
Post-COVID innovation in postgraduate medical education: Insights from five countries
Submitted: 8 August 2025
Accepted: 18 November 2025
Published online: 7 April, TAPS 2026, 11(2), 4-8
https://doi.org/10.29060/TAPS.2026-11-2/GP3842
Dujeepa D. Samarasekera1, Chung-Hsien Chaou2, Ardi Findyartini3, Jamuna Vadivelu4, Malcolm Mahadevan5, Yang Faridah Abdul Aziz6, Faith Chia7, Yeo Su Ping1 & Lee Shuh Shing1
1Centre for Medical Education (CenMED), Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Department of Emergency Medicine & Medical Education Research Center, Chang Gung Memorial Hospital, Linkou Branch, Taiwan; 3Department of Medical Education, Faculty of Medicine, University of Indonesia, Indonesia; 4Medical Education and Research Development Unit (MERDU), Faculty of Medicine, University of Malaya, Malaysia; 5Department of Emergency Medicine, National University Hospital, National University Health System (NUHS), Singapore; 6Department of Biomedical Imaging & Medical Education and Research Unit, Faculty of Medicine, University of Malaya, Malaysia; 7Department of Rheumatology, Allergy and Immunology, Tan Tock Seng Hospital, Singapore
Abstract
Introduction: The COVID-19 pandemic significantly impacted postgraduate medical education (PGME). This led to rapid adaptations to ensure training continuity and to develop competent healthcare professionals.
Methods: This descriptive study focusses on the sustainable innovations made in Indonesia, Malaysia, Singapore, Taiwan and the USA PGME residency training. Draft country sections were written by co-authors with direct, current knowledge of postgraduate training in those settings.
Results: Key lessons emerged from curricular adjustments, digital transformation, operational agility, assessments, and faculty development. Curriculum changes included integrating pandemic-specific content, such as COVID-19 management and public health priorities, into training programs. Singapore’s rapid revision efforts and Indonesia’s compulsory topic introduction are typical examples. Despite movement restrictions and constraints on clinical training, innovative solutions like simulations and telemedicine preserved skill development. Digital transformation played a crucial role, with countries adopting virtual platforms and hybrid simulation models. Technology-driven innovations like augmented reality and teleconsultation expanded training scopes. However, challenges like engagement, transitioning faculty to remote learning systems and unstable internet connectivity remained challenges. Operational agility was demonstrated through cross-institutional collaborations. Assessment formats evolved, with hybrid models and virtual logbooks introduced to maintain educational standards. Accreditation processes were adapted, with flexibility granted in assessment delivery while ensuring quality. Faculty development was accelerated with Singapore leveraging international trends to ensure resilience in local training programs.
Conclusion: The pandemic instigated a paradigm shift from reactive adaptation to proactive transformation in PGME, positioning systems as global exemplars of how medical education can evolve amidst complexity and incorporate necessary changes envisioning long-term strengthening of the systems.
Practice Highlights
PGME adaptation during COVID-19 pandemic and transformation post pandemic is supported by:
- Implementation of operational agility by placing residents in diverse environments and fostering national collaborations to sustain training.
- Integration of simulations and telemedicine to maintain skill development amid constraints during crisis situations.
- Development of teleconsultation and hybrid learning models to enhance inclusivity, accessibility, and resilience in medical education.
- Adoption of flexible models to accredit and sustain quality of training and accreditation of programmes.
- Evolvement of assessment and accreditation with hybrid models and virtual tools to preserve educational standards and flexibility.
I. INTRODUCTION
The COVID-19 pandemic has profoundly impacted postgraduate medical education (PGME) worldwide. The challenges and opportunities have led to significant transformations in how medical training is delivered (Sklar, 2020). This manuscript examines the experiences and adaptations to PGME in Singapore, Indonesia, Malaysia, Taiwan, and the USA. Draft country sections were written by co-authors with direct, contemporary knowledge of postgraduate training in each setting (authors are listed under Notes on Contributors). We used a shared template (curriculum changes; clinical exposure; digital transformation; assessments; faculty development; operational agility) to ensure comparability. Country drafts were iteratively edited centrally to harmonise scope and remove duplication. This manuscript is a descriptive synthesis of these country reports and the peer-reviewed literature cited.
A. Curricular Adjustments and Clinical Exposure
The onset of COVID-19 served as a catalyst for revising PGME curricula across the globe. In Singapore, the curriculum was quickly adjusted to include COVID-19 management and public health priorities. The curriculum in internal medicine and infectious diseases was updated to cover outbreak containment, infection prevention, and control. Emergency medicine and surgical specialties underwent targeted curricular revisions to embed pandemic-specific protocols and essential skills (Oon et al, 2023).
In Indonesia, while the curriculum remained largely unchanged, COVID-19 management became a compulsory knowledge area, with online courses and skills training introduced to equip residents for frontline duties. Residents gained competencies in global health problem management, highlighting the need for an integrated curriculum approach.
Malaysia adopted remote learning platforms for curricular delivery, introducing virtual ward rounds and telemedicine consultations. Training e-portfolios were developed to record and review trainee progress systematically. This shift presented new training opportunities, allowing engagement in telehealth and familiarisation with hospital delivery systems.
Taiwan leveraged its experience from previous outbreaks to make pandemic-related curricular adjustments, including telemedicine. Their curriculum stability stemmed from existing frameworks that allowed swift incorporation of new competencies such as video-assisted intubations.
In the USA, tele-supervision and tele-health were integrated into curricula, accommodating training disruptions with an emphasis on tele-consultation skills. The ACGME’s flexibility enabled programs to maintain educational continuity despite the challenges.
Clinical exposure faced challenges due to movement restrictions and infection control measures. In Singapore, inter-hospital rotations were halted. This limited the breadth of exposure but ensured procedural training through simulations and telemedicine. Indonesia encountered similar constraints. In addition to this, residents were developed as frontline healthcare workers combating the pandemic in the healthcare system. These circumstances led to urgent and creative adaptations in teaching and supervision formats to support skill acquisition. Cognitive components were taught online, while skill development was conducted in person in various possible and safe forms. These online learning methods have been further developed and integrated into current residency training programmes (Balakrishnan et al., 2020).
B. Digital Transformation in Teaching
The pandemic catalysed a rapid digital transformation in PGME, redefining teaching methodologies across countries. Singapore quickly transitioned to virtual platforms for didactic sessions, ensuring continuity and increasing accessibility. Simulation-based learning adapted to hybrid models, preserving educational value while meeting safety requirements. Emerging technologies like augmented reality have redefined surgical training, providing scalable educational models (Balakrishnan et al., 2020) (Renaud et al., 2021).
Indonesia embraced online learning, integrating video learning and flipped classrooms for cognitive acquisitions. However, engagement challenges persisted due to unstable internet connections and multitasking of both the consultants and residents during online sessions. Practical skill development continued in clinical settings with enhanced simulations and adapted supervision system.
Malaysia’s teaching innovations partially replaced face-to-face interactions with a hybrid approach, enhancing attendance monitoring and assessment efficiency. However, the “hidden curriculum” often delivered through personal interactions was less effectively communicated online (Yusoff et al., 2020).
Taiwan’s use of virtual simulations and online OSCEs (Objective Structured Clinical Examinations) allowed for skill development in an online environment. Challenges included financial limitations and resistance to change. Although most faculty members and students have become accustomed to online courses and virtual meetings in the post-pandemic era, face-to-face interaction still offers irreplaceable benefits, particularly in communication, engagement, and collaborative learning.
During the COVID-19 pandemic, postgraduate programmes across the USA reported a rapid expansion of both remote didactic sessions and tele-health patient encounters, though adoption varied widely across specialties. Psychiatry, internal medicine and paediatrics shifted substantial portions of clinical care and teaching online, whereas procedure-intensive fields such as surgery and obstetrics transitioned more selectively. Programme evaluations highlight that learning outcomes were most positive when virtual teaching incorporated interactive case discussions, small-group sessions, and real-time feedback rather than passive online lectures. Concurrently, the ACGME issued time-limited flexibilities on supervision and clinical learning environments, endorsing tele-supervision in appropriate contexts while safeguarding procedural competency standards. These experiences have accelerated national discussions on how tele-education and tele-supervision can be safely integrated into residency training. The ACGME’s ongoing review of its Common Program Requirements aims to include evidence-informed guidance on remote education, supervision, and competency assessment. Going forward, US training programmes are encouraged to document the impact of these modalities on trainee performance, patient outcomes, and wellbeing to inform sustainable, equitable models of postgraduate medical education.
C. Operational Agility and Workforce Planning
The pandemic presented unprecedented challenges for PGME operational management, requiring adaptive strategies to sustain training and healthcare delivery. Singapore implemented a “fostering” approach, integrating residents into alternative hospital environments to maintain clinical exposure. This model enriched training and spurred national coordination of residency programs, fostering cross-institutional collaborations. This is now ongoing and residents from different sponsoring Institutions (SI) have the opportunity to train and use learning resources from another Sis (Renaud et al., 2021).
Indonesia and Malaysia adapted their operational frameworks for remote learning, employing proctoring systems and modifying assessment methods. While these adaptations ensured quality, challenges remained in creating learning resources and encouraging faculty transition to online formats.
Taiwan maintained operational stability by leveraging past outbreak management experiences, while the USA’s ACGME allowed temporary emergency statuses for flexibility in training requirements.
D. Assessment and Accreditation
Assessment and accreditation processes were restructured to accommodate pandemic constraints while maintaining educational integrity. In Singapore, summative assessments shifted to hybrid formats, preserving fairness and rigour. Virtual logbooks and electronic portfolios were introduced, enriching formative assessment ecosystems.
Indonesia’s accreditation processes were simplified, conducting online exams with real-time monitoring. Malaysia faced accreditation delays due to SOP adjustments for virtual formats but integrated online assessments into credentialing processes.
Taiwan’s credentialing remained stable, with minor shifts toward competency-based medical education. Relevant assessment tools, such as milestones and Entrustable Professional Activities (EPAs), have been widely adopted across various specialty training programs nationwide. The USA maintained accreditation standards, adapting supervision practices and reporting on pandemic impacts in PGME activities.
E. Educational Innovations
The pandemic drove enduring innovations in PGME, including teleconsultation and hybrid learning models. The observed differences map to four system-level features. First, health system structure focusing on centralised systems (e.g., Singapore’s national clusters) were able to coordinate cross-institutional resources faster than highly fragmented systems. Second, resource availability determined technological sophistication (high in Singapore/US, constrained in parts of Indonesia/Malaysia). Third, accreditation flexibility and governance (e.g., ACGME guidance vs local regulator timelines) influenced how quickly assessments could be adapted. Finally, learning culture and prior outbreak experience (Taiwan’s SARS legacy) shaped faculty and trainee readiness to adopt remote modalities. Recognising these drivers helps tailor recommendations: resource-intensive tech works where funding and digital literacy permit, whereas low-cost simulation and task-sharing strategies are more applicable in lower-resource settings.
F. Faculty Development and Pedagogical Shifts
The global transformation in faculty development was accelerated by the pandemic, compelling educators to rethink teaching, assessment, and mentorship delivery. Singapore harnessed international innovations to enhance local faculty development, adopting flipped classroom models and microlearning inspired by global trends.
Participation in international faculty development programs enriched local practices, building faculty champions who guided reforms and shared Singapore’s innovations on global platforms. The USA encouraged programs to document faculty adaptation, recognising resilience as crucial to PGME sustainability.
By observing and adapting international best practices, local institutions weathered the pandemic’s educational storm and emerged with a more agile, inclusive, and scholarly approach to faculty development.
G. Postgraduate Medical Education in the Post-Covid Era
The COVID-19 pandemic disrupted traditional models of postgraduate medical education, prompting rapid shifts towards digital learning. Initially driven by necessity, these changes have since evolved into permanent components of contemporary curricula, reflecting the adaptability of residents, faculty, and institutions.
During the pandemic, clinical exposure was significantly curtailed, and the informal curriculum typically acquired through in-person interactions and experiential learning was diluted. In response, digital simulations, telemedicine, and virtual case-based discussions were introduced to bridge the gap. While these tools could not fully replicate the complexity of real patient care, they laid the groundwork for blended learning models that are now being refined and embedded into routine training.
Faculty development became a priority, with short, focused programmes in digital pedagogy helping educators gain confidence and competence in online teaching. Peer support networks and institutional incentives have further encouraged sustained engagement. These efforts have led to more inclusive and flexible teaching approaches, better suited to diverse learner needs.
Assessment practices also underwent transformation. Hybrid models combining online and in-person evaluations were trialled and are now being formalised, offering greater adaptability while maintaining rigour. Cross-institutional collaborations, initially formed to share resources during the crisis, have matured into structured partnerships that enhance access and quality across programmes.
Today, interactive digital platforms, gamification, and real-time feedback mechanisms are routinely used to foster engagement and recreate aspects of the informal curriculum. Augmented reality and high-fidelity simulations are increasingly integrated into clinical skills training, complementing supervised patient encounters. These innovations are not temporary fixes but strategic enhancements to educational delivery.
Equity remains a central concern. Institutions are investing in infrastructure and inclusive teaching strategies to ensure all trainees regardless of background can participate fully and benefit equally. The pandemic revealed gaps, but it also accelerated progress towards more resilient, responsive, and equitable systems.
Postgraduate medical education has not simply recovered it has reoriented. The adaptations made under pressure have become embedded practices, shaping a future that is more flexible, collaborative, and inclusive.
II. CONCLUSION
The COVID-19 pandemic influenced and accelerated innovations both necessary and lasting transformations in postgraduate medical education. Our cross-country comparison shows that the nature and scale of innovations were shaped by health-system structure, resource/digital readiness, accreditation flexibility and learning culture. Future resilience will depend on tailoring strategies to these systemic features investing in scalable, equity-minded digital solutions where resources permit, and prioritising low-cost, high-impact simulation and regional collaborations in lower-resourced settings.
Notes on Contributors
Yang Faridah Abdul Aziz, Chung-Hsien Chaou, Faith Chia, Ardi Findyartini, Malcolm Mahadevan Jamuna Vadivelu drafted the respective portion for their countries and subsequently, the manuscript was combined and edited by Dujeepa Samarasekera, Lee Shuh Shing and Yeo Su Ping. All the authors read the final version and provided their suggestions and/or approvals.
Acknowledgement
We would like to thank Prof Timothy Brigham and Prof Lynne Kirk for their perspectives on the initiatives rolled out in the United States of America during the pandemic.
Funding
There is no funding for this study.
Declaration of Interest
The authors declare no conflict of interest.
References
Ashokka, B., Ong, S. Y., Tay, K. H., Loh, N. H. W., Gee, C. F., & Samarasekera, D. D. (2020). Coordinated responses of academic medical centres to pandemics: Sustaining medical education during COVID-19. Medical Teacher, 42(7), 762-771. https://doi.org/10.1080/0142159X.2020.1757634
Oon, J. E. L., Mok, S. F., Samarasekera, D. D., & Teunissen, P. (2023). Training infectious diseases senior residents during COVID-19: The impact and the lessons learnt. Medical Teacher, 45(9), 1005-1011. https://doi.org/10.1080/0142159X.2023.2168182
Renaud, C. J., Chen, Z. X., Yuen, H. W., Tan, L. L., Te Pan, T. L., & Samarasekera, D. D. (2021). Impact of COVID-19 on health profession education in Singapore: Adoption of innovative strategies and contingencies across the educational continuum. The Asia Pacific Scholar, 6(3), 14-23. https://doi.org/10.29060/TAPS.2021-6-3/RA2346
Sklar, D. P. (2020). COVID-19: Lessons from the disaster that can improve health professions education. Academic Medicine, 95(11), 1631-1633. https://doi.org/10.1097/ACM.0000000000003547
Yusoff, M. S. B., Hadie, S. N. H., Mohamad, I., Draman, N., Al-Aarifin, I. M., Rahman, W. F. W. A., … & Yaacob, N. A. (2020). Sustainable medical teaching and learning during the COVID-19 pandemic: Surviving the new normal. The Malaysian Journal of Medical Sciences: MJMS, 27(3), 137-142. https://doi.org/10.21315/mjms2020.27.3.14
*Dujeepa D. Samarasekera
Yong Loo Lin School of Medicine,
National University of Singapore, Singapore
10 Medical Drive, Singapore 117597
Email: dujeepa@nus.edu.sg
Submitted: 23 September 2025
Accepted: 20 November 2025
Published online: 7 April, TAPS 2026, 11(2), 127-128
https://doi.org/10.29060/TAPS.2026-11-2/LE3891
Nghia Phu Nguyen1,2 & Phillip Tran1,3
1College of Health Sciences, Nam Can Tho University, Vietnam; 2Cardiovascular Research Laboratories, Methodist Hospital, Merrillville, Indiana, United States of America; 3Yavapai Regional Medical Centre, Prescott, Arizona, United States of America
Dear Editor,
The recent article by Kreepala et al. provides valuable insights into factors influencing the duration of answering multiple-choice questions (MCQs) in medical examinations (Kreepala et al., 2025). The authors identified word count, question difficulty, language, visual aids, and exam environment as important determinants of test-taking time (Kreepala et al., 2025). These findings resonate strongly with our experiences from medical education in Vietnam, where English has increasingly become the medium of instruction.
In our setting, both Vietnamese and international medical students are non-native English speakers. While they possess adequate medical knowledge, the language of the examination itself often represents a substantial barrier. This is particularly evident in anatomy courses that integrate clinical applications and imaging, where examination items are frequently written as long case-based scenarios. Such stems in English, especially when containing complex syntax or uncommon terminology, consume disproportionate time for comprehension before reasoning can be applied. As a result, even well-prepared students may spend excessive time reading rather than problem solving, frequently resorting to guessing when exam time runs short. Such observations reinforce the conclusion of Kreepala et al. (2025) that language is a major determinant of MCQ duration.
The broader significance of this issue is supported by a recent systematic review synthesizing evidence from 49 studies with over 14,500 students worldwide (Hamad et al., 2025). The review demonstrated that using a foreign language as the primary medium of medical education impedes comprehension of textbooks, lectures, and assessments, leading to poorer outcomes, increased stress, and higher dropout rates (Hamad et al., 2025). It further noted that language barriers can hinder communication with patients in the native language, thereby compromising the quality of care (Hamad et al., 2025). These findings emphasize that language challenges affect not only examination performance but also long-term educational and professional competencies.
Given this evidence, exam designers and curriculum planners in non-native English contexts should carefully consider the linguistic load of MCQ assessments. Simplifying question wording, avoiding unnecessary complexity, and providing glossaries of key terms may help ensure that MCQs measure medical competence rather than English proficiency.
This study highlights an often overlooked aspect of assessment design. Further research in Vietnam and similar settings could compare student performance and timing across English and native-language versions of the same test to quantify this effect more precisely.
Notes on Contributors
Phu Nghia Nguyen conceptualised and drafted the letter, and approved the final version for submission.
Phillip Tran contributed to critical revision of the letter for clarity and intellectual content, and approved the final version for submission.
Funding
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Interest
The authors have no conflicts of interest to disclose.
