
An online programme in teaching and assessing critical thinking for medical faculty

Submitted: 4 October 2022
Accepted: 5 December 2022
Published online: 4 April, TAPS 2023, 8(2), 66-69
https://doi.org/10.29060/TAPS.2023-8-2/SC2894
Simon Field1, Pat Croskerry2, Susan Love3, & Peggy Alexiadis Brown4
1Undergraduate Medical Education and Emergency Medicine, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 2Critical Thinking Program, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 3Faculty Development, Continuing Professional Development, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 4Dalhousie Medicine New Brunswick, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada
Abstract
Introduction: For all clinical providers in healthcare, decision-making is a critical feature of everything they do. Every day physicians engage in clinical decision-making where knowledge, evidence, experience, and interpretation of clinical data are used to produce decisions, yet, it is fair to say that most do not have an explicit insight or understanding of this complex process. In particular, few will have training in teaching and assessing the cognitive and affective factors that underlie clinical decision-making.
Methods: To foster an increased awareness and understanding of these factors, the Dalhousie Critical Thinking Program was established with the mandate to develop and deliver curriculum for critical thinking in the 4-year undergraduate program. To assist teaching faculty with the goal and objectives of the program, the Teaching and Assessing Critical Thinking Program (TACT) was introduced.
Results: Using the dual process model as a platform for decision-making, this program introduces general principles of critical thinking and provides tools to teach learners how to strengthen their critical thinking skills. To offer flexible learning, an online approach was chosen for delivery of the program.
Conclusion: To date, we have offered eleven iterations of Part 1 to a total of 261 participants and six iterations of Part 2 to a total of 89 participants. Evaluations show the online approach to content delivery was well received and the content to be of practical use.
Keywords: Critical Thinking, Clinical Decision-Making, Faculty Development, Asynchronous Learning
I. INTRODUCTION
This paper provides a review of a two-part Teaching and Assessing Critical Thinking (TACT) program which was developed to help faculty understand vulnerability to bias and the role of metacognitive processes in clinical decision-making. The objective of the TACT program is to better prepare faculty to teach learners these important skills. In this paper, we describe how it was implemented, how participants perceived the program, and what changes were needed to address this important hidden ‘soft’ skill within the clinical setting.
II. METHODS
Physicians are constantly required to interpret information when they interact with patients, communicate with colleagues, review medical histories and laboratory reports, conduct physical exams, review the medical literature, and attend rounds. All of these clinical activities demand a sustained level of accuracy, clarity, and especially rationality. Critical thinking (CT) does not guarantee rationality but is one of its more important features and is essential for the role of physician.
Reliable and accurate diagnosis is the barometer of good clinical decision-making and will have a direct impact on treatment outcomes and patient safety. One in 20 (or roughly 12 million) American adult outpatients are affected by diagnostic errors every year. The overall number of fatalities associated with diagnostic failure is not known, but it is estimated that 40,000 – 80,000 deaths occur annually in hospitalised patients in the USA due to diagnostic failure.
A number of studies have shown that training in the development of CT skills in undergraduate students is effective. (Abrami et al., 2015) However, given that most faculty in medical schools today will not have had explicit CT training, specific initiatives in teaching it seem appropriate, not only for the faculty themselves but, importantly, for the students they teach.
To better prepare learners, Dalhousie’s Faculty of Medicine established the Critical Thinking Program in 2012. The program incorporated principles from the Foundation for Critical Thinking into a general model of clinical reasoning (Croskerry, 2018). The Dalhousie critical thinking curriculum reflects a consensus in the current medical literature that the dual process model (System 1 and System 2) is the most appropriate platform for reviewing the clinical decision-making process (See Figure 1).
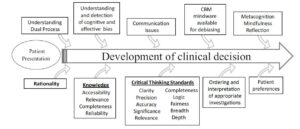
Figure 1. The Dalhousie University model for clinical decision making. (Reproduced with Permission)
A key component in the delivery of this curriculum is helping faculty develop the skills they will need to teach and mentor critical thinking in the clinical environment. Most educators have limited understanding of the advances in medical decision-making and how to best teach critical thinking and clinical reasoning.
The TACT Program comprises two distinct courses: TACT 1 and TACT 2. The program is structured to develop a sound knowledge of critical thinking principles in TACT 1, followed by a focus on teaching and learning in TACT 2. TACT 1 centres on three main themes: How Physicians Make Decisions, Cognitive and Affective Biases, and Cognitive Debiasing Strategies. TACT 2 centres on two main themes: Fundamentals of Medical Education and Strategies for Teaching and Assessing CT. In TACT 2, participants choose one of four elective options: Evidence Based Medicine, Competency Based Medical Education, Medical Humanities, or Curriculum Development.
The TACT Program uses an asynchronous online approach to reach Dalhousie faculty who are distributed across the Canadian Maritime Provinces. This approach mediates potential barriers for participation such as distance and time constraints and allows for individualised learning experiences while building an interactive online community of practice experience (Cook & Steinert, 2013). We use a combination of curricular tools including online didactic lectures, independent study activities, webinars, and discussion boards.
To date (Winter 2022), we have held 11 iterations of TACT 1 and 6 iterations of TACT 2, with 163 of 261 participants completing TACT 1 and 78 of 89 registrants completing TACT 2.
Of those who completed TACT 1, 55 % went on to enrol in TACT 2.
We initially developed the TACT Program for Dalhousie faculty (primarily physicians); however, due to growing interest in the topic, we have opened enrolment to include participants from around the world, including the United States, Mexico, United Kingdom, Australia, New Zealand, Turkey and Brazil. We also opened enrolment to participants from a variety of health professions and other fields of study. By opening the program to participants with diverse backgrounds in practice and location we have increased the diversity of perspectives and the richness of reflections posted to the discussion boards.
