
Developing a holistic healthcare practitioner for a sustainable future
Published online: 6 January, TAPS 2026, 11(1), 1-3
https://doi.org/10.29060/TAPS.2026-11-1/EV11N1
We are delighted to present this fourth thematic issue of The Asia Pacific Scholar (TAPS) on Developing a Holistic Healthcare Practitioner for a Sustainable Future. This issue encapsulates a wealth of contributions from authors across regions and disciplines, reflecting the shared agency in addressing the changing landscape of healthcare. Authors were invited to explore how sustainability, inclusivity, and innovation could be interwoven into the formation of the modern practitioner. In response, 14 thought-provoking papers were submitted and accepted. These papers explored the vital shift from siloed clinical training toward education that integrates empathy, well-being, interprofessional collaboration, and environmental consciousness.
Amid rising global healthcare demands, technological innovation and disruption, and environmental and psychological stressors, there is a pressing need to evolve health professions education. We need to train practitioners who are not only clinically competent but also emotionally intelligent, team-oriented, reflective, and resilient as well as being equipped to address both individual and planetary health.
This issue features three overarching themes:
- Holistic practice and environmental concerns,
- Faculty development and self-care, and
- Curriculum advancement for future-ready healthcare professionals.
A. Theme 1: Holistic Practitioner and Environmental Concerns
Healthcare is increasingly shaped by ecological crises and shifting societal values. Ramachandran et al. present an insightful discussion on the multilayered nature of developing holistic practitioners. They contrast public and private health education models and stress the importance of aligning training with international standards while remaining deeply connected to local community needs. Their Malaysian case study underscores the importance of strong scientific grounding coupled with empathetic and technological capabilities, alongside ecological awareness. Importantly, they recognise that individual practitioners may vary in their strengths, hence advocating for a unified and complementary workforce where collective skills fulfil holistic objectives.
Woodall et al. explore the art and challenge of reflective practice during rural placements. Their study, involving educators such as doctors and nurses, reveals several enablers for deep reflection: fostering trust, embracing multidisciplinary collaboration, prioritising rural healthcare contexts, and encouraging meaningful reflective activities. A key inhibitor was the overuse of superficial reflection assessments. They also found that students’ life experiences and prior engagement with reflective practices could either enrich or limit their capacity for introspection.
The growing connection between climate change and psychological toll is examined by Teoh and Azim. They highlight how climate-related stressors impact mental health and urge the integration of planetary health into healthcare education.
B. Theme 2: Faculty Development and Self-Care
Health professionals must be equipped to care not only for others, but also for themselves. Al Rashid and Rajagopalan argue for personal development programs (PDPs) that strengthen emotional intelligence and communication within the healthcare workforce.
Ong et al. provide preliminary evidence on the use of a theatre-based medical humanities program in Singapore. Designed for faculty development, this approach suggests that exposure to medical humanities supports professional identity formation, builds communities of practice, and fosters emotional resilience.
Susilo et al. report on a qualitative study evaluating a workshop for Indonesian medical students that incorporates reflective and collaborative learning. Their findings identified five dimensions critical to developing resilience, particularly during crises like COVID-19. These include faith, endurance, adaptability, recoverability, and a sense of life calling. It was noted that resilience strategies are vital for healthcare workers navigating high-stress environments.
Krasner contributes to this discussion with a clear proposition, namely a thriving workforce leads to better patient outcomes. He introduces the globally adopted Mindful Practice in Medicine (MPiM) program which integrates contemplative methods and narrative medicine and focuses on empowering professionals to flourish, encouraging competencies like self-awareness, compassionate listening, and emotional regulation. This underscores the value of institutional support for such initiatives. Hassed echoes this call in his article on integrating mindfulness as a core curriculum initiative under Monash University’s Health Enhancement Program (HEP). This curriculum component enhances students’ coping and communication skills throughout their medical training.
Koh et al. share findings from their application of action research and Entrustable Professional Activities (EPAs) to enhance a pharmacy pre-registration program. Their iterative process identified several areas for improvement, which include refining documentation, optimising indirect patient care experiences, auditing assessments, and streamlining administrative protocols. This framework offers a valuable model for tailoring workplace-based training programs to better serve community health needs while improving professional readiness.
The article by Azim and Teoh explores the imbalance between patient care demands and the well-being of healthcare workers. The authors highlight the escalating mental health burden on medical students and junior doctors, who face distinct stressors – from academic pressure to overwhelming workloads. The paper advocates for a holistic and sustainable approach to supporting healthcare providers, including normalising help-seeking, modelling healthy behaviour by senior staff, and integrating evidence-based strategies like motivational interviewing. Ultimately, the authors argue that high-quality, sustainable care is inseparable from the psychological health of those delivering it.
C. Theme 3: Curriculum Advancement for Future Ready Healthcare Professionals
Curriculum innovation is essential to prepare practitioners for the complexities of modern healthcare. Lau describes how the National University of Singapore has responded to rapid technological advances, shifting demographics, and escalating care demands via the Common Curriculum Healthcare Professional Education (CCHPE), structured around five pillars including socio-ecological health, digital and data literacy, and interprofessional professionalism. The curriculum’s emphasis on experiential learning, such as Longitudinal Patient Experience and virtual case collaboration, equips graduates to thrive in modern, team-based care settings. van der Merwe and van Vuuren explore the use of theoretical frameworks in curriculum design, applying the theory of planned behaviour to scaffold communication skills training in an interprofessional South African context. Their findings emphasise the importance of shaping behavioural intentions and perceptions of control, particularly in nurturing cultural sensitivity and adaptability in team settings.
Omotoso and Peter consider the role of technology in transforming anatomical science education. With students increasingly using technologically driven learning tools, these authors advocate for a blended approach that embraces digital platforms while preserving core teaching principles. Their vision supports flexible and autonomous learning, aligning curriculum design with evolving student expectations.
Phang et al. offer a practical advancement in assessment tools by developing a Singapore-specific version of the Professionalism Mini Evaluation Exercise (P-MEX). Adapted from the mini-CEX, the P-MEX evaluates professionalism in terms of patient care, interprofessional relationship skills, and reflective practice. This tool reflects the growing need for culturally sensitive assessments that resonate with regional medical education contexts.
D. Conclusion
This thematic issue emphasises critical perspectives on preparing healthcare professionals for an uncertain and complex future. It highlights the necessity of providing practitioners with resilience, ecological awareness, emotional intelligence, and technological adaptability. At the heart of these discussions is the aspiration to develop a healthcare workforce that embodies holistic care. This can be summed up as a practitioner who cares for the individual, the community, and the planet with equal compassion and competence.
We thank the authors for their insightful contributions and the reviewers and editorial team for their dedication. May this issue inspire deeper dialogue, practical transformation, and a continued journey toward holistic, sustainable healthcare education.
Marcus A. Henning
Centre for Medical and Health Sciences Education, Faculty of Medical and Health Sciences,
University of Auckland, New Zealand
Mabel Yap
Director (Professional Training and Assessment Standards),
Education Director Office, Ministry of Health, Singapore
Submitted: 21 December 2024
Accepted: 14 May 2025
Published online: 6 January, TAPS 2026, 11(1), 4-8
https://doi.org/10.29060/TAPS.2026-11-1/GP3610
Ganesh Ramachandran1, Aung Ko Ko Min2 & Vivian Fernandez1
1School of Medicine, Faculty of Health & Medical Sciences, Taylor’s University, Malaysia; 2Faculty of Medicine, MAHSA University, Malaysia
Abstract
Introduction: The provision of higher education has been for the longest time the responsibility of the state. With increasing demands for places in institutions of higher learning, there has been increasing involvement of the non-public (private) sector in this area. The extent of this involvement is wide and encompasses both nonprofessional and professional qualifications. This involvement has brought the issue of ensuring that graduates from the non-public sector institutions are on par with their public sector counterparts.
Methods: This paper looks at strategies that are in place or that may be employed to ensure that the non-public sector plays its part in developing holistic and fit for purpose healthcare practitioners with a primary focus on the Malaysian doctor. It is largely based on the local landscape, referring to global standards, expectations and recommendations.
Results: Developing a holistic healthcare practitioner begins with appropriate selection and delivering accredited standardised training and assessment.
Conclusion: It is expected that these strategies are similar for all healthcare professionals, and that adhering to the required measures will meet the expectations of the primary stakeholder, the patient.
Practice Highlights
- A holistic healthcare professional is knowledgeable, skilled and will have the required affective attributes to provide safe, high quality and empathetic healthcare with an emphasis on prevention of disease and staying healthy.
- This requires the selection of appropriate candidates, standardised training and assessment to produce a fit for needs practitioner.
- Defined standards will ensure that we are able to meet this aim more effectively.
I. INTRODUCTION
The Good Medical Practice Guide of the Malaysian Medical Council (2019) states that “the doctor is traditionally held in esteem by society as a highly qualified professional who is expected to serve his fellow human beings in a dedicated and selfless manner. His opinion on matters, not just medical, is often sought and received with respect.
As such while theoretical knowledge, practical and clinical skills are a given requirement for a doctor or any healthcare professional, these must be complemented by a good standard of soft skills that are necessary to meet the demands of the end users, primarily the patient, family and the employing authority (AlThukair & Rattray, 2023).
II. DEVELOPING A HOLISTIC HEALTHCARE PRACTITIONER
Traditionally, tertiary education as a whole and tertiary education leading to a professional qualification in particular has always been within the realm of the public sector or the state.
This has changed because of increasing demands and “democratisation” of all areas of education including higher education. Regulations have been modified to attract international students and develop “educational hubs” in some countries. Economic considerations have resulted in decreased funding of public sector institutions making them unable to meet demands and appear inefficient in delivery, paving the way for the non-public or private sector.
The non-public sector contribution to higher education may be in the form of government aided institutions, not-for-profit institutions and for-profit institutions.
In developed economies such as the United Kingdom and the United States of America, private higher education providers comprise about 3% and 23% respectively of total enrolment. This is in contrast to Asia where as much as 80% depend on the private sector for higher education. In India, more than 50% of students are enrolled in private institutions. Korea reports figures as high as 85%, and in Malaysia up to 52% are enrolled in private institutions. Almost all of these are for profit institutions.
A study by the United Kingdom’s Centre for Global Higher Education looked at for-profit providers in six countries (USA, Germany, Australia, Poland, Japan, and Chile) and reported that the standards in these institutions tend to be inferior to that of a public institution. This finding gives rise to the possibility that standards in these institutions may be more malleable and that is worrisome for countries where the numbers seeking private higher education is high. This situation, if not addressed, will be detrimental to the healthcare provisions in the country in the middle and long term.
Inevitably, the perception of private institutions is usually negative. They are perceived to be for profit and not particularly interested in quality, without any positive impact for the stakeholders and community. However, this is not entirely accurate. In many countries including Malaysia, these providers are regulated and must meet the standards of the accreditation agency in the country. In the case of Malaysia, it is the Malaysian Qualifications Agency and for medicine the standards are determined by the Malaysian Medical Council and contained in a document called the Standards for Undergraduate Medical Education (2nd edition 2022). All medical schools are regularly monitored, and accreditation is a requirement for recognition and registration with the council prior to employment as interns.
Having more medical schools will address the need for more locally qualified doctors and meet the needs of an increasing population. Prospective students will have increased choices in terms of institutions they choose to attend.
In the long run it will reduce dependence on an expatriate workforce by providing local doctors for a local populace. Job opportunities for qualified specialist staff will also increase with healthy competition between the public and private sectors.
Private institutions are also able to operate without too much dependence on policies driven by politics of the land and may be able to introduce more cutting-edge teaching and learning technologies because of financial viability and less red tape.
On the other hand, private institutions must always guard against being overwhelmed by the for-profit motive and must ensure that standards are not diluted. The institution must ensure employment of adequate numbers of trained academics to prevent any compromise in teaching, while investing in physical infrastructure, laboratory equipment, simulators, cadavers and prosected specimens among others. These schools may not be able to address the needs of the whole community because they are likely to be situated in urban and affluent environments and may contribute to a lack of racial diversity among the student population.
Additionally, unplanned expansion may also result in excessive numbers which may lead to a reflex moratorium on new schools, this in turn may impact numbers down the line leading to a shortage of doctors as seen in Malaysia currently.
A robust accrediting body and medical council which sets standards and guards against the above is always required to ensure compliance. In the Malaysian landscape this is largely in place to ensure standards of all local graduates from the public and private educational sector. Evidence from the Ministry of Health Malaysia seems to indicate that most attrition is due to mental health and coping issues as well as disciplinary matters such as non-completion of logbooks and tardiness in fulfilment of required duties. This means that checks and balances regarding theoretical and practical competence are largely in place, with the problems being related to attitudes, resilience and expected standards of conduct. This is a real challenge and must be addressed to ensure holistic medical practice.
A holistic healthcare practitioner is one who takes consideration of all the patient’s needs as far as possible when delivering care. This implies a practitioner who is theoretically and practically sound with the necessary soft skills to provide care for the patient under their charge. The practitioner must also be resilient, mindful and be aware of the expectations of the community they serve in.
While many of us assume that our stakeholders want healthcare providers that are competent and fit for purpose in terms of expertise, it appears that there are unmet needs in many encounters.
Patients want to be treated as a person not a number. They want community-based care that addresses social issues and family involvement in decision making. Patients also expect affordable care, destigmatisation of certain types of diseases, and avoiding stereotyping (Natafgi et al., 2022).
This then is the expectation, and the challenge is how we meet these. The Institute of Medicine (National Academies of Science, Engineering, and Medicine, Washington USA) in 2019 has outlined the six aims to improve health care delivery. It emphasises safety, effectiveness, equity, efficiency, timeliness, and a patient centred focus (Torralba & Katz, 2020) which broadly resonates with patient expectations outlined previously.
The BMJ in 2002 posed two questions to its readers, “what makes a good doctor?” and “how can we make one?” Answers varied but some important takeaways regarding a good doctor were that
- A good doctor had to be a good human being.
- A good doctor had to be one that genuinely liked people and wanted to help them.
- A good doctor had to be special in some way, extra dedicated, extra humane or extra selfless.
- A good doctor had to take care of themselves first.
- A good doctor had to find medicine fun, fascinating, and stimulating (Rizo, 2002).
Producing a good doctor appears to be more challenging. It is a given that providing quality healthcare requires quality medical education. Correspondingly, providing quality medical education depends on
- good student selection mechanisms.
- attracting and maintaining highly qualified academic and practice staff.
- designing a curriculum that is current and reviewed regularly to ensure active learning, problem solving, and critical thinking with appropriate use of technology grounded in real life examples.
- basing curriculum design and renewal on multiple stakeholder feedback and on real time performance of graduates in the workplace.
- a high standard of cognitive and psychomotor learning coupled with affective attributes of safe, ethical, and empathetic practice.
- designing valid assessments that ensure achievement of learning outcomes in the area of cognitive, psychomotor and affective skills.
- adequate investment in infrastructure in terms of classrooms, laboratories, libraries and clinical teaching sites that are all equipped to provide quality teaching and learning.
- developing links with other institutions of learning and practice to benchmark standards and provide opportunities for internships and elective placements in preparation for their future careers.
- incorporating quality assurance in all aspects of teaching, learning and assessment.
All of these are generally the norm and are contained in accreditation standards which are based on the recommendations of the World Federation of Medical Education.
In effect, all medical schools, public or private need to commit to producing a competent practitioner who is knowledgeable, skilled, and has the necessary positive affective attributes to deliver holistic care. We have got it right to a large extent in the areas of cognitive and psychomotor competence which are tangible and measurable. The affective competencies in terms of soft skills, resilience, coping mechanisms, and mental health are something that we all continue to work on. It is less tangible and is ever changing because of the changing expectations of all stakeholders. To ensure a competent professional we also have to take into consideration the environmental and animal health issues that have an increasing impact on our health. There is a need to refine our curriculums to move from one that emphasises treatment to one that emphasises prevention and staying healthy. Additionally, incorporation of digital skills and the utilisation of artificial intelligence is another space that needs to be explored and incorporated into the curriculum aiming to create a holistic and complete healthcare professional.
This will require the implementation of a minimum acceptable standard for entry that is based on a set of acceptable qualifications, or a standardised entrance test. Selection of a student should also take into account affective attributes, needs background, and aptitude. This entails the use of interviews, multiple mini-interviews and aptitude tests in the selection process. Complying to a required curriculum standard with a common exit examination for all medical schools will help achieve the above targets (Aftab et al., 2021).
We will also need to explore and incorporate elements of the one health curriculum, preventive medical care and digital competencies into an already packed curriculum in a meaningful and practical manner.
Different countries and institutions are on different stages of this path but what is evident is that there is an acknowledgement of the need to set a common minimum standard of entry, competency and outcome.

Figure 1. Attributes and the regulatory mechanisms to achieve this aim. Solid arrows are the processes in place and dotted arrows are the processes in progress.
III. CONCLUSION
In conclusion, the Shushruta Samhita an ancient Indian text of surgery, harking back to 400 BC perhaps put it well by saying “A physician well versed in the principles of the science of medicine but incompetent in the art because of want of practice, as well as the physician, experienced in his art but short on the knowledge of Ayurveda, is like a one-winged bird that is incapable of soaring high in the sky”.
This statement encompasses the requirements expected of a holistic practitioner and is time tested across the ages. This is the holy grail we all aspire to whether in the public or private sector of medical education. By and large, we have the regulations and mechanisms required in place. Continuous quality enhancement and working together will enhance standards in our aspiration to produce holistic, balanced graduates who are global and flexible in their outlook and employability.
Notes on Contributors
All authors were involved in the literature review, writing, editing and proof reading of this article. The concept is attributed to GR the first author. All authors have approved the final version of this article.
Acknowledgement
The authors thank the faulty leadership for permission to write and submit this article.
Funding
There was no funding support involved.
Declaration of Interest
All authors are from private universities that provide an accredited undergraduate medical programme in Malaysia.
References
Aftab, W., Khan, M., Rego, S., Chavan, N., Rahman-Shepherd, A., Sharma, I., Wu, S., Zeinali, Z., Hasan, R., & Siddiqi, S. (2021). Variations in regulations to control standards for training and licensing of physicians: A multi-country comparison. Human Resources for Health, 19, Article 91. https://doi.org/10.1186/s12960-021-00629-5
AlThukair, D., & Rattray, J. (2023). What makes a high-quality medical education and graduate? The Saudi Arabia labor market’s perspective. In Innovations in higher education teaching and learning (pp. 67-83). https://doi.org/10.1108/s2055-364120230000054004
Natafgi, N., Ladeji, O., Blackwell, S., Hong, Y. D., Graham, G., Cort, M., & Mullins, C. D. (2022). Similar values, different expectations: How do patients and providers view ‘health’ and perceive the healthcare experience? Health Expectations, 25(4), 1517-1528. https://doi.org/10.1111/hex.13493
Rizo, C. A. (2002). What’s a good doctor and how do you make one? BMJ, 325(7366), 711. https://doi.org/10.1136/bmj.325.7366.711
Torralba, K. M. D., & Katz, J. D. (2020). Quality of medical care begins with quality of medical education. Clinical Rheumatology, 39(3), 617-618. https://doi.org/10.1007/s10067-019-04902-w
*Ganesh Ramachandran
School of Medicine,
Faculty of Health and Medical Sciences,
Taylor’s University, Malaysia
+6 012 373 2201
Email: Ganesh.Ramachandran@taylors.edu.my
Submitted: 29 January 2025
Accepted: 16 April 2025
Published online: 6 January, TAPS 2026, 11(1), 9-13
https://doi.org/10.29060/TAPS.2026-11-1/GP3651
Michael Krasner
Department of Medicine, University of Rochester School of Medicine and Dentistry, United States of America
Abstract
Introduction: The growing prevalence of burnout among healthcare professionals has emerged as a global crisis, adversely affecting individual well-being, patient care, and healthcare systems while imposing significant economic burdens. Addressing this systemic problem requires innovative, scalable interventions that target the root causes of burnout. Mindful Practice in Medicine (MPIM), developed at the University of Rochester School of Medicine and Dentistry, represents a promising approach. MPIM fosters self-awareness, emotional intelligence, teamwork, and compassion. With over 20 years of evidence-based implementation, MPIM has demonstrated substantial improvements in clinician well-being, burnout, empathy, teamwork, and patient-centered care.
Methods: This global perspective highlights the program’s global impact through case studies of MPIM-trained facilitators who have embeded these programs into undergraduate, graduate, and postgraduate medical education as well as into institutional healthcare systems.
Results: Examples from Switzerland, the United States, the United Kingdom, Australia, and Canada illustrate MPIM’s adaptability and effectiveness for fostering systemic cultural changes, restoring joy in medicine, and promoting organisational resilience.
Conclusion: These efforts underscore the potential of MPIM to catalyse a global paradigm shift in healthcare, improving outcomes for both professionals and patients. Further research and strategic scaling are necessary to maximise MPIM’s reach and sustainability and to address the intertwined crises of professional burnout and healthcare quality.
Practice Highlights
- MPIM programs integrates contemplative practices, narrative medicine, and appreciative inquiry.
- MPIM demonstrates sustainable improvement in burnout, wellness, teamwork, and patient centered care.
- MPIM facilitators have implemented global programs across the medical training and care continuum.
- MPIM interventions can be scaled to address individual and systemic health professional challenges.
- MPIM may help provide solutions for improving healthcare quality and health professional wellbeing.
Everybody complains about the weather, but nobody does anything about it.
Charles Dudley Warner
I. THE PROBLEM OF HEALTH PROFESSIONAL BURNOUT AND WELLBEING
Awareness of physician and health professional burnout and efforts to promote their well-being have gained significant attention in recent years, especially as the COVID-19 pandemic underscored the critical role of physician wellbeing in achieving healthcare’s mission of providing quality patient care. Burnout, a work-related syndrome characterised by emotional exhaustion, depersonalisation, and a reduced sense of personal accomplishment, has become a global public health crisis. More than 50% of physicians, both in training and in practice, exhibit burnout symptoms, leading to negative impacts on patient care, healthcare systems, and health professionals’ mental health, compromising professionalism and care quality, and imposing substantial economic costs. The worldwide economic impact is difficult to assess but estimates six years ago from within the United States healthcare system amounted to $4.6 billion, or approximately $7,600 per employed physician annually (Han et al., 2019).
The drivers of health professional burnout are not rooted in the health professional’s individual shortfalls, a lack of resilience, or insufficient experience managing complex personal, interpersonal, and medical dynamics within the complicated maze found in healthcare systems. Rather, it is derived primarily from systemic issues including excessive workloads, inefficient processes, administrative burdens, work-life conflicts, and a lack of organisational support and control over workplace decisions (West et al., 2018). Demographic factors also contribute, with burnout rates higher among female and younger physicians. Addressing this crisis thus requires organisational level strategies like redesigning work processes and increasing clinical support as well as fostering a culture of supportive leadership and collaboration.
Yet, many interventions developed in response to this crisis fall short of addressing these systemic and medical cultural challenges. Among such interventions that show promise are mindfulness-based stress reduction programs, small-group community building programs, and initiatives to promote meaning and connection in the workplace. These interventions, primarily individually oriented, have demonstrated tangible benefits when aligned with the specific drivers of burnout and hold the potential to mitigate its widespread effects and enhance both physician well-being and healthcare system performance. However, in many ways they are not designed nor intended to specifically address systemic issues, and thus far have failed to improve causal structural and cultural factors (Shanafelt, 2021).
II. MINDFUL PRACTICE IN MEDICINE/FLOURISHING IN MEDICINE
This Global Perspective discusses an intervention called Mindful Practice in Medicine (MPIM). In addition to empirically published evidence on its salutary effects on physician burnout and wellbeing and its demonstrated flexibility, the work of a growing number of trained MPIM facilitators worldwide has begun to address the systemic, organisational, and medical culture changes needed to begin to have an impact on this epidemic and move healthcare systems toward healthier, stabler, and higher quality. This report presents an overview of MPIM programs and training, and a sampling of how its trained facilitators impact systems of medicine across the continuum of undergraduate, graduate, and post-graduate medical education, as well as within academic healthcare educational and delivery culture.
MPIM/Flourishing in Medicine, developed at the University of Rochester School of Medicine and Dentistry 20 years ago, provides educational skills training designed to empower health professionals and organisations to thrive by restoring joy in medicine, fostering community, and promoting excellence in healthcare. Through interactive in-person and online workshops, seminars, and presentations, these programs serve physicians, medical educators, trainees, other health professionals, and leaders within the healthcare ecosystem at individual, organisational, and institutional levels. The approach emphasises self-awareness, emotional intelligence, deep listening, interpersonal dynamics, teamwork, and compassion, while actively engaging participants with a focus on relationship-centered care.
Rooted in a biopsychosocial framework, MPIM integrates contemplative and awareness-building practices, narrative medicine, and appreciative inquiry to enhance clinician well-being, relational dynamics, individual and group resilience, and quality of patient care. Research conducted at the University of Rochester and replicated globally demonstrates significant improvements in well-being, burnout, empathy, teamwork, work satisfaction, and a stronger psychosocial orientation in patient care delivery. Participants consistently highlight the program’s emphasis on its ability to foster collegial community, the contemplative practices, narrative medicine skills, the application of appreciative inquiry, and a focus on self-care as keys to its effectiveness in transforming both individual and organisational healthcare experiences. (Epstein et al., 2022; Krasner et al., 2009). Several thousand health professionals worldwide have participated in this training with nearly two hundred completing facilitator or advanced teacher training. The following examples highlight a few interventions and programs that MPIM teacher trainees have implemented in their medical communities across the globe. These demonstrate real-world responses to the crisis in healthcare systems and medical culture across a continuum of medical education.
MPIM is being implemented globally with adaptations that align with diverse cultural and educational contexts, ensuring its relevance and effectiveness in various healthcare environments. Unlike conventional mindfulness programs, MPIM is specifically designed for the medical professional, integrating self-awareness, emotional intelligence, and relationship-centered care into clinical practice. Its flexibility allows trained facilitators to tailor interventions to local healthcare systems, addressing both individual well-being and systemic cultural challenges. By embedding mindfulness-based principles within medical education and institutional frameworks, MPIM goes beyond individual stress reduction, acting as a catalyst for systemic change in healthcare, ultimately improving physician well-being, team dynamics, and patient care quality on a global scale. Figure 1 shows the global presence of mindful practice in medicine programmes.

Figure 1. Global presence of mindful practice in medicine programs (locations of intensive workshops or advanced teacher trainees)
III. GLOBAL APPLICATIONS ACROSS LEVELS OF MEDICAL EDUCATION
A. Undergraduate Medical Training, University of Fribourg, Switzerland
Dr. Raphael Bonvin, an MPIM Advanced Teacher Training graduate, came to the University of Fribourg Faculty of Science and Medicine to improve academic performance by addressing the intrinsic motivations of undergraduate medical students. Directing the second half of the six-year undergraduate medical education curriculum, he has embedded pedagogy and programs influenced by MPIM. The new curriculum highlights contemplative practices, self-awareness and self-care, mind-body medicine, and a humanistic approach to assessments that focus on formative assessment as a primary motivator of the development of individual learning plans with the goal of improved preparation for graduate medical training and the practice of medicine. Outcomes to date of this curricular redesign, now in its fifth year, demonstrate this program as leading Swiss medical schools’ federal licensing exam scores that reflect clinical skills and knowledge. The undergraduate medical education at Fribourg also demonstrates significantly improved sense of autonomy and efficacy among graduates who have now moved on to graduate medical training programs.
B. School of Medicine, The University of Missouri Kansas City, USA
Dr. Jodi Jackson, an MPIM Advanced Teacher Training graduate, created the Mindfulness in Medicine Scholars Program, now in its second full year. It is a yearlong training program for a combined group of undergraduate medical students and medical school faculty with a goal of enhancing self-awareness, professional relationships, quality of medical care, and personal wellness, leading to a designation for the students of Distinction in Mindfulness in Medicine upon graduation. The program is based directly on the MPIM formal curriculum and taught over a ten-month period. Outcomes to date (not yet published) have demonstrated significant improvements in self-efficacy, mindfulness, and burnout for students, and improvements in mindfulness and burnout for faculty.
C. University of Warwick Medical School, West Midlands, UK
Dr. Majid Khan, an MPIM Advanced Teacher Training graduate, and Dr. Manuel Villareal, an MPIM Facilitator Training graduate, along with their colleague Dr. Petra Hanson, have developed an MPIM program for graduate medical education general practitioner trainees in the United Kingdom. They have demonstrated not only feasibility for this program but also significant improvements in burnout, wellbeing, engagement, stress, and mindfulness. Based on these findings they are implementing a more widespread integration of this MPIM program into other graduate medical training programs at their institution.
D. Barwon Health, Geelong, Victoria, Australia
Based on his experience as an MPIM Advanced Teacher Training graduate, and to introduce MPIM to clinician members of his hospital staff, Dr. Ross Carne has created an MPIM-informed program called Belonging in Medicine which is delivered as a post-graduate educational experience within a community hospital setting. Feedback from the first few cohorts of this program include a request for more MPIM-informed programming for medical staff, a strong recommendation of the program to physicians more junior in training to support their professional development and health, and a greater sense of connection of participants with their colleagues, their work, and themselves.
