
An exploratory study of the relationships among physical health, competitiveness, stress, motivation, and grade attainment: Pre-medical and health science students

Published online: 4 September, TAPS 2018, 3(3), 5-16
DOI: https://doi.org/10.29060/TAPS.2018-3-3/OA1054
Marcus A. Henning1, Christian U. Krägeloh2, Roger Booth3, Erin M. Hill4, Julie Chen5, Craig Webster1,6
1Centre for Medical and Health Sciences Education, University of Auckland, New Zealand; 2Department of Psychology, Auckland University of Technology, New Zealand, 3Molecular Medicine & Pathology, Faculty of Medical and Health Sciences, University of Auckland, New Zealand; 4Department of Psychology, West Chester University, United States of America; 5Department of Family Medicine and Primary Care, Bau Institute of Medical and Health Sciences Education, Li Ka Shing Faculty of Medicine, The University of Hong Kong; 6Department of Anaesthesiology, University of Auckland, New Zealand
Abstract
This study highlights the use of multi-factor analytical approaches in the investigation of students’ academic performance and their well-being. The aim of the study was to explore the relationships among physical health, competitiveness, perceived stress, motivation, and academic achievement in pre-medical and health science students. Responses were elicited from 339 students preparing for medical and other health science programmes. Questionnaires obtained information regarding gender, age, grade achievement, perceived stress, motivation, physical health, and competitiveness. Due to the subtle gender differences evident in the literature and substantiated by the findings in this study, two structural equation models were generated, one representing male students and the other female students. In general, the illustrated models showed a positive relationship between physical health and enjoyment of competition. Next, physical health was negatively associated with perceived stress, which showed a negative association with self-efficacy and a positive association with test anxiety. Enjoyment of competition was positively associated with self-efficacy. Grade achievement was positively associated with self-efficacy. The models suggest that students, as a whole, experiencing good physical health report less perceived stress and less test anxiety, and more self-efficacy which are associated with positive grade outcomes. These models give insights into how physical health and learning variables may influence grade outcome providing scope for further research into how these relationships impact learning environments, team behaviours, and professional training.
Keywords: Biomedical and Health Science Students, New Zealand, Motivation, Physical Health, Competitiveness, Academic Achievement
Practice Highlights
- The derived structural equation models were able to systematically explore the relationships among physical health, competitiveness, perceived stress, motivational beliefs, and consider their impact on grade attainment among first-year pre-medical and health science students.
- The structural equation models indicated that physical health significantly co-varied with enjoyment of competition and that there was a significant negative association with perceived stress.
- Enjoyment of competition formed predictive relationships with self-efficacy and intrinsic value for female students and with only self-efficacy for male students.
- Perceived stress, and the motivational belief variables of self-efficacy, test anxiety, and intrinsic value were identified in this study in relation to the prediction of academic achievement.
I. INTRODUCTION
The learning environment of medical and health sciences students consists of numerous opportunities and challenges. When studying medicine and other health sciences, students are entering a phase in their educational lives that requires them to be self-directed, adult learners adopting evidence-based reasoning (Spencer & Jordan, 1999). However, in this stimulating learning environment challenges emerge, that require them to cope with stress, maintain good physical health, while ensuring that they stay motivated, and achieve good grades (Hojat, Gonnella, Erdmann, & Vogel, 2003). A further important issue that is often ignored is how competitiveness factors may stimulate or impair learning, and this is particularly pertinent in medicine given that medical students are often cited as being highly competitive and aiming for high academic achievement (Hilliard, 1995).
The aim of this study was to examine the interactions between different types of factors linked with learning that are relevant to these first-year biomedical and health science students, many of whom are competing for admission to medical school and other professional programmes. Furthermore, we explored how their perceptions of physical health, perceived stress, motivation and competitiveness could be linked with their academic achievement. This was an exploratory study investigating the relationships between certain key variables targeting learning behaviour, well-being, and grade outcome, with the view to understanding how these variables influence each other to further promote student well-being and academic performance.
A. Physical health
Physical health has been associated with: coping with daily activities, dependence on medicinal substances and medical aids, levels of energy and fatigue, notions of mobility, experiences of pain and discomfort, ability to work, and levels of sleep and rest (World Health Organisation, 1996). One issue often documented in relation to medical students is their problems with maintaining healthy sleep patterns. In their study Samaranayake, Arroll, and Fernando (2014) found that 39% of the medical students that they surveyed reported significant problems with sleep. In addition to sleep issues, Tanaka, Mizuno, Fukuda, Shigihara, and Watanabe (2008) reported that 20% of the medical students surveyed in their study experienced significant levels of fatigue, as measured by the Chalder Fatigue Scale. Of those students who experienced fatigue, Tanaka et al. also found significant issues associated with eating patterns, school attendance, feelings of satisfaction and being attentive to what was taught in the lectures. Eating problems and sedentary behaviours amongst medical students have also been reported elsewhere thus increasing the risk of cardio-vascular problems later in life (Kulkarni, 2016; Rustagi, Taneja, Mishra, & Ingle, 2011). Similar findings on the high prevalence of coronary heart disease risk factors amongst medical students have been further reported (Ibrahim et al., 2014).
B. Perceived stress
Perceived stress is related to how much a person recognizes an incident to be demanding (Cohen, Kamarck, & Mermelstein, 1983). It has been documented that the experience of undue stress and issues related to the retention of first-year students are common phenomena (Chester, Burton, Xenos, & Elgar, 2013; Friedlander, Reid, Shupak, & Cribbie, 2007). In one study (Park et al., 2012), a feedback loop was indicated when researching the interactions between motivation, grade achievement and stress in medical students. Moreover, Park et al. proposed that a reciprocal relationship occurs between stress and motivation and that motivation is somewhat moderated by both stress and academic performance. One of the practical implications of this study was to develop applicable stress management methods that directly promote motivation. Some of the reasons provided to explain the experience of high levels of stress and issues related to retention include: coping with the transition from high school to university; increased academic demand for self-directed learning approaches; adjusting to a new and larger learning environment; changes in social support systems; fear of failure; fear of anonymity; peer competition; financial strains for students no longer living at home; and transportation changes (Friedlander et al., 2007; Moffat, McConnachie, Ross, & Morrison, 2004).