References
Hamad, A. A., Mustaffa, D. B., Alnajjar, A. Z., Amro, R., Deameh, M. G., Amin, B., & Alkhawaldeh, I. M. (2025). Decolonizing medical education: A systematic review of educational language barriers in countries using foreign languages for instruction. BMC Medical Education, 25(1), 701. https://doi.org/10.1186/s12909-025-07251-2
Kreepala, C., Thongsombat, S., Wattanavaekin, K., Danjittrong, T., Keeratibharat, N., & Juntararuangtong, T. (2025). Understanding the factors affecting duration in answering MCQ examination: The students’ perspective. The Asia Pacific Scholar, 10(2), 57–64. https://doi.org/10.29060/TAPS.2025-10-2/OA3332
*Nghia Phu Nguyen, M. D.
College of Health Sciences,
Nam Can Tho University,
168 Nguyen Van Cu Street,
An Binh Ward, Can Tho City, Vietnam
Email: npnghia@nctu.edu.vn
Submitted: 3 October 2025
Accepted: 29 October 2025
Published online: 7 April, TAPS 2026, 11(2), 129-130
https://doi.org/10.29060/TAPS.2026-11-2/LE3898
Nghia Phu Nguyen
College of Health Sciences, Nam Can Tho University, Vietnam
Dear Editor,
The rapid emergence of large language models (LLMs) in medical education has transformed the process of generating multiple-choice questions (MCQs). Recent literature has comprehensively summarised the classical flaws in MCQ design, including weak distractors, convergence errors, incomplete stems, and the importance of systematic post-hoc item analysis (Steele et al., 2025). It has also highlighted that, even as generative AI becomes integrated into assessment design, expert review remains indispensable to ensure validity, reliability, and cognitive depth (Elzayyat et al., 2025).
As generative AI becomes integrated into the question-writing process, these flaws are emerging as factors that can compromise the quality and fairness of assessments. My review of AI-generated questions reveals several recurring problems that pose real risks to assessment quality. Weak distractors are common: they may be implausible, overly brief, include absolute terms that reduce discrimination, or contrast sharply with the correct option in length and detail, making the correct answer identifiable even without content knowledge. Word overlap or convergence, in which key terms from the stem are repeated in answer choices, often serves as another unintended cue. Another frequent flaw is the over-explained correct option, which goes beyond simple identification and provides additional functional characteristics that are absent in other distractors. Finally, bias in answer distribution has also been observed; for example, the correct answer appeared disproportionately less often in option A, which may create predictable patterns and encourage strategic guessing. Although computer-based assessments typically randomise question and option order, reducing the impact of such bias, it could still influence small-scale paper-based tests such as in-course assessments, where students may exploit positional patterns.
These problems are not minor. If they are ignored, they can reduce the fairness of exams, make test scores less meaningful, and allow poor-quality questions to become available. As AI-generated content becomes more common, educators need to be cautious and actively involved in checking its quality. Questions created by AI should always be carefully reviewed by humans before being used in any exam. Each item should be examined for the quality and plausibility of distractors, the balance of language, possible cues that reveal the answer, and the overall distribution of correct options. AI should be seen only as a tool to support question development, not as a replacement for human judgment. Careful and systematic review is essential if we want to maintain the quality, fairness, and credibility of assessments in the era of generative AI.
Notes on Contributors
Nghia Phu Nguyen conceptualised and drafted the letter, contributed to critical revision of the letter for clarity and intellectual content, and approved the final version for submission.
Funding
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Interest
The authors have no conflicts of interest to disclose.
References
Elzayyat, M., Mohammad, J. N., & Zaqout, S. (2025). Assessing LLM-generated vs. expert-created clinical anatomy MCQs: A student perception-based comparative study in medical education. Medical Education Online, 30(1), 2554678. https://doi.org/10.1080/10872981.2025.2554678
Steele, S., Nayak, N., Mohamed, Y., & Panigrahi, D. (2025). The generation and use of medical MCQs: A narrative review. Advances in Medical Education and Practice, 16, 1331-1340. https://doi.org/10.2147/AMEP.S513119
*Nghia Phu Nguyen, M. D.
College of Health Sciences,
Nam Can Tho University,
168 Nguyen Van Cu Street,
An Binh Ward, Can Tho City, Vietnam
Email: npnghia@nctu.edu.vn
Submitted: 29 November 2024
Accepted: 22 September 2025
Published online: 7 April, TAPS 2026, 11(2), 102-113
https://doi.org/10.29060/TAPS.2026-11-2/OA3754
Juveria Arjumand1, Syed Muhammad Azfar2, Syeda Rubaba Azim3 & Rania Alkhadragy1,4
1Centre of Medical Education, School of Medicine, University of Dundee, United Kingdom; 2Department of Orthopaedic Surgery, Liaqat College of Medicine and Dentistry, Pakistan; 3Department of Medical Education, Dow University of Health Sciences, Pakistan; 4Suez Canal University, Egypt
Abstract
Introduction: The necessity for evaluating the effectiveness of medical education departments (DME) arises from the rapid technological advancements, frequent updates in healthcare paradigms and increasing societal demands. Such evaluations are crucial to understand how DMEs influence the future healthcare workforce and the quality of healthcare delivery. This research aims to explore the functions, procedures, and potential areas for innovation and improvement within DMEs.
Methods: A qualitative study was conducted at Liaquat College of Medicine and Dentistry’s Department of Medical Education, involving two focus groups of seven faculty members each. Participants included both junior and senior faculty. One session was held in person and the online one via Zoom. This was followed by inductive reflexive Thematic analysis.
Results: The study identified several strengths within the Liaquat College of Medicine and Dentistry DME, including robust faculty development programmes and strong student support services. However, areas of concern were highlighted such as research infrastructure and interdisciplinary connections. While faculty members expressed their satisfaction with the provided academic support services, they have reported the need for improving available research resources and faculty development programmes.
Conclusion: The study underscores the significant role of DMEs in medical education and suggests fostering joint research projects, encouraging faculty development, and enhancing student support services. Implementing these recommendations is crucial for advancing medical education and maintaining high standards of excellence. Continuous examination and implementation of these suggestions will ensure that DMEs can adapt to and meet the challenges of an ever-evolving healthcare landscape.
Keywords: Medical Education Department, Qualitative Study, Action Research, Focus Group
Practice Highlights
- Establish regular interdisciplinary workshops to foster innovative solutions in Medical Education.
- Provide training on innovative teaching techniques with emphasis on Technology Enhanced Learning integration.
- Introduce financial and non-financial rewards to motivate faculty for exceptional contribution.
- Provide comprehensive research training and encourage faculty participation in research activities.
- Develop a systematic student feedback process to continuously enhance teaching strategies and support services.
I. INTRODUCTION
A. Importance and Roles of Department of Medical Education (DME)
Medical education is an interdisciplinary specialty essential for the efficient operation of medical school. The roles of the Medical Education department vary based on institutional principles (Al Sheikh et al., 2022). A primary function of medical education department is to equip teaching staff with the necessary skills for effective role performance (Varpio et al., 2014). This includes course design experience, teaching practices, student assessment expertise, and instructional material development (Yusoff et al., 2014). A comprehensive faculty development programme, with clear goals and dedication, helps nurturing confident and competent staff who can support students’ career progression (Steinert et al., 2005).
The DME should also engage medical teachers in medical education research (Davis et al., 2005) and stimulate intra-departmental research and innovation. This can lead to proposals for action research to improve the teaching and learning environment (Yusoff et al., 2014). Additionally, the DME should organise educational activities that facilitate students’ engagement (Yusoff et al., 2014). These activities should address both personal and professional development, with emphasis on self-directed learning. The latter supports students to maximise their potential and strengthen their commitment to the medical field (Yusoff et al., 2010).
B. Worldwide Impact of DMEs in Medical Colleges
Departments of Medical Education (DMEs) have become integral in medical institutions globally (Alsheikh et al., 2022). DME evolution is shifting from the need to establish one to an increased public expectation (Davis et al., 2005).
The scope of DME activities varies expanding to undergraduates, postgraduates and continuing medical education. However, still flexibility is the key when planning for staffing at DME (Davis et al., 2005).
A study in four African medical universities revealed that medical education departments significantly enhance faculty abilities and student learning, support innovative teaching strategies, and advocate for improved assessment techniques (Kiguli-Malwadde et al., 2015). At the University of Michigan Medical School, DME has increased faculty engagement in scholarly activities through the Medical Education Scholars Program, fostering educational leadership and collaboration among faculty. This network has strengthened interdepartmental collaborations and reinforced education as a crucial element of faculty professional identity (Gruppen, 2004).
C. Context in Pakistan
In Pakistan, medical education requires significant reforms due to outdated practices and resource limitations (Nasim, 2011). Siddiqui & Shaikh (2014) noted a disconnect between basic and clinical sciences, with students lacking early patient contact. Khan et al. (2020) highlighted the need for systemic changes to maintain educational quality. Establishing DMEs is crucial for managing medical education systems (Latif & Wajid, 2018). However, challenges include inadequate infrastructure, qualified personnel, and resistance from management (Latif & Wajid, 2018). The Pakistan Medical and Dental Counsil (PMDC) and Higher Education Commission (HEC) have failed to provide clear guidelines for DME roles and responsibilities, complicating their establishment. The PMDC mandated the establishment of DMEs for accreditation in 2008, but many institutions struggle due to unclear guidelines and lack of skilled educators (Ali & Shamim, 2014). DMEs must develop strategic plans and align tasks with institutional goals. Faculty development programmes should be targeted and resource-efficient (Ali & Shamim, 2014). There is a significant need for faculty training in various skills, including self-directed learning, educational leadership, and research (Anwar & Humayun, 2015). Despite advancements, medical education and research in Pakistan are hindered by low funding and inadequate publication practices (Ghaffar et al., 2013). Improved assessment procedures and centralised evaluation offices are necessary for enhancing educational standards (Ali & Shamim, 2014).
At Liaquat College of Medicine and Dentistry (LCMD), institution under study, the DME was established in 2011. It oversees undergraduate and postgraduate education, continuing professional development, and dental education. The department is responsible for curriculum planning, design, implementation, and monitoring. It also supports educational innovation through instructional techniques and student skill development. The DME collaborates in research programme evaluation and quality assurance of assessments, aligning with local, regional, and international medical councils and accreditation bodies (LCMD, 2023). To enhance the department’s practices, an action research project was conducted to explore faculty perspectives on the DME’s role. Action research involves a cyclical process of collaboration for improving traditional procedures and is effective for identifying issues and generating workable solutions (Meyer, 2000). This study focuses on faculty expectations from the DME at LCMD and their suggestions for future endeavors.
Successful change involves consulting stakeholders to elucidate the need for improvement, considering their input in planning, and involving them as team members with full ownership (Lindberg, 1998). Understanding faculty perceptions is crucial for sustainable change, helping align faculty expectations with the department’s scope and filling any gaps (Khalid, 2013).
D. Need for Change
There is a practical-knowledge gap in the literature regarding the effectiveness of DMEs. While many studies focus on theoretical aspects and expected roles, there is a need for practical investigations into current practices (Al Shawwa, 2012; AlSheikh et al., 2022; Al-Wardy, 2008; Batool et al., 2018; Davis et al., 2005; Gruppen, 2008; Khalid, 2013; Kiguli-Malwadde et al., 2015). This study aims to address this gap by evaluating existing practices and identifying areas for improvement.
E. Research Questions
The study will address the following research questions:
- What is the faculty’s perception of the roles of the medical education department?
- What are the positive and negative experiences of working with a medical education department?
- How should the medical education department function in the future?
II. METHODS
This study adopts a qualitative approach which aligns with the study’s aim at addressing and improving current practices in the Department of Medical Education (DME). The latter requires a comprehensive understanding of the research context and culture to tailor recommendations effectively. Participatory epistemology was adopted emphasising that knowledge is co-constructed through cooperation rather than imparted by researchers (Torre, 2009). This approach values participants’ lived experiences and insights, aiming to produce context-specific and practical knowledge to address real-world issues. This collaborative method, particularly relevant in medical education, involves continuous interaction between researchers, academics, students, and administrators, fostering an environment where knowledge evolves through ongoing dialogue and mutual learning (Peralta, 2017).
The study employs an action research approach, which involves the researcher in a structured process of planning, implementing, and reflecting on actions to bring about positive changes in a specific context (Meyer, 2000). Action research is well-suited for exploring and improving practices within the DME, as it emphasises collaboration, reflection, and iterative cycles to understand and enhance real-world practices (Soh et al., 2011). This methodology is increasingly used in health and education settings due to its applicability, stakeholder involvement, and focus on continuous development.
Action research in this study involves two main stages. Stage 1 consists of focus group discussions with faculty members to gather their opinions and recommendations for improvement. Focus groups facilitate the exchange and development of ideas among participants, generating diverse viewpoints essential for the study’s goals (Cleary et al., 2014). Stage 2 involves collecting and analysing the potential solutions identified in the focus groups for feasibility, with recommendations shared with stakeholders for review and further action.
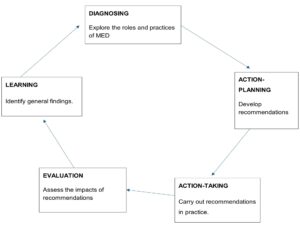
Figure 1. Five stages of action research (Everd, 1978)
A voluntary sampling technique was used to recruit participants. All faculty members were informed about the study’s objectives and invited to participate via email, resulting in 14 respondents. These participants were divided into two focus groups. Each focus group (n=7) included a mix of male and female participants with varying teaching experiences, ensuring a balanced representation of perspectives.
The first discussion took place in person, while the second was conducted online via Zoom. Each session lasted between 60 and 80 minutes, allowing for thorough exploration of the topics without causing participant fatigue (Tang et al., 1995). The discussions were guided by a set of open-ended questions designed to elicit detailed responses regarding the roles, practices, and improvement suggestions for the DME.
Transcripts of the discussions were analysed using thematic analysis (TA), using Braun & Clarke (2012). TA’s flexibility and accessibility make it suitable for novice researchers and for studies aiming to generate reports based on participants’ perceptions and viewpoints. The analysis followed Braun and Clarke’s (2006) six-phase framework, involving familiarisation with the data, generating initial codes, theme development, refining themes, defining themes and producing the report. This approach ensured a systematic and thorough examination of the data, leading to a comprehensive understanding of the issues and potential solutions within the DME.
A. Researcher Position and Ethical Considerations
Ethical approval was obtained from both Liaquat College of Medicine and Dentistry with the reference number IRB/M-000037/22 and the University of Dundee with reference number SMED REC 22/64. Participants were provided with an information sheet and consent form, ensuring informed consent, confidentiality, and anonymity (Illing, 2013). Data was securely stored, and pseudonyms were used to protect participants’ identities.
III. RESULTS
Two focus groups were conducted including 14 participants, 7 in each discussion. Thereafter transcripts were analysed using thematic analysis. Codes lead to themes, then further refinement was done, until finally reduced to 4 themes and 14 subthemes.

Figure 2. Mind map of themes and sub-themes
When presenting participants’ quotes “p5FG1” refers to participant number 5 in first focus group discussion.
A. Theme 1: Department Role and Activities
The Medical Education Department should encompass all important responsibilities such as teaching, research, and service providing, as well as supporting staff career development. However, the balance of these activities may vary within departments. When discussed the current state and impact of the medical education department in the college, the participants appreciated its role and activities. Hence two themes were generated.
1. Positive impact:
Participants highlighted the positive impact of the Medical Education Department and echoed department’s responsibility in improving teaching skills, supporting innovative approaches, encouraging interdisciplinary collaboration, and establishing a friendly and inclusive atmosphere for faculty members.
“The department’s current situation is pretty impressive. It has made great progress in improving medical education quality.” – p5FG1
“The department has played a critical role in raising medical education standards.” – p6FG2
2. Collaborative role:
Participants stressed the need for more communication and collaboration with other departments.
“While there have been some collaborative initiatives, I believe there is still potential for development.” – p6FG1
Especially, Collaborative opportunities for curriculum development among faculty members will not only bring diverse expertise, comprehensive approach, innovation, and creativity but will also enhance their engagement and sense of ownership.
“They should hold brainstorming sessions, curriculum mapping exercises, and curriculum review meetings to discuss ideas and viewpoints.” – p2FG2
B. Theme 2: Faculty Development
Faculty development initiatives planned by the college’s medical education department seem satisfactory. However, faculty members stressed the need to include innovative and trendy topics i.e., creative pedagogy, technology informed teaching practices and leadership and communication skills for the workshops.
1. Need for training for professional excellence:
The faculty believes that they have a legitimate need for pedagogical training.
“As I have decided to pursue my carrier as a medical teacher and for that yes I need to develop some pedagogical knowledge and skills.” – p3FG1
“We’re eager to succeed in our professions, these training can positively impact our carriers.” – p5FG2
2. Nature and scope of activities:
Participants highlighted the need to introduce new and updated topics in relevance faculty development activities (FDA) with emphasis on participants’ engagement and interactivity.
“But sometimes I feel that these workshops should also consider our educational needs like research and leadership skills.” – p4FG1
“More interactive and active learning techniques would help us understand the content and would be more beneficial in its application.” – p7FG1
3. Motivation to participate:
Most participants thought that faculty members’ contributions to these faculty development events should be acknowledged in some way, hence motivating them to participate.
“Like for young doctors like me, who are struggling to find some balance between family and work, the institute must consider some incentives or recognitions in any form. That I think can keep us motivated.” – p1FG1
4. Roadblocks to faculty development:
Despite the advantages of faculty development workshops mentioned, participants still highlighted some barriers to their development i.e., duration, challenging commitments.
“After the hectic clinical schedule, I sometimes literally drag myself for the workshops. I would suggest planning short duration workshops.” – p6FG1
“After fulfilling my teaching and clinical commitments, despite understanding its (FDA) importance, I hardly wish to spare any time for it.” – p3FG2
5. Challenges to the adaptation to new practices:
Adaptation to new practices can occur at various levels like content, pedagogical and assessment adaptations. Participants focused on pedagogical training, especially for the introduction of new integrated curriculum. One of the members responded as follows.
“…then there is the issue of matching our existing resources to the new curriculum’s requirements. This requires reconsideration of our lesson ideas, assessments, and even classroom layouts.” – p4FG2
C. Theme 3: Inadequate Contributions Towards Research
MEDs play an important role in creating a culture of research (i.e. prevailing attitudes, values, and practices regarding research activities) by innovating, developing new methodologies to medical education, and disseminating their findings (Al-Wardy, 2008). However, the participants seem quite unsatisfied with the current research culture of the institute.
“Well! I think this needs attention, as the research resources are not adequate.” – p5FG1
1. Workload balance:
Faculty find it difficult to balance between clinical and teaching responsibilities while conducting research work. Research work needs more commitment.
“The rigorous clinical workload leaves us with little time and energy to devote to research. Balancing clinical commitments and research can be difficult.” – p6FG2
2. Training and skills:
They also feel the need for research support offices to help and motivate the researchers and teach them research skills like conducting sound literature search strategies, data collection, analysis etc.
“I can see that faculty members who do not obtain proper research training usually have to struggle to initiate and carry out research projects.” – p7FG1
3. Limited resources:
Resources include financial as well as research resources. They feel that restricted financial and research resources (databases, journals, and libraries) are big impediments to the development of research culture in their institute.
