
A dramaturgical analysis of a paediatric team handover

Submitted: 2 November 2020
Accepted: 8 February 2021
Published online: 5 October, TAPS 2021, 6(4), 37-48
https://doi.org/10.29060/TAPS.2021-6-4/OA2425
Stephen Bradley1, Aaron Ooi2, Kerry Stafford3, Shuvayon Mukherjee1 & Marcus A. Henning4
1Department of Paediatrics, Lakes District Health Board, New Zealand; 2Department of Paediatrics, Waikato District Health Board, New Zealand; 3Department of Paediatrics, Christchurch Hospital, New Zealand; 4Centre for Medical and Health Sciences Education, University of Auckland, New Zealand
Abstract
Introduction: The paediatric team handover process is a crucial workplace practice and comprises the transfer of patient information from one shift to another involving medical professionals and students. A qualitative study was performed to analyse the feasibility, functionality, benefits and limitations of the dramaturgical approach when applied to examining a handover session.
Methods: Data relating to one handover were collected and analysed from video and audio recordings, notes created by two independent observers and a de-identified copy of the handover sheet.
Results: The dramaturgical constructs and subsequent findings allowed us to make informed inferences about the dynamics of the handover procedure. The directors/lead actors consisted of a consultant and a registrar. One consultant was transitory and the remaining 12 attendees were either major support, support or bit actors. The students (bit actors/audience) were included when a learning point was emphasised. The script was informal and improvised as the discussion emphasised certain facets of patient care or accentuated learning points. The staging involved the seating arrangement, a whiteboard, computer screen and ongoing data presentation. The performance suggested a handover of two halves: one emphasising learning and the other allocation of patient care responsibility.
Conclusion: We concluded that the real-life drama occurring within a handover was feasibly analysed, with its functionality demonstrated, using the dramaturgical investigative system. The multifaceted recordings enabled researchers to review the ‘authentic’ handover system without censorship. These findings have implications for educational and organisational research.
Keywords: Dramaturgical, Handover, Paediatric, Methodology
Practice Highlights
- Dramaturgical methodology provided a unique, authentic and detailed analysis of the handover.
- The dramaturgical research methodology used to evaluate the handover was feasible and functional.
- This research methodology can be used to analyse education within similar team based settings.
- This research methodology can be applied to the team handovers and other complex health meetings.
- This research methodology identifies important clinical/educational roles and dynamics within teams.
I. INTRODUCTION
Hospital team handovers involve effective transfer of information and responsibility from one health professional to another, ensuring continuity of patient care (Australian Medical Association Limited, 2006; Hilligoss & Cohen, 2011). The level of communication needs to be comprehensive, unambiguous and coherent so that patient information is easily understood, thus optimising patient care through the meaningful and efficient transfer of patient information (Fujikawa et al., 2021). This is crucial given the ramifications for optimising patient care and minimising potential treatment error, including miscued transfer of knowledge, insertion of faulty or misleading information, treatment delay, and poor patient outcomes (Arora et al., 2005; Bomba & Prakash, 2005). To explore the nuances occurring in handover practice from organisational behaviour and educational perspectives, different methodological approaches need to be developed.
In this paper, we propose that the dramaturgical approach can optimally analyse handover dynamics, as it is an integrated, pragmatic and multidimensional approach. This approach uses multi-source feedback from video and audio recordings, observer records, and transcripts of analysis. The dramaturgical approach argues that the individuals present in the activity assume different roles that influence the way they communicate and behave (Canary et al., 2008; Goffman, 1959; Henderson, 2005). Using this approach, the handover activity can be analysed much like a drama or element of theatre. The dramaturgical approach has the potential to offer insights into the clinical and educational handover components, much like the insights drawn when applying this approach to analysing healthcare simulations (Crea, 2017), decision-making aspects of an emergency department triage (Forde, 2014), and behaviour of radiographers and their patients (Murphy, 2009). This analytical approach enables the researcher to be present at the moment of the occurrence, rather than relying on retrospective data obtained when subsequently interviewing participants. Interviews can be a powerful means of obtaining information, but require participants to accurately retell their experiences of the activity (DiCicco‐Bloom & Crabtree, 2006). The dramaturgical approach tells it for what it is, and allows researchers the ability to see and hear the authentic process of communication (Goffman, 1959; Murphy, 2009). We surmised that the dramaturgical approach would be a more comprehensive evaluative system and thus well suited for collecting observational data that could inform training and development initiatives within hospital systems.
The research aim of this study was to explore the feasibility and functionality of the dramaturgical methodological system of analysis not yet applied to the handover procedure.
The research questions driving this study include:
- How can the dramaturgical approach feasibly be applied to the handover system?
- How does the dramaturgical approach describe the functional dynamics of the handover procedure?
- What are the benefits and limitations associated with applying this research methodology?