C. Motivation, competitiveness and gender
In general it can be inferred that medical and health science students are likely to be highly motivated given the demanding admissions requirement for studying and entry into medical school and other professional courses. For example, at the University of Auckland, entry into medicine or other health science degrees is largely contingent upon a high level of academic attainment in their first year of study in the Biomedical Common Year or Overlapping Year 1 programme (The University of Auckland, 2015). Motivation studies in medical education have tended to describe ways of measuring motivation in reference to medical students and trying to understand how medical students learn (Henning et al., 2011; Kusurkar, Ten Cate, Van Asperen, & Croiset, 2011; Lonka et al., 2008; Sobral, 2004). Very few studies have tried to link motivation with academic achievement (Kusurkar, 2012) and of those studies very few have generated convincing arguments regarding such a link (Henning et al., 2011). However, the first-year experience requires cultivation of motivational beliefs, such as self-efficacy, and this is likely to positively influence educational outcomes and academic persistence (Elliott, 2014). Additionally studies in the general educational literature also suggest substantive links between motivation variables, such as self-efficacy, intrinsic value, test anxiety, and academic outcome (Pintrich, 2003; Pintrich & De Groot, 1990; Pintrich & Zusho, 2007).
Less is known about how competition affects academic attainment, although there is a convincing argument linking the experience of competition with stress. For example, there are reports regarding this pre-medical student group in New Zealand as being potentially at risk of lowered life satisfaction and stress-induced difficulties due to the uncertainty of being accepted into medicine and because of the highly competitive environment that precedes acceptance into the medical programme (Samaranayake & Fernando, 2011).
A further, potentially important, demographic factor influencing the experience and expression of the feelings of anxiety, stress and confidence is that of gender. For example, it has been consistently shown that female students are more likely to show high levels of test anxiety and stress, and lower levels of confidence than their male peers (Blanch, Hall, Roter, & Frankel, 2008; Henning et al., 2013; Hojat, Glaser, Xu, Veloski, & Christian, 1999; Papier, Ahmed, Lee, & Wiseman, 2014). In addition, Hibbard and Buhrmester (2010) investigated the two sides of competition, namely competing to win (creating a zero-sum outcome) versus competing to excel, which focuses more on ‘personal development’. In their study, they found that the impact of competitiveness on developing well-being and social relationships was linked to type of competitiveness and gender. In terms of gender, Hibbard and Buhrmester revealed that competing to win created both “internalizing and externalizing problems among females, but mainly related to externalizing problems only among males (p. 420).” In addition they reported that competing to win was linked to dissension in social relationships and problems with developing empathy for females. In contrast, competing to excel, was linked to forming positive social relationships and higher self-esteem for both males and females.
D. Aim of study
The overall aim of the current paper is to explore the relationships among physical health, competitiveness, perceived stress, motivation, and grade attainment in pre-medical and health science students. More specifically, this was a preliminary study to further explore and understand how these variables may impact each other to better support students with specific interventions, such as developing stress management approaches that promote students’ motivation and physical health when learning to strive in highly competitive courses.
II. METHODS
A. Participants
All students (N=1036) studying in a population health course within the Biomedical Common Year or Overlapping Year 1 programme were invited to participate in this survey. This programme consists of numerous core first-year courses and one general education course, with the aim of preparing students for a Bachelor of Health Science, Bachelor of Pharmacy, Bachelor of Optometry and other programmes (The University of Auckland, 2015). Students aiming for entry into courses such as medicine and other health-related courses attend this programme, and hence the distinction between medical students and health science students has not yet been established and such a distinction eventuates at the end of this year of study. In addition, to be granted an interview for entry into the Medical programme, students need to attain overall grades of ‘B+’ or greater.
B. Procedure
Students were provided with an email outlining the study and an invitation to participate in the survey by the phase director. Students were informed about the study in late July 2015 and two reminder emails were sent out. The grade for their Population Health paper relates to their course completion in semester 1 (ending June 29, 2015). Therefore, the survey was conducted after course completion and after this grade had been released to students. Anonymity was maintained throughout the process, and the phase director was unaware of who the study participants were. Participants were able to withdraw from the study up to the time of questionnaire submission. They were also able to put their name into a draw to win a $100 supermarket voucher, but their disclosed contact details for the draw were not able to be connected to their responses to the questionnaire. Data were collected online using a Google Forms questionnaire (Google.com, 2015).
C. Measure
1) Demographic and background details
Several measures were obtained from University records: (1) age in years; (2) gender; and (3) academic grade for Population Health (POPLHLTH 111), one of the core courses in the Biomedical Common Year or Overlapping Year 1.
2) Physical Health domain of the World Health Organisation Quality of Life (WHOQOL) Questionnaire
The physical health domain is one of four domains measured by 26-item version of the WHOQOL questionnaire (BREF version) (Krägeloh et al., 2011; Krägeloh et al., 2013). This scale has 7 items measuring: activities of daily living, dependence on medicinal substances and medical aids, energy and fatigue, mobility, pain and discomfort, sleep and rest, and work capacity (World Health Organisation, 1996) All items are presented on a 5-point Likert scale with varying anchors with high scores (after re-scoring negatively worded items) representing higher levels of quality of life.
