
Perceptions of postgraduate students on the use of portfolio in the paediatrics department
Submitted: 28 August 2023
Accepted: 12 July 2024
Published online: 1 October, TAPS 2024, 9(4),81-83
https://doi.org/10.29060/TAPS.2024-9-4/CS3229
Tayzar Hein1, Nilar Lwin2 & Ye Phyo Aung1
1Department of Medical Education, Defence Services Medical Academy, Myanmar; 2Department of Child Health, Defence Services Obstetrics, Gynaecology & Children’s Hospital, Myanmar
I. INTRODUCTION
Portfolios, as structured collections of documentation, not only showcase a student’s learning progress and achievements but also foster a self-directed approach to assessing their own performance and setting future goal (Birgin & Adnan, 2007). Existing literature predominantly addresses the broader usage of portfolios across various disciplines, underscoring their role in enhancing reflective practice and competency-based assessments (David et al., 2001). Although portfolios in paediatrics department provide advantages, their implementation encounters substantial obstacles. These include the substantial time and effort required to maintain them, the need for clear guidelines from faculty, and a varying degree of acceptance among students and faculty, who may prefer traditional assessment methods. This study specifically aims to address these challenges by exploring the perceptions of postgraduate students on the use of portfolios in the paediatrics department at the Defence Services Medical Academy.
II. METHODS
Ethical permission for this study was granted in July 2022. The research was conducted over a six-month period from September 2022 to February 2023 within the Paediatrics Department at the Defence Services Medical Academy. To explore the experiences and perceptions of portfolio use in paediatric education, we employed purposive sampling to select six postgraduate paediatric students. We acknowledge the limitations of a small sample size. However, the focus was to gain a preliminary understanding and not to reach data saturation. The study utilised a qualitative research design (Creswell & Creswell, 2017), incorporating focus group discussions to facilitate in-depth dialogue and collect rich qualitative data. Although initially described as employing a ‘grounded theory’ approach, it is more accurate to characterise the methodology as exploratory qualitative research. Data collection involved structured focus group discussions, which were carefully designed to prompt reflection on the students’ experiences with portfolio learning. Data analysis was conducted using manual coding in conjunction with MAXQDA software, facilitating the organisation and thematic analysis of focus group transcripts.
III. RESULTS
The data analysis revealed four key themes regarding the use of portfolios in assessing competencies in the paediatrics department.
A. Theme 1: Value of Portfolios in Assessing Competencies
One participant stated, “Portfolios allowed me to reflect on my learning and track my progress towards meeting my competencies.” Another participant added, “It was helpful to have a structured way of documenting my experiences and reflecting on my strengths and areas for improvement.” The participants also noted that the use of portfolios provided an opportunity for self-directed learning and development.
B. Theme 2: Time and Effort Required
One participant stated, “It was challenging to find the time to update my portfolio regularly, especially with other demands on my time.” Another participant added, “The process of compiling evidence and reflecting on my experiences was more time-consuming than I anticipated.” The participants noted that clear guidelines and expectations were necessary to ensure the success of the portfolio assessment process.
C. Theme 3: Need for Feedback and Support
One participant stated, “I appreciated receiving feedback from my supervisors on my portfolio, as it helped me to identify areas for improvement and set goals for the future.” Another participant added, “It was helpful to have regular check-ins with my supervisors to discuss my progress and receive support and guidance.” The participants noted that faculty members needed to be trained in providing feedback and support to ensure the success of the portfolio assessment process.
D. Theme 4: Limited Impact on Career Development
One participant stated, “While portfolios were helpful in documenting my progress towards meeting my competencies, they did not have a significant impact on my career development.” Another participant added, “Portfolios were a useful assessment tool, but they did not provide me with opportunities for networking or career advancement.” The participants noted that additional career development opportunities were necessary to complement the use of portfolios.
IV. DISCUSSION
A. Implications for Practice
Building on the insights from this study, the paediatrics department is encouraged to integrate portfolio assessment into its curriculum. The findings corroborate with a study who noted that portfolio use enhances self-directed learning and the documentation of competencies (Jimoyiannis & Tsiotakis, 2016). The comprehensive nature of portfolios allows students to systematically track their progress and reflect on their learning journey, fostering a deeper engagement with educational content. Implementing such assessments can not only enhance learning autonomy but also promote critical reflection among postgraduate paediatric students. This could lead to more personalised educational experiences and potentially improve competency acquisition.
B. Implications for Research
While this study provides preliminary insights into the effectiveness of portfolio assessments, it also underscores a significant gap in the literature regarding long-term impacts on learning outcomes and career progression within paediatric education. To provide a thorough assessment of the practical advantages and drawbacks of portfolio-based learning, studies could use longitudinal designs to follow the professional development of those who have participated in it.
C. Addressing Limitations and Strengthening the Argument
The study is limited by its focus on a small cohort of postgraduate students within one department, which restricts the generalisability of the findings. Moreover, the exploratory nature of the research calls for cautious interpretation. The enthusiasm and perceived benefits reported by participants align with broader educational theories emphasising active learning and continuous assessment (Trowler, 2010).
V. CONCLUSION
In conclusion, this study has provided valuable insights into the perceptions of postgraduate students on the use of portfolios in the paediatrics department. The findings suggest that portfolios can be a valuable assessment tool, but clear guidelines and expectations, as well as feedback and support from faculty members, are necessary to ensure its success.
Notes on Contributors
Dr. Tayzar Hein has played a pivotal role as the main author in this research study, contributing significantly to the conception, design, and execution of the investigation into the perceptions of postgraduate students regarding the use of portfolios in the paediatrics department.
In the early stages of the research, Dr. Nilar Lwin played a crucial role in conceptualising and designing the study. Her insights and experience contributed to shaping the research questions and methodology, ensuring a comprehensive exploration of the subject matter.
As a co-author, Dr. Yephyo Aung has been actively involved in the ethical approval process, emphasising the importance of adhering to ethical standards in research. His commitment to ethical considerations has been instrumental in maintaining the credibility and integrity of the study.
Acknowledgement
We extend our sincere appreciation to all those who contributed to the completion of this research study, particularly acknowledging individuals and organisations whose support, guidance, and contributions were instrumental in the research process.
Ethical Approval
Ethics approval was granted by the Ethical Review Committee of the DSMA, Ethical Review Board (2/ ERB/ 2022).
Funding
This research is entirely self-funded, as there is currently no external financial support available for the project, necessitating the coverage of all expenses independently.
Declaration of Interest
The authors of this research study declare that there are no conflicts of interest that could potentially influence or bias the outcomes, interpretations, or conclusions of the study. A conflict of interest is defined as any financial, consultant, institutional, or other relationships that may pose a risk of bias or conflict with the objectivity and integrity of the research.
References
Birgin, O., & Adnan, B. (2007). The use of portfolio to assess student’s performance. Journal of Turkish Science Education, 4(2), 75-90. https://www.tused.org/index.php/tused/article/view/673
Creswell, J. W., & Creswell, J. D. (2017). Research design: Qualitative, quantitative, and mixed methods approaches (5th ed.). Sage Publications. https://spada.uns.ac.id/pluginfile.php/510378/ mod_resource/content/1/creswell.pdf
David, M. F. B., Davis, M., Harden, R., Howie, P., Ker, J., & Pippard, M. (2001). AMEE Medical Education Guide No. 24: Portfolios as a method of student assessment. Medical Teacher, 23(6), 535-551. https://doi.org/10.1080/01421590120090952
Jimoyiannis, A., & Tsiotakis, P. (2016). Self-directed learning in e-portfolios: Analysing students’ performance and learning presence. EAI Endorsed Transactions on e-Learning, 3(10), e7. https://doi.org/10.4108/eai.10-3-2016.151120
Trowler, V. (2010). Student engagement literature review. The Higher Education Academy, 11(1), 1-15.
*Tayzar Hein
No.94, D-1, Pyay Road,
Mingaladon Township,
Yangon, Myanmar
Postal code – 11021
+95 95188093
Email: dr.tayzarhein@gmail.com
Submitted: 14 December 2023
Accepted: 14 May 2024
Published online: 1 October, TAPS 2024, 9(4), 76-80
https://doi.org/10.29060/TAPS.2024-9-4/CS3215
Vanda Wen Teng Ho1 & Kay Choong See2
1Division of Geriatric Medicine, Department of Medicine, National University Hospital, Singapore; 2Division of Respiratory and Critical Care Medicine, Department of Medicine, National University Hospital, Singapore
I. INTRODUCTION
Residents are vital to the medical workforce, especially for overnight call duties. Transitioning from junior roles to handling overnight calls as senior residents (SRs) can be anxiety-inducing, leading to decline in cognitive performance and fatigue (Weiss et al., 2016). These pose concerns for patient safety and quality of supervision, as SRs often serve as the most senior staff on-site overnight. However, calls offer valuable training opportunities, fostering autonomy, decision-making skills, and preparation for future consultant roles. The challenge is to ensure that overnight calls are safe for both patients and physicians while being conducive to learning.
During the COVID-19 pandemic, the health system’s reallocation of manpower substantially increased the workload. While there remains conflicting evidence on the optimal on-call arrangement, the Accreditation Council for Graduate Medical Education stipulates a maximum of 24 consecutive hours of direct patient care to safeguard against negative effects of chronic sleep deprivation (Nasca et al., 2010). In our tertiary hospital, two medical SRs performed stay-in overnight calls ranging from 15 to 21 hours (1700-0800h on weekdays and 1100-0800h on weekends). Before each call, SRs started work at 0700h. One SR was in-charge of the intensive care unit (ICU) and the other was on the general medicine floor. During each call, the ICU SR was responsible for supervising 2 stay-in junior residents, 2-5 new patient admissions and 20 existing ICU patients; the general medicine SR was responsible for supervising a team of four stay-in junior residents, 30-50 new patient admissions, and 100-150 existing inpatients. After each call, SRs would continue with the morning ward rounds before ending work. SRs could seek help by calling the duty consultant, who stayed out of hospital.
With limited data on SRs’ call experiences during the pandemic, understanding their perceptions and attitudes would be essential for system improvement and preparation for future challenges. Therefore, we aimed to explore the perceptions, attitudes, and practices of SRs with regards to overnight stay-in calls during the COVID-19 pandemic, as well as avenues for improvements in the call system.
II. METHODS
An electronic survey was conducted via monthly email invitation to SRs in the internal medicine department of a 1,200-bed tertiary university hospital between November 2021 and January 2022. All SRs approached had at least three calls per month. Each email invitation was sent to 40 SRs who consisted of the hospital’s on-call medicine pool. Consent was exempt as this was an anonymised survey (NHG DSRB reference number: 2021/00413). Participants were asked to provide their opinions on various aspects of these calls using a 5-point Likert scale. Monthly prompts to complete the survey were issued.
III. RESULTS
Out of the 40 medical SRs surveyed, 20 responded (50% rate). Their education backgrounds were split between the United Kingdom (n=7) and Singapore (n=13). All trained and worked as SRs in the same hospital group for 4-9 years (median 5 years). The specialties represented included advanced internal medicine (4 respondents), endocrinology (4 respondents), geriatric medicine (3 respondents), neurology (2 respondents), rheumatology (2 respondents), and one respondent each from respiratory and critical care medicine, haematology, infectious diseases. Two participants declined to state their specialty.
In terms of perception, SRs generally agreed that calls contributed to their development as specialists and were essential to their training. They found the learning experience during calls to be valuable for exposure to diverse cases, different from their specialist training which mostly occurred during daytime clinical work. In terms of attitude, most SRs felt prepared and confident for their calls. However, around one-quarter expressed doubts about handling difficult call situations. Many SRs believed that the patient experience overnight could be greatly improved. Nearly half perceived overnight patient care quality as compromised, with 95% noting a decline post-call. While the majority felt safe on-call, fifteen SRs agreed that they would ask for help on-call. Worryingly, only 55% were comfortable doing so and 60% preferred having more supervision during calls.
For potential improvements (Fig 1), SRs were asked to rank various choices on a 5-point Likert scale. These choices were specific to overnight calls. Most SRs agreed that the educational value of calls could be enhanced, and they would prefer to have fewer calls during their training. Around two-thirds disagreed with the idea that certain specialties should have more calls or that consultants should perform stay-in calls. Detailed results can be found in the Appendix.
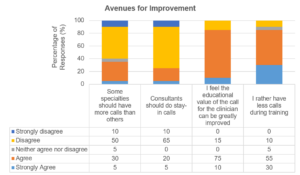
Figure 1. Avenues for improvement for senior residents’ call experience
IV. DISCUSSION
Our survey indicates that SRs felt prepared and recognised the educational value of overnight calls, but there is a clear need for enhanced learning experiences and supervision. Research on junior residents had shown that having in-house overnight hospitalists led to fewer barriers in contacting supervising physicians (Catalanotti et al., 2021) and improved the educational quality of calls (Trowbridge et al., 2010). However, SRs have varying preferences for such supervision, suggesting a need to explore the most suitable form of oversight.
Concerns about compromised patient care during and post-call periods suggest the negative impact of sleep deprivation on performance. Sleep deprivation can impact performance, and the debate around optimal work hours and call types continues, as shorter calls have not demonstrated improved outcomes (Schuh et al., 2011). Alternatives like increasing SRs on call each night should be considered while balancing frequency and stress levels. A larger survey on more hospitalists and SRs from other specialties is needed to confirm these findings and develop appropriate improvements to the on-call system.
V. CONCLUSION
Although the survey was relatively small and limited to one internal medicine department, the findings provide valuable insights for efforts to enhance SRs’ call experiences. Overall, SRs feel confident and safe during overnight calls, but further research is needed to explore and improve three areas: (1) call supervision; (2) learning value of calls; and (3) quality of patient care during and post-call. Graduate medical education programs must prioritise training excellence, resident well-being, and patient care. Our survey revealed challenges associated with overnight calls during a period of high workload marked by the COVID-19 pandemic, which we hope can stimulate the development and study of appropriate interventions.
Notes on Contributors
VWTH and KCS jointly conceptualised this study. VWTH conducted the study, wrote the manuscript, and analysed the data. KCS provided oversight during the study conduct and reviewed the manuscript.
Ethical Approval
This study has been approved by the National Health Group Domain Specific Review Board (reference number: 2021/00413).
Acknowledgement
The authors would like to thank the participating SRs for their responses.
Funding
This study has no funding sources.
Declaration of Interest
There are no interests to declare.
References
Catalanotti, J. S., O’Connor, A. B., Kisielewski, M., Chick, D. A., & Fletcher, K. E. (2021). Barriers to accessing nighttime supervisors: A national survey of internal medicine residents. Journal of General Internal Medicine, 36(7), 1974-1979. https://doi.org/10.1007/s11606-020-06516-4
Nasca, T. J., Day, S. H., & Amis, E. S., Jr. (2010). The new recommendations on duty hours from the ACGME task force. The New England Journal of Medicine, 363(2), e3. https://doi.org/10.1056/NEJMsb1005800
Schuh, L. A., Khan, M. A., Harle, H., Southerland, A. M., Hicks, W. J., Falchook, A., Schultz, L., & Finney, G. R. (2011). Pilot trial of IOM duty hour recommendations in neurology residency programs: Unintended consequences. Neurology, 77(9), 883-887. https://doi.org/10.1212/WNL.0b013e31822c61c3
Trowbridge, R. L., Almeder, L., Jacquet, M., & Fairfield, K. M. (2010). The effect of overnight in-house attending coverage on perceptions of care and education on a general medical service. Journal of Graduate Medical Education, 2(1), 53-56. https://doi.org/10.4300/jgme-d-09-00056.1
Weiss, P., Kryger, M., & Knauert, M. (2016). Impact of extended duty hours on medical trainees. Sleep Health, 2(4), 309-315. https://doi.org/10.1016/j.sleh.2016.08.003
*Dr Vanda Ho
Division of Geriatric Medicine,
Department of Medicine,
National University Health System ,
Tower Block Level 10, 1E Kent Ridge Rd
Singapore 119228
Email: vanda_wt_ho@nuhs.edu.sg
Submitted: 25 October 2023
Accepted: 3 April 2024
Published online: 1 October, TAPS 2024, 9(4), 71-75
https://doi.org/10.29060/TAPS.2024-9-4/CS3161
Sulthan Al Rashid1, Syed Ziaur Rahman2, Santosh R Patil3 & Mohmed Isaqali Karobari4
1Department of Pharmacology, Saveetha Medical College and Hospital, Saveetha Institute of Medical and Technical Sciences (SIMATS), India; 2Department of Pharmacology, Jawaharlal Nehru Medical College, Aligarh Muslim University, India; 3Department of Oral Medicine and Radiology, Chhattisgarh Dental College & Research Institute, India; 4Dental Research Unit – Centre for Global Health Research, Saveetha Medical College and Hospital, Saveetha Institute of Medical and Technical Sciences (SIMATS), India
I. INTRODUCTION
Concept maps serve as teaching and learning tools that appear to assist medical students in cultivating critical thinking skills. This is attributed to the adaptability of the tool, acting as a facilitator for knowledge integration and a method for both learning and teaching. The extensive array of contexts, purposes, and approaches in utilising Concept maps and tools to evaluate critical thinking enhances our confidence in the consistent positive effects (Fonseca et al., 2023).
