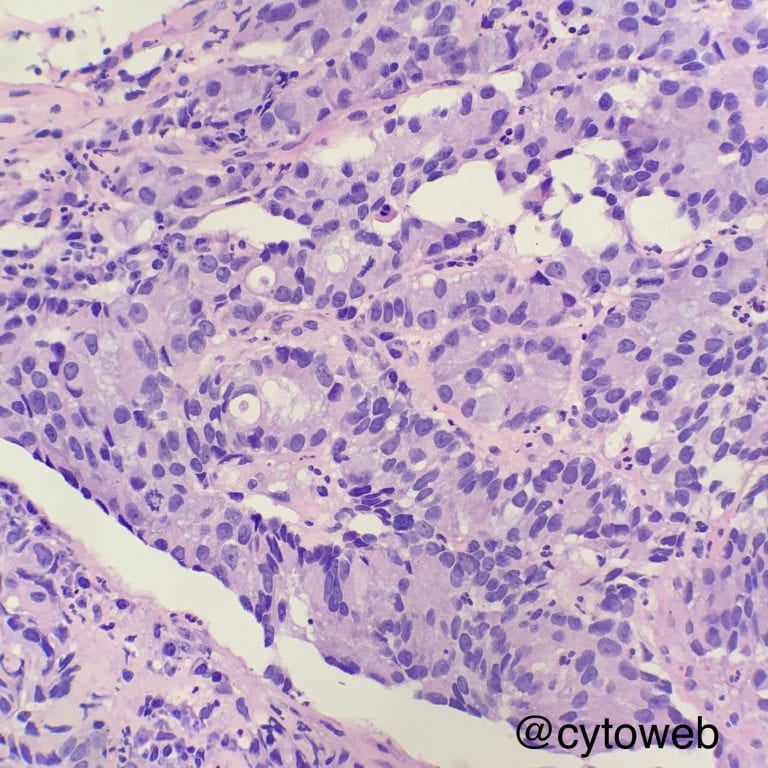
The disordered architecture (overlapping cells) and atypical cytologic features (mild nuclear pleomorphism, nuclear membrane irregularity) should prompt consideration of malignancy. The common primary malignant tumours of the lung include adenocarcinoma, squamous cell carcinoma and small cell carcinoma. Small cell carcinoma is ruled out in this instance because of the low N:C ratio of the cells in this specimen, leaving two main diagnoses:
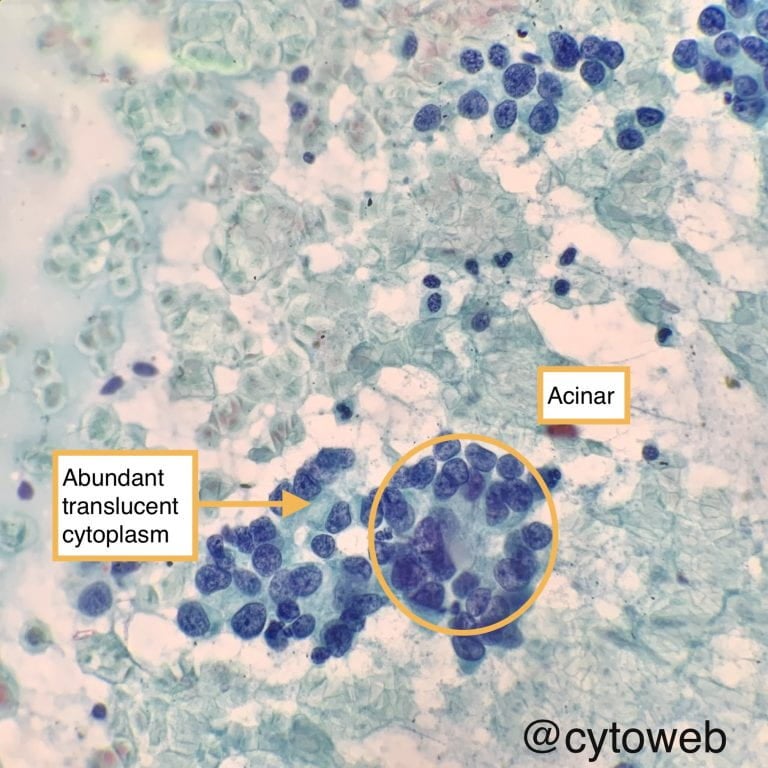
- Adenocarcinoma
- Sheets, acini and papillae with fibrovascular core
- Finely textured chromatin
- Eccentric nuclei
- Abundant, translucent, vacuolated cytoplasm
- Squamous cell carcinoma
- Sheets with nuclei streaming in parallel fashion
- Coarsely textured chromatin
- Dense cytoplasm if keratinised cells are present (Robin blue on DQ, orangeophilic on PAP)
- Bizarrely shaped individual keratinised cells, if present (tadpole or fibre cells)
It should also be noted that the lung is a frequent site of metastases, in particular carcinoma from the visceral organs. The common sources of malignancy include the colorectum, kidney, breast, female genital tract, prostate, urinary system, upper gastrointestinal tract, pancreatobiliary tract, liver and thyroid.