3) Revised Competitiveness Index
This 14-item instrument measured students’ intention to win in interpersonal situations (Houston, Harris, McIntire, & Francis, 2002). There are two scales which measure enjoyment of competition (9 items) and contentiousness (5 items), with the latter scale measuring aspects of avoidance and dislike of conflict situations. All items are presented on a 5-point Likert scale (1 = never true to 5 = always true) with 9 items reversed scored: Items 4, 6, 7, 8, 10, 11, 12, 13, and 14.
4) Perceived Stress Scale
This 10-item instrument measured the degree to which students perceived their lives to be stressful based on their life experiences in certain situations (Cohen et al., 1983; Cohen, Kamarck, & Mermelstein, 1994). Students were instructed to respond to how often they felt over the last month: upset, in control, nervous, confident or angered. All items are presented on a 5-point Likert scale (1 = never to 5 = always). Three reversals were instigated for items 4, 5, 7, and 8.
5) Motivated Strategies for Learning Questionnaire
Twenty two items were taken from the motivational beliefs scale, a questionnaire designed and applied by Pintrich and De Groot (1990). Three scales were incorporated measuring aspects of self-efficacy (9 items), intrinsic value (9 items), and test anxiety (4 items). Students were instructed to respond to the items on a 5-point Likert scale (1 = never true to 5 = always true) in reference to their perceptions of their behaviour in the Biomedical Common Year or Overlapping Year 1 programme.
D) Data analysis
First, the response rate (n/N) was calculated as a percentage measure. Second, statistics were presented that described the demographic and academic achievement details of the participants. These descriptive statistics were collected to consider the characteristics of the acquired sample of participants in relation to the student population. Third, the domains within the instruments were appraised in terms of their internal consistency using Cronbach’s alpha coefficients. Lastly, structural equation modelling was incorporated to consider the interrelationships among the four questionnaire measures of physical health, competitiveness, perceived stress, and motivation beliefs. Given the evidence from the literature concerning gender-based differences in these areas of measurement (Blanch et al., 2008; Henning et al., 2013; Hojat et al., 1999; Papier et al., 2014), two structural equation models (SEMs) were conducted for each gender group. The SEMs were conducted using the software AMOS v20. As chi-square values tend to become inflated with increases in sample size (Marsh, Balla, & McDonald, 1988), model fits were evaluated using a combination of goodness-of-fit indices: root mean square error of approximation (RMSEA), comparative fit index (CFI), and standardized root mean square residual (SRMR). Following the accepted guidelines (Hu & Bentler, 1998), model fits were considered acceptable if RMSEA < 0.06, SRMR < 0.08, and CFI close to 0.95 or higher. To ensure that the analysis of the model parameters were stable and that the assumption of multivariate normality was not violated we implemented a Bootstrap method when calculating the confidence intervals and regressions weights (Byrne, 2010). We surmised this was a prudent statistical approach given the male and female models yielded markedly different sample sizes. Consequently, the regression weights were obtained using maximum likelihood bootstrapping with 1,000 samples. Additionally, bias-corrected 95% confidence intervals were calculated for the regression weights
III. RESULTS
A. Response rate and participant data
Three hundred and thirty nine students (n=339) completed the online survey resulting in a response rate of 33%. The average age of the sample was 18.98 years (SD = 2.80) with 75% of respondents being female. Academic achievement grades for the sample were equally spread across all grade allocations (A=31%, B=37%, C=17%, D=2%, other=13%). Table 1 provides demographic and academic achievement details for the sample and population. Some differences were noted, such as the sample group tend to be younger, with a higher proportion of female students, and their achievement scores were higher. However, upon inspection the distributions of the sample data did not indicate any major irregularities.
| Sample | Population | ||
| Age (years) | Mean | 18.94 | 19.6 |
| SD | 2.8 | 2.80 | |
| Gender (%) | Female | 75% | 65% |
| Male | 25% | 35% | |
| Ethnicity (%) | Asian | 42% | 49% |
| Māori | 7% | 5% | |
| New Zealand European | 35% | 33% | |
| Other | 8% | 6% | |
| Pacific | 8% | 6% | |
| Self-reported POPLHLTH grade (%) | A | 31% | 23% |
| B | 37% | 36% | |
| C | 17% | 28% | |
| D | 2% | 11% | |
| Other | 13% | 2% |
Table 1. Demographic and academic achievement details of the sample versus the population
The means and standard deviations for the variables of interest (Table 2), namely physical health, perceived stress, and motivational beliefs were comparable with other studies in the area (Henning et al., 2011; Henning et al., 2013; Roberti, Harrington, & Storch, 2006). The competitiveness scores were also well-matched, although trending lower than cited elsewhere (Harris & Houston, 2010; Houston et al., 2002).
|
Measures |
Domains | Mean | SD |
| WHOQOL questionnaire (BREF version) | Physical Health | 3.72 | 0.62 |
| Revised Competitiveness Index | Enjoyment of competition | 27.79 | 7.97 |
| Contentiousness | 13.92 | 4.67 | |
| MSLQ | Self-efficacy | 3.35 | 0.69 |
| Test anxiety | 3.16 | 1.00 | |
| Intrinsic value | 4.19 | 0.52 | |
| Perceived Stress Scale | 20.24 | 7.33 |
Table 2. Means and standard deviations (SD) of the measures used in the study
In reference to internal consistency, all Cronbach measures met acceptable standards (Field, 2005): physical health (α =.77), perceived Stress Scale (α =.86), the competitiveness scales of enjoyment of competition (α =.91) and contentiousness (α =.83), and the motivational beliefs scales for intrinsic value (α =.83), self-efficacy (α =.90), and test anxiety (α =.84).
