molecular Biology |
T+P |
22 |
61.32 |
5.98 |
22 |
70.31 |
5.68 |
0.000* |
|
Transfusion Medicine |
T+P |
22 |
66.68 |
6.84 |
22 |
69.87 |
6.20 |
0.163 |
Table 1. Comparison of results among undergraduates
*Paired sample T-test p < 0.05; T-theory, P-practical, C-clinical
IV. DISCUSSION
Online teaching was a big challenge to Sri Lankan undergraduates and teachers due to inadequate internet and infrastructural facilities for online teaching at the beginning of the COVID-19 pandemic. There was no other substitution except to conduct lectures online to provide continuous education during the lockdown. Therefore, this study was carried out to analyse the effectiveness of online teaching and student performances in selected batches of the FAHS, University of Ruhuna, Sri Lanka.
The mean value of the students’ marks for the several theoretical subjects was comparable in both groups. These findings show that the undergraduates in all three courses have appropriately adhered to the online method, and it may probably show the adherence of the lecturers to the technology. Indeed, free access to the LEARN platform may provide a huge impact on the results and the high information literacy of the undergraduates and lecturers may be the reason for it (Sample survey division, 2021). Though poor internet facilities disturbed and demotivated the undergraduates, the opportunity to listen to video recordings repeatedly may have mitigated the effect of this barrier. The reasons for the higher marks scored by the students who learned via Zoom than physical mode might be the favourable environment that prevailed by listening to lectures at their homes; fewer travel costs and time; the opportunity to have a better conversation with lecturers; having more time for self-learning/studying; and minimum disturbances from colleagues.
However, the mean value for the practical and clinical subjects was significantly low among the online group compared to the physical group. The clinical component is an essential part of the nursing undergraduate since it is vital to have adequate clinical exposure to gain competence to work in a real patient situation. Mainly, students learn how to handle patients with various disease conditions during their clinical practices. Furthermore, undergraduates can apply their theoretical knowledge in a real patient environment (e.g. evidenced-based practice); understand real patient matters; get technical and caring skills through interaction with patients and healthcare workers; and develop empathetic attitudes. Undergraduates did not get an opportunity to continue their clinical attachments as done previously due to the COVID-19 outbreak in Sri Lanka. During their clinical placements, they had to face several internal (fear, anxiety, etc.) and external (maintaining distance, lockdowns, close contacts, PPEs, etc.) constraints. It may be the reason for the lower performance.
However, another study conducted with final-year medical students found that some part of clinical exposure can be gained by providing online interactive learning materials (Ariyananda et al., 2022). Simulations are the recommended method for students to develop their clinical skills (Koukourikos et al., 2021) but these methods are not very popular in Sri Lanka due to the high cost of such kind of manikin. Likewise, practical subjects are essential to have a factual environment to get adequate training and robust hands-on skills. Nursing procedures/practical was not conducted due to the closure of the university and the limitations of close contact. This may also reduce the practical skills of nursing undergraduates. Under the pharmacy department, a significant difference was observed for the subject of Pharmaceutical Chemistry 1, which contains a lot of physical interactive parts. In the Zoom platform, it was difficult to conduct that much of interactive sessions with limited resources. That might be the reason for the difference. However, MLS and pharmacy departments have provided recorded practical sessions which may be the reason for the different results among departments.
In the study conducted in one faculty of the University of Ruhuna, a low number of participants were limitations of the study. A mixed-method study approach with a larger sample was recommended and further recommendations were made to assess the experience of undergraduates and lecturers.
V. CONCLUSION
Mode of teaching had not impacted the theoretical course units of undergraduates whereas practical/interactive session-based course units and clinical appointments had a greater impact on the mode of teaching. The findings can act as a primer for the development of an action plan to support university undergraduates’ academic and clinical works during pandemics. Further, the findings of this study would be helpful in robust the quality of online teaching methods in future pandemics.
Note on Contributors
TDS and EW contributed to the data analysis, manuscript drafting, and final editing of the revised manuscript. PW and SK contributed to the data analysis and manuscript drafting. ES and KY contributed to the data analysis. All authors read and approved the final revised manuscript.
Ethical Approval
Ethical approval was obtained from the Ethics Review Committee, Faculty of Allied Health Sciences, University of Ruhuna, Galle, Sri Lanka (Ref. no. 200.01.2023). Permission was obtained from the Dean/Faculty of Allied Health Sciences, University of Ruhuna, Assistant registrar/Faculty of Allied Health Sciences, University of Ruhuna, and Heads of the Department of Nursing, Department of Medical Laboratory Science, and Department of Pharmacy/Faculty of Allied Health Sciences, University of Ruhuna.
Data Availability
Data sets analysed during the current study would be available from the corresponding author upon reasonable request.
Acknowledgement
The authors are grateful to the Dean, Assistant Registrar, and the three Heads of the departments mentioned above for granting permission. Further, Ms. Chithra Ranasinghe, a Former WHO consultant is acknowledged for her contribution to language editing.
Funding
The authors received no funding for this study.
Declaration of Interest
The authors declare that they have no competing interests.
References
Ariyananda, P. L., Chin, J. H., Raman, R. K., Athif, A. L., Tan, Y. Y., & Hafiz, M. (2022). Online learning during the COVID pandemic lockdown: A cross sectional study among medical students. The Asia Pacific Scholar, 7(3), 46-50. https://doi.org/10.29060/taps.2022-7-3/sc2715
Hayashi, R., Garcia, M., Maddawin, A., & Hewagamage, K. P. (2020). Online Learning in Sri Lanka’s Higher Education Institutions during the COVID-19 Pandemic. Asian Development Bank. https://doi.org/10.22617/brf200260-2
Koukourikos, K., Tsaloglidou, A., Kourkouta, L., Papathanasiou, I. V., Iliadis, C., Fratzana, A., & Panagiotou, A. (2021). Simulation in clinical nursing education. Acta Informatica Medica, 29(1), 15-20. https://doi.org/10.5455/aim.2021.29.15-20
Sample Survey Division. (2021). Computer Literacy Statistics 2021 Annual Bulletin. Department of Census and Statistics. http://www.statistics.gov.lk/Resource/en/ComputerLiteracy/Bulletins/AnnualBuletinComputerLiteracy-2021.pdf
*Thamudi Sundarapperuma
Department of Nursing,
Faculty of Allied Health Sciences,
University of Ruhuna,
Galle, 80 000, Sri Lanka
+94 71 31 86 524
Email: chamudi2006@yahoo.com,
thamudids@ahs.ruh.ac.lk
Submitted: 24 January 2023
Accepted: 2 August 2023
Published online: 2 January, TAPS 2024, 9(1), 42-48
https://doi.org/10.29060/TAPS.2024-9-1/SC2997
Rahizan Zainuldin1 & Heidi Siew Khoon Tan1,2
1Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore; 2Pre-Professional Education Office, Tan Tock Seng Hospital, Singapore
Abstract
Introduction: Singapore Institute of Technology’s undergraduate (UG) occupational therapy (OT) and physiotherapy (PT) programs are one of the first implementors of Entrustable Professional Activities (EPAs) in the respective allied health professions training. The aim of the paper is to report the outcomes of the first year of EPAs implementation in clinical practice education (CPE) and share next steps refining implementation.
Methods: A quality improvement (QI) study using the Plan-Do-Check-Act (PDCA) cycle was conducted. UG OT Year 2 and Year 3 students, UG PT Year 3 students and their clinical educators (CEs) who experienced the use of EPAs for the first time were surveyed at the end of the clinical block.
Results: There was generally high agreement (>70% agreed or strongly agreed) among all groups in using EPAs to better understand the learning objectives of CPE and practice expectations as future entry-level practitioners at conditional-registration. More than 70% of OT respondents but less than 50% PT respondents found the EPA assessment forms easy to use. Less than 60% of both program CEs did not include colleagues for EPA assessments. 55% of both OT and PT CEs found the EPA training and resources adequate. Overall, PT respondents showed lower agreement than OT respondents in five survey items.
Conclusion: The first implementation cycle of EPA in the undergraduate OT and PT CPE had mixed acceptability to the EPA assessment tools. Three strategic changes were made for the second implementation cycle., i.e., redesign of EPA-based assessment forms, training focus and ‘just-in-time’ training with streamlined resources.
Keywords: Clinical Training, Entrustable Professional Activities, Occupational Therapy, Physiotherapy, Undergraduate, Workplace-based Assessment
I. INTRODUCTION
In 2021, the occupational therapy (OT) and physiotherapy (PT) undergraduate programs at Singapore Institute of Technology (SIT) added a novel assessment, Entrustable Professional Activities (EPAs), to the extant competency-based assessment tools in clinical practice education (CPE). EPAs are units of professional activities entrusted to a learner determined by five levels of supervision, once the learner has demonstrated the required competence (ten Cate & Taylor, 2020). OT EPAs and PT EPAs (Zainuldin & Tan, 2021) were developed and introduced to SIT CPE as part of the Ministry of Health’s review of healthcare professions’ training standards. EPA-based assessments are relevant in CPE where students perform professional activities at workplace, supervised by onsite clinical educators (CEs). Previous CPEs assessed only OT and PT student competencies using the validated Student Practice Evaluation Form-Revised Edition (SPEF-R) (Turpin et al., 2011) and the Clinical Competency and Reasoning Assessment (CCRA), respectively. Conceptually, the pairing of EPAs with SPEF-R or CCRA potentially offer CEs an opportunity to empower students through graduated levels of entrustment supported by appropriate proficiency levels. Operationally, EPA assessment does not add new activities. OT and PT CEs can utilise routine observations of students’ tasks, case discussions and case-notes documentation as sources to inform entrustment levels in EPAs.
No EPA implementation in any OT and PT curricula has been documented. At SIT, EPA implementation in CPE needs evaluation. Recognising that implementing process changes requires an iterative approach, SIT embarked on a quality improvement study using the Plan-Do-Check-Act (PDCA) cycle. This paper reports the results of operationalising EPAs for the first time in OT and PT CPE, including the use of EPA-based assessment forms. The Methods section describes the Plan and Do, followed by the Results section reporting outcomes of the Check and the Discussion section highlighting the Act to improve implementation.