E. University of Calgary Cumming School of Medicine, Calgary, Alberta, Canada
Dr. Todd Hill and Dr. Ward Flemon, both MPIM Facilitator Training graduates, have engaged senior leadership at their institution to support the training of a critical number of MPIM facilitators within their institution with the goal of embedding MPIM-informed programs vertically and longitudinally into the healthcare institution at every level (undergraduate, graduate, and post-graduate medical education as well as more broadly across other health professional teams such as behavioral health, nursing, public health, and community health). Over the past several years over one-hundred thirty faculty physicians and medical trainees have undergone MPIM Core Training, and sixteen faculty have recently completed the MPIM Facilitator Training and are now developing and implementing MPIM-informed interventions that are supported by senior administration leadership within their academic medical center to improve the institutional culture, the work experience of health professionals, and the quality of care delivered to patients.
IV. CONCLUSION
The increasing prevalence of burnout among healthcare professionals jeopardises the well-being of the practitioners, adversely affects patient care, and imposes significant economic burdens on healthcare systems. Addressing this issue necessitates creative and comprehensive organisational strategies that impact underlying systemic and cultural factors. The healthcare system globally finds itself in the initial stages of developing feasible, effective, and scalable interventions to address this problem, and requires more efforts to succeed.
The MPIM program, with its flexibility, broad applications as demonstrated in this Global Perspective across educational domains within medical training and healthcare delivery, and its global presence, represents one such intervention. MPIM programs integrate individual and group skills training that are relevant to the multiple layers of stakeholders within Medicine and focuses not solely on individual factors. As a result of MPIM’s impact on the experience of learners from levels of students to seasoned clinicians, it also function as a systemic change dynamic, creating ripples of effects horizontally (to other learners at the participant’s level), as well as vertically (to teams and staff as well as leadership and management), and thereby effects positive changes within the nested relationships in healthcare systems (the patients, the colleagues, the staff, the leaders, the management, and the larger community).
The challenges of scaling this program to impact larger numbers of healthcare systems and communities are significant, but not unsolvable. More research is required to consolidate MPIM’s feasibility and scalability as well as its impact on end points such as quality measures of patient care, sustainability of health professional wellbeing improvements, diminished job turnover, and demonstrable healthcare cost benefits. However daunting these challenges seem, the examples featured in this perspective provide a foundation for solutions. Equipping committed and trained health professionals with the facilitation and orgainsational skills and experience to design MPIM interventions tailored to their specific community’s needs provide the key. These efforts have the potential for more widespread acceptance, impact, and improvements in the experience of care and the experience of caring for both the patients we serve, and the professionals we are.
Notes on Contributors
Michael Krasner contributed to the conception of the work, the acquisition of data for the work, drafts the work or revising it critically for important intellectual content, approves the final version to be published, and agrees to be accountable for all aspects of the work.
Acknowledgement
The author acknowledges the commitment and creativity of the colleagues mentioned, listed in alphabetical order: Raphael Bonvin, M.D., Ross Carne, M.B.B.S., M.D., Ward Flemons, M.D., Todd Hill, Ph.D., Jodi Jackson, M.D., Majid Khan, M.D., & Manuel Villareal, M.D.
Funding
There is no funding involved.
Declaration of Interest
The author declares that there are no conflicts of interest.
References
Epstein, R. M., Marshall, F., Sanders, M., & Krasner, M. S. (2022). Effect of an intensive mindful practice workshop on patient-centered compassionate care, clinician well-being, work engagement, and teamwork. Journal of Continuing Education in the Health Professions, 42(1), 19-27. https://doi.org/10.1097/CEH.0000000000000379
Han, S., Shanafelt, T. D., Sinsky, C. A., Awad, K. M., Dyrbye, L. N., Fiscus, L. C., Trockel, M., & Goh, J. (2019). Estimating the attributable cost of physician burnout in the United States. Annals of Internal Medicine, 170(11), 784-790. https://doi.org/10.7326/M18-1422
Krasner, M. S., Epstein, R. M., Beckman, H., Suchman, A. L., Chapman, B., Mooney, C. J., & Quill, T. E. (2009). Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA, 302(12), 1284-1293. https://doi.org/10.1001/jama.2009.1384
Shanafelt, T. D. (2021). Physician well-being 2.0: Where are we and where are we going? Mayo Clinic Proceedings, 96(10), 2682-2693. https://doi.org/10.1016/j.mayocp.2021.06.005
West, C. P., Dyrbye, L. N., & Shanafelt, T. D. (2018). Physician burnout: Contributors, consequences and solutions. Journal of Internal Medicine, 283(6), 516-529. https://doi.org/10.1111/joim.12752
*Michael Krasner
601 Elmwood Ave,
Rochester, NY 14642,
United States
Email: m.krasner@medmal.com
Submitted: 28 March 2025
Accepted: 16 April 2025
Published online: 6 January, TAPS 2026, 11(1), 14-17
https://doi.org/10.29060/TAPS.2026-11-1/GP3708
Tang Ching Lau
Dean’s Office, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: The healthcare landscape is evolving rapidly, driven by technological advancements, an aging population, and the increasing complexity of patient care. The National University of Singapore (NUS)’s Common Curriculum for Healthcare Professional Education (CCHPE) is a comprehensive framework designed to foster collaboration, communication, and shared decision-making among future healthcare leaders. This article explores how NUS Medicine’s curriculum prepares students for the challenges of modern healthcare through a multi-disciplinary approach, with a focus on Singapore’s unique healthcare context.
Methods: NUS Medicine employs several strategies including: (1) Curriculum design with the CCHPE structured around five pillars that integrate multi-disciplinary perspectives; (2) Educational Strategies through the implementation of Interprofessional Education (IPE) initiatives, Longitudinal Patient Experience (LPE) programs, use of technology and digital tools, as well as the assessment and feedback mechanisms to foster collaboration among students of different healthcare disciplines; and (3) Stakeholder Management though relationship building and ensuring leadership support.
Results: The CCHPE enhances teamwork, communication, and patient outcomes, preparing graduates to thrive in team-based healthcare environments. NUS Medicine graduates are known for their ability to effectively work in multi-disciplinary teams, contributing to high standards of care in Singapore.
Conclusion: NUS Medicine’s CCHPE emphasises the importance of collaboration in modern healthcare, preparing students to meet complex healthcare challenges, and is essential for ensuring that our graduates are able to meet the demand for high-quality, team-based care in Singapore.
Practice Highlights
- Interprofessional Education (IPE) Initiatives involve joint training sessions and collaborative projects among students from different healthcare disciplines.
- Longitudinal Patient Experience (LPE) provides interdisciplinary experiential learning through home visits over one year.
- Utilising digital platforms and tools for collaborative learning, including virtual case discussions and online modules.
- Assessment with regular feedback to students on teamwork and communication skills, as well as conducting reflective practices to enhance learning.
- Agile Curriculum is designed with regular reviews and updates to adapt to evolving healthcare needs and technologies.
I. INTRODUCTION
The healthcare landscape is evolving rapidly, driven by technological advancements, an aging population, and the increasing complexity of patient care. In Singapore, the National University of Singapore (NUS) Yong Loo Lin School of Medicine has been a pioneer in medical education, adopting innovative approaches to train healthcare professionals who can work effectively in multi-disciplinary teams. Central to this effort is the school’s Common Curriculum for Healthcare Professional Education (CCHPE), a comprehensive framework designed to foster collaboration, communication, and shared decision-making among future healthcare leaders. This article explores how NUS Medicine’s curriculum prepares students for the challenges of modern healthcare through a multi-disciplinary approach, with a focus on Singapore’s unique healthcare context.
Healthcare delivery today requires the coordinated efforts of diverse professionals, including doctors, nurses, pharmacists, and allied health workers. Research consistently shows that effective teamwork in healthcare leads to better patient outcomes, reduced medical errors, and improved patient satisfaction (Brandt et al., 2019; Reeves et al., 2017). In Singapore, where the healthcare system is renowned for its efficiency and quality, the demand for collaborative practice is further amplified by an aging population, rising chronic disease burden, and the need for cost-effective solutions.
Recognising these challenges, NUS Medicine has embraced Interprofessional Education (IPE), where students from different healthcare disciplines learn together to develop the skills necessary for collaborative practice. The school’s Common Curriculum for Healthcare Professional Education (CCHPE) serves as a model for integrating multi-disciplinary learning into medical education, ensuring that graduates are equipped to thrive in team-based healthcare environments.
II. CURRICULUM STRUCTURE
The CCHPE is a cornerstone of NUS Medicine’s educational strategy. It is designed to provide students with a strong foundation in medical knowledge while emphasising the importance of collaboration, communication, and systems thinking. The curriculum is structured around five pillars, each addressing specific learning objectives with a focus on integrating multi-disciplinary perspectives.
A. Pillar 1 – Socio-Ecological Determinants of Health
This pillar introduces students to the social, ecological, and behavioral determinants of health, emphasising their influence on health and illness. Students learn to develop empathy for individuals embedded in various settings and systems that impact their health. This pillar aligns with Singapore’s Healthier SG initiative, which promotes population health through a life-course approach and targeted health measures for specific segments of society. By understanding these determinants, students are better equipped to address the root causes of health issues and work collaboratively to improve community health outcomes.
B. Pillar 2 – Professional Practice 1: The Foundations of Health Professionalism
In this pillar, students explore the professional attributes that underpin the identity of healthcare professionals, including compassion, honesty, integrity, empathy, responsibility, and respect. They learn to apply ethical principles to practical healthcare scenarios and understand the legal and regulatory frameworks that govern the health professions. This pillar also emphasises the importance of therapeutic communication and adopting a person-centered approach in professional practice, which is critical for building trust and rapport with patients and their families.
C. Pillar 3 – Professional Practice 2: Basic Skills in Health Professionalism
Building on the foundations of professionalism, this pillar focuses on developing interpersonal skills, cultural competence, and teamwork. Students learn to collaborate effectively in healthcare delivery, apply ethical reasoning, and navigate the ethical and regulatory considerations that arise in the context of vulnerable populations and health systems. They also learn to apply principles of conflict resolution and constructive feedback, which are essential for fostering a collaborative and supportive work environment.
D. Pillar 4 – Data Literacy for Healthcare
In an era of data-driven healthcare, this pillar equips students with the skills to evaluate clinical evidence, understand study designs, and recognise sources of bias in data analysis. Students learn to calculate and interpret basic statistical tests, enabling them to make informed decisions based on data. This pillar is particularly relevant in Singapore, where the integration of data and technology is a key component of the Healthier SG initiative.
E. Pillar 5 – Digital Literacy for Healthcare
The final pillar focuses on developing students’ ability to apply computational thinking and use digital tools safely and effectively. In a rapidly digitising healthcare landscape, this pillar prepares students to leverage technology to improve practice and outcomes. It aligns with Singapore’s vision of becoming a global leader in healthcare innovation, as outlined in the Healthcare 2020 Masterplan.
III. METHODS
NUS Medicine employs several strategies to ensure that its curriculum fosters effective collaboration among healthcare professionals:
A. Interprofessional Education (IPE) Initiatives
Students from medicine, nursing, pharmacy, and allied health programs participate in joint training sessions and collaborative projects. These activities are designed to break down silos and promote mutual respect among disciplines (Reeves et al., 2019).
B. Longitudinal Patient Experience (LPE)
As part of their interdisciplinary experiential learning, students from the four healthcare professions are grouped together to visit patients in their homes and living environments over a one-year period. This program allows students to apply concepts learned in class to real-world situations, fostering a person-centered approach to care.
C. Technology and Digital Tools
NUS Medicine leverages digital platforms to facilitate collaborative learning. Virtual case discussions and online modules allow students to engage with peers from different disciplines, even outside the classroom (Masters et al., 2020).
D. Assessment and Feedback
Students receive regular feedback on their teamwork and communication skills, helping them identify areas for improvement. Reflective practices, such as reflective writing and debriefing sessions, further enhance learning (Ramani & Krackov, 2019).
The CCHPE is likely to have a profound impact on NUS Medicine graduates and the broader healthcare system. Studies have shown that interprofessional education improves teamwork, communication, and patient outcomes (Reeves et al., 2019). In Singapore, graduates of NUS Medicine are known for their ability to work effectively in multi-disciplinary teams, contributing to the high standards of care that the country is renowned for.
IV. STRATEGIES AND RESULTS
Implementing a multi-disciplinary curriculum like the CCHPE is not without its challenges. However, NUS Medicine has identified key strategies to address these obstacles:
A. Building Relationships and Trust Among Faculties and Administrators
- Challenge: Different faculties and departments may have varying priorities and teaching styles, which can hinder collaboration.
- Solution: NUS Medicine emphasises relationship-building and trust among educators and administrators. Regular communication and mutual support are key to ensuring the success of the curriculum.
B. Ensuring Senior Leadership Support
- Challenge: Without strong support from senior leadership, it can be difficult to align resources and priorities across disciplines.
- Solution: NUS Medicine has secured strong backing from senior leadership, which has been instrumental in driving the curriculum forward and ensuring its sustainability.
C. Adapting to Evolving Needs
- Challenge: The healthcare landscape is constantly evolving, requiring the curriculum to adapt to new challenges and technologies.
- Solution: The curriculum is designed to be agile, with regular reviews and updates to ensure it remains relevant. Faculty members are encouraged to be flexible and responsive to emerging needs.
D. Integrating Evaluation and Research
- Challenge: Measuring the effectiveness of a multi-disciplinary curriculum can be complex.
- Solution: NUS Medicine has built evaluation and research into the curriculum from the outset, allowing for continuous improvement based on data-driven insights.
V. CONCLUSION
Looking ahead, NUS Medicine aims to expand its interprofessional training opportunities and strengthen partnerships with healthcare institutions. By doing so, it will continue to produce graduates who are not only skilled clinicians but also effective collaborators and innovators.
The NUS Yong Loo Lin School of Medicine’s Common Curriculum for Healthcare Professional Education (CCHPE) represents a forward-thinking approach to medical education, emphasising the importance of collaboration in modern healthcare. By integrating multi-disciplinary learning into every aspect of the curriculum, NUS Medicine is preparing its students to meet the challenges of an increasingly complex healthcare system. In Singapore, where the demand for high-quality, team-based care is greater than ever, this approach is not just beneficial—it is essential. As other institutions look to NUS Medicine as a model, the school’s commitment to innovation and collaboration will continue to shape the future of healthcare education.
Notes on Contributors
Adjunct Professor Lau Tang Ching contributes to the conception and writing of the initial draft, and revising it critically for important intellectual content, approves the final version to be published, and agrees to be accountable for all aspects of the work.
Funding
No funding was received.
Declaration of Interest
The author has no conflict of interest, including financial, consultant, institutional and other relationships that might lead to bias.
References
Brandt, B., Lutfiyya, M. N., King, J. A., & Chioreso, C. (2019). A scoping review of interprofessional collaborative practice and education using the lens of the Triple Aim. Journal of Interprofessional Care, 28(5), 393-399. https://doi.org/10.3109/13561820.2014.906391
Motola, I., Devine, L. A., Chung, H. S., Sullivan, J. E., & Issenberg, S. B. (2020). Simulation in healthcare education: A best evidence practical guide. AMEE Guide No. 82. Medical Teacher, 35(10), e1511-e1530. https://doi.org/10.3109/0142159X.2013.818632
Masters, K., Ellaway, R. H., Topps, D., Archibald, D., & Hogue, R. J. (2020). Mobile technologies in medical education: AMEE Guide No. 105. Medical Teacher, 38(6), 537-549. https://doi.org/10.3109/0142159X.2016.1141190
Ramani, S., & Krackov, S. K. (2019). Twelve tips for giving feedback effectively in the clinical environment. Medical Teacher, 34(10), 787-791. https://doi.org/10.3109/0142159x.2012.684916
Reeves, S., Fletcher, S., Barr, H., Birch, I., Boet, S., Davies, N., McFayden, A., Rivera, J., & Kitto, S. (2019). A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Medical Teacher, 38(7), 656-668. https://doi.org/10.3109/0142159x.2016.1173663
*Lau Tang Ching
1E Kent Ridge Road
NUHS Tower Block, Level 11,
NUS Yong Loo Lin School of Medicine,
Singapore 119228
Email: mdcltc@nus.edu.sg
Submitted: 16 November 2024
Accepted: 7 February 2025
Published online: 6 January, TAPS 2026, 11(1), 18-21
https://doi.org/10.29060/TAPS.2026-11-1/GP3573
Dayo Rotimi Omotoso1 & Joy Oyiza Peter2
1Department of Human Anatomy, Faculty of Basic Medical Sciences, Redeemer’s University, Ede, Nigeria; 2Department of Educational Technology, Faculty of Education, University of Ilorin, Ilorin, Nigeria
Abstract
Introduction: The application of modern and innovative technology into anatomical science education has been on a rapid increase globally in recent years with the anatomy tutors and students playing important and complementary roles in the process of the integration.
Methods: This narrative perspective presents the current state of technological applications adopted in anatomy education in medical colleges in Africa and the roles of the anatomy tutors and students in the process.
Results: The role of the anatomy tutors in African medical colleges include facilitation of technological integration into anatomy education and curriculum, promotion of active learning in anatomy, design of innovative assessment strategies, provision of relevant technological support, and advocate for provision of resources and infrastructure. Similarly, the trainees played important roles in the process of technological integration into anatomy education in Africa which include increased acceptability of technology for anatomy learning, utilisation and validation of innovative assessment methods, peer-advocacy for technology-driven learning, and bridging the technological gap.
Conclusion: The active participation of both the tutors and students in the adoption of technological solutions and tools will continue to enhance the quality of anatomical science pedagogy across African medical colleges.
Practice Highlights
- Application of technology in anatomy education has been on a rapid increase globally.
- Technology applications are used in anatomy education to complement traditional methods.
- Tutors and students in Africa have played vital roles in the adoption of technology for anatomy education.
- Technological applications are currently re-shaping anatomy education landscape to improve learning outcomes.
- Application of technology in anatomy education should be promoted to further enhance learning.
I. INTRODUCTION
Anatomy is a foundational discipline in medical education which is required in the training of medical and allied health students in order to gain requisite knowledge and professional competence. Hence, anatomical science content remains a pivotal component of the academic curricula of all sub-disciplines of the medical sciences (Hildebrandt, 2019). The provision of quality education (including medical education) is one (number 4) of the United Nations’ sustainable development goals (SDGs) targeted at ensuring equitable and inclusive quality education for all. Technological advancements of the past decade have been applied to facilitate educational processes. Hence, digital technologies have been identified as important tools that would facilitate the achievement of the SDG 4.
The integration of technology has resulted in major evolution in anatomical pedagogy leading to a wide array of positive outcomes. In essence, the use of modern and innovative technological applications by the anatomy tutors and students for teaching and learning processes has resulted in satisfactory outcomes (Patra et al., 2022). In several African medical colleges, the characteristic cadaveric-based learning is being augmented with technological applications in order to improve learning outcomes and to prepare the students for the emerging medical professional practice (Owolabi et al., 2022). Additionally, technology-driven interactive learning strategies that ensure online delivery of learning resources are being explored for histology education. These strategies, which have enabled the trainees to complete learning outcomes while not physically present in classrooms or laboratories, have further helped to solve associated cognitive challenges of histology learning (Meyer, 2023).
The transition from the conventional classroom to technological-driven anatomy teaching and learning became prevalent during the coronavirus disease 19 (COVID-19) pandemic when medical colleges were shut down around the world (Omotoso, 2023). In essence, both the anatomy tutors and students necessarily played a complementary role in the adoption of the technological applications to sustain anatomy education. The current study presents the perspective on the role of the anatomy tutors and students in the application of technology for anatomy education in medical colleges across Africa.
II. METHODS
Based on the appraisal of the current practices and existing literature, the authors have developed the narrative perspective on the role of tutors and students in the emerging process of application of technology for anatomy education in African medical colleges.
III. RESULTS
The anatomy tutors and students are the most important stakeholders at the centre of the process of application of technology for anatomy education in African medical colleges. Regardless of the identified beneficial impact of technological adoption in anatomy education, the acceptability and successful integration of technology into anatomical science pedagogy in African medical colleges largely depend on the roles of the anatomy tutors and students in the process.
IV. DISCUSSION
A. Roles of African Tutors in the Application of Technology into Anatomy Education
Anatomy tutors in medical colleges across Africa have played the following crucial roles in the integration of technology into anatomical science pedagogy:
1) Facilitate technological integration into anatomy education: Anatomy tutors are the key players in facilitating the adoption of technology into anatomical science pedagogy. In essence, anatomy tutors in African medical colleges act the crucial linkages that connect the students to technology-based learning strategies as a complement to the conventional cadaver-based anatomy learning. In addition, technological applications such as virtual microscopy are being explored in the delivery of histology education to enhance the teaching and learning process by enabling continuous interaction with unlimited numbers of high-quality, digitised histological sections. In essence, the African anatomists are generally technology inclined and are helping to facilitate the integration of technology into anatomy education in African medical colleges.
2) Design of innovative anatomy curriculum: The incorporation of technology into anatomy pedagogy entails an integration of innovative and technological-based strategies into the conventional anatomy curriculum for health profession students. This process is currently driven by the anatomy tutors in African medical colleges by ensuring that digital technological applications are tailored to achieve the learning objectives and expected outcomes of anatomy modules. The tutors further drive the students’ knowledge of emerging anatomy education concepts in the updated curriculum through digital applications in complement to conventional physical learning.
3) Promote active learning and student engagement: Active learning, which emphasises students’ participation and interaction, is a key pedagogical strategy which is currently enabled by technology in anatomical education. Anatomy tutors encourage the students to engage with digital applications like virtual reality (VR)-based anatomy models or interactive anatomy applications, thereby fostering more hands-on approach to anatomy learning in order to improve learning experiences and satisfaction.
4) Design and utilise innovative assessment strategies: The strategies for students’ assessment in anatomical science are steadily evolving due to integration of technological-enhanced methods with the utilisation of these innovative methods essentially dependent on the tutors to drive the process. Technology-driven assessments such as computer-based test (CBT), conducted on online platforms or learning management systems (LMS), have been adopted to execute the conventional assessments including short answer questions, multiple choice questions, and objective structured practical examination (OSPE) with comparable or improved outcomes and satisfaction.
5) Provide mentorship and technological support: Due to the socio-economic background, some students in African medical colleges may not be compliant with the modern digital technologies used for educational purposes. The anatomy tutors act as mentors and instructors that provide support for the students to overcome the barriers associated with technological literacy. In this role, anatomy tutors offer both academic and technological support to help the students use modern technological applications for anatomy learning.
6) Advocate for provision of infrastructure and resources: The application of technology in anatomical science pedagogy requires robust infrastructure such as regular internet connectivity, computer laboratories, VR laboratory, virtual platforms such LMS and so on. Anatomy tutors play a crucial role in advocating for institutional support toward the provision of requisite infrastructure and resources to drive the technology-based anatomy learning environment. In many African medical colleges, infrastructural deficits pose significant barriers to technological integration.
7) Act as technology advocates and change agents: Another role of the anatomy tutors is the promotion of paradigm shift towards acceptability of technology as an effective tool for anatomical science education. Essentially, the African medical colleges have always adopted the conventional cadaver-based anatomy learning. The recent application of technology in anatomy pedagogy has attracted some concerns, especially the uncertainty of its effectiveness and efficiency compared to the conventional methods. However, with the scientific findings of comparable effectiveness of technological-driven anatomy learning, advocacy now revolves around its adoption as a complement and not replacement to conventional methods of learning.
B. Roles of African Students in Application of Technology for Anatomy Education
Anatomy trainees are the major end-users of the technological applications and hence, positioned as the key determinants of how the applications would be utilised in classrooms, laboratories, or clinical settings for anatomy learning. Therefore, the roles of the African trainees in driving the technological-based anatomical science pedagogy include:
1) Adoption of digital applications for improved anatomy learning outcomes: Students in African medical colleges act as early adopters of technological applications that could enhance anatomy learning. Virtual anatomy platforms like the Visible Body and Complete Anatomy are currently used to complement the traditional cadaver-based learning and technological tools such as 3D anatomy apps, virtual dissection tables, and online simulations have become increasingly popular in medical schools across the continent.
2) Utilisation and validation of innovative assessment methods: The advancement of digital technology has enabled the development of more interactive and objective assessments strategies in anatomy pedagogy. Essentially, the anatomy trainees are central to the pilot testing and deployment of these technology-driven assessment strategies for anatomical science. In addition, the anatomy trainees provide critical feedback on the effectiveness and efficiency of the technology-driven assessment tools. This feedback is required for their improvement and validation for consequent integration into the overall assessment strategies.
3) Peer-advocacy for technology-driven learning: Recent technological advancements have further impacted anatomy education due to the more technological-compliance of the emerging trainees. As such, anatomy trainees have become more inclined to online learning than conventional classroom learning with reported satisfactory or even improved outcomes. The trainees actively learn through online anatomy resources or virtual dissection simulations in order to sustain anatomy education when the physical classroom learning was not accessible.
4) Bridging the technology gap: Despite the growing availability of digital tools, there remain challenges in accessing technological resources in many African medical colleges, particularly in remote and under-funded institutions. The anatomy trainees have risen to the responsibility of bridging this gap by setting-up initiatives to share access to digital anatomy tools through shared devices or group licenses for online platforms.
V. CONCLUSION
Technology applications applied in anatomical science learning and assessment are actively complementing the traditional methods in Africa medical colleges thereby gradually transforming the anatomy education landscape in Africa. Anatomy tutors play crucial roles in the utilisation of the technology for facilitation and learning to complement the traditional method of delivering anatomy education. The students have similarly adopted innovative technological tools to achieve self-directed and flexible anatomy learning. The active participation of both the tutors and students in the adoption of technological solutions and tools will continue to enhance the quality of anatomical science pedagogy across African medical colleges.
Notes on Contributors
DRO conceptualised the study, participated in literature search, manuscript drafting, manuscript editing, final review and approval of the manuscript.
JOP participated in literature search, manuscript drafting, manuscript editing, final review and approval of the manuscript.
Acknowledgement
The authors would like to acknowledge the support from the staff of Department of Human Anatomy, Faculty of Basic Medical Sciences, Redeemer’s University, Ede, Nigeria.
Funding
This work has not received any external funding.
Declaration of Interest
The authors declare no conflict of interest for this study.
References
Hildebrandt, S. (2019). The role of history and ethics of anatomy in medical education. Anatomical Science Education, 12(4), 425-431. https://doi.org/10.1002/ase.1852
Meyer, G. T. (2023). Online, interactive, digital visualisation resources that enhance histology education. In: S. Border, P. M. Rea, & I. D. Keenan (Eds.), Biomedical Visualisation: Advances in Experimental Medicine and Biology (vol 1421., pp. 125-160). Springer. https://doi.org/10.1007/978-3-031-30379-1_6
Omotoso, D. R. (2023). Adoption of online classes for anatomy learning during coronavirus disease 2019 pandemic – participation, perception and preference of basic medical students of a Nigerian University. National Journal of Clinical Anatomy, 12, 121-126. https://doi.org/10.4103/NJCA.NJCA_48_23
Owolabi, J., Ojiambo, R., Seifu, D., Nishimwe, A., Masimbi, O., Okorie, C. E., Ineza, D., & Bekele, A. (2022). African medical educators and anatomy teachers’ perceptions and acceptance of the anatomage table as an edtech and innovation: a qualitative study. Advances in Medical Education and Practice, 12, 619-625. https://doi.org/10.2147/AMEP.S358702
Patra, A., Asghar, A., Chaudhary, P., & Ravi, K. S. (2022). Integration of innovative educational technologies in anatomy teaching: New normal in anatomy education. Surgical and Radiological Anatomy, 44(1), 25-32. https://doi.org/10.1007/s00276-021-02868-6
*Dayo Rotimi Omotoso
Department of Human Anatomy,
Faculty of Basic Medical Sciences,
Redeemer’s University, Ede,
Nigeria.
+2348034779886
dayohmts@gmail.com
Submitted: 28 January 2025
Accepted: 16 June 2025
Published online: 6 January, TAPS 2026, 11(1), 22-31
https://doi.org/10.29060/TAPS.2026-11-1/OA3633
Hannah Woodall1,2, Linda Furness1,2, Robert Heffernan1,2, Kay Brumpton1, Janani Pinidiyapathirage1,2 & Brendan Carrigan1,2
1Rural Clinical School, Griffith University, Toowoomba, Australia; 2Rural Medical Education Australia, Toowoomba, Australia
Abstract
Introduction: Reflection offers many benefits for medical students, improving self-awareness and integration of theory into real situations. However, like any skill, reflection must be learned and practiced. Reflective learning is also influenced by the workplace, particularly in students’ clinical training years. This study explored the factors perceived by educators to influence reflective learning amongst medical students undertaking a rural longitudinal integrated clerkship (LIC).
Methods: All educators within the LIC program were invited to participate. Educators come from both a medical and nursing background. Two focus groups (FG) were conducted. FG were facilitated by experienced researchers. Transcripts were analysed by two researchers using Braun and Clark’s approach to thematic analysis.
Results: Eleven educators participated in two focus groups (six medical educators; five nursing educators). Educators perceived that reflective learning was influenced at three levels: student, educator and institution. These findings aligned with workplace learning theory. Educator and institutional influences were identified as “affordances” which support or hinder reflection. Supportive affordances included labelling of reflection, multidisciplinary collaborative learning, and the longitudinal nature of the rural model. Hindering affordances included using artificial reflective assessments. Educators also identified characteristics of the individual student which may contribute to student decision-making about reflection.
