
Developing a blended learning orientation programme for junior doctors in Neonatology
Submitted: 19 October 2023
Accepted: 25 March 2024
Published online: 2 July, TAPS 2024, 9(3), 58-60
https://doi.org/10.29060/TAPS.2024-9-3/CS3159
Wing Yee Tong1, Bin Huey Quek1, Arif Tyebally2 & Cristelle Chow3
1Department of Neonatology, KK Women and Children’s Hospital, Singapore; 2Emergency Medicine, KK Women and Children’s Hospital, Singapore; 3Department of Paediatrics, KK Women and Children’s Hospital, Singapore
I. INTRODUCTION
Neonatology is considered a ‘niche’ paediatric subspecialty. Most junior doctors posted to the department have limited prior exposure to the neonatal population, and require quick and effective training to help them function safely on the clinical floor. In recent years, postgraduate medical teaching has found the use of blended learning to be effective (Liu et al., 2016). Blended learning is defined as a combination of classroom face-time with online teaching approaches, and there is currently paucity of literature on its efficacy in ‘up-skilling’ relatively inexperienced healthcare professionals in a subspecialty setting. Hence, the aim of this study was to design and evaluate the efficacy of a blended-learning orientation programme in improving neonatal clinical knowledge and procedural skills amongst junior doctors.
II. METHODS
A. Study Setting and Participants
This study was set in the largest academic tertiary paediatric hospital in Singapore.
B. Curriculum Development
We adopted the Kern’s six-step approach for curriculum development (Thomas et al., 2022), as it systematically identifies and addresses learner needs, and its cyclical nature also allows for constant modifications and improvements.
1) Step 1: Problem identification and general needs assessment
We conducted a quantitative survey to identify the general issues with our current programme, which consisted of daily face-to-face, largely didactic lectures over the first month of the posting. We noticed that many junior doctors missed teaching sessions due to work obligations, resulting in ‘piecemeal’ and ineffective learning. The one-month programme was also considered excessively lengthy.
2) Step 2: Targeted needs assessment
Most junior doctors considered themselves to be ‘novice’ learners in neonatology. This emphasised the importance of starting with foundational teaching concepts to avoid overwhelming them. Junior doctors also preferred interactive learning methods.
3) Step 3: Goals and objectives
Our main objective was for the junior doctors to be competent and safe members of the clinical team, with basic neonatal clinical knowledge and the ability to perform and assist in neonatal procedures.
4) Step 4: Educational strategies: Course content development
We identified a list of core topics and procedural skills which formed the programme curriculum (Figure 1).
The teaching format was changed from mainly didactic lectures to case-based scenarios in both online and face-to-face sessions, as this has been shown to better motivate students towards self-directed learning and develop problem-solving skills. Case-based scenarios would also facilitate greater peer discussion and interactivity amongst learners in the face-to-face sessions.
We worked with IT specialists to convert specific topics to six online learning modules, and included interactive components such as clickable elements and narration to better engage learners (Choules, 2007). Each module was designed to be completed within 30 minutes.
For neonatal procedural skills, learners were expected to watch online demonstration videos created by the department prior to attending hands-on practical sessions.
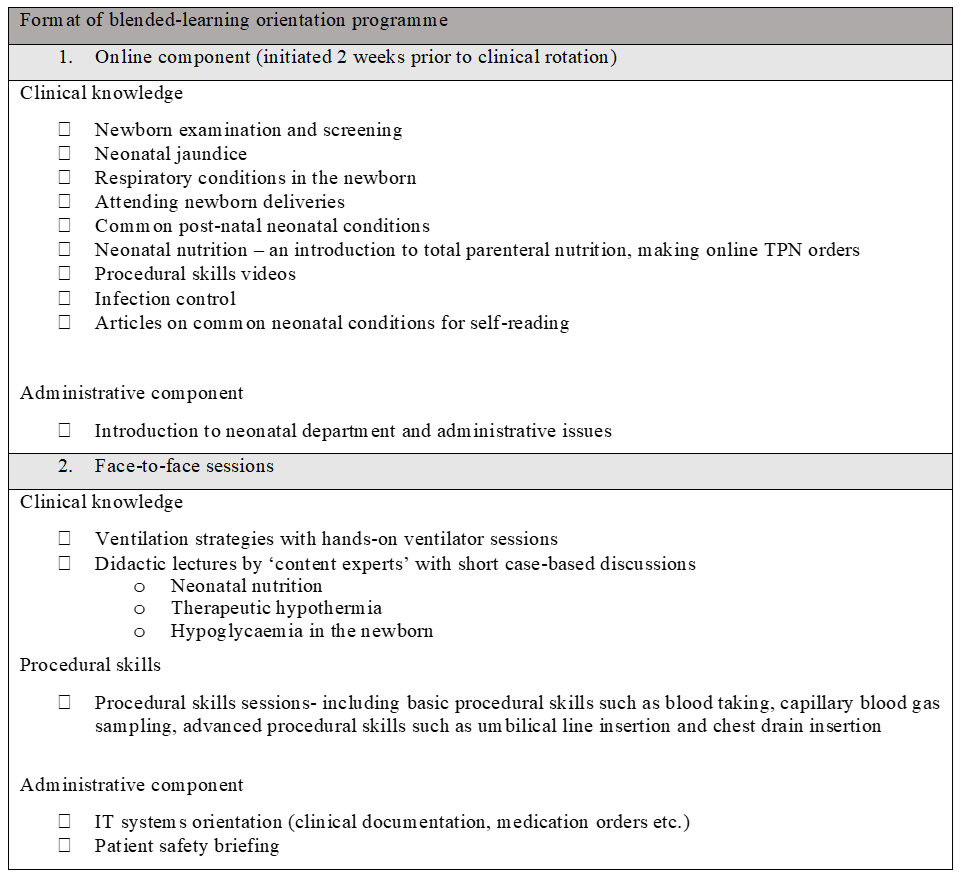
Figure 1. Outline of blended-learning orientation programme
5) Step 5: Implementation
The blended learning programme was implemented with junior doctors across two batches from July 2022 to January 2023. Majority were from post-graduate year three to five, with approximately half having no prior working experience in neonatology. All participated in the face-to-face sessions and completed the online modules.
We used our institution’s online learning management system to deliver the e-learning modules, and department faculty members conducted the face-to-face sessions. Designated ‘protected teaching time’ was implemented to facilitate attendance during office hours.
6) Step 6: Evaluation and feedback
We designed a pre-and-post-programme assessment consisting of 24 multiple-choice questions covering the following aspects – (1) clinical scenarios with interpretation of laboratory and radiological results, (2) factual knowledge and (3) questions on procedural skills.
The junior doctors also completed an online survey which assessed the learners’ perceptions on blended learning. Consent for the survey data to be used for research was implied in their participation.
III. RESULTS
The junior doctors had a positive experience with blended learning. All participants agreed that the learning content was relevant and appropriate for their level of experience. Almost all participants felt that there was ease of access to the online learning modules, with minimal technical issues. Learners also found specific online modules such as respiratory conditions ‘useful’, but enjoyed the face-to-face nature of sessions such as ventilatory strategies, as it gave them the opportunity to clarify doubts with their facilitator. Overall, the duration of the face-to-face orientation sessions was halved, and there was a significant improvement in the mean MCQ score.
IV. DISCUSSION
A blended learning programme designed for novice learners in Neonatology is effective in preparing junior doctors for clinical work.
Learning theories suggest that adult learners are motivated to invest time in learning if they understand its relevance (Taylor & Hamdy, 2013). The shift towards case-based learning bridges theory and practice, and motivates participation in clinical decision-making. This is an effective form of learning as demonstrated by an improvement in the mean post-test MCQ score of the participants. The experience was also deemed a positive one in qualitative feedback. In addition, the accessibility of online modules provided learners with autonomy to control their pace of learning. However, it is important to strike the right balance between online and classroom teaching, as learners still value the interactivity offered by face-to-face teaching.
We should work to create a supportive infrastructure to support blended learning methods by training more clinician-educators in online learning approaches and designing ‘reusable’ learning resources, which can be modified and integrated into other medical courses in future (Singh et al., 2021).
The limitations of our study include reliance on multiple choice tests to assess knowledge, and a lack of formal evaluation of procedural skills. Competency-based evaluations, as well as practical skills evaluations can be implemented in future runs to evaluate the efficacy of the courses.
V. CONCLUSION
Technology enhanced learning is fast becoming an integral part of medical education. Through this study, we demonstrate that blended learning programmes can be successfully integrated into the training of junior doctors in a subspecialty setting.
Notes on Contributors
WT led the design and conceptualisation of this work, implemented the education programme, and drafted the manuscript. BQ provided feedback and guidance on creating the content of the education programme. CC provided guidance on the evaluation of teaching programme. CC, AT and BQ provided feedback on the manuscript. All authors approve the publishing of this manuscript.
Funding
The authors received a Singhealth Duke-NUS Academic Medicine Education Institute Education Grant 2021 (funding number EING2205) to support the development of curriculum content for our programme.
Declaration of Interest
All authors declare that there are no conflicts of interest.
References
Choules, A. P. (2007). The use of elearning in medical education: A review of the current situation. Postgraduate Medical Journal, 83(978), 212-216. https://doi.org/10.1136/pgmj.2006.05 4189
Liu, Q., Peng, W., Zhang, F., Hu, R., Li, Y., & Yan, W. (2016). The effectiveness of blended learning in health professions: Systematic review and meta-analysis. Journal of Medical Internet Research, 18(1), e2.
Singh, J., Steele, K., & Singh, L. (2021). Combining the best of online and face-to-face learning: Hybrid and blended learning approach for COVID-19, post vaccine, & post-pandemic world. Journal of Educational Technology Systems, 50(2), 140-171. https://doi.org/10.1177/00472395211047865
Taylor, D. C., & Hamdy, H. (2013). Adult learning theories: Implications for learning and teaching in medical education: AMEE Guide No. 83. Medical Teacher, 35(11), e1561-e1572. https://doi.org/10.3109/0142159x.2013.828153
Thomas, P. A., Kern, D. E., Hughes, M. T., Tackett, S. A., & Chen, B. Y. (Eds.). (2022). Curriculum development for medical education: A six-step approach. Johns Hopkins University Press.
*Tong Wing Yee
100 Bukit Timah Road
Singapore 229899
Email: tong.wing.yee@singhealth.com.sg
Submitted: 19 September 2023
Accepted: 9 January 2024
Published online: 2 July, TAPS 2024, 9(3), 61-63
https://doi.org/10.29060/TAPS.2024-9-3/CS3137
Yoshikazu Asada1, Chikusa Muraoka2, Katsuhisa Waseda3 & Chikako Kawahara4
1Medical Education Center, Jichi Medical University, Japan; 2School of Health Sciences, Fujita Health University, Japan; 3Medical Education Center, Aichi Medical University, Japan; 4Department of Medical Education, Showa University, Japan
I. INTRODUCTION
The COVID-19 epidemic has prompted the spread of ICT-based education, with many university classes being conducted remotely. Some education systems use asynchronous tools such as learning management systems (LMSs); others use synchronous tools such as web conference systems. This trend has affected not only lectures but also exercises among students and clinical practice. Game-based education is no exception, and classes that require direct face-to-face interaction have become difficult to implement. Escape rooms (ERs) are one example of game-based education.
ERs are defined as “live-action team-based games where players discover clues, solve puzzles, and accomplish tasks in one or more rooms in order to accomplish a specific goal (usually escaping from the room) in a limited amount of time” (Nicholson, 2015). Originally intended for entertainment purposes, ERs now also serve educational purposes (Davis et al., 2022). As an educational tool, ERs are mainly used for teaching specific content knowledge and content-related skills, general skills, and affective goals (Veldkamp et al., 2020). In addition, since ERs are categorised as game-based education, they are also useful for motivating students.
ERs may be conducted either face-to-face or online. Online-based ERs, known as “Digital Educational Escape Rooms” (DEERs), have become common since the COVID-19 pandemic (Makri et al., 2021). DEERs combine the (1) possibility of digital and analog hybrid style, (2) the potential to provide immediate feedback, and (3) the suitability for some learning objectives such as social skills.
This study is intended to design and develop DEERs based on Moodle and Zoom for teaching basic professionalism, with a focus on peer collaboration for medical students.
II. METHODS
The authors made an online-based DEER with Moodle LMS and used it for teaching team communication and reviewing basic CPR knowledge for second-year undergraduate medical students. In this case, students solve asynchronous DEER challenges in Moodle through synchronous discussion in Zoom breakout rooms.