Clues to metastases:
- Relevant history and imaging findings (e.g. bilateral lung nodules suggests metastases vs solitary lung mass)
- Morphology of some common metastase:
- Colorectum: columnar cells (picket fence appearance), cigar-shaped nuclei with nuclear palisading, background dirty necrosis
- Breast (lobular variant): single file arrangement with mucin-containing intracytoplasmic lumina
- Kidney (clear cell variant): large cells with abundant clear / vacuolated cytoplasm and poorly defined cell membranes
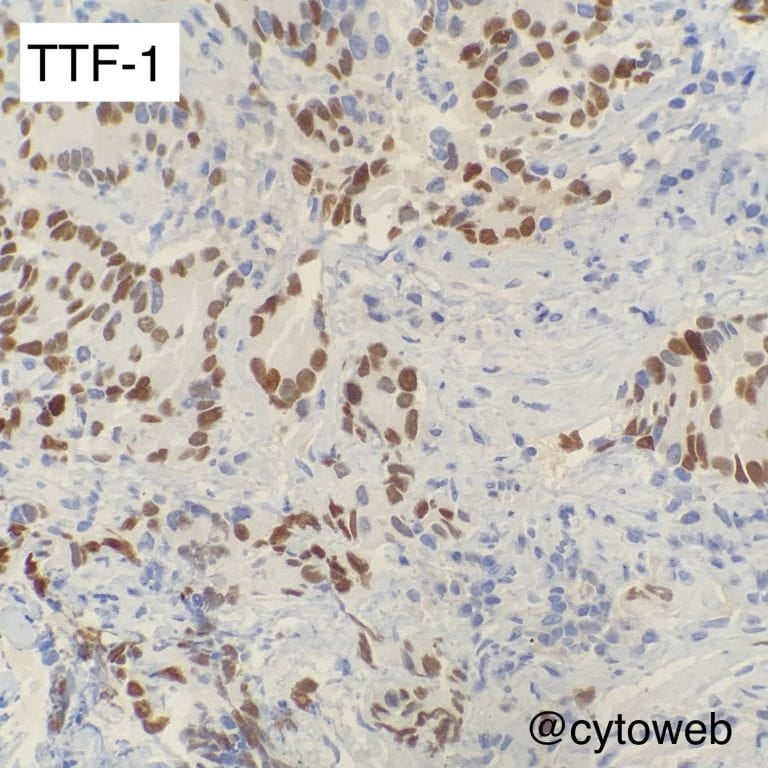
- Immunohistochemistry: some useful markers to suggest possible sites of tumour origin
- TTF-1: primary lung adenocarcinoma, thyroid and small cell carcinoma of any site
- PAX8: thyroid, renal, female genital tract
- ER: breast and female genital tract (a subset of tumours)
- GATA3: urinary system, breast, some endocrine tumours (e.g. parathyroid, paraganglioma)
- CDX2: gastrointestinal tract (in general, diffuse for colorectum, patchy for upper tract and pancreatic tumours)