II. METHODS
A. Phenomenon of Interest
Feasibility, functionality and quality were informed by examples taken from one handover involving team discussion regarding patients admitted to a general paediatric ward (20 beds) and a Special Care Baby Unit (8 cots) in a New Zealand secondary-level hospital (Hensher et al., 2006).
B. Sample/Participants
All the health professionals and medical students involved in one handover were asked to volunteer for the study, with eligibility determined by consent and approval from hospital management. Informed consent was obtained after eligible participants read a detailed information sheet, provided by an administrator, followed by a consent form that they then signed.
C. Data Collection
Data were obtained from several sources.
- Five video cameras were situated in the handover room to obtain multiple angles of the handover. Two audio recorders were placed in the room and served as the primary sources of data for transcription.
- The final transcription of events was checked by all authors using data from the cameras.
- Notes on the salient aspects of handover interactions were made by two present ‘unknown’ observers (i.e., one medical student and one medical educationalist).
A diagram of the seating positions of each participant was constructed (see Figure 1).
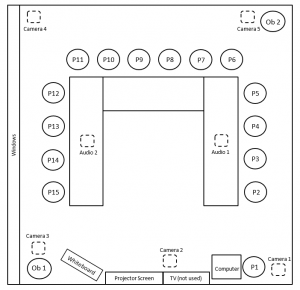
Figure 1: Handover room layout depicting seating arrangements, participants (P1-P15, with original position participants sat in), 2 observers (Ob1 and Ob2) and equipment.
D. Ethical Considerations
Confidentiality of the key informants was maintained by the following criteria:
- All participants were given an anonymised label (P1 to P15).
- All patients discussed within the handover were anonymised (labelled 1 to 36) and identifiable information was deleted from patient reports.
- Several hospital employees involved in the study were not present at the handover and transcription was conducted by an uninvolved third party.
-
-
E. Data Analysis
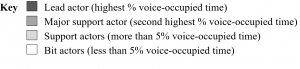
To test the feasibility of the dramaturgical approach, a framework was adapted exploring the perspectives of the actors and audience, the script, the staging and the overall performance (Canary et al., 2008; Crea, 2017; Henderson, 2005). Delineation of roles within the handover (Preves & Stephenson, 2009; Schell, 2016) identified the following ‘actors’: lead, major support, support, and bit actors. The perceived director was involved in the leading and facilitation of the handover (Goffman, 1959). The audience was defined as observers or those actors minimally involved in the main discussion (Canary et al., 2008; Hays & Weinert, 2006). Other factors considered in the analysis included scripting, staging, and performance analysis (Hays & Weinert, 2006).
We scrutinised the data using a deductive thematic content analysis based on dramaturgy criteria (Elo & Kyngäs, 2008). The usefulness of voice-occupied time (VOT) was appraised and VOT was defined as the total time a participant spoke during the entire handover divided by the total duration of the handover, expressed as a percentage. The utility of a timeline considered the dynamics connected to scene development. Lastly, the trustworthiness of the qualitative data analysis protocol was audited (Elo et al., 2014).
III. RESULTS
The following data were used to assess the feasibility, functionality and quality of the dramaturgical process. For full data details, please refer to Figshare (2020).
A. Actors and Audience
The handover involved 15 participants (Table 1).

Table 1: Roles and number of participants and observers present in handover.
The VOT analysis (see Table 2) was useful in quantifying participation as aligned with perceived roles. The participant with the highest VOT was deemed to be the lead actor, while the second highest VOT was classified as the major supporting actor. Participants with VOTs of greater than 5% were defined as supporting actors, and participants who had VOTs of less than 5% were judged to be bit actors and audience. Accordingly, the lead consultant (the initial director) (P13) and the senior registrar (P3), who each had more than 15% of the VOT, were judged to be the lead and major support actors respectively. Eight (53%) of the participants were identified to be present as bit actors or audience.
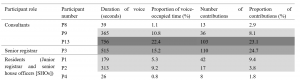
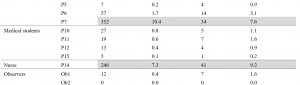

Table 2: Percentage of voice occupied time (VOT) and number of contributions per participant.
A separate analysis was conducted counting the number of contributions (clearly-heard comments) each handover participant made, with a total of 446 contributions quantified during the handover. This was correlated with the VOT and provided a point of comparison to identify crucial facets of the handover drama.
B. Roles
The utility of the dramaturgical approach was also demonstrated in identifying the roles of handover members. It was ascertained that the three consultants had distinct roles. The lead actor (P13) was the consultant on the ward that week. She led the beginning of the handover, directed the flow of discussion and took on a major teaching role. The second consultant (P9), who had been on call overnight, contributed important information and was involved in teaching. The third consultant (P8) sought information about suitable patients for teaching, but contributed little to the discussions.
A further key role identified was the senior registrar (P3), who contributed little to the handover until the dramatic time when a phone call interrupted the handover. After the departure of the lead consultant (P13), she acquired the major support actor role, but did so in a very business-like manner to ensure that all patients were discussed and a safe plan established.
