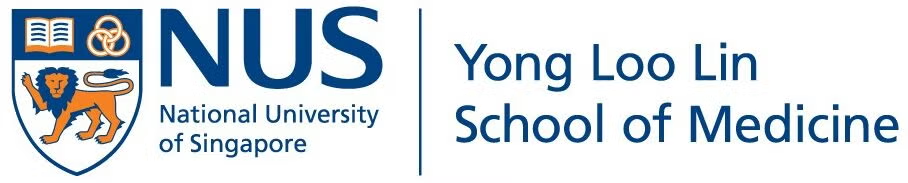
The important morphologic differential diagnosis to consider include:
1. Primary thyroid carcinoma – papillary thyroid carcinoma; possibly with dedifferentiation to anaplastic carcinoma
2. Metastatic poorly differentiated carcinoma
3. Treatment induced atypia
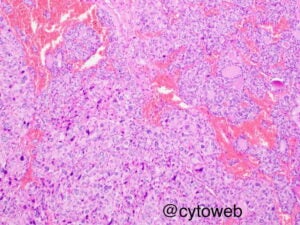
The presence of significant cytologic atypia in any thyroid FNA sample should not render an unequivocal benign diagnosis; think about malignancy, think hard!
Anaplastic carcinoma of the thyroid is an important consideration based on the cytomorphology. However, the young age of the patient and the clinical history of neck irradiation and systemic chemotherapy makes anaplastic carcinoma less likely. There was also no rapid enlargement of the thyroid nodules in this case which is a hallmark of anaplastic carcinoma.
The diagnosis of metastatic carcinoma is less likely due to the young age of the patient and lack of significant clinical history of a primary cancer elsewhere.
Lymphomatous involvement (particularly Hodgkin) of the thyroid is also less likely because the atypical cells are present as single cells and as part of the follicles. No small lymphocytes are present in the background.
Treatment induced atypia may be considered because of the history of both radiation therapy and chemotherapy.