The learning objectives were to “learn collaboratively with peers” and to “understand concepts related to interpersonal relationships and interpersonal behaviour.” Before the class, students submitted a short report on the important elements that are required for team medicine, which they had learned as first-year students. The class was 100 minutes in length. The first 10 minutes were used for orientation. The next 60 minutes were used for DEERs. Within 60 minutes, a hint for solving DEERs was provided via Google Documents; authors added the hint as time went on. After the game, 30 minutes were used for reflection, including the explanation of the DEER answers and the basic lectures. Despite the existence of two aforementioned learning objectives, the time limits made it particularly hard to assess students’ achievement. Therefore, after the class, a report was assigned on the topic “points to keep in mind when sharing information and communicating with your team online through the game experience.”
There were three stages to the DEER. A total game design is shown in Figure 1. The first stage consisted of a 360o virtual room. Students had to explore the virtual room and solve two riddles. In this stage, some hints were hidden on the ceiling or the floor. Students had to find them by looking around the room. After solving the riddles, students inputted the answer to Moodle. If the answer was wrong, they had to wait one minute before inputting another answer. The second stage began after the two riddles. This stage had four puzzles related to CPR, such as concerning the placement of AED or metronome tempo of chest compression. Since the students learned about CPR when they were first-year students, these four puzzles were reviewed their understanding. The third stage was after the four CPR puzzles. In the third stage, students had to gather all the clues to clear the game.
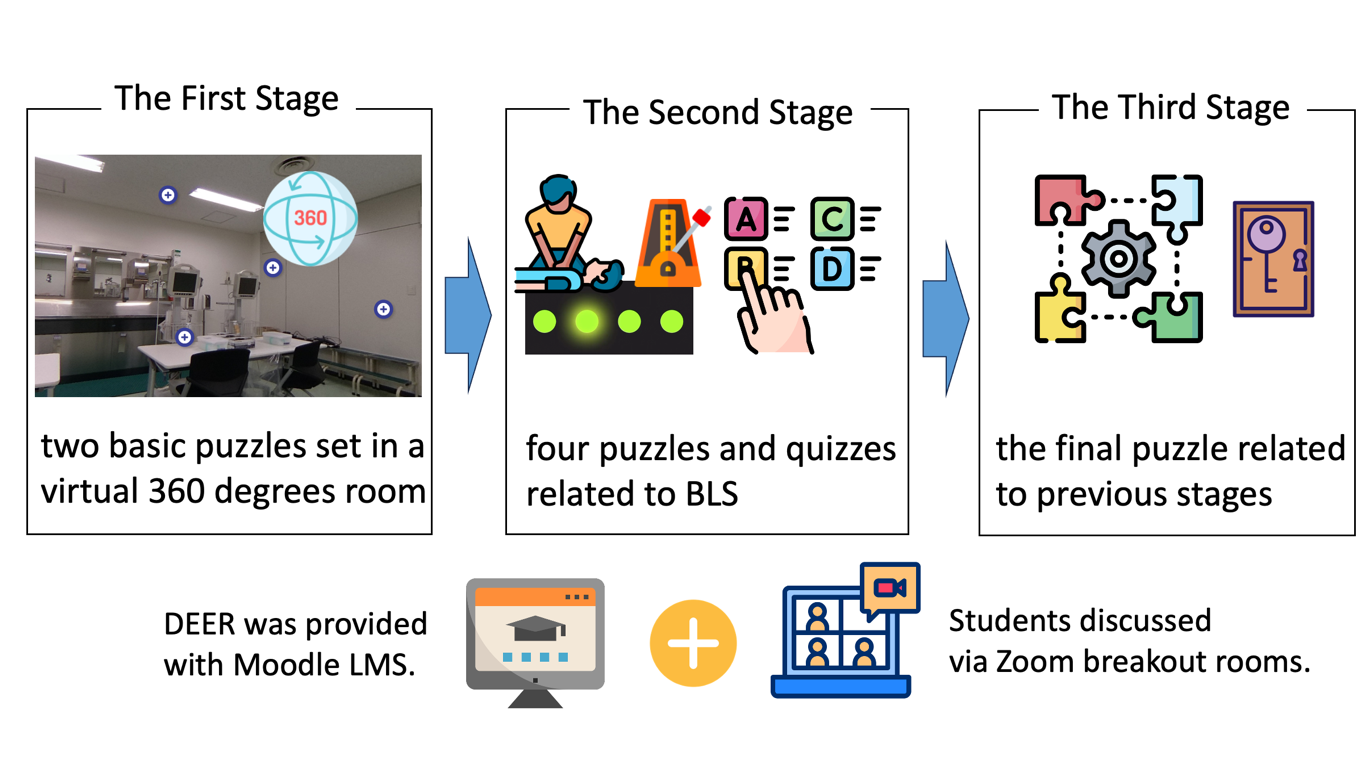
Figure 1. A total game design
Program evaluation was based on students’ achievement results from the Moodle log and their comments from the questionnaires.
III. RESULTS
There were 29 groups, and each one had three to four students. While five groups were able to solve the riddle completely, one group could not even reach stage two. Moodle log data and questionnaires suggested that the difficulty of the riddles was appropriate, since only 8% of participants answered that the first stage was difficult, and other groups used about 15 minutes for the first stage from the logs.
In some groups, students turned off their cameras and solved the riddles individually. In this case, they shared almost nothing but the answers, and very little about the process for solving puzzles and riddles. In other groups, students turned on their cameras and shared the screen. In contrast to the previous groups, they solved the puzzles and riddles through live discussions.
IV. DISCUSSION
Some groups could not complete the DEERs, and one group could not reach stage two. In the group that could not finish stage one, students did not share the process of solving riddles. Moreover, they turned off their cameras, which made it difficult to define how they were approaching the tasks. The communication style of students potentially affects their achievement level. It is also connected to their learning objectives.
Despite the difficulty of teaching skills and attitude only with asynchronous distance learning, some scope exists for interactive content, for example, by having the students choose the correct tempo for chest compressions by sound with live discussion and feedback from others. Of course, it will be more effective to use face-to-face simulations to check psychomotor skills.
In this case, gathering students’ learning logs was easy since DEER was provided with Moodle. In addition, observing how students discuss in online was possible, since Zoom can track the activity status in breakout rooms. Although the design, development, and implementation of the DEERs will be complicated, the hybrid-style DEER, such as using LMS with synchronous classes, might make DEERs more attractive. Furthermore, it makes collection of a variety of data, such as the timestamp of answer, pattern of the failure, and manner of online communication, possible. These data would be useful to assess students and provide feedback to them.
V. CONCLUSION
DEERs are potentially useful for engaging student communication and discussion even in the online synchronous class. In the future, it will be possible to provide an integrated learning experience with a more appropriate difficulty level by accumulating Moodle log data and student recognition data.
Notes on Contributors
YA and CM designed and developed DEER. They also analysed the results.
KW and CK managed the class and facilitated the breakout room.
All authors have read and approved the final manuscript.
Acknowledgement
The authors would like to acknowledge the contributions of all participants.
Funding
This work was supported by FOST (Foundation for the Fusion of Science and Technology) 2019 and 2022 Research Grants.
Declaration of Interest
All authors declare no conflicts of interest.
References
Davis, K., Lo, H. Y., Lichliter, R., Wallin, K., Elegores, G., Jacobson, S., & Doughty, C. (2022). Twelve tips for creating an escape room activity for medical education. Medical Teacher, 44(4), 366–371. https://doi.org/10.1080/0142159X.2021.1909715
Makri, A., Vlachopoulos, D., & Martina, R. A. (2021). Digital escape rooms as innovative pedagogical tools in education: A systematic literature review. Sustainability, 13(8), Article 4587. https://doi.org/10.3390/su13084587
Nicholson, S. (2015, May 24). Peeking behind the locked door: A survey of escape room facilities. http://scottnicholson.com/pubs/erfacwhite.pdf
Veldkamp, A., van de Grint, L., Knippels, M. P. J., & van Joolingen, W. R. (2020). Escape education: A systematic review on escape rooms in education. Educational Research Review, 31, Article 100364. https://doi.org/10.1016/j.edurev.2020.100364
*Yoshikazu Asada
Medical Education Center
Jichi Medical University
3311-1, Yakushiji, Shimotsuke,
Tochigi, Japan
+81-285-58-7067
Email: yasada@jichi.ac.jp
Submitted: 13 September 2023
Accepted: 4 March 2024
Published online: 2 July, TAPS 2024, 9(3), 64-66
https://doi.org/10.29060/TAPS.2024-9-3/CS3138
Jayabharathi Krishnan, Sara Kashkouli Rahmanzadeh & S. Thameem Dheen
Department of Anatomy, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
I. INTRODUCTION
In preclinical years, histology, which is the study of the microscopic structures of tissue and organs, aids students in understanding the normal morphology of cell and tissue organisation in organs and differentiating their pathological changes (Hussein & Raad, 2015). The study of histology is important as it provides the fundamental basis of anatomical knowledge. Students have adapted to a new learning environment, particularly after the COVID-19 outbreak, by utilising autonomous learning strategies, including online and digital learning, as histology requires visual interpretation that is developed by continuous practice (Yohannan et al., 2019). Given this, we have created a virtual histology platform using our existing tool: the National University of Singapore – Human Anatomy Learning resOurce (NUS-HALO). NUS- HALO is an online platform with digital images and videos and has emerged as a novel tool in transforming anatomy teaching and learning. By integrating cutting-edge, high-definition histology images and relevant learning materials, the histology component of NUS-HALO offers a platform that aids students to excel in histology (Darici et al., 2021).
The NUS-HALO platform aids student learning of histology. Histology resources are organised systematically, along with pertinent teaching resources and explanations, to help students better comprehend each histological slide. Furthermore, during their third year of medical school, when students are introduced to pathology, they must use their earlier understanding of normal histology to identify pathological changes.
II. METHODS
Our team included three technical and five academic staff members. The digitisation of histology sections, selected from our existing collection in the Department, was done using Aperio software, and the digital images were saved on a server to be accessed later for teaching. Overall, images from 160 histology slides comprising 13 organ systems were digitised, each taking about 90 minutes to digitise. These images were clustered with the previously saved images (200 images from seven organ systems) and selected for NUS-HALO’s histology arm. The histology slides were carefully chosen to obtain low- and high-magnification images. The images were labelled to give students a clear understanding of each organ system and its critical features.
III. DISCUSSION
NUS-HALO offers a platform that aids student learning of histology. Histology resources are organised systematically, along with pertinent teaching resources and explanations, to help students better comprehend each histological slide. Furthermore, during their third year of medical school, when students are introduced to pathology, they must use their earlier understanding of normal histology to identify pathological changes.
HALO’s histology resources can be seamlessly integrated with what students learn during their anatomy and physiology classes. The use of this tool allows for a holistic understanding where students are able to correlate the microscopic histological structures with macroscopic anatomical features and physiological functions. Informal feedback that has been obtained from both staff and students has been overwhelmingly positive, highlighting the ease of use and quality of the resources available on the platform. A notable outcome has been the informal feedback received by students, stating that the platform has aided their examination preparation. However, continued and more formal gathering of feedback is essential for the platform’s ongoing improvement.
Future enhancements of the platform include using more diverse slide samples, and more interactive elements such as self-evaluation guides to enhance student’s experience and the effectiveness of NUS-HALO. Self-evaluation guides that are currently being considered include identification exercises, where students name structures on slides, and interpretive questions that can test their understanding of how histological changes might relate to pathological conditions. These tools will reinforce learning and enable students to track their progress.
A. Pedagogical Framework of Digital Histology on NUS-HALO
The resources on the NUS-HALO webpage were organised as follows:
1) Categorisation of Histology Images:
Images were organised based on the organ system they belong to (e.g., respiratory, digestive). Each image was annotated with labels and identification markers highlighting fundamental structures and features.
2) Integration of Teaching Resources:
Short notes describing salient features of the sections were embedded alongside the corresponding histology images to provide students with further explanations.
3) Navigation and User Interface:
The resources were organised to facilitate easy navigation, with a search function, intuitive m menus, and clear headings.