“Faculty and students encounter problems performing strong investigations and generating significant findings without access to advanced laboratory equipment, research databases, and specialised research rooms.” – p4FG2
4. Motivation for research:
The institutional culture of a medical college can influence the emphasis and support for research efforts. If the college does not emphasise research or does not have a supportive research culture, faculty members may not receive appropriate recognition, incentives, or resources to engage in research. This can demotivate staff and result in low quality of research work. For instance, one of the participants said:
“Be it any field, lack of incentives, awards, and acknowledgment for research accomplishments might discourage academics and students from actively participating in research activities.” – p7FG2
D. Theme 4: Student Support Services
Planning and providing instructional activities that encourage students’ involvement in learning is another duty of the Medical Education Department. Yusoff. et. al (2014) argued that, to guarantee that medical students are engaged in their study, it is necessary to prepare and teach them to do so. Thus, at both the personal and professional levels, student development activities are essential and fundamental part of nurturing and preparing students for learning in the medical field.
1. Academic support:
The faculty agreed that students needed help and direction in their academic endeavours and appreciate the students’ services of the department.
“The current state of advising services, in my opinion, is fairly good. The department includes resolute advisers and mentors who help students with many aspects of their academic and personal lives. They are easily accessible and eager to respond to students’ problems and questions.” – p1FG1
2. Advisory of study:
The conversation emphasised the significance of addressing students’ emotional and mental health.
“There is a need for improved mental health support. Additional information and guidance on managing stress, building resilience, and obtaining counselling services would be great.” – p5FG2
The importance of educating medical students for their future careers options was underlined by the faculty.
3. Communication and feedback:
Establishing a successful mentoring programme requires thorough programme evaluation. As the programme’s focus, students’ expectations must be considered while evaluating the programme’s effectiveness in terms of its outcomes (Jayalakshmi et. al., 2011). Participants strongly felt that there is a need for a formalised feedback process to collect student perspectives and issues.
“Clearer communication lines, faster response times, and more proactive guidance suited to students’ specific needs and objectives would be advantageous.” – p4FG1
IV. DISCUSSION
A. Staff Perception of the Roles of the Medical Education Department
Staff generally perceive the Medical Education Department (MED) positively, particularly regarding its support for faculty development and student services. Faculty members appreciate the department’s commitment to assisting in teaching initiatives by offering tools, courses, and training opportunities, which help them enhance their teaching skills and stay current with pedagogical practices. This support contributes to providing high-quality education to students, contrasting findings by Latif & Wajid (2018), who reported difficulties in establishing DMEs due to a lack of consensus on their roles. Participants noted that MED encourages conference attendance and fosters professional development, benefiting both individual careers and institutional networking, research collaboration, and communication skills (Kamal et al., 2022). Additionally, MED’s role in organising extracurricular activities and mentorship programmes maximises students’ educational experiences, promoting personal development and teamwork (Yusoff et al., 2014). Khalid (2013) and Kiguli-Malwadde et al. (2015) found faculty viewing MED as a positive change and an agent of educational innovation. Rahman et al. (2019) reported faculty transfer knowledge from MED activities and use them in pedagogical and assessment techniques, hence classified them as beneficial activities. However, it was reported in other studies that faculty felt threatened by MED’s activities, perceiving them as taking over the curriculum (Batool, 2018).
Despite these positives, there is limited awareness among administration and students about MED’s role, leading to under-utilisation of its resources and lack of collaboration. Hence DMEs should actively promote their services through newsletters, workshops, and engagement with student and faculty organisations. Raising awareness ensures that MED’s resources and support reach those who can benefit, and therefore improve the educational experience for all involved stakeholders (Rahman et al., 2019; Khalid, 2013).
B. Staff Positive and Negative Experiences While Working with a Medical Education Department
Faculty members at LCMD view faculty development activities positively, appreciating their focus on teaching methods, assessment techniques, and curriculum development. Junior faculty members, in particular, value these activities as they transition from students to competent instructors, developing teaching abilities, communication skills, and interdepartmental collaboration through these programmes (Thorndyke et al., 2006; Whitcomb, 2004).
However, barriers include time constraints due to faculty members’ multiple responsibilities, passive learning methods in workshops, and a lack of incentives for participation. Studies in India found similar limitations, with debates on the effectiveness of incentives for attending workshops (Adkoli & Sood, 2009; Singh et al., 2008; Srinivas & Adkoli, 2009). While some argue for monetary incentives, others caution against misaligned motivations and ethical issues (Jessani et al., 2020).
Participants expressed dissatisfaction with research activities, with the limited research funding, lack of institutional support, and insufficient collaboration. Medical education research is essential for understanding teaching and learning in medicine, fostering innovation, and developing critical thinking skills (Magan, 2018; Susiani et al., 2018). Challenges include securing funding, lack of resources, and institutional prioritisation of clinical skills over educational research (Ghaffar et al., 2013; Sabzwari et al., 2009).
Regarding student services, faculty members are satisfied with advisory and mentoring activities but suggest improvements. Effective mentoring involves role modeling, career development advice, and direct interaction, evaluated through student feedback (Nimmons et al., 2019). The Kirkpatrick model offers a framework for assessing mentoring programme effectiveness, though evaluations should extend to the organisational level (Nimmons et al., 2019; Smidt et al., 2009).
C. How Should the Medical Education Department Function in the Future?
To address time constraints, MED should offer flexible scheduling for faculty development activities, including evening and weekend classes, and online resources. Integrating these activities into ongoing events and establishing mentorship programmes can further support faculty development. Journal clubs can promote knowledge exchange and research interest, addressing time constraints through peer group discussions (Bhattacharya, 2017; Linzer et al., 1988).
Active learning methods, such as workshops, case studies, and role-play, should be incorporated into faculty development programmes, underpinned by Knowles’ adult learning theory principles to promote internal motivation and self-directed learning (Kaufman, 2003; Norcini et al., 2005; Steinert et al., 2000). Monetary incentives and recognition for contributions should be allocated to motivate participation, with a framework for regular evaluation of teachers’ performance (Adkoli & Sood, 2009; Shah et al., 2018; Srinivas & Adkoli, 2009).
Customised workshops, though challenging, can be facilitated through self-assessed pathways like the COINNS model, identifying key issues and opportunities for professional development (Swanwick & McKimm, 2010). Research training, financial support, and acknowledgment for research accomplishments are crucial for fostering a research culture. Creating research support offices can streamline research processes, mentor researchers, uncover funding opportunities, and support collaborative research (Albanese et al., 2001; Eder & Pierce, 2011; Gisondi et al., 2022).
For student support, more academic services like stress management and study skills activities are needed. Ensuring student engagement and development through well-planned instructional activities can improve outcomes (Prebble et al., 2004; Yusoff et al., 2014). Resilience workshops and cognitive-behavioral training can address the mental and physical health pressures faced by medical students (Rogers, 2016).
V. CONCLUSION
This action research study highlights several key findings and recommendations based on faculty perceptions of their medical education department’s practices and policies. Faculty members expressed a positive attitude towards current policies, indicating a strong foundation for further advancements. However, the need for greater collaboration through multidisciplinary projects and cross-departmental connections was emphasised to enhance overall efficacy.
While existing faculty development programmes meet some demands, a stronger focus on motivational rewards is necessary to maintain participation and commitment. Incentives or acknowledgment for outstanding achievements can renew faculty devotion to departmental goals. Faculty development should also include interactive workshops on advanced pedagogical methods, technological integration, interdisciplinary teaching partnerships, and assessment strategies. These workshops ensure that faculty stay updated with educational advancements, benefiting both teachers and students.
Concerns about workload and its impact on research and scholarship were noted. Addressing the lack of research-related training and resources is crucial to fostering an academic culture of inquiry. Providing skill-enhancement programmes and seeking additional funding can empower faculty to pursue research initiatives.
Lastly, while faculty are satisfied with academic mentoring and support services, the student feedback system needs improvement. A more organised and proactive mechanism is required to effectively capture student insights and ensure continuous improvement.
A. Study Recommendations
Study recommends encouraging regular interactions with other departments via interdisciplinary/ multidisciplinary workshops; providing innovative pedagogical techniques; fostering Financial and Non-Financial Incentives. The latter could be planned by implementing a merit-based system, which rewards exceptional contributions with stipends, bonuses, and research funding. Recognising outstanding faculty annually for their achievements is a key in inspiring others and igniting their motivation. Moreover, aiming at improving DME practices, institutional research profile should be strengthened by organising research activities focused on grant writing, research publication, data analysis.
B. Study Limitations
Being localised to a single institute limits data generalisability. The findings are specific to unique context and may not apply to other institutions (Braydon-Miller et al., 2003). Voluntary faculty participation introduces selection bias, as the sample may not represent all faculty viewpoints (Gill, 2020; Berndt, 2020). Additionally, the study focused on faculty opinions, potentially missing insights from other stakeholders such as students, graduates, and recruiters, which could provide a more comprehensive understanding of the department’s strengths and areas for improvement.
Notes on Contributors
Dr Juveria Arjumand contributed to conceived the study, drafted the study proposal, conducted online Zoom focus group discussion, analysed the data as per her master proposal, and prepared the manuscript for submission.
Dr Syed Muhammad Azfar obtained ethical approval and assisted in conducting focus group discussion and data collection.
Dr Rubaba Azim assisted in conducting focus group discussions and data collection.
Dr Rania Alkhadragy reviewed the study proposal, planned for study design, followed data collection and analysis, gave critical review and edited the final version of the manuscript.
All authors read and approved the final manuscript.
Ethical Approval
Ethical approval was issued from Liaquat College of Medicine and Dentistry with the reference number IRB/M-000037/22 and from University of Dundee with the reference number SMED REC 22/64.
Data Availability
All relevant data are within the manuscript. Data has sensitive information form participants’ quotes that should not be publicly available.
Acknowledgement
We would like to thank all the faculty members at LCMD who participated in the study.
Funding
The author did not receive any funding to conduct this study.
Declaration of Interest
All authors have no conflict of interest.
References
Adkoli, B. V., & Sood, R. (2009). Faculty development and medical education units in India: A survey. National Medical Journal of India, 22(1), 28-32. https://pubmed.ncbi.nlm.nih.gov/19761158/
Al Shawwa, L. A. (2012). The establishment and roles of the medical education department in the faculty of medicine, King Abdul Aziz University, Jeddah Saudi Arabia. Oman Medical Journal, 27(1), 4. https://doi.org/10.5001/omj.2012.02
Albanese, M. A., Dottl, S., & Nowacek, G. A. (2001). Offices of research in medical education: Accomplishments and added value contributions. Teaching and Learning in Medicine, 13(4), 258-267. https://doi.org/10.1207/s15328015tlm1304_08
Ali, S. M., & Shamim, M. S. (2014). Way forward for departments of medical education in Pakistan. Journal Pakistan Medical Association, 64(7), 732-733. https://doi.org/10.12669/pjms.314.8575
AlSheikh, M. H., Zaini, R., Abdalla, M. E., & Magzoub, M. E. (2022). The wicked role of the medical education department. Health Professions Education, 8(1), 3-8. https://doi.org/10.55890/2452-3011.1014
Al-Wardy, N. M. (2008). Medical education units: History, functions, and organisation. Sultan Qaboos University Medical Journal, 8(2), 149.
Anwar, M. I., & Humayun, A. (2015). Faculty development – Looking through different lenses. Pakistan Armed Forces Medical Journal, 65(1), 110-117. https://pafmj.org/PAFMJ/article/view/701
Batool, S., Raza, M. A., & Khan, R. A. (2018). Roles of medical education department: What are expectations of the faculty? Pakistan Journal of Medical Sciences, 34(4), 864. https://doi.org/10.12669/pjms.344.14609
Berndt, A. E. (2020). Sampling methods. Journal of Human Lactation, 36(2), 224-226. https://doi.org/10.1177/0890334420906850
Bhattacharya, S. (2017). Journal club and post-graduate medical education. Indian Journal of Plastic Surgery, 50(3), 302-305. https://doi.org/10.4103/ijps.ijps_222_17
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101. https://doi.org/10.1191/1478088706qp063oa
Braun, V., & Clarke, V. (2012). Thematic analysis. In H. Cooper (Ed.), APA handbook of research methods in psychology (Vol. 2, pp. 57-71). American Psychological Association. https://psycnet.apa.org/doi/10.1037/13620-004
Brydon-Miller, M., Greenwood, D., & Maguire, P. (2003). Why action research? Action Research, 1(1), 9-28. https://doi.org/10.1177/14767503030011002
Cleary, M., Horsfall, J., & Hayter, M. (2014). Data collection and sampling in qualitative research: Does size matter? Journal of Advanced Nursing, 70(3), 473-475. https://doi.org/10.1111/jan.12163
Davis, M. H., Karunathilake, I., & Harden, R. M. (2005). AMEE education guide no. 28: The development and role of departments of medical education. Medical Teacher, 27(8), 665-675. https://doi.org/10.1080/01421590500398788
Eder, M., & Pierce, J. R. (2011). Innovations in faculty development: Study of a research assistance unit designed to assist clinician-educators with research. Southern Medical Journal, 104(9), 647-650. https://doi.org/10.1097/smj.0b013e3182294e82
Evered, R. D., & Susman, G. I. (1978). An assessment of the scientific merits of action research. Administrative Science Quarterly, 23(4), 582-603. https://doi.org/10.2307/2392581
Ghaffar, A., Zaidi, S., Qureshi, H., & Hafeez, A. (2013). Medical education and research in Pakistan. The Lancet, 381(9885), 2234-2236. https://doi.org/10.1016/s0140-6736(13)60146-4
Gill, S. L. (2020). Qualitative sampling methods. Journal of Human Lactation, 36(4), 579-581. https://doi.org/10.1177/0890334420949218
Gisondi, M. A., Michael, S., Li-Sauerwine, S., Brazil, V., Caretta-Weyer, H. A., Issenberg, B., … & Chan, T. M. (2022). The purpose, design, and promise of medical education research labs. Academic Medicine, 97(9), 1281-1288. https://doi.org/10.1097/acm.0000000000004746
Gruppen, L. (2008). Creating and sustaining centres for medical education research and development. Medical Education, 42(2), 121-123. https://doi.org/10.1111/j.1365-2923.2007.02931.x
Gruppen, L. D. (2004). The department of medical education at the University of Michigan Medical School: A case study in medical education research productivity. Academic Medicine, 79(10), 997-1002. https://doi.org/10.1097/00001888-200410000-00023
Illing, J. (2013). Thinking about research: Theoretical perspectives, ethics, and scholarship. In T. Swanwick (Ed.), Understanding medical education: Evidence, theory, and practice (2nd ed., pp. 331-348). Chichester: Wiley Blackwell. https://doi.org/10.1002/9781118472361.ch24
Jessani, N. S., Valmeekanathan, A., Babcock, C. M., & Ling, B. (2020). Academic incentives for enhancing faculty engagement with decision-makers – Considerations and recommendations from one School of Public Health. Humanities and Social Sciences Communications, 7(1), 1-13. https://doi.org/10.1057/s41599-020-00629-1
Kamal, M., Bhargava, S., & Katyal, S. (2022). Role of conferences and continuing medical education (CME) in post-graduate anaesthesia education. Indian Journal of Anaesthesia, 66(1), 82. https://doi.org/10.4103/ija.ija_1102_21
Kaufman, D. M. (2003). Applying educational theory in practice. British Medical Journal, 326(7382), 213-216. https://doi.org/10.1136/bmj.326.7382.213
Khalid, T. (2013). Faculty perceptions about roles and functions of a department of medical education. Journal of College of Physicians and Surgeons Pakistan, 23(1), 56-61. https://pesquisa.bvsalud.org/portal/resource/pt/emr-140581
Khan, A. W., Sethi, A., Wajid, G., & Yasmeen, R. (2020). Challenges towards quality assurance of basic medical education in Pakistan. Pakistan Journal of Medical Sciences, 36(2), 4. https://doi.org/10.12669/pjms.36.2.1319
Kiguli-Malwadde, E., Talib, Z. M., Wohltjen, H., Connors, S. C., Gandari, J., Banda, S. S., & Van Schalkwyk, S. C. (2015). Medical education departments: A study of four medical schools in Sub-Saharan Africa. British Medical Council medical education, 15(1), 1-9. https://doi.org/10.1186/s12909-015-0398-y
Latif, M. Z., & Wajid, G. (2018). Reforming medical education in Pakistan through strengthening departments of medical education. Pakistan Journal of Medical Sciences, 34(6), 1439. https://doi.org/10.12669/pjms.346.15942
Liaquat College of Medicine and Dentistry [LCMD]. (2023). Department of health professions education. Retrieved January 22, 2023, from https://www.lcmd.edu.pk/dhpe
Lindberg, M. A. (1998). The process of change: Stories of the journey. Academic Medicine, 73(9), S4-S10. https://doi.org/10.1097/00001888-199809000-00029
Linzer, M., Brown, J., Frazier, L., Delong, E., & Siegel, W. (1988). Impact of a medical journal club on house-staff reading habits, knowledge, and critical appraisal skills. A randomized control trials. The Journal of the American Medical Association, 260(17), 2537-2541. https://doi.org/10.1001/jama.260.17.2537
Magan, D. (2018). Importance of research in medical education. Journal of Medical Education, 17(3). https://brieflands.com/articles/jme-105647
Meyer, J. (2000). Using qualitative methods in health-related action research. British Medical Journal, 320(7228), 178-181. https://doi.org/10.7748/nop.12.1.22.s12
Nasim, M. (2011). Medical education needs to change in Pakistan. Journal of the Pakistan Medical Association, 61(8), 808. https://europepmc.org/article/med/22356007
Nimmons, D., Giny, S., & Rosenthal, J. (2019). Medical student mentoring programs: Current insights. Advances in Medical Education and Practice, 10, 113-123. https://doi.org/10.2147/amep.s154974
Norcini, J., Burdick, W., & Morahan, P. (2005). The FAIMER Institute: Creating international networks of medical educators. Medical Teacher, 27(3), 214-218. https://doi.org/10.1080/01421590500126379
Peralta, K. J. (2017). Toward a deeper appreciation of participatory epistemology in community-based participatory research. PRISM: A Journal of Regional Engagement, 6(1), 4. https://encompass.eku.edu/prism/vol6/iss1/4/
Prebble, T., Hargraves, H., Leach, L., Naidoo, K., Suddaby, G., & Zepke, N. (2004). Impact of student support services and academic development programmes on student outcomes in undergraduate tertiary study: A synthesis of the research: Report to the Ministry of Education. Wellington: Ministry of Education. https://rb.gy/fd8mpf
Rahman, S., Talukder, M. H. K., & Alam, K. K. (2019). Activities of Medical Education Unit (MEU) in medical colleges of Bangladesh and some challenges faced. Bangladesh Journal of Medical Education, 10(2), 12-18. https://doi.org/10.3329/bjme.v10i2.44637
Rogers, D. (2016). Which educational interventions improve healthcare professionals’ resilience? Medical Teacher, 38(12), 1236-1241. https://doi.org/10.1080/0142159x.2016.1210111
Sabzwari, S., Kauser, S., & Khuwaja, A. K. (2009). Experiences, attitudes and barriers towards research amongst junior faculty of Pakistani medical universities. BMC Medical Education, 9(1), 1-7. https://doi.org/10.1186/1472-6920-9-68
Shah, N., Tabassum, A., & Shah, N. (2018). A needs assessment for faculty development at two medical colleges of Dow University of Health Sciences, Karachi. Pakistan Journal of Medical Sciences, 34(6), 1386. https://doi.org/10.12669/pjms.346.16302
Siddiqui, F. G., & Shaikh, N. A. (2014). Challenges and issues in medical education in Pakistan. Journal of Liaquat University of Medical Health Sciences, 13(3), 91-92.