II. METHODS
A. CPE Structure
OT CPE consists of four blocks of seven weeks each and interspersed between academic modules in Years 2, 3 and 4. PT CPE consists of five consequent blocks (four core and one elective) of six weeks each, begins only after all academic modules are completed in Year 3 and continues to Year 4. OT and PT students complete different clinical settings for each CPE block.
B. Participants and Study Design
OT Year 2 and Year 3 students, PT Year 3 students and their CEs who experienced EPA use for the first time were surveyed at the end of a clinical block. An online EPA survey is incorporated with routine post placement feedback for both students and CEs, therefore no consent was required. The QI study was exempt from ethics review (SIT Institutional Review Board, No. 2022122). Survey results were extracted from February to December 2021.
C. PDCA Cycle: Plan-Do
OT and PT have five core EPAs each. EPA-based assessment activities are short practice observations, entrustment-based discussions and case-notes evaluations. These activities serve as sources of information (SOIs), or workplace-based assessments (WBAs) in OT CPE, to inform entrustment decision-making. OT CE assesses EPAs by documenting in a single patient case form with all three WBAs per EPA. PT CE assesses EPAs for every patient case anchored by three different SOI forms with written justifications. OT and PT CEs and students were trained on nuts and bolts of EPAs and on using WBA/SOI forms in CE training workshops and student pre-CPE briefing, respectively.
Each OT EPA requires a total of six patient cases entrusted to students at Level 3 entrustment (indirect supervision) across four CPE blocks. Each PT EPA requires six cases at Level 3 entrustment at each core clinical block, which totals 24 cases by end of the program. Appendix 1 and 2 provides visualisation of EPA implementation across multiple CPE blocks.
The EPA survey has ten items. The first eight items are scored on a 4-point Likert-scale (strongly disagree-strongly agree). The final two questions seek qualitative feedback on benefits and challenges and suggestions for improvements. Unless indicated, items are phrased in the same manner in both student and CE surveys.
D. Data Collection and Analysis
Data were counted as proportions of respondents who agreed (pooled response from ‘agree’ and ‘strongly agree’) and proportions disagreed (pooled from ‘disagree’ and ‘strongly disagree’). The authors grouped the qualitative narrative into benefits and challenges.
III. RESULTS
A. PDCA Cycle: Check
There were 99.0% response rate from OT Year 2 students (105/106), 97.7% from Year 3 OT students (85/87), 93.2% from PT Year 3 students (137/147), 98.5% from OT CEs (199/202) and 92.5% from PT CEs (247/267). Proportion of respondents who agreed with each item statement is shown in Table 1. Data on item scores for each student and CE are available at online repository, http://doi.org/10.6084/m9.figshare.21941288
|
Survey Items |
OT Year 3 students |
OT Year 2 students |
PT Year 3 students |
OT CEs
|
PT CEs
|
|
(n = 85) |
(n = 105) |
(n = 137) |
(n = 199) |
(n = 247) |
|
|
Q1 – Using EPAs in CPE helps me better understand and meet future conditional-registration requirements.
|
90.6 |
98.1 |
75.2 |
89.4 |
71.7 |
|
Q2 – The EPA documents help me to better understand the learning objectives in CPE.
|
84.7 |
98.1 |
72.3 |
75.9 |
71.7 |
|
Q3 – The WBA/SOI forms are easy to use.
|
76.5 |
85.7 |
38.7 |
73.4 |
47.8 |
|
Q4 – CE: The WBA/SOI forms are adequate for me to determine students’ competence and entrustment level. / Student: The WBAs/SOIs help me to better gauge my progress and level of competence.
|
91.8 |
97.1 |
70.1 |
72.9 |
64.6 |
|
Q5 – I understand the connection between OT EPAs and SPEF-R2 competencies or PT EPAs and CCRA.
|
84.7 |
97.1 |
72.3 |
69.8 |
83.0 |
|
Q6 – CE: I use the EPA documents explicitly with students during clinical teaching and assessment. / Student: I use the EPA documents to guide my learning goals during CPE.
|
62.4 |
92.4 |
51.1 |
87.9 |
59.1 |
|
Q7 – CE: I involve other colleagues in doing WBAs/SOIs to calibrate students’ entrustment level. / Student: Besides my CE, I also received feedback from other OTs or other PTs who were involved in my WBAs/SOIs.
|
44.7 |
66.7 |
54.0 |
58.8 |
45.3 |
|
Q8 – I feel the current briefing/training/resources are adequate for me to incorporate the use of EPAs in CPE. |
70.6 |
89.5 |
56.2 |
55.3 |
55.9 |
Table 1. Proportion of OT and PT students and CEs who agree with the EPA survey items
PT CEs and students were almost unanimous that SOI forms were difficult to use (Q3). Common to OT and PT CEs, many did not involve colleagues in EPAs (Q7) and felt that training to understand EPAs was inadequate (Q8).
Qualitatively, both disciplines benefitted from the use of WBA/SOI forms to scaffold learning through structured feedback and action plans when addressing identified competency gaps. Feedback from OT and PT students below closely exemplified the appreciation:
“EPAs allow me to track my progress over the weeks and transfer my reflections into action when given the opportunity to receive objective and qualitative feedback from the EPA form.”
OT Student#45
“The discussions with the CE on what to do if the situation was different made me realise the importance of planning even for the worst-case scenario…enabled me to identify the gaps in knowledge and skills that had to be worked on.”
PT Student#67
However, PT groups cited complicated forms design and copious paperwork from numerous SOIs time-consuming and stressful. Ambivalence on its practicality was best summed by PT CE#31, “As a first-time user of the SOIs, I found it quite difficult to navigate the forms, took me some tries to understand how I can determine the students’ competence and entrustment level. As there were many forms, it was quite confusing, and hence stressful and time-consuming. Otherwise, they are useful tools.”
The most common challenge among OT CEs was assessing certain EPAs, such as planning care transition, in some settings. “Some EPAs are harder to do in some settings, for example, in the hands therapy setting; it is harder to do the handover/discharge EPA as there are less of these patients.” (OT CE#32). Calling for more support, one CE suggested “SIT go through a round of training on the different EPAs and give relevant case examples to help us better understand them.” (OT CE#4).
IV. DISCUSSION
Response rates were excellent. The convergence of high agreement rates with narrative feedback on using EPAs and WBA/SOIs for teaching/learning, understanding the CPE learning objectives and meeting practice expectations as future entry-level practitioners suggest early indication that EPAs may facilitate SIT OT and PT students transit to new practitioners. The positive experience in this regard resonated with other EPA survey on final-year dietetics students and their clinical supervisors in Australia (Bramley et al., 2021). Practical challenges with the SOI forms, resulting in onerous and time-consuming evidence collection; low levels in involving colleagues in EPA assessments; and inadequate EPA training/resources for CEs were identified as key areas for change in both disciplines.
A. PDCA Cycle: Act
First, to reduce assessment burden, WBA and SOI forms were redesigned and harmonised in preparation towards a standardised EPA online assessment system currently developed in-house. Multiple WBA/SOI forms were combined into a single-page checklist form with a small open-ended section. A checklist was similarly suggested for nursing EPAs assessment, citing convenience as a reason (Lau et al., 2020). On the single-page form, CEs tick entrustment levels for each WBA/SOI associated to each EPA with all EPAs on the same page. The only narrative section is where CEs describe key justifications supporting their entrustment decisions, followed by students’ reflections. Second, to bridge assessment expectations among clinicians and increase propensity to share EPA assessments with colleagues, EPA training was refined to emphasise balance of supervision control with autonomy and clearer definitions between entrustment levels 2 (direct supervision) and 3 (indirect supervision) through case examples. Third, ‘just-in-time’ refresher training was added to activate volition in assessing EPAs. Toolkits containing briefing videos and streamlined resources in short bites, such as 3-minute videos, powtoons, form samplers and frequently-asked-questions, were released for OT and PT CEs closer to placement block. PT CEs also received a refresher at early weeks of every placement block.
V. CONCLUSION
The PDCA cycle is used to inform and make iterative adaptations to each cycle of EPA implementation. The Plan-Do stage completed the first implementation cycle of EPA in the undergraduate OT and PT CPE in 2021. The Check stage revealed mixed experiences to EPA use. The lowest agreement was the ease of using SOI forms among PT students and CEs. While EPAs were accepted as teaching and learning tools, CEs did not involve colleagues in EPA assessments. Training on EPA assessment for CEs was inadequate. Consequently, the Act stage yielded changes in form design, training focus and streamlined resources for the next implementation cycle.
Notes on Contributors
Rahizan Zainuldin (RZ) led the design of the quality improvement and implementation of EPAs, submitted the study to SIT IRB, analysed and interpreted both quantitative and qualitative data for the PT CPE, prepared the manuscript, wrote the initial draft and finalised for submission.
Heidi Siew Khoon Tan (HSKT) led the design of the EPA survey, analysed and interpreted both quantitative and qualitative data for the OT CPE, provided a critical review of the manuscript, and concurred on the final version.
Ethical Approval
The QI study was exempt from ethics review (SIT Institutional Review Board, No. 2022122).
Data Availability
Data on item scores for each student and CE are available at online repository, publicly accessed at http://doi.org/ 10.6084/m9.figshare.21941288. While the data is available for readers’ perusal and no permission from the authors is needed, please write an email of intention to use the data for any purposes to the corresponding author.
Acknowledgement
We would like to acknowledge the OT and PT CPE committee members who have contributed in the planning and implementation of the EPA. We would also like to thank Ms Annie Wang Haiyan, Manager, Academic Programmes Administration, SIT, for uploading the survey on and extracting the survey results from the online assessment portal of our Clinical Practice Education portal.
Funding
No funding source is provided.
Declaration of Interest
Rahizan Zainuldin and Heidi Siew Khoon Tan disclose there is no conflict of interest of any form.