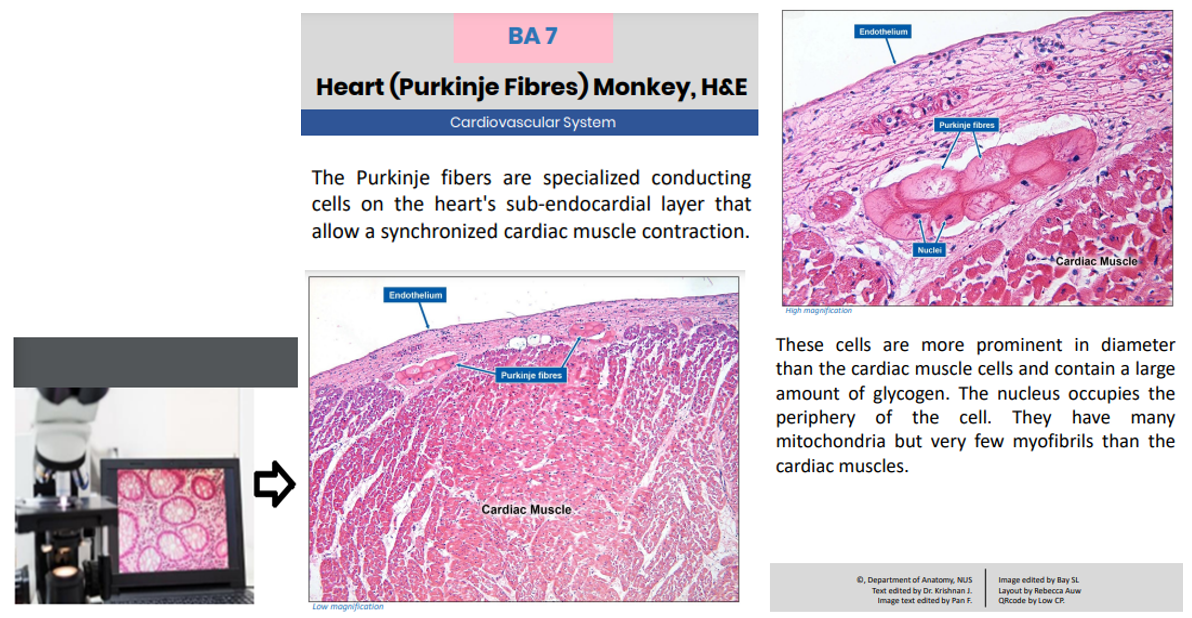
Figure 1: Showing high-quality images captured and uploaded for student access (leftmost). Image showing information available to students when they select digitised slides.
IV. CONCLUSION
The advent of computer-aided digital media and images has significantly impacted medical education, including image-intensive histology. Digitising histology slides appears cost-effective as it reduces the need for microscope maintenance and preparation of glass slides when damaged and manpower costs. This tool serves as an additional learning resource that students can access in conjuction with their existing histology lectures or practical lessons.
In the future, digital histology can be enhanced by incorporating augmented and virtual reality and artificial intelligence to provide students with an enhanced, immersive, and interactive learning experience.
Note on Contributors
Dr. Jayabharathi Krishnan, Dr. Sara Kashkouli Rahmanzadeh, and Professor S. Thameem Dheen are content experts on the Histology aspect of NUS-HALO. All authors contributed equally to this manuscript.
Acknowledgement
The authors would like to acknowledge the technical staff: Ms . Pan Feng, Ms. Bay SL, Ms. Rebecca Auw, and Mr. Low CP from the Department of Anatomy, Yong Loo Lin School of Medicine, for their technical support. The authors would sincerely like to thank the Department of Pathology for contributing to developing the digitalised images.
Funding
The authors did not receive any funding for this study.
Declaration of Interest
The authors do not have any conflict of interest.
References
Darici, D., Reissner, C., Brockhaus, J., & Missler, M. (2021). Implementation of a fully digital histology course in the anatomical teaching curriculum during covid-19 pandemic. Annals of Anatomy – Anatomischer Anzeiger, 236, Article 151718. https://doi.org/10.1016/j.aanat.2021.151718
Hussein, I. H., & Raad, M. (2015). Once upon a microscopic slide: The story of histology. Journal of Cytology & Histology, 6(6), Article 1000377. https://doi.org/10.4172/2157-7099.1000377
Yohannan, D. G., Oommen, A. M., Umesan, K. G., Raveendran, V. L., Sreedhar, L. S., Anish, T. S., Hortsch, M., & Krishnapillai, R. (2019). Overcoming barriers in a traditional medical education system by the stepwise, evidence-based introduction of a modern learning technology. Medical Science Educator, 29(3), 803–817. https://doi.org/10.1007/s40670-019-00759-5
*DR K JAYABHARATHI
Department of Anatomy
Yong Loo Lin School of Medicine
MD10, 4 Medical Drive
Singapore 117594
Email: antkj@nus.edu.sg
Submitted: 19 August 2023
Accepted: 21 December 2023
Published online: 2 July, TAPS 2024, 9(3), 41-49
https://doi.org/10.29060/TAPS.2024-9-3/SC3111
Rosy Swee Cheng Tay1, Debby Regina Wegner2, Li Siong Lim3, Joshua Ting4 & Shu Ting Ong5
1University of Glasgow Singapore, Singapore; 2Singapore Institute of Technology, Singapore; 3Singapore Institute of Technology, Singapore; 4Alexandra Health, Singapore; 5Gleaneagles Hospital, Singapore
Abstract
Introduction: The Singapore Institute of Technology-University of Glasgow (SIT-UofG) Nursing Programme has traditionally taken a didactic teaching approach in the delivery of the Evidence-Based Practice (EBP) module. A hybrid approach was introduced using Game-Based Learning (GBL) to encourage active learning through gameplay.
Methods: A Randomised Controlled Trial (RCT) was undertaken encompassing a cohort of 100 Nursing students taking the EBP module in their first year at the Singapore Institute of Technology (SIT) in the 2021/22 academic year. The experimental group (n=27) worked through the online GBL intervention and the EBP module, while the control group (n=27) took the EBP module alone. The GBL included five Learning Quests and three case studies.
Results: High levels of satisfaction were reported by both the experimental group (n=22) and the control group (n=15) on the traditional content and delivery of the EBP module. High levels of engagement were reported by the experimental group on the GBL intervention; a one-sample statistics analysis confirming a significant level of engagement (p<0.001). A Mann-Whitney U Test, however, found no significant difference in the Continuous Assessment (CA) scores of the two groups (p=0.507 and 0.461).
Conclusion: The introduction of GBL designed to deliver educational content directly associated with the learning outcomes increased the nursing student engagement in the EBP module. These findings and discoveries can be utilised to improve the GBL intervention to the EBP module to have a more positive impact the student CA scores and therefore on student learning.
Keywords: Evidence-Based Teaching, Evidence-Based Practice (EBP), Nursing Education, Game-Based Learning (GBL), Teaching and Learning EBP, Nursing Students, Gamification
I. INTRODUCTION
The Singapore Institute of Technology-University of Glasgow (SIT-UofG) Nursing Programme has traditionally taken a didactic teaching approach in the delivery of the Evidence-Based Practice (EBP) module. Numerous undergraduate nursing programmes have taken a similar approach aimed at preparing students to be informed knowledge generators, rather than the more effective savvy consumers of research, or “evidence users” (Melnyk & Fineout-Overholt, 2019). These undergraduate nursing programmes continue to teach “traditional” nursing research courses that fail to address many of the skills, attitudes, and critical knowledge needed to foster EBP, doing little to promote the development of competencies critical for engaging in EBP in clinical contexts (Davidson & Candy, 2016).
EBP is mandated by the Singapore Nursing Board as a key entry to nursing practice competency (Singapore Nursing Board, n.d.) and yet new graduate nurses still lack the knowledge, skills, and attitudes that nurture EBP. In addition, the COVID-19 pandemic brought about unprecedented challenges when classes moved from face-to-face to online, with one of the side-effects being a marked deterioration in the active engagement of the students in their classes. Active engagement is seen as critically pertinent to the learning development of nursing students in preparing them to be future-ready graduates.
Gamification, or the application of game design elements like levels and badges to non-game activities, has been avidly adopted to support contextual teaching and learning, assignments, and assessments in efforts to strengthen student creativity and retention (Caponetto et.al., 2014). Although, as reported by Tavares (2022), results have been varied, Game-Based Learning (GBL) is being increasingly utilized in nursing education. The aim of this short communication is to describe the development and evaluation of an innovative teaching strategy to evaluate student satisfaction, perception, level of engagement, and overall achievement of the learning outcomes via the gamification of the EBP module.
II. METHODS
A Randomised Controlled Trial (RCT) was undertaken using the 100 Nursing students taking the EBP module in their first year at the Singapore Institute of Technology (SIT) in Trimester 3 of the 2021/22 academic year. All the students were invited to participate in the study and complete the Informed Consent form. The participants were randomized into either the experimental/ intervention group (n=27) or the control group (n=27).
The control group attended the traditional EBP module made up of lectures, workshops, and seminars. The intervention group completed both the EBP module and the GBL intervention. The web-based, mobile-optimized GBL was composed of five levels or Learning Quests (LQs) and three case studies. The LQs followed six different EBP steps (Melnyk & Fineout-Overholt, 2019), with each LQ calling for increasing levels of knowledge and proficiency to cultivate a spirit of inquiry for the undergraduate nursing students. The intervention group was informed to access the GBL only after the key EBP concepts and teaching were delivered to both groups.
Two surveys were used to evaluate participant satisfaction, perception, level of engagement, and overall achievement of the learning outcomes. At the end of the trimester, a university-wide Module and Teaching Feedback survey (Appendix 1) was used to assess how satisfied both groups were with teaching and learning within the EBP module. The GBL Module Learning Outcomes Feedback survey was to get a sense of how the intervention group evaluated the effectiveness of the four main GBL outcomes (Appendix 2).
III. RESULTS
A total of 54 students out of the 100 (54%) taking the EBP module agreed to participate in this study. A total of 22 (81.5%) participants from the intervention group and 15 (55.6%) from the control group completed the surveys. There was a 44.4% attrition from the control group.
A. Grade Performance
There were two types of Continuous Assessment (CA) used – a group presentation worth 40% of the total grade, and an individual essay worth 60%. For the group presentation the mean score and standard deviation of the intervention group was 79.56 (3.70) and the control group was 78.70 (4.03). For the essay, the mean score and standard deviation of the intervention group was 69.6 (11.93) and for the control group was 67.81 (10.76). The Mann Whitney U Test found that there was no significance difference between the CA scores of the intervention and control groups (p = 0.507 and 0.461).
B. Level of Satisfaction
Overall, there was a high level of satisfaction for the EBP module for both groups (intervention: 95.5%; control: 93.3%) with no significant difference (p=0.658) found between the two groups.
C. Level of Perception
Both groups demonstrated similar positive perceptions about the EBP module. 5 themes emerged from the thematic analysis of the open-ended questions (Table 1)
D. Level of Engagement
The GBL was reported by the students to have deepened their learning of EBP. 4 themes emerged from a thematic analysis of the open-ended questions (Table 1).
|
Level of Perception |
|
1) Achieving learning outcomes · ‘A step-by-step guide allow recapping throughout the module’ · ‘A good flow of module delivery and depth’
2) Systematic approach to learning EBP · ‘I learnt how to systematically search for relevant articles via various databases’ · ‘A good approach to critique articles to gather most relevant evidence’
3) Appreciating the guidance · ‘EBP requires a lot of teamwork with good input from faculty. The journey was tough but the outcome was satisfying’ · ‘Prompt feedback with clear explanations were given by faculty’
4) Scaffolding to thesis · ‘Foundational learning scaffolds well to the Honours Thesis’ · ‘Gives a good head start to the writing of Honours Thesis’
5) Seeking clarity · ‘Standardize teaching and instructions to manage expectations’ · ‘Move the learning to game-based learning’ |
|
Level of Engagement |
|
1) Applied learning · ‘The game provided opportunities to apply and enhanced my learning’ · ‘The case studies/questions provided opportunities to apply what I have learned’
2) Clear understanding of the EBP concepts/process · ‘Interactivity of game allow better learning of concepts and engagement’ · ‘Reinforcement of key concepts via quests. Learnt more than what was taught during lessons’
3) Level of engagement and interactivity · ‘The activities were helpful as assessments…a good way to enhance learning’ · ‘A more game-based approach to quests for more engagement’
4) Enhancing user experience and interface · ‘The user interface was a bit hard…especially when the case scenarios were squeezed all the way to the left side of the screen’ · ‘Hard to navigate between articles. Can provide side by side scrolling for better navigation’ |
Table 1. Themes and associated subthemes
Note. This table lists the themes and associated subthemes that were identified from the student responses to the open-ended questions under perception and engagement. Selected student comments are included.
IV. DISCUSSION
There were several key findings from the development of GBL for the EBP module. Although no significant difference was found on the CA grade performance between the groups, both groups expressed a high level of satisfaction upon completing the EBP module.
Despite facing challenges with the usual didactic approach of teaching and learning of EBP, participants expressed appreciation to the faculty for the close stepwise guidance and prompt feedback in facilitating synergistic class teamwork. The systematic flow helped create a positive perception of the module delivery. This well-structured learning scaffold also provided a solid foundation for writing their Honours Thesis.
Gamification using case studies provided good interactivity for applied learning to enhance student engagement and learning. With regards to the interface itself, the navigation of the case studies via the user interface was found to be challenging, so side-by-side scrolling can be considered to improve future user experience. Standardizing teaching and instructional methods to manage student expectations can also be considered, as there was definite support for moving the EBP module towards game-based learning.