Roles were highlighted participants’ costumes. The doctors and students in the handover wore smart-casual attire. Several clearly had available stethoscopes, whilst the nurse wore a uniform.
C. Script
The script was found to be a useful informal source of information. Whilst close attention was given to the handover sheet containing patient details, it was clear that participants improvised. The dramaturgical analysis established that the patients cared for by the paediatric team were the subjects of the performance. Patients were referred to respectfully, and the discussion was focused on their daily requirements.
D. Staging
The room (Figure 1) was notable for the horseshoe-shaped arrangement of tables and chairs, which enabled the researchers to evaluate visibility of participants and their access to technological equipment. The notion of staging also enabled researchers to establish the activities that occurred within the room (on-stage) as opposed to those outside the room (off-stage).
E. Props
The most significant prop was the handover sheet (or script) listing the patients’ names, demographic data, their medical issues, and initiated investigations and plan.
F. Performance
1) Scenes: The scenes could be classified as follows. These were the prologue, three acts, and an epilogue represented as 14 distinct scenes (Table 3). We were able to identify each new scene arising at the point of a significant incident in the handover discussion.
|
Act |
Scene number |
Scene name |
Major theme of scene |
Description of scene |
Actors with VOT within scene |
|
Prologue. |
1 |
“Nice to meet you.” |
Setting the scene. |
First four handover members arrive (P3, P12, P13, P14). New SHO arrives (P6) and receives brief orientation. Remaining handover members arrive (P1, P2, P4, P5, P7, P9, P10, P11). Meet member of research team (Ob 1). |
P3, P6, P12, P13, P14, Ob 1 |
|
Act 1 – The beginning of handover. |
2 |
“Can we just get going?” |
Introductions. |
Each member of team states their name and role. |
P1, P2, P3, P4, P5, P6, P7, P9, P10, P11, P12, P13, P14 |
|
3 |
“Fire away!” |
Start of night handover. |
Lead consultant (P13) initiates handover. Night SHO (P2) utilises handover sheet as a prompt to discuss cases encountered during the night. P8 enters room. |
P2, P8, P13 |
|
|
4 |
“Patient 21, a baby.” |
Focus on a sick child. |
Case of specific child who deteriorated during the night presented, becoming a significant aspect of discussion. Four most senior members of the team (P3, P8, P9, P13) contribute to this discussion. P15 enters room. P2 completes handover of relevant patients, exits thereafter. |
P1, P2, P3, P8, P9, P13 |
|
|
Act 2 – Educational moments and the climax.
|
5 |
“Can I just interrupt?” |
Planning for assessment. |
Consultant (P8) requests patients for examination purposes (principal reason for P8 attending handover), exits thereafter. |
P8, P13 |
|
6 |
“What other things would you like to tell us?” |
Educational moment arising from handover. |
Consultant (P9) presents case of a specific child with alleged non accidental injury, with subsequent educational moment (P13 and P9 acting as prompts for discussion and sources of information respectively). |
P1, P4, P9, P13, P14 |
|
|
7 |
“Is there any learning for us from that one?” |
Further educational moment. |
Lengthy discussion focussed around a ‘difficult’ case. Consultant (P13) uses words “And herein is the learning”, stands up and uses whiteboard to discuss differentials and poses questions to individual team members. P9 serves as a source of clinical information. On-call SHO phone rings and SHO (P5) exits room, followed by senior registrar (P3) from whom help is sought. P9 exits room. |
P1, P3, P4, P5, P6, P7, P9, P10, P11, P12, P13, P14, P15 |
|
|
8 |
“I will need to divide them up.” |
Focus on workload for patients on inpatient ward. |
Resumption of systematically working through inpatients on the handover sheet to generate management plans, with input obtained from residents and students who had seen children the previous day. |
P1, P3, P7, P13 |
|
|
9 |
“Just been phoned from ED!” |
Dramatic intervention – a sick child in the Emergency Department (ED). |
Interruption of handover to discuss a seriously unwell child who requires specialist attention in ED (climax). P13 states: “Emergent patient care always takes priority”. Lead consultant (P13) exits with on-call SHO (P5). |
P1, P3, P5, P13, P14 |
|
|
Act 3 – The business end of handover. |
10 |
“So, shall we go back up to …?” |
Focus on workload for patients on inpatient ward. |
Resumption of systematically working through inpatients on the handover sheet to generate management plans, with input obtained from residents and students who had seen children the previous day. Senior registrar (P3) now leads the handover discussion with regular, brief contributions. |
P1, P3, P7, P11, P14 |
|
11 |
“OK. Umm and SCBU…” |
Focus on workload for neonates in the Special Care Baby Unit (SCBU). |
Systematic working through SCBU patients on the handover sheet to generate management plans, with input obtained from residents and students who had seen children the previous day. |
P3, P7, P14 |
|
|
12 |
“And then… chase results.” |
Focus on chasing up outstanding laboratory results. |
Systematic working through patients on handover sheet who have outstanding laboratory results to be followed up. |
P1, P3, P7, P14 |
|
|
Epilogue. |
13 |
“So, what are you doing now?” |
Discussion about participants’ day plans. |
Senior registrar (P3) checks with members of team their understanding of their roles for the day. |
P1, P3, P4, P6, P7 |
|
14 |
“Yeah, sweet… done!” |
Conclusion. |
Completion of handover as evidenced by verbal and body language cues as members of team exit the room. |
P3 |
Table 3: Acts and scenes within the handover
2) Entrances and exits: Easily demarcated entrance and exit points of the handover were identified. P1 arrived 5 minutes before the handover commenced, prepared the computer, and then left and returned with the remainder of the handover team. This initial entrance represented the entire group arriving, with a prologue consisting of set up and early introductions (Scene 1).