References
Bramley, A. L., Thomas, C. J., McKenna, L., & Itsiopoulos, C. (2021). E-portfolios and entrustable professional activities to support competency-based education in dietetics. Nursing and Health Sciences, 23(1), 148-156. https://doi.org/10.1111/nhs.12774
Lau, S. T., Ang, E., Samarasekera, D. D., & Shorey, S. (2020). Evaluation of an undergraduate nursing entrustable professional activities framework: An exploratory qualitative research. Nurse Education Today, 87, Article 104343. https://doi.org/10.1016/j.nedt.2020.104343
ten Cate, O., & Taylor, D. R. (2020). The recommended description of an entrustable professional activity: AMEE Guide No. 140. Medical Teacher 43(10), 1106-1114. https://doi.org/10.1080/0142159X.2020.1838465
Turpin, M., Fitzgerald, C., & Rodger, S. (2011). Development of the Student Practice Evaluation Form Revised Edition Package. Australian Occupational Therapy Journal, 58(2), 67-73. https://doi.org/10.1111/j.1440-1630.2010.00890.x
Zainuldin, R., & Tan, H. Y. (2021). Development of entrustable professional activities for a physiotherapy undergraduate programme in Singapore. Physiotherapy, 112, 64-71. https://doi.org/10.1016/j.physio.2021.03.017
*Rahizan Zainuldin
10 Dover Road,
Singapore 138683
+6596522418
Email: Rahizan.Zainuldin@singaporetech.edu.sg
Submitted: 5 April 2023
Accepted: 17 August 2023
Published online: 2 January, TAPS 2024, 9(1), 28-35
https://doi.org/10.29060/TAPS.2024-9-1/OA3035
Aminda Faizura Omar, Tun Yasmin Iffah Mohd Suria Affandi, Mohd Isyrafuddin Ismail, Mas Suryalis Ahmad & Ilham Wan Mokhtar
Comprehensive Care Centre of Studies, Faculty of Dentistry, Universiti Teknologi MARA, Malaysia
Abstract
Introduction: This study was undertaken to investigate students’ perceptions of innovation-integrated learning, adopted as an alternative approach for special care dentistry (SCD) training.
Methods: Ninety final-year dental students from the 2021 cohort were divided into eight groups to complete an innovation project dedicated to eight categories of patients with special health care needs. Discussion and final presentations, involving related experts were conducted remotely via an online platform. Then, students were invited to answer a validated online feedback survey on their perceptions of the learning approach.
Results: The response rate for the feedback survey was 91.1% (n=82). Most students agreed that the activity was interesting, improved their knowledge and understanding of SCD, allowed engagement between peers, supported sharing of ideas and experiences, encouraged student–lecturer interactions, and enhanced knowledge integration and application. Students also expressed that the activity enhanced creativity and innovation, instilled an interest and positive attitude toward learning SCD, and encouraged teamwork. However, a few students noted facing some limitations in completing their projects (i.e., technological challenges and reduced physical access to purchase materials). Around half felt neutral about having an increased workload from this activity. Moreover, perceptions differed regarding time and financial commitments, as well as supervisors’ and patients’ involvement during the project development process.
Conclusion: Students perceived that the innovation-oriented learning activity, was beneficial in multiple aspects of SCD training.
Keywords: Innovation, Learning, Dental Students, Perception
Practice Highlights
- We have developed a new integrated teaching method via the utilisation of innovation development for special needs groups.
- Students’ perceptions of this learning method were explored using both quantitative and qualitative methods via an online feedback questionnaire.
- Overall, students positively responded to the teaching method when it came to improving their knowledge and understanding of SCD, engagement between peers, sharing of ideas and experiences, student–lecturer interactions, and knowledge integration and application.
- This novel teaching method achieves the highest level of Bloom’s Taxonomy which is to create something new.
I. INTRODUCTION
Special care dentistry (SCD) involves managing patients with special health care needs, such as those with physical, intellectual, psychological impairments as well as complex medical conditions (Royal Australasian College of Dental Surgeons, 2021). At the undergraduate level, many teaching and learning activities have been conducted to provide students with learning experience in this area of patient care. These activities include lectures, community-based learning, simulation exercises and clinical training (Ahmad, Mokhtar, et al., 2020; Mohamed Rohani & Mohd Nor, 2021). Students who received training in SCD were found to have demonstrated better comfort and attitudes in managing patients with special health care needs (Mohamed Rohani et al., 2021).
However, these learning activities may be compromised by situations that limit face-to-face interactions, either among students, between teacher and learners, as well as with the patients. Such situations may happen due to disease (such as the recent COVID-19 pandemic), geographical barriers and accessibility issues (Amir et al., 2020). It was found that limitations of dental training that requires physical contact may compromise students’ learning experience, thus affecting their competency, knowledge and confidence in patient care (Chang et al., 2021).
Meanwhile, it has become incumbent on dental education providers to prepare future graduates with essential skills that are deemed beneficial for practicing health care professionals. These skills include innovation, leadership, critical thinking and enterpreneurial abilities (Malaysian Dental Council, 2021). Acquisition of these abilities have been associated with many aspects of personal and professional development including emotional intelligence and practice management (Saleem et al., 2019; Wang et al., 2020).
In view of the various challenges and demands of the current (and future) educational environment and healthcare needs, an innovation-integrated educational approach was developed and adopted as an alternative teaching and learning method to teach SCD. This approach, undertaken mostly remotely using an online learning platform, involved the integration of students’ cognitive function, psychomotor ability, and affective skills through the development of innovative products to address oral health issues experienced by the different categories of patients with special health care needs. As a novel educational approach, assessment of its effectiveness is therefore essential. This study was undertaken to investigate students’ perceptions of the innovation-integrated learning, conducted remotely via an online platform, developed during the COVID-19 pandemic, as an alternative approach for SCD training.
II. METHODS
A. Study design
This was a descriptive, cross-sectional, quantitative and qualitative study, using a validated online feedback questionnaire involving the final-year undergraduate students of the Bachelor of Dental Surgery program of the Faculty of Dentistry, Universiti Teknologi MARA.
B. Study Population
Because this module is a compulsory component of the final-year undergraduate dental curriculum (Faculty of Dentistry, 2022), all students were required to be involved with the group innovation project. However, participation in the online feedback survey was voluntary. At the beginning of the semester, the students were made aware of the study and that their participation in the innovation program and the research were treated separately.
All students who agreed to participate in the online feedback survey provided informed consent, attached to the information sheet supplied to all potential participants via their official university email. To avoid coercion, students were provided with an explanation in the information sheet that their participation was entirely voluntary and anonymous. Those who wished not to participate in the online feedback survey would not be penalised, and they could withdraw their participation at any point without having to provide a justification.
C. Study Instrument
The questionnaire used for the online feedback survey was adopted from the study by Rowe and Wood (2008). It was content-validated by a panel of 2 experts in dental education before its use in the main survey. From the item-level content validatiy index (I-CVI) for each item as well as a summation of the I-CVI divided by the number of average (S-CVI/Ave), a score of 1 was obtained for both indices as the panelists rated all items with a score of 3 or 4. The questionnaire consisted of nine items about the perception of students towards this teaching method, measured using a 5-point Likert scale (strongly disagree, disagree, neutral, agree, and strongly agree). Open-ended questions were included at the end of the questionnaire to further explore students’ perceptions of the learning activities.
D. Study Conduct
For the group innovation project, all final-year students (n=90) were divided into eight groups, based on their assigned clinical groupings. Each group was assigned to an academic or clinical specialist in SCD, who acted as a supervisor. Eight categories of patients with special health care needs were identified and randomly allocated to the different groups. The categories of patients were 1) hearing disability, 2) speech disability, 3) visual disability, 4) geriatric, 5) Down syndrome, 6) autism, 7) cerebral palsy, and 8) dementia.
Students were given three months to develop innovative products. They were expected to engage with their supervisors during the whole development process, which involved 1) identification of health complications related to the condition and its impact on oral health, 2) understanding of issues related to patients’ oral health care; 3) creation of a prototype to address the related oral health–related complications. Because all students were at the time subjected to restrictions in having physical classes due to COVID-19 (Samat et al., 2020), large-group discussions and final presentations were undertaken remotely online.
At the end of this group activity, an online presentation, judged by experts in related fields, was conducted as a form of assessment, as well as constructive feedback on improvements and the marketability of the product. Students were then invited to participate in the online feedback questionnaire, which was distributed via their official university email. An English language questionnaire was used as the respondents were undergraduate dental students with a good command and understanding of the language. A reminder email was sent a week later, with another reminder sent the following week.
E. Data Analysis
To maximise the outcome, quantitative data were simplified into a 3-point Likert scale (agree, neutral, and disagree). Using SPSS version 27, the frequency of the data was analysed to compare students’ responses for each item. For analysis of the benefits, the nine items of the questionnaire were further categorised into different themes: Theme 1—Acceptance of the teaching method concept (Item 1), Theme 2—Effectiveness of teaching method (Items 2, 3, 6, and 7), Theme 3—Important role of supervisors (Items 4, 5, and 8), and Theme 4—Impact on students’ workload (Item 9).
For the qualitative component, data were analysed via thematic analysis involving open and closed coding. Emerging themes were then identified based on these codes, which were then validated through comparisons amongst researchers.
F. Ethical Approval
Ethics approval was obtained from the Research Ethics Committee (REC) Universiti Teknologi MARA, Malaysia, in accordance with the Declaration of Helsinki (REC12/2021 [MR 1004]).