This development of GBL for the EBP module was an innovative hybrid approach to the teaching pedagogy of the educational and healthcare institutions in Singapore. The employment of both didactic and GBL teaching and learning served to enhance the learning experience of the students and helped clarify the future translation of EBP into their respective clinical practice. While the feedback from the intervention group indicated the GBL interface can be improved, the high levels of satisfaction and engagement experienced by this group demonstrated the incorporation of game mechanics in the design of a teaching-learning process can help engage learners in a more productive learning experience.
With no significant difference between the grades of the two groups, it could be argued that the nursing students are already being well guided and supported by Faculty in the teaching and learning of EBP and that the intervention was built upon a firm foundation. Leveraging upon authentic digital learning with a sound pedagogical approach, however, can help to further promote critical thinking, active engagement, and positive learning experiences for the nursing students. Future enhancement to the GBL intervention can consider levelling up the basis of gamifying learning for higher immersive learning experience. As there was a high attrition from the control group of 44.4%, future studies can consider a larger sample size for better generalizability. As this study only employed the GBL after the key concepts and teaching of EBP was delivered, future studies can consider the teaching and learning pedagogy of GBL along with seminar sessions to evaluate its viability.
V. CONCLUSION
This research project was carried out at the Singapore Institute of Technology to assess the impact of a GBL intervention on teaching and learning in the EBP module for nursing students. Despite no significant differences in grades between the groups, the results show the intervention had a positive impact on the student engagement, satisfaction, and perception of the learning experience, offering an excellent option of combining traditional didactic teaching with the innovative approach of GBL to enhance the EBP teaching and learning of undergraduate nursing students and healthcare professionals in both educational and healthcare institutions.
Notes on Contributors
Assistant Professor Rosy Tay Swee Cheng spearheaded the development of this research project, conducted the survey and data analysis, contributed to the conception, drafted, and critically revised the manuscript.
Ms. Debby Regina Wegener is a Senior Librarian and assisted with the development of a part of this research project, and critically revised the manuscript.
Mr. Lim Li Siong is a Senior Educational Developer in CoLEAD and coordinated the development of the research project and contributed to the critical review of the manuscript.
Mr. Joshua Ting is a Staff Nurse, Alexandra Health and played a key role in the development, conducted the survey and data analysis of this research project, and assisted in the critical review of the manuscript.
Ms. Ong Shu Ting is a Staff Nurse, Gleneagles Hospital and played a key role in the development, conducted the survey and data analysis of this research project, and assisted in the critical review of the manuscript.
All authors gave their final approval and agreed to be accountable for all aspects of the work.
Ethical Approval
Ethical approval approved by Singapore Institute of Technology (SIT) Review Board (IRB Project No. 2021157).
Data Availability
As per institutional policy, research dataset is available on reasonable request to the corresponding author.
Acknowledgement
The authors would like to thank Adjunct Associate Professor Edward Poon, Singapore Institute of Technology (SIT) for his invaluable support to the research project and Tam Yew Chung, Centre for Learning Environment and Assessment Development (CoLEAD), SIT for his advice and invaluable support in navigating the funding process.
Funding
Funding (WBS Code: P-ALI-A203-0008) was received from Applied Learning and Innovation Grant (ALIGN), CoLEAD, SIT for the development of this web-based EBP game-based learning.
Declaration of Interest
The authors declare no conflict of interest.
References
Caponetto, I., Earp, J., & Ott, M. (2014). Gamification and education: A literature review. European Conference on Games Based Learning, 1, 50–57.
Davidson, S. J., & Candy, L. (2016). Teaching EBP using game-based learning: Improving the student experience. Worldviews on Evidence-Based Nursing, 13(4), 285–293. https://doi.org/10.1111/wvn.12152
Melnyk, B. M., & Fineout-Overholt, E. (2019). Evidence-based practice in nursing & healthcare: A guide to best practice (4th ed.). Wolters Kluwer.
Singapore Nursing Board. (n.d.). Guidelines and Standards. https://www.healthprofessionals.gov.sg/snb/guidelines-and-standards
Tavares, N. (2022). The use and impact of game-based learning on the learning experience and knowledge retention of nursing undergraduate students: A systematic literature review. Nurse Education Today, 117, Article 105484. https://doi.org/10.1016/j.nedt.2022.105484
*Rosy Tay Swee Cheng
University of Glasgow, Singapore,
10 Dover Drive, Singapore 138683
+65 6592 4521
Email: rosy.tay@glasgow.ac.uk
Submitted: 11 December 2023
Accepted: 18 March 2024
Published online: 2 July, TAPS 2024, 9(3), 67-69
https://doi.org/10.29060/TAPS.2024-9-3/CS3189
Galvin Sim Siang Lin1, Wen Wu Tan2, Yook Shiang Ng1 & Kelvin I. Afrashtehfar3
1Department of Restorative Dentistry, Kulliyyah of Dentistry, International Islamic University Malaysia, Malaysia; 2Department of Dental Public Health, Faculty of Dentistry, Asian Institute of Medicine, Science and Technology (AIMST) University, Malaysia; 3Evidence-Based Practice Unit, Clinical Sciences Department, College of Dentistry, Ajman University, United Arab Emirates
I. INTRODUCTION
The landscape of health profession education, particularly dental education, is evolving to equip students with essential contemporary knowledge and skills for competent dental practice. Within this context, dental materials science plays a pivotal role in undergraduate dental programs, providing the foundation for understanding the materials used in clinical dentistry. However, traditional teaching approaches relies on didactic lectures, often rendering this multidisciplinary subject seem dry and challenging (Soni et al., 2021). Students also face difficulties in grasping the practical applications of materials science in clinical dentistry within the confines of passive didactic lectures.
Recognising these limitations, there is a growing need for innovative pedagogical strategies shifting from teacher-centred to student-centred approaches, fostering active learning. Problem-based learning (PBL), case-based learning (CBL), and team-based learning (TBL) emerge as alternatives. While PBL involves open-inquiry scenarios, it can be time-consuming. CBL, a guided inquiry method, recreates clinical settings, with the teacher as a facilitator. Meanwhile, TBL, introduced in the 1970s, is a teacher-centred approach fostering active learning through student engagement (Michaelsen et al., 2004). Despite their efficacy, their application in dental materials science courses remains underrepresented. This gap represents a significant deficiency in dental education, especially given the critical role of dental professionals in selecting and justifying the use of appropriate materials in clinical cases. This study addresses this gap by comparing the academic performance of undergraduate dental students in dental materials science courses, utilising a hybrid TBL-CBL approach against traditional didactic lectures.
II. METHODS
The study received approval from the local institutional ethics committee (approval code AUHEC/FOD/ 2022/28). The preclinical course comprised four modules taught over two semesters (One academic year consists of 2 semesters). A quasi-experimental design involved 74 second-year dental students, comparing continuous assessment scores between didactic lectures (pre-test) and hybrid TBL-CBL (post-test) introduced in the third module. Excluding the first module and final assessment in the fourth module, only scores from modules 2 and 3 were compared. Content validation involved group discussion and consensus among faculty members ensuring question difficulty alignment with learning outcomes. Hybrid TBL-CBL was conducted in seminar rooms with students randomly assigned to groups. Pre-reading materials, including PowerPoint slides from prior lectures were given. The process encompassed a 15-minute introduction, Readiness Assurance Process (iRAT and tRAT), application activities, and a debriefing session. Data collection involved an unbiased faculty member anonymously obtaining consent for module 2 and module 3 assessment scores, evaluated against grading criteria. Descriptive statistics analysed demographic background, while the Wilcoxon test assessed academic performance using IBM SPSS software with a significance level set at 0.05.
III. RESULTS
54 females (73%) and 20 males (27%) consented to assessment score collection. Mean scores increased significantly (p=0.001) from 61.89±15.67 to 67.35±12.57 after hybrid TBL-CBL, with both female and male scores rising. However, male academic improvement was not statistically significant (p=0.130). Following hybrid TBL-CBL, 13 initially failing students in traditional lectures passed (p=0.020). Assessment grades depicted a notable increase in ‘A’ grades (8.1% to 20.3%) and a decrease in ‘D’ and ‘F’ grades (23.0% to 6.7%). These findings underscore the positive impact of hybrid TBL-CBL on academic outcomes and the successful remediation of initially struggling students.
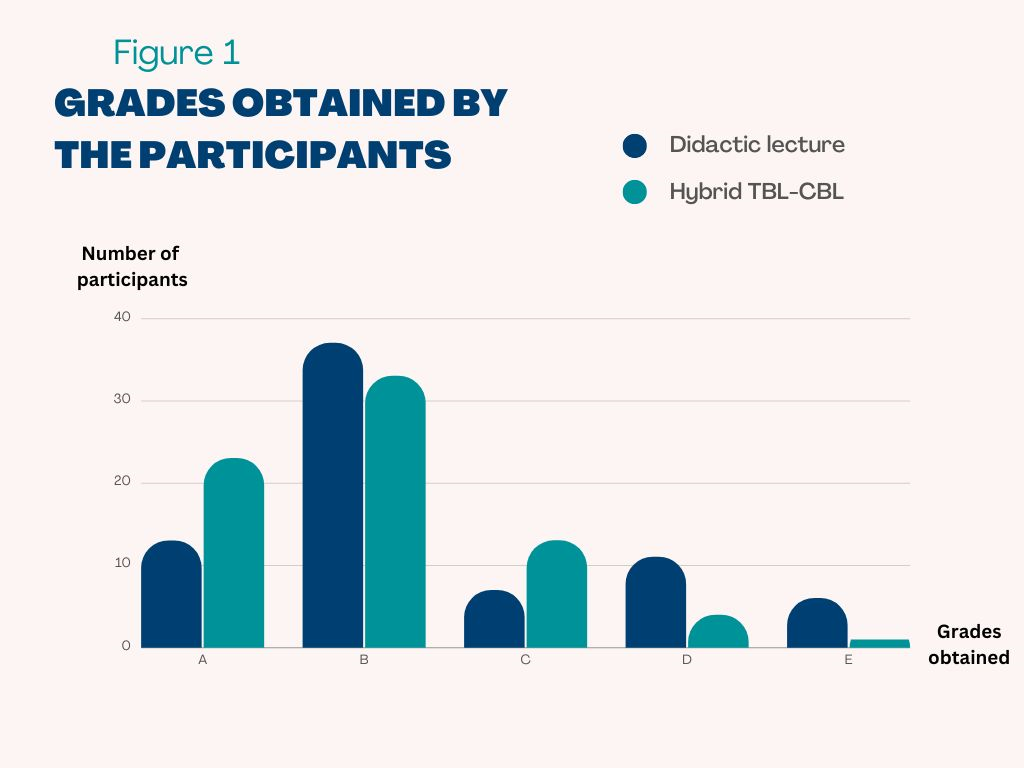
Figure 1. Assessment grades of students before and after the implementation of hybrid TBL-CBL
IV. DISCUSSION
In contrast to traditional didactic lectures, the hybrid TBL-CBL approach requires active student participation in group discussions, case analysis, and feedback sessions. After implementing hybrid TBL-CBL in module 3, significant improvement in students’ comprehension of dental materials science was observed through higher assessment scores. This finding is consistent with other research suggesting that both TBL and CBL improve students’ knowledge retention and learning experiences through active group learning, leading to better academic performance (Ulfa et al., 2021). Students are expected to participate more actively in group discussions and learn better from the prior knowledge they gained through pre-reading materials, which helps them perform well in collaborative learning. Both TBL and CBL involve dividing students into small groups, which provides the opportunity to be more interactive and engage in discussion among each other. Unlike the passive nature of large lecture-based teaching, which often leads to “lecture ennui” among students due to one-way communication.
The current study revealed that both male and female students showed improvement in their mean assessment scores following the implementation of hybrid TBL-CBL approach. However, the improvement was not significant among male students. It is plausible that female students perceived the hybrid TBL-CBL sessions more positively, leading to increased engagement and learning (Das et al., 2019). Conversely, male students frequently attend TBL sessions less prepared and feel that their assessment scores do not accurately represent their level of knowledge. Nevertheless, female students tend to learn in a collaborative, dependent, and participatory manner, whereas male students lean towards independent and competitive ways (Mahamod et al., 2010). Thus, the authors postulated that female students would benefit more from peer learning in hybrid TBL-CBL sessions than male students.
One limitation of the present study is that a comparison of assessment scores among higher-performing and low-performing students were not performed. Although there was no statistically significant increase in the academic performance of male students, it is important to note that this may be because there were fewer male students than female students, which may hinder our ability to detect significant differences. Since the present study utilised a one-group pre- and post-test research design, it is likely that students’ interactions with teachers and learning styles may have an impact on their assessment scores. Moreover, the effectiveness of the present hybrid TBL-CBL would be further supported by randomised control research including a larger sample size in different institutions across the nation.
