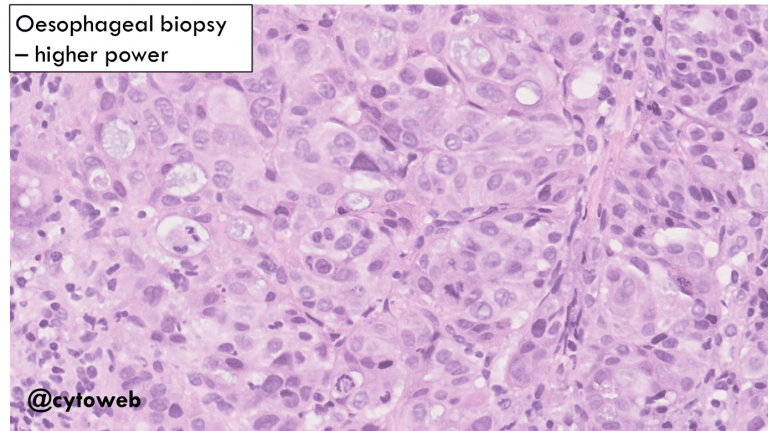
The malignant cells show features of adenocarcinoma.
Elimination of “suspects” based on the options in the Bethesda System for Reporting Thyroid Cytopathology:
The appearance of the tumour cells is NOT typical of primary thyroid carcinoma (follicular carcinoma, papillary thyroid carcinoma, medullary thyroid carcinoma or anaplastic carcinoma).
Possible remaining options:
- Metastatic malignancy: This is the favoured diagnosis as a second distinct population of benign thyroid cells are admixed with the carcinoma (see below).
- Poorly differentiated carcinoma (of the thyroid): this is often associated with differentiated carcinoma, which we may consider given the patient’s self-reported history of a previous thyroid operation.
Note: Dysphagia may be seen in advanced thyroid carcinoma but is not common.
Possible primary sources of a metastatic adenocarcinoma to the thyroid to consider:
- Lung adenocarcinoma
- Renal cell carcinoma (not likely the clear cell type)
- Breast carcinoma (invasive carcinoma of no special type)
- Gastrointestinal tract/pancreatobiliary adenocarcinoma
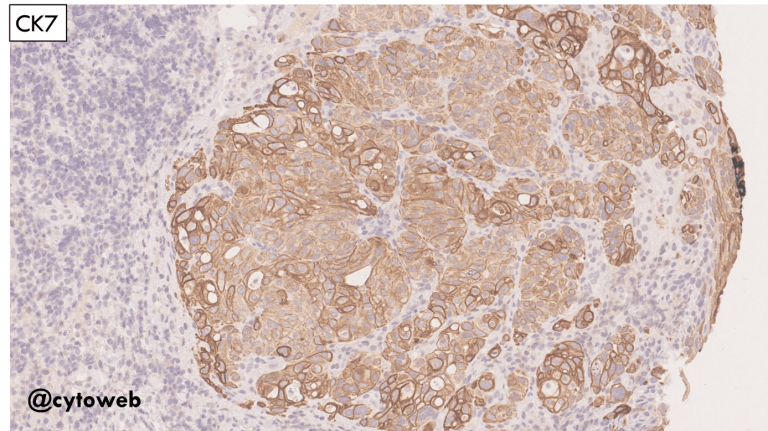
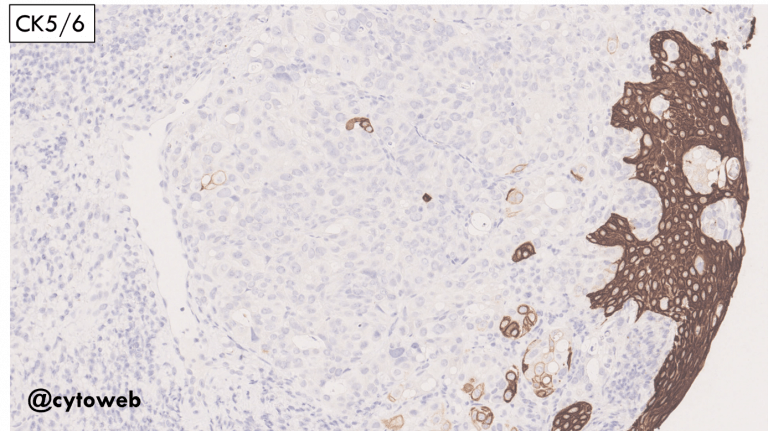
Knowledge of relevant clinical history and immunocytochemistry on cell block would be very helpful in the DDx.