B. Structural Equation Modelling
Based on previous literature (e.g., Chester et al., 2013; Friedlander et al., 2007; Henning, Krägeloh, Hawken, Zhao, & Doherty, 2010; Hilliard, 1995; Hussain, Guppy, Robertson, & Temple, 2013; Lonka et al., 2008; Papier et al., 2014; Samaranayake & Fernando, 2011), an a priori model was specified that was then tested using structural equation modelling. The criterion variable was the students’ grades on the course Population Health, where scores varied from 0 (fail) to 9 (A+). The outcome variable, ‘Grade’ was assumed to be linked to the variances in the motivational variables test anxiety, self-efficacy, and intrinsic value, which created a potential predictive relationship with perceived stress, and in turn by physical health. Enjoyment of competition and contentiousness were treated as personality trait variables affecting the three motivational belief variables.
Models were tested twice, separately for males and females. The values obtained for RMSEA, SRMRand CFI indicated that the model fits were acceptable. For females, fits were RMSEA = 0.036, CFI = 0.993and SRMR = 0.033. For males, the fits were RMSEA = 0.027, CFI = 0.996and SRMR = 0.056.
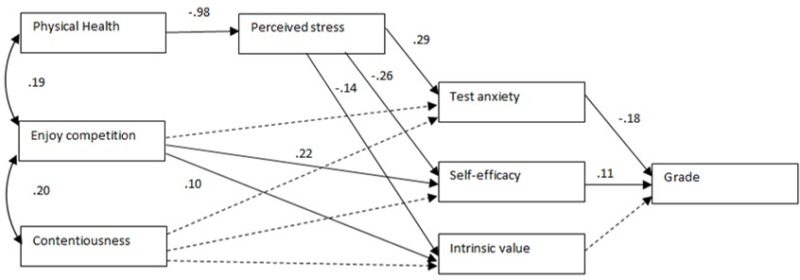
Figure 1. Path diagram of the tested structural equation model for female students only. The path coefficients were shown only when statistically significant (p<.05). For non-significant relationships, directive arrows are shown with dashed lines.
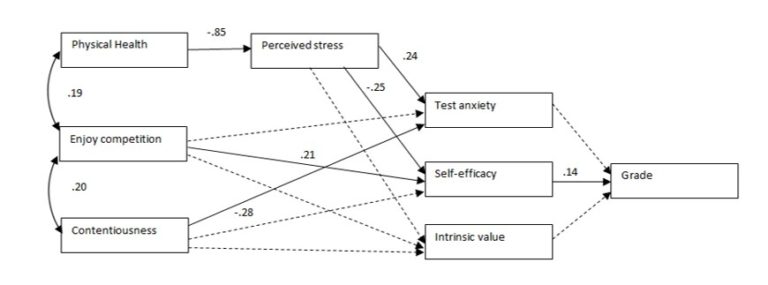
Figure 2. Path diagram of the tested structural equation model for male students only. The path coefficients were shown only when statistically significant (p<.05). For non-significant relationships, directive arrows are shown with dashed lines.
During the process of model specification, modification indices were inspected, and as a result, enjoyment of competition was correlated with contentiousness and enjoyment of competition with physical health. Additionally, the error variances of the three motivation variables test anxiety, self-efficacy, and intrinsic value were allowed to be correlated. No other error variances were correlated.
Figures 1 and 2 show the path diagrams for female and male students respectively, for the physical domain. The path coefficients are shown for significant relationships only. The bias-corrected 95% confidence intervals for the regression weights (path coefficients) obtained using the maximum likelihood bootstrapping approach are shown in Table 3.
For female students (Figure 1), physical health was significantly associated with perceived stress, which significantly explained test anxiety, self-efficacy, and intrinsic value. Contentiousness was not a significant predictor of any of the three motivational beliefs, and enjoyment of competition significantly predicted test anxiety and intrinsic value. Both test anxiety and self-efficacy predicted grade outcome.
For male students (Figure 2), physical health was significantly associated with perceived stress, which significantly explained test anxiety and self-efficacy, but not intrinsic value. Contentiousness was a significant predictor of test anxiety, and enjoyment of competition significantly predicted test anxiety but not intrinsic value. Only self-efficacy predicted grade outcome.
|
Path |
Group | Lower | Upper |
| Physical QOL -> Perceived Stress | Female | -1.18 | -0.78 |
| Male | -1.14 | -0.58 | |
| Enjoy competition -> Test anxiety | Female | -0.10 | 0.01 |
| Male | -0.05 | 0.11 | |
| Enjoy competition -> Self-efficacy | Female | 0.13 | 0.34 |
| Male | 0.02 | 0.36 | |
| Enjoy competition -> Intrinsic value | Female | 0.03 | 0.19 |
| Male | -0.04 | 0.33 | |
| Contentiousness -> Test anxiety | Female | -0.10 | 0.10 |
| Male | -0.38 | -0.17 | |
| Contentiousness -> Self-efficacy | Female | -0.23 | 0.10 |
| Male | -0.39 | 0.05 | |
| Contentiousness -> Intrinsic value | Female | -0.15 | 0.12 |
| Male | -0.36 | 0.14 | |
| Perceived stress -> Test anxiety | Female | 0.21 | 0.35 |
| Male | 0.14 | 0.33 | |
| Perceived stress -> Self-efficacy | Female | -0.35 | -0.15 |
| Male | -0.44 | -0.05 | |
| Perceived stress -> Intrinsic value | Female | -0.21 | -0.05 |
| Male | -0.41 | 0.06 | |
| Test anxiety -> Grade | Female | -0.25 | -0.10 |
| Male | -0.24 | 0.13 | |
| Self-efficacy -> Grade | Female | 0.04 | 0.17 |
| Male | 0.01 | 0.28 | |
| Intrinsic value -> Grade | Female | -0.07 | 0.10 |
| Male | -0.16 |
0.14 |
Table 3. Lower and upper ends of bias-corrected 95% confidence intervals of the regression weights of the directional paths of the SEM. Confidence intervals are shown separately for females and males.