Singh, T., Bansal, P., & Sharma, M. (2008). A need and necessity for faculty development: The role of medical education units in the Indian context. South East Asian Journal of Medical Education, 2(1), 2-6. https://doi.org/10.4038/seajme.v2i1.484
Smidt, A., Balandin, S., Sigafoos, J., & Reed, V. A. (2009). The Kirkpatrick model: A useful tool for evaluating training outcomes. Journal of Intellectual and Developmental Disability, 34(3), 266-274. https://doi.org/10.1080/13668250903093125
Soh, K. L., Davidson, P. M., Leslie, G., & Rahman, A. B. A. (2011). Action research studies in the intensive care setting: A systematic review. International Journal of Nursing Studies, 48(2), 258-268. https://doi.org/10.1016/j.ijnurstu.2010.09.014
Srinivas, D. K., & Adkoli, B. V. (2009). Faculty development in medical education in India: The need of the day. Al Ameen Journal of Medical Sciences, 2(1), 6-13. https://www.cabidigitallibrary.org/doi/full/10.5555/20103114268
Steinert, Y., Cruess, S., Cruess, R., & Snell, L. (2005). Faculty development for teaching and evaluating professionalism: From programme design to curriculum change. Medical Education, 39(2), 127-136. https://doi.org/10.1111/j.1365-2929.2004.02069.x
Susiani, T. S., Salimi, M., & Hidayah, R. (2018). Research based learning (RBL): How to improve critical thinking skills? Social Human Science Web of Conferences, 42, 00042. https://doi.org/10.1051/shsconf/20184200042
Tang, K. C., Davis, A., Sullivan, S., & Fisher, J. (1995). A review of 5 existing guidelines for planning focus groups in GP research. Australian Family Physician, 24(2), 184-186. https://europepmc.org/article/med/7880138
Thorndyke, L. E., Gusic, M. E., George, J. H., Quillen, D. A., & Milner, R. J. (2006). Empowering junior faculty: Penn State’s faculty development and mentoring program. Academic Medicine, 81(7), 668-673. https://doi.org/10.1097/01.acm.0000232424.88922.df
Torre, M. E. (2009). Participatory action research and critical race theory: Fueling spaces for nos-otras to research. The Urban Review, 41, 106-120. https://doi.org/10.1007/s11256-008-0097-7
Varpio, L., Bidlake, E., Humphrey-Murto, S., Sutherland, S., & Hamstra, S. J. (2014). Key considerations for the success of medical education research and innovation units in Canada: Unit director perceptions. Advances in Health Sciences Education, 19(3), 361-377. https://doi.org/10.1007/s10459-013-9479-z
Whitcomb, M. E., & Cohen, J. J. (2004). The future of primary care medicine. New England Journal of Medicine, 351(7), 710-712.
Wolcott, L. L., & Betts, K. S. (1999). What’s in it for me? Incentives for faculty participation in distance education. Journal of Distance Education, 14(2), 34-49. https://www.ijede.ca/index.php/jde/article/download/156/340?inline=1
Yusoff, M. S. B., Rahim, A. F. A., & Jaafar, R. (2014). Medical education department roles and initiatives towards achieving APEX agenda. Education in Medicine Journal, 6(2), e1-e7. https://doi.org/10.5959/eimj.v6i2.261
Yusoff, M. S. B., Rahim, A. F. A., Noor, A. R., Yaacob, N., & Hussin, Z. (2010). Evaluation of medical students’ perception towards the Big Sib Programme in the School of Medical Sciences, USM. Education in Medicine Journal, 2(1), e2-e11.
*Dr Rania Alkhadragy
University of Dundee,
Nethergate Dundee,
Scotland, United Kingdom
Email: ryalkhadragy@dundee.ac.uk
Published online: 7 April, TAPS 2026, 11(2), 1-3
https://doi.org/10.29060/TAPS.2026-11-2/EV11N2
Artificial intelligence (AI) is now a part of all areas of academic work. Journal reviewers and editors have noticed that more manuscripts are being written with the help of AI, specifically generative AI (GenAI), and reviews are being improved through chatbots. To make things more cost-efficient and effective, editorial workflows now include automated screening. The question is no longer if GenAI will affect scholarship. It already does! The key question is, how can we ensure authors are the primary agents of their conceptions and, thus, motivate authors to write articles in a transparent manner that authentically represents their own ideas.
Recent discussions across leading journal editorial boards reflect both optimism and caution. Commentaries in The Lancet Infectious Diseases warn that large language models may generate confident but flawed critiques, amplify bias and hallucinate references (Donker, 2023). Such systems lack epistemic responsibility. They predict language. They do not understand method. Peer review, however, is a moral and scholarly act. It demands judgement, accountability and contextual reasoning. Similarly, discussions in Health Affairs Scholar and Critical Care highlight GenAI’s growing presence in peer review processes. GenAI may assist with triage, language refinement, and detection of plagiarism or reporting omissions. Yet it cannot replace human oversight (Bauchner & Rivara, 2024; Cheng, Sun, Liu, Wu & Li, 2024). These perspectives are not anti-technology. They are pro-accountability. They call for stewardship. Major journal organisations now articulate consistent policy principles. The International Committee of Medical Journal Editors (ICMJE, 2024), the World Association of Medical Editors (Zielinski et al., 2024), the Committee on Publication Ethics (COPE Council, n.d.), and others converge on several points. GenAI tools cannot be authors. Authorship requires responsibility, the ability to declare conflicts of interest, and legal accountability. GenAI meets none of these criteria.
The key is transparency. This can be achieved if authors are required to identify the GenAI tool (e.g., ChatGPT, Claude, Gemini, and Microsoft Copilot) and its version. The JAMA Network further requires the author to describe how GenAI contributed to writing and or analysis (Flanagin et al., 2024). Disclosure is now part of scholarly honesty, which requires a sense of responsibility. The British Medical Journal and The Lancet adopt similar positions. GenAI may assist in writing or editing, but it cannot generate scientific insight, interpret data independently, or substitute researcher judgement (BMJ, 2024; The Lancet, n.d.). Confidentiality remains central. As for reviewers, they must not upload unpublished manuscripts into publicly available GenAI platforms. The National Institutes of Health (NIH, 2023) has formalised this requirement through revised nondisclosure agreements. The integrity of peer review depends on trust. That trust cannot be compromised for convenience. Human accountability remains the anchor.
Yet policy clarity does not eliminate deeper tensions.
First, enforcement remains uncertain. Disclosure depends largely on author and reviewer honesty. Detection tools are imperfect. Investing in digital literacy and understanding the GenAI technologies by journal editors should be the way forward rather than prohibiting them.
Second, GenAI use raises questions of equity. For many medical educators specially in the Asia-Pacific region where English is the second language, GenAI can improve clarity and confidence. For some others, access to expensive GenAI tools may widen disparities. Responsible governance must consider inclusion, not merely control.
Third, we must confront the educational implications. In medical education scholarship, GenAI shapes how learners write, search, and reflect. Editorial policies therefore signal curricular values. If we treat GenAI only as threat, we model fear. If we treat it uncritically as a cost-efficient mechanism, we risk eroding critical thinking. We must instead teach discernment. GenAI literacy should become part of scholarly professionalism. Basil et al. (2026) have conducted a comprehensive review of the impact of GenAI in health profession education and one of their policy suggestions is to regularly audit GenAI policies due to the evolving nature of GenAI technology.
At its heart, this moment is not about technology. It is about identity and professionalism. What does it mean to be an author? A reviewer? An editor? GenAI can assist with language, much like the use of a human proof-reader in the past. However, it cannot assume responsibility for truth as that would mislead and mask the true authorship of the idea being presented. That responsibility remains human.
For The Asia Pacific Scholar, the way forward is balanced and transparent. We should require clear disclosure of GenAI use in manuscript preparation. We should prohibit uploading confidential material into unsecured systems. We should allow cautious use for language improvement when declared. This is also important as English is not the first language of most of the scholars in the region. Journals may employ licensed GenAI tools for plagiarism detection or reviewer matching however with human oversight. It is important that we should preserve human judgement in decisions that shape academic careers and patient care.
GenAI is here to stay. And further to this, we need to be mindful of the dynamic nature of the development of AI technology, as Bennani (2024) amongst many others inform the academic world of the impending advent of artificial general intelligence (AGI). The idea of AGI being to make AI decisions more autonomous thus requiring greater vigilance to ensure these technological changes continue to align with human values of integrity and professionalism. Our task is not surrender, nor resistance for its own sake. It is stewardship and to continue to be well informed. As such, we must guide its use in ways that strengthen scholarship, protect integrity and support our diverse academic community across the Asia-Pacific region.
Technology can accelerate manuscript generation and reviews. However, it cannot replace wisdom.
And wisdom remains our responsibility!
Dujeepa D. Samarasekera
Centre for Medical Education (CenMED), NUS Yong Loo Lin School of Medicine,
National University of Singapore, Singapore
Marcus A. Henning
Centre for Medical and Health Sciences Education, Faculty of Medical and Health Sciences,
University of Auckland, New Zealand
Basil, M., Ahmed, W., Hajeomar, R., Strawbridge, J., Lynch, M., & Mukhalalati, B. (2026). A scoping review of the use of generative artificial intelligence tools in health profession education. BMC Medical Education, 26, Article 291. https://doi.org/10.1186/s12909-025-08527-3
Bauchner, H., & Rivara, F. P. (2024). Use of artificial intelligence and the future of peer review. Health Affairs Scholar, 2(5), qxae058. https://doi.org/10.1093/haschl/qxae058
Bennani, T. (2024). Advancing Healthcare with GenerativeAI: A Multifaceted Approach to Reliable Medical Information and Innovation (Doctoral dissertation, Massachusetts Institute of Technology). https://hdl.handle.net/1721.1/156048
BMJ. (2024). AI use. BMJ. https://www.bmj.com/content/ai-use
Cheng, K., Sun, Z., Liu, X., Wu, H., & Li, C. (2024). Generative artificial intelligence is infiltrating peer review process. Critical Care, 28(1), 149. https://doi.org/10.1186/s13054-024-04933-z
COPE Council. (n.d.). COPE position – Authorship and AI – English. Committee on Publication Ethics. https://doi.org/10.24318/cCVRZBms
Donker, T. (2023). The dangers of using large language models for peer review. The Lancet Infectious Diseases, 23(7), 781. https://doi.org/10.1016/S1473-3099(23)00290-6
Flanagin, A., Pirracchio, R., Khera, R., Berkwits, M., Hswen, Y., & Bibbins-Domingo, K. (2024). Reporting use of AI in research and scholarly publication—JAMA Network Guidance. Jama, 331(13), 1096-1098. https://doi.org/10.1001/jama.2024.3471
International Committee of Medical Journal Editors (ICMJE). (2024). Recommendations for the conduct, reporting, editing and publication of scholarly work in medical journals (revised in January 2024): A Korean translation. The Ewha Medical Journal, 47(4). https://doi.org/10.12771/emj.2024.e48
National Institutes of Health (NIH). (2023). The Use of Generative Artificial Intelligence Technologies is Prohibited for the NIH Peer Review Process. https://grants.nih.gov/grants/guide/notice-files/NOT-OD-23-149.html
The Lancet. (n.d.). Editorial Policies. The Lancet. https://www.thelancet.com/editorial-policies
Zielinski, C., Winker, M. A., Aggarwal, R., Ferris, L. E., Heinemann, M., Lapeña, J. F., … & WAME Board. (2024). Chatbots, generative AI, and scholarly manuscripts: WAME recommendations on chatbots and generative artificial intelligence in relation to scholarly publications. Current Medical Research and Opinion, 40(1), 11-13. https://doi.org/10.1080/03007995.2023.2286102
Submitted: 14 April 2025
Accepted: 19 August 2025
Published online: 7 April, TAPS 2026, 11(2), 134-136
https://doi.org/10.29060/TAPS.2026-11-2/II3751
Dexter Chai Yih Haur1, Lee Shuh Shing2, Yeo Su Ping2, Goh Zi Qing2 & Han Ting Jillian Yeo2
1School of Humanities and Interdisciplinary Studies, Ngee Ann Polytechnic, Singapore; 2Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
I. INTRODUCTION
Surveys/ Questionnaires are one of the most commonly used tools in data collection, enabling researchers to analyse different patterns or trends and ultimately, contribute to the advancement of evidence-based educational practices (Wilson et al., 2023). However, conducting surveys presents several challenges that can compromise data quality and reliability of data collected. This paper draws on our institutional experience in conducting educational surveys, sharing both successes and challenges. We aim to explore the factors influencing survey participation, strategies adopted to address them, and emerging opportunities in survey design.
II. CHALLENGES AND FACTORS IMPACTING SURVEY RESPONSE RATES
Despite their utility, surveys face challenges that can be broadly categorised as participant-related and survey structure-related. Participant-related challenges include response bias, low motivation, and incomplete or inaccurate answers, all of which can compromise data validity, reliability, and representativeness (Phillips et al., 2017). Low response rates further increase the risk of non-response bias. Survey structure-related issues, such as poorly framed questions or excessively lengthy surveys, can reduce engagement and completion rates. Technical barriers and survey fatigue further contribute to low response quality.
This contention aligns with the scholarly discourse presented by Saleh and Bista (2017), elucidating the multifaceted nature of factors influencing survey response rates. Drawing upon the theoretical framework of social exchange theory, which posits that human behaviour is directed by the anticipation of reciprocation, Saleh and Bista (2017) explained that survey response rates hinge upon an array of factors which includes the following: (a) incentives (rewards in increasing survey participants), (b) authority (credibility of the agencies which conducted the survey), (c) survey design (length and types of the question in the survey) and (d) ethical considerations (data privacy, and anonymity).
III. INSTITUTIONAL STRATEGIES TO MITIGATE CHALLENGES
In the past year, Centre for Medical Education (CenMED) conducted multiple educational research involving surveys. Guided by an understanding of response rate determinants, we focused on improving two key domains: design and administration. We prioritised brevity, targeting surveys that could be completed within 10–15 minutes. A mixture of open and closed-ended questions – multiple choice, sliders, ranking, etc. – kept respondents engaged while minimising cognitive load. We limited the number of items to under 50 to avoid fatigue. Questions were concise and clearly worded. Surveys were hosted on Qualtrics with no identifiable data collected, and ethical standards were upheld with Internal Review Board approval before administration.
To improve reach and uptake, we enlisted key faculty members to disseminate the surveys and framed invitation emails to highlight the relevance and value of participation. Despite these measures, we continued to observe lower-than-expected response rates. Deeper examination revealed that survey fatigue – exacerbated by repeated requests and overlapping topics – reduced participant enthusiasm. Generic email blasts lacked the personal engagement necessary to motivate participation.
To circumvent survey fatigue and improve perceptions of surveys, the Centre collaborates with the Dean’s Office to streamline administration process and prevent topic overlap. Recognising the influence of authority figures, key faculty members such as medical educationalists, Vice Dean (Education) or Phase Coordinators, were enlisted to encourage participation during face-to-face sessions. This approach provided a direct personalised appeal to enhance the perceived importance and value of the survey. Additionally, to further facilitate the survey participation, the team provided protected time and space during face-to-face session for respondents to complete the survey.
With this, the team successfully boosted response rates to a satisfactory level. Other than participant-related, and survey structure-related challenges, organisations-related challenges could be one of the contributing factors to low response rates especially in a highly research-focused university. Streamlining processes to eliminate redundancy in survey administration helps improve perceptions of surveys and reduce survey fatigue.
IV. EMERGING OPPORTUNITIES IN SURVEY DESIGN
A. Artificial Intelligence (AI)
One significant area of innovation lies in the use of Artificial Intelligence (AI) to support various stages of the survey lifecycle. AI can facilitate the development of adaptive questionnaires that adjust in real time based on a respondent’s previous answers, thereby improving relevance and reducing cognitive fatigue. Natural language processing capabilities allow for more efficient analysis of open-ended responses. Predictive analytics can help researchers identify trends in responses and patterns of dropout or incomplete data. As described by Paduraru et al. (2024), this enabled for better allocation of resources (e.g. manpower) as AI agents will be able to facilitate the process of questionnaire development, data collection and survey data analysis.
B. Open Data Sharing
Open data sharing in research refers to the practice of making research data freely accessible to other researchers and the public. Open data sharing in research not only enhances collaboration and transparency but also plays a crucial role in improving survey responses. By making survey data openly accessible, researchers can build upon existing datasets, reducing the need for repetitive surveys and minimising respondent fatigue. This approach allows for more robust meta-analyses, enabling a deeper understanding of trends without overburdening participants with multiple survey requests. Additionally, shared data fosters greater trust and engagement among respondents, as they see their contributions being utilised effectively to drive meaningful research outcomes.
C. Social Media
Social media platforms offer a powerful avenue for survey administration, enabling researchers to reach diverse and geographically dispersed populations efficiently. Platforms like Facebook, Twitter, LinkedIn, and Instagram allow for targeted survey distribution through organic posts, paid advertisements, and community groups. Features such as polls, direct messaging, and embedded survey links enhance accessibility and engagement, encouraging higher response rates. Additionally, social media analytics provide real-time insights into respondent demographics and engagement patterns, allowing for adaptive survey strategies. By leveraging these platforms, researchers can improve outreach, increase participation, and gather timely data while minimising costs.
D. Gamification
Gamification can enhance survey administration by incorporating game-like elements to increase engagement and response rates. Features such as points, badges and progress bars make the survey experience more enjoyable, reducing respondent fatigue and encouraging completion. Personalised challenges, leaderboards, and instant feedback can further motivate participation, especially in longer surveys. By integrating storytelling and immersive design, researchers can create a more engaging environment that keeps respondents interested while maintaining data quality. Gamification not only enhances the user experience but also helps mitigate dropouts, making it a valuable strategy for improving survey administration.
V. CONCLUSION
Survey questionnaires remain vital tools in medical education research. Yet, the challenges surrounding participation demand thoughtful design and contextual strategies. Our institutional experience highlights the importance of reducing respondent burden, personalising outreach, and integrating surveys into existing workflows.
Looking ahead, innovations in AI, open data sharing, and social media offer promising avenues for improving data collection. Importantly, while our strategies have shown success within our context, we acknowledge they may not be directly transferable to other institutions. Adaptation to local contexts remains essential. Ultimately, survey success lies in balancing methodological rigour with human-centred design – facilitating meaningful research that benefits both educators and learners.
Notes on Contributors
Dexter Chai drafted the first manuscript and subsequently, the manuscript was edited by Lee Shuh Shing, Yeo Su Ping, Goh Zi Qing and Han Ting Jillian Yeo.