Conclusion: This study provides a deeper understanding about educator experiences of reflective learning within LIC settings. The findings provide insights into the ways in which educators, educational institutions and student workplace settings may support or hinder reflective practice. This study also highlighted the potential for the LIC model to support reflective practice.
Keywords: Reflective Practice, Undergraduate Medical Education, Rural Medical Education, Longitudinal Integrated Clerkship, Workplace Learning
Practice Highlights
- Educator factors including labelling and positive modelling of reflection may support reflective learning in clinical settings. Modelling of negative attitudes to reflection may hinder reflection in such settings.
- Institutional factors including the LIC model, allowing time for reflective activities and prioritising activities which promote genuine reflection may support reflection in clinical placements. Conversely, allowing limited time for reflection and focussing on written reflective activities may hinder reflection in these same settings.
- Despite educator and institutional factors, students must still choose to engage in reflection.
I. INTRODUCTION
Reflection is a vital skill for medical students, particularly as they transition from theoretical learning environments into clinical settings (Greenhill et al., 2017). In clinical settings, students must learn to translate theory into practice and integrate ethics, communication, professionalism, and culture into real-life situations (Malau-Aduli et al., 2020; Schön, 1995). Reflection supports students to make this transition and become reflective practitioners.
The relationship between reflection and learning is well established (Sandars, 2009). Dewey (1910) proposed that knowledge is created through reflection on experience, through which learners resolve doubt and make sense of situations. This early work has been reshaped, and advanced, with reflection recently defined as: “a metacognitive process that occurs before, during and after situations with the purpose of developing greater understanding of both the self and the situation so that future encounters with the situation are informed from previous encounters” (Sandars, 2009).
This definition proposes a broad understanding of reflection as “thinking about thinking” (metacognition) which occurs at all stages of an experience (before, during and after) (Flavell, 1979; Sandars, 2009). This definition recognises that reflection considers the situation, empirical knowledge and the drivers of the actions of “self” (Sandars, 2009). Such reflection allows past experience to shape future encounters (Kolb, 2014). Through reflection, students actively consider their experiences and examine their skills, beliefs, or assumptions to make sense of complex situations (Bradbury et al., 2010; Chambers et al., 2011; Fernandez et al., 2015; Sandars, 2009). This process moves beyond introspective reflection, instead requiring students to participate in “critical reflection”, whereby learners critically and intentionally consider their experience, knowledge and practice to shape and improve future encounters (Ash & Clayton, 2009).
Reflection is not an automatic or passive process, but requires time, willingness, and skills (Ash and Clayton, 2009; Chambers et al., 2011). Current reflective learning education has been criticised for its reliance on formulaic and written reflections, which may lead to contrived, inauthentic attempts (de la Croix & Veen, 2018). Similarly, while reflective models and frameworks (e.g. Boud, Driscoll or Gibbs) provide useful tools, a narrow focus on reflective models or assessment matrices can paradoxically reduce opportunities for authentic reflection (Boud et al., 1985; Dewey, 1910; Driscoll, 1994; Gathu, 2022; Gibbs, 1988). Evidence increasingly supports diverse reflective methods to enable learners to identify their own personal systems for reflection (de la Croix & Veen, 2018; MacAskill et al., 2023).
Student reflective learning is also impacted by the transition from university-based to workplace-based learning that occurs as students move into clinical settings. Workplace learning is a cooperative process between workplace and learner (Billett, 2001, 2016). In this duality, the workplace or clinical placement offers “affordances” such as formal training, mentoring or the underlying values and culture of the organisation, which may enable or hinder learning (Billett, 2001, 2016). However for meaningful learning to occur, a learner must elect to engage with these workplace opportunities (Billett, 2001). Engagement decisions may be shaped by many factors, including knowledge, values and motivations (Billett, 2001). Where these factors align with what the workplace affords, skill development and mastery will be promoted (Billett, 2001).
Our study was conducted within the context of a rural Longitudinal Integrated Clerkship (LIC) for medical students in Queensland, Australia. Rural longitudinal placements have been reported to foster reflective practice amongst students (Bates et al., 2013; Daly et al., 2013; Gaufberg et al., 2014; Greenhill & Poncelet, 2013; Nyaradi et al., 2025). However, educators in our program have expressed concerns that student reflections were often superficial and may not foster lifelong reflective practice. Given these concerns, a greater understanding of educator perspectives on student reflection is needed.
The student perspective in this context has been explored previously and identified that students valued scaffolding of reflective activities to assist them in learning to reflect, particularly at the beginning of their placement or where they were unsure what to reflect on in a specific situation (MacAskill et al., 2024). However, to gain a more comprehensive view of the placement setting, the perspectives of educators must be considered. Educators bring experience drawn from multiple student cohorts and observe student educational, clinical and interpersonal interactions over the course of a year (Hirsh et al., 2007; Norris et al., 2009). In the rural LIC context, these insights are gained not only through their formal work as educators but also through their roles as health professionals co-located with the students in small rural hospitals. This external perspective provided by educators offers valuable insights into the development of reflective practices and abilities of the students during their clinical placement. This study aimed to identify the factors that educators perceive as influencing reflective learning within a rural LIC program. Additionally, it explores effective methods for supporting student reflection and facilitating the development of authentic reflective practice.
II. METHODS
A. Setting
This study explored reflective learning in the Griffith University “Longlook” program, a rural LIC in south-east Queensland, Australia. Medical students in the Griffith Medical program, a four-year postgraduate medical degree, can elect to participate in Longlook for one or both of their clinical years (years three and four). Longlook students are placed in rural locations for one or two years and meet learning goals across multiple disciplines within a longitudinal placement rather than through isolated blocks (Fuller et al., 2021). Students live in communal accommodation within these rural locations.
The Longlook model affords students continuity of relationships with supervising clinicians and patients (Fuller et al., 2021; The Consortium of Longitudinal Integrated Clerkships [CLIC], 2020; Worley et al., 2016). Approximately 50 students participate in this program each year at one of eight rural clinical training sites (Carrigan et al., 2023).
Longlook is unique in being delivered in partnership with a rural not-for profit organisation, Rural Medical Education Australia (RMEA). Students are supported by generalist educators from both a medical and nursing background who are co-located with students in the hospital sites. Longlook medical educators are rural generalists, who are trained as general practitioners and also provide care within emergency medicine and/or obstetrics, anaesthetics or other hospital services within their local setting (Department of Health and Aged Care [DHAC], 2021). Longlook clinical nurse educators have advanced training to work in rural generalist hospitals and support education delivery within the LIC. Both nursing and medical educators attend monthly training sessions with the students at a central location throughout the academic year in addition to supporting medical students at their respective local sites.
Griffith University medical students are taught and practice reflective practice framed through the MaRIS model. MaRIS applies contemplative pedagogy to medical student teaching to foster a culture of affective reflection (Chan et al., 2020). The year 3 and 4 curricula include two forms of reflective assessment. The first is a written reflection on the student’s topic of choice, completed by all students in both year levels. The second is a series of case presentations (twenty-four in year 3 and six in year 4) which include reflection on the case as well as consideration of ethical, legal, professional or other non-biomedical issues.
B. Research Team
The research team has broad experience across medical education and clinical practice. HW is an academic GP. KB, BC and RH are clinicians and medical educators who have been involved in the development and implementation of the Longlook program. BC and RH lead the 3rd and 4th year student programs. LF is an occupational therapist with expertise in education and reflective learning within the allied health context. JP is an experienced health researcher and RMEA director of research. The research team reflected upon the assumptions brought to the study, namely that reflective learning is important but existing approaches do not appear to engage students in genuine reflection. The background of research team members allows an active interpretation of the results based on experience within medical education and clinical practice (Olmos-Vega et al., 2023).
C. Participants
All educators within the Longlook program were invited to participate (eight medical educators, six nursing educators). Participants were not recruited from outside of this program due to the challenges of comparing this unique context with other education settings.
D. Study Design
A constructivist case study research paradigm was used to ensure methodological congruence and forefront the experiences and voices of the research participants. Constructivist perspectives reflected the desire to explore the participants’ constructions of their lived experiences as educators (Shannon-Baker, 2023). The case study approach enabled the team to understand and describe the experiences of educators within the setting of a rural LIC by purposively selecting educators within the program (Hall et al., 2008). In accordance with the constructivist approach, semi-structured focus groups were used to capture educators’ collective experiences and enable rich data generation based on interactions between participants (Gill & Baillie, 2018).
Two focus groups were conducted between August and December 2022. The potential for power differentials between medical and nursing educators led to the decision to separate focus groups, ensuring that the perspectives of both groups could be explored freely. The medical educator (ME) focus group was conducted by a ME, while the clinical nurse educator (NE) focus group was facilitated by a clinical nurse educator. Focus groups lasted approximately one hour and were conducted in person during student teaching days. Informed written consent was obtained from all participants prior to the focus group. The focus groups explored educator views on reflective learning activities, an evaluation of current reflective methods, and how reflective learning could be improved. The interview guide is attached in Appendix 1.
Focus group data recordings were transcribed using Sonix™ and uploaded to NVivo™ for coding. Braun and Clarke’s 6-step approach to thematic analysis was adopted to generate codes and themes inductively from the transcribed data, aligning with the qualitative approach to data generation and in keeping with the constructivist paradigm underpinning the research design (Braun & Clarke, 2006). Two researchers (HW and LF) worked independently on analysis before coming together to define and decide on the most significant themes, applying the principals of thematic analysis in a non-linear and iterative way.
The research team sought to ensure the trustworthiness of the data through acknowledging their own background and assumptions, providing thick descriptions of the data and its context, and through independent analysis by team members from different backgrounds (Ahmed, 2024).
E. Ethics
Ethical approval was obtained from the Griffith University Human Research Ethics Committee (GU 2021/376).
III. RESULTS
Eleven educators were recruited to participate in this study, including six with a medical background, and five with a nursing background. Factors perceived by educators to impact student reflective practice occurred at three levels: student, educator and institution.
A. Student Factors
The student’s pre-clinical life experience and innate ability to reflect appeared to impact their ability to engage in reflective practice. Educators perceived that some students were already skilled in reflection, while for others it was a new and challenging concept. They also perceived that student’s life experience and self-awareness impacted on their ability to reflect.
“You’re teaching, for some people, something that they’re doing already and then for others, … you are actually trying to teach, you know, an unnatural kind of process.” ME3
“Everybody has really different life experiences and the way that they bring those life experiences to the way that they either talk to somebody or treat a patient or think about, diagnose, diagnostics or anything like that, you know, all of those life experiences will contribute to that in some way. So I guess it’s just also that self-awareness of who you are and where you came from and how that’s influencing the way that you are interacting and thinking about other people as well.” NE4
“An increasing number of students that come rural, actually, it is a practice for them, and they will actually journal and reflect on their day most days… I don’t know whether something that they’re, they’ve been taught to do in years one and two, or whether it’s something that they’ve it’s just been a practice of theirs from something else” NE5
Educators perceived clinical exposure as significantly impacting the quality of student reflections, with students new to the placement reflecting on the newness of their experience, while students who had been on the placement for several weeks or months reflected on their capabilities and strategies for improving their practice. Educators witnessed the evolution of student’s reflective skills and described deepening complexity of reflections, incorporating the socio-cultural context of rural healthcare, during the LIC program.
“At the beginning, the reflection was just, this is all new and different. And now the reflection is more about what was done well and how they contributed and how they could do better or could do things differently.” ME1
“By the end of it, they’ve learnt so much that the reflective practice is actually more where they’re thinking…They’re now more thinking about reflecting on their practice and how they’re going to be a better doctor.” NE2
“I think with the rural generalist model, when people are learning in these kind of, in rural towns, that application to a bigger context is a bit probably easier for them to learn and to see. So we probably do have an opportunity to actually get them to understand that more and reflect on that more.” ME6
Educators also described informal reflection occurring outside of the clinical environment. The immersion in a rural LIC setting and shared accommodation was felt to provide greater informal opportunities for reflection.
“I think about the students in the accommodation building this year and I think about the students in the accommodation building last year, and last year there was lots of reflective practice, just informally, in the accommodation building. This year, it was very limited, and that’s, you know, different personalities” ME1
“I wonder within the rural context whether our students are naturally doing it [reflecting] at night when they go home and talk to each other a little bit anyway.” ME6
B. Educator Factors
Educators recognised the importance of role modelling and their own reflective practice to support student reflection. The approach and attitude of medical educators towards reflection was felt to be particularly significant. Educators linked this with the “hidden curriculum”; the informal learning that occurs through witnessing attitudes and behaviours of educators and supervisors (Hafferty & O’Donnell, 2014).
“I wonder if the groaning about, and negativity to reflective practice is in the hidden curriculum in that as a profession, we groan and have a negative attitude to reflective practice.” ME2
“I’m not sure whether we as doctors do as much active reflecting as we probably should as well and show how important that is.” ME6
“It [reflection] probably also needs to be better embraced amongst the medical community itself. Because, yeah, because there’s a lot of doctors out there that’ll think it’s a bit airy fairy or bit of a waste of time. And I suppose when you’re trying to be a doctor, a doctor’s opinion is going to have a higher standing than a nurse’s opinion” NE4
Educators also acknowledged that reflection is not always labelled when it occurs, which may impact student reflective activities.
“I hear lots of philosophical conversations coming from my colleagues with medical students… I’ve never heard any of them termed as reflection.” ME3
“You asked if we use the word reflection, and I think we all try and shy away from it.” ME5
Educators reported that educators and students engaging in collaborative reflection provided a positive influence, as an example of educators modelling reflection.
“One thing I try and do with the students is every week we catch up and I ask them all the question, “What was the most interesting thing you saw this week?” …. I always try and do one as well to model firstly that I’m still learning. This was interesting to me because I missed the diagnosis, actually, and I need to work on that or for whatever reason and be part of the collective “we’re all learning together” ME5
Collaborative reflection as part of multidisciplinary educator teams was also considered significant. Educators from different disciplines are involved in the Longlook program, with educators proposing that different disciplines may bring different reflective skills. Nurse educators identified that they may be able to contribute more to this aspect of student learning and wondered if medical educators may benefit from professional development in this area.
“Perhaps the nurse educators are better positioned to talk to them about reflective practice …Because perhaps the medical educators don’t do it well, either.” NE5
“If there are some struggling, because [medical educator] doesn’t have the time. Maybe I could just work with them… What’s been going on? Have that sort of informal thing just to prompt them to reflect a little bit more” NE4
“Maybe …some professional development for the medical educators as well, just to see how comfortable they are with it” NE5
Participants identified that this process of learning together requires a safe learning environment in which trust and vulnerability from both sides allows educators and students to learn to reflect together.
“Because they’re [students] so used to being such high performers, being in a position where you’re not performing so well definitely puts them in a vulnerable position…” NE1
“I think that depends on trust. That’s probably the key thing. And the relationship that exists, so it wouldn’t be a natural thing at the start of a year to do it with an educator.” ME3
C. Institutional Factors
Finally, educators identified organisational factors related to the university curriculum which impacted student reflective learning. Time constraints within the medical school program meant that reflective activities were omitted when time was tight.
“When you’ve only got like two hours to get through six people [presenting case-based discussions], you may not be able to sort of expand on some of those reflections, as interesting as they might be to discuss as a group.” NE1
Educators felt that students required institutions, assessors and educators to set clear expectations for reflection.
“We could probably do a better job of actually setting that standard with orientation” ME2
“Do it [reflective teaching] as a sort of combined nurse-educator to the students reflective practice session. “This is what we’re going to expect for the year.” Maybe then they’ll start off a little bit better instead of gradually getting better if they know what we are expecting. NE3
Educators also expressed concern that assessing reflection may create an engineered environment that may reduce the opportunities for deep reflective learning.
“I do worry that in assessment that people will just write the minimum of what they have to do because they don’t see it as a priority.” ME6
“I think the main thing about doing it as a formal assessment is that it’s hard to actually sit down and put it in writing in a formal way that the university wants to hear, basically, though. Doing it as a practice is a good thing, but having to write it like an assignment makes it hard work.” NE2
“It should be sort of mandated that in some capacity they do it, but maybe not so much in a “you’ve got to do it and I’ve got to tick the box and say that, you know, you’ve passed or whatever” ME5
Educators instead suggested reflective activities to focus on real-world situations to encourage authentic reflection.
“Why are we doing this as a single one off reflective about a random event that may or may not be true and we just add reflection onto a true in situ real world case and assess it across an entire year” ME1
“Could they knock off one of the CEXs [clinical evaluation exercises] and have a reflective piece like that is just a reflection for each block that they do? NE3
IV. DISCUSSION
This study identified student, educator and institutional factors that were perceived by educators to enable or inhibit student reflective learning. Enabling factors included labelling of reflection, provision of a trusting environment, multidisciplinary collaborative reflective learning, allowing time for reflective activities and the longitudinal nature of the rural model. Inhibiting factors included the use of artificial reflective assessments. Two elements were identified which may either inhibit or enable reflective learning: student factors (both life experience and experience of reflection) and modelling. Students’ previous positive experiences of reflection or established life experience was perceived to enhance student reflection. Conversely, reflective activities may be inhibited by a student’s lack of experience or previous negative experiences of reflection. In addition, modelling could be inhibitory or enabling depending on whether positive or negative attitudes towards reflection were modelled to students.
A. Workplace Reflective Learning
Educator insights align with workplace learning theory which describes “affordances” through which workplaces support or hinder learning (Billett, 2001, 2016). The educator and institutional factors identified can be viewed as “affordances” for reflective learning. Educator modelling and labelling of reflective practice in the clinical setting provide opportunities for students to learn. Similarly, the development of a trusting environment, allowing time for reflection and encouraging real-world reflections provide opportunities for students to reflect.
However, workplace learning theory also recognises that, despite the number and quality of affordances, individuals have choice about whether to engage in learning activities (Billett, 2001, 2016). Educators identified student factors which may improve engagement with reflection. This study was conducted in a post-graduate medical program with students from diverse backgrounds and with different experiences and reflective skills. These elements may impact individual decisions to engage. This observation aligns with workplace learning theory’s identification that, even with the same affordances, learners may make different choices when it comes to engagement.
B. Educator Reflective Ability
Educators strongly focused on the impact of their own practice in these focus groups, identifying areas for improvement in their clinical and educator roles. Medical educators highlighted the impact of their own, often negative, views of reflection and failure to label reflective activities. Nurse educators realised that they may have a key role in reflective learning and identified practical strategies to increase their involvement.
These insights arose through profound reflective discussions during the focus groups. Educators reflected deeply on their own challenges, experiences and struggles with reflection. They reflected on the impact of their own practice and attitudes on their students. Educators then collectively discussed changes to future practice including modelling positive examples of reflection, labelling reflective activity or actively participating in student reflective activities. While this process occurred in an iterative and conversational manner, it clearly demonstrates reflective skills. However, this process was not labelled as reflection at any point in either group.
This demonstration of reflective ability is especially meaningful since educators, particularly medical educators, expressed concerns that they lacked reflective skills. The focus group discussions suggest that educators have reflective skills but may not be attuned to recognise reflection when it occurs.
C. The Rural LIC Model
The rural LIC model was identified as an affordance for reflective learning. The long-term student-educator and student-student relationships in the rural LIC setting were felt to enable the development of a trusting environment in which students and educators feel safe to reflect honestly. The rural longitudinal setting was also felt to enable greater opportunities for reflection through communal living arrangements. These benefits were seen as supporting reflection in medical students and align with previously reported benefits of the LIC model including relationship continuity, a holistic perspective on the patient and their experience, and self-awareness (Carrigan et al., 2023; Gaufberg et al., 2014; Mylopoulos et al., 2020; Purea et al., 2022).
D. Limitations
This study considered the educator perspective only. A study exploring the student perspective in this setting has previously been published (MacAskill et al., 2024).
The limited sample size of this study was related to the limited pool of educators in this program. Limitations in numbers of rural medical educators is a widespread problem. Most medical educators are located in urban centres (McGrail et al., 2023). Given the unique context of this study (rural LIC), it was not possible to recruit more widely within different programs.
E. Future Research
The significance of the LIC model in this setting highlights an important lesson for medical education more broadly. This study demonstrates the importance of trust for reflection, and how these elements are facilitated through models such as the LIC. Further study is needed to explore how trust can be developed in the context of shorter-term student-educator relationships. This study also did not include a comparator group within a more traditional block-mode setting but this may be a useful area for future enquiry. Further studies to explore reflection within other LIC models and within other collaborative multidisciplinary learning environments would be useful to more fully understand the role of such models in reflective learning. Finally, further study to explore the drivers of student engagement in reflective learning would improve our understanding of why some students do not engage despite affordances.
F. Implications for Practice
This study was conducted to identify how reflective practice could be improved in this rural medical education setting. Educators identified that students who are not naturally reflective, lack life experience or exhibit limited self-awareness were less likely to engage in reflective practice. Engagement may also relate to educator factors such as the labelling of reflective activities and students experiencing modelling of positive attitudes towards reflection.
Educators identified that the relationships formed through the rural LIC model may support students to reflect but also noted that educators should ensure that they label reflection where it occurs, and model positive and authentic reflective practice to their students. This study also highlighted the potential strengths of different clinical disciplines and emphasised the benefits of multidisciplinary educator teams. Encouraging nurse and medical educators to teach and reflect together may improve reflective skills of the educator and student cohort.
V. CONCLUSION
This study sought the perspectives of educators on student reflective learning within a rural longitudinal integrated clerkship. Findings aligned with workplace learning theory, with “affordances” identified which facilitated or hindered reflective learning. These affordances predominantly related to educator factors including modelling and labelling of reflection, and institutional factors including the time allowed for reflection and the nature of reflective activities. Elements of a rural LIC model provide affordances to develop deeper reflective learning and highlight the extended opportunities provided by this model.
Notes on Contributors
Hannah Woodall designed the study with Robert Heffernan, Kay Brumpton, Janani Pinidiyapathirage and Brendan Carrigan. Hannah Woodall was responsible for data collection and worked with Linda Furness to analyse the data. Hannah Woodall was responsible for development and editing of the manuscript.
Linda Furness worked with Hannah Woodall to analyse the data and was involved in interpreting the results. Robert Heffernan was involved in conceptualisation of the study and interpretation of the data. Kay Brumpton was involved in study design and development of study materials. Kay Brumpton participated in making sense of the data, contributing theoretical background to the analysis. Janani Pinidiyapathirage was involved in development of the study protocol and materials and contributed to interpreting the data. Brendan Carrigan was involved in study development and interpretation of the collected data. All authors have read and approved the final manuscript.
Ethical Approval
Ethical approval for the study was obtained from the Griffith University Human Research Ethics Committee (GU 2021/376).
Data Availability
The datasets analysed during the current study are not publicly available due to participants’ potential identifiability due to the small dataset. Data is available from the corresponding author on reasonable request.
Acknowledgement
The writers acknowledge Dr Claire D Nicholls (University of Southern Queensland) for her assistance in reviewing the research methods section of this manuscript.
Funding
The authors would like to acknowledge the funding received through the Rural Health Multidisciplinary Training (RHMT) program grant of the Australian Government that supported the salaries of HW, LF, RH, KB, JP and BC during this study.
Declaration of Interest
The authors declare that they have no competing interests.
References
Ahmed, S. K. (2024). The pillars of trustworthiness in qualitative research. Journal of Medicine, Surgery, and Public Health, 2, Article 100051. https://doi.org/10.1016/j.glmedi.2024.100051
Ash, S. L. & Clayton, P.H. (2009). Generating, deepening, and documenting learning: The power of critical reflection in applied learning. Journal of Applied Learning in Higher Education, 1(1), 25-48. https://doi.org/10.57186/jalhe_2009_v1a2p25-48
Department of Health and Aged Care. (2021). National rural generalist pathway. Australian Government. https://www.health.gov.au/initiatives-and-programs/national-rural-generalist-pathway
Bates, J., Konkin, J., Suddards, C., Dobson, S., & Pratt, D. (2013). Student perceptions of assessment and feedback in longitudinal integrated clerkships. Medical Education, 47(4), 362-374. https://doi.org/10.1111/medu.12087
Billett, S. (2001). Learning through work: Workplace affordances and individual engagement. Journal of Workplace Learning, 13(5), 209-214. https://doi.org/10.1108/EUM0000000005548
Billett, S. (2016). Learning through health care work: Premises, contributions and practices. Medical Education, 50(1), 124-131. https://doi.org/10.1111/medu.12848
Boud, D., Keogh, R., & Walker, D. (Eds.). (1985). Reflection: Turning experience into learning. Taylor & Francis Group. https://lccn.loc.gov/84016507
Bradbury, H., Frost, N., Kilminster, S., & Zukas, M. (2010). Beyond reflective practice: New approaches to professional lifelong learning. Routledge. https://doi.org/10.4324/9780203873175
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101. https://doi.org/10.1191/1478088706qp063oa
Carrigan, B., Bass, L., Pinidiyapathirage, J., Walters, S., Woodall, H., & Brumpton, K. (2023). Connectivity is the key to longer rural placement: Retaining students on rural longitudinal integrated clerkships. Medical Teacher, 46(2), 225-231. https://doi.org/10.1080/0142159X.2023.2243025
Chambers, S. L. K., Brosnan, C., & Hassell, A. B. (2011). Introducing medical students to reflective practice. Education for Primary Care, 22(2), 100-105. https://doi.org/10.1080/14739879.2011.11493975
Chan, K. D., Humphreys, L., Mey, A., Holland, C., Wu, C., & Rogers, G. D. (2020). Beyond communication training: The MaRIS model for developing medical students’ human capabilities and personal resilience. Medical Teacher, 42(2), 187-195. https://doi.org/10.1080/0142159x.2019.1670340
Daly, M., Roberts, C., Kumar, K., & Perkins, D. (2013). Longitudinal integrated rural placements: A social learning systems perspective. Medical Education, 47(4), 352-361. https://doi.org/10.1111/medu.12097
de la Croix, A., & Veen, M. (2018). The reflective zombie: Problematizing the conceptual framework of reflection in medical education. Perspectives on Medical Education, 7(6), 394-400. https://doi.org/10.1007/s40037-018-0479-9
Dewey, J. (1910). How we think. D C Heath. https://doi.org/10.1037/10903-000
Driscoll, M. P. (1994). Psychology of learning for instruction. Allyn & Bacon.
Fernandez, S. C., Chelliah, K. K., & Halim, L. (2015). A peek into oneself: Reflective writing amongst undergraduate medical imaging students. Reflective Practice, 16(1), 109-122. https://doi.org/10.1080/14623943.2014.982524
Flavell, J. H. (1979). Metacognition and cognitive monitoring: A new area of cognitive–developmental inquiry. American Psychologist, 34(10), 906. https://doi.org/10.1037/0003-066X.34.10.906
Fuller, L., Lawson, M., & Beattie, J. (2021). The impact of clerkship model and clinical setting on medical student’s participation in the clinical workplace: A comparison of rural LIC and rural block rotation experience. Medical Teacher, 43(3), 307-313. https://doi.org/10.1080/0142159x.2020.1839032
Gathu, C. (2022). Facilitators and barriers of reflective learning in postgraduate medical education: A narrative review. Journal of Medical Education and Curricular Development, 9. https://doi.org/10.1177/23821205221096106
Gaufberg, E., Hirsh, D., Krupat, E., Ogur, B., Pelletier, S., Reiff, D., & Bor, D. (2014). Into the future: Patient-centredness endures in longitudinal integrated clerkship graduates. Medical Education, 48(6), 572-582. https://doi.org/10.1111/medu.12413
Gibbs, G. (1988). Learning by doing: A guide to teaching and learning methods. Great Britain Further Education.
Gill, P., & Baillie, J. (2018). Interviews and focus groups in qualitative research: An update for the digital age. British Dental Journal, 225(7), 668-672. https://doi.org/10.1038/sj.bdj.2018.815
Greenhill, J., & Poncelet, A. N. (2013). Transformative learning through longitudinal integrated clerkships. Medical Education, 47(4), 336-339. https://doi.org/10.1111/medu.12139
Greenhill, J., Richards, J. N., Mahoney, S., Campbell, N., & Walters, L. (2017). Transformative learning in medical education: Context matters, a South Australian longitudinal study. Journal of Transformative Education, 16(1), 58-75. https://doi.org/10.1177/1541344617715710
Hafferty, F. W., & O’Donnell, J. F. (2014). The hidden curriculum in health professional education. Dartmouth College Press. https://muse.jhu.edu/book/36816.
Hall, S. L., Forrester, S., & Borsz, M. (2008). A constructivist case study examining the leadership development of undergraduate students in campus recreational sports. Journal of College Student Development, 49(2), 125-140. https://doi.org./10.1353/csd.2008.0010
Kolb, D. (2014). Experiential learning: Experience as the source of learning and development, second edition (2nd edition ed.). PH Professional Business.