In the realm of medical education, employing concept maps as a learning strategy can prove to be beneficial (Torre et al., 2023). Concept maps, visual representations of learners’ understanding of a set of concepts, have proven to be valuable tools in medical education (Novak & Cañas, 2008). The integration of concept maps as a teaching strategy allows for the depiction and exploration of the relationships among various medical concepts (Ruiz-Primo & Shavelson, 1996). In our instructional approach, instructors employ concept maps during lectures (Appendix 1), emphasising the interconnectedness of key concepts. Students actively participate in creating their own concept maps, facilitating collaborative learning. This flexible approach accommodates diverse learning styles, with students using both concept map notes and textbooks. The final evaluation includes an assessment of students based on their application of concepts outlined in the concept maps, contributing to a well-rounded and adaptable learning experience in medical education.
In this study, we aimed to assess the impact of utilising the concept map teaching technique in conjunction with concept map notes on the academic performance of students.
II. METHODS
In the field of medical education, the adoption of Competency-Based Medical Education (CBME) introduced by the National Medical Commission (NMC) for the MBBS 2019 batch has led to the implementation of various innovative teaching approaches. This research, conducted with the approval of the Institutional Review Board (IRB) under the reference number 020/09/2023/Faculty/SRB/SMCH, focuses on comparing the academic outcomes of two MBBS batches of Saveetha Medical College and Hospital.
We evaluated the first-year results of the 2020 MBBS batch, which did not receive concept map teaching, and compared them with the first-year results of the 2021 MBBS batch, where concept map teaching was implemented. Students are encouraged to create concept map notes on A3 white sheets, as illustrated in Appendix 2. Furthermore, “subject-wise Saveetha Maps” were developed, incorporating handwritten notes taken by students on each topic.
Generally, it was advised to all the included students to carry on with the books and concept map notes. Furthermore, if they encounter any difficulty in referring the books, they are advised to make use of the concept map notes. In our educational setup, we promoted the combined use of concept maps notes and books for all the students. All students received their compiled handwritten notes, which include all the topics included in their particular subject, as a part of the final evaluation during summative assessment at the end of academic year, and their performance was examined by the examiners.
III. RESULTS
Performance of both the 2020 MBBS batch and the 2021 MBBS batch was assessed. To compare the percentages of first-year results of the 2020 MBBS batch (without concept map) and first-year results of the 2021 MBBS batch (with concept map), a t-test was used, and the results were highly significant (P <0.001) (Table 1 and Appendix 3).
|
Percentage |
N |
Mean |
SD |
t value |
P value |
|
First-year results of the 2021 MBBS batch (with concept map) |
248 |
75.7100 |
7.70000 |
14.953 |
<0.001* |
|
First-year results of the 2020 MBBS batch (without concept map) |
249 |
62.7800 |
11.25000 |
Table 1. Mean comparison for percentages of first-year results of the 2021 MBBS batch (with concept map) and the first-year results of the 2020 MBBS batch (without concept map)
IV. DISCUSSION
For students and physicians who are pursuing a career in medicine, teaching via concept maps has been proven to be an effective tool. However, there has been a lack of exploration regarding its integration with students’ personally crafted concept map notes. The initial year of the curriculum encompasses subjects such as anatomy, physiology, and biochemistry. Our investigation revealed that the average percentage of first-year results for the 2021 MBBS batch, which had been exposed to the concept mapping teaching technique, was 75.7%. In contrast, the mean percentage of first-year results for the 2020 MBBS batch, which had not been exposed to the concept mapping technique, was 62.8%. The disparity in results proved to be statistically significant (P <0.001) as indicated in Table 1 and Appendix 3.
This shows the very good effectiveness of the concept map teaching technique supplemented with students handwritten notes over conventional teaching methods like PowerPoint lectures on students’ academic performance (Niamtu, 2001).
Based on our experience, we wish to emphasise that elucidating key concepts through concept map lectures may prove beneficial for slow learners. Given the extensive topics in the MBBS curriculum, this approach may enable slow learners to prepare for exams more efficiently. Further research should be conducted to see the effect of concept maps on the learning capacity of slow learners. On the other hand, quick learners may leverage the advantage of quickly summarising and identifying main points from these handwritten concept map notes, complementing their book reading efforts. Substituting conventional teaching methods with the concept map teaching approach, enhanced by students’ handwritten concept map notes, significantly improves academic performance.
V. CONCLUSION
According to the findings of our study, we deduce that substituting conventional teaching methods with the concept map teaching approach, enhanced by students’ personally crafted concept map notes, leads to a more significant enhancement in students’ academic performance. In future studies, students may be classified into slow learners and fast learners depending upon the results of the previous year’s final examination and the feedback should be collected from the students in regards to the concept maps teaching approach.
Note on Contributors
Sulthan Al Rashid contributed to the concept, scientific content, data collection, statistical analysis, and manuscript preparation.
Syed Ziaur Rahman helped with the manuscript writing, editing, and proofreading.
Santosh R Patil helped with the review and editing of the manuscript.
Mohmed Isaqali Karobari helped with the review and editing of the manuscript.
The final manuscript has been read and approved by all the authors.
Ethical Approval
This study was conducted after IRB approval (020/09/2023/Faculty/SRB/SMCH).
Acknowledgement
The authors would like to acknowledge the director and medical education unit of Saveetha Medical College and Hospital for providing the details of MBBS students exam results to do this educational research.
Funding
For this study, the authors were not given any funding.
Declaration of Interest
The authors claim to have no conflicts of interest.
References
Fonseca, M., Marvão, P., Oliveira, B., Heleno, B., Carreiro-Martins, P., Neuparth, N., & Rendas, A. (2023). The effectiveness of concept mapping as a tool for developing critical thinking in undergraduate medical education – A BEME systematic review: BEME Guide No. 81. Medical Teacher, 1-14. https://doi.org/10.1080/0142159X.2023.2281248
Niamtu, J. (2001). The power of PowerPoint. Plastic and Reconstructive Surgery, 108(2), 466-484. https://doi.org/10.1097/00006534-200108000-00030
Novak, J. D., & Cañas, A. J. (2008). The theory underlying concept maps and how to construct and use them. Florida Institute for Human and Machine Cognition, 1-36.
Ruiz-Primo, M. A., & Shavelson, R. J. (1996). Problems and issues in the use of concept maps in science assessment tasks [Doctoral dissertation, Brigham Young University]. Provo UT.
Torre, D., German, D., Daley, B., & Taylor, D. (2023). Concept mapping: An aid to teaching and learning: AMEE Guide No. 157. Medical Teacher, 45(5), 455-463. https://doi.org/10.1080/0142159X.2023.2182176
*Sulthan Al Rashid
Department of Pharmacology,
Saveetha Medical College and Hospital,
Saveetha Institute of Medical & Technical Sciences (SIMATS),
Chennai, Tamil Nadu, India
+919629696523
Email: sulthanalrashid@gmail.com
Submitted: 31 January 2024
Accepted: 22 July 2024
Published online: 1 October, TAPS 2024, 9(4), 68-70
https://doi.org/10.29060/TAPS.2024-9-4/PV3238
Ardi Findyartini1,2 & Azis Muhammad Putera2
1Department of Medical Education, Faculty of Medicine, Universitas Indonesia, Indonesia; 2Medical Education Center, Indonesian Medical Education and Research Institute, Faculty of Medicine, Universitas Indonesia, Indonesia
I. ON PROFESSIONAL IDENTITY FORMATION
Professionalism in medicine can be considered as attributes, behaviours, and identity of the professionals who put the needs of their patients and the community they serve above their individual needs. The concept of professionalism is dynamic and might be perceived differently over time, in different contexts, and by different fields, although some ground values like excellence, competence, and altruism might persist.
Identity formation is an inseparable part of professionalism as it underlines the importance of “being” in addition to the essence of “behaving”. Professional identity formation (PIF) in medical education is both an active psychological process conducted by individuals in internalising their values and others’ expectations. It is also a dynamic socialisation process allowing an individual to be part of the professional community with increasing roles and recognitions. This applies for both medical students who grow to become medical professionals and for medical teachers who probably juggle their different identities as clinicians/researchers to be able to enact their roles as teachers (Cruess et al., 2014).
There is no “one-size-fits-all” rule as to how their PIF should be navigated, as PIF is a journey unique to each individual. The students need to be supported to form their identity from the stage where they just follow the rules to become individuals who can internalise values and expectations from their professional community as an integral part of themselves. The medical teachers, on the other hand, still have to develop their professional identities as teachers and educators in addition to their other identities.
II. CULTURE: WHY DOES IT MATTER?
Given the importance of individual and socialisation processes in PIF, we suggest that it is time for us to consider the influence of cultural factors in students’ and teachers’ PIF. It has been well-established that culture plays a pivotal role in how education is designed, developed, and delivered systematically. However, the frameworks by which medical curricula and faculty development programs are developed, as well as literature informing the commonly understood concepts of PIF, often stem from Western countries. Recent understanding of culture, professionalism, and PIF acknowledges that professionalism is context-specific, with notable differences between norms adopted by the contemporary Western world and in non-Western settings (Al-Rumayyan et al., 2017). Herewith, we use Hofstede’s cultural framework to discuss this matter, where countries are characterised by spectrums of hierarchy, collectivism, uncertainty avoidance, long vs short term orientation, femininity vs masculinity, and self-indulgence and restraint (Hofstede, 2001).
For instance, our research highlights the importance of culture in the PIF of medical teachers. Four main factors seemed to influence the PIF of medical teachers in our settings: an interplay between internal values and external influences, empowerment of teachers’ roles by early socialisation, experiential workplace learning, and future prospects of their careers as teachers. Looking deeper, we identified several relatively unexplored factors influencing the PIF of our teachers: the importance of divine values and religious beliefs, influence of family, and how their roles are recognised by the society (Wahid et al, 2021).
The influence of religious beliefs and societal recognition on PIF seems to be predominant in Arabic and Islamic countries, something that may not be predominant in Western countries. The strong religious influence built a perception of teaching as an act of good deed and opportunity to enact one’s faith in God, cultivating the motivation to pursue a teaching career. From Hofstede’s framework viewpoint, familial influence plays a critical role in a collectivist society like ours, as proven in our study where the participants’ decision to be medical teachers was strongly influenced by also considering coexisting personal roles in the family (especially evident in female teachers). The existence of a family member acting as a role model and internal decision making in the family also supported the decision to pursue a teaching career (Wahid et al., 2021).
The communality in collectivistic society was also notable, since societal recognition was deemed as a reward to develop oneself professionally, showing a stronger emphasis on social relationship as opposed to the Western counterpart which might put more emphasis on individual values and self-fulfilment. The importance of socialisation was evident as many admitted that early in their teaching careers, they would often shadow their seniors, engage in faculty development programs, and nurture their identity by engaging with students and patients. Interacting with fellow teachers helped them to grow professionally and remind them of their roots, creating a valuable interplay between their internal motivation and external influences. This shows an important implication for faculty development (FD) programs: since FD plays an important societal role in supporting the teachers’ PIF, FD programs should be developed with an emphasis on workplace and social learning (Wahid et al., 2021).
Our study among medical students also emphasises the need to address cultural factors such as high power distance, uncertainty avoidance, and collectivism. Our findings suggest that the role of the learning environment is pertinent. In a hierarchical setting with large power distance like ours, we found that socialisation through the hidden curriculum might result in negative role-modelling, which might hinder students’ professional development. The hierarchical and collectivistic settings also influenced students’ responses to professional dilemmas, causing internal conflicts and confusion as to how they should act later on when misconducts are normalised by their hierarchical environment. Considering the study context, teachers have a great role on students’ PIF through good role modelling and facilitation for students in dealing with ethical and professional dilemmas during their learning process, especially in clinical practice. A practical implication is how our students preferred a more structured approach and clear guidance to develop reflective skills and feedback-seeking behaviour in this setting with high uncertainty avoidance compared with other settings (Findyartini et al., 2022).
Our findings suggest that PIF is indeed a fluid process and socialisation is essential. Many students admitted as they got involved further in their medical education journey and continuously reflected on their experience, they were able to understand the complexity of their PIF more. Many were aware about their psychological journey into becoming a professional and how they continuously internalise the traits expected of a professional. External influences like the hidden curriculum, the learning environment, and the behaviours of their peers seemed to intercalate with their initial motivations through continuous socialisation forms, showing a dynamic psychosocial transition (Findyartini et al., 2022).
III. RETHINKING CULTURE AND PIF: THE IMPLICATIONS
We propose two major ways by which culture influences PIF. First, it dynamically influences the societal expectation of professional traits. This should pose some questions, like what kind of professionals does the community need? How does the community currently, and probably in the near future, perceive what a professional is? By this first understanding of ours, it is then pertinent to continuously reflect and identify the needs of the community in defining the traits of a professional. Thus, simply adopting findings from Western literature might not be beneficial and results must be interpreted contextually, and this should call for further studies on professional identity formation in diverse socio-cultural contexts. We would also like to reiterate that professionalism is a temporal and contextual concept, and this will be continuously reinterpreted and redefined with influence from scientific breakthroughs, industrialisation, and globalisation.
Second, we think of culture as a subtle yet powerful force saliently affecting the process to reach the intended outcome i.e professional identity, as elaborated before. Culture exerts substantial influence on the development process itself, and this is where culture operating on individual and institutional levels, we argue, plays a critical role. Take, for example, our findings on how our students preferred a more direct, structure-driven, and clear guidance in navigating their professional development, or how our teachers were greatly driven by religious beliefs and familial motivation. The communality informs how curriculum for students and FD programs for teachers could be developed. The concepts of intertwining roles of each unique individual student/teacher and the socialisation process involving the learning environment, role models and relevant experiences play a pivotal role in this matter. Curricula and FD program should be developed around the concept of the target as subjects with their own internal values and preferred ways of thinking and doing influenced by the communities of practice around them. We would like to also underscore that the PIF of students and teachers are very much interrelated and we expect that students’ PIF will be highly facilitated by the teachers whose PIF as educator is well internalised.
To summarise, we would like to reemphasise the role of culture and understanding of cultural diversity in the context of PIF. We urge students, teachers, and educators to look at and understand culture as a subtle force driving the aim and process to be professionals. Since socialisation is central in the identity development of both teachers and students, special attention should be given to first reflect and identify cultural values in different levels, most importantly the institution, to develop culturally-sensitive curriculum and faculty development programs.
Notes on Contributors
Ardi Findyartini (AF) currently serves as a Professor of Medical Education and the Head of Medical Education Center, IMERI, Faculty of Medicine, Universitas Indonesia. AF led the study, developed the ideas, wrote, and critically revised the manuscript.
Azis Muhammad Putera (AMP) is a researcher at the Medical Education Center, IMERI, Faculty of Medicine, Universitas Indonesia. AMP developed the ideas, wrote, and critically revised the manuscript.
Acknowledgement
The authors would like to thank all teaching and academic staffs of the Department of Medical Education, Faculty of Medicine, Universitas Indonesia, as well as the researchers, research assistants, research interns, and administrative staffs at the Medical Education Center, IMERI, Faculty of Medicine, Universitas Indonesia for the great collaboration by which this paper can be produced.
Funding
The authors received no funding for this work.
Declaration of Interest
The authors declare no competing nor conflict of interests.
References
Al-Rumayyan, A., Van Mook, W. N. K. A., Magzoub, M. E., Al-Eraky, M. M., Ferwana, M., Khan, M. A., & Dolmans, D. (2017). Medical professionalism frameworks across non-Western cultures: A narrative overview. Medical Teacher, 39(sup1), S8–S14. https://doi.org/10.1080/0142159X.2016.1254740
Cruess, R. L., Cruess, S. R., Boudreau, J. D., Snell, L., & Steinert, Y. (2014). Reframing medical education to support professional identity formation. Academic Medicine: Journal of the Association of American Medical Colleges, 89(11), 1446–1451. https://doi.org/10.1097/ACM.0000000000000427
Findyartini, A., Greviana, N., Felaza, E., Faruqi, M., Zahratul, T. A., & Firdausy, M. A. (2022). Professional identity formation of medical students: A mixed-methods study in a hierarchical and collectivist culture. BMC Medical Education, 22(1), 443. https://doi.org/10.1186/s12909-022-03393-9
Hofstede, G. (2001). Culture’s consequence: Comparing values, behaviors, institutions, and organisations across nations. Sage Publications. https://doi.org/10.1016/S0005-7967(02)00184-5
Wahid, M. H., Findyartini, A., Soemantri, D., Mustika, R., Felaza, E., Steinert, Y., Samarasekera, D. D., Greviana, N., Hidayah, R. N., Khoiriyah, U., & Soeselo, D. A. (2021). Professional identity formation of medical teachers in a non-Western setting. Medical Teacher, 43(8), 868–873. https://doi.org/10.1080/0142159X.2021.1922657
*Ardi Findyartini
Faculty of Medicine,
University of Indonesia
Salemba 6 Central Jakarta 10430
+62 21 3901814
Email: ardi.findyartini@ui.ac.id
Submitted: 7 October 2023
Accepted: 19 June 2024
Published online: 1 October, TAPS 2024, 9(4), 65-67
https://doi.org/10.29060/TAPS.2024-9-4/PV3154
Justin Wen Hao Leong*, Yu Bin Tan* & Bochao Jiang
Department of Gastroenterology and Hepatology, Singapore General Hospital, Singapore
*Co-first authors
I. INTRODUCTION
“Teach them this art, if they want to learn it, without fee or indenture; to impart precept, oral instruction, and all other instruction”- Hippocratic Oath
Since time memorial, the very act of teaching has been intertwined with that of being a physician. In so far that this tradition is found inscribed in the Hippocratic Corpus dating to the 5th century BC. Beyond a calling and a duty, the sharing of experience and expertise is also a rewarding aspect of our roles of doctors. In a climate of ever-increasing demands of knowledge and clinical load, it is imperative we hold on to this aspect closely, and simultaneously look to and embrace new mediums to assist medical educators to meet the current challenges. In this article, we share our experience on how we can incorporate X, formerly known as Twitter, as an extra tool to facilitate teaching on the go during ward rounds and promote self-reflection after.