III. RESULTS
A total of 82 out of 90 students returned the questionnaire, giving a response rate of 91.1%. The frequency of responses for each question or item, categorised into the different themes, is shown in Table 1.
|
Items |
Questions |
Themes |
Negative (%) |
Neutral (%) |
Positive (%) |
|
Item 1 |
The program is an interesting new teaching method to learn about Special Care Dentistry. |
Acceptance of teaching methods/ concept |
1.2 |
8.5 |
91.3 |
|
Item 2 |
The program has provided me a clear understanding of the Special Care Dentistry concept. |
Effectiveness of teaching method |
1.2 |
9.8 |
89.0 |
|
Item 3 |
The teaching method managed to integrate the knowledge and clinical implication in Special Care Dentistry. |
1.2 |
4.9 |
93.9 |
|
|
Item 6 |
The method of teaching allows me to interact effectively with my fellow group mate and the rest of the batch. |
2.4 |
7.3 |
91.3 |
|
|
Item 7 |
The teaching method supports ideas and experience sharing between students |
0.0 |
2.4 |
97.6 |
|
|
Item 4 |
The supervisors encourage and accept different opinion. |
Important role of supervisors |
0.0 |
3.7 |
96.3 |
|
Item 5 |
The teaching method provide opportunities for discussion between students and supervisors. |
2.4 |
2.4 |
95.2 |
|
|
Item 8 |
The supervisors explained the purpose of the program well and structured. |
0.0 |
7.3 |
92.7 |
|
|
Item 9 |
The teaching method increase the workload of students compared to classroom learning. |
Impact on students’ workload |
7.3 |
53.7 |
39.1 |
Table 1. Frequency of responses for items, categorised into different themes.
Overall, most students provided positive responses regarding activity acceptance and effectiveness and the supporting role of supervisors. However, slightly more than half of the students felt neutral about the learning activity causing an increased workload compared to classroom learning.
The thematic analysis of qualitative data yielded multiple themes that can be categorised into three main areas: 1) benefits of this education method, 2) limitations of this learning intervention, and 3) differing opinions on the integration of the group innovation project into the dental curriculum.
A. Benefits of The Study
Within this area, the students expressed four main themes.
1) Enhances creativity and innovation: Most students felt that this teaching method had enhanced their creativity in finding methods to manage patients with special dental needs as well as in developing innovations for the group of interest.
“This integrated learning helps me with my creativity and critical thinking so we could create an innovation that is appropriate with the current technology.”
Student 10
2) Improves knowledge and understanding of SCD: Using innovation in teaching made students delve into the subject matter, thus improving their knowledge of their patients and gaining a deeper understanding of SCD.
“A good approach indeed. I have a chance to challenge my understanding and gain new information from my friends, supervisors, and postgraduate students. This helped me develop a new way of thinking and find good literature on SCD.”
Student 35
Subtheme 1: Encourages independent information-gathering about SCD
Some students noted that they had to rely on the resources they had and work by themselves due to the pandemic, which made them more independent when researching topics about SCD.
“In my opinion, this teaching method is helpful to help the students to understand the special needs module by asking the student to develop products according to the difficulties of the disabilities required.”
Student 25
Subtheme 2: Development of critical thinking and problem-solving skills in SCD
By giving students the task of developing information, they were forced to solve problems the special interest group faced. Therefore, students believed this made them learn better critical thinking and problem-solving skills.
“Good to brainstorm ideas and put us in their shoes in order to address their different needs.”
Student 74
3) Instils interest and positive attitudes towards learning SCD: Due to their minimal patient experience, most students felt this task made them more interested in their special interest group, which improved their attitudes to learning SCD.
“The integrated learning approach gives me ideas on how situations should be handled in real life on aspects like the expectation from special care patients and preparedness as a future dentist to have a special care patient.”
Student 12
4) Encourages teamwork: Some students noted that, even with the isolation, they felt that this type of teaching method had encouraged them to work more closely with not only their teammates but supervisors as well.
“Innovative program. Good. Made students and supervisors unite as teammates.”
Student 62
B. Limitations of this Learning Intervention
Regarding limitations, two themes were noted.
1) Technological challenges: Several students experienced poor internet connection throughout the process, which hindered their efficiency.
”Very helpful, but internet connection and environment are some of the barriers for me for not study effectively, I prefer face-to-face learning approach. ”
Student 72
2) Reduced physical access to purchasing of materials: The movement control order that was implemented throughout most of the pandemic left most students restricted from being able to access appropriate materials from local or distant suppliers.
“We faced problems buying materials due to the movement control order.”
Student 77
C. Differing Opinions on the Integration of the Group Innovation Project into the Dental Curriculum
Students had differing opinions on the following aspects.
1) Time commitment and workload: Despite the lack of face-to-face sessions, some students believed they were given adequate time to create and execute ideas comfortably.
“Since the project is given so much earlier than the deadline, we are able to create a better project without feeling any burden in completing the module.”
Student 36
However, a handful of students felt they needed more time to be able to have performed better for the task.
“It is an interesting method and helpful to learn special care dentistry, but it is quite time-consuming, and we have restrictions due to COVID-19.”
Student 65
2) Financial demands: Depending on the type of innovation they designed, some students felt that the funding provided was not sufficient for them to prepare a good product.
“Some innovations need to create prototype only because low budget, but it is understandable.”
Student 74
However, a few students believed the financial assistance was enough for them to complete their innovation.
“The funding provided was sufficient.”
Student 43
3) Guidance from supervisors: Many students noted that their supervisor provided ample guidance throughout the project.
“Excellent. Students and supervisors can communicate and deliver knowledge well through this method.”
Student 19
“Our supervisor introduced us to some deaf patients. So we were able to get the patient’s feedback on our product.”
Student 52
However, some students believed the transition from face-to-face to online consultations was not ideal for the guidance they needed.
“However, there is lacking in communication and discussion between students and supervisors as this is still new to some students.”
Student 47
4) Exposure to SCD practice: Because the students were supposed to have exposure to special care patients in their final year, they believed that this teaching module was sufficient to help them understand patients.
“I think this method actually gives a realistic overview of how to work with patients.”
Student 43
On the other hand, a few felt that clinical sessions were more beneficial for them to apply the knowledge they have.
“In my opinion, direct exposure to SND patients would be better so we can apply the knowledge and innovation.”
Student 76
IV. DISCUSSION
This study involved the undergraduate teaching of SCD for students in a Malaysian dental school. In Malaysia, SCD education has yet to become a compulsory component of the five-year undergraduate curriculum (Naimie et al., 2020). This may be related to various barriers to providing training in this area of dentistry, including a lack of clinical expertise and educational resources (Ahmad et al., 2014). Despite this, Universiti Teknlologi MARA, Malaysia has taken a proactive approach to provide training in SCD, at both undergraduate and postgraduate levels (https://dentistry. uitm.edu.my/index.php/en/). For undergraduate students, teaching and learning of SCD are provided in the final year, as part of the Comprehensive Care Dentistry course (Faculty of Dentistry, 2022). Students undergo a series of lectures, hands-on demonstrations, problem-based learning, tutorials, a clinical rotation in the SCD specialist clinic, and a community engagement activity project (Faculty of Dentistry, 2022).
Although various teaching and learning interventions have been successfully conducted in the undergraduate training of SCD in previous years (Naimie et al., 2020), the transition from face-to-face training to online distance learning imposed on higher learning institutions in this country during the COVID-19 pandemic (Halim et al., 2021) may lead to compromised learning experiences. This is especially pertinent for SCD training, which involves clinical exposure to various groups of patients (Dougall et al., 2014). As clinical training was limited at that point of time, alternative teaching and learning approaches were designed to ensure students were exposed to issues in managing patients with special health care needs, which in this case was achieved by developing an innovative product to address patients’ difficulty in maintaining satisfactory oral health.
This study found that students demonstrated favorable responses toward acceptance of such an education intervention. With dental students experiencing physical and mental health deterioration with online distance learning during the COVID-19 pandemic (Lestari et al., 2022), it was encouraging to observe that students in this study found the learning activities interesting. They also opined that the educational method enhanced creativity and innovative skills, which are the highest level of learning domains (Bloom et al., 1964; Miller, 1990). Therefore, acceptance of this training approach has positive implications for its future development and implementation in the undergraduate dental curriculum.
Various benefits of this learning activity, as reported by students in this study, also further supports the use of innovation-integrated learning for teaching SCD. Participants cited improved knowledge and understanding of SCD, which has been reported as lacking among members of the dental fraternity around the world (Ahmad et al., 2015; Borromeo et al., 2018; Mandasari et al., 2021). They also opined that this learning intervention allowed integration of SCD theory and clinical practice, supporting its effectiveness, which is comparable to a similar approach previously undertaken via face-to-face learning (Ahmad et al., 2020).
The enhanced student attitude and interest in learning SCD reported in this study suggest a positive impact of learning that could potentially be translated into practice. Those with educational experience in SCD have been found to feel more comfortable and positive in managing patients with special health care needs (Mohamed Rohani et al., 2021). Dental practitioners who received exposure to SCD during university education were also more likely to have provided care to these patients, in comparison with their colleagues without such training experience (Alumran et al., 2018).
To further enhance students’ attitudes and interest in learning, the role of academicians as supervisors is integral. Academicians who play an effective role could influence students’ active engagement in learning, guide students in achieving learning goals, and enhance their overall learning experience (Sølvik & Glenna, 2021). It was evident in the present study that despite being conducted virtually, this learning activity was successful in encouraging engagement between students and supervisors. Some students also reported receiving assistance from their supervisors in gaining access to patients, whose feedback was sought for improvement of their products. This is an encouraging finding, given previous studies reporting negative implications of virtual and remote learning on student–teacher relationships (Halim et al., 2021). To ensure that all students receive quality supervision, the faculty must monitor the roles and engagement of every academician, especially during learning activities that involve remote delivery.
Besides improving student–teacher engagement, this learning activity was also beneficial in enhancing peer interactions and teamwork, while allowing sharing of experiences and ideas between students. Although social interaction and group dynamics in learning have been reportedly compromised during the COVID-19 pandemic (Walker & Koralesky, 2021), this education activity was perceived to have overcome this issue. Enhanced teamwork and communication brought about by this activity could provide opportunities for students to develop professionalism, which is integral to the practice of dentistry. Teamwork and effective communication are especially important in the practice of SCD, where multidisciplinary collaboration is mandatory in addressing patients’ complex health care needs (Glassman et al., 2016). The development of skills (e.g., independent information-gathering, critical thinking, problem-solving skills) reported by the study participants is also beneficial in preparing them as competent practitioners who can function at a high level of professionalism.