MacAskill, W., Chua, W., Woodall, H., & Pinidiyapathirage, J. (2023). Beyond the written reflection: A systematic review and qualitative synthesis of creative approaches to reflective learning amongst medical students. Perspectives on Medical Education, 12(1), 361-371. https://doi.org/10.5334/pme.914
MacAskill, W., Woodall, H., Nicholls, C. D., Brumpton, K., & Pinidiyapathirage, J. (2024). Enhancing reflective practice using prompts in Online Submission of Case Reports (OSCAR): An exploratory study among medical students in rural longitudinal integrated clerkships. Perspectives on Medical Education, 13(1), 654-665. https://doi.org/10.5334/pme.1416
Malau-Aduli, B. S., Roche, P., Adu, M., Jones, K., Alele, F., & Drovandi, A. (2020). Perceptions and processes influencing the transition of medical students from pre-clinical to clinical training. BMC Medical Education, 20(1), 279. https://doi.org/10.1186/s12909-020-02186-2
McGrail, M. R., Doyle, Z., Fuller, L., Gupta, T. S., Shires, L., & Walters, L. (2023). The pathway to more rural doctors: The role of universities. Medical Journal of Australia, 219(S3), S8-S13. https://doi.org/10.5694/mja2.52021
Mylopoulos, M., Kulasegaram, K., Weyman, K., Bernstein, S., & Martimianakis, M. A. (2020). Same but different: Exploring mechanisms of learning in a longitudinal integrated clerkship. Academic Medicine, 95(3), 411-416. https://doi.org/10.1097/ACM.0000000000002960
Olmos-Vega, F. M., Stalmeijer, R. E., Varpio, L., & Kahlke, R. (2023). A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Medical Teacher, 45(3), 241-251. https://doi.org/10.1080/0142159X.2022.2057287
Purea, P., Brumpton, K., Kumar, K., & Pinidiyapathirage, J. (2022). Exploring the learning environment afforded by an Aboriginal community controlled health service in a rural longitudinal integrated clerkship. Education for Primary Care, 33(4), 214-220. https://doi.org/10.1080/14739879.2022.2054371
Sandars, J. (2009). The use of reflection in medical education: AMEE Guide No. 44. Medical Teacher, 31(8), 685-695. http://doi.org/10.1080/01421590903050374
Schön, D. A. (1995). Reflective practitioner: How professionals think in action. Taylor and Francis Group. https://doi.org/10.4324/9781315237473
Shannon-Baker, P. (2023). Philosophical underpinnings of mixed methods research in education. In R. J. Tierney, F. Rizvi, & K. Ercikan (Eds.), International encyclopaedia of education (4th ed., pp. 380-389). Elsevier. https://doi.org/10.1016/B978-0-12-818630-5.11037-1
The Consortium of Longitudinal Integrated Clerkships. (2020). CLIC – The Consortium of Longitudinal Integrated Clerkships. CLIC. https://clicmeded.com
Worley, P., Couper, I., Strasser, R., Graves, L., Cummings, B. A., Woodman, R., Stagg, P., & Hirsh, D. (2016). A typology of longitudinal integrated clerkships. Medical Education, 50(9), 922-932. https://doi.org/10.1111/medu.13084
*Hannah Woodall
190 Hume Street, Toowoomba, QLD, 4350
Email: h.woodall@griffith.edu.au
Submitted: 28 February 2025
Accepted: 24 June 2025
Published online: 6 January, TAPS 2026, 11(1), 32-43
https://doi.org/10.29060/TAPS.2026-11-1/OA3683
Sei Keng Koh1,2, Li Wen Loo1,2, Zhining Goh1,3, Dujeepa D. Samarasekera4, Carolyn Ching Ching Ho1, Paul John Gallagher5, Wai Keung Chui5 & Camilla Ming Lee Wong1,6
1Chief Pharmacist’s Office, Ministry of Health, Singapore; 2Division of Pharmacy, Singapore General Hospital, Singapore; 3Department of Pharmacy, Ng Teng Feng General Hospital, Singapore; 4Centre for Medical Education, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 5Department of Pharmacy and Pharmaceutical Sciences, National University of Singapore, Singapore; 6Division of Allied Health & Pharmacy, Sengkang Health, Singapore
Abstract
Introduction: An action research-guided national pre-registration pharmacist (pre-reg) training programme was implemented in two phases: July 2023 to January 2024, and May 2024 to January 2025. The programme is based on professional activities (PAs) required for independent practice, aligning with the Singapore Development Framework for Pharmacists’ competency standards. Workplace-based assessments (WBAs) graded using a supervision scale form the assessment framework.
Objective: This study aims to evaluate the appropriateness of PAs for training and assessment while gathering feedback on user experience.
Methods: Pre-regs and preceptors were selected through purposive sampling with randomisation. Data was collected via online surveys and group interviews. Interviews were conducted separately for pre-regs and preceptors using similar question guides, and audio-recorded, transcribed, then thematically analysed.
Results: Responses from 14 pre-regs and 16 preceptors during Phase One highlighted the strengths, challenges, and recommendations for improving PAs and WBA templates. Pre-regs felt the framework supports a seamless transition to post-course training, while preceptors recognised their role in ensuring that pre-regs attain appropriate supervision levels. The framework was positively received, with well-performing elements retained and areas for improvement identified. Insights gained from action research informed refinements to the framework. Action research for Phase Two is ongoing, with results forthcoming.
Conclusion: The study’s findings led to framework modifications for Phase Two implementation from May 2024. Adjustments were made to individual PAs and WBA forms, with consolidated guidance provided in a user toolkit for dissemination.
Keywords: Action Research, Pre-registration Pharmacist Training, Entrustable Professional Activities
Practice Highlights
- Professional Activities (PA) for direct and indirect patient care (pharmaceutical companies and regulatory authority), were developed for the national pre-registration pharmacists (pre-regs) training and assessment framework and implemented in phases.
- Action research approach was used to identify areas of improvement for framework enhancement.
- Key areas of enhancement encompass three main aspects: improving the clarity of PA documents, validity of the indirect patient care PAs, and assessment tools and administrative processes; strengthening preceptors’ skills in conducting workplace-based assessments (WBAs), and enhancing pre-registration pharmacists’ engagement with PAs and WBAs.
- A Pre-Registration Training Advisory Committee will be appointed to support the full implementation of the framework in May 2025.
I. INTRODUCTION
In Singapore, pharmacy graduates must complete 12 months of pre-registration training to be eligible for registration with the Singapore Pharmacy Council (SPC). Training for local graduates is divided into two segments: Pre-reg 1 (PR1), a 22-week programme within the National University of Singapore (NUS) Bachelor of Pharmacy (Honours) course and Pre-reg 2 (PR2), a 30-week post-course programme (Figure 1). PR1 rotations are completed in primary care (i.e. retail pharmacy or polyclinic) and either an indirect patient care setting (i.e. pharmaceutical company or regulatory authority) or community hospital. The training was guided by the SPC Competency Standards Framework which articulates 301 competency standards across nine functional areas (Singapore Pharmacy Council, 2010).

Figure 1. Overview of a Pre-Registration Pharmacist’s Journey
In 2020, the Chief Pharmacist’s Office introduced the Development Framework for Pharmacists (DFP), defining competency continuum from foundation to advanced practice across eight key roles aligned with NUS educational outcomes (Ministry of Health, Chief Pharmacist’s Office, 2024) (Figure 2).
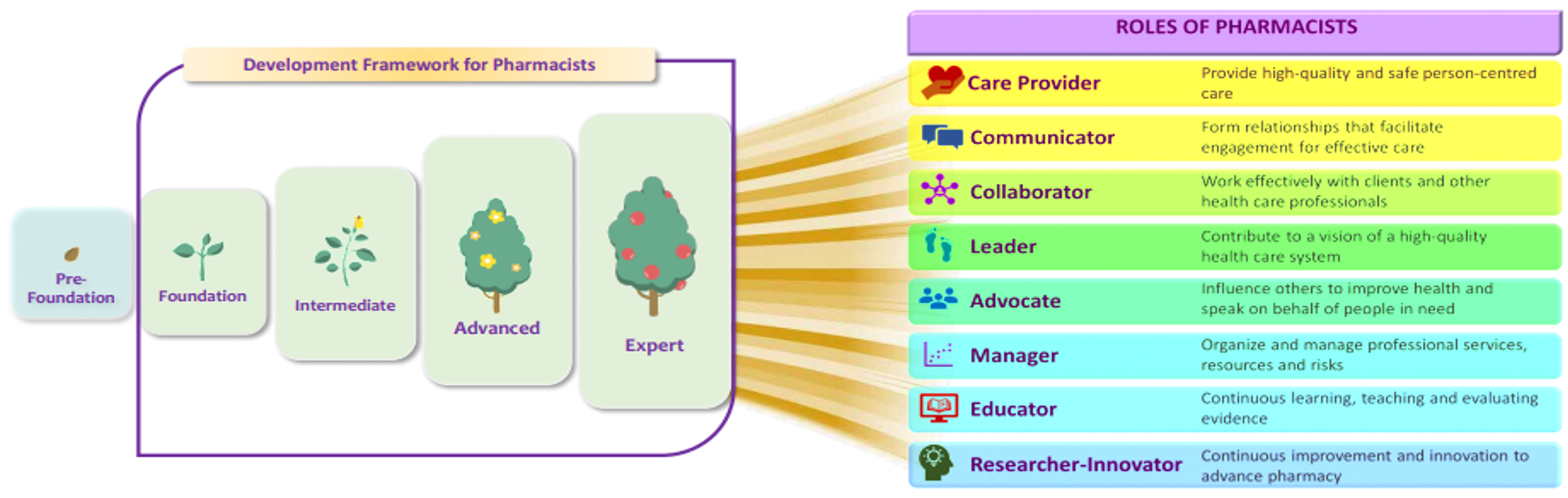
Copyright © Ministry of Health, Singapore (2024). Version 2.0: June 2024
Figure 2. Continuum of Competency for Development of Pharmacists Towards 8 Key Roles
To facilitate a seamless transition from school to workplace, the Pre-registration Competency Standards Framework Review Committee (PRCSFRC) was appointed in 2021 to align educational outcomes and pre-registration training with the DFP. The committee developed a training and assessment framework with key features including:
- Competency blueprint for Day-1 Pharmacists adapted from DFP standards
- 10 Professional Activities (PAs) proposed as macro-outcomes for training (Table 1)
- Workplace-based assessments as main assessment modality
- A 5-level supervision scale to guide progression towards independent practice (Figure 3)
|
Professional Activities for Pre-Registration Pharmacists Training |
|
|
1 |
Develop and implement a care plan |
|
2 |
Accurate supply of health products |
|
3 |
Educate patients on the appropriate use of health products |
|
4 |
Respond to drug information or health product enquiry |
|
5 |
Collaborative partnerships with patients, and the pharmacy and interprofessional teams |
|
6 |
Develop a Continuous Professional Development (CPD) plan |
|
7 |
Prepare documents for regulatory decision making and/or compliance |
|
8 |
Handle/manage the activities relating to the roles of a Responsible Person for the licences/regulatory requirements |
|
9 |
Support project planning and data analysis |
|
10 |
Develop communication materials for healthcare professionals and public |
Table 1. Professional Activities for Phase-1 Pre-Registration Pharmacists Training

Figure 3. Supervision Scale Used for Assessing Pre-registration Pharmacists’ Professional Activities
This framework uses PAs adapted from Entrustable Professional Activities (EPAs) (Cate, 2018). EPAs are units of professional work that can be fully entrusted to an individual trainee, once they have demonstrated the needed ability to execute them unsupervised, and this requires the integration of multiple competencies (Cate, 2005). The impetus to adopt PAs for training and assessment included the potential of an EPA-based curriculum to link clinical training and assessment to the actual work that pharmacists do on a day-to-day basis (Hennus et al., 2022). This approach also provides scaffolding for workplace-based training by offering a safe and evidence-based way to facilitate the development of skills and knowledge (Richardson, 2024). EPAs are gaining attention as a practical method to assess competencies in pharmacy practice (Abeyaratne & Galbraith, 2024). Countries like USA, UK and Australia have developed core EPAs for their pharmacy graduates and for pre-registration training (Abeyaratne & Galbraith, 2023; Abeyaratne & Galbraith, 2024; Haines et al., 2017; Richardson, 2024). EPAs were also implemented locally in medical, nursing and allied health professions (Goh et al., 2015; Lau et al., 2020; Zainuldin & Tan, 2023a; Zainuldin & Tan, 2023b; Zhou et al., 2022).
The framework was implemented in phases, with Phase 1 involving 15 pre-registration pharmacists undergoing their PR1 rotations in July to September 2023 and November 2023 to January 2024. Phase 2 followed up with Phase 1 participants and included the entire second cohort of BPharm (Hons) students entering PR1. Action Research was used to identify problems, design solutions, and evaluate the impact of these solutions.
The research aims were to:
- Review the appropriateness of entry-to-practice pharmacists’ scope of practice as described in the PAs and
- Gather feedback on the assessment framework from preceptors and pre-registration pharmacists.
II. METHODS
A. Research Design
Practical Action Research was employed as a research strategy, coupled with both qualitative and quantitative content analysis. The research model is operational (technical), adopting an iterative approach of “Plan-Act-Observe-Reflect” (George, 2024). For the quantitative analysis, online surveys were disseminated to both pre-registration pharmacists (pre-reg) and their preceptors at the end of each rotation. The survey questions focused on three broad areas of (i) Content validity and reliability, (ii) Process and (iii) Comfort and Confidence. The qualitative analysis included group interviews with the pre-regs and their preceptors at the end of each rotation.
The survey and interview questions were developed based on the objectives of the action research cycle, informed by literature on EPAs. These were then validated by sharing with content experts from the pre-registration training and development committee and piloted with the first cycle collection of data. The questions relevant items were then enhanced for the subsequent cycles. This pretesting of the interview questions helped to identify unclear or ambiguous statements (Castillo-Montoya, 2016; Dikko, 2016).
B. Setting
The study was conducted in multiple sites across Singapore. Participating sites for indirect patient care included three pharmaceutical multinational companies. Participating sites for direct patient care included three retail pharmacy chains and one polyclinic (primary care) group.
C. Sample and Sampling Method
Pre-regs were posted to the training sites by the university. Fifteen pre-regs posted to the study sites for both rotations were invited via email to participate in the study. Nine female and six male pre-regs (n=15) were recruited. Twenty-four preceptors trained in the new framework were assigned to supervise these 15 pre-regs and invited to participate in the study. Each pre-reg is assigned one preceptor per rotation block, while each preceptor may precept up to two pre-regs per rotation block. Nineteen preceptors participated in the study.
D. Data Collection and Analysis
Data for this study was collected via an anonymous electronic survey, with responses analysed using descriptive statistics. Following the survey, group interviews were conducted both face-to-face and virtually. Qualitative data were obtained from free-text responses within the survey as well as from in-depth, audio-recorded group interviews, which were transcribed verbatim. Group interviews were held separately for pre-registration pharmacists (PRPs) and preceptors, utilising the same semi-structured interview guide to ensure consistency across cohorts. Each interview was facilitated by two trained pharmacist interviewers. To enhance credibility and trustworthiness, all transcripts underwent member-checking and peer debriefing. Coding was conducted inductively, with two researchers independently coding the transcripts before reconciling any discrepancies through consensus meetings. Thematic analysis was undertaken to interpret the qualitative data, enabling the identification of nuanced themes that complemented the broader trends observed in the survey findings.
E. Ethical Considerations
This study was approved by both the Singapore Health Services (SingHealth) and NUS Institution Review Boards. Informed consent was obtained from the pre-regs and preceptors. Participation in the study was purely voluntary.
III. RESULTS
A. Online Survey Results
Fourteen (93%) pre-regs and 16 (84%) preceptors responded to the online survey. One pre-reg did not respond despite multiple reminders. Majority of the pre-regs (13/14, 92.9%) agreed that the framework prepared them well for their future role as a pharmacist. They felt that the PAs adequately described the scope of work of a pharmacist and the supervision levels were pegged appropriately for entry-to-practice. Preceptors assessed them fairly and they had the resources and support that they needed from the institutions. There was uncertainty about the ease and efficiency of the system for submission of assessment outcomes and inputs; as well as pre-regs being able to pass rotations under the framework. Survey results are in Table 2.
|
No |
Question |
Rating* |
Pre-Registration Pharmacists (n=14) (%) |
Question |
Rating* |
Preceptor (n=16) (%) |
|
1 |
I feel that the revised training and assessment framework will prepare me well for my future role as a pharmacist. |
SA |
2 (14.3) |
I feel that the revised training and assessment framework will prepare pre-registration pharmacists well for their future role as a pharmacist. |
SA |
3 (18.8) |
|
A |
11 (78.6) |
A |
13 (81.2) |
|||
|
UN |
1 (7.1) |
UN |
0 |
|||
|
DA |
0 |
DA |
0 |
|||
|
SDA |
0 |
SDA |
0 |
|||
|
2 |
The Professional Activities define the scope of work of an entry-level pharmacist well. |
SA |
1 (7.1) |
The Professional Activities adequately define the scope of work of an entry-level pharmacist well. |
SA |
3 (18.8) |
|
A |
12 (85.7) |
A |
11 (68.8) |
|||
|
UN |
1 (7.1) |
UN |
2 (12.5) |
|||
|
DA |
0 |
DA |
0 |
|||
|
SDA |
0 |
SDA |
0 |
|||
|
3 |
I believe the Professional Activities will be assessed appropriately and sufficiently to reflect my actual performance ability. |
SA |
1 (7.1) |
The Professional Activities are pegged at an appropriate level for entry to pharmacy practice. |
SA |
2 (12.5) |
|
A |
11 (78.6) |
A |
13 (81.3) |
|||
|
UN |
2 (14.3) |
UN |
1 (6.3) |
|||
|
DA |
0 |
DA |
0 |
|||
|
SDA |
0 |
SDA |
0 |
|||
|
4 |
I believe the preceptors will be fair when assessing me. |
SA |
4 (28.6) |
I believe I will be able to assess my pre-registration pharmacists fairly. |
SA |
3 (18.8) |
|
A |
10 (71.4) |
A |
13 (81.3) |
|||
|
UN |
0 |
UN |
0 |
|||
|
DA |
0 |
DA |
0 |
|||
|
SDA |
0 |
SDA |
0 |
|||
|
5 |
I have a good working knowledge of how the revised training and assessment framework works.
|
SA |
1 (7.1) |
I have a good working knowledge of how the revised training and assessment framework works. |
SA |
1 (6.3) |
|
A |
8 (57.1) |
A |
14 (87.5) |
|||
|
UN |
5 (35.7) |
UN |
1 (6.3) |
|||
|
DA |
0 |
DA |
0 |
|||
|
SDA |
0 |
SDA |
0 |
|||
|
6 |
I believe the training site will be adequately resourced to deliver pre-reg training using the revised framework (e.g. time given for assessments, sufficient number of preceptors). |
SA |
1 (7.1) |
My training site is adequately resourced to deliver pre-registration training using the revised framework. |
SA |
3 (18.8) |
|
A |
10 (71.4) |
A |
8 (50.0) |
|||
|
UN |
3 (21.5) |
UN |
2 (12.5) |
|||
|
DA |
0 |
DA |
3 (18.8) |
|||
|
SDA |
0 |
SDA |
0 |
|||
|
7 |
I am confident that I will get adequate help and guidance from my preceptors to manage the workload with the revised training and assessment framework. |
SA |
2 (14.3) |
I am confident that my pre-registration pharmacists will get adequate help and guidance to manage the case loads with the revised assessment framework. |
SA |
2 (12.5) |
|
A |
8 (57.1) |
A |
12 (75.0) |
|||
|
UN |
4 (28.6) |
UN |
2 (12.5) |
|||
|
DA |
0 |
DA |
0 |
|||
|
SDA |
0 |
SDA |
0 |
|||
|
8 |
There is an easy and efficient system of submission online, after assessments and evaluations are completed. |
SA |
2 (14.3) |
There is an easy and efficient system of submissions after assessments and evaluations are completed. |
SA |
1 (6.3) |
|
A |
5 (35.7) |
A |
4 (25.0) |
|||
|
UN |
6 (42.9) |
UN |
10 (2.5) |
|||
|
DA |
0 |
DA |
1 (6.3) |
|||
|
SDA |
1 (7.1) |
SDA |
0 |
|||
|
9 |
I am confident about passing this rotation under the revised training and assessment framework. |
SA |
1 (7.1) |
I am confident about my pre-registration pharmacists passing this rotation under the revised training and assessment framework. |
SA |
2 (12.5) |
|
A |
7 (50.0) |
A |
11 (68.8) |
|||
|
UN |
6 (42.9) |
UN |
3 (18.8) |
|||
|
DA |
0 |
DA |
0 |
|||
|
SDA |
0 |
SDA |
0 |
Rating*: Strongly Agreed (SA), Agree (A), Unsure/Neutral (UN), Disagreed (DA), Strongly disagreed (SDA)
Table 2. Results for Online Survey (Pre-Registration Pharmacists and Preceptors)
Qualitative comments were sought from pre-regs and preceptors on their perceived benefits and concerns of the PA-based framework compared to the previous competency-based one. For benefits, pre-regs felt that there was more interaction with patients and preceptors. They appreciated the use of real-life case scenarios and discussions for assessment. The PAs encouraged critical thinking and are comprehensive in defining the scope of work of a pharmacist. The PAs also helped to reflect their real competency level and areas for improvement. The preceptors were supportive of the training and assessment framework. The supervision scale was clearer and more intuitive than the previous rating scale of “Competent” or “Not Competent”. Furthermore, as pre-regs were trained to do the activities commonly performed by pharmacists, preceptors felt that pre-regs would be better prepared for their future roles as registered pharmacists. The training and assessment framework was noted to be better structured compared to the previous framework.
Some pre-regs were concerned about their ability to perform and complete training requirements. The training workload was perceived to be higher, and more preparation work was required to collate learning logs and WBAs. There were also concerns whether they could complete all assignments in a timely manner. Preceptors were concerned with inter-rater variability as WBAs were perceived to be subjective. They found the training framework to be more resource-intensive in terms of manpower and time. There were more documentation requirements. There was confusion on the various WBA tools, types of cases and complexities of cases that could be used for assessment. Preceptors also shared that implementation of the revised framework varied across institutions and the process for document submission to SPC was unclear.
B. Group Interviews
Thirteen interview sessions with 34 participants were conducted between September 2023 and January 2024. Four group interviews were conducted with 15 pre-regs (100%), and six were conducted with 19 preceptors (19/24, 79.2%). Two preceptors and one pre-reg had individual interviews due to conflicting schedules.
C. Theme 1: Validity and Reliability
1) Professional Activities for Direct Patient Care:
Both preceptors and pre-regs agreed that the PAs for direct patient care were clear and appropriate. The six PAs accurately represented the competencies of a Day-1 pharmacist, and no revisions were suggested. However, there were differing views on the following:
a) The core categories under PA 2 (Accurate Supply of Medications) were not applicable to all settings.
“Medicines, quite easy…but the wound management part…Very limited chance, almost sometimes none, depends on the luck, that there will be wound dressing questions.” – Preceptor1
b) There were differing opinions on appropriateness of the passing criteria of Level 3C for PA3 (Educate Patients).
“A 3C and a 4 requires a lot of trust… so I feel that (3C) is a bit too high for PR1”- Preceptor9
“Because I can’t expect them to go into PR2 without a 3C level or so… I did have an expectation of them to be at this level.”- Preceptor7
“I feel…the gradings were quite tough (to achieve)” – Pre-reg13
c) The number of evidence required e.g. 10 case notes for PA1 (Develop and Implement a Care Plan) may not be sufficient. However, preceptors mitigated the concern with WBAs that were formally introduced with the framework.
“I think 10 (SOAP notes) is definitely not enough for me to do a very good evaluation”- Preceptor1
“But we have the new system (WBAs). I’ll argue that you get a better understanding of the student’s actual scope of knowledge…It’s one thing when you have all of the notes on your side and you just craft out the best (written) answer (SOAP), it’s another to be able to test that on the spot to see if they actually know more”- Preceptor6
“For direct patient care.. I feel that because of the new framework, I actually learn more.. like you get to apply what you learn in real life” – Pre-reg5
2) Professional Activities for Indirect Patient Care:
The five PAs for indirect patient care demonstrated poor validity due to the diverse functions pharmacists perform in the industry sector. PAs 7 and 8 were focused on regulatory affairs and restricted some pre-regs’ exposure to other significant industry roles such as marketing and pharmacovigilance. This narrow focus could also limit the number of companies eligible to serve as training sites. Furthermore, PA8 which addressed the roles of the Responsible Person lacked clarity, particularly in its supporting tasks and assessment criteria.
The value proposition of having an indirect patient care rotation as part of registration requirement was raised.
“Are we expecting that all of them would be doing regulatory…to be doing commercial…what is that functional competency we want to train the (pre-regs) on?” – Preceptor18
“…we really need to scope this pharma industry attachment… because if this is the trend moving forward…to scope them as more of an introduction of indirect (patient care)… How indirect patient care actually is important role in your direct patient care”- Preceptor19
“Basically, I feel it’s too streamlined already…like we are all funnelled into the RA role only…although there might be people like me who want to do other stuffs like commercial marketing, medical affairs etc” – Pre-reg10
3) Professional Activity on Developing a Continuous Professional Development (CPD) Plan:
PA6 (Developing a CPD Plan) required greater clarity in terms of its conduct and the template to be used. Several preceptors were unsure how to assess the CPD plans and to guide their pre-regs in developing one. Preceptors also proposed to reduce the number of CPD reviews over the 22-week training period.
“…the CPD, which (my pre-reg) needs to do in the beginning, in the mid and then at the end. It seems to be just repeating only.”- Preceptor10
“ For my student, she doesn’t really know what a CPD entails… she didn’t really know exactly how to fill it in. So when she did fill it in, understandably it was quite general. So she just copied paste…doesn’t really know what she needs to know”- Preceptor1
“Can I ask if CPD is really necessary?” – Pre-reg1
“Actually I am thinking for the final CPD, it can be better formatted…in the sense that we know there is a part on future learning plan and action plan…but it’s already our final week, so we don’t know how applicable it is to us – like we draft a learning plan, but when will we get to execute it” – Pre-reg6
4) Assessments and Supervision Scale:
The supervision scale was found to be intuitive and descriptive as it reflected how independence and supervision is accorded for work. It was preferred over the “Competent or Not Yet Competent” (C/NYC) rating in the previous assessment framework.
“I think C/NYC is like there’s no gray (area)…Most time…it’s not really to the extent that it’s NYC, so yeah, you just end up with a C…I think (the supervision scale) is real…you’ll be managing them like that in the workplace”- Preceptor7
“ I think [the supervision scale] is better …clearer to the PRPs as well…”“I feel my student has more progress …she’s at 3A…Let’s try to progress her to 3B…there was no such articulation [in the previous framework]” – Preceptor1
There was varied interpretation on the “minimum number for WBAs to be completed satisfactorily”. Some preceptors performed the minimum number regardless of assessment outcomes while others aimed to achieve the required passing criteria for all WBAs. There were also concerns about assessor variability affecting the assessment outcomes. Some pre-regs felt that the ratings were not reflective of their actual competencies as the preceptors would just give them the minimum rating for them to pass.
“For the same assessment, one preceptor may grade me as 3B, but to another preceptor, I may be a 3A” – Pre-reg8
“Because no matter how we perform, I feel eventually our preceptor will just pass us by giving us the bare minimum score required”- Pre-reg10
Mini-CEXes and Case-based discussions were conducted in a variety of ways due to a lack of understanding of the purpose of different assessment methods. Multi-source feedback (MSF) contributed to the administrative load for indirect patient care preceptors.
“How do you decide if this is a mini-CEX and this one is a CBD… in the end what I did was like CBD is (for) more complex cases then mini-CEX is (for) easier (cases)?” – Preceptor9
5) Mindset Shift:
Preceptors were unclear of the mindset shift required for prospective decision making that integrated learner attributes – agency, reliability, integrity, humility and capability (ARICH), when using the supervision scale under the revised framework.
“The new framework is actually very content(-based), it doesn’t focus a lot on attitude actually. So if they can get the content done, but their attitude is very poor, I think…we can still pass them actually, but their attitude will be reflected in the comments”- Preceptor12
D. Theme 2: Process
Both preceptors and pre-regs welcomed the change. Pre-regs felt that the revised framework would facilitate a smoother transition to post-course pre-registration training. The preceptors found the revised framework rewarding as it allowed them to be part of the pre-regs’ developmental journey. Pre-regs were viewed as a key success factor for the implementation of the revised framework to be successful and should be empowered to exercise their agency with proper preparation.
The initial implementation process was described as “messy”, and some participants felt “stressful” due to the perceived increase in workload and documentation requirements. Better clarity was needed in terms of the assessment requirements and different types of WBAs to be used.
E. Theme 3: Comfort and Confidence
1) Framework:
Pre-regs were comfortable with the framework and were confident that it would prepare them well for post-course pre-registration training. Preceptors welcomed the change and felt that the framework was learner-centric.
“Compared to the previous (framework)…good change yes…there’s really a lot more feedback…that is now in black and white…For the preceptor, more time-consuming. But I guess if we think in terms of learner-centric kind of role it’s good for the learners.”- Preceptor11
However, they were concerned about scalability due to resourcing concerns.
“Now (phased implementation) is maybe one or two (PRPs on the revised framework per rotation). It’s still fine, but I think really eight at one go…is gonna be pretty overwhelming… And then I think the volume might dilute the effort to give feedback after a while.”- Preceptor13
Preceptors further suggested for cross-learning amongst institutions on framework and WBA implementation, and for more resource materials to be included in the implementation toolkit.
2) Defensibility of Training Decisions:
Preceptors highlighted concerns on the defensibility of training decisions and felt compelled to pass pre-regs due to potential implications related to remediation and its consequences on training capacity and delay in graduation.