IV. DISCUSSION
The derived SEMs were able to systematically explore the relationships among physical health, competitiveness, perceived stress, motivational beliefs, and consider their impact on grade attainment among first-year pre-medical and health science students. The models considered all potential variable options and measures outlined in the Measures section above. These combinations were informed by prior work conducted in this research area (e.g., Chester et al., 2013; Friedlander et al., 2007; Henning, Krägeloh, Hawken, Zhao, & Doherty, 2010; Henning et al., 2011; Hilliard, 1995; Hussain et al., 2013; Lonka et al., 2008; Papier et al., 2014; Samaranayake & Fernando, 2011). In this study, we have also focused purely on physical health as a hard endpoint outcome variable and focused on the interactions between salient factors rather than creating a binary logistic argument and approach (Henning et al., 2017).
In the emergent model, the variables that resulted in the best fits included the exogenous variables physical health and measures of competitiveness. The process variables encompassed a global sense of perceived stress and motivational beliefs linked to self-efficacy, test anxiety, and intrinsic value. The outcome variable was the acquired Population Health grade on a pre-medical and health science degree course. Hence the model was able to identify and derive links among students’ characteristics, their experience of stress and motivation, and their grade achievement.
A. Exogenous variables: Physical health and competitiveness
Physical health and levels of competitiveness were considered as specific student attributes and this was reinforced by the best-fitted SEMs. The SEMs indicated that physical health significantly co-varied with enjoyment of competition and that there was a significant negative association with perceived stress. This suggests that physical health problems reported by students are likely interacting with stress, although the direction of effect cannot be directly inferred. Stress may impact physical health or vice versa. Nonetheless, physical health is a multidimensional variable and hence further research may need to consider more specific aspects of physical health relevant to this population, such as issues associated with sleep and fatigue (Samaranayake et al., 2014; Tanaka et al., 2008) with potential links with lifestyle choices (Kulkarni, 2016; Rustagi et al., 2011; Tanaka et al., 2008). The indirect effects and powerful predictive relationships between physical health, perceived stress and motivation are evidenced in our findings; however this relationship differed between male and female students with respect to grade achievement. These gender differences will be unpacked later in the discussion.
The notion of competitiveness employed in this study was derived from trait theory (Harris & Houston, 2010). In this study, competitiveness was seen more as a personal characteristic rather than a learned behaviour suggesting that this trait would be enhanced in certain circumstances that reflects a strong intention to succeed in competitive interpersonal situations (Musson, Sandal, & Helmreich, 2004). It is also related to the notion of conscientiousness or a strong sense of persistence in achieving one’s goals (Musson et al., 2004), which in turn relates to the competitive student environment of the biomedical sciences course. In their paper, Houston and colleagues (2002) developed two factors of competitiveness: enjoyment of competitiveness and contentiousness, with the latter concept describing a sense of defiance.
The findings of our study suggest that enjoyment of competition formed predictive relationships with self-efficacy and intrinsic value for female students and with only self-efficacy for male students. For the male data only, contentiousness formed a significant predictive relationship with test anxiety. It is likely that students who enjoy a sense of competition will do better academically, and this is consistent with our belief that students studying in the medical and health sciences are highly competitive and that the learning environment will likely escalate this behaviour (Coles, 1998; Rohe et al., 2006). In one study (Hancock, 2001), students were found to be more test anxious when they are more sensitive to competitive environments, agreeing somewhat with the results of the present study suggesting that the male students were more defiant (less sensitive) and thus less test anxious. One indirect effect on academic achievement was noted for enjoyment of competition only and this was via self-efficacy for both male and female students suggesting a significant interplay between enjoyment of competition and self- efficacy in terms of their predictive relationship with academic achievement.
B. Process variables: Perceived stress and motivation
Four factors were identified in this study in relation to the prediction of academic achievement. These included perceived stress, and the motivational belief variables of self-efficacy, test anxiety, and intrinsic value. According to the SEMs, perceived stress had an antecedent impact on the three motivational belief variables. Perceived stress was positively related to test anxiety and negatively associated with self-efficacy for all students.
Perceived stress can be seen as a generalized form of stress. Cohen and colleagues (1983) developed a global measure describing the impact that situational stressors may have on someone in their everyday life. The findings in our study showed that students who experienced relatively higher levels of everyday life stress are disadvantaged when it comes to developing their motivational beliefs as students. It could be inferred that the environment that one lives in as a person within society inevitably has an impact on the ‘student life’. However, differences were noted in the findings between male and female students, such that for male students there was no predictive relationship between perceived stress and intrinsic value, suggesting that the pre-medical and health science learning environment has differential effects on men and women, or there are differential perceived learning experiences being formed between the two groups. Differences between medical male and female student groups have been reported elsewhere in the literature but at a later level of education (Henning et al., 2013).
The findings further showed that the perceived stress impacted not only test anxiety but also had associations with self-efficacy and intrinsic value, although for male students the association between perceived stress and intrinsic value was not significant. Lee, Bong and Kim (2014) proposed that heightened stress is linked to the deployment of maladaptive strategies and that perceived stress affects educational competency. There is the potential for a feedback process that can create high levels of stress if students have lowered levels of expectancy about doing well and lowered confidence but at the same time value their course of study. In the SEMs in this present study, the optimal models do not account for this feedback mechanism and we would assume there are feedback links between the variables cited. Nonetheless, more research is required to fully explore the shape, direction and magnitude of these connections.