V. CONCLUSION
The hybrid TBL-CBL enhanced academic performance over traditional lectures, particularly benefiting female students. While promising for dental materials science education, future studies are needed to assess its efficacy across healthcare fields and diverse health professional student populations.
Notes on Contributors
Galvin Sim Siang Lin designed the study, performed data collection, drafted the manuscript and approved the final manuscript.
Wen Wu Tan performed data analysis, drafted and approved the final manuscript.
Yook Shiang Ng drafted, read and approved the final manuscript.
Kelvin I. Afrashtehfar gave critical feedback, read and approved the final manuscript.
Ethical Approval
The present study was approved by the Asian Institute of Medicine, Science and Technology (AIMST) University Human Ethics Committee (AUHEC) with ethical approval code AUHEC/FOD/2022/28.
Data Availability
The data supporting the findings of this study are available within the article, but raw data of this study are available from the corresponding author on request.
Acknowledgement
The authors would like to thank the participants of this study.
Funding
The study received no funding.
Declaration of Interest
All authors have no conflicts of interest.
References
Das, S., Nandi, K., Baruah, P., Sarkar, S. K., Goswami, B., & Koner, B. C. (2019). Is learning outcome after team based learning influenced by gender and academic standing? Biochemistry and Molecular Biology Education, 47(1), 58-66. https://doi.org/10.1002/bmb.21197
Mahamod, Z., Embi, M. A., Yunus, M. M., Lubis, M. A., & Chong, O. S. (2010). Comparative learning styles of Malay language among native and non-native students. Procedia – Social and Behavioral Sciences, 9, 1042-1047. https://doi.org/10.1016/j.sbspro.2010.12.283
Michaelsen, L. K., Knight, A. B., & Fink, L. D. (2004). Team-based Learning: A transformative use of small groups in college teaching. Stylus Pub. https://books.google.com.my/books?id=Hj OdPwAACAAJ
Soni, V., Kotsane, D. F., Moeno, S., & Molepo, J. (2021). Perceptions of students on a stand-alone dental materials course in a revised dental curriculum. European Journal of Dental Education, 25(1), 117-123. https://doi.org/10.1111/eje.12582
Ulfa, Y., Igarashi, Y., Takahata, K., Shishido, E., & Horiuchi, S. (2021). A comparison of team-based learning and lecture-based learning on clinical reasoning and classroom engagement: A cluster randomized controlled trial. BMC Medical Education, 21(1), 444. https://doi.org/10.1186/s12909-021-02881-8
*Galvin Sim Siang Lin
Department of Restorative Dentistry,
Kulliyyah of Dentistry,
International Islamic University Malaysia,
25200, Kuantan, Pahang, Malaysia
Email: galvin@iium.edu.my
Submitted: 15 September 2023
Accepted: 17 November 2023
Published online: 2 April, TAPS 2024, 9(2),101-104
https://doi.org/10.29060/TAPS.2024-9-2/CS3140
Claudia Ng & Aishah Moore
Medical Education Unit, National School of Medicine (Sydney Campus), University of Notre Dame, Australia
I. INTRODUCTION
Despite agreement on the importance of Interprofessional education (IPE) for health professional education (HPE), best practice in developing and implementing IPE remains ambiguous. Students are important stakeholders and can be allies in IPE, but much of their potential in the development of curricula remains untapped.
In 2022, the University of Notre Dame, Australia (UNDA) partnered with the University of Tasmania (UTAS) to engage students in the co-design, implementation, and delivery of a program to support the development of interprofessional practice for preclinical medical students from the Doctor of Medicine (MD) and final year paramedicine students. The COVID-19 pandemic was a catalyst to re-imagine different ways of learning and teaching in this area. This paper aims to describe the process of and opportunities for involving students as partners (SaP).
II. METHODS
Expressions of interest were invited from student cohorts attending a previous iteration of the program. Four student partners across the professions were recruited.
A collaborative workshop provided an initial opportunity for student and staff partnership. The workshop intended to nurture relationships through dialogue and reflection. Student evaluations from previous programs were reviewed and themes were highlighted for discussion. Opportunities were provided for students and educators from both professions to express individual opinions and perspectives from their own experiences of the program.
The major themes that arose from the student experience were the importance of experiential learning through simulation and the importance of having dedicated time for clinical skills practice. The opportunity to engage in interprofessional education was a consistent theme. Educators and student partners discussed the meaning of “success” in an interprofessional program and whether certain pedagogical models and program design could enhance learner outcomes.
III. OUTCOMES
Engagement of students occurred in various ways (Figure 1) and resulted in co-developed learning outcomes for an updated Rural Trauma week (RTW), focusing on the assessment and management of the patient, understanding the differing roles of each profession, and the impact of communication and teamwork of interprofessional teams on patient outcomes.
Students co-designed and reviewed the sequence of program elements. The program commenced with building the learner’s knowledge base through online delivery of lectures and pre-reading materials.
Student partners were also involved in the development of learning activities, including case-based discussions. The case-based discussions intended to provide opportunities for the application and integration of knowledge from the pre-reading and lecture materials. The content was developed alongside an expert clinician, with academic faculty members providing feedback. Students co-facilitated the case-based discussions with an expert faculty partner.
Specific hands-on skills practice was delivered using an interprofessional, near-peer model for facilitation, with final-year paramedicine students acting as tutors for pre-clinical medical students, under the supervision of expert facilitators.
The week culminated in simulation scenarios, with paramedicine and medical students working alongside each other to better understand the role of each profession and the impact of communication on the patient journey as they managed a range of presentations.
Finally, student partners considered approaches for the evaluation of the program, reviewed the evaluation instrument, and suggested how to optimise response rates. Participating students from both professions rated the interprofessional approach used in RTW highly, with the simulation session being rated Above Average and Excellent by 95% of students. Student partners were similarly positive when reflecting on their experiences.

Figure 1. Opportunities for SaP in IPE
IV. DISCUSSION
There is an emerging impact when cultivating learner agency is prime, and meaningful learning relationships between students and staff develop (Matthews, 2018). Students have potential to be partners in learning and teaching in higher education, becoming more than just passive consumers, acting as change agents to help bring about educational transformation (Healey et al., 2014).
The faculties desired to engage students as partners in the reimagination of RTW. Cook-Sather et al. (2014) described student and staff partnership as “a collaborative, reciprocal process through which all participants have the opportunity to contribute equally but not necessarily in the same ways”. It is a disruptive cultural shift from institutions making decisions to a more collaborative mindset where staff and students are working in partnership as colleagues and collaborators with shared goals (Matthews, 2018). Students may not be content or pedagogical experts, but their expertise lies in their lived experience of being a student. They understand learner needs and how the learning experience can be enriched. In our case study, one of our medical student partners had worked as a paramedic before studying medicine. His paramedic experience provided unique perspectives to the discussions and planning.
“As a former paramedic now studying medicine, I have experienced how each side appears mysterious to the other in what they actually do, or how they contribute to the patient. Our attempts in writing these cases have been to broach this gap, which I felt was received very well.” – Medical Student Partner
Engaging students of both professions in the co-design and delivery of the program also fostered further interprofessional collaboration which is an important step to interprofessional practice. Collaboration between Australian medicine and paramedicine undergraduates is uncommon. Although interprofessional practice is seen to be increasingly important in health care, health systems remain fragmented in the face of increasing complexity. Application of SaP in our example fostered staff-student relationships within a profession, but also between students and staff from other professions leading to an increased sense of interprofessional collaboration.
The use of SaP pedagogy is lacking in inter-institutional and cross-disciplinary initiatives (Mercer-Mapstone et al., 2017). Whilst our case study provides an “outcomes-focused” example of SaP’s application in IPE, translation of theoretical aspects of SaP into an HPE context can benefit from better integration of scholarship from other disciplines where the “process” of SaP has been further developed (Barradell & Bell, 2021).
V. CONCLUSION
Students can have a powerful influence on shaping health professional education through shared success in preparation for interprofessional practice. Engaging students as partners in the co-design of a cross-institutional, interprofessional education activity was a valuable experience for staff and students. Students can be an important ally in interprofessional education. The ideas of “respect, reciprocity, and shared responsibility” in student partnership will provide a foundation for the same values to be shared in interprofessional practice.
Notes on Contributors
Dr Claudia Ng is a lecturer in the MD Program at the University of Notre Dame Australia (UNDA) and is currently completing a Masters in Health Professional Education. Claudia co-authored this manuscript and presented at the Asia Pacific Medical Educators Conference in 2023.
Dr Aishah Moore is Co-Head of Curriculum, MD Program at the University of Notre Dame Australia and a General Practitioner. Aishah co-authored this manuscript.
Acknowledgement
Dr Samuel Bulford is a sessional academic at UNDA and an expert facilitator in the RTW program. Mr David Donato is a lecturer in Paramedicine at UTAS and an expert facilitator in the RTW program. SB and DD contributed to the collaborative workshop. Dr Gisselle Gallego is the Senior Research Fellow at the University of Notre Dame, providing input into research design and analysis of qualitative data arising from the project.
Student Partners, Sidney Flego, Katarina Needham, Matthew Dowsett, and Anthony Salole were involved in the co-design and facilitation of the RTW 2022.
Professor Michael Brydon, UNDA, Associate Professor Andrew Dean, UNDA, and Ms Suzanne Avis oversaw the running of the 2022 RTW program.
The facilitators and staff at Lithgow Clinical School and UTAS Campus were involved in the logistics and running of the program.
Funding
The project was funded by a UNDA Seed Grant for Scholarship of Teaching and Learning in 2022.
Declaration of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
Barradell, S., & Bell, A. (2021). Is health professional education making the most of the idea of ‘students as partners’? Insights from a qualitative research synthesis. Advances in Health Sciences Education: Theory and Practice, 26(2), 513-580. https://doi.org/10.1007/s10459-020-09998-3
Cook-Sather, A., Bovill, C., & Felten, P. (2014). Engaging students as partners in learning and teaching: A guide for faculty (1st ed.). Wiley.
Healey, M., Flint, A., & Harrington, K. (2014). Engagement through partnership: students as partners in learning and teaching in higher education. York: HEA. https://advance-he.ac.uk/knowledge-hub/engagement-through-partnership-students-partners-learning-and-teaching-higher
Matthews, K. E. (2018). Engaging students as participants and partners: An argument for partnership with students in higher education research on student success. International Journal of Chinese Education, 7(1), 42-64. https://doi.org/10.1163/22125868-12340089
Mercer-Mapstone, L., Dvorakova, S. L., Matthews, K. E., Abbot, S., Cheng, B., Felten, P., Knorr, K., Marquis, E., Shammas, R., & Swaim, K. (2017). A systematic literature review of students as partners in higher education. International Journal for Students As Partners, 1(1), 15–37. https://doi.org/10.15173/ijsap.v1i1.3119
*Dr Claudia Ng
The University of Notre Dame Australia
School of Medicine
160 Oxford St Darlinghurst
NSW Australia 2010
Email: claudia.ng@nd.edu.au
Submitted: 4 November 2023
Accepted: 20 November 2023
Published online: 2 April, TAPS 2024, 9(2),98-100
https://doi.org/10.29060/TAPS.2024-9-2/PV3165
John Norcini
Department of Psychiatry, SUNY Upstate Medical University, United States of America
I. INTRODUCTION
Over the past 25 years, the Asia Pacific region has seen striking growth in the scholarship of health professions education, and it is poised to continue its development. A window into the past and a glimpse of the future can be found in the meetings of the Asia Pacific Medical Education Conference (APMEC), which recently celebrated its 25th anniversary. To frame my personal observations, a word cloud was created using the titles of the plenaries, keynotes, and symposia of the 2003, 2004, and 2006 conferences and another was created using the titles from 2021, 2022, and 2023. When comparing these two clouds (an exercise akin to interpreting inkblots), three themes emerged: interprofessional education and practice (IPEP), the scholarship of teaching and learning (SoTL), and the growing role of technology.
Interprofessional Education and Practice. In the first three conferences, the most common word was ‘medical’ and in the last three it was ‘education’. This parallels developments in the field, which started with a focus entirely on medical education, expanded to all the health professions, and in its most recent iteration, turned to interprofessional education. The reason for this latest development is research showing that interprofessional practice results in better patient outcomes, improved efficiency of care, and increased satisfaction among providers (Reeves et al., 2017).
One of the biggest barriers to IPEP is social closure, defined by Mackert (2012) as the “process of drawing boundaries, constructing identities, and building communities in order to monopolize scarce resources for one’s own group, thereby excluding others from using them.” (Mackert, 2012). Each profession has an educational model that encompasses as much of practice as possible, and they compete over ownership at the boundaries. This limits interprofessional cooperation and the opportunity for joint training.