“It’s difficult for us not to pass them because it means we need to extend them. Then what are we going to do? Logistically, I think you all know it is very difficult” – Preceptor2
“Once bitten, twice shy. (I document) like everything… if they are going to have issues then I have to bring up the details.” – Preceptor5
IV. DISCUSSION
The revised training and assessment approach uses professional activities (PAs) to frame the assessment, akin to the Entrustable Professional Activities (EPA) approach developed by Cate (2018). In a scoping review conducted by Hennus et al. (2002), the authors found that most programmes used a mix of logics to establish a framework of EPAs. These logics could be categorised into four broad areas: i) service provision, ii) procedures, iii) disease or patient group, and iv) non-EPAs that are unsuitable for summative entrustment decisions but are important as they describe the abilities physicians require to effectively meet healthcare needs (e.g., developing a CPD plan, PA6).
We chose a mixed logic approach to develop our PAs as pharmacists can practise in various settings. The “mixed logic approach” refers to the use of multiple design logics (e.g., task-based, setting-based, developmental) to develop professional activities. We link this to Hennus et al.’s (2022) framework on EPA design and align it with the iterative, participatory principles of action research (Plan-Act-Observe-Reflect). In Singapore, slightly more than half (approximately 55%) of our locally registered pharmacists work in patient care areas (tertiary hospitals, polyclinics, and retail pharmacies), while the remaining work in indirect patient care areas such as pharmaceutical industries and regulatory bodies (data provided by SPC). The Committee thus envisioned a training system whereby pharmacists from both settings could collaborate and co-develop outcomes for a holistic training programme for our local graduates. For harmonisation across all training sites, PAs for indirect patient care areas were developed. As not all professional activities fit the descriptors of an EPA as described by Cate and Taylor (2020), we have chosen to describe them as professional activities instead of EPAs. PAs 1 to 6 were adapted from those used for new pharmacy graduates in USA (Haines et al., 2017) and the general level training of junior pharmacists in a local academic medical centre since 2019, whereas PAs 7 to 10 were developed by local domain experts from the pharmaceutical industry and regulatory authority.
The results of our study showed that PAs for direct patient care were valid and mostly pegged appropriately to entry to practice level pharmacists. There were concerns about the supervision level for PA3 which some preceptors felt that it was pegged beyond an entry level pharmacist. Preceptors felt that it would be difficult to achieve the suggested level within a short duration of 11 weeks especially when this is the first pre-licensing assessment in their undergraduate days. To the best of our knowledge, there have been no PAs developed for pharmacists working in pharmaceutical companies. It was challenging to develop PAs due to the diverse roles pharmacists can play in the indirect patient care areas. Hence, preceptors felt that PAs 7 and 8 were too restrictive. Furthermore, the value preposition of having an indirect patient care rotation was unclear. Henceforth, there were varied opinions on what would constitute indirect patient care PAs. As SPC has not implemented CPD yet, PA6 will need to be refined further for clarity.
As WBAs were not widely used in all participating training institutions, there were varying comfort levels and understanding amongst preceptors and pre-regs in using mini-CEX and CBD for assessments. Resourcing for manpower, contact time with pre-regs and documentation were cited as key concerns among the preceptors. Similar concerns were raised by Massie and Ali (2015), who suggested approaches to alleviate these issues, including clarifying the purpose of WBA, mandatory training to reduce inter-rater variability and increasing trainees’ engagement with the WBA tools, building training time into preceptors’ responsibilities, as well as improving accessibility to WBA forms with tablet/smartphone applications (Massie & Ali, 2015; So et al., 2024).
The pre-regs’ concerns about inter-rater variability were valid concerns as it may impact the reliability of the revised training and assessment framework. This was subsequently mitigated with additional training sessions for preceptors and several preceptor townhalls to address queries and concerns. Further Phase 2 research is required to understand the preceptors’ concerns with ‘failure-to-fail’ and ensuring defensibility of their decisions as these may potentially compromise the quality of pre-regs who exit the programme and contribute to unpleasant training experience for preceptors through an onerous documentation workload.
The initial implementation process was highlighted as “messy”. Submission of training documents to SPC was done manually as the online registration system was not updated for the revised framework. Moving forward, the registration system will be renewed to support the submission of the training documents in a seamless manner. To mitigate the initial confusion and understanding of PA requirements, SPC will collaborate with NUS to conduct detailed briefing sessions for pre-regs in the subsequent phases of implementation. This is to better enable the students to drive their own learning during rotations, as highlighted by preceptors.
Overall, preceptors and PRPs welcomed the change and are supportive of the revised framework. Many felt that the change was a clearer reflection of the daily work as a pharmacist. The Committee had reviewed the key study findings and proposed the following recommendations and action plans which were implemented prior to Phase 2:
- The Indirect Patient Care PAs were further refined for clarity and to broaden the scope beyond regulatory affairs.
- The number of CPD plan reviews for PR1 were reduced from six to four.
- The number of documents for SPC submission was streamlined to ease administrative burden.
- The toolkit was updated to reflect changes made and included frequently asked questions, providing both pre-regs and preceptors with comprehensive information.
- Emphasis on WBAs was increased at the national faculty development workshops that were conducted to upskill existing preceptors.
- SPC worked with NUS to conduct more in-depth briefing sessions prior to the start of their PR1 training, to better prepare pre-regs to navigate the training requirements.
- SPC established a Pre-Registration Training Advisory Committee to better support preceptors in the implementation of the framework.
- SPC will commence an annual faculty development event for preceptors to share best-practices.
A. Limitation
This study is limited to the context settings of the participating PR1 rotation sites and has a small sample size, thereby limiting the generalisability of findings.
V. CONCLUSION
A robust training and assessment framework, incorporating meaningful placement experiences, is essential for pre-regs to develop and demonstrate their competence for professional practise. This study shares our experience of implementing PAs in pre-registration training across both direct and indirect care settings, and how action research guided our phased framework implementation. The findings may benefit other international pharmacy institutions implementing EPA frameworks. As this framework is newly established, longitudinal monitoring of PRPs’ post-training performance will be necessary to validate its effectiveness in developing the required workforce and to inform further programme refinements.
Notes on Contributors
Sei Keng Koh was involved in the conceptualisation of this paper, writing and revision.
Li Wen Loo was involved in the conceptualisation of this paper, interviewing, data analysis, writing and revision.
Zhining Goh was involved in the conceptualisation of this paper, interviewing, data analysis and revision of manuscript.
Dujeepa D. Samarasekera was involved in the design of the research methodology and in the revision of the manuscript.
Carolyn Ching Ching Ho was involved in the revision of manuscript.
Paul John Gallanger was involved in the revision of the manuscript.
Wai Keung Chui was involved in the revision of the manuscript.
Camilla Ming Lee Wong was involved in the revision of the manuscript.
Ethical Approval
Ethical approval was obtained from the Institutional Review Boards of the Singapore Health Services (CIRB ref: 2023/2393) and the National University of Singapore.
Data Availability
No data was given to share transcript data and analysis.
Acknowledgement
We thank the Singapore Pharmacy Council, the Pre-Registration Training Standards Committee, the preceptors and pre-registration pharmacists for their support in this research study.
We thank Mr Richmond Ng from the Singapore Pharmacy Council for his assistance with the data extraction.
Funding
There is no funding support for this study.
Declaration of Interest
All authors have no potential conflicts of interest.
References
Abeyaratne, C., & Galbraith, K. (2023). A review of entrustable professional activities in pharmacy education. American Journal of Pharmaceutical Education, 87(3), ajpe8871. https://doi.org/10.5688/ajpe8872
Abeyaratne, C., & Galbraith, K. (2024). Implementation and evaluation of entrustable professional activities for a pharmacy intern training program in Australia. American Journal of Pharmaceutical Education, 88(12), 101308. https://doi.org/10.1016/j.ajpe.2024.101308
Castillo-Montoya, M. (2016). Preparing for interview research: The interview protocol refinement framework. The Qualitative Report, 21(5), 811–831. https://doi.org/10.46743/2160-3715/2016.2337
Cate, O. T. (2005). Entrustability of professional activities and competency-based training. Medical Education, 39(12), 1176–1177. https://doi.org/10.1111/j.1365-2929.2005.02341.x
Cate, O. T. (2018). A primer on entrustable professional activities. Korean Journal of Medical Education, 30(1), 1–10. https://doi.org/10.3946/kjme.2018.76
Cate, O. T., & Taylor, D. R. (2020). The recommended description of an entrustable professional activity: AMEE Guide No. 140. Medical Teacher, 43(10), 1106–1114. https://doi.org/10.1080/0142159x.2020.1838465
Dikko, M. (2016). Establishing construct validity and reliability: Pilot testing of a qualitative interview for research in Takaful (Islamic Insurance). The Qualitative Report, 21(3), 521–528. https://doi.org/10.46743/2160-3715/2016.2243
George, T. (2024). What is action research? Definitions and examples. Retrieved February 9, 2025, from https://www.scribbr.com/methodology/action-research/
Goh, D. L., Samarasekera, D. D., & Jacobs, J. L. (2015). Implementing entrustable professional activities at Yong Loo Lin School of Medicine Singapore undergraduate medical education program. South‐East Asian Journal of Medical Education, 9(1), 5. https://doi.org/10.4038/seajme.v9i1.90
Haines, S. T., Pittenger, A. L., Stolte, S. K., Plaza, C. M., Gleason, B. L., Kantorovich, A., McCollum, M., Trujillo, J. M., Copeland, D. A., Lacroix, M. M., Masuda, Q. N., Mbi, P., Medina, M. S., & Miller, S. M. (2017). Core entrustable professional activities for new pharmacy graduates. American Journal of Pharmaceutical Education, 81(1), S2. https://doi.org/10.5688/ajpe811s2
Hennus, M. P., Van Dam, M., Gauthier, S., Taylor, D. R., & Cate, O. T. (2022). The logic behind entrustable professional activity frameworks: A scoping review of the literature. Medical Education, 56(9), 881–891. https://doi.org/10.1111/medu.14806
Lau, S. T., Ang, E., Samarasekera, D. D., & Shorey, S. (2020). Development of undergraduate nursing entrustable professional activities to enhance clinical care and practice. Nurse Education Today, 87, 104347. https://doi.org/10.1016/j.nedt.2020.104347
Massie, J., & Ali, J. M. (2015). Workplace-based assessment: A review of user perceptions and strategies to address the identified shortcomings. Advances in Health Sciences Education, 21(2), 455–473. https://doi.org/10.1007/s10459-015-9614-0
Ministry of Health, Chief Pharmacist’s Office. (2024). Development Framework for Pharmacists (DFP).
Richardson, C. L. (2024). Entrustable professional activities: A new approach to supervising trainee pharmacists on clinical placements. Retrieved February 9, 2025, from https://pharmaceutical-journal.com/article/ld/entrustable-professional-activities-a-new-approach-to-supervising-trainee-pharmacists-on-clinical-placements
Singapore Pharmacy Council. (2010, March). Competency standards for Singapore pharmacists.
So, H., Choi, Y., Chan, P., Chan, A. K., Ng, G. W., & Wong, G. K. (2024). Workplace-based assessments: What, why, and how to implement? Hong Kong Medical Journal, 30(3), 250–254. https://doi.org/10.12809/hkmj2311361
Zainuldin, R., & Tan, H. Y. (2023a). Entrustable professional activities developed for allied health entry-level programs across a national level training standards framework in Singapore. PubMed, 52(2), 104–112. https://pubmed.ncbi.nlm.nih.gov/37269028
Zainuldin, R., & Tan, H. S. K. (2023b). Entrustable professional activities implementation in undergraduate allied health therapy programs. The Asia Pacific Scholar, 9(1), 42–48. https://doi.org/10.29060/taps.2024-9-1/sc2997
Zhou, W., Poh, C. L., Chan, H. L., & Shorey, S. (2022). Development of entrustable professional activities for advanced practice nurses education. Nurse Education Today, 116, 105462. https://doi.org/10.1016/j.nedt.2022.105462
*Sei Keng Koh
Division of Pharmacy, Singapore General Hospital
Level 9, SingHealth Tower
10 Hospital Blvd, Singapore 168582
+65-81251901
Email: koh.sei.keng@sgh.com.sg
Submitted: 6 December 2024
Accepted: 14 May 2025
Published online: 6 January, TAPS 2026, 11(1), 44-54
https://doi.org/10.29060/TAPS.2026-11-1/OA3596
Anke van der Merwe & Corlia Janse van Vuuren
School of Health and Rehabilitation Sciences, Faculty of Health Sciences, University of the Free State, South Africa
Abstract
Introduction: Although effective healthcare communication is widely acknowledged as essential, a significant gap remains in practical communication training for healthcare students. The Theory of Planned Behaviour (TPB) provides a framework for designing communication activities that positively influence healthcare students’ attitudes towards and perceived control over their communication skills. TPB also incorporates societal expectations around healthcare communication, encouraging students to apply their learned skills effectively. This study aimed to explore students’ experiences of interprofessional healthcare communication activities structured around the TPB within an interprofessional healthcare curriculum.
Methods: A qualitative descriptive study design was used to assess communication skill development among first- to third-year healthcare students participating in an interprofessional curriculum. Data were collected via an annual institutional module evaluation and anecdotal feedback and analysed thematically under the TPB’s key constructs: attitudes, subjective norms, and perceived behavioural control.
Results: Students reported positive experiences with communication-based activities, particularly those that involved real-world applications. Feedback indicated that interprofessional group activities and community engagement significantly improved students’ perceived communication efficacy, although some challenges in managing group dynamics were noted.
Conclusion: Intentionally integrating communication skills training within an interprofessional curriculum to create behavioral intention positively impacts students’ attitudes, motivation, and ability to communicate effectively in diverse healthcare settings. The TPB framework supports the purposeful design of communication-based activities, fostering a more patient-centered approach among future healthcare professionals. Further research should investigate the long-term effects of this curricular approach on professional communication practice.
Keywords: Healthcare Communication, Interprofessional Education, Theory of Planned Behaviour, Curriculum Development
Practice Highlights
- Real-world communication activities enhance students’ confidence and skills through application.
- Interprofessional group work fosters communication skills related to teamwork and adaptability.
- TPB-guided communication activities increase students’ motivation for patient-centred communication.
- Continuous feedback supports the sustainable development of communication skills.
I. INTRODUCTION
Despite the recognised importance of effective healthcare communication, a substantial gap persists in the practical training of communication skills among healthcare students and professionals. Approximately half of the participants in a recent study reported limited exposure to health communication training, highlighting deficits in both skills and awareness of barriers affecting interpersonal health communication (Zota et al., 2023). Current curricula emphasise theoretical knowledge but often neglect practical applications, limiting healthcare providers’ ability to navigate diverse linguistic and cultural patient needs, especially in multilingual societies where language barriers can lead to miscommunication, misdiagnoses, and treatment errors (Mangal & Farmer, 2023; Organi et al., 2024). Compounded by limited access to interpreter services in resource-constrained settings, these barriers increase healthcare costs, delay treatments, and compromise patient safety (Organi et al., 2024).
While healthcare providers play a vital role in promoting informed decision-making through the informed consent process for assessment and treatment interventions, they often struggle to simplify complex medical language to accommodate varying patient health literacy levels- sometimes their own (Guo et al., 2020; Mirza & Tabani, 2018). Effective communication is essential for ensuring that patients fully understand their healthcare situation, which is crucial not only for fostering a strong patient-provider relationship but also for enabling truly informed decision-making (Mirza & Tabani, 2018). Literature thus highlights the critical role of communication skill development in healthcare training (Gilligan et al., 2021; Hagiwara et al., 2019; Medendorp et al., 2021; Stamer et al., 2023). Simulation-based learning is particularly emphasised as an effective method to address gaps in communication skills, especially in areas such as obtaining informed consent (Baby et al., 2018; Medendorp et al., 2021). The rise of digital platforms, however, introduces a need for additional training in digital health communication, considering ethical and legal risks (Etheredge & Fabian, 2022). In response, the practical development of a variety of communication skills is critical for future healthcare professionals (Del Riccio et al., 2023; Fliorent et al., 2023; Neuhauser & Kreps, 2003; Pang et al., 2023).
Research further indicates that fit-for-purpose communication positively impacts patient satisfaction, trust, and treatment adherence (Bennet & Lyons, 2011; Houbby et al., 2020). Structured communication training has been associated with improved patient interactions and better management of challenging interactions (Baby et al., 2018; Bachmann et al., 2022; Hagiwara et al., 2019). Effective communication is also instrumental in advancing health literacy, essential for meeting the United Nations Sustainable Development Goals (UN, 2024). Nevertheless, barriers to healthcare access persist, further complicated by an aging population that challenges global efforts to alleviate healthcare professional shortages (Pang et al., 2023). These complexities, in addition to the reported decline in communication skills, as healthcare professionals progress in their studies (Ha & Longnecker, 2010), highlight the need for the early and longitudinal integration of communication skills development into health curricula to empower students to engage effectively with diverse patient populations (Gilligan et al., 2021).
Despite the growing emphasis on communication in healthcare education, practical application is still limited, particularly in pre-clinical years (Madhavanprabhakaran et al., 2015; Nicolaides et al., 2018). To address this gap, the School of Health and Rehabilitation Sciences (SoHRS) at the University of the Free State (UFS) in South Africa embarked on an interprofessional curriculum initiative, comprising one module a year, that spans the four undergraduate years (van der Merwe & Janse van Vuuren, 2024). Students from the following departments participate in the interprofessional curriculum: Biokinetics, Dietetics, Occupational therapy, Optometry, and Physiotherapy. The first- to third-year modules specifically explore various aspects related to being a healthcare professional including but not limited to a structured progression of communication skills training. Students enrolled in this interprofessional curriculum are from the departments of biokinetics, dietetics, occupational therapy, optometry, and physiotherapy allowing varied perspectives within the curriculum. The detailed process of curriculum development has been described previously (van der Merwe & Janse van Vuuren, 2024) whereas this article will focus only on the intentionally scaffolded and implemented communication-based content from the first- to third-year of study through the lens of the Theory of planned behaviour (TPB).
A. Theoretical Framework: Theory of Planned Behaviour
This literature review explores the significance of healthcare communication skills, and their intentional curricular integration grounded in the Theory of Planned Behaviour (TPB). The TPB posits that an individual’s behavioural intention is influenced by their attitude towards the behaviour, the expectation and attitude of the significant other or group of people toward the behaviour known as the subjective norms, and the individual’s perceived behavioural control namely how difficult or easy they view the performance of the behaviour (Ajzen, 1991; Asare, 2015). The TPB has been previously applied in healthcare research to understand and predict behaviours, such as diagnostic radiographers’ adherence to radiation protection best practices (Lewis et al., 2021) as well as predicting nurses’ intentions and actual use of oxygen therapy in COVID-19 (Dehsorkhi et al., 2023). The TPB highlights the importance of attitudes, subjective norms, and perceived behavioural control in potentially fostering effective training transfer to clinical practice. Within the context of healthcare communication, TPB may help understand and predict how students’ attitudes, the influence of their peers and lecturers, and their confidence in their communication abilities may affect their communication practices.
1) Subjective Norm:
In South Africa, as in many other countries, healthcare professionals are held to high standards by society and regulatory bodies (Hompashe et al., 2021; HPCSA, 2025). The Health Professions Council of South Africa (HPCSA) sets minimum training standards for institutions offering healthcare programmes and requires that all registered professionals adhere to a strict code of conduct. Central to these standards is the expectation of effective patient communication (Hompashe et al., 2021; HPCSA, 2025). Higher education institutions such as the one where the study was performed also emphasise the importance of developing communication skills in their graduates. Coupled with the societal expectation of a healthcare professional who can professionally, but also effectively and clearly communicate with a diverse patient population (Amirthalingam et al., 2022; Hagiwara et al., 2019; Hompashe et al., 2021), the importance of and expectations regarding healthcare communication is clear. Aligned with the TPB, these professional and societal expectations would act as a strong motivator for healthcare students to adjust their communication behaviour through intentional skill development to ensure they satisfy societal and regulatory body expectations.
2) Perceived Behavioural Control:
The authors viewed the student’s perceived control over their communication abilities, as well as their perceived difficulty in demonstrating effective communication to be directly impacted by their educational environment. The impact of the educator is therefore situated within the intentional design of transformational learning spaces where students are guided and supported to develop the required communication skills (Mahdy et al., 2020; Pillay et al., 2019). Within the described interprofessional curriculum (van der Merwe & Janse van Vuuren, 2024), opportunities for gaining theoretical knowledge, the provision of both educator and peer feedback as well as the practical application of learnt skills in various settings were created to allow students to manage and mitigate any perceived barriers, they might experience towards developing their communication skills (Figure 1).
3) Attitude Towards Behaviour:
Student’s expectations and evaluation of their applied communication abilities were explored through the intentional application of the learned communication skills within a community setting (Figure 1). Additionally, students explored their changing attitudes toward their communication abilities through interprofessional class engagement, closely simulating the interprofessional nature of their future healthcare environment (Pillay et al., 2019). Healthcare students acknowledge the importance of collaborative teamwork in achieving optimal patient outcomes (Pillay et al., 2019), while their commitment to improving the well-being of individuals under their care serves as a key motivator for their engagement with provided educational content and learning opportunities (Kassab et al., 2022). By directly engaging with both their peers and the community they will serve during their later study years, students are afforded the opportunity of real-life implementation of their learned skills for the betterment of society.
B. Conceptual Framework
Applying the TPB in communication training involves addressing students’ attitudes toward communication, reinforcing positive subjective norms, and enhancing their perceived control over performing communication tasks. In line with the TPB, the authors considered the interplay between the various TPB elements and intentionally selected and designed activities, content, and assessments to better prepare students for real-world communication challenges. The authors mapped communication-based activities throughout the interprofessional modules from the first- to third year of study (Figure 1).
With an initial first step of any behavioural change being that of the participant’s motivation to change (Ajzen, 1991; Asare, 2015), it was deemed essential to ensure students were introduced to the importance and value of effective communication within the healthcare field from their first year of study. Additionally, to minimise potential cognitive overload the content was scaffolded, as illustrated in Figure 1, to gradually expose students to increasingly challenging concepts and activities.

HC: Healthcare
HPCSA: Health Professions Council of South Africa
Figure 1. Conceptual framework of the curricular mapping of communication-based activities
Activities included didactic lectures, practical demonstrations, and the application of learned skills in various contexts (Figure 1). Assessment was aligned to both modular outcomes and took a practical format by including simulation-based assessments, submitted video recordings where the desired skills were showcased, as well as a social media artifact aimed at communicating healthcare science to the public.
Developing communication skills in undergraduate healthcare students is vital for improving both patient care and public health outcomes. Grounded in the TPB, purposely planned interventions for healthcare communication training may assist students in increasing their intention to practice and develop this essential skill. This study therefore aimed to explore, through the application of the TPB, the experiences of healthcare students’ interprofessional communication skills training as embedded within the aforementioned interprofessional healthcare curriculum.
II. METHODS
A qualitative descriptive research design was employed to gain an in-depth understanding of the communication-related experiences of undergraduate healthcare students. This approach allowed for an exploration of participants’ perspectives, offering a nuanced view of the perceived effectiveness and impact of the communication activities embedded within each study year’s interprofessional module.
Before study commencement ethical approval was obtained from the General/Human Research Ethics Committee (UFS-HSD2021/0921/21) at the UFS. All first- to third-year students enrolled in the relevant interprofessional modules, as they were introduced between 2022 and 2024, were informed about the study via an information leaflet sent to their institutional email accounts and invited to participate. Students were informed that participation is voluntary, and they could withdraw at any stage without any repercussions. The annual UFS module evaluation survey was made available through the institutional Learning Management System at the end of the academic year to all students enrolled in the respective modules (Table 1).
|
Module |
Year |
Number of enrolled students |
|
SHRS1500 |
2022 |
135 |
|
2023 |
125 |
|
|
2024 |
109 |
|
|
SHRS2600 |
2023 |
141 |
|
2024 |
123 |
|
|
SHRS3700 |
2024 |
121 |
Table 1. Student enrolments 2022 to 2024
Qualitative data were collected from all students enrolled in the respective modules through two processes namely an annual institutional module evaluation (2022 and 2023) as well as voluntarily provided anecdotal feedback (2024). The survey included open-ended questions to gather narrative accounts of student participants’ module experiences and to capture any provided suggestions. Verbal feedback was provided by students to the researcher directly following activity engagement answering the question “How did you experience the communication-based activity?”.
The primary author (AvM) repeatedly reviewed both the typed responses to open-ended survey questions and the verbatim transcriptions of students’ verbal feedback to identify and extract aspects related to students’ experiences of communication-based activities presented in the interprofessional modules. All data were thematically analysed by the AvM through deductive In vivo coding (Saldaña, 2018) under the predetermined themes of the TPB namely subjective norm, attitude towards behaviour, and perceived behavioural control, and subsequently checked by the second author (CvV).
III. RESULTS
Module evaluation response rates, although varied between years and student groups (Table 2), remained low. Additional verbal feedback from students following communication activities supplemented module evaluation data.
|
Module |
Year |
Responses rate |
|
SHRS1500 |
2022 |
30% (n=41; N=135) |
|
2023 |
30% (n=22; N=125) |
|
|
SHRS2600 |
2023 |
7% (n=10; N=142) |
Table 2. Response rates on module evaluation survey (2022, 2023)
The three TPB elements served as themes namely subjective norm, attitude towards behaviour, and perceived behavioural control, and yielded a total of eight categories (Figure 2).

Figure 2. Thematic analysis of qualitative data
Quotes supporting the identified themes and categories (Figure 2) are presented in Table 3.
|
Theme |
Category |
Quote |
|
Subjective norm |
Professional expectations & development
|
“We learned about things that nobody really tells you to do, it is just expected from you in your immediate workplace.” (SHRS1500, 2022).
“It taught me how to manage a variety of problem scenarios in the healthcare environment; hence, I feel more confident in the fact that I will learn how to be the best OT for my future clients” (SHRS1500, 2023).
“I am more conscious of problem-solving during communication, finding a solution with my patient.” (SHRS2600, 2024).
“It was a challenge to present it in layman’s terms” (SHRS3700, 2024).
“I was a person who went through life with a tunnel vision mindset, which made me dismiss anything that wasn’t related to my goal but now I AM very mindful of most things in my life.” (SHRS1500, 2023). |
|
Interprofessional communication
|
“l enjoy working with my group and l am grateful that l got to learn more about our different culture and customs.” (SHRS1500, 2023). |
|
|
Attitude towards behaviour
|
Real-world application
|
“It is really beneficial to learn about how to cooperate and communicate with other in a professional manner.” (SHRS1500, 2022).
“That we got to interview people during our visits and that helped me see that I need to work more on my verbal communication skills.” (SHRS1500, 2022).
“We were faced with reality.” (SHRS2600, 2023).
“I liked where we got to see the communities and interact with them, to get better perspective with what most communities struggle with.” (SHRS1500, 2022).
“Through engaging case visits from special guests and dynamic discussions, I’ve come to understand just how important it is to respect the diverse backgrounds, beliefs, and values.” (SHRS1500, 2023).
“The only thing I really did not like was the times we had to interview parents, we did not really understand what we were doing.” (SHRS1500, 2023). |
|
Perceived behavioural control
|
External perspectives
|
“I liked that we had multiple speakers from their respective fields” (SHRS1500, 2023).
“That is my take-home message, we can always change how our health system is structured since we are the ones that are the upcoming health professionals. We can always change..we can like make a difference in our health system.” (SHRS1500, 2023).
“It was also insightful to get input and feedback from someone who knows nothing about the research or the specific field. Sometimes we as students (who are so familiar with our “language” we are taught), struggle to have an objective view.” (SHRS3700, 2024).
“To realise how much I have evolved from the person I was, to the person I am today is absolutely incredible…I will always remember the life lesson that I learned from a quote I heard through the week – “nothing good comes from comfort zones” and I am committed to living by those words.” (SHRS1500, 2023). |
|
Practical application |
“..integrate real-life situations into our learning. Attending class and theory only prepare us to a certain extent, but physical involvement opens our minds, critical thinking, and perceptions to what we will really be facing once we are in the working field.” (SHRS1500, 2023).
“The classes give structure for us to know what to do and how.” (SHRS2600, 2024).
“I liked the fact that we were challenged intellectually and that we had the chance to engage with other soon-to-be primary healthcare professionals as well as those that already are.” (SHRS1500, 2022).
“The in-class role-playing made the simulation assessment more comfortable as we knew what to expect.” (SHRS2600, 2024). |
|
|
Group collaboration |
“I like the groups because we were able to build a trusting environment and a supportive one.” (SHRS1500, 2022).
“I also disliked the amount of group work, it made it difficult at times to fully engage in the content as it required a lot of excessive delegation and trying to improve mutual understanding.” (SHRS1500, 2023). |
|
|
Lecturer-student communication |
“It was always clear what was expected from us.” (SHRS1500, 2022).
“Every contact session week I would panic a bit because I automatically felt intimidated by the content just by reading the schedule but every single time without fail the lecturer guided us through every single step and I learned so much from it.” (SHRS1500, 2023). |
Table 3. Supporting quotes per theme
A. Subjective Norm
Students reported that, through practical engagement, they were allowed to develop essential professional skills expected of them in their future work environments (Table 3).