A gender difference was also noted in connection with the variable ‘Test anxiety’ such that test anxiety negatively predicted grade outcomes for female students only. Pintrich and Zusho (2007) stated in their paper that there is little evidence suggesting a difference between males and females in academic achievement. Nonetheless, in a further study, Henning and colleagues (2013) found differences between male and female medical students in their fourth and fifth years of study in reference to self-efficacy and test anxiety, with female students being more test anxious and less self-efficacious.
C. Grade outcome
In the present study, grade outcome was directly associated with the motivational variables test anxiety and self-efficacy for female students and only self-efficacy for male students. This suggests a difference in the way male students report their level of test anxiety or respond to the competitive factors within the learning environment. And this difference may be linked to the notion of sensitivity to the learning environment (Hancock, 2001); however further research is required to unpack this difference.
Similar to the present study, Pintrich and De Groot (1990) found strong associations between the motivational belief variables of self-efficacy, intrinsic value and test anxiety with grade outcome. Similarly, Henning et al. (2011) reported that written grade scores in a medical examination were related to these aspects of motivational beliefs in addition to aspects of self-regulation. However, the current findings showed that intrinsic value does not have a significant association with grade achievement suggesting that further research could investigate whether the role of extrinsic value is significant.
D. Limitations of the study and implications for educational research
The major limitation of this study is the response rate of 33%, although this is considered within the acceptable range for a purposive online survey (Nulty, 2008; Sax, Gilmartin, & Bryant, 2003). Nonetheless, the grade, age and gender distributions appear to be reasonable suggesting that any potential biases in the makeup of the sample are unlikely to change the interrelationships shown in the SEMs, but this potential limitation should nonetheless be acknowledged.
In this study, the illustrative models (Figures 1 and 2) suggest that students, in general, who have good physical health experiences will report less perceived stress, less test anxiety, and more self-efficacy and this then associates with positive grade outcomes. The results suggest that students who experience high levels of physical health will do better academically and this is partly explained because their motivational belief systems are enhanced. There are also subtle differences evident in the findings between the predictive relationships shown for the female students as opposed to their male peers, suggesting that ongoing work needs to be applied in ensuring equitable gender learning experiences. Moreover, physical health was chosen as the illustrative exemplar; however, similar linkages could also be explored in terms of psychological, social and environmental well-being.
From an educational perspective, these results suggest a conundrum, because, once selected into medical school, the educational ethos changes to one of collaboration and interprofessional practice, which could be perceived as antithetical to individual competitiveness (Reagan & Blakemore, 2009). The learning environment selects highly competitive students and then requires them to become collaborative or at least to appear so. A further area of research that will likely stem from this study is the type of competitiveness instilled in this year of study, whether this is in the form of ‘competing to win’ versus ‘competing to excel’ (Hibbard & Buhrmester, 2010). In this study, we only considered aspects of ‘enjoyment’ and ‘contentiousness’, whereas the study of competitive intention may yield interesting results that may prove to be invaluable in understanding the development of empathy and refining assessment protocols in this pre-medical and health science course, such as instilling more collaborative based assessment. Clearly, more work is needed to tease out these connections, which are likely best studied by longitudinal studies to assess prospective influences on later behaviours as professionals.
V. Conclusion
Physical health and competitiveness characteristics were considered in this paper and the findings clearly show that ‘enjoyment of competition’ is linked with motivational beliefs especially self-efficacy and intrinsic value, and eventually academic outcome. Simply put, students who enjoy competition have more interest in their subject, are more confident, and do better. From a functional perspective, it can be inferred that more competitive students will do better, although there is evidence to suggest that competitiveness leads to performance learning rather than mastery learning at the undergraduate level (Harackiewicz, Barron, Tauer, & Elliot, 2002). Interestingly, our findings showed that competitiveness had a positive relationship with intrinsic value for female students, indicating that the source of their competition may have an intrinsic form which is a positive outcome. However, further research needs to assess the influence of extrinsic value mechanisms and links with mastery versus performance learning (Harackiewicz et al., 2002).
Notes on Contributors
Marcus A. Henning is an associate professor in the Centre for Medical and Health Sciences Education at the University of Auckland, New Zealand.
Christian U. Krägeloh is an associate professor in the Department of Psychology at AUT University, New Zealand.
Roger Booth is an associate professor in molecular medicine and pathology, in the Faculty of Medical and Health Sciences at the University of Auckland, New Zealand.
Erin M. Hill is an assistant professor in the Department of Psychology at West Chester University, United States of America.
Julie Chen is an assistant professor in the Department of Family Medicine and Primary Care and Institute of Medical and Health Sciences Education, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong.
Craig Webster is a senior lecturer in the Centre for Medical and Health Sciences Education at the University of Auckland, New Zealand.
Ethical Approval
Ethics approval for the collection and use of data was obtained from the University of Auckland Human Participants Ethics Committee (Ref. 010641).
Acknowledgements
This paper was presented in part as an e-poster at APMEC conference, Singapore, January 2017 and, for which the authors won a Merit award.
Declaration of Interest
The authors declared no competing interest.
References
Blanch, D. C., Hall, J. A., Roter, D. L., & Frankel, R. M. (2008). Medical student gender and issues of confidence. Patient Education and Counseling, 72(3), 374-381.
https://doi.org/10.1016/j.pec.2008.05.021.
Byrne, B. M. (2010). Structural Equation Modeling with AMOS: Basic concepts, applications and programming (2nd ed.). New York: Routledge.
Chester, A., Burton, L. J., Xenos, S., & Elgar, K. (2013). Peer mentoring: Supporting successful transition for first year undergraduate psychology students. Australian Journal of Psychology, 65(1), 30-37.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 385-396.
Cohen, S., Kamarck, T., & Mermelstein, R. (1994). Perceived stress scale. Measuring stress: A guide for health and social scientists. Retrieved from
http://mindgarden.com/documents/PerceivedStressScale.pdf.