Ethical Approval
Ethical approval is not required for this article as no human participant data was collected/presented.
Funding
The authors did not receive any funding for this article.
Declaration of Interest
The authors would like to declare that they do not have any conflict of interest.
References
Paduraru, C. I., Cristea, R., & Stefanescu, A. (2024). Adaptive questionnaire design using AI agents for people profiling. International Conference on Agents and Artificial Intelligence, 3, 633-640. https://doi.org/10.5220/0012379600003636
Phillips, A. W., Friedman, B. T., Utrankar, A., Ta, A. Q., Reddy, S. T., & Durning, S. J. (2017). Surveys of health professions trainees: Prevalence, response rates, and predictive factors to guide researchers. Academic Medicine, 92(2), 222-228. https://doi.org/10.1097/acm.0000000000001334
Saleh, A., & Bista, K. (2017). Examining factors impacting online survey response rates in educational research: Perceptions of graduate students. Journal of Multi-Disciplinary Evaluation, 13(29), 63-74. https://doi.org/10.56645/jmde.v13i29.487
Wilson, A. B., Brooks, W. S., Edwards, D. N., Deaver, J., Surd, J. A., Pirlo, O. J., Byrd, W. A., Meyer, E. R., Beresheim, A., Cuskey, S. L., Tsintolas, J. G., Norrell, E. S., Fisher, H. C., Skaggs, C. W., Mysak, D., Levin, S. R., Escutia Rosas, C. E., Cale, A. S., Karim, M. N., … Lufler, R. S. (2023). Survey response rates in health sciences education research: A 10‐year meta‐analysis. Anatomical Sciences Education, 17(1), 11-23. https://doi.org/10.1002/ase.2345
*Dexter Chai Yih Haur
School of Humanities and Interdisciplinary Studies,
Ngee Ann Polytechnic, Singapore
Email: trexed89@gmail.com
Submitted: 7 July 2025
Accepted: 3 November 2025
Published online: 7 April, TAPS 2026, 11(2), 118-126
https://doi.org/10.29060/TAPS.2026-11-2/SC3813
Lean Heong Foo1,3,4, Pei Yuan Chan2,3,4, Jeen Nee Lui2,3,4 & Marianne Meng Ann Ong1,3,4
1Periodontic Unit, 2Endodontic Unit, Department of Restorative Dentistry, National Dental Centre Singapore, Singapore; 3National Dental Research Institute Singapore, National Dental Centre Singapore, Singapore; 4Oral Health Academic Clinical Programme, Duke-NUS Medical School, Singapore
Abstract
Introduction: Team-Based Learning (TBL), grounded in constructivist learning theory, promotes active engagement among learners. This study aimed to explore postgraduate residents’ perceptions and attitudes toward learning about periodontal-endodontic lesions using TBL as an educational method.
Methods: A total of 8 Periodontic residents and 11 Endodontic residents received pre-reading articles related to periodontal-endodontic lesions. On the day of the workshop, they were divided into four mixed-specialty groups. They completed individual and group readiness assurance tests, followed by facilitated discussions on three simulated clinical cases. Feedback was collected through an online anonymous survey that included 32 Team-Based Learning Student Assessment Instrument (TBL-SAI) items, eight on programme content, four on skills contributions, seven on faculty, and four on learning outcomes, all scored on a 5-point Likert scale (1-strongly disagree to 5-strongly agree) and analysed with descriptive and Cronbach’s alpha analysis.
Results: Fifteen of 19 residents attended the workshop. TBL-SAI scores (max 40) reflected strong accountability, with overall mean scores around 29 across both Periodontic and Endodontic residents. Learning preference scores (max 80) averaged approximately 50, and student satisfaction scores (max 40) were similarly positive, averaging just under 30. Programme content, learning outcomes, and faculty performance received high ratings, with mean scores above 4 out of 5. Internal consistency was strong across all subscales (Cronbach’s alpha: 0.69–0.99). Qualitative feedback highlighted the value of clinical case applications in enhancing engagement and understanding.
Conclusion: Residents reported positive perceptions of Team-Based Learning, noting high engagement, accountability, and satisfaction. The findings support its effectiveness as a valuable instructional approach in postgraduate dental education.
Keywords: Dental Education, Endodontics, Periodontics, Residency, Team-Based Learning
I. INTRODUCTION
Team-Based Learning (TBL) is an instructional strategy that promotes active, collaborative learning and encourages students to take responsibility for their education by engaging deeply with content, peers, and instructors. The TBL process includes three core phases: pre-reading, readiness assurance (individual and group), and application. The application phase uses the 4S framework—significant problem, same problem, specific choice, and simultaneous reporting—to drive critical discussion, often resembling a faculty-facilitated debate. TBL has demonstrated positive results in pre-clinical dental education, with improved diagnostic skills and examination scores (Pileggi & O’Neill, 2008). However, most available research focuses on undergraduate learners. There is a lack of data on how TBL impacts dental postgraduate students, who are typically mature, self-directed learners. The aim of this study was to address this gap by exploring residents’ perceptions and attitudes toward learning complex, interdisciplinary topics—specifically periodontal-endodontic lesions—through the Team-Based Learning (TBL) approach, given the diagnostic and treatment challenges these lesions often present in clinical practice.
II. METHODS
A. Study Design and Population
This descriptive study was exempted from formal Centralised Institutional Review Board review by SingHealth Institutional Review Board. The study included all 19 postgraduate residents from the National University of Singapore’s three-year Master of Dental Surgery programme through convenient sampling–11 in Endodontics (four first-year, three second-year, four third-year) and eight in Periodontics (three first-year, three second-year, two third-year), and absentees of the workshop were excluded. No formal sample size calculation was conducted due to the small, fixed cohort size. Despite the small sample size (n=19) limiting generalizability, this pilot study aimed to gain preliminary insights into residents’ perceptions of Team-Based Learning for complex topics like periodontal-endodontic lesions.
B. Team-Based Learning (TBL) Workshop
A 4.5-hour TBL workshop was conducted on 7th December 2022. Two weeks prior, participants received pre-reading materials, including 14 journal articles and a book chapter covering key aspects of periodontal-endodontic lesions, such as diagnosis, radiographic features, and the updated classification system (Herrera et al., 2018).
On the workshop day, participants completed a seven-question Individual Readiness Assurance Test (IRAT) to assess their foundational knowledge in diagnosis, investigation, and management. They were then divided into four teams to complete the same questions as a Team Readiness Assurance Test (TRAT), administered via Google Forms (https://www.google.com/forms/about/) and Fyrebox (www.fyrebox.com) facilitate efficient data collection and real-time feedback during the workshop. This was followed by three clinical case discussions designed using the 4S framework–significant problem, same problem, specific choice, and simultaneous reporting–to apply pre-reading concepts to clinical scenarios.
Verbal consent was obtained, and participants completed an anonymous online survey. Using a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), they responded to 32 TBL-SAI items (TBL-SAI) (Mennenga, 2012), eight other questions on the course content, four on skills, seven on faculty, and four on learning outcomes. Participants also rated workshop components as ‘Poor’, ‘Fair’, ‘Satisfactory’, ‘Very Good’, or ‘Excellent’, and selected their favourite component. and answered two open-ended questions on the most useful aspects and suggestions for improvement. The TBL-SAI included three subscales: accountability (≥25), learning preference (≥49), and satisfaction (≥28), with a total score >102 indicating positive perception. Permission was obtained to adapt the instrument (Mennenga, 2012), excluding item 31 (“I think Team-Based Learning helped me to improve my grade”) due to the non-graded nature of the workshop. Qualitative data was collected through open-ended questions on valuable workshop moments and suggestions for improvement, and were thematically reviewed to identify common reflections, without formal qualitative analysis. Data was collected anonymously and analysed using descriptive statistics. Cronbach’s alpha assessed the instrument’s reliability.
III. RESULTS
A. Study Population Demographics
Fifteen out of 19 participants attended the workshop, with two absentees from each of the Periodontics and Endodontics residency programmes. The 15 participants were divided into four teams, with balanced representation of year one, two, and three residents in each group. All participants (four males and 11 females, mean age 28.3 ±2.326, range 25-34) responded to the post-workshop survey (100% response rate). The average IRAT score was 67.6±12.6, and the TRAT score was 80.4±6.8 (Appendix 1). All data is deposited at Figshare at
(https://doi.org/10.6084/m9.figshare.28366964).
B. Workshop Ratings
Participants rated the workshop components highly. Pre-reading materials were rated ‘very good’ or ‘excellent’ by 73.3% (11/15), IRAT by 80% (12/15), TRAT by 93.3% (14/15), and clinical case application by 80% (12/15). Most (93.3%) chose the clinical case discussion as their favourite component.
C. TBL-SAI Results
The cohort’s mean TBL-SAI score was 109 ± 0.98, indicating a strong positive perception (Table 1, Appendix 2, Appendix 3 and Appendix 4).
1. Accountability
Periodontic residents scored highest in year 3 (30.5 ± 2.1). Endodontic residents in year 1 (34.0 ± 4.4). Combined cohort mean was 30.1 ± 2.1. Cronbach’s alpha was 0.83 (Periodontics) and 0.75 (Endodontics), indicating good internal consistency. Most residents (86.7%) prepared beforehand and contributed actively.
2. Preference for Lecture or TBL Subscale
Periodontic residents showed consistent preference (mean 50.7 ± 4.1). Endodontic residents varied. Year three scored highest (53.3 ± 6.1). Combined mean: 49.8 ± 13.5. Cronbach’s alpha was 0.69 (Periodontics) and 0.78 (Endodontics). Most (86.7%) reported better understanding and retention through TBL.
3. Student Satisfaction Subscale
Periodontics year three residents had a mean score of 30.0 ± 2.8, resulting in an overall mean of 28.3 ± 1.9, while Endodontics year three scored slightly lower at 29.3 ± 0.0 resulting mean of 29.6 ± 9.5 for the Endodontic residents. The overall cohort mean was 29.1 ± 1.9. Cronbach’s alpha analysis showed 0.69 (Periodontics), 0.68 (Endodontics). Most (86.7%) found the workshop enjoyable and effective; 93.3% preferred learning in teams. Only one participant viewed TBL negatively.
D. Programme Content
Programme content was rated highly for both Periodontic and Endodontic residents (4.3 ± 0.5; 4.6 ± 0.5, total mean 4.6 ± 0.5). Cronbach’s alpha was notably high at 0.94 for Periodontic residents and 0.98 for Endodontic residents, indicating excellent internal consistency. All agreed materials and objectives were appropriate.
E. Programme Learning
Learning subscale scored slightly lower for both groups (Periodontics 3.6 ± 0.8, Endodontics 4.0 ± 1.0, total mean 3.9 ± 0.9), The Cronbach’s alpha values for the programme learning subscale were 0.95 for Periodontic residents and 0.99 for Endodontic residents. Majority of the participants (12/15, 80%) agreed they could apply the knowledge to their work respectively.
F. Faculty
Both Periodontic and Endodontic residents scored highly for the faculty performance (4.5 ± 0.5; 4.4 ± 0.5, total mean 4.4 ± 0.5). Cronbach’s alpha values were 0.98 for Periodontic residents and 0.96 for Endodontic residents, all participants unanimously agreed faculty were engaging and communicated clearly.
G. Qualitative Feedback
Majority (12/15, 80%) of the participants valued clinical cases and group discussion. One participant quoted “enjoyed the interactive sessions”, while another praised the “use of TBL pedagogy for active learning”. One participant said, “Case discussions, hearing from my colleagues as well as supervisors on various treatment options”. Suggestions included more time for discussion and aligning articles discussed with pre-reading.
IV. DISCUSSION
This descriptive study explored postgraduate residents’ perceptions of Team-Based Learning (TBL) in teaching the diagnosis and management of periodontal-endodontic lesions. The positive reception of TBL among residents may be attributed to its focus on clinical relevance, active participation, and peer collaboration.
Both Periodontic and Endodontic residents preferred TBL over traditional lectures (scores>49), consistent with previous studies (Takeuchi et al., 2015). Qualitative feedback emphasized the value of real-life case discussions and interactive sessions, supporting the idea that TBL fosters engagement and critical thinking aligned with adult learning principles. The format encouraged residents to take ownership of their learning while benefiting from team-based decision-making following constructivist learning theory, where exposure to differing viewpoints during discussion facilitates deeper understanding (Hrynchak & Batty, 2012).
Despite overall satisfaction, suggestions for longer discussion time and better alignment of pre-reading with session content indicate a need for improved facilitation and onboarding. Slightly lower preferences among Endodontic residents may reflect differences in prior exposure. High ratings for faculty support and the effectiveness of mixed-level resident teams further highlight the importance of guided facilitation and peer learning. Mixing junior and senior residents within teams promoted mentorship and dynamic learning, reflecting real-world clinical team structures. This structure leverages diverse academic levels to enhance small-group learning outcomes. These findings support TBL as a relevant and effective approach in dental residency education, promoting clinical reasoning, interdisciplinary learning, and professional development.
The 32-item TBL-SAI and 22-item programme surveys may have contributed to survey fatigue and response bias; shortening these in future studies could enhance data quality. Although the study lacked a control group and relied on self-reported data from a small cohort, bias was minimized by assuring participants that responses would not affect exam results. Peer evaluation was excluded due to the single-session format.
|
Items |
Periodontic Residents |
Endodontic Residents |
Whole Cohort |
|
Accountability (Max: 40, mean± s.d.) |
28.3 ± 2.8 |
31.3 ± 3.1 |
30.1 ± 2.1 |
|
Cronbach’s alpha |
0.83 |
0.75 |
0.81 |
|
Preference for Lecture / TBL (Max: 80, mean± s.d.) |
50.7 ± 4.1 |
49.2±6.2 |
49.8 ± 13.5 |
|
Cronbach’s alpha |
0.69 |
0.78 |
0.74 |
|
Student Satisfaction (Max: 40, mean± s.d.) |
28.3 ± 1.9 |
29.3 ± 0.0 |
29.1 ± 1.9 |
|
Cronbach’s alpha |
0.69 |
0.68 |
0.66 |
|
Programme Content (Max: 5, mean± s.d.) |
4.3 ± 0.5 |
4.6 ± 0.5 |
4.6 ± 0.5 |
|
Cronbach’s alpha |
0.94 |
0.98 |
0.96 |
|
Programme Learning (Max: 5, mean± s.d.) |
3.6 ± 0.8 |
4.0 ± 1.0 |
3.9 ± 0.9 |
|
Cronbach’s alpha |
0.95 |
0.99 |
0.98 |
|
Faculty (Max: 5, mean± s.d.) |
4.5 ± 0.5 |
4.4 ± 0.5 |
4.4 ± 0.5 |
|
Cronbach’s alpha |
0.98 |
0.96 |
0.97 |
Table 1. Learners’ feedback and Cronbach’s alpha scores based on Team-Based Learning student assessment instrument, programme content, programme learning and faculty
Future research could incorporate independent faculty follow-up to assess residents’ clinical performance in diagnosing and managing periodontal-endodontic lesions (Kirkpatrick Level 3). Despite its limitations, this study suggested that TBL can be an effective approach for teaching interdisciplinary topics in dentistry. It fostered active engagement, deepened learning, and reinforcing the power of structured peer-supported learning in postgraduate education.
V. CONCLUSION
Residents reported positive perceptions of Team-Based Learning (TBL), with high scores for accountability, engagement, and satisfaction. Consistent quantitative outcomes and corroborating qualitative feedback reinforce its effectiveness. Real-life cases enhanced clinical relevance and critical thinking, while TBL’s collaborative format promoted interdisciplinary learning—ultimately strengthening clinical preparedness and teamwork among dental residents.
Notes on Contributors
Dr Lean Heong Foo is a Consultant Periodontist in Department of Restorative Dentistry, National Dental Centre Singapore. LHF reviewed the literature, contributed to the study conception, data acquisition, data analysis, drafted and critically revised the manuscript.
Dr Pei Yuan Chan is a Senior Consultant Endodontist in Department of Restorative Dentistry, National Dental Centre Singapore and Associate Director, Master of Dental Surgery Endodontic Residency programme. PYC contributed to the study conception, data acquisition, and critically revised the manuscript.
Dr Jeen Nee Lui is a Senior Consultant Endodontist in National Dental Centre Singapore. JNL contributed to the data acquisition and critically revised the manuscript.
Dr Marianne Meng Ann Ong is a Senior Consultant Periodontist in National Dental Centre Singapore Associate Director, Master of Dental Surgery Periodontics Residency programme. MO contributed to the data acquisition and critically revised the manuscript.
All authors gave their final approval and agreed to be accountable for all aspects of the work.
Ethical Approval
This study was exempted from formal Centralised Institutional Board review by SingHealth Institutional Review Board (CIRB Ref: 2024-4153).
Data Availability
Data is deposited at Figshare repository (https://doi.org/10.6084/m9.figshare.28366964).
Acknowledgment
We wish to express our appreciation to the National University of Singapore, Faculty of Dentistry for their support in enabling MDS resident participation in this workshop.
We would also like to thank Ms Geraldine Tan and Ms Liu Yanting from National Dental Centre Singapore, ACP Education, for their help in data preparation and collection.
Funding
There was no funding involved in the preparation of the manuscript.
Declaration of Interest
The authors declare no conflict of interest.
References
Foo, L. H., Chan, P. Y., Lui, J. N., & Ong, M. M. A. (2025). Perceptions of Team-Based Learning among Periodontic and Endodontic postgraduate residents. [Data set]. Figshare. https://doi.org/10.6084/m9.figshare.28182398
Herrera, D., Retamal-Valdes, B., Alonso, B., & Feres, M. (2018). Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. Journal of Clinical Periodontology, 89 Suppl 1, S85-S102. https://doi.org/10.1002/JPER.16-0642
Hrynchak, P., & Batty, H. (2012). The educational theory basis of Team-Based Learning. Medical Teacher, 34(10), 796-801. https://doi.org/10.3109/0142159X.2012.687120
Mennenga, H. A. (2012). Development and psychometric testing of the Team-Based Learning student assessment instrument. Nurse Educator, 37(4), 168-172. https://doi.org/10.1097/NNE.0b013e31825a87cc
Pileggi, R., & O’Neill, P. N. (2008). Team-Based Learning using an audience response system: An innovative method of teaching diagnosis to undergraduate dental students. Journal of Dental Education, 72(10), 1182-1188. https://www.ncbi.nlm.nih.gov/pubmed/18923099
Takeuchi, H., Omoto, K., Okura, K., Tajima, T., Suzuki, Y., Hosoki, M., Koori, M., Shigemoto, S., Ueda, M., Nishigawa, K., Rodis, O. M., & Matsuka, Y. (2015). Effects of Team-Based Learning on fixed prosthodontic education in a Japanese School of Dentistry. Journal of Dental Education, 79(4), 417-423. https://www.ncbi.nlm.nih.gov/pubmed/25838013
*Foo Lean Heong
National Dental Centre Singapore,
5, Second Hospital Avenue,
Singapore 168938
Email: foo.lean.heong@singhealth.com.sg
Submitted: 16 March 2025
Accepted: 11 September 2025
Published online: 7 April, TAPS 2026, 11(2), 49-53
https://doi.org/10.29060/TAPS.2026-11-2/OA3593
Clarisse Chu1, Rehena Sultana2, Neville Wei Yang Teo1 & Abhilash Balakrishnan1
1Department of Otorhinolaryngology – Head and Neck Surgery, Singapore General Hospital, Singapore; 2Centre for Quantitative Medicine, Duke-NUS Medical School, Singapore
Abstract
Introduction: The ACGME-I Singapore Otorhinolaryngology residency programme started in 2011. Our first Exit MCQ Examinations were held at the start of the fifth year of residency, in 2015. Its questions are developed by the American Boards and modified by Singapore’s regulatory bodies to ensure relevance to local clinical practice. In contrast, Otorhinolaryngology residents in both Singapore and the USA take the same Otorhinolaryngology Training Examination (OTE) annually. Otorhinolaryngology residents in Singapore sit for the OTE in their first to fourth years of the five-year residency programme.