Challenges reported by students while undergoing this learning activity (technological difficulties and reduced physical access to purchase materials) demand the attention of faculty and supervisors to be more proactive in addressing the related issues. Nevertheless, with allowance of physical classes recently, this issue would not compromised students’ learning experience should the faculty decide to continue such this approach. Differing opinions about time constraints, heavy workloads, and increased financial demands expressed by students in this study require further investigation and planning by the faculty to ensure that the students receive adequate assistance to support their learning process. Feedback from patients regarding the developed innovative products could be gained through the conduct of proper research that assesses the effectiveness and benefit of the intervention. Consequently, students’ innovative ideas could be further developed for commercialisation, thus equipping them with entreperneurial skills, which is highly recommended to be taught in the higher education curriculum (Tuononen et al., 2022).
This study also indicates that integrating innovation in the teaching and learning of SCD supports many aspects of student learning that targets the recommended core contents as recommended in the IADH guidelines. These contents include 1) Identifying and addressing access and barriers to oral health faced by people with special needs (Domain 2), 2) Demonstrating appropriate communication skills when managing patients with special needs (Domain 4), 3) Understanding the impact of impairments, disabilities and systemic conditions on oral health and functions (Domain 5), as well as 4) Developing and applying effective methods when managing patient with special needs, including in planning oral health education program and designing interventions for clinical treatment (Domain 6) (Daly et al., 2014).
This study is limited by the non-participation of some students, whose responses were not included in the investigation. Nevertheless, the high response rate indicates the representativeness of the study population, hence supporting the validity of the study findings.
The results of this study provided important information for program developers, faculty, and the dental education fraternity at large. It identified the potential of innovation-integrated learning, for providing SCD training to undergraduate students, including in circumstances that may limit physical access to education.
V. CONCLUSION
Students’ acceptance of this teaching method proves it is sufficient and beneficial in improving their creativity and innovation, enhancing their knowledge and understanding of SCD, instilling interest and positive attitudes in learning SCD, and encouraging teamwork and effective communication between peers and supervisors. However, they provided differing opinions on the impact of the learning activity on their workload, time and financial demands, and exposure to SCD practice. Some faced technological challenges and reduced physical access to purchase materials.
Notes on Contributors
Aminda F. Omar was involved in literature search, data acquisitions and analysis and the manuscript preparation.
Tun Yasmin Iffah Mohd Suria Affandi was involved in data acquisitions and analysis.
Mohd Isyrafuddin Ismail was involved indata acquisition.
Mas S. Ahmad was involved in study conception and design, data analysis, manuscript editing and review.
Ilham W. Mokhtar was involved in the study conception and design and manuscript review.
All the authors approved the final version of the manuscript publication.
Ethical Approval
Ethics approval was obtained from the Research Ethics Committee (REC) Universiti Teknologi MARA, Malaysia in accordance with the Declaration of Helsinki (REC12/2021 [MR 1004]).
Data Availability
As per the requirement of the local ethics, data will be kept in an enclosed and dedicated facility in the faculty building.
Acknowledgement
The authors wish to thank the dental students from Universiti Teknologi MARA, Malaysia for participating in this study. The authors confirm that no financial support was received to fund this work. The authors also confirm they have no interests to declare.
Funding
No funding was provided for this study.
Declaration of Interest
There are no conflicts of interests.
References
Ahmad, M. S., Mokhtar, I. W., & Khan, N. L. A. (2020). Extramural oral health educational program involving individuals with disabilities: Impact on dental students’ professionalism. Journal of International Society of Preventive & Community Dentistry, 10(3), 323-328. https://doi.org/10.4103/jispcd.JISPCD_74_20
Ahmad, M. S., Radhi, D. S. M., Rusle, F. F., Zul, M. F., Jalaluddin, J., & Baharuddin, I. H. (2020). Photodentistry – An innovative approach to improving students’ empathy and learning experiences in comprehensive patient care. Journal of Dental Education, 84(11), 1219-1229. https://doi.org/10.1002/jdd.12295
Ahmad, M. S., Razak, I. A., & Borromeo, G. L. (2014). Undergraduate education in special needs dentistry in Malaysian and Australian dental schools. Journal of Dental Education, 78(8), 1154-1161.
Ahmad, M. S., Razak, I. A., & Borromeo, G. L. (2015). Special needs dentistry: Perception, attitudes and educational experience of Malaysian dental students. European Journal of Dental Education, 19(1), 44-52. https://doi.org/10.1111/eje.12101
Alumran, A., Almulhim, L., Almolhim, B., Bakodah, S., Aldossary, H., & Alakrawi, Z. (2018). Preparedness and willingness of dental care providers to treat patients with special needs. Clinical, Cosmetic and Investigational Dentistry, 10, 231-236. https://doi.org/10.2147/CCIDE.S178114
Amir, L. R., Tanti, I., Maharani, D. A., Wimardhani, Y. S., Julia, V., Sulijaya, B., & Puspitawati, R. (2020). Student perspective of classroom and distance learning during COVID-19 pandemic in the undergraduate dental study program Universitas Indonesia. BMC Medical Education, 20(1), Article 392. https://doi.org/10.1186/s12909-020-02312-0
Bloom, B. S., College, C. O., & Examiners, U. (1964). Taxonomy of educational objectives (Vol. 2). Longmans.
Borromeo, G. L., Ahmad, M. S., Buckley, S., Bozanic, M., Cao, A., Al-Dabbagh, M., & Athale, A. (2018). Perception of Special Needs Dentistry education and practice amongst Australian dental auxiliary students. European Journal of Dental Education, 22(3), e321-e326. https://doi.org/10.1111/eje.12296
Chang, T.-Y., Hsu, M.-L., Kwon, J.-S., Kusdhany, M. F. L. S., & Hong, G. (2021). Effect of online learning for dental education in Asia during the pandemic of COVID-19. Journal of Dental Sciences, 16(4), 1095-1101. https://doi.org/10.1016/j.jds.2021.06. 006
Daly, B., Boyle, C., Mc Pherson, A., & Thompson, S. (2014). Core content for a curriculum in Special Care Dentistry at the undergraduate level mapped to the learning outcomes for “Preparing for practice” (GDC-UK, 2011). British Society for Disability and Oral Health, March, 1–23.
Dougall, A., Thompson, S. A., Faulks, D., Ting, G., & Nunn, J. (2014). Guidance for the core content of a curriculum in Special Care Dentistry at the undergraduate level. European Journal of Dental Education, 18(1), 39-43. https://doi.org/10.1111/eje.12054
Faculty of Dentistry. (2022). DS240- Bachelor of Dental Surgery Program Structure. Retrieved from https://dentistry.uitm.edu.my/index.php/en/programme/programme-offered/2-uncategorised/67-ds240-programme-structure
Glassman, P., Harrington, M., Namakian, M., & Subar, P. (2016). Interprofessional collaboration in improving oral health for special populations. Dental Clinics of North America, 60(4), 843-855. https://doi.org/10.1016/j.cden.2016.05.004
Halim, M., Noorani, T., Karobari, M., & Kamaruddin, N. (2021). COVID-19 and dental education: A Malaysian perspective. Journal of International Oral Health, 13(3), 201-206. https://doi.org/10.4103/jioh.jioh_8_21
Lestari, W., Yazid, N. H., Azhar, Z. N., Ismail, A., & Sukotjo, C. (2022). Impact of COVID-19 on Malaysian dental students’ physical, mental, financial and academic concerns. BMC Oral Health, 22(1), Article 46. https://doi.org/10.1186/s12903-022-02081-w
Malaysian Dental Council. (2021). Code of Practice for Programme Accreditation – Undergraduate dental degree. (2019, effective, April 1, 2021). http://mdc.moh.gov.my/modules/mastop_publish/?tac=COPPA
Mandasari, M., Rahmayanti, F., Derbi, H., & Wimardhani, Y. S. (2021). Special care dentistry perception among dentists in Jakarta: An online survey study. PloS ONE, 16(4): e0249727. https://doi.org/10.1371/journal.pone.0249727
Miller, G. E. (1990). The assessment of clinical skills/competence /performance. Academic Medicine, 65(9), S63-S67. https://doi.org/10.1097/00001888-199009000-00045
Mohamed Rohani, M., Ahmad Fuad, N., Ahmad, M. S., & Esa, R. (2021). Impact of the special care dentistry education on Malaysian students’ attitudes, self-efficacy and intention to treat people with learning disability. European Journal of Dental Education, 26(4), 741-749. https://doi.org/10.1111/eje.12756
Mohamed Rohani, M., & Mohd Nor, N. A. (2021). Dental students’ perception on Disability Equality Training as part of the special care dentistry curriculum. Journal of Dental Education, 85(5), 690-698. https://doi.org/10.1002/jdd.12528
Naimie, Z., Ahmad, N., Shoaib, L., Safii, S., & Mohamed Rohani, M. (2020). Curriculum for Special Care Dentistry: Are we there yet? Journal of International Oral Health, 12(1), 1-7. https://doi.org/10.4103/jioh.jioh_146_19
Rowe, A. D., & Wood, L. N. (2008). Student perceptions and preferences for feedback. Asian Social Science, 4(3), 78-88. https://doi.org/10.5539/ass.v4n3p78
Royal Australasian College of Dental Surgeons. (2021). Specialist Dental Practice. https://racds.org/sdp/
Saleem, Z., Sethi, A., Hassan, M., & Wajahat, M. (2019). Assessments of dental students’ entrepreneurial self-efficacy to aid practice management. Health Professions Educator Journal, 2(2), 54-59. https://doi.org/10.53708/hpej.v2i2.105
Samat, M. F., Awang, N. A., Hussin, S. N. A., & Mat Nawi, F. A. (2020). Online distance learning amidst Covid-19 pandemic among university students. Asian Journal of University Education 16(3), 220-233. https://doi.org/10.24191/ajue.v16i3.9787
Sølvik, R. M., & Glenna, A. E. H. (2021). Teachers’ potential to promote students’ deeper learning in whole-class teaching: An observation study in Norwegian classrooms. Journal of Educational Change, 23, 343-369. https://doi.org/10.1007/s10833-021-09420-8
Tuononen, T., Hyytinen, H., Kleemola, K., Hailikari, T., Männikkö, I., & Toom, A. (2022). Systematic review of learning generic skills in higher education—Enhancing and impeding factors. Frontiers in Education, 7, 1-13. https://doi.org/10.3389/feduc.2022.885917
Walker, K. A., & Koralesky, K. E. (2021). Student and instructor perceptions of engagement after the rapid online transition of teaching due to COVID‐19. Natural Sciences Education, 50(1), e20038. https://doi.org/10.1002/nse2.20038
Wang, J., Peng, B., Zhou, H., & Zhang, J. H. (2020). Dentists’ entrepreneurial intention and associated factors in public hospitals in major cities in Guangdong (South China): A cross-sectional study. BMC Oral Health, 20, 334 https://doi.org/10.1186/s12903-020-01331-z
*Ilham Wan Mokhtar
Faculty of Dentistry, Universiti Teknologi MARA,
47000, Jln Hospital, Sungai Buloh
Selangor, Malaysia
Email: ilham@uitm.edu.my
Submitted: 30 January 2023
Accepted: 2 August 2023
Published online: 2 January, TAPS 2024, 9(1), 20-27
https://doi.org/10.29060/TAPS.2024-9-1/OA2999
Mitsumi Masuda, Naomi Kimura & Akemi Nakagaki
Graduate School of Nursing, Nagoya City University, Japan
Abstract
Introduction: The level of BLS achievement at the end of basic education is not clear, so to develop a BLS training program using QCPR LearnerⓇ and to verify its effectiveness.