The interprofessional nature of the module and module groups allowed students the opportunity to get to develop teamwork and interprofessional communication skills (Table 3).
B. Attitude Towards Behaviour
The real-world application of communication skills in a community setting was generally described as a positive experience, though it was accompanied by some uncertainty and revealed areas for improvement (Table 3).
C. Perceived Behavioural Control
Activities presented by or including external guests were mentioned to have a positive impact on students through providing a real-world perspective (Table 3).
The allowance for students to, both in class and in assessment activities, practically apply learned communication skills was mentioned repeatedly as a positive aspect in the development of these essential skills (Table 3).
As shown in Table 3 the inclusion of group work activities, although fostering the development of a supportive environment, did challenge some students, most notably in finding a common understanding during class activities.
An essential aspect highlighted in this study was that the communication extended beyond the taught skills, but also to the lecturer-student communication relationship (Table 3).
IV. DISCUSSION
This study aimed to explore the experiences of students participating in purposefully designed communication-based activities hosted within an interprofessional healthcare curriculum. The TPB framework used in this curriculum allowed the authors to purposefully design communication-based teachings and activities to foster behavioural intention on the part of undergraduate healthcare students to best incorporate learned communication skills and appreciate the value thereof within their future practice (Bennett & Lyons, 2011). The findings reveal that by integrating TPB elements – attitudes, subjective norms, and perceived behavioural control—into a healthcare education framework, students reported increased confidence, skill retention, and adaptability in real-world interactions. These results align with prior studies demonstrating the positive effects of structured communication training on healthcare students’ self-efficacy and readiness for patient-centred care (Bachmann et al., 2022; Vogel, Meyer, & Harendza, 2018).
Healthcare professionals are expected to be increasingly adaptable, driven by both the evolving demands of the healthcare environment and societal expectations for effective communication within the profession. Even though the healthcare landscape has changed dramatically over the past few years, the importance of effective and clear healthcare communication within a diverse patient population remains central to optimal patient management (Paget et al., 2011; Skolnik & Butler, 2014). Previous studies have noted challenges related to language and cultural barriers in healthcare often leading to miscommunication, delays in treatment, and poorer health outcomes (Organi et al., 2024; Zota et al., 2023). Not only limited to this study’s context but also from a global perspective, effective intercultural engagement is, therefore, an essential skill expected from healthcare professionals, necessitating the development thereof during the undergraduate study years (Madhavanprabhakaran et al., 2015; Nicolaides et al., 2018; Pillay et al., 2019). This does not imply mastery of all cultural nuances but rather an understanding of the principles necessary for managing diverse patient interactions effectively.
Effective health communication is grounded in a shared decision model, which emphasises the patient’s understanding of proposed management options and aligns with society’s expectation that healthcare communication be collaborative, fostering a partnership between healthcare professionals and patients (Ha and Longnecker, 2010; Paget et al., 2011; Zota et al., 2023). However, healthcare professionals’ reliance on an information-based approach where information on symptoms and treatment options is provided with limited consideration of the patient’s perspective, understanding, or emotional response remains a challenge (Ha & Longnecker, 2010; Zota et al., 2023). Clear, accessible information through, amongst others, employing lay terms in healthcare communication significantly enhances patient understanding by making information clearer, facilitating informed decision-making, reducing anxiety, building trust, and preventing misunderstandings (Guo et al., 2022; Paget et al., 2011; Skolnik & Butler, 2014). However, participants in this study noted struggling to communicate healthcare information in a simplified manner, highlighting the need for additional attention being given to the development of this essential skill.
Considering the collaborative nature of healthcare, this study highlighted the value of interprofessional communication-based engagement in preparing students for the world of work. Participants reported that working alongside peers from diverse health disciplines provided valuable exposure to different perspectives, reinforcing the importance of clear communication, teamwork, and adaptability. Interprofessional learning experiences have been reported to foster a shared understanding of patient needs and enhance collaborative problem-solving, skills that are vital in patient-centred models of care (Madhavanprabhakaran et al., 2015; Nicolaides et al., 2018). Allowing students the opportunity to engage with and learn from one another further ensures exposure to varied personal, professional, and cultural perspectives and managing the received input accordingly. The value of interprofessional engagement has further been highlighted in promoting resilience and adaptability (Gilligan et al., 2021; Pillay et al., 2019), by allowing students to communicate effectively across different professional contexts, aligning with the professional and societal expectations of qualified healthcare professionals. The importance of the early integration of interprofessional activities and community engagement spanning across study years has also been emphasised (Bennett & Lyons, 2011; Thibault, 2020) with this current study’s participants expressing the value of learning how to co-operate and respectfully communicate with others. The authors believe that positive experiences in interprofessional communication will lead healthcare students to engage more confidently and positively in future interprofessional interactions.
The study’s findings indicated that participants’ attitudes towards communication were positively influenced through practical community-based interactions, potentially translating to feelings of perceived behavioural control. Although some students reported uncertainty when engaging in real-world communication activities, most expressed increasing confidence and were able to identify areas for improvements related to their communication abilities. Aligned with previous research, it is suggested that if students perceive positive communication outcomes and consider those positive outcomes to be more likely, they will place more value on working toward achieving those outcomes (Bennett & Lyons, 2011; Dehsorkhi et al., 2023; Lewis et al., 2021). Consequently, it is hypothesised that students will be more inclined to engage in improved communication behaviours, with potentially improved skills transferred to clinical settings.
A scaffolded teaching and learning approach aimed to assist students in gradually developing their communication skills by providing opportunities to continuously build knowledge and allow engagement (Van de Pol et al., 2010). This scaffolded learning approach also aimed to prevent cognitive overload by breaking complex communication tasks and skill acquisition into manageable steps, allowing students to focus on mastering each element gradually (Sweller, 2010; Van Merriënboer & Kirschner, 2018). The intentional transition from theoretical understanding to real-world application also allowed students to engage in hands-on practice optimising their learning and potentially effecting behavioural change (Kurtz, Silverman, Benson, & Draper, 2003). Berkhof et al. (2011) underscore this by showing that repeated exposure to communication training enhances students’ skills in empathy and active listening, while also equipping students to manage emotionally charged patient interactions more effectively.
Through establishing a curricular space that encouraged the exchange of diverse perspectives and incorporated both peer and educator feedback, students were empowered to address and overcome perceived barriers to their communication-based learning, potentially enhancing their behavioural control over time. Additionally, exposure to varied viewpoints—through content presenters, assessors, and feedback providers—aimed to foster the development of critical thinking skills and a deeper understanding of the subject matter (Bedford & Barnes, 2024). Aligned with published recommendations, communication-based activities in this curriculum also emphasised diverse forms of interaction such as simulation and role-play, aiming to further assist students in overcoming communication barriers by providing practical experience in effective person-centred communication (Bennett & Lyons, 2011; De Sousa Mata et al., 2021). This practical approach encourages active student participation, enabling them to practice key skills and fostering behaviour change (De Sousa Mata et al., 2021).
The inclusion of group work activities was mostly experienced as positive in developing a different communication skill set. However, some students expressed frustration with groupwork activities especially when navigating diverse opinions and communication styles. These challenges reflect findings by Vacheishvili (2021) and Wilson et al. (2018) who note that while group work fosters teamwork skills, it can also be difficult to manage if group work activities are not selected with care. Considering the collaborative nature of healthcare practice, developing communication skills within a group setting may contribute to the resilience and flexibility required as students develop the skills to mediate conflicts and balance differing viewpoints, ultimately enhancing their adaptability in future professional settings (Paget et al., 2011; Vacheishvili, 2021; Wilson et al., 2018).
The perceived impact of educator-student communication as a model for professional behaviour and academic support was also highlighted in this study. Positive educator-student communication and feedback were frequently cited by participants as contributing to their confidence and clarity in the learning process, a finding corroborated by Kassab et al. (2022) linking educator engagement with increased student motivation and self-efficacy in healthcare training. Educator feedback provided students with practical guidance, while the supportive learning environment encouraged open dialogue, both of which are key for developing reflective healthcare practitioners (van der Merwe et al., 2024).
V. CONCLUSION
This study highlights the value of, through consideration of the TPB, embedding interprofessional, practical communication-based activities in healthcare education to facilitate behavioural intention towards patient-centred communication. Findings suggest that practical, real-world communication activities helped students develop the expected healthcare communication skills. Additionally, results indicated that the intentional communication-based activities positively influenced students’ attitudes toward patient-centred communication. By incorporating a range of communication-based activities paired with continuous feedback, students were consistently supported across multiple study years, helping them to develop and sustain essential communication skills. This ongoing reinforcement positively impacted participants’ sense of behavioural control, as they gained confidence in their ability to perform these skills effectively in practice. The study underscores that to ensure healthcare graduates can communicate in an adaptable, culturally sensitive, and collaborative way, purposefully integrating communication-based activities to affect potential behavioural change is essential. Future research into the long-term effects of such training on professional performance and patient outcomes is recommended.
Notes on Contributors
AvM coordinates the curricular implementation. All authors contributed equally to the manuscript conceptualisation, data checking, and proofreading of the manuscript. All authors have read and approved the manuscript.
Ethical Approval
Before the commencement of the study approval was granted by the General/Human Research Ethics Committee (UFS-HSD2021/0921/21) at the University of the Free State, ensuring that all guidelines for research including human participants were adhered to. Informed consent was obtained from all individual participants included in the study.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgement
The authors wish to acknowledge the participating students for their valuable feedback. The authors acknowledge the use of OpenAI’s ChatGPT to provide language and grammar feedback in the discussion section during the preparation of the final manuscript.
Funding
No funding was received for this study.
Declaration of Interest
The authors have no conflict of interest to declare.
References
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. https://doi.org/10.1016/0749-5978(91)90020-t
Amirthalingam, S. D., Ramasamy, S., & Aznal, S. S. H. S. (2023). Gamification through collaborative learning in medical education. The Asia Pacific Scholar, 8(3), 45–49. https://doi.org/10.29060/taps.2023-8-3/sc2921
Asare, M. (2015). Using the theory of planned behavior to determine the condom use behavior among college students. American Journal of Health Studies, 30(1), 43-50. https://pubmed.ncbi.nlm.nih.gov/26512197/
Baby, M., Gale, C., & Swain, N. (2018). Communication skills training in the management of patient aggression and violence in healthcare. Aggression and Violent Behaviour, 39, 67-82. https://doi.org/10.1016/j.avb.2018.02.004
Bachmann, C., Pettit, J., & Rosenbaum, M. (2022). Developing communication curricula in healthcare education: An evidence-based guide. Patient Education and Counseling, 105(2), 2320-2327. https://doi.org/10.1016/j.pec.2021.11.016
Bedford, A., & Barnes, N. (2024). A call for different perspectives. Historical Thinking, Culture, and Education, 1(1), 110-114. https://doi.org/10.12685/htce.1317
Bennett, K. S., & Lyons, Z. (2011). Communication skills in medical education: An integrated approach. Education Research and Perspectives, 38(2), 45-56. https://www.researchgate.net/publication/267977840_Communication_Skills_in_Medical_Education_An_Integrated_Approach
Berkhof, M., van Rijssen, H. J., Schellart, A. J., Anema, J. R., & van der Beek, A. J. (2011). Effective training strategies for teaching communication skills to physicians: An overview of systematic reviews. Patient Education and Counseling, 84(2), 152-162. https://doi.org/10.1016/j.pec.2010.06.010
Dehsorkhi, H. F., Shamami, M. A., Hayat, A. A., & Rokni, J. (2023). Predicting training transfer of oxygen therapy during COVID-19: Theory of planned behavior application. Journal of Health and Nursing Management, 33(4), 250-258. https://doi.org/10.32598/jhnm.33.4.2468
Del Riccio, M., Costantini, L., Guasconi, M., Casella, G., Fanfani, A., Cosma, C., Mindrican, P., Bonaccorsi, G., Corradini, E., Artioli, G., Sarli, L., Laverack, G., Rondini, E., & Martucci, G. (2023). Role and challenges to digital technologies in community health promotion programs in Italy during the COVID-19 pandemic: A multiple embedded case study protocol. PubMed, 94(1), e2023019. https://doi.org/10.23750/abm.v94i1.14109
De Sousa Mata, Á. N., De Azevedo, K. P. M., Braga, L. P., De Medeiros, G. C. B. S., De Oliveira Segundo, V. H., Bezerra, I. N. M., Pimenta, I. D. S. F., Nicolás, I. M., & Piuvezam, G. (2021). Training in communication skills for self-efficacy of health professionals: A systematic review. Human Resources for Health, 19(1). https://doi.org/10.1186/s12960-021-00574-3
Etheredge, H., & Fabian, J. (2022). Communication in healthcare: Global challenges in the 21st century. Hamostaseologie, 42(1), 29-35. https://doi.org/10.1055/a-1685-7096
Fliorent, R., Mistry, S., Javaid, K., et al. (2023). Skin of color is underrepresented on Instagram: Assessing South Jersey Skin Talk as an educational tool to increase awareness. Cureus, 15(10), e47388. https://doi.org/10.7759/cureus.47388
Gilligan, C., Powell, M., Lynagh, M. C., Ward, B. M., Lonsdale, C., Harvey, P., James, E. L., Rich, D., Dewi, S. P., Nepal, S., Cro, H. A., & Silverman, J. (2021). Interventions for improving medical students’ interpersonal communication in medical consultations. Cochrane Database of Systematic Reviews, 2021(2), CD012418. https://doi.org/10.1002/14651858.CD012418.pub2
Guo, Y., Qiu, W., Wang, Y., & Cohen, T. (2021). Automated lay language summarization of biomedical scientific reviews. Proceedings of the Thirty-Fifth Association for the Advancement of Artificial Intelligence Conference. 35(1), 160-168. https://doi.org/10.1609/aaai.v35i1.16089
Ha, J. F., & Longnecker, N. (2010). Doctor-patient communication: A review. Ochsner Journal, 10(1), 38–43. https://pubmed.ncbi.nlm.nih.gov/21603354/
Hagiwara, N., Elston Lafata, J., Mezuk, B., Vrana, S. R., & Fetters, M. D. (2019). Detecting implicit racial bias in provider communication behaviors to reduce disparities in healthcare: Challenges, solutions, and future directions for provider communication training. Patient Education and Counseling, 102(9), 1738-1743. https://doi.org/10.1016/j.pec.2019.04.023
Health Professions Council of South Africa. (2025, June 13). New and updated ethical guidelines. https://www.hpcsa-blogs.co.za/new-and-updated-ethical-guidelines/
Hompashe, D. M., Gerdtham, U. G., Christian, C. S., Smith, A., & Burger, R. (2021). ‘The nurse did not even greet me’: How informed versus non-informed patients evaluate health systems responsiveness in South Africa. BMJ Global Health, 6(4), e004360. https://doi.org/10.1136/bmjgh-2020-004360
Houbby, N., Abdelwahed, A., & Kumar, S. (2020). A reflection on Imperial College London’s Community Action Project. Education for Primary Care. 31(3), 186-187. https://doi.org/10.1080/14739879.2020.1744191
Kassab, S. E., Taylor, D., & Hamdy, H. (2022). Student engagement in health professions education: AMEE Guide No. 152. Medical Teacher, 45(9), 949-965. https://doi.org/10.1080/0142159X.2022.2137018
Kurtz, S. M., Silverman, J. D., Benson, J., & Draper, J. (2003). Marrying content and process in clinical method teaching: Enhancing the Calgary–Cambridge guides. Academic Medicine, 78(8), 802-809. https://doi.org/10.1097/00001888-200308000-00011
Lewis, S., Downing, C., & Hayre, C. M. (2021). Using the theory of planned behaviour to determine radiation protection among South African diagnostic radiographers: A cross-sectional survey. Journal of Medical Radiation Sciences, 69(1), 47-55. https://doi.org/10.1002/jmrs.537
Madhavanprabhakaran, G., Al-Khasawneh, E., & Wittmann, L. (2015). Perceived benefits of preclinical simulation-based training on clinical learning outcomes among Omani undergraduate nursing students. Sultan Qaboos University Medical Journal, 15(1), e105-e111. https://pubmed.ncbi.nlm.nih.gov/25685368/
Mahdy, Z. A., Maaya, M., Atan, I. K., et al. (2020). Simulation in healthcare in the realm of Education 4.0. Sains Malaysiana, 49(8), 1987-1993. https://doi.org/10.17576/jsm-2020-4908-21
Mangal, J. P., & Farmer, B. S. (2023). Language barriers in healthcare. In Advances in medical education, research, and ethics (AMERE) book series (pp. 113–129). https://doi.org/10.4018/978-1-6684-5493-0.ch007
Medendorp, N. M., van den Heuvel, L. M., Han, P. K. J., Hillen, M. A., & Smets, E. M. A. (2021). Communication skills training for healthcare professionals in providing genetic counseling: A scoping literature review. Patient Education and Counseling, 104(1), 27-39. https://doi.org/10.1016/j.pec.2020.07.018
Mirza, S. N., & Tabani, U. (2018). The rhetoric of healthcare professionals: Infectious communication and its effects. Madridge Journal of Internal and Emergency Medicine, 2(1), 45-47. https://doi.org/10.18689/mjiem-1000108
Neuhauser, L., & Kreps, G. L. (2003). Rethinking communication in the e-health era. Journal of Health Psychology, 8(1), 7-23. https://doi.org/10.1177/1359105303008001426
Nicolaides, M., Cardillo, L., Theodoulou, I., Hanrahan, J., Tsoulfas, G., Athanasiou, T., Papalois, A., & Sideris, M. (2018). Developing a novel framework for non-technical skills learning strategies for undergraduates: A systematic review. Annals of Medicine and Surgery, 36, 29-40. https://doi.org/10.1016/j.amsu.2018.10.005
Paget, L., Han, P., Nedza, S., Kurtz, P., Racine, E., Russell, S., Santa, J., Schuman, M. J., Simha, J., & Von Kohorn, I. (2011). Patient clinician communication: Basic principles and expectations – NAM. (n.d.). NAM. https://nam.edu/perspectives-2011-patient-cliniciancommunication-basic-principles-and-expectations/
Pang, T. Y., Lee, T. K., & Murshed, M. (2023). Towards a new paradigm for digital health training and education in Australia: Exploring the implication of the fifth industrial revolution. Applied Sciences, 13(11), 6854. https://doi.org/10.3390/app13116854
Pillay, J. D., Ally, F., & Govender, N. (2019). Exploring opportunities for embedding graduate attributes in a first-year undergraduate anatomy course for allied health students. BMC Medical Education, 19(1). https://doi.org/10.1186/s12909-019-1777-6
Saldaña, J., & Omasta, M. (2018). Analyzing interviews: Condensing and coding. In Qualitative research: Analysing life (pp. 117-140).
Organi, Z. K., Nazarenia, M., & Aghaee, F. (2024). Understanding the challenges of language barriers in healthcare. Advances in Medical Education, Research, and Ethics, 3(3), 28-35. https://doi.org/10.61838/kman.isslp.3.3.5
Skolnik, P. J., & Butler, N. (2014). The patient’s and patient family’s perspective. In Patient Safety in Surgery (pp. 403–408). https://doi.org/10.1007/978-1-4471-4369-7_28
Stamer, T., Steinhäuser, J., & Flägel, K. (2023). Artificial intelligence supporting the training of communication skills in the education of health care professions: Scoping review. Journal of Medical Internet Research, 25, e43311. https://doi.org/10.2196/43311
Sweller, J. (2010). Cognitive load theory: Recent theoretical advances. In Plass, J. L., Moreno, R., & Brünken, R. (Eds.), Cognitive load theory. Cambridge University Press. https://doi.org/10.1017/CBO9780511844744.004
Thibault, G. E. (2020). The future of health professions education: Emerging trends in the United States. FASEB BioAdvances, 2, 685-694. https://doi.org/10.1096/fba.2020-00061
United Nations. (2024). Goal 3 | Department of Economic and Social Affairs. (n.d.). https://sdgs.un.org/goals/goal3
Vacheishvili, N. (2021). Collaborative communication as an effective strategy in education. Proceedings of the Strategic Communications Today: Existing Challenges and Opportunities Conference. https://www.researchgate.net/publication/353606348_Collaborative_Communication_as_an_Effective_Strategy_in_Education#fullTextFileContent
van de Pol, J., Volman, M., & Beishuizen, J. (2010). Scaffolding in teacher–student interaction: A decade of research. Educational Psychology Review, 22(3), 271-296. https://doi.org/10.1007/s10648-010-9127-6
van der Merwe, A., & Janse van Vuuren, C. (2024). Creating transformational learning experiences for 21st century healthcare students through pre-clinical skills training at a South African university. BMC Medical Education, 24(198). https://doi.org/10.1186/s12909-024-05177-9
van der Merwe, A., Serekoane, M., & du Plooy, S. (2024). Situating pluralism in biomedical healthcare practices: Lessons from the ethnomedical approach. SoTL in the South, 8(2), 49-65. https://doi.org/10.36615/sotls.v8i2.397
Van Merriënboer, J. J. G., Kirschner, P. A., & Frèrejean, J. (2024). Ten steps to complex learning. https://doi.org/10.4324/9781003322481
Vogel, D., Meyer, M., & Harendza, S. (2018). Verbal and non-verbal communication skills including empathy during history taking of undergraduate medical students. BMC Medical Education, 18, 157. https://doi.org/10.1186/s12909-018-1260-9
Wilson, K. J., Brickman, P., & Brame, C. J. (2018). Group work. CBE—Life Sciences Education, 17(1), fe1. https://doi.org/10.1187/cbe.17-12-0258
Zota, D., Diamantis, D. V., Katsas, K., Karnaki, P., Tsiampalis, T., Sakowski, P., Christophi, C. A., Ioannidou, E., Darias-Curvo, S., & Batury, V.-L. (2023). Essential skills for health communication, barriers, facilitators and the need for training: Perceptions of healthcare professionals from seven European countries. Healthcare, 11(14), 2058. https://doi.org/10.3390/healthcare11142058
*Anke van der Merwe
205 Nelson Mandela Drive,
Park West, Bloemfontein, 9301
Email: gonzalesa@ufs.ac.za
Submitted: 16 October 2024
Accepted: 16 June 2025
Published online: 6 January, TAPS 2026, 11(1), 55-68
https://doi.org/10.29060/TAPS.2026-11-1/OA3543
Jie Kie Phang1,2, Yu Heng Kwan1,2, Sungwon Yoon2 & Warren Fong1,3,4
1Department of Rheumatology and Immunology, Singapore General Hospital, Singapore; 2Program in Health Services and Systems Research, Duke-NUS Medical School, Singapore; 3Office of Education, Duke-NUS Medical School, Singapore; 4Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract
Introduction: There are limited medical professionalism assessment tools that are adapted for Singapore. We aimed to evaluate the validity, reliability and feasibility of the Singapore version of the Professionalism Mini-Evaluation Exercise (P-MEX) for assessment of professionalism of residents at a teaching hospital in Singapore.
Methods: We collected assessment data from residents from July 2019 to January 2020. Content validity was evaluated through cognitive debriefing interviews (CDIs). Construct validity was evaluated using a priori hypothesis with another comparator instrument. Structural validity was assessed through both confirmatory factor analysis (CFA) using the original four-factor model and exploratory factor analysis (EFA). Internal consistency was assessed using Cronbach’s alpha.
Results: CDIs conducted with nine faculty supported content validity of the Singapore version of P-MEX. The cross-sectional data demonstrated satisfactory construct validity (83% of hypotheses met) and good internal consistency (Cronbach’s alpha ranged from 0.72 to 0.93). The CFA of the original four-factor model of the P-MEX did not obtain meet all the acceptable fit of indexes. EFA suggested a two-factor model—the first factor had an eigenvalue of 8.52 and explained 73.8% of the variance, while the second factor had an eigenvalue of 1.90 and explained 26.2% of the variance.
Conclusion: This study supports the content validity, construct validity, internal consistency of the Singapore version of P-MEX in assessing medical professionalism in the local residency training programme. However, there was no conclusive support for the original four-factor model of the P-MEX. EFA identified 2 main factors, which appeared to encompass “Patient care and inter-professional relationship skills” and “Reflective skills”.
Keywords: Professionalism, Singapore, Validation, Assessment
Practice Highlights
- This study supports the content validity, construct validity, internal consistency of the Singapore version of P-MEX in assessing medical professionalism in the local residency training programme.
- Future research should examine the structural validity of the modified P-MEX in different samples of medical trainees as confirmatory factor analysis (CFA) of the original four-factor model of the P-MEX did not obtain meet all the acceptable fit of indexes.
- Medical educators in the region with similar multi-cultural backgrounds can consider using the Singapore version of P-MEX to assess medical professionalism among trainees.
I. INTRODUCTION
Listed as one of the core competencies in the Accreditation Council for Graduate Medical Education (ACGME) curriculum (Swing, 2007), medical professionalism is being increasingly emphasised in medical training for both undergraduates and postgraduates as part of their development of a professional identity (Cruess & Cruess, 2006; Cruess et al., 2015; Swick et al., 1999). Unprofessional behaviour during residency training has been shown to predict future disciplinary actions of doctors (Papadakis et al., 2008). Fortunately, there is evidence to suggest that remediation of unprofessional behaviour has been effective (Guerrasio et al., 2014; Zbieranowski et al., 2013). Various training programmes have been developed in the hope to teach and train professionalism among the residents (Lumlertgul et al., 2009). The ability to evaluate the level of medical professionalism is imperative to determine the effectiveness of the training programmes aiming to instil medical professionalism among residents (Hawkins et al., 2009). Furthermore, assessment supports the development of the professional identity and allows for early remediation of residents displaying unprofessional behaviour (Cruess et al., 2015; Cruess et al., 2019).
Previous studies have identified professionalism as a complex multi-dimensional social construct, thus making geographical location and culture important considerations in the assessment of professionalism (Cruess et al., 2010; Ho et al., 2011). Importantly, there is evidence on geographical and regional variations in the attitudes, beliefs and behaviours constituting medical professionalism (Chandratilake et al., 2012). Following the Ottawa consensus conference, it has been advised that re-validation of assessment tools be performed when used in new cultural contexts (Hodges et al., 2011). The Professionalism Mini- Evaluation Exercise (P-MEX), developed in Canada (Cruess et al., 2006), is one of the promising observer-based tools that can be used for assessment of medical professionalism -in the workplace (Hawkins et al., 2009; Kwan et al., 2018). This allows us to assess the Does of Millers pyramid (Miller, 1990). Since its conception, the P-MEX has been piloted in Japan, Finland, Iran, Turkey and Switzerland (Amirhajlou et al., 2019; Bajwa et al., 2021; Karukivi et al., 2015; Taşçı et al., 2023; Tsugawa et al., 2009), but there are no studies validating the P-MEX in the multi-ethnic Southeast Asia region. Singapore is a multi-ethnic country, comprising of predominantly Chinese (74%), followed by Malays (13%) and Indians (9%) (Noor & Leong, 2013). Previous study has shown that the definition of medical professionalism differs even among two Chinese cultural contexts (Ho et al., 2014), thus highlighting the need to adapt the P-MEX when using it in a new socio-cultural context.
The current assessment tool in the Singapore residency programme includes the MOHH C1 form, which contains 6 general questions on medical professionalism such as (1) Accepts responsibility and follows through on tasks, (2) Responds to patient’s unique characteristics and needs equitably, (3) Demonstrates care and concern for the patient/family, (4) Communicates effectively with patient/family, (5) Communicates and works effectively with other healthcare professionals, and (6) Demonstrates integrity and ethical behaviour. However, the P-MEX, consisting of 24 observable behaviours that were distilled from the original 142 behaviours, allowed for assessors to evaluate as many attributes of a professional doctor with the smallest number of behaviours (Cruess et al., 2006). The explicit observable behaviours allow for more objective assessments of professionalism as compared to the more general items of the MOHH C1 form. Previously, our Delphi study had demonstrated consensus regarding the relevance of the Singapore version of P-MEX with 23 items to be used in Singapore for evaluation of medical professionalism among residents (Fong et al., 2020). The aim of the present study was to evaluate the validity and reliability of the Singapore version of the P-MEX for assessment of medical professionalism of residents at a teaching hospital in Singapore.
II. METHODS
A. Study Settings and Participants
We conducted two studies examining- (1) content validity of the Singapore version of the P-MEX using cognitive debriefing interviews (CDIs) and (2) construct validity, reliability and feasibility of the Singapore version of the P-MEX in a cross-sectional study among residents in the SingHealth residency programme in the Singapore General Hospital. Within the SingHealth residency programme, foreign medical graduates constitute 13.7% of the residents (unpublished data). SingHealth Residency offers 30 programmes, of which 21 are accredited by the Accreditation Council of Graduate Medical Education – International (ACGME-I), and 9 are accredited by the Joint Committee of Specialist Training (JCST) (SingHealth, 2024). ACGME-I is the extension of the accreditation model of ACGME internationally (Arrighi et al., 2024).
All study protocols were approved by the SingHealth Centralised Institutional Review Board (IRB) (Reference number: 2016/3009 and 2019/2431). For the first study investigating content validity of the Singapore version of the P-MEX using CDIs, written consent was obtained from all participants before study commencement. For the second study investigating construct validity, reliability as well as feasibility of the Singapore version of the P-MEX in a cross-sectional study, waiver of documentation of informed consent was granted.