Multiple specialities have described a positive association between in-training examination and final board MCQ examination pass rates. Our study aims to demonstrate that that OTE scores may serve as predictors of performance in our local Exit MCQ Examination.
Methods: A retrospective review was performed of all 24 Otorhinolaryngology residents who entered and took the Exit MCQ Examination at a single institution’s residency programme between 2016 to 2023.
Results: 75% (18/24) passed the Exit MCQ Examination in their first sitting. Univariate logistic regression analyses showed lower OTE stanines in the fourth year of residency was significantly associated with failing the Exit MCQ Examination. Youden’s index showed attaining an OTE stanine <4 in the fourth year of residency training was most associated with failing the Exit MCQ Examination.
Conclusion: OTE scores may be a better predictor of Exit MCQ performance in the fourth year of residency. Optimal OTE score targets for each year of residency were established.
Keywords: Health Profession Education, Board Examinations, Assessments, Otorhinolaryngology, Residency, ACGME
Practice Highlights
- The OTE serves as an important goalpost for resident learning as they work towards specialist accreditation.
- Our findings will facilitate the identification of residents at risk of performing poorly in the final Exit MCQ Examination, such that remediation measures can be instituted early.
I. INTRODUCTION
Medical education is important for doctors in training throughout their years in residency and beyond. A key tenet of medical education is the use of regular examinations and assessments. They serve multiple functions such as evaluating the retention of medical knowledge, the clinical competencies, and tracking of residents’ progress. Multiple specialities such as Anaesthesia, General Surgery, and Internal Medicine have established a positive correlation between in-training examination performance and pass rates amongst their residents in the final board examinations (McDonald et al., 2020; Patzkowski et al., 2023; Stain et al., 2021).
The Accreditation Council for Graduate Medical Education – International (ACGME-I) Singapore Otorhinolaryngology residency programme was started in 2011 to provide a comprehensive and holistic training programme for prospective Otorhinolaryngologists in Singapore. Our first Exit Multiple-Choice-Question (MCQ) examinations were held at the start of the fifth year of residency, in 2015 (Ministry of Health Singapore, 2023).
There are two summative assessments in Singapore’s five-year Otorhinolaryngology residency programme, namely the Master of Medicine (Otorhinolaryngology) (MMed(ORL)) Examination and the Exit Examinations (Figure 1). Residents usually take the MMed(ORL) Examination in their second year. This is set by the Division of Graduate Medical Studies (DGMS), part of the National University of Singapore. It currently comprises an Objective Structured Clinical Examination (OSCE) and Oral Examination (Division of Graduate Medical Studies, Yong Loo Lin School of Medicine, 2024). Residents have to pass the MMed(ORL) Examination by the fourth year of residency in order to sit for the Exit Examinations.
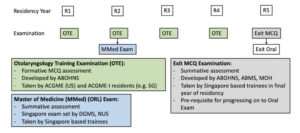
Figure 1. Background of Assessments in Singapore’s Otorhinolaryngology Residency Programme (ABOHNS: American Board of Otorhinolaryngology – Head and Neck Surgery; ACGME: Accreditation Council for Graduate Medical Education; DGMS: Division of Graduate Medical Studies; NUS: National University of Singapore; ABMS: American Board of Medical Specialities; MOH: Ministry of Health)
The Exit MCQ Examination is the first of the two-part Exit Examination comprising both the MCQ and Oral Examinations. Residents take the Exit MCQ Examination at the start of the fifth year of residency. Candidates are required to pass the MCQ in order to be eligible for the Oral Examination at the end of the same year of residency. It is colloquially known as the Exit Examination because it is a regulatory requirement before a resident can complete (and therefore “exit”) specialist training and subsequently obtain specialist accreditation in Singapore. The Exit MCQ Examination is developed by the American Board of Otorhinolaryngology – Head and Neck Surgery (ABOHNS), ACGME-I and Ministry of Health (MOH) Singapore. Its questions are based on the established blueprint used by the three regulatory bodies, and modified to ensure relevance to local clinical practice (ACGME International, 2024).
On the other hand, Otorhinolaryngology residents in the United States of America (USA) take the Board Examinations developed by ABOHNS following completion of specialty training in an ACGME accredited residency programme (Cantrell & Goldstein, 1999; Miller, 2007).
The Otorhinolaryngology Training Examination (OTE) is an MCQ assessment developed by the ABOHNS. It is a formative assessment, and is conducted on an annual basis, to assess Otorhinolaryngology residents’ clinical knowledge. Unlike the Exit MCQ Examination, residents in both Singapore and the USA take the same OTE with the same set of questions. Otorhinolaryngology residents in Singapore sit for the OTE in their first to fourth years, while those in the USA sit for the OTE in their second to fifth years of the five-year residency programme (Puscas, 2019).
Our study aims to demonstrate a similar relationship amongst Otorhinolaryngology residents in Singapore’s largest healthcare cluster, that OTE scores can be used to predict performance in our local Exit MCQ Examination. This enables medical educators to identify residents who are at risk of failing the Exit MCQ Examination and institute remediation programmes early.
II. METHODS
A retrospective review was performed of the examination results of all 24 Otorhinolaryngology residents from our healthcare cluster who entered and took the Exit MCQ Examination between 2016 and 2023. Approval from the SingHealth Institutional Review Board (IRB) was obtained for a waiver of informed consent (IRB reference number 2024-3953). All data was de-identified to ensure anonymity.
Each individual resident’s performance in the OTEs from year one to four of residency and the subsequent Exit MCQ Examination was included in the analysis. The profile and educational background of the individual residents were also obtained. These include their age, gender, primary medical education and the numbers of years spent as a practising medical doctor.
The OTE performance across the first to fourth years of residency is reported in terms of stanines, where raw test scores are converted to a 9-point standard scale across a bell curved distribution of all residents across the same residency training year. An OTE stanine of 9 is the highest, while a stanine of 1 was the lowest – i.e., best and poorest performance respectively. The results of the Exit MCQ Examination are binary, either pass or fail.
Frequencies (proportions) were used to summarise variables. The effects of various factors on Exit MCQ Examination performance was evaluated using logistic regression analyses and association from logistic regression analyses were expressed as odds ratio with 95% confidence interval (CI). Receiver operating characteristic (ROC) curves were also calculated to predict the OTE stanines most associated with a pass result in the Exit MCQ Examination. SPSS for Windows version 25 was used in the analyses.
III. RESULTS
Between 2016 to 2023, 24 Otorhinolaryngology residents in our healthcare cluster entered and took the Exit MCQ Examination. 45.8% (11/24) were male and 54.2% (13/24) were female. 95.8% (23/24) underwent their undergraduate medical training in Singapore, while 4.2% (1/24) studied overseas. The mean post-graduate year at exits was 8.7 ± 2.3 years. 75% (18/24) passed the Exit MCQ Examination in their first sitting (Table 1).
|
Residents’ Characteristics |
N=24 |
|
Final Exit MCQ Performance (first sitting); N(%) |
|
|
Passed |
18 (75%) |
|
Failed |
6 (25%) |
|
Gender; N(%) |
|
|
Male |
11 (45.8%) |
|
Female |
13 (54.2%) |
|
Medical School; N(%) |
|
|
Singapore |
23 (95.8%) |
|
Non-Singapore |
1 (4.2%) |
|
Post-Graduate Year at time of Exits; mean ± SD |
8.7 ± 2.3 |
Table 1. Summary Table of Residents’ Characteristics
Univariate analyses demonstrated lower OTE stanines in the second (OR 0.44, 95% CI 0.20-0.97, p<0.05) and fourth (OR 0.35, 95% CI 0.13-0.99, p<0.05) years of residency were significantly associated with failing the Exit MCQ Examination. There was no significant association between OTE stanines and Exit MCQ Examination performance in the first (OR 0.09, 95% CI 0.008-1.13, p=0.06) and third (OR 0.68, 95% CI 0.35-1.32, p=0.25) years of residency. There was no significant association between gender (Fisher’s exact test p=1.00), medical school (Fisher’s exact test p=0.25) and Exit MCQ Examination performance.
Receiver Operating Characteristic (ROC) curve analysis was used to evaluate the predictive power of OTE stanine scores in identifying residents who would pass the Exit MCQ Examination. For each potential stanine cut-off in Years 1–4, we calculated the sensitivity (true positive rate) and specificity (true negative rate) for predicting a pass outcome. The ROC curve plots these values, and the Area Under the Curve (AUC) quantifies discriminatory ability. To determine the most effective cut-off for each year, we applied the Youden Index (J = sensitivity + specificity − 1). The stanine cut-off with the highest Youden Index was selected as the optimal threshold, balancing the risk of false positives and false negatives. For example, in Year 4, a stanine cut-off of ≥4 yielded the highest Youden Index (J = 0.67), meaning this threshold had the best combined sensitivity and specificity for predicting Exit MCQ success. Similarly, in Year 2, a stanine cut-off of ≥3 yielded the highest Youden Index (J = 0.50). In Year 1, a stanine cut-off of ≥2 yielded the highest Youden Index (J = 0.72). Residents scoring below this threshold may benefit from targeted remediation. In Year 3, no stanine cut-off could not be established, as the maximum Youden Index observed was low (J = 0.30).
Additionally, we noted that all residents who obtained OTE stanines >4 in both their second or fourth years of residency passed the Exit MCQ Examination on their first attempt.
IV. DISCUSSION
The OTE is recommended by the ABOHNS as a practice test for residents prior to sitting for primary certification (American Board Examinations) to be qualified as board-certified. Our study aimed to refine the utility of the OTE by assessing whether there were predictive values to stanine levels in Singapore residents sitting for the MCQ component of the specialist Exit Examinations. In this respect, our study demonstrated a positive correlation between OTE stanines and Exit MCQ Examination performance. However, this only applied to the OTE stanines in the second and fourth years of residency and not the other years. Given that the OTE is a formative assessment with no penalty for suboptimal performance, low scores may not correlate with residents’ academic knowledge.
It is worthwhile to note that in the second year of residency, residents sit for the MMed(ORL) Examination, which is a summative assessment, about one month after the OTE examination. Similarly, Year-4 residents sitting for the OTE have to sit for the Exit MCQ Examination, which determines eligibility for taking the Exit Oral Examination, in about six months’ time. As the OTE is conducted relatively closer to these high-stakes examinations, residents would be undertaking more extensive preparation, and hence their OTE stanines would be more reflective of their academic performance.
Additionally, using Youden’s index, we identified OTE score targets which residents can aim to meet at each year of residency. For each stanine, the sensitivity and specificity for failing the Exit MCQ Examination were determined. The stanine with the highest sensitivity and specificity was deemed the cut off. Our analysis showed that residents should aim to achieve OTE stanines of ≥3 in their second year and ≥4 in their fourth year of residency to reduce their risk of failing the Exit MCQ Examination. Faculty can then work with residents to develop individualised learning plans to achieve these concrete academic goals.
Our study had a small sample size (n=24), drawn from a single healthcare cluster in Singapore. This limited sample size reduces the effect size of our analysis. Despite this limitation, our results provide a preliminary insight into OTE scores as predictors of performance in our local Exit MCQ Examination. In the future, we aim to expand it to the two other healthcare clusters in Singapore for a larger pool of candidates, for increased statistical power and to determine the broader applicability of our conclusions.
V. CONCLUSION
Continuous assessment tools, such as the OTE, serve as key milestones and reference points for residents to take stock of their own academic performance as they work towards specialist accreditation. Our findings will facilitate the identification of residents at risk of performing poorly in the final Exit MCQ Examination, such that remediation measures can be instituted early.
Notes on Contributors
Clarisse Chu reviewed the literature, performed data analysis and wrote the manuscript.
Rehena Ganguly designed the study, performed data analysis and developed the manuscript.
Neville Wei Yang Teo advised design of the study and gave critical feedback to the writing of the manuscript.
Abhilash Balakrishnan reviewed the literature, advised design of the study and gave critical feedback to the writing of the manuscript.
All authors have read and approved the final manuscript.
Ethical Approval
Approval from the SingHealth Institutional Review Board (IRB) was obtained for waiver of informed consent (IRB reference number 2024-3953).
Data Availability
The data relevant to the study is not publicly available, so as to protect our residents’ confidentiality. Although there are no specific descriptors about each resident, the small number of residents per year could lead to the examination results being narrowed down to specific residents.
Our Graduate Medical Office does not share survey results with programmes if there are fewer than 4 respondents each year. Similarly, we would not share the information as there are multiple years where the residents taking the OTE are less than 4 in their year of graduation.
Funding
There are no funding source(s) for this paper or research study.
Declaration of Interest
There are no financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest.
References
ACGME International. (2017). Otolaryngology Milestones for Singapore. ACGME International. https://www.acgme-i.org/globalassets/acgme-international/specialties/otolaryngology/otolaryngology_milestones_for_singapore.pdf
Cantrell, R. W., & Goldstein, J. C. (1999). The American Board of Otolaryngology, 1924–1999: 75 years of excellence. Archives of Otolaryngology–Head & Neck Surgery, 125(10), 1071–1079. https://doi.org/10.1001/archotol.125.10.1071-a
Division of Graduate Medical Studies, Yong Loo Lin School of Medicine. (2024). Master of Medicine (Otorhinolaryngology) examination. National University of Singapore. https://medicine.nus.edu.sg/dgms/master-of-medicine/otorhinolaryngology/
McDonald, F. S., Jurich, D., Duhigg, L. M., Paniagua, M., Chick, D., Wells, M., Williams, A., & Alguire, P. (2020). Correlations between the USMLE Step examinations, American College of Physicians In-Training Examination, and ABIM Internal Medicine Certification Examination. Academic Medicine, 95(9), 1388–1395. https://doi.org/10.1097/ACM.0000000000003382
Miller, R. H. (2007). Certification and maintenance of certification in otolaryngology–head and neck surgery. Otolaryngologic Clinics of North America, 40(6), 1347–1357. https://doi.org/10.1016/j.otc.2007.07.010
Ministry of Health Singapore. (2023). SAB: Otorhinolaryngology examination (2024). Ministry of Health Singapore. https://www.healthprofessionals.gov.sg/sab/specialist-examination/otorhinolaryngology-examination-(2024)
Patzkowski, M. S., Hauser, J. M., Liu, M., Herrera, G. F., Highland, K. B., & Capener, D. C. (2023). Medical school clinical knowledge exam scores, not demographic or other factors, associated with residency in-training exam performance. Military Medicine, 188(1–2), e388–e391. https://doi.org/10.1093/milmed/usab332
Puscas, L. (2019). Junior otolaryngology resident in-service exams predict written board exam passage. The Laryngoscope, 129(1), 124–128. https://doi.org/10.1002/lary.27515
Stain, S. C., Matthews, J. B., Ata, A., Adams, D. B., Chen, H., & Potts, J. R. (2021). US Medical Licensing Exam performance and American Board of Surgery qualifying and certifying examinations. Journal of the American College of Surgeons, 233(6), 722–729. https://doi.org/10.1016/j.jamcollsurg.2021.08.674
*A/Prof Abhilash Balakrishnan
31 Third Hospital Ave
Singapore General Hospital
Singapore 168753
Email: balakrishnan@singhealth.com.sg
Submitted: 6 February 2025
Accepted: 24 September 2025
Published online: 7 April, TAPS 2026, 11(2), 131-133
https://doi.org/10.29060/TAPS.2026-11-2/II3665
Pacifico Eric Eusebio Calderon1,2,3
1St. Luke’s Medical Center, 2National Children’s Hospital, Quezon City, Philippines; 3Faculty of Laws, University College London, United Kingdom
I. INTRODUCTION
Artificial intelligence (AI) is now a familiar presence in healthcare. Frequently introduced as a means of augmenting clinical work, it also invites reflection on how the character of medical practice is evolving. AI may influence not only clinical decision-making (Byrne, 2023), but also the production of medical knowledge, the framing of ethical questions, and the assignment of responsibility when outcomes are uncertain, or contested (Aquino, 2023). As these technologies become embedded in the routines of care, they may begin to reshape prevailing conceptions of clinical judgement, moral attentiveness, and professional responsibility.
This article reflects on how the increasing integration of AI into clinical settings may be subtly reconfiguring the ethical landscape of medicine and considers how such shifts might be addressed in ethics education. It critiques three domains in which new tensions emerge: the erosion of space for moral discernment, epistemic injustice within data-driven systems, and the fragmentation of responsibility across increasingly distributed environments.
In place of technical prescriptions, the paper invites educators to reflect on the kinds of moral sensibilities we seek to cultivate in those learning to practise medicine—whether students, trainees, or professionals in continuing formation. How might ethical capacities be fostered in healthcare systems increasingly configured by technologies that clinicians do not design and cannot fully control? What dispositions might be required to remain attentive, critical, and responsive within datafied systems of care?
These questions are pursued through a series of reflections on how AI is reshaping attentiveness, knowledge, and responsibility—and on how ethics education might engage with these shifts with nuance and care.
II. PRESERVING ATTENTIVENESS IN ALGORITHMIC ENCOUNTERS
The clinical encounter between doctor and patient remains foundational to medical practice. Such moments are rarely straightforward. They require not only clinical reasoning but also the capacity to navigate uncertainty, emotional nuance, and what is often unspoken. Ethical significance in these situations is not always immediately visible; it may emerge in a hesitation, a glance, or an absence that nonetheless invites moral attention. Attending to these subtleties requires what might be called moral attentiveness: the ability to notice what might otherwise be missed, and to recognise that ethical meaning is not always legible within procedural norms.
This form of attentiveness finds philosophical resonance in Tronto’s (1993) articulation of care as relational, situated, and responsive to particular needs. On this view, good care cannot be reduced to procedural fidelity or technical adequacy. It involves a willingness to remain present, to slow down, and to engage meaningfully with the lived experience of the person before us.
Yet this space for attentiveness may be increasingly constrained by the integration of AI systems into clinical work (Dalton-Brown, 2020). Many such systems are designed to promote speed, consistency, and institutional efficiency. They may generate clinical suggestions before a patient is even seen, structure how documentation is produced, and guide decisions in ways that encourage adherence to predefined pathways (Byrne, 2023). Whilst these tools may support workflow, their underlying logic can narrow the reflective space needed for ethical discernment. When clinical attention is structured in advance by algorithmic cues, the opportunity to pause, to wonder, or to respond to the unexpected may begin to contract (Dalton-Brown, 2020).