Coles, R. (1998). The moral education of medical students. Academic Medicine, 73(1), 55-57.
Elliott, D. C. (2014). Trailblazing: Exploring first-generation college students’ self-efficacy beliefs and academic adjustment. Journal of The First-Year Experience & Students in Transition, 26(2), 29-49.
Field, A. P. (2005). Discovering statistics using SPSS: And sex, drugs and rock’n’roll (2nd ed.). London, United Kingdom: SAGE.
Friedlander, L. J., Reid, G. J., Shupak, N., & Cribbie, R. (2007). Social support, self-esteem, and stress as predictors of adjustment to university among first-year undergraduates. Journal of College Student Development, 48(3), 259-274.
Google.com. (2015). Homepage. Retrieved February 13, 2015, from https://www.google.co.nz/forms/about/.
Hancock, D. R. (2001). Effects of test anxiety and evaluative threat on students’ achievement and motivation. The Journal of Educational Research, 94(5), 284-290.
Harackiewicz, J. M., Barron, K. E., Tauer, J. M., & Elliot, A. J. (2002). Predicting success in college: A longitudinal study of achievement goals and ability measures as predictors of interest and performance from freshman year through graduation. Journal of Educational Psychology, 94(3), 562.
Harris, P. B., & Houston, J. M. (2010). A reliability analysis of the revised competitiveness index 1. Psychological Reports, 106(3), 870-874.
Henning, M. A., Krägeloh, C. U., Hawken, S., Zhao, Y., & Doherty, I. (2010). Quality of life and motivation to learn: A study of medical students. Issues in Educational Research, 20(3), 244-256.
Henning, M. A., Krägeloh, C. U., Booth, R., Hill, E. M., Chen, J., & Webster, C. S. (2017). Profiling potential medical students and exploring determinants of career choice. The Asia-Pacific Scholar, 2(1). Retrieved from http://theasiapacificscholar.org/profiling-potential-medical-students-and-exploring-determinants-of-career-choice-2/.
Henning, M. A., Krägeloh, C. U., Hawken, S. J., Doherty, I., Zhao, Y., & Shulruf, B. (2011). Motivation to learn, quality of life and estimated academic achievement: Medical students studying in New Zealand. Medical Science Educator, 21(2), 142-150.
Henning, M. A., Krägeloh, C. U., Manalo, E., Doherty, I., Lamdin, R., & Hawken, S. J. (2013). Medical students in early clinical training and achievement motivation: Variations according to gender, enrolment status, and age. Medical Science Educator, 23(1), 6-15.
Hibbard, D. R., & Buhrmester, D. (2010). Competitiveness, gender, and adjustment among adolescents. Sex Roles, 63(5-6), 412-424.
Hilliard, R. I. (1995). How do medical students learn: medical student learning styles and factors that affect these learning styles. Teaching and Learning in Medicine: An International Journal, 7(4), 201-210.
Hojat, M., Glaser, K., Xu, G., Veloski, J. J., & Christian, E. B. (1999). Gender comparisons of medical students’ psychosocial profiles. Medical Education, 33, 342-349. https://doi.org/10.1046/j.1365-2923.1999.00331.x.
Hojat, M., Gonnella, J. S., Erdmann, J. B., & Vogel, W. H. (2003). Medical students’ cognitive appraisal of stressful life events as related to personality, physical wellbeing, and academic performance: A longitudinal study. Personality and Individual Differences, 35(1), 219-235.
Houston, J., Harris, P., McIntire, S., & Francis, D. (2002). Revising the competitiveness index using factor analysis. Psychological Reports, 90(1), 31-34.
Hu, L.-t., & Bentler, P. M. (1998). Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods, 3(4), 424-453.
Hussain, R., Guppy, M., Robertson, S., & Temple, E. (2013). Physical and mental health perspectives of first year undergraduate rural university students. BMC Public Health, 13(1), 848.
Ibrahim, N. K., Mahnashi, M., Al-Dhaheri, A., Al-Zahrani, B., Al-Wadie, E., Aljabri, M., . . . Bashawri, J. (2014). Risk factors of coronary heart disease among medical students in King Abdulaziz University, Jeddah, Saudi Arabia. BMC Public Health, 14(1), 411.
Krägeloh, C. U., Henning, M. A., Hawken, S., Zhao, Y., Shepherd, D., & Billington, R. (2011). Validation of the WHOQOL-BREF quality of life questionnaire for use with medical students. Education for Health, 24(2), 545. Retrieved from http://educationforhealth.net/publishedarticles/article_print_545.pdf.
Krägeloh, C. U., Kersten, P., Billington, D. R., Hsu, P. H.-C., Shepherd, D., Landon, J., & Feng, X. J. (2013). Validation of the WHOQOL-BREF quality of life questionnaire for general use in New Zealand: Confirmatory factor analysis and Rasch analysis. Quality of Life Research, 22(6), 1451-1457.
Kulkarni, M. V. (2016). Lifestyle disease risk behaviour among Medical Students in Central India. Panacea Journal of Medical Sciences, 6(2), 92-95.
Kusurkar, R. (2012). Motivation in medical students. Oisterwijk, Netherlands: Uitgeverij BOXPress
Kusurkar, R., Ten Cate, T. J., Van Asperen, M., & Croiset, G. (2011). Motivation as an independent and a dependent variable in medical education: A review of the literature. Medical Teacher, 33(5), e242-e262.
Lee, J., Bong, M., & Kim, S.-i. (2014). Interaction between task values and self-efficacy on maladaptive achievement strategy use. Educational Psychology, 34(5), 538-560.