II. THE MEDIUM
X is a leading social medial platform with up to 541 million monthly users (Musk, 2023). Users can create posts, with each post limited to 280 characters with spaces. The term tweetorial, a neologism combining “tweet” and “tutorial”, is a consecutive series of posts that provide coverage of a given topic. One common format of a tweetorial involves the author creating a multi-post thread about a topic, providing a content outline followed by a brief discussion of the topic with links to various societal guidelines or papers. The user interface allows hashtags, images, and weblinks to be embedded into the posts.
Whilst some naysayers have decried the character limit by saying that it eschews complexity, conversely, it is precisely in the form of such brevity that makes it invaluable. For it is this very brevity that forces key information to be distilled in bite-sized teaching points (Breu, 2020).
Increasingly, physicians have been using the platform to disseminate research, share ideas and discuss topics. In the field of gastroenterology, popular hashtags include #Livertwitter or #GITwitter, with several physicians such as @drkeithsiau, @stevenbollipo, @AustinChiangMD from the United Kingdom, Australia and the United States respectively amassing followers of up to 118 thousand with each post on average being viewed thousands of times. The global scale and reach of X is undeniable; despite this, the posts remain personable and accessible, as readers are able to interact with the authors of these directly by liking, reposting, quoting, commenting or bookmarking them.
Whilst these have led to many discourses on the general use of social media in medical education, the ‘how-to’ of incorporating the use of X as a means of teaching on the run to residents and understanding its role in learning theory has not been expounded upon. In this reflection, we share how we can incorporate this medium in the immediacy of facilitating teaching on the run and the learning theories that underpin this.
III. SETTING THE STAGE
Teaching is a pre-planned learning activity, and even teaching on the run in a busy clinical setting can be planned. The crux as educators is firstly, to be keenly aware of the ever-evolving learning needs of our residents, and secondly, to amalgamate the two seemingly antithetical spheres of ‘running to do’ and ‘pausing to teach’ by having on hand an armamentarium of teaching posts that cover the gamut of core and common topics.
One way to be attuned to the learning needs of our residents is to refer to the programme-specific entrustable professional activities (EPAs). First introduced in the Netherlands in 2005, EPAs are discrete and professional core tasks that are speciality-specific. They are independently executable, observable in practice and measurable in output (Ten Cate, 2005). The EPAs clearly defines the need of the residents and across EPAs, span the breath of the content and desired outcomes after graduation from a specific residency programme.
For the educator, recognising the EPAs and imbibing the same shared mental model as our residents, coupled with pre-prepared content provides the chance to deliver a teaching point on a topic on-the-go whenever a given opportunity arises. The aim here is the immediacy of the educational intervention, to guide and stimulate learning in the here and now – to set the stage to seize the teaching moment.
IV. SEIZING THE MOMENT
Whilst covering the inpatient gastroenterology service, our team had a new admission – a young man with a history of chronic pancreatitis had just been admitted for complaints of abdominal pain. He appeared cachexic and was hunched up in bed in pain. After obtaining a history, performing a physical examination and ensuring that the appropriate investigations and medications were ordered, we came together for a short huddle. Just a few weeks prior, we had authored a tweetorial on chronic pancreatitis, covering the definition, pathophysiology, aetiology, diagnostic algorithm, imaging features and complications including pain, malnutrition, exocrine deficiency and cancer.
In the huddle, each member of the team came together, took out their smartphones and independently accessed the given thread on X. We then in a succinct fashion, embarked on a discussion of chronic pancreatitis with the tweetorial providing a scaffold for the discussion.
In cognitive learning theory, the locus of learning is the internal environment of the learner and his or her cognitive structures. The learner uses cognitive tools, including insight, information processing, perception and memory to lock-in the learning by assigning meaning to certain actions. One of the most important aspects of cognitive learning is the development of critical thinking through reflection. This process of reflection can either be a reflection ‘on’ action, where the learner reflects on a situation that has happened, or a reflection ‘in’ action where the learner reflects about the action in the moment, as they are performed. The core, here then, is in seizing the immediacy of such encounters, such that the reflection and synthesising of new knowledge will always be one of reflection ‘in’ action and allow the immediate synapse of what is gleaned to what is previously known.
Before we broke off our huddle to continue with our rounds, our residents could now articulate that more than a patient with a history of chronic pancreatitis presenting with abdominal pain, we had encountered a patient with hereditary pancreatitis with imaging features of pancreatic calcification, ductal lithiasis and intermittent Amman Type B pain who may benefit from a trial of neuromodulators. They then bookmarked the tweet for future reference, and within it, its attendant link to a clinical review paper on chronic pancreatitis for further reading.
V. REFLECTING AND PROPAGATING
Finally, our residents were encouraged to reflect on the topic towards the end of the day (reflection ‘on’ action) by reposting the thread on X and sharing their learning points with regard to the patient encounter and the topic. There were also encouraged to tag fellow residents in the team to further encourage discourse and craft their own new tweetorials on pertinent topics pertinent topics to maximise the use of X as a learning tool (Forgie, 2013).
The spirit of reflection the provides the transition from a cognitivist orientation to a humanist orientation of learning. Within this framework, learning is viewed as a personal act to achieve one’s own full potential with goal that is self-directed and autonomous. This has three main characteristics, firstly, personal involvement by the learner, secondly, learning that is self-initiated, and lastly, learning that is self-evaluated. Taken together, the combination of these three reflects the growth of an independent learner.
The creation of tweetorials by learners thus fosters the development of additional knowledge translation skills by training the learner to first dive deeper into the topic, synthesise knowledge, distil it and lastly, package it with brevity (Tsang, 2023). The learner-created tweetorial then takes on a life of its own online, allowing its own interactions and comments allowing the student to engage in critical thinking and constructive feedback online which in turn transitions into self-evaluation.
VI. CONCLUSION
The traditional Bloom’s taxonomy of remember, understand, apply, analyse, evaluate and create serves as a valuable framework for learning and X, if used appropriately, can be an excellent teaching tool to achieve these educational goals. Initially, the learner ‘consumes’ a tweet in a cognitivist framework, but by bringing the immediacy of the clinical encounter head-on into the screens of their smartphones, the use of X then fast tracks them into applying this new-found knowledge in the current clinical encounter. After the encounter, the learning then shifts into a humanist orientation with the vision of an independent, self-driven and self-critical learner that creates new work; and through this process, take their own steps toward becoming a teacher on the run with an X-tra tool.
Notes on Contributors
Justin Leong and Tan Yu Bin conceptualised the work, drafted the work, revised it and gave final approval of the version to be published. Jiang Bochao drafted the work, revised it and gave final approval of the version to be published.
Funding
There were no funding sources in this paper.
Declaration of Interest
No potential conflicts of interests relevant to this article was reported.
References
Breu, A. C. (2020). From tweetstorm to tweetorials: Threaded tweets as a tool for medical education and knowledge dissemination. Seminars in Nephrology, 40(3), 273-278. https://doi.org/10.1016/j.semnephrol.2020.04.005
Forgie, S. E., Duff, J. P., & Ross, S. (2013). Twelve tips for using Twitter as a learning tool in medical education. Medical Teacher, 35(1), 8-14. https://doi.org/10.3109/0142159X.2012.746448
Musk, E. [@elonmusk]. (2023, July 29). ? monthly users reach new high in 2023. [Image attached] [Post]. X. https://twitter.com/elonmusk/status/1684978651857596429
Ten Cate, O. (2005). Entrustability of professional activities and competency-based training. Medical Education, 39(12),1176-1177. https://doi.org/10.1111/j.1365-2929.2005.02341.x
Tsang, R., & Pinder, K.E. (2023). The #Tweetorial: An underutilised teaching tool in undergraduate medical education? Medical Science Educator, 33, 583–587. https://doi.org/10.1007/s40670-023-01764-5
*Justin Wen Hao Leong
31 Third Hospital Ave,
Singapore 168753
Email: justinleongwenhao@gmail.com
Submitted: 3 January 2023
Accepted: 29 May 2024
Published online: 1 October, TAPS 2024, 9(4), 1-5
https://doi.org/10.29060/TAPS.2024-9-4/GP2940
Sengkhoun Lim1, Steve Vilhem2, Sambath Cheab1, Laura Goldman3, Aklinn Nhem1, Ponndara Ith1 & Youttiroung Bounchan1
1University of Health Sciences, Cambodia; 2Institute of Humanities in Medicine CHUV, Switzerland; 3Boston University, United States of America
Abstract
Introduction: There is a global call for transforming medical education to meet evolving healthcare needs. However, navigating the challenges of educational change in resource-limited contexts requires key stakeholders, from leaders to educators and students, to adopt innovative approaches. This paper presents practical examples of such innovations from the University of Health Sciences (UHS) in Cambodia’s experiences, followed by discussions on enabled and hindered factors of their initiation, implementation, and sustainability. This paper also aims to inspire future medical education innovations.
Methods: This paper relied on internal document reviews, including strategic plans, project proposals & planning, course syllabi, and evaluation reports, and the collective working experiences of co-authors in initiating, implementing, and leading these innovations.
Results: Three innovative projects at UHS illustrated how creative ideas are put into practice, including (1) The elective International Programme (IP) with a dual objective of training local trainers while preparing students for international mobility, (2) The Master of Health Professions Education (MHPE), a cost-effective faculty development programme delivered in-person at UHS campus by faculty of a university partner, and (3) Peer-assisted Learning (PAL), a student-led initiative to promote learning skills.
Conclusion: Medical education innovations are needed in resource-limited contexts. The success of these initiatives resulted from multi-factors, notably long-term strategic planning, supportive leadership, active partnerships, policy commitment, local champions, resourcefulness, and student engagement. The late adoption of technology-enhanced learning, the necessity for robust faculty development programmes, and early investment in student leaders, coupled with post-graduate retention planning, represent challenges that present strategic opportunities.
Practice Highlights
- Medical education innovations are needed in a resource-limited country like Cambodia.
- Piloting before widespread implementation allows for tailoring to a specific local context.
- Long-term partnerships between external experts and internal faculty foster contextualisation, local capacity-building, and stakeholder buy-in.
- Continuous and supportive leadership with strategic planning is essential for driving and sustaining educational innovations.
- Identifying and nurturing local champions to carry out innovations is key to sustainability.
I. INTRODUCTION
The 1910 Flexner report inspired the transformation of medical education to a science and knowledge-based curriculum. A century later, an influential Lancet report called for transforming health professions education to meet changing population healthcare needs (Frenk et al., 2010). However, in resource-limited contexts, doctor training has not kept pace with public health challenges like an increase of chronic diseases. Moving away from the Flexnerian model presents significant challenges to the status quo because it involves leadership, technical, financial, and administrative commitments, specifically in Cambodia (Lim et al., 2024). To address these issues, key stakeholders, from leaders to educators and students, must adopt innovative approaches to medical education that are culturally and contextually appropriate.
This paper showcases three innovations that exemplify how creative ideas are put into practice at the university level: the elective programme, faculty development, and student-led initiative. Innovation, by definition, refers to the ability to introduce novel and useful ideas within a specific context. These examples are considered new and beneficial for stakeholders in the Cambodian context. The first two are practices adapted from other countries, while the last is an initiative of, by, and for students from within the university. The “Triple I” model of three phases of initiation, implementation, and institutionalisation, is used to discuss these innovations, especially the challenges to sustainability (Fullan, 2015). This paper also aims to inspire future innovations in medical education.
II. THREE INNOVATIONS IN MEDICAL EDUCATION
University of Health Sciences (UHS) is the oldest and largest state-owned university of health sciences in Cambodia. In late 2001, UHS became a public administrative institution entrusted by the Ministry of Health to be a leading university in medical education reforms. Below are three medical education innovations at UHS.
A. Elective Programme
Launched in 2013 by UHS-Faculty of Medicine (FoM) with financial and technical assistance from development partners, especially France, the International Programme (IP) is a tool for educational innovation and strengthening international relationships. This 3-year elective programme annually selects 60 outstanding students during their clinical phase (years 4-6). The IP has a dual objective: training of trainers (ToT) and student preparation for international mobility. To achieve these goals, UHS brings foreign professors from partner universities to role model a new generation of Cambodian trainers in modern teaching. Students actively engage in four main activities: academic training, language courses, research methodology, and socio-cultural activities. Visiting professors teach IP undergraduate students in the mornings and post-graduate residents in the afternoons to maximise their in-country time. Local trainers co-train with these professors in their respective disciplines to learn new teaching methods. French, English, and Khmer languages are mediums of instruction.
The IP has functioned as a pilot initiative, introducing student-centered learning, simulation-based education, and standardized assessment to the medical curriculum. These approaches have been well-received by faculty and students. In 2017, case-based learning (CBL) and simulation were scaled up to all students at FoM. The IP is considered an achievement because of its contribution to UHS’s strategic goals: educational innovation, ToT, and strengthening international relations. Presently, UHS has a pool of at least 60 trainers in CBL and simulation at FoM. Furthermore, the IP model was replicated within UHS’s nursing and pharmacy programmes in 2015 and 2018, respectively.
B. Faculty Development Programme
Faculty development (FD) is key to supporting educators in their multifaceted roles. UHS has invested in FD programmes to equip faculty with knowledge and skills, specifically responding to reforms in health professions education (HPE). A key initiative was a 2-year Master of Health Professions Education (MHPE) programme, offered in partnership with University of the Philippines (UP)-Manila from 2011 to 2016. Funded by the WHO and French Cooperation, the programme catered to two cohorts of 28 health professionals, including doctors, dentists, pharmacists, nurses, and medical laboratory technicians.
The programme’s hybrid delivery model was a historical first at UHS. It combined intensive 5-day on-site sessions led by visiting UP-Manila faculty, followed by distance learning modules. The MHPE programme is not only for individual professional development but also institutional development. While the programme faced challenges with language barriers, inter-professional learning, and technology limitations, it yielded positive outcomes in local human resource development in HPE. Eight students graduated with master’s degrees, while 12 received diplomas. Many graduates now contribute significantly to UHS, staffing the pedagogy unit and different faculties.
Building on local expertise, those MHPE graduates embarked on own FD programme development at UHS, beginning with a mandatory 4-day basic pedagogy course for all educators in 2015. The pedagogy unit has trained over 518 teachers in basic pedagogy. Currently, UHS’s FD programmes include short courses and workshops; strategically tailored to address national, institutional, and teacher needs. These programmes focus on competency-based course development, lesson planning, writing MCQs, and practical teaching skills (e.g., interactive lectures, small group, and simulation-based facilitation). For sustainability, UHS prioritises FD initiatives that are competency-based, cost-effective, and fit to the Cambodian context. Most FD programmes are now designed and delivered in Khmer by local trainers. UHS still collaborates with international partners to develop different FD programmes, especially for new HPE topics like interprofessional education (IPE).
C. Student-led Initiative
The value of students as active partners in education is well-established. Recognizing this notion, UHS actively promotes student engagement, particularly student roles in teaching. Through the Global Health through Education Training and Service (GHETS) grant (2016-2022), six cohorts of 56 students participated in the Essential Skills in Medical Education (ESME) online course. A group of student champions from the first cohort (including two authors: SL and SC) partnered with UHS-Medical Student Association (MSA) to launch the Peer-assisted Learning (PAL) club. PAL initially began as a 3-month extra-curricular course designed to integrate learning skills with basic science subjects. It has currently evolved into a hub for student-led initiatives, offering the Annual Medical Education Conference (AMEC), training courses, workshops, and socio-cultural events. Most activities were postponed during the pandemic, and some were restarted by UHS-MSA in 2023.
III. DISCUSSION
The “Triple I” model describes three phases of educational change over time (Fullan, 2015). The first phase is initiation, an attempt to embrace innovations. The second phase is implementation, the process of putting ideas into action. The third phase is institutionalisation when innovations become routine. The goal of change is institutionalisation; however, it does not occur without innovative adoptions being successfully initiated and implemented. This model is a conceptual framework used to discuss enabled and hindered factors in medical education innovations at UHS, Cambodia.
Active collaboration with development partners drives educational change at national and institutional levels in Cambodia (Lim et al., 2024). The IP and FD are examples of technical cooperation, directly contributing to the university’s long-term goals of educational innovation, human resource capacity-building, and international relations strengthening. Aligning innovations with organisational goals, shared beliefs, and core values is crucial for acceptability and implementation effectiveness (Century et al., 2012). Such partnerships hold particular significance in resource-limited contexts. Through external expertise and funding, medical schools can overcome barriers such as stakeholder buy-in, technical and resource constraints.