Methods: A quantitative descriptive study design was used. The developed BLS program was implemented for 81 fourth-year students at the school of nursing. The program consisted of 2 minutes of training per student and real-time feedback by QCPR LearnerⓇ as well as feedback among students and from faculty members and was conducted twice for each student. Evaluation was conducted from three aspects: learner response and program evaluation both using questionnaires, learning achievement of QCPR score.
Results: The mean values of learners’ responses before and after the program were: attention, 4.32 before and 4.59 after; relevance, 4.48 before and 4.75 after; confidence, 2.32 before and 3.78 after; and satisfaction, 2.12 before and 3.41 after, which increased significantly after the program. The QCPR LearnerⓇ scores increased significantly from 74.08 for the first time to 86.76 for the second time. In the free response, some respondents stated that “visualisation of the procedure by the application improved my skills.”
Conclusion: The results of the evaluation from three aspects showed that this program was effective in improving students’ motivation to learn and skills.
Keywords: Basic Life Support, Real-Time Feedback, Basic Nursing Education, Simulation Training, QCPR Learner
Practice Highlights
- Real-time feedback application was effective in increasing motivation to learn and BLS skills.
- QCPR LearnerⓇ can be easily installed on the learner’s device, making it suitable for self-learning.
I. INTRODUCTION
A “chain of life support” is necessary to save the lives of individuals in life-threatening situations such as cardiac arrest or asphyxiation, or in imminent danger of such situations, and to lead them back to society (Japan Resuscitation Council, 2020). When a person is unresponsive, it is important to immediately report suspected cardiac arrest and provide basic life support (BLS), which involves a series of procedures to support breathing and circulation including cardiopulmonary resuscitation (CPR) with chest compressions and artificial respiration and the use of an automated external defibrillator (AED). Prompt initiation of CPR by bystanders is essential to improve the survival rate of individuals in cardiac arrest and prompt BLS plays a major role in their reintegration into society. The international consensus on CPR has recently been revised after five years (Nolan et al., 2015), with the updated Japan Resuscitation Council Resuscitation Guidelines published in 2020 (Japan Resuscitation Council, 2020). This guideline includes detailed guidance on compression depth and rhythm of cardiac massage, with improved quality of cardiac massage highlighted as particularly important in increasing survival following cardiac arrest. Effective education and training are important as quality CPR requires accurate compression depth, rhythm, and ventilation volume.
Studies of BLS simulations for nursing students have reported learning effects in students who had prior knowledge of BLS (Requena-Mullor et al, 2021). However, visual assessment is reported to be inaccurate in assessing quality of CPR (Brennan et al., 2016). Accordingly, the Resuscitation Guidelines 2020 include game-based learning, virtual reality, full mastery learning, iterative learning, and on-site simulation, which did not receive significant attention in the Resuscitation Guidelines 2015 (Japan Resuscitation Council, 2015). The new learning styles advocated by the revised Resuscitation Guidelines are expected to further promote the development and effectiveness of teaching materials. In educational settings, devices that can objectively evaluate CPR skills have been developed as a means of increasing educational effectiveness, with teaching materials that provide real-time feedback increasingly being used. In recent years, the use of feedback devices in BLS training for medical personnel has been shown to improve CPR skills (Abella et al., 2007; Lin et al., 2018; Otero-Agra et al., 2019; Semeraro et al., 2019); however, feedback devices for CPR have not previously been evaluated in prelicensure nursing students.
Accordingly, we focused on QCPR Little Anne, a cardiopulmonary resuscitation simulator that incorporates a feedback device into CPR training, and QCPR LearnerⓇ, a dedicated application that allows learners to check their performance. QCPR LearnerⓇ can be used in conjunction with QCPR Little Anne to obtain objective feedback on the quality of CPR from a smartphone or tablet PC. In the basic nursing curriculum, students are required to acquire BLS skills by the time they graduate from the program. The present study therefore aimed to develop a BLS training program with real-time feedback incorporating QCPR Little Anne and QCPR LearnerⓇ to enhance emergency response skills in a basic nursing education program. The BLS training program was evaluated according to three aspects: learner response including satisfaction, learning achievement, and overall program evaluation. QCPR is not a skill that can be experienced routinely in clinical practice. In addition, for nursing students, it is a skill that they may not always be able to experience during clinical practice. Objective feedback on the quality of QCPR would help students to further improve their skills through repeated self-leaning.
II. METHODS
A. Program Overview
In the BLS training program, participants were required to study until they achieved a score of 100 on a test of items related to BLS in the online educational tool Nursing Skills as a prerequisite for program participation. This is because in simulation education, it is important to learn practically based on an understanding of knowledge. Those who fulfilled the conditions for participation participated in the program, and a pretest and simulation training assignments were conducted.
B. Study Participants
The present study comprised fourth-year undergraduate nursing students in the School of Nursing at Nagoya City University in Japan. All students consented to participation in the present study.
C. Training Program Development
The development process of the program used in the present study is described below. CPR is one of the essential skills for both nursing students and health care providers. In clinical settings, BLS training has been shown to be effective in allowing trainees to respond quickly in situations requiring BLS (Kuyt et al., 2021; Shin et al., 2015). However, the effectiveness of BLS education in basic nursing curricula has not been adequately examined despite BLS being a requirement for graduation. In recent years, teaching materials have been developed that allow real-time visualisation of performance using cardiopulmonary resuscitation simulators that incorporate feedback devices. As BLS education is required by nursing students before graduation, visualisation of skills through real-time feedback may represent a useful addition to BLS training.
The following learning objectives for the program were set with reference to the skills required of nursing students at graduation (Ministry of Health, Labor and Welfare, 2021) and the BLS provider course conducted by the ACLS Association of Japan (American Heart Association, 2016). Goal 1: Be able to perform an initial assessment of an injured or unwell individual following a witnessed collapse. Goal 2: Be able to request support from the emergency response system. Goal 3: Be able to immediately perform CPR. Goal 4: Be able to promptly use an automated external defibrillator (AED). The program focused on how to respond as a bystander following a witnessed collapse of a patient and included BLS training for in-hospital cardiac arrest as an algorithmic simulation that assumes an actual situation. During the program design, interviews were conducted with nurses with extensive BLS teaching experience and experts in simulation education to confirm the appropriateness and validity of the content. In addition, a pilot test was conducted by researchers and nursing faculty with experience in BLS education for nursing students.
The specific program flow was as follows. An orientation and pre-test were given to participants who met the prerequisites. The simulation used one QCPR Little Anne per group of three to four participants. Each facilitator was assigned one or two groups. After a 10-minute briefing, the participants were divided into groups. Group members took turns and each person performed two 5-minute simulations. Each simulation consisted of preparation, practical (two minutes), and feedback. QCPR LearnerⓇ real-time feedback consisted of overall score, compression depth, and ventilation rate (Laerdal, 2022). Performers were also advised of the observations of the group members and facilitators. A 20-minute debriefing was held after all participants had completed the simulation. The evaluation was conducted from three aspects: learner response including satisfaction and program evaluation, as Level 1 response of Kirkpatrick’s four-level evaluation method (Gagne et al., 2005), and learning achievement, as Level 2 learning.
D. Data Collection
1) Survey Contents:
As a pre-test, a test consisting of five questions was evaluated the learners’ knowledge before the program. The pre-test was created based on a test of items related to BLS in the online educational tool Nursing Skills, with correct answer scoring one point. Learner responses were assessed before and after the program using a self-administered, anonymous learner response sheet. The response sheet consisted of questions regarding attention, relevance, confidence, and satisfaction on a 5-point Likert scale with reference to previous research (Hirakawa et al., 2018) on the Kirkpatrick’s Four-Level Training Evaluation Model (Alzahrani, 2016) was originally developed. Participants were also given the opportunity to provide free-response statements. As a measure of learning achievement, the overall score for each applicant was used in the study analysis. A Class Evaluation Scale for Nursing Skills Practice (Mochizuki & Nagano, 1999) was administered after the program to allow evaluation of the overall program. The class evaluation scale is a scale consisting of 39 questions on six subscales.
2) Survey Method:
Prior to the start of the exercise, the pre-tasks were reviewed, and a pre-test and response sheet were administered. After the program, response sheets and class evaluation scales were distributed to all participants. The response sheets and class evaluation scales were collected anonymously. Data collection was conducted in September 2020.
E. Data Analysis
For quantitative data, the correspondence t-test was used to compare test scores and an independent t-test was used to compare data from learner response sheets. Descriptive statistics were used for program evaluations. For qualitative data, free-response statements and class evaluation scores were categorised to maintain semantic content. Codes, subcategories, and categories were checked between researchers to enhance the veracity of the analysis. Quantitative data were analysed using SPSS ver. 28.0.