B. Content Validity
We conducted CDIs to assess the content validity of the 23-item Singapore version of P-MEX from June 2019 to July 2019. Nine faculty who were core faculty in the residency programme were recruited using convenience sampling while ensuring representation of both genders and a range of duration of experience in the assessment of medical professionalism. Faculty chosen had to have performed assessments of medical professionalism of residents within the past one year. After viewing a video showing a resident displaying unprofessional behaviours, faculty were asked to complete the modified P-MEX assessment form in the presence of an interviewer unaided and were invited to comment on the necessity and relevance of items, instructions and response format through interview. During the interview, the faculty explained the reasons for their answers to each item, and commented on any ambiguities in the items, instructions, and response options. For example, for the question on “listened actively to patients”, we probed on (i) the meaning of the phrase ‘listened actively’, (ii) any different way to reword the phrase ‘listened actively’ based on the description, and (iii) the reason for choosing the response option (i.e., Exceeded expectations, Met expectations, Below expectations, Unacceptable, Not Applicable). The faculty were also asked whether any important issues had been omitted. We iteratively modified the items based on findings in CDIs via discussions with the study team until faculty reported no significant difficulty.
C. Cross-Sectional Study for Validation
Potential assessors (core faculty in residency programs and senior residents) in Endocrinology, Gastroenterology, Geriatric Medicine, Internal Medicine, Obstetrics & Gynaecology, Oncology, Rehabilitation Medicine, Rheumatology, and Respiratory Medicine specialties were sent an invitation via email introducing the study objectives and the study procedures. Depending on the faculty’s preference, hardcopy or electronic assessment forms were provided upon agreement to participate in the study. Prior to the study, assessors were given a short briefing on the use of the assessment forms, with descriptors of the items explained to the assessors. Residents were evaluated using the 23-item Singapore version of P-MEX forms from July 2019 to January 2020. Repeated assessments on the same resident were allowed as there was no identifiers collected to track the residents assessed. The P-MEX was conducted using direct observation of the resident by faculty as part of their workplace-based assessments. Immediate feedback was not compulsory, but it was encouraged especially if there were critical incidents observed. The online forms were made available to faculty through an app and could be accessed conveniently when performing the direct observations.
Responses for selected items from comparator instruments were collected. Faculty were also asked to provide feedback after completing the assessment using the Singapore version of P-MEX through hardcopy or online survey, depending on faculty’s preference.
D. Singapore Version of P-MEX
The P-MEX assessed four different domains of medical professionalism: doctor-patient relationship, reflective skills, time management, and inter-professional relationship (Cruess et al., 2006). Each category contained 3 to 8 items, with a total of 23 items. The score for each item was calculated based on a four-point rating scale (4=Exceeded expectations, 3= Met expectations, 2= Below expectations, 1= Unacceptable). There was also a “Not applicable” option for each item. There is also a global question assessing the overall professional performance during the specific encounter at the end of the assessment form. Demographics information such as the level of the trainee (e.g. Medical officer, Year 1-3 Resident, Year 1-3 Senior resident) was collected as part of the P-MEX.
E. Comparator Instrument
There is no dedicated instrument to assess medical professionalism in residency programmes in Singapore. Therefore, selected questions which were deemed to encompass medical professionalism from the current assessment tool used in residency programmes (MOHH C1 form) was included as comparator instrument. The questions included- (1) Accepts responsibility and follows through on tasks, (2) Responds to patient’s unique characteristics and needs equitably, (3) Demonstrates care and concern for the patient/family, (4) Communicates effectively with patient/family, (5) Communicates and works effectively with other healthcare professionals, and (6) Demonstrates integrity and ethical behaviour. The questions were evaluated using a 9-point Likert scale (1-3: Unsatisfactory, 4-6: Satisfactory, 7-9: Superior).
F. Feedback from Assessors
The assessors’ feedback on the Singapore version of P-MEX was evaluated using the following questions using a 5-point Likert scale- (1) “Is this assessment tool (P-MEX) better than current tools used in your programme in terms of assessing medical professionalism?” (1=Very much better, 2= A little better, 3=Neutral, 4= A little worse, 5=Very much worse); (2) “Is this assessment tool (P-MEX) easy to complete?” (1=Very easy, 2= Fairly easy, 3=Neutral, 4= Fairly hard, 5=Very hard); and (3) “Are the behaviours assessed in the P-MEX reasonable and appropriate for the assessment of medical professionalism?” (1=Very reasonable and appropriate, 2= Fairly reasonable and appropriate, 3=Neutral, 4, Fairly unreasonable and inappropriate, 5=Very unreasonable and inappropriate).
G. Data Analysis
Construct validity was tested using the following a priori hypothesis:
- Total score of the Singapore version of P-MEX items in the doctor-patient relationship domain is positively and highly correlated with “Responds to patient’s unique characteristics and needs equitably”
- Total score of the Singapore version of P-MEX items in the doctor-patient relationship domain is positively and highly correlated with “Demonstrates care and concern for the patient/family”
- Total score of the Singapore version of P-MEX items in the doctor-patient relationship domain is positively and highly correlated with “Communicates effectively with patient/family”
- Total score of the Singapore version of P-MEX items in the time management domain is positively and moderately correlated with “Accepts responsibility and follows through on tasks”
- Total score of the Singapore version of P-MEX items in the inter-professional relationship domain is positively and highly correlated with “Communicates and works effectively with other healthcare professionals”
- The Singapore version of P-MEX global question score is positively and highly correlated with “Demonstrates integrity and ethical behaviour”
The correlation between P-MEX and comparator instrument was evaluated using Spearman’s rank correlation coefficient (rs). High (rs = 0.5-0.8) and moderate (rs = 0.3-0.5) correlation coefficients suggest that the scores from 2 instruments are correlated, whereas low (rs ≤ 0.3) correlation coefficients suggest that the PROMs are measuring different constructs (Cohen, 2016). Convergent validity is supported when at least 75% of the results are in accordance with the hypotheses (Prinsen et al., 2018). We adjusted the p values using Bonferroni’s correction to reduce the likelihood of Type I errors (Curtin & Schulz, 1998), and p values < 0.00833 were considered significant.
Structural validity was determined by first carrying out confirmatory factor analysis (CFA) through structural equation modelling to test model fit of the original four-factor model as observed in previous study on development of the P-MEX (Cruess et al., 2006). Modification indices (MIs) indicate how much the model fit will be improved after adding a new path to the model. MIs > 10 warranted covariance of error terms (Cole et al., 2005). Various goodness-of-fit indices were used to estimate the model fit, namely (1) x2, (2) Comparative-of-Fit Index (CFI), (3) Tucker-Lewis Index (TLI), (4) Root mean square error of approximation (RMSEA). A model is considered to fit the data well when the x2 value is not significant; CFI and TLI >0.9; RMSEA < 0.1030. Standardised factor loadings were also examined.
In the case of less than acceptable model fit with the original four-domain model in CFA, exploratory factor analysis (EFA) would be conducted using the principal axis/factors method to extract factors, allowing for oblique rotation, without specifying the number of factors a priori. Value of the eigenvalues, proportion of variance explained, and cumulative variance explained would be examined. Factors with eigenvalue >1 or factors that explained >10% of the proportion of variance or cumulative variance of >75% would be retained. Factor loadings would be examined after determining the appropriate number of factors. In this step, any item with a factor loading less than 0.5 would be removed (Arifin & Yusoff, 2016).
Reliability refers to the overall consistency of the measure (Mokkink et al., 2018). In this study, reliability was assessed using internal consistency, assuming all items within a single sub-domain measured a single construct. Internal consistency is supported when Cronbach’s alpha ≥0.70.
We conducted the data analysis and factor analysis using Stata SE15.0 (Stata-Corp, College Station, TX, USA).
III. RESULTS
A. Content Validity
We conducted CDIs with nine faculty (33% male, median age 35 years old, age range from 31 to 38 years old, 89% Chinese, median year as faculty 5 years, years as faculty ranging from 1 to 10 years). The faculty were from rheumatology (n=2), obstetrics and gynaecology (n=2), respiratory and critical care medicine (n=2), renal (n=1), gastroenterology (n=1), advanced internal medicine (n=1) specialties. Overall, faculty found the P-MEX to be relevant in assessing medical professionalism without any missing concepts. However, changes to the description for 10 items were made after 7 CDIs. The main issues raised during the CDIs could be categorised into 2 main categories:
- Difficulty understanding/ misinterpretation of the intent of the question. To address this, we provided alternative terms, some of which were elicited from the faculty.
- Inappropriate examples in description of behaviour: To address this, we provided alternative examples derived from the faculty (Table 1).
The above-mentioned modifications were tested on two subsequent faculty. The faculty reported ease of comprehension with the modified P-MEX, and thus no further modifications were made.
B. Cross-Sectional Study for Validation
We received a total of 208 P-MEX assessment forms, of which 86% (n=178) assessed junior residents, and 14% (n=30) assessed senior residents. The mean (SD) number of years post-graduation for the resident was 3.4 (2.3). For all the 23 items, “met expectations” was the most frequent rating (Table 2). 6.3% (n=13) of the assessments identified behaviours that were unacceptable or below expectations, particularly in the item “solicited feedback” (n=7). 94% (n=195) of the evaluations were done based on ward activity, with the rest performed in the clinic, operating theatre or emergency room setting. Items with more than 10% ratings as “not applicable” were ‘solicited feedback’ (18.3%) and ‘admitted errors’ (13.0%).
C. Construct Validity
83% (5 out of 6) of the a priori hypotheses were met. There were significant associations between the P-MEX and the comparator instrument (all p values <0.01), with Spearman’s rank correlation coefficient ranging from 0.472 to 0.633 (Table 3).
D. Structural Validity
The CFA of the original four-factor model of the P-MEX did not meet all the acceptable fit of indexes, with x2= 573.349, CFI=0.856, TLI=0.824, and RMSEA=0.093 (Figure 1).
Given the poor fit of our data to the four-factor model, we decided to investigate the factor structure of the Singapore version of the P-MEX in the present sample by means of an EFA. EFA strongly suggested a two-factor model—the first factor had an eigenvalue of 8.52 and explained 73.8% of the variance, while the second factor had an eigenvalue of 1.90 and explained 26.2% of the variance. Three items (6. Advocated on behalf of a patient; 13. Maintained composure in a difficult situation; 22. Used health resources appropriately) had factor loadings <0.5 in the EFA. Table 4 presents the two-factor model for the present study. Factor 1 consisted of seventeen items with loadings of 0.5 or above: Listened actively to patients (factor loading 0.76); Showed interest in patients as a person (factor loading 0.62); Recognised and met patient needs (factor loading 0.72); Extended his/herself to meet patient needs(factor loading 0.66); Ensured continuity of patient care(factor loading 0.57); Maintained appropriate boundaries(factor loading 0.56); Communicated effectively with patient (factor loading 0.74); Demonstrated awareness of limitations(factor loading 0.77); Was on time(factor loading 0.53); Completed tasks in a reliable fashion(factor loading 0.71); Was available to colleagues(factor loading 0.57); Maintained appropriate appearance(factor loading 0.67); Addressed own gaps in knowledge and skills(factor loading 0.77); Demonstrated respect for colleagues(factor loading 0.83); Avoided derogatory language(factor loading 0.62); Maintained patient confidentiality(factor loading 0.65); Demonstrated collegiality(factor loading 0.73). Factor 2 consisted of three items with loadings of 0.5 or above: Admitted errors/omissions (factor loading 0.67); Solicited feedback (factor loading 0.55); Accepted feedback (factor loading 0.64).
E. Reliability
Cronbach’s alpha for the doctor-patient relationship, reflective, time management, and inter-professional relationship domains were 0.84, 0.72, 0.81 and 0.82 respectively, which implies that the original four domains of the P-MEX had satisfactory internal consistency.
Cronbach’s alpha for the 2-factor model were 0.93 and 0.72 respectively, which implies that the 2-factor model of the Singapore version of the P-MEX obtained from EFA had satisfactory internal consistency.
F. Feedback from Assessors
A total of 81 assessors (median number of years as faculty=4, range from 2 to 39) provided feedback on the Singapore version of P-MEX. Among the 81 assessors, 56 (69%) of the faculty considered the Singapore version of P-MEX to be better than current tools in terms of assessing medical professionalism. For the question regarding the ease of completion of the Singapore version of P-MEX, 57 (70%) deemed that the P-MEX to be very easy or fairly easy to complete. Lastly, 71 (88%) of the faculty deemed that the behaviours assessed in the Singapore version of P-MEX to be reasonable and appropriate for the assessment of medical professionalism.
|
Item |
Original description |
Issues raised (number of faculty who reported difficulty) |
Modifications |
Modified description |
|
Domain: Doctor-patient relationship skills |
||||
|
Ensured continuity of patient care |
Ensured proper hand-over of care of patient, e.g. at handover rounds in the evening or when discharging the patient to the care of another doctor
|
Unsure if the question was only applicable during transfer of care (n=1) |
Added “proper follow-up of patient” |
Ensured proper hand-over of care of patient (e.g. at handover rounds in the evening or when discharging the patient to the care of another doctor) or proper follow-up of patient |
|
Advocated on behalf of a patient |
Spoke up in support of the patient – e.g. made an appeal on behalf of the patient to get subsidy for medical care |
Unsure whether the making an appeal on behalf of the patient would be applicable in local context, suggested that better example would be standing by the patient during a conflict in the treatment plan between the patient and family (n=5) |
Added the example “making known the wishes of the patient when there is a conflict of opinion in the treatment plan between family members and patient” |
Spoke up in support of the patient’s opinion, interests, priorities and concerns – e.g. made an appeal on behalf of the patient to get subsidy for medical care; making known the wishes of the patient when they is a conflict of opinion in the treatment plan between family members and patient
|
|
Maintained appropriate boundaries |
Aware of and behaved appropriately according to social, religious and cultural norms in our multi-ethnic and multi-religious country. E.g. neither overly friendly or unfriendly to patients and colleagues
|
Commented that the example provided may be inappropriate as being unfriendly may be keeping appropriate distance (n=5) |
Removed the example “neither overly friendly or unfriendly to patients and colleagues” |
Aware of and behaved appropriately according to social, religious and cultural norms in our multi-ethnic and multi-religious country |
|
Communicated effectively with patient |
Explained with empathy the diagnosis of the disease, treatment options (including alternatives), risks and benefits, and ensured that patients understood
|
Commented that clarity is more important than empathy in communication (n=1) |
Changed “explained with empathy” to “explained with empathy and clarity” |
Explained with empathy and clarity the diagnosis of the disease, treatment options (including alternatives), risks and benefits, and ensured that patients understood |
|
Domain: Reflective skills |
||||
|
Solicited feedback |
Actively asked for feedback on his/her actions or management of patients
|
Unsure if the question was asking about soliciting feedback from who (n=4) |
Added “from colleagues” |
Actively asked for feedback from colleagues on his/her actions or management of patients |
|
Accepted feedback |
Open to criticisms and comments and had the humility to learn from feedback
|
Unsure if the question was asking about accepting feedback from who (n=2) |
Added “from patients and/ or colleagues” |
Open to criticisms and comments and had the humility to learn from feedback from patients and/ or colleagues |
|
Domain: Inter-professional relationship skills |
||||
|
Maintained appropriate appearance |
Maintained appropriate appearance Appeared clean, neat, groomed and dressed modestly
|
Unsure about the meaning of “modestly” (n=2) |
Changed “modestly” to “appropriately (i.e convey a professional image)” |
Appeared clean, neat, groomed and dressed appropriately (i.e convey a professional image) |
|
Addressed own gaps in knowledge and skills |
Kept up to date in medical knowledge and skills. E.g. by reading journals, attending courses and conferences |
Commented that it would be good if the trainee can “understand gaps in knowledge and skills” (n=2) |
Added “Recognised gaps in his/her knowledge” |
Recognised gaps in his/her knowledge and kept up to date in medical knowledge and skills. E.g. by reading journals, attending courses and conferences
|
|
Demonstrated respect for colleagues |
Listened to their professional opinion and did not oppose colleagues in public |
Commented that “did not oppose colleagues in public” was inappropriate as doctors should be speaking up when there are differing opinion (n=5) |
Changed “did not oppose colleagues in public” to “resolved difference of opinions in a professional and non-confrontational manner”
|
Listened to professional opinion of healthcare team and resolved difference of opinions in a professional and non-confrontational manner |
|
Avoided derogatory language |
Did not ridicule, insult or use foul language when talking about patients or colleagues |
Commented that avoiding derogatory language was more important when talking to patients and colleagues (n=2)
|
Changed “when talking about patients or colleagues” to “when talking to patients or colleagues”
|
Did not ridicule, insult or use foul language when talking to patients or colleagues |
Table 1. Issues raised during the CDIs and modifications made to the P-MEX
|
Item |
Not applicable |
Unacceptable |
Below expectations |
Met expectations |
Exceeded expectations |
|
Domain: Doctor-patient relationship skills |
|||||
|
Listened actively to patients |
0 (0) |
0 (0) |
0 (0) |
151 (72.6) |
57 (27.4) |
|
Showed interest in patients as a person |
1 (0.5) |
0 (0) |
1 (0.5) |
145 (69.7) |
61 (29.3) |
|
Recognised and met patient needs |
0 (0) |
0 (0) |
3 (1.4) |
147 (70.7) |
58 (27.9) |
|
Extended his/herself to meet patient needs |
0 (0) |
0 (0) |
2 (1.0) |
154 (74.0) |
52 (25.0) |
|
Ensured continuity of patient care |
1 (0.5) |
0 (0) |
3 (1.4) |
131 (63.0) |
73 (35.1) |
|
Advocated on behalf of a patient |
5 (2.4) |
0 (0) |
3 (1.4) |
155 (74.5) |
45 (21.6) |
|
Maintained appropriate boundaries |
6 (3.0) |
0 (0) |
2 (1.0) |
151 (72.6) |
49 (23.6) |
|
Communicated effectively with patient |
0 (0) |
0 (0) |
3 (1.4) |
159 (76.4) |
48 (23.1) |
|
Domain: Reflective skills |
|||||
|
Demonstrated awareness of limitations |
0 (0) |
0 (0) |
1 (0.5) |
159 (76.4) |
48 (23.1) |
|
Admitted errors/omissions |
27 (13.0) |
0 (0) |
3 (1.4) |
142 (68.3) |
36 (17.3) |
|
Solicited feedback |
38 (18.3) |
0 (0) |
7 (3.4) |
139 (66.8) |
24 (11.5) |
|
Accepted feedback |
15 (7.2) |
0 (0) |
3 (1.4) |
159 (76.4) |
31 (14.9) |
|
Maintained composure in a difficult situation |
17 (8.2) |
0 (0) |
4 (1.9) |
147 (70.7) |
40 (19.2) |
|
Domain: Time management |
|||||
|
Was on time |
0 (0) |
0 (0) |
1 (0.5) |
137 (65.9) |
70 (33.7) |
|
Completed tasks in a reliable fashion |
1 (0.5) |
0 (0) |
2 (1.0) |
115 (55.3) |
90 (43.3) |
|
Was available to colleagues |
2 (1.0) |
0 (0) |
3 (1.4) |
131 (63.0) |
72 (34.6) |
|
Domain: Inter-professional relationship skills |
|||||
|
Maintained appropriate appearance |
0 (0) |
0 (0) |
1 (0.5) |
141 (67.8) |
66 (31.7) |
|
Addressed own gaps in knowledge and skills |
2 (1.0) |
0 (0) |
4 (1.9) |
167 (80.3) |
35 (16.8) |
|
Demonstrated respect for colleagues |
0 (0) |
0 (0) |
2 (1.0) |
133 (63.9) |
73 (35.1) |
|
Avoided derogatory language |
2 (1.0) |
0 (0) |
0 (0) |
142 (68.3) |
64 (30.8) |
|
Maintained patient confidentiality |
1 (0.5) |
0 (0) |
1 (0.5) |
152 (73.1) |
54 (26.0) |
|
Used health resources appropriately |
4 (1.9) |
0 (0) |
1 (0.5) |
173 (83.2) |
30 (14.4) |
|
Demonstrated collegiality |
0 (0) |
0 (0) |
1 (0.5) |
134 (64.4) |
73 (35.1) |
Table 2. Distribution of score (n%) for the 208 P-MEX assessment forms received
|
P-MEX components |
Question from comparator instrument |
Hypothesis |
Spearman correlation |
Confirmation |
|
Doctor-patient relationship domain |
Responds to patient’s unique characteristics and needs equitably |
High (+) |
0.633* |
Yes |
|
Doctor-patient relationship domain |
Demonstrates care and concern for the patient/family |
High (+) |
0.580* |
Yes |
|
Doctor-patient relationship domain |
Communicates effectively with patient/family |
High (+) |
0.617* |
Yes |
|
Time management domain |
Accepts responsibility and follows through on tasks |
Moderate (+) |
0.472* |
Yes |
|
Inter-professional relationship domain |
Communicates and works effectively with other healthcare professionals |
High (+) |
0.498* |
No |
|
Global score |
Demonstrates integrity and ethical behaviour |
High (+) |
0.545* |
Yes |
*p<0.00833 as corrected using Bonferroni’s correction; (+) and (-) indicate the direction of correlations.
Table 3. Construct validity of the P-MEX
|
Item |
Factor 1 |
Factor 2 |
Uniqueness |
|
Listened actively to patients |
0.76 |
|
0.42 |
|
Showed interest in patients as a person |
0.62 |
|
0.61 |
|
Recognised and met patient needs |
0.72 |
|
0.47 |
|
Extended his/herself to meet patient needs |
0.66 |
|
0.56 |
|
Ensured continuity of patient care |
0.57 |
|
0.67 |
|
Advocated on behalf of a patient |
a |
|
0.82 |
|
Maintained appropriate boundaries |
0.56 |
|
0.68 |
|
Communicated effectively with patient |
0.74 |
|
0.45 |
|
Demonstrated awareness of limitations |
0.77 |
|
0.41 |
|
Admitted errors/omissions |
|
0.67 |
0.53 |
|
Solicited feedback |
|
0.55 |
0.62 |
|
Accepted feedback |
|
0.64 |
0.55 |
|
Maintained composure in a difficult situation |
a |
|
0.62 |
|
Was on time |
0.71 |
|
0.42 |
|
Completed tasks in a reliable fashion |
0.57 |
|
0.63 |
|
Was available to colleagues |
0.67 |
|
0.50 |
|
Maintained appropriate appearance |
0.77 |
|
0.37 |
|
Addressed own gaps in knowledge and skills |
0.53 |
|
0.57 |
|
Demonstrated respect for colleagues |
0.83 |
|
0.26 |
|
Avoided derogatory language |
0.62 |
|
0.59 |
|
Maintained patient confidentiality |
0.65 |
|
0.57 |
|
Used health resources appropriately |
a |
|
0.85 |
|
Demonstrated collegiality |
0.73 |
|
0.43 |
a represent loading <0 .5
Table 4. Factor loadings (pattern matrix) and unique variances of the P-MEX items in exploratory factor analysis
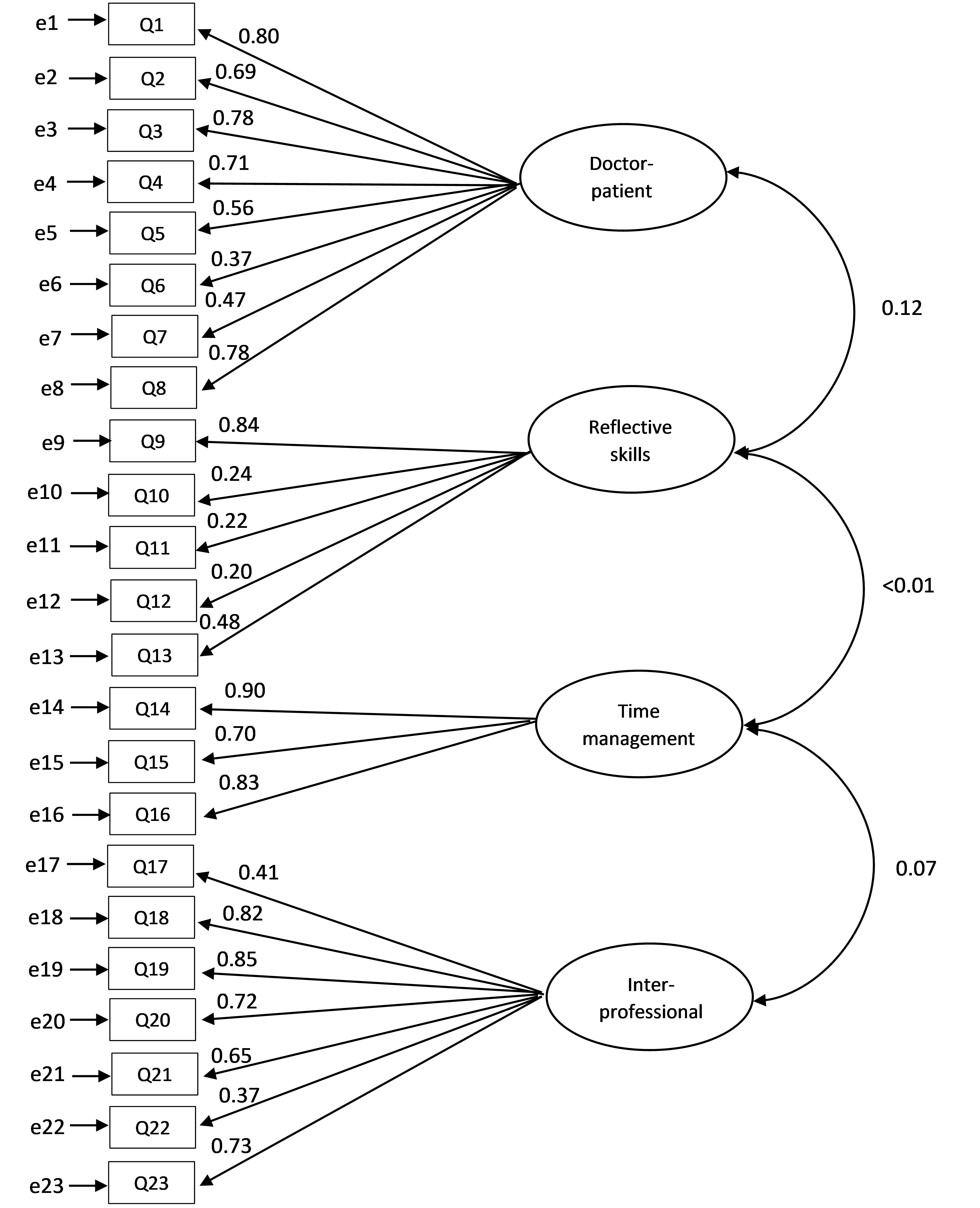
Figure 1. Confirmatory factor analysis (CFA) through structural equation modelling of the P-MEX. Latent variables are shown in ellipses, while observed variables are shown in rectangles. Directed arrows represent causal relationship among variables, while double-headed arrows represent correlations between variables. The numbers beside the arrows indicate the standard path coefficients.
IV. DISCUSSION
This study is the first to validate the psychometric properties of the Singapore version of P-MEX. The CDIs indicate that the Singapore version of P-MEX was generally deemed by faculty to be easy to understand, relevant and comprehensive. Feedback by assessors on the Singapore P-MEX were largely positive, with majority of assessors saying that the Singapore version of P-MEX was better than current assessment tools used in their respective programmes for the assessment of medical professionalism. The study also involved faculty and senior residents as assessors to reflect real-life situations that took place in the assessment of residents. This is important as 360-degree assessments and workplace-based assessments often involve both faculty and senior residents.
The four-factor CFA had a poor fit. Based on the EFA with a two-factor structure, three items (Advocated on behalf of a patient; Maintained composure in a difficult situation; Used health resources appropriately) had factor loadings less than 0.5, thus these 3 items could be removed in future assessments. Two of the items (Advocated on behalf of a patient; Used health resources appropriately) also did not reach consensus for either inclusion or exclusion into the questionnaire in a previous Delphi study (Fong et al., 2020). In the two-factor structure, factor 1 appeared to encompass “Patient care and inter-professional relationship skills” while factor 2 appeared to encompass “Reflective skills”. Previously, the structural validity of the four-factor model of the P-MEX has been supported in various studies (Tsugawa et al., 2011), and this divergence in structural validity observed in our sample may imply that the measure of medical professionalism may differ even among Asian countries. It might be beneficial for medical organisations with different cultural backgrounds to conduct a factor analysis with their data independently prior to use. The lack of fit to the four-factor structure could also be because psychometric properties of some items measured more than one latent construct. For example, while ‘Demonstrated awareness of limitations’ showed reflective skills, it could also be an important marker of appropriate patient care and inter-professional relationship, where the resident sought help from more experienced colleagues when needed. Items under time management, inter-professional relationship and doctor-patient relationship also came together to measure the same construct, which appeared to encompass “Patient care and inter-professional relationship skills”. With Singapore’s rapidly aging population, the rise in numbers of patients with chronic diseases and complex conditions warrant healthcare professionals across different specialties to work in multidisciplinary teams and contribute their unique expertise to improve the quality of patient care (Tan et al., 2021; Zheng et al., 2016). As such, items measuring time management, inter-professional relationship and doctor-patient relationship might overlap and be viewed as one entity instead of individual segments.