Innovations utilizing existing or external resources are more likely to gain approval from university leaders. Student engagement can positively enhance the university’s reputation on the international and national stage. UHS continues supporting PAL student-led activities, which were initially cost-free and run by highly motivated student volunteers, despite not aligning directly with strategic priorities and may not be perceived as needed by stakeholders.
Innovation characteristics influence the process of putting ideas into action. Relevant stakeholders may struggle to perceive the necessity for change because needs are often unclear at the beginning of innovation. Educational change is inherently complex, demanding shifts in educational philosophy, teaching strategies, and even skillsets. While this complexity poses implementation challenges, it also results in greater change because more is being attempted (Fullan, 2015). The IP was initially co-led with international experts, and local stakeholders ensured contextual and cultural relevance through co-creation and co-teaching. The IP marked a radical departure from the status quo, transitioning from teacher-centered to student-centered instruction. This shift presented significant challenges to many UHS teachers whose teaching practices rely on didactic lectures. Considerable efforts are needed to increase faculty buy-in, commitment, and capacity-building. Placing teachers as co-trainers alongside visiting professors is one way to overcome these challenges and contribute to the success.
Piloting is another enabling factor in which innovations are tested before committing to their full adoption. The IP, FD, and PAL all started as small-scale, elective experimentations before scaling up to benefit all.
Sustainability remains a persistent challenge in resource-limited contexts. Innovative projects will likely cease after a few years of implementation due to a lack of financial, technical, or stakeholder commitment. At UHS, the IP, FD, and PAL are examples of sustainable innovations. Several factors contribute to sustainability. Changing university policies is key to ensuring medical schools engage in long-term transformation (Bland et al., 2000). These three initiatives were built into organisational and programme structures through policy change, budgeting, or academic calendar. For instance, UHS incorporated PAL student-led activities into its 5-year strategic plan (2019-2023) and allocated a small stipend for student peer-teaching. Additionally, students receive recognition through certificates and further opportunities. PAL is sustained through MSA, an established organisational structure at UHS.
Strong leadership is paramount for driving and sustaining innovations (Bland et al., 2000). Beyond mere initiation, innovation implementation requires ongoing evaluation, revision, and expansion plans to sustain success. UHS strategic plans (2014-2018 and 2019-2023) made public commitment by setting clear indicators for innovative activities such as the IP and FD. These programmes had local leaders do hard work overtime. Empowering local champions to carry out innovations is key to sustainability. UHS exemplifies this through proactive approaches such as identifying and training faculty and student leaders, providing them opportunities to engage in impactful work. Notably, most FD programmes at UHS are now developed and conducted in Khmer by local trainers, underscoring institutional commitment to local capacity-building and sustainability.
Many challenges still exist. The university’s late adoption of technology-enhanced learning hindered its response to the COVID-19 pandemic, causing disruptions when moving to distance learning. Limited resources add another layer of complexity. To ensure effectiveness and sustainability, UHS must invest in technology-enhanced and robust FD programmes, especially in the context of transitioning toward competency-based medical education. Securing funding can be achieved through collaborative partnerships and increased budgets from UHS itself. Investing in student leaders early holds promise; however, results may not be immediately apparent. It takes a bird’s view to allocate resources to develop future leaders, and a transition plan is needed to retain these student champions at UHS after their graduation.
IV. CONCLUSION
Medical education innovations are needed in a resource-limited country like Cambodia. UHS strategically launched three small-scale programmes to meet institutional goals in medical education reforms. The sustainability of these programmes is due to several factors. Leveraging both internal and external resources, including development partners, local faculty and students, enabled knowledge transfer, and maximised resources. Long-term partnerships between international experts and local faculty resulted in contextualisation, capacity-building, and stakeholder buy-in at the home institution. Identifying and nurturing leaders and champions among faculty and students was a key feature alongside piloting innovations, allowing for local adaptations before scaling up. The challenges facing the university can be strategically turned into further opportunities.
Notes on Contributors
Sengkhoun Lim conceptualized and designed the study, collected and analyzed data, and wrote the manuscript.
Steve Vilhem analyzed data and drafted the International Programme part.
Sambath Cheab provided input on the initial study design and participated in data collection and analysis.
Laura N. Goldman provided guidance on manuscript writing, contributed to the discussion section, and edited the whole manuscript into plain English.
Aklinn Nhem provided source documents, validated information, gave feedback, and proofread.
Ponndara Ith validated information, gave feedback, proofread, and edited the text.
Youttiroung Bounchan provided source documents, validated information, gave feedback, proofread, and edited the manuscript. All authors have read and approved the final manuscript.
Acknowledgement
The authors thank Professor Vonthanak Saphonn, Rector of the University of Health Sciences, for his continuous and supportive leadership in these medical education innovations and Professor Mam Bunsocheat for his contributions to the International Programme at the University of Health Sciences, Cambodia.
Funding
There is no funding involved for this paper.
Declaration of Interest
The authors report no conflict of interest.
References
Bland, C. J., Starnaman, S., Wersal, L., Moorehead-Rosenberg, L., Zonia, S., & Henry, R. (2000). Curricular change in medical schools: How to succeed. Academic medicine, 75(6), 575–594. https://doi.org/10.1097/00001888-200006000-00006
Century, J., Cassata, A., Rudnick, M., & Freeman, C. (2012). Measuring enactment of innovations and the factors that affect implementation and sustainability: Moving toward common language and shared conceptual understanding. The Journal of Behavioral Health Services & Research, 39(4), 343–361. https://doi.org/10.1007/s11414-012-9287-x
Frenk, J., Chen, L., Bhutta, Z. A., Cohen, J., Crisp, N., Evans, T., Fineberg, H., Garcia, P., Ke, Y., Kelley, P., Kistnasamy, B., Meleis, A., Naylor, D., Pablos-Mendez, A., Reddy, S., Scrimshaw, S., Sepulveda, J., Serwadda, D., & Zurayk, H. (2010). Health professionals for a new century: Transforming education to strengthen health systems in an interdependent world. The Lancet, 376(9756), 1923–1958. https://doi.org/10.1016/S0140-6736 (10) 61854-5
Fullan, M. (2015). The new meaning of educational change (5th ed.). Teachers College Press.
Lim, S., Cheab, S., Goldman, L. N., Ith, P., & Bounchan, Y. (2024). The past, present and future of medical education in Cambodia. Medical Teacher, 46(6), 842-848. https://doi.org/10.1080/014 2159X.2024.2327490
*Sengkhoun Lim
73 Preah Monivong Blvd (93),
Phnom Penh, Cambodia
+855 92 222 622
Email: sengkhounlim@ymail.com
Submitted: 17 January 2024
Accepted: 14 May 2024
Published online: 1 October, TAPS 2024, 9(4), 57-60
https://doi.org/10.29060/TAPS.2024-9-4/SC3234
Nicole Huiyi Ong1, Boon Chong Kwok2,3, Siti Munirah Aman4, Steven Michael Dans Macabasco5 & Wai Pong Wong2
1Department of Physiotherapy, Singapore General Hospital, Singapore; 2Health and Social Sciences, Singapore Institute of Technology, Singapore; 3Rehabilitation, Clinical Pilates Family Physiotherapy, Singapore; 4Department of Rehabilitation, Outram Community Hospital, Singapore; 5Rehabilitation, NTUC Eldercare, Singapore
Abstract
Introduction: Clinical practice education is an important curriculum in developing physiotherapy students to professionals. This curriculum is largely dependent on clinical educators. Although traits of effective clinical educators had been studied in Western population, it was unclear if the Asian population would yield similar traits. Hence, we studied perspectives of students and academic educators to identify top five core traits of an effective clinical educator. The findings will then help guide policy development for clinical educator training and development.
Methods: A survey was circulated to physiotherapy students and academic educators through convenience sampling. We studied 16 traits – enthusiasm, availability, clarity, clinical competence / knowledge, feedback skills, organisational skills, professionalism, well prepared, scholarly activity, non-judgemental, respect students’ autonomy / independence, sincerity, listening skills, evidence-based practice, role model, and awareness of students’ learning needs.
Results: The top five traits identified by students and academic educators were similar in four traits – clinical competency / knowledge, clarity, feedback skills, and enthusiasm, and differed in the choice of “non-judgemental” by students and “awareness of students’ learning needs” by academic educators. Interestingly, when the top six traits were considered instead of five, students and academic educators identified the same traits but in different ranked orders.
Conclusion: The study found six common core traits of an effective clinical educator from the perspectives of students and academic educators. Continuing education development for clinical educators should focus on these six traits prior to other 10 sub-traits.
Keywords: Training, Development, Education, Allied Health, Entrustable Professional Activities, Mentoring
I. INTRODUCTION
Clinical Practice Education (CPE) is a core component in undergraduate allied health studies, partnering clinicians with additional role as a Clinical Educator (CE) (Gibson et al., 2019). A study evaluating effective residency teaching for doctors identified 15 traits that a CE should possess, which are enthusiasm, competence-knowledge, clarity, availability, non-judgemental, independence, feedback skills, role model, professionalism, sincere, organised, well-prepared, evidence-based practice, scholarly activity and listening skills (Buchel & Edwards, 2005). A recent study found that being aware of the learning needs of students could be the 16th trait a CE should possess (Francis et al., 2016). Considering recent shift towards the use of the Entrustable Professional Activity framework for work place competency review at student and professional levels (Kwok et al., 2023), it is important to consider which top five traits are considered core competence of a CE as defined by the pinnacle of entrustment at Level 5.
Perspectives of critical traits of an effective CE might differ between students, CEs and academic educators (AEs). Students in early years of undergraduate study and CEs identified similar top five traits of an ideal CE (Cross, 1995). In the study by Cross (1995), CEs should be approachable, possess good communication skills, be knowledgeable and demonstrate enthusiasm in teaching, including clinical competency (Cross, 1995). Competency of CEs was similarly desired among academic educators, alongside “being approachable” and “good communicator”, whereas two differences were noted as compared to CEs and students, which were “interested in learning process of the students” and “concerned about patient care” (Cross, 1995). It is possible that among the Asian population, competency of the CEs would be similarly desired. Recent studies might have considered different trait terms as compared to the classic study, for instance, “learning process” was likely subsumed under “learning needs” (Francis et al., 2016). It is unclear whether the Asian population will present with different trait ranking as compared to Western population.
Therefore, this study was undertaken to identify the top five essential traits of an effective CE. In view of notable differences between perspectives of students and AEs in past literature, this study explored similarities and differences of perspectives between students and AEs. In addition, we explored what gaps might exist in developing CEs. In this study, the AEs, all of whom used to be CEs, could provide useful and important inputs on the traits required of a CE. The findings would then provide directions for future policy development pertaining to clinical education and professional supervision.
II. METHODS
A. Study Design
A survey was conducted through convenience sampling. The study was conducted between March to December 2022. The study was approved by the Institutional Review Board of the Singapore Institute of Technology (SIT-IRB-2022031).
B. Participants
Students in the third year of undergraduate physiotherapy programme and AEs of the physiotherapy faculty (as of April 2022) were involved in the survey. Large variations in response rate exists in convenience sampling, so we projected at least 50% response rate for the students and also the AEs. Students who had withdrawn from the programme were excluded. Associate faculty educators were excluded because they were only involved in ad hoc teaching sessions. Informed consent was sought at the beginning of the survey and digitally recorded.
C. Procedures
The survey described the 16 traits that contribute to an effective CE, which provided participants with knowledge about each trait, which was externally validated by five physiotherapists from the public and private sectors with experience ranging from eight to 25 years. The demographic data included student identification numbers to ensure that each response was unique. Thereafter, the data was de-identified to ensure anonymity during data analysis. As the sample size for the AEs was small, no personal data was collected to ensure anonymity. A survey invitation including a standardised survey link was distributed via email to all eligible participants. Participants were then asked to rank the 16 traits from 1 to 16, with 1 being the most important trait and 16 being the least important. Survey items were not randomised. The online survey was hosted on the secured Qualtrics Survey System (Qualtrics XM, 333 W. River Park Drive, Provo, UT 84604 USA). Student participants were first notified via email, followed by four reminder notifications, two months apart, via the cohort group chat on WhatsApp. AEs were first notified via email, followed by two reminder notifications via WhatsApp three months apart.
D. Statistical Analysis
Data analyses were performed using IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, N.Y., USA). Continuous variables are presented with means (standard deviations) and categorical variables with counts (percentages). Friedman test was used to analyse the mean rank of each trait. Then Kendall’s coefficient of concordance (Kendall’s W) was used to test the level of agreement among students for the mean ranks of the traits, as well as among AEs. The level of agreement was interpreted based on common recommendation and should yield statistical significance at p < 0.05.
III. RESULTS
A total of 81 students completed the survey (response rate of 46.6%) and a total of five AEs completed the survey (response rate of 41.7%). The average age, mean (standard deviation), of the students is 24.5 (4.1) years, and 52 of them are female (64.2%). The traits were ranked and presented in Table 1. Among the top five traits, there were four similar traits found between students and AEs, which were clinical competency / knowledge, clarity, feedback skills, and enthusiasm. The students ranked “non-judgemental” within the top five traits, whereas the AEs identified “awareness of students’ learning needs”. If the top six traits were considered, both students and AEs yielded similar traits. In the traits ranking, the students showed fair level of agreement, approximating closely to moderate agreement, Kendall’s W = 0.38, p < 0.001, while AEs showed moderate level of agreement, Kendall’s W = 0.51, p = 0.001.
|
Rank |
Students (n = 81) |
Academic Educators (n = 5) |
||
|
Traits |
Mean rank |
Traits |
Mean rank |
|
|
1 |
Clinical competency / knowledge |
4.51 |
Awareness of students’ learning needs |
3.20 |
|
2 |
Non-judgemental |
4.78 |
Feedback skills |
4.00 |
|
3 |
Clarity |
4.94 |
Clinical competency / knowledge |
4.20 |
|
4 |
Feedback skills |
5.01 |
Enthusiasm |
5.60 |
|
5 |
Enthusiasm |
7.06 |
Clarity |
6.80 |
|
6 |
Awareness of students’ learning needs |
7.27 |
Non-judgemental |
7.00 |
|
7 |
Availability |
7.93 |
Role model |
7.60 |
|
8 |
Sincerity |
8.56 |
Professionalism |
8.00 |
|
9 |
Respect students’ autonomy / independence |
8.68 |
Listening skills |
8.60 |
|
10 |
Listening skills |
9.35 |
Respect students’ autonomy / independence |
9.80 |
|
11 |
Professionalism |
9.51 |
Well prepared |
10.20 |
|
12 |
Organisational skills |
9.56 |
Organisational skills |
10.40 |
|
13 |
Role model |
10.23 |
Availability |
10.80 |
|
14 |
Well prepared |
11.69 |
Sincerity |
11.20 |
|
15 |
Evidence-based practice |
11.75 |
Evidence-based practice |
13.00 |
|
16 |
Scholarly activity |
15.19 |
Scholarly activity |
15.60 |
|
Table 1. Ranking of clinical educator traits by students and academic educators |
||||
IV. DISCUSSION
The study was initiated to identify the top five traits an effective CE should possess through the perspectives of students and AEs. The students and AEs differed only in the selection of one trait. Interestingly, when the top six traits were considered, students and AEs were aligned in traits selection and only differed in the ranking of traits. These six traits were 1) clinical competence / knowledge, 2) non-judgemental, 3) clarity, 4) feedback skills, 5) enthusiasm in teaching, and 6) awareness of students’ learning needs. The level of agreement found among students was fair and among the AEs was moderate for the rankings of traits in this study.
A few differences were observed in the top five traits as compared to western culture. Four traits were similar to those identified in the past – clinical competence / knowledge, clarity, feedback skills and enthusiasm in teaching (Cross, 1995). Whilst “clinical competence / knowledge” was ranked first by the students, we caution that these traits must be complemented by appropriate “feedback skills” and “clear communication”. A key difference between students and AEs was the identification of “non-judgemental” and “awareness of students’ learning needs” in the top five traits. The differences between students and AEs were essentially non-existent if we recognise top six traits as core competencies of an effective CE as compared to five traits. In view that the AEs were also past CEs, the rankings by the AEs provide valuable insights and could be used to align the students’ expectations.
The study found two common traits that were ranked lower among students and AEs – evidence-based practice and scholarly activity. It is possible that the students and AEs have assumed that “evidence-based practice” was a part of “clinical competency”, given the fact that “evidence-based practice” is essential in clinical practice. Moving forward, it would be of interest to study the perspectives of the students and AEs with regards to “evidence-based practice” in clinical education. Future research could explore the traits as “must have”, “should have” and good-to-have” categories, which could help identify the critical traits (“must have”).
The study has a few limitations. Although self-reported survey could lead to response bias, we did not detect similar responses in consecutive order during data inspection. Next, we set out to collect 50% response rate, unfortunately, we were slightly away from the target as some respondents did not complete or withdrew their participation. As such, the sample size of the AEs was small and so perspectives from the AEs might require careful considerations. The study also did not allow for qualitative inputs from the respondents to explore other traits that were not listed. Lastly, we were unable to engage participation from CEs as the survey was not compulsory as part of their role.
V. CONCLUSION
This study identified six core traits an effective CE should possess. These traits are clinical competence / knowledge, non-judgemental, clarity, feedback skills, enthusiasm in teaching, and awareness of students’ learning needs. We identified that evidence-based practice and scholarly activity traits were potential gaps in career development of CEs as they were ranked lower among students and AEs.