Prior to starting the TACT Program, we asked participants to complete a survey measuring their current knowledge of teaching and assessing CT, and motivation for taking the course.
Participants reported little satisfaction with previous knowledge in CT (Mean: 2.67 ± 0.84 on a Likert Scale of 1 (not at all satisfied) to 5 (very satisfied)). The following themes were identified as motivators for taking the TACT Program — a desire to: learn, improve clinical reasoning by increasing knowledge, understand the impact of critical thinking, provide better clinical care, decrease diagnostic error, and become a better educator.
We administered a summative evaluation following both TACT 1 and TACT 2. For TACT 1, 75% (121/162) completed the final evaluation and for TACT 2, 90% (63/70). In the summative evaluation, we asked participants to rate their course in a number of areas from course delivery to the effectiveness of increasing their knowledge and comfort in teaching critical thinking. Consent to data collection was implied as part of the administration of the evaluation. We found that participants were very satisfied with delivery methods.
III. RESULTS
A. What Did We Learn about the Participants?
All participants taking the TACT Program shared a similar motivation: the intent to improve their critical thinking skills and to teaching others. Steinert et al. (2002) found that faculty are more likely to enrol in an online program if they believe it would meet a perceived need. Our participants identified a desire to improve their own practice, confidence and awareness, to make the unconscious conscious, and to develop the language to name, identify and act on cognitive biases and those circumstances that create biases. This enabled them to better teach and mentor CT.
Participants also identified the value of communicating with others who offered a different perspective on clinical work and life experiences.
Physicians may not readily share/disclose mistakes they make in the clinical setting. In medical training environments, overconfidence and reluctance to admit mistakes are often the norm, which may work against fostering a culture of reflection (Brezis et al., 2016). Due to the confidentiality of the discussion boards, our participants could freely reflect on what factors contribute to errors they have made/seen and share those lessons with peers without fear of loss of reputation and embarrassment.
B. What Did We Learn about the Delivery?
We found that the online delivery was successful in reaching a broad base of participants. Some participants appreciated the mode of delivery as well.
A benefit of online courses is the ease with which faculty can control their pace of instruction. When asked, we found that 97.4% of respondents identified they would do more faculty development programs online.
When we reviewed the online tracking statistics, we found that our participants were accessing materials at all hours. Participants, each with their own learning style, appreciated the mix of interactivity and self-study the online format offered.
IV. DISCUSSION
Ideally, we would like to know how effectively participants in the TACT program incorporated the teaching principles into their own practices in the real clinical world. However, it is very challenging methodologically to do this, and it appears the best we can do is to ask about participant impressions and insight into their experience.
It appeared that the TACT program provided a rich opportunity for participants to interact and share their quest to understand and refine the metacognitive aspects associated with their clinical decision-making and critical thinking processes. It also provided our participants with the language to describe and teach these processes to trainees.
V. CONCLUSION
In summary, the TACT program shows promise in engaging distributed faculty to further their curiosity and interest in how to improve, teach and foster critical thinking skills within medical education and in their own practice. We recognise that although this online asynchronous mode of delivery may not be appropriate to meet the diverse learning styles of all potential participants, the favourable reviews we have received from our program graduates highlighted that the flexible interactivity with the content contributed to the success of the TACT program.
Notes on Contributor
Simon Field assisted in the initial development of the TACT program and contributed to the data analysis and writing of the article.
Pat Croskerry was a founding member of the Critical Thinking Advisory Group, and contributed to the development of the TACT program and to the writing of the article.
Susan Love has been an active contributor to the running of the TACT program, designed the survey tools, collected and analyzed qualitative and quantitative data from the program evaluation, and contributed to the writing of the article.
Peggy Alexiadis Brown collected and analyzed qualitative and quantitative data from the program evaluation survey tools, and contributed to the writing of the article.
All authors have reviewed and approved the final manuscript.
Ethical Approval
The data gathered for this article was collected anonymously as part of Program Evaluation, and a written waiver has been obtained stating that it is exempt from full institutional Research Ethics approval.
Acknowledgement
We acknowledge the valuable support and contribution of Deirdre Harvey and other members of the Critical Thinking Advisory Group. For further information on how to implement a similar program in your region, please feel free to contact us.
Funding
There is no funding associated with this project.
Declaration of Interest
None of the authors have any conflicts of interest to declare, and they do not receive any financial assistance or funding for their participation in the TACT program.
References
Abrami, P. C., Bernard, R. M., Borokhovski, E., Waddington, D. I., Wade, C. A., & Persson, T. (2015). Strategies for teaching students to think critically: A meta-analysis. Review of Educational Research, 85(2), 275-314. https://doi.org/10.3102%2F0034654314551063
Brezis, M., Orkin-Bedolach, Y., Fink, D., & Kiderman, A. (2016). Does physician’s training induce overconfidence that hampers disclosing errors? Journal of Patient Safety, 15(4) 296-298. https://doi.org/10.1097/pts.0000000000000255
Cook, D. A., & Steinert, Y. (2013). Online learning for faculty development: a review of the literature. Medical Teacher, 35(11), 930-937. https://doi.org/10.3109/0142159X.2013.827328
Croskerry, P. (2018). A model for clinical decision-making in medicine. Medical Science Educator, 27(Suppl 1), S9-S13. https://doi.org/10.1007/s40670-017-0499-9
Steinert, Y. L., McLeod, P. J., Conochie, L., & Nasmith, L. (2002). An online discussion for medical faculty: An experiment that failed. Academic Medicine., 77(9), 939-940. https://doi.org/10.1097/00001888-200209000-00046
*Simon Field
Dept of Emergency Medicine,
Dalhousie University, Halifax,
Nova Scotia, Canada
Email: simonfield@dal.ca
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