Social closure has been institutionalised through the regulatory processes (i.e., accreditation and licensure/registration) used in many countries. These fix the boundaries of the professions and the nature of training and practice. Regulation ensures initial competence but makes it challenging to develop shared competencies across the professions. Moreover, there are few regulatory requirements for keeping up with changing practice and even fewer ways to acknowledge the acquisition of additional competencies after formal training.
Digital badges or micro-credentials are one way to approach the issue of social closure. They are circumscribed credentials based on shorter educational experiences followed by assessment. They can be part of existing broad educational and regulatory processes, complement them, or replace them in part. These credentials can be applied across professions and throughout careers.
Micro-credentials can support the development of IPEP by increasing access and shifting the focus from what the professions can do, to what patients and healthcare systems need. The fact that different professions experience the same educational process leads to comparability across providers regardless of discipline, less siloed regulation, and increased interprofessional collaboration. Furthermore, it offers a pathway for practitioners who seek to upgrade their skills or acquire new competencies.
The scholarship of teaching and learning. The second theme that emerged from a comparison of the word clouds was the scholarship of teaching and learning (SoTL). ‘Curriculum’ and ‘assessment’ were prominent in the first APMEC conferences, but they vanished recently, with ‘learning’, ‘scholarship’, and ‘educator’ being more prominent. In my view, this shift signifies the growing role of SoTL.
The goal of SOTL is to improve student learning by identifying effective teaching practices and disseminating those practices. It is a relatively new field of scholarship that has nine attributes: “committed engagement in action, critique-based, disciplinary, context-oriented, critical enquiry process, continuous deep reflection, dynamic process, shared publicly, and learning focused.” (Mirhosseini et al., 2018).
A recent edition of the Asia Pacific Scholar exemplifies this work (Lee & Norcini, 2023). It included studies that addressed topics such as community based interprofessional education, cultural awareness training in the emergency room, approaches to vaccine hesitancy, innovative oral exams for occupational therapy students, and coaching programs for faculty members.
Technology. The third theme that emerged from the comparison of the word clouds was technology. ‘eLearning’, prevalent in the early days of the conference, has disappeared to be replaced by ‘technology’. In my view, this signifies its growing role in health professions education and assessment. To pursue this further, Bard (Google’s AI chatbot) was asked, “What effect will technology have on education in the health professions?” Below is Bard’s response, edited for British spelling and for length by removing examples.
“Technology is already having a significant impact on education in the health professions, and this trend is only going to accelerate in the coming years. Here are some of the key ways in which technology is transforming health professions education
- Increased use of e-learning and simulation provides students access to high-quality educational resources and experiences, regardless of location or time constraints.
- Technology can be used to create personalised learning experiences for each student.
- Technology can be used to facilitate interprofessional collaboration between students and healthcare professionals from different disciplines.
- Technology can be used to collect and analyse data on student learning and performance.
Overall, technology is making health professions education more accessible, personalised, and effective.
Here are some of the potential benefits of using technology in health professions education:
- Improved access to education: Technology can help to break down barriers to access to education, such as distance, time constraints, and financial resources.
- Increased student engagement: Technology can be used to create more engaging and interactive learning experiences.
- Improved learning outcomes: Technology can be used to personalise learning, provide feedback, and track student progress.
- Better preparation for practice: Technology can be used to simulate real-world clinical scenarios and help students to develop the skills they need to be successful practitioners.
However, there are also some potential challenges associated with the use of technology in health professions education, such as:
- Cost: Technology can be expensive to purchase and maintain
- Digital divide: Not all students have equal access to technology resources
- Technical challenges: Technology can be complex and difficult to use
- Quality control: It is important to ensure that technology-enhanced learning resources are high-quality and effective
Overall, the benefits of using technology in health professions education outweigh the challenges. However, it is important to use technology thoughtfully and strategically to ensure that it is used to enhance learning, not replace it.” (Bard, 10/30/2023)
This is an impressive performance by Bard, and it offers a small preview of what technology may do. The ideas are not novel, but a wide range of thinking was summarised in a systematic fashion within seconds. This is just the beginning for generative artificial intelligence but it is clear that technology will reshape educational practice and scholarship. It also raises important questions about how we interact with it going forward.
II. SUMMARY
APMEC’s history provides a means of describing the dramatic growth in health professions education in the Asia Pacific region. The past 25 years have seen the focus of research expand from its start in medical education through all the health professions to IPEP. To drive this growth, new forms of scholarship have taken root. With its strong emphasis on context, SoTL enhances the relevance of this research to the cultures and practices of the region. Finally, technology, and our relationship with it, will have profound effects going forward. Taken together, these trends lay the groundwork for future work that will serve the needs of the region and have sizeable influences beyond it.
Note on Contributor
John Norcini wrote the paper.
Funding
No funding was involved.
Declaration of Interest
There are no conflicts to declare.
References
Lee, S. S., & Norcini, J. (2023). Celebrating excellence in the scholarship of teaching and learning. The Asia Pacific Scholar, 8(2), 1-3. https://doi.org/10.29060/TAPS.2023-8-2/EV8N2
Mackert, J. (2012). Social Closure. Oxford University Press.
Mirhosseini, F., Mehrdad, N., Bigdeli, S., Peyravi, H., Khoddam, H. (2018). Exploring the concept of scholarship of teaching and learning (SoTL): Concept analysis. Medical Journal of The Islamic Republic of Iran, 32(1), 553-560. https://doi.org/10.14196/mjiri. 32.96
Reeves, S., Pelone, F., Harrison, R., Goldman, J., & Zwarenstein, M. (2017). Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database of Systematic Reviews, 6. https://doi.org/10.1002/14651858.CD0000 72.pub3
*John Norcini
Upstate University Hospital
750 East Adams Street
Syracuse, NY 13210
Email: John.norcini@gmail.com
Submitted: 30 June 2023
Accepted: 19 October 2023
Published online: 2 April, TAPS 2024, 9(2), 95-97
https://doi.org/10.29060/TAPS.2024-9-2/PV3075
Gabriel Tse Feng Chong1,2
1Singapore Armed Forces HQ Medical Corps, Singapore; 2Dental Specialist Accreditation Committee (Dental Public Health), Singapore
There is growing awareness of the need to include humanities in educating dental students at the undergraduate/pre-doctoral level (Marti et al., 2019). However, there appears to be no literature discussing or advocating the inclusion of humanities for the training of dental specialists. Dental Public Health (DPH) is one such dental specialty where its trainees and practitioners would benefit from an inclusion of humanities in its pedagogy.
This author opines that exposure to humanities (which includes, but is not limited to, literature – both fiction and non-fiction, art, history, narrative dentistry/medicine, philosophy, ethics, and medical anthropology) that touch on dental themes can make a DPH trainee/practitioner more rounded; able to empathise better with the individuals that his/her policies and programs would affect; become even more persuasive in health promotion efforts; and more articulate in their advocacy efforts with stakeholders and policy makers.
Unfortunately, the curriculum of most DPH training programs (in English speaking jurisdictions) do not include humanities apart from the inclusion of ethics in North American programs. Perhaps the roots of this problem can be traced back to the dental undergraduate/pre-doctoral level where the typical training is predominately focused on biomedical subjects. The result is “few dental schools have implemented humanities in their dental education” and where humanities are taught, ethics tend to form the bulk (Marti et al., 2019). At the postgraduate specialty-training level, this traditional segregation between what are considered ‘sciences’ on one hand, and ‘humanities’ on the other hand, are already ingrained for most dental specialties. However, the DPH curriculum is different from the sister dental specialties because the trainee is required to understand for instance: sociology, health-related behaviors, the interactions of social, cultural and political variables (including age, gender, socioeconomic status, culture, religion, ethnicity and globalisation) on public health, health inequities, and the provision of health services. In essence, the DPH curriculum aims to re-orientate the trainee from a biomedical model of care to a biopsychosocial model of care. As such, the DPH curriculum is a natural starting point for the inclusion of humanities in the training of dental specialists.
There are some foreseeable barriers to implement humanities in the DPH training curriculum – (i) the possible lack of DPH educators and practitioners who are well-versed or at least comfortable with humanities and this itself may be a barrier to even commencing the addition of humanities into the pedagogy, and (ii) finding the time and space to include humanities into the voluminous curriculum that the DPH trainee is expected to cover in a relatively short amount of time. One suggestion to resolve the former barrier is cross-disciplinary training, where dental and/or public health schools can reach across to educators and researchers in the humanities departments to co-develop the DPH-humanities curriculum and training materials. The latter barrier can perhaps be tackled by infusing readings and discussions on humanities into the DPH curriculum that already require the trainee to adopt a biopsychosocial approach to healthcare and where humanities would be natural additional skillsets for inclusion in the DPH trainees’/practitioners’ toolbox.
Oral health inequities exist in most, if not all, societies. The burden and resultant impact of dental caries is largely borne by those who are disadvantaged and underserved. This is true even of an affluent country in Asia-Pacific like Singapore with a highly educated populace with very good healthcare system, infrastructure, and policies. Singapore enjoys (i) an universal community water fluoridation program covering 100% of Singapore’s population, (ii) public health education to increase awareness and health literacy by actors, such as, the Ministry of Health (MOH) and Health Promotion Board (HPB), (iii) free dental care to school children up to 18 years of age, and (iv) an extensive network of dental clinics in the private and public sector (Chong & Tseng, 2011). Despite all these benefits, the burden of poor oral health is mainly carried by members of lower socioeconomic groups and certain racial groups (Chong & Tseng, 2011).
Humanities can also challenge the lens through which a DPH trainee/practitioner views oral health problems. For instance, even the current epidemiological trends of dental caries was not always the case. For example, if we were to go back in time to about the late 18th century, dental caries in Europe was largely a disease of the affluent. This is even mentioned in a gastronomical literature text ‘The Physiology of Taste’, written by Brillat-Savarin (published in 1825), in which the author describes the poor oral health of his fellow diners. He writes “what then if the mouth is neither fresh nor pretty? And what shall be said of those monstrous chasms which open up to reveal pits that would seem bottomless, if it were not for the sight of shapeless, time-corroded stumps?” (Chong, 2012).
What caused the epidemiological shift such that dental caries was no longer a disease of the affluent but became one of the poor? This is because until about the late 18th century, sugar was not yet widely available to the masses for consumption frequently and/or in large quantities so as to cause widespread decay. For example, in England, the annual consumption of sugar per capita increased from almost zero in the 17th century to 1.8kg in 1704 to 8.2kg in 1800, and finally to 40.8kg by the mid-19th century (Chong, 2012). Several factors have been identified as the causes of increased consumption of sugar during this period: increased disposable income due to the industrial revolution; the availability of processed foods and beverages; and the change in dietary habits to add sugar as a sweetener to tea and coffee (Chong, 2012).
This historical trend is important for the modern DPH trainee/practitioner because it approximates ecological studies and supports our modern understanding that the intake of dietary sugars is the most important risk factor for developing dental caries. This should focus DPH trainees’/practitioners’ efforts to tackle the Social Determinants of Health (including the commercial determinants, such as the health risks posed by the sugar and fast-food industries). Furthermore, the 180-degree shift in the epidemiology of dental caries should serve as a reminder that what is the norm of today can be changed drastically in the future, and therefore improvements at a societal-level are possible.
Despite being the most prevalent chronic disease condition globally, dental caries is seldom reported in the news save for the rare occasions where it is extremely headlines worthy, such as the case where a 12-year old American boy (Deamonte Driver) passed away because of an untreated tooth abscess arising from dental caries (Otto, 2017). In this regard, DPH trainees and practitioners can utilise the humanities (in the form of literature, narrative dentistry, and art) as useful media to showcase the plight of the poor and the injustice of oral health inequities. This is needful because sometimes key stakeholders and policy makers (who usually do not have healthcare backgrounds) may not quite comprehend or relate to quantitative data, whereas the narrative aspects such as the description of the individuals’ experience can be very emotive to nudge those stakeholders and policy makers towards the right direction. Editors and reporters of traditional media channels are more likely to publish articles and editorial pieces that are deemed ‘headlines worthy’ with a compelling story to tell.
To highlight the potential power of humanities in telling a story, the author would like to quote a passage from the novel ‘Les Miserables’ by Victor Hugo (originally published in 1862), that depicts the emotional and physical pain of those who were forced to sell their teeth out of dire economic circumstances; which was a fairly common practice in European society of that time.
Excerpt from Les Miserables (Hugo, 1982, p. 177 – 178):
He was an itinerant dentist selling sets of false teeth, opiates, powders, and elixirs… seeing Fantine laugh, the dentist cried:
‘You’ve got a fine set of teeth, my lass. If you’d care to sell me your two incisors I’ll pay you a gold napoleon for each.’