Notes on Contributors
NHO was involved in study conceptualisation, data collection, data analysis, data interpretation and drafting manuscript.
BCK was involved in study conceptualisation, data analysis, data interpretation, drafting manuscript and final revision of manuscript.
SMA was involved in study conceptualisation, data collection and revising the manuscript.
SMDM was involved in study conceptualisation, data collection and revising the manuscript.
WPW initiated the study conceptualisation, project administration, data interpretation and review of the drafted manuscript.
Ethical Approval
The study was approved by the Institutional Review Board of the Singapore Institute of Technology (SIT-IRB-2022031).
Data Availability
Based on the ethics approval, data will not be shared on a repository. The anonymised dataset can be obtained from the corresponding author with reasonable request.
Acknowledgement
The authors thank the physiotherapy students and educators from the Singapore Institute of Technology for their study participation.
Funding
This study is unfunded.
Declaration of Interest
None of the authors has any conflict or financial interest to declare.
References
Buchel, T. L., & Edwards, F. D. (2005). Characteristics of effective clinical teachers. Family Medicine, 37(1), 30-35. https://www.ncbi.nlm.nih.gov/pubmed/15619153
Cross, V. (1995). Perceptions of the ideal clinical educator in physiotherapy education. Physiotherapy, 81(9), 506-513. https://doi.org/10.1016/S0031-9406(05)66680-1
Francis, A., Hills, C., MacDonald-Wicks, L., Johnston, C., James, D., Surjan, Y., & Warren-Forward, H. (2016). Characteristics of an ideal practice educator: Perspectives from practice educators in diagnostic radiography, nuclear medicine, nutrition and dietetics, occupational therapy and physiotherapy and radiation therapy. Radiography, 22(4), 287-294. https://doi.org/10.1016/j.radi.2016.04.001
Gibson, S. J., Porter, J., Anderson, A., Bryce, A., Dart, J., Kellow, N., Meiklejohn, S., Volders, E., Young, A., & Palermo, C. (2019). Clinical educators’ skills and qualities in allied health: A systematic review. Medical Education, 53(5), 432-442. https://doi.org/10.1111/medu.13782
Kwok, B. C., Zulimran, M., & Sue, P. (2023). Re-designing performance management for healthcare – The performance empowerment, advancement and career excellence (PEACE) system. International Journal of Productivity and Performance Management, 72(7), 2183-2193. https://doi.org/10.1108/IJPPM-12-2022-0610
*Boon Chong Kwok
10 Dover Drive,
Singapore Institute of Technology,
Singapore 138683
96916703
Email: boonchong.kwok@singaporetech.edu.sg /
kwokboonchong@gmail.com
Submitted: 19 December 2023
Accepted: 26 April 2024
Published online: 1 October, TAPS 2024, 9(4), 50-56
https://doi.org/10.29060/TAPS.2024-9-4/SC3194
Craig S. Webster1, Jack Forsythe2, Antonia Verstappen1, Phillippa Poole3, Tim Wilkinson4 & Marcus A. Henning1
1Centre for Medical and Health Sciences Education, School of Medicine, University of Auckland, Auckland, New Zealand; 2Auckland District Health Board, Te Whatu Ora, Auckland, New Zealand; 3School of Medicine, University of Auckland, Auckland, New Zealand; 4Education Unit, University of Otago, Christchurch, New Zealand
Abstract
Introduction: A valid, longitudinal approach is critical for service planning in healthcare and to understand career choice in medical graduates.
Methods: We quantitatively analysed self-reported influences underlying career choice in a national cohort of medical graduates over the first five years of their careers. Participants rated career influences on importance across 26 items using a 5-point Likert scale (1=not at all, 5=a great deal).
Results: We included 659 New Zealand medical graduates (mean 25.4 years old, 376 F, 283 M) from the University of Auckland and the University of Otago, graduating in 2012 and 2013 (85% response rate). Responses were linked longitudinally over their post-graduate years 1, 3 and 5, and underwent principal component analyses. At graduation the factor rated as the most important in career choice had a mean (SD) item score of 3.9 (0.7) and comprised: Medical School Experiences; Specialty Experience; Mentors; and Self-Appraisal – consistent with graduates securing initial employment. Factors which explained the most variance in career choice over the five years after graduation indicated that the costs of medical school and further training were consistently rated as the least important in career choices, while flexibility in working hours were consistently rated as the most important. Factors remained relatively stable over time, showing variation in scores of only a median of 0.5 Likert points, indicating further opportunities for career choice research.
Conclusion: Our results regarding costs of medical training are reassuring, and suggest that greater flexibility in working hours may attract graduates to underserved specialties.
Keywords: Medical Education, Career Choice, Career Influences, Cost, Debt, Measurement, Medical Graduates, National Longitudinal Study, Working Hours, Work Culture
I. INTRODUCTION
A common strategic aim of medical schools throughout the world is to supply the range of graduates who will best meet the healthcare needs of their communities (Gorman, 2018). However, fulfilling this aim is far from straight-forward, with perhaps the most critical difficulty involving understanding the influences that underlie career choice in medical graduates and how these vary over time.
The financial burden of completing medical school and further training has been one of the most widely studied influences underlying career choice, with suggestions that rising costs may encourage graduates to pursue specialties perceived to be more highly paid, often in cities, thus undersupplying primary healthcare and rural locations. However, in New Zealand medical graduates are otherwise free to choose their preferred career path and choices may be influenced by many things other than training costs and debt, including personal interest, employment conditions, specialty availability and lifestyle preferences (Webster et al., 2020; Webster et al., 2017).
Therefore, in the following, we analyse the self-reported influences underlying career choice in a national cohort of medical school graduates during the first five years of their careers using quantitative data drawn from the existing longitudinal Medical Schools Outcomes Database (MSOD).
II. METHODS
The MSOD project is a bi-national longitudinal questionnaire study that aims to improve healthcare delivery in Australia and New Zealand (Poole et al., 2019). At graduation and in postgraduate years (PGY), graduates are asked to specify their preferred area(s) of medicine, and complete a schedule of influencing items, indicating the degree to which each was important in their choice, using a 5-point Likert scale with anchors of 1 (not at all) to 5 (a great deal) – see Supplementary Table 1 for full question set.
A. Data Analysis
We conducted a series of principal component analyses (SPSS v27, IBM Corporation, New York) of the responses to the 26 influencing item questions at each time point to identify factors within responses, and describe them over time.
III. RESULTS
Data from a national cohort of 659 New Zealand medical school graduates who had graduated from the University of Auckland and the University of Otago in 2012 and 2013 were included. The response rate for completed questionnaires in the Exit cohort was 85% – representing a sampling margin of error of only 1% at the 95% level of confidence. The mean (SD) age of participants in the cohort was 25.4 (2.7) years, with a higher proportion of female graduates (376 F vs 283 M). Over the next five years, this Exit cohort self-reported on the same set of influences underlying career choice at PGY1, PGY3 and PGY5 – maintaining a response rate between 53% and 56%, and a sampling margin of error of 3%.
We used conventional settings during analysis, comprising varimax rotation and suppression of loadings below 0.3. The Kaiser-Meyer-Olkin measure of sampling adequacy across time points demonstrated a median (range) of 0.77 (0.75 to 0.82), indicating distinct and reliable factors at each time point. In addition, Bartlett’s test of sphericity was highly significant at each time point, (2338<c2<3498, p<0.0001), demonstrating correlation with little redundancy in items (Kaiser, 1974).
|
Influencing items* |
Factor numbers and item loadings |
||||
|
|
A: Exit (yrs 2012 and 2013) |
||||
|
|
1 |
2 |
3 |
4 |
5 |
|
Costs Voc. Training |
0.855 |
||||
|
Costs Med. School |
0.832 |
||||
|
Insurance Risk |
0.675 |
||||
|
Parents/Relatives |
0.536 |
||||
|
Prestige |
0.528 |
||||
|
Training Yrs |
0.508 |
||||
|
Financial Prospects |
0.463 |
||||
|
Research/Teaching |
0.442 |
||||
|
Location |
0.440 |
||||
|
Flexible Hrs |
0.862 |
||||
|
Working Hrs |
0.838 |
||||
|
Domestic Circum. |
0.633 |
||||
|
Work Culture |
0.416 |
||||
|
Career Prospects |
0.725 |
||||
|
Procedural Work |
0.698 |
||||
|
Job Security |
0.555 |
||||
|
Voc. Training Avail. |
0.409 |
||||
|
Med. School Exp. |
0.836 |
||||
|
Specialty Exp. |
0.787 |
||||
|
Mentors |
0.752 |
||||
|
Self-Appraisal |
0.388 |
||||
|
Typical Patients |
0.643 |
||||
|
Helping People |
0.642 |
||||
|
Intel. Content |
0.532 |
||||
|
Variance explained, % |
15.8 |
11.1 |
9.5 |
9.3 |
7.3 |
|
Factor score, mean (SD)** |
2.3 (0.7) |
3.6 (0.8) |
3.3 (0.9) |
3.9 (0.7) |
3.8 (0.7) |
|
|
B: PGY1 (yrs 2013 and 2014) |
||||
|
|
2 |
1 |
4 |
3 |
5 |
|
Working Hrs |
0.847 |
||||
|
Flexible Hrs |
0.831 |
||||
|
Domestic Circum. |
0.673 |
||||
|
Training Yrs |
0.538 |
||||
|
Voc. Training Avail. |
0.494 |
||||
|
Location |
0.411 |
||||
|
Job Security |
0.391 |
||||
|
Costs Voc. Training |
0.836 |
||||
|
Costs Med. School |
0.765 |
||||
|
Insurance Risk |
0.673 |
||||
|
Research/Teaching |
0.547 |
||||
|
Specialty Exp. |
0.791 |
||||
|
Med. School Exp. |
0.777 |
||||
|
Training Exp./Doc. |
0.590 |
||||
|
Helping People |
0.393 |
||||
|
Post-Grad. Work |
0.302 |
||||
|
Prestige |
0.730 |
||||
|
Financial Prospects |
0.712 |
||||
|
Procedural Work |
0.576 |
||||
|
Intel. Content |
0.604 |
||||
|
Career Prospects |
0.566 |
||||
|
Work Culture |
0.451 |
||||
|
Typical Patients |
0.395 |
||||
|
Self-Appraisal |
0.368 |
||||
|
Variance explained, % |
12.4 |
11.4 |
9.2 |
8.8 |
8.3 |
|
Factor score, mean (SD)** |
3.1 (0.8) |
1.8 (0.7) |
3.6 (0.7) |
2.7 (0.9) |
3.6 (0.6) |
|
|
C: PGY3 (yrs 2015 and 2016) |
||||
|
|
1 |
2 |
5 |
4 |
3 |
|
Costs Voc. Training |
0.806 |
||||
|
Costs Med. School |
0.803 |
||||
|
Financial Prospects |
0.635 |
||||
|
Prestige |
0.621 |
||||
|
Insurance Risk |
0.596 |
||||
|
Career Prospects |
0.544 |
||||
|
Job Security |
0.511 |
||||
|
Research/Teaching |
0.367 |
||||
|
Flexible Hrs |
0.849 |
||||
|
Working Hrs |
0.827 |
||||
|
Domestic Circum. |
0.732 |
||||
|
Voc. Training Avail. |
0.399 |
||||
|
Intel. Content |
0.669 |
||||
|
Training Exp./Doc. |
0.581 |
||||
|
Work Culture |
0.576 |
||||
|
Post-Grad. Work |
0.558 |
||||
|
Typical Patients |
0.540 |
||||
|
Self-Appraisal |
0.451 |
||||
|
Procedural Work |
0.374 |
||||
|
Specialty Exp. |
0.911 |
||||
|
Med. School Exp. |
0.892 |
||||
|
Training Yrs |
0.521 |
||||
|
Location |
0.476 |
||||
|
Helping People |
0.464 |
||||
|
Variance explained, % |
13.7 |
13.1 |
11.5 |
7.5 |
5.4 |
|
Factor score, mean (SD)** |
2.3 (0.7) |
3.4 (0.9) |
3.8 (0.6) |
3.1 (1.2) |
3.1 (0.7) |
|
|
D: PGY5 (yrs 2017 and 2018) |
||||
|
|
2 |
3 |
1 |
5 |
4 |
|
Flexible Hrs |
0.822 |
||||
|
Working Hrs |
0.791 |
||||
|
Domestic Circum. |
0.687 |
||||
|
Location |
0.454 |
||||
|
Career Prospects |
0.790 |
||||
|
Prestige |
0.633 |
||||
|
Job Security |
0.613 |
||||
|
Financial Prospects |
0.604 |
||||
|
Procedural Work |
0.521 |
||||
|
Research/Teaching |
0.508 |
||||
|
Voc. Training Avail. |
0.355 |
||||
|
Costs Voc. Training |
0.859 |
||||
|
Costs Med. School |
0.831 |
||||
|
Insurance Risk |
0.604 |
||||
|
Training Yrs |
|
0.563 |
|||
|
Parents/Relatives |
0.350 |
||||
|
Typical Patients |
0.600 |
||||
|
Helping People |
0.585 |
||||
|
Intel. Content |
0.562 |
||||
|
Self-Appraisal |
0.507 |
||||
|
Work Culture |
0.464 |
||||
|
Training Exp./Doc. |
0.432 |
||||
|
Post-Grad. Work |
0.429 |
||||
|
Specialty Exp. |
0.896 |
||||
|
Med. School Exp. |
0.881 |
||||
|
Variance explained, % |
12.1 |
11.3 |
11.1 |
8.3 |
7.8 |
|
Factor score, mean (SD)** |
3.4 (0.9) |
2.8 (0.7) |
1.8 (0.7) |
3.9 (0.6) |
2.9 (1.2) |
|
*See Supplementary Table 1 for full item descriptors **Mean (SD) of 5-point Likert scores making up factor |
|||||
Table 1. Principal component analyses of influences underlying career choice in medical graduates to five years after graduation
Table 1 shows the results of the principal component analyses, demonstrating well-formed factors at each time point. Factors are reported in the descending order of their variance explained (VE), and with a factor score, being the mean (SD) of the Likert question scores making up the factor. The VE is a measure of the amount of variability in the participants’ responses that can be explained by the factor, hence higher levels of VE indicate agreement by a larger number of graduates. The factor score indicates the degree to which graduates consider the factor to be important or unimportant in their choices.
For example, at Exit from medical school (Table 1A), Factor 1 accounts for the largest VE (15.8%), comprising the 9 question items that are, on average, the least influential in determining career choice for graduates, with a factor score of 2.3 (out of 5). These least influential items are: Costs of Vocational Training; Costs of Medical School; Insurance Risk; Parents/Relatives; Prestige; Training Years; Financial Prospects; Research/Teaching; and Location. By contrast, Factor 4 at Exit, with the highest factor score of 3.9 and explaining 9.3% of the variance, contains the 4 items rated as the most influential by graduates in determining career choice. These most influential items are: Medical School Experiences; Specialty Experience; Mentors; and Self-Appraisal. These results are consistent with new graduates making the most of their abilities and opportunities to secure their first healthcare role. Other factors at Exit fall within these two extremes.
It is worth noting that the item Parent/Relatives fails to load over the 0.3 threshold on any factor at PGY1 or PGY3 (hence does not appear). Some change in factor structures over time do occur, reflecting changing priorities for graduates. For example, Factor 2 at Exit has a relatively high factor score of 3.6 (VE=11.1%) indicating that the items Flexible Hours, Working Hours, Domestic Circumstances, and Work Culture are important for new graduates. However, by PGY1 (Table 1B) this factor then picks up the items of Training Years, Vocational Training Availability, Location and Job Security, and becomes important to a greater number of graduates by becoming the factor with the largest variance explained (VE=12.4%). This result suggests that graduates are adjusting to their new working lives and are planning for their futures in terms of further training.
Factor 1 and Factor 2 consistently demonstrate high levels of variance explained and contain a common core of three influencing items. Factor 1, with a median (range) score of 2.1 (1.8 to 2.3) across all time points, continues to describe influences on career choice rated as the least important for medical graduates, and consistently contains the items Costs of Vocational Training, Costs of Medical School, and Insurance Risk. By contrast, Factor 2 is consistently rated as relatively important, with a median (range) score of 3.4 (3.1 to 3.6) across time points, and consistently contains the items Flexible Hours, Working Hours, and Domestic Circumstances.
Our results demonstrate the existence of well-formed factors in the MSOD data at each time point. Despite some change in factor structure over time, the scores for each factor remain relatively stable, with a median (range) variation in scores of only 0.5 (0.3 to 1.0) Likert points. Table 1 contains results which allow substantial scope for hypothesis formation and future research, including targeted work to better understand the decision points in the critical first five years of a graduate’s career.
IV. DISCUSSION
Better understanding the influences underlying career choice in medical graduates is a strategically important and practical concern when aiming to match graduate production with professional and community needs. This study is the among the first to conduct a quantitative analysis of the self-reported influences underlying medical graduate career choice in a prospective, national cohort of the same graduates over the critical first five years of their careers.
The financial burden of completing medical school and vocational training is one of the most widely studied influences in career choice for medical graduates. It is therefore reassuring that our findings demonstrate that these costs are among the least influential considerations at all time points in the five years after graduation for our cohort.
