Answer. E: None of the above, i.e. all four of these entities should be considered and assessed for as part of the workup for a clear cell tumour of the pancreas.
In this particular case, the cell block stained negatively for neuroendocrine markers CD56, synaptophysin, chromogranin, favouring against PNET, as well as melanocytic markers HMB45 and melan A, favouring against PEComa (‘clear cell sugar tumour’). Tumour stained positively for cytokeratins, inhibin and CAIX, with negativity for PAX8.
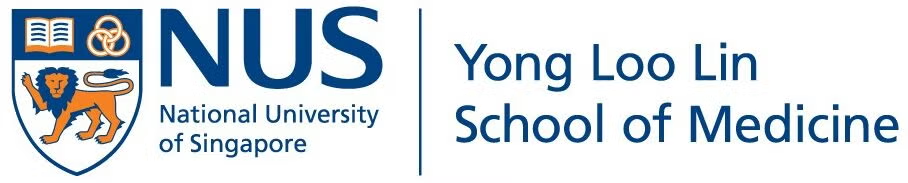
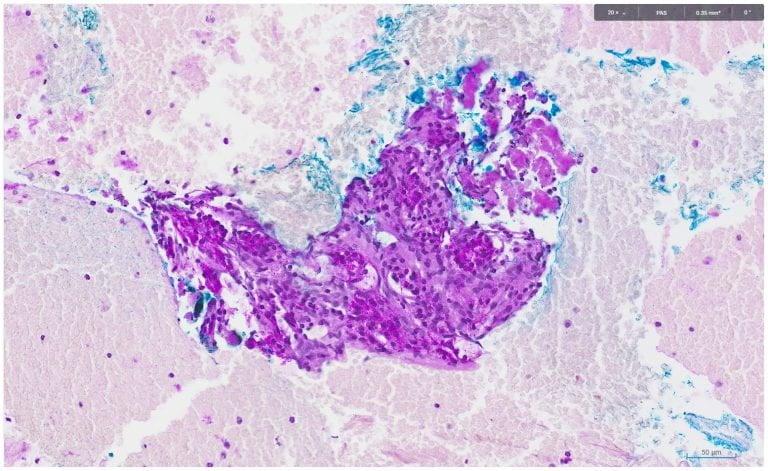
PAS and DPAS staining showed the following:
The overall cyto-histo-morphology and immuno-histochemical findings favour a diagnosis of serous cystadenoma.
Serous cystadenoma cytology typically consists of lesional groups with poor cohesiveness and architectural integrity, even less so than neuroendocrine tumours. Yields are often paucicellular, with abundant ‘stripped’ nuclei and loose groups or acini. Nuclei are usually small, round and uniform with chromatin that may have a degree of neuroendocrine-like hyperchromasia and granularity, though not as prominent.
The lesions are usually cystic, though solid tumours have been described. They stain positively for GLUT1, inhibin and CAIX, with these results potentially leading to diagnostic confusion with adrenal and renal-derivation tumours hence the need to utilise a wider panel of markers and clinical-histomorphological correlation in conjunction with the immunohistochemistry.
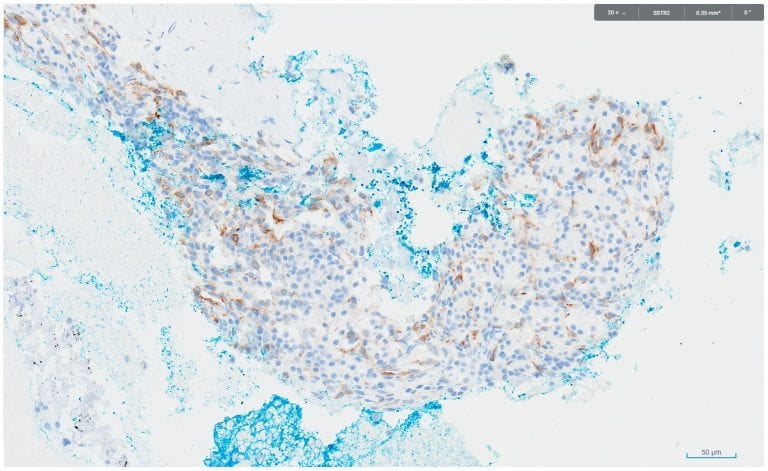
While they are negative for traditional neuroendocrine markers, somatostain receptor expression has been described, which can lead to positive uptake on Dotatate scanning, leading to further potential confusion with neuroendocrine tumours. In this case the tumour showed positive immunostaining for SSTR2.
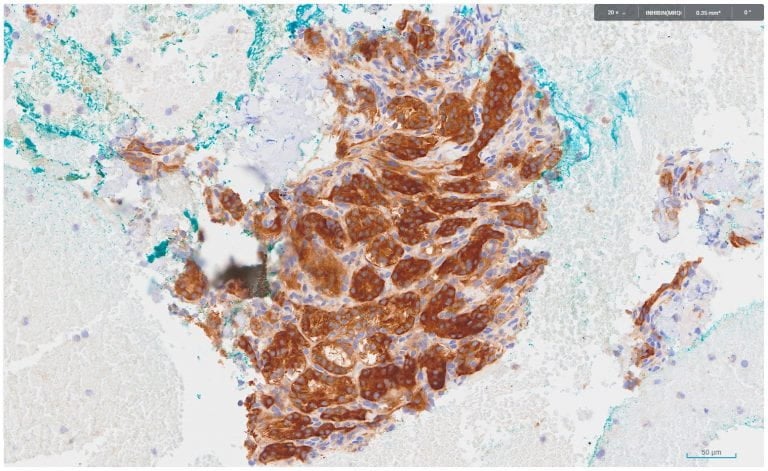
Additional images:
Inhibin (Immunoperoxidase 20x)
SSTR2 (Immunoperoxidase 20x)