‘What are my incisors?’
‘Your two top front teeth.’
‘How horrible!’ exclaimed Fantine.
‘Two napoleons,’ grumbled a toothless old woman standing near. ‘She’s in luck!’
Fantine fled, covering her ears to shut out the man’s hoarse voice as he shouted after her:
‘Think it over, my girl. Two napoleons are worth having. If you change your mind you’ll find me this evening at the Tillac d’argent.’…
When Marguerite entered Fantine’s room next morning… she found her seated cold and shivering on her bed… and it seemed that she had aged ten years overnight.
‘Lord preserve us!’ cried Marguerite, ‘What’s the matter with you?’
‘Nothing is the matter with me,’ said Fantine, ‘I’m happy. My baby isn’t going to die of that dreadful disease for lack of medicine.’
She pointed to two napoleons that lay gleaming on the table.
‘A fortune,’ murmured Marguerite. ‘A fortune! Where did you get them?’
‘I earned them,’ said Fantine.
She smiled as she said it, and the candle lighted her face. It was a bloodstained smile. There were flecks of blood at the corners of her mouth and a wide gap beneath her upper lip.
Notes on Contributors
The author conceived the ideas stated in this personal review article and wrote the manuscript.
Funding
The author declares that no financial support was received for this personal view article.
Declaration of Interest
The author declares that there is no potential conflict of interest.
References
Chong, G. T. F. (2012). Jean-Anthelme Brillat-Savarin’s 1825 treatise on the mouth and ingestion. Singapore Dental Journal, 33(1), 31-36. https://doi.org/10.1016/j.sdj.2012.10.002
Chong, G. T. F., & Tseng, P. (2011). A review of the uses of fluoride and outcomes of dental caries control in Singapore. Singapore Dental Journal, 32(1), 14-18. https://doi.org/10.1016/ S0377-5291(12)70011-1
Hugo, V. (1982). Les Miserables. Penguin Classics.
Marti, K. C., Mylonas, A. I., MacEacher, M., & Gruppen, L. (2019). Humanities in predoctoral dental education: A scoping review. Journal of Dental Education, 83(10), 1174-1198. https://doi.org/10.21815/JDE.019.126
Otto, M. (2017, June 13). How can a child die of toothache in the US? The Guardian. https://www.theguardian.com/inequality/2017 /jun/13/healthcare-gap-how-can-a-child-die-of-toothache-in-the-us
*Gabriel Chong
Singapore Armed Forces HQ Medical Corps,
701 Transit Rd,
Singapore 778910
Email: g.chong@mail.com
Submitted: 6 May 2023
Accepted: 12 September 2023
Published online: 2 April, TAPS 2024, 9(2), 92-94
https://doi.org/10.29060/TAPS.2024-9-2/PV3054
Bhuvan KC1 & Pathiyil Ravi Shankar2
1School of Clinical Sciences, Faculty of Health, Queensland University of Technology, Australia; 2IMU Centre for Education, International Medical University, Malaysia
I. INTRODUCTION
Learning spaces can be physical, virtual, or hybrid spaces where students engage with the learning material and interact with peers and facilitators. Traditionally, learning spaces used to be classrooms, lecture halls, laboratories, and libraries and would include a teacher and students working inside a fixed space using a blackboard/whiteboard, PowerPoint projector, boards, and flexible/fixed seating arrangements. With the advancement in educational methodologies and incorporation of technology and newer applications, learning spaces now include simulated laboratories, online learning platforms, and virtual and augmented reality-based platforms. Using virtual spaces students can interact and learn from wherever they are living/staying.
The healthcare sector has a demand for personalised and precision medicine, teleconsultation, artificial intelligence (AI)-assisted devices and programs, health/clinical applications, health informatics, and robotics along with the need for healthcare and clinical services and medicines. However, there has not been enough research and discussion around the built-in environment i.e., learning spaces in health sciences education and the activities of teaching and learning (Temple, 2007). Against this backdrop, we need to examine how students use learning spaces to interact and engage with the learning material in our current environment and think about how we can optimise the learning spaces for active learning and make them more impactful and future-ready.
II. LEARNING SPACES
Learning spaces in health sciences must consider the unique needs of these subjects in terms of teaching and learning activities, student engagement, and hands-on sessions. Learning spaces design are domain specific and must cater to the teaching and learning needs of the discipline. Designing learning spaces for health sciences is challenging. Learning space can have a significant impact on teaching and learning experiences. A well-designed learning space can help students in many ways:
- It can promote student engagement, is always inviting and comfortable, and stimulating for students. They can sit together and discuss a case or work on a project (Wilson & Randall, 2012).
- A nice and comfortable multi-purpose space can help students engage in project work. They can move the seating to suit their group’s needs, write on the table surface, and whiteboards and discuss, charge their laptops, and use the internet to interact in virtual spaces. Interactive classrooms could make instruction more efficient and effective. More research is needed on the effect of learning space design on students’ engagement and the outcomes of teaching and learning. Health sciences students engage in formal and informal learning, peer support and discussion, clinical case practice and use different diagnostic equipment.
- A well-designed and well-equipped classroom can allow teachers to design workshops and activities that engage students in groups. A flexible learning space can help teachers be more creative and innovative in their approach. Flexible learning spaces provide pedagogical opportunities and support innovative practices that are not easily provided by traditional learning spaces (Benade, 2019). Health Sciences schools must think of ways to design and use learning spaces to promote active learning and help students learn clinical decision-making, required skills, therapeutic reasoning, clinical examinations, and other important practical skills.
- A well-designed learning space can promote collaboration and enhance creativity among the students. A learning space where students can interact face to face, bring their devices, and use tables, boards, and other tools will promote better collaboration and learning. However, one significant challenge is to have enough collaborative learning rooms to accommodate students; multipurpose tables, boards, and other teaching aids and devices are important given that space is at a premium, especially in urban centres (Jamieson, 2003; Van Joolingen et al., 2005). Hybrid learning spaces may partly address this problem.
III. DESIGNING A COLLABORATIVE LEARNING SPACE
To design a collaborative learning space for health sciences we must examine how learning occurs. Active learning plays an important role. There is extensive use of technology in learning. We use interactive whiteboards, create personalised learning environments, wireless networks and the internet, interactive software such as PollEverywhere, Slido and MyDispense, games, applications, etc. to engage with learners in a physical, virtual, or hybrid environment. So, our first consideration is to have a learning space that is flexible, accommodative, supports technologies used for teaching and learning, and is sustainable. Some steps that we can include in our planning and design of learning space can be:
1) Define the learning objectives: The first key consideration while designing a learning space is to look at the programme learning objective. We need to evaluate what students want to achieve in terms of learning outcomes and what skills do they need to acquire for that programme/subject. For campuses running multiple programmes collaboration across the discipline is needed during the planning stage to look at learning spaces that can work for multiple disciplines. Health sciences students gain specialised skills for patient care, including clinical competence, interdisciplinary collaboration, ethics, cultural sensitivity, and patient communication.
2) Consider the size and layout: The learning space must have adequate room to fit all the pupils in the group, necessary furnishings, and equipment. Consider the programme’s enrolment and the activities that the learners will take part in. The layout should encourage student collaboration and active learning.
3) Utilise technology: Technology plays a significant role in modern-day learning. Our subjects/programmes are managed via online platforms like Moodle, CANVAS, Blackboard, etc. Post-COVID Universities/ Schools are running their programmes in a hybrid fashion. Integrating the latest technology, especially the information and communication technology (ICT) based applications and built-in system seems to be vital when we deliver our programmes through online platforms. Tests are run via online quizzes and electronic assessment platforms.
4) Flexibility in learning spaces: Flexibility is the key consideration when designing a learning space in modern classrooms. These learning spaces must be customisable to accommodate the various learning requirements of the students in a flexible learning environment.
5) Optimise lighting and acoustics: Lighting and acoustics are critical factors that can impact learning. It is important when we want to use a virtual environment for immersive learning or play a video to demonstrate 3D- anatomical illustrations. Ensure the learning space has adequate lighting, and acoustics are optimised to minimise noise levels and distractions.
6) Emphasise sustainability: When designing the learning space, sustainability should be a top priority. To lessen the environmental impact and foster a healthy learning environment, incorporate sustainable materials and designs.
7) Encourage collaboration: Active learning requires collaboration, which is a crucial component. Think about including group tables, breakout rooms, and collaborative learning spaces.
8) Customisation of learning spaces: Learning spaces (formal or informal) must be accommodative. For example, a learning space must fit multiple activities like workshops, lectures, problem-based learning, small group discussions, simulation activities, etc. Thus, having flexible elements like collapsible walls, movable desks and chairs, computers on wheels, and foldable furniture and equipment will be ideal from a customisation perspective.
IV. CHALLENGES IN DESIGNING LEARNING SPACES
Learning space design is challenging especially for health and medical sciences programmes because of the specialisation and the complexities of the curriculum and its requirements. It is even more challenging for resource limited settings where universities and schools are struggling to deliver high quality teaching and learning even in traditional environments. These challenges are manifold:
1) Health sciences curricula are content-rich but traditionally taught didactically. Designing learning spaces, crucial for activities like problem-based learning, clinical skill practice, and immersive anatomy learning, presents challenges due to their specialised requirements. Altering spaces to these needs is complex.
2) Keeping the learning spaces human centred is another challenge given the rapidly changing teaching and learning delivery methods brought about by information technology. The pedagogy must be the priority and technology must support it and make it more efficient.
3) Designing learning spaces involves multiple priorities. There are elements like curriculum/content requirement, disability access, collaborative learning, and use of technology. Creating a learning space balancing these elements is a challenge, especially for educational institutions in low resource settings.
4) Designing adaptable learning environments that embrace evolving technologies and teaching methods is complex. A versatile collaborative space, equipped with tables, chairs, digital tools, and virtual platforms, must serve diverse students and activities. This challenge is intensified in resource-limited settings, where maintaining physical and virtual elements, costly online resources, and internet quality pose additional hurdles.
V. CONCLUSION
Learning spaces need proper focus. Health science programs are undergoing major structural transformations. Thus, our learning space must be coordinated with active learning pedagogy and philosophy. While designing learning spaces we must consider flexibility, comfort, technology, collaboration, and safety to build a collaborative and futuristic learning space that allows students to engage with their learning content and achieve the required learning outcomes.
Notes on Contributors
BKC contributed to the conceptualisation of the manuscript, wrote the first draft, revised the subsequent draft, and contributed to the final draft. PRS contributed to the conceptualisation of the manuscript and critically revised the first draft. He contributed to the subsequent revision and finalisation of the manuscript.
Funding
The authors did not receive any funding for this article.
Declaration of Interest
The authors would like to declare that they do not have any conflict of interest.
References
Benade, L. (2019). Flexible learning spaces: Designed for inclusion? New Zealand Journal of Education Studies, 54(1), 53-68.
Jamieson, P. (2003). Designing more effective on‐campus teaching and learning spaces: a role for academic developers. International Journal for Academic Development, 8(1-2), 119-133. https://doi.org/10.1080/1360144042000277991
Temple, P. (2007). Learning spaces for the 21st century: A review of the literature. Retrieved from https://www.advance-he.ac.uk/knowledge-hub/learning-spaces-21st-century
Van Joolingen, W. R., de Jong, T., Lazonder, A. W., Savelsbergh, E. R., & Manlove, S. (2005). Co-Lab: Research and development of an online learning environment for collaborative scientific discovery learning. Computers in Human Behavior, 21(4), 671-688. https://doi.org/10.1016/j.chb.2004.10.039
Wilson, G., & Randall, M. (2012). The implementation and evaluation of a new learning space: a pilot study. Research in Learning Technology, 20(2), 14431. https://doi.org/10.3402/rlt.v20i0.14431
*Bhuvan KC
Discipline of Pharmacy, School of Clinical Sciences,
Queensland University of Technology,
2 George Street, Brisbane, Qld, Australia
Email: kc.bhuvan@qut.edu.au
Submitted: 17 August 2023
Accepted: 21 December 2023
Published online: 2 April, TAPS 2024, 9(2), 87-91
https://doi.org/10.29060/TAPS.2024-9-2/SC3114
Isharyah Sunarno1,2, Budu Mannyu2,3, Suryani As’ad2,4, Sri Asriyani2,5, Irawan Yusuf 2,6, Rina Masadah2,7 & Agussalim Bukhari2,4
1Department of Obstetrics and Gynecology, Faculty of Medicine, Hasanuddin University, Indonesia; 2Department of Medical Education, Faculty of Medicine, Hasanuddin University, Indonesia; 3Department of Ophthalmology, Faculty of Medicine, Hasanuddin University, Indonesia; 4Department of Clinical Nutrition, Faculty of Medicine, Hasanuddin University, Indonesia; 5Department of Radiology, Faculty of Medicine, Hasanuddin University, Indonesia; 6Department of Physiology, Faculty of Medicine, Hasanuddin University, Indonesia; 7Department of Pathological Anatomy, Faculty of Medicine, Hasanuddin University, Indonesia
Abstract
Introduction: The study aimed to ascertain how the faculty at the Faculty of Medicine, Hasanuddin University perceived their role as a tutor during a problem-based learning activity during the academic phase of medical education, based on the length of time they acted as a tutor.