Factor 2 in the present study consistently contains the items Flexible Hours, Working Hours and Domestic Circumstances, and is rated as important over the first five years of graduates’ careers. Flexibility around working hours and a desire to practice part-time has traditionally been thought of as largely important for female medical graduates (Heiliger & Hingstman, 2000). However, this is no longer the case, with many male graduates in recent decades also desiring more lifestyle-friendly working arrangements allowing the flexibility to spend more time with family (Heiliger & Hingstman, 2000). Taken together with the evidence that the costs of medical school and further training are the least influential in career choice, our results therefore strongly suggest that the ability to offer greater flexibility in working hours is likely to be useful in recruiting medical graduates to underserved specialties.
It is a practical and pressing necessity that healthcare workforce planning is guided by the best available evidence. A strength of the current study is the ability to link the same participants longitudinally, thus eliminating an important source of bias. Women in the current study made up 57% of medical graduate respondents, reflecting the fact that in recent years in New Zealand and Australia female graduates have outnumbered male graduates. A further strength is the high response rates, yielding a sampling margin of error of only 3% or less at all time points, which compares favourably with many questionnaire studies of medical graduates.
V. CONCLUSION
Despite widespread concern over rising debt levels and the cost of medical school, our results are reassuring in that the costs of medical school and vocational training were consistently rated as the least important influences in career choice. Our results also suggest that offering greater flexibility around working hours may assist in attracting medical graduates to underserved specialties. Our description of well-formed factors in the influences underlying career choice in the national MSOD questionnaire data provides a useful basis for further research to better understand key decision points in the critical first five years of graduates’ careers.
Notes on Contributors
Craig Webster was involved in the conceptualisation of this paper, data analysis, writing and revision.
Jack Forsythe was involved in the conceptualisation of this paper, data analysis, writing and revision.
Antonia Verstappen was involved in accessing data for this paper, writing and revision.
Phillippa Poole was involved in the writing and revision of this paper.
Tim Wilkinson was involved in the writing and revision of this paper.
Marcus Henning was involved in the writing and revision of this paper.
Ethical Approval
This study was carried out in accordance with all regulations of the host organisations and with the approvals of the Human Participants Ethics Committees of the University of Auckland (approval numbers 022388 and 018456) and the University of Otago (approval number 07-155), New Zealand. All participants gave written informed consent to participate in the study, including for anonymised aggregated data to be published.
Data Availability
The ethics approval for the longitudinal MSOD project currently does not permit the sharing of non-aggregated data. However, this restriction is under review and so non-aggregated data may be available from the corresponding author in the near future.
Acknowledgement
We thank the Health Career Pathways Project, Faculty of Medical and Health Sciences, University of Auckland, and the Medical Schools Outcomes Database Longitudinal Tracking Project at the University of Auckland and the University of Otago for assistance and data access.
Funding
JF received a summer studentship stipend from the Faculty of Medical and Health Sciences, University of Auckland, New Zealand in support of this research. The Medical Schools Outcomes Database Longitudinal Tracking Project is supported by a grant from Health Workforce New Zealand.
Declaration of Interest
All authors have no potential conflicts of interest.
References
Gorman, D. (2018). Matching the production of doctors with national needs. Medical Education, 52(1), 103-113. https://doi.org/10.1111/medu.13369
Heiliger, P. J., & Hingstman, L. (2000). Career preferences and the work-family balance in medicine: Gender differences among medical specialists. Social Science and Medicine, 50(9), 1235-1246. https://doi.org/10.1016/s0277-9536(99)00363-9
Kaiser, H. F. (1974). An index of factorial simplicity. Psychometrika, 39, 31–36. https://doi.org/10.1007/BF02291575
Poole, P., Wilkinson, T. J., Bagg, W., Freegard, J., Hyland, F., Jo, C. E., Kool, B., Roberts, E., Rudland, J., Smith, B., & Verstappen, A. (2019). Developing New Zealand’s medical workforce: Realising the potential of longitudinal career tracking. New Zealand Medical Journal, 132(1495), 65-73.
Webster, C. S., Ling, C., Barrow, M., Poole, P., & Henning, M. (2017). A cross-disciplinary assessment of student loans debt, financial support for study and career preferences upon graduation. New Zealand Medical Journal, 130(1459), 43-53.
Webster, C. S., McKillop, A., Bennett, W., & Bagg, W. A. (2020). A qualitative and semiquantitative exploration of the experience of a rural and regional clinical placement programme. Medical Science Educator, 30(2), 783-789. https://doi.org/10.1007/s40670-020-00949-6
*Craig Webster
Centre for Medical and Health Sciences Education,
School of Medicine, University of Auckland,
Private Bag 92-019
Auckland 1142, New Zealand
+649 923 6525
Email: c.webster@auckland.ac.nz
Submitted: 12 December 2023
Accepted: 25 March 2024
Published online: 1 October, TAPS 2024, 9(4), 40-49
https://doi.org/10.29060/TAPS.2024-9-4/SC3254
Vivien Lee1, Jeffrey Jiang1, Anna Szücs1, V Vien Lee1, Low Si Hui2, Faith Teo1, Jose M Valderas1 & Victor Loh1
1Division of Family Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2National University Polyclinics, Singapore
Abstract
Introduction: Globally, persons with disabilities (PWD) face structural and social barriers to inclusive healthcare. Medical schools, as crucibles of medical professional identity formation, have the responsibility to foster person-centredness toward all patients, including PWD, among her graduates. We co-designed with PWD a “Communications with Persons with Disabilities” workshop and evaluated its impact.
Methods: The workshop enlisted PWD as patient educators, occurred within the third-year undergraduate Family Medicine posting, and was designed to positively impact communications skills and attitudes toward PWD. Students (n=135) were surveyed pre- and post- workshop following a mixed-methods approach (demographic data, Attitude Towards Disabled Persons (ATDP)-O scale, feedback questions, and post-workshop free reflections). Descriptive analysis was used for demographic and feedback questions, and thematic analysis for reflections. Paired t-test was used to evaluate change in ATDP-O scores.
Results: There were 69 survey respondents (51.11%). Most students agreed that communications training with PWD could be strengthened in medical school, and that the workshop was relevant to their future medical career (n=68, 98.55%). Attitudes towards PWD significantly improved after the workshop (ATDP-O change: +9.29 points (12.7%), p <0.001). Student reflections included attitudes, such as the importance of seeing the person beyond the disability, and a call for action towards inclusivity and accessibility of care for PWD.
Conclusion: Students’ attitudes were positively affected by involving PWD in the curriculum. Further research is needed for assessing the impact of how a longitudinal PWD curriculum could affect medical trainees and improve social inclusiveness in healthcare practice.
Keywords: Medical Education, Communication, Persons with Disabilities, Disability, Social Inclusiveness, Student Attitudes, Person Centred Care, Active Learning
I. INTRODUCTION
Globally, persons with disabilities (PWD) face structural and social barriers to inclusive healthcare. In Singapore, few are comfortable with direct personal interaction with PWD (National Council of Social Service Singapore, 2019).
With respect to medical education, different disability curriculum from didactic lectures to longitudinal patient experiences have been described (Ali et al., 2023). Overall evidence suggests that more frequent and positive contact with PWD increased positive attitudes (Ali et al., 2023; National Council of Social Service Singapore, 2019).
Medical schools, as crucibles of medical professional identity formation, have the responsibility to foster person-centredness toward all patients, including PWD, among her graduates. In July 2022, the National University of Singapore’s Division of Family Medicine developed with PWD, piloted and assessed a four-hour experiential workshop for third-year medical students called “Communication with PWD” in July 2022.
The four-hour workshop was prefaced by pre-event reading materials. A plenary started on site learning, followed by fishbowl discussions where student volunteers took turns to perform a clinical consultation with PWD who enacted scripted role-plays. There was a ratio of one tutor and PWD to a group of ten to fifteen students. Each student would encounter three broad categories of disability (vision, hearing, mobility) during the fishbowl sessions. Students interacted with PWD after each role play. Reflections and debrief by tutors would close the workshop.
This study aimed to evaluate the workshop’s impact on students’ attitudes towards PWD for: (Q1) differences in pre-workshop attitudes towards PWD between male and female medical students; (Q2) within-person changes in students’ overall attitudes towards PWD pre-post workshop; (Q3) associations between pre-workshop attitudes towards PWD and personal experience with PWD; and (Q4) exploration of how the workshop has affected students’ attitudes towards caring for PWDs.
II. METHODS
A. Study Design
This study had a mixed methods design including a pre- and post-intervention survey (quantitative), and reflections (qualitative). Students attending the 3rd and 4th Family Medicine Rotation (January to March 2023) of Academic Year 2022/23 were invited to participate in the study. The questionnaire was administered in person. Students completed the questionnaires independently. A waiver of consent was applied for reflections.
B. Survey
The pre-workshop questionnaire comprised demographic information and the 20-item Attitude Towards Disabled Persons (ATDP)-O scale (Yuker et al., 1960). The questions were scored on six-point Likert scale from “I disagree very much” (-3) to “I agree very much” (+3). The post-workshop questionnaire comprised the ATDP-O scale and feedback questions.
We used the original ATDP-O form as it had been used in other studies on medical students (Arabi et al., 2021) and was deemed reliable (reliability coefficient .80) and valid by prior psychometric analyses (Yuker et al., 1960). Performance in local context was assessed through cognitive testing with five randomly selected medical students who were classmates of study participants and excluded from the study sample.
C. Reflections
Student reflection sheets included a single open-ended statement: “Please pen a question or a reflection you’d like to share from the session today”. Reflections were transcribed verbatim and de-identified before analysis. All reflections were used to limit selection bias.
D. Data Analysis
Numeric data was analysed by R software (version 4.31). Internal consistency of the scale in our study sample was measured with Cronbach’s alpha. We used two samples independent unpaired t-test to evaluate Q1 (differences in baseline ATDP-O scores between males and females), two samples paired t-test to evaluate Q2 (change in pre-post workshop ATDP-O scores), and two samples independent unpaired t-tests, Welch’s t-tests and Spearman’s correlation tests to evaluate Q3 (difference in baseline ATDP-O scores across different types/levels of contact with PWD). In the evaluation of Q3, two samples independent unpaired t-test was used when two groups have similar sample sizes or similar variances while Welch’s t-test was used when there’s unequal variances or disparate sample sizes between two groups. Spearman’s correlation was used to analyse associations with ordinal variables.
Student reflections were analysed thematically. Four researchers (VLE, VVL, AS, FT) reviewed the data and generated initial codes independently. Multiple discussions were conducted to explore different perspectives and increasingly develop codes. Based on codes generated, potential themes and subthemes were developed over several iterations. Final themes and subthemes were reviewed in relation to the entire dataset.
III. RESULTS
Of 135 students invited, 69 students consented to the study and completed both the pre- and post-workshop questionnaire. The results are summarised (Table 1a and 1b).
Cognitive testing confirmed that students had no difficulties understanding questions nor suggested any edits for clarification. The internal consistency of the scale was α = 0.72 (pre-workshop) and α = 0.78 (post-workshop).
(Q1) Female gender had a significantly higher baseline ATDP-O scores (p = 0.028).
(Q2) There was a significant improvement of 9.29 points (12.7%) in the ATDP-O score post workshop (p <0.001).
(Q3) Previous experience of training to care for PWD (p<0.001) and previous experience caring for PWD (p = 0.033) had significantly lower baseline ATDP-O scores.
|
Results |
Number (%) |
ATDP-O baseline score Mean (SD) |
Statistics |
||
|
Overall |
N=69 |
72.71 (10.46) |
|
||
|
By age (Mean = 21.59, SD = 0.96) |
Pearson’s r(67) = – 0.02, p = .857 |
||||
|
By gender |
|||||
|
Female |
37 (53.62%) |
75.32 (8.61) |
t(67) = 2.30, p = .025*
|
||
|
Male |
32 (46.38%) |
69.69 (11.69) |
|||
|
By ethnicity |
|||||
|
Chinese |
56 (81.16%) |
73.18 (10.20) |
F(2, 66) = 1.64, p = .201 |
||
|
Indian |
12 (17.39%) |
69.33 (11.18) |
|||
|
Others |
1 (1.45%) |
87.00 (.) |
|||
|
Self-reported disability |
|||||
|
No |
66 (95.65%) |
72.74 (10.59) |
t(2) = 0.14, p = .900 |
||
|
Yes |
3 (4.35%) |
72.00 (8.89) |
|||
|
Self-reported training to care for PWD |
|||||
|
No |
67 (97.10%) |
73.06 (10.42) |
t(7) = 7.45, p < .001* |
||
|
Yes |
3 (4.35%) |
61.00 (1.41) |
|||
|
Self-reported frequency of care for PWD (ranked variable ranging from never = 1 to often = 4) |
|||||
|
Never |
34 (49.28%) |
75.7 (9.5) |
Spearman’s rho(67) = – 0.26, p = .033* |
||
|
Rarely |
22 (31.88%) |
69.8 (11.8) |
|||
|
Sometimes |
12 (17.39%) |
69.5 (9) |
|||
|
Often |
1 (1.45%) |
75 (.) |
|||
|
Self-reported knowledge of PWD who is important to them |
|||||
|
No |
53 (76.81%) |
73.57 (10.95) |
t(67) = 1.24, p = .219
|
||
|
Yes |
16 (23.19%) |
69.88 (8.34) |
|||
|
Self-rated likelihood of pursuing career in Family Medicine (ranked variable ranging from very unlikely = 1 to very likely = 5) |
|||||
|
Very likely |
9 (13.04%) |
72.1 (10) |
Spearman’s rho(67) = 0.03 , p = .803 |
||
|
Likely |
18 (26.09%) |
73.2 (11.5) |
|||
|
Undecided |
37 (53.62%) |
73.5 (10.3) |
|||
|
Unlikely |
4 (5.80%) |
63.5 (8.9) |
|||
|
Very unlikely |
1 (1.45%) |
78 (.) |
|||
|
Do you feel your education about persons with disabilities in medical school has been adequate so far? |
|||||
|
Agree |
1 (1.45%) |
– |
– |
||
|
Neither disagree nor agree |
19 (27.54%) |
– |
– |
||
|
Disagree |
42 (60.87%) |
– |
– |
||
|
Strongly disagree |
7 (10.14%) |
– |
– |
||
|
Would you find it important to include education and training on persons with disabilities? |
|||||
|
Strongly agree |
23 (33.33%) |
– |
– |
||
|
Agree |
39 (56.52%) |
– |
– |
||
|
Neither disagree nor agree |
5 (7.25%) |
– |
– |
||
|
Disagree |
1 (1.45%) |
– |
– |
||
|
Strongly disagree |
1 (1.45%) |
– |
– |
||
|
Do you feel that the education provided during the Communications with Persons with Disabilities workshop was relevant to your future career as doctors? |
|||||
|
Strongly agree |
45 (65.22%) |
– |
– |
||
|
Agree |
23 (33.33%) |
– |
– |
||
Table 1a. Baseline ATDP-O scores and curriculum feedback
|
Results |
ATDP-O score Mean (SD) |
Pre-Post workshop comparison statistics |
|
Descriptive statistics |
||
|
Pre-workshop ATDP-O score |
72.71 (10.46) |
t(68) = 8.69, p < .001*
|
|
Post-workshop ATDP-O score |
82.00 (11.46) |
|
|
Difference in ATDP-O scores |
||
|
Overall sample |
9.29 (8.88) |
t(68) = 8.69, p < .001 |
|
By age (Mean = 21.59, SD = 0.96) |
Pearson’s r(67) = – 0.06, p = .643 |
|
|
By gender |
||
|
Female |
8.62 (9.33) |
t(67) = – 0.67, p = .505 |
|
Male |
10.06 (8.41) |
|
|
By ethnicity |
||
|
Chinese |
9.02 (9.45) |
F(2, 66) = 0.15, p = .859 |
|
Indian |
10.33 (6.21) |
|
|
Others |
12.00 (.) |
|
|
Self-reported disability |
||
|
No |
9.50 (8.06) |
t(2) = 0.36, p = .752 |
|
Yes |
4.67 (23.12) |
|
|
Self-reported training to care for PWD |
||
|
No |
9.09 (8.92) |
t(1) = – 2.17, p = .230 |
|
Yes |
16.00 (4.24) |
|
|
Self-reported frequency of care for PWD (ranked variable ranging from never = 1 to often = 4) |
||
|
Never |
8.8 (6.1) |
Spearman’s rho(67) = 0.05, p = .678 |
|
Rarely |
11.5 (9.1) |
|
|
Sometimes |
9.4 (10.8) |
|
|
Often |
-22 (.) |
|
|
Self-reported knowledge of PWD who is important to them |
||
|
No |
10.72 (7.61) |
t(67) = 2.52, p = .014*
|
|
Yes |
4.56 (11.20) |
|
|
Self-rated likelihood of pursuing career in Family Medicine (ranked variable ranging from very unlikely = 1 to very likely = 5) |
||
|
Very likely |
10.4 (9.2) |
Spearman’s rho(67) = 0.07, p = .547 |
|
Likely |
10.9 (7.8) |
|
|
Undecided |
7.9 (9.5) |
|
|
Unlikely |
11.5 (9.3) |
|
|
Very unlikely |
11 (.) |
|
Table 1b. Difference in ATDP-O scores post workshop
Most students found the workshop a positive experience and reported feelings of thankfulness and inspiration towards patient educators. Four themes emerged from the students’ post-workshop reflections, of which we highlight those related to attitudes – Humanizing mindsets towards PWD (Theme 1) and Call for action towards inclusivity and accessibility (Theme 2). The other themes were Knowledge and Skills, as students included knowledge and communication skills they acquired during the workshop (Appendix 1 and 2).