Lonka, K., Sharafi, P., Karlgren, K., Masiello, I., Nieminen, J., Birgegård, G., & Josephson, A. (2008). MED NORD-A tool for measuring medical students’ wellbeing and study orientations. Medical Teacher, 30(1), 72 – 79.
https://doi.org/10.1080/01421590701769555.
Marsh, H. W., Balla, J. R., & McDonald, R. P. (1988). Goodness-of-fit indexes in confirmatory factor analysis: The effect of sample size. Psychological Bulletin, 103(3), 391-410.
Moffat, K. J., McConnachie, A., Ross, S., & Morrison, J. M. (2004). First year medical student stress and coping in a problem‐based learning medical curriculum. Medical Education, 38(5), 482-491.
Musson, D. M., Sandal, G., & Helmreich, R. L. (2004). Personality characteristics and trait clusters in final stage astronaut selection. Aviation, Space, and Environmental Medicine, 75(4), 342-349.
Nulty, D. D. (2008). The adequacy of response rates to online and paper surveys: What can be done? Assessment & Evaluation in Higher Education, 33(3), 301-314.
Papier, K., Ahmed, F., Lee, P., & Wiseman, J. (2015). Stress and dietary behaviour among first-year university students in Australia: Sex differences. Nutrition, 31(2), 324-330.
Park, J., Chung, S., An, H., Park, S., Lee, C., Kim, S. Y., . . . Kim, K.-S. (2012). A structural model of stress, motivation, and academic performance in medical students. Psychiatry Investigation, 9(2), 143-149.
Pintrich, P. R. (2003). A motivational science perspective on the role of student motivation in learning and teaching contexts. Journal of Educational Psychology, 95(4), 667-686.
Pintrich, P. R., & De Groot, E. V. (1990). Motivational and self-regulated learning components of classroom academic performance. Journal of Educational Psychology, 82(1), 33-40.
Pintrich, P. R., & Zusho, A. (2007). Student motivation and self-regulated learning in the college classroom. In R. P. Perry, & J. C. Smart (Eds.), The scholarship of teaching and learning in higher education: An evidence-based perspective, 731-810. Dordrecht, The Netherlands: Springer.
Reagan, J., & Blakemore, L. C. (2009). Competitiveness Can Undermine Team Goals. Virtual Mentor, 11(5), 368-372.
Roberti, J. W., Harrington, L. N., & Storch, E. A. (2006). Further psychometric support for the 10‐item version of the perceived stress scale. Journal of College Counseling, 9(2), 135-147.
Rohe, D. E., Barrier, P. A., Clark, M. M., Cook, D. A., Vickers, K. S., & Decker, P. A. (2006). The benefits of pass-fail grading on stress, mood, and group cohesion in medical students. Paper presented at the Mayo Clinic Proceedings.
Rustagi, N., Taneja, D. K., Mishra, P., & Ingle, G. K. (2011). Cardiovascular risk behavior among students of a Medical College in Delhi. Indian Journal of Community Medicine, 36(1), 51-53.
Samaranayake, C. B., Arroll, B., & Fernando, A. T. (2014). Sleep disorders, depression, anxiety and satisfaction with life among young adults: a survey of university students in Auckland, New Zealand. The New Zealand Medical Journal (Online), 127(1399), 13-22.
Samaranayake, C. B., & Fernando, A. T. (2011). Satisfaction with life and depression among medical students in Auckland, New Zealand. Women, 20(1341), 17-45.
Sax, L. J., Gilmartin, S. K., & Bryant, A. N. (2003). Assessing response rates and nonresponse bias in web and paper surveys. Research in Higher Education, 44(4), 409-432.
Sobral, D. T. (2004). What kind of motivation drives medical students’ learning quests? Medical Education, 38(9), 950-957.
Spencer, J. A., & Jordan, R. K. (1999). Learner centred approaches in medical education. BMJ, 318(7193), 1280-1283.
Tanaka, M., Mizuno, K., Fukuda, S., Shigihara, Y., & Watanabe, Y. (2008). Relationships between dietary habits and the prevalence of fatigue in medical students. Nutrition, 24(10), 985-989. The University of Auckland. (2015). Biomedical Common Year or Overlapping Year. Retrieved from http://www.science.auckland.ac.nz/en/about/our-programmes/op-biomed-common-year.html.
World Health Organisation. (1996). WHOQOL-BREF: Introduction, administration, scoring and generic version of the assessment. Retrieved from
http://www.who.int/mental_health/media/en/76.pdf?ua=1.
*Marcus A. Henning
Centre for Medical and Health Sciences Education
The University of Auckland
Private Bag 92019
Auckland 1142
New Zealand
E-mail: m.henning@auckland.ac.nz
Fax: 0064 9 3737204
Announcements
- Best Reviewer Awards 2025
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2025.
Refer here for the list of recipients. - Most Accessed Article 2025
The Most Accessed Article of 2025 goes to Analyses of self-care agency and mindset: A pilot study on Malaysian undergraduate medical students.
Congratulations, Dr Reshma Mohamed Ansari and co-authors! - Best Article Award 2025
The Best Article Award of 2025 goes to From disparity to inclusivity: Narrative review of strategies in medical education to bridge gender inequality.
Congratulations, Dr Han Ting Jillian Yeo and co-authors! - Best Reviewer Awards 2024
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2024.
Refer here for the list of recipients. - Most Accessed Article 2024
The Most Accessed Article of 2024 goes to Persons with Disabilities (PWD) as patient educators: Effects on medical student attitudes.
Congratulations, Dr Vivien Lee and co-authors! - Best Article Award 2024
The Best Article Award of 2024 goes to Achieving Competency for Year 1 Doctors in Singapore: Comparing Night Float or Traditional Call.
Congratulations, Dr Tan Mae Yue and co-authors! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors.