An example of a dramatic exit and re-entrance of two doctors (P3, P5) was noted during Scenes 7 and 9, which proved to be a major incident, as the phone call off-stage notified them of a critical case. Following this, the lead consultant (P13) exited with a SHO (P5) and the director role was handed to the senior registrar (P3). This altered the handover significantly and came at a time when the handover had moved from a largely educational milieu to a more work-like role.
See Figure 2 for a time-line regarding the Handover.
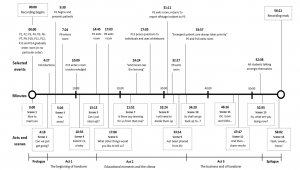
Figure 2: Timeline of acts, scenes and selected events
3) Additional observations: Multiple data collection methods enhanced the dramaturgical method, through clarifying inaudible audio data. Entrances and exits did not always prompt comments on the audio recording, but were noted from the video recordings. A critical incident occurred when the lead consultant established an educational role and used the whiteboard for teaching – the impact of this would not have been so apparent without a video recording.
IV. DISCUSSION
The studied handover was attended by multiple professionals and students, and had several purposes, focussing on the safe exchange of knowledge and responsibility for a group of patients with variable clinical conditions and acuity (Australian Medical Association Limited, 2006; Hilligoss & Cohen, 2011). We argued that the dramaturgical approach would be a valuable method for analysing the dynamics of this handover. To evaluate the effectiveness of this research approach, we focussed on the feasibility, functionality and quality of the dramaturgy approach.
A. Feasibility
The dramaturgical perspective argues that individuals “play different roles as ‘actors’ and engage in ‘performances’ in order to shape their ‘definition of the situation’” (Canary et al., 2008, p. 155). We applied the metaphor of ‘life as drama’ to this handover. The findings and information gleaned from this handover demonstrated that a dramaturgy approach embedded within a case study methodology can be applied to a complex team handover.
Obtaining consent from all handover attendees in a manner that did not impact on the handover itself required significant pre-planning by the research team and cooperation from the department. In their systematic review, Flory and Emanuel (2004) examined methods for improving the consent process and for increasing participant understanding. One recommendation centred on employing significant person-to-person contact as an optimal method to improve understanding. To avoid undue power dynamics, a senior consultant at this hospital involved in the study was not involved in the administrative process, and this prevented any direct involvement in the recruitment and data collection processes, thus minimising inducement and conflict of interest.
Patients are often particularly vulnerable in this type of research, as they may not fully understand their legal or ethical rights (Sankar et al., 2003). We were cognisant of this when considering our research design. To maintain confidentiality of patients, we de-identified patient details, using a numbering system and only referred to patients by their number code to minimise release of personal medical information.
We established that the dramaturgical approach was able to feasibly capture both verbal and non-verbal elements of the discourse. To capture this wide range of information, we used multiple methods of data collection creating greater accuracy of the handover. Other studies have used different research approaches. Using grounded theory and content analysis, Behara et al. (2005) studied five North American Emergency Departments using ethnographic observations, and emphasised the active participation of handover members in co-construction of their understanding about the patients who were considered in the handover. The use of ethnographic observation has some resonance with this study, although, in this study, we created an ‘a priori’ framework for analysis using the dramaturgical components. The dramaturgical method allowed us to structure our analysis. Several researchers (Donnelly et al., 2019; Ooi et al., 2020) have used inductive techniques to analyse semi-structured interview data, and these studies provided useful perceptions of team handovers in New Zealand hospitals. The advantage of using interviews is that professionals interviewed have time to reflect on the salient aspects of the handover; however, a disadvantage is that the interviewees can censor and forget key elements of the process.
B. Functionality
In this section, we address the second research question focussed on describing the functional dynamics of the handover.