Methods: This was prospective observational research with an explanatory sequential mixed-method design, which was performed at the Undergraduate Medical Study Program, Faculty of Medicine, Hasanuddin University, from January 2023 until May 2023. Research subjects were divided into two groups: a) the Novice group and b) the Expert group. Quantitative data were collected by giving a questionnaire containing six categories with 35 questions and distributed by Google form. An independent t-test was used to compare the faculty’s perception, with a p-value <.05 significant. Followed by Focus Group Discussion (FGD) for qualitative data, which then were analysed by thematic analysis. The last stage is integrating quantitative and qualitative data.
Results: There were statistically significant differences in seven issues between the two groups. Most of the tutors in both groups had favorable opinions, except for the expert group’s disagreement with the passive role of the tutor in the tutorial group. Eight positive and twelve negative perceptions were found in the FGD.
Conclusion: Most tutors positively perceived their role in PBL, with the expert group having more dependable opinions and well-reasoned suggestions.
Keywords: Problem-Based Learning, Undergraduate Medical Education, Focus Group Discussion
I. INTRODUCTION
The transition from teacher-centered to student-centered learning occurs with the introduction of active learning based on the needs of the students. The majority of effective active learning activities in the classroom were created in small groups using the Problem-Based Learning (PBL) approach. PBL has no worse outcomes in terms of academic performance and is more effective than conventional methods at enhancing social and communication skills, problem-solving abilities, and self-learning abilities, and allows the students to collaborate while integrating science, theory, and practice (Trullàs et al., 2022; Wiggins et al., 2017). A tutor or a facilitator is a pertinent element for the success of tutorial activities in PBL, thus evaluating periodically their perception and understanding about PBL activities, will help determine the need for resource development at the faculty level. Based on the aforementioned background, the author is intrigued to understand how the faculty at the Undergraduate Faculty of Medicine at Hasanuddin University perceived their role as a tutor during a PBL activity based on the duration they acted as a tutor.
II. METHODS
Short-case PBL tutorial is the model being implemented in our institution. An explanatory sequential mixed-methods observational prospective design study was carried out from January 2023 to May 2023. Informed consent was obtained from all the participants (ethics approval recommendation number: 99/UN4.6.4.5.31/PP36/2022). The study was conducted in three stages (Figure 1):
A. Stage 1
Gathering quantitative data via a survey disseminated using Google form, after which the information was analysed using SPSS version 25. The Likert scale, which ranged from 1 (extremely disagree) to 5 (extremely agree), was used to evaluate the 35 items in the questionnaire that served as the study’s primary data collection tool (Table 1 which is openly available on Figshare). The validity and reliability test for the study’s questionnaire was carried out as the first step and the Pearson Correlation was used to examine the outcome; all questions were valid with Cronbach’s α .951. The next step was to collect data through convenience sampling. Inclusion criteria were lecturers who: have attended training to become PBL tutors, are actively involved in PBL activities, and are willing to participate in the research projects to completion. Exclusion criteria were lecturers who were not familiar with the Google form application. Subjects with other commitments that prevented them from finishing the research activities and with a conflict of interest in continuing the study were considered dropouts. The research participants were split into two groups: the novice group (participants who served as tutors for less than five years) and the expert group (participants who served as tutors for five years or more). The Slovin formula was used to determine the minimum sample size, and the result was 32 people for each group. Characteristics of the study subjects were presented descriptively. An independent t-test was used to compare the faculty’s perception of their role as a tutor during a problem-based learning activity, with a p-value <.05 significant.
B. Stage 2
Focus Group Discussions (FGD) were held to collect qualitative data. The participants in the FGD were divided into two groups using the identical criteria utilised for the quantitative group categorisation, and each group consisted of six subjects. Each participant received a set of open-ended questions to be discussed during the FGD. All events and discussions were recorded, and then all conversations were transcribed using the VERBATIM app. MAXQDA 2020 was then used to tag and categorise the data. Thematic analysis was used to assess qualitative data. We used an audit trail and triangulation during data collection and conducted a peer review during data analysis to ensure the validity of the qualitative data.
C. Stage 3
Integrating quantitative and qualitative data was performed by linking data, followed by integration at the interpretation and reporting level which was conducted by integration through a narrative with a weaving approach.
III. RESULTS
A. Characteristics of the Subjects
The subjects in the novice groups were all under 45 years old, but the expert group was predominately made up of older faculty members. Both groups were predominately female. At the time of the research, medical doctors dominated the novice group, but the expert group included people with a range of educational backgrounds. Characteristics of the study subjects are openly available in Table 2 on Figshare.
B. Quantitative Data
Seven question items from four categories significantly differed between the novice and expert groups as shown in Table 3 which is openly available on Figshare.
C. Qualitative Data
Thematic analysis from the FGD revealed that the expert group only has negative perceptions, whereas the novice group has both negative and positive perceptions. The data are openly available in Table 4 on Figshare.
D. Integration of Quantitative and Qualitative Data
Faculty staff has the same perception about almost all concepts about the role of a PBL tutor, except for seven concepts that were statistically significantly different (Figure 1):
1) PBL as Pedagogical Method: Q5 (group tutorials help students share experiences) and Q9 (PBL is a great tool for student learning) were significantly different, with the majority of the novice group agreeing with it while the majority of the expert group were extremely agreeable. Nevertheless, while the novice had a positive perspective shown in the discussion, the expert expressly stated that “(PBL) increased the (student’s) ability to discuss but not the depth of knowledge.”
2) Supervising Problem Processing in Tutorial Groups: Q12 (I function as a resource person in the group) and Q13 (I participate in creating a positive work environment for the group) were significantly different, with most of the novice group agreeing to the concept while the majority of the expert group were extremely agreeable. The novice group stated in the FGD that “PBL is very effective for building students’ analytical skills because the students can interact with each other to express their opinions and find key problem-solving strategies.” Both groups had the same perception that some tutors attended the PBL activities “just as a formality.” Q17 (I am sensitive to the wishes of the students regarding their need for support) was also significantly different, with most participants in both groups agreeing that tutors are sensitive to the student’s need for support, but 5.71% of the novices extremely disagreed. In contrast, none of the experts in the expert group disagreed with the concept. From the FGD results, the expert group suggested that the “tutor should give feedback and guidance to the students”.
3) Potential Barriers to Student Learning in PBL: the majority of both groups agreed that the group size is just right from a tutorial point of view (Q24), but the novice group had a wide range of responses (from extremely disagree to extremely agree), while 77.14% of the expert group agreed. “Six to eight students in one PBL group” is an elaborate suggestion made by the expert group as a result of the FGD.
4) There was a statistically significant difference between the two groups regarding the role of the tutor, which is usually passive in the tutorial group (Q29), with the expert group’s consensus on the matter being unfavorable, whereas the novice group’s responses were evenly split between neutral and disagree. The FGD’s results revealed that the novice merely stated, “If the students had a misleading concept, the tutor could not be kept silent,” whereas the expert suggested, “The tutor should be the chairman of the group discussion,” and “Questions and keywords must be made by the tutor.”
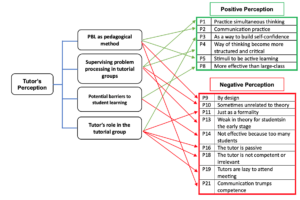
Figure 1. Integration of Quantitative and Qualitative Data
IV. DISCUSSION
PBL can be regarded as a multidisciplinary method that allows the learners to resolve real-life problems and situations in every aspect, learn how to construct new information meaningfully, put away the understanding of ready-to-use knowledge, and acquire critical thinking skills. Problem processing or facilitation is a challenging task (Aydogmus & Mutlu, 2019). Since PBL can be used in specific topics and can break up the monotony of traditional didactic teaching, it has become a popular alternative teaching strategy for undergraduate medical students. It can also be used as a method of integrated teaching. Overall, it is a great tool for students learning (Gadicherla et al., 2022).
The group size is one of the possible obstacles to students’ learning in PBL. All students will not be able to participate in a team that is too big. A team that is too small could not have enough members to address the learning objectives or enough diverse opinions to guarantee a robust discussion. The tutor should be aware of how the participants play their roles, noting those who do not contribute to debates or who are silent. Therefore, they must pay close attention to what is happening in the group process to intervene and provide feedback, promoting the participants’ individual and group progress. The tutor can assist the student in identifying their requirements through motivated evaluations and simple feedback, fostering the growth of self-confidence, autonomy, and, ultimately, integration into group dynamics. PBL teams ideally consist of 6–10 students (Dent et al., 2017).
V. CONCLUSION
Aside from seven concepts, both groups mostly had positive perceptions about their role as tutors, with the expert group having more dependable opinions and well-reasoned suggestions.
Notes on Contributors
Isharyah Sunarno made the following contributions to the study: conceptualised, created the initial draft and study design, investigated and collected data, conducted formal analysis, looked for research references, performed critical revision of the article, reviewed and edited the article, and approved the study’s final published version.
The following are the contributions Budu Mannyu made to the study: provided insights into the methodology, suggested research references, served as a peer reviewer of the study’s findings, performed critical revision of the article, and gave his approval of the final draft to be published.
Suryani As’ad contributed the following to the study: she offered insights into the methodology, proposed research references, served as a peer reviewer of the study’s findings, revised the article critically, and approved the final draft of the manuscript to be published.
The study benefited from Sri Asriyani’s efforts, which included: suggestion for research references, peer review of the study’s findings, and performed critical revision of the article.
The following contributions were made to the study by Irawan Yusuf: peer reviewing of the result, supervising the research activities, and critical editing of the publication.
The following are the contributions Rina Masadah contributed to the study: provided ideas into the original draft, supervised the research activities, and edited the publication critically.
Agussalim Bukhari made the following contributions to the study: offered insights into the methodology, oversaw the research activities, critically revised the final version of the article.
Ethical Approval
The study was approved by the Research Ethical Committee Faculty of Medicine Hasanuddin University with recommendation number: 99/UN4.6.4.5.31/PP36/ 2022.
Data Availability
The authors confirm that the data supporting the findings of this study are available within the article and its Supplementary material for research instrument in https://doi.org/10.6084/m9.figshare.23646918
Acknowledgement
Authors would like to express our sincere gratitude to all the tutors who participated in this study. A special appreciation is given to Ichlas Nanang Affandi and A. Tenri Rustam from the Psychology Study Program, Faculty of Medicine, Hasanuddin University for their valuable support throughout the research process, including their role as the facilitator of the FGD. We also would like to thank Andriany Qanitha and the CRP team from Faculty of Medicine, Hasanuddin University for their support in developing the manuscript. We are also grateful to the Department of Medical Education, Faculty of Medicine, Hasanuddin University for providing us with the resources and support we needed to complete this study.
Funding
This research received no external funding.
Declaration of Interest
The authors declare no conflict of interest.
References
Aydogmus, M., & Mutlu, A. (2019). Problem-based learning studies: A content analysis. Turkish Studies-Educational Sciences, 14(4), 1615–1630. https://doi.org/10.29228/turkishstudies.23012
Dent, J. A., Harden, R. M., & Hunt, D. (2017). A practical guide for medical teachers (5th ed.). Elsevier.
Gadicherla, S., Kulkarni, A., Rao, C., & Rao, M. Y. (2022). Perception and acceptance of problem-based learning as a teaching-learning method among undergraduate medical students and faculty. Azerbaijan Medical Journal, 62(03), 975–982.
Trullàs, J. C., Blay, C., Sarri, E., & Pujol, R. (2022). Effectiveness of problem-based learning methodology in undergraduate medical education: A scoping review. BMC Medical Education, 22(1), 1–12. https://doi.org/10.1186/s12909-022-03154-8
Wiggins, B. L., Eddy, S. L., Wener-Fligner, L., Freisem, K., Grunspan, D. Z., Theobald, E. J., Timbrook, J., & Crowe, A. J. (2017). ASPECT: A survey to assess student perspective of engagement in an active-learning classroom. CBE Life Sciences Education, 16(2), 1–13. https://doi.org/10.1187/cbe.16-08-0244
*Isharyah Sunarno
Jl. Perintis Kemerdekaan Km. 11,
Faculty of Medicine, Hasanuddin University
+62411-585859
Email: isharyahsunarno@gmail.com
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