Our study had identified professional lapses in 6.3% of the residents. This was comparable to the study by Papadakis et al (Papadakis et al., 2008), where 4.8% of the residents were noted to have low professionalism ratings in their assessments across all years of residency training. This was also consistent with the overall incidence of unprofessional behaviour that has been flagged up by faculty in disciplinary meetings, ranging between 1% to 3% of the cohort of residents from 2015 to 2019 (unpublished data). Also, only 13 cases (4.1%) of Singapore Medical Council (SMC) disciplinary tribunals involved junior doctors from 1979 to 2017 (Norman et al., 2021).
Medical unprofessionalism may be associated with suboptimal patient care. Therefore it is imperative for healthcare organizations to invest in efforts to improve medical professionalism. There is currently no validated instrument to assess medical professionalism in residency programmes in Singapore. The Singapore version of P-MEX validated in this study may be useful to bridge this gap, and allows provision of feedback to residents for improvement in medical professionalism (Hawkins et al., 2009). Assessment may also help to measure the effectiveness of educational programs that aim to instil medical professionalism (Hawkins et al., 2009), which are increasingly common in medical education (Lee et al., 2007; Macneill et al., 2020).
This study has several limitations. Firstly, we were unable to determine the reproducibility of the average score of the residents using the Singapore version of P-MEX by the generalisability theory as the IRB did not allow for any identifiers to be collected. Therefore, we were unable to track the residents assessed. Future studies will need to be performed to determine the number of evaluations needed to obtain a satisfactory dependability coefficient for the Singapore version of P-MEX. Secondly, as we did not collect data after remediation on medical professionalism, we were unable to determine the responsiveness of the Singapore version of P-MEX to remediation in our population. Thirdly, the participants in the CDIs and cross-sectional study were recruited using convenience sampling and the participants were mainly from medical disciplines. Coupled with the possibility that faculty members who are more interested in medical professionalism may be more likely to participate, this could skew the results because the sample may not be representative of the entire faculty and resident population. Moreover, the narrow distribution of the P-MEX scores has a halo effect on all items which limits variability and co-variability. However, the concentration of the P-MEX scores near the ceiling suggests that the most of the participants are professional, which is supported by previous study (Papadakis et al., 2008). Lastly, we used the same sample for CFA and EFA due to the small sample size, which may lead to overfitting. Future research should consider larger and more diverse samples involving more specialties to improve generalizability and robustness of results.
V. CONCLUSION
This study supports the content validity, construct validity, internal consistency and feasibility of the Singapore version of P-MEX in assessing medical professionalism in the local residency training programme. However, this study did not provide conclusive support for the original four-factor model of the P-MEX, and the EFA identified 2 main factors in our sample, which appeared to encompass “Patient care and inter-professional relationship skills” and “Reflective skills”. Future research should examine the structural validity of the P-MEX in different samples of medical trainees. Medical educators in the region with similar multi-cultural backgrounds can consider using the Singapore version of P-MEX to assess medical professionalism among trainees.
Notes on Contributors
WF, YHK, SWY conceptualised the study design, and drafted the survey questionnaire. WF, YHK and JKP acquired the data. WF, YHK, SWY and JKP wrote the initial manuscript draft. All authors critically reviewed and approved the final manuscript.
Ethical Approval
The SingHealth Centralised Institutional Review Board approved this study (Reference Number: 2016/3009 and 2019/2431).
Data Availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request. Data is not deposited in repository due to privacy concerns.
Acknowledgement
The authors thank all the participants for their time and contribution to the study.
Funding
This research was supported by SingHealth Duke-NUS Medicine Academic Clinical Programme Education Support Programme Grant (Ref No: 03/FY2017/P2/03-A47). Funder was not involved in the design, delivery or submission of the research.
Declaration of Interest
The authors declare that they have no competing interests.
References
Amirhajlou, L., Bidari, A., Alipour, F., Yaseri, M., Vaziri, S., Rezai, M., Tavakoli, N., Farsi, D., Yasinzadeh, A. R., Mosaddegh, R., & Hashemi, A. (2019). Validity, reliability and acceptability of Professionalism Mini-Evaluation Exercise (P-MEX) for emergency medicine residency training. Journal of Medical Ethics and History of Medicine, 12. https://doi.org/10.18502/jmehm.v12i12.1641
Arifin, W. N., & Yusoff, M. S. B. (2016). Confirmatory factor analysis of the Universiti Sains Malaysia emotional quotient inventory among medical students in Malaysia. Sage Open, 6(2), 2158244016650240. https://doi.org/10.1177/2158244016650240
Arrighi, J. A., Lewis, L. C., & Nasca, T. J. (2024). The Role of ACGME International in enhancing opportunities of residents for advanced subspecialty training. Journal of Graduate Medical Education, 16(2), 237-240. https://doi.org/10.4300/jgme-d-24-00150.1
Bajwa, N. M., Nendaz, M. R., Posfay-Barbe, K. M., Yudkowsky, R., & Park, Y. S. (2021). A meaningful and actionable professionalism assessment: Validity evidence for the Professionalism Mini-Evaluation Exercise (P-MEX) across 8 years. Academic Medicine, 96(11S), S151-S157. https://doi.org/10.1097/ACM.0000000000004286
Chandratilake, M., McAleer, S., & Gibson, J. (2012). Cultural similarities and differences in medical professionalism: A multi‐region study. Medical Education, 46(3), 257-266. https://doi.org/10.1111/j.1365-2923.2011.04153.x
Cohen, J. (2016). A power primer. https://doi.org/10.1037/14805-018
Cole, J. C., Motivala, S. J., Khanna, D., Lee, J. Y., Paulus, H. E., & Irwin, M. R. (2005). Validation of single‐factor structure and scoring protocol for the Health Assessment Questionnaire‐Disability Index. Arthritis Care & Research: Official Journal of the American College of Rheumatology, 53(4), 536-542. https://doi.org/10.1002/art.21325
Cruess, R., McIlroy, J. H., Cruess, S., Ginsburg, S., & Steinert, Y. (2006). The professionalism mini-evaluation exercise: A preliminary investigation. Academic Medicine, 81(10), S74-S78.
Cruess, R. L., & Cruess, S. R. (2006). Teaching professionalism: General principles. Medical Teacher, 28(3), 205-208. https://doi.org/10.1080/01421590600643653
Cruess, R. L., Cruess, S. R., Boudreau, J. D., Snell, L., & Steinert, Y. (2015). A schematic representation of the professional identity formation and socialization of medical students and residents: A guide for medical educators. Academic Medicine, 90(6), 718-725. https://doi.org/10.1097/ACM.0000000000000700
Cruess, S. R., Cruess, R. L., & Steinert, Y. (2010). Teaching professionalism across cultural and national borders: Lessons learned from an AMEE workshop. Medical Teacher, 32(5), 371-374. https://doi.org/10.3109/01421591003692730
Cruess, S. R., Cruess, R. L., & Steinert, Y. (2019). Supporting the development of a professional identity: General principles. Medical Teacher, 41(6), 641-649. https://doi.org/10.1080/0142159X.2018.1536260
Curtin, F., & Schulz, P. (1998). Multiple correlations and Bonferroni’s correction. Biological Psychiatry, 44(8), 775-777. https://doi.org/10.1016/S0006-3223(98)00043-2
Fong, W., Kwan, Y. H., Yoon, S., Phang, J. K., Thumboo, J., Leung, Y. Y., & Ng, S. C. (2020). Assessment of medical professionalism using the Professionalism Mini Evaluation Exercise (P-MEX) in a multi-ethnic society: A Delphi study. BMC Medical Education, 20, 1-9. https://doi.org/10.1186/s12909-020-02147-9
Guerrasio, J., Garrity, M. J., & Aagaard, E. M. (2014). Learner deficits and academic outcomes of medical students, residents, fellows, and attending physicians referred to a remediation program, 2006–2012. Academic Medicine, 89(2), 352-358. https://doi.org/10.1097/ACM.0000000000000122
Hawkins, R. E., Katsufrakis, P. J., Holtman, M. C., & Clauser, B. E. (2009). Assessment of medical professionalism: Who, what, when, where, how, and… why? Medical Teacher, 31(4), 348-361. https://doi.org/10.1080/01421590902887404
Ho, M. J., Yu, K. H., Hirsh, D., Huang, T. S., & Yang, P. C. (2011). Does one size fit all? Building a framework for medical professionalism. Academic Medicine, 86(11), 1407-1414. https://doi.org/10.1097/ACM.0b013e31823059d1
Ho, M. J., Yu, K. H., Pan, H., Norris, J. L., Liang, Y. S., Li, J. N., & Hirsh, D. (2014). A tale of two cities: Understanding the differences in medical professionalism between two Chinese cultural contexts. Academic Medicine, 89(6), 944-950. https://doi.org/10.1097/ACM.0000000000000240
Hodges, B. D., Ginsburg, S., Cruess, R., Cruess, S., Delport, R., Hafferty, F., Ho, M. J., Holmboe, E., Holtman, M., Ohbu, S., Rees, C., Cate, O. T., Tsugawa, Y., Mook, W.V., Wilkinson, T., & Wade, W. (2011). Assessment of professionalism: Recommendations from the Ottawa 2010 Conference. Medical Teacher, 33(5), 354-363. https://doi.org/10.3109/0142159X.2011.577300
Karukivi, M., Kortekangas-Savolainen, O., Saxén, U., & Haapasalo-Pesu, K. M. (2015). Professionalism Mini-Evaluation Exercise in Finland: A preliminary investigation introducing the Finnish version of the P-MEX instrument. Journal of Advances in Medical Education & Professionalism, 3(4), 154.
Kwan, Y. H., Png, K., Phang, J. K., Leung, Y. Y., Goh, H., Seah, Y., Thumboo, J., Ng, S. C., Fong, W., & Lie, D. (2018). A systematic review of the quality and utility of observer-based instruments for assessing medical professionalism. Journal of Graduate Medical Education, 10(6), 629-638. https://doi.org/10.4300/JGME-D-18-00086.1
Lee, A. G., Beaver, H. A., Boldt, H. C., Olson, R., Oetting, T. A., Abramoff, M., & Carter, K. (2007). Teaching and assessing professionalism in ophthalmology residency training programs. Survey of Ophthalmology, 52(3), 300-314. https://doi.org/10.1016/j.survophthal.2007.02.003
Lumlertgul, N., Kijpaisalratana, N., Pityaratstian, N., & Wangsaturaka, D. (2009). Cinemeducation: A pilot student project using movies to help students learn medical professionalism. Medical Teacher, 31(7), e327-e332. https://doi.org/10.1080/01421590802637941
Macneill, P., Joseph, R., Lysaght, T., Samarasekera, D. D., & Hooi, S. C. (2020). A professionalism program in medical education and training – From broad values to specific applications: YLL School of Medicine, Singapore. Medical Teacher, 42(5), 561-571. https://doi.org/10.1080/0142159X.2020.1714021
Miller, G. E. (1990). The assessment of clinical skills/competence/performance. Academic Medicine, 65(9), S63-67.
Mokkink, L. B., De Vet, H. C., Prinsen, C. A., Patrick, D. L., Alonso, J., Bouter, L. M., & Terwee, C. B. (2018). COSMIN risk of bias checklist for systematic reviews of patient-reported outcome measures. Quality of Life Research, 27, 1171-1179. https://doi.org/10.1007/s11136-017-1765-4
Noor, N. M., & Leong, C.-H. (2013). Multiculturalism in Malaysia and Singapore: Contesting models. International Journal of Intercultural Relations, 37(6), 714-726. https://doi.org/10.1016/j.ijintrel.2013.09.009
Norman, N. B. M., Soo, J. M. P., Lam, M. Y. K., & Thirumoorthy, T. (2021). Unprofessional behaviour of junior doctors: A retrospective analysis of outcomes by the Singapore Medical Council disciplinary tribunals. Singapore Medical Journal, 62(3), 120. https://doi.org/10.11622/smedj.2020021
Papadakis, M. A., Arnold, G. K., Blank, L. L., Holmboe, E. S., & Lipner, R. S. (2008). Performance during internal medicine residency training and subsequent disciplinary action by state licensing boards. Annals of Internal Medicine, 148(11), 869-876. https://doi.org/10.7326/0003-4819-148-11-200806030-00009
Prinsen, C. A., Mokkink, L. B., Bouter, L. M., Alonso, J., Patrick, D. L., De Vet, H. C., & Terwee, C. B. (2018). COSMIN guideline for systematic reviews of patient-reported outcome measures. Quality of Life Research, 27, 1147-1157. https://doi.org/10.1007/s11136-018-1798-3
SingHealth. (2024). Why SingHealth Residency.
Swick, H. M., Szenas, P., Danoff, D., & Whitcomb, M. E. (1999). Teaching professionalism in undergraduate medical education. Jama, 282(9), 830-832. https://doi.org/10.1001/jama.282.9.830
Swing, S. R. (2007). The ACGME outcome project: Retrospective and prospective. Medical Teacher, 29(7), 648-654. https://doi.org/10.1080/01421590701392903
Tan, C. C., Lam, C. S., Matchar, D. B., Zee, Y. K., & Wong, J. E. (2021). Singapore’s health-care system: Key features, challenges, and shifts. The Lancet, 398(10305), 1091-1104.
Taşçı, A. İ., Akdeniz, E., Gülpınar, M. A., Danacıoğlu, Y. O., Sarı, E. E., Yaşar, L., Karandere, F., & Ferahman, S. (2023). Adaptation of the professionalism mini-evaluation exercise instrument into Turkish: A validity and reliability study. BMC Medical Education, 23(1), 698. https://doi.org/10.1186/s12909-023-04675-6
Tsugawa, Y., Ohbu, S., Cruess, R., Cruess, S., Okubo, T., Takahashi, O., Tokuda, Y., Heist, B., Bito, S., Itoh, T., Aoki, A., Chiba, T., & Fukui, T. (2011). Introducing the Professionalism Mini-Evaluation Exercise (P-MEX) in Japan: Results from a multicenter, cross-sectional study. Academic Medicine, 86(8), 1026-1031. https://doi.org/10.1097/ACM.0b013e3182222ba0
Tsugawa, Y., Tokuda, Y., Ohbu, S., Okubo, T., Cruess, R., Cruess, S., Ohde, S., Okada, S., Hayashida, N., & Fukui, T. (2009). Professionalism mini‐evaluation exercise for medical residents in Japan: A pilot study. Medical Education, 43(10), 968-978. https://doi.org/10.1111/j.1365-2923.2009.03437.x
Zbieranowski, I., Takahashi, S. G., Verma, S., & Spadafora, S. M. (2013). Remediation of residents in difficulty: A retrospective 10-year review of the experience of a postgraduate board of examiners. Academic Medicine, 88(1), 111-116. https://doi.org/10.1097/ACM.0b013e3182764cb6
Zheng, R. M., Sim, Y. F., & Koh, G. C.-H. (2016). Attitudes towards interprofessional collaboration among primary care physicians and nurses in Singapore. Journal of Interprofessional Care, 30(4), 505-511. https://doi.org/10.3109/13561820.2016.1160039
*Warren Fong
Academia, Level 4, 20 College Road, Singapore 169856
Email: gmsfwsw@nus.edu.sg
Submitted: 31 January 2025
Accepted: 16 June 2025
Published online: 6 January, TAPS 2026, 11(1), 74-78
https://doi.org/10.29060/TAPS.2026-11-1/SC3658
Astrid Pratidina Susilo1, Ervin Dyah Ayu Masita Dewi1, Satrio Utomo2 & Jasmine Aulia Sabrina2
1Department of Medical Education and Bioethics, Faculty of Medicine, Universitas Surabaya, Indonesia; 2Bachelor Program of Medical Education, Faculty of Medicine, Universitas Surabaya, Indonesia
Abstract
Introduction: Limited resources have caused many challenges in health care. Health workers faced dilemmas that potentially cause burnout. Medical students must be strengthened with resilience when facing dilemmas. This study aimed to investigate Indonesian students’ strategies for strengthening resilience after participating in a bioethics workshop based on reflective and collaborative principles.
Methods: A bioethics workshop based on reflective and collaborative principles without didactic elements was conducted with 30 medical students. We collected quantitative data from the Adapted Version of the Adult Personal Resilience Questionnaire and qualitative data from the students’ reflections on strategies to strengthen resilience. Descriptive statistics and thematic analysis were used to analyse the quantitative and qualitative data, respectively.
Results: Thirty students participated in the study. The total score of the resilience questionnaire was 4.28 (SD 0.39), indicating that the students perceived themselves as having a moderate-to-high level of resilience for all items. The following four themes from the qualitative analysis were identified: faith, adaptation, self-management, and relationships.
Conclusion: Indonesian students’ strategies for strengthening resilience are related to faith, adaptation, self-management, and relationships. Although without a didactic approach, the reflective and collaborative learning in this workshop can raise medical students’ awareness of strategies for building resilience and provided an opportunity for students to reflect on their resilience level.
Keywords: Resilience, Reflective Learning, Collaborative Learning, Self-Management, Relationships, Faith, Mixed-Method Approach
I. INTRODUCTION
During the corona virus disease 2019 (COVID-19) pandemic, many healthcare professionals worldwide experienced burnout for several reasons, such as a high workload, fear of getting infected, and passing on the infection to family members. They also faced ethical dilemmas, were compelled to make challenging decisions about which patients to focus on during resource scarcity, and experienced hopelessness about not being able to help all the patients. They had to “play God without God’s power,” determine who could be admitted for care, and who had to be left behind. Previous studies have shown that the situation was overwhelming, and healthcare professionals were unprepared to face it (Ningrum & Missel, 2023).
Beyond the COVID-19 pandemic, healthcare resource scarcity is a reality that healthcare professionals frequently encounter. Therefore, it is essential to prepare future healthcare professionals to be able to decide on resource allocation during resource scarcity and build their resilience to face unpredictable situations (Dewi et al., 2023). Resilience refers to one’s ability to “spring back into shape,” that is, recover quickly from challenges by using a positive coping mechanism. Resilience is multidimensional and can be learned. Nurturing resilience is more than a mere one-point process. It is a longitudinal process that requires practice and perseverance (Calo et al., 2024).
Most resilience education includes didactic content that introduces theories and strategies related to resilience, such as mindfulness or meditation practices (Calo et al., 2024).As students naturally have coping mechanisms and can learn from each other, we developed a workshop to raise awareness of resilience based on reflective (Calo et al., 2024) and collaborative learning principles (Yang, 2023). We asked the students to complete a questionnaire to reflect on their resilience levels and subsequently engage in discussions with peers. To investigate whether this educational approach can raise students’ awareness of resilience, we explored the students’ key takeaways from this workshop using the following research question: what are the students’ strategies to strengthen resilience after attending a workshop based on reflective and collaborative principles?
II. METHODS
This study was conducted in a private medical school in East Java, Indonesia. We developed a one-day bioethics workshop tailored to address the gaps highlighted by previous study (Dewi et al., 2023) with three objectives. First, we aimed to improve students’ decision-making skills in ethical decisions. Second, we introduced the communication skills necessary to discuss with patients and their families. Third, we attempted to raise students’ awareness of developing resilience. This study focuses on the third objective. The participants were third- and fourth-year pre-clinical phase medical students who were selected using a random sampling approach. Although they have not yet experienced significant real-patient encounters, they had a basic understanding of bioethics and doctor-patient communication skills, while modules on resilience were not yet included in the curriculum. All participants were informed about the study goals and procedures and signed written consent forms.
During the session on resilience, which lasted one hour, the students engaged in several activities. They reflected on their resilience levels by completing a questionnaire. This activity was based on the principle of reflective learning. Subsequently, considering the ethical dilemma of resource scarcity, the students discussed in pairs how to mitigate burnout due to such a dilemmatic situation and how to strengthen their resilience. The method was based on the collaborative learning principle. Finally, the students shared their strategies to strengthen their resilience as medical students.
We collected the quantitative and qualitative data from the questionnaire and students’ reflections, respectively. This study used the Adapted Version of Adult Personal Resilience Questionnaire, translated to Indonesian, and used in a study to explore physicians’ resilience in remote areas (Handoyo et al., 2021). The questionnaire had a 5-point Likert scale (1=strongly disagree, 2=disagree, 3=neutral, 4=agree, 5=strongly agree). We modified the Indonesian version and validated the content with three experts (two medical educationalists and one psychiatrist). The experts scored the relevance of each item to measure resilience (1=highly irrelevant, 2=irrelevant, 3=relevant, and 4=highly relevant). Only those items for which all experts scored 4 were included. The final questionnaire consisted of 19 items, with a Cronbach’s alpha of 0.848. Data from the questionnaire were descriptively analysed using SPSS 26 while the qualitative data were analysed using a thematic analysis approach. Two researchers independently coded and developed themes and discussed them until a consensus was achieved.
III. RESULTS
Thirty students (11 male and 19 female) participated in the study. The total score of the resilience questionnaire was 4.28 (SD 0.39), indicating that the students perceived themselves as having a moderate-to-high level of resilience for all items.
|
No. |
Item |
Mean |
Standard Deviation (SD) |
|
Determination |
|||
|
1 |
Once I set a goal, I am determined to achieve it. |
4.10 |
0.89 |
|
2 |
I persevere at the things I decide, despite difficulties. |
4.27 |
0.69 |
|
3 |
Being determined is an important part of my character. |
4.23 |
0.86 |
|
4 |
I keep trying for the things I want until I reach them. |
4.37 |
0.62 |
|
|
Subtotal |
4.24 |
0.54 |
|
Endurance |
|||
|
5 |
I am able to live through difficult times |
4.23 |
0.77 |
|
6 |
I can withstand difficult situations. |
4.30 |
0.84 |
|
7 |
I can endure the problems that life brings. |
4.23 |
0.86 |
|
8 |
I can endure even when I am attacked |
4.00 |
0.87 |
|
|
Subtotal |
4.19 |
0.69 |
|
Adaptability |
|||
|
9 |
I have the ability to adapt to difficult situations. |
3.73 |
1.02 |
|
10 |
I can change to fit into many kinds of circumstances |
3.90 |
0.80 |
|
11 |
I can find ways to adapt to unexpected conditions. |
3.97 |
0.62 |
|
|
Subtotal |
3.87 |
0.67 |
|
Recuperability |
|||
|
12 |
I recover from any misfortune that happens to me. |
3.93 |
0.74 |
|
13 |
I am able to bounce back from any kind of adversity. |
3.93 |
0.74 |
|
14 |
I can recover from any type of problem. |
3.97 |
1.00 |
|
|
Subtotal |
3.94 |
0.66 |
|
Life Calling |
|||
|
15 |
I believe that God has a purpose in placing me here. |
4.80 |
0.48 |
|
16 |
God has always guided me through my life. |
4.73 |
0.58 |
|
17 |
God would never allow me to walk through life alone. |
4.77 |
0.68 |
|
18 |
Even in difficult situations, God has been there to guide me. |
4.83 |
0.46 |
|
19 |
I believe that God is ever-present, in everything I do |
4.93 |
0.25 |
|
|
Subtotal |
4.81 |
0.36 |
|
Total |
4.28 |
0.39 |
Table 1. Participants’ Resilience as Measured in the Adapted Version of the Adult Personal Resilience Questionnaire
Four themes emerged from the qualitative analysis: faith, adaptation, self-management, and relationships. Each theme was described and relevant examples of quotes to illustrate them are provided below.
A. Faith
The participants implied that resilience was related to their faith in God. They believed that God would not give them a “test” that was more difficult than their ability to handle it. The importance of believing that God will give the strength to deal with every problem was strongly emphasised. Additionally, the participants mentioned striving to be “Ikhlas” (sincere) and repeatedly accepting their reality as strategies to improve resilience. For example, Student 3 wrote, “I will accept the reality and handle every situation with sincerity.”
B. Adaptation
Participants believed that they could increase their resilience through ongoing practice. Thus, self-motivation and self-confidence were essential factors. They mentioned strategies, such as stepping out of their comfort zones, trying new things, and improving their perseverance and recoverability. For instance, Student 25 mentioned “Practice to challenge oneself toward change” as a strategy for resilience.
C. Self-Management
Participants reported that self-management is important in achieving resilience. They need to understand their limits as well as learn how to manage stress, emotions, and time. Students also mentioned meditation, journal writing, and rest as self-management strategies that improved resilience. They argued that a balance between logic and feelings increases one’s resilience.
D. Relationship
Students were aware of the fact that they need friends and colleagues to share, collaborate with, and make decisions. They need to have friends with a positive attitude, surround themselves with individuals with a positive outlook, and participate in volunteering activities. Student 8 shared, “Do not push yourself; try to share your problems with your friends.”
IV. DISCUSSION
The study findings revealed that the workshop based on reflective and collaborative learning principles can raise students’ awareness of effective strategies to strengthen their resilience. Two themes were in line with the constructs in the questionnaire: “faith” and “adaptation”. “Faith” is a fairly similar concept to “life calling” while “adaption” reflected other subscales in the questionnaire, such as “determination” and “recuperability” (Handoyo et al., 2021). This resemblance suggested that students were inspired when they reflected on the questionnaire in which they scored themselves on a relatively high scale of 3 or above for all items. The reflection process exposed them to the concept of resilience.
However, “self-management” and “relationships” were not reflected in the questionnaire responses, but found in pair discussions and personal reflections. Beyond what they learned while completing the questionnaire, the students gained new ideas through discussions with their peers. Collaborative learning raised the students’ awareness, as they learned from each other’s perspectives during the discussion (Yang, 2023).
Overall, the students’ ideas were in line with the findings of previous research on strengthening resilience (Calo et al., 2024) and covered diverse aspects. In their writing, they could indicate the dynamics of the strengthening resilience through internal adaptation, relationships with others, and views from a faith perspective. “Adaptation” and “self-management” reflected the strategies for improving resilience which comes from within. The “relationship” aspect suggested the students’ need for other people in their lives as a critical support system in strengthening resilience. Finally, “faith” showed that the students viewed God’s influence as essential for nurturing resilience.
This study has certain limitations. First, the workshop focusing on resilience was short (only one hour) as it was embedded in a larger workshop aimed at enhancing the students’ decision-making skills in ethical dilemmas. A longitudinal workshop may yield different results. Second, the qualitative data were based on the students’ writing, which was influenced by their ability to express themselves. Interviews may have yielded different results.
Despite this constraint, the findings showed that a workshop based on reflective and collaborative learning, without a didactic approach, could raise medical students’ awareness of strategies to build resilience. This finding is important in providing alternative strategies to strengthen resilience in medical education, particularly when time is constrained. Future studies need to explore the transfer of learning, that is, to what extent students apply what they are aware of in actual practice and how it can improve their resilience levels. Additionally, it is essential to examine whether improved awareness of resilience will enhance medical students’ abilities to face ethical dilemmas in future clinical practice.
V. CONCLUSION
Although without a lecture, a workshop based on reflective and collaborative learning could raise medical students’ awareness of strategies to build resilience. Students’ have ideas of strategies which fall into four categories: faith, adaptation, self-management, and relationship.
Notes on Contributors
Astrid Pratidina Susilo conceptualised the study, organised the workshop, collected and analysed the data, and drafted the manuscript.
Ervin Dyah Ayu Masita Dewi conceptualised the study, organised the workshop, analysed the data, and drafted the manuscript.
Satrio Utomo organised the workshop, collected the data, and reviewed the manuscript.
Jasmine Aulia Sabrina organised the workshop, collected the data, and reviewed the manuscript.
Ethical Approval
Ethical approval was obtained from the University Surabaya Ethical Committee (approval no.297/KE/I/2024).
Data Availability
Data were in Indonesian and can be made available upon personal request.
Acknowledgement
We would to thank all the students who participated in the workshops and the experts who validated the questionnaire. We would like to thank Editage (www.editage.com) for English language editing.
Funding
This study was supported by a research grant from the Universitas Surabaya (N0.165/SP-Lit/LPPM-01/Int/FK/XI/2023).
Declaration of Interest
The authors declare no conflicts of interest.
References
Calo, M., Judd, B., & Peiris, C. (2024). Grit, resilience and growth-mindset interventions in health professional students: A systematic review and meta-analysis. Medical Education, 58(8), 902–919. https://doi.org/10.1111/medu.15391
Dewi, E. D. A. M., Matter, L., Susilo, A. P., & Krumeich, A. (2023). A qualitative study on patients’ selection in the scarcity of resources in the COVID-19 pandemic in a communal culture. Developing World Bioethics, 10, 84–92. https://doi.org/10.1111/dewb.12438
Handoyo, N. E., Rahayu, G. R., Claramita, M., Keraf, M. K. P. A., Octrisdey, K., Yuniarti, K. W., Ash, J., & Schuwirth, L. (2021). Developing personal resilience questionnaire for rural doctors: An indigenous approach study in Indonesia. BMC Psychology, 9(158). https://doi.org/10.1186/s40359-021-00666-8
Ningrum, A. P., & Missel, M. (2023). Urip iku urup (life is lit) by service to others: A qualitative study of frontline healthcare workers’ lived experiences providing patient care in Indonesia’s COVID-19-designated hospital. BMC Health Services Research, 23(262). https://doi.org/10.1186/s12913-023-09257-2
Yang, X. (2023). A historical review of collaborative learning and cooperative learning. TechTrends, 67(4), 718–728. https://doi.org/10.1007/s11528-022-00823-9
*Ervin Dyah Ayu Masita Dewi
Faculty of Medicine, Universitas Surabaya
Jalan Raya Kalirungkut, Surabaya,
60293, Indonesia
+62-85865256147
Email: ervin_dyah@staff.ubaya.ac.id
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