III. RESULTS
A. Overview of Study Participants
A total of 81 students participated in the present study after provided informed consent. Valid responses were obtained from 78 students (96.2%) for the first response sheet, from 80 students (98.8%) for the second response sheet, and from 78 students (96.2%) for the overall class evaluation form. The mean score on pre-test was 4.57 ± 0.67.
B. Learner Reactions
Comparisons of scores from the pre- and post-program response sheets are shown in Table 1 (Masuda, 2023). Significantly increases in all four assessed areas were observed after the program: interest (t= −2.74; P = 0.01), relevance (t= −2.926; P = 0.00), confidence (t= −10.45; P = 0.00), and satisfaction (t=−8.12; p = 0.00). The four items on the response sheets were strongly and positively correlated with interest and satisfaction (pre: r = 0.51; post: r = 0.58) and confidence and satisfaction (pre: r = 0.87; post: r = 0.74) before and after the program, respectively.
|
|
Pre-program group (n=78) |
Post-Program group (n=80) |
t |
p |
||
|
|
M |
SD |
M |
SD |
||
|
Attention to learning BLS |
4.32 |
.69 |
4.59 |
.52 |
-2.73 |
.01 |
|
Are relevance to learning BLS |
4.48 |
.66 |
4.75 |
.49 |
-2.92 |
.00 |
|
I am confident in my BLS skills |
2.32 |
1.02 |
3.78 |
.71 |
-10.45 |
.00 |
|
I am satisfied with my current BLS skills |
2.12 |
1.08 |
3.41 |
.92 |
-8.12 |
.00 |
Table 1. Learners’ responses to BLS in the pre- and post-program
Independent t-test: M = mean, SD = standard deviation
The free-response statements were summarised resulting in 116 codes, 17 subcategories, and four categories. Responses related to subcategories and “categories” are shown below (Table 2: Masuda, 2023). The most frequent positive responses were those related to the effectiveness of QCPR Learner. Examples of statements representative of categories and subcategories are provided below.
Visualisation of the appropriateness of the technique clarified my issues, I can improve by checking my current level with the application and “Visualisation of the technique with the application improved my skills”. Comments related to the effectiveness of QCPR Learner informed the “I improved my skills through repetitive practice training” category consisting of subcategory statements such as I improved my skills through repetitive training, and my skills improved through practical training. The category “Learned the elements of techniques necessary for QCPR” consisted of statements informing subcategories such as using the back mask was difficult and I was able to learn a series of BLS techniques. The category “I realised that the effectiveness of BLS is enhanced through group cooperation” included the subcategory “I was able to enhance my skills with my group members, including encouragement and feedback from members”. Statements informing the “Increased motivation to learn” category included I enjoyed improving my skills, I am glad I participated, I gained confidence, and if something happens, I will be able to implement BLS.
|
Subcategory |
Category |
|
Visualising the appropriateness of the technique helped clarify issues |
Skills improved through visualisation of techniques by application |
|
Enjoyed learning while improving the accuracy of skills |
|
|
The use of the app increased my motivation |
|
|
The application allowed me to see my current level of skill so that I can improve |
|
|
Practical training improved my skills |
Skills improved through repetitive practice training |
|
The content was designed for practical use |
|
|
I was able to acquire skills through repetitive training |
|
|
Skills improved through repetitive training |
|
|
Correct use of BM is difficult |
Learned the elements of techniques required for QCPR |
|
Learned how to use the back mask |
|
|
I was able to learn a series of BLS techniques |
|
|
Realised that BLS requires physical strength |
|
|
I was able to perform high-quality CPR by working together as a group. |
Realised that BLS is more effective when working in a group |
|
I was able to enhance my skills with my group members |
|
|
I learned that BLS is more effective when we work together as a group |
|
|
I was able to improve my skills in a fun way |
Increased motivation to learn |
|
If something happened, I would be able to perform it. |
|
|
If something happens, I will be confused, but I will be able to cooperate with others |
|
|
I gained confidence |
|
|
I am glad to have participated |
Table 2. Categories related to learner response
C. Learning Achievement
The second test scores on QCPR Learner were significantly higher than the first test scores (t = −4.78; P = 0.00) (Table3).
D. Program Evaluation
Regarding the class evaluation scale administered after the program, the subscale “Time allocation and difficulty of content” scored 59.49 ± 6.12, “Delivery and guidance/advice” scored 33.77± 2.21, “Use and innovation of teaching materials” scored 9.27 ± 1.02, “Demonstration” scored 26.21 ± 4.71, “Interaction among students” scored 9.64 ± 0.84, and “Attitude and response to students and exercises” scored 43.29 ± 3.30 (Table 4).
|
|
|
|
|
n=78 |
||
|
|
1st QCPR |
2nd QCPR |
t |
P |
||
|
|
M |
SD |
M |
SD |
||
|
QCPR score |
74.08 |
23.53 |
86.76 |
14.29 |
-4.78 |
0.00 |
Table 3. Pre- and post-QCPR score changes
Paired-samples t-test: M = mean, SD = standard deviation
|
n=79 |
||
|
|
M |
SD |
|
Time allocation and difficulty of the content |
59.49 |
6.12 |
|
Delivery and guidance/advice |
33.77 |
2.21 |
|
Use and innovation of teaching materials |
9.27 |
1.02 |
|
Demonstration |
26.21 |
4.71 |
|
Interaction among students |
9.64 |
.84 |
|
Attitude and response to students and exercises |
43.29 |
3.30 |
Table 4. Evaluation of a class evaluation scale for nursing skills practice
Subjects were asked to respond to an open-ended question regarding their evaluation of the program, resulting in 29 codes, 10 subcategories, and six categories. Responses related to subcategories and “categories” are shown below (Table 5). Statements related to evaluation of the program content and facilitators informed the category “The facilitator’s involvement was good” consisting of statements representative of the subcategories the entire program was clear and concise, and the facilitator created an easygoing atmosphere. The category “The program time and content were just right” consisted of subcategories informed by statements such as the time of the program was just right, and the amount of the program was just right. There were a few opinions regarding the content of the program and the instructors such as there were some problems with the application, more specific explanations would have been better, and there were too many hours spent on the exercise.
|
Subcategory |
Category |
|
The entire program was clear and concise |
The facilitators involvement was good |
|
The Facilitators created an easygoing atmosphere |
|
|
The time of the program was just right |
The program time and content were just right |
|
The amount of program was just right |
|
|
There were some problems with the application |
There was a glitch in the application |
|
More specific explanations would have been better |
More specific explanations would have been better |
|
There were too many hours spent on the exercise |
|
|
The time commitment was too much |
The time commitment was too much |
Table 5. Categories related to evaluation of the program
IV. DISCUSSION
A. Evaluating Programs from the Perspective of Learner Responses
The results of the response sheets administered before and after the program demonstrated a significant increase in all items. BLS skills are technical items in the nursing education curriculum designated by the Ministry of Health, Labor and Welfare (Ministry of Health, Labor and Welfare, 2021) that may be required in clinical practice. The implementation of simulations of potential future scenarios promotes student motivation (Hae-Kyoung, 2021). and simulations are known to be an effective learning method for putting theoretical knowledge into practice and reducing fear before encountering real situations (Carrero- Planells et al, 2021). The students were highly satisfied with the simulation in the present study as they had completed their clinical training, had an image of the clinical situation, and recognised that it was a necessary skill for post-graduates.
In addition, a correlation was observed between interest in BLS and satisfaction with BLS, and between confidence and satisfaction with BLS. The findings indicate that it is necessary to select subjects that are already interested in BLS and likely to have greater satisfaction with BLS training and to structure BLS programs in a way that leads to confidence and satisfaction with BLS skills.
Many participants in the present study gave positive evaluations of the program, such as “Visualisation of the technique by the application helped me improve my skills.” The effectiveness of visual feedback has been shown to be effective in improving skills in previous studies in other fields (Unell et al., 2021; Yamamoto et al., 2019). The QCPR LearnerⓇ used in this study also make it clear at a glance whether the current skill of the self is appropriate, due to is visualised the CPR situation in real time. For example, by following the application parameters while performing chest compressions, the learner was able to learn how to utilise his/her own body functions accurately while performing the CPR. Thus, we believe that the real-time visual feedback was a challenge for the learners and helped them to improve their skills.
The learners also realised that visualisation and repetitive training using the QCPR LearnerⓇ helped them learn the elements of the technique necessary for high-quality CPR and that the effectiveness of BLS was enhanced through group cooperation. Furthermore, this may have led to increased motivation to learn. The ARCS model (Keller, 2010), a model for improving motivation to learn proposed by John Keller in 1983 (Keller, 1987), describes the following actions that educators should take to improve and maintain learner motivation: attention, relevance, confidence, and satisfaction. From the components of the “Increased motivation to learn” category identified in the present study, the following subcategories were developed: I enjoyed improving my skills, if something happens, I will be able to implement BLS, I gained confidence, and I am glad I participated.
Considering the four aspects of the ARCS model, “Enjoyed” corresponds to attention, “Will be able to implement” to relevance, “Gained confidence” to confidence, and “Glad to have participated” to satisfaction. A key finding of the present study was the importance of simulating all four aspects of the ARCS model, as evidenced by the increased motivation to learn among participating nursing students.
B. Learning Effectiveness in terms of Learning Attainment
Our program used QCPR Little Anne and QCPR LearnerⓇ to improve BLS skills, with feedback given according to the application score after the first implementation. As a result, significantly higher scores were obtained in the second session. Previous studies have reported that visual feedback enables students to perform challenging procedures such as ensuring the correct depth of chest compressions (Baldi et al., 2017). In our program, students were able to visually perceive them own BLS skills as numerical values indicating weaknesses and areas for improvement, thereby leading to improved BLS skills.
C. Program Evaluation
Program feedback, time allocation and difficulty level of the content, communication of significance and objectives, guidance and advice, use and innovation of teaching materials, demonstration, interaction among students, and attitude and response to students and exercises were all highly evaluated in the present study. The program was conducted in small groups after the students watched a demonstration video with clearly stated objectives and goals. We believe this approach increased student motivation to learn BLS skills. The program also received positive feedback from the facilitators and group members during individual training and the facilitators provided timely advice, which led to skill improvement. These results indicate that the program provided appropriate conditions for the acquisition of BLS skills.