We found that dramaturgical methods provided a useful lens to analyse the way the actors and their roles interacted with the staging. For example, the handover was clearly orchestrated by designated and perceived roles of the lead actor (P13) and the major support actor (P3). Our method of utilising VOT allowed us to evaluate the reasons why some actors within the handover participated more or less, with findings clearly showing that the handover was directed by P13, until she left the room and then P3 became the dominant driver of the performance. This finding is consistent with the work of Donnelly, who described the critical nature of the team handover leader’s role in ensuring safe and equitable outcomes for patients by “running meetings smoothly and respectfully” (Donnelly et al., 2019, p. 611).
The interruption caused by the critical case in Scene 9 highlighted the importance of patient safety and care in handover function (Australian Medical Association Limited, 2006), which took priority over ensuring equal voice contribution of the handover attendees. The impact of handover members having differing levels of clinical experience within a team has been noted as an important contributor to handover dynamics (Behara et al., 2005; Hilligoss & Cohen, 2011). We documented a degree of audience segregation (Canary et al., 2008; Murphy, 2009) within the handover, in that, within specific scenes, some actors were markedly involved, whilst others, particularly the bit actors, were effectively the audience and were relatively uninvolved unless prompted by the director or major support actor.
The video analysis permitted us to regard this handover as more akin to an unscripted improvisation (Sawyer, 2004; Schryer et al., 2003) based on the handover sheet. Hilligoss and Cohen (2011, p. 95) have described handovers as “routines grounded in human memory for habits”, and the handover sheet provided a routine document to be worked through. The dramaturgical framework allowed us to visually consider the layout of the room (or stage) (Goffman, 1959; Murphy, 2009). Kinahan (2017), in her qualitative analysis of seating positions within an educational context, reported that different seating positions likely yield different outcomes. The horseshoe-formation structure used in this handover likely promoted more participant engagement.
Lastly, the dramaturgical approach allowed us to segment the analysis in terms of acts and scenes (Henderson, 2005). This was useful as it allowed us to determine if there were specific activity patterns or key events arising within this handover. Hilligoss and Cohen (2011, p. 95) stated that research “examines how micro patterns of activity in [handover] are embedded in, shaped by, and ultimately produce effects on the larger system of hospital activities”. The handover had a prologue in which members had a brief period of social contact, an important element of handover (Hilligoss & Cohen, 2011; Nugus et al., 2017) which initiates formalising the community of practice (Bradley et al., 2018; Egan & Jaye, 2009).
The functionality of the dramaturgical approach can be easily demonstrated within Acts 2 and 3. Act 2 centred on discussion regarding two patients who presented diagnostic uncertainty, and provided the platform for opportunistic teaching, with significant emphasis and time spent on these patients. However, it was clear from our analysis that these teaching moments resulted in a single focus when all team members were effectively engaged through use of directed questioning. The importance of learning within handover has been described (Hilligoss & Cohen, 2011; Ooi et al., 2020; Paradis & Sutkin, 2017). Specifically, the use of brief opportunistic learning related to appropriate patients has been suggested as a useful strategy within handover (Bradley et al., 2018; Ooi et al., 2020). Nonetheless, it was unclear to the researchers whether the teaching initiatives seen in this handover represent typical behaviour, or whether participant activity may have been influenced by the study itself (Paradis & Sutkin, 2017). Act 2 revealed a subsequent shift from a focus on education to patient care, demonstrating that patients continued to receive emergency treatment when required. This reflected an understanding that the participation of the team at handover did not compromise the ongoing provision of medical care for other patients (Australian Medical Association Limited, 2006).
A further change in focus was observed in Act 3, with a focus on the requirement to discuss briefly the remaining 28 patients on the sheet. Our analysis demonstrated a shift to much briefer discussions, reflecting the need to work in a timely manner. This suggested a shift in the handover from a community of practice with at least partly an educational focus to that of a formal work group (Egan & Jaye, 2009; Wenger & Snyder, 1999). The need to pace the handover and to balance the conflicting functions has been noted in other studies (Donnelly et al., 2019; Horsky et al., 2015).
C. Quality Appraisal of the Research Methodology
The dramaturgical approach created a formalised structure from which authentic workplace activity could be identified. In comparison to other qualitative methods, the advantages were the rich, untainted data obtained. The findings of semi structured interviews conducted with the participants involved in this handover are published in a further report (Ooi et al., 2020) and builds on other existing findings published to date within other specialties (Donnelly et al., 2019). The findings of the Ooi et al study were informative as they allowed probing, using semi-structured interviews, into the perceptions of the handover participants after the handover had taken place. These findings are useful in the understanding participants’ views on team dynamics, modes of communication, and the opportunities for learning. Similarly using an interview approach to gathering data, Bradley et al. (2018) was able to develop a set of themes that could be used to describe the handover process, namely informal learning (comprising opportunistic learning, implicit learning, and reflective learning) and formal and deliberative learning. Gathering data using the interview approach enables a deliberative process whereby the participants have time to reflect on their educational and clinical experience associated with the handover. Nevertheless, as aforementioned, it also allows participants to censor their thoughts and memories of the handover (Knox & Burkard, 2009) and may not capture the authoritative complexity of what has occurred in a multifaceted meeting. Therefore, the dramaturgical process could be viewed as authentic ‘in the moment’ research whilst an interview perspective is memory driven, retrospective and reflective.