This shift presents a challenge not only for practice but also for pedagogy. If AI systems increasingly shape how care is delivered, then ethics education must consider how to support learners in sustaining forms of attentiveness that resist automation. What pedagogical approaches might preserve interpretive openness in contexts structured around procedural closure? This may call for renewed emphasis on cultivating presence, responsiveness, and moral imagination (Tronto, 1993)—qualities that remain vital to ethical practice but are difficult to codify, even harder to delegate to machines.
III. RECOGNISING EXCLUSIONS IN DATA-DRIVEN KNOWLEDGE
AI systems are often introduced with the promise of improving efficiency, promoting consistency, and mitigating bias or human error in clinical practice (Byrne, 2023). Yet the data on which such systems rely on is rarely neutral. Most are developed in high-resource environments and trained on datasets that reflect the clinical norms, priorities, and assumptions of those contexts. As a result, some experiences of illness are amplified, whilst others are excluded, distorted, or remain unrecognised altogether (Aquino, 2023). These exclusions are not merely technical gaps but carry ethical implications, shaping whose suffering is acknowledged and whose is not.
This form of marginalisation has been theorised by Fricker (2007) as epistemic injustice: harm that arises when individuals or groups are excluded from contributing to shared knowledge, or when their insights are misrepresented, dismissed, or devalued. In healthcare, for instance, this may occur when symptoms presented by certain populations are not recognised by AI systems trained on different demographics, or when non-standard forms of expression—whether cultural context, embodied experience, or vernacular language—are treated as deviations rather than legitimate sources of insight.
For learners, the effects of these omissions may unfold incrementally. What is consistently absent from training tools may come to feel irrelevant; what is frequently represented may appear normative. Over time, these patterns can come to shape how clinicians perceive credibility, construct clinical knowledge, and attend to suffering. The narrowing of epistemic horizons is rarely intentional, but it has moral consequences (Fricker, 2007). Certain voices come to dominate, and some forms of distress remain invisible within algorithmic frames (Aquino, 2023).
Ethics education might respond by fostering what could be described as epistemic humility: an awareness that all systems of knowledge, however advanced, can be partial and situated. This involves not only recognising what is missing but also cultivating the capacity to dwell with uncertainty and remain attentive to the margins of representation. Especially in global or resource-constrained settings—where imported AI systems may misrepresent local realities—this disposition is not only prudent, but also pedagogically essential. The task is not to reject such tools outright, but to approach them with critical distance, sustained attentiveness, and moral care.
IV. NAVIGATING RESPONSIBILITY IN DISTRIBUTED SYSTEMS
The deeper integration of AI into medical work is also reshaping how professional responsibility is perceived. AI is often viewed as a form of support—something that augments rather than replaces the clinician (Byrne, 2023). Yet in practice, the distinction between assistance and authority may be far from straightforward. When outputs appear confident and their reasoning opaque, clinicians may feel compelled to defer, even in the presence of doubt.
Efficiency is frequently presented as the primary feature of such tools. Yet efficiency is rarely neutral. It tends to reflect the priorities of institutions—throughput, documentation, predictability—rather than the relational demands of ethical care. The logic of efficiency that underpins many AI systems often aligns with these institutional imperatives. In doing so, it may shift the moral orientation of practice away from responsiveness to particular needs and toward standardised procedures. As Tronto (1993) reminds us, responsibility is not simply the performance of tasks; it involves attentiveness to needs that unfold slowly or resist resolution. When time saved is redirected toward institutional metrics, the more reflective dimensions of medical work may be compromised.
Within such systems, responsibility can become fragmented and elusive. Clinical decisions often arise through a convergence of human reasoning, algorithmic suggestion, and organisational structure (Aquino, 2023). Yet when outcomes are contested, accountability frequently reverts to the individual clinician. For learners, this may create a disorienting professional ethical terrain. They are expected to exercise moral judgement in contexts that may increasingly constrain their agency.
In response, ethics education might offer more than abstract principles. It can support learners in reflecting on what it means to assume responsibility in conditions where control is partial and in navigating situations where the line between autonomous professional judgement and systemic compliance is blurred. Discernment—understood here as the capacity to act with care in the face of uncertainty, complexity, or constraint—becomes central to this pedagogical task. It is perhaps not a matter of identifying the right answer, but of cultivating the sensitivity to decide well when clarity is elusive.
V. CONCLUDING REFLECTIONS
The discussion has traced how the integration of AI into clinical practice may be reshaping the moral contours of medicine—not through sudden rupture, but through subtler shifts in how clinicians attend, decide, and take responsibility. It explored three such developments: the narrowing of interpretive space in clinical encounters; the exclusions embedded in data infrastructures; and the dispersal of professional responsibility across distributed systems. These changes do not call for rejection, but for careful recalibration—one that sustains moral attentiveness, epistemic humility, and ethical discernment within systems increasingly structured around speed, efficiency, and procedural logic. Each domain also opens space for pedagogical reflection, prompting us to ask not only how we teach ethics, but what kinds of moral sensibilities we hope to preserve.
What forms of teaching might support the cultivation of these capacities? How might empirical inquiry illuminate the lived ethical consequences of AI integration across diverse institutional and cultural contexts? And how can educators, ethicists, clinicians, and curriculum designers engage in shared dialogue about the values we wish to uphold amid technological transformation? Much, however, remains unsettled. The task ahead may lie in cultivating–in learners, and in ourselves as educators– a disposition to remain with ethical demands that technological systems cannot resolve. Such a pedagogy would rest not on certainty but on reflective presence, epistemic humility, and a sustained attentiveness to the forms of care we still hope to practise in a world increasingly shaped by algorithmic reasoning.
Notes on Contributors
The author solely conceptualised, drafted, and revised the manuscript.
Ethical Approval
As this is a theoretical study, it does not involve human participants or data collection. Accordingly, ethical approval was not applicable.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Interest
The author declares no conflict of interest.
References
Aquino, Y. S. J. (2023). Making decisions: Bias in artificial intelligence and data-driven diagnostic tools. Australian Journal of General Practice, 52(7), 439–444. https://doi.org/10.31128/AJGP-12-22-6630
Byrne, M. F., Parsa, N., Greenhill, A. T., Chahal, D., Ahmad, O., & Bagci, U. (Eds.). (2023). AI in clinical medicine: A practical guide for healthcare professionals. John Wiley & Sons.
Dalton-Brown, S. (2020). The ethics of medical AI and the physician–patient relationship. Cambridge Quarterly of Healthcare Ethics, 29(1), 115–121. https://doi.org/10.1017/S0963180119000847
Fricker, M. (2007). Epistemic injustice: Power and the ethics of knowing. Oxford University Press. https://doi.org/10.1093/acprof:oso/9780198237907.001.0001
Tronto, J. (2020). Moral boundaries: A political argument for an ethic of care. Routledge. https://doi.org/10.4324/9781003070672
*Pacifico Eric Eusebio Calderon
Faculty of Laws, University College London
4-8 Endsleigh Gardens,
London WC1H 0EG
United Kingdom
Email: pacifico.calderon.24@ucl.ac.uk
Submitted: 8 April 2025
Accepted: 27 August 2025
Published online: 7 April, TAPS 2026, 11(2), 81-88
https://doi.org/10.29060/TAPS.2026-11-2/OA3714
Vy Van Thao Ngan Nguyen & Nguyen Bao Phuc Diep
School of Nursing and Medical Technology, The University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam
Abstract
Introduction: Self-efficacy significantly impacts academic performance and clinical competence in healthcare education. Students need to develop confidence and adaptability to handle unpredictable situations in high-pressure fields like anaesthesia nursing. While global studies emphasise self-efficacy’s role in clinical training, research on Vietnamese nursing students is limited. This study aimed to evaluate the clinical self-efficacy beliefs of anaesthesia nursing students to understand their confidence levels and identify factors influencing this.
Methods: A cross-sectional descriptive study was conducted from February to June 2024, with Stratified sampling of 205 third- and fourth-year anaesthesia nursing students at the University of Medicine and Pharmacy in Ho Chi Minh City. The Self-Efficacy in Clinical Performance (SECP) scale was used to evaluate students’ self-efficacy, and the Critical Thinking Disposition Inventory for Medical College Students (CTDI-M) measured critical thinking disposition.
Results: The overall clinical self-efficacy score for students was 105.4±12.87. A statistically significant positive correlation was found between self-efficacy and critical thinking disposition among students (rs = 0.37, p < 0.001). Furthermore, a significant linear regression analysis indicated that critical thinking disposition (coefficient = 8.6, p < 0.001), attitudes regarding the characteristics of anaesthesia nursing students (coefficient = 0.9, p < 0.001), and academic year (coefficient = 6.1, p < 0.001) are significant predictors of clinical self-efficacy.
Conclusion: Integrating the promotion of critical thinking, addressing specific attitudes, and considering students’ academic progression into clinical training programmes is essential. This has important implications for developing training programmes that enhance essential skills and better prepare students for their professional careers.
Keywords: Anaesthesia Nursing Students, Clinical Self-Efficacy, Critical Thinking Disposition, Clinical Practice
Practice Highlights
- Anaesthesia nursing students demonstrated a moderate level of self-efficacy in clinical practice, highlighting the need for targeted interventions to enhance their confidence and competency.
- A significant positive correlation was identified between self-efficacy and critical thinking disposition (p = 0.001), suggesting that students with stronger critical thinking skills tend to have higher confidence in clinical settings.
- Strengthening critical thinking skills and positive attitudes concerning professional characteristics may serve as a key strategy to enhance clinical self-efficacy among anaesthesia nursing students, improving their readiness for professional practice.
I. INTRODUCTION
In nursing education, the concepts of self-efficacy and critical thinking are essential for developing competent practitioners who can make sound clinical decisions.
Self-efficacy, as defined by Bandura, refers to an individual’s belief in their ability to perform the behaviours required to achieve specific outcomes (Bandura, 1991). Higher self-efficacy in nursing correlates with improved clinical performance, motivation, job satisfaction, and patient care outcomes (Köseoglu, 2015; Shorey & Lopez, 2021). Nursing students, especially those in the Anaesthesia specialisation, face unique clinical challenges, including high-pressure hospital environments, which necessitate strong self-efficacy to manage professional responsibilities and emergencies (Albooghobeish et al., 2023). Additionally, errors in this field can lead to serious consequences for both patients and practitioners, including legal issues and psychological trauma.
Critical thinking is equally vital, as it involves the objective analysis of information necessary for effective clinical decision-making (Nederland, 2010; Yildirim et al., 2012). This is particularly important for nurse anaesthesia students, who must cultivate strong critical thinking skills to navigate the complexities of anaesthesia care. They need to make quick and accurate decisions in unpredictable situations during operations (Burns et al., 2013; Scott Imus et al., 2017).
Moreover, transitioning from classroom learning to clinical practice presents significant challenges for students. Numerous studies have highlighted the connection between critical thinking skills and confidence in clinical practice. Students who possess strong critical thinking abilities are more likely to demonstrate greater confidence in making clinical decisions and performing nursing tasks (Albooghobeish et al., 2023; Dehghani et al., 2011; İşeri et al., 2023; Sahebi & Barkhordari-Sharifabad, 2023; Salimi et al., 2017). This connection not only enhances students’ clinical experiences but also creates a bridge between theory and practice.
Some Research indicates that educational interventions, such as simulation-based learning and case-based learning platforms, can enhance essential competencies in nursing education, especially having positively impacted nursing students’ self-efficacy and clinical performance (Azizi et al., 2022).
Despite the recognised importance of self-efficacy and critical thinking in nursing education, there is a notable lack of research specifically focused on anaesthesia nursing students, particularly in Vietnam. Understanding the relationship between these constructs is crucial for developing targeted educational strategies that enhance clinical competence. Therefore, the research question focuses on whether there is a relationship between students’ clinical self-efficacy and their critical thinking disposition, as well as the factors that influence this relationship.
The University of Medicine and Pharmacy in Ho Chi Minh City (UMP HCMC) is a leading institution for training anaesthesia nursing professionals in southern Vietnam, emphasising the importance of assessing and enhancing students’ self-efficacy and critical thinking skills.
This study aims to evaluate the levels of self-efficacy and critical thinking disposition among third- and fourth-year anaesthesia nursing students at UMP HCMC. Additionally, it seeks to examine the relationship between these variables and their combined impact on clinical performance. The findings are expected to inform curriculum development and instructional methodologies, ultimately improving the preparedness of anaesthesia nursing students for clinical practice. This, in turn, will contribute to enhancing the quality of training and support the comprehensive development of students, ensuring they meet the demands of the profession in the near future.
II. METHODS
A. Design and Setting
This cross-sectional research employed an exploratory, descriptive, and quantitative study design that utilised a structured questionnaire to gain insights into nursing students’ perspectives. It was conducted at the School of Nursing and Medical Technology at the University of Medicine and Pharmacy in Ho Chi Minh City from February 2024 to June 2024.
B. Sample
This study involved 205 students enrolled in the anaesthesia nursing degree programme at the University of Medicine and Pharmacy in Ho Chi Minh City, Vietnam. The sample size was determined through a two-step process: first, an initial sample size for the mean was calculated, and then Cochran’s formula for finite populations was applied to make the necessary correction. A stratified random sampling method was employed, based on the academic year, to ensure proportional representation. Since the curriculum for this four-year programme requires students to begin clinical practice related to their major in their third year, we stratified the population of eligible students into two groups: third-year students and fourth-year students. Simple random sampling was then applied within each stratum to select participants until the required sample size for that stratum was reached. This process resulted in 53% of the participants (110 students) being in their third year, accurately reflecting their proportion within the total student population. Only students who provided informed consent were included in the study.
C. Instruments
This study evaluated the self-efficacy of nursing students in the clinical practice environment using the Self-Efficacy for Clinical Performance (SECP) scale (Cheraghi et al., 2009). The translation and back-translation technique was used to convert the English version to Vietnamese, and four experts assessed the content validity with a CVI (content validity index) of 1. The SECP scale includes 37 questions divided into four subcategories: Assessment (12 items), Diagnosis and Planning (9 items), Implementation (10 items), and Evaluation (6 items). Each item on the questionnaire is rated on a Likert scale ranging from 1 (not relevant) to 5 (very relevant). The total score is calculated by summing the ratings for all questions, with possible scores ranging from a minimum of 37 to a maximum of 148. A higher score reflects greater self-efficacy. The questionnaire demonstrated a high Cronbach’s alpha coefficient of 0.96 in a pilot test, indicating strong reliability.
This study also utilised the Critical Thinking Disposition Inventory for Medical College Students (CTDI-M) to assess critical thinking skills. Developed by Wang et al. in 2019 (Wang et al., 2019), the inventory consists of 18 items categorised into three factors: open-mindedness, systematic/analytical thinking, and truth-seeking. To adapt the instrument for the Vietnamese context, a translation and back-translation methodology was employed. The content validity of the translated instrument was then independently assessed by four experts, who collectively assigned a Content Validity Index (CVI) of 0.9. Participants respond using a Likert scale that ranges from 1 (strongly disagree) to 5 (strongly agree). The overall score for each factor is calculated by averaging the scores of the relevant questions. The questionnaire achieved a Cronbach’s alpha of 0.85, indicating good reliability.
To evaluate the internal reliability of the questionnaire, a pilot study was conducted with 25 students from the anaesthesia nursing programme at the University of Medicine and Pharmacy in Ho Chi Minh City. We employed a stratified simple random sampling method to select participants, ensuring the sample was representative of the different academic years (third and fourth year) engaged in clinically relevant practice. The study included only students who provided informed consent and did not participate in the main study.
D. Data Analysis
The study data were processed using Stata 15.0, a statistical software. The first step involved analysing background variables through descriptive statistics, which included calculating the mean, standard deviation, percentiles, and ranges for all parameters. To examine the relationship between sociodemographic characteristics and nursing students’ self-efficacy and critical thinking, we used one-way analysis with the Kruskal-Wallis test and the Mann-Whitney U test. Spearman’s correlation was employed to identify the relationship among the main variables. We set the threshold for statistical significance at p < 0.05. Finally, we used multivariate linear regression to predict self-efficacy in clinical practice based on several independent variables.
III. RESULTS
A. Participant Characteristics
In the study, 74.1% of the participants were women. The youngest student was 21 years old, while the oldest was 30, with an average age of 21.69 years (± 1.01 years). The majority of the students (95.1%) identified as belonging to the Kinh ethnic group, which is the predominant ethnic group in Vietnam. Additionally, more than half of the participants (65.9%) did not identify with any specific religious affiliation. Third-year students made up the largest proportion of participants at 53.7%, while fourth-year students accounted for 46.3%. Moreover, the average score of students’ attitudes towards the professional characteristics of anaesthesia nursing students in clinical practice was 27.50 ± 3.80, with a minimum score of 16 and a maximum score of 33.
|
Variables |
N (%) |
|
|
Academic year |
3rd year |
110 (53.7) |
|
4th year |
95 (46.3) |
|
|
Gender |
Men |
53 (25.9) |
|
Women |
152 (74.1) |
|
|
Ethnicity |
Kinh |
195 (95.1) |
|
Others |
10 (4.9) |
|
|
Religion |
Atheists |
135 (65.9) |
|
Buddhist |
43 (21) |
|
|
Christian |
24 (11.7) |
|
|
Others |
3 (1.4) |
|
|
Mean ± SD |
||
|
Age |
21.7 1,01 |
|
|
Attitude Concerning Characteristics of Anaesthesia Nursing Students |
27.5 1,01 |
|
Table 1. Participant Characteristics (N = 205)
B. Descriptive Statistics of Self-Efficacy for Clinical Practice, Critical Thinking Disposition, and Associated Factors
|
Variables |
Min – Max |
Mean ± SD or Mean (IQR)+ |
|
Critical Thinking Disposition |
1.1 – 5.0 |
3.7 ± 0.47 |
|
Open-mindedness+ |
1.1 – 5.0 |
3,8 (3.4-4.0) |
|
Truth-seeking+ |
1.0 – 5.0 |
3,7 (3.4-4.0) |
|
Systematicity+ |
1.2 – 5.0 |
3,7 (3.3-4.0) |
|
Self-Efficacy for Clinical Practice |
75-148 |
105,4± 12,87 |
|
Assessment+ |
24-48 |
34.7 (31-37) |
|
Diagnosis and Planning+ |
14-36 |
24.4 (22-27) |
|
Implementation+ |
20-20 |
29.9 (28-32) |
|
Evaluation+ |
12-24 |
16.5 (14-18) |
+ Nonnormal distribution
IQR: interquartile range
Table 2. Descriptive Analysis of Critical Thinking Disposition and Self-Efficacy for Clinical Practice of Nursing Students (N = 205)
Regarding critical thinking disposition, the students exhibited relatively strong critical thinking skills, demonstrated by an average score of 3.7 ± 0.47. Among the various categories of critical thinking dispositions, “open-mindedness” received the highest average score of 3.8, with an interquartile range (IQR) of 3.4 to 4.0. In terms of self-efficacy, the total score was 105.4 ± 12.87. The highest score was obtained in the area of “Assessment” (mean = 34.7, IQR = 31-37), while the lowest score was in “Evaluation” (mean = 16.5, IQR = 14-18).
|
Variables |
Self-Efficacy for Clinical Practice rs (p< 0.01) |
||||
|
Assessment |
Diagnosis and Planning |
Implementation |
Evaluation |
SECP |
|
|
Critical Thinking Disposition |
0.33 |
0.31 |
0.30 |
0.36 |
0.37 |
|
Open-mindedness |
0.26 |
0.20 |
0.22 |
0.20 |
0.24 |
|
Truth-seeking |
0.28 |
0.30 |
0.29 |
0.33 |
0.34 |
|
Systematicity |
0.33 |
0.33 |
0.30 |
0.43 |
0.40 |
Table 3. The Correlation Between Self-Efficacy for Clinical Practice and Critical Thinking Disposition (N=205)
The results presented in Table 3 show a significant positive correlation between nursing students’ self-efficacy in clinical practice and their disposition toward critical thinking (rs = 0.37, p < 0.0001). There are also notable relationships with factors associated with critical thinking (p < 0.001). The highest score was recorded in the area of “Systematicity” (rs = 0.40, p < 0.001), while the lowest score was noted in “Open-mindedness” (rs = 0.24, p < 0.001). Additionally, the strongest correlation was found between the “Systematicity” aspect of critical thinking disposition and self-efficacy in “Evaluation” (rs = 0.43, p < 0.001). Conversely, the weakest scores were observed for the “Open-mindedness” disposition concerning the “Evaluation” skill (rs = 0.20, p < 0.001), as well as the “Diagnosis and Planning” skill of self-efficacy (rs = 0.20, p < 0.001).
