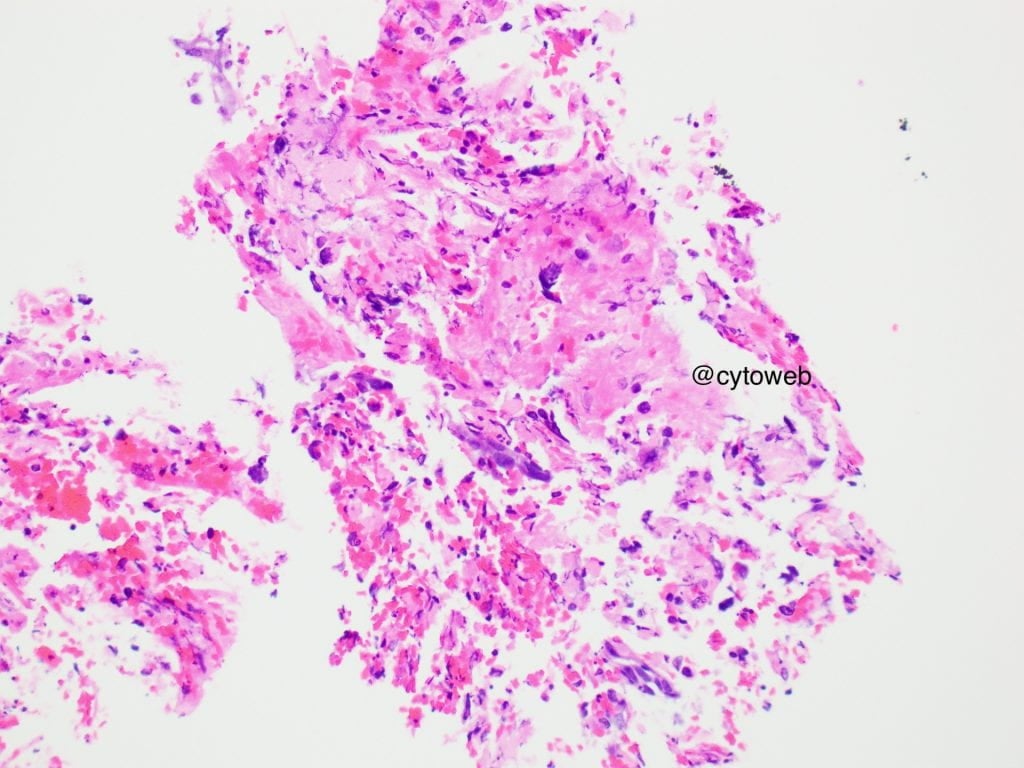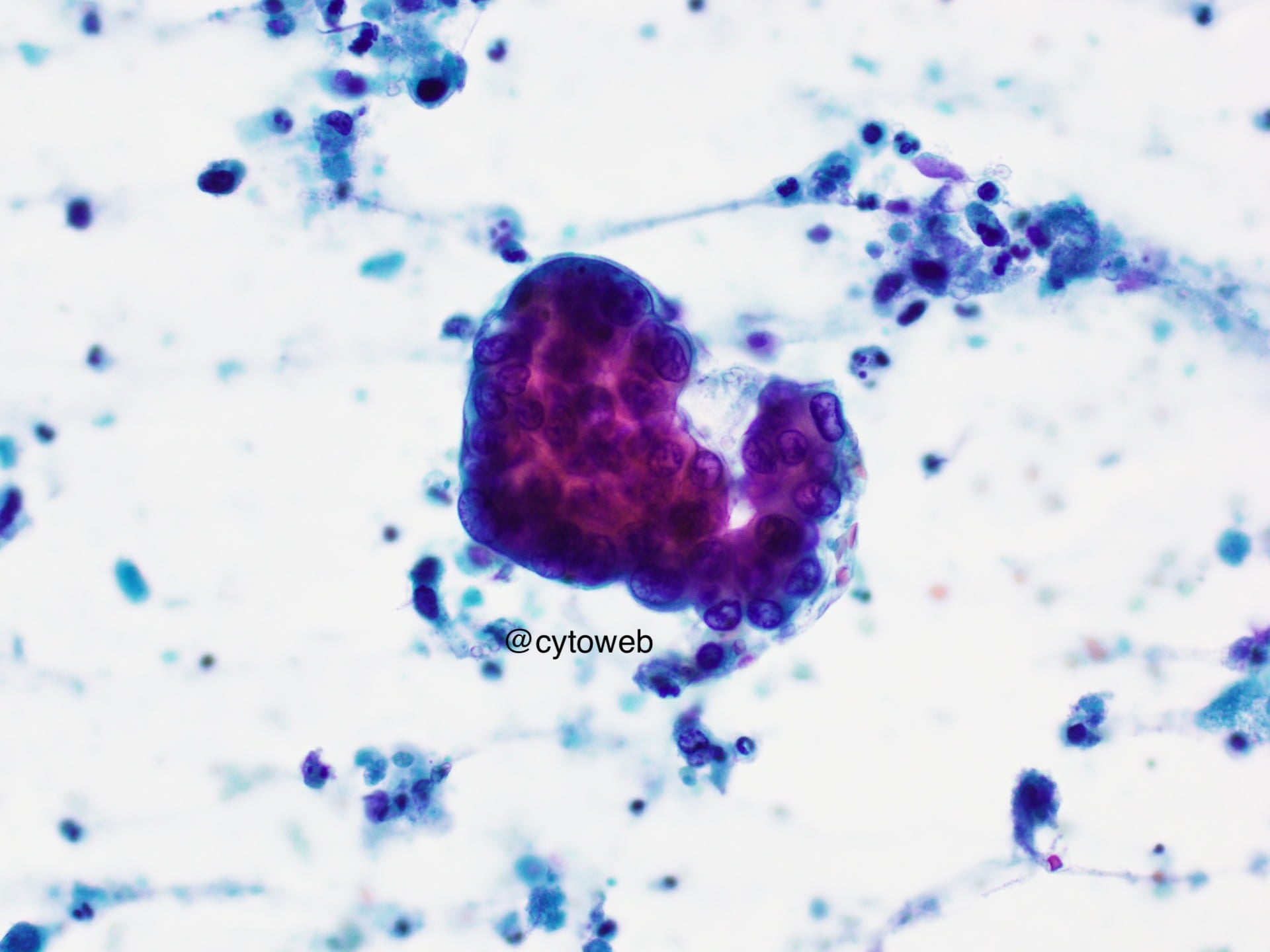
- Small clusters and single dispersed plasmacytoid cells
- Oval vesicular nuclei, coarse chromatin and moderate nuclear pleomorphism
- Moderate amounts of cytoplasm
- Necrotic background
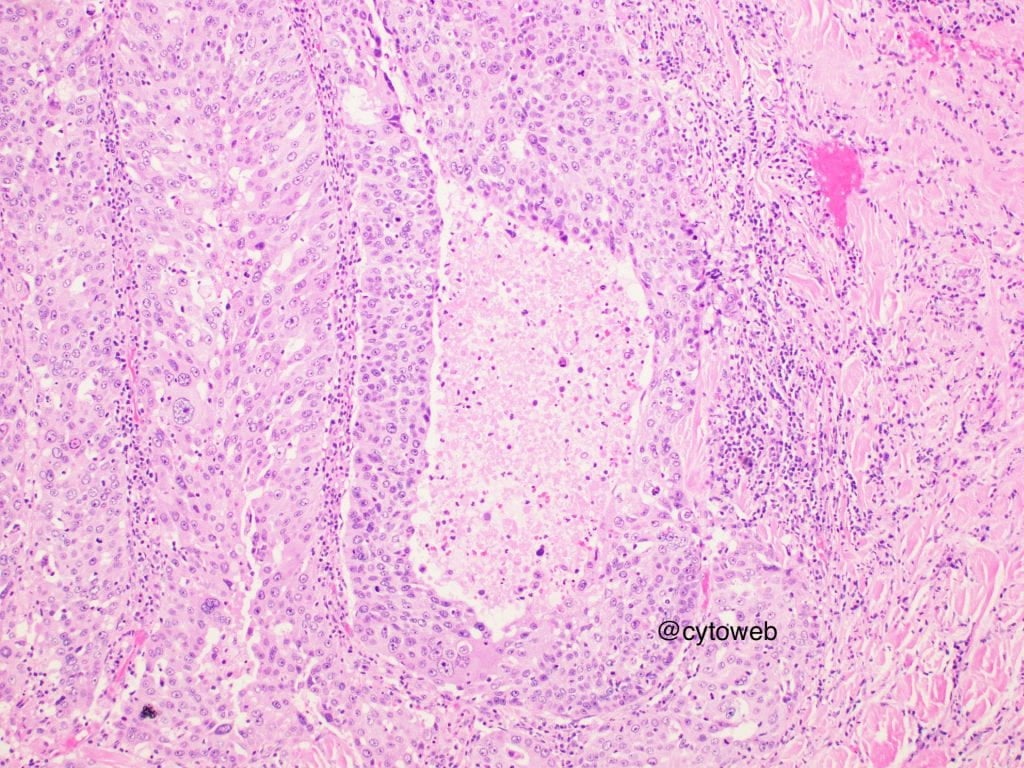
Commentary: Provisionally, the diagnosis is a high grade carcinoma.