The optimal approach is to use the dramaturgical system to capture the objective evidence of what actually happened in the handover, and then to use interview data to consider how the participants frame their reflections of what happened. Using both systems would be highly informative in terms of illustrating congruity or incongruity between what happened, what participants thought had happened, and participants’ consequential deliberations regarding their educational and clinical experiences. Using both research systems would benefit handovers, as they would complement each other. To gather data from a larger sample source, using a self-report questionnaire may be valuable once the theoretical domains are established. However, it is acknowledged that designing and developing a questionnaire that is fit for purpose takes careful planning and a rigorous research process (Rattray & Jones, 2007).
A major limitation of the dramaturgical approach taken was the presence of the observers, cameras and audio recording devices and the knowledge of being observed. The Hawthorne effect has been noted as an important aspect of studies as it infers that the perception of special attention may influence behaviour (Paradis & Sutkin, 2017). The research team was uncertain whether the strong emphasis within this handover on teaching reflected the usual practice of the paediatricians involved, but acknowledged that some of the handover participants were aware that two of the researchers were involved in previous research in this area (Ooi et al., 2020), which could have contributed to conciliatory behaviour. One further area of concern was conflict of interest or undue influence. The handover we studied occurred within a hospital at which one of the researchers is both Clinical Director and a paediatrician, and where two others are previous or current members of the paediatric team. None of these three doctors was present in the room during the study, but we acknowledge a potential conflict of interest, which could have altered participants’ behaviour. However, we felt that we had instigated safeguards to minimise this influence, such as having two independent observers within the handover and asking an administrator to contact handover participants with regards to participation and consent. In addition, we also believe in the professionalism of the participants as their main concern in the handover was the authentic transfer of patient information to ensure optimal patient care. It is likely that a mixed-methods approach would be the optimal method for describing the explicit and implicit nature of the handover process.
Our system of analysis created a triangulation method drawing information from the video and audio recordings taken from differing angles, the subsequent transcription of the audio recording, and the notes from two independent observers (medical student and medical educationalist). We were also able to collect data on the room layout (Figure 1) and the handover sheet. We found the data from the video source invaluable in identifying which participants were speaking and in detecting dialogue that was not clearly audible from the audio recording. Once the transcript was agreed on, we found analysis of the video sources and the recordings of the two observers critical to understanding the dynamics within the handover. The video allowed us to identify non-verbal behaviours such as the entrances and exits of staff where this was not otherwise referenced in the audio recording. An entire sequence of teaching occurred when one participant used the whiteboard, and this would not have been appreciated from use of the audio source only. Rees et al., 2013) used video and audio recordings to collect data relating to bedside teaching of medical students, but did not use a structured method of analysis; nonetheless, they found the video useful in capturing linguistic and para-linguistic information, although they noted the difficulty in capturing subtle non‐verbal communication (e.g. smiles).
V. CONCLUSION
This feasibility study has demonstrated that a dramaturgical method had immense utility when analysing the complexity of a paediatric handover meeting. A discussion as to its functionality, benefits and limitations is also provided and we believe that this approach has generated a deep understanding of this handover’s dynamics and highlighted key aspects of the handover’s function, with implications for educational and organisational research.
Further studies could be designed relating to the dramaturgical method. These could be directed to other team handovers in either paediatric or other specialties, and in different health systems to broaden the understanding of processes that occur within these complex meetings. Examples of other such meetings are Multi-Disciplinary patient related meetings, ward rounds, radiology meetings and educational meetings such as Grand Rounds and workshops. Further research could be broadened to include semi-structured interviews of handover participants to gain further understanding of handover members’ reactions to the handovers they have participated in.
Notes on Contributors
Stephen Bradly is a consultant paediatrician (MBChB, FRACP, MClinEd), Clinical Lead, Medical Education, Lakes District Health Board, New Zealand. He reviewed the literature, co-designed the study, analysed the transcripts and co-wrote the manuscript.
Aaron Ooi is a registrar and teaching fellow (MBChB, DipPaed, PGDipClinEd), Waikato District Health Board, New Zealand. He reviewed the literature, co-designed the study, analysed the transcripts and co-wrote the manuscript.
Kerry Stafford is a senior house officer (BMBS), Department of Paediatrics, Christchurch Hospital, Canterbury District Health Board, New Zealand. She reviewed the literature, co-designed the study, analysed the transcripts and contributed to the manuscript.
Shuvayon Mukherjee was a fifth year medical student (BSc) at the time of the study, University of Auckland, New Zealand and on clinical attachment at the Department of Paediatrics, Rotorua Hospital, Lakes District Health Board. He reviewed the literature, co-designed the study, conducted the interviews, analysed the transcripts and contributed to the manuscript.