This study employed linear regression analyses to investigate the impact of several factors on students’ self-efficacy in clinical practice. The model satisfied the assumptions of multicollinearity and homoscedasticity, ensuring the reliability of the regression estimates. Table 4 presents the confidence intervals for the predictors of self-efficacy.
|
Variables |
Coef. |
SE |
t |
p |
95% Conf. Interval |
|
Critical thinking disposition |
8.6 |
2.0 |
4.28 |
0.000 |
4.6 – 12.5 |
|
Attitude Concerning Characteristics of Anaesthesia Nursing Students |
0.9 |
0.2 |
4.42 |
0.000 |
0.4 – 0.9 |
|
Academic year |
6.1 |
1.6 |
3.82 |
0.000 |
2.9 – 9.2 |
F = 23.6 (p <0.0001), R2 = 0.26, VIF = 1.01 – 1.07, Const = 40.2
Table 4. Factors Affecting Anaesthesia Nursing Students’ Self-Efficacy for Clinical Practice (N = 205)
Three key factors, including academic year (p < 0.0001), attitudes toward the characteristics of Anaesthesia Nursing students (p < 0.0001), and critical thinking disposition (p < 0.0001), emerged as crucial determinants in predicting overall clinical self-efficacy. According to the model, each one-point increase in critical thinking disposition and attitude toward professional attributes increases self-efficacy by 8.6 and 0.9 points, respectively. Additionally, an increase in self-efficacy would necessitate an increase of 6.1 units in the academic year. The model was significant and accounted for 26% of the variance in self-efficacy (F = 23.6, p < 0.0001, VIF = 1.1).
IV. DISCUSSION
A. Clinical Self-Efficacy among Anaesthesia Nursing Students
After collecting and analysing the data, the research team found that students’ self-efficacy scores were at a moderate level. A study by Vũ Thị Thu Hà in Vietnam reported that approximately 78.8% of nursing students displayed only a moderate level of confidence during clinical practice (Vũ et al., 2023). Similarly, research conducted by Phan Hoang Trong found that the highest percentage of students (55.6%) exhibited moderate levels of confidence (Trong et al., 2023). These findings offer an overview of the current state of nursing students’ self-efficacy perceptions in clinical practice. Additionally, the results of this study align with several international studies. For instance, Zahra reported an overall self-efficacy perception score of 102.40 ± 21.57 among 194 nursing students (Sahebi & Barkhordari-Sharifabad, 2023). A study conducted in China on third-year nursing students reported a mean self-efficacy score of 23.62 ± 3.98 out of a possible 40, indicating a relatively low perception of self-efficacy (Jin & Lv, 2018). In contrast, some international studies have demonstrated higher self-efficacy levels among nursing students. For example, research conducted on 214 nursing students in the United Arab Emirates revealed that approximately 56% of students exhibited high self-efficacy (Tirgari, 2018). Additionally, various studies in Iran indicated that nursing students demonstrated a high level of self-efficacy during clinical training (Motahari et al., 2020; Sajadi & Mehrabi, 2019). One possible explanation for this discrepancy could be the differences in cultural and educational contexts, which may significantly influence self-efficacy perceptions. In Vietnam, traditional educational paradigms often emphasise theoretical knowledge over practical application, potentially limiting opportunities for students to develop confidence in real-world clinical scenarios. Additionally, cultural factors such as a tendency towards modesty or a hierarchical educational system might lead students to express moderate rather than high self-efficacy, even if their competence is higher.
B. Factors Influencing Students’ Clinical Self-Efficacy
The analysis results indicated a correlation coefficient of rs = 0.37 (p < 0.0001) between self-efficacy and critical thinking disposition among anaesthesia nursing students. Several studies have also demonstrated a positive correlation between clinical self-efficacy and critical thinking in nursing students. For example, research conducted by Orujlu and Hemmati Maslakpak found a significant positive correlation (rs = 0.42; p = 0.002) (Orujlu & Hemmati Maslakpak, 2017). Another study by Özge İşeri revealed a positive correlation between perceived self-efficacy and critical thinking disposition among nurses working in the operating room (rs = 0.213; p < 0.05) (İşeri et al., 2023). For anaesthesia nursing, where split-second decisions can have profound consequences, strong critical thinking skills are not merely an academic asset but a crucial component of clinical confidence and effective patient care. When students can objectively analyse information and make sound judgments, their belief in their ability to perform tasks in complex and high-pressure situations naturally increases. This highlights the clear need for nursing education programmes to integrate training that focuses on critical thinking and self-efficacy in clinical practice.
Furthermore, Self-efficacy among anaesthesia students regarding their professional characteristics during clinical practice showed a positive correlation (rs = 0.30; p < 0.0001). This finding aligns with research by Esra Türker and Özlem Ülkü Bulut (2023), which explored the relationship between self-efficacy and the attitudes of nursing students in clinical settings (Esra & Özlem Ülkü, 2023). Additionally, a study by Azza Fathi Ibrahim (2019) revealed that nursing students who reported high satisfaction with their clinical environment also exhibited elevated levels of self-efficacy in various clinical learning activities and tasks (Ibrahim et al., 2019). Therefore, it is essential for nursing students to receive a thorough and accurate orientation before entering clinical practice. Clinical instructors should encourage students to take on challenging tasks to enhance their perception of self-efficacy.
The analysis results also indicated a statistically significant difference in the self-efficacy of students in clinical practice based on their “Academic Year” (p = 0.0002). Research conducted by Esra Türker also supported this finding, showing that as students progressed through their grade levels, their self-efficacy in clinical practice improved (Esra & Özlem Ülkü, 2023). This can be attributed to increased clinical exposure and practical experience, which provide more opportunities for students to handle diverse situations and solidify their skills, thereby boosting their confidence. Besides, two studies conducted in Turkey revealed that students with more clinical experience had higher perceptions of self-efficacy in their clinical practice compared to those with less experience (Karahan Okuroğlu, 2022; Terry & Peck, 2020).
The linear regression model identified three significant predictors of self-efficacy in clinical practice: academic year, critical thinking disposition, and attitudes towards the characteristics of Anaesthesia Nursing students. Among these variables, critical thinking disposition had the most substantial impact, surpassing both academic year and professional attitude. This finding once again emphasises the essential role that critical thinking skills play in shaping students’ confidence and competence in clinical settings. Therefore, promoting the development of critical thinking and professional identity in nursing education may be an important strategy for enhancing clinical self-efficacy.
This study reveals crucial implications for enhancing self-efficacy among anaesthesia nursing students, underscoring a clear need for pedagogical advancements. Nurse educators should prioritise integrating innovative teaching strategies, including high-fidelity simulation, problem-based learning, and case-based learning. These methods provide a safe environment for students to apply theoretical knowledge, cultivate critical thinking through decision-making, and receive immediate feedback, boosting their confidence. Clinical instructors are equally vital, needing to consistently provide assessment of progress and strategically encourage students to undertake incrementally challenging clinical tasks aligned with their academic year. Furthermore, a comprehensive orientation to clinical practice is essential to clarify expectations, mitigate anxiety, and foster a positive attitude towards anaesthesia nursing. These combined interventions are critical for cultivating capable and confident nursing professionals.
While rigorous attempts were made to conduct the research accurately, the study acknowledges inherent limitations. This study utilised a cross-sectional design, limiting causal inference and the ability to track changes in self-efficacy and critical thinking over time. Data was collected through self-report questionnaires, which could introduce bias due to socially desirable responses. Furthermore, the research was conducted at a single university, restricting the generalisability of the findings to other nursing programmes or cultural contexts outside of Vietnam.
Future research should use longitudinal designs to track the development of self-efficacy and critical thinking throughout the anaesthesia nursing programme. This approach will reveal how these constructs evolve and the impact of educational interventions. Moreover, mixed-methods research, including qualitative approaches like interviews, could provide deeper insights into factors influencing self-efficacy and the challenges students face in clinical practice. Lastly, evaluating the effectiveness of simulation- or case-based learning interventions on improving self-efficacy and critical thinking would be valuable for evidence-based curriculum development.
V. CONCLUSION
The study found that anaesthesia nursing students exhibited a moderate level of self-efficacy in clinical practice. This indicates a need for targeted interventions aimed at enhancing their confidence and competency in clinical settings.
A significant finding of the study was the positive correlation between self-efficacy in clinical practice and critical thinking disposition, with critical thinking having the most substantial impact among the factors examined. This underscores the vital role that critical thinking skills play in developing clinical confidence and decision-making abilities in anaesthesia nursing students. In light of these findings, curriculum improvements should focus on fostering critical thinking skills to optimise self-efficacy during clinical training. Enhancing critical thinking can be a key strategy for better preparing students for professional practice. Future research should explore longitudinal changes in self-efficacy and evaluate the effectiveness of interventions specifically designed to improve clinical competence.
Notes on Contributors
The Lead Author conceived the study, designed the experimental methodology, oversaw data collection, performed the primary statistical analysis, drafted the initial manuscript and contributed significantly to the interpretation of the results and the overall structure and content of the paper.
The Contributing Author assisted in the development of the experimental design and data collection protocols, conducted key experiments and contributed to data curation and preliminary analysis.
Ethical Approval
This study was approved by the ethics review committee of the University of Medicine and Pharmacy of Ho Chi Minh City (IRB No. 339/HDDD-DHYD) in 2024. The researcher informed the participants about the project and its purpose. The students who agreed to participate were requested to sign a form known as “Commitment to Participating in Research”. This form confirmed that the students understood the information provided and participated voluntarily.
Data Availability
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request. Specific datasets are available on the Figshare repository:
https://doi.org/10.6084/m9.figshare.28845323.
Acknowledgement
The authors express gratitude to KOICA and the University of Medicine and Pharmacy in Ho Chi Minh City.
Funding
There is currently no funding available for this study.
Declaration of Interest
There are no conflicts of interest, including financial, consulting, institutional, and other relationships that could lead to bias or a conflict of interest.
References
Albooghobeish, M., Saidkhani, V., Angali, K. A., & Farzaneh, M. (2023). Clinical decision-making and self-efficacy skills in anesthesiology nursing students: A cross-sectional study. Shiraz E-Medical Journal, 24(4), e134178. https://doi.org/10.5812/semj-134178
Azizi, M., Ramezani, G., Karimi, E., Hayat, A. A., Faghihi, S. A., & Keshavarzi, M. H. (2022). A comparison of the effects of teaching through simulation and the traditional method on nursing students’ self-efficacy skills and clinical performance: A quasi-experimental study. BMC Nursing, 21, 283. https://doi.org/10.1186/s12912-022-01065-z
Bandura, A. (1991). Self-efficacy mechanism in physiological activation and health-promoting behavior. In J. Madden, IV (Ed.), Neurobiology of learning, emotion and affect (pp. 229-269). New York: Raven.
Burns, S., Mendel, S., Fisher, R., Cooper, K., & Fisher, M. (2013). Critical thinking in nurse anaesthesia education: A pilot study. Journal of Curriculum Teaching, 2(1), 83-90. http://dx.doi.org/10.5430/jct.v2n1p83
Cheraghi, F., Hassani, P., Yaghmaei, F., & Alavi‐Majed, H. (2009). Developing a valid and reliable self‐efficacy in clinical performance scale. International Nursing Review, 56(2), 214-221. https://doi.org/10.1111/j.1466-7657.2008.00685.x
Dehghani, M., Sani, H. J., Pakmehr, H., & Malekzadeh, A. (2011). Relationship between students’ critical thinking and self-efficacy beliefs in Ferdowsi University of Mashhad, Iran. Procedia-Social Behavioral Sciences, 15, 2952-2955. https://doi.org/10.1016/j.sbspro.2011.04.221
Esra, T., & Özlem Ülkü, B. (2023). Academic self-efficacy and attitudes to clinical practices of nursing students. Lokman Hekim Health Sciences, 3(3), 201-210. https://doi.org/10.14744/lhhs.2023.90001
Ibrahim, A. F., Abdelaziz, T. M., & Akel, D. T. (2019). The relationship between undergraduate nursing students’ satisfaction about clinical learning environment and their competency self-efficacy. Journal of Nursing Education Practice, 9(11), 92. https://doi.org/10.5430/jnep.v9n11p92
İşeri, Ö., Atasayar, B., & Ursavas, F. (2023). Investigation of the relationship between emotional self-efficacy and critical thinking disposition in surgical nurses. Journal of Health and Nursing Management / Sağlık ve Hemşirelik Yönetimi Dergisi, 10(1), 29-37. https://doi.org/10.54304/shyd.2023.32848
Jin, Y., & Lv, X. (2018). Self-efficacy among third-year nursing students: A questionnaire study [Degree Thesis, University of Gavle].
Karahan Okuroğlu, G. (2022). Hemşirelik Öğrencilerinin Klinik Performanslarına İlişkin Öz Yeterliklerinin Akademik Öz Yeterlikleri ve Akademik Başarıları ile İlişkisi: Tanımlayıcı Araştırma [The relationship between Nursing students’ self-efficacy regarding clinical performance and their academic self-efficacy and academic success: A descriptive study]. Turkish Clinics Journal of Nursing Sciences / Turkiye Klinikleri Journal of Nursing Sciences, 14(1), 125-31. https://doi.org/10.5336/nurses.2021-83326
Köseoglu, Y. (2015). Self-efficacy and academic achievement – A case from Turkey. Journal of Education Practice, 6(29), 131-141. https://eric.ed.gov/?id=EJ1081281
Motahari, M., Rahimibashar, M., & GHasemnegad, S. (2020). The relationship between clinical self-efficacy and academic achievement motivation in nursing students. Research in Medical Education, 12(2), 10-20.
Nederland, G. G. Z. (2010). Een inventarisatie van personeel in de geestelijke gezondheidszorg [A survey of personnel in mental health care]. Dutch Medical Healthcare Association / GGZ Nederland: Utrecht, The Netherlands.
Orujlu, S., & Hemmati Maslakpak, M. (2017). Assessing the relationship between critical thinking and self-efficacy of nursing student. Journal of Nursing Education, 5(6), 11-17. http://dx.doi.org/10.21859/jne-05062
Sahebi, Z., & Barkhordari-Sharifabad, M. (2023). Spiritual care competency and its relationship with clinical self-efficacy in nursing students. BMC Medical Education, 23(1), 937. https://doi.org/10.1186/s12909-023-04937-3
Sajadi, M., & Mehrabi, F. (2019). Relationship between clinical environment stressors and nursing students self-efficacy in clinical performance. Journal of Nursing Education, 8(2), 44-50. http://jne.ir/article-1-1011-en.html
Salimi, H. R., Pourebrahimi, M., & Hoseinabadi-Farahani, M. J. (2017). Clinical self-efficacy, dimensions and related factors among nursing students. Iranian Journal of Psychiatric Nursing, 5, 1-7. http://dx.doi.org/10.21859/ijpn-05021
Scott Imus, F., Burns, S., & Donna, M. W. M. (2017). Self-efficacy and graduate education in a nurse anaesthesia program: A pilot study. AANA Journal, 85(3), 205-216.
Shorey, S., & Lopez, V. (2021). Self-Efficacy in a nursing context. In G. Haugan & M. Eriksson (Eds.), Health promotion in health care – Vital theories research (pp. 145-158). Springer. https://doi.org/10.1007/978-3-030-63135-2
Terry, D., & Peck, B. (2020). Factors that impact measures of grit among nursing students: A journey emblematic of the koi fish. European Journal of Investigation in Health, Psychology and Education, 10(2), 564-574. https://doi.org/10.3390/ejihpe10020041
Tirgari, B. (2018). Study of clinical self-efficacy and belongingness to clinical environment in undergraduate nursing students of Razi School of Nursing and Midwifery, Kerman University of Medical Sciences. Journal of Nursing Education, 7(6), 31-38. http://jne.ir/article-1-1021-en.html
Trọng, P. H., Tiên, H. M., & Phương, H. T. T. (2023). Mức Độ Tự Tin Của Sinh Viên Điều Dưỡng Khi Thực Hành Đặt Nội Khí Quản Và Các Yếu Tố Liên Quan [Level of confidence among Nursing students when practicing Endotracheal Intubation and related factors]. Vietnam Medical Journal / Tạp chí Y học Việt Nam, 531(1), 179-182. https://doi.org/10.51298/vmj.v531i1.6945
Vũ, T. T. H., Vũ, V. Đ., Vũ, T. T. H., Nguyễn, T. T. C., Hoàng, M. P., Đặng, T. T. T., & Đặng, T. Đ. (2023). Mức độ tự tin trong thực hành kỹ năng lâm sàng của sinh viên điều dưỡng tại một số trường cao đẳng khu vực Tây Nguyên năm 2023 [Levels of confidence in clinical skills practice among nursing students at some colleges in the Central Highlands region in 2023]. Journal of Nursing Science / Tạp chí Khoa học Điều dưỡng, 6(05), 55-63. https://doi.org/10.54436/jns.2023.05.715
Wang, X., Sun, X., Huang, T., He, R., Hao, W., & Zhang, L. J. B. M. E. (2019). Development and validation of the critical thinking disposition inventory for Chinese medical college students (CTDI-M). BMC Medical Education,19, 200. https://doi.org/10.1186/s12909-019-1593-z
Yildirim, B., Özkahraman, Ş., & Ersoy, S. (2012). Investigation of critical thinking disposition in nurses working in public hospitals. International Journal of Business, Humanities and Technology, 2(3), 61-67. https://www.ijbhtnet.com/journals/Vol_2_No_3_May_2012/9.pdf
*Vy Van Thao Ngan Nguyen
School of Nursing and Medical Technology,
The University of Medicine and Pharmacy
at Ho Chi Minh City,
201 Nguyen Chi Thanh Street, Ward 12,
District 5, Ho Chi Minh City, Vietnam
Email: silver.clover219@ump.edu.vn
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