A. Theme 1 – Humanising Mindset towards Persons with Disabilities
Students expressed attitudes of empathy, sensitivity, and humanising care through viewing PWD as individuals beyond their disabilities. A student reflected
“Being able to speak to members of these respective communities helped me to understand how empowered PWD can be… It is essential that [PWD] are treated as exactly that, [and] not characterised by their disabilities.”
On providing care for PWD, students noted the distinction between empathy and sympathy, and highlighted the importance of empathy instead of pity. As summed up by a student,
“Not to sympathise but to empathise. Not to see them and pity them”
B. Theme 2 – Call for Action towards Inclusivity and Accessibility
Concurrent with attitudes expressed in the reflections, students discussed the need to improve inclusivity and accessibility from an individual and societal perspective. One student wrote,
“As doctors, we need to try our best to alleviate their disease burden, and at the same time, make their journey to accessing healthcare more seamless with less barriers.”
Beyond self-improvement, students were aware of the need to shift their own perspectives of disability from a medical to a social model. Students also reflected the need for greater national efforts towards societal inclusivity for PWD. A student reflected,
“I think policymakers and organisations should periodically involve PWD to [better] take their needs into consideration as they have the right to integrate into our society just as much as everyone else.”
IV. DISCUSSION
Our study showed positive change in attitudes towards PWD among medical students after a workshop with improvement of 9.29 points in the ATDP-O score (Table 1b), reinforced by their post-workshop reflections. To our knowledge, this is the first study in Asia evaluating an educational intervention focusing on communications skills training with PWD. Based on student reflections, the communications workshop was effective in developing knowledge and communication skills, prompting the key attitudes of humanizing care, and a call for action towards societal inclusivity and accessibility towards PWD.
We intentionally had PWD co-designing the workshop and playing key roles as patient educators. Student reflections support these curriculum design decisions. Our work coheres with literature that a contact-based approach with PWD would be impactful: reducing anxiety and improving empathy levels, rather than more theoretical approaches to promote attitudes towards PWD (Arabi et al., 2021).
Our study corroborates the widely reported result that female gender positively influenced baseline attitudes towards PWD in medical students (Satchidanand et al., 2012). A possible explanation is females having a propensity to exhibit more empathetic feelings toward others. There is a greater change in attitudes in males than females after the workshop, but this change is not significant.
In contrast to prior research that consistently associated increased contact with PWD with more positive attitudes (Satchidanand et al., 2012), we found that having previous experience with PWD influenced baseline ATDP-O scores negatively (Table 1a). Moreover, there was a significantly smaller change in ATDP-O scores if they knew a PWD who is important to them (Table 1b). A possible explanation is “caregiver fatigue” due to unavailability of support to allow adequate care for PWD (Arabi et al., 2021). The type of previous experience may thus be key factors in shaping current attitudes towards PWDs.
This study has several limitations. We cannot determine if positive change in attitudes post-workshop would translate into changes in clinical practice in the future. The survey was not compulsory for students, potentially leading to selection bias. We tried to overcome the selection bias by including all student reflections.
V. CONCLUSION
There was significant improvement in students’ attitudes towards PWD post-workshop, as shown through the ADTP-O score and reflection analysis. Medical students benefit particularly from the fishbowl discussions which allows students to interact with persons with disability, growing our future generations of healthcare professionals who humanise care.
Notes on Contributors
Author VLE conceptualised the study, developed the methodology, conducted the investigation, did the formal analysis and visualization of data, wrote the original draft, reviewed and edited the manuscript. Author JJ conceptualized the study, developed the methodology and original draft, reviewed and edited the manuscript. Author AS developed the methodology, did the formal analysis of data, reviewed and edited the manuscript. Author VVL did the formal analysis of data, wrote the original draft, reviewed and edited the manuscript. Author LSH did the formal analysis and visualization of data. Author FT did the formal analysis, reviewed and edited the manuscript. Author JMV supervised the conceptualization and methodology of the study, reviewed and edited the manuscript. VLO supervised the conceptualization of the study, developed the methodology, reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the National University of Singapore on 11 November 2022 (NUS-IRB-2022-608).
Data Availability
Quantitative data repository can be freely accessed at: https://doi.org/10.6084/m9.figshare.24013134
Qualitative data repository can be freely accessed at: https://doi.org/10.6084/m9.figshare.24051195
Funding
There was no funding for this research study.
Declaration of Interest
Authors VLE, JJ and VLO are tutors in the “Communications with Persons with Disabilities” workshop. There are otherwise no other conflicts of interest.
References
Ali, A., Nguyen, J., Dennett, L., Goez, H., & Rashid, M. (2023). A scoping review for designing a disability curriculum and its impact for medical students. Canadian Medical Education Journal, 14(3), 75–86. https://doi.org/10.36834/cmej.74411
Arabi, H., Adarmouch, L., & Ahmed Eladip, G. (2021). The assessment of student doctors’ attitude towards disabled people after teaching them a module. Acta Bio-Medica: Atenei Parmensis, 92(2), e2021059. https://doi.org/10.23750/abm.v92i2.9547
National Council of Social Service Singapore. (2019). Public Attitudes Towards Persons with Disabilities 2019. https://www.ncss.gov.sg/docs/default-source/ncss-publications-doc/pdfdocument/public-attitudes-towards-persons-with-disabilities-2019-infographics.pdf
Satchidanand, N., Gunukula, S. K., Lam, W. Y., McGuigan, D., New, I., Symons, A. B., Withiam-Leitch, M., & Akl, E. A. (2012). Attitudes of healthcare students and professionals toward patients with physical disability: A systematic review. American Journal of Physical Medicine & Rehabilitation, 91(6), 533–545. https://doi.org/10.1097/PHM.0b013e3182555ea4
Yuker, H. E., Block, J. R., & Campbell, W. J. (1960). A scale to measure attitudes toward disabled persons. In Human Resources Study Number 5. Human Resources Foundation.
*Vivien Lee
1E Kent Ridge Rd,
Singapore 119228
Email: vivienl@nus.edu.sg
Submitted: 3 April 2024
Accepted: 22 July 2024
Published online: 1 October, TAPS 2024, 9(4), 33-39
https://doi.org/10.29060/TAPS.2024-9-4/OA3282
Meltem Saygılı1, Aysun Kandemir Türe1 & Şirin Özkan2
1Department of Health Management, Kırıkkale University, Kırıkkale, Türkiye; 2Department of Medical Services and Techniques, Vocational School of Health Services, Uludag University, Türkiye
Abstract
Introduction: Many societal changes threaten the sustainability of health systems. Entrepreneurs play a significant role in creating sustainable innovations necessary for development and structural change. This study aimed to evaluate how university students studying health sciences perceive individual entrepreneurship during the COVID-19 pandemic and to explore the impact of COVID-19-related hopelessness on their perception of entrepreneurship.
Methods: Six hundred eighty-one undergraduate students from the faculty of health sciences in Türkiye, participated in the study. The Individual Entrepreneurship Perception Scale and Beck Hopelessness Scale were used to collect data.
Results: The results revealed that the students’ perception of individual entrepreneurship was high, while their hopelessness levels were moderate. In addition, a moderate negative relationship was found between the students’ hopelessness levels and their perception of individual entrepreneurship. The regression analysis showed that the students’ hopelessness levels and sub-dimensions (hope, loss of motivation, and future expectation) accounted for 26.3% of the total variance in individual entrepreneurship perception. Increased hopelessness regarding the sub-dimensions of hope, loss of motivation, and expectations for the future decreased their individual entrepreneurship perceptions.
Conclusions: These findings suggest that individual entrepreneurship perception among health sciences students could be negatively impacted during extraordinary periods related to health crises like pandemics. Developing hope, motivation, and expectations for the future is crucial to enhancing individual entrepreneurship perception among health sciences students.
Keywords: Individual Entrepreneurship Perception, Hopelessness, Health Sciences, University Students, COVID-19 Pandemic
Practice Highlights
- University education plays a critical role in developing students’ perceptions of entrepreneurship.
- Students’ perceptions of entrepreneurship are affected by changing environmental conditions.
- The COVID-19 pandemic has led to a significant increase in awareness of Healthcare Entrepreneurship.
- The COVID-19 pandemic has negatively affected students’ expectations and hopes for the future.
- Health sciences students experienced the psychological effects of the pandemic more intensely.
I. INTRODUCTION
Entrepreneurs are described as individuals who “implement bold new ideas from the outset, taking on the risks of the business or venture that enables innovation to happen” (Suryavanshi et al., 2020). Entrepreneurship education seeks to provide students with in-depth knowledge, motivation, and skills to increase entrepreneurial intentions’ success in various settings (Sampene et al., 2023). In developing economies such as Türkiye, government efforts to improve unemployment conditions are directed towards developing students’ positive attitudes towards entrepreneurship and increasing their interest in self-employment.
Universities are crucial in developing students’ entrepreneurial intentions (Bagheri, 2018). It is critical to examine and develop the entrepreneurial potential of university students trained to fulfill important roles in the field of health services in the future. This is because students and newly graduated healthcare professionals with entrepreneurial skills are now needed to develop innovative healthcare delivery models that can improve the quality of healthcare services, improve treatment outcomes, and reduce the cost of care (Fashami et al., 2021; Mohamed et al., 2023). It is stated that healthcare is one of the main industrial areas where user entrepreneurship takes place worldwide (Schiavone et al., 2020) and the pandemic environment brings unique opportunities for entrepreneurs, especially in healthcare. However, research shows that fear and worry due to the COVID-19 pandemic are making the future workforce anxious and hopeless about their professional futures (Duplaga & Grysztar, 2021; Tao et al., 2023). In such an environment, it is predicted that university students, especially those who are trained to work in health service delivery, may act in different ways in their decisions about their professional future.
Because an individual’s perception of current conditions can significantly, positively, or negatively affect the formation of entrepreneurial intentions and the likelihood of starting an enterprise (Krichen & Chaabouni, 2022). Considering the increasing entrepreneurship opportunities in healthcare and the negative effects of the COVID-19 pandemic on healthcare services, it has become important to address the entrepreneurship perceptions of students who will serve in this field in the future and to evaluate the hopelessness experienced. When the literature was examined, no other research addressing entrepreneurship in the context of hopelessness was found. Therefore, we believe that our research findings will make a valuable contribution to filling this gap in the literature.
A. Universities, Health Sciences Education and Entrepreneurship
Recent years have focused on the role of universities in industrial competitiveness and their impact on social change (Hart & Rodgers, 2023), and universities in teaching and initiating entrepreneurship have emerged as leading actors. Recent research examining students’ attitudes toward entrepreneurship reveals that universities have a critical role in developing entrepreneurial spirit and perceptions of entrepreneurship in students (Krichen & Chaabouni, 2022; Liao et al., 2022; Sampene et al., 2023). Moreover, university students now value real experience more and prefer universities that offer entrepreneurship opportunities and experiences (Taneja et al., 2024).
Universities providing education in healthcare have traditionally emphasised vocational training and unfortunately, there are very few university programs with curricula that focus on innovation and entrepreneurship in healthcare (Suryavanshi et al., 2020). Consequently, most newly graduated physicians and other healthcare professionals start their careers without the knowledge, experience, and courage to integrate their medical knowledge with the healthcare business world, and thus are unable to commercialise new healthcare delivery methods (Boore & Porter, 2011).
B. Hopelessness Experienced by Students Due to the COVID-19 Pandemic and Perception of Individual Entrepreneurship
Students are one of the groups that experience the psychological effects of the pandemic most intensely (Marahwa et al., 2022). Studies conducted with students during the pandemic period showed that students experienced higher levels of anxiety and depressive symptoms due to uncertainties about the future and the negative effects of the pandemic on their educational lives (Alnıaçık et al., 2021; Hajinasab et al., 2022; Kaplan Serin & Doğan, 2023; Zhang et al., 2021). Moreover, it was also determined that students’ hopelessness levels were higher in the first wave of the pandemic and during the quarantine period and decreased with normalisation (Tao et al., 2023). In addition, it has been found that students who are educated in the field of health and have clinical experience are more anxious and hopeless than undergraduate students who are educated outside the field of health (Pretorius, 2021). Although entrepreneurship is a future-oriented orientation and is perceived as the ability to turn negative situations into opportunities, it is estimated that the psychological effects of COVID-19 may negatively affect entrepreneurial intention in students. Therefore, this study aims to examine the effect of hopelessness experienced by health sciences faculty students during the COVID-19 pandemic on their perception of individual entrepreneurship.
II. METHODS
A. Sampling and Participants and Data Collection
The study was conducted with university students studying at the Faculty of Health Sciences in Türkiye. The faculty consists of six departments, namely Physiotherapy and Rehabilitation, Health Management, Social Work, Nutrition and Dietetics, Child Development and Nursing, and has 2335 students. The sample size required for the study was calculated using the formula (n=[z²xp(1-p)/d²]/1+[z²xp(1-p)/d²N]) and it was determined that a minimum of 337 participants would be sufficient with a 5% error level and 95% confidence level. Participants were selected using a simple random sampling technique and volunteerism was taken as a basis in obtaining the data. The study was conducted between April and May 2022 and 681 valid questionnaires were returned from the participating students.
Data were collected using the socio-demographic information form, Individual Entrepreneurship Perception Scale, and Beck Hopelessness Scale. The Individual Entrepreneurship Perception Scale is a 5-point Likert scale consisting of 31 items and six sub-dimensions: planning, locus of control, self-confidence, communication, motivation, and self-discipline. This scale was developed by Incik and Uzun in 2017 to assess university students’ perceptions of entrepreneurship. The reliability coefficients (Cronbach’s Alpha) of the sub-dimensions of the Individual Entrepreneurship Perception Scale and the total scale were found to be 0.80, 0.84, 0.75, 0.75, 0.75, 0.72, 0.75, 0.60 and 0.92, respectively (Incik & Uzun, 2017). For this study, it was determined that the Cronbach Alpha values of the Individual Entrepreneurship Perception Scale ranged between 0.69 and 0.93 (Table 2).
The Hopelessness Scale was initially developed by Beck et al. in 1974 and subsequently adapted into Turkish by Durak and Palabıyıkoğlu in 1994. This scale comprises 20 items divided into three sub-dimensions: expectations for the future, loss of motivation, and hope. Each question in the scale requires a ‘yes’ or ‘no’ response, and the maximum achievable score is 20. An increase in the overall score denotes a higher level of hopelessness. The reliability coefficients for the sub-dimensions of the scale were calculated to be 0.78, 0.72, and 0.72, respectively (Durak & Palabıyıkoğlu, 1994). Table 2 presents the Cronbach’s alpha coefficients for the sub-dimensions and the scale, which were found to be 0.75, 0.77, 0.74, and 0.88, respectively.
B. Statistical Analysis
The statistical analyses used were performed in SPSS v23.0. Descriptive analyses such as percentage, mean, standard deviation, reliability analysis (Cronbach’s Alpha), and normality tests were performed to obtain the results. To test the normal distribution, kurtosis, and skewness values were calculated for each scale’s sub-dimensions and total scores. It was determined that the values obtained were in the range of -1.5 to +1.5 and the data showed a normal distribution (Tabachnick & Fidell, 2013). The results of the analysis are presented in Table 2. In addition, multiple linear regression analysis was used to investigate the relationship between hopelessness and students’ perception of individual entrepreneurship.