Marcus A. Henning is an associate professor (BA, MA, MBus, PhD), Centre for Medical and Health Sciences Education, University of Auckland, New Zealand. He reviewed the literature, co-designed the study, conducted the interviews, analysed the transcripts and co-wrote the manuscript. He is the corresponding author for this manuscript*.
Ethical Approval
Ethics approval was obtained from the University of Auckland Human Participants Ethics Committee (UAHPEC) on 26 June 2018. The reference protocol number is 121483.
Data Availability
The anonymised data set is available on https://figshare.com/s/2985a2e3047594816d88 Figshare (2020), with URL details below.
Due to the nature of the video and audio recording containing identifying information, these have not been made public. Requests for these can be directed to the corresponding author if required.
Acknowledgement
We wish to thank the participants in the handover that we studied, who graciously allowed our observation of them working hard to provide excellent care for their patients. We are also grateful to Brenda Flood, who efficiently and capably transcribed the handover.
Funding
A grant to meet the cost of transcription was received from the Stolwyk Trust, Lakes District Health Board.
Declaration of Interest
The authors declare no conflicts of interest.
References
Arora, V., Johnson, J., Lovinger, D., Humphrey, H., & Meltzer, D. (2005). Communication failures in patient sign-out and suggestions for improvement: A critical incident analysis. BMJ Quality & Safety, 14(6), 401-407. https://doi.org/10.1136/qshc.2005.015107
Australian Medical Association Limited. (2006). Safe handover: Safe patients. Guidance on clinical handover for clinicians and managers. http://ama.com.au/sites/default/files/documents/Clinical_Handover_0.pdf
Behara, R., Wears, R. L., Perry, S. J., Eisenberg, E., Murphy, L., Vanderhoef, M., Shapiro, M., Beach, C., Croskerry, P., & Cosby, K. (2005). A conceptual framework for studying the safety of transitions in emergency care. In K. Henricksen, J. Balttles, & E. Marks (Eds.), Advances in patient safety: From research to implementation (Vol. 2, pp. 309-321). Agency for Healthcare Research and Quality.
Bomba, D. T., & Prakash, R. (2005). A description of handover processes in an Australian public hospital. Australian Health Review, 29(1), 68-79. https://doi.org/10.1071/AH050068
Bradley, S. K., Egan, J., & Henning, M. A. (2018). Paediatric team handover: A time to learn? New Zealand Medical Journal, 131(1476), 70-80. https://assets-global.website-files.com/5e332a62c703f653182faf47/5e332a62c703f63e992fd3f5_Bradley-FINAL.pdf
Canary, D. J., Cody, M. J., & Manusov, V. L. (2008). Interpersonal communication: A goals based approach. Bedford/St. Martin’s.
Crea, T. (2017). Narrative dramaturgy and sense making in healthcare simulation. In D. Nestel, B. Jolly, M. Kelly, & M. Watson (Eds.), Healthcare Simulation Education: Evidence, Theory and Practice (pp. 54-59). John Wiley and Sons.
DiCicco‐Bloom, B., & Crabtree, B. F. (2006). The qualitative research interview. Medical Education, 40(4), 314-321. https://doi.org/10.1111/j.1365-2929.2006.02418.x
Donnelly, S., Dinesh, D., Dew, K., & Stubbe, M. (2019). The handover room: A qualitative enquiry into the experience of morning clinical handover for acute medical teams. Internal medicine journal, 49(5), 607-614. https://doi.org/10.1111/imj.14142
Egan, T., & Jaye, C. (2009). Communities of clinical practice: The social organization of clinical learning. Health, 13(1), 107-125. https://doi.org/10.1177/1363459308097363
Elo, S., Kääriäinen, M., Kanste, O., Pölkki, T., Utriainen, K., & Kyngäs, H. (2014). Qualitative content analysis: A focus on trustworthiness. SAGE Open, 4(1), 2158244014522633. https://doi.org/10.1177/2158244014522633
Elo, S., & Kyngäs, H. (2008). The qualitative content analysis process. Journal of Advanced Nursing, 62(1), 107-115. https://doi.org/10.1111/j.1365-2648.2007.04569.x
Figshare. (2020). Handover notes – Observer 1 (Anonymised).docx. https://figshare.com/s/2985a2e3047594816d88
Flory, J., & Emanuel, E. (2004). Interventions to improve research participants’ understanding in informed consent for research: A systematic review. Journal of the American Medical Association, 292(13), 1593-1601. https://doi.org/10.1001/jama.292.13.1593
Forde, C. A. (2014). Emergency medicine triage as the intersection of storytelling, decision-making, and dramaturgy. University of South Florida. https://scholarcommons.usf.edu/etd/5354/
Fujikawa, H., Son, D., & Eto, M. (2021). Are residents learners or workers? A historical perspective in Japan. The Asia Pacific Scholar, 6(1), 122-124. https://doi.org/10.29060/TAPS.2021-6-1/PV2339
Goffman, E. (1959). The Presentation of Self in Everyday Life. Anchor Books.