In the results of the free description, most of the participants were positive about the facilitator’s involvement and the duration and content of the program. On the other hand, some participants felt that the program was too time-consuming, albeit only slightly. This may be attributable to the extra time required to change clothes due to coronavirus precautions. In addition, some participants expressed a desire for more practice. The QCPR LearnerⓇ used in this program can be easily installed on the learner’s own device. We therefore believe that methods that allow self-study at any time may satisfy the desire to learn and lead to skill improvement. Regarding the device, one participant stated “There was a problem with the application”; however, this was expected and could be avoided as a spare device had been prepared in advance. We were able to confirm once again that preparing in advance for anticipated problems and responses to them is an important factor for success when using such devices.
V. CONCLUSION
The results of the present study demonstrate that visualisation of skill improvement using an application that provides real-time feedback was effective in increasing motivation to learn and improving BLS skills. This led some of the learners to request further training. Although it is possible to increase the training time per person by increasing the program duration or the number of simulations, this is limited by cost and manpower. Accordingly, it is necessary to establish a self-learning system that enables learning at any time.
Notes on Contributors
Mitsumi Masuda, Naomi Kimura, and Akemi Nakagaki contributed to all process of this research and read and approved the final manuscript.
Dr. Mitsumi Masuda, PhD, RN, is an associate professor at the Graduate School of Nursing, Nagoya City University. She reviewed the literature, designed the study, performed data collection, data analysis and wrote the manuscript.
Dr. Naomi Kimura, PhD, RN, MW, is an assistant professor at the Graduate School of Nursing, Nagoya City University. She developed the methodological framework for the study, performed data collection, data analysis and gave critical feedback to the writing of the manuscript.
Dr. Akemi Nakagaki, PhD, RN, MW, is an associate professor at the Graduate School of Nursing, Nagoya City University. She performed data collection and data analysis. All the authors have read and approved the final manuscript.
Ethical Approval
The present study was conducted with the approval of the Research Ethics Review Committee of Nagoya City University (approval number: 20011-3). The research subjects were informed orally and in writing of the purpose, methods, protection of personal information, respect for their free will, that the submitted assignments would be processed for research after class evaluation so that individuals would not be identified, and that they would not be involved in any individual class evaluation.
Data Availability
Datasets generated and/or analysed during the current study are available from the following URL:
https://doi.org/10.6084/m9.figshare.21918864.v1
Acknowledgement
We would like to thank all the nursing students who willingly cooperated in the present study.
Declaration of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interests.
Funding Statement
This study was completed without the support of the funding.
References
Abella, B. S., Elizabeth, D. P., Myklebust, H., Barry, A. M., O’Hearn, N., Vanden Hoek, T. L., & Becker, L. B. (2007). CPR quality improvement during in-hospital cardiac arrest using a real-time audiovisual feedback system. Resuscitation, 73(1), 54-61. https://doi.org/10.1016/j.resuscitation.2006.10.027
Alzahrani, A. R. (2016). Kirkpatrick’s four-level training evaluation model. International Journal of Scientific and Engineer ing Research, 7(5), 66-69.
American Heart Association. (2016). Basic life support instructor manual for instructor-led training. American Heart Association.
Baldi, M. E., Cornara, S., Contri, E., Epis, F., Fina, D., Zelaschi, B., Dossena, C., Fichtner, F., Tonani, M., Di Maggio, M., Zambaiti, E., & Somaschini, A. (2017). Real-time visual feedback during training improves laypersons’ CPR quality: A randomized controlled manikin study. Canadian Journal of Emergency Medi- cine, 19(6), 480-487. https://doi.org/10.1017/cem.2016.410
Brennan, E. E., McGraw, R. C., & Brooks, S. C. (2016). Accuracy of instructor assessment of chest compression quality during simulated resuscitation. Canadian Journal of Emergency Medicine, 18(4), 276-282. https://doi.org/10.1017/cem.2015.104
Carrero-Planells, A., Pol-Castaneda, S., Candida, M., Alamillos-Guardiola, M. C., Prieto-Alomar, M., Tomas-Sanchez, M., & Moreno-Mulet, C. (2021). Students and teachers’ satisfaction and perspectives on high-fidelity simulation for learning fundamental nursing procedures: A mixed-method study. Nurse Education Today, 104, Article 104981. https://doi.org/10.1016/j.nedt.2021.104981
Gagne, R. M., Wager, W. W., Golas, K. C., Keller, J. M., & Russell, J. D. (2005). Principles of instructional design (5th ed.). Cengage Learning.
Hae-Kyoung, S., & Son, H. K. (2021). The effects of simulation problem-based learning on the empathy, attitudes toward caring for the elderly, and team efficacy of undergraduate health profession students. International Journal of Environmental Research and Public Health, 18(18), 1-13. https://doi.org/10.3390/ijerph18189658
Hirakawa, Y., Yahiro, Y., Fukano, K., Nakamura, M., Maruyama, T., Usui, Y., & Aoki, N. (2018). Student’s evaluation on simulation learning in perioperative nursing. Journal of Japan Association for Simulation-Based Education in Healthcare Professionals, 6, 36-40.
Japan Resuscitation Council. (2015). JRC resuscitation guideline 2015. IGAKU-SHOIN Ltd.
Japan Resuscitation Council. (2020). JRC Resuscitation Guideline 2020. IGAKU-SHOIN Ltd.
Keller, J. M. (2010). Motivational design for learning and performance: The ARCS model approach (1st ed.). Springer.
Keller, J. M. (1987). Development and use of the ARCS model of instructional design. Journal of Instructional Development, 10(3), 2-10.
Kuyt, K., Mullen, M., Fullwood, C., Chang, T. P., Fenwick, J., Withey, V., & MacKinnon, R. J. (2021). The assessment of a manikin-based low-dose, high-frequency cardiac resuscitation quality improvement program in early UK adopter hospitals. Advances in Simulation, 6(14), 1-12. https://doi.org/10.1186/s410 77-021-00168
Laerdal. (2022). Products & services. Laerdal. Retrieved November 1, 2022, from https://laerdal.force.com/HelpCenter/s/ article/QCPR-App-feedback-symbols-and-scoring
Lin, Y., Cheng, A., Grant, V. J., Currie, G. R., & Hecker, K. G. (2018). Improving CPR quality with distributed practice and real-time feedback in pediatric healthcare providers – A randomized controlled trial. Resuscitation, 130, 6-12. https://doi.org/10.1016/ j.resuscitation.2018.06.025
Masuda, M. (2023). Real-time feedback in basic nursing education: Evaluation of basic life support training programs [Data set]. Figshare. https://doi.org/10.6084/m9.figshare. 2191886 4.v1
Mochizuki, M., & Nagano, M. (2015). Classroom process evaluation scale for nursing skills exercises. IGAKU Ltd.
Ministry of Health, Labour and Welfare. (2021). Operational guidelines for the technical intern training program relating to specific occupations and operations regarding the standards for the occupation ‘care worker’. Retrieved November 30, 2022, from https://www.jspcun.or.jp/wp/wp-content/uploads/2021/03/guideli ne_2020.11.26.pdf
Nolan, J. P., Hazinski, M. F., Aickin, R., Bhanji, F., Billi, J. E., Callaway, C. W., Castren, M., de Caen, A. R., Ferrer, J. M., Finn, J. C., Gent, L. M., Griffin, R. E., Iverson, S., Lang, E., Lim, S. H., Maconochie, I. K., Montgomery, W. H., Morley, P. T., Nadkarni, V. M., & Zideman, D. A. (2015). Part 1: Executive summary: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation, 95, e1-31. https://doi.org/10.10 16/j.resuscitation.2015.07.039
Otero-Agra, M., Barcala-Furelos, R., Besada-Saavedra, I., Peixoto-Pino, L., Martiínez-Isasi, S., & Rodriíguez-Nunúñez, A. (2019). Let the kids play: Gamification as a CPR training methodology in secondary school students. A quasi-experimental manikin simulation study. Emergency Medicine Journal, 36(11), 653-659. https://doi.org/10.1136/emermed-2018-208108
Requena-Mullor, M. D. M., Alarcón-Rodríguez, R., Ventura-Miranda, M. I., & García-González, J. (2021). Effects of a clinical simulation course about basic life support on undergraduate nursing students’ learning. International Journal of Environmental Research and Public Health, 18(4), Article 1409. https://doi.org/10.3390/ijerph18041409
Semeraro, F., Frisoli, A., Loconsole, C., Mastronicola, N., Stroppa, F., Ristagno, G., Scapigliati, A., Marchetti, L., & Cerchaiari, E. (2019). Kids (learn how to) save lives in the school with the serious game Relive. Resuscitation, 36(11), 653-659. https://doi.org/10.1016/j.resuscitation.2017.04.038
Shin, N., Tonaka, K., Dosaka, A. (2015). Study of educational effects of BLS training for each number of attempts – from the result of analysis of a participant questionnaire. The Bulletin of Keio University Health Center, 33, 115-121.
Unell, A., Eisenstat, Z. M., Braun, A., Gandhi, A., Gilad‑Gutnick, S., Ben‑Ami, S., & Sinha, P. (2021). Influence of visual feedback persistence on visuo‑motor skill improvement. Scientific Reports, 11, Article 17347. https://doi.org/10.1038/s41598-021-9
Yamamoto, R., Akizuki, K., Kanai, Y., Nakano, W., Kobayashi, Y., Ohashi, Y. (2019). Differences in skill level influence the effects of visual feedback on motor learning. Journal of Physical Therapy Science, 31(11), 939–945. https://doi.org/10.1589/jpts.31.939
*Mitsumi Masuda
Nagoya City University,
1, Kawasumi, Mizuho-cho,
Mizuho-ku, Nagoya, 467-8601, Japan
+81-52-853-8063
E-mail: m.masuda@med.nagoya-cu.ac.jp
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