III. RESULTS
The study involved students with an average age of 21.3 years, ranging from 18 to 44 years old. 86% of the participants were female students, and the majority (52.3%) reported a grade point average of 3 or above (with a scale of 0 to 4). 68.3% of the students lived in the city center with their families. Among the students’ mothers, 37.7% had a primary school graduate degree, and 81.4% were not working. On the other hand, 32.2% of the students’ fathers had a high school graduate degree, and 78.4% were actively working. Most of the students (68.3%) stayed in dormitories. Regarding career plans after graduation, most students expressed their interest in working in a health institution (public or private). At the same time, only 15.6% said they wanted to start their own business. 15% of the students were still undecided about their work plans (Table 1).
|
Variables |
n |
% |
Variables |
n |
% |
|
Department |
Place of Residence Outside Education |
||||
|
Health Management (HM) |
122 |
17.9 |
City Centre |
465 |
68.3 |
|
Nursing (HEM) |
124 |
18.3 |
District |
171 |
25.1 |
|
Child Development (CDE) |
114 |
16.7 |
Village |
45 |
6.6 |
|
Nutrition and Dietetics (ND) |
116 |
17.0 |
Education Level of Mother |
||
|
Physiotherapy and Rehabilitation (FTR) |
140 |
20.6 |
Illiterate |
23 |
3.4 |
|
Social Work (SW) |
65 |
9.5 |
Primary School |
257 |
37.7 |
|
Classroom |
Middle School |
171 |
25.1 |
||
|
Grade 1 |
159 |
23.4 |
High School |
178 |
26.2 |
|
Grade 2 |
188 |
27.6 |
University |
52 |
7.6 |
|
Grade 3 |
165 |
24.2 |
Education Level of Father |
||
|
Grade 4 |
169 |
24.8 |
Primary School |
173 |
25.4 |
|
Gender |
Middle School |
141 |
20.7 |
||
|
Woman |
585 |
85.9 |
High School |
219 |
32.2 |
|
Male |
96 |
14.1 |
University |
148 |
21.7 |
|
Age |
Employment Status of Mother |
||||
|
18-20 years old |
277 |
40.7 |
Working |
127 |
18.6 |
|
21-22 years old |
272 |
39.9 |
Not working |
554 |
81.4 |
|
23 years and older |
132 |
19.4 |
Employment Status of Father |
||
|
Academic Average |
Working |
534 |
78.4 |
||
|
2.99 and below |
260 |
38.2 |
Not working |
147 |
21.6 |
|
3 and above |
356 |
52.3 |
Income Status |
||
|
Total |
616 |
90.5 |
Scholarship |
190 |
27.9 |
|
Not specified |
65 |
9.5 |
Tuition loan |
211 |
31.0 |
|
Career Future Plan After Graduation |
Working |
51 |
7.5 |
||
|
I will definitely be working in an organization (public-private) |
225 |
33.0 |
Only my family supports me |
229 |
33.6 |
|
Where Do You Live During Your Education? |
|||||
|
I tend to be an employee in an organization (public-private) |
240 |
35.2 |
Dormitory |
465 |
68.3 |
|
Undecided |
102 |
15.1 |
Apart |
171 |
25.1 |
|
I tend to start my own business. I have my own business |
114 |
16.7 |
Home+ Staying with my family |
45 |
6.6 |
|
Total |
681 |
100 |
Total |
681 |
100 |
Table 1. Sociodemographic characteristics of the students
|
Variables |
Cronbach’s Alpha |
Mean |
SD |
Skewness |
Kurtosis |
|
Planning |
0.770 |
21.72 |
3.82 |
-0.271 |
0.233 |
|
Focus of Control |
0.810 |
30.96 |
4.73 |
1.141 |
1.157 |
|
Self Confidence |
0.792 |
23.42 |
3.86 |
-0.231 |
0.772 |
|
Communication |
0.694 |
15.54 |
2.57 |
0.880 |
0.424 |
|
Motivation |
0.709 |
15.18 |
2.78 |
-0.559 |
0.596 |
|
Self-Discipline |
0.726 |
11.14 |
2.31 |
-0.306 |
-0.031 |
|
Individual Entrepreneurship Perception Scale Total Score |
0.937 |
117.95 |
16.85 |
-0.406 |
0.899 |
|
Hope |
0.739 |
3.01 |
2.09 |
0.292 |
-0.991 |
|
Loss of Motivation |
0.766 |
3.76 |
2.33 |
0.295 |
-0.971 |
|
Future Expectations |
0.750 |
2.28 |
1.71 |
0.157 |
-1.273 |
|
Beck Hopelessness Scale Total Score |
0.885 |
9.06 |
5.36 |
0.232 |
-0.981 |
Table 2. Average scores of the participants from the Individual Entrepreneurship Perception Scale and Beck Hopelessness Scale
The data above show the mean scores of the participants obtained from the Individual Perception of Entrepreneurship Scale and Beck Hopelessness Scale used for the research. Despite the difficulties brought on by the pandemic and other negative experiences, students within the health sciences field scored high in individual entrepreneurship perception (Mean: 117.95±16.84 Min:44-Max:155). The study also found that the student’s level of hopelessness was moderate (Mean: 9.06±5.36 Min:0-Max:20) (Table 2).
|
Variables |
B |
SE |
β |
t |
p |
VIF |
|
(Constant) |
131.996 |
1.113 |
|
118.644 |
<.001 |
|
|
1. Hope |
-19.278 |
2.611 |
-.342 |
-7.383 |
<.001 |
1.974 |
|
2. Loss of Motivation |
-6.568 |
2.659 |
-.114 |
-2.470 |
.014 |
1.949 |
|
3. Future Expectations |
-5.830 |
2.589 |
-.119 |
-2.252 |
.025 |
2.547 |
|
R =0.513 R² =0.263 F =80.449 p<0.001 Durbin Watson=1.895 |
|
|||||
Table 3. Multiple Linear Regression Analysis results on hopelessness levels and its effect on individual entrepreneurship perception
*Criterion: Perception of Individual Entrepreneurship
In Table 3, the regression model proved significant and reliable (F=80.449; p<0.001), with the hopelessness levels and sub-dimensions of the participants accounting for 26.3% of the total variance in individual entrepreneurship perception. The study found that the participants’ hopelessness perceptions about the sub-dimensions of hope (t=-7.383; p<0.001), loss of motivation (t=-2.470; p=0.014), and expectations for the future (t=-2.252; p=0.025) had a statistically significant impact on their individual entrepreneurship perceptions. As participants’ levels of hopelessness increased, their individual entrepreneurship perceptions decreased. Based on the standardised regression coefficient (β), the predictor variables’ relative order of importance on individual entrepreneurship perception is hope (β=-0.342), expectations about the future (β=-0.119), and loss of motivation (β=-0.114) shown in Table 3.
IV. DISCUSSION
The results obtained from this study; health sciences students have a positive outlook on individual entrepreneurship despite the challenges created by the adverse conditions due to the pandemic. Studies conducted among health sciences students in Türkiye before the pandemic revealed that students’ perceptions of individual entrepreneurship were at a moderate level (Baltacı & Baydin, 2023; Göktekin et al., 2022). According to these results, it can be said that the pandemic process increased the awareness of individual entrepreneurship in students studying in the field of health sciences. This is a phenomenon that should be considered in discussions about current market trends and potential business opportunities.
In addition, this research revealed that students had moderate levels of hopelessness during the pandemic period. Although this result is slightly higher than the findings of a previous study conducted with associate degree students in Türkiye during the pandemic (Okur & Şentürk, 2022); similar results were obtained in studies conducted with undergraduate students of the faculty of health sciences in the international literature (Pretorius, 2021).
Finally, regression analysis findings showed that participants’ hopelessness levels and their sub-dimensions collectively explained 26.3% of the total variance in their individual entrepreneurship perceptions. This result suggests that hopelessness significantly affects students’ perceptions of entrepreneurship. Similarly, a study conducted with Chinese university students supports these findings by showing that the COVID-19 pandemic had a significant and negative impact on students’ entrepreneurial intentions and behaviors (Wang et al., 2023). However, this regression analysis result also implies that hopelessness caused by negative emotions during the pandemic cannot alone determine students’ perceptions of individual entrepreneurship. Other factors that may affect the individual entrepreneurship perceptions of students studying in the field of health sciences in similar health crises such as the COVID-19 pandemic should also be investigated.
Although it is stated that the pandemic period is full of opportunities for health entrepreneurship, it should be taken into consideration that entrepreneurial intention/perception is affected by many environmental factors. The related literature points out that ‘hope’ is a critical source of motivation for individuals who want to become entrepreneurs (Gódány et al., 2021). However, studies conducted during the pandemic period revealed that students perceived a high level of individual entrepreneurship risk (Krichen & Chaabouni, 2022). On the other hand, studies show that fear and anxiety caused by the COVID-19 pandemic negatively affect students’ perceptions of entrepreneurship (Loan et al., 2021). In particular, health sciences students are reported to experience higher levels of anxiety compared to other students studying in non-health fields, which leads to hopelessness and changes in career plans (Alnıaçık et al., 2021). Therefore, the results of this study are supported by the findings of previous studies.
V. CONCLUSION
Our research has shown that students who are trained to provide health services during periods of extraordinary health crises such as pandemics may experience hopelessness about their professional future and that students’ perceptions of individual entrepreneurship are negatively affected by this situation. The content and purpose of the university education received play a critical role in the development of students’ individual entrepreneurship perceptions.
Therefore, entrepreneurship courses should be carefully integrated into the curricula of all students studying in the field of health sciences, students should be motivated to take the course and encouraged to become entrepreneurs. In addition, interviews, company visits, and project studies with successful health entrepreneurs during similar crisis periods can increase students’ interest in health entrepreneurship and reduce their level of hopelessness. For a more comprehensive understanding of the relationships examined in the study, the inclusion of qualitative research methods in future studies may increase the depth of the analysis.
Notes on Contributors
MS, reviewed the literature, designed the research, analyzed data, co-wrote the manuscript, critically reviewed and edited the manuscript, and then read it through before final approval.
AKT, co-wrote the manuscript, and critically reviewed and edited the manuscript.
ŞÖ, prepared the manuscript for publication, critically reviewed, and edited the manuscript.
Ethical Approval
This study was conducted according to the ethical standards of the 1964 Declaration of Helsinki. Approval was obtained from Kırıkkale University Faculty of Health Sciences (Date: 30.03.2022; Number: E.88159) and Kırıkkale University Non-Interventional Research Ethics Committee (Date: 07.04.2022, Decision No: 2022.04.13).
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgment
All authors would like to thank all participants.
Funding
No financial support was received from any institution or organisation in the conduct and publication of this research.
Declaration of Interest
There is no conflict of interest between the authors.
References
Alnıaçık, E., Of, M., Balkaş, J., Tülemez, S., Mirzayev, M., & Alfarra, H. (2021). The effects of university students’ psychological resilience and hopelessness on their perception of career future during the pandemic process. Business & Management Studies: An International Journal, 9(1), 248-266. https://doi.org/10.15295/bmij.v9i1.1757
Bagheri, A. (2018). University students’ entrepreneurial intentions: Does education make a difference? In N. Faghih, & M. Zali (Eds.), Entrepreneurship education and research in the Middle East and North Africa (MENA) perspectives on trends, policy and educational environment: Contributions to management science (pp. 131-154). Springer. https://doi.org/10.1007/978-3-319-90394-1_8
Baltacı, N., & Baydin, N. Ü. (2023). Analysis of individual innovativeness, entrepreneurship, curiosity, and exploration characteristics of nursing students. Journal of Inönü University Vocational School of Health Services, 11(2), 1440-1454. https://doi.org/10.33715/inonusaglik.1164998
Beck, A. T., Weissman, A., Lester, D., & Trexler, L. (1974). The measurement of pessimism: The hopelessness scale. Journal of Consulting and Clinical Psychology, 42(6), 861-865. https://doi.org/10.1037/h0037562
Boore, J., & Porter, S. (2011). Education for entrepreneurship in nursing. Nurse Education Today, 31(2), 184-191. https://doi.org/10.1016/j.nedt.2010.05.016
Duplaga, M., & Grysztar, M. (2021). The association between future anxiety, health literacy and the perception of the COVID-19 pandemic: A cross-sectional study. Healthcare, 9(1), 1–18. https://doi.org/10.3390/healthcare9010043
Durak, A., & Palabıyıkoğlu, R. (1994). Beck hopelessness scale validity study. Crisis Journal, 2(2), 311-319. https://doi.org/10.1501/Kriz_0000000071
Fashami, F. M., Nili, M., Farahani, A. V., Shaikh, N., Dwibedi, N., & Madhavan, S. S. (2021). Determining the entrepreneurial and intrapreneurial intentions of student pharmacists in Iran. American Journal of Pharmaceutical Education, 85(2), 113-122. https://doi.org/10.5688/ajpe8080
Gódány, Z., Machová, R., Mura, L., & Zsigmond, T. (2021). Entrepreneurship motivation in the 21st century in terms of pull and push factors. TEM Journal-Technology Education Management Informatics, 10(1), 334-342.https://doi.org/10.18421/TEM101-42
Göktekin, Z., Aslan, R., & Yildiz, E. (2022). Determination of the entrepreneurship levels of the students of the faculty of health sciences and the factors affecting these levels. Ahi Evran University Journal of Institute of Social Sciences, 8(2), 379-392. https://doi.org/10.31592/aeusbed.907637
Hajinasab, N., Amiri, M., Sharifi, M., Sanati, T., Dolatabadi, Z., & Amiri-Farahani, L. (2022). The relationship between social support and hopelessness among Iranian students during Coronavirus disease 2019 (COVID-19) pandemic. The Open Public Health Journal, 15(1), 1-9. https://doi.org/10.2174/18749445-v15-e2209290
Hart, P. F., & Rodgers, W. (2023). Competition, competitiveness, and competitive advantage in higher education institutions: A systematic literature review. Studies in Higher Education, 1–25. https://doi.org/10.1080/03075079.2023.2293926
Incik, E. Y., & Uzun, N. B. (2017). Validity and reliability study of individual entrepreneurship perception scale. Mustafa Kemal University Journal of Institute of Social Sciences, 14(39), 471-485. https://dergipark.org.tr/tr/pub/mkusbed/issue/31632/331276
Kaplan Serin, E., & Doğan, R. (2023). The relationship between anxiety and hopelessness levels among nursing students during the COVID-19 pandemic and related factors. OMEGA-J Death Dying, 87(3), 793-813. https://doi.org/10.1177/00302228211029144
Krichen, K., & Chaabouni, H. (2022). Entrepreneurial intention of academic students in the time of COVID-19 pandemic. Journal of Small Business and Enterprise Development, 29(1), 106-126. https://doi.org/10.1108/JSBED-03-2021-0110
Liao, Y. K., Nguyen, V. H. A., Chi, H. K., & Nguyen, H. H. (2022). Unraveling the direct and indirect effects of entrepreneurial education and mindset on entrepreneurial intention: The moderating role of entrepreneurial passion. Global Business and Organizational Excellence, 41(3), 23-40. https://doi.org/10.1002/joe.22151
Loan, L. T., Doanh, D. C., Thang, H. N., Nga, N. T. V., Van, P. T., & Hoa, P. T. (2021). Entrepreneurial behaviour: The effects of the fear and anxiety of COVID-19 and business opportunity recognition. Entrepreneurial Business and Economics Review, 9(3), 7-23. https://doi.org/10.15678/EBER.2021.090301
Marahwa, P., Makota, P., Chikomo, D. T., Chakanyuka, T., Ruvai, T., Osafo, K. S., Huang, T., & Chen, L. (2022). The psychological impact of COVID-19 on university students in China and Africa. PLoS ONE, 17(8), Article e0270824. https://doi.org/10.1371/journal.pone.0270824
Mohamed, M. E., Elshaer, I. A., Azazz, A. M., & Younis, N. S. (2023). Born not made: The impact of six entrepreneurial personality dimensions on entrepreneurial intention: Evidence from healthcare higher education students. Sustainability, 15(3), 2266-2278. https://doi.org/10.3390/su15032266
Okur, E., & Şentürk, A. Y. (2022). Coronavirus anxiety in vocational school students studying in the field of health in the coronavirus pandemic period. Journal of Adnan Menderes University Faculty of Health Sciences, 9(3), 499-512. https://doi.org/10.46237/amusbfd.978275
Pretorius, T. L. (2021). Depression among health care students in the time of COVID-19: The mediating role of resilience in the hopelessness–depression relationship. South African Journal of Psychology, 51(2), 269-278. https://doi.org/10.1177/0081246321994452
Sampene, A. K., Li, C., Khan, A., Agyeman, F. O., & Opoku, R. K. (2023). Yes! I want to be an entrepreneur: A study on university students’ entrepreneurship intentions through the theory of planned behavior. Current Psychology, 42(25), 21578-21596. https://doi.org/10.1007/s12144-022-03161-4
Saygılı, M., Kandemir Türe, A., & Özkan, Ş. (2022). The effect of hopelessness on individual entrepreneurship perception in health science students. Research Square. https://doi.org/10.21203/rs.3.rs-2381250/v1
Schiavone, F., Tutore, I., & Cucari, N. (2020). How digital user innovators become entrepreneurs: A sociomaterial analysis. Technology Analysis & Strategic Management, 32(6), 683-696. https://doi.org/10.1080/09537325.2019.1696955
Suryavanshi, T., Lambert, S., Lal, S., Chin, A., & Chan, T. M. (2020). Entrepreneurship and innovation in health sciences education: A scoping review. Medical Science Educator, 30, 1797-1809. https://doi.org/10.1007/s40670-020-01050-8
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Pearson Education.
Taneja, M., Kiran, R., & Bose, S. C. (2024). Assessing entrepreneurial intentions through experiential learning, entrepreneurial self-efficacy, and entrepreneurial attitude. Studies in Higher Education, 49(1), 98-118. https://doi.org/10.1080/03075079.2023.2223219
Tao, Y., Niu, H., Hou, W., Zhang, L., & Ying, R. (2023). Hopelessness during and after the COVID‐19 pandemic lockdown among Chinese college students: A longitudinal network analysis. Journal of Clinical Psychology, 79(3), 748-761. https://doi.org/10.1002/jclp.23439
Wang, J., Xu, M., Li, X., & Ni, Y. (2023). A latent class analysis of hopelessness in relation to depression and trauma during the COVID-19 pandemic in China. Journal of Affective Disorders, 329, 81-87. https://doi.org/10.1016/j.jad.2023.02.077
Zhang, Y., Bao, X., Yan, J., Miao, H., & Guo, C. (2021). Anxiety and depression in Chinese students during the COVID-19 pandemic: A meta-analysis. Frontiers in Public Health, 9, Article 697642. https://doi.org/10.3389/fpubh.2021.697642
*Meltem Saygılı
Department of Health Management,
Prof. Dr. Fuat Sezgin Health Campus
Faculty of Health Sciences
Kırıkkale University
71450 Merkez/Kırıkkale, Türkiye
+90 318 3423738/7732
Email: meltemsaygili@kku.edu.tr
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