Hays, M. M., & Weinert, C. (2006). A dramaturgical analysis of shift report patterns with cost implications: A case study. Nursing Economics, 24(5), 253.
Henderson, A. (2005). The value of integrating interpretive research approaches in the exposition of healthcare context. Journal of Advanced Nursing, 52(5), 554-560. https://doi.org/10.1111/j.1365-2648.2005.03622.x
Hensher, M., Price, M., & Adomakoh, S. (2006). Referral hospitals. In D. T. Jamison, J. G. Breman, A. R. Measham, G. Alleyne, M. Claeson, D. B. Evans, P. J. Mills, & P. Musgrove (Eds.), Disease control priorities in developing countries (2nd ed., pp. 1229-1243). Oxford University Press.
Hilligoss, B., & Cohen, M. D. (2011). Hospital handoffs as multifunctional situated routines: Implications for researchers and administrators. In L. H. Friedman, J. Goes, & G. T. Savage (Eds.), Biennial review of health care management (Vol. 11, pp. 91-132). Emerald Group Publishing Limited. https://doi.org//10.1108/S1474-8231(2011)0000011008
Horsky, J., Suh, E. H., Sayan, O., & Patel, V. (2015). Uncertainty, case complexity and the content of verbal handoffs at the emergency department. AMIA Annual Symposium Proceedings.
Kinahan, M. P. (2017). Teachers and seating arrangements and assignments: A qualitative study [Doctoral thesis, Northeastern University]. https://repository.library.northeastern.edu/files/neu:cj82q019x/fulltext.pdf
Knox, S., & Burkard, A. W. (2009). Qualitative research interviews. Psychotherapy research, 19(4-5), 566-575. https://doi.org/10.1080/10503300802702105
Murphy, F. (2009). Act, scene, agency: The drama of medical imaging. Radiography, 15(1), 34-39. https://doi.org/10.1016/j.radi.2007.09.006
Nugus, P., McCarthy, S., Holdgate, A., Braithwaite, J., Schoenmakers, A., & Wagner, C. (2017). Packaging patients and handing them over: Communication context and persuasion in the emergency department. Annals of Emergency Medicine, 69(2), 210-217. e212. https://doi.org/10.1016/j.annemergmed.2016.08.456
Ooi, A., Bradley, S., Mukherjee, S., Stafford, K., & Henning, M. A. (2020). Facilitating educational experiences in a paediatric handover: A qualitative case study. Journal of Paediatrics Child Health, 56(9), 1426-1431. https://doi.org/10.1111/jpc.14964
Paradis, E., & Sutkin, G. (2017). Beyond a good story: from hawthorne effect to reactivity in health professions education research. Medical Education, 51(1), 31-39. https://doi.org/10.1111/medu.13122
Preves, S., & Stephenson, D. (2009). The classroom as stage: Impression management in collaborative teaching. Teaching Sociology, 37(3), 245-256. https://doi.org/10.1177/0092055X0903700303
Rattray, J., & Jones, M. C. (2007). Essential elements of questionnaire design and development. Journal of Clinical Nursing, 16(2), 234-243. https://doi.org/10.1111/j.1365-2702.2006.01573.x
Rees, C. E., Ajjawi, R., & Monrouxe, L. V. (2013). The construction of power in family medicine bedside teaching: A video observation study. Medical Education, 47(2), 154-165. https://doi.org/10.1111/medu.12055
Sankar, P., Mora, S., Merz, J. F., & Jones, N. L. (2003). Patient perspectives of medical confidentiality: A review of the literature. Journal of General Internal Medicine, 18(8), 659-669. https://doi.org/10.1046/j.1525-1497.2003.20823.x
Sawyer, R. K. (2004). Creative teaching: Collaborative discussion as disciplined improvisation. Educational Researcher, 33(2), 12-20. https://doi.org/10.3102/0013189X033002012
Schell, H. (2016). Casting revealed: A guide for film directors. Routledge.
Schryer, C. F., Lingard, L., Spafford, M., & Garwood, K. (2003). Structure and agency in medical case presentations. In B. C & R. D (Eds.), Writing selves/writing societies: Research from activity perspectives (pp. 62-96). The WAC Clearing House. https://wac.colostate.edu/books/selves_societies/schryer/schryer.pdf
Wenger, E. C., & Snyder, W. M. (2000). Communities of practice: The organizational frontier. Retrieved June 22, 2019, from https://hbr.org/2000/01/communities-of-practice-the-organizational-frontier
*Marcus A. Henning
The University of Auckland,
Private Bag 92019,
Auckland 1142,
New Zealand,
Contact No: 0064 923 7392
Email: m.henning@auckland.ac.nz
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