In the salivary gland, the differential diagnoses include:
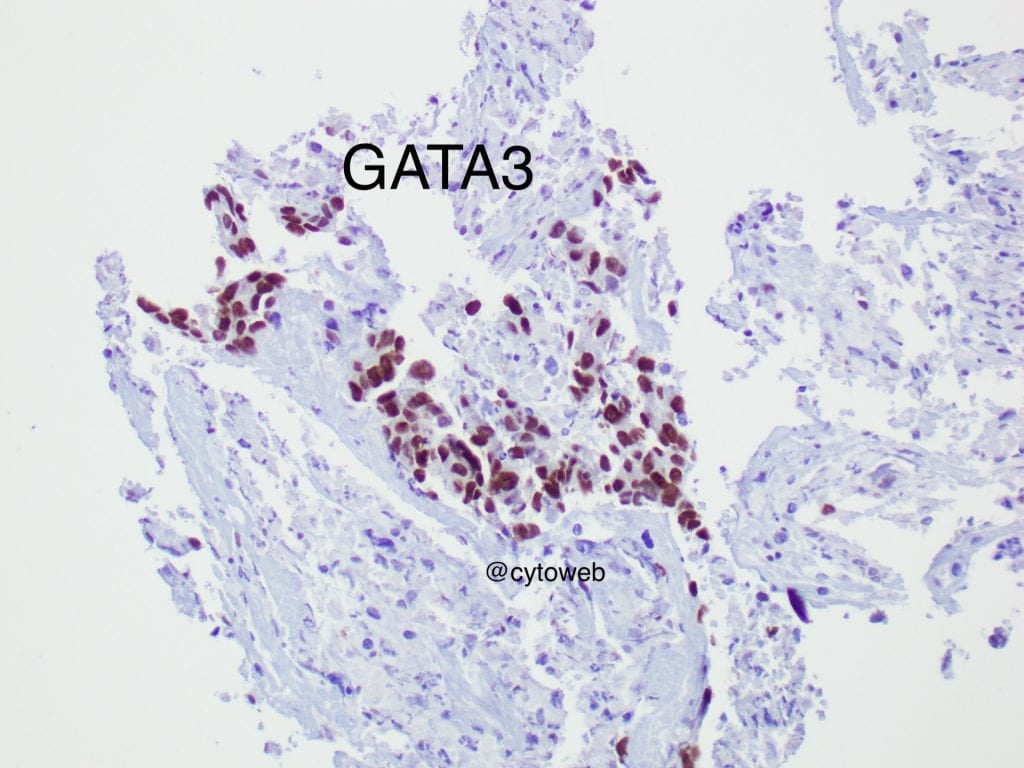
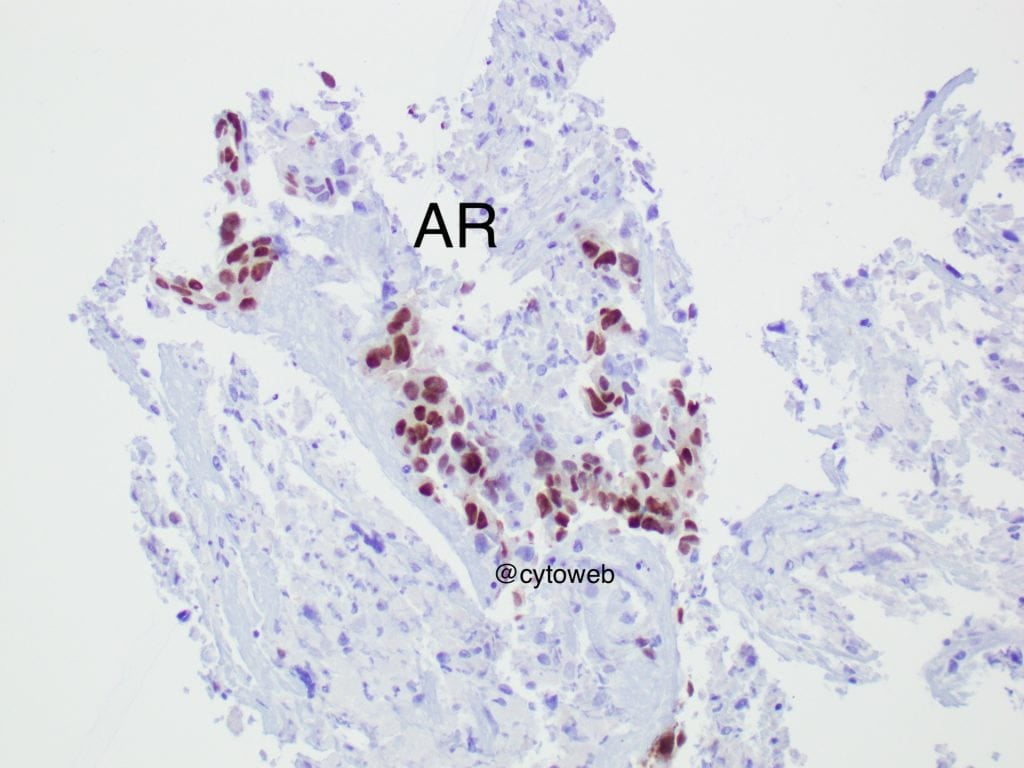
- Salivary duct carcinoma
- High grade mucoepidermoid carcinoma
- High grade myoepithelial carcinoma
- Adenocarcinoma, NOS
- Metastasis
Distinction of these entities may not be possible based on morphology and the use of immunocytochemistry could further refine the diagnosis. Hence, additional sampling for a cell block should be obtained from the FNA procedure, whenever a clinically aggressive salivary gland lesion is suspected. If further diagnostic characterisation is not possible, the tumour may be signed out as a "high grade carcinoma". Importantly, even if the carcinoma cannot be specifically typed, the high grade nature of the tumour should be conveyed to the clinician so that radical surgery can be planned accordingly.
In the salivary gland, a high grade malignant tumour may arise de novo or due to high grade transformation of a low grade malignancy e.g. adenoid cystic carcinoma or a benign tumour like pleomorphic adenoma. A distinct lower grade / benign component may be present on